User login
An epidemic of fear and misinformation
As I write this, the 2019 novel coronavirus* continues to spread, exceeding 59,000 cases and 1,300 deaths worldwide. With it spreads fear. In the modern world of social media, misinformation spreads even faster than disease.

The news about a novel and deadly illness crowds out more substantial worries. Humans are not particularly good at assessing risk or responding rationally and consistently to it. Risk is hard to fully define. If you look up “risk” in Merriam Webster’s online dictionary, you get the simple definition of “possibility of loss or injury; peril.” If you look up risk in Wikipedia, you get 12 pages of explanation and 8 more pages of links and references.
People handle risk differently. Some people are more risk adverse than others. Some get a pleasurable thrill from risk, whether a slot machine or a parachute jump. Most people really don’t comprehend small probabilities, with tens of billions of dollars spent annually on U.S. lotteries.
Because 98% of people who get COVID-19 are recovering, this is not an extinction-level event or the zombie apocalypse. It is a major health hazard, and one where morbidity and mortality might be assuaged by an early and effective public health response, including the population’s adoption of good habits such as hand washing, cough etiquette, and staying home when ill.
Three key factors may help reduce the fear factor.
One key factor is accurate communication of health information to the public. This has been severely harmed in the last few years by the promotion of gossip on social media, such as Facebook, within newsfeeds without any vetting, along with a smaller component of deliberate misinformation from untraceable sources. Compare this situation with the decision in May 1988 when Surgeon General C. Everett Koop chose to snail mail a brochure on AIDS to every household in America. It was unprecedented. One element of this communication is the public’s belief that government and health care officials will responsibly and timely convey the information. There are accusations that the Chinese government initially impeded early warnings about COVID-19. Dr. Koop, to his great credit and lifesaving leadership, overcame queasiness within the Reagan administration about issues of morality and taste in discussing some of the HIV information. Alas, no similar leadership occurred in the decade of the 2010s when deaths from the opioid epidemic in the United States skyrocketed to claim more lives annually than car accidents or suicide.

A second factor is the credibility of the scientists. Antivaxxers, climate change deniers, and mercenary scientists have severely damaged that credibility of science, compared with the trust in scientists 50 years ago during the Apollo moon shot.
A third factor is perspective. Poor journalism and clickbait can focus excessively on the rare events as news. Airline crashes make the front page while fatal car accidents, claiming a hundred times more lives annually, don’t even merit a story in local media. Someone wins the lottery weekly but few pay attention to those suffering from gambling debts.
Influenza is killing many times more people than the 2019 novel coronavirus, but the news is focused on cruise ships. In the United States, influenza annually will strike tens of millions, with about 10 per 1,000 hospitalized and 0.5 per 1,000 dying. The novel coronavirus is more lethal. SARS (a coronavirus epidemic in 2003) had 8,000 cases with a mortality rate of 96 per 1,000 while the novel 2019 strain so far is killing about 20 per 1,000. That value may be an overestimate, because there may be a significant fraction of COVID-19 patients with symptoms mild enough that they do not seek medical care and do not get tested and counted.
For perspective, in 1952 the United States reported 50,000 cases of polio (meningitis or paralytic) annually with 3,000 deaths. As many as 95% of cases of poliovirus infection have no or mild symptoms and would not have been reported, so the case fatality rate estimate is skewed. In the 1950s, the United States averaged about 500,000 cases of measles per year, with about 500 deaths annually for a case fatality rate of about 1 per 1,000 in a population that was well nourished with good medical care. In malnourished children without access to modern health care, the case fatality rate can be as high as 100 per 1,000, which is why globally measles killed 142,000 people in 2018, a substantial improvement from 536,000 deaths globally in 2000, but still a leading killer of children worldwide. Vaccines had reduced the annual death toll of polio and measles in the U.S. to zero.
In comparison, in this country the annual incidences are about 70,000 overdose deaths, 50,000 suicides, and 40,000 traffic deaths.
Reassurance is the most common product sold by pediatricians. We look for low-probability, high-impact bad things. Usually we don’t find them and can reassure parents that the child will be okay. Sometimes we spot a higher-risk situation and intervene. My job is to worry professionally so that parents can worry less.
COVID-19 worries me, but irrational people worry me more. The real enemies are fear, disinformation, discrimination, and economic warfare.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
*This article was updated 2/21/2020.
As I write this, the 2019 novel coronavirus* continues to spread, exceeding 59,000 cases and 1,300 deaths worldwide. With it spreads fear. In the modern world of social media, misinformation spreads even faster than disease.
The news about a novel and deadly illness crowds out more substantial worries. Humans are not particularly good at assessing risk or responding rationally and consistently to it. Risk is hard to fully define. If you look up “risk” in Merriam Webster’s online dictionary, you get the simple definition of “possibility of loss or injury; peril.” If you look up risk in Wikipedia, you get 12 pages of explanation and 8 more pages of links and references.
People handle risk differently. Some people are more risk adverse than others. Some get a pleasurable thrill from risk, whether a slot machine or a parachute jump. Most people really don’t comprehend small probabilities, with tens of billions of dollars spent annually on U.S. lotteries.
Because 98% of people who get COVID-19 are recovering, this is not an extinction-level event or the zombie apocalypse. It is a major health hazard, and one where morbidity and mortality might be assuaged by an early and effective public health response, including the population’s adoption of good habits such as hand washing, cough etiquette, and staying home when ill.
Three key factors may help reduce the fear factor.
One key factor is accurate communication of health information to the public. This has been severely harmed in the last few years by the promotion of gossip on social media, such as Facebook, within newsfeeds without any vetting, along with a smaller component of deliberate misinformation from untraceable sources. Compare this situation with the decision in May 1988 when Surgeon General C. Everett Koop chose to snail mail a brochure on AIDS to every household in America. It was unprecedented. One element of this communication is the public’s belief that government and health care officials will responsibly and timely convey the information. There are accusations that the Chinese government initially impeded early warnings about COVID-19. Dr. Koop, to his great credit and lifesaving leadership, overcame queasiness within the Reagan administration about issues of morality and taste in discussing some of the HIV information. Alas, no similar leadership occurred in the decade of the 2010s when deaths from the opioid epidemic in the United States skyrocketed to claim more lives annually than car accidents or suicide.
A second factor is the credibility of the scientists. Antivaxxers, climate change deniers, and mercenary scientists have severely damaged that credibility of science, compared with the trust in scientists 50 years ago during the Apollo moon shot.
A third factor is perspective. Poor journalism and clickbait can focus excessively on the rare events as news. Airline crashes make the front page while fatal car accidents, claiming a hundred times more lives annually, don’t even merit a story in local media. Someone wins the lottery weekly but few pay attention to those suffering from gambling debts.
Influenza is killing many times more people than the 2019 novel coronavirus, but the news is focused on cruise ships. In the United States, influenza annually will strike tens of millions, with about 10 per 1,000 hospitalized and 0.5 per 1,000 dying. The novel coronavirus is more lethal. SARS (a coronavirus epidemic in 2003) had 8,000 cases with a mortality rate of 96 per 1,000 while the novel 2019 strain so far is killing about 20 per 1,000. That value may be an overestimate, because there may be a significant fraction of COVID-19 patients with symptoms mild enough that they do not seek medical care and do not get tested and counted.
For perspective, in 1952 the United States reported 50,000 cases of polio (meningitis or paralytic) annually with 3,000 deaths. As many as 95% of cases of poliovirus infection have no or mild symptoms and would not have been reported, so the case fatality rate estimate is skewed. In the 1950s, the United States averaged about 500,000 cases of measles per year, with about 500 deaths annually for a case fatality rate of about 1 per 1,000 in a population that was well nourished with good medical care. In malnourished children without access to modern health care, the case fatality rate can be as high as 100 per 1,000, which is why globally measles killed 142,000 people in 2018, a substantial improvement from 536,000 deaths globally in 2000, but still a leading killer of children worldwide. Vaccines had reduced the annual death toll of polio and measles in the U.S. to zero.
In comparison, in this country the annual incidences are about 70,000 overdose deaths, 50,000 suicides, and 40,000 traffic deaths.
Reassurance is the most common product sold by pediatricians. We look for low-probability, high-impact bad things. Usually we don’t find them and can reassure parents that the child will be okay. Sometimes we spot a higher-risk situation and intervene. My job is to worry professionally so that parents can worry less.
COVID-19 worries me, but irrational people worry me more. The real enemies are fear, disinformation, discrimination, and economic warfare.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
*This article was updated 2/21/2020.
As I write this, the 2019 novel coronavirus* continues to spread, exceeding 59,000 cases and 1,300 deaths worldwide. With it spreads fear. In the modern world of social media, misinformation spreads even faster than disease.
The news about a novel and deadly illness crowds out more substantial worries. Humans are not particularly good at assessing risk or responding rationally and consistently to it. Risk is hard to fully define. If you look up “risk” in Merriam Webster’s online dictionary, you get the simple definition of “possibility of loss or injury; peril.” If you look up risk in Wikipedia, you get 12 pages of explanation and 8 more pages of links and references.
People handle risk differently. Some people are more risk adverse than others. Some get a pleasurable thrill from risk, whether a slot machine or a parachute jump. Most people really don’t comprehend small probabilities, with tens of billions of dollars spent annually on U.S. lotteries.
Because 98% of people who get COVID-19 are recovering, this is not an extinction-level event or the zombie apocalypse. It is a major health hazard, and one where morbidity and mortality might be assuaged by an early and effective public health response, including the population’s adoption of good habits such as hand washing, cough etiquette, and staying home when ill.
Three key factors may help reduce the fear factor.
One key factor is accurate communication of health information to the public. This has been severely harmed in the last few years by the promotion of gossip on social media, such as Facebook, within newsfeeds without any vetting, along with a smaller component of deliberate misinformation from untraceable sources. Compare this situation with the decision in May 1988 when Surgeon General C. Everett Koop chose to snail mail a brochure on AIDS to every household in America. It was unprecedented. One element of this communication is the public’s belief that government and health care officials will responsibly and timely convey the information. There are accusations that the Chinese government initially impeded early warnings about COVID-19. Dr. Koop, to his great credit and lifesaving leadership, overcame queasiness within the Reagan administration about issues of morality and taste in discussing some of the HIV information. Alas, no similar leadership occurred in the decade of the 2010s when deaths from the opioid epidemic in the United States skyrocketed to claim more lives annually than car accidents or suicide.
A second factor is the credibility of the scientists. Antivaxxers, climate change deniers, and mercenary scientists have severely damaged that credibility of science, compared with the trust in scientists 50 years ago during the Apollo moon shot.
A third factor is perspective. Poor journalism and clickbait can focus excessively on the rare events as news. Airline crashes make the front page while fatal car accidents, claiming a hundred times more lives annually, don’t even merit a story in local media. Someone wins the lottery weekly but few pay attention to those suffering from gambling debts.
Influenza is killing many times more people than the 2019 novel coronavirus, but the news is focused on cruise ships. In the United States, influenza annually will strike tens of millions, with about 10 per 1,000 hospitalized and 0.5 per 1,000 dying. The novel coronavirus is more lethal. SARS (a coronavirus epidemic in 2003) had 8,000 cases with a mortality rate of 96 per 1,000 while the novel 2019 strain so far is killing about 20 per 1,000. That value may be an overestimate, because there may be a significant fraction of COVID-19 patients with symptoms mild enough that they do not seek medical care and do not get tested and counted.
For perspective, in 1952 the United States reported 50,000 cases of polio (meningitis or paralytic) annually with 3,000 deaths. As many as 95% of cases of poliovirus infection have no or mild symptoms and would not have been reported, so the case fatality rate estimate is skewed. In the 1950s, the United States averaged about 500,000 cases of measles per year, with about 500 deaths annually for a case fatality rate of about 1 per 1,000 in a population that was well nourished with good medical care. In malnourished children without access to modern health care, the case fatality rate can be as high as 100 per 1,000, which is why globally measles killed 142,000 people in 2018, a substantial improvement from 536,000 deaths globally in 2000, but still a leading killer of children worldwide. Vaccines had reduced the annual death toll of polio and measles in the U.S. to zero.
In comparison, in this country the annual incidences are about 70,000 overdose deaths, 50,000 suicides, and 40,000 traffic deaths.
Reassurance is the most common product sold by pediatricians. We look for low-probability, high-impact bad things. Usually we don’t find them and can reassure parents that the child will be okay. Sometimes we spot a higher-risk situation and intervene. My job is to worry professionally so that parents can worry less.
COVID-19 worries me, but irrational people worry me more. The real enemies are fear, disinformation, discrimination, and economic warfare.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
*This article was updated 2/21/2020.
An unusual ‘retirement’ option
Whether “retirement” is withdrawing from one’s occupation or from an active working life, it is of utmost importance to not let one’s mind degenerate. Some individuals move on to gathering new intellectual skills by attending new educational courses or meetings, some travel, some become semiprofessional golfers or fishermen, and some find other forms of personal extension. I now serve to develop cost-saving medical programs for county jails in the state of Texas while attempting to improve the overall quality of inmate care.
Initially I was a pediatrician in Houston with special training in allergy and immunology, but because of a medical problem I was forced to abandon my first love – primary pediatrics. My move to a small town at the age of 40 required me to reevaluate my professional life, and I opted to provide care only in my allergy and immunology specialty.
However, living in a small town is different from life in a metropolis, and it was not uncommon for doctors to be asked to assist the community. A number of years ago, our county judge asked if I would help evaluate why our county jail was spending so much money. After several attempts to refuse, I eventually did evaluate the program there, and was flabbergasted by how much money was being wasted. I made some rather simple suggestions as how to correct the problem, but when no primary care doctor stepped forward to implement the changes and run the jail medical program, I became its medical director. When we saved $120,000 the first year, even I was astounded.
While I continued to run my private practice, I did accept other small community’s offers to look into their county jails’ programs. I found that their problems in cost control and quality of health care mirrored those I found in the first jail, and they were easily solvable if the county judge and the local sheriff wanted solutions. I also found that politics makes strange bedfellows, as the saying goes, and often the obvious changes were met with obstruction in one form or another. Nonetheless, I found that I could serve these communities in addition to my individual patients. When it was time for retirement, I continued to have a real desire to make the towns around which I lived and my own community more livable. So
In most things, I found that the same business philosophy and personal medical approach I learned in my pediatrics training and as a private practitioner applied to the jail system. Let me mention some specifics. Using generic medicines was less expensive than using brand names. The diagnoses which patients claimed when they entered jail might or might not be correct, so reevaluating the diagnosis and treatment was appropriate as soon as possible. Hospital and ED visits should be limited to patients’ medically requiring them rather than using the ED as a screening tool.
But I did come to understand that medical care in the county jail is different from medical care outside an incarcerated facility in that sometimes the prisoners had their own reasons for seeking medical care. This was complicated by the fact that often there were critically ill patients presenting to county jails. So carefully established criteria and protocols were an absolute necessity to save lives.
Let me expand on the topic of seeking medical care by the inmate-patients. A relatively small number of these individuals required immediate emergency treatment, without which they could not do well: The diabetic who was not taking his insulin, the out-of-control paranoid schizophrenic who decided he was cured and therefore was unattended, the alcoholic or drug addict who would develop delirium tremens if medications were stopped abruptly. These people had to be identified as quickly as possible and correctly treated. Confounding the problem was the fact that many, and I repeat many, individuals try to use the medical route to manipulate their incarceration environment. I called this the B problem: beds, blankets, barter, buzz, better food, and be out of here. They might claim an illness existed, and often they might believe it did.
A related situation might exist when individuals would demand psychiatric and pain medications, often in large quantities, when they in fact had not taken them for some time in the outside world. Often these patients were addicts, and of course this could create an entire other relationship with the medical team. A third example would be the claim of hypoglycemia so that the prisoner would receive more frequent meals.
