User login
In-Office Diagnostic Needle Arthroscopy: Understanding the Potential Value for the US Healthcare System
Take-Home Points
- In-office diagnostic needle arthroscopy is a minimally invasive, rapid method for identification of intra-articular joint pathology.
- Cost savings of a significant value can be realized to both the patient and healthcare system via small-bore needle arthroscopy as opposed to MRI.
- Diagnostic needle arthroscopy can lead to quicker identification of pathology than MRI.
- Diagnostic needle arthroscopy can reduce the number of undue "formal" surgical diagnostic arthroscopies.
- Standardization of image quality of small bore arthroscopy may pose benefits to the variable quality of MRI.
Patient satisfaction and healthcare costs have taken a leading role in today’s health care market. Patient satisfaction, often categorized as the "patient experience," can be measured on numerous levels, such as access to healthcare professionals and diagnostic testing, wait time for appointments, and timely test results. Furthermore, patients’ having a full understanding of their pathology and treatment options may correlate with their overall satisfaction. Some metrics are subjective, but procedure costs are objective.
The algorithm for treating patients who present with knee or shoulder pathology to an orthopedic office involves taking a thorough history, performing a physical examination, and, in many cases, obtaining diagnostic imaging. After arriving at a diagnosis, the physician plans the patient’s treatment. In most cases in which magnetic resonance imaging (MRI) is required, the process can take 2 to 3 weeks.1
Surgical knee arthroscopy is one of the most common procedures in the United States.2,3 Worldwide, more than 2 million knee arthroscopies are performed yearly.4 For most procedures, the decision to treat is based on physical examination findings, and the diagnosis is confirmed with MRI. MRI has 86% sensitivity and 91% specificity for diagnosing ligamentous and meniscal tears.5 However, regular use of MRI has led to increased healthcare expenditures and a larger financial burden for patients, which can delay diagnosis.6
Since 2000, MRI use in the United States has risen significantly—by 10% over a 10-year period.7 According to a 2013 population analysis, 107 in 1000 US inhabitants had an MRI yearly.8
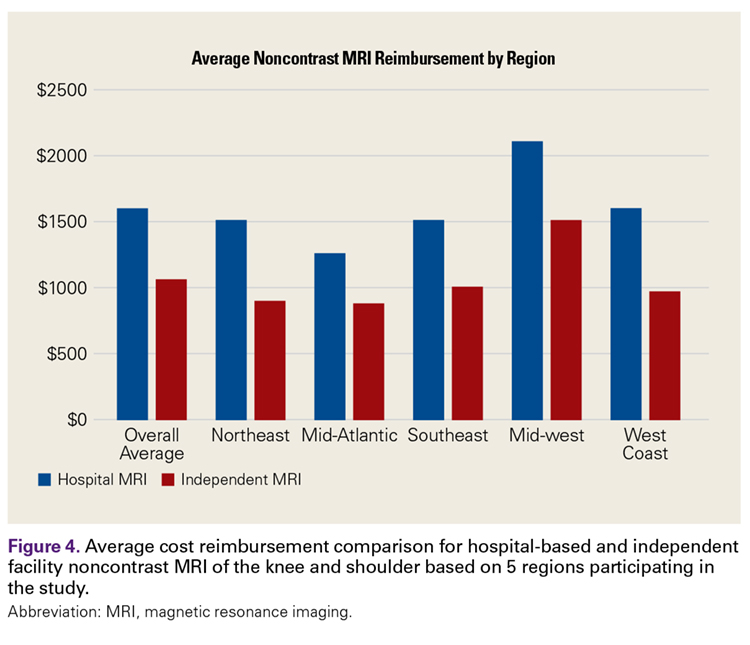
MRI costs vary widely because of several factors, including state/regional consideration, scanning in a hospital or an independent facility, and use of contrast and arthrography. In a 2017 study of the variation in noncontrast MRI costs at 71 hospitals and 26 independent facilities in Iowa, Westermann and colleagues9 found that, excluding radiologist interpretation fees, the mean MRI technical component cost to consumers was US $1874 (SD, $694; range, $500-$4000).
Patient factors may preclude use of MRI (Table).
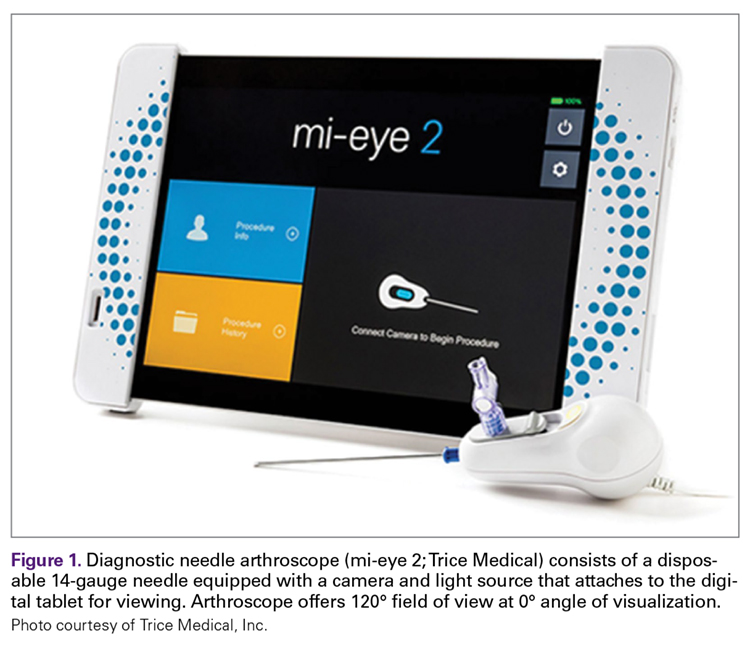
Small-bore needle arthroscopy is a cost-effective alternative diagnostic tool with efficacy and accuracy similar to those of MRI and standard arthroscopy for intra-articular pathologies.6,11 The procedure is performed with a disposable handpiece equipped with an internal light source and optics; this handpiece attaches to a reusable tablet for ease of transportation and visualization (Figure 1).
In 2014, Voigt and colleagues6 reported a significant net healthcare system cost saving with use of a small-needle arthroscope for diagnostic testing. The saving was estimated at $115 million to $177 million for simple isolation of medial meniscus pathology—or, more specifically, for appropriate care after more accurate visualization with the diagnostic needle arthroscope coupled with a decrease in false positives compared with MRI use. Other factors include the economic impact of the patient’s lost work hours, often associated with the time off needed for the MRI and for the follow-up visit for review of results.
Methods
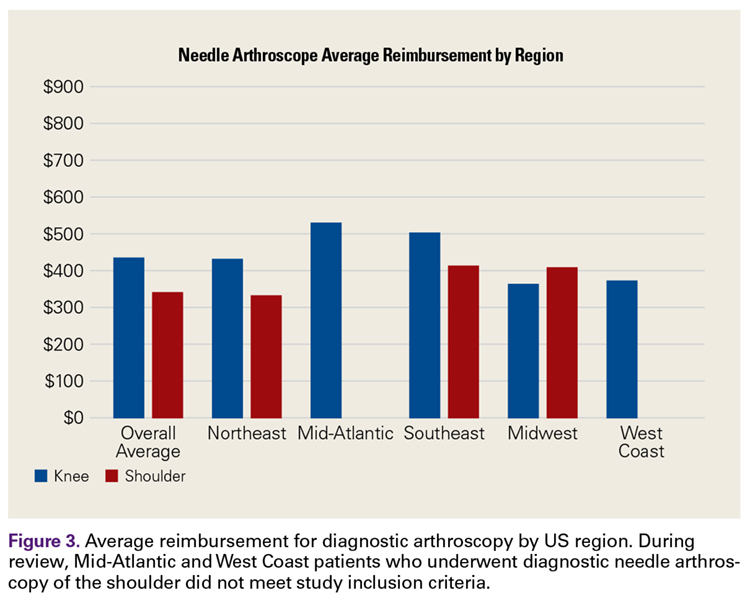
We retrospectively reviewed the patient charts for 200 in-office knee and shoulder diagnostic needle arthroscopies performed by 5 surgeons over a 12-month period and examined the costs. Medicare, Medicaid, worker’s compensation, self-pay, and motor vehicle cases were excluded to provide uniformity across commercial insurance payers. Only the reimbursement amounts for Current Procedural Terminology codes 29870 (diagnostic knee arthroscopy) and 29805 (diagnostic shoulder arthroscopy) were examined. Geographical differences in commercial payer reimbursements were considered. The 5 surgeons who submitted data for this study practice in different parts of the United States—the Northeast, the Mid-Atlantic, the Southeast, the Midwest, and the West Coast. Similarly, the costs of outpatient and inpatient MRI and MRA were reported by each physician based on regional rates. MRI reimbursement was considered only if the MRI magnet was 1.5 Tesla or stronger.
Results
We reviewed 200 (175 knee, 25 shoulder) in-office diagnostic needle arthroscopies of patients with commercial insurances. Average reimbursement was calculated across all commercial payers for both knee and shoulder arthroscopies (Figure 2).
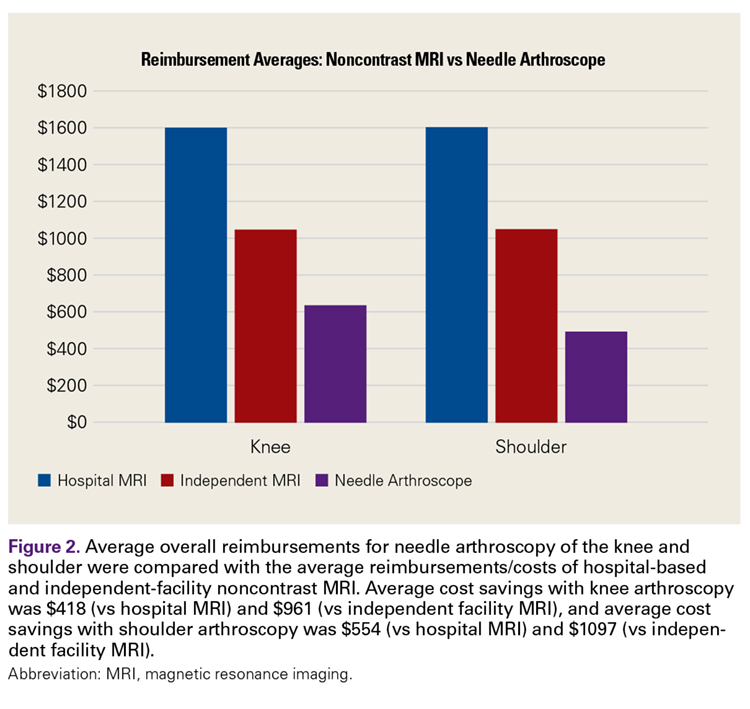
For in-office diagnostic needle arthroscopy of the knee, average reimbursement was $628.92 (range, $340-$1391). For in-office diagnostic needle arthroscopy of the shoulder, average reimbursement was $492.38 (range, $471-$593). Outpatient MRI without contrast of the knee or shoulder averaged $1047 (range, $565-$2100) (Figure 3).
Discussion
Over the past decade, the combination of health and economics has often driven patient care and consumer demand. With rising deductibles and variations in secondary insurance carriers, patients often base healthcare decisions on their financial impact. Conversely, physicians are often in the difficult position of treating patients who are hesitant to obtain medical imaging out of financial concern. In addition, physicians and patients routinely are concerned about delays in care and timely reporting of test results. A patient’s ability to quickly obtain test results and start a course of definitive treatment may affect the patient’s perception of the overall healthcare experience with the physician, as has been noted in popular healthcare polls, such as Press-Ganey.13
Diagnostic needle arthroscopy performed in an office can yield a cost saving over MRI. Our review revealed in-office needle arthroscopy of the knee provided an average cost saving of $418.08 over standard MRI performed in an outpatient facility (Figure 3). That saving more than doubled, to $961.08, when MRI was performed in a hospital. Similarly, in-office needle arthroscopy of the shoulder provided an average cost saving of $554.62 over standard MRI. This saving also increased substantially, to $1097.62, over hospital MRI. An additional cost saving of $100 to $350 was found for knee or shoulder diagnostic needle arthroscopy over MRA.
Other factors affect the economic benefit of diagnostic needle arthroscopy over standard MRI. Having the procedure performed the same day as the presenting office visit can save the patient time and allow the physician to create a medical treatment plan sooner. In addition, the patient (and the insurance company) can save costs by avoiding a later office visit for review of MRI findings. Time spent going to MRI follow-up visits potentially can be analyzed as lost wages or as time lost from other segments of life. For the patient, this time can be defined as value hours. Last, there is a cost saving in avoiding nonoperative treatments in cases in which the initial definitive diagnosis would have called for surgical intervention. Accordingly, for patients who cannot undergo MRI, obtaining information on intra-articular pathology in the office may also decrease unnecessary "traditional" diagnostic arthroscopy in the operating room. Therefore, patients who do not require true formal arthroscopy to determine lack of pertinent intra-articular pathology can avoid unnecessary anesthesia, time off work, and associated healthcare expenses.
This study had several limitations. First, evaluating more cases would have increased the strength of the findings. Second, the large number of knee cases relative to shoulder cases may have been a by-product of the practice makeup of the surgeons rather than a matter of preference with this relatively new technology. However, the significant gap in cost savings between needle arthroscope and MRI cannot be discounted, and it provides a window on the potential cost savings the healthcare system can realize. Furthermore, analysis of payments made by the commercial payers in each state may have revealed a reimbursement fluctuation. The largest challenge in this study was the extreme variation in MRI costs. According to the literature, MRI of the upper or lower extremity ranges in cost from $500 to $4000.4 In addition, this cost is often negotiated between the patient and the MRI facility if the patient is willing to work outside insurance, which potentially can alter the overall average MRI cost.
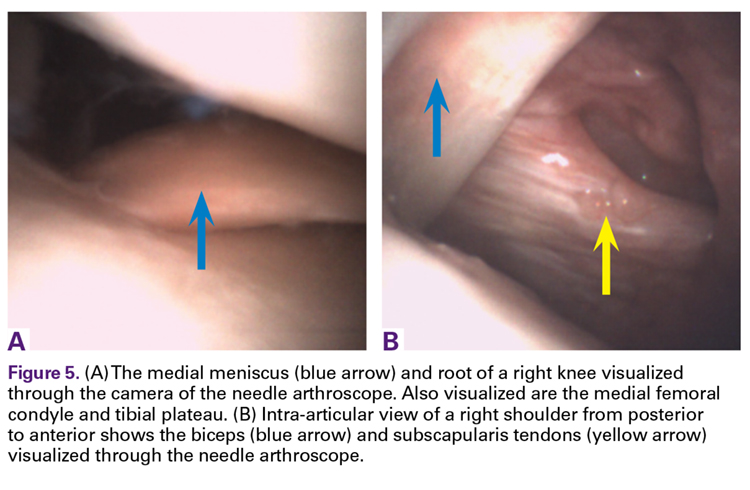
The last points to consider are the reliability of users and the reproducibility of in-office diagnostic needle arthroscopy. Much as with true surgical arthroscopy and other diagnostic imaging practices, this procedure has a learning curve. We know that the number of successful diagnoses will increase with training and repetition, but so far there are no data on the number of procedures needed for proficiency. However, diagnostic needle arthroscopy images are of high quality and are static across users (Figures 5A, 5B). By contrast, the quality of MRI in the United States varies with the quality of the magnets used in individual facilities.
Conclusion
In-office diagnostic needle arthroscopy is a cost-effective and reproducible procedure with potential cost and quality-of-life benefits for commercial payers and patients. Although further study of long-term cost savings for the health care system is needed, significant value was realized in this 200-patient retrospective review. Minimum savings of $418 and $554.62 were realized for noncontrast knee and shoulder MRIs, respectively, in independent facilities. Those cost savings more than doubled in hospital-based facilities: $961.08 and $1097.62, respectively, for knee and shoulder noncontrast MRIs.
For More on In-office Arthroscopy...
Don’t miss Dr. Sean McMillan’s “Innovative Technique Update: In-Office Arthroscopy: My Technique and Results” at the upcoming Innovative Techniques® Knee, Hip, and Shoulder Course in Las Vegas. 29.5 CME/MOC available. Learn more
1. O’Donnell J. Trice Medical literature. #4-10-0032 Rev A.
2. Kim S, Bosque J, Meehan JP, Jamali A, Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am. 2011;93(11):994-1000.
3. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Rep. 2009;(11):1-25.
4. Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ. 2017;(357):j1982.
5. Crawford R, Walley G, Bridgman S, Maffulli N. Magnetic resonance imaging versus arthroscopy in the diagnosis of knee pathology, concentrating on meniscal lesions and ACL tears: a systematic review. Br Med Bull. 2007;(84):5-23.
6. Voigt JD, Mosier M, Huber B. Diagnostic needle arthroscopy and the economics of improved diagnostic accuracy: a cost analysis. Appl Health Econ Health Policy. 2014;12(5):523-535.
7. Sharpe RE Jr, Levin DC, Parker L, Rao VM. The recent reversal of the growth trend in MRI: a harbinger of the future? J Am Coll Radiol. 2013;10(8):599-602.
8. Organisation for Economic Cooperation and Development (OECD). 46. Magnetic resonance imaging (MRI) exams, total per 1 000 population. OECD website. http://dx.doi.org/10.1787/mri-exam-total-table-2014-1-en. Published June 30, 2014. Accessed August 14, 2017.
9. Westermann RW, Schick C, Graves CM, Duchman KR, Weinstein SL. What does a shoulder MRI cost the consumer? Clin Orthop Relat Res. 2017;475(3):580-584.
10. Thakkar RS, Thakkar SC, Srikumaran U, McFarland EG, Fayad LM. Complications of rotator cuff surgery—the role of post-operative imaging in patient care. Br J Radiol. 2014;87(1039):20130630.
11. Gramas DA, Antounian FS, Peterfy CG, Genant HK, Lane NE. Assessment of needle arthroscopy, standard arthroscopy, physical examination, and magnetic resonance imaging in knee pain: a pilot study. J Clin Rheumatol. 1995;1(1):26-34.
12. McMillan S, Saini S, Alyea E, Ford EA. Office-based needle arthroscopy: a standardized diagnostic approach to the knee. Arthrosc Tech. 2017.
13. Keeping me waiting: medical practice wait times and patient satisfaction [white paper]. South Bend, IN: Press Ganey; 2010. https://helpandtraining.pressganey.com/Documents_secure/Medical%20Practices/White%20Papers/Keep_Me_Waiting.pdf. Published 2010. Accessed August 14, 2017.
Take-Home Points
- In-office diagnostic needle arthroscopy is a minimally invasive, rapid method for identification of intra-articular joint pathology.
- Cost savings of a significant value can be realized to both the patient and healthcare system via small-bore needle arthroscopy as opposed to MRI.
- Diagnostic needle arthroscopy can lead to quicker identification of pathology than MRI.
- Diagnostic needle arthroscopy can reduce the number of undue "formal" surgical diagnostic arthroscopies.
- Standardization of image quality of small bore arthroscopy may pose benefits to the variable quality of MRI.
Patient satisfaction and healthcare costs have taken a leading role in today’s health care market. Patient satisfaction, often categorized as the "patient experience," can be measured on numerous levels, such as access to healthcare professionals and diagnostic testing, wait time for appointments, and timely test results. Furthermore, patients’ having a full understanding of their pathology and treatment options may correlate with their overall satisfaction. Some metrics are subjective, but procedure costs are objective.
The algorithm for treating patients who present with knee or shoulder pathology to an orthopedic office involves taking a thorough history, performing a physical examination, and, in many cases, obtaining diagnostic imaging. After arriving at a diagnosis, the physician plans the patient’s treatment. In most cases in which magnetic resonance imaging (MRI) is required, the process can take 2 to 3 weeks.1
Surgical knee arthroscopy is one of the most common procedures in the United States.2,3 Worldwide, more than 2 million knee arthroscopies are performed yearly.4 For most procedures, the decision to treat is based on physical examination findings, and the diagnosis is confirmed with MRI. MRI has 86% sensitivity and 91% specificity for diagnosing ligamentous and meniscal tears.5 However, regular use of MRI has led to increased healthcare expenditures and a larger financial burden for patients, which can delay diagnosis.6
Since 2000, MRI use in the United States has risen significantly—by 10% over a 10-year period.7 According to a 2013 population analysis, 107 in 1000 US inhabitants had an MRI yearly.8
MRI costs vary widely because of several factors, including state/regional consideration, scanning in a hospital or an independent facility, and use of contrast and arthrography. In a 2017 study of the variation in noncontrast MRI costs at 71 hospitals and 26 independent facilities in Iowa, Westermann and colleagues9 found that, excluding radiologist interpretation fees, the mean MRI technical component cost to consumers was US $1874 (SD, $694; range, $500-$4000).
Patient factors may preclude use of MRI (Table).
Small-bore needle arthroscopy is a cost-effective alternative diagnostic tool with efficacy and accuracy similar to those of MRI and standard arthroscopy for intra-articular pathologies.6,11 The procedure is performed with a disposable handpiece equipped with an internal light source and optics; this handpiece attaches to a reusable tablet for ease of transportation and visualization (Figure 1).
In 2014, Voigt and colleagues6 reported a significant net healthcare system cost saving with use of a small-needle arthroscope for diagnostic testing. The saving was estimated at $115 million to $177 million for simple isolation of medial meniscus pathology—or, more specifically, for appropriate care after more accurate visualization with the diagnostic needle arthroscope coupled with a decrease in false positives compared with MRI use. Other factors include the economic impact of the patient’s lost work hours, often associated with the time off needed for the MRI and for the follow-up visit for review of results.
Methods
We retrospectively reviewed the patient charts for 200 in-office knee and shoulder diagnostic needle arthroscopies performed by 5 surgeons over a 12-month period and examined the costs. Medicare, Medicaid, worker’s compensation, self-pay, and motor vehicle cases were excluded to provide uniformity across commercial insurance payers. Only the reimbursement amounts for Current Procedural Terminology codes 29870 (diagnostic knee arthroscopy) and 29805 (diagnostic shoulder arthroscopy) were examined. Geographical differences in commercial payer reimbursements were considered. The 5 surgeons who submitted data for this study practice in different parts of the United States—the Northeast, the Mid-Atlantic, the Southeast, the Midwest, and the West Coast. Similarly, the costs of outpatient and inpatient MRI and MRA were reported by each physician based on regional rates. MRI reimbursement was considered only if the MRI magnet was 1.5 Tesla or stronger.
Results
We reviewed 200 (175 knee, 25 shoulder) in-office diagnostic needle arthroscopies of patients with commercial insurances. Average reimbursement was calculated across all commercial payers for both knee and shoulder arthroscopies (Figure 2).
For in-office diagnostic needle arthroscopy of the knee, average reimbursement was $628.92 (range, $340-$1391). For in-office diagnostic needle arthroscopy of the shoulder, average reimbursement was $492.38 (range, $471-$593). Outpatient MRI without contrast of the knee or shoulder averaged $1047 (range, $565-$2100) (Figure 3).
Discussion
Over the past decade, the combination of health and economics has often driven patient care and consumer demand. With rising deductibles and variations in secondary insurance carriers, patients often base healthcare decisions on their financial impact. Conversely, physicians are often in the difficult position of treating patients who are hesitant to obtain medical imaging out of financial concern. In addition, physicians and patients routinely are concerned about delays in care and timely reporting of test results. A patient’s ability to quickly obtain test results and start a course of definitive treatment may affect the patient’s perception of the overall healthcare experience with the physician, as has been noted in popular healthcare polls, such as Press-Ganey.13
Diagnostic needle arthroscopy performed in an office can yield a cost saving over MRI. Our review revealed in-office needle arthroscopy of the knee provided an average cost saving of $418.08 over standard MRI performed in an outpatient facility (Figure 3). That saving more than doubled, to $961.08, when MRI was performed in a hospital. Similarly, in-office needle arthroscopy of the shoulder provided an average cost saving of $554.62 over standard MRI. This saving also increased substantially, to $1097.62, over hospital MRI. An additional cost saving of $100 to $350 was found for knee or shoulder diagnostic needle arthroscopy over MRA.
Other factors affect the economic benefit of diagnostic needle arthroscopy over standard MRI. Having the procedure performed the same day as the presenting office visit can save the patient time and allow the physician to create a medical treatment plan sooner. In addition, the patient (and the insurance company) can save costs by avoiding a later office visit for review of MRI findings. Time spent going to MRI follow-up visits potentially can be analyzed as lost wages or as time lost from other segments of life. For the patient, this time can be defined as value hours. Last, there is a cost saving in avoiding nonoperative treatments in cases in which the initial definitive diagnosis would have called for surgical intervention. Accordingly, for patients who cannot undergo MRI, obtaining information on intra-articular pathology in the office may also decrease unnecessary "traditional" diagnostic arthroscopy in the operating room. Therefore, patients who do not require true formal arthroscopy to determine lack of pertinent intra-articular pathology can avoid unnecessary anesthesia, time off work, and associated healthcare expenses.
This study had several limitations. First, evaluating more cases would have increased the strength of the findings. Second, the large number of knee cases relative to shoulder cases may have been a by-product of the practice makeup of the surgeons rather than a matter of preference with this relatively new technology. However, the significant gap in cost savings between needle arthroscope and MRI cannot be discounted, and it provides a window on the potential cost savings the healthcare system can realize. Furthermore, analysis of payments made by the commercial payers in each state may have revealed a reimbursement fluctuation. The largest challenge in this study was the extreme variation in MRI costs. According to the literature, MRI of the upper or lower extremity ranges in cost from $500 to $4000.4 In addition, this cost is often negotiated between the patient and the MRI facility if the patient is willing to work outside insurance, which potentially can alter the overall average MRI cost.
The last points to consider are the reliability of users and the reproducibility of in-office diagnostic needle arthroscopy. Much as with true surgical arthroscopy and other diagnostic imaging practices, this procedure has a learning curve. We know that the number of successful diagnoses will increase with training and repetition, but so far there are no data on the number of procedures needed for proficiency. However, diagnostic needle arthroscopy images are of high quality and are static across users (Figures 5A, 5B). By contrast, the quality of MRI in the United States varies with the quality of the magnets used in individual facilities.
Conclusion
In-office diagnostic needle arthroscopy is a cost-effective and reproducible procedure with potential cost and quality-of-life benefits for commercial payers and patients. Although further study of long-term cost savings for the health care system is needed, significant value was realized in this 200-patient retrospective review. Minimum savings of $418 and $554.62 were realized for noncontrast knee and shoulder MRIs, respectively, in independent facilities. Those cost savings more than doubled in hospital-based facilities: $961.08 and $1097.62, respectively, for knee and shoulder noncontrast MRIs.
For More on In-office Arthroscopy...
Don’t miss Dr. Sean McMillan’s “Innovative Technique Update: In-Office Arthroscopy: My Technique and Results” at the upcoming Innovative Techniques® Knee, Hip, and Shoulder Course in Las Vegas. 29.5 CME/MOC available. Learn more
Take-Home Points
- In-office diagnostic needle arthroscopy is a minimally invasive, rapid method for identification of intra-articular joint pathology.
- Cost savings of a significant value can be realized to both the patient and healthcare system via small-bore needle arthroscopy as opposed to MRI.
- Diagnostic needle arthroscopy can lead to quicker identification of pathology than MRI.
- Diagnostic needle arthroscopy can reduce the number of undue "formal" surgical diagnostic arthroscopies.
- Standardization of image quality of small bore arthroscopy may pose benefits to the variable quality of MRI.
Patient satisfaction and healthcare costs have taken a leading role in today’s health care market. Patient satisfaction, often categorized as the "patient experience," can be measured on numerous levels, such as access to healthcare professionals and diagnostic testing, wait time for appointments, and timely test results. Furthermore, patients’ having a full understanding of their pathology and treatment options may correlate with their overall satisfaction. Some metrics are subjective, but procedure costs are objective.
The algorithm for treating patients who present with knee or shoulder pathology to an orthopedic office involves taking a thorough history, performing a physical examination, and, in many cases, obtaining diagnostic imaging. After arriving at a diagnosis, the physician plans the patient’s treatment. In most cases in which magnetic resonance imaging (MRI) is required, the process can take 2 to 3 weeks.1
Surgical knee arthroscopy is one of the most common procedures in the United States.2,3 Worldwide, more than 2 million knee arthroscopies are performed yearly.4 For most procedures, the decision to treat is based on physical examination findings, and the diagnosis is confirmed with MRI. MRI has 86% sensitivity and 91% specificity for diagnosing ligamentous and meniscal tears.5 However, regular use of MRI has led to increased healthcare expenditures and a larger financial burden for patients, which can delay diagnosis.6
Since 2000, MRI use in the United States has risen significantly—by 10% over a 10-year period.7 According to a 2013 population analysis, 107 in 1000 US inhabitants had an MRI yearly.8
MRI costs vary widely because of several factors, including state/regional consideration, scanning in a hospital or an independent facility, and use of contrast and arthrography. In a 2017 study of the variation in noncontrast MRI costs at 71 hospitals and 26 independent facilities in Iowa, Westermann and colleagues9 found that, excluding radiologist interpretation fees, the mean MRI technical component cost to consumers was US $1874 (SD, $694; range, $500-$4000).
Patient factors may preclude use of MRI (Table).
Small-bore needle arthroscopy is a cost-effective alternative diagnostic tool with efficacy and accuracy similar to those of MRI and standard arthroscopy for intra-articular pathologies.6,11 The procedure is performed with a disposable handpiece equipped with an internal light source and optics; this handpiece attaches to a reusable tablet for ease of transportation and visualization (Figure 1).
