User login
Are You Delivering on the Promise of Higher Quality?
One hospitalist-led pilot project produced a 61% decrease in heart failure readmission rates. Another resulted in a 33% drop in all-cause readmissions. The numbers might be impressive, but what do they really say about how hospitalists have influenced healthcare quality?
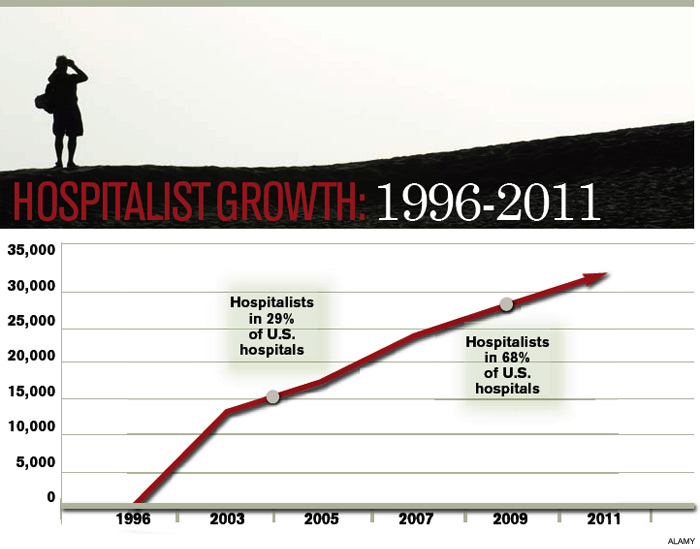
When HM emerged 15 years ago, advocates pitched the fledgling physician specialty as a model of efficient inpatient care, and subsequent findings that the concept led to reductions in length of stay encouraged more hospitals to bolster their staff with the newcomers. With a rising emphasis on quality and patient safety over the past decade, and the new era of pay-for-performance, the hospitalist model of care has expanded to embrace improved quality of care as a chief selling point.
Measuring quality is no easy task, however, and researchers still debate the relative merits of metrics like 30-day readmission rates and inpatient mortality. "Without question, quality measurement is an imperfect science, and all measures will contain some level of imprecision and bias," concluded a recent commentary in Health Affairs.1
Against that backdrop, relatively few studies have looked broadly at the contributions of hospital medicine. Most interventions have been individually tailored to a hospital or instituted at only a few sites, precluding large-scale, head-to-head comparisons.
And so the question remains: Has hospital medicine lived up to its promise on quality?
The Evidence
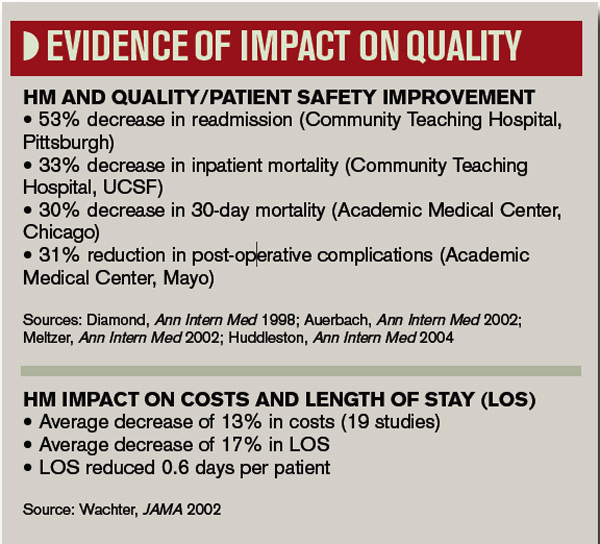
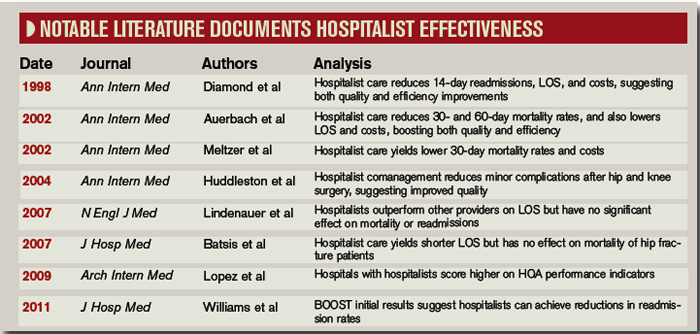
In one of the few national surveys of HM’s impact on patient care, a yearlong comparison of more than 3,600 hospitals found that the roughly 40% that employed hospitalists scored better on multiple Hospital Quality Alliance indicators. The 2009 Archives of Internal Medicine study suggested that hospitals with hospitalists outperformed their counterparts in quality metrics for acute myocardial infarction, pneumonia, overall disease treatment and diagnosis, and counseling and prevention. Congestive heart failure was the only category of the five reviewed that lacked a statistically significant difference.2
A separate editorial, however, argued that the study’s data were not persuasive enough to support the conclusion that hospitalists bring a higher quality of care to the table.3 And even less can be said about the national impact of HM on newly elevated metrics, such as readmission rates. The obligation to gather evidence, in fact, is largely falling upon hospitalists themselves, and the multitude of research abstracts from SHM’s annual meeting in May suggests that plenty of physician scientists are taking the responsibility seriously. Among the presentations, a study led by David Boyte, MD, assistant professor of medicine at Duke University and a hospitalist at Durham Regional Hospital, found that a multidisciplinary approach greatly improved one hospital unit’s 30-day readmission rates for heart failure patients. After a three-month pilot in the cardiac nursing unit, readmission rates fell to 10.7% from 27.6%.4
Although the multidisciplinary effort has included doctors, nurses, nutritionists, pharmacists, unit managers, and other personnel, Dr. Boyte says the involvement of hospitalists has been key to the project’s success. "We feel like we were the main participants who could see the whole picture from a patient-centered perspective," he says. "We were the glue; we were the center node of all the healthcare providers." Based on that dramatic improvement, Dr. Boyte says, the same interventional protocol has been rolled out in three other medical surgical units, and the hospital is using a similar approach to address AMI readmission rates.
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions; www.hospitalmedicine.org/boost )—by far the largest study of how HM is impacting readmission rates—has amassed data from more than 20 hospitals, with more expected from a growing roster of participants. So far, however, the project has only released data from six pilot sites describing the six-month periods before and after the project’s start. Among those sites, initial results suggest that readmission rates fell by an average of more than 20%, to 11.2% from 14.2%.5
Though the early numbers are encouraging, experts say rates from a larger group of participants at the one-year mark will be more telling, as will direct comparisons between BOOST units and nonparticipating counterparts at the same hospitals. Principal investigator Mark Williams, MD, FHM, professor and chief of the division of hospital medicine at the Northwestern University Feinberg School of Medicine in Chicago, says researchers still need to clean up that data before they’re ready to share it publicly.
In the meantime, some individual BOOST case studies are suggesting that hospitalist-led changes could pay big dividends. To help create cohesiveness and a sense of ownership within its HM program, St. Mary’s Health Center in St. Louis started a 20-bed hospitalist unit in 2008. Philip Vaidyan, MD, FACP, head of the hospitalist program and practice group leader for IPC: The Hospitalist Company at St. Mary’s, says one unit, 3 West, has since functioned as a lab for testing new ideas that are then introduced hospitalwide.
One early change was to bring all of the unit’s care providers together, from doctors and nurses to the unit-based case manager and social worker, for 9 a.m. handoff meetings. "We have this collective brain to find unique solutions," Dr. Vaidyan says. After seeing positive trends on length of stay, 30-day readmission rates, and patient satisfaction scores, St. Mary’s upgraded to a 32-bed hospitalist unit in early 2009. That same year, the 525-bed community teaching hospital was accepted into the BOOST program.
The hospitalist unit’s improved quality scores continued under BOOST, leading to a 33% reduction in readmission rates from 2008 to 2010 (to 10.5% from 15.7%). Rates for a nonhospitalist unit, by contrast, hovered around 17%. "For reducing readmissions, people may think that you have to have a higher length of stay," Dr. Vaidyan says. But the unit trended toward a lower length of stay, in addition to its reduced 30-day readmissions and improved patient satisfaction scores.

Flush with success, the 10 physicians and four nurse practitioners in the hospitalist program have since begun spreading their best practices to the rest of the hospital units. "Hospitalists are in the best ‘sweet spot,’ " Dr. Vaidyan says, "partnering with all of the disciplines, bringing them together, and keeping everybody on the same page."
Ironically, pinpointing the contribution of hospitalists is harder when their changes produce an ecological effect throughout an entire institution, says Siddhartha Singh, MD, MS, associate chief medical officer of Medical College Physicians, the adult practice for Medical College of Wisconsin in Milwaukee. Even so, he stresses that the impact of the two dozen hospitalists at Medical College Physicians has been felt.
"Coinciding with and following the introduction of our hospitalist program in 2004, we have noticed dramatic decreases in our length of stay throughout medicine services," he says. The same has held true for inpatient mortality. "And that, we feel, is attributable to the standardization of processes introduced by the hospitalist group." Multidisciplinary rounds; whiteboards in patient rooms; and standardized admission orders, prophylactic treatments, and discharge processes—"all of this would’ve been impossible, absolutely impossible, without the hospitalist," he says.
Over the past decade, Dr. Singh’s assessment has been echoed by several studies suggesting that individual hospitalist programs have brought significant improvements in quality measures, such as complication rates and inpatient mortality. In 2002, for example, Andrew Auerbach, MD, MPH, at the University of California San Francisco Medical Center, led a study that compared HM care with that of community physicians in a community-based teaching hospital. Patients cared for by hospitalists, the study found, had a lower risk of death during the hospitalization, as well as at 30 days and 60 days after discharge.6

A separate report by David Meltzer, MD, PhD, and colleagues at the University of Chicago found that an HM program in an academic general medicine service led to a 30% reduction in 30-day mortality rates during its second year of operation.7 And a 2004 study led by Jeanne Huddleston, MD, at the Mayo Clinic College of Medicine in Rochester, Minn., found that a hospitalist-orthopedic co-management model (versus care by orthopedic surgeons with medical consultation) led to more patients being discharged with no complications after elective hip or knee surgery.8 Hospitalist co-management also reduced the rate of minor complications, but had no effect on actual length of stay or cost.
A subsequent study by the same group, however, documented improved efficiency of care through the HM model, but no effect on the mortality of hip fracture patients up to one year after discharge.9 Multiple studies of hospitalist programs, in fact, have seen increased efficiency but little or no impact on inpatient mortality, leading researchers to broadly conclude that such programs can decrease resource use without compromising quality.
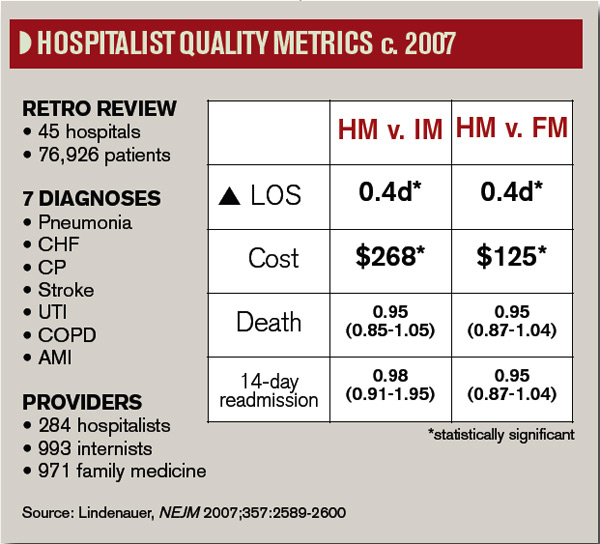
In 2007, a retrospective study of nearly 77,000 patients admitted to 45 hospitals with one of seven common diagnoses compared the care delivered by hospitalists, general internists, and family physicians.10 Although the study authors found that hospitalist care yielded a small drop in length of stay, they saw no difference in the inpatient mortality rates or 14-day readmission rates. More recently, mortality has become ensnared in controversy over its reliability as an accurate indicator of quality.

-Shai Gavi, DO, MPH, chief, section of hospital medicine, assistant professor, Stony Brook University School of Medicine, Brookhaven, N.Y.
Half of the Equation
Despite a lack of ideal metrics, another promising sign for HM might be the model’s exportability. Lee Kheng Hock, MMed, senior consultant and head of the Department of Family Medicine and Continuing Care at Singapore General Hospital, says the 1,600-bed hospital began experimenting with the hospitalist model when officials realized the existing care system wasn’t sustainable. Amid an aging population and increasingly complex and fragmented care, Hock views the hospitalist movement as a natural evolution of the healthcare system to meet the needs of a changing environment.
In a recent study, Hock and his colleagues used the hospital’s administrative database to examine the resource use and outcomes of patients cared for in 2008 by family medicine hospitalists or by specialists.11 The comparison, based on several standard metrics, found no significant improvements in quality, with similar inpatient mortality rates and 30-day, all-cause, unscheduled readmission rates regardless of the care delivery method. The study, though, revealed a significantly shorter hospital stay (4.4 days vs. 5.3 days) and lower costs per patient for those cared for by hospitalists ($2,250 vs. $2,500).11
Hock points out that, like his study, most analyses of hospitalist programs have shown an improvement in length of stay and cost of care without any increase in mortality and morbidity. If value equals quality divided by cost, he says, it stands to reason that quality must increase as overall value remains the same but costs decrease.
"The main difference is that the patients received undivided attention from a well-rounded generalist physician who is focused on providing holistic general medical care," Hock says, adding that "it is really a no-brainer that the outcome would be different."
Patients Rule
Other measures like the effectiveness of communication and seamlessness of handoffs often are assessed through their impacts on patient outcomes. But Sunil Kripalani, MD, MSc, SFHM, chief of the section of hospital medicine and an associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., says communication is now a primary focal point in Medicare’s new hospital value-based purchasing program (VBP). Within VBP’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) component, worth 30% of a hospital’s sum score, four of the 10 survey-based measures deal directly with communication. Patients’ overall rating and recommendation of hospitals likely will reflect their satisfaction with communication as well. Dr. Kripalani says it’s inevitable that hospitals—and hospitalists—will pay more attention to communication ratings as patients become judges of quality.
The expertise of hospitalists in handling challenging patients also leads to improved quality over time, says Shai Gavi, DO, MPH, chief of the section of hospital medicine and assistant professor of clinical medicine at Stony Brook University School of Medicine in Brookhaven, N.Y. Hospitalists, he says, excel in handling such high-stakes medical issues as gastrointestinal bleeding, pancreatitis, sepsis, and pain management that can quickly impact patient outcomes if not addressed properly and proficiently. "I think there’s significant value to having people who do this on a pretty frequent basis," he says.
And because of their broad day-to-day interactions, Dr. Gavi says, hospitalists are natural choices for committees focused on improving quality. "When we sit on committees, people often look to us for answers and directions because they know we’re on the front lines and we’ve interfaced with all of the services in the hospital," he says. "You have a good view of the whole hospital operation from A to Z, and I think that’s pretty unique to hospitalists."
The Verdict
In a recent issue brief by Lisa Sprague, principal policy analyst at the National Health Policy Forum, she asserts, "Hospitalists have the undeniable advantage of being there when a crisis occurs, when a patient is ready for discharge, and so on."12
So is "being there" the defining concept of hospital medicine, as she subsequently suggests?
Based on both scientific and anecdotal evidence, the contribution of hospitalists to healthcare quality might be better summarized as "being involved." Whether as innovators, navigators, physician champions, the "sweet spot" of interdepartmental partnerships, the "glue" of multidisciplinary teams, or the nuclei of performance committees, hospitalists are increasingly described as being in the middle of efforts to improve quality. On this basis, the discipline appears to be living up to expectations, though experts say more research is needed to better assess the impacts of HM on quality.
Dr. Vaidyan says hospitalists are particularly well positioned to understand what constitutes ideal care from the perspective of patients. "They want to be treated well: That’s patient satisfaction," he says. "They want to have their chief complaint—why they came to the hospital—properly addressed, so you need a coordinated care team. They want to go home early and don’t want come back: That’s low length of stay and a reduction in 30-day readmissions. And they don’t want any hospital-acquired complications."
Treating patients better, then, should be reflected by improved quality, even if the participation of hospitalists cannot be precisely quantified. "Being involved is something that may be difficult to measure," Dr. Gavi says, "but nonetheless, it has an important impact." TH
Bryn Nelson is a medical writer based in Seattle.
References
- Pronovost PJ, Lilford R. Analysis & commentary: A roadmap for improving the performance of performance measures. Health Aff (Millwood). 2011;30(4):569-73.
- López L, Hicks LS, Cohen AP, McKean S, Weissman JS. Hospitalists and the quality of care in hospitals. Arch Intern Med. 2009;169(15):1389-1394.
- Centor RM, Taylor BB. Do hospitalists improve quality? Arch Intern Med. 2009;169(15):1351-1352.
- Boyte D, Verma L, Wightman M. A multidisciplinary approach to reducing heart failure readmissions. J Hosp Med. 2011;6(4)Supp 2:S14.
- Williams MV, Hansen L, Greenwald J, Howell E, et al. BOOST: impact of a quality improvement project to reduce rehospitalizations. J Hosp Med. 2011;6(4) Supp 2:S88. BOOST: impact of a quality improvement project to reduce rehospitalizations.
- Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859-865.
- Meltzer D, Manning WG, Morrison J, et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(1):866-874.
- Huddleston JM, Hall K, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty. Ann Intern Med. 2004;141(1):28-38.
- Batsis JA, Phy MP, Melton LJ, et al. Effects of a hospitalist care model on mortality of elderly patients with hip fractures. J Hosp Med. 2007;2(4): 219–225.
- Lindenauer PK, Rothberg MB, Pekow PS, et al. Outcomes of care by hospitalists, general internists, and family physicians. N Eng J Med. 2007;357:2589-2600.
- Hock Lee K, Yang Y, Soong Yang K, Chi Ong B, Seong Ng H. Bringing generalists into the hospital: outcomes of a family medicine hospitalist model in Singapore. J Hosp Med. 2011;6(3):115-121.
- Sprague L. The hospitalist: better value in inpatient care? National Health Policy Forum website. Available at: www.nhpf.org/library/issue-briefs/IB842_Hospitalist_03-30-11.pdf. Accessed June 28, 2011.
One hospitalist-led pilot project produced a 61% decrease in heart failure readmission rates. Another resulted in a 33% drop in all-cause readmissions. The numbers might be impressive, but what do they really say about how hospitalists have influenced healthcare quality?
When HM emerged 15 years ago, advocates pitched the fledgling physician specialty as a model of efficient inpatient care, and subsequent findings that the concept led to reductions in length of stay encouraged more hospitals to bolster their staff with the newcomers. With a rising emphasis on quality and patient safety over the past decade, and the new era of pay-for-performance, the hospitalist model of care has expanded to embrace improved quality of care as a chief selling point.
Measuring quality is no easy task, however, and researchers still debate the relative merits of metrics like 30-day readmission rates and inpatient mortality. "Without question, quality measurement is an imperfect science, and all measures will contain some level of imprecision and bias," concluded a recent commentary in Health Affairs.1
Against that backdrop, relatively few studies have looked broadly at the contributions of hospital medicine. Most interventions have been individually tailored to a hospital or instituted at only a few sites, precluding large-scale, head-to-head comparisons.
And so the question remains: Has hospital medicine lived up to its promise on quality?
The Evidence
In one of the few national surveys of HM’s impact on patient care, a yearlong comparison of more than 3,600 hospitals found that the roughly 40% that employed hospitalists scored better on multiple Hospital Quality Alliance indicators. The 2009 Archives of Internal Medicine study suggested that hospitals with hospitalists outperformed their counterparts in quality metrics for acute myocardial infarction, pneumonia, overall disease treatment and diagnosis, and counseling and prevention. Congestive heart failure was the only category of the five reviewed that lacked a statistically significant difference.2
A separate editorial, however, argued that the study’s data were not persuasive enough to support the conclusion that hospitalists bring a higher quality of care to the table.3 And even less can be said about the national impact of HM on newly elevated metrics, such as readmission rates. The obligation to gather evidence, in fact, is largely falling upon hospitalists themselves, and the multitude of research abstracts from SHM’s annual meeting in May suggests that plenty of physician scientists are taking the responsibility seriously. Among the presentations, a study led by David Boyte, MD, assistant professor of medicine at Duke University and a hospitalist at Durham Regional Hospital, found that a multidisciplinary approach greatly improved one hospital unit’s 30-day readmission rates for heart failure patients. After a three-month pilot in the cardiac nursing unit, readmission rates fell to 10.7% from 27.6%.4
Although the multidisciplinary effort has included doctors, nurses, nutritionists, pharmacists, unit managers, and other personnel, Dr. Boyte says the involvement of hospitalists has been key to the project’s success. "We feel like we were the main participants who could see the whole picture from a patient-centered perspective," he says. "We were the glue; we were the center node of all the healthcare providers." Based on that dramatic improvement, Dr. Boyte says, the same interventional protocol has been rolled out in three other medical surgical units, and the hospital is using a similar approach to address AMI readmission rates.
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions; www.hospitalmedicine.org/boost )—by far the largest study of how HM is impacting readmission rates—has amassed data from more than 20 hospitals, with more expected from a growing roster of participants. So far, however, the project has only released data from six pilot sites describing the six-month periods before and after the project’s start. Among those sites, initial results suggest that readmission rates fell by an average of more than 20%, to 11.2% from 14.2%.5
Though the early numbers are encouraging, experts say rates from a larger group of participants at the one-year mark will be more telling, as will direct comparisons between BOOST units and nonparticipating counterparts at the same hospitals. Principal investigator Mark Williams, MD, FHM, professor and chief of the division of hospital medicine at the Northwestern University Feinberg School of Medicine in Chicago, says researchers still need to clean up that data before they’re ready to share it publicly.
In the meantime, some individual BOOST case studies are suggesting that hospitalist-led changes could pay big dividends. To help create cohesiveness and a sense of ownership within its HM program, St. Mary’s Health Center in St. Louis started a 20-bed hospitalist unit in 2008. Philip Vaidyan, MD, FACP, head of the hospitalist program and practice group leader for IPC: The Hospitalist Company at St. Mary’s, says one unit, 3 West, has since functioned as a lab for testing new ideas that are then introduced hospitalwide.
One early change was to bring all of the unit’s care providers together, from doctors and nurses to the unit-based case manager and social worker, for 9 a.m. handoff meetings. "We have this collective brain to find unique solutions," Dr. Vaidyan says. After seeing positive trends on length of stay, 30-day readmission rates, and patient satisfaction scores, St. Mary’s upgraded to a 32-bed hospitalist unit in early 2009. That same year, the 525-bed community teaching hospital was accepted into the BOOST program.
The hospitalist unit’s improved quality scores continued under BOOST, leading to a 33% reduction in readmission rates from 2008 to 2010 (to 10.5% from 15.7%). Rates for a nonhospitalist unit, by contrast, hovered around 17%. "For reducing readmissions, people may think that you have to have a higher length of stay," Dr. Vaidyan says. But the unit trended toward a lower length of stay, in addition to its reduced 30-day readmissions and improved patient satisfaction scores.
Flush with success, the 10 physicians and four nurse practitioners in the hospitalist program have since begun spreading their best practices to the rest of the hospital units. "Hospitalists are in the best ‘sweet spot,’ " Dr. Vaidyan says, "partnering with all of the disciplines, bringing them together, and keeping everybody on the same page."
Ironically, pinpointing the contribution of hospitalists is harder when their changes produce an ecological effect throughout an entire institution, says Siddhartha Singh, MD, MS, associate chief medical officer of Medical College Physicians, the adult practice for Medical College of Wisconsin in Milwaukee. Even so, he stresses that the impact of the two dozen hospitalists at Medical College Physicians has been felt.
"Coinciding with and following the introduction of our hospitalist program in 2004, we have noticed dramatic decreases in our length of stay throughout medicine services," he says. The same has held true for inpatient mortality. "And that, we feel, is attributable to the standardization of processes introduced by the hospitalist group." Multidisciplinary rounds; whiteboards in patient rooms; and standardized admission orders, prophylactic treatments, and discharge processes—"all of this would’ve been impossible, absolutely impossible, without the hospitalist," he says.
Over the past decade, Dr. Singh’s assessment has been echoed by several studies suggesting that individual hospitalist programs have brought significant improvements in quality measures, such as complication rates and inpatient mortality. In 2002, for example, Andrew Auerbach, MD, MPH, at the University of California San Francisco Medical Center, led a study that compared HM care with that of community physicians in a community-based teaching hospital. Patients cared for by hospitalists, the study found, had a lower risk of death during the hospitalization, as well as at 30 days and 60 days after discharge.6
A separate report by David Meltzer, MD, PhD, and colleagues at the University of Chicago found that an HM program in an academic general medicine service led to a 30% reduction in 30-day mortality rates during its second year of operation.7 And a 2004 study led by Jeanne Huddleston, MD, at the Mayo Clinic College of Medicine in Rochester, Minn., found that a hospitalist-orthopedic co-management model (versus care by orthopedic surgeons with medical consultation) led to more patients being discharged with no complications after elective hip or knee surgery.8 Hospitalist co-management also reduced the rate of minor complications, but had no effect on actual length of stay or cost.
A subsequent study by the same group, however, documented improved efficiency of care through the HM model, but no effect on the mortality of hip fracture patients up to one year after discharge.9 Multiple studies of hospitalist programs, in fact, have seen increased efficiency but little or no impact on inpatient mortality, leading researchers to broadly conclude that such programs can decrease resource use without compromising quality.
In 2007, a retrospective study of nearly 77,000 patients admitted to 45 hospitals with one of seven common diagnoses compared the care delivered by hospitalists, general internists, and family physicians.10 Although the study authors found that hospitalist care yielded a small drop in length of stay, they saw no difference in the inpatient mortality rates or 14-day readmission rates. More recently, mortality has become ensnared in controversy over its reliability as an accurate indicator of quality.
-Shai Gavi, DO, MPH, chief, section of hospital medicine, assistant professor, Stony Brook University School of Medicine, Brookhaven, N.Y.
Half of the Equation
Despite a lack of ideal metrics, another promising sign for HM might be the model’s exportability. Lee Kheng Hock, MMed, senior consultant and head of the Department of Family Medicine and Continuing Care at Singapore General Hospital, says the 1,600-bed hospital began experimenting with the hospitalist model when officials realized the existing care system wasn’t sustainable. Amid an aging population and increasingly complex and fragmented care, Hock views the hospitalist movement as a natural evolution of the healthcare system to meet the needs of a changing environment.
In a recent study, Hock and his colleagues used the hospital’s administrative database to examine the resource use and outcomes of patients cared for in 2008 by family medicine hospitalists or by specialists.11 The comparison, based on several standard metrics, found no significant improvements in quality, with similar inpatient mortality rates and 30-day, all-cause, unscheduled readmission rates regardless of the care delivery method. The study, though, revealed a significantly shorter hospital stay (4.4 days vs. 5.3 days) and lower costs per patient for those cared for by hospitalists ($2,250 vs. $2,500).11
Hock points out that, like his study, most analyses of hospitalist programs have shown an improvement in length of stay and cost of care without any increase in mortality and morbidity. If value equals quality divided by cost, he says, it stands to reason that quality must increase as overall value remains the same but costs decrease.
