User login
MDedge conference coverage features onsite reporting of the latest study results and expert perspectives from leading researchers.
Atogepant prevents episodic migraine in some difficult-to-treat cases
BOSTON – , according to findings from a study presented at the 2023 annual meeting of the American Academy of Neurology.
Initial results from the double-blind ELEVATE trial showed the oral atogepant group had significantly fewer mean monthly migraine days (MMD) compared with a placebo group. There was also a significant difference in the number of participants who achieved 50% or greater reduction in the number of mean MMDs and a significant reduction in acute medication use days compared with the placebo group, according to Patricia Pozo-Rosich, MD, PhD, a headache specialist in the neurology department and director of the headache and craniofacial pain clinical unit and the Migraine Adaptive Brain Center at the Vall d’Hebron University Hospital in Barcelona, and colleagues.

The oral calcitonin gene-related peptide (CGRP) receptor antagonist is currently approved in the United States by the Food and Drug Administration as a preventative for both episodic and chronic migraine.
Results from ELEVATE
Overall, ELEVATE’s initial efficacy analysis population consisted of 309 adults aged between 18 and 80 years from North America and Europe with episodic migraine who had 4-14 MMDs and had treatment failure with at least two classes of conventional oral medication. After a 28-day screening period, participants received either 60 mg of oral atogepant once per day (154 participants) or a placebo (155 participants). In the efficacy analysis population, 56.0% of participants had failed two oral migraine preventative medication classes, while 44.0% failed three or more classes of medication. Dr. Pozo-Rosich noted that participants were taking a number of different oral preventatives across different medication classes, including flunarizine, beta blockers, topiramate, and amitriptyline, but data are not yet available on which participants had received certain combinations of oral medications.
“[T]hese people have already taken some type of prevention, so they’re not naive patients,” she said. “They’re usually more or less well treated in the sense of having had a contact with specialists or a general neurologist, someone that actually tries to do some prevention.”
The researchers examined change from MMDs at baseline and at 12 weeks as a primary outcome, with 50% or greater MMD reduction, change in mean monthly headache days, and change in acute medication use days as secondary outcomes. Regarding the different acute medications used, Dr. Pozo-Rosich said the main three types were analgesics, nonsteroid anti-inflammatory drugs, and triptans, with participants excluded from the trial if they were taking opioids.
The results showed participants in the atogepant group had significantly fewer mean MMDs compared with the placebo group at 12 weeks compared with baseline (–4.20 vs. –1.85 days; P < .0001). Researchers also found statistically significant improvement in the atogepant group for 50% or greater reduction in MMD, change in mean monthly headache days, and change in acute medication use days across 12 weeks of treatment compared with the placebo group. While the specific data analyses for secondary outcomes were not conducted in the initial analysis, Dr. Pozo-Rosich said the numbers “correlate with the primary outcome” as seen in other migraine trials.
Compared with the placebo group, participants in the atogepant group had higher rates of constipation (10.3% vs. 2.5%), COVID-19 (9.6% vs. 8.3%), and nausea (7.1% vs. 3.2%), while the placebo group had a higher rate of nasopharyngitis (5.1% vs. 7.6%).*
Migraine is a prevalent and undertreated disease, and patients around the world with migraine are in need of treatment options that are both safe and effective, Dr. Pozo-Rosich said in an interview. “[E]ven in these hard-to-treat or difficult-to-treat migraine patients, you have a drug that works, and is safe, and well tolerated and effective,” she said.
That’s “kind of good news for all of us,” she said. Patients “need this type of good news and solution,” she explained, because they may not tolerate or have access to injectable medications. Atogepant would also give clinicians have another option to offer patients with difficult-to-treat migraine cases, she noted. “It makes life easier for many physicians and many patients for many different reasons,” she said.
Dr. Pozo-Rosich said the likely next step in the research is to conduct the main analysis as well as post hoc analyses with accumulated data from pathology trials “to understand patterns of response, understand the sustainability of the response, [and] adherence to the treatment in the long term.”
‘Exciting that it works well’ in difficult-to-treat patients
Commenting on the study, Alan M. Rapoport, MD, clinical professor of neurology at University of California, Los Angeles, and past president of the International Headache Society, agreed that better options in migraine treatment and prevention are needed.
“We needed something that was going to be better than what we had before,” he said.
Dr. Rapoport noted the study was well designed with strongly positive results. “It looks like it’s an effective drug, and it looks really good in that it’s effective for people that have failed all these preventives that have very little hope for the future,” he said.
He specifically praised the inclusion of older participants in the population. “You never see a study on 80-year-olds,” he said, “but I like that, because they felt it would be safe. There are 80-year-old patients – fewer of them than 40-year-old patients – but there are 80-year-old patients who still have migraine, so I’m really glad they put older patients in it,” he said.
For atogepant, he noted that “some patients won’t get the side effects, and some patients will tolerate the side effects because it’s working really well.” While the study was not a head-to-head comparison against other oral migraine preventatives, he pointed out the high rate of constipation among participants in the trial setting may be a warning sign of future issues, as seen with other CGRP receptor agonists.
“I can tell you that with erenumab, the monoclonal antibody that was injected in the double-blind studies, they didn’t find any significant increase in constipation,” he explained. However, some clinicians using erenumab in the real world have reported up to 20% of their patients are constipated. “It’s not good that they’re reporting 10% are constipated” in the study, he said.
Overall, “all you can really say is it does work well,” Dr. Rapoport said. “It’s exciting that it works well in such difficult-to-treat patients, and it does come with some side effects.”
Dr. Pozo-Rosich reports serving as a consultant and developing education materials for AbbVie, Eli Lilly, Novartis, Teva Pharmaceuticals, and Pfizer. Dr. Rapoport is the editor-in-chief of Neurology Reviews; he reports being a consultant for AbbVie, the developer of atogepant. The ELEVATE trial is supported by AbbVie.
*Correction, 5/4/23: An earlier version of this article misstated the percentage of COVID-positive patients in the study population.
BOSTON – , according to findings from a study presented at the 2023 annual meeting of the American Academy of Neurology.
Initial results from the double-blind ELEVATE trial showed the oral atogepant group had significantly fewer mean monthly migraine days (MMD) compared with a placebo group. There was also a significant difference in the number of participants who achieved 50% or greater reduction in the number of mean MMDs and a significant reduction in acute medication use days compared with the placebo group, according to Patricia Pozo-Rosich, MD, PhD, a headache specialist in the neurology department and director of the headache and craniofacial pain clinical unit and the Migraine Adaptive Brain Center at the Vall d’Hebron University Hospital in Barcelona, and colleagues.
The oral calcitonin gene-related peptide (CGRP) receptor antagonist is currently approved in the United States by the Food and Drug Administration as a preventative for both episodic and chronic migraine.
Results from ELEVATE
Overall, ELEVATE’s initial efficacy analysis population consisted of 309 adults aged between 18 and 80 years from North America and Europe with episodic migraine who had 4-14 MMDs and had treatment failure with at least two classes of conventional oral medication. After a 28-day screening period, participants received either 60 mg of oral atogepant once per day (154 participants) or a placebo (155 participants). In the efficacy analysis population, 56.0% of participants had failed two oral migraine preventative medication classes, while 44.0% failed three or more classes of medication. Dr. Pozo-Rosich noted that participants were taking a number of different oral preventatives across different medication classes, including flunarizine, beta blockers, topiramate, and amitriptyline, but data are not yet available on which participants had received certain combinations of oral medications.
“[T]hese people have already taken some type of prevention, so they’re not naive patients,” she said. “They’re usually more or less well treated in the sense of having had a contact with specialists or a general neurologist, someone that actually tries to do some prevention.”
The researchers examined change from MMDs at baseline and at 12 weeks as a primary outcome, with 50% or greater MMD reduction, change in mean monthly headache days, and change in acute medication use days as secondary outcomes. Regarding the different acute medications used, Dr. Pozo-Rosich said the main three types were analgesics, nonsteroid anti-inflammatory drugs, and triptans, with participants excluded from the trial if they were taking opioids.
The results showed participants in the atogepant group had significantly fewer mean MMDs compared with the placebo group at 12 weeks compared with baseline (–4.20 vs. –1.85 days; P < .0001). Researchers also found statistically significant improvement in the atogepant group for 50% or greater reduction in MMD, change in mean monthly headache days, and change in acute medication use days across 12 weeks of treatment compared with the placebo group. While the specific data analyses for secondary outcomes were not conducted in the initial analysis, Dr. Pozo-Rosich said the numbers “correlate with the primary outcome” as seen in other migraine trials.
Compared with the placebo group, participants in the atogepant group had higher rates of constipation (10.3% vs. 2.5%), COVID-19 (9.6% vs. 8.3%), and nausea (7.1% vs. 3.2%), while the placebo group had a higher rate of nasopharyngitis (5.1% vs. 7.6%).*
Migraine is a prevalent and undertreated disease, and patients around the world with migraine are in need of treatment options that are both safe and effective, Dr. Pozo-Rosich said in an interview. “[E]ven in these hard-to-treat or difficult-to-treat migraine patients, you have a drug that works, and is safe, and well tolerated and effective,” she said.
That’s “kind of good news for all of us,” she said. Patients “need this type of good news and solution,” she explained, because they may not tolerate or have access to injectable medications. Atogepant would also give clinicians have another option to offer patients with difficult-to-treat migraine cases, she noted. “It makes life easier for many physicians and many patients for many different reasons,” she said.
Dr. Pozo-Rosich said the likely next step in the research is to conduct the main analysis as well as post hoc analyses with accumulated data from pathology trials “to understand patterns of response, understand the sustainability of the response, [and] adherence to the treatment in the long term.”
‘Exciting that it works well’ in difficult-to-treat patients
Commenting on the study, Alan M. Rapoport, MD, clinical professor of neurology at University of California, Los Angeles, and past president of the International Headache Society, agreed that better options in migraine treatment and prevention are needed.
“We needed something that was going to be better than what we had before,” he said.
Dr. Rapoport noted the study was well designed with strongly positive results. “It looks like it’s an effective drug, and it looks really good in that it’s effective for people that have failed all these preventives that have very little hope for the future,” he said.
He specifically praised the inclusion of older participants in the population. “You never see a study on 80-year-olds,” he said, “but I like that, because they felt it would be safe. There are 80-year-old patients – fewer of them than 40-year-old patients – but there are 80-year-old patients who still have migraine, so I’m really glad they put older patients in it,” he said.
For atogepant, he noted that “some patients won’t get the side effects, and some patients will tolerate the side effects because it’s working really well.” While the study was not a head-to-head comparison against other oral migraine preventatives, he pointed out the high rate of constipation among participants in the trial setting may be a warning sign of future issues, as seen with other CGRP receptor agonists.
“I can tell you that with erenumab, the monoclonal antibody that was injected in the double-blind studies, they didn’t find any significant increase in constipation,” he explained. However, some clinicians using erenumab in the real world have reported up to 20% of their patients are constipated. “It’s not good that they’re reporting 10% are constipated” in the study, he said.
Overall, “all you can really say is it does work well,” Dr. Rapoport said. “It’s exciting that it works well in such difficult-to-treat patients, and it does come with some side effects.”
Dr. Pozo-Rosich reports serving as a consultant and developing education materials for AbbVie, Eli Lilly, Novartis, Teva Pharmaceuticals, and Pfizer. Dr. Rapoport is the editor-in-chief of Neurology Reviews; he reports being a consultant for AbbVie, the developer of atogepant. The ELEVATE trial is supported by AbbVie.
*Correction, 5/4/23: An earlier version of this article misstated the percentage of COVID-positive patients in the study population.
BOSTON – , according to findings from a study presented at the 2023 annual meeting of the American Academy of Neurology.
Initial results from the double-blind ELEVATE trial showed the oral atogepant group had significantly fewer mean monthly migraine days (MMD) compared with a placebo group. There was also a significant difference in the number of participants who achieved 50% or greater reduction in the number of mean MMDs and a significant reduction in acute medication use days compared with the placebo group, according to Patricia Pozo-Rosich, MD, PhD, a headache specialist in the neurology department and director of the headache and craniofacial pain clinical unit and the Migraine Adaptive Brain Center at the Vall d’Hebron University Hospital in Barcelona, and colleagues.
The oral calcitonin gene-related peptide (CGRP) receptor antagonist is currently approved in the United States by the Food and Drug Administration as a preventative for both episodic and chronic migraine.
Results from ELEVATE
Overall, ELEVATE’s initial efficacy analysis population consisted of 309 adults aged between 18 and 80 years from North America and Europe with episodic migraine who had 4-14 MMDs and had treatment failure with at least two classes of conventional oral medication. After a 28-day screening period, participants received either 60 mg of oral atogepant once per day (154 participants) or a placebo (155 participants). In the efficacy analysis population, 56.0% of participants had failed two oral migraine preventative medication classes, while 44.0% failed three or more classes of medication. Dr. Pozo-Rosich noted that participants were taking a number of different oral preventatives across different medication classes, including flunarizine, beta blockers, topiramate, and amitriptyline, but data are not yet available on which participants had received certain combinations of oral medications.
“[T]hese people have already taken some type of prevention, so they’re not naive patients,” she said. “They’re usually more or less well treated in the sense of having had a contact with specialists or a general neurologist, someone that actually tries to do some prevention.”
The researchers examined change from MMDs at baseline and at 12 weeks as a primary outcome, with 50% or greater MMD reduction, change in mean monthly headache days, and change in acute medication use days as secondary outcomes. Regarding the different acute medications used, Dr. Pozo-Rosich said the main three types were analgesics, nonsteroid anti-inflammatory drugs, and triptans, with participants excluded from the trial if they were taking opioids.
The results showed participants in the atogepant group had significantly fewer mean MMDs compared with the placebo group at 12 weeks compared with baseline (–4.20 vs. –1.85 days; P < .0001). Researchers also found statistically significant improvement in the atogepant group for 50% or greater reduction in MMD, change in mean monthly headache days, and change in acute medication use days across 12 weeks of treatment compared with the placebo group. While the specific data analyses for secondary outcomes were not conducted in the initial analysis, Dr. Pozo-Rosich said the numbers “correlate with the primary outcome” as seen in other migraine trials.
Compared with the placebo group, participants in the atogepant group had higher rates of constipation (10.3% vs. 2.5%), COVID-19 (9.6% vs. 8.3%), and nausea (7.1% vs. 3.2%), while the placebo group had a higher rate of nasopharyngitis (5.1% vs. 7.6%).*
Migraine is a prevalent and undertreated disease, and patients around the world with migraine are in need of treatment options that are both safe and effective, Dr. Pozo-Rosich said in an interview. “[E]ven in these hard-to-treat or difficult-to-treat migraine patients, you have a drug that works, and is safe, and well tolerated and effective,” she said.
That’s “kind of good news for all of us,” she said. Patients “need this type of good news and solution,” she explained, because they may not tolerate or have access to injectable medications. Atogepant would also give clinicians have another option to offer patients with difficult-to-treat migraine cases, she noted. “It makes life easier for many physicians and many patients for many different reasons,” she said.
Dr. Pozo-Rosich said the likely next step in the research is to conduct the main analysis as well as post hoc analyses with accumulated data from pathology trials “to understand patterns of response, understand the sustainability of the response, [and] adherence to the treatment in the long term.”
‘Exciting that it works well’ in difficult-to-treat patients
Commenting on the study, Alan M. Rapoport, MD, clinical professor of neurology at University of California, Los Angeles, and past president of the International Headache Society, agreed that better options in migraine treatment and prevention are needed.
“We needed something that was going to be better than what we had before,” he said.
Dr. Rapoport noted the study was well designed with strongly positive results. “It looks like it’s an effective drug, and it looks really good in that it’s effective for people that have failed all these preventives that have very little hope for the future,” he said.
He specifically praised the inclusion of older participants in the population. “You never see a study on 80-year-olds,” he said, “but I like that, because they felt it would be safe. There are 80-year-old patients – fewer of them than 40-year-old patients – but there are 80-year-old patients who still have migraine, so I’m really glad they put older patients in it,” he said.
For atogepant, he noted that “some patients won’t get the side effects, and some patients will tolerate the side effects because it’s working really well.” While the study was not a head-to-head comparison against other oral migraine preventatives, he pointed out the high rate of constipation among participants in the trial setting may be a warning sign of future issues, as seen with other CGRP receptor agonists.
