User login
ATV injuries: where risk taking and medical helplessness collide
I. Hate. ATVs.
The modern world is full of potentially dangerous things that we regulate – sometimes by the knowledge of the person giving it (medication) or by age (tobacco, alcohol, cars). Or sometimes we simply ban something altogether (illicit drugs).
After years of neurology practice, I’ve learned to hate ATVs. Outside of firearms, I don’t think I’ve seen any gadget that has such a devastating effect on young lives.

My first medical encounter with one was 20-some years ago during my neurosurgery rotation. It was a man in his mid-20s. He was young, muscular, and clearly in excellent condition. And here he was, flaccid below the neck, and permanently on a ventilator.
I sat at the nurses station for a long time, looking at him and thinking about how a young life can go so horribly wrong so quickly. He hadn’t been drunk at the time. He’d simply had a wreck, the cause of which I never found out. After a few days, he was shipped off to a long-term ventilator facility, and I never saw him again.
Cars are dangerous, too, but are bigger and have gadgets to try to improve safety. ATVs are exposed, with only minimal, if any, protection for their riders. Their use is most typically by the young, meaning a disproportionate number of serious injuries will affect those at the beginning of adulthood.
Sadly, banning ATVs won’t stop injuries. There will always be people who do risky things in the name of being daring and having fun.
What’s changed is that 100 years ago they’d likely have died of their injuries soon afterward. Today they’ll probably survive, debilitated long term because of medical advancements.
These are the situations where I feel helpless. There are all kinds of horrible diseases we handle that have no known cause or cure. That’s one kind of helpless. But the ones with easily avoidable risk factors (ATVs, illegal drugs, tobacco) that occur are just plain frustrating for us and tragic for the patients and families.
In the land of the free, freedom to endanger your own life and health are pretty deeply entrenched. The best we can do is present people with the facts and let them make informed decisions about risky behaviors (sadly, the young often believe they’re immortal). If we ban ATVs, we still won’t stop people from making bad decisions on motorcycles or in cars, or with firearms or illegal drugs.
Like so much in medicine, there are no easy answers, and there likely never will be.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I. Hate. ATVs.
The modern world is full of potentially dangerous things that we regulate – sometimes by the knowledge of the person giving it (medication) or by age (tobacco, alcohol, cars). Or sometimes we simply ban something altogether (illicit drugs).
After years of neurology practice, I’ve learned to hate ATVs. Outside of firearms, I don’t think I’ve seen any gadget that has such a devastating effect on young lives.
My first medical encounter with one was 20-some years ago during my neurosurgery rotation. It was a man in his mid-20s. He was young, muscular, and clearly in excellent condition. And here he was, flaccid below the neck, and permanently on a ventilator.
I sat at the nurses station for a long time, looking at him and thinking about how a young life can go so horribly wrong so quickly. He hadn’t been drunk at the time. He’d simply had a wreck, the cause of which I never found out. After a few days, he was shipped off to a long-term ventilator facility, and I never saw him again.
Cars are dangerous, too, but are bigger and have gadgets to try to improve safety. ATVs are exposed, with only minimal, if any, protection for their riders. Their use is most typically by the young, meaning a disproportionate number of serious injuries will affect those at the beginning of adulthood.
Sadly, banning ATVs won’t stop injuries. There will always be people who do risky things in the name of being daring and having fun.
What’s changed is that 100 years ago they’d likely have died of their injuries soon afterward. Today they’ll probably survive, debilitated long term because of medical advancements.
These are the situations where I feel helpless. There are all kinds of horrible diseases we handle that have no known cause or cure. That’s one kind of helpless. But the ones with easily avoidable risk factors (ATVs, illegal drugs, tobacco) that occur are just plain frustrating for us and tragic for the patients and families.
In the land of the free, freedom to endanger your own life and health are pretty deeply entrenched. The best we can do is present people with the facts and let them make informed decisions about risky behaviors (sadly, the young often believe they’re immortal). If we ban ATVs, we still won’t stop people from making bad decisions on motorcycles or in cars, or with firearms or illegal drugs.
Like so much in medicine, there are no easy answers, and there likely never will be.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I. Hate. ATVs.
The modern world is full of potentially dangerous things that we regulate – sometimes by the knowledge of the person giving it (medication) or by age (tobacco, alcohol, cars). Or sometimes we simply ban something altogether (illicit drugs).
After years of neurology practice, I’ve learned to hate ATVs. Outside of firearms, I don’t think I’ve seen any gadget that has such a devastating effect on young lives.
My first medical encounter with one was 20-some years ago during my neurosurgery rotation. It was a man in his mid-20s. He was young, muscular, and clearly in excellent condition. And here he was, flaccid below the neck, and permanently on a ventilator.
I sat at the nurses station for a long time, looking at him and thinking about how a young life can go so horribly wrong so quickly. He hadn’t been drunk at the time. He’d simply had a wreck, the cause of which I never found out. After a few days, he was shipped off to a long-term ventilator facility, and I never saw him again.
Cars are dangerous, too, but are bigger and have gadgets to try to improve safety. ATVs are exposed, with only minimal, if any, protection for their riders. Their use is most typically by the young, meaning a disproportionate number of serious injuries will affect those at the beginning of adulthood.
Sadly, banning ATVs won’t stop injuries. There will always be people who do risky things in the name of being daring and having fun.
What’s changed is that 100 years ago they’d likely have died of their injuries soon afterward. Today they’ll probably survive, debilitated long term because of medical advancements.
These are the situations where I feel helpless. There are all kinds of horrible diseases we handle that have no known cause or cure. That’s one kind of helpless. But the ones with easily avoidable risk factors (ATVs, illegal drugs, tobacco) that occur are just plain frustrating for us and tragic for the patients and families.
In the land of the free, freedom to endanger your own life and health are pretty deeply entrenched. The best we can do is present people with the facts and let them make informed decisions about risky behaviors (sadly, the young often believe they’re immortal). If we ban ATVs, we still won’t stop people from making bad decisions on motorcycles or in cars, or with firearms or illegal drugs.
Like so much in medicine, there are no easy answers, and there likely never will be.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.

The EHR Report: The vortex that sucks you in
Recently, a colleague of ours described the office electronic health record as “the vortex that sucks you in.” This statement occurred during a departmental meeting focused on physician burnout. When members of the department were asked about what things they felt contributed to a feeling of dissatisfaction with work, the electronic health record quickly emerged as a common denominator of dissatisfaction. There were certainly other contributors – the changing and challenging medical environment, fighting with insurance companies, decreased autonomy over practice decisions – but far and away the most cited contributor to dissatisfaction among members of the department was the EHR.
The reasons that EHRs have led to dissatisfaction seem to have changed over the last few years. Initially, physicians found it difficult to suddenly adapt practice styles developed over many years to the new world of electronic documentation. Suddenly they needed to type (or in the case of many, hunt and peck) notes into the history of present illness and fit patient histories into templates seemingly developed by engineers rather than physicians. Now, while most of us have adapted to the logistics of the EHR, there is no escaping the increasing demands for more and more information. There is also ongoing frustration with the lack of control in deciding whether information is relevant for the patient, as well as disparity between the promise and expectation of what electronic records should deliver and what we experience each day in front of us.

Given the degree to which EHRs are contributing to physician dissatisfaction and burnout, it is incumbent upon us to figure out ways to make the EHR work better for clinicians. The literature describes burnout as “a syndrome characterized by a loss of enthusiasm for work (emotional exhaustion), feelings of cynicism (depersonalization), and a low sense of personal accomplishment.” In a recent study, almost half of all physicians described at least one symptom of burnout. Interestingly, physician burnout is greatest in primary care specialties. Surprisingly, compared with other working adults in the United States, physicians are more likely to have symptoms of burnout (38% vs 28%) as well as express dissatisfaction with their work-life balance (40% vs. 23%).1 This issue is important because burnout – in addition to its negative effects on physicians’ experience and quality of life – can erode the quality of the care they give, increase the risk of medical errors, and lead to early ending of lifelong careers.2 The literature suggests that the high prevalence of burnout among U.S. physicians means that “the problem lies more with the system and environment in which physicians work rather than being due to innate vulnerabilities in a few susceptible individuals.” Not surprisingly, we have received letters from readers of our column over many years discussing how the entry of EHRs into their practice was a critical influence in their decisions to retire early.
In our discussion after the department meeting, several physicians described the need to do charting at night from home in order to have their work accomplished for the next day. This is not surprising to any of us who work in primary care and use EHRs. The ability to have access to the EHR anytime and from anywhere is a classic double-edged sword. It is certainly convenient to be able to complete our charting from home without having to stay late in the office on nights and weekends. Unfortunately, bringing work home also erodes into time that could otherwise be spent with family and pursuing other interests.
This is just one of many frustrations. Another common issue is superfluous documentation on the part of specialists. Often, the information is entered by physician extenders or using canned macros to “pad” the note. Sifting through paragraphs of this irrelevant – and sometimes inaccurate – information in consultant notes devalues the integrity of the interaction. It also minimizes the time that was actually spent in the office doing the real hard work of medicine instead of the rudimentary work of documenting things that were either never said or mentioned briefly in passing.
The week after our department meeting was the first week of work for our new interns. Rounding in one of our nursing homes, I handed the intern a patient’s chart and began to explain how the chart was organized – where the orders, progress notes, and labs were located in the chart. The intern had an odd smile on her face. I asked her what was wrong. She replied, “I didn’t know anyone still had paper charts; how do you enter a note there?”
So we come full circle. You can’t miss what you never had. Younger physicians do not resent the EHR, nor can they perceive the EHR to be contributing to discontent. That is not to say that it does not contribute; it is just difficult to identify problems when the way things are is what you have always known. The issue of EHRs contributing to physician burnout is real, and we need to learn more about its causes. Please email us with your thoughts about the aspects of EHRs that you find most frustrating or challenging. Our goal in hearing from you is that it is only by knowing the challenges that we face that we can begin to formulate solutions to overcome those challenges and together make tomorrow’s practice better than today’s.
References
1. Shanafelt TD et al. Burnout and satisfaction with work-life balance among U.S. physicians relative to the general U.S. population. Arch Intern Med. 2012;172(18):1377-85.
2. Shanafelt TD, Balch CM, Bechamps G et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records.
Recently, a colleague of ours described the office electronic health record as “the vortex that sucks you in.” This statement occurred during a departmental meeting focused on physician burnout. When members of the department were asked about what things they felt contributed to a feeling of dissatisfaction with work, the electronic health record quickly emerged as a common denominator of dissatisfaction. There were certainly other contributors – the changing and challenging medical environment, fighting with insurance companies, decreased autonomy over practice decisions – but far and away the most cited contributor to dissatisfaction among members of the department was the EHR.
The reasons that EHRs have led to dissatisfaction seem to have changed over the last few years. Initially, physicians found it difficult to suddenly adapt practice styles developed over many years to the new world of electronic documentation. Suddenly they needed to type (or in the case of many, hunt and peck) notes into the history of present illness and fit patient histories into templates seemingly developed by engineers rather than physicians. Now, while most of us have adapted to the logistics of the EHR, there is no escaping the increasing demands for more and more information. There is also ongoing frustration with the lack of control in deciding whether information is relevant for the patient, as well as disparity between the promise and expectation of what electronic records should deliver and what we experience each day in front of us.
Given the degree to which EHRs are contributing to physician dissatisfaction and burnout, it is incumbent upon us to figure out ways to make the EHR work better for clinicians. The literature describes burnout as “a syndrome characterized by a loss of enthusiasm for work (emotional exhaustion), feelings of cynicism (depersonalization), and a low sense of personal accomplishment.” In a recent study, almost half of all physicians described at least one symptom of burnout. Interestingly, physician burnout is greatest in primary care specialties. Surprisingly, compared with other working adults in the United States, physicians are more likely to have symptoms of burnout (38% vs 28%) as well as express dissatisfaction with their work-life balance (40% vs. 23%).1 This issue is important because burnout – in addition to its negative effects on physicians’ experience and quality of life – can erode the quality of the care they give, increase the risk of medical errors, and lead to early ending of lifelong careers.2 The literature suggests that the high prevalence of burnout among U.S. physicians means that “the problem lies more with the system and environment in which physicians work rather than being due to innate vulnerabilities in a few susceptible individuals.” Not surprisingly, we have received letters from readers of our column over many years discussing how the entry of EHRs into their practice was a critical influence in their decisions to retire early.
In our discussion after the department meeting, several physicians described the need to do charting at night from home in order to have their work accomplished for the next day. This is not surprising to any of us who work in primary care and use EHRs. The ability to have access to the EHR anytime and from anywhere is a classic double-edged sword. It is certainly convenient to be able to complete our charting from home without having to stay late in the office on nights and weekends. Unfortunately, bringing work home also erodes into time that could otherwise be spent with family and pursuing other interests.
This is just one of many frustrations. Another common issue is superfluous documentation on the part of specialists. Often, the information is entered by physician extenders or using canned macros to “pad” the note. Sifting through paragraphs of this irrelevant – and sometimes inaccurate – information in consultant notes devalues the integrity of the interaction. It also minimizes the time that was actually spent in the office doing the real hard work of medicine instead of the rudimentary work of documenting things that were either never said or mentioned briefly in passing.
The week after our department meeting was the first week of work for our new interns. Rounding in one of our nursing homes, I handed the intern a patient’s chart and began to explain how the chart was organized – where the orders, progress notes, and labs were located in the chart. The intern had an odd smile on her face. I asked her what was wrong. She replied, “I didn’t know anyone still had paper charts; how do you enter a note there?”
So we come full circle. You can’t miss what you never had. Younger physicians do not resent the EHR, nor can they perceive the EHR to be contributing to discontent. That is not to say that it does not contribute; it is just difficult to identify problems when the way things are is what you have always known. The issue of EHRs contributing to physician burnout is real, and we need to learn more about its causes. Please email us with your thoughts about the aspects of EHRs that you find most frustrating or challenging. Our goal in hearing from you is that it is only by knowing the challenges that we face that we can begin to formulate solutions to overcome those challenges and together make tomorrow’s practice better than today’s.
References
1. Shanafelt TD et al. Burnout and satisfaction with work-life balance among U.S. physicians relative to the general U.S. population. Arch Intern Med. 2012;172(18):1377-85.
2. Shanafelt TD, Balch CM, Bechamps G et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records.
Recently, a colleague of ours described the office electronic health record as “the vortex that sucks you in.” This statement occurred during a departmental meeting focused on physician burnout. When members of the department were asked about what things they felt contributed to a feeling of dissatisfaction with work, the electronic health record quickly emerged as a common denominator of dissatisfaction. There were certainly other contributors – the changing and challenging medical environment, fighting with insurance companies, decreased autonomy over practice decisions – but far and away the most cited contributor to dissatisfaction among members of the department was the EHR.
The reasons that EHRs have led to dissatisfaction seem to have changed over the last few years. Initially, physicians found it difficult to suddenly adapt practice styles developed over many years to the new world of electronic documentation. Suddenly they needed to type (or in the case of many, hunt and peck) notes into the history of present illness and fit patient histories into templates seemingly developed by engineers rather than physicians. Now, while most of us have adapted to the logistics of the EHR, there is no escaping the increasing demands for more and more information. There is also ongoing frustration with the lack of control in deciding whether information is relevant for the patient, as well as disparity between the promise and expectation of what electronic records should deliver and what we experience each day in front of us.
Given the degree to which EHRs are contributing to physician dissatisfaction and burnout, it is incumbent upon us to figure out ways to make the EHR work better for clinicians. The literature describes burnout as “a syndrome characterized by a loss of enthusiasm for work (emotional exhaustion), feelings of cynicism (depersonalization), and a low sense of personal accomplishment.” In a recent study, almost half of all physicians described at least one symptom of burnout. Interestingly, physician burnout is greatest in primary care specialties. Surprisingly, compared with other working adults in the United States, physicians are more likely to have symptoms of burnout (38% vs 28%) as well as express dissatisfaction with their work-life balance (40% vs. 23%).1 This issue is important because burnout – in addition to its negative effects on physicians’ experience and quality of life – can erode the quality of the care they give, increase the risk of medical errors, and lead to early ending of lifelong careers.2 The literature suggests that the high prevalence of burnout among U.S. physicians means that “the problem lies more with the system and environment in which physicians work rather than being due to innate vulnerabilities in a few susceptible individuals.” Not surprisingly, we have received letters from readers of our column over many years discussing how the entry of EHRs into their practice was a critical influence in their decisions to retire early.
In our discussion after the department meeting, several physicians described the need to do charting at night from home in order to have their work accomplished for the next day. This is not surprising to any of us who work in primary care and use EHRs. The ability to have access to the EHR anytime and from anywhere is a classic double-edged sword. It is certainly convenient to be able to complete our charting from home without having to stay late in the office on nights and weekends. Unfortunately, bringing work home also erodes into time that could otherwise be spent with family and pursuing other interests.
This is just one of many frustrations. Another common issue is superfluous documentation on the part of specialists. Often, the information is entered by physician extenders or using canned macros to “pad” the note. Sifting through paragraphs of this irrelevant – and sometimes inaccurate – information in consultant notes devalues the integrity of the interaction. It also minimizes the time that was actually spent in the office doing the real hard work of medicine instead of the rudimentary work of documenting things that were either never said or mentioned briefly in passing.
The week after our department meeting was the first week of work for our new interns. Rounding in one of our nursing homes, I handed the intern a patient’s chart and began to explain how the chart was organized – where the orders, progress notes, and labs were located in the chart. The intern had an odd smile on her face. I asked her what was wrong. She replied, “I didn’t know anyone still had paper charts; how do you enter a note there?”
So we come full circle. You can’t miss what you never had. Younger physicians do not resent the EHR, nor can they perceive the EHR to be contributing to discontent. That is not to say that it does not contribute; it is just difficult to identify problems when the way things are is what you have always known. The issue of EHRs contributing to physician burnout is real, and we need to learn more about its causes. Please email us with your thoughts about the aspects of EHRs that you find most frustrating or challenging. Our goal in hearing from you is that it is only by knowing the challenges that we face that we can begin to formulate solutions to overcome those challenges and together make tomorrow’s practice better than today’s.
References
1. Shanafelt TD et al. Burnout and satisfaction with work-life balance among U.S. physicians relative to the general U.S. population. Arch Intern Med. 2012;172(18):1377-85.
2. Shanafelt TD, Balch CM, Bechamps G et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University, Philadelphia. Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is also a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records.