"The main difference is that the patients received undivided attention from a well-rounded generalist physician who is focused on providing holistic general medical care," Hock says, adding that "it is really a no-brainer that the outcome would be different."
Patients Rule
Other measures like the effectiveness of communication and seamlessness of handoffs often are assessed through their impacts on patient outcomes. But Sunil Kripalani, MD, MSc, SFHM, chief of the section of hospital medicine and an associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., says communication is now a primary focal point in Medicare’s new hospital value-based purchasing program (VBP). Within VBP’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) component, worth 30% of a hospital’s sum score, four of the 10 survey-based measures deal directly with communication. Patients’ overall rating and recommendation of hospitals likely will reflect their satisfaction with communication as well. Dr. Kripalani says it’s inevitable that hospitals—and hospitalists—will pay more attention to communication ratings as patients become judges of quality.
The expertise of hospitalists in handling challenging patients also leads to improved quality over time, says Shai Gavi, DO, MPH, chief of the section of hospital medicine and assistant professor of clinical medicine at Stony Brook University School of Medicine in Brookhaven, N.Y. Hospitalists, he says, excel in handling such high-stakes medical issues as gastrointestinal bleeding, pancreatitis, sepsis, and pain management that can quickly impact patient outcomes if not addressed properly and proficiently. "I think there’s significant value to having people who do this on a pretty frequent basis," he says.
And because of their broad day-to-day interactions, Dr. Gavi says, hospitalists are natural choices for committees focused on improving quality. "When we sit on committees, people often look to us for answers and directions because they know we’re on the front lines and we’ve interfaced with all of the services in the hospital," he says. "You have a good view of the whole hospital operation from A to Z, and I think that’s pretty unique to hospitalists."
The Verdict
In a recent issue brief by Lisa Sprague, principal policy analyst at the National Health Policy Forum, she asserts, "Hospitalists have the undeniable advantage of being there when a crisis occurs, when a patient is ready for discharge, and so on."12
So is "being there" the defining concept of hospital medicine, as she subsequently suggests?
Based on both scientific and anecdotal evidence, the contribution of hospitalists to healthcare quality might be better summarized as "being involved." Whether as innovators, navigators, physician champions, the "sweet spot" of interdepartmental partnerships, the "glue" of multidisciplinary teams, or the nuclei of performance committees, hospitalists are increasingly described as being in the middle of efforts to improve quality. On this basis, the discipline appears to be living up to expectations, though experts say more research is needed to better assess the impacts of HM on quality.
Dr. Vaidyan says hospitalists are particularly well positioned to understand what constitutes ideal care from the perspective of patients. "They want to be treated well: That’s patient satisfaction," he says. "They want to have their chief complaint—why they came to the hospital—properly addressed, so you need a coordinated care team. They want to go home early and don’t want come back: That’s low length of stay and a reduction in 30-day readmissions. And they don’t want any hospital-acquired complications."
Treating patients better, then, should be reflected by improved quality, even if the participation of hospitalists cannot be precisely quantified. "Being involved is something that may be difficult to measure," Dr. Gavi says, "but nonetheless, it has an important impact." TH
Bryn Nelson is a medical writer based in Seattle.
References
- Pronovost PJ, Lilford R. Analysis & commentary: A roadmap for improving the performance of performance measures. Health Aff (Millwood). 2011;30(4):569-73.
- López L, Hicks LS, Cohen AP, McKean S, Weissman JS. Hospitalists and the quality of care in hospitals. Arch Intern Med. 2009;169(15):1389-1394.
- Centor RM, Taylor BB. Do hospitalists improve quality? Arch Intern Med. 2009;169(15):1351-1352.
- Boyte D, Verma L, Wightman M. A multidisciplinary approach to reducing heart failure readmissions. J Hosp Med. 2011;6(4)Supp 2:S14.
- Williams MV, Hansen L, Greenwald J, Howell E, et al. BOOST: impact of a quality improvement project to reduce rehospitalizations. J Hosp Med. 2011;6(4) Supp 2:S88. BOOST: impact of a quality improvement project to reduce rehospitalizations.
- Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859-865.
- Meltzer D, Manning WG, Morrison J, et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(1):866-874.
- Huddleston JM, Hall K, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty. Ann Intern Med. 2004;141(1):28-38.
- Batsis JA, Phy MP, Melton LJ, et al. Effects of a hospitalist care model on mortality of elderly patients with hip fractures. J Hosp Med. 2007;2(4): 219–225.
- Lindenauer PK, Rothberg MB, Pekow PS, et al. Outcomes of care by hospitalists, general internists, and family physicians. N Eng J Med. 2007;357:2589-2600.
- Hock Lee K, Yang Y, Soong Yang K, Chi Ong B, Seong Ng H. Bringing generalists into the hospital: outcomes of a family medicine hospitalist model in Singapore. J Hosp Med. 2011;6(3):115-121.
- Sprague L. The hospitalist: better value in inpatient care? National Health Policy Forum website. Available at: www.nhpf.org/library/issue-briefs/IB842_Hospitalist_03-30-11.pdf. Accessed June 28, 2011.
One hospitalist-led pilot project produced a 61% decrease in heart failure readmission rates. Another resulted in a 33% drop in all-cause readmissions. The numbers might be impressive, but what do they really say about how hospitalists have influenced healthcare quality?
When HM emerged 15 years ago, advocates pitched the fledgling physician specialty as a model of efficient inpatient care, and subsequent findings that the concept led to reductions in length of stay encouraged more hospitals to bolster their staff with the newcomers. With a rising emphasis on quality and patient safety over the past decade, and the new era of pay-for-performance, the hospitalist model of care has expanded to embrace improved quality of care as a chief selling point.
Measuring quality is no easy task, however, and researchers still debate the relative merits of metrics like 30-day readmission rates and inpatient mortality. "Without question, quality measurement is an imperfect science, and all measures will contain some level of imprecision and bias," concluded a recent commentary in Health Affairs.1
Against that backdrop, relatively few studies have looked broadly at the contributions of hospital medicine. Most interventions have been individually tailored to a hospital or instituted at only a few sites, precluding large-scale, head-to-head comparisons.
And so the question remains: Has hospital medicine lived up to its promise on quality?
The Evidence
In one of the few national surveys of HM’s impact on patient care, a yearlong comparison of more than 3,600 hospitals found that the roughly 40% that employed hospitalists scored better on multiple Hospital Quality Alliance indicators. The 2009 Archives of Internal Medicine study suggested that hospitals with hospitalists outperformed their counterparts in quality metrics for acute myocardial infarction, pneumonia, overall disease treatment and diagnosis, and counseling and prevention. Congestive heart failure was the only category of the five reviewed that lacked a statistically significant difference.2
A separate editorial, however, argued that the study’s data were not persuasive enough to support the conclusion that hospitalists bring a higher quality of care to the table.3 And even less can be said about the national impact of HM on newly elevated metrics, such as readmission rates. The obligation to gather evidence, in fact, is largely falling upon hospitalists themselves, and the multitude of research abstracts from SHM’s annual meeting in May suggests that plenty of physician scientists are taking the responsibility seriously. Among the presentations, a study led by David Boyte, MD, assistant professor of medicine at Duke University and a hospitalist at Durham Regional Hospital, found that a multidisciplinary approach greatly improved one hospital unit’s 30-day readmission rates for heart failure patients. After a three-month pilot in the cardiac nursing unit, readmission rates fell to 10.7% from 27.6%.4
Although the multidisciplinary effort has included doctors, nurses, nutritionists, pharmacists, unit managers, and other personnel, Dr. Boyte says the involvement of hospitalists has been key to the project’s success. "We feel like we were the main participants who could see the whole picture from a patient-centered perspective," he says. "We were the glue; we were the center node of all the healthcare providers." Based on that dramatic improvement, Dr. Boyte says, the same interventional protocol has been rolled out in three other medical surgical units, and the hospital is using a similar approach to address AMI readmission rates.
SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions; www.hospitalmedicine.org/boost )—by far the largest study of how HM is impacting readmission rates—has amassed data from more than 20 hospitals, with more expected from a growing roster of participants. So far, however, the project has only released data from six pilot sites describing the six-month periods before and after the project’s start. Among those sites, initial results suggest that readmission rates fell by an average of more than 20%, to 11.2% from 14.2%.5
Though the early numbers are encouraging, experts say rates from a larger group of participants at the one-year mark will be more telling, as will direct comparisons between BOOST units and nonparticipating counterparts at the same hospitals. Principal investigator Mark Williams, MD, FHM, professor and chief of the division of hospital medicine at the Northwestern University Feinberg School of Medicine in Chicago, says researchers still need to clean up that data before they’re ready to share it publicly.
In the meantime, some individual BOOST case studies are suggesting that hospitalist-led changes could pay big dividends. To help create cohesiveness and a sense of ownership within its HM program, St. Mary’s Health Center in St. Louis started a 20-bed hospitalist unit in 2008. Philip Vaidyan, MD, FACP, head of the hospitalist program and practice group leader for IPC: The Hospitalist Company at St. Mary’s, says one unit, 3 West, has since functioned as a lab for testing new ideas that are then introduced hospitalwide.
One early change was to bring all of the unit’s care providers together, from doctors and nurses to the unit-based case manager and social worker, for 9 a.m. handoff meetings. "We have this collective brain to find unique solutions," Dr. Vaidyan says. After seeing positive trends on length of stay, 30-day readmission rates, and patient satisfaction scores, St. Mary’s upgraded to a 32-bed hospitalist unit in early 2009. That same year, the 525-bed community teaching hospital was accepted into the BOOST program.
The hospitalist unit’s improved quality scores continued under BOOST, leading to a 33% reduction in readmission rates from 2008 to 2010 (to 10.5% from 15.7%). Rates for a nonhospitalist unit, by contrast, hovered around 17%. "For reducing readmissions, people may think that you have to have a higher length of stay," Dr. Vaidyan says. But the unit trended toward a lower length of stay, in addition to its reduced 30-day readmissions and improved patient satisfaction scores.
Flush with success, the 10 physicians and four nurse practitioners in the hospitalist program have since begun spreading their best practices to the rest of the hospital units. "Hospitalists are in the best ‘sweet spot,’ " Dr. Vaidyan says, "partnering with all of the disciplines, bringing them together, and keeping everybody on the same page."
Ironically, pinpointing the contribution of hospitalists is harder when their changes produce an ecological effect throughout an entire institution, says Siddhartha Singh, MD, MS, associate chief medical officer of Medical College Physicians, the adult practice for Medical College of Wisconsin in Milwaukee. Even so, he stresses that the impact of the two dozen hospitalists at Medical College Physicians has been felt.
"Coinciding with and following the introduction of our hospitalist program in 2004, we have noticed dramatic decreases in our length of stay throughout medicine services," he says. The same has held true for inpatient mortality. "And that, we feel, is attributable to the standardization of processes introduced by the hospitalist group." Multidisciplinary rounds; whiteboards in patient rooms; and standardized admission orders, prophylactic treatments, and discharge processes—"all of this would’ve been impossible, absolutely impossible, without the hospitalist," he says.
Over the past decade, Dr. Singh’s assessment has been echoed by several studies suggesting that individual hospitalist programs have brought significant improvements in quality measures, such as complication rates and inpatient mortality. In 2002, for example, Andrew Auerbach, MD, MPH, at the University of California San Francisco Medical Center, led a study that compared HM care with that of community physicians in a community-based teaching hospital. Patients cared for by hospitalists, the study found, had a lower risk of death during the hospitalization, as well as at 30 days and 60 days after discharge.6
A separate report by David Meltzer, MD, PhD, and colleagues at the University of Chicago found that an HM program in an academic general medicine service led to a 30% reduction in 30-day mortality rates during its second year of operation.7 And a 2004 study led by Jeanne Huddleston, MD, at the Mayo Clinic College of Medicine in Rochester, Minn., found that a hospitalist-orthopedic co-management model (versus care by orthopedic surgeons with medical consultation) led to more patients being discharged with no complications after elective hip or knee surgery.8 Hospitalist co-management also reduced the rate of minor complications, but had no effect on actual length of stay or cost.
A subsequent study by the same group, however, documented improved efficiency of care through the HM model, but no effect on the mortality of hip fracture patients up to one year after discharge.9 Multiple studies of hospitalist programs, in fact, have seen increased efficiency but little or no impact on inpatient mortality, leading researchers to broadly conclude that such programs can decrease resource use without compromising quality.
In 2007, a retrospective study of nearly 77,000 patients admitted to 45 hospitals with one of seven common diagnoses compared the care delivered by hospitalists, general internists, and family physicians.10 Although the study authors found that hospitalist care yielded a small drop in length of stay, they saw no difference in the inpatient mortality rates or 14-day readmission rates. More recently, mortality has become ensnared in controversy over its reliability as an accurate indicator of quality.
-Shai Gavi, DO, MPH, chief, section of hospital medicine, assistant professor, Stony Brook University School of Medicine, Brookhaven, N.Y.
Half of the Equation
Despite a lack of ideal metrics, another promising sign for HM might be the model’s exportability. Lee Kheng Hock, MMed, senior consultant and head of the Department of Family Medicine and Continuing Care at Singapore General Hospital, says the 1,600-bed hospital began experimenting with the hospitalist model when officials realized the existing care system wasn’t sustainable. Amid an aging population and increasingly complex and fragmented care, Hock views the hospitalist movement as a natural evolution of the healthcare system to meet the needs of a changing environment.
In a recent study, Hock and his colleagues used the hospital’s administrative database to examine the resource use and outcomes of patients cared for in 2008 by family medicine hospitalists or by specialists.11 The comparison, based on several standard metrics, found no significant improvements in quality, with similar inpatient mortality rates and 30-day, all-cause, unscheduled readmission rates regardless of the care delivery method. The study, though, revealed a significantly shorter hospital stay (4.4 days vs. 5.3 days) and lower costs per patient for those cared for by hospitalists ($2,250 vs. $2,500).11
Hock points out that, like his study, most analyses of hospitalist programs have shown an improvement in length of stay and cost of care without any increase in mortality and morbidity. If value equals quality divided by cost, he says, it stands to reason that quality must increase as overall value remains the same but costs decrease.
"The main difference is that the patients received undivided attention from a well-rounded generalist physician who is focused on providing holistic general medical care," Hock says, adding that "it is really a no-brainer that the outcome would be different."
Patients Rule
Other measures like the effectiveness of communication and seamlessness of handoffs often are assessed through their impacts on patient outcomes. But Sunil Kripalani, MD, MSc, SFHM, chief of the section of hospital medicine and an associate professor of medicine at Vanderbilt University Medical Center in Nashville, Tenn., says communication is now a primary focal point in Medicare’s new hospital value-based purchasing program (VBP). Within VBP’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) component, worth 30% of a hospital’s sum score, four of the 10 survey-based measures deal directly with communication. Patients’ overall rating and recommendation of hospitals likely will reflect their satisfaction with communication as well. Dr. Kripalani says it’s inevitable that hospitals—and hospitalists—will pay more attention to communication ratings as patients become judges of quality.
The expertise of hospitalists in handling challenging patients also leads to improved quality over time, says Shai Gavi, DO, MPH, chief of the section of hospital medicine and assistant professor of clinical medicine at Stony Brook University School of Medicine in Brookhaven, N.Y. Hospitalists, he says, excel in handling such high-stakes medical issues as gastrointestinal bleeding, pancreatitis, sepsis, and pain management that can quickly impact patient outcomes if not addressed properly and proficiently. "I think there’s significant value to having people who do this on a pretty frequent basis," he says.
And because of their broad day-to-day interactions, Dr. Gavi says, hospitalists are natural choices for committees focused on improving quality. "When we sit on committees, people often look to us for answers and directions because they know we’re on the front lines and we’ve interfaced with all of the services in the hospital," he says. "You have a good view of the whole hospital operation from A to Z, and I think that’s pretty unique to hospitalists."
The Verdict
In a recent issue brief by Lisa Sprague, principal policy analyst at the National Health Policy Forum, she asserts, "Hospitalists have the undeniable advantage of being there when a crisis occurs, when a patient is ready for discharge, and so on."12
So is "being there" the defining concept of hospital medicine, as she subsequently suggests?
Based on both scientific and anecdotal evidence, the contribution of hospitalists to healthcare quality might be better summarized as "being involved." Whether as innovators, navigators, physician champions, the "sweet spot" of interdepartmental partnerships, the "glue" of multidisciplinary teams, or the nuclei of performance committees, hospitalists are increasingly described as being in the middle of efforts to improve quality. On this basis, the discipline appears to be living up to expectations, though experts say more research is needed to better assess the impacts of HM on quality.
Dr. Vaidyan says hospitalists are particularly well positioned to understand what constitutes ideal care from the perspective of patients. "They want to be treated well: That’s patient satisfaction," he says. "They want to have their chief complaint—why they came to the hospital—properly addressed, so you need a coordinated care team. They want to go home early and don’t want come back: That’s low length of stay and a reduction in 30-day readmissions. And they don’t want any hospital-acquired complications."
Treating patients better, then, should be reflected by improved quality, even if the participation of hospitalists cannot be precisely quantified. "Being involved is something that may be difficult to measure," Dr. Gavi says, "but nonetheless, it has an important impact." TH
Bryn Nelson is a medical writer based in Seattle.
References
- Pronovost PJ, Lilford R. Analysis & commentary: A roadmap for improving the performance of performance measures. Health Aff (Millwood). 2011;30(4):569-73.
- López L, Hicks LS, Cohen AP, McKean S, Weissman JS. Hospitalists and the quality of care in hospitals. Arch Intern Med. 2009;169(15):1389-1394.
- Centor RM, Taylor BB. Do hospitalists improve quality? Arch Intern Med. 2009;169(15):1351-1352.
- Boyte D, Verma L, Wightman M. A multidisciplinary approach to reducing heart failure readmissions. J Hosp Med. 2011;6(4)Supp 2:S14.
- Williams MV, Hansen L, Greenwald J, Howell E, et al. BOOST: impact of a quality improvement project to reduce rehospitalizations. J Hosp Med. 2011;6(4) Supp 2:S88. BOOST: impact of a quality improvement project to reduce rehospitalizations.
- Auerbach AD, Wachter RM, Katz P, Showstack J, Baron RB, Goldman L. Implementation of a voluntary hospitalist service at a community teaching hospital: improved clinical efficiency and patient outcomes. Ann Intern Med. 2002;137(11):859-865.
- Meltzer D, Manning WG, Morrison J, et al. Effects of physician experience on costs and outcomes on an academic general medicine service: results of a trial of hospitalists. Ann Intern Med. 2002;137(1):866-874.
- Huddleston JM, Hall K, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty. Ann Intern Med. 2004;141(1):28-38.
- Batsis JA, Phy MP, Melton LJ, et al. Effects of a hospitalist care model on mortality of elderly patients with hip fractures. J Hosp Med. 2007;2(4): 219–225.
- Lindenauer PK, Rothberg MB, Pekow PS, et al. Outcomes of care by hospitalists, general internists, and family physicians. N Eng J Med. 2007;357:2589-2600.
- Hock Lee K, Yang Y, Soong Yang K, Chi Ong B, Seong Ng H. Bringing generalists into the hospital: outcomes of a family medicine hospitalist model in Singapore. J Hosp Med. 2011;6(3):115-121.
- Sprague L. The hospitalist: better value in inpatient care? National Health Policy Forum website. Available at: www.nhpf.org/library/issue-briefs/IB842_Hospitalist_03-30-11.pdf. Accessed June 28, 2011.
It Takes a Village
Gregory Misky, MD, has been a hospitalist for 12 years, first at a community hospital and for the past seven years at the University of Colorado Denver. In recent years, his frustration has grown over the challenges of discharge planning, care transitions, and preventing readmissions for vulnerable, disadvantaged patients, including the uninsured, underinsured, and medically indigent.
“There’s a big elephant in the room that we’re not talking about, and that elephant is having babies,” he says. “Access is such a big problem for these patients and, as a hospitalist, it’s just not OK to me anymore. I need to be proactive about finding solutions.”
Dr. Misky’s concerns led him to do research with mentor Eric Coleman, MD, the university’s creator of the Care Transitions Program (www.caretransitions.org), studying patients who lacked primary-care physicians (PCPs) or timely PCP follow-up, and their resulting higher rates of readmissions.1 Dr. Misky also helped develop care pathways, including post-discharge care, for VTE patients, a “common, costly, and dangerous” condition. He is working with a hospitalist colleague to explore how electronic health records (EHR) might be used to help trigger post-discharge follow-up for at-risk patients.
University of Colorado Hospital (UCH), a 425-bed urban academic tertiary-care center, is not the designated safety net hospital for metro Denver, yet 28% to 32% of patients discharged from its medical services are uninsured, Dr. Misky says. He finds that academic physicians at UCH are not always able to take on large numbers of uninsured patients in their clinics, given the productivity demands they face, while the hospital has not been able to participate in systemwide, comprehensive national models for improving care transitions, such as SHM’s Project BOOST (www.hospitalmedicine.org/boost) or Boston Medical Center’s Project RED (www.bu.edu/fammed/projectred/).
Dr. Misky is in discussions with local community services, such as the Metro Community Provider Network (MCPN) of clinics for underserved patients, and exploring the development of a collaborative model for integrating post-hospital care between UCH and MCPN. “A lot of our ideas are still very exploratory—trying to get the key providers to the table to talk about what these approaches might look like,” Dr. Misky explains. “I’ve been part of ongoing meetings, and I think similar kinds of conversations are happening at many levels at UCH, but there’s not a unified, consensus approach to care transitions—and that’s a problem. But I’m in the midst of it all, trying to highlight the issues and explore solutions.”
—Patricia Rutherford, RN, MS, vice president, Institute for Healthcare Improvement
Dr. Misky says every hospital-based provider—hospitalist, nurses, social workers—feels the same frustration and worry about the level of care when indigent patients are discharged to the community. Uninsured patients can run into problems post-hospitalization and return to the ED for their primary care because they lack other options, he says. “Without established liaisons to the community clinics,” he notes, “it can take three or four months for a new indigent patient to get seen at one.”
Disproportional Issues of the Uninsured
Hospitalists at San Francisco General Hospital, which is the safety-net provider for the Bay Area, are looking at similar issues, says Jeff Critchfield, MD, division chief of hospital medicine. “What we know about the uninsured is that they have a wealth of other challenges and barriers that they bring to the table,” he says. “First of all, un- and underinsured patients are more likely to have chronic illnesses, to be hospitalized for those illnesses, and then to be rehospitalized after discharge.”
Other issues disproportionally impacting uninsured or indigent patients include low literacy, low healthcare literacy, language barriers, cross-cultural barriers, substance abuse and mental health issues, homelessness or marginal housing, transportation barriers, and “social isolation, which also plagues our population and, I believe, places patients at risk, as does depression,” says Dr. Critchfield’s colleague Michelle Schneidermann, MD.
One-third of San Francisco General’s patients are uninsured and 40% have Medi-Cal (California’s version of Medicaid), which basically means they are underinsured.
“California has 19 safety-net hospitals, with 6% of the state’s inpatient beds but 50% of its uninsured population. So that’s what we do,” Dr. Critchfield says. But almost any hospital or hospitalist will see many of the same issues and problems, just not in the same proportions. “These are patients who can be most frustrating to hospitalists, requiring a disproportionate amount of our time,” he says, adding the greatest difficulty is helping these patients understand and follow post-discharge care plans. But if someone is ill enough to need acute hospitalization and is later discharged back to the street, readmission should not be a surprise. “We’ve done that experiment for many years, and we know how it turns out,” he says.
Dr. Schneidermann serves as medical director of San Francisco General’s medical respite program, a 45-bed emergency shelter that accepts homeless or marginally housed patients in need of follow-up care following discharge from any of the city’s acute-care hospitals. Research has shown that the programs can have a major effect on keeping discharged patients off the street, reducing their rates of rehospitalization by as much as 50%.2,3
“We know that homeless patients have longer lengths of hospital stay because their discharges are fraught with problems,” she says. A homeless patient hospitalized with a blood clot potentially could be kept in the hospital for a week while transitioning from heparin to Coumadin, while similar patients with community support might get discharged in a day.
“We are also fortunate to have a program called Healthy San Francisco,” which isn’t a health insurance program per se but since 2007 has provided access to outpatient, inpatient, and preventive care and medications for indigent patients, Dr. Schneidermann says. Sponsored by the city’s Department of Public Health, it is accessed through 32 medical homes located in both public and private clinics. The hospitalists’ goal is to have a follow-up appointment set with a receiving provider at the time of discharge. “It doesn’t always happen, but that’s the goal,” she explains. “Someone, by name, who has accepted the referral.”
Dr. Critchfield is running a randomized controlled trial of the hospital’s interventions to stem the tide of readmissions in patients 60 and older; many of these patients share the same indigent demographics of the rest of San Francisco General’s caseload, although most patients 65 and older qualify for Medicare. He describes the program as a hybrid of Project RED and Dr. Coleman’s Care Transitions Program, although it targets patients who speak English, Spanish, Cantonese, and Mandarin.
How many Americans are uninsured today is a moving target in the context of healthcare reform and its uncertain future, but the number increased to 53 million in 2007 from 42 million in 1998.4 The number of hospitalizations of uninsured patients also grew to 2.3 million from 1.8 million in the same time period, an increase of 31%, while total hospitalizations were increasing by 13%. A May 2011 research brief from the U.S. Department of Health and Human Services estimates that uncompensated costs of hospital care incurred for uninsured patients total $73 billion per year.5
The homeless in shelters or on the street number about 630,000 on any given evening, and 1.5 million Americans experienced homelessness last year, says Sabrina Edgington, MSSW, program and policy specialist at the National Health Care for the Homeless Council in Nashville, Tenn. That said, 30% of the U.S. homeless have health insurance. Uninsured patients are less likely to receive necessary diagnostic tests and labs while in the hospital, and they face limited access and longer wait times—even in the facilities that are willing to take them.7 Research published in the Journal of Hospital Medicine finds that uninsured or Medicaid patients with three common conditions are more likely to die in the hospital than insured patients.8 A 2008 national sample survey of physicians found that “most U.S. physicians limit their care of medically indigent patients.”9 Other recent research suggests that readmission rates are affected by race and by site of care—with hospitals serving a higher proportion of black patients also having higher readmission rates.10
“This is not a hospital problem—it’s a communitywide problem. So there’s not just a hospital solution; it will take the whole village,” says Patricia Rutherford, RN, MS, vice president of the Institute for Healthcare Improvement (IHI), which sponsors initiatives targeting care transitions.
The major national care-transitions programs that assist hospitals with addressing rehospitalizations all share similar objectives, Rutherford says, and all could be helpful in improving hospitals’ responses to indigent patients. The recognized programs include IHI’s STAAR (State Action on Avoidable Rehospitalizations: www.ihi.org/IHI/Programs), a multistate, multistakeholder quality improvement (QI) program; Project BOOST; Project RED; Dr. Coleman’s Care Transitions Project; the nursing-based Transitional Care Model (www.transitionalcare.info); and the American College of Cardiology’s Hospital to Home (www.cardiosource.org).

