User login
What’s New in Diffuse Large B-cell Lymphoma?
Diffuse large B-cell lymphoma (DLBCL) is the most diagnosed non-Hodgkin lymphoma (NHL), accounting for up to one-third of cases. For many decades, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) has been the standard first-line treatment approach for eligible patients in the first-line setting, resulting in long-term remissions in about two-thirds of patients. However, as our understanding of the biologic heterogeneity of this disease has advanced with the ability to perform more sophisticated molecular testing at diagnosis, researchers have been able to identify high-risk patient subtypes with suboptimal outcomes. While survival outcomes among low-risk patient subgroups are favorable with first-line immunochemotherapy, the majority of high-risk patients will experience relapse and often succumb to their disease.
Given the poor outcomes among patients with relapsed or refractory (R/R) DLBCL, there has been a massive research effort over the last decade to improve survival in this setting. Many experts agree that the approval of chimeric antigen receptor (CAR) T-cell therapy was the first major victory in this uphill battle. First approved in October of 2017, axicabtagene ciloleucel was the first of the 3 currently available commercial CAR T-cell therapy constructs to be approved in the third-line setting for DLBCL. Compared to historical controls, CAR T-cell therapy is associated with significant improvement in patient survival with complete response (CR) rates of 40%-50% compared to <20% with standard salvage immunochemotherapy.
Following approval in the third-line setting, these agents were quickly expedited to second-line therapy with pivotal trials demonstrating superiority with CAR T-cell therapy in the second line compared to salvage immunochemotherapy followed by autologous stem cell transplant. In 2022 the ZUMA-7 study reported a 24-month event-free survival (EFS) of 41% with axicabtagene ciloleucel compared to 16% with standard of care, and the TRANSFORM study documented a median EFS not yet reached with lisocabtagene ciloleucel compared to 2.3 months with standard of care. Despite these drastic improvements in patient outcomes, more than half of patients will still fail CAR T-cell therapy and require further systemic therapy.
Thankfully, this year has seen even more advancement in the treatment landscape of R/R DLBCL with two new commercially approved agents in yet another novel therapeutic category: bispecific antibodies. The following is a description of the newest data leading to the latest approvals by the US Food and Drug Administration.
Bispecific antibodies (BsAbs) are an off-the-shelf product that activate endogenous immune cells by cotargeting both tumor antigens as well as host T cells or natural killer cells. Several different experimental agents with varying constructs are under active observation in a wide variety of both hematologic and solid malignancies. Specifically within the realm of B-cell NHL, however, this class of agents is extremely promising and possibly represents the next significant milestone in the treatment of lymphoma.
The toxicity profile of these agents has been reliably predictable in most early phase clinical studies and is related predominantly to T-cell overactivation. The most commonly reported adverse events consist of cytokine release syndrome (CRS) as well as neutropenia, anemia, and hypophosphatemia. While neurologic toxicity has been reported, the incidence is low, and the mechanism is thought to be different than that reported with CAR T-cell therapy given that BsAbs are not likely to cross the blood–brain barrier.
Epcoritamab is a subcutaneously administered bispecific antibody that targets CD3 and CD20 in a 1:1 ratio and activates T cells to destroy CD20-expressing malignant cells. The recent EPCORE NHL-1 clinical trial investigated epcoritamab monotherapy in R/R mature B-cell lymphomas. This agent is administered with a step-up dosing strategy seen consistently across the BsAb drug class. Patients receive a first priming dose of 0.16 mg on cycle 1 day 1, followed by an intermediate dose of 0.8 mg on cycle 1 day 8, followed by the first full dose of 48 mg on cycle 1 day 15. Subsequent doses are administered once weekly for cycles 1-3 followed by every 2 weeks for cycles 4-9, and every 4 weeks starting with cycle 10.
The study enrolled 157 patients globally with median age of 64 and 3 median prior lines of antilymphoma therapy. Nearly 40% of patients had received at least 4 prior lines of therapy, and 83% of patients were refractory to last systemic therapy. Thirty-nine percent of patients had received prior CAR T-cell therapy; 75% of these patients developed progressive disease within 6 months of CAR T-cell therapy.
Among patients treated in the study, the results were as follows:
CR rate 39% with an overall response rate (ORR) of 63%
Duration of response 12 months; duration of objective response not reached in patients with CR
Duration of CR 12 months
Median PFS 4.4 months; median OS not reached
Time to CR of 2.7 months
Toxicity profile was notable for the following:
Any grade CRS in 50%, grade ≥3 in 2.5%
Most CRS occurs with first full dose on cycle 1 day 15 with median time to onset of 20 hours and median time to resolution of 48 hours
Any grade neutropenia in 22%, grade ≥3 in 15%, febrile neutropenia in 2.5%
Any grade anemia in 18%, grade ≥3 in 10%
Injection site reaction, any grade, in 20%
Any grade neurotoxicity in 6%, grade ≥3 in 1 patient (0.6%)
Epcoritamab was granted accelerated approval on May 19, 2023, for use in patients with R/R DLBCL who have received at least 2 prior lines of systemic therapy.
Glofitamab is the more recently approved BsAb for DLBCL. This agent is distinguished by its 2:1 binding configuration that confers bivalency for the CD20 binding site. Glofitamab is delivered intravenously and requires pretreatment with obinutuzumab 1000 mg 7 days before the first dose. With a similar step-up dosing strategy, patients receive a priming dose of 2.5mg on cycle 1 day 8, an intermediate dose of 10mg on cycle 1 day 15, and a first full dose of 30mg on cycle 2 day 1. Subsequent treatments are administered every 21 days for up to 12 cycles.
The open-label phase 1-2 clinical trial of glofitamab monotherapy enrolled 155 patients with a median age of 66 and 3 median prior lines of therapy. Thirty-three percent of patients had received prior CAR T-cell therapy, and 86% were refractory to last line of therapy with 30% refractory to CAR T-cell therapy.
Results were as follows:
CR rate of 39%, ORR 52%
Median duration of CR not reached, median duration of objective response 18.4 months
Median PFS 4.9 months, median OS not reached
Toxicity profile demonstrated the following:
Any grade CRS 66%, grade ≥ 2 in 18%
Median time to onset 13.5 hours from cycle 1 day 8, median duration 30.5 hours
Any grade neutropenia in 38%, grade ≥ 3 in 27%
Grade ≥ 2 neurologic event in 15%
Glofitamab received accelerated approval from the FDA on June 15, 2023, with an identical indication to epcoritamab.
The introduction of BsAbs in DLBCL has highlighted some important issues. Will BsAbs supplant CAR T-cell therapy in DLBCL? Experts can be found on both sides of this debate. BsAbs circumvent the logistics surrounding the production of CAR T-cell therapy products and can, for the large part, be administered in the outpatient setting. However, CAR T-cell therapy has significantly longer follow-up times, which speaks to the curative potential of these agents even in the third-line setting. BsAbs, some may argue, seem to carry a more favorable toxicity profile with the CRS mitigation strategies. However, we still have much to learn about the downstream side effects with prolonged T-cell activation and the potential for T-cell exhaustion.
Finally, with the continued development of new agents in this arena, the art of sequencing therapies will become ever more important. What is the efficacy of CAR T-cell therapy after BsAb exposure? Can BsAbs be used as bridging therapy to a curative option with CAR T-cell therapy? With longer-term follow-up in several years, will we see late relapses after CR with BsAbs? Ongoing clinical trials investigating combination strategies and CAR T-cell therapy consolidation with BsAbs will hopefully eventually clarify some of these questions.
Diffuse large B-cell lymphoma (DLBCL) is the most diagnosed non-Hodgkin lymphoma (NHL), accounting for up to one-third of cases. For many decades, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) has been the standard first-line treatment approach for eligible patients in the first-line setting, resulting in long-term remissions in about two-thirds of patients. However, as our understanding of the biologic heterogeneity of this disease has advanced with the ability to perform more sophisticated molecular testing at diagnosis, researchers have been able to identify high-risk patient subtypes with suboptimal outcomes. While survival outcomes among low-risk patient subgroups are favorable with first-line immunochemotherapy, the majority of high-risk patients will experience relapse and often succumb to their disease.
Given the poor outcomes among patients with relapsed or refractory (R/R) DLBCL, there has been a massive research effort over the last decade to improve survival in this setting. Many experts agree that the approval of chimeric antigen receptor (CAR) T-cell therapy was the first major victory in this uphill battle. First approved in October of 2017, axicabtagene ciloleucel was the first of the 3 currently available commercial CAR T-cell therapy constructs to be approved in the third-line setting for DLBCL. Compared to historical controls, CAR T-cell therapy is associated with significant improvement in patient survival with complete response (CR) rates of 40%-50% compared to <20% with standard salvage immunochemotherapy.
Following approval in the third-line setting, these agents were quickly expedited to second-line therapy with pivotal trials demonstrating superiority with CAR T-cell therapy in the second line compared to salvage immunochemotherapy followed by autologous stem cell transplant. In 2022 the ZUMA-7 study reported a 24-month event-free survival (EFS) of 41% with axicabtagene ciloleucel compared to 16% with standard of care, and the TRANSFORM study documented a median EFS not yet reached with lisocabtagene ciloleucel compared to 2.3 months with standard of care. Despite these drastic improvements in patient outcomes, more than half of patients will still fail CAR T-cell therapy and require further systemic therapy.
Thankfully, this year has seen even more advancement in the treatment landscape of R/R DLBCL with two new commercially approved agents in yet another novel therapeutic category: bispecific antibodies. The following is a description of the newest data leading to the latest approvals by the US Food and Drug Administration.
Bispecific antibodies (BsAbs) are an off-the-shelf product that activate endogenous immune cells by cotargeting both tumor antigens as well as host T cells or natural killer cells. Several different experimental agents with varying constructs are under active observation in a wide variety of both hematologic and solid malignancies. Specifically within the realm of B-cell NHL, however, this class of agents is extremely promising and possibly represents the next significant milestone in the treatment of lymphoma.
The toxicity profile of these agents has been reliably predictable in most early phase clinical studies and is related predominantly to T-cell overactivation. The most commonly reported adverse events consist of cytokine release syndrome (CRS) as well as neutropenia, anemia, and hypophosphatemia. While neurologic toxicity has been reported, the incidence is low, and the mechanism is thought to be different than that reported with CAR T-cell therapy given that BsAbs are not likely to cross the blood–brain barrier.
Epcoritamab is a subcutaneously administered bispecific antibody that targets CD3 and CD20 in a 1:1 ratio and activates T cells to destroy CD20-expressing malignant cells. The recent EPCORE NHL-1 clinical trial investigated epcoritamab monotherapy in R/R mature B-cell lymphomas. This agent is administered with a step-up dosing strategy seen consistently across the BsAb drug class. Patients receive a first priming dose of 0.16 mg on cycle 1 day 1, followed by an intermediate dose of 0.8 mg on cycle 1 day 8, followed by the first full dose of 48 mg on cycle 1 day 15. Subsequent doses are administered once weekly for cycles 1-3 followed by every 2 weeks for cycles 4-9, and every 4 weeks starting with cycle 10.
The study enrolled 157 patients globally with median age of 64 and 3 median prior lines of antilymphoma therapy. Nearly 40% of patients had received at least 4 prior lines of therapy, and 83% of patients were refractory to last systemic therapy. Thirty-nine percent of patients had received prior CAR T-cell therapy; 75% of these patients developed progressive disease within 6 months of CAR T-cell therapy.
Among patients treated in the study, the results were as follows:
CR rate 39% with an overall response rate (ORR) of 63%
Duration of response 12 months; duration of objective response not reached in patients with CR
Duration of CR 12 months
Median PFS 4.4 months; median OS not reached
Time to CR of 2.7 months
Toxicity profile was notable for the following:
Any grade CRS in 50%, grade ≥3 in 2.5%
Most CRS occurs with first full dose on cycle 1 day 15 with median time to onset of 20 hours and median time to resolution of 48 hours
Any grade neutropenia in 22%, grade ≥3 in 15%, febrile neutropenia in 2.5%
Any grade anemia in 18%, grade ≥3 in 10%
Injection site reaction, any grade, in 20%
Any grade neurotoxicity in 6%, grade ≥3 in 1 patient (0.6%)
Epcoritamab was granted accelerated approval on May 19, 2023, for use in patients with R/R DLBCL who have received at least 2 prior lines of systemic therapy.
Glofitamab is the more recently approved BsAb for DLBCL. This agent is distinguished by its 2:1 binding configuration that confers bivalency for the CD20 binding site. Glofitamab is delivered intravenously and requires pretreatment with obinutuzumab 1000 mg 7 days before the first dose. With a similar step-up dosing strategy, patients receive a priming dose of 2.5mg on cycle 1 day 8, an intermediate dose of 10mg on cycle 1 day 15, and a first full dose of 30mg on cycle 2 day 1. Subsequent treatments are administered every 21 days for up to 12 cycles.
The open-label phase 1-2 clinical trial of glofitamab monotherapy enrolled 155 patients with a median age of 66 and 3 median prior lines of therapy. Thirty-three percent of patients had received prior CAR T-cell therapy, and 86% were refractory to last line of therapy with 30% refractory to CAR T-cell therapy.
Results were as follows:
CR rate of 39%, ORR 52%
Median duration of CR not reached, median duration of objective response 18.4 months
Median PFS 4.9 months, median OS not reached
Toxicity profile demonstrated the following:
Any grade CRS 66%, grade ≥ 2 in 18%
Median time to onset 13.5 hours from cycle 1 day 8, median duration 30.5 hours
Any grade neutropenia in 38%, grade ≥ 3 in 27%
Grade ≥ 2 neurologic event in 15%
Glofitamab received accelerated approval from the FDA on June 15, 2023, with an identical indication to epcoritamab.
The introduction of BsAbs in DLBCL has highlighted some important issues. Will BsAbs supplant CAR T-cell therapy in DLBCL? Experts can be found on both sides of this debate. BsAbs circumvent the logistics surrounding the production of CAR T-cell therapy products and can, for the large part, be administered in the outpatient setting. However, CAR T-cell therapy has significantly longer follow-up times, which speaks to the curative potential of these agents even in the third-line setting. BsAbs, some may argue, seem to carry a more favorable toxicity profile with the CRS mitigation strategies. However, we still have much to learn about the downstream side effects with prolonged T-cell activation and the potential for T-cell exhaustion.
Finally, with the continued development of new agents in this arena, the art of sequencing therapies will become ever more important. What is the efficacy of CAR T-cell therapy after BsAb exposure? Can BsAbs be used as bridging therapy to a curative option with CAR T-cell therapy? With longer-term follow-up in several years, will we see late relapses after CR with BsAbs? Ongoing clinical trials investigating combination strategies and CAR T-cell therapy consolidation with BsAbs will hopefully eventually clarify some of these questions.
Diffuse large B-cell lymphoma (DLBCL) is the most diagnosed non-Hodgkin lymphoma (NHL), accounting for up to one-third of cases. For many decades, R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) has been the standard first-line treatment approach for eligible patients in the first-line setting, resulting in long-term remissions in about two-thirds of patients. However, as our understanding of the biologic heterogeneity of this disease has advanced with the ability to perform more sophisticated molecular testing at diagnosis, researchers have been able to identify high-risk patient subtypes with suboptimal outcomes. While survival outcomes among low-risk patient subgroups are favorable with first-line immunochemotherapy, the majority of high-risk patients will experience relapse and often succumb to their disease.
Given the poor outcomes among patients with relapsed or refractory (R/R) DLBCL, there has been a massive research effort over the last decade to improve survival in this setting. Many experts agree that the approval of chimeric antigen receptor (CAR) T-cell therapy was the first major victory in this uphill battle. First approved in October of 2017, axicabtagene ciloleucel was the first of the 3 currently available commercial CAR T-cell therapy constructs to be approved in the third-line setting for DLBCL. Compared to historical controls, CAR T-cell therapy is associated with significant improvement in patient survival with complete response (CR) rates of 40%-50% compared to <20% with standard salvage immunochemotherapy.
Following approval in the third-line setting, these agents were quickly expedited to second-line therapy with pivotal trials demonstrating superiority with CAR T-cell therapy in the second line compared to salvage immunochemotherapy followed by autologous stem cell transplant. In 2022 the ZUMA-7 study reported a 24-month event-free survival (EFS) of 41% with axicabtagene ciloleucel compared to 16% with standard of care, and the TRANSFORM study documented a median EFS not yet reached with lisocabtagene ciloleucel compared to 2.3 months with standard of care. Despite these drastic improvements in patient outcomes, more than half of patients will still fail CAR T-cell therapy and require further systemic therapy.
Thankfully, this year has seen even more advancement in the treatment landscape of R/R DLBCL with two new commercially approved agents in yet another novel therapeutic category: bispecific antibodies. The following is a description of the newest data leading to the latest approvals by the US Food and Drug Administration.
Bispecific antibodies (BsAbs) are an off-the-shelf product that activate endogenous immune cells by cotargeting both tumor antigens as well as host T cells or natural killer cells. Several different experimental agents with varying constructs are under active observation in a wide variety of both hematologic and solid malignancies. Specifically within the realm of B-cell NHL, however, this class of agents is extremely promising and possibly represents the next significant milestone in the treatment of lymphoma.
The toxicity profile of these agents has been reliably predictable in most early phase clinical studies and is related predominantly to T-cell overactivation. The most commonly reported adverse events consist of cytokine release syndrome (CRS) as well as neutropenia, anemia, and hypophosphatemia. While neurologic toxicity has been reported, the incidence is low, and the mechanism is thought to be different than that reported with CAR T-cell therapy given that BsAbs are not likely to cross the blood–brain barrier.
Epcoritamab is a subcutaneously administered bispecific antibody that targets CD3 and CD20 in a 1:1 ratio and activates T cells to destroy CD20-expressing malignant cells. The recent EPCORE NHL-1 clinical trial investigated epcoritamab monotherapy in R/R mature B-cell lymphomas. This agent is administered with a step-up dosing strategy seen consistently across the BsAb drug class. Patients receive a first priming dose of 0.16 mg on cycle 1 day 1, followed by an intermediate dose of 0.8 mg on cycle 1 day 8, followed by the first full dose of 48 mg on cycle 1 day 15. Subsequent doses are administered once weekly for cycles 1-3 followed by every 2 weeks for cycles 4-9, and every 4 weeks starting with cycle 10.
The study enrolled 157 patients globally with median age of 64 and 3 median prior lines of antilymphoma therapy. Nearly 40% of patients had received at least 4 prior lines of therapy, and 83% of patients were refractory to last systemic therapy. Thirty-nine percent of patients had received prior CAR T-cell therapy; 75% of these patients developed progressive disease within 6 months of CAR T-cell therapy.
Among patients treated in the study, the results were as follows:
CR rate 39% with an overall response rate (ORR) of 63%
Duration of response 12 months; duration of objective response not reached in patients with CR
Duration of CR 12 months
Median PFS 4.4 months; median OS not reached
Time to CR of 2.7 months
Toxicity profile was notable for the following:
Any grade CRS in 50%, grade ≥3 in 2.5%
Most CRS occurs with first full dose on cycle 1 day 15 with median time to onset of 20 hours and median time to resolution of 48 hours
Any grade neutropenia in 22%, grade ≥3 in 15%, febrile neutropenia in 2.5%
Any grade anemia in 18%, grade ≥3 in 10%
Injection site reaction, any grade, in 20%
Any grade neurotoxicity in 6%, grade ≥3 in 1 patient (0.6%)
Epcoritamab was granted accelerated approval on May 19, 2023, for use in patients with R/R DLBCL who have received at least 2 prior lines of systemic therapy.
Glofitamab is the more recently approved BsAb for DLBCL. This agent is distinguished by its 2:1 binding configuration that confers bivalency for the CD20 binding site. Glofitamab is delivered intravenously and requires pretreatment with obinutuzumab 1000 mg 7 days before the first dose. With a similar step-up dosing strategy, patients receive a priming dose of 2.5mg on cycle 1 day 8, an intermediate dose of 10mg on cycle 1 day 15, and a first full dose of 30mg on cycle 2 day 1. Subsequent treatments are administered every 21 days for up to 12 cycles.
The open-label phase 1-2 clinical trial of glofitamab monotherapy enrolled 155 patients with a median age of 66 and 3 median prior lines of therapy. Thirty-three percent of patients had received prior CAR T-cell therapy, and 86% were refractory to last line of therapy with 30% refractory to CAR T-cell therapy.
Results were as follows:
CR rate of 39%, ORR 52%
Median duration of CR not reached, median duration of objective response 18.4 months
Median PFS 4.9 months, median OS not reached
Toxicity profile demonstrated the following:
Any grade CRS 66%, grade ≥ 2 in 18%
Median time to onset 13.5 hours from cycle 1 day 8, median duration 30.5 hours
Any grade neutropenia in 38%, grade ≥ 3 in 27%
Grade ≥ 2 neurologic event in 15%
Glofitamab received accelerated approval from the FDA on June 15, 2023, with an identical indication to epcoritamab.
The introduction of BsAbs in DLBCL has highlighted some important issues. Will BsAbs supplant CAR T-cell therapy in DLBCL? Experts can be found on both sides of this debate. BsAbs circumvent the logistics surrounding the production of CAR T-cell therapy products and can, for the large part, be administered in the outpatient setting. However, CAR T-cell therapy has significantly longer follow-up times, which speaks to the curative potential of these agents even in the third-line setting. BsAbs, some may argue, seem to carry a more favorable toxicity profile with the CRS mitigation strategies. However, we still have much to learn about the downstream side effects with prolonged T-cell activation and the potential for T-cell exhaustion.
Finally, with the continued development of new agents in this arena, the art of sequencing therapies will become ever more important. What is the efficacy of CAR T-cell therapy after BsAb exposure? Can BsAbs be used as bridging therapy to a curative option with CAR T-cell therapy? With longer-term follow-up in several years, will we see late relapses after CR with BsAbs? Ongoing clinical trials investigating combination strategies and CAR T-cell therapy consolidation with BsAbs will hopefully eventually clarify some of these questions.
Human frailty is a cash cow
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.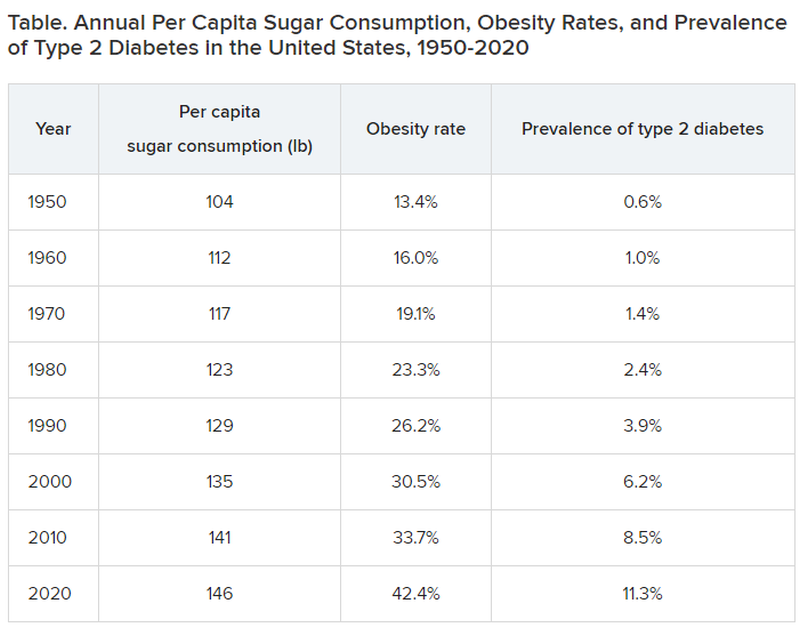
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Doctor, if you are caring for patients with diabetes, I sure hope you know more about it than I do. The longer I live, it seems, the less I understand.
In a free society, people can do what they want, and that’s great except when it isn’t. That’s why societies develop ethics and even public laws if ethics are not strong enough to protect us from ourselves and others.
Sugar, sugar
When I was growing up in small-town Alabama during the Depression and World War II, we called it sugar diabetes. Eat too much sugar, you got fat; your blood sugar went up, and you spilled sugar into your urine. Diabetes was fairly rare, and so was obesity. Doctors treated it by limiting the intake of sugar (and various sweet foods), along with attempting weight loss. If that didn’t do the trick, insulin injections.
From then until now, note these trends.
Type 2 diabetes was diagnosed even more infrequently before 1950:
- 1920: 0.2% of the population
- 1930: 0.3% of the population
- 1940: 0.4% of the population
In 2020, although 11.3% of the population was diagnosed with type 2 diabetes, the unknown undiagnosed proportion could be much higher.
Notice a correlation between sugar consumption and prevalence of diabetes? Of course, correlation is not causation, but at the same time, it sure as hell is not negation. Such concordance can be considered hypothesis generating. It may not be true causation, but it’s a good bet when 89% of people with diabetes have overweight or obesity.
