User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Genetic testing in the PICU prompts meaningful changes in care
according to a new study presented at the Society of Critical Care Medicine’s 2023 Critical Care Congress.
“We have had a lot of success using genome sequencing to help not only with diagnosis, but also changes in management,” lead author Katherine Rodriguez, MD, a pediatric critical care fellow physician at Rady Children’s Hospital, San Diego, told this news organization.
However, data on the use of rapid whole genome sequencing (rWGS) in the pediatric intensive care unit (PICU) are limited, and data from multiple institutions are lacking, Dr. Rodriguez said. In the current study, data from multiple hospitals allowed the researchers to examine differences in management across institutions, she said.
Dr. Rodriguez, with principal investigator Nicole Coufal, MD, also of Rady Children’s, and colleagues conducted the study at three children’s hospitals from March 2019 to July 2022. The study population included 80 children whose origin of illness was uncertain. The patients underwent rWGS testing in the PICU or cardiac ICU setting. The patients ranged in age from 0 to 17 years; 64% were younger than 1 year, (mean age, 2.8 years); 56% were male, and 59% were White.
After rWGS testing, 65% of the children were positive for a genetic variant. The data prompted changes to care for 42% of these patients; 38% of the changes occurred during the patient’s PICU stay, including medication changes and procedures that were either avoided or completed.
The remaining 62% of the changes were subacute and affected management for the remainder of the child’s hospitalization and after discharge, Dr. Rodriguez explained in her presentation.
The average turnaround time for the testing was 10 days, which is important to an intensivist, who may have been hesitant to order tests because of the time involved, Dr. Rodriguez said. The current study shows that “we can get test results in a reasonable time to make meaningful changes in care,” she told this news organization.
Choosing which patients to test can be a challenge for clinicians, Dr. Rodriguez acknowledged. “We have gotten a sense of which patients are likely to have diagnostic or not diagnostic genomes, but it is also a gut feeling,” she said.
“If this child is your patient and you are concerned, if they seem sicker than expected, or have a concerning family history, then send the test,” she said. “It is becoming more affordable, and can come back quickly enough to guide treatment while the patient is still in the ICU.”
In the current study, the greatest diagnostic utility appeared in patients with cardiac symptoms, such as congenital heart disease, sudden cardiac arrest, or suspected channelopathy, Dr. Rodriguez said in her presentation.
Patients with suspected neurological disease had a 50% rate of molecular diagnosis. “Interestingly, 74% of patients with respiratory disease where an underlying genetic etiology was suspected received a molecular diagnosis,” although rWGS was not applied to general populations with RSV or other respiratory illnesses, she said.
In her presentation, Dr. Rodriguez shared examples of how genetic testing had a dramatic impact on patient survival. In one case, a 14-year-old girl presented in cardiac arrest and was found to have new-onset dilated cardiomyopathy. Whether the etiology was acquired or infectious and possibly reversible or genetic was unclear, she said.
“A diagnostic genome result within 48 hours indicated a genetic etiology,” she said. The patient was listed for heart transplant despite the incomplete infectious workup, and received a successful heart transplant 1 week after admission, Dr. Rodriguez said.
Guidelines for which PICU patients should undergo genetic testing do not yet exist, Dr. Rodriguez told this news organization. “We are trying to find some more meaningful parameters where we can say that a patient has a high pretest possibility of a genetic condition,” she said.
“Increasing availability of rWGS can significantly impact patient care and assist families in making difficult decisions during times of critical illness,” she said.
Insurance coverage and testing access are improving, said Dr. Rodriguez. Medicaid policies exist for neonates/infants in the ICU in several states, including Oregon, California, Michigan, Maryland, and Louisiana, she said. In some areas, hospitals may pay for testing for these children if insurance will not, she added.
Dr. Rodriguez and colleagues are continuing to enroll patients in a prospective study of the impact of rWGS, with the addition of a fourth study site and inclusion of family surveys. “We also will be looking at a secondary analysis of cost savings and benefits,” she said.
Ultimately, the current study should be empowering to physicians, “especially if they don’t have good access to geneticists,” Dr. Rodriguez said in an interview.
The study received no outside funding. Dr. Rodriguez reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new study presented at the Society of Critical Care Medicine’s 2023 Critical Care Congress.
“We have had a lot of success using genome sequencing to help not only with diagnosis, but also changes in management,” lead author Katherine Rodriguez, MD, a pediatric critical care fellow physician at Rady Children’s Hospital, San Diego, told this news organization.
However, data on the use of rapid whole genome sequencing (rWGS) in the pediatric intensive care unit (PICU) are limited, and data from multiple institutions are lacking, Dr. Rodriguez said. In the current study, data from multiple hospitals allowed the researchers to examine differences in management across institutions, she said.
Dr. Rodriguez, with principal investigator Nicole Coufal, MD, also of Rady Children’s, and colleagues conducted the study at three children’s hospitals from March 2019 to July 2022. The study population included 80 children whose origin of illness was uncertain. The patients underwent rWGS testing in the PICU or cardiac ICU setting. The patients ranged in age from 0 to 17 years; 64% were younger than 1 year, (mean age, 2.8 years); 56% were male, and 59% were White.
After rWGS testing, 65% of the children were positive for a genetic variant. The data prompted changes to care for 42% of these patients; 38% of the changes occurred during the patient’s PICU stay, including medication changes and procedures that were either avoided or completed.
The remaining 62% of the changes were subacute and affected management for the remainder of the child’s hospitalization and after discharge, Dr. Rodriguez explained in her presentation.
The average turnaround time for the testing was 10 days, which is important to an intensivist, who may have been hesitant to order tests because of the time involved, Dr. Rodriguez said. The current study shows that “we can get test results in a reasonable time to make meaningful changes in care,” she told this news organization.
Choosing which patients to test can be a challenge for clinicians, Dr. Rodriguez acknowledged. “We have gotten a sense of which patients are likely to have diagnostic or not diagnostic genomes, but it is also a gut feeling,” she said.
“If this child is your patient and you are concerned, if they seem sicker than expected, or have a concerning family history, then send the test,” she said. “It is becoming more affordable, and can come back quickly enough to guide treatment while the patient is still in the ICU.”
In the current study, the greatest diagnostic utility appeared in patients with cardiac symptoms, such as congenital heart disease, sudden cardiac arrest, or suspected channelopathy, Dr. Rodriguez said in her presentation.
Patients with suspected neurological disease had a 50% rate of molecular diagnosis. “Interestingly, 74% of patients with respiratory disease where an underlying genetic etiology was suspected received a molecular diagnosis,” although rWGS was not applied to general populations with RSV or other respiratory illnesses, she said.
In her presentation, Dr. Rodriguez shared examples of how genetic testing had a dramatic impact on patient survival. In one case, a 14-year-old girl presented in cardiac arrest and was found to have new-onset dilated cardiomyopathy. Whether the etiology was acquired or infectious and possibly reversible or genetic was unclear, she said.
“A diagnostic genome result within 48 hours indicated a genetic etiology,” she said. The patient was listed for heart transplant despite the incomplete infectious workup, and received a successful heart transplant 1 week after admission, Dr. Rodriguez said.
Guidelines for which PICU patients should undergo genetic testing do not yet exist, Dr. Rodriguez told this news organization. “We are trying to find some more meaningful parameters where we can say that a patient has a high pretest possibility of a genetic condition,” she said.
“Increasing availability of rWGS can significantly impact patient care and assist families in making difficult decisions during times of critical illness,” she said.
Insurance coverage and testing access are improving, said Dr. Rodriguez. Medicaid policies exist for neonates/infants in the ICU in several states, including Oregon, California, Michigan, Maryland, and Louisiana, she said. In some areas, hospitals may pay for testing for these children if insurance will not, she added.
Dr. Rodriguez and colleagues are continuing to enroll patients in a prospective study of the impact of rWGS, with the addition of a fourth study site and inclusion of family surveys. “We also will be looking at a secondary analysis of cost savings and benefits,” she said.
Ultimately, the current study should be empowering to physicians, “especially if they don’t have good access to geneticists,” Dr. Rodriguez said in an interview.
The study received no outside funding. Dr. Rodriguez reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new study presented at the Society of Critical Care Medicine’s 2023 Critical Care Congress.
“We have had a lot of success using genome sequencing to help not only with diagnosis, but also changes in management,” lead author Katherine Rodriguez, MD, a pediatric critical care fellow physician at Rady Children’s Hospital, San Diego, told this news organization.
However, data on the use of rapid whole genome sequencing (rWGS) in the pediatric intensive care unit (PICU) are limited, and data from multiple institutions are lacking, Dr. Rodriguez said. In the current study, data from multiple hospitals allowed the researchers to examine differences in management across institutions, she said.
Dr. Rodriguez, with principal investigator Nicole Coufal, MD, also of Rady Children’s, and colleagues conducted the study at three children’s hospitals from March 2019 to July 2022. The study population included 80 children whose origin of illness was uncertain. The patients underwent rWGS testing in the PICU or cardiac ICU setting. The patients ranged in age from 0 to 17 years; 64% were younger than 1 year, (mean age, 2.8 years); 56% were male, and 59% were White.
After rWGS testing, 65% of the children were positive for a genetic variant. The data prompted changes to care for 42% of these patients; 38% of the changes occurred during the patient’s PICU stay, including medication changes and procedures that were either avoided or completed.
The remaining 62% of the changes were subacute and affected management for the remainder of the child’s hospitalization and after discharge, Dr. Rodriguez explained in her presentation.
The average turnaround time for the testing was 10 days, which is important to an intensivist, who may have been hesitant to order tests because of the time involved, Dr. Rodriguez said. The current study shows that “we can get test results in a reasonable time to make meaningful changes in care,” she told this news organization.
Choosing which patients to test can be a challenge for clinicians, Dr. Rodriguez acknowledged. “We have gotten a sense of which patients are likely to have diagnostic or not diagnostic genomes, but it is also a gut feeling,” she said.
“If this child is your patient and you are concerned, if they seem sicker than expected, or have a concerning family history, then send the test,” she said. “It is becoming more affordable, and can come back quickly enough to guide treatment while the patient is still in the ICU.”
In the current study, the greatest diagnostic utility appeared in patients with cardiac symptoms, such as congenital heart disease, sudden cardiac arrest, or suspected channelopathy, Dr. Rodriguez said in her presentation.
Patients with suspected neurological disease had a 50% rate of molecular diagnosis. “Interestingly, 74% of patients with respiratory disease where an underlying genetic etiology was suspected received a molecular diagnosis,” although rWGS was not applied to general populations with RSV or other respiratory illnesses, she said.
In her presentation, Dr. Rodriguez shared examples of how genetic testing had a dramatic impact on patient survival. In one case, a 14-year-old girl presented in cardiac arrest and was found to have new-onset dilated cardiomyopathy. Whether the etiology was acquired or infectious and possibly reversible or genetic was unclear, she said.
“A diagnostic genome result within 48 hours indicated a genetic etiology,” she said. The patient was listed for heart transplant despite the incomplete infectious workup, and received a successful heart transplant 1 week after admission, Dr. Rodriguez said.
Guidelines for which PICU patients should undergo genetic testing do not yet exist, Dr. Rodriguez told this news organization. “We are trying to find some more meaningful parameters where we can say that a patient has a high pretest possibility of a genetic condition,” she said.
“Increasing availability of rWGS can significantly impact patient care and assist families in making difficult decisions during times of critical illness,” she said.
Insurance coverage and testing access are improving, said Dr. Rodriguez. Medicaid policies exist for neonates/infants in the ICU in several states, including Oregon, California, Michigan, Maryland, and Louisiana, she said. In some areas, hospitals may pay for testing for these children if insurance will not, she added.
Dr. Rodriguez and colleagues are continuing to enroll patients in a prospective study of the impact of rWGS, with the addition of a fourth study site and inclusion of family surveys. “We also will be looking at a secondary analysis of cost savings and benefits,” she said.
Ultimately, the current study should be empowering to physicians, “especially if they don’t have good access to geneticists,” Dr. Rodriguez said in an interview.
The study received no outside funding. Dr. Rodriguez reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM SCCM 2023
Herbal combination tames active UC in small study
AURORA, COLO. –
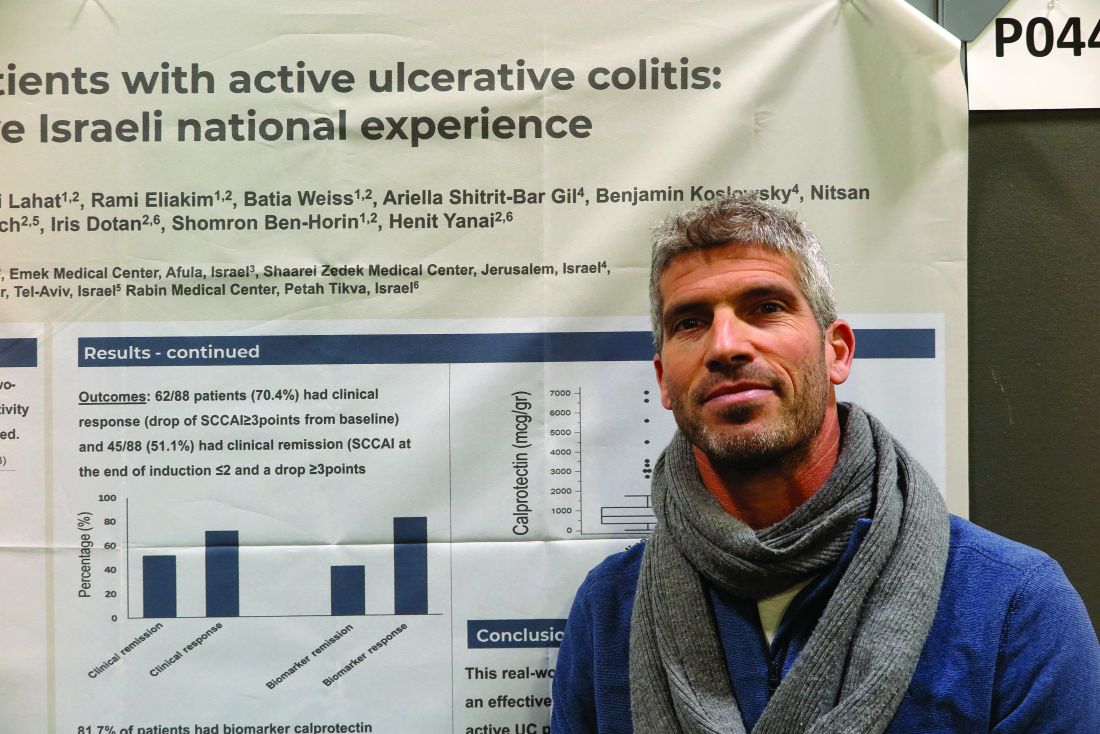
Among 42 patients randomized on a 2:1 basis to receive either an enteric-coated pill containing 3 g of curcumin and qing-dai (CurQD) or placebo for 8 weeks, 43% of those assigned to receive the combination met the co-primary endpoint of a significant reduction in disease activity and objective evidence of response, compared with 8% of those assigned to placebo, reported Shomron Ben-Horin, MD, of Sheba Medical Center in Tel Aviv, Israel, and colleagues.
“In this randomized multicenter placebo-controlled trial, combination CurQD was found effective for inducing remission in active UC patients, including biologic-experienced patients,” they wrote in a scientific poster presented at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Nice spice
Curcumin is a polyphenolic compound derived from the spice turmeric that has been shown to have antioxidative and anti-inflammatory properties. Qing-dai (QD), also known as indigo naturalis, has been used in traditional Chinese medicine as an anti-inflammatory. Both agents are available over the counter in the United States, and have been on the market in Israel as a combination since 2016, said coauthor Nir Salomon, a certified herbalist at Sheba Medical Center.