Law & Medicine: Discovery rule and statute of limitations
Question: In July 2002, a patient in California underwent surgery for a herniated T8-9 disk, but the surgeon instead removed the T6-7 and T7-8 disks. On Sept. 11, 2002, the surgeon discussed with the patient the MRI findings showing his mistake. On Sept. 17, 2003, the patient filed a malpractice lawsuit, just 6 days beyond California’s 1-year limitations period. California subscribes to the discovery rule, that is, a cause of action accrues only when a claimant discovers or should have discovered injury was the result of negligence.
Which of the following choices is best?
A. The lawsuit filed Sept. 17, 2003, is time barred, as the negligent surgery took place in July 2002.
B. On its face, the lawsuit was filed too late, being 1 year and 6 days after the Sept. 11, 2002, discussion date.
C. The lawsuit was timely filed, so long as the claimant can prove he was out of town for more than 6 days of that year.
D. The patient should sue as an action in battery, which has a longer statute of limitations.
E. All choices except A are correct.
Answer: E. At common law, there was no time limit that barred a plaintiff from bringing a claim, although an equitable doctrine of laches existed to foreclose an action that had long lapsed. Statutory changes in the law now require that lawsuits be brought in a timely manner so that the evidence remains fresh, accurate, and reliable.

Another reason is to provide repose to the wrongdoer, that is, relief from worrying for an indefinite period of time whether a lawsuit will be brought. This time period, during which a lawsuit must be filed or it will be barred, is termed the statute of limitations. It is 2 years for the tort of negligence in most jurisdictions, with states such as California and Tennessee placing a 1-year limit on medical malpractice claims. In California, the running of the statute is tolled (temporarily halted) for the days a claimant is out of state.
The above case scenario is taken from Kaplan v. Mamelak,1 where the plaintiff’s lawsuit was not barred to allow him to identify the number of days he was out of town. The court also permitted a cause of action in battery, which is covered under a longer statute of limitations, as well as one sounding in malpractice.
Patients who are injured from malpractice may not always be aware that a negligent act had taken place, and some injuries may remain latent for a long period. Recognizing this, statutes of limitation emphasize the date when the plaintiff first discovered that the injury resulted from negligence. This is termed the discovery rule.
Stated more formally, the limitations period commences at the time the cause of action (negligence or other wrongs) accrues, and this usually means when the claimant knew (actual knowledge) or should have known (constructive knowledge).
The rule, in the words of one court, is meant to balance the need for “prompt assertion of claims” against a policy “favoring adjudication of claims on the merits and ensuring that a party with a valid claim will be given an opportunity to present it.”
As is typical of other jurisdictions, Hawaii sought to clarify the discovery rule in a series of court cases, beginning with Yoshizaki v. Hilo Hospital,2 where the court deemed a cause of action “does not begin to run until the plaintiff knew or should have known of the defendant’s negligence.”
Subsequently, Hawaii’s Intermediate Court of Appeals explained that the state’s 2-year limitations statute commences when the plaintiff discovers, or through the use of reasonable diligence should have discovered, 1) the damage; 2) the violation of the duty; and 3) the causal connection between the violation of the duty and the damage.3
The court subsequently held that the rule prevents the running of the limitations period until “the plaintiff [has] knowledge of those facts which are necessary for an actionable claim.”4 In 1999, the Hawaii Supreme Court clarified that it was “factual knowledge,” rather than “legal knowledge,” that starts the clock running, and that legal knowledge of a defendant’s negligence was not required.5
More recently, litigation over the time barring of claims was evident in Moon v. Rhode,6 where Dr. Clarissa Rhode and Central Illinois Radiological Associates were sued for negligently misreading a patient’s CT scans.
The 90-year-old patient, Kathryn Moon, was admitted to Proctor Hospital May 18, 2009, and died 11 days later following surgery and complications of fluid overload and a pneumoperitoneum. Dr. Rhode, a radiologist, interpreted two CT scans, which an independent expert in 2013 determined were negligently misread. A lawsuit was then brought against Dr. Rhode, who was not a named defendant when the plaintiff had timely filed a medical negligence action back in 2011 against the surgeon and the attending doctor.
The court of appeals held that the discovery rule can be applied to wrongful death and survival actions, and that the statute of limitations begins to run when the plaintiff knows or should have known that the death was “wrongfully caused.” However, this did not necessarily mean knowledge of a specific defendant’s negligent conduct or knowledge of the existence of a cause of action.
The court stated: “Plaintiff filed his complaint long after he became possessed with sufficient information, which put him on inquiry to determine whether actionable conduct was involved.” The court ruled that the relevant inquiry was not when the plaintiff became aware that Dr. Rhode may have committed medical negligence, but when any defendant may have committed medical negligence against the patient Kathryn. The case is currently on appeal to the Supreme Court of Illinois.
In addition to the discovery rule, other situations may toll the limitations period. One example is fraudulent concealment of a right of action, where the statute may be tolled during the period of concealment. And in all jurisdictions, the running of the time period is halted in malpractice complaints involving treatment of a minor until that minor reaches a certain age, such as age of majority, or after a stipulated number of years, for example, 6 years.
Occasionally, a health care provider may overlook an important tolling provision. California, for example, has a rule that any “payment” made to an injured party must be accompanied by a written statement regarding the applicable statute of limitations.
In the recent Coastal Surgical Institute v. Blevins case,7 the defendant surgeon made a payment of $4,118.23 for medical expenses incurred by an unrepresented plaintiff, but had neglected to attach a release or a written notice regarding the statute of limitations. The plaintiff subsequently decided to file a lawsuit, even though more than a year – the statutory period – had lapsed.
Under the facts, the limitation period was tolled, and the trial court allowed the case to go forward, ultimately finding liability and awarding damages of $500,000, later reduced to $285,114. The court of appeals affirmed the decision.
This case has prompted MIEC, a malpractice insurance carrier, to emphasize putting in writing the restrictions imposed by the limitations statute to any unrepresented patient. MIEC also warned that the term “payment” might be construed liberally, citing case examples that include a free counseling session and the provision of specialized care for a student injured by a school’s gym equipment.
References
1. Kaplan v. Mamelak, 162 Cal. App. 4th 637 (2008).
2. Yoshizaki v. Hilo Hospital, 433 P.2d 220 (1967).
3. Jacoby v. Kaiser Foundation Hospital, 622 P.2d 613 (1981).
4. Yamaguchi v. Queen’s Medical Center, 648 P.2d 689 (1982).
5. Buck v. Miles, 971 P.2d 717 (1999).
6. Moon v. Rhode, IL. 2015 App. 3d 130613.
7. Coastal Surgical Institute v. Blevins, 232 Cal. App. 4th 1321 (2015).
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. It is adapted from the author’s book, “Medical Malpractice: Understanding the Law, Managing the Risk” (2006). For additional information, readers may contact the author at siang@hawaii.edu.
Question: In July 2002, a patient in California underwent surgery for a herniated T8-9 disk, but the surgeon instead removed the T6-7 and T7-8 disks. On Sept. 11, 2002, the surgeon discussed with the patient the MRI findings showing his mistake. On Sept. 17, 2003, the patient filed a malpractice lawsuit, just 6 days beyond California’s 1-year limitations period. California subscribes to the discovery rule, that is, a cause of action accrues only when a claimant discovers or should have discovered injury was the result of negligence.
Which of the following choices is best?
A. The lawsuit filed Sept. 17, 2003, is time barred, as the negligent surgery took place in July 2002.
B. On its face, the lawsuit was filed too late, being 1 year and 6 days after the Sept. 11, 2002, discussion date.
C. The lawsuit was timely filed, so long as the claimant can prove he was out of town for more than 6 days of that year.
D. The patient should sue as an action in battery, which has a longer statute of limitations.
E. All choices except A are correct.
Answer: E. At common law, there was no time limit that barred a plaintiff from bringing a claim, although an equitable doctrine of laches existed to foreclose an action that had long lapsed. Statutory changes in the law now require that lawsuits be brought in a timely manner so that the evidence remains fresh, accurate, and reliable.
Another reason is to provide repose to the wrongdoer, that is, relief from worrying for an indefinite period of time whether a lawsuit will be brought. This time period, during which a lawsuit must be filed or it will be barred, is termed the statute of limitations. It is 2 years for the tort of negligence in most jurisdictions, with states such as California and Tennessee placing a 1-year limit on medical malpractice claims. In California, the running of the statute is tolled (temporarily halted) for the days a claimant is out of state.
The above case scenario is taken from Kaplan v. Mamelak,1 where the plaintiff’s lawsuit was not barred to allow him to identify the number of days he was out of town. The court also permitted a cause of action in battery, which is covered under a longer statute of limitations, as well as one sounding in malpractice.
Patients who are injured from malpractice may not always be aware that a negligent act had taken place, and some injuries may remain latent for a long period. Recognizing this, statutes of limitation emphasize the date when the plaintiff first discovered that the injury resulted from negligence. This is termed the discovery rule.
Stated more formally, the limitations period commences at the time the cause of action (negligence or other wrongs) accrues, and this usually means when the claimant knew (actual knowledge) or should have known (constructive knowledge).
The rule, in the words of one court, is meant to balance the need for “prompt assertion of claims” against a policy “favoring adjudication of claims on the merits and ensuring that a party with a valid claim will be given an opportunity to present it.”
As is typical of other jurisdictions, Hawaii sought to clarify the discovery rule in a series of court cases, beginning with Yoshizaki v. Hilo Hospital,2 where the court deemed a cause of action “does not begin to run until the plaintiff knew or should have known of the defendant’s negligence.”
Subsequently, Hawaii’s Intermediate Court of Appeals explained that the state’s 2-year limitations statute commences when the plaintiff discovers, or through the use of reasonable diligence should have discovered, 1) the damage; 2) the violation of the duty; and 3) the causal connection between the violation of the duty and the damage.3
The court subsequently held that the rule prevents the running of the limitations period until “the plaintiff [has] knowledge of those facts which are necessary for an actionable claim.”4 In 1999, the Hawaii Supreme Court clarified that it was “factual knowledge,” rather than “legal knowledge,” that starts the clock running, and that legal knowledge of a defendant’s negligence was not required.5
More recently, litigation over the time barring of claims was evident in Moon v. Rhode,6 where Dr. Clarissa Rhode and Central Illinois Radiological Associates were sued for negligently misreading a patient’s CT scans.
The 90-year-old patient, Kathryn Moon, was admitted to Proctor Hospital May 18, 2009, and died 11 days later following surgery and complications of fluid overload and a pneumoperitoneum. Dr. Rhode, a radiologist, interpreted two CT scans, which an independent expert in 2013 determined were negligently misread. A lawsuit was then brought against Dr. Rhode, who was not a named defendant when the plaintiff had timely filed a medical negligence action back in 2011 against the surgeon and the attending doctor.
The court of appeals held that the discovery rule can be applied to wrongful death and survival actions, and that the statute of limitations begins to run when the plaintiff knows or should have known that the death was “wrongfully caused.” However, this did not necessarily mean knowledge of a specific defendant’s negligent conduct or knowledge of the existence of a cause of action.
The court stated: “Plaintiff filed his complaint long after he became possessed with sufficient information, which put him on inquiry to determine whether actionable conduct was involved.” The court ruled that the relevant inquiry was not when the plaintiff became aware that Dr. Rhode may have committed medical negligence, but when any defendant may have committed medical negligence against the patient Kathryn. The case is currently on appeal to the Supreme Court of Illinois.
In addition to the discovery rule, other situations may toll the limitations period. One example is fraudulent concealment of a right of action, where the statute may be tolled during the period of concealment. And in all jurisdictions, the running of the time period is halted in malpractice complaints involving treatment of a minor until that minor reaches a certain age, such as age of majority, or after a stipulated number of years, for example, 6 years.
Occasionally, a health care provider may overlook an important tolling provision. California, for example, has a rule that any “payment” made to an injured party must be accompanied by a written statement regarding the applicable statute of limitations.
In the recent Coastal Surgical Institute v. Blevins case,7 the defendant surgeon made a payment of $4,118.23 for medical expenses incurred by an unrepresented plaintiff, but had neglected to attach a release or a written notice regarding the statute of limitations. The plaintiff subsequently decided to file a lawsuit, even though more than a year – the statutory period – had lapsed.
Under the facts, the limitation period was tolled, and the trial court allowed the case to go forward, ultimately finding liability and awarding damages of $500,000, later reduced to $285,114. The court of appeals affirmed the decision.
This case has prompted MIEC, a malpractice insurance carrier, to emphasize putting in writing the restrictions imposed by the limitations statute to any unrepresented patient. MIEC also warned that the term “payment” might be construed liberally, citing case examples that include a free counseling session and the provision of specialized care for a student injured by a school’s gym equipment.
References
1. Kaplan v. Mamelak, 162 Cal. App. 4th 637 (2008).
2. Yoshizaki v. Hilo Hospital, 433 P.2d 220 (1967).
3. Jacoby v. Kaiser Foundation Hospital, 622 P.2d 613 (1981).
4. Yamaguchi v. Queen’s Medical Center, 648 P.2d 689 (1982).
5. Buck v. Miles, 971 P.2d 717 (1999).
6. Moon v. Rhode, IL. 2015 App. 3d 130613.
7. Coastal Surgical Institute v. Blevins, 232 Cal. App. 4th 1321 (2015).
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. It is adapted from the author’s book, “Medical Malpractice: Understanding the Law, Managing the Risk” (2006). For additional information, readers may contact the author at siang@hawaii.edu.
Question: In July 2002, a patient in California underwent surgery for a herniated T8-9 disk, but the surgeon instead removed the T6-7 and T7-8 disks. On Sept. 11, 2002, the surgeon discussed with the patient the MRI findings showing his mistake. On Sept. 17, 2003, the patient filed a malpractice lawsuit, just 6 days beyond California’s 1-year limitations period. California subscribes to the discovery rule, that is, a cause of action accrues only when a claimant discovers or should have discovered injury was the result of negligence.
Which of the following choices is best?
A. The lawsuit filed Sept. 17, 2003, is time barred, as the negligent surgery took place in July 2002.
B. On its face, the lawsuit was filed too late, being 1 year and 6 days after the Sept. 11, 2002, discussion date.
C. The lawsuit was timely filed, so long as the claimant can prove he was out of town for more than 6 days of that year.
D. The patient should sue as an action in battery, which has a longer statute of limitations.
E. All choices except A are correct.
Answer: E. At common law, there was no time limit that barred a plaintiff from bringing a claim, although an equitable doctrine of laches existed to foreclose an action that had long lapsed. Statutory changes in the law now require that lawsuits be brought in a timely manner so that the evidence remains fresh, accurate, and reliable.
Another reason is to provide repose to the wrongdoer, that is, relief from worrying for an indefinite period of time whether a lawsuit will be brought. This time period, during which a lawsuit must be filed or it will be barred, is termed the statute of limitations. It is 2 years for the tort of negligence in most jurisdictions, with states such as California and Tennessee placing a 1-year limit on medical malpractice claims. In California, the running of the statute is tolled (temporarily halted) for the days a claimant is out of state.
The above case scenario is taken from Kaplan v. Mamelak,1 where the plaintiff’s lawsuit was not barred to allow him to identify the number of days he was out of town. The court also permitted a cause of action in battery, which is covered under a longer statute of limitations, as well as one sounding in malpractice.
Patients who are injured from malpractice may not always be aware that a negligent act had taken place, and some injuries may remain latent for a long period. Recognizing this, statutes of limitation emphasize the date when the plaintiff first discovered that the injury resulted from negligence. This is termed the discovery rule.
Stated more formally, the limitations period commences at the time the cause of action (negligence or other wrongs) accrues, and this usually means when the claimant knew (actual knowledge) or should have known (constructive knowledge).
The rule, in the words of one court, is meant to balance the need for “prompt assertion of claims” against a policy “favoring adjudication of claims on the merits and ensuring that a party with a valid claim will be given an opportunity to present it.”
As is typical of other jurisdictions, Hawaii sought to clarify the discovery rule in a series of court cases, beginning with Yoshizaki v. Hilo Hospital,2 where the court deemed a cause of action “does not begin to run until the plaintiff knew or should have known of the defendant’s negligence.”
Subsequently, Hawaii’s Intermediate Court of Appeals explained that the state’s 2-year limitations statute commences when the plaintiff discovers, or through the use of reasonable diligence should have discovered, 1) the damage; 2) the violation of the duty; and 3) the causal connection between the violation of the duty and the damage.3
The court subsequently held that the rule prevents the running of the limitations period until “the plaintiff [has] knowledge of those facts which are necessary for an actionable claim.”4 In 1999, the Hawaii Supreme Court clarified that it was “factual knowledge,” rather than “legal knowledge,” that starts the clock running, and that legal knowledge of a defendant’s negligence was not required.5
More recently, litigation over the time barring of claims was evident in Moon v. Rhode,6 where Dr. Clarissa Rhode and Central Illinois Radiological Associates were sued for negligently misreading a patient’s CT scans.
The 90-year-old patient, Kathryn Moon, was admitted to Proctor Hospital May 18, 2009, and died 11 days later following surgery and complications of fluid overload and a pneumoperitoneum. Dr. Rhode, a radiologist, interpreted two CT scans, which an independent expert in 2013 determined were negligently misread. A lawsuit was then brought against Dr. Rhode, who was not a named defendant when the plaintiff had timely filed a medical negligence action back in 2011 against the surgeon and the attending doctor.
The court of appeals held that the discovery rule can be applied to wrongful death and survival actions, and that the statute of limitations begins to run when the plaintiff knows or should have known that the death was “wrongfully caused.” However, this did not necessarily mean knowledge of a specific defendant’s negligent conduct or knowledge of the existence of a cause of action.
The court stated: “Plaintiff filed his complaint long after he became possessed with sufficient information, which put him on inquiry to determine whether actionable conduct was involved.” The court ruled that the relevant inquiry was not when the plaintiff became aware that Dr. Rhode may have committed medical negligence, but when any defendant may have committed medical negligence against the patient Kathryn. The case is currently on appeal to the Supreme Court of Illinois.
In addition to the discovery rule, other situations may toll the limitations period. One example is fraudulent concealment of a right of action, where the statute may be tolled during the period of concealment. And in all jurisdictions, the running of the time period is halted in malpractice complaints involving treatment of a minor until that minor reaches a certain age, such as age of majority, or after a stipulated number of years, for example, 6 years.
Occasionally, a health care provider may overlook an important tolling provision. California, for example, has a rule that any “payment” made to an injured party must be accompanied by a written statement regarding the applicable statute of limitations.
In the recent Coastal Surgical Institute v. Blevins case,7 the defendant surgeon made a payment of $4,118.23 for medical expenses incurred by an unrepresented plaintiff, but had neglected to attach a release or a written notice regarding the statute of limitations. The plaintiff subsequently decided to file a lawsuit, even though more than a year – the statutory period – had lapsed.
Under the facts, the limitation period was tolled, and the trial court allowed the case to go forward, ultimately finding liability and awarding damages of $500,000, later reduced to $285,114. The court of appeals affirmed the decision.
This case has prompted MIEC, a malpractice insurance carrier, to emphasize putting in writing the restrictions imposed by the limitations statute to any unrepresented patient. MIEC also warned that the term “payment” might be construed liberally, citing case examples that include a free counseling session and the provision of specialized care for a student injured by a school’s gym equipment.
References
1. Kaplan v. Mamelak, 162 Cal. App. 4th 637 (2008).
2. Yoshizaki v. Hilo Hospital, 433 P.2d 220 (1967).
3. Jacoby v. Kaiser Foundation Hospital, 622 P.2d 613 (1981).
4. Yamaguchi v. Queen’s Medical Center, 648 P.2d 689 (1982).
5. Buck v. Miles, 971 P.2d 717 (1999).
6. Moon v. Rhode, IL. 2015 App. 3d 130613.
7. Coastal Surgical Institute v. Blevins, 232 Cal. App. 4th 1321 (2015).
Dr. Tan is emeritus professor of medicine and a former adjunct professor of law at the University of Hawaii. This article is meant to be educational and does not constitute medical, ethical, or legal advice. It is adapted from the author’s book, “Medical Malpractice: Understanding the Law, Managing the Risk” (2006). For additional information, readers may contact the author at siang@hawaii.edu.