“I can tell you that with erenumab, the monoclonal antibody that was injected in the double-blind studies, they didn’t find any significant increase in constipation,” he explained. However, some clinicians using erenumab in the real world have reported up to 20% of their patients are constipated. “It’s not good that they’re reporting 10% are constipated” in the study, he said.
Overall, “all you can really say is it does work well,” Dr. Rapoport said. “It’s exciting that it works well in such difficult-to-treat patients, and it does come with some side effects.”
Dr. Pozo-Rosich reports serving as a consultant and developing education materials for AbbVie, Eli Lilly, Novartis, Teva Pharmaceuticals, and Pfizer. Dr. Rapoport is the editor-in-chief of Neurology Reviews; he reports being a consultant for AbbVie, the developer of atogepant. The ELEVATE trial is supported by AbbVie.
*Correction, 5/4/23: An earlier version of this article misstated the percentage of COVID-positive patients in the study population.
FROM AAN 2023
Meta-analysis examines cancer risk concern for JAK inhibitors
MANCHESTER, ENGLAND – Janus kinase (JAK) inhibitors may be associated with a higher risk for cancer relative to tumor necrosis factor (TNF) inhibitors, according to a meta-analysis reported at the annual meeting of the British Society for Rheumatology.
Looking at all phase 2, 3, and 4 trials and long-term extension studies across the indications of rheumatoid arthritis, psoriatic arthritis, psoriasis, axial spondyloarthritis, inflammatory bowel disease, and atopic dermatitis, the risk ratio for any cancer developing was 1.63 when compared with anti-TNF therapy (95% confidence interval, 1.27-2.09).
By comparison, JAK inhibitor use was not significantly associated with any greater risk for cancer than methotrexate (RR, 1.06; 95% confidence interval, 0.58-1.94) or placebo (RR, 1.16; 95% CI, 0.75-1.80).
“Our data suggests that rather than JAK inhibitors necessarily being harmful, it could be more a case of TNF inhibitors being protective,” said Christopher Stovin, MBChB, a specialist registrar in rheumatology at the Princess Royal University Hospital, King’s College Hospital NHS Trust, London.
“We should stress that these are rare events in our study, roughly around 1 in every 100 patient-years of exposure,” Dr. Stovin said.
“Despite having over 80,000 years of patient exposure, the median follow-up duration for JAK inhibitors was still only 118 weeks, which for cancers [that] obviously have long latency periods is still a relatively small duration of time,” the researcher added.

“People worry about the drugs. But there is a possibility that [a] disturbed immune system plays a role per se in development of cancers,” consultant rheumatologist Anurag Bharadwaj, MD, DM, said in an interview.
“Although there are studies which attribute increased risk of cancer to different DMARDs [disease-modifying antirheumatic drugs] and biologics like TNF, but on other hand, it’s maybe that we are giving these drugs to patients who have got more serious immunological disease,” suggested Bharadwaj, who serves as the clinical lead for rheumatology at Basildon (England) Hospital, Mid & South Essex Foundation Trust.
“So, a possibility may be that the more severe or the more active the immunological inflammatory disease, the higher the chance of cancer, and these are the patients who go for the stronger medications,” Dr. Bharadwaj said.
There is an “immunological window of opportunity” when treating these inflammatory diseases, said Dr. Bharadwaj, noting that the first few months of treatment are vital. “For all immunological diseases, the more quickly you bring the immunological abnormality down, the chances of long-term complications go down, including [possibly that the] chances of cancer go down, chances of cardiovascular disease go down, and chances of lung disease go down. Hit it early, hit it hard.”
Concern over a possible higher risk for cancer with JAK inhibitors than with TNF inhibitors was raised following the release of data from the ORAL Surveillance trial, a postmarketing trial of tofacitinib (Xeljanz) that had been mandated by the Food and Drug Administration.
“This was a study looking at the coprimary endpoints of malignancy and major adverse cardiovascular events, and it was enriched with patients over the age of 50, with one additional cardiac risk factor, designed to amplify the detection of these rare events,” Dr. Stovin said.
“There was a signal of an increased risk of malignancy in the tofacitinib group, and this led to the FDA issuing a [boxed warning for all licensed JAK inhibitors] at that time,” he added.
Dr. Stovin and colleagues aimed to determine what, if any, cancer risk was associated with all available JAK inhibitors relative to placebo, TNF inhibitors, and methotrexate.
In all, data from 62 randomized controlled trials and 14 long-term extension studies were included in the meta-analysis, accounting for 82,366 patient years of follow-up. The JAK inhibitors analyzed included tofacitinib, baricitinib (Olumiant), upadacitinib (Rinvoq), filgotinib (Jyseleca), and peficitinib (Smyraf). (Filgotinib and peficitinib have not been approved by the FDA.)
The researchers performed sensitivity analyses that excluded cancers detected within the first 6 months of treatment, the use of higher than licensed JAK inhibitor doses, and patients with non-rheumatoid arthritis diagnoses, but the results remained largely unchanged, Dr. Stovin reported.
“Perhaps not surprisingly, when we removed ORAL Surveillance” from the analysis comparing JAK inhibitors and TNF inhibitors, “we lost statistical significance,” he said.
“Longitudinal observational data is needed but currently remains limited,” Dr. Stovin concluded.
Dr. Stovin and Dr. Bharadwaj reported no relevant financial relationships. The meta-analysis was independently supported. Dr. Bharadwaj was not involved in the study and provided comment ahead of the presentation.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND – Janus kinase (JAK) inhibitors may be associated with a higher risk for cancer relative to tumor necrosis factor (TNF) inhibitors, according to a meta-analysis reported at the annual meeting of the British Society for Rheumatology.
Looking at all phase 2, 3, and 4 trials and long-term extension studies across the indications of rheumatoid arthritis, psoriatic arthritis, psoriasis, axial spondyloarthritis, inflammatory bowel disease, and atopic dermatitis, the risk ratio for any cancer developing was 1.63 when compared with anti-TNF therapy (95% confidence interval, 1.27-2.09).
By comparison, JAK inhibitor use was not significantly associated with any greater risk for cancer than methotrexate (RR, 1.06; 95% confidence interval, 0.58-1.94) or placebo (RR, 1.16; 95% CI, 0.75-1.80).
“Our data suggests that rather than JAK inhibitors necessarily being harmful, it could be more a case of TNF inhibitors being protective,” said Christopher Stovin, MBChB, a specialist registrar in rheumatology at the Princess Royal University Hospital, King’s College Hospital NHS Trust, London.
“We should stress that these are rare events in our study, roughly around 1 in every 100 patient-years of exposure,” Dr. Stovin said.
“Despite having over 80,000 years of patient exposure, the median follow-up duration for JAK inhibitors was still only 118 weeks, which for cancers [that] obviously have long latency periods is still a relatively small duration of time,” the researcher added.
“People worry about the drugs. But there is a possibility that [a] disturbed immune system plays a role per se in development of cancers,” consultant rheumatologist Anurag Bharadwaj, MD, DM, said in an interview.
“Although there are studies which attribute increased risk of cancer to different DMARDs [disease-modifying antirheumatic drugs] and biologics like TNF, but on other hand, it’s maybe that we are giving these drugs to patients who have got more serious immunological disease,” suggested Bharadwaj, who serves as the clinical lead for rheumatology at Basildon (England) Hospital, Mid & South Essex Foundation Trust.
“So, a possibility may be that the more severe or the more active the immunological inflammatory disease, the higher the chance of cancer, and these are the patients who go for the stronger medications,” Dr. Bharadwaj said.
There is an “immunological window of opportunity” when treating these inflammatory diseases, said Dr. Bharadwaj, noting that the first few months of treatment are vital. “For all immunological diseases, the more quickly you bring the immunological abnormality down, the chances of long-term complications go down, including [possibly that the] chances of cancer go down, chances of cardiovascular disease go down, and chances of lung disease go down. Hit it early, hit it hard.”
Concern over a possible higher risk for cancer with JAK inhibitors than with TNF inhibitors was raised following the release of data from the ORAL Surveillance trial, a postmarketing trial of tofacitinib (Xeljanz) that had been mandated by the Food and Drug Administration.
“This was a study looking at the coprimary endpoints of malignancy and major adverse cardiovascular events, and it was enriched with patients over the age of 50, with one additional cardiac risk factor, designed to amplify the detection of these rare events,” Dr. Stovin said.
“There was a signal of an increased risk of malignancy in the tofacitinib group, and this led to the FDA issuing a [boxed warning for all licensed JAK inhibitors] at that time,” he added.
Dr. Stovin and colleagues aimed to determine what, if any, cancer risk was associated with all available JAK inhibitors relative to placebo, TNF inhibitors, and methotrexate.
In all, data from 62 randomized controlled trials and 14 long-term extension studies were included in the meta-analysis, accounting for 82,366 patient years of follow-up. The JAK inhibitors analyzed included tofacitinib, baricitinib (Olumiant), upadacitinib (Rinvoq), filgotinib (Jyseleca), and peficitinib (Smyraf). (Filgotinib and peficitinib have not been approved by the FDA.)
The researchers performed sensitivity analyses that excluded cancers detected within the first 6 months of treatment, the use of higher than licensed JAK inhibitor doses, and patients with non-rheumatoid arthritis diagnoses, but the results remained largely unchanged, Dr. Stovin reported.
“Perhaps not surprisingly, when we removed ORAL Surveillance” from the analysis comparing JAK inhibitors and TNF inhibitors, “we lost statistical significance,” he said.
“Longitudinal observational data is needed but currently remains limited,” Dr. Stovin concluded.
Dr. Stovin and Dr. Bharadwaj reported no relevant financial relationships. The meta-analysis was independently supported. Dr. Bharadwaj was not involved in the study and provided comment ahead of the presentation.
A version of this article first appeared on Medscape.com.
MANCHESTER, ENGLAND – Janus kinase (JAK) inhibitors may be associated with a higher risk for cancer relative to tumor necrosis factor (TNF) inhibitors, according to a meta-analysis reported at the annual meeting of the British Society for Rheumatology.
Looking at all phase 2, 3, and 4 trials and long-term extension studies across the indications of rheumatoid arthritis, psoriatic arthritis, psoriasis, axial spondyloarthritis, inflammatory bowel disease, and atopic dermatitis, the risk ratio for any cancer developing was 1.63 when compared with anti-TNF therapy (95% confidence interval, 1.27-2.09).
By comparison, JAK inhibitor use was not significantly associated with any greater risk for cancer than methotrexate (RR, 1.06; 95% confidence interval, 0.58-1.94) or placebo (RR, 1.16; 95% CI, 0.75-1.80).
“Our data suggests that rather than JAK inhibitors necessarily being harmful, it could be more a case of TNF inhibitors being protective,” said Christopher Stovin, MBChB, a specialist registrar in rheumatology at the Princess Royal University Hospital, King’s College Hospital NHS Trust, London.
“We should stress that these are rare events in our study, roughly around 1 in every 100 patient-years of exposure,” Dr. Stovin said.
“Despite having over 80,000 years of patient exposure, the median follow-up duration for JAK inhibitors was still only 118 weeks, which for cancers [that] obviously have long latency periods is still a relatively small duration of time,” the researcher added.
“People worry about the drugs. But there is a possibility that [a] disturbed immune system plays a role per se in development of cancers,” consultant rheumatologist Anurag Bharadwaj, MD, DM, said in an interview.
“Although there are studies which attribute increased risk of cancer to different DMARDs [disease-modifying antirheumatic drugs] and biologics like TNF, but on other hand, it’s maybe that we are giving these drugs to patients who have got more serious immunological disease,” suggested Bharadwaj, who serves as the clinical lead for rheumatology at Basildon (England) Hospital, Mid & South Essex Foundation Trust.
“So, a possibility may be that the more severe or the more active the immunological inflammatory disease, the higher the chance of cancer, and these are the patients who go for the stronger medications,” Dr. Bharadwaj said.
There is an “immunological window of opportunity” when treating these inflammatory diseases, said Dr. Bharadwaj, noting that the first few months of treatment are vital. “For all immunological diseases, the more quickly you bring the immunological abnormality down, the chances of long-term complications go down, including [possibly that the] chances of cancer go down, chances of cardiovascular disease go down, and chances of lung disease go down. Hit it early, hit it hard.”
Concern over a possible higher risk for cancer with JAK inhibitors than with TNF inhibitors was raised following the release of data from the ORAL Surveillance trial, a postmarketing trial of tofacitinib (Xeljanz) that had been mandated by the Food and Drug Administration.
“This was a study looking at the coprimary endpoints of malignancy and major adverse cardiovascular events, and it was enriched with patients over the age of 50, with one additional cardiac risk factor, designed to amplify the detection of these rare events,” Dr. Stovin said.
“There was a signal of an increased risk of malignancy in the tofacitinib group, and this led to the FDA issuing a [boxed warning for all licensed JAK inhibitors] at that time,” he added.
Dr. Stovin and colleagues aimed to determine what, if any, cancer risk was associated with all available JAK inhibitors relative to placebo, TNF inhibitors, and methotrexate.
In all, data from 62 randomized controlled trials and 14 long-term extension studies were included in the meta-analysis, accounting for 82,366 patient years of follow-up. The JAK inhibitors analyzed included tofacitinib, baricitinib (Olumiant), upadacitinib (Rinvoq), filgotinib (Jyseleca), and peficitinib (Smyraf). (Filgotinib and peficitinib have not been approved by the FDA.)
The researchers performed sensitivity analyses that excluded cancers detected within the first 6 months of treatment, the use of higher than licensed JAK inhibitor doses, and patients with non-rheumatoid arthritis diagnoses, but the results remained largely unchanged, Dr. Stovin reported.
“Perhaps not surprisingly, when we removed ORAL Surveillance” from the analysis comparing JAK inhibitors and TNF inhibitors, “we lost statistical significance,” he said.
“Longitudinal observational data is needed but currently remains limited,” Dr. Stovin concluded.
Dr. Stovin and Dr. Bharadwaj reported no relevant financial relationships. The meta-analysis was independently supported. Dr. Bharadwaj was not involved in the study and provided comment ahead of the presentation.
A version of this article first appeared on Medscape.com.
AT BSR 2023
Small study finds IPL-radiofrequency combination effective for dry eye disease
PHOENIX – and improved meibum quality in both upper and lower eyelids, results from an ongoing, novel study showed.
Dry eye disease affects a large proportion of people in the United States “and the factors that contribute to that are certainly not going away,” lead study author James G. Chelnis MD, said at the annual conference of the American Society for Laser Medicine and Surgery, where he presented the results during an abstract session. “Prepandemic, we used to have meetings in person; now most are on a computer screen,” a common risk factor for worsening dry eyes, he said. Telltale dry eye symptoms include blurry vision, irritation, and corneal damage – mostly caused by meibomian gland dysfunction – which impacts the quality and quantity of meibum secreted. Common treatments include warm compresses, doxycycline, and artificial tears.

While some studies have shown IPL is helpful in treating dry eye disease caused by meibomian gland dysfunction, little information is available on its use alone or in combination with topical RF to preserve and improve the function of meibomian glands, said Dr. Chelnis, an ophthalmic plastic surgeon in New York City. “The theory here is that the radiofrequency would be able to vibrate the water molecules inside the meibomian glands, which would allow you to turn over the meibum faster, as well as improve the blink reflex response by building supporting collagen,” he said. “Our novel study explores the ability of this combined modality treatment to improve upon meibomian gland health.”
Study design, results
Dr. Chelnis and his colleagues enrolled 11 individuals with a previous diagnosis of dry eye disease and meibomian gland dysfunction with Ocular Surface Disease Index (OSDI) survey scores higher than 23, which indicate at least moderate dry eye symptoms. Inclusion criteria were being 22 years of age or older, signs of meibomian gland dysfunction as detected by biomicroscopy, a modified meibomian gland score over 12 in the lower eyelid of at least one eye, and type I-IV skin.
All patients received four treatments (each 2 weeks apart) of IPL to the lower eyelid, surrounding malar region, and nose, followed by 7 minutes of topical RF treatments at 1 MHz and 4 MHz extending to the inferior, lateral, and superior orbital rim. Evaluation of meibomian gland expression and quality of meibum upon expression was conducted following each treatment session, with a final evaluation 4 weeks after the final treatment session.
Meibum quality was evaluated on a scale of 0-3 representing clear (0), cloudy (1), inspissated (2), and blocked (3) meibum, respectively.
