User login
Management of adults with syncope
Syncope is characterized by sudden transient loss of consciousness due to cerebral hypoperfusion and is typically associated with an inability to maintain postural tone. There are many different causes and clinical presentations of syncope and the incidence varies depending on the population. Estimated lifetime prevalence rates are as high as 41% for a single episode of syncope, with recurrent syncope occurring in 13.5% of the general population. Incidence follows a trimodal distribution with peaks at age 20, 60, and 80 years for both men and women. The National Hospital Ambulatory Medical Care Survey reported 6.7 million episodes of syncope in the emergency department, which is where most patients with syncope initially present. However, patients may also present to the primary care outpatient setting, and providers should be equipped for initial evaluation and management.
Previous and current treatment guidelines
Although there have been general reviews published by general and specialty societies, there were no comprehensive guidelines on the evaluation and management of syncope until recently. The 2017 guideline from the American College of Cardiology, American Heart Association, and Heart Rhythm Society is intended to provide guidance on evaluation and management of syncope, specifically in the context of different clinical settings, specific causes, or selected circumstances.1
What primary care providers should know
A detailed history and physical exam should be performed in all patients with syncope. Useful details include the setting in which syncope occurs, prodromal symptoms, witness reports, postevent symptoms, comorbidities, medication use, past medical history, and family history. The physical exam should include orthostatic vital signs, cardiac exam, neurologic exam, and any other relevant systems. A resting 12-lead ECG in the initial evaluation is recommended to detect underlying arrhythmia or structural heart disease (Class I recommendation – strong).
There are many different causes of syncope (see Table 1). Vasovagal syncope, a form of reflex syncope mediated by the vasovagal reflex, is the most common cause of syncope and a frequent reason for emergency department visits. There is often a prodrome of diaphoresis, warmth, nausea, and/or pallor, often followed by fatigue. The diagnosis can be made by the history, physical exam, and eyewitness observation.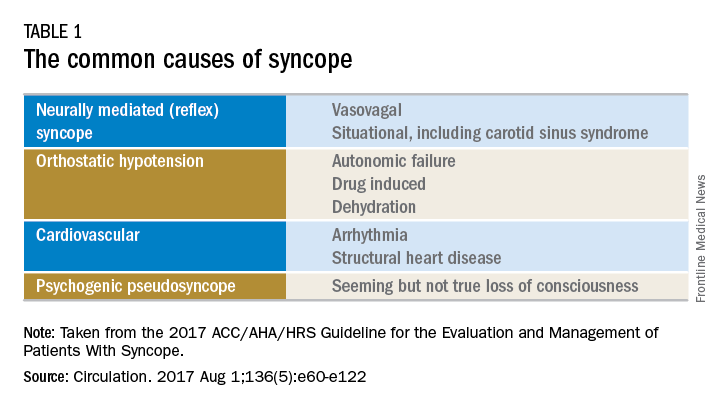
Once the initial evaluation is complete, further evaluation and management depends on the presence of risk factors presented in Table 2. Outpatient management is reasonable for patients with presumptive reflex-mediated syncope when there is an absence of serious medical conditions such as cardiac disease or comorbid neurologic disease. While hospital-based evaluation has not been shown to improve outcomes in patients with a low risk profile, hospital-based evaluation and treatment are recommended for patients presenting with syncope who have a serious medical condition potentially relevant to the cause of syncope.2 Serious medical conditions that require hospital management include arrhythmia, cardiac ischemia, severe aortic stenosis, hypertrophic cardiomyopathy, aortic dissection, acute heart failure, severe anemia, or major traumatic injury. Finally, patients with intermediate risk may benefit from an observational protocol in the emergency department.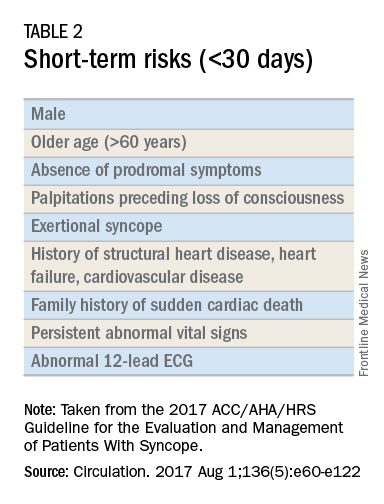
Routine and comprehensive laboratory testing is not useful in syncope work-up (Class III recommendation – no benefit). Routine cardiac imaging is not recommended unless a cardiac etiology is suspected and routine neurological imaging and EEG are not recommended in the absence of focal neurologic findings. Additional work-up may be indicated if initial evaluation suggests a more specific etiology. If the initial evaluation suggests neurogenic orthostatic hypotension but the diagnosis is not clear, then referral for an autonomic evaluation is reasonable. If reflex syncope is suspected, tilt-table testing may be helpful to confirm the diagnosis. Lastly, if a cardiovascular etiology is suspected, it is recommended that the patient have cardiac monitoring in the acute care setting. In this later group, stress testing, transthoracic echocardiogram, electrophysiology study, and/or MRI or CT may be useful. Electrophysiologic testing is reasonable in patients with suspected arrhythmia as the etiology for syncope (Class IIa recommendation – moderate strength). The guideline provides a convenient summary algorithm to approach the initial and subsequent evaluations for syncope based on the initial evaluation and presenting symptoms.

Special populations
There are specific considerations for certain populations. In the pediatric population, the vast majority of syncopal episodes are reflex syncope but breath-holding spells should also be considered. In the geriatric population, particularly individuals older than 75 years, the incidence of syncope is high, the differential diagnosis is broad, and the diagnosis may be imprecise given amnesia, falls, lack of witnesses, and polypharmacy. In this group, morbidity is high because of multimorbidity and frailty. A careful history and physical exam with orthostatic vital signs is important, as is a multidisciplinary approach with geriatric consultation when needed.

Summary
Syncope is a common clinical syndrome often presenting to the emergency department or primary care setting. There are many causes, the most common being vasovagal syncope. In the initial evaluation, providers should perform a detailed history and physical exam, check orthostatic signs and perform a 12-lead ECG. Patients can be evaluated and managed safely in the outpatient setting in the absence of risk factors. Routine comprehensive laboratory testing and cardiac imaging are often not needed. For patients with defined risk factors, a more detailed evaluation in the hospital is recommended.
Dr. Li is a second-year resident in the family medicine residency program in the department of family and community medicine at the Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the departments of family and community medicine and physiology at the Sidney Kimmel Medical College. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. Shen W, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation. 2017 Aug 1;136(5):e60-e122. doi: 10.1161/CIR.0000000000000499. Epub 2017 Mar 9.
2. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-85.
Syncope is characterized by sudden transient loss of consciousness due to cerebral hypoperfusion and is typically associated with an inability to maintain postural tone. There are many different causes and clinical presentations of syncope and the incidence varies depending on the population. Estimated lifetime prevalence rates are as high as 41% for a single episode of syncope, with recurrent syncope occurring in 13.5% of the general population. Incidence follows a trimodal distribution with peaks at age 20, 60, and 80 years for both men and women. The National Hospital Ambulatory Medical Care Survey reported 6.7 million episodes of syncope in the emergency department, which is where most patients with syncope initially present. However, patients may also present to the primary care outpatient setting, and providers should be equipped for initial evaluation and management.
Previous and current treatment guidelines
Although there have been general reviews published by general and specialty societies, there were no comprehensive guidelines on the evaluation and management of syncope until recently. The 2017 guideline from the American College of Cardiology, American Heart Association, and Heart Rhythm Society is intended to provide guidance on evaluation and management of syncope, specifically in the context of different clinical settings, specific causes, or selected circumstances.1
What primary care providers should know
A detailed history and physical exam should be performed in all patients with syncope. Useful details include the setting in which syncope occurs, prodromal symptoms, witness reports, postevent symptoms, comorbidities, medication use, past medical history, and family history. The physical exam should include orthostatic vital signs, cardiac exam, neurologic exam, and any other relevant systems. A resting 12-lead ECG in the initial evaluation is recommended to detect underlying arrhythmia or structural heart disease (Class I recommendation – strong).
There are many different causes of syncope (see Table 1). Vasovagal syncope, a form of reflex syncope mediated by the vasovagal reflex, is the most common cause of syncope and a frequent reason for emergency department visits. There is often a prodrome of diaphoresis, warmth, nausea, and/or pallor, often followed by fatigue. The diagnosis can be made by the history, physical exam, and eyewitness observation.
Once the initial evaluation is complete, further evaluation and management depends on the presence of risk factors presented in Table 2. Outpatient management is reasonable for patients with presumptive reflex-mediated syncope when there is an absence of serious medical conditions such as cardiac disease or comorbid neurologic disease. While hospital-based evaluation has not been shown to improve outcomes in patients with a low risk profile, hospital-based evaluation and treatment are recommended for patients presenting with syncope who have a serious medical condition potentially relevant to the cause of syncope.2 Serious medical conditions that require hospital management include arrhythmia, cardiac ischemia, severe aortic stenosis, hypertrophic cardiomyopathy, aortic dissection, acute heart failure, severe anemia, or major traumatic injury. Finally, patients with intermediate risk may benefit from an observational protocol in the emergency department.
Routine and comprehensive laboratory testing is not useful in syncope work-up (Class III recommendation – no benefit). Routine cardiac imaging is not recommended unless a cardiac etiology is suspected and routine neurological imaging and EEG are not recommended in the absence of focal neurologic findings. Additional work-up may be indicated if initial evaluation suggests a more specific etiology. If the initial evaluation suggests neurogenic orthostatic hypotension but the diagnosis is not clear, then referral for an autonomic evaluation is reasonable. If reflex syncope is suspected, tilt-table testing may be helpful to confirm the diagnosis. Lastly, if a cardiovascular etiology is suspected, it is recommended that the patient have cardiac monitoring in the acute care setting. In this later group, stress testing, transthoracic echocardiogram, electrophysiology study, and/or MRI or CT may be useful. Electrophysiologic testing is reasonable in patients with suspected arrhythmia as the etiology for syncope (Class IIa recommendation – moderate strength). The guideline provides a convenient summary algorithm to approach the initial and subsequent evaluations for syncope based on the initial evaluation and presenting symptoms.
Special populations
There are specific considerations for certain populations. In the pediatric population, the vast majority of syncopal episodes are reflex syncope but breath-holding spells should also be considered. In the geriatric population, particularly individuals older than 75 years, the incidence of syncope is high, the differential diagnosis is broad, and the diagnosis may be imprecise given amnesia, falls, lack of witnesses, and polypharmacy. In this group, morbidity is high because of multimorbidity and frailty. A careful history and physical exam with orthostatic vital signs is important, as is a multidisciplinary approach with geriatric consultation when needed.
Summary
Syncope is a common clinical syndrome often presenting to the emergency department or primary care setting. There are many causes, the most common being vasovagal syncope. In the initial evaluation, providers should perform a detailed history and physical exam, check orthostatic signs and perform a 12-lead ECG. Patients can be evaluated and managed safely in the outpatient setting in the absence of risk factors. Routine comprehensive laboratory testing and cardiac imaging are often not needed. For patients with defined risk factors, a more detailed evaluation in the hospital is recommended.
Dr. Li is a second-year resident in the family medicine residency program in the department of family and community medicine at the Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the departments of family and community medicine and physiology at the Sidney Kimmel Medical College. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. Shen W, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation. 2017 Aug 1;136(5):e60-e122. doi: 10.1161/CIR.0000000000000499. Epub 2017 Mar 9.
2. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-85.
Syncope is characterized by sudden transient loss of consciousness due to cerebral hypoperfusion and is typically associated with an inability to maintain postural tone. There are many different causes and clinical presentations of syncope and the incidence varies depending on the population. Estimated lifetime prevalence rates are as high as 41% for a single episode of syncope, with recurrent syncope occurring in 13.5% of the general population. Incidence follows a trimodal distribution with peaks at age 20, 60, and 80 years for both men and women. The National Hospital Ambulatory Medical Care Survey reported 6.7 million episodes of syncope in the emergency department, which is where most patients with syncope initially present. However, patients may also present to the primary care outpatient setting, and providers should be equipped for initial evaluation and management.
Previous and current treatment guidelines
Although there have been general reviews published by general and specialty societies, there were no comprehensive guidelines on the evaluation and management of syncope until recently. The 2017 guideline from the American College of Cardiology, American Heart Association, and Heart Rhythm Society is intended to provide guidance on evaluation and management of syncope, specifically in the context of different clinical settings, specific causes, or selected circumstances.1
What primary care providers should know
A detailed history and physical exam should be performed in all patients with syncope. Useful details include the setting in which syncope occurs, prodromal symptoms, witness reports, postevent symptoms, comorbidities, medication use, past medical history, and family history. The physical exam should include orthostatic vital signs, cardiac exam, neurologic exam, and any other relevant systems. A resting 12-lead ECG in the initial evaluation is recommended to detect underlying arrhythmia or structural heart disease (Class I recommendation – strong).
There are many different causes of syncope (see Table 1). Vasovagal syncope, a form of reflex syncope mediated by the vasovagal reflex, is the most common cause of syncope and a frequent reason for emergency department visits. There is often a prodrome of diaphoresis, warmth, nausea, and/or pallor, often followed by fatigue. The diagnosis can be made by the history, physical exam, and eyewitness observation.
Once the initial evaluation is complete, further evaluation and management depends on the presence of risk factors presented in Table 2. Outpatient management is reasonable for patients with presumptive reflex-mediated syncope when there is an absence of serious medical conditions such as cardiac disease or comorbid neurologic disease. While hospital-based evaluation has not been shown to improve outcomes in patients with a low risk profile, hospital-based evaluation and treatment are recommended for patients presenting with syncope who have a serious medical condition potentially relevant to the cause of syncope.2 Serious medical conditions that require hospital management include arrhythmia, cardiac ischemia, severe aortic stenosis, hypertrophic cardiomyopathy, aortic dissection, acute heart failure, severe anemia, or major traumatic injury. Finally, patients with intermediate risk may benefit from an observational protocol in the emergency department.