In 2014, Voigt and colleagues6 reported a significant net healthcare system cost saving with use of a small-needle arthroscope for diagnostic testing. The saving was estimated at $115 million to $177 million for simple isolation of medial meniscus pathology—or, more specifically, for appropriate care after more accurate visualization with the diagnostic needle arthroscope coupled with a decrease in false positives compared with MRI use. Other factors include the economic impact of the patient’s lost work hours, often associated with the time off needed for the MRI and for the follow-up visit for review of results.
Methods
We retrospectively reviewed the patient charts for 200 in-office knee and shoulder diagnostic needle arthroscopies performed by 5 surgeons over a 12-month period and examined the costs. Medicare, Medicaid, worker’s compensation, self-pay, and motor vehicle cases were excluded to provide uniformity across commercial insurance payers. Only the reimbursement amounts for Current Procedural Terminology codes 29870 (diagnostic knee arthroscopy) and 29805 (diagnostic shoulder arthroscopy) were examined. Geographical differences in commercial payer reimbursements were considered. The 5 surgeons who submitted data for this study practice in different parts of the United States—the Northeast, the Mid-Atlantic, the Southeast, the Midwest, and the West Coast. Similarly, the costs of outpatient and inpatient MRI and MRA were reported by each physician based on regional rates. MRI reimbursement was considered only if the MRI magnet was 1.5 Tesla or stronger.
Results
We reviewed 200 (175 knee, 25 shoulder) in-office diagnostic needle arthroscopies of patients with commercial insurances. Average reimbursement was calculated across all commercial payers for both knee and shoulder arthroscopies (Figure 2).
For in-office diagnostic needle arthroscopy of the knee, average reimbursement was $628.92 (range, $340-$1391). For in-office diagnostic needle arthroscopy of the shoulder, average reimbursement was $492.38 (range, $471-$593). Outpatient MRI without contrast of the knee or shoulder averaged $1047 (range, $565-$2100) (Figure 3).
Discussion
Over the past decade, the combination of health and economics has often driven patient care and consumer demand. With rising deductibles and variations in secondary insurance carriers, patients often base healthcare decisions on their financial impact. Conversely, physicians are often in the difficult position of treating patients who are hesitant to obtain medical imaging out of financial concern. In addition, physicians and patients routinely are concerned about delays in care and timely reporting of test results. A patient’s ability to quickly obtain test results and start a course of definitive treatment may affect the patient’s perception of the overall healthcare experience with the physician, as has been noted in popular healthcare polls, such as Press-Ganey.13
Diagnostic needle arthroscopy performed in an office can yield a cost saving over MRI. Our review revealed in-office needle arthroscopy of the knee provided an average cost saving of $418.08 over standard MRI performed in an outpatient facility (Figure 3). That saving more than doubled, to $961.08, when MRI was performed in a hospital. Similarly, in-office needle arthroscopy of the shoulder provided an average cost saving of $554.62 over standard MRI. This saving also increased substantially, to $1097.62, over hospital MRI. An additional cost saving of $100 to $350 was found for knee or shoulder diagnostic needle arthroscopy over MRA.
Other factors affect the economic benefit of diagnostic needle arthroscopy over standard MRI. Having the procedure performed the same day as the presenting office visit can save the patient time and allow the physician to create a medical treatment plan sooner. In addition, the patient (and the insurance company) can save costs by avoiding a later office visit for review of MRI findings. Time spent going to MRI follow-up visits potentially can be analyzed as lost wages or as time lost from other segments of life. For the patient, this time can be defined as value hours. Last, there is a cost saving in avoiding nonoperative treatments in cases in which the initial definitive diagnosis would have called for surgical intervention. Accordingly, for patients who cannot undergo MRI, obtaining information on intra-articular pathology in the office may also decrease unnecessary "traditional" diagnostic arthroscopy in the operating room. Therefore, patients who do not require true formal arthroscopy to determine lack of pertinent intra-articular pathology can avoid unnecessary anesthesia, time off work, and associated healthcare expenses.
This study had several limitations. First, evaluating more cases would have increased the strength of the findings. Second, the large number of knee cases relative to shoulder cases may have been a by-product of the practice makeup of the surgeons rather than a matter of preference with this relatively new technology. However, the significant gap in cost savings between needle arthroscope and MRI cannot be discounted, and it provides a window on the potential cost savings the healthcare system can realize. Furthermore, analysis of payments made by the commercial payers in each state may have revealed a reimbursement fluctuation. The largest challenge in this study was the extreme variation in MRI costs. According to the literature, MRI of the upper or lower extremity ranges in cost from $500 to $4000.4 In addition, this cost is often negotiated between the patient and the MRI facility if the patient is willing to work outside insurance, which potentially can alter the overall average MRI cost.
The last points to consider are the reliability of users and the reproducibility of in-office diagnostic needle arthroscopy. Much as with true surgical arthroscopy and other diagnostic imaging practices, this procedure has a learning curve. We know that the number of successful diagnoses will increase with training and repetition, but so far there are no data on the number of procedures needed for proficiency. However, diagnostic needle arthroscopy images are of high quality and are static across users (Figures 5A, 5B). By contrast, the quality of MRI in the United States varies with the quality of the magnets used in individual facilities.
Conclusion
In-office diagnostic needle arthroscopy is a cost-effective and reproducible procedure with potential cost and quality-of-life benefits for commercial payers and patients. Although further study of long-term cost savings for the health care system is needed, significant value was realized in this 200-patient retrospective review. Minimum savings of $418 and $554.62 were realized for noncontrast knee and shoulder MRIs, respectively, in independent facilities. Those cost savings more than doubled in hospital-based facilities: $961.08 and $1097.62, respectively, for knee and shoulder noncontrast MRIs.
For More on In-office Arthroscopy...
Don’t miss Dr. Sean McMillan’s “Innovative Technique Update: In-Office Arthroscopy: My Technique and Results” at the upcoming Innovative Techniques® Knee, Hip, and Shoulder Course in Las Vegas. 29.5 CME/MOC available. Learn more
1. O’Donnell J. Trice Medical literature. #4-10-0032 Rev A.
2. Kim S, Bosque J, Meehan JP, Jamali A, Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am. 2011;93(11):994-1000.
3. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Rep. 2009;(11):1-25.
4. Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ. 2017;(357):j1982.
5. Crawford R, Walley G, Bridgman S, Maffulli N. Magnetic resonance imaging versus arthroscopy in the diagnosis of knee pathology, concentrating on meniscal lesions and ACL tears: a systematic review. Br Med Bull. 2007;(84):5-23.
6. Voigt JD, Mosier M, Huber B. Diagnostic needle arthroscopy and the economics of improved diagnostic accuracy: a cost analysis. Appl Health Econ Health Policy. 2014;12(5):523-535.
7. Sharpe RE Jr, Levin DC, Parker L, Rao VM. The recent reversal of the growth trend in MRI: a harbinger of the future? J Am Coll Radiol. 2013;10(8):599-602.
8. Organisation for Economic Cooperation and Development (OECD). 46. Magnetic resonance imaging (MRI) exams, total per 1 000 population. OECD website. http://dx.doi.org/10.1787/mri-exam-total-table-2014-1-en. Published June 30, 2014. Accessed August 14, 2017.
9. Westermann RW, Schick C, Graves CM, Duchman KR, Weinstein SL. What does a shoulder MRI cost the consumer? Clin Orthop Relat Res. 2017;475(3):580-584.
10. Thakkar RS, Thakkar SC, Srikumaran U, McFarland EG, Fayad LM. Complications of rotator cuff surgery—the role of post-operative imaging in patient care. Br J Radiol. 2014;87(1039):20130630.
11. Gramas DA, Antounian FS, Peterfy CG, Genant HK, Lane NE. Assessment of needle arthroscopy, standard arthroscopy, physical examination, and magnetic resonance imaging in knee pain: a pilot study. J Clin Rheumatol. 1995;1(1):26-34.
12. McMillan S, Saini S, Alyea E, Ford EA. Office-based needle arthroscopy: a standardized diagnostic approach to the knee. Arthrosc Tech. 2017.
13. Keeping me waiting: medical practice wait times and patient satisfaction [white paper]. South Bend, IN: Press Ganey; 2010. https://helpandtraining.pressganey.com/Documents_secure/Medical%20Practices/White%20Papers/Keep_Me_Waiting.pdf. Published 2010. Accessed August 14, 2017.
1. O’Donnell J. Trice Medical literature. #4-10-0032 Rev A.
2. Kim S, Bosque J, Meehan JP, Jamali A, Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am. 2011;93(11):994-1000.
3. Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Rep. 2009;(11):1-25.
4. Siemieniuk RAC, Harris IA, Agoritsas T, et al. Arthroscopic surgery for degenerative knee arthritis and meniscal tears: a clinical practice guideline. BMJ. 2017;(357):j1982.
5. Crawford R, Walley G, Bridgman S, Maffulli N. Magnetic resonance imaging versus arthroscopy in the diagnosis of knee pathology, concentrating on meniscal lesions and ACL tears: a systematic review. Br Med Bull. 2007;(84):5-23.
6. Voigt JD, Mosier M, Huber B. Diagnostic needle arthroscopy and the economics of improved diagnostic accuracy: a cost analysis. Appl Health Econ Health Policy. 2014;12(5):523-535.
7. Sharpe RE Jr, Levin DC, Parker L, Rao VM. The recent reversal of the growth trend in MRI: a harbinger of the future? J Am Coll Radiol. 2013;10(8):599-602.
8. Organisation for Economic Cooperation and Development (OECD). 46. Magnetic resonance imaging (MRI) exams, total per 1 000 population. OECD website. http://dx.doi.org/10.1787/mri-exam-total-table-2014-1-en. Published June 30, 2014. Accessed August 14, 2017.
9. Westermann RW, Schick C, Graves CM, Duchman KR, Weinstein SL. What does a shoulder MRI cost the consumer? Clin Orthop Relat Res. 2017;475(3):580-584.
10. Thakkar RS, Thakkar SC, Srikumaran U, McFarland EG, Fayad LM. Complications of rotator cuff surgery—the role of post-operative imaging in patient care. Br J Radiol. 2014;87(1039):20130630.
11. Gramas DA, Antounian FS, Peterfy CG, Genant HK, Lane NE. Assessment of needle arthroscopy, standard arthroscopy, physical examination, and magnetic resonance imaging in knee pain: a pilot study. J Clin Rheumatol. 1995;1(1):26-34.
12. McMillan S, Saini S, Alyea E, Ford EA. Office-based needle arthroscopy: a standardized diagnostic approach to the knee. Arthrosc Tech. 2017.
13. Keeping me waiting: medical practice wait times and patient satisfaction [white paper]. South Bend, IN: Press Ganey; 2010. https://helpandtraining.pressganey.com/Documents_secure/Medical%20Practices/White%20Papers/Keep_Me_Waiting.pdf. Published 2010. Accessed August 14, 2017.

Phototherapy Coding and Documentation in the Time of Biologics
In this era of biologics for psoriasis with ever-increasing effectiveness and safety as well as patients who have less and less time to visit the physician's office, it would seem that the days of in-office UV treatments would be numbered. However, rumors of the demise of phototherapy may be greatly exaggerated. Phototherapy is still one of the safest and most cost-effective treatments for psoriasis and other dermatoses.1 Its use often is a prerequisite for biologic therapy, and it may be the only therapeutic option for certain subsets of patients, such as children, pregnant women, and immunosuppressed patients. Moreover, narrowband UVB technology has breathed new life into phototherapy, with better efficacy and less long-term risk. Although the utilization of psoralen plus UVA (PUVA) light therapy has indeed decreased over the last 2 decades, the use of UVB therapies continues to increase dramatically.2
Phototherapy Codes
There are 4 chief Current Procedural Terminology (CPT) codes for reporting phototherapy services: (1) 96900: actinotherapy (UV light treatment); (2) 96910: photochemotherapy, tar, and UVB (Goeckerman treatment) or petrolatum and UVB; (3) 96912: photochemotherapy and PUVA; and (4) 96913: photochemotherapy (Goeckerman and/or PUVA) for severe photoresponsive dermatoses requiring at least 4 to 8 hours of care under direct supervision of the physician.3
There is lack of specificity of the CPT code descriptions for phototherapy. Moreover, insurer guidance for documentation for phototherapy is vague to nonexistent, and of course whenever the use of any medical service increases, insurer scrutiny is sure to follow. Therefore, it is not surprising that dermatology practices have reported that private insurers as well as Medicare are auditing medical records for phototherapy treatments.4 In fact, recently we have seen a Midwest private insurer demand payment from dermatologists for hundreds of 96910 phototherapy services, which the insurer asserted should have been coded as 96900 because topical therapies were not applied by the dermatology staff. The insurer did not just evaluate medical records but also contacted patients directly and asked how services had been provided. Clearly, more detailed guidance for dermatologists and insurers on documentation and performance standards for each phototherapy service is needed.
Existing coding guidance for phototherapy indicates that actinotherapy (96900) defines the basic service of treating a patient with a UV light unit.5 Actinotherapy does not involve application of topical medications while the patient is in the office.
In contrast, photochemotherapy (96910) implies addition of a chemo agent to phototherapy. Despite the somewhat nonspecific nature of the code descriptor, it is apparent that application of photoenhancing agents such as tar, petrolatum, or distillates of petrolatum meet the requirements of 96910. The Coder's Desk Reference for Procedures 2017 describes 96910 as "the physician uses photosensitizing chemicals and light rays to treat skin ailments."6 Application of light-enhancing topical products should occur within the office by either staff or the patient. In fact, examination of practice expense data from the Centers for Medicare & Medicaid Services indicated that the 96910 code includes payment for clinical staff time to apply topical products as well as the cost of the topical agent(s).7
The PUVA code 96912 is defined by the use of photosensitizing psoralen medication, which can be administered topically or orally, followed by UVA treatment. In my experience, PUVA has similar performance standards with in-office application of psoralen, if applicable. If application of topical photoenhancing products occurs outside the office, the requirements of photochemotherapy are not met, and 96900 should be reported.
The 96913 code defines prolonged phototherapy service with intensive topical therapy requirements and multiple phototherapy sessions per day.3 This code is rarely reported (average of fewer than 100 times in the Medicare population per year), and most insurers do not reimburse this service.
Protecting Yourself From an Audit
In my experience, review of private insurer audits of phototherapy services has yielded important lessons. First, having a written standard operating procedure in place regarding the performance of phototherapy services and how application of topicals will be handled has been helpful in audit defense. The other key to beating audits for phototherapy services is to have detailed documentation or a flowchart in the medical record regarding the topical agent and the light administration. The medical record should include what topical agent was applied, if any; whether the topical agent was applied in the office; where the topical product was applied; and who applied the topical product. Sometimes topical product application by a physician or staff is not feasible because of patient preference or the site of application. If the patient applied the topical, document that assistance was offered and refused, along with what type of UV light was used and the dosage. Inclusion of these elements in the medical record provides a clear picture of the delivery of the phototherapy service and will aid in responding to medical record audit.
Final Thoughts
Phototherapy is a critical treatment modality that continues to be utilized frequently in the expanding armamentarium of treatments for dermatoses. Phototherapy is performed almost exclusively by dermatologists and allows dermatologists to offer a unique level of care and value in the treatment of skin disease. Careful documentation, a written standard operating procedure, and adherence to proper performance standards will allow dermatologists to be compensated fairly for this important treatment modality and pass audits that are likely to occur.
- Lapolla W, Yentzer BA, Bagel J, et al. A review of phototherapy protocols for psoriasis treatment. J Am Acad Dermatol. 2011;64:936-949.
- Simpson GL, Yelverton CB, Rittenberg S, et al. Do utilization management controls for phototherapy increase the prescription of biologics? J Dermatolog Treat. 2006;17:359-361.
- Current Procedural Terminology 2017, Professional Edition. Chicago IL: American Medical Association; 2016.
- American Academy of Dermatology Association. Insurers review billing for photochemotherapy (CPT 96910). Derm Coding Consult. Spring 2009;13:4.
- American Academy of Dermatology Association. Coding Q&A's. Derm Coding Consult. Spring 2007;11:5, 7, 8.
- Coders' Desk Reference for Procedures 2017. Chicago, IL: Optum360; 2017.
- Relative Value Scale Update Committee Database. Chicago, IL: American Medical Association; 2016.
In this era of biologics for psoriasis with ever-increasing effectiveness and safety as well as patients who have less and less time to visit the physician's office, it would seem that the days of in-office UV treatments would be numbered. However, rumors of the demise of phototherapy may be greatly exaggerated. Phototherapy is still one of the safest and most cost-effective treatments for psoriasis and other dermatoses.1 Its use often is a prerequisite for biologic therapy, and it may be the only therapeutic option for certain subsets of patients, such as children, pregnant women, and immunosuppressed patients. Moreover, narrowband UVB technology has breathed new life into phototherapy, with better efficacy and less long-term risk. Although the utilization of psoralen plus UVA (PUVA) light therapy has indeed decreased over the last 2 decades, the use of UVB therapies continues to increase dramatically.2
Phototherapy Codes
There are 4 chief Current Procedural Terminology (CPT) codes for reporting phototherapy services: (1) 96900: actinotherapy (UV light treatment); (2) 96910: photochemotherapy, tar, and UVB (Goeckerman treatment) or petrolatum and UVB; (3) 96912: photochemotherapy and PUVA; and (4) 96913: photochemotherapy (Goeckerman and/or PUVA) for severe photoresponsive dermatoses requiring at least 4 to 8 hours of care under direct supervision of the physician.3
There is lack of specificity of the CPT code descriptions for phototherapy. Moreover, insurer guidance for documentation for phototherapy is vague to nonexistent, and of course whenever the use of any medical service increases, insurer scrutiny is sure to follow. Therefore, it is not surprising that dermatology practices have reported that private insurers as well as Medicare are auditing medical records for phototherapy treatments.4 In fact, recently we have seen a Midwest private insurer demand payment from dermatologists for hundreds of 96910 phototherapy services, which the insurer asserted should have been coded as 96900 because topical therapies were not applied by the dermatology staff. The insurer did not just evaluate medical records but also contacted patients directly and asked how services had been provided. Clearly, more detailed guidance for dermatologists and insurers on documentation and performance standards for each phototherapy service is needed.
Existing coding guidance for phototherapy indicates that actinotherapy (96900) defines the basic service of treating a patient with a UV light unit.5 Actinotherapy does not involve application of topical medications while the patient is in the office.
In contrast, photochemotherapy (96910) implies addition of a chemo agent to phototherapy. Despite the somewhat nonspecific nature of the code descriptor, it is apparent that application of photoenhancing agents such as tar, petrolatum, or distillates of petrolatum meet the requirements of 96910. The Coder's Desk Reference for Procedures 2017 describes 96910 as "the physician uses photosensitizing chemicals and light rays to treat skin ailments."6 Application of light-enhancing topical products should occur within the office by either staff or the patient. In fact, examination of practice expense data from the Centers for Medicare & Medicaid Services indicated that the 96910 code includes payment for clinical staff time to apply topical products as well as the cost of the topical agent(s).7
The PUVA code 96912 is defined by the use of photosensitizing psoralen medication, which can be administered topically or orally, followed by UVA treatment. In my experience, PUVA has similar performance standards with in-office application of psoralen, if applicable. If application of topical photoenhancing products occurs outside the office, the requirements of photochemotherapy are not met, and 96900 should be reported.
The 96913 code defines prolonged phototherapy service with intensive topical therapy requirements and multiple phototherapy sessions per day.3 This code is rarely reported (average of fewer than 100 times in the Medicare population per year), and most insurers do not reimburse this service.
Protecting Yourself From an Audit
In my experience, review of private insurer audits of phototherapy services has yielded important lessons. First, having a written standard operating procedure in place regarding the performance of phototherapy services and how application of topicals will be handled has been helpful in audit defense. The other key to beating audits for phototherapy services is to have detailed documentation or a flowchart in the medical record regarding the topical agent and the light administration. The medical record should include what topical agent was applied, if any; whether the topical agent was applied in the office; where the topical product was applied; and who applied the topical product. Sometimes topical product application by a physician or staff is not feasible because of patient preference or the site of application. If the patient applied the topical, document that assistance was offered and refused, along with what type of UV light was used and the dosage. Inclusion of these elements in the medical record provides a clear picture of the delivery of the phototherapy service and will aid in responding to medical record audit.
Final Thoughts
Phototherapy is a critical treatment modality that continues to be utilized frequently in the expanding armamentarium of treatments for dermatoses. Phototherapy is performed almost exclusively by dermatologists and allows dermatologists to offer a unique level of care and value in the treatment of skin disease. Careful documentation, a written standard operating procedure, and adherence to proper performance standards will allow dermatologists to be compensated fairly for this important treatment modality and pass audits that are likely to occur.
In this era of biologics for psoriasis with ever-increasing effectiveness and safety as well as patients who have less and less time to visit the physician's office, it would seem that the days of in-office UV treatments would be numbered. However, rumors of the demise of phototherapy may be greatly exaggerated. Phototherapy is still one of the safest and most cost-effective treatments for psoriasis and other dermatoses.1 Its use often is a prerequisite for biologic therapy, and it may be the only therapeutic option for certain subsets of patients, such as children, pregnant women, and immunosuppressed patients. Moreover, narrowband UVB technology has breathed new life into phototherapy, with better efficacy and less long-term risk. Although the utilization of psoralen plus UVA (PUVA) light therapy has indeed decreased over the last 2 decades, the use of UVB therapies continues to increase dramatically.2
Phototherapy Codes
There are 4 chief Current Procedural Terminology (CPT) codes for reporting phototherapy services: (1) 96900: actinotherapy (UV light treatment); (2) 96910: photochemotherapy, tar, and UVB (Goeckerman treatment) or petrolatum and UVB; (3) 96912: photochemotherapy and PUVA; and (4) 96913: photochemotherapy (Goeckerman and/or PUVA) for severe photoresponsive dermatoses requiring at least 4 to 8 hours of care under direct supervision of the physician.3
There is lack of specificity of the CPT code descriptions for phototherapy. Moreover, insurer guidance for documentation for phototherapy is vague to nonexistent, and of course whenever the use of any medical service increases, insurer scrutiny is sure to follow. Therefore, it is not surprising that dermatology practices have reported that private insurers as well as Medicare are auditing medical records for phototherapy treatments.4 In fact, recently we have seen a Midwest private insurer demand payment from dermatologists for hundreds of 96910 phototherapy services, which the insurer asserted should have been coded as 96900 because topical therapies were not applied by the dermatology staff. The insurer did not just evaluate medical records but also contacted patients directly and asked how services had been provided. Clearly, more detailed guidance for dermatologists and insurers on documentation and performance standards for each phototherapy service is needed.
Existing coding guidance for phototherapy indicates that actinotherapy (96900) defines the basic service of treating a patient with a UV light unit.5 Actinotherapy does not involve application of topical medications while the patient is in the office.
In contrast, photochemotherapy (96910) implies addition of a chemo agent to phototherapy. Despite the somewhat nonspecific nature of the code descriptor, it is apparent that application of photoenhancing agents such as tar, petrolatum, or distillates of petrolatum meet the requirements of 96910. The Coder's Desk Reference for Procedures 2017 describes 96910 as "the physician uses photosensitizing chemicals and light rays to treat skin ailments."6 Application of light-enhancing topical products should occur within the office by either staff or the patient. In fact, examination of practice expense data from the Centers for Medicare & Medicaid Services indicated that the 96910 code includes payment for clinical staff time to apply topical products as well as the cost of the topical agent(s).7
The PUVA code 96912 is defined by the use of photosensitizing psoralen medication, which can be administered topically or orally, followed by UVA treatment. In my experience, PUVA has similar performance standards with in-office application of psoralen, if applicable. If application of topical photoenhancing products occurs outside the office, the requirements of photochemotherapy are not met, and 96900 should be reported.
The 96913 code defines prolonged phototherapy service with intensive topical therapy requirements and multiple phototherapy sessions per day.3 This code is rarely reported (average of fewer than 100 times in the Medicare population per year), and most insurers do not reimburse this service.
Protecting Yourself From an Audit
In my experience, review of private insurer audits of phototherapy services has yielded important lessons. First, having a written standard operating procedure in place regarding the performance of phototherapy services and how application of topicals will be handled has been helpful in audit defense. The other key to beating audits for phototherapy services is to have detailed documentation or a flowchart in the medical record regarding the topical agent and the light administration. The medical record should include what topical agent was applied, if any; whether the topical agent was applied in the office; where the topical product was applied; and who applied the topical product. Sometimes topical product application by a physician or staff is not feasible because of patient preference or the site of application. If the patient applied the topical, document that assistance was offered and refused, along with what type of UV light was used and the dosage. Inclusion of these elements in the medical record provides a clear picture of the delivery of the phototherapy service and will aid in responding to medical record audit.
Final Thoughts
Phototherapy is a critical treatment modality that continues to be utilized frequently in the expanding armamentarium of treatments for dermatoses. Phototherapy is performed almost exclusively by dermatologists and allows dermatologists to offer a unique level of care and value in the treatment of skin disease. Careful documentation, a written standard operating procedure, and adherence to proper performance standards will allow dermatologists to be compensated fairly for this important treatment modality and pass audits that are likely to occur.
- Lapolla W, Yentzer BA, Bagel J, et al. A review of phototherapy protocols for psoriasis treatment. J Am Acad Dermatol. 2011;64:936-949.
- Simpson GL, Yelverton CB, Rittenberg S, et al. Do utilization management controls for phototherapy increase the prescription of biologics? J Dermatolog Treat. 2006;17:359-361.
- Current Procedural Terminology 2017, Professional Edition. Chicago IL: American Medical Association; 2016.
- American Academy of Dermatology Association. Insurers review billing for photochemotherapy (CPT 96910). Derm Coding Consult. Spring 2009;13:4.
- American Academy of Dermatology Association. Coding Q&A's. Derm Coding Consult. Spring 2007;11:5, 7, 8.
- Coders' Desk Reference for Procedures 2017. Chicago, IL: Optum360; 2017.
- Relative Value Scale Update Committee Database. Chicago, IL: American Medical Association; 2016.
- Lapolla W, Yentzer BA, Bagel J, et al. A review of phototherapy protocols for psoriasis treatment. J Am Acad Dermatol. 2011;64:936-949.
- Simpson GL, Yelverton CB, Rittenberg S, et al. Do utilization management controls for phototherapy increase the prescription of biologics? J Dermatolog Treat. 2006;17:359-361.
- Current Procedural Terminology 2017, Professional Edition. Chicago IL: American Medical Association; 2016.
- American Academy of Dermatology Association. Insurers review billing for photochemotherapy (CPT 96910). Derm Coding Consult. Spring 2009;13:4.
- American Academy of Dermatology Association. Coding Q&A's. Derm Coding Consult. Spring 2007;11:5, 7, 8.
- Coders' Desk Reference for Procedures 2017. Chicago, IL: Optum360; 2017.
- Relative Value Scale Update Committee Database. Chicago, IL: American Medical Association; 2016.

One Diagnosis and Modifier -25: Appropriate or Audit Target?
An established patient comes into your office with a painful new lesion on the hand. He thinks it may be a wart. You take a focused history of the lesion, do a physical examination, and confirm the diagnosis of verruca vulgaris. You discuss treatment options, risks, and the benefits of treatment, as well as the pathophysiology of warts. The decision is made to proceed that same day with cryosurgical destruction, which is performed. You feel that billing both an office visit with an appended modifier -25 and the benign destruction code 17110 is warranted, but your biller says only the procedure should be reported. Who is correct?
Modifier -25 use has come under increased scrutiny by insurers and regulators. There is a perception that this modifier is frequently used inappropriately or unnecessarily. In fact, the Office of Inspector General reported that 35% of claims using modifier -25 that Medicare allowed did not meet the requirements. The Office of Inspector General has recommended that the “[Centers for Medicare & Medicaid Services] should work with carriers to reduce the number of claims submitted using modifier -25” and “include modifier -25 reviews in their medical review strategies.”1 Translation: More chart reviews and audits! In my discussions with insurer medical directors, they point to the single diagnosis modifier -25 as likely abused and feel that its use in this context is almost never appropriate. Their audits have been focused on this aspect of dermatologists’ coding. In addition, some private insurers have started to discount reimbursement for office visits billed with modifier -25 by 50% to account for the level of perceived overuse.2
The Current Procedural Terminology description of modifier -25 is relatively clear: Modifier -25 is used to facilitate billing of evaluation and management (E/M) services on the day of a procedure for which separate payment may be made.3 This modifier indicates that a significant, separately identifiable E/M service was performed by the same physician on the day of a procedure. To appropriately bill both the E/M service and the procedure, the physician must indicate that the patient’s condition required an E/M service “above and beyond the usual pre- and post-operative work of a procedure.”4 However, it is largely left up to the physician to decide what constitutes the significant, separately identifiable E/M service.
As dermatologists, we all report modifier -25 appropriately as part of our daily practice. Performance of a medically necessary procedure on the same day as an E/M service generally is done to facilitate a prompt diagnosis or streamline treatment of a complex condition. Providing distinct medically necessary services on the same date allows physicians to provide effective and efficient high-quality care, in many cases saving patients a return visit. The most common scenario for using modifier -25 involves multiple concerns and multiple diagnoses, some of which are not associated with a procedure(s) that is performed on the same date of service. With multiple diagnoses, it is straightforward to demonstrate the separate E/M service associated with the nonprocedure-related diagnosis code(s); however, with one diagnosis for both the office visit and the procedure, clear documentation of the separate and identifiable E/M service is critical and is dependent on understanding what is included in the global surgical package.