“What we have here is a combination of these two compounds that are specifically sourced – the gut-directed curcumin, which we developed, and the specifically-sourced QD, and we use them in a specific protocol with a formulation suitable for moderate to severe disease,” he said in an interview.
Mr. Salomon and colleagues in Israel and in Athens, Greece, tested CurQD in a two-part trial. The first part was a 4-week open-label study of CurQD in 10 patients with active UC defined by a Simple Clinical Colitis Activity Index (SCCAI) score of 5 or greater and a modified Mayo endoscopic subscore of 2 or greater.
Part 2 was the placebo-controlled trial described before, with 42 patients with active UC. For 49% of these patients immunomodulatory and/or biologic therapies had failed to induce or maintain remissions.
A total of 43% of patients assigned to CurQD met the primary combined endpoint of a reduction in SCCAI of at least 3 points and objective evidence of response, consisting of either a Mayo endoscopic subscore improvement of 1 or greater, or at least 50% reduction in calprotectin.
In all, 85.7% of patients assigned to CurQD had a clinical response, compared with 30.7% of those assigned to placebo (P < .001).
In addition, 75% of patients on CurQD had endoscopic improvement, compared with 20% on placebo (P = .036), and more patients on the combined supplement had at least 50% reductions in calprotectin levels (46.4% vs. 15.4%, respectively), although the difference did not reach statistical significance.
Patients randomized to CurQD had significantly better resolution of rectal bleeding by day 12 (P value not shown).
Eight additional weeks of maintenance on curcumin alone resulted in 93% retention at week 16 of clinical response, 80% retention of remissions, and 40% maintenance of clinical biomarker responses.
CurQD, but not placebo, was associated with activation of the aryl-hydrocarbon receptor (AhR) pathway. AhR is a nuclear receptor that has been implicated as a mediator of inflammatory bowel disease.
“Induction of AhR merits further study as [a] potential treatment target in active UC,” the investigators wrote.
Small molecule
“This is a very promising and nicely conducted trial. Previously there are separate trials both determining potential mechanisms of action as well as efficacy of curcumin and Qing Dai separately in this population. This is a nice study that uses the combination in patients with mild to moderate UC,” said Ashwin N. Ananthakrishnan, MBBS, MPH, a gastroenterology physician and researcher at Massachusetts General Hospital in Boston.
“Immunosuppressive treatments are very effective in our patients with IBD but there remains concern (particularly for patients) about the consequences of immunosuppression including risk of treatment associated cancer. Thus, there is a lot of interest in rigorous studies of nonimmunosuppressive treatments that may still be effective in relieving objective inflammation (apart from just symptomatic improvement). This study provides a nice evidence base for that. There remain multiple limitations including small sample size, potential generalizability to other populations, and importantly whether the efficacy is driven by curcumin or Qing Dai,” he said in reply to a request for independent commentary.
Dr. Ananthakrishnan was not involved in the study.
“This is great work! We are also studying Qing Dai/indigo naturalis and have developed a single small molecule that works similarly to this therapy,” Matt Davidson, PhD, of Azora Therapeutics in Encino, Calif., said in an online chat section of the meeting website.
In a separate scientific poster presented at the meeting, Dr. Davidson and Julie Saiki, PhD, also from Azora, reported that their company is developing a novel synthetic small molecule prodrug of indirubin, an AhR agonist derived from indigo that is purported to maximize colonic exposure while minimizing systemic exposure.
In mouse models of colitis, oral administration of the prodrug significantly reduced Disease Activity Index and weight loss similar in magnitude to the active compound indirubin, they reported.
The study was supported by Sheba Medical Center. Mr. Salomon disclosed speaking fees from various companies and has received consulting fees and has an equity position in EvNature, the manufacturer of CurQD. Dr. Ananthakrishnan reported having no disclosures relative to the study. Dr. Davidson is CEO and cofounder of Avora Therapeutics.
AURORA, COLO. –
Among 42 patients randomized on a 2:1 basis to receive either an enteric-coated pill containing 3 g of curcumin and qing-dai (CurQD) or placebo for 8 weeks, 43% of those assigned to receive the combination met the co-primary endpoint of a significant reduction in disease activity and objective evidence of response, compared with 8% of those assigned to placebo, reported Shomron Ben-Horin, MD, of Sheba Medical Center in Tel Aviv, Israel, and colleagues.
“In this randomized multicenter placebo-controlled trial, combination CurQD was found effective for inducing remission in active UC patients, including biologic-experienced patients,” they wrote in a scientific poster presented at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Nice spice
Curcumin is a polyphenolic compound derived from the spice turmeric that has been shown to have antioxidative and anti-inflammatory properties. Qing-dai (QD), also known as indigo naturalis, has been used in traditional Chinese medicine as an anti-inflammatory. Both agents are available over the counter in the United States, and have been on the market in Israel as a combination since 2016, said coauthor Nir Salomon, a certified herbalist at Sheba Medical Center.
“What we have here is a combination of these two compounds that are specifically sourced – the gut-directed curcumin, which we developed, and the specifically-sourced QD, and we use them in a specific protocol with a formulation suitable for moderate to severe disease,” he said in an interview.
Mr. Salomon and colleagues in Israel and in Athens, Greece, tested CurQD in a two-part trial. The first part was a 4-week open-label study of CurQD in 10 patients with active UC defined by a Simple Clinical Colitis Activity Index (SCCAI) score of 5 or greater and a modified Mayo endoscopic subscore of 2 or greater.
Part 2 was the placebo-controlled trial described before, with 42 patients with active UC. For 49% of these patients immunomodulatory and/or biologic therapies had failed to induce or maintain remissions.
A total of 43% of patients assigned to CurQD met the primary combined endpoint of a reduction in SCCAI of at least 3 points and objective evidence of response, consisting of either a Mayo endoscopic subscore improvement of 1 or greater, or at least 50% reduction in calprotectin.
In all, 85.7% of patients assigned to CurQD had a clinical response, compared with 30.7% of those assigned to placebo (P < .001).
In addition, 75% of patients on CurQD had endoscopic improvement, compared with 20% on placebo (P = .036), and more patients on the combined supplement had at least 50% reductions in calprotectin levels (46.4% vs. 15.4%, respectively), although the difference did not reach statistical significance.
Patients randomized to CurQD had significantly better resolution of rectal bleeding by day 12 (P value not shown).
Eight additional weeks of maintenance on curcumin alone resulted in 93% retention at week 16 of clinical response, 80% retention of remissions, and 40% maintenance of clinical biomarker responses.
CurQD, but not placebo, was associated with activation of the aryl-hydrocarbon receptor (AhR) pathway. AhR is a nuclear receptor that has been implicated as a mediator of inflammatory bowel disease.
“Induction of AhR merits further study as [a] potential treatment target in active UC,” the investigators wrote.
Small molecule
“This is a very promising and nicely conducted trial. Previously there are separate trials both determining potential mechanisms of action as well as efficacy of curcumin and Qing Dai separately in this population. This is a nice study that uses the combination in patients with mild to moderate UC,” said Ashwin N. Ananthakrishnan, MBBS, MPH, a gastroenterology physician and researcher at Massachusetts General Hospital in Boston.
“Immunosuppressive treatments are very effective in our patients with IBD but there remains concern (particularly for patients) about the consequences of immunosuppression including risk of treatment associated cancer. Thus, there is a lot of interest in rigorous studies of nonimmunosuppressive treatments that may still be effective in relieving objective inflammation (apart from just symptomatic improvement). This study provides a nice evidence base for that. There remain multiple limitations including small sample size, potential generalizability to other populations, and importantly whether the efficacy is driven by curcumin or Qing Dai,” he said in reply to a request for independent commentary.
Dr. Ananthakrishnan was not involved in the study.
“This is great work! We are also studying Qing Dai/indigo naturalis and have developed a single small molecule that works similarly to this therapy,” Matt Davidson, PhD, of Azora Therapeutics in Encino, Calif., said in an online chat section of the meeting website.
In a separate scientific poster presented at the meeting, Dr. Davidson and Julie Saiki, PhD, also from Azora, reported that their company is developing a novel synthetic small molecule prodrug of indirubin, an AhR agonist derived from indigo that is purported to maximize colonic exposure while minimizing systemic exposure.
In mouse models of colitis, oral administration of the prodrug significantly reduced Disease Activity Index and weight loss similar in magnitude to the active compound indirubin, they reported.
The study was supported by Sheba Medical Center. Mr. Salomon disclosed speaking fees from various companies and has received consulting fees and has an equity position in EvNature, the manufacturer of CurQD. Dr. Ananthakrishnan reported having no disclosures relative to the study. Dr. Davidson is CEO and cofounder of Avora Therapeutics.
AURORA, COLO. –
Among 42 patients randomized on a 2:1 basis to receive either an enteric-coated pill containing 3 g of curcumin and qing-dai (CurQD) or placebo for 8 weeks, 43% of those assigned to receive the combination met the co-primary endpoint of a significant reduction in disease activity and objective evidence of response, compared with 8% of those assigned to placebo, reported Shomron Ben-Horin, MD, of Sheba Medical Center in Tel Aviv, Israel, and colleagues.
“In this randomized multicenter placebo-controlled trial, combination CurQD was found effective for inducing remission in active UC patients, including biologic-experienced patients,” they wrote in a scientific poster presented at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Nice spice
Curcumin is a polyphenolic compound derived from the spice turmeric that has been shown to have antioxidative and anti-inflammatory properties. Qing-dai (QD), also known as indigo naturalis, has been used in traditional Chinese medicine as an anti-inflammatory. Both agents are available over the counter in the United States, and have been on the market in Israel as a combination since 2016, said coauthor Nir Salomon, a certified herbalist at Sheba Medical Center.
“What we have here is a combination of these two compounds that are specifically sourced – the gut-directed curcumin, which we developed, and the specifically-sourced QD, and we use them in a specific protocol with a formulation suitable for moderate to severe disease,” he said in an interview.
Mr. Salomon and colleagues in Israel and in Athens, Greece, tested CurQD in a two-part trial. The first part was a 4-week open-label study of CurQD in 10 patients with active UC defined by a Simple Clinical Colitis Activity Index (SCCAI) score of 5 or greater and a modified Mayo endoscopic subscore of 2 or greater.
Part 2 was the placebo-controlled trial described before, with 42 patients with active UC. For 49% of these patients immunomodulatory and/or biologic therapies had failed to induce or maintain remissions.
A total of 43% of patients assigned to CurQD met the primary combined endpoint of a reduction in SCCAI of at least 3 points and objective evidence of response, consisting of either a Mayo endoscopic subscore improvement of 1 or greater, or at least 50% reduction in calprotectin.
In all, 85.7% of patients assigned to CurQD had a clinical response, compared with 30.7% of those assigned to placebo (P < .001).
In addition, 75% of patients on CurQD had endoscopic improvement, compared with 20% on placebo (P = .036), and more patients on the combined supplement had at least 50% reductions in calprotectin levels (46.4% vs. 15.4%, respectively), although the difference did not reach statistical significance.
Patients randomized to CurQD had significantly better resolution of rectal bleeding by day 12 (P value not shown).
Eight additional weeks of maintenance on curcumin alone resulted in 93% retention at week 16 of clinical response, 80% retention of remissions, and 40% maintenance of clinical biomarker responses.
CurQD, but not placebo, was associated with activation of the aryl-hydrocarbon receptor (AhR) pathway. AhR is a nuclear receptor that has been implicated as a mediator of inflammatory bowel disease.
“Induction of AhR merits further study as [a] potential treatment target in active UC,” the investigators wrote.
Small molecule
“This is a very promising and nicely conducted trial. Previously there are separate trials both determining potential mechanisms of action as well as efficacy of curcumin and Qing Dai separately in this population. This is a nice study that uses the combination in patients with mild to moderate UC,” said Ashwin N. Ananthakrishnan, MBBS, MPH, a gastroenterology physician and researcher at Massachusetts General Hospital in Boston.
“Immunosuppressive treatments are very effective in our patients with IBD but there remains concern (particularly for patients) about the consequences of immunosuppression including risk of treatment associated cancer. Thus, there is a lot of interest in rigorous studies of nonimmunosuppressive treatments that may still be effective in relieving objective inflammation (apart from just symptomatic improvement). This study provides a nice evidence base for that. There remain multiple limitations including small sample size, potential generalizability to other populations, and importantly whether the efficacy is driven by curcumin or Qing Dai,” he said in reply to a request for independent commentary.
Dr. Ananthakrishnan was not involved in the study.
“This is great work! We are also studying Qing Dai/indigo naturalis and have developed a single small molecule that works similarly to this therapy,” Matt Davidson, PhD, of Azora Therapeutics in Encino, Calif., said in an online chat section of the meeting website.
In a separate scientific poster presented at the meeting, Dr. Davidson and Julie Saiki, PhD, also from Azora, reported that their company is developing a novel synthetic small molecule prodrug of indirubin, an AhR agonist derived from indigo that is purported to maximize colonic exposure while minimizing systemic exposure.
In mouse models of colitis, oral administration of the prodrug significantly reduced Disease Activity Index and weight loss similar in magnitude to the active compound indirubin, they reported.
The study was supported by Sheba Medical Center. Mr. Salomon disclosed speaking fees from various companies and has received consulting fees and has an equity position in EvNature, the manufacturer of CurQD. Dr. Ananthakrishnan reported having no disclosures relative to the study. Dr. Davidson is CEO and cofounder of Avora Therapeutics.
AT THE CROHN’S & COLITIS CONGRESS
Adult stem cells can heal intractable perianal Crohn’s fistulae
AURORA, COLO. – Perianal Crohn’s disease with fistula is notoriously difficult to treat and can make patients’ lives miserable, but a new, minimally invasive approach involving local injection of mesenchymal stem cells is both safe and, in a significant proportion of patients, highly effective, according to a colorectal surgeon.
“It’s a really debilitating phenotype, a spectrum of phenotypes,” Amy Lightner, MD, of the Cleveland Clinic said at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Although some patients have minimal symptoms, others may require multiple setons to aid in drainage and healing, while others may require fistulotomy, endorectal advancement flap, intersphincteric fistula tract (LIFT) procedure, diversion, or proctectomy.

“Why is it so difficult to treat? Well, part of it is that this is an anatomic defect, and this is why 90% of patients will come to the operating room and will see their surgeons on a frequent basis. The other part of that is that we have medical therapies to treat these fistulas but they’re really largely ineffective, because there is that anatomical defect, the hole there that needs to be closed,” Dr. Lightner said.
Up to 20% of patients may require a permanent stoma, and an additional 20% may require temporary fecal diversion.
Mesenchymal stem cells (MSC) are derived from bone marrow, fat stores, or umbilical cord tissues. Unlike embryonic stem cells, which have the ability to metamorphose into a multitude of other cell types, mesenchymal stem cells are differentiated “adult” cells.
They work by secreting anti-inflammatory cytokines and recruiting immune cells to stimulate tissue repair and healing. The cells are delivered in a minimally invasive outpatient setting, and there is no risk of incontinence compared with more invasive procedures such as fistulotomy or advancement flaps.
Effective and safe
MSCs were first used in Spain in 2003 to successfully treat a young women with a complex fistula with five perianal tracts converging into a rectovaginal fistula. The investigators injected a single dose of 9 x 106 MSCs into the site, and the fistula healed within 3 months.
Since then in multiple clinical trials involving more than 400 patients, injection of MSCs has resulted in fistula closure and complete healing by 8-12 weeks in 50%-85% of patients, Dr. Lightner said.
The treatment effect is also durable, she said, pointing to data from the ADMIRE-CD study, in which 51.5% of Crohn’s disease patients with treatment-refractory complex perianal fistula were healed at 24 weeks following injection of adipose-derived stem cells, compared with 35.6% of controls. At 1 year of follow-up, respective rates of healing were 56.3% vs. 38.6%.