Routine and comprehensive laboratory testing is not useful in syncope work-up (Class III recommendation – no benefit). Routine cardiac imaging is not recommended unless a cardiac etiology is suspected and routine neurological imaging and EEG are not recommended in the absence of focal neurologic findings. Additional work-up may be indicated if initial evaluation suggests a more specific etiology. If the initial evaluation suggests neurogenic orthostatic hypotension but the diagnosis is not clear, then referral for an autonomic evaluation is reasonable. If reflex syncope is suspected, tilt-table testing may be helpful to confirm the diagnosis. Lastly, if a cardiovascular etiology is suspected, it is recommended that the patient have cardiac monitoring in the acute care setting. In this later group, stress testing, transthoracic echocardiogram, electrophysiology study, and/or MRI or CT may be useful. Electrophysiologic testing is reasonable in patients with suspected arrhythmia as the etiology for syncope (Class IIa recommendation – moderate strength). The guideline provides a convenient summary algorithm to approach the initial and subsequent evaluations for syncope based on the initial evaluation and presenting symptoms.
Special populations
There are specific considerations for certain populations. In the pediatric population, the vast majority of syncopal episodes are reflex syncope but breath-holding spells should also be considered. In the geriatric population, particularly individuals older than 75 years, the incidence of syncope is high, the differential diagnosis is broad, and the diagnosis may be imprecise given amnesia, falls, lack of witnesses, and polypharmacy. In this group, morbidity is high because of multimorbidity and frailty. A careful history and physical exam with orthostatic vital signs is important, as is a multidisciplinary approach with geriatric consultation when needed.
Summary
Syncope is a common clinical syndrome often presenting to the emergency department or primary care setting. There are many causes, the most common being vasovagal syncope. In the initial evaluation, providers should perform a detailed history and physical exam, check orthostatic signs and perform a 12-lead ECG. Patients can be evaluated and managed safely in the outpatient setting in the absence of risk factors. Routine comprehensive laboratory testing and cardiac imaging are often not needed. For patients with defined risk factors, a more detailed evaluation in the hospital is recommended.
Dr. Li is a second-year resident in the family medicine residency program in the department of family and community medicine at the Sidney Kimmel Medical College at Thomas Jefferson University, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the departments of family and community medicine and physiology at the Sidney Kimmel Medical College. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health.
References
1. Shen W, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. Circulation. 2017 Aug 1;136(5):e60-e122. doi: 10.1161/CIR.0000000000000499. Epub 2017 Mar 9.
2. Soteriades ES, Evans JC, Larson MG, et al. Incidence and prognosis of syncope. N Engl J Med. 2002;347(12):878-85.
Treatment of low bone density or osteoporosis to prevent fractures in men and women
Osteoporosis is defined by a clinically diagnosed fragility fracture or a bone mineral density (BMD) of at least 2.5 SD below the mean for young female adults, usually measured by dual-energy x-ray absorptiometry. Risk factors include age, female sex, post-menopause, hypogonadism or premature ovarian failure, history of cigarette smoking or alcohol consumption (3 or more drinks daily), rheumatoid arthritis, or medications including glucocorticoids, anticoagulants, anticonvulsants, and aromatase inhibitors.
This guideline update focuses on treatment with bisphosphonates (alendronate, risedronate, ibandronate, zoledronic acid) and denosumab. Denosumab, a human monoclonal antibody against RANK-ligand, approved by the Food and Drug Administration for treatment of osteoporosis, has been added to the list of allowed medications since publication of the 2008 guideline. Several therapies have been excluded from the update, including calcitonin, which is no longer widely used for osteoporosis treatment, and etidronate and pamidronate, neither of which are FDA-approved for the prevention of fractures or treatment of osteoporosis. It should be noted that the evidence continues to be insufficient regarding the effectiveness of therapies to prevent fractures or to treat osteoporosis in men.
Bisphosphonates are associated with mild upper GI symptoms, atypical subtrochanteric fracture, and rare osteonecrosis of the jaw. There is no significant association between bisphosphonate use and total cardiovascular adverse events. Evidence is insufficient to associate bisphosphonates with increased cancer risk. Zoledronic acid is associated with atrial fibrillation, arthritis/arthralgias, headaches, hypocalcemia, influenza-like symptoms, and an increased incidence of uveitis/episcleritis. Denosumab is associated with mild upper GI symptoms, rash/eczema, and cellulitis.
While in the past additional medications were recommended for osteoporosis, the current guidelines recommend against using raloxifene, ibandronate, teriparatide, menopausal estrogen therapy, or menopausal estrogen plus progesterone therapy for first-line pharmacologic treatment.
The overall effect of calcium, vitamin D, or exercise alone on fracture risk is uncertain. Calcium and vitamin D may be added to treatment regimens, as a majority of trials with bisphosphonate therapy added this supplementation. Dosages should be considered because excessive dosing has been associated with hypercalcemia. Although previous data suggested an association between calcium supplementation and increased risk for myocardial infarction, moderate-quality evidence shows no association, though there is a risk of kidney stones.
Recommendation: Women who have osteoporosis and receive pharmacologic treatment should be treated for 5 years (weak recommendation; low-quality evidence). The evidence to determine the length of treatment is not strong, so recommendation is an extrapolation from existing evidence. High-risk patients may benefit from more than 5 years of treatment. Data suggests that patients treated with alendronate who had preexisting fractures or those with a BMD of –2.5 or less after 5 years of initial therapy may benefit from continued treatment, because these patients experienced a decreased incidence of new clinical vertebral fractures.
Recommendation: Pharmacologic treatment with bisphosphonates to reduce the risk for vertebral fracture can be offered to men who have clinically recognized osteoporosis (weak recommendation, low-quality evidence). No evidence suggests that outcomes associated with pharmacologic treatment would differ between men and women if based on similar BMDs.
Recommendation: Bone density monitoring is not recommended during the 5-year pharmacologic treatment period for osteoporosis in women (weak recommendation, low-quality evidence). Data showed that most women with normal dual-energy x-ray absorptiometry scores did not progress to osteoporosis within 15 years. Data also does not support monitoring BMD during the initial 5 years of treatment in patients taking pharmacologic agents to treat osteoporosis. Several studies showed that women treated with antiresorptive treatment benefited from reduced fractures with treatment even if BMD did not increase.
Only 10% of women with normal or mild osteopenia develop osteoporosis within 15 years; 10% of women with moderate osteopenia develop osteoporosis within 5 years, and 10% of women with advanced osteopenia develop osteoporosis within 1 year.
Recommendation: The decision about whether to treat osteopenic women older then 65 years of age who are at a high risk for fracture should be based on a discussion of with the patient about their risk of fracture and the risk and benefits of treatment. Clinicians can use their judgment regarding the qualitative risk for fracture, or a validated tool such as the FRAX tool that gives 10-year risk of any major osteoporotic fracture and of hip fracture. The FRAX site recommends consideration of treatment for individuals with low bone mass (T-score between –1.0 and –2.5 at the femoral neck or spine) and a 10-year probability of a hip fracture of at least 3% or a 10-year probability of a major osteoporosis-related fracture greater than 20%.
Bottom line:
Clinicians should offer pharmacologic treatment with alendronate, risedronate, zoledronic acid, or denosumab to reduce the risk of hip and vertebral fractures in women who have known osteoporosis diagnosed as a T score less than –2.5 or those with a fragility fracture. Pharmacologic therapy should be used for 5 years; however, high risk patients may benefit from longer treatment. There is no benefit to bone density monitoring during the 5-year pharmacologic treatment period. In addition, bisphosphonates should be considered in men who have clinically recognized osteoporosis.
Reference:
Qaseem, A, Forciea, MA, McLean RM, Denberg TD. Treatment of Low Bone Density or Osteoporosis to Prevent Fractures in Men and Women: A Clinical Practice Guideline Update From the American College of Physicians. Ann Int Med. 2017;166(11):818-39.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Meizinger is a second year resident in the Family Medicine Residency Program at Abington Jefferson Health.
Osteoporosis is defined by a clinically diagnosed fragility fracture or a bone mineral density (BMD) of at least 2.5 SD below the mean for young female adults, usually measured by dual-energy x-ray absorptiometry. Risk factors include age, female sex, post-menopause, hypogonadism or premature ovarian failure, history of cigarette smoking or alcohol consumption (3 or more drinks daily), rheumatoid arthritis, or medications including glucocorticoids, anticoagulants, anticonvulsants, and aromatase inhibitors.
This guideline update focuses on treatment with bisphosphonates (alendronate, risedronate, ibandronate, zoledronic acid) and denosumab. Denosumab, a human monoclonal antibody against RANK-ligand, approved by the Food and Drug Administration for treatment of osteoporosis, has been added to the list of allowed medications since publication of the 2008 guideline. Several therapies have been excluded from the update, including calcitonin, which is no longer widely used for osteoporosis treatment, and etidronate and pamidronate, neither of which are FDA-approved for the prevention of fractures or treatment of osteoporosis. It should be noted that the evidence continues to be insufficient regarding the effectiveness of therapies to prevent fractures or to treat osteoporosis in men.
Bisphosphonates are associated with mild upper GI symptoms, atypical subtrochanteric fracture, and rare osteonecrosis of the jaw. There is no significant association between bisphosphonate use and total cardiovascular adverse events. Evidence is insufficient to associate bisphosphonates with increased cancer risk. Zoledronic acid is associated with atrial fibrillation, arthritis/arthralgias, headaches, hypocalcemia, influenza-like symptoms, and an increased incidence of uveitis/episcleritis. Denosumab is associated with mild upper GI symptoms, rash/eczema, and cellulitis.
While in the past additional medications were recommended for osteoporosis, the current guidelines recommend against using raloxifene, ibandronate, teriparatide, menopausal estrogen therapy, or menopausal estrogen plus progesterone therapy for first-line pharmacologic treatment.
The overall effect of calcium, vitamin D, or exercise alone on fracture risk is uncertain. Calcium and vitamin D may be added to treatment regimens, as a majority of trials with bisphosphonate therapy added this supplementation. Dosages should be considered because excessive dosing has been associated with hypercalcemia. Although previous data suggested an association between calcium supplementation and increased risk for myocardial infarction, moderate-quality evidence shows no association, though there is a risk of kidney stones.
Recommendation: Women who have osteoporosis and receive pharmacologic treatment should be treated for 5 years (weak recommendation; low-quality evidence). The evidence to determine the length of treatment is not strong, so recommendation is an extrapolation from existing evidence. High-risk patients may benefit from more than 5 years of treatment. Data suggests that patients treated with alendronate who had preexisting fractures or those with a BMD of –2.5 or less after 5 years of initial therapy may benefit from continued treatment, because these patients experienced a decreased incidence of new clinical vertebral fractures.
Recommendation: Pharmacologic treatment with bisphosphonates to reduce the risk for vertebral fracture can be offered to men who have clinically recognized osteoporosis (weak recommendation, low-quality evidence). No evidence suggests that outcomes associated with pharmacologic treatment would differ between men and women if based on similar BMDs.
Recommendation: Bone density monitoring is not recommended during the 5-year pharmacologic treatment period for osteoporosis in women (weak recommendation, low-quality evidence). Data showed that most women with normal dual-energy x-ray absorptiometry scores did not progress to osteoporosis within 15 years. Data also does not support monitoring BMD during the initial 5 years of treatment in patients taking pharmacologic agents to treat osteoporosis. Several studies showed that women treated with antiresorptive treatment benefited from reduced fractures with treatment even if BMD did not increase.
Only 10% of women with normal or mild osteopenia develop osteoporosis within 15 years; 10% of women with moderate osteopenia develop osteoporosis within 5 years, and 10% of women with advanced osteopenia develop osteoporosis within 1 year.
Recommendation: The decision about whether to treat osteopenic women older then 65 years of age who are at a high risk for fracture should be based on a discussion of with the patient about their risk of fracture and the risk and benefits of treatment. Clinicians can use their judgment regarding the qualitative risk for fracture, or a validated tool such as the FRAX tool that gives 10-year risk of any major osteoporotic fracture and of hip fracture. The FRAX site recommends consideration of treatment for individuals with low bone mass (T-score between –1.0 and –2.5 at the femoral neck or spine) and a 10-year probability of a hip fracture of at least 3% or a 10-year probability of a major osteoporosis-related fracture greater than 20%.
Bottom line:
Clinicians should offer pharmacologic treatment with alendronate, risedronate, zoledronic acid, or denosumab to reduce the risk of hip and vertebral fractures in women who have known osteoporosis diagnosed as a T score less than –2.5 or those with a fragility fracture. Pharmacologic therapy should be used for 5 years; however, high risk patients may benefit from longer treatment. There is no benefit to bone density monitoring during the 5-year pharmacologic treatment period. In addition, bisphosphonates should be considered in men who have clinically recognized osteoporosis.
Reference:
Qaseem, A, Forciea, MA, McLean RM, Denberg TD. Treatment of Low Bone Density or Osteoporosis to Prevent Fractures in Men and Women: A Clinical Practice Guideline Update From the American College of Physicians. Ann Int Med. 2017;166(11):818-39.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Meizinger is a second year resident in the Family Medicine Residency Program at Abington Jefferson Health.
Osteoporosis is defined by a clinically diagnosed fragility fracture or a bone mineral density (BMD) of at least 2.5 SD below the mean for young female adults, usually measured by dual-energy x-ray absorptiometry. Risk factors include age, female sex, post-menopause, hypogonadism or premature ovarian failure, history of cigarette smoking or alcohol consumption (3 or more drinks daily), rheumatoid arthritis, or medications including glucocorticoids, anticoagulants, anticonvulsants, and aromatase inhibitors.
This guideline update focuses on treatment with bisphosphonates (alendronate, risedronate, ibandronate, zoledronic acid) and denosumab. Denosumab, a human monoclonal antibody against RANK-ligand, approved by the Food and Drug Administration for treatment of osteoporosis, has been added to the list of allowed medications since publication of the 2008 guideline. Several therapies have been excluded from the update, including calcitonin, which is no longer widely used for osteoporosis treatment, and etidronate and pamidronate, neither of which are FDA-approved for the prevention of fractures or treatment of osteoporosis. It should be noted that the evidence continues to be insufficient regarding the effectiveness of therapies to prevent fractures or to treat osteoporosis in men.
