User login
Seen or viewed: A black hematologist’s perspective
After a long day in hematology clinic, I skimmed the inpatient list to see if any of my patients had been admitted. Seeing Ms. Short’s name (changed for privacy), a delightful African American woman I met during my early days of fellowship, had me making the trek to the hospital. She was living with multiple myeloma complicated by extramedullary manifestations that had significantly impacted her quality of life.

During our first encounter, she showed me a growing left subscapular mass the size of an orange that was erythematous, hot, painful, and irritated. As an enthusiastic first-year fellow, I wanted to be aggressive in addressing her concerns in response to her obvious distress about this mass. Ultimately, she left clinic with antibiotics and an appointment with radiation oncology to see if they could use radiation to shrink the subscapular mass.
When I went back in to discuss the plan with her, she grabbed my hand, looked me in my eyes and said: “Thank you, I’ve been mentioning this for a while and you’re the first person to get something done about it.” In that moment I knew that she felt seen.
By the time I made it over to the hospital, she was getting settled in her room to start another cycle of cytoreductive chemotherapy.
“I told them I had a Black doctor!” she exclaimed as I walked into her hospital room. “I was looking for you today in clinic ... I kept telling them I had a Black doctor, but the nurses kept telling me no, that there were only Black nurse practitioners.” She had repeatedly told the staff that I, her “Black doctor,” did indeed exist, and she went on to describe me as “you know, the [heavy-chested] and short Black doctor I saw early this fall.” To this day, her description still makes me chuckle.
Though I laughed at her description, it hurt that I had worked in a clinic for 6 months yet was invisible. Initially disappointed, I left Ms. Short’s room with a smile on my face, energized and encouraged.
My time with Ms. Short prompted me to ruminate on my experience as a Black physician. To put it in perspective, 5% of all physicians are Black, 2% are Black women, and 2.3% are oncologists, even though African Americans make up 13% of the general U.S. population. I reside in a space where I am simultaneously scrutinized because I am one of the few (or the only) Black physicians in the building, and yet I am invisible because my colleagues and coworkers routinely ignore my presence.
Black physicians, let alone hematologists, are so rare that nurses often cannot fathom that a Black woman could be more than a nurse practitioner. Sadly, this is the tip of the iceberg of some of the negative experiences I, and other Black doctors, have had.
How I present myself must be carefully curated to make progress in my career. My peers and superiors seem to hear me better when my hair is straight and not in its naturally curly state. My introversion has been interpreted as being standoffish or disinterested. Any tone other than happy is interpreted as “aggressive” or “angry”. Talking “too much” to Black support staff was reported to my program, as it was viewed as suspicious, disruptive, and “appearances matter”.
I am also expected to be nurturing in ways that White physicians are not required to be. In my presence, White physicians have denigrated an entire patient population that is disproportionately Black by calling them “sicklers.” If there is an interpersonal conflict, I must think about the long-term consequences of voicing my perspective. My non-Black colleagues do not have to think about these things.
Imagine dealing with this at work, then on your commute home being worried about the reality that you may be pulled over and become the next name on the ever-growing list of Black women and men murdered at the hands of police. The cognitive and emotional impact of being invisible is immense and cumulative over the years.
My Blackness creates a bias of inferiority that cannot be overcome by respectability, compliance, professionalism, training, and expertise. This is glaringly apparent on both sides of the physician-patient relationship. Black patients’ concerns are routinely overlooked and dismissed, as seen with Ms. Short, and are reflected in the Black maternal death rate, pain control in Black versus White patients, and personal experience as a patient and an advocate for my family members.
Patients have looked me in the face and said, “all lives matter,” displaying their refusal to recognize that systematic racism and inequality exist. These facts and experiences are the antithesis of “primum non nocere.”
Sadly, my and Ms. Short’s experiences are not singular ones, and racial bias in medicine is a diagnosed, but untreated cancer. Like the malignancies I treat, ignoring the problem has not made it go away; therefore, it continues to fester and spread, causing more destruction. It is of great importance and concern that all physicians recognize, reflect, and correct their implicit biases not only toward their patients, but also colleagues and trainees.
It seems that health care professionals can talk the talk, as many statements have been made against racism and implicit bias in medicine, but can we take true and meaningful action to begin the journey to equity and justice?
I would like to thank Adrienne Glover, MD, MaKenzie Hodge, MD, Maranatha McLean, MD, and Darion Showell, MD, for our stimulating conversations that helped me put pen to paper. I’d also like to thank my family for being my editors.
Daphanie D. Taylor, MD, is a hematology/oncology fellow PGY-6 at Levine Cancer Institute, Charlotte, N.C.
References and further reading
Roy L. “‘It’s My Calling To Change The Statistics’: Why We Need More Black Female Physicians.” Forbes Magazine, 27 Feb. 2020.
“Diversity in Medicine: Facts and Figures 2019.” Association of American Medical Colleges, 2019.
“Facts & Figures: Diversity in Oncology.” American Society of Clinical Oncology. 2020 Jan 16.
After a long day in hematology clinic, I skimmed the inpatient list to see if any of my patients had been admitted. Seeing Ms. Short’s name (changed for privacy), a delightful African American woman I met during my early days of fellowship, had me making the trek to the hospital. She was living with multiple myeloma complicated by extramedullary manifestations that had significantly impacted her quality of life.
During our first encounter, she showed me a growing left subscapular mass the size of an orange that was erythematous, hot, painful, and irritated. As an enthusiastic first-year fellow, I wanted to be aggressive in addressing her concerns in response to her obvious distress about this mass. Ultimately, she left clinic with antibiotics and an appointment with radiation oncology to see if they could use radiation to shrink the subscapular mass.
When I went back in to discuss the plan with her, she grabbed my hand, looked me in my eyes and said: “Thank you, I’ve been mentioning this for a while and you’re the first person to get something done about it.” In that moment I knew that she felt seen.
By the time I made it over to the hospital, she was getting settled in her room to start another cycle of cytoreductive chemotherapy.
“I told them I had a Black doctor!” she exclaimed as I walked into her hospital room. “I was looking for you today in clinic ... I kept telling them I had a Black doctor, but the nurses kept telling me no, that there were only Black nurse practitioners.” She had repeatedly told the staff that I, her “Black doctor,” did indeed exist, and she went on to describe me as “you know, the [heavy-chested] and short Black doctor I saw early this fall.” To this day, her description still makes me chuckle.
Though I laughed at her description, it hurt that I had worked in a clinic for 6 months yet was invisible. Initially disappointed, I left Ms. Short’s room with a smile on my face, energized and encouraged.
My time with Ms. Short prompted me to ruminate on my experience as a Black physician. To put it in perspective, 5% of all physicians are Black, 2% are Black women, and 2.3% are oncologists, even though African Americans make up 13% of the general U.S. population. I reside in a space where I am simultaneously scrutinized because I am one of the few (or the only) Black physicians in the building, and yet I am invisible because my colleagues and coworkers routinely ignore my presence.
Black physicians, let alone hematologists, are so rare that nurses often cannot fathom that a Black woman could be more than a nurse practitioner. Sadly, this is the tip of the iceberg of some of the negative experiences I, and other Black doctors, have had.
How I present myself must be carefully curated to make progress in my career. My peers and superiors seem to hear me better when my hair is straight and not in its naturally curly state. My introversion has been interpreted as being standoffish or disinterested. Any tone other than happy is interpreted as “aggressive” or “angry”. Talking “too much” to Black support staff was reported to my program, as it was viewed as suspicious, disruptive, and “appearances matter”.
I am also expected to be nurturing in ways that White physicians are not required to be. In my presence, White physicians have denigrated an entire patient population that is disproportionately Black by calling them “sicklers.” If there is an interpersonal conflict, I must think about the long-term consequences of voicing my perspective. My non-Black colleagues do not have to think about these things.
Imagine dealing with this at work, then on your commute home being worried about the reality that you may be pulled over and become the next name on the ever-growing list of Black women and men murdered at the hands of police. The cognitive and emotional impact of being invisible is immense and cumulative over the years.
My Blackness creates a bias of inferiority that cannot be overcome by respectability, compliance, professionalism, training, and expertise. This is glaringly apparent on both sides of the physician-patient relationship. Black patients’ concerns are routinely overlooked and dismissed, as seen with Ms. Short, and are reflected in the Black maternal death rate, pain control in Black versus White patients, and personal experience as a patient and an advocate for my family members.
Patients have looked me in the face and said, “all lives matter,” displaying their refusal to recognize that systematic racism and inequality exist. These facts and experiences are the antithesis of “primum non nocere.”
Sadly, my and Ms. Short’s experiences are not singular ones, and racial bias in medicine is a diagnosed, but untreated cancer. Like the malignancies I treat, ignoring the problem has not made it go away; therefore, it continues to fester and spread, causing more destruction. It is of great importance and concern that all physicians recognize, reflect, and correct their implicit biases not only toward their patients, but also colleagues and trainees.
It seems that health care professionals can talk the talk, as many statements have been made against racism and implicit bias in medicine, but can we take true and meaningful action to begin the journey to equity and justice?
I would like to thank Adrienne Glover, MD, MaKenzie Hodge, MD, Maranatha McLean, MD, and Darion Showell, MD, for our stimulating conversations that helped me put pen to paper. I’d also like to thank my family for being my editors.
Daphanie D. Taylor, MD, is a hematology/oncology fellow PGY-6 at Levine Cancer Institute, Charlotte, N.C.
References and further reading
Roy L. “‘It’s My Calling To Change The Statistics’: Why We Need More Black Female Physicians.” Forbes Magazine, 27 Feb. 2020.
“Diversity in Medicine: Facts and Figures 2019.” Association of American Medical Colleges, 2019.
“Facts & Figures: Diversity in Oncology.” American Society of Clinical Oncology. 2020 Jan 16.
After a long day in hematology clinic, I skimmed the inpatient list to see if any of my patients had been admitted. Seeing Ms. Short’s name (changed for privacy), a delightful African American woman I met during my early days of fellowship, had me making the trek to the hospital. She was living with multiple myeloma complicated by extramedullary manifestations that had significantly impacted her quality of life.
During our first encounter, she showed me a growing left subscapular mass the size of an orange that was erythematous, hot, painful, and irritated. As an enthusiastic first-year fellow, I wanted to be aggressive in addressing her concerns in response to her obvious distress about this mass. Ultimately, she left clinic with antibiotics and an appointment with radiation oncology to see if they could use radiation to shrink the subscapular mass.
When I went back in to discuss the plan with her, she grabbed my hand, looked me in my eyes and said: “Thank you, I’ve been mentioning this for a while and you’re the first person to get something done about it.” In that moment I knew that she felt seen.
By the time I made it over to the hospital, she was getting settled in her room to start another cycle of cytoreductive chemotherapy.
“I told them I had a Black doctor!” she exclaimed as I walked into her hospital room. “I was looking for you today in clinic ... I kept telling them I had a Black doctor, but the nurses kept telling me no, that there were only Black nurse practitioners.” She had repeatedly told the staff that I, her “Black doctor,” did indeed exist, and she went on to describe me as “you know, the [heavy-chested] and short Black doctor I saw early this fall.” To this day, her description still makes me chuckle.
Though I laughed at her description, it hurt that I had worked in a clinic for 6 months yet was invisible. Initially disappointed, I left Ms. Short’s room with a smile on my face, energized and encouraged.
My time with Ms. Short prompted me to ruminate on my experience as a Black physician. To put it in perspective, 5% of all physicians are Black, 2% are Black women, and 2.3% are oncologists, even though African Americans make up 13% of the general U.S. population. I reside in a space where I am simultaneously scrutinized because I am one of the few (or the only) Black physicians in the building, and yet I am invisible because my colleagues and coworkers routinely ignore my presence.
Black physicians, let alone hematologists, are so rare that nurses often cannot fathom that a Black woman could be more than a nurse practitioner. Sadly, this is the tip of the iceberg of some of the negative experiences I, and other Black doctors, have had.
How I present myself must be carefully curated to make progress in my career. My peers and superiors seem to hear me better when my hair is straight and not in its naturally curly state. My introversion has been interpreted as being standoffish or disinterested. Any tone other than happy is interpreted as “aggressive” or “angry”. Talking “too much” to Black support staff was reported to my program, as it was viewed as suspicious, disruptive, and “appearances matter”.
I am also expected to be nurturing in ways that White physicians are not required to be. In my presence, White physicians have denigrated an entire patient population that is disproportionately Black by calling them “sicklers.” If there is an interpersonal conflict, I must think about the long-term consequences of voicing my perspective. My non-Black colleagues do not have to think about these things.
Imagine dealing with this at work, then on your commute home being worried about the reality that you may be pulled over and become the next name on the ever-growing list of Black women and men murdered at the hands of police. The cognitive and emotional impact of being invisible is immense and cumulative over the years.
My Blackness creates a bias of inferiority that cannot be overcome by respectability, compliance, professionalism, training, and expertise. This is glaringly apparent on both sides of the physician-patient relationship. Black patients’ concerns are routinely overlooked and dismissed, as seen with Ms. Short, and are reflected in the Black maternal death rate, pain control in Black versus White patients, and personal experience as a patient and an advocate for my family members.
Patients have looked me in the face and said, “all lives matter,” displaying their refusal to recognize that systematic racism and inequality exist. These facts and experiences are the antithesis of “primum non nocere.”
Sadly, my and Ms. Short’s experiences are not singular ones, and racial bias in medicine is a diagnosed, but untreated cancer. Like the malignancies I treat, ignoring the problem has not made it go away; therefore, it continues to fester and spread, causing more destruction. It is of great importance and concern that all physicians recognize, reflect, and correct their implicit biases not only toward their patients, but also colleagues and trainees.
It seems that health care professionals can talk the talk, as many statements have been made against racism and implicit bias in medicine, but can we take true and meaningful action to begin the journey to equity and justice?
I would like to thank Adrienne Glover, MD, MaKenzie Hodge, MD, Maranatha McLean, MD, and Darion Showell, MD, for our stimulating conversations that helped me put pen to paper. I’d also like to thank my family for being my editors.
Daphanie D. Taylor, MD, is a hematology/oncology fellow PGY-6 at Levine Cancer Institute, Charlotte, N.C.
References and further reading
Roy L. “‘It’s My Calling To Change The Statistics’: Why We Need More Black Female Physicians.” Forbes Magazine, 27 Feb. 2020.
“Diversity in Medicine: Facts and Figures 2019.” Association of American Medical Colleges, 2019.
“Facts & Figures: Diversity in Oncology.” American Society of Clinical Oncology. 2020 Jan 16.
What Tom Brady and Patrick Mahomes can teach us about physicians
Warning: This article will be about Tom Brady. If you love Tom Brady, hate Tom Brady, previously loved and now hate Tom Brady, I’m just warning you so you’ll be in the right frame of mind to continue. (If you don’t know who Tom Brady is, he’s Gisele’s husband).

Brady, who plays for the Tampa Bay Buccaneers, has played in the NFL for 21 seasons, an unbelievable number given the average career for a quarterback is 3 years. He’s 43 years old and was the oldest player in a Super Bowl, ever. He faced Patrick Mahomes, the quarterback for the opposing Kansas City Chiefs. Mahomes is one of the most athletic and talented quarterbacks of all time, and Mahomes is nearly 20 years younger than Brady. Yet, in a shot heard around the NFL world, Brady won.
But, was a Brady victory so shocking? Hot-shot residents may have a lot of moxie and talent, but experienced doctors often prevail by simply making sound decisions and avoiding mistakes. In our department, we’ve been discussing this lately: We’re hiring two dermatologists and we’re fortunate to have some amazing candidates apply. Some, like Mahomes, are young all-stars with outstanding ability and potential, right out of residency. Others, Brady-like, have been in practice for years and are ready to move to a new franchise.
Our medical group’s experiences are probably similar to many practices: New physicians out of residency often bring energy, inspiration, and ease with the latest therapies, devices, and surgical techniques. Yet, they sometimes struggle with efficiency and unforced errors. Experienced physicians might not know what’s hot, but they can often see where the best course of action lies, understanding not only the physiology but also the patient in ways that only experience can teach you. Fortunately, for those like me who’ve crossed midlife, there doesn’t seem to be an upper limit to experience – it is possible to keep getting better. Yes, I’m just like Tom Brady. (I wrote this article just to print that line.)
Some of the best doctors I’ve ever seen in action were emeritus physicians. In medical school at Wake Forest University, one of my professors was Dr. Eben Alexander. A retired neurosurgeon, he taught a case-based critical thinking skills class. I recall his brilliant insight and coaching, working through cases that had nothing to do with the brain or with surgery. He used his vast experience and wisdom to teach us how to practice medicine. He was, at that time, nearly 90 years old. Despite having been retired for decades, he was still writing articles and editing journals. He was inspiring. For a minute, he had me thinking I’d like to be a neurosurgeon, so I could be just like Eben Alexander. I did not, but I learned things from him that still impact my practice as a dermatologist today.
I’m sure you’ve had similar experiences of older colleagues or mentors who were the best doctor in the clinic or the O.R. They are the Dr. Anthony Faucis, not just practicing, but leading while in their 8th or 9th decade. We are all so fortunate that they keep playing.
We’ve not made our final choices on whom to hire, but with two positions, I expect we’ll choose both a young doctor and an experienced one to add to our team. It will be fun to watch and learn from them. Just like it will be fun to watch Tom Brady in the Super Bowl again next year.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Warning: This article will be about Tom Brady. If you love Tom Brady, hate Tom Brady, previously loved and now hate Tom Brady, I’m just warning you so you’ll be in the right frame of mind to continue. (If you don’t know who Tom Brady is, he’s Gisele’s husband).
Brady, who plays for the Tampa Bay Buccaneers, has played in the NFL for 21 seasons, an unbelievable number given the average career for a quarterback is 3 years. He’s 43 years old and was the oldest player in a Super Bowl, ever. He faced Patrick Mahomes, the quarterback for the opposing Kansas City Chiefs. Mahomes is one of the most athletic and talented quarterbacks of all time, and Mahomes is nearly 20 years younger than Brady. Yet, in a shot heard around the NFL world, Brady won.
But, was a Brady victory so shocking? Hot-shot residents may have a lot of moxie and talent, but experienced doctors often prevail by simply making sound decisions and avoiding mistakes. In our department, we’ve been discussing this lately: We’re hiring two dermatologists and we’re fortunate to have some amazing candidates apply. Some, like Mahomes, are young all-stars with outstanding ability and potential, right out of residency. Others, Brady-like, have been in practice for years and are ready to move to a new franchise.
Our medical group’s experiences are probably similar to many practices: New physicians out of residency often bring energy, inspiration, and ease with the latest therapies, devices, and surgical techniques. Yet, they sometimes struggle with efficiency and unforced errors. Experienced physicians might not know what’s hot, but they can often see where the best course of action lies, understanding not only the physiology but also the patient in ways that only experience can teach you. Fortunately, for those like me who’ve crossed midlife, there doesn’t seem to be an upper limit to experience – it is possible to keep getting better. Yes, I’m just like Tom Brady. (I wrote this article just to print that line.)
Some of the best doctors I’ve ever seen in action were emeritus physicians. In medical school at Wake Forest University, one of my professors was Dr. Eben Alexander. A retired neurosurgeon, he taught a case-based critical thinking skills class. I recall his brilliant insight and coaching, working through cases that had nothing to do with the brain or with surgery. He used his vast experience and wisdom to teach us how to practice medicine. He was, at that time, nearly 90 years old. Despite having been retired for decades, he was still writing articles and editing journals. He was inspiring. For a minute, he had me thinking I’d like to be a neurosurgeon, so I could be just like Eben Alexander. I did not, but I learned things from him that still impact my practice as a dermatologist today.
I’m sure you’ve had similar experiences of older colleagues or mentors who were the best doctor in the clinic or the O.R. They are the Dr. Anthony Faucis, not just practicing, but leading while in their 8th or 9th decade. We are all so fortunate that they keep playing.
We’ve not made our final choices on whom to hire, but with two positions, I expect we’ll choose both a young doctor and an experienced one to add to our team. It will be fun to watch and learn from them. Just like it will be fun to watch Tom Brady in the Super Bowl again next year.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Warning: This article will be about Tom Brady. If you love Tom Brady, hate Tom Brady, previously loved and now hate Tom Brady, I’m just warning you so you’ll be in the right frame of mind to continue. (If you don’t know who Tom Brady is, he’s Gisele’s husband).
