User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Fall Vaccine Updates From the Advisory Committee on Immunization Practices: New Recommendations
This transcript has been edited for clarity.
This episode of Medicine Matters reviews highlights from the Advisory Committee on Immunization Practices’ (ACIP’s) October 2024 meeting, with new recommendations for pneumococcal, COVID, and meningococcal B (Men B) vaccines, as well as a safety update for maternal RSV vaccination.
Pneumococcal Vaccination and New Lower Age-Based Recommendations
New age-based recommendation. ACIP has lowered the age for routine vaccination with the pneumococcal conjugate vaccine (PCV) from age 65 down to age 50, but only with PCV. Review of data revealed that more than half of those in the 50- to 64-year-old age group already had a risk indication to receive a PCV dose. In addition, rates of invasive pneumococcal disease peak at younger ages in Black patients compared with White patients. The rate of invasive pneumococcal disease (IPD) among Black adults aged 50 or older exceeds the average rate of IPD for all adults aged 65 or older. The goal of this age-based change is to reduce disease in demographic groups with the highest burden of disease.
The new expanded age-based recommendation applies only to vaccination with PCV. Conjugate vaccines trigger memory B-cell production and therefore induce greater long-term immunity. New research is now focusing on higher-valent PCV vaccines. Two 24-valent pneumococcal conjugate vaccines and one 31-valent pneumococcal conjugate vaccine are now in advanced stages of development.
Risk-based recommendation. A risk-based recommendation for ages 19 through 49 years still applies to those with certain medical conditions, including diabetes; chronic heart, lung, liver, or kidney disease; and also for those with immunocompromising conditions. Risk-based recommendations are harder to implement particularly because many vaccines are now administered in pharmacies and pharmacists don’t know the patients as well as their physicians do, so it’s harder for them to know who should get the vaccine if the recommendation is based on risk.
COVID-19 Vaccines With Additional Dose Recommendations
Everyone 6 months or older is recommended to receive a dose of the updated 2024-2025 COVID vaccine. An additional updated COVID vaccine dose is now recommended for everyone aged 65 or older, and for those aged 6 months or older with immunocompromising (moderate or severe) conditions. Review of data revealed that 1 in 6 patients hospitalized with COVID have an immunocompromising condition, and 70% of COVID hospitalizations are in those aged 65 or older. This older age group also has the highest death rates due to COVID-19. We know that vaccination protection wanes with time. Data from previous studies show that additional vaccine doses provide additional protection. Additional doses are now being recommended for those at highest risk.
Timing of additional doses. This second dose is recommended at 6 months after the last updated COVID-19 vaccine dose. However, the additional dose can be given as early as 2 months after the last dose. Those who recently had COVID-19 can wait 3 months before getting an additional vaccine dose. This flexibility allows patients to maximize additional protection by timing additional doses around travel and life events, such as weddings, family get-togethers, or chemotherapy.
Those with immunocompromising conditions may receive more doses. Patients with immunocompromising conditions can receive even more additional doses, if recommended by their physician, under shared clinical decision-making.
Meningococcal Vaccines
Meningococcal disease is rare but deadly. The disease can progress rapidly. As many as 10%-15% of people with meningococcal infection die, even with appropriate antibiotic therapy. And for those who survive, about 20% suffer long-term sequalae (cognitive deficits, hearing loss, limb amputations).
Aligning Men B vaccine dosing intervals. The new ACIP vote applies only to Men B vaccines, of which there are two: one by GSK (brand name Bexsero), and the other by Wyeth, a Pfizer subsidiary (brand name Trumenba). The two MenB vaccine products are not interchangeable. The same type of MenB vaccine has to be used to complete the series.
The MenB vaccines initially had different dosing schedules and now they don’t. ACIP voted to harmonize and align the dosing schedule for the two different MenB products to mirror recent FDA (Food and Drug Administration) labeling updates. So now the dosing recommendations for both MenB vaccines are the same: either two doses given 6 months apart to healthy adolescents and young adults, or a three-dose series given at zero, 1-2 months, and 6 months for those at high risk or for those who want to optimize rapid protection (for example, if they are starting the series within 6 months of going off to college). But understand that the current recommendation for MenB vaccination for healthy adolescents and young adults is based on shared clinical decision-making, preferably for those aged 16-18.
MenACWY. Two doses of MenACWY are routinely recommended, with the first dose at age 11-12 and a second dose at age 16. The MenACWY vaccines are interchangeable.
Implementation challenges and new pentavalent vaccines. Having to use the same MenB vaccine product for all doses in a patient’s series is difficult. It’s even more difficult when the patient needs both MenACWY and MenB vaccinations.
Adding to the complexity is a new pentavalent vaccine from Pfizer (brand name Penbraya) that combines MenACWY with the MenB vaccine. And another pentavalent vaccine version by GSK is up for regulatory decision in February 2025.
The work group did say that they plan to take a fresh look at the meningococcal vaccination schedule. Let’s hope it gets simpler, so more to come on that.
Respiratory Syncytial Virus (RSV) Vaccines
Current RSV vaccine recommendations for older adults. RSV vaccine has both age- and risk-based recommendations. Now, everyone aged 75 or older needs a dose of RSV vaccine. Adults aged 60-75 with risk factors for severe RSV are also recommended to receive a dose of RSV vaccine, but not adults without these risk factors. The conditions associated with increased risk for severe RSV disease include lung disease, heart disease, immune compromise, diabetes, obesity with BMI (body mass index) of 40 or higher, neurologic or neuromuscular conditions, chronic kidney disease, liver disorders, and hematologic disorders. Frailty, as well as living in a nursing home or other long-term care facility, are other risk factors for severe RSV disease. Those aged 60-75 without these risk factors are no longer recommended to receive it.
Three RSV vaccines. We now have three RSV vaccine to choose from. Two are protein subunit vaccines. One is by Pfizer (brand name Abrysvo) that does not contain an adjuvant. The other protein-based RSV vaccine by GSK (brand name Arexvy) does contain an adjuvant. The third RSV vaccine by Moderna (brand name mRESVIA) uses an mRNA platform, and durability of protection is still unclear. However, recent studies now suggest that the RSV protein subunit vaccines confer 36 months of protection rather than only 24 months.
All three RSV vaccines are licensed for those aged 60 or older. The age indication for GSK’s RSV vaccine, Arexvy, has already been lowered by the FDA to age 50. FDA recently lowered the age approval for Abrysvo to age 18 for those at high risk. However, ACIP has not yet expanded its age recommendations for getting these vaccines. One of the main hesitations is vaccine safety concerns. FDA›s safety update presented to ACIP still suggests an increased risk for Guillain-Barré syndrome with both protein-based RSV vaccines among those aged 65 or older. Fortunately, the risk is rare: less than 10 cases per million vaccinations.
RSV immunization for infant protection. RSV season starts in October and goes through March. We now have two new ways to protect babies. One is a maternal RSV vaccine, given at 32-36 weeks of pregnancy to moms who will deliver their babies during RSV season. But only Pfizer’s RSV vaccine (brand name Abrysvo, without an adjuvant) can be given during pregnancy.
A maternal RSV vaccine safety update, presented at ACIP, was reassuring. Abrysvo was not associated with increased risk for preterm birth or small gestational age at birth.
Nirsevimab, a long-acting monoclonal antibody, can be given to infants. Nirsevimab is indicated for all babies under 8 months of age entering their first RSV season.
People who received a maternal RSV vaccine during a previous pregnancy are not recommended to receive additional doses during subsequent pregnancies. However, infants born to women who were vaccinated during a prior pregnancy should receive nirsevimab.
Sandra Adamson Fryhofer, Adjunct Clinical Associate Professor of Medicine, Emory University School of Medicine, Atlanta, Georgia, has disclosed conflicts of interest with the American Medical Association, the Medical Association of Atlanta, ACIP, and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This episode of Medicine Matters reviews highlights from the Advisory Committee on Immunization Practices’ (ACIP’s) October 2024 meeting, with new recommendations for pneumococcal, COVID, and meningococcal B (Men B) vaccines, as well as a safety update for maternal RSV vaccination.
Pneumococcal Vaccination and New Lower Age-Based Recommendations
New age-based recommendation. ACIP has lowered the age for routine vaccination with the pneumococcal conjugate vaccine (PCV) from age 65 down to age 50, but only with PCV. Review of data revealed that more than half of those in the 50- to 64-year-old age group already had a risk indication to receive a PCV dose. In addition, rates of invasive pneumococcal disease peak at younger ages in Black patients compared with White patients. The rate of invasive pneumococcal disease (IPD) among Black adults aged 50 or older exceeds the average rate of IPD for all adults aged 65 or older. The goal of this age-based change is to reduce disease in demographic groups with the highest burden of disease.
The new expanded age-based recommendation applies only to vaccination with PCV. Conjugate vaccines trigger memory B-cell production and therefore induce greater long-term immunity. New research is now focusing on higher-valent PCV vaccines. Two 24-valent pneumococcal conjugate vaccines and one 31-valent pneumococcal conjugate vaccine are now in advanced stages of development.
Risk-based recommendation. A risk-based recommendation for ages 19 through 49 years still applies to those with certain medical conditions, including diabetes; chronic heart, lung, liver, or kidney disease; and also for those with immunocompromising conditions. Risk-based recommendations are harder to implement particularly because many vaccines are now administered in pharmacies and pharmacists don’t know the patients as well as their physicians do, so it’s harder for them to know who should get the vaccine if the recommendation is based on risk.
COVID-19 Vaccines With Additional Dose Recommendations
Everyone 6 months or older is recommended to receive a dose of the updated 2024-2025 COVID vaccine. An additional updated COVID vaccine dose is now recommended for everyone aged 65 or older, and for those aged 6 months or older with immunocompromising (moderate or severe) conditions. Review of data revealed that 1 in 6 patients hospitalized with COVID have an immunocompromising condition, and 70% of COVID hospitalizations are in those aged 65 or older. This older age group also has the highest death rates due to COVID-19. We know that vaccination protection wanes with time. Data from previous studies show that additional vaccine doses provide additional protection. Additional doses are now being recommended for those at highest risk.
Timing of additional doses. This second dose is recommended at 6 months after the last updated COVID-19 vaccine dose. However, the additional dose can be given as early as 2 months after the last dose. Those who recently had COVID-19 can wait 3 months before getting an additional vaccine dose. This flexibility allows patients to maximize additional protection by timing additional doses around travel and life events, such as weddings, family get-togethers, or chemotherapy.
Those with immunocompromising conditions may receive more doses. Patients with immunocompromising conditions can receive even more additional doses, if recommended by their physician, under shared clinical decision-making.
Meningococcal Vaccines
Meningococcal disease is rare but deadly. The disease can progress rapidly. As many as 10%-15% of people with meningococcal infection die, even with appropriate antibiotic therapy. And for those who survive, about 20% suffer long-term sequalae (cognitive deficits, hearing loss, limb amputations).
Aligning Men B vaccine dosing intervals. The new ACIP vote applies only to Men B vaccines, of which there are two: one by GSK (brand name Bexsero), and the other by Wyeth, a Pfizer subsidiary (brand name Trumenba). The two MenB vaccine products are not interchangeable. The same type of MenB vaccine has to be used to complete the series.
The MenB vaccines initially had different dosing schedules and now they don’t. ACIP voted to harmonize and align the dosing schedule for the two different MenB products to mirror recent FDA (Food and Drug Administration) labeling updates. So now the dosing recommendations for both MenB vaccines are the same: either two doses given 6 months apart to healthy adolescents and young adults, or a three-dose series given at zero, 1-2 months, and 6 months for those at high risk or for those who want to optimize rapid protection (for example, if they are starting the series within 6 months of going off to college). But understand that the current recommendation for MenB vaccination for healthy adolescents and young adults is based on shared clinical decision-making, preferably for those aged 16-18.
MenACWY. Two doses of MenACWY are routinely recommended, with the first dose at age 11-12 and a second dose at age 16. The MenACWY vaccines are interchangeable.
Implementation challenges and new pentavalent vaccines. Having to use the same MenB vaccine product for all doses in a patient’s series is difficult. It’s even more difficult when the patient needs both MenACWY and MenB vaccinations.
Adding to the complexity is a new pentavalent vaccine from Pfizer (brand name Penbraya) that combines MenACWY with the MenB vaccine. And another pentavalent vaccine version by GSK is up for regulatory decision in February 2025.
The work group did say that they plan to take a fresh look at the meningococcal vaccination schedule. Let’s hope it gets simpler, so more to come on that.
Respiratory Syncytial Virus (RSV) Vaccines
Current RSV vaccine recommendations for older adults. RSV vaccine has both age- and risk-based recommendations. Now, everyone aged 75 or older needs a dose of RSV vaccine. Adults aged 60-75 with risk factors for severe RSV are also recommended to receive a dose of RSV vaccine, but not adults without these risk factors. The conditions associated with increased risk for severe RSV disease include lung disease, heart disease, immune compromise, diabetes, obesity with BMI (body mass index) of 40 or higher, neurologic or neuromuscular conditions, chronic kidney disease, liver disorders, and hematologic disorders. Frailty, as well as living in a nursing home or other long-term care facility, are other risk factors for severe RSV disease. Those aged 60-75 without these risk factors are no longer recommended to receive it.
Three RSV vaccines. We now have three RSV vaccine to choose from. Two are protein subunit vaccines. One is by Pfizer (brand name Abrysvo) that does not contain an adjuvant. The other protein-based RSV vaccine by GSK (brand name Arexvy) does contain an adjuvant. The third RSV vaccine by Moderna (brand name mRESVIA) uses an mRNA platform, and durability of protection is still unclear. However, recent studies now suggest that the RSV protein subunit vaccines confer 36 months of protection rather than only 24 months.
All three RSV vaccines are licensed for those aged 60 or older. The age indication for GSK’s RSV vaccine, Arexvy, has already been lowered by the FDA to age 50. FDA recently lowered the age approval for Abrysvo to age 18 for those at high risk. However, ACIP has not yet expanded its age recommendations for getting these vaccines. One of the main hesitations is vaccine safety concerns. FDA›s safety update presented to ACIP still suggests an increased risk for Guillain-Barré syndrome with both protein-based RSV vaccines among those aged 65 or older. Fortunately, the risk is rare: less than 10 cases per million vaccinations.
RSV immunization for infant protection. RSV season starts in October and goes through March. We now have two new ways to protect babies. One is a maternal RSV vaccine, given at 32-36 weeks of pregnancy to moms who will deliver their babies during RSV season. But only Pfizer’s RSV vaccine (brand name Abrysvo, without an adjuvant) can be given during pregnancy.