Bisphosphonates are associated with mild upper GI symptoms, atypical subtrochanteric fracture, and rare osteonecrosis of the jaw. There is no significant association between bisphosphonate use and total cardiovascular adverse events. Evidence is insufficient to associate bisphosphonates with increased cancer risk. Zoledronic acid is associated with atrial fibrillation, arthritis/arthralgias, headaches, hypocalcemia, influenza-like symptoms, and an increased incidence of uveitis/episcleritis. Denosumab is associated with mild upper GI symptoms, rash/eczema, and cellulitis.
While in the past additional medications were recommended for osteoporosis, the current guidelines recommend against using raloxifene, ibandronate, teriparatide, menopausal estrogen therapy, or menopausal estrogen plus progesterone therapy for first-line pharmacologic treatment.
The overall effect of calcium, vitamin D, or exercise alone on fracture risk is uncertain. Calcium and vitamin D may be added to treatment regimens, as a majority of trials with bisphosphonate therapy added this supplementation. Dosages should be considered because excessive dosing has been associated with hypercalcemia. Although previous data suggested an association between calcium supplementation and increased risk for myocardial infarction, moderate-quality evidence shows no association, though there is a risk of kidney stones.
Recommendation: Women who have osteoporosis and receive pharmacologic treatment should be treated for 5 years (weak recommendation; low-quality evidence). The evidence to determine the length of treatment is not strong, so recommendation is an extrapolation from existing evidence. High-risk patients may benefit from more than 5 years of treatment. Data suggests that patients treated with alendronate who had preexisting fractures or those with a BMD of –2.5 or less after 5 years of initial therapy may benefit from continued treatment, because these patients experienced a decreased incidence of new clinical vertebral fractures.
Recommendation: Pharmacologic treatment with bisphosphonates to reduce the risk for vertebral fracture can be offered to men who have clinically recognized osteoporosis (weak recommendation, low-quality evidence). No evidence suggests that outcomes associated with pharmacologic treatment would differ between men and women if based on similar BMDs.
Recommendation: Bone density monitoring is not recommended during the 5-year pharmacologic treatment period for osteoporosis in women (weak recommendation, low-quality evidence). Data showed that most women with normal dual-energy x-ray absorptiometry scores did not progress to osteoporosis within 15 years. Data also does not support monitoring BMD during the initial 5 years of treatment in patients taking pharmacologic agents to treat osteoporosis. Several studies showed that women treated with antiresorptive treatment benefited from reduced fractures with treatment even if BMD did not increase.
Only 10% of women with normal or mild osteopenia develop osteoporosis within 15 years; 10% of women with moderate osteopenia develop osteoporosis within 5 years, and 10% of women with advanced osteopenia develop osteoporosis within 1 year.
Recommendation: The decision about whether to treat osteopenic women older then 65 years of age who are at a high risk for fracture should be based on a discussion of with the patient about their risk of fracture and the risk and benefits of treatment. Clinicians can use their judgment regarding the qualitative risk for fracture, or a validated tool such as the FRAX tool that gives 10-year risk of any major osteoporotic fracture and of hip fracture. The FRAX site recommends consideration of treatment for individuals with low bone mass (T-score between –1.0 and –2.5 at the femoral neck or spine) and a 10-year probability of a hip fracture of at least 3% or a 10-year probability of a major osteoporosis-related fracture greater than 20%.
Bottom line:
Clinicians should offer pharmacologic treatment with alendronate, risedronate, zoledronic acid, or denosumab to reduce the risk of hip and vertebral fractures in women who have known osteoporosis diagnosed as a T score less than –2.5 or those with a fragility fracture. Pharmacologic therapy should be used for 5 years; however, high risk patients may benefit from longer treatment. There is no benefit to bone density monitoring during the 5-year pharmacologic treatment period. In addition, bisphosphonates should be considered in men who have clinically recognized osteoporosis.
Reference:
Qaseem, A, Forciea, MA, McLean RM, Denberg TD. Treatment of Low Bone Density or Osteoporosis to Prevent Fractures in Men and Women: A Clinical Practice Guideline Update From the American College of Physicians. Ann Int Med. 2017;166(11):818-39.
Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Meizinger is a second year resident in the Family Medicine Residency Program at Abington Jefferson Health.

The EHR Report: Communication, social media, and legal vulnerability
Social media is now a part of everyday life. From Twitter, with its 140 character limit, to Facebook to Linkedin, there is a world of possibilities for communicating with friends, family, colleagues, and others online. Communication is good, but electronic media is a minefield for medical professionals who do not think carefully before they post.
The stories in the news about health care professionals who have posted obviously inflammatory material online, perhaps in a fit of rage, and have had their careers impacted or ended are just the tip of the iceberg. HIPAA violations have received a good deal of attention, with a well-known example being the doctor who was accused of posting a selfie with Joan Rivers, who was unconscious on the operating table. These examples, however, represent obvious violations of HIPAA and are infractions that most physicians would readily identify. Other examples may not be as obvious.
We know of one case where a nurse on the staff of a physicians’ office posted on Facebook that work was grueling that day because he felt under the weather with suspected flu. This may seem, at first, to be an innocuous communication. And that’s all it was, until, the son of an immunosuppressed man who had an appointment at that doctor’s office was flabbergasted to hear from a mutual friend that one of the nurses in the office was at work despite having the flu. He demanded to speak with the office manager and made sure that his father was not seen by that nurse. It may seem like an unlikely coincidence, but, in medical-legal circles, unlikely events occur all the time.

Many people who use social media will check in or post when they are out with friends or colleagues blowing off steam. For example, you might post something on social media about a holiday party you are attending. But, consider what happens if, at work the next day, something goes wrong, your care is called into question, and a lawsuit ensues. Your post may be innocent, but it now falls into the hands of the patient’s attorney. When you are having your deposition taken, the lawyer pulls your social media post out of a stack of papers and grills you about where you were, what you were doing, how late you stayed out, whether you were drinking, how much, and so on. Maybe you explain to him that you were only at the holiday party for an hour and did not have a single drink. That attorney, however, is not required to take your word for it and can ask you who you were with. All of a sudden, your friends and colleagues are being served with subpoenas for their depositions and being examined about what you did that night. Possibly, the lawyer is sending a subpoena for your credit card receipt and the restaurant’s billing records to determine what you ordered that night.
You should never rely on the false assumption that even “private” messages sent directly to other people will truly remain private. One of us was recently involved in a case where this worked to our advantage. A 30-year-old woman claimed that her family doctor never recommended that she see a gastroenterologist. A friend of the patient testified in a deposition that the two of them had discussed her medical care in private messages on Facebook. After the court ordered that the patient turn over her private Facebook messages, we learned that she told her friend that the doctor had indeed made the recommendation for her to see that specialist.
This cautionary tale doesn’t just apply to social media. Keep in mind that, if you are involved in litigation, attorneys can subpoena the records from your cellular phone provider. All cell phone text message are archived by the cellular provider and can be retrieved under subpoena. You may innocently be blowing off steam to a spouse or friend about a difficult patient or bad outcome but later have those text messages used against you in litigation.
The various social media platforms can be great tools for all kinds of professionals to share interesting information and further their professional development. However, everybody, especially the medical professional, needs to think before they post or send a message. We must also remember that, once information is out in cyberspace, it remains there and can never be truly erased. In other words, you can never unring the proverbial bell. It is important to think about the potential impact of that communication before posting and electronically communicating. Only communicate something that you would be comfortable defending in court.
Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Mr. Shear is an associate attorney in the health care department at Marshall Dennehey Warner Coleman & Goggin in Pittsburgh. He represents physicians, medical professionals, and hospitals in medical malpractice actions.
Social media is now a part of everyday life. From Twitter, with its 140 character limit, to Facebook to Linkedin, there is a world of possibilities for communicating with friends, family, colleagues, and others online. Communication is good, but electronic media is a minefield for medical professionals who do not think carefully before they post.
The stories in the news about health care professionals who have posted obviously inflammatory material online, perhaps in a fit of rage, and have had their careers impacted or ended are just the tip of the iceberg. HIPAA violations have received a good deal of attention, with a well-known example being the doctor who was accused of posting a selfie with Joan Rivers, who was unconscious on the operating table. These examples, however, represent obvious violations of HIPAA and are infractions that most physicians would readily identify. Other examples may not be as obvious.
We know of one case where a nurse on the staff of a physicians’ office posted on Facebook that work was grueling that day because he felt under the weather with suspected flu. This may seem, at first, to be an innocuous communication. And that’s all it was, until, the son of an immunosuppressed man who had an appointment at that doctor’s office was flabbergasted to hear from a mutual friend that one of the nurses in the office was at work despite having the flu. He demanded to speak with the office manager and made sure that his father was not seen by that nurse. It may seem like an unlikely coincidence, but, in medical-legal circles, unlikely events occur all the time.
Many people who use social media will check in or post when they are out with friends or colleagues blowing off steam. For example, you might post something on social media about a holiday party you are attending. But, consider what happens if, at work the next day, something goes wrong, your care is called into question, and a lawsuit ensues. Your post may be innocent, but it now falls into the hands of the patient’s attorney. When you are having your deposition taken, the lawyer pulls your social media post out of a stack of papers and grills you about where you were, what you were doing, how late you stayed out, whether you were drinking, how much, and so on. Maybe you explain to him that you were only at the holiday party for an hour and did not have a single drink. That attorney, however, is not required to take your word for it and can ask you who you were with. All of a sudden, your friends and colleagues are being served with subpoenas for their depositions and being examined about what you did that night. Possibly, the lawyer is sending a subpoena for your credit card receipt and the restaurant’s billing records to determine what you ordered that night.
You should never rely on the false assumption that even “private” messages sent directly to other people will truly remain private. One of us was recently involved in a case where this worked to our advantage. A 30-year-old woman claimed that her family doctor never recommended that she see a gastroenterologist. A friend of the patient testified in a deposition that the two of them had discussed her medical care in private messages on Facebook. After the court ordered that the patient turn over her private Facebook messages, we learned that she told her friend that the doctor had indeed made the recommendation for her to see that specialist.
This cautionary tale doesn’t just apply to social media. Keep in mind that, if you are involved in litigation, attorneys can subpoena the records from your cellular phone provider. All cell phone text message are archived by the cellular provider and can be retrieved under subpoena. You may innocently be blowing off steam to a spouse or friend about a difficult patient or bad outcome but later have those text messages used against you in litigation.
The various social media platforms can be great tools for all kinds of professionals to share interesting information and further their professional development. However, everybody, especially the medical professional, needs to think before they post or send a message. We must also remember that, once information is out in cyberspace, it remains there and can never be truly erased. In other words, you can never unring the proverbial bell. It is important to think about the potential impact of that communication before posting and electronically communicating. Only communicate something that you would be comfortable defending in court.
Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Mr. Shear is an associate attorney in the health care department at Marshall Dennehey Warner Coleman & Goggin in Pittsburgh. He represents physicians, medical professionals, and hospitals in medical malpractice actions.
Social media is now a part of everyday life. From Twitter, with its 140 character limit, to Facebook to Linkedin, there is a world of possibilities for communicating with friends, family, colleagues, and others online. Communication is good, but electronic media is a minefield for medical professionals who do not think carefully before they post.
The stories in the news about health care professionals who have posted obviously inflammatory material online, perhaps in a fit of rage, and have had their careers impacted or ended are just the tip of the iceberg. HIPAA violations have received a good deal of attention, with a well-known example being the doctor who was accused of posting a selfie with Joan Rivers, who was unconscious on the operating table. These examples, however, represent obvious violations of HIPAA and are infractions that most physicians would readily identify. Other examples may not be as obvious.
We know of one case where a nurse on the staff of a physicians’ office posted on Facebook that work was grueling that day because he felt under the weather with suspected flu. This may seem, at first, to be an innocuous communication. And that’s all it was, until, the son of an immunosuppressed man who had an appointment at that doctor’s office was flabbergasted to hear from a mutual friend that one of the nurses in the office was at work despite having the flu. He demanded to speak with the office manager and made sure that his father was not seen by that nurse. It may seem like an unlikely coincidence, but, in medical-legal circles, unlikely events occur all the time.
Many people who use social media will check in or post when they are out with friends or colleagues blowing off steam. For example, you might post something on social media about a holiday party you are attending. But, consider what happens if, at work the next day, something goes wrong, your care is called into question, and a lawsuit ensues. Your post may be innocent, but it now falls into the hands of the patient’s attorney. When you are having your deposition taken, the lawyer pulls your social media post out of a stack of papers and grills you about where you were, what you were doing, how late you stayed out, whether you were drinking, how much, and so on. Maybe you explain to him that you were only at the holiday party for an hour and did not have a single drink. That attorney, however, is not required to take your word for it and can ask you who you were with. All of a sudden, your friends and colleagues are being served with subpoenas for their depositions and being examined about what you did that night. Possibly, the lawyer is sending a subpoena for your credit card receipt and the restaurant’s billing records to determine what you ordered that night.
You should never rely on the false assumption that even “private” messages sent directly to other people will truly remain private. One of us was recently involved in a case where this worked to our advantage. A 30-year-old woman claimed that her family doctor never recommended that she see a gastroenterologist. A friend of the patient testified in a deposition that the two of them had discussed her medical care in private messages on Facebook. After the court ordered that the patient turn over her private Facebook messages, we learned that she told her friend that the doctor had indeed made the recommendation for her to see that specialist.
This cautionary tale doesn’t just apply to social media. Keep in mind that, if you are involved in litigation, attorneys can subpoena the records from your cellular phone provider. All cell phone text message are archived by the cellular provider and can be retrieved under subpoena. You may innocently be blowing off steam to a spouse or friend about a difficult patient or bad outcome but later have those text messages used against you in litigation.