One might think that as a pediatrician I was ill prepared to treat adults, and in fact, there was much review of the general medical care needed when I began this program. However, the internists and family physicians in town were glad to assist me whenever I encountered a difficult patient. When hospitalizations were required, the inpatient always was covered by one of the internists on hospital staff. Quite frankly, the doctors seemed pleased to not be dealing with this group of individuals as much as they had in the past.
On a slightly different note, skills honed during my pediatric career were extremely valuable. Children, particularly young children, do not verbally communicate with their parents or their doctor particularly well, so pediatricians are well trained in the skill of observation. The patient who claims a guard hurt his shoulder so badly during an altercation that he cannot move it is found out when he easily whips his arms over his head when asked to remove his shirt. It is not uncommon for an individual to demand antidepressant medications from the medical staff, but when evaluated more thoroughly and for a longer period of time, the patient ends up laughing, even denying any suicidal ideation or any other sign of depression. One also deals with a lot of adolescent behavior from the inmates, such as the individuals who say that unless they don’t get their way (more food) they are not going to take their medications and thus get sicker. That’s Adolescent Medicine 101.
Some of the modalities I utilized in modifying the jail programs will be familiar to every practicing pediatrician. I educate; I teach; I train. Parents of my asthmatic patients had to know what medications to keep handy and when to use them. It is pretty easy to see how that relates to jail medicine. Many patients come into jail with inhalers and with a diagnosis of asthma. Some have the condition, and some do not. By training jail and medical staff how to observe breathing patterns and by performing pulse oximetry, we eliminated a large number of unnecessary ED visits, and we often made the diagnosis of hyperventilation syndrome rather than misdiagnosed asthma.
Jail medicine is a large part of the cost of housing inmates. I did consultation work for a large urban jail, and we saved over $7 million in 1 year. In a medium-sized jail, the cost-savings after a 4-month consultation was over $300,000. This is a lot of money to me, and I suspect is to you, too. Just as in our general communities, we have enough resources to provide medical care and to provide a high level of care for all. However, we cannot waste money by providing inappropriate care or overtesting or overtreating. The medical care must be what treats the disease the patient actually has ... nothing more and nothing less!
If it sounds as if I am cynical about inmate patients, that is not true. However, I am realistic that no one wishes to be in jail. I realize that the medical route is just one that prisoners can and do use to modify their situation. I understand that the medical staff within a jail needs constant education and supervision at first, and with time they become more astute – just like a physician in this arena – at distinguishing the very serious from the mildly serious from malingering. In spite of this, we doctors also can be fooled. However, through constant vigilance and constant education we can get better.
Jail medicine is not for everyone in retirement. Heck, it is not for everyone ever. I found it interesting because it required me to match my diagnostic skills against the diseases and the psychodynamics of individuals who often – not always – made that diagnosis more difficult. Diagnosing illness and curing it – isn’t this why we all went into medicine?
Dr. Yoffe is a retired pediatrician specializing in allergy and immunology who resides in Brenham, Tex. Email him at pdnews@mdedge.com.
This article was updated 2/13/2020.
Whether “retirement” is withdrawing from one’s occupation or from an active working life, it is of utmost importance to not let one’s mind degenerate. Some individuals move on to gathering new intellectual skills by attending new educational courses or meetings, some travel, some become semiprofessional golfers or fishermen, and some find other forms of personal extension. I now serve to develop cost-saving medical programs for county jails in the state of Texas while attempting to improve the overall quality of inmate care.
Initially I was a pediatrician in Houston with special training in allergy and immunology, but because of a medical problem I was forced to abandon my first love – primary pediatrics. My move to a small town at the age of 40 required me to reevaluate my professional life, and I opted to provide care only in my allergy and immunology specialty.
However, living in a small town is different from life in a metropolis, and it was not uncommon for doctors to be asked to assist the community. A number of years ago, our county judge asked if I would help evaluate why our county jail was spending so much money. After several attempts to refuse, I eventually did evaluate the program there, and was flabbergasted by how much money was being wasted. I made some rather simple suggestions as how to correct the problem, but when no primary care doctor stepped forward to implement the changes and run the jail medical program, I became its medical director. When we saved $120,000 the first year, even I was astounded.
While I continued to run my private practice, I did accept other small community’s offers to look into their county jails’ programs. I found that their problems in cost control and quality of health care mirrored those I found in the first jail, and they were easily solvable if the county judge and the local sheriff wanted solutions. I also found that politics makes strange bedfellows, as the saying goes, and often the obvious changes were met with obstruction in one form or another. Nonetheless, I found that I could serve these communities in addition to my individual patients. When it was time for retirement, I continued to have a real desire to make the towns around which I lived and my own community more livable. So
In most things, I found that the same business philosophy and personal medical approach I learned in my pediatrics training and as a private practitioner applied to the jail system. Let me mention some specifics. Using generic medicines was less expensive than using brand names. The diagnoses which patients claimed when they entered jail might or might not be correct, so reevaluating the diagnosis and treatment was appropriate as soon as possible. Hospital and ED visits should be limited to patients’ medically requiring them rather than using the ED as a screening tool.
But I did come to understand that medical care in the county jail is different from medical care outside an incarcerated facility in that sometimes the prisoners had their own reasons for seeking medical care. This was complicated by the fact that often there were critically ill patients presenting to county jails. So carefully established criteria and protocols were an absolute necessity to save lives.
Let me expand on the topic of seeking medical care by the inmate-patients. A relatively small number of these individuals required immediate emergency treatment, without which they could not do well: The diabetic who was not taking his insulin, the out-of-control paranoid schizophrenic who decided he was cured and therefore was unattended, the alcoholic or drug addict who would develop delirium tremens if medications were stopped abruptly. These people had to be identified as quickly as possible and correctly treated. Confounding the problem was the fact that many, and I repeat many, individuals try to use the medical route to manipulate their incarceration environment. I called this the B problem: beds, blankets, barter, buzz, better food, and be out of here. They might claim an illness existed, and often they might believe it did.
A related situation might exist when individuals would demand psychiatric and pain medications, often in large quantities, when they in fact had not taken them for some time in the outside world. Often these patients were addicts, and of course this could create an entire other relationship with the medical team. A third example would be the claim of hypoglycemia so that the prisoner would receive more frequent meals.
One might think that as a pediatrician I was ill prepared to treat adults, and in fact, there was much review of the general medical care needed when I began this program. However, the internists and family physicians in town were glad to assist me whenever I encountered a difficult patient. When hospitalizations were required, the inpatient always was covered by one of the internists on hospital staff. Quite frankly, the doctors seemed pleased to not be dealing with this group of individuals as much as they had in the past.
On a slightly different note, skills honed during my pediatric career were extremely valuable. Children, particularly young children, do not verbally communicate with their parents or their doctor particularly well, so pediatricians are well trained in the skill of observation. The patient who claims a guard hurt his shoulder so badly during an altercation that he cannot move it is found out when he easily whips his arms over his head when asked to remove his shirt. It is not uncommon for an individual to demand antidepressant medications from the medical staff, but when evaluated more thoroughly and for a longer period of time, the patient ends up laughing, even denying any suicidal ideation or any other sign of depression. One also deals with a lot of adolescent behavior from the inmates, such as the individuals who say that unless they don’t get their way (more food) they are not going to take their medications and thus get sicker. That’s Adolescent Medicine 101.
Some of the modalities I utilized in modifying the jail programs will be familiar to every practicing pediatrician. I educate; I teach; I train. Parents of my asthmatic patients had to know what medications to keep handy and when to use them. It is pretty easy to see how that relates to jail medicine. Many patients come into jail with inhalers and with a diagnosis of asthma. Some have the condition, and some do not. By training jail and medical staff how to observe breathing patterns and by performing pulse oximetry, we eliminated a large number of unnecessary ED visits, and we often made the diagnosis of hyperventilation syndrome rather than misdiagnosed asthma.
Jail medicine is a large part of the cost of housing inmates. I did consultation work for a large urban jail, and we saved over $7 million in 1 year. In a medium-sized jail, the cost-savings after a 4-month consultation was over $300,000. This is a lot of money to me, and I suspect is to you, too. Just as in our general communities, we have enough resources to provide medical care and to provide a high level of care for all. However, we cannot waste money by providing inappropriate care or overtesting or overtreating. The medical care must be what treats the disease the patient actually has ... nothing more and nothing less!
If it sounds as if I am cynical about inmate patients, that is not true. However, I am realistic that no one wishes to be in jail. I realize that the medical route is just one that prisoners can and do use to modify their situation. I understand that the medical staff within a jail needs constant education and supervision at first, and with time they become more astute – just like a physician in this arena – at distinguishing the very serious from the mildly serious from malingering. In spite of this, we doctors also can be fooled. However, through constant vigilance and constant education we can get better.
Jail medicine is not for everyone in retirement. Heck, it is not for everyone ever. I found it interesting because it required me to match my diagnostic skills against the diseases and the psychodynamics of individuals who often – not always – made that diagnosis more difficult. Diagnosing illness and curing it – isn’t this why we all went into medicine?
Dr. Yoffe is a retired pediatrician specializing in allergy and immunology who resides in Brenham, Tex. Email him at pdnews@mdedge.com.
This article was updated 2/13/2020.
Whether “retirement” is withdrawing from one’s occupation or from an active working life, it is of utmost importance to not let one’s mind degenerate. Some individuals move on to gathering new intellectual skills by attending new educational courses or meetings, some travel, some become semiprofessional golfers or fishermen, and some find other forms of personal extension. I now serve to develop cost-saving medical programs for county jails in the state of Texas while attempting to improve the overall quality of inmate care.
Initially I was a pediatrician in Houston with special training in allergy and immunology, but because of a medical problem I was forced to abandon my first love – primary pediatrics. My move to a small town at the age of 40 required me to reevaluate my professional life, and I opted to provide care only in my allergy and immunology specialty.
However, living in a small town is different from life in a metropolis, and it was not uncommon for doctors to be asked to assist the community. A number of years ago, our county judge asked if I would help evaluate why our county jail was spending so much money. After several attempts to refuse, I eventually did evaluate the program there, and was flabbergasted by how much money was being wasted. I made some rather simple suggestions as how to correct the problem, but when no primary care doctor stepped forward to implement the changes and run the jail medical program, I became its medical director. When we saved $120,000 the first year, even I was astounded.
While I continued to run my private practice, I did accept other small community’s offers to look into their county jails’ programs. I found that their problems in cost control and quality of health care mirrored those I found in the first jail, and they were easily solvable if the county judge and the local sheriff wanted solutions. I also found that politics makes strange bedfellows, as the saying goes, and often the obvious changes were met with obstruction in one form or another. Nonetheless, I found that I could serve these communities in addition to my individual patients. When it was time for retirement, I continued to have a real desire to make the towns around which I lived and my own community more livable. So
In most things, I found that the same business philosophy and personal medical approach I learned in my pediatrics training and as a private practitioner applied to the jail system. Let me mention some specifics. Using generic medicines was less expensive than using brand names. The diagnoses which patients claimed when they entered jail might or might not be correct, so reevaluating the diagnosis and treatment was appropriate as soon as possible. Hospital and ED visits should be limited to patients’ medically requiring them rather than using the ED as a screening tool.
But I did come to understand that medical care in the county jail is different from medical care outside an incarcerated facility in that sometimes the prisoners had their own reasons for seeking medical care. This was complicated by the fact that often there were critically ill patients presenting to county jails. So carefully established criteria and protocols were an absolute necessity to save lives.
Let me expand on the topic of seeking medical care by the inmate-patients. A relatively small number of these individuals required immediate emergency treatment, without which they could not do well: The diabetic who was not taking his insulin, the out-of-control paranoid schizophrenic who decided he was cured and therefore was unattended, the alcoholic or drug addict who would develop delirium tremens if medications were stopped abruptly. These people had to be identified as quickly as possible and correctly treated. Confounding the problem was the fact that many, and I repeat many, individuals try to use the medical route to manipulate their incarceration environment. I called this the B problem: beds, blankets, barter, buzz, better food, and be out of here. They might claim an illness existed, and often they might believe it did.
A related situation might exist when individuals would demand psychiatric and pain medications, often in large quantities, when they in fact had not taken them for some time in the outside world. Often these patients were addicts, and of course this could create an entire other relationship with the medical team. A third example would be the claim of hypoglycemia so that the prisoner would receive more frequent meals.
One might think that as a pediatrician I was ill prepared to treat adults, and in fact, there was much review of the general medical care needed when I began this program. However, the internists and family physicians in town were glad to assist me whenever I encountered a difficult patient. When hospitalizations were required, the inpatient always was covered by one of the internists on hospital staff. Quite frankly, the doctors seemed pleased to not be dealing with this group of individuals as much as they had in the past.
On a slightly different note, skills honed during my pediatric career were extremely valuable. Children, particularly young children, do not verbally communicate with their parents or their doctor particularly well, so pediatricians are well trained in the skill of observation. The patient who claims a guard hurt his shoulder so badly during an altercation that he cannot move it is found out when he easily whips his arms over his head when asked to remove his shirt. It is not uncommon for an individual to demand antidepressant medications from the medical staff, but when evaluated more thoroughly and for a longer period of time, the patient ends up laughing, even denying any suicidal ideation or any other sign of depression. One also deals with a lot of adolescent behavior from the inmates, such as the individuals who say that unless they don’t get their way (more food) they are not going to take their medications and thus get sicker. That’s Adolescent Medicine 101.
Some of the modalities I utilized in modifying the jail programs will be familiar to every practicing pediatrician. I educate; I teach; I train. Parents of my asthmatic patients had to know what medications to keep handy and when to use them. It is pretty easy to see how that relates to jail medicine. Many patients come into jail with inhalers and with a diagnosis of asthma. Some have the condition, and some do not. By training jail and medical staff how to observe breathing patterns and by performing pulse oximetry, we eliminated a large number of unnecessary ED visits, and we often made the diagnosis of hyperventilation syndrome rather than misdiagnosed asthma.
Jail medicine is a large part of the cost of housing inmates. I did consultation work for a large urban jail, and we saved over $7 million in 1 year. In a medium-sized jail, the cost-savings after a 4-month consultation was over $300,000. This is a lot of money to me, and I suspect is to you, too. Just as in our general communities, we have enough resources to provide medical care and to provide a high level of care for all. However, we cannot waste money by providing inappropriate care or overtesting or overtreating. The medical care must be what treats the disease the patient actually has ... nothing more and nothing less!
If it sounds as if I am cynical about inmate patients, that is not true. However, I am realistic that no one wishes to be in jail. I realize that the medical route is just one that prisoners can and do use to modify their situation. I understand that the medical staff within a jail needs constant education and supervision at first, and with time they become more astute – just like a physician in this arena – at distinguishing the very serious from the mildly serious from malingering. In spite of this, we doctors also can be fooled. However, through constant vigilance and constant education we can get better.
Jail medicine is not for everyone in retirement. Heck, it is not for everyone ever. I found it interesting because it required me to match my diagnostic skills against the diseases and the psychodynamics of individuals who often – not always – made that diagnosis more difficult. Diagnosing illness and curing it – isn’t this why we all went into medicine?
Dr. Yoffe is a retired pediatrician specializing in allergy and immunology who resides in Brenham, Tex. Email him at pdnews@mdedge.com.
This article was updated 2/13/2020.
Make the Diagnosis - March 2020
The patient’s biopsy showed sparse and grouped and slightly enlarged atypical stained mononuclear cells in mostly perifollicular areas with focal epidermotropism. CD30 staining was positive. She responded to potent topical steroids.
The etiology of LyP is unknown. It is unclear whether the proliferation of T-cells is a benign and chronic disorder, or an indolent T-cell malignancy.
In addition, 10% of LyP cases are associated with anaplastic large-cell lymphoma, cutaneous T-cell lymphoma (mycosis fungoides), or Hodgkin lymphoma. Borderline cases are those that overlap LyP and lymphoma.