A maternal RSV vaccine safety update, presented at ACIP, was reassuring. Abrysvo was not associated with increased risk for preterm birth or small gestational age at birth.
Nirsevimab, a long-acting monoclonal antibody, can be given to infants. Nirsevimab is indicated for all babies under 8 months of age entering their first RSV season.
People who received a maternal RSV vaccine during a previous pregnancy are not recommended to receive additional doses during subsequent pregnancies. However, infants born to women who were vaccinated during a prior pregnancy should receive nirsevimab.
Sandra Adamson Fryhofer, Adjunct Clinical Associate Professor of Medicine, Emory University School of Medicine, Atlanta, Georgia, has disclosed conflicts of interest with the American Medical Association, the Medical Association of Atlanta, ACIP, and Medscape.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This episode of Medicine Matters reviews highlights from the Advisory Committee on Immunization Practices’ (ACIP’s) October 2024 meeting, with new recommendations for pneumococcal, COVID, and meningococcal B (Men B) vaccines, as well as a safety update for maternal RSV vaccination.
Pneumococcal Vaccination and New Lower Age-Based Recommendations
New age-based recommendation. ACIP has lowered the age for routine vaccination with the pneumococcal conjugate vaccine (PCV) from age 65 down to age 50, but only with PCV. Review of data revealed that more than half of those in the 50- to 64-year-old age group already had a risk indication to receive a PCV dose. In addition, rates of invasive pneumococcal disease peak at younger ages in Black patients compared with White patients. The rate of invasive pneumococcal disease (IPD) among Black adults aged 50 or older exceeds the average rate of IPD for all adults aged 65 or older. The goal of this age-based change is to reduce disease in demographic groups with the highest burden of disease.
The new expanded age-based recommendation applies only to vaccination with PCV. Conjugate vaccines trigger memory B-cell production and therefore induce greater long-term immunity. New research is now focusing on higher-valent PCV vaccines. Two 24-valent pneumococcal conjugate vaccines and one 31-valent pneumococcal conjugate vaccine are now in advanced stages of development.
Risk-based recommendation. A risk-based recommendation for ages 19 through 49 years still applies to those with certain medical conditions, including diabetes; chronic heart, lung, liver, or kidney disease; and also for those with immunocompromising conditions. Risk-based recommendations are harder to implement particularly because many vaccines are now administered in pharmacies and pharmacists don’t know the patients as well as their physicians do, so it’s harder for them to know who should get the vaccine if the recommendation is based on risk.
COVID-19 Vaccines With Additional Dose Recommendations
Everyone 6 months or older is recommended to receive a dose of the updated 2024-2025 COVID vaccine. An additional updated COVID vaccine dose is now recommended for everyone aged 65 or older, and for those aged 6 months or older with immunocompromising (moderate or severe) conditions. Review of data revealed that 1 in 6 patients hospitalized with COVID have an immunocompromising condition, and 70% of COVID hospitalizations are in those aged 65 or older. This older age group also has the highest death rates due to COVID-19. We know that vaccination protection wanes with time. Data from previous studies show that additional vaccine doses provide additional protection. Additional doses are now being recommended for those at highest risk.
Timing of additional doses. This second dose is recommended at 6 months after the last updated COVID-19 vaccine dose. However, the additional dose can be given as early as 2 months after the last dose. Those who recently had COVID-19 can wait 3 months before getting an additional vaccine dose. This flexibility allows patients to maximize additional protection by timing additional doses around travel and life events, such as weddings, family get-togethers, or chemotherapy.
Those with immunocompromising conditions may receive more doses. Patients with immunocompromising conditions can receive even more additional doses, if recommended by their physician, under shared clinical decision-making.
Meningococcal Vaccines
Meningococcal disease is rare but deadly. The disease can progress rapidly. As many as 10%-15% of people with meningococcal infection die, even with appropriate antibiotic therapy. And for those who survive, about 20% suffer long-term sequalae (cognitive deficits, hearing loss, limb amputations).
Aligning Men B vaccine dosing intervals. The new ACIP vote applies only to Men B vaccines, of which there are two: one by GSK (brand name Bexsero), and the other by Wyeth, a Pfizer subsidiary (brand name Trumenba). The two MenB vaccine products are not interchangeable. The same type of MenB vaccine has to be used to complete the series.
The MenB vaccines initially had different dosing schedules and now they don’t. ACIP voted to harmonize and align the dosing schedule for the two different MenB products to mirror recent FDA (Food and Drug Administration) labeling updates. So now the dosing recommendations for both MenB vaccines are the same: either two doses given 6 months apart to healthy adolescents and young adults, or a three-dose series given at zero, 1-2 months, and 6 months for those at high risk or for those who want to optimize rapid protection (for example, if they are starting the series within 6 months of going off to college). But understand that the current recommendation for MenB vaccination for healthy adolescents and young adults is based on shared clinical decision-making, preferably for those aged 16-18.
MenACWY. Two doses of MenACWY are routinely recommended, with the first dose at age 11-12 and a second dose at age 16. The MenACWY vaccines are interchangeable.
Implementation challenges and new pentavalent vaccines. Having to use the same MenB vaccine product for all doses in a patient’s series is difficult. It’s even more difficult when the patient needs both MenACWY and MenB vaccinations.
Adding to the complexity is a new pentavalent vaccine from Pfizer (brand name Penbraya) that combines MenACWY with the MenB vaccine. And another pentavalent vaccine version by GSK is up for regulatory decision in February 2025.
The work group did say that they plan to take a fresh look at the meningococcal vaccination schedule. Let’s hope it gets simpler, so more to come on that.
Respiratory Syncytial Virus (RSV) Vaccines
Current RSV vaccine recommendations for older adults. RSV vaccine has both age- and risk-based recommendations. Now, everyone aged 75 or older needs a dose of RSV vaccine. Adults aged 60-75 with risk factors for severe RSV are also recommended to receive a dose of RSV vaccine, but not adults without these risk factors. The conditions associated with increased risk for severe RSV disease include lung disease, heart disease, immune compromise, diabetes, obesity with BMI (body mass index) of 40 or higher, neurologic or neuromuscular conditions, chronic kidney disease, liver disorders, and hematologic disorders. Frailty, as well as living in a nursing home or other long-term care facility, are other risk factors for severe RSV disease. Those aged 60-75 without these risk factors are no longer recommended to receive it.
Three RSV vaccines. We now have three RSV vaccine to choose from. Two are protein subunit vaccines. One is by Pfizer (brand name Abrysvo) that does not contain an adjuvant. The other protein-based RSV vaccine by GSK (brand name Arexvy) does contain an adjuvant. The third RSV vaccine by Moderna (brand name mRESVIA) uses an mRNA platform, and durability of protection is still unclear. However, recent studies now suggest that the RSV protein subunit vaccines confer 36 months of protection rather than only 24 months.
All three RSV vaccines are licensed for those aged 60 or older. The age indication for GSK’s RSV vaccine, Arexvy, has already been lowered by the FDA to age 50. FDA recently lowered the age approval for Abrysvo to age 18 for those at high risk. However, ACIP has not yet expanded its age recommendations for getting these vaccines. One of the main hesitations is vaccine safety concerns. FDA›s safety update presented to ACIP still suggests an increased risk for Guillain-Barré syndrome with both protein-based RSV vaccines among those aged 65 or older. Fortunately, the risk is rare: less than 10 cases per million vaccinations.
RSV immunization for infant protection. RSV season starts in October and goes through March. We now have two new ways to protect babies. One is a maternal RSV vaccine, given at 32-36 weeks of pregnancy to moms who will deliver their babies during RSV season. But only Pfizer’s RSV vaccine (brand name Abrysvo, without an adjuvant) can be given during pregnancy.
A maternal RSV vaccine safety update, presented at ACIP, was reassuring. Abrysvo was not associated with increased risk for preterm birth or small gestational age at birth.
Nirsevimab, a long-acting monoclonal antibody, can be given to infants. Nirsevimab is indicated for all babies under 8 months of age entering their first RSV season.
People who received a maternal RSV vaccine during a previous pregnancy are not recommended to receive additional doses during subsequent pregnancies. However, infants born to women who were vaccinated during a prior pregnancy should receive nirsevimab.
Sandra Adamson Fryhofer, Adjunct Clinical Associate Professor of Medicine, Emory University School of Medicine, Atlanta, Georgia, has disclosed conflicts of interest with the American Medical Association, the Medical Association of Atlanta, ACIP, and Medscape.
A version of this article first appeared on Medscape.com.
Digital Danger: How Cyberattacks Put Patients at Risk
On September 27, 2024, UMC Health System in Lubbock, Texas, experienced an IT outage because of a cybersecurity incident that temporarily diverted patients to other healthcare facilities. So far, in 2024, there have been 386 cyberattacks on healthcare organizations. These high-impact ransomware attacks disrupt and delay patient care.
In recent years, many healthcare systems, including Scripps Health, Universal Health Services, Vastaamo, Sky Lakes, and the University of Vermont, have paid millions — even tens of millions — to recover data after a cyberattack or data breach. When healthcare systems come under cyber fire, the impact extends far past disrupting workflows and compromising data, patient safety can be also be compromised, vital information may be lost, and imaging and lab results can go missing or be held for ransom, making physicians’ job difficult or impossible.
In fact, cyberattacks on hospitals are far more common than you may realize. A new report issued by Ponemon and Proofpoint found that 92% of healthcare organizations have experienced a cyberattack in the past 12 months. Even more sobering is that about half of the organizations affected suffered disruptions in patient care.
Healthcare Systems = ‘Soft Targets’
Healthcare systems are a “soft target” for hackers for several reasons, pointed out Matthew Radolec, vice president, incident response and cloud operations at Varonis, a data security company. “One, they’re usually an amalgamation of many healthcare systems that are interconnected,” said Radolec. “A lot of hospitals are connected to other hospitals or connected to educational institutions, which means their computer vulnerabilities are shared ... and if they have an issue, it could very easily spread to your network.”
Another factor is the cost of securing data. “[With hospitals], they’ll say that a dollar spent on security is a dollar not spent on patient care,” said Radolec. “So the idea of investing in security is really tough from a budget standpoint…they’re choosing between a new MRI machine or better antivirus, backups, or data security.”
Because of the wealth of private data and healthcare information they maintain, hospitals are considered “high impact” for cybercriminals. Attackers know that if they get a foothold in a hospital, it’s more likely to pay — and pay quickly, Radolec told this news organization. Hospitals are also likely to have cyber insurance to help cover the cost of having their data stolen, encrypted, and ransomed.
The 2024 Microsoft Digital Defense Report also found that the bad actors are more sophisticated and better resourced and can challenge even the best cybersecurity. Improved defenses may not be good enough, and the sheer volume of attacks must be met with effective deterrence and government solutions that impose consequences for cybercriminals.
Vulnerable Users
Whether through a phishing email or text, password attack, or web attack, “the moment a ‘threat actor’ gets into your institution and gets credentials ... that’s the Nirvana state of a threat actor,” warned Ryan Witt, chair of the healthcare customer advisory board and vice president of Industry Solutions at Proofpoint, a cybersecurity platform. “They have those credentials and will go into deep reconnaissance mode. It often takes healthcare up to 6 months to even ascertain whether somebody’s actually in the network.” During that time, the hacker is learning how the institution works, what job functions matter, and how best to plan their attack.
“Attackers are getting in because they’re buying databases of usernames and passwords. And they’re trying them by the millions,” added Radolec. “For a sophisticated actor, all it takes is time and motivation. They have the skills. It’s just a matter of how persistent they want to be.”
Certain hospital staff are also more likely to be targeted by cyberhackers than others. “About 10% of a healthcare organization’s user base is much more vulnerable for all sorts of reasons — how they work, the value of their job title and job function, and therefore their access to systems,” said Witt.
High-profile staff are more likely to be targeted than those in lower-level positions; the so-called “CEO attack” is typical. However, staff in other hospital departments are also subject to cybercriminals, including hospice departments/hospice organizations and research arms of hospitals.
The Impact of Cyberattacks on Patients
Physicians and healthcare execs may have considered cybersecurity more of a compliance issue than a true threat to patients in the past. But this attitude is rapidly changing. “We are starting to see a very clear connection between a cyber event and how it can impact patient care and patient safety,” said Witt.
According to the Proofpoint report, cyber breaches can severely affect patient care. In 2024:
- 56% of respondents saw a delay in patient tests/procedures
- 53% experienced increased patient complications from medical procedures
- 52% noted a longer patient length of stay
- 44% saw an increase in patient transfers to other facilities
- 28% had an increase in mortality rate
What Hospitals and Physicians Can Do
Fortunately, hospitals can take measures to better protect their data and their patients. One strategy is segmenting networks to reduce the amount of data or systems one person or system can access. Educating staff about the dangers of phishing and spoofing emails also help protect organizations from ransomware attacks. Having staff avoid reusing passwords and updating logins and passwords frequently helps.
Most hospitals also need more robust security controls. Physicians and healthcare facilities must also embrace the cybersecurity controls found in other industries, said Witt. “Multifactor authentication is one of those things that can cause us frustration,” he said. “The controls can seem onerous, but they’re really valuable overall…and should become standard practice.”
Doctors can also prepare for a ransomware attack and protect patients by practicing some “old-school” medicine, like using paper systems and maintaining good patient notes — often, those notes are synced locally as well as offsite, so you’d be able to access them even during a data breach. “It’s smart to write prescriptions on pads sometimes,” said Radolec. “Don’t forget how to do those things because that will make you more resilient in the event of a ransomware attack.”
A Continuing Threat
Cyberattacks will continue. “When you look at the high likelihood [of success] and the soft target, you end up with ... a perfect storm,” said Radolec. “Hospitals have a lot of vulnerabilities. They have to keep operations going just to receive income, but also to deliver care to people.”
That means that the burden is on healthcare organizations — including physicians, nurses, staff, and C-level execs — to help keep the “security” in cybersecurity. “We are all part of the cybersecurity defense,” said Witt. Helping to maintain that defense has become a critical aspect of caring for patients.
A version of this article first appeared on Medscape.com.
On September 27, 2024, UMC Health System in Lubbock, Texas, experienced an IT outage because of a cybersecurity incident that temporarily diverted patients to other healthcare facilities. So far, in 2024, there have been 386 cyberattacks on healthcare organizations. These high-impact ransomware attacks disrupt and delay patient care.