Dr. Lightner also cited a case report of a patient whose fistula remained healed 4 years after receiving MSCs for refractory perianal Crohn’s fistulas.
Although MSCs are derived from healthy donors, they do not bear cellular surface antigens that would instigate a destructive host immune response, and to date, there have been no reports from clinical trials of systemic infections or complications. The most frequently reported adverse events have been injection-site pain in about 12%-15% of patients, and perianal abscess in 5%-13%, with similar frequencies in treatment and control groups.
Dr. Lightner and colleagues are currently exploring additional indications for stem cell therapy with MSCs, including other complex fistula phenotypes, intestinal Crohn’s disease, and ulcerative colitis.
Other approaches
In a separate presentation, James D. Lewis, MD, MSCE, of the University of Pennsylvania in Philadelphia talked about what would be needed to achieve a “medical moonshot” with the goal of curing inflammatory bowel disease (IBD), and touched on hematopoietic stem cell transplants as a potential option for patients with chronic, severe, and intractable disease.
One of his patients was a woman in her 60s who was diagnosed with stricturing and penetrating Crohn’s disease in her 30s, with the disease involving the ileum and entire colon. She had previously undergone three small bowel resections and a partial colon resection, and had never experienced remission despite taking steroids, azathioprine, methotrexate, four anti-TNF drugs, ustekinumab (Stelara), and vedolizumab (Entyvio).
Following an autologous hematopoietic stem cell transplant, she had a Simple Endoscopic Score for Crohn’s Disease (SES-CD) of 0. Her course was complicated by demand ischemia and acute kidney injury.
An IBD specialist who was not involved in either study commented in an interview that both MSCs and stem cell transplants show promise for treatment-refractory IBD,
“Both approaches are very promising, but stem cell transplants for IBD haven’t been formally studied yet so the data aren’t as strong, but there is promise for the future,” said Berkeley N. Limketkai, MD, PhD, from the University of California, Los Angeles.
“The challenges, however, are also the morbidity associated with actually undergoing such procedures,” he continued. Short- and long-term morbidities associated with hematopoietic stem cell transplants may include mucositis; hemorrhagic cystitis; prolonged, severe pancytopenia; infection; graft-versus-host disease; graft failure; pulmonary complications, veno-occlusive disease of the liver; and thrombotic microangiopathy.
Dr. Limketkai said that over time as the protocols for stem cell transplants in IBD improve, the benefits for select patients may more clearly outweigh the risks.
Dr. Lightner’s work is supported by the Leona M. and Harry B. Helmsley Charitable Trust and the American Society of Colon and Rectal Surgery. She disclosed consulting fees from Boomerang Medical, Mesoblast Limited, Ossium Health, and Takeda Pharmaceuticals USA. Dr. Lewis’ work is supported by grants from the National Institutes of Health, and from AbbVie, Takeda, Janssen, and Nestlé Health Science. He has also served as a consultant to and data safety monitoring board member for several entities. Dr. Limketkai disclosed consulting for Azora Therapeutics.
AURORA, COLO. – Perianal Crohn’s disease with fistula is notoriously difficult to treat and can make patients’ lives miserable, but a new, minimally invasive approach involving local injection of mesenchymal stem cells is both safe and, in a significant proportion of patients, highly effective, according to a colorectal surgeon.
“It’s a really debilitating phenotype, a spectrum of phenotypes,” Amy Lightner, MD, of the Cleveland Clinic said at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Although some patients have minimal symptoms, others may require multiple setons to aid in drainage and healing, while others may require fistulotomy, endorectal advancement flap, intersphincteric fistula tract (LIFT) procedure, diversion, or proctectomy.
“Why is it so difficult to treat? Well, part of it is that this is an anatomic defect, and this is why 90% of patients will come to the operating room and will see their surgeons on a frequent basis. The other part of that is that we have medical therapies to treat these fistulas but they’re really largely ineffective, because there is that anatomical defect, the hole there that needs to be closed,” Dr. Lightner said.
Up to 20% of patients may require a permanent stoma, and an additional 20% may require temporary fecal diversion.
Mesenchymal stem cells (MSC) are derived from bone marrow, fat stores, or umbilical cord tissues. Unlike embryonic stem cells, which have the ability to metamorphose into a multitude of other cell types, mesenchymal stem cells are differentiated “adult” cells.
They work by secreting anti-inflammatory cytokines and recruiting immune cells to stimulate tissue repair and healing. The cells are delivered in a minimally invasive outpatient setting, and there is no risk of incontinence compared with more invasive procedures such as fistulotomy or advancement flaps.
Effective and safe
MSCs were first used in Spain in 2003 to successfully treat a young women with a complex fistula with five perianal tracts converging into a rectovaginal fistula. The investigators injected a single dose of 9 x 106 MSCs into the site, and the fistula healed within 3 months.
Since then in multiple clinical trials involving more than 400 patients, injection of MSCs has resulted in fistula closure and complete healing by 8-12 weeks in 50%-85% of patients, Dr. Lightner said.
The treatment effect is also durable, she said, pointing to data from the ADMIRE-CD study, in which 51.5% of Crohn’s disease patients with treatment-refractory complex perianal fistula were healed at 24 weeks following injection of adipose-derived stem cells, compared with 35.6% of controls. At 1 year of follow-up, respective rates of healing were 56.3% vs. 38.6%.
Dr. Lightner also cited a case report of a patient whose fistula remained healed 4 years after receiving MSCs for refractory perianal Crohn’s fistulas.
Although MSCs are derived from healthy donors, they do not bear cellular surface antigens that would instigate a destructive host immune response, and to date, there have been no reports from clinical trials of systemic infections or complications. The most frequently reported adverse events have been injection-site pain in about 12%-15% of patients, and perianal abscess in 5%-13%, with similar frequencies in treatment and control groups.
Dr. Lightner and colleagues are currently exploring additional indications for stem cell therapy with MSCs, including other complex fistula phenotypes, intestinal Crohn’s disease, and ulcerative colitis.
Other approaches
In a separate presentation, James D. Lewis, MD, MSCE, of the University of Pennsylvania in Philadelphia talked about what would be needed to achieve a “medical moonshot” with the goal of curing inflammatory bowel disease (IBD), and touched on hematopoietic stem cell transplants as a potential option for patients with chronic, severe, and intractable disease.
One of his patients was a woman in her 60s who was diagnosed with stricturing and penetrating Crohn’s disease in her 30s, with the disease involving the ileum and entire colon. She had previously undergone three small bowel resections and a partial colon resection, and had never experienced remission despite taking steroids, azathioprine, methotrexate, four anti-TNF drugs, ustekinumab (Stelara), and vedolizumab (Entyvio).
Following an autologous hematopoietic stem cell transplant, she had a Simple Endoscopic Score for Crohn’s Disease (SES-CD) of 0. Her course was complicated by demand ischemia and acute kidney injury.
An IBD specialist who was not involved in either study commented in an interview that both MSCs and stem cell transplants show promise for treatment-refractory IBD,
“Both approaches are very promising, but stem cell transplants for IBD haven’t been formally studied yet so the data aren’t as strong, but there is promise for the future,” said Berkeley N. Limketkai, MD, PhD, from the University of California, Los Angeles.
“The challenges, however, are also the morbidity associated with actually undergoing such procedures,” he continued. Short- and long-term morbidities associated with hematopoietic stem cell transplants may include mucositis; hemorrhagic cystitis; prolonged, severe pancytopenia; infection; graft-versus-host disease; graft failure; pulmonary complications, veno-occlusive disease of the liver; and thrombotic microangiopathy.
Dr. Limketkai said that over time as the protocols for stem cell transplants in IBD improve, the benefits for select patients may more clearly outweigh the risks.
Dr. Lightner’s work is supported by the Leona M. and Harry B. Helmsley Charitable Trust and the American Society of Colon and Rectal Surgery. She disclosed consulting fees from Boomerang Medical, Mesoblast Limited, Ossium Health, and Takeda Pharmaceuticals USA. Dr. Lewis’ work is supported by grants from the National Institutes of Health, and from AbbVie, Takeda, Janssen, and Nestlé Health Science. He has also served as a consultant to and data safety monitoring board member for several entities. Dr. Limketkai disclosed consulting for Azora Therapeutics.
AURORA, COLO. – Perianal Crohn’s disease with fistula is notoriously difficult to treat and can make patients’ lives miserable, but a new, minimally invasive approach involving local injection of mesenchymal stem cells is both safe and, in a significant proportion of patients, highly effective, according to a colorectal surgeon.
“It’s a really debilitating phenotype, a spectrum of phenotypes,” Amy Lightner, MD, of the Cleveland Clinic said at the annual Crohn’s & Colitis Congress®, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Although some patients have minimal symptoms, others may require multiple setons to aid in drainage and healing, while others may require fistulotomy, endorectal advancement flap, intersphincteric fistula tract (LIFT) procedure, diversion, or proctectomy.
“Why is it so difficult to treat? Well, part of it is that this is an anatomic defect, and this is why 90% of patients will come to the operating room and will see their surgeons on a frequent basis. The other part of that is that we have medical therapies to treat these fistulas but they’re really largely ineffective, because there is that anatomical defect, the hole there that needs to be closed,” Dr. Lightner said.
Up to 20% of patients may require a permanent stoma, and an additional 20% may require temporary fecal diversion.
Mesenchymal stem cells (MSC) are derived from bone marrow, fat stores, or umbilical cord tissues. Unlike embryonic stem cells, which have the ability to metamorphose into a multitude of other cell types, mesenchymal stem cells are differentiated “adult” cells.
They work by secreting anti-inflammatory cytokines and recruiting immune cells to stimulate tissue repair and healing. The cells are delivered in a minimally invasive outpatient setting, and there is no risk of incontinence compared with more invasive procedures such as fistulotomy or advancement flaps.
Effective and safe
MSCs were first used in Spain in 2003 to successfully treat a young women with a complex fistula with five perianal tracts converging into a rectovaginal fistula. The investigators injected a single dose of 9 x 106 MSCs into the site, and the fistula healed within 3 months.
Since then in multiple clinical trials involving more than 400 patients, injection of MSCs has resulted in fistula closure and complete healing by 8-12 weeks in 50%-85% of patients, Dr. Lightner said.
The treatment effect is also durable, she said, pointing to data from the ADMIRE-CD study, in which 51.5% of Crohn’s disease patients with treatment-refractory complex perianal fistula were healed at 24 weeks following injection of adipose-derived stem cells, compared with 35.6% of controls. At 1 year of follow-up, respective rates of healing were 56.3% vs. 38.6%.
Dr. Lightner also cited a case report of a patient whose fistula remained healed 4 years after receiving MSCs for refractory perianal Crohn’s fistulas.
Although MSCs are derived from healthy donors, they do not bear cellular surface antigens that would instigate a destructive host immune response, and to date, there have been no reports from clinical trials of systemic infections or complications. The most frequently reported adverse events have been injection-site pain in about 12%-15% of patients, and perianal abscess in 5%-13%, with similar frequencies in treatment and control groups.
Dr. Lightner and colleagues are currently exploring additional indications for stem cell therapy with MSCs, including other complex fistula phenotypes, intestinal Crohn’s disease, and ulcerative colitis.
Other approaches
In a separate presentation, James D. Lewis, MD, MSCE, of the University of Pennsylvania in Philadelphia talked about what would be needed to achieve a “medical moonshot” with the goal of curing inflammatory bowel disease (IBD), and touched on hematopoietic stem cell transplants as a potential option for patients with chronic, severe, and intractable disease.
One of his patients was a woman in her 60s who was diagnosed with stricturing and penetrating Crohn’s disease in her 30s, with the disease involving the ileum and entire colon. She had previously undergone three small bowel resections and a partial colon resection, and had never experienced remission despite taking steroids, azathioprine, methotrexate, four anti-TNF drugs, ustekinumab (Stelara), and vedolizumab (Entyvio).
Following an autologous hematopoietic stem cell transplant, she had a Simple Endoscopic Score for Crohn’s Disease (SES-CD) of 0. Her course was complicated by demand ischemia and acute kidney injury.
An IBD specialist who was not involved in either study commented in an interview that both MSCs and stem cell transplants show promise for treatment-refractory IBD,
“Both approaches are very promising, but stem cell transplants for IBD haven’t been formally studied yet so the data aren’t as strong, but there is promise for the future,” said Berkeley N. Limketkai, MD, PhD, from the University of California, Los Angeles.
“The challenges, however, are also the morbidity associated with actually undergoing such procedures,” he continued. Short- and long-term morbidities associated with hematopoietic stem cell transplants may include mucositis; hemorrhagic cystitis; prolonged, severe pancytopenia; infection; graft-versus-host disease; graft failure; pulmonary complications, veno-occlusive disease of the liver; and thrombotic microangiopathy.
Dr. Limketkai said that over time as the protocols for stem cell transplants in IBD improve, the benefits for select patients may more clearly outweigh the risks.
Dr. Lightner’s work is supported by the Leona M. and Harry B. Helmsley Charitable Trust and the American Society of Colon and Rectal Surgery. She disclosed consulting fees from Boomerang Medical, Mesoblast Limited, Ossium Health, and Takeda Pharmaceuticals USA. Dr. Lewis’ work is supported by grants from the National Institutes of Health, and from AbbVie, Takeda, Janssen, and Nestlé Health Science. He has also served as a consultant to and data safety monitoring board member for several entities. Dr. Limketkai disclosed consulting for Azora Therapeutics.
AT CROHN’S & COLITIS CONGRESS

Expert gives tips on less-discussed dermatologic diseases
ORLANDO – , according to Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington.
These semi-forsaken diseases are important not to miss and can “also be quite challenging when we think about their management,” he said at the ODAC Dermatology, Aesthetic & Surgical Conference.

Dr. Friedman, also director of the GW dermatology residency program, reviewed several of these diseases – along with tips for management – during a session at the meeting.
. It does not always have the classic ring pattern for which it is best known, he said. And in patients with darker skin tones, it is characterized by more of a brown or black color, rather than the pink-red color.
Dr. Friedman said that despite a kind of “Pavlovian response” linking GA with diabetes, this link might not be as strong as the field has come to believe, since the studies on which this belief was based included a patient population with narrow demographics. “Maybe GA and type 1 diabetes aren’t necessarily connected,” he said.
Dyslipidemia, on the other hand, has a strong connection with GA, he said. The disease is also linked to thyroid disease and is linked with malignancy, especially in older patients with generalized or atypical presentations of GA, he said.
Spontaneous resolution of the disease is seen within 2 years for 50% to 75% of patients, so “no treatment may be the best treatment,” but antimalarials can be effective, Dr. Friedman said. “I use antimalarials frequently in my practice,” he said. “The key is, they take time to work (4-5 months),” which should be explained to patients.
Antibiotics, he said, can be “somewhat effective,” but in the case of doxycycline at least, the disease can resolve within weeks but then may return when treatment is stopped.
There is some evidence to support using biologics and more recently, Janus kinase (JAK) inhibitors, off-label, to treat GA. Efficacy has been seen with the tumor necrosis factor (TNF) blocker infliximab and with the JAK inhibitor tofacitinib, he said.
Lichen planus (LP). This is another common disease that can go off-script with its presentation. The disease is often described with the “six P’s” indicating the following characteristics: pruritic, polygonal, planar or flat-topped, purple papules, and plaques. But LP “didn’t read the textbook,” Dr. Friedman said.
“The clinical presentation of lichen planus can be quite broad,” he said. “The P’s aren’t always followed as there are a variety of colors and configurations which can be witnessed.”
With LP, there is a clear association with dyslipidemia and diabetes, so “asking the right questions is going to be important” when talking to the patient. There is also a higher risk of autoimmune diseases, especially of the thyroid type, associated with LP, he said.
No treatment has been Food and Drug Administration approved for LP, but some are expected in the future, he said.
For now, he emphasized creativity in the management of patients with LP. “I love oral retinoids for this,” he said. Antimalarials and methotrexate are also options.
