User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Local hospitals still have a role in treating severe stroke
a new study has shown.

In the RACECAT trial, functional outcomes were similar for patients suspected of having a large-vessel occlusion stroke who were located in areas not currently served by a comprehensive stroke center, whether they were first taken to a local primary stroke center or whether they were transported over a longer distance to a comprehensive center.
“Under the particular conditions in our study where we had a very well-organized system, a ‘mothership’ transfer protocol for patients with suspected large-vessel occlusion has not proven superior over the ‘drip-and-ship’ protocol, but the opposite is also true,” lead investigator Marc Ribo, MD, concluded.
Dr. Ribo, assistant professor of neurology at Hospital Vall d’Hebron, Barcelona, presented the RACECAT results at the European Stroke Organisation–World Stroke Organisation (ESO-WSO) Conference 2020.
Dr. Ribo said in an interview that there is a feeling among the stroke community that patients with a suspected large-vessel occlusion should be transferred directly to a comprehensive stroke center capable of performing endovascular thrombectomy, even if there is a nearer, smaller primary stroke center where patients are usually taken first for thrombolysis.
“Many stroke neurologists believe we are losing time by sending patients with severe stroke to a local hospital and that we should skip this step, but this is controversial area,” he commented. “Our findings suggest that we should not automatically bypass local stroke centers.”
Dr. Ribo pointed out that the local centers performed very well in the study, with very fast “in/out” times for patients who were subsequently transferred for thrombectomy.
“On the basis of our results, we recommend that if a local stroke center can perform well like ours did – if they are within the time indicators for treating and transferring patients – then they should keep receiving these patients. But if they are not performing well in this regard, then they should probably be bypassed,” he commented.
The RACECAT trial was well received by stroke experts at an ESO-WSO 2020 press conference at which it was discussed.
Stefan Kiechl, MD, Medical University Innsbruck (Austria), described the trial as “outstanding,” adding: “It has addressed a very important question. It is a big achievement in stroke medicine.”
Patrik Michel, MD, Lausanne (Switzerland) University Hospital, said that “this is a very important and highly sophisticated trial in terms of design and execution. The message is that it doesn’t matter which pathway is used, but it is important to have a well-organized network with highly trained paramedics.”
RACECAT
The RACECAT trial was conducted in the Catalonia region of Spain. Twenty-seven hospitals participated, including 7 comprehensive stroke centers and 20 local stroke centers.
The trial included stroke patients with suspected large-vessel occlusion stroke, as determined on the basis of evaluation by paramedics using the criteria of a Rapid Arterial Occlusion Evaluation (RACE) scale score above 4 and on the basis of a call to a vascular neurologist. For inclusion in the study, patients had to be in a geographical area not served by a comprehensive stroke center and to have an estimated arrival time to a comprehensive center of less than 7 hours from symptom onset in order that thrombectomy would be possible.
Of 7,475 stroke code patients evaluated, 1,401 met the inclusion criteria and were randomly assigned to be transferred to a local hospital or to a comprehensive stroke center farther away.
Baseline characteristics were similar between the two groups. The patients had severe strokes with an average National Institutes of Health Stroke Scale score of 17. It was later confirmed that 46% of the patients enrolled in the study had a large-vessel occlusion stroke.
Results showed that time from symptom onset to hospital arrival was 142 minutes for those taken to a local center and 216 minutes for those taken to a comprehensive stroke center. Of those taken to a local hospital, 86% arrived within 4 hours of symptom onset and so were potential candidates for thrombolysis, compared with 76% of those taken to a comprehensive center.
Of the patients taken to a local hospital, 60% were given thrombolysis versus 43% of those taken immediately to a comprehensive center. On the other hand, 50% of patients who were taken directly to a comprehensive center underwent thrombectomy, compared with 40% who were first taken to a local center.
For patients who received thrombolysis, time to tissue plasminogen activator administration was 120 minutes for those treated at a local hospital versus 155 minutes for those taken directly to a comprehensive center.
For patients who received thrombectomy, time from symptom onset to groin puncture was 270 minutes if they were first taken to a local hospital and were then transferred, versus 214 minutes for those taken directly to the comprehensive center.
The primary efficacy endpoint was functional outcome using Modified Rankin Scale (mRS) shift analysis at 90 days for ischemic stroke patients. This showed a “completely flat” result, Dr. Ribo reported, with an adjusted hazard ratio of 1.029 for patients taken to a comprehensive center in comparison with those taken to a local center.
“There was absolutely no trend towards benefit in one group over the other,” he said.
What about hemorrhagic stroke?
The study also evaluated functional outcomes for the whole population enrolled. “If we make the decision just based on thrombectomy-eligible patients, we may harm the rest of the patients, so we did this study to look at the whole population of severe stroke patients,” Dr. Ribo said.
Of the study population, 25% of patients were found to have had a hemorrhagic stroke.
“The problem is, at the prehospital level, it is impossible to know if a patient is having a large-vessel occlusion ischemic stroke or a hemorrhagic stroke,” Dr. Ribo explained. “We have to make a decision for the whole population, and while a longer transport time to get to a comprehensive stroke center might help a patient with a large-vessel occlusion ischemic stroke, it might not be so appropriate for patients with a hemorrhagic stroke who need to have their blood pressure stabilized as soon as possible.”
For the whole population, the mRS shift analysis at 90 days was also neutral, with an aHR of 0.965.
When considering only patients with hemorrhagic stroke, the adjusted hazard ratio for the mRS shift analysis at 90 days was 1.216, which was still nonsignificant (95% confidence interval, 0.864-1.709). This included a nonsignificant increase in mortality among those taken directly to a comprehensive center.
“If we had better tools for a certain diagnosis in the field, then we could consider taking large-vessel occlusion ischemic stroke patients to a comprehensive center and hemorrhagic stroke patients to the local stroke center, but so far, we don’t have this option apart from a few places using mobile stroke units with CT scanners,” Dr. Ribo noted.
Transfer times to comprehensive centers in the study ranged from 30 minutes to 2.5 hours. “There might well be a difference in outcomes for short and long transfers, and we may be able to offer different transfer protocols in these different situations, and we are looking at that, but the study was only stopped in June, and we haven’t had a chance to analyze those results yet,” Dr. Ribo added.
Complications during transport occurred in 0.5% of those taken to a local hospital and in 1% of those taken directly to a comprehensive center. “We were concerned about complications with longer transfers, but these numbers are quite low. Intubations were very low – just one patient taken to a local center, versus three or four in the longer transfer group,” he added.
For both local and comprehensive centers, treatment times were impressive in the study. For local hospitals, the average in/out time was just 60 minutes for patients who went to a comprehensive center; for patients receiving thrombolysis, the average door to needle time was around 30 minutes.
Time to thrombectomy in the comprehensive center for patients transferred from a local hospital was also very fast, with an average door to groin puncture time of less than 40 minutes. “This shows we have a very well-oiled system,” Dr. Ribo said.
“There is always going to be a balance between a quicker time to thrombolysis by taking a patient to the closest hospital but a quicker time to thrombectomy if patients are taken straight to the comprehensive center,” he concluded. “But in our system, where we are achieving fast treatment and transfer times, our results show that patients had timely access to reperfusion therapies regardless of transfer protocol, and under these circumstances, it is fine for the emergency services to take stroke patients to the closest stroke center.”
Results applicable elsewhere?
During the discussion at an ESO-WSO 2020 press conference, other experts pointed out that the Catalonia group is a leader in this field, being the pioneers of the RACE score used in this study for paramedics to identify suspected large-vessel occlusions. This led to questions about the applicability of the results.
“The performance by paramedics was very good using the RACE scale, and the performance times were very impressive. Are these results applicable elsewhere?” Dr. Kiechl asked.
Dr. Ribo said the combination of the RACE score and a call with a vascular neurologist was of “great value” in identifying appropriate patients. Half of the patients selected in this way for the trial were confirmed to have a large-vessel occlusion. “That is a good result,” he added.
He noted that the performance of the local hospitals improved dramatically during the study. “They had an incentive to work on their times. They could have lost most of their stroke patients if their results came out worse. We told them they had an opportunity to show that they have a role in treating these patients, and they took that opportunity.”
Dr. Ribo said there were lessons here for those involved in acute stroke care. “When creating stroke transfer policies in local networks, the performances of individual centers need to be taken into account. If primary stroke centers are motivated and can work in a well-coordinated way and perform to within the recommended times, then they can keep receiving stroke code patients. This should be possible in most developed countries.”
Noting that the in/out time of 60 minutes at local hospitals was “very impressive,” Dr. Kiechl asked how such fast times were achieved.
Dr. Ribo responded that, to a great extent, this was because of ambulance staff. “We have trained the paramedics to anticipate a second transfer after delivering the patient to the local hospital so they can prepare for this rather than waiting for a second call.”
Dr. Ribo pointed out that there were other advantages in taking patients to local centers first. “For those that do not need to be transferred on, they will be closer to relatives. It is very difficult for the family if the patient is hundreds of miles away. And there may be a cost advantage. We did look at costs, but haven’t got that data yet.”
He said: “If local stroke centers do not treat so many stroke code patients, they will lose their expertise, and that will be detrimental to the remaining patients who are taken there. We want to try to maintain a good standard of stroke care across a decent spread of hospitals—not just a couple of major comprehensive centers,” he added.
Commenting on the study, Jesse Dawson, MD, University of Glasgow, who was chair of the plenary session at which the study was presented, said: “RACECAT is very interesting but needs a lot of thought to dissect. My takeaway is that we know that time to reperfusion is key, and we need to get these times as low as possible, but we don’t need to chase a particular care pathway. Thus, if your country/geography suits ‘drip and ship’ better, this is acceptable. If direct to endovascular is possible or you are close to such a center, then this is ideal. But within those paradigms, be as fast as possible.”
He added that results of the subgroups with regard to transfer time will be helpful.
The RACECAT study was funded by Fundacio Ictus Malaltia Vascular.
A version of this article originally appeared on Medscape.com.
a new study has shown.
In the RACECAT trial, functional outcomes were similar for patients suspected of having a large-vessel occlusion stroke who were located in areas not currently served by a comprehensive stroke center, whether they were first taken to a local primary stroke center or whether they were transported over a longer distance to a comprehensive center.
“Under the particular conditions in our study where we had a very well-organized system, a ‘mothership’ transfer protocol for patients with suspected large-vessel occlusion has not proven superior over the ‘drip-and-ship’ protocol, but the opposite is also true,” lead investigator Marc Ribo, MD, concluded.
Dr. Ribo, assistant professor of neurology at Hospital Vall d’Hebron, Barcelona, presented the RACECAT results at the European Stroke Organisation–World Stroke Organisation (ESO-WSO) Conference 2020.
Dr. Ribo said in an interview that there is a feeling among the stroke community that patients with a suspected large-vessel occlusion should be transferred directly to a comprehensive stroke center capable of performing endovascular thrombectomy, even if there is a nearer, smaller primary stroke center where patients are usually taken first for thrombolysis.
“Many stroke neurologists believe we are losing time by sending patients with severe stroke to a local hospital and that we should skip this step, but this is controversial area,” he commented. “Our findings suggest that we should not automatically bypass local stroke centers.”
Dr. Ribo pointed out that the local centers performed very well in the study, with very fast “in/out” times for patients who were subsequently transferred for thrombectomy.
“On the basis of our results, we recommend that if a local stroke center can perform well like ours did – if they are within the time indicators for treating and transferring patients – then they should keep receiving these patients. But if they are not performing well in this regard, then they should probably be bypassed,” he commented.
The RACECAT trial was well received by stroke experts at an ESO-WSO 2020 press conference at which it was discussed.
Stefan Kiechl, MD, Medical University Innsbruck (Austria), described the trial as “outstanding,” adding: “It has addressed a very important question. It is a big achievement in stroke medicine.”
Patrik Michel, MD, Lausanne (Switzerland) University Hospital, said that “this is a very important and highly sophisticated trial in terms of design and execution. The message is that it doesn’t matter which pathway is used, but it is important to have a well-organized network with highly trained paramedics.”
RACECAT
The RACECAT trial was conducted in the Catalonia region of Spain. Twenty-seven hospitals participated, including 7 comprehensive stroke centers and 20 local stroke centers.
The trial included stroke patients with suspected large-vessel occlusion stroke, as determined on the basis of evaluation by paramedics using the criteria of a Rapid Arterial Occlusion Evaluation (RACE) scale score above 4 and on the basis of a call to a vascular neurologist. For inclusion in the study, patients had to be in a geographical area not served by a comprehensive stroke center and to have an estimated arrival time to a comprehensive center of less than 7 hours from symptom onset in order that thrombectomy would be possible.
Of 7,475 stroke code patients evaluated, 1,401 met the inclusion criteria and were randomly assigned to be transferred to a local hospital or to a comprehensive stroke center farther away.
Baseline characteristics were similar between the two groups. The patients had severe strokes with an average National Institutes of Health Stroke Scale score of 17. It was later confirmed that 46% of the patients enrolled in the study had a large-vessel occlusion stroke.
Results showed that time from symptom onset to hospital arrival was 142 minutes for those taken to a local center and 216 minutes for those taken to a comprehensive stroke center. Of those taken to a local hospital, 86% arrived within 4 hours of symptom onset and so were potential candidates for thrombolysis, compared with 76% of those taken to a comprehensive center.
Of the patients taken to a local hospital, 60% were given thrombolysis versus 43% of those taken immediately to a comprehensive center. On the other hand, 50% of patients who were taken directly to a comprehensive center underwent thrombectomy, compared with 40% who were first taken to a local center.
For patients who received thrombolysis, time to tissue plasminogen activator administration was 120 minutes for those treated at a local hospital versus 155 minutes for those taken directly to a comprehensive center.
For patients who received thrombectomy, time from symptom onset to groin puncture was 270 minutes if they were first taken to a local hospital and were then transferred, versus 214 minutes for those taken directly to the comprehensive center.
The primary efficacy endpoint was functional outcome using Modified Rankin Scale (mRS) shift analysis at 90 days for ischemic stroke patients. This showed a “completely flat” result, Dr. Ribo reported, with an adjusted hazard ratio of 1.029 for patients taken to a comprehensive center in comparison with those taken to a local center.
“There was absolutely no trend towards benefit in one group over the other,” he said.
What about hemorrhagic stroke?
The study also evaluated functional outcomes for the whole population enrolled. “If we make the decision just based on thrombectomy-eligible patients, we may harm the rest of the patients, so we did this study to look at the whole population of severe stroke patients,” Dr. Ribo said.
Of the study population, 25% of patients were found to have had a hemorrhagic stroke.
“The problem is, at the prehospital level, it is impossible to know if a patient is having a large-vessel occlusion ischemic stroke or a hemorrhagic stroke,” Dr. Ribo explained. “We have to make a decision for the whole population, and while a longer transport time to get to a comprehensive stroke center might help a patient with a large-vessel occlusion ischemic stroke, it might not be so appropriate for patients with a hemorrhagic stroke who need to have their blood pressure stabilized as soon as possible.”
For the whole population, the mRS shift analysis at 90 days was also neutral, with an aHR of 0.965.
When considering only patients with hemorrhagic stroke, the adjusted hazard ratio for the mRS shift analysis at 90 days was 1.216, which was still nonsignificant (95% confidence interval, 0.864-1.709). This included a nonsignificant increase in mortality among those taken directly to a comprehensive center.
“If we had better tools for a certain diagnosis in the field, then we could consider taking large-vessel occlusion ischemic stroke patients to a comprehensive center and hemorrhagic stroke patients to the local stroke center, but so far, we don’t have this option apart from a few places using mobile stroke units with CT scanners,” Dr. Ribo noted.
Transfer times to comprehensive centers in the study ranged from 30 minutes to 2.5 hours. “There might well be a difference in outcomes for short and long transfers, and we may be able to offer different transfer protocols in these different situations, and we are looking at that, but the study was only stopped in June, and we haven’t had a chance to analyze those results yet,” Dr. Ribo added.
Complications during transport occurred in 0.5% of those taken to a local hospital and in 1% of those taken directly to a comprehensive center. “We were concerned about complications with longer transfers, but these numbers are quite low. Intubations were very low – just one patient taken to a local center, versus three or four in the longer transfer group,” he added.
For both local and comprehensive centers, treatment times were impressive in the study. For local hospitals, the average in/out time was just 60 minutes for patients who went to a comprehensive center; for patients receiving thrombolysis, the average door to needle time was around 30 minutes.
Time to thrombectomy in the comprehensive center for patients transferred from a local hospital was also very fast, with an average door to groin puncture time of less than 40 minutes. “This shows we have a very well-oiled system,” Dr. Ribo said.
“There is always going to be a balance between a quicker time to thrombolysis by taking a patient to the closest hospital but a quicker time to thrombectomy if patients are taken straight to the comprehensive center,” he concluded. “But in our system, where we are achieving fast treatment and transfer times, our results show that patients had timely access to reperfusion therapies regardless of transfer protocol, and under these circumstances, it is fine for the emergency services to take stroke patients to the closest stroke center.”
Results applicable elsewhere?
During the discussion at an ESO-WSO 2020 press conference, other experts pointed out that the Catalonia group is a leader in this field, being the pioneers of the RACE score used in this study for paramedics to identify suspected large-vessel occlusions. This led to questions about the applicability of the results.
“The performance by paramedics was very good using the RACE scale, and the performance times were very impressive. Are these results applicable elsewhere?” Dr. Kiechl asked.
Dr. Ribo said the combination of the RACE score and a call with a vascular neurologist was of “great value” in identifying appropriate patients. Half of the patients selected in this way for the trial were confirmed to have a large-vessel occlusion. “That is a good result,” he added.
He noted that the performance of the local hospitals improved dramatically during the study. “They had an incentive to work on their times. They could have lost most of their stroke patients if their results came out worse. We told them they had an opportunity to show that they have a role in treating these patients, and they took that opportunity.”
Dr. Ribo said there were lessons here for those involved in acute stroke care. “When creating stroke transfer policies in local networks, the performances of individual centers need to be taken into account. If primary stroke centers are motivated and can work in a well-coordinated way and perform to within the recommended times, then they can keep receiving stroke code patients. This should be possible in most developed countries.”
Noting that the in/out time of 60 minutes at local hospitals was “very impressive,” Dr. Kiechl asked how such fast times were achieved.
Dr. Ribo responded that, to a great extent, this was because of ambulance staff. “We have trained the paramedics to anticipate a second transfer after delivering the patient to the local hospital so they can prepare for this rather than waiting for a second call.”
Dr. Ribo pointed out that there were other advantages in taking patients to local centers first. “For those that do not need to be transferred on, they will be closer to relatives. It is very difficult for the family if the patient is hundreds of miles away. And there may be a cost advantage. We did look at costs, but haven’t got that data yet.”
He said: “If local stroke centers do not treat so many stroke code patients, they will lose their expertise, and that will be detrimental to the remaining patients who are taken there. We want to try to maintain a good standard of stroke care across a decent spread of hospitals—not just a couple of major comprehensive centers,” he added.
Commenting on the study, Jesse Dawson, MD, University of Glasgow, who was chair of the plenary session at which the study was presented, said: “RACECAT is very interesting but needs a lot of thought to dissect. My takeaway is that we know that time to reperfusion is key, and we need to get these times as low as possible, but we don’t need to chase a particular care pathway. Thus, if your country/geography suits ‘drip and ship’ better, this is acceptable. If direct to endovascular is possible or you are close to such a center, then this is ideal. But within those paradigms, be as fast as possible.”
He added that results of the subgroups with regard to transfer time will be helpful.
The RACECAT study was funded by Fundacio Ictus Malaltia Vascular.
A version of this article originally appeared on Medscape.com.
a new study has shown.
In the RACECAT trial, functional outcomes were similar for patients suspected of having a large-vessel occlusion stroke who were located in areas not currently served by a comprehensive stroke center, whether they were first taken to a local primary stroke center or whether they were transported over a longer distance to a comprehensive center.
“Under the particular conditions in our study where we had a very well-organized system, a ‘mothership’ transfer protocol for patients with suspected large-vessel occlusion has not proven superior over the ‘drip-and-ship’ protocol, but the opposite is also true,” lead investigator Marc Ribo, MD, concluded.
Dr. Ribo, assistant professor of neurology at Hospital Vall d’Hebron, Barcelona, presented the RACECAT results at the European Stroke Organisation–World Stroke Organisation (ESO-WSO) Conference 2020.
Dr. Ribo said in an interview that there is a feeling among the stroke community that patients with a suspected large-vessel occlusion should be transferred directly to a comprehensive stroke center capable of performing endovascular thrombectomy, even if there is a nearer, smaller primary stroke center where patients are usually taken first for thrombolysis.
“Many stroke neurologists believe we are losing time by sending patients with severe stroke to a local hospital and that we should skip this step, but this is controversial area,” he commented. “Our findings suggest that we should not automatically bypass local stroke centers.”
Dr. Ribo pointed out that the local centers performed very well in the study, with very fast “in/out” times for patients who were subsequently transferred for thrombectomy.
“On the basis of our results, we recommend that if a local stroke center can perform well like ours did – if they are within the time indicators for treating and transferring patients – then they should keep receiving these patients. But if they are not performing well in this regard, then they should probably be bypassed,” he commented.
The RACECAT trial was well received by stroke experts at an ESO-WSO 2020 press conference at which it was discussed.
Stefan Kiechl, MD, Medical University Innsbruck (Austria), described the trial as “outstanding,” adding: “It has addressed a very important question. It is a big achievement in stroke medicine.”
Patrik Michel, MD, Lausanne (Switzerland) University Hospital, said that “this is a very important and highly sophisticated trial in terms of design and execution. The message is that it doesn’t matter which pathway is used, but it is important to have a well-organized network with highly trained paramedics.”
RACECAT
The RACECAT trial was conducted in the Catalonia region of Spain. Twenty-seven hospitals participated, including 7 comprehensive stroke centers and 20 local stroke centers.
The trial included stroke patients with suspected large-vessel occlusion stroke, as determined on the basis of evaluation by paramedics using the criteria of a Rapid Arterial Occlusion Evaluation (RACE) scale score above 4 and on the basis of a call to a vascular neurologist. For inclusion in the study, patients had to be in a geographical area not served by a comprehensive stroke center and to have an estimated arrival time to a comprehensive center of less than 7 hours from symptom onset in order that thrombectomy would be possible.
Of 7,475 stroke code patients evaluated, 1,401 met the inclusion criteria and were randomly assigned to be transferred to a local hospital or to a comprehensive stroke center farther away.