What did the entire medical, public health, government, agriculture, nursing, food manufacturing, marketing, advertising, restaurant, and education constituencies do about this as it was happening? They observed, documented, gave lip service, and wrung their hands in public a bit. I do not believe that this is an organized active conspiracy; it would take too many players cooperating over too long a period of time. But it certainly may be a passive conspiracy, and primary care physicians and their patients are trapped.
The proper daily practice of medicine consists of one patient, one physician, one moment, and one decision. Let it be a shared decision, informed by the best evidence and taking cost into consideration. That encounter represents an opportunity, a responsibility, and a conundrum.
Individual health is subsumed under the collective health of the public. As such, a patient’s health is out of the control of both physician and patient; instead, patients are the beneficiaries or victims of the “marketplace.” Humans are frail and easily taken advantage of by the brilliant and highly motivated strategic planning and execution of Big Agriculture, Big Food, Big Pharma, Big Marketing, and Big Money-Driven Medicine and generally failed by Big Government, Big Public Health, Big Education, Big Psychology, and Big Religion.
Rethinking diabetes
Consider diabetes as one of many examples. What a terrific deal for capitalism. then it discovers (invents) long-term, very expensive, compelling treatments to slim us down, with no end in sight, and still without ever understanding the true nature of diabetes.
Gary Taubes’s great new book, “Rethinking Diabetes: What Science Reveals About Diet, Insulin, and Successful Treatments,” is being published by Alfred A. Knopf in early 2024.
It is 404 pages of (dense) text, with 401 numbered references and footnotes, a bibliography of 790 references, alphabetically arranged for easy cross-checking, and a 25-page index.
Remember Mr. Taubes’s earlier definitive historical treatises: “Good Calories, Bad Calories” (2007), “Why We Get Fat” (2010), “The Case Against Sugar” (2016), and “The Case for Keto” (2020)?
This new book is more like “Good Calories, Bad Calories”: long, dense, detailed, definitive, and of great historical reference value, including original research information from other countries in other languages. The author told me that the many early research reference sources were available only in German and that his use of generative artificial intelligence as an assistant researcher was of great value.
Nonphysician author Mr. Taubes uses his deep understanding of science and history to inform his long-honed talents of impartial investigative journalism as he attempts to understand and then explain why after all these years, the medical scientific community still does not have a sound consensus about the essence of diabetes, diet, insulin, and proper prevention and treatment at a level that is actually effective – amazing and so sad.
To signal these evolved and evolving conflicts, the book includes the following chapters:
- “Rise of the Carbohydrate-Rich and Very-Low-Carbohydrate Diets”
- “The Fear of Fat and High-Fat Diets”
- “Insulin and The End of Carbohydrate Restriction and Low Blood Sugar”
Yes, it is difficult. Imagine the bookend segments: “The Nature of Medical Knowledge” and “The Conflicts of Evidence-Based Medicine.” There is also a detailed discussion of good versus bad science spanning three long chapters.
If all that reads like a greatly confused mess to you then you’re beginning to understand. If you are a fan of an unbiased explication of the evolution of understanding the ins and outs of scientific history in richly documented detail, this is a book for you. It’s not a quick nor easy read. And don’t expect to discover whether the newest wonder drugs for weight loss and control of diabetes will be the long-term solution for people with obesity and diabetes worldwide.
Obesity and overweight are major risk factors for type 2 diabetes. About 90% of patients with diabetes have either overweight or obesity. Thus, the complications of these two conditions, which largely overlap, include atherosclerotic cardiovascular disease; myocardial infarction; stroke; hypertension; metabolic syndrome; lower-extremity gangrene; chronic kidney disease; retinopathy; glaucoma; cataracts; disabling osteoarthritis; breast, endometrial, colon, and other cancers; fatty liver; sleep apnea; and peripheral neuropathy. These diseases create a major lucrative business for a wide swathe of medical and surgical specialties, plus hospital, clinic, device, pharmaceutical, and food industries.
In summary, we’ve just been through 40 years of failure to recognize the sugar-elephant in the room and intervene with serious preventive efforts. Forty years of fleshing out both the populace and the American medical-industrial complex (AMIC). Talk about a sweet spot. The only successful long-term treatment of obesity (and with it, diabetes) is prevention. Don’t emphasize losing weight. Focus on preventing excessive weight gain, right now, for the population, beginning with yourselves. Otherwise, we continue openly to perpetuate a terrific deal for the AMIC, a travesty for everyone else. Time for some industrial grade penance and a course correction.
Meanwhile, here we are living out Big Pharma’s dream of a big populace, produced by the agriculture and food industries, enjoyed by capitalism after failures of education, medicine, and public health: a seemingly endless supply of people living with big complications who are ready for big (expensive, new) medications to fix the world’s big health problems.
Dr. Lundberg is editor in chief, Cancer Commons. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Morning vs. afternoon exercise debate: A false dichotomy
Should we be exercising in the morning or afternoon? Before a meal or after a meal?
Popular media outlets, researchers, and clinicians seem to love these debates. I hate them. For me, it’s a false dichotomy. A false dichotomy is when people argue two sides as if only one option exists. A winner must be crowned, and a loser exists. But
Some but not all research suggests that morning fasted exercise may be the best time of day and condition to work out for weight control and training adaptations. Morning exercise may be a bit better for logistical reasons if you like to get up early. Some of us are indeed early chronotypes who rise early, get as much done as we can, including all our fitness and work-related activities, and then head to bed early (for me that is about 10 PM). Getting an early morning workout seems to fit with our schedules as morning larks.
But if you are a late-day chronotype, early exercise may not be in sync with your low morning energy levels or your preference for leisure-time activities later in the day. And lots of people with diabetes prefer to eat and then exercise. Late chronotypes are less physically active in general, compared with early chronotypes, and those who train in the morning tend to have better training adherence and expend more energy overall throughout the day. According to Dr. Normand Boulé from the University of Alberta, Edmonton, who presented on the topic of exercise time of day at the recent scientific sessions of the American Diabetes Association in San Diego, morning exercise in the fasted state tends to be associated with higher rates of fat oxidation, better weight control, and better skeletal muscle adaptations over time, compared with exercise performed later in the day. Dr Boulé also proposed that fasted exercise might be superior for training adaptations and long-term glycemia if you have type 2 diabetes.
But the argument for morning-only exercise falls short when we look specifically at postmeal glycemia, according to Dr. Jenna Gillen from the University of Toronto, who faced off against Dr. Boulé at a debate at the meeting and also publishes on the topic. She pointed out that mild to moderate intensity exercising done soon after meals typically results in fewer glucose spikes after meals in people with diabetes, and her argument is supported by at least one recent meta-analysis where postmeal walking was best for improving glycemia in those with prediabetes and type 2 diabetes.
The notion that postmeal or afternoon exercise is best for people with type 2 diabetes is also supported by a recent reexamination of the original Look AHEAD Trial of over 2,400 adults with type 2 diabetes, wherein the role of lifestyle intervention on cardiovascular outcomes was the original goal. In this recent secondary analysis of the Look AHEAD Trial, those most active in the afternoon (between 1:43 p.m. and 5:00 p.m.) had the greatest improvements in their overall glucose control after 1 year of the intensive lifestyle intervention, compared with exercise at other times of day. Afternoon exercisers were also more likely to have complete “remission” of their diabetes, as defined by no longer needing any glucose-lowering agents to control their glucose levels. But this was not a study that was designed for determining whether exercise time of day matters for glycemia because the participants were not randomly assigned to a set time of day for their activity, and glycemic control was not the primary endpoint (cardiovascular events were).
But hold on a minute. I said this was a false-dichotomy argument. It is. Just because it may or may not be “better” for your glucose to exercise in the morning vs. afternoon, if you have diabetes, it doesn’t mean you have to choose one or the other. You could choose neither (okay, that’s bad), both, or you could alternate between the two. For me this argument is like saying; “There only one time of day to save money”; “to tell a joke”; “to eat a meal” (okay, that’s another useless debate); or “do my laundry” (my mother once told me it’s technically cheaper after 6 p.m.!).
I live with diabetes, and I take insulin. I like how morning exercise in the form of a run with my dog wakes me up, sets me up for the day with positive thoughts, helps generate lots of creative ideas, and perhaps more importantly for me, it tends not to result in hypoglycemia because my insulin on board is lowest then.
Exercise later in the day is tricky when taking insulin because it tends to result in a higher insulin “potency effect” with prandial insulins. However, I still like midday activity and late-day exercise. For example, taking an activity break after lunch blunts the rise in my glucose and breaks up my prolonged sitting time in the office. After-dinner exercise allows me to spend a little more time with my wife, dog, or friends outdoors as the hot summer day begins to cool off. On Monday nights, I play basketball because that’s the only time we can book the gymnasium and that may not end until 9:45 p.m. (15 minutes before I want to go to bed; if you remember, I am a lark). That can result in two frustrating things related to my diabetes: It can cause an immediate rise in my glucose because of a competitive stress response and then a drop in my glucose overnight when I’m sleeping. But I still do it. I know that the training I’m doing at any point of the day will benefit me in lots of little ways, and I think we all need to take as many opportunities to be physically active as we possibly can. My kids and I coin this our daily “fitness opportunities,” and it does not matter to me if its morning, noon, or night!
It’s time to make the headlines and arguments stop. There is no wrong time of day to exercise. At least not in my opinion.
Dr. Riddle is a full professor in the school of kinesiology and health science at York University and senior scientist at LMC Diabetes & Endocrinology, both in Toronto. He has disclosed financial relationships with Dexcom, Eli Lilly, Indigo Diabetes, Insulet, Novo Nordisk, Sanofi, Supersapiens, and Zucara Therapeutics.
A version of this article first appeared on Medscape.com.
Should we be exercising in the morning or afternoon? Before a meal or after a meal?
Popular media outlets, researchers, and clinicians seem to love these debates. I hate them. For me, it’s a false dichotomy. A false dichotomy is when people argue two sides as if only one option exists. A winner must be crowned, and a loser exists. But
Some but not all research suggests that morning fasted exercise may be the best time of day and condition to work out for weight control and training adaptations. Morning exercise may be a bit better for logistical reasons if you like to get up early. Some of us are indeed early chronotypes who rise early, get as much done as we can, including all our fitness and work-related activities, and then head to bed early (for me that is about 10 PM). Getting an early morning workout seems to fit with our schedules as morning larks.
But if you are a late-day chronotype, early exercise may not be in sync with your low morning energy levels or your preference for leisure-time activities later in the day. And lots of people with diabetes prefer to eat and then exercise. Late chronotypes are less physically active in general, compared with early chronotypes, and those who train in the morning tend to have better training adherence and expend more energy overall throughout the day. According to Dr. Normand Boulé from the University of Alberta, Edmonton, who presented on the topic of exercise time of day at the recent scientific sessions of the American Diabetes Association in San Diego, morning exercise in the fasted state tends to be associated with higher rates of fat oxidation, better weight control, and better skeletal muscle adaptations over time, compared with exercise performed later in the day. Dr Boulé also proposed that fasted exercise might be superior for training adaptations and long-term glycemia if you have type 2 diabetes.
But the argument for morning-only exercise falls short when we look specifically at postmeal glycemia, according to Dr. Jenna Gillen from the University of Toronto, who faced off against Dr. Boulé at a debate at the meeting and also publishes on the topic. She pointed out that mild to moderate intensity exercising done soon after meals typically results in fewer glucose spikes after meals in people with diabetes, and her argument is supported by at least one recent meta-analysis where postmeal walking was best for improving glycemia in those with prediabetes and type 2 diabetes.
The notion that postmeal or afternoon exercise is best for people with type 2 diabetes is also supported by a recent reexamination of the original Look AHEAD Trial of over 2,400 adults with type 2 diabetes, wherein the role of lifestyle intervention on cardiovascular outcomes was the original goal. In this recent secondary analysis of the Look AHEAD Trial, those most active in the afternoon (between 1:43 p.m. and 5:00 p.m.) had the greatest improvements in their overall glucose control after 1 year of the intensive lifestyle intervention, compared with exercise at other times of day. Afternoon exercisers were also more likely to have complete “remission” of their diabetes, as defined by no longer needing any glucose-lowering agents to control their glucose levels. But this was not a study that was designed for determining whether exercise time of day matters for glycemia because the participants were not randomly assigned to a set time of day for their activity, and glycemic control was not the primary endpoint (cardiovascular events were).
But hold on a minute. I said this was a false-dichotomy argument. It is. Just because it may or may not be “better” for your glucose to exercise in the morning vs. afternoon, if you have diabetes, it doesn’t mean you have to choose one or the other. You could choose neither (okay, that’s bad), both, or you could alternate between the two. For me this argument is like saying; “There only one time of day to save money”; “to tell a joke”; “to eat a meal” (okay, that’s another useless debate); or “do my laundry” (my mother once told me it’s technically cheaper after 6 p.m.!).
I live with diabetes, and I take insulin. I like how morning exercise in the form of a run with my dog wakes me up, sets me up for the day with positive thoughts, helps generate lots of creative ideas, and perhaps more importantly for me, it tends not to result in hypoglycemia because my insulin on board is lowest then.
Exercise later in the day is tricky when taking insulin because it tends to result in a higher insulin “potency effect” with prandial insulins. However, I still like midday activity and late-day exercise. For example, taking an activity break after lunch blunts the rise in my glucose and breaks up my prolonged sitting time in the office. After-dinner exercise allows me to spend a little more time with my wife, dog, or friends outdoors as the hot summer day begins to cool off. On Monday nights, I play basketball because that’s the only time we can book the gymnasium and that may not end until 9:45 p.m. (15 minutes before I want to go to bed; if you remember, I am a lark). That can result in two frustrating things related to my diabetes: It can cause an immediate rise in my glucose because of a competitive stress response and then a drop in my glucose overnight when I’m sleeping. But I still do it. I know that the training I’m doing at any point of the day will benefit me in lots of little ways, and I think we all need to take as many opportunities to be physically active as we possibly can. My kids and I coin this our daily “fitness opportunities,” and it does not matter to me if its morning, noon, or night!
It’s time to make the headlines and arguments stop. There is no wrong time of day to exercise. At least not in my opinion.
Dr. Riddle is a full professor in the school of kinesiology and health science at York University and senior scientist at LMC Diabetes & Endocrinology, both in Toronto. He has disclosed financial relationships with Dexcom, Eli Lilly, Indigo Diabetes, Insulet, Novo Nordisk, Sanofi, Supersapiens, and Zucara Therapeutics.
A version of this article first appeared on Medscape.com.
Should we be exercising in the morning or afternoon? Before a meal or after a meal?
Popular media outlets, researchers, and clinicians seem to love these debates. I hate them. For me, it’s a false dichotomy. A false dichotomy is when people argue two sides as if only one option exists. A winner must be crowned, and a loser exists. But
Some but not all research suggests that morning fasted exercise may be the best time of day and condition to work out for weight control and training adaptations. Morning exercise may be a bit better for logistical reasons if you like to get up early. Some of us are indeed early chronotypes who rise early, get as much done as we can, including all our fitness and work-related activities, and then head to bed early (for me that is about 10 PM). Getting an early morning workout seems to fit with our schedules as morning larks.
But if you are a late-day chronotype, early exercise may not be in sync with your low morning energy levels or your preference for leisure-time activities later in the day. And lots of people with diabetes prefer to eat and then exercise. Late chronotypes are less physically active in general, compared with early chronotypes, and those who train in the morning tend to have better training adherence and expend more energy overall throughout the day. According to Dr. Normand Boulé from the University of Alberta, Edmonton, who presented on the topic of exercise time of day at the recent scientific sessions of the American Diabetes Association in San Diego, morning exercise in the fasted state tends to be associated with higher rates of fat oxidation, better weight control, and better skeletal muscle adaptations over time, compared with exercise performed later in the day. Dr Boulé also proposed that fasted exercise might be superior for training adaptations and long-term glycemia if you have type 2 diabetes.
But the argument for morning-only exercise falls short when we look specifically at postmeal glycemia, according to Dr. Jenna Gillen from the University of Toronto, who faced off against Dr. Boulé at a debate at the meeting and also publishes on the topic. She pointed out that mild to moderate intensity exercising done soon after meals typically results in fewer glucose spikes after meals in people with diabetes, and her argument is supported by at least one recent meta-analysis where postmeal walking was best for improving glycemia in those with prediabetes and type 2 diabetes.
The notion that postmeal or afternoon exercise is best for people with type 2 diabetes is also supported by a recent reexamination of the original Look AHEAD Trial of over 2,400 adults with type 2 diabetes, wherein the role of lifestyle intervention on cardiovascular outcomes was the original goal. In this recent secondary analysis of the Look AHEAD Trial, those most active in the afternoon (between 1:43 p.m. and 5:00 p.m.) had the greatest improvements in their overall glucose control after 1 year of the intensive lifestyle intervention, compared with exercise at other times of day. Afternoon exercisers were also more likely to have complete “remission” of their diabetes, as defined by no longer needing any glucose-lowering agents to control their glucose levels. But this was not a study that was designed for determining whether exercise time of day matters for glycemia because the participants were not randomly assigned to a set time of day for their activity, and glycemic control was not the primary endpoint (cardiovascular events were).
But hold on a minute. I said this was a false-dichotomy argument. It is. Just because it may or may not be “better” for your glucose to exercise in the morning vs. afternoon, if you have diabetes, it doesn’t mean you have to choose one or the other. You could choose neither (okay, that’s bad), both, or you could alternate between the two. For me this argument is like saying; “There only one time of day to save money”; “to tell a joke”; “to eat a meal” (okay, that’s another useless debate); or “do my laundry” (my mother once told me it’s technically cheaper after 6 p.m.!).
I live with diabetes, and I take insulin. I like how morning exercise in the form of a run with my dog wakes me up, sets me up for the day with positive thoughts, helps generate lots of creative ideas, and perhaps more importantly for me, it tends not to result in hypoglycemia because my insulin on board is lowest then.
Exercise later in the day is tricky when taking insulin because it tends to result in a higher insulin “potency effect” with prandial insulins. However, I still like midday activity and late-day exercise. For example, taking an activity break after lunch blunts the rise in my glucose and breaks up my prolonged sitting time in the office. After-dinner exercise allows me to spend a little more time with my wife, dog, or friends outdoors as the hot summer day begins to cool off. On Monday nights, I play basketball because that’s the only time we can book the gymnasium and that may not end until 9:45 p.m. (15 minutes before I want to go to bed; if you remember, I am a lark). That can result in two frustrating things related to my diabetes: It can cause an immediate rise in my glucose because of a competitive stress response and then a drop in my glucose overnight when I’m sleeping. But I still do it. I know that the training I’m doing at any point of the day will benefit me in lots of little ways, and I think we all need to take as many opportunities to be physically active as we possibly can. My kids and I coin this our daily “fitness opportunities,” and it does not matter to me if its morning, noon, or night!
It’s time to make the headlines and arguments stop. There is no wrong time of day to exercise. At least not in my opinion.
Dr. Riddle is a full professor in the school of kinesiology and health science at York University and senior scientist at LMC Diabetes & Endocrinology, both in Toronto. He has disclosed financial relationships with Dexcom, Eli Lilly, Indigo Diabetes, Insulet, Novo Nordisk, Sanofi, Supersapiens, and Zucara Therapeutics.
A version of this article first appeared on Medscape.com.
First-line therapy in T2D: Has metformin been ‘dethroned’?
Initially approved by the U.S. Food and Drug Administration (FDA) in 1994, metformin has been the preferred first-line glucose-lowering agent for patients with type 2 diabetes (T2D) owing to its effectiveness, low hypoglycemia risk, weight neutrality, long clinical track record of safety, and affordability. However, the advent of newer glucose-lowering agents with evidence-based cardiovascular (CV) and renal benefits calls into question whether metformin should continue to be the initial pharmacotherapy for all patients with T2D.
Cardiovascular outcome trials transform standard of care
In 2008, the FDA issued guidance to industry to ensure that CV risk is more thoroughly addressed during development of T2D therapies. This guidance document required dedicated trials to establish CV safety of new glucose-lowering therapies. Findings from subsequent cardiovascular outcome trials (CVOTs) and subsequent large renal and heart failure (HF) outcome trials have since prompted frequent and substantial updates to major guidelines. On the basis of recent evidence from CVOT and renal trials, contemporary clinical practice guidelines have transitioned from a traditional glucocentric treatment approach to a holistic management approach that emphasizes organ protection through heart-kidney-metabolic risk reduction.
Per the 2008 FDA guidance, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagonlike peptide-1 (GLP-1) receptor agonists, and sodium-glucose cotransporter-2 (SGLT2) inhibitors were evaluated in large dedicated CVOTs. Findings from several CVOTs established GLP-1 receptor agonist and SGLT2 inhibitor CV safety, and unexpectedly demonstrated reduced rates of major adverse cardiovascular events (MACE) relative to placebo. The LEADER and EMPA-REG OUTCOME trials were the first CVOTs to report cardioprotective benefits of the GLP-1 receptor agonist liraglutide and the SGLT2 inhibitor empagliflozin, respectively. The LEADER trial reported a 13% significant relative risk reduction for its primary composite MACE outcome, and the EMPA-REG OUTCOME trial similarly reported a 14% relative risk reduction for MACE. After CVOTs on other GLP-1 receptor agonists and SGLT2 inhibitors reported CV benefit, clinical practice guidelines began to recommend use of these agents in at-risk patients to mitigate CV risk.
During the period when most CVOTs were designed and conducted, a majority of trial participants were receiving metformin at baseline. Inclusion of a small subset of metformin-naive participants in these trials allowed for several post hoc and meta-analyses investigating the impact of background metformin use on the overall CV benefits reported. Depending on the trial, baseline metformin use in large GLP-1 receptor agonist CVOTs ranged from 66% to 81%. For instance, 76% of participants in the LEADER trial were receiving metformin at baseline, but a post hoc analysis found no heterogeneity for the observed CV benefit based on background metformin use. Similarly, a subgroup analysis of pooled data from the SUSTAIN-6 and PIONEER 6 trials of injectable and oral formulations of semaglutide, respectively, reported similar CV outcomes for participants, regardless of concomitant metformin use. When looking at the GLP-1 receptor agonist class overall, a meta-analysis of seven CVOTs, which included participants with established atherosclerotic cardiovascular disease (ASCVD) and those with multiple ASCVD risk factors, concluded that GLP-1 receptor agonist therapy reduced the overall incidence of MACE in participants not receiving concomitant metformin at baseline.
Similar analyses have examined the impact of background metformin use on CV outcomes with SGLT2 inhibitors. An analysis of EMPA-REG OUTCOME found that empagliflozin improved CV outcomes and reduced mortality irrespective of background metformin, sulfonylurea, or insulin use. Of note, this analysis suggested a greater risk reduction for incident or worsening nephropathy in patients not on concomitant metformin (hazard ratio, 0.47; 95% confidence interval, 0.37-0.59; P = .01), when compared with those taking metformin at baseline (HR, 0.68; 95% CI, 0.58-0.79; P = .01). In addition, a meta-analysis of six large outcome trials found consistent benefits of SGLT2 inhibition on CV, kidney, and mortality outcomes regardless of background metformin treatment. Therefore, although CVOTs on GLP-1 receptor agonists and SGLT2 inhibitors were not designed to assess the impact of background metformin use on CV outcomes, available evidence supports the CV benefits of these agents independent of metformin use.
Individualizing care to attain cardiorenal-metabolic goals
Three dedicated SGLT2 inhibitor renal outcome trials have been published to date: CREDENCE, DAPA-CKD, and EMPA-KIDNEY. All three studies confirmed the positive secondary renal outcomes observed in SGLT2 inhibitor CVOTs: reduced progression of kidney disease, HF-associated hospital admissions, and CV-related death. The observed renal and CV benefits from the CREDENCE trial were consistent across different levels of kidney function. Similarly, a meta-analysis of five SGLT2 inhibitor trials of patients with HF demonstrated a decreased risk for CV-related death and admission for HF, irrespective of baseline heart function. The ongoing FLOW is the first dedicated kidney-outcome trial to evaluate the effectiveness of a GLP-1 receptor agonist (semaglutide) in slowing the progression and worsening of chronic kidney disease (CKD) in patients with T2D.
As previously noted, findings from the LEADER and EMPA-REG OUTCOME trials demonstrated the beneficial effects of GLP-1 receptor agonists and SGLT2 inhibitors not only on MACE but also on secondary HF and kidney disease outcomes. These findings have supported a series of dedicated HF and kidney outcome trials further informing the standard of care for patients with these key comorbidities. Indeed, the American Diabetes Association’s 2023 Standards of Care in Diabetes updated its recommendations and algorithm for the use of glucose-lowering medications in the management of T2D. The current ADA recommendations stress cardiorenal risk reduction while concurrently achieving and maintaining glycemic and weight management goals. On the basis of evolving outcome trial data, GLP-1 receptor agonists and SGLT2 inhibitors with evidence of benefit are recommended for patients with established or at high risk for ASCVD. Further, the Standards preferentially recommend SGLT2 inhibitors for patients with HF and/or CKD. Because evidence suggests no heterogeneity of benefit based on hemoglobin A1c for MACE outcomes with GLP-1 receptor agonists and no heterogeneity of benefit for HF or CKD benefits with SGLT2 inhibitors, these agents are recommended for cardiorenal risk reduction regardless of the need to lower glucose.