The various social media platforms can be great tools for all kinds of professionals to share interesting information and further their professional development. However, everybody, especially the medical professional, needs to think before they post or send a message. We must also remember that, once information is out in cyberspace, it remains there and can never be truly erased. In other words, you can never unring the proverbial bell. It is important to think about the potential impact of that communication before posting and electronically communicating. Only communicate something that you would be comfortable defending in court.
Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Mr. Shear is an associate attorney in the health care department at Marshall Dennehey Warner Coleman & Goggin in Pittsburgh. He represents physicians, medical professionals, and hospitals in medical malpractice actions.
Management of chronic insomnia in adults
Most adults experience problems with sleep from time to time, and 6%-10% meet diagnostic criteria for chronic insomnia. Many of these patients present to their primary care clinicians looking for help. This clinical practice guideline from the American College of Physicians provides recommendations based on a review of studies published during the previous decade, which were assessed in terms of the strength of the recommendation and the quality of evidence. The guideline resulted in two recommendations:
1: All adult patients should receive cognitive behavioral therapy for insomnia (CBT-I) as the initial treatment for chronic insomnia. (strong recommendation)
2: Clinicians should use a shared decision-making approach discussing the benefits, harms, and costs of short-term use of medications, to decide whether to add pharmacological therapy in adults with chronic insomnia in whom cognitive behavioral therapy for insomnia (CBT-I) alone was unsuccessful. (weak recommendation)
Cognitive behavioral therapy for insomnia (CBT-I)
Cognitive behavioral therapy for insomnia encompasses a variety of measures that aim to change patients’ habits and beliefs associated with sleep. These measures include general “sleep hygiene” interventions, as well as stimulus control, sleep restriction, relaxation training, and cognitive reframing. With sleep hygiene, patients are educated about environmental factors that affect sleep, such as avoiding caffeine late in the day, limiting alcohol intake, having a regular sleep schedule, avoiding napping, the importance of exercise, and the importance of a quiet dark room in which to sleep. Examples of stimulus control include going to bed only when sleepy, and avoiding reading and watching TV in the bedroom. Sleep restriction limits the time in bed with strict sleep and wake-up times, gradually increasing time in bed as sleep efficiency improves.
Clinicians may find it surprising that this guideline makes such a strong, clear case for the primacy of behavioral measures in the treatment of chronic insomnia. The authors make a number of points in support of this position.
First, the effects of behavioral interventions appear to be robust – at least comparable to the short-term effects of medications – and often significantly better. For example, various studies of CBT-I show a decrease in sleep onset latency (how long it takes to fall asleep after going to bed) of between 12 and 31 minutes and an increase in total sleep time of 40 minutes. This compares favorably to the short-term effects of commonly used sleep medications.
Second, the effects of behavioral interventions are long-lasting compared with medications, which are usually approved for only short-term use, lose effectiveness over time, and have no benefit at all once they’re no longer being taken. Finally, there appear to be no harms associated with CBT-I, compared with significant adverse effects of medications.
One challenge is that access to effective behavioral interventions for insomnia can be an issue. On the other hand, a number of behavioral delivery methods were examined, and found to be effective, including in-person individual or group therapy, telephone- or Web-based modules or apps, and self-help books. An editorial accompanying the guidelines calls for efforts to increase the availability of behavioral modalities for insomnia.
Pharmacologic therapy
The recommendation to use pharmacologic therapy for insomnia is much more qualified than that for CBT-I, with language about shared decision-making, discussion of risks and benefits, emphasis on short-term use, and a provision that it be used only after an unsatisfactory trial of CBT-I alone. In addition, this recommendation is classified as “weak,” and the associated evidence “low-quality.” Medications reviewed included eszopiclone, zaleplon, zolpidem, orexin receptor antagonist, melatonin, ramelteon, and benzodiazepines.
There are several reasons why pharmacologic therapy is deemphasized. First, as noted above, the effects of commonly used medications are modest. As an example, typical patients with chronic insomnia will have sleep-onset latency of 60-70 minutes. Medications reviewed for this guideline decreased this time by approximately 10-20 minutes in short-term studies, so patients still took 40-60 minutes to fall asleep. Similar modest short-term effects were seen in terms of increasing total sleep time.
A second issue with pharmacologic therapy is that while many patients with chronic insomnia seek to use medications long term, the available studies have tended to look only at short-term use, and those studies with longer duration show a diminution of medication effect over time.
Finally, there are significant adverse effects associated with sedative-hypnotic medications, including somnolence, anxiety, confusion, and disturbance in attention. This is problematic, considering that these are precisely the symptoms that patients may be hoping to avoid when they take medications to help them sleep. Even patients who may not feel impaired often show demonstrable deficits in attention and performance following use of sleep medications; this issue is reflected in the boxed warnings that accompany several commonly prescribed agents.
It is noted in the evidence reviews that there are differences among the available medications. The nonbenzodiazepine hypnotics eszopiclone and zolpidem as well as the orexin receptor antagonist suvorexant improved short-term sleep quality, though the effect was small and there was significant evidence of harm as described above. Benzodiazepine hypnotics, melatonin agonists, and antidepressants studied had little or low-quality evidence to support efficacy on improving sleep. For melatonin and ramelteon, the evidence review notes that adverse effects did not differ between the medication and the placebo groups, though two open-label longer-term studies showed evidence of adverse effects with ramelteon. It is also important to note that patients studied in medication trials were mostly healthy middle-aged individuals; it is possible that the side effects of sleep medications may be greater in those who are older or more infirm.
Bottom line
This guideline from the American College of Physicians strongly endorses the use of tailored cognitive behavioral therapy modalities for the initial treatment of patients with chronic insomnia. Medications are given a weak recommendation for a limited back-up role.
Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
Qaseem A, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016;165:125-33.
Brasure M. Psychological and Behavioral Interventions for Managing Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:113-24.
Wilt TJ, et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:103-12.
Most adults experience problems with sleep from time to time, and 6%-10% meet diagnostic criteria for chronic insomnia. Many of these patients present to their primary care clinicians looking for help. This clinical practice guideline from the American College of Physicians provides recommendations based on a review of studies published during the previous decade, which were assessed in terms of the strength of the recommendation and the quality of evidence. The guideline resulted in two recommendations:
1: All adult patients should receive cognitive behavioral therapy for insomnia (CBT-I) as the initial treatment for chronic insomnia. (strong recommendation)
2: Clinicians should use a shared decision-making approach discussing the benefits, harms, and costs of short-term use of medications, to decide whether to add pharmacological therapy in adults with chronic insomnia in whom cognitive behavioral therapy for insomnia (CBT-I) alone was unsuccessful. (weak recommendation)
Cognitive behavioral therapy for insomnia (CBT-I)
Cognitive behavioral therapy for insomnia encompasses a variety of measures that aim to change patients’ habits and beliefs associated with sleep. These measures include general “sleep hygiene” interventions, as well as stimulus control, sleep restriction, relaxation training, and cognitive reframing. With sleep hygiene, patients are educated about environmental factors that affect sleep, such as avoiding caffeine late in the day, limiting alcohol intake, having a regular sleep schedule, avoiding napping, the importance of exercise, and the importance of a quiet dark room in which to sleep. Examples of stimulus control include going to bed only when sleepy, and avoiding reading and watching TV in the bedroom. Sleep restriction limits the time in bed with strict sleep and wake-up times, gradually increasing time in bed as sleep efficiency improves.
Clinicians may find it surprising that this guideline makes such a strong, clear case for the primacy of behavioral measures in the treatment of chronic insomnia. The authors make a number of points in support of this position.
First, the effects of behavioral interventions appear to be robust – at least comparable to the short-term effects of medications – and often significantly better. For example, various studies of CBT-I show a decrease in sleep onset latency (how long it takes to fall asleep after going to bed) of between 12 and 31 minutes and an increase in total sleep time of 40 minutes. This compares favorably to the short-term effects of commonly used sleep medications.
Second, the effects of behavioral interventions are long-lasting compared with medications, which are usually approved for only short-term use, lose effectiveness over time, and have no benefit at all once they’re no longer being taken. Finally, there appear to be no harms associated with CBT-I, compared with significant adverse effects of medications.
One challenge is that access to effective behavioral interventions for insomnia can be an issue. On the other hand, a number of behavioral delivery methods were examined, and found to be effective, including in-person individual or group therapy, telephone- or Web-based modules or apps, and self-help books. An editorial accompanying the guidelines calls for efforts to increase the availability of behavioral modalities for insomnia.
Pharmacologic therapy
The recommendation to use pharmacologic therapy for insomnia is much more qualified than that for CBT-I, with language about shared decision-making, discussion of risks and benefits, emphasis on short-term use, and a provision that it be used only after an unsatisfactory trial of CBT-I alone. In addition, this recommendation is classified as “weak,” and the associated evidence “low-quality.” Medications reviewed included eszopiclone, zaleplon, zolpidem, orexin receptor antagonist, melatonin, ramelteon, and benzodiazepines.
There are several reasons why pharmacologic therapy is deemphasized. First, as noted above, the effects of commonly used medications are modest. As an example, typical patients with chronic insomnia will have sleep-onset latency of 60-70 minutes. Medications reviewed for this guideline decreased this time by approximately 10-20 minutes in short-term studies, so patients still took 40-60 minutes to fall asleep. Similar modest short-term effects were seen in terms of increasing total sleep time.
A second issue with pharmacologic therapy is that while many patients with chronic insomnia seek to use medications long term, the available studies have tended to look only at short-term use, and those studies with longer duration show a diminution of medication effect over time.
Finally, there are significant adverse effects associated with sedative-hypnotic medications, including somnolence, anxiety, confusion, and disturbance in attention. This is problematic, considering that these are precisely the symptoms that patients may be hoping to avoid when they take medications to help them sleep. Even patients who may not feel impaired often show demonstrable deficits in attention and performance following use of sleep medications; this issue is reflected in the boxed warnings that accompany several commonly prescribed agents.
It is noted in the evidence reviews that there are differences among the available medications. The nonbenzodiazepine hypnotics eszopiclone and zolpidem as well as the orexin receptor antagonist suvorexant improved short-term sleep quality, though the effect was small and there was significant evidence of harm as described above. Benzodiazepine hypnotics, melatonin agonists, and antidepressants studied had little or low-quality evidence to support efficacy on improving sleep. For melatonin and ramelteon, the evidence review notes that adverse effects did not differ between the medication and the placebo groups, though two open-label longer-term studies showed evidence of adverse effects with ramelteon. It is also important to note that patients studied in medication trials were mostly healthy middle-aged individuals; it is possible that the side effects of sleep medications may be greater in those who are older or more infirm.
Bottom line
This guideline from the American College of Physicians strongly endorses the use of tailored cognitive behavioral therapy modalities for the initial treatment of patients with chronic insomnia. Medications are given a weak recommendation for a limited back-up role.
Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
Qaseem A, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016;165:125-33.
Brasure M. Psychological and Behavioral Interventions for Managing Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:113-24.
Wilt TJ, et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:103-12.
Most adults experience problems with sleep from time to time, and 6%-10% meet diagnostic criteria for chronic insomnia. Many of these patients present to their primary care clinicians looking for help. This clinical practice guideline from the American College of Physicians provides recommendations based on a review of studies published during the previous decade, which were assessed in terms of the strength of the recommendation and the quality of evidence. The guideline resulted in two recommendations:
1: All adult patients should receive cognitive behavioral therapy for insomnia (CBT-I) as the initial treatment for chronic insomnia. (strong recommendation)
2: Clinicians should use a shared decision-making approach discussing the benefits, harms, and costs of short-term use of medications, to decide whether to add pharmacological therapy in adults with chronic insomnia in whom cognitive behavioral therapy for insomnia (CBT-I) alone was unsuccessful. (weak recommendation)
Cognitive behavioral therapy for insomnia (CBT-I)
Cognitive behavioral therapy for insomnia encompasses a variety of measures that aim to change patients’ habits and beliefs associated with sleep. These measures include general “sleep hygiene” interventions, as well as stimulus control, sleep restriction, relaxation training, and cognitive reframing. With sleep hygiene, patients are educated about environmental factors that affect sleep, such as avoiding caffeine late in the day, limiting alcohol intake, having a regular sleep schedule, avoiding napping, the importance of exercise, and the importance of a quiet dark room in which to sleep. Examples of stimulus control include going to bed only when sleepy, and avoiding reading and watching TV in the bedroom. Sleep restriction limits the time in bed with strict sleep and wake-up times, gradually increasing time in bed as sleep efficiency improves.
Clinicians may find it surprising that this guideline makes such a strong, clear case for the primacy of behavioral measures in the treatment of chronic insomnia. The authors make a number of points in support of this position.
First, the effects of behavioral interventions appear to be robust – at least comparable to the short-term effects of medications – and often significantly better. For example, various studies of CBT-I show a decrease in sleep onset latency (how long it takes to fall asleep after going to bed) of between 12 and 31 minutes and an increase in total sleep time of 40 minutes. This compares favorably to the short-term effects of commonly used sleep medications.
Second, the effects of behavioral interventions are long-lasting compared with medications, which are usually approved for only short-term use, lose effectiveness over time, and have no benefit at all once they’re no longer being taken. Finally, there appear to be no harms associated with CBT-I, compared with significant adverse effects of medications.
One challenge is that access to effective behavioral interventions for insomnia can be an issue. On the other hand, a number of behavioral delivery methods were examined, and found to be effective, including in-person individual or group therapy, telephone- or Web-based modules or apps, and self-help books. An editorial accompanying the guidelines calls for efforts to increase the availability of behavioral modalities for insomnia.
Pharmacologic therapy
The recommendation to use pharmacologic therapy for insomnia is much more qualified than that for CBT-I, with language about shared decision-making, discussion of risks and benefits, emphasis on short-term use, and a provision that it be used only after an unsatisfactory trial of CBT-I alone. In addition, this recommendation is classified as “weak,” and the associated evidence “low-quality.” Medications reviewed included eszopiclone, zaleplon, zolpidem, orexin receptor antagonist, melatonin, ramelteon, and benzodiazepines.