Following treatment, meibomian gland expression and meibum quality improved in all eyelids in all 11 patients. Specifically, in the right eye, the number of upper lid expressible glands increased from an average of 13 to 27.9 and the number of lower lid expressible glands increased from an average of 14.6 to 28.2; and in the left eye, the number of upper lid expressible glands increased from an average of 13.3 to 27.3 and the number of lower lid expressible glands increased from an average of 14.8 to 26.8 (P < .001 for all associations).
The overall percentage improvement in meibomian gland expression in the right eye was 82.7% for the upper lids and 136.6% for the lower lids, and in the left eye, 82.9% for the upper lids, and 112.2% for the lower lids.
When comparing upper against lower lids, meibomian gland expression increased 124.4% and 82.8%, respectively. Meibum quality improved in all four eyelids, although upper eyelids displayed a superior improvement compared with lower eyelids.
“We are finding that combining IPL plus RF produces a more complete and comprehensive improvement in the quality of their meibomian gland health, and as such, their dry eyes,” with “a large decrease in their symptom profile,” he concluded.
More patients to be studied
Dr. Chelnis acknowledged certain limitations of the study, including the small number of patients, but he and his colleagues have added an additional clinical site to expand the sample size. “Larger scale studies are needed to evaluate long-term effectiveness of IPL plus RF as well as a comparison with other treatment options.”
During a question-and-answer session Mathew M. Avram, MD, JD, director of laser, cosmetics, and dermatologic surgery at Massachusetts General Hospital, Boston, who served as one of the abstract session moderators, asked Dr. Chelnis to comment on what the mechanism of action of the IPL-RF combination in improving meibomian gland health.
“It’s not fully understood, but part of it is improved vascularity at the lid margin,” said Dr. Chelnis, who holds a faculty position in the department of ophthalmology at Icahn School of Medicine at Mount Sinai, New York. “Your ocular surface is sort of like your screen door; it catches everything that’s in the environment. An increase in vascularity and immunologic cytokines occurs in response to that. If you’re looking at the eye with a slit lamp, you can see a lot of vascularity that occurs at the lid margin and crowds the meibomian glands. When you decrease that crowding and immunogenic response, you move towards a normally functioning lid margin.”
Dr. Chelnis disclosed that he is a consultant to or an adviser for Lumenis, Horizon Therapeutics, and Soniquence.
PHOENIX – and improved meibum quality in both upper and lower eyelids, results from an ongoing, novel study showed.
Dry eye disease affects a large proportion of people in the United States “and the factors that contribute to that are certainly not going away,” lead study author James G. Chelnis MD, said at the annual conference of the American Society for Laser Medicine and Surgery, where he presented the results during an abstract session. “Prepandemic, we used to have meetings in person; now most are on a computer screen,” a common risk factor for worsening dry eyes, he said. Telltale dry eye symptoms include blurry vision, irritation, and corneal damage – mostly caused by meibomian gland dysfunction – which impacts the quality and quantity of meibum secreted. Common treatments include warm compresses, doxycycline, and artificial tears.
While some studies have shown IPL is helpful in treating dry eye disease caused by meibomian gland dysfunction, little information is available on its use alone or in combination with topical RF to preserve and improve the function of meibomian glands, said Dr. Chelnis, an ophthalmic plastic surgeon in New York City. “The theory here is that the radiofrequency would be able to vibrate the water molecules inside the meibomian glands, which would allow you to turn over the meibum faster, as well as improve the blink reflex response by building supporting collagen,” he said. “Our novel study explores the ability of this combined modality treatment to improve upon meibomian gland health.”
Study design, results
Dr. Chelnis and his colleagues enrolled 11 individuals with a previous diagnosis of dry eye disease and meibomian gland dysfunction with Ocular Surface Disease Index (OSDI) survey scores higher than 23, which indicate at least moderate dry eye symptoms. Inclusion criteria were being 22 years of age or older, signs of meibomian gland dysfunction as detected by biomicroscopy, a modified meibomian gland score over 12 in the lower eyelid of at least one eye, and type I-IV skin.
All patients received four treatments (each 2 weeks apart) of IPL to the lower eyelid, surrounding malar region, and nose, followed by 7 minutes of topical RF treatments at 1 MHz and 4 MHz extending to the inferior, lateral, and superior orbital rim. Evaluation of meibomian gland expression and quality of meibum upon expression was conducted following each treatment session, with a final evaluation 4 weeks after the final treatment session.
Meibum quality was evaluated on a scale of 0-3 representing clear (0), cloudy (1), inspissated (2), and blocked (3) meibum, respectively.
Following treatment, meibomian gland expression and meibum quality improved in all eyelids in all 11 patients. Specifically, in the right eye, the number of upper lid expressible glands increased from an average of 13 to 27.9 and the number of lower lid expressible glands increased from an average of 14.6 to 28.2; and in the left eye, the number of upper lid expressible glands increased from an average of 13.3 to 27.3 and the number of lower lid expressible glands increased from an average of 14.8 to 26.8 (P < .001 for all associations).
The overall percentage improvement in meibomian gland expression in the right eye was 82.7% for the upper lids and 136.6% for the lower lids, and in the left eye, 82.9% for the upper lids, and 112.2% for the lower lids.
When comparing upper against lower lids, meibomian gland expression increased 124.4% and 82.8%, respectively. Meibum quality improved in all four eyelids, although upper eyelids displayed a superior improvement compared with lower eyelids.
“We are finding that combining IPL plus RF produces a more complete and comprehensive improvement in the quality of their meibomian gland health, and as such, their dry eyes,” with “a large decrease in their symptom profile,” he concluded.
More patients to be studied
Dr. Chelnis acknowledged certain limitations of the study, including the small number of patients, but he and his colleagues have added an additional clinical site to expand the sample size. “Larger scale studies are needed to evaluate long-term effectiveness of IPL plus RF as well as a comparison with other treatment options.”
During a question-and-answer session Mathew M. Avram, MD, JD, director of laser, cosmetics, and dermatologic surgery at Massachusetts General Hospital, Boston, who served as one of the abstract session moderators, asked Dr. Chelnis to comment on what the mechanism of action of the IPL-RF combination in improving meibomian gland health.
“It’s not fully understood, but part of it is improved vascularity at the lid margin,” said Dr. Chelnis, who holds a faculty position in the department of ophthalmology at Icahn School of Medicine at Mount Sinai, New York. “Your ocular surface is sort of like your screen door; it catches everything that’s in the environment. An increase in vascularity and immunologic cytokines occurs in response to that. If you’re looking at the eye with a slit lamp, you can see a lot of vascularity that occurs at the lid margin and crowds the meibomian glands. When you decrease that crowding and immunogenic response, you move towards a normally functioning lid margin.”
Dr. Chelnis disclosed that he is a consultant to or an adviser for Lumenis, Horizon Therapeutics, and Soniquence.
PHOENIX – and improved meibum quality in both upper and lower eyelids, results from an ongoing, novel study showed.
Dry eye disease affects a large proportion of people in the United States “and the factors that contribute to that are certainly not going away,” lead study author James G. Chelnis MD, said at the annual conference of the American Society for Laser Medicine and Surgery, where he presented the results during an abstract session. “Prepandemic, we used to have meetings in person; now most are on a computer screen,” a common risk factor for worsening dry eyes, he said. Telltale dry eye symptoms include blurry vision, irritation, and corneal damage – mostly caused by meibomian gland dysfunction – which impacts the quality and quantity of meibum secreted. Common treatments include warm compresses, doxycycline, and artificial tears.
While some studies have shown IPL is helpful in treating dry eye disease caused by meibomian gland dysfunction, little information is available on its use alone or in combination with topical RF to preserve and improve the function of meibomian glands, said Dr. Chelnis, an ophthalmic plastic surgeon in New York City. “The theory here is that the radiofrequency would be able to vibrate the water molecules inside the meibomian glands, which would allow you to turn over the meibum faster, as well as improve the blink reflex response by building supporting collagen,” he said. “Our novel study explores the ability of this combined modality treatment to improve upon meibomian gland health.”
Study design, results
Dr. Chelnis and his colleagues enrolled 11 individuals with a previous diagnosis of dry eye disease and meibomian gland dysfunction with Ocular Surface Disease Index (OSDI) survey scores higher than 23, which indicate at least moderate dry eye symptoms. Inclusion criteria were being 22 years of age or older, signs of meibomian gland dysfunction as detected by biomicroscopy, a modified meibomian gland score over 12 in the lower eyelid of at least one eye, and type I-IV skin.
All patients received four treatments (each 2 weeks apart) of IPL to the lower eyelid, surrounding malar region, and nose, followed by 7 minutes of topical RF treatments at 1 MHz and 4 MHz extending to the inferior, lateral, and superior orbital rim. Evaluation of meibomian gland expression and quality of meibum upon expression was conducted following each treatment session, with a final evaluation 4 weeks after the final treatment session.
Meibum quality was evaluated on a scale of 0-3 representing clear (0), cloudy (1), inspissated (2), and blocked (3) meibum, respectively.
Following treatment, meibomian gland expression and meibum quality improved in all eyelids in all 11 patients. Specifically, in the right eye, the number of upper lid expressible glands increased from an average of 13 to 27.9 and the number of lower lid expressible glands increased from an average of 14.6 to 28.2; and in the left eye, the number of upper lid expressible glands increased from an average of 13.3 to 27.3 and the number of lower lid expressible glands increased from an average of 14.8 to 26.8 (P < .001 for all associations).
The overall percentage improvement in meibomian gland expression in the right eye was 82.7% for the upper lids and 136.6% for the lower lids, and in the left eye, 82.9% for the upper lids, and 112.2% for the lower lids.
When comparing upper against lower lids, meibomian gland expression increased 124.4% and 82.8%, respectively. Meibum quality improved in all four eyelids, although upper eyelids displayed a superior improvement compared with lower eyelids.
“We are finding that combining IPL plus RF produces a more complete and comprehensive improvement in the quality of their meibomian gland health, and as such, their dry eyes,” with “a large decrease in their symptom profile,” he concluded.
More patients to be studied
Dr. Chelnis acknowledged certain limitations of the study, including the small number of patients, but he and his colleagues have added an additional clinical site to expand the sample size. “Larger scale studies are needed to evaluate long-term effectiveness of IPL plus RF as well as a comparison with other treatment options.”
During a question-and-answer session Mathew M. Avram, MD, JD, director of laser, cosmetics, and dermatologic surgery at Massachusetts General Hospital, Boston, who served as one of the abstract session moderators, asked Dr. Chelnis to comment on what the mechanism of action of the IPL-RF combination in improving meibomian gland health.
“It’s not fully understood, but part of it is improved vascularity at the lid margin,” said Dr. Chelnis, who holds a faculty position in the department of ophthalmology at Icahn School of Medicine at Mount Sinai, New York. “Your ocular surface is sort of like your screen door; it catches everything that’s in the environment. An increase in vascularity and immunologic cytokines occurs in response to that. If you’re looking at the eye with a slit lamp, you can see a lot of vascularity that occurs at the lid margin and crowds the meibomian glands. When you decrease that crowding and immunogenic response, you move towards a normally functioning lid margin.”
Dr. Chelnis disclosed that he is a consultant to or an adviser for Lumenis, Horizon Therapeutics, and Soniquence.
AT ASLMS 2023
Hybrid ablation superior for persistent AFib: CEASE-AF
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”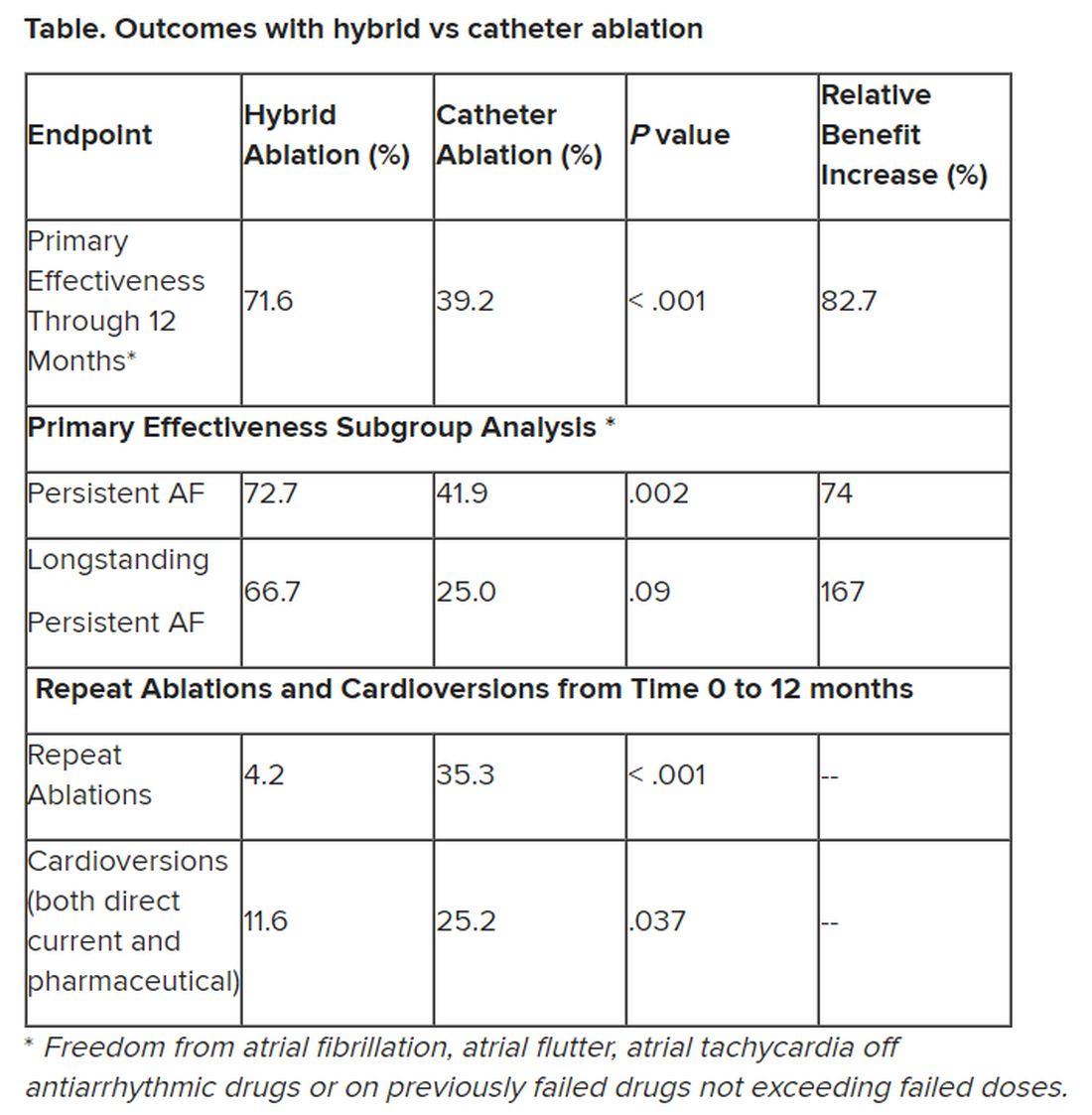
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
BARCELONA – Staged hybrid ablation provided superior freedom from atrial arrhythmias compared with endocardial catheter ablation alone, including the need for repeat ablations in patients with advanced atrial fibrillation (AF), new data show.
“We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase, so this is a huge difference,” concluded cardiac surgeon Nicholas Doll, MD, PhD, Schüchtermann Clinic, Bad Rothenfelde, Germany.
Dr. Doll presented the 12-month follow up results of the Combined Endoscopic Epicardial and Percutaneous Endocardial Ablation Versus Repeated Catheter Ablation in Persistent and Longstanding Persistent Atrial Fibrillation (CEASE-AF) trial at the European Heart Rhythm Association 2023 Congress, held recently in Barcelona and virtually.
He said CEASE-AF is the largest multicenter randomized clinical trial comparing these two approaches for control of atrial arrhythmias.
Safety outcomes were numerically higher in the hybrid ablation (HA) group of the trial but not statistically different from the catheter ablation (CA) group.
Unstable wavefront
As background, Dr. Doll explained that in advanced AF, there is a high degree of endocardial-epicardial dissociation with unstable wavefront propagation transitioning between the endocardial and epicardial surfaces. Endocardial mapping and ablation alone may be insufficient to address the mechanism of AF.
“So, the hypothesis of the CEASE-AF study was a minimally invasive hybrid ablation approach which combines endocardial and epicardial ablation to achieve superior effectiveness when compared to endocardial catheter ablation alone,” he said.