Baseline characteristics were similar between the two groups. The patients had severe strokes with an average National Institutes of Health Stroke Scale score of 17. It was later confirmed that 46% of the patients enrolled in the study had a large-vessel occlusion stroke.
Results showed that time from symptom onset to hospital arrival was 142 minutes for those taken to a local center and 216 minutes for those taken to a comprehensive stroke center. Of those taken to a local hospital, 86% arrived within 4 hours of symptom onset and so were potential candidates for thrombolysis, compared with 76% of those taken to a comprehensive center.
Of the patients taken to a local hospital, 60% were given thrombolysis versus 43% of those taken immediately to a comprehensive center. On the other hand, 50% of patients who were taken directly to a comprehensive center underwent thrombectomy, compared with 40% who were first taken to a local center.
For patients who received thrombolysis, time to tissue plasminogen activator administration was 120 minutes for those treated at a local hospital versus 155 minutes for those taken directly to a comprehensive center.
For patients who received thrombectomy, time from symptom onset to groin puncture was 270 minutes if they were first taken to a local hospital and were then transferred, versus 214 minutes for those taken directly to the comprehensive center.
The primary efficacy endpoint was functional outcome using Modified Rankin Scale (mRS) shift analysis at 90 days for ischemic stroke patients. This showed a “completely flat” result, Dr. Ribo reported, with an adjusted hazard ratio of 1.029 for patients taken to a comprehensive center in comparison with those taken to a local center.
“There was absolutely no trend towards benefit in one group over the other,” he said.
What about hemorrhagic stroke?
The study also evaluated functional outcomes for the whole population enrolled. “If we make the decision just based on thrombectomy-eligible patients, we may harm the rest of the patients, so we did this study to look at the whole population of severe stroke patients,” Dr. Ribo said.
Of the study population, 25% of patients were found to have had a hemorrhagic stroke.
“The problem is, at the prehospital level, it is impossible to know if a patient is having a large-vessel occlusion ischemic stroke or a hemorrhagic stroke,” Dr. Ribo explained. “We have to make a decision for the whole population, and while a longer transport time to get to a comprehensive stroke center might help a patient with a large-vessel occlusion ischemic stroke, it might not be so appropriate for patients with a hemorrhagic stroke who need to have their blood pressure stabilized as soon as possible.”
For the whole population, the mRS shift analysis at 90 days was also neutral, with an aHR of 0.965.
When considering only patients with hemorrhagic stroke, the adjusted hazard ratio for the mRS shift analysis at 90 days was 1.216, which was still nonsignificant (95% confidence interval, 0.864-1.709). This included a nonsignificant increase in mortality among those taken directly to a comprehensive center.
“If we had better tools for a certain diagnosis in the field, then we could consider taking large-vessel occlusion ischemic stroke patients to a comprehensive center and hemorrhagic stroke patients to the local stroke center, but so far, we don’t have this option apart from a few places using mobile stroke units with CT scanners,” Dr. Ribo noted.
Transfer times to comprehensive centers in the study ranged from 30 minutes to 2.5 hours. “There might well be a difference in outcomes for short and long transfers, and we may be able to offer different transfer protocols in these different situations, and we are looking at that, but the study was only stopped in June, and we haven’t had a chance to analyze those results yet,” Dr. Ribo added.
Complications during transport occurred in 0.5% of those taken to a local hospital and in 1% of those taken directly to a comprehensive center. “We were concerned about complications with longer transfers, but these numbers are quite low. Intubations were very low – just one patient taken to a local center, versus three or four in the longer transfer group,” he added.
For both local and comprehensive centers, treatment times were impressive in the study. For local hospitals, the average in/out time was just 60 minutes for patients who went to a comprehensive center; for patients receiving thrombolysis, the average door to needle time was around 30 minutes.
Time to thrombectomy in the comprehensive center for patients transferred from a local hospital was also very fast, with an average door to groin puncture time of less than 40 minutes. “This shows we have a very well-oiled system,” Dr. Ribo said.
“There is always going to be a balance between a quicker time to thrombolysis by taking a patient to the closest hospital but a quicker time to thrombectomy if patients are taken straight to the comprehensive center,” he concluded. “But in our system, where we are achieving fast treatment and transfer times, our results show that patients had timely access to reperfusion therapies regardless of transfer protocol, and under these circumstances, it is fine for the emergency services to take stroke patients to the closest stroke center.”
Results applicable elsewhere?
During the discussion at an ESO-WSO 2020 press conference, other experts pointed out that the Catalonia group is a leader in this field, being the pioneers of the RACE score used in this study for paramedics to identify suspected large-vessel occlusions. This led to questions about the applicability of the results.
“The performance by paramedics was very good using the RACE scale, and the performance times were very impressive. Are these results applicable elsewhere?” Dr. Kiechl asked.
Dr. Ribo said the combination of the RACE score and a call with a vascular neurologist was of “great value” in identifying appropriate patients. Half of the patients selected in this way for the trial were confirmed to have a large-vessel occlusion. “That is a good result,” he added.
He noted that the performance of the local hospitals improved dramatically during the study. “They had an incentive to work on their times. They could have lost most of their stroke patients if their results came out worse. We told them they had an opportunity to show that they have a role in treating these patients, and they took that opportunity.”
Dr. Ribo said there were lessons here for those involved in acute stroke care. “When creating stroke transfer policies in local networks, the performances of individual centers need to be taken into account. If primary stroke centers are motivated and can work in a well-coordinated way and perform to within the recommended times, then they can keep receiving stroke code patients. This should be possible in most developed countries.”
Noting that the in/out time of 60 minutes at local hospitals was “very impressive,” Dr. Kiechl asked how such fast times were achieved.
Dr. Ribo responded that, to a great extent, this was because of ambulance staff. “We have trained the paramedics to anticipate a second transfer after delivering the patient to the local hospital so they can prepare for this rather than waiting for a second call.”
Dr. Ribo pointed out that there were other advantages in taking patients to local centers first. “For those that do not need to be transferred on, they will be closer to relatives. It is very difficult for the family if the patient is hundreds of miles away. And there may be a cost advantage. We did look at costs, but haven’t got that data yet.”
He said: “If local stroke centers do not treat so many stroke code patients, they will lose their expertise, and that will be detrimental to the remaining patients who are taken there. We want to try to maintain a good standard of stroke care across a decent spread of hospitals—not just a couple of major comprehensive centers,” he added.
Commenting on the study, Jesse Dawson, MD, University of Glasgow, who was chair of the plenary session at which the study was presented, said: “RACECAT is very interesting but needs a lot of thought to dissect. My takeaway is that we know that time to reperfusion is key, and we need to get these times as low as possible, but we don’t need to chase a particular care pathway. Thus, if your country/geography suits ‘drip and ship’ better, this is acceptable. If direct to endovascular is possible or you are close to such a center, then this is ideal. But within those paradigms, be as fast as possible.”
He added that results of the subgroups with regard to transfer time will be helpful.
The RACECAT study was funded by Fundacio Ictus Malaltia Vascular.
A version of this article originally appeared on Medscape.com.
FROM ESO-WSO 2020
Sjögren’s symptom clusters may identify treatment options
Patients with Sjögren’s syndrome can be categorized into four distinct symptom clusters – independent of age, sex, and some disease manifestations – that may both improve symptom relief and aid in the development of targeted therapies, investigators reported.

Analysis of data from a survey conducted by the Sjögren’s Foundation identified four symptom clusters based on the grouping of five common characteristics: anxiety, depression, pain, fatigue, and dryness, Sara S. McCoy, MD, of the University of Wisconsin–Madison, and colleagues reported.
“Verification of features unique to each Sjögren’s cluster might provide guidance for future cluster-targeted therapy,” Dr. McCoy said in an oral abstract presentation during the virtual annual meeting of the American College of Rheumatology.
The dearth of Food and Drug Administration–approved disease-modifying therapies for Sjögren’s syndrome can be attributed in part to the small number of patients with extraglandular disease manifestations, the heterogeneity of disease, and the failure of available therapy to improve common symptoms such as fatigue, dryness, quality-of-life decrements, anxiety and depression, she said.
Symptom clusters verify smaller study’s findings
Dr. McCoy and colleagues explored whether symptom clusters identified in a 2019 study from the United Kingdom would apply to a larger U.S. population.
In the U.K. study, Jessica R. Tarn, PhD, and colleagues performed a hierarchical cluster analysis to identify subgroups among 608 patients in the U.K. Primary Sjögren’s Syndrome Registry and in 396 patients in two independent validation cohorts from Norway and France.
They identified four subgroups they categorized as low symptom burden, high symptom burden, dryness dominant with fatigue, and pain dominant with fatigue, and reported that the groups showed significant difference in serum and transcriptomic markers.
In the U.S. study, McCoy et al. sought to verify the symptom-based cluster and report on differences in key measures between the groups. They used data from a survey by the Sjögren’s Foundation of 2,961 adults with self-reported Sjögren’s syndrome. The investigators then used an unsupervised hierarchical clustering method to identify the optimal phenotypically similar clusters based on patient-reported severity of anxiety (from never to daily), depression (never to daily), pain on a visual analog scale (0 to 10), fatigue on a VAS, and dryness on a VAS. They collected data on demographics, medications, quality of life, and Sjögren’s-specific symptom frequency and systemic manifestations within each cluster, and identified cluster differences controlled for age, sex, race, and Social Security disability.
They identified four symptom-based clusters from 2,806 participants for whom complete data on the five key symptoms were available:
- Cluster 1 patients (prevalence, 30%) had high symptom burden in all categories.
- Cluster 2 patients (22%) had high anxiety and depression (22%), with some fatigue.
- Cluster 3 patients (34%) had predominant high dryness and fatigue.
- Cluster 4 patients (14%) had low symptom burden.
“We found that clusters differed in Sjögren’s-specific symptoms,” Dr. McCoy said.
For example, patients in the high-symptom-burden cluster had, as the name implies, an overall higher burden of symptoms among all major ocular, oral, and other dryness symptoms, as well as systemic organ system symptoms, whereas patients in the low-symptom-burden group consistently had the lowest levels of symptoms across the spectrum.
“We also noticed significant differences in systemic medication use. High symptom burden and high dryness and fatigue had higher use of systemic therapies targeting dryness, as might be expected,” she said.
The highest corticosteroid use was in the high-symptom-burden group, while hydroxychloroquine use was highest in the high-anxiety/depression group. Antidepressant use was also high in these two groups.
In addition, 35% of patients in the high-symptom-burden group used prescription opioid analgesics, compared with just 7% in the low-symptom-burden group.
The categories from low to high symptom burden also significantly correlated with quality-of-life measures, including Social Security Disability enrollment, emotional burden of disease, effects of disease on independence, and effects of Sjögren’s on relationships with family and friends (P < .001 for all).
Systemic manifestations of disease differed significantly among the groups for inflammatory arthritis, interstitial lung disease, and neuropathy, but there were no significant differences in the incidence of leukopenia or lymphoma.
The investigators plan to perform symptom-based cluster analysis with validated Sjögren’s syndrome populations, and propose studies to define phenotypic features of distinct clusters “to better define subsets of this heterogeneous disease, and ultimately inform targeted therapy,” Dr. McCoy concluded.
Opportunity to tailor practice and research
During the question-and-answer period following the presentation, Gabriela Hernandez-Molina, MD, of the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán in Mexico City, commented that “fatigue and pain might be also attributed to other comorbidities in these patients such as fibromyalgia,” and asked Dr. McCoy to comment on that.
“That’s exactly what we’re driving at,” Dr. McCoy replied. “Fatigue and pain frequently affect how patients experience their disease, and it would be beneficial to take this into account when we evaluate patients, and also for the studies that we’re performing, as well as future ‘-omic’ studies – transcriptomics and what-not – there’s potential here to take that type of patient we frequently see and try to tailor our clinical practice and our research to clearly what we’re seeing in practice, which is these other comorbidities.”
Dana DiRenzo, MD, from Johns Hopkins University, Baltimore, who moderated the session, asked how the information is changing the management of patients with Sjögren’s syndrome in clinic.
Dr. McCoy said that the study was based on self-reported data that can introduce bias, and that she and colleagues plan to validate the results before applying them to clinical care.
The study was supported by grants from the National Institutes of Health and the University of Wisconsin. Dr. McCoy disclosed consulting fees from Novartis and Bristol-Myers Squibb. Dr. Hernandez-Molina and Dr. DiRenzo reported no relevant disclosures.
SOURCE: McCoy SS et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 1504.
Patients with Sjögren’s syndrome can be categorized into four distinct symptom clusters – independent of age, sex, and some disease manifestations – that may both improve symptom relief and aid in the development of targeted therapies, investigators reported.
Analysis of data from a survey conducted by the Sjögren’s Foundation identified four symptom clusters based on the grouping of five common characteristics: anxiety, depression, pain, fatigue, and dryness, Sara S. McCoy, MD, of the University of Wisconsin–Madison, and colleagues reported.
“Verification of features unique to each Sjögren’s cluster might provide guidance for future cluster-targeted therapy,” Dr. McCoy said in an oral abstract presentation during the virtual annual meeting of the American College of Rheumatology.
The dearth of Food and Drug Administration–approved disease-modifying therapies for Sjögren’s syndrome can be attributed in part to the small number of patients with extraglandular disease manifestations, the heterogeneity of disease, and the failure of available therapy to improve common symptoms such as fatigue, dryness, quality-of-life decrements, anxiety and depression, she said.
Symptom clusters verify smaller study’s findings
Dr. McCoy and colleagues explored whether symptom clusters identified in a 2019 study from the United Kingdom would apply to a larger U.S. population.
In the U.K. study, Jessica R. Tarn, PhD, and colleagues performed a hierarchical cluster analysis to identify subgroups among 608 patients in the U.K. Primary Sjögren’s Syndrome Registry and in 396 patients in two independent validation cohorts from Norway and France.
They identified four subgroups they categorized as low symptom burden, high symptom burden, dryness dominant with fatigue, and pain dominant with fatigue, and reported that the groups showed significant difference in serum and transcriptomic markers.
In the U.S. study, McCoy et al. sought to verify the symptom-based cluster and report on differences in key measures between the groups. They used data from a survey by the Sjögren’s Foundation of 2,961 adults with self-reported Sjögren’s syndrome. The investigators then used an unsupervised hierarchical clustering method to identify the optimal phenotypically similar clusters based on patient-reported severity of anxiety (from never to daily), depression (never to daily), pain on a visual analog scale (0 to 10), fatigue on a VAS, and dryness on a VAS. They collected data on demographics, medications, quality of life, and Sjögren’s-specific symptom frequency and systemic manifestations within each cluster, and identified cluster differences controlled for age, sex, race, and Social Security disability.
They identified four symptom-based clusters from 2,806 participants for whom complete data on the five key symptoms were available:
- Cluster 1 patients (prevalence, 30%) had high symptom burden in all categories.
- Cluster 2 patients (22%) had high anxiety and depression (22%), with some fatigue.
- Cluster 3 patients (34%) had predominant high dryness and fatigue.
- Cluster 4 patients (14%) had low symptom burden.
“We found that clusters differed in Sjögren’s-specific symptoms,” Dr. McCoy said.
For example, patients in the high-symptom-burden cluster had, as the name implies, an overall higher burden of symptoms among all major ocular, oral, and other dryness symptoms, as well as systemic organ system symptoms, whereas patients in the low-symptom-burden group consistently had the lowest levels of symptoms across the spectrum.
“We also noticed significant differences in systemic medication use. High symptom burden and high dryness and fatigue had higher use of systemic therapies targeting dryness, as might be expected,” she said.
The highest corticosteroid use was in the high-symptom-burden group, while hydroxychloroquine use was highest in the high-anxiety/depression group. Antidepressant use was also high in these two groups.
In addition, 35% of patients in the high-symptom-burden group used prescription opioid analgesics, compared with just 7% in the low-symptom-burden group.
The categories from low to high symptom burden also significantly correlated with quality-of-life measures, including Social Security Disability enrollment, emotional burden of disease, effects of disease on independence, and effects of Sjögren’s on relationships with family and friends (P < .001 for all).
Systemic manifestations of disease differed significantly among the groups for inflammatory arthritis, interstitial lung disease, and neuropathy, but there were no significant differences in the incidence of leukopenia or lymphoma.
The investigators plan to perform symptom-based cluster analysis with validated Sjögren’s syndrome populations, and propose studies to define phenotypic features of distinct clusters “to better define subsets of this heterogeneous disease, and ultimately inform targeted therapy,” Dr. McCoy concluded.
Opportunity to tailor practice and research
During the question-and-answer period following the presentation, Gabriela Hernandez-Molina, MD, of the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán in Mexico City, commented that “fatigue and pain might be also attributed to other comorbidities in these patients such as fibromyalgia,” and asked Dr. McCoy to comment on that.
“That’s exactly what we’re driving at,” Dr. McCoy replied. “Fatigue and pain frequently affect how patients experience their disease, and it would be beneficial to take this into account when we evaluate patients, and also for the studies that we’re performing, as well as future ‘-omic’ studies – transcriptomics and what-not – there’s potential here to take that type of patient we frequently see and try to tailor our clinical practice and our research to clearly what we’re seeing in practice, which is these other comorbidities.”
Dana DiRenzo, MD, from Johns Hopkins University, Baltimore, who moderated the session, asked how the information is changing the management of patients with Sjögren’s syndrome in clinic.
Dr. McCoy said that the study was based on self-reported data that can introduce bias, and that she and colleagues plan to validate the results before applying them to clinical care.
The study was supported by grants from the National Institutes of Health and the University of Wisconsin. Dr. McCoy disclosed consulting fees from Novartis and Bristol-Myers Squibb. Dr. Hernandez-Molina and Dr. DiRenzo reported no relevant disclosures.
SOURCE: McCoy SS et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 1504.
Patients with Sjögren’s syndrome can be categorized into four distinct symptom clusters – independent of age, sex, and some disease manifestations – that may both improve symptom relief and aid in the development of targeted therapies, investigators reported.
Analysis of data from a survey conducted by the Sjögren’s Foundation identified four symptom clusters based on the grouping of five common characteristics: anxiety, depression, pain, fatigue, and dryness, Sara S. McCoy, MD, of the University of Wisconsin–Madison, and colleagues reported.
“Verification of features unique to each Sjögren’s cluster might provide guidance for future cluster-targeted therapy,” Dr. McCoy said in an oral abstract presentation during the virtual annual meeting of the American College of Rheumatology.
The dearth of Food and Drug Administration–approved disease-modifying therapies for Sjögren’s syndrome can be attributed in part to the small number of patients with extraglandular disease manifestations, the heterogeneity of disease, and the failure of available therapy to improve common symptoms such as fatigue, dryness, quality-of-life decrements, anxiety and depression, she said.
Symptom clusters verify smaller study’s findings
Dr. McCoy and colleagues explored whether symptom clusters identified in a 2019 study from the United Kingdom would apply to a larger U.S. population.
In the U.K. study, Jessica R. Tarn, PhD, and colleagues performed a hierarchical cluster analysis to identify subgroups among 608 patients in the U.K. Primary Sjögren’s Syndrome Registry and in 396 patients in two independent validation cohorts from Norway and France.
They identified four subgroups they categorized as low symptom burden, high symptom burden, dryness dominant with fatigue, and pain dominant with fatigue, and reported that the groups showed significant difference in serum and transcriptomic markers.
In the U.S. study, McCoy et al. sought to verify the symptom-based cluster and report on differences in key measures between the groups. They used data from a survey by the Sjögren’s Foundation of 2,961 adults with self-reported Sjögren’s syndrome. The investigators then used an unsupervised hierarchical clustering method to identify the optimal phenotypically similar clusters based on patient-reported severity of anxiety (from never to daily), depression (never to daily), pain on a visual analog scale (0 to 10), fatigue on a VAS, and dryness on a VAS. They collected data on demographics, medications, quality of life, and Sjögren’s-specific symptom frequency and systemic manifestations within each cluster, and identified cluster differences controlled for age, sex, race, and Social Security disability.
They identified four symptom-based clusters from 2,806 participants for whom complete data on the five key symptoms were available:
- Cluster 1 patients (prevalence, 30%) had high symptom burden in all categories.
- Cluster 2 patients (22%) had high anxiety and depression (22%), with some fatigue.
- Cluster 3 patients (34%) had predominant high dryness and fatigue.
- Cluster 4 patients (14%) had low symptom burden.
“We found that clusters differed in Sjögren’s-specific symptoms,” Dr. McCoy said.
For example, patients in the high-symptom-burden cluster had, as the name implies, an overall higher burden of symptoms among all major ocular, oral, and other dryness symptoms, as well as systemic organ system symptoms, whereas patients in the low-symptom-burden group consistently had the lowest levels of symptoms across the spectrum.
“We also noticed significant differences in systemic medication use. High symptom burden and high dryness and fatigue had higher use of systemic therapies targeting dryness, as might be expected,” she said.
The highest corticosteroid use was in the high-symptom-burden group, while hydroxychloroquine use was highest in the high-anxiety/depression group. Antidepressant use was also high in these two groups.
In addition, 35% of patients in the high-symptom-burden group used prescription opioid analgesics, compared with just 7% in the low-symptom-burden group.
The categories from low to high symptom burden also significantly correlated with quality-of-life measures, including Social Security Disability enrollment, emotional burden of disease, effects of disease on independence, and effects of Sjögren’s on relationships with family and friends (P < .001 for all).
Systemic manifestations of disease differed significantly among the groups for inflammatory arthritis, interstitial lung disease, and neuropathy, but there were no significant differences in the incidence of leukopenia or lymphoma.
The investigators plan to perform symptom-based cluster analysis with validated Sjögren’s syndrome populations, and propose studies to define phenotypic features of distinct clusters “to better define subsets of this heterogeneous disease, and ultimately inform targeted therapy,” Dr. McCoy concluded.
Opportunity to tailor practice and research
During the question-and-answer period following the presentation, Gabriela Hernandez-Molina, MD, of the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán in Mexico City, commented that “fatigue and pain might be also attributed to other comorbidities in these patients such as fibromyalgia,” and asked Dr. McCoy to comment on that.
“That’s exactly what we’re driving at,” Dr. McCoy replied. “Fatigue and pain frequently affect how patients experience their disease, and it would be beneficial to take this into account when we evaluate patients, and also for the studies that we’re performing, as well as future ‘-omic’ studies – transcriptomics and what-not – there’s potential here to take that type of patient we frequently see and try to tailor our clinical practice and our research to clearly what we’re seeing in practice, which is these other comorbidities.”
Dana DiRenzo, MD, from Johns Hopkins University, Baltimore, who moderated the session, asked how the information is changing the management of patients with Sjögren’s syndrome in clinic.