In recent years, many healthcare systems, including Scripps Health, Universal Health Services, Vastaamo, Sky Lakes, and the University of Vermont, have paid millions — even tens of millions — to recover data after a cyberattack or data breach. When healthcare systems come under cyber fire, the impact extends far past disrupting workflows and compromising data, patient safety can be also be compromised, vital information may be lost, and imaging and lab results can go missing or be held for ransom, making physicians’ job difficult or impossible.
In fact, cyberattacks on hospitals are far more common than you may realize. A new report issued by Ponemon and Proofpoint found that 92% of healthcare organizations have experienced a cyberattack in the past 12 months. Even more sobering is that about half of the organizations affected suffered disruptions in patient care.
Healthcare Systems = ‘Soft Targets’
Healthcare systems are a “soft target” for hackers for several reasons, pointed out Matthew Radolec, vice president, incident response and cloud operations at Varonis, a data security company. “One, they’re usually an amalgamation of many healthcare systems that are interconnected,” said Radolec. “A lot of hospitals are connected to other hospitals or connected to educational institutions, which means their computer vulnerabilities are shared ... and if they have an issue, it could very easily spread to your network.”
Another factor is the cost of securing data. “[With hospitals], they’ll say that a dollar spent on security is a dollar not spent on patient care,” said Radolec. “So the idea of investing in security is really tough from a budget standpoint…they’re choosing between a new MRI machine or better antivirus, backups, or data security.”
Because of the wealth of private data and healthcare information they maintain, hospitals are considered “high impact” for cybercriminals. Attackers know that if they get a foothold in a hospital, it’s more likely to pay — and pay quickly, Radolec told this news organization. Hospitals are also likely to have cyber insurance to help cover the cost of having their data stolen, encrypted, and ransomed.
The 2024 Microsoft Digital Defense Report also found that the bad actors are more sophisticated and better resourced and can challenge even the best cybersecurity. Improved defenses may not be good enough, and the sheer volume of attacks must be met with effective deterrence and government solutions that impose consequences for cybercriminals.
Vulnerable Users
Whether through a phishing email or text, password attack, or web attack, “the moment a ‘threat actor’ gets into your institution and gets credentials ... that’s the Nirvana state of a threat actor,” warned Ryan Witt, chair of the healthcare customer advisory board and vice president of Industry Solutions at Proofpoint, a cybersecurity platform. “They have those credentials and will go into deep reconnaissance mode. It often takes healthcare up to 6 months to even ascertain whether somebody’s actually in the network.” During that time, the hacker is learning how the institution works, what job functions matter, and how best to plan their attack.
“Attackers are getting in because they’re buying databases of usernames and passwords. And they’re trying them by the millions,” added Radolec. “For a sophisticated actor, all it takes is time and motivation. They have the skills. It’s just a matter of how persistent they want to be.”
Certain hospital staff are also more likely to be targeted by cyberhackers than others. “About 10% of a healthcare organization’s user base is much more vulnerable for all sorts of reasons — how they work, the value of their job title and job function, and therefore their access to systems,” said Witt.
High-profile staff are more likely to be targeted than those in lower-level positions; the so-called “CEO attack” is typical. However, staff in other hospital departments are also subject to cybercriminals, including hospice departments/hospice organizations and research arms of hospitals.
The Impact of Cyberattacks on Patients
Physicians and healthcare execs may have considered cybersecurity more of a compliance issue than a true threat to patients in the past. But this attitude is rapidly changing. “We are starting to see a very clear connection between a cyber event and how it can impact patient care and patient safety,” said Witt.
According to the Proofpoint report, cyber breaches can severely affect patient care. In 2024:
- 56% of respondents saw a delay in patient tests/procedures
- 53% experienced increased patient complications from medical procedures
- 52% noted a longer patient length of stay
- 44% saw an increase in patient transfers to other facilities
- 28% had an increase in mortality rate
What Hospitals and Physicians Can Do
Fortunately, hospitals can take measures to better protect their data and their patients. One strategy is segmenting networks to reduce the amount of data or systems one person or system can access. Educating staff about the dangers of phishing and spoofing emails also help protect organizations from ransomware attacks. Having staff avoid reusing passwords and updating logins and passwords frequently helps.
Most hospitals also need more robust security controls. Physicians and healthcare facilities must also embrace the cybersecurity controls found in other industries, said Witt. “Multifactor authentication is one of those things that can cause us frustration,” he said. “The controls can seem onerous, but they’re really valuable overall…and should become standard practice.”
Doctors can also prepare for a ransomware attack and protect patients by practicing some “old-school” medicine, like using paper systems and maintaining good patient notes — often, those notes are synced locally as well as offsite, so you’d be able to access them even during a data breach. “It’s smart to write prescriptions on pads sometimes,” said Radolec. “Don’t forget how to do those things because that will make you more resilient in the event of a ransomware attack.”
A Continuing Threat
Cyberattacks will continue. “When you look at the high likelihood [of success] and the soft target, you end up with ... a perfect storm,” said Radolec. “Hospitals have a lot of vulnerabilities. They have to keep operations going just to receive income, but also to deliver care to people.”
That means that the burden is on healthcare organizations — including physicians, nurses, staff, and C-level execs — to help keep the “security” in cybersecurity. “We are all part of the cybersecurity defense,” said Witt. Helping to maintain that defense has become a critical aspect of caring for patients.
A version of this article first appeared on Medscape.com.
On September 27, 2024, UMC Health System in Lubbock, Texas, experienced an IT outage because of a cybersecurity incident that temporarily diverted patients to other healthcare facilities. So far, in 2024, there have been 386 cyberattacks on healthcare organizations. These high-impact ransomware attacks disrupt and delay patient care.
In recent years, many healthcare systems, including Scripps Health, Universal Health Services, Vastaamo, Sky Lakes, and the University of Vermont, have paid millions — even tens of millions — to recover data after a cyberattack or data breach. When healthcare systems come under cyber fire, the impact extends far past disrupting workflows and compromising data, patient safety can be also be compromised, vital information may be lost, and imaging and lab results can go missing or be held for ransom, making physicians’ job difficult or impossible.
In fact, cyberattacks on hospitals are far more common than you may realize. A new report issued by Ponemon and Proofpoint found that 92% of healthcare organizations have experienced a cyberattack in the past 12 months. Even more sobering is that about half of the organizations affected suffered disruptions in patient care.
Healthcare Systems = ‘Soft Targets’
Healthcare systems are a “soft target” for hackers for several reasons, pointed out Matthew Radolec, vice president, incident response and cloud operations at Varonis, a data security company. “One, they’re usually an amalgamation of many healthcare systems that are interconnected,” said Radolec. “A lot of hospitals are connected to other hospitals or connected to educational institutions, which means their computer vulnerabilities are shared ... and if they have an issue, it could very easily spread to your network.”
Another factor is the cost of securing data. “[With hospitals], they’ll say that a dollar spent on security is a dollar not spent on patient care,” said Radolec. “So the idea of investing in security is really tough from a budget standpoint…they’re choosing between a new MRI machine or better antivirus, backups, or data security.”
Because of the wealth of private data and healthcare information they maintain, hospitals are considered “high impact” for cybercriminals. Attackers know that if they get a foothold in a hospital, it’s more likely to pay — and pay quickly, Radolec told this news organization. Hospitals are also likely to have cyber insurance to help cover the cost of having their data stolen, encrypted, and ransomed.
The 2024 Microsoft Digital Defense Report also found that the bad actors are more sophisticated and better resourced and can challenge even the best cybersecurity. Improved defenses may not be good enough, and the sheer volume of attacks must be met with effective deterrence and government solutions that impose consequences for cybercriminals.
Vulnerable Users
Whether through a phishing email or text, password attack, or web attack, “the moment a ‘threat actor’ gets into your institution and gets credentials ... that’s the Nirvana state of a threat actor,” warned Ryan Witt, chair of the healthcare customer advisory board and vice president of Industry Solutions at Proofpoint, a cybersecurity platform. “They have those credentials and will go into deep reconnaissance mode. It often takes healthcare up to 6 months to even ascertain whether somebody’s actually in the network.” During that time, the hacker is learning how the institution works, what job functions matter, and how best to plan their attack.
“Attackers are getting in because they’re buying databases of usernames and passwords. And they’re trying them by the millions,” added Radolec. “For a sophisticated actor, all it takes is time and motivation. They have the skills. It’s just a matter of how persistent they want to be.”
Certain hospital staff are also more likely to be targeted by cyberhackers than others. “About 10% of a healthcare organization’s user base is much more vulnerable for all sorts of reasons — how they work, the value of their job title and job function, and therefore their access to systems,” said Witt.
High-profile staff are more likely to be targeted than those in lower-level positions; the so-called “CEO attack” is typical. However, staff in other hospital departments are also subject to cybercriminals, including hospice departments/hospice organizations and research arms of hospitals.
The Impact of Cyberattacks on Patients
Physicians and healthcare execs may have considered cybersecurity more of a compliance issue than a true threat to patients in the past. But this attitude is rapidly changing. “We are starting to see a very clear connection between a cyber event and how it can impact patient care and patient safety,” said Witt.
According to the Proofpoint report, cyber breaches can severely affect patient care. In 2024:
- 56% of respondents saw a delay in patient tests/procedures
- 53% experienced increased patient complications from medical procedures
- 52% noted a longer patient length of stay
- 44% saw an increase in patient transfers to other facilities
- 28% had an increase in mortality rate
What Hospitals and Physicians Can Do
Fortunately, hospitals can take measures to better protect their data and their patients. One strategy is segmenting networks to reduce the amount of data or systems one person or system can access. Educating staff about the dangers of phishing and spoofing emails also help protect organizations from ransomware attacks. Having staff avoid reusing passwords and updating logins and passwords frequently helps.
Most hospitals also need more robust security controls. Physicians and healthcare facilities must also embrace the cybersecurity controls found in other industries, said Witt. “Multifactor authentication is one of those things that can cause us frustration,” he said. “The controls can seem onerous, but they’re really valuable overall…and should become standard practice.”
Doctors can also prepare for a ransomware attack and protect patients by practicing some “old-school” medicine, like using paper systems and maintaining good patient notes — often, those notes are synced locally as well as offsite, so you’d be able to access them even during a data breach. “It’s smart to write prescriptions on pads sometimes,” said Radolec. “Don’t forget how to do those things because that will make you more resilient in the event of a ransomware attack.”
A Continuing Threat
Cyberattacks will continue. “When you look at the high likelihood [of success] and the soft target, you end up with ... a perfect storm,” said Radolec. “Hospitals have a lot of vulnerabilities. They have to keep operations going just to receive income, but also to deliver care to people.”
That means that the burden is on healthcare organizations — including physicians, nurses, staff, and C-level execs — to help keep the “security” in cybersecurity. “We are all part of the cybersecurity defense,” said Witt. Helping to maintain that defense has become a critical aspect of caring for patients.
A version of this article first appeared on Medscape.com.
When Your Malpractice Insurer Investigates You: What to Know
When psychiatrist Paul Sartain, MD (not his real name), received a letter from his state’s medical board, he was concerned. A patient’s family complained that he made sexual advances to a young woman he treated for psychotic depression.
“There was absolutely no evidence, and the claims were vague,” he said. “I think the family was angry at me and with the system — the woman had not gotten better.” Sartain reviewed his medical records and then called his malpractice insurer.
The insurer asked about his involvement with the patient’s case, if there was anything credible to the patient’s complaint, and if he had thorough documentation. Then, the carrier offered Sartain his choice of several attorneys who could represent him. The medical board ultimately closed the case with no findings against him, and the patient’s family never sued him.
“If I’m wrongly accused, I’m defended (by the carrier). If I had stolen money or had a sexual relationship with the patient, then you’re acting outside the bounds of what is protected (by the carrier),” he said.
How Medical Board and Malpractice Insurer Investigations Differ
Medical board complaints differ from malpractice claims, in which patients seek damages. The investigation process also varies.
When a patient reports a doctor to a state medical board, they may also sue the doctor for monetary damages in civil court. The medical board responds to patient complaints made directly to them, but it also may also initiate its own investigations. Those can be prompted by a malpractice claim resolution, with a court verdict against the doctor, or a settlement recorded in the National Practitioner Data Bank.
Malpractice insurers may offer limited legal representation for medical board investigations, requiring the doctor to report the medical board issue to them before the doctor takes any action. Often, they will cover up to $50,000 in defense costs but not cover any subsequent medical board fines or required classes or medical board fees.
When a doctor contacts the carrier about a medical board investigation, the carrier may ask for the medical board document and the medical records, said Alex Keoskey, a partner in Frier Levitt’s life sciences group.
The carrier may want to ask about the patient, staff members involved, the doctor’s background, if there have been previous medical board investigations or lawsuits against this doctor, and the doctor’s opinion of the allegations. The doctor should be transparent with the carrier, Keoskey said.
Some carriers conduct more in-depth investigations, examining record-keeping, prescription practices, patient consent processes, and continuing medical education status. That’s because the medical board may inquire about these as well should its own investigation expand.
Not all carriers explore cases like these, even if reimbursing for defense costs, said Karen Frisella, director of professional liability claims at BETA Healthcare Group in California. In her experience, a licensing investigation usually follows a claim resolution that was already worked up by the carrier. If a complaint was made directly to the licensing board without an accompanying liability claim, the carrier’s ability to initiate an investigation on the incident depends on the policy terms or coverage available.
“Typically, a professional liability policy requires that the insured report a claim to trigger coverage. The carrier can’t unilaterally decide to open a claim,” she said. A licensing board investigation is not a claim by definition and therefore does not provide a mechanism for the carrier to open a liability claim file, she added.
If the medical board ultimately restricts the doctor’s license or puts the doctor on probation, that becomes public, and the underwriting department may then look into it.
Malpractice insurers routinely monitor licensing board discipline notices. A reprimand or restrictions on a doctor’s license could trigger a review of the physician’s future insurability and lead to higher premiums or even nonrenewal, Frisella said.
If a carrier investigates a reported claim and determines there are issues with the care rendered, whether there is an accompanying medical board action, that also can affect underwriting decisions, Frisella said.
Who Is Your Attorney Really Working for?
The doctor should understand whose interests the attorney represents. In a medical board claim, the attorney — even if defense is paid by the carrier — represents the doctor.
Frisella said her organization provides pass-through coverage, meaning it reimburses the doctor for medical board defense costs. “Because the carrier isn’t directing the medical board defense, it is not generally privy to the work product.”