This prospective clinical trial randomized patients 2:1 at nine sites in five countries to HA (n = 102) or CA (n = 52). All had left atrial diameter of 4 cm to 6 cm and persistent AF for up to 1 year or longstanding persistent AF for greater than 1 year up to 10 years.
Any patient with a previous ablation procedure, BMI greater than 35 kg/m2, or left ventricular ejection fraction less than 30% was excluded.
For HA, stage 1 consisted of epicardial lesions for pulmonary vein isolation (PVI) plus the posterior wall box plus left atrial appendage exclusion using the AtriClip (AtriCure Inc.) left atrial appendage exclusion device. Stage 2 involved endocardial mapping and catheter ablation to address gaps.
For CA, the index procedure involved catheter-mediated PVI plus repeat endocardial ablation as clinically indicated. For both HA and CA, additional ablation techniques and lesions were allowed for nonparoxysmal AF.
The HA timeline was the first stage, index procedure at time 0 (n = 102), a 90-day blanking period, and then the second stage, endocardial procedure at 90 to 180 days from the index procedure (n = 93).
For the CA arm of the trial, endocardial catheter ablation was performed on a minimal endocardial lesion set at time 0. Then after a 90-day blanking period, repeat catheter ablation was performed if clinically indicated (6/52).
Repeat ablations and electrical or pharmaceutical cardioversions were allowed during the 12-month follow-up period from time 0.
The primary efficacy endpoint was freedom from AF, atrial flutter, or atrial tachycardia of greater than 30 seconds through 12 months in the absence of class I/III antiarrhythmic drugs except ones that previously had failed, at doses not exceeding those previously failed doses. The safety endpoint was a composite rate of major complications over the course of the study.
Even with relatively modest cohort sizes, the HA and CA arms of the trial were well matched at baseline for age (approximately 60 years), gender (75.5% and 73.1% male, respectively), BMI (29.7 and 29.8 kg/m2), and persistent AF (79.4% and 82.7%).
The groups had persistent AF for 2.94 ± 3.29 years and 3.34 ± 3.52 years, respectively. The mean left atrial size was 4.7 ± 0.5 cm for the HA group and 4.7 ± 0.4 cm for the CA group.
Outcomes favored hybrid ablation over catheter ablation, the researchers reported. “We never would have expected these huge differences,” Dr. Doll told the congress. “We have seen that hybrid ablation resulted in 32.4% absolute benefit increase in effectiveness and 83% relative benefit increase.”
Subgroup analyses were consistent with the primary endpoint, but he said they would not be published because the trial was not powered for such comparisons.
Still, he noted that “there are only slightly reduced outcomes in the long-standing [persistent AF subgroup] in a really challenging patient arm, and we still have a success rate of 67%.” And the repeat ablations in about one-third of patients in the CA arm and need for cardioversions in about one quarter of them may have implications for reduced quality of life.
The total procedure duration was higher for the hybrid group at 336.4 ± 97 minutes, taking into account the index procedure plus the second stage procedure, vs. endocardial ablation at 251.9 ± 114 minutes, which includes the index procedure plus any repeat ablations (HA vs AF total duration, P < .001). Overall fluoroscopy time was approximately 8 minutes shorter for the HA arm.
Complications were assessed for 30 days post index procedure and 30 days post second stage procedure for the HA arm and for 30 days post index procedure and any repeat ablation for the CA arm.
The HA arm showed a complication rate of 7.8% vs. 5.8% for the CA arm (P = .751). Two patients in the former and three patients in the latter group had more than one major complication. There was one death in the HA group 93 days after the index procedure, and it was adjudicated as unrelated to the procedure.
“If you look back in the past, other studies showed a ... higher complication rate in the hybrid arm, so we feel very comfortable with these complication rates, which [are] very low and almost comparable,” Dr. Doll said.
Limitations of the study included symptom-driven electrocardiogram monitoring performed at unscheduled visits. Also, ablation beyond PVI in the CA arm and PVI/posterior box in the HA arm was not standardized and was performed according to standard practices in the participating countries.
“Success of epicardial-endocardial approach emphasizes the role of the collaborative heart team approach in the treatment of nonparoxysmal atrial fibrillation, and if I sum it up together, we can do it better” together, Dr. Doll advised.
‘Exceptional’ trial
After Dr. Doll’s presentation, appointed discussant Stylianos Tzeis, MD, PhD, head of the cardiology clinic and electrophysiology and pacing department at Mitera Hospital in Athens, congratulated the investigators and called CEASE-AF “an exceptional trial. It was really challenging to enroll patients in such a randomized controlled clinical trial.”
But Dr. Tzeis questioned whether pitting CA against HA was a fair comparison.
“Were the ablation targets similar between the two groups?” he asked. He noted that for the HA group, in the first stage the patients had PVI, posterior wall isolation, exclusion of the left atrial appendage, and additional lesions at the discretion of the operator. Ninety percent proceeded to the second stage, which was endocardial catheter ablation with verification of posterior wall isolation and PVI and additional lesions made if needed.
In the CA group, repeat catheter ablation could be performed after the 90-day blanking period if clinically indicated. “Please take note that only 10% were offered the second ablation. So at least in my perspective, this was a comparison of a two-stage approach versus a single-stage approach with a much more aggressive ablation protocol in the hybrid ablation group as compared to the endocardial group,” he said.
Seeing the higher success rate of the HA group in achieving the primary efficacy endpoint of freedom from all arrhythmias at 12 months, Dr. Tzeis asked, “Does this reflect the superiority of the epi-endo approach, or does it reflect the suboptimal performance of the catheter ablation approach?”
There was a 40% success rate in the CA patient population, a cohort that he deemed “not the most challenging persistent AF population in the world”: those with left atrial diameter of 47 millimeters and with 80% having an AF duration less than 12 months.
He also noted that “the average duration of the catheter ablation for the PVI in the vast majority of cases was 4 hours, which does not reflect what really happens in the everyday practice.”
All those critiques having been advanced, Dr. Tzeis said, “Definitely do not doubt my first comment that the authors should be congratulated, and I strongly believe that the main objective has been achieved to bring electrophysiologist and cardiac surgeons ... closer.”
The study sponsor was AtriCure Inc. with collaboration of Cardialysis BV. Doll has received consulting fees or royalties and/or has ownership or stockholder interest in AtriCure. Tzeis reports no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
AT EHRA 2023
Ablation for atrial fibrillation may protect the aging brain
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – , new research suggests.
Investigators found adults who had previously undergone catheter ablation were significantly less likely to be cognitively impaired during the 2-year study period, compared with those who receive medical management alone.
“Catheter ablation is intended to stop atrial fibrillation and restore the normal rhythm of the heart. By doing so, there is an improved cerebral hemodynamic profile,” said Bahadar S. Srichawla, DO, department of neurology, University of Massachusetts, Worcester.
“Thus, long-term cognitive outcomes may be improved due to improved blood flow to the brain by restoring the normal rhythm of the heart,” he added.
This research was presented at the 2023 annual meeting of the American Academy of Neurology.
Heart-brain connection
The study involved 887 older adults (mean age 75; 49% women) with atrial fibrillation participating in the SAGE-AF (Systematic Assessment of Geriatric Elements) study. A total of 193 (22%) participants underwent catheter ablation prior to enrollment. These individuals more frequently had an implantable cardiac device (46% vs. 28%, P < .001) and persistent atrial fibrillation (31% vs. 23%, P < .05).
Cognitive function was assessed using the Montreal Cognitive Assessment (MoCA) tool at baseline and 1 and 2 years, with cognitive impairment defined as a MoCA score of 23 or below. Individuals who had catheter ablation had an average MoCA score of 25, compared with an average score of 23 in those who didn’t have catheter ablation.
After adjusting for potential confounding factors such as heart disease, renal disease, sleep apnea, and atrial fibrillation risk score, those who underwent catheter ablation were 36% less likely to develop cognitive impairment over 2 years than those who were treated only with medication (adjusted odds ratio, 0.64; 95% CI, 0.46-0.88).
During his presentation, Dr. Srichawla noted there is a hypothesis that individuals who are anticoagulated with warfarin may be prone to cerebral microbleeds and may be more cognitively impaired over time.
However, in a subgroup analysis, “cognitive function was similar at 2-year follow-up in those anticoagulated with warfarin, compared with all other anticoagulants. However, it should be noted that in this study, a direct head-to-head comparison was not done,” Dr. Srichawla told attendees.
“In patients with atrial fibrillation, catheter ablation should be discussed as a potential treatment strategy, particularly in patients who have or are at risk for cognitive decline and dementia,” Dr. Srichawla said.
Intriguing findings
Commenting on the research, Percy Griffin, PhD, Alzheimer’s Association director of scientific engagement, said the study is “intriguing and adds to what we know from previous research connecting cardiovascular and cognitive health.”
“However, there are limitations to this study,” Dr. Griffin said, “including its predominantly White cohort and the use of only neuropsychiatric testing to diagnose dementia. More research is needed to fully understand the impact of atrial fibrillation on cognitive outcomes in all people.”
“It’s well known that the heart and the brain are intimately connected. Individuals experiencing any cardiovascular issues should speak to their doctor,” Dr. Griffin added.
Shaheen Lakhan, MD, PhD, a neurologist and researcher in Boston, agreed. “If you ever get up too quickly and feel woozy, that is your brain not getting enough blood flow and you are getting all the warning signs to correct that – or else! Similarly, with atrial fibrillation, the heart is contracting, but not effectively pumping blood to the brain,” he said.
“This line of research shows that correcting the abnormal heart rhythm by zapping the faulty circuit with a catheter is actually better for your brain health than just taking medications alone,” added Dr. Lakhan, who was not involved with the study.
The study had no commercial funding. Dr. Srichawla, Dr. Griffin, and Dr. Lakhan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2023
Psilocybin promising for body dysmorphic disorder
WASHINGTON – Psilocybin is safe and effective in patients with body dysmorphic disorder (BDD), preliminary findings of a small pilot study show.
“The results suggest that psilocybin appears to be relatively safe and potentially helpful for people with BDD, and that it has a broader scope than just depression,” study investigator Franklin Schneier, MD, codirector of the Anxiety Disorders Clinic, New York State Psychiatric Institute, and special lecturer in psychiatry at Columbia University Medical Center in New York City, told this news organization.
So far, psilocybin has mostly been examined in clinical trials among patients with major depression. Dr. Schneier said he is aware of only a single case in the literature of its use in BDD: a patient who self-treated with psilocybin and reported symptom improvement.
The current study was presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Few treatment options
Patients with BDD are preoccupied with a body part they perceive as ugly or defective, “and not just mildly so,” said Dr. Schneier. “It bothers them to the extreme such that they may obsess about it on and off all day long.”
Such patients may engage in compulsive behaviors like constantly checking themselves in the mirror, and going to great lengths to conceal the body part they feel is defective. “They often seek out cosmetic procedures that objectively aren’t warranted,” said Dr. Schneier.
BDD patients often have comorbid depression, and many attempt suicide. As with other anxiety and depressive disorders, BDD is twice as prevalent in women vs. men, said Dr. Schneier.
Selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioral therapy (CBT) are the only approved therapies for BDD.
The investigators thought there may be a good chance BDD patients could benefit from psilocybin. Psilocybin alters bodily self-awareness, which “might shake up people’s beliefs about their abnormal body perceptions,” said Dr. Schneier.
There’s also some suggestion that psilocybin relaxes inflexible thinking, he added. “People with BDD have very rigid beliefs about their body distortions that aren’t easily swayed by logic.”
The study included 12 adults (8 women, 4 men) with a mean age of 34 years and moderate to severe BDD who failed at least one SSRI course and had had BDD for an average of 21 years.
Participants had preliminary sessions with a therapist familiar with psilocybin who prepared them psychologically and discussed what to expect from the experience. On the day of the intervention, subjects took a single 25 mg oral dose of synthetic psilocybin in a comfortable setting.
Therapists were present for the next 8 hours to answer questions and support subjects through the experience.
High response rate
The primary efficacy outcome was change in the BDD Yale-Brown Obsessive Compulsive Disorder Scale Modified (BDD-YBOCS) total score.
The mean baseline BDD-YBOCS score was 29.17. Researchers regularly assessed this score in the following weeks.
At 12 weeks, BDD-YBOCS scores decreased significantly from baseline (P < .001) with a large effect size (partial eta squared = .54).
However, said Dr. Schneier, what really stood out was the proportion of responders. At week 12, seven (58%) of the 12 participants were responders, as defined by a 30% or greater decrease in the BDD-YBOCS score. Of these, three were “almost symptom-free,” he added.
A number of secondary outcomes, including conviction of belief, disability, and negative affect, also significantly improved.
It’s too early to determine if additional treatment is required. The investigators plan to follow-up with the cohort at 1 year.
Although exciting, these early results warrant caution, said Dr. Schneier. “On the one hand, this is a sample of people who have struggled for a long time and have failed previous therapies, so that’s good. But on the other hand, it’s an open trial with no placebo group, and everyone has high expectations, so we don’t know how much of a placebo effect there was.”
Most adverse events, including headaches and fatigue, were mild and resolved within the first week after dosing, and there were no serious adverse events.
Based on these findings, Dr. Schneier said controlled trials of psilocybin in BDD are warranted.
Need for scientific rigor
Commenting on the research, Charles B. Nemeroff, MD, PhD, professor and chair, department of psychiatry and behavioral sciences, University of Texas at Austin, said while promising, psilocybin is “not for everyone” and patients need to be closely screened.

“We want to know their medical history and if they have a family history of schizophrenia or bipolar disorder. We don’t know whether these [psychedelic] medicines might trigger an episode.”
Dr. Nemeroff also noted there’s a risk of “troubling” side effects from the drug.
“My view is psilocybin clearly has therapeutic effects and we need to apply scientific rigor as we would any medicine in order to determine the risk/benefit ratio,” said Dr. Nemeroff, who was not associated with this psilocybin trial.
In addition, psilocybin is being tested in conditions other than BDD and major depression, including anorexia nervosa, postpartum depression, and alcohol use disorder, he added.
The study received funding from COMPASS Pathways PLC.
Dr. Nemeroff reports he has received research support from the NIH and Stanley Medical Research Institute; served as a consultant for Bracket (Clintara), Fortress Biotech, Intra-Cellular Therapies, Janssen Research and Development, Magstim, Navitor Pharmaceuticals, Sunovion Pharmaceuticals, Taisho Pharmaceuticals, Takeda, TC MSO, and Xhale; served on scientific advisory boards for the American Foundation for Suicide Prevention, the Anxiety and Depression Association of America, Bracket (Clintara), Brain and Behavior Research Foundation, Laureate Institute for Brain Research, Skyland Trail, and Xhale; is a stockholder in AbbVie, Antares, BI Gen Holdings, Celgene, OPKO Health, Seattle Genetics, and Xhale; serves on the board of directors for the American Foundation for Suicide Prevention, Anxiety and Depression Association of America, and Gratitude America; has received income or equity of $10,000 or more from American Psychiatric Publishing, Bracket (Clintara), Magstim, CME Outfitters, and Intra-Cellular Therapies; and holds patents on a method and devices for transdermal delivery of lithium and a method of assessing antidepressant drug therapy via transport inhibition of monoamine neurotransmitters by ex vivo assay.
A version of this article first appeared on Medscape.com.
WASHINGTON – Psilocybin is safe and effective in patients with body dysmorphic disorder (BDD), preliminary findings of a small pilot study show.
“The results suggest that psilocybin appears to be relatively safe and potentially helpful for people with BDD, and that it has a broader scope than just depression,” study investigator Franklin Schneier, MD, codirector of the Anxiety Disorders Clinic, New York State Psychiatric Institute, and special lecturer in psychiatry at Columbia University Medical Center in New York City, told this news organization.
So far, psilocybin has mostly been examined in clinical trials among patients with major depression. Dr. Schneier said he is aware of only a single case in the literature of its use in BDD: a patient who self-treated with psilocybin and reported symptom improvement.
The current study was presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Few treatment options
Patients with BDD are preoccupied with a body part they perceive as ugly or defective, “and not just mildly so,” said Dr. Schneier. “It bothers them to the extreme such that they may obsess about it on and off all day long.”
Such patients may engage in compulsive behaviors like constantly checking themselves in the mirror, and going to great lengths to conceal the body part they feel is defective. “They often seek out cosmetic procedures that objectively aren’t warranted,” said Dr. Schneier.