Brady, who plays for the Tampa Bay Buccaneers, has played in the NFL for 21 seasons, an unbelievable number given the average career for a quarterback is 3 years. He’s 43 years old and was the oldest player in a Super Bowl, ever. He faced Patrick Mahomes, the quarterback for the opposing Kansas City Chiefs. Mahomes is one of the most athletic and talented quarterbacks of all time, and Mahomes is nearly 20 years younger than Brady. Yet, in a shot heard around the NFL world, Brady won.
But, was a Brady victory so shocking? Hot-shot residents may have a lot of moxie and talent, but experienced doctors often prevail by simply making sound decisions and avoiding mistakes. In our department, we’ve been discussing this lately: We’re hiring two dermatologists and we’re fortunate to have some amazing candidates apply. Some, like Mahomes, are young all-stars with outstanding ability and potential, right out of residency. Others, Brady-like, have been in practice for years and are ready to move to a new franchise.
Our medical group’s experiences are probably similar to many practices: New physicians out of residency often bring energy, inspiration, and ease with the latest therapies, devices, and surgical techniques. Yet, they sometimes struggle with efficiency and unforced errors. Experienced physicians might not know what’s hot, but they can often see where the best course of action lies, understanding not only the physiology but also the patient in ways that only experience can teach you. Fortunately, for those like me who’ve crossed midlife, there doesn’t seem to be an upper limit to experience – it is possible to keep getting better. Yes, I’m just like Tom Brady. (I wrote this article just to print that line.)
Some of the best doctors I’ve ever seen in action were emeritus physicians. In medical school at Wake Forest University, one of my professors was Dr. Eben Alexander. A retired neurosurgeon, he taught a case-based critical thinking skills class. I recall his brilliant insight and coaching, working through cases that had nothing to do with the brain or with surgery. He used his vast experience and wisdom to teach us how to practice medicine. He was, at that time, nearly 90 years old. Despite having been retired for decades, he was still writing articles and editing journals. He was inspiring. For a minute, he had me thinking I’d like to be a neurosurgeon, so I could be just like Eben Alexander. I did not, but I learned things from him that still impact my practice as a dermatologist today.
I’m sure you’ve had similar experiences of older colleagues or mentors who were the best doctor in the clinic or the O.R. They are the Dr. Anthony Faucis, not just practicing, but leading while in their 8th or 9th decade. We are all so fortunate that they keep playing.
We’ve not made our final choices on whom to hire, but with two positions, I expect we’ll choose both a young doctor and an experienced one to add to our team. It will be fun to watch and learn from them. Just like it will be fun to watch Tom Brady in the Super Bowl again next year.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Don’t fear patients reading their clinical notes: Opinion
Doctors are learning about new rules coming this April that encourage open and transparent communication among patients, families, and clinicians. The rules, putting into effect the bipartisan 21st Century Cures Act, mandate offering patients access to notes (“open notes”) written by clinicians in electronic medical records.
A recent article from this news organization noted that for many doctors this represents both a sudden and troubling change in practice. For others, the rules codify what they have been doing as a matter of routine for a decade. Spurred by the OpenNotes movement, at least 55 million Americans are already offered access to their clinical notes, including, since 2013, more than 9 million veterans with access to the Blue Button function in Veterans Affairs practices and hospitals.
The practice is spreading beyond the United States to other countries, including Canada, Sweden, Norway, Estonia, and the United Kingdom.
In this commentary, we review what patients, clinicians, and policymakers have been learning about open notes.
The patient experience
What do patients experience? In a survey of more than 22,000 patients who read notes in three diverse health systems, more than 90% reported having a good grasp of what their doctors and other clinicians had written, and very few (3%) reported being very confused by what they read. About two-thirds described reading their notes as very important for taking care of their health, remembering details of their visits and their care plans, and understanding why a medication was prescribed.
Indeed, in a clinically exciting finding, 14% of survey respondents reported that reading their notes made them more likely to take their medications as their doctors wished. With about half of Americans with chronic illness failing to take their medicines as prescribed, which sometimes leads to compromised outcomes and associated unnecessary costs (estimated at $300 billion annually), these reports of increased adherence should be taken very seriously.
Some doctors anticipate that open notes will erode patient communication. A growing body of research reveals just the opposite. In multiple surveys, patients describe open notes as “extending the visit,” strengthening collaboration and teamwork with their doctor. Quite possibly, the invitation to read notes may in itself increase trust. Such benefits appear especially pronounced among patients who are older, less educated, are persons of color or Hispanic, or who do not speak English at home.
And in several studies, more than a third of patients also report sharing their notes with others, with older and chronically ill patients in particular sharing access with family and friends who are their care partners.
On the other hand, a small minority of patients (5%) do report being more worried by what they read. It’s unknown whether this is because they are better informed about their care or because baseline anxiety levels increase. Doctors expect also that some patients, particularly those with cancer or serious mental illness, will be upset by their notes. So far, evidence does not support that specific concern.
Conversely, withholding, delaying, or blocking notes may be a source of anxiety or even stigmatization. When clinicians find themselves worried about sharing notes, we suggest that they discuss with their patients the benefits and risks. Recall also that transparency facilitates freedom of choice; patients make their own decision, and quite a few choose to leave notes unread.
Finding mistakes early and preventing harm are important goals for health care, and open notes can make care safer. Inevitably, medical records contain errors, omissions, and inaccuracies. In a large patient survey, 21% reported finding an error in their notes, and 42% perceived the error to be serious.
Moreover, 25% of doctors with more than a year’s experience with open notes reported patients finding errors that they (the doctors) considered “serious.” In 2015, the National Academy of Medicine cited open notes as a mechanism for improving diagnostic accuracy. In regard to possible legal action from patients, most attorneys, patients, and doctors agree that more transparent communication will build trust overall and, if anything, diminish litigation. We know of no instances so far of lawsuits deriving from open notes.
The physician experience
Doctors may worry that open notes will impede workflow, that they will be compelled to “dumb down” their documentation to avoid causing offense or anxiety, and that patients will demand changes to what is written. Here, extensive survey research should allay such fears and expectations. In a survey of more than 1,600 clinicians with at least 1 year of experience with open notes, reports of disruption to workflow were uncommon.

Most doctors (84%) reported that patients contacted them with questions about their notes “less than monthly or never.” Approximately two-thirds (62%) reported spending the same amount of time writing visit notes.
After implementing open notes, many doctors do report being more mindful about their documentation. For example, 41% reported changing how they used language such as “patient denies” or “noncompliant,” and 18% reported changing their use of medical jargon or abbreviations. Might these changes undermine the utility of medical notes? A majority of doctors surveyed (78%) said no, reporting that, after implementing open notes, the value of their documentation was the same or better.
Innovations spotlight difficult and often longstanding challenges. Open notes highlight the complex role of medical records in preserving privacy, especially in the spectrum of abuse, whether domestic or involving elders, children or sexual transgressions. For families with adolescents, issues concerning confidentiality can become a two-way street, and federal and state rules at times provide conflicting and idiosyncratic guidance. It is important to emphasize that the new rules permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties.
Perhaps think of open notes as a new medicine designed to help the vast majority of those who use it but with side effects and even contraindications for a few. Doctors can step in to minimize risks to vulnerable individuals, and imaginative and creative solutions to complex issues may emerge. In a growing number of practices serving adolescents, clinicians can now create two notes, with some elements of care visible on a patient portal and others held privately or visible only to the adolescent.
The shared experience
Overall, when it comes to documenting sensitive social information, open notes may act as a useful catalyst prompting deeper discussion about personal details clinically important to record, as opposed to those perhaps best left unwritten.
The implementation of open notes nationwide calls for exciting explorations. How can transparent systems maximize benefits for targeted populations in diverse settings? For patients with mental illness, can notes become part of the therapy? Given that care partners often report more benefit from reading notes than do patients themselves, how can they be mobilized to maximize their contributions to those acutely ill on hospital floors, or to family members with Alzheimer’s or in long-term care facilities?
How can we harness emerging technologies to translate notes and medical records into other languages or support lower literacy levels, while preserving the clinical detail in the notes? Should patients contribute to their own notes, cogenerating them with their clinicians? Experiments for “OurNotes” interventions are underway, and early reports from both patients and doctors hold considerable promise.
Ownership of medical records is evolving. Once firmly held by clinicians, electronic technologies have rapidly led to what may best be viewed currently as joint ownership by clinicians and patients. As apps evolve further and issues with interoperability of records diminish, it is likely that patients will eventually take control. Then it will be up to patients what to carry in their records. Clinicians will advise, but patients will decide.
The new rules herald clear changes in the fabric of care, and after a decade of study we anticipate that the benefits well outweigh the harms. But in the short run, it’s wrong to predict an avalanche. Two decades ago, when patient portals first revealed laboratory test findings to patients, doctors expected cataclysmic change in their practices. It did not occur. The vast majority of patients who registered on portals benefited and few disturbed their doctors.
Similarly, after notes were first unblinded by the OpenNotes research teams, the question we were asked most commonly by the primary care doctors who volunteered was whether the computers were actually displaying their notes. Even though many patients read them carefully, the doctors heard little from them. Clinicians have now reported the same experience in several subsequent studies.
Patients are resourceful, turning quickly to friends or the Internet for answers to their questions. They know how busy doctors are and don’t want to bother them if at all possible. When notes do trigger questions, the time taken to respond is probably offset by silence from other patients finding answers to their own questions in notes they read.
We believe that clinicians should embrace the spirit of the rules and also view them as HIPAA catching up with a computerized universe. As the new practice takes hold, ambiguities will diminish as further experience and research evolve. Warner V. Slack, MD, the first doctor to ask patients to talk to computers, opined that patients are the “largest and least utilized resource in health care.” Open and transparent communication through electronic medical records may mobilize patients (and their families) far more effectively. Patients will almost certainly benefit. Remembering Dr. Slack’s prophecy, we believe that clinicians will too.
A version of this article first appeared on Medscape.com.
Doctors are learning about new rules coming this April that encourage open and transparent communication among patients, families, and clinicians. The rules, putting into effect the bipartisan 21st Century Cures Act, mandate offering patients access to notes (“open notes”) written by clinicians in electronic medical records.
A recent article from this news organization noted that for many doctors this represents both a sudden and troubling change in practice. For others, the rules codify what they have been doing as a matter of routine for a decade. Spurred by the OpenNotes movement, at least 55 million Americans are already offered access to their clinical notes, including, since 2013, more than 9 million veterans with access to the Blue Button function in Veterans Affairs practices and hospitals.
The practice is spreading beyond the United States to other countries, including Canada, Sweden, Norway, Estonia, and the United Kingdom.
In this commentary, we review what patients, clinicians, and policymakers have been learning about open notes.
The patient experience
What do patients experience? In a survey of more than 22,000 patients who read notes in three diverse health systems, more than 90% reported having a good grasp of what their doctors and other clinicians had written, and very few (3%) reported being very confused by what they read. About two-thirds described reading their notes as very important for taking care of their health, remembering details of their visits and their care plans, and understanding why a medication was prescribed.
Indeed, in a clinically exciting finding, 14% of survey respondents reported that reading their notes made them more likely to take their medications as their doctors wished. With about half of Americans with chronic illness failing to take their medicines as prescribed, which sometimes leads to compromised outcomes and associated unnecessary costs (estimated at $300 billion annually), these reports of increased adherence should be taken very seriously.
Some doctors anticipate that open notes will erode patient communication. A growing body of research reveals just the opposite. In multiple surveys, patients describe open notes as “extending the visit,” strengthening collaboration and teamwork with their doctor. Quite possibly, the invitation to read notes may in itself increase trust. Such benefits appear especially pronounced among patients who are older, less educated, are persons of color or Hispanic, or who do not speak English at home.
And in several studies, more than a third of patients also report sharing their notes with others, with older and chronically ill patients in particular sharing access with family and friends who are their care partners.
On the other hand, a small minority of patients (5%) do report being more worried by what they read. It’s unknown whether this is because they are better informed about their care or because baseline anxiety levels increase. Doctors expect also that some patients, particularly those with cancer or serious mental illness, will be upset by their notes. So far, evidence does not support that specific concern.
Conversely, withholding, delaying, or blocking notes may be a source of anxiety or even stigmatization. When clinicians find themselves worried about sharing notes, we suggest that they discuss with their patients the benefits and risks. Recall also that transparency facilitates freedom of choice; patients make their own decision, and quite a few choose to leave notes unread.
Finding mistakes early and preventing harm are important goals for health care, and open notes can make care safer. Inevitably, medical records contain errors, omissions, and inaccuracies. In a large patient survey, 21% reported finding an error in their notes, and 42% perceived the error to be serious.
Moreover, 25% of doctors with more than a year’s experience with open notes reported patients finding errors that they (the doctors) considered “serious.” In 2015, the National Academy of Medicine cited open notes as a mechanism for improving diagnostic accuracy. In regard to possible legal action from patients, most attorneys, patients, and doctors agree that more transparent communication will build trust overall and, if anything, diminish litigation. We know of no instances so far of lawsuits deriving from open notes.
The physician experience
Doctors may worry that open notes will impede workflow, that they will be compelled to “dumb down” their documentation to avoid causing offense or anxiety, and that patients will demand changes to what is written. Here, extensive survey research should allay such fears and expectations. In a survey of more than 1,600 clinicians with at least 1 year of experience with open notes, reports of disruption to workflow were uncommon.
Most doctors (84%) reported that patients contacted them with questions about their notes “less than monthly or never.” Approximately two-thirds (62%) reported spending the same amount of time writing visit notes.
After implementing open notes, many doctors do report being more mindful about their documentation. For example, 41% reported changing how they used language such as “patient denies” or “noncompliant,” and 18% reported changing their use of medical jargon or abbreviations. Might these changes undermine the utility of medical notes? A majority of doctors surveyed (78%) said no, reporting that, after implementing open notes, the value of their documentation was the same or better.
Innovations spotlight difficult and often longstanding challenges. Open notes highlight the complex role of medical records in preserving privacy, especially in the spectrum of abuse, whether domestic or involving elders, children or sexual transgressions. For families with adolescents, issues concerning confidentiality can become a two-way street, and federal and state rules at times provide conflicting and idiosyncratic guidance. It is important to emphasize that the new rules permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties.
Perhaps think of open notes as a new medicine designed to help the vast majority of those who use it but with side effects and even contraindications for a few. Doctors can step in to minimize risks to vulnerable individuals, and imaginative and creative solutions to complex issues may emerge. In a growing number of practices serving adolescents, clinicians can now create two notes, with some elements of care visible on a patient portal and others held privately or visible only to the adolescent.
The shared experience
Overall, when it comes to documenting sensitive social information, open notes may act as a useful catalyst prompting deeper discussion about personal details clinically important to record, as opposed to those perhaps best left unwritten.
The implementation of open notes nationwide calls for exciting explorations. How can transparent systems maximize benefits for targeted populations in diverse settings? For patients with mental illness, can notes become part of the therapy? Given that care partners often report more benefit from reading notes than do patients themselves, how can they be mobilized to maximize their contributions to those acutely ill on hospital floors, or to family members with Alzheimer’s or in long-term care facilities?
How can we harness emerging technologies to translate notes and medical records into other languages or support lower literacy levels, while preserving the clinical detail in the notes? Should patients contribute to their own notes, cogenerating them with their clinicians? Experiments for “OurNotes” interventions are underway, and early reports from both patients and doctors hold considerable promise.
Ownership of medical records is evolving. Once firmly held by clinicians, electronic technologies have rapidly led to what may best be viewed currently as joint ownership by clinicians and patients. As apps evolve further and issues with interoperability of records diminish, it is likely that patients will eventually take control. Then it will be up to patients what to carry in their records. Clinicians will advise, but patients will decide.
The new rules herald clear changes in the fabric of care, and after a decade of study we anticipate that the benefits well outweigh the harms. But in the short run, it’s wrong to predict an avalanche. Two decades ago, when patient portals first revealed laboratory test findings to patients, doctors expected cataclysmic change in their practices. It did not occur. The vast majority of patients who registered on portals benefited and few disturbed their doctors.
Similarly, after notes were first unblinded by the OpenNotes research teams, the question we were asked most commonly by the primary care doctors who volunteered was whether the computers were actually displaying their notes. Even though many patients read them carefully, the doctors heard little from them. Clinicians have now reported the same experience in several subsequent studies.
Patients are resourceful, turning quickly to friends or the Internet for answers to their questions. They know how busy doctors are and don’t want to bother them if at all possible. When notes do trigger questions, the time taken to respond is probably offset by silence from other patients finding answers to their own questions in notes they read.
We believe that clinicians should embrace the spirit of the rules and also view them as HIPAA catching up with a computerized universe. As the new practice takes hold, ambiguities will diminish as further experience and research evolve. Warner V. Slack, MD, the first doctor to ask patients to talk to computers, opined that patients are the “largest and least utilized resource in health care.” Open and transparent communication through electronic medical records may mobilize patients (and their families) far more effectively. Patients will almost certainly benefit. Remembering Dr. Slack’s prophecy, we believe that clinicians will too.
A version of this article first appeared on Medscape.com.
Doctors are learning about new rules coming this April that encourage open and transparent communication among patients, families, and clinicians. The rules, putting into effect the bipartisan 21st Century Cures Act, mandate offering patients access to notes (“open notes”) written by clinicians in electronic medical records.
A recent article from this news organization noted that for many doctors this represents both a sudden and troubling change in practice. For others, the rules codify what they have been doing as a matter of routine for a decade. Spurred by the OpenNotes movement, at least 55 million Americans are already offered access to their clinical notes, including, since 2013, more than 9 million veterans with access to the Blue Button function in Veterans Affairs practices and hospitals.
The practice is spreading beyond the United States to other countries, including Canada, Sweden, Norway, Estonia, and the United Kingdom.
In this commentary, we review what patients, clinicians, and policymakers have been learning about open notes.
The patient experience
What do patients experience? In a survey of more than 22,000 patients who read notes in three diverse health systems, more than 90% reported having a good grasp of what their doctors and other clinicians had written, and very few (3%) reported being very confused by what they read. About two-thirds described reading their notes as very important for taking care of their health, remembering details of their visits and their care plans, and understanding why a medication was prescribed.
Indeed, in a clinically exciting finding, 14% of survey respondents reported that reading their notes made them more likely to take their medications as their doctors wished. With about half of Americans with chronic illness failing to take their medicines as prescribed, which sometimes leads to compromised outcomes and associated unnecessary costs (estimated at $300 billion annually), these reports of increased adherence should be taken very seriously.
Some doctors anticipate that open notes will erode patient communication. A growing body of research reveals just the opposite. In multiple surveys, patients describe open notes as “extending the visit,” strengthening collaboration and teamwork with their doctor. Quite possibly, the invitation to read notes may in itself increase trust. Such benefits appear especially pronounced among patients who are older, less educated, are persons of color or Hispanic, or who do not speak English at home.
And in several studies, more than a third of patients also report sharing their notes with others, with older and chronically ill patients in particular sharing access with family and friends who are their care partners.
On the other hand, a small minority of patients (5%) do report being more worried by what they read. It’s unknown whether this is because they are better informed about their care or because baseline anxiety levels increase. Doctors expect also that some patients, particularly those with cancer or serious mental illness, will be upset by their notes. So far, evidence does not support that specific concern.
Conversely, withholding, delaying, or blocking notes may be a source of anxiety or even stigmatization. When clinicians find themselves worried about sharing notes, we suggest that they discuss with their patients the benefits and risks. Recall also that transparency facilitates freedom of choice; patients make their own decision, and quite a few choose to leave notes unread.
Finding mistakes early and preventing harm are important goals for health care, and open notes can make care safer. Inevitably, medical records contain errors, omissions, and inaccuracies. In a large patient survey, 21% reported finding an error in their notes, and 42% perceived the error to be serious.
Moreover, 25% of doctors with more than a year’s experience with open notes reported patients finding errors that they (the doctors) considered “serious.” In 2015, the National Academy of Medicine cited open notes as a mechanism for improving diagnostic accuracy. In regard to possible legal action from patients, most attorneys, patients, and doctors agree that more transparent communication will build trust overall and, if anything, diminish litigation. We know of no instances so far of lawsuits deriving from open notes.