The 2023 update to the American Association of Clinical Endocrinology Consensus Statement: Type 2 Diabetes Management Algorithm similarly recommends the use of GLP-1 receptor agonists and SGLT2 inhibitors to improve cardiorenal outcomes. To further emphasize the importance of prescribing agents with proven organ-protective benefits, the AACE consensus statement provides a complications-centric algorithm to guide therapeutic decisions for risk reduction in patients with key comorbidities (for instance, ASCVD, HF, CKD) and a separate glucocentric algorithm to guide selection and intensification of glucose-lowering agents in patients without key comorbidities to meet individualized glycemic targets. Within the complications-centric algorithm, AACE recommends GLP-1 receptor agonists and SGLT2 inhibitors as first-line treatment for cardiorenal risk reduction regardless of background metformin use or A1c level.
In addition to the emphasis on the use of GLP-1 receptor agonists and SGLT2 inhibitors for organ protection, guidelines now recommend SGLT2 inhibitors as the standard-of-care therapy in patients with T2D and CKD with an estimated glomerular filtration rate ≥ 20 mL/min per 1.73 m2, and irrespective of ejection fraction or a diagnosis of diabetes in the setting of HF. Overall, a common thread within current guidelines is the importance of individualized therapy based on patient- and medication-specific factors.
Optimizing guideline-directed medical therapy
Results from the DISCOVER trial found that GLP-1 receptor agonist and SGLT2 inhibitor use was less likely in the key patient subgroups most likely to benefit from therapy, including patients with peripheral artery disease and CKD. Factors contributing to underutilization of newer cardiorenal protective glucose-lowering therapies range from cost and access barriers to clinician-level barriers (for example, lack of knowledge on CKD, lack of familiarity with CKD practice guidelines). Addressing these issues and helping patients work through financial and other access barriers is essential to optimize the utilization of these therapies and improve cardiorenal and metabolic outcomes.
So, has metformin been “dethroned” as a first-line therapy for T2D? As is often the case in medicine, the answer depends on the individual patient and clinical situation. Metformin remains an important first-line treatment in combination with lifestyle interventions to help patients with T2D without key cardiorenal comorbidities achieve individualized glycemic targets. However, based on evidence demonstrating cardiorenal protective benefits and improved glycemia and weight loss, GLP-1 agonists and SGLT2 inhibitors may be considered as first-line treatment for patients with T2D with or at high risk for ASCVD, HF, or CKD, regardless of the need for additional glucose-lowering agents and independent of background metformin. Ultimately, the choice of first-line therapy for patients with T2D should be informed by individualized treatment goals, preferences, and cost-related access. Continued efforts to increase patient access to GLP-1 receptor agonists and SGLT2 inhibitors as first-line treatment when indicated are essential to ensure optimal treatment and outcomes.
Dr. Neumiller is professor, department of pharmacotherapy, Washington State University, Spokane. He disclosed ties with Bayer, Boehringer Ingelheim, and Eli Lilly. Dr. Alicic is clinical professor, department of medicine, University of Washington; and associate director of research, Inland Northwest Washington, Providence St. Joseph Health, Spokane. She disclosed ties with Providence St. Joseph Health, Boehringer Ingelheim/Lilly, and Bayer.
A version of this article appeared on Medscape.com.
Initially approved by the U.S. Food and Drug Administration (FDA) in 1994, metformin has been the preferred first-line glucose-lowering agent for patients with type 2 diabetes (T2D) owing to its effectiveness, low hypoglycemia risk, weight neutrality, long clinical track record of safety, and affordability. However, the advent of newer glucose-lowering agents with evidence-based cardiovascular (CV) and renal benefits calls into question whether metformin should continue to be the initial pharmacotherapy for all patients with T2D.
Cardiovascular outcome trials transform standard of care
In 2008, the FDA issued guidance to industry to ensure that CV risk is more thoroughly addressed during development of T2D therapies. This guidance document required dedicated trials to establish CV safety of new glucose-lowering therapies. Findings from subsequent cardiovascular outcome trials (CVOTs) and subsequent large renal and heart failure (HF) outcome trials have since prompted frequent and substantial updates to major guidelines. On the basis of recent evidence from CVOT and renal trials, contemporary clinical practice guidelines have transitioned from a traditional glucocentric treatment approach to a holistic management approach that emphasizes organ protection through heart-kidney-metabolic risk reduction.
Per the 2008 FDA guidance, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagonlike peptide-1 (GLP-1) receptor agonists, and sodium-glucose cotransporter-2 (SGLT2) inhibitors were evaluated in large dedicated CVOTs. Findings from several CVOTs established GLP-1 receptor agonist and SGLT2 inhibitor CV safety, and unexpectedly demonstrated reduced rates of major adverse cardiovascular events (MACE) relative to placebo. The LEADER and EMPA-REG OUTCOME trials were the first CVOTs to report cardioprotective benefits of the GLP-1 receptor agonist liraglutide and the SGLT2 inhibitor empagliflozin, respectively. The LEADER trial reported a 13% significant relative risk reduction for its primary composite MACE outcome, and the EMPA-REG OUTCOME trial similarly reported a 14% relative risk reduction for MACE. After CVOTs on other GLP-1 receptor agonists and SGLT2 inhibitors reported CV benefit, clinical practice guidelines began to recommend use of these agents in at-risk patients to mitigate CV risk.
During the period when most CVOTs were designed and conducted, a majority of trial participants were receiving metformin at baseline. Inclusion of a small subset of metformin-naive participants in these trials allowed for several post hoc and meta-analyses investigating the impact of background metformin use on the overall CV benefits reported. Depending on the trial, baseline metformin use in large GLP-1 receptor agonist CVOTs ranged from 66% to 81%. For instance, 76% of participants in the LEADER trial were receiving metformin at baseline, but a post hoc analysis found no heterogeneity for the observed CV benefit based on background metformin use. Similarly, a subgroup analysis of pooled data from the SUSTAIN-6 and PIONEER 6 trials of injectable and oral formulations of semaglutide, respectively, reported similar CV outcomes for participants, regardless of concomitant metformin use. When looking at the GLP-1 receptor agonist class overall, a meta-analysis of seven CVOTs, which included participants with established atherosclerotic cardiovascular disease (ASCVD) and those with multiple ASCVD risk factors, concluded that GLP-1 receptor agonist therapy reduced the overall incidence of MACE in participants not receiving concomitant metformin at baseline.
Similar analyses have examined the impact of background metformin use on CV outcomes with SGLT2 inhibitors. An analysis of EMPA-REG OUTCOME found that empagliflozin improved CV outcomes and reduced mortality irrespective of background metformin, sulfonylurea, or insulin use. Of note, this analysis suggested a greater risk reduction for incident or worsening nephropathy in patients not on concomitant metformin (hazard ratio, 0.47; 95% confidence interval, 0.37-0.59; P = .01), when compared with those taking metformin at baseline (HR, 0.68; 95% CI, 0.58-0.79; P = .01). In addition, a meta-analysis of six large outcome trials found consistent benefits of SGLT2 inhibition on CV, kidney, and mortality outcomes regardless of background metformin treatment. Therefore, although CVOTs on GLP-1 receptor agonists and SGLT2 inhibitors were not designed to assess the impact of background metformin use on CV outcomes, available evidence supports the CV benefits of these agents independent of metformin use.
Individualizing care to attain cardiorenal-metabolic goals
Three dedicated SGLT2 inhibitor renal outcome trials have been published to date: CREDENCE, DAPA-CKD, and EMPA-KIDNEY. All three studies confirmed the positive secondary renal outcomes observed in SGLT2 inhibitor CVOTs: reduced progression of kidney disease, HF-associated hospital admissions, and CV-related death. The observed renal and CV benefits from the CREDENCE trial were consistent across different levels of kidney function. Similarly, a meta-analysis of five SGLT2 inhibitor trials of patients with HF demonstrated a decreased risk for CV-related death and admission for HF, irrespective of baseline heart function. The ongoing FLOW is the first dedicated kidney-outcome trial to evaluate the effectiveness of a GLP-1 receptor agonist (semaglutide) in slowing the progression and worsening of chronic kidney disease (CKD) in patients with T2D.
As previously noted, findings from the LEADER and EMPA-REG OUTCOME trials demonstrated the beneficial effects of GLP-1 receptor agonists and SGLT2 inhibitors not only on MACE but also on secondary HF and kidney disease outcomes. These findings have supported a series of dedicated HF and kidney outcome trials further informing the standard of care for patients with these key comorbidities. Indeed, the American Diabetes Association’s 2023 Standards of Care in Diabetes updated its recommendations and algorithm for the use of glucose-lowering medications in the management of T2D. The current ADA recommendations stress cardiorenal risk reduction while concurrently achieving and maintaining glycemic and weight management goals. On the basis of evolving outcome trial data, GLP-1 receptor agonists and SGLT2 inhibitors with evidence of benefit are recommended for patients with established or at high risk for ASCVD. Further, the Standards preferentially recommend SGLT2 inhibitors for patients with HF and/or CKD. Because evidence suggests no heterogeneity of benefit based on hemoglobin A1c for MACE outcomes with GLP-1 receptor agonists and no heterogeneity of benefit for HF or CKD benefits with SGLT2 inhibitors, these agents are recommended for cardiorenal risk reduction regardless of the need to lower glucose.
The 2023 update to the American Association of Clinical Endocrinology Consensus Statement: Type 2 Diabetes Management Algorithm similarly recommends the use of GLP-1 receptor agonists and SGLT2 inhibitors to improve cardiorenal outcomes. To further emphasize the importance of prescribing agents with proven organ-protective benefits, the AACE consensus statement provides a complications-centric algorithm to guide therapeutic decisions for risk reduction in patients with key comorbidities (for instance, ASCVD, HF, CKD) and a separate glucocentric algorithm to guide selection and intensification of glucose-lowering agents in patients without key comorbidities to meet individualized glycemic targets. Within the complications-centric algorithm, AACE recommends GLP-1 receptor agonists and SGLT2 inhibitors as first-line treatment for cardiorenal risk reduction regardless of background metformin use or A1c level.
In addition to the emphasis on the use of GLP-1 receptor agonists and SGLT2 inhibitors for organ protection, guidelines now recommend SGLT2 inhibitors as the standard-of-care therapy in patients with T2D and CKD with an estimated glomerular filtration rate ≥ 20 mL/min per 1.73 m2, and irrespective of ejection fraction or a diagnosis of diabetes in the setting of HF. Overall, a common thread within current guidelines is the importance of individualized therapy based on patient- and medication-specific factors.
Optimizing guideline-directed medical therapy
Results from the DISCOVER trial found that GLP-1 receptor agonist and SGLT2 inhibitor use was less likely in the key patient subgroups most likely to benefit from therapy, including patients with peripheral artery disease and CKD. Factors contributing to underutilization of newer cardiorenal protective glucose-lowering therapies range from cost and access barriers to clinician-level barriers (for example, lack of knowledge on CKD, lack of familiarity with CKD practice guidelines). Addressing these issues and helping patients work through financial and other access barriers is essential to optimize the utilization of these therapies and improve cardiorenal and metabolic outcomes.
So, has metformin been “dethroned” as a first-line therapy for T2D? As is often the case in medicine, the answer depends on the individual patient and clinical situation. Metformin remains an important first-line treatment in combination with lifestyle interventions to help patients with T2D without key cardiorenal comorbidities achieve individualized glycemic targets. However, based on evidence demonstrating cardiorenal protective benefits and improved glycemia and weight loss, GLP-1 agonists and SGLT2 inhibitors may be considered as first-line treatment for patients with T2D with or at high risk for ASCVD, HF, or CKD, regardless of the need for additional glucose-lowering agents and independent of background metformin. Ultimately, the choice of first-line therapy for patients with T2D should be informed by individualized treatment goals, preferences, and cost-related access. Continued efforts to increase patient access to GLP-1 receptor agonists and SGLT2 inhibitors as first-line treatment when indicated are essential to ensure optimal treatment and outcomes.
Dr. Neumiller is professor, department of pharmacotherapy, Washington State University, Spokane. He disclosed ties with Bayer, Boehringer Ingelheim, and Eli Lilly. Dr. Alicic is clinical professor, department of medicine, University of Washington; and associate director of research, Inland Northwest Washington, Providence St. Joseph Health, Spokane. She disclosed ties with Providence St. Joseph Health, Boehringer Ingelheim/Lilly, and Bayer.
A version of this article appeared on Medscape.com.
Initially approved by the U.S. Food and Drug Administration (FDA) in 1994, metformin has been the preferred first-line glucose-lowering agent for patients with type 2 diabetes (T2D) owing to its effectiveness, low hypoglycemia risk, weight neutrality, long clinical track record of safety, and affordability. However, the advent of newer glucose-lowering agents with evidence-based cardiovascular (CV) and renal benefits calls into question whether metformin should continue to be the initial pharmacotherapy for all patients with T2D.
Cardiovascular outcome trials transform standard of care
In 2008, the FDA issued guidance to industry to ensure that CV risk is more thoroughly addressed during development of T2D therapies. This guidance document required dedicated trials to establish CV safety of new glucose-lowering therapies. Findings from subsequent cardiovascular outcome trials (CVOTs) and subsequent large renal and heart failure (HF) outcome trials have since prompted frequent and substantial updates to major guidelines. On the basis of recent evidence from CVOT and renal trials, contemporary clinical practice guidelines have transitioned from a traditional glucocentric treatment approach to a holistic management approach that emphasizes organ protection through heart-kidney-metabolic risk reduction.
Per the 2008 FDA guidance, dipeptidyl peptidase-4 (DPP-4) inhibitors, glucagonlike peptide-1 (GLP-1) receptor agonists, and sodium-glucose cotransporter-2 (SGLT2) inhibitors were evaluated in large dedicated CVOTs. Findings from several CVOTs established GLP-1 receptor agonist and SGLT2 inhibitor CV safety, and unexpectedly demonstrated reduced rates of major adverse cardiovascular events (MACE) relative to placebo. The LEADER and EMPA-REG OUTCOME trials were the first CVOTs to report cardioprotective benefits of the GLP-1 receptor agonist liraglutide and the SGLT2 inhibitor empagliflozin, respectively. The LEADER trial reported a 13% significant relative risk reduction for its primary composite MACE outcome, and the EMPA-REG OUTCOME trial similarly reported a 14% relative risk reduction for MACE. After CVOTs on other GLP-1 receptor agonists and SGLT2 inhibitors reported CV benefit, clinical practice guidelines began to recommend use of these agents in at-risk patients to mitigate CV risk.
During the period when most CVOTs were designed and conducted, a majority of trial participants were receiving metformin at baseline. Inclusion of a small subset of metformin-naive participants in these trials allowed for several post hoc and meta-analyses investigating the impact of background metformin use on the overall CV benefits reported. Depending on the trial, baseline metformin use in large GLP-1 receptor agonist CVOTs ranged from 66% to 81%. For instance, 76% of participants in the LEADER trial were receiving metformin at baseline, but a post hoc analysis found no heterogeneity for the observed CV benefit based on background metformin use. Similarly, a subgroup analysis of pooled data from the SUSTAIN-6 and PIONEER 6 trials of injectable and oral formulations of semaglutide, respectively, reported similar CV outcomes for participants, regardless of concomitant metformin use. When looking at the GLP-1 receptor agonist class overall, a meta-analysis of seven CVOTs, which included participants with established atherosclerotic cardiovascular disease (ASCVD) and those with multiple ASCVD risk factors, concluded that GLP-1 receptor agonist therapy reduced the overall incidence of MACE in participants not receiving concomitant metformin at baseline.
Similar analyses have examined the impact of background metformin use on CV outcomes with SGLT2 inhibitors. An analysis of EMPA-REG OUTCOME found that empagliflozin improved CV outcomes and reduced mortality irrespective of background metformin, sulfonylurea, or insulin use. Of note, this analysis suggested a greater risk reduction for incident or worsening nephropathy in patients not on concomitant metformin (hazard ratio, 0.47; 95% confidence interval, 0.37-0.59; P = .01), when compared with those taking metformin at baseline (HR, 0.68; 95% CI, 0.58-0.79; P = .01). In addition, a meta-analysis of six large outcome trials found consistent benefits of SGLT2 inhibition on CV, kidney, and mortality outcomes regardless of background metformin treatment. Therefore, although CVOTs on GLP-1 receptor agonists and SGLT2 inhibitors were not designed to assess the impact of background metformin use on CV outcomes, available evidence supports the CV benefits of these agents independent of metformin use.
Individualizing care to attain cardiorenal-metabolic goals
Three dedicated SGLT2 inhibitor renal outcome trials have been published to date: CREDENCE, DAPA-CKD, and EMPA-KIDNEY. All three studies confirmed the positive secondary renal outcomes observed in SGLT2 inhibitor CVOTs: reduced progression of kidney disease, HF-associated hospital admissions, and CV-related death. The observed renal and CV benefits from the CREDENCE trial were consistent across different levels of kidney function. Similarly, a meta-analysis of five SGLT2 inhibitor trials of patients with HF demonstrated a decreased risk for CV-related death and admission for HF, irrespective of baseline heart function. The ongoing FLOW is the first dedicated kidney-outcome trial to evaluate the effectiveness of a GLP-1 receptor agonist (semaglutide) in slowing the progression and worsening of chronic kidney disease (CKD) in patients with T2D.
As previously noted, findings from the LEADER and EMPA-REG OUTCOME trials demonstrated the beneficial effects of GLP-1 receptor agonists and SGLT2 inhibitors not only on MACE but also on secondary HF and kidney disease outcomes. These findings have supported a series of dedicated HF and kidney outcome trials further informing the standard of care for patients with these key comorbidities. Indeed, the American Diabetes Association’s 2023 Standards of Care in Diabetes updated its recommendations and algorithm for the use of glucose-lowering medications in the management of T2D. The current ADA recommendations stress cardiorenal risk reduction while concurrently achieving and maintaining glycemic and weight management goals. On the basis of evolving outcome trial data, GLP-1 receptor agonists and SGLT2 inhibitors with evidence of benefit are recommended for patients with established or at high risk for ASCVD. Further, the Standards preferentially recommend SGLT2 inhibitors for patients with HF and/or CKD. Because evidence suggests no heterogeneity of benefit based on hemoglobin A1c for MACE outcomes with GLP-1 receptor agonists and no heterogeneity of benefit for HF or CKD benefits with SGLT2 inhibitors, these agents are recommended for cardiorenal risk reduction regardless of the need to lower glucose.
The 2023 update to the American Association of Clinical Endocrinology Consensus Statement: Type 2 Diabetes Management Algorithm similarly recommends the use of GLP-1 receptor agonists and SGLT2 inhibitors to improve cardiorenal outcomes. To further emphasize the importance of prescribing agents with proven organ-protective benefits, the AACE consensus statement provides a complications-centric algorithm to guide therapeutic decisions for risk reduction in patients with key comorbidities (for instance, ASCVD, HF, CKD) and a separate glucocentric algorithm to guide selection and intensification of glucose-lowering agents in patients without key comorbidities to meet individualized glycemic targets. Within the complications-centric algorithm, AACE recommends GLP-1 receptor agonists and SGLT2 inhibitors as first-line treatment for cardiorenal risk reduction regardless of background metformin use or A1c level.
In addition to the emphasis on the use of GLP-1 receptor agonists and SGLT2 inhibitors for organ protection, guidelines now recommend SGLT2 inhibitors as the standard-of-care therapy in patients with T2D and CKD with an estimated glomerular filtration rate ≥ 20 mL/min per 1.73 m2, and irrespective of ejection fraction or a diagnosis of diabetes in the setting of HF. Overall, a common thread within current guidelines is the importance of individualized therapy based on patient- and medication-specific factors.
Optimizing guideline-directed medical therapy
Results from the DISCOVER trial found that GLP-1 receptor agonist and SGLT2 inhibitor use was less likely in the key patient subgroups most likely to benefit from therapy, including patients with peripheral artery disease and CKD. Factors contributing to underutilization of newer cardiorenal protective glucose-lowering therapies range from cost and access barriers to clinician-level barriers (for example, lack of knowledge on CKD, lack of familiarity with CKD practice guidelines). Addressing these issues and helping patients work through financial and other access barriers is essential to optimize the utilization of these therapies and improve cardiorenal and metabolic outcomes.
So, has metformin been “dethroned” as a first-line therapy for T2D? As is often the case in medicine, the answer depends on the individual patient and clinical situation. Metformin remains an important first-line treatment in combination with lifestyle interventions to help patients with T2D without key cardiorenal comorbidities achieve individualized glycemic targets. However, based on evidence demonstrating cardiorenal protective benefits and improved glycemia and weight loss, GLP-1 agonists and SGLT2 inhibitors may be considered as first-line treatment for patients with T2D with or at high risk for ASCVD, HF, or CKD, regardless of the need for additional glucose-lowering agents and independent of background metformin. Ultimately, the choice of first-line therapy for patients with T2D should be informed by individualized treatment goals, preferences, and cost-related access. Continued efforts to increase patient access to GLP-1 receptor agonists and SGLT2 inhibitors as first-line treatment when indicated are essential to ensure optimal treatment and outcomes.
Dr. Neumiller is professor, department of pharmacotherapy, Washington State University, Spokane. He disclosed ties with Bayer, Boehringer Ingelheim, and Eli Lilly. Dr. Alicic is clinical professor, department of medicine, University of Washington; and associate director of research, Inland Northwest Washington, Providence St. Joseph Health, Spokane. She disclosed ties with Providence St. Joseph Health, Boehringer Ingelheim/Lilly, and Bayer.
A version of this article appeared on Medscape.com.
A step forward in diabetic foot disease management
As we navigate the ever-evolving landscape of diabetic foot disease management, The goal is to create a common language of risk that is easily related from clinician to clinician to patient.
Whatever language we use, though, the problem we face is vast:
- Diabetic foot ulcers affect approximately 18.6 million people worldwide and 1.6 million in the United States each year.
- They are associated with high rates of premature death, with a 5-year mortality rate of 30%. This rate is greater than 70% for those with above-foot amputations, worse than all but the most aggressive cancers.
- The direct costs of treating diabetic foot ulcers in the United States is estimated at $9 billion-$13 billion annually.
- Over 550 million people worldwide have diabetes, with 18.6 million developing foot ulcers annually. Up to 34% of those with diabetes will develop a foot ulcer.
- About 20% of those with a diabetic foot ulcer will undergo amputation, a major cause of which is infection, which affects 50% of foot ulcers.
- Up to 20% of those with a foot ulcer require hospitalization, with 15%-20% undergoing amputation. Inequities exist in diabetes-related foot complications:
- –Rates of major amputation are higher in non-Hispanic Black, Hispanic, and Native American populations, compared with non-Hispanic White populations.
- –Non-Hispanic Black and Hispanic populations present with more advanced ulcers and peripheral artery disease, and are more likely to undergo amputation without revascularization attempt.
The IWGDF, a multidisciplinary team of international experts, has recently updated its guidelines. This team, comprising endocrinologists, internal medicine physicians, physiatrists, podiatrists, and vascular surgeons from across the globe, has worked tirelessly to provide us with a comprehensive guide to managing diabetes-related foot ulcers.
The updated guidelines address five critical clinical questions, each with up to 13 important outcomes. The systematic review that underpins these guidelines identified 149 eligible studies, assessing 28 different systems. This exhaustive research has led to the development of seven key recommendations that address the clinical questions and consider the existence of different clinical settings.
One of the significant updates in the 2023 guidelines is the recommendation of SINBAD – site, ischemia, neuropathy, bacterial infection, area, and depth – as the priority wound classification system for people with diabetes and a foot ulcer. This system is particularly useful for interprofessional communication, describing each composite variable, and conducting clinical audits using the full score. However, the guidelines also recommend the use of other, more specific assessment systems for infection and peripheral artery disease from the Infectious Diseases Society of America/IWGDF when resources and an appropriate level of expertise exist.
The introduction of the Wound, Ischemia and Foot Infection (WIfI) classification system in the guidelines is also a noteworthy development. This system is crucial in assessing perfusion and the likely benefit of revascularization in a person with diabetes and a foot ulcer. By assessing the level of wound ischemia and infection, we can make informed decisions about the need for vascular intervention, which can significantly affect the patient’s outcome. This can be done simply by classifying each of the three categories of wound, ischemia, or foot infection as none, mild, moderate, or severe. By simplifying the very dynamic comorbidities of tissue loss, ischemia, and infection into a usable and predictive scale, it helps us to communicate risk across disciplines. This has been found to be highly predictive of healing, amputation, and mortality.