If a patient files a malpractice claim, however, the attorney ultimately represents the insurance company.
“The panel counsel who works for the insurer does not work for the doctor, and that’s always important to remember,” Keoskey said. While the attorney will do their best to aggressively defend the doctor, “he’s going to protect the insurer’s interest before the doctor’s.”
Physicians who find any conflict of interest with their insurer should seek counsel.
Such conflicts could include:
- Disagreements over the case’s ultimate worth. For example, a physician might want a case to settle for less than their carrier is willing to pay.
- The legal judgment may exceed the carrier’s policy limits, or there are punitive damages or allegations of criminal acts that the insurer does not cover.
In these cases, the insurance company should recommend the doctor get personal counsel. They will send a reservation of rights letter saying they will defend the doctor for now, but if the facts show the doctor committed some type of misconduct, they may decline coverage, said Keoskey. Some states, including California, require that the carrier pay for this independent counsel.
Unless there is a conflict of interest, though, having a personal attorney just makes the situation more complicated, said Frisella.
A version of this article first appeared on Medscape.com.
When psychiatrist Paul Sartain, MD (not his real name), received a letter from his state’s medical board, he was concerned. A patient’s family complained that he made sexual advances to a young woman he treated for psychotic depression.
“There was absolutely no evidence, and the claims were vague,” he said. “I think the family was angry at me and with the system — the woman had not gotten better.” Sartain reviewed his medical records and then called his malpractice insurer.
The insurer asked about his involvement with the patient’s case, if there was anything credible to the patient’s complaint, and if he had thorough documentation. Then, the carrier offered Sartain his choice of several attorneys who could represent him. The medical board ultimately closed the case with no findings against him, and the patient’s family never sued him.
“If I’m wrongly accused, I’m defended (by the carrier). If I had stolen money or had a sexual relationship with the patient, then you’re acting outside the bounds of what is protected (by the carrier),” he said.
How Medical Board and Malpractice Insurer Investigations Differ
Medical board complaints differ from malpractice claims, in which patients seek damages. The investigation process also varies.
When a patient reports a doctor to a state medical board, they may also sue the doctor for monetary damages in civil court. The medical board responds to patient complaints made directly to them, but it also may also initiate its own investigations. Those can be prompted by a malpractice claim resolution, with a court verdict against the doctor, or a settlement recorded in the National Practitioner Data Bank.
Malpractice insurers may offer limited legal representation for medical board investigations, requiring the doctor to report the medical board issue to them before the doctor takes any action. Often, they will cover up to $50,000 in defense costs but not cover any subsequent medical board fines or required classes or medical board fees.
When a doctor contacts the carrier about a medical board investigation, the carrier may ask for the medical board document and the medical records, said Alex Keoskey, a partner in Frier Levitt’s life sciences group.
The carrier may want to ask about the patient, staff members involved, the doctor’s background, if there have been previous medical board investigations or lawsuits against this doctor, and the doctor’s opinion of the allegations. The doctor should be transparent with the carrier, Keoskey said.
Some carriers conduct more in-depth investigations, examining record-keeping, prescription practices, patient consent processes, and continuing medical education status. That’s because the medical board may inquire about these as well should its own investigation expand.
Not all carriers explore cases like these, even if reimbursing for defense costs, said Karen Frisella, director of professional liability claims at BETA Healthcare Group in California. In her experience, a licensing investigation usually follows a claim resolution that was already worked up by the carrier. If a complaint was made directly to the licensing board without an accompanying liability claim, the carrier’s ability to initiate an investigation on the incident depends on the policy terms or coverage available.
“Typically, a professional liability policy requires that the insured report a claim to trigger coverage. The carrier can’t unilaterally decide to open a claim,” she said. A licensing board investigation is not a claim by definition and therefore does not provide a mechanism for the carrier to open a liability claim file, she added.
If the medical board ultimately restricts the doctor’s license or puts the doctor on probation, that becomes public, and the underwriting department may then look into it.
Malpractice insurers routinely monitor licensing board discipline notices. A reprimand or restrictions on a doctor’s license could trigger a review of the physician’s future insurability and lead to higher premiums or even nonrenewal, Frisella said.
If a carrier investigates a reported claim and determines there are issues with the care rendered, whether there is an accompanying medical board action, that also can affect underwriting decisions, Frisella said.
Who Is Your Attorney Really Working for?
The doctor should understand whose interests the attorney represents. In a medical board claim, the attorney — even if defense is paid by the carrier — represents the doctor.
Frisella said her organization provides pass-through coverage, meaning it reimburses the doctor for medical board defense costs. “Because the carrier isn’t directing the medical board defense, it is not generally privy to the work product.”
If a patient files a malpractice claim, however, the attorney ultimately represents the insurance company.
“The panel counsel who works for the insurer does not work for the doctor, and that’s always important to remember,” Keoskey said. While the attorney will do their best to aggressively defend the doctor, “he’s going to protect the insurer’s interest before the doctor’s.”
Physicians who find any conflict of interest with their insurer should seek counsel.
Such conflicts could include:
- Disagreements over the case’s ultimate worth. For example, a physician might want a case to settle for less than their carrier is willing to pay.
- The legal judgment may exceed the carrier’s policy limits, or there are punitive damages or allegations of criminal acts that the insurer does not cover.
In these cases, the insurance company should recommend the doctor get personal counsel. They will send a reservation of rights letter saying they will defend the doctor for now, but if the facts show the doctor committed some type of misconduct, they may decline coverage, said Keoskey. Some states, including California, require that the carrier pay for this independent counsel.
Unless there is a conflict of interest, though, having a personal attorney just makes the situation more complicated, said Frisella.
A version of this article first appeared on Medscape.com.
When psychiatrist Paul Sartain, MD (not his real name), received a letter from his state’s medical board, he was concerned. A patient’s family complained that he made sexual advances to a young woman he treated for psychotic depression.
“There was absolutely no evidence, and the claims were vague,” he said. “I think the family was angry at me and with the system — the woman had not gotten better.” Sartain reviewed his medical records and then called his malpractice insurer.
The insurer asked about his involvement with the patient’s case, if there was anything credible to the patient’s complaint, and if he had thorough documentation. Then, the carrier offered Sartain his choice of several attorneys who could represent him. The medical board ultimately closed the case with no findings against him, and the patient’s family never sued him.
“If I’m wrongly accused, I’m defended (by the carrier). If I had stolen money or had a sexual relationship with the patient, then you’re acting outside the bounds of what is protected (by the carrier),” he said.
How Medical Board and Malpractice Insurer Investigations Differ
Medical board complaints differ from malpractice claims, in which patients seek damages. The investigation process also varies.
When a patient reports a doctor to a state medical board, they may also sue the doctor for monetary damages in civil court. The medical board responds to patient complaints made directly to them, but it also may also initiate its own investigations. Those can be prompted by a malpractice claim resolution, with a court verdict against the doctor, or a settlement recorded in the National Practitioner Data Bank.
Malpractice insurers may offer limited legal representation for medical board investigations, requiring the doctor to report the medical board issue to them before the doctor takes any action. Often, they will cover up to $50,000 in defense costs but not cover any subsequent medical board fines or required classes or medical board fees.
When a doctor contacts the carrier about a medical board investigation, the carrier may ask for the medical board document and the medical records, said Alex Keoskey, a partner in Frier Levitt’s life sciences group.
The carrier may want to ask about the patient, staff members involved, the doctor’s background, if there have been previous medical board investigations or lawsuits against this doctor, and the doctor’s opinion of the allegations. The doctor should be transparent with the carrier, Keoskey said.
Some carriers conduct more in-depth investigations, examining record-keeping, prescription practices, patient consent processes, and continuing medical education status. That’s because the medical board may inquire about these as well should its own investigation expand.
Not all carriers explore cases like these, even if reimbursing for defense costs, said Karen Frisella, director of professional liability claims at BETA Healthcare Group in California. In her experience, a licensing investigation usually follows a claim resolution that was already worked up by the carrier. If a complaint was made directly to the licensing board without an accompanying liability claim, the carrier’s ability to initiate an investigation on the incident depends on the policy terms or coverage available.
“Typically, a professional liability policy requires that the insured report a claim to trigger coverage. The carrier can’t unilaterally decide to open a claim,” she said. A licensing board investigation is not a claim by definition and therefore does not provide a mechanism for the carrier to open a liability claim file, she added.
If the medical board ultimately restricts the doctor’s license or puts the doctor on probation, that becomes public, and the underwriting department may then look into it.
Malpractice insurers routinely monitor licensing board discipline notices. A reprimand or restrictions on a doctor’s license could trigger a review of the physician’s future insurability and lead to higher premiums or even nonrenewal, Frisella said.
If a carrier investigates a reported claim and determines there are issues with the care rendered, whether there is an accompanying medical board action, that also can affect underwriting decisions, Frisella said.
Who Is Your Attorney Really Working for?
The doctor should understand whose interests the attorney represents. In a medical board claim, the attorney — even if defense is paid by the carrier — represents the doctor.
Frisella said her organization provides pass-through coverage, meaning it reimburses the doctor for medical board defense costs. “Because the carrier isn’t directing the medical board defense, it is not generally privy to the work product.”
If a patient files a malpractice claim, however, the attorney ultimately represents the insurance company.
“The panel counsel who works for the insurer does not work for the doctor, and that’s always important to remember,” Keoskey said. While the attorney will do their best to aggressively defend the doctor, “he’s going to protect the insurer’s interest before the doctor’s.”
Physicians who find any conflict of interest with their insurer should seek counsel.
Such conflicts could include:
- Disagreements over the case’s ultimate worth. For example, a physician might want a case to settle for less than their carrier is willing to pay.
- The legal judgment may exceed the carrier’s policy limits, or there are punitive damages or allegations of criminal acts that the insurer does not cover.
In these cases, the insurance company should recommend the doctor get personal counsel. They will send a reservation of rights letter saying they will defend the doctor for now, but if the facts show the doctor committed some type of misconduct, they may decline coverage, said Keoskey. Some states, including California, require that the carrier pay for this independent counsel.
Unless there is a conflict of interest, though, having a personal attorney just makes the situation more complicated, said Frisella.
A version of this article first appeared on Medscape.com.
The Rise of Sham Peer Reviews
While a medical peer review occurs once a patient, fellow doctor, or staff member reports that a physician failed to treat a patient up to standards or acted improperly, a “sham peer review” is undertaken for ulterior motives.
They’re typically undertaken due to professional competition or institutional politics rather than to promote quality care or uphold professional standards.
Physicians should be concerned. In a soon-to-be-published Medscape report on peer reviews, 56% of US physicians surveyed expressed higher levels of concern that a peer review could be misused to punish a physician for reasons unrelated to the matter being reviewed.
This is a troublesome issue, and many doctors may not be aware of it or how often it occurs.
“The biggest misconception about sham peer reviews is a denial of how pervasive they are,” said Andy Schlafly, general counsel for the Association of American Physicians and Surgeons (AAPS), which offers a free legal consultation service for physicians facing a sham peer review. “Many hospital administrations are as dangerous to good physicians as street gangs can be in a crime-ridden neighborhood.”
“Physicians should become aware of whether sham peer reviews are prevalent at their hospital and, if so, those physicians should look to practice somewhere else,” Schlafly said in an interview.
Unfortunately, there are limited data on how often this happens. When it does, it can be a career killer, said Lawrence Huntoon, MD, PhD, who has run the AAPS sham peer review hotline for over 20 years.
The physicians at the most risk for a sham peer review tend to be those who work for large hospital systems — as this is one way for hospitals to get rid of the doctors they don’t want to retain on staff, Huntoon said.
“Hospitals want a model whereby every physician on the medical staff is an employee,” Huntoon added. “This gives them complete power and control over these physicians, including the way they practice and how many patients they see per day, which, for some, is 20-50 a day to generate sufficient revenue.”
Complaints are generally filed via incident reporting software.
“The complaint could be that the physician is ‘disruptive,’ which can include facial expression, tone of voice, and body language — for example, ‘I found his facial expression demeaning’ or ‘I found her tone condescending’ — and this can be used to prosecute a doctor,” Huntoon said.
After the complaint is filed, the leaders of a hospital’s peer review committee meet to discuss the incident, followed by a panel of fellow physicians convened to review the matter. Once the date for a meeting is set, the accused doctor is allowed to testify, offer evidence, and have attorney representation.
The entire experience can take a physician by surprise.
“A sham peer review is difficult to prepare for because no physician thinks this is going to happen to them,” said Laurie L. York, a medical law attorney in Austin, Texas.
York added that there may also be a misperception of what is actually happening.
“When a physician becomes aware of an investigation, it initially may look like a regular peer review, and the physician may feel there has been a ‘misunderstanding’ that they can make right by explaining things,” York said. “The window of opportunity to shut down a sham peer review happens quickly. That’s why the physician needs the help of an experienced attorney as early in the process as possible.”
If You’re a Victim of a Sham Peer Review
Be vigilant. The most important thing you should think about when it comes to sham peer reviews is that this can, indeed, happen to you, Huntoon said. “I’ve written articles to help educate physicians about the tactics that are used,” he said. “You need to be educated and read medical staff bylaws to know your rights before something bad happens.”
Stay in your job. No matter what, if you’re under review, do not resign your position, no matter how difficult this may be. “A resignation during a sham peer review triggers an adverse report to the National Practitioner Data Bank [NPDB],” Schlafly said. The NPDB is a flagging system created by Congress to improve healthcare quality and reduce healthcare fraud and abuse. “A resignation also waives the physician’s right to contest the unfair review. In addition, leverage to negotiate a favorable settlement is lost if the physician simply resigns.”
Get a lawyer on board early. This is the only way to protect your rights. “Don’t wait a year to get an attorney involved,” Huntoon said. But this also can’t be any lawyer. It’s critical to find someone who specializes in sham peer reviews, so be sure to ask about their experience in handling peer review matters in hospitals and how knowledgeable they are about databank reporting requirements. “Sometimes, doctors will hire a malpractice attorney with no knowledge of what happens with sham peer reviews, and they may give bad advice,” he said. “Others may hire an employment attorney and that attorney will be up on employment law but has no experience with peer review matters in hospitals.”
Given the seriousness of a sham peer review, following these guidelines can help.
Contact the AAPA right away. There are things that can be done early on like getting a withdrawal of the request for corrective action as well as obtaining a preliminary injunction. Preparing for the fallout that may occur can be just as challenging.