The physician experience
Doctors may worry that open notes will impede workflow, that they will be compelled to “dumb down” their documentation to avoid causing offense or anxiety, and that patients will demand changes to what is written. Here, extensive survey research should allay such fears and expectations. In a survey of more than 1,600 clinicians with at least 1 year of experience with open notes, reports of disruption to workflow were uncommon.
Most doctors (84%) reported that patients contacted them with questions about their notes “less than monthly or never.” Approximately two-thirds (62%) reported spending the same amount of time writing visit notes.
After implementing open notes, many doctors do report being more mindful about their documentation. For example, 41% reported changing how they used language such as “patient denies” or “noncompliant,” and 18% reported changing their use of medical jargon or abbreviations. Might these changes undermine the utility of medical notes? A majority of doctors surveyed (78%) said no, reporting that, after implementing open notes, the value of their documentation was the same or better.
Innovations spotlight difficult and often longstanding challenges. Open notes highlight the complex role of medical records in preserving privacy, especially in the spectrum of abuse, whether domestic or involving elders, children or sexual transgressions. For families with adolescents, issues concerning confidentiality can become a two-way street, and federal and state rules at times provide conflicting and idiosyncratic guidance. It is important to emphasize that the new rules permit information blocking if there is clear evidence that doing so “will substantially reduce the risk of harm” to patients or to other third parties.
Perhaps think of open notes as a new medicine designed to help the vast majority of those who use it but with side effects and even contraindications for a few. Doctors can step in to minimize risks to vulnerable individuals, and imaginative and creative solutions to complex issues may emerge. In a growing number of practices serving adolescents, clinicians can now create two notes, with some elements of care visible on a patient portal and others held privately or visible only to the adolescent.
The shared experience
Overall, when it comes to documenting sensitive social information, open notes may act as a useful catalyst prompting deeper discussion about personal details clinically important to record, as opposed to those perhaps best left unwritten.
The implementation of open notes nationwide calls for exciting explorations. How can transparent systems maximize benefits for targeted populations in diverse settings? For patients with mental illness, can notes become part of the therapy? Given that care partners often report more benefit from reading notes than do patients themselves, how can they be mobilized to maximize their contributions to those acutely ill on hospital floors, or to family members with Alzheimer’s or in long-term care facilities?
How can we harness emerging technologies to translate notes and medical records into other languages or support lower literacy levels, while preserving the clinical detail in the notes? Should patients contribute to their own notes, cogenerating them with their clinicians? Experiments for “OurNotes” interventions are underway, and early reports from both patients and doctors hold considerable promise.
Ownership of medical records is evolving. Once firmly held by clinicians, electronic technologies have rapidly led to what may best be viewed currently as joint ownership by clinicians and patients. As apps evolve further and issues with interoperability of records diminish, it is likely that patients will eventually take control. Then it will be up to patients what to carry in their records. Clinicians will advise, but patients will decide.
The new rules herald clear changes in the fabric of care, and after a decade of study we anticipate that the benefits well outweigh the harms. But in the short run, it’s wrong to predict an avalanche. Two decades ago, when patient portals first revealed laboratory test findings to patients, doctors expected cataclysmic change in their practices. It did not occur. The vast majority of patients who registered on portals benefited and few disturbed their doctors.
Similarly, after notes were first unblinded by the OpenNotes research teams, the question we were asked most commonly by the primary care doctors who volunteered was whether the computers were actually displaying their notes. Even though many patients read them carefully, the doctors heard little from them. Clinicians have now reported the same experience in several subsequent studies.
Patients are resourceful, turning quickly to friends or the Internet for answers to their questions. They know how busy doctors are and don’t want to bother them if at all possible. When notes do trigger questions, the time taken to respond is probably offset by silence from other patients finding answers to their own questions in notes they read.
We believe that clinicians should embrace the spirit of the rules and also view them as HIPAA catching up with a computerized universe. As the new practice takes hold, ambiguities will diminish as further experience and research evolve. Warner V. Slack, MD, the first doctor to ask patients to talk to computers, opined that patients are the “largest and least utilized resource in health care.” Open and transparent communication through electronic medical records may mobilize patients (and their families) far more effectively. Patients will almost certainly benefit. Remembering Dr. Slack’s prophecy, we believe that clinicians will too.
A version of this article first appeared on Medscape.com.
What to do if an employee tests positive for COVID-19
An increasingly common question I’m receiving is:
As always, it depends, but here is some general advice: The specifics will vary depending on state/local laws, or your particular situation.
First, you need to determine the level of exposure, and whether it requires action. According to the Centers for Disease Control and Prevention, actionable exposure occurs 2 days prior to the onset of illness, and lasts 10 days after onset.
If action is required, you’ll need to determine who needs to quarantine and who needs to be tested. Vaccinated employees who have been exposed to suspected or confirmed COVID-19 are not required to quarantine or be tested if they are fully vaccinated and have remained asymptomatic since the exposure. Those employees should, however, follow all the usual precautions (masks, social distancing, handwashing, etc.) with increased diligence. Remind them that no vaccine is 100% effective, and suggest they self-monitor for symptoms (fever, cough, shortness of breath, etc.)
All other exposed employees should be tested. A negative test means an individual was not infected at the time the sample was collected, but that does not mean an individual will not get sick later. Some providers are retesting on days 5 and 7 post exposure.
Some experts advise that you monitor exposed employees (vaccinated or not) yourself, with daily temperature readings and inquiries regarding symptoms, and perhaps a daily pulse oximetry check, for 14 days following exposure. Document these screenings in writing. Anyone testing positive or developing a fever or other symptoms should, of course, be sent home and seek medical treatment as necessary.
Employees who develop symptoms or test positive for COVID-19 should remain out of work until all CDC “return-to-work” criteria are met. At this writing, the basic criteria include:
- At least 10 days pass after symptoms first appeared
- At least 24 hours pass after last fever without the use of fever-reducing medications
- Cough, shortness of breath, and any other symptoms improve
Anyone who is significantly immunocompromised may need more time at home, and probably consultation with an infectious disease specialist.
Your facility should be thoroughly cleaned after the exposure. Close off all areas used by the sick individual, and clean and disinfect all areas such as offices, doorknobs, bathrooms, common areas, and shared electronic equipment. Of course, the cleaners should wear gowns, gloves, masks, and goggles. Some practices are hiring cleaning crews to professionally disinfect their offices. Once the area has been disinfected, it can be reopened for use. Workers without close contact with the person who is sick can return to work immediately after disinfection.
If the potential infected area is widespread and cannot be isolated to a room or rooms where doors can be shut, it may be prudent to temporarily close your office, send staff home, and divert patients to other locations if they cannot be rescheduled. Once your facility is cleaned and disinfected and staff have been cleared, your office may reopen.
Use enhanced precautions for any staff or patients who are immunocompromised, or otherwise fall into the high-risk category, to keep them out of the path of potential exposure areas and allow them to self-quarantine if they desire.

You should continue following existing leave policies (paid time off, vacation, sick, short-term disability, leave of absence, Family and Medical Leave Act, and Americans with Disabilities Act). If the employee was exposed at work, contact your workers’ compensation carrier regarding lost wages. Unless your state laws specify otherwise, you are under no obligation to pay beyond your policies, but you may do so if you choose.
Of course, you can take proactive steps to prevent unnecessary exposure and avoid closures in the first place; for example:
- Call patients prior to their visit, or question them upon arrival, regarding fever, shortness of breath, and other COVID-19 symptoms.
- Check employees’ temperatures every morning.
- Check patients’ temperatures as they enter the office.
- Require everyone, patients and employees alike, to wear face coverings.
- Ask patients to leave friends and family members at home.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
An increasingly common question I’m receiving is:
As always, it depends, but here is some general advice: The specifics will vary depending on state/local laws, or your particular situation.
First, you need to determine the level of exposure, and whether it requires action. According to the Centers for Disease Control and Prevention, actionable exposure occurs 2 days prior to the onset of illness, and lasts 10 days after onset.
If action is required, you’ll need to determine who needs to quarantine and who needs to be tested. Vaccinated employees who have been exposed to suspected or confirmed COVID-19 are not required to quarantine or be tested if they are fully vaccinated and have remained asymptomatic since the exposure. Those employees should, however, follow all the usual precautions (masks, social distancing, handwashing, etc.) with increased diligence. Remind them that no vaccine is 100% effective, and suggest they self-monitor for symptoms (fever, cough, shortness of breath, etc.)
All other exposed employees should be tested. A negative test means an individual was not infected at the time the sample was collected, but that does not mean an individual will not get sick later. Some providers are retesting on days 5 and 7 post exposure.
Some experts advise that you monitor exposed employees (vaccinated or not) yourself, with daily temperature readings and inquiries regarding symptoms, and perhaps a daily pulse oximetry check, for 14 days following exposure. Document these screenings in writing. Anyone testing positive or developing a fever or other symptoms should, of course, be sent home and seek medical treatment as necessary.
Employees who develop symptoms or test positive for COVID-19 should remain out of work until all CDC “return-to-work” criteria are met. At this writing, the basic criteria include:
- At least 10 days pass after symptoms first appeared
- At least 24 hours pass after last fever without the use of fever-reducing medications
- Cough, shortness of breath, and any other symptoms improve
Anyone who is significantly immunocompromised may need more time at home, and probably consultation with an infectious disease specialist.
Your facility should be thoroughly cleaned after the exposure. Close off all areas used by the sick individual, and clean and disinfect all areas such as offices, doorknobs, bathrooms, common areas, and shared electronic equipment. Of course, the cleaners should wear gowns, gloves, masks, and goggles. Some practices are hiring cleaning crews to professionally disinfect their offices. Once the area has been disinfected, it can be reopened for use. Workers without close contact with the person who is sick can return to work immediately after disinfection.
If the potential infected area is widespread and cannot be isolated to a room or rooms where doors can be shut, it may be prudent to temporarily close your office, send staff home, and divert patients to other locations if they cannot be rescheduled. Once your facility is cleaned and disinfected and staff have been cleared, your office may reopen.
Use enhanced precautions for any staff or patients who are immunocompromised, or otherwise fall into the high-risk category, to keep them out of the path of potential exposure areas and allow them to self-quarantine if they desire.
You should continue following existing leave policies (paid time off, vacation, sick, short-term disability, leave of absence, Family and Medical Leave Act, and Americans with Disabilities Act). If the employee was exposed at work, contact your workers’ compensation carrier regarding lost wages. Unless your state laws specify otherwise, you are under no obligation to pay beyond your policies, but you may do so if you choose.
Of course, you can take proactive steps to prevent unnecessary exposure and avoid closures in the first place; for example:
- Call patients prior to their visit, or question them upon arrival, regarding fever, shortness of breath, and other COVID-19 symptoms.
- Check employees’ temperatures every morning.
- Check patients’ temperatures as they enter the office.
- Require everyone, patients and employees alike, to wear face coverings.
- Ask patients to leave friends and family members at home.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
An increasingly common question I’m receiving is:
As always, it depends, but here is some general advice: The specifics will vary depending on state/local laws, or your particular situation.
First, you need to determine the level of exposure, and whether it requires action. According to the Centers for Disease Control and Prevention, actionable exposure occurs 2 days prior to the onset of illness, and lasts 10 days after onset.
If action is required, you’ll need to determine who needs to quarantine and who needs to be tested. Vaccinated employees who have been exposed to suspected or confirmed COVID-19 are not required to quarantine or be tested if they are fully vaccinated and have remained asymptomatic since the exposure. Those employees should, however, follow all the usual precautions (masks, social distancing, handwashing, etc.) with increased diligence. Remind them that no vaccine is 100% effective, and suggest they self-monitor for symptoms (fever, cough, shortness of breath, etc.)
All other exposed employees should be tested. A negative test means an individual was not infected at the time the sample was collected, but that does not mean an individual will not get sick later. Some providers are retesting on days 5 and 7 post exposure.
Some experts advise that you monitor exposed employees (vaccinated or not) yourself, with daily temperature readings and inquiries regarding symptoms, and perhaps a daily pulse oximetry check, for 14 days following exposure. Document these screenings in writing. Anyone testing positive or developing a fever or other symptoms should, of course, be sent home and seek medical treatment as necessary.
Employees who develop symptoms or test positive for COVID-19 should remain out of work until all CDC “return-to-work” criteria are met. At this writing, the basic criteria include:
- At least 10 days pass after symptoms first appeared
- At least 24 hours pass after last fever without the use of fever-reducing medications
- Cough, shortness of breath, and any other symptoms improve
Anyone who is significantly immunocompromised may need more time at home, and probably consultation with an infectious disease specialist.
Your facility should be thoroughly cleaned after the exposure. Close off all areas used by the sick individual, and clean and disinfect all areas such as offices, doorknobs, bathrooms, common areas, and shared electronic equipment. Of course, the cleaners should wear gowns, gloves, masks, and goggles. Some practices are hiring cleaning crews to professionally disinfect their offices. Once the area has been disinfected, it can be reopened for use. Workers without close contact with the person who is sick can return to work immediately after disinfection.
If the potential infected area is widespread and cannot be isolated to a room or rooms where doors can be shut, it may be prudent to temporarily close your office, send staff home, and divert patients to other locations if they cannot be rescheduled. Once your facility is cleaned and disinfected and staff have been cleared, your office may reopen.
Use enhanced precautions for any staff or patients who are immunocompromised, or otherwise fall into the high-risk category, to keep them out of the path of potential exposure areas and allow them to self-quarantine if they desire.
You should continue following existing leave policies (paid time off, vacation, sick, short-term disability, leave of absence, Family and Medical Leave Act, and Americans with Disabilities Act). If the employee was exposed at work, contact your workers’ compensation carrier regarding lost wages. Unless your state laws specify otherwise, you are under no obligation to pay beyond your policies, but you may do so if you choose.
Of course, you can take proactive steps to prevent unnecessary exposure and avoid closures in the first place; for example:
- Call patients prior to their visit, or question them upon arrival, regarding fever, shortness of breath, and other COVID-19 symptoms.
- Check employees’ temperatures every morning.
- Check patients’ temperatures as they enter the office.
- Require everyone, patients and employees alike, to wear face coverings.
- Ask patients to leave friends and family members at home.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

X-ray vision: Using AI to maximize the value of radiographic images
Artificial intelligence (AI) is expected to one day affect the entire continuum of cancer care – from screening and risk prediction to diagnosis, risk stratification, treatment selection, and follow-up, according to an expert in the field.

Hugo J.W.L. Aerts, PhD, director of the AI in Medicine Program at Brigham and Women’s Hospital in Boston, described studies using AI for some of these purposes during a presentation at the AACR Virtual Special Conference: Artificial Intelligence, Diagnosis, and Imaging (Abstract IA-06).
In one study, Dr. Aerts and colleagues set out to determine whether a convolutional neural network (CNN) could extract prognostic information from chest radiographs. The researchers tested this theory using patients from two trials – the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial and the National Lung Screening Trial (NLST).
The team developed a CNN, called CXR-risk, and tested whether it could predict the longevity and prognosis of patients in the PLCO (n = 52,320) and NLST (n = 5,493) trials over a 12-year time period, based only on chest radiographs. No clinical information, demographics, radiographic interpretations, duration of follow-up, or censoring were provided to the deep-learning system.
CXR-risk output was stratified into five categories of radiographic risk scores for probability of death, from 0 (very low likelihood of mortality) to 1 (very high likelihood of mortality).
The investigators found a graded association between radiographic risk score and mortality. The very-high-risk group had mortality rates of 53.0% (PLCO) and 33.9% (NLST). In both trials, this was significantly higher than for the very-low-risk group. The unadjusted hazard ratio was 18.3 in the PCLO data set and 15.2 in the NLST data set (P < .001 for both).
This association was maintained after adjustment for radiologists’ findings (e.g., a lung nodule) and risk factors such as age, gender, and comorbid illnesses like diabetes. The adjusted HR was 4.8 in the PCLO data set and 7.0 in the NLST data set (P < .001 for both).
In both data sets, individuals in the very-high-risk group were significantly more likely to die of lung cancer. The aHR was 11.1 in the PCLO data set and 8.4 in the NSLT data set (P < .001 for both).
This might be expected for people who were interested in being screened for lung cancer. However, patients in the very-high-risk group were also more likely to die of cardiovascular illness (aHR, 3.6 for PLCO and 47.8 for NSLT; P < .001 for both) and respiratory illness (aHR, 27.5 for PLCO and 31.9 for NLST; P ≤ .001 for both).
With this information, a clinician could initiate additional testing and/or utilize more aggressive surveillance measures. If an oncologist considered therapy for a patient with newly diagnosed cancer, treatment choices and stratification for adverse events would be more intelligently planned.
Using AI to predict the risk of lung cancer
In another study, Dr. Aerts and colleagues developed and validated a CNN called CXR-LC, which was based on CXR-risk. The goal of this study was to see if CXR-LC could predict long-term incident lung cancer using data available in the EHR, including chest radiographs, age, sex, and smoking status.
The CXR-LC model was developed using data from the PLCO trial (n = 41,856) and was validated in smokers from the PLCO trial (n = 5,615; 12-year follow-up) as well as heavy smokers from the NLST trial (n = 5,493; 6-year follow-up).
Results showed that CXR-LC was able to predict which patients were at highest risk for developing lung cancer.
CXR-LC had better discrimination for incident lung cancer than did Medicare eligibility in the PLCO data set (area under the curve, 0.755 vs. 0.634; P < .001). And the performance of CXR-LC was similar to that of the PLCOM2012 risk score in both the PLCO data set (AUC, 0.755 vs. 0.751) and the NLST data set (AUC, 0.659 vs. 0.650).
When they were compared in screening populations of equal size, CXR-LC was more sensitive than Medicare eligibility criteria in the PLCO data set (74.9% vs. 63.8%; P = .012) and missed 30.7% fewer incident lung cancer diagnoses.
AI as a substitute for specialized testing and consultation
In a third study, Dr. Aerts and colleagues used a CNN to predict cardiovascular risk by assessing coronary artery calcium (CAC) from clinically obtained, readily available CT scans.
Ordinarily, identifying CAC – an accurate predictor of cardiovascular events – requires specialized expertise (manual measurement and cardiologist interpretation), time (estimated at 20 minutes/scan), and equipment (ECG-gated cardiac CT scan and special software).
In this study, the researchers used a fully end-to-end automated system with analytic time measured in less than 2 seconds.
The team trained and tuned their CNN using the Framingham Heart Study Offspring and Third Generation cohorts (n = 1,636), which included asymptomatic patients with high-quality, cardiac-gated CT scans for CAC quantification.
The researchers then tested the CNN on two asymptomatic and two symptomatic cohorts:
- Asymptomatic Framingham Heart Study participants (n = 663) in whom the outcome measures were cardiovascular disease and death.
- Asymptomatic NLST participants (n = 14,959) in whom the outcome measure was atherosclerotic cardiovascular death.
- Symptomatic PROMISE study participants with stable chest pain (n = 4,021) in whom the outcome measures were all-cause mortality, MI, and hospitalization for unstable angina.
- Symptomatic ROMICAT-II study patients with acute chest pain (n = 441) in whom the outcome measure was acute coronary syndrome at 28 days.
Among 5,521 subjects across all testing cohorts with cardiac-gated and nongated chest CT scans, the CNN and expert reader interpretations agreed on the CAC risk scores with a high level of concordance (kappa, 0.71; concordance rate, 0.79).
There was a very high Spearman’s correlation of 0.92 (P < .0001) and substantial agreement between automatically and manually calculated CAC risk groups, substantiating robust risk prediction for cardiovascular disease across multiple clinical scenarios.
Dr. Aerts commented that, among the NLST participants who had the highest risk of developing lung cancer, the risk of cardiovascular death was as high as the risk of death from lung cancer.
Using AI to assess patient outcomes
In an unpublished study, Dr. Aerts and colleagues used AI in an attempt to determine whether changes in measurements of subcutaneous adipose tissue (SAT), visceral adipose tissue (VAT), and skeletal muscle mass would provide clues about treatment outcomes in lung cancer patients.
The researchers developed a deep learning model using data from 1,129 patients at Massachusetts General and Brigham and Women’s Hospitals, measuring SAT, VAT, and muscle mass. The team applied the measurement system to a population of 12,128 outpatients and calculated z scores for SAT, VAT, and muscle mass to determine “normal” values.