We use WIfI every day across our system. An example might include a patient we recently treated:
A 76-year-old woman presented with a wound to her left foot. Her past medical history revealed type 2 diabetes, peripheral neuropathy, and documented peripheral artery disease with prior bilateral femoral-popliteal bypass conducted at an external facility. In addition to gangrenous changes to her fourth toe, she displayed erythema and lymphangitic streaking up her dorsal foot. While she was afebrile, her white cell count was 13,000/mcL. Radiographic examinations did not show signs of osteomyelitis. Noninvasive vascular evaluations revealed an ankle brachial index of 0.4 and a toe pressure of 10 mm Hg. An aortogram with a lower-extremity runoff arteriogram confirmed the obstruction of her left femoral-popliteal bypass.
Taking these results into account, her WIfI score was determined as: wound 2 (moderate), ischemia 3 (severe), foot infection 2 (moderate, no sepsis), translating to a clinical stage 4. This denotes a high risk for major amputation.
Following a team discussion, she was taken to the operating room for an initial debridement of her infection which consisted of a partial fourth ray resection to the level of the mid-metatarsal. Following control of the infection, she received a vascular assessment which ultimately constituted a femoral to distal anterior tibial bypass. Following both of these, she was discharged on a negative-pressure wound therapy device, receiving a split-thickness skin graft 4 weeks later.
The guidelines also emphasize the need for specific training, skills, and experience to ensure the accuracy of the recommended systems for characterizing foot ulcers. The person applying these systems should be appropriately trained and, according to their national or regional standards, should have the knowledge, expertise, and skills necessary to manage people with a diabetes-related foot ulcer.
As we continue to navigate the complexities of diabetes-related foot disease, these guidelines serve as a valuable compass, guiding our decisions and actions. They remind us of the importance of continuous learning, collaboration, and the application of evidence-based practice in our work.
I encourage you to delve into these guidelines. Let’s use them to improve our practice, enhance our communication, and, ultimately, provide better care for our patients.
Dr. Armstrong is professor of surgery, director of limb preservation, University of Southern California, Los Angeles. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
As we navigate the ever-evolving landscape of diabetic foot disease management, The goal is to create a common language of risk that is easily related from clinician to clinician to patient.
Whatever language we use, though, the problem we face is vast:
- Diabetic foot ulcers affect approximately 18.6 million people worldwide and 1.6 million in the United States each year.
- They are associated with high rates of premature death, with a 5-year mortality rate of 30%. This rate is greater than 70% for those with above-foot amputations, worse than all but the most aggressive cancers.
- The direct costs of treating diabetic foot ulcers in the United States is estimated at $9 billion-$13 billion annually.
- Over 550 million people worldwide have diabetes, with 18.6 million developing foot ulcers annually. Up to 34% of those with diabetes will develop a foot ulcer.
- About 20% of those with a diabetic foot ulcer will undergo amputation, a major cause of which is infection, which affects 50% of foot ulcers.
- Up to 20% of those with a foot ulcer require hospitalization, with 15%-20% undergoing amputation. Inequities exist in diabetes-related foot complications:
- –Rates of major amputation are higher in non-Hispanic Black, Hispanic, and Native American populations, compared with non-Hispanic White populations.
- –Non-Hispanic Black and Hispanic populations present with more advanced ulcers and peripheral artery disease, and are more likely to undergo amputation without revascularization attempt.
The IWGDF, a multidisciplinary team of international experts, has recently updated its guidelines. This team, comprising endocrinologists, internal medicine physicians, physiatrists, podiatrists, and vascular surgeons from across the globe, has worked tirelessly to provide us with a comprehensive guide to managing diabetes-related foot ulcers.
The updated guidelines address five critical clinical questions, each with up to 13 important outcomes. The systematic review that underpins these guidelines identified 149 eligible studies, assessing 28 different systems. This exhaustive research has led to the development of seven key recommendations that address the clinical questions and consider the existence of different clinical settings.
One of the significant updates in the 2023 guidelines is the recommendation of SINBAD – site, ischemia, neuropathy, bacterial infection, area, and depth – as the priority wound classification system for people with diabetes and a foot ulcer. This system is particularly useful for interprofessional communication, describing each composite variable, and conducting clinical audits using the full score. However, the guidelines also recommend the use of other, more specific assessment systems for infection and peripheral artery disease from the Infectious Diseases Society of America/IWGDF when resources and an appropriate level of expertise exist.
The introduction of the Wound, Ischemia and Foot Infection (WIfI) classification system in the guidelines is also a noteworthy development. This system is crucial in assessing perfusion and the likely benefit of revascularization in a person with diabetes and a foot ulcer. By assessing the level of wound ischemia and infection, we can make informed decisions about the need for vascular intervention, which can significantly affect the patient’s outcome. This can be done simply by classifying each of the three categories of wound, ischemia, or foot infection as none, mild, moderate, or severe. By simplifying the very dynamic comorbidities of tissue loss, ischemia, and infection into a usable and predictive scale, it helps us to communicate risk across disciplines. This has been found to be highly predictive of healing, amputation, and mortality.
We use WIfI every day across our system. An example might include a patient we recently treated:
A 76-year-old woman presented with a wound to her left foot. Her past medical history revealed type 2 diabetes, peripheral neuropathy, and documented peripheral artery disease with prior bilateral femoral-popliteal bypass conducted at an external facility. In addition to gangrenous changes to her fourth toe, she displayed erythema and lymphangitic streaking up her dorsal foot. While she was afebrile, her white cell count was 13,000/mcL. Radiographic examinations did not show signs of osteomyelitis. Noninvasive vascular evaluations revealed an ankle brachial index of 0.4 and a toe pressure of 10 mm Hg. An aortogram with a lower-extremity runoff arteriogram confirmed the obstruction of her left femoral-popliteal bypass.
Taking these results into account, her WIfI score was determined as: wound 2 (moderate), ischemia 3 (severe), foot infection 2 (moderate, no sepsis), translating to a clinical stage 4. This denotes a high risk for major amputation.
Following a team discussion, she was taken to the operating room for an initial debridement of her infection which consisted of a partial fourth ray resection to the level of the mid-metatarsal. Following control of the infection, she received a vascular assessment which ultimately constituted a femoral to distal anterior tibial bypass. Following both of these, she was discharged on a negative-pressure wound therapy device, receiving a split-thickness skin graft 4 weeks later.
The guidelines also emphasize the need for specific training, skills, and experience to ensure the accuracy of the recommended systems for characterizing foot ulcers. The person applying these systems should be appropriately trained and, according to their national or regional standards, should have the knowledge, expertise, and skills necessary to manage people with a diabetes-related foot ulcer.
As we continue to navigate the complexities of diabetes-related foot disease, these guidelines serve as a valuable compass, guiding our decisions and actions. They remind us of the importance of continuous learning, collaboration, and the application of evidence-based practice in our work.
I encourage you to delve into these guidelines. Let’s use them to improve our practice, enhance our communication, and, ultimately, provide better care for our patients.
Dr. Armstrong is professor of surgery, director of limb preservation, University of Southern California, Los Angeles. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
As we navigate the ever-evolving landscape of diabetic foot disease management, The goal is to create a common language of risk that is easily related from clinician to clinician to patient.
Whatever language we use, though, the problem we face is vast:
- Diabetic foot ulcers affect approximately 18.6 million people worldwide and 1.6 million in the United States each year.
- They are associated with high rates of premature death, with a 5-year mortality rate of 30%. This rate is greater than 70% for those with above-foot amputations, worse than all but the most aggressive cancers.
- The direct costs of treating diabetic foot ulcers in the United States is estimated at $9 billion-$13 billion annually.
- Over 550 million people worldwide have diabetes, with 18.6 million developing foot ulcers annually. Up to 34% of those with diabetes will develop a foot ulcer.
- About 20% of those with a diabetic foot ulcer will undergo amputation, a major cause of which is infection, which affects 50% of foot ulcers.
- Up to 20% of those with a foot ulcer require hospitalization, with 15%-20% undergoing amputation. Inequities exist in diabetes-related foot complications:
- –Rates of major amputation are higher in non-Hispanic Black, Hispanic, and Native American populations, compared with non-Hispanic White populations.
- –Non-Hispanic Black and Hispanic populations present with more advanced ulcers and peripheral artery disease, and are more likely to undergo amputation without revascularization attempt.
The IWGDF, a multidisciplinary team of international experts, has recently updated its guidelines. This team, comprising endocrinologists, internal medicine physicians, physiatrists, podiatrists, and vascular surgeons from across the globe, has worked tirelessly to provide us with a comprehensive guide to managing diabetes-related foot ulcers.
The updated guidelines address five critical clinical questions, each with up to 13 important outcomes. The systematic review that underpins these guidelines identified 149 eligible studies, assessing 28 different systems. This exhaustive research has led to the development of seven key recommendations that address the clinical questions and consider the existence of different clinical settings.
One of the significant updates in the 2023 guidelines is the recommendation of SINBAD – site, ischemia, neuropathy, bacterial infection, area, and depth – as the priority wound classification system for people with diabetes and a foot ulcer. This system is particularly useful for interprofessional communication, describing each composite variable, and conducting clinical audits using the full score. However, the guidelines also recommend the use of other, more specific assessment systems for infection and peripheral artery disease from the Infectious Diseases Society of America/IWGDF when resources and an appropriate level of expertise exist.
The introduction of the Wound, Ischemia and Foot Infection (WIfI) classification system in the guidelines is also a noteworthy development. This system is crucial in assessing perfusion and the likely benefit of revascularization in a person with diabetes and a foot ulcer. By assessing the level of wound ischemia and infection, we can make informed decisions about the need for vascular intervention, which can significantly affect the patient’s outcome. This can be done simply by classifying each of the three categories of wound, ischemia, or foot infection as none, mild, moderate, or severe. By simplifying the very dynamic comorbidities of tissue loss, ischemia, and infection into a usable and predictive scale, it helps us to communicate risk across disciplines. This has been found to be highly predictive of healing, amputation, and mortality.
We use WIfI every day across our system. An example might include a patient we recently treated:
A 76-year-old woman presented with a wound to her left foot. Her past medical history revealed type 2 diabetes, peripheral neuropathy, and documented peripheral artery disease with prior bilateral femoral-popliteal bypass conducted at an external facility. In addition to gangrenous changes to her fourth toe, she displayed erythema and lymphangitic streaking up her dorsal foot. While she was afebrile, her white cell count was 13,000/mcL. Radiographic examinations did not show signs of osteomyelitis. Noninvasive vascular evaluations revealed an ankle brachial index of 0.4 and a toe pressure of 10 mm Hg. An aortogram with a lower-extremity runoff arteriogram confirmed the obstruction of her left femoral-popliteal bypass.
Taking these results into account, her WIfI score was determined as: wound 2 (moderate), ischemia 3 (severe), foot infection 2 (moderate, no sepsis), translating to a clinical stage 4. This denotes a high risk for major amputation.
Following a team discussion, she was taken to the operating room for an initial debridement of her infection which consisted of a partial fourth ray resection to the level of the mid-metatarsal. Following control of the infection, she received a vascular assessment which ultimately constituted a femoral to distal anterior tibial bypass. Following both of these, she was discharged on a negative-pressure wound therapy device, receiving a split-thickness skin graft 4 weeks later.
The guidelines also emphasize the need for specific training, skills, and experience to ensure the accuracy of the recommended systems for characterizing foot ulcers. The person applying these systems should be appropriately trained and, according to their national or regional standards, should have the knowledge, expertise, and skills necessary to manage people with a diabetes-related foot ulcer.
As we continue to navigate the complexities of diabetes-related foot disease, these guidelines serve as a valuable compass, guiding our decisions and actions. They remind us of the importance of continuous learning, collaboration, and the application of evidence-based practice in our work.
I encourage you to delve into these guidelines. Let’s use them to improve our practice, enhance our communication, and, ultimately, provide better care for our patients.
Dr. Armstrong is professor of surgery, director of limb preservation, University of Southern California, Los Angeles. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
A Review of Evidence and Safety for First-Line JAKi Use in PsA

Janus kinase inhibitors (JAKi) are a novel class of oral, targeted small-molecule inhibitors that are increasingly used to treat several different autoimmune conditions. In terms of rheumatologic indications, the FDA first approved tofacitinib (TOF) for use in moderate to severe rheumatoid arthritis (RA) unresponsive to methotrexate therapy. Eleven years later, the indications for JAKi use have expanded to include ulcerative colitis, ankylosing spondylitis, and psoriatic arthritis (PsA), among other diseases. As with any new therapeutic mechanism, there are questions as to how JAKi should be incorporated into the treatment paradigm of PsA. In this article, we briefly review the efficacy and safety data of these agents and discuss our approach to their use in PsA.
Two JAKi are currently FDA approved for the treatment of PsA: tofacitinib (TOF) and upadacitinib (UPA). Other JAKi, such as filgotinib and peficitinib, are only approved outside the United States and will not be discussed here.
TOF was originally studied in skin psoriasis (PsO) before 2 pivotal studies demonstrated efficacy in PsA. TOF or adalimumab (ADA) were compared with placebo in patients who had failed conventional synthetic disease-modifying antirheumatic drugs (DMARD).1 ACR20 response was superior with TOF 5 mg twice daily (BID) (50%) and 10 mg BID (61%) vs placebo (33%), and it was comparable to ADA (52%), which was used in this study as an active comparator. The overall rate of adverse events was similar with both doses of TOF when compared with ADA; however, patients taking TOF had numerically more cases of cancer, serious infection, and herpes zoster.
Another study evaluated TOF compared with placebo in patients with PsA who had an inadequate response to tumor necrosis factor inhibitor (TNFi) therapy.2 The study showed an ACR20 response of 50% in patients taking TOF 5 mg BID and 47% in patients taking 10 mg BID, compared with 24% in those taking placebo. Patients who received the 10 mg TOF dose continuously had higher rates of adverse events compared to TOF 5 mg, placebo, and patients who crossed over from placebo to TOF at either dose. In the TOF groups, there were cases of serious infection and herpes zoster, as well as 2 patients with major adverse cardiovascular events (MACE). Following review of these data, the FDA approved only the 5 mg BID dose, and later an 11-mg daily extended-release formulation that was pharmacokinetically similar.
The efficacy for UPA in PsA was shown in 2 pivotal phase 3 trials. SELECT-PsA1 compared UPA at 2 doses, 15 mg and 30 mg daily, vs placebo and vs ADA in patients with biologic DMARD (bDMARD)-naïve PsA.3 This trial demonstrated superiority of UPA in the ACR20 response at both doses (71% and 79%, respectively) compared with placebo (36%). The 15-mg dose of UPA was comparable to ADA (65%), while the 30-mg dose achieved superiority compared to ADA. Secondary outcomes including skin activity, patient-reported symptoms, and inhibition of radiographic progression were also superior in UPA compared with placebo and similar or greater with UPA compared with ADA, depending on the specific outcome.4 SELECT-PsA2 compared UPA 15 mg, 30 mg, and placebo in patients with prior incomplete response or intolerance to a bDMARD.5 At week 12 of the study, patients taking UPA 15 mg and 30 mg had an ACR20 response of 57% and 64%, respectively, compared with placebo (24%). At week 24, minimal disease activity was achieved by 25% of patients taking UPA 15 mg and 29% of patients taking UPA 30 mg, which was superior to placebo (3%).
Both studies found a significant increase in infections, including serious infections, at the 30-mg UPA dose compared with the placebo and adalimumab groups. Cytopenia and elevated creatine kinase (CK) level also occurred more frequently in the UPA 30-mg group. Rates of cancer were low overall and comparable between the patients treated with UPA and ADA. Given the higher incidence of adverse events with the 30-mg dose and the relatively similar efficacy, the sponsor elected to submit only the lower dose to the FDA for approval.
In the last few years, concerns for safety with JAKi use grew after the publication of data from the ORAL SURVEILLANCE trial, an FDA-mandated, post-approval safety study of TOF in RA. In this trial, patients with active RA over 50 years of age and with at least 1 additional cardiovascular risk factor were randomized to TOF at 1 of 2 doses, 5 mg or 10 mg BID, or a TNFi.6 This trial was designed as a noninferiority study, and TOF did not meet the noninferiority threshold compared to TNFi, with hazard ratios of 1.33 and 1.48 for MACE and malignancy, respectively. The results of this trial prompted the FDA to add a black box warning to the label for all JAKi, pointing out the risk of malignancy and MACE, as well as infection, mortality, and thrombosis.
In the ORAL SURVEILLANCE trial, the increased risk of MACE and malignancy was primarily seen in the study patients with high risk for a cardiovascular event. To address the question of whether a similar risk profile exists when using JAKi to treat PsA, or whether this is a disease-specific process related to RA, a post hoc analysis of 3 PsA trials and 7 PsO trials of patients treated with TOF was conducted.7 The analysis found that patients with a history of atherosclerotic cardiovascular disease (ASCVD) or metabolic syndrome, or patients at high risk for ASCVD (score > 20%) had increased incidence rates of MACE compared with those with low risk scores for ASCVD. Interestingly, as in RA, increased incidence rates of malignancy were seen in patients with preexisting or at high risk for ASCVD.
While the FDA recommends JAKi use in patients who have failed or are inappropriate for treatment with a TNFi, we would consider the use of JAKi for first-line therapy in PsA on an individual basis. One advantage of JAKi is their efficacy across multiple PsA domains, including peripheral arthritis, axial disease, enthesitis, dactylitis, and skin disease (although the approved dose of TOF was not statistically effective for PsO in the pivotal trials). Based on this efficacy, we believe that patients with overlapping, multifaceted disease may benefit the most from these medications. Patient risk factors and comorbidities are a prominent consideration in our use of JAKi to ensure safety, as the risk for MACE and malignancy is informed partly by baseline cardiovascular status. In younger patients without cardiovascular risk factors, JAKi may be a strong candidate for first-line therapy, particularly in patients averse to subcutaneous or intravenous therapy. We do counsel all patients on the increased risk of infection, and we do recommend inactivated herpes zoster vaccination in previously unvaccinated patients planning to start JAKi therapy.
On the horizon are the development of novel, oral agents targeting tyrosine kinase 2 (TYK2), which is a member of the JAK family of signaling proteins. In fact, the TYK2 inhibitor deucravacitinib was approved by the FDA in 2022 for the treatment of PsO. TYK2 inhibitors appear to have the advantage of a more selective mechanism of action, with fewer off-target effects. There were fewer adverse events in the deucravacitinib trials, which led to its prompt PsO authorization, and the FDA approval for the drug did not include the same black box warning that appears in the label for other JAKi.8 A phase 2 study showed early promise for the efficacy and safety of deucravacitinib in PsA.9 Further investigation will be needed to better understand the role of deucravacitinib and other TYK2 inhibitors being developed for the treatment of PsA. In the meantime, JAKi continue to be a prominent consideration for first-line PsA therapy in a carefully selected patient population.
Mease P, Hall S, FitzGerald O, et al. Tofacitinib or adalimumab versus placebo for psoriatic arthritis. N Engl J Med. 2017;377(16):1537-1550.
Gladman D, Rigby W, Azevedo VF, et al. Tofacitinib for psoriatic arthritis in patients with an inadequate response to TNF inhibitors. N Engl J Med. 2017;377(16):1525-1536.
McInnes IB, Anderson JK, Magrey M, et al. Trial of upadacitinib and adalimumab for psoriatic arthritis. N Engl J Med. 2021;384(13):1227-1239.
McInnes IB, Kato K, Magrey M, et al. Efficacy and safety of upadacitinib in patients with psoriatic arthritis: 2-year results from the phase 3 SELECT-PsA 1 study. Rheumatol Ther. 2023;10(1):275-292.
Mease PJ, Lertratanakul A, Anderson JK, et al. Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2. Ann Rheum Dis. 2021;80(3):312-320.
Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316-326.
Kristensen LE, Strober B, Poddubnyy D, et al. Association between baseline cardiovascular risk and incidence rates of major adverse cardiovascular events and malignancies in patients with psoriatic arthritis and psoriasis receiving tofacitinib. Ther Adv Musculoskelet Dis. 2023;15:1759720X221149965.
Dolgin E. TYK2-blocking agent showcases power of atypical kinase. Nat Biotechnol. 2022;40(12):1701-1704.
Mease PJ, Deodhar AA, van der Heijde D, et al. Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a phase II trial in psoriatic arthritis. Ann Rheum Dis. 2022;81(6):815-822.
Janus kinase inhibitors (JAKi) are a novel class of oral, targeted small-molecule inhibitors that are increasingly used to treat several different autoimmune conditions. In terms of rheumatologic indications, the FDA first approved tofacitinib (TOF) for use in moderate to severe rheumatoid arthritis (RA) unresponsive to methotrexate therapy. Eleven years later, the indications for JAKi use have expanded to include ulcerative colitis, ankylosing spondylitis, and psoriatic arthritis (PsA), among other diseases. As with any new therapeutic mechanism, there are questions as to how JAKi should be incorporated into the treatment paradigm of PsA. In this article, we briefly review the efficacy and safety data of these agents and discuss our approach to their use in PsA.
Two JAKi are currently FDA approved for the treatment of PsA: tofacitinib (TOF) and upadacitinib (UPA). Other JAKi, such as filgotinib and peficitinib, are only approved outside the United States and will not be discussed here.
TOF was originally studied in skin psoriasis (PsO) before 2 pivotal studies demonstrated efficacy in PsA. TOF or adalimumab (ADA) were compared with placebo in patients who had failed conventional synthetic disease-modifying antirheumatic drugs (DMARD).1 ACR20 response was superior with TOF 5 mg twice daily (BID) (50%) and 10 mg BID (61%) vs placebo (33%), and it was comparable to ADA (52%), which was used in this study as an active comparator. The overall rate of adverse events was similar with both doses of TOF when compared with ADA; however, patients taking TOF had numerically more cases of cancer, serious infection, and herpes zoster.
Another study evaluated TOF compared with placebo in patients with PsA who had an inadequate response to tumor necrosis factor inhibitor (TNFi) therapy.2 The study showed an ACR20 response of 50% in patients taking TOF 5 mg BID and 47% in patients taking 10 mg BID, compared with 24% in those taking placebo. Patients who received the 10 mg TOF dose continuously had higher rates of adverse events compared to TOF 5 mg, placebo, and patients who crossed over from placebo to TOF at either dose. In the TOF groups, there were cases of serious infection and herpes zoster, as well as 2 patients with major adverse cardiovascular events (MACE). Following review of these data, the FDA approved only the 5 mg BID dose, and later an 11-mg daily extended-release formulation that was pharmacokinetically similar.
The efficacy for UPA in PsA was shown in 2 pivotal phase 3 trials. SELECT-PsA1 compared UPA at 2 doses, 15 mg and 30 mg daily, vs placebo and vs ADA in patients with biologic DMARD (bDMARD)-naïve PsA.3 This trial demonstrated superiority of UPA in the ACR20 response at both doses (71% and 79%, respectively) compared with placebo (36%). The 15-mg dose of UPA was comparable to ADA (65%), while the 30-mg dose achieved superiority compared to ADA. Secondary outcomes including skin activity, patient-reported symptoms, and inhibition of radiographic progression were also superior in UPA compared with placebo and similar or greater with UPA compared with ADA, depending on the specific outcome.4 SELECT-PsA2 compared UPA 15 mg, 30 mg, and placebo in patients with prior incomplete response or intolerance to a bDMARD.5 At week 12 of the study, patients taking UPA 15 mg and 30 mg had an ACR20 response of 57% and 64%, respectively, compared with placebo (24%). At week 24, minimal disease activity was achieved by 25% of patients taking UPA 15 mg and 29% of patients taking UPA 30 mg, which was superior to placebo (3%).
Both studies found a significant increase in infections, including serious infections, at the 30-mg UPA dose compared with the placebo and adalimumab groups. Cytopenia and elevated creatine kinase (CK) level also occurred more frequently in the UPA 30-mg group. Rates of cancer were low overall and comparable between the patients treated with UPA and ADA. Given the higher incidence of adverse events with the 30-mg dose and the relatively similar efficacy, the sponsor elected to submit only the lower dose to the FDA for approval.
In the last few years, concerns for safety with JAKi use grew after the publication of data from the ORAL SURVEILLANCE trial, an FDA-mandated, post-approval safety study of TOF in RA. In this trial, patients with active RA over 50 years of age and with at least 1 additional cardiovascular risk factor were randomized to TOF at 1 of 2 doses, 5 mg or 10 mg BID, or a TNFi.6 This trial was designed as a noninferiority study, and TOF did not meet the noninferiority threshold compared to TNFi, with hazard ratios of 1.33 and 1.48 for MACE and malignancy, respectively. The results of this trial prompted the FDA to add a black box warning to the label for all JAKi, pointing out the risk of malignancy and MACE, as well as infection, mortality, and thrombosis.