Insurer payment for procedures includes local or topical anesthesia, the surgical service/procedure itself, immediate postoperative care including dictating the operative note, meeting/discussing the patient’s procedure with family and other physicians, evaluating the patient in postanesthesia/recovery area, and writing orders for the patient. This group of services is called the global surgical package. For minor procedures (ie, those with either 0- or 10-day global periods), the surgical package also includes same-day E/M associated with the decision to perform surgery. An appropriate history and physical examination, as well as the discussion of differential diagnosis, treatment options, and risk and benefits of treatments, are all included in the payment of a minor procedure itself. Therefore, if an E/M service is performed on the same day as a minor procedure to decide whether to proceed with the minor surgical procedure, this E/M service cannot be separately reported. Moreover, the fact that the patient is new to the physician is not sufficient to allow reporting of an E/M service with such a minor procedure. For major procedures (ie, those with 90-day postoperative periods), the decision for surgery is excluded from the global surgical package.
Therefore, it is clear that the clinical scenario for verruca vulgaris treatment as described at the start of this article does not meet criteria for an office visit billed in addition to the destruction. The E/M services performed prior to the patient’s verruca vulgaris treatment are integral to and necessary for the decision to perform the procedure. Making and confirming the diagnosis of a condition or lesion prior to a procedure either by physical evaluation or by interpretation of a pathology report is part of the evaluation required to make the decision to proceed with a particular procedure.
There are clinical scenarios in which a physician can support additional E/M services beyond that of the procedure with just one diagnosis. If a patient presents with warts on the hand and face with resultant cryosurgical destruction done on the hand and a prescription for imiquimod to be used on the face to induce immunologic clearance of viral infection and decrease the risk of scarring, it is clear that a significant and separately identifiable E/M service exists. The evaluation of the facial warts and the prescription of medication and discussion of the risks, benefits, and therapeutic effects of that prescription is definitely distinct from the procedure. Similarly, if an evaluation of a patient with a rash results in only a diagnostic biopsy with no separate cognitive services other than the decision to perform the biopsy, an office visit charge in addition to the biopsy charge would not be warranted. However, if in addition to the biopsy the rash also is treated with topical or systemic steroids because of pruritus or a more extensive evaluation for systemic complications is required, an office visit charge is appropriate.
The frequent use of modifier -25 is a critical part of a high-quality and cost-effective dermatology practice. Same-day performance of E/M services and minor procedures allows for more rapid and efficient diagnosis and treatment of various conditions as well as minimizing unnecessary office visits. However, modifier -25 use, particularly in the context of the same diagnosis for the office visit and the procedure, is under intense insurer scrutiny. Careful and complete documentation of the additional E/M service provided, including the additional history, physical examination results, and treatment considerations above and beyond those typically required by the minor procedure, will reduce the likelihood of redeterminations from reviews and audits. Understanding Medicare guidelines and National Correct Coding Initiative recommendations will help keep the dermatologist out of hot water.5
- Levinson DR. Use of modifier 25. Office of Inspector General website. https://oig.hhs.gov/oei/reports/oei-07-03-00470.pdf. Published November 2005. Accessed January 31, 2017.
- Modifier tables. Tufts Health Plan website. https://tuftshealthplan.com/documents/providers/payment-policies/modifier-tables-payment-policy. Revised April 2016. Accessed February 24, 2017.
- Current Procedural Terminology 2017, Professional Edition. Chicago, IL: American Medical Association; 2016.
- Centers for Medicare & Medicaid Services. Payment for evaluation and management services provided during global period of surgery. MLN Matters. May 19, 2006. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM5025.pdf. Updated November 1, 2012. Accessed January 31, 2017.
- National Correct Coding Initiative Policy Manual for Medicare Services—Effective January 1, 2017. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/Downloads/2017-NCCI-Policy-Manual.zip. Accessed February 24, 2017.
An established patient comes into your office with a painful new lesion on the hand. He thinks it may be a wart. You take a focused history of the lesion, do a physical examination, and confirm the diagnosis of verruca vulgaris. You discuss treatment options, risks, and the benefits of treatment, as well as the pathophysiology of warts. The decision is made to proceed that same day with cryosurgical destruction, which is performed. You feel that billing both an office visit with an appended modifier -25 and the benign destruction code 17110 is warranted, but your biller says only the procedure should be reported. Who is correct?
Modifier -25 use has come under increased scrutiny by insurers and regulators. There is a perception that this modifier is frequently used inappropriately or unnecessarily. In fact, the Office of Inspector General reported that 35% of claims using modifier -25 that Medicare allowed did not meet the requirements. The Office of Inspector General has recommended that the “[Centers for Medicare & Medicaid Services] should work with carriers to reduce the number of claims submitted using modifier -25” and “include modifier -25 reviews in their medical review strategies.”1 Translation: More chart reviews and audits! In my discussions with insurer medical directors, they point to the single diagnosis modifier -25 as likely abused and feel that its use in this context is almost never appropriate. Their audits have been focused on this aspect of dermatologists’ coding. In addition, some private insurers have started to discount reimbursement for office visits billed with modifier -25 by 50% to account for the level of perceived overuse.2
The Current Procedural Terminology description of modifier -25 is relatively clear: Modifier -25 is used to facilitate billing of evaluation and management (E/M) services on the day of a procedure for which separate payment may be made.3 This modifier indicates that a significant, separately identifiable E/M service was performed by the same physician on the day of a procedure. To appropriately bill both the E/M service and the procedure, the physician must indicate that the patient’s condition required an E/M service “above and beyond the usual pre- and post-operative work of a procedure.”4 However, it is largely left up to the physician to decide what constitutes the significant, separately identifiable E/M service.
As dermatologists, we all report modifier -25 appropriately as part of our daily practice. Performance of a medically necessary procedure on the same day as an E/M service generally is done to facilitate a prompt diagnosis or streamline treatment of a complex condition. Providing distinct medically necessary services on the same date allows physicians to provide effective and efficient high-quality care, in many cases saving patients a return visit. The most common scenario for using modifier -25 involves multiple concerns and multiple diagnoses, some of which are not associated with a procedure(s) that is performed on the same date of service. With multiple diagnoses, it is straightforward to demonstrate the separate E/M service associated with the nonprocedure-related diagnosis code(s); however, with one diagnosis for both the office visit and the procedure, clear documentation of the separate and identifiable E/M service is critical and is dependent on understanding what is included in the global surgical package.
Insurer payment for procedures includes local or topical anesthesia, the surgical service/procedure itself, immediate postoperative care including dictating the operative note, meeting/discussing the patient’s procedure with family and other physicians, evaluating the patient in postanesthesia/recovery area, and writing orders for the patient. This group of services is called the global surgical package. For minor procedures (ie, those with either 0- or 10-day global periods), the surgical package also includes same-day E/M associated with the decision to perform surgery. An appropriate history and physical examination, as well as the discussion of differential diagnosis, treatment options, and risk and benefits of treatments, are all included in the payment of a minor procedure itself. Therefore, if an E/M service is performed on the same day as a minor procedure to decide whether to proceed with the minor surgical procedure, this E/M service cannot be separately reported. Moreover, the fact that the patient is new to the physician is not sufficient to allow reporting of an E/M service with such a minor procedure. For major procedures (ie, those with 90-day postoperative periods), the decision for surgery is excluded from the global surgical package.
Therefore, it is clear that the clinical scenario for verruca vulgaris treatment as described at the start of this article does not meet criteria for an office visit billed in addition to the destruction. The E/M services performed prior to the patient’s verruca vulgaris treatment are integral to and necessary for the decision to perform the procedure. Making and confirming the diagnosis of a condition or lesion prior to a procedure either by physical evaluation or by interpretation of a pathology report is part of the evaluation required to make the decision to proceed with a particular procedure.
There are clinical scenarios in which a physician can support additional E/M services beyond that of the procedure with just one diagnosis. If a patient presents with warts on the hand and face with resultant cryosurgical destruction done on the hand and a prescription for imiquimod to be used on the face to induce immunologic clearance of viral infection and decrease the risk of scarring, it is clear that a significant and separately identifiable E/M service exists. The evaluation of the facial warts and the prescription of medication and discussion of the risks, benefits, and therapeutic effects of that prescription is definitely distinct from the procedure. Similarly, if an evaluation of a patient with a rash results in only a diagnostic biopsy with no separate cognitive services other than the decision to perform the biopsy, an office visit charge in addition to the biopsy charge would not be warranted. However, if in addition to the biopsy the rash also is treated with topical or systemic steroids because of pruritus or a more extensive evaluation for systemic complications is required, an office visit charge is appropriate.
The frequent use of modifier -25 is a critical part of a high-quality and cost-effective dermatology practice. Same-day performance of E/M services and minor procedures allows for more rapid and efficient diagnosis and treatment of various conditions as well as minimizing unnecessary office visits. However, modifier -25 use, particularly in the context of the same diagnosis for the office visit and the procedure, is under intense insurer scrutiny. Careful and complete documentation of the additional E/M service provided, including the additional history, physical examination results, and treatment considerations above and beyond those typically required by the minor procedure, will reduce the likelihood of redeterminations from reviews and audits. Understanding Medicare guidelines and National Correct Coding Initiative recommendations will help keep the dermatologist out of hot water.5
An established patient comes into your office with a painful new lesion on the hand. He thinks it may be a wart. You take a focused history of the lesion, do a physical examination, and confirm the diagnosis of verruca vulgaris. You discuss treatment options, risks, and the benefits of treatment, as well as the pathophysiology of warts. The decision is made to proceed that same day with cryosurgical destruction, which is performed. You feel that billing both an office visit with an appended modifier -25 and the benign destruction code 17110 is warranted, but your biller says only the procedure should be reported. Who is correct?
Modifier -25 use has come under increased scrutiny by insurers and regulators. There is a perception that this modifier is frequently used inappropriately or unnecessarily. In fact, the Office of Inspector General reported that 35% of claims using modifier -25 that Medicare allowed did not meet the requirements. The Office of Inspector General has recommended that the “[Centers for Medicare & Medicaid Services] should work with carriers to reduce the number of claims submitted using modifier -25” and “include modifier -25 reviews in their medical review strategies.”1 Translation: More chart reviews and audits! In my discussions with insurer medical directors, they point to the single diagnosis modifier -25 as likely abused and feel that its use in this context is almost never appropriate. Their audits have been focused on this aspect of dermatologists’ coding. In addition, some private insurers have started to discount reimbursement for office visits billed with modifier -25 by 50% to account for the level of perceived overuse.2
The Current Procedural Terminology description of modifier -25 is relatively clear: Modifier -25 is used to facilitate billing of evaluation and management (E/M) services on the day of a procedure for which separate payment may be made.3 This modifier indicates that a significant, separately identifiable E/M service was performed by the same physician on the day of a procedure. To appropriately bill both the E/M service and the procedure, the physician must indicate that the patient’s condition required an E/M service “above and beyond the usual pre- and post-operative work of a procedure.”4 However, it is largely left up to the physician to decide what constitutes the significant, separately identifiable E/M service.
As dermatologists, we all report modifier -25 appropriately as part of our daily practice. Performance of a medically necessary procedure on the same day as an E/M service generally is done to facilitate a prompt diagnosis or streamline treatment of a complex condition. Providing distinct medically necessary services on the same date allows physicians to provide effective and efficient high-quality care, in many cases saving patients a return visit. The most common scenario for using modifier -25 involves multiple concerns and multiple diagnoses, some of which are not associated with a procedure(s) that is performed on the same date of service. With multiple diagnoses, it is straightforward to demonstrate the separate E/M service associated with the nonprocedure-related diagnosis code(s); however, with one diagnosis for both the office visit and the procedure, clear documentation of the separate and identifiable E/M service is critical and is dependent on understanding what is included in the global surgical package.
Insurer payment for procedures includes local or topical anesthesia, the surgical service/procedure itself, immediate postoperative care including dictating the operative note, meeting/discussing the patient’s procedure with family and other physicians, evaluating the patient in postanesthesia/recovery area, and writing orders for the patient. This group of services is called the global surgical package. For minor procedures (ie, those with either 0- or 10-day global periods), the surgical package also includes same-day E/M associated with the decision to perform surgery. An appropriate history and physical examination, as well as the discussion of differential diagnosis, treatment options, and risk and benefits of treatments, are all included in the payment of a minor procedure itself. Therefore, if an E/M service is performed on the same day as a minor procedure to decide whether to proceed with the minor surgical procedure, this E/M service cannot be separately reported. Moreover, the fact that the patient is new to the physician is not sufficient to allow reporting of an E/M service with such a minor procedure. For major procedures (ie, those with 90-day postoperative periods), the decision for surgery is excluded from the global surgical package.
Therefore, it is clear that the clinical scenario for verruca vulgaris treatment as described at the start of this article does not meet criteria for an office visit billed in addition to the destruction. The E/M services performed prior to the patient’s verruca vulgaris treatment are integral to and necessary for the decision to perform the procedure. Making and confirming the diagnosis of a condition or lesion prior to a procedure either by physical evaluation or by interpretation of a pathology report is part of the evaluation required to make the decision to proceed with a particular procedure.
There are clinical scenarios in which a physician can support additional E/M services beyond that of the procedure with just one diagnosis. If a patient presents with warts on the hand and face with resultant cryosurgical destruction done on the hand and a prescription for imiquimod to be used on the face to induce immunologic clearance of viral infection and decrease the risk of scarring, it is clear that a significant and separately identifiable E/M service exists. The evaluation of the facial warts and the prescription of medication and discussion of the risks, benefits, and therapeutic effects of that prescription is definitely distinct from the procedure. Similarly, if an evaluation of a patient with a rash results in only a diagnostic biopsy with no separate cognitive services other than the decision to perform the biopsy, an office visit charge in addition to the biopsy charge would not be warranted. However, if in addition to the biopsy the rash also is treated with topical or systemic steroids because of pruritus or a more extensive evaluation for systemic complications is required, an office visit charge is appropriate.
The frequent use of modifier -25 is a critical part of a high-quality and cost-effective dermatology practice. Same-day performance of E/M services and minor procedures allows for more rapid and efficient diagnosis and treatment of various conditions as well as minimizing unnecessary office visits. However, modifier -25 use, particularly in the context of the same diagnosis for the office visit and the procedure, is under intense insurer scrutiny. Careful and complete documentation of the additional E/M service provided, including the additional history, physical examination results, and treatment considerations above and beyond those typically required by the minor procedure, will reduce the likelihood of redeterminations from reviews and audits. Understanding Medicare guidelines and National Correct Coding Initiative recommendations will help keep the dermatologist out of hot water.5
- Levinson DR. Use of modifier 25. Office of Inspector General website. https://oig.hhs.gov/oei/reports/oei-07-03-00470.pdf. Published November 2005. Accessed January 31, 2017.
- Modifier tables. Tufts Health Plan website. https://tuftshealthplan.com/documents/providers/payment-policies/modifier-tables-payment-policy. Revised April 2016. Accessed February 24, 2017.
- Current Procedural Terminology 2017, Professional Edition. Chicago, IL: American Medical Association; 2016.
- Centers for Medicare & Medicaid Services. Payment for evaluation and management services provided during global period of surgery. MLN Matters. May 19, 2006. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM5025.pdf. Updated November 1, 2012. Accessed January 31, 2017.
- National Correct Coding Initiative Policy Manual for Medicare Services—Effective January 1, 2017. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/Downloads/2017-NCCI-Policy-Manual.zip. Accessed February 24, 2017.
- Levinson DR. Use of modifier 25. Office of Inspector General website. https://oig.hhs.gov/oei/reports/oei-07-03-00470.pdf. Published November 2005. Accessed January 31, 2017.
- Modifier tables. Tufts Health Plan website. https://tuftshealthplan.com/documents/providers/payment-policies/modifier-tables-payment-policy. Revised April 2016. Accessed February 24, 2017.
- Current Procedural Terminology 2017, Professional Edition. Chicago, IL: American Medical Association; 2016.
- Centers for Medicare & Medicaid Services. Payment for evaluation and management services provided during global period of surgery. MLN Matters. May 19, 2006. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/MM5025.pdf. Updated November 1, 2012. Accessed January 31, 2017.
- National Correct Coding Initiative Policy Manual for Medicare Services—Effective January 1, 2017. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/Downloads/2017-NCCI-Policy-Manual.zip. Accessed February 24, 2017.
Practice Points
- Modifier -25 use is appropriate and critical for high-quality, efficient dermatology care.
- Correct use and documentation can help avoid loss of audits associated with modifier -25.

Coding Changes for 2017
All physicians will see changes in reimbursement in 2017. A new president with a new agenda makes for an interesting time ahead for health care in the United States. However, in this time of flux, there is one constant: the Final Rule, an informal term for the annual update on how the Medicare system will function and how much you will get paid for what you do.1 The document is 393 pages and outlines what is new in the Medicare system, with lots of supplements giving granular details about physician work, overhead, and supply and labor costs. In this column, I have taken the liberty of dissecting the Final Rule for you and to bring attention to its high and low points for dermatologists.
Changes in Relative Value Units
The conversion factor has gone up, meaning you will be paid a bit more this year for what you do; it is not enough to account for inflation or the increasing cost of unfunded mandates, but it is better than nothing. Although the conversion factor was $35.8043 in 2016, it increased by more than 0.2% on January 1, 2017, to $35.8887.1 How is this conversion factor calculated? We go up 0.5% due to MACRA (Medicare Access and CHIP Reauthorization Act), down 0.013% due to budget neutrality, down 0.07% due to multiple procedure payment reduction changes, and down another 0.18% due to the misvalued code target.1 The misvalued code target is related to targets established by statute for 2016 to 2018 and payment rates are reduced across the board if they are not met.
If payments suffer from reductions in work value, they may not happen all at once. If the Centers for Medicare & Medicaid Services (CMS) reduce total relative value units (RVUs) by more than 20%, reductions will take place over at least 2 years with a single year drop maximum of 19%.1 Unfortunately, such limits do not apply to revised codes, which can take as big a hit as the CMS cares to make.
Changes to Global Periods
In 2015, we learned that 10- and 90-day global periods would be eliminated in 2017 and 2018, respectively, with great concern on the part of the government about the number and level of evaluation and management services embedded in these codes. The implementation of global policy elimination was prohibited by MACRA and the CMS was required to develop and implement a process to gather data on services furnished in the global period from a representative sample of physicians, which they will use to value surgical services beginningin 2019.1 The CMS decided to capture this data with a new set of time-based G codes (which would be onerous for all practicing physicians), not just the unlucky folks who were to be the sample mandated under MACRA.2 During the comment period, it became obvious to the CMS that this concept was flawed for many reasons and it decided to hold a town hall meeting at the CMS headquarters on August 25, 2016, on data collection on resources used in furnishing global services in which 90 minutes of live testimony in the morning was followed by another 90 minutes by telephone in the afternoon.3 This meeting, which I attended, resulted in the CMS changing the all-practitioner reporting program to a specified sample with others allowed to opt in. Practitioners in groups of less than 10 are exempt, and only physicians in Florida, Kentucky, Louisiana, Nevada, New Jersey, North Dakota, Ohio, Oregon, and Rhode Island must capture data beginning in July 2017.1 These data only have to be captured on codes that are used by more than 100 practitioners and are furnished at least 10,000 times or have allowed charges of greater than $10,000,000 annually. If you are lucky enough to live in one of the testing states, you must start on July 1 but can start before July 1 if you wish. Practitioners in smaller practices or in other geographic areas are encouraged to report data if feasible but are not required to do so. Current Procedural Terminology (CPT) code 99024 will be used for reporting postoperative services rather than the proposed onerous set of G codes, and reporting will not be required for preoperative visits included in the global package or for services not related to the patient’s visit.
Changes to Chronic Care Management
There are new and modified chronic care management codes that are not of use to you unless you are the primary provider for the patient and you and the patient meet multiple stringent requirements.4 The patient must have multiple illnesses, use multiple medications, be unable to perform activities of daily living, require a caregiver, and/or have repeat admissions or emergency department visits. Typical adult patients who receive complex chronic care management services are treated with 3 or more prescription medications and may be receiving other types of therapeutic interventions (eg, physical therapy, occupational therapy). Typical pediatric patients receive 3 or more therapeutic interventions (eg, medications, nutritional support, respiratory therapy). All patients have 2 or more chronic continuous or episodic health conditions that are expected to last at least 12 months or until the death of the patient and place the patient at serious risk for death, acute exacerbation/decompensation, or functional decline.4
Changes to Moderate Sedation Codes
The economic value of providing moderate sedation (eg, drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation) used to be embedded in a variety of CPT codes, which is no longer the case in 2017. Diazepam or similar drugs swallowed or dissolved under the tongue are not included. The new CPT codes 99151, 99152, 99153, 99155, 99156, and 99157 are not to be used to report administration of medications for pain control or minimal sedation (anxiolysis). An independent trained observer, an individual who is qualified to monitor the patient during the procedure and who has no other duties (eg, assisting at surgery) during the procedure, must be present. If you are thinking of using these codes, read the entire section in the CPT manual,4 check your state laws, and consult your malpractice carrier and perhaps even your health care attorney.
Changes to Nail Procedure Codes
Current Procedural Terminology code 11752 (excision of nail and nail matrix, partial or complete [eg, ingrown or deformed nail], for permanent removal; with amputation of tuft of distal phalanx) is now gone, while base code 11750 remains. If you are doing nail surgery and removing underlying bone, instead use code 26236 (partial excision [craterization, saucerization, or diaphysectomy] bone [eg, osteomyelitis]; distal phalanx of finger), 28124 (partial excision [craterization, saucerization, sequestrectomy, or diaphysectomy] bone [eg, osteomyelitis or bossing]; phalanx of toe), or other codes in the same section of the CPT manual if they more precisely describe the procedure performed.
Changes to Slide Consultation Codes
The slide consultation codes 88321 (consultation and report on referred slides prepared elsewhere), 88323 (consultation and report on referred material requiring preparation of slides), and 88325 (consultation, comprehensive, with review of records and specimens, with report on referred material) were revalued this year, with the first 2 showing no change but the latter showing an increase in value from 2.50 to 2.85 RVUs.1 None are meant to be routine. If you have every slide looked at by someone else for “quality assurance reasons,” the consultation is not reportable. If you use these consultation codes too often, the CMS might have concerns about fraud and abuse. Visit http://data.cms.gov to see how you compare to your peers.
Changes to Reflectance Confocal Microscopy Codes
Reflectance confocal microscopy had new codes for 2016, which were carrier priced, and in 2017 they have real RVUs per the CMS. The payments for these codes have a national average reimbursement of $161.85 for 96931 (reflectance confocal microscopy for cellular and subcellular imaging of skin; image acquisition and interpretation and report, first lesion), $104.80 for 96932 (image acquisition only, first lesion), and $45.94 for 96933 (interpretation and report only, first lesion).5 The respective add-on codes have values of $83.26 for 96934 (image acquisition and interpretation and report, each additional lesion [list separately in addition to code for primary procedure]), $35.17 for 96935 (image acquisition only, each additional lesion [list separately in addition to code for primary procedure]), and $43.78 for 96936 (interpretation and report only, each additional lesion [list separately in addition to code for primary procedure]).
Other Coding Changes
There are a whole bunch of new codes in the “Genomic Sequencing Procedures and Other Molecular Multianalyte Assays” (MMAAs) section of CPT. The important thing for you to remember is these codes are for the laboratory performing the assay to report, not the physician ordering it. There is a new Appendix O for proprietary laboratory analysis MMAAs, including those that do not have a Category I code. These MMAAs are identified in Appendix O by a 4-digit number followed by the letter M.4
There are some revisions to psychotherapy codes 90832 to 90847. These codes are outside our scope of practice and should only be used by psychiatrists, social workers, psychologists, or other appropriate mental health workers.
Final Thoughts
It has not been a breakout year for telehealth and we still do not have payment for store-and-forward teledermatology, except in a few designated rural areas. With the advent of the rhetoric we have heard after the presidential election, any speculation on what will happen to the brave new world of the merit-based incentive payment system, alternative payment models, and other regulations are anyone’s guess.
- Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2017; Medicare Advantage Bid Pricing Data Release; Medicare Advantage and Part D Medical Loss Ratio Data Release; Medicare Advantage Provider Network Requirements; Expansion of Medicare Diabetes Prevention Program Model; Medicare Shared Savings Program Requirements. Fed Regist. 2016;81(220):80170-80562. To be codified at 42 CFR § 405, 410, 411, 414, 417, 422, 423, 424, 425, and 460.
- Siegel DM. The Proposed Rule and payments for 2017: the good, the bad, and the ugly. Cutis. 2016;98:245-248.
- Data collection on resources used in furnishing global services town hall CY 2017 Medicare physician fee schedule Proposed Rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/CY2017-PFS-FR-Townhall.pdf. Published August 25, 2016. Accessed January 4, 2017.
- Current Procedural Terminology 2017, Professional Edition. Chicago, IL: American Medical Association; 2016.
- Addendum B—relative value units and related information used in CY 2017 final rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/CY2017-PFS-FR-Addenda.zip. Accessed January 23, 2017.
All physicians will see changes in reimbursement in 2017. A new president with a new agenda makes for an interesting time ahead for health care in the United States. However, in this time of flux, there is one constant: the Final Rule, an informal term for the annual update on how the Medicare system will function and how much you will get paid for what you do.1 The document is 393 pages and outlines what is new in the Medicare system, with lots of supplements giving granular details about physician work, overhead, and supply and labor costs. In this column, I have taken the liberty of dissecting the Final Rule for you and to bring attention to its high and low points for dermatologists.
Changes in Relative Value Units
The conversion factor has gone up, meaning you will be paid a bit more this year for what you do; it is not enough to account for inflation or the increasing cost of unfunded mandates, but it is better than nothing. Although the conversion factor was $35.8043 in 2016, it increased by more than 0.2% on January 1, 2017, to $35.8887.1 How is this conversion factor calculated? We go up 0.5% due to MACRA (Medicare Access and CHIP Reauthorization Act), down 0.013% due to budget neutrality, down 0.07% due to multiple procedure payment reduction changes, and down another 0.18% due to the misvalued code target.1 The misvalued code target is related to targets established by statute for 2016 to 2018 and payment rates are reduced across the board if they are not met.
If payments suffer from reductions in work value, they may not happen all at once. If the Centers for Medicare & Medicaid Services (CMS) reduce total relative value units (RVUs) by more than 20%, reductions will take place over at least 2 years with a single year drop maximum of 19%.1 Unfortunately, such limits do not apply to revised codes, which can take as big a hit as the CMS cares to make.
Changes to Global Periods
In 2015, we learned that 10- and 90-day global periods would be eliminated in 2017 and 2018, respectively, with great concern on the part of the government about the number and level of evaluation and management services embedded in these codes. The implementation of global policy elimination was prohibited by MACRA and the CMS was required to develop and implement a process to gather data on services furnished in the global period from a representative sample of physicians, which they will use to value surgical services beginningin 2019.1 The CMS decided to capture this data with a new set of time-based G codes (which would be onerous for all practicing physicians), not just the unlucky folks who were to be the sample mandated under MACRA.2 During the comment period, it became obvious to the CMS that this concept was flawed for many reasons and it decided to hold a town hall meeting at the CMS headquarters on August 25, 2016, on data collection on resources used in furnishing global services in which 90 minutes of live testimony in the morning was followed by another 90 minutes by telephone in the afternoon.3 This meeting, which I attended, resulted in the CMS changing the all-practitioner reporting program to a specified sample with others allowed to opt in. Practitioners in groups of less than 10 are exempt, and only physicians in Florida, Kentucky, Louisiana, Nevada, New Jersey, North Dakota, Ohio, Oregon, and Rhode Island must capture data beginning in July 2017.1 These data only have to be captured on codes that are used by more than 100 practitioners and are furnished at least 10,000 times or have allowed charges of greater than $10,000,000 annually. If you are lucky enough to live in one of the testing states, you must start on July 1 but can start before July 1 if you wish. Practitioners in smaller practices or in other geographic areas are encouraged to report data if feasible but are not required to do so. Current Procedural Terminology (CPT) code 99024 will be used for reporting postoperative services rather than the proposed onerous set of G codes, and reporting will not be required for preoperative visits included in the global package or for services not related to the patient’s visit.
Changes to Chronic Care Management
There are new and modified chronic care management codes that are not of use to you unless you are the primary provider for the patient and you and the patient meet multiple stringent requirements.4 The patient must have multiple illnesses, use multiple medications, be unable to perform activities of daily living, require a caregiver, and/or have repeat admissions or emergency department visits. Typical adult patients who receive complex chronic care management services are treated with 3 or more prescription medications and may be receiving other types of therapeutic interventions (eg, physical therapy, occupational therapy). Typical pediatric patients receive 3 or more therapeutic interventions (eg, medications, nutritional support, respiratory therapy). All patients have 2 or more chronic continuous or episodic health conditions that are expected to last at least 12 months or until the death of the patient and place the patient at serious risk for death, acute exacerbation/decompensation, or functional decline.4
Changes to Moderate Sedation Codes
The economic value of providing moderate sedation (eg, drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation) used to be embedded in a variety of CPT codes, which is no longer the case in 2017. Diazepam or similar drugs swallowed or dissolved under the tongue are not included. The new CPT codes 99151, 99152, 99153, 99155, 99156, and 99157 are not to be used to report administration of medications for pain control or minimal sedation (anxiolysis). An independent trained observer, an individual who is qualified to monitor the patient during the procedure and who has no other duties (eg, assisting at surgery) during the procedure, must be present. If you are thinking of using these codes, read the entire section in the CPT manual,4 check your state laws, and consult your malpractice carrier and perhaps even your health care attorney.