There are several reasons why pharmacologic therapy is deemphasized. First, as noted above, the effects of commonly used medications are modest. As an example, typical patients with chronic insomnia will have sleep-onset latency of 60-70 minutes. Medications reviewed for this guideline decreased this time by approximately 10-20 minutes in short-term studies, so patients still took 40-60 minutes to fall asleep. Similar modest short-term effects were seen in terms of increasing total sleep time.
A second issue with pharmacologic therapy is that while many patients with chronic insomnia seek to use medications long term, the available studies have tended to look only at short-term use, and those studies with longer duration show a diminution of medication effect over time.
Finally, there are significant adverse effects associated with sedative-hypnotic medications, including somnolence, anxiety, confusion, and disturbance in attention. This is problematic, considering that these are precisely the symptoms that patients may be hoping to avoid when they take medications to help them sleep. Even patients who may not feel impaired often show demonstrable deficits in attention and performance following use of sleep medications; this issue is reflected in the boxed warnings that accompany several commonly prescribed agents.
It is noted in the evidence reviews that there are differences among the available medications. The nonbenzodiazepine hypnotics eszopiclone and zolpidem as well as the orexin receptor antagonist suvorexant improved short-term sleep quality, though the effect was small and there was significant evidence of harm as described above. Benzodiazepine hypnotics, melatonin agonists, and antidepressants studied had little or low-quality evidence to support efficacy on improving sleep. For melatonin and ramelteon, the evidence review notes that adverse effects did not differ between the medication and the placebo groups, though two open-label longer-term studies showed evidence of adverse effects with ramelteon. It is also important to note that patients studied in medication trials were mostly healthy middle-aged individuals; it is possible that the side effects of sleep medications may be greater in those who are older or more infirm.
Bottom line
This guideline from the American College of Physicians strongly endorses the use of tailored cognitive behavioral therapy modalities for the initial treatment of patients with chronic insomnia. Medications are given a weak recommendation for a limited back-up role.
Dr. Clark is associate director of the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Thomas Jefferson University, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
Qaseem A, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016;165:125-33.
Brasure M. Psychological and Behavioral Interventions for Managing Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:113-24.
Wilt TJ, et al. Pharmacologic Treatment of Insomnia Disorder: An Evidence Report for a Clinical Practice Guideline by the American College of Physicians. Ann Intern Med. 2016;165:103-12.
Clinical Guidelines: ADA 2017 Standards of Medical Care in Diabetes
In 2012, 29.1 million Americans, or 9.3% of the population, had diabetes. Of this number, 21 million were diagnosed, and 8.1 million were undiagnosed. Each year almost 1.5 million Americans receive a new diagnosis of diabetes. The management of diabetes relies upon excellent primary care. Each year the American Diabetes Association reviews new evidence and publishes an updated Standards of Care in the January issue of Diabetes Care. Here we give a short overview of the guidelines with emphasis on fundamentals and changes in the standards over the past year.
Self-management education and support, nutrition therapy, and physical activity
All patients should participate in ongoing diabetes self-management education (DSME) to facilitate the knowledge, skills, and abilities necessary to obtain optimal self-care and incorporate the needs, goals, and life experiences of the person with diabetes as they face new challenges throughout a lifetime of diabetes.
In addition, each patient should receive individualized medical nutrition therapy (MNT) provided by a registered dietitian with knowledge regarding diabetes-specific MNT. Most patients should increase aerobic physical activity to 150 min/week. Providers should encourage patients to reduce the amount of time spent sedentary by briefly standing, walking, or performing other light physical activities every 30 minutes.
Glycemic targets
A reasonable hemoglobin A1c goal for many diabetic nonpregnant adults is less than 7%. A less stringent goal under 8% may be appropriate for patients with a history of severe hypoglycemia, limited life expectancy, advanced microvascular and macrovascular complications, and extensive comorbid conditions. HbA1c measurements should be done at diagnosis and routinely to monitor glycemic control. To aid in achieving glycemic targets, self-monitoring blood glucose (SMBG) allows patients to evaluate their individual response to therapy. Integrating SMBG data into diabetes management can help guide MNT, adjust medications, determine physical activity requirements, and prevent hypoglycemia. Individuals at risk for hypoglycemia should be asked about symptomatic and asymptomatic hypoglycemia at each encounter and counseled regarding treatment of hypoglycemic events.

Obesity management
There is strong and consistent evidence that obesity management may be beneficial in the treatment of type 2 diabetes. For overweight and obese patients with type 2 diabetes, interventions should be high intensity (more than 16 sessions in 6 months) and focus on diet, physical activity, and behavioral therapy designed to achieve a greater than 5% weight loss (energy deficit of 500-750 kcal/day).
For select patients, weight loss medications may be effective as adjuncts to lifestyle changes. When choosing additional pharmacologic interventions to improve glycemic control in overweight or obese patients, providers should use medications that promote weight loss or are weight neutral including metformin, sodium-glucose cotransporter-2 (SGLT-2) inhibitors, glucagon-like peptide-1 (GLP-1) agonists, and dipeptidyl peptidase-4 inhibitors (DPP-4) versus those that cause weight gain such as insulin secretagogues, thiazolidinediones, and insulin.
Metabolic surgery should be recommended to patients with type 2 diabetes and body mass index above 40 kg/m2 (BMI above 37.5 kg/m2 in Asian Americans), regardless of adequate glycemic control and for patients with BMI above 35 kg/m2 (more than 32.5 kg/m2 in Asian Americans) without adequate glycemic control despite lifestyle modifications and optimal medical therapy. Metabolic surgery should be considered for appropriate candidates with BMIs as low as 30 if hyperglycemia is inadequately controlled despite optical medical control by either oral or injectable medications.
CV disease and risk management: BP, lipids, antiplatelet therapy, and glycemic medication management
Atherosclerotic cardiovascular disease is the leading cause of morbidity and mortality for individuals with diabetes. Screening for atherosclerotic cardiovascular disease is not recommended; rather, the emphasis is on careful risk factor management.
If systolic blood pressure (SBP) is confirmed to be above 140 mm Hg and/or the diastolic blood pressure (DBP) is confirmed to be above 90 mm Hg, pharmacologic therapy should be initiated. A meta-analysis of randomized trials of adults with type 2 diabetes comparing intensive blood pressure targets (upper limit of 130 mm Hg SBP and 80 mm Hg DBP) with standard targets (upper limit of 140-160 mm Hg SBP and 85-100 mm Hg DBP) found no significant reduction in mortality or nonfatal MI. There was a statistically significant, 35% relative risk (RR) reduction in stroke with intensive targets, but intensive targets were associated with an increased risk for adverse events such as hypotension and syncope. Recommendations suggest that antihypertension treatment in adults with diabetes without albuminuria should include any of the classes of medication demonstrated to reduce cardiovascular events in patients with diabetes, such as ACE inhibitors, angiotensin receptor blockers (ARBs), thiazide-like diuretics, or dihydropyridine calcium-channel blockers. ACE inhibitors and ARBs continue to be recommended as first-line medications for the treatment of hypertension in patients with diabetes and elevated urine albumin/creatinine ratios (above 30 mg/g creatinine). The standards also suggest consideration of administering one or more antihypertensive medications at bedtime, which may improve cardiovascular outcomes.
For patients aged 40-75 years who have diabetes without additional atherosclerotic CV disease risk factors, a moderate-intensity statin should be considered. If there are additional cardiovascular risk factors, then a high-intensity statin should be considered. For patients who are younger than 40 years of age and have diabetes with additional atherosclerotic CV disease risk factors, a less strong recommendation is to consider using moderate-intensity or high-intensity statins. For patients older than 75 years with diabetes without additional atherosclerotic CV disease risk factors, consider using moderate-intensity statin therapy; high-intensity statin therapy may be considered in older adults with risk factors for atherosclerotic cardiovascular disease.
Both women and men who are at least 50 years old and have diabetes with at least one additional cardiovascular risk factor should consider taking daily aspirin therapy (75-162 mg/day) if they do not have any risk for excessive bleeding.
In patients with long-standing suboptimally controlled type 2 diabetes and established atherosclerotic CV disease, empagliflozin or liraglutide should be considered as they have been shown to reduce cardiovascular and all-cause mortality when added to standard care.

Microvascular disease and foot care
Large prospective studies have demonstrated that optimized glucose control can reduce the onset and progression of diabetic microvascular complications. Diabetic kidney disease occurs in about 20%-40% of persons with diabetes. Annual screening includes estimated glomerular filtration rate and spot urine albumin-to-creatinine ratio. Treatment includes ACE inhibitors or ARBs in addition to a target blood pressure of under 140/90 mm Hg.
Diabetic retinopathy screening includes a dilated eye exam by an eye care professional. Treatment includes laser photocoagulation therapy for high risk nonproliferative retinopathy or proliferative retinopathy, or intravitreal injections of antivascular endothelial growth factor agents for central-involved diabetic macular edema.
Diabetic peripheral neuropathy screening includes annual 10-g monofilament and 128-HZ tuning fork vibration sensation. Medications for painful diabetic neuropathy may include gabapentin, pregabalin, duloxetine, and other agents.
Neuropathy and vascular disease are contributors to diabetic foot ulcers and amputation. A comprehensive foot examination along with appropriate risk factor oriented history to include neuropathic and vascular components (pulses, claudication) should be performed annually, while all patients with diabetes should have their feet checked at every visit.
Older adults
Prioritizing treatment goals in older adults is important in this heterogeneous population. Cardiovascular risk factor treatment is likely to be beneficial.
In setting HbA1c goals, functional status, and comorbid conditions should be considered. Metformin can still be a first-line agent for many older adults with type 2 diabetes, with consideration to renal status (creatinine clearance above 30 mL/min per 1.73 m2) and heart failure. DPP-4s have few side effects and low risk of hypoglycemia. GLP-1 receptor agonists have a low risk of hypoglycemia but may be associated with GI side effects and weight loss. SGLT-2 inhibitors have a low risk of hypoglycemia, and attention should be paid to renal thresholds for use. Thiazolidinediones should be used cautiously in those with heart failure or at elevated fracture risk. Sulfonylureas should be used cautiously because of their elevated risk of hypoglycemia. When used, a short-acting sulfonylurea – such as glipizide – is preferred, as long-acting sulfonylureas are contraindicated because of even greater hypoglycemic risk. Single-injection basal insulin may be appropriate for many with ease of use and efficacy.
The bottom line
Diabetes is a rapidly changing field and each year the American Diabetes Association updates the Standards of Medical Care document to be consistent with the latest evidence. Highlights of the standards include emphasis on diabetes self-management education, individualized glycemic goal setting, obesity management, setting blood pressure targets to less than 140/90 mm Hg, as well as statins and daily aspirin for most people with diabetes. In addition, ADA now recommends the use of specific antihyperglycemic medications to reduce cardiovascular and all-cause mortality in patients with diabetes and established cardiovascular disease.
Reference
American Diabetes Association Standards of Medical Care in Diabetes – 2017. Diabetes Care 2017; 40 (sup 1):S1-S138
Dr. Skolnik is professor of family and community medicine, Temple University School of Medicine, Philadelphia, and associate director, Family Medicine Residency Program, Abington-Jefferson Health, Abington, Pa. Dr. Johnson is associate professor at the University of North Dakota School of Medicine and Health Sciences, and practices at the Altru Diabetes Center, Grand Forks. Ms. Neuman practices at St. Mark’s Hospital, Salt Lake City.
In 2012, 29.1 million Americans, or 9.3% of the population, had diabetes. Of this number, 21 million were diagnosed, and 8.1 million were undiagnosed. Each year almost 1.5 million Americans receive a new diagnosis of diabetes. The management of diabetes relies upon excellent primary care. Each year the American Diabetes Association reviews new evidence and publishes an updated Standards of Care in the January issue of Diabetes Care. Here we give a short overview of the guidelines with emphasis on fundamentals and changes in the standards over the past year.
Self-management education and support, nutrition therapy, and physical activity
All patients should participate in ongoing diabetes self-management education (DSME) to facilitate the knowledge, skills, and abilities necessary to obtain optimal self-care and incorporate the needs, goals, and life experiences of the person with diabetes as they face new challenges throughout a lifetime of diabetes.
In addition, each patient should receive individualized medical nutrition therapy (MNT) provided by a registered dietitian with knowledge regarding diabetes-specific MNT. Most patients should increase aerobic physical activity to 150 min/week. Providers should encourage patients to reduce the amount of time spent sedentary by briefly standing, walking, or performing other light physical activities every 30 minutes.
Glycemic targets
A reasonable hemoglobin A1c goal for many diabetic nonpregnant adults is less than 7%. A less stringent goal under 8% may be appropriate for patients with a history of severe hypoglycemia, limited life expectancy, advanced microvascular and macrovascular complications, and extensive comorbid conditions. HbA1c measurements should be done at diagnosis and routinely to monitor glycemic control. To aid in achieving glycemic targets, self-monitoring blood glucose (SMBG) allows patients to evaluate their individual response to therapy. Integrating SMBG data into diabetes management can help guide MNT, adjust medications, determine physical activity requirements, and prevent hypoglycemia. Individuals at risk for hypoglycemia should be asked about symptomatic and asymptomatic hypoglycemia at each encounter and counseled regarding treatment of hypoglycemic events.
Obesity management
There is strong and consistent evidence that obesity management may be beneficial in the treatment of type 2 diabetes. For overweight and obese patients with type 2 diabetes, interventions should be high intensity (more than 16 sessions in 6 months) and focus on diet, physical activity, and behavioral therapy designed to achieve a greater than 5% weight loss (energy deficit of 500-750 kcal/day).
For select patients, weight loss medications may be effective as adjuncts to lifestyle changes. When choosing additional pharmacologic interventions to improve glycemic control in overweight or obese patients, providers should use medications that promote weight loss or are weight neutral including metformin, sodium-glucose cotransporter-2 (SGLT-2) inhibitors, glucagon-like peptide-1 (GLP-1) agonists, and dipeptidyl peptidase-4 inhibitors (DPP-4) versus those that cause weight gain such as insulin secretagogues, thiazolidinediones, and insulin.