In one case Dr. Friedman saw, nothing seemed to work: light therapy for a year; metronidazole; isotretinoin; halobetasol/tazarotene lotion; and the TNF-blocker adalimumab either weren’t effective or resulted in complications in the patient.
Knowing the recent implication of the interleukin (IL)-17 pathway in the pathophysiology of LP, he then tried the anti-IL17 antibody secukinumab. “This patient had a pretty robust response to treatment,” Dr. Friedman said. “He was very excited. The problem, as always, is access, especially for off-label therapies.”
Tumid lupus erythematosus. This disease is characterized by erythematous, edematous, nonscarring plaques on sun-exposed sites. For treatment, Dr. Friedman said antimalarials can be up to 90% effective, sometimes with rapid resolution of the lesions.
“You want to dose below that 5 mg per kg of true body weight to limit the small potential for ocular toxicity over time,” he said. And, he emphasized, “always combine treatment with good sun-protective measures.”
Dr. Friedman reported financial relationships with Sanova, Pfizer, Novartis, and other companies.
ORLANDO – , according to Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington.
These semi-forsaken diseases are important not to miss and can “also be quite challenging when we think about their management,” he said at the ODAC Dermatology, Aesthetic & Surgical Conference.
Dr. Friedman, also director of the GW dermatology residency program, reviewed several of these diseases – along with tips for management – during a session at the meeting.
. It does not always have the classic ring pattern for which it is best known, he said. And in patients with darker skin tones, it is characterized by more of a brown or black color, rather than the pink-red color.
Dr. Friedman said that despite a kind of “Pavlovian response” linking GA with diabetes, this link might not be as strong as the field has come to believe, since the studies on which this belief was based included a patient population with narrow demographics. “Maybe GA and type 1 diabetes aren’t necessarily connected,” he said.
Dyslipidemia, on the other hand, has a strong connection with GA, he said. The disease is also linked to thyroid disease and is linked with malignancy, especially in older patients with generalized or atypical presentations of GA, he said.
Spontaneous resolution of the disease is seen within 2 years for 50% to 75% of patients, so “no treatment may be the best treatment,” but antimalarials can be effective, Dr. Friedman said. “I use antimalarials frequently in my practice,” he said. “The key is, they take time to work (4-5 months),” which should be explained to patients.
Antibiotics, he said, can be “somewhat effective,” but in the case of doxycycline at least, the disease can resolve within weeks but then may return when treatment is stopped.
There is some evidence to support using biologics and more recently, Janus kinase (JAK) inhibitors, off-label, to treat GA. Efficacy has been seen with the tumor necrosis factor (TNF) blocker infliximab and with the JAK inhibitor tofacitinib, he said.
Lichen planus (LP). This is another common disease that can go off-script with its presentation. The disease is often described with the “six P’s” indicating the following characteristics: pruritic, polygonal, planar or flat-topped, purple papules, and plaques. But LP “didn’t read the textbook,” Dr. Friedman said.
“The clinical presentation of lichen planus can be quite broad,” he said. “The P’s aren’t always followed as there are a variety of colors and configurations which can be witnessed.”
With LP, there is a clear association with dyslipidemia and diabetes, so “asking the right questions is going to be important” when talking to the patient. There is also a higher risk of autoimmune diseases, especially of the thyroid type, associated with LP, he said.
No treatment has been Food and Drug Administration approved for LP, but some are expected in the future, he said.
For now, he emphasized creativity in the management of patients with LP. “I love oral retinoids for this,” he said. Antimalarials and methotrexate are also options.
In one case Dr. Friedman saw, nothing seemed to work: light therapy for a year; metronidazole; isotretinoin; halobetasol/tazarotene lotion; and the TNF-blocker adalimumab either weren’t effective or resulted in complications in the patient.
Knowing the recent implication of the interleukin (IL)-17 pathway in the pathophysiology of LP, he then tried the anti-IL17 antibody secukinumab. “This patient had a pretty robust response to treatment,” Dr. Friedman said. “He was very excited. The problem, as always, is access, especially for off-label therapies.”
Tumid lupus erythematosus. This disease is characterized by erythematous, edematous, nonscarring plaques on sun-exposed sites. For treatment, Dr. Friedman said antimalarials can be up to 90% effective, sometimes with rapid resolution of the lesions.
“You want to dose below that 5 mg per kg of true body weight to limit the small potential for ocular toxicity over time,” he said. And, he emphasized, “always combine treatment with good sun-protective measures.”
Dr. Friedman reported financial relationships with Sanova, Pfizer, Novartis, and other companies.
ORLANDO – , according to Adam Friedman, MD, professor and chair of dermatology at George Washington University, Washington.
These semi-forsaken diseases are important not to miss and can “also be quite challenging when we think about their management,” he said at the ODAC Dermatology, Aesthetic & Surgical Conference.
Dr. Friedman, also director of the GW dermatology residency program, reviewed several of these diseases – along with tips for management – during a session at the meeting.
. It does not always have the classic ring pattern for which it is best known, he said. And in patients with darker skin tones, it is characterized by more of a brown or black color, rather than the pink-red color.
Dr. Friedman said that despite a kind of “Pavlovian response” linking GA with diabetes, this link might not be as strong as the field has come to believe, since the studies on which this belief was based included a patient population with narrow demographics. “Maybe GA and type 1 diabetes aren’t necessarily connected,” he said.
Dyslipidemia, on the other hand, has a strong connection with GA, he said. The disease is also linked to thyroid disease and is linked with malignancy, especially in older patients with generalized or atypical presentations of GA, he said.
Spontaneous resolution of the disease is seen within 2 years for 50% to 75% of patients, so “no treatment may be the best treatment,” but antimalarials can be effective, Dr. Friedman said. “I use antimalarials frequently in my practice,” he said. “The key is, they take time to work (4-5 months),” which should be explained to patients.
Antibiotics, he said, can be “somewhat effective,” but in the case of doxycycline at least, the disease can resolve within weeks but then may return when treatment is stopped.
There is some evidence to support using biologics and more recently, Janus kinase (JAK) inhibitors, off-label, to treat GA. Efficacy has been seen with the tumor necrosis factor (TNF) blocker infliximab and with the JAK inhibitor tofacitinib, he said.
Lichen planus (LP). This is another common disease that can go off-script with its presentation. The disease is often described with the “six P’s” indicating the following characteristics: pruritic, polygonal, planar or flat-topped, purple papules, and plaques. But LP “didn’t read the textbook,” Dr. Friedman said.
“The clinical presentation of lichen planus can be quite broad,” he said. “The P’s aren’t always followed as there are a variety of colors and configurations which can be witnessed.”
With LP, there is a clear association with dyslipidemia and diabetes, so “asking the right questions is going to be important” when talking to the patient. There is also a higher risk of autoimmune diseases, especially of the thyroid type, associated with LP, he said.
No treatment has been Food and Drug Administration approved for LP, but some are expected in the future, he said.
For now, he emphasized creativity in the management of patients with LP. “I love oral retinoids for this,” he said. Antimalarials and methotrexate are also options.
In one case Dr. Friedman saw, nothing seemed to work: light therapy for a year; metronidazole; isotretinoin; halobetasol/tazarotene lotion; and the TNF-blocker adalimumab either weren’t effective or resulted in complications in the patient.
Knowing the recent implication of the interleukin (IL)-17 pathway in the pathophysiology of LP, he then tried the anti-IL17 antibody secukinumab. “This patient had a pretty robust response to treatment,” Dr. Friedman said. “He was very excited. The problem, as always, is access, especially for off-label therapies.”
Tumid lupus erythematosus. This disease is characterized by erythematous, edematous, nonscarring plaques on sun-exposed sites. For treatment, Dr. Friedman said antimalarials can be up to 90% effective, sometimes with rapid resolution of the lesions.
“You want to dose below that 5 mg per kg of true body weight to limit the small potential for ocular toxicity over time,” he said. And, he emphasized, “always combine treatment with good sun-protective measures.”
Dr. Friedman reported financial relationships with Sanova, Pfizer, Novartis, and other companies.
AT ODAC 2023
Expert offers insights on pediatric dermatology emergencies
ORLANDO – The eruption spread away from the head and her transaminase levels were “dramatic,” in the 700s, said Kalyani S. Marathe, MD, MPH, associate professor of dermatology and pediatrics at the University of Cincinnati.
Dr. Marathe, director of the division of dermatology at Cincinnati Children’s Hospital, reviewed this case in a presentation on pediatric dermatologic emergencies at the ODAC Dermatology, Aesthetic & Surgery Conference, pointing out potential pitfalls and important aspects that might require swift action.

The patient was diagnosed with drug reaction with eosinophilia and systemic symptoms (DRESS).
Facial involvement is common in pediatric cases of DRESS, but edema of the face is less common in children than adults, Dr. Marathe said.
Antiepileptic medications are the most common cause of DRESS, followed by antibiotics – most often, vancomycin and trimethoprim/sulfamethoxazole, she said. But sometimes the trigger is not clear, she noted, recalling a vexing case she once saw in which IV contrast was eventually identified as the cause.
When DRESS is suspected, she said, lab work should be done during the acute eruption and after resolution. This should include CBC, liver function tests, creatinine, and urinalysis, and human herpesvirus 6 (HHV-6) and thyroid testing.
Treatment typically includes supportive care, unless symptoms are systemic, or if there is impending liver failure, when steroids, cyclosporine, or IVIG can be used.
Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN): Mortality rates when these diseases overlap is 4%, Dr. Marathe said. Clues to diagnosing this other medication-induced condition include involvement of the palms and the soles of the feet; presence of the Nikolsky sign in which the top layers of the skin slip away from the lower layers when rubbed; mucosal involvement, which often precedes cutaneous involvement; and these symptoms occurring within the first 8 weeks of taking a medication, which are most commonly antibiotics and anti-epileptics.
Dr. Marathe underscored how important it is to get ophthalmology involved right away, because of the risk of vision loss. Amniotic membrane transfer to the eye at the time of diagnosis has been found to produce dramatically better outcomes, she said. The membrane has anti-inflammatory and antiscarring properties and can promote wound healing on the surface of the eye.
“I would recommend getting your ophthalmology team on board early because they have to advocate for these patients,” she said.
Corticosteroids and IVIG can improve ocular outcomes, but cyclosporine is associated with better mortality outcomes, she said. Emerging data on etanercept has also led to more use of that drug, she said.
Erythema multiforme (EM): unlike urticaria, multiforme EM can have mucosal involvement, Dr. Marathe said. Clinicians should look for three zones of color: A central duskiness, a rim of pallor, and a ring of erythema.
EM is triggered by a virus, which is usually herpes simplex virus (HSV). But she added that HSV is not always found. “So, there are certainly other triggers out there that we just haven’t identified,” she said.
If HSV is suspected, oral acyclovir is effective, she noted.
Other cases might not be as straightforward. Dr. Marathe said that during her fellowship, she saw a patient with EM that was controlled only by IVIG, so it was administered every 3 months. In that case, the trigger was never found.
Multisystem inflammatory syndrome in children (MIS-C): This syndrome can follow COVID-19 infection, and usually presents with 3-5 days of fever after COVID has resolved. It can include gastrointestinal, cardiorespiratory, and neurocognitive symptoms.
The skin presentation is mainly a morbilliform pattern, but clinicians might also see conjunctival involvement, mucosal involvement, and “COVID toes,” painful red or purple lesions on the toes.
Treatment is usually IVIG and systemic corticosteroids, with the treatment course depending on the severity.
MIS-C was initially thought to be Kawasaki’s disease, another autoinflammatory disorder, which is related but distinct, Dr. Marathe said.
Patients with MIS-C “are usually going to have COVID-positive antibodies,” she said. But since almost everybody may have COVID antibodies, “it’s not usually a helpful test for you now. But early on, that’s what we used as helpful indicator.”
Dr. Marathe reported no relevant financial relationships.
ORLANDO – The eruption spread away from the head and her transaminase levels were “dramatic,” in the 700s, said Kalyani S. Marathe, MD, MPH, associate professor of dermatology and pediatrics at the University of Cincinnati.
Dr. Marathe, director of the division of dermatology at Cincinnati Children’s Hospital, reviewed this case in a presentation on pediatric dermatologic emergencies at the ODAC Dermatology, Aesthetic & Surgery Conference, pointing out potential pitfalls and important aspects that might require swift action.
The patient was diagnosed with drug reaction with eosinophilia and systemic symptoms (DRESS).
Facial involvement is common in pediatric cases of DRESS, but edema of the face is less common in children than adults, Dr. Marathe said.
Antiepileptic medications are the most common cause of DRESS, followed by antibiotics – most often, vancomycin and trimethoprim/sulfamethoxazole, she said. But sometimes the trigger is not clear, she noted, recalling a vexing case she once saw in which IV contrast was eventually identified as the cause.
When DRESS is suspected, she said, lab work should be done during the acute eruption and after resolution. This should include CBC, liver function tests, creatinine, and urinalysis, and human herpesvirus 6 (HHV-6) and thyroid testing.
Treatment typically includes supportive care, unless symptoms are systemic, or if there is impending liver failure, when steroids, cyclosporine, or IVIG can be used.
Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN): Mortality rates when these diseases overlap is 4%, Dr. Marathe said. Clues to diagnosing this other medication-induced condition include involvement of the palms and the soles of the feet; presence of the Nikolsky sign in which the top layers of the skin slip away from the lower layers when rubbed; mucosal involvement, which often precedes cutaneous involvement; and these symptoms occurring within the first 8 weeks of taking a medication, which are most commonly antibiotics and anti-epileptics.
Dr. Marathe underscored how important it is to get ophthalmology involved right away, because of the risk of vision loss. Amniotic membrane transfer to the eye at the time of diagnosis has been found to produce dramatically better outcomes, she said. The membrane has anti-inflammatory and antiscarring properties and can promote wound healing on the surface of the eye.
“I would recommend getting your ophthalmology team on board early because they have to advocate for these patients,” she said.
Corticosteroids and IVIG can improve ocular outcomes, but cyclosporine is associated with better mortality outcomes, she said. Emerging data on etanercept has also led to more use of that drug, she said.
Erythema multiforme (EM): unlike urticaria, multiforme EM can have mucosal involvement, Dr. Marathe said. Clinicians should look for three zones of color: A central duskiness, a rim of pallor, and a ring of erythema.
EM is triggered by a virus, which is usually herpes simplex virus (HSV). But she added that HSV is not always found. “So, there are certainly other triggers out there that we just haven’t identified,” she said.
If HSV is suspected, oral acyclovir is effective, she noted.
Other cases might not be as straightforward. Dr. Marathe said that during her fellowship, she saw a patient with EM that was controlled only by IVIG, so it was administered every 3 months. In that case, the trigger was never found.
Multisystem inflammatory syndrome in children (MIS-C): This syndrome can follow COVID-19 infection, and usually presents with 3-5 days of fever after COVID has resolved. It can include gastrointestinal, cardiorespiratory, and neurocognitive symptoms.
The skin presentation is mainly a morbilliform pattern, but clinicians might also see conjunctival involvement, mucosal involvement, and “COVID toes,” painful red or purple lesions on the toes.
Treatment is usually IVIG and systemic corticosteroids, with the treatment course depending on the severity.
MIS-C was initially thought to be Kawasaki’s disease, another autoinflammatory disorder, which is related but distinct, Dr. Marathe said.
Patients with MIS-C “are usually going to have COVID-positive antibodies,” she said. But since almost everybody may have COVID antibodies, “it’s not usually a helpful test for you now. But early on, that’s what we used as helpful indicator.”
Dr. Marathe reported no relevant financial relationships.
ORLANDO – The eruption spread away from the head and her transaminase levels were “dramatic,” in the 700s, said Kalyani S. Marathe, MD, MPH, associate professor of dermatology and pediatrics at the University of Cincinnati.