Changes to Nail Procedure Codes
Current Procedural Terminology code 11752 (excision of nail and nail matrix, partial or complete [eg, ingrown or deformed nail], for permanent removal; with amputation of tuft of distal phalanx) is now gone, while base code 11750 remains. If you are doing nail surgery and removing underlying bone, instead use code 26236 (partial excision [craterization, saucerization, or diaphysectomy] bone [eg, osteomyelitis]; distal phalanx of finger), 28124 (partial excision [craterization, saucerization, sequestrectomy, or diaphysectomy] bone [eg, osteomyelitis or bossing]; phalanx of toe), or other codes in the same section of the CPT manual if they more precisely describe the procedure performed.
Changes to Slide Consultation Codes
The slide consultation codes 88321 (consultation and report on referred slides prepared elsewhere), 88323 (consultation and report on referred material requiring preparation of slides), and 88325 (consultation, comprehensive, with review of records and specimens, with report on referred material) were revalued this year, with the first 2 showing no change but the latter showing an increase in value from 2.50 to 2.85 RVUs.1 None are meant to be routine. If you have every slide looked at by someone else for “quality assurance reasons,” the consultation is not reportable. If you use these consultation codes too often, the CMS might have concerns about fraud and abuse. Visit http://data.cms.gov to see how you compare to your peers.
Changes to Reflectance Confocal Microscopy Codes
Reflectance confocal microscopy had new codes for 2016, which were carrier priced, and in 2017 they have real RVUs per the CMS. The payments for these codes have a national average reimbursement of $161.85 for 96931 (reflectance confocal microscopy for cellular and subcellular imaging of skin; image acquisition and interpretation and report, first lesion), $104.80 for 96932 (image acquisition only, first lesion), and $45.94 for 96933 (interpretation and report only, first lesion).5 The respective add-on codes have values of $83.26 for 96934 (image acquisition and interpretation and report, each additional lesion [list separately in addition to code for primary procedure]), $35.17 for 96935 (image acquisition only, each additional lesion [list separately in addition to code for primary procedure]), and $43.78 for 96936 (interpretation and report only, each additional lesion [list separately in addition to code for primary procedure]).
Other Coding Changes
There are a whole bunch of new codes in the “Genomic Sequencing Procedures and Other Molecular Multianalyte Assays” (MMAAs) section of CPT. The important thing for you to remember is these codes are for the laboratory performing the assay to report, not the physician ordering it. There is a new Appendix O for proprietary laboratory analysis MMAAs, including those that do not have a Category I code. These MMAAs are identified in Appendix O by a 4-digit number followed by the letter M.4
There are some revisions to psychotherapy codes 90832 to 90847. These codes are outside our scope of practice and should only be used by psychiatrists, social workers, psychologists, or other appropriate mental health workers.
Final Thoughts
It has not been a breakout year for telehealth and we still do not have payment for store-and-forward teledermatology, except in a few designated rural areas. With the advent of the rhetoric we have heard after the presidential election, any speculation on what will happen to the brave new world of the merit-based incentive payment system, alternative payment models, and other regulations are anyone’s guess.
All physicians will see changes in reimbursement in 2017. A new president with a new agenda makes for an interesting time ahead for health care in the United States. However, in this time of flux, there is one constant: the Final Rule, an informal term for the annual update on how the Medicare system will function and how much you will get paid for what you do.1 The document is 393 pages and outlines what is new in the Medicare system, with lots of supplements giving granular details about physician work, overhead, and supply and labor costs. In this column, I have taken the liberty of dissecting the Final Rule for you and to bring attention to its high and low points for dermatologists.
Changes in Relative Value Units
The conversion factor has gone up, meaning you will be paid a bit more this year for what you do; it is not enough to account for inflation or the increasing cost of unfunded mandates, but it is better than nothing. Although the conversion factor was $35.8043 in 2016, it increased by more than 0.2% on January 1, 2017, to $35.8887.1 How is this conversion factor calculated? We go up 0.5% due to MACRA (Medicare Access and CHIP Reauthorization Act), down 0.013% due to budget neutrality, down 0.07% due to multiple procedure payment reduction changes, and down another 0.18% due to the misvalued code target.1 The misvalued code target is related to targets established by statute for 2016 to 2018 and payment rates are reduced across the board if they are not met.
If payments suffer from reductions in work value, they may not happen all at once. If the Centers for Medicare & Medicaid Services (CMS) reduce total relative value units (RVUs) by more than 20%, reductions will take place over at least 2 years with a single year drop maximum of 19%.1 Unfortunately, such limits do not apply to revised codes, which can take as big a hit as the CMS cares to make.
Changes to Global Periods
In 2015, we learned that 10- and 90-day global periods would be eliminated in 2017 and 2018, respectively, with great concern on the part of the government about the number and level of evaluation and management services embedded in these codes. The implementation of global policy elimination was prohibited by MACRA and the CMS was required to develop and implement a process to gather data on services furnished in the global period from a representative sample of physicians, which they will use to value surgical services beginningin 2019.1 The CMS decided to capture this data with a new set of time-based G codes (which would be onerous for all practicing physicians), not just the unlucky folks who were to be the sample mandated under MACRA.2 During the comment period, it became obvious to the CMS that this concept was flawed for many reasons and it decided to hold a town hall meeting at the CMS headquarters on August 25, 2016, on data collection on resources used in furnishing global services in which 90 minutes of live testimony in the morning was followed by another 90 minutes by telephone in the afternoon.3 This meeting, which I attended, resulted in the CMS changing the all-practitioner reporting program to a specified sample with others allowed to opt in. Practitioners in groups of less than 10 are exempt, and only physicians in Florida, Kentucky, Louisiana, Nevada, New Jersey, North Dakota, Ohio, Oregon, and Rhode Island must capture data beginning in July 2017.1 These data only have to be captured on codes that are used by more than 100 practitioners and are furnished at least 10,000 times or have allowed charges of greater than $10,000,000 annually. If you are lucky enough to live in one of the testing states, you must start on July 1 but can start before July 1 if you wish. Practitioners in smaller practices or in other geographic areas are encouraged to report data if feasible but are not required to do so. Current Procedural Terminology (CPT) code 99024 will be used for reporting postoperative services rather than the proposed onerous set of G codes, and reporting will not be required for preoperative visits included in the global package or for services not related to the patient’s visit.
Changes to Chronic Care Management
There are new and modified chronic care management codes that are not of use to you unless you are the primary provider for the patient and you and the patient meet multiple stringent requirements.4 The patient must have multiple illnesses, use multiple medications, be unable to perform activities of daily living, require a caregiver, and/or have repeat admissions or emergency department visits. Typical adult patients who receive complex chronic care management services are treated with 3 or more prescription medications and may be receiving other types of therapeutic interventions (eg, physical therapy, occupational therapy). Typical pediatric patients receive 3 or more therapeutic interventions (eg, medications, nutritional support, respiratory therapy). All patients have 2 or more chronic continuous or episodic health conditions that are expected to last at least 12 months or until the death of the patient and place the patient at serious risk for death, acute exacerbation/decompensation, or functional decline.4
Changes to Moderate Sedation Codes
The economic value of providing moderate sedation (eg, drug-induced depression of consciousness during which patients respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation) used to be embedded in a variety of CPT codes, which is no longer the case in 2017. Diazepam or similar drugs swallowed or dissolved under the tongue are not included. The new CPT codes 99151, 99152, 99153, 99155, 99156, and 99157 are not to be used to report administration of medications for pain control or minimal sedation (anxiolysis). An independent trained observer, an individual who is qualified to monitor the patient during the procedure and who has no other duties (eg, assisting at surgery) during the procedure, must be present. If you are thinking of using these codes, read the entire section in the CPT manual,4 check your state laws, and consult your malpractice carrier and perhaps even your health care attorney.
Changes to Nail Procedure Codes
Current Procedural Terminology code 11752 (excision of nail and nail matrix, partial or complete [eg, ingrown or deformed nail], for permanent removal; with amputation of tuft of distal phalanx) is now gone, while base code 11750 remains. If you are doing nail surgery and removing underlying bone, instead use code 26236 (partial excision [craterization, saucerization, or diaphysectomy] bone [eg, osteomyelitis]; distal phalanx of finger), 28124 (partial excision [craterization, saucerization, sequestrectomy, or diaphysectomy] bone [eg, osteomyelitis or bossing]; phalanx of toe), or other codes in the same section of the CPT manual if they more precisely describe the procedure performed.
Changes to Slide Consultation Codes
The slide consultation codes 88321 (consultation and report on referred slides prepared elsewhere), 88323 (consultation and report on referred material requiring preparation of slides), and 88325 (consultation, comprehensive, with review of records and specimens, with report on referred material) were revalued this year, with the first 2 showing no change but the latter showing an increase in value from 2.50 to 2.85 RVUs.1 None are meant to be routine. If you have every slide looked at by someone else for “quality assurance reasons,” the consultation is not reportable. If you use these consultation codes too often, the CMS might have concerns about fraud and abuse. Visit http://data.cms.gov to see how you compare to your peers.
Changes to Reflectance Confocal Microscopy Codes
Reflectance confocal microscopy had new codes for 2016, which were carrier priced, and in 2017 they have real RVUs per the CMS. The payments for these codes have a national average reimbursement of $161.85 for 96931 (reflectance confocal microscopy for cellular and subcellular imaging of skin; image acquisition and interpretation and report, first lesion), $104.80 for 96932 (image acquisition only, first lesion), and $45.94 for 96933 (interpretation and report only, first lesion).5 The respective add-on codes have values of $83.26 for 96934 (image acquisition and interpretation and report, each additional lesion [list separately in addition to code for primary procedure]), $35.17 for 96935 (image acquisition only, each additional lesion [list separately in addition to code for primary procedure]), and $43.78 for 96936 (interpretation and report only, each additional lesion [list separately in addition to code for primary procedure]).
Other Coding Changes
There are a whole bunch of new codes in the “Genomic Sequencing Procedures and Other Molecular Multianalyte Assays” (MMAAs) section of CPT. The important thing for you to remember is these codes are for the laboratory performing the assay to report, not the physician ordering it. There is a new Appendix O for proprietary laboratory analysis MMAAs, including those that do not have a Category I code. These MMAAs are identified in Appendix O by a 4-digit number followed by the letter M.4
There are some revisions to psychotherapy codes 90832 to 90847. These codes are outside our scope of practice and should only be used by psychiatrists, social workers, psychologists, or other appropriate mental health workers.
Final Thoughts
It has not been a breakout year for telehealth and we still do not have payment for store-and-forward teledermatology, except in a few designated rural areas. With the advent of the rhetoric we have heard after the presidential election, any speculation on what will happen to the brave new world of the merit-based incentive payment system, alternative payment models, and other regulations are anyone’s guess.
- Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2017; Medicare Advantage Bid Pricing Data Release; Medicare Advantage and Part D Medical Loss Ratio Data Release; Medicare Advantage Provider Network Requirements; Expansion of Medicare Diabetes Prevention Program Model; Medicare Shared Savings Program Requirements. Fed Regist. 2016;81(220):80170-80562. To be codified at 42 CFR § 405, 410, 411, 414, 417, 422, 423, 424, 425, and 460.
- Siegel DM. The Proposed Rule and payments for 2017: the good, the bad, and the ugly. Cutis. 2016;98:245-248.
- Data collection on resources used in furnishing global services town hall CY 2017 Medicare physician fee schedule Proposed Rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/CY2017-PFS-FR-Townhall.pdf. Published August 25, 2016. Accessed January 4, 2017.
- Current Procedural Terminology 2017, Professional Edition. Chicago, IL: American Medical Association; 2016.
- Addendum B—relative value units and related information used in CY 2017 final rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/CY2017-PFS-FR-Addenda.zip. Accessed January 23, 2017.
- Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2017; Medicare Advantage Bid Pricing Data Release; Medicare Advantage and Part D Medical Loss Ratio Data Release; Medicare Advantage Provider Network Requirements; Expansion of Medicare Diabetes Prevention Program Model; Medicare Shared Savings Program Requirements. Fed Regist. 2016;81(220):80170-80562. To be codified at 42 CFR § 405, 410, 411, 414, 417, 422, 423, 424, 425, and 460.
- Siegel DM. The Proposed Rule and payments for 2017: the good, the bad, and the ugly. Cutis. 2016;98:245-248.
- Data collection on resources used in furnishing global services town hall CY 2017 Medicare physician fee schedule Proposed Rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/CY2017-PFS-FR-Townhall.pdf. Published August 25, 2016. Accessed January 4, 2017.
- Current Procedural Terminology 2017, Professional Edition. Chicago, IL: American Medical Association; 2016.
- Addendum B—relative value units and related information used in CY 2017 final rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/Downloads/CY2017-PFS-FR-Addenda.zip. Accessed January 23, 2017.
Practice Points
- The conversion factor has increased more than 0.2%, which means you will be paid a bit more this year.
- Review Current Procedural Terminology codes carefully for pain control or moderate sedation as well as nail surgery and slide consultation.
- Reflectance confocal microscopy now has relative value units assigned by the Centers for Medicare & Medicaid Services.

A Potpourri of Things to Do Correctly
When you pick up the Current Procedural Terminology (CPT) manual and read it, you may wonder what certain terms mean and how they may be looked at by payers and auditors. As your eyes glaze over from reading mind-numbing descriptions, a few points should be obvious, but conversations with friends, colleagues, and US Office of Inspector General and Centers for Medicare &
Excisions
For excisions (11400–11646), size is easy to determine. You measure the longest diameter of the lesion and the smallest margin required based on your judgment. The sum of the diameter and twice the margin is your lesion size. For benign lesions, the margin can be as small as 0 to 1 mm. For malignancies, it might be 5 to 9 mm for a melanoma in situ, 1 cm or more for an invasive melanoma with similar margins for squamous cell carcinoma, and somewhat less than 1 cm for basal cell carcinomas and more than 1 cm for Merkel cell carcinomas or spindle cell neoplasms.
There are times when you may delay a repair for medical reasons, which you would document in the medical record, but if you systematically delay a repair overnight to avoid the multiple procedure payment reduction, you may become “a person of interest,” which is a bad thing.
The shave removal codes (11300–11313) do not require repair and hemostasis is included. The size of the lesion determines the size of the lesion reported, and margins are not included. Hemostasis is included in the value of the CPT code and is not separately reportable.
It is not uncommon for a patient, usually one well known to you, to present with another skin cancer that has classic clinical findings. You review options with your patient and proceed to take one of the following approaches.
Option 1: You can tangentially remove or curette the tumor bulk and send the specimen for pathology review. At the same time, you curette and cauterize the base. In this case, you should hold your bill and await pathology. If the lesion is malignant, you would report the appropriate malignant destruction code (17260–17286) only. If it is benign, you would report a biopsy based on site or a benign destruction (17110) if for some reason the destruction was medically necessary. If it is an actinic keratosis, you could report either a biopsy or a premalignant destruction (17000).
Option 2: You perform a full-thickness excision of the lesion with a margin to remove it and send the specimen for pathology review. You should hold your bill and await pathology. If the lesion is malignant, you would report the appropriate malignant excision (11600–11646) and repair as discussed above. If it is benign, you would report the appropriate benign excision (11400–11446) and repair as discussed above.
If a shave, excision, or destruction is performed, a biopsy of the tissue should never be reported separately simply because the tissue may be sent to the laboratory. In other words, a biopsy is not separately reportable when another procedure was done at the same site on the same day.
Biopsy
Biopsies come in 2 varieties: general and site specific. All dermatologists are familiar with the basic skin biopsy codes 11110 and 11101 (biopsy of skin, subcutaneous tissue and/or mucous membrane [including simple closure], unless otherwise listed). Many are not aware of site-specific biopsy codes that often are more appropriate and should be used when their localization is more precise than the general skin biopsy.
Biopsies of the nail unit (eg, plate, bed, matrix, hyponychium, proximal and lateral nail folds) are reported using CPT code 11755. A simple nail clipping for culture or periodic acid–Schiff stain is not a nail biopsy and should not be separately reported from the evaluation and management component of the visit.
The lip biopsy code (40490) is used appropriately when the vermilion is sampled, not the skin around it. If the skin and vermilion are contiguously sampled, only report 40490. Specific codes exist for the vestibule of the mouth (40808), the anterior two-thirds (41100) and posterior one-third (41105) of the tongue, the floor (41108) and roof (42100) of the mouth, and the salivary glands by needle (42400) or by incision (42405).
The penis can be biopsied on the surface (54100) or deep structures can be sampled (54105), though the latter is uncommon in dermatology practices. The vulva can be sampled with codes comparable to general biopsy, with 54605 for the first biopsy and 54606 used for each additional one.
An incisional biopsy of the eyelid margin is reported with 67810, while conjunctival biopsy is reported with 68100; 68510 describes a lacrimal gland biopsy. The ear, not to be left out, has its own biopsy codes, with 69100 for the external ear and 69105 for the auditory canal.
Clipping of hair or tape stripping of skin (similar to nail clipping described above) are not biopsies and are not separately reportable, as the work involved is considered incident to the cognitive visit taking place.
Final Thoughts
These points should all be fairly straightforward—yes, the skin biopsy includes mucosa, but if a mucosal site such as the mouth has a more specific code, then that code is correct—and the simplest test for the clinician is to ask yourself, “If I were reviewing the claim, what would I expect to see?” As always, document what you do, do what you document, and report that which is medically necessary.
When you pick up the Current Procedural Terminology (CPT) manual and read it, you may wonder what certain terms mean and how they may be looked at by payers and auditors. As your eyes glaze over from reading mind-numbing descriptions, a few points should be obvious, but conversations with friends, colleagues, and US Office of Inspector General and Centers for Medicare &
Excisions
For excisions (11400–11646), size is easy to determine. You measure the longest diameter of the lesion and the smallest margin required based on your judgment. The sum of the diameter and twice the margin is your lesion size. For benign lesions, the margin can be as small as 0 to 1 mm. For malignancies, it might be 5 to 9 mm for a melanoma in situ, 1 cm or more for an invasive melanoma with similar margins for squamous cell carcinoma, and somewhat less than 1 cm for basal cell carcinomas and more than 1 cm for Merkel cell carcinomas or spindle cell neoplasms.
There are times when you may delay a repair for medical reasons, which you would document in the medical record, but if you systematically delay a repair overnight to avoid the multiple procedure payment reduction, you may become “a person of interest,” which is a bad thing.
The shave removal codes (11300–11313) do not require repair and hemostasis is included. The size of the lesion determines the size of the lesion reported, and margins are not included. Hemostasis is included in the value of the CPT code and is not separately reportable.
It is not uncommon for a patient, usually one well known to you, to present with another skin cancer that has classic clinical findings. You review options with your patient and proceed to take one of the following approaches.
Option 1: You can tangentially remove or curette the tumor bulk and send the specimen for pathology review. At the same time, you curette and cauterize the base. In this case, you should hold your bill and await pathology. If the lesion is malignant, you would report the appropriate malignant destruction code (17260–17286) only. If it is benign, you would report a biopsy based on site or a benign destruction (17110) if for some reason the destruction was medically necessary. If it is an actinic keratosis, you could report either a biopsy or a premalignant destruction (17000).
Option 2: You perform a full-thickness excision of the lesion with a margin to remove it and send the specimen for pathology review. You should hold your bill and await pathology. If the lesion is malignant, you would report the appropriate malignant excision (11600–11646) and repair as discussed above. If it is benign, you would report the appropriate benign excision (11400–11446) and repair as discussed above.
If a shave, excision, or destruction is performed, a biopsy of the tissue should never be reported separately simply because the tissue may be sent to the laboratory. In other words, a biopsy is not separately reportable when another procedure was done at the same site on the same day.
Biopsy
Biopsies come in 2 varieties: general and site specific. All dermatologists are familiar with the basic skin biopsy codes 11110 and 11101 (biopsy of skin, subcutaneous tissue and/or mucous membrane [including simple closure], unless otherwise listed). Many are not aware of site-specific biopsy codes that often are more appropriate and should be used when their localization is more precise than the general skin biopsy.
Biopsies of the nail unit (eg, plate, bed, matrix, hyponychium, proximal and lateral nail folds) are reported using CPT code 11755. A simple nail clipping for culture or periodic acid–Schiff stain is not a nail biopsy and should not be separately reported from the evaluation and management component of the visit.
The lip biopsy code (40490) is used appropriately when the vermilion is sampled, not the skin around it. If the skin and vermilion are contiguously sampled, only report 40490. Specific codes exist for the vestibule of the mouth (40808), the anterior two-thirds (41100) and posterior one-third (41105) of the tongue, the floor (41108) and roof (42100) of the mouth, and the salivary glands by needle (42400) or by incision (42405).
The penis can be biopsied on the surface (54100) or deep structures can be sampled (54105), though the latter is uncommon in dermatology practices. The vulva can be sampled with codes comparable to general biopsy, with 54605 for the first biopsy and 54606 used for each additional one.
An incisional biopsy of the eyelid margin is reported with 67810, while conjunctival biopsy is reported with 68100; 68510 describes a lacrimal gland biopsy. The ear, not to be left out, has its own biopsy codes, with 69100 for the external ear and 69105 for the auditory canal.
Clipping of hair or tape stripping of skin (similar to nail clipping described above) are not biopsies and are not separately reportable, as the work involved is considered incident to the cognitive visit taking place.
Final Thoughts
These points should all be fairly straightforward—yes, the skin biopsy includes mucosa, but if a mucosal site such as the mouth has a more specific code, then that code is correct—and the simplest test for the clinician is to ask yourself, “If I were reviewing the claim, what would I expect to see?” As always, document what you do, do what you document, and report that which is medically necessary.
When you pick up the Current Procedural Terminology (CPT) manual and read it, you may wonder what certain terms mean and how they may be looked at by payers and auditors. As your eyes glaze over from reading mind-numbing descriptions, a few points should be obvious, but conversations with friends, colleagues, and US Office of Inspector General and Centers for Medicare &
Excisions
For excisions (11400–11646), size is easy to determine. You measure the longest diameter of the lesion and the smallest margin required based on your judgment. The sum of the diameter and twice the margin is your lesion size. For benign lesions, the margin can be as small as 0 to 1 mm. For malignancies, it might be 5 to 9 mm for a melanoma in situ, 1 cm or more for an invasive melanoma with similar margins for squamous cell carcinoma, and somewhat less than 1 cm for basal cell carcinomas and more than 1 cm for Merkel cell carcinomas or spindle cell neoplasms.
There are times when you may delay a repair for medical reasons, which you would document in the medical record, but if you systematically delay a repair overnight to avoid the multiple procedure payment reduction, you may become “a person of interest,” which is a bad thing.
The shave removal codes (11300–11313) do not require repair and hemostasis is included. The size of the lesion determines the size of the lesion reported, and margins are not included. Hemostasis is included in the value of the CPT code and is not separately reportable.
It is not uncommon for a patient, usually one well known to you, to present with another skin cancer that has classic clinical findings. You review options with your patient and proceed to take one of the following approaches.
Option 1: You can tangentially remove or curette the tumor bulk and send the specimen for pathology review. At the same time, you curette and cauterize the base. In this case, you should hold your bill and await pathology. If the lesion is malignant, you would report the appropriate malignant destruction code (17260–17286) only. If it is benign, you would report a biopsy based on site or a benign destruction (17110) if for some reason the destruction was medically necessary. If it is an actinic keratosis, you could report either a biopsy or a premalignant destruction (17000).
Option 2: You perform a full-thickness excision of the lesion with a margin to remove it and send the specimen for pathology review. You should hold your bill and await pathology. If the lesion is malignant, you would report the appropriate malignant excision (11600–11646) and repair as discussed above. If it is benign, you would report the appropriate benign excision (11400–11446) and repair as discussed above.
If a shave, excision, or destruction is performed, a biopsy of the tissue should never be reported separately simply because the tissue may be sent to the laboratory. In other words, a biopsy is not separately reportable when another procedure was done at the same site on the same day.
Biopsy
Biopsies come in 2 varieties: general and site specific. All dermatologists are familiar with the basic skin biopsy codes 11110 and 11101 (biopsy of skin, subcutaneous tissue and/or mucous membrane [including simple closure], unless otherwise listed). Many are not aware of site-specific biopsy codes that often are more appropriate and should be used when their localization is more precise than the general skin biopsy.
Biopsies of the nail unit (eg, plate, bed, matrix, hyponychium, proximal and lateral nail folds) are reported using CPT code 11755. A simple nail clipping for culture or periodic acid–Schiff stain is not a nail biopsy and should not be separately reported from the evaluation and management component of the visit.
The lip biopsy code (40490) is used appropriately when the vermilion is sampled, not the skin around it. If the skin and vermilion are contiguously sampled, only report 40490. Specific codes exist for the vestibule of the mouth (40808), the anterior two-thirds (41100) and posterior one-third (41105) of the tongue, the floor (41108) and roof (42100) of the mouth, and the salivary glands by needle (42400) or by incision (42405).
The penis can be biopsied on the surface (54100) or deep structures can be sampled (54105), though the latter is uncommon in dermatology practices. The vulva can be sampled with codes comparable to general biopsy, with 54605 for the first biopsy and 54606 used for each additional one.
An incisional biopsy of the eyelid margin is reported with 67810, while conjunctival biopsy is reported with 68100; 68510 describes a lacrimal gland biopsy. The ear, not to be left out, has its own biopsy codes, with 69100 for the external ear and 69105 for the auditory canal.
Clipping of hair or tape stripping of skin (similar to nail clipping described above) are not biopsies and are not separately reportable, as the work involved is considered incident to the cognitive visit taking place.
Final Thoughts
These points should all be fairly straightforward—yes, the skin biopsy includes mucosa, but if a mucosal site such as the mouth has a more specific code, then that code is correct—and the simplest test for the clinician is to ask yourself, “If I were reviewing the claim, what would I expect to see?” As always, document what you do, do what you document, and report that which is medically necessary.
Practice Points
- A biopsy is not separately reportable when another procedure was done at the same site on the same day (eg, shave, excision, destruction).
- Use site-specific biopsy codes when their localization is more precise than the general skin biopsy.
- A simple nail clipping for culture or periodic acid-Schiff stain is not a nail biopsy and should not be separately reported from the evaluation and management component of the visit.
Everything You Need to Know About the Bundled Payments for Care Improvement Initiative

As far back as 1983 —13 years before the birth of HM—Medicare created what was then called an “inpatient prospective payment system,” which essentially let Medicare pay a fixed amount for the entirety of a hospital stay, based on diagnosis. Then in 1991, the Centers for Medicare & Medicaid Services (CMS) introduced one payment for coronary artery bypass graft surgery, and even included 90-day readmission in the check.
Fast forward to the past 10 years when accountable care organizations (ACOs) and value-based purchasing (VBP) have been the focus of HM executives looking to take the lead in how to make bundled payments work for them.
The Bundled Payments for Care Improvement (BPCI) initiative was introduced by CMS’s Center for Medicare & Medicaid Innovation (CMMI) in 2011 and is now compiling its first data sets for the next frontier of payments for episodic care.
For rank-and-file hospitalists who have felt inundated by the regulations and promised payment reforms from ACOs and VBPs, why is this program so important?
“The reason this is so special is that it is one of the few CMS programs that allows providers to be in the driver’s seat,” says Kerry Weiner, MD, chief medical officer of acute and post-acute services at TeamHealth-IPC The Hospitalist Company. “They have the opportunity to be accountable and to actually be the designers of reengineering care. The other programs that you just mentioned, like value-based purchasing, largely originate from health systems or the federal government and dictate the principles and the metrics that as a provider you’re going to be evaluated upon.
“This model, the bundled model, gives us the flexibility, scale and brackets of risk that we want to accept and thereby gives us a lot more control over what physicians and physician groups can manage successfully.”
BPCI might be a game-changer for HM because it’s the first of the bundled-payment initiatives that truly falls direct to the care provided by hospitalists. In short, the plan covers 48 defined episodes of care and would parse out payments for those episodes in a holistic—and some say more appropriate—way. Currently, a hospitalist would get paid for a patient’s stay in the hospital and a primary-care physician (PCP) could be paid for some follow-up. If the patient ends up back in the hospital quickly, the hospitalist could get paid again and, upon discharge, a PCP could, too.
But under BPCI, pay would be determined based on the episode of care. The details of who gets paid what and the rules that apply are all likely to evolve, of course, but it’s hoped the basic premise of bundled payments would lower the overall cost of healthcare.
How It Works
Under the Patient Protection and Affordable Care Act (ACA) of 2009, it was mandated that the government establish a five-year pilot program by 2013 that bundled payments for inpatient care, according to the American Hospital Association.
The program has now ramped up to include more than 650 participating organization, not including thousands of physicians that then partner with those groups, over four models. The initiative covers defined episodes of care, both medical and surgical, that begin at the time of inpatient admission and stretch 30, 60 or 90 days post-discharge.
And hospitalists are poised to take the lead on how payment models, especially bundled payments, are shaped over the next few years, says John Nelson, MD, MHM, a co-founder and past president of SHM and and principal in Nelson Flores Hospital Medicine Consultants in Bellevue, Wash. Nelson says his consulting firm has seen an uptick in calls over the past two years dealing with alternative payment models (APMs).
“Hospitalists find themselves at a vitally important nexus of performance and success on new payment models,” he adds.

Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners in Darien, Conn., agrees that BPCI and future iterations of bundled payment programs “are likely to be a potent driver of an evolving hospitalist specialty.” His hypothesis is that APMs such as BPCI are an important way for Medicare to reach its stated goal of having 50% of its fee-for-service payments running through APMs by the end of 2018. To further entice that process, physicians who document at least 25% of their revenue as coming through APMs will get a 5% bonus.
“The stakes are high now,” says Dr. Whitcomb, a past SHM president whose employer is an Awardee Convener in the BPCI initiative, meaning it administers the program. “Medicare [has] laid out the
course for the next two and a half, three years and beyond… It will be crucial for hospitalists to have a path to participate broadly in APMs..”