Patients typically present with crops of asymptomatic erythematous to brown papules that may become pustular, vesicular, or necrotic. Lesions tend to resolve within 2-8 weeks with or without scarring. The trunk and extremities are commonly affected. The condition tends to be chronic over months to years. The waxing and waning course is characteristic of LyP. Constitutional symptoms are generally absent in cases not associated with systemic disease.

Histopathologic examination reveals a dense wedge-shaped dermal infiltrate of atypical lymphocytes along with numerous eosinophils and neutrophils. Epidermotropism may be present and lymphocytes stain positive for CD30+. Vessels in the dermis may exhibit fibrin deposition and red blood cell extravasation. Histologically, LyP can be classified as Type A to E. These subtypes are determined by the size and type of atypical cells, location and amount of infiltrate, and staining of CD30 and CD8.
The differential diagnosis of LyP includes pityriasis lichenoides, anaplastic large cell lymphoma, cutaneous T-cell lymphoma, folliculitis, arthropod assault, Langerhans cell histiocytosis, and leukemia cutis. Treatment is symptomatic. Mild forms of LyP can many times be managed with superpotent topical corticosteroids. Bexarotene gel has been used for early lesions. For more widespread or persistent disease, intralesional corticosteroids, phototherapy (UVB or PUVA), tetracycline antibiotics, and methotrexate have been reported to be effective. Refractory cases may respond to interferon alpha or oral bexarotene. Routine evaluations are recommended as patients may be at increased risk for the development of lymphoma.
This case and photo were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
The patient’s biopsy showed sparse and grouped and slightly enlarged atypical stained mononuclear cells in mostly perifollicular areas with focal epidermotropism. CD30 staining was positive. She responded to potent topical steroids.
The etiology of LyP is unknown. It is unclear whether the proliferation of T-cells is a benign and chronic disorder, or an indolent T-cell malignancy.
In addition, 10% of LyP cases are associated with anaplastic large-cell lymphoma, cutaneous T-cell lymphoma (mycosis fungoides), or Hodgkin lymphoma. Borderline cases are those that overlap LyP and lymphoma.
Patients typically present with crops of asymptomatic erythematous to brown papules that may become pustular, vesicular, or necrotic. Lesions tend to resolve within 2-8 weeks with or without scarring. The trunk and extremities are commonly affected. The condition tends to be chronic over months to years. The waxing and waning course is characteristic of LyP. Constitutional symptoms are generally absent in cases not associated with systemic disease.
Histopathologic examination reveals a dense wedge-shaped dermal infiltrate of atypical lymphocytes along with numerous eosinophils and neutrophils. Epidermotropism may be present and lymphocytes stain positive for CD30+. Vessels in the dermis may exhibit fibrin deposition and red blood cell extravasation. Histologically, LyP can be classified as Type A to E. These subtypes are determined by the size and type of atypical cells, location and amount of infiltrate, and staining of CD30 and CD8.
The differential diagnosis of LyP includes pityriasis lichenoides, anaplastic large cell lymphoma, cutaneous T-cell lymphoma, folliculitis, arthropod assault, Langerhans cell histiocytosis, and leukemia cutis. Treatment is symptomatic. Mild forms of LyP can many times be managed with superpotent topical corticosteroids. Bexarotene gel has been used for early lesions. For more widespread or persistent disease, intralesional corticosteroids, phototherapy (UVB or PUVA), tetracycline antibiotics, and methotrexate have been reported to be effective. Refractory cases may respond to interferon alpha or oral bexarotene. Routine evaluations are recommended as patients may be at increased risk for the development of lymphoma.
This case and photo were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.
The patient’s biopsy showed sparse and grouped and slightly enlarged atypical stained mononuclear cells in mostly perifollicular areas with focal epidermotropism. CD30 staining was positive. She responded to potent topical steroids.
The etiology of LyP is unknown. It is unclear whether the proliferation of T-cells is a benign and chronic disorder, or an indolent T-cell malignancy.
In addition, 10% of LyP cases are associated with anaplastic large-cell lymphoma, cutaneous T-cell lymphoma (mycosis fungoides), or Hodgkin lymphoma. Borderline cases are those that overlap LyP and lymphoma.
Patients typically present with crops of asymptomatic erythematous to brown papules that may become pustular, vesicular, or necrotic. Lesions tend to resolve within 2-8 weeks with or without scarring. The trunk and extremities are commonly affected. The condition tends to be chronic over months to years. The waxing and waning course is characteristic of LyP. Constitutional symptoms are generally absent in cases not associated with systemic disease.
Histopathologic examination reveals a dense wedge-shaped dermal infiltrate of atypical lymphocytes along with numerous eosinophils and neutrophils. Epidermotropism may be present and lymphocytes stain positive for CD30+. Vessels in the dermis may exhibit fibrin deposition and red blood cell extravasation. Histologically, LyP can be classified as Type A to E. These subtypes are determined by the size and type of atypical cells, location and amount of infiltrate, and staining of CD30 and CD8.
The differential diagnosis of LyP includes pityriasis lichenoides, anaplastic large cell lymphoma, cutaneous T-cell lymphoma, folliculitis, arthropod assault, Langerhans cell histiocytosis, and leukemia cutis. Treatment is symptomatic. Mild forms of LyP can many times be managed with superpotent topical corticosteroids. Bexarotene gel has been used for early lesions. For more widespread or persistent disease, intralesional corticosteroids, phototherapy (UVB or PUVA), tetracycline antibiotics, and methotrexate have been reported to be effective. Refractory cases may respond to interferon alpha or oral bexarotene. Routine evaluations are recommended as patients may be at increased risk for the development of lymphoma.
This case and photo were submitted by Dr. Bilu Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to dermnews@mdedge.com.

Be alert for embezzlement
With myriad complex, high-tech problems facing private practice in this modern era, I am periodically reminded by long-time readers to revisit some of the low-tech issues that will always require our attention.

Few are lower tech (in most cases) and more easily overlooked than theft from within. Embezzlement remains far more common in medical offices than generally assumed – and it often occurs in full view of physicians who think everything is fine. Most embezzlers are not skillful or discreet; their transgressions may go undetected for years, simply because no one suspects it is happening.
Detecting fraud is an inexact science. There is no textbook approach that one can follow, but a few simple measures will prevent or expose the most common forms:
- Make it more difficult. Theft and embezzlement are usually products of opportunity, so minimize those opportunities. No one person should be in charge of the entire bookkeeping process: The person who enters charges should be different from the one who enters payments. The one who writes checks or makes electronic fund transfers should not balance the books, and so on. Internal audits should be done on a regular basis, and all employees should know that. Your accountant can help.
- Reconcile cash receipts daily. Embezzlement does not require sophisticated technology; the most common form is simply taking cash out of the till. In a typical scenario, a patient pays a copay of $15 in cash; the receptionist records the payment as $5, and pockets the rest. Make sure a receipt is generated for every cash transaction, and that someone other than the person accepting cash reconciles the charges, receipts, and cash totals daily.
- Inventory your stock. Cash isn’t the only susceptible commodity. If you sell cosmetics or other products, inventory your stock frequently. And office personnel are not the only potential thieves: Last year, a locum tenens physician down the street conspired with a receptionist to take cash transactions for cosmetic neurotoxins and fillers “off the books” and split the spoils. That office was being ripped off twice; first for the neurotoxin and filler materials themselves, and then for the cash proceeds.
- Separate all accounting duties. Another popular ploy is false invoicing for imaginary supplies. A friend’s experience provides a good example (retold with his permission): His bookkeeper wrote sizable checks to herself, disguising them in the ledger as payments to vendors commonly used by his practice. Since the same employee also balanced the checkbook, she got away with it for years. “It wasn’t at all clever,” he told me, “and I’m embarrassed to admit that it happened to me.” Once again, separation of duties is the key to prevention. One employee should enter invoices into the data system, another should issue the check or make the electronic transfer, and a third should match invoices to goods and services received.
- Verify expense reports. False expense reporting is a subset of the fake invoice scam. When an employee asks for reimbursement of expenses, make sure those expenses are real.
- Consider computer safeguards. Computers facilitate a lot of financial chores, but they also consolidate financial data in one place, where it is potentially accessible to anybody, anywhere. Your computer vendor should be aware of this, and there should be safeguards built into your system. Ask about them. If they aren’t there, ask why.
- Hire honest employees. All applicants look great on paper, so check their references; and with their permission, you can run background checks for a few dollars on any of several public information web sites. My columns on hiring are available on the MDedge Dermatology website.
- Look for “red flags.” Examples include employees who refuse to take vacations, because someone else will have do their work or who insist on posting expenses that are a coworker’s responsibility, “just to be nice.” Anyone obviously living beyond his or her means merits suspicion as well.
- Consider bonding your employees. Dishonesty bonds are relatively inexpensive, and provide assurance of some measure of recovery if your safeguards fail. Also, just knowing that your staff is bonded will scare off most dishonest applicants. One effective screen is a question on your employment application: “Would you object to being bonded?”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
With myriad complex, high-tech problems facing private practice in this modern era, I am periodically reminded by long-time readers to revisit some of the low-tech issues that will always require our attention.
Few are lower tech (in most cases) and more easily overlooked than theft from within. Embezzlement remains far more common in medical offices than generally assumed – and it often occurs in full view of physicians who think everything is fine. Most embezzlers are not skillful or discreet; their transgressions may go undetected for years, simply because no one suspects it is happening.
Detecting fraud is an inexact science. There is no textbook approach that one can follow, but a few simple measures will prevent or expose the most common forms:
- Make it more difficult. Theft and embezzlement are usually products of opportunity, so minimize those opportunities. No one person should be in charge of the entire bookkeeping process: The person who enters charges should be different from the one who enters payments. The one who writes checks or makes electronic fund transfers should not balance the books, and so on. Internal audits should be done on a regular basis, and all employees should know that. Your accountant can help.
- Reconcile cash receipts daily. Embezzlement does not require sophisticated technology; the most common form is simply taking cash out of the till. In a typical scenario, a patient pays a copay of $15 in cash; the receptionist records the payment as $5, and pockets the rest. Make sure a receipt is generated for every cash transaction, and that someone other than the person accepting cash reconciles the charges, receipts, and cash totals daily.
- Inventory your stock. Cash isn’t the only susceptible commodity. If you sell cosmetics or other products, inventory your stock frequently. And office personnel are not the only potential thieves: Last year, a locum tenens physician down the street conspired with a receptionist to take cash transactions for cosmetic neurotoxins and fillers “off the books” and split the spoils. That office was being ripped off twice; first for the neurotoxin and filler materials themselves, and then for the cash proceeds.
- Separate all accounting duties. Another popular ploy is false invoicing for imaginary supplies. A friend’s experience provides a good example (retold with his permission): His bookkeeper wrote sizable checks to herself, disguising them in the ledger as payments to vendors commonly used by his practice. Since the same employee also balanced the checkbook, she got away with it for years. “It wasn’t at all clever,” he told me, “and I’m embarrassed to admit that it happened to me.” Once again, separation of duties is the key to prevention. One employee should enter invoices into the data system, another should issue the check or make the electronic transfer, and a third should match invoices to goods and services received.
- Verify expense reports. False expense reporting is a subset of the fake invoice scam. When an employee asks for reimbursement of expenses, make sure those expenses are real.
- Consider computer safeguards. Computers facilitate a lot of financial chores, but they also consolidate financial data in one place, where it is potentially accessible to anybody, anywhere. Your computer vendor should be aware of this, and there should be safeguards built into your system. Ask about them. If they aren’t there, ask why.
- Hire honest employees. All applicants look great on paper, so check their references; and with their permission, you can run background checks for a few dollars on any of several public information web sites. My columns on hiring are available on the MDedge Dermatology website.
- Look for “red flags.” Examples include employees who refuse to take vacations, because someone else will have do their work or who insist on posting expenses that are a coworker’s responsibility, “just to be nice.” Anyone obviously living beyond his or her means merits suspicion as well.
- Consider bonding your employees. Dishonesty bonds are relatively inexpensive, and provide assurance of some measure of recovery if your safeguards fail. Also, just knowing that your staff is bonded will scare off most dishonest applicants. One effective screen is a question on your employment application: “Would you object to being bonded?”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
With myriad complex, high-tech problems facing private practice in this modern era, I am periodically reminded by long-time readers to revisit some of the low-tech issues that will always require our attention.
Few are lower tech (in most cases) and more easily overlooked than theft from within. Embezzlement remains far more common in medical offices than generally assumed – and it often occurs in full view of physicians who think everything is fine. Most embezzlers are not skillful or discreet; their transgressions may go undetected for years, simply because no one suspects it is happening.
Detecting fraud is an inexact science. There is no textbook approach that one can follow, but a few simple measures will prevent or expose the most common forms:
- Make it more difficult. Theft and embezzlement are usually products of opportunity, so minimize those opportunities. No one person should be in charge of the entire bookkeeping process: The person who enters charges should be different from the one who enters payments. The one who writes checks or makes electronic fund transfers should not balance the books, and so on. Internal audits should be done on a regular basis, and all employees should know that. Your accountant can help.
- Reconcile cash receipts daily. Embezzlement does not require sophisticated technology; the most common form is simply taking cash out of the till. In a typical scenario, a patient pays a copay of $15 in cash; the receptionist records the payment as $5, and pockets the rest. Make sure a receipt is generated for every cash transaction, and that someone other than the person accepting cash reconciles the charges, receipts, and cash totals daily.
- Inventory your stock. Cash isn’t the only susceptible commodity. If you sell cosmetics or other products, inventory your stock frequently. And office personnel are not the only potential thieves: Last year, a locum tenens physician down the street conspired with a receptionist to take cash transactions for cosmetic neurotoxins and fillers “off the books” and split the spoils. That office was being ripped off twice; first for the neurotoxin and filler materials themselves, and then for the cash proceeds.
- Separate all accounting duties. Another popular ploy is false invoicing for imaginary supplies. A friend’s experience provides a good example (retold with his permission): His bookkeeper wrote sizable checks to herself, disguising them in the ledger as payments to vendors commonly used by his practice. Since the same employee also balanced the checkbook, she got away with it for years. “It wasn’t at all clever,” he told me, “and I’m embarrassed to admit that it happened to me.” Once again, separation of duties is the key to prevention. One employee should enter invoices into the data system, another should issue the check or make the electronic transfer, and a third should match invoices to goods and services received.
- Verify expense reports. False expense reporting is a subset of the fake invoice scam. When an employee asks for reimbursement of expenses, make sure those expenses are real.
- Consider computer safeguards. Computers facilitate a lot of financial chores, but they also consolidate financial data in one place, where it is potentially accessible to anybody, anywhere. Your computer vendor should be aware of this, and there should be safeguards built into your system. Ask about them. If they aren’t there, ask why.
- Hire honest employees. All applicants look great on paper, so check their references; and with their permission, you can run background checks for a few dollars on any of several public information web sites. My columns on hiring are available on the MDedge Dermatology website.
- Look for “red flags.” Examples include employees who refuse to take vacations, because someone else will have do their work or who insist on posting expenses that are a coworker’s responsibility, “just to be nice.” Anyone obviously living beyond his or her means merits suspicion as well.
- Consider bonding your employees. Dishonesty bonds are relatively inexpensive, and provide assurance of some measure of recovery if your safeguards fail. Also, just knowing that your staff is bonded will scare off most dishonest applicants. One effective screen is a question on your employment application: “Would you object to being bonded?”
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

Helping patients at the end of their lives
My wife thinks I am a little morbid, because I still read the local Sunday newspaper not to catch up on the news, and certainly not for the ads, but mostly to read the obituaries.

All of us have elderly patients, and I am growing old with many of my older patients. Now after treating many thousands of patients whom I have grown to know well, it is not unusual to see an obituary of someone my office staff and I know in the newspaper on a weekly basis.