When they applied the norms to surgical lung cancer data sets from the Boston Lung Cancer Study (n = 437) and TRACERx study (n = 394), the researchers found that smokers had lower adiposity and lower muscle mass than never-smokers.
More importantly, over time, among lung cancer patients who lost greater than 5% of VAT, SAT, and muscle mass, those patients with the greatest SAT loss (P < .0001) or VAT loss (P = .0015) had the lowest lung cancer–specific survival in the TRACERx study. There was no significant impairment of lung cancer-specific survival for patients who experienced skeletal muscle loss (P = .23).
The same observation was made for overall survival among patients enrolled in the Boston Lung Cancer Study, using the 5% threshold. Overall survival was significantly worse with increasing VAT loss (P = .0023) and SAT loss (P = .0082) but not with increasing skeletal muscle loss (P = .3).
The investigators speculated about whether the correlation between body composition and clinical outcome could yield clues about tumor biology. To test this, the researchers used the RNA sequencing–based ORACLE risk score in lung cancer patients from TRACERx. There was a high correlation between higher ORACLE risk scores and lower VAT and SAT, suggesting that measures of adiposity on CT were reflected in tumor biology patterns on an RNA level in lung cancer patients. There was no such correlation between ORACLE risk scores and skeletal muscle mass.
Wonderment ... tempered by concern and challenges
AI has awe-inspiring potential to yield actionable and prognostically important information from data mining the EHR and extracting the vast quantities of information from images. In some cases (like CAC), it is information that is “hiding in plain sight.” However, Dr. Aerts expressed several cautions, some of which have already plagued AI.
He referenced the Gartner Hype Cycle, which provides a graphic representation of five phases in the life cycle of emerging technologies. The “innovation trigger” is followed by a “peak of inflated expectations,” a “trough of disillusionment,” a “slope of enlightenment,” and a “plateau of productivity.”
Dr. Aerts noted that, in recent years, AI has seemed to fall into the trough of disillusionment, but it may be entering the slope of enlightenment on the way to the plateau of productivity.
His research highlighted several examples of productivity in radiomics in cancer patients and those who are at high risk of developing cancer.
In Dr. Aerts’s opinion, a second concern is replication of AI research results. He noted that, among 400 published studies, only 6% of authors shared the codes that would enable their findings to be corroborated. About 30% shared test data, and 54% shared “pseudocodes,” but transparency and reproducibility are problems for the acceptance and broad implementation of AI.
Dr. Aerts endorsed the Modelhub initiative (www.modelhub.ai), a multi-institutional initiative to advance reproducibility in the AI field and advance its full potential.
However, there are additional concerns about the implementation of radiomics and, more generally, data mining from clinicians’ EHRs to personalize care.
Firstly, it may be laborious and difficult to explain complex, computer-based risk stratification models to patients. Hereditary cancer testing is an example of a risk assessment test that requires complicated explanations that many clinicians relegate to genetics counselors – when patients elect to see them. When a model is not explainable, it undermines the confidence of patients and their care providers, according to an editorial related to the CXR-LC study.
Another issue is that uptake of lung cancer screening, in practice, has been underutilized by individuals who meet current, relatively straightforward Medicare criteria. Despite the apparently better accuracy of the CXR-LC deep-learning model, its complexity and limited access could constitute an additional barrier for the at-risk individuals who should avail themselves of screening.
Furthermore, although age and gender are accurate in most circumstances, there is legitimate concern about the accuracy of, for example, smoking history data and comorbid conditions in current EHRs. Who performs the laborious curation of the input in an AI model to assure its accuracy for individual patients?
Finally, it is unclear how scalable and applicable AI will be to medically underserved populations (e.g., smaller, community-based, free-standing, socioeconomically disadvantaged or rural health care institutions). There are substantial initial and maintenance costs that may limit AI’s availability to some academic institutions and large health maintenance organizations.
As the concerns and challenges are addressed, it will be interesting to see where and when the plateau of productivity for AI in cancer care occurs. When it does, many cancer patients will benefit from enhanced care along the continuum of the complex disease they and their caregivers seek to master.
Dr. Aerts disclosed relationships with Onc.AI outside the presented work.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Artificial intelligence (AI) is expected to one day affect the entire continuum of cancer care – from screening and risk prediction to diagnosis, risk stratification, treatment selection, and follow-up, according to an expert in the field.
Hugo J.W.L. Aerts, PhD, director of the AI in Medicine Program at Brigham and Women’s Hospital in Boston, described studies using AI for some of these purposes during a presentation at the AACR Virtual Special Conference: Artificial Intelligence, Diagnosis, and Imaging (Abstract IA-06).
In one study, Dr. Aerts and colleagues set out to determine whether a convolutional neural network (CNN) could extract prognostic information from chest radiographs. The researchers tested this theory using patients from two trials – the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial and the National Lung Screening Trial (NLST).
The team developed a CNN, called CXR-risk, and tested whether it could predict the longevity and prognosis of patients in the PLCO (n = 52,320) and NLST (n = 5,493) trials over a 12-year time period, based only on chest radiographs. No clinical information, demographics, radiographic interpretations, duration of follow-up, or censoring were provided to the deep-learning system.
CXR-risk output was stratified into five categories of radiographic risk scores for probability of death, from 0 (very low likelihood of mortality) to 1 (very high likelihood of mortality).
The investigators found a graded association between radiographic risk score and mortality. The very-high-risk group had mortality rates of 53.0% (PLCO) and 33.9% (NLST). In both trials, this was significantly higher than for the very-low-risk group. The unadjusted hazard ratio was 18.3 in the PCLO data set and 15.2 in the NLST data set (P < .001 for both).
This association was maintained after adjustment for radiologists’ findings (e.g., a lung nodule) and risk factors such as age, gender, and comorbid illnesses like diabetes. The adjusted HR was 4.8 in the PCLO data set and 7.0 in the NLST data set (P < .001 for both).
In both data sets, individuals in the very-high-risk group were significantly more likely to die of lung cancer. The aHR was 11.1 in the PCLO data set and 8.4 in the NSLT data set (P < .001 for both).
This might be expected for people who were interested in being screened for lung cancer. However, patients in the very-high-risk group were also more likely to die of cardiovascular illness (aHR, 3.6 for PLCO and 47.8 for NSLT; P < .001 for both) and respiratory illness (aHR, 27.5 for PLCO and 31.9 for NLST; P ≤ .001 for both).
With this information, a clinician could initiate additional testing and/or utilize more aggressive surveillance measures. If an oncologist considered therapy for a patient with newly diagnosed cancer, treatment choices and stratification for adverse events would be more intelligently planned.
Using AI to predict the risk of lung cancer
In another study, Dr. Aerts and colleagues developed and validated a CNN called CXR-LC, which was based on CXR-risk. The goal of this study was to see if CXR-LC could predict long-term incident lung cancer using data available in the EHR, including chest radiographs, age, sex, and smoking status.
The CXR-LC model was developed using data from the PLCO trial (n = 41,856) and was validated in smokers from the PLCO trial (n = 5,615; 12-year follow-up) as well as heavy smokers from the NLST trial (n = 5,493; 6-year follow-up).
Results showed that CXR-LC was able to predict which patients were at highest risk for developing lung cancer.
CXR-LC had better discrimination for incident lung cancer than did Medicare eligibility in the PLCO data set (area under the curve, 0.755 vs. 0.634; P < .001). And the performance of CXR-LC was similar to that of the PLCOM2012 risk score in both the PLCO data set (AUC, 0.755 vs. 0.751) and the NLST data set (AUC, 0.659 vs. 0.650).
When they were compared in screening populations of equal size, CXR-LC was more sensitive than Medicare eligibility criteria in the PLCO data set (74.9% vs. 63.8%; P = .012) and missed 30.7% fewer incident lung cancer diagnoses.
AI as a substitute for specialized testing and consultation
In a third study, Dr. Aerts and colleagues used a CNN to predict cardiovascular risk by assessing coronary artery calcium (CAC) from clinically obtained, readily available CT scans.
Ordinarily, identifying CAC – an accurate predictor of cardiovascular events – requires specialized expertise (manual measurement and cardiologist interpretation), time (estimated at 20 minutes/scan), and equipment (ECG-gated cardiac CT scan and special software).
In this study, the researchers used a fully end-to-end automated system with analytic time measured in less than 2 seconds.
The team trained and tuned their CNN using the Framingham Heart Study Offspring and Third Generation cohorts (n = 1,636), which included asymptomatic patients with high-quality, cardiac-gated CT scans for CAC quantification.
The researchers then tested the CNN on two asymptomatic and two symptomatic cohorts:
- Asymptomatic Framingham Heart Study participants (n = 663) in whom the outcome measures were cardiovascular disease and death.
- Asymptomatic NLST participants (n = 14,959) in whom the outcome measure was atherosclerotic cardiovascular death.
- Symptomatic PROMISE study participants with stable chest pain (n = 4,021) in whom the outcome measures were all-cause mortality, MI, and hospitalization for unstable angina.
- Symptomatic ROMICAT-II study patients with acute chest pain (n = 441) in whom the outcome measure was acute coronary syndrome at 28 days.
Among 5,521 subjects across all testing cohorts with cardiac-gated and nongated chest CT scans, the CNN and expert reader interpretations agreed on the CAC risk scores with a high level of concordance (kappa, 0.71; concordance rate, 0.79).
There was a very high Spearman’s correlation of 0.92 (P < .0001) and substantial agreement between automatically and manually calculated CAC risk groups, substantiating robust risk prediction for cardiovascular disease across multiple clinical scenarios.
Dr. Aerts commented that, among the NLST participants who had the highest risk of developing lung cancer, the risk of cardiovascular death was as high as the risk of death from lung cancer.
Using AI to assess patient outcomes
In an unpublished study, Dr. Aerts and colleagues used AI in an attempt to determine whether changes in measurements of subcutaneous adipose tissue (SAT), visceral adipose tissue (VAT), and skeletal muscle mass would provide clues about treatment outcomes in lung cancer patients.
The researchers developed a deep learning model using data from 1,129 patients at Massachusetts General and Brigham and Women’s Hospitals, measuring SAT, VAT, and muscle mass. The team applied the measurement system to a population of 12,128 outpatients and calculated z scores for SAT, VAT, and muscle mass to determine “normal” values.
When they applied the norms to surgical lung cancer data sets from the Boston Lung Cancer Study (n = 437) and TRACERx study (n = 394), the researchers found that smokers had lower adiposity and lower muscle mass than never-smokers.
More importantly, over time, among lung cancer patients who lost greater than 5% of VAT, SAT, and muscle mass, those patients with the greatest SAT loss (P < .0001) or VAT loss (P = .0015) had the lowest lung cancer–specific survival in the TRACERx study. There was no significant impairment of lung cancer-specific survival for patients who experienced skeletal muscle loss (P = .23).
The same observation was made for overall survival among patients enrolled in the Boston Lung Cancer Study, using the 5% threshold. Overall survival was significantly worse with increasing VAT loss (P = .0023) and SAT loss (P = .0082) but not with increasing skeletal muscle loss (P = .3).
The investigators speculated about whether the correlation between body composition and clinical outcome could yield clues about tumor biology. To test this, the researchers used the RNA sequencing–based ORACLE risk score in lung cancer patients from TRACERx. There was a high correlation between higher ORACLE risk scores and lower VAT and SAT, suggesting that measures of adiposity on CT were reflected in tumor biology patterns on an RNA level in lung cancer patients. There was no such correlation between ORACLE risk scores and skeletal muscle mass.
Wonderment ... tempered by concern and challenges
AI has awe-inspiring potential to yield actionable and prognostically important information from data mining the EHR and extracting the vast quantities of information from images. In some cases (like CAC), it is information that is “hiding in plain sight.” However, Dr. Aerts expressed several cautions, some of which have already plagued AI.
He referenced the Gartner Hype Cycle, which provides a graphic representation of five phases in the life cycle of emerging technologies. The “innovation trigger” is followed by a “peak of inflated expectations,” a “trough of disillusionment,” a “slope of enlightenment,” and a “plateau of productivity.”
Dr. Aerts noted that, in recent years, AI has seemed to fall into the trough of disillusionment, but it may be entering the slope of enlightenment on the way to the plateau of productivity.
His research highlighted several examples of productivity in radiomics in cancer patients and those who are at high risk of developing cancer.
In Dr. Aerts’s opinion, a second concern is replication of AI research results. He noted that, among 400 published studies, only 6% of authors shared the codes that would enable their findings to be corroborated. About 30% shared test data, and 54% shared “pseudocodes,” but transparency and reproducibility are problems for the acceptance and broad implementation of AI.
Dr. Aerts endorsed the Modelhub initiative (www.modelhub.ai), a multi-institutional initiative to advance reproducibility in the AI field and advance its full potential.
However, there are additional concerns about the implementation of radiomics and, more generally, data mining from clinicians’ EHRs to personalize care.
Firstly, it may be laborious and difficult to explain complex, computer-based risk stratification models to patients. Hereditary cancer testing is an example of a risk assessment test that requires complicated explanations that many clinicians relegate to genetics counselors – when patients elect to see them. When a model is not explainable, it undermines the confidence of patients and their care providers, according to an editorial related to the CXR-LC study.
Another issue is that uptake of lung cancer screening, in practice, has been underutilized by individuals who meet current, relatively straightforward Medicare criteria. Despite the apparently better accuracy of the CXR-LC deep-learning model, its complexity and limited access could constitute an additional barrier for the at-risk individuals who should avail themselves of screening.
Furthermore, although age and gender are accurate in most circumstances, there is legitimate concern about the accuracy of, for example, smoking history data and comorbid conditions in current EHRs. Who performs the laborious curation of the input in an AI model to assure its accuracy for individual patients?
Finally, it is unclear how scalable and applicable AI will be to medically underserved populations (e.g., smaller, community-based, free-standing, socioeconomically disadvantaged or rural health care institutions). There are substantial initial and maintenance costs that may limit AI’s availability to some academic institutions and large health maintenance organizations.
As the concerns and challenges are addressed, it will be interesting to see where and when the plateau of productivity for AI in cancer care occurs. When it does, many cancer patients will benefit from enhanced care along the continuum of the complex disease they and their caregivers seek to master.
Dr. Aerts disclosed relationships with Onc.AI outside the presented work.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Artificial intelligence (AI) is expected to one day affect the entire continuum of cancer care – from screening and risk prediction to diagnosis, risk stratification, treatment selection, and follow-up, according to an expert in the field.
Hugo J.W.L. Aerts, PhD, director of the AI in Medicine Program at Brigham and Women’s Hospital in Boston, described studies using AI for some of these purposes during a presentation at the AACR Virtual Special Conference: Artificial Intelligence, Diagnosis, and Imaging (Abstract IA-06).
In one study, Dr. Aerts and colleagues set out to determine whether a convolutional neural network (CNN) could extract prognostic information from chest radiographs. The researchers tested this theory using patients from two trials – the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer Screening Trial and the National Lung Screening Trial (NLST).
The team developed a CNN, called CXR-risk, and tested whether it could predict the longevity and prognosis of patients in the PLCO (n = 52,320) and NLST (n = 5,493) trials over a 12-year time period, based only on chest radiographs. No clinical information, demographics, radiographic interpretations, duration of follow-up, or censoring were provided to the deep-learning system.
CXR-risk output was stratified into five categories of radiographic risk scores for probability of death, from 0 (very low likelihood of mortality) to 1 (very high likelihood of mortality).
The investigators found a graded association between radiographic risk score and mortality. The very-high-risk group had mortality rates of 53.0% (PLCO) and 33.9% (NLST). In both trials, this was significantly higher than for the very-low-risk group. The unadjusted hazard ratio was 18.3 in the PCLO data set and 15.2 in the NLST data set (P < .001 for both).
This association was maintained after adjustment for radiologists’ findings (e.g., a lung nodule) and risk factors such as age, gender, and comorbid illnesses like diabetes. The adjusted HR was 4.8 in the PCLO data set and 7.0 in the NLST data set (P < .001 for both).
In both data sets, individuals in the very-high-risk group were significantly more likely to die of lung cancer. The aHR was 11.1 in the PCLO data set and 8.4 in the NSLT data set (P < .001 for both).
This might be expected for people who were interested in being screened for lung cancer. However, patients in the very-high-risk group were also more likely to die of cardiovascular illness (aHR, 3.6 for PLCO and 47.8 for NSLT; P < .001 for both) and respiratory illness (aHR, 27.5 for PLCO and 31.9 for NLST; P ≤ .001 for both).
With this information, a clinician could initiate additional testing and/or utilize more aggressive surveillance measures. If an oncologist considered therapy for a patient with newly diagnosed cancer, treatment choices and stratification for adverse events would be more intelligently planned.
Using AI to predict the risk of lung cancer
In another study, Dr. Aerts and colleagues developed and validated a CNN called CXR-LC, which was based on CXR-risk. The goal of this study was to see if CXR-LC could predict long-term incident lung cancer using data available in the EHR, including chest radiographs, age, sex, and smoking status.
The CXR-LC model was developed using data from the PLCO trial (n = 41,856) and was validated in smokers from the PLCO trial (n = 5,615; 12-year follow-up) as well as heavy smokers from the NLST trial (n = 5,493; 6-year follow-up).
Results showed that CXR-LC was able to predict which patients were at highest risk for developing lung cancer.
CXR-LC had better discrimination for incident lung cancer than did Medicare eligibility in the PLCO data set (area under the curve, 0.755 vs. 0.634; P < .001). And the performance of CXR-LC was similar to that of the PLCOM2012 risk score in both the PLCO data set (AUC, 0.755 vs. 0.751) and the NLST data set (AUC, 0.659 vs. 0.650).
When they were compared in screening populations of equal size, CXR-LC was more sensitive than Medicare eligibility criteria in the PLCO data set (74.9% vs. 63.8%; P = .012) and missed 30.7% fewer incident lung cancer diagnoses.
AI as a substitute for specialized testing and consultation
In a third study, Dr. Aerts and colleagues used a CNN to predict cardiovascular risk by assessing coronary artery calcium (CAC) from clinically obtained, readily available CT scans.
Ordinarily, identifying CAC – an accurate predictor of cardiovascular events – requires specialized expertise (manual measurement and cardiologist interpretation), time (estimated at 20 minutes/scan), and equipment (ECG-gated cardiac CT scan and special software).
In this study, the researchers used a fully end-to-end automated system with analytic time measured in less than 2 seconds.
The team trained and tuned their CNN using the Framingham Heart Study Offspring and Third Generation cohorts (n = 1,636), which included asymptomatic patients with high-quality, cardiac-gated CT scans for CAC quantification.
The researchers then tested the CNN on two asymptomatic and two symptomatic cohorts:
- Asymptomatic Framingham Heart Study participants (n = 663) in whom the outcome measures were cardiovascular disease and death.
- Asymptomatic NLST participants (n = 14,959) in whom the outcome measure was atherosclerotic cardiovascular death.
- Symptomatic PROMISE study participants with stable chest pain (n = 4,021) in whom the outcome measures were all-cause mortality, MI, and hospitalization for unstable angina.
- Symptomatic ROMICAT-II study patients with acute chest pain (n = 441) in whom the outcome measure was acute coronary syndrome at 28 days.
Among 5,521 subjects across all testing cohorts with cardiac-gated and nongated chest CT scans, the CNN and expert reader interpretations agreed on the CAC risk scores with a high level of concordance (kappa, 0.71; concordance rate, 0.79).
There was a very high Spearman’s correlation of 0.92 (P < .0001) and substantial agreement between automatically and manually calculated CAC risk groups, substantiating robust risk prediction for cardiovascular disease across multiple clinical scenarios.
Dr. Aerts commented that, among the NLST participants who had the highest risk of developing lung cancer, the risk of cardiovascular death was as high as the risk of death from lung cancer.
Using AI to assess patient outcomes
In an unpublished study, Dr. Aerts and colleagues used AI in an attempt to determine whether changes in measurements of subcutaneous adipose tissue (SAT), visceral adipose tissue (VAT), and skeletal muscle mass would provide clues about treatment outcomes in lung cancer patients.
The researchers developed a deep learning model using data from 1,129 patients at Massachusetts General and Brigham and Women’s Hospitals, measuring SAT, VAT, and muscle mass. The team applied the measurement system to a population of 12,128 outpatients and calculated z scores for SAT, VAT, and muscle mass to determine “normal” values.