Outpatient parenteral antimicrobial therapy for homeless patients saves lives, cuts costs
Prolonged hospitalizations for complicated patients with severe infections who need long courses of intravenous antibiotics, are common in many institutions.
Outpatient parenteral antimicrobial therapy (OPAT) is a safe and cost-effective way to administer intravenous (IV) antimicrobial therapy to patients with the potential to decrease hospital length of stay (LOS). OPAT programs train motivated patients in self-administration of IV medications at home, in a stable environment. Ideally, infectious disease (ID) consultation should be involved to determine appropriate candidates for OPAT as well as a suitable drug regimen and duration of therapy.

A potential barrier to successful utilization of OPAT programs is the need for stable housing at discharge for home infusion services.
Challenge facing homeless patients
There is very little published data regarding the use of OPAT at a medical respite facility for homeless patients. This may be due to perceived concerns of difficulty in administering OPAT to these disadvantaged patients for multiple reasons such as unstable or no housing, inability to stay engaged in medical care, and underlying mental illness and substance abuse problems. In particular, active substance abuse, specifically injection drug use (IDU), is a significant problem.
Traditionally, homeless patients requiring ongoing parenteral therapy have remained inpatient for the duration of their course, which can cause significant inpatient discharge delays and increased LOS. Recommending long-term parenteral therapy as an inpatient for all patients who are homeless or have a history of IDU can lead to prolonged hospitalizations, increased health care costs and contribute to conflicts between patients and staff.
Our study, recently published in the Journal of Hospital Medicine (J Hosp Med. 2016 Apr 27. doi: 10.1002/jhm.2597), aimed to evaluate our experience with administering OPAT to homeless patients at a medical respite facility and to determine if patients could complete a successful treatment course of antibiotics for a variety of illnesses.
We demonstrated that 87% of homeless patients were able to complete a defined course of antibiotic therapy, and 64% were successfully treated with OPAT at medical respite. To our knowledge this is the first study evaluating this specific population (including those with homelessness, mental illness, substance abuse) in which OPAT was received at medical respite.
Our rate of adverse events was 7%, similar to other OPAT studies in the published literature. Our total readmission rate of 30% was similar to what current literature suggests. Our data suggest that providing OPAT to homeless patients is feasible at a medical respite facility with care coordination between members of a multidisciplinary team, including nursing, home infusion pharmacist, and ID clinic.
Partnering with medical respite programs is important, as home infusion services are not available otherwise to homeless patients. The recommendation for ID consultation is beneficial to determine candidacy for OPAT, including close scrutiny of social behaviors in the OPAT patient selection process, and can assist with transitions in care from inpatient to outpatient setting.
Homeless IDU patients remain a challenging population to treat with long term IV antibiotics. However, in certain circumstances, IDU alone may not be a reason to fully exclude someone from OPAT candidacy. Careful review of substance abuse history and evaluation of psychosocial factors are needed. Furthermore, an evaluation of the patient’s willingness to comply with care agreements while inpatient and at medical respite, and ensuring appropriate resources for chemical dependency treatment are needed. Early consideration of oral antimicrobial options if the patient is readmitted for complications/non-adherence should be encouraged.
Medical respite programs
Treating homeless IDU patients with OPAT is possible under close supervision at medical respite. Our patients sign an agreement to refrain from using their IV access for drug use. Security seals are used on all connections and tubing to prevent tampering. The IV access sites are inspected daily, and ID providers are contacted to discuss any patients suspicious of tampering with their IV to determine plan of care – either readmission or transition to oral antibiotics.
Medical respite programs are gaining in popularity in the United States. Medical respite can help engage patients in follow-up care and provide linkage to housing, mental health, and chemical dependency services. Many programs support harm reduction IDU practices and offer referrals for substance abuse treatment programs, which are not typically offered during inpatient admission in most hospitals.
Medical respite may continue to be a site of OPAT expansion, as there is continued pressure to discharge nonacute patients from the hospital. Moving forward, it may be beneficial for hospitals, public health departments, and communities to support these programs, which can assist with close monitoring of homeless patients receiving OPAT.
There are ongoing challenges for housed IDU patients who require OPAT, as medical respite placement and home infusion are generally not options, and skilled nursing facility placement can be difficult. Careful review of substance abuse history; evaluation of psychosocial factors, such as housing status; mental health history; and outpatient support systems are needed.
Again, ID consultation is highly recommended to determine appropriate IV therapy, and if possible, early transition to oral antimicrobial therapy, as well as duration of treatment for specific illnesses on a case-by-case basis. Close follow-up is needed to ensure patient compliance with prescribed antimicrobial regimen, sometimes requiring weekly visits.
OPAT is effective for many patients, and it is optimal to utilize ID consultation to determine appropriate candidates – particularly among homeless and IDU patients. OPAT can be successful in a closely monitored medical respite setting for homeless patients with multiple comorbidities, with the help of a multidisciplinary team. Medical respite OPAT can decrease LOS in patients who would otherwise require long hospitalizations, resulting in overall cost savings.
Shireesha Dhanireddy, MD, is medical director of the infectious disease clinic at Harborview Medical Center, Seattle. Alison Beieler, PA-C, MPAS, runs the OPAT program in the infectious disease clinic at Harborview Medical Center.
Prolonged hospitalizations for complicated patients with severe infections who need long courses of intravenous antibiotics, are common in many institutions.
Outpatient parenteral antimicrobial therapy (OPAT) is a safe and cost-effective way to administer intravenous (IV) antimicrobial therapy to patients with the potential to decrease hospital length of stay (LOS). OPAT programs train motivated patients in self-administration of IV medications at home, in a stable environment. Ideally, infectious disease (ID) consultation should be involved to determine appropriate candidates for OPAT as well as a suitable drug regimen and duration of therapy.
A potential barrier to successful utilization of OPAT programs is the need for stable housing at discharge for home infusion services.
Challenge facing homeless patients
There is very little published data regarding the use of OPAT at a medical respite facility for homeless patients. This may be due to perceived concerns of difficulty in administering OPAT to these disadvantaged patients for multiple reasons such as unstable or no housing, inability to stay engaged in medical care, and underlying mental illness and substance abuse problems. In particular, active substance abuse, specifically injection drug use (IDU), is a significant problem.
Traditionally, homeless patients requiring ongoing parenteral therapy have remained inpatient for the duration of their course, which can cause significant inpatient discharge delays and increased LOS. Recommending long-term parenteral therapy as an inpatient for all patients who are homeless or have a history of IDU can lead to prolonged hospitalizations, increased health care costs and contribute to conflicts between patients and staff.
Our study, recently published in the Journal of Hospital Medicine (J Hosp Med. 2016 Apr 27. doi: 10.1002/jhm.2597), aimed to evaluate our experience with administering OPAT to homeless patients at a medical respite facility and to determine if patients could complete a successful treatment course of antibiotics for a variety of illnesses.
We demonstrated that 87% of homeless patients were able to complete a defined course of antibiotic therapy, and 64% were successfully treated with OPAT at medical respite. To our knowledge this is the first study evaluating this specific population (including those with homelessness, mental illness, substance abuse) in which OPAT was received at medical respite.
Our rate of adverse events was 7%, similar to other OPAT studies in the published literature. Our total readmission rate of 30% was similar to what current literature suggests. Our data suggest that providing OPAT to homeless patients is feasible at a medical respite facility with care coordination between members of a multidisciplinary team, including nursing, home infusion pharmacist, and ID clinic.
Partnering with medical respite programs is important, as home infusion services are not available otherwise to homeless patients. The recommendation for ID consultation is beneficial to determine candidacy for OPAT, including close scrutiny of social behaviors in the OPAT patient selection process, and can assist with transitions in care from inpatient to outpatient setting.
Homeless IDU patients remain a challenging population to treat with long term IV antibiotics. However, in certain circumstances, IDU alone may not be a reason to fully exclude someone from OPAT candidacy. Careful review of substance abuse history and evaluation of psychosocial factors are needed. Furthermore, an evaluation of the patient’s willingness to comply with care agreements while inpatient and at medical respite, and ensuring appropriate resources for chemical dependency treatment are needed. Early consideration of oral antimicrobial options if the patient is readmitted for complications/non-adherence should be encouraged.
Medical respite programs
Treating homeless IDU patients with OPAT is possible under close supervision at medical respite. Our patients sign an agreement to refrain from using their IV access for drug use. Security seals are used on all connections and tubing to prevent tampering. The IV access sites are inspected daily, and ID providers are contacted to discuss any patients suspicious of tampering with their IV to determine plan of care – either readmission or transition to oral antibiotics.
Medical respite programs are gaining in popularity in the United States. Medical respite can help engage patients in follow-up care and provide linkage to housing, mental health, and chemical dependency services. Many programs support harm reduction IDU practices and offer referrals for substance abuse treatment programs, which are not typically offered during inpatient admission in most hospitals.
Medical respite may continue to be a site of OPAT expansion, as there is continued pressure to discharge nonacute patients from the hospital. Moving forward, it may be beneficial for hospitals, public health departments, and communities to support these programs, which can assist with close monitoring of homeless patients receiving OPAT.
There are ongoing challenges for housed IDU patients who require OPAT, as medical respite placement and home infusion are generally not options, and skilled nursing facility placement can be difficult. Careful review of substance abuse history; evaluation of psychosocial factors, such as housing status; mental health history; and outpatient support systems are needed.
Again, ID consultation is highly recommended to determine appropriate IV therapy, and if possible, early transition to oral antimicrobial therapy, as well as duration of treatment for specific illnesses on a case-by-case basis. Close follow-up is needed to ensure patient compliance with prescribed antimicrobial regimen, sometimes requiring weekly visits.
OPAT is effective for many patients, and it is optimal to utilize ID consultation to determine appropriate candidates – particularly among homeless and IDU patients. OPAT can be successful in a closely monitored medical respite setting for homeless patients with multiple comorbidities, with the help of a multidisciplinary team. Medical respite OPAT can decrease LOS in patients who would otherwise require long hospitalizations, resulting in overall cost savings.
Shireesha Dhanireddy, MD, is medical director of the infectious disease clinic at Harborview Medical Center, Seattle. Alison Beieler, PA-C, MPAS, runs the OPAT program in the infectious disease clinic at Harborview Medical Center.
Prolonged hospitalizations for complicated patients with severe infections who need long courses of intravenous antibiotics, are common in many institutions.
Outpatient parenteral antimicrobial therapy (OPAT) is a safe and cost-effective way to administer intravenous (IV) antimicrobial therapy to patients with the potential to decrease hospital length of stay (LOS). OPAT programs train motivated patients in self-administration of IV medications at home, in a stable environment. Ideally, infectious disease (ID) consultation should be involved to determine appropriate candidates for OPAT as well as a suitable drug regimen and duration of therapy.
A potential barrier to successful utilization of OPAT programs is the need for stable housing at discharge for home infusion services.
Challenge facing homeless patients
There is very little published data regarding the use of OPAT at a medical respite facility for homeless patients. This may be due to perceived concerns of difficulty in administering OPAT to these disadvantaged patients for multiple reasons such as unstable or no housing, inability to stay engaged in medical care, and underlying mental illness and substance abuse problems. In particular, active substance abuse, specifically injection drug use (IDU), is a significant problem.
Traditionally, homeless patients requiring ongoing parenteral therapy have remained inpatient for the duration of their course, which can cause significant inpatient discharge delays and increased LOS. Recommending long-term parenteral therapy as an inpatient for all patients who are homeless or have a history of IDU can lead to prolonged hospitalizations, increased health care costs and contribute to conflicts between patients and staff.
Our study, recently published in the Journal of Hospital Medicine (J Hosp Med. 2016 Apr 27. doi: 10.1002/jhm.2597), aimed to evaluate our experience with administering OPAT to homeless patients at a medical respite facility and to determine if patients could complete a successful treatment course of antibiotics for a variety of illnesses.
We demonstrated that 87% of homeless patients were able to complete a defined course of antibiotic therapy, and 64% were successfully treated with OPAT at medical respite. To our knowledge this is the first study evaluating this specific population (including those with homelessness, mental illness, substance abuse) in which OPAT was received at medical respite.
Our rate of adverse events was 7%, similar to other OPAT studies in the published literature. Our total readmission rate of 30% was similar to what current literature suggests. Our data suggest that providing OPAT to homeless patients is feasible at a medical respite facility with care coordination between members of a multidisciplinary team, including nursing, home infusion pharmacist, and ID clinic.
Partnering with medical respite programs is important, as home infusion services are not available otherwise to homeless patients. The recommendation for ID consultation is beneficial to determine candidacy for OPAT, including close scrutiny of social behaviors in the OPAT patient selection process, and can assist with transitions in care from inpatient to outpatient setting.
Homeless IDU patients remain a challenging population to treat with long term IV antibiotics. However, in certain circumstances, IDU alone may not be a reason to fully exclude someone from OPAT candidacy. Careful review of substance abuse history and evaluation of psychosocial factors are needed. Furthermore, an evaluation of the patient’s willingness to comply with care agreements while inpatient and at medical respite, and ensuring appropriate resources for chemical dependency treatment are needed. Early consideration of oral antimicrobial options if the patient is readmitted for complications/non-adherence should be encouraged.
Medical respite programs
Treating homeless IDU patients with OPAT is possible under close supervision at medical respite. Our patients sign an agreement to refrain from using their IV access for drug use. Security seals are used on all connections and tubing to prevent tampering. The IV access sites are inspected daily, and ID providers are contacted to discuss any patients suspicious of tampering with their IV to determine plan of care – either readmission or transition to oral antibiotics.
Medical respite programs are gaining in popularity in the United States. Medical respite can help engage patients in follow-up care and provide linkage to housing, mental health, and chemical dependency services. Many programs support harm reduction IDU practices and offer referrals for substance abuse treatment programs, which are not typically offered during inpatient admission in most hospitals.
Medical respite may continue to be a site of OPAT expansion, as there is continued pressure to discharge nonacute patients from the hospital. Moving forward, it may be beneficial for hospitals, public health departments, and communities to support these programs, which can assist with close monitoring of homeless patients receiving OPAT.
There are ongoing challenges for housed IDU patients who require OPAT, as medical respite placement and home infusion are generally not options, and skilled nursing facility placement can be difficult. Careful review of substance abuse history; evaluation of psychosocial factors, such as housing status; mental health history; and outpatient support systems are needed.
Again, ID consultation is highly recommended to determine appropriate IV therapy, and if possible, early transition to oral antimicrobial therapy, as well as duration of treatment for specific illnesses on a case-by-case basis. Close follow-up is needed to ensure patient compliance with prescribed antimicrobial regimen, sometimes requiring weekly visits.
OPAT is effective for many patients, and it is optimal to utilize ID consultation to determine appropriate candidates – particularly among homeless and IDU patients. OPAT can be successful in a closely monitored medical respite setting for homeless patients with multiple comorbidities, with the help of a multidisciplinary team. Medical respite OPAT can decrease LOS in patients who would otherwise require long hospitalizations, resulting in overall cost savings.
Shireesha Dhanireddy, MD, is medical director of the infectious disease clinic at Harborview Medical Center, Seattle. Alison Beieler, PA-C, MPAS, runs the OPAT program in the infectious disease clinic at Harborview Medical Center.