Dr. Marathe, director of the division of dermatology at Cincinnati Children’s Hospital, reviewed this case in a presentation on pediatric dermatologic emergencies at the ODAC Dermatology, Aesthetic & Surgery Conference, pointing out potential pitfalls and important aspects that might require swift action.
The patient was diagnosed with drug reaction with eosinophilia and systemic symptoms (DRESS).
Facial involvement is common in pediatric cases of DRESS, but edema of the face is less common in children than adults, Dr. Marathe said.
Antiepileptic medications are the most common cause of DRESS, followed by antibiotics – most often, vancomycin and trimethoprim/sulfamethoxazole, she said. But sometimes the trigger is not clear, she noted, recalling a vexing case she once saw in which IV contrast was eventually identified as the cause.
When DRESS is suspected, she said, lab work should be done during the acute eruption and after resolution. This should include CBC, liver function tests, creatinine, and urinalysis, and human herpesvirus 6 (HHV-6) and thyroid testing.
Treatment typically includes supportive care, unless symptoms are systemic, or if there is impending liver failure, when steroids, cyclosporine, or IVIG can be used.
Stevens-Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN): Mortality rates when these diseases overlap is 4%, Dr. Marathe said. Clues to diagnosing this other medication-induced condition include involvement of the palms and the soles of the feet; presence of the Nikolsky sign in which the top layers of the skin slip away from the lower layers when rubbed; mucosal involvement, which often precedes cutaneous involvement; and these symptoms occurring within the first 8 weeks of taking a medication, which are most commonly antibiotics and anti-epileptics.
Dr. Marathe underscored how important it is to get ophthalmology involved right away, because of the risk of vision loss. Amniotic membrane transfer to the eye at the time of diagnosis has been found to produce dramatically better outcomes, she said. The membrane has anti-inflammatory and antiscarring properties and can promote wound healing on the surface of the eye.
“I would recommend getting your ophthalmology team on board early because they have to advocate for these patients,” she said.
Corticosteroids and IVIG can improve ocular outcomes, but cyclosporine is associated with better mortality outcomes, she said. Emerging data on etanercept has also led to more use of that drug, she said.
Erythema multiforme (EM): unlike urticaria, multiforme EM can have mucosal involvement, Dr. Marathe said. Clinicians should look for three zones of color: A central duskiness, a rim of pallor, and a ring of erythema.
EM is triggered by a virus, which is usually herpes simplex virus (HSV). But she added that HSV is not always found. “So, there are certainly other triggers out there that we just haven’t identified,” she said.
If HSV is suspected, oral acyclovir is effective, she noted.
Other cases might not be as straightforward. Dr. Marathe said that during her fellowship, she saw a patient with EM that was controlled only by IVIG, so it was administered every 3 months. In that case, the trigger was never found.
Multisystem inflammatory syndrome in children (MIS-C): This syndrome can follow COVID-19 infection, and usually presents with 3-5 days of fever after COVID has resolved. It can include gastrointestinal, cardiorespiratory, and neurocognitive symptoms.
The skin presentation is mainly a morbilliform pattern, but clinicians might also see conjunctival involvement, mucosal involvement, and “COVID toes,” painful red or purple lesions on the toes.
Treatment is usually IVIG and systemic corticosteroids, with the treatment course depending on the severity.
MIS-C was initially thought to be Kawasaki’s disease, another autoinflammatory disorder, which is related but distinct, Dr. Marathe said.
Patients with MIS-C “are usually going to have COVID-positive antibodies,” she said. But since almost everybody may have COVID antibodies, “it’s not usually a helpful test for you now. But early on, that’s what we used as helpful indicator.”
Dr. Marathe reported no relevant financial relationships.
AT ODAC 2023
Which populations should be screened for cervical cancer?
Montrouge, France – Whether you are a cisgender woman or a transgender man who has kept his uterus, regardless of the sex of your partner, and even if you are a woman who is no longer sexually active, you must take part in cervical cancer screening. This is the reminder issued by Julia Maruani, MD, a medical gynecologist in Marseille, France, at a press conference ahead of the 46th meeting of the French Colposcopy and Cervical-Vaginal Diseases Society (SFCPCV).
Cervical screening currently targets asymptomatic, immunocompetent, and sexually active women between ages 25 and 65 years.
Sex between women
There is a widely held belief that only men can transmit human papillomavirus (HPV). “If you are in a sexual relationship with a man, then yes, you can get HPV from him. But it’s also possible for HPV to be transmitted in a sexual relationship between two women via touch, bodily fluids, or sex toys,” said Dr. Maruani, who pointed out that 20% of lesbians and 30% of bisexual women are HPV carriers.
Because women who have sexual relationships with other women have the mistaken view that their demographic is less affected, they are less likely to take part in cervical screening. They also present more often with advanced lesions and with cancer because of the lack of screening in this group.
Transgender men
Dr. Maruani defines transgender men as “women who have changed gender and who have become men.” Why are they affected by cervical screening? Not all of them are. Those who’ve had their uterus removed no longer have a cervix, so this screening doesn’t affect them. But hysterectomies are rarely performed, as they’re not required in most European countries to legally change gender.
The figures are concerning: 27% of transgender men are screened versus 60% of cisgender females.
“For this demographic, specialist gynecology appointments are hard to come by. Sitting in a women’s waiting room is not easy,” said Dr. Maruani, recalling that often discussion about the transition phase takes up the entire appointment time. It’s also usually the case that any medical problems or health care prevention issues not related to the topic of transitioning are not discussed.
Moreover, the online appointment-booking software doesn’t allow transgender men who have kept their cervix and legally identify as men to make an appointment. “Gynecologists must disable this default option,” said Dr. Maruani.
Likewise, transgender men will not receive an invitation to take part in cervical or breast cancer screening, as they are identified as male by social security services and screening sites. Furthermore, in what Dr. Maruani referred to as an “administrative head-scratcher that needs to change,” some medical procedures are not funded for men.
Yet the risk of contracting HPV is higher among transgender men than in the rest of the population because of different sexual practices in this demographic, as well as the propensity to have multiple sexual partners. The risk of finding abnormalities on cytology screening is greater.
Although data regarding cancer are lacking, “if screening is inadequate but the risk of infection with HPV is great, logic tells us that there will be more lesions, more cancer” in this demographic, said Dr. Maruani.
Celibate women
Nowadays, screening drops with age in women, especially after menopause. This is especially true for women who are no longer sexually active. Another preconceived notion to be addressed is that women who are no longer sexually active no longer need screening. But this concept completely goes against the natural history of HPV infection. “There are years, at least 5, between infection and the development of precancerous lesions. There is a further 5 years between a precancerous lesion and cancer,” said Dr. Maruani.
A woman could still be at risk even 20 years after contracting HPV. Approximately 80% of women are exposed to HPV, and 5%-10% have a persistent infection that could lead to the development of precancerous lesions.
“So, a woman who is no longer sexually active can’t stop participating in cervical screening, especially since there aren’t any symptoms until a fairly advanced stage of cancer.” No longer having sex does not mean that screening can be stopped.
What treatment is appropriate for partners of a woman who is no longer sexually active? None. During the press conference, the specialists agreed that a positive HPV test would be of importance to her partner. Even so, they recalled that the infection would generally be an old one and that the woman’s partner (whether male or female) would therefore have probably already been exposed to it. Patients should also be reminded that, in the past, cytology testing did not look for HPV, so the virus could already have been there. According to these specialists, you don’t need to change your sexual habits, just continue to monitor yourself.
This article was translated from the Medscape French edition and a version first appeared on Medscape.com.
Montrouge, France – Whether you are a cisgender woman or a transgender man who has kept his uterus, regardless of the sex of your partner, and even if you are a woman who is no longer sexually active, you must take part in cervical cancer screening. This is the reminder issued by Julia Maruani, MD, a medical gynecologist in Marseille, France, at a press conference ahead of the 46th meeting of the French Colposcopy and Cervical-Vaginal Diseases Society (SFCPCV).
Cervical screening currently targets asymptomatic, immunocompetent, and sexually active women between ages 25 and 65 years.
Sex between women
There is a widely held belief that only men can transmit human papillomavirus (HPV). “If you are in a sexual relationship with a man, then yes, you can get HPV from him. But it’s also possible for HPV to be transmitted in a sexual relationship between two women via touch, bodily fluids, or sex toys,” said Dr. Maruani, who pointed out that 20% of lesbians and 30% of bisexual women are HPV carriers.
Because women who have sexual relationships with other women have the mistaken view that their demographic is less affected, they are less likely to take part in cervical screening. They also present more often with advanced lesions and with cancer because of the lack of screening in this group.
Transgender men
Dr. Maruani defines transgender men as “women who have changed gender and who have become men.” Why are they affected by cervical screening? Not all of them are. Those who’ve had their uterus removed no longer have a cervix, so this screening doesn’t affect them. But hysterectomies are rarely performed, as they’re not required in most European countries to legally change gender.
The figures are concerning: 27% of transgender men are screened versus 60% of cisgender females.
“For this demographic, specialist gynecology appointments are hard to come by. Sitting in a women’s waiting room is not easy,” said Dr. Maruani, recalling that often discussion about the transition phase takes up the entire appointment time. It’s also usually the case that any medical problems or health care prevention issues not related to the topic of transitioning are not discussed.
Moreover, the online appointment-booking software doesn’t allow transgender men who have kept their cervix and legally identify as men to make an appointment. “Gynecologists must disable this default option,” said Dr. Maruani.
Likewise, transgender men will not receive an invitation to take part in cervical or breast cancer screening, as they are identified as male by social security services and screening sites. Furthermore, in what Dr. Maruani referred to as an “administrative head-scratcher that needs to change,” some medical procedures are not funded for men.
Yet the risk of contracting HPV is higher among transgender men than in the rest of the population because of different sexual practices in this demographic, as well as the propensity to have multiple sexual partners. The risk of finding abnormalities on cytology screening is greater.
Although data regarding cancer are lacking, “if screening is inadequate but the risk of infection with HPV is great, logic tells us that there will be more lesions, more cancer” in this demographic, said Dr. Maruani.
Celibate women
Nowadays, screening drops with age in women, especially after menopause. This is especially true for women who are no longer sexually active. Another preconceived notion to be addressed is that women who are no longer sexually active no longer need screening. But this concept completely goes against the natural history of HPV infection. “There are years, at least 5, between infection and the development of precancerous lesions. There is a further 5 years between a precancerous lesion and cancer,” said Dr. Maruani.
A woman could still be at risk even 20 years after contracting HPV. Approximately 80% of women are exposed to HPV, and 5%-10% have a persistent infection that could lead to the development of precancerous lesions.
“So, a woman who is no longer sexually active can’t stop participating in cervical screening, especially since there aren’t any symptoms until a fairly advanced stage of cancer.” No longer having sex does not mean that screening can be stopped.
What treatment is appropriate for partners of a woman who is no longer sexually active? None. During the press conference, the specialists agreed that a positive HPV test would be of importance to her partner. Even so, they recalled that the infection would generally be an old one and that the woman’s partner (whether male or female) would therefore have probably already been exposed to it. Patients should also be reminded that, in the past, cytology testing did not look for HPV, so the virus could already have been there. According to these specialists, you don’t need to change your sexual habits, just continue to monitor yourself.
This article was translated from the Medscape French edition and a version first appeared on Medscape.com.
Montrouge, France – Whether you are a cisgender woman or a transgender man who has kept his uterus, regardless of the sex of your partner, and even if you are a woman who is no longer sexually active, you must take part in cervical cancer screening. This is the reminder issued by Julia Maruani, MD, a medical gynecologist in Marseille, France, at a press conference ahead of the 46th meeting of the French Colposcopy and Cervical-Vaginal Diseases Society (SFCPCV).
Cervical screening currently targets asymptomatic, immunocompetent, and sexually active women between ages 25 and 65 years.
Sex between women
There is a widely held belief that only men can transmit human papillomavirus (HPV). “If you are in a sexual relationship with a man, then yes, you can get HPV from him. But it’s also possible for HPV to be transmitted in a sexual relationship between two women via touch, bodily fluids, or sex toys,” said Dr. Maruani, who pointed out that 20% of lesbians and 30% of bisexual women are HPV carriers.
Because women who have sexual relationships with other women have the mistaken view that their demographic is less affected, they are less likely to take part in cervical screening. They also present more often with advanced lesions and with cancer because of the lack of screening in this group.
Transgender men
Dr. Maruani defines transgender men as “women who have changed gender and who have become men.” Why are they affected by cervical screening? Not all of them are. Those who’ve had their uterus removed no longer have a cervix, so this screening doesn’t affect them. But hysterectomies are rarely performed, as they’re not required in most European countries to legally change gender.
The figures are concerning: 27% of transgender men are screened versus 60% of cisgender females.
“For this demographic, specialist gynecology appointments are hard to come by. Sitting in a women’s waiting room is not easy,” said Dr. Maruani, recalling that often discussion about the transition phase takes up the entire appointment time. It’s also usually the case that any medical problems or health care prevention issues not related to the topic of transitioning are not discussed.
Moreover, the online appointment-booking software doesn’t allow transgender men who have kept their cervix and legally identify as men to make an appointment. “Gynecologists must disable this default option,” said Dr. Maruani.
Likewise, transgender men will not receive an invitation to take part in cervical or breast cancer screening, as they are identified as male by social security services and screening sites. Furthermore, in what Dr. Maruani referred to as an “administrative head-scratcher that needs to change,” some medical procedures are not funded for men.
Yet the risk of contracting HPV is higher among transgender men than in the rest of the population because of different sexual practices in this demographic, as well as the propensity to have multiple sexual partners. The risk of finding abnormalities on cytology screening is greater.
Although data regarding cancer are lacking, “if screening is inadequate but the risk of infection with HPV is great, logic tells us that there will be more lesions, more cancer” in this demographic, said Dr. Maruani.
Celibate women
Nowadays, screening drops with age in women, especially after menopause. This is especially true for women who are no longer sexually active. Another preconceived notion to be addressed is that women who are no longer sexually active no longer need screening. But this concept completely goes against the natural history of HPV infection. “There are years, at least 5, between infection and the development of precancerous lesions. There is a further 5 years between a precancerous lesion and cancer,” said Dr. Maruani.
A woman could still be at risk even 20 years after contracting HPV. Approximately 80% of women are exposed to HPV, and 5%-10% have a persistent infection that could lead to the development of precancerous lesions.
“So, a woman who is no longer sexually active can’t stop participating in cervical screening, especially since there aren’t any symptoms until a fairly advanced stage of cancer.” No longer having sex does not mean that screening can be stopped.
What treatment is appropriate for partners of a woman who is no longer sexually active? None. During the press conference, the specialists agreed that a positive HPV test would be of importance to her partner. Even so, they recalled that the infection would generally be an old one and that the woman’s partner (whether male or female) would therefore have probably already been exposed to it. Patients should also be reminded that, in the past, cytology testing did not look for HPV, so the virus could already have been there. According to these specialists, you don’t need to change your sexual habits, just continue to monitor yourself.
This article was translated from the Medscape French edition and a version first appeared on Medscape.com.
Dermatologists address cultural competence and unconscious biases in the specialty
ORLANDO – When he was applying for residency, Omar N. Qutub, MD, eagerly arrived at his first interview of the day. But he was quickly thrown off his game.
The interviewer, he said, spent a surprising amount of time asking about his ethnicity and his last name. “I think I spent about 3-5 minutes in the first interview talking about my last name,” said Dr. Qutub, who practices in Portland, Ore., during a session titled “unconscious bias and microaggressions in dermatology” at the ODAC Dermatology, Aesthetic and Surgical Conference. “I really would have rather talked about my research interests.” The interaction threw him off for the rest of the interview process, he said.