Dr. Whitcomb says BPCI is the program that should excite hospitalists most because it is more applicable to them moving forward than ACOs, heralded by many healthcare executives several years ago as the future of payment reform.
“With a focus on ambulatory care, ACOs have not broadly involved hospitalists,” he says. “If you look at the State of Hospital Medicine surveys, you look at how many hospitalists are meaningfully working at a system level on ACOs and committees and so forth to improve the performance of the ACO, and it’s very low.”
In fact, just 13.9% of HM groups serving adults only had formed or were participating in a functioning ACO, according to SHM’s 2014 State of Hospital Medicine report. Another 6% were in the process of forming or participating, the paper reported.
“ACOs have not yet widely worked alongside hospitalist teams to optimize where patients go after hospitalization, which is arguably the most important way to deal with post-acute-care utilization” Dr. Whitcomb adds. “whereas nearly all hospitalists working in bundle payments are focusing on a ‘high-value’ transition out of the hospital.”
Improving Care

While BPCI is focused on payment structure, the program could breed process improvements as well as improve care, says hospitalist Patrick Conway, MD, MHM, MSc, CMS’s chief medical officer and deputy administrator for innovation and quality.
“In addition to assessing the quality of patient outcomes and patient experience, CMS is also monitoring for unintended consequences, including whether there is an increase in the number of specific clinical episodes [such as specific elective surgeries] that would not have been expected in the absence of BPCI,” Dr. Conway says. “CMS can audit and intervene if it detects unintended negative consequences for beneficiaries.”
Dr. Whitcomb says two main ways that hospitalists can use BPCI to calculate value is by having better metrics on post-acute facility utilization and reduced readmission.

Immediate past SHM President Robert Harrington Jr., MD, SFHM, says that BPCI is a major stepping stone to merging quality and payment, along the lines of using Physician Quality Reporting System (PQRS) data in the value-based payment modifier.
“CMS is saying to all of us in the provider world, ‘We want to get out of the business of unit economics, and we want to start paying for episodes of care and providers should be at risk for quality outcomes,” he says. “BPCI, to me, is one of the rungs in the ladder.”
Dr. Harrington, chief medical officer at Reliant Post-Acute Care Solutions in Atlanta, says that the program’s inclusion of acute-care hospitals, skilled nursing facilities (SNFs), physician group practices, long-term care hospitals, inpatient rehabilitation facilities, and home health agencies working together is what differentiates it from past attempts at payment reform.
“Population health is sort of where this is headed,” he adds. “You sit in a CFO seat at a hospital or healthcare system right now, and five years ago, they’d buy an MRI machine and they wanted throughput through that MRI machine and they wanted as many people run through that MRI machine in the fee-for-service world as they could get to go through that machine. Nowadays, you start to look at it from a population health standpoint and the CFO is going to say to you, ‘I don’t want anybody going through that MRI machine unless they have to.’
“So it’s a total reversal of perspective when hospitals either become joined at the hip with the payors or become the payors and they start taking risk on population health and I think BPCI is one way that Medicare has allowed all of us to test the waters and get comfortable with that.”
Getting Involved
Dr. Weiner is aware that some hospitalists are nervous about bundled payments because their reimbursement is, in part based on care provided outside of their control. Take a surgical procedure where a hospitalist managing the post-surgery care is left to deal with any potential mistakes made. Or the process works fine until there is poor management by ambulatory care once the patient is discharged.
“That is the reason this program exists,” he says. “It poses the question, who is going to be accountable for the care outside of the traditional site of care that providers have been practicing in, your traditional boundaries? I would argue that physicians are more or are just as valuable as any other segment of the healthcare system in managing the transitions of care and in managing the gaps in the system.”
Given how HM has moved into post-discharge care via SNFs and other post-acute care facilities in recent years, Dr. Weiner says that while hospitalists can’t actually deliver all of the care in an “episode,” they can shepherd that process.
Hospitalists “have control over where the patient goes after they leave the acute-care facility, for example,” he says. “They write the orders on what level of care is needed, and they should have the intimate knowledge about what’s available in their community to ensure the patient gets the best care possible. As long as they have the accountability and the power to direct care, then they have the ability to negotiate and recommend care that is best for the patient, so they can select the better facilities in the community, the better agencies in the community, the better resources in the community to ensure that there is better care once the patient leaves the hospital.”
Dr. Conway suggests HM practitioners view BPCI as a model based on “quality and value.” He says early participants helped define clinical episodes, length of episode, and risk track, making the program better suited to address the actual needs of hospitalists.
“I would encourage hospital medicine physicians and care teams to view bundled payment models as an opportunity for them and their patients for better care and smarter spending,” he adds. “CMS continues to explore ways to pay for value and not just volume. Many of the organizations that are participating in BPCI have partnered with their physician communities and established gainsharing agreement. …Most importantly, this model focuses on care coordination for patients across episodes of care.
And that’s the key for Dr. Weiner.
Hospitalists who embrace BPCI can shape it as the predominant inpatient funding model for hospitals over the next five or 10 years. HM administrators and practitioners who don’t seize the opportunity to flesh out the program tacitly cede control to people outside the hospital who may not tailor the program nearly as well, he says.
“Those who have accountability in the end, the systems, the people, the entities, the providers that have the ability, the accountability for it will ultimately design it,” Dr. Weiner adds. “I think physicians, especially hospitalists, should be at that table. We should play an active role in designing the system.” TH
Richard Quinn is a freelance writer in New Jersey.
The ABCs of $$$s

- APM: Alternative payment models. The catch-all phrase for a variety of programs and initiatives that are outside the traditional fee-for-service model.
- MACRA: Medicare Access & CHIP Reauthorization Act of 2015. The act ended the hated sustainable growth rate (SGR) formula and combined CMS’s existing quality reporting programs under one system.
- MIPS: Merit-Based Incentive Payment System. The new program combines parts of the Physician Quality Reporting System (PQRS), the value modifier (VM, or value-based payment modifier/VBPM), and the Medicare electronic health record (EHR) incentive program into a single program.
Source: Centers for Medicare & Medicaid Services
—By Richard Quinn
As far back as 1983 —13 years before the birth of HM—Medicare created what was then called an “inpatient prospective payment system,” which essentially let Medicare pay a fixed amount for the entirety of a hospital stay, based on diagnosis. Then in 1991, the Centers for Medicare & Medicaid Services (CMS) introduced one payment for coronary artery bypass graft surgery, and even included 90-day readmission in the check.
Fast forward to the past 10 years when accountable care organizations (ACOs) and value-based purchasing (VBP) have been the focus of HM executives looking to take the lead in how to make bundled payments work for them.
The Bundled Payments for Care Improvement (BPCI) initiative was introduced by CMS’s Center for Medicare & Medicaid Innovation (CMMI) in 2011 and is now compiling its first data sets for the next frontier of payments for episodic care.
For rank-and-file hospitalists who have felt inundated by the regulations and promised payment reforms from ACOs and VBPs, why is this program so important?
“The reason this is so special is that it is one of the few CMS programs that allows providers to be in the driver’s seat,” says Kerry Weiner, MD, chief medical officer of acute and post-acute services at TeamHealth-IPC The Hospitalist Company. “They have the opportunity to be accountable and to actually be the designers of reengineering care. The other programs that you just mentioned, like value-based purchasing, largely originate from health systems or the federal government and dictate the principles and the metrics that as a provider you’re going to be evaluated upon.
“This model, the bundled model, gives us the flexibility, scale and brackets of risk that we want to accept and thereby gives us a lot more control over what physicians and physician groups can manage successfully.”
BPCI might be a game-changer for HM because it’s the first of the bundled-payment initiatives that truly falls direct to the care provided by hospitalists. In short, the plan covers 48 defined episodes of care and would parse out payments for those episodes in a holistic—and some say more appropriate—way. Currently, a hospitalist would get paid for a patient’s stay in the hospital and a primary-care physician (PCP) could be paid for some follow-up. If the patient ends up back in the hospital quickly, the hospitalist could get paid again and, upon discharge, a PCP could, too.
But under BPCI, pay would be determined based on the episode of care. The details of who gets paid what and the rules that apply are all likely to evolve, of course, but it’s hoped the basic premise of bundled payments would lower the overall cost of healthcare.
How It Works
Under the Patient Protection and Affordable Care Act (ACA) of 2009, it was mandated that the government establish a five-year pilot program by 2013 that bundled payments for inpatient care, according to the American Hospital Association.
The program has now ramped up to include more than 650 participating organization, not including thousands of physicians that then partner with those groups, over four models. The initiative covers defined episodes of care, both medical and surgical, that begin at the time of inpatient admission and stretch 30, 60 or 90 days post-discharge.
And hospitalists are poised to take the lead on how payment models, especially bundled payments, are shaped over the next few years, says John Nelson, MD, MHM, a co-founder and past president of SHM and and principal in Nelson Flores Hospital Medicine Consultants in Bellevue, Wash. Nelson says his consulting firm has seen an uptick in calls over the past two years dealing with alternative payment models (APMs).
“Hospitalists find themselves at a vitally important nexus of performance and success on new payment models,” he adds.
Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners in Darien, Conn., agrees that BPCI and future iterations of bundled payment programs “are likely to be a potent driver of an evolving hospitalist specialty.” His hypothesis is that APMs such as BPCI are an important way for Medicare to reach its stated goal of having 50% of its fee-for-service payments running through APMs by the end of 2018. To further entice that process, physicians who document at least 25% of their revenue as coming through APMs will get a 5% bonus.
“The stakes are high now,” says Dr. Whitcomb, a past SHM president whose employer is an Awardee Convener in the BPCI initiative, meaning it administers the program. “Medicare [has] laid out the
course for the next two and a half, three years and beyond… It will be crucial for hospitalists to have a path to participate broadly in APMs..”
Dr. Whitcomb says BPCI is the program that should excite hospitalists most because it is more applicable to them moving forward than ACOs, heralded by many healthcare executives several years ago as the future of payment reform.
“With a focus on ambulatory care, ACOs have not broadly involved hospitalists,” he says. “If you look at the State of Hospital Medicine surveys, you look at how many hospitalists are meaningfully working at a system level on ACOs and committees and so forth to improve the performance of the ACO, and it’s very low.”
In fact, just 13.9% of HM groups serving adults only had formed or were participating in a functioning ACO, according to SHM’s 2014 State of Hospital Medicine report. Another 6% were in the process of forming or participating, the paper reported.
“ACOs have not yet widely worked alongside hospitalist teams to optimize where patients go after hospitalization, which is arguably the most important way to deal with post-acute-care utilization” Dr. Whitcomb adds. “whereas nearly all hospitalists working in bundle payments are focusing on a ‘high-value’ transition out of the hospital.”
Improving Care
While BPCI is focused on payment structure, the program could breed process improvements as well as improve care, says hospitalist Patrick Conway, MD, MHM, MSc, CMS’s chief medical officer and deputy administrator for innovation and quality.
“In addition to assessing the quality of patient outcomes and patient experience, CMS is also monitoring for unintended consequences, including whether there is an increase in the number of specific clinical episodes [such as specific elective surgeries] that would not have been expected in the absence of BPCI,” Dr. Conway says. “CMS can audit and intervene if it detects unintended negative consequences for beneficiaries.”
Dr. Whitcomb says two main ways that hospitalists can use BPCI to calculate value is by having better metrics on post-acute facility utilization and reduced readmission.
Immediate past SHM President Robert Harrington Jr., MD, SFHM, says that BPCI is a major stepping stone to merging quality and payment, along the lines of using Physician Quality Reporting System (PQRS) data in the value-based payment modifier.
“CMS is saying to all of us in the provider world, ‘We want to get out of the business of unit economics, and we want to start paying for episodes of care and providers should be at risk for quality outcomes,” he says. “BPCI, to me, is one of the rungs in the ladder.”
Dr. Harrington, chief medical officer at Reliant Post-Acute Care Solutions in Atlanta, says that the program’s inclusion of acute-care hospitals, skilled nursing facilities (SNFs), physician group practices, long-term care hospitals, inpatient rehabilitation facilities, and home health agencies working together is what differentiates it from past attempts at payment reform.
“Population health is sort of where this is headed,” he adds. “You sit in a CFO seat at a hospital or healthcare system right now, and five years ago, they’d buy an MRI machine and they wanted throughput through that MRI machine and they wanted as many people run through that MRI machine in the fee-for-service world as they could get to go through that machine. Nowadays, you start to look at it from a population health standpoint and the CFO is going to say to you, ‘I don’t want anybody going through that MRI machine unless they have to.’
“So it’s a total reversal of perspective when hospitals either become joined at the hip with the payors or become the payors and they start taking risk on population health and I think BPCI is one way that Medicare has allowed all of us to test the waters and get comfortable with that.”
Getting Involved
Dr. Weiner is aware that some hospitalists are nervous about bundled payments because their reimbursement is, in part based on care provided outside of their control. Take a surgical procedure where a hospitalist managing the post-surgery care is left to deal with any potential mistakes made. Or the process works fine until there is poor management by ambulatory care once the patient is discharged.
“That is the reason this program exists,” he says. “It poses the question, who is going to be accountable for the care outside of the traditional site of care that providers have been practicing in, your traditional boundaries? I would argue that physicians are more or are just as valuable as any other segment of the healthcare system in managing the transitions of care and in managing the gaps in the system.”
Given how HM has moved into post-discharge care via SNFs and other post-acute care facilities in recent years, Dr. Weiner says that while hospitalists can’t actually deliver all of the care in an “episode,” they can shepherd that process.
Hospitalists “have control over where the patient goes after they leave the acute-care facility, for example,” he says. “They write the orders on what level of care is needed, and they should have the intimate knowledge about what’s available in their community to ensure the patient gets the best care possible. As long as they have the accountability and the power to direct care, then they have the ability to negotiate and recommend care that is best for the patient, so they can select the better facilities in the community, the better agencies in the community, the better resources in the community to ensure that there is better care once the patient leaves the hospital.”
Dr. Conway suggests HM practitioners view BPCI as a model based on “quality and value.” He says early participants helped define clinical episodes, length of episode, and risk track, making the program better suited to address the actual needs of hospitalists.
“I would encourage hospital medicine physicians and care teams to view bundled payment models as an opportunity for them and their patients for better care and smarter spending,” he adds. “CMS continues to explore ways to pay for value and not just volume. Many of the organizations that are participating in BPCI have partnered with their physician communities and established gainsharing agreement. …Most importantly, this model focuses on care coordination for patients across episodes of care.
And that’s the key for Dr. Weiner.
Hospitalists who embrace BPCI can shape it as the predominant inpatient funding model for hospitals over the next five or 10 years. HM administrators and practitioners who don’t seize the opportunity to flesh out the program tacitly cede control to people outside the hospital who may not tailor the program nearly as well, he says.
“Those who have accountability in the end, the systems, the people, the entities, the providers that have the ability, the accountability for it will ultimately design it,” Dr. Weiner adds. “I think physicians, especially hospitalists, should be at that table. We should play an active role in designing the system.” TH
Richard Quinn is a freelance writer in New Jersey.
The ABCs of $$$s
- APM: Alternative payment models. The catch-all phrase for a variety of programs and initiatives that are outside the traditional fee-for-service model.
- MACRA: Medicare Access & CHIP Reauthorization Act of 2015. The act ended the hated sustainable growth rate (SGR) formula and combined CMS’s existing quality reporting programs under one system.
- MIPS: Merit-Based Incentive Payment System. The new program combines parts of the Physician Quality Reporting System (PQRS), the value modifier (VM, or value-based payment modifier/VBPM), and the Medicare electronic health record (EHR) incentive program into a single program.
Source: Centers for Medicare & Medicaid Services
—By Richard Quinn
As far back as 1983 —13 years before the birth of HM—Medicare created what was then called an “inpatient prospective payment system,” which essentially let Medicare pay a fixed amount for the entirety of a hospital stay, based on diagnosis. Then in 1991, the Centers for Medicare & Medicaid Services (CMS) introduced one payment for coronary artery bypass graft surgery, and even included 90-day readmission in the check.
Fast forward to the past 10 years when accountable care organizations (ACOs) and value-based purchasing (VBP) have been the focus of HM executives looking to take the lead in how to make bundled payments work for them.
The Bundled Payments for Care Improvement (BPCI) initiative was introduced by CMS’s Center for Medicare & Medicaid Innovation (CMMI) in 2011 and is now compiling its first data sets for the next frontier of payments for episodic care.
For rank-and-file hospitalists who have felt inundated by the regulations and promised payment reforms from ACOs and VBPs, why is this program so important?
“The reason this is so special is that it is one of the few CMS programs that allows providers to be in the driver’s seat,” says Kerry Weiner, MD, chief medical officer of acute and post-acute services at TeamHealth-IPC The Hospitalist Company. “They have the opportunity to be accountable and to actually be the designers of reengineering care. The other programs that you just mentioned, like value-based purchasing, largely originate from health systems or the federal government and dictate the principles and the metrics that as a provider you’re going to be evaluated upon.
“This model, the bundled model, gives us the flexibility, scale and brackets of risk that we want to accept and thereby gives us a lot more control over what physicians and physician groups can manage successfully.”
BPCI might be a game-changer for HM because it’s the first of the bundled-payment initiatives that truly falls direct to the care provided by hospitalists. In short, the plan covers 48 defined episodes of care and would parse out payments for those episodes in a holistic—and some say more appropriate—way. Currently, a hospitalist would get paid for a patient’s stay in the hospital and a primary-care physician (PCP) could be paid for some follow-up. If the patient ends up back in the hospital quickly, the hospitalist could get paid again and, upon discharge, a PCP could, too.
But under BPCI, pay would be determined based on the episode of care. The details of who gets paid what and the rules that apply are all likely to evolve, of course, but it’s hoped the basic premise of bundled payments would lower the overall cost of healthcare.
How It Works
Under the Patient Protection and Affordable Care Act (ACA) of 2009, it was mandated that the government establish a five-year pilot program by 2013 that bundled payments for inpatient care, according to the American Hospital Association.
The program has now ramped up to include more than 650 participating organization, not including thousands of physicians that then partner with those groups, over four models. The initiative covers defined episodes of care, both medical and surgical, that begin at the time of inpatient admission and stretch 30, 60 or 90 days post-discharge.
And hospitalists are poised to take the lead on how payment models, especially bundled payments, are shaped over the next few years, says John Nelson, MD, MHM, a co-founder and past president of SHM and and principal in Nelson Flores Hospital Medicine Consultants in Bellevue, Wash. Nelson says his consulting firm has seen an uptick in calls over the past two years dealing with alternative payment models (APMs).
“Hospitalists find themselves at a vitally important nexus of performance and success on new payment models,” he adds.
Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners in Darien, Conn., agrees that BPCI and future iterations of bundled payment programs “are likely to be a potent driver of an evolving hospitalist specialty.” His hypothesis is that APMs such as BPCI are an important way for Medicare to reach its stated goal of having 50% of its fee-for-service payments running through APMs by the end of 2018. To further entice that process, physicians who document at least 25% of their revenue as coming through APMs will get a 5% bonus.
“The stakes are high now,” says Dr. Whitcomb, a past SHM president whose employer is an Awardee Convener in the BPCI initiative, meaning it administers the program. “Medicare [has] laid out the
course for the next two and a half, three years and beyond… It will be crucial for hospitalists to have a path to participate broadly in APMs..”
Dr. Whitcomb says BPCI is the program that should excite hospitalists most because it is more applicable to them moving forward than ACOs, heralded by many healthcare executives several years ago as the future of payment reform.
“With a focus on ambulatory care, ACOs have not broadly involved hospitalists,” he says. “If you look at the State of Hospital Medicine surveys, you look at how many hospitalists are meaningfully working at a system level on ACOs and committees and so forth to improve the performance of the ACO, and it’s very low.”
In fact, just 13.9% of HM groups serving adults only had formed or were participating in a functioning ACO, according to SHM’s 2014 State of Hospital Medicine report. Another 6% were in the process of forming or participating, the paper reported.
“ACOs have not yet widely worked alongside hospitalist teams to optimize where patients go after hospitalization, which is arguably the most important way to deal with post-acute-care utilization” Dr. Whitcomb adds. “whereas nearly all hospitalists working in bundle payments are focusing on a ‘high-value’ transition out of the hospital.”
Improving Care
While BPCI is focused on payment structure, the program could breed process improvements as well as improve care, says hospitalist Patrick Conway, MD, MHM, MSc, CMS’s chief medical officer and deputy administrator for innovation and quality.
“In addition to assessing the quality of patient outcomes and patient experience, CMS is also monitoring for unintended consequences, including whether there is an increase in the number of specific clinical episodes [such as specific elective surgeries] that would not have been expected in the absence of BPCI,” Dr. Conway says. “CMS can audit and intervene if it detects unintended negative consequences for beneficiaries.”
Dr. Whitcomb says two main ways that hospitalists can use BPCI to calculate value is by having better metrics on post-acute facility utilization and reduced readmission.
Immediate past SHM President Robert Harrington Jr., MD, SFHM, says that BPCI is a major stepping stone to merging quality and payment, along the lines of using Physician Quality Reporting System (PQRS) data in the value-based payment modifier.
“CMS is saying to all of us in the provider world, ‘We want to get out of the business of unit economics, and we want to start paying for episodes of care and providers should be at risk for quality outcomes,” he says. “BPCI, to me, is one of the rungs in the ladder.”
Dr. Harrington, chief medical officer at Reliant Post-Acute Care Solutions in Atlanta, says that the program’s inclusion of acute-care hospitals, skilled nursing facilities (SNFs), physician group practices, long-term care hospitals, inpatient rehabilitation facilities, and home health agencies working together is what differentiates it from past attempts at payment reform.
“Population health is sort of where this is headed,” he adds. “You sit in a CFO seat at a hospital or healthcare system right now, and five years ago, they’d buy an MRI machine and they wanted throughput through that MRI machine and they wanted as many people run through that MRI machine in the fee-for-service world as they could get to go through that machine. Nowadays, you start to look at it from a population health standpoint and the CFO is going to say to you, ‘I don’t want anybody going through that MRI machine unless they have to.’
“So it’s a total reversal of perspective when hospitals either become joined at the hip with the payors or become the payors and they start taking risk on population health and I think BPCI is one way that Medicare has allowed all of us to test the waters and get comfortable with that.”
Getting Involved
Dr. Weiner is aware that some hospitalists are nervous about bundled payments because their reimbursement is, in part based on care provided outside of their control. Take a surgical procedure where a hospitalist managing the post-surgery care is left to deal with any potential mistakes made. Or the process works fine until there is poor management by ambulatory care once the patient is discharged.
“That is the reason this program exists,” he says. “It poses the question, who is going to be accountable for the care outside of the traditional site of care that providers have been practicing in, your traditional boundaries? I would argue that physicians are more or are just as valuable as any other segment of the healthcare system in managing the transitions of care and in managing the gaps in the system.”
Given how HM has moved into post-discharge care via SNFs and other post-acute care facilities in recent years, Dr. Weiner says that while hospitalists can’t actually deliver all of the care in an “episode,” they can shepherd that process.
Hospitalists “have control over where the patient goes after they leave the acute-care facility, for example,” he says. “They write the orders on what level of care is needed, and they should have the intimate knowledge about what’s available in their community to ensure the patient gets the best care possible. As long as they have the accountability and the power to direct care, then they have the ability to negotiate and recommend care that is best for the patient, so they can select the better facilities in the community, the better agencies in the community, the better resources in the community to ensure that there is better care once the patient leaves the hospital.”
Dr. Conway suggests HM practitioners view BPCI as a model based on “quality and value.” He says early participants helped define clinical episodes, length of episode, and risk track, making the program better suited to address the actual needs of hospitalists.
“I would encourage hospital medicine physicians and care teams to view bundled payment models as an opportunity for them and their patients for better care and smarter spending,” he adds. “CMS continues to explore ways to pay for value and not just volume. Many of the organizations that are participating in BPCI have partnered with their physician communities and established gainsharing agreement. …Most importantly, this model focuses on care coordination for patients across episodes of care.
And that’s the key for Dr. Weiner.
Hospitalists who embrace BPCI can shape it as the predominant inpatient funding model for hospitals over the next five or 10 years. HM administrators and practitioners who don’t seize the opportunity to flesh out the program tacitly cede control to people outside the hospital who may not tailor the program nearly as well, he says.
“Those who have accountability in the end, the systems, the people, the entities, the providers that have the ability, the accountability for it will ultimately design it,” Dr. Weiner adds. “I think physicians, especially hospitalists, should be at that table. We should play an active role in designing the system.” TH
Richard Quinn is a freelance writer in New Jersey.
The ABCs of $$$s
- APM: Alternative payment models. The catch-all phrase for a variety of programs and initiatives that are outside the traditional fee-for-service model.
- MACRA: Medicare Access & CHIP Reauthorization Act of 2015. The act ended the hated sustainable growth rate (SGR) formula and combined CMS’s existing quality reporting programs under one system.
- MIPS: Merit-Based Incentive Payment System. The new program combines parts of the Physician Quality Reporting System (PQRS), the value modifier (VM, or value-based payment modifier/VBPM), and the Medicare electronic health record (EHR) incentive program into a single program.
Source: Centers for Medicare & Medicaid Services
—By Richard Quinn

The Proposed Rule and Payments for 2017: The Good, the Bad, and the Ugly
Just as Charlie Brown looks forward to the coming of the Great Pumpkin each Halloween, those of us who dance in the minefields of payment policy await the publication of the Proposed Rule, more formally known as the “Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2017.”1,2 You could read the entire tome—a mere 316 pages (excluding the hundreds of pages of granular supplement data discussed in the last few columns)—or simply read what I have outlined as the good, the bad, and the ugly for the Proposed Rule for 2017.
The Good
In 2017, dermatology will increase its share of the pie by 1% to $3.505 billion of a total $89.467 billion expected to be expended for physician services.1 The effect on individual providers will vary by geographic location and practice mix. Half is from the 0.5% increase that has come to all physicians across the board as mandated by the Medicare Access and CHIP Reauthorization Act (MACRA).3
Current Procedural Terminology (CPT) codes for reflectance confocal microscopy (96931–96936) will have Centers for Medicare & Medicaid Services valuations beginning in 2017, and individuals performing this service should be able to report it and be paid for their efforts.1 The values are below the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC) recommendations.
The Bad
Payment rates for 2017 will be based on a conversion factor of 35.7751,1 a drop from the 2016 conversion factor of 35.8043. Cuts will be made for some specialties. Gastroenterology, nephrology, neurosurgery, radiology, urology, and radiation therapy centers will take a 1% hit; ophthalmology, pathology, and vascular surgery will take 2% cuts; and interventional radiology will lose 7%.1 A special case within dermatology and pathology is a 15% cut to the technical component of slide preparation for CPT code 883054 due to a redefinition of the valuation of eosin stains.2 While the accuracy and precision of the value of these practice expense inputs can be debated, the government by definition makes the rules and involved specialties had an opportunity to appeal this change through the comment process that ended on September 6, 2016. The government can take comments into account, but substantial changes usually are not made from the Proposed Rule to the Final Rule, which usually arrives around the beginning of November; however, in an election year, the Final Rule can be a few weeks late.
The Ugly
The government will increase its unfunded mandates with the creation of new Medicare G codes (global services codes) that will allow the government to track the provision of postoperative care for all 010 and 090 global service periods (Table 1). The codes look mostly at time and do not clearly take into account the severity or complexity of the conditions being cared for and will be reported on claim forms as an unfunded mandate with more confusion and cost.1 Because not all claim-paying intermediaries are likely to have these G codes smoothly set up in their systems, there will still be a cost to filing the claim. Unless changes occur in the Final Rule, which is unlikely, there will be no payment for the time and effort of submitting these claims. The goal of the US Government is to hone in on postoperative services and parse them down so they can cut payments wherever possible beginning in 2019.1 Everyone wants to save money, from the consumer5 to the payer, and the ultimate payer is playing hardball. Additional validation efforts likely will lower physician fee-for-service payments further.

The US Government also is taking a shot at what they call “misvalued services” that have not had recent refinement within the RUC process.1 The work list for 2017 includes a number of 000 global period codes where additional evaluation and management services are reported using modifier -25, which implies a substantial, separately identifiable cognitive service performed by the same physician on the day of a procedure above and beyond other services provided or beyond the usual preservice and postservice care associated with the procedure that was performed. Although codes such as biopsies (11100 and 11101) and premalignant destructions (17000–17004) have an adjustment built in and dermatologists who provide services on the same day are actually penalized for the multiple built-in reductions that are already additive, the government is concerned that 19% of the 000 global services were billed more than 50% of the time with an evaluation and management code with modifier -25. Eighty-three codes met the criteria for which the government believes it may be overpaying1; the codes of interest to dermatology are shown in Table 2.1

The refinement of global periods will be an ongoing exercise through 2017, and beyond, with results likely to play an important role in the 2019 fee schedule. These global period reviews combined with some Stark law refinement relating the leasing of space at market rates while disallowing the landlord physician from receiving patient referrals from the tenant may also affect practitioner income.1,6 I never cease to be amazed that former Congressman Fortney Hillman “Pete” Stark (D), who has an antikickback scheme that keeps expanding, never went after the banking and brokerage industries. The founder of the $1.1 billion Security National Bank, a small bank in Walnut Creek, California,7 never focused on regulating banks. In his 40-year congressional career, he decided physicians make better targets. His efforts have not helped physicians but have helped lawyers, as he is quick to acknowledge.8
Final Thoughts
I end this column with an appeal to the dermatologists of America. Go to the American Academy of Dermatology Association Political Action Committee website (https://skinpac.org/), the home page for the only political action committee that represents the dermatology specialty, and consider making a donation. Emergency medicine physicians created the “Giving a Shift” campaign, which is a donation to their national political action committee of one shift’s earnings, and most of us could easily donate a half day’s income, as the only way to potentially change the increasingly onerous burdens on practitioners is through political action. As we say at RUC meetings, you can eat lunch or be lunch. The choice is yours.
- Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2017; Medicare Advantage Pricing Data Release; Medicare Advantage and Part D Medical Low Ratio Data Release; Medicare Advantage Provider Network Requirements; Expansion of Medicare Diabetes Prevention Program Model. Fed Regist. 2016;81(136):46162-46476. To be codified at 42 CFR §405, 410, 411, et al. https://www.gpo.gov/fdsys/pkg/FR-2016-07-15/pdf/2016-16097.pdf. Accessed September 7, 2016.
- Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2017. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1654-P.html. Accessed September 7, 2016.
- Text of the Medicare Access and CHIP Reauthorization Act of 2015. GovTrack website. https://www.govtrack.us/congress/bills/114/hr2/text. Accessed September 9, 2016.
- Kaplan KJ. Proposed Medicare 2017 reimbursement schedule whacks biopsy payments; digital pathology payments up. Digital Pathology Blog website. http://tissuepathology.com/2016/07/20/proposed-medicare-2017-reimbursement-schedule-whacks-biopsy-payments-digital-pathology-payments-up/#ixzz4HEqBLgzu. Published July 20, 2016. Accessed September 7, 2016.
- Abelson R. Cost, not choice, is top concern of health insurance customers. The New York Times. http://www.nytimes.com/2016/08/13/business/cost-not-choice-is-top-concern-of-health-insurance-customers.html?_r=0. Published August 12, 2016. Accessed September 7, 2016.
- Stark Law website. http://starklaw.org/. Accessed September 7, 2016.
- Pete Stark. Freedom From Religion website. https://ffrf.org/news/day/dayitems/item/14800-pete-stark. Accessed September 19, 2016.
- Adamy J. Pete Stark: Law regulating doctors mostly helped lawyers. The Wall Street Journal. October 22, 2014. http://blogs.wsj.com/washwire/2014/10/22/pete-stark-law-regulating-doctors-mostly-helped-lawyers/. Accessed September 19, 2016.
Just as Charlie Brown looks forward to the coming of the Great Pumpkin each Halloween, those of us who dance in the minefields of payment policy await the publication of the Proposed Rule, more formally known as the “Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2017.”1,2 You could read the entire tome—a mere 316 pages (excluding the hundreds of pages of granular supplement data discussed in the last few columns)—or simply read what I have outlined as the good, the bad, and the ugly for the Proposed Rule for 2017.
The Good
In 2017, dermatology will increase its share of the pie by 1% to $3.505 billion of a total $89.467 billion expected to be expended for physician services.1 The effect on individual providers will vary by geographic location and practice mix. Half is from the 0.5% increase that has come to all physicians across the board as mandated by the Medicare Access and CHIP Reauthorization Act (MACRA).3
Current Procedural Terminology (CPT) codes for reflectance confocal microscopy (96931–96936) will have Centers for Medicare & Medicaid Services valuations beginning in 2017, and individuals performing this service should be able to report it and be paid for their efforts.1 The values are below the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC) recommendations.
The Bad
Payment rates for 2017 will be based on a conversion factor of 35.7751,1 a drop from the 2016 conversion factor of 35.8043. Cuts will be made for some specialties. Gastroenterology, nephrology, neurosurgery, radiology, urology, and radiation therapy centers will take a 1% hit; ophthalmology, pathology, and vascular surgery will take 2% cuts; and interventional radiology will lose 7%.1 A special case within dermatology and pathology is a 15% cut to the technical component of slide preparation for CPT code 883054 due to a redefinition of the valuation of eosin stains.2 While the accuracy and precision of the value of these practice expense inputs can be debated, the government by definition makes the rules and involved specialties had an opportunity to appeal this change through the comment process that ended on September 6, 2016. The government can take comments into account, but substantial changes usually are not made from the Proposed Rule to the Final Rule, which usually arrives around the beginning of November; however, in an election year, the Final Rule can be a few weeks late.
The Ugly
The government will increase its unfunded mandates with the creation of new Medicare G codes (global services codes) that will allow the government to track the provision of postoperative care for all 010 and 090 global service periods (Table 1). The codes look mostly at time and do not clearly take into account the severity or complexity of the conditions being cared for and will be reported on claim forms as an unfunded mandate with more confusion and cost.1 Because not all claim-paying intermediaries are likely to have these G codes smoothly set up in their systems, there will still be a cost to filing the claim. Unless changes occur in the Final Rule, which is unlikely, there will be no payment for the time and effort of submitting these claims. The goal of the US Government is to hone in on postoperative services and parse them down so they can cut payments wherever possible beginning in 2019.1 Everyone wants to save money, from the consumer5 to the payer, and the ultimate payer is playing hardball. Additional validation efforts likely will lower physician fee-for-service payments further.
The US Government also is taking a shot at what they call “misvalued services” that have not had recent refinement within the RUC process.1 The work list for 2017 includes a number of 000 global period codes where additional evaluation and management services are reported using modifier -25, which implies a substantial, separately identifiable cognitive service performed by the same physician on the day of a procedure above and beyond other services provided or beyond the usual preservice and postservice care associated with the procedure that was performed. Although codes such as biopsies (11100 and 11101) and premalignant destructions (17000–17004) have an adjustment built in and dermatologists who provide services on the same day are actually penalized for the multiple built-in reductions that are already additive, the government is concerned that 19% of the 000 global services were billed more than 50% of the time with an evaluation and management code with modifier -25. Eighty-three codes met the criteria for which the government believes it may be overpaying1; the codes of interest to dermatology are shown in Table 2.1
The refinement of global periods will be an ongoing exercise through 2017, and beyond, with results likely to play an important role in the 2019 fee schedule. These global period reviews combined with some Stark law refinement relating the leasing of space at market rates while disallowing the landlord physician from receiving patient referrals from the tenant may also affect practitioner income.1,6 I never cease to be amazed that former Congressman Fortney Hillman “Pete” Stark (D), who has an antikickback scheme that keeps expanding, never went after the banking and brokerage industries. The founder of the $1.1 billion Security National Bank, a small bank in Walnut Creek, California,7 never focused on regulating banks. In his 40-year congressional career, he decided physicians make better targets. His efforts have not helped physicians but have helped lawyers, as he is quick to acknowledge.8
Final Thoughts
I end this column with an appeal to the dermatologists of America. Go to the American Academy of Dermatology Association Political Action Committee website (https://skinpac.org/), the home page for the only political action committee that represents the dermatology specialty, and consider making a donation. Emergency medicine physicians created the “Giving a Shift” campaign, which is a donation to their national political action committee of one shift’s earnings, and most of us could easily donate a half day’s income, as the only way to potentially change the increasingly onerous burdens on practitioners is through political action. As we say at RUC meetings, you can eat lunch or be lunch. The choice is yours.
Just as Charlie Brown looks forward to the coming of the Great Pumpkin each Halloween, those of us who dance in the minefields of payment policy await the publication of the Proposed Rule, more formally known as the “Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2017.”1,2 You could read the entire tome—a mere 316 pages (excluding the hundreds of pages of granular supplement data discussed in the last few columns)—or simply read what I have outlined as the good, the bad, and the ugly for the Proposed Rule for 2017.
The Good
In 2017, dermatology will increase its share of the pie by 1% to $3.505 billion of a total $89.467 billion expected to be expended for physician services.1 The effect on individual providers will vary by geographic location and practice mix. Half is from the 0.5% increase that has come to all physicians across the board as mandated by the Medicare Access and CHIP Reauthorization Act (MACRA).3
Current Procedural Terminology (CPT) codes for reflectance confocal microscopy (96931–96936) will have Centers for Medicare & Medicaid Services valuations beginning in 2017, and individuals performing this service should be able to report it and be paid for their efforts.1 The values are below the American Medical Association/Specialty Society Relative Value Scale Update Committee (RUC) recommendations.
The Bad
Payment rates for 2017 will be based on a conversion factor of 35.7751,1 a drop from the 2016 conversion factor of 35.8043. Cuts will be made for some specialties. Gastroenterology, nephrology, neurosurgery, radiology, urology, and radiation therapy centers will take a 1% hit; ophthalmology, pathology, and vascular surgery will take 2% cuts; and interventional radiology will lose 7%.1 A special case within dermatology and pathology is a 15% cut to the technical component of slide preparation for CPT code 883054 due to a redefinition of the valuation of eosin stains.2 While the accuracy and precision of the value of these practice expense inputs can be debated, the government by definition makes the rules and involved specialties had an opportunity to appeal this change through the comment process that ended on September 6, 2016. The government can take comments into account, but substantial changes usually are not made from the Proposed Rule to the Final Rule, which usually arrives around the beginning of November; however, in an election year, the Final Rule can be a few weeks late.
The Ugly
The government will increase its unfunded mandates with the creation of new Medicare G codes (global services codes) that will allow the government to track the provision of postoperative care for all 010 and 090 global service periods (Table 1). The codes look mostly at time and do not clearly take into account the severity or complexity of the conditions being cared for and will be reported on claim forms as an unfunded mandate with more confusion and cost.1 Because not all claim-paying intermediaries are likely to have these G codes smoothly set up in their systems, there will still be a cost to filing the claim. Unless changes occur in the Final Rule, which is unlikely, there will be no payment for the time and effort of submitting these claims. The goal of the US Government is to hone in on postoperative services and parse them down so they can cut payments wherever possible beginning in 2019.1 Everyone wants to save money, from the consumer5 to the payer, and the ultimate payer is playing hardball. Additional validation efforts likely will lower physician fee-for-service payments further.
The US Government also is taking a shot at what they call “misvalued services” that have not had recent refinement within the RUC process.1 The work list for 2017 includes a number of 000 global period codes where additional evaluation and management services are reported using modifier -25, which implies a substantial, separately identifiable cognitive service performed by the same physician on the day of a procedure above and beyond other services provided or beyond the usual preservice and postservice care associated with the procedure that was performed. Although codes such as biopsies (11100 and 11101) and premalignant destructions (17000–17004) have an adjustment built in and dermatologists who provide services on the same day are actually penalized for the multiple built-in reductions that are already additive, the government is concerned that 19% of the 000 global services were billed more than 50% of the time with an evaluation and management code with modifier -25. Eighty-three codes met the criteria for which the government believes it may be overpaying1; the codes of interest to dermatology are shown in Table 2.1
The refinement of global periods will be an ongoing exercise through 2017, and beyond, with results likely to play an important role in the 2019 fee schedule. These global period reviews combined with some Stark law refinement relating the leasing of space at market rates while disallowing the landlord physician from receiving patient referrals from the tenant may also affect practitioner income.1,6 I never cease to be amazed that former Congressman Fortney Hillman “Pete” Stark (D), who has an antikickback scheme that keeps expanding, never went after the banking and brokerage industries. The founder of the $1.1 billion Security National Bank, a small bank in Walnut Creek, California,7 never focused on regulating banks. In his 40-year congressional career, he decided physicians make better targets. His efforts have not helped physicians but have helped lawyers, as he is quick to acknowledge.8
Final Thoughts
I end this column with an appeal to the dermatologists of America. Go to the American Academy of Dermatology Association Political Action Committee website (https://skinpac.org/), the home page for the only political action committee that represents the dermatology specialty, and consider making a donation. Emergency medicine physicians created the “Giving a Shift” campaign, which is a donation to their national political action committee of one shift’s earnings, and most of us could easily donate a half day’s income, as the only way to potentially change the increasingly onerous burdens on practitioners is through political action. As we say at RUC meetings, you can eat lunch or be lunch. The choice is yours.
- Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2017; Medicare Advantage Pricing Data Release; Medicare Advantage and Part D Medical Low Ratio Data Release; Medicare Advantage Provider Network Requirements; Expansion of Medicare Diabetes Prevention Program Model. Fed Regist. 2016;81(136):46162-46476. To be codified at 42 CFR §405, 410, 411, et al. https://www.gpo.gov/fdsys/pkg/FR-2016-07-15/pdf/2016-16097.pdf. Accessed September 7, 2016.
- Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2017. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1654-P.html. Accessed September 7, 2016.
- Text of the Medicare Access and CHIP Reauthorization Act of 2015. GovTrack website. https://www.govtrack.us/congress/bills/114/hr2/text. Accessed September 9, 2016.
- Kaplan KJ. Proposed Medicare 2017 reimbursement schedule whacks biopsy payments; digital pathology payments up. Digital Pathology Blog website. http://tissuepathology.com/2016/07/20/proposed-medicare-2017-reimbursement-schedule-whacks-biopsy-payments-digital-pathology-payments-up/#ixzz4HEqBLgzu. Published July 20, 2016. Accessed September 7, 2016.
- Abelson R. Cost, not choice, is top concern of health insurance customers. The New York Times. http://www.nytimes.com/2016/08/13/business/cost-not-choice-is-top-concern-of-health-insurance-customers.html?_r=0. Published August 12, 2016. Accessed September 7, 2016.
- Stark Law website. http://starklaw.org/. Accessed September 7, 2016.
- Pete Stark. Freedom From Religion website. https://ffrf.org/news/day/dayitems/item/14800-pete-stark. Accessed September 19, 2016.
- Adamy J. Pete Stark: Law regulating doctors mostly helped lawyers. The Wall Street Journal. October 22, 2014. http://blogs.wsj.com/washwire/2014/10/22/pete-stark-law-regulating-doctors-mostly-helped-lawyers/. Accessed September 19, 2016.
- Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2017; Medicare Advantage Pricing Data Release; Medicare Advantage and Part D Medical Low Ratio Data Release; Medicare Advantage Provider Network Requirements; Expansion of Medicare Diabetes Prevention Program Model. Fed Regist. 2016;81(136):46162-46476. To be codified at 42 CFR §405, 410, 411, et al. https://www.gpo.gov/fdsys/pkg/FR-2016-07-15/pdf/2016-16097.pdf. Accessed September 7, 2016.
- Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2017. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1654-P.html. Accessed September 7, 2016.
- Text of the Medicare Access and CHIP Reauthorization Act of 2015. GovTrack website. https://www.govtrack.us/congress/bills/114/hr2/text. Accessed September 9, 2016.
- Kaplan KJ. Proposed Medicare 2017 reimbursement schedule whacks biopsy payments; digital pathology payments up. Digital Pathology Blog website. http://tissuepathology.com/2016/07/20/proposed-medicare-2017-reimbursement-schedule-whacks-biopsy-payments-digital-pathology-payments-up/#ixzz4HEqBLgzu. Published July 20, 2016. Accessed September 7, 2016.
- Abelson R. Cost, not choice, is top concern of health insurance customers. The New York Times. http://www.nytimes.com/2016/08/13/business/cost-not-choice-is-top-concern-of-health-insurance-customers.html?_r=0. Published August 12, 2016. Accessed September 7, 2016.
- Stark Law website. http://starklaw.org/. Accessed September 7, 2016.
- Pete Stark. Freedom From Religion website. https://ffrf.org/news/day/dayitems/item/14800-pete-stark. Accessed September 19, 2016.
- Adamy J. Pete Stark: Law regulating doctors mostly helped lawyers. The Wall Street Journal. October 22, 2014. http://blogs.wsj.com/washwire/2014/10/22/pete-stark-law-regulating-doctors-mostly-helped-lawyers/. Accessed September 19, 2016.
Practice Points
- The Proposed Rule outlines the probable payment levels for calendar year 2017.
- The rule also announces how the Medicare Access and CHIP Reauthorization Act (MACRA) may be implemented.
Work Intensity and IWPUT
After reading the July 2016 column on global periods and Current Procedural Terminology (CPT) code 99024,1 you may be wondering why you get paid what you do and how the procedure and visits all link together, which is associated with work intensity.
When CPT codes are given a value, the determination of the value of the work is performed via a survey process carried out by specialties for presentation to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which is used by the Centers for Medicare & Medicaid Services (CMS) to help determine relative value units (RVUs) that determine payment. The work RVU (wRVU) is typically around half of the total RVU for each CPT code. The value is based on multiple factors including the time to perform the service, the technical skill needed, the physical effort involved, mental effort and judgment, and stress under which the physician works due to the potential risks to the patient.2 A series of instruments and calculations have been used to determine a value called intraservice work per unit of time (IWPUT), which is used to examine the intraservice (skin-to-skin) work of a procedure relative to similar procedures.
Calculating the IWPUT
To determine the IWPUT value of a procedure, a formula is used to subtract all the preservice and postservice work and look at what is left based on the total RVUs for the procedure, which can be mathematically presented using the following construct: total wRVUs (the complete work you provide in performing the service) is the sum of preservice work (eg, evaluation and management [E&M] services, preparatory work [eg, scrub, dress, wait]), intraservice (skin-to-skin) work, immediate postservice work (eg, dressings, prescriptions, instructions given by the physician), and postoperative work at E&M visits (eg, hospital days, discharge day, global follow-up visits).
All of these activities defined as E&M services are simply subtracted from the total wRVU, while wRVUs for preservice and postservice work that is not linked to a CPT global period are calculated by simply subtracting the product of each specified time by their intensity (eg, day prior evaluation, same day evaluation, and immediate post have an intensity of 0.0224, while scrub/preparation has an intensity of 0.0081),3 leaving you with intraservice (skin-to-skin) work. This intraservice work is divided by the intraservice time to give you IWPUT. For more information on the concept as well as the process and controversies, an excellent review is available from the CMS.4
Understanding the IWPUT
The procedure with the highest IWPUT value in all of medicine is an emergency endotracheal intubation (CPT code 31500), which has a value of 0.4061.5 The procedure is short and intense, and if it fails, the patient is dead. All other procedures have lower IWPUT values. For example, a small malignant excision on the trunk, arms, or legs (CPT code 11600) has an IWPUT of 0.0324, while a laparoscopic cholecystectomy with exploration of the common duct (CPT code 47564) has an IWPUT of 0.0737.5 These small values have been the drivers behind much of the Relative Value Scale Update Committee’s valuation process for more than a decade. Some specialists who perform mostly 90-day global procedures wanted IWPUT to be the critical validation factor in the process, which led to problems for the first few years of this century. It may seem obvious that if there are 2 ways to fix a broken leg, the more complex one would likely have a higher IWPUT. Because IWPUT is a pure number with no values attached, this assumption would seem reasonable. If we compare a malignant excision to a benign one, we would expect higher intensity for the malignant one, as we are going deeper and have more concerns about clear margins and recurrences. Within a group of similar procedures, these pure numbers can be useful to validate a proposed value. More wRVUs in a shorter time period would result in a higher IWPUT; however, anomalies arise. There are eleven 000 global period CPT codes, ten 010 codes, and one hundred ninety 090 codes with negative IWPUTs, implying the skin-to-skin work has a value less than 0, which is an illogical conclusion. The more logical conclusion is that the codes are overloaded with preservice and postservice times. The real travesty is when one begins to compare apples to oranges—glaucoma surgery to belly surgery, endoscopy to skin surgery, or any other comparison you can come up with—taking a number that can be used to evaluate intensity between similar procedures and generalizing across all procedures, a concept that has never been validated. The wRVUs themselves define the relativity, but in many instances the IWPUT has been used in the process to justify forcing values lower based on cross-specialty comparisons, which may lead some to think we need better measures, as has been reported in the literature.6-8 Reform likely will happen, but for now we must work within the constraints of this tiny number, the IWPUT.
Obtaining the IWPUT
You are probably wondering, “How can I learn the IWPUT for the codes I use?” You probably do not want or need to other than to gain an understanding of how they have been misused. Purchase a subscription to the Resource-Based Relative Value Scale (RBRVS) DataManager Online or access the data for free through the CMS website (https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1654-P.html) by downloading the CY 2017 PFS Proposed Rule Addenda, which gives you total RVUs for all CPT codes, and the CY 2017 PFS Proposed Rule Physician Time, which gives you the preservice, intraservice, and postservice times for all CPT codes.
Using CPT code 11600 as an example, the total wRVU is 1.63, while preservice evaluation time is 10 minutes, intraservice time is 10 minutes, and immediate postservice time is 5 minutes. There is also 1 global follow-up visit, a CPT 99213, built in with a wRVU of 0.97 that determines the total value of the code. Using the IWPUT formula, we have the following: {1.63 – [(10 × 0.0224) + (5 × 0.0224) + 0.97]} / 10 = 0.0324.
These data also are useful if you are negotiating a contract based on RVUs, so learn a bit more about why you get paid what you are paid.
The Importance of IWPUT
Those interested in the academic discourse behind IWPUT should consult the literature,3,9 which is open source and freely available, but for now we will concentrate on why IWPUT is an important concept. As global periods are reevaluated under the Medicare Access and CHIP Reauthorization Act of 2015,10 the removal of global period visits will cause changes in the IWPUT value of codes, which will make them outliers and therefore targeted for resurvey and revaluation. The intent of the CMS is to cut reimbursement under our fee-for-service system, so there will be pain for physicians who have flourished under the current policy. To avoid inappropriate decreases in reimbursement, we should all keep accurate records of which global postoperative services are indeed provided, which leads us back to CPT code 99024. If it is not tracked, then it may not be seen as having been done. So be sure to use it.
Remember that if you do what you document, document what you do, and report medically necessary CPT codes, you should have nothing to worry about for now.
- Siegel DM. Global visits, 99024, and MACRA: 3 things you should think about and lose sleep over but probably do not. Cutis. 2016;98:43-44, 46.
- Overview of the RBRVS. American Medical Association website. http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/the-resource-based-relative-value-scale/overview-of-rbrvs.page. Accessed July 14, 2016.
- Mabry CD, McCann BC, Harris JA, et al. The use of intraservice work per unit of time (IWPUT) and the building block method (BBM) for the calculation of surgical work. Ann Surg. 2005;241:929-938; discussion 938-940.
- Wynn BO, Burgette LF, Mulcahy AW, et al. Development of a Model for the Validation of Work Relative Value Units for the Medicare Physician Fee Schedule. Santa Monica, CA: RAND Corporation; 2015. http://www.rand.org/content/dam/rand/pubs/research_reports/RR600/RR662/RAND_RR662.pdf. Accessed July 18, 2016.
- RBRVS DataManager Online. American Medical Association. https://commerce.ama-assn .org/store/catalog/productDetail.jsp?product_ id=prod280002&navAction=push. Accessed July 20, 2016.
- Horner RD, Szaflarski JP, Ying J, et al. Physician work intensity among medical specialties: emerging evidence on its magnitude and composition. Med Care. 2011;49:1007-1111.
- Jacobson CJ Jr, Bolon S, Elder N, et al. Temporal and subjective work demands in office-based patient care: an exploration of the dimensions of physician work intensity. Med Care. 2011;49:52-58.
- Horner RD, Szaflarski JP, Jacobson CJ, et al. Clinical work intensity among physician specialties: how might we assess it? what do we find? Med Care. 2011;49:108-113.
- Zwolak RM, Trout HH 3rd. Vascular surgery and the Resource-based Relative Value Scale five-year review. J Vasc Surg. 1997;25:1077-1086.
- Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
After reading the July 2016 column on global periods and Current Procedural Terminology (CPT) code 99024,1 you may be wondering why you get paid what you do and how the procedure and visits all link together, which is associated with work intensity.
When CPT codes are given a value, the determination of the value of the work is performed via a survey process carried out by specialties for presentation to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which is used by the Centers for Medicare & Medicaid Services (CMS) to help determine relative value units (RVUs) that determine payment. The work RVU (wRVU) is typically around half of the total RVU for each CPT code. The value is based on multiple factors including the time to perform the service, the technical skill needed, the physical effort involved, mental effort and judgment, and stress under which the physician works due to the potential risks to the patient.2 A series of instruments and calculations have been used to determine a value called intraservice work per unit of time (IWPUT), which is used to examine the intraservice (skin-to-skin) work of a procedure relative to similar procedures.
Calculating the IWPUT
To determine the IWPUT value of a procedure, a formula is used to subtract all the preservice and postservice work and look at what is left based on the total RVUs for the procedure, which can be mathematically presented using the following construct: total wRVUs (the complete work you provide in performing the service) is the sum of preservice work (eg, evaluation and management [E&M] services, preparatory work [eg, scrub, dress, wait]), intraservice (skin-to-skin) work, immediate postservice work (eg, dressings, prescriptions, instructions given by the physician), and postoperative work at E&M visits (eg, hospital days, discharge day, global follow-up visits).
All of these activities defined as E&M services are simply subtracted from the total wRVU, while wRVUs for preservice and postservice work that is not linked to a CPT global period are calculated by simply subtracting the product of each specified time by their intensity (eg, day prior evaluation, same day evaluation, and immediate post have an intensity of 0.0224, while scrub/preparation has an intensity of 0.0081),3 leaving you with intraservice (skin-to-skin) work. This intraservice work is divided by the intraservice time to give you IWPUT. For more information on the concept as well as the process and controversies, an excellent review is available from the CMS.4
Understanding the IWPUT
The procedure with the highest IWPUT value in all of medicine is an emergency endotracheal intubation (CPT code 31500), which has a value of 0.4061.5 The procedure is short and intense, and if it fails, the patient is dead. All other procedures have lower IWPUT values. For example, a small malignant excision on the trunk, arms, or legs (CPT code 11600) has an IWPUT of 0.0324, while a laparoscopic cholecystectomy with exploration of the common duct (CPT code 47564) has an IWPUT of 0.0737.5 These small values have been the drivers behind much of the Relative Value Scale Update Committee’s valuation process for more than a decade. Some specialists who perform mostly 90-day global procedures wanted IWPUT to be the critical validation factor in the process, which led to problems for the first few years of this century. It may seem obvious that if there are 2 ways to fix a broken leg, the more complex one would likely have a higher IWPUT. Because IWPUT is a pure number with no values attached, this assumption would seem reasonable. If we compare a malignant excision to a benign one, we would expect higher intensity for the malignant one, as we are going deeper and have more concerns about clear margins and recurrences. Within a group of similar procedures, these pure numbers can be useful to validate a proposed value. More wRVUs in a shorter time period would result in a higher IWPUT; however, anomalies arise. There are eleven 000 global period CPT codes, ten 010 codes, and one hundred ninety 090 codes with negative IWPUTs, implying the skin-to-skin work has a value less than 0, which is an illogical conclusion. The more logical conclusion is that the codes are overloaded with preservice and postservice times. The real travesty is when one begins to compare apples to oranges—glaucoma surgery to belly surgery, endoscopy to skin surgery, or any other comparison you can come up with—taking a number that can be used to evaluate intensity between similar procedures and generalizing across all procedures, a concept that has never been validated. The wRVUs themselves define the relativity, but in many instances the IWPUT has been used in the process to justify forcing values lower based on cross-specialty comparisons, which may lead some to think we need better measures, as has been reported in the literature.6-8 Reform likely will happen, but for now we must work within the constraints of this tiny number, the IWPUT.
Obtaining the IWPUT
You are probably wondering, “How can I learn the IWPUT for the codes I use?” You probably do not want or need to other than to gain an understanding of how they have been misused. Purchase a subscription to the Resource-Based Relative Value Scale (RBRVS) DataManager Online or access the data for free through the CMS website (https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1654-P.html) by downloading the CY 2017 PFS Proposed Rule Addenda, which gives you total RVUs for all CPT codes, and the CY 2017 PFS Proposed Rule Physician Time, which gives you the preservice, intraservice, and postservice times for all CPT codes.
Using CPT code 11600 as an example, the total wRVU is 1.63, while preservice evaluation time is 10 minutes, intraservice time is 10 minutes, and immediate postservice time is 5 minutes. There is also 1 global follow-up visit, a CPT 99213, built in with a wRVU of 0.97 that determines the total value of the code. Using the IWPUT formula, we have the following: {1.63 – [(10 × 0.0224) + (5 × 0.0224) + 0.97]} / 10 = 0.0324.
These data also are useful if you are negotiating a contract based on RVUs, so learn a bit more about why you get paid what you are paid.
The Importance of IWPUT
Those interested in the academic discourse behind IWPUT should consult the literature,3,9 which is open source and freely available, but for now we will concentrate on why IWPUT is an important concept. As global periods are reevaluated under the Medicare Access and CHIP Reauthorization Act of 2015,10 the removal of global period visits will cause changes in the IWPUT value of codes, which will make them outliers and therefore targeted for resurvey and revaluation. The intent of the CMS is to cut reimbursement under our fee-for-service system, so there will be pain for physicians who have flourished under the current policy. To avoid inappropriate decreases in reimbursement, we should all keep accurate records of which global postoperative services are indeed provided, which leads us back to CPT code 99024. If it is not tracked, then it may not be seen as having been done. So be sure to use it.
Remember that if you do what you document, document what you do, and report medically necessary CPT codes, you should have nothing to worry about for now.
After reading the July 2016 column on global periods and Current Procedural Terminology (CPT) code 99024,1 you may be wondering why you get paid what you do and how the procedure and visits all link together, which is associated with work intensity.
When CPT codes are given a value, the determination of the value of the work is performed via a survey process carried out by specialties for presentation to the American Medical Association/Specialty Society Relative Value Scale Update Committee, which is used by the Centers for Medicare & Medicaid Services (CMS) to help determine relative value units (RVUs) that determine payment. The work RVU (wRVU) is typically around half of the total RVU for each CPT code. The value is based on multiple factors including the time to perform the service, the technical skill needed, the physical effort involved, mental effort and judgment, and stress under which the physician works due to the potential risks to the patient.2 A series of instruments and calculations have been used to determine a value called intraservice work per unit of time (IWPUT), which is used to examine the intraservice (skin-to-skin) work of a procedure relative to similar procedures.