ACO Insider: Not ready for an ACO? Think CPC+
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”

As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”
As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.
The Centers for Medicare & Medicaid Services in April announced its newest initiative, Comprehensive Primary Care Plus, to target primary care practices of varying capabilities to participate in an innovative payment model designed to support the delivery of comprehensive primary care that rewards value and quality.
“Strengthening primary care is critical to an effective health care system,” said Patrick Conway, MD, CMS deputy administrator and chief medical officer. “By supporting primary care doctors and clinicians to spend time with patients, serve patients’ needs outside of the office visit, and better coordinate care with specialists, we can continue to build a health care system that results in healthier people and smarter spending of our health care dollars.”
As readers of this column know, these are also the engines of accountable care organization success. So, if you and your patient-centered medical home are not in a Medicare ACO, this gets you going on high-value activities – and pays you monthly to do it.
The rub is that once you are in the Medicare Shared Savings Program, you can’t continue with this initiative. But, it’s a great “on ramp” to prep you for ACO success. You get monthly payments instead of waiting 18 months for shared savings that you may or may not get under the Medicare Shared Savings Program.
CPC+ is an advanced primary medical home model, created from lessons learned in the Comprehensive Primary Care Initiative and the Multi-Payer Advanced Primary Care Practice Demonstration. Similar to these programs, multi-payer engagement is an essential component of the model.
In the CPC+ model, the CMS intends to nationally solicit a variety of payers committed to strengthening primary care in up to 20 regions and accept up to 5,000 practices to participate in those regions. The CPC+ program is further evidence that primary care should not only be a fundamental component to moving our health care system to one that awards clinicians based on the quality, not quantity, of care they give patients, but that payment redesign must provide flexibility to accommodate the diverse needs of primary care practices.
What to know about payment
To provide this flexibility and to attract practices of varying capabilities and levels of experience, the CPC+ program offers two tracks with different payment options, which include a monthly care management fee, comprehensive primary care payments, and performance-based incentive payments.
In track 1, the CMS will pay practices a risk-adjusted prospective monthly care management fee ($15 per beneficiary per month [PBPM] average across four risk tiers), in addition to the fee-for-service payments under the Medicare Physician Fee Schedule for activities.
In track 2, the Medicare monthly care management fees will average $28 PBPM across five risk tiers, which includes a $100 care management fee to support care for patients with the most complex needs. Instead of full Medicare fee-for-service payments for evaluation and management services, track 2 practices will receive a hybrid of reduced Medicare fee-for-service payments and up-front comprehensive primary care payments for those services.
In addition, the CMS is providing incentive payments at $2.50 PBPM for track 1 and $4 PBPM for track 2, based on practice performance on utilization metrics and quality, measured at the practice level. While these payments are prepaid at the beginning of a performance year, they are subject to recoupment if the practice does not meet thresholds for quality and utilization performance.
What to know about participation
To participate, your practice must be located within 1 of the 20 regional geographic areas selected by the CMS and must serve not only Medicare beneficiaries, but patients covered by one or more additional participating payers.
You may apply for either track 1 or track 2, but participation for the entire 5-year period will be within a single track.
All practices will be expected to deliver a set of five comprehensive primary care functions and have certified electronic health record technology capabilities. Track 2 practices will be expected to focus on a core set of advance capabilities for health information technology and must submit a letter of support from their health IT vendors. The CMS may require a track 2 applicant to participate in track 1.
Participating in the CPC+ program limits your ability to fully participate in or utilize other CMS initiatives, models, or demonstrations, however – including the Medicare Shared Savings Program and Next Generation ACO, or bill for the chronic care management fee. This is a big trade-off for practices well down the value transformation path, but an opportunity for those getting started.
Although the shift to payment for improved population health can herald the golden age of primary care, you cannot default on this opportunity through inaction. It is urgent that you choose a path to value-care delivery. CPC+ provides the ability for greater cash flow and flexibility for primary care practices to deliver high-quality, whole-person patient-centered care.
Mr. Bobbitt is head of the health law group at the Smith Anderson law firm in Raleigh, N.C. He is president of Value Health Partners, LLC, a health care strategic consulting company. He has years of experience assisting physicians to form integrated delivery systems and prepare for the value-based compensation era. Mr. Parker is a member of the health law group at Smith Anderson and works with Mr. Bobbitt to guide physicians regarding preparing for value-based care. This article is meant to be educational and does not constitute legal advice. For additional information, readers may contact the author at bbobbitt@smithlaw.com or 919-821-6612.

Choosing the transaxillary or supraclavicular approach for neurogenic TOS
The transaxillary approach has its advantages
I began my vascular fellowship at UCLA on July 1, 1986 – the previous day I was a chief surgery resident running a VA general surgery service where my last emergency case that evening was an abdominal peroneal resection for perforated rectal cancer! I was delighted to begin my fellowship, and learned that on Tuesdays I would be operating with Herb Machleder, MD – the expert on thoracic outlet syndrome (TOS) who perfected the transaxillary approach. I remembered his service from when I was an intern holding the patient arm up by cradling it my arms while he and the fellow removed the rib and identified each structure—subclavius tendon, subclavian vein, anterior scalene muscle, subclavian artery brachial plexus and any other abnormal band or structure present. The rib was removed in entirety to ensure an excellent outcome and to prevent any possibility of recurrence from scarring to the brachial plexus to a portion of retained rib. Dr. Machleder then went on to design a rib retractor to better support the arm and afford superb visibility.
As I began my career, I included transaxillary first rib resection as part of my practice for all forms of TOS, except when we needed to replace the subclavian artery because of an aneurysm or thrombosis. In those instances, we would employ the supraclavicular approach with an infraclavicular incision when necessary. In my 5 years as chief of the division of vascular surgery at UCLA (1998-2003), we saw many patients with TOS thanks to the legacy and practice of Dr. Machleder. We performed approximately 300 such operations between three of us and saw probably three to four times as many patients in clinic who did not need surgery to treat their TOS or other conditions.

When I arrived at Johns Hopkins as department chair in 2003, a robust thoracic outlet program did not exist there, so we began one. By the time I left in 2014, we were seeing 5-7 new patients per week and were operating on 125 per year, of which half were neurogenic. Ying Wei Lum, MD, and Maggie Arnold, MD, are continuing that practice at Johns Hopkins today.
The most important point about the “approach” for neurogenic thoracic outlet syndrome is whether or not you should operate. At Johns Hopkins, we only operated on about a third of those who presented to us with neurogenic symptoms, as 60%-70% will get better with a thoracic outlet–focused physical therapy regimen. We developed a protocol for this, which we actually handed to the patients as the prescription as they came from all over for our opinion on their conditions. We are doing the same at UC Davis.
We have published a great deal about patients who do not do as well with the surgical approach to neurogenic TOS. These patients include those over the age of 40 and those who have had symptoms for more than 10 years, as they tend to be quite debilitated and never quite recover fully from the operation.1 A scalene block with lidocaine can predict success in patients with the operation, and I use it in older patients or those with multiple complaints.2 At UC Davis, our pain service can perform the block with ultrasound guidance, which is easier for the patient.
Other patients who do not do well with the surgical approach to neurogenic TOS include those with other comorbidities such as cervical spine disease and shoulder abnormalities or injuries, as well as those with a severe dependence on pain medication due to such medical issues as complex pain syndrome or myofasciitis caused by comorbid diseases.3
These patients cannot adequately perform the requisite postoperative physical therapy to completely improve, and some can take up to a year to get range of motion and strength back. We also found that patients who smoke get recurrent disease due to scarring.
At both UC Davis and Johns Hopkins, we created a YouTube video for patients to educate them on the procedure and expected results. The need for postoperative physical therapy should be emphasized in all patients. Some require more therapy than others, which means taking time off from work to focus on the therapy and not performing other activities until the pain and discomfort are gone and strength is back. In another study we performed, we found that if patients did improve the first year, they were more likely to stay symptom free over many years.
While we were doing a transaxillary rib resection case at UC Davis, my team, which includes my partner Misty Humphries, MD, created a list of the top 10 reasons that the transaxillary approach is preferred for neurogenic thoracic outlet syndrome:
1. The scar is less noticeable and painful for the patient than the scar in the supraclavicular fossa, allowing the patient to start physical therapy 2 weeks after surgery.
2. The Machleder retractor makes visualization easy and stable, and allows all members of the team to see the anatomy.
3. The brachial plexus does not have to be retracted and is out of harm’s way, so no temporary palsies are seen in the postoperative period.
4. The subclavius tendon can be seen in entirety and the anterior portion of the rib is easy to completely remove.
5. The subclavian vein can be seen in entirety and defines the anterior portion of the dissection.
6. Once the anterior scalenectomy muscle is cut, the subclavian artery naturally retracts cephalad and is no longer near the rib when it is to be removed.
7. The posterior portion of the rib can be completely removed by readjusting the retraction and a second cut can be done safely with either the rib cutter or the first rib rongeur. It is essential to remove the rib posteriorly behind the nerve root so the arm is adducted and the nerve does not come in contact with the remaining rib, as we feel that leads to increased recurrences.
8. Two operating surgeons can address the rib from their side of the table and completely resect the rib, depending on the patient’s soft bony anatomy, by angling the instruments from either side.
9. Even large muscular or obese patients can be safely approached from the axilla utilizing the Machleder retractor and a lighted retractor.
10. The transaxillary approach can be taught through the teaching video we have made and through the ability for both surgeons to see because of the retractor.
Some of my favorite memories as a vascular surgeon were operating on Tuesdays with Dr. Machleder – similar to Tuesdays with Morrie.4 Not only did we remove ribs safely and completely, but he also taught me philosophy of surgery and of life. I hope I am doing the same with my team as we remove ribs now on Thursday – “Thursdays with Freischlag” – at UC Davis.
Dr. Freischlag is vice chancellor for human health sciences and dean of the school of medicine at the University of California, Davis. She had no relevant disclosures.
References
1. J Vasc Surg. 2012;55(5):1370-5.
2. Curr Treat Options Cardiovasc Med. 2009;11(2):176-83.
3. J Vasc Surg. 2012;56(4):1061-7.
Use a supraclavicular approach: My way is best!
The best sense we have of the pathophysiology of neurogenic (NTOS) is that the scalene triangle is “too tight” with regard to what it contains – the brachial plexus and the subclavian artery. Whether this is due to the triangle being too small or the nerves being “too large” (inflammation) is unknown. Supporting the former theory are observations that the anterior scalene muscle is frequently inflamed and/or chronically injured.1 but others have suggested that the first rib is abnormally located or elevated.2 In addition, some have suggested that inflammatory tissue surrounding the plexus contributes to the process, at least for chronic cases.3
Given the fact that at least two of the three parts of the triangle, plus tissue surrounding the plexus itself, have all been implicated in the disease process, why not choose an approach that allows correction of all potential causes? The transaxillary approach has been used for decades for this condition, but can only decompress the base of the triangle (first rib) and, to varying degrees, only part of the anterior scalene. It does not allow thorough exploration of the nerves. The supraclavicular approach (and the supraclavicular half of paraclavicular excision) addresses these concerns. First, the anterior scalene muscle is essentially entirely removed. With proper technique it is completely visible from the scalene tubercle to its origin at the spine. This approach also allows removal of all muscular and associated tissue medially, completely clearing the parietal pleura at the apex of the lung, at least theoretically reducing the chances of scar tissue arising from residual tissue here.