The experience is an example of how the field has a ways to go in acquiring cultural competence and in overcoming unconscious biases, said Dr. Qutub. In 2020, a review in Clinics in Dermatology referred to a report that dermatology was the second-least diverse medical specialty, only behind orthopedic surgery, because of its low numbers of residents and faculty from groups underrepresented in medicine.
“We really need to put cultural competency at the forefront in order to do better for our patients,” he said.
Adam Friedman, MD, professor and chair of dermatology and director of the residency program at George Washington University, Washington, who also spoke during the session, said that the process of diversifying the field has to go deeper than the resident interviewing process. “If we just focus on trying to increase the diversity of our applicant pool for residents, it’s too late.”
Nada Elbuluk, MD, associate professor of dermatology at the University of Southern California, Los Angeles, pointed to USC’s Derm RISES initiative, a service program that aims to reach inner-city students through education in the sciences, starting from kindergarten to 12th grade. The program also includes premed undergraduate and medical students, “with the goal of increasing exposure to the sciences, medicine, and dermatology,” according to the USC website. “It’s crucial to begin the process early to get a high yield of students who reach medical school and eventually dermatology, she said, because of the inevitable attrition at each level of the education process.

“It’s incredibly rewarding,” added Dr. Elbuluk, who is also director of the dermatology diversity and inclusion program at USC. “And we get these thank-you letters back from students who [say], ‘I didn’t know I could be a doctor.’ ”
In another presentation, Kavita Mariwalla, MD, who practices in West Islip, N.Y., provided tips on boosting cultural competence during aesthetic consults.
One was to “know your fillers,” she said, noting that fillers have different effects on different skin tones, because of differences in fibroblast content, and fat cells will interact with fillers in different ways across skin tones.
Another is to “understand the shortfall of facial canons,” the idea that you can divide a face into sections that can be viewed and enhanced discretely. This concept was based on a White European model and has to be expanded when considering other ethnicities, Dr. Mariwalla said.
Overgeneralizing categories is another pitfall, she said. “Asian” is a term that covers countries from India to Japan, but within that category are a multitude of notions and nuances about aesthetics, and dermatologists have to be sensitive to all of them.
When meeting with a patient, Dr. Mariwalla said, asking the typical “Where are you from?” is not a helpful question. Instead, she suggested asking: “What is your cultural background? Can you tell me more about what your expectations are?”
“I ask for pictures,” she said. “I want to know what they looked like as a kid. I want to know what their family looks like. And I always hand patients a mirror. Patients will say to me: ‘I want to do what you think.’ It’s not about what I think, because what I see, and what you see in your magnifying mirror, are totally different things.”
After the session ended, a member of the audience, Sharon Stokes, MD, a dermatologist in the Orlando area, provided her view of the presentations, noting that it was an important discussion.
“I think it’s past time in medicine for cultural diversity training and awareness for physicians to understand their patients better and getting to know them – and how to even approach the patient and not to offensively and microaggressively approach the patient,” she said.
Dr. Elbuluk reported relevant relationships with Avita, Incyte, Beiersdorf, and other companies. Dr. Friedman reported financial relationships with Sanova, Pfizer, Novartis and other companies. Dr. Mariwalla reported relevant financial relationships with Abbvie, Sanofi, Regeneron and other companies. Dr. Qutub reported no relevant financial relationships. Dr. Qutub is the ODAC director of equity, diversity, and inclusion.
ORLANDO – When he was applying for residency, Omar N. Qutub, MD, eagerly arrived at his first interview of the day. But he was quickly thrown off his game.
The interviewer, he said, spent a surprising amount of time asking about his ethnicity and his last name. “I think I spent about 3-5 minutes in the first interview talking about my last name,” said Dr. Qutub, who practices in Portland, Ore., during a session titled “unconscious bias and microaggressions in dermatology” at the ODAC Dermatology, Aesthetic and Surgical Conference. “I really would have rather talked about my research interests.” The interaction threw him off for the rest of the interview process, he said.
The experience is an example of how the field has a ways to go in acquiring cultural competence and in overcoming unconscious biases, said Dr. Qutub. In 2020, a review in Clinics in Dermatology referred to a report that dermatology was the second-least diverse medical specialty, only behind orthopedic surgery, because of its low numbers of residents and faculty from groups underrepresented in medicine.
“We really need to put cultural competency at the forefront in order to do better for our patients,” he said.
Adam Friedman, MD, professor and chair of dermatology and director of the residency program at George Washington University, Washington, who also spoke during the session, said that the process of diversifying the field has to go deeper than the resident interviewing process. “If we just focus on trying to increase the diversity of our applicant pool for residents, it’s too late.”
Nada Elbuluk, MD, associate professor of dermatology at the University of Southern California, Los Angeles, pointed to USC’s Derm RISES initiative, a service program that aims to reach inner-city students through education in the sciences, starting from kindergarten to 12th grade. The program also includes premed undergraduate and medical students, “with the goal of increasing exposure to the sciences, medicine, and dermatology,” according to the USC website. “It’s crucial to begin the process early to get a high yield of students who reach medical school and eventually dermatology, she said, because of the inevitable attrition at each level of the education process.
“It’s incredibly rewarding,” added Dr. Elbuluk, who is also director of the dermatology diversity and inclusion program at USC. “And we get these thank-you letters back from students who [say], ‘I didn’t know I could be a doctor.’ ”
In another presentation, Kavita Mariwalla, MD, who practices in West Islip, N.Y., provided tips on boosting cultural competence during aesthetic consults.
One was to “know your fillers,” she said, noting that fillers have different effects on different skin tones, because of differences in fibroblast content, and fat cells will interact with fillers in different ways across skin tones.
Another is to “understand the shortfall of facial canons,” the idea that you can divide a face into sections that can be viewed and enhanced discretely. This concept was based on a White European model and has to be expanded when considering other ethnicities, Dr. Mariwalla said.
Overgeneralizing categories is another pitfall, she said. “Asian” is a term that covers countries from India to Japan, but within that category are a multitude of notions and nuances about aesthetics, and dermatologists have to be sensitive to all of them.
When meeting with a patient, Dr. Mariwalla said, asking the typical “Where are you from?” is not a helpful question. Instead, she suggested asking: “What is your cultural background? Can you tell me more about what your expectations are?”
“I ask for pictures,” she said. “I want to know what they looked like as a kid. I want to know what their family looks like. And I always hand patients a mirror. Patients will say to me: ‘I want to do what you think.’ It’s not about what I think, because what I see, and what you see in your magnifying mirror, are totally different things.”
After the session ended, a member of the audience, Sharon Stokes, MD, a dermatologist in the Orlando area, provided her view of the presentations, noting that it was an important discussion.
“I think it’s past time in medicine for cultural diversity training and awareness for physicians to understand their patients better and getting to know them – and how to even approach the patient and not to offensively and microaggressively approach the patient,” she said.
Dr. Elbuluk reported relevant relationships with Avita, Incyte, Beiersdorf, and other companies. Dr. Friedman reported financial relationships with Sanova, Pfizer, Novartis and other companies. Dr. Mariwalla reported relevant financial relationships with Abbvie, Sanofi, Regeneron and other companies. Dr. Qutub reported no relevant financial relationships. Dr. Qutub is the ODAC director of equity, diversity, and inclusion.
ORLANDO – When he was applying for residency, Omar N. Qutub, MD, eagerly arrived at his first interview of the day. But he was quickly thrown off his game.
The interviewer, he said, spent a surprising amount of time asking about his ethnicity and his last name. “I think I spent about 3-5 minutes in the first interview talking about my last name,” said Dr. Qutub, who practices in Portland, Ore., during a session titled “unconscious bias and microaggressions in dermatology” at the ODAC Dermatology, Aesthetic and Surgical Conference. “I really would have rather talked about my research interests.” The interaction threw him off for the rest of the interview process, he said.
The experience is an example of how the field has a ways to go in acquiring cultural competence and in overcoming unconscious biases, said Dr. Qutub. In 2020, a review in Clinics in Dermatology referred to a report that dermatology was the second-least diverse medical specialty, only behind orthopedic surgery, because of its low numbers of residents and faculty from groups underrepresented in medicine.
“We really need to put cultural competency at the forefront in order to do better for our patients,” he said.
Adam Friedman, MD, professor and chair of dermatology and director of the residency program at George Washington University, Washington, who also spoke during the session, said that the process of diversifying the field has to go deeper than the resident interviewing process. “If we just focus on trying to increase the diversity of our applicant pool for residents, it’s too late.”
Nada Elbuluk, MD, associate professor of dermatology at the University of Southern California, Los Angeles, pointed to USC’s Derm RISES initiative, a service program that aims to reach inner-city students through education in the sciences, starting from kindergarten to 12th grade. The program also includes premed undergraduate and medical students, “with the goal of increasing exposure to the sciences, medicine, and dermatology,” according to the USC website. “It’s crucial to begin the process early to get a high yield of students who reach medical school and eventually dermatology, she said, because of the inevitable attrition at each level of the education process.
“It’s incredibly rewarding,” added Dr. Elbuluk, who is also director of the dermatology diversity and inclusion program at USC. “And we get these thank-you letters back from students who [say], ‘I didn’t know I could be a doctor.’ ”
In another presentation, Kavita Mariwalla, MD, who practices in West Islip, N.Y., provided tips on boosting cultural competence during aesthetic consults.
One was to “know your fillers,” she said, noting that fillers have different effects on different skin tones, because of differences in fibroblast content, and fat cells will interact with fillers in different ways across skin tones.
Another is to “understand the shortfall of facial canons,” the idea that you can divide a face into sections that can be viewed and enhanced discretely. This concept was based on a White European model and has to be expanded when considering other ethnicities, Dr. Mariwalla said.
Overgeneralizing categories is another pitfall, she said. “Asian” is a term that covers countries from India to Japan, but within that category are a multitude of notions and nuances about aesthetics, and dermatologists have to be sensitive to all of them.
When meeting with a patient, Dr. Mariwalla said, asking the typical “Where are you from?” is not a helpful question. Instead, she suggested asking: “What is your cultural background? Can you tell me more about what your expectations are?”
“I ask for pictures,” she said. “I want to know what they looked like as a kid. I want to know what their family looks like. And I always hand patients a mirror. Patients will say to me: ‘I want to do what you think.’ It’s not about what I think, because what I see, and what you see in your magnifying mirror, are totally different things.”
After the session ended, a member of the audience, Sharon Stokes, MD, a dermatologist in the Orlando area, provided her view of the presentations, noting that it was an important discussion.
“I think it’s past time in medicine for cultural diversity training and awareness for physicians to understand their patients better and getting to know them – and how to even approach the patient and not to offensively and microaggressively approach the patient,” she said.
Dr. Elbuluk reported relevant relationships with Avita, Incyte, Beiersdorf, and other companies. Dr. Friedman reported financial relationships with Sanova, Pfizer, Novartis and other companies. Dr. Mariwalla reported relevant financial relationships with Abbvie, Sanofi, Regeneron and other companies. Dr. Qutub reported no relevant financial relationships. Dr. Qutub is the ODAC director of equity, diversity, and inclusion.
AT ODAC 2023
Dermatopathologist reflects on the early history of melanoma
SAN DIEGO – Evidence of melanoma in the ancient past is rare, but according to James W. Patterson, MD, .
“Radiocarbon dating indicated that these mummies were 2,400 years old,” Dr. Patterson, professor emeritus of pathology and dermatology at the University of Virginia, Charlottesville, said at the annual Cutaneous Malignancy Update.
John Hunter, a famous British surgeon who lived from 1728 to 1793, had the first known reported encounter with melanoma in 1787. “He thought it was a form of cancerous fungus,” said Dr. Patterson, a former president of the American Board of Dermatology. “That tumor was preserved in the Hunterian Museum of the Royal College of Surgeons in London, and in 1968 it was reexamined and turned out to be melanoma.”
René Laënnec, the French physician who invented the stethoscope in 1816, is believed to be the first person to lecture on melanoma while a medical student in 1804. The lecture was published about a year later. He originated the term “melanose” (becoming black), a French word derived from the Greek language, to describe metastatic melanoma and reported metastasis to the lungs. During the early part of his career, Dr. Laënnec had studied dissection in the laboratory of the French anatomist and military surgeon Guillaume Dupuytren, best known for his description of Dupuytren’s contracture. Dr. Dupuytren took exception to Dr. Laënnec’s publication about melanoma and called foul.
“As sometimes happens these days, there was some rivalry between these two outstanding physicians of their time,” Dr. Patterson said at the meeting, hosted by Scripps MD Anderson Cancer Center. “Dupuytren was unhappy that Laënnec took credit for this because he claimed credit for originally describing melanoma. He claimed that Laënnec stole the idea from his lectures. I’m not sure that issue was ever resolved.”
In 1820, William Norris, a general practitioner from Stourbridge, England, published the first English language report of melanoma in the Edinburgh Medical and Surgical Journal. “The report was titled ‘A case of fungoid disease,’ so it appears that melanoma was often regarded as a fungal infection back then,” Dr. Patterson said. In the report, Dr. Norris described the tumor in a 59-year-old man as “nearly half the size of a hen’s egg, of a deep brown color, of a firm and fleshy feel, [and] ulcerated on its surface.” Dr. Norris authored a later work titled “Eight cases of melanosis, with pathological and therapeutical remarks on that disease.”
In 1840, a full 2 decades following the first published report from Dr. Norris, the British surgeon Samuel Cooper published a book titled “First Lines of Theory and Practice of Surgery,” in which he described patients with advanced stage melanoma as untreatable and postulated that the only chance for survival was early removal of the tumor.
Dr. Patterson reported having no relevant disclosures.
SAN DIEGO – Evidence of melanoma in the ancient past is rare, but according to James W. Patterson, MD, .
“Radiocarbon dating indicated that these mummies were 2,400 years old,” Dr. Patterson, professor emeritus of pathology and dermatology at the University of Virginia, Charlottesville, said at the annual Cutaneous Malignancy Update.
John Hunter, a famous British surgeon who lived from 1728 to 1793, had the first known reported encounter with melanoma in 1787. “He thought it was a form of cancerous fungus,” said Dr. Patterson, a former president of the American Board of Dermatology. “That tumor was preserved in the Hunterian Museum of the Royal College of Surgeons in London, and in 1968 it was reexamined and turned out to be melanoma.”
René Laënnec, the French physician who invented the stethoscope in 1816, is believed to be the first person to lecture on melanoma while a medical student in 1804. The lecture was published about a year later. He originated the term “melanose” (becoming black), a French word derived from the Greek language, to describe metastatic melanoma and reported metastasis to the lungs. During the early part of his career, Dr. Laënnec had studied dissection in the laboratory of the French anatomist and military surgeon Guillaume Dupuytren, best known for his description of Dupuytren’s contracture. Dr. Dupuytren took exception to Dr. Laënnec’s publication about melanoma and called foul.
“As sometimes happens these days, there was some rivalry between these two outstanding physicians of their time,” Dr. Patterson said at the meeting, hosted by Scripps MD Anderson Cancer Center. “Dupuytren was unhappy that Laënnec took credit for this because he claimed credit for originally describing melanoma. He claimed that Laënnec stole the idea from his lectures. I’m not sure that issue was ever resolved.”
In 1820, William Norris, a general practitioner from Stourbridge, England, published the first English language report of melanoma in the Edinburgh Medical and Surgical Journal. “The report was titled ‘A case of fungoid disease,’ so it appears that melanoma was often regarded as a fungal infection back then,” Dr. Patterson said. In the report, Dr. Norris described the tumor in a 59-year-old man as “nearly half the size of a hen’s egg, of a deep brown color, of a firm and fleshy feel, [and] ulcerated on its surface.” Dr. Norris authored a later work titled “Eight cases of melanosis, with pathological and therapeutical remarks on that disease.”