“After this situation, the doctor is damaged goods,” Huntoon said. “What hospital will want to hire damaged goods to be part of their medical staff? Finding employment is going to be challenging and opening your own practice may also be difficult because the insurers have access to data bank reports.”
Ultimately, the best advice Huntoon can offer is to do your best to stay one step ahead of any work issues that could even lead to a sham peer review.
“Try and shield yourself from a sham peer review and be prepared should it happen,” he said. “I’ve seen careers end in the blink of an eye — wrongfully.”
A version of this article first appeared on Medscape.com.
While a medical peer review occurs once a patient, fellow doctor, or staff member reports that a physician failed to treat a patient up to standards or acted improperly, a “sham peer review” is undertaken for ulterior motives.
They’re typically undertaken due to professional competition or institutional politics rather than to promote quality care or uphold professional standards.
Physicians should be concerned. In a soon-to-be-published Medscape report on peer reviews, 56% of US physicians surveyed expressed higher levels of concern that a peer review could be misused to punish a physician for reasons unrelated to the matter being reviewed.
This is a troublesome issue, and many doctors may not be aware of it or how often it occurs.
“The biggest misconception about sham peer reviews is a denial of how pervasive they are,” said Andy Schlafly, general counsel for the Association of American Physicians and Surgeons (AAPS), which offers a free legal consultation service for physicians facing a sham peer review. “Many hospital administrations are as dangerous to good physicians as street gangs can be in a crime-ridden neighborhood.”
“Physicians should become aware of whether sham peer reviews are prevalent at their hospital and, if so, those physicians should look to practice somewhere else,” Schlafly said in an interview.
Unfortunately, there are limited data on how often this happens. When it does, it can be a career killer, said Lawrence Huntoon, MD, PhD, who has run the AAPS sham peer review hotline for over 20 years.
The physicians at the most risk for a sham peer review tend to be those who work for large hospital systems — as this is one way for hospitals to get rid of the doctors they don’t want to retain on staff, Huntoon said.
“Hospitals want a model whereby every physician on the medical staff is an employee,” Huntoon added. “This gives them complete power and control over these physicians, including the way they practice and how many patients they see per day, which, for some, is 20-50 a day to generate sufficient revenue.”
Complaints are generally filed via incident reporting software.
“The complaint could be that the physician is ‘disruptive,’ which can include facial expression, tone of voice, and body language — for example, ‘I found his facial expression demeaning’ or ‘I found her tone condescending’ — and this can be used to prosecute a doctor,” Huntoon said.
After the complaint is filed, the leaders of a hospital’s peer review committee meet to discuss the incident, followed by a panel of fellow physicians convened to review the matter. Once the date for a meeting is set, the accused doctor is allowed to testify, offer evidence, and have attorney representation.
The entire experience can take a physician by surprise.
“A sham peer review is difficult to prepare for because no physician thinks this is going to happen to them,” said Laurie L. York, a medical law attorney in Austin, Texas.
York added that there may also be a misperception of what is actually happening.
“When a physician becomes aware of an investigation, it initially may look like a regular peer review, and the physician may feel there has been a ‘misunderstanding’ that they can make right by explaining things,” York said. “The window of opportunity to shut down a sham peer review happens quickly. That’s why the physician needs the help of an experienced attorney as early in the process as possible.”
If You’re a Victim of a Sham Peer Review
Be vigilant. The most important thing you should think about when it comes to sham peer reviews is that this can, indeed, happen to you, Huntoon said. “I’ve written articles to help educate physicians about the tactics that are used,” he said. “You need to be educated and read medical staff bylaws to know your rights before something bad happens.”
Stay in your job. No matter what, if you’re under review, do not resign your position, no matter how difficult this may be. “A resignation during a sham peer review triggers an adverse report to the National Practitioner Data Bank [NPDB],” Schlafly said. The NPDB is a flagging system created by Congress to improve healthcare quality and reduce healthcare fraud and abuse. “A resignation also waives the physician’s right to contest the unfair review. In addition, leverage to negotiate a favorable settlement is lost if the physician simply resigns.”
Get a lawyer on board early. This is the only way to protect your rights. “Don’t wait a year to get an attorney involved,” Huntoon said. But this also can’t be any lawyer. It’s critical to find someone who specializes in sham peer reviews, so be sure to ask about their experience in handling peer review matters in hospitals and how knowledgeable they are about databank reporting requirements. “Sometimes, doctors will hire a malpractice attorney with no knowledge of what happens with sham peer reviews, and they may give bad advice,” he said. “Others may hire an employment attorney and that attorney will be up on employment law but has no experience with peer review matters in hospitals.”
Given the seriousness of a sham peer review, following these guidelines can help.
Contact the AAPA right away. There are things that can be done early on like getting a withdrawal of the request for corrective action as well as obtaining a preliminary injunction. Preparing for the fallout that may occur can be just as challenging.
“After this situation, the doctor is damaged goods,” Huntoon said. “What hospital will want to hire damaged goods to be part of their medical staff? Finding employment is going to be challenging and opening your own practice may also be difficult because the insurers have access to data bank reports.”
Ultimately, the best advice Huntoon can offer is to do your best to stay one step ahead of any work issues that could even lead to a sham peer review.
“Try and shield yourself from a sham peer review and be prepared should it happen,” he said. “I’ve seen careers end in the blink of an eye — wrongfully.”
A version of this article first appeared on Medscape.com.
While a medical peer review occurs once a patient, fellow doctor, or staff member reports that a physician failed to treat a patient up to standards or acted improperly, a “sham peer review” is undertaken for ulterior motives.
They’re typically undertaken due to professional competition or institutional politics rather than to promote quality care or uphold professional standards.
Physicians should be concerned. In a soon-to-be-published Medscape report on peer reviews, 56% of US physicians surveyed expressed higher levels of concern that a peer review could be misused to punish a physician for reasons unrelated to the matter being reviewed.
This is a troublesome issue, and many doctors may not be aware of it or how often it occurs.
“The biggest misconception about sham peer reviews is a denial of how pervasive they are,” said Andy Schlafly, general counsel for the Association of American Physicians and Surgeons (AAPS), which offers a free legal consultation service for physicians facing a sham peer review. “Many hospital administrations are as dangerous to good physicians as street gangs can be in a crime-ridden neighborhood.”
“Physicians should become aware of whether sham peer reviews are prevalent at their hospital and, if so, those physicians should look to practice somewhere else,” Schlafly said in an interview.
Unfortunately, there are limited data on how often this happens. When it does, it can be a career killer, said Lawrence Huntoon, MD, PhD, who has run the AAPS sham peer review hotline for over 20 years.
The physicians at the most risk for a sham peer review tend to be those who work for large hospital systems — as this is one way for hospitals to get rid of the doctors they don’t want to retain on staff, Huntoon said.
“Hospitals want a model whereby every physician on the medical staff is an employee,” Huntoon added. “This gives them complete power and control over these physicians, including the way they practice and how many patients they see per day, which, for some, is 20-50 a day to generate sufficient revenue.”
Complaints are generally filed via incident reporting software.
“The complaint could be that the physician is ‘disruptive,’ which can include facial expression, tone of voice, and body language — for example, ‘I found his facial expression demeaning’ or ‘I found her tone condescending’ — and this can be used to prosecute a doctor,” Huntoon said.
After the complaint is filed, the leaders of a hospital’s peer review committee meet to discuss the incident, followed by a panel of fellow physicians convened to review the matter. Once the date for a meeting is set, the accused doctor is allowed to testify, offer evidence, and have attorney representation.
The entire experience can take a physician by surprise.
“A sham peer review is difficult to prepare for because no physician thinks this is going to happen to them,” said Laurie L. York, a medical law attorney in Austin, Texas.
York added that there may also be a misperception of what is actually happening.
“When a physician becomes aware of an investigation, it initially may look like a regular peer review, and the physician may feel there has been a ‘misunderstanding’ that they can make right by explaining things,” York said. “The window of opportunity to shut down a sham peer review happens quickly. That’s why the physician needs the help of an experienced attorney as early in the process as possible.”
If You’re a Victim of a Sham Peer Review
Be vigilant. The most important thing you should think about when it comes to sham peer reviews is that this can, indeed, happen to you, Huntoon said. “I’ve written articles to help educate physicians about the tactics that are used,” he said. “You need to be educated and read medical staff bylaws to know your rights before something bad happens.”
Stay in your job. No matter what, if you’re under review, do not resign your position, no matter how difficult this may be. “A resignation during a sham peer review triggers an adverse report to the National Practitioner Data Bank [NPDB],” Schlafly said. The NPDB is a flagging system created by Congress to improve healthcare quality and reduce healthcare fraud and abuse. “A resignation also waives the physician’s right to contest the unfair review. In addition, leverage to negotiate a favorable settlement is lost if the physician simply resigns.”
Get a lawyer on board early. This is the only way to protect your rights. “Don’t wait a year to get an attorney involved,” Huntoon said. But this also can’t be any lawyer. It’s critical to find someone who specializes in sham peer reviews, so be sure to ask about their experience in handling peer review matters in hospitals and how knowledgeable they are about databank reporting requirements. “Sometimes, doctors will hire a malpractice attorney with no knowledge of what happens with sham peer reviews, and they may give bad advice,” he said. “Others may hire an employment attorney and that attorney will be up on employment law but has no experience with peer review matters in hospitals.”
Given the seriousness of a sham peer review, following these guidelines can help.
Contact the AAPA right away. There are things that can be done early on like getting a withdrawal of the request for corrective action as well as obtaining a preliminary injunction. Preparing for the fallout that may occur can be just as challenging.
“After this situation, the doctor is damaged goods,” Huntoon said. “What hospital will want to hire damaged goods to be part of their medical staff? Finding employment is going to be challenging and opening your own practice may also be difficult because the insurers have access to data bank reports.”
Ultimately, the best advice Huntoon can offer is to do your best to stay one step ahead of any work issues that could even lead to a sham peer review.
“Try and shield yourself from a sham peer review and be prepared should it happen,” he said. “I’ve seen careers end in the blink of an eye — wrongfully.”
A version of this article first appeared on Medscape.com.
At Last, a Nasal Epinephrine Spray
This summer, the US Food and Drug Administration (FDA) fast-tracked approval of the first-in-its-class nasal epinephrine (neffy). It’s a very welcome addition to our anaphylaxis treatment armamentarium. In healthy volunteers, neffy achieved similar serum epinephrine levels, rises in blood pressure, and pulse compared with IM epinephrine.
The Need for Neffy
It was just a few days ago that I saw a new patient with fire ant anaphylaxis. The last time he tried to use an injectable epinephrine pen, he made two mistakes. First, he placed the wrong end against his thigh, and when it did not inject, he depressed it with his thumb — in other words, he injected his thumb with epinephrine. Of course, that cannot happen with neffy.
I recall a few years ago, a child experienced anaphylaxis but the parent was hesitant to administer the EAI (epinephrine autoinjector). The parent drove to the emergency room but was delayed by traffic, and by the time they reached the ER, the patient had suffered a respiratory arrest and passed away.
Patients are not the only ones who are hesitant to administer epinephrine. Some clinicians do not treat anaphylaxis appropriately. As an allergist, I see patients after-the-fact for diagnosis and management. Patients often tell me of systemic allergic reactions treated with IV antihistamines/corticosteroids and even sometimes with nebulized beta agonists, but not epinephrine.
My opinion is that it’s not just needle phobia. As I mentioned, in my Medscape commentary “Injectable Epinephrine: An Epidemic of Misuse,” I believe it’s due to a misunderstanding of the guidelines and a sense that epinephrine is a potent medication to be used sparingly. Clinicians and patients must understand that epinephrine is a naturally occurring hormone and administration leads to serum levels seen under other natural circumstances (eg, stress — the fight-or-flight surge). The aforementioned article also includes a patient handout, “Don’t Fear Epinephrine,” which I encourage you to read and distribute.
The potential benefits of neffy are clear:
- It should overcome fear of injection ergo being more likely to be used, and used earlier, by both patient/family member and clinicians.
- It’s easier to carry than many larger devices (though not the AUVI-Q).
- It cannot be injected incorrectly.
- Expiration is 8 months longer than the EAI.
- There are no pharmacist substitutions (as there is no equivalent device).
Potential Problems With Neffy and Some Suggested Solutions
As promising and beneficial as it is, I wonder about a few training issues. In the office, patients can be trained with a (reusable) injectable epinephrine trainer but not with a nasal spray device trainer in the office (an important alternative is a small model of a nose in the office for patient education). A training device should also be included in the neffy prescription, as with the EAI.
Neffy and Patients With Nasal Polyps or Nasal Surgery
It’s more complicated than that neffy cannot be used with patients who have had nasal polyps or nasal surgery. It’s really about how much healthy nasal mucosa is required for absorption. Nasal surgery may be simple or complex. Nasal polyps may be obstructive or resolved with nasal steroid or biologic therapy. Nasal polyps affect 2% of the population, but 35% of pediatric food allergy (FA) patients develop allergic rhinitis (AR), and these AR symptoms present even when not triggered by FA. AR is present at baseline in patients with FA. How does this influence neffy absorption? For FA patients who have anaphylactic reactions with severe nasal reactions, neffy absorption could be further compromised, something that has not been studied.
Insurance Coverage
As we don’t yet know the comparative efficacy of neffy in anaphylactic episodes, it’s likely that patients, especially with more severe food sensitivities, will be prescribed both the nasal and IM devices. The question remains whether insurance will cover both.
In “mild cases,” I suspect that doctors might be more inclined to prescribe neffy.
Conclusion
Delay in epinephrine use is frequent despite the clear indication during anaphylactic episodes, which in turn increases risk for mortality. Neffy will probably save many lives.
Dr. Stadtmauer serves on the advisory board of Medscape. He is in private practice in New York City and is affiliated with the Mount Sinai School of Medicine.
A version of this article first appeared on Medscape.com.
This summer, the US Food and Drug Administration (FDA) fast-tracked approval of the first-in-its-class nasal epinephrine (neffy). It’s a very welcome addition to our anaphylaxis treatment armamentarium. In healthy volunteers, neffy achieved similar serum epinephrine levels, rises in blood pressure, and pulse compared with IM epinephrine.
The Need for Neffy
It was just a few days ago that I saw a new patient with fire ant anaphylaxis. The last time he tried to use an injectable epinephrine pen, he made two mistakes. First, he placed the wrong end against his thigh, and when it did not inject, he depressed it with his thumb — in other words, he injected his thumb with epinephrine. Of course, that cannot happen with neffy.