Second, although no research has yet implicated the middle scalene (scalenus medius, which does not translate perfectly), many patients have impressively bulky musculature at this site. The middle scalene is also completely resected while approaching the first rib; perhaps removing this as well contributes to the excellent results we see today.
Third, the entire portion of the rib involved in NTOS (and the entire rib altogether if a paraclavicular approach is used) is very easily removed using this approach, as are any cervical ribs or Roos bands. Everything is seen, and everything can be evaluated and resected. Finally, many consider full neurolysis of the brachial plexus in this area an important part of the procedure. This is based on low-grade evidence only,3 but in the author’s experience, the incidence of improvement or cure seems to be higher, and recurrence rates lower, than with less-complete operations.
Parenthetically, related to this issue is that of visualization and education. The primary goal is ensuring the best outcome for the patient. Visualization is, by far, best if a supraclavicular approach is used. This is beneficial clinically by ensuring the most complete decompression of the nerves and avoidance of complications, but also is extremely helpful with regard to educating residents and fellows, learning the anatomy, identifying aberrant structures, and so on. Even with the best techniques (including a head- or retractor-mounted camera), no one can see what’s going on during a transaxillary approach except for the operator.
If the supraclavicular approach allows better access to and removal of all the potentially involved components causing NTOS, why doesn’t everyone use it? One answer is that the potential complication rate may be higher. Both the long thoracic and phrenic nerves are very much more at risk using this approach than using the transaxillary approach, and, on the left side, the risk of thoracic duct injury is higher. It must be conceded that published results, in general, do not show significant differences in outcomes between the two approaches.4 However, many would interpret this as a type II error, combined with the “fuzziness” of diagnosis and evaluation of outcomes this field has labored under. However, the opposite interpretation should be considered – there are no definitive data showing any higher complication rate between the two approaches. This debate likely is answerable in the same fashion as many other such debates in our field – someone who is good at the transaxillary approach will do a better job than someone who is not, and someone who is good at the supraclavicular approach will do a better job than someone who is not.
Is a prospective trial indicated? In theory, yes. However, the relative rarity of this condition, the fact that most surgeons follow almost exclusively one or the other technique, and the categorical nature of the outcome variable make such a trial relatively impractical. Pending this, the best suggestion is obviously to pick the best TOS surgeon you can find and have him or her fix the problem in the way they are most experienced!
Dr. Illig is professor of surgery and director, division of vascular surgery, and associate chair, faculty development and mentoring, University of South Florida, Morsani College of Medicine, Tampa, Fla. He had no relevant disclosures.
References
2. Thoracic Outlet Syndrome. London: Springer 2013; 319-21.
The transaxillary approach has its advantages
I began my vascular fellowship at UCLA on July 1, 1986 – the previous day I was a chief surgery resident running a VA general surgery service where my last emergency case that evening was an abdominal peroneal resection for perforated rectal cancer! I was delighted to begin my fellowship, and learned that on Tuesdays I would be operating with Herb Machleder, MD – the expert on thoracic outlet syndrome (TOS) who perfected the transaxillary approach. I remembered his service from when I was an intern holding the patient arm up by cradling it my arms while he and the fellow removed the rib and identified each structure—subclavius tendon, subclavian vein, anterior scalene muscle, subclavian artery brachial plexus and any other abnormal band or structure present. The rib was removed in entirety to ensure an excellent outcome and to prevent any possibility of recurrence from scarring to the brachial plexus to a portion of retained rib. Dr. Machleder then went on to design a rib retractor to better support the arm and afford superb visibility.
As I began my career, I included transaxillary first rib resection as part of my practice for all forms of TOS, except when we needed to replace the subclavian artery because of an aneurysm or thrombosis. In those instances, we would employ the supraclavicular approach with an infraclavicular incision when necessary. In my 5 years as chief of the division of vascular surgery at UCLA (1998-2003), we saw many patients with TOS thanks to the legacy and practice of Dr. Machleder. We performed approximately 300 such operations between three of us and saw probably three to four times as many patients in clinic who did not need surgery to treat their TOS or other conditions.
When I arrived at Johns Hopkins as department chair in 2003, a robust thoracic outlet program did not exist there, so we began one. By the time I left in 2014, we were seeing 5-7 new patients per week and were operating on 125 per year, of which half were neurogenic. Ying Wei Lum, MD, and Maggie Arnold, MD, are continuing that practice at Johns Hopkins today.
The most important point about the “approach” for neurogenic thoracic outlet syndrome is whether or not you should operate. At Johns Hopkins, we only operated on about a third of those who presented to us with neurogenic symptoms, as 60%-70% will get better with a thoracic outlet–focused physical therapy regimen. We developed a protocol for this, which we actually handed to the patients as the prescription as they came from all over for our opinion on their conditions. We are doing the same at UC Davis.
We have published a great deal about patients who do not do as well with the surgical approach to neurogenic TOS. These patients include those over the age of 40 and those who have had symptoms for more than 10 years, as they tend to be quite debilitated and never quite recover fully from the operation.1 A scalene block with lidocaine can predict success in patients with the operation, and I use it in older patients or those with multiple complaints.2 At UC Davis, our pain service can perform the block with ultrasound guidance, which is easier for the patient.
Other patients who do not do well with the surgical approach to neurogenic TOS include those with other comorbidities such as cervical spine disease and shoulder abnormalities or injuries, as well as those with a severe dependence on pain medication due to such medical issues as complex pain syndrome or myofasciitis caused by comorbid diseases.3
These patients cannot adequately perform the requisite postoperative physical therapy to completely improve, and some can take up to a year to get range of motion and strength back. We also found that patients who smoke get recurrent disease due to scarring.
At both UC Davis and Johns Hopkins, we created a YouTube video for patients to educate them on the procedure and expected results. The need for postoperative physical therapy should be emphasized in all patients. Some require more therapy than others, which means taking time off from work to focus on the therapy and not performing other activities until the pain and discomfort are gone and strength is back. In another study we performed, we found that if patients did improve the first year, they were more likely to stay symptom free over many years.
While we were doing a transaxillary rib resection case at UC Davis, my team, which includes my partner Misty Humphries, MD, created a list of the top 10 reasons that the transaxillary approach is preferred for neurogenic thoracic outlet syndrome:
1. The scar is less noticeable and painful for the patient than the scar in the supraclavicular fossa, allowing the patient to start physical therapy 2 weeks after surgery.
2. The Machleder retractor makes visualization easy and stable, and allows all members of the team to see the anatomy.
3. The brachial plexus does not have to be retracted and is out of harm’s way, so no temporary palsies are seen in the postoperative period.
4. The subclavius tendon can be seen in entirety and the anterior portion of the rib is easy to completely remove.
5. The subclavian vein can be seen in entirety and defines the anterior portion of the dissection.
6. Once the anterior scalenectomy muscle is cut, the subclavian artery naturally retracts cephalad and is no longer near the rib when it is to be removed.
7. The posterior portion of the rib can be completely removed by readjusting the retraction and a second cut can be done safely with either the rib cutter or the first rib rongeur. It is essential to remove the rib posteriorly behind the nerve root so the arm is adducted and the nerve does not come in contact with the remaining rib, as we feel that leads to increased recurrences.
8. Two operating surgeons can address the rib from their side of the table and completely resect the rib, depending on the patient’s soft bony anatomy, by angling the instruments from either side.
9. Even large muscular or obese patients can be safely approached from the axilla utilizing the Machleder retractor and a lighted retractor.
10. The transaxillary approach can be taught through the teaching video we have made and through the ability for both surgeons to see because of the retractor.
Some of my favorite memories as a vascular surgeon were operating on Tuesdays with Dr. Machleder – similar to Tuesdays with Morrie.4 Not only did we remove ribs safely and completely, but he also taught me philosophy of surgery and of life. I hope I am doing the same with my team as we remove ribs now on Thursday – “Thursdays with Freischlag” – at UC Davis.
Dr. Freischlag is vice chancellor for human health sciences and dean of the school of medicine at the University of California, Davis. She had no relevant disclosures.
References
1. J Vasc Surg. 2012;55(5):1370-5.
2. Curr Treat Options Cardiovasc Med. 2009;11(2):176-83.
3. J Vasc Surg. 2012;56(4):1061-7.
Use a supraclavicular approach: My way is best!
The best sense we have of the pathophysiology of neurogenic (NTOS) is that the scalene triangle is “too tight” with regard to what it contains – the brachial plexus and the subclavian artery. Whether this is due to the triangle being too small or the nerves being “too large” (inflammation) is unknown. Supporting the former theory are observations that the anterior scalene muscle is frequently inflamed and/or chronically injured.1 but others have suggested that the first rib is abnormally located or elevated.2 In addition, some have suggested that inflammatory tissue surrounding the plexus contributes to the process, at least for chronic cases.3
Given the fact that at least two of the three parts of the triangle, plus tissue surrounding the plexus itself, have all been implicated in the disease process, why not choose an approach that allows correction of all potential causes? The transaxillary approach has been used for decades for this condition, but can only decompress the base of the triangle (first rib) and, to varying degrees, only part of the anterior scalene. It does not allow thorough exploration of the nerves. The supraclavicular approach (and the supraclavicular half of paraclavicular excision) addresses these concerns. First, the anterior scalene muscle is essentially entirely removed. With proper technique it is completely visible from the scalene tubercle to its origin at the spine. This approach also allows removal of all muscular and associated tissue medially, completely clearing the parietal pleura at the apex of the lung, at least theoretically reducing the chances of scar tissue arising from residual tissue here.
Second, although no research has yet implicated the middle scalene (scalenus medius, which does not translate perfectly), many patients have impressively bulky musculature at this site. The middle scalene is also completely resected while approaching the first rib; perhaps removing this as well contributes to the excellent results we see today.
Third, the entire portion of the rib involved in NTOS (and the entire rib altogether if a paraclavicular approach is used) is very easily removed using this approach, as are any cervical ribs or Roos bands. Everything is seen, and everything can be evaluated and resected. Finally, many consider full neurolysis of the brachial plexus in this area an important part of the procedure. This is based on low-grade evidence only,3 but in the author’s experience, the incidence of improvement or cure seems to be higher, and recurrence rates lower, than with less-complete operations.
Parenthetically, related to this issue is that of visualization and education. The primary goal is ensuring the best outcome for the patient. Visualization is, by far, best if a supraclavicular approach is used. This is beneficial clinically by ensuring the most complete decompression of the nerves and avoidance of complications, but also is extremely helpful with regard to educating residents and fellows, learning the anatomy, identifying aberrant structures, and so on. Even with the best techniques (including a head- or retractor-mounted camera), no one can see what’s going on during a transaxillary approach except for the operator.
If the supraclavicular approach allows better access to and removal of all the potentially involved components causing NTOS, why doesn’t everyone use it? One answer is that the potential complication rate may be higher. Both the long thoracic and phrenic nerves are very much more at risk using this approach than using the transaxillary approach, and, on the left side, the risk of thoracic duct injury is higher. It must be conceded that published results, in general, do not show significant differences in outcomes between the two approaches.4 However, many would interpret this as a type II error, combined with the “fuzziness” of diagnosis and evaluation of outcomes this field has labored under. However, the opposite interpretation should be considered – there are no definitive data showing any higher complication rate between the two approaches. This debate likely is answerable in the same fashion as many other such debates in our field – someone who is good at the transaxillary approach will do a better job than someone who is not, and someone who is good at the supraclavicular approach will do a better job than someone who is not.
Is a prospective trial indicated? In theory, yes. However, the relative rarity of this condition, the fact that most surgeons follow almost exclusively one or the other technique, and the categorical nature of the outcome variable make such a trial relatively impractical. Pending this, the best suggestion is obviously to pick the best TOS surgeon you can find and have him or her fix the problem in the way they are most experienced!
Dr. Illig is professor of surgery and director, division of vascular surgery, and associate chair, faculty development and mentoring, University of South Florida, Morsani College of Medicine, Tampa, Fla. He had no relevant disclosures.
References
2. Thoracic Outlet Syndrome. London: Springer 2013; 319-21.
The transaxillary approach has its advantages
I began my vascular fellowship at UCLA on July 1, 1986 – the previous day I was a chief surgery resident running a VA general surgery service where my last emergency case that evening was an abdominal peroneal resection for perforated rectal cancer! I was delighted to begin my fellowship, and learned that on Tuesdays I would be operating with Herb Machleder, MD – the expert on thoracic outlet syndrome (TOS) who perfected the transaxillary approach. I remembered his service from when I was an intern holding the patient arm up by cradling it my arms while he and the fellow removed the rib and identified each structure—subclavius tendon, subclavian vein, anterior scalene muscle, subclavian artery brachial plexus and any other abnormal band or structure present. The rib was removed in entirety to ensure an excellent outcome and to prevent any possibility of recurrence from scarring to the brachial plexus to a portion of retained rib. Dr. Machleder then went on to design a rib retractor to better support the arm and afford superb visibility.
As I began my career, I included transaxillary first rib resection as part of my practice for all forms of TOS, except when we needed to replace the subclavian artery because of an aneurysm or thrombosis. In those instances, we would employ the supraclavicular approach with an infraclavicular incision when necessary. In my 5 years as chief of the division of vascular surgery at UCLA (1998-2003), we saw many patients with TOS thanks to the legacy and practice of Dr. Machleder. We performed approximately 300 such operations between three of us and saw probably three to four times as many patients in clinic who did not need surgery to treat their TOS or other conditions.
When I arrived at Johns Hopkins as department chair in 2003, a robust thoracic outlet program did not exist there, so we began one. By the time I left in 2014, we were seeing 5-7 new patients per week and were operating on 125 per year, of which half were neurogenic. Ying Wei Lum, MD, and Maggie Arnold, MD, are continuing that practice at Johns Hopkins today.
The most important point about the “approach” for neurogenic thoracic outlet syndrome is whether or not you should operate. At Johns Hopkins, we only operated on about a third of those who presented to us with neurogenic symptoms, as 60%-70% will get better with a thoracic outlet–focused physical therapy regimen. We developed a protocol for this, which we actually handed to the patients as the prescription as they came from all over for our opinion on their conditions. We are doing the same at UC Davis.
We have published a great deal about patients who do not do as well with the surgical approach to neurogenic TOS. These patients include those over the age of 40 and those who have had symptoms for more than 10 years, as they tend to be quite debilitated and never quite recover fully from the operation.1 A scalene block with lidocaine can predict success in patients with the operation, and I use it in older patients or those with multiple complaints.2 At UC Davis, our pain service can perform the block with ultrasound guidance, which is easier for the patient.
Other patients who do not do well with the surgical approach to neurogenic TOS include those with other comorbidities such as cervical spine disease and shoulder abnormalities or injuries, as well as those with a severe dependence on pain medication due to such medical issues as complex pain syndrome or myofasciitis caused by comorbid diseases.3
These patients cannot adequately perform the requisite postoperative physical therapy to completely improve, and some can take up to a year to get range of motion and strength back. We also found that patients who smoke get recurrent disease due to scarring.
At both UC Davis and Johns Hopkins, we created a YouTube video for patients to educate them on the procedure and expected results. The need for postoperative physical therapy should be emphasized in all patients. Some require more therapy than others, which means taking time off from work to focus on the therapy and not performing other activities until the pain and discomfort are gone and strength is back. In another study we performed, we found that if patients did improve the first year, they were more likely to stay symptom free over many years.
While we were doing a transaxillary rib resection case at UC Davis, my team, which includes my partner Misty Humphries, MD, created a list of the top 10 reasons that the transaxillary approach is preferred for neurogenic thoracic outlet syndrome:
1. The scar is less noticeable and painful for the patient than the scar in the supraclavicular fossa, allowing the patient to start physical therapy 2 weeks after surgery.
2. The Machleder retractor makes visualization easy and stable, and allows all members of the team to see the anatomy.
3. The brachial plexus does not have to be retracted and is out of harm’s way, so no temporary palsies are seen in the postoperative period.
4. The subclavius tendon can be seen in entirety and the anterior portion of the rib is easy to completely remove.
5. The subclavian vein can be seen in entirety and defines the anterior portion of the dissection.
6. Once the anterior scalenectomy muscle is cut, the subclavian artery naturally retracts cephalad and is no longer near the rib when it is to be removed.
7. The posterior portion of the rib can be completely removed by readjusting the retraction and a second cut can be done safely with either the rib cutter or the first rib rongeur. It is essential to remove the rib posteriorly behind the nerve root so the arm is adducted and the nerve does not come in contact with the remaining rib, as we feel that leads to increased recurrences.
8. Two operating surgeons can address the rib from their side of the table and completely resect the rib, depending on the patient’s soft bony anatomy, by angling the instruments from either side.
9. Even large muscular or obese patients can be safely approached from the axilla utilizing the Machleder retractor and a lighted retractor.
10. The transaxillary approach can be taught through the teaching video we have made and through the ability for both surgeons to see because of the retractor.
Some of my favorite memories as a vascular surgeon were operating on Tuesdays with Dr. Machleder – similar to Tuesdays with Morrie.4 Not only did we remove ribs safely and completely, but he also taught me philosophy of surgery and of life. I hope I am doing the same with my team as we remove ribs now on Thursday – “Thursdays with Freischlag” – at UC Davis.
Dr. Freischlag is vice chancellor for human health sciences and dean of the school of medicine at the University of California, Davis. She had no relevant disclosures.
References
1. J Vasc Surg. 2012;55(5):1370-5.
2. Curr Treat Options Cardiovasc Med. 2009;11(2):176-83.
3. J Vasc Surg. 2012;56(4):1061-7.
Use a supraclavicular approach: My way is best!
The best sense we have of the pathophysiology of neurogenic (NTOS) is that the scalene triangle is “too tight” with regard to what it contains – the brachial plexus and the subclavian artery. Whether this is due to the triangle being too small or the nerves being “too large” (inflammation) is unknown. Supporting the former theory are observations that the anterior scalene muscle is frequently inflamed and/or chronically injured.1 but others have suggested that the first rib is abnormally located or elevated.2 In addition, some have suggested that inflammatory tissue surrounding the plexus contributes to the process, at least for chronic cases.3
Given the fact that at least two of the three parts of the triangle, plus tissue surrounding the plexus itself, have all been implicated in the disease process, why not choose an approach that allows correction of all potential causes? The transaxillary approach has been used for decades for this condition, but can only decompress the base of the triangle (first rib) and, to varying degrees, only part of the anterior scalene. It does not allow thorough exploration of the nerves. The supraclavicular approach (and the supraclavicular half of paraclavicular excision) addresses these concerns. First, the anterior scalene muscle is essentially entirely removed. With proper technique it is completely visible from the scalene tubercle to its origin at the spine. This approach also allows removal of all muscular and associated tissue medially, completely clearing the parietal pleura at the apex of the lung, at least theoretically reducing the chances of scar tissue arising from residual tissue here.
Second, although no research has yet implicated the middle scalene (scalenus medius, which does not translate perfectly), many patients have impressively bulky musculature at this site. The middle scalene is also completely resected while approaching the first rib; perhaps removing this as well contributes to the excellent results we see today.
Third, the entire portion of the rib involved in NTOS (and the entire rib altogether if a paraclavicular approach is used) is very easily removed using this approach, as are any cervical ribs or Roos bands. Everything is seen, and everything can be evaluated and resected. Finally, many consider full neurolysis of the brachial plexus in this area an important part of the procedure. This is based on low-grade evidence only,3 but in the author’s experience, the incidence of improvement or cure seems to be higher, and recurrence rates lower, than with less-complete operations.
Parenthetically, related to this issue is that of visualization and education. The primary goal is ensuring the best outcome for the patient. Visualization is, by far, best if a supraclavicular approach is used. This is beneficial clinically by ensuring the most complete decompression of the nerves and avoidance of complications, but also is extremely helpful with regard to educating residents and fellows, learning the anatomy, identifying aberrant structures, and so on. Even with the best techniques (including a head- or retractor-mounted camera), no one can see what’s going on during a transaxillary approach except for the operator.
If the supraclavicular approach allows better access to and removal of all the potentially involved components causing NTOS, why doesn’t everyone use it? One answer is that the potential complication rate may be higher. Both the long thoracic and phrenic nerves are very much more at risk using this approach than using the transaxillary approach, and, on the left side, the risk of thoracic duct injury is higher. It must be conceded that published results, in general, do not show significant differences in outcomes between the two approaches.4 However, many would interpret this as a type II error, combined with the “fuzziness” of diagnosis and evaluation of outcomes this field has labored under. However, the opposite interpretation should be considered – there are no definitive data showing any higher complication rate between the two approaches. This debate likely is answerable in the same fashion as many other such debates in our field – someone who is good at the transaxillary approach will do a better job than someone who is not, and someone who is good at the supraclavicular approach will do a better job than someone who is not.
Is a prospective trial indicated? In theory, yes. However, the relative rarity of this condition, the fact that most surgeons follow almost exclusively one or the other technique, and the categorical nature of the outcome variable make such a trial relatively impractical. Pending this, the best suggestion is obviously to pick the best TOS surgeon you can find and have him or her fix the problem in the way they are most experienced!
Dr. Illig is professor of surgery and director, division of vascular surgery, and associate chair, faculty development and mentoring, University of South Florida, Morsani College of Medicine, Tampa, Fla. He had no relevant disclosures.
References
2. Thoracic Outlet Syndrome. London: Springer 2013; 319-21.

How we can support our LGBTQ patients
This past month has been a difficult one. The violence committed against people on the basis of presumed sexual orientation, color of skin, religion, and occupation has been difficult to make sense of. These tragic and horrible events highlight the continued need to focus on building inclusive environments and fostering communication between people with different backgrounds, points of view, and life experiences.
Several of my past articles have touched on the need to create inclusive environments for our LGBTQ (lesbian, gay, bisexual, transgender, questioning) patients, but have not included direct input from youth. With this in mind, I sat down with several youth from our local youth LGBTQ center in Ohio to ask them how we as health care providers could be more supportive of our patients.