—Amy Boutwell, MD, MPP, hospitalist, Newton (Mass.) Wellesley Hospital, president, Collaborative Healthcare Strategies
Most of these “well-established, evidence-based interventions,” including BOOST, will be given preference in applications for grants from the federal Community-Based Care Transitions Program (CCTP). The program recently committed $500 million to support community-based coalitions that include hospitals that are working with community partners to create seamless care transitions. “It’s most important that hospitalists are integrally involved with these care-transition teams—if not leading them,” Rutherford says.
BOOST’s approach is built on a major change-management strategy to reconstruct hospitals’ care transitions and discharge processes from the ground up, says Tina Budnitz, MPH, the project’s director at SHM (see “Discharge Improvement,” p. 7.) “The first thing we do, we literally get out pens and paper and chart what happens before patients get into the hospital and what happens after they are discharged, all of the services that touch them—or should,” she says. “The planning process occurs on many levels, with all of the stakeholders in the community looking at the process map and seeing where people fall off and end up readmitted.”
—Jeff Critchfield, MD, division chief of hospital medicine, San Francisco General Hospital
SHM is planning to launch several new BOOST cohorts for participating hospitals this fall, along with a wider range of technical support, Budnitz says.
The Cross-Setting Team
Research on care transitions for uninsured or indigent patients “is not very robust,” observes Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Newton, Mass., former director of health policy at IHI and president of Collaborative Healthcare Strategies. “We don’t have the information we need, but there are great opportunities to improve our research base,” she explains.
Dr. Boutwell is a big fan of the “cross-setting team,” which brings together around a conference table professionals who work in different care settings, including the hospital, long-term care, and home-based care. She says it’s her job “to make sure patients are safe upon discharge, but if the community is under-resourced for primary-care physicians, if the patient is uninsured and we can’t find a PCP, the hospitalist and cross-setting team need to say, ‘We just can’t accept that.’ ”
What Do HM’s Community Partners Think About the Problem?

Lori J. Heim, MD, FAAFP, board chair of the American Academy of Family Physicians, a family physician in Vass, N.C., and hospitalist at Scotland Memorial Hospital in Laurinburg, N.C., says the unassigned patient who lacks a PCP might be the hardest issue to overcome in improving care transitions.
“We have a lot of members who volunteer at free clinics. Others are part of revolving lists of physicians willing to take unassigned call and accept referrals of indigent patients from the hospital,” Dr. Heim says. “If you look at the number of primary-care practices that are barely surviving, most hospitalists I know are very cognizant of how financially strapped family practice and general internist physicians are these days.”
It isn’t always clear who benefits financially from improved care transitions, particularly for indigent patients, Dr. Heim says. But the growth of patient-centered medical homes through the rollout of national healthcare reform, opportunities for community clinics to become those medical homes, and the wider dissemination of electronic medical records are all important components of the changes that need to take place.
“I would encourage hospitalists to be involved with their hospital leadership on these issues and have ongoing communication with community physicians. Both sides need to think more in terms of the systemic demands,” she says. “Often the ED doctor or the hospitalist knows about these issues and can help hospital leaders understand potential solutions for uninsured patients.–LB
A proper handoff should be done in a way that helps the patient and the physician providing the follow-up care. “But you won’t know what that is unless you ask the people you’re sending patients to how you’re doing,” she explains. “When we routinely review readmitted patients in cross-setting groups, it quickly breaks down the mindset that we in the hospital did everything we could have done to make the discharge successful.”
Dr. Boutwell recommends that hospitalists avoid thinking of these issues in a vacuum, as medical-clinical issues that only doctors can fix. “Because you can’t,” she says. “I would never ask an individual hospitalist to reduce readmissions. It requires a multidisciplinary, all-hands-on-deck approach by the hospital. This is different and more exciting than other quality-improvement efforts.” What’s more, she says, the day is coming—and soon—when failing to manage these readmissions will be a bad business proposition for the hospital (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
IHI’s STAAR Initiative is working with coalitions of providers in Massachusetts, Michigan, Ohio, and Washington. One of those coalitions, Detroit CARR (Community Action to Reduce Rehospitalizations), convened by MPRO, a Michigan-based quality-improvement organization, is a great example of a cross-continuum team involving five inner-city hospitals, Dr. Boutwell says.
“CARR has really dug deeply into the needs of vulnerable patients in one of America’s most economically challenged communities, with a high proportion of Medicaid, uninsured, and disabled patients” and a shrinking population, she says. Many rehospitalizations are related to socio-economics. “The CARR coalition is meeting with the homeless shelters, the food pantries, and the faith-based agencies,” she says. “They’re really getting at the root of significant issues in their community.”
Nancy Vecchioni, RN, MSN, CPHQ, vice present of Medicare operations at MPRO, says CARR involves more than just healthcare providers; it also brings community agencies together with them to take ownership of the patient. Organizations that a year ago weren’t talking to each other are now meeting regularly to focus on the most vulnerable patients, reviewing cases of rehospitalized homeless patients, and sharing their experiences. Rehospitalized patients are being interviewed, using a prepared script (see Figure 1, p. 34), which allows the patient to tell their story. The information is shared within the coalition.
Each hospital has its own transition team, with post-acute providers, physicians, home health agencies, and community service providers, Vecchioni says. For patients who can’t get in to see a PCP within five days of discharge, some hospitals are opening continuity clinics. Others give patients three- to 30-day supplies of needed medications. “There’s no magic bullet—it’s just a different way of looking at how we do this work,” she adds. “Every day we see new barriers. But we’ve already seen a 5% overall reduction in readmissions. And I think hospitalists can be the champions and leaders of these efforts.”
Hospitalists have to raise the bar for themselves, Dr. Schneidermann says, “doing our best while recognizing we can only do so much. There is a lot we can learn from geriatrics, starting with truly embracing the multidisciplinary team.” If hospitalists feel like they are functioning in isolation, she says, they need to look around. “Are these kinds of interdisciplinary meetings happening? If so, join them. If not, light a fire. Convert your frustrating experiences with patients into action.” TH
Larry Beresford is a freelance medical writer based in California.
References
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5:392-397.
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
- Kertesz SG, Posner MA, O’Connell JJ, et al. Post-hospital medical respite care and hospital readmission of homeless persons. J Prev Inter Community. 2009;37:129-142.
- Nagamine M, Stocks C, Merrill C. Trends in uninsured hospital stays, 1998-2007. Health Care Cost & Utilization Project (HCUP) Statistical Brief #88. May 2010.
- U.S. Department of Health and Human Services. ASPE Research Brief. The value of health insurance: few of the uninsured have adequate resources to pay potential hospital bills. May 2011.
- U.S. Department of Housing and Urban Development. The Annual Housing Assessment Report to Congress, 2009.
- Kellerman A, Coleman M. Care without Coverage: Too Little, Too Late. Report by Institute of Medicine, May 2002.
- Hasan O, Orav EJ, Hicks LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8):452-459.
- Chirayath HT, Wentworth AL. Constraints to caring: Service to medically indigent patients by allopathic and osteopathic physicians. J Health Care Poor Underserved. 2008;19:500-511.
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675-681.
- Buchanan D, Rohr L, Kehoe L, Glick SB, Jain S. Changing attitudes toward homeless people. J Gen Intern Med. 2004;19(5 Pt 2):566-568.
Liability and Compliance Issues

Hospitalists and other experts say medical/legal liability for indigent patients resulting from readmissions has not been a major focus of their care-transitions initiatives. Even as bundled care models will give hospitals greater financial responsibility for episodes of care across settings, getting sued by patients is not said to be a major concern.
“What we try to do is put together the most robust plan of care that we can for patients, whether insured or not,” says Jeff Critchfield, MD, chief of hospital medicine and medical director of risk management at San Francisco General Hospital. “The tone of the conversation for patients without insurance is different—because the options are fewer. We may have to keep these patients longer because of the absence of options. But rarely does risk management come into it. We don’t get sued by these patients, so that’s not a driving force.”
State and local regulations and Medicare conditions of participation also define expectations for hospitals regarding the care of indigent patients who present at the hospital with acute medical needs. In Los Angeles, a controversy emerged in 2005 when several hospitals were accused of dumping homeless patients on skid row. Local governments responded by approving a $100 million plan to provide homeless shelters across Los Angeles County; in 2008, the same public officials passed an ordinance making it illegal for hospitals to discharge homeless patients to the streets without their consent.
There can be liability issues for any patient who gets transferred out of the hospital and the transition is not a good one, Dr. Critchfield adds, “but I try to think about this population the same as any other.”—LB
Gregory Misky, MD, has been a hospitalist for 12 years, first at a community hospital and for the past seven years at the University of Colorado Denver. In recent years, his frustration has grown over the challenges of discharge planning, care transitions, and preventing readmissions for vulnerable, disadvantaged patients, including the uninsured, underinsured, and medically indigent.
“There’s a big elephant in the room that we’re not talking about, and that elephant is having babies,” he says. “Access is such a big problem for these patients and, as a hospitalist, it’s just not OK to me anymore. I need to be proactive about finding solutions.”
Dr. Misky’s concerns led him to do research with mentor Eric Coleman, MD, the university’s creator of the Care Transitions Program (www.caretransitions.org), studying patients who lacked primary-care physicians (PCPs) or timely PCP follow-up, and their resulting higher rates of readmissions.1 Dr. Misky also helped develop care pathways, including post-discharge care, for VTE patients, a “common, costly, and dangerous” condition. He is working with a hospitalist colleague to explore how electronic health records (EHR) might be used to help trigger post-discharge follow-up for at-risk patients.
University of Colorado Hospital (UCH), a 425-bed urban academic tertiary-care center, is not the designated safety net hospital for metro Denver, yet 28% to 32% of patients discharged from its medical services are uninsured, Dr. Misky says. He finds that academic physicians at UCH are not always able to take on large numbers of uninsured patients in their clinics, given the productivity demands they face, while the hospital has not been able to participate in systemwide, comprehensive national models for improving care transitions, such as SHM’s Project BOOST (www.hospitalmedicine.org/boost) or Boston Medical Center’s Project RED (www.bu.edu/fammed/projectred/).
Dr. Misky is in discussions with local community services, such as the Metro Community Provider Network (MCPN) of clinics for underserved patients, and exploring the development of a collaborative model for integrating post-hospital care between UCH and MCPN. “A lot of our ideas are still very exploratory—trying to get the key providers to the table to talk about what these approaches might look like,” Dr. Misky explains. “I’ve been part of ongoing meetings, and I think similar kinds of conversations are happening at many levels at UCH, but there’s not a unified, consensus approach to care transitions—and that’s a problem. But I’m in the midst of it all, trying to highlight the issues and explore solutions.”
—Patricia Rutherford, RN, MS, vice president, Institute for Healthcare Improvement
Dr. Misky says every hospital-based provider—hospitalist, nurses, social workers—feels the same frustration and worry about the level of care when indigent patients are discharged to the community. Uninsured patients can run into problems post-hospitalization and return to the ED for their primary care because they lack other options, he says. “Without established liaisons to the community clinics,” he notes, “it can take three or four months for a new indigent patient to get seen at one.”
Disproportional Issues of the Uninsured
Hospitalists at San Francisco General Hospital, which is the safety-net provider for the Bay Area, are looking at similar issues, says Jeff Critchfield, MD, division chief of hospital medicine. “What we know about the uninsured is that they have a wealth of other challenges and barriers that they bring to the table,” he says. “First of all, un- and underinsured patients are more likely to have chronic illnesses, to be hospitalized for those illnesses, and then to be rehospitalized after discharge.”
Other issues disproportionally impacting uninsured or indigent patients include low literacy, low healthcare literacy, language barriers, cross-cultural barriers, substance abuse and mental health issues, homelessness or marginal housing, transportation barriers, and “social isolation, which also plagues our population and, I believe, places patients at risk, as does depression,” says Dr. Critchfield’s colleague Michelle Schneidermann, MD.
One-third of San Francisco General’s patients are uninsured and 40% have Medi-Cal (California’s version of Medicaid), which basically means they are underinsured.
“California has 19 safety-net hospitals, with 6% of the state’s inpatient beds but 50% of its uninsured population. So that’s what we do,” Dr. Critchfield says. But almost any hospital or hospitalist will see many of the same issues and problems, just not in the same proportions. “These are patients who can be most frustrating to hospitalists, requiring a disproportionate amount of our time,” he says, adding the greatest difficulty is helping these patients understand and follow post-discharge care plans. But if someone is ill enough to need acute hospitalization and is later discharged back to the street, readmission should not be a surprise. “We’ve done that experiment for many years, and we know how it turns out,” he says.
Dr. Schneidermann serves as medical director of San Francisco General’s medical respite program, a 45-bed emergency shelter that accepts homeless or marginally housed patients in need of follow-up care following discharge from any of the city’s acute-care hospitals. Research has shown that the programs can have a major effect on keeping discharged patients off the street, reducing their rates of rehospitalization by as much as 50%.2,3
“We know that homeless patients have longer lengths of hospital stay because their discharges are fraught with problems,” she says. A homeless patient hospitalized with a blood clot potentially could be kept in the hospital for a week while transitioning from heparin to Coumadin, while similar patients with community support might get discharged in a day.
“We are also fortunate to have a program called Healthy San Francisco,” which isn’t a health insurance program per se but since 2007 has provided access to outpatient, inpatient, and preventive care and medications for indigent patients, Dr. Schneidermann says. Sponsored by the city’s Department of Public Health, it is accessed through 32 medical homes located in both public and private clinics. The hospitalists’ goal is to have a follow-up appointment set with a receiving provider at the time of discharge. “It doesn’t always happen, but that’s the goal,” she explains. “Someone, by name, who has accepted the referral.”
Dr. Critchfield is running a randomized controlled trial of the hospital’s interventions to stem the tide of readmissions in patients 60 and older; many of these patients share the same indigent demographics of the rest of San Francisco General’s caseload, although most patients 65 and older qualify for Medicare. He describes the program as a hybrid of Project RED and Dr. Coleman’s Care Transitions Program, although it targets patients who speak English, Spanish, Cantonese, and Mandarin.
How many Americans are uninsured today is a moving target in the context of healthcare reform and its uncertain future, but the number increased to 53 million in 2007 from 42 million in 1998.4 The number of hospitalizations of uninsured patients also grew to 2.3 million from 1.8 million in the same time period, an increase of 31%, while total hospitalizations were increasing by 13%. A May 2011 research brief from the U.S. Department of Health and Human Services estimates that uncompensated costs of hospital care incurred for uninsured patients total $73 billion per year.5
The homeless in shelters or on the street number about 630,000 on any given evening, and 1.5 million Americans experienced homelessness last year, says Sabrina Edgington, MSSW, program and policy specialist at the National Health Care for the Homeless Council in Nashville, Tenn. That said, 30% of the U.S. homeless have health insurance. Uninsured patients are less likely to receive necessary diagnostic tests and labs while in the hospital, and they face limited access and longer wait times—even in the facilities that are willing to take them.7 Research published in the Journal of Hospital Medicine finds that uninsured or Medicaid patients with three common conditions are more likely to die in the hospital than insured patients.8 A 2008 national sample survey of physicians found that “most U.S. physicians limit their care of medically indigent patients.”9 Other recent research suggests that readmission rates are affected by race and by site of care—with hospitals serving a higher proportion of black patients also having higher readmission rates.10
“This is not a hospital problem—it’s a communitywide problem. So there’s not just a hospital solution; it will take the whole village,” says Patricia Rutherford, RN, MS, vice president of the Institute for Healthcare Improvement (IHI), which sponsors initiatives targeting care transitions.
The major national care-transitions programs that assist hospitals with addressing rehospitalizations all share similar objectives, Rutherford says, and all could be helpful in improving hospitals’ responses to indigent patients. The recognized programs include IHI’s STAAR (State Action on Avoidable Rehospitalizations: www.ihi.org/IHI/Programs), a multistate, multistakeholder quality improvement (QI) program; Project BOOST; Project RED; Dr. Coleman’s Care Transitions Project; the nursing-based Transitional Care Model (www.transitionalcare.info); and the American College of Cardiology’s Hospital to Home (www.cardiosource.org).
—Amy Boutwell, MD, MPP, hospitalist, Newton (Mass.) Wellesley Hospital, president, Collaborative Healthcare Strategies
Most of these “well-established, evidence-based interventions,” including BOOST, will be given preference in applications for grants from the federal Community-Based Care Transitions Program (CCTP). The program recently committed $500 million to support community-based coalitions that include hospitals that are working with community partners to create seamless care transitions. “It’s most important that hospitalists are integrally involved with these care-transition teams—if not leading them,” Rutherford says.
BOOST’s approach is built on a major change-management strategy to reconstruct hospitals’ care transitions and discharge processes from the ground up, says Tina Budnitz, MPH, the project’s director at SHM (see “Discharge Improvement,” p. 7.) “The first thing we do, we literally get out pens and paper and chart what happens before patients get into the hospital and what happens after they are discharged, all of the services that touch them—or should,” she says. “The planning process occurs on many levels, with all of the stakeholders in the community looking at the process map and seeing where people fall off and end up readmitted.”
—Jeff Critchfield, MD, division chief of hospital medicine, San Francisco General Hospital
SHM is planning to launch several new BOOST cohorts for participating hospitals this fall, along with a wider range of technical support, Budnitz says.
The Cross-Setting Team
Research on care transitions for uninsured or indigent patients “is not very robust,” observes Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Newton, Mass., former director of health policy at IHI and president of Collaborative Healthcare Strategies. “We don’t have the information we need, but there are great opportunities to improve our research base,” she explains.
Dr. Boutwell is a big fan of the “cross-setting team,” which brings together around a conference table professionals who work in different care settings, including the hospital, long-term care, and home-based care. She says it’s her job “to make sure patients are safe upon discharge, but if the community is under-resourced for primary-care physicians, if the patient is uninsured and we can’t find a PCP, the hospitalist and cross-setting team need to say, ‘We just can’t accept that.’ ”
What Do HM’s Community Partners Think About the Problem?
Lori J. Heim, MD, FAAFP, board chair of the American Academy of Family Physicians, a family physician in Vass, N.C., and hospitalist at Scotland Memorial Hospital in Laurinburg, N.C., says the unassigned patient who lacks a PCP might be the hardest issue to overcome in improving care transitions.
“We have a lot of members who volunteer at free clinics. Others are part of revolving lists of physicians willing to take unassigned call and accept referrals of indigent patients from the hospital,” Dr. Heim says. “If you look at the number of primary-care practices that are barely surviving, most hospitalists I know are very cognizant of how financially strapped family practice and general internist physicians are these days.”
It isn’t always clear who benefits financially from improved care transitions, particularly for indigent patients, Dr. Heim says. But the growth of patient-centered medical homes through the rollout of national healthcare reform, opportunities for community clinics to become those medical homes, and the wider dissemination of electronic medical records are all important components of the changes that need to take place.
“I would encourage hospitalists to be involved with their hospital leadership on these issues and have ongoing communication with community physicians. Both sides need to think more in terms of the systemic demands,” she says. “Often the ED doctor or the hospitalist knows about these issues and can help hospital leaders understand potential solutions for uninsured patients.–LB
A proper handoff should be done in a way that helps the patient and the physician providing the follow-up care. “But you won’t know what that is unless you ask the people you’re sending patients to how you’re doing,” she explains. “When we routinely review readmitted patients in cross-setting groups, it quickly breaks down the mindset that we in the hospital did everything we could have done to make the discharge successful.”
Dr. Boutwell recommends that hospitalists avoid thinking of these issues in a vacuum, as medical-clinical issues that only doctors can fix. “Because you can’t,” she says. “I would never ask an individual hospitalist to reduce readmissions. It requires a multidisciplinary, all-hands-on-deck approach by the hospital. This is different and more exciting than other quality-improvement efforts.” What’s more, she says, the day is coming—and soon—when failing to manage these readmissions will be a bad business proposition for the hospital (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
IHI’s STAAR Initiative is working with coalitions of providers in Massachusetts, Michigan, Ohio, and Washington. One of those coalitions, Detroit CARR (Community Action to Reduce Rehospitalizations), convened by MPRO, a Michigan-based quality-improvement organization, is a great example of a cross-continuum team involving five inner-city hospitals, Dr. Boutwell says.
“CARR has really dug deeply into the needs of vulnerable patients in one of America’s most economically challenged communities, with a high proportion of Medicaid, uninsured, and disabled patients” and a shrinking population, she says. Many rehospitalizations are related to socio-economics. “The CARR coalition is meeting with the homeless shelters, the food pantries, and the faith-based agencies,” she says. “They’re really getting at the root of significant issues in their community.”
Nancy Vecchioni, RN, MSN, CPHQ, vice present of Medicare operations at MPRO, says CARR involves more than just healthcare providers; it also brings community agencies together with them to take ownership of the patient. Organizations that a year ago weren’t talking to each other are now meeting regularly to focus on the most vulnerable patients, reviewing cases of rehospitalized homeless patients, and sharing their experiences. Rehospitalized patients are being interviewed, using a prepared script (see Figure 1, p. 34), which allows the patient to tell their story. The information is shared within the coalition.
Each hospital has its own transition team, with post-acute providers, physicians, home health agencies, and community service providers, Vecchioni says. For patients who can’t get in to see a PCP within five days of discharge, some hospitals are opening continuity clinics. Others give patients three- to 30-day supplies of needed medications. “There’s no magic bullet—it’s just a different way of looking at how we do this work,” she adds. “Every day we see new barriers. But we’ve already seen a 5% overall reduction in readmissions. And I think hospitalists can be the champions and leaders of these efforts.”
Hospitalists have to raise the bar for themselves, Dr. Schneidermann says, “doing our best while recognizing we can only do so much. There is a lot we can learn from geriatrics, starting with truly embracing the multidisciplinary team.” If hospitalists feel like they are functioning in isolation, she says, they need to look around. “Are these kinds of interdisciplinary meetings happening? If so, join them. If not, light a fire. Convert your frustrating experiences with patients into action.” TH
Larry Beresford is a freelance medical writer based in California.
References
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5:392-397.
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
- Kertesz SG, Posner MA, O’Connell JJ, et al. Post-hospital medical respite care and hospital readmission of homeless persons. J Prev Inter Community. 2009;37:129-142.
- Nagamine M, Stocks C, Merrill C. Trends in uninsured hospital stays, 1998-2007. Health Care Cost & Utilization Project (HCUP) Statistical Brief #88. May 2010.
- U.S. Department of Health and Human Services. ASPE Research Brief. The value of health insurance: few of the uninsured have adequate resources to pay potential hospital bills. May 2011.
- U.S. Department of Housing and Urban Development. The Annual Housing Assessment Report to Congress, 2009.
- Kellerman A, Coleman M. Care without Coverage: Too Little, Too Late. Report by Institute of Medicine, May 2002.
- Hasan O, Orav EJ, Hicks LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8):452-459.
- Chirayath HT, Wentworth AL. Constraints to caring: Service to medically indigent patients by allopathic and osteopathic physicians. J Health Care Poor Underserved. 2008;19:500-511.
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675-681.
- Buchanan D, Rohr L, Kehoe L, Glick SB, Jain S. Changing attitudes toward homeless people. J Gen Intern Med. 2004;19(5 Pt 2):566-568.
Liability and Compliance Issues
Hospitalists and other experts say medical/legal liability for indigent patients resulting from readmissions has not been a major focus of their care-transitions initiatives. Even as bundled care models will give hospitals greater financial responsibility for episodes of care across settings, getting sued by patients is not said to be a major concern.
“What we try to do is put together the most robust plan of care that we can for patients, whether insured or not,” says Jeff Critchfield, MD, chief of hospital medicine and medical director of risk management at San Francisco General Hospital. “The tone of the conversation for patients without insurance is different—because the options are fewer. We may have to keep these patients longer because of the absence of options. But rarely does risk management come into it. We don’t get sued by these patients, so that’s not a driving force.”
State and local regulations and Medicare conditions of participation also define expectations for hospitals regarding the care of indigent patients who present at the hospital with acute medical needs. In Los Angeles, a controversy emerged in 2005 when several hospitals were accused of dumping homeless patients on skid row. Local governments responded by approving a $100 million plan to provide homeless shelters across Los Angeles County; in 2008, the same public officials passed an ordinance making it illegal for hospitals to discharge homeless patients to the streets without their consent.
There can be liability issues for any patient who gets transferred out of the hospital and the transition is not a good one, Dr. Critchfield adds, “but I try to think about this population the same as any other.”—LB
Gregory Misky, MD, has been a hospitalist for 12 years, first at a community hospital and for the past seven years at the University of Colorado Denver. In recent years, his frustration has grown over the challenges of discharge planning, care transitions, and preventing readmissions for vulnerable, disadvantaged patients, including the uninsured, underinsured, and medically indigent.
“There’s a big elephant in the room that we’re not talking about, and that elephant is having babies,” he says. “Access is such a big problem for these patients and, as a hospitalist, it’s just not OK to me anymore. I need to be proactive about finding solutions.”
Dr. Misky’s concerns led him to do research with mentor Eric Coleman, MD, the university’s creator of the Care Transitions Program (www.caretransitions.org), studying patients who lacked primary-care physicians (PCPs) or timely PCP follow-up, and their resulting higher rates of readmissions.1 Dr. Misky also helped develop care pathways, including post-discharge care, for VTE patients, a “common, costly, and dangerous” condition. He is working with a hospitalist colleague to explore how electronic health records (EHR) might be used to help trigger post-discharge follow-up for at-risk patients.
University of Colorado Hospital (UCH), a 425-bed urban academic tertiary-care center, is not the designated safety net hospital for metro Denver, yet 28% to 32% of patients discharged from its medical services are uninsured, Dr. Misky says. He finds that academic physicians at UCH are not always able to take on large numbers of uninsured patients in their clinics, given the productivity demands they face, while the hospital has not been able to participate in systemwide, comprehensive national models for improving care transitions, such as SHM’s Project BOOST (www.hospitalmedicine.org/boost) or Boston Medical Center’s Project RED (www.bu.edu/fammed/projectred/).
Dr. Misky is in discussions with local community services, such as the Metro Community Provider Network (MCPN) of clinics for underserved patients, and exploring the development of a collaborative model for integrating post-hospital care between UCH and MCPN. “A lot of our ideas are still very exploratory—trying to get the key providers to the table to talk about what these approaches might look like,” Dr. Misky explains. “I’ve been part of ongoing meetings, and I think similar kinds of conversations are happening at many levels at UCH, but there’s not a unified, consensus approach to care transitions—and that’s a problem. But I’m in the midst of it all, trying to highlight the issues and explore solutions.”
—Patricia Rutherford, RN, MS, vice president, Institute for Healthcare Improvement
Dr. Misky says every hospital-based provider—hospitalist, nurses, social workers—feels the same frustration and worry about the level of care when indigent patients are discharged to the community. Uninsured patients can run into problems post-hospitalization and return to the ED for their primary care because they lack other options, he says. “Without established liaisons to the community clinics,” he notes, “it can take three or four months for a new indigent patient to get seen at one.”