When they applied the norms to surgical lung cancer data sets from the Boston Lung Cancer Study (n = 437) and TRACERx study (n = 394), the researchers found that smokers had lower adiposity and lower muscle mass than never-smokers.
More importantly, over time, among lung cancer patients who lost greater than 5% of VAT, SAT, and muscle mass, those patients with the greatest SAT loss (P < .0001) or VAT loss (P = .0015) had the lowest lung cancer–specific survival in the TRACERx study. There was no significant impairment of lung cancer-specific survival for patients who experienced skeletal muscle loss (P = .23).
The same observation was made for overall survival among patients enrolled in the Boston Lung Cancer Study, using the 5% threshold. Overall survival was significantly worse with increasing VAT loss (P = .0023) and SAT loss (P = .0082) but not with increasing skeletal muscle loss (P = .3).
The investigators speculated about whether the correlation between body composition and clinical outcome could yield clues about tumor biology. To test this, the researchers used the RNA sequencing–based ORACLE risk score in lung cancer patients from TRACERx. There was a high correlation between higher ORACLE risk scores and lower VAT and SAT, suggesting that measures of adiposity on CT were reflected in tumor biology patterns on an RNA level in lung cancer patients. There was no such correlation between ORACLE risk scores and skeletal muscle mass.
Wonderment ... tempered by concern and challenges
AI has awe-inspiring potential to yield actionable and prognostically important information from data mining the EHR and extracting the vast quantities of information from images. In some cases (like CAC), it is information that is “hiding in plain sight.” However, Dr. Aerts expressed several cautions, some of which have already plagued AI.
He referenced the Gartner Hype Cycle, which provides a graphic representation of five phases in the life cycle of emerging technologies. The “innovation trigger” is followed by a “peak of inflated expectations,” a “trough of disillusionment,” a “slope of enlightenment,” and a “plateau of productivity.”
Dr. Aerts noted that, in recent years, AI has seemed to fall into the trough of disillusionment, but it may be entering the slope of enlightenment on the way to the plateau of productivity.
His research highlighted several examples of productivity in radiomics in cancer patients and those who are at high risk of developing cancer.
In Dr. Aerts’s opinion, a second concern is replication of AI research results. He noted that, among 400 published studies, only 6% of authors shared the codes that would enable their findings to be corroborated. About 30% shared test data, and 54% shared “pseudocodes,” but transparency and reproducibility are problems for the acceptance and broad implementation of AI.
Dr. Aerts endorsed the Modelhub initiative (www.modelhub.ai), a multi-institutional initiative to advance reproducibility in the AI field and advance its full potential.
However, there are additional concerns about the implementation of radiomics and, more generally, data mining from clinicians’ EHRs to personalize care.
Firstly, it may be laborious and difficult to explain complex, computer-based risk stratification models to patients. Hereditary cancer testing is an example of a risk assessment test that requires complicated explanations that many clinicians relegate to genetics counselors – when patients elect to see them. When a model is not explainable, it undermines the confidence of patients and their care providers, according to an editorial related to the CXR-LC study.
Another issue is that uptake of lung cancer screening, in practice, has been underutilized by individuals who meet current, relatively straightforward Medicare criteria. Despite the apparently better accuracy of the CXR-LC deep-learning model, its complexity and limited access could constitute an additional barrier for the at-risk individuals who should avail themselves of screening.
Furthermore, although age and gender are accurate in most circumstances, there is legitimate concern about the accuracy of, for example, smoking history data and comorbid conditions in current EHRs. Who performs the laborious curation of the input in an AI model to assure its accuracy for individual patients?
Finally, it is unclear how scalable and applicable AI will be to medically underserved populations (e.g., smaller, community-based, free-standing, socioeconomically disadvantaged or rural health care institutions). There are substantial initial and maintenance costs that may limit AI’s availability to some academic institutions and large health maintenance organizations.
As the concerns and challenges are addressed, it will be interesting to see where and when the plateau of productivity for AI in cancer care occurs. When it does, many cancer patients will benefit from enhanced care along the continuum of the complex disease they and their caregivers seek to master.
Dr. Aerts disclosed relationships with Onc.AI outside the presented work.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
FROM AACR: AI, DIAGNOSIS, AND IMAGING 2021
The importance of family acceptance for LGBTQ youth
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults. 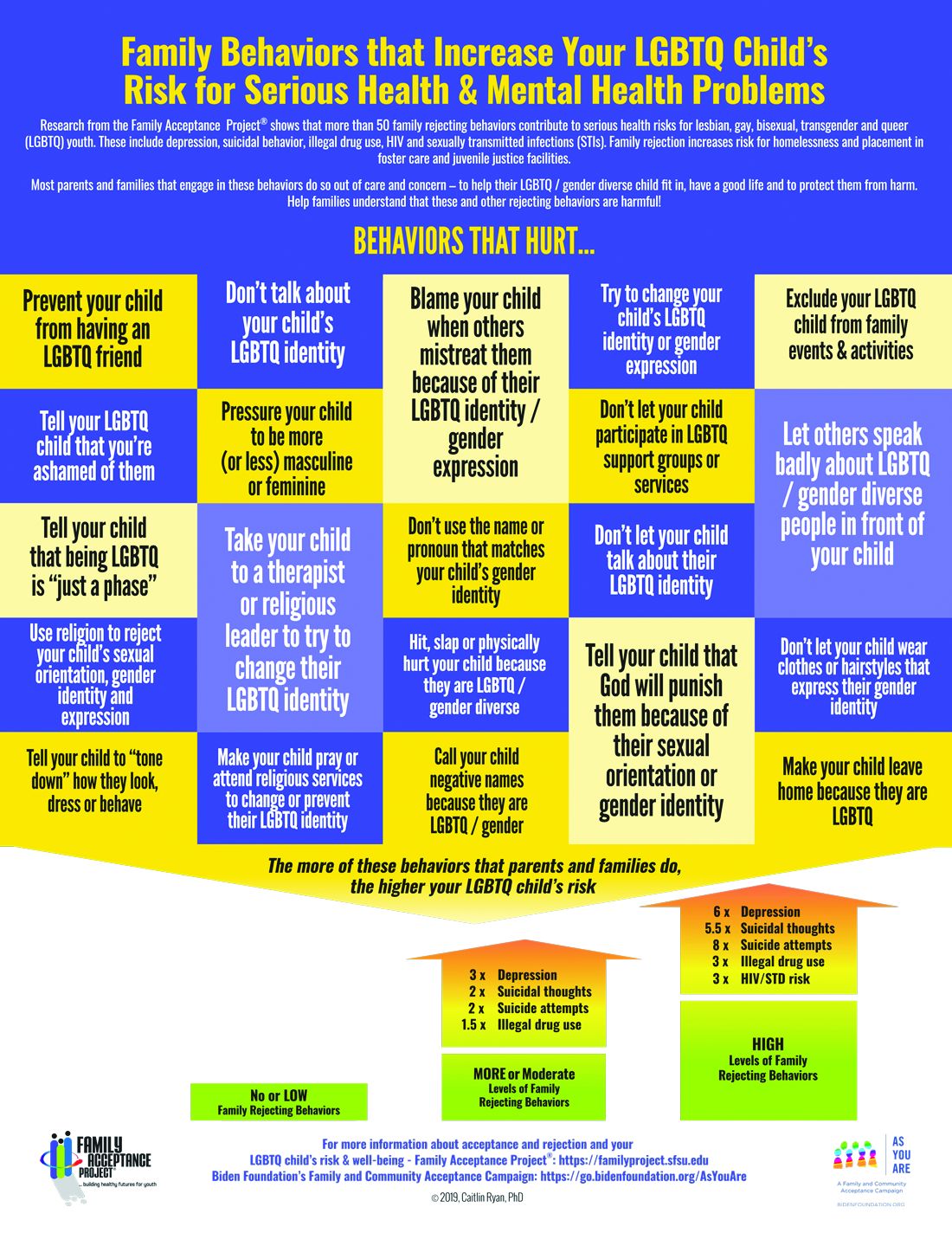
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.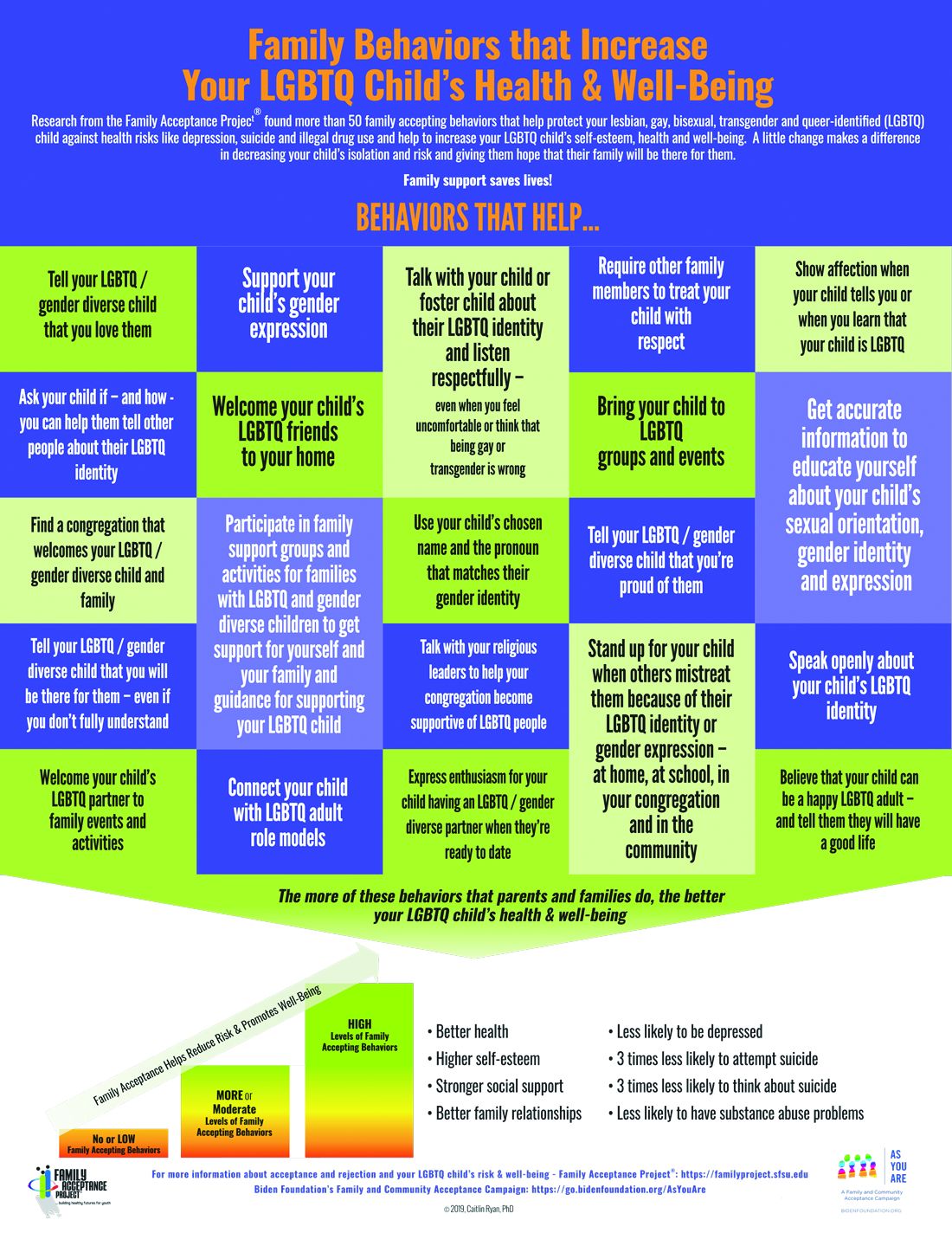
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6

To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults.
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6
To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
It is well established that LGBTQ individuals experience more health disparities compared with their cisgender, heterosexual counterparts. In general, LGBTQ adolescents and young adults have higher levels of depression, suicide attempts, and substance use than those of their heterosexual peers. However, a key protective factor is family acceptance and support. By encouraging families to modify and change behaviors that are experienced by their LGBTQ children as rejecting and to engage in supportive and affirming behaviors, providers can help families to decrease risk and promote healthy outcomes for LGBTQ youth and young adults.
We all know that a supportive family can make a difference for any child, but this is especially true for LGBTQ youth and is critical during a pandemic when young people are confined with families and separated from peers and supportive adults outside the home. Several research studies show that family support can improve outcomes related to suicide, depression, homelessness, drug use, and HIV in LGBTQ young people. Family acceptance improves health outcomes, while rejection undermines family relationships and worsens both health and other serious outcomes such as homelessness and placement in custodial care. Pediatricians can help their patients by educating parents and caregivers with LGBTQ children about the critical role of family support – both those who see themselves as accepting and those who believe that being gay or transgender is wrong and are struggling with parenting a child who identifies as LGBTQ or who is gender diverse.
The Family Acceptance Project (FAP) at San Francisco State University conducted the first research on LGBTQ youth and families, developed the first evidence-informed family support model, and has published a range of studies and evidence-based resources that demonstrate the harm caused by family rejection, validate the importance of family acceptance, and provide guidance to increase family support. FAP’s research found that parents and caregivers that engage in rejecting behaviors are typically motivated by care and concern and by trying to protect their children from harm. They believe such behaviors will help their LGBTQ children fit in, have a good life, meet cultural and religious expectations, and be respected by others.1 FAP’s research identified and measured more than 50 rejecting behaviors that parents and caregivers use to respond to their LGBTQ children. Some of these commonly expressed rejecting behaviors include ridiculing and making disparaging comments about their child and other LGBTQ people; excluding them from family activities; blaming their child when others mistreat them because they are LGBTQ; blocking access to LGBTQ resources including friends, support groups, and activities; and trying to change their child’s sexual orientation and gender identity.2 LGBTQ youth experience these and other such behaviors as hurtful, harmful, and traumatic and may feel that they need to hide or repress their identity which can affect their self-esteem, increase isolation, depression, and risky behaviors.3 Providers working with families of LGBTQ youth should focus on shared goals, such as reducing risk and having a happy, healthy child. Most parents love their children and fear for their well-being. However, many are uninformed about their child’s gender identity and sexual orientation and don’t know how to nurture and support them.
In FAP’s initial study, LGB young people who reported higher levels of family rejection had substantially higher rates of attempted suicide, depression, illegal drug use, and unprotected sex.4 These rates were even more significant among Latino gay and bisexual men.4 Those who are rejected by family are less likely to want to have a family or to be parents themselves5 and have lower educational and income levels.6
To reduce risk, pediatricians should ask LGBTQ patients about family rejecting behaviors and help parents and caregivers to identify and understand the effect of such behaviors to reduce health risks and conflict that can lead to running away, expulsion, and removal from the home. Even decreasing rejecting behaviors to moderate levels can significantly improve negative outcomes.5
Caitlin Ryan, PhD, and her team also identified and measured more than 50 family accepting behaviors that help protect against risk and promote well-being. They found that young adults who experience high levels of family acceptance during adolescence report significantly higher levels of self-esteem, social support, and general health with much lower levels of depression, suicidality, and substance abuse.7 Family accepting and supportive behaviors include talking with the child about their LGBTQ identity; advocating for their LGBTQ child when others mistreat them; requiring other family members to treat their LGBTQ child with respect; and supporting their child’s gender identity.5 FAP has developed an evidence-informed family support model and multilingual educational resources for families, providers, youth and religious leaders to decrease rejection and increase family support. These are available in print copies and for download at familyproject.sfsu.edu.
In addition, Dr. Ryan and colleagues1,4,8 recommend the following guidance for providers:
- Ask LGBTQ adolescents about family reactions to their sexual orientation, gender identity, and expression, and refer to LGBTQ community support programs and for supportive counseling, as needed.
- Identify LGBTQ community support programs and online resources to educate parents about how to help their children. Parents need culturally relevant peer support to help decrease rejection and increase family support.
- Advise parents that negative reactions to their adolescent’s LGBTQ identity may negatively impact their child’s health and mental health while supportive and affirming reactions promote well-being.
- Advise parents and caregivers to modify and change family rejecting behaviors that increase their child’s risk for suicide, depression, substance abuse ,and risky sexual behaviors.
- Expand anticipatory guidance to include information on the need for support and the link between family rejection and negative health problems.
- Provide guidance on sexual orientation and gender identity as part of normative child development during well-baby and early childhood care.
- Use FAP’s multilingual family education booklets and Healthy Futures poster series in family and patient education and provide these materials in clinical and community settings. FAP’s Healthy Futures posters include a poster guidance, a version on family acceptance, a version on family rejection and a family acceptance version for conservative families and settings. They are available in camera-ready art in four sizes in English and Spanish and are forthcoming in five Asian languages: familyproject.sfsu.edu/poster.
Dr. Lawlis is assistant professor of pediatrics at the University of Oklahoma Health Sciences Center, Oklahoma City, and an adolescent medicine specialist at OU Children’s. She has no relevant financial disclosures.
Resources
• Family Acceptance Project – consultation and training; evidence-based educational materials for families, providers, religious leaders and youth.
• PFLAG – peer support for parents and friends with LGBTQ children in all states and several other countries.
References
1. Ryan C. Generating a revolution in prevention, wellness & care for LGBT children & youth. Temple Political & Civil Rights Law Review. 2014;23(2):331-44.
2. Ryan C. Healthy Futures Poster Series – Family Accepting & Rejecting Behaviors That Impact LGBTQ Children’s Health & Well-Being. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2019.
3. Ryan C. Family Acceptance Project: Culturally grounded framework for supporting LGBTQ children and youth. J Am Acad Child Adolesc Psychiatr. 2019;58(10):S58-9.
4. Ryan C et al. Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346-52.
5. Ryan C. Supportive families, healthy children: Helping families with lesbian, gay, bisexual & transgender children. In: Family Acceptance Project Marian Wright Edelman Institute SFSU, ed. San Francisco, CA2009.
6. Ryan C et al. Parent-initiated sexual orientation change efforts with LGBT adolescents: Implications for young adult mental health and adjustment. J Homosexuality. 2020;67(2):159-73.
7. Ryan C et al. Family acceptance in adolescence and the health of LGBT young adults. J Child Adolesc Psychiatr Nursing. 2010;23(4):205-13. 8. Substance Abuse and Mental Health Services Administration. A Practitioner’s Guide: Helping Families to Support Their LGBT Children. In: Administration SAaMhS, ed. Vol PEP14-LGBTKIDS. Rockville, MD: HHS Publication; 2014.
Child ‘Mis’behavior – What’s ‘mis’ing?
“What kind of parent are you? Why don’t you straighten him out!” rants the woman being jostled in the grocery store by your patient. “Easy for you to say,” thinks your patient’s frazzled and now insulted parent.

Blaming the parent for an out-of-control child has historically been a common refrain of neighbors, relatives, and even strangers. But considering child behavior as resulting from both parent and child factors is central to the current transactional model of child development. In this model, mismatch of the parent’s and child’s response patterns is seen as setting them up for chronically rough interactions around parent requests/demands. A parent escalating quickly from a briefly stated request to a tirade may create more tension paired with an anxious child who takes time to act, for example. Once a parent (and ultimately the child) recognize patterns in what leads to conflict, they can become more proactive in predicting and negotiating these situations. Ross Greene, PhD, explains this in his book “The Explosive Child,” calling the method Collaborative Problem Solving (now Collaborative & Proactive Solutions or CPS).
While there are general principles parents can use to modify what they consider “mis”behaviors, these methods often do not account for the “missing” skills of the individual child (and parent) predisposing to those “mis”takes. Thinking of misbehaviors as being because of a kind of “learning disability” in the child rather than willful defiance can help cool off interactions by instead focusing on solving the underlying problem.
What kinds of “gaps in skills” set a child up for defiant or explosive reactions? If you think about what features of children, and parent-child relationships are associated with harmonious interactions this becomes evident. Children over 3 who are patient, easygoing, flexible or adaptable, and good at transitions and problem-solving can delay gratification and tolerate frustration, regulate their emotions, explain their desires, and multitask. They are better at reading the parent’s needs and intent and tend to interpret requests as positive or at least neutral and are more likely to comply with parent requests without a fuss.