Here are some of their suggestions:
• “Trust your patients. … Respect that I am knowledgeable about my body.”
Youth in the group stated that they want providers who listen to and trust what they say. Youth reported that they trust that their medical providers are experts in medicine and the care of patients, but they are the experts on themselves.
• “Don’t blame the hormones. Don’t blame things on puberty. … It’s not just a phase.”
Youth reported that they often get frustrated when providers assume that their sexual orientation or gender identity is “just a phase.” While adolescence can be a time of experimentation, it is important to acknowledge and respect youth’s emerging identities.
• “Know your patients. Educate yourselves.”
Many youth reported that while they are happy to share their stories, they do not want to be put in the role of having to educate their providers about the basics.
Youth expect that their providers have a general understanding of LGBTQ terminology and health care needs. They are happy to answer specific questions, but expect a degree of cultural competency from their providers.
• “Don’t push birth control. Don’t make assumptions about my behaviors; ask me first.”
Many female-bodied youth had the perception that providers make assumptions about their sexual orientation (assuming they are heterosexual), sexual behaviors, and risk of unintended pregnancy and sexually transmitted diseases.
Youth reported that they are open to conversations about reproductive health and safe sex, but get turned off when providers incorrectly assume they are heterosexual and in need of birth control. Asking about sexual attraction and the gender of partners as a routine part of any adolescent sexual history can help providers avoid these mistakes.
• “Have a discussion versus telling people what to do. Tell me why you are checking things and what they mean.”
Youth reported that they were interested in being active participants in their health care visits. They stated that if labs are being checked, they want to know why and what the results mean. When medications are prescribed or lifestyle changes are recommended, they want to discuss why these changes are necessary and have some input as to how these changes happen.
• “I like to have my privacy respected. It can be uncomfortable talking about things with my parents in the room.”
Many youth reported privacy and one-on-one time with their providers being important. They reported being uncomfortable or embarrassed talking about certain topics in front of their parents and valued providers who respected their privacy.
Private time with patients is not meant to cut parents out of the visit; rather it is meant to be a time when patients can openly discuss concerns with their providers and begin to take ownership of their health and bodies.
Many of the suggestions above are helpful in the care of all youth, regardless of sexual orientation and gender identity. Most of the qualities youth were looking for in providers were related to communication and respect and are in keeping with current research and guidelines on creating youth friendly services. Following these suggestions, and continuing to find ways to include youth in our conversations to improve health care, are just a few ways we can make youth feel more comfortable in this setting and hopefully begin to achieve health equity for all youth.
Acknowledgments
I appreciate the youth at Kaleidoscope Youth Center for giving their time and continually helping me improve the care I provide to all patients and allowing me to share this information with others.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
This past month has been a difficult one. The violence committed against people on the basis of presumed sexual orientation, color of skin, religion, and occupation has been difficult to make sense of. These tragic and horrible events highlight the continued need to focus on building inclusive environments and fostering communication between people with different backgrounds, points of view, and life experiences.
Several of my past articles have touched on the need to create inclusive environments for our LGBTQ (lesbian, gay, bisexual, transgender, questioning) patients, but have not included direct input from youth. With this in mind, I sat down with several youth from our local youth LGBTQ center in Ohio to ask them how we as health care providers could be more supportive of our patients.
Here are some of their suggestions:
• “Trust your patients. … Respect that I am knowledgeable about my body.”
Youth in the group stated that they want providers who listen to and trust what they say. Youth reported that they trust that their medical providers are experts in medicine and the care of patients, but they are the experts on themselves.
• “Don’t blame the hormones. Don’t blame things on puberty. … It’s not just a phase.”
Youth reported that they often get frustrated when providers assume that their sexual orientation or gender identity is “just a phase.” While adolescence can be a time of experimentation, it is important to acknowledge and respect youth’s emerging identities.
• “Know your patients. Educate yourselves.”
Many youth reported that while they are happy to share their stories, they do not want to be put in the role of having to educate their providers about the basics.
Youth expect that their providers have a general understanding of LGBTQ terminology and health care needs. They are happy to answer specific questions, but expect a degree of cultural competency from their providers.
• “Don’t push birth control. Don’t make assumptions about my behaviors; ask me first.”
Many female-bodied youth had the perception that providers make assumptions about their sexual orientation (assuming they are heterosexual), sexual behaviors, and risk of unintended pregnancy and sexually transmitted diseases.
Youth reported that they are open to conversations about reproductive health and safe sex, but get turned off when providers incorrectly assume they are heterosexual and in need of birth control. Asking about sexual attraction and the gender of partners as a routine part of any adolescent sexual history can help providers avoid these mistakes.
• “Have a discussion versus telling people what to do. Tell me why you are checking things and what they mean.”
Youth reported that they were interested in being active participants in their health care visits. They stated that if labs are being checked, they want to know why and what the results mean. When medications are prescribed or lifestyle changes are recommended, they want to discuss why these changes are necessary and have some input as to how these changes happen.
• “I like to have my privacy respected. It can be uncomfortable talking about things with my parents in the room.”
Many youth reported privacy and one-on-one time with their providers being important. They reported being uncomfortable or embarrassed talking about certain topics in front of their parents and valued providers who respected their privacy.
Private time with patients is not meant to cut parents out of the visit; rather it is meant to be a time when patients can openly discuss concerns with their providers and begin to take ownership of their health and bodies.
Many of the suggestions above are helpful in the care of all youth, regardless of sexual orientation and gender identity. Most of the qualities youth were looking for in providers were related to communication and respect and are in keeping with current research and guidelines on creating youth friendly services. Following these suggestions, and continuing to find ways to include youth in our conversations to improve health care, are just a few ways we can make youth feel more comfortable in this setting and hopefully begin to achieve health equity for all youth.
Acknowledgments
I appreciate the youth at Kaleidoscope Youth Center for giving their time and continually helping me improve the care I provide to all patients and allowing me to share this information with others.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
This past month has been a difficult one. The violence committed against people on the basis of presumed sexual orientation, color of skin, religion, and occupation has been difficult to make sense of. These tragic and horrible events highlight the continued need to focus on building inclusive environments and fostering communication between people with different backgrounds, points of view, and life experiences.
Several of my past articles have touched on the need to create inclusive environments for our LGBTQ (lesbian, gay, bisexual, transgender, questioning) patients, but have not included direct input from youth. With this in mind, I sat down with several youth from our local youth LGBTQ center in Ohio to ask them how we as health care providers could be more supportive of our patients.
Here are some of their suggestions:
• “Trust your patients. … Respect that I am knowledgeable about my body.”
Youth in the group stated that they want providers who listen to and trust what they say. Youth reported that they trust that their medical providers are experts in medicine and the care of patients, but they are the experts on themselves.
• “Don’t blame the hormones. Don’t blame things on puberty. … It’s not just a phase.”
Youth reported that they often get frustrated when providers assume that their sexual orientation or gender identity is “just a phase.” While adolescence can be a time of experimentation, it is important to acknowledge and respect youth’s emerging identities.
• “Know your patients. Educate yourselves.”
Many youth reported that while they are happy to share their stories, they do not want to be put in the role of having to educate their providers about the basics.
Youth expect that their providers have a general understanding of LGBTQ terminology and health care needs. They are happy to answer specific questions, but expect a degree of cultural competency from their providers.
• “Don’t push birth control. Don’t make assumptions about my behaviors; ask me first.”
Many female-bodied youth had the perception that providers make assumptions about their sexual orientation (assuming they are heterosexual), sexual behaviors, and risk of unintended pregnancy and sexually transmitted diseases.
Youth reported that they are open to conversations about reproductive health and safe sex, but get turned off when providers incorrectly assume they are heterosexual and in need of birth control. Asking about sexual attraction and the gender of partners as a routine part of any adolescent sexual history can help providers avoid these mistakes.
• “Have a discussion versus telling people what to do. Tell me why you are checking things and what they mean.”
Youth reported that they were interested in being active participants in their health care visits. They stated that if labs are being checked, they want to know why and what the results mean. When medications are prescribed or lifestyle changes are recommended, they want to discuss why these changes are necessary and have some input as to how these changes happen.
• “I like to have my privacy respected. It can be uncomfortable talking about things with my parents in the room.”
Many youth reported privacy and one-on-one time with their providers being important. They reported being uncomfortable or embarrassed talking about certain topics in front of their parents and valued providers who respected their privacy.
Private time with patients is not meant to cut parents out of the visit; rather it is meant to be a time when patients can openly discuss concerns with their providers and begin to take ownership of their health and bodies.
Many of the suggestions above are helpful in the care of all youth, regardless of sexual orientation and gender identity. Most of the qualities youth were looking for in providers were related to communication and respect and are in keeping with current research and guidelines on creating youth friendly services. Following these suggestions, and continuing to find ways to include youth in our conversations to improve health care, are just a few ways we can make youth feel more comfortable in this setting and hopefully begin to achieve health equity for all youth.
Acknowledgments
I appreciate the youth at Kaleidoscope Youth Center for giving their time and continually helping me improve the care I provide to all patients and allowing me to share this information with others.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.

Me? Address social determinants of health? How?
When I heard the American Academy of Pediatrics call for pediatricians to address poverty and social determinants of health, I – and maybe you, too – thought, “Great idea. But how am I, as a practicing pediatrician, supposed to help with such overwhelming and socially determined factors?”
It seems that the best way to reduce poverty, homelessness, and inadequate education is to advocate and vote to maintain or expand proven social programs. But there are also more proximal “relational” (relationship) factors we can address. The Adverse Childhood Experiences (ACE) study showed that the number of ACEs reported in their pasts by adults has a nearly linear relationship to long-term morbidities, including suicide, depression, obesity, smoking, substance abuse, heart disease, and early death. The ACE events during childhood – besides lack of food – came from the child’s relationships: abuse (emotional, physical, or sexual) and family dysfunction (mother abused; loss of a caregiver through divorce, separation, or death; household members with alcohol or substance abuse, mental illness, or time in prison).

The most important step you can take to prevent your patients from ACEs is detection. You have to ask parents, either verbally or with a screening tool about current factors that could be harmful to the child. You may think, “My patients don’t have these problems,” but abuse, intimate partner violence (IPV), depression, substance use, and loss occur in families of all kinds and means. Even the presence of food insecurity and imprisonment in some of my “put together” families has surprised me.
There are a number of tools available to screen for individual factors such as parental depression (Edinburgh Postnatal Screening, Patient Health Questionnaire-2 and -4), IPV, substance use (CRAFFT, which stands for Car, Relax, Alone, Forget, Friends, Trouble), and food insecurity. Tools covering multiple risk factors also are available on paper (Safe Environment for Every Kid [SEEK], Survey of Well-being of Young Children [SWYC]) or online (CHADIS). Rather than being overly intrusive, parents report accepting these questions as representing your caring about them as well as their child.
Coverage for screening and counseling for depression and IPV is mandated by the Affordable Care Act. As of July 2016, screening for maternal depression by pediatricians is paid for by Medicaid and many other insurers, often as part of the well-child visit, according to the Center for Medicaid and CHIP Services’ Informational Bulletin of May 11, 2016. For patient-centered medical homes, there is a mandate for referral and care coordination (AHRQ Publication No.11-M005-EF, December 2010). New value-based payment mechanisms are likely to pay you based on such screening and referral processes (e.g. New York), so we had best prepare (“Value-Based Payment Models for Medicaid Child Health Services,” Report to the Schuyler Center for Analysis and Advocacy and the United Hospital Fund, July 13, 2016).
But what to do when the screen or questions reveal a problem? Your first impulse is likely to be to refer. But unlike referrals for a physical health issue such as severe anemia for which the parent calls the hematologist immediately, in the case of these touchy, embarrassing, or emotionally charged problems, accepting help may not be so easy. It may be the financially critical partner who is the substance user or the mother herself who is too depressed to move towards help. For problems such as lack of food or the need to get a GED (general education development), the referral may be successful by supplying phone numbers. Referrals for IPV, one of the most common (greater than 29%) and damaging ACEs to the child, who is exposed to violence and often abused, have been found to mainly fail from simply making a referral.
Just as for a positive blood screen, for a referral to be effective more information is needed. In the case of a family stressor, you need to find out the nature and extent of the problem, the immediacy of the danger, and what has been done so far to reduce it. Research now shows that the most effective way to collect this information is using motivational interviewing (MI) techniques that nonjudgmentally determine not just the facts, but engage parents in weighing the pros and cons of changing the status quo, their readiness to change, the types of interventions that might be acceptable, and what would tell them that it was time to act. When using MI, you are actually doing more than making a referral, you are beginning to address the problem you uncovered.