Dr. McCoy said that the study was based on self-reported data that can introduce bias, and that she and colleagues plan to validate the results before applying them to clinical care.
The study was supported by grants from the National Institutes of Health and the University of Wisconsin. Dr. McCoy disclosed consulting fees from Novartis and Bristol-Myers Squibb. Dr. Hernandez-Molina and Dr. DiRenzo reported no relevant disclosures.
SOURCE: McCoy SS et al. Arthritis Rheumatol. 2020;72(suppl 10), Abstract 1504.
FROM ACR 2020
Methotrexate and hydroxychloroquine split on cardiovascular outcomes in RA
No significant differences in major adverse cardiovascular events (MACE) emerged between methotrexate and hydroxychloroquine (HCQ) treatment in a comparison of adults 65 years or older with rheumatoid arthritis. However, researchers reported some elevation in risk for stroke in the methotrexate group and for myocardial infarction and heart failure in the HCQ group.
The primary outcome, a composite of MI, stroke, or cardiovascular death, had an incidence of 23.39 per 1,000 person-years in the methotrexate group versus 24.33 in the HCQ group in this observational study of nearly 60,000 people.
“These results suggest an importance of looking at different individual events of cardiovascular disease rather than the whole ‘CV’ disease only,” Seoyoung Kim, MD, said in an interview. “The other important thing is that the mortality was not significantly different between the two groups.”
For example, the researchers reported 256 cardiovascular-related deaths in the methotrexate group and 263 such deaths in the HCQ cohort.
Addressing a recognized risk
“It is well known that patients with rheumatoid arthritis have excessive morbidity and mortality,” Dr. Kim, of the division of rheumatology at Brigham and Women’s Hospital and associate professor of medicine at Harvard Medical School in Boston, said at the virtual annual meeting of the American College of Rheumatology.
Among prior studies in this area, the Cardiovascular Inflammation Reduction Trial (CIRT) found no significant reduction in cardiovascular events among people taking methotrexate versus placebo. However, the study of 4,786 people was not specific to RA, Dr. Kim said. The lack of efficacy on this endpoint prompted researchers to stop CIRT early.
“So what does the conclusion of the CIRT trial mean for rheumatoid arthritis patients?” Dr. Kim asked.
To find out, she and colleagues compared risk of MACE among participants newly starting either methotrexate or HCQ. The study included 59,329 people aged 65 and older who were identified through Medicare claims data from 2008 to 2016. Mean age was 74 years, and 80% were women.
The investigators used propensity score matching to control for multiple covariates for demographics, other medications, and comorbidities. Use of other medications was similar between groups, including glucocorticoids, NSAIDs, and statins. Baseline cardiovascular morbidities likewise were well balanced, Dr. Kim said.
The hazard ratio for the primary MACE outcome was 0.96 (95% confidence interval, 0.86-1.08).
Secondary outcomes
MI was less common in the methotrexate group, for example, with an incidence of 8.49 per 1,000 person-years versus 10.68 per 1,000 person-years in the HCQ cohort. This finding was statically significant, Dr. Kim said, with a hazard ratio of 0.80 favoring methotrexate.
Heart failure also occurred less often in the methotrexate cohort, with an incidence rate of 8.57 per 1,000 person-years versus a rate of 14.24 in the HCQ group. The hazard ratio again favored methotrexate at 0.60.
In contrast, strokes were more common with methotrexate than with (incidence of 7.94 vs. 6.01 per 1,000 person-years).
Another secondary outcome, all-cause mortality, was not significantly different between groups. There were 821 deaths in the methotrexate group (28.65 per 1,000 person-years) and 796 deaths in the HCQ group (31.33 per 1,000 person-years).
Studying causality next?
Session moderator Maya Buch, MD, PhD, professor of rheumatology at the University of Manchester (England), asked Dr. Kim why she found significant differences in some secondary outcomes but not the primary composite endpoint.

“When we think of cardiovascular diseases, we tend to think of them all developing through the same mechanism. But perhaps the exact mechanism might not be identical,” Dr. Kim replied. The findings do not suggest causality because the study was observational, she added, “but maybe this will lead to a randomized, controlled trial.”
When asked for comment, Dr. Buch said that the study was “interesting” and “suggestive of differences in type of MACE between the two drugs evaluated,” but that there should be caution in interpreting the findings because of the lack of detailed information on RA disease and activity in claims databases, in addition to other factors, even though the investigators made adjustments for known differences through propensity score matching.
The division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital supported the study. Dr. Kim has received support for Brigham and Women’s Hospital for unrelated research from Pfizer, AbbVie, Roche, and Bristol-Myers Squibb. Several other coauthors reported having financial relationships with pharmaceutical companies that make drugs for RA. Dr. Buch had no relevant disclosures.
SOURCE: He M et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 1993.
No significant differences in major adverse cardiovascular events (MACE) emerged between methotrexate and hydroxychloroquine (HCQ) treatment in a comparison of adults 65 years or older with rheumatoid arthritis. However, researchers reported some elevation in risk for stroke in the methotrexate group and for myocardial infarction and heart failure in the HCQ group.
The primary outcome, a composite of MI, stroke, or cardiovascular death, had an incidence of 23.39 per 1,000 person-years in the methotrexate group versus 24.33 in the HCQ group in this observational study of nearly 60,000 people.
“These results suggest an importance of looking at different individual events of cardiovascular disease rather than the whole ‘CV’ disease only,” Seoyoung Kim, MD, said in an interview. “The other important thing is that the mortality was not significantly different between the two groups.”
For example, the researchers reported 256 cardiovascular-related deaths in the methotrexate group and 263 such deaths in the HCQ cohort.
Addressing a recognized risk
“It is well known that patients with rheumatoid arthritis have excessive morbidity and mortality,” Dr. Kim, of the division of rheumatology at Brigham and Women’s Hospital and associate professor of medicine at Harvard Medical School in Boston, said at the virtual annual meeting of the American College of Rheumatology.
Among prior studies in this area, the Cardiovascular Inflammation Reduction Trial (CIRT) found no significant reduction in cardiovascular events among people taking methotrexate versus placebo. However, the study of 4,786 people was not specific to RA, Dr. Kim said. The lack of efficacy on this endpoint prompted researchers to stop CIRT early.
“So what does the conclusion of the CIRT trial mean for rheumatoid arthritis patients?” Dr. Kim asked.
To find out, she and colleagues compared risk of MACE among participants newly starting either methotrexate or HCQ. The study included 59,329 people aged 65 and older who were identified through Medicare claims data from 2008 to 2016. Mean age was 74 years, and 80% were women.
The investigators used propensity score matching to control for multiple covariates for demographics, other medications, and comorbidities. Use of other medications was similar between groups, including glucocorticoids, NSAIDs, and statins. Baseline cardiovascular morbidities likewise were well balanced, Dr. Kim said.
The hazard ratio for the primary MACE outcome was 0.96 (95% confidence interval, 0.86-1.08).
Secondary outcomes
MI was less common in the methotrexate group, for example, with an incidence of 8.49 per 1,000 person-years versus 10.68 per 1,000 person-years in the HCQ cohort. This finding was statically significant, Dr. Kim said, with a hazard ratio of 0.80 favoring methotrexate.
Heart failure also occurred less often in the methotrexate cohort, with an incidence rate of 8.57 per 1,000 person-years versus a rate of 14.24 in the HCQ group. The hazard ratio again favored methotrexate at 0.60.
In contrast, strokes were more common with methotrexate than with (incidence of 7.94 vs. 6.01 per 1,000 person-years).
Another secondary outcome, all-cause mortality, was not significantly different between groups. There were 821 deaths in the methotrexate group (28.65 per 1,000 person-years) and 796 deaths in the HCQ group (31.33 per 1,000 person-years).
Studying causality next?
Session moderator Maya Buch, MD, PhD, professor of rheumatology at the University of Manchester (England), asked Dr. Kim why she found significant differences in some secondary outcomes but not the primary composite endpoint.
“When we think of cardiovascular diseases, we tend to think of them all developing through the same mechanism. But perhaps the exact mechanism might not be identical,” Dr. Kim replied. The findings do not suggest causality because the study was observational, she added, “but maybe this will lead to a randomized, controlled trial.”
When asked for comment, Dr. Buch said that the study was “interesting” and “suggestive of differences in type of MACE between the two drugs evaluated,” but that there should be caution in interpreting the findings because of the lack of detailed information on RA disease and activity in claims databases, in addition to other factors, even though the investigators made adjustments for known differences through propensity score matching.
The division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital supported the study. Dr. Kim has received support for Brigham and Women’s Hospital for unrelated research from Pfizer, AbbVie, Roche, and Bristol-Myers Squibb. Several other coauthors reported having financial relationships with pharmaceutical companies that make drugs for RA. Dr. Buch had no relevant disclosures.
SOURCE: He M et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 1993.
No significant differences in major adverse cardiovascular events (MACE) emerged between methotrexate and hydroxychloroquine (HCQ) treatment in a comparison of adults 65 years or older with rheumatoid arthritis. However, researchers reported some elevation in risk for stroke in the methotrexate group and for myocardial infarction and heart failure in the HCQ group.
The primary outcome, a composite of MI, stroke, or cardiovascular death, had an incidence of 23.39 per 1,000 person-years in the methotrexate group versus 24.33 in the HCQ group in this observational study of nearly 60,000 people.
“These results suggest an importance of looking at different individual events of cardiovascular disease rather than the whole ‘CV’ disease only,” Seoyoung Kim, MD, said in an interview. “The other important thing is that the mortality was not significantly different between the two groups.”
For example, the researchers reported 256 cardiovascular-related deaths in the methotrexate group and 263 such deaths in the HCQ cohort.
Addressing a recognized risk
“It is well known that patients with rheumatoid arthritis have excessive morbidity and mortality,” Dr. Kim, of the division of rheumatology at Brigham and Women’s Hospital and associate professor of medicine at Harvard Medical School in Boston, said at the virtual annual meeting of the American College of Rheumatology.
Among prior studies in this area, the Cardiovascular Inflammation Reduction Trial (CIRT) found no significant reduction in cardiovascular events among people taking methotrexate versus placebo. However, the study of 4,786 people was not specific to RA, Dr. Kim said. The lack of efficacy on this endpoint prompted researchers to stop CIRT early.
“So what does the conclusion of the CIRT trial mean for rheumatoid arthritis patients?” Dr. Kim asked.
To find out, she and colleagues compared risk of MACE among participants newly starting either methotrexate or HCQ. The study included 59,329 people aged 65 and older who were identified through Medicare claims data from 2008 to 2016. Mean age was 74 years, and 80% were women.
The investigators used propensity score matching to control for multiple covariates for demographics, other medications, and comorbidities. Use of other medications was similar between groups, including glucocorticoids, NSAIDs, and statins. Baseline cardiovascular morbidities likewise were well balanced, Dr. Kim said.
The hazard ratio for the primary MACE outcome was 0.96 (95% confidence interval, 0.86-1.08).
Secondary outcomes
MI was less common in the methotrexate group, for example, with an incidence of 8.49 per 1,000 person-years versus 10.68 per 1,000 person-years in the HCQ cohort. This finding was statically significant, Dr. Kim said, with a hazard ratio of 0.80 favoring methotrexate.
Heart failure also occurred less often in the methotrexate cohort, with an incidence rate of 8.57 per 1,000 person-years versus a rate of 14.24 in the HCQ group. The hazard ratio again favored methotrexate at 0.60.
In contrast, strokes were more common with methotrexate than with (incidence of 7.94 vs. 6.01 per 1,000 person-years).
Another secondary outcome, all-cause mortality, was not significantly different between groups. There were 821 deaths in the methotrexate group (28.65 per 1,000 person-years) and 796 deaths in the HCQ group (31.33 per 1,000 person-years).
Studying causality next?
Session moderator Maya Buch, MD, PhD, professor of rheumatology at the University of Manchester (England), asked Dr. Kim why she found significant differences in some secondary outcomes but not the primary composite endpoint.
“When we think of cardiovascular diseases, we tend to think of them all developing through the same mechanism. But perhaps the exact mechanism might not be identical,” Dr. Kim replied. The findings do not suggest causality because the study was observational, she added, “but maybe this will lead to a randomized, controlled trial.”
When asked for comment, Dr. Buch said that the study was “interesting” and “suggestive of differences in type of MACE between the two drugs evaluated,” but that there should be caution in interpreting the findings because of the lack of detailed information on RA disease and activity in claims databases, in addition to other factors, even though the investigators made adjustments for known differences through propensity score matching.
The division of pharmacoepidemiology and pharmacoeconomics at Brigham and Women’s Hospital supported the study. Dr. Kim has received support for Brigham and Women’s Hospital for unrelated research from Pfizer, AbbVie, Roche, and Bristol-Myers Squibb. Several other coauthors reported having financial relationships with pharmaceutical companies that make drugs for RA. Dr. Buch had no relevant disclosures.
SOURCE: He M et al. Arthritis Rheumatol. 2020;72(suppl 10): Abstract 1993.
FROM ACR 2020
‘Test all patients with cancer’: One in eight have inherited mutations
These findings come from the largest study of its kind so far, conducted in nearly 3,000 patients with a wide range of cancer stages and types, including breast, colorectal, lung, ovarian, pancreatic, bladder, prostate, and endometrial cancers.
“This study tells us that the clinical practice guidelines are not very sensitive for identifying who does or doesn’t have a genetic mutation that is predisposing them to cancer,” commented first author Niloy Jewell Samadder, MD, director of the high-risk cancer clinic at the Mayo Clinic in Phoenix.
Finding a genetic mutation can alter clinical management of the cancer.
“This really does open up treatment and management options that might not have been accessible to these patients,” Dr. Samadder emphasized.
The results were published online on Oct. 30 in JAMA Oncology and were presented simultaneously at the American Society of Human Genetics. Dr. Samadder discussed details of the study in a video posted on YouTube.
A clinician not involved in the study said the new results should lead to changes in practice.
“For cancer patients, I think the debate is over. We should test everybody,” Peter Beitsch, MD, surgical oncologist at the Dallas Surgical Group, said in an interview.
The Mayo Clinic is changing its daily practice at all four of its cancer centers. The changes will begin in the first quarter of 2021 at its Arizona campus.
“Every cancer patient who comes to Mayo Clinic will be offered genomic evaluation that includes genetic testing to identify if they have an underlying genetic mutation that predisposes to their cancer and [helps physicians decide] how to incorporate that knowledge into designing the best surgical and treatment options for that patient and their family,” Dr. Samadder said.
Study details
The study included 2,984 patients with cancer who were receiving care for a variety of solid tumor cancers at Mayo Clinic cancer centers in Arizona, Florida, Minnesota, and a community cancer center in Wisconsin.
Patients were tested for about 84 genes using next-generation sequencing provided by Invitae.
Among participants, 13.3% (n = 397) tested positive for pathogenic mutations. Of these, about 70% (282 of 397 patients) carried moderate- and high-penetrance genes that increased their risk for cancer. For almost 28.2% (n = 42) of patients with high-penetrance mutations, changes were made in treatment as a result of genetic testing. These included changes in surgical management, immunotherapy, chemotherapy, or enrollment in a clinical trial for which they may otherwise have not been eligible.
Researchers also compared their universal testing approach with targeted testing recommended in guidelines from the National Comprehensive Cancer Network, the National Society of Genetic Counselors, and the American College of Medical Genetics.
They identified pathogenic mutations in 192 patients whose mutations would have been missed using guideline-recommended criteria, such as tumor pathology or family history. This represents 6.4% of all participants in the study (192 of 2,984 patients) and 48.4% of patients who tested positive for pathogenic mutations (397 of 2,984 patients).
“Genetic testing is underutilized in cancer care, both for patients and for their families, often due to outdated guidelines that restrict testing to a narrow group of high-risk patients. All cancer patients should have access to complete genetic information that can guide their care and inform their families’ health,” coauthor Robert Nussbaum, MD, chief medical officer of Invitae, said in a statement.
Some clinicians have been pushing for genetic testing of all patients with cancer, including Dr. Beitsch, who was lead author of a similar study in breast cancer patients published last year in the Journal of Oncology. That article made waves when the authors concluded that all breast cancer patients should have expanded panel genetic testing.
This new Mayo Clinic study extends the findings in breast cancer to “all cancer patients, not just breast cancer patients,” Dr. Beitsch said in an interview.
Long-running debate
The new findings and opinions add to a long-running debate in oncology over the role of genetic testing and screening for pathogenic mutations.
Part of the debate about genetic testing has hinged on the question of costs, said Dr. Beitsch. When genetic testing first became available, it was conducted by hand, and costs were often prohibitive. Since then, genetic testing has been automated using next-generation sequencing, and the cost has decreased considerably.
“The Invitae cash price for an 80-plus gene panel is $250. That’s [the cost of] a mani-pedi in Dallas. I don’t discount that it’s a lot of money for a lot of people. Yes, it’s expensive, but it’s a lot less expensive than it used to be,” Dr. Beitsch said.
Another issue is that doctors are not entirely sure how to manage variants of uncertain significance (VUSs) when they are found. In the Mayo Clinic study, about half (47.4%; n = 1415) of participants had VUSs. The authors noted that these results are consistent with past studies.
Dr. Beitsch said that VUSs are a matter of education. To date, only about 2% of VUSs have been associated with cancer. The remainder, about 98%, do not affect treatment for patients who have already been diagnosed with cancer.
“We all have VUSs. They’re just minor variations in a gene. The vast majority of them have no consequence and don’t alter the function of the gene,” he said. “I tell everybody to ignore the VUSs [when found in patients with cancer]. Do not act on them at all. We just need to educate everybody to make sure they don’t get stressed about it.”
These comments echo guidance from the American Society of Breast Surgeons, which says that VUSs are DNA sequences that are not clinically actionable. This type of result needs to be considered as inconclusive, and patient management should not be influenced by such results.
However, VUSs are more significant if they are found in individuals who do not have cancer but who have a strong family history of cancer. In such cases, clinicians should be more aware, Dr. Beitsch emphasized.
“Patients who have a VUS and don’t have a cancer should absolutely pay more attention to their health. They got tested for a reason, and that reason is usually strong family history,” Dr. Beitsch said.
He added that a major advantage of genetic testing is that it can enable cascade genetic testing of family members. Identifying pathogenic mutations in family members can lead them to undergo screening to detect early cancers, and preventive measures can be taken that may be lifesaving.
In the Mayo Clinic study, researchers offered genetic testing to family members of patients who tested positive for a pathogenic mutation. Testing was available free of charge for up to 90 days after a participant tested positive. In addition, family members were shown an educational video.
Nevertheless, only 17.6% (n = 70) of patients with pathogenic mutations had family members who underwent testing. Among these, 45% (79 of 176) of family members who were tested were found to carry pathogenic mutations.
“This really told us that financial barriers are not the only barrier to families understanding and undergoing preventive testing,” Dr. Samadder said. “There are probably a number of other barriers – socioeconomic or emotional – that we have to deal with.”
Genetic testing was provided by Invitae. The study was supported by several grants, including a Mayo Transform the Practice Grant, and by Mayo Clinic’s Center for Individualized Medicine. Two coauthors are employees of Invitae. Dr. Beitsch reported participating in a study 2 years ago that was funded by Invitae. He currently receives no financial support from Invitae. Several authors report receiving fees from one or more of the following companies: Pfizer, Maze Therapeutics, Genome Medical, Astellas, and Merck.
This article first appeared on Medscape.com.
These findings come from the largest study of its kind so far, conducted in nearly 3,000 patients with a wide range of cancer stages and types, including breast, colorectal, lung, ovarian, pancreatic, bladder, prostate, and endometrial cancers.
“This study tells us that the clinical practice guidelines are not very sensitive for identifying who does or doesn’t have a genetic mutation that is predisposing them to cancer,” commented first author Niloy Jewell Samadder, MD, director of the high-risk cancer clinic at the Mayo Clinic in Phoenix.
Finding a genetic mutation can alter clinical management of the cancer.
“This really does open up treatment and management options that might not have been accessible to these patients,” Dr. Samadder emphasized.
The results were published online on Oct. 30 in JAMA Oncology and were presented simultaneously at the American Society of Human Genetics. Dr. Samadder discussed details of the study in a video posted on YouTube.
A clinician not involved in the study said the new results should lead to changes in practice.
“For cancer patients, I think the debate is over. We should test everybody,” Peter Beitsch, MD, surgical oncologist at the Dallas Surgical Group, said in an interview.
The Mayo Clinic is changing its daily practice at all four of its cancer centers. The changes will begin in the first quarter of 2021 at its Arizona campus.
“Every cancer patient who comes to Mayo Clinic will be offered genomic evaluation that includes genetic testing to identify if they have an underlying genetic mutation that predisposes to their cancer and [helps physicians decide] how to incorporate that knowledge into designing the best surgical and treatment options for that patient and their family,” Dr. Samadder said.
Study details
The study included 2,984 patients with cancer who were receiving care for a variety of solid tumor cancers at Mayo Clinic cancer centers in Arizona, Florida, Minnesota, and a community cancer center in Wisconsin.
Patients were tested for about 84 genes using next-generation sequencing provided by Invitae.
Among participants, 13.3% (n = 397) tested positive for pathogenic mutations. Of these, about 70% (282 of 397 patients) carried moderate- and high-penetrance genes that increased their risk for cancer. For almost 28.2% (n = 42) of patients with high-penetrance mutations, changes were made in treatment as a result of genetic testing. These included changes in surgical management, immunotherapy, chemotherapy, or enrollment in a clinical trial for which they may otherwise have not been eligible.
Researchers also compared their universal testing approach with targeted testing recommended in guidelines from the National Comprehensive Cancer Network, the National Society of Genetic Counselors, and the American College of Medical Genetics.
They identified pathogenic mutations in 192 patients whose mutations would have been missed using guideline-recommended criteria, such as tumor pathology or family history. This represents 6.4% of all participants in the study (192 of 2,984 patients) and 48.4% of patients who tested positive for pathogenic mutations (397 of 2,984 patients).
“Genetic testing is underutilized in cancer care, both for patients and for their families, often due to outdated guidelines that restrict testing to a narrow group of high-risk patients. All cancer patients should have access to complete genetic information that can guide their care and inform their families’ health,” coauthor Robert Nussbaum, MD, chief medical officer of Invitae, said in a statement.
Some clinicians have been pushing for genetic testing of all patients with cancer, including Dr. Beitsch, who was lead author of a similar study in breast cancer patients published last year in the Journal of Oncology. That article made waves when the authors concluded that all breast cancer patients should have expanded panel genetic testing.