What? No kid you know is great at all of these? These skills, at best variable, develop with maturation. Some are part of temperament, considered normal variation in personality. For example, so-called difficult temperament includes low adaptability, high-intensity reactions, low regularity, tendency to withdraw, and negative mood. But in the extreme, weaknesses in these skills are core to or comorbid with diagnosable mental health disorders. Defiance and irritable responses are criteria for oppositional defiant disorder (ODD), and less severe categories called aggressive/oppositional problem or variation. ODD is often found in children diagnosed with ADHD (65%), Tourette’s (15%-65%), depression (70% if severe), bipolar disorder (85%), OCD, anxiety (45%), autism, and language-processing disorders (55%), or trauma. These conditions variably include lower emotion regulation, poorer executive functioning including poor task shifting and impulsivity, obsessiveness, lower expressive and receptive communication skills, and less social awareness that facilitates harmonious problem solving.
The basic components of the CPS approach to addressing parent-child conflict sound intuitive but defining them clearly is important when families are stuck. There are three levels of plans. If the problem is an emergency or nonnegotiable, e.g., child hurting the cat, it may call for Plan A – parent-imposed solutions, sometimes with consequences or rewards. As children mature, Plan A should be used less frequently. If solving the problem is not a top life priority, Plan C – postponing action, may be appropriate. Plan C highlights that behavior change is a long-term project and “picking your fights” is important.
The biggest value of CPS for resolving behavior problems comes from intermediate Plan B. In Plan B the first step of problem solving for parents facing child defiance or upset is to empathically and nonjudgmentally figure out the child’s concern. Questions such as “I’ve noticed that when I remind you that it is trash night you start shouting. What’s up with that?” then patiently asking about the who, what, where, and when of their concern and checking to ensure understanding. Specificity is important as well as noting times when the reaction occurs or not.
Once the child’s concern is clear, e.g., feeling that the demand to take out the trash now interrupts his games during the only time his friends are online, the parents should echo the child’s concern then express their own concern about how the behavior is affecting them and others, potentially including the child; e.g., mother is so upset by the shouting that she can’t sleep, and worry that the child is not learning responsibility, and then checking for child understanding.
Finally, the parent invites brainstorming for a solution that addresses both of their concerns, first asking the child for suggestions, aiming for a strategy that is realistic and specific. Children reluctant to make suggestions may need more time and the parent may be wondering “if there is a way for both of our concerns to be addressed.” Solutions chosen are then tried for several weeks, success tracked, and needed changes negotiated.
For parents, using a collaborative approach to dealing with their child’s behavior takes skills they may not have at the moment, or ever. Especially under the stresses of COVID-19 lockdown, taking a step back from an encounter to consider lack of a skill to turn off the video game promptly when a Zoom meeting starts is challenging. Parents may also genetically share the child’s predisposing ADHD, anxiety, depression, OCD, or weakness in communication or social sensitivity.
Sometimes part of the solution for a conflict is for the parent to reduce expectations. This requires understanding and accepting the child’s cognitive or emotional limitations. Reducing expectations is ideally done before a request rather than by giving in after it, which reinforces protests. For authoritarian adults rigid in their belief that parents are boss, changing expectations can be tough and can feel like losing control or failing as a leader. One benefit of working with a CPS coach (see livesinthebalance.org or ThinkKids.org) is to help parents identify their own limitations.
Predicting the types of demands that tend to create conflict, such as to act immediately or be flexible about options, allows parents to prioritize those requests for calmer moments or when there is more time for discussion. Reviewing a checklist of common gaps in skills and creating a list of expectations and triggers that are difficult for the child helps the family be more proactive in developing solutions. Authors of CPS have validated a checklist of skill deficits, “Thinking Skills Inventory,” to facilitate detection of gaps that is educational plus useful for planning specific solutions.
CPS has been shown in randomized trials with both parent groups and in home counseling to be as effective as Parent Training in reducing oppositional behavior and reducing maternal stress, with effects lasting even longer.
CPS Plan B notably has no reward or punishment components as it assumes the child wants to behave acceptably but can’t; has the “will but not the skill.” When skill deficits are worked around the child is satisfied with complying and pleasing the parents. The idea of a “function” of the misbehavior for the child of gaining attention or reward or avoiding consequences is reinterpreted as serving to communicate the problem the child is having trouble in meeting the parent’s demand. When the parent understands and helps the child solve the problem his/her misbehavior is no longer needed. A benefit of the communication and mutual problem solving used in CPS is on not only improving behavior but empowering parents and children, building parental empathy, and improving child skills.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
Reference
Greene RW et al. A transactional model of oppositional behavior: Underpinnings of the Collaborative Problem Solving approach. J Psychosom Res. 2003;55(1):67-75.
“What kind of parent are you? Why don’t you straighten him out!” rants the woman being jostled in the grocery store by your patient. “Easy for you to say,” thinks your patient’s frazzled and now insulted parent.
Blaming the parent for an out-of-control child has historically been a common refrain of neighbors, relatives, and even strangers. But considering child behavior as resulting from both parent and child factors is central to the current transactional model of child development. In this model, mismatch of the parent’s and child’s response patterns is seen as setting them up for chronically rough interactions around parent requests/demands. A parent escalating quickly from a briefly stated request to a tirade may create more tension paired with an anxious child who takes time to act, for example. Once a parent (and ultimately the child) recognize patterns in what leads to conflict, they can become more proactive in predicting and negotiating these situations. Ross Greene, PhD, explains this in his book “The Explosive Child,” calling the method Collaborative Problem Solving (now Collaborative & Proactive Solutions or CPS).
While there are general principles parents can use to modify what they consider “mis”behaviors, these methods often do not account for the “missing” skills of the individual child (and parent) predisposing to those “mis”takes. Thinking of misbehaviors as being because of a kind of “learning disability” in the child rather than willful defiance can help cool off interactions by instead focusing on solving the underlying problem.
What kinds of “gaps in skills” set a child up for defiant or explosive reactions? If you think about what features of children, and parent-child relationships are associated with harmonious interactions this becomes evident. Children over 3 who are patient, easygoing, flexible or adaptable, and good at transitions and problem-solving can delay gratification and tolerate frustration, regulate their emotions, explain their desires, and multitask. They are better at reading the parent’s needs and intent and tend to interpret requests as positive or at least neutral and are more likely to comply with parent requests without a fuss.
What? No kid you know is great at all of these? These skills, at best variable, develop with maturation. Some are part of temperament, considered normal variation in personality. For example, so-called difficult temperament includes low adaptability, high-intensity reactions, low regularity, tendency to withdraw, and negative mood. But in the extreme, weaknesses in these skills are core to or comorbid with diagnosable mental health disorders. Defiance and irritable responses are criteria for oppositional defiant disorder (ODD), and less severe categories called aggressive/oppositional problem or variation. ODD is often found in children diagnosed with ADHD (65%), Tourette’s (15%-65%), depression (70% if severe), bipolar disorder (85%), OCD, anxiety (45%), autism, and language-processing disorders (55%), or trauma. These conditions variably include lower emotion regulation, poorer executive functioning including poor task shifting and impulsivity, obsessiveness, lower expressive and receptive communication skills, and less social awareness that facilitates harmonious problem solving.
The basic components of the CPS approach to addressing parent-child conflict sound intuitive but defining them clearly is important when families are stuck. There are three levels of plans. If the problem is an emergency or nonnegotiable, e.g., child hurting the cat, it may call for Plan A – parent-imposed solutions, sometimes with consequences or rewards. As children mature, Plan A should be used less frequently. If solving the problem is not a top life priority, Plan C – postponing action, may be appropriate. Plan C highlights that behavior change is a long-term project and “picking your fights” is important.
The biggest value of CPS for resolving behavior problems comes from intermediate Plan B. In Plan B the first step of problem solving for parents facing child defiance or upset is to empathically and nonjudgmentally figure out the child’s concern. Questions such as “I’ve noticed that when I remind you that it is trash night you start shouting. What’s up with that?” then patiently asking about the who, what, where, and when of their concern and checking to ensure understanding. Specificity is important as well as noting times when the reaction occurs or not.
Once the child’s concern is clear, e.g., feeling that the demand to take out the trash now interrupts his games during the only time his friends are online, the parents should echo the child’s concern then express their own concern about how the behavior is affecting them and others, potentially including the child; e.g., mother is so upset by the shouting that she can’t sleep, and worry that the child is not learning responsibility, and then checking for child understanding.
Finally, the parent invites brainstorming for a solution that addresses both of their concerns, first asking the child for suggestions, aiming for a strategy that is realistic and specific. Children reluctant to make suggestions may need more time and the parent may be wondering “if there is a way for both of our concerns to be addressed.” Solutions chosen are then tried for several weeks, success tracked, and needed changes negotiated.
For parents, using a collaborative approach to dealing with their child’s behavior takes skills they may not have at the moment, or ever. Especially under the stresses of COVID-19 lockdown, taking a step back from an encounter to consider lack of a skill to turn off the video game promptly when a Zoom meeting starts is challenging. Parents may also genetically share the child’s predisposing ADHD, anxiety, depression, OCD, or weakness in communication or social sensitivity.
Sometimes part of the solution for a conflict is for the parent to reduce expectations. This requires understanding and accepting the child’s cognitive or emotional limitations. Reducing expectations is ideally done before a request rather than by giving in after it, which reinforces protests. For authoritarian adults rigid in their belief that parents are boss, changing expectations can be tough and can feel like losing control or failing as a leader. One benefit of working with a CPS coach (see livesinthebalance.org or ThinkKids.org) is to help parents identify their own limitations.
Predicting the types of demands that tend to create conflict, such as to act immediately or be flexible about options, allows parents to prioritize those requests for calmer moments or when there is more time for discussion. Reviewing a checklist of common gaps in skills and creating a list of expectations and triggers that are difficult for the child helps the family be more proactive in developing solutions. Authors of CPS have validated a checklist of skill deficits, “Thinking Skills Inventory,” to facilitate detection of gaps that is educational plus useful for planning specific solutions.
CPS has been shown in randomized trials with both parent groups and in home counseling to be as effective as Parent Training in reducing oppositional behavior and reducing maternal stress, with effects lasting even longer.
CPS Plan B notably has no reward or punishment components as it assumes the child wants to behave acceptably but can’t; has the “will but not the skill.” When skill deficits are worked around the child is satisfied with complying and pleasing the parents. The idea of a “function” of the misbehavior for the child of gaining attention or reward or avoiding consequences is reinterpreted as serving to communicate the problem the child is having trouble in meeting the parent’s demand. When the parent understands and helps the child solve the problem his/her misbehavior is no longer needed. A benefit of the communication and mutual problem solving used in CPS is on not only improving behavior but empowering parents and children, building parental empathy, and improving child skills.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
Reference
Greene RW et al. A transactional model of oppositional behavior: Underpinnings of the Collaborative Problem Solving approach. J Psychosom Res. 2003;55(1):67-75.
“What kind of parent are you? Why don’t you straighten him out!” rants the woman being jostled in the grocery store by your patient. “Easy for you to say,” thinks your patient’s frazzled and now insulted parent.
Blaming the parent for an out-of-control child has historically been a common refrain of neighbors, relatives, and even strangers. But considering child behavior as resulting from both parent and child factors is central to the current transactional model of child development. In this model, mismatch of the parent’s and child’s response patterns is seen as setting them up for chronically rough interactions around parent requests/demands. A parent escalating quickly from a briefly stated request to a tirade may create more tension paired with an anxious child who takes time to act, for example. Once a parent (and ultimately the child) recognize patterns in what leads to conflict, they can become more proactive in predicting and negotiating these situations. Ross Greene, PhD, explains this in his book “The Explosive Child,” calling the method Collaborative Problem Solving (now Collaborative & Proactive Solutions or CPS).
While there are general principles parents can use to modify what they consider “mis”behaviors, these methods often do not account for the “missing” skills of the individual child (and parent) predisposing to those “mis”takes. Thinking of misbehaviors as being because of a kind of “learning disability” in the child rather than willful defiance can help cool off interactions by instead focusing on solving the underlying problem.
What kinds of “gaps in skills” set a child up for defiant or explosive reactions? If you think about what features of children, and parent-child relationships are associated with harmonious interactions this becomes evident. Children over 3 who are patient, easygoing, flexible or adaptable, and good at transitions and problem-solving can delay gratification and tolerate frustration, regulate their emotions, explain their desires, and multitask. They are better at reading the parent’s needs and intent and tend to interpret requests as positive or at least neutral and are more likely to comply with parent requests without a fuss.
What? No kid you know is great at all of these? These skills, at best variable, develop with maturation. Some are part of temperament, considered normal variation in personality. For example, so-called difficult temperament includes low adaptability, high-intensity reactions, low regularity, tendency to withdraw, and negative mood. But in the extreme, weaknesses in these skills are core to or comorbid with diagnosable mental health disorders. Defiance and irritable responses are criteria for oppositional defiant disorder (ODD), and less severe categories called aggressive/oppositional problem or variation. ODD is often found in children diagnosed with ADHD (65%), Tourette’s (15%-65%), depression (70% if severe), bipolar disorder (85%), OCD, anxiety (45%), autism, and language-processing disorders (55%), or trauma. These conditions variably include lower emotion regulation, poorer executive functioning including poor task shifting and impulsivity, obsessiveness, lower expressive and receptive communication skills, and less social awareness that facilitates harmonious problem solving.
The basic components of the CPS approach to addressing parent-child conflict sound intuitive but defining them clearly is important when families are stuck. There are three levels of plans. If the problem is an emergency or nonnegotiable, e.g., child hurting the cat, it may call for Plan A – parent-imposed solutions, sometimes with consequences or rewards. As children mature, Plan A should be used less frequently. If solving the problem is not a top life priority, Plan C – postponing action, may be appropriate. Plan C highlights that behavior change is a long-term project and “picking your fights” is important.
The biggest value of CPS for resolving behavior problems comes from intermediate Plan B. In Plan B the first step of problem solving for parents facing child defiance or upset is to empathically and nonjudgmentally figure out the child’s concern. Questions such as “I’ve noticed that when I remind you that it is trash night you start shouting. What’s up with that?” then patiently asking about the who, what, where, and when of their concern and checking to ensure understanding. Specificity is important as well as noting times when the reaction occurs or not.
Once the child’s concern is clear, e.g., feeling that the demand to take out the trash now interrupts his games during the only time his friends are online, the parents should echo the child’s concern then express their own concern about how the behavior is affecting them and others, potentially including the child; e.g., mother is so upset by the shouting that she can’t sleep, and worry that the child is not learning responsibility, and then checking for child understanding.
Finally, the parent invites brainstorming for a solution that addresses both of their concerns, first asking the child for suggestions, aiming for a strategy that is realistic and specific. Children reluctant to make suggestions may need more time and the parent may be wondering “if there is a way for both of our concerns to be addressed.” Solutions chosen are then tried for several weeks, success tracked, and needed changes negotiated.
For parents, using a collaborative approach to dealing with their child’s behavior takes skills they may not have at the moment, or ever. Especially under the stresses of COVID-19 lockdown, taking a step back from an encounter to consider lack of a skill to turn off the video game promptly when a Zoom meeting starts is challenging. Parents may also genetically share the child’s predisposing ADHD, anxiety, depression, OCD, or weakness in communication or social sensitivity.
Sometimes part of the solution for a conflict is for the parent to reduce expectations. This requires understanding and accepting the child’s cognitive or emotional limitations. Reducing expectations is ideally done before a request rather than by giving in after it, which reinforces protests. For authoritarian adults rigid in their belief that parents are boss, changing expectations can be tough and can feel like losing control or failing as a leader. One benefit of working with a CPS coach (see livesinthebalance.org or ThinkKids.org) is to help parents identify their own limitations.
Predicting the types of demands that tend to create conflict, such as to act immediately or be flexible about options, allows parents to prioritize those requests for calmer moments or when there is more time for discussion. Reviewing a checklist of common gaps in skills and creating a list of expectations and triggers that are difficult for the child helps the family be more proactive in developing solutions. Authors of CPS have validated a checklist of skill deficits, “Thinking Skills Inventory,” to facilitate detection of gaps that is educational plus useful for planning specific solutions.
CPS has been shown in randomized trials with both parent groups and in home counseling to be as effective as Parent Training in reducing oppositional behavior and reducing maternal stress, with effects lasting even longer.
CPS Plan B notably has no reward or punishment components as it assumes the child wants to behave acceptably but can’t; has the “will but not the skill.” When skill deficits are worked around the child is satisfied with complying and pleasing the parents. The idea of a “function” of the misbehavior for the child of gaining attention or reward or avoiding consequences is reinterpreted as serving to communicate the problem the child is having trouble in meeting the parent’s demand. When the parent understands and helps the child solve the problem his/her misbehavior is no longer needed. A benefit of the communication and mutual problem solving used in CPS is on not only improving behavior but empowering parents and children, building parental empathy, and improving child skills.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
Reference
Greene RW et al. A transactional model of oppositional behavior: Underpinnings of the Collaborative Problem Solving approach. J Psychosom Res. 2003;55(1):67-75.
The lost year – even for common respiratory viruses
In this column in September 2020, you read how common respiratory viruses’ seasons are usually so predictable, each virus arising, peaking, and then dying out in a predictable virus parade (Figure 1).1 Well, the predictable virus seasonal pattern was lost in 2020. Since March of 2020, it is striking how little activity was detected for the usual seasonal viruses in Kansas City after mid-March 2020 (Figure 2).2 So, my concern in September 2020 for possible rampant coinfections of common viruses with or in tandem with SARS-CoV-2 did not pan out. That said, the seasons for non–SARS-CoV-2 viruses did change; I just didn’t expect they would nearly disappear.
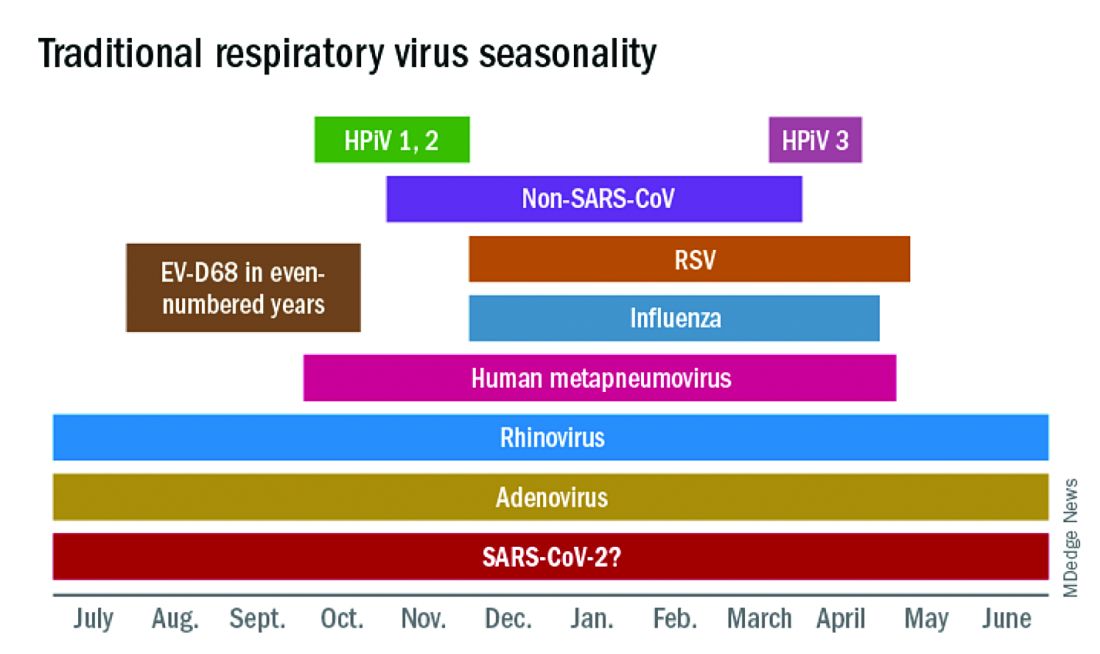
The 2020 winter-spring. In the first quarter (the last part of the overall 2019-2020 respiratory viral season), viral detections were chugging along as usual up to mid-March (Figure 2); influenza, respiratory syncytial virus (RSV), and rhinovirus were the big players.