Disproportional Issues of the Uninsured
Hospitalists at San Francisco General Hospital, which is the safety-net provider for the Bay Area, are looking at similar issues, says Jeff Critchfield, MD, division chief of hospital medicine. “What we know about the uninsured is that they have a wealth of other challenges and barriers that they bring to the table,” he says. “First of all, un- and underinsured patients are more likely to have chronic illnesses, to be hospitalized for those illnesses, and then to be rehospitalized after discharge.”
Other issues disproportionally impacting uninsured or indigent patients include low literacy, low healthcare literacy, language barriers, cross-cultural barriers, substance abuse and mental health issues, homelessness or marginal housing, transportation barriers, and “social isolation, which also plagues our population and, I believe, places patients at risk, as does depression,” says Dr. Critchfield’s colleague Michelle Schneidermann, MD.
One-third of San Francisco General’s patients are uninsured and 40% have Medi-Cal (California’s version of Medicaid), which basically means they are underinsured.
“California has 19 safety-net hospitals, with 6% of the state’s inpatient beds but 50% of its uninsured population. So that’s what we do,” Dr. Critchfield says. But almost any hospital or hospitalist will see many of the same issues and problems, just not in the same proportions. “These are patients who can be most frustrating to hospitalists, requiring a disproportionate amount of our time,” he says, adding the greatest difficulty is helping these patients understand and follow post-discharge care plans. But if someone is ill enough to need acute hospitalization and is later discharged back to the street, readmission should not be a surprise. “We’ve done that experiment for many years, and we know how it turns out,” he says.
Dr. Schneidermann serves as medical director of San Francisco General’s medical respite program, a 45-bed emergency shelter that accepts homeless or marginally housed patients in need of follow-up care following discharge from any of the city’s acute-care hospitals. Research has shown that the programs can have a major effect on keeping discharged patients off the street, reducing their rates of rehospitalization by as much as 50%.2,3
“We know that homeless patients have longer lengths of hospital stay because their discharges are fraught with problems,” she says. A homeless patient hospitalized with a blood clot potentially could be kept in the hospital for a week while transitioning from heparin to Coumadin, while similar patients with community support might get discharged in a day.
“We are also fortunate to have a program called Healthy San Francisco,” which isn’t a health insurance program per se but since 2007 has provided access to outpatient, inpatient, and preventive care and medications for indigent patients, Dr. Schneidermann says. Sponsored by the city’s Department of Public Health, it is accessed through 32 medical homes located in both public and private clinics. The hospitalists’ goal is to have a follow-up appointment set with a receiving provider at the time of discharge. “It doesn’t always happen, but that’s the goal,” she explains. “Someone, by name, who has accepted the referral.”
Dr. Critchfield is running a randomized controlled trial of the hospital’s interventions to stem the tide of readmissions in patients 60 and older; many of these patients share the same indigent demographics of the rest of San Francisco General’s caseload, although most patients 65 and older qualify for Medicare. He describes the program as a hybrid of Project RED and Dr. Coleman’s Care Transitions Program, although it targets patients who speak English, Spanish, Cantonese, and Mandarin.
How many Americans are uninsured today is a moving target in the context of healthcare reform and its uncertain future, but the number increased to 53 million in 2007 from 42 million in 1998.4 The number of hospitalizations of uninsured patients also grew to 2.3 million from 1.8 million in the same time period, an increase of 31%, while total hospitalizations were increasing by 13%. A May 2011 research brief from the U.S. Department of Health and Human Services estimates that uncompensated costs of hospital care incurred for uninsured patients total $73 billion per year.5
The homeless in shelters or on the street number about 630,000 on any given evening, and 1.5 million Americans experienced homelessness last year, says Sabrina Edgington, MSSW, program and policy specialist at the National Health Care for the Homeless Council in Nashville, Tenn. That said, 30% of the U.S. homeless have health insurance. Uninsured patients are less likely to receive necessary diagnostic tests and labs while in the hospital, and they face limited access and longer wait times—even in the facilities that are willing to take them.7 Research published in the Journal of Hospital Medicine finds that uninsured or Medicaid patients with three common conditions are more likely to die in the hospital than insured patients.8 A 2008 national sample survey of physicians found that “most U.S. physicians limit their care of medically indigent patients.”9 Other recent research suggests that readmission rates are affected by race and by site of care—with hospitals serving a higher proportion of black patients also having higher readmission rates.10
“This is not a hospital problem—it’s a communitywide problem. So there’s not just a hospital solution; it will take the whole village,” says Patricia Rutherford, RN, MS, vice president of the Institute for Healthcare Improvement (IHI), which sponsors initiatives targeting care transitions.
The major national care-transitions programs that assist hospitals with addressing rehospitalizations all share similar objectives, Rutherford says, and all could be helpful in improving hospitals’ responses to indigent patients. The recognized programs include IHI’s STAAR (State Action on Avoidable Rehospitalizations: www.ihi.org/IHI/Programs), a multistate, multistakeholder quality improvement (QI) program; Project BOOST; Project RED; Dr. Coleman’s Care Transitions Project; the nursing-based Transitional Care Model (www.transitionalcare.info); and the American College of Cardiology’s Hospital to Home (www.cardiosource.org).
—Amy Boutwell, MD, MPP, hospitalist, Newton (Mass.) Wellesley Hospital, president, Collaborative Healthcare Strategies
Most of these “well-established, evidence-based interventions,” including BOOST, will be given preference in applications for grants from the federal Community-Based Care Transitions Program (CCTP). The program recently committed $500 million to support community-based coalitions that include hospitals that are working with community partners to create seamless care transitions. “It’s most important that hospitalists are integrally involved with these care-transition teams—if not leading them,” Rutherford says.
BOOST’s approach is built on a major change-management strategy to reconstruct hospitals’ care transitions and discharge processes from the ground up, says Tina Budnitz, MPH, the project’s director at SHM (see “Discharge Improvement,” p. 7.) “The first thing we do, we literally get out pens and paper and chart what happens before patients get into the hospital and what happens after they are discharged, all of the services that touch them—or should,” she says. “The planning process occurs on many levels, with all of the stakeholders in the community looking at the process map and seeing where people fall off and end up readmitted.”
—Jeff Critchfield, MD, division chief of hospital medicine, San Francisco General Hospital
SHM is planning to launch several new BOOST cohorts for participating hospitals this fall, along with a wider range of technical support, Budnitz says.
The Cross-Setting Team
Research on care transitions for uninsured or indigent patients “is not very robust,” observes Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Newton, Mass., former director of health policy at IHI and president of Collaborative Healthcare Strategies. “We don’t have the information we need, but there are great opportunities to improve our research base,” she explains.
Dr. Boutwell is a big fan of the “cross-setting team,” which brings together around a conference table professionals who work in different care settings, including the hospital, long-term care, and home-based care. She says it’s her job “to make sure patients are safe upon discharge, but if the community is under-resourced for primary-care physicians, if the patient is uninsured and we can’t find a PCP, the hospitalist and cross-setting team need to say, ‘We just can’t accept that.’ ”
What Do HM’s Community Partners Think About the Problem?
Lori J. Heim, MD, FAAFP, board chair of the American Academy of Family Physicians, a family physician in Vass, N.C., and hospitalist at Scotland Memorial Hospital in Laurinburg, N.C., says the unassigned patient who lacks a PCP might be the hardest issue to overcome in improving care transitions.
“We have a lot of members who volunteer at free clinics. Others are part of revolving lists of physicians willing to take unassigned call and accept referrals of indigent patients from the hospital,” Dr. Heim says. “If you look at the number of primary-care practices that are barely surviving, most hospitalists I know are very cognizant of how financially strapped family practice and general internist physicians are these days.”
It isn’t always clear who benefits financially from improved care transitions, particularly for indigent patients, Dr. Heim says. But the growth of patient-centered medical homes through the rollout of national healthcare reform, opportunities for community clinics to become those medical homes, and the wider dissemination of electronic medical records are all important components of the changes that need to take place.
“I would encourage hospitalists to be involved with their hospital leadership on these issues and have ongoing communication with community physicians. Both sides need to think more in terms of the systemic demands,” she says. “Often the ED doctor or the hospitalist knows about these issues and can help hospital leaders understand potential solutions for uninsured patients.–LB
A proper handoff should be done in a way that helps the patient and the physician providing the follow-up care. “But you won’t know what that is unless you ask the people you’re sending patients to how you’re doing,” she explains. “When we routinely review readmitted patients in cross-setting groups, it quickly breaks down the mindset that we in the hospital did everything we could have done to make the discharge successful.”
Dr. Boutwell recommends that hospitalists avoid thinking of these issues in a vacuum, as medical-clinical issues that only doctors can fix. “Because you can’t,” she says. “I would never ask an individual hospitalist to reduce readmissions. It requires a multidisciplinary, all-hands-on-deck approach by the hospital. This is different and more exciting than other quality-improvement efforts.” What’s more, she says, the day is coming—and soon—when failing to manage these readmissions will be a bad business proposition for the hospital (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
IHI’s STAAR Initiative is working with coalitions of providers in Massachusetts, Michigan, Ohio, and Washington. One of those coalitions, Detroit CARR (Community Action to Reduce Rehospitalizations), convened by MPRO, a Michigan-based quality-improvement organization, is a great example of a cross-continuum team involving five inner-city hospitals, Dr. Boutwell says.
“CARR has really dug deeply into the needs of vulnerable patients in one of America’s most economically challenged communities, with a high proportion of Medicaid, uninsured, and disabled patients” and a shrinking population, she says. Many rehospitalizations are related to socio-economics. “The CARR coalition is meeting with the homeless shelters, the food pantries, and the faith-based agencies,” she says. “They’re really getting at the root of significant issues in their community.”
Nancy Vecchioni, RN, MSN, CPHQ, vice present of Medicare operations at MPRO, says CARR involves more than just healthcare providers; it also brings community agencies together with them to take ownership of the patient. Organizations that a year ago weren’t talking to each other are now meeting regularly to focus on the most vulnerable patients, reviewing cases of rehospitalized homeless patients, and sharing their experiences. Rehospitalized patients are being interviewed, using a prepared script (see Figure 1, p. 34), which allows the patient to tell their story. The information is shared within the coalition.
Each hospital has its own transition team, with post-acute providers, physicians, home health agencies, and community service providers, Vecchioni says. For patients who can’t get in to see a PCP within five days of discharge, some hospitals are opening continuity clinics. Others give patients three- to 30-day supplies of needed medications. “There’s no magic bullet—it’s just a different way of looking at how we do this work,” she adds. “Every day we see new barriers. But we’ve already seen a 5% overall reduction in readmissions. And I think hospitalists can be the champions and leaders of these efforts.”
Hospitalists have to raise the bar for themselves, Dr. Schneidermann says, “doing our best while recognizing we can only do so much. There is a lot we can learn from geriatrics, starting with truly embracing the multidisciplinary team.” If hospitalists feel like they are functioning in isolation, she says, they need to look around. “Are these kinds of interdisciplinary meetings happening? If so, join them. If not, light a fire. Convert your frustrating experiences with patients into action.” TH
Larry Beresford is a freelance medical writer based in California.
References
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5:392-397.
- Buchanan D, Doblin B, Sai T, Garcia P. The effects of respite care for homeless patients: a cohort study. Am J Public Health. 2006;96:1278-1281.
- Kertesz SG, Posner MA, O’Connell JJ, et al. Post-hospital medical respite care and hospital readmission of homeless persons. J Prev Inter Community. 2009;37:129-142.
- Nagamine M, Stocks C, Merrill C. Trends in uninsured hospital stays, 1998-2007. Health Care Cost & Utilization Project (HCUP) Statistical Brief #88. May 2010.
- U.S. Department of Health and Human Services. ASPE Research Brief. The value of health insurance: few of the uninsured have adequate resources to pay potential hospital bills. May 2011.
- U.S. Department of Housing and Urban Development. The Annual Housing Assessment Report to Congress, 2009.
- Kellerman A, Coleman M. Care without Coverage: Too Little, Too Late. Report by Institute of Medicine, May 2002.
- Hasan O, Orav EJ, Hicks LS. Insurance status and hospital care for myocardial infarction, stroke, and pneumonia. J Hosp Med. 2010;5(8):452-459.
- Chirayath HT, Wentworth AL. Constraints to caring: Service to medically indigent patients by allopathic and osteopathic physicians. J Health Care Poor Underserved. 2008;19:500-511.
- Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675-681.
- Buchanan D, Rohr L, Kehoe L, Glick SB, Jain S. Changing attitudes toward homeless people. J Gen Intern Med. 2004;19(5 Pt 2):566-568.
Liability and Compliance Issues
Hospitalists and other experts say medical/legal liability for indigent patients resulting from readmissions has not been a major focus of their care-transitions initiatives. Even as bundled care models will give hospitals greater financial responsibility for episodes of care across settings, getting sued by patients is not said to be a major concern.
“What we try to do is put together the most robust plan of care that we can for patients, whether insured or not,” says Jeff Critchfield, MD, chief of hospital medicine and medical director of risk management at San Francisco General Hospital. “The tone of the conversation for patients without insurance is different—because the options are fewer. We may have to keep these patients longer because of the absence of options. But rarely does risk management come into it. We don’t get sued by these patients, so that’s not a driving force.”
State and local regulations and Medicare conditions of participation also define expectations for hospitals regarding the care of indigent patients who present at the hospital with acute medical needs. In Los Angeles, a controversy emerged in 2005 when several hospitals were accused of dumping homeless patients on skid row. Local governments responded by approving a $100 million plan to provide homeless shelters across Los Angeles County; in 2008, the same public officials passed an ordinance making it illegal for hospitals to discharge homeless patients to the streets without their consent.
There can be liability issues for any patient who gets transferred out of the hospital and the transition is not a good one, Dr. Critchfield adds, “but I try to think about this population the same as any other.”—LB
Policy Corner: ACA provides multiple pathways to develop and support ACOs
“ACO” is probably the most common acronym to come out of the Affordable Care Act of 2010 (ACA). Over the last several months, much of the public dialogue has focused on the confusion surrounding the “ACO Proposed Rule.” And now there are three new ACO initiatives, which were announced in May by the Centers for Medicare & Medicaid Services (CMS).
So, what’s the difference? And what does it mean for hospitalists?
The ACA provides multiple pathways to develop and support ACOs, or accountable-care organizations. The proposed rule released in March 2011 was for the Medicare Shared Savings Program (MSSP). Through this program, healthcare providers can join together in ACOs to integrate and coordinate services in return for a share of any savings to the Medicare program. These ACOs will be rewarded for lowering growth in Medicare costs while meeting performance standards on quality of care and putting patients first.
Three other initiatives from the newly created Center for Medicare and Medicaid Innovation give providers a broad range of options and support, and reflect the varying needs of providers in embarking on delivery system reforms. They are:
- Pioneer ACO Model: Provides a faster path for mature ACOs that already have begun coordinating care for patients. This model is estimated to save Medicare as much as $430 million over three years through better managing care for beneficiaries and eliminating duplication. It is designed to move away from the fee-for-service (FFS) payment model more quickly than its MSSP counterpart. In year three of the program, Pioneer ACOs that have shown savings over the first two years will be eligible to move to a population-based payment model. The MSSP version is based completely on FFS.
- Advance Payment ACO Initiative: Would allow certain ACOs participating in the MSSP access to a portion of their shared savings up front, helping providers make the infrastructure and staff investments crucial to successful ACOs.
- Accelerated Development Learning Sessions: These sessions will provide the executive leadership teams from existing or emerging ACO entities the opportunity to learn about essential ACO functions and ways to build capacity needed to achieve better care, better health, and lower costs through integrated care models. Three sessions will be offered in the fall: San Francisco in September, Philadelphia in October, and Atlanta in November. For more info, visit https://acoregister.rti.org.
For more information about ACOs, visit www.healthcare.gov.
How hospitalists will be impacted under the ACO model is largely up to the individual hospitalists. Hospitalists are uniquely positioned to lead the system-level changes and quality-improvement (QI) efforts that will be critical to ACO success, and will bring significant value to the ACO model due to the central role that many hospitalists play in promoting team-based care, care coordination, and improving transitions of care. All of these roles are critical to delivering higher-quality care more efficiently.
CMS has provided detailed information on the above programs via Healthcare.gov. SHM submitted comments on the Medicare Shared Savings Program and the Advance Payment ACO Initiative, which can be found in the Advocacy section of www.hospitalmedicine.org under “SHM Letters.” TH
“ACO” is probably the most common acronym to come out of the Affordable Care Act of 2010 (ACA). Over the last several months, much of the public dialogue has focused on the confusion surrounding the “ACO Proposed Rule.” And now there are three new ACO initiatives, which were announced in May by the Centers for Medicare & Medicaid Services (CMS).
So, what’s the difference? And what does it mean for hospitalists?
The ACA provides multiple pathways to develop and support ACOs, or accountable-care organizations. The proposed rule released in March 2011 was for the Medicare Shared Savings Program (MSSP). Through this program, healthcare providers can join together in ACOs to integrate and coordinate services in return for a share of any savings to the Medicare program. These ACOs will be rewarded for lowering growth in Medicare costs while meeting performance standards on quality of care and putting patients first.
Three other initiatives from the newly created Center for Medicare and Medicaid Innovation give providers a broad range of options and support, and reflect the varying needs of providers in embarking on delivery system reforms. They are:
- Pioneer ACO Model: Provides a faster path for mature ACOs that already have begun coordinating care for patients. This model is estimated to save Medicare as much as $430 million over three years through better managing care for beneficiaries and eliminating duplication. It is designed to move away from the fee-for-service (FFS) payment model more quickly than its MSSP counterpart. In year three of the program, Pioneer ACOs that have shown savings over the first two years will be eligible to move to a population-based payment model. The MSSP version is based completely on FFS.
- Advance Payment ACO Initiative: Would allow certain ACOs participating in the MSSP access to a portion of their shared savings up front, helping providers make the infrastructure and staff investments crucial to successful ACOs.
- Accelerated Development Learning Sessions: These sessions will provide the executive leadership teams from existing or emerging ACO entities the opportunity to learn about essential ACO functions and ways to build capacity needed to achieve better care, better health, and lower costs through integrated care models. Three sessions will be offered in the fall: San Francisco in September, Philadelphia in October, and Atlanta in November. For more info, visit https://acoregister.rti.org.
For more information about ACOs, visit www.healthcare.gov.
How hospitalists will be impacted under the ACO model is largely up to the individual hospitalists. Hospitalists are uniquely positioned to lead the system-level changes and quality-improvement (QI) efforts that will be critical to ACO success, and will bring significant value to the ACO model due to the central role that many hospitalists play in promoting team-based care, care coordination, and improving transitions of care. All of these roles are critical to delivering higher-quality care more efficiently.
CMS has provided detailed information on the above programs via Healthcare.gov. SHM submitted comments on the Medicare Shared Savings Program and the Advance Payment ACO Initiative, which can be found in the Advocacy section of www.hospitalmedicine.org under “SHM Letters.” TH
“ACO” is probably the most common acronym to come out of the Affordable Care Act of 2010 (ACA). Over the last several months, much of the public dialogue has focused on the confusion surrounding the “ACO Proposed Rule.” And now there are three new ACO initiatives, which were announced in May by the Centers for Medicare & Medicaid Services (CMS).
So, what’s the difference? And what does it mean for hospitalists?
The ACA provides multiple pathways to develop and support ACOs, or accountable-care organizations. The proposed rule released in March 2011 was for the Medicare Shared Savings Program (MSSP). Through this program, healthcare providers can join together in ACOs to integrate and coordinate services in return for a share of any savings to the Medicare program. These ACOs will be rewarded for lowering growth in Medicare costs while meeting performance standards on quality of care and putting patients first.
Three other initiatives from the newly created Center for Medicare and Medicaid Innovation give providers a broad range of options and support, and reflect the varying needs of providers in embarking on delivery system reforms. They are:
- Pioneer ACO Model: Provides a faster path for mature ACOs that already have begun coordinating care for patients. This model is estimated to save Medicare as much as $430 million over three years through better managing care for beneficiaries and eliminating duplication. It is designed to move away from the fee-for-service (FFS) payment model more quickly than its MSSP counterpart. In year three of the program, Pioneer ACOs that have shown savings over the first two years will be eligible to move to a population-based payment model. The MSSP version is based completely on FFS.
- Advance Payment ACO Initiative: Would allow certain ACOs participating in the MSSP access to a portion of their shared savings up front, helping providers make the infrastructure and staff investments crucial to successful ACOs.
- Accelerated Development Learning Sessions: These sessions will provide the executive leadership teams from existing or emerging ACO entities the opportunity to learn about essential ACO functions and ways to build capacity needed to achieve better care, better health, and lower costs through integrated care models. Three sessions will be offered in the fall: San Francisco in September, Philadelphia in October, and Atlanta in November. For more info, visit https://acoregister.rti.org.
For more information about ACOs, visit www.healthcare.gov.
How hospitalists will be impacted under the ACO model is largely up to the individual hospitalists. Hospitalists are uniquely positioned to lead the system-level changes and quality-improvement (QI) efforts that will be critical to ACO success, and will bring significant value to the ACO model due to the central role that many hospitalists play in promoting team-based care, care coordination, and improving transitions of care. All of these roles are critical to delivering higher-quality care more efficiently.
CMS has provided detailed information on the above programs via Healthcare.gov. SHM submitted comments on the Medicare Shared Savings Program and the Advance Payment ACO Initiative, which can be found in the Advocacy section of www.hospitalmedicine.org under “SHM Letters.” TH
Discharge improvement
If you’re a hospitalist interested in reducing readmissions in your hospital, the time to act is now.
Project BOOST (Better Outcomes for Older Adults through Safe Transitions), SHM’s groundbreaking program designed to help hospitals reduce unplanned readmissions, is now accepting applications for two new cohorts: one national and another specific to California. The deadline for applications is August 1.
Now with 85 sites as part of the national community, Project BOOST will introduce new sites across the country in the fall. In addition to the national cohort, Project BOOST will also establish a new cohort in California, with discounted tuition through grants from three healthcare groups in the state.
“It’s a great time to apply,” says Stephanie Rennke, MD, assistant clinical professor of medicine at the University of California San Francisco Medical Center. “We are at the cusp of a lot of big changes in health reform. The time to address readmissions is now. Hospitals will have to address this, and BOOST is one way to do that.”

—Stephanie Rennke, MD, assistant clinical professor of medicine, University of California San Francisco Medical Center
Applications are submitted online (www.hospitalmedicine.org/boost) and evaluated based on whether improving discharge and care transitions is a high priority at the institution. Applications must be accompanied by a letter of support from an executive sponsor within the applicant’s hospital.
Once accepted into the program, BOOST participants pay a tuition fee of $28,000. Thanks to the support of the California HealthCare Foundation, the L.A. Care Health Plan, and the Hospital Association of Southern California, sites in California are eligible for reduced tuition based on site location and availability of funds.
For Dr. Rennke, the link between healthcare reform and readmissions is clear, along with the repercussions for hospitals. Most notably, the discharge process affects multiple quality issues, including “patient satisfaction, provider satisfaction and improving communication from hospital to home.”
“Hospitals need to realize healthcare reform is coming,” says Dr. Rennke, who previously served as a Project BOOST site team member and now works as a BOOST mentor. “Not only is reducing readmissions the right thing to do, it will also have a financial impact for hospitals that don’t address it. … It’s going to be of paramount importance to address the discharge process.”
National Growth
Since it was initially developed through a grant from the John A. Hartford Foundation, Project BOOST has spread to hospitals across the country and received widespread attention throughout the healthcare community.
At the time of Project BOOST’s inception in 2008, readmissions already were an intractable and costly issue for hospitals. The next year, research coauthored by Project BOOST principal investigator Mark V. Williams, MD, FHM, and published in the New England Journal of Medicine revealed that unplanned readmissions cost Medicare $17.4 billion annually.
Project BOOST’s pilot cohort consisted of six hospital sites. The program’s growth accelerated quickly, and it soon added another 24 sites and, later, two statewide programs in Michigan and Illinois.
The popularity of Project BOOST among hospitals has captured the attention of media and other organizations as well:
- This year, Kaiser Health News featured the work of Atlanta’s Piedmont Hospital to reduce readmissions using Project BOOST in an article focusing on the impact of healthcare reform laws on hospital readmissions.
- The Bassett Healthcare Network, a Project BOOST site in upstate New York, has earned the Hospital Association of New York State’s prestigious 2011 HANYS Pinnacle Award for Quality and Safety for the group’s care-transition work. The award was presented to Bassett Healthcare Network chief executives in June.
- In California, the Kaiser Permanente West LA BOOST Team was recognized with an award from Dr. Benjamin Chu, president of Southern California Kaiser Foundation Health Plan.
- In December 2010, Dr. Williams and hospitalist Matthew Schreiber, CMO of Piedmont Hospital, shared their experiences with Project BOOST at a national conference hosted by the Centers for Medicare & Medicaid Services (CMS).
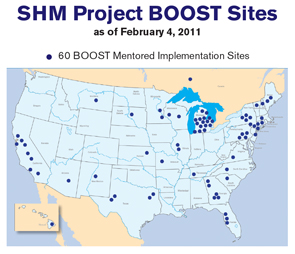
The Project BOOST Process
Once a site is accepted as a Project BOOST site, the site leader receives an information package and access to the Project BOOST online repository for recording and uploading readmission data. Then, each Project BOOST cohort performs an in-person conference. Networking and personal interaction are an important part of sharing challenges and successes in reducing readmissions. The conference also includes training on root-cause analysis and process mapping, a required step for application of the new Community Based Care Transitions Program (CCTP), part of the Affordable Care Act.
Each site leader is assigned a Project BOOST mentor, a national expert on reducing readmissions to the hospital. The mentor conducts a site visit to the hospital to meet the entire team in person and better understand the discharge challenges first-hand.
Over the course of the year, through regularly scheduled telephone calls, the mentor works with the Project BOOST team to best apply the program to the needs of the specific hospital. Mentors also help answer questions related to project planning, toolkit materials, data collection, implementation, and analysis.
In Dr. Rennke’s case, the process helped augment and guide UCSF’s current discharge program. Having multiple team members from different disciplines made distributing the work and implementation easier.
“Overall, we knew this was going to be doable because we incorporated Project BOOST into an already existing discharge process,” Dr. Rennke says.
Readmissions in the Crosshairs
The impacts of preventable readmissions on patient safety and efficiency of care in the hospital have made the issue a heated one in public policy. Earlier this year, the U.S. Department of Health and Human Services announced the creation of Partnership for Patients, a $1 billion initiative to address “quality, safety, and affordability of healthcare for all Americans.” SHM was one of the first medical societies to sign on to the “Partnership for Patients Pledge.”
One of the partnership’s two major goals is to reduce hospital readmissions by 20%. According to the Partnership for Patients website, “achieving this goal would mean more than 1.6 million patients would recover from illness without suffering a preventable complication requiring rehospitalization within 30 days of discharge.”
The government is backing up this goal with funding for hospitals with concrete plans to reduce readmissions. Under the Affordable Care Act of 2010—commonly known as the healthcare reform law—Medicare created the five-year CCTP earlier this year. The program provides $500 million to collaborative partnerships between hospitals and community-based organizations to implement care-transition services for Medicare beneficiaries, many of whom are at high risk of readmission.