BDD patients often have comorbid depression, and many attempt suicide. As with other anxiety and depressive disorders, BDD is twice as prevalent in women vs. men, said Dr. Schneier.
Selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioral therapy (CBT) are the only approved therapies for BDD.
The investigators thought there may be a good chance BDD patients could benefit from psilocybin. Psilocybin alters bodily self-awareness, which “might shake up people’s beliefs about their abnormal body perceptions,” said Dr. Schneier.
There’s also some suggestion that psilocybin relaxes inflexible thinking, he added. “People with BDD have very rigid beliefs about their body distortions that aren’t easily swayed by logic.”
The study included 12 adults (8 women, 4 men) with a mean age of 34 years and moderate to severe BDD who failed at least one SSRI course and had had BDD for an average of 21 years.
Participants had preliminary sessions with a therapist familiar with psilocybin who prepared them psychologically and discussed what to expect from the experience. On the day of the intervention, subjects took a single 25 mg oral dose of synthetic psilocybin in a comfortable setting.
Therapists were present for the next 8 hours to answer questions and support subjects through the experience.
High response rate
The primary efficacy outcome was change in the BDD Yale-Brown Obsessive Compulsive Disorder Scale Modified (BDD-YBOCS) total score.
The mean baseline BDD-YBOCS score was 29.17. Researchers regularly assessed this score in the following weeks.
At 12 weeks, BDD-YBOCS scores decreased significantly from baseline (P < .001) with a large effect size (partial eta squared = .54).
However, said Dr. Schneier, what really stood out was the proportion of responders. At week 12, seven (58%) of the 12 participants were responders, as defined by a 30% or greater decrease in the BDD-YBOCS score. Of these, three were “almost symptom-free,” he added.
A number of secondary outcomes, including conviction of belief, disability, and negative affect, also significantly improved.
It’s too early to determine if additional treatment is required. The investigators plan to follow-up with the cohort at 1 year.
Although exciting, these early results warrant caution, said Dr. Schneier. “On the one hand, this is a sample of people who have struggled for a long time and have failed previous therapies, so that’s good. But on the other hand, it’s an open trial with no placebo group, and everyone has high expectations, so we don’t know how much of a placebo effect there was.”
Most adverse events, including headaches and fatigue, were mild and resolved within the first week after dosing, and there were no serious adverse events.
Based on these findings, Dr. Schneier said controlled trials of psilocybin in BDD are warranted.
Need for scientific rigor
Commenting on the research, Charles B. Nemeroff, MD, PhD, professor and chair, department of psychiatry and behavioral sciences, University of Texas at Austin, said while promising, psilocybin is “not for everyone” and patients need to be closely screened.
“We want to know their medical history and if they have a family history of schizophrenia or bipolar disorder. We don’t know whether these [psychedelic] medicines might trigger an episode.”
Dr. Nemeroff also noted there’s a risk of “troubling” side effects from the drug.
“My view is psilocybin clearly has therapeutic effects and we need to apply scientific rigor as we would any medicine in order to determine the risk/benefit ratio,” said Dr. Nemeroff, who was not associated with this psilocybin trial.
In addition, psilocybin is being tested in conditions other than BDD and major depression, including anorexia nervosa, postpartum depression, and alcohol use disorder, he added.
The study received funding from COMPASS Pathways PLC.
Dr. Nemeroff reports he has received research support from the NIH and Stanley Medical Research Institute; served as a consultant for Bracket (Clintara), Fortress Biotech, Intra-Cellular Therapies, Janssen Research and Development, Magstim, Navitor Pharmaceuticals, Sunovion Pharmaceuticals, Taisho Pharmaceuticals, Takeda, TC MSO, and Xhale; served on scientific advisory boards for the American Foundation for Suicide Prevention, the Anxiety and Depression Association of America, Bracket (Clintara), Brain and Behavior Research Foundation, Laureate Institute for Brain Research, Skyland Trail, and Xhale; is a stockholder in AbbVie, Antares, BI Gen Holdings, Celgene, OPKO Health, Seattle Genetics, and Xhale; serves on the board of directors for the American Foundation for Suicide Prevention, Anxiety and Depression Association of America, and Gratitude America; has received income or equity of $10,000 or more from American Psychiatric Publishing, Bracket (Clintara), Magstim, CME Outfitters, and Intra-Cellular Therapies; and holds patents on a method and devices for transdermal delivery of lithium and a method of assessing antidepressant drug therapy via transport inhibition of monoamine neurotransmitters by ex vivo assay.
A version of this article first appeared on Medscape.com.
WASHINGTON – Psilocybin is safe and effective in patients with body dysmorphic disorder (BDD), preliminary findings of a small pilot study show.
“The results suggest that psilocybin appears to be relatively safe and potentially helpful for people with BDD, and that it has a broader scope than just depression,” study investigator Franklin Schneier, MD, codirector of the Anxiety Disorders Clinic, New York State Psychiatric Institute, and special lecturer in psychiatry at Columbia University Medical Center in New York City, told this news organization.
So far, psilocybin has mostly been examined in clinical trials among patients with major depression. Dr. Schneier said he is aware of only a single case in the literature of its use in BDD: a patient who self-treated with psilocybin and reported symptom improvement.
The current study was presented as part of the Anxiety and Depression Association of America Anxiety & Depression conference.
Few treatment options
Patients with BDD are preoccupied with a body part they perceive as ugly or defective, “and not just mildly so,” said Dr. Schneier. “It bothers them to the extreme such that they may obsess about it on and off all day long.”
Such patients may engage in compulsive behaviors like constantly checking themselves in the mirror, and going to great lengths to conceal the body part they feel is defective. “They often seek out cosmetic procedures that objectively aren’t warranted,” said Dr. Schneier.
BDD patients often have comorbid depression, and many attempt suicide. As with other anxiety and depressive disorders, BDD is twice as prevalent in women vs. men, said Dr. Schneier.
Selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioral therapy (CBT) are the only approved therapies for BDD.
The investigators thought there may be a good chance BDD patients could benefit from psilocybin. Psilocybin alters bodily self-awareness, which “might shake up people’s beliefs about their abnormal body perceptions,” said Dr. Schneier.
There’s also some suggestion that psilocybin relaxes inflexible thinking, he added. “People with BDD have very rigid beliefs about their body distortions that aren’t easily swayed by logic.”
The study included 12 adults (8 women, 4 men) with a mean age of 34 years and moderate to severe BDD who failed at least one SSRI course and had had BDD for an average of 21 years.
Participants had preliminary sessions with a therapist familiar with psilocybin who prepared them psychologically and discussed what to expect from the experience. On the day of the intervention, subjects took a single 25 mg oral dose of synthetic psilocybin in a comfortable setting.
Therapists were present for the next 8 hours to answer questions and support subjects through the experience.
High response rate
The primary efficacy outcome was change in the BDD Yale-Brown Obsessive Compulsive Disorder Scale Modified (BDD-YBOCS) total score.
The mean baseline BDD-YBOCS score was 29.17. Researchers regularly assessed this score in the following weeks.
At 12 weeks, BDD-YBOCS scores decreased significantly from baseline (P < .001) with a large effect size (partial eta squared = .54).
However, said Dr. Schneier, what really stood out was the proportion of responders. At week 12, seven (58%) of the 12 participants were responders, as defined by a 30% or greater decrease in the BDD-YBOCS score. Of these, three were “almost symptom-free,” he added.
A number of secondary outcomes, including conviction of belief, disability, and negative affect, also significantly improved.
It’s too early to determine if additional treatment is required. The investigators plan to follow-up with the cohort at 1 year.
Although exciting, these early results warrant caution, said Dr. Schneier. “On the one hand, this is a sample of people who have struggled for a long time and have failed previous therapies, so that’s good. But on the other hand, it’s an open trial with no placebo group, and everyone has high expectations, so we don’t know how much of a placebo effect there was.”
Most adverse events, including headaches and fatigue, were mild and resolved within the first week after dosing, and there were no serious adverse events.
Based on these findings, Dr. Schneier said controlled trials of psilocybin in BDD are warranted.
Need for scientific rigor
Commenting on the research, Charles B. Nemeroff, MD, PhD, professor and chair, department of psychiatry and behavioral sciences, University of Texas at Austin, said while promising, psilocybin is “not for everyone” and patients need to be closely screened.
“We want to know their medical history and if they have a family history of schizophrenia or bipolar disorder. We don’t know whether these [psychedelic] medicines might trigger an episode.”
Dr. Nemeroff also noted there’s a risk of “troubling” side effects from the drug.
“My view is psilocybin clearly has therapeutic effects and we need to apply scientific rigor as we would any medicine in order to determine the risk/benefit ratio,” said Dr. Nemeroff, who was not associated with this psilocybin trial.
In addition, psilocybin is being tested in conditions other than BDD and major depression, including anorexia nervosa, postpartum depression, and alcohol use disorder, he added.
The study received funding from COMPASS Pathways PLC.
Dr. Nemeroff reports he has received research support from the NIH and Stanley Medical Research Institute; served as a consultant for Bracket (Clintara), Fortress Biotech, Intra-Cellular Therapies, Janssen Research and Development, Magstim, Navitor Pharmaceuticals, Sunovion Pharmaceuticals, Taisho Pharmaceuticals, Takeda, TC MSO, and Xhale; served on scientific advisory boards for the American Foundation for Suicide Prevention, the Anxiety and Depression Association of America, Bracket (Clintara), Brain and Behavior Research Foundation, Laureate Institute for Brain Research, Skyland Trail, and Xhale; is a stockholder in AbbVie, Antares, BI Gen Holdings, Celgene, OPKO Health, Seattle Genetics, and Xhale; serves on the board of directors for the American Foundation for Suicide Prevention, Anxiety and Depression Association of America, and Gratitude America; has received income or equity of $10,000 or more from American Psychiatric Publishing, Bracket (Clintara), Magstim, CME Outfitters, and Intra-Cellular Therapies; and holds patents on a method and devices for transdermal delivery of lithium and a method of assessing antidepressant drug therapy via transport inhibition of monoamine neurotransmitters by ex vivo assay.
A version of this article first appeared on Medscape.com.
AT ADAA 2023
Phase 3 study of new levodopa/carbidopa delivery system meets all efficacy endpoints
BOSTON – presented at the 2023 annual meeting of the American Academy of Neurology.
When compared with optimized oral immediate-release medication, the delivery system, called ND0612 (NeuroDerm, Rehovot, Israel), improved ON time without troublesome dyskinesias while improving symptoms according to ratings from both patients and clinicians, according to Alberto J. Espay, MD, professor of neurology and director of the Gardner Family Center for Parkinson’s Disease and Movement Disorders, University of Cincinnati.

The new delivery system addresses the challenge of reducing the variability in levodopa plasma concentrations, a major factor in motor fluctuations and diminishing benefit from orally administered drug, according to Dr. Espay. He said that continuous infusion strategies have long been sought as a method to preserve levodopa efficacy.
BouNDless findings
There were two phases to this multinational trial, called BouNDless. In the first, an open-label run-in phase, 381 patients with Parkinson’s disease were dose titrated for optimization of oral immediate-release levodopa and carbidopa. They were then optimized for the same drugs delivered with ND0612. The study was conducted over 12 weeks; 122 patients left the study after this phase due to adverse events, lack of efficacy, or withdrawal of consent.
In the second phase, the 259 remaining patients were randomized to the continuous infusion arm or to immediate release oral therapy. In this double-blind, double-dummy phase, those randomized to the ND0612 infusion also received oral placebos. Those randomized to oral therapy received a placebo infusion. Efficacy and safety were assessed at the end of 12 weeks.
At the end of phase 1, the ON time increased by about 3 hours when levodopa-carbidopa dosing was optimized on either delivery method. Dr. Espay attributed the improvement to the value of optimized dosing even in patients with relatively advanced disease.
However, for the purposes of the double-blind comparison, this improvement in ON time provided a new baseline for comparison of the two delivery methods. This is important for interpreting the primary result, which was a 1.72-hour difference in ON time at the end of the study. The difference was created when ON time was maintained with ND0612 continuous drug delivery but eroded in the group randomized to oral immediate-release treatment.
Several secondary endpoints supported the greater efficacy of continuous subcutaneous delivery. These included lower OFF time (0.50 vs. 1.90 hours), less accumulation of disability on the United Parkinson’s Disease Rating Scale part II-M-EDL (-0.30 vs. +2.75 points), and greater improvement on the Patient Global Impression of Change (+0.31 vs. +0.70 points), and the Clinical Global Impression of change (+0.31 vs. +0.77 points). The differences were highly statistically significant (all P < .0001).
The patients participating in the double-blind phase of the study were similar with a mean age of 63.5 years in both groups and time since Parkinson’s disease diagnosis (> 9 years). The median ON time without troublesome dyskinesias was about 12 hours at baseline in both groups and the median OFF time was about 3.5 hours.
The higher rate of treatment-related adverse events in the ND0612 group (67.2% vs. 52.7%) was largely explained by the greater rate of infusion site reactions (57.0% vs. 42.7%). The rates of severe reactions in the two groups were the same (0.8%), but both mild (43.8% vs. 36.6%) and moderate (12.5% vs. 5.3%) reactions occurred more commonly in the group receiving active therapy.
“Infusion reactions are the Achilles heel of all subcutaneous therapies,” acknowledged Dr. Espay, who expects other infusion systems in development to share this risk. He suggested that the clinical impact can be attenuated to some degree by rotating infusion sites.
BeyoND extension study
Data from an open-label extension (OLE) of the phase 2b BeyoND trial were also presented at the AAN meeting and generated generally similar results. Largely a safety study, there was no active control in the initial BeyoND or the BeyoND OLE. In BeyoND, the improvement in ON time from baseline was even greater than that seen in BouNDless, but, again, the optimization of dosing in the BouNDless run-in established a greater baseline of disease control.
In the OLE of BeyoND, presented by Aaron Ellenbogen, DO, a neurologist in Farmington, Mich., one of the notable findings was the retention of patients. After 2 years of follow-up, 82% completed at least 2 years of follow-up and 66.7% have now remained on treatment for at least 3 years. Dr. Ellenbogen maintains that this retention rate provides compelling evidence of a favorable benefit-to-risk ratio.
Fulfilling an unmet need
The favorable efficacy data from this trial represent “a big advance,” according to Ihtsham Ul Haq, MD, chief, movement disorders division, University of Miami, who was reached for comment. He noted that continuous infusion delivery has been anticipated for some time, and he expects these types of systems to fulfill an unmet need.
“This will be a useful option in a carefully selected group of patients,” said Dr. Haq, who considers the types of improvement in ON time to be highly clinically meaningful.
However, he cautioned that the nodules created by injection site reactions might limit the utility of this treatment option in at least some patients. Wearing the external device might also be a limiting factor for some patients.
In complex Parkinson’s disease, a stage that can be reached fairly rapidly in some patients but might take 15 years or more in others, all of the options involve a careful benefit-to-risk calculation, according to Dr. Haq. Deep brain stimulation is among the most effective options, but continuous infusion might appeal to some patients for delaying this procedure or as an alternative.
“We need multiple options for these types of patients, and it appears that continuous infusion will be one of them,” Dr. Haq said.
Dr. Espay has financial relationships with Acadia, Acorda, Amneal, AskBio, Bexion, Kyowa Kirin, Neuroderm, Neurocrine, and Sunovion. Dr. Ellenbogen has financial relationships with Allergan, Acorda, Supernus, and Teva. Dr. Haq reports no potential conflicts of interest.
BOSTON – presented at the 2023 annual meeting of the American Academy of Neurology.
When compared with optimized oral immediate-release medication, the delivery system, called ND0612 (NeuroDerm, Rehovot, Israel), improved ON time without troublesome dyskinesias while improving symptoms according to ratings from both patients and clinicians, according to Alberto J. Espay, MD, professor of neurology and director of the Gardner Family Center for Parkinson’s Disease and Movement Disorders, University of Cincinnati.
The new delivery system addresses the challenge of reducing the variability in levodopa plasma concentrations, a major factor in motor fluctuations and diminishing benefit from orally administered drug, according to Dr. Espay. He said that continuous infusion strategies have long been sought as a method to preserve levodopa efficacy.
BouNDless findings
There were two phases to this multinational trial, called BouNDless. In the first, an open-label run-in phase, 381 patients with Parkinson’s disease were dose titrated for optimization of oral immediate-release levodopa and carbidopa. They were then optimized for the same drugs delivered with ND0612. The study was conducted over 12 weeks; 122 patients left the study after this phase due to adverse events, lack of efficacy, or withdrawal of consent.