In the ORAL SURVEILLANCE trial, the increased risk of MACE and malignancy was primarily seen in the study patients with high risk for a cardiovascular event. To address the question of whether a similar risk profile exists when using JAKi to treat PsA, or whether this is a disease-specific process related to RA, a post hoc analysis of 3 PsA trials and 7 PsO trials of patients treated with TOF was conducted.7 The analysis found that patients with a history of atherosclerotic cardiovascular disease (ASCVD) or metabolic syndrome, or patients at high risk for ASCVD (score > 20%) had increased incidence rates of MACE compared with those with low risk scores for ASCVD. Interestingly, as in RA, increased incidence rates of malignancy were seen in patients with preexisting or at high risk for ASCVD.
While the FDA recommends JAKi use in patients who have failed or are inappropriate for treatment with a TNFi, we would consider the use of JAKi for first-line therapy in PsA on an individual basis. One advantage of JAKi is their efficacy across multiple PsA domains, including peripheral arthritis, axial disease, enthesitis, dactylitis, and skin disease (although the approved dose of TOF was not statistically effective for PsO in the pivotal trials). Based on this efficacy, we believe that patients with overlapping, multifaceted disease may benefit the most from these medications. Patient risk factors and comorbidities are a prominent consideration in our use of JAKi to ensure safety, as the risk for MACE and malignancy is informed partly by baseline cardiovascular status. In younger patients without cardiovascular risk factors, JAKi may be a strong candidate for first-line therapy, particularly in patients averse to subcutaneous or intravenous therapy. We do counsel all patients on the increased risk of infection, and we do recommend inactivated herpes zoster vaccination in previously unvaccinated patients planning to start JAKi therapy.
On the horizon are the development of novel, oral agents targeting tyrosine kinase 2 (TYK2), which is a member of the JAK family of signaling proteins. In fact, the TYK2 inhibitor deucravacitinib was approved by the FDA in 2022 for the treatment of PsO. TYK2 inhibitors appear to have the advantage of a more selective mechanism of action, with fewer off-target effects. There were fewer adverse events in the deucravacitinib trials, which led to its prompt PsO authorization, and the FDA approval for the drug did not include the same black box warning that appears in the label for other JAKi.8 A phase 2 study showed early promise for the efficacy and safety of deucravacitinib in PsA.9 Further investigation will be needed to better understand the role of deucravacitinib and other TYK2 inhibitors being developed for the treatment of PsA. In the meantime, JAKi continue to be a prominent consideration for first-line PsA therapy in a carefully selected patient population.
Janus kinase inhibitors (JAKi) are a novel class of oral, targeted small-molecule inhibitors that are increasingly used to treat several different autoimmune conditions. In terms of rheumatologic indications, the FDA first approved tofacitinib (TOF) for use in moderate to severe rheumatoid arthritis (RA) unresponsive to methotrexate therapy. Eleven years later, the indications for JAKi use have expanded to include ulcerative colitis, ankylosing spondylitis, and psoriatic arthritis (PsA), among other diseases. As with any new therapeutic mechanism, there are questions as to how JAKi should be incorporated into the treatment paradigm of PsA. In this article, we briefly review the efficacy and safety data of these agents and discuss our approach to their use in PsA.
Two JAKi are currently FDA approved for the treatment of PsA: tofacitinib (TOF) and upadacitinib (UPA). Other JAKi, such as filgotinib and peficitinib, are only approved outside the United States and will not be discussed here.
TOF was originally studied in skin psoriasis (PsO) before 2 pivotal studies demonstrated efficacy in PsA. TOF or adalimumab (ADA) were compared with placebo in patients who had failed conventional synthetic disease-modifying antirheumatic drugs (DMARD).1 ACR20 response was superior with TOF 5 mg twice daily (BID) (50%) and 10 mg BID (61%) vs placebo (33%), and it was comparable to ADA (52%), which was used in this study as an active comparator. The overall rate of adverse events was similar with both doses of TOF when compared with ADA; however, patients taking TOF had numerically more cases of cancer, serious infection, and herpes zoster.
Another study evaluated TOF compared with placebo in patients with PsA who had an inadequate response to tumor necrosis factor inhibitor (TNFi) therapy.2 The study showed an ACR20 response of 50% in patients taking TOF 5 mg BID and 47% in patients taking 10 mg BID, compared with 24% in those taking placebo. Patients who received the 10 mg TOF dose continuously had higher rates of adverse events compared to TOF 5 mg, placebo, and patients who crossed over from placebo to TOF at either dose. In the TOF groups, there were cases of serious infection and herpes zoster, as well as 2 patients with major adverse cardiovascular events (MACE). Following review of these data, the FDA approved only the 5 mg BID dose, and later an 11-mg daily extended-release formulation that was pharmacokinetically similar.
The efficacy for UPA in PsA was shown in 2 pivotal phase 3 trials. SELECT-PsA1 compared UPA at 2 doses, 15 mg and 30 mg daily, vs placebo and vs ADA in patients with biologic DMARD (bDMARD)-naïve PsA.3 This trial demonstrated superiority of UPA in the ACR20 response at both doses (71% and 79%, respectively) compared with placebo (36%). The 15-mg dose of UPA was comparable to ADA (65%), while the 30-mg dose achieved superiority compared to ADA. Secondary outcomes including skin activity, patient-reported symptoms, and inhibition of radiographic progression were also superior in UPA compared with placebo and similar or greater with UPA compared with ADA, depending on the specific outcome.4 SELECT-PsA2 compared UPA 15 mg, 30 mg, and placebo in patients with prior incomplete response or intolerance to a bDMARD.5 At week 12 of the study, patients taking UPA 15 mg and 30 mg had an ACR20 response of 57% and 64%, respectively, compared with placebo (24%). At week 24, minimal disease activity was achieved by 25% of patients taking UPA 15 mg and 29% of patients taking UPA 30 mg, which was superior to placebo (3%).
Both studies found a significant increase in infections, including serious infections, at the 30-mg UPA dose compared with the placebo and adalimumab groups. Cytopenia and elevated creatine kinase (CK) level also occurred more frequently in the UPA 30-mg group. Rates of cancer were low overall and comparable between the patients treated with UPA and ADA. Given the higher incidence of adverse events with the 30-mg dose and the relatively similar efficacy, the sponsor elected to submit only the lower dose to the FDA for approval.
In the last few years, concerns for safety with JAKi use grew after the publication of data from the ORAL SURVEILLANCE trial, an FDA-mandated, post-approval safety study of TOF in RA. In this trial, patients with active RA over 50 years of age and with at least 1 additional cardiovascular risk factor were randomized to TOF at 1 of 2 doses, 5 mg or 10 mg BID, or a TNFi.6 This trial was designed as a noninferiority study, and TOF did not meet the noninferiority threshold compared to TNFi, with hazard ratios of 1.33 and 1.48 for MACE and malignancy, respectively. The results of this trial prompted the FDA to add a black box warning to the label for all JAKi, pointing out the risk of malignancy and MACE, as well as infection, mortality, and thrombosis.
In the ORAL SURVEILLANCE trial, the increased risk of MACE and malignancy was primarily seen in the study patients with high risk for a cardiovascular event. To address the question of whether a similar risk profile exists when using JAKi to treat PsA, or whether this is a disease-specific process related to RA, a post hoc analysis of 3 PsA trials and 7 PsO trials of patients treated with TOF was conducted.7 The analysis found that patients with a history of atherosclerotic cardiovascular disease (ASCVD) or metabolic syndrome, or patients at high risk for ASCVD (score > 20%) had increased incidence rates of MACE compared with those with low risk scores for ASCVD. Interestingly, as in RA, increased incidence rates of malignancy were seen in patients with preexisting or at high risk for ASCVD.
While the FDA recommends JAKi use in patients who have failed or are inappropriate for treatment with a TNFi, we would consider the use of JAKi for first-line therapy in PsA on an individual basis. One advantage of JAKi is their efficacy across multiple PsA domains, including peripheral arthritis, axial disease, enthesitis, dactylitis, and skin disease (although the approved dose of TOF was not statistically effective for PsO in the pivotal trials). Based on this efficacy, we believe that patients with overlapping, multifaceted disease may benefit the most from these medications. Patient risk factors and comorbidities are a prominent consideration in our use of JAKi to ensure safety, as the risk for MACE and malignancy is informed partly by baseline cardiovascular status. In younger patients without cardiovascular risk factors, JAKi may be a strong candidate for first-line therapy, particularly in patients averse to subcutaneous or intravenous therapy. We do counsel all patients on the increased risk of infection, and we do recommend inactivated herpes zoster vaccination in previously unvaccinated patients planning to start JAKi therapy.
On the horizon are the development of novel, oral agents targeting tyrosine kinase 2 (TYK2), which is a member of the JAK family of signaling proteins. In fact, the TYK2 inhibitor deucravacitinib was approved by the FDA in 2022 for the treatment of PsO. TYK2 inhibitors appear to have the advantage of a more selective mechanism of action, with fewer off-target effects. There were fewer adverse events in the deucravacitinib trials, which led to its prompt PsO authorization, and the FDA approval for the drug did not include the same black box warning that appears in the label for other JAKi.8 A phase 2 study showed early promise for the efficacy and safety of deucravacitinib in PsA.9 Further investigation will be needed to better understand the role of deucravacitinib and other TYK2 inhibitors being developed for the treatment of PsA. In the meantime, JAKi continue to be a prominent consideration for first-line PsA therapy in a carefully selected patient population.
Mease P, Hall S, FitzGerald O, et al. Tofacitinib or adalimumab versus placebo for psoriatic arthritis. N Engl J Med. 2017;377(16):1537-1550.
Gladman D, Rigby W, Azevedo VF, et al. Tofacitinib for psoriatic arthritis in patients with an inadequate response to TNF inhibitors. N Engl J Med. 2017;377(16):1525-1536.
McInnes IB, Anderson JK, Magrey M, et al. Trial of upadacitinib and adalimumab for psoriatic arthritis. N Engl J Med. 2021;384(13):1227-1239.
McInnes IB, Kato K, Magrey M, et al. Efficacy and safety of upadacitinib in patients with psoriatic arthritis: 2-year results from the phase 3 SELECT-PsA 1 study. Rheumatol Ther. 2023;10(1):275-292.
Mease PJ, Lertratanakul A, Anderson JK, et al. Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2. Ann Rheum Dis. 2021;80(3):312-320.
Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316-326.
Kristensen LE, Strober B, Poddubnyy D, et al. Association between baseline cardiovascular risk and incidence rates of major adverse cardiovascular events and malignancies in patients with psoriatic arthritis and psoriasis receiving tofacitinib. Ther Adv Musculoskelet Dis. 2023;15:1759720X221149965.
Dolgin E. TYK2-blocking agent showcases power of atypical kinase. Nat Biotechnol. 2022;40(12):1701-1704.
Mease PJ, Deodhar AA, van der Heijde D, et al. Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a phase II trial in psoriatic arthritis. Ann Rheum Dis. 2022;81(6):815-822.
Mease P, Hall S, FitzGerald O, et al. Tofacitinib or adalimumab versus placebo for psoriatic arthritis. N Engl J Med. 2017;377(16):1537-1550.
Gladman D, Rigby W, Azevedo VF, et al. Tofacitinib for psoriatic arthritis in patients with an inadequate response to TNF inhibitors. N Engl J Med. 2017;377(16):1525-1536.
McInnes IB, Anderson JK, Magrey M, et al. Trial of upadacitinib and adalimumab for psoriatic arthritis. N Engl J Med. 2021;384(13):1227-1239.
McInnes IB, Kato K, Magrey M, et al. Efficacy and safety of upadacitinib in patients with psoriatic arthritis: 2-year results from the phase 3 SELECT-PsA 1 study. Rheumatol Ther. 2023;10(1):275-292.
Mease PJ, Lertratanakul A, Anderson JK, et al. Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2. Ann Rheum Dis. 2021;80(3):312-320.
Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316-326.
Kristensen LE, Strober B, Poddubnyy D, et al. Association between baseline cardiovascular risk and incidence rates of major adverse cardiovascular events and malignancies in patients with psoriatic arthritis and psoriasis receiving tofacitinib. Ther Adv Musculoskelet Dis. 2023;15:1759720X221149965.
Dolgin E. TYK2-blocking agent showcases power of atypical kinase. Nat Biotechnol. 2022;40(12):1701-1704.
Mease PJ, Deodhar AA, van der Heijde D, et al. Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a phase II trial in psoriatic arthritis. Ann Rheum Dis. 2022;81(6):815-822.
Plant-based or animal-based diet: Which is better?
This transcript has been edited for clarity.
Dr. Jain: I’m Akshay Jain, an endocrinologist in Vancouver. This is Dr. Christopher Gardner, a nutritional scientist at Stanford. He is the author of many publications, including the widely cited SWAP-MEAT study. He was also a presenter at the American Diabetes Association conference in San Diego in 2023.
We’ll be talking about his work and the presentation that he did classifying different kinds of diets as well as the pluses and minuses of a plant-based diet versus an animal-based diet. Welcome, Dr Gardner.
Dr. Gardner: Glad to be here.
Dr. Jain: Let’s get right into this. There’s obviously been a large amount of talk, both in the lay media and in the scientific literature, on plant-based diets versus animal-based diets.
Dr. Gardner: I think this is one of those false dichotomies. It’s really not all one or all the other. Two of my favorite sayings are “with what” and “instead of what.” You may be thinking, I’m really going to go for animal based. I know it’s low carb. I have diabetes. I know animal foods have few carbs in them.
That’s true. But think of some of the more and the less healthy animal foods. Yogurt is a great choice for an animal food. Fish is a great choice for an animal food with omega-3s. Chicken McNuggets, not so much.
Then, you switch to the plant side and say: “I’ve heard all these people talking about a whole-food, plant-based diet. That sounds great. I’m thinking broccoli and chickpeas.”
I know there’s somebody out there saying: “I just had a Coke. Isn’t that plant based? I just had a pastry. Isn’t that full of plants?” It doesn’t really take much to think about this, but it’s not as dichotomous as animal versus plant.
Dr. Jain: There is, obviously, a good understanding regarding what actually constitutes the diet. Initially, people were saying that animal-based diets are really bad from a cardiovascular perspective. But now, some studies are suggesting that it may not be true. What’s your take on that?
Dr. Gardner: Again, if you think “with what” or “instead of what,” microbiome is a super-hot topic. That’s really fiber and fermented food, which are only plants. Saturated fat, despite all the controversy, raises your blood cholesterol. It’s more prevalent in animal foods than in plant foods.
Are there any great nutrients in animal foods? Sure. There’s calcium in dairy products for osteoporosis. There’s iron. Actually, people can get too much iron, which can be a pro-oxidant in levels that are too high.
The American Heart Association, in particular, which I’m very involved with, came out with new guidelines in 2021. It was very plant focused. The top of the list was vegetables, fruits, whole grains, and protein. When it came to protein, it was mostly from lentils, beans, and grains.
Dr. Jain: That’s good to know. Let’s talk about protein. We often hear about how somebody on a plant-based diet only can never have all the essential amino acids and the amount of protein that one needs. Whether it’s for general everyday individuals or even more so for athletes or bodybuilders, you cannot get enough good-quality protein from a plant-based diet.
Is there any truth to that? If not, what would you suggest for everyday individuals on a plant-based diet?
Dr. Gardner: This one drives me nuts. Please stop obsessing about protein. This isn’t a very scientific answer, but go watch the documentary Game Changers, which is all about vegan athletes. There are some pretty hokey things in that film that are very unscientific.
Let’s go back to basics, since we only have a couple of minutes together. It is a myth that plants don’t have all the amino acids, including all nine essential amino acids. I have several YouTube rants about this if anybody wants to search “Gardner Stanford protein.” All plant foods have all nine essential amino acids and all 20 amino acids.
There is a modest difference. Grains tend to be a little low in lysine, and beans tend to be a little low in methionine. Part of this has to do with how much of a difference is a little low. If you go to protein requirements that were written up in 2005 by the Institute of Medicine, you’ll see that the estimated average requirement for adults is 0.66 g/kg of body weight.
If we recommended the estimated average requirement for everyone, and everyone got it, by definition, half the population would be deficient. We have recommended daily allowances. The recommended daily allowances include two standard deviations above the estimated average requirement. Why would we do that? It’s a population approach.
If that’s the goal and everybody got it, you’d actually still have the tail of the normal distribution that would be deficient, which would be about 2.5%. The flip side of that argument is how many would exceed their requirement? That’s 97.5% of the population who would exceed their requirement if they got the recommended daily allowance.
The recommended daily allowance translates to about 45 g of protein per day for women and about 55 g of protein per day for men. Today, men and women in the United States get 80 g, 90 g, and 100 g of protein per day. What I hear them say is: “I’m not sure if I need the recommended daily allowance. I feel like I’m extra special or I’m above the curve and I want to make sure I’m getting enough.”
The recommended daily allowance already has a safety buffer in it. It was designed that way.
Let’s flip to athletes just for a second. Athletes want to be more muscular and make sure they’re supporting their activity. Americans get 1.2-1.5 g of protein per kg of body weight per day, which is almost double.
Athletes don’t eat as many calories as the average American does. If they’re working out to be muscular, they’re not eating 2,000 or 2,500 calories per day. I have a Rose Bowl football player teaching assistant from a Human Nutrition class at Stanford. He logged what he was eating for his football workouts. He was eating 5,000 calories per day. He was getting 250 g of protein per day, without any supplements or shakes.
I really do think this whole protein thing is a myth. As long as you get a reasonable amount of variety in your diet, there is no problem meeting your protein needs. Vegetarians? Absolutely no problem because they’re getting dairy and some eggs and things. Even vegans are likely fine. They would have to pay a little more attention to this, but I know many very strong, healthy vegans.
Dr. Jain: This is so helpful, Dr Gardner. I know that many clinicians, including myself, will find this very helpful, including when we talk to our patients and counsel them on their requirements. Thanks for sharing that.
Final question for you. We know people who are on either side of the extreme: either completely plant based or completely animal based. For a majority of us that have some kind of a happy medium, what would your suggestions be as far as the macronutrient distribution that you would recommend from a mixed animal- and plant-based diet? What would be the ideal recommendations here?
Dr. Gardner: We did a huge weight loss study with people with prediabetes. It was as low in carbs as people could go and as low in fat as people could go. That didn’t end up being the ketogenic level or the low-fat, vegan level. That ended up being much more moderate.
We found that people were successful either on low carb or low fat. Interestingly, on both diets, protein was very similar. Let’s not get into that since we just did a lot of protein. The key was a healthy low carb or a healthy low fat. I actually think we have a lot of wiggle room there. Let me build on what you said just a moment ago.
I really don’t think you need to be vegan to be healthy. We prefer the term whole food, plant based. If you’re getting 70% or 80% of your food from plants, you’re fine. If you really want to get the last 5%, 10%, or 15% all from plants, the additional benefit is not going to be large. You might want to do that for the environment or animal rights and welfare, but from a health perspective, a whole-food, plant-based diet leaves room for some yogurt, fish, and maybe some eggs for breakfast instead of those silly high-carb breakfasts that most Americans eat.
I will say that animal foods have no fiber. Given what a hot topic the microbiome is these days, the higher and higher you get in animal food, it’s going to be really hard to get antioxidants, most of which are in plants, and very hard to get enough fiber, which is good for the microbiome.
That’s why I tend to follow along the lines of a whole-food, plant-based diet that leaves some room for meat and animal-sourced foods, which you could leave out and be fine. I wouldn’t go in the opposite direction to the all-animal side.
Dr. Jain: That was awesome. Thank you so much, Dr Gardner. Final pearl of wisdom here. When clinicians like us see patients with diabetes, what should be the final take-home message that we can counsel our patients about?
Dr. Gardner: That’s a great question. I don’t think it’s really so much animal or plants; it’s actually type of carbohydrate. There’s a great paper out of JAMA in 2019 or 2020 by Shan and colleagues. They looked at the proportion of calories from proteins, carbs, and fats over about 20 years, and they looked at the subtypes.
Very interestingly, protein from animal foods is about 10% of calories; from plants, about 5%; mono-, poly-, and saturated fats are all about 10% of calories; and high-quality carbohydrates are about 10% of calories. What’s left is 40% of calories from crappy carbohydrates. We eat so many calories from added sugars and refined grains, and those are plant-based. Added sugars and refined grains are plant-based.
In terms of a lower-carbohydrate diet, there is an immense amount of room for cutting back on that 40%. What would you do with that? Would you eat more animal food? Would you eat more plant food? This is where I think we have a large amount of wiggle room. If the patients could get rid of all or most of that 40%, they could pick some eggs, yogurt, fish, and some high-fat foods. They could pick avocados, nuts, seeds, and olive oil or they could have more broccoli, chickpeas, tempeh, and tofu.
There really is a large amount of wiggle room. The key – can we please get rid of the elephant in the room, which is plant food – is all that added sugar and refined grain.
Dr. Jain is an endocrinologist and clinical instructor University of British Columbia, Vancouver. Dr. Gardner is a professor of medicine at Stanford (Calif.) University. Dr. Jain reported numerous conflicts of interest with various companies; Dr. Gardner reported receiving research funding from Beyond Meat.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Dr. Jain: I’m Akshay Jain, an endocrinologist in Vancouver. This is Dr. Christopher Gardner, a nutritional scientist at Stanford. He is the author of many publications, including the widely cited SWAP-MEAT study. He was also a presenter at the American Diabetes Association conference in San Diego in 2023.
We’ll be talking about his work and the presentation that he did classifying different kinds of diets as well as the pluses and minuses of a plant-based diet versus an animal-based diet. Welcome, Dr Gardner.
Dr. Gardner: Glad to be here.
Dr. Jain: Let’s get right into this. There’s obviously been a large amount of talk, both in the lay media and in the scientific literature, on plant-based diets versus animal-based diets.
Dr. Gardner: I think this is one of those false dichotomies. It’s really not all one or all the other. Two of my favorite sayings are “with what” and “instead of what.” You may be thinking, I’m really going to go for animal based. I know it’s low carb. I have diabetes. I know animal foods have few carbs in them.
That’s true. But think of some of the more and the less healthy animal foods. Yogurt is a great choice for an animal food. Fish is a great choice for an animal food with omega-3s. Chicken McNuggets, not so much.
Then, you switch to the plant side and say: “I’ve heard all these people talking about a whole-food, plant-based diet. That sounds great. I’m thinking broccoli and chickpeas.”
I know there’s somebody out there saying: “I just had a Coke. Isn’t that plant based? I just had a pastry. Isn’t that full of plants?” It doesn’t really take much to think about this, but it’s not as dichotomous as animal versus plant.
Dr. Jain: There is, obviously, a good understanding regarding what actually constitutes the diet. Initially, people were saying that animal-based diets are really bad from a cardiovascular perspective. But now, some studies are suggesting that it may not be true. What’s your take on that?
Dr. Gardner: Again, if you think “with what” or “instead of what,” microbiome is a super-hot topic. That’s really fiber and fermented food, which are only plants. Saturated fat, despite all the controversy, raises your blood cholesterol. It’s more prevalent in animal foods than in plant foods.
Are there any great nutrients in animal foods? Sure. There’s calcium in dairy products for osteoporosis. There’s iron. Actually, people can get too much iron, which can be a pro-oxidant in levels that are too high.
The American Heart Association, in particular, which I’m very involved with, came out with new guidelines in 2021. It was very plant focused. The top of the list was vegetables, fruits, whole grains, and protein. When it came to protein, it was mostly from lentils, beans, and grains.
Dr. Jain: That’s good to know. Let’s talk about protein. We often hear about how somebody on a plant-based diet only can never have all the essential amino acids and the amount of protein that one needs. Whether it’s for general everyday individuals or even more so for athletes or bodybuilders, you cannot get enough good-quality protein from a plant-based diet.
Is there any truth to that? If not, what would you suggest for everyday individuals on a plant-based diet?
Dr. Gardner: This one drives me nuts. Please stop obsessing about protein. This isn’t a very scientific answer, but go watch the documentary Game Changers, which is all about vegan athletes. There are some pretty hokey things in that film that are very unscientific.
Let’s go back to basics, since we only have a couple of minutes together. It is a myth that plants don’t have all the amino acids, including all nine essential amino acids. I have several YouTube rants about this if anybody wants to search “Gardner Stanford protein.” All plant foods have all nine essential amino acids and all 20 amino acids.
There is a modest difference. Grains tend to be a little low in lysine, and beans tend to be a little low in methionine. Part of this has to do with how much of a difference is a little low. If you go to protein requirements that were written up in 2005 by the Institute of Medicine, you’ll see that the estimated average requirement for adults is 0.66 g/kg of body weight.
If we recommended the estimated average requirement for everyone, and everyone got it, by definition, half the population would be deficient. We have recommended daily allowances. The recommended daily allowances include two standard deviations above the estimated average requirement. Why would we do that? It’s a population approach.
If that’s the goal and everybody got it, you’d actually still have the tail of the normal distribution that would be deficient, which would be about 2.5%. The flip side of that argument is how many would exceed their requirement? That’s 97.5% of the population who would exceed their requirement if they got the recommended daily allowance.