In 1840, a full 2 decades following the first published report from Dr. Norris, the British surgeon Samuel Cooper published a book titled “First Lines of Theory and Practice of Surgery,” in which he described patients with advanced stage melanoma as untreatable and postulated that the only chance for survival was early removal of the tumor.
Dr. Patterson reported having no relevant disclosures.
SAN DIEGO – Evidence of melanoma in the ancient past is rare, but according to James W. Patterson, MD, .
“Radiocarbon dating indicated that these mummies were 2,400 years old,” Dr. Patterson, professor emeritus of pathology and dermatology at the University of Virginia, Charlottesville, said at the annual Cutaneous Malignancy Update.
John Hunter, a famous British surgeon who lived from 1728 to 1793, had the first known reported encounter with melanoma in 1787. “He thought it was a form of cancerous fungus,” said Dr. Patterson, a former president of the American Board of Dermatology. “That tumor was preserved in the Hunterian Museum of the Royal College of Surgeons in London, and in 1968 it was reexamined and turned out to be melanoma.”
René Laënnec, the French physician who invented the stethoscope in 1816, is believed to be the first person to lecture on melanoma while a medical student in 1804. The lecture was published about a year later. He originated the term “melanose” (becoming black), a French word derived from the Greek language, to describe metastatic melanoma and reported metastasis to the lungs. During the early part of his career, Dr. Laënnec had studied dissection in the laboratory of the French anatomist and military surgeon Guillaume Dupuytren, best known for his description of Dupuytren’s contracture. Dr. Dupuytren took exception to Dr. Laënnec’s publication about melanoma and called foul.
“As sometimes happens these days, there was some rivalry between these two outstanding physicians of their time,” Dr. Patterson said at the meeting, hosted by Scripps MD Anderson Cancer Center. “Dupuytren was unhappy that Laënnec took credit for this because he claimed credit for originally describing melanoma. He claimed that Laënnec stole the idea from his lectures. I’m not sure that issue was ever resolved.”
In 1820, William Norris, a general practitioner from Stourbridge, England, published the first English language report of melanoma in the Edinburgh Medical and Surgical Journal. “The report was titled ‘A case of fungoid disease,’ so it appears that melanoma was often regarded as a fungal infection back then,” Dr. Patterson said. In the report, Dr. Norris described the tumor in a 59-year-old man as “nearly half the size of a hen’s egg, of a deep brown color, of a firm and fleshy feel, [and] ulcerated on its surface.” Dr. Norris authored a later work titled “Eight cases of melanosis, with pathological and therapeutical remarks on that disease.”
In 1840, a full 2 decades following the first published report from Dr. Norris, the British surgeon Samuel Cooper published a book titled “First Lines of Theory and Practice of Surgery,” in which he described patients with advanced stage melanoma as untreatable and postulated that the only chance for survival was early removal of the tumor.
Dr. Patterson reported having no relevant disclosures.
AT MELANOMA 2023
New ‘reference regimen’ in metastatic pancreatic cancer?
(mPDAC) in a global phase 3 trial dubbed NAPOLI-3.
Liposomal irinotecan (Onivyde) plus 5-fluorouracil/leucovorin and oxaliplatin (together known as NALIRIFOX) extended both overall and progression-free survival compared with gemcitabine plus nab-paclitaxel when used as first-line therapy in treatment-naive patients with mPDAC.
“These results support the NALIRIFOX regimen as a new regimen for the first-line treatment of patients with metastatic PDAC,” said lead study author Zev A. Wainberg, MD, professor of medicine at University of California, Los Angeles (UCLA) and codirector of the UCLA GI Oncology Program. “This study indicates that the more aggressive chemotherapy approach should be considered for those patients who are able to tolerate it.”
The findings were presented at the ASCO Gastrointestinal Cancers Symposium 2023.
Liposomal irinotecan administered with 5-fluorouracil/leucovorin has been approved in both the United States and Europe for patients with mPDAC who experience disease progression after treatment with gemcitabine-based therapy. This new trial investigated the approach as a first-line option.
It involved 770 patients who were randomly assigned to one of two treatment arms: NALIRIFOX (liposomal irinotecan 50 mg/m2, 5-fluorouracil 2400 mg/m2, leucovorin 400 mg/m2, and oxaliplatin 60 mg/m2; days 1 and 15 of 28-day cycle) or gemcitabine 1,000 mg/m2 plus nab-paclitaxel 125 mg/m2 (days 1, 8, and 15 of 28-day cycle).
Most patients in both study arms were male (53.3% and 59.4% for liposomal irinotecan/NALIRIFOX recipient vs. the control group, respectively), had at least three metastatic sites (38.9% and 36.4%), had liver metastases (80.2% and 80.4%), and had their main tumor located outside the head of the pancreas (61.6% and 59.7%).
Most patients (65% in both arms) were treated outside of North America and East Asia.
“This is truly a global study, enrolling in over 20 countries, with a mix of both academic and community centers,” said Dr. Wainberg.
At a median follow-up of 16.1 months, 544 events had occurred.
“The study met its primary endpoint of overall survival by improving the median from 9.2 months with gemcitabine plus nab-paclitaxel to 11.1 months with NALIFIROX-treated group,” said Dr. Wainberg. “The hazard ratio was 0.84, with a P value of .04.”
Significant improvement was also observed in progression-free survival: 7.4 months for NALIFIROX vs. 5.6 months for gemcitabine plus nab-paclitaxel (hazard ratio, 0.69; P < .0001).
The overall response rate for liposomal irinotecan/NALIRIFOX vs. nab-paclitaxel/gemcitabine was 41.8% vs. 36.2%, and the complete response rate was 0.3% in both arms.
Dr. Wainberg noted that about half of the patients in both groups underwent subsequent anticancer therapy (50.5% vs. 54.4%); this included systemic treatments, surgery, and radiation therapy.
Grade 3/4 treatment-emergent adverse events reported in ≥ 10% of patients in both groups included diarrhea (20.3% vs. 4.5%), nausea (11.9% vs. 2.6%), hypokalemia (15.1% vs. 4.0%), anemia (10.5% vs. 17.4%), and neutropenia (14.1% vs. 24.5%).
“When one looks at the nuances in the patients and the toxicity profiles, we can see these two regimens have very different toxicity profiles,” Dr. Wainberg said. “There was also less peripheral neuropathy seen in the NALIRIFOX arm relative to the nab-paclitaxel/gemcitabine arm.”
The differences in the toxicity profiles were related to the mechanisms of action, Dr. Wainberg explained. “No new safety concerns with the NALIRIFOX regimen were identified.”
New reference regimen
Dr. Wainberg concluded that the NALIRIFOX regimen can be considered the new reference regimen for first-line treatment of metastatic pancreatic adenocarcinoma. “Hopefully it’s something we can build off of in the future.”
Discussant for this paper, Laura Goff, MD, MSCI, associate professor of medicine and the executive medical director for the Cancer Patient Care Center at Vanderbilt Ingram Cancer Center, Nashville, Tenn., agreed.
For “fit patients, these results support the NALIRIFOX regimen as the new reference regimen for first-line treatment of metastatic pancreatic adenocarcinoma,” she said.
“It is the new standard for fit patients,” she added.
She also agreed with the authors’ conclusion that NALIRIFOX demonstrated clinically meaningful and statistically significant improvements in overall and progression-free survival compared with nab-paclitaxel/gemcitabine.
“The safety profile of NALIRFOX was manageable and consistent with the treatment components,” she said. “Both regimens had high toxicity rates, but their toxicity profiles were different.”
Dr. Goff pointed out that high rates of toxicity were seen in both arms, “despite the reputation that gemcitabine/nab-paclitaxel is a significantly easier regimen to tolerate. I would argue that these data do not necessarily support that.”
The study was funded by Ipsen. Dr. Wainberg reported relationships with Amgen, Arcus Bioscience, AstraZeneca/MedImmune, Bayer, Bristol-Myers Squibb, Daiichi Sankyo/Astra Zeneca, Ipsen, Lilly, Merck, Novartis, Pfizer, Plexxikon, PureTech, QED Therapeutics, Seattle Genetics. Dr. Goff reported relationships with Agios, ASLAN Pharmaceuticals, AstraZeneca, Basilea, BeiGene, Boehringer Ingelheim, Bristol-Myers Squibb, Exelixis, Genentech, Merck, and QED Therapeutics. Most of the other sudy authors had disclosures.
A version of this article first appeared on Medscape.com.
(mPDAC) in a global phase 3 trial dubbed NAPOLI-3.
Liposomal irinotecan (Onivyde) plus 5-fluorouracil/leucovorin and oxaliplatin (together known as NALIRIFOX) extended both overall and progression-free survival compared with gemcitabine plus nab-paclitaxel when used as first-line therapy in treatment-naive patients with mPDAC.
“These results support the NALIRIFOX regimen as a new regimen for the first-line treatment of patients with metastatic PDAC,” said lead study author Zev A. Wainberg, MD, professor of medicine at University of California, Los Angeles (UCLA) and codirector of the UCLA GI Oncology Program. “This study indicates that the more aggressive chemotherapy approach should be considered for those patients who are able to tolerate it.”
The findings were presented at the ASCO Gastrointestinal Cancers Symposium 2023.
Liposomal irinotecan administered with 5-fluorouracil/leucovorin has been approved in both the United States and Europe for patients with mPDAC who experience disease progression after treatment with gemcitabine-based therapy. This new trial investigated the approach as a first-line option.
It involved 770 patients who were randomly assigned to one of two treatment arms: NALIRIFOX (liposomal irinotecan 50 mg/m2, 5-fluorouracil 2400 mg/m2, leucovorin 400 mg/m2, and oxaliplatin 60 mg/m2; days 1 and 15 of 28-day cycle) or gemcitabine 1,000 mg/m2 plus nab-paclitaxel 125 mg/m2 (days 1, 8, and 15 of 28-day cycle).
Most patients in both study arms were male (53.3% and 59.4% for liposomal irinotecan/NALIRIFOX recipient vs. the control group, respectively), had at least three metastatic sites (38.9% and 36.4%), had liver metastases (80.2% and 80.4%), and had their main tumor located outside the head of the pancreas (61.6% and 59.7%).
Most patients (65% in both arms) were treated outside of North America and East Asia.
“This is truly a global study, enrolling in over 20 countries, with a mix of both academic and community centers,” said Dr. Wainberg.
At a median follow-up of 16.1 months, 544 events had occurred.
“The study met its primary endpoint of overall survival by improving the median from 9.2 months with gemcitabine plus nab-paclitaxel to 11.1 months with NALIFIROX-treated group,” said Dr. Wainberg. “The hazard ratio was 0.84, with a P value of .04.”
Significant improvement was also observed in progression-free survival: 7.4 months for NALIFIROX vs. 5.6 months for gemcitabine plus nab-paclitaxel (hazard ratio, 0.69; P < .0001).
The overall response rate for liposomal irinotecan/NALIRIFOX vs. nab-paclitaxel/gemcitabine was 41.8% vs. 36.2%, and the complete response rate was 0.3% in both arms.
Dr. Wainberg noted that about half of the patients in both groups underwent subsequent anticancer therapy (50.5% vs. 54.4%); this included systemic treatments, surgery, and radiation therapy.
Grade 3/4 treatment-emergent adverse events reported in ≥ 10% of patients in both groups included diarrhea (20.3% vs. 4.5%), nausea (11.9% vs. 2.6%), hypokalemia (15.1% vs. 4.0%), anemia (10.5% vs. 17.4%), and neutropenia (14.1% vs. 24.5%).
“When one looks at the nuances in the patients and the toxicity profiles, we can see these two regimens have very different toxicity profiles,” Dr. Wainberg said. “There was also less peripheral neuropathy seen in the NALIRIFOX arm relative to the nab-paclitaxel/gemcitabine arm.”
The differences in the toxicity profiles were related to the mechanisms of action, Dr. Wainberg explained. “No new safety concerns with the NALIRIFOX regimen were identified.”
New reference regimen
Dr. Wainberg concluded that the NALIRIFOX regimen can be considered the new reference regimen for first-line treatment of metastatic pancreatic adenocarcinoma. “Hopefully it’s something we can build off of in the future.”
Discussant for this paper, Laura Goff, MD, MSCI, associate professor of medicine and the executive medical director for the Cancer Patient Care Center at Vanderbilt Ingram Cancer Center, Nashville, Tenn., agreed.
For “fit patients, these results support the NALIRIFOX regimen as the new reference regimen for first-line treatment of metastatic pancreatic adenocarcinoma,” she said.
“It is the new standard for fit patients,” she added.
She also agreed with the authors’ conclusion that NALIRIFOX demonstrated clinically meaningful and statistically significant improvements in overall and progression-free survival compared with nab-paclitaxel/gemcitabine.
“The safety profile of NALIRFOX was manageable and consistent with the treatment components,” she said. “Both regimens had high toxicity rates, but their toxicity profiles were different.”
Dr. Goff pointed out that high rates of toxicity were seen in both arms, “despite the reputation that gemcitabine/nab-paclitaxel is a significantly easier regimen to tolerate. I would argue that these data do not necessarily support that.”
The study was funded by Ipsen. Dr. Wainberg reported relationships with Amgen, Arcus Bioscience, AstraZeneca/MedImmune, Bayer, Bristol-Myers Squibb, Daiichi Sankyo/Astra Zeneca, Ipsen, Lilly, Merck, Novartis, Pfizer, Plexxikon, PureTech, QED Therapeutics, Seattle Genetics. Dr. Goff reported relationships with Agios, ASLAN Pharmaceuticals, AstraZeneca, Basilea, BeiGene, Boehringer Ingelheim, Bristol-Myers Squibb, Exelixis, Genentech, Merck, and QED Therapeutics. Most of the other sudy authors had disclosures.
A version of this article first appeared on Medscape.com.
(mPDAC) in a global phase 3 trial dubbed NAPOLI-3.
Liposomal irinotecan (Onivyde) plus 5-fluorouracil/leucovorin and oxaliplatin (together known as NALIRIFOX) extended both overall and progression-free survival compared with gemcitabine plus nab-paclitaxel when used as first-line therapy in treatment-naive patients with mPDAC.
“These results support the NALIRIFOX regimen as a new regimen for the first-line treatment of patients with metastatic PDAC,” said lead study author Zev A. Wainberg, MD, professor of medicine at University of California, Los Angeles (UCLA) and codirector of the UCLA GI Oncology Program. “This study indicates that the more aggressive chemotherapy approach should be considered for those patients who are able to tolerate it.”
The findings were presented at the ASCO Gastrointestinal Cancers Symposium 2023.
Liposomal irinotecan administered with 5-fluorouracil/leucovorin has been approved in both the United States and Europe for patients with mPDAC who experience disease progression after treatment with gemcitabine-based therapy. This new trial investigated the approach as a first-line option.
It involved 770 patients who were randomly assigned to one of two treatment arms: NALIRIFOX (liposomal irinotecan 50 mg/m2, 5-fluorouracil 2400 mg/m2, leucovorin 400 mg/m2, and oxaliplatin 60 mg/m2; days 1 and 15 of 28-day cycle) or gemcitabine 1,000 mg/m2 plus nab-paclitaxel 125 mg/m2 (days 1, 8, and 15 of 28-day cycle).
Most patients in both study arms were male (53.3% and 59.4% for liposomal irinotecan/NALIRIFOX recipient vs. the control group, respectively), had at least three metastatic sites (38.9% and 36.4%), had liver metastases (80.2% and 80.4%), and had their main tumor located outside the head of the pancreas (61.6% and 59.7%).
Most patients (65% in both arms) were treated outside of North America and East Asia.
“This is truly a global study, enrolling in over 20 countries, with a mix of both academic and community centers,” said Dr. Wainberg.
At a median follow-up of 16.1 months, 544 events had occurred.
“The study met its primary endpoint of overall survival by improving the median from 9.2 months with gemcitabine plus nab-paclitaxel to 11.1 months with NALIFIROX-treated group,” said Dr. Wainberg. “The hazard ratio was 0.84, with a P value of .04.”