Metabolic surgery should be recommended to patients with type 2 diabetes and body mass index above 40 kg/m2 (BMI above 37.5 kg/m2 in Asian Americans), regardless of adequate glycemic control and for patients with BMI above 35 kg/m2 (more than 32.5 kg/m2 in Asian Americans) without adequate glycemic control despite lifestyle modifications and optimal medical therapy. Metabolic surgery should be considered for appropriate candidates with BMIs as low as 30 if hyperglycemia is inadequately controlled despite optical medical control by either oral or injectable medications.
CV disease and risk management: BP, lipids, antiplatelet therapy, and glycemic medication management
Atherosclerotic cardiovascular disease is the leading cause of morbidity and mortality for individuals with diabetes. Screening for atherosclerotic cardiovascular disease is not recommended; rather, the emphasis is on careful risk factor management.
If systolic blood pressure (SBP) is confirmed to be above 140 mm Hg and/or the diastolic blood pressure (DBP) is confirmed to be above 90 mm Hg, pharmacologic therapy should be initiated. A meta-analysis of randomized trials of adults with type 2 diabetes comparing intensive blood pressure targets (upper limit of 130 mm Hg SBP and 80 mm Hg DBP) with standard targets (upper limit of 140-160 mm Hg SBP and 85-100 mm Hg DBP) found no significant reduction in mortality or nonfatal MI. There was a statistically significant, 35% relative risk (RR) reduction in stroke with intensive targets, but intensive targets were associated with an increased risk for adverse events such as hypotension and syncope. Recommendations suggest that antihypertension treatment in adults with diabetes without albuminuria should include any of the classes of medication demonstrated to reduce cardiovascular events in patients with diabetes, such as ACE inhibitors, angiotensin receptor blockers (ARBs), thiazide-like diuretics, or dihydropyridine calcium-channel blockers. ACE inhibitors and ARBs continue to be recommended as first-line medications for the treatment of hypertension in patients with diabetes and elevated urine albumin/creatinine ratios (above 30 mg/g creatinine). The standards also suggest consideration of administering one or more antihypertensive medications at bedtime, which may improve cardiovascular outcomes.
For patients aged 40-75 years who have diabetes without additional atherosclerotic CV disease risk factors, a moderate-intensity statin should be considered. If there are additional cardiovascular risk factors, then a high-intensity statin should be considered. For patients who are younger than 40 years of age and have diabetes with additional atherosclerotic CV disease risk factors, a less strong recommendation is to consider using moderate-intensity or high-intensity statins. For patients older than 75 years with diabetes without additional atherosclerotic CV disease risk factors, consider using moderate-intensity statin therapy; high-intensity statin therapy may be considered in older adults with risk factors for atherosclerotic cardiovascular disease.
Both women and men who are at least 50 years old and have diabetes with at least one additional cardiovascular risk factor should consider taking daily aspirin therapy (75-162 mg/day) if they do not have any risk for excessive bleeding.
In patients with long-standing suboptimally controlled type 2 diabetes and established atherosclerotic CV disease, empagliflozin or liraglutide should be considered as they have been shown to reduce cardiovascular and all-cause mortality when added to standard care.
Microvascular disease and foot care
Large prospective studies have demonstrated that optimized glucose control can reduce the onset and progression of diabetic microvascular complications. Diabetic kidney disease occurs in about 20%-40% of persons with diabetes. Annual screening includes estimated glomerular filtration rate and spot urine albumin-to-creatinine ratio. Treatment includes ACE inhibitors or ARBs in addition to a target blood pressure of under 140/90 mm Hg.
Diabetic retinopathy screening includes a dilated eye exam by an eye care professional. Treatment includes laser photocoagulation therapy for high risk nonproliferative retinopathy or proliferative retinopathy, or intravitreal injections of antivascular endothelial growth factor agents for central-involved diabetic macular edema.
Diabetic peripheral neuropathy screening includes annual 10-g monofilament and 128-HZ tuning fork vibration sensation. Medications for painful diabetic neuropathy may include gabapentin, pregabalin, duloxetine, and other agents.
Neuropathy and vascular disease are contributors to diabetic foot ulcers and amputation. A comprehensive foot examination along with appropriate risk factor oriented history to include neuropathic and vascular components (pulses, claudication) should be performed annually, while all patients with diabetes should have their feet checked at every visit.
Older adults
Prioritizing treatment goals in older adults is important in this heterogeneous population. Cardiovascular risk factor treatment is likely to be beneficial.
In setting HbA1c goals, functional status, and comorbid conditions should be considered. Metformin can still be a first-line agent for many older adults with type 2 diabetes, with consideration to renal status (creatinine clearance above 30 mL/min per 1.73 m2) and heart failure. DPP-4s have few side effects and low risk of hypoglycemia. GLP-1 receptor agonists have a low risk of hypoglycemia but may be associated with GI side effects and weight loss. SGLT-2 inhibitors have a low risk of hypoglycemia, and attention should be paid to renal thresholds for use. Thiazolidinediones should be used cautiously in those with heart failure or at elevated fracture risk. Sulfonylureas should be used cautiously because of their elevated risk of hypoglycemia. When used, a short-acting sulfonylurea – such as glipizide – is preferred, as long-acting sulfonylureas are contraindicated because of even greater hypoglycemic risk. Single-injection basal insulin may be appropriate for many with ease of use and efficacy.
The bottom line
Diabetes is a rapidly changing field and each year the American Diabetes Association updates the Standards of Medical Care document to be consistent with the latest evidence. Highlights of the standards include emphasis on diabetes self-management education, individualized glycemic goal setting, obesity management, setting blood pressure targets to less than 140/90 mm Hg, as well as statins and daily aspirin for most people with diabetes. In addition, ADA now recommends the use of specific antihyperglycemic medications to reduce cardiovascular and all-cause mortality in patients with diabetes and established cardiovascular disease.
Reference
American Diabetes Association Standards of Medical Care in Diabetes – 2017. Diabetes Care 2017; 40 (sup 1):S1-S138
Dr. Skolnik is professor of family and community medicine, Temple University School of Medicine, Philadelphia, and associate director, Family Medicine Residency Program, Abington-Jefferson Health, Abington, Pa. Dr. Johnson is associate professor at the University of North Dakota School of Medicine and Health Sciences, and practices at the Altru Diabetes Center, Grand Forks. Ms. Neuman practices at St. Mark’s Hospital, Salt Lake City.
In 2012, 29.1 million Americans, or 9.3% of the population, had diabetes. Of this number, 21 million were diagnosed, and 8.1 million were undiagnosed. Each year almost 1.5 million Americans receive a new diagnosis of diabetes. The management of diabetes relies upon excellent primary care. Each year the American Diabetes Association reviews new evidence and publishes an updated Standards of Care in the January issue of Diabetes Care. Here we give a short overview of the guidelines with emphasis on fundamentals and changes in the standards over the past year.
Self-management education and support, nutrition therapy, and physical activity
All patients should participate in ongoing diabetes self-management education (DSME) to facilitate the knowledge, skills, and abilities necessary to obtain optimal self-care and incorporate the needs, goals, and life experiences of the person with diabetes as they face new challenges throughout a lifetime of diabetes.
In addition, each patient should receive individualized medical nutrition therapy (MNT) provided by a registered dietitian with knowledge regarding diabetes-specific MNT. Most patients should increase aerobic physical activity to 150 min/week. Providers should encourage patients to reduce the amount of time spent sedentary by briefly standing, walking, or performing other light physical activities every 30 minutes.
Glycemic targets
A reasonable hemoglobin A1c goal for many diabetic nonpregnant adults is less than 7%. A less stringent goal under 8% may be appropriate for patients with a history of severe hypoglycemia, limited life expectancy, advanced microvascular and macrovascular complications, and extensive comorbid conditions. HbA1c measurements should be done at diagnosis and routinely to monitor glycemic control. To aid in achieving glycemic targets, self-monitoring blood glucose (SMBG) allows patients to evaluate their individual response to therapy. Integrating SMBG data into diabetes management can help guide MNT, adjust medications, determine physical activity requirements, and prevent hypoglycemia. Individuals at risk for hypoglycemia should be asked about symptomatic and asymptomatic hypoglycemia at each encounter and counseled regarding treatment of hypoglycemic events.
Obesity management
There is strong and consistent evidence that obesity management may be beneficial in the treatment of type 2 diabetes. For overweight and obese patients with type 2 diabetes, interventions should be high intensity (more than 16 sessions in 6 months) and focus on diet, physical activity, and behavioral therapy designed to achieve a greater than 5% weight loss (energy deficit of 500-750 kcal/day).
For select patients, weight loss medications may be effective as adjuncts to lifestyle changes. When choosing additional pharmacologic interventions to improve glycemic control in overweight or obese patients, providers should use medications that promote weight loss or are weight neutral including metformin, sodium-glucose cotransporter-2 (SGLT-2) inhibitors, glucagon-like peptide-1 (GLP-1) agonists, and dipeptidyl peptidase-4 inhibitors (DPP-4) versus those that cause weight gain such as insulin secretagogues, thiazolidinediones, and insulin.
Metabolic surgery should be recommended to patients with type 2 diabetes and body mass index above 40 kg/m2 (BMI above 37.5 kg/m2 in Asian Americans), regardless of adequate glycemic control and for patients with BMI above 35 kg/m2 (more than 32.5 kg/m2 in Asian Americans) without adequate glycemic control despite lifestyle modifications and optimal medical therapy. Metabolic surgery should be considered for appropriate candidates with BMIs as low as 30 if hyperglycemia is inadequately controlled despite optical medical control by either oral or injectable medications.
CV disease and risk management: BP, lipids, antiplatelet therapy, and glycemic medication management
Atherosclerotic cardiovascular disease is the leading cause of morbidity and mortality for individuals with diabetes. Screening for atherosclerotic cardiovascular disease is not recommended; rather, the emphasis is on careful risk factor management.
If systolic blood pressure (SBP) is confirmed to be above 140 mm Hg and/or the diastolic blood pressure (DBP) is confirmed to be above 90 mm Hg, pharmacologic therapy should be initiated. A meta-analysis of randomized trials of adults with type 2 diabetes comparing intensive blood pressure targets (upper limit of 130 mm Hg SBP and 80 mm Hg DBP) with standard targets (upper limit of 140-160 mm Hg SBP and 85-100 mm Hg DBP) found no significant reduction in mortality or nonfatal MI. There was a statistically significant, 35% relative risk (RR) reduction in stroke with intensive targets, but intensive targets were associated with an increased risk for adverse events such as hypotension and syncope. Recommendations suggest that antihypertension treatment in adults with diabetes without albuminuria should include any of the classes of medication demonstrated to reduce cardiovascular events in patients with diabetes, such as ACE inhibitors, angiotensin receptor blockers (ARBs), thiazide-like diuretics, or dihydropyridine calcium-channel blockers. ACE inhibitors and ARBs continue to be recommended as first-line medications for the treatment of hypertension in patients with diabetes and elevated urine albumin/creatinine ratios (above 30 mg/g creatinine). The standards also suggest consideration of administering one or more antihypertensive medications at bedtime, which may improve cardiovascular outcomes.
For patients aged 40-75 years who have diabetes without additional atherosclerotic CV disease risk factors, a moderate-intensity statin should be considered. If there are additional cardiovascular risk factors, then a high-intensity statin should be considered. For patients who are younger than 40 years of age and have diabetes with additional atherosclerotic CV disease risk factors, a less strong recommendation is to consider using moderate-intensity or high-intensity statins. For patients older than 75 years with diabetes without additional atherosclerotic CV disease risk factors, consider using moderate-intensity statin therapy; high-intensity statin therapy may be considered in older adults with risk factors for atherosclerotic cardiovascular disease.
Both women and men who are at least 50 years old and have diabetes with at least one additional cardiovascular risk factor should consider taking daily aspirin therapy (75-162 mg/day) if they do not have any risk for excessive bleeding.
In patients with long-standing suboptimally controlled type 2 diabetes and established atherosclerotic CV disease, empagliflozin or liraglutide should be considered as they have been shown to reduce cardiovascular and all-cause mortality when added to standard care.
Microvascular disease and foot care
Large prospective studies have demonstrated that optimized glucose control can reduce the onset and progression of diabetic microvascular complications. Diabetic kidney disease occurs in about 20%-40% of persons with diabetes. Annual screening includes estimated glomerular filtration rate and spot urine albumin-to-creatinine ratio. Treatment includes ACE inhibitors or ARBs in addition to a target blood pressure of under 140/90 mm Hg.
Diabetic retinopathy screening includes a dilated eye exam by an eye care professional. Treatment includes laser photocoagulation therapy for high risk nonproliferative retinopathy or proliferative retinopathy, or intravitreal injections of antivascular endothelial growth factor agents for central-involved diabetic macular edema.
Diabetic peripheral neuropathy screening includes annual 10-g monofilament and 128-HZ tuning fork vibration sensation. Medications for painful diabetic neuropathy may include gabapentin, pregabalin, duloxetine, and other agents.
Neuropathy and vascular disease are contributors to diabetic foot ulcers and amputation. A comprehensive foot examination along with appropriate risk factor oriented history to include neuropathic and vascular components (pulses, claudication) should be performed annually, while all patients with diabetes should have their feet checked at every visit.
Older adults
Prioritizing treatment goals in older adults is important in this heterogeneous population. Cardiovascular risk factor treatment is likely to be beneficial.