This new Mayo Clinic study extends the findings in breast cancer to “all cancer patients, not just breast cancer patients,” Dr. Beitsch said in an interview.
Long-running debate
The new findings and opinions add to a long-running debate in oncology over the role of genetic testing and screening for pathogenic mutations.
Part of the debate about genetic testing has hinged on the question of costs, said Dr. Beitsch. When genetic testing first became available, it was conducted by hand, and costs were often prohibitive. Since then, genetic testing has been automated using next-generation sequencing, and the cost has decreased considerably.
“The Invitae cash price for an 80-plus gene panel is $250. That’s [the cost of] a mani-pedi in Dallas. I don’t discount that it’s a lot of money for a lot of people. Yes, it’s expensive, but it’s a lot less expensive than it used to be,” Dr. Beitsch said.
Another issue is that doctors are not entirely sure how to manage variants of uncertain significance (VUSs) when they are found. In the Mayo Clinic study, about half (47.4%; n = 1415) of participants had VUSs. The authors noted that these results are consistent with past studies.
Dr. Beitsch said that VUSs are a matter of education. To date, only about 2% of VUSs have been associated with cancer. The remainder, about 98%, do not affect treatment for patients who have already been diagnosed with cancer.
“We all have VUSs. They’re just minor variations in a gene. The vast majority of them have no consequence and don’t alter the function of the gene,” he said. “I tell everybody to ignore the VUSs [when found in patients with cancer]. Do not act on them at all. We just need to educate everybody to make sure they don’t get stressed about it.”
These comments echo guidance from the American Society of Breast Surgeons, which says that VUSs are DNA sequences that are not clinically actionable. This type of result needs to be considered as inconclusive, and patient management should not be influenced by such results.
However, VUSs are more significant if they are found in individuals who do not have cancer but who have a strong family history of cancer. In such cases, clinicians should be more aware, Dr. Beitsch emphasized.
“Patients who have a VUS and don’t have a cancer should absolutely pay more attention to their health. They got tested for a reason, and that reason is usually strong family history,” Dr. Beitsch said.
He added that a major advantage of genetic testing is that it can enable cascade genetic testing of family members. Identifying pathogenic mutations in family members can lead them to undergo screening to detect early cancers, and preventive measures can be taken that may be lifesaving.
In the Mayo Clinic study, researchers offered genetic testing to family members of patients who tested positive for a pathogenic mutation. Testing was available free of charge for up to 90 days after a participant tested positive. In addition, family members were shown an educational video.
Nevertheless, only 17.6% (n = 70) of patients with pathogenic mutations had family members who underwent testing. Among these, 45% (79 of 176) of family members who were tested were found to carry pathogenic mutations.
“This really told us that financial barriers are not the only barrier to families understanding and undergoing preventive testing,” Dr. Samadder said. “There are probably a number of other barriers – socioeconomic or emotional – that we have to deal with.”
Genetic testing was provided by Invitae. The study was supported by several grants, including a Mayo Transform the Practice Grant, and by Mayo Clinic’s Center for Individualized Medicine. Two coauthors are employees of Invitae. Dr. Beitsch reported participating in a study 2 years ago that was funded by Invitae. He currently receives no financial support from Invitae. Several authors report receiving fees from one or more of the following companies: Pfizer, Maze Therapeutics, Genome Medical, Astellas, and Merck.
This article first appeared on Medscape.com.
These findings come from the largest study of its kind so far, conducted in nearly 3,000 patients with a wide range of cancer stages and types, including breast, colorectal, lung, ovarian, pancreatic, bladder, prostate, and endometrial cancers.
“This study tells us that the clinical practice guidelines are not very sensitive for identifying who does or doesn’t have a genetic mutation that is predisposing them to cancer,” commented first author Niloy Jewell Samadder, MD, director of the high-risk cancer clinic at the Mayo Clinic in Phoenix.
Finding a genetic mutation can alter clinical management of the cancer.
“This really does open up treatment and management options that might not have been accessible to these patients,” Dr. Samadder emphasized.
The results were published online on Oct. 30 in JAMA Oncology and were presented simultaneously at the American Society of Human Genetics. Dr. Samadder discussed details of the study in a video posted on YouTube.
A clinician not involved in the study said the new results should lead to changes in practice.
“For cancer patients, I think the debate is over. We should test everybody,” Peter Beitsch, MD, surgical oncologist at the Dallas Surgical Group, said in an interview.
The Mayo Clinic is changing its daily practice at all four of its cancer centers. The changes will begin in the first quarter of 2021 at its Arizona campus.
“Every cancer patient who comes to Mayo Clinic will be offered genomic evaluation that includes genetic testing to identify if they have an underlying genetic mutation that predisposes to their cancer and [helps physicians decide] how to incorporate that knowledge into designing the best surgical and treatment options for that patient and their family,” Dr. Samadder said.
Study details
The study included 2,984 patients with cancer who were receiving care for a variety of solid tumor cancers at Mayo Clinic cancer centers in Arizona, Florida, Minnesota, and a community cancer center in Wisconsin.
Patients were tested for about 84 genes using next-generation sequencing provided by Invitae.
Among participants, 13.3% (n = 397) tested positive for pathogenic mutations. Of these, about 70% (282 of 397 patients) carried moderate- and high-penetrance genes that increased their risk for cancer. For almost 28.2% (n = 42) of patients with high-penetrance mutations, changes were made in treatment as a result of genetic testing. These included changes in surgical management, immunotherapy, chemotherapy, or enrollment in a clinical trial for which they may otherwise have not been eligible.
Researchers also compared their universal testing approach with targeted testing recommended in guidelines from the National Comprehensive Cancer Network, the National Society of Genetic Counselors, and the American College of Medical Genetics.
They identified pathogenic mutations in 192 patients whose mutations would have been missed using guideline-recommended criteria, such as tumor pathology or family history. This represents 6.4% of all participants in the study (192 of 2,984 patients) and 48.4% of patients who tested positive for pathogenic mutations (397 of 2,984 patients).
“Genetic testing is underutilized in cancer care, both for patients and for their families, often due to outdated guidelines that restrict testing to a narrow group of high-risk patients. All cancer patients should have access to complete genetic information that can guide their care and inform their families’ health,” coauthor Robert Nussbaum, MD, chief medical officer of Invitae, said in a statement.
Some clinicians have been pushing for genetic testing of all patients with cancer, including Dr. Beitsch, who was lead author of a similar study in breast cancer patients published last year in the Journal of Oncology. That article made waves when the authors concluded that all breast cancer patients should have expanded panel genetic testing.
This new Mayo Clinic study extends the findings in breast cancer to “all cancer patients, not just breast cancer patients,” Dr. Beitsch said in an interview.
Long-running debate
The new findings and opinions add to a long-running debate in oncology over the role of genetic testing and screening for pathogenic mutations.
Part of the debate about genetic testing has hinged on the question of costs, said Dr. Beitsch. When genetic testing first became available, it was conducted by hand, and costs were often prohibitive. Since then, genetic testing has been automated using next-generation sequencing, and the cost has decreased considerably.
“The Invitae cash price for an 80-plus gene panel is $250. That’s [the cost of] a mani-pedi in Dallas. I don’t discount that it’s a lot of money for a lot of people. Yes, it’s expensive, but it’s a lot less expensive than it used to be,” Dr. Beitsch said.
Another issue is that doctors are not entirely sure how to manage variants of uncertain significance (VUSs) when they are found. In the Mayo Clinic study, about half (47.4%; n = 1415) of participants had VUSs. The authors noted that these results are consistent with past studies.
Dr. Beitsch said that VUSs are a matter of education. To date, only about 2% of VUSs have been associated with cancer. The remainder, about 98%, do not affect treatment for patients who have already been diagnosed with cancer.
“We all have VUSs. They’re just minor variations in a gene. The vast majority of them have no consequence and don’t alter the function of the gene,” he said. “I tell everybody to ignore the VUSs [when found in patients with cancer]. Do not act on them at all. We just need to educate everybody to make sure they don’t get stressed about it.”
These comments echo guidance from the American Society of Breast Surgeons, which says that VUSs are DNA sequences that are not clinically actionable. This type of result needs to be considered as inconclusive, and patient management should not be influenced by such results.
However, VUSs are more significant if they are found in individuals who do not have cancer but who have a strong family history of cancer. In such cases, clinicians should be more aware, Dr. Beitsch emphasized.
“Patients who have a VUS and don’t have a cancer should absolutely pay more attention to their health. They got tested for a reason, and that reason is usually strong family history,” Dr. Beitsch said.
He added that a major advantage of genetic testing is that it can enable cascade genetic testing of family members. Identifying pathogenic mutations in family members can lead them to undergo screening to detect early cancers, and preventive measures can be taken that may be lifesaving.
In the Mayo Clinic study, researchers offered genetic testing to family members of patients who tested positive for a pathogenic mutation. Testing was available free of charge for up to 90 days after a participant tested positive. In addition, family members were shown an educational video.
Nevertheless, only 17.6% (n = 70) of patients with pathogenic mutations had family members who underwent testing. Among these, 45% (79 of 176) of family members who were tested were found to carry pathogenic mutations.
“This really told us that financial barriers are not the only barrier to families understanding and undergoing preventive testing,” Dr. Samadder said. “There are probably a number of other barriers – socioeconomic or emotional – that we have to deal with.”
Genetic testing was provided by Invitae. The study was supported by several grants, including a Mayo Transform the Practice Grant, and by Mayo Clinic’s Center for Individualized Medicine. Two coauthors are employees of Invitae. Dr. Beitsch reported participating in a study 2 years ago that was funded by Invitae. He currently receives no financial support from Invitae. Several authors report receiving fees from one or more of the following companies: Pfizer, Maze Therapeutics, Genome Medical, Astellas, and Merck.
This article first appeared on Medscape.com.
Don’t miss postpartum thyroiditis
All patients with postpartum depression should be screened for thyroid dysfunction, as postpartum thyroiditis is often missed and misdiagnosed, according to Christine Kessler, CNS, ANP.
Postpartum thyroiditis (PPT) is “an inflammatory, autoimmune thyroid condition,” Ms. Kessler said at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education. This dysfunction can involve high or low thyroid-stimulating hormone and may occur during the first postpartum year in women who were euthyroid prior to pregnancy. Women with PPT will be thyroid peroxidase (TPO) antibody positive. Postpartum thyroiditis also can occur after a miscarriage.
PPT can occur when the immune system rebounds after pregnancy following immune suppression during pregnancy. “Autoimmune destruction of the thyroid gland leads to initial release of stored thyroid hormone,” Ms. Kessler said. Notably, “patients with a predisposition for Hashimoto’s will have an attack on the thyroid gland. Don’t miss this in your patients.”
PPT is the most common endocrine disease in premenopausal women, with an incidence of 8%-14% in the United States, noted Ms. Kessler, a nurse practitioner in private practice in Virginia. However, the symptoms are often attributed to anxiety, depression, or the stress of new motherhood.
Women with PPT have positive thyroid peroxidase antibodies, said Ms. Kessler, and the higher the antibody, the higher the risk for PPT. Other risk factors include the presence of autoimmune disorders prior to pregnancy, a patient or family history of thyroid dysfunction, and a history of PPT.
Roughly one-third of women with PPT present with hyperthyroidism alone, another third present with hypothyroidism alone, and another third have the classic presentation of PPT, which starts with a transient hyperthyroid phase that usually occurs 1-4 months post partum, followed by a hypothyroid phase and euthyroid phase that is usually achieved within the first 12-18 months post partum, she said.
Patients presenting with PPT in the hyperthyroid phase display symptoms including insomnia, anxiety, irritability, heat intolerance, fatigue, and palpitations, Ms. Kessler said. These women “are often told they have postpartum depression; they aren’t sleeping well, and they feel like they are failing as a mom.”
Patients in the hypothyroid phase may present with fatigue, depression, cold intolerance, dry skin, impaired concentration, and paresthesias, she noted.
Treatment for PPT depends on the stage patients are in when they present. For patients in the hyperthyroid phase, Ms. Kessler recommended beta-blockers for relief of symptoms including tremor and palpitations, but these should be tapered as symptoms decrease. “There is no need for antithyroid drugs for women in the hyperthyroid phase.”
For patients presenting in the hypothyroid phase, Ms. Kessler recommended levothyroxine for 6-12 months if needed, but the drug should be tapered and discontinued after PPT, as about 80% of patients will become euthyroid. However, approximately 50% of women with PPT will develop hypothyroidism in 2-10 years, so ongoing follow-up is essential for these patients.
Ms. Kessler disclosed serving as an adviser/speaker for Novo Nordisk, serving as a speaker for Salix and Acella, and serving as National Study Chair of probiotic use with antibiotics for Clarion Brand. Global Academy and this news organization are owned by the same parent company.
All patients with postpartum depression should be screened for thyroid dysfunction, as postpartum thyroiditis is often missed and misdiagnosed, according to Christine Kessler, CNS, ANP.
Postpartum thyroiditis (PPT) is “an inflammatory, autoimmune thyroid condition,” Ms. Kessler said at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education. This dysfunction can involve high or low thyroid-stimulating hormone and may occur during the first postpartum year in women who were euthyroid prior to pregnancy. Women with PPT will be thyroid peroxidase (TPO) antibody positive. Postpartum thyroiditis also can occur after a miscarriage.
PPT can occur when the immune system rebounds after pregnancy following immune suppression during pregnancy. “Autoimmune destruction of the thyroid gland leads to initial release of stored thyroid hormone,” Ms. Kessler said. Notably, “patients with a predisposition for Hashimoto’s will have an attack on the thyroid gland. Don’t miss this in your patients.”
PPT is the most common endocrine disease in premenopausal women, with an incidence of 8%-14% in the United States, noted Ms. Kessler, a nurse practitioner in private practice in Virginia. However, the symptoms are often attributed to anxiety, depression, or the stress of new motherhood.
Women with PPT have positive thyroid peroxidase antibodies, said Ms. Kessler, and the higher the antibody, the higher the risk for PPT. Other risk factors include the presence of autoimmune disorders prior to pregnancy, a patient or family history of thyroid dysfunction, and a history of PPT.
Roughly one-third of women with PPT present with hyperthyroidism alone, another third present with hypothyroidism alone, and another third have the classic presentation of PPT, which starts with a transient hyperthyroid phase that usually occurs 1-4 months post partum, followed by a hypothyroid phase and euthyroid phase that is usually achieved within the first 12-18 months post partum, she said.
Patients presenting with PPT in the hyperthyroid phase display symptoms including insomnia, anxiety, irritability, heat intolerance, fatigue, and palpitations, Ms. Kessler said. These women “are often told they have postpartum depression; they aren’t sleeping well, and they feel like they are failing as a mom.”
Patients in the hypothyroid phase may present with fatigue, depression, cold intolerance, dry skin, impaired concentration, and paresthesias, she noted.
Treatment for PPT depends on the stage patients are in when they present. For patients in the hyperthyroid phase, Ms. Kessler recommended beta-blockers for relief of symptoms including tremor and palpitations, but these should be tapered as symptoms decrease. “There is no need for antithyroid drugs for women in the hyperthyroid phase.”
For patients presenting in the hypothyroid phase, Ms. Kessler recommended levothyroxine for 6-12 months if needed, but the drug should be tapered and discontinued after PPT, as about 80% of patients will become euthyroid. However, approximately 50% of women with PPT will develop hypothyroidism in 2-10 years, so ongoing follow-up is essential for these patients.
Ms. Kessler disclosed serving as an adviser/speaker for Novo Nordisk, serving as a speaker for Salix and Acella, and serving as National Study Chair of probiotic use with antibiotics for Clarion Brand. Global Academy and this news organization are owned by the same parent company.
All patients with postpartum depression should be screened for thyroid dysfunction, as postpartum thyroiditis is often missed and misdiagnosed, according to Christine Kessler, CNS, ANP.
Postpartum thyroiditis (PPT) is “an inflammatory, autoimmune thyroid condition,” Ms. Kessler said at the Metabolic & Endocrine Disease Summit by Global Academy for Medical Education. This dysfunction can involve high or low thyroid-stimulating hormone and may occur during the first postpartum year in women who were euthyroid prior to pregnancy. Women with PPT will be thyroid peroxidase (TPO) antibody positive. Postpartum thyroiditis also can occur after a miscarriage.
PPT can occur when the immune system rebounds after pregnancy following immune suppression during pregnancy. “Autoimmune destruction of the thyroid gland leads to initial release of stored thyroid hormone,” Ms. Kessler said. Notably, “patients with a predisposition for Hashimoto’s will have an attack on the thyroid gland. Don’t miss this in your patients.”
PPT is the most common endocrine disease in premenopausal women, with an incidence of 8%-14% in the United States, noted Ms. Kessler, a nurse practitioner in private practice in Virginia. However, the symptoms are often attributed to anxiety, depression, or the stress of new motherhood.
Women with PPT have positive thyroid peroxidase antibodies, said Ms. Kessler, and the higher the antibody, the higher the risk for PPT. Other risk factors include the presence of autoimmune disorders prior to pregnancy, a patient or family history of thyroid dysfunction, and a history of PPT.
Roughly one-third of women with PPT present with hyperthyroidism alone, another third present with hypothyroidism alone, and another third have the classic presentation of PPT, which starts with a transient hyperthyroid phase that usually occurs 1-4 months post partum, followed by a hypothyroid phase and euthyroid phase that is usually achieved within the first 12-18 months post partum, she said.
Patients presenting with PPT in the hyperthyroid phase display symptoms including insomnia, anxiety, irritability, heat intolerance, fatigue, and palpitations, Ms. Kessler said. These women “are often told they have postpartum depression; they aren’t sleeping well, and they feel like they are failing as a mom.”
Patients in the hypothyroid phase may present with fatigue, depression, cold intolerance, dry skin, impaired concentration, and paresthesias, she noted.
Treatment for PPT depends on the stage patients are in when they present. For patients in the hyperthyroid phase, Ms. Kessler recommended beta-blockers for relief of symptoms including tremor and palpitations, but these should be tapered as symptoms decrease. “There is no need for antithyroid drugs for women in the hyperthyroid phase.”
For patients presenting in the hypothyroid phase, Ms. Kessler recommended levothyroxine for 6-12 months if needed, but the drug should be tapered and discontinued after PPT, as about 80% of patients will become euthyroid. However, approximately 50% of women with PPT will develop hypothyroidism in 2-10 years, so ongoing follow-up is essential for these patients.
Ms. Kessler disclosed serving as an adviser/speaker for Novo Nordisk, serving as a speaker for Salix and Acella, and serving as National Study Chair of probiotic use with antibiotics for Clarion Brand. Global Academy and this news organization are owned by the same parent company.
FROM MEDS 2020
Tofacitinib effective for ankylosing spondylitis in phase 3
Patients with active ankylosing spondylitis (AS) experienced rapid clinical response to the oral Janus kinase (JAK) inhibitor tofacitinib (Xeljanz) in a phase 3, randomized, double-blind, placebo-controlled study.
Tofacitinib was significantly more effective than was placebo at primary and secondary endpoints. Adverse events were more frequent with tofacitinib than with placebo, but there were no new safety risks.
Results were presented at the virtual annual meeting of the American College of Rheumatology by Atul Deodhar, MD, medical director of rheumatology clinics at Oregon Health and Science University, Portland.
At week 16, 56.4% of patients who received tofacitinib met ASAS20 criteria (Assessment of Ankylosing Spondylitis, a validated measure of 20% improvement), compared with 29.4% in the placebo group (P < .0001). The percentage of ASAS40 responders at week 16 was also significantly greater with tofacitinib (40.6%) than placebo (12.5%) (P < .0001).
The trial, sponsored by Pfizer, enrolled 269 adults with active AS who had a poor response to or were intolerant of at least two NSAIDs. Most in the active treatment and placebo groups were men (about 85%); the average age was 41 years. Most (77%) had no prior exposure to biologic disease-modifying antirheumatic drugs.
“Symptom duration was about 13 years,” Dr. Deodhar said.
In the 4-month double-blind phase, patients were randomly assigned in a 1:1 ratio to receive either tofacitinib 5 mg twice a day or placebo. After 16 weeks, all patients received open-label tofacitinib until week 48.
Safety was a secondary endpoint, Dr. Deodhar said.
In the tofacitinib group, 72 patients (54.1%) experienced adverse events (AEs), compared with 70 patients in the placebo group (51.5%). Two patients in the treatment group experienced severe AEs; none in the placebo group did so. In the treatment group, three patients left the trial because of AEs; in the placebo group, one patient did so.
The most common AEs were upper respiratory tract infection and nasopharyngitis.
“There were no unexpected side effects in this study,” Dr. Deodhar said. He noted that the risks were similar to known risks for those taking the drug for rheumatoid arthritis and psoriatic arthritis.
With tofacitinib there were no deaths, thromboembolic events, malignancies, major cardiac events, or gastrointestinal perforation. By week 48, three patients in the tofacitinib group had nonserious herpes zoster versus one in the placebo group.
“There’s a lot of hand-wringing” about why a JAK inhibitor would be effective for AS, inasmuch as it does not target the tumor necrosis factor [TNF] pathway or interleukin-17,” Dr. Deodhar said.
“Somehow, JAK inhibitor drugs are downstream, affecting several cytokines that we know are important in the pathogenesis and the phenotypic expression of the disease,” he said.
Sonali Khandelwal, MD, of Rush University, Chicago, who did not take part in the research, said in an interview that tofacitinib holds promise as a much-needed option.
“JAK inhibitors have been used with success in RA, and it is reassuring to see these phase 3 data for AS,” especially for those patients whose disease was not well controlled with other approved agents, she said.
She added that oral administration is a plus for patients.
“AS, like all other chronic rheumatologic conditions, has no cure,” Dr. Khandelwal noted. “The advent of biologics has changed the course of these conditions, but not one drug works for everyone.”
She said it would be helpful if future trials were to compare the safety and efficacy of tofacitinib with those of biologics that have already been approved for AS, such as anti-TNF agents and IL-17 antagonists.
The study was sponsored by Pfizer. Dr. Deodhar reported relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, and UCB. Dr. Khandelwal disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Patients with active ankylosing spondylitis (AS) experienced rapid clinical response to the oral Janus kinase (JAK) inhibitor tofacitinib (Xeljanz) in a phase 3, randomized, double-blind, placebo-controlled study.
Tofacitinib was significantly more effective than was placebo at primary and secondary endpoints. Adverse events were more frequent with tofacitinib than with placebo, but there were no new safety risks.
Results were presented at the virtual annual meeting of the American College of Rheumatology by Atul Deodhar, MD, medical director of rheumatology clinics at Oregon Health and Science University, Portland.