The MI process strengthens the trust in your relationship with the parent, starting with reflecting on the issue (“It sounds as though you don’t always feel safe at home”), empathizing (“That must be really scary. I am sorry you are going through that”), and assessing (“May I try to help you with this?”).
After collecting the pros and cons for making a change, either in the interview or via the screening tool SEEK Plus in CHADIS, your job is to help the parent weigh them (“On the one hand you love him and need his income, but on the other hand you are so afraid that you can’t sleep and your children are too nervous to concentrate in school.”) Then you need to elicit what would be enough to move them (“How will you know when it is time to act?”) and to assess readiness to change (“What kinds of help would you be open to?”), then offer that kind of help (“I would like to connect you to a professional who has a lot of experience helping people in your situation. Is it okay if we call her right now?”). Provide written contact information, of course, but actually assisting by calling the appropriate resource or even doing a “warm handoff” in person is more effective.
Obviously, to make an effective referral, we need resources assembled in advance for the most common issues. UnitedWay.org is a good place to include on your list.
Our job, however, is not over with an “accepted” referral. Most referrals are not kept, help is never received, and risk to the child is not averted. There are many potential barriers to families’ accessing help – time off work, money, transportation, or child care – but difficulty generating the courage to change is understandable and may resolve only gradually with your work and support. It is wise to tell the parent that “I (or someone on your staff) will check in on how this goes, okay?”
Making a follow-up appointment with you is important, even if you feel helpless to do more than refer. Why? A return visit is a chance to show that you care, to be sure they went, and to get information on the quality and appropriateness of the care provided so you can support it or refer elsewhere. Perhaps most importantly, it shows that you do not reject them for revealing what they may see as personal failure or immoral behavior so that you can continue caring for and monitoring their at-risk child.
What if they decline help, no resources are to be found, or the damage has already occurred? You still have valuable help to provide. Our goal is to ameliorate the impact of the stressors on the child now and in the future. Just as relational factors can stress the child, improving supportive relationships is key to reducing their effects. Parents with ACE risk factors are often self-absorbed in their pain, using smoking, substances, or alcohol to dampen it and moving from one troubled relationship to another in response to past trauma; thus they are emotionally unavailable to the child.
You can help them by focusing on the wonders of their child, encouraging daily individual time for play, and modeling Reach Out and Read as a supportive, calm activity they can do even when stressed. You can encourage the practice of mindfulness – an exercise of letting thoughts pass over them without judgment while breathing rhythmically – for stressed parents and school-aged children. It has been shown to be an effective intervention for recovering from past as well as current stress. Children also should receive any needed mental health care.
An emotionally available, supportive, nurturing parent is the most important protective factor for the child’s development of emotion regulation, resilience, and the ability to cope with adversity throughout their life. Referring parents to services such as home visiting, Healthy Steps, or parent-child therapy to build these skills has evidence for improving relational health. Helping the parents avoid ACEs for their children and assisting them in ameliorating them, if they occur, are important investments in long-term health that you can provide.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
When I heard the American Academy of Pediatrics call for pediatricians to address poverty and social determinants of health, I – and maybe you, too – thought, “Great idea. But how am I, as a practicing pediatrician, supposed to help with such overwhelming and socially determined factors?”
It seems that the best way to reduce poverty, homelessness, and inadequate education is to advocate and vote to maintain or expand proven social programs. But there are also more proximal “relational” (relationship) factors we can address. The Adverse Childhood Experiences (ACE) study showed that the number of ACEs reported in their pasts by adults has a nearly linear relationship to long-term morbidities, including suicide, depression, obesity, smoking, substance abuse, heart disease, and early death. The ACE events during childhood – besides lack of food – came from the child’s relationships: abuse (emotional, physical, or sexual) and family dysfunction (mother abused; loss of a caregiver through divorce, separation, or death; household members with alcohol or substance abuse, mental illness, or time in prison).
The most important step you can take to prevent your patients from ACEs is detection. You have to ask parents, either verbally or with a screening tool about current factors that could be harmful to the child. You may think, “My patients don’t have these problems,” but abuse, intimate partner violence (IPV), depression, substance use, and loss occur in families of all kinds and means. Even the presence of food insecurity and imprisonment in some of my “put together” families has surprised me.
There are a number of tools available to screen for individual factors such as parental depression (Edinburgh Postnatal Screening, Patient Health Questionnaire-2 and -4), IPV, substance use (CRAFFT, which stands for Car, Relax, Alone, Forget, Friends, Trouble), and food insecurity. Tools covering multiple risk factors also are available on paper (Safe Environment for Every Kid [SEEK], Survey of Well-being of Young Children [SWYC]) or online (CHADIS). Rather than being overly intrusive, parents report accepting these questions as representing your caring about them as well as their child.
Coverage for screening and counseling for depression and IPV is mandated by the Affordable Care Act. As of July 2016, screening for maternal depression by pediatricians is paid for by Medicaid and many other insurers, often as part of the well-child visit, according to the Center for Medicaid and CHIP Services’ Informational Bulletin of May 11, 2016. For patient-centered medical homes, there is a mandate for referral and care coordination (AHRQ Publication No.11-M005-EF, December 2010). New value-based payment mechanisms are likely to pay you based on such screening and referral processes (e.g. New York), so we had best prepare (“Value-Based Payment Models for Medicaid Child Health Services,” Report to the Schuyler Center for Analysis and Advocacy and the United Hospital Fund, July 13, 2016).
But what to do when the screen or questions reveal a problem? Your first impulse is likely to be to refer. But unlike referrals for a physical health issue such as severe anemia for which the parent calls the hematologist immediately, in the case of these touchy, embarrassing, or emotionally charged problems, accepting help may not be so easy. It may be the financially critical partner who is the substance user or the mother herself who is too depressed to move towards help. For problems such as lack of food or the need to get a GED (general education development), the referral may be successful by supplying phone numbers. Referrals for IPV, one of the most common (greater than 29%) and damaging ACEs to the child, who is exposed to violence and often abused, have been found to mainly fail from simply making a referral.
Just as for a positive blood screen, for a referral to be effective more information is needed. In the case of a family stressor, you need to find out the nature and extent of the problem, the immediacy of the danger, and what has been done so far to reduce it. Research now shows that the most effective way to collect this information is using motivational interviewing (MI) techniques that nonjudgmentally determine not just the facts, but engage parents in weighing the pros and cons of changing the status quo, their readiness to change, the types of interventions that might be acceptable, and what would tell them that it was time to act. When using MI, you are actually doing more than making a referral, you are beginning to address the problem you uncovered.
The MI process strengthens the trust in your relationship with the parent, starting with reflecting on the issue (“It sounds as though you don’t always feel safe at home”), empathizing (“That must be really scary. I am sorry you are going through that”), and assessing (“May I try to help you with this?”).
After collecting the pros and cons for making a change, either in the interview or via the screening tool SEEK Plus in CHADIS, your job is to help the parent weigh them (“On the one hand you love him and need his income, but on the other hand you are so afraid that you can’t sleep and your children are too nervous to concentrate in school.”) Then you need to elicit what would be enough to move them (“How will you know when it is time to act?”) and to assess readiness to change (“What kinds of help would you be open to?”), then offer that kind of help (“I would like to connect you to a professional who has a lot of experience helping people in your situation. Is it okay if we call her right now?”). Provide written contact information, of course, but actually assisting by calling the appropriate resource or even doing a “warm handoff” in person is more effective.
Obviously, to make an effective referral, we need resources assembled in advance for the most common issues. UnitedWay.org is a good place to include on your list.
Our job, however, is not over with an “accepted” referral. Most referrals are not kept, help is never received, and risk to the child is not averted. There are many potential barriers to families’ accessing help – time off work, money, transportation, or child care – but difficulty generating the courage to change is understandable and may resolve only gradually with your work and support. It is wise to tell the parent that “I (or someone on your staff) will check in on how this goes, okay?”
Making a follow-up appointment with you is important, even if you feel helpless to do more than refer. Why? A return visit is a chance to show that you care, to be sure they went, and to get information on the quality and appropriateness of the care provided so you can support it or refer elsewhere. Perhaps most importantly, it shows that you do not reject them for revealing what they may see as personal failure or immoral behavior so that you can continue caring for and monitoring their at-risk child.
What if they decline help, no resources are to be found, or the damage has already occurred? You still have valuable help to provide. Our goal is to ameliorate the impact of the stressors on the child now and in the future. Just as relational factors can stress the child, improving supportive relationships is key to reducing their effects. Parents with ACE risk factors are often self-absorbed in their pain, using smoking, substances, or alcohol to dampen it and moving from one troubled relationship to another in response to past trauma; thus they are emotionally unavailable to the child.
You can help them by focusing on the wonders of their child, encouraging daily individual time for play, and modeling Reach Out and Read as a supportive, calm activity they can do even when stressed. You can encourage the practice of mindfulness – an exercise of letting thoughts pass over them without judgment while breathing rhythmically – for stressed parents and school-aged children. It has been shown to be an effective intervention for recovering from past as well as current stress. Children also should receive any needed mental health care.
An emotionally available, supportive, nurturing parent is the most important protective factor for the child’s development of emotion regulation, resilience, and the ability to cope with adversity throughout their life. Referring parents to services such as home visiting, Healthy Steps, or parent-child therapy to build these skills has evidence for improving relational health. Helping the parents avoid ACEs for their children and assisting them in ameliorating them, if they occur, are important investments in long-term health that you can provide.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
When I heard the American Academy of Pediatrics call for pediatricians to address poverty and social determinants of health, I – and maybe you, too – thought, “Great idea. But how am I, as a practicing pediatrician, supposed to help with such overwhelming and socially determined factors?”
It seems that the best way to reduce poverty, homelessness, and inadequate education is to advocate and vote to maintain or expand proven social programs. But there are also more proximal “relational” (relationship) factors we can address. The Adverse Childhood Experiences (ACE) study showed that the number of ACEs reported in their pasts by adults has a nearly linear relationship to long-term morbidities, including suicide, depression, obesity, smoking, substance abuse, heart disease, and early death. The ACE events during childhood – besides lack of food – came from the child’s relationships: abuse (emotional, physical, or sexual) and family dysfunction (mother abused; loss of a caregiver through divorce, separation, or death; household members with alcohol or substance abuse, mental illness, or time in prison).
The most important step you can take to prevent your patients from ACEs is detection. You have to ask parents, either verbally or with a screening tool about current factors that could be harmful to the child. You may think, “My patients don’t have these problems,” but abuse, intimate partner violence (IPV), depression, substance use, and loss occur in families of all kinds and means. Even the presence of food insecurity and imprisonment in some of my “put together” families has surprised me.
There are a number of tools available to screen for individual factors such as parental depression (Edinburgh Postnatal Screening, Patient Health Questionnaire-2 and -4), IPV, substance use (CRAFFT, which stands for Car, Relax, Alone, Forget, Friends, Trouble), and food insecurity. Tools covering multiple risk factors also are available on paper (Safe Environment for Every Kid [SEEK], Survey of Well-being of Young Children [SWYC]) or online (CHADIS). Rather than being overly intrusive, parents report accepting these questions as representing your caring about them as well as their child.
Coverage for screening and counseling for depression and IPV is mandated by the Affordable Care Act. As of July 2016, screening for maternal depression by pediatricians is paid for by Medicaid and many other insurers, often as part of the well-child visit, according to the Center for Medicaid and CHIP Services’ Informational Bulletin of May 11, 2016. For patient-centered medical homes, there is a mandate for referral and care coordination (AHRQ Publication No.11-M005-EF, December 2010). New value-based payment mechanisms are likely to pay you based on such screening and referral processes (e.g. New York), so we had best prepare (“Value-Based Payment Models for Medicaid Child Health Services,” Report to the Schuyler Center for Analysis and Advocacy and the United Hospital Fund, July 13, 2016).
But what to do when the screen or questions reveal a problem? Your first impulse is likely to be to refer. But unlike referrals for a physical health issue such as severe anemia for which the parent calls the hematologist immediately, in the case of these touchy, embarrassing, or emotionally charged problems, accepting help may not be so easy. It may be the financially critical partner who is the substance user or the mother herself who is too depressed to move towards help. For problems such as lack of food or the need to get a GED (general education development), the referral may be successful by supplying phone numbers. Referrals for IPV, one of the most common (greater than 29%) and damaging ACEs to the child, who is exposed to violence and often abused, have been found to mainly fail from simply making a referral.
Just as for a positive blood screen, for a referral to be effective more information is needed. In the case of a family stressor, you need to find out the nature and extent of the problem, the immediacy of the danger, and what has been done so far to reduce it. Research now shows that the most effective way to collect this information is using motivational interviewing (MI) techniques that nonjudgmentally determine not just the facts, but engage parents in weighing the pros and cons of changing the status quo, their readiness to change, the types of interventions that might be acceptable, and what would tell them that it was time to act. When using MI, you are actually doing more than making a referral, you are beginning to address the problem you uncovered.
The MI process strengthens the trust in your relationship with the parent, starting with reflecting on the issue (“It sounds as though you don’t always feel safe at home”), empathizing (“That must be really scary. I am sorry you are going through that”), and assessing (“May I try to help you with this?”).
After collecting the pros and cons for making a change, either in the interview or via the screening tool SEEK Plus in CHADIS, your job is to help the parent weigh them (“On the one hand you love him and need his income, but on the other hand you are so afraid that you can’t sleep and your children are too nervous to concentrate in school.”) Then you need to elicit what would be enough to move them (“How will you know when it is time to act?”) and to assess readiness to change (“What kinds of help would you be open to?”), then offer that kind of help (“I would like to connect you to a professional who has a lot of experience helping people in your situation. Is it okay if we call her right now?”). Provide written contact information, of course, but actually assisting by calling the appropriate resource or even doing a “warm handoff” in person is more effective.
Obviously, to make an effective referral, we need resources assembled in advance for the most common issues. UnitedWay.org is a good place to include on your list.
Our job, however, is not over with an “accepted” referral. Most referrals are not kept, help is never received, and risk to the child is not averted. There are many potential barriers to families’ accessing help – time off work, money, transportation, or child care – but difficulty generating the courage to change is understandable and may resolve only gradually with your work and support. It is wise to tell the parent that “I (or someone on your staff) will check in on how this goes, okay?”
Making a follow-up appointment with you is important, even if you feel helpless to do more than refer. Why? A return visit is a chance to show that you care, to be sure they went, and to get information on the quality and appropriateness of the care provided so you can support it or refer elsewhere. Perhaps most importantly, it shows that you do not reject them for revealing what they may see as personal failure or immoral behavior so that you can continue caring for and monitoring their at-risk child.
What if they decline help, no resources are to be found, or the damage has already occurred? You still have valuable help to provide. Our goal is to ameliorate the impact of the stressors on the child now and in the future. Just as relational factors can stress the child, improving supportive relationships is key to reducing their effects. Parents with ACE risk factors are often self-absorbed in their pain, using smoking, substances, or alcohol to dampen it and moving from one troubled relationship to another in response to past trauma; thus they are emotionally unavailable to the child.
You can help them by focusing on the wonders of their child, encouraging daily individual time for play, and modeling Reach Out and Read as a supportive, calm activity they can do even when stressed. You can encourage the practice of mindfulness – an exercise of letting thoughts pass over them without judgment while breathing rhythmically – for stressed parents and school-aged children. It has been shown to be an effective intervention for recovering from past as well as current stress. Children also should receive any needed mental health care.
An emotionally available, supportive, nurturing parent is the most important protective factor for the child’s development of emotion regulation, resilience, and the ability to cope with adversity throughout their life. Referring parents to services such as home visiting, Healthy Steps, or parent-child therapy to build these skills has evidence for improving relational health. Helping the parents avoid ACEs for their children and assisting them in ameliorating them, if they occur, are important investments in long-term health that you can provide.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.

Vegetarian diets 101
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.

The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.
The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
In the era where obesity is the No. 1 health crisis affecting people of all ages, physicians are often faced with questions regarding restricted diets or a patient may report that they are “vegetarian” in their history. Although new trendy diets appear all the time, “vegetarian inclined” diets are among the most common. A study conducted in 2008 identified that approximately 10% of Americans age 18 and older consumed a vegetarian diet.1 It is important to know the basics so that you can offer some guidance and look for possible deficiencies that may result from an altered diet.
Studies show that children who follow a vegetarian diet have normal growth and development but tend to be leaner than their omnivore counterparts.2 A healthy diet consumed in childhood lessens the risk for chronic diseases and promotes optimal growth and development. But altered or restricted diets in adolescents can be tricky because teens are actively growing and therefore usually need greater amounts of vital nutrients. So guidance is important to avoid common mistakes.
The simplest way to remember what is appropriate in a vegetarian diet is the restriction on intake of any food that once had a mother and a father. The vegetarian diet is further divided based on what it includes or excludes. Although the below list is not complete, it outlines the more common vegetarian diets:
• Vegan. This diet restricts intake of any animal product.
• Macrobiotics. This diet consists of whole grain, brown rice, fruits, and vegetables, and restricts intake of white meat or fish to twice a week.
• Lacto-vegetarian. This diet is one which allows milk products.
• Ovo vegetarian. – This diet allows eggs, but no meat, dairy, or fish.
• Pescitarian. This diet restricts meats, dairy, and eggs, but allows fish.
• Semi-vegetarian. This diet just restricts eating meat.
It is important to encourage anyone wishing to follow a vegetarian diet to fully research and understand what it entails. Health.gov under “dietary guidelines 2015-2020” is a wonderful reference to help understand how much of vital nutrients should be consumed to promote healthy eating habits and prevent deficiencies.
The key nutrients to discuss with patients are intake of protein, iron, calcium, vitamin B12, and vitamin D. Inadequate or incorrect intake can lead to deficiency of the vital nutrients that likely will result in disease.
Protein is a necessary nutrient because it provides the essential amino acids necessary for growth and repair. When animal protein breaks down, it provides all of the essential amino acids, unlike plant protein which can be deficient in some of the amino acids. Because each source of plant protein varies in the amino acid it is deficient in, it is important to have a mixed source of protein to ensure adequate intake. The soy bean has comparable amounts of protein to animal protein. Other sources of protein are legumes, grain, cereal, eggs, nuts, Greek yogurt, cottage cheese, but these are less digestible so greater consumption is needed to meet the daily requirements. Deficiency in protein can result in impaired growth.
Iron that is obtained from animals or meat sources has heme component, which makes it easier to absorb. Iron obtained from plants does not contain heme component and therefore is more difficult to absorb. Ascorbic acid (vitamin C) helps nonheme iron to be absorbed, but must be taken with an iron source to be effective. Therefore, vitamin C–containing foods such as fruits and vegetables should be consumed at every meal to assist in iron absorption. Deficiency in iron can lead to anemia and reduced energy.
Calcium is an important nutrient for bone formation, and deficiency can lead to increased risk for fracture and osteoporosis later in life. Its excretion and absorption can be affected by other nutrients, such as iron and zinc, present during digestion. Milk and dairy products are the most common source for calcium intake, but there are other calcium sources such as kale, broccoli, and food fortified with calcium such as cereal and orange juice. These foods can be better sources of calcium than supplements because they allow for better absorption.
Vitamin D is needed for calcium and phosphorus absorption, which is important for proper bone formation. Vitamin D is found in dairy products, fortified food and beverages, and exposure to the sun. Those living in colder climates and of darker pigmentation are at greater risk of deficiency so supplementation is usually necessary. Deficiency of vitamin D can lead to rickets.
Vitamin B12 is found in meat, fish, and dairy products, but not in plants. Intake of B12 is likely to be deficient in vegans because they do not consume most of those sources. Vegans are at a significant risk of vitamin B12 deficiency3 which can lead to macrocytosis, anemia, and decreased energy.
Educating families on healthy eating is essential at any visit. A good understanding of the possible deficiencies that can occur with restricted diets will allow for proper guidance and avoidable diseases.
References
1. Stahler C. “How Many Youth Are Vegetarian? The Vegetarian Resource Group Asks in a 2010 National Poll.”
2. Pediatrics. 1989 Sep;84(3):475-81.
3. J Am Diet Assoc. 2003 Jun;103(6):771-5.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