I recall a few years ago, a child experienced anaphylaxis but the parent was hesitant to administer the EAI (epinephrine autoinjector). The parent drove to the emergency room but was delayed by traffic, and by the time they reached the ER, the patient had suffered a respiratory arrest and passed away.
Patients are not the only ones who are hesitant to administer epinephrine. Some clinicians do not treat anaphylaxis appropriately. As an allergist, I see patients after-the-fact for diagnosis and management. Patients often tell me of systemic allergic reactions treated with IV antihistamines/corticosteroids and even sometimes with nebulized beta agonists, but not epinephrine.
My opinion is that it’s not just needle phobia. As I mentioned, in my Medscape commentary “Injectable Epinephrine: An Epidemic of Misuse,” I believe it’s due to a misunderstanding of the guidelines and a sense that epinephrine is a potent medication to be used sparingly. Clinicians and patients must understand that epinephrine is a naturally occurring hormone and administration leads to serum levels seen under other natural circumstances (eg, stress — the fight-or-flight surge). The aforementioned article also includes a patient handout, “Don’t Fear Epinephrine,” which I encourage you to read and distribute.
The potential benefits of neffy are clear:
- It should overcome fear of injection ergo being more likely to be used, and used earlier, by both patient/family member and clinicians.
- It’s easier to carry than many larger devices (though not the AUVI-Q).
- It cannot be injected incorrectly.
- Expiration is 8 months longer than the EAI.
- There are no pharmacist substitutions (as there is no equivalent device).
Potential Problems With Neffy and Some Suggested Solutions
As promising and beneficial as it is, I wonder about a few training issues. In the office, patients can be trained with a (reusable) injectable epinephrine trainer but not with a nasal spray device trainer in the office (an important alternative is a small model of a nose in the office for patient education). A training device should also be included in the neffy prescription, as with the EAI.
Neffy and Patients With Nasal Polyps or Nasal Surgery
It’s more complicated than that neffy cannot be used with patients who have had nasal polyps or nasal surgery. It’s really about how much healthy nasal mucosa is required for absorption. Nasal surgery may be simple or complex. Nasal polyps may be obstructive or resolved with nasal steroid or biologic therapy. Nasal polyps affect 2% of the population, but 35% of pediatric food allergy (FA) patients develop allergic rhinitis (AR), and these AR symptoms present even when not triggered by FA. AR is present at baseline in patients with FA. How does this influence neffy absorption? For FA patients who have anaphylactic reactions with severe nasal reactions, neffy absorption could be further compromised, something that has not been studied.
Insurance Coverage
As we don’t yet know the comparative efficacy of neffy in anaphylactic episodes, it’s likely that patients, especially with more severe food sensitivities, will be prescribed both the nasal and IM devices. The question remains whether insurance will cover both.
In “mild cases,” I suspect that doctors might be more inclined to prescribe neffy.
Conclusion
Delay in epinephrine use is frequent despite the clear indication during anaphylactic episodes, which in turn increases risk for mortality. Neffy will probably save many lives.
Dr. Stadtmauer serves on the advisory board of Medscape. He is in private practice in New York City and is affiliated with the Mount Sinai School of Medicine.
A version of this article first appeared on Medscape.com.
This summer, the US Food and Drug Administration (FDA) fast-tracked approval of the first-in-its-class nasal epinephrine (neffy). It’s a very welcome addition to our anaphylaxis treatment armamentarium. In healthy volunteers, neffy achieved similar serum epinephrine levels, rises in blood pressure, and pulse compared with IM epinephrine.
The Need for Neffy
It was just a few days ago that I saw a new patient with fire ant anaphylaxis. The last time he tried to use an injectable epinephrine pen, he made two mistakes. First, he placed the wrong end against his thigh, and when it did not inject, he depressed it with his thumb — in other words, he injected his thumb with epinephrine. Of course, that cannot happen with neffy.
I recall a few years ago, a child experienced anaphylaxis but the parent was hesitant to administer the EAI (epinephrine autoinjector). The parent drove to the emergency room but was delayed by traffic, and by the time they reached the ER, the patient had suffered a respiratory arrest and passed away.
Patients are not the only ones who are hesitant to administer epinephrine. Some clinicians do not treat anaphylaxis appropriately. As an allergist, I see patients after-the-fact for diagnosis and management. Patients often tell me of systemic allergic reactions treated with IV antihistamines/corticosteroids and even sometimes with nebulized beta agonists, but not epinephrine.
My opinion is that it’s not just needle phobia. As I mentioned, in my Medscape commentary “Injectable Epinephrine: An Epidemic of Misuse,” I believe it’s due to a misunderstanding of the guidelines and a sense that epinephrine is a potent medication to be used sparingly. Clinicians and patients must understand that epinephrine is a naturally occurring hormone and administration leads to serum levels seen under other natural circumstances (eg, stress — the fight-or-flight surge). The aforementioned article also includes a patient handout, “Don’t Fear Epinephrine,” which I encourage you to read and distribute.
The potential benefits of neffy are clear:
- It should overcome fear of injection ergo being more likely to be used, and used earlier, by both patient/family member and clinicians.
- It’s easier to carry than many larger devices (though not the AUVI-Q).
- It cannot be injected incorrectly.
- Expiration is 8 months longer than the EAI.
- There are no pharmacist substitutions (as there is no equivalent device).
Potential Problems With Neffy and Some Suggested Solutions
As promising and beneficial as it is, I wonder about a few training issues. In the office, patients can be trained with a (reusable) injectable epinephrine trainer but not with a nasal spray device trainer in the office (an important alternative is a small model of a nose in the office for patient education). A training device should also be included in the neffy prescription, as with the EAI.
Neffy and Patients With Nasal Polyps or Nasal Surgery
It’s more complicated than that neffy cannot be used with patients who have had nasal polyps or nasal surgery. It’s really about how much healthy nasal mucosa is required for absorption. Nasal surgery may be simple or complex. Nasal polyps may be obstructive or resolved with nasal steroid or biologic therapy. Nasal polyps affect 2% of the population, but 35% of pediatric food allergy (FA) patients develop allergic rhinitis (AR), and these AR symptoms present even when not triggered by FA. AR is present at baseline in patients with FA. How does this influence neffy absorption? For FA patients who have anaphylactic reactions with severe nasal reactions, neffy absorption could be further compromised, something that has not been studied.
Insurance Coverage
As we don’t yet know the comparative efficacy of neffy in anaphylactic episodes, it’s likely that patients, especially with more severe food sensitivities, will be prescribed both the nasal and IM devices. The question remains whether insurance will cover both.
In “mild cases,” I suspect that doctors might be more inclined to prescribe neffy.
Conclusion
Delay in epinephrine use is frequent despite the clear indication during anaphylactic episodes, which in turn increases risk for mortality. Neffy will probably save many lives.
Dr. Stadtmauer serves on the advisory board of Medscape. He is in private practice in New York City and is affiliated with the Mount Sinai School of Medicine.
A version of this article first appeared on Medscape.com.
The Bad News Behind the Rise in Locum Tenens
I’ve worked locum tenens off and on since 1982. Flexible schedules allowed me to write several books, pursue a parallel career as a medical journalist, lead medical missions in the Philippines, and develop modest expertise as an underwater photographer.
But the recent rise in locum tenens practitioners signals trouble for medicine.
A Multibillion-Dollar Industry
Roughly 52,000 US doctors work locum tenens full or part time. In annual reports by CHG Healthcare, two thirds of healthcare facilities surveyed report using locums and more than half expect to maintain or increase their use in 2024.
Another measure of the industry’s growth is that membership of The National Association of Locum Tenens Organizations (NALTO), formed in 2001 to lead this fledgling industry, has doubled since 2019. Currently, NALTO has 148 member agencies.
Why Locums?
What used to be the preserve of older physicians transitioning to retirement is now becoming a career choice. According to the 2024 Survey of Locum Tenens Physicians and Advanced Practice Professionals by AMN Healthcare, 81% of respondents said they started taking locum tenens assignments immediately after finishing medical training or in mid-career. What entices doctors to move from place to place, repeatedly adapt to new facilities and electronic medical records, live in cheap hotels, and work without paid vacations, health insurance, or retirement benefits?
Supplemental income is one reason. But the elephant in the room is clearly burnout. Rates of burnout in practicing doctors and physicians-in-training have exceeded 50%. Burnout results in medical errors, malpractice suits, and increased healthcare costs.
A recent Doximity poll of 7590 physicians revealed that 63% would not want their children to pursue a medical career. And in a Medscape survey of 7000 physicians, a third of docs under 40 would not choose medicine again if they had a do-over. If a career in medicine brings high income and privileged status, why do so many physicians regret it and discourage their children from taking the same path?
Where Is Marcus Welby, MD?
Private practice is an endangered species that no one is trying to save. According to a 2022 AMA survey, 44% of physicians owned their practices compared with 76% of physicians in the 1980s. Even fewer younger physicians are choosing private practice. Among physicians under 45 years of age, only 32% owned their practices. Most physicians are now employees, not employers. They have lost control over their duties and work hours.
In 2022, barely 13% of physicians were in solo practice. The iconic Dr Marcus Welby of the 1970s TV series has transmuted from an idealized physician to an implausible figure. (My medical students have never heard of him.)
Hospitals and health systems have purchased many private medical groups. Private-equity companies own close to 1000 physician practices and staff up to 40% of emergency rooms. For these firms, profits are paramount.
Canary in a Coal Mine
Locum tenens offers physicians unprecedented flexibility where they work, when they work, and how much they work. It provides an escape from overwhelming and unsatisfying clinical practice. While some physicians have fled to nonclinical careers, locums physicians can practice medicine without the burdens of administration, hospital politics, and ever-increasing overhead.
The locum tenens paradox is that its successful growth indicates a deteriorating traditional healthcare model. Locum tenens is not the problem, but it’s also not the solution. At best, locums is a pair of crutches that helps the current system limp along.
Healthcare is increasingly controlled by those who prioritize profit, not patients. If physicians become nothing more than complicit cogs in a dysfunctional system, burnout will fester. The profession will fail to attract the best and the brightest, the doctor shortage will increase, and the quality of patient care will decline. Everyone will suffer.
It’s already happening.
Andrew Wilner is an associate professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported conflicts of interest from Accordant Health Services.
A version of this article first appeared on Medscape.com.
I’ve worked locum tenens off and on since 1982. Flexible schedules allowed me to write several books, pursue a parallel career as a medical journalist, lead medical missions in the Philippines, and develop modest expertise as an underwater photographer.
But the recent rise in locum tenens practitioners signals trouble for medicine.
A Multibillion-Dollar Industry
Roughly 52,000 US doctors work locum tenens full or part time. In annual reports by CHG Healthcare, two thirds of healthcare facilities surveyed report using locums and more than half expect to maintain or increase their use in 2024.
Another measure of the industry’s growth is that membership of The National Association of Locum Tenens Organizations (NALTO), formed in 2001 to lead this fledgling industry, has doubled since 2019. Currently, NALTO has 148 member agencies.
Why Locums?
What used to be the preserve of older physicians transitioning to retirement is now becoming a career choice. According to the 2024 Survey of Locum Tenens Physicians and Advanced Practice Professionals by AMN Healthcare, 81% of respondents said they started taking locum tenens assignments immediately after finishing medical training or in mid-career. What entices doctors to move from place to place, repeatedly adapt to new facilities and electronic medical records, live in cheap hotels, and work without paid vacations, health insurance, or retirement benefits?
Supplemental income is one reason. But the elephant in the room is clearly burnout. Rates of burnout in practicing doctors and physicians-in-training have exceeded 50%. Burnout results in medical errors, malpractice suits, and increased healthcare costs.
A recent Doximity poll of 7590 physicians revealed that 63% would not want their children to pursue a medical career. And in a Medscape survey of 7000 physicians, a third of docs under 40 would not choose medicine again if they had a do-over. If a career in medicine brings high income and privileged status, why do so many physicians regret it and discourage their children from taking the same path?
Where Is Marcus Welby, MD?
Private practice is an endangered species that no one is trying to save. According to a 2022 AMA survey, 44% of physicians owned their practices compared with 76% of physicians in the 1980s. Even fewer younger physicians are choosing private practice. Among physicians under 45 years of age, only 32% owned their practices. Most physicians are now employees, not employers. They have lost control over their duties and work hours.
In 2022, barely 13% of physicians were in solo practice. The iconic Dr Marcus Welby of the 1970s TV series has transmuted from an idealized physician to an implausible figure. (My medical students have never heard of him.)
Hospitals and health systems have purchased many private medical groups. Private-equity companies own close to 1000 physician practices and staff up to 40% of emergency rooms. For these firms, profits are paramount.
Canary in a Coal Mine
Locum tenens offers physicians unprecedented flexibility where they work, when they work, and how much they work. It provides an escape from overwhelming and unsatisfying clinical practice. While some physicians have fled to nonclinical careers, locums physicians can practice medicine without the burdens of administration, hospital politics, and ever-increasing overhead.
The locum tenens paradox is that its successful growth indicates a deteriorating traditional healthcare model. Locum tenens is not the problem, but it’s also not the solution. At best, locums is a pair of crutches that helps the current system limp along.
Healthcare is increasingly controlled by those who prioritize profit, not patients. If physicians become nothing more than complicit cogs in a dysfunctional system, burnout will fester. The profession will fail to attract the best and the brightest, the doctor shortage will increase, and the quality of patient care will decline. Everyone will suffer.
It’s already happening.
Andrew Wilner is an associate professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported conflicts of interest from Accordant Health Services.
A version of this article first appeared on Medscape.com.
I’ve worked locum tenens off and on since 1982. Flexible schedules allowed me to write several books, pursue a parallel career as a medical journalist, lead medical missions in the Philippines, and develop modest expertise as an underwater photographer.
But the recent rise in locum tenens practitioners signals trouble for medicine.
A Multibillion-Dollar Industry
Roughly 52,000 US doctors work locum tenens full or part time. In annual reports by CHG Healthcare, two thirds of healthcare facilities surveyed report using locums and more than half expect to maintain or increase their use in 2024.
Another measure of the industry’s growth is that membership of The National Association of Locum Tenens Organizations (NALTO), formed in 2001 to lead this fledgling industry, has doubled since 2019. Currently, NALTO has 148 member agencies.
Why Locums?