At week 16, 56.4% of patients who received tofacitinib met ASAS20 criteria (Assessment of Ankylosing Spondylitis, a validated measure of 20% improvement), compared with 29.4% in the placebo group (P < .0001). The percentage of ASAS40 responders at week 16 was also significantly greater with tofacitinib (40.6%) than placebo (12.5%) (P < .0001).
The trial, sponsored by Pfizer, enrolled 269 adults with active AS who had a poor response to or were intolerant of at least two NSAIDs. Most in the active treatment and placebo groups were men (about 85%); the average age was 41 years. Most (77%) had no prior exposure to biologic disease-modifying antirheumatic drugs.
“Symptom duration was about 13 years,” Dr. Deodhar said.
In the 4-month double-blind phase, patients were randomly assigned in a 1:1 ratio to receive either tofacitinib 5 mg twice a day or placebo. After 16 weeks, all patients received open-label tofacitinib until week 48.
Safety was a secondary endpoint, Dr. Deodhar said.
In the tofacitinib group, 72 patients (54.1%) experienced adverse events (AEs), compared with 70 patients in the placebo group (51.5%). Two patients in the treatment group experienced severe AEs; none in the placebo group did so. In the treatment group, three patients left the trial because of AEs; in the placebo group, one patient did so.
The most common AEs were upper respiratory tract infection and nasopharyngitis.
“There were no unexpected side effects in this study,” Dr. Deodhar said. He noted that the risks were similar to known risks for those taking the drug for rheumatoid arthritis and psoriatic arthritis.
With tofacitinib there were no deaths, thromboembolic events, malignancies, major cardiac events, or gastrointestinal perforation. By week 48, three patients in the tofacitinib group had nonserious herpes zoster versus one in the placebo group.
“There’s a lot of hand-wringing” about why a JAK inhibitor would be effective for AS, inasmuch as it does not target the tumor necrosis factor [TNF] pathway or interleukin-17,” Dr. Deodhar said.
“Somehow, JAK inhibitor drugs are downstream, affecting several cytokines that we know are important in the pathogenesis and the phenotypic expression of the disease,” he said.
Sonali Khandelwal, MD, of Rush University, Chicago, who did not take part in the research, said in an interview that tofacitinib holds promise as a much-needed option.
“JAK inhibitors have been used with success in RA, and it is reassuring to see these phase 3 data for AS,” especially for those patients whose disease was not well controlled with other approved agents, she said.
She added that oral administration is a plus for patients.
“AS, like all other chronic rheumatologic conditions, has no cure,” Dr. Khandelwal noted. “The advent of biologics has changed the course of these conditions, but not one drug works for everyone.”
She said it would be helpful if future trials were to compare the safety and efficacy of tofacitinib with those of biologics that have already been approved for AS, such as anti-TNF agents and IL-17 antagonists.
The study was sponsored by Pfizer. Dr. Deodhar reported relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, and UCB. Dr. Khandelwal disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Patients with active ankylosing spondylitis (AS) experienced rapid clinical response to the oral Janus kinase (JAK) inhibitor tofacitinib (Xeljanz) in a phase 3, randomized, double-blind, placebo-controlled study.
Tofacitinib was significantly more effective than was placebo at primary and secondary endpoints. Adverse events were more frequent with tofacitinib than with placebo, but there were no new safety risks.
Results were presented at the virtual annual meeting of the American College of Rheumatology by Atul Deodhar, MD, medical director of rheumatology clinics at Oregon Health and Science University, Portland.
At week 16, 56.4% of patients who received tofacitinib met ASAS20 criteria (Assessment of Ankylosing Spondylitis, a validated measure of 20% improvement), compared with 29.4% in the placebo group (P < .0001). The percentage of ASAS40 responders at week 16 was also significantly greater with tofacitinib (40.6%) than placebo (12.5%) (P < .0001).
The trial, sponsored by Pfizer, enrolled 269 adults with active AS who had a poor response to or were intolerant of at least two NSAIDs. Most in the active treatment and placebo groups were men (about 85%); the average age was 41 years. Most (77%) had no prior exposure to biologic disease-modifying antirheumatic drugs.
“Symptom duration was about 13 years,” Dr. Deodhar said.
In the 4-month double-blind phase, patients were randomly assigned in a 1:1 ratio to receive either tofacitinib 5 mg twice a day or placebo. After 16 weeks, all patients received open-label tofacitinib until week 48.
Safety was a secondary endpoint, Dr. Deodhar said.
In the tofacitinib group, 72 patients (54.1%) experienced adverse events (AEs), compared with 70 patients in the placebo group (51.5%). Two patients in the treatment group experienced severe AEs; none in the placebo group did so. In the treatment group, three patients left the trial because of AEs; in the placebo group, one patient did so.
The most common AEs were upper respiratory tract infection and nasopharyngitis.
“There were no unexpected side effects in this study,” Dr. Deodhar said. He noted that the risks were similar to known risks for those taking the drug for rheumatoid arthritis and psoriatic arthritis.
With tofacitinib there were no deaths, thromboembolic events, malignancies, major cardiac events, or gastrointestinal perforation. By week 48, three patients in the tofacitinib group had nonserious herpes zoster versus one in the placebo group.
“There’s a lot of hand-wringing” about why a JAK inhibitor would be effective for AS, inasmuch as it does not target the tumor necrosis factor [TNF] pathway or interleukin-17,” Dr. Deodhar said.
“Somehow, JAK inhibitor drugs are downstream, affecting several cytokines that we know are important in the pathogenesis and the phenotypic expression of the disease,” he said.
Sonali Khandelwal, MD, of Rush University, Chicago, who did not take part in the research, said in an interview that tofacitinib holds promise as a much-needed option.
“JAK inhibitors have been used with success in RA, and it is reassuring to see these phase 3 data for AS,” especially for those patients whose disease was not well controlled with other approved agents, she said.
She added that oral administration is a plus for patients.
“AS, like all other chronic rheumatologic conditions, has no cure,” Dr. Khandelwal noted. “The advent of biologics has changed the course of these conditions, but not one drug works for everyone.”
She said it would be helpful if future trials were to compare the safety and efficacy of tofacitinib with those of biologics that have already been approved for AS, such as anti-TNF agents and IL-17 antagonists.
The study was sponsored by Pfizer. Dr. Deodhar reported relationships with AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Eli Lilly, Galapagos, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, and UCB. Dr. Khandelwal disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM ACR 2020
Virtual AHA 2020 may influence template for postpandemic scientific sessions
Cardiologists are already old hands at virtual meetings this year and are fast becoming experts on Zoom and other teleconferencing platforms, if not on how to unmute their microphones.
With expectations perhaps elevated and the new communications genre’s novelty on the wane, the American Heart Association (AHA) Scientific Sessions 2020 has a chance to both innovate with familiar formats and captivate with the field’s latest research findings.
Although the virtual AHA 2020 might not satisfy longings for face-to-face networking, shop talk, or kidding around over coffee, it will feature many traditional elements of the live conferences adapted for ear buds and small screens. They include late-breaking science (LBS) presentations and panel discussions, poster and live oral abstract presentations, meet-the-trialist talks, fireside-chat discussion forums, early career events, and satellite symposia.
The event may well hold lessons for future iterations of AHA Scientific Sessions in the postpandemic world, which some foresee as, potentially, an amalgam of the time-honored live format and a robust, complementary online presence.

“I can’t commit to exactly what AHA sessions will look like next November; I think that’s still being looked at,” the organization’s president-elect Donald M. Lloyd-Jones, MD, ScM, chair of the AHA Committee on Scientific Sessions Programming, told theheart.org | Medscape Cardiology.
There’s no debating that a live conference is valuable “for career networking and other opportunities, so I don’t think we can do without it. That has to be an important part of it,” he said. “When we can safely, of course.”
Still, “the virtual platform democratizes, right? I mean, it just allows greater access for a broader audience, and I think that’s important, too,” said Lloyd-Jones, MD, Northwestern University Feinberg School of Medicine, Chicago.
“I don’t think we’ll ever go completely back to it being all in-person,” he said. “I think the world has changed, and we’ll have to adapt our platforms to recognize that.”
Online, at least, meeting registrants will get a better look at Anthony Fauci, MD, than one might from the middle rows of a vast ballroom-turned-auditorium. Fauci is scheduled to speak on “Public Health and Scientific Challenges” during the Main Event Session “Latest Insights on COVID 19 and Cardiovascular Disease,” slated for the meeting’s final day.
Fauci has directed the National Institute of Allergy and Infectious Diseases (NIAID) since 1984, and has been celebrated for his leadership roles in the battles against AIDS and Ebola virus. Today, his name is close to a household word for his service as a prominent though embattled member of the White House Coronavirus Task Force.
The virtual AHA sessions will feature a core collection of LBS presentations from often high-profile clinical trials and other studies the organization deems worthy of special attention. There are nine such presentations arrayed across the meeting’s five days — from Friday, November 13 to Tuesday, November 17 — at times listed in this story and throughout the AHA Scientific Session program synched with the Central Standard Time (CST) zone of the AHA’s home office in Dallas.
Late-Breaking Science 1. Friday, November 13, 10:30 AM - 11:30 AM CST
The LBS sessions launch with the GALACTIC-HF trial, which — the world recently learned — may expand the burgeoning list of meds shown to improve clinical outcomes in chronic heart failure (HF) with reduced ejection fraction (HFrEF).
In cursory top-line results announced last month, those in the trial of more than 8000 patients who were randomly assigned to receive omecamtiv mecarbil (Amgen/Cytokinetics/Servier) showed a slight but significant benefit for the primary end point of cardiovascular (CV) death or HF events. The hazard ratio (HR), compared with standard care, was 0.92 (95% CI, 0.86 - 0.99; P = .025), noted a press release from Amgen.
Among the announcement’s few other details was a short take on safety outcomes: no difference in risk for “adverse events, including major ischemic cardiac events,” between the active and control groups. The presentation is sure to provide further insights and caveats, if any, along with other information crucial to the study’s interpretation.
Next on the schedule is the closely watched AFFIRM-AHF, billed as the first major outcomes trial of iron administration to iron-deficient patients with acute HF. It randomly assigned more than 1000 such patients to receive IV ferric carboxymaltose or a placebo. The first dose was given in-hospital and subsequent doses at home for 24 weeks or until patients were no longer iron deficient. They were followed to 1 year for the primary end point of recurrent HF hospitalizations or CV death.
The session wraps with the VITAL Rhythm trial, a substudy of the doubly randomized VITAL trial that explored the effects of vitamin D and omega-3 fatty acid supplementation on CV and cancer risk in more than 25,000 patients in the community. The substudy explored the effects of two active therapies, a preparation of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) (Omacor, Reliant Pharmaceuticals) or vitamin D3 supplements, on new-onset atrial fibrillation (AF) as the primary end point; it also looked at risk for sudden death.
Late-Breaking Science 2. Friday, November 13, 12:00 PM - 1:00 PM CST
Dominating the session in two presentations, the (TIPS)-3 trial explored a polypill primary-prevention strategy and daily aspirin with vitamin D supplementation in three separate placebo-controlled comparisons in more than 5700 “intermediate risk” participants 55 years and older, mostly in developing countries.
The daily polypill in this trial is a combination of hydrochlorothiazide 25 mg, atenolol 100 mg, ramipril 10 mg, and simvastatin 40 mg; aspirin was given at 75 mg daily and vitamin D at 60,000 IU monthly.
The participants are followed for a primary end point composed of major CV disease, HF, resuscitated cardiac arrest, or ischemia-driven revascularization for the polypill comparison; CV events or cancer for the aspirin comparison; and fracture risk for the vitamin D component of the trial.
In the Swedish Cardiopulmonary Bioimage Study (SCAPIS), presented third in the session, a random sample of adults from throughout Sweden, projected at about 30,000, underwent a 2-day evaluation for metabolic risk factors plus ultrasound and coronary and lung CT scans. The group has been followed for risks for myocardial infarction (MI), sudden death, and other cardiac diseases; and chronic obstructive pulmonary disease (COPD) and other lung disorders.
Late-Breaking Science 3. Saturday, November 14, 12:00 PM - 1:00 PM CST
The field may learn more mechanistically about MI associated with nonobstructed coronary arteries (MINOCA) than ever before from the Heart Attack Research Program-Imaging Study (HARP). The observational study is enrolling a projected 450 patients with suspected MI and ischemic symptoms who were referred for cardiac catheterization.
Their evaluation includes coronary optical coherence tomographic (OCT) scanning and cardiac magnetic resonance (CMR) imaging for evidence of coronary plaque disruption as the primary end point. The patients are to be followed for 10 years for a composite of death, unstable angina, stroke, recurrent MI, diagnostic or interventional catheterization, and cardiac hospitalization.
The major direct oral anticoagulant (DOAC) comparisons with warfarin in atrial fibrillation (AF) didn’t include many patients with prosthetic valve implants. In contrast, the RIVER trial enrolled 1005 adults with either persistent or paroxysmal AF and bioprosthetic mitral valves and assigned them to rivaroxaban 20 mg or the vitamin K antagonist.
The presentation will include the noninferiority primary outcome of major clinical events, which is stroke, transient ischemic attack (TIA), major bleeding, death from any cause, valve thrombosis, other systemic embolism, or HF hospitalization over 12 months.
This session also includes ALPHEUS, a trial pitting ticagrelor (Brilinta/Brilique, AstraZeneca) against mainstay clopidogrel in a setting that is mostly uncharted for such comparisons, elective percutaneous coronary intervention (PCI).
About 1900 patients with stable coronary disease were randomly assigned to a month of treatment with either agent on top of continuous aspirin. The primary end point is PCI-related MI or myocardial injury within 48 hours of the procedure.
Late-Breaking Science 4. Sunday, November 15, 9:00 AM - 10:00 AM CST
The Self-Assessment Method for Statin Side-effects Or Nocebo (SAMSON) trial may be one of the AHA 2020 frontrunners for early buzz and anticipation. So it’s with some irony that it’s also among the smallest of the LBS studies, at 60 patients, which was nonetheless considered sufficient due to its unusual design.
SAMSON is the latest and perhaps most rigorous attempt to clarify whether symptoms, especially muscle pain or discomfort, attributed to statins by many patients are pharmacologic in origin or, rather, a nocebo effect from negative expectations about statin side effects.
The study patients, all of whom had previously halted statins because of side effects, were assigned to follow three separate regimens, each for month, in a randomized order; they did that four times, for a total of 12 months. The regimens consisted of atorvastatin 20 mg daily, a placebo, or neither.
Patients kept daily logs of any perceived side effects. Parity between side effects experienced on the statin and the placebo would point to a nocebo effect, whereas a significant excess on atorvastatin would suggest they are direct drug effects.
The session also features two randomized trials each on a unique omega-3 fatty acid preparation for either secondary prevention or high-risk primary prevention, in both cases compared with a corn-oil placebo.
The Omega-3 Fatty Acids in Elderly Patients with Myocardial Infarction (OMEMI) trial randomly assigned more than 1000 elderly post-MI patients to take Pikasol (Orkla Care) at 1.8 g EPA and DHA per day or the placebo. It looked for all-cause mortality, nonfatal MI, stroke, revascularization, or hospitalization for new or worsened HF over 24 months.
The STRENGTH trial, with a planned enrollment of about 13,000 high-vascular-risk patients, looked primarily at the effect of daily treatment with Epanova (AstraZeneca), which also contains DHA and EPA, on the composite of CV death, nonfatal MI or stroke, coronary revascularization, and hospitalization for unstable angina. The trial was halted early for low likelihood of benefit, AstraZeneca announced in January of this year.
Late-Breaking Science 5. Sunday, November 15, 7:15 PM - 8:30 PM CST
Slated for the session is the primary analysis of the PIONEER 3 trial, conducted in the United States, Europe, and Japan. It compared the BuMA Supreme biodegradable drug-coated stent (SinoMed) with the durable Xience (Abbott Vascular) and Promus (Boston Scientific) drug-eluting stents. The trial followed more than 1600 patients treated for chronic stable angina or acute coronary syndrome (ACS) for the 1-year composite of cardiac death, target-vessel-related MI, and clinically driven target-lesion revascularization.
Late-Breaking Science 6. Monday, November 16, 9:00 AM - 10:00 AM CST
The EARLY-AF trial enrolled 303 patients with symptomatic paroxysmal or persistent AF suitable for catheter ablation, assigning them to pulmonary vein isolation (PVI) by cryoablation using the Arctic Front (Medtronic) system or antiarrhythmic drug therapy for rhythm control. The primary end point is time to recurrence of AF, atrial flutter, or atrial tachycardia, whether symptomatic or asymptomatic, as determined by implantable loop recorder. Patients will also be followed for symptoms and arrhythmia burden.
Also in the session, the SEARCH-AF study randomized almost 400 patients undergoing cardiac surgery who were engaged subacutely with one of two commercial portable cardiac rhythm monitoring devices (CardioSTAT, Icentia; or SEEQ, Medtronic) or, alternatively, to receive usual postoperative care
The patients, considered to be at high risk for stroke with no history of AF, were followed for the primary end point of cumulative burden of AF or atrial flutter exceeding 6 minutes or documentation of either arrhythmia by 12-lead ECG within 30 days.
Two other studies in the session look at different approaches to AF screening, one using a handheld ECG monitor in the primary care setting and the other wearable monitors in the form of a patch or wristband. The VITAL-AF presentation is titled “Screening for Atrial Fibrillation in Older Adults at Primary Care Visits Using Single Lead Electrocardiograms.” The other presentation, on the study mSToPS, is called “Three-Year Clinical Outcomes in a Nationwide, Randomized, Pragmatic Clinical Trial of Atrial Fibrillation Screening — Mhealth Screening to Prevent Strokes.”
Late-Breaking Science 7. Monday, November 16, 7:00 PM - 8:30 PM CST
In the randomized FIDELIO-DKD trial with more than 5700 patients with type 2 diabetes and associated kidney disease, those assigned to the novel mineralocorticoid receptor antagonist (MRA) finerenone (Bayer) showed an 18% drop in risk for adverse renal events, including death from renal causes (P = .001), over a median of 2.6 years. That primary outcome was previously presented in detail at a nephrology meeting and published in the New England Journal of Medicine in October.
Patients on the MRA showed a similar reduction in a composite CV-event end point, it was also reported at that time. A follow-up presentation at the AHA sessions promises to dive deeper into the trial’s CV outcomes.
In the RAPID-CTCA study, slated next for the session, 1749 patients with suspected or confirmed intermediate-risk ACS were randomly assigned to undergo computed tomographic coronary angiography (CTCA) for guiding treatment decisions or a standard-of-care strategy. It followed patients for the primary end point of death or nonfatal MI over 1 year.
Rilonacept (Arcalyst, Kiniksa/Regeneron) is an interleukin-1α and -1β inhibitor used in several autoinflammatory diseases that went unsuccessfully before regulators for the treatment of gout. The RHAPSODY trial has now explored its use against recurrent pericarditis in a randomized trial that entered 86 patients 12 years and older who had previously experienced at least three episodes.
In top-line results reported to investors in June, patients assigned to receive the drug instead of placebo in weekly injections showed a 96% drop in risk for pericarditis recurrence and “no or minimal pain” on more than 90% of days in the trial. A full presentation is expected during this LBS session.
Also on the schedule is the THALES study, which led the US Food and Drug Administration (FDA) to expand indications for ticagrelor to include stroke prevention in patients with a history of acute ischemic stroke or high-risk TIA based on the trial’s primary results published in July.
In THALES, more than 11,000 patients with mild to moderate acute noncardiogenic ischemic stroke or TIA were randomly assigned within 24 hours to start on daily aspirin with or without ticagrelor given as a 180 mg loading dose followed by 90 mg twice daily for 30 days.
At the end of a month, it was reported, those on dual antiplatelet therapy showed a 17% risk reduction (P = .02) for the primary end point of stroke or death, at the cost of a slight but significant increase in “severe” bleeding (0.5% vs 0.1%; P = .001).
The session is to conclude with two related studies that fell victim in part to the COVID-19 pandemic, both of which explored sotagliflozin (Zynquista, Sanofi/Lexicon), an inhibitor of both sodium-glucose cotransporters 1 and 2 (SGLT1 and SGLT2, respectively) in patients with type 2 diabetes.
SOLOIST-WHF had entered 1222 such patients hospitalized with urgent or worsening HF at 466 centers and randomly assigned them to receive sotagliflozin or placebo; they were followed for the composite of CV death or HF events. SCORED reached an enrollment of 10,584 patients with diabetes and chronic kidney disease at 754 hospitals, following them for the same primary end point.
Lexicon announced in March that the trials would be “closed out early” because of the unavailability of funding “together with uncertainties relating to the COVID-19 pandemic on the trials.” The LBS presentation is expected to include analyses of available data; SOLOIST-WHF launched in summer 2018 and SCORED began in November 2017.
Late-Breaking Science 8. Tuesday, November 17, 9:00 AM - 10:00 AM CST
Most of this LBS session is devoted to the AHA COVID-19 Cardiovascular Disease registry, which is looking at the hospital journey, clinical course, and outcomes of patients hospitalized with SARS-CoV-2 infections at centers participating in the organization’s Get With The Guidelines (GWTG) quality-improvement program. As of September, the registry included data from more than 15,000 patients.
Scheduled presentations include a summary of the registry’s design and initial results; an analysis of racial and ethnic variation in therapy and clinical outcomes; an exploration of how body mass index influenced outcomes, including death, use of mechanical ventilation, and cardiovascular end points, in patients with COVID-19; and a deep dive into the relation between CV disease and clinical outcomes in the cohort.
The last of this LBS block’s five talks will cover the randomized Influenza Vaccine to Effectively Stop Cardio Thoracic Events and Decompensated Heart Failure (INVESTED) trial, which compared vaccination with high-dose trivalent influenza vaccine or a standard-dose quadrivalent vaccine in 5388 adults with a history of hospitalization for either MI or HF. Patients were required to have at least one other CV risk factor, such as older age, reduced left ventricular ejection fraction, or diabetes.
INVESTED tracked the patients at 190 centers across an initial pilot flu season and three subsequent flu seasons for the primary end point of death from any cause or cardiopulmonary hospitalization.
The trial is one of at least three that have been looking at the effect of flu vaccination on cardiovascular outcomes; results from the other two — IAMI, with more than 2500 participants, and RCT-IVVE, with an enrollment of 4871 — are planned for presentation in 2021, theheart.org | Medscape Cardiology recently reported.