Calculating the IWPUT
To determine the IWPUT value of a procedure, a formula is used to subtract all the preservice and postservice work and look at what is left based on the total RVUs for the procedure, which can be mathematically presented using the following construct: total wRVUs (the complete work you provide in performing the service) is the sum of preservice work (eg, evaluation and management [E&M] services, preparatory work [eg, scrub, dress, wait]), intraservice (skin-to-skin) work, immediate postservice work (eg, dressings, prescriptions, instructions given by the physician), and postoperative work at E&M visits (eg, hospital days, discharge day, global follow-up visits).
All of these activities defined as E&M services are simply subtracted from the total wRVU, while wRVUs for preservice and postservice work that is not linked to a CPT global period are calculated by simply subtracting the product of each specified time by their intensity (eg, day prior evaluation, same day evaluation, and immediate post have an intensity of 0.0224, while scrub/preparation has an intensity of 0.0081),3 leaving you with intraservice (skin-to-skin) work. This intraservice work is divided by the intraservice time to give you IWPUT. For more information on the concept as well as the process and controversies, an excellent review is available from the CMS.4
Understanding the IWPUT
The procedure with the highest IWPUT value in all of medicine is an emergency endotracheal intubation (CPT code 31500), which has a value of 0.4061.5 The procedure is short and intense, and if it fails, the patient is dead. All other procedures have lower IWPUT values. For example, a small malignant excision on the trunk, arms, or legs (CPT code 11600) has an IWPUT of 0.0324, while a laparoscopic cholecystectomy with exploration of the common duct (CPT code 47564) has an IWPUT of 0.0737.5 These small values have been the drivers behind much of the Relative Value Scale Update Committee’s valuation process for more than a decade. Some specialists who perform mostly 90-day global procedures wanted IWPUT to be the critical validation factor in the process, which led to problems for the first few years of this century. It may seem obvious that if there are 2 ways to fix a broken leg, the more complex one would likely have a higher IWPUT. Because IWPUT is a pure number with no values attached, this assumption would seem reasonable. If we compare a malignant excision to a benign one, we would expect higher intensity for the malignant one, as we are going deeper and have more concerns about clear margins and recurrences. Within a group of similar procedures, these pure numbers can be useful to validate a proposed value. More wRVUs in a shorter time period would result in a higher IWPUT; however, anomalies arise. There are eleven 000 global period CPT codes, ten 010 codes, and one hundred ninety 090 codes with negative IWPUTs, implying the skin-to-skin work has a value less than 0, which is an illogical conclusion. The more logical conclusion is that the codes are overloaded with preservice and postservice times. The real travesty is when one begins to compare apples to oranges—glaucoma surgery to belly surgery, endoscopy to skin surgery, or any other comparison you can come up with—taking a number that can be used to evaluate intensity between similar procedures and generalizing across all procedures, a concept that has never been validated. The wRVUs themselves define the relativity, but in many instances the IWPUT has been used in the process to justify forcing values lower based on cross-specialty comparisons, which may lead some to think we need better measures, as has been reported in the literature.6-8 Reform likely will happen, but for now we must work within the constraints of this tiny number, the IWPUT.
Obtaining the IWPUT
You are probably wondering, “How can I learn the IWPUT for the codes I use?” You probably do not want or need to other than to gain an understanding of how they have been misused. Purchase a subscription to the Resource-Based Relative Value Scale (RBRVS) DataManager Online or access the data for free through the CMS website (https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1654-P.html) by downloading the CY 2017 PFS Proposed Rule Addenda, which gives you total RVUs for all CPT codes, and the CY 2017 PFS Proposed Rule Physician Time, which gives you the preservice, intraservice, and postservice times for all CPT codes.
Using CPT code 11600 as an example, the total wRVU is 1.63, while preservice evaluation time is 10 minutes, intraservice time is 10 minutes, and immediate postservice time is 5 minutes. There is also 1 global follow-up visit, a CPT 99213, built in with a wRVU of 0.97 that determines the total value of the code. Using the IWPUT formula, we have the following: {1.63 – [(10 × 0.0224) + (5 × 0.0224) + 0.97]} / 10 = 0.0324.
These data also are useful if you are negotiating a contract based on RVUs, so learn a bit more about why you get paid what you are paid.
The Importance of IWPUT
Those interested in the academic discourse behind IWPUT should consult the literature,3,9 which is open source and freely available, but for now we will concentrate on why IWPUT is an important concept. As global periods are reevaluated under the Medicare Access and CHIP Reauthorization Act of 2015,10 the removal of global period visits will cause changes in the IWPUT value of codes, which will make them outliers and therefore targeted for resurvey and revaluation. The intent of the CMS is to cut reimbursement under our fee-for-service system, so there will be pain for physicians who have flourished under the current policy. To avoid inappropriate decreases in reimbursement, we should all keep accurate records of which global postoperative services are indeed provided, which leads us back to CPT code 99024. If it is not tracked, then it may not be seen as having been done. So be sure to use it.
Remember that if you do what you document, document what you do, and report medically necessary CPT codes, you should have nothing to worry about for now.
- Siegel DM. Global visits, 99024, and MACRA: 3 things you should think about and lose sleep over but probably do not. Cutis. 2016;98:43-44, 46.
- Overview of the RBRVS. American Medical Association website. http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/the-resource-based-relative-value-scale/overview-of-rbrvs.page. Accessed July 14, 2016.
- Mabry CD, McCann BC, Harris JA, et al. The use of intraservice work per unit of time (IWPUT) and the building block method (BBM) for the calculation of surgical work. Ann Surg. 2005;241:929-938; discussion 938-940.
- Wynn BO, Burgette LF, Mulcahy AW, et al. Development of a Model for the Validation of Work Relative Value Units for the Medicare Physician Fee Schedule. Santa Monica, CA: RAND Corporation; 2015. http://www.rand.org/content/dam/rand/pubs/research_reports/RR600/RR662/RAND_RR662.pdf. Accessed July 18, 2016.
- RBRVS DataManager Online. American Medical Association. https://commerce.ama-assn .org/store/catalog/productDetail.jsp?product_ id=prod280002&navAction=push. Accessed July 20, 2016.
- Horner RD, Szaflarski JP, Ying J, et al. Physician work intensity among medical specialties: emerging evidence on its magnitude and composition. Med Care. 2011;49:1007-1111.
- Jacobson CJ Jr, Bolon S, Elder N, et al. Temporal and subjective work demands in office-based patient care: an exploration of the dimensions of physician work intensity. Med Care. 2011;49:52-58.
- Horner RD, Szaflarski JP, Jacobson CJ, et al. Clinical work intensity among physician specialties: how might we assess it? what do we find? Med Care. 2011;49:108-113.
- Zwolak RM, Trout HH 3rd. Vascular surgery and the Resource-based Relative Value Scale five-year review. J Vasc Surg. 1997;25:1077-1086.
- Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
- Siegel DM. Global visits, 99024, and MACRA: 3 things you should think about and lose sleep over but probably do not. Cutis. 2016;98:43-44, 46.
- Overview of the RBRVS. American Medical Association website. http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/the-resource-based-relative-value-scale/overview-of-rbrvs.page. Accessed July 14, 2016.
- Mabry CD, McCann BC, Harris JA, et al. The use of intraservice work per unit of time (IWPUT) and the building block method (BBM) for the calculation of surgical work. Ann Surg. 2005;241:929-938; discussion 938-940.
- Wynn BO, Burgette LF, Mulcahy AW, et al. Development of a Model for the Validation of Work Relative Value Units for the Medicare Physician Fee Schedule. Santa Monica, CA: RAND Corporation; 2015. http://www.rand.org/content/dam/rand/pubs/research_reports/RR600/RR662/RAND_RR662.pdf. Accessed July 18, 2016.
- RBRVS DataManager Online. American Medical Association. https://commerce.ama-assn .org/store/catalog/productDetail.jsp?product_ id=prod280002&navAction=push. Accessed July 20, 2016.
- Horner RD, Szaflarski JP, Ying J, et al. Physician work intensity among medical specialties: emerging evidence on its magnitude and composition. Med Care. 2011;49:1007-1111.
- Jacobson CJ Jr, Bolon S, Elder N, et al. Temporal and subjective work demands in office-based patient care: an exploration of the dimensions of physician work intensity. Med Care. 2011;49:52-58.
- Horner RD, Szaflarski JP, Jacobson CJ, et al. Clinical work intensity among physician specialties: how might we assess it? what do we find? Med Care. 2011;49:108-113.
- Zwolak RM, Trout HH 3rd. Vascular surgery and the Resource-based Relative Value Scale five-year review. J Vasc Surg. 1997;25:1077-1086.
- Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
Practice Points
- Intraservice work per unit of time (IWPUT) examines skin-to-skin work of a procedure.
- The removal of global period visits will cause changes in the IWPUT of codes.
Global Visits, 99024, and MACRA: 3 Things You Should Think About and Lose Sleep Over But Probably Do Not
How does the global period affect dermatologists?
Global period is a term used to describe what is included in the payment for performance of a procedure using Current Procedural Terminology (CPT) codes. These global periods can either be 0 (000), 10 (010), or 90 (090) days. In dermatology, we have all three. Most codes used by dermatologists fall under global periods of 0 and 10 days, while 90-day codes are used for all adjacent tissue transfers and split- and full-thickness grafts. In documents listing global periods for CPT codes,1 you also may see “XXX” when the global period concept does not apply to a particular code, “YYY” when the payer decides on whether a global period applies and what it will be, and “ZZZ” when a certain code is an add-on to another service and is therefore included in the global period for that service.
The contents of a service are defined by the global period. Although the procedure itself is an obvious component, CPT codes with a global period of 000 (eg, biopsy of a skin lesion, simple repairs) have no preoperative or postoperative periods, and an evaluation and management (E&M) service usually is not payable if it was done in relation to the procedure. If the patient returns the following day for any reason, including concerns about the procedure itself, these visits may be reported separately.
For CPT codes with global periods of 010 (eg, excisions, intermediate and complex repairs, destructions), there also is no preoperative period and a visit on the day of the procedure generally is not payable as a separate service. The day of the procedure and the 10 days after are included in the global period, and any visits relating to the procedure on that day and the 10 days following the procedure are not payable separately. Typically, the value of one 99212 or 99213 E&M visit is included in the payment for the procedure.
For CPT codes with global periods of 090, the day before the procedure, the day of the procedure, and 90 days following the procedure are all included. Typically, more than one established patient visit along with hospital management and discharge planning where deemed necessary by the Centers for Medicare & Medicaid Services (CMS) are included, which seems straightforward, but there is a sort of paradox here. An initial evaluation by the surgeon who determines the need for the 090 code (by definition, 090 means major surgery and major surgery means 090) can be separately reported for E&M using modifier -57 (decision for surgery), which means the surgeon seeing the hot abdomen in the emergency department can report an E&M code in addition to the procedure, as can the surgeon who decides to repair a defect after removal of a skin tumor with a flap or graft. The same is not applicable if one performs a simple repair (included with benign or malignant excisions) following Mohs micrographic surgery or an intermediate or complex repair after any form of skin cancer removal. In any event, you are making a decision about what repair is best for the patient and sharing that with him/her while obtaining patient consent, but only 090 codes allow the capture of the decision to perform the procedure.
Which modifiers can you use on the same day as a procedure during the global period?
All is not lost if you perform other activities on the same day as the procedure or during the global period if those other activities are unrelated, which means complications of the procedure cannot be separately reported. If the unrelated cognitive work is reported on the day of a procedure with an E&M code, it should be accompanied by modifier -25 (significant, separately identifiable E&M service by the same physician or other qualified health care professional on the same day of the procedure or other service). If you have an E&M visit unrelated to the procedure within the global period, report it using modifier -24 (unrelated E&M service by the same physician or other qualified health care professional during a postoperative period).
If you perform another procedure on the same day as the primary one, you can use modifier -51 (multiple procedures) to let the payer know you provided other services that are separately reportable. If you do multiples of the same procedure, use modifier -59 (distinct procedural service) to let the payer know that you indeed did multiple procedures and did not submit a typographical error. Modifier -59 also is used when you perform a pair of procedures on separate and distinct lesions that would be disallowed by Mutually Exclusive Edits if done on a single lesion. For example, if you perform a biopsy of a lesion and immediately curette it, you should wait for the pathology report; if the lesion is malignant, only the destruction should be reported, and if it is benign, the only medically necessary service was the biopsy. When biopsy and curettage are performed on 2 separate lesions on the same date of service, payer software will disallow the biopsy charge unless a -59 modifier is attached to indicate that the biopsy was performed on a separate lesion. Medicare has introduced the -XS modifier, which is planned to be phased in to replace the -59 modifier for Medicare patients,2 if and when the CMS sets up their systems to accept the modifier.
If you repeat a procedure during the global period (eg, reexcision for a positive margin), it is appropriate to use modifier -58 (staged or related procedure or service by the same physician or other qualified health care professional during the postoperative period). If an unrelated procedure is performed during the global period, such as removing another lesion at a different site, modifier -79 (unrelated procedure or service by the same physician or other qualified health care professional during the postoperative period) lets you report it.
There are 2 available modifiers that you might think twice before using. Modifier -76 (repeat procedure or service by same physician or other qualified health care professional) may be used if, for example, a wound opens and you have to sew it up again. The more common usage is more pedestrian; a second electrocardiogram reading on the same day is a common use.3 Modifier -78 (unplanned return to the operating/procedure room by the same physician or other qualified health care professional following initial procedure for a related procedure during the postoperative period) is used when something goes awry, such as an aneurysm repair that is bleeding postoperatively, necessitating a trip back to the operating room.4
How might these modifiers be used in dermatology? One example may be if a wound dehisces or needs to be seen for a bleeding issue that might necessitate opening and exploring the wound; if a patient has one of these problems after fixing the plumbing and hits himself with a wrench, use of these modifiers is reasonable. On the other hand, if the patient is waiting in your office to be picked up and the problem happens, using these modifiers may not be the wisest thing to do. Let common sense prevail!
What is CPT code 99024?
Likely a code you have never used in your private office, the descriptor for 99024 states “postoperative follow-up visit, normally included in the surgical package, to indicate that an E&M service was performed during a postoperative period for a reason(s) related to the original procedure,” which translates to “here for an included visit so why am I billing this and having the cost of a claim with no reimbursement?” Why indeed. You may be using it as a space holder—one more check and balance so no patient leaves the office without a superbill or its electronic equivalent being submitted to your billing staff—or you may simply never use it. The CMS is interested in it as a way to see if the visits embedded in global periods actually take place. This is especially important as CMS is legally mandated under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA)5 to see if these visits actually take place.6 There are billions of dollars paid out for visits that are part of the global package and this code is one way the government may track them. If you are not using this code at all, you might consider it, even if you do not submit a claim. Your staff will know you did not forget to report a service and the reporting of the code by you internally and it lets you document for the billing side of the practice that they were there and a code report has been performed and not simply forgotten.
Final Thoughts
Following this discussion of global periods and CPT code 99024, you may be wondering why you get paid what you do and how the visits all link together. The buzzword is intensity, and we will explore that concept and IWPUT (intraservice work per unit of time), which I have coined as meaning “I Will Persevere Until Then,” in the next column.
- Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016. Addendum B—Relative Value Units and Related Information Used in CY 2016 Final Rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched?Downloads?CY2016-PFS-FC-Addenda.zip. Updated November 5, 2015. Accessed June 1, 2016.
- Modifier 59 article. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/downloads/modifier59.pdf. Accessed June 20, 2016.
- Modifier dictionary FAQ. American College of Emergency Physicians website. https://www.acep.org/Physician-Resources/Practice-Resources/Administration/Financial-Issues-/-Reimbursement/Modifier-Dictionary-FAQ/. Updated April 2014. Accessed June 2, 2016.
- Modifier 78 fact sheet. Wisconsin Physicians Service Insurance Corporation website. http://wpsmedicare.com/j8macpartb/resources/modifiers/modifier-78.shtml. Accessed June 2, 2016.
- Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
- Medicare Learning Network. Collecting data on global surgery as required by MACRA: listening session. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Outreach-and-Education/Outreach/NPC/Downloads/2016-01-20-MACRA-Transcript.pdf. Posted January 20, 2016. Accessed June 2, 2016.
How does the global period affect dermatologists?
Global period is a term used to describe what is included in the payment for performance of a procedure using Current Procedural Terminology (CPT) codes. These global periods can either be 0 (000), 10 (010), or 90 (090) days. In dermatology, we have all three. Most codes used by dermatologists fall under global periods of 0 and 10 days, while 90-day codes are used for all adjacent tissue transfers and split- and full-thickness grafts. In documents listing global periods for CPT codes,1 you also may see “XXX” when the global period concept does not apply to a particular code, “YYY” when the payer decides on whether a global period applies and what it will be, and “ZZZ” when a certain code is an add-on to another service and is therefore included in the global period for that service.
The contents of a service are defined by the global period. Although the procedure itself is an obvious component, CPT codes with a global period of 000 (eg, biopsy of a skin lesion, simple repairs) have no preoperative or postoperative periods, and an evaluation and management (E&M) service usually is not payable if it was done in relation to the procedure. If the patient returns the following day for any reason, including concerns about the procedure itself, these visits may be reported separately.
For CPT codes with global periods of 010 (eg, excisions, intermediate and complex repairs, destructions), there also is no preoperative period and a visit on the day of the procedure generally is not payable as a separate service. The day of the procedure and the 10 days after are included in the global period, and any visits relating to the procedure on that day and the 10 days following the procedure are not payable separately. Typically, the value of one 99212 or 99213 E&M visit is included in the payment for the procedure.
For CPT codes with global periods of 090, the day before the procedure, the day of the procedure, and 90 days following the procedure are all included. Typically, more than one established patient visit along with hospital management and discharge planning where deemed necessary by the Centers for Medicare & Medicaid Services (CMS) are included, which seems straightforward, but there is a sort of paradox here. An initial evaluation by the surgeon who determines the need for the 090 code (by definition, 090 means major surgery and major surgery means 090) can be separately reported for E&M using modifier -57 (decision for surgery), which means the surgeon seeing the hot abdomen in the emergency department can report an E&M code in addition to the procedure, as can the surgeon who decides to repair a defect after removal of a skin tumor with a flap or graft. The same is not applicable if one performs a simple repair (included with benign or malignant excisions) following Mohs micrographic surgery or an intermediate or complex repair after any form of skin cancer removal. In any event, you are making a decision about what repair is best for the patient and sharing that with him/her while obtaining patient consent, but only 090 codes allow the capture of the decision to perform the procedure.
Which modifiers can you use on the same day as a procedure during the global period?
All is not lost if you perform other activities on the same day as the procedure or during the global period if those other activities are unrelated, which means complications of the procedure cannot be separately reported. If the unrelated cognitive work is reported on the day of a procedure with an E&M code, it should be accompanied by modifier -25 (significant, separately identifiable E&M service by the same physician or other qualified health care professional on the same day of the procedure or other service). If you have an E&M visit unrelated to the procedure within the global period, report it using modifier -24 (unrelated E&M service by the same physician or other qualified health care professional during a postoperative period).
If you perform another procedure on the same day as the primary one, you can use modifier -51 (multiple procedures) to let the payer know you provided other services that are separately reportable. If you do multiples of the same procedure, use modifier -59 (distinct procedural service) to let the payer know that you indeed did multiple procedures and did not submit a typographical error. Modifier -59 also is used when you perform a pair of procedures on separate and distinct lesions that would be disallowed by Mutually Exclusive Edits if done on a single lesion. For example, if you perform a biopsy of a lesion and immediately curette it, you should wait for the pathology report; if the lesion is malignant, only the destruction should be reported, and if it is benign, the only medically necessary service was the biopsy. When biopsy and curettage are performed on 2 separate lesions on the same date of service, payer software will disallow the biopsy charge unless a -59 modifier is attached to indicate that the biopsy was performed on a separate lesion. Medicare has introduced the -XS modifier, which is planned to be phased in to replace the -59 modifier for Medicare patients,2 if and when the CMS sets up their systems to accept the modifier.
If you repeat a procedure during the global period (eg, reexcision for a positive margin), it is appropriate to use modifier -58 (staged or related procedure or service by the same physician or other qualified health care professional during the postoperative period). If an unrelated procedure is performed during the global period, such as removing another lesion at a different site, modifier -79 (unrelated procedure or service by the same physician or other qualified health care professional during the postoperative period) lets you report it.
There are 2 available modifiers that you might think twice before using. Modifier -76 (repeat procedure or service by same physician or other qualified health care professional) may be used if, for example, a wound opens and you have to sew it up again. The more common usage is more pedestrian; a second electrocardiogram reading on the same day is a common use.3 Modifier -78 (unplanned return to the operating/procedure room by the same physician or other qualified health care professional following initial procedure for a related procedure during the postoperative period) is used when something goes awry, such as an aneurysm repair that is bleeding postoperatively, necessitating a trip back to the operating room.4
How might these modifiers be used in dermatology? One example may be if a wound dehisces or needs to be seen for a bleeding issue that might necessitate opening and exploring the wound; if a patient has one of these problems after fixing the plumbing and hits himself with a wrench, use of these modifiers is reasonable. On the other hand, if the patient is waiting in your office to be picked up and the problem happens, using these modifiers may not be the wisest thing to do. Let common sense prevail!
What is CPT code 99024?
Likely a code you have never used in your private office, the descriptor for 99024 states “postoperative follow-up visit, normally included in the surgical package, to indicate that an E&M service was performed during a postoperative period for a reason(s) related to the original procedure,” which translates to “here for an included visit so why am I billing this and having the cost of a claim with no reimbursement?” Why indeed. You may be using it as a space holder—one more check and balance so no patient leaves the office without a superbill or its electronic equivalent being submitted to your billing staff—or you may simply never use it. The CMS is interested in it as a way to see if the visits embedded in global periods actually take place. This is especially important as CMS is legally mandated under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA)5 to see if these visits actually take place.6 There are billions of dollars paid out for visits that are part of the global package and this code is one way the government may track them. If you are not using this code at all, you might consider it, even if you do not submit a claim. Your staff will know you did not forget to report a service and the reporting of the code by you internally and it lets you document for the billing side of the practice that they were there and a code report has been performed and not simply forgotten.
Final Thoughts
Following this discussion of global periods and CPT code 99024, you may be wondering why you get paid what you do and how the visits all link together. The buzzword is intensity, and we will explore that concept and IWPUT (intraservice work per unit of time), which I have coined as meaning “I Will Persevere Until Then,” in the next column.
How does the global period affect dermatologists?
Global period is a term used to describe what is included in the payment for performance of a procedure using Current Procedural Terminology (CPT) codes. These global periods can either be 0 (000), 10 (010), or 90 (090) days. In dermatology, we have all three. Most codes used by dermatologists fall under global periods of 0 and 10 days, while 90-day codes are used for all adjacent tissue transfers and split- and full-thickness grafts. In documents listing global periods for CPT codes,1 you also may see “XXX” when the global period concept does not apply to a particular code, “YYY” when the payer decides on whether a global period applies and what it will be, and “ZZZ” when a certain code is an add-on to another service and is therefore included in the global period for that service.
The contents of a service are defined by the global period. Although the procedure itself is an obvious component, CPT codes with a global period of 000 (eg, biopsy of a skin lesion, simple repairs) have no preoperative or postoperative periods, and an evaluation and management (E&M) service usually is not payable if it was done in relation to the procedure. If the patient returns the following day for any reason, including concerns about the procedure itself, these visits may be reported separately.
For CPT codes with global periods of 010 (eg, excisions, intermediate and complex repairs, destructions), there also is no preoperative period and a visit on the day of the procedure generally is not payable as a separate service. The day of the procedure and the 10 days after are included in the global period, and any visits relating to the procedure on that day and the 10 days following the procedure are not payable separately. Typically, the value of one 99212 or 99213 E&M visit is included in the payment for the procedure.
For CPT codes with global periods of 090, the day before the procedure, the day of the procedure, and 90 days following the procedure are all included. Typically, more than one established patient visit along with hospital management and discharge planning where deemed necessary by the Centers for Medicare & Medicaid Services (CMS) are included, which seems straightforward, but there is a sort of paradox here. An initial evaluation by the surgeon who determines the need for the 090 code (by definition, 090 means major surgery and major surgery means 090) can be separately reported for E&M using modifier -57 (decision for surgery), which means the surgeon seeing the hot abdomen in the emergency department can report an E&M code in addition to the procedure, as can the surgeon who decides to repair a defect after removal of a skin tumor with a flap or graft. The same is not applicable if one performs a simple repair (included with benign or malignant excisions) following Mohs micrographic surgery or an intermediate or complex repair after any form of skin cancer removal. In any event, you are making a decision about what repair is best for the patient and sharing that with him/her while obtaining patient consent, but only 090 codes allow the capture of the decision to perform the procedure.
Which modifiers can you use on the same day as a procedure during the global period?
All is not lost if you perform other activities on the same day as the procedure or during the global period if those other activities are unrelated, which means complications of the procedure cannot be separately reported. If the unrelated cognitive work is reported on the day of a procedure with an E&M code, it should be accompanied by modifier -25 (significant, separately identifiable E&M service by the same physician or other qualified health care professional on the same day of the procedure or other service). If you have an E&M visit unrelated to the procedure within the global period, report it using modifier -24 (unrelated E&M service by the same physician or other qualified health care professional during a postoperative period).
If you perform another procedure on the same day as the primary one, you can use modifier -51 (multiple procedures) to let the payer know you provided other services that are separately reportable. If you do multiples of the same procedure, use modifier -59 (distinct procedural service) to let the payer know that you indeed did multiple procedures and did not submit a typographical error. Modifier -59 also is used when you perform a pair of procedures on separate and distinct lesions that would be disallowed by Mutually Exclusive Edits if done on a single lesion. For example, if you perform a biopsy of a lesion and immediately curette it, you should wait for the pathology report; if the lesion is malignant, only the destruction should be reported, and if it is benign, the only medically necessary service was the biopsy. When biopsy and curettage are performed on 2 separate lesions on the same date of service, payer software will disallow the biopsy charge unless a -59 modifier is attached to indicate that the biopsy was performed on a separate lesion. Medicare has introduced the -XS modifier, which is planned to be phased in to replace the -59 modifier for Medicare patients,2 if and when the CMS sets up their systems to accept the modifier.
If you repeat a procedure during the global period (eg, reexcision for a positive margin), it is appropriate to use modifier -58 (staged or related procedure or service by the same physician or other qualified health care professional during the postoperative period). If an unrelated procedure is performed during the global period, such as removing another lesion at a different site, modifier -79 (unrelated procedure or service by the same physician or other qualified health care professional during the postoperative period) lets you report it.
There are 2 available modifiers that you might think twice before using. Modifier -76 (repeat procedure or service by same physician or other qualified health care professional) may be used if, for example, a wound opens and you have to sew it up again. The more common usage is more pedestrian; a second electrocardiogram reading on the same day is a common use.3 Modifier -78 (unplanned return to the operating/procedure room by the same physician or other qualified health care professional following initial procedure for a related procedure during the postoperative period) is used when something goes awry, such as an aneurysm repair that is bleeding postoperatively, necessitating a trip back to the operating room.4
How might these modifiers be used in dermatology? One example may be if a wound dehisces or needs to be seen for a bleeding issue that might necessitate opening and exploring the wound; if a patient has one of these problems after fixing the plumbing and hits himself with a wrench, use of these modifiers is reasonable. On the other hand, if the patient is waiting in your office to be picked up and the problem happens, using these modifiers may not be the wisest thing to do. Let common sense prevail!
What is CPT code 99024?
Likely a code you have never used in your private office, the descriptor for 99024 states “postoperative follow-up visit, normally included in the surgical package, to indicate that an E&M service was performed during a postoperative period for a reason(s) related to the original procedure,” which translates to “here for an included visit so why am I billing this and having the cost of a claim with no reimbursement?” Why indeed. You may be using it as a space holder—one more check and balance so no patient leaves the office without a superbill or its electronic equivalent being submitted to your billing staff—or you may simply never use it. The CMS is interested in it as a way to see if the visits embedded in global periods actually take place. This is especially important as CMS is legally mandated under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA)5 to see if these visits actually take place.6 There are billions of dollars paid out for visits that are part of the global package and this code is one way the government may track them. If you are not using this code at all, you might consider it, even if you do not submit a claim. Your staff will know you did not forget to report a service and the reporting of the code by you internally and it lets you document for the billing side of the practice that they were there and a code report has been performed and not simply forgotten.
Final Thoughts
Following this discussion of global periods and CPT code 99024, you may be wondering why you get paid what you do and how the visits all link together. The buzzword is intensity, and we will explore that concept and IWPUT (intraservice work per unit of time), which I have coined as meaning “I Will Persevere Until Then,” in the next column.
- Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016. Addendum B—Relative Value Units and Related Information Used in CY 2016 Final Rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched?Downloads?CY2016-PFS-FC-Addenda.zip. Updated November 5, 2015. Accessed June 1, 2016.
- Modifier 59 article. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/downloads/modifier59.pdf. Accessed June 20, 2016.
- Modifier dictionary FAQ. American College of Emergency Physicians website. https://www.acep.org/Physician-Resources/Practice-Resources/Administration/Financial-Issues-/-Reimbursement/Modifier-Dictionary-FAQ/. Updated April 2014. Accessed June 2, 2016.
- Modifier 78 fact sheet. Wisconsin Physicians Service Insurance Corporation website. http://wpsmedicare.com/j8macpartb/resources/modifiers/modifier-78.shtml. Accessed June 2, 2016.
- Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
- Medicare Learning Network. Collecting data on global surgery as required by MACRA: listening session. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Outreach-and-Education/Outreach/NPC/Downloads/2016-01-20-MACRA-Transcript.pdf. Posted January 20, 2016. Accessed June 2, 2016.
- Revisions to Payment Policies under the Physician Fee Schedule and Other Revisions to Part B for CY 2016. Addendum B—Relative Value Units and Related Information Used in CY 2016 Final Rule. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched?Downloads?CY2016-PFS-FC-Addenda.zip. Updated November 5, 2015. Accessed June 1, 2016.
- Modifier 59 article. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/downloads/modifier59.pdf. Accessed June 20, 2016.
- Modifier dictionary FAQ. American College of Emergency Physicians website. https://www.acep.org/Physician-Resources/Practice-Resources/Administration/Financial-Issues-/-Reimbursement/Modifier-Dictionary-FAQ/. Updated April 2014. Accessed June 2, 2016.
- Modifier 78 fact sheet. Wisconsin Physicians Service Insurance Corporation website. http://wpsmedicare.com/j8macpartb/resources/modifiers/modifier-78.shtml. Accessed June 2, 2016.
- Medicare Access and CHIP Reauthorization Act of 2015, HR 2, 114th Cong, 1st Sess (2015).
- Medicare Learning Network. Collecting data on global surgery as required by MACRA: listening session. Centers for Medicare & Medicaid Services website. https://www.cms.gov/Outreach-and-Education/Outreach/NPC/Downloads/2016-01-20-MACRA-Transcript.pdf. Posted January 20, 2016. Accessed June 2, 2016.
Practice Points
- Global period refers to payment for performance of a procedure and can be either 0 (000), 10 (010), or 90 (090) days. Most codes used by dermatologists fall under global periods of 0 and 10 days.
- Modifiers can be used if you perform other activities on the same day as the procedure or during the global period if those other activities are unrelated.
- Current Procedural Terminology code 99024 allows you to document for the billing side of the practice that the patient was there for a postoperative visit and may be a useful way to let payers know the visit occurred.
Electronic Health Records, Autocoding, and Ewe: Don’t Be a Sheep!
Sheep are thought of as nervous animals, a good target for predators. You do not want to be a sheep. Unfortunately, many electronic health record (EHR) programs make you a target for audits and requests for the return of payments for a variety of reasons. Although you likely are aware of the uses of modifier -25, it is the abuses—either intentional or accidental—that can bring an audit your way. The use of modifier -25 was previously reviewed in Cutis.1 Despite the availability of this excellent review, I have found that there is still great confusion about both the use of modifier -25 and the selection of the correct evaluation and management (E&M) code when used.
When to Bill for E&M
Based on recent discussions with colleagues in the New York area who have been audited, an easy way to bring on a request for medical records is to report an E&M 100% of the time with a procedure. In these instances, every single E&M was performed on the same visit as a dermatologic procedure, most commonly biopsies(Current Procedural Terminology [CPT] code 11100, 11101) and premalignant destructions (CPT code 17000, 17003, 17004), which is in contrast with typical practitioners who perform an E&M approximately 70% of the time (RUC rationale; American Medical Association RBRVS Data Manager; May 12, 2016). One circumstance involved the reporting of E&M services 100% of the time when performed during the same visit as Mohs micrographic surgery (CPT code 17311–17315), a surprising frequency considering that the typical same day use of a code for this procedure with an E&M in the Medicare population is less than 25%.
According to the National Correct Coding Initiative Policy Manual for Medicare Services, procedures with a global period of 90 days are defined as major surgical procedures,2 which only include adjacent tissue transfers and grafts for dermatology. If an E&M is performed on the same date of service as one of these procedures to decide whether to perform the procedure, the E&M can be reported separately using modifier -57. Other preoperative E&M services provided on the same date of service as a major surgical procedure are included in the global payment for the procedure and are not reported separately.2
All other procedures dermatologists perform generally are considered minor, which are defined as having a global period of 0 or 10 days. Because the decision to perform a minor procedure is included in the payment for the procedure, E&M services should not be reported separately from the minor procedure. However, “a significant and separately identifiable E&M service unrelated to the decision to perform the minor surgical procedure is separately reportable with modifier 25. The E&M service and minor surgical procedure do not require different diagnoses. If a minor surgical procedure is performed on a new patient, the same rules for reporting E&M services apply.”2
Documentation Guidelines
These guidelines seem straightforward, but as with so much else where the government is involved, the devil is in the details. When making coding decisions, you may consult the documentation guidelines from either 19953 or 1997,4 which are available for download on the Centers for Medicare & Medicaid Services (CMS) website (https://www.cms.gov/outreach-and-education/medicare-learning-network-MLN/MLNedwebguide/emdoc.html). The 1995 guidelines are less empiric and offer more flexibility, while the 1997 guidelines rely on number of “bullets” as examination elements.
1995 Guidelines
According to the 1995 documentation guidelines, the levels of E&M services are based on 4 types of examination that are defined as follows: (1) problem focused, a limited examination of the affected body area or organ system; (2) expanded problem focused, a limited examination of the affected body area or organ system and other symptomatic or related organ system(s); (3) detailed, an extended examination of the affected body area(s) and other symptomatic or related organ system(s); and (4) comprehensive, a general multisystem examination or complete examination of a single organ system.3 Detailed history is the fuzziest part of the coding universe. Some insurers take an approach that you need to examine 2 to 7 organ systems and 4 distinct lesions in 4 body areas, which is discussed in audit tools available from some Medicare intermediaries (Advancing the Business of Healthcare forum; April 10, 2014). As a result, the 12-bullet examination from the 1997 documentation guidelines may be more suitable for a new level 3 or established level 4 visit. For a comprehensive examination, the 1995 criteria allow for a complete examination of a single organ system such as the full-body skin examination with the patient completely undressed, which is medically necessary in our melanoma patients.
For purposes of examination, 9 body areas are recognized in the 1995 guidelines,3 along with more than a dozen organ systems of which the skin is of most interest to dermatologists.
According to the 1995 guidelines,3 the extent of examinations performed and documented is dependent upon clinical judgment and the nature of the presenting problem(s) and range from focused examinations of single body areas to general multisystem or complete single organ system examinations. Specific abnormal and relevant negative findings of the examination of the affected or symptomatic body area(s) or organ system(s) should be documented. Although a notation of normal is sufficient, abnormal without elaboration is insufficient, and abnormal or unexpected findings of the examination of the unaffected or asymptomatic body area(s) or organ system(s) should be described. The medical record for a general multisystem examination should include findings involving approximately 8 or more of the 12 organ systems.
An expanded problem focused examination under the 1995 guidelines could be as simple as “Scar on cancer excision site on left cheek soft and supple. No cervical adenopathy.” There is some confusion regarding detailed examinations, and one consultant went as far as calling the guidelines “vague,”5 while others such as a Medicare intermediary make a quantum leap that if a comprehensive general system examination includes 8 to 12 organ systems, one step below should include 2 to 7 organ systems.6 In essence, the payer makes the rules here.
1997 Guidelines
According to the 1997 documentation guidelines, count bullets that are examination elements, which can be either general or single organ system.4 (A table showing the bullets for the examination elements is available from the CMS.4) For each type of examination, apply the following: problem focused examination requires 1 to 5 elements identified by a bullet, expanded problem focused examination needs at least 6, detailed examination requires at least 12, and comprehensive examination requires all elements identified by a bullet with documentation of every element in each box with a shaded border and at least 1 element in each box with an unshaded border.4 Although you may do more writing when using the 1997 guidelines, you can easily count up bullets and these guidelines are amenable to template examinations on paper and obviously easily coded into EHR software that will do the bullet counting for you.
Unfortunately, this is where a ewe becomes a sheep, ripe for hunting for a number of reasons. First, just because you documented an E&M service does not mean it is medically necessary. Do you really need vital signs for every visit? If you are a meaningful EHR user working on penalty avoidance, you may capture examination data for meaningful use that is not medically necessary but cannot be parsed out by the autocoder in your EHR. As a result, simply do a quick manual audit of your notes to see if you are overcoding, which becomes second nature if you do it often.
The second trap, which brings us back to modifier -25, is when you perform a procedure the same day as your E&M or vice versa. Every procedure we do within the Resource-Based Relative Value Scale contains preservice time, which includes review of materials relevant to the procedure, examination of the area, and all preparation (eg, marking, time out, anesthesia, scrub and drape) before the surgery begins. The detailed vignettes are available to those involved in the Relative Value Scale Update Committee process and to the rest of the world in a subscription product called the RBRVS DataManager Online, which is produced by the American Medical Association. Unfortunately, the American Medical Association is not accepting new subscriptions to this product, as it has decided to outsource most of its coding resources to Optum360, one of the many arms of UnitedHealth Group, and will not have a replacement product until after June 30, 2016.7
In essence, if you (and your EHR) are counting bullets and then treating the body area in question, you are double-dipping, as the examination of the area is included in the procedure. So if you are heading toward a CPT 99213-25 with 6 bullets, one of which is on the left arm, and you perform a 0- or 10-day global procedure on that arm, you are down to 5 bullets, which drops your level of examination to problem focused. Remember, you need only 2 of 3—history, examination, and decision making—to be at or above that need for that particular level of reporting. If only one of your history or decision making is at or above the needed level for a 99213, the loss of a single bullet drops you down to a 99212! An audit where a handful of medical records are pulled and a request for money back on the universe of payments the insurer has paid is always unpleasant and you should, if you get a request for same, follow all the rules and timelines outlined by the payer. If you knowingly behaved in a risky fashion, consult a good attorney.
Of course, you may argue that the effort needed for the E&M work for the procedure was above and beyond what is typical for the service, which can be a hard standard to meet. Although the CMS requires a “significant and separately identifiable E&M service” as noted above and a separate diagnosis is not needed, the onus is on you to prove it. It is much easier to have a separate diagnosis that stands on its own, which will probably make an audit less common (unless you do it too often).
Final Thoughts
In summary, document what you do, do what you document, and report what is medically necessary. Keep watch over your EHR to be sure it is not overcoding for you. You do not want to be a ewe!
- Alam M. Modifier -25 use in dermatology. Cutis. 2015;95:76-77.
- National Correct Coding Initiative Policy Manual for Medicare Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 2016. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/Downloads/2016-NCCI-Policy-Manual.zip. Accessed May 6, 2016.
- 1995 Documentation Guidelines for Evaluation and Management Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 1995. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuideDownloads/95Docguidelines.pdf. Accessed May 6, 2016.
- 1997 Documentation Guidelines for Evaluation and Management Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 1997. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed May 6, 2016.
- E/M FAQ #19. E/M University website. http://www.emuniversity.com/FAQ/EMFAQ19.html. Accessed May 4, 2016.
- In the E/M documentation guidelines, what does “more detail” regarding the exam mean, and what is the difference between an expanded problem-focused exam and detailed exam? Palmetto GBA website. http://www.palmettogba.com/palmetto/providers.nsf/DocsCat/Providers~Railroad%2Medicare~Resources~FAQs~EM%20Help%20Center~8EELQD7181?open&navmenu=%7C%7C. Updated March 2, 2016. Accessed May 4, 2016.
- AMA website. http://info.commerce.ama-assn.org/online-coding-home. Accessed May 4, 2016.
Sheep are thought of as nervous animals, a good target for predators. You do not want to be a sheep. Unfortunately, many electronic health record (EHR) programs make you a target for audits and requests for the return of payments for a variety of reasons. Although you likely are aware of the uses of modifier -25, it is the abuses—either intentional or accidental—that can bring an audit your way. The use of modifier -25 was previously reviewed in Cutis.1 Despite the availability of this excellent review, I have found that there is still great confusion about both the use of modifier -25 and the selection of the correct evaluation and management (E&M) code when used.
When to Bill for E&M
Based on recent discussions with colleagues in the New York area who have been audited, an easy way to bring on a request for medical records is to report an E&M 100% of the time with a procedure. In these instances, every single E&M was performed on the same visit as a dermatologic procedure, most commonly biopsies(Current Procedural Terminology [CPT] code 11100, 11101) and premalignant destructions (CPT code 17000, 17003, 17004), which is in contrast with typical practitioners who perform an E&M approximately 70% of the time (RUC rationale; American Medical Association RBRVS Data Manager; May 12, 2016). One circumstance involved the reporting of E&M services 100% of the time when performed during the same visit as Mohs micrographic surgery (CPT code 17311–17315), a surprising frequency considering that the typical same day use of a code for this procedure with an E&M in the Medicare population is less than 25%.
According to the National Correct Coding Initiative Policy Manual for Medicare Services, procedures with a global period of 90 days are defined as major surgical procedures,2 which only include adjacent tissue transfers and grafts for dermatology. If an E&M is performed on the same date of service as one of these procedures to decide whether to perform the procedure, the E&M can be reported separately using modifier -57. Other preoperative E&M services provided on the same date of service as a major surgical procedure are included in the global payment for the procedure and are not reported separately.2
All other procedures dermatologists perform generally are considered minor, which are defined as having a global period of 0 or 10 days. Because the decision to perform a minor procedure is included in the payment for the procedure, E&M services should not be reported separately from the minor procedure. However, “a significant and separately identifiable E&M service unrelated to the decision to perform the minor surgical procedure is separately reportable with modifier 25. The E&M service and minor surgical procedure do not require different diagnoses. If a minor surgical procedure is performed on a new patient, the same rules for reporting E&M services apply.”2
Documentation Guidelines
These guidelines seem straightforward, but as with so much else where the government is involved, the devil is in the details. When making coding decisions, you may consult the documentation guidelines from either 19953 or 1997,4 which are available for download on the Centers for Medicare & Medicaid Services (CMS) website (https://www.cms.gov/outreach-and-education/medicare-learning-network-MLN/MLNedwebguide/emdoc.html). The 1995 guidelines are less empiric and offer more flexibility, while the 1997 guidelines rely on number of “bullets” as examination elements.
1995 Guidelines
According to the 1995 documentation guidelines, the levels of E&M services are based on 4 types of examination that are defined as follows: (1) problem focused, a limited examination of the affected body area or organ system; (2) expanded problem focused, a limited examination of the affected body area or organ system and other symptomatic or related organ system(s); (3) detailed, an extended examination of the affected body area(s) and other symptomatic or related organ system(s); and (4) comprehensive, a general multisystem examination or complete examination of a single organ system.3 Detailed history is the fuzziest part of the coding universe. Some insurers take an approach that you need to examine 2 to 7 organ systems and 4 distinct lesions in 4 body areas, which is discussed in audit tools available from some Medicare intermediaries (Advancing the Business of Healthcare forum; April 10, 2014). As a result, the 12-bullet examination from the 1997 documentation guidelines may be more suitable for a new level 3 or established level 4 visit. For a comprehensive examination, the 1995 criteria allow for a complete examination of a single organ system such as the full-body skin examination with the patient completely undressed, which is medically necessary in our melanoma patients.
For purposes of examination, 9 body areas are recognized in the 1995 guidelines,3 along with more than a dozen organ systems of which the skin is of most interest to dermatologists.
According to the 1995 guidelines,3 the extent of examinations performed and documented is dependent upon clinical judgment and the nature of the presenting problem(s) and range from focused examinations of single body areas to general multisystem or complete single organ system examinations. Specific abnormal and relevant negative findings of the examination of the affected or symptomatic body area(s) or organ system(s) should be documented. Although a notation of normal is sufficient, abnormal without elaboration is insufficient, and abnormal or unexpected findings of the examination of the unaffected or asymptomatic body area(s) or organ system(s) should be described. The medical record for a general multisystem examination should include findings involving approximately 8 or more of the 12 organ systems.
An expanded problem focused examination under the 1995 guidelines could be as simple as “Scar on cancer excision site on left cheek soft and supple. No cervical adenopathy.” There is some confusion regarding detailed examinations, and one consultant went as far as calling the guidelines “vague,”5 while others such as a Medicare intermediary make a quantum leap that if a comprehensive general system examination includes 8 to 12 organ systems, one step below should include 2 to 7 organ systems.6 In essence, the payer makes the rules here.
1997 Guidelines
According to the 1997 documentation guidelines, count bullets that are examination elements, which can be either general or single organ system.4 (A table showing the bullets for the examination elements is available from the CMS.4) For each type of examination, apply the following: problem focused examination requires 1 to 5 elements identified by a bullet, expanded problem focused examination needs at least 6, detailed examination requires at least 12, and comprehensive examination requires all elements identified by a bullet with documentation of every element in each box with a shaded border and at least 1 element in each box with an unshaded border.4 Although you may do more writing when using the 1997 guidelines, you can easily count up bullets and these guidelines are amenable to template examinations on paper and obviously easily coded into EHR software that will do the bullet counting for you.
Unfortunately, this is where a ewe becomes a sheep, ripe for hunting for a number of reasons. First, just because you documented an E&M service does not mean it is medically necessary. Do you really need vital signs for every visit? If you are a meaningful EHR user working on penalty avoidance, you may capture examination data for meaningful use that is not medically necessary but cannot be parsed out by the autocoder in your EHR. As a result, simply do a quick manual audit of your notes to see if you are overcoding, which becomes second nature if you do it often.
The second trap, which brings us back to modifier -25, is when you perform a procedure the same day as your E&M or vice versa. Every procedure we do within the Resource-Based Relative Value Scale contains preservice time, which includes review of materials relevant to the procedure, examination of the area, and all preparation (eg, marking, time out, anesthesia, scrub and drape) before the surgery begins. The detailed vignettes are available to those involved in the Relative Value Scale Update Committee process and to the rest of the world in a subscription product called the RBRVS DataManager Online, which is produced by the American Medical Association. Unfortunately, the American Medical Association is not accepting new subscriptions to this product, as it has decided to outsource most of its coding resources to Optum360, one of the many arms of UnitedHealth Group, and will not have a replacement product until after June 30, 2016.7
In essence, if you (and your EHR) are counting bullets and then treating the body area in question, you are double-dipping, as the examination of the area is included in the procedure. So if you are heading toward a CPT 99213-25 with 6 bullets, one of which is on the left arm, and you perform a 0- or 10-day global procedure on that arm, you are down to 5 bullets, which drops your level of examination to problem focused. Remember, you need only 2 of 3—history, examination, and decision making—to be at or above that need for that particular level of reporting. If only one of your history or decision making is at or above the needed level for a 99213, the loss of a single bullet drops you down to a 99212! An audit where a handful of medical records are pulled and a request for money back on the universe of payments the insurer has paid is always unpleasant and you should, if you get a request for same, follow all the rules and timelines outlined by the payer. If you knowingly behaved in a risky fashion, consult a good attorney.
Of course, you may argue that the effort needed for the E&M work for the procedure was above and beyond what is typical for the service, which can be a hard standard to meet. Although the CMS requires a “significant and separately identifiable E&M service” as noted above and a separate diagnosis is not needed, the onus is on you to prove it. It is much easier to have a separate diagnosis that stands on its own, which will probably make an audit less common (unless you do it too often).
Final Thoughts
In summary, document what you do, do what you document, and report what is medically necessary. Keep watch over your EHR to be sure it is not overcoding for you. You do not want to be a ewe!
Sheep are thought of as nervous animals, a good target for predators. You do not want to be a sheep. Unfortunately, many electronic health record (EHR) programs make you a target for audits and requests for the return of payments for a variety of reasons. Although you likely are aware of the uses of modifier -25, it is the abuses—either intentional or accidental—that can bring an audit your way. The use of modifier -25 was previously reviewed in Cutis.1 Despite the availability of this excellent review, I have found that there is still great confusion about both the use of modifier -25 and the selection of the correct evaluation and management (E&M) code when used.
When to Bill for E&M
Based on recent discussions with colleagues in the New York area who have been audited, an easy way to bring on a request for medical records is to report an E&M 100% of the time with a procedure. In these instances, every single E&M was performed on the same visit as a dermatologic procedure, most commonly biopsies(Current Procedural Terminology [CPT] code 11100, 11101) and premalignant destructions (CPT code 17000, 17003, 17004), which is in contrast with typical practitioners who perform an E&M approximately 70% of the time (RUC rationale; American Medical Association RBRVS Data Manager; May 12, 2016). One circumstance involved the reporting of E&M services 100% of the time when performed during the same visit as Mohs micrographic surgery (CPT code 17311–17315), a surprising frequency considering that the typical same day use of a code for this procedure with an E&M in the Medicare population is less than 25%.
According to the National Correct Coding Initiative Policy Manual for Medicare Services, procedures with a global period of 90 days are defined as major surgical procedures,2 which only include adjacent tissue transfers and grafts for dermatology. If an E&M is performed on the same date of service as one of these procedures to decide whether to perform the procedure, the E&M can be reported separately using modifier -57. Other preoperative E&M services provided on the same date of service as a major surgical procedure are included in the global payment for the procedure and are not reported separately.2
All other procedures dermatologists perform generally are considered minor, which are defined as having a global period of 0 or 10 days. Because the decision to perform a minor procedure is included in the payment for the procedure, E&M services should not be reported separately from the minor procedure. However, “a significant and separately identifiable E&M service unrelated to the decision to perform the minor surgical procedure is separately reportable with modifier 25. The E&M service and minor surgical procedure do not require different diagnoses. If a minor surgical procedure is performed on a new patient, the same rules for reporting E&M services apply.”2
Documentation Guidelines
These guidelines seem straightforward, but as with so much else where the government is involved, the devil is in the details. When making coding decisions, you may consult the documentation guidelines from either 19953 or 1997,4 which are available for download on the Centers for Medicare & Medicaid Services (CMS) website (https://www.cms.gov/outreach-and-education/medicare-learning-network-MLN/MLNedwebguide/emdoc.html). The 1995 guidelines are less empiric and offer more flexibility, while the 1997 guidelines rely on number of “bullets” as examination elements.
1995 Guidelines
According to the 1995 documentation guidelines, the levels of E&M services are based on 4 types of examination that are defined as follows: (1) problem focused, a limited examination of the affected body area or organ system; (2) expanded problem focused, a limited examination of the affected body area or organ system and other symptomatic or related organ system(s); (3) detailed, an extended examination of the affected body area(s) and other symptomatic or related organ system(s); and (4) comprehensive, a general multisystem examination or complete examination of a single organ system.3 Detailed history is the fuzziest part of the coding universe. Some insurers take an approach that you need to examine 2 to 7 organ systems and 4 distinct lesions in 4 body areas, which is discussed in audit tools available from some Medicare intermediaries (Advancing the Business of Healthcare forum; April 10, 2014). As a result, the 12-bullet examination from the 1997 documentation guidelines may be more suitable for a new level 3 or established level 4 visit. For a comprehensive examination, the 1995 criteria allow for a complete examination of a single organ system such as the full-body skin examination with the patient completely undressed, which is medically necessary in our melanoma patients.
For purposes of examination, 9 body areas are recognized in the 1995 guidelines,3 along with more than a dozen organ systems of which the skin is of most interest to dermatologists.
According to the 1995 guidelines,3 the extent of examinations performed and documented is dependent upon clinical judgment and the nature of the presenting problem(s) and range from focused examinations of single body areas to general multisystem or complete single organ system examinations. Specific abnormal and relevant negative findings of the examination of the affected or symptomatic body area(s) or organ system(s) should be documented. Although a notation of normal is sufficient, abnormal without elaboration is insufficient, and abnormal or unexpected findings of the examination of the unaffected or asymptomatic body area(s) or organ system(s) should be described. The medical record for a general multisystem examination should include findings involving approximately 8 or more of the 12 organ systems.
An expanded problem focused examination under the 1995 guidelines could be as simple as “Scar on cancer excision site on left cheek soft and supple. No cervical adenopathy.” There is some confusion regarding detailed examinations, and one consultant went as far as calling the guidelines “vague,”5 while others such as a Medicare intermediary make a quantum leap that if a comprehensive general system examination includes 8 to 12 organ systems, one step below should include 2 to 7 organ systems.6 In essence, the payer makes the rules here.
1997 Guidelines
According to the 1997 documentation guidelines, count bullets that are examination elements, which can be either general or single organ system.4 (A table showing the bullets for the examination elements is available from the CMS.4) For each type of examination, apply the following: problem focused examination requires 1 to 5 elements identified by a bullet, expanded problem focused examination needs at least 6, detailed examination requires at least 12, and comprehensive examination requires all elements identified by a bullet with documentation of every element in each box with a shaded border and at least 1 element in each box with an unshaded border.4 Although you may do more writing when using the 1997 guidelines, you can easily count up bullets and these guidelines are amenable to template examinations on paper and obviously easily coded into EHR software that will do the bullet counting for you.
Unfortunately, this is where a ewe becomes a sheep, ripe for hunting for a number of reasons. First, just because you documented an E&M service does not mean it is medically necessary. Do you really need vital signs for every visit? If you are a meaningful EHR user working on penalty avoidance, you may capture examination data for meaningful use that is not medically necessary but cannot be parsed out by the autocoder in your EHR. As a result, simply do a quick manual audit of your notes to see if you are overcoding, which becomes second nature if you do it often.
The second trap, which brings us back to modifier -25, is when you perform a procedure the same day as your E&M or vice versa. Every procedure we do within the Resource-Based Relative Value Scale contains preservice time, which includes review of materials relevant to the procedure, examination of the area, and all preparation (eg, marking, time out, anesthesia, scrub and drape) before the surgery begins. The detailed vignettes are available to those involved in the Relative Value Scale Update Committee process and to the rest of the world in a subscription product called the RBRVS DataManager Online, which is produced by the American Medical Association. Unfortunately, the American Medical Association is not accepting new subscriptions to this product, as it has decided to outsource most of its coding resources to Optum360, one of the many arms of UnitedHealth Group, and will not have a replacement product until after June 30, 2016.7
In essence, if you (and your EHR) are counting bullets and then treating the body area in question, you are double-dipping, as the examination of the area is included in the procedure. So if you are heading toward a CPT 99213-25 with 6 bullets, one of which is on the left arm, and you perform a 0- or 10-day global procedure on that arm, you are down to 5 bullets, which drops your level of examination to problem focused. Remember, you need only 2 of 3—history, examination, and decision making—to be at or above that need for that particular level of reporting. If only one of your history or decision making is at or above the needed level for a 99213, the loss of a single bullet drops you down to a 99212! An audit where a handful of medical records are pulled and a request for money back on the universe of payments the insurer has paid is always unpleasant and you should, if you get a request for same, follow all the rules and timelines outlined by the payer. If you knowingly behaved in a risky fashion, consult a good attorney.
Of course, you may argue that the effort needed for the E&M work for the procedure was above and beyond what is typical for the service, which can be a hard standard to meet. Although the CMS requires a “significant and separately identifiable E&M service” as noted above and a separate diagnosis is not needed, the onus is on you to prove it. It is much easier to have a separate diagnosis that stands on its own, which will probably make an audit less common (unless you do it too often).
Final Thoughts
In summary, document what you do, do what you document, and report what is medically necessary. Keep watch over your EHR to be sure it is not overcoding for you. You do not want to be a ewe!
- Alam M. Modifier -25 use in dermatology. Cutis. 2015;95:76-77.
- National Correct Coding Initiative Policy Manual for Medicare Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 2016. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/Downloads/2016-NCCI-Policy-Manual.zip. Accessed May 6, 2016.
- 1995 Documentation Guidelines for Evaluation and Management Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 1995. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuideDownloads/95Docguidelines.pdf. Accessed May 6, 2016.
- 1997 Documentation Guidelines for Evaluation and Management Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 1997. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed May 6, 2016.
- E/M FAQ #19. E/M University website. http://www.emuniversity.com/FAQ/EMFAQ19.html. Accessed May 4, 2016.
- In the E/M documentation guidelines, what does “more detail” regarding the exam mean, and what is the difference between an expanded problem-focused exam and detailed exam? Palmetto GBA website. http://www.palmettogba.com/palmetto/providers.nsf/DocsCat/Providers~Railroad%2Medicare~Resources~FAQs~EM%20Help%20Center~8EELQD7181?open&navmenu=%7C%7C. Updated March 2, 2016. Accessed May 4, 2016.
- AMA website. http://info.commerce.ama-assn.org/online-coding-home. Accessed May 4, 2016.
- Alam M. Modifier -25 use in dermatology. Cutis. 2015;95:76-77.
- National Correct Coding Initiative Policy Manual for Medicare Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 2016. https://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/Downloads/2016-NCCI-Policy-Manual.zip. Accessed May 6, 2016.
- 1995 Documentation Guidelines for Evaluation and Management Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 1995. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuideDownloads/95Docguidelines.pdf. Accessed May 6, 2016.
- 1997 Documentation Guidelines for Evaluation and Management Services. Baltimore, MD: Centers for Medicare & Medicaid Services; 1997. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNEdWebGuide/Downloads/97Docguidelines.pdf. Accessed May 6, 2016.
- E/M FAQ #19. E/M University website. http://www.emuniversity.com/FAQ/EMFAQ19.html. Accessed May 4, 2016.
- In the E/M documentation guidelines, what does “more detail” regarding the exam mean, and what is the difference between an expanded problem-focused exam and detailed exam? Palmetto GBA website. http://www.palmettogba.com/palmetto/providers.nsf/DocsCat/Providers~Railroad%2Medicare~Resources~FAQs~EM%20Help%20Center~8EELQD7181?open&navmenu=%7C%7C. Updated March 2, 2016. Accessed May 4, 2016.
- AMA website. http://info.commerce.ama-assn.org/online-coding-home. Accessed May 4, 2016.
Practice Points
- Know when to bill for evaluation and management (E&M) services performed on the same visit as a dermatologic procedure.
- Consult documentation guidelines from the Centers for Medicare & Medicaid Services when making coding decisions about E&M services.
- Watch that your electronic health record program is not overcoding.