To Dr. Rennke, the attention to reducing readmissions is an extension of her responsibility as a caregiver. “Our responsibility doesn’t end when the patient leaves the hospital,” she says. TH
Brendon Shank is SHM’s assistant vice president of communications.
If you’re a hospitalist interested in reducing readmissions in your hospital, the time to act is now.
Project BOOST (Better Outcomes for Older Adults through Safe Transitions), SHM’s groundbreaking program designed to help hospitals reduce unplanned readmissions, is now accepting applications for two new cohorts: one national and another specific to California. The deadline for applications is August 1.
Now with 85 sites as part of the national community, Project BOOST will introduce new sites across the country in the fall. In addition to the national cohort, Project BOOST will also establish a new cohort in California, with discounted tuition through grants from three healthcare groups in the state.
“It’s a great time to apply,” says Stephanie Rennke, MD, assistant clinical professor of medicine at the University of California San Francisco Medical Center. “We are at the cusp of a lot of big changes in health reform. The time to address readmissions is now. Hospitals will have to address this, and BOOST is one way to do that.”
—Stephanie Rennke, MD, assistant clinical professor of medicine, University of California San Francisco Medical Center
Applications are submitted online (www.hospitalmedicine.org/boost) and evaluated based on whether improving discharge and care transitions is a high priority at the institution. Applications must be accompanied by a letter of support from an executive sponsor within the applicant’s hospital.
Once accepted into the program, BOOST participants pay a tuition fee of $28,000. Thanks to the support of the California HealthCare Foundation, the L.A. Care Health Plan, and the Hospital Association of Southern California, sites in California are eligible for reduced tuition based on site location and availability of funds.
For Dr. Rennke, the link between healthcare reform and readmissions is clear, along with the repercussions for hospitals. Most notably, the discharge process affects multiple quality issues, including “patient satisfaction, provider satisfaction and improving communication from hospital to home.”
“Hospitals need to realize healthcare reform is coming,” says Dr. Rennke, who previously served as a Project BOOST site team member and now works as a BOOST mentor. “Not only is reducing readmissions the right thing to do, it will also have a financial impact for hospitals that don’t address it. … It’s going to be of paramount importance to address the discharge process.”
National Growth
Since it was initially developed through a grant from the John A. Hartford Foundation, Project BOOST has spread to hospitals across the country and received widespread attention throughout the healthcare community.
At the time of Project BOOST’s inception in 2008, readmissions already were an intractable and costly issue for hospitals. The next year, research coauthored by Project BOOST principal investigator Mark V. Williams, MD, FHM, and published in the New England Journal of Medicine revealed that unplanned readmissions cost Medicare $17.4 billion annually.
Project BOOST’s pilot cohort consisted of six hospital sites. The program’s growth accelerated quickly, and it soon added another 24 sites and, later, two statewide programs in Michigan and Illinois.
The popularity of Project BOOST among hospitals has captured the attention of media and other organizations as well:
- This year, Kaiser Health News featured the work of Atlanta’s Piedmont Hospital to reduce readmissions using Project BOOST in an article focusing on the impact of healthcare reform laws on hospital readmissions.
- The Bassett Healthcare Network, a Project BOOST site in upstate New York, has earned the Hospital Association of New York State’s prestigious 2011 HANYS Pinnacle Award for Quality and Safety for the group’s care-transition work. The award was presented to Bassett Healthcare Network chief executives in June.
- In California, the Kaiser Permanente West LA BOOST Team was recognized with an award from Dr. Benjamin Chu, president of Southern California Kaiser Foundation Health Plan.
- In December 2010, Dr. Williams and hospitalist Matthew Schreiber, CMO of Piedmont Hospital, shared their experiences with Project BOOST at a national conference hosted by the Centers for Medicare & Medicaid Services (CMS).
The Project BOOST Process
Once a site is accepted as a Project BOOST site, the site leader receives an information package and access to the Project BOOST online repository for recording and uploading readmission data. Then, each Project BOOST cohort performs an in-person conference. Networking and personal interaction are an important part of sharing challenges and successes in reducing readmissions. The conference also includes training on root-cause analysis and process mapping, a required step for application of the new Community Based Care Transitions Program (CCTP), part of the Affordable Care Act.
Each site leader is assigned a Project BOOST mentor, a national expert on reducing readmissions to the hospital. The mentor conducts a site visit to the hospital to meet the entire team in person and better understand the discharge challenges first-hand.
Over the course of the year, through regularly scheduled telephone calls, the mentor works with the Project BOOST team to best apply the program to the needs of the specific hospital. Mentors also help answer questions related to project planning, toolkit materials, data collection, implementation, and analysis.
In Dr. Rennke’s case, the process helped augment and guide UCSF’s current discharge program. Having multiple team members from different disciplines made distributing the work and implementation easier.
“Overall, we knew this was going to be doable because we incorporated Project BOOST into an already existing discharge process,” Dr. Rennke says.
Readmissions in the Crosshairs
The impacts of preventable readmissions on patient safety and efficiency of care in the hospital have made the issue a heated one in public policy. Earlier this year, the U.S. Department of Health and Human Services announced the creation of Partnership for Patients, a $1 billion initiative to address “quality, safety, and affordability of healthcare for all Americans.” SHM was one of the first medical societies to sign on to the “Partnership for Patients Pledge.”
One of the partnership’s two major goals is to reduce hospital readmissions by 20%. According to the Partnership for Patients website, “achieving this goal would mean more than 1.6 million patients would recover from illness without suffering a preventable complication requiring rehospitalization within 30 days of discharge.”
The government is backing up this goal with funding for hospitals with concrete plans to reduce readmissions. Under the Affordable Care Act of 2010—commonly known as the healthcare reform law—Medicare created the five-year CCTP earlier this year. The program provides $500 million to collaborative partnerships between hospitals and community-based organizations to implement care-transition services for Medicare beneficiaries, many of whom are at high risk of readmission.
To Dr. Rennke, the attention to reducing readmissions is an extension of her responsibility as a caregiver. “Our responsibility doesn’t end when the patient leaves the hospital,” she says. TH
Brendon Shank is SHM’s assistant vice president of communications.
If you’re a hospitalist interested in reducing readmissions in your hospital, the time to act is now.
Project BOOST (Better Outcomes for Older Adults through Safe Transitions), SHM’s groundbreaking program designed to help hospitals reduce unplanned readmissions, is now accepting applications for two new cohorts: one national and another specific to California. The deadline for applications is August 1.
Now with 85 sites as part of the national community, Project BOOST will introduce new sites across the country in the fall. In addition to the national cohort, Project BOOST will also establish a new cohort in California, with discounted tuition through grants from three healthcare groups in the state.
“It’s a great time to apply,” says Stephanie Rennke, MD, assistant clinical professor of medicine at the University of California San Francisco Medical Center. “We are at the cusp of a lot of big changes in health reform. The time to address readmissions is now. Hospitals will have to address this, and BOOST is one way to do that.”
—Stephanie Rennke, MD, assistant clinical professor of medicine, University of California San Francisco Medical Center
Applications are submitted online (www.hospitalmedicine.org/boost) and evaluated based on whether improving discharge and care transitions is a high priority at the institution. Applications must be accompanied by a letter of support from an executive sponsor within the applicant’s hospital.
Once accepted into the program, BOOST participants pay a tuition fee of $28,000. Thanks to the support of the California HealthCare Foundation, the L.A. Care Health Plan, and the Hospital Association of Southern California, sites in California are eligible for reduced tuition based on site location and availability of funds.
For Dr. Rennke, the link between healthcare reform and readmissions is clear, along with the repercussions for hospitals. Most notably, the discharge process affects multiple quality issues, including “patient satisfaction, provider satisfaction and improving communication from hospital to home.”
“Hospitals need to realize healthcare reform is coming,” says Dr. Rennke, who previously served as a Project BOOST site team member and now works as a BOOST mentor. “Not only is reducing readmissions the right thing to do, it will also have a financial impact for hospitals that don’t address it. … It’s going to be of paramount importance to address the discharge process.”
National Growth
Since it was initially developed through a grant from the John A. Hartford Foundation, Project BOOST has spread to hospitals across the country and received widespread attention throughout the healthcare community.
At the time of Project BOOST’s inception in 2008, readmissions already were an intractable and costly issue for hospitals. The next year, research coauthored by Project BOOST principal investigator Mark V. Williams, MD, FHM, and published in the New England Journal of Medicine revealed that unplanned readmissions cost Medicare $17.4 billion annually.
Project BOOST’s pilot cohort consisted of six hospital sites. The program’s growth accelerated quickly, and it soon added another 24 sites and, later, two statewide programs in Michigan and Illinois.
The popularity of Project BOOST among hospitals has captured the attention of media and other organizations as well:
- This year, Kaiser Health News featured the work of Atlanta’s Piedmont Hospital to reduce readmissions using Project BOOST in an article focusing on the impact of healthcare reform laws on hospital readmissions.
- The Bassett Healthcare Network, a Project BOOST site in upstate New York, has earned the Hospital Association of New York State’s prestigious 2011 HANYS Pinnacle Award for Quality and Safety for the group’s care-transition work. The award was presented to Bassett Healthcare Network chief executives in June.
- In California, the Kaiser Permanente West LA BOOST Team was recognized with an award from Dr. Benjamin Chu, president of Southern California Kaiser Foundation Health Plan.
- In December 2010, Dr. Williams and hospitalist Matthew Schreiber, CMO of Piedmont Hospital, shared their experiences with Project BOOST at a national conference hosted by the Centers for Medicare & Medicaid Services (CMS).
The Project BOOST Process
Once a site is accepted as a Project BOOST site, the site leader receives an information package and access to the Project BOOST online repository for recording and uploading readmission data. Then, each Project BOOST cohort performs an in-person conference. Networking and personal interaction are an important part of sharing challenges and successes in reducing readmissions. The conference also includes training on root-cause analysis and process mapping, a required step for application of the new Community Based Care Transitions Program (CCTP), part of the Affordable Care Act.
Each site leader is assigned a Project BOOST mentor, a national expert on reducing readmissions to the hospital. The mentor conducts a site visit to the hospital to meet the entire team in person and better understand the discharge challenges first-hand.
Over the course of the year, through regularly scheduled telephone calls, the mentor works with the Project BOOST team to best apply the program to the needs of the specific hospital. Mentors also help answer questions related to project planning, toolkit materials, data collection, implementation, and analysis.
In Dr. Rennke’s case, the process helped augment and guide UCSF’s current discharge program. Having multiple team members from different disciplines made distributing the work and implementation easier.
“Overall, we knew this was going to be doable because we incorporated Project BOOST into an already existing discharge process,” Dr. Rennke says.
Readmissions in the Crosshairs
The impacts of preventable readmissions on patient safety and efficiency of care in the hospital have made the issue a heated one in public policy. Earlier this year, the U.S. Department of Health and Human Services announced the creation of Partnership for Patients, a $1 billion initiative to address “quality, safety, and affordability of healthcare for all Americans.” SHM was one of the first medical societies to sign on to the “Partnership for Patients Pledge.”
One of the partnership’s two major goals is to reduce hospital readmissions by 20%. According to the Partnership for Patients website, “achieving this goal would mean more than 1.6 million patients would recover from illness without suffering a preventable complication requiring rehospitalization within 30 days of discharge.”
The government is backing up this goal with funding for hospitals with concrete plans to reduce readmissions. Under the Affordable Care Act of 2010—commonly known as the healthcare reform law—Medicare created the five-year CCTP earlier this year. The program provides $500 million to collaborative partnerships between hospitals and community-based organizations to implement care-transition services for Medicare beneficiaries, many of whom are at high risk of readmission.
To Dr. Rennke, the attention to reducing readmissions is an extension of her responsibility as a caregiver. “Our responsibility doesn’t end when the patient leaves the hospital,” she says. TH
Brendon Shank is SHM’s assistant vice president of communications.
What Is Your Value?

For those of you who attended Bob Wachter’s talk at HM11 in Dallas, you learned that Bob drives a particular model of a popular SUV made by a well-known Japanese manufacturer. When he was in the market for a vehicle, he decided he wanted to buy an SUV. He acknowledged there were certainly less expensive SUVs on the market, along with more expensive alternatives.
So why did he choose to purchase that particular model? Was it the color, the seat warmers, or the keyless entry system? The answer is simple: He decided to purchase the popular SUV because he thought it was the best value for his dollar.
I have this vision of Bob, head cocked to one side, with his index finger resting against his chin and a text bubble above his head reading, “What is the quality of this vehicle and what is the price tag?”
These are decisions all of us make in our everyday lives. I make the same value judgment when I pull into the gasoline station to purchase gas (regular or premium?) or when I go to the grocery store (brand-name or generic orange juice?). But we know that higher cost doesn’t always mean higher quality. Think American-made automobiles versus Japanese-made vehicles in the 1970s and ’80s.
Along those same lines, let’s think about the U.S. healthcare system in 2011. America is trying to move its healthcare toward a value-based system. How do we receive the best healthcare for the—many times taxpayer—dollar? I am a taxpayer and I am all for higher-quality healthcare for my dollars.
At HM11, I heard from many supporters of healthcare reform, but I also heard many people vilify the government’s efforts at reforming our healthcare system. Just about everyone agreed that the future is uncertain. The current healthcare system certainly values hospitalists. It is hard to argue with the facts. In less than 15 years, our healthcare system has created jobs for more than 30,000 hospitalists, the majority of whom require nonclinical revenue from hospitals to meet expenses. The latest SHM-MGMA data show that the average hospitalist full-time equivalent (FTE) receives more than $131,500 of nonclinical revenue (primarily from hospitals) annually.
Payors of healthcare are no different than Bob when it comes to purchasing a car, or me when it comes to purchasing orange juice. Payors will pay for hospitalists as long as they perceive value in their investment.
But what is the basis of this notion that hospitalists are high-value healthcare providers, and is it justified? At HM11, I heard about the continued rise in hospitalist salaries. Higher costs mean we will have to increase quality if we hope to achieve the same value (value=quality/cost).
Don’t Worry, Share Your Data
I have listened to many presentations about healthcare value, quality, and cost. My perception is that it makes the most sense if it is personal. I live in Massachusetts, and my state government has been aggressive at helping everyone understand the quality and the cost of care being delivered at our hospitals. For example, our state government generates a massive annual report that describes the quality and cost of healthcare being delivered at individual hospitals; a PDF of the report is available at www.mass.gov. (For full disclosure, I work at Beth Israel Deaconess Medical Center [BIDMC] in Boston and I serve on a Massachusetts Department of Public Health Stroke Advisory Committee.)
The annual report shows there is not as much of a direct relationship between quality and cost as one would like to see. But I applaud Massachusetts for producing this report. Recognizing and understanding a problem is the first step in creating a solution to the problem. One cannot create a value-based system without understanding the existing quality and cost.
This is one of the reasons why, several years ago, the BIDMC leadership posted my hospital’s quality data online for public consumption (www.bidmc.org/QualityandSafety.aspx). The BIDMC website even features a short video of hospitalist Ken Sands, MD, who also happens to be the vice president of quality at BIDMC, telling you about the hospital quality data. Before the hospital posted this data online, most of our hospital staff and providers, let alone our patients and their families, were unaware of the data. BIDMC is not the only hospital who does this. I understand Cedars-Sinai Medical Center in Los Angeles and Dartmouth-Hitchcock Medical Center in New Hampshire have long shared their quality data publicly.
But the truth is, if you look hard enough, you can find these data for just about all acute-care hospitals in the country. Start with Medicare’s Hospital Compare website (www.hospitalcompare.hhs.gov). However, BIDMC and others have simply made it easier to find the data by putting it directly on their websites.
Policy of Transparency
An interesting thing happened over the past decade at BIDMC. In 1997, there were no hospitalists who cared for BIDMC patients. Today, hospitalists manage nearly 100% of the patients hospitalized on our large medical service.
When you look at the data being reported by BIDMC and the state of Massachusetts about nonsurgical conditions, doesn’t that reflect the care being provided by the hospitalists who work at BIDMC? I imagine that is what will run through my CEO and CFO’s minds when we discuss the hospitalist budget this summer. They will ask themselves, “What is the value of our hospitalists? What is the quality of their care? How much do they cost us?”
Some of you might be in a similar position. Do your hospitalists now provide the bulk of the care at your hospital? Are your hospital’s data being publicly reported? I think the answer is a resounding “yes” for many of you.
Allow me to ask this question: What are you doing to collect data to understand the quality and cost of your hospitalist program? Wouldn’t you rather know this information before your hospital or state government tells you?
As the director of my hospitalist group, I spearhead our group efforts to better understand the quality of care we provide. This proactive, introspective approach is essential, especially if hospitalist groups around the country hope to continue being perceived as “high value” providers.
I am interested in hearing from you about your efforts to understand the care being provided by your hospitalists. Feel free to email me at JosephLi@HospitalMedicine.org. TH
Dr. Li is president of SHM.
For those of you who attended Bob Wachter’s talk at HM11 in Dallas, you learned that Bob drives a particular model of a popular SUV made by a well-known Japanese manufacturer. When he was in the market for a vehicle, he decided he wanted to buy an SUV. He acknowledged there were certainly less expensive SUVs on the market, along with more expensive alternatives.
So why did he choose to purchase that particular model? Was it the color, the seat warmers, or the keyless entry system? The answer is simple: He decided to purchase the popular SUV because he thought it was the best value for his dollar.
I have this vision of Bob, head cocked to one side, with his index finger resting against his chin and a text bubble above his head reading, “What is the quality of this vehicle and what is the price tag?”
These are decisions all of us make in our everyday lives. I make the same value judgment when I pull into the gasoline station to purchase gas (regular or premium?) or when I go to the grocery store (brand-name or generic orange juice?). But we know that higher cost doesn’t always mean higher quality. Think American-made automobiles versus Japanese-made vehicles in the 1970s and ’80s.
Along those same lines, let’s think about the U.S. healthcare system in 2011. America is trying to move its healthcare toward a value-based system. How do we receive the best healthcare for the—many times taxpayer—dollar? I am a taxpayer and I am all for higher-quality healthcare for my dollars.
At HM11, I heard from many supporters of healthcare reform, but I also heard many people vilify the government’s efforts at reforming our healthcare system. Just about everyone agreed that the future is uncertain. The current healthcare system certainly values hospitalists. It is hard to argue with the facts. In less than 15 years, our healthcare system has created jobs for more than 30,000 hospitalists, the majority of whom require nonclinical revenue from hospitals to meet expenses. The latest SHM-MGMA data show that the average hospitalist full-time equivalent (FTE) receives more than $131,500 of nonclinical revenue (primarily from hospitals) annually.
Payors of healthcare are no different than Bob when it comes to purchasing a car, or me when it comes to purchasing orange juice. Payors will pay for hospitalists as long as they perceive value in their investment.
But what is the basis of this notion that hospitalists are high-value healthcare providers, and is it justified? At HM11, I heard about the continued rise in hospitalist salaries. Higher costs mean we will have to increase quality if we hope to achieve the same value (value=quality/cost).
Don’t Worry, Share Your Data
I have listened to many presentations about healthcare value, quality, and cost. My perception is that it makes the most sense if it is personal. I live in Massachusetts, and my state government has been aggressive at helping everyone understand the quality and the cost of care being delivered at our hospitals. For example, our state government generates a massive annual report that describes the quality and cost of healthcare being delivered at individual hospitals; a PDF of the report is available at www.mass.gov. (For full disclosure, I work at Beth Israel Deaconess Medical Center [BIDMC] in Boston and I serve on a Massachusetts Department of Public Health Stroke Advisory Committee.)
The annual report shows there is not as much of a direct relationship between quality and cost as one would like to see. But I applaud Massachusetts for producing this report. Recognizing and understanding a problem is the first step in creating a solution to the problem. One cannot create a value-based system without understanding the existing quality and cost.
This is one of the reasons why, several years ago, the BIDMC leadership posted my hospital’s quality data online for public consumption (www.bidmc.org/QualityandSafety.aspx). The BIDMC website even features a short video of hospitalist Ken Sands, MD, who also happens to be the vice president of quality at BIDMC, telling you about the hospital quality data. Before the hospital posted this data online, most of our hospital staff and providers, let alone our patients and their families, were unaware of the data. BIDMC is not the only hospital who does this. I understand Cedars-Sinai Medical Center in Los Angeles and Dartmouth-Hitchcock Medical Center in New Hampshire have long shared their quality data publicly.
But the truth is, if you look hard enough, you can find these data for just about all acute-care hospitals in the country. Start with Medicare’s Hospital Compare website (www.hospitalcompare.hhs.gov). However, BIDMC and others have simply made it easier to find the data by putting it directly on their websites.
Policy of Transparency
An interesting thing happened over the past decade at BIDMC. In 1997, there were no hospitalists who cared for BIDMC patients. Today, hospitalists manage nearly 100% of the patients hospitalized on our large medical service.
When you look at the data being reported by BIDMC and the state of Massachusetts about nonsurgical conditions, doesn’t that reflect the care being provided by the hospitalists who work at BIDMC? I imagine that is what will run through my CEO and CFO’s minds when we discuss the hospitalist budget this summer. They will ask themselves, “What is the value of our hospitalists? What is the quality of their care? How much do they cost us?”
Some of you might be in a similar position. Do your hospitalists now provide the bulk of the care at your hospital? Are your hospital’s data being publicly reported? I think the answer is a resounding “yes” for many of you.
Allow me to ask this question: What are you doing to collect data to understand the quality and cost of your hospitalist program? Wouldn’t you rather know this information before your hospital or state government tells you?
As the director of my hospitalist group, I spearhead our group efforts to better understand the quality of care we provide. This proactive, introspective approach is essential, especially if hospitalist groups around the country hope to continue being perceived as “high value” providers.
I am interested in hearing from you about your efforts to understand the care being provided by your hospitalists. Feel free to email me at JosephLi@HospitalMedicine.org. TH
Dr. Li is president of SHM.
For those of you who attended Bob Wachter’s talk at HM11 in Dallas, you learned that Bob drives a particular model of a popular SUV made by a well-known Japanese manufacturer. When he was in the market for a vehicle, he decided he wanted to buy an SUV. He acknowledged there were certainly less expensive SUVs on the market, along with more expensive alternatives.
So why did he choose to purchase that particular model? Was it the color, the seat warmers, or the keyless entry system? The answer is simple: He decided to purchase the popular SUV because he thought it was the best value for his dollar.
I have this vision of Bob, head cocked to one side, with his index finger resting against his chin and a text bubble above his head reading, “What is the quality of this vehicle and what is the price tag?”
These are decisions all of us make in our everyday lives. I make the same value judgment when I pull into the gasoline station to purchase gas (regular or premium?) or when I go to the grocery store (brand-name or generic orange juice?). But we know that higher cost doesn’t always mean higher quality. Think American-made automobiles versus Japanese-made vehicles in the 1970s and ’80s.
Along those same lines, let’s think about the U.S. healthcare system in 2011. America is trying to move its healthcare toward a value-based system. How do we receive the best healthcare for the—many times taxpayer—dollar? I am a taxpayer and I am all for higher-quality healthcare for my dollars.
At HM11, I heard from many supporters of healthcare reform, but I also heard many people vilify the government’s efforts at reforming our healthcare system. Just about everyone agreed that the future is uncertain. The current healthcare system certainly values hospitalists. It is hard to argue with the facts. In less than 15 years, our healthcare system has created jobs for more than 30,000 hospitalists, the majority of whom require nonclinical revenue from hospitals to meet expenses. The latest SHM-MGMA data show that the average hospitalist full-time equivalent (FTE) receives more than $131,500 of nonclinical revenue (primarily from hospitals) annually.
Payors of healthcare are no different than Bob when it comes to purchasing a car, or me when it comes to purchasing orange juice. Payors will pay for hospitalists as long as they perceive value in their investment.
But what is the basis of this notion that hospitalists are high-value healthcare providers, and is it justified? At HM11, I heard about the continued rise in hospitalist salaries. Higher costs mean we will have to increase quality if we hope to achieve the same value (value=quality/cost).
Don’t Worry, Share Your Data
I have listened to many presentations about healthcare value, quality, and cost. My perception is that it makes the most sense if it is personal. I live in Massachusetts, and my state government has been aggressive at helping everyone understand the quality and the cost of care being delivered at our hospitals. For example, our state government generates a massive annual report that describes the quality and cost of healthcare being delivered at individual hospitals; a PDF of the report is available at www.mass.gov. (For full disclosure, I work at Beth Israel Deaconess Medical Center [BIDMC] in Boston and I serve on a Massachusetts Department of Public Health Stroke Advisory Committee.)
The annual report shows there is not as much of a direct relationship between quality and cost as one would like to see. But I applaud Massachusetts for producing this report. Recognizing and understanding a problem is the first step in creating a solution to the problem. One cannot create a value-based system without understanding the existing quality and cost.
This is one of the reasons why, several years ago, the BIDMC leadership posted my hospital’s quality data online for public consumption (www.bidmc.org/QualityandSafety.aspx). The BIDMC website even features a short video of hospitalist Ken Sands, MD, who also happens to be the vice president of quality at BIDMC, telling you about the hospital quality data. Before the hospital posted this data online, most of our hospital staff and providers, let alone our patients and their families, were unaware of the data. BIDMC is not the only hospital who does this. I understand Cedars-Sinai Medical Center in Los Angeles and Dartmouth-Hitchcock Medical Center in New Hampshire have long shared their quality data publicly.
But the truth is, if you look hard enough, you can find these data for just about all acute-care hospitals in the country. Start with Medicare’s Hospital Compare website (www.hospitalcompare.hhs.gov). However, BIDMC and others have simply made it easier to find the data by putting it directly on their websites.
Policy of Transparency
An interesting thing happened over the past decade at BIDMC. In 1997, there were no hospitalists who cared for BIDMC patients. Today, hospitalists manage nearly 100% of the patients hospitalized on our large medical service.
When you look at the data being reported by BIDMC and the state of Massachusetts about nonsurgical conditions, doesn’t that reflect the care being provided by the hospitalists who work at BIDMC? I imagine that is what will run through my CEO and CFO’s minds when we discuss the hospitalist budget this summer. They will ask themselves, “What is the value of our hospitalists? What is the quality of their care? How much do they cost us?”
Some of you might be in a similar position. Do your hospitalists now provide the bulk of the care at your hospital? Are your hospital’s data being publicly reported? I think the answer is a resounding “yes” for many of you.
Allow me to ask this question: What are you doing to collect data to understand the quality and cost of your hospitalist program? Wouldn’t you rather know this information before your hospital or state government tells you?
As the director of my hospitalist group, I spearhead our group efforts to better understand the quality of care we provide. This proactive, introspective approach is essential, especially if hospitalist groups around the country hope to continue being perceived as “high value” providers.
I am interested in hearing from you about your efforts to understand the care being provided by your hospitalists. Feel free to email me at JosephLi@HospitalMedicine.org. TH
Dr. Li is president of SHM.
Marriage of Necessity
Doctors and hospitals need each other. Healthcare reform is requiring hospitals to rely more heavily on physicians to help them meet quality, safety, and efficiency goals. But in return, doctors are demanding more financial security and a larger role in hospital leadership.