Influenza. In most years, influenza type B leads off and is quickly replaced by type A only to see B reemerge to end influenza season in March-April. In early 2020, both influenza type A and influenza type B cocirculated nearly equally, but both dropped like a rock in mid-March (Figure 2).2 Neither type has been seen since with the exception of sporadic detections – perhaps being false positives.
RSV. In the usual year in temperate mid-latitudes of the northern hemisphere, RSV season usually starts in early December, peaks in January-March, and declines gradually until the end of RSV season in April (Figure 1). In southern latitudes, RSV is less seasonal, being present most of the year, but peaking in “winter” months.3 But in 2020, RSV also disappeared in mid-March and has yet to reappear.
Other viruses. Small bumps in detection of parainfluenza of varying types usually frame influenza season, one B bump in early autumn and another in April-May. In most years, human metapneumovirus is detected on and off, with worse years at 2- to 3-year intervals. Adenovirus occurs year-round with bumps as children get back to school in autumn. Yet in 2020, almost no parainfluenza, adenovirus, common coronaviruses, or human metapneumovirus were detected in either spring or autumn. This was supposed to be a banner summer-autumn for EV-D68 – but almost none was detected. Interestingly, the cockroach of viruses, rhinovirus, has its usual year (Figure 2).
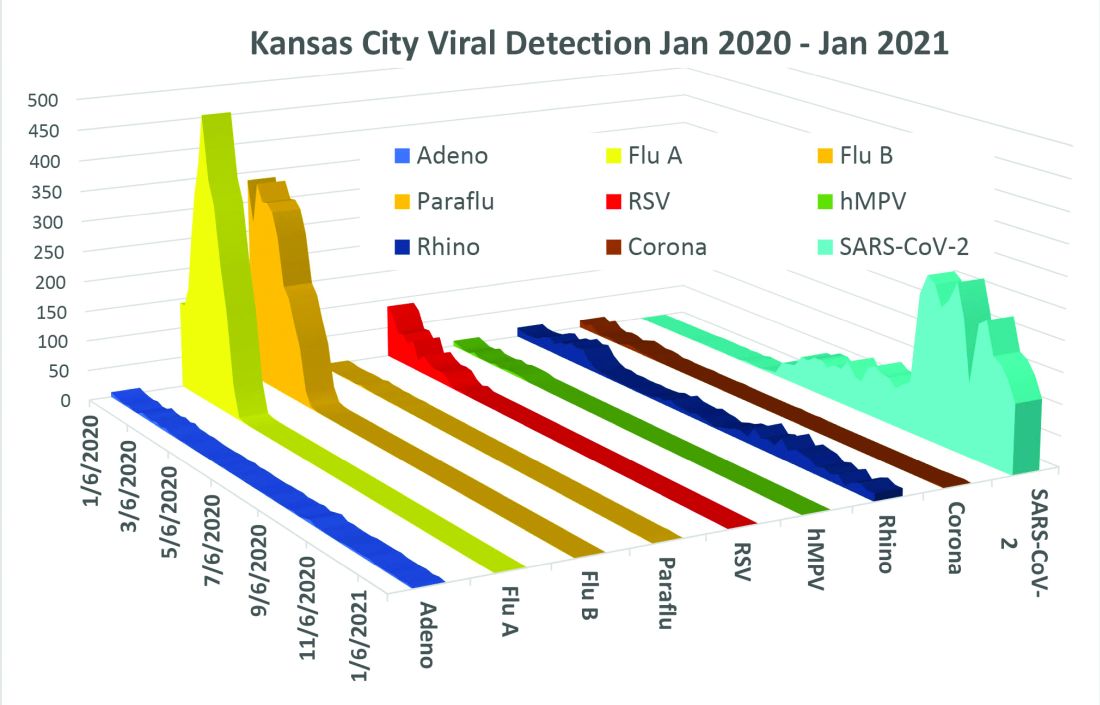
What happened? Intense social mitigation interventions, including social distancing and closing daycares and schools, were likely major factors.4 For influenza, vaccine may have helped but uptake was not remarkably better than most prior years. There may have been “viral competition,”where a new or highly transmissible virus outcompetes less-transmissible viruses with lower affinity for respiratory receptors.5,6 Note that SARS-CoV-2 has very high affinity for the ACE2 receptor and has been highly prevalent. So, SARS-CoV-2 could fit the theoretical mold for a virus that outcompetes others.
Does it matter for the future? Blunted 2019-2020 and nearly absent 2020-2021 respiratory virus season may have set the stage for intense 2021-2022 rebounds for the non–SARS-CoV-2 viruses. We now have two whole and one partial birth cohort with no experience with seasonal respiratory viruses, including EV-D68 (and nonrespiratory viruses too – like norovirus, parechovirus, and other enteroviruses). Most viruses have particularly bad seasons every 2-3 years, thought to be caused by increasing accumulation of susceptible individuals in consecutive birth cohorts until a critical mass of susceptible individuals is achieved. The excess in susceptible individuals means that each contagious case is likely to expose one or more susceptible individuals, enhancing transmission and infection numbers in an ever-extending ripple effect. We have never had this many children aged under 3 years with no immunity to influenza, RSV, etc. So unless mother nature is kind (when has that happened lately?), expect rebound years for seasonal viruses as children return to daycare/schools and as social mitigation becomes less necessary in the waning pandemic.

Options? If you ramped up telehealth visits for the pandemic, that may be a saving grace, i.e., more efficiency so more “visits” can be completed per day, and less potential contact in reception rooms between well and ill children. And if there was ever a time to really intensify efforts to immunize all our pediatric patients, the next two seasons are just that. Adding a bit of a warning to families with young children also seems warranted. If they understand that, while 2021-2022 will be better for SARS-CoV-2, it is likely going to be worse for the other viruses.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. Harrison CJ. 2020-2021 respiratory viral season: Onset, presentations, and testing likely to differ in pandemic, Pediatric News: September 17, 2020.
2. Olsen SJ et al. MMWR Morb Mortal Wkly Rep. 2020;69:1305-9.
3. Respiratory Syncytial Virus Surveillance. http://www.floridahealth.gov/diseases-and-conditions/respiratory-syncytial-virus/_documents/2021-w4-rsv-summary.pdf
4. Baker RE et al. PNAS. Dec 2020 117;(48):30547-53.
5. Sema Nickbakhsh et al. PNAS. Dec 2019 116;(52):27142-50.
6. Kirsten M et al. PNAS. Mar 2020 117;(13):6987.
In this column in September 2020, you read how common respiratory viruses’ seasons are usually so predictable, each virus arising, peaking, and then dying out in a predictable virus parade (Figure 1).1 Well, the predictable virus seasonal pattern was lost in 2020. Since March of 2020, it is striking how little activity was detected for the usual seasonal viruses in Kansas City after mid-March 2020 (Figure 2).2 So, my concern in September 2020 for possible rampant coinfections of common viruses with or in tandem with SARS-CoV-2 did not pan out. That said, the seasons for non–SARS-CoV-2 viruses did change; I just didn’t expect they would nearly disappear.
The 2020 winter-spring. In the first quarter (the last part of the overall 2019-2020 respiratory viral season), viral detections were chugging along as usual up to mid-March (Figure 2); influenza, respiratory syncytial virus (RSV), and rhinovirus were the big players.
Influenza. In most years, influenza type B leads off and is quickly replaced by type A only to see B reemerge to end influenza season in March-April. In early 2020, both influenza type A and influenza type B cocirculated nearly equally, but both dropped like a rock in mid-March (Figure 2).2 Neither type has been seen since with the exception of sporadic detections – perhaps being false positives.
RSV. In the usual year in temperate mid-latitudes of the northern hemisphere, RSV season usually starts in early December, peaks in January-March, and declines gradually until the end of RSV season in April (Figure 1). In southern latitudes, RSV is less seasonal, being present most of the year, but peaking in “winter” months.3 But in 2020, RSV also disappeared in mid-March and has yet to reappear.
Other viruses. Small bumps in detection of parainfluenza of varying types usually frame influenza season, one B bump in early autumn and another in April-May. In most years, human metapneumovirus is detected on and off, with worse years at 2- to 3-year intervals. Adenovirus occurs year-round with bumps as children get back to school in autumn. Yet in 2020, almost no parainfluenza, adenovirus, common coronaviruses, or human metapneumovirus were detected in either spring or autumn. This was supposed to be a banner summer-autumn for EV-D68 – but almost none was detected. Interestingly, the cockroach of viruses, rhinovirus, has its usual year (Figure 2).
What happened? Intense social mitigation interventions, including social distancing and closing daycares and schools, were likely major factors.4 For influenza, vaccine may have helped but uptake was not remarkably better than most prior years. There may have been “viral competition,”where a new or highly transmissible virus outcompetes less-transmissible viruses with lower affinity for respiratory receptors.5,6 Note that SARS-CoV-2 has very high affinity for the ACE2 receptor and has been highly prevalent. So, SARS-CoV-2 could fit the theoretical mold for a virus that outcompetes others.
Does it matter for the future? Blunted 2019-2020 and nearly absent 2020-2021 respiratory virus season may have set the stage for intense 2021-2022 rebounds for the non–SARS-CoV-2 viruses. We now have two whole and one partial birth cohort with no experience with seasonal respiratory viruses, including EV-D68 (and nonrespiratory viruses too – like norovirus, parechovirus, and other enteroviruses). Most viruses have particularly bad seasons every 2-3 years, thought to be caused by increasing accumulation of susceptible individuals in consecutive birth cohorts until a critical mass of susceptible individuals is achieved. The excess in susceptible individuals means that each contagious case is likely to expose one or more susceptible individuals, enhancing transmission and infection numbers in an ever-extending ripple effect. We have never had this many children aged under 3 years with no immunity to influenza, RSV, etc. So unless mother nature is kind (when has that happened lately?), expect rebound years for seasonal viruses as children return to daycare/schools and as social mitigation becomes less necessary in the waning pandemic.
Options? If you ramped up telehealth visits for the pandemic, that may be a saving grace, i.e., more efficiency so more “visits” can be completed per day, and less potential contact in reception rooms between well and ill children. And if there was ever a time to really intensify efforts to immunize all our pediatric patients, the next two seasons are just that. Adding a bit of a warning to families with young children also seems warranted. If they understand that, while 2021-2022 will be better for SARS-CoV-2, it is likely going to be worse for the other viruses.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. Harrison CJ. 2020-2021 respiratory viral season: Onset, presentations, and testing likely to differ in pandemic, Pediatric News: September 17, 2020.
2. Olsen SJ et al. MMWR Morb Mortal Wkly Rep. 2020;69:1305-9.
3. Respiratory Syncytial Virus Surveillance. http://www.floridahealth.gov/diseases-and-conditions/respiratory-syncytial-virus/_documents/2021-w4-rsv-summary.pdf
4. Baker RE et al. PNAS. Dec 2020 117;(48):30547-53.
5. Sema Nickbakhsh et al. PNAS. Dec 2019 116;(52):27142-50.
6. Kirsten M et al. PNAS. Mar 2020 117;(13):6987.
In this column in September 2020, you read how common respiratory viruses’ seasons are usually so predictable, each virus arising, peaking, and then dying out in a predictable virus parade (Figure 1).1 Well, the predictable virus seasonal pattern was lost in 2020. Since March of 2020, it is striking how little activity was detected for the usual seasonal viruses in Kansas City after mid-March 2020 (Figure 2).2 So, my concern in September 2020 for possible rampant coinfections of common viruses with or in tandem with SARS-CoV-2 did not pan out. That said, the seasons for non–SARS-CoV-2 viruses did change; I just didn’t expect they would nearly disappear.
The 2020 winter-spring. In the first quarter (the last part of the overall 2019-2020 respiratory viral season), viral detections were chugging along as usual up to mid-March (Figure 2); influenza, respiratory syncytial virus (RSV), and rhinovirus were the big players.
Influenza. In most years, influenza type B leads off and is quickly replaced by type A only to see B reemerge to end influenza season in March-April. In early 2020, both influenza type A and influenza type B cocirculated nearly equally, but both dropped like a rock in mid-March (Figure 2).2 Neither type has been seen since with the exception of sporadic detections – perhaps being false positives.
RSV. In the usual year in temperate mid-latitudes of the northern hemisphere, RSV season usually starts in early December, peaks in January-March, and declines gradually until the end of RSV season in April (Figure 1). In southern latitudes, RSV is less seasonal, being present most of the year, but peaking in “winter” months.3 But in 2020, RSV also disappeared in mid-March and has yet to reappear.
Other viruses. Small bumps in detection of parainfluenza of varying types usually frame influenza season, one B bump in early autumn and another in April-May. In most years, human metapneumovirus is detected on and off, with worse years at 2- to 3-year intervals. Adenovirus occurs year-round with bumps as children get back to school in autumn. Yet in 2020, almost no parainfluenza, adenovirus, common coronaviruses, or human metapneumovirus were detected in either spring or autumn. This was supposed to be a banner summer-autumn for EV-D68 – but almost none was detected. Interestingly, the cockroach of viruses, rhinovirus, has its usual year (Figure 2).
What happened? Intense social mitigation interventions, including social distancing and closing daycares and schools, were likely major factors.4 For influenza, vaccine may have helped but uptake was not remarkably better than most prior years. There may have been “viral competition,”where a new or highly transmissible virus outcompetes less-transmissible viruses with lower affinity for respiratory receptors.5,6 Note that SARS-CoV-2 has very high affinity for the ACE2 receptor and has been highly prevalent. So, SARS-CoV-2 could fit the theoretical mold for a virus that outcompetes others.
Does it matter for the future? Blunted 2019-2020 and nearly absent 2020-2021 respiratory virus season may have set the stage for intense 2021-2022 rebounds for the non–SARS-CoV-2 viruses. We now have two whole and one partial birth cohort with no experience with seasonal respiratory viruses, including EV-D68 (and nonrespiratory viruses too – like norovirus, parechovirus, and other enteroviruses). Most viruses have particularly bad seasons every 2-3 years, thought to be caused by increasing accumulation of susceptible individuals in consecutive birth cohorts until a critical mass of susceptible individuals is achieved. The excess in susceptible individuals means that each contagious case is likely to expose one or more susceptible individuals, enhancing transmission and infection numbers in an ever-extending ripple effect. We have never had this many children aged under 3 years with no immunity to influenza, RSV, etc. So unless mother nature is kind (when has that happened lately?), expect rebound years for seasonal viruses as children return to daycare/schools and as social mitigation becomes less necessary in the waning pandemic.
Options? If you ramped up telehealth visits for the pandemic, that may be a saving grace, i.e., more efficiency so more “visits” can be completed per day, and less potential contact in reception rooms between well and ill children. And if there was ever a time to really intensify efforts to immunize all our pediatric patients, the next two seasons are just that. Adding a bit of a warning to families with young children also seems warranted. If they understand that, while 2021-2022 will be better for SARS-CoV-2, it is likely going to be worse for the other viruses.
Dr. Harrison is professor of pediatrics and pediatric infectious diseases at Children’s Mercy Hospitals and Clinics, Kansas City, Mo. He said he had no relevant financial disclosures. Email him at pdnews@mdedge.com.
References
1. Harrison CJ. 2020-2021 respiratory viral season: Onset, presentations, and testing likely to differ in pandemic, Pediatric News: September 17, 2020.
2. Olsen SJ et al. MMWR Morb Mortal Wkly Rep. 2020;69:1305-9.
3. Respiratory Syncytial Virus Surveillance. http://www.floridahealth.gov/diseases-and-conditions/respiratory-syncytial-virus/_documents/2021-w4-rsv-summary.pdf
4. Baker RE et al. PNAS. Dec 2020 117;(48):30547-53.
5. Sema Nickbakhsh et al. PNAS. Dec 2019 116;(52):27142-50.
6. Kirsten M et al. PNAS. Mar 2020 117;(13):6987.
COVID-19: Helping patients overcome what might feel like an existential crisis
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.

Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.
Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
Way back in the spring of last year, I wrote about a pandemic of posttraumatic stress disorder that would descend upon us because of COVID-19. At the time, we were told that, by summer – June or July 2020 – all the steps we needed to take to stay ahead of the virus, including remaining socially distant, and yes, even wearing masks, would be over. Life would get back to normal.
Little did we know that a national plan for our safety, including making sure that we had enough masks and PPE, would not be forthcoming, and that so many thousands of Americans would perish, leaving millions of distraught families and friends.
So many people are suffering. Mothers, for example, are struggling to balance remote schooling with additional child care and domestic work. More than 2 million women left the U.S. workforce last year between February 2020 and October 2020, according to a report by the National Women’s Law Center. Even before COVID-19, loneliness among young adults was considered a domestic epidemic – and the social isolation forced by the pandemic has worsened those trends, research shows. These trends are creating so much more anxiety, depression, despair, and yes, even PTSD. As mental health professionals, we have a lot of work to do in educating people about coping skills and in providing treatments when appropriate.
Experiences take on new meaning
One day a friend and professional colleague called me, and he sounded quite distraught. He had not been able to reach his primary care physician and thought that, as a physician, I might have some insights about his symptoms. He began telling me that something really strange was happening whenever he walked around outside with his mask on. He couldn’t breathe with it on, he told me. In addition, his eyes teared up, his nose started running, and his eyeglasses fogged up so much that he couldn’t see where he was going. He was really anxious, nervous, and felt a great sense of despair – and disorientation. He did not fully understand what was happening and didn’t know whether those disorienting symptoms were mask-related or whether he was incubating some yet undiagnosed illness.
I addressed his concerns in the moment by assuring him that I, too, had been experiencing similar challenges with fogged-up glasses and a runny nose; many people were experiencing some of the same things. I explained that even I had called an allergist to find out whether I might be allergic to some component in the mask and whether he had seen those symptoms in his practice.
Albeit, those issues tied to masks are relatively minor, compared with the enormous psychological toll this pandemic has taken on some people. But it’s clear that different people suffer different effects in light of the marked changes in life and lifestyles caused by the pandemic.
‘It’s something else’
Two people I know, both professionals, recently told me that in their social lives they constantly feel tired and anxious, and that their concentration has diminished. They worry more about their futures, they told me separately. (They don’t know each other.) They reported going through daily life “like being on automatic.” Both said they were far too irritable and reported feeling that social isolation had dulled their thinking.
They said they were not depressed; “it’s something else.” I reassured them both that this would pass with time and suggested that they work at not socially isolating – to the extent that they can – during the pandemic. I also encouraged them to get vaccinated and to talk with a professional if their malaise was altering their level of functioning.
So far, more than 475,000 people in the United States have died of COVID-19, and thousands continue to suffer. People are saying goodbye to loved ones on iPads, and watching news stories about hospitals at overcapacity and refrigeration units storing bodies. Meanwhile, health care workers, many of whom are putting their lives and those of their families at risk, are reporting increased levels of burnout – and moral injury.
Value of relaxation techniques
We know that the latest mitigation measures advised by the Centers for Disease Control and Prevention must continue during the COVID-19 vaccination process. The new CDC guidelines on the value of double masking make sense and should be followed. However, even as we learn more about the virus and how to stop its spread, we must recognize that social distancing is not the same as social isolation. We must continue to do what we can to maintain social relationships and keep open the lines of communication, including the use of virtual tools. I am pleased to see the growth of telemedicine during the pandemic. When applicable, telemedicine allows greater medical and mental health care without the stress of travel and the risk of exposure to more people than necessary.
, whether it’s hypnosis, mindfulness, transcendental meditation, or deep breathing exercises. For the more advanced therapies, guided imagery can help patients develop a sense of calm and equanimity.
For those who are not skilled in relaxation techniques, YouTube offers some excellent programs that teach relaxation and mindfulness. Another thing I do is talk regularly with people I know and sometimes with people I know I’ll disagree with – just to keep my brain active. I also try to learn new things in my spare time to establish new brain pathways and stay mentally active.
The pain and grief tied to the pandemic are unlike anything we’ve ever experienced. Our training as psychiatrists, psychologists, and other mental health care professionals makes us all uniquely suited to assist patients as they process these traumatic times. We must step forward and do so.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (Kettlehole Publishing, 2019). He has no conflicts of interest.