We send sympathy cards, sometimes I write a personal note to the spouse or family, and several times a year, some of my staff and I will go to the funeral or memorial ceremony.
I usually ask if they died well, comfortably with family, or better yet, suddenly, dropping dead like a stone. This is the unspoken, though usually unrealized, goal of many of us from the world of medicine.
All physicians who have been surrounded by death, some horrible deaths, want to die well. I think it is difficult to do, although my mother came close.
One day when dropping off her best little friend (my 10-year-old daughter), she said “look here, I’ve got a knot in my belly button.” I felt the blood rushing to my head and before I could stop her, she showed me her Sister Mary Joseph nodule, a sign of metastatic internal malignancy. I sat stunned as she looked at me; her eyes showed she already knew my answer.
She lasted at home for 6 weeks, went into hospice, and died 36 hours later.
The last morning before she died, I took my daughter to see her before school. She woke up and called her “sugar” and had her climb into bed with her and snuggle. I got choked up and tearful and started telling her how much I loved her and how sorry I was and how much we would miss her. She looked over at me, and with anger in her voice, told me to be quiet, and explained that death comes to everyone eventually and just to get over it. In retrospect, I understand now that I was not helping her die well.
I am telling this story to bring up a point about professionalism. , this becomes important as the life cycle ends. Aged patients sometimes start blossoming with skin cancers. You must carefully gauge how much “treatment” a patient really needs.
You have a conflict. You get paid to diagnose and treat skin cancers. You must shift roles and become the patient’s protector, and treat the patient as if he or she was your parent. Less, sometimes much less, is often more. Perhaps you only biopsy and treat rapidly growing cancers that endanger crucial structures. You ignore the noninvasive tumors on the trunk and extremities. It is a fine and difficult line to walk.
Patients know they are dying, and at certain stages of grieving will want everything possible done, especially if it is visible. Skin wounds, even from curetting, salves, and cryotherapy, can be painful and sometimes disabling. You must resist unnecessary treatments, temporize if possible, discuss quality time with the patient and the family, and reach a consensus on how aggressive not to be. You must help them die well.
You are not only a healer, but as a master physician you – yes, even you the dermatologist – must also be a helpful guide at the end of life. I am sad to see patients, my old friends, in the newspaper, but feel secretly satisfied if I have spared them unnecessary suffering.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at dermnews@mdedge.com.
My wife thinks I am a little morbid, because I still read the local Sunday newspaper not to catch up on the news, and certainly not for the ads, but mostly to read the obituaries.
All of us have elderly patients, and I am growing old with many of my older patients. Now after treating many thousands of patients whom I have grown to know well, it is not unusual to see an obituary of someone my office staff and I know in the newspaper on a weekly basis.
We send sympathy cards, sometimes I write a personal note to the spouse or family, and several times a year, some of my staff and I will go to the funeral or memorial ceremony.
I usually ask if they died well, comfortably with family, or better yet, suddenly, dropping dead like a stone. This is the unspoken, though usually unrealized, goal of many of us from the world of medicine.
All physicians who have been surrounded by death, some horrible deaths, want to die well. I think it is difficult to do, although my mother came close.
One day when dropping off her best little friend (my 10-year-old daughter), she said “look here, I’ve got a knot in my belly button.” I felt the blood rushing to my head and before I could stop her, she showed me her Sister Mary Joseph nodule, a sign of metastatic internal malignancy. I sat stunned as she looked at me; her eyes showed she already knew my answer.
She lasted at home for 6 weeks, went into hospice, and died 36 hours later.
The last morning before she died, I took my daughter to see her before school. She woke up and called her “sugar” and had her climb into bed with her and snuggle. I got choked up and tearful and started telling her how much I loved her and how sorry I was and how much we would miss her. She looked over at me, and with anger in her voice, told me to be quiet, and explained that death comes to everyone eventually and just to get over it. In retrospect, I understand now that I was not helping her die well.
I am telling this story to bring up a point about professionalism. , this becomes important as the life cycle ends. Aged patients sometimes start blossoming with skin cancers. You must carefully gauge how much “treatment” a patient really needs.
You have a conflict. You get paid to diagnose and treat skin cancers. You must shift roles and become the patient’s protector, and treat the patient as if he or she was your parent. Less, sometimes much less, is often more. Perhaps you only biopsy and treat rapidly growing cancers that endanger crucial structures. You ignore the noninvasive tumors on the trunk and extremities. It is a fine and difficult line to walk.
Patients know they are dying, and at certain stages of grieving will want everything possible done, especially if it is visible. Skin wounds, even from curetting, salves, and cryotherapy, can be painful and sometimes disabling. You must resist unnecessary treatments, temporize if possible, discuss quality time with the patient and the family, and reach a consensus on how aggressive not to be. You must help them die well.
You are not only a healer, but as a master physician you – yes, even you the dermatologist – must also be a helpful guide at the end of life. I am sad to see patients, my old friends, in the newspaper, but feel secretly satisfied if I have spared them unnecessary suffering.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at dermnews@mdedge.com.
My wife thinks I am a little morbid, because I still read the local Sunday newspaper not to catch up on the news, and certainly not for the ads, but mostly to read the obituaries.
All of us have elderly patients, and I am growing old with many of my older patients. Now after treating many thousands of patients whom I have grown to know well, it is not unusual to see an obituary of someone my office staff and I know in the newspaper on a weekly basis.
We send sympathy cards, sometimes I write a personal note to the spouse or family, and several times a year, some of my staff and I will go to the funeral or memorial ceremony.
I usually ask if they died well, comfortably with family, or better yet, suddenly, dropping dead like a stone. This is the unspoken, though usually unrealized, goal of many of us from the world of medicine.
All physicians who have been surrounded by death, some horrible deaths, want to die well. I think it is difficult to do, although my mother came close.
One day when dropping off her best little friend (my 10-year-old daughter), she said “look here, I’ve got a knot in my belly button.” I felt the blood rushing to my head and before I could stop her, she showed me her Sister Mary Joseph nodule, a sign of metastatic internal malignancy. I sat stunned as she looked at me; her eyes showed she already knew my answer.
She lasted at home for 6 weeks, went into hospice, and died 36 hours later.
The last morning before she died, I took my daughter to see her before school. She woke up and called her “sugar” and had her climb into bed with her and snuggle. I got choked up and tearful and started telling her how much I loved her and how sorry I was and how much we would miss her. She looked over at me, and with anger in her voice, told me to be quiet, and explained that death comes to everyone eventually and just to get over it. In retrospect, I understand now that I was not helping her die well.
I am telling this story to bring up a point about professionalism. , this becomes important as the life cycle ends. Aged patients sometimes start blossoming with skin cancers. You must carefully gauge how much “treatment” a patient really needs.
You have a conflict. You get paid to diagnose and treat skin cancers. You must shift roles and become the patient’s protector, and treat the patient as if he or she was your parent. Less, sometimes much less, is often more. Perhaps you only biopsy and treat rapidly growing cancers that endanger crucial structures. You ignore the noninvasive tumors on the trunk and extremities. It is a fine and difficult line to walk.
Patients know they are dying, and at certain stages of grieving will want everything possible done, especially if it is visible. Skin wounds, even from curetting, salves, and cryotherapy, can be painful and sometimes disabling. You must resist unnecessary treatments, temporize if possible, discuss quality time with the patient and the family, and reach a consensus on how aggressive not to be. You must help them die well.
You are not only a healer, but as a master physician you – yes, even you the dermatologist – must also be a helpful guide at the end of life. I am sad to see patients, my old friends, in the newspaper, but feel secretly satisfied if I have spared them unnecessary suffering.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Write to him at dermnews@mdedge.com.
Like a hot potato
Most of us did our postgraduate training in tertiary medical centers, ivory towers of medicine often attached to or closely affiliated with medical schools. These are the places where the buck stops. Occasionally, a very complex patient might be sent to another tertiary center that claims to have a supersubspecialist, a one-of-a-kind physician with nationally recognized expertise. But for most patients, the tertiary medical center is the end of the line, and his or her physicians must manage with the resources at hand. They may confer with one another but there is no place for them to pass the buck.

But most of us who chose primary care left the comforting cocoon of the teaching hospital complex when we finished our training. Those first few months and years in the hinterland can be angst producing. Until we have established our own personal networks of consultants and mentors, patients with more than run-of-the-mill complaints may prompt us to reach for the phone or fire off an email call for help to our recently departed mother ship.
It can take awhile to establish the self-confidence – or at least the appearance of self-confidence – that physicians are expected to exude. But even after years of experience, none of us wants to watch a patient die or suffer preventable complications under our care when we know there is another facility that can provide a higher lever of care just an ambulance ride or short helicopter trip away.
Our primary concern is of course assuring that our patient is receiving the best care. How quickly we reach for the phone to refer out the most fragile patients depends on several factors. Do we practice in a community that has a historic reputation of having a low threshold for malpractice suits? How well do we know the patient and her family? Have we had time to establish bidirectional trust?
Is the patient’s diagnosis one that we feel comfortable with or is the diagnosis one that we believe could quickly deteriorate without warning? For example, a recently published study revealed that 20% of pediatric trauma patients were overtriaged and that the mechanism of injury – firearms or motor vehicle accidents – appeared to have an outsized influence in the triage decision (Trauma Surg Acute Care Open. 2019 Dec 29. doi: 10.1136/tsaco-2019-000300).

Because I have no experience with firearm injuries and minimal experience with motor vehicle injuries I can understand why the emergency medical technicians might be quick to ship these patients to the trauma center. However, I hope that, were I offered better training and more opportunities to gain experience with these types of injuries, I would have a lower overtriage percentage.
Which begs the question of what is an acceptable rate of overtriage or overreferral? It’s the same old question of how many normal appendixes should one remove to avoid a fatal outcome. Each of us arrives at a given clinical crossroads with our own level of experience and comfort level.
But in the final analysis it boils down to a personal decision and our own basic level of anxiety. Let’s face it, some of us worry more than others. Physicians come in all shades of anxiety. A hot potato in your hands may feel only room temperature to me.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Most of us did our postgraduate training in tertiary medical centers, ivory towers of medicine often attached to or closely affiliated with medical schools. These are the places where the buck stops. Occasionally, a very complex patient might be sent to another tertiary center that claims to have a supersubspecialist, a one-of-a-kind physician with nationally recognized expertise. But for most patients, the tertiary medical center is the end of the line, and his or her physicians must manage with the resources at hand. They may confer with one another but there is no place for them to pass the buck.
But most of us who chose primary care left the comforting cocoon of the teaching hospital complex when we finished our training. Those first few months and years in the hinterland can be angst producing. Until we have established our own personal networks of consultants and mentors, patients with more than run-of-the-mill complaints may prompt us to reach for the phone or fire off an email call for help to our recently departed mother ship.
It can take awhile to establish the self-confidence – or at least the appearance of self-confidence – that physicians are expected to exude. But even after years of experience, none of us wants to watch a patient die or suffer preventable complications under our care when we know there is another facility that can provide a higher lever of care just an ambulance ride or short helicopter trip away.
Our primary concern is of course assuring that our patient is receiving the best care. How quickly we reach for the phone to refer out the most fragile patients depends on several factors. Do we practice in a community that has a historic reputation of having a low threshold for malpractice suits? How well do we know the patient and her family? Have we had time to establish bidirectional trust?
Is the patient’s diagnosis one that we feel comfortable with or is the diagnosis one that we believe could quickly deteriorate without warning? For example, a recently published study revealed that 20% of pediatric trauma patients were overtriaged and that the mechanism of injury – firearms or motor vehicle accidents – appeared to have an outsized influence in the triage decision (Trauma Surg Acute Care Open. 2019 Dec 29. doi: 10.1136/tsaco-2019-000300).
Because I have no experience with firearm injuries and minimal experience with motor vehicle injuries I can understand why the emergency medical technicians might be quick to ship these patients to the trauma center. However, I hope that, were I offered better training and more opportunities to gain experience with these types of injuries, I would have a lower overtriage percentage.
Which begs the question of what is an acceptable rate of overtriage or overreferral? It’s the same old question of how many normal appendixes should one remove to avoid a fatal outcome. Each of us arrives at a given clinical crossroads with our own level of experience and comfort level.
But in the final analysis it boils down to a personal decision and our own basic level of anxiety. Let’s face it, some of us worry more than others. Physicians come in all shades of anxiety. A hot potato in your hands may feel only room temperature to me.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Most of us did our postgraduate training in tertiary medical centers, ivory towers of medicine often attached to or closely affiliated with medical schools. These are the places where the buck stops. Occasionally, a very complex patient might be sent to another tertiary center that claims to have a supersubspecialist, a one-of-a-kind physician with nationally recognized expertise. But for most patients, the tertiary medical center is the end of the line, and his or her physicians must manage with the resources at hand. They may confer with one another but there is no place for them to pass the buck.
But most of us who chose primary care left the comforting cocoon of the teaching hospital complex when we finished our training. Those first few months and years in the hinterland can be angst producing. Until we have established our own personal networks of consultants and mentors, patients with more than run-of-the-mill complaints may prompt us to reach for the phone or fire off an email call for help to our recently departed mother ship.
It can take awhile to establish the self-confidence – or at least the appearance of self-confidence – that physicians are expected to exude. But even after years of experience, none of us wants to watch a patient die or suffer preventable complications under our care when we know there is another facility that can provide a higher lever of care just an ambulance ride or short helicopter trip away.
Our primary concern is of course assuring that our patient is receiving the best care. How quickly we reach for the phone to refer out the most fragile patients depends on several factors. Do we practice in a community that has a historic reputation of having a low threshold for malpractice suits? How well do we know the patient and her family? Have we had time to establish bidirectional trust?
Is the patient’s diagnosis one that we feel comfortable with or is the diagnosis one that we believe could quickly deteriorate without warning? For example, a recently published study revealed that 20% of pediatric trauma patients were overtriaged and that the mechanism of injury – firearms or motor vehicle accidents – appeared to have an outsized influence in the triage decision (Trauma Surg Acute Care Open. 2019 Dec 29. doi: 10.1136/tsaco-2019-000300).
Because I have no experience with firearm injuries and minimal experience with motor vehicle injuries I can understand why the emergency medical technicians might be quick to ship these patients to the trauma center. However, I hope that, were I offered better training and more opportunities to gain experience with these types of injuries, I would have a lower overtriage percentage.
Which begs the question of what is an acceptable rate of overtriage or overreferral? It’s the same old question of how many normal appendixes should one remove to avoid a fatal outcome. Each of us arrives at a given clinical crossroads with our own level of experience and comfort level.
But in the final analysis it boils down to a personal decision and our own basic level of anxiety. Let’s face it, some of us worry more than others. Physicians come in all shades of anxiety. A hot potato in your hands may feel only room temperature to me.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
The Mississippi solution
I agree wholeheartedly with Dr. William G. Wilkoff’s doubts that an increase in medical schools/students and/or foreign medical graduates is the answer to the physician shortage felt by many areas of the country (Letters From Maine, “Help Wanted,” Nov. 2019, page 19). All you have to do is look at the glut of physicians – and just about any other profession – in metropolitan areas versus rural America, and ask basic questions regarding why those doctors practice where they do. You will quickly discover that most are willing to trade the possibility of a higher salary in areas where their presence is more needed to achieve more school choices, jobs for a spouse, and likely a more favorable call schedule. Something more attractive than salary or the prospect of more “elbow room” is desired.
Here in Mississippi we may have found an answer to the problem. A few years ago our state legislature started the Mississippi Rural Health Scholarship Program that pays for recipients to attend a state-run medical school on scholarship in exchange for agreeing to practice at least 4 years in a rural area of the state (less than 20k population) following their primary care residency (family medicine, pediatrics, ob.gyn., med-peds, internal medicine, and, recently added, psychiatry). Although a recent increase in the number of pediatric residency slots at our state’s sole program will no doubt also have a positive effect to this end, such a scholarship program as the one implemented by Mississippi is the best way to compete with the various intangibles that lead people to choose bigger cities over rural areas of the state to practice their trade. Once there, many – like myself – will find that such a practice is not only a good business decision but often is a wonderful place to raise a family. Meanwhile, our own practice just added a fourth physician as a result of said Rural Health Scholarship Program, and we could not be more satisfied with the result.
I agree wholeheartedly with Dr. William G. Wilkoff’s doubts that an increase in medical schools/students and/or foreign medical graduates is the answer to the physician shortage felt by many areas of the country (Letters From Maine, “Help Wanted,” Nov. 2019, page 19). All you have to do is look at the glut of physicians – and just about any other profession – in metropolitan areas versus rural America, and ask basic questions regarding why those doctors practice where they do. You will quickly discover that most are willing to trade the possibility of a higher salary in areas where their presence is more needed to achieve more school choices, jobs for a spouse, and likely a more favorable call schedule. Something more attractive than salary or the prospect of more “elbow room” is desired.
Here in Mississippi we may have found an answer to the problem. A few years ago our state legislature started the Mississippi Rural Health Scholarship Program that pays for recipients to attend a state-run medical school on scholarship in exchange for agreeing to practice at least 4 years in a rural area of the state (less than 20k population) following their primary care residency (family medicine, pediatrics, ob.gyn., med-peds, internal medicine, and, recently added, psychiatry). Although a recent increase in the number of pediatric residency slots at our state’s sole program will no doubt also have a positive effect to this end, such a scholarship program as the one implemented by Mississippi is the best way to compete with the various intangibles that lead people to choose bigger cities over rural areas of the state to practice their trade. Once there, many – like myself – will find that such a practice is not only a good business decision but often is a wonderful place to raise a family. Meanwhile, our own practice just added a fourth physician as a result of said Rural Health Scholarship Program, and we could not be more satisfied with the result.
I agree wholeheartedly with Dr. William G. Wilkoff’s doubts that an increase in medical schools/students and/or foreign medical graduates is the answer to the physician shortage felt by many areas of the country (Letters From Maine, “Help Wanted,” Nov. 2019, page 19). All you have to do is look at the glut of physicians – and just about any other profession – in metropolitan areas versus rural America, and ask basic questions regarding why those doctors practice where they do. You will quickly discover that most are willing to trade the possibility of a higher salary in areas where their presence is more needed to achieve more school choices, jobs for a spouse, and likely a more favorable call schedule. Something more attractive than salary or the prospect of more “elbow room” is desired.
Here in Mississippi we may have found an answer to the problem. A few years ago our state legislature started the Mississippi Rural Health Scholarship Program that pays for recipients to attend a state-run medical school on scholarship in exchange for agreeing to practice at least 4 years in a rural area of the state (less than 20k population) following their primary care residency (family medicine, pediatrics, ob.gyn., med-peds, internal medicine, and, recently added, psychiatry). Although a recent increase in the number of pediatric residency slots at our state’s sole program will no doubt also have a positive effect to this end, such a scholarship program as the one implemented by Mississippi is the best way to compete with the various intangibles that lead people to choose bigger cities over rural areas of the state to practice their trade. Once there, many – like myself – will find that such a practice is not only a good business decision but often is a wonderful place to raise a family. Meanwhile, our own practice just added a fourth physician as a result of said Rural Health Scholarship Program, and we could not be more satisfied with the result.
The power of an odd couple
The time has come for good men and women to unite and rise up against a common foe. For too long nurses and doctors have labored under the tyranny of a dictator who claimed to help them provide high-quality care for their patients while at the same time cutting their paperwork to nil. But like most autocrats he failed to engage his subjects in a meaningful dialogue as each new version of his promised improvements rolled off the drawing board. When the caregivers were slow to adopt these new nonsystems he offered them financial incentives and issued threats to their survival. Although they were warned that there might be uncomfortable adjustment periods, the caregivers were promised that the steep learning curves would level out and their professional lives would again be valued and productive.

Of course, the dictator is not a single person but a motley and disorganized conglomerate of user- and patient-unfriendly electronic health record nonsystems. Ask almost any nurse or physician for her feelings about computer-based medical record systems, and you will hear tales of long hours, disengagement, and frustration. Caregivers are unhappy at all levels, and patients have grown tired of their nurses and physicians spending most of their time looking at computer screens.
You certainly have heard this all before. But you are hearing it in hospital hallways and grocery store checkout lines as a low rumble of discontent emerging from separate individuals, not as a well-articulated and widely distributed voice of physicians as a group. To some extent this relative silence is because there is no such group, at least not in same mold as a labor union. The term “labor union” may make you uncomfortable. But given the current climate in medicine, unionizing may be the best and only way to effect change.
But organizing to effect change in the workplace isn’t part of the physician genome. In the 1960s, a group of house officers in Boston engaged in a heal-in to successfully improve their salaries and working conditions. But over the ensuing half century physicians have remained tragically silent in the face of a changing workplace landscape in which they have gone from being independent owner operators in control of their destinies to becoming employees feeling powerless to improve their working conditions. This perceived impotence has escalated in the face of the challenge posed by the introduction of dysfunctional EHRs.

Ironically, a solution is at almost every physician’s elbow. In a recent New York Times opinion piece Theresa Brown and Stephen Bergman acknowledge that physicians don’t seem prepared to mount a meaningful response to the challenge to the failed promise of EHRs (“Doctors, Nurses and the Paperwork Crisis That Could Unite Them,” Dec. 31, 2019). They point out that, over the last half century, physicians have remained isolated on the sidelines, finding just enough voice to grumble. Nurses have in a variety of situations organized to effect change in their working conditions – in some cases by forming labor unions.
The authors of this op-ed piece, a physician and a nurse, make a strong argument that the time has come for nurses and doctors shake off the shackles of their stereotypic roles and join in creating a loud, forceful, and effective voice to demand a working environment in which the computer functions as an asset and no longer as the terrible burden it has become. Neither group has the power to do it alone, but together they may be able to turn the tide. For physicians it will probably mean venturing several steps outside of their comfort zone. But working shoulder to shoulder with nurses may provide the courage to speak out.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
The time has come for good men and women to unite and rise up against a common foe. For too long nurses and doctors have labored under the tyranny of a dictator who claimed to help them provide high-quality care for their patients while at the same time cutting their paperwork to nil. But like most autocrats he failed to engage his subjects in a meaningful dialogue as each new version of his promised improvements rolled off the drawing board. When the caregivers were slow to adopt these new nonsystems he offered them financial incentives and issued threats to their survival. Although they were warned that there might be uncomfortable adjustment periods, the caregivers were promised that the steep learning curves would level out and their professional lives would again be valued and productive.
Of course, the dictator is not a single person but a motley and disorganized conglomerate of user- and patient-unfriendly electronic health record nonsystems. Ask almost any nurse or physician for her feelings about computer-based medical record systems, and you will hear tales of long hours, disengagement, and frustration. Caregivers are unhappy at all levels, and patients have grown tired of their nurses and physicians spending most of their time looking at computer screens.
You certainly have heard this all before. But you are hearing it in hospital hallways and grocery store checkout lines as a low rumble of discontent emerging from separate individuals, not as a well-articulated and widely distributed voice of physicians as a group. To some extent this relative silence is because there is no such group, at least not in same mold as a labor union. The term “labor union” may make you uncomfortable. But given the current climate in medicine, unionizing may be the best and only way to effect change.
But organizing to effect change in the workplace isn’t part of the physician genome. In the 1960s, a group of house officers in Boston engaged in a heal-in to successfully improve their salaries and working conditions. But over the ensuing half century physicians have remained tragically silent in the face of a changing workplace landscape in which they have gone from being independent owner operators in control of their destinies to becoming employees feeling powerless to improve their working conditions. This perceived impotence has escalated in the face of the challenge posed by the introduction of dysfunctional EHRs.
Ironically, a solution is at almost every physician’s elbow. In a recent New York Times opinion piece Theresa Brown and Stephen Bergman acknowledge that physicians don’t seem prepared to mount a meaningful response to the challenge to the failed promise of EHRs (“Doctors, Nurses and the Paperwork Crisis That Could Unite Them,” Dec. 31, 2019). They point out that, over the last half century, physicians have remained isolated on the sidelines, finding just enough voice to grumble. Nurses have in a variety of situations organized to effect change in their working conditions – in some cases by forming labor unions.
The authors of this op-ed piece, a physician and a nurse, make a strong argument that the time has come for nurses and doctors shake off the shackles of their stereotypic roles and join in creating a loud, forceful, and effective voice to demand a working environment in which the computer functions as an asset and no longer as the terrible burden it has become. Neither group has the power to do it alone, but together they may be able to turn the tide. For physicians it will probably mean venturing several steps outside of their comfort zone. But working shoulder to shoulder with nurses may provide the courage to speak out.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
The time has come for good men and women to unite and rise up against a common foe. For too long nurses and doctors have labored under the tyranny of a dictator who claimed to help them provide high-quality care for their patients while at the same time cutting their paperwork to nil. But like most autocrats he failed to engage his subjects in a meaningful dialogue as each new version of his promised improvements rolled off the drawing board. When the caregivers were slow to adopt these new nonsystems he offered them financial incentives and issued threats to their survival. Although they were warned that there might be uncomfortable adjustment periods, the caregivers were promised that the steep learning curves would level out and their professional lives would again be valued and productive.
Of course, the dictator is not a single person but a motley and disorganized conglomerate of user- and patient-unfriendly electronic health record nonsystems. Ask almost any nurse or physician for her feelings about computer-based medical record systems, and you will hear tales of long hours, disengagement, and frustration. Caregivers are unhappy at all levels, and patients have grown tired of their nurses and physicians spending most of their time looking at computer screens.
You certainly have heard this all before. But you are hearing it in hospital hallways and grocery store checkout lines as a low rumble of discontent emerging from separate individuals, not as a well-articulated and widely distributed voice of physicians as a group. To some extent this relative silence is because there is no such group, at least not in same mold as a labor union. The term “labor union” may make you uncomfortable. But given the current climate in medicine, unionizing may be the best and only way to effect change.
But organizing to effect change in the workplace isn’t part of the physician genome. In the 1960s, a group of house officers in Boston engaged in a heal-in to successfully improve their salaries and working conditions. But over the ensuing half century physicians have remained tragically silent in the face of a changing workplace landscape in which they have gone from being independent owner operators in control of their destinies to becoming employees feeling powerless to improve their working conditions. This perceived impotence has escalated in the face of the challenge posed by the introduction of dysfunctional EHRs.
Ironically, a solution is at almost every physician’s elbow. In a recent New York Times opinion piece Theresa Brown and Stephen Bergman acknowledge that physicians don’t seem prepared to mount a meaningful response to the challenge to the failed promise of EHRs (“Doctors, Nurses and the Paperwork Crisis That Could Unite Them,” Dec. 31, 2019). They point out that, over the last half century, physicians have remained isolated on the sidelines, finding just enough voice to grumble. Nurses have in a variety of situations organized to effect change in their working conditions – in some cases by forming labor unions.
The authors of this op-ed piece, a physician and a nurse, make a strong argument that the time has come for nurses and doctors shake off the shackles of their stereotypic roles and join in creating a loud, forceful, and effective voice to demand a working environment in which the computer functions as an asset and no longer as the terrible burden it has become. Neither group has the power to do it alone, but together they may be able to turn the tide. For physicians it will probably mean venturing several steps outside of their comfort zone. But working shoulder to shoulder with nurses may provide the courage to speak out.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Should supplemental MRI be used in otherwise average-risk women with extremely dense breasts?
While the frequency of dense breasts decreases with age, approximately 10% of women in the United States have extremely dense breasts (Breast Imaging, Reporting, and Data System [BI-RADS] category D), and another 40% have heterogeneously dense breasts (BI-RADS category C).1 Women with dense breasts have both an increased risk for developing breast cancer and reduced mammographic sensitivity for breast cancer detection compared with women who have nondense breasts.2
These 2 observations have led the majority of states to pass legislation requiring that women with dense breasts be informed of their breast density, and most require that providers discuss these results with their patients. Thoughtful clinicians who review the available literature, however, will find sparse evidence on which to counsel patients as to next steps.
Now, a recent trial adds to our knowledge about supplemental magnetic resonance imaging (MRI) breast screening in women with extremely dense breasts.
DENSE trial offers high-quality data
Bakker and colleagues studied women aged 50 to 74 who were participating in a Netherlands population-based biennial mammography screening program.3 They enrolled average-risk women with extremely dense breasts who had a negative screening digital mammogram into the Dense Tissue and Early Breast Neoplasm Screening (DENSE) multicenter trial. The women were randomly assigned to receive either continued biennial digital mammography or supplemental breast MRI.
The primary outcome was the between-group difference in the development of interval breast cancers—that is, breast cancers detected by women or their providers between rounds of screening mammography. Interval breast cancers were chosen as the primary outcome for 2 reasons:
- interval cancers appear to be more aggressive tumors than those cancers detected by screening mammography
- interval cancers can be identified over a shorter time interval, making them easier to study than outcomes such as breast cancer mortality, which typically require more than a decade to identify.
The DENSE trial’s secondary outcomes included recall rates from MRI, cancer detection rates on MRI, positive predictive value of MRIs requiring biopsy, and breast cancer characteristics (size, stage) diagnosed in the different groups.
Between-group difference in incidence of interval cancers
A total of 40,373 women with extremely dense breasts were screened; 8,061 of these were randomly assigned to receive breast MRI and 32,312 to continued mammography only (1:4 cluster randomization) across 12 mammography centers in the Netherlands. Among the women assigned to the MRI group, 59% actually underwent MRI (4,783 of the 8,061).
The interval cancer rate in the mammography-only group was 5.0 per 1,000 screenings (95% confidence interval [CI], 4.3–5.8), while the interval cancer rate in the MRI-assigned group was 2.5 per 1,000 screenings (95% CI, 1.6–3.8) (TABLE 1).3
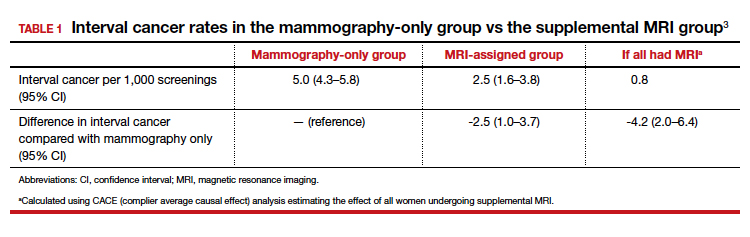
Key secondary outcomes
Of the women who underwent supplemental MRI, 9.49% were recalled for additional imaging, follow-up, or biopsy. Of the 4,783 women who had an MRI, 300 (6.3%) underwent a breast biopsy, and 79 breast cancers (1.65%) were detected. Sixty-four of these cancers were invasive, and 15 were ductal carcinoma in situ (DCIS). Among women who underwent a biopsy for an MRI-detected abnormality, the positive predictive value was 26.3%.
Tumor characteristics. For women who developed breast cancer during the study, both tumor size at diagnosis and tumor stage (early vs late) were described. TABLE 2 shows these results in the women who had their breast cancer detected on MRI, those in the MRI-assigned group who developed interval cancer, and those in the mammography-only group who had interval cancers.3 Overall, tumor size was smaller in the interval group who underwent MRI compared with those who underwent mammography only.
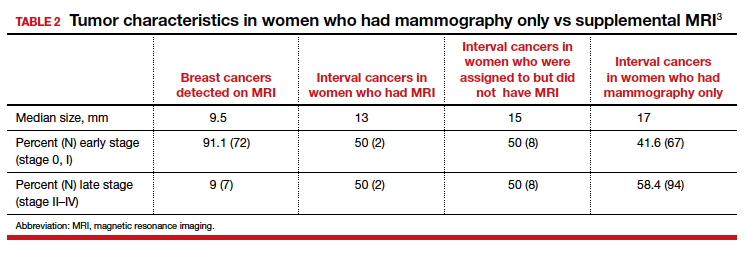
Continue to: Study contributes valuable data, but we need more on long-term outcomes...
Study contributes valuable data, but we need more on long-term outcomes
The trial by Bakker and colleagues employed a solid study design as women were randomly assigned to supplemental MRI screening or ongoing biennial mammography, and nearly all cancers were identified in the short-term of follow-up. In addition, very few women were lost to follow-up, and secondary outcomes, including false-positive rates, were collected to help providers and patients better understand some of the potential downsides of supplemental screening.
The substantial reduction in interval cancers (50% in the intent-to-screen analysis and 84% in the women who actually underwent supplemental MRI) was highly statistically significant (P<.001). While there were substantially fewer interval cancers in the MRI-assigned group, the interval cancers that did occur were of similar stage as those in the women assigned to the mammography-only group (TABLE 2).
Data demonstrate that interval cancers appear to be more aggressive than screen-detected cancers.4 While reducing interval cancers should be a good thing overall, it remains unproven that using supplemental MRI in all women with dense breasts would reduce breast cancer specific mortality, all-cause mortality, or the risk of more invasive treatments (for example, the need for chemotherapy or requirement for mastectomy).
On the other hand, using routine supplemental breast MRI in women with extremely dense breasts would result in very substantial use of resources, including cost, radiologist time, provider time, and machine time. In the United States, approximately 49 million women are aged 50 to 74.5 Breast MRI charges commonly range from $1,000 to $4,000. If the 4.9 million women with extremely dense breasts underwent supplemental MRI this year, the approximate cost would be somewhere between $4.9 and $19.5 billion for imaging alone. This does not include callbacks, biopsies, or provider time for ordering, interpreting, and arranging for follow-up.
While the reduction in interval cancers seen in this study is promising, more assurance of improvement in important outcomes—such as reduced mortality or reduced need for more invasive breast cancer treatments—should precede any routine change in practice.
Unanswered questions
This study did not address a number of other important questions, including:
Should MRI be done with every round of breast cancer screening given the possibility of prevalence bias? Prevalence bias can be defined as more cancers detected in the first round of MRI screening with possible reduced benefit in future rounds of screening. The study authors indicated that they will continue to analyze the study results to see what occurs in the next round of screening.
Is there a similar impact on decreased interval cancers in women undergoing annual mammography or in women screened between ages 40 and 49? This study was conducted in women aged 50 to 74 undergoing mammography every 2 years. In the United States, annual mammography in women aged 40 to 49 is frequently recommended.
What effect does supplemental MRI screening have in women with heterogeneously dense breasts, which represents 40% of the population? The US Food and Drug Administration recommends that all women with dense breasts be counseled regarding options for management.6
Do these results translate to the more racially and ethnically diverse populations of the United States? In the Netherlands, where this study was conducted, 85% to 90% of women are either Dutch or of western European origin. Women of different racial and ancestral backgrounds have biologically different breast cancers and cancer risk (for example, higher rates of triple-negative breast cancers in African American women; 10-fold higher rates of BRCA pathogenic variants in Ashkenazi Jewish women).
Continue to: Use validated tools to assess risk comprehensively...
Use validated tools to assess risk comprehensively
Women aged 50 to 74 with extremely dense breasts have reduced interval cancers following a normal biennial mammogram if supplemental MRI is offered, but the long-term benefit of identifying these cancers earlier is unclear. Until more data are available on important long-term outcomes (such as breast cancer mortality and need for more invasive treatments), providers should consider breast density in the context of a more comprehensive assessment of breast cancer risk using a validated breast cancer risk assessment tool.
I prefer the modified version of the International Breast Cancer Intervention Study (IBIS) tool, which is readily available online (https://ibis.ikonopedia.com/).7 This tool incorporates several breast cancer risk factors, including reproductive risk factors, body mass index, BRCA gene status, breast density, and family history. The tool takes 1 to 2 minutes to complete and provides an estimate of a woman’s 10-year risk and lifetime risk of breast cancer.
If the lifetime risk exceeds 20%, I offer the patient supplemental MRI screening, consistent with current recommendations of the National Comprehensive Cancer Network and the American Cancer Society.8,9 I generally recommend starting breast imaging screening 7 to 10 years prior to the youngest breast cancer occurrence in the family, with mammography starting no earlier than age 30 and MRI no earlier than age 25. Other validated tools also can be used.10-13
Incorporating breast density and other important risk factors allows a more comprehensive analysis upon which to counsel women about the value (benefits and harms) of breast imaging.8
- Sprague BL, Gagnon RE, Burt V, et al. Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst. 2014;106:dju255. doi: 10.1093/jcni/dju255.
- Boyd NF, Guo H, Martin LJ, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356:227-236.
- Bakker MF, de Lange SV, Pijnappel RM, et al; for the DENSE Trial Study Group. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102.
- Drukker CA, Schmidt MK, Rutgers EJT, et al. Mammographic screening detects low-risk tumor biology breast cancers. Breast Cancer Res Treat. 2014;144:103-111.
- Statista website. Resident population of the United States by sex and age as of July 1, 2018. https://www.statista.com/statistics/241488/population-of-the-us-by-sex-and-age. Accessed January 6, 2020.
- US Food and Drug Administration website. Mammography: what you need to know. https://www.fda.gov/consumers/consumer-updates/mammography-what-you-need-know. Accessed January 13, 2020.
- IBIS (International Breast Cancer Intervention Study) website. Online Tyrer-Cuzick Model Breast Cancer Risk Evaluation Tool. ibis.ikonopedia.com. Accessed January 13, 2020.
- Bevers TB, Anderson BO, Bonaccio E, et al; National Comprehensive Cancer Network. Breast cancer screening and diagnosis: NCCN practice guidelines in oncology. JNCCN. 2009;7:1060-1096.
- Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
- Antoniou AC, Cunningham AP, Peto J, et al. The BOADICEA model of genetic susceptibility to breast and ovarian cancers: updates and extensions. Br J Cancer. 2008;98:1457-1466.
- Claus EB, Risch N, Thompson WD. Autosomal dominant inheritance of early-onset breast cancer: implications for risk prediction. Cancer. 1994;73:643-651.
- Parmigiani G, Berry D, Aguilar O. Determining carrier probabilities for breast cancer-susceptibility genes BRCA1 and BRCA2. Am J Hum Genet. 1998;62:145-158.
- Tyrer J, Duffy SW, Cuzick J. A breast cancer prediction model incorporating familial and personal risk factors. Stat Med. 2004;23:1111-1130.
Mark D. Pearlman, MD
Director, Cancer Genetics and Breast Health
S. Jan Behrman Professor, Department of Obstetrics and Gynecology
University of Michigan Medical School
Ann Arbor, Michigan
Committee Member, National Comprehensive Cancer Network
Writing Group for Breast Cancer Screening and Diagnosis
OBG Management Contributing Editor
The author reports no financial relationships relevant to this article.
Mark D. Pearlman, MD
Director, Cancer Genetics and Breast Health
S. Jan Behrman Professor, Department of Obstetrics and Gynecology
University of Michigan Medical School
Ann Arbor, Michigan
Committee Member, National Comprehensive Cancer Network
Writing Group for Breast Cancer Screening and Diagnosis
OBG Management Contributing Editor
The author reports no financial relationships relevant to this article.
Mark D. Pearlman, MD
Director, Cancer Genetics and Breast Health
S. Jan Behrman Professor, Department of Obstetrics and Gynecology
University of Michigan Medical School
Ann Arbor, Michigan
Committee Member, National Comprehensive Cancer Network
Writing Group for Breast Cancer Screening and Diagnosis
OBG Management Contributing Editor
The author reports no financial relationships relevant to this article.
While the frequency of dense breasts decreases with age, approximately 10% of women in the United States have extremely dense breasts (Breast Imaging, Reporting, and Data System [BI-RADS] category D), and another 40% have heterogeneously dense breasts (BI-RADS category C).1 Women with dense breasts have both an increased risk for developing breast cancer and reduced mammographic sensitivity for breast cancer detection compared with women who have nondense breasts.2
These 2 observations have led the majority of states to pass legislation requiring that women with dense breasts be informed of their breast density, and most require that providers discuss these results with their patients. Thoughtful clinicians who review the available literature, however, will find sparse evidence on which to counsel patients as to next steps.
Now, a recent trial adds to our knowledge about supplemental magnetic resonance imaging (MRI) breast screening in women with extremely dense breasts.
DENSE trial offers high-quality data
Bakker and colleagues studied women aged 50 to 74 who were participating in a Netherlands population-based biennial mammography screening program.3 They enrolled average-risk women with extremely dense breasts who had a negative screening digital mammogram into the Dense Tissue and Early Breast Neoplasm Screening (DENSE) multicenter trial. The women were randomly assigned to receive either continued biennial digital mammography or supplemental breast MRI.
The primary outcome was the between-group difference in the development of interval breast cancers—that is, breast cancers detected by women or their providers between rounds of screening mammography. Interval breast cancers were chosen as the primary outcome for 2 reasons:
- interval cancers appear to be more aggressive tumors than those cancers detected by screening mammography
- interval cancers can be identified over a shorter time interval, making them easier to study than outcomes such as breast cancer mortality, which typically require more than a decade to identify.
The DENSE trial’s secondary outcomes included recall rates from MRI, cancer detection rates on MRI, positive predictive value of MRIs requiring biopsy, and breast cancer characteristics (size, stage) diagnosed in the different groups.
Between-group difference in incidence of interval cancers
A total of 40,373 women with extremely dense breasts were screened; 8,061 of these were randomly assigned to receive breast MRI and 32,312 to continued mammography only (1:4 cluster randomization) across 12 mammography centers in the Netherlands. Among the women assigned to the MRI group, 59% actually underwent MRI (4,783 of the 8,061).
The interval cancer rate in the mammography-only group was 5.0 per 1,000 screenings (95% confidence interval [CI], 4.3–5.8), while the interval cancer rate in the MRI-assigned group was 2.5 per 1,000 screenings (95% CI, 1.6–3.8) (TABLE 1).3
Key secondary outcomes
Of the women who underwent supplemental MRI, 9.49% were recalled for additional imaging, follow-up, or biopsy. Of the 4,783 women who had an MRI, 300 (6.3%) underwent a breast biopsy, and 79 breast cancers (1.65%) were detected. Sixty-four of these cancers were invasive, and 15 were ductal carcinoma in situ (DCIS). Among women who underwent a biopsy for an MRI-detected abnormality, the positive predictive value was 26.3%.
Tumor characteristics. For women who developed breast cancer during the study, both tumor size at diagnosis and tumor stage (early vs late) were described. TABLE 2 shows these results in the women who had their breast cancer detected on MRI, those in the MRI-assigned group who developed interval cancer, and those in the mammography-only group who had interval cancers.3 Overall, tumor size was smaller in the interval group who underwent MRI compared with those who underwent mammography only.
Continue to: Study contributes valuable data, but we need more on long-term outcomes...
Study contributes valuable data, but we need more on long-term outcomes
The trial by Bakker and colleagues employed a solid study design as women were randomly assigned to supplemental MRI screening or ongoing biennial mammography, and nearly all cancers were identified in the short-term of follow-up. In addition, very few women were lost to follow-up, and secondary outcomes, including false-positive rates, were collected to help providers and patients better understand some of the potential downsides of supplemental screening.
The substantial reduction in interval cancers (50% in the intent-to-screen analysis and 84% in the women who actually underwent supplemental MRI) was highly statistically significant (P<.001). While there were substantially fewer interval cancers in the MRI-assigned group, the interval cancers that did occur were of similar stage as those in the women assigned to the mammography-only group (TABLE 2).
Data demonstrate that interval cancers appear to be more aggressive than screen-detected cancers.4 While reducing interval cancers should be a good thing overall, it remains unproven that using supplemental MRI in all women with dense breasts would reduce breast cancer specific mortality, all-cause mortality, or the risk of more invasive treatments (for example, the need for chemotherapy or requirement for mastectomy).
On the other hand, using routine supplemental breast MRI in women with extremely dense breasts would result in very substantial use of resources, including cost, radiologist time, provider time, and machine time. In the United States, approximately 49 million women are aged 50 to 74.5 Breast MRI charges commonly range from $1,000 to $4,000. If the 4.9 million women with extremely dense breasts underwent supplemental MRI this year, the approximate cost would be somewhere between $4.9 and $19.5 billion for imaging alone. This does not include callbacks, biopsies, or provider time for ordering, interpreting, and arranging for follow-up.
While the reduction in interval cancers seen in this study is promising, more assurance of improvement in important outcomes—such as reduced mortality or reduced need for more invasive breast cancer treatments—should precede any routine change in practice.
Unanswered questions
This study did not address a number of other important questions, including:
Should MRI be done with every round of breast cancer screening given the possibility of prevalence bias? Prevalence bias can be defined as more cancers detected in the first round of MRI screening with possible reduced benefit in future rounds of screening. The study authors indicated that they will continue to analyze the study results to see what occurs in the next round of screening.
Is there a similar impact on decreased interval cancers in women undergoing annual mammography or in women screened between ages 40 and 49? This study was conducted in women aged 50 to 74 undergoing mammography every 2 years. In the United States, annual mammography in women aged 40 to 49 is frequently recommended.
What effect does supplemental MRI screening have in women with heterogeneously dense breasts, which represents 40% of the population? The US Food and Drug Administration recommends that all women with dense breasts be counseled regarding options for management.6
Do these results translate to the more racially and ethnically diverse populations of the United States? In the Netherlands, where this study was conducted, 85% to 90% of women are either Dutch or of western European origin. Women of different racial and ancestral backgrounds have biologically different breast cancers and cancer risk (for example, higher rates of triple-negative breast cancers in African American women; 10-fold higher rates of BRCA pathogenic variants in Ashkenazi Jewish women).
Continue to: Use validated tools to assess risk comprehensively...
Use validated tools to assess risk comprehensively
Women aged 50 to 74 with extremely dense breasts have reduced interval cancers following a normal biennial mammogram if supplemental MRI is offered, but the long-term benefit of identifying these cancers earlier is unclear. Until more data are available on important long-term outcomes (such as breast cancer mortality and need for more invasive treatments), providers should consider breast density in the context of a more comprehensive assessment of breast cancer risk using a validated breast cancer risk assessment tool.
I prefer the modified version of the International Breast Cancer Intervention Study (IBIS) tool, which is readily available online (https://ibis.ikonopedia.com/).7 This tool incorporates several breast cancer risk factors, including reproductive risk factors, body mass index, BRCA gene status, breast density, and family history. The tool takes 1 to 2 minutes to complete and provides an estimate of a woman’s 10-year risk and lifetime risk of breast cancer.
If the lifetime risk exceeds 20%, I offer the patient supplemental MRI screening, consistent with current recommendations of the National Comprehensive Cancer Network and the American Cancer Society.8,9 I generally recommend starting breast imaging screening 7 to 10 years prior to the youngest breast cancer occurrence in the family, with mammography starting no earlier than age 30 and MRI no earlier than age 25. Other validated tools also can be used.10-13
Incorporating breast density and other important risk factors allows a more comprehensive analysis upon which to counsel women about the value (benefits and harms) of breast imaging.8
While the frequency of dense breasts decreases with age, approximately 10% of women in the United States have extremely dense breasts (Breast Imaging, Reporting, and Data System [BI-RADS] category D), and another 40% have heterogeneously dense breasts (BI-RADS category C).1 Women with dense breasts have both an increased risk for developing breast cancer and reduced mammographic sensitivity for breast cancer detection compared with women who have nondense breasts.2
These 2 observations have led the majority of states to pass legislation requiring that women with dense breasts be informed of their breast density, and most require that providers discuss these results with their patients. Thoughtful clinicians who review the available literature, however, will find sparse evidence on which to counsel patients as to next steps.
Now, a recent trial adds to our knowledge about supplemental magnetic resonance imaging (MRI) breast screening in women with extremely dense breasts.
DENSE trial offers high-quality data
Bakker and colleagues studied women aged 50 to 74 who were participating in a Netherlands population-based biennial mammography screening program.3 They enrolled average-risk women with extremely dense breasts who had a negative screening digital mammogram into the Dense Tissue and Early Breast Neoplasm Screening (DENSE) multicenter trial. The women were randomly assigned to receive either continued biennial digital mammography or supplemental breast MRI.
The primary outcome was the between-group difference in the development of interval breast cancers—that is, breast cancers detected by women or their providers between rounds of screening mammography. Interval breast cancers were chosen as the primary outcome for 2 reasons:
- interval cancers appear to be more aggressive tumors than those cancers detected by screening mammography
- interval cancers can be identified over a shorter time interval, making them easier to study than outcomes such as breast cancer mortality, which typically require more than a decade to identify.
The DENSE trial’s secondary outcomes included recall rates from MRI, cancer detection rates on MRI, positive predictive value of MRIs requiring biopsy, and breast cancer characteristics (size, stage) diagnosed in the different groups.
Between-group difference in incidence of interval cancers
A total of 40,373 women with extremely dense breasts were screened; 8,061 of these were randomly assigned to receive breast MRI and 32,312 to continued mammography only (1:4 cluster randomization) across 12 mammography centers in the Netherlands. Among the women assigned to the MRI group, 59% actually underwent MRI (4,783 of the 8,061).
The interval cancer rate in the mammography-only group was 5.0 per 1,000 screenings (95% confidence interval [CI], 4.3–5.8), while the interval cancer rate in the MRI-assigned group was 2.5 per 1,000 screenings (95% CI, 1.6–3.8) (TABLE 1).3
Key secondary outcomes
Of the women who underwent supplemental MRI, 9.49% were recalled for additional imaging, follow-up, or biopsy. Of the 4,783 women who had an MRI, 300 (6.3%) underwent a breast biopsy, and 79 breast cancers (1.65%) were detected. Sixty-four of these cancers were invasive, and 15 were ductal carcinoma in situ (DCIS). Among women who underwent a biopsy for an MRI-detected abnormality, the positive predictive value was 26.3%.
Tumor characteristics. For women who developed breast cancer during the study, both tumor size at diagnosis and tumor stage (early vs late) were described. TABLE 2 shows these results in the women who had their breast cancer detected on MRI, those in the MRI-assigned group who developed interval cancer, and those in the mammography-only group who had interval cancers.3 Overall, tumor size was smaller in the interval group who underwent MRI compared with those who underwent mammography only.
Continue to: Study contributes valuable data, but we need more on long-term outcomes...
Study contributes valuable data, but we need more on long-term outcomes
The trial by Bakker and colleagues employed a solid study design as women were randomly assigned to supplemental MRI screening or ongoing biennial mammography, and nearly all cancers were identified in the short-term of follow-up. In addition, very few women were lost to follow-up, and secondary outcomes, including false-positive rates, were collected to help providers and patients better understand some of the potential downsides of supplemental screening.
The substantial reduction in interval cancers (50% in the intent-to-screen analysis and 84% in the women who actually underwent supplemental MRI) was highly statistically significant (P<.001). While there were substantially fewer interval cancers in the MRI-assigned group, the interval cancers that did occur were of similar stage as those in the women assigned to the mammography-only group (TABLE 2).
Data demonstrate that interval cancers appear to be more aggressive than screen-detected cancers.4 While reducing interval cancers should be a good thing overall, it remains unproven that using supplemental MRI in all women with dense breasts would reduce breast cancer specific mortality, all-cause mortality, or the risk of more invasive treatments (for example, the need for chemotherapy or requirement for mastectomy).
On the other hand, using routine supplemental breast MRI in women with extremely dense breasts would result in very substantial use of resources, including cost, radiologist time, provider time, and machine time. In the United States, approximately 49 million women are aged 50 to 74.5 Breast MRI charges commonly range from $1,000 to $4,000. If the 4.9 million women with extremely dense breasts underwent supplemental MRI this year, the approximate cost would be somewhere between $4.9 and $19.5 billion for imaging alone. This does not include callbacks, biopsies, or provider time for ordering, interpreting, and arranging for follow-up.
While the reduction in interval cancers seen in this study is promising, more assurance of improvement in important outcomes—such as reduced mortality or reduced need for more invasive breast cancer treatments—should precede any routine change in practice.
Unanswered questions
This study did not address a number of other important questions, including:
Should MRI be done with every round of breast cancer screening given the possibility of prevalence bias? Prevalence bias can be defined as more cancers detected in the first round of MRI screening with possible reduced benefit in future rounds of screening. The study authors indicated that they will continue to analyze the study results to see what occurs in the next round of screening.
Is there a similar impact on decreased interval cancers in women undergoing annual mammography or in women screened between ages 40 and 49? This study was conducted in women aged 50 to 74 undergoing mammography every 2 years. In the United States, annual mammography in women aged 40 to 49 is frequently recommended.
What effect does supplemental MRI screening have in women with heterogeneously dense breasts, which represents 40% of the population? The US Food and Drug Administration recommends that all women with dense breasts be counseled regarding options for management.6
Do these results translate to the more racially and ethnically diverse populations of the United States? In the Netherlands, where this study was conducted, 85% to 90% of women are either Dutch or of western European origin. Women of different racial and ancestral backgrounds have biologically different breast cancers and cancer risk (for example, higher rates of triple-negative breast cancers in African American women; 10-fold higher rates of BRCA pathogenic variants in Ashkenazi Jewish women).
Continue to: Use validated tools to assess risk comprehensively...
Use validated tools to assess risk comprehensively
Women aged 50 to 74 with extremely dense breasts have reduced interval cancers following a normal biennial mammogram if supplemental MRI is offered, but the long-term benefit of identifying these cancers earlier is unclear. Until more data are available on important long-term outcomes (such as breast cancer mortality and need for more invasive treatments), providers should consider breast density in the context of a more comprehensive assessment of breast cancer risk using a validated breast cancer risk assessment tool.
I prefer the modified version of the International Breast Cancer Intervention Study (IBIS) tool, which is readily available online (https://ibis.ikonopedia.com/).7 This tool incorporates several breast cancer risk factors, including reproductive risk factors, body mass index, BRCA gene status, breast density, and family history. The tool takes 1 to 2 minutes to complete and provides an estimate of a woman’s 10-year risk and lifetime risk of breast cancer.
If the lifetime risk exceeds 20%, I offer the patient supplemental MRI screening, consistent with current recommendations of the National Comprehensive Cancer Network and the American Cancer Society.8,9 I generally recommend starting breast imaging screening 7 to 10 years prior to the youngest breast cancer occurrence in the family, with mammography starting no earlier than age 30 and MRI no earlier than age 25. Other validated tools also can be used.10-13
Incorporating breast density and other important risk factors allows a more comprehensive analysis upon which to counsel women about the value (benefits and harms) of breast imaging.8
- Sprague BL, Gagnon RE, Burt V, et al. Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst. 2014;106:dju255. doi: 10.1093/jcni/dju255.
- Boyd NF, Guo H, Martin LJ, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356:227-236.
- Bakker MF, de Lange SV, Pijnappel RM, et al; for the DENSE Trial Study Group. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102.
- Drukker CA, Schmidt MK, Rutgers EJT, et al. Mammographic screening detects low-risk tumor biology breast cancers. Breast Cancer Res Treat. 2014;144:103-111.
- Statista website. Resident population of the United States by sex and age as of July 1, 2018. https://www.statista.com/statistics/241488/population-of-the-us-by-sex-and-age. Accessed January 6, 2020.
- US Food and Drug Administration website. Mammography: what you need to know. https://www.fda.gov/consumers/consumer-updates/mammography-what-you-need-know. Accessed January 13, 2020.
- IBIS (International Breast Cancer Intervention Study) website. Online Tyrer-Cuzick Model Breast Cancer Risk Evaluation Tool. ibis.ikonopedia.com. Accessed January 13, 2020.
- Bevers TB, Anderson BO, Bonaccio E, et al; National Comprehensive Cancer Network. Breast cancer screening and diagnosis: NCCN practice guidelines in oncology. JNCCN. 2009;7:1060-1096.
- Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
- Antoniou AC, Cunningham AP, Peto J, et al. The BOADICEA model of genetic susceptibility to breast and ovarian cancers: updates and extensions. Br J Cancer. 2008;98:1457-1466.
- Claus EB, Risch N, Thompson WD. Autosomal dominant inheritance of early-onset breast cancer: implications for risk prediction. Cancer. 1994;73:643-651.
- Parmigiani G, Berry D, Aguilar O. Determining carrier probabilities for breast cancer-susceptibility genes BRCA1 and BRCA2. Am J Hum Genet. 1998;62:145-158.
- Tyrer J, Duffy SW, Cuzick J. A breast cancer prediction model incorporating familial and personal risk factors. Stat Med. 2004;23:1111-1130.
- Sprague BL, Gagnon RE, Burt V, et al. Prevalence of mammographically dense breasts in the United States. J Natl Cancer Inst. 2014;106:dju255. doi: 10.1093/jcni/dju255.
- Boyd NF, Guo H, Martin LJ, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356:227-236.
- Bakker MF, de Lange SV, Pijnappel RM, et al; for the DENSE Trial Study Group. Supplemental MRI screening for women with extremely dense breast tissue. N Engl J Med. 2019;381:2091-2102.
- Drukker CA, Schmidt MK, Rutgers EJT, et al. Mammographic screening detects low-risk tumor biology breast cancers. Breast Cancer Res Treat. 2014;144:103-111.
- Statista website. Resident population of the United States by sex and age as of July 1, 2018. https://www.statista.com/statistics/241488/population-of-the-us-by-sex-and-age. Accessed January 6, 2020.
- US Food and Drug Administration website. Mammography: what you need to know. https://www.fda.gov/consumers/consumer-updates/mammography-what-you-need-know. Accessed January 13, 2020.
- IBIS (International Breast Cancer Intervention Study) website. Online Tyrer-Cuzick Model Breast Cancer Risk Evaluation Tool. ibis.ikonopedia.com. Accessed January 13, 2020.
- Bevers TB, Anderson BO, Bonaccio E, et al; National Comprehensive Cancer Network. Breast cancer screening and diagnosis: NCCN practice guidelines in oncology. JNCCN. 2009;7:1060-1096.
- Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57:75-89.
- Antoniou AC, Cunningham AP, Peto J, et al. The BOADICEA model of genetic susceptibility to breast and ovarian cancers: updates and extensions. Br J Cancer. 2008;98:1457-1466.
- Claus EB, Risch N, Thompson WD. Autosomal dominant inheritance of early-onset breast cancer: implications for risk prediction. Cancer. 1994;73:643-651.
- Parmigiani G, Berry D, Aguilar O. Determining carrier probabilities for breast cancer-susceptibility genes BRCA1 and BRCA2. Am J Hum Genet. 1998;62:145-158.
- Tyrer J, Duffy SW, Cuzick J. A breast cancer prediction model incorporating familial and personal risk factors. Stat Med. 2004;23:1111-1130.
Tumor Necrosis Factor Inhibitors May Reduce Cardiovascular Morbidity in Patients With Psoriasis
The connection between psoriasis and increased major adverse cardiovascular events (MACEs) has been well studied. 1,2 Although treatment of psoriasis can improve skin and joint symptoms, it is less clear whether therapies may mitigate the increased risk for cardiovascular comorbidities. Tumor necrosis factor (TNF) inhibitors in particular have been studied with great interest given the role of TNF in vascular and metabolic functions. 3 Using a retrospective cohort design, Wu and colleagues 4 examined if treatment with TNF inhibitors in patients with psoriasis would be associated with a lower risk for MACEs compared to phototherapy. Results suggested a significantly lower hazard of MACEs in patients using TNF inhibitors vs patients treated with phototherapy (adjusted hazard ratio, 0.77; P = .046). Moreover, based on these findings, they calculated that treating approximately 161 patients with TNF inhibitors rather than phototherapy would result in 1 less MACE per year overall. 4
Patients with psoriasis have been shown to have a greater noncalcified coronary plaque burden and prevalence of high-risk plaque compared to healthy patients.5 Lerman and colleagues5 measured the coronary plaque burden of 105 patients with psoriasis and 25 healthy volunteers using coronary computed tomography angiography. Although the patients were on average 10 years younger and had lower cardiovascular risk as measured by traditional risk scores, patients with psoriasis were found to have a greater noncalcified coronary plaque burden compared to 100 patients with hyperlipidemia. This burden was associated with an increased prevalence of high-risk plaques. Furthermore, in patients followed for 1 year, improvements in psoriasis severity were associated with reductions in noncalcified coronary plaque burden, though this finding was across all treatment modalities. However, there was no significant difference in calcified coronary plaque burden associated with reduced psoriasis severity.5
Moreover, Pina et al6 conducted a prospective study evaluating the use of the TNF inhibitor adalimumab to improve endothelial function and arterial stiffness in patients with moderate to severe psoriasis. Among 29 patients, they found a significant improvement in endothelial function as measured by flow-mediated dilatation after 6 months of adalimumab therapy, with a mean increase from 6.19% to 7.46% (P=.008). They also reported decreases in arterial stiffness by pulse wave velocity (P=.03). Despite a small sample size, these findings provide 2 potential mechanisms by which TNF inhibitor therapy may reduce the risk for cardiovascular events.6
A retrospective cohort study evaluating data from the Kaiser Permanente Southern California health plan assessed whether TNF inhibitor therapy was associated with a lower risk for MACE in patients with psoriasis.7 A total of 18,194 patients were included; of these, 1463 received TNF inhibitor therapy for at least 2 months. After controlling for other variables, including age at psoriasis diagnosis, sex, race/ethnicity, and other cardiovascular risk factors (eg, history of smoking or alcohol use; use of clopidogrel, antihypertensive agents, antihyperlipidemics, or anticoagulants), patients in the TNF inhibitor cohort demonstrated a significantly lower MACE hazard ratio compared to patients treated with topicals (hazard ratio, 0.80; 95% confidence interval, 0.66-0.98; P<.05).7
Conversely, a randomized, placebo-controlled trial of 107 patients found no difference in vascular inflammation of the ascending aorta and the carotids after 16 weeks of adalimumab treatment vs placebo. In this study, however, most patients had only moderate psoriasis based on a mean psoriasis area and severity index score of 9.8.8 Given studies finding higher risk burden in patients with more severe skin disease,2 it is possible that the effect of TNF inhibitor therapy may not be as pronounced in patients with less skin involvement. There was a significant effect on C-reactive protein levels in patients receiving TNF inhibitor therapy compared to placebo at 16 weeks (P=.012), suggesting TNF does play some role in systemic inflammation, and it is possible it may exert cardiovascular effects through a mechanism other than vascular inflammation.8
A second double-blind, randomized trial reported similar results.9 Among 97 patients randomized to receive adalimumab, placebo, or phototherapy, no significant difference in vascular inflammation was found after 12 weeks of therapy. In contrast, levels of C-reactive protein, IL-6, and glycoprotein acetylation were markedly reduced. The authors also reported adverse effects of adalimumab therapy on lipid metabolism with reduced cholesterol efflux capacity, a marker of ability of high-density-lipoprotein particles to perform reverse cholesterol transport, and high-density-lipoprotein particles, suggesting these effects may counteract some of the anti-inflammatory effects of TNF inhibitors.9
A growing body of data regarding the effect of TNF inhibitors on cardiovascular morbidity in patients with psoriasis is being collected, but no strong conclusions can be made. Given the disconnect of findings across these studies, it is possible that we have yet to elucidate the full mechanism by which TNF inhibitors may affect cardiovascular health. However, there may be additional confounding factors or patient characteristics at play. More large, prospective, randomized, controlled studies are needed to further understand this relationship.
- Ogdie A, Yu Y, Haynes K, et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: a population-based cohort study. Ann Rheum Dis. 2015;74:326-332.
- Ahlehoff O, Gislason GH, Charlot M, et al. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med. 2011;270:147-157.
- Kölliker Frers RA, Bisoendial RJ, Montoya SF, et al. Psoriasis and cardiovascular risk: immune-mediated crosstalk between metabolic, vascular, and autoimmune inflammation. Int J Cardiol Metab Endocr. 2015;6:43-54.
- Wu JJ, Sundaram M, Cloutier M, et al. The risk of cardiovascular events in psoriasis patients treated with tumor necrosis factor-α inhibitors versus phototherapy: an observational cohort study. J Am Acad Dermatol. 2018;79:60-68.
- Lerman JB, Joshi AA, Chaturvedi A, et al. Coronary plaque characterization in psoriasis reveals high-risk features that improve after treatment in a prospective observational study. Circulation. 2017;136:263-276.
- Pina T, Corrales A, Lopez-Mejias R, et al. Anti-tumor necrosis factor-α therapy improves endothelial function and arterial stiffness in patients with moderate to severe psoriasis: a 6 month prospective study. J Dermatol. 2016;43:1267-1272.
- Wu JJ, Joshi AA, Reddy SP, et al. Anti-inflammatory therapy with tumor necrosis factor inhibitors is associated with reduced risk of major adverse cardiovascular events in psoriasis [published online March 24, 2018]. J Eur Acad Dermatol Venereol. doi:10.1111/jdv.14951.
- Bissonnette R, Harel F, Krueger JG, et al. TNF-α antagonist and vascular inflammation patients with psoriasis vulgaris: a randomized placebo-controlled study. J Invest Dermatol. 2017;137:1638-1645 .
- Mehta NN, Shin DB, Joshi AA, et al. Effect of 2 psoriasis treatments on vascular inflammation and novel inflammatory cardiovascular biomarkers: a randomized placebo-controlled trial. Circ Cardiovasc Imaging. 2018;11:e007394.
The connection between psoriasis and increased major adverse cardiovascular events (MACEs) has been well studied. 1,2 Although treatment of psoriasis can improve skin and joint symptoms, it is less clear whether therapies may mitigate the increased risk for cardiovascular comorbidities. Tumor necrosis factor (TNF) inhibitors in particular have been studied with great interest given the role of TNF in vascular and metabolic functions. 3 Using a retrospective cohort design, Wu and colleagues 4 examined if treatment with TNF inhibitors in patients with psoriasis would be associated with a lower risk for MACEs compared to phototherapy. Results suggested a significantly lower hazard of MACEs in patients using TNF inhibitors vs patients treated with phototherapy (adjusted hazard ratio, 0.77; P = .046). Moreover, based on these findings, they calculated that treating approximately 161 patients with TNF inhibitors rather than phototherapy would result in 1 less MACE per year overall. 4
Patients with psoriasis have been shown to have a greater noncalcified coronary plaque burden and prevalence of high-risk plaque compared to healthy patients.5 Lerman and colleagues5 measured the coronary plaque burden of 105 patients with psoriasis and 25 healthy volunteers using coronary computed tomography angiography. Although the patients were on average 10 years younger and had lower cardiovascular risk as measured by traditional risk scores, patients with psoriasis were found to have a greater noncalcified coronary plaque burden compared to 100 patients with hyperlipidemia. This burden was associated with an increased prevalence of high-risk plaques. Furthermore, in patients followed for 1 year, improvements in psoriasis severity were associated with reductions in noncalcified coronary plaque burden, though this finding was across all treatment modalities. However, there was no significant difference in calcified coronary plaque burden associated with reduced psoriasis severity.5
Moreover, Pina et al6 conducted a prospective study evaluating the use of the TNF inhibitor adalimumab to improve endothelial function and arterial stiffness in patients with moderate to severe psoriasis. Among 29 patients, they found a significant improvement in endothelial function as measured by flow-mediated dilatation after 6 months of adalimumab therapy, with a mean increase from 6.19% to 7.46% (P=.008). They also reported decreases in arterial stiffness by pulse wave velocity (P=.03). Despite a small sample size, these findings provide 2 potential mechanisms by which TNF inhibitor therapy may reduce the risk for cardiovascular events.6
A retrospective cohort study evaluating data from the Kaiser Permanente Southern California health plan assessed whether TNF inhibitor therapy was associated with a lower risk for MACE in patients with psoriasis.7 A total of 18,194 patients were included; of these, 1463 received TNF inhibitor therapy for at least 2 months. After controlling for other variables, including age at psoriasis diagnosis, sex, race/ethnicity, and other cardiovascular risk factors (eg, history of smoking or alcohol use; use of clopidogrel, antihypertensive agents, antihyperlipidemics, or anticoagulants), patients in the TNF inhibitor cohort demonstrated a significantly lower MACE hazard ratio compared to patients treated with topicals (hazard ratio, 0.80; 95% confidence interval, 0.66-0.98; P<.05).7
Conversely, a randomized, placebo-controlled trial of 107 patients found no difference in vascular inflammation of the ascending aorta and the carotids after 16 weeks of adalimumab treatment vs placebo. In this study, however, most patients had only moderate psoriasis based on a mean psoriasis area and severity index score of 9.8.8 Given studies finding higher risk burden in patients with more severe skin disease,2 it is possible that the effect of TNF inhibitor therapy may not be as pronounced in patients with less skin involvement. There was a significant effect on C-reactive protein levels in patients receiving TNF inhibitor therapy compared to placebo at 16 weeks (P=.012), suggesting TNF does play some role in systemic inflammation, and it is possible it may exert cardiovascular effects through a mechanism other than vascular inflammation.8
A second double-blind, randomized trial reported similar results.9 Among 97 patients randomized to receive adalimumab, placebo, or phototherapy, no significant difference in vascular inflammation was found after 12 weeks of therapy. In contrast, levels of C-reactive protein, IL-6, and glycoprotein acetylation were markedly reduced. The authors also reported adverse effects of adalimumab therapy on lipid metabolism with reduced cholesterol efflux capacity, a marker of ability of high-density-lipoprotein particles to perform reverse cholesterol transport, and high-density-lipoprotein particles, suggesting these effects may counteract some of the anti-inflammatory effects of TNF inhibitors.9
A growing body of data regarding the effect of TNF inhibitors on cardiovascular morbidity in patients with psoriasis is being collected, but no strong conclusions can be made. Given the disconnect of findings across these studies, it is possible that we have yet to elucidate the full mechanism by which TNF inhibitors may affect cardiovascular health. However, there may be additional confounding factors or patient characteristics at play. More large, prospective, randomized, controlled studies are needed to further understand this relationship.
The connection between psoriasis and increased major adverse cardiovascular events (MACEs) has been well studied. 1,2 Although treatment of psoriasis can improve skin and joint symptoms, it is less clear whether therapies may mitigate the increased risk for cardiovascular comorbidities. Tumor necrosis factor (TNF) inhibitors in particular have been studied with great interest given the role of TNF in vascular and metabolic functions. 3 Using a retrospective cohort design, Wu and colleagues 4 examined if treatment with TNF inhibitors in patients with psoriasis would be associated with a lower risk for MACEs compared to phototherapy. Results suggested a significantly lower hazard of MACEs in patients using TNF inhibitors vs patients treated with phototherapy (adjusted hazard ratio, 0.77; P = .046). Moreover, based on these findings, they calculated that treating approximately 161 patients with TNF inhibitors rather than phototherapy would result in 1 less MACE per year overall. 4
Patients with psoriasis have been shown to have a greater noncalcified coronary plaque burden and prevalence of high-risk plaque compared to healthy patients.5 Lerman and colleagues5 measured the coronary plaque burden of 105 patients with psoriasis and 25 healthy volunteers using coronary computed tomography angiography. Although the patients were on average 10 years younger and had lower cardiovascular risk as measured by traditional risk scores, patients with psoriasis were found to have a greater noncalcified coronary plaque burden compared to 100 patients with hyperlipidemia. This burden was associated with an increased prevalence of high-risk plaques. Furthermore, in patients followed for 1 year, improvements in psoriasis severity were associated with reductions in noncalcified coronary plaque burden, though this finding was across all treatment modalities. However, there was no significant difference in calcified coronary plaque burden associated with reduced psoriasis severity.5
Moreover, Pina et al6 conducted a prospective study evaluating the use of the TNF inhibitor adalimumab to improve endothelial function and arterial stiffness in patients with moderate to severe psoriasis. Among 29 patients, they found a significant improvement in endothelial function as measured by flow-mediated dilatation after 6 months of adalimumab therapy, with a mean increase from 6.19% to 7.46% (P=.008). They also reported decreases in arterial stiffness by pulse wave velocity (P=.03). Despite a small sample size, these findings provide 2 potential mechanisms by which TNF inhibitor therapy may reduce the risk for cardiovascular events.6
A retrospective cohort study evaluating data from the Kaiser Permanente Southern California health plan assessed whether TNF inhibitor therapy was associated with a lower risk for MACE in patients with psoriasis.7 A total of 18,194 patients were included; of these, 1463 received TNF inhibitor therapy for at least 2 months. After controlling for other variables, including age at psoriasis diagnosis, sex, race/ethnicity, and other cardiovascular risk factors (eg, history of smoking or alcohol use; use of clopidogrel, antihypertensive agents, antihyperlipidemics, or anticoagulants), patients in the TNF inhibitor cohort demonstrated a significantly lower MACE hazard ratio compared to patients treated with topicals (hazard ratio, 0.80; 95% confidence interval, 0.66-0.98; P<.05).7
Conversely, a randomized, placebo-controlled trial of 107 patients found no difference in vascular inflammation of the ascending aorta and the carotids after 16 weeks of adalimumab treatment vs placebo. In this study, however, most patients had only moderate psoriasis based on a mean psoriasis area and severity index score of 9.8.8 Given studies finding higher risk burden in patients with more severe skin disease,2 it is possible that the effect of TNF inhibitor therapy may not be as pronounced in patients with less skin involvement. There was a significant effect on C-reactive protein levels in patients receiving TNF inhibitor therapy compared to placebo at 16 weeks (P=.012), suggesting TNF does play some role in systemic inflammation, and it is possible it may exert cardiovascular effects through a mechanism other than vascular inflammation.8
A second double-blind, randomized trial reported similar results.9 Among 97 patients randomized to receive adalimumab, placebo, or phototherapy, no significant difference in vascular inflammation was found after 12 weeks of therapy. In contrast, levels of C-reactive protein, IL-6, and glycoprotein acetylation were markedly reduced. The authors also reported adverse effects of adalimumab therapy on lipid metabolism with reduced cholesterol efflux capacity, a marker of ability of high-density-lipoprotein particles to perform reverse cholesterol transport, and high-density-lipoprotein particles, suggesting these effects may counteract some of the anti-inflammatory effects of TNF inhibitors.9
A growing body of data regarding the effect of TNF inhibitors on cardiovascular morbidity in patients with psoriasis is being collected, but no strong conclusions can be made. Given the disconnect of findings across these studies, it is possible that we have yet to elucidate the full mechanism by which TNF inhibitors may affect cardiovascular health. However, there may be additional confounding factors or patient characteristics at play. More large, prospective, randomized, controlled studies are needed to further understand this relationship.
- Ogdie A, Yu Y, Haynes K, et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: a population-based cohort study. Ann Rheum Dis. 2015;74:326-332.
- Ahlehoff O, Gislason GH, Charlot M, et al. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med. 2011;270:147-157.
- Kölliker Frers RA, Bisoendial RJ, Montoya SF, et al. Psoriasis and cardiovascular risk: immune-mediated crosstalk between metabolic, vascular, and autoimmune inflammation. Int J Cardiol Metab Endocr. 2015;6:43-54.
- Wu JJ, Sundaram M, Cloutier M, et al. The risk of cardiovascular events in psoriasis patients treated with tumor necrosis factor-α inhibitors versus phototherapy: an observational cohort study. J Am Acad Dermatol. 2018;79:60-68.
- Lerman JB, Joshi AA, Chaturvedi A, et al. Coronary plaque characterization in psoriasis reveals high-risk features that improve after treatment in a prospective observational study. Circulation. 2017;136:263-276.
- Pina T, Corrales A, Lopez-Mejias R, et al. Anti-tumor necrosis factor-α therapy improves endothelial function and arterial stiffness in patients with moderate to severe psoriasis: a 6 month prospective study. J Dermatol. 2016;43:1267-1272.
- Wu JJ, Joshi AA, Reddy SP, et al. Anti-inflammatory therapy with tumor necrosis factor inhibitors is associated with reduced risk of major adverse cardiovascular events in psoriasis [published online March 24, 2018]. J Eur Acad Dermatol Venereol. doi:10.1111/jdv.14951.
- Bissonnette R, Harel F, Krueger JG, et al. TNF-α antagonist and vascular inflammation patients with psoriasis vulgaris: a randomized placebo-controlled study. J Invest Dermatol. 2017;137:1638-1645 .
- Mehta NN, Shin DB, Joshi AA, et al. Effect of 2 psoriasis treatments on vascular inflammation and novel inflammatory cardiovascular biomarkers: a randomized placebo-controlled trial. Circ Cardiovasc Imaging. 2018;11:e007394.
- Ogdie A, Yu Y, Haynes K, et al. Risk of major cardiovascular events in patients with psoriatic arthritis, psoriasis and rheumatoid arthritis: a population-based cohort study. Ann Rheum Dis. 2015;74:326-332.
- Ahlehoff O, Gislason GH, Charlot M, et al. Psoriasis is associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. J Intern Med. 2011;270:147-157.
- Kölliker Frers RA, Bisoendial RJ, Montoya SF, et al. Psoriasis and cardiovascular risk: immune-mediated crosstalk between metabolic, vascular, and autoimmune inflammation. Int J Cardiol Metab Endocr. 2015;6:43-54.
- Wu JJ, Sundaram M, Cloutier M, et al. The risk of cardiovascular events in psoriasis patients treated with tumor necrosis factor-α inhibitors versus phototherapy: an observational cohort study. J Am Acad Dermatol. 2018;79:60-68.
- Lerman JB, Joshi AA, Chaturvedi A, et al. Coronary plaque characterization in psoriasis reveals high-risk features that improve after treatment in a prospective observational study. Circulation. 2017;136:263-276.
- Pina T, Corrales A, Lopez-Mejias R, et al. Anti-tumor necrosis factor-α therapy improves endothelial function and arterial stiffness in patients with moderate to severe psoriasis: a 6 month prospective study. J Dermatol. 2016;43:1267-1272.
- Wu JJ, Joshi AA, Reddy SP, et al. Anti-inflammatory therapy with tumor necrosis factor inhibitors is associated with reduced risk of major adverse cardiovascular events in psoriasis [published online March 24, 2018]. J Eur Acad Dermatol Venereol. doi:10.1111/jdv.14951.
- Bissonnette R, Harel F, Krueger JG, et al. TNF-α antagonist and vascular inflammation patients with psoriasis vulgaris: a randomized placebo-controlled study. J Invest Dermatol. 2017;137:1638-1645 .
- Mehta NN, Shin DB, Joshi AA, et al. Effect of 2 psoriasis treatments on vascular inflammation and novel inflammatory cardiovascular biomarkers: a randomized placebo-controlled trial. Circ Cardiovasc Imaging. 2018;11:e007394.