Just how far are they willing to take their mutual relationship to meet their individual needs? A new report by professional services company PwC (formerly PricewaterhouseCoopers) examines the mindsets of potential partners, including an online survey of more than 1,000 doctors and in-depth interviews with 28 healthcare executives. The results suggest plenty of opportunities for alignment, though perhaps also the need for serious pre-marriage counseling.
“From Courtship to Marriage Part II” (www.PwC.com/us/PhysicianHospitalAlignment) follows an initial report that emphasizes the element of trust that’s necessary for any doctor-hospital alignment to succeed. This time around, the sequel is focusing on more concrete steps needed to take the budding relationship to the next level and sustain it. In particular, the new report focuses on sharing power (governance), sharing resources (compensation), and sharing outcomes (guidelines).
The PwC report preempts the naysayers by acknowledging at the outset that “hospitals and physicians have been to the altar before, but many of those marriages ended in divorce.” So what’s different from the 1990s, that decade of broken marriages doomed by the irreconcilable differences over capitation?
“Number one is that back in the ’90s, there wasn’t a clear consensus in defining and determining what is quality,” says Warren Skea, a director in the PwC Health Enterprise Growth Practice. In the intervening years, he says, membership societies—SHM among them—and nonprofit organizations, such as the National Quality Forum, have helped address the need to define and measure healthcare quality. The Centers for Medicare & Medicaid Services (CMS) followed up by adopting and implementing some of those measures in programs, including hospital value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
Another missing component in the ’90s, Skea says, was an adequate set of tools for gauging quality. “Even if we did agree what quality was, we couldn’t go back in there and measure it in a valid way,” he explains. “We just didn’t have that capacity.”
A third lesson learned the hard way is that decision-making should involve all physicians, from primary-care doctors to specialists. That power-sharing will be critical, Skea says, as reimbursement models move away from fee-for-service, transaction-based compensation methods and toward paying for outcomes and quality. Silos of care are out, and transitioning patients across a continuum of care is definitely in.
Sound familiar? It should, and the similarity to the hospitalist job description isn’t lost on Skea. “I think hospitalists have served as a very good illustrative example of how physicians can add value to that efficiency equation, improve quality, increase [good] outcomes—all of those things,” he says. In fact, Skea says, the question now is how the quarterback role assumed by hospitalists can be translated or projected to the larger industry and other settings (e.g. outpatient clinics, home care rehabilitation, and continuing care facilities).
Accountable-care organizations (ACOs) are a hot topic in any discussion of better patient transitions and closer doctor-hospital alignments, but they’re hardly the only wedding chapels in town. The new report sketches out the corresponding amenities of a comanagement model and provider-owned plan, and Skea notes that part of the new Center for Medicare & Medicaid Innovation’s mandate will be to investigate other promising methods for encouraging providers to work together.
Leaders, Partners
For most doctors, according to the survey, working together means making joint decisions. More than 90% said they should be involved in “hospital governance activities such as serving on boards, being in management, and taking part in performance.”
“That didn’t surprise me at all; there’s a huge appetite for physicians to be involved in strategic governance and oversight,” Skea says. “That’s where hospitalists have been really good: taking it to that next level of strategy and leadership.”
Next to compensation, he says, governance is the biggest issue for many hospital-affiliated physicians. One wrinkle, however, is what the report’s authors heard from hospital executives. “There’s a recognition by hospital executives that they need those physicians in those governance roles,” Skea says. But the executives felt that more physicians should be trained and educated in business and financial decision-making.
Some of the training strategies, he says, are homegrown. One hospital client, for example, is providing its physicians with courses in statistical analysis, financial modeling, and change management, and referring to the educational package as “MBA in a box.” Other hospitals are steering their physicians toward outside sources of instruction. SHM’s four-day Leadership Academy (www.hospitalmedicine.org/leadership) offers another resource for hospitalists seeking more prominent roles within their institutions.
Along with a desire for more power-sharing, doctors looking to a hospital setting have clearly indicated that they expect to hold their own financially. According to the survey, 83% of doctors considering hospital employment expect to be paid as much as or more than they are currently earning.
And therein lies another potential sticking point. Based on past experience, doctors might expect that hospitals’ financial resources will still allow them to maximize their compensation. But as health reform plays out, Skea cautions, “everybody is going to have to do more with less.”
Compromise Ahead
But other survey results hint at the potential for compromise. According to the report, physicians agreed that half of their compensation should be a fixed salary, while the remaining half could be based on meeting productivity, quality, patient satisfaction, and cost-of-care goals, with the potential for performance rewards. “This shows that physicians realize the health system is changing to track and reward performance and that they can influence the quality and cost of care delivery at the institutional level,” the report states.
And as for the guidelines doctors follow while delivering healthcare, 62% of those surveyed believe nationally accepted guidelines should guide the way they practice medicine; 30% prefer local guidelines.
Skea says he was a bit surprised that nearly 1 in 3 doctors are still resistant to national guidelines, though he believes that number is on the wane. After an initial pushback, he says, doctors seem to be gravitating toward the national standards, due in part to physician societies taking active roles in the discussions.
So what should hospitalists take away from all of this? Skea says they should continue to highlight and demonstrate the value they provide in standardizing care, measuring quality, and improving efficiencies in the four walls of the hospital. “They’ve had a track record, I think they have the mindset, and they’ve had the relationship with hospital executives,” he says.
Hospitalists likely will be called upon to help educate their physician colleagues in other specialties. Because of their background and history of success, Skea says, “they could be one of the real leaders and catalysts for change within an ACO or some of these other more integrated and aligned delivery models, and then move into governance.”
With a little assistance, perhaps this marriage might work after all. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Doctors and hospitals need each other. Healthcare reform is requiring hospitals to rely more heavily on physicians to help them meet quality, safety, and efficiency goals. But in return, doctors are demanding more financial security and a larger role in hospital leadership.
Just how far are they willing to take their mutual relationship to meet their individual needs? A new report by professional services company PwC (formerly PricewaterhouseCoopers) examines the mindsets of potential partners, including an online survey of more than 1,000 doctors and in-depth interviews with 28 healthcare executives. The results suggest plenty of opportunities for alignment, though perhaps also the need for serious pre-marriage counseling.
“From Courtship to Marriage Part II” (www.PwC.com/us/PhysicianHospitalAlignment) follows an initial report that emphasizes the element of trust that’s necessary for any doctor-hospital alignment to succeed. This time around, the sequel is focusing on more concrete steps needed to take the budding relationship to the next level and sustain it. In particular, the new report focuses on sharing power (governance), sharing resources (compensation), and sharing outcomes (guidelines).
The PwC report preempts the naysayers by acknowledging at the outset that “hospitals and physicians have been to the altar before, but many of those marriages ended in divorce.” So what’s different from the 1990s, that decade of broken marriages doomed by the irreconcilable differences over capitation?
“Number one is that back in the ’90s, there wasn’t a clear consensus in defining and determining what is quality,” says Warren Skea, a director in the PwC Health Enterprise Growth Practice. In the intervening years, he says, membership societies—SHM among them—and nonprofit organizations, such as the National Quality Forum, have helped address the need to define and measure healthcare quality. The Centers for Medicare & Medicaid Services (CMS) followed up by adopting and implementing some of those measures in programs, including hospital value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
Another missing component in the ’90s, Skea says, was an adequate set of tools for gauging quality. “Even if we did agree what quality was, we couldn’t go back in there and measure it in a valid way,” he explains. “We just didn’t have that capacity.”
A third lesson learned the hard way is that decision-making should involve all physicians, from primary-care doctors to specialists. That power-sharing will be critical, Skea says, as reimbursement models move away from fee-for-service, transaction-based compensation methods and toward paying for outcomes and quality. Silos of care are out, and transitioning patients across a continuum of care is definitely in.
Sound familiar? It should, and the similarity to the hospitalist job description isn’t lost on Skea. “I think hospitalists have served as a very good illustrative example of how physicians can add value to that efficiency equation, improve quality, increase [good] outcomes—all of those things,” he says. In fact, Skea says, the question now is how the quarterback role assumed by hospitalists can be translated or projected to the larger industry and other settings (e.g. outpatient clinics, home care rehabilitation, and continuing care facilities).
Accountable-care organizations (ACOs) are a hot topic in any discussion of better patient transitions and closer doctor-hospital alignments, but they’re hardly the only wedding chapels in town. The new report sketches out the corresponding amenities of a comanagement model and provider-owned plan, and Skea notes that part of the new Center for Medicare & Medicaid Innovation’s mandate will be to investigate other promising methods for encouraging providers to work together.
Leaders, Partners
For most doctors, according to the survey, working together means making joint decisions. More than 90% said they should be involved in “hospital governance activities such as serving on boards, being in management, and taking part in performance.”
“That didn’t surprise me at all; there’s a huge appetite for physicians to be involved in strategic governance and oversight,” Skea says. “That’s where hospitalists have been really good: taking it to that next level of strategy and leadership.”
Next to compensation, he says, governance is the biggest issue for many hospital-affiliated physicians. One wrinkle, however, is what the report’s authors heard from hospital executives. “There’s a recognition by hospital executives that they need those physicians in those governance roles,” Skea says. But the executives felt that more physicians should be trained and educated in business and financial decision-making.
Some of the training strategies, he says, are homegrown. One hospital client, for example, is providing its physicians with courses in statistical analysis, financial modeling, and change management, and referring to the educational package as “MBA in a box.” Other hospitals are steering their physicians toward outside sources of instruction. SHM’s four-day Leadership Academy (www.hospitalmedicine.org/leadership) offers another resource for hospitalists seeking more prominent roles within their institutions.
Along with a desire for more power-sharing, doctors looking to a hospital setting have clearly indicated that they expect to hold their own financially. According to the survey, 83% of doctors considering hospital employment expect to be paid as much as or more than they are currently earning.
And therein lies another potential sticking point. Based on past experience, doctors might expect that hospitals’ financial resources will still allow them to maximize their compensation. But as health reform plays out, Skea cautions, “everybody is going to have to do more with less.”
Compromise Ahead
But other survey results hint at the potential for compromise. According to the report, physicians agreed that half of their compensation should be a fixed salary, while the remaining half could be based on meeting productivity, quality, patient satisfaction, and cost-of-care goals, with the potential for performance rewards. “This shows that physicians realize the health system is changing to track and reward performance and that they can influence the quality and cost of care delivery at the institutional level,” the report states.
And as for the guidelines doctors follow while delivering healthcare, 62% of those surveyed believe nationally accepted guidelines should guide the way they practice medicine; 30% prefer local guidelines.
Skea says he was a bit surprised that nearly 1 in 3 doctors are still resistant to national guidelines, though he believes that number is on the wane. After an initial pushback, he says, doctors seem to be gravitating toward the national standards, due in part to physician societies taking active roles in the discussions.
So what should hospitalists take away from all of this? Skea says they should continue to highlight and demonstrate the value they provide in standardizing care, measuring quality, and improving efficiencies in the four walls of the hospital. “They’ve had a track record, I think they have the mindset, and they’ve had the relationship with hospital executives,” he says.
Hospitalists likely will be called upon to help educate their physician colleagues in other specialties. Because of their background and history of success, Skea says, “they could be one of the real leaders and catalysts for change within an ACO or some of these other more integrated and aligned delivery models, and then move into governance.”
With a little assistance, perhaps this marriage might work after all. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Doctors and hospitals need each other. Healthcare reform is requiring hospitals to rely more heavily on physicians to help them meet quality, safety, and efficiency goals. But in return, doctors are demanding more financial security and a larger role in hospital leadership.
Just how far are they willing to take their mutual relationship to meet their individual needs? A new report by professional services company PwC (formerly PricewaterhouseCoopers) examines the mindsets of potential partners, including an online survey of more than 1,000 doctors and in-depth interviews with 28 healthcare executives. The results suggest plenty of opportunities for alignment, though perhaps also the need for serious pre-marriage counseling.
“From Courtship to Marriage Part II” (www.PwC.com/us/PhysicianHospitalAlignment) follows an initial report that emphasizes the element of trust that’s necessary for any doctor-hospital alignment to succeed. This time around, the sequel is focusing on more concrete steps needed to take the budding relationship to the next level and sustain it. In particular, the new report focuses on sharing power (governance), sharing resources (compensation), and sharing outcomes (guidelines).
The PwC report preempts the naysayers by acknowledging at the outset that “hospitals and physicians have been to the altar before, but many of those marriages ended in divorce.” So what’s different from the 1990s, that decade of broken marriages doomed by the irreconcilable differences over capitation?
“Number one is that back in the ’90s, there wasn’t a clear consensus in defining and determining what is quality,” says Warren Skea, a director in the PwC Health Enterprise Growth Practice. In the intervening years, he says, membership societies—SHM among them—and nonprofit organizations, such as the National Quality Forum, have helped address the need to define and measure healthcare quality. The Centers for Medicare & Medicaid Services (CMS) followed up by adopting and implementing some of those measures in programs, including hospital value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
Another missing component in the ’90s, Skea says, was an adequate set of tools for gauging quality. “Even if we did agree what quality was, we couldn’t go back in there and measure it in a valid way,” he explains. “We just didn’t have that capacity.”
A third lesson learned the hard way is that decision-making should involve all physicians, from primary-care doctors to specialists. That power-sharing will be critical, Skea says, as reimbursement models move away from fee-for-service, transaction-based compensation methods and toward paying for outcomes and quality. Silos of care are out, and transitioning patients across a continuum of care is definitely in.
Sound familiar? It should, and the similarity to the hospitalist job description isn’t lost on Skea. “I think hospitalists have served as a very good illustrative example of how physicians can add value to that efficiency equation, improve quality, increase [good] outcomes—all of those things,” he says. In fact, Skea says, the question now is how the quarterback role assumed by hospitalists can be translated or projected to the larger industry and other settings (e.g. outpatient clinics, home care rehabilitation, and continuing care facilities).
Accountable-care organizations (ACOs) are a hot topic in any discussion of better patient transitions and closer doctor-hospital alignments, but they’re hardly the only wedding chapels in town. The new report sketches out the corresponding amenities of a comanagement model and provider-owned plan, and Skea notes that part of the new Center for Medicare & Medicaid Innovation’s mandate will be to investigate other promising methods for encouraging providers to work together.
Leaders, Partners
For most doctors, according to the survey, working together means making joint decisions. More than 90% said they should be involved in “hospital governance activities such as serving on boards, being in management, and taking part in performance.”
“That didn’t surprise me at all; there’s a huge appetite for physicians to be involved in strategic governance and oversight,” Skea says. “That’s where hospitalists have been really good: taking it to that next level of strategy and leadership.”
Next to compensation, he says, governance is the biggest issue for many hospital-affiliated physicians. One wrinkle, however, is what the report’s authors heard from hospital executives. “There’s a recognition by hospital executives that they need those physicians in those governance roles,” Skea says. But the executives felt that more physicians should be trained and educated in business and financial decision-making.
Some of the training strategies, he says, are homegrown. One hospital client, for example, is providing its physicians with courses in statistical analysis, financial modeling, and change management, and referring to the educational package as “MBA in a box.” Other hospitals are steering their physicians toward outside sources of instruction. SHM’s four-day Leadership Academy (www.hospitalmedicine.org/leadership) offers another resource for hospitalists seeking more prominent roles within their institutions.
Along with a desire for more power-sharing, doctors looking to a hospital setting have clearly indicated that they expect to hold their own financially. According to the survey, 83% of doctors considering hospital employment expect to be paid as much as or more than they are currently earning.
And therein lies another potential sticking point. Based on past experience, doctors might expect that hospitals’ financial resources will still allow them to maximize their compensation. But as health reform plays out, Skea cautions, “everybody is going to have to do more with less.”
Compromise Ahead
But other survey results hint at the potential for compromise. According to the report, physicians agreed that half of their compensation should be a fixed salary, while the remaining half could be based on meeting productivity, quality, patient satisfaction, and cost-of-care goals, with the potential for performance rewards. “This shows that physicians realize the health system is changing to track and reward performance and that they can influence the quality and cost of care delivery at the institutional level,” the report states.
And as for the guidelines doctors follow while delivering healthcare, 62% of those surveyed believe nationally accepted guidelines should guide the way they practice medicine; 30% prefer local guidelines.
Skea says he was a bit surprised that nearly 1 in 3 doctors are still resistant to national guidelines, though he believes that number is on the wane. After an initial pushback, he says, doctors seem to be gravitating toward the national standards, due in part to physician societies taking active roles in the discussions.
So what should hospitalists take away from all of this? Skea says they should continue to highlight and demonstrate the value they provide in standardizing care, measuring quality, and improving efficiencies in the four walls of the hospital. “They’ve had a track record, I think they have the mindset, and they’ve had the relationship with hospital executives,” he says.
Hospitalists likely will be called upon to help educate their physician colleagues in other specialties. Because of their background and history of success, Skea says, “they could be one of the real leaders and catalysts for change within an ACO or some of these other more integrated and aligned delivery models, and then move into governance.”
With a little assistance, perhaps this marriage might work after all. TH
Bryn Nelson is a freelance medical writer based in Seattle.
POLICY CORNER: SHM Pledges Support to Patient-Safety Initiative

On April 12, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius joined the Centers for Medicare & Medicaid Services (CMS) administrator Donald Berwick, MD, in announcing a major patient-safety initiative bringing together hospitals, clinicians, consumers, employers, federal and state governments, and many more groups around two common goals: reducing harm caused to patients in hospitals and reducing hospital readmissions.
SHM was one of the first physician groups to sign on to the Pledge of Support, which aims to reduce hospital-acquired conditions by 40% and decrease preventable readmissions within 30 days of discharge by 20%, both by the end of 2013.
The pledge includes specific expectations for each of the different healthcare entities signing on. By signing, SHM agrees on behalf of hospitalists that they will work together to redesign activities within the hospital to reduce harm, learn from experiences and share best practices, and engage with patients and families to implement practices that foster more patient-centered care that improves safety, communication, and care coordination.
HHS is committing a total of $1 billion from the Patient Protection and Affordable Care Act of 2010 (ACA) to support hospitals and other providers in their efforts to reach these goals. Of the funding, $500 million will come through the Community-Based Care Transitions Program (CCTP) created in the ACA to help community-based organizations partnering with eligible hospitals to improve transitions between settings of care. The other $500 million will come from the Centers for Medicare and Medicaid Innovation (CMMI) to test different models of improving patient care, patient engagement, and collaboration in order to reduce hospital-acquired conditions and improve care transitions nationwide.
The partnership takes the best ideas from the public and private sectors and accelerates their spread to achieve a safer, higher-quality healthcare system for all Americans. It aligns Dr. Berwick’s triple aim (improve care, improve people’s health, and reduce the overall cost of healthcare) with SHM’s efforts to improve quality and patient safety through innovation and collaboration.
SHM’s Project BOOST (www.hospitalmedicine.org/boost) is listed in the solicitation for applications for the CCTP, and SHM’s VTE resource room is among the resources posted on the partnership website.
For more information on the initiative, visit www.healthcare.gov. TH
On April 12, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius joined the Centers for Medicare & Medicaid Services (CMS) administrator Donald Berwick, MD, in announcing a major patient-safety initiative bringing together hospitals, clinicians, consumers, employers, federal and state governments, and many more groups around two common goals: reducing harm caused to patients in hospitals and reducing hospital readmissions.
SHM was one of the first physician groups to sign on to the Pledge of Support, which aims to reduce hospital-acquired conditions by 40% and decrease preventable readmissions within 30 days of discharge by 20%, both by the end of 2013.
The pledge includes specific expectations for each of the different healthcare entities signing on. By signing, SHM agrees on behalf of hospitalists that they will work together to redesign activities within the hospital to reduce harm, learn from experiences and share best practices, and engage with patients and families to implement practices that foster more patient-centered care that improves safety, communication, and care coordination.
HHS is committing a total of $1 billion from the Patient Protection and Affordable Care Act of 2010 (ACA) to support hospitals and other providers in their efforts to reach these goals. Of the funding, $500 million will come through the Community-Based Care Transitions Program (CCTP) created in the ACA to help community-based organizations partnering with eligible hospitals to improve transitions between settings of care. The other $500 million will come from the Centers for Medicare and Medicaid Innovation (CMMI) to test different models of improving patient care, patient engagement, and collaboration in order to reduce hospital-acquired conditions and improve care transitions nationwide.
The partnership takes the best ideas from the public and private sectors and accelerates their spread to achieve a safer, higher-quality healthcare system for all Americans. It aligns Dr. Berwick’s triple aim (improve care, improve people’s health, and reduce the overall cost of healthcare) with SHM’s efforts to improve quality and patient safety through innovation and collaboration.
SHM’s Project BOOST (www.hospitalmedicine.org/boost) is listed in the solicitation for applications for the CCTP, and SHM’s VTE resource room is among the resources posted on the partnership website.
For more information on the initiative, visit www.healthcare.gov. TH
On April 12, U.S. Department of Health and Human Services (HHS) Secretary Kathleen Sebelius joined the Centers for Medicare & Medicaid Services (CMS) administrator Donald Berwick, MD, in announcing a major patient-safety initiative bringing together hospitals, clinicians, consumers, employers, federal and state governments, and many more groups around two common goals: reducing harm caused to patients in hospitals and reducing hospital readmissions.
SHM was one of the first physician groups to sign on to the Pledge of Support, which aims to reduce hospital-acquired conditions by 40% and decrease preventable readmissions within 30 days of discharge by 20%, both by the end of 2013.
The pledge includes specific expectations for each of the different healthcare entities signing on. By signing, SHM agrees on behalf of hospitalists that they will work together to redesign activities within the hospital to reduce harm, learn from experiences and share best practices, and engage with patients and families to implement practices that foster more patient-centered care that improves safety, communication, and care coordination.
HHS is committing a total of $1 billion from the Patient Protection and Affordable Care Act of 2010 (ACA) to support hospitals and other providers in their efforts to reach these goals. Of the funding, $500 million will come through the Community-Based Care Transitions Program (CCTP) created in the ACA to help community-based organizations partnering with eligible hospitals to improve transitions between settings of care. The other $500 million will come from the Centers for Medicare and Medicaid Innovation (CMMI) to test different models of improving patient care, patient engagement, and collaboration in order to reduce hospital-acquired conditions and improve care transitions nationwide.
The partnership takes the best ideas from the public and private sectors and accelerates their spread to achieve a safer, higher-quality healthcare system for all Americans. It aligns Dr. Berwick’s triple aim (improve care, improve people’s health, and reduce the overall cost of healthcare) with SHM’s efforts to improve quality and patient safety through innovation and collaboration.
SHM’s Project BOOST (www.hospitalmedicine.org/boost) is listed in the solicitation for applications for the CCTP, and SHM’s VTE resource room is among the resources posted on the partnership website.
For more information on the initiative, visit www.healthcare.gov. TH
The Future of Better Patient Care

GRAPEVINE, Texas—Hospitalist Michael Monge, MD, of Cogent Healthcare in San Bernardino, Calif., watched an instructor squeeze the lubricating gel on the transponder and press it gently, but firmly, into the crook of a woman’s arm. Veins practically popped off an ultrasound monitor, serving as a literal road map for vascular access.
And he thought: Wouldn’t it be great if I had this technology all the time, just like I remember from my residency?
“A lot of my ER attendings were able to do a study at the bedside in a manner of minutes, not 30 or 45 minutes,” says Dr. Monge, who practices at Saint Bernardine Medical Center. “If they saw something abnormal, sure enough, they got the full study. But they were able to get that glimpse. Ultimately, it’s just better patient care.”
Dr. Monge’s ultrasound lesson was a first for the SHM annual meeting. In past years, training on ultrasounds was wrapped into the “Medical Procedures for the Hospitalist” pre-course. But at HM11, thanks to the growing prevalence and portability of the technology, the training was expanded into its own half-day pre-course, appropriately dubbed “Portable Ultrasound for the Hospitalist.”
“The ultrasound will be the stethoscope of the 21st century,” says Mark Ault, director of the Division of General Internal Medicine and assistant chairman for clinical affairs of the Department of Medicine at Cedars-Sinai Medical Center in Los Angeles. “And the goal will be to have an ultrasound in the hands of every internist.”
Only time will tell whether portable ultrasound becomes as commonplace as Dr. Ault envisions, but what is clear is that the evolution of the technology makes it widely applicable to hospitalists, says Bradley Rosen, MD, MBA, medical director of the Inpatient Specialty Program (ISP) at Cedars-Sinai Medical Center.
Pricing is one such example. In years past, ultrasound machines were bulky and costly, with price tags in the hundreds of thousands of dollars. Now, portable units, depending on the number of transducers and functionality, can come as low as $20,000, though more-advanced machines quickly jump into the $40,000 to $60,000 range.
Still, Dr. Rosen views the practical uses of the technology as almost endless, and could include vascular access, placing central and PICC lines, and insertion and removal of catheters. Most hospitalists, however, continue to have limited experience with portable ultrasound, meaning those interested in learning more likely have to seek out physicians in other departments to provide the training and mentorship required. Dr. Rosen suggests working with ED physicians, OB-GYNs, and radiologists, although he notes you should be careful to be clear that the HM community is not looking to supplant anyone, or take billing opportunities away.
Hospitalists “don’t know how to use it, and people don’t know where to go to learn how to use it,” he says. “This is a starting point that will allow people … to take these ideas back and, hopefully, generate enough of a critical mass that it becomes a louder and louder chorus asking for this technology.”
GRAPEVINE, Texas—Hospitalist Michael Monge, MD, of Cogent Healthcare in San Bernardino, Calif., watched an instructor squeeze the lubricating gel on the transponder and press it gently, but firmly, into the crook of a woman’s arm. Veins practically popped off an ultrasound monitor, serving as a literal road map for vascular access.
And he thought: Wouldn’t it be great if I had this technology all the time, just like I remember from my residency?
“A lot of my ER attendings were able to do a study at the bedside in a manner of minutes, not 30 or 45 minutes,” says Dr. Monge, who practices at Saint Bernardine Medical Center. “If they saw something abnormal, sure enough, they got the full study. But they were able to get that glimpse. Ultimately, it’s just better patient care.”
Dr. Monge’s ultrasound lesson was a first for the SHM annual meeting. In past years, training on ultrasounds was wrapped into the “Medical Procedures for the Hospitalist” pre-course. But at HM11, thanks to the growing prevalence and portability of the technology, the training was expanded into its own half-day pre-course, appropriately dubbed “Portable Ultrasound for the Hospitalist.”
“The ultrasound will be the stethoscope of the 21st century,” says Mark Ault, director of the Division of General Internal Medicine and assistant chairman for clinical affairs of the Department of Medicine at Cedars-Sinai Medical Center in Los Angeles. “And the goal will be to have an ultrasound in the hands of every internist.”
Only time will tell whether portable ultrasound becomes as commonplace as Dr. Ault envisions, but what is clear is that the evolution of the technology makes it widely applicable to hospitalists, says Bradley Rosen, MD, MBA, medical director of the Inpatient Specialty Program (ISP) at Cedars-Sinai Medical Center.