The recommended daily allowance translates to about 45 g of protein per day for women and about 55 g of protein per day for men. Today, men and women in the United States get 80 g, 90 g, and 100 g of protein per day. What I hear them say is: “I’m not sure if I need the recommended daily allowance. I feel like I’m extra special or I’m above the curve and I want to make sure I’m getting enough.”
The recommended daily allowance already has a safety buffer in it. It was designed that way.
Let’s flip to athletes just for a second. Athletes want to be more muscular and make sure they’re supporting their activity. Americans get 1.2-1.5 g of protein per kg of body weight per day, which is almost double.
Athletes don’t eat as many calories as the average American does. If they’re working out to be muscular, they’re not eating 2,000 or 2,500 calories per day. I have a Rose Bowl football player teaching assistant from a Human Nutrition class at Stanford. He logged what he was eating for his football workouts. He was eating 5,000 calories per day. He was getting 250 g of protein per day, without any supplements or shakes.
I really do think this whole protein thing is a myth. As long as you get a reasonable amount of variety in your diet, there is no problem meeting your protein needs. Vegetarians? Absolutely no problem because they’re getting dairy and some eggs and things. Even vegans are likely fine. They would have to pay a little more attention to this, but I know many very strong, healthy vegans.
Dr. Jain: This is so helpful, Dr Gardner. I know that many clinicians, including myself, will find this very helpful, including when we talk to our patients and counsel them on their requirements. Thanks for sharing that.
Final question for you. We know people who are on either side of the extreme: either completely plant based or completely animal based. For a majority of us that have some kind of a happy medium, what would your suggestions be as far as the macronutrient distribution that you would recommend from a mixed animal- and plant-based diet? What would be the ideal recommendations here?
Dr. Gardner: We did a huge weight loss study with people with prediabetes. It was as low in carbs as people could go and as low in fat as people could go. That didn’t end up being the ketogenic level or the low-fat, vegan level. That ended up being much more moderate.
We found that people were successful either on low carb or low fat. Interestingly, on both diets, protein was very similar. Let’s not get into that since we just did a lot of protein. The key was a healthy low carb or a healthy low fat. I actually think we have a lot of wiggle room there. Let me build on what you said just a moment ago.
I really don’t think you need to be vegan to be healthy. We prefer the term whole food, plant based. If you’re getting 70% or 80% of your food from plants, you’re fine. If you really want to get the last 5%, 10%, or 15% all from plants, the additional benefit is not going to be large. You might want to do that for the environment or animal rights and welfare, but from a health perspective, a whole-food, plant-based diet leaves room for some yogurt, fish, and maybe some eggs for breakfast instead of those silly high-carb breakfasts that most Americans eat.
I will say that animal foods have no fiber. Given what a hot topic the microbiome is these days, the higher and higher you get in animal food, it’s going to be really hard to get antioxidants, most of which are in plants, and very hard to get enough fiber, which is good for the microbiome.
That’s why I tend to follow along the lines of a whole-food, plant-based diet that leaves some room for meat and animal-sourced foods, which you could leave out and be fine. I wouldn’t go in the opposite direction to the all-animal side.
Dr. Jain: That was awesome. Thank you so much, Dr Gardner. Final pearl of wisdom here. When clinicians like us see patients with diabetes, what should be the final take-home message that we can counsel our patients about?
Dr. Gardner: That’s a great question. I don’t think it’s really so much animal or plants; it’s actually type of carbohydrate. There’s a great paper out of JAMA in 2019 or 2020 by Shan and colleagues. They looked at the proportion of calories from proteins, carbs, and fats over about 20 years, and they looked at the subtypes.
Very interestingly, protein from animal foods is about 10% of calories; from plants, about 5%; mono-, poly-, and saturated fats are all about 10% of calories; and high-quality carbohydrates are about 10% of calories. What’s left is 40% of calories from crappy carbohydrates. We eat so many calories from added sugars and refined grains, and those are plant-based. Added sugars and refined grains are plant-based.
In terms of a lower-carbohydrate diet, there is an immense amount of room for cutting back on that 40%. What would you do with that? Would you eat more animal food? Would you eat more plant food? This is where I think we have a large amount of wiggle room. If the patients could get rid of all or most of that 40%, they could pick some eggs, yogurt, fish, and some high-fat foods. They could pick avocados, nuts, seeds, and olive oil or they could have more broccoli, chickpeas, tempeh, and tofu.
There really is a large amount of wiggle room. The key – can we please get rid of the elephant in the room, which is plant food – is all that added sugar and refined grain.
Dr. Jain is an endocrinologist and clinical instructor University of British Columbia, Vancouver. Dr. Gardner is a professor of medicine at Stanford (Calif.) University. Dr. Jain reported numerous conflicts of interest with various companies; Dr. Gardner reported receiving research funding from Beyond Meat.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Dr. Jain: I’m Akshay Jain, an endocrinologist in Vancouver. This is Dr. Christopher Gardner, a nutritional scientist at Stanford. He is the author of many publications, including the widely cited SWAP-MEAT study. He was also a presenter at the American Diabetes Association conference in San Diego in 2023.
We’ll be talking about his work and the presentation that he did classifying different kinds of diets as well as the pluses and minuses of a plant-based diet versus an animal-based diet. Welcome, Dr Gardner.
Dr. Gardner: Glad to be here.
Dr. Jain: Let’s get right into this. There’s obviously been a large amount of talk, both in the lay media and in the scientific literature, on plant-based diets versus animal-based diets.
Dr. Gardner: I think this is one of those false dichotomies. It’s really not all one or all the other. Two of my favorite sayings are “with what” and “instead of what.” You may be thinking, I’m really going to go for animal based. I know it’s low carb. I have diabetes. I know animal foods have few carbs in them.
That’s true. But think of some of the more and the less healthy animal foods. Yogurt is a great choice for an animal food. Fish is a great choice for an animal food with omega-3s. Chicken McNuggets, not so much.
Then, you switch to the plant side and say: “I’ve heard all these people talking about a whole-food, plant-based diet. That sounds great. I’m thinking broccoli and chickpeas.”
I know there’s somebody out there saying: “I just had a Coke. Isn’t that plant based? I just had a pastry. Isn’t that full of plants?” It doesn’t really take much to think about this, but it’s not as dichotomous as animal versus plant.
Dr. Jain: There is, obviously, a good understanding regarding what actually constitutes the diet. Initially, people were saying that animal-based diets are really bad from a cardiovascular perspective. But now, some studies are suggesting that it may not be true. What’s your take on that?
Dr. Gardner: Again, if you think “with what” or “instead of what,” microbiome is a super-hot topic. That’s really fiber and fermented food, which are only plants. Saturated fat, despite all the controversy, raises your blood cholesterol. It’s more prevalent in animal foods than in plant foods.
Are there any great nutrients in animal foods? Sure. There’s calcium in dairy products for osteoporosis. There’s iron. Actually, people can get too much iron, which can be a pro-oxidant in levels that are too high.
The American Heart Association, in particular, which I’m very involved with, came out with new guidelines in 2021. It was very plant focused. The top of the list was vegetables, fruits, whole grains, and protein. When it came to protein, it was mostly from lentils, beans, and grains.
Dr. Jain: That’s good to know. Let’s talk about protein. We often hear about how somebody on a plant-based diet only can never have all the essential amino acids and the amount of protein that one needs. Whether it’s for general everyday individuals or even more so for athletes or bodybuilders, you cannot get enough good-quality protein from a plant-based diet.
Is there any truth to that? If not, what would you suggest for everyday individuals on a plant-based diet?
Dr. Gardner: This one drives me nuts. Please stop obsessing about protein. This isn’t a very scientific answer, but go watch the documentary Game Changers, which is all about vegan athletes. There are some pretty hokey things in that film that are very unscientific.
Let’s go back to basics, since we only have a couple of minutes together. It is a myth that plants don’t have all the amino acids, including all nine essential amino acids. I have several YouTube rants about this if anybody wants to search “Gardner Stanford protein.” All plant foods have all nine essential amino acids and all 20 amino acids.
There is a modest difference. Grains tend to be a little low in lysine, and beans tend to be a little low in methionine. Part of this has to do with how much of a difference is a little low. If you go to protein requirements that were written up in 2005 by the Institute of Medicine, you’ll see that the estimated average requirement for adults is 0.66 g/kg of body weight.
If we recommended the estimated average requirement for everyone, and everyone got it, by definition, half the population would be deficient. We have recommended daily allowances. The recommended daily allowances include two standard deviations above the estimated average requirement. Why would we do that? It’s a population approach.
If that’s the goal and everybody got it, you’d actually still have the tail of the normal distribution that would be deficient, which would be about 2.5%. The flip side of that argument is how many would exceed their requirement? That’s 97.5% of the population who would exceed their requirement if they got the recommended daily allowance.
The recommended daily allowance translates to about 45 g of protein per day for women and about 55 g of protein per day for men. Today, men and women in the United States get 80 g, 90 g, and 100 g of protein per day. What I hear them say is: “I’m not sure if I need the recommended daily allowance. I feel like I’m extra special or I’m above the curve and I want to make sure I’m getting enough.”
The recommended daily allowance already has a safety buffer in it. It was designed that way.
Let’s flip to athletes just for a second. Athletes want to be more muscular and make sure they’re supporting their activity. Americans get 1.2-1.5 g of protein per kg of body weight per day, which is almost double.
Athletes don’t eat as many calories as the average American does. If they’re working out to be muscular, they’re not eating 2,000 or 2,500 calories per day. I have a Rose Bowl football player teaching assistant from a Human Nutrition class at Stanford. He logged what he was eating for his football workouts. He was eating 5,000 calories per day. He was getting 250 g of protein per day, without any supplements or shakes.
I really do think this whole protein thing is a myth. As long as you get a reasonable amount of variety in your diet, there is no problem meeting your protein needs. Vegetarians? Absolutely no problem because they’re getting dairy and some eggs and things. Even vegans are likely fine. They would have to pay a little more attention to this, but I know many very strong, healthy vegans.
Dr. Jain: This is so helpful, Dr Gardner. I know that many clinicians, including myself, will find this very helpful, including when we talk to our patients and counsel them on their requirements. Thanks for sharing that.
Final question for you. We know people who are on either side of the extreme: either completely plant based or completely animal based. For a majority of us that have some kind of a happy medium, what would your suggestions be as far as the macronutrient distribution that you would recommend from a mixed animal- and plant-based diet? What would be the ideal recommendations here?
Dr. Gardner: We did a huge weight loss study with people with prediabetes. It was as low in carbs as people could go and as low in fat as people could go. That didn’t end up being the ketogenic level or the low-fat, vegan level. That ended up being much more moderate.
We found that people were successful either on low carb or low fat. Interestingly, on both diets, protein was very similar. Let’s not get into that since we just did a lot of protein. The key was a healthy low carb or a healthy low fat. I actually think we have a lot of wiggle room there. Let me build on what you said just a moment ago.
I really don’t think you need to be vegan to be healthy. We prefer the term whole food, plant based. If you’re getting 70% or 80% of your food from plants, you’re fine. If you really want to get the last 5%, 10%, or 15% all from plants, the additional benefit is not going to be large. You might want to do that for the environment or animal rights and welfare, but from a health perspective, a whole-food, plant-based diet leaves room for some yogurt, fish, and maybe some eggs for breakfast instead of those silly high-carb breakfasts that most Americans eat.
I will say that animal foods have no fiber. Given what a hot topic the microbiome is these days, the higher and higher you get in animal food, it’s going to be really hard to get antioxidants, most of which are in plants, and very hard to get enough fiber, which is good for the microbiome.
That’s why I tend to follow along the lines of a whole-food, plant-based diet that leaves some room for meat and animal-sourced foods, which you could leave out and be fine. I wouldn’t go in the opposite direction to the all-animal side.
Dr. Jain: That was awesome. Thank you so much, Dr Gardner. Final pearl of wisdom here. When clinicians like us see patients with diabetes, what should be the final take-home message that we can counsel our patients about?
Dr. Gardner: That’s a great question. I don’t think it’s really so much animal or plants; it’s actually type of carbohydrate. There’s a great paper out of JAMA in 2019 or 2020 by Shan and colleagues. They looked at the proportion of calories from proteins, carbs, and fats over about 20 years, and they looked at the subtypes.
Very interestingly, protein from animal foods is about 10% of calories; from plants, about 5%; mono-, poly-, and saturated fats are all about 10% of calories; and high-quality carbohydrates are about 10% of calories. What’s left is 40% of calories from crappy carbohydrates. We eat so many calories from added sugars and refined grains, and those are plant-based. Added sugars and refined grains are plant-based.
In terms of a lower-carbohydrate diet, there is an immense amount of room for cutting back on that 40%. What would you do with that? Would you eat more animal food? Would you eat more plant food? This is where I think we have a large amount of wiggle room. If the patients could get rid of all or most of that 40%, they could pick some eggs, yogurt, fish, and some high-fat foods. They could pick avocados, nuts, seeds, and olive oil or they could have more broccoli, chickpeas, tempeh, and tofu.
There really is a large amount of wiggle room. The key – can we please get rid of the elephant in the room, which is plant food – is all that added sugar and refined grain.
Dr. Jain is an endocrinologist and clinical instructor University of British Columbia, Vancouver. Dr. Gardner is a professor of medicine at Stanford (Calif.) University. Dr. Jain reported numerous conflicts of interest with various companies; Dr. Gardner reported receiving research funding from Beyond Meat.
A version of this article first appeared on Medscape.com.
Biofeedback Training Is a Good Alternative to Preventive Medication for Migraine and Tension-Type Headache


What types of headache and other illnesses respond to biofeedback training?
Migraine affects about 12% of the US and most Western populations, and is 3 times more common in women than men. Migraine can be treated with a variety of strategies that include medications and nonpharmacologic therapies such as biofeedback, as well as other behavioral therapies and devices. Biofeedback refers to the use of instrumentation to monitor and display physiologic responses that the patient may not be aware of so that they can be “modified” in a more adaptive direction. Feedback gives immediate objective information and is usually combined with a relaxation-based therapy. The most common biofeedback treatments for migraine include feeding back muscle activity in the face and neck to help people relax contracted muscles and teach them a “low-arousal” response; they learn to increase finger temperature, which coincides with modifying the “stress” nervous system. Biofeedback has been shown to be helpful for migraine and tension-type headache. It is also helpful to decrease anxiety and stress levels and lower blood pressure.
Can patients use biofeedback treatments in conjunction with migraine medication?
Research has shown that migraine, in particular higher-frequency migraine, is best treated by a combination of medications and behavioral strategies. Biofeedback is a good option for use in conjunction with medication for migraine.
Who is trained to provide biofeedback treatments?
Biofeedback for migraine is something usually performed by psychologists and other professionals with specialized training. Many practitioners are certified by the Biofeedback Certification Institute of America (BCIA). It is important to find an experienced biofeedback practitioner who also has some expertise in treating headache disorders.
How are biofeedback treatments performed?
Biofeedback is a therapy that follows a learning model whereby the patient gradually learns a self-regulation skill that impacts their headaches.
Patients come to an office, typically once per week, where they are attached to instruments that measure physical responses associated with migraine. The patient typically sits in a comfortable chair or recliner, and numerous physiologic responses are monitored with surface electrodes.
When treating headache, sensors are typically placed on the head and neck to monitor muscle responses and a thermistor is placed on a finger to measure temperature. Feedback is given via visual cues (computer graphics) or a change in auditory tone as the patient is taught various relaxation techniques.
Patients use the feedback to learn a physiologic relaxation response that may be beneficial for their headache management. Most of the research on biofeedback is related to treatment to prevent migraine; however, these techniques can be helpful to use during an acute attack, ideally paired with an acute care migraine medication.
Can children with migraine have biofeedback treatments as well?
Most children typically have a lower frequency of migraine than adults, although some have frequent migraines with associated disability and are candidates for preventive medication (although no medications are yet approved for children by the US Food and Drug Association). Most children are good candidates for behavioral therapies such as biofeedback. There are many computer games utilized in biofeedback training that children easily learn to modify physical responses. There are some fairly recent data suggesting that behavioral treatments, some of which include biofeedback, are effective strategies for children and may be more effective than preventive medication.
What other types of illnesses could benefit from biofeedback training?
There are data showing that biofeedback therapy can be helpful for anxiety disorders, insomnia, and functional bowel disorders and may help in modifying high blood pressure. It can also be a very effective stress-management strategy.
Do you refer some of your patients with migraine to a psychologist for biofeedback treatments?
Yes, but it is always good for the referring physician to check on the credentials of the person performing the biofeedback treatment. Some headache specialists might do it themselves, but we do not. It takes a while—at least several sessions—and psychologists are better at it. Patients’ perspectives are also important. We communicate with the referred biofeedback treatment specialist to get more insight on the patient. For example, some patients are anxious and depressed, and they are not sleeping at night. The doctor we referred the patient to may recommend an antidepressant for the patient to help address those issues. It is a team effort.
What is the average cost per treatment?
The costs vary throughout the country and range from $75 to $400 per session. Insurance coverage varies.
How many times should a patient go in for treatment?
Most protocols are about 10 to 12 sessions, depending on patient response.
Have there been clinical trials on biofeedback treatments/devices?
There have been many clinical trials that have been positive, so there is good evidence that biofeedback can be an effective treatment for migraine and tension-type headache. There are many types of biofeedback devices that measure different modalities. The most common one used in migraine is measuring scalp muscle contraction with surface electromyography or measuring peripheral blood flow with a temperature gauge. The goals are to relax muscles and learn to increase finger temperature, which is related to decreased arousal of the sympathetic nervous system or stress system. Other modalities include learning to modulate brain waves (electroencephalography or neurofeedback) and certain cardiovascular measures that reduce the stress response by a different mechanism. The goal is for patients to learn a low arousal response that they can utilize in their natural environment. Certain breathing techniques and visualization exercises are also helpful, but biofeedback refers to using physiologic recording equipment to help learn to change physical responses related to headache disorder.
Over our years of experience, we have found that biofeedback can help a large percentage of our patients with migraine and tension-type headache, and it is associated with almost no adverse events.
What types of headache and other illnesses respond to biofeedback training?
Migraine affects about 12% of the US and most Western populations, and is 3 times more common in women than men. Migraine can be treated with a variety of strategies that include medications and nonpharmacologic therapies such as biofeedback, as well as other behavioral therapies and devices. Biofeedback refers to the use of instrumentation to monitor and display physiologic responses that the patient may not be aware of so that they can be “modified” in a more adaptive direction. Feedback gives immediate objective information and is usually combined with a relaxation-based therapy. The most common biofeedback treatments for migraine include feeding back muscle activity in the face and neck to help people relax contracted muscles and teach them a “low-arousal” response; they learn to increase finger temperature, which coincides with modifying the “stress” nervous system. Biofeedback has been shown to be helpful for migraine and tension-type headache. It is also helpful to decrease anxiety and stress levels and lower blood pressure.
Can patients use biofeedback treatments in conjunction with migraine medication?
Research has shown that migraine, in particular higher-frequency migraine, is best treated by a combination of medications and behavioral strategies. Biofeedback is a good option for use in conjunction with medication for migraine.
Who is trained to provide biofeedback treatments?
Biofeedback for migraine is something usually performed by psychologists and other professionals with specialized training. Many practitioners are certified by the Biofeedback Certification Institute of America (BCIA). It is important to find an experienced biofeedback practitioner who also has some expertise in treating headache disorders.
How are biofeedback treatments performed?
Biofeedback is a therapy that follows a learning model whereby the patient gradually learns a self-regulation skill that impacts their headaches.
Patients come to an office, typically once per week, where they are attached to instruments that measure physical responses associated with migraine. The patient typically sits in a comfortable chair or recliner, and numerous physiologic responses are monitored with surface electrodes.
When treating headache, sensors are typically placed on the head and neck to monitor muscle responses and a thermistor is placed on a finger to measure temperature. Feedback is given via visual cues (computer graphics) or a change in auditory tone as the patient is taught various relaxation techniques.
Patients use the feedback to learn a physiologic relaxation response that may be beneficial for their headache management. Most of the research on biofeedback is related to treatment to prevent migraine; however, these techniques can be helpful to use during an acute attack, ideally paired with an acute care migraine medication.
Can children with migraine have biofeedback treatments as well?
Most children typically have a lower frequency of migraine than adults, although some have frequent migraines with associated disability and are candidates for preventive medication (although no medications are yet approved for children by the US Food and Drug Association). Most children are good candidates for behavioral therapies such as biofeedback. There are many computer games utilized in biofeedback training that children easily learn to modify physical responses. There are some fairly recent data suggesting that behavioral treatments, some of which include biofeedback, are effective strategies for children and may be more effective than preventive medication.
What other types of illnesses could benefit from biofeedback training?
There are data showing that biofeedback therapy can be helpful for anxiety disorders, insomnia, and functional bowel disorders and may help in modifying high blood pressure. It can also be a very effective stress-management strategy.
Do you refer some of your patients with migraine to a psychologist for biofeedback treatments?
Yes, but it is always good for the referring physician to check on the credentials of the person performing the biofeedback treatment. Some headache specialists might do it themselves, but we do not. It takes a while—at least several sessions—and psychologists are better at it. Patients’ perspectives are also important. We communicate with the referred biofeedback treatment specialist to get more insight on the patient. For example, some patients are anxious and depressed, and they are not sleeping at night. The doctor we referred the patient to may recommend an antidepressant for the patient to help address those issues. It is a team effort.
What is the average cost per treatment?
The costs vary throughout the country and range from $75 to $400 per session. Insurance coverage varies.
How many times should a patient go in for treatment?
Most protocols are about 10 to 12 sessions, depending on patient response.
Have there been clinical trials on biofeedback treatments/devices?
There have been many clinical trials that have been positive, so there is good evidence that biofeedback can be an effective treatment for migraine and tension-type headache. There are many types of biofeedback devices that measure different modalities. The most common one used in migraine is measuring scalp muscle contraction with surface electromyography or measuring peripheral blood flow with a temperature gauge. The goals are to relax muscles and learn to increase finger temperature, which is related to decreased arousal of the sympathetic nervous system or stress system. Other modalities include learning to modulate brain waves (electroencephalography or neurofeedback) and certain cardiovascular measures that reduce the stress response by a different mechanism. The goal is for patients to learn a low arousal response that they can utilize in their natural environment. Certain breathing techniques and visualization exercises are also helpful, but biofeedback refers to using physiologic recording equipment to help learn to change physical responses related to headache disorder.
Over our years of experience, we have found that biofeedback can help a large percentage of our patients with migraine and tension-type headache, and it is associated with almost no adverse events.
What types of headache and other illnesses respond to biofeedback training?
Migraine affects about 12% of the US and most Western populations, and is 3 times more common in women than men. Migraine can be treated with a variety of strategies that include medications and nonpharmacologic therapies such as biofeedback, as well as other behavioral therapies and devices. Biofeedback refers to the use of instrumentation to monitor and display physiologic responses that the patient may not be aware of so that they can be “modified” in a more adaptive direction. Feedback gives immediate objective information and is usually combined with a relaxation-based therapy. The most common biofeedback treatments for migraine include feeding back muscle activity in the face and neck to help people relax contracted muscles and teach them a “low-arousal” response; they learn to increase finger temperature, which coincides with modifying the “stress” nervous system. Biofeedback has been shown to be helpful for migraine and tension-type headache. It is also helpful to decrease anxiety and stress levels and lower blood pressure.
Can patients use biofeedback treatments in conjunction with migraine medication?
Research has shown that migraine, in particular higher-frequency migraine, is best treated by a combination of medications and behavioral strategies. Biofeedback is a good option for use in conjunction with medication for migraine.
Who is trained to provide biofeedback treatments?
Biofeedback for migraine is something usually performed by psychologists and other professionals with specialized training. Many practitioners are certified by the Biofeedback Certification Institute of America (BCIA). It is important to find an experienced biofeedback practitioner who also has some expertise in treating headache disorders.
How are biofeedback treatments performed?
Biofeedback is a therapy that follows a learning model whereby the patient gradually learns a self-regulation skill that impacts their headaches.
Patients come to an office, typically once per week, where they are attached to instruments that measure physical responses associated with migraine. The patient typically sits in a comfortable chair or recliner, and numerous physiologic responses are monitored with surface electrodes.
When treating headache, sensors are typically placed on the head and neck to monitor muscle responses and a thermistor is placed on a finger to measure temperature. Feedback is given via visual cues (computer graphics) or a change in auditory tone as the patient is taught various relaxation techniques.
Patients use the feedback to learn a physiologic relaxation response that may be beneficial for their headache management. Most of the research on biofeedback is related to treatment to prevent migraine; however, these techniques can be helpful to use during an acute attack, ideally paired with an acute care migraine medication.
Can children with migraine have biofeedback treatments as well?