In the second phase, the 259 remaining patients were randomized to the continuous infusion arm or to immediate release oral therapy. In this double-blind, double-dummy phase, those randomized to the ND0612 infusion also received oral placebos. Those randomized to oral therapy received a placebo infusion. Efficacy and safety were assessed at the end of 12 weeks.
At the end of phase 1, the ON time increased by about 3 hours when levodopa-carbidopa dosing was optimized on either delivery method. Dr. Espay attributed the improvement to the value of optimized dosing even in patients with relatively advanced disease.
However, for the purposes of the double-blind comparison, this improvement in ON time provided a new baseline for comparison of the two delivery methods. This is important for interpreting the primary result, which was a 1.72-hour difference in ON time at the end of the study. The difference was created when ON time was maintained with ND0612 continuous drug delivery but eroded in the group randomized to oral immediate-release treatment.
Several secondary endpoints supported the greater efficacy of continuous subcutaneous delivery. These included lower OFF time (0.50 vs. 1.90 hours), less accumulation of disability on the United Parkinson’s Disease Rating Scale part II-M-EDL (-0.30 vs. +2.75 points), and greater improvement on the Patient Global Impression of Change (+0.31 vs. +0.70 points), and the Clinical Global Impression of change (+0.31 vs. +0.77 points). The differences were highly statistically significant (all P < .0001).
The patients participating in the double-blind phase of the study were similar with a mean age of 63.5 years in both groups and time since Parkinson’s disease diagnosis (> 9 years). The median ON time without troublesome dyskinesias was about 12 hours at baseline in both groups and the median OFF time was about 3.5 hours.
The higher rate of treatment-related adverse events in the ND0612 group (67.2% vs. 52.7%) was largely explained by the greater rate of infusion site reactions (57.0% vs. 42.7%). The rates of severe reactions in the two groups were the same (0.8%), but both mild (43.8% vs. 36.6%) and moderate (12.5% vs. 5.3%) reactions occurred more commonly in the group receiving active therapy.
“Infusion reactions are the Achilles heel of all subcutaneous therapies,” acknowledged Dr. Espay, who expects other infusion systems in development to share this risk. He suggested that the clinical impact can be attenuated to some degree by rotating infusion sites.
BeyoND extension study
Data from an open-label extension (OLE) of the phase 2b BeyoND trial were also presented at the AAN meeting and generated generally similar results. Largely a safety study, there was no active control in the initial BeyoND or the BeyoND OLE. In BeyoND, the improvement in ON time from baseline was even greater than that seen in BouNDless, but, again, the optimization of dosing in the BouNDless run-in established a greater baseline of disease control.
In the OLE of BeyoND, presented by Aaron Ellenbogen, DO, a neurologist in Farmington, Mich., one of the notable findings was the retention of patients. After 2 years of follow-up, 82% completed at least 2 years of follow-up and 66.7% have now remained on treatment for at least 3 years. Dr. Ellenbogen maintains that this retention rate provides compelling evidence of a favorable benefit-to-risk ratio.
Fulfilling an unmet need
The favorable efficacy data from this trial represent “a big advance,” according to Ihtsham Ul Haq, MD, chief, movement disorders division, University of Miami, who was reached for comment. He noted that continuous infusion delivery has been anticipated for some time, and he expects these types of systems to fulfill an unmet need.
“This will be a useful option in a carefully selected group of patients,” said Dr. Haq, who considers the types of improvement in ON time to be highly clinically meaningful.
However, he cautioned that the nodules created by injection site reactions might limit the utility of this treatment option in at least some patients. Wearing the external device might also be a limiting factor for some patients.
In complex Parkinson’s disease, a stage that can be reached fairly rapidly in some patients but might take 15 years or more in others, all of the options involve a careful benefit-to-risk calculation, according to Dr. Haq. Deep brain stimulation is among the most effective options, but continuous infusion might appeal to some patients for delaying this procedure or as an alternative.
“We need multiple options for these types of patients, and it appears that continuous infusion will be one of them,” Dr. Haq said.
Dr. Espay has financial relationships with Acadia, Acorda, Amneal, AskBio, Bexion, Kyowa Kirin, Neuroderm, Neurocrine, and Sunovion. Dr. Ellenbogen has financial relationships with Allergan, Acorda, Supernus, and Teva. Dr. Haq reports no potential conflicts of interest.
BOSTON – presented at the 2023 annual meeting of the American Academy of Neurology.
When compared with optimized oral immediate-release medication, the delivery system, called ND0612 (NeuroDerm, Rehovot, Israel), improved ON time without troublesome dyskinesias while improving symptoms according to ratings from both patients and clinicians, according to Alberto J. Espay, MD, professor of neurology and director of the Gardner Family Center for Parkinson’s Disease and Movement Disorders, University of Cincinnati.
The new delivery system addresses the challenge of reducing the variability in levodopa plasma concentrations, a major factor in motor fluctuations and diminishing benefit from orally administered drug, according to Dr. Espay. He said that continuous infusion strategies have long been sought as a method to preserve levodopa efficacy.
BouNDless findings
There were two phases to this multinational trial, called BouNDless. In the first, an open-label run-in phase, 381 patients with Parkinson’s disease were dose titrated for optimization of oral immediate-release levodopa and carbidopa. They were then optimized for the same drugs delivered with ND0612. The study was conducted over 12 weeks; 122 patients left the study after this phase due to adverse events, lack of efficacy, or withdrawal of consent.
In the second phase, the 259 remaining patients were randomized to the continuous infusion arm or to immediate release oral therapy. In this double-blind, double-dummy phase, those randomized to the ND0612 infusion also received oral placebos. Those randomized to oral therapy received a placebo infusion. Efficacy and safety were assessed at the end of 12 weeks.
At the end of phase 1, the ON time increased by about 3 hours when levodopa-carbidopa dosing was optimized on either delivery method. Dr. Espay attributed the improvement to the value of optimized dosing even in patients with relatively advanced disease.
However, for the purposes of the double-blind comparison, this improvement in ON time provided a new baseline for comparison of the two delivery methods. This is important for interpreting the primary result, which was a 1.72-hour difference in ON time at the end of the study. The difference was created when ON time was maintained with ND0612 continuous drug delivery but eroded in the group randomized to oral immediate-release treatment.
Several secondary endpoints supported the greater efficacy of continuous subcutaneous delivery. These included lower OFF time (0.50 vs. 1.90 hours), less accumulation of disability on the United Parkinson’s Disease Rating Scale part II-M-EDL (-0.30 vs. +2.75 points), and greater improvement on the Patient Global Impression of Change (+0.31 vs. +0.70 points), and the Clinical Global Impression of change (+0.31 vs. +0.77 points). The differences were highly statistically significant (all P < .0001).
The patients participating in the double-blind phase of the study were similar with a mean age of 63.5 years in both groups and time since Parkinson’s disease diagnosis (> 9 years). The median ON time without troublesome dyskinesias was about 12 hours at baseline in both groups and the median OFF time was about 3.5 hours.
The higher rate of treatment-related adverse events in the ND0612 group (67.2% vs. 52.7%) was largely explained by the greater rate of infusion site reactions (57.0% vs. 42.7%). The rates of severe reactions in the two groups were the same (0.8%), but both mild (43.8% vs. 36.6%) and moderate (12.5% vs. 5.3%) reactions occurred more commonly in the group receiving active therapy.
“Infusion reactions are the Achilles heel of all subcutaneous therapies,” acknowledged Dr. Espay, who expects other infusion systems in development to share this risk. He suggested that the clinical impact can be attenuated to some degree by rotating infusion sites.
BeyoND extension study
Data from an open-label extension (OLE) of the phase 2b BeyoND trial were also presented at the AAN meeting and generated generally similar results. Largely a safety study, there was no active control in the initial BeyoND or the BeyoND OLE. In BeyoND, the improvement in ON time from baseline was even greater than that seen in BouNDless, but, again, the optimization of dosing in the BouNDless run-in established a greater baseline of disease control.
In the OLE of BeyoND, presented by Aaron Ellenbogen, DO, a neurologist in Farmington, Mich., one of the notable findings was the retention of patients. After 2 years of follow-up, 82% completed at least 2 years of follow-up and 66.7% have now remained on treatment for at least 3 years. Dr. Ellenbogen maintains that this retention rate provides compelling evidence of a favorable benefit-to-risk ratio.
Fulfilling an unmet need
The favorable efficacy data from this trial represent “a big advance,” according to Ihtsham Ul Haq, MD, chief, movement disorders division, University of Miami, who was reached for comment. He noted that continuous infusion delivery has been anticipated for some time, and he expects these types of systems to fulfill an unmet need.
“This will be a useful option in a carefully selected group of patients,” said Dr. Haq, who considers the types of improvement in ON time to be highly clinically meaningful.
However, he cautioned that the nodules created by injection site reactions might limit the utility of this treatment option in at least some patients. Wearing the external device might also be a limiting factor for some patients.
In complex Parkinson’s disease, a stage that can be reached fairly rapidly in some patients but might take 15 years or more in others, all of the options involve a careful benefit-to-risk calculation, according to Dr. Haq. Deep brain stimulation is among the most effective options, but continuous infusion might appeal to some patients for delaying this procedure or as an alternative.
“We need multiple options for these types of patients, and it appears that continuous infusion will be one of them,” Dr. Haq said.
Dr. Espay has financial relationships with Acadia, Acorda, Amneal, AskBio, Bexion, Kyowa Kirin, Neuroderm, Neurocrine, and Sunovion. Dr. Ellenbogen has financial relationships with Allergan, Acorda, Supernus, and Teva. Dr. Haq reports no potential conflicts of interest.
FROM AAN 2023
Registry data ‘reassure’ on biologics’ heart attack risk in rheumatoid arthritis
MANCHESTER, ENGLAND – Rheumatoid arthritis patients are no more likely to have a heart attack if they are treated with an interleukin-6 inhibitor (IL-6i) than if they are treated with a tumor necrosis factor inhibitor (TNFi), according to data presented at the British Society for Rheumatology annual meeting.
Results of a large analysis from the long-running British Society for Rheumatology Biologics Register–Rheumatoid Arthritis (BSRBR-RA) found no statistical difference in the rate of myocardial infarction (MI), considering treatment in almost 21,000 patients. The overall propensity-score adjusted hazard ratio for MI risk comparing TNFi and IL-6i was 0.77, but the 95% confidence interval crossed the line for statistical significance.
“This result reassures patients and clinical teams about the long-term treatment effects on myocardial infarction in a real-world setting,” said Tian Zixing, a PhD student at the University of Manchester (England).

“Patients with rheumatoid arthritis have an increased risk of myocardial infarction, compared to the general population,” Ms. Tian explained. However, this risk has been “considerably improved” with biologic treatment of rheumatoid arthritis, notably with the TNFi drugs vs. nonbiologic disease-modifying antirheumatic drugs.
The reasoning behind the current analysis was to see if there was any risk associated with IL-6i, as these drugs have been noted to increase low-density cholesterol levels, which in turn can raise the risk for MI.
The study population consisted of all patients registered in the BSRBR-RA over the past 20 years who had started treatment with one of the many TNFi drugs available in the UK – adalimumab (Humira and biosimilars), etanercept (Enbrel), infliximab (Remicade and biosimilars), certolizumab pegol (Cimzia), and golimumab (Simponi) – or the two available drugs that target the effects of IL-6 – tocilizumab (RoActemra, but Actemra in the U.S.), which targets IL-6 itself, and sarilumab (Kevzara), which targets the IL-6 receptor.
Clinical follow-up forms, death certificates, and patient reports confirmed by the clinical team were used to identify patients who experienced a MI, but only MIs that occurred while on treatment were counted.
More than 30,000 lines of therapy in 20,898 patients were recorded. Ms. Tian noted that most (> 90%) patients had been treated with a TNFi across all lines of therapy.
“It is very important to consider the treatment sequence,” she said. “Most patients start first-line treatment with a TNF inhibitor, with only a few patients starting an IL-6 inhibitor,” she noted. “IL-6 inhibitors are more commonly used in the later stages of disease, when more cardiovascular risk factors have accumulated.”
Thus, to ensure that the MI risk was fairly evaluated, the statistical analyses compared TNFi and IL-6i according to the line of treatment. “That means only patients on their first-line treatment will be compared to each other, and only those on their second-line treatment will be compared to each other, and so on,” Ms. Tian explained.
Baseline characteristics were broadly similar for patients treated with TNFi and IL-6i drugs, except for hyperlipidemia, which was higher in patients treated with an IL-6i. Nevertheless, there was no suggestion of any difference in the MI rates after adjustment for cardiovascular risk factors.
There are a lot of strengths to these data, but of course the possibilities of residual confounding and confounding by indication exist, Ms. Tian said. There were also missing data that had to be imputed.
“There has been quite a bit around interleukin-1 blockers being cardiovascular protective,” observed Kenneth Baker, MBChB, PhD, who chaired the RA oral abstracts session during which Ms. Tian presented the findings.
“IL-6 is quite good at suppressing CRP [C-reactive protein],” added Dr. Baker, a senior clinical research fellow at Newcastle University and honorary consultant rheumatologist at Freeman Hospital, both in Newcastle upon Tyne, England.
“You’ve hypothesized or extrapolated that the differences in the lipid levels may not be relevant,” he said to Ms. Tian, “but do you think there might be an extra element going on here?” Maybe IL-6i drugs such as tocilizumab are better at suppressing inflammation, and that counterbalances the effects on lipids, he suggested.
Ms. Tian and Dr. Baker disclosed no relevant financial relationships. The BSRBR-RA is managed by the University of Manchester on behalf of the British Society for Rheumatology. The registry is supported by funding from multiple pharmaceutical companies, including AbbVie, Amgen, Celltrion Healthcare, Eli Lilly, Galapagos, Pfizer, Samsung Bioepis, and Sanofi, and in the past Hospira, Merck Sharp & Dohme, Roche, Sandoz, SOBI, and UCB.
A version of this article originally appeared on Medscape.com.
MANCHESTER, ENGLAND – Rheumatoid arthritis patients are no more likely to have a heart attack if they are treated with an interleukin-6 inhibitor (IL-6i) than if they are treated with a tumor necrosis factor inhibitor (TNFi), according to data presented at the British Society for Rheumatology annual meeting.
Results of a large analysis from the long-running British Society for Rheumatology Biologics Register–Rheumatoid Arthritis (BSRBR-RA) found no statistical difference in the rate of myocardial infarction (MI), considering treatment in almost 21,000 patients. The overall propensity-score adjusted hazard ratio for MI risk comparing TNFi and IL-6i was 0.77, but the 95% confidence interval crossed the line for statistical significance.
“This result reassures patients and clinical teams about the long-term treatment effects on myocardial infarction in a real-world setting,” said Tian Zixing, a PhD student at the University of Manchester (England).
“Patients with rheumatoid arthritis have an increased risk of myocardial infarction, compared to the general population,” Ms. Tian explained. However, this risk has been “considerably improved” with biologic treatment of rheumatoid arthritis, notably with the TNFi drugs vs. nonbiologic disease-modifying antirheumatic drugs.
The reasoning behind the current analysis was to see if there was any risk associated with IL-6i, as these drugs have been noted to increase low-density cholesterol levels, which in turn can raise the risk for MI.
The study population consisted of all patients registered in the BSRBR-RA over the past 20 years who had started treatment with one of the many TNFi drugs available in the UK – adalimumab (Humira and biosimilars), etanercept (Enbrel), infliximab (Remicade and biosimilars), certolizumab pegol (Cimzia), and golimumab (Simponi) – or the two available drugs that target the effects of IL-6 – tocilizumab (RoActemra, but Actemra in the U.S.), which targets IL-6 itself, and sarilumab (Kevzara), which targets the IL-6 receptor.
Clinical follow-up forms, death certificates, and patient reports confirmed by the clinical team were used to identify patients who experienced a MI, but only MIs that occurred while on treatment were counted.
More than 30,000 lines of therapy in 20,898 patients were recorded. Ms. Tian noted that most (> 90%) patients had been treated with a TNFi across all lines of therapy.
“It is very important to consider the treatment sequence,” she said. “Most patients start first-line treatment with a TNF inhibitor, with only a few patients starting an IL-6 inhibitor,” she noted. “IL-6 inhibitors are more commonly used in the later stages of disease, when more cardiovascular risk factors have accumulated.”