Late-Breaking Science 9. Tuesday, November 17, 12:00 PM - 1:00 PM CST
The conference’s concluding LBS session features three studies that relied on technologic strategies for modifying patient compliance and other care behaviors and one that used human-centered design principles to develop a group-care model aimed improving the management of diabetes, hypertension, and other noncommunicable diseases in economically disadvantaged regions of Kenya.
The EPIC-HF trial tested a strategy for improving HFrEF medication-plan engagement by use of a video and documents delivered to patients several times by email or text prior to their follow-up clinic appointments. The strategy was compared with usual care for its effect on HF-medication optimization over 1 month and 1 year in a total of 306 patients.
Following EPIC-HF on the schedule is the MYROAD trial, looking at the efficacy of discharge instructions provided to patients with acute HF as an audio recording that they and their physicians could replay on demand, the idea being to increase adherence to the instructions. The trial’s 1073 patients were assigned to the novel strategy or usual care and followed for HF rehospitalization within 30 days.
MYROAD is to be followed by a presentation entitled “Digital Care Transformation: One-Year Report of >5,000 Patients Enrolled in a Remote Algorithm-Based CV Risk Management Program to Achieve Optimal Lipid and Hypertension Control.”
Rounding out the LBS session: the Bridging Income Generation With Group Integrated Care (BIGPIC) program, a pilot study that developed and executed “a healthcare delivery model targeting health behaviors, medication adherence, and financial barriers to accessing healthcare” in four rural counties in Kenya.
The model features locally developed plans, tailored for regional needs, that are said to “combine the benefits of microfinance with the peer support available through group medical care to enhance management of hypertension and diabetes.” The microfinance component is aimed at improving household economies to alleviate the financial burden of care and clinic attendance, and for the health effects of improved quality of life.
The study randomized 2890 adults with diabetes or prediabetes to one of four groups: usual care plus microfinance group support, group medical visits only or combined with microfinance group support, or usual care only. They were followed for changes in systolic blood pressure and CV-risk score over 12 months.
Lloyd-Jones and Fauci declared no conflicts.
This article first appeared on Medscape.com.
Cardiologists are already old hands at virtual meetings this year and are fast becoming experts on Zoom and other teleconferencing platforms, if not on how to unmute their microphones.
With expectations perhaps elevated and the new communications genre’s novelty on the wane, the American Heart Association (AHA) Scientific Sessions 2020 has a chance to both innovate with familiar formats and captivate with the field’s latest research findings.
Although the virtual AHA 2020 might not satisfy longings for face-to-face networking, shop talk, or kidding around over coffee, it will feature many traditional elements of the live conferences adapted for ear buds and small screens. They include late-breaking science (LBS) presentations and panel discussions, poster and live oral abstract presentations, meet-the-trialist talks, fireside-chat discussion forums, early career events, and satellite symposia.
The event may well hold lessons for future iterations of AHA Scientific Sessions in the postpandemic world, which some foresee as, potentially, an amalgam of the time-honored live format and a robust, complementary online presence.
“I can’t commit to exactly what AHA sessions will look like next November; I think that’s still being looked at,” the organization’s president-elect Donald M. Lloyd-Jones, MD, ScM, chair of the AHA Committee on Scientific Sessions Programming, told theheart.org | Medscape Cardiology.
There’s no debating that a live conference is valuable “for career networking and other opportunities, so I don’t think we can do without it. That has to be an important part of it,” he said. “When we can safely, of course.”
Still, “the virtual platform democratizes, right? I mean, it just allows greater access for a broader audience, and I think that’s important, too,” said Lloyd-Jones, MD, Northwestern University Feinberg School of Medicine, Chicago.
“I don’t think we’ll ever go completely back to it being all in-person,” he said. “I think the world has changed, and we’ll have to adapt our platforms to recognize that.”
Online, at least, meeting registrants will get a better look at Anthony Fauci, MD, than one might from the middle rows of a vast ballroom-turned-auditorium. Fauci is scheduled to speak on “Public Health and Scientific Challenges” during the Main Event Session “Latest Insights on COVID 19 and Cardiovascular Disease,” slated for the meeting’s final day.
Fauci has directed the National Institute of Allergy and Infectious Diseases (NIAID) since 1984, and has been celebrated for his leadership roles in the battles against AIDS and Ebola virus. Today, his name is close to a household word for his service as a prominent though embattled member of the White House Coronavirus Task Force.
The virtual AHA sessions will feature a core collection of LBS presentations from often high-profile clinical trials and other studies the organization deems worthy of special attention. There are nine such presentations arrayed across the meeting’s five days — from Friday, November 13 to Tuesday, November 17 — at times listed in this story and throughout the AHA Scientific Session program synched with the Central Standard Time (CST) zone of the AHA’s home office in Dallas.
Late-Breaking Science 1. Friday, November 13, 10:30 AM - 11:30 AM CST
The LBS sessions launch with the GALACTIC-HF trial, which — the world recently learned — may expand the burgeoning list of meds shown to improve clinical outcomes in chronic heart failure (HF) with reduced ejection fraction (HFrEF).
In cursory top-line results announced last month, those in the trial of more than 8000 patients who were randomly assigned to receive omecamtiv mecarbil (Amgen/Cytokinetics/Servier) showed a slight but significant benefit for the primary end point of cardiovascular (CV) death or HF events. The hazard ratio (HR), compared with standard care, was 0.92 (95% CI, 0.86 - 0.99; P = .025), noted a press release from Amgen.
Among the announcement’s few other details was a short take on safety outcomes: no difference in risk for “adverse events, including major ischemic cardiac events,” between the active and control groups. The presentation is sure to provide further insights and caveats, if any, along with other information crucial to the study’s interpretation.
Next on the schedule is the closely watched AFFIRM-AHF, billed as the first major outcomes trial of iron administration to iron-deficient patients with acute HF. It randomly assigned more than 1000 such patients to receive IV ferric carboxymaltose or a placebo. The first dose was given in-hospital and subsequent doses at home for 24 weeks or until patients were no longer iron deficient. They were followed to 1 year for the primary end point of recurrent HF hospitalizations or CV death.
The session wraps with the VITAL Rhythm trial, a substudy of the doubly randomized VITAL trial that explored the effects of vitamin D and omega-3 fatty acid supplementation on CV and cancer risk in more than 25,000 patients in the community. The substudy explored the effects of two active therapies, a preparation of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) (Omacor, Reliant Pharmaceuticals) or vitamin D3 supplements, on new-onset atrial fibrillation (AF) as the primary end point; it also looked at risk for sudden death.
Late-Breaking Science 2. Friday, November 13, 12:00 PM - 1:00 PM CST
Dominating the session in two presentations, the (TIPS)-3 trial explored a polypill primary-prevention strategy and daily aspirin with vitamin D supplementation in three separate placebo-controlled comparisons in more than 5700 “intermediate risk” participants 55 years and older, mostly in developing countries.
The daily polypill in this trial is a combination of hydrochlorothiazide 25 mg, atenolol 100 mg, ramipril 10 mg, and simvastatin 40 mg; aspirin was given at 75 mg daily and vitamin D at 60,000 IU monthly.
The participants are followed for a primary end point composed of major CV disease, HF, resuscitated cardiac arrest, or ischemia-driven revascularization for the polypill comparison; CV events or cancer for the aspirin comparison; and fracture risk for the vitamin D component of the trial.
In the Swedish Cardiopulmonary Bioimage Study (SCAPIS), presented third in the session, a random sample of adults from throughout Sweden, projected at about 30,000, underwent a 2-day evaluation for metabolic risk factors plus ultrasound and coronary and lung CT scans. The group has been followed for risks for myocardial infarction (MI), sudden death, and other cardiac diseases; and chronic obstructive pulmonary disease (COPD) and other lung disorders.
Late-Breaking Science 3. Saturday, November 14, 12:00 PM - 1:00 PM CST
The field may learn more mechanistically about MI associated with nonobstructed coronary arteries (MINOCA) than ever before from the Heart Attack Research Program-Imaging Study (HARP). The observational study is enrolling a projected 450 patients with suspected MI and ischemic symptoms who were referred for cardiac catheterization.
Their evaluation includes coronary optical coherence tomographic (OCT) scanning and cardiac magnetic resonance (CMR) imaging for evidence of coronary plaque disruption as the primary end point. The patients are to be followed for 10 years for a composite of death, unstable angina, stroke, recurrent MI, diagnostic or interventional catheterization, and cardiac hospitalization.
The major direct oral anticoagulant (DOAC) comparisons with warfarin in atrial fibrillation (AF) didn’t include many patients with prosthetic valve implants. In contrast, the RIVER trial enrolled 1005 adults with either persistent or paroxysmal AF and bioprosthetic mitral valves and assigned them to rivaroxaban 20 mg or the vitamin K antagonist.
The presentation will include the noninferiority primary outcome of major clinical events, which is stroke, transient ischemic attack (TIA), major bleeding, death from any cause, valve thrombosis, other systemic embolism, or HF hospitalization over 12 months.
This session also includes ALPHEUS, a trial pitting ticagrelor (Brilinta/Brilique, AstraZeneca) against mainstay clopidogrel in a setting that is mostly uncharted for such comparisons, elective percutaneous coronary intervention (PCI).
About 1900 patients with stable coronary disease were randomly assigned to a month of treatment with either agent on top of continuous aspirin. The primary end point is PCI-related MI or myocardial injury within 48 hours of the procedure.
Late-Breaking Science 4. Sunday, November 15, 9:00 AM - 10:00 AM CST
The Self-Assessment Method for Statin Side-effects Or Nocebo (SAMSON) trial may be one of the AHA 2020 frontrunners for early buzz and anticipation. So it’s with some irony that it’s also among the smallest of the LBS studies, at 60 patients, which was nonetheless considered sufficient due to its unusual design.
SAMSON is the latest and perhaps most rigorous attempt to clarify whether symptoms, especially muscle pain or discomfort, attributed to statins by many patients are pharmacologic in origin or, rather, a nocebo effect from negative expectations about statin side effects.
The study patients, all of whom had previously halted statins because of side effects, were assigned to follow three separate regimens, each for month, in a randomized order; they did that four times, for a total of 12 months. The regimens consisted of atorvastatin 20 mg daily, a placebo, or neither.
Patients kept daily logs of any perceived side effects. Parity between side effects experienced on the statin and the placebo would point to a nocebo effect, whereas a significant excess on atorvastatin would suggest they are direct drug effects.
The session also features two randomized trials each on a unique omega-3 fatty acid preparation for either secondary prevention or high-risk primary prevention, in both cases compared with a corn-oil placebo.
The Omega-3 Fatty Acids in Elderly Patients with Myocardial Infarction (OMEMI) trial randomly assigned more than 1000 elderly post-MI patients to take Pikasol (Orkla Care) at 1.8 g EPA and DHA per day or the placebo. It looked for all-cause mortality, nonfatal MI, stroke, revascularization, or hospitalization for new or worsened HF over 24 months.
The STRENGTH trial, with a planned enrollment of about 13,000 high-vascular-risk patients, looked primarily at the effect of daily treatment with Epanova (AstraZeneca), which also contains DHA and EPA, on the composite of CV death, nonfatal MI or stroke, coronary revascularization, and hospitalization for unstable angina. The trial was halted early for low likelihood of benefit, AstraZeneca announced in January of this year.
Late-Breaking Science 5. Sunday, November 15, 7:15 PM - 8:30 PM CST
Slated for the session is the primary analysis of the PIONEER 3 trial, conducted in the United States, Europe, and Japan. It compared the BuMA Supreme biodegradable drug-coated stent (SinoMed) with the durable Xience (Abbott Vascular) and Promus (Boston Scientific) drug-eluting stents. The trial followed more than 1600 patients treated for chronic stable angina or acute coronary syndrome (ACS) for the 1-year composite of cardiac death, target-vessel-related MI, and clinically driven target-lesion revascularization.
Late-Breaking Science 6. Monday, November 16, 9:00 AM - 10:00 AM CST
The EARLY-AF trial enrolled 303 patients with symptomatic paroxysmal or persistent AF suitable for catheter ablation, assigning them to pulmonary vein isolation (PVI) by cryoablation using the Arctic Front (Medtronic) system or antiarrhythmic drug therapy for rhythm control. The primary end point is time to recurrence of AF, atrial flutter, or atrial tachycardia, whether symptomatic or asymptomatic, as determined by implantable loop recorder. Patients will also be followed for symptoms and arrhythmia burden.
Also in the session, the SEARCH-AF study randomized almost 400 patients undergoing cardiac surgery who were engaged subacutely with one of two commercial portable cardiac rhythm monitoring devices (CardioSTAT, Icentia; or SEEQ, Medtronic) or, alternatively, to receive usual postoperative care
The patients, considered to be at high risk for stroke with no history of AF, were followed for the primary end point of cumulative burden of AF or atrial flutter exceeding 6 minutes or documentation of either arrhythmia by 12-lead ECG within 30 days.
Two other studies in the session look at different approaches to AF screening, one using a handheld ECG monitor in the primary care setting and the other wearable monitors in the form of a patch or wristband. The VITAL-AF presentation is titled “Screening for Atrial Fibrillation in Older Adults at Primary Care Visits Using Single Lead Electrocardiograms.” The other presentation, on the study mSToPS, is called “Three-Year Clinical Outcomes in a Nationwide, Randomized, Pragmatic Clinical Trial of Atrial Fibrillation Screening — Mhealth Screening to Prevent Strokes.”
Late-Breaking Science 7. Monday, November 16, 7:00 PM - 8:30 PM CST
In the randomized FIDELIO-DKD trial with more than 5700 patients with type 2 diabetes and associated kidney disease, those assigned to the novel mineralocorticoid receptor antagonist (MRA) finerenone (Bayer) showed an 18% drop in risk for adverse renal events, including death from renal causes (P = .001), over a median of 2.6 years. That primary outcome was previously presented in detail at a nephrology meeting and published in the New England Journal of Medicine in October.
Patients on the MRA showed a similar reduction in a composite CV-event end point, it was also reported at that time. A follow-up presentation at the AHA sessions promises to dive deeper into the trial’s CV outcomes.
In the RAPID-CTCA study, slated next for the session, 1749 patients with suspected or confirmed intermediate-risk ACS were randomly assigned to undergo computed tomographic coronary angiography (CTCA) for guiding treatment decisions or a standard-of-care strategy. It followed patients for the primary end point of death or nonfatal MI over 1 year.
Rilonacept (Arcalyst, Kiniksa/Regeneron) is an interleukin-1α and -1β inhibitor used in several autoinflammatory diseases that went unsuccessfully before regulators for the treatment of gout. The RHAPSODY trial has now explored its use against recurrent pericarditis in a randomized trial that entered 86 patients 12 years and older who had previously experienced at least three episodes.
In top-line results reported to investors in June, patients assigned to receive the drug instead of placebo in weekly injections showed a 96% drop in risk for pericarditis recurrence and “no or minimal pain” on more than 90% of days in the trial. A full presentation is expected during this LBS session.
Also on the schedule is the THALES study, which led the US Food and Drug Administration (FDA) to expand indications for ticagrelor to include stroke prevention in patients with a history of acute ischemic stroke or high-risk TIA based on the trial’s primary results published in July.
In THALES, more than 11,000 patients with mild to moderate acute noncardiogenic ischemic stroke or TIA were randomly assigned within 24 hours to start on daily aspirin with or without ticagrelor given as a 180 mg loading dose followed by 90 mg twice daily for 30 days.
At the end of a month, it was reported, those on dual antiplatelet therapy showed a 17% risk reduction (P = .02) for the primary end point of stroke or death, at the cost of a slight but significant increase in “severe” bleeding (0.5% vs 0.1%; P = .001).
The session is to conclude with two related studies that fell victim in part to the COVID-19 pandemic, both of which explored sotagliflozin (Zynquista, Sanofi/Lexicon), an inhibitor of both sodium-glucose cotransporters 1 and 2 (SGLT1 and SGLT2, respectively) in patients with type 2 diabetes.
SOLOIST-WHF had entered 1222 such patients hospitalized with urgent or worsening HF at 466 centers and randomly assigned them to receive sotagliflozin or placebo; they were followed for the composite of CV death or HF events. SCORED reached an enrollment of 10,584 patients with diabetes and chronic kidney disease at 754 hospitals, following them for the same primary end point.
Lexicon announced in March that the trials would be “closed out early” because of the unavailability of funding “together with uncertainties relating to the COVID-19 pandemic on the trials.” The LBS presentation is expected to include analyses of available data; SOLOIST-WHF launched in summer 2018 and SCORED began in November 2017.
Late-Breaking Science 8. Tuesday, November 17, 9:00 AM - 10:00 AM CST
Most of this LBS session is devoted to the AHA COVID-19 Cardiovascular Disease registry, which is looking at the hospital journey, clinical course, and outcomes of patients hospitalized with SARS-CoV-2 infections at centers participating in the organization’s Get With The Guidelines (GWTG) quality-improvement program. As of September, the registry included data from more than 15,000 patients.
Scheduled presentations include a summary of the registry’s design and initial results; an analysis of racial and ethnic variation in therapy and clinical outcomes; an exploration of how body mass index influenced outcomes, including death, use of mechanical ventilation, and cardiovascular end points, in patients with COVID-19; and a deep dive into the relation between CV disease and clinical outcomes in the cohort.
The last of this LBS block’s five talks will cover the randomized Influenza Vaccine to Effectively Stop Cardio Thoracic Events and Decompensated Heart Failure (INVESTED) trial, which compared vaccination with high-dose trivalent influenza vaccine or a standard-dose quadrivalent vaccine in 5388 adults with a history of hospitalization for either MI or HF. Patients were required to have at least one other CV risk factor, such as older age, reduced left ventricular ejection fraction, or diabetes.
INVESTED tracked the patients at 190 centers across an initial pilot flu season and three subsequent flu seasons for the primary end point of death from any cause or cardiopulmonary hospitalization.
The trial is one of at least three that have been looking at the effect of flu vaccination on cardiovascular outcomes; results from the other two — IAMI, with more than 2500 participants, and RCT-IVVE, with an enrollment of 4871 — are planned for presentation in 2021, theheart.org | Medscape Cardiology recently reported.
Late-Breaking Science 9. Tuesday, November 17, 12:00 PM - 1:00 PM CST
The conference’s concluding LBS session features three studies that relied on technologic strategies for modifying patient compliance and other care behaviors and one that used human-centered design principles to develop a group-care model aimed improving the management of diabetes, hypertension, and other noncommunicable diseases in economically disadvantaged regions of Kenya.
The EPIC-HF trial tested a strategy for improving HFrEF medication-plan engagement by use of a video and documents delivered to patients several times by email or text prior to their follow-up clinic appointments. The strategy was compared with usual care for its effect on HF-medication optimization over 1 month and 1 year in a total of 306 patients.
Following EPIC-HF on the schedule is the MYROAD trial, looking at the efficacy of discharge instructions provided to patients with acute HF as an audio recording that they and their physicians could replay on demand, the idea being to increase adherence to the instructions. The trial’s 1073 patients were assigned to the novel strategy or usual care and followed for HF rehospitalization within 30 days.
MYROAD is to be followed by a presentation entitled “Digital Care Transformation: One-Year Report of >5,000 Patients Enrolled in a Remote Algorithm-Based CV Risk Management Program to Achieve Optimal Lipid and Hypertension Control.”
Rounding out the LBS session: the Bridging Income Generation With Group Integrated Care (BIGPIC) program, a pilot study that developed and executed “a healthcare delivery model targeting health behaviors, medication adherence, and financial barriers to accessing healthcare” in four rural counties in Kenya.
The model features locally developed plans, tailored for regional needs, that are said to “combine the benefits of microfinance with the peer support available through group medical care to enhance management of hypertension and diabetes.” The microfinance component is aimed at improving household economies to alleviate the financial burden of care and clinic attendance, and for the health effects of improved quality of life.
The study randomized 2890 adults with diabetes or prediabetes to one of four groups: usual care plus microfinance group support, group medical visits only or combined with microfinance group support, or usual care only. They were followed for changes in systolic blood pressure and CV-risk score over 12 months.
Lloyd-Jones and Fauci declared no conflicts.
This article first appeared on Medscape.com.
Cardiologists are already old hands at virtual meetings this year and are fast becoming experts on Zoom and other teleconferencing platforms, if not on how to unmute their microphones.
With expectations perhaps elevated and the new communications genre’s novelty on the wane, the American Heart Association (AHA) Scientific Sessions 2020 has a chance to both innovate with familiar formats and captivate with the field’s latest research findings.
Although the virtual AHA 2020 might not satisfy longings for face-to-face networking, shop talk, or kidding around over coffee, it will feature many traditional elements of the live conferences adapted for ear buds and small screens. They include late-breaking science (LBS) presentations and panel discussions, poster and live oral abstract presentations, meet-the-trialist talks, fireside-chat discussion forums, early career events, and satellite symposia.
The event may well hold lessons for future iterations of AHA Scientific Sessions in the postpandemic world, which some foresee as, potentially, an amalgam of the time-honored live format and a robust, complementary online presence.
“I can’t commit to exactly what AHA sessions will look like next November; I think that’s still being looked at,” the organization’s president-elect Donald M. Lloyd-Jones, MD, ScM, chair of the AHA Committee on Scientific Sessions Programming, told theheart.org | Medscape Cardiology.
There’s no debating that a live conference is valuable “for career networking and other opportunities, so I don’t think we can do without it. That has to be an important part of it,” he said. “When we can safely, of course.”
Still, “the virtual platform democratizes, right? I mean, it just allows greater access for a broader audience, and I think that’s important, too,” said Lloyd-Jones, MD, Northwestern University Feinberg School of Medicine, Chicago.
“I don’t think we’ll ever go completely back to it being all in-person,” he said. “I think the world has changed, and we’ll have to adapt our platforms to recognize that.”
Online, at least, meeting registrants will get a better look at Anthony Fauci, MD, than one might from the middle rows of a vast ballroom-turned-auditorium. Fauci is scheduled to speak on “Public Health and Scientific Challenges” during the Main Event Session “Latest Insights on COVID 19 and Cardiovascular Disease,” slated for the meeting’s final day.
Fauci has directed the National Institute of Allergy and Infectious Diseases (NIAID) since 1984, and has been celebrated for his leadership roles in the battles against AIDS and Ebola virus. Today, his name is close to a household word for his service as a prominent though embattled member of the White House Coronavirus Task Force.
The virtual AHA sessions will feature a core collection of LBS presentations from often high-profile clinical trials and other studies the organization deems worthy of special attention. There are nine such presentations arrayed across the meeting’s five days — from Friday, November 13 to Tuesday, November 17 — at times listed in this story and throughout the AHA Scientific Session program synched with the Central Standard Time (CST) zone of the AHA’s home office in Dallas.