Most children typically have a lower frequency of migraine than adults, although some have frequent migraines with associated disability and are candidates for preventive medication (although no medications are yet approved for children by the US Food and Drug Association). Most children are good candidates for behavioral therapies such as biofeedback. There are many computer games utilized in biofeedback training that children easily learn to modify physical responses. There are some fairly recent data suggesting that behavioral treatments, some of which include biofeedback, are effective strategies for children and may be more effective than preventive medication.
What other types of illnesses could benefit from biofeedback training?
There are data showing that biofeedback therapy can be helpful for anxiety disorders, insomnia, and functional bowel disorders and may help in modifying high blood pressure. It can also be a very effective stress-management strategy.
Do you refer some of your patients with migraine to a psychologist for biofeedback treatments?
Yes, but it is always good for the referring physician to check on the credentials of the person performing the biofeedback treatment. Some headache specialists might do it themselves, but we do not. It takes a while—at least several sessions—and psychologists are better at it. Patients’ perspectives are also important. We communicate with the referred biofeedback treatment specialist to get more insight on the patient. For example, some patients are anxious and depressed, and they are not sleeping at night. The doctor we referred the patient to may recommend an antidepressant for the patient to help address those issues. It is a team effort.
What is the average cost per treatment?
The costs vary throughout the country and range from $75 to $400 per session. Insurance coverage varies.
How many times should a patient go in for treatment?
Most protocols are about 10 to 12 sessions, depending on patient response.
Have there been clinical trials on biofeedback treatments/devices?
There have been many clinical trials that have been positive, so there is good evidence that biofeedback can be an effective treatment for migraine and tension-type headache. There are many types of biofeedback devices that measure different modalities. The most common one used in migraine is measuring scalp muscle contraction with surface electromyography or measuring peripheral blood flow with a temperature gauge. The goals are to relax muscles and learn to increase finger temperature, which is related to decreased arousal of the sympathetic nervous system or stress system. Other modalities include learning to modulate brain waves (electroencephalography or neurofeedback) and certain cardiovascular measures that reduce the stress response by a different mechanism. The goal is for patients to learn a low arousal response that they can utilize in their natural environment. Certain breathing techniques and visualization exercises are also helpful, but biofeedback refers to using physiologic recording equipment to help learn to change physical responses related to headache disorder.
Over our years of experience, we have found that biofeedback can help a large percentage of our patients with migraine and tension-type headache, and it is associated with almost no adverse events.
An Atypical Discussion of the Link Between Metabolic Syndrome and Type 2 Diabetes—and the Use of Precision Medicine to Treat the Whole Patient
Metabolic syndrome, type 2 diabetes mellitus (T2DM), and the “diabetes syndrome,” are interrelated, serious health conditions that share common risk factors and mechanisms. While they are each distinct conditions, a significant association exists between them, with metabolic syndrome often being considered a precursor to the development of typical T2DM.
Metabolic syndrome is a cluster of individual metabolic abnormalities that includes a combination of risk factors such as abdominal obesity, high blood pressure, elevated insulin levels, high triglyceride levels, and low levels of high-density lipoprotein (HDL) cholesterol related to genes and epigenetic changes associated with insulin resistance. These risk factors increase the likelihood of developing cardiovascular diseases, such as heart disease and stroke, and, when combined with significant damage to β -cell function and the influence of concordant environmental precipitants, result in hyperglycemia/overt diabetes—classically defined as T2DM.
It is estimated that there will be a staggering 3.1 billion people living with T2DM by 2050, according to a recent article in The Lancet. This devastating number will place a heavy burden on the health care system.
However, this typical pathophysiologic definition of T2DM is imprecise. Twenty percent of patients with T2DM have islet-cell antibodies that are typical of the immune destruction of β-cells in patients with type 1 diabetes mellitus (T1DM). Furthermore, approximately 40% of patients with T1DM have insulin resistance.
Thus, to better understand and distinguish the disease processes unique to each individual, we have defined a new beta cell classification for all forms of diabetes mellitus (DM). In this classification, there are 4 common pathophysiologic causes of all DM (including classic T2DM), with resultant damage to the β-cells (ie, genetic and epigenetic changes, inflammation, an abnormal environment, and insulin resistance), which results in 11 mechanisms of hyperglycemia, represented as “the egregious eleven” in Figure 1.
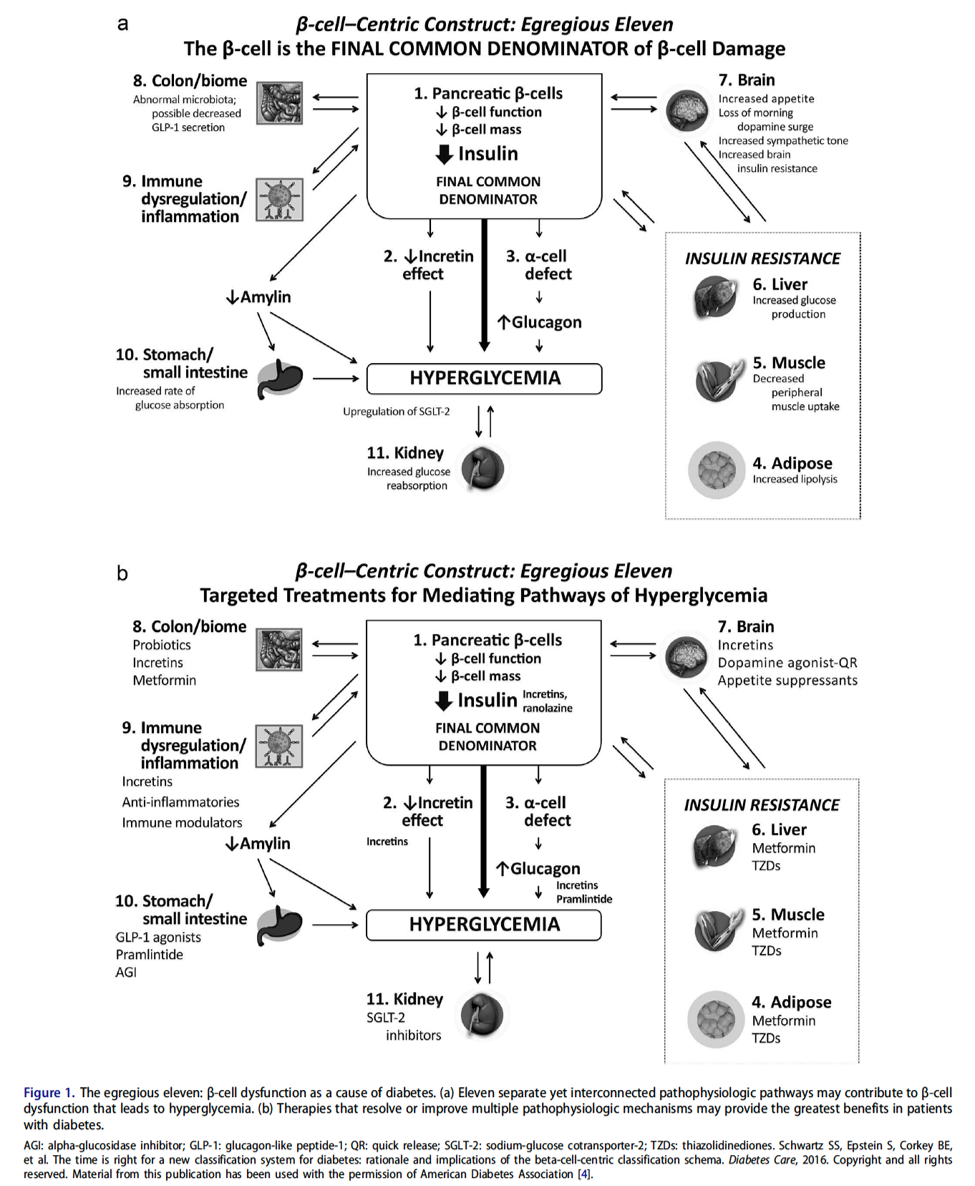
Additionally, Figure 2 illustrates the association between overlapping genes/epigenetic changes responsible for DM and the increased susceptibility to developing various microvascular complications commonly observed in all forms of DM, including classic T2DM. These complications, now recognized as components of the diabetes syndrome, encompass a range of conditions with shared interrelated pathophysiologic mechanisms, such as arteriosclerotic vascular disease (ASVD), dementia, some cancers, nonalcoholic fatty liver disease or nonalcoholic steatohepatitis (NAFLD/NASH), or psoriasis.
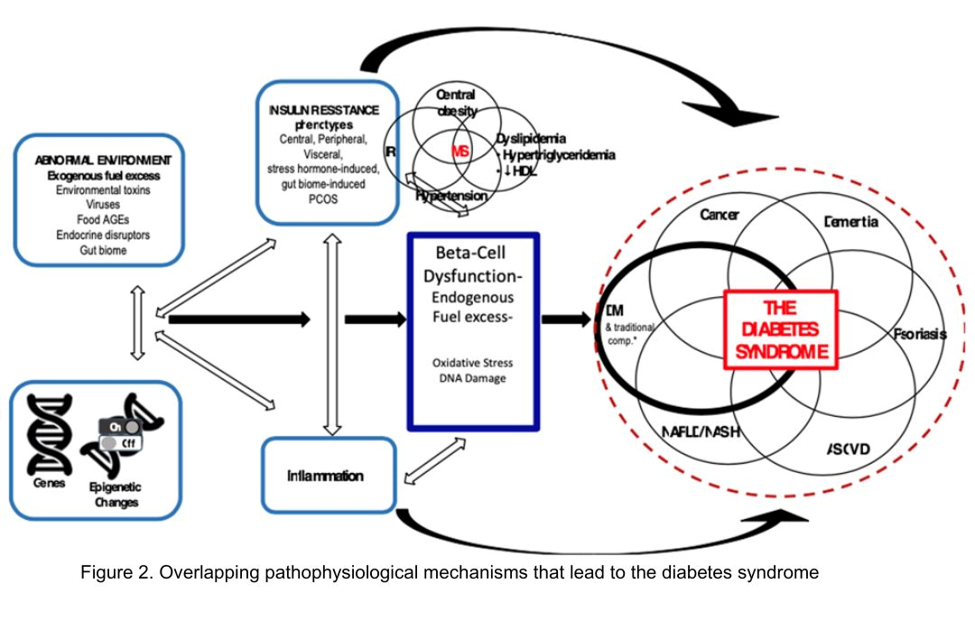
The likelihood of developing a specific type of DM, with classic complications or associated conditions, is contingent on an individual’s genes, epigenetic factors, inflammation, insulin resistance, and environmental exposures over time. It has now been postulated that these factors can be identified in a particular individual by a set of genomics, metabolomics, proteomics, and markers of these processes.
This more precise approach has the added benefit of giving rise to a more accurate individualization of therapy—precision medicine.
Precision medicine is an approach to healthcare that considers an individual's specific characteristics, such as genetic makeup, lifestyle, and environmental factors, to tailor medical treatments and interventions. In the context of this discussion on T2DM, precision medicine’s goal is to provide targeted therapies and interventions based on an individual's unique -omic profile to improve treatment outcomes and minimize side effects. An additional benefit of precision medicine use in diabetes syndrome is giving the diabetes specialist the opportunity to treat the whole patient, looking for complications and associated conditions earlier via defining the presence or absence of various markers of their individual pathophysiology. Additionally, we have come to recognize that many of the medications for treating T2DM (eg, glucagon-like peptide 1 receptor agonists [GLP-1 RA], dipeptidyl peptidase 4 inhibitors [DPP-4 inhibitors], sodium-glucose cotransporter-2 inhibitors [SGLT-2 inhibitors], metformin, Cycloset [bromocriptine mesylate]) can offer other benefits for the patient—treating not only multiple mechanisms of hyperglycemia (the egregious eleven: use the fewest number of agents in combination to treat the most number of mechanisms of hyperglycemia) but also recognize that they can prevent and treat the complications and associated conditions of the diabetes syndrome: cardiovascular, renal, liver, some cancers, psoriasis, and dementia.
The classic link between metabolic syndrome and T2DM is important to consider when applying precision medicine approaches to the management of T2DM. Here are some examples of how precision medicine is being applied in the management of T2DM:
Genetic testing: Genetic testing can help identify specific genetic variants or mutations that may influence an individual's risk of developing T2DM or their response to certain medications. By understanding a person's genetic predisposition, clinicians can make more informed decisions about treatment options and develop personalized strategies for their patients.
Pharmacogenomics: Certain genetic variations can impact how a person metabolizes and responds to specific diabetes medications. By analyzing an individual's genetic profile, medications that are more likely to be effective and have fewer adverse effects for that patient may be selected.
Continuous glucose monitoring (CGM): CGM devices provide real-time information about an individual’s blood glucose levels, allowing for more precise management of diabetes. By continuously monitoring glucose levels, patterns can be identified, allowing for adjustments to medication dosages, dietary recommendations, and lifestyle modifications on an individualized basis.
Lifestyle interventions: Precision medicine also recognizes that lifestyle factors play a crucial role in the development and management of T2DM. Lifestyle interventions, such as diet and exercise plans, based on an individual's preferences, metabolic profile, and response to different interventions can be personalized (ie, some individuals may benefit more from a low-carbohydrate diet, while others may respond better to a Mediterranean-style diet).
Predictive modeling and risk stratification: Precision medicine leverages data analytics and predictive modeling to assess an individual's risk of developing complications associated with T2DM. By analyzing various factors such as medical history, genetics, lifestyle, and biomarkers, individuals who are at a higher risk of developing complications can be identified, and their treatment plans can be tailored accordingly. Precision medicine enables early identification of individuals who are at a higher risk of developing T2DM based on their metabolic syndrome status.
In summary, precision medicine for T2DM considers the link between metabolic syndrome and diabetes syndrome to develop personalized approaches for prevention, early intervention, and treatment. By understanding an individual's metabolic and genetic profile, targeted strategies to optimize management and improve outcomes for patients with metabolic syndrome and those at risk of developing diabetes can be implemented.
It is important to note that while precision medicine holds promise in improving diabetes management, it is still an evolving field, and its widespread implementation is not yet fully realized. Collaboration between clinicians, researchers, and technological advancements will continue to drive the progress of precision medicine in T2DM management.
Metabolic syndrome, type 2 diabetes mellitus (T2DM), and the “diabetes syndrome,” are interrelated, serious health conditions that share common risk factors and mechanisms. While they are each distinct conditions, a significant association exists between them, with metabolic syndrome often being considered a precursor to the development of typical T2DM.
Metabolic syndrome is a cluster of individual metabolic abnormalities that includes a combination of risk factors such as abdominal obesity, high blood pressure, elevated insulin levels, high triglyceride levels, and low levels of high-density lipoprotein (HDL) cholesterol related to genes and epigenetic changes associated with insulin resistance. These risk factors increase the likelihood of developing cardiovascular diseases, such as heart disease and stroke, and, when combined with significant damage to β -cell function and the influence of concordant environmental precipitants, result in hyperglycemia/overt diabetes—classically defined as T2DM.
It is estimated that there will be a staggering 3.1 billion people living with T2DM by 2050, according to a recent article in The Lancet. This devastating number will place a heavy burden on the health care system.
However, this typical pathophysiologic definition of T2DM is imprecise. Twenty percent of patients with T2DM have islet-cell antibodies that are typical of the immune destruction of β-cells in patients with type 1 diabetes mellitus (T1DM). Furthermore, approximately 40% of patients with T1DM have insulin resistance.
Thus, to better understand and distinguish the disease processes unique to each individual, we have defined a new beta cell classification for all forms of diabetes mellitus (DM). In this classification, there are 4 common pathophysiologic causes of all DM (including classic T2DM), with resultant damage to the β-cells (ie, genetic and epigenetic changes, inflammation, an abnormal environment, and insulin resistance), which results in 11 mechanisms of hyperglycemia, represented as “the egregious eleven” in Figure 1.
Additionally, Figure 2 illustrates the association between overlapping genes/epigenetic changes responsible for DM and the increased susceptibility to developing various microvascular complications commonly observed in all forms of DM, including classic T2DM. These complications, now recognized as components of the diabetes syndrome, encompass a range of conditions with shared interrelated pathophysiologic mechanisms, such as arteriosclerotic vascular disease (ASVD), dementia, some cancers, nonalcoholic fatty liver disease or nonalcoholic steatohepatitis (NAFLD/NASH), or psoriasis.
The likelihood of developing a specific type of DM, with classic complications or associated conditions, is contingent on an individual’s genes, epigenetic factors, inflammation, insulin resistance, and environmental exposures over time. It has now been postulated that these factors can be identified in a particular individual by a set of genomics, metabolomics, proteomics, and markers of these processes.
This more precise approach has the added benefit of giving rise to a more accurate individualization of therapy—precision medicine.
Precision medicine is an approach to healthcare that considers an individual's specific characteristics, such as genetic makeup, lifestyle, and environmental factors, to tailor medical treatments and interventions. In the context of this discussion on T2DM, precision medicine’s goal is to provide targeted therapies and interventions based on an individual's unique -omic profile to improve treatment outcomes and minimize side effects. An additional benefit of precision medicine use in diabetes syndrome is giving the diabetes specialist the opportunity to treat the whole patient, looking for complications and associated conditions earlier via defining the presence or absence of various markers of their individual pathophysiology. Additionally, we have come to recognize that many of the medications for treating T2DM (eg, glucagon-like peptide 1 receptor agonists [GLP-1 RA], dipeptidyl peptidase 4 inhibitors [DPP-4 inhibitors], sodium-glucose cotransporter-2 inhibitors [SGLT-2 inhibitors], metformin, Cycloset [bromocriptine mesylate]) can offer other benefits for the patient—treating not only multiple mechanisms of hyperglycemia (the egregious eleven: use the fewest number of agents in combination to treat the most number of mechanisms of hyperglycemia) but also recognize that they can prevent and treat the complications and associated conditions of the diabetes syndrome: cardiovascular, renal, liver, some cancers, psoriasis, and dementia.
The classic link between metabolic syndrome and T2DM is important to consider when applying precision medicine approaches to the management of T2DM. Here are some examples of how precision medicine is being applied in the management of T2DM:
Genetic testing: Genetic testing can help identify specific genetic variants or mutations that may influence an individual's risk of developing T2DM or their response to certain medications. By understanding a person's genetic predisposition, clinicians can make more informed decisions about treatment options and develop personalized strategies for their patients.
Pharmacogenomics: Certain genetic variations can impact how a person metabolizes and responds to specific diabetes medications. By analyzing an individual's genetic profile, medications that are more likely to be effective and have fewer adverse effects for that patient may be selected.
Continuous glucose monitoring (CGM): CGM devices provide real-time information about an individual’s blood glucose levels, allowing for more precise management of diabetes. By continuously monitoring glucose levels, patterns can be identified, allowing for adjustments to medication dosages, dietary recommendations, and lifestyle modifications on an individualized basis.
Lifestyle interventions: Precision medicine also recognizes that lifestyle factors play a crucial role in the development and management of T2DM. Lifestyle interventions, such as diet and exercise plans, based on an individual's preferences, metabolic profile, and response to different interventions can be personalized (ie, some individuals may benefit more from a low-carbohydrate diet, while others may respond better to a Mediterranean-style diet).
Predictive modeling and risk stratification: Precision medicine leverages data analytics and predictive modeling to assess an individual's risk of developing complications associated with T2DM. By analyzing various factors such as medical history, genetics, lifestyle, and biomarkers, individuals who are at a higher risk of developing complications can be identified, and their treatment plans can be tailored accordingly. Precision medicine enables early identification of individuals who are at a higher risk of developing T2DM based on their metabolic syndrome status.
In summary, precision medicine for T2DM considers the link between metabolic syndrome and diabetes syndrome to develop personalized approaches for prevention, early intervention, and treatment. By understanding an individual's metabolic and genetic profile, targeted strategies to optimize management and improve outcomes for patients with metabolic syndrome and those at risk of developing diabetes can be implemented.
It is important to note that while precision medicine holds promise in improving diabetes management, it is still an evolving field, and its widespread implementation is not yet fully realized. Collaboration between clinicians, researchers, and technological advancements will continue to drive the progress of precision medicine in T2DM management.
Metabolic syndrome, type 2 diabetes mellitus (T2DM), and the “diabetes syndrome,” are interrelated, serious health conditions that share common risk factors and mechanisms. While they are each distinct conditions, a significant association exists between them, with metabolic syndrome often being considered a precursor to the development of typical T2DM.
Metabolic syndrome is a cluster of individual metabolic abnormalities that includes a combination of risk factors such as abdominal obesity, high blood pressure, elevated insulin levels, high triglyceride levels, and low levels of high-density lipoprotein (HDL) cholesterol related to genes and epigenetic changes associated with insulin resistance. These risk factors increase the likelihood of developing cardiovascular diseases, such as heart disease and stroke, and, when combined with significant damage to β -cell function and the influence of concordant environmental precipitants, result in hyperglycemia/overt diabetes—classically defined as T2DM.
It is estimated that there will be a staggering 3.1 billion people living with T2DM by 2050, according to a recent article in The Lancet. This devastating number will place a heavy burden on the health care system.
However, this typical pathophysiologic definition of T2DM is imprecise. Twenty percent of patients with T2DM have islet-cell antibodies that are typical of the immune destruction of β-cells in patients with type 1 diabetes mellitus (T1DM). Furthermore, approximately 40% of patients with T1DM have insulin resistance.
Thus, to better understand and distinguish the disease processes unique to each individual, we have defined a new beta cell classification for all forms of diabetes mellitus (DM). In this classification, there are 4 common pathophysiologic causes of all DM (including classic T2DM), with resultant damage to the β-cells (ie, genetic and epigenetic changes, inflammation, an abnormal environment, and insulin resistance), which results in 11 mechanisms of hyperglycemia, represented as “the egregious eleven” in Figure 1.
Additionally, Figure 2 illustrates the association between overlapping genes/epigenetic changes responsible for DM and the increased susceptibility to developing various microvascular complications commonly observed in all forms of DM, including classic T2DM. These complications, now recognized as components of the diabetes syndrome, encompass a range of conditions with shared interrelated pathophysiologic mechanisms, such as arteriosclerotic vascular disease (ASVD), dementia, some cancers, nonalcoholic fatty liver disease or nonalcoholic steatohepatitis (NAFLD/NASH), or psoriasis.
The likelihood of developing a specific type of DM, with classic complications or associated conditions, is contingent on an individual’s genes, epigenetic factors, inflammation, insulin resistance, and environmental exposures over time. It has now been postulated that these factors can be identified in a particular individual by a set of genomics, metabolomics, proteomics, and markers of these processes.
This more precise approach has the added benefit of giving rise to a more accurate individualization of therapy—precision medicine.
Precision medicine is an approach to healthcare that considers an individual's specific characteristics, such as genetic makeup, lifestyle, and environmental factors, to tailor medical treatments and interventions. In the context of this discussion on T2DM, precision medicine’s goal is to provide targeted therapies and interventions based on an individual's unique -omic profile to improve treatment outcomes and minimize side effects. An additional benefit of precision medicine use in diabetes syndrome is giving the diabetes specialist the opportunity to treat the whole patient, looking for complications and associated conditions earlier via defining the presence or absence of various markers of their individual pathophysiology. Additionally, we have come to recognize that many of the medications for treating T2DM (eg, glucagon-like peptide 1 receptor agonists [GLP-1 RA], dipeptidyl peptidase 4 inhibitors [DPP-4 inhibitors], sodium-glucose cotransporter-2 inhibitors [SGLT-2 inhibitors], metformin, Cycloset [bromocriptine mesylate]) can offer other benefits for the patient—treating not only multiple mechanisms of hyperglycemia (the egregious eleven: use the fewest number of agents in combination to treat the most number of mechanisms of hyperglycemia) but also recognize that they can prevent and treat the complications and associated conditions of the diabetes syndrome: cardiovascular, renal, liver, some cancers, psoriasis, and dementia.
The classic link between metabolic syndrome and T2DM is important to consider when applying precision medicine approaches to the management of T2DM. Here are some examples of how precision medicine is being applied in the management of T2DM:
Genetic testing: Genetic testing can help identify specific genetic variants or mutations that may influence an individual's risk of developing T2DM or their response to certain medications. By understanding a person's genetic predisposition, clinicians can make more informed decisions about treatment options and develop personalized strategies for their patients.
Pharmacogenomics: Certain genetic variations can impact how a person metabolizes and responds to specific diabetes medications. By analyzing an individual's genetic profile, medications that are more likely to be effective and have fewer adverse effects for that patient may be selected.
Continuous glucose monitoring (CGM): CGM devices provide real-time information about an individual’s blood glucose levels, allowing for more precise management of diabetes. By continuously monitoring glucose levels, patterns can be identified, allowing for adjustments to medication dosages, dietary recommendations, and lifestyle modifications on an individualized basis.
Lifestyle interventions: Precision medicine also recognizes that lifestyle factors play a crucial role in the development and management of T2DM. Lifestyle interventions, such as diet and exercise plans, based on an individual's preferences, metabolic profile, and response to different interventions can be personalized (ie, some individuals may benefit more from a low-carbohydrate diet, while others may respond better to a Mediterranean-style diet).