Thus, to ensure that the MI risk was fairly evaluated, the statistical analyses compared TNFi and IL-6i according to the line of treatment. “That means only patients on their first-line treatment will be compared to each other, and only those on their second-line treatment will be compared to each other, and so on,” Ms. Tian explained.
Baseline characteristics were broadly similar for patients treated with TNFi and IL-6i drugs, except for hyperlipidemia, which was higher in patients treated with an IL-6i. Nevertheless, there was no suggestion of any difference in the MI rates after adjustment for cardiovascular risk factors.
There are a lot of strengths to these data, but of course the possibilities of residual confounding and confounding by indication exist, Ms. Tian said. There were also missing data that had to be imputed.
“There has been quite a bit around interleukin-1 blockers being cardiovascular protective,” observed Kenneth Baker, MBChB, PhD, who chaired the RA oral abstracts session during which Ms. Tian presented the findings.
“IL-6 is quite good at suppressing CRP [C-reactive protein],” added Dr. Baker, a senior clinical research fellow at Newcastle University and honorary consultant rheumatologist at Freeman Hospital, both in Newcastle upon Tyne, England.
“You’ve hypothesized or extrapolated that the differences in the lipid levels may not be relevant,” he said to Ms. Tian, “but do you think there might be an extra element going on here?” Maybe IL-6i drugs such as tocilizumab are better at suppressing inflammation, and that counterbalances the effects on lipids, he suggested.
Ms. Tian and Dr. Baker disclosed no relevant financial relationships. The BSRBR-RA is managed by the University of Manchester on behalf of the British Society for Rheumatology. The registry is supported by funding from multiple pharmaceutical companies, including AbbVie, Amgen, Celltrion Healthcare, Eli Lilly, Galapagos, Pfizer, Samsung Bioepis, and Sanofi, and in the past Hospira, Merck Sharp & Dohme, Roche, Sandoz, SOBI, and UCB.
A version of this article originally appeared on Medscape.com.
MANCHESTER, ENGLAND – Rheumatoid arthritis patients are no more likely to have a heart attack if they are treated with an interleukin-6 inhibitor (IL-6i) than if they are treated with a tumor necrosis factor inhibitor (TNFi), according to data presented at the British Society for Rheumatology annual meeting.
Results of a large analysis from the long-running British Society for Rheumatology Biologics Register–Rheumatoid Arthritis (BSRBR-RA) found no statistical difference in the rate of myocardial infarction (MI), considering treatment in almost 21,000 patients. The overall propensity-score adjusted hazard ratio for MI risk comparing TNFi and IL-6i was 0.77, but the 95% confidence interval crossed the line for statistical significance.
“This result reassures patients and clinical teams about the long-term treatment effects on myocardial infarction in a real-world setting,” said Tian Zixing, a PhD student at the University of Manchester (England).
“Patients with rheumatoid arthritis have an increased risk of myocardial infarction, compared to the general population,” Ms. Tian explained. However, this risk has been “considerably improved” with biologic treatment of rheumatoid arthritis, notably with the TNFi drugs vs. nonbiologic disease-modifying antirheumatic drugs.
The reasoning behind the current analysis was to see if there was any risk associated with IL-6i, as these drugs have been noted to increase low-density cholesterol levels, which in turn can raise the risk for MI.
The study population consisted of all patients registered in the BSRBR-RA over the past 20 years who had started treatment with one of the many TNFi drugs available in the UK – adalimumab (Humira and biosimilars), etanercept (Enbrel), infliximab (Remicade and biosimilars), certolizumab pegol (Cimzia), and golimumab (Simponi) – or the two available drugs that target the effects of IL-6 – tocilizumab (RoActemra, but Actemra in the U.S.), which targets IL-6 itself, and sarilumab (Kevzara), which targets the IL-6 receptor.
Clinical follow-up forms, death certificates, and patient reports confirmed by the clinical team were used to identify patients who experienced a MI, but only MIs that occurred while on treatment were counted.
More than 30,000 lines of therapy in 20,898 patients were recorded. Ms. Tian noted that most (> 90%) patients had been treated with a TNFi across all lines of therapy.
“It is very important to consider the treatment sequence,” she said. “Most patients start first-line treatment with a TNF inhibitor, with only a few patients starting an IL-6 inhibitor,” she noted. “IL-6 inhibitors are more commonly used in the later stages of disease, when more cardiovascular risk factors have accumulated.”
Thus, to ensure that the MI risk was fairly evaluated, the statistical analyses compared TNFi and IL-6i according to the line of treatment. “That means only patients on their first-line treatment will be compared to each other, and only those on their second-line treatment will be compared to each other, and so on,” Ms. Tian explained.
Baseline characteristics were broadly similar for patients treated with TNFi and IL-6i drugs, except for hyperlipidemia, which was higher in patients treated with an IL-6i. Nevertheless, there was no suggestion of any difference in the MI rates after adjustment for cardiovascular risk factors.
There are a lot of strengths to these data, but of course the possibilities of residual confounding and confounding by indication exist, Ms. Tian said. There were also missing data that had to be imputed.
“There has been quite a bit around interleukin-1 blockers being cardiovascular protective,” observed Kenneth Baker, MBChB, PhD, who chaired the RA oral abstracts session during which Ms. Tian presented the findings.
“IL-6 is quite good at suppressing CRP [C-reactive protein],” added Dr. Baker, a senior clinical research fellow at Newcastle University and honorary consultant rheumatologist at Freeman Hospital, both in Newcastle upon Tyne, England.
“You’ve hypothesized or extrapolated that the differences in the lipid levels may not be relevant,” he said to Ms. Tian, “but do you think there might be an extra element going on here?” Maybe IL-6i drugs such as tocilizumab are better at suppressing inflammation, and that counterbalances the effects on lipids, he suggested.
Ms. Tian and Dr. Baker disclosed no relevant financial relationships. The BSRBR-RA is managed by the University of Manchester on behalf of the British Society for Rheumatology. The registry is supported by funding from multiple pharmaceutical companies, including AbbVie, Amgen, Celltrion Healthcare, Eli Lilly, Galapagos, Pfizer, Samsung Bioepis, and Sanofi, and in the past Hospira, Merck Sharp & Dohme, Roche, Sandoz, SOBI, and UCB.
A version of this article originally appeared on Medscape.com.
AT BSR 2023
Guidelines for assessing cancer risk may need updating
The authors of the clinical trial suggest that these guidelines may need to be revised.
Individuals with hereditary breast and ovarian cancer (HBOC) have an 80% lifetime risk of breast cancer and are at greater risk of ovarian cancer, pancreatic cancer, prostate cancer, and melanoma. Those with Lynch syndrome (LS) have an 80% lifetime risk of colorectal cancer, a 60% lifetime risk of endometrial cancer, and heightened risk of upper gastrointestinal, urinary tract, skin, and other tumors, said study coauthor N. Jewel Samadder, MD in a statement.
The National Cancer Control Network has guidelines for determining family risk for colorectal cancer and breast, ovarian, and pancreatic cancer to identify individuals who should be screened for LS and HBOC, but these rely on personal and family health histories.
“These criteria were created at a time when genetic testing was cost prohibitive and thus aimed to identify those at the greatest chance of being a mutation carrier in the absence of population-wide whole-exome sequencing. However, [LS and HBOC] are poorly identified in current practice, and many patients are not aware of their cancer risk,” said Dr. Samadder, professor of medicine and coleader of the precision oncology program at the Mayo Clinic Comprehensive Cancer Center, Phoenix, in the statement.
Whole-exome sequencing covers only protein-coding regions of the genome, which is less than 2% of the total genome but includes more than 85% of known disease-related genetic variants, according to Emily Gay, who presented the trial results (Abstract 5768) on April 18 at the annual meeting of the American Association for Cancer Research.
“In recent years, the cost of whole-exome sequencing has been rapidly decreasing, allowing us to complete this test on saliva samples from thousands, if not tens of thousands of patients covering large populations and large health systems,” said Ms. Gay, a genetic counseling graduate student at the University of Arizona, during her presentation.
She described results from the TAPESTRY clinical trial, with 44,306 participants from Mayo Clinic centers in Arizona, Florida, and Minnesota, who were identified as definitely or likely to be harboring pathogenic mutations and consented to whole-exome sequencing from saliva samples. They used electronic health records to determine whether patients would satisfy the testing criteria from NCCN guidelines.
The researchers identified 1.24% of participants to be carriers of HBOC or LS. Of the HBOC carriers, 62.8% were female, and of the LS carriers, 62.6% were female. The percentages of HBOC and LS carriers who were White were 88.6 and 94.5, respectively. The median age of both groups was 57 years. Of HBOC carriers, 47.3% had personal histories of cancers; for LS carries, the percentage was 44.2.
Of HBOC carriers, 49.1% had been previously unaware of their genetic condition, while an even higher percentage of patients with LS – 59.3% – fell into that category. Thirty-two percent of those with HBOC and 56.2% of those with LS would not have qualified for screening using the relevant NCCN guidelines.
“Most strikingly,” 63.8% of individuals with mutations in the MSH6 gene and 83.7% of those mutations in the PMS2 gene would not have met NCCN criteria, Ms. Gay said.
Having a cancer type not known to be related to a genetic syndrome was a reason for 58.6% of individuals failing to meet NCCN guidelines, while 60.5% did not meet the guidelines because of an insufficient number of relatives known to have a history of cancer, and 63.3% did not because they had no personal history of cancer. Among individuals with a pathogenic mutation who met NCCN criteria, 34% were not aware of their condition.
“This suggests that the NCCN guidelines are underutilized in clinical practice, potentially due to the busy schedule of clinicians or because the complexity of using these criteria,” said Ms. Gay.
The numbers were even more striking among minorities: “There is additional data analysis and research needed in this area, but based on our preliminary findings, we saw that nearly 50% of the individuals who are [part of an underrepresented minority group] did not meet criteria, compared with 32% of the white cohort,” said Ms. Gay.
Asked what new NCCN guidelines should be, Ms. Gay replied: “I think maybe limiting the number of relatives that you have to have with a certain type of cancer, especially as we see families get smaller and smaller, especially in the United States – that family data isn’t necessarily available or as useful. And then also, I think, incorporating in the size of a family into the calculation, so more of maybe a point-based system like we see with other genetic conditions rather than a ‘yes you meet or no, you don’t.’ More of a range to say ‘you fall on the low-risk, medium-risk, or high-risk stage,’” said Ms. Gay.
During the Q&A period, session cochair Andrew Godwin, PhD, who is a professor of molecular oncology and pathology at University of Kansas Medical Center, Kansas City, said he wondered if whole-exome sequencing was capable of picking up cancer risk mutations that standard targeted tests don’t look for.
Dr. Samadder, who was in the audience, answered the question, saying that targeted tests are actually better at picking up some types of mutations like intronic mutations, single-nucleotide polymorphisms, and deletions.
“There are some limitations to whole-exome sequencing. Our estimate here of 1.2% [of participants carrying HBOC or LS mutations] is probably an underestimate. There are additional variants that exome sequencing probably doesn’t pick up easily or as well. That’s why we qualify that exome sequencing is a screening test, not a diagnostic,” he continued.
Ms. Gay and Dr. Samadder have no relevant financial disclosures. Dr. Godwin has financial relationships with Clara Biotech, VITRAC Therapeutics, and Sinochips Diagnostics.
The authors of the clinical trial suggest that these guidelines may need to be revised.
Individuals with hereditary breast and ovarian cancer (HBOC) have an 80% lifetime risk of breast cancer and are at greater risk of ovarian cancer, pancreatic cancer, prostate cancer, and melanoma. Those with Lynch syndrome (LS) have an 80% lifetime risk of colorectal cancer, a 60% lifetime risk of endometrial cancer, and heightened risk of upper gastrointestinal, urinary tract, skin, and other tumors, said study coauthor N. Jewel Samadder, MD in a statement.
The National Cancer Control Network has guidelines for determining family risk for colorectal cancer and breast, ovarian, and pancreatic cancer to identify individuals who should be screened for LS and HBOC, but these rely on personal and family health histories.
“These criteria were created at a time when genetic testing was cost prohibitive and thus aimed to identify those at the greatest chance of being a mutation carrier in the absence of population-wide whole-exome sequencing. However, [LS and HBOC] are poorly identified in current practice, and many patients are not aware of their cancer risk,” said Dr. Samadder, professor of medicine and coleader of the precision oncology program at the Mayo Clinic Comprehensive Cancer Center, Phoenix, in the statement.
Whole-exome sequencing covers only protein-coding regions of the genome, which is less than 2% of the total genome but includes more than 85% of known disease-related genetic variants, according to Emily Gay, who presented the trial results (Abstract 5768) on April 18 at the annual meeting of the American Association for Cancer Research.
“In recent years, the cost of whole-exome sequencing has been rapidly decreasing, allowing us to complete this test on saliva samples from thousands, if not tens of thousands of patients covering large populations and large health systems,” said Ms. Gay, a genetic counseling graduate student at the University of Arizona, during her presentation.
She described results from the TAPESTRY clinical trial, with 44,306 participants from Mayo Clinic centers in Arizona, Florida, and Minnesota, who were identified as definitely or likely to be harboring pathogenic mutations and consented to whole-exome sequencing from saliva samples. They used electronic health records to determine whether patients would satisfy the testing criteria from NCCN guidelines.
The researchers identified 1.24% of participants to be carriers of HBOC or LS. Of the HBOC carriers, 62.8% were female, and of the LS carriers, 62.6% were female. The percentages of HBOC and LS carriers who were White were 88.6 and 94.5, respectively. The median age of both groups was 57 years. Of HBOC carriers, 47.3% had personal histories of cancers; for LS carries, the percentage was 44.2.
Of HBOC carriers, 49.1% had been previously unaware of their genetic condition, while an even higher percentage of patients with LS – 59.3% – fell into that category. Thirty-two percent of those with HBOC and 56.2% of those with LS would not have qualified for screening using the relevant NCCN guidelines.
“Most strikingly,” 63.8% of individuals with mutations in the MSH6 gene and 83.7% of those mutations in the PMS2 gene would not have met NCCN criteria, Ms. Gay said.
Having a cancer type not known to be related to a genetic syndrome was a reason for 58.6% of individuals failing to meet NCCN guidelines, while 60.5% did not meet the guidelines because of an insufficient number of relatives known to have a history of cancer, and 63.3% did not because they had no personal history of cancer. Among individuals with a pathogenic mutation who met NCCN criteria, 34% were not aware of their condition.
“This suggests that the NCCN guidelines are underutilized in clinical practice, potentially due to the busy schedule of clinicians or because the complexity of using these criteria,” said Ms. Gay.
The numbers were even more striking among minorities: “There is additional data analysis and research needed in this area, but based on our preliminary findings, we saw that nearly 50% of the individuals who are [part of an underrepresented minority group] did not meet criteria, compared with 32% of the white cohort,” said Ms. Gay.
Asked what new NCCN guidelines should be, Ms. Gay replied: “I think maybe limiting the number of relatives that you have to have with a certain type of cancer, especially as we see families get smaller and smaller, especially in the United States – that family data isn’t necessarily available or as useful. And then also, I think, incorporating in the size of a family into the calculation, so more of maybe a point-based system like we see with other genetic conditions rather than a ‘yes you meet or no, you don’t.’ More of a range to say ‘you fall on the low-risk, medium-risk, or high-risk stage,’” said Ms. Gay.
During the Q&A period, session cochair Andrew Godwin, PhD, who is a professor of molecular oncology and pathology at University of Kansas Medical Center, Kansas City, said he wondered if whole-exome sequencing was capable of picking up cancer risk mutations that standard targeted tests don’t look for.
Dr. Samadder, who was in the audience, answered the question, saying that targeted tests are actually better at picking up some types of mutations like intronic mutations, single-nucleotide polymorphisms, and deletions.
“There are some limitations to whole-exome sequencing. Our estimate here of 1.2% [of participants carrying HBOC or LS mutations] is probably an underestimate. There are additional variants that exome sequencing probably doesn’t pick up easily or as well. That’s why we qualify that exome sequencing is a screening test, not a diagnostic,” he continued.
Ms. Gay and Dr. Samadder have no relevant financial disclosures. Dr. Godwin has financial relationships with Clara Biotech, VITRAC Therapeutics, and Sinochips Diagnostics.
The authors of the clinical trial suggest that these guidelines may need to be revised.