What used to be the preserve of older physicians transitioning to retirement is now becoming a career choice. According to the 2024 Survey of Locum Tenens Physicians and Advanced Practice Professionals by AMN Healthcare, 81% of respondents said they started taking locum tenens assignments immediately after finishing medical training or in mid-career. What entices doctors to move from place to place, repeatedly adapt to new facilities and electronic medical records, live in cheap hotels, and work without paid vacations, health insurance, or retirement benefits?
Supplemental income is one reason. But the elephant in the room is clearly burnout. Rates of burnout in practicing doctors and physicians-in-training have exceeded 50%. Burnout results in medical errors, malpractice suits, and increased healthcare costs.
A recent Doximity poll of 7590 physicians revealed that 63% would not want their children to pursue a medical career. And in a Medscape survey of 7000 physicians, a third of docs under 40 would not choose medicine again if they had a do-over. If a career in medicine brings high income and privileged status, why do so many physicians regret it and discourage their children from taking the same path?
Where Is Marcus Welby, MD?
Private practice is an endangered species that no one is trying to save. According to a 2022 AMA survey, 44% of physicians owned their practices compared with 76% of physicians in the 1980s. Even fewer younger physicians are choosing private practice. Among physicians under 45 years of age, only 32% owned their practices. Most physicians are now employees, not employers. They have lost control over their duties and work hours.
In 2022, barely 13% of physicians were in solo practice. The iconic Dr Marcus Welby of the 1970s TV series has transmuted from an idealized physician to an implausible figure. (My medical students have never heard of him.)
Hospitals and health systems have purchased many private medical groups. Private-equity companies own close to 1000 physician practices and staff up to 40% of emergency rooms. For these firms, profits are paramount.
Canary in a Coal Mine
Locum tenens offers physicians unprecedented flexibility where they work, when they work, and how much they work. It provides an escape from overwhelming and unsatisfying clinical practice. While some physicians have fled to nonclinical careers, locums physicians can practice medicine without the burdens of administration, hospital politics, and ever-increasing overhead.
The locum tenens paradox is that its successful growth indicates a deteriorating traditional healthcare model. Locum tenens is not the problem, but it’s also not the solution. At best, locums is a pair of crutches that helps the current system limp along.
Healthcare is increasingly controlled by those who prioritize profit, not patients. If physicians become nothing more than complicit cogs in a dysfunctional system, burnout will fester. The profession will fail to attract the best and the brightest, the doctor shortage will increase, and the quality of patient care will decline. Everyone will suffer.
It’s already happening.
Andrew Wilner is an associate professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported conflicts of interest from Accordant Health Services.
A version of this article first appeared on Medscape.com.
Nutrition and Medical Education
How comfortable are you giving nutritional advice to your patients? When you offer it are you basing your advice on something you learned during medical school or your training? Was it included in a course devoted to nutrition? Did you learn it later as part of continuing medical education course (CME)? Or was it just something you just picked up from your experience seeing patients (osmosis)? It is very unlikely that a significant portion, or any part for that matter, of your medical training was devoted to nutrition. It certainly wasn’t during my training.
I recently read an interview with Emily M. Broad Leib, JD, faculty director of the Harvard School Center for Health Law and Policy Innovation, Cambridge, Massachusetts, who would like to correct that deficiency. She feels doctors need to know more about food and that acquiring that knowledge should be a significant component of their formal training.

In the interview, Leib said that “roughly 86% of physicians report they do not feel adequately trained to answer basic questions on diet or nutrition.” She also notes that while “72% of entering medical students report they believe food is important to health” less than 50% retained this belief after graduation.
Leib and associates feel they have recently reached a milestone in their efforts to include nutrition in the mainstream of medical education this fall by publishing a paper that demonstrates “consensus on doctor-approved nutritional standard for medical schools and residency programs.”
36 Recommended Competencies
Curious about what these nutrition experts chose to include in medical training, I decided to drill down into the list of 36 consensus-driven competencies they had agreed upon.
It was an interesting voyage into a forest of redundancies, many of which can be boiled down to having the student demonstrate that he/she understands that what we eat is important to our health and that there is a complex web of relationships connecting our society to the food consume.
Some of the recommended competencies I found make perfect sense. For example the student/trainee should be able to take a diet and food history and be able to interpret lab values and anthropometric measurements and be able to discuss the patient’s weight and diet with sensitivity while keeping in mind his/her own biases about food.
Some other recommendations are more problematic, for example, “performs a comprehensive nutrition-focused physical examination” or “demonstrates knowledge of how to create culinary nutrition SMART [Specific, Measurable, Achievable, Relevant, and Time-Bound] goals for personal use and for patient care” or “provides brief counseling interventions to help patients decrease visceral adiposity or reduce the risk of metabolic syndrome.” Including competencies like these demonstrates a lack of understanding of the time restraints and realities of a primary care physician’s life and training.
Instead of simply reinforcing the prospective physician’s preexisting assumption that food and health are entwined and discussing when and how to consult a nutrition expert, these 36 competencies seem to be an attempt to create fast-tracked part-time dietitians and nutrition advocates out of medical students and trainees who already believe that nutrition is important for health but also have a very full plate of clinical responsibilities ahead of them.
The study that Leib quotes — that 72% of medical students believed food was important in health while after graduation only 50% of agreed — doesn’t necessarily mean that professors are preaching that food was unimportant. It is more likely by the end of medical school the students have seen that food must share the spotlight with numerous other factors that influence their patients’ health.
‘A More Appropriate Focus’
In my experience, diet and lifestyle counseling done well is extremely time consuming and best done by people for whom that is their specialty. A more appropriate focus for a list of nutritional competencies for physicians in training would be for the student to achieve an understanding of when and how to consult a dietitian and then how to support and evaluate the dietitian’s recommendations to the patient.
Finally, I don’t think we can ignore a serious public relations problem that hangs like a cloud over the nutrition advocacy community. It is the same one that casts a shadow on the medical community as well. It is a common perception among the lay public that nutritionists (and physicians) are always changing their recommendations when it comes to food. What is believable? Just think about eggs, red wine, or introducing peanuts to infants, to name just a few. And what about the food pyramids that seem to have been rebuilt every several years? The problem is compounded when some “credentialed” nutritionists and physicians continue to make dietary pronouncements with only a shred of evidence or poorly documented anecdotal observations.
The first of the 36 competencies I reviewed reads: “Provide evidence-based, culturally sensitive nutrition and food recommendations for the prevention and treatment of disease.” When it comes to nutrition the “evidence” can be tough to come by. The natural experiments in which individuals and populations had extremely limited access to a certain nutrients (eg, scurvy) don’t occur very often. Animal studies don’t always extrapolate to humans. And, observational studies concerning diet often have co-factors that are difficult to control and must run over time courses that can tax even the most patient researchers.
I certainly applaud Leib and associates for promoting their primary goal of including more about of the relationship between food and health in the medical school and trainee curriculum. But I must voice a caution to be careful to keep it truly evidence-based and in a format that acknowledges the realities of the life and education of a primary care provider.
The best nutritional advice I ever received in my training was from an older pediatric professor who suggested that a healthy diet consisted of everything in moderation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
How comfortable are you giving nutritional advice to your patients? When you offer it are you basing your advice on something you learned during medical school or your training? Was it included in a course devoted to nutrition? Did you learn it later as part of continuing medical education course (CME)? Or was it just something you just picked up from your experience seeing patients (osmosis)? It is very unlikely that a significant portion, or any part for that matter, of your medical training was devoted to nutrition. It certainly wasn’t during my training.
I recently read an interview with Emily M. Broad Leib, JD, faculty director of the Harvard School Center for Health Law and Policy Innovation, Cambridge, Massachusetts, who would like to correct that deficiency. She feels doctors need to know more about food and that acquiring that knowledge should be a significant component of their formal training.
In the interview, Leib said that “roughly 86% of physicians report they do not feel adequately trained to answer basic questions on diet or nutrition.” She also notes that while “72% of entering medical students report they believe food is important to health” less than 50% retained this belief after graduation.
Leib and associates feel they have recently reached a milestone in their efforts to include nutrition in the mainstream of medical education this fall by publishing a paper that demonstrates “consensus on doctor-approved nutritional standard for medical schools and residency programs.”
36 Recommended Competencies
Curious about what these nutrition experts chose to include in medical training, I decided to drill down into the list of 36 consensus-driven competencies they had agreed upon.
It was an interesting voyage into a forest of redundancies, many of which can be boiled down to having the student demonstrate that he/she understands that what we eat is important to our health and that there is a complex web of relationships connecting our society to the food consume.
Some of the recommended competencies I found make perfect sense. For example the student/trainee should be able to take a diet and food history and be able to interpret lab values and anthropometric measurements and be able to discuss the patient’s weight and diet with sensitivity while keeping in mind his/her own biases about food.
Some other recommendations are more problematic, for example, “performs a comprehensive nutrition-focused physical examination” or “demonstrates knowledge of how to create culinary nutrition SMART [Specific, Measurable, Achievable, Relevant, and Time-Bound] goals for personal use and for patient care” or “provides brief counseling interventions to help patients decrease visceral adiposity or reduce the risk of metabolic syndrome.” Including competencies like these demonstrates a lack of understanding of the time restraints and realities of a primary care physician’s life and training.
Instead of simply reinforcing the prospective physician’s preexisting assumption that food and health are entwined and discussing when and how to consult a nutrition expert, these 36 competencies seem to be an attempt to create fast-tracked part-time dietitians and nutrition advocates out of medical students and trainees who already believe that nutrition is important for health but also have a very full plate of clinical responsibilities ahead of them.
The study that Leib quotes — that 72% of medical students believed food was important in health while after graduation only 50% of agreed — doesn’t necessarily mean that professors are preaching that food was unimportant. It is more likely by the end of medical school the students have seen that food must share the spotlight with numerous other factors that influence their patients’ health.
‘A More Appropriate Focus’
In my experience, diet and lifestyle counseling done well is extremely time consuming and best done by people for whom that is their specialty. A more appropriate focus for a list of nutritional competencies for physicians in training would be for the student to achieve an understanding of when and how to consult a dietitian and then how to support and evaluate the dietitian’s recommendations to the patient.
Finally, I don’t think we can ignore a serious public relations problem that hangs like a cloud over the nutrition advocacy community. It is the same one that casts a shadow on the medical community as well. It is a common perception among the lay public that nutritionists (and physicians) are always changing their recommendations when it comes to food. What is believable? Just think about eggs, red wine, or introducing peanuts to infants, to name just a few. And what about the food pyramids that seem to have been rebuilt every several years? The problem is compounded when some “credentialed” nutritionists and physicians continue to make dietary pronouncements with only a shred of evidence or poorly documented anecdotal observations.
The first of the 36 competencies I reviewed reads: “Provide evidence-based, culturally sensitive nutrition and food recommendations for the prevention and treatment of disease.” When it comes to nutrition the “evidence” can be tough to come by. The natural experiments in which individuals and populations had extremely limited access to a certain nutrients (eg, scurvy) don’t occur very often. Animal studies don’t always extrapolate to humans. And, observational studies concerning diet often have co-factors that are difficult to control and must run over time courses that can tax even the most patient researchers.
I certainly applaud Leib and associates for promoting their primary goal of including more about of the relationship between food and health in the medical school and trainee curriculum. But I must voice a caution to be careful to keep it truly evidence-based and in a format that acknowledges the realities of the life and education of a primary care provider.
The best nutritional advice I ever received in my training was from an older pediatric professor who suggested that a healthy diet consisted of everything in moderation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
How comfortable are you giving nutritional advice to your patients? When you offer it are you basing your advice on something you learned during medical school or your training? Was it included in a course devoted to nutrition? Did you learn it later as part of continuing medical education course (CME)? Or was it just something you just picked up from your experience seeing patients (osmosis)? It is very unlikely that a significant portion, or any part for that matter, of your medical training was devoted to nutrition. It certainly wasn’t during my training.
I recently read an interview with Emily M. Broad Leib, JD, faculty director of the Harvard School Center for Health Law and Policy Innovation, Cambridge, Massachusetts, who would like to correct that deficiency. She feels doctors need to know more about food and that acquiring that knowledge should be a significant component of their formal training.
In the interview, Leib said that “roughly 86% of physicians report they do not feel adequately trained to answer basic questions on diet or nutrition.” She also notes that while “72% of entering medical students report they believe food is important to health” less than 50% retained this belief after graduation.
Leib and associates feel they have recently reached a milestone in their efforts to include nutrition in the mainstream of medical education this fall by publishing a paper that demonstrates “consensus on doctor-approved nutritional standard for medical schools and residency programs.”
36 Recommended Competencies
Curious about what these nutrition experts chose to include in medical training, I decided to drill down into the list of 36 consensus-driven competencies they had agreed upon.
It was an interesting voyage into a forest of redundancies, many of which can be boiled down to having the student demonstrate that he/she understands that what we eat is important to our health and that there is a complex web of relationships connecting our society to the food consume.
Some of the recommended competencies I found make perfect sense. For example the student/trainee should be able to take a diet and food history and be able to interpret lab values and anthropometric measurements and be able to discuss the patient’s weight and diet with sensitivity while keeping in mind his/her own biases about food.
Some other recommendations are more problematic, for example, “performs a comprehensive nutrition-focused physical examination” or “demonstrates knowledge of how to create culinary nutrition SMART [Specific, Measurable, Achievable, Relevant, and Time-Bound] goals for personal use and for patient care” or “provides brief counseling interventions to help patients decrease visceral adiposity or reduce the risk of metabolic syndrome.” Including competencies like these demonstrates a lack of understanding of the time restraints and realities of a primary care physician’s life and training.
Instead of simply reinforcing the prospective physician’s preexisting assumption that food and health are entwined and discussing when and how to consult a nutrition expert, these 36 competencies seem to be an attempt to create fast-tracked part-time dietitians and nutrition advocates out of medical students and trainees who already believe that nutrition is important for health but also have a very full plate of clinical responsibilities ahead of them.
The study that Leib quotes — that 72% of medical students believed food was important in health while after graduation only 50% of agreed — doesn’t necessarily mean that professors are preaching that food was unimportant. It is more likely by the end of medical school the students have seen that food must share the spotlight with numerous other factors that influence their patients’ health.
‘A More Appropriate Focus’
In my experience, diet and lifestyle counseling done well is extremely time consuming and best done by people for whom that is their specialty. A more appropriate focus for a list of nutritional competencies for physicians in training would be for the student to achieve an understanding of when and how to consult a dietitian and then how to support and evaluate the dietitian’s recommendations to the patient.