Predictive modeling and risk stratification: Precision medicine leverages data analytics and predictive modeling to assess an individual's risk of developing complications associated with T2DM. By analyzing various factors such as medical history, genetics, lifestyle, and biomarkers, individuals who are at a higher risk of developing complications can be identified, and their treatment plans can be tailored accordingly. Precision medicine enables early identification of individuals who are at a higher risk of developing T2DM based on their metabolic syndrome status.
In summary, precision medicine for T2DM considers the link between metabolic syndrome and diabetes syndrome to develop personalized approaches for prevention, early intervention, and treatment. By understanding an individual's metabolic and genetic profile, targeted strategies to optimize management and improve outcomes for patients with metabolic syndrome and those at risk of developing diabetes can be implemented.
It is important to note that while precision medicine holds promise in improving diabetes management, it is still an evolving field, and its widespread implementation is not yet fully realized. Collaboration between clinicians, researchers, and technological advancements will continue to drive the progress of precision medicine in T2DM management.
Circulating Tumor DNA Testing and Liquid Biopsy: The Future for Precision Medicine and Guided Targeted Therapy for Breast Cancer?

The current standard for breast cancer screening (for non–high-risk patients) is an annual or semiannual mammogram for women aged 40 and older.1 However, mammography-based screening can give false-positive or false-negative results. This can lead to excessive use of invasive tissue biopsies and unnecessary exposure to ionizing radiation—which can also become expensive and time-consuming for patients.2
Both normal and cancerous cells shed cell-free DNA (cfDNA) into the blood circulation.3 Circulating tumor DNA (ctDNA) are fragments of DNA derived from tumor cells that circulate in the blood together with cfDNA. The ctDNA originates directly from a tumor or from circulating tumor cells (and carries information from the tumor cell genome), whereas cfDNA enters the bloodstream after apoptosis or necrosis and carries genome-wide DNA information. The amount of ctDNA in the blood has been shown to be elevated in patients with cancer.3 Different cancers release varying levels of ctDNA; the amount of ctDNA released depends on the number of tumor cells that are in senescence vs undergoing apoptosis.4
The possibility of incorporating this biomarker obtained from a “liquid biopsy” is currently being studied and will hopefully become a standard of care for breast cancer screening and monitoring. The liquid biopsy detects ctDNA that has been released into the bloodstream from tumor regions and helps identify intratumoral heterogeneity and clonal evolution.5 Additionally, sequencing tumor DNA has opened new possibilities for precision oncology.6 Detection of somatic gene mutations, amplifications, and gene fusions helps to deliver targeted therapies.6 Analysis of potential somatic mutations in ctDNA, in combination with cfDNA levels, can help capture clinically relevant information beyond single genetic alterations and tumor fraction, potentially improving the accuracy of early detection and screening for breast cancer.
Recent advances in ctDNA testing technology have made it more accurate and reliable. ctDNA testing has several benefits, including early detection of cancer (detecting ctDNA at low levels)7; monitoring of tumor dynamics, therapeutic response, and residual disease8; as well as analysis of the evolution of genetic or epigenetic alterations characterizing the tumor.9 Its noninvasiveness, rapidity, and low cost allow for longitudinal monitoring of cancer in real time, potentially capturing tumor heterogeneity.10,11
The liquid biopsy potentially can give more options for therapeutic monitoring for breast cancer and may mirror clinically relevant genetic alterations that occur in all tumor tissues. Liquid biopsy offers many advantages. It allows for the detection of minimal residual disease and micrometastatic disease that may be difficult to detect with a traditional tissue biopsy.12 Liquid biopsy detects ctDNA that has been released into the bloodstream from multiple tumor regions and allows the possibility of identifying intratumoral heterogeneity and clonal evolution.5 It can also detect small quantitative variations within the blood, enabling real-time surveillance.
The liquid biopsy can offer earlier and easier access to some tumor-based genetic information at any given timepoint and can replace a tumor tissue biopsy in some cases, helping to avoid delays and complications of a solid tumor invasive biopsy procedure. This is especially relevant in the metastatic setting, in which ctDNA might be the only available genetic material from tumors.13 Tissue biopsy can only provide a static and spatially limited view of the disease at the time of sampling; ctDNA analysis could potentially reflect the genetic alterations that occur in all metastatic breast cancer sites over time.14,15 Furthermore, machine learning of multi-gene signatures, obtained from ctDNA, can possibly identify complex biological features, including measures of tumor proliferation and estrogen receptor signaling, similar to direct tumor tissue DNA or RNA profiling.16
ctDNA testing is currently being studied to monitor patients who have been diagnosed with breast cancer. Small retrospective studies have shown that detection of ctDNA in plasma, after patients have completed therapy for early-stage breast cancer, is associated with a very high risk of relapse.17
Ongoing studies are examining the tailoring of adjuvant treatment based on ctDNA. If these trials are successful, certain aspects of adjuvant treatment could be lessened, or omitted, for patients who have undetectable ctDNA or intensified for patients who have detectable ctDNA after definitive treatments. This could personalize treatment specifically to the patient.
The detection and persistence of ctDNA in the middle of neoadjuvant systemic therapy may have the potential to negatively predict response to treatment and identify patients who will not achieve pathologic complete response. This may have the potential to aid in clinical decision-making for treatment escalation in these nonresponders.18
Despite these distinct characteristics, the low levels of ctDNA found in early-stage disease, along with the lack of ctDNA shedding from some tumors, can further complicate or impede detection of recurrence in early-stage breast cancer. Testing is further complicated by hematologic genetic alterations.5 The limitation of ctDNA approaches is that these techniques only detect known mutations in certain genes, so patients without these mutations could be overlooked, limiting the application of this technology.19
Overall, ctDNA testing represents a promising area of research for the diagnosis, treatment, and monitoring of breast cancer. While more research is needed to fully understand its potential, the advances in this technology are certainly exciting and could lead to significant improvements in patient outcomes. It is hopeful that in the near future, ctDNA testing from liquid biopsy could become a standard of care in breast cancer screening, ultimately helping clinicians to personalize treatment therapies and improve patient outcomes when treating patients with breast cancer.
1. Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599-1614.
2. Zubor P, Kubatka P, Kajo K, et al. Why the gold standard approach by mammography demands extension by multiomics? Application of liquid biopsy miRNA profiles to breast cancer disease management. Int J Mol Sci. 2019;20(12):E2878.
3. Thierry AR, El Messaoudi S, Gahan PB, Anker P, Stroun M. Origins, structures, and functions of circulating DNA in oncology. Cancer Metastasis Rev. 2016;35(3):347-376.
4. Rostami A, Lambie M, Yu CW, Stambolic V, Waldron JN, Bratman SV. Senescence, necrosis, and apoptosis govern circulating cell-free DNA release kinetics. Cell Rep. 2020;31(13):107830.
5. De Rubis G, Rajeev Krishnan S, Bebawy M. Liquid biopsies in cancer diagnosis, monitoring, and prognosis. Trends Pharmacol Sci. 2019;40(3):172-186.
6. Mateo J, Chakravarty D, Dienstmann R, et al. A framework to rank genomic alterations as targets for cancer precision medicine: the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT). Ann Oncol. 2018;29:1895-1902.
7. Wang J, Han X, Sun Y. DNA methylation signatures in circulating cell-free DNA as biomarkers for the early detection of cancer. Sci China Life Sci. 2017;60(4):356-362.
8. Dawson S-J, Tsui DWY, Murtaza M, et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N Engl J Med. 2013;368(13):1199-1209.
9. Diaz Jr LA, Bardelli A. Liquid biopsies: genotyping circulating tumor DNA. J Clin Oncol. 2014;32(6):579-586.
10. Oxnard GR, Paweletz CP, Kuang Y, et al. Noninvasive detection of response and resistance in EGFR-mutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA. Clin Cancer Res. 2014;20(6):1698-1705.
11. Jamal-Hanjani M, Wilson GA, Horswell S, et al. Detection of ubiquitous and heterogeneous mutations in cell-free DNA from patients with early-stage non-small-cell lung cancer. Ann Oncol. 2016;27(5):862-867.
12. Fiala C, Diamandis EP. Utility of circulating tumor DNA in cancer diagnostics with
13. Xia Y, Fan C, Hoadley KA, Parker JS, Perou CM. Genetic determinants of the molecular portraits of epithelial cancers. Nat Commun. 2019;10(1):5666.
14. Wan JCM, Massie C, Garcia-Corbacho J, et al. Liquid biopsies come of age: towards implementation of circulating tumour DNA. Nat Rev Cancer. 2017;17(4):223-238.
15. Boldrin E, Nardo G, Zulato E, et al. Detection of loss of heterozygosity in cfDNA of advanced EGFR- or KRAS-mutated non-small-cell lung cancer patients. Int J Mol Sci. 2019;21(1):66.
16. Prat A, Brasó-Maristany F, Martínez-Sáez O, et al. Circulating tumor DNA reveals complex biological features with clinical relevance in metastatic breast cancer. Nat Commun. 2023;14(1):1157.
17. Coombes RC, Page K, Salari R, et al. Personalized detection of circulating tumor DNA antedates breast cancer metastatic recurrence. Clin Cancer Res. 2019;25(14):4255-4263.
18. Zhou Q, Gampenrieder SP, Frantal S, et al. Persistence of ctDNA in patients with breast cancer during neoadjuvant treatment is a significant predictor of poor tumor response. Clin Cancer Res. 2022;28(4):697-707.
19. Lin C, Liu X, Zheng B, Ke R, Tzeng C-M. Liquid biopsy, ctDNA diagnosis through NGS. Life (Basel). 2021;11(9):890.
The current standard for breast cancer screening (for non–high-risk patients) is an annual or semiannual mammogram for women aged 40 and older.1 However, mammography-based screening can give false-positive or false-negative results. This can lead to excessive use of invasive tissue biopsies and unnecessary exposure to ionizing radiation—which can also become expensive and time-consuming for patients.2
Both normal and cancerous cells shed cell-free DNA (cfDNA) into the blood circulation.3 Circulating tumor DNA (ctDNA) are fragments of DNA derived from tumor cells that circulate in the blood together with cfDNA. The ctDNA originates directly from a tumor or from circulating tumor cells (and carries information from the tumor cell genome), whereas cfDNA enters the bloodstream after apoptosis or necrosis and carries genome-wide DNA information. The amount of ctDNA in the blood has been shown to be elevated in patients with cancer.3 Different cancers release varying levels of ctDNA; the amount of ctDNA released depends on the number of tumor cells that are in senescence vs undergoing apoptosis.4
The possibility of incorporating this biomarker obtained from a “liquid biopsy” is currently being studied and will hopefully become a standard of care for breast cancer screening and monitoring. The liquid biopsy detects ctDNA that has been released into the bloodstream from tumor regions and helps identify intratumoral heterogeneity and clonal evolution.5 Additionally, sequencing tumor DNA has opened new possibilities for precision oncology.6 Detection of somatic gene mutations, amplifications, and gene fusions helps to deliver targeted therapies.6 Analysis of potential somatic mutations in ctDNA, in combination with cfDNA levels, can help capture clinically relevant information beyond single genetic alterations and tumor fraction, potentially improving the accuracy of early detection and screening for breast cancer.
Recent advances in ctDNA testing technology have made it more accurate and reliable. ctDNA testing has several benefits, including early detection of cancer (detecting ctDNA at low levels)7; monitoring of tumor dynamics, therapeutic response, and residual disease8; as well as analysis of the evolution of genetic or epigenetic alterations characterizing the tumor.9 Its noninvasiveness, rapidity, and low cost allow for longitudinal monitoring of cancer in real time, potentially capturing tumor heterogeneity.10,11
The liquid biopsy potentially can give more options for therapeutic monitoring for breast cancer and may mirror clinically relevant genetic alterations that occur in all tumor tissues. Liquid biopsy offers many advantages. It allows for the detection of minimal residual disease and micrometastatic disease that may be difficult to detect with a traditional tissue biopsy.12 Liquid biopsy detects ctDNA that has been released into the bloodstream from multiple tumor regions and allows the possibility of identifying intratumoral heterogeneity and clonal evolution.5 It can also detect small quantitative variations within the blood, enabling real-time surveillance.
The liquid biopsy can offer earlier and easier access to some tumor-based genetic information at any given timepoint and can replace a tumor tissue biopsy in some cases, helping to avoid delays and complications of a solid tumor invasive biopsy procedure. This is especially relevant in the metastatic setting, in which ctDNA might be the only available genetic material from tumors.13 Tissue biopsy can only provide a static and spatially limited view of the disease at the time of sampling; ctDNA analysis could potentially reflect the genetic alterations that occur in all metastatic breast cancer sites over time.14,15 Furthermore, machine learning of multi-gene signatures, obtained from ctDNA, can possibly identify complex biological features, including measures of tumor proliferation and estrogen receptor signaling, similar to direct tumor tissue DNA or RNA profiling.16
ctDNA testing is currently being studied to monitor patients who have been diagnosed with breast cancer. Small retrospective studies have shown that detection of ctDNA in plasma, after patients have completed therapy for early-stage breast cancer, is associated with a very high risk of relapse.17
Ongoing studies are examining the tailoring of adjuvant treatment based on ctDNA. If these trials are successful, certain aspects of adjuvant treatment could be lessened, or omitted, for patients who have undetectable ctDNA or intensified for patients who have detectable ctDNA after definitive treatments. This could personalize treatment specifically to the patient.
The detection and persistence of ctDNA in the middle of neoadjuvant systemic therapy may have the potential to negatively predict response to treatment and identify patients who will not achieve pathologic complete response. This may have the potential to aid in clinical decision-making for treatment escalation in these nonresponders.18
Despite these distinct characteristics, the low levels of ctDNA found in early-stage disease, along with the lack of ctDNA shedding from some tumors, can further complicate or impede detection of recurrence in early-stage breast cancer. Testing is further complicated by hematologic genetic alterations.5 The limitation of ctDNA approaches is that these techniques only detect known mutations in certain genes, so patients without these mutations could be overlooked, limiting the application of this technology.19
Overall, ctDNA testing represents a promising area of research for the diagnosis, treatment, and monitoring of breast cancer. While more research is needed to fully understand its potential, the advances in this technology are certainly exciting and could lead to significant improvements in patient outcomes. It is hopeful that in the near future, ctDNA testing from liquid biopsy could become a standard of care in breast cancer screening, ultimately helping clinicians to personalize treatment therapies and improve patient outcomes when treating patients with breast cancer.
The current standard for breast cancer screening (for non–high-risk patients) is an annual or semiannual mammogram for women aged 40 and older.1 However, mammography-based screening can give false-positive or false-negative results. This can lead to excessive use of invasive tissue biopsies and unnecessary exposure to ionizing radiation—which can also become expensive and time-consuming for patients.2
Both normal and cancerous cells shed cell-free DNA (cfDNA) into the blood circulation.3 Circulating tumor DNA (ctDNA) are fragments of DNA derived from tumor cells that circulate in the blood together with cfDNA. The ctDNA originates directly from a tumor or from circulating tumor cells (and carries information from the tumor cell genome), whereas cfDNA enters the bloodstream after apoptosis or necrosis and carries genome-wide DNA information. The amount of ctDNA in the blood has been shown to be elevated in patients with cancer.3 Different cancers release varying levels of ctDNA; the amount of ctDNA released depends on the number of tumor cells that are in senescence vs undergoing apoptosis.4
The possibility of incorporating this biomarker obtained from a “liquid biopsy” is currently being studied and will hopefully become a standard of care for breast cancer screening and monitoring. The liquid biopsy detects ctDNA that has been released into the bloodstream from tumor regions and helps identify intratumoral heterogeneity and clonal evolution.5 Additionally, sequencing tumor DNA has opened new possibilities for precision oncology.6 Detection of somatic gene mutations, amplifications, and gene fusions helps to deliver targeted therapies.6 Analysis of potential somatic mutations in ctDNA, in combination with cfDNA levels, can help capture clinically relevant information beyond single genetic alterations and tumor fraction, potentially improving the accuracy of early detection and screening for breast cancer.
Recent advances in ctDNA testing technology have made it more accurate and reliable. ctDNA testing has several benefits, including early detection of cancer (detecting ctDNA at low levels)7; monitoring of tumor dynamics, therapeutic response, and residual disease8; as well as analysis of the evolution of genetic or epigenetic alterations characterizing the tumor.9 Its noninvasiveness, rapidity, and low cost allow for longitudinal monitoring of cancer in real time, potentially capturing tumor heterogeneity.10,11
The liquid biopsy potentially can give more options for therapeutic monitoring for breast cancer and may mirror clinically relevant genetic alterations that occur in all tumor tissues. Liquid biopsy offers many advantages. It allows for the detection of minimal residual disease and micrometastatic disease that may be difficult to detect with a traditional tissue biopsy.12 Liquid biopsy detects ctDNA that has been released into the bloodstream from multiple tumor regions and allows the possibility of identifying intratumoral heterogeneity and clonal evolution.5 It can also detect small quantitative variations within the blood, enabling real-time surveillance.
The liquid biopsy can offer earlier and easier access to some tumor-based genetic information at any given timepoint and can replace a tumor tissue biopsy in some cases, helping to avoid delays and complications of a solid tumor invasive biopsy procedure. This is especially relevant in the metastatic setting, in which ctDNA might be the only available genetic material from tumors.13 Tissue biopsy can only provide a static and spatially limited view of the disease at the time of sampling; ctDNA analysis could potentially reflect the genetic alterations that occur in all metastatic breast cancer sites over time.14,15 Furthermore, machine learning of multi-gene signatures, obtained from ctDNA, can possibly identify complex biological features, including measures of tumor proliferation and estrogen receptor signaling, similar to direct tumor tissue DNA or RNA profiling.16
ctDNA testing is currently being studied to monitor patients who have been diagnosed with breast cancer. Small retrospective studies have shown that detection of ctDNA in plasma, after patients have completed therapy for early-stage breast cancer, is associated with a very high risk of relapse.17
Ongoing studies are examining the tailoring of adjuvant treatment based on ctDNA. If these trials are successful, certain aspects of adjuvant treatment could be lessened, or omitted, for patients who have undetectable ctDNA or intensified for patients who have detectable ctDNA after definitive treatments. This could personalize treatment specifically to the patient.
The detection and persistence of ctDNA in the middle of neoadjuvant systemic therapy may have the potential to negatively predict response to treatment and identify patients who will not achieve pathologic complete response. This may have the potential to aid in clinical decision-making for treatment escalation in these nonresponders.18
Despite these distinct characteristics, the low levels of ctDNA found in early-stage disease, along with the lack of ctDNA shedding from some tumors, can further complicate or impede detection of recurrence in early-stage breast cancer. Testing is further complicated by hematologic genetic alterations.5 The limitation of ctDNA approaches is that these techniques only detect known mutations in certain genes, so patients without these mutations could be overlooked, limiting the application of this technology.19
Overall, ctDNA testing represents a promising area of research for the diagnosis, treatment, and monitoring of breast cancer. While more research is needed to fully understand its potential, the advances in this technology are certainly exciting and could lead to significant improvements in patient outcomes. It is hopeful that in the near future, ctDNA testing from liquid biopsy could become a standard of care in breast cancer screening, ultimately helping clinicians to personalize treatment therapies and improve patient outcomes when treating patients with breast cancer.
1. Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599-1614.
2. Zubor P, Kubatka P, Kajo K, et al. Why the gold standard approach by mammography demands extension by multiomics? Application of liquid biopsy miRNA profiles to breast cancer disease management. Int J Mol Sci. 2019;20(12):E2878.
3. Thierry AR, El Messaoudi S, Gahan PB, Anker P, Stroun M. Origins, structures, and functions of circulating DNA in oncology. Cancer Metastasis Rev. 2016;35(3):347-376.
4. Rostami A, Lambie M, Yu CW, Stambolic V, Waldron JN, Bratman SV. Senescence, necrosis, and apoptosis govern circulating cell-free DNA release kinetics. Cell Rep. 2020;31(13):107830.
5. De Rubis G, Rajeev Krishnan S, Bebawy M. Liquid biopsies in cancer diagnosis, monitoring, and prognosis. Trends Pharmacol Sci. 2019;40(3):172-186.
6. Mateo J, Chakravarty D, Dienstmann R, et al. A framework to rank genomic alterations as targets for cancer precision medicine: the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT). Ann Oncol. 2018;29:1895-1902.
7. Wang J, Han X, Sun Y. DNA methylation signatures in circulating cell-free DNA as biomarkers for the early detection of cancer. Sci China Life Sci. 2017;60(4):356-362.
8. Dawson S-J, Tsui DWY, Murtaza M, et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N Engl J Med. 2013;368(13):1199-1209.
9. Diaz Jr LA, Bardelli A. Liquid biopsies: genotyping circulating tumor DNA. J Clin Oncol. 2014;32(6):579-586.
10. Oxnard GR, Paweletz CP, Kuang Y, et al. Noninvasive detection of response and resistance in EGFR-mutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA. Clin Cancer Res. 2014;20(6):1698-1705.
11. Jamal-Hanjani M, Wilson GA, Horswell S, et al. Detection of ubiquitous and heterogeneous mutations in cell-free DNA from patients with early-stage non-small-cell lung cancer. Ann Oncol. 2016;27(5):862-867.
12. Fiala C, Diamandis EP. Utility of circulating tumor DNA in cancer diagnostics with
13. Xia Y, Fan C, Hoadley KA, Parker JS, Perou CM. Genetic determinants of the molecular portraits of epithelial cancers. Nat Commun. 2019;10(1):5666.
14. Wan JCM, Massie C, Garcia-Corbacho J, et al. Liquid biopsies come of age: towards implementation of circulating tumour DNA. Nat Rev Cancer. 2017;17(4):223-238.
15. Boldrin E, Nardo G, Zulato E, et al. Detection of loss of heterozygosity in cfDNA of advanced EGFR- or KRAS-mutated non-small-cell lung cancer patients. Int J Mol Sci. 2019;21(1):66.
16. Prat A, Brasó-Maristany F, Martínez-Sáez O, et al. Circulating tumor DNA reveals complex biological features with clinical relevance in metastatic breast cancer. Nat Commun. 2023;14(1):1157.
17. Coombes RC, Page K, Salari R, et al. Personalized detection of circulating tumor DNA antedates breast cancer metastatic recurrence. Clin Cancer Res. 2019;25(14):4255-4263.
18. Zhou Q, Gampenrieder SP, Frantal S, et al. Persistence of ctDNA in patients with breast cancer during neoadjuvant treatment is a significant predictor of poor tumor response. Clin Cancer Res. 2022;28(4):697-707.
19. Lin C, Liu X, Zheng B, Ke R, Tzeng C-M. Liquid biopsy, ctDNA diagnosis through NGS. Life (Basel). 2021;11(9):890.
1. Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599-1614.
2. Zubor P, Kubatka P, Kajo K, et al. Why the gold standard approach by mammography demands extension by multiomics? Application of liquid biopsy miRNA profiles to breast cancer disease management. Int J Mol Sci. 2019;20(12):E2878.
3. Thierry AR, El Messaoudi S, Gahan PB, Anker P, Stroun M. Origins, structures, and functions of circulating DNA in oncology. Cancer Metastasis Rev. 2016;35(3):347-376.
4. Rostami A, Lambie M, Yu CW, Stambolic V, Waldron JN, Bratman SV. Senescence, necrosis, and apoptosis govern circulating cell-free DNA release kinetics. Cell Rep. 2020;31(13):107830.
5. De Rubis G, Rajeev Krishnan S, Bebawy M. Liquid biopsies in cancer diagnosis, monitoring, and prognosis. Trends Pharmacol Sci. 2019;40(3):172-186.
6. Mateo J, Chakravarty D, Dienstmann R, et al. A framework to rank genomic alterations as targets for cancer precision medicine: the ESMO Scale for Clinical Actionability of molecular Targets (ESCAT). Ann Oncol. 2018;29:1895-1902.
7. Wang J, Han X, Sun Y. DNA methylation signatures in circulating cell-free DNA as biomarkers for the early detection of cancer. Sci China Life Sci. 2017;60(4):356-362.
8. Dawson S-J, Tsui DWY, Murtaza M, et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N Engl J Med. 2013;368(13):1199-1209.
9. Diaz Jr LA, Bardelli A. Liquid biopsies: genotyping circulating tumor DNA. J Clin Oncol. 2014;32(6):579-586.
10. Oxnard GR, Paweletz CP, Kuang Y, et al. Noninvasive detection of response and resistance in EGFR-mutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA. Clin Cancer Res. 2014;20(6):1698-1705.
11. Jamal-Hanjani M, Wilson GA, Horswell S, et al. Detection of ubiquitous and heterogeneous mutations in cell-free DNA from patients with early-stage non-small-cell lung cancer. Ann Oncol. 2016;27(5):862-867.