Individuals with hereditary breast and ovarian cancer (HBOC) have an 80% lifetime risk of breast cancer and are at greater risk of ovarian cancer, pancreatic cancer, prostate cancer, and melanoma. Those with Lynch syndrome (LS) have an 80% lifetime risk of colorectal cancer, a 60% lifetime risk of endometrial cancer, and heightened risk of upper gastrointestinal, urinary tract, skin, and other tumors, said study coauthor N. Jewel Samadder, MD in a statement.
The National Cancer Control Network has guidelines for determining family risk for colorectal cancer and breast, ovarian, and pancreatic cancer to identify individuals who should be screened for LS and HBOC, but these rely on personal and family health histories.
“These criteria were created at a time when genetic testing was cost prohibitive and thus aimed to identify those at the greatest chance of being a mutation carrier in the absence of population-wide whole-exome sequencing. However, [LS and HBOC] are poorly identified in current practice, and many patients are not aware of their cancer risk,” said Dr. Samadder, professor of medicine and coleader of the precision oncology program at the Mayo Clinic Comprehensive Cancer Center, Phoenix, in the statement.
Whole-exome sequencing covers only protein-coding regions of the genome, which is less than 2% of the total genome but includes more than 85% of known disease-related genetic variants, according to Emily Gay, who presented the trial results (Abstract 5768) on April 18 at the annual meeting of the American Association for Cancer Research.
“In recent years, the cost of whole-exome sequencing has been rapidly decreasing, allowing us to complete this test on saliva samples from thousands, if not tens of thousands of patients covering large populations and large health systems,” said Ms. Gay, a genetic counseling graduate student at the University of Arizona, during her presentation.
She described results from the TAPESTRY clinical trial, with 44,306 participants from Mayo Clinic centers in Arizona, Florida, and Minnesota, who were identified as definitely or likely to be harboring pathogenic mutations and consented to whole-exome sequencing from saliva samples. They used electronic health records to determine whether patients would satisfy the testing criteria from NCCN guidelines.
The researchers identified 1.24% of participants to be carriers of HBOC or LS. Of the HBOC carriers, 62.8% were female, and of the LS carriers, 62.6% were female. The percentages of HBOC and LS carriers who were White were 88.6 and 94.5, respectively. The median age of both groups was 57 years. Of HBOC carriers, 47.3% had personal histories of cancers; for LS carries, the percentage was 44.2.
Of HBOC carriers, 49.1% had been previously unaware of their genetic condition, while an even higher percentage of patients with LS – 59.3% – fell into that category. Thirty-two percent of those with HBOC and 56.2% of those with LS would not have qualified for screening using the relevant NCCN guidelines.
“Most strikingly,” 63.8% of individuals with mutations in the MSH6 gene and 83.7% of those mutations in the PMS2 gene would not have met NCCN criteria, Ms. Gay said.
Having a cancer type not known to be related to a genetic syndrome was a reason for 58.6% of individuals failing to meet NCCN guidelines, while 60.5% did not meet the guidelines because of an insufficient number of relatives known to have a history of cancer, and 63.3% did not because they had no personal history of cancer. Among individuals with a pathogenic mutation who met NCCN criteria, 34% were not aware of their condition.
“This suggests that the NCCN guidelines are underutilized in clinical practice, potentially due to the busy schedule of clinicians or because the complexity of using these criteria,” said Ms. Gay.
The numbers were even more striking among minorities: “There is additional data analysis and research needed in this area, but based on our preliminary findings, we saw that nearly 50% of the individuals who are [part of an underrepresented minority group] did not meet criteria, compared with 32% of the white cohort,” said Ms. Gay.
Asked what new NCCN guidelines should be, Ms. Gay replied: “I think maybe limiting the number of relatives that you have to have with a certain type of cancer, especially as we see families get smaller and smaller, especially in the United States – that family data isn’t necessarily available or as useful. And then also, I think, incorporating in the size of a family into the calculation, so more of maybe a point-based system like we see with other genetic conditions rather than a ‘yes you meet or no, you don’t.’ More of a range to say ‘you fall on the low-risk, medium-risk, or high-risk stage,’” said Ms. Gay.
During the Q&A period, session cochair Andrew Godwin, PhD, who is a professor of molecular oncology and pathology at University of Kansas Medical Center, Kansas City, said he wondered if whole-exome sequencing was capable of picking up cancer risk mutations that standard targeted tests don’t look for.
Dr. Samadder, who was in the audience, answered the question, saying that targeted tests are actually better at picking up some types of mutations like intronic mutations, single-nucleotide polymorphisms, and deletions.
“There are some limitations to whole-exome sequencing. Our estimate here of 1.2% [of participants carrying HBOC or LS mutations] is probably an underestimate. There are additional variants that exome sequencing probably doesn’t pick up easily or as well. That’s why we qualify that exome sequencing is a screening test, not a diagnostic,” he continued.
Ms. Gay and Dr. Samadder have no relevant financial disclosures. Dr. Godwin has financial relationships with Clara Biotech, VITRAC Therapeutics, and Sinochips Diagnostics.
FROM AACR 2023
Novel neural cell therapy: A cure for focal epilepsy?
BOSTON – (MTLE) in the first-in-human test of the novel therapy.
“It is notable that the early significant seizure reduction observed in this study appears to be durable in these first two patients treated with a single administration of NRTX-1001,” principal investigator Robert Beach, MD, PhD, said in a news release.
“It is also encouraging that the first patient has been free from disabling seizures from the second month on and has shown improved memory performance on multiple cognitive tests, as memory problems can be an issue for individuals with drug-resistant MTLE,” said Dr. Beach, chief of epilepsy and professor of neurology at State University of New York, Syracuse.
The findings were presented at the annual meeting of the American Academy of Neurology.
Restorative not destructive
NRTX-1001 therapy (Neurona Therapeutics) is a one-time dose of an injectable suspension of high-purity inhibitory interneurons that secrete the inhibitory neurotransmitter gamma-aminobutyric acid (GABA). The interneurons are intended to integrate and innervate on-target, providing long-term GABAergic inhibition to repair hyperexcitable neural networks.
Preclinical work in animal models of epilepsy has provided strong support for both the safety and the efficacy of boosting inhibition in the seizure focus using implanted human inhibitory interneurons.
This therapy is “potentially restorative instead of just destructive, like epilepsy surgery,” study investigator David Spencer, MD, professor of neurology and director of the Comprehensive Epilepsy Center, Oregon Health & Science University in Portland, said during a press briefing.
In the first two patients, the cells were implanted in the seizure focus using MRI guidance through a tiny opening in the back of the skull. The patients recovered overnight and went home the next day.
The first patient had a 9-year history of drug-resistant epilepsy and was averaging 30 seizures per month at baseline. Testing confirmed that the seizures were coming from a single focus on the right temporal lobe. The implant was uncomplicated, and the cells were delivered to the seizure focus on target.
To date, there have been no serious or unexpected adverse events from the implant. At 9 months of follow-up the patient has had a 93% reduction in seizures overall and is free of all seizures causing impairment of awareness, “which was the most debilitating seizure type for this patient,” Dr. Spencer noted.
Studies of brain metabolism in the area of the implant have shown favorable markers of increased inhibition and decreased inflammation. Cognitive testing at 6 months showed no worsening of memory function or cognition. And, in fact, there were some mild improvements, he said.
The second patient had an 8-year history of drug-resistant epilepsy, averaging 14 focal seizures per month at baseline. Testing also confirmed seizure onset in a single focus in the right temporal lobe and the cells were again implanted without complication on target. Five months after treatment, the patient has had a 94% reduction in seizures and no serious adverse events.
‘Hot off the press’
Epilepsy affects about 3.5 million people in the United States. About two-thirds of people with epilepsy get good control of their seizures using antiseizure medication.
For seizures that are uncontrolled with medication, identifying the seizure focus and removing it surgically can often result in seizure freedom in a high proportion of patients. But not all patients are candidates for epilepsy surgery, and for those who can have it the surgery itself carries some risks, including diminished cognition and memory.
“While these are still early days, we’re encouraged by the positive safety findings so far, and the early seizure responses” with neural cell therapy, Dr. Spencer told reporters.
Given the positive results in the first two patients, additional patients will be treated “with careful safety review all along the way. This is going to be rolling out over the next several years,” Dr. Spencer said. Patient recruitment is underway at epilepsy centers across the United States.
Briefing moderator Natalia Rost, MD, MPH, chair of the AAN science committee, said, “This is a true example of emerging science. It’s literally hot off the press,” and the preliminary results are “very promising.”
Dr. Rost, chief of the stroke division at Massachusetts General Hospital in Boston, noted that this type of cell therapy implant is “very novel and representative of where the field is moving, when no traditional solutions exist for common neurological problems.”
The study was sponsored by Neurona Therapeutics and funded in part by the California Institute for Regenerative Medicine. Dr. Beach and Dr. Spencer report no relevant financial relationships. Several investigators are employees of Neurona Therapeutics. Dr. Rost reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – (MTLE) in the first-in-human test of the novel therapy.
“It is notable that the early significant seizure reduction observed in this study appears to be durable in these first two patients treated with a single administration of NRTX-1001,” principal investigator Robert Beach, MD, PhD, said in a news release.
“It is also encouraging that the first patient has been free from disabling seizures from the second month on and has shown improved memory performance on multiple cognitive tests, as memory problems can be an issue for individuals with drug-resistant MTLE,” said Dr. Beach, chief of epilepsy and professor of neurology at State University of New York, Syracuse.
The findings were presented at the annual meeting of the American Academy of Neurology.
Restorative not destructive
NRTX-1001 therapy (Neurona Therapeutics) is a one-time dose of an injectable suspension of high-purity inhibitory interneurons that secrete the inhibitory neurotransmitter gamma-aminobutyric acid (GABA). The interneurons are intended to integrate and innervate on-target, providing long-term GABAergic inhibition to repair hyperexcitable neural networks.
Preclinical work in animal models of epilepsy has provided strong support for both the safety and the efficacy of boosting inhibition in the seizure focus using implanted human inhibitory interneurons.
This therapy is “potentially restorative instead of just destructive, like epilepsy surgery,” study investigator David Spencer, MD, professor of neurology and director of the Comprehensive Epilepsy Center, Oregon Health & Science University in Portland, said during a press briefing.
In the first two patients, the cells were implanted in the seizure focus using MRI guidance through a tiny opening in the back of the skull. The patients recovered overnight and went home the next day.
The first patient had a 9-year history of drug-resistant epilepsy and was averaging 30 seizures per month at baseline. Testing confirmed that the seizures were coming from a single focus on the right temporal lobe. The implant was uncomplicated, and the cells were delivered to the seizure focus on target.
To date, there have been no serious or unexpected adverse events from the implant. At 9 months of follow-up the patient has had a 93% reduction in seizures overall and is free of all seizures causing impairment of awareness, “which was the most debilitating seizure type for this patient,” Dr. Spencer noted.
Studies of brain metabolism in the area of the implant have shown favorable markers of increased inhibition and decreased inflammation. Cognitive testing at 6 months showed no worsening of memory function or cognition. And, in fact, there were some mild improvements, he said.
The second patient had an 8-year history of drug-resistant epilepsy, averaging 14 focal seizures per month at baseline. Testing also confirmed seizure onset in a single focus in the right temporal lobe and the cells were again implanted without complication on target. Five months after treatment, the patient has had a 94% reduction in seizures and no serious adverse events.
‘Hot off the press’
Epilepsy affects about 3.5 million people in the United States. About two-thirds of people with epilepsy get good control of their seizures using antiseizure medication.
For seizures that are uncontrolled with medication, identifying the seizure focus and removing it surgically can often result in seizure freedom in a high proportion of patients. But not all patients are candidates for epilepsy surgery, and for those who can have it the surgery itself carries some risks, including diminished cognition and memory.
“While these are still early days, we’re encouraged by the positive safety findings so far, and the early seizure responses” with neural cell therapy, Dr. Spencer told reporters.
Given the positive results in the first two patients, additional patients will be treated “with careful safety review all along the way. This is going to be rolling out over the next several years,” Dr. Spencer said. Patient recruitment is underway at epilepsy centers across the United States.
Briefing moderator Natalia Rost, MD, MPH, chair of the AAN science committee, said, “This is a true example of emerging science. It’s literally hot off the press,” and the preliminary results are “very promising.”
Dr. Rost, chief of the stroke division at Massachusetts General Hospital in Boston, noted that this type of cell therapy implant is “very novel and representative of where the field is moving, when no traditional solutions exist for common neurological problems.”
The study was sponsored by Neurona Therapeutics and funded in part by the California Institute for Regenerative Medicine. Dr. Beach and Dr. Spencer report no relevant financial relationships. Several investigators are employees of Neurona Therapeutics. Dr. Rost reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
BOSTON – (MTLE) in the first-in-human test of the novel therapy.
“It is notable that the early significant seizure reduction observed in this study appears to be durable in these first two patients treated with a single administration of NRTX-1001,” principal investigator Robert Beach, MD, PhD, said in a news release.
“It is also encouraging that the first patient has been free from disabling seizures from the second month on and has shown improved memory performance on multiple cognitive tests, as memory problems can be an issue for individuals with drug-resistant MTLE,” said Dr. Beach, chief of epilepsy and professor of neurology at State University of New York, Syracuse.
The findings were presented at the annual meeting of the American Academy of Neurology.
Restorative not destructive
NRTX-1001 therapy (Neurona Therapeutics) is a one-time dose of an injectable suspension of high-purity inhibitory interneurons that secrete the inhibitory neurotransmitter gamma-aminobutyric acid (GABA). The interneurons are intended to integrate and innervate on-target, providing long-term GABAergic inhibition to repair hyperexcitable neural networks.
Preclinical work in animal models of epilepsy has provided strong support for both the safety and the efficacy of boosting inhibition in the seizure focus using implanted human inhibitory interneurons.
This therapy is “potentially restorative instead of just destructive, like epilepsy surgery,” study investigator David Spencer, MD, professor of neurology and director of the Comprehensive Epilepsy Center, Oregon Health & Science University in Portland, said during a press briefing.
In the first two patients, the cells were implanted in the seizure focus using MRI guidance through a tiny opening in the back of the skull. The patients recovered overnight and went home the next day.
The first patient had a 9-year history of drug-resistant epilepsy and was averaging 30 seizures per month at baseline. Testing confirmed that the seizures were coming from a single focus on the right temporal lobe. The implant was uncomplicated, and the cells were delivered to the seizure focus on target.
To date, there have been no serious or unexpected adverse events from the implant. At 9 months of follow-up the patient has had a 93% reduction in seizures overall and is free of all seizures causing impairment of awareness, “which was the most debilitating seizure type for this patient,” Dr. Spencer noted.
Studies of brain metabolism in the area of the implant have shown favorable markers of increased inhibition and decreased inflammation. Cognitive testing at 6 months showed no worsening of memory function or cognition. And, in fact, there were some mild improvements, he said.
The second patient had an 8-year history of drug-resistant epilepsy, averaging 14 focal seizures per month at baseline. Testing also confirmed seizure onset in a single focus in the right temporal lobe and the cells were again implanted without complication on target. Five months after treatment, the patient has had a 94% reduction in seizures and no serious adverse events.
‘Hot off the press’
Epilepsy affects about 3.5 million people in the United States. About two-thirds of people with epilepsy get good control of their seizures using antiseizure medication.
For seizures that are uncontrolled with medication, identifying the seizure focus and removing it surgically can often result in seizure freedom in a high proportion of patients. But not all patients are candidates for epilepsy surgery, and for those who can have it the surgery itself carries some risks, including diminished cognition and memory.
“While these are still early days, we’re encouraged by the positive safety findings so far, and the early seizure responses” with neural cell therapy, Dr. Spencer told reporters.
Given the positive results in the first two patients, additional patients will be treated “with careful safety review all along the way. This is going to be rolling out over the next several years,” Dr. Spencer said. Patient recruitment is underway at epilepsy centers across the United States.
Briefing moderator Natalia Rost, MD, MPH, chair of the AAN science committee, said, “This is a true example of emerging science. It’s literally hot off the press,” and the preliminary results are “very promising.”
Dr. Rost, chief of the stroke division at Massachusetts General Hospital in Boston, noted that this type of cell therapy implant is “very novel and representative of where the field is moving, when no traditional solutions exist for common neurological problems.”
The study was sponsored by Neurona Therapeutics and funded in part by the California Institute for Regenerative Medicine. Dr. Beach and Dr. Spencer report no relevant financial relationships. Several investigators are employees of Neurona Therapeutics. Dr. Rost reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AAN 2023