Terrorist Activity: Are You Ready?
I was relaxing after work in my local American Legion a few weeks ago when a quiet young man entered with a backpack. He set it down to use the restroom, and when he returned a few minutes later, he picked up the backpack and walked away. After he left, a group of us discussed how lax we were about this situation. Yes, it was probably innocent—but what if it wasn’t? A sign over the bar reads, “Don’t let anyone leave a stranger.” The purpose of that sign is, of course, to make everyone feel welcome, but these days I think it also means to be aware of your surroundings. I have seen too many American flags at half-staff this year to overlook a potential tragedy.
Today, clinicians must be prepared for all possible emergencies, including terrorism. Acts of terrorism (as the word implies) are designed to instill terror and panic, disrupt security and communication systems, destroy property, and kill or injure innocent civilians.
Recent terrorist attacks in 2016, while shocking in their brutality, were not inconceivable—public locations where large groups gather are logical targets. Terrorists often target high-traffic areas, such as airports or shopping malls, where they can quickly disappear into a crowd if necessary (hence the concern circling the Olympic Games to be held in Brazil this month).
Attacks at restaurants, airports, and other public “hot spots” are especially frightening. With terrorist attack locations in the past year ranging from nightclubs (the Pulse Nightclub shooting in Orlando, Florida, left 49 dead) to restaurants (a bomb in Dhaka, Bangladesh, killed 20) to conference rooms (a shooting in San Bernardino, California, left 14 dead and 21 injured), it’s clear that the fundamental message terrorists want to send is: You are not safe—anywhere!
While organized events and big crowds are a bull’s-eye for terrorists, our personal surroundings have risk factors, too. Because a terrorist attack can happen anywhere at any time, you need to be prepared by knowing what to do and how to maximize your chances of survival.
As this year’s attacks exemplify, we shouldn’t assume we understand the “logic” or thinking of terrorist organizations or individuals. Preparation for a terrorist attack boils down to being aware of the warning signs and being cautious and alert. Terrorists use a range of weapons and tactics, including bombs, arson, hijacking, and kidnapping (see Table).1,2
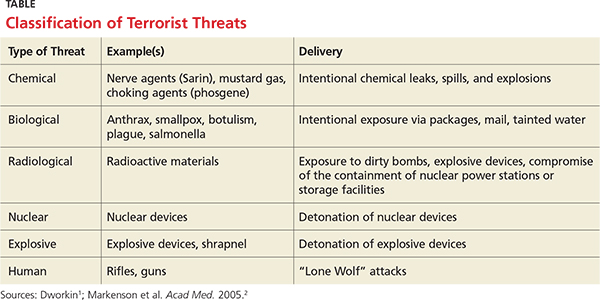
According to Dr. Howard Mell, an EMS director in North Carolina, the overwhelming majority of gunfire in the emergency department—or anywhere—is not the result of an active shooter. Most gunfire is targeted at a specific goal (ie, escaping or avoiding capture) or person. However, should there be an active shooter, he recommends three steps to take: Run (if the path is open), hide (if your exit is blocked), or fight (if there are no other alternatives).3
Wherever you are, always have multiple potential escape routes in mind. If you run, leave all belongings behind. Help others escape if possible, and take steps to prevent others from entering once you have left the area.
If you are unable to run, decide where to hide. If possible, barricade the area; if you are in a room, turn out the lights and stay away from the door. Be silent and put your cell phone on silent. While you are hiding, prepare to fight.
Fighting is the last resort. Act aggressively and improvise weapons to use against the assailant. If you have family, friends, or colleagues with you, put them to work!
When law enforcement officers arrive, understand that their job is to go right to the source and contain the danger. Keep your hands visible at all times, with fingers spread. Do not grab them for protection, and avoid yelling or pointing. Be prepared to give the authorities any pertinent information (eg, shooter description, last known location, direction of travel, or weapons seen).
Many health care facilities and organizations have valuable disaster and terrorism training programs, which include emergency evacuation procedures. I encourage you to take advantage of them, particularly if you travel internationally.4
Continue for personal preparedness >>
This is about personal preparedness. While I am not promoting paranoia, I do believe the risk for terrorist activity has increased in recent years.
I therefore urge you to have a healthy suspicion when you see or hear people
• Asking unusual questions about safety procedures at work
• Engaging in behaviors that provoke suspicion
• Loitering, parking, or standing in the same area over multiple days
• Attempting to disguise themselves from visit to visit
• Obtaining unusual quantities of weapons, ammunition, or explosive precursors
• Wearing clothing not appropriate for the season
• Leaving items, including backpacks or packages, unattended
• Leaving anonymous threats via telephone or e-mail
If after conducting a risk assessment of your surroundings, you believe you could (directly or indirectly) be impacted by terrorism, you must implement evacuation plans, notification of appropriate personnel, and personal safety measures.
In the event of a terrorist incident, remain calm, follow the advice of local emergency officials, and follow radio, television, and cell phone updates for news and instructions. 5
If an attack occurs near you or your home, here are practical steps you can take: Check for injuries. Give first aid and get help for seriously injured people. Check for damage using a flashlight—do not light matches or candles, or use electrical switches. Check for fires, fire hazards, and other household hazards. Sniff for gas leaks, starting at the water heater. If you smell gas or suspect a leak, turn off the main gas valve, open windows, and evacuate quickly. Shut off any damaged utilities, and confine or secure your pets. Call your family contact—but do not use the telephone again unless it is a life-threatening emergency. Cell phones may or may not be working. Check on your neighbors, especially those who are elderly or disabled.
Terrorist attacks leave citizens concerned about future incidents of terrorism in the United States and their potential impact. They raise ambiguity about what might happen next and increase stress levels. You can take steps to prepare for terrorist attacks and reduce the stress you may feel, now and later, should an emergency arise. Taking preparatory action can reassure you, your family, and your children that you have a measure of control—even in the face of terrorism. If you have additional suggestions for terrorist defense preparation, you can email your ideas to PAEditor@frontlinemedcom.com.
References
1. Dworkin RW. Preparing hospitals, doctors, and nurses for a terrorist attack. Hudson Institute. www.hudson.org/content/researchattach ments/attachment/291/dworkin_white_paper.pdf. Accessed July 6, 2016.
2. Markenson F, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):517-526.
3. Mell HK. Run, hide, fight: how to react when there’s gunfire in the emergency department. ACEP NOW. June 21, 2016. www.acepnow.com/react-theres-gunfire-emergency-department/?elq_mid=10369&elq_cid=5274988. Accessed July 6, 2016.
4. Uniformed Services University of the Health Sciences, Center for the Study of Traumatic Stress. Workplace preparedness for terrorism. www.cstsonline.org/assets/media/docu ments/CSTS_report_sloan_workplace_prepare_terrorism_preparedness.pdf. Accessed July 6, 2016.
5. American Red Cross. Terrorism Preparedness. www.redcross.org/prepare/disaster/terrorism. Accessed July 6, 2016.
I was relaxing after work in my local American Legion a few weeks ago when a quiet young man entered with a backpack. He set it down to use the restroom, and when he returned a few minutes later, he picked up the backpack and walked away. After he left, a group of us discussed how lax we were about this situation. Yes, it was probably innocent—but what if it wasn’t? A sign over the bar reads, “Don’t let anyone leave a stranger.” The purpose of that sign is, of course, to make everyone feel welcome, but these days I think it also means to be aware of your surroundings. I have seen too many American flags at half-staff this year to overlook a potential tragedy.
Today, clinicians must be prepared for all possible emergencies, including terrorism. Acts of terrorism (as the word implies) are designed to instill terror and panic, disrupt security and communication systems, destroy property, and kill or injure innocent civilians.
Recent terrorist attacks in 2016, while shocking in their brutality, were not inconceivable—public locations where large groups gather are logical targets. Terrorists often target high-traffic areas, such as airports or shopping malls, where they can quickly disappear into a crowd if necessary (hence the concern circling the Olympic Games to be held in Brazil this month).
Attacks at restaurants, airports, and other public “hot spots” are especially frightening. With terrorist attack locations in the past year ranging from nightclubs (the Pulse Nightclub shooting in Orlando, Florida, left 49 dead) to restaurants (a bomb in Dhaka, Bangladesh, killed 20) to conference rooms (a shooting in San Bernardino, California, left 14 dead and 21 injured), it’s clear that the fundamental message terrorists want to send is: You are not safe—anywhere!
While organized events and big crowds are a bull’s-eye for terrorists, our personal surroundings have risk factors, too. Because a terrorist attack can happen anywhere at any time, you need to be prepared by knowing what to do and how to maximize your chances of survival.
As this year’s attacks exemplify, we shouldn’t assume we understand the “logic” or thinking of terrorist organizations or individuals. Preparation for a terrorist attack boils down to being aware of the warning signs and being cautious and alert. Terrorists use a range of weapons and tactics, including bombs, arson, hijacking, and kidnapping (see Table).1,2
According to Dr. Howard Mell, an EMS director in North Carolina, the overwhelming majority of gunfire in the emergency department—or anywhere—is not the result of an active shooter. Most gunfire is targeted at a specific goal (ie, escaping or avoiding capture) or person. However, should there be an active shooter, he recommends three steps to take: Run (if the path is open), hide (if your exit is blocked), or fight (if there are no other alternatives).3
Wherever you are, always have multiple potential escape routes in mind. If you run, leave all belongings behind. Help others escape if possible, and take steps to prevent others from entering once you have left the area.
If you are unable to run, decide where to hide. If possible, barricade the area; if you are in a room, turn out the lights and stay away from the door. Be silent and put your cell phone on silent. While you are hiding, prepare to fight.
Fighting is the last resort. Act aggressively and improvise weapons to use against the assailant. If you have family, friends, or colleagues with you, put them to work!
When law enforcement officers arrive, understand that their job is to go right to the source and contain the danger. Keep your hands visible at all times, with fingers spread. Do not grab them for protection, and avoid yelling or pointing. Be prepared to give the authorities any pertinent information (eg, shooter description, last known location, direction of travel, or weapons seen).
Many health care facilities and organizations have valuable disaster and terrorism training programs, which include emergency evacuation procedures. I encourage you to take advantage of them, particularly if you travel internationally.4
Continue for personal preparedness >>
This is about personal preparedness. While I am not promoting paranoia, I do believe the risk for terrorist activity has increased in recent years.
I therefore urge you to have a healthy suspicion when you see or hear people
• Asking unusual questions about safety procedures at work
• Engaging in behaviors that provoke suspicion
• Loitering, parking, or standing in the same area over multiple days
• Attempting to disguise themselves from visit to visit
• Obtaining unusual quantities of weapons, ammunition, or explosive precursors
• Wearing clothing not appropriate for the season
• Leaving items, including backpacks or packages, unattended
• Leaving anonymous threats via telephone or e-mail
If after conducting a risk assessment of your surroundings, you believe you could (directly or indirectly) be impacted by terrorism, you must implement evacuation plans, notification of appropriate personnel, and personal safety measures.
In the event of a terrorist incident, remain calm, follow the advice of local emergency officials, and follow radio, television, and cell phone updates for news and instructions. 5
If an attack occurs near you or your home, here are practical steps you can take: Check for injuries. Give first aid and get help for seriously injured people. Check for damage using a flashlight—do not light matches or candles, or use electrical switches. Check for fires, fire hazards, and other household hazards. Sniff for gas leaks, starting at the water heater. If you smell gas or suspect a leak, turn off the main gas valve, open windows, and evacuate quickly. Shut off any damaged utilities, and confine or secure your pets. Call your family contact—but do not use the telephone again unless it is a life-threatening emergency. Cell phones may or may not be working. Check on your neighbors, especially those who are elderly or disabled.
Terrorist attacks leave citizens concerned about future incidents of terrorism in the United States and their potential impact. They raise ambiguity about what might happen next and increase stress levels. You can take steps to prepare for terrorist attacks and reduce the stress you may feel, now and later, should an emergency arise. Taking preparatory action can reassure you, your family, and your children that you have a measure of control—even in the face of terrorism. If you have additional suggestions for terrorist defense preparation, you can email your ideas to PAEditor@frontlinemedcom.com.
References
1. Dworkin RW. Preparing hospitals, doctors, and nurses for a terrorist attack. Hudson Institute. www.hudson.org/content/researchattach ments/attachment/291/dworkin_white_paper.pdf. Accessed July 6, 2016.
2. Markenson F, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):517-526.
3. Mell HK. Run, hide, fight: how to react when there’s gunfire in the emergency department. ACEP NOW. June 21, 2016. www.acepnow.com/react-theres-gunfire-emergency-department/?elq_mid=10369&elq_cid=5274988. Accessed July 6, 2016.
4. Uniformed Services University of the Health Sciences, Center for the Study of Traumatic Stress. Workplace preparedness for terrorism. www.cstsonline.org/assets/media/docu ments/CSTS_report_sloan_workplace_prepare_terrorism_preparedness.pdf. Accessed July 6, 2016.
5. American Red Cross. Terrorism Preparedness. www.redcross.org/prepare/disaster/terrorism. Accessed July 6, 2016.
I was relaxing after work in my local American Legion a few weeks ago when a quiet young man entered with a backpack. He set it down to use the restroom, and when he returned a few minutes later, he picked up the backpack and walked away. After he left, a group of us discussed how lax we were about this situation. Yes, it was probably innocent—but what if it wasn’t? A sign over the bar reads, “Don’t let anyone leave a stranger.” The purpose of that sign is, of course, to make everyone feel welcome, but these days I think it also means to be aware of your surroundings. I have seen too many American flags at half-staff this year to overlook a potential tragedy.
Today, clinicians must be prepared for all possible emergencies, including terrorism. Acts of terrorism (as the word implies) are designed to instill terror and panic, disrupt security and communication systems, destroy property, and kill or injure innocent civilians.
Recent terrorist attacks in 2016, while shocking in their brutality, were not inconceivable—public locations where large groups gather are logical targets. Terrorists often target high-traffic areas, such as airports or shopping malls, where they can quickly disappear into a crowd if necessary (hence the concern circling the Olympic Games to be held in Brazil this month).
Attacks at restaurants, airports, and other public “hot spots” are especially frightening. With terrorist attack locations in the past year ranging from nightclubs (the Pulse Nightclub shooting in Orlando, Florida, left 49 dead) to restaurants (a bomb in Dhaka, Bangladesh, killed 20) to conference rooms (a shooting in San Bernardino, California, left 14 dead and 21 injured), it’s clear that the fundamental message terrorists want to send is: You are not safe—anywhere!
While organized events and big crowds are a bull’s-eye for terrorists, our personal surroundings have risk factors, too. Because a terrorist attack can happen anywhere at any time, you need to be prepared by knowing what to do and how to maximize your chances of survival.
As this year’s attacks exemplify, we shouldn’t assume we understand the “logic” or thinking of terrorist organizations or individuals. Preparation for a terrorist attack boils down to being aware of the warning signs and being cautious and alert. Terrorists use a range of weapons and tactics, including bombs, arson, hijacking, and kidnapping (see Table).1,2
According to Dr. Howard Mell, an EMS director in North Carolina, the overwhelming majority of gunfire in the emergency department—or anywhere—is not the result of an active shooter. Most gunfire is targeted at a specific goal (ie, escaping or avoiding capture) or person. However, should there be an active shooter, he recommends three steps to take: Run (if the path is open), hide (if your exit is blocked), or fight (if there are no other alternatives).3
Wherever you are, always have multiple potential escape routes in mind. If you run, leave all belongings behind. Help others escape if possible, and take steps to prevent others from entering once you have left the area.
If you are unable to run, decide where to hide. If possible, barricade the area; if you are in a room, turn out the lights and stay away from the door. Be silent and put your cell phone on silent. While you are hiding, prepare to fight.
Fighting is the last resort. Act aggressively and improvise weapons to use against the assailant. If you have family, friends, or colleagues with you, put them to work!
When law enforcement officers arrive, understand that their job is to go right to the source and contain the danger. Keep your hands visible at all times, with fingers spread. Do not grab them for protection, and avoid yelling or pointing. Be prepared to give the authorities any pertinent information (eg, shooter description, last known location, direction of travel, or weapons seen).
Many health care facilities and organizations have valuable disaster and terrorism training programs, which include emergency evacuation procedures. I encourage you to take advantage of them, particularly if you travel internationally.4
Continue for personal preparedness >>
This is about personal preparedness. While I am not promoting paranoia, I do believe the risk for terrorist activity has increased in recent years.
I therefore urge you to have a healthy suspicion when you see or hear people
• Asking unusual questions about safety procedures at work
• Engaging in behaviors that provoke suspicion
• Loitering, parking, or standing in the same area over multiple days
• Attempting to disguise themselves from visit to visit
• Obtaining unusual quantities of weapons, ammunition, or explosive precursors
• Wearing clothing not appropriate for the season
• Leaving items, including backpacks or packages, unattended
• Leaving anonymous threats via telephone or e-mail
If after conducting a risk assessment of your surroundings, you believe you could (directly or indirectly) be impacted by terrorism, you must implement evacuation plans, notification of appropriate personnel, and personal safety measures.
In the event of a terrorist incident, remain calm, follow the advice of local emergency officials, and follow radio, television, and cell phone updates for news and instructions. 5
If an attack occurs near you or your home, here are practical steps you can take: Check for injuries. Give first aid and get help for seriously injured people. Check for damage using a flashlight—do not light matches or candles, or use electrical switches. Check for fires, fire hazards, and other household hazards. Sniff for gas leaks, starting at the water heater. If you smell gas or suspect a leak, turn off the main gas valve, open windows, and evacuate quickly. Shut off any damaged utilities, and confine or secure your pets. Call your family contact—but do not use the telephone again unless it is a life-threatening emergency. Cell phones may or may not be working. Check on your neighbors, especially those who are elderly or disabled.
Terrorist attacks leave citizens concerned about future incidents of terrorism in the United States and their potential impact. They raise ambiguity about what might happen next and increase stress levels. You can take steps to prepare for terrorist attacks and reduce the stress you may feel, now and later, should an emergency arise. Taking preparatory action can reassure you, your family, and your children that you have a measure of control—even in the face of terrorism. If you have additional suggestions for terrorist defense preparation, you can email your ideas to PAEditor@frontlinemedcom.com.
References
1. Dworkin RW. Preparing hospitals, doctors, and nurses for a terrorist attack. Hudson Institute. www.hudson.org/content/researchattach ments/attachment/291/dworkin_white_paper.pdf. Accessed July 6, 2016.
2. Markenson F, DiMaggio C, Redlener I. Preparing health professions students for terrorism, disaster, and public health emergencies: core competencies. Acad Med. 2005;80(6):517-526.
3. Mell HK. Run, hide, fight: how to react when there’s gunfire in the emergency department. ACEP NOW. June 21, 2016. www.acepnow.com/react-theres-gunfire-emergency-department/?elq_mid=10369&elq_cid=5274988. Accessed July 6, 2016.
4. Uniformed Services University of the Health Sciences, Center for the Study of Traumatic Stress. Workplace preparedness for terrorism. www.cstsonline.org/assets/media/docu ments/CSTS_report_sloan_workplace_prepare_terrorism_preparedness.pdf. Accessed July 6, 2016.
5. American Red Cross. Terrorism Preparedness. www.redcross.org/prepare/disaster/terrorism. Accessed July 6, 2016.