Late-Breaking Science 1. Friday, November 13, 10:30 AM - 11:30 AM CST
The LBS sessions launch with the GALACTIC-HF trial, which — the world recently learned — may expand the burgeoning list of meds shown to improve clinical outcomes in chronic heart failure (HF) with reduced ejection fraction (HFrEF).
In cursory top-line results announced last month, those in the trial of more than 8000 patients who were randomly assigned to receive omecamtiv mecarbil (Amgen/Cytokinetics/Servier) showed a slight but significant benefit for the primary end point of cardiovascular (CV) death or HF events. The hazard ratio (HR), compared with standard care, was 0.92 (95% CI, 0.86 - 0.99; P = .025), noted a press release from Amgen.
Among the announcement’s few other details was a short take on safety outcomes: no difference in risk for “adverse events, including major ischemic cardiac events,” between the active and control groups. The presentation is sure to provide further insights and caveats, if any, along with other information crucial to the study’s interpretation.
Next on the schedule is the closely watched AFFIRM-AHF, billed as the first major outcomes trial of iron administration to iron-deficient patients with acute HF. It randomly assigned more than 1000 such patients to receive IV ferric carboxymaltose or a placebo. The first dose was given in-hospital and subsequent doses at home for 24 weeks or until patients were no longer iron deficient. They were followed to 1 year for the primary end point of recurrent HF hospitalizations or CV death.
The session wraps with the VITAL Rhythm trial, a substudy of the doubly randomized VITAL trial that explored the effects of vitamin D and omega-3 fatty acid supplementation on CV and cancer risk in more than 25,000 patients in the community. The substudy explored the effects of two active therapies, a preparation of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) (Omacor, Reliant Pharmaceuticals) or vitamin D3 supplements, on new-onset atrial fibrillation (AF) as the primary end point; it also looked at risk for sudden death.
Late-Breaking Science 2. Friday, November 13, 12:00 PM - 1:00 PM CST
Dominating the session in two presentations, the (TIPS)-3 trial explored a polypill primary-prevention strategy and daily aspirin with vitamin D supplementation in three separate placebo-controlled comparisons in more than 5700 “intermediate risk” participants 55 years and older, mostly in developing countries.
The daily polypill in this trial is a combination of hydrochlorothiazide 25 mg, atenolol 100 mg, ramipril 10 mg, and simvastatin 40 mg; aspirin was given at 75 mg daily and vitamin D at 60,000 IU monthly.
The participants are followed for a primary end point composed of major CV disease, HF, resuscitated cardiac arrest, or ischemia-driven revascularization for the polypill comparison; CV events or cancer for the aspirin comparison; and fracture risk for the vitamin D component of the trial.
In the Swedish Cardiopulmonary Bioimage Study (SCAPIS), presented third in the session, a random sample of adults from throughout Sweden, projected at about 30,000, underwent a 2-day evaluation for metabolic risk factors plus ultrasound and coronary and lung CT scans. The group has been followed for risks for myocardial infarction (MI), sudden death, and other cardiac diseases; and chronic obstructive pulmonary disease (COPD) and other lung disorders.
Late-Breaking Science 3. Saturday, November 14, 12:00 PM - 1:00 PM CST
The field may learn more mechanistically about MI associated with nonobstructed coronary arteries (MINOCA) than ever before from the Heart Attack Research Program-Imaging Study (HARP). The observational study is enrolling a projected 450 patients with suspected MI and ischemic symptoms who were referred for cardiac catheterization.
Their evaluation includes coronary optical coherence tomographic (OCT) scanning and cardiac magnetic resonance (CMR) imaging for evidence of coronary plaque disruption as the primary end point. The patients are to be followed for 10 years for a composite of death, unstable angina, stroke, recurrent MI, diagnostic or interventional catheterization, and cardiac hospitalization.
The major direct oral anticoagulant (DOAC) comparisons with warfarin in atrial fibrillation (AF) didn’t include many patients with prosthetic valve implants. In contrast, the RIVER trial enrolled 1005 adults with either persistent or paroxysmal AF and bioprosthetic mitral valves and assigned them to rivaroxaban 20 mg or the vitamin K antagonist.
The presentation will include the noninferiority primary outcome of major clinical events, which is stroke, transient ischemic attack (TIA), major bleeding, death from any cause, valve thrombosis, other systemic embolism, or HF hospitalization over 12 months.
This session also includes ALPHEUS, a trial pitting ticagrelor (Brilinta/Brilique, AstraZeneca) against mainstay clopidogrel in a setting that is mostly uncharted for such comparisons, elective percutaneous coronary intervention (PCI).
About 1900 patients with stable coronary disease were randomly assigned to a month of treatment with either agent on top of continuous aspirin. The primary end point is PCI-related MI or myocardial injury within 48 hours of the procedure.
Late-Breaking Science 4. Sunday, November 15, 9:00 AM - 10:00 AM CST
The Self-Assessment Method for Statin Side-effects Or Nocebo (SAMSON) trial may be one of the AHA 2020 frontrunners for early buzz and anticipation. So it’s with some irony that it’s also among the smallest of the LBS studies, at 60 patients, which was nonetheless considered sufficient due to its unusual design.
SAMSON is the latest and perhaps most rigorous attempt to clarify whether symptoms, especially muscle pain or discomfort, attributed to statins by many patients are pharmacologic in origin or, rather, a nocebo effect from negative expectations about statin side effects.
The study patients, all of whom had previously halted statins because of side effects, were assigned to follow three separate regimens, each for month, in a randomized order; they did that four times, for a total of 12 months. The regimens consisted of atorvastatin 20 mg daily, a placebo, or neither.
Patients kept daily logs of any perceived side effects. Parity between side effects experienced on the statin and the placebo would point to a nocebo effect, whereas a significant excess on atorvastatin would suggest they are direct drug effects.
The session also features two randomized trials each on a unique omega-3 fatty acid preparation for either secondary prevention or high-risk primary prevention, in both cases compared with a corn-oil placebo.
The Omega-3 Fatty Acids in Elderly Patients with Myocardial Infarction (OMEMI) trial randomly assigned more than 1000 elderly post-MI patients to take Pikasol (Orkla Care) at 1.8 g EPA and DHA per day or the placebo. It looked for all-cause mortality, nonfatal MI, stroke, revascularization, or hospitalization for new or worsened HF over 24 months.
The STRENGTH trial, with a planned enrollment of about 13,000 high-vascular-risk patients, looked primarily at the effect of daily treatment with Epanova (AstraZeneca), which also contains DHA and EPA, on the composite of CV death, nonfatal MI or stroke, coronary revascularization, and hospitalization for unstable angina. The trial was halted early for low likelihood of benefit, AstraZeneca announced in January of this year.
Late-Breaking Science 5. Sunday, November 15, 7:15 PM - 8:30 PM CST
Slated for the session is the primary analysis of the PIONEER 3 trial, conducted in the United States, Europe, and Japan. It compared the BuMA Supreme biodegradable drug-coated stent (SinoMed) with the durable Xience (Abbott Vascular) and Promus (Boston Scientific) drug-eluting stents. The trial followed more than 1600 patients treated for chronic stable angina or acute coronary syndrome (ACS) for the 1-year composite of cardiac death, target-vessel-related MI, and clinically driven target-lesion revascularization.
Late-Breaking Science 6. Monday, November 16, 9:00 AM - 10:00 AM CST
The EARLY-AF trial enrolled 303 patients with symptomatic paroxysmal or persistent AF suitable for catheter ablation, assigning them to pulmonary vein isolation (PVI) by cryoablation using the Arctic Front (Medtronic) system or antiarrhythmic drug therapy for rhythm control. The primary end point is time to recurrence of AF, atrial flutter, or atrial tachycardia, whether symptomatic or asymptomatic, as determined by implantable loop recorder. Patients will also be followed for symptoms and arrhythmia burden.
Also in the session, the SEARCH-AF study randomized almost 400 patients undergoing cardiac surgery who were engaged subacutely with one of two commercial portable cardiac rhythm monitoring devices (CardioSTAT, Icentia; or SEEQ, Medtronic) or, alternatively, to receive usual postoperative care
The patients, considered to be at high risk for stroke with no history of AF, were followed for the primary end point of cumulative burden of AF or atrial flutter exceeding 6 minutes or documentation of either arrhythmia by 12-lead ECG within 30 days.
Two other studies in the session look at different approaches to AF screening, one using a handheld ECG monitor in the primary care setting and the other wearable monitors in the form of a patch or wristband. The VITAL-AF presentation is titled “Screening for Atrial Fibrillation in Older Adults at Primary Care Visits Using Single Lead Electrocardiograms.” The other presentation, on the study mSToPS, is called “Three-Year Clinical Outcomes in a Nationwide, Randomized, Pragmatic Clinical Trial of Atrial Fibrillation Screening — Mhealth Screening to Prevent Strokes.”
Late-Breaking Science 7. Monday, November 16, 7:00 PM - 8:30 PM CST
In the randomized FIDELIO-DKD trial with more than 5700 patients with type 2 diabetes and associated kidney disease, those assigned to the novel mineralocorticoid receptor antagonist (MRA) finerenone (Bayer) showed an 18% drop in risk for adverse renal events, including death from renal causes (P = .001), over a median of 2.6 years. That primary outcome was previously presented in detail at a nephrology meeting and published in the New England Journal of Medicine in October.
Patients on the MRA showed a similar reduction in a composite CV-event end point, it was also reported at that time. A follow-up presentation at the AHA sessions promises to dive deeper into the trial’s CV outcomes.
In the RAPID-CTCA study, slated next for the session, 1749 patients with suspected or confirmed intermediate-risk ACS were randomly assigned to undergo computed tomographic coronary angiography (CTCA) for guiding treatment decisions or a standard-of-care strategy. It followed patients for the primary end point of death or nonfatal MI over 1 year.
Rilonacept (Arcalyst, Kiniksa/Regeneron) is an interleukin-1α and -1β inhibitor used in several autoinflammatory diseases that went unsuccessfully before regulators for the treatment of gout. The RHAPSODY trial has now explored its use against recurrent pericarditis in a randomized trial that entered 86 patients 12 years and older who had previously experienced at least three episodes.
In top-line results reported to investors in June, patients assigned to receive the drug instead of placebo in weekly injections showed a 96% drop in risk for pericarditis recurrence and “no or minimal pain” on more than 90% of days in the trial. A full presentation is expected during this LBS session.
Also on the schedule is the THALES study, which led the US Food and Drug Administration (FDA) to expand indications for ticagrelor to include stroke prevention in patients with a history of acute ischemic stroke or high-risk TIA based on the trial’s primary results published in July.
In THALES, more than 11,000 patients with mild to moderate acute noncardiogenic ischemic stroke or TIA were randomly assigned within 24 hours to start on daily aspirin with or without ticagrelor given as a 180 mg loading dose followed by 90 mg twice daily for 30 days.
At the end of a month, it was reported, those on dual antiplatelet therapy showed a 17% risk reduction (P = .02) for the primary end point of stroke or death, at the cost of a slight but significant increase in “severe” bleeding (0.5% vs 0.1%; P = .001).
The session is to conclude with two related studies that fell victim in part to the COVID-19 pandemic, both of which explored sotagliflozin (Zynquista, Sanofi/Lexicon), an inhibitor of both sodium-glucose cotransporters 1 and 2 (SGLT1 and SGLT2, respectively) in patients with type 2 diabetes.
SOLOIST-WHF had entered 1222 such patients hospitalized with urgent or worsening HF at 466 centers and randomly assigned them to receive sotagliflozin or placebo; they were followed for the composite of CV death or HF events. SCORED reached an enrollment of 10,584 patients with diabetes and chronic kidney disease at 754 hospitals, following them for the same primary end point.
Lexicon announced in March that the trials would be “closed out early” because of the unavailability of funding “together with uncertainties relating to the COVID-19 pandemic on the trials.” The LBS presentation is expected to include analyses of available data; SOLOIST-WHF launched in summer 2018 and SCORED began in November 2017.
Late-Breaking Science 8. Tuesday, November 17, 9:00 AM - 10:00 AM CST
Most of this LBS session is devoted to the AHA COVID-19 Cardiovascular Disease registry, which is looking at the hospital journey, clinical course, and outcomes of patients hospitalized with SARS-CoV-2 infections at centers participating in the organization’s Get With The Guidelines (GWTG) quality-improvement program. As of September, the registry included data from more than 15,000 patients.
Scheduled presentations include a summary of the registry’s design and initial results; an analysis of racial and ethnic variation in therapy and clinical outcomes; an exploration of how body mass index influenced outcomes, including death, use of mechanical ventilation, and cardiovascular end points, in patients with COVID-19; and a deep dive into the relation between CV disease and clinical outcomes in the cohort.
The last of this LBS block’s five talks will cover the randomized Influenza Vaccine to Effectively Stop Cardio Thoracic Events and Decompensated Heart Failure (INVESTED) trial, which compared vaccination with high-dose trivalent influenza vaccine or a standard-dose quadrivalent vaccine in 5388 adults with a history of hospitalization for either MI or HF. Patients were required to have at least one other CV risk factor, such as older age, reduced left ventricular ejection fraction, or diabetes.
INVESTED tracked the patients at 190 centers across an initial pilot flu season and three subsequent flu seasons for the primary end point of death from any cause or cardiopulmonary hospitalization.
The trial is one of at least three that have been looking at the effect of flu vaccination on cardiovascular outcomes; results from the other two — IAMI, with more than 2500 participants, and RCT-IVVE, with an enrollment of 4871 — are planned for presentation in 2021, theheart.org | Medscape Cardiology recently reported.
Late-Breaking Science 9. Tuesday, November 17, 12:00 PM - 1:00 PM CST
The conference’s concluding LBS session features three studies that relied on technologic strategies for modifying patient compliance and other care behaviors and one that used human-centered design principles to develop a group-care model aimed improving the management of diabetes, hypertension, and other noncommunicable diseases in economically disadvantaged regions of Kenya.
The EPIC-HF trial tested a strategy for improving HFrEF medication-plan engagement by use of a video and documents delivered to patients several times by email or text prior to their follow-up clinic appointments. The strategy was compared with usual care for its effect on HF-medication optimization over 1 month and 1 year in a total of 306 patients.
Following EPIC-HF on the schedule is the MYROAD trial, looking at the efficacy of discharge instructions provided to patients with acute HF as an audio recording that they and their physicians could replay on demand, the idea being to increase adherence to the instructions. The trial’s 1073 patients were assigned to the novel strategy or usual care and followed for HF rehospitalization within 30 days.
MYROAD is to be followed by a presentation entitled “Digital Care Transformation: One-Year Report of >5,000 Patients Enrolled in a Remote Algorithm-Based CV Risk Management Program to Achieve Optimal Lipid and Hypertension Control.”
Rounding out the LBS session: the Bridging Income Generation With Group Integrated Care (BIGPIC) program, a pilot study that developed and executed “a healthcare delivery model targeting health behaviors, medication adherence, and financial barriers to accessing healthcare” in four rural counties in Kenya.
The model features locally developed plans, tailored for regional needs, that are said to “combine the benefits of microfinance with the peer support available through group medical care to enhance management of hypertension and diabetes.” The microfinance component is aimed at improving household economies to alleviate the financial burden of care and clinic attendance, and for the health effects of improved quality of life.
The study randomized 2890 adults with diabetes or prediabetes to one of four groups: usual care plus microfinance group support, group medical visits only or combined with microfinance group support, or usual care only. They were followed for changes in systolic blood pressure and CV-risk score over 12 months.
Lloyd-Jones and Fauci declared no conflicts.
This article first appeared on Medscape.com.
Poverty raises depression risk in patients with cystic fibrosis
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.

“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
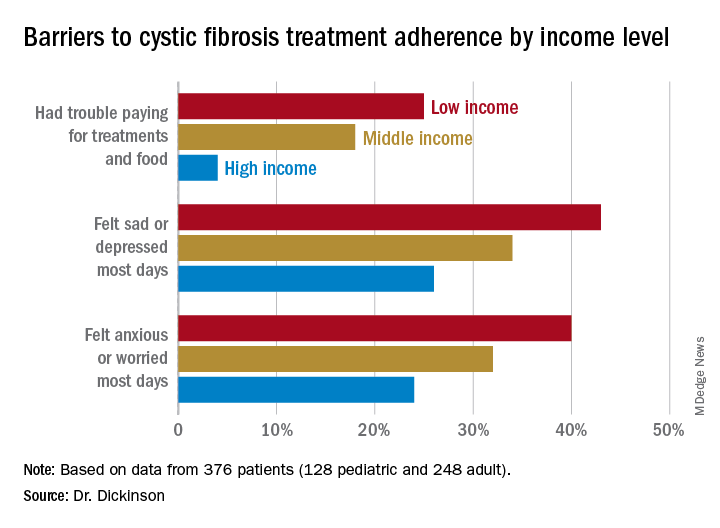
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
Poor people with chronic illness have greater difficulty managing their disease than do their better-off counterparts, and a new study confirms this reality for patients with cystic fibrosis.
and anxiety symptoms, according to a new cross-sectional study. The data were drawn from the Cystic Fibrosis Foundation’s Success with Therapies Research Consortium.
“Assessing the special challenges that individuals with lower SES face, including financial barriers, is essential to understand how we can address the unique combinations of adherence barriers. In other chronic disorders, financial barriers or lower socioeconomic status is associated with nonadherence, but this relationship has not been well established in cystic fibrosis,” said Kimberly Dickinson, MD, MPH, of Johns Hopkins University, Baltimore, during her presentation of the results at the virtual North American Cystic Fibrosis Conference.
“I’ve always thought that my patients in the poorer population were doing worse, and I think this demonstrates that that’s true,” said Robert Giusti, MD, in an interview. Dr. Giusti is a clinical professor of pediatrics at the New York University and director of the Pediatric Cystic Fibrosis Center in New York. He was not involved in the study.
“These are very pertinent issues, especially if you think about the pandemic, and some of the issues related to mental health. It just highlights the importance of socioeconomic status and screening for some of the known risk factors so that we can develop interventions or programs to provide equitable care to all of our cystic fibrosis patients,” said Ryan Perkins, MD, who moderated the session where the study was presented. He is a pediatric and adult pulmonary fellow at Boston Children’s Hospital and Brigham and Women’s Hospital, also in Boston.
The researchers looked retrospectively at 1 year’s worth of pharmacy refill receipts and number of times prescriptions were refilled versus the number of times prescribed, then calculated medicinal possession ratios. This was cross-referenced with annual household income and insurance status of patients with CF at 12 pediatric and 9 adult CF care centers, for a total of 376 patients (128 pediatric and 248 adult).
In this population, 32% of participants had public or no insurance, 68% had private or military insurance. The public/no insurance group was more likely than the private/military insurance group to report having trouble paying for treatments, food, or critical expenses related to CF care (23.3% vs. 12.1%, respectively); feeling symptoms on most days of depression (42.5% vs. 31.3%) or anxiety (40.0% vs. 28.5%); and experiencing conflict or stress with loved ones over treatments (30.0% vs. 20.3%) (P < .05 for all).
In all, 35% had a household income less than $40,000 per year, 33% between $44,000 and $100,000, and 32% higher than $100,000. The low-income group had a lower composite medication possession ratio (0.41) than the middle- (0.44) or high-income (0.52) groups, were more likely to have trouble paying for treatments, food, or treatment-related expenses (25%, 18%, 4%, respectively); were more likely most days to report symptoms of depression (43%, 34%, 26%) or anxiety (40%, 32%, 24%), and to have concerns about whether treatments were effective (42%, 27%, 29%). They were more likely to not be able to maintain a daily schedule or routine for treatments (28%, 22%, 14%).
The study showed that adherence barriers and suboptimal adherence are issues that cross all socioeconomic categories, though they were more problematic in the lowest bracket. Greater anxiety and depression among lower income individuals and those with private or no insurance was a key finding, according to Dr. Dickinson. “It highlights the importance of screening for mental health comorbidities that may impact non-adherence,” she said.
The study received funding from the Cystic Fibrosis Foundation. Dr. Dickinson, Dr. Giusti, and Dr. Perkins have no relevant financial disclosures.
FROM NACFC 2020
.
Home care for bortezomib safe and reduces hospital visits in myeloma patients
Home administration of bortezomib (Velcade), as a once or twice-weekly subcutaneous self-injection is safe in patients with myeloma, significantly reducing hospital visits, and likely improving quality of life, a study shows.
The majority (43 of 52 patients) successfully self-administered bortezomib and completed the course. Also, hospital visits for those on the so-called Homecare programme reduced by 50%, with most visits comprising a fortnightly drug pickup from the drive-through pharmacy.
The work was presented as a poster by lead author and researcher, Kanchana De Abrew, hematology consultant at University Hospital Southampton NHS Foundation Trust, at this year’s virtual British Society of Haematology (BSH) meeting. De Abrew conducted the study while at Queen Alexandra Hospital, Portsmouth.
“We wanted to minimize patient visits to hospital because with travel time and waiting time, patients can easily find a visit takes up a whole morning, so this relates to their quality of life as well as having financial implications for patients,” Dr. De Abrew said in an interview. It also reduced the impact on day units and improved capacity for other services.
Dr. De Abrew noted that the study was conducted in the pre-COVID-19 era, but that the current enhanced threat of infection only served to reinforce the benefits of self-administration at home and avoiding unnecessary hospital visits.
“This project could easily be set up in other hospitals and some other centers have already contacted us about this. It might suit rural areas,” she added.
‘Safe and effective’
Dr. Matthew Jenner, consultant hematologist for University Hospital Southampton NHS Foundation Trust, who was not involved in the study, remarked that the study demonstrated another way to deliver bortezomib outside of hospital in addition to home care services that require trained nurses to administer treatment. “With a modest amount of training of the patient and family, it is both a safe and effective way of delivering treatment. This reduces hospital visits for the patient and frees up much needed capacity for heavily stretched chemotherapy units, creating space for other newer treatments that require hospital attendance.
“It is of benefit all round to both the patients undertaking self-administration and those who benefit from improved capacity,” added Dr. Jenner.
Avoiding hospital visits
Myeloma patients are already immunosuppressed prior to treatment and then this worsens once on treatment. Once they are sitting in a clinic environment they are surrounded by similarly immunosuppressed patients, so their risk is heightened further.
Figures suggest myeloma cases are on the increase. Annually, the United Kingdom sees around 5,800 new cases of myeloma and incidence increased by a significant 32% between the periods of 1993-1995 and 2015-2017. These figures were reflected in the patient numbers at the Queen Alexandra Hospital where the study was carried out. Many patients receive bortezomib, which forms the backbone of four National Institute for Health and Care Excellence (NICE) approved regimens.