In setting HbA1c goals, functional status, and comorbid conditions should be considered. Metformin can still be a first-line agent for many older adults with type 2 diabetes, with consideration to renal status (creatinine clearance above 30 mL/min per 1.73 m2) and heart failure. DPP-4s have few side effects and low risk of hypoglycemia. GLP-1 receptor agonists have a low risk of hypoglycemia but may be associated with GI side effects and weight loss. SGLT-2 inhibitors have a low risk of hypoglycemia, and attention should be paid to renal thresholds for use. Thiazolidinediones should be used cautiously in those with heart failure or at elevated fracture risk. Sulfonylureas should be used cautiously because of their elevated risk of hypoglycemia. When used, a short-acting sulfonylurea – such as glipizide – is preferred, as long-acting sulfonylureas are contraindicated because of even greater hypoglycemic risk. Single-injection basal insulin may be appropriate for many with ease of use and efficacy.
The bottom line
Diabetes is a rapidly changing field and each year the American Diabetes Association updates the Standards of Medical Care document to be consistent with the latest evidence. Highlights of the standards include emphasis on diabetes self-management education, individualized glycemic goal setting, obesity management, setting blood pressure targets to less than 140/90 mm Hg, as well as statins and daily aspirin for most people with diabetes. In addition, ADA now recommends the use of specific antihyperglycemic medications to reduce cardiovascular and all-cause mortality in patients with diabetes and established cardiovascular disease.
Reference
American Diabetes Association Standards of Medical Care in Diabetes – 2017. Diabetes Care 2017; 40 (sup 1):S1-S138
Dr. Skolnik is professor of family and community medicine, Temple University School of Medicine, Philadelphia, and associate director, Family Medicine Residency Program, Abington-Jefferson Health, Abington, Pa. Dr. Johnson is associate professor at the University of North Dakota School of Medicine and Health Sciences, and practices at the Altru Diabetes Center, Grand Forks. Ms. Neuman practices at St. Mark’s Hospital, Salt Lake City.
Clinical Guidelines: Hospital-acquired and ventilator-associated pneumonia
Hospital-acquired pneumonia (HAP) is pneumonia that presents at least 48 hours after admission to the hospital. In contrast, ventilator-associated pneumonia (VAP), is pneumonia that clinically presents 48 hours after endotracheal intubation. Together, these are some of the most common hospital-acquired infections in the United States and pose a considerable burden on hospitals nationwide.
The Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) recently updated their management guidelines for HAP and VAP with a goal of striking a balance between providing appropriate early antibiotic coverage and avoiding unnecessary treatment that can lead to adverse effects such as Clostridium difficile infections and development of antibiotic resistance.1 This update eliminated the concept of Healthcare Associated Pneumonia (HCAP), often used for patients in skilled care facilities, because newer evidence has shown that patients who had met these criteria did not have a higher incidence of multidrug resistant pathogens; rather, they have microbial etiologies and sensitivities that are similar to adults with community acquired pneumonia (CAP).
Hospital-acquired pneumonia

Reasons to cover for MRSA in HAP:
Risk factors:
• IV antibiotic treatment within 90 days
• Treatment in a unit where the prevalence of MRSA is greater than 20% or unknown
• Prior detection of MRSA by culture or nonculture screening (weaker risk factor)
High risk of mortality: • Septic shock
• Need for ventilator support
MRSA should be covered with use of either vancomycin or linezolid in these cases.
In addition, patients with HAP should be covered for Pseudomonas aeruginosa and other gram-negative bacilli. For patients with risk factors for pseudomonas or other gram-negative infection or a high risk for mortality, then two antipseudomonal antibiotics from different classes are recommended, such as piperacillin-tazobactam/tobramycin or cefepime/amikacin.
Use two antipseudomonal antibiotics in HAP if the patient has these risk factors:
Pseudomonas risk factors:
• IV antibiotic treatment within 90 days
• Structural lung disease increasing the risk of gram-negative infection (bronchiectasis, cystic fibrosis)
• High-quality gram stain from respiratory specimen showing predominant and numerous gram-negative bacilli
High risk of mortality:
• Septic shock
• Need for ventilator support
Ventilator-associated pneumonia
General management of VAP is similar to HAP in that empiric treatment should be tailored to the local distribution and susceptibilities of pathogens based on each hospital’s antibiogram. All regimens should cover for S. aureus, P. aeruginosa, and other gram-negative bacilli based on the risk of mortality associated with the need for ventilator support. MSSA should be covered for VAP unless the patient has methicillin-resistant risk factors (see below).
MRSA should be covered for VAP if:
• Patient has had IV antibiotic use within past 90 days
• Hospital unit has greater than 10%-20% of S. aureus isolates are MRSA or MRSA prevalence unknown
Only one antipseudomonal agent should be used unless there are one of the following characteristics present, as described below.
Use two antipseudomonal agents in VAP if:
• Prior IV antibiotic use within 90 days
• Septic shock at time of VAP
• Acute respiratory distress syndrome preceding VAP
• 5 or more days of hospitalization prior to the occurrence of VAP
• Acute renal replacement therapy prior to VAP onset
• Greater than 10% of gram-negative isolates are resistant to an agent being considered for monotherapy
• Local antibiotic susceptibility rates unknown
In both HAP and VAP, antibiotics should be de-escalated to those with a narrower spectrum after initial empiric therapy, ideally within 72 hours and based on sputum or blood culture results. The guidelines support obtaining noninvasive sputum cultures in patients with VAP (endotracheal aspirates) and HAP (spontaneous expectoration, induced sputum, or nasotracheal suctioning in a patient who is unable to cooperate to produce a sputum sample). Patients who are improving clinically may be switched to appropriate oral therapy based on the susceptibility of an identified organism. Another key change is that of the standard duration of therapy. Previously, patients were treated for up to 2-3 weeks with antibiotics. The new IDSA/ATS guidelines recommend that patients should be treated with 7 days of antibiotics rather than a longer course.
The bottom line
Empiric therapy for HAP and VAP should be tailored to each hospital’s local pathogen distribution and antimicrobial susceptibilities, as detailed in an antibiogram. In HAP and VAP, empiric antibiotics should cover for S. aureus, but it only needs to target MRSA if risk factors are present, prevalence is greater than 20% or unknown, and – if HAP – a high risk of mortality. P. aeruginosa and other gram-negative bacilli should also be covered in empiric regimens. Dual antipseudomonal antibiotics is only recommended to be used in HAP if there are specific pseudomonal risk factors or a high risk of mortality. They should be used in VAP if there are multidrug-resistant risk factors present or there is a high/unknown prevalence of resistant organisms. All antibiotic regimens should be deescalated rather than maintained, and both HAP and VAP patients ought to be treated for 7 days.
References
1. Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016 Sep 1;63(5):557-82.
2. Beardsley JR, Williamson JC, Johnson JW, Ohl CA, Karchmer TB, Bowton DL. Using local microbiologic data to develop institution-specific guidelines for the treatment of hospital-acquired pneumonia. Chest. 2006 Sep;130(3):787-93.
Dr. Botti is a second-year resident in the family medicine residency program department of family and community medicine at Jefferson Medical College, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the department of family and community medicine and department of physiology at Jefferson Medical College, Philadelphia. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia.
Hospital-acquired pneumonia (HAP) is pneumonia that presents at least 48 hours after admission to the hospital. In contrast, ventilator-associated pneumonia (VAP), is pneumonia that clinically presents 48 hours after endotracheal intubation. Together, these are some of the most common hospital-acquired infections in the United States and pose a considerable burden on hospitals nationwide.
The Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) recently updated their management guidelines for HAP and VAP with a goal of striking a balance between providing appropriate early antibiotic coverage and avoiding unnecessary treatment that can lead to adverse effects such as Clostridium difficile infections and development of antibiotic resistance.1 This update eliminated the concept of Healthcare Associated Pneumonia (HCAP), often used for patients in skilled care facilities, because newer evidence has shown that patients who had met these criteria did not have a higher incidence of multidrug resistant pathogens; rather, they have microbial etiologies and sensitivities that are similar to adults with community acquired pneumonia (CAP).
Hospital-acquired pneumonia
Reasons to cover for MRSA in HAP:
Risk factors:
• IV antibiotic treatment within 90 days
• Treatment in a unit where the prevalence of MRSA is greater than 20% or unknown
• Prior detection of MRSA by culture or nonculture screening (weaker risk factor)
High risk of mortality: • Septic shock
• Need for ventilator support
MRSA should be covered with use of either vancomycin or linezolid in these cases.
In addition, patients with HAP should be covered for Pseudomonas aeruginosa and other gram-negative bacilli. For patients with risk factors for pseudomonas or other gram-negative infection or a high risk for mortality, then two antipseudomonal antibiotics from different classes are recommended, such as piperacillin-tazobactam/tobramycin or cefepime/amikacin.
Use two antipseudomonal antibiotics in HAP if the patient has these risk factors:
Pseudomonas risk factors:
• IV antibiotic treatment within 90 days
• Structural lung disease increasing the risk of gram-negative infection (bronchiectasis, cystic fibrosis)
• High-quality gram stain from respiratory specimen showing predominant and numerous gram-negative bacilli
High risk of mortality:
• Septic shock
• Need for ventilator support
Ventilator-associated pneumonia
General management of VAP is similar to HAP in that empiric treatment should be tailored to the local distribution and susceptibilities of pathogens based on each hospital’s antibiogram. All regimens should cover for S. aureus, P. aeruginosa, and other gram-negative bacilli based on the risk of mortality associated with the need for ventilator support. MSSA should be covered for VAP unless the patient has methicillin-resistant risk factors (see below).
MRSA should be covered for VAP if:
• Patient has had IV antibiotic use within past 90 days
• Hospital unit has greater than 10%-20% of S. aureus isolates are MRSA or MRSA prevalence unknown
Only one antipseudomonal agent should be used unless there are one of the following characteristics present, as described below.
Use two antipseudomonal agents in VAP if:
• Prior IV antibiotic use within 90 days
• Septic shock at time of VAP
• Acute respiratory distress syndrome preceding VAP
• 5 or more days of hospitalization prior to the occurrence of VAP
• Acute renal replacement therapy prior to VAP onset
• Greater than 10% of gram-negative isolates are resistant to an agent being considered for monotherapy
• Local antibiotic susceptibility rates unknown
In both HAP and VAP, antibiotics should be de-escalated to those with a narrower spectrum after initial empiric therapy, ideally within 72 hours and based on sputum or blood culture results. The guidelines support obtaining noninvasive sputum cultures in patients with VAP (endotracheal aspirates) and HAP (spontaneous expectoration, induced sputum, or nasotracheal suctioning in a patient who is unable to cooperate to produce a sputum sample). Patients who are improving clinically may be switched to appropriate oral therapy based on the susceptibility of an identified organism. Another key change is that of the standard duration of therapy. Previously, patients were treated for up to 2-3 weeks with antibiotics. The new IDSA/ATS guidelines recommend that patients should be treated with 7 days of antibiotics rather than a longer course.
The bottom line
Empiric therapy for HAP and VAP should be tailored to each hospital’s local pathogen distribution and antimicrobial susceptibilities, as detailed in an antibiogram. In HAP and VAP, empiric antibiotics should cover for S. aureus, but it only needs to target MRSA if risk factors are present, prevalence is greater than 20% or unknown, and – if HAP – a high risk of mortality. P. aeruginosa and other gram-negative bacilli should also be covered in empiric regimens. Dual antipseudomonal antibiotics is only recommended to be used in HAP if there are specific pseudomonal risk factors or a high risk of mortality. They should be used in VAP if there are multidrug-resistant risk factors present or there is a high/unknown prevalence of resistant organisms. All antibiotic regimens should be deescalated rather than maintained, and both HAP and VAP patients ought to be treated for 7 days.
References
1. Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016 Sep 1;63(5):557-82.
2. Beardsley JR, Williamson JC, Johnson JW, Ohl CA, Karchmer TB, Bowton DL. Using local microbiologic data to develop institution-specific guidelines for the treatment of hospital-acquired pneumonia. Chest. 2006 Sep;130(3):787-93.
Dr. Botti is a second-year resident in the family medicine residency program department of family and community medicine at Jefferson Medical College, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the department of family and community medicine and department of physiology at Jefferson Medical College, Philadelphia. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia.
Hospital-acquired pneumonia (HAP) is pneumonia that presents at least 48 hours after admission to the hospital. In contrast, ventilator-associated pneumonia (VAP), is pneumonia that clinically presents 48 hours after endotracheal intubation. Together, these are some of the most common hospital-acquired infections in the United States and pose a considerable burden on hospitals nationwide.
The Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS) recently updated their management guidelines for HAP and VAP with a goal of striking a balance between providing appropriate early antibiotic coverage and avoiding unnecessary treatment that can lead to adverse effects such as Clostridium difficile infections and development of antibiotic resistance.1 This update eliminated the concept of Healthcare Associated Pneumonia (HCAP), often used for patients in skilled care facilities, because newer evidence has shown that patients who had met these criteria did not have a higher incidence of multidrug resistant pathogens; rather, they have microbial etiologies and sensitivities that are similar to adults with community acquired pneumonia (CAP).
Hospital-acquired pneumonia
Reasons to cover for MRSA in HAP:
Risk factors:
• IV antibiotic treatment within 90 days
• Treatment in a unit where the prevalence of MRSA is greater than 20% or unknown
• Prior detection of MRSA by culture or nonculture screening (weaker risk factor)
High risk of mortality: • Septic shock
• Need for ventilator support
MRSA should be covered with use of either vancomycin or linezolid in these cases.
In addition, patients with HAP should be covered for Pseudomonas aeruginosa and other gram-negative bacilli. For patients with risk factors for pseudomonas or other gram-negative infection or a high risk for mortality, then two antipseudomonal antibiotics from different classes are recommended, such as piperacillin-tazobactam/tobramycin or cefepime/amikacin.
Use two antipseudomonal antibiotics in HAP if the patient has these risk factors:
Pseudomonas risk factors:
• IV antibiotic treatment within 90 days
• Structural lung disease increasing the risk of gram-negative infection (bronchiectasis, cystic fibrosis)
• High-quality gram stain from respiratory specimen showing predominant and numerous gram-negative bacilli
High risk of mortality:
• Septic shock
• Need for ventilator support
Ventilator-associated pneumonia
General management of VAP is similar to HAP in that empiric treatment should be tailored to the local distribution and susceptibilities of pathogens based on each hospital’s antibiogram. All regimens should cover for S. aureus, P. aeruginosa, and other gram-negative bacilli based on the risk of mortality associated with the need for ventilator support. MSSA should be covered for VAP unless the patient has methicillin-resistant risk factors (see below).