Finally, I don’t think we can ignore a serious public relations problem that hangs like a cloud over the nutrition advocacy community. It is the same one that casts a shadow on the medical community as well. It is a common perception among the lay public that nutritionists (and physicians) are always changing their recommendations when it comes to food. What is believable? Just think about eggs, red wine, or introducing peanuts to infants, to name just a few. And what about the food pyramids that seem to have been rebuilt every several years? The problem is compounded when some “credentialed” nutritionists and physicians continue to make dietary pronouncements with only a shred of evidence or poorly documented anecdotal observations.
The first of the 36 competencies I reviewed reads: “Provide evidence-based, culturally sensitive nutrition and food recommendations for the prevention and treatment of disease.” When it comes to nutrition the “evidence” can be tough to come by. The natural experiments in which individuals and populations had extremely limited access to a certain nutrients (eg, scurvy) don’t occur very often. Animal studies don’t always extrapolate to humans. And, observational studies concerning diet often have co-factors that are difficult to control and must run over time courses that can tax even the most patient researchers.
I certainly applaud Leib and associates for promoting their primary goal of including more about of the relationship between food and health in the medical school and trainee curriculum. But I must voice a caution to be careful to keep it truly evidence-based and in a format that acknowledges the realities of the life and education of a primary care provider.
The best nutritional advice I ever received in my training was from an older pediatric professor who suggested that a healthy diet consisted of everything in moderation.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
New Drug Options Abound for Duchenne Muscular Dystrophy
SAVANNAH, GEORGIA — When Ann & Robert H. Lurie Children’s Hospital of Chicago pediatric neurologist Nancy L. Kuntz, MD, was a fellow about 45 years ago, there were few more devastating diagnoses than Duchenne muscular dystrophy (DMD).
“The rule of thumb was that they would stop walking by age 10 and probably die around age 20, and there was not much we could do,” Kuntz told colleagues at the American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) 2024.
Now, “In the last 8 years, we’ve seen eight different therapies that are FDA-approved specifically for Duchenne, and many more are in the pipeline,” said session moderator Kathryn Mosher, MD, a pediatric physical medicine and rehabilitation physician at Akron Children’s Hospital, Akron, Ohio.
This is both good news and a new challenge for clinicians: Which of these treatments are best for which patients? Kuntz said the traditional therapy of corticosteroids is still crucial. However, “there are still families begging to not use steroids, or refusing to use steroids, just not filling the prescriptions,” she said.
Beware of Parents Who Reject Steroids
The failure to use steroids “breaks your heart” because data show their impact on “really important functions like walking and being able to get up from the ground,” she said. “You can add months and years to life with this treatment.”
However, “while we have shown that using corticosteroids makes a difference, I don’t think that we’ve really worked out the best age at which to start the steroids, or the dosing schedule, or even the type of steroids,” she cautioned.
In an accompanying presentation about therapy for DMD, pediatric neurologist Craig M. Zaidman, MD, of Washington University in St. Louis, Missouri, cautioned that “daily steroids make a big impact on your growth and particularly on your height.”
In particular, the corticosteroid deflazacort has been linked to more cataracts than prednisone and less weight gain and height growth. “They really don’t grow, they don’t get taller, and they also don’t gain weight. They look like little boys when they’re 13 years old.”
Deflazacort or Vamorolone?
Vamorolone (Agamree) is a cheaper corticosteroid alternative to deflazacort (Emflaza), and a 2024 study showed no difference in functional outcomes over 48 weeks, he said. Also, daily vamorolone does a better job of preserving height growth than daily prednisone, he said, and he’s seen less risk for vertebral fractures.
Where do newer drugs fit in? One crucial thing to know about the new generation of targeted therapies is that they’re often mutation-dependent, Kuntz said. They may only work in patients with certain mutations, or mutations may lead to more side effects.
“You should have the exact mutation of your patient, and then you can look and see what they’re eligible for,” she said.
$700,000 a Year for Givinostat
Zaidman highlighted the newly approved givinostat (Duvyzat), a histone deacetylase inhibitor approved for boys 6 years or older. The cost is $700,000 a year, he said, and it’s been linked to less decline in four-stair climb per a double-blind, placebo-controlled, phase 3 trial.
The drug can cause side effects such as reducing platelets, boosting triglycerides, and inducing gastrointestinal problems. “When you drop the dose, these problems go away,” he said.
Does givinostat work? While trial data are challenging to interpret, they do suggest that patients “will lose skill, but they might not lose two or three skills they otherwise would have,” Zaidman said. “To me, that’s quite compelling.”
As for exon-skipping therapies, another new-generation option for DMD, he noted that “these drugs are on the market based on their accelerated approval. We will never have the perfect phase 3, randomized, controlled, long-term trial for these. It’s just not going to come. This is what we get.”
Mosher disclosed the advisory board (Sarepta Therapeutics, Pfizer, Reata Pharmaceuticals, and PTC). Kuntz disclosed advisory board (Astellas Pharma, Inc., argenx, Catalyst, Entrada Therapeutics, Genentech, and Novartis), exchange expert on-demand program (Sarepta Therapeutics), speaker (Genentech, Sarepta Therapeutics, and Solid), and research funding (Astellas Pharma, Inc., argenx, Biogen, Catalyst, Genentech, Novartis, and Sarepta Therapeutics). Zaidman disclosed speaking/advisor/consulting (Sarepta Therapeutics and Optum) and research funding (Novartis and Biogen).
A version of this article appeared on Medscape.com.
SAVANNAH, GEORGIA — When Ann & Robert H. Lurie Children’s Hospital of Chicago pediatric neurologist Nancy L. Kuntz, MD, was a fellow about 45 years ago, there were few more devastating diagnoses than Duchenne muscular dystrophy (DMD).
“The rule of thumb was that they would stop walking by age 10 and probably die around age 20, and there was not much we could do,” Kuntz told colleagues at the American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) 2024.
Now, “In the last 8 years, we’ve seen eight different therapies that are FDA-approved specifically for Duchenne, and many more are in the pipeline,” said session moderator Kathryn Mosher, MD, a pediatric physical medicine and rehabilitation physician at Akron Children’s Hospital, Akron, Ohio.
This is both good news and a new challenge for clinicians: Which of these treatments are best for which patients? Kuntz said the traditional therapy of corticosteroids is still crucial. However, “there are still families begging to not use steroids, or refusing to use steroids, just not filling the prescriptions,” she said.
Beware of Parents Who Reject Steroids
The failure to use steroids “breaks your heart” because data show their impact on “really important functions like walking and being able to get up from the ground,” she said. “You can add months and years to life with this treatment.”
However, “while we have shown that using corticosteroids makes a difference, I don’t think that we’ve really worked out the best age at which to start the steroids, or the dosing schedule, or even the type of steroids,” she cautioned.
In an accompanying presentation about therapy for DMD, pediatric neurologist Craig M. Zaidman, MD, of Washington University in St. Louis, Missouri, cautioned that “daily steroids make a big impact on your growth and particularly on your height.”
In particular, the corticosteroid deflazacort has been linked to more cataracts than prednisone and less weight gain and height growth. “They really don’t grow, they don’t get taller, and they also don’t gain weight. They look like little boys when they’re 13 years old.”
Deflazacort or Vamorolone?
Vamorolone (Agamree) is a cheaper corticosteroid alternative to deflazacort (Emflaza), and a 2024 study showed no difference in functional outcomes over 48 weeks, he said. Also, daily vamorolone does a better job of preserving height growth than daily prednisone, he said, and he’s seen less risk for vertebral fractures.
Where do newer drugs fit in? One crucial thing to know about the new generation of targeted therapies is that they’re often mutation-dependent, Kuntz said. They may only work in patients with certain mutations, or mutations may lead to more side effects.
“You should have the exact mutation of your patient, and then you can look and see what they’re eligible for,” she said.
$700,000 a Year for Givinostat
Zaidman highlighted the newly approved givinostat (Duvyzat), a histone deacetylase inhibitor approved for boys 6 years or older. The cost is $700,000 a year, he said, and it’s been linked to less decline in four-stair climb per a double-blind, placebo-controlled, phase 3 trial.
The drug can cause side effects such as reducing platelets, boosting triglycerides, and inducing gastrointestinal problems. “When you drop the dose, these problems go away,” he said.
Does givinostat work? While trial data are challenging to interpret, they do suggest that patients “will lose skill, but they might not lose two or three skills they otherwise would have,” Zaidman said. “To me, that’s quite compelling.”
As for exon-skipping therapies, another new-generation option for DMD, he noted that “these drugs are on the market based on their accelerated approval. We will never have the perfect phase 3, randomized, controlled, long-term trial for these. It’s just not going to come. This is what we get.”
Mosher disclosed the advisory board (Sarepta Therapeutics, Pfizer, Reata Pharmaceuticals, and PTC). Kuntz disclosed advisory board (Astellas Pharma, Inc., argenx, Catalyst, Entrada Therapeutics, Genentech, and Novartis), exchange expert on-demand program (Sarepta Therapeutics), speaker (Genentech, Sarepta Therapeutics, and Solid), and research funding (Astellas Pharma, Inc., argenx, Biogen, Catalyst, Genentech, Novartis, and Sarepta Therapeutics). Zaidman disclosed speaking/advisor/consulting (Sarepta Therapeutics and Optum) and research funding (Novartis and Biogen).
A version of this article appeared on Medscape.com.
SAVANNAH, GEORGIA — When Ann & Robert H. Lurie Children’s Hospital of Chicago pediatric neurologist Nancy L. Kuntz, MD, was a fellow about 45 years ago, there were few more devastating diagnoses than Duchenne muscular dystrophy (DMD).
“The rule of thumb was that they would stop walking by age 10 and probably die around age 20, and there was not much we could do,” Kuntz told colleagues at the American Association of Neuromuscular & Electrodiagnostic Medicine (AANEM) 2024.
Now, “In the last 8 years, we’ve seen eight different therapies that are FDA-approved specifically for Duchenne, and many more are in the pipeline,” said session moderator Kathryn Mosher, MD, a pediatric physical medicine and rehabilitation physician at Akron Children’s Hospital, Akron, Ohio.
This is both good news and a new challenge for clinicians: Which of these treatments are best for which patients? Kuntz said the traditional therapy of corticosteroids is still crucial. However, “there are still families begging to not use steroids, or refusing to use steroids, just not filling the prescriptions,” she said.
Beware of Parents Who Reject Steroids
The failure to use steroids “breaks your heart” because data show their impact on “really important functions like walking and being able to get up from the ground,” she said. “You can add months and years to life with this treatment.”
However, “while we have shown that using corticosteroids makes a difference, I don’t think that we’ve really worked out the best age at which to start the steroids, or the dosing schedule, or even the type of steroids,” she cautioned.
In an accompanying presentation about therapy for DMD, pediatric neurologist Craig M. Zaidman, MD, of Washington University in St. Louis, Missouri, cautioned that “daily steroids make a big impact on your growth and particularly on your height.”
In particular, the corticosteroid deflazacort has been linked to more cataracts than prednisone and less weight gain and height growth. “They really don’t grow, they don’t get taller, and they also don’t gain weight. They look like little boys when they’re 13 years old.”
Deflazacort or Vamorolone?
Vamorolone (Agamree) is a cheaper corticosteroid alternative to deflazacort (Emflaza), and a 2024 study showed no difference in functional outcomes over 48 weeks, he said. Also, daily vamorolone does a better job of preserving height growth than daily prednisone, he said, and he’s seen less risk for vertebral fractures.
Where do newer drugs fit in? One crucial thing to know about the new generation of targeted therapies is that they’re often mutation-dependent, Kuntz said. They may only work in patients with certain mutations, or mutations may lead to more side effects.
“You should have the exact mutation of your patient, and then you can look and see what they’re eligible for,” she said.
$700,000 a Year for Givinostat
Zaidman highlighted the newly approved givinostat (Duvyzat), a histone deacetylase inhibitor approved for boys 6 years or older. The cost is $700,000 a year, he said, and it’s been linked to less decline in four-stair climb per a double-blind, placebo-controlled, phase 3 trial.
The drug can cause side effects such as reducing platelets, boosting triglycerides, and inducing gastrointestinal problems. “When you drop the dose, these problems go away,” he said.
Does givinostat work? While trial data are challenging to interpret, they do suggest that patients “will lose skill, but they might not lose two or three skills they otherwise would have,” Zaidman said. “To me, that’s quite compelling.”
As for exon-skipping therapies, another new-generation option for DMD, he noted that “these drugs are on the market based on their accelerated approval. We will never have the perfect phase 3, randomized, controlled, long-term trial for these. It’s just not going to come. This is what we get.”
Mosher disclosed the advisory board (Sarepta Therapeutics, Pfizer, Reata Pharmaceuticals, and PTC). Kuntz disclosed advisory board (Astellas Pharma, Inc., argenx, Catalyst, Entrada Therapeutics, Genentech, and Novartis), exchange expert on-demand program (Sarepta Therapeutics), speaker (Genentech, Sarepta Therapeutics, and Solid), and research funding (Astellas Pharma, Inc., argenx, Biogen, Catalyst, Genentech, Novartis, and Sarepta Therapeutics). Zaidman disclosed speaking/advisor/consulting (Sarepta Therapeutics and Optum) and research funding (Novartis and Biogen).
A version of this article appeared on Medscape.com.
FROM AANEM 2024
Skin Fungal Infections Increasing in the United States
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
. Tinea unguium, tinea pedis, and tinea corporis were among the most common infections.
METHODOLOGY:
- Researchers analyzed data from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 2005 to 2016, to evaluate trends in the prevalence of SCFIs during this period.
- The analysis included over 13 billion ambulatory visits to nonfederally funded community, office-based physician practices, and emergency or outpatient departments in the United States, with an estimated 1,104,258,333 annual average.
- The Jonckheere-Terpstra nonparametric test for trend was used to determine the pattern of SCFI prevalence over the 12-year period.
TAKEAWAY:
- SCFIs constituted approximately 0.54% of all annual ambulatory visits, with an estimated 6,001,852 visits for SCFIs per year and over 72 million total visits for the infections during the study period.
- Tinea unguium, tinea pedis, and tinea corporis were the most common infections, comprising 20.5%, 12.2%, and 12.0% of the total visits, respectively.
- Researchers noted an increasing trend in annual SCFIs (P = .03).
IN PRACTICE:
“We observed a