“Patients are living longer so in the early 2000s patients had a life expectancy of 2-3 years, whereas now patients live for around 5 years. Also, the scope and lines of treatments have increased a lot. Over 50% of patients are likely to have bortezomib at some point in their management,” explained Dr. De Abrew.
Bortezomib is given once or twice weekly as a subcutaneous injection, and this usually continues for approximately 6-8 months with four to six cycles. Administering the drug in hospital requires around a half-hour slot placing considerable burden on the hematology day unit resources, and this can adversely affect the patient experience with waiting times and the need for frequent hospital visits.
Patient or relatives taught to self-administer at home
In 2017, clinical nurse specialists taught suitable patients to self-administer bortezomib in the Homecare protocol. Patients collected a 2-week supply of the drug. The protocol aimed to improve patient quality of life by reducing hospital visits, and increasing capacity in the hematology day unit. Since the start of the programme in 2017, the majority (71) of myeloma patients at Portsmouth have been treated through the Homecare program.
Dr. De Abrew conducted a retrospective review of patients who received bortezomib between January and October 2019 aimed at determining the effectiveness of the Homecare programme. To this end, she measured the proportion able to commence the Homecare protocol; the proportion successful in completing treatment on the Homecare protocol; the amount of additional clinical nurse specialist time required to support the Homecare protocol; and the number of associated adverse incidents.
A total of 52 bortezomib-treated patients were included in the study. Patients were excluded if they were on a different combination of drugs that required hospital visits, or inpatient care for other reasons. Three patients ceased the drug – two because of toxicity, and one because of rapid progression. The average age of patients was 74 years, and 55.8% were using bortezomib as first-line, 36.5% second-line, and the remainder third-line or more.
The vast majority started the Homecare protocol (45/52), and 25 self-administered and 17 received a relative’s help. A total of 43 completed the self-administration protocol with two reverting to hospital assistance. Bortezomib was given for four to six cycles lasting around 6-8 months.
Clinical nurse specialists trained 38 patients for home care, with an average training time of 43 minutes. Two of these patients were considered unsuitable for self-administration. The remainder were trained by ward nurses or did not require training having received bortezomib previously.
A total of 20 patients required additional clinical nurse specialist time requiring an average of 55 minutes. Of those requiring additional support: Seven needed retraining; two needed the first dose delivered by a nurse specialist; two requested help from the hematology unit; and nine wanted general extra support – for example, help with injection site queries (usually administered to the abdominal area), reassurance during administration, syringe queries, administrative queries, and queries around spillages.
“Importantly, patients always have the phone number of the nurse specialist at hand. But most people managed okay, and even if they needed additional support they still got there,” remarked Dr. De Abrew.
In terms of adverse events, there were six in total. These included three reported spillages (with no harm caused), and three experienced injection site incidents (rash, pain). “We found a low number of reported adverse events,” she said.
Dr. De Abrew added that generally, many more medications were being converted to subcutaneous formulations in myeloma and other hematology conditions. “Perhaps these results could inform self-administration of other drugs. In hematology, we get so many new drugs come through every year, but we don’t get the increased resources to manage this in the day units. Broadening self-administration could really help with capacity as well as improve quality of life for the patients.
“These results show that it can be done!” she said.
Dr. De Abrew declared no relevant conflicts of interest. Dr. Jenner declared receiving honoraria from Janssen, which manufactures branded Velcade (bortezomib).
A version of this story originally appeared on Medscape.com.
Home administration of bortezomib (Velcade), as a once or twice-weekly subcutaneous self-injection is safe in patients with myeloma, significantly reducing hospital visits, and likely improving quality of life, a study shows.
The majority (43 of 52 patients) successfully self-administered bortezomib and completed the course. Also, hospital visits for those on the so-called Homecare programme reduced by 50%, with most visits comprising a fortnightly drug pickup from the drive-through pharmacy.
The work was presented as a poster by lead author and researcher, Kanchana De Abrew, hematology consultant at University Hospital Southampton NHS Foundation Trust, at this year’s virtual British Society of Haematology (BSH) meeting. De Abrew conducted the study while at Queen Alexandra Hospital, Portsmouth.
“We wanted to minimize patient visits to hospital because with travel time and waiting time, patients can easily find a visit takes up a whole morning, so this relates to their quality of life as well as having financial implications for patients,” Dr. De Abrew said in an interview. It also reduced the impact on day units and improved capacity for other services.
Dr. De Abrew noted that the study was conducted in the pre-COVID-19 era, but that the current enhanced threat of infection only served to reinforce the benefits of self-administration at home and avoiding unnecessary hospital visits.
“This project could easily be set up in other hospitals and some other centers have already contacted us about this. It might suit rural areas,” she added.
‘Safe and effective’
Dr. Matthew Jenner, consultant hematologist for University Hospital Southampton NHS Foundation Trust, who was not involved in the study, remarked that the study demonstrated another way to deliver bortezomib outside of hospital in addition to home care services that require trained nurses to administer treatment. “With a modest amount of training of the patient and family, it is both a safe and effective way of delivering treatment. This reduces hospital visits for the patient and frees up much needed capacity for heavily stretched chemotherapy units, creating space for other newer treatments that require hospital attendance.
“It is of benefit all round to both the patients undertaking self-administration and those who benefit from improved capacity,” added Dr. Jenner.
Avoiding hospital visits
Myeloma patients are already immunosuppressed prior to treatment and then this worsens once on treatment. Once they are sitting in a clinic environment they are surrounded by similarly immunosuppressed patients, so their risk is heightened further.
Figures suggest myeloma cases are on the increase. Annually, the United Kingdom sees around 5,800 new cases of myeloma and incidence increased by a significant 32% between the periods of 1993-1995 and 2015-2017. These figures were reflected in the patient numbers at the Queen Alexandra Hospital where the study was carried out. Many patients receive bortezomib, which forms the backbone of four National Institute for Health and Care Excellence (NICE) approved regimens.
“Patients are living longer so in the early 2000s patients had a life expectancy of 2-3 years, whereas now patients live for around 5 years. Also, the scope and lines of treatments have increased a lot. Over 50% of patients are likely to have bortezomib at some point in their management,” explained Dr. De Abrew.
Bortezomib is given once or twice weekly as a subcutaneous injection, and this usually continues for approximately 6-8 months with four to six cycles. Administering the drug in hospital requires around a half-hour slot placing considerable burden on the hematology day unit resources, and this can adversely affect the patient experience with waiting times and the need for frequent hospital visits.
Patient or relatives taught to self-administer at home
In 2017, clinical nurse specialists taught suitable patients to self-administer bortezomib in the Homecare protocol. Patients collected a 2-week supply of the drug. The protocol aimed to improve patient quality of life by reducing hospital visits, and increasing capacity in the hematology day unit. Since the start of the programme in 2017, the majority (71) of myeloma patients at Portsmouth have been treated through the Homecare program.
Dr. De Abrew conducted a retrospective review of patients who received bortezomib between January and October 2019 aimed at determining the effectiveness of the Homecare programme. To this end, she measured the proportion able to commence the Homecare protocol; the proportion successful in completing treatment on the Homecare protocol; the amount of additional clinical nurse specialist time required to support the Homecare protocol; and the number of associated adverse incidents.
A total of 52 bortezomib-treated patients were included in the study. Patients were excluded if they were on a different combination of drugs that required hospital visits, or inpatient care for other reasons. Three patients ceased the drug – two because of toxicity, and one because of rapid progression. The average age of patients was 74 years, and 55.8% were using bortezomib as first-line, 36.5% second-line, and the remainder third-line or more.
The vast majority started the Homecare protocol (45/52), and 25 self-administered and 17 received a relative’s help. A total of 43 completed the self-administration protocol with two reverting to hospital assistance. Bortezomib was given for four to six cycles lasting around 6-8 months.
Clinical nurse specialists trained 38 patients for home care, with an average training time of 43 minutes. Two of these patients were considered unsuitable for self-administration. The remainder were trained by ward nurses or did not require training having received bortezomib previously.
A total of 20 patients required additional clinical nurse specialist time requiring an average of 55 minutes. Of those requiring additional support: Seven needed retraining; two needed the first dose delivered by a nurse specialist; two requested help from the hematology unit; and nine wanted general extra support – for example, help with injection site queries (usually administered to the abdominal area), reassurance during administration, syringe queries, administrative queries, and queries around spillages.
“Importantly, patients always have the phone number of the nurse specialist at hand. But most people managed okay, and even if they needed additional support they still got there,” remarked Dr. De Abrew.
In terms of adverse events, there were six in total. These included three reported spillages (with no harm caused), and three experienced injection site incidents (rash, pain). “We found a low number of reported adverse events,” she said.
Dr. De Abrew added that generally, many more medications were being converted to subcutaneous formulations in myeloma and other hematology conditions. “Perhaps these results could inform self-administration of other drugs. In hematology, we get so many new drugs come through every year, but we don’t get the increased resources to manage this in the day units. Broadening self-administration could really help with capacity as well as improve quality of life for the patients.
“These results show that it can be done!” she said.
Dr. De Abrew declared no relevant conflicts of interest. Dr. Jenner declared receiving honoraria from Janssen, which manufactures branded Velcade (bortezomib).
A version of this story originally appeared on Medscape.com.
Home administration of bortezomib (Velcade), as a once or twice-weekly subcutaneous self-injection is safe in patients with myeloma, significantly reducing hospital visits, and likely improving quality of life, a study shows.
The majority (43 of 52 patients) successfully self-administered bortezomib and completed the course. Also, hospital visits for those on the so-called Homecare programme reduced by 50%, with most visits comprising a fortnightly drug pickup from the drive-through pharmacy.
The work was presented as a poster by lead author and researcher, Kanchana De Abrew, hematology consultant at University Hospital Southampton NHS Foundation Trust, at this year’s virtual British Society of Haematology (BSH) meeting. De Abrew conducted the study while at Queen Alexandra Hospital, Portsmouth.
“We wanted to minimize patient visits to hospital because with travel time and waiting time, patients can easily find a visit takes up a whole morning, so this relates to their quality of life as well as having financial implications for patients,” Dr. De Abrew said in an interview. It also reduced the impact on day units and improved capacity for other services.
Dr. De Abrew noted that the study was conducted in the pre-COVID-19 era, but that the current enhanced threat of infection only served to reinforce the benefits of self-administration at home and avoiding unnecessary hospital visits.
“This project could easily be set up in other hospitals and some other centers have already contacted us about this. It might suit rural areas,” she added.
‘Safe and effective’
Dr. Matthew Jenner, consultant hematologist for University Hospital Southampton NHS Foundation Trust, who was not involved in the study, remarked that the study demonstrated another way to deliver bortezomib outside of hospital in addition to home care services that require trained nurses to administer treatment. “With a modest amount of training of the patient and family, it is both a safe and effective way of delivering treatment. This reduces hospital visits for the patient and frees up much needed capacity for heavily stretched chemotherapy units, creating space for other newer treatments that require hospital attendance.
“It is of benefit all round to both the patients undertaking self-administration and those who benefit from improved capacity,” added Dr. Jenner.
Avoiding hospital visits
Myeloma patients are already immunosuppressed prior to treatment and then this worsens once on treatment. Once they are sitting in a clinic environment they are surrounded by similarly immunosuppressed patients, so their risk is heightened further.
Figures suggest myeloma cases are on the increase. Annually, the United Kingdom sees around 5,800 new cases of myeloma and incidence increased by a significant 32% between the periods of 1993-1995 and 2015-2017. These figures were reflected in the patient numbers at the Queen Alexandra Hospital where the study was carried out. Many patients receive bortezomib, which forms the backbone of four National Institute for Health and Care Excellence (NICE) approved regimens.
“Patients are living longer so in the early 2000s patients had a life expectancy of 2-3 years, whereas now patients live for around 5 years. Also, the scope and lines of treatments have increased a lot. Over 50% of patients are likely to have bortezomib at some point in their management,” explained Dr. De Abrew.
Bortezomib is given once or twice weekly as a subcutaneous injection, and this usually continues for approximately 6-8 months with four to six cycles. Administering the drug in hospital requires around a half-hour slot placing considerable burden on the hematology day unit resources, and this can adversely affect the patient experience with waiting times and the need for frequent hospital visits.
Patient or relatives taught to self-administer at home
In 2017, clinical nurse specialists taught suitable patients to self-administer bortezomib in the Homecare protocol. Patients collected a 2-week supply of the drug. The protocol aimed to improve patient quality of life by reducing hospital visits, and increasing capacity in the hematology day unit. Since the start of the programme in 2017, the majority (71) of myeloma patients at Portsmouth have been treated through the Homecare program.
Dr. De Abrew conducted a retrospective review of patients who received bortezomib between January and October 2019 aimed at determining the effectiveness of the Homecare programme. To this end, she measured the proportion able to commence the Homecare protocol; the proportion successful in completing treatment on the Homecare protocol; the amount of additional clinical nurse specialist time required to support the Homecare protocol; and the number of associated adverse incidents.
A total of 52 bortezomib-treated patients were included in the study. Patients were excluded if they were on a different combination of drugs that required hospital visits, or inpatient care for other reasons. Three patients ceased the drug – two because of toxicity, and one because of rapid progression. The average age of patients was 74 years, and 55.8% were using bortezomib as first-line, 36.5% second-line, and the remainder third-line or more.
The vast majority started the Homecare protocol (45/52), and 25 self-administered and 17 received a relative’s help. A total of 43 completed the self-administration protocol with two reverting to hospital assistance. Bortezomib was given for four to six cycles lasting around 6-8 months.
Clinical nurse specialists trained 38 patients for home care, with an average training time of 43 minutes. Two of these patients were considered unsuitable for self-administration. The remainder were trained by ward nurses or did not require training having received bortezomib previously.
A total of 20 patients required additional clinical nurse specialist time requiring an average of 55 minutes. Of those requiring additional support: Seven needed retraining; two needed the first dose delivered by a nurse specialist; two requested help from the hematology unit; and nine wanted general extra support – for example, help with injection site queries (usually administered to the abdominal area), reassurance during administration, syringe queries, administrative queries, and queries around spillages.
“Importantly, patients always have the phone number of the nurse specialist at hand. But most people managed okay, and even if they needed additional support they still got there,” remarked Dr. De Abrew.
In terms of adverse events, there were six in total. These included three reported spillages (with no harm caused), and three experienced injection site incidents (rash, pain). “We found a low number of reported adverse events,” she said.
Dr. De Abrew added that generally, many more medications were being converted to subcutaneous formulations in myeloma and other hematology conditions. “Perhaps these results could inform self-administration of other drugs. In hematology, we get so many new drugs come through every year, but we don’t get the increased resources to manage this in the day units. Broadening self-administration could really help with capacity as well as improve quality of life for the patients.
“These results show that it can be done!” she said.
Dr. De Abrew declared no relevant conflicts of interest. Dr. Jenner declared receiving honoraria from Janssen, which manufactures branded Velcade (bortezomib).
A version of this story originally appeared on Medscape.com.
What happened to melanoma care during COVID-19 sequestration
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.

This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.

Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”

“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
Initial evidence suggests that the , Rebecca I. Hartman, MD, MPH, said at a virtual forum on cutaneous malignancies jointly presented by Postgraduate Institute for Medicine and Global Academy for Medication Education.
This is not what National Comprehensive Cancer Network officials expected when they issued short-term recommendations on how to manage cutaneous melanoma during the first wave of the COVID-19 pandemic. Those recommendations for restriction of care, which Dr. Hartman characterized as “pretty significant changes from how we typically practice melanoma care in the U.S.,” came at a time when there was justifiable concern that the first COVID-19 surge would strain the U.S. health care system beyond the breaking point.
The rationale given for the NCCN recommendations was that most time-to-treat studies have shown no adverse patient outcomes for 90-day delays in treatment, even for thicker melanomas. But those studies, all retrospective, have been called into question. And the first real-world data on the impact of care restrictions during the lockdown, reported by Italian dermatologists, highlights adverse effects with potentially far-reaching consequences, noted Dr. Hartman, director of melanoma epidemiology at Brigham and Women’s Hospital and a dermatologist, Harvard University, Boston.
Analysis of the impact of lockdown-induced delays in melanoma care is not merely an academic exercise, she added. While everyone hopes that the spring 2020 COVID-19 shelter-in-place was a once-in-a-lifetime event, there’s no guarantee that will be the case. Moreover, the lockdown provides a natural experiment addressing the possible consequences of melanoma care delays on patient outcomes, a topic that for ethical reasons could never be addressed in a randomized trial.
The short-term NCCN recommendations included the use of excisional biopsies for melanoma diagnosis whenever possible; and delay of up to 3 months for wide local excision of in situ melanoma, any invasive melanoma with negative margins, and even T1 melanomas with positive margins provided the bulk of the lesion had been excised. The guidance also suggested delaying sentinel lymph node biopsy (SLNB), along with increased use of neoadjuvant therapy in patients with clinically palpable regional lymph nodes in order to delay surgery for up to 8 weeks. Single-agent systemic therapy at the least-frequent dosing was advised in order to minimize toxicity and reduce the need for additional health care resources: for example, nivolumab (Opdivo) at 480 mg every 4 weeks instead of every 2 weeks, and pembrolizumab (Keytruda) at 400 mg every 6 weeks, rather than every 3 weeks.
So, that’s what the NCCN recommended. Here’s what actually happened during shelter-in-place as captured in Dr. Hartman’s survey of 18 U.S. members of the Melanoma Prevention Working Group, all practicing dermatology in centers particularly hard-hit in the first wave of the pandemic: In-person new melanoma patient visits plunged from an average of 4.83 per week per provider to 0.83 per week. Telemedicine visits with new melanoma patients went from zero prepandemic to 0.67 visits per week per provider, which doesn’t come close to making up for the drop in in-person visits. Interestingly, two respondents reported turning to gene-expression profile testing for patient prognostication because of delays in SLNB.
Wide local excision was delayed by an average of 6 weeks in roughly one-third of melanoma patients with early tumor stage disease, regardless of margin status. For patients with stage T1b disease, wide local excision was typically performed on time during shelter-in-place; however, SLNB was delayed by an average of 5 weeks in 22% of patients with positive margins and 28% of those with negative margins. In contrast, 80% of patients with more advanced T2-T4 melanoma underwent on-schedule definitive management with wide local excision and SLNB, Dr. Hartman reported.
Critics have taken issue with the NCCN’s conclusion that most time-to-treatment studies show no harm arising from 90-day treatment delays. A review of the relevant published literature by Dr. Hartman’s Harvard colleagues, published in July, found that the evidence is mixed. “There is insufficient evidence to definitively conclude that delayed wide resection after gross removal of the primary melanoma is without harm,” they concluded in the review.
Spanish dermatologists performed a modeling study in order to estimate the potential impact of COVID-19 lockdowns on 5- and 10-year survival of melanoma patients. Using the growth rate of a random sample of 1,000 melanomas to model estimates of tumor thickness after various delays, coupled with American Joint Committee on Cancer survival data for different T stages, they estimated that 5-year survival would be reduced from 94.2% to 92.3% with a 90-day delay in diagnosis, and that 10-year survival would drop from 90.0% to 87.6%.
But that’s merely modeling. Francesco Ricci, MD, PhD, and colleagues from the melanoma unit at the Istituto Dermopatico dell’Immacolata, Rome, have provided a first look at the real-world impact of the lockdown. In the prelockdown period of January through March 9th, 2020, the referral center averaged 2.3 new melanoma diagnoses per day. During the Rome lockdown, from March 10th through May 3rd, this figure dropped to a mean of 0.6 melanoma diagnoses per day. Postlockdown, from May 4th to June 6th, the average climbed to 1.3 per day. The rate of newly diagnosed nodular melanoma was 5.5-fold greater postlockdown, compared with prelockdown; the rate of ulcerated melanoma was 4.9-fold greater.
“We can hypothesize that this may have been due to delays in diagnosis and care,” Dr. Hartman commented. “This is important because we know that nodular melanoma as well as ulceration tend to have a worse prognosis in terms of mortality.”
The mean Breslow thickness of newly diagnosed melanomas was 0.88 mm prelockdown, 0.66 mm during lockdown, and 1.96 mm postlockdown. The investigators speculated that the reduced Breslow thickness of melanomas diagnosed during lockdown might be explained by a greater willingness of more health-conscious people to defy the shelter-in-place instructions because of their concern about a suspicious skin lesion. “Though it is way too early to gauge the consequences of such diagnostic delay, should this issue be neglected, dermatologists and their patients may pay a higher price later with increased morbidity, mortality, and financial burden,” according to the investigators.
Dr. Hartman observed that it will be important to learn whether similar experiences occurred elsewhere during lockdown.
Another speaker, John M. Kirkwood, MD, said he has seen several melanoma patients referred from outside centers who had delays of up to 3 months in sentinel lymph node management of T2 and T3 tumors during lockdown who now have widespread metastatic disease.
“Now, is that anecdotal? I don’t know, it’s just worrisome to me,” commented Dr. Kirkwood, professor of medicine, dermatology, and translational science at the University of Pittsburgh.
Merrick Ross, MD, professor of surgical oncology at M.D. Anderson Cancer Center, Houston, recalled, “There was a period of time [during the lockdown] when we weren’t allowed to do certain elective procedures, if you want to call cancer surgery elective.”
“It’s too soon to talk about outcomes because a lot of patients are still in the process of being treated after what I would consider a significant delay in diagnosis,” the surgeon added.
An audience member asked if there will be an opportunity to see data on the damage done by delaying melanoma management as compared to lives saved through the lockdown for COVID-19. Dr. Ross replied that M.D. Anderson is in the midst of an institution-wide study analyzing the delay in diagnosis of a range of cancers.
“In our melanoma center it is absolutely clear, although we’re still collecting data, that the median tumor thickness is much higher since the lockdown,” Dr. Ross commented.
Dr. Hartman said she and her coinvestigators in the Melanoma Prevention Working Group are attempting to tally up the damage done via the lockdown by delaying melanoma diagnosis and treatment. But she agreed with the questioner that the most important thing is overall net lives saved through shelter-in-place.
“I’m sure that, separately, nondermatologists – perhaps infectious disease doctors and internists – are looking at how many lives were saved by the lockdown policy. So I do think all that data will come out,” Dr. Hartman predicted.
She reported having no financial conflicts regarding her presentation.
Global Academy for Medical Education and this news organization are owned by the same company.
SOURCE: Hartman, R. Cutaneous malignancies forum.
REPORTING FROM THE CUTANEOUS MALIGNANCIES FORUM