Significant improvement was also observed in progression-free survival: 7.4 months for NALIFIROX vs. 5.6 months for gemcitabine plus nab-paclitaxel (hazard ratio, 0.69; P < .0001).
The overall response rate for liposomal irinotecan/NALIRIFOX vs. nab-paclitaxel/gemcitabine was 41.8% vs. 36.2%, and the complete response rate was 0.3% in both arms.
Dr. Wainberg noted that about half of the patients in both groups underwent subsequent anticancer therapy (50.5% vs. 54.4%); this included systemic treatments, surgery, and radiation therapy.
Grade 3/4 treatment-emergent adverse events reported in ≥ 10% of patients in both groups included diarrhea (20.3% vs. 4.5%), nausea (11.9% vs. 2.6%), hypokalemia (15.1% vs. 4.0%), anemia (10.5% vs. 17.4%), and neutropenia (14.1% vs. 24.5%).
“When one looks at the nuances in the patients and the toxicity profiles, we can see these two regimens have very different toxicity profiles,” Dr. Wainberg said. “There was also less peripheral neuropathy seen in the NALIRIFOX arm relative to the nab-paclitaxel/gemcitabine arm.”
The differences in the toxicity profiles were related to the mechanisms of action, Dr. Wainberg explained. “No new safety concerns with the NALIRIFOX regimen were identified.”
New reference regimen
Dr. Wainberg concluded that the NALIRIFOX regimen can be considered the new reference regimen for first-line treatment of metastatic pancreatic adenocarcinoma. “Hopefully it’s something we can build off of in the future.”
Discussant for this paper, Laura Goff, MD, MSCI, associate professor of medicine and the executive medical director for the Cancer Patient Care Center at Vanderbilt Ingram Cancer Center, Nashville, Tenn., agreed.
For “fit patients, these results support the NALIRIFOX regimen as the new reference regimen for first-line treatment of metastatic pancreatic adenocarcinoma,” she said.
“It is the new standard for fit patients,” she added.
She also agreed with the authors’ conclusion that NALIRIFOX demonstrated clinically meaningful and statistically significant improvements in overall and progression-free survival compared with nab-paclitaxel/gemcitabine.
“The safety profile of NALIRFOX was manageable and consistent with the treatment components,” she said. “Both regimens had high toxicity rates, but their toxicity profiles were different.”
Dr. Goff pointed out that high rates of toxicity were seen in both arms, “despite the reputation that gemcitabine/nab-paclitaxel is a significantly easier regimen to tolerate. I would argue that these data do not necessarily support that.”
The study was funded by Ipsen. Dr. Wainberg reported relationships with Amgen, Arcus Bioscience, AstraZeneca/MedImmune, Bayer, Bristol-Myers Squibb, Daiichi Sankyo/Astra Zeneca, Ipsen, Lilly, Merck, Novartis, Pfizer, Plexxikon, PureTech, QED Therapeutics, Seattle Genetics. Dr. Goff reported relationships with Agios, ASLAN Pharmaceuticals, AstraZeneca, Basilea, BeiGene, Boehringer Ingelheim, Bristol-Myers Squibb, Exelixis, Genentech, Merck, and QED Therapeutics. Most of the other sudy authors had disclosures.
A version of this article first appeared on Medscape.com.
AT ASCO GI 2023
SUNLIGHT shows new standard of care in refractory metastatic CRC
SAN FRANCISCO – ,” say the trial investigators. An expert not involved in the study predicted that it will change clinical practice.
The results show that adding bevacizumab to trifluridine (FTD)/tipiracil (TPI) significantly improved survival, compared with those who received FTD/TPI alone. Median overall survival was 10.8 months in the investigational arm vs 7.5 months among controls (hazard ratio, 0.61; P < .001).
Adding bevacizumab also did not increase the risk for serious adverse events or events that led to treatment discontinuation, the researchers noted.
The new data were presented by Josep Tabernero, MD, PhD, head of the department of medical oncology, Vall d’Hebron University Hospital, and director of the Vall d’Hebron Institute of Oncology, Barcelona, at the ASCO Gastrointestinal Cancers Symposium 2023. He concluded that bevacizumab added to FTD/TPI “represents a new standard of care for the treatment of patients with refractory metastatic colorectal cancer who had previously progressed after two lines of therapy.”
Discussant for the abstract, Dustin Deming, MD, an associate professor in the division of hematology, medical oncology and palliative care at the University of Wisconsin–Madison, said the findings showed very “exciting advantages in progression-free and overall survival.” He agreed that “FTD/TPI and bevacizumab should be considered the preferred nontargeted regimen in the refractory setting” and added that “this trial does change standard clinical practice.”
Dr. Deming also said that this has implications for future clinical trials because these results create a new standard for control arms.
Improvement in all endpoints
FTD/TPI, which is marketed as Lonsurf, is already approved as a monotherapy for third-line use in refractory metastatic colorectal cancer, and bevacizumab is an established anticancer agent that targets vascular endothelial growth factor and inhibits angiogenesis, he explained. The combination of bevacizumab plus FTD/TPI has previously produced encouraging results in the treatment of refractory metastatic colorectal cancer in smaller phase 2 randomized and single-arm studies.
“The phase 3 SUNLIGHT study was designed to confirm the efficacy and safety of FTD/TPI plus bevacizumab, as compared with FTD/TPI alone, in patients with refractory metastatic colorectal cancer following two chemotherapy regimens,” said Dr. Tabernero.
The cohort included 492 patients who were randomly assigned to receive either FTD/TPI plus bevacizumab (FTD/TPI 35 mg/m2 twice daily on days 1-5 and 8-12 [28-day cycle] and bevacizumab 5 mg/kg on days 1 and 15) or FTD/TPI alone.
Across both arms, most patients (72%) had already received prior treatment with bevacizumab.
At 6 months, the overall survival rate was 77% with the combination therapy versus 61% with the control therapy, and after 12 months, the overall survival rate was 43% versus 30%.
Median progression-free survival was 5.6 months in the treatment arm versus 2.4 months in the control arm (HR, 0.44; P < .001). At 6 months, progression-free survival was 43% versus 16%, respectively, and at 12 months, it was 16% versus 1%.
Both overall response rate and disease control rate were also superior in the investigational arm. The overall response rate was 6.3% versus 0.0% in the control arm, with an absolute gain of 5.4% (P = .004). Similarly, the absolute gain for disease control rate was 29.6% (76.6% vs. 47.0%; P < .001).
For quality of life, worsening in global health status in the investigational arm was significantly delayed, compared with the control arm (8.5 months vs. 4.7 months; HR, 0.50; P < .001), as was worsening to an Eastern Cooperative Oncology Group performance status of 2 or greater (9.3 months vs. 6.3 months; HR, 0.54; P < .001).
When looking at toxicity, Tabernero reported that there were no treatment-related deaths and the rates of severe adverse events were similar in both groups: 72% in the FTD/TPI plus bevacizumab group versus 70% among controls.
“The safety profile was manageable and consistent with the individual safety profiles of FTD/TPI plus bevacizumab,” said Dr. Tabernero.
Overall, adverse events were comparable in both groups, except for slightly higher rates in the bevacizumab plus FTD/TPI arm for hypertension (10% vs. 2%), nausea (37% vs. 27%), and neutropenia (62% vs. 51%).
The study was sponsored by Taiho Oncology, manufacturer of Lonsurf (trifluridine plus tipiracil). Dr. Tabernero and Dr. Deming both reported relationships with numerous pharmaceutical companies. Several of the study authors also reported conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – ,” say the trial investigators. An expert not involved in the study predicted that it will change clinical practice.
The results show that adding bevacizumab to trifluridine (FTD)/tipiracil (TPI) significantly improved survival, compared with those who received FTD/TPI alone. Median overall survival was 10.8 months in the investigational arm vs 7.5 months among controls (hazard ratio, 0.61; P < .001).
Adding bevacizumab also did not increase the risk for serious adverse events or events that led to treatment discontinuation, the researchers noted.
The new data were presented by Josep Tabernero, MD, PhD, head of the department of medical oncology, Vall d’Hebron University Hospital, and director of the Vall d’Hebron Institute of Oncology, Barcelona, at the ASCO Gastrointestinal Cancers Symposium 2023. He concluded that bevacizumab added to FTD/TPI “represents a new standard of care for the treatment of patients with refractory metastatic colorectal cancer who had previously progressed after two lines of therapy.”
Discussant for the abstract, Dustin Deming, MD, an associate professor in the division of hematology, medical oncology and palliative care at the University of Wisconsin–Madison, said the findings showed very “exciting advantages in progression-free and overall survival.” He agreed that “FTD/TPI and bevacizumab should be considered the preferred nontargeted regimen in the refractory setting” and added that “this trial does change standard clinical practice.”
Dr. Deming also said that this has implications for future clinical trials because these results create a new standard for control arms.
Improvement in all endpoints
FTD/TPI, which is marketed as Lonsurf, is already approved as a monotherapy for third-line use in refractory metastatic colorectal cancer, and bevacizumab is an established anticancer agent that targets vascular endothelial growth factor and inhibits angiogenesis, he explained. The combination of bevacizumab plus FTD/TPI has previously produced encouraging results in the treatment of refractory metastatic colorectal cancer in smaller phase 2 randomized and single-arm studies.
“The phase 3 SUNLIGHT study was designed to confirm the efficacy and safety of FTD/TPI plus bevacizumab, as compared with FTD/TPI alone, in patients with refractory metastatic colorectal cancer following two chemotherapy regimens,” said Dr. Tabernero.
The cohort included 492 patients who were randomly assigned to receive either FTD/TPI plus bevacizumab (FTD/TPI 35 mg/m2 twice daily on days 1-5 and 8-12 [28-day cycle] and bevacizumab 5 mg/kg on days 1 and 15) or FTD/TPI alone.
Across both arms, most patients (72%) had already received prior treatment with bevacizumab.
At 6 months, the overall survival rate was 77% with the combination therapy versus 61% with the control therapy, and after 12 months, the overall survival rate was 43% versus 30%.
Median progression-free survival was 5.6 months in the treatment arm versus 2.4 months in the control arm (HR, 0.44; P < .001). At 6 months, progression-free survival was 43% versus 16%, respectively, and at 12 months, it was 16% versus 1%.
Both overall response rate and disease control rate were also superior in the investigational arm. The overall response rate was 6.3% versus 0.0% in the control arm, with an absolute gain of 5.4% (P = .004). Similarly, the absolute gain for disease control rate was 29.6% (76.6% vs. 47.0%; P < .001).
For quality of life, worsening in global health status in the investigational arm was significantly delayed, compared with the control arm (8.5 months vs. 4.7 months; HR, 0.50; P < .001), as was worsening to an Eastern Cooperative Oncology Group performance status of 2 or greater (9.3 months vs. 6.3 months; HR, 0.54; P < .001).
When looking at toxicity, Tabernero reported that there were no treatment-related deaths and the rates of severe adverse events were similar in both groups: 72% in the FTD/TPI plus bevacizumab group versus 70% among controls.
“The safety profile was manageable and consistent with the individual safety profiles of FTD/TPI plus bevacizumab,” said Dr. Tabernero.
Overall, adverse events were comparable in both groups, except for slightly higher rates in the bevacizumab plus FTD/TPI arm for hypertension (10% vs. 2%), nausea (37% vs. 27%), and neutropenia (62% vs. 51%).
The study was sponsored by Taiho Oncology, manufacturer of Lonsurf (trifluridine plus tipiracil). Dr. Tabernero and Dr. Deming both reported relationships with numerous pharmaceutical companies. Several of the study authors also reported conflicts of interest.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – ,” say the trial investigators. An expert not involved in the study predicted that it will change clinical practice.
The results show that adding bevacizumab to trifluridine (FTD)/tipiracil (TPI) significantly improved survival, compared with those who received FTD/TPI alone. Median overall survival was 10.8 months in the investigational arm vs 7.5 months among controls (hazard ratio, 0.61; P < .001).
Adding bevacizumab also did not increase the risk for serious adverse events or events that led to treatment discontinuation, the researchers noted.
The new data were presented by Josep Tabernero, MD, PhD, head of the department of medical oncology, Vall d’Hebron University Hospital, and director of the Vall d’Hebron Institute of Oncology, Barcelona, at the ASCO Gastrointestinal Cancers Symposium 2023. He concluded that bevacizumab added to FTD/TPI “represents a new standard of care for the treatment of patients with refractory metastatic colorectal cancer who had previously progressed after two lines of therapy.”
Discussant for the abstract, Dustin Deming, MD, an associate professor in the division of hematology, medical oncology and palliative care at the University of Wisconsin–Madison, said the findings showed very “exciting advantages in progression-free and overall survival.” He agreed that “FTD/TPI and bevacizumab should be considered the preferred nontargeted regimen in the refractory setting” and added that “this trial does change standard clinical practice.”
Dr. Deming also said that this has implications for future clinical trials because these results create a new standard for control arms.
Improvement in all endpoints
FTD/TPI, which is marketed as Lonsurf, is already approved as a monotherapy for third-line use in refractory metastatic colorectal cancer, and bevacizumab is an established anticancer agent that targets vascular endothelial growth factor and inhibits angiogenesis, he explained. The combination of bevacizumab plus FTD/TPI has previously produced encouraging results in the treatment of refractory metastatic colorectal cancer in smaller phase 2 randomized and single-arm studies.
“The phase 3 SUNLIGHT study was designed to confirm the efficacy and safety of FTD/TPI plus bevacizumab, as compared with FTD/TPI alone, in patients with refractory metastatic colorectal cancer following two chemotherapy regimens,” said Dr. Tabernero.
The cohort included 492 patients who were randomly assigned to receive either FTD/TPI plus bevacizumab (FTD/TPI 35 mg/m2 twice daily on days 1-5 and 8-12 [28-day cycle] and bevacizumab 5 mg/kg on days 1 and 15) or FTD/TPI alone.
Across both arms, most patients (72%) had already received prior treatment with bevacizumab.
At 6 months, the overall survival rate was 77% with the combination therapy versus 61% with the control therapy, and after 12 months, the overall survival rate was 43% versus 30%.
Median progression-free survival was 5.6 months in the treatment arm versus 2.4 months in the control arm (HR, 0.44; P < .001). At 6 months, progression-free survival was 43% versus 16%, respectively, and at 12 months, it was 16% versus 1%.
Both overall response rate and disease control rate were also superior in the investigational arm. The overall response rate was 6.3% versus 0.0% in the control arm, with an absolute gain of 5.4% (P = .004). Similarly, the absolute gain for disease control rate was 29.6% (76.6% vs. 47.0%; P < .001).
For quality of life, worsening in global health status in the investigational arm was significantly delayed, compared with the control arm (8.5 months vs. 4.7 months; HR, 0.50; P < .001), as was worsening to an Eastern Cooperative Oncology Group performance status of 2 or greater (9.3 months vs. 6.3 months; HR, 0.54; P < .001).
When looking at toxicity, Tabernero reported that there were no treatment-related deaths and the rates of severe adverse events were similar in both groups: 72% in the FTD/TPI plus bevacizumab group versus 70% among controls.
“The safety profile was manageable and consistent with the individual safety profiles of FTD/TPI plus bevacizumab,” said Dr. Tabernero.
Overall, adverse events were comparable in both groups, except for slightly higher rates in the bevacizumab plus FTD/TPI arm for hypertension (10% vs. 2%), nausea (37% vs. 27%), and neutropenia (62% vs. 51%).
The study was sponsored by Taiho Oncology, manufacturer of Lonsurf (trifluridine plus tipiracil). Dr. Tabernero and Dr. Deming both reported relationships with numerous pharmaceutical companies. Several of the study authors also reported conflicts of interest.
A version of this article first appeared on Medscape.com.
AT ASCO GI 2023