MRSA should be covered for VAP if:
• Patient has had IV antibiotic use within past 90 days
• Hospital unit has greater than 10%-20% of S. aureus isolates are MRSA or MRSA prevalence unknown
Only one antipseudomonal agent should be used unless there are one of the following characteristics present, as described below.
Use two antipseudomonal agents in VAP if:
• Prior IV antibiotic use within 90 days
• Septic shock at time of VAP
• Acute respiratory distress syndrome preceding VAP
• 5 or more days of hospitalization prior to the occurrence of VAP
• Acute renal replacement therapy prior to VAP onset
• Greater than 10% of gram-negative isolates are resistant to an agent being considered for monotherapy
• Local antibiotic susceptibility rates unknown
In both HAP and VAP, antibiotics should be de-escalated to those with a narrower spectrum after initial empiric therapy, ideally within 72 hours and based on sputum or blood culture results. The guidelines support obtaining noninvasive sputum cultures in patients with VAP (endotracheal aspirates) and HAP (spontaneous expectoration, induced sputum, or nasotracheal suctioning in a patient who is unable to cooperate to produce a sputum sample). Patients who are improving clinically may be switched to appropriate oral therapy based on the susceptibility of an identified organism. Another key change is that of the standard duration of therapy. Previously, patients were treated for up to 2-3 weeks with antibiotics. The new IDSA/ATS guidelines recommend that patients should be treated with 7 days of antibiotics rather than a longer course.
The bottom line
Empiric therapy for HAP and VAP should be tailored to each hospital’s local pathogen distribution and antimicrobial susceptibilities, as detailed in an antibiogram. In HAP and VAP, empiric antibiotics should cover for S. aureus, but it only needs to target MRSA if risk factors are present, prevalence is greater than 20% or unknown, and – if HAP – a high risk of mortality. P. aeruginosa and other gram-negative bacilli should also be covered in empiric regimens. Dual antipseudomonal antibiotics is only recommended to be used in HAP if there are specific pseudomonal risk factors or a high risk of mortality. They should be used in VAP if there are multidrug-resistant risk factors present or there is a high/unknown prevalence of resistant organisms. All antibiotic regimens should be deescalated rather than maintained, and both HAP and VAP patients ought to be treated for 7 days.
References
1. Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016 Sep 1;63(5):557-82.
2. Beardsley JR, Williamson JC, Johnson JW, Ohl CA, Karchmer TB, Bowton DL. Using local microbiologic data to develop institution-specific guidelines for the treatment of hospital-acquired pneumonia. Chest. 2006 Sep;130(3):787-93.
Dr. Botti is a second-year resident in the family medicine residency program department of family and community medicine at Jefferson Medical College, Philadelphia. Dr. Mills is assistant residency program director and assistant professor in the department of family and community medicine and department of physiology at Jefferson Medical College, Philadelphia. Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia.
Treatment of depression – nonpharmacologic vs. pharmacologic
Major depressive disorder (MDD) affects 16% of adults in the United States at some point in their lives. It is one of the most important causes of disability, time off from work, and personal distress, accounting for more than 8 million office visits per year.
Recent information shows that while 8% of the population screens positive for depression, only a quarter of those with depression receive treatment. Most patients with depression are cared for by primary care physicians, not psychiatrists.1 It is important that primary care physicians are familiar with the range of evidence-based treatments for depression and their relative efficacy. Most patients with depression receive antidepressant medication and less than one-third of patients receive some form of psychotherapy.1 The American College of Physicians guideline reviews the evidence regarding the relative efficacy and safety of second-generation antidepressants and nonpharmacologic treatment of depression.2

Outcomes evaluated in this guideline include response, remission, functional capacity, quality of life, reduction of suicidality or hospitalizations, and harms.
The pharmacotherapy treatment of depression, as assessed in this guideline, are second-generation antidepressants (SGAs), which include selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, and selective serotonin norepinephrine reuptake inhibitors. Previous reviews have shown that the SGAs have similar efficacy and safety with the side effects varying among the different medications; common side effects include constipation, diarrhea, nausea, decreased sexual ability, dizziness, headache, insomnia, and fatigue.
The strongest evidence, rated as moderate quality, comes from trials comparing SGAs to a form of psychotherapy called cognitive-behavioral therapy (CBT). CBT uses the technique of “collaborative empiricism” to question patients maladaptive beliefs, and by examining those beliefs, help patients to take on interpretations of reality that are less biased by their initial negative thoughts. Through these “cognitive” exercises, patients begin to take on healthier, more-adaptive approaches to the social, physical, and emotional challenges in their lives. These interpretations are then “tested” in the real world, the behavioral aspect of CBT. Studies that ranged in time from 8 to 52 weeks in patients with MDD showed SGAs and CBT to have equal efficacy with regard to response and remission of depression to therapy. Combining SGA and CBT, compared with SGA alone, did not show a difference in outcomes of response to therapy or remission of depression, though patients who received both therapies had some improved efficacy in work function.
When SGAs were compared with interpersonal therapy, psychodynamic therapy, St. John’s wort, acupuncture, and exercise, there was low-quality evidence that these interventions performed with equal efficacy to SGAs. Two trials of exercise, compared with sertraline, had moderate-quality evidence showing similar efficacy between the two treatments.
When patients have an incomplete response to initial treatment with an SGA, there was no difference in response or remission when using a strategy of switching from one SGA to another versus switching to cognitive therapy. Similarly, with regard to augmentation, CBT appears to work equally to augmenting initial SGA therapy with bupropion or buspirone.
The guidelines discuss that, with regard to adverse effects, while the discontinuation rates of SGAs and CBT are similar, CBT likely has fewer side effects. In addition, it is important to recognize that CBT has lower relapse rate associated with its use than do SGAs. This is presumably because once a skill set is developed when learning CBT, those skills can continue to be used long term.
The bottom line
Most patients who experience depression are cared for by their primary care physician. Treatments for depression include psychotherapy, complementary and alternative medicine (CAM), exercise, and pharmacotherapy. After discussion with the patient, the American College of Physicians recommends choosing either cognitive-behavioral therapy or second-generation antidepressants when treating depression.
References
1. Olfson M, Blanco C, Marcus SC. Treatment of Adult Depression in the United States. JAMA Intern Med. 2016 Oct;176(10):1482-91.
2. Qaseem A, et al. Nonpharmacologic Versus Pharmacologic Treatment of Adult Patients With Major Depressive Disorder: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016 Mar 1;164:350-59.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Aaron Sutton is a behavioral therapy consultant in the family medicine residency program at Abington Memorial Hospital.
Major depressive disorder (MDD) affects 16% of adults in the United States at some point in their lives. It is one of the most important causes of disability, time off from work, and personal distress, accounting for more than 8 million office visits per year.
Recent information shows that while 8% of the population screens positive for depression, only a quarter of those with depression receive treatment. Most patients with depression are cared for by primary care physicians, not psychiatrists.1 It is important that primary care physicians are familiar with the range of evidence-based treatments for depression and their relative efficacy. Most patients with depression receive antidepressant medication and less than one-third of patients receive some form of psychotherapy.1 The American College of Physicians guideline reviews the evidence regarding the relative efficacy and safety of second-generation antidepressants and nonpharmacologic treatment of depression.2
Outcomes evaluated in this guideline include response, remission, functional capacity, quality of life, reduction of suicidality or hospitalizations, and harms.
The pharmacotherapy treatment of depression, as assessed in this guideline, are second-generation antidepressants (SGAs), which include selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, and selective serotonin norepinephrine reuptake inhibitors. Previous reviews have shown that the SGAs have similar efficacy and safety with the side effects varying among the different medications; common side effects include constipation, diarrhea, nausea, decreased sexual ability, dizziness, headache, insomnia, and fatigue.
The strongest evidence, rated as moderate quality, comes from trials comparing SGAs to a form of psychotherapy called cognitive-behavioral therapy (CBT). CBT uses the technique of “collaborative empiricism” to question patients maladaptive beliefs, and by examining those beliefs, help patients to take on interpretations of reality that are less biased by their initial negative thoughts. Through these “cognitive” exercises, patients begin to take on healthier, more-adaptive approaches to the social, physical, and emotional challenges in their lives. These interpretations are then “tested” in the real world, the behavioral aspect of CBT. Studies that ranged in time from 8 to 52 weeks in patients with MDD showed SGAs and CBT to have equal efficacy with regard to response and remission of depression to therapy. Combining SGA and CBT, compared with SGA alone, did not show a difference in outcomes of response to therapy or remission of depression, though patients who received both therapies had some improved efficacy in work function.
When SGAs were compared with interpersonal therapy, psychodynamic therapy, St. John’s wort, acupuncture, and exercise, there was low-quality evidence that these interventions performed with equal efficacy to SGAs. Two trials of exercise, compared with sertraline, had moderate-quality evidence showing similar efficacy between the two treatments.
When patients have an incomplete response to initial treatment with an SGA, there was no difference in response or remission when using a strategy of switching from one SGA to another versus switching to cognitive therapy. Similarly, with regard to augmentation, CBT appears to work equally to augmenting initial SGA therapy with bupropion or buspirone.
The guidelines discuss that, with regard to adverse effects, while the discontinuation rates of SGAs and CBT are similar, CBT likely has fewer side effects. In addition, it is important to recognize that CBT has lower relapse rate associated with its use than do SGAs. This is presumably because once a skill set is developed when learning CBT, those skills can continue to be used long term.
The bottom line
Most patients who experience depression are cared for by their primary care physician. Treatments for depression include psychotherapy, complementary and alternative medicine (CAM), exercise, and pharmacotherapy. After discussion with the patient, the American College of Physicians recommends choosing either cognitive-behavioral therapy or second-generation antidepressants when treating depression.
References
1. Olfson M, Blanco C, Marcus SC. Treatment of Adult Depression in the United States. JAMA Intern Med. 2016 Oct;176(10):1482-91.
2. Qaseem A, et al. Nonpharmacologic Versus Pharmacologic Treatment of Adult Patients With Major Depressive Disorder: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016 Mar 1;164:350-59.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Aaron Sutton is a behavioral therapy consultant in the family medicine residency program at Abington Memorial Hospital.
Major depressive disorder (MDD) affects 16% of adults in the United States at some point in their lives. It is one of the most important causes of disability, time off from work, and personal distress, accounting for more than 8 million office visits per year.
Recent information shows that while 8% of the population screens positive for depression, only a quarter of those with depression receive treatment. Most patients with depression are cared for by primary care physicians, not psychiatrists.1 It is important that primary care physicians are familiar with the range of evidence-based treatments for depression and their relative efficacy. Most patients with depression receive antidepressant medication and less than one-third of patients receive some form of psychotherapy.1 The American College of Physicians guideline reviews the evidence regarding the relative efficacy and safety of second-generation antidepressants and nonpharmacologic treatment of depression.2
Outcomes evaluated in this guideline include response, remission, functional capacity, quality of life, reduction of suicidality or hospitalizations, and harms.
The pharmacotherapy treatment of depression, as assessed in this guideline, are second-generation antidepressants (SGAs), which include selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, and selective serotonin norepinephrine reuptake inhibitors. Previous reviews have shown that the SGAs have similar efficacy and safety with the side effects varying among the different medications; common side effects include constipation, diarrhea, nausea, decreased sexual ability, dizziness, headache, insomnia, and fatigue.
The strongest evidence, rated as moderate quality, comes from trials comparing SGAs to a form of psychotherapy called cognitive-behavioral therapy (CBT). CBT uses the technique of “collaborative empiricism” to question patients maladaptive beliefs, and by examining those beliefs, help patients to take on interpretations of reality that are less biased by their initial negative thoughts. Through these “cognitive” exercises, patients begin to take on healthier, more-adaptive approaches to the social, physical, and emotional challenges in their lives. These interpretations are then “tested” in the real world, the behavioral aspect of CBT. Studies that ranged in time from 8 to 52 weeks in patients with MDD showed SGAs and CBT to have equal efficacy with regard to response and remission of depression to therapy. Combining SGA and CBT, compared with SGA alone, did not show a difference in outcomes of response to therapy or remission of depression, though patients who received both therapies had some improved efficacy in work function.
When SGAs were compared with interpersonal therapy, psychodynamic therapy, St. John’s wort, acupuncture, and exercise, there was low-quality evidence that these interventions performed with equal efficacy to SGAs. Two trials of exercise, compared with sertraline, had moderate-quality evidence showing similar efficacy between the two treatments.
When patients have an incomplete response to initial treatment with an SGA, there was no difference in response or remission when using a strategy of switching from one SGA to another versus switching to cognitive therapy. Similarly, with regard to augmentation, CBT appears to work equally to augmenting initial SGA therapy with bupropion or buspirone.
The guidelines discuss that, with regard to adverse effects, while the discontinuation rates of SGAs and CBT are similar, CBT likely has fewer side effects. In addition, it is important to recognize that CBT has lower relapse rate associated with its use than do SGAs. This is presumably because once a skill set is developed when learning CBT, those skills can continue to be used long term.
The bottom line
Most patients who experience depression are cared for by their primary care physician. Treatments for depression include psychotherapy, complementary and alternative medicine (CAM), exercise, and pharmacotherapy. After discussion with the patient, the American College of Physicians recommends choosing either cognitive-behavioral therapy or second-generation antidepressants when treating depression.
References
1. Olfson M, Blanco C, Marcus SC. Treatment of Adult Depression in the United States. JAMA Intern Med. 2016 Oct;176(10):1482-91.
2. Qaseem A, et al. Nonpharmacologic Versus Pharmacologic Treatment of Adult Patients With Major Depressive Disorder: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med. 2016 Mar 1;164:350-59.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Aaron Sutton is a behavioral therapy consultant in the family medicine residency program at Abington Memorial Hospital.