Pricing is one such example. In years past, ultrasound machines were bulky and costly, with price tags in the hundreds of thousands of dollars. Now, portable units, depending on the number of transducers and functionality, can come as low as $20,000, though more-advanced machines quickly jump into the $40,000 to $60,000 range.
Still, Dr. Rosen views the practical uses of the technology as almost endless, and could include vascular access, placing central and PICC lines, and insertion and removal of catheters. Most hospitalists, however, continue to have limited experience with portable ultrasound, meaning those interested in learning more likely have to seek out physicians in other departments to provide the training and mentorship required. Dr. Rosen suggests working with ED physicians, OB-GYNs, and radiologists, although he notes you should be careful to be clear that the HM community is not looking to supplant anyone, or take billing opportunities away.
Hospitalists “don’t know how to use it, and people don’t know where to go to learn how to use it,” he says. “This is a starting point that will allow people … to take these ideas back and, hopefully, generate enough of a critical mass that it becomes a louder and louder chorus asking for this technology.”
GRAPEVINE, Texas—Hospitalist Michael Monge, MD, of Cogent Healthcare in San Bernardino, Calif., watched an instructor squeeze the lubricating gel on the transponder and press it gently, but firmly, into the crook of a woman’s arm. Veins practically popped off an ultrasound monitor, serving as a literal road map for vascular access.
And he thought: Wouldn’t it be great if I had this technology all the time, just like I remember from my residency?
“A lot of my ER attendings were able to do a study at the bedside in a manner of minutes, not 30 or 45 minutes,” says Dr. Monge, who practices at Saint Bernardine Medical Center. “If they saw something abnormal, sure enough, they got the full study. But they were able to get that glimpse. Ultimately, it’s just better patient care.”
Dr. Monge’s ultrasound lesson was a first for the SHM annual meeting. In past years, training on ultrasounds was wrapped into the “Medical Procedures for the Hospitalist” pre-course. But at HM11, thanks to the growing prevalence and portability of the technology, the training was expanded into its own half-day pre-course, appropriately dubbed “Portable Ultrasound for the Hospitalist.”
“The ultrasound will be the stethoscope of the 21st century,” says Mark Ault, director of the Division of General Internal Medicine and assistant chairman for clinical affairs of the Department of Medicine at Cedars-Sinai Medical Center in Los Angeles. “And the goal will be to have an ultrasound in the hands of every internist.”
Only time will tell whether portable ultrasound becomes as commonplace as Dr. Ault envisions, but what is clear is that the evolution of the technology makes it widely applicable to hospitalists, says Bradley Rosen, MD, MBA, medical director of the Inpatient Specialty Program (ISP) at Cedars-Sinai Medical Center.
Pricing is one such example. In years past, ultrasound machines were bulky and costly, with price tags in the hundreds of thousands of dollars. Now, portable units, depending on the number of transducers and functionality, can come as low as $20,000, though more-advanced machines quickly jump into the $40,000 to $60,000 range.
Still, Dr. Rosen views the practical uses of the technology as almost endless, and could include vascular access, placing central and PICC lines, and insertion and removal of catheters. Most hospitalists, however, continue to have limited experience with portable ultrasound, meaning those interested in learning more likely have to seek out physicians in other departments to provide the training and mentorship required. Dr. Rosen suggests working with ED physicians, OB-GYNs, and radiologists, although he notes you should be careful to be clear that the HM community is not looking to supplant anyone, or take billing opportunities away.
Hospitalists “don’t know how to use it, and people don’t know where to go to learn how to use it,” he says. “This is a starting point that will allow people … to take these ideas back and, hopefully, generate enough of a critical mass that it becomes a louder and louder chorus asking for this technology.”
HM=Improved Patient Care

GRAPEVINE, Texas—The most successful companies tend to have superior branding. Starbucks owns coffee. Disney owns family fun. And hospitalists own patient-safety and quality-improvement (QI) initiatives within their hospitals.
“We were pretty confident that if we embraced this, we would have a clear running field to ourselves,” says Robert Wachter, MD, MHM, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president, and author of the Wachter’s World blog. “No other physician field would do the same thing, and by owning the patient-safety field, we would distinguish ourselves.”
Now comes the really hard part, though.
Three keynote speakers at HM11—Dr. Wachter, AMA President Cecil Wilson, MD, and Robert Kocher, MD, a healthcare policy advisor to President Obama—pointed to hospitalists as the physician cohort that can help shepherd the conceptual reform passed last year by Congress into daily practice in America’s hospitals. And all three also point to HM’s role at the vanguard of patient safety as a primary reason why.
Hurdles will arise, Dr. Wilson says. A solo practitioner most of his career, he says hospitalists can play a key role in the coming years as more patients receive insurance, but looming doctor shortages could stymie the cause. While many caution that the flood of newly insured patients will overburden primary-care physicians (PCPs), the expected shortage of physicians will plague HM as well.
“Hospitalists are primary-care physicians; the vast majority of them are general internists,” Dr. Wilson says. “… So when we say that the number of people who are going into primary care, particularly general internal medicine, is reducing, that reduces not only the pool of physicians in the community, but also the hospitalist pool. We’re in that boat together.”
Dr. Kocher, director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., says hospitalists are in the best position to push for on-the-ground reform as they are the doctors who bridge all hospital departments, floors, and wards. He sees four broad areas where HM can take a particularly leading role:

- Increasing labor productivity. HM’s role as a link between specialties from cardiology to the pharmacy makes HM a natural conduit to push institutional values from a unique vantage point.
- Driving decision-making. Whether it’s recommending less costly drugs with similar outcomes, questioning whether expensive test batteries are truly necessary or being done for fear of missing something, or pausing to ask whether a “90-year-old hip replacement patient should receive orthopedic implants that will last far longer than their grandkids will be alive,” hospitalists can use their data to be a common-sense lynchpin of daily operations.
- Using technology to lower delivery costs. Many insurance companies are willing to enter into risk-based contracts with hospitals, but some hospital executives worry whether they will be able to perform well enough to justify the risk. “Hospitalists can help say, ‘We can do this. We can hit the thresholds.’ ”
- Shifting compensation models from “selling work RVUs to selling years of health.”
“The biggest thing [hospitalists] should begin doing,” Dr. Kocher adds, “is stop thinking about units of work, or RVUs, and start thinking about how much better patients can be by virtue of the care they’re delivering, how many readmissions are they avoiding, how many core measures/outcomes are they hitting, how much better is the patient experience, and how much smoother is the handoff.”
The push to improve quality and show better outcomes, of course, is intrinsically tied to payment reform. Bundled payments that reimburse a set fee for a case from pre-admission to a preset post-discharge deadline worry some hospitalists, who fear how the payments will be divvied up and who will be in charge of said payment decisions. Dr. Kocher says that even when the initial rules are set, the system is likely to evolve.
However, the hospitalist’s role as a driver of QI positions the field well, all three speakers noted. By quarterbacking patient handoffs and continuing to be seen by hospital executives as quality and safety leaders, HM groups can make the argument that they are worth the financial support they ask for in negotiations. Dr. Wachter adds that while quality research has become a staple of academics and residents, hospitalists should look to now tie value to the equation, effectively linking better patient outcomes to HM’s bottom line.
“There’s no question that physicians that can care for patients more efficiently, in a higher-quality way, in hospitals at lower costs, are going to do better no matter how the system evolves,” Dr. Kocher says. “I’m positive, as long as hospitalists are confident—and I think they should be—that they can deliver, more consistently, better care than those who aren’t hospitalists practicing in hospitals … and they’re going to do better economically.”
GRAPEVINE, Texas—The most successful companies tend to have superior branding. Starbucks owns coffee. Disney owns family fun. And hospitalists own patient-safety and quality-improvement (QI) initiatives within their hospitals.
“We were pretty confident that if we embraced this, we would have a clear running field to ourselves,” says Robert Wachter, MD, MHM, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president, and author of the Wachter’s World blog. “No other physician field would do the same thing, and by owning the patient-safety field, we would distinguish ourselves.”
Now comes the really hard part, though.
Three keynote speakers at HM11—Dr. Wachter, AMA President Cecil Wilson, MD, and Robert Kocher, MD, a healthcare policy advisor to President Obama—pointed to hospitalists as the physician cohort that can help shepherd the conceptual reform passed last year by Congress into daily practice in America’s hospitals. And all three also point to HM’s role at the vanguard of patient safety as a primary reason why.
Hurdles will arise, Dr. Wilson says. A solo practitioner most of his career, he says hospitalists can play a key role in the coming years as more patients receive insurance, but looming doctor shortages could stymie the cause. While many caution that the flood of newly insured patients will overburden primary-care physicians (PCPs), the expected shortage of physicians will plague HM as well.
“Hospitalists are primary-care physicians; the vast majority of them are general internists,” Dr. Wilson says. “… So when we say that the number of people who are going into primary care, particularly general internal medicine, is reducing, that reduces not only the pool of physicians in the community, but also the hospitalist pool. We’re in that boat together.”
Dr. Kocher, director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., says hospitalists are in the best position to push for on-the-ground reform as they are the doctors who bridge all hospital departments, floors, and wards. He sees four broad areas where HM can take a particularly leading role:
- Increasing labor productivity. HM’s role as a link between specialties from cardiology to the pharmacy makes HM a natural conduit to push institutional values from a unique vantage point.
- Driving decision-making. Whether it’s recommending less costly drugs with similar outcomes, questioning whether expensive test batteries are truly necessary or being done for fear of missing something, or pausing to ask whether a “90-year-old hip replacement patient should receive orthopedic implants that will last far longer than their grandkids will be alive,” hospitalists can use their data to be a common-sense lynchpin of daily operations.
- Using technology to lower delivery costs. Many insurance companies are willing to enter into risk-based contracts with hospitals, but some hospital executives worry whether they will be able to perform well enough to justify the risk. “Hospitalists can help say, ‘We can do this. We can hit the thresholds.’ ”
- Shifting compensation models from “selling work RVUs to selling years of health.”
“The biggest thing [hospitalists] should begin doing,” Dr. Kocher adds, “is stop thinking about units of work, or RVUs, and start thinking about how much better patients can be by virtue of the care they’re delivering, how many readmissions are they avoiding, how many core measures/outcomes are they hitting, how much better is the patient experience, and how much smoother is the handoff.”
The push to improve quality and show better outcomes, of course, is intrinsically tied to payment reform. Bundled payments that reimburse a set fee for a case from pre-admission to a preset post-discharge deadline worry some hospitalists, who fear how the payments will be divvied up and who will be in charge of said payment decisions. Dr. Kocher says that even when the initial rules are set, the system is likely to evolve.
However, the hospitalist’s role as a driver of QI positions the field well, all three speakers noted. By quarterbacking patient handoffs and continuing to be seen by hospital executives as quality and safety leaders, HM groups can make the argument that they are worth the financial support they ask for in negotiations. Dr. Wachter adds that while quality research has become a staple of academics and residents, hospitalists should look to now tie value to the equation, effectively linking better patient outcomes to HM’s bottom line.
“There’s no question that physicians that can care for patients more efficiently, in a higher-quality way, in hospitals at lower costs, are going to do better no matter how the system evolves,” Dr. Kocher says. “I’m positive, as long as hospitalists are confident—and I think they should be—that they can deliver, more consistently, better care than those who aren’t hospitalists practicing in hospitals … and they’re going to do better economically.”
GRAPEVINE, Texas—The most successful companies tend to have superior branding. Starbucks owns coffee. Disney owns family fun. And hospitalists own patient-safety and quality-improvement (QI) initiatives within their hospitals.
“We were pretty confident that if we embraced this, we would have a clear running field to ourselves,” says Robert Wachter, MD, MHM, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president, and author of the Wachter’s World blog. “No other physician field would do the same thing, and by owning the patient-safety field, we would distinguish ourselves.”
Now comes the really hard part, though.
Three keynote speakers at HM11—Dr. Wachter, AMA President Cecil Wilson, MD, and Robert Kocher, MD, a healthcare policy advisor to President Obama—pointed to hospitalists as the physician cohort that can help shepherd the conceptual reform passed last year by Congress into daily practice in America’s hospitals. And all three also point to HM’s role at the vanguard of patient safety as a primary reason why.
Hurdles will arise, Dr. Wilson says. A solo practitioner most of his career, he says hospitalists can play a key role in the coming years as more patients receive insurance, but looming doctor shortages could stymie the cause. While many caution that the flood of newly insured patients will overburden primary-care physicians (PCPs), the expected shortage of physicians will plague HM as well.
“Hospitalists are primary-care physicians; the vast majority of them are general internists,” Dr. Wilson says. “… So when we say that the number of people who are going into primary care, particularly general internal medicine, is reducing, that reduces not only the pool of physicians in the community, but also the hospitalist pool. We’re in that boat together.”
Dr. Kocher, director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., says hospitalists are in the best position to push for on-the-ground reform as they are the doctors who bridge all hospital departments, floors, and wards. He sees four broad areas where HM can take a particularly leading role:
- Increasing labor productivity. HM’s role as a link between specialties from cardiology to the pharmacy makes HM a natural conduit to push institutional values from a unique vantage point.
- Driving decision-making. Whether it’s recommending less costly drugs with similar outcomes, questioning whether expensive test batteries are truly necessary or being done for fear of missing something, or pausing to ask whether a “90-year-old hip replacement patient should receive orthopedic implants that will last far longer than their grandkids will be alive,” hospitalists can use their data to be a common-sense lynchpin of daily operations.
- Using technology to lower delivery costs. Many insurance companies are willing to enter into risk-based contracts with hospitals, but some hospital executives worry whether they will be able to perform well enough to justify the risk. “Hospitalists can help say, ‘We can do this. We can hit the thresholds.’ ”
- Shifting compensation models from “selling work RVUs to selling years of health.”
“The biggest thing [hospitalists] should begin doing,” Dr. Kocher adds, “is stop thinking about units of work, or RVUs, and start thinking about how much better patients can be by virtue of the care they’re delivering, how many readmissions are they avoiding, how many core measures/outcomes are they hitting, how much better is the patient experience, and how much smoother is the handoff.”
The push to improve quality and show better outcomes, of course, is intrinsically tied to payment reform. Bundled payments that reimburse a set fee for a case from pre-admission to a preset post-discharge deadline worry some hospitalists, who fear how the payments will be divvied up and who will be in charge of said payment decisions. Dr. Kocher says that even when the initial rules are set, the system is likely to evolve.
However, the hospitalist’s role as a driver of QI positions the field well, all three speakers noted. By quarterbacking patient handoffs and continuing to be seen by hospital executives as quality and safety leaders, HM groups can make the argument that they are worth the financial support they ask for in negotiations. Dr. Wachter adds that while quality research has become a staple of academics and residents, hospitalists should look to now tie value to the equation, effectively linking better patient outcomes to HM’s bottom line.
“There’s no question that physicians that can care for patients more efficiently, in a higher-quality way, in hospitals at lower costs, are going to do better no matter how the system evolves,” Dr. Kocher says. “I’m positive, as long as hospitalists are confident—and I think they should be—that they can deliver, more consistently, better care than those who aren’t hospitalists practicing in hospitals … and they’re going to do better economically.”
HM11 BREAKOUT SESSIONS OVERVIEW





QUALITY
Utilizing Technology to Improve the Clinical and Operational Performance of Hospitalists
SPEAKERS: Jason Stein, MD, SFHM, associate vice chair for quality, Department of Medicine, Bryce Gartland, MD, FHM, associate director, section of hospital medicine, Emory University School of Medicine, Atlanta
In an age of increasing technology, just getting technology into a hospital isn’t the answer. It’s about integrating it into practice to improve care.
At Emory, the marriage of “low-tech solutions” and patented data displays has resulted in what Drs. Stein and Gartland call an accountable-care unit (ACU). The unit-based team features geographic ownership and structured interdisciplinary bedside rounds (SIBR). Perhaps more important, the unit generates real-time data captured on monitors, allowing teams of hospitalists, nonphysician providers (NPPs), residents, interns, and social workers to “visually digest immense amounts of information in a very short time period,” Dr. Gartland said.
Dr. Stein defined an ACU as a bounded geographic inpatient area responsible for the clinical, service, and cost outcomes it produces. To help manage beds, Emory instituted a system called “e-Bed,” a McKesson system that tracks room availability. The system shows whether rooms are occupied, being cleaned, or somewhere in between. It has icons to show whether patients are elsewhere in the hospital for treatment, as well as clinical data capacities. Unit teams round together and use a portable workstation or tablet computer to input clinical data, notes, or other comments into real-time dashboards that can then show everything from VTE prophylaxis to whether a patient is at high risk for falls.
The project has been in the works for several years, and Dr. Garltand noted that any hospitalists looking to push similar initiatives at their institution need to ensure that they have buy-in from providers and a commitment to seeing the project through.
“Timing is everything,” he said. “If we tried to force this … a few years ago, it would not have worked.”
PRACTICE MANAGEMENT
Recruiting and Retaining Hospitalists: Developing a Talent Facilitation Framework
SPEAKERS: Patrick Kneeland, MD, hospitalist, Providence Regional Medical Center, Everett, Wash.; Christine Kneeland, COO, Center Partners, Fort Collins, Colo.; Niraj Sehgal, associate professor of medicine, associate chair for quality and safety, Department of Medicine, University of California at San Francisco
Lincoln Godfrey, DO, a hospitalist at Baxter Regional Medical Center in Mountain Home, Ark., was sitting and listening to strategies to lure and keep hospitalists when his hospital CEO sent him a text asking how his recruiting efforts were going with a would-be hire.
“I said I’d get back to him,” Dr. Godfrey jokes.
The C-suite’s passion is understandable, though, as the fight to hire experienced staff outside of major markets continues to stymie many HM groups. Dr. Godfrey says he can’t hire anybody without first getting them to the Ozark Mountains to learn the hospital, its people, and its community.
“There’s going to be a limited talent pool of people who will come at all,” he says. “But I don’t get anybody who doesn’t work with us for a bit first.”
Christine Kneeland—Dr. Kneeland’s mother—said HM leaders tasked with their group’s personnel duties should focus on a few main concepts:
- Think outside the bank. Some physicians look only to earn as much as they can as quickly as they can, but many seek personal and professional satisfaction.
- Engagement is instrumental. A one-day orientation program for a lifetime job doesn’t sound like enough, does it?
In the coming years, hiring managers will have to focus on “millennials”—the generation of doctors born between 1977 and 1999—which Christine Kneeland described as tech-savvy doctors interested in a blended lifestyle of work and leisure. And while some might not agree with or understand their perspective, they’d better get used to it, she said. “The millennials are here, the workplace has changed, and they are leading that change,” she added. “Just embrace it.”
QUALITY
Patient Satisfaction: Tips for Improving Your HCAHPS Scores
MODERATORS: Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; Steven Deitelzweig, MD, MMM, SFHM, system chairman, Department of Hospital Medicine, regional vice president of medical affairs, Ochsner Health System, New Orleans
Patient satisfaction scores are a big deal right now, as many HM groups tie the scores to compensation and the federal government tethers the scores and a portion of hospital payment through the value-based purchasing (VBP) program.
So how does a hospitalist improve their HCAHPS score? Here’s what the experts said:
- Personalize things. Give a business card with a picture. Sit down. Smile. Ask the patient if they understand what you’ve said, and don’t get frustrated if they don’t.
- First and last. Make good impressions when introducing yourself to the patient and when it’s time to discharge or transition them to a different facility. “When the hospitalist hands a patient off,” Dr. Whitcomb said, “it doesn’t cut it to pull out your brochure of 40 practitioners when the patient asks, ‘Who am I going to see tomorrow?’”
- Be professional. Don’t vent about workplace issues in front of patients. Dr. Deitelzweig illustrated the point with the case of an elderly patient who got out of bed to help a practitioner they heard complaining about a heavy workload. The patient fell.
- Creative use of white space. Consider using in-room white boards to help keep patients informed of a day’s care plan.
David Jaworski, MD, director of the hospitalist service at Windham Hospital in Willimantic, Conn., says honesty was a key piece of advice he gleaned from the session.
“I think one of the things people appreciate the most when they’re in the hospital is being honest about our uncertainties,” he says. “I have had more people thank me for saying, ‘I don’t know, but we will find out by doing this, this, and this.’ ”
ACADEMIC
The Role of Hospital Medicine in Adapting to the New ACGME Requirements
SPEAKER: Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center, New Orleans
The new Accreditation Council for Graduate Medical Education (ACGME) work-hour rules that take effect July 1 have received a lot of attention since they were announced last summer. The guideline that has attracted the bulk of the attention limits intern shifts to 16 hours, with upper-level residents capped at 24 consecutive hours, with four hours of administrative follow-on allowed with the caveat that strategic napping is “strongly suggested.”
“I’m all for work hours,” said Dr. Wiese, immediate past president of SHM. “It’s the right thing to do; it’s safer. But I think we have to be careful we don’t super-fragment the system or double the intensity of the system. And on both of those plates, if you don’t do it right, what you end up with is people who will be ill-prepared.”
Dr. Wiese said an easy way to question the validity of one ACGME rule is to examine the guideline that limits a first-year resident’s census to 10 patients. He wondered which scenario offers more teaching opportunities: a roster of six chest-pain cases, two pneumonia cases, and two similarly familiar or relatively safe cases, or a resident with only four cases but each one having multiple comorbidities and complex decisions?
The new rules provide hospitals and HM groups an opportunity to change their way of thinking, adds Jeffrey Schnipper, MD, MPH, FHM, of Brigham and Women’s Hospital and Massachusetts General Hospital in Boston. “Every program has to change its entire way of doing business anyway, so let’s be at the table and say, ‘Well, while you’re redesigning your entire program, let’s inject patent safety and quality of care, and good pedagogy into the system,’” he says.
CLINICAL
Skin is In: Dermatological Images Every Hospitalist Should Recognize
MODERATOR: Paul Aronowitz, MD, FACP, internal medicine residency program director, California Pacific Medical Center, San Francisco
A patient comes into the ED with a blistering skin condition, but the diagnosis escapes the triage doctor on the case. The problem turns out to be bullosis diabeticorum, but the ED doc doesn’t know that yet and pushes to add a patient to the upstairs HM roster.
“The ED will usually try to admit because they’re worried [the patient has] some terrible drug eruption, but they can actually go home,” Dr. Aronowitz explained. “Hospitalists can help tell the difference.”
HM groups shouldn’t work to become amateur dermatologists, Dr. Aronowitz added. However, given that many hospitalists find themselves confronted by dermatologic cases several times a month, a rudimentary pedigree is a good idea to help sift out which cases require admission and which would take up bed space required for others.
He referred to it as knowing enough to know whether you know enough. “For sure, a hospitalist can diagnose a hypersensitivity reaction from a classic drug like Dilantin,” Dr. Aronowitz said, “and then stop the drug, because that would be one of the best things they could do.”
The session exposed hospitalists to dozens of images of skin conditions theymight come across in daily rounds, from snakebites to drug reactions to argyria.
“The idea is to help hospitalists recognize what’s serious and what’s not,” he said. “If you recognize those initial cutaneous clues, you can guide your antibiotic therapy, or whether you need antibiotics.”
CAREER
This Disease Is Easy; It’s the Patient Who’s Difficult
Speaker: Susan Block, chair, Department of Psychosocial Oncology and Palliative Care at Dana Farber Cancer Institute, Boston
Every physician will have their “button pushed” by a patient now and then, and hospitalists are in the unfortunate position of having little or no previous relationship with most patients, according to Dr. Block, a national expert in physician-patient conflict resolution who said “interpersonal challenges are an onerous part” of the job.
“We want to make sure we provide really good care to these patients, but it can be very challenging,” she said, noting that between 10% and 30% of patients in the healthcare setting present with difficult behaviors.
Whether it’s an empowered patient, a traumatized patient, an intrusive family member, or a patient with clear psychosocial issues, Dr. Block explained that “these patients can make physicians feel lousy. … Being aware of that and trying to stop that process is one of the key issues in professionalism and competence in working with difficult patients.”
She also warned hospitalists to recognize when they become a “magnet” for difficult patients, as many times the expert in the group will become the “go-to” doc. “I don’t think anyone can take care of a large panel of these patients; it’s just too much,” she said, noting you have to negotiate some limits or you will “burn out and lose perspective.”
Many doctors are very uncomfortable with scared or crying patients, Dr. Block said, explaining these are some of her most difficult patients. “Show me a patient in the hospital who isn’t scared,” she said. “Even it they aren’t, they are scared of dying.”
Other sources of workplace discomfort include the dependent or “needy” patient, the suspicious patient, and the extremely pushy patient. Dr. Block suggested setting clear boundaries with patients; she also noted physicians should be ready and willing to identify and reflect on your own emotions so that “you have the capacity to get perspective on the problem and keep yourself from being part of the problem.
“Limit-setting is one of the most therapeutic things you can do with difficult patients,” she said. “It feels to us as a form of sadism, as though we are punishing patients. But for many patients, the most dangerous, scary, and dysfunctional thing you can do for patients is not set limits.”
CLINICAL
The Art of Clinical Problem-Solving: Mystery Cases
SPEAKER: Gupreet Dhaliwal, MD, University of California at San Francisco
Humility, patience, and practice: Those are the keys to improving one’s clinical diagnostic skills, according to Dr. Dhaliwal, an acclaimed educator and clinician at UCSF who walked a packed room through two blind cases and encouraged hospitalists to work hard at their craft.
“If you want to reach your maximum potential, you have to view it the same way we do other things, the same way a great musician rehearses and a great soccer player scrimmages,” he said. “All of us are busy, but you either have to increase the number of cases you put your mind through, or you take the cases you have and you analyze them, you seek feedback, you try to improve the process around the diagnostic.
“The message isn’t always fun, because both of those things equal more work, but there is no way to hide it because there is no field in which people get better without more work.”
Dr. Dhaliwal says hospitalists should be “humble about diagnosis.” He explained that the more experienced people become, the more we shift from analytical reasoning, “thinking hard like we did when we were students and residents,” to intuitive reasoning, which “is basically saying, ‘I recognize a pattern, this is an old friend, I’ve seen gout before.’ I think any of us can be guilty of forgetting that it has pitfalls. And there is a whole list of cognitive biases that are associated with moving fast and building patterns.”
He also believes hospitalists who dedicate themselves to clinical greatness can parlay such improvement in the quality realm. “Every one of us has used diagnosis as a core part of our identity, but in terms of getting the community or other stakeholders behind improving diagnosis or improving judgment, I think the umbrella of quality and reducing diagnostic errors is the most appealing and most logical,” he says. “I think we start to take for granted we are good at it, but I think there are ways many of us, especially if we work at it, can become great at it.”
CLINICAL
The How, When, and Why of Noninvasive Ventilation
SPEAKER: Eric Siegal, MD, SFHM, critical care fellow, University of Wisconsin School of Medicine, Madison
Dr. Siegal’s review of literature in front of a packed crowd provided a road map to Noninvasive Positive Pressure Ventilation (NPPV) usage. In the end, NPPV should be a hospitalist’s first choice for patients with hypercarbic COPD exacerbations, and likely in patients with acute cardiogenic pulmonary edema, hypoxemic respiratory failure, immunocompromised patients, and pre-intubation patients.
Dr. Siegal stressed the use of NPPV in COPD, which has been studied thoroughly and “held up to repeated scrutiny.”
“If you put people on NPPV instead of intubating them … mortality is halved, intubation rate is less than half, treatment failure is much lower, you have a third of the complications, and huge reductions in length of stay,” Dr. Siegal said.
In the absence of contraindications, he stressed, NPPV should be the first line of therapy for patients with hypercarbic COPD exacerbations. “In fact, I would argue that you really should be asking yourself, ‘Why can’t I put these patients on NPPV?’ ” he asked, “because this has really shown to be life-saving.”
Dr. Siegal also explored recent findings on NPPV in acute cardiogenic pulmonary edema patients, which surprisingly showed “no better than supplemental oxygen.” He concluded that if your patient is not hypercarbic, “there is no advantage to adding pressure support.” He also said the benefit is more robust in ACPE patients who have acute coronary syndrome.
Dr. Siegal advised hospitalists to pick the right patients, start NPPV therapy early, and if the patient doesn’t improve within one or two hours, “it’s time to move on.”
QUALITY
Utilizing Technology to Improve the Clinical and Operational Performance of Hospitalists
SPEAKERS: Jason Stein, MD, SFHM, associate vice chair for quality, Department of Medicine, Bryce Gartland, MD, FHM, associate director, section of hospital medicine, Emory University School of Medicine, Atlanta
In an age of increasing technology, just getting technology into a hospital isn’t the answer. It’s about integrating it into practice to improve care.
At Emory, the marriage of “low-tech solutions” and patented data displays has resulted in what Drs. Stein and Gartland call an accountable-care unit (ACU). The unit-based team features geographic ownership and structured interdisciplinary bedside rounds (SIBR). Perhaps more important, the unit generates real-time data captured on monitors, allowing teams of hospitalists, nonphysician providers (NPPs), residents, interns, and social workers to “visually digest immense amounts of information in a very short time period,” Dr. Gartland said.
Dr. Stein defined an ACU as a bounded geographic inpatient area responsible for the clinical, service, and cost outcomes it produces. To help manage beds, Emory instituted a system called “e-Bed,” a McKesson system that tracks room availability. The system shows whether rooms are occupied, being cleaned, or somewhere in between. It has icons to show whether patients are elsewhere in the hospital for treatment, as well as clinical data capacities. Unit teams round together and use a portable workstation or tablet computer to input clinical data, notes, or other comments into real-time dashboards that can then show everything from VTE prophylaxis to whether a patient is at high risk for falls.
The project has been in the works for several years, and Dr. Garltand noted that any hospitalists looking to push similar initiatives at their institution need to ensure that they have buy-in from providers and a commitment to seeing the project through.
“Timing is everything,” he said. “If we tried to force this … a few years ago, it would not have worked.”
PRACTICE MANAGEMENT
Recruiting and Retaining Hospitalists: Developing a Talent Facilitation Framework
SPEAKERS: Patrick Kneeland, MD, hospitalist, Providence Regional Medical Center, Everett, Wash.; Christine Kneeland, COO, Center Partners, Fort Collins, Colo.; Niraj Sehgal, associate professor of medicine, associate chair for quality and safety, Department of Medicine, University of California at San Francisco
Lincoln Godfrey, DO, a hospitalist at Baxter Regional Medical Center in Mountain Home, Ark., was sitting and listening to strategies to lure and keep hospitalists when his hospital CEO sent him a text asking how his recruiting efforts were going with a would-be hire.
“I said I’d get back to him,” Dr. Godfrey jokes.
The C-suite’s passion is understandable, though, as the fight to hire experienced staff outside of major markets continues to stymie many HM groups. Dr. Godfrey says he can’t hire anybody without first getting them to the Ozark Mountains to learn the hospital, its people, and its community.
“There’s going to be a limited talent pool of people who will come at all,” he says. “But I don’t get anybody who doesn’t work with us for a bit first.”
Christine Kneeland—Dr. Kneeland’s mother—said HM leaders tasked with their group’s personnel duties should focus on a few main concepts:
- Think outside the bank. Some physicians look only to earn as much as they can as quickly as they can, but many seek personal and professional satisfaction.
- Engagement is instrumental. A one-day orientation program for a lifetime job doesn’t sound like enough, does it?
In the coming years, hiring managers will have to focus on “millennials”—the generation of doctors born between 1977 and 1999—which Christine Kneeland described as tech-savvy doctors interested in a blended lifestyle of work and leisure. And while some might not agree with or understand their perspective, they’d better get used to it, she said. “The millennials are here, the workplace has changed, and they are leading that change,” she added. “Just embrace it.”
QUALITY
Patient Satisfaction: Tips for Improving Your HCAHPS Scores
MODERATORS: Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; Steven Deitelzweig, MD, MMM, SFHM, system chairman, Department of Hospital Medicine, regional vice president of medical affairs, Ochsner Health System, New Orleans
Patient satisfaction scores are a big deal right now, as many HM groups tie the scores to compensation and the federal government tethers the scores and a portion of hospital payment through the value-based purchasing (VBP) program.
So how does a hospitalist improve their HCAHPS score? Here’s what the experts said:
- Personalize things. Give a business card with a picture. Sit down. Smile. Ask the patient if they understand what you’ve said, and don’t get frustrated if they don’t.
- First and last. Make good impressions when introducing yourself to the patient and when it’s time to discharge or transition them to a different facility. “When the hospitalist hands a patient off,” Dr. Whitcomb said, “it doesn’t cut it to pull out your brochure of 40 practitioners when the patient asks, ‘Who am I going to see tomorrow?’”
- Be professional. Don’t vent about workplace issues in front of patients. Dr. Deitelzweig illustrated the point with the case of an elderly patient who got out of bed to help a practitioner they heard complaining about a heavy workload. The patient fell.
- Creative use of white space. Consider using in-room white boards to help keep patients informed of a day’s care plan.
David Jaworski, MD, director of the hospitalist service at Windham Hospital in Willimantic, Conn., says honesty was a key piece of advice he gleaned from the session.
“I think one of the things people appreciate the most when they’re in the hospital is being honest about our uncertainties,” he says. “I have had more people thank me for saying, ‘I don’t know, but we will find out by doing this, this, and this.’ ”
ACADEMIC
The Role of Hospital Medicine in Adapting to the New ACGME Requirements
SPEAKER: Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center, New Orleans
The new Accreditation Council for Graduate Medical Education (ACGME) work-hour rules that take effect July 1 have received a lot of attention since they were announced last summer. The guideline that has attracted the bulk of the attention limits intern shifts to 16 hours, with upper-level residents capped at 24 consecutive hours, with four hours of administrative follow-on allowed with the caveat that strategic napping is “strongly suggested.”
“I’m all for work hours,” said Dr. Wiese, immediate past president of SHM. “It’s the right thing to do; it’s safer. But I think we have to be careful we don’t super-fragment the system or double the intensity of the system. And on both of those plates, if you don’t do it right, what you end up with is people who will be ill-prepared.”
Dr. Wiese said an easy way to question the validity of one ACGME rule is to examine the guideline that limits a first-year resident’s census to 10 patients. He wondered which scenario offers more teaching opportunities: a roster of six chest-pain cases, two pneumonia cases, and two similarly familiar or relatively safe cases, or a resident with only four cases but each one having multiple comorbidities and complex decisions?
The new rules provide hospitals and HM groups an opportunity to change their way of thinking, adds Jeffrey Schnipper, MD, MPH, FHM, of Brigham and Women’s Hospital and Massachusetts General Hospital in Boston. “Every program has to change its entire way of doing business anyway, so let’s be at the table and say, ‘Well, while you’re redesigning your entire program, let’s inject patent safety and quality of care, and good pedagogy into the system,’” he says.
CLINICAL
Skin is In: Dermatological Images Every Hospitalist Should Recognize
MODERATOR: Paul Aronowitz, MD, FACP, internal medicine residency program director, California Pacific Medical Center, San Francisco
A patient comes into the ED with a blistering skin condition, but the diagnosis escapes the triage doctor on the case. The problem turns out to be bullosis diabeticorum, but the ED doc doesn’t know that yet and pushes to add a patient to the upstairs HM roster.
“The ED will usually try to admit because they’re worried [the patient has] some terrible drug eruption, but they can actually go home,” Dr. Aronowitz explained. “Hospitalists can help tell the difference.”
HM groups shouldn’t work to become amateur dermatologists, Dr. Aronowitz added. However, given that many hospitalists find themselves confronted by dermatologic cases several times a month, a rudimentary pedigree is a good idea to help sift out which cases require admission and which would take up bed space required for others.
He referred to it as knowing enough to know whether you know enough. “For sure, a hospitalist can diagnose a hypersensitivity reaction from a classic drug like Dilantin,” Dr. Aronowitz said, “and then stop the drug, because that would be one of the best things they could do.”
The session exposed hospitalists to dozens of images of skin conditions theymight come across in daily rounds, from snakebites to drug reactions to argyria.
“The idea is to help hospitalists recognize what’s serious and what’s not,” he said. “If you recognize those initial cutaneous clues, you can guide your antibiotic therapy, or whether you need antibiotics.”
CAREER
This Disease Is Easy; It’s the Patient Who’s Difficult
Speaker: Susan Block, chair, Department of Psychosocial Oncology and Palliative Care at Dana Farber Cancer Institute, Boston
Every physician will have their “button pushed” by a patient now and then, and hospitalists are in the unfortunate position of having little or no previous relationship with most patients, according to Dr. Block, a national expert in physician-patient conflict resolution who said “interpersonal challenges are an onerous part” of the job.
“We want to make sure we provide really good care to these patients, but it can be very challenging,” she said, noting that between 10% and 30% of patients in the healthcare setting present with difficult behaviors.
Whether it’s an empowered patient, a traumatized patient, an intrusive family member, or a patient with clear psychosocial issues, Dr. Block explained that “these patients can make physicians feel lousy. … Being aware of that and trying to stop that process is one of the key issues in professionalism and competence in working with difficult patients.”
She also warned hospitalists to recognize when they become a “magnet” for difficult patients, as many times the expert in the group will become the “go-to” doc. “I don’t think anyone can take care of a large panel of these patients; it’s just too much,” she said, noting you have to negotiate some limits or you will “burn out and lose perspective.”
Many doctors are very uncomfortable with scared or crying patients, Dr. Block said, explaining these are some of her most difficult patients. “Show me a patient in the hospital who isn’t scared,” she said. “Even it they aren’t, they are scared of dying.”
Other sources of workplace discomfort include the dependent or “needy” patient, the suspicious patient, and the extremely pushy patient. Dr. Block suggested setting clear boundaries with patients; she also noted physicians should be ready and willing to identify and reflect on your own emotions so that “you have the capacity to get perspective on the problem and keep yourself from being part of the problem.
“Limit-setting is one of the most therapeutic things you can do with difficult patients,” she said. “It feels to us as a form of sadism, as though we are punishing patients. But for many patients, the most dangerous, scary, and dysfunctional thing you can do for patients is not set limits.”
CLINICAL
The Art of Clinical Problem-Solving: Mystery Cases
SPEAKER: Gupreet Dhaliwal, MD, University of California at San Francisco
Humility, patience, and practice: Those are the keys to improving one’s clinical diagnostic skills, according to Dr. Dhaliwal, an acclaimed educator and clinician at UCSF who walked a packed room through two blind cases and encouraged hospitalists to work hard at their craft.
“If you want to reach your maximum potential, you have to view it the same way we do other things, the same way a great musician rehearses and a great soccer player scrimmages,” he said. “All of us are busy, but you either have to increase the number of cases you put your mind through, or you take the cases you have and you analyze them, you seek feedback, you try to improve the process around the diagnostic.
“The message isn’t always fun, because both of those things equal more work, but there is no way to hide it because there is no field in which people get better without more work.”
Dr. Dhaliwal says hospitalists should be “humble about diagnosis.” He explained that the more experienced people become, the more we shift from analytical reasoning, “thinking hard like we did when we were students and residents,” to intuitive reasoning, which “is basically saying, ‘I recognize a pattern, this is an old friend, I’ve seen gout before.’ I think any of us can be guilty of forgetting that it has pitfalls. And there is a whole list of cognitive biases that are associated with moving fast and building patterns.”
He also believes hospitalists who dedicate themselves to clinical greatness can parlay such improvement in the quality realm. “Every one of us has used diagnosis as a core part of our identity, but in terms of getting the community or other stakeholders behind improving diagnosis or improving judgment, I think the umbrella of quality and reducing diagnostic errors is the most appealing and most logical,” he says. “I think we start to take for granted we are good at it, but I think there are ways many of us, especially if we work at it, can become great at it.”
CLINICAL
The How, When, and Why of Noninvasive Ventilation
SPEAKER: Eric Siegal, MD, SFHM, critical care fellow, University of Wisconsin School of Medicine, Madison
Dr. Siegal’s review of literature in front of a packed crowd provided a road map to Noninvasive Positive Pressure Ventilation (NPPV) usage. In the end, NPPV should be a hospitalist’s first choice for patients with hypercarbic COPD exacerbations, and likely in patients with acute cardiogenic pulmonary edema, hypoxemic respiratory failure, immunocompromised patients, and pre-intubation patients.
Dr. Siegal stressed the use of NPPV in COPD, which has been studied thoroughly and “held up to repeated scrutiny.”
“If you put people on NPPV instead of intubating them … mortality is halved, intubation rate is less than half, treatment failure is much lower, you have a third of the complications, and huge reductions in length of stay,” Dr. Siegal said.
In the absence of contraindications, he stressed, NPPV should be the first line of therapy for patients with hypercarbic COPD exacerbations. “In fact, I would argue that you really should be asking yourself, ‘Why can’t I put these patients on NPPV?’ ” he asked, “because this has really shown to be life-saving.”
Dr. Siegal also explored recent findings on NPPV in acute cardiogenic pulmonary edema patients, which surprisingly showed “no better than supplemental oxygen.” He concluded that if your patient is not hypercarbic, “there is no advantage to adding pressure support.” He also said the benefit is more robust in ACPE patients who have acute coronary syndrome.
Dr. Siegal advised hospitalists to pick the right patients, start NPPV therapy early, and if the patient doesn’t improve within one or two hours, “it’s time to move on.”
QUALITY
Utilizing Technology to Improve the Clinical and Operational Performance of Hospitalists
SPEAKERS: Jason Stein, MD, SFHM, associate vice chair for quality, Department of Medicine, Bryce Gartland, MD, FHM, associate director, section of hospital medicine, Emory University School of Medicine, Atlanta
In an age of increasing technology, just getting technology into a hospital isn’t the answer. It’s about integrating it into practice to improve care.
At Emory, the marriage of “low-tech solutions” and patented data displays has resulted in what Drs. Stein and Gartland call an accountable-care unit (ACU). The unit-based team features geographic ownership and structured interdisciplinary bedside rounds (SIBR). Perhaps more important, the unit generates real-time data captured on monitors, allowing teams of hospitalists, nonphysician providers (NPPs), residents, interns, and social workers to “visually digest immense amounts of information in a very short time period,” Dr. Gartland said.
Dr. Stein defined an ACU as a bounded geographic inpatient area responsible for the clinical, service, and cost outcomes it produces. To help manage beds, Emory instituted a system called “e-Bed,” a McKesson system that tracks room availability. The system shows whether rooms are occupied, being cleaned, or somewhere in between. It has icons to show whether patients are elsewhere in the hospital for treatment, as well as clinical data capacities. Unit teams round together and use a portable workstation or tablet computer to input clinical data, notes, or other comments into real-time dashboards that can then show everything from VTE prophylaxis to whether a patient is at high risk for falls.
The project has been in the works for several years, and Dr. Garltand noted that any hospitalists looking to push similar initiatives at their institution need to ensure that they have buy-in from providers and a commitment to seeing the project through.
“Timing is everything,” he said. “If we tried to force this … a few years ago, it would not have worked.”
PRACTICE MANAGEMENT
Recruiting and Retaining Hospitalists: Developing a Talent Facilitation Framework
SPEAKERS: Patrick Kneeland, MD, hospitalist, Providence Regional Medical Center, Everett, Wash.; Christine Kneeland, COO, Center Partners, Fort Collins, Colo.; Niraj Sehgal, associate professor of medicine, associate chair for quality and safety, Department of Medicine, University of California at San Francisco
Lincoln Godfrey, DO, a hospitalist at Baxter Regional Medical Center in Mountain Home, Ark., was sitting and listening to strategies to lure and keep hospitalists when his hospital CEO sent him a text asking how his recruiting efforts were going with a would-be hire.
“I said I’d get back to him,” Dr. Godfrey jokes.
The C-suite’s passion is understandable, though, as the fight to hire experienced staff outside of major markets continues to stymie many HM groups. Dr. Godfrey says he can’t hire anybody without first getting them to the Ozark Mountains to learn the hospital, its people, and its community.
“There’s going to be a limited talent pool of people who will come at all,” he says. “But I don’t get anybody who doesn’t work with us for a bit first.”
Christine Kneeland—Dr. Kneeland’s mother—said HM leaders tasked with their group’s personnel duties should focus on a few main concepts:
- Think outside the bank. Some physicians look only to earn as much as they can as quickly as they can, but many seek personal and professional satisfaction.
- Engagement is instrumental. A one-day orientation program for a lifetime job doesn’t sound like enough, does it?
In the coming years, hiring managers will have to focus on “millennials”—the generation of doctors born between 1977 and 1999—which Christine Kneeland described as tech-savvy doctors interested in a blended lifestyle of work and leisure. And while some might not agree with or understand their perspective, they’d better get used to it, she said. “The millennials are here, the workplace has changed, and they are leading that change,” she added. “Just embrace it.”
QUALITY
Patient Satisfaction: Tips for Improving Your HCAHPS Scores
MODERATORS: Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; Steven Deitelzweig, MD, MMM, SFHM, system chairman, Department of Hospital Medicine, regional vice president of medical affairs, Ochsner Health System, New Orleans
Patient satisfaction scores are a big deal right now, as many HM groups tie the scores to compensation and the federal government tethers the scores and a portion of hospital payment through the value-based purchasing (VBP) program.
So how does a hospitalist improve their HCAHPS score? Here’s what the experts said:
- Personalize things. Give a business card with a picture. Sit down. Smile. Ask the patient if they understand what you’ve said, and don’t get frustrated if they don’t.
- First and last. Make good impressions when introducing yourself to the patient and when it’s time to discharge or transition them to a different facility. “When the hospitalist hands a patient off,” Dr. Whitcomb said, “it doesn’t cut it to pull out your brochure of 40 practitioners when the patient asks, ‘Who am I going to see tomorrow?’”
- Be professional. Don’t vent about workplace issues in front of patients. Dr. Deitelzweig illustrated the point with the case of an elderly patient who got out of bed to help a practitioner they heard complaining about a heavy workload. The patient fell.
- Creative use of white space. Consider using in-room white boards to help keep patients informed of a day’s care plan.
David Jaworski, MD, director of the hospitalist service at Windham Hospital in Willimantic, Conn., says honesty was a key piece of advice he gleaned from the session.
“I think one of the things people appreciate the most when they’re in the hospital is being honest about our uncertainties,” he says. “I have had more people thank me for saying, ‘I don’t know, but we will find out by doing this, this, and this.’ ”
ACADEMIC
The Role of Hospital Medicine in Adapting to the New ACGME Requirements
SPEAKER: Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center, New Orleans
The new Accreditation Council for Graduate Medical Education (ACGME) work-hour rules that take effect July 1 have received a lot of attention since they were announced last summer. The guideline that has attracted the bulk of the attention limits intern shifts to 16 hours, with upper-level residents capped at 24 consecutive hours, with four hours of administrative follow-on allowed with the caveat that strategic napping is “strongly suggested.”
“I’m all for work hours,” said Dr. Wiese, immediate past president of SHM. “It’s the right thing to do; it’s safer. But I think we have to be careful we don’t super-fragment the system or double the intensity of the system. And on both of those plates, if you don’t do it right, what you end up with is people who will be ill-prepared.”
Dr. Wiese said an easy way to question the validity of one ACGME rule is to examine the guideline that limits a first-year resident’s census to 10 patients. He wondered which scenario offers more teaching opportunities: a roster of six chest-pain cases, two pneumonia cases, and two similarly familiar or relatively safe cases, or a resident with only four cases but each one having multiple comorbidities and complex decisions?
The new rules provide hospitals and HM groups an opportunity to change their way of thinking, adds Jeffrey Schnipper, MD, MPH, FHM, of Brigham and Women’s Hospital and Massachusetts General Hospital in Boston. “Every program has to change its entire way of doing business anyway, so let’s be at the table and say, ‘Well, while you’re redesigning your entire program, let’s inject patent safety and quality of care, and good pedagogy into the system,’” he says.
CLINICAL
Skin is In: Dermatological Images Every Hospitalist Should Recognize
MODERATOR: Paul Aronowitz, MD, FACP, internal medicine residency program director, California Pacific Medical Center, San Francisco
A patient comes into the ED with a blistering skin condition, but the diagnosis escapes the triage doctor on the case. The problem turns out to be bullosis diabeticorum, but the ED doc doesn’t know that yet and pushes to add a patient to the upstairs HM roster.
“The ED will usually try to admit because they’re worried [the patient has] some terrible drug eruption, but they can actually go home,” Dr. Aronowitz explained. “Hospitalists can help tell the difference.”
HM groups shouldn’t work to become amateur dermatologists, Dr. Aronowitz added. However, given that many hospitalists find themselves confronted by dermatologic cases several times a month, a rudimentary pedigree is a good idea to help sift out which cases require admission and which would take up bed space required for others.
He referred to it as knowing enough to know whether you know enough. “For sure, a hospitalist can diagnose a hypersensitivity reaction from a classic drug like Dilantin,” Dr. Aronowitz said, “and then stop the drug, because that would be one of the best things they could do.”
The session exposed hospitalists to dozens of images of skin conditions theymight come across in daily rounds, from snakebites to drug reactions to argyria.
“The idea is to help hospitalists recognize what’s serious and what’s not,” he said. “If you recognize those initial cutaneous clues, you can guide your antibiotic therapy, or whether you need antibiotics.”
CAREER
This Disease Is Easy; It’s the Patient Who’s Difficult
Speaker: Susan Block, chair, Department of Psychosocial Oncology and Palliative Care at Dana Farber Cancer Institute, Boston
Every physician will have their “button pushed” by a patient now and then, and hospitalists are in the unfortunate position of having little or no previous relationship with most patients, according to Dr. Block, a national expert in physician-patient conflict resolution who said “interpersonal challenges are an onerous part” of the job.
“We want to make sure we provide really good care to these patients, but it can be very challenging,” she said, noting that between 10% and 30% of patients in the healthcare setting present with difficult behaviors.
Whether it’s an empowered patient, a traumatized patient, an intrusive family member, or a patient with clear psychosocial issues, Dr. Block explained that “these patients can make physicians feel lousy. … Being aware of that and trying to stop that process is one of the key issues in professionalism and competence in working with difficult patients.”
She also warned hospitalists to recognize when they become a “magnet” for difficult patients, as many times the expert in the group will become the “go-to” doc. “I don’t think anyone can take care of a large panel of these patients; it’s just too much,” she said, noting you have to negotiate some limits or you will “burn out and lose perspective.”
Many doctors are very uncomfortable with scared or crying patients, Dr. Block said, explaining these are some of her most difficult patients. “Show me a patient in the hospital who isn’t scared,” she said. “Even it they aren’t, they are scared of dying.”
Other sources of workplace discomfort include the dependent or “needy” patient, the suspicious patient, and the extremely pushy patient. Dr. Block suggested setting clear boundaries with patients; she also noted physicians should be ready and willing to identify and reflect on your own emotions so that “you have the capacity to get perspective on the problem and keep yourself from being part of the problem.
“Limit-setting is one of the most therapeutic things you can do with difficult patients,” she said. “It feels to us as a form of sadism, as though we are punishing patients. But for many patients, the most dangerous, scary, and dysfunctional thing you can do for patients is not set limits.”
CLINICAL
The Art of Clinical Problem-Solving: Mystery Cases
SPEAKER: Gupreet Dhaliwal, MD, University of California at San Francisco
Humility, patience, and practice: Those are the keys to improving one’s clinical diagnostic skills, according to Dr. Dhaliwal, an acclaimed educator and clinician at UCSF who walked a packed room through two blind cases and encouraged hospitalists to work hard at their craft.
“If you want to reach your maximum potential, you have to view it the same way we do other things, the same way a great musician rehearses and a great soccer player scrimmages,” he said. “All of us are busy, but you either have to increase the number of cases you put your mind through, or you take the cases you have and you analyze them, you seek feedback, you try to improve the process around the diagnostic.
“The message isn’t always fun, because both of those things equal more work, but there is no way to hide it because there is no field in which people get better without more work.”
Dr. Dhaliwal says hospitalists should be “humble about diagnosis.” He explained that the more experienced people become, the more we shift from analytical reasoning, “thinking hard like we did when we were students and residents,” to intuitive reasoning, which “is basically saying, ‘I recognize a pattern, this is an old friend, I’ve seen gout before.’ I think any of us can be guilty of forgetting that it has pitfalls. And there is a whole list of cognitive biases that are associated with moving fast and building patterns.”
He also believes hospitalists who dedicate themselves to clinical greatness can parlay such improvement in the quality realm. “Every one of us has used diagnosis as a core part of our identity, but in terms of getting the community or other stakeholders behind improving diagnosis or improving judgment, I think the umbrella of quality and reducing diagnostic errors is the most appealing and most logical,” he says. “I think we start to take for granted we are good at it, but I think there are ways many of us, especially if we work at it, can become great at it.”
CLINICAL
The How, When, and Why of Noninvasive Ventilation
SPEAKER: Eric Siegal, MD, SFHM, critical care fellow, University of Wisconsin School of Medicine, Madison
Dr. Siegal’s review of literature in front of a packed crowd provided a road map to Noninvasive Positive Pressure Ventilation (NPPV) usage. In the end, NPPV should be a hospitalist’s first choice for patients with hypercarbic COPD exacerbations, and likely in patients with acute cardiogenic pulmonary edema, hypoxemic respiratory failure, immunocompromised patients, and pre-intubation patients.
Dr. Siegal stressed the use of NPPV in COPD, which has been studied thoroughly and “held up to repeated scrutiny.”
“If you put people on NPPV instead of intubating them … mortality is halved, intubation rate is less than half, treatment failure is much lower, you have a third of the complications, and huge reductions in length of stay,” Dr. Siegal said.
In the absence of contraindications, he stressed, NPPV should be the first line of therapy for patients with hypercarbic COPD exacerbations. “In fact, I would argue that you really should be asking yourself, ‘Why can’t I put these patients on NPPV?’ ” he asked, “because this has really shown to be life-saving.”
Dr. Siegal also explored recent findings on NPPV in acute cardiogenic pulmonary edema patients, which surprisingly showed “no better than supplemental oxygen.” He concluded that if your patient is not hypercarbic, “there is no advantage to adding pressure support.” He also said the benefit is more robust in ACPE patients who have acute coronary syndrome.
Dr. Siegal advised hospitalists to pick the right patients, start NPPV therapy early, and if the patient doesn’t improve within one or two hours, “it’s time to move on.”