State of the evidence: Treatment-resistant depression in children and adolescents
Case
Max was a 17-year-old boy and avid video gamer who, predating COVID-19, was within a major depressive episode and continued to meet criteria through the duration of COVID-19 quarantine. He lives with his mother, who is a single mom and is working hard in a variety of jobs through the pandemic. Max had little motivation to engage in sports or other activities, and despite doing well enough in school, he spent much of his days escaping into video games and social media, where his friends communicated and bonded the most. He has had very little response to complete trials of two different selective serotonin reuptake inhibitors (SSRIs), and the off-label attempts at a serotonin-norepinephrine reuptake inhibitor and bupropion augmentation of an SSRI, as extrapolated by his pediatrician from adult data on treatment-resistant depression. He had ongoing supportive psychotherapy and his mother and pediatrician were wary of changing that relationship, as they were just happy he would engage at all. His shy nature made him very wary of attending any programs or groups. He had no other diagnosis including anxiety, substance abuse disorder, or learning disorder.
Case discussion
As a child and adolescent psychiatrist embedded in primary care practices, I (like you) am seeing more and more parents, children, and families struggling with depression through the course of this unprecedented and challenging year.

Max presented to me with his mother at the request of his primary care physician because within the course of many medication trials, it had been over 6 months of persistent symptoms without an end in sight for him, his family, or his primary care provider (PCP).
His diagnosis was treatment-resistant depression and his PCP was grasping at adult strategies to manage this all with additional psychopharmacology. As a consulting child-and-adolescent psychiatrist in primary care, how could I help the PCP? I too worry if there is anything that I can do to shift depression once standard treatments fail, and when the idea of engaging in behavioral activation or other pro-health activities is just too much for a depressed adolescent to bear. I weigh that with what is known about the evidence, and the good data driving us beyond medication solutions. I often find that it can be helpful to reiterate the following points to providers and families.
First, what to know about depression in kids
Depression looks different at different ages in children. In school-aged children, it’s widely known that irritability or psychosomatic symptoms (frequent headaches and stomach aches) can be the first preverbal signs of an emerging anxiety and depressive disorder in children. In adolescents, one would maybe expect more typical melancholic adult-like symptoms of depression; however, there is mounting evidence that adolescents actually present with more classically “atypical symptoms” of depression (low motivation, weight gain, escapism to sleep or video games, as with Max) with less persistence across setting (home, work, school) compared with adults (“Diagnosing Depression in Children and Adolescents” by Glen R. Elliott, PhD, MD, from The Carlat Child Psychiatry Report, November 2015, Antidepressant Use in Children).In addition, major life stressors (the breakup of a romantic relationship, failing a class, bullying) can be perceived as more permanent, and suicidal thinking can be acute and lethal in these contexts. With Max, it was accepted by all who were supporting him that he was struggling with depression, which is the first step in managing this well.
The idea of the designated patient
Often left out in a discussion of pediatric patients is the family. As a designated patient, much of our focus is on improving the symptoms of the patient in front of us. Parents direct their gaze at the child as the one with the condition who needs support. First following identification of depression, I find that a reframe of a diagnosis can be useful. Family systems theory approaches a child with a depression diagnosis, and says, that if one family member changes, even in a small way, a family as a system is forced to change. With a sense of an external locus of control, we often are left with a patient and parent feeling stuck. To provide a reorientation to the parents, ask how they are feeling. Can they get treatment for depression knowing the biology of the condition or consider making behavioral changes of their own and as a family? Can they consider family psychotherapy so they can cope better and break some cycles of maladaptive engagement shared across a family? These kinds of reorientations can be useful to shift the idea of treatment from the designated patient (the child) and medication options (limited data for kids who aren’t responding to them) to a family approach. Making the depression management strategy a family affair can help the entire family shift from seeing the only option as medications or interventions exclusively directed at a child. The Vermont Center for Children, Youth, and Families at the University of Vermont Medical Center has many pioneering developments in addressing family-based approaches to mental health concerns in the pediatric population, and can serve as a source of inspiration for this shift in discussing depression.
Practical strategies for the pediatrician
Medications can be useful for treating child and adolescent depression, but there is also strong evidence for psychotherapy, working with the child’s school and family, and different forms of behavioral activation (exercise, mindfulness, yoga, and other positive activities). Medications, if one is looking at standard of care treatment and Food and Drug Administration approval exclusively, is limited in scope and should not be the only intervention considered, as described in the case above.
In “The Use of Medication in Treating Childhood and Adolescent Depression: Information for Patients and Families,” which is a practical guide prepared by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, it is noted that Prozac and Lexapro are approved medications, as follows:
- Antidepressant medications can be effective in relieving the symptoms of depression for some children and adolescents. One antidepressant – fluoxetine, or Prozac – a medicine in the category of SSRIs, has been approved by the FDA for treating depression in children 8 years of age and older. Escitalopram, or Lexapro, has also been approved by the FDA for treating adolescents 12 years of age and older.
- About “60 percent of children and adolescents will respond to initial treatment with medication,” which leaves many children needing further interventions. “Of those who don’t [respond], a significant number may respond to another medication but also may respond to the addition of a form of psychotherapy called cognitive behavioral therapy (CBT).”
It is common, as in the case above, that a connection with a therapist or support is valued over the specific modality even if it’s not showing improvement or outcomes. It is important to consider CBT as a form of evidence-based treatment for children with depression and to cite the famous “Treatment for Adolescents with Depression Study (TADS)” funded by the National Institute of Mental Health, published in 2004, that shows the following findings: “After 12 weeks of treatment, 71 percent of the patients who received the combination of medication and CBT were much improved.” In looking at the group that does not improve with medications alone, adolescents in particular can have more gains with the addition of CBT.
Tracking progress, little by little
Often we reflexively ask parents of depressed children: Are they better? And we ask the child: How do you feel? It can be difficult for parents to reflect on that, or see progress or gains from appointment to appointment. I suggest trying to use structured measures and tools to frame a discussion with progress on medication and treatment such as what is available at the Mood Treatment Center website.I also suggest apps such as Mood Kit,which is for mood tracking with some CBT exercises in addition to behavioral activation strategies for children and parents. It can be useful to have families take some ownership of tracking their moods and what may be playing into them. In particular with the pandemic, we can reflect on how much isolation or socialization, activities, sleep, eating habits, and exercise can affect us and make corresponding behavioral changes as a family to improve our own coping. Depression itself can be like glasses clouding one’s vision in gray, and that can also cloud one’s review of progress. When we hear comments such as “nothing gets better” from a child or parent, it may be helpful to try to track any contributing factors to a persistent low mood and acknowledge any slow and steady progress.
In summary, we can strive as providers to maximize our approach to depression in children and adolescents beyond the limited FDA-approved medications, or extrapolating adult data to children. If we emphasize the evidence-based practice of CBT and other interventions in addition to encouraging a tracking and review of outcomes measures with parents and families, we can empower them to make meaningful change in both perspectives and behaviors that can perpetuate depressive states.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington.
Case
Max was a 17-year-old boy and avid video gamer who, predating COVID-19, was within a major depressive episode and continued to meet criteria through the duration of COVID-19 quarantine. He lives with his mother, who is a single mom and is working hard in a variety of jobs through the pandemic. Max had little motivation to engage in sports or other activities, and despite doing well enough in school, he spent much of his days escaping into video games and social media, where his friends communicated and bonded the most. He has had very little response to complete trials of two different selective serotonin reuptake inhibitors (SSRIs), and the off-label attempts at a serotonin-norepinephrine reuptake inhibitor and bupropion augmentation of an SSRI, as extrapolated by his pediatrician from adult data on treatment-resistant depression. He had ongoing supportive psychotherapy and his mother and pediatrician were wary of changing that relationship, as they were just happy he would engage at all. His shy nature made him very wary of attending any programs or groups. He had no other diagnosis including anxiety, substance abuse disorder, or learning disorder.
Case discussion
As a child and adolescent psychiatrist embedded in primary care practices, I (like you) am seeing more and more parents, children, and families struggling with depression through the course of this unprecedented and challenging year.
Max presented to me with his mother at the request of his primary care physician because within the course of many medication trials, it had been over 6 months of persistent symptoms without an end in sight for him, his family, or his primary care provider (PCP).
His diagnosis was treatment-resistant depression and his PCP was grasping at adult strategies to manage this all with additional psychopharmacology. As a consulting child-and-adolescent psychiatrist in primary care, how could I help the PCP? I too worry if there is anything that I can do to shift depression once standard treatments fail, and when the idea of engaging in behavioral activation or other pro-health activities is just too much for a depressed adolescent to bear. I weigh that with what is known about the evidence, and the good data driving us beyond medication solutions. I often find that it can be helpful to reiterate the following points to providers and families.
First, what to know about depression in kids
Depression looks different at different ages in children. In school-aged children, it’s widely known that irritability or psychosomatic symptoms (frequent headaches and stomach aches) can be the first preverbal signs of an emerging anxiety and depressive disorder in children. In adolescents, one would maybe expect more typical melancholic adult-like symptoms of depression; however, there is mounting evidence that adolescents actually present with more classically “atypical symptoms” of depression (low motivation, weight gain, escapism to sleep or video games, as with Max) with less persistence across setting (home, work, school) compared with adults (“Diagnosing Depression in Children and Adolescents” by Glen R. Elliott, PhD, MD, from The Carlat Child Psychiatry Report, November 2015, Antidepressant Use in Children).In addition, major life stressors (the breakup of a romantic relationship, failing a class, bullying) can be perceived as more permanent, and suicidal thinking can be acute and lethal in these contexts. With Max, it was accepted by all who were supporting him that he was struggling with depression, which is the first step in managing this well.
The idea of the designated patient
Often left out in a discussion of pediatric patients is the family. As a designated patient, much of our focus is on improving the symptoms of the patient in front of us. Parents direct their gaze at the child as the one with the condition who needs support. First following identification of depression, I find that a reframe of a diagnosis can be useful. Family systems theory approaches a child with a depression diagnosis, and says, that if one family member changes, even in a small way, a family as a system is forced to change. With a sense of an external locus of control, we often are left with a patient and parent feeling stuck. To provide a reorientation to the parents, ask how they are feeling. Can they get treatment for depression knowing the biology of the condition or consider making behavioral changes of their own and as a family? Can they consider family psychotherapy so they can cope better and break some cycles of maladaptive engagement shared across a family? These kinds of reorientations can be useful to shift the idea of treatment from the designated patient (the child) and medication options (limited data for kids who aren’t responding to them) to a family approach. Making the depression management strategy a family affair can help the entire family shift from seeing the only option as medications or interventions exclusively directed at a child. The Vermont Center for Children, Youth, and Families at the University of Vermont Medical Center has many pioneering developments in addressing family-based approaches to mental health concerns in the pediatric population, and can serve as a source of inspiration for this shift in discussing depression.
Practical strategies for the pediatrician
Medications can be useful for treating child and adolescent depression, but there is also strong evidence for psychotherapy, working with the child’s school and family, and different forms of behavioral activation (exercise, mindfulness, yoga, and other positive activities). Medications, if one is looking at standard of care treatment and Food and Drug Administration approval exclusively, is limited in scope and should not be the only intervention considered, as described in the case above.
In “The Use of Medication in Treating Childhood and Adolescent Depression: Information for Patients and Families,” which is a practical guide prepared by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, it is noted that Prozac and Lexapro are approved medications, as follows:
- Antidepressant medications can be effective in relieving the symptoms of depression for some children and adolescents. One antidepressant – fluoxetine, or Prozac – a medicine in the category of SSRIs, has been approved by the FDA for treating depression in children 8 years of age and older. Escitalopram, or Lexapro, has also been approved by the FDA for treating adolescents 12 years of age and older.
- About “60 percent of children and adolescents will respond to initial treatment with medication,” which leaves many children needing further interventions. “Of those who don’t [respond], a significant number may respond to another medication but also may respond to the addition of a form of psychotherapy called cognitive behavioral therapy (CBT).”
It is common, as in the case above, that a connection with a therapist or support is valued over the specific modality even if it’s not showing improvement or outcomes. It is important to consider CBT as a form of evidence-based treatment for children with depression and to cite the famous “Treatment for Adolescents with Depression Study (TADS)” funded by the National Institute of Mental Health, published in 2004, that shows the following findings: “After 12 weeks of treatment, 71 percent of the patients who received the combination of medication and CBT were much improved.” In looking at the group that does not improve with medications alone, adolescents in particular can have more gains with the addition of CBT.
Tracking progress, little by little
Often we reflexively ask parents of depressed children: Are they better? And we ask the child: How do you feel? It can be difficult for parents to reflect on that, or see progress or gains from appointment to appointment. I suggest trying to use structured measures and tools to frame a discussion with progress on medication and treatment such as what is available at the Mood Treatment Center website.I also suggest apps such as Mood Kit,which is for mood tracking with some CBT exercises in addition to behavioral activation strategies for children and parents. It can be useful to have families take some ownership of tracking their moods and what may be playing into them. In particular with the pandemic, we can reflect on how much isolation or socialization, activities, sleep, eating habits, and exercise can affect us and make corresponding behavioral changes as a family to improve our own coping. Depression itself can be like glasses clouding one’s vision in gray, and that can also cloud one’s review of progress. When we hear comments such as “nothing gets better” from a child or parent, it may be helpful to try to track any contributing factors to a persistent low mood and acknowledge any slow and steady progress.
In summary, we can strive as providers to maximize our approach to depression in children and adolescents beyond the limited FDA-approved medications, or extrapolating adult data to children. If we emphasize the evidence-based practice of CBT and other interventions in addition to encouraging a tracking and review of outcomes measures with parents and families, we can empower them to make meaningful change in both perspectives and behaviors that can perpetuate depressive states.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington.
Case
Max was a 17-year-old boy and avid video gamer who, predating COVID-19, was within a major depressive episode and continued to meet criteria through the duration of COVID-19 quarantine. He lives with his mother, who is a single mom and is working hard in a variety of jobs through the pandemic. Max had little motivation to engage in sports or other activities, and despite doing well enough in school, he spent much of his days escaping into video games and social media, where his friends communicated and bonded the most. He has had very little response to complete trials of two different selective serotonin reuptake inhibitors (SSRIs), and the off-label attempts at a serotonin-norepinephrine reuptake inhibitor and bupropion augmentation of an SSRI, as extrapolated by his pediatrician from adult data on treatment-resistant depression. He had ongoing supportive psychotherapy and his mother and pediatrician were wary of changing that relationship, as they were just happy he would engage at all. His shy nature made him very wary of attending any programs or groups. He had no other diagnosis including anxiety, substance abuse disorder, or learning disorder.
Case discussion
As a child and adolescent psychiatrist embedded in primary care practices, I (like you) am seeing more and more parents, children, and families struggling with depression through the course of this unprecedented and challenging year.
Max presented to me with his mother at the request of his primary care physician because within the course of many medication trials, it had been over 6 months of persistent symptoms without an end in sight for him, his family, or his primary care provider (PCP).
His diagnosis was treatment-resistant depression and his PCP was grasping at adult strategies to manage this all with additional psychopharmacology. As a consulting child-and-adolescent psychiatrist in primary care, how could I help the PCP? I too worry if there is anything that I can do to shift depression once standard treatments fail, and when the idea of engaging in behavioral activation or other pro-health activities is just too much for a depressed adolescent to bear. I weigh that with what is known about the evidence, and the good data driving us beyond medication solutions. I often find that it can be helpful to reiterate the following points to providers and families.
First, what to know about depression in kids
Depression looks different at different ages in children. In school-aged children, it’s widely known that irritability or psychosomatic symptoms (frequent headaches and stomach aches) can be the first preverbal signs of an emerging anxiety and depressive disorder in children. In adolescents, one would maybe expect more typical melancholic adult-like symptoms of depression; however, there is mounting evidence that adolescents actually present with more classically “atypical symptoms” of depression (low motivation, weight gain, escapism to sleep or video games, as with Max) with less persistence across setting (home, work, school) compared with adults (“Diagnosing Depression in Children and Adolescents” by Glen R. Elliott, PhD, MD, from The Carlat Child Psychiatry Report, November 2015, Antidepressant Use in Children).In addition, major life stressors (the breakup of a romantic relationship, failing a class, bullying) can be perceived as more permanent, and suicidal thinking can be acute and lethal in these contexts. With Max, it was accepted by all who were supporting him that he was struggling with depression, which is the first step in managing this well.
The idea of the designated patient
Often left out in a discussion of pediatric patients is the family. As a designated patient, much of our focus is on improving the symptoms of the patient in front of us. Parents direct their gaze at the child as the one with the condition who needs support. First following identification of depression, I find that a reframe of a diagnosis can be useful. Family systems theory approaches a child with a depression diagnosis, and says, that if one family member changes, even in a small way, a family as a system is forced to change. With a sense of an external locus of control, we often are left with a patient and parent feeling stuck. To provide a reorientation to the parents, ask how they are feeling. Can they get treatment for depression knowing the biology of the condition or consider making behavioral changes of their own and as a family? Can they consider family psychotherapy so they can cope better and break some cycles of maladaptive engagement shared across a family? These kinds of reorientations can be useful to shift the idea of treatment from the designated patient (the child) and medication options (limited data for kids who aren’t responding to them) to a family approach. Making the depression management strategy a family affair can help the entire family shift from seeing the only option as medications or interventions exclusively directed at a child. The Vermont Center for Children, Youth, and Families at the University of Vermont Medical Center has many pioneering developments in addressing family-based approaches to mental health concerns in the pediatric population, and can serve as a source of inspiration for this shift in discussing depression.
Practical strategies for the pediatrician
Medications can be useful for treating child and adolescent depression, but there is also strong evidence for psychotherapy, working with the child’s school and family, and different forms of behavioral activation (exercise, mindfulness, yoga, and other positive activities). Medications, if one is looking at standard of care treatment and Food and Drug Administration approval exclusively, is limited in scope and should not be the only intervention considered, as described in the case above.
In “The Use of Medication in Treating Childhood and Adolescent Depression: Information for Patients and Families,” which is a practical guide prepared by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, it is noted that Prozac and Lexapro are approved medications, as follows:
- Antidepressant medications can be effective in relieving the symptoms of depression for some children and adolescents. One antidepressant – fluoxetine, or Prozac – a medicine in the category of SSRIs, has been approved by the FDA for treating depression in children 8 years of age and older. Escitalopram, or Lexapro, has also been approved by the FDA for treating adolescents 12 years of age and older.
- About “60 percent of children and adolescents will respond to initial treatment with medication,” which leaves many children needing further interventions. “Of those who don’t [respond], a significant number may respond to another medication but also may respond to the addition of a form of psychotherapy called cognitive behavioral therapy (CBT).”
It is common, as in the case above, that a connection with a therapist or support is valued over the specific modality even if it’s not showing improvement or outcomes. It is important to consider CBT as a form of evidence-based treatment for children with depression and to cite the famous “Treatment for Adolescents with Depression Study (TADS)” funded by the National Institute of Mental Health, published in 2004, that shows the following findings: “After 12 weeks of treatment, 71 percent of the patients who received the combination of medication and CBT were much improved.” In looking at the group that does not improve with medications alone, adolescents in particular can have more gains with the addition of CBT.
Tracking progress, little by little
Often we reflexively ask parents of depressed children: Are they better? And we ask the child: How do you feel? It can be difficult for parents to reflect on that, or see progress or gains from appointment to appointment. I suggest trying to use structured measures and tools to frame a discussion with progress on medication and treatment such as what is available at the Mood Treatment Center website.I also suggest apps such as Mood Kit,which is for mood tracking with some CBT exercises in addition to behavioral activation strategies for children and parents. It can be useful to have families take some ownership of tracking their moods and what may be playing into them. In particular with the pandemic, we can reflect on how much isolation or socialization, activities, sleep, eating habits, and exercise can affect us and make corresponding behavioral changes as a family to improve our own coping. Depression itself can be like glasses clouding one’s vision in gray, and that can also cloud one’s review of progress. When we hear comments such as “nothing gets better” from a child or parent, it may be helpful to try to track any contributing factors to a persistent low mood and acknowledge any slow and steady progress.
In summary, we can strive as providers to maximize our approach to depression in children and adolescents beyond the limited FDA-approved medications, or extrapolating adult data to children. If we emphasize the evidence-based practice of CBT and other interventions in addition to encouraging a tracking and review of outcomes measures with parents and families, we can empower them to make meaningful change in both perspectives and behaviors that can perpetuate depressive states.
Dr. Pawlowski is an adult, adolescent, and child psychiatrist at the University of Vermont Medical Center and assistant professor of psychiatry at the Larner College of Medicine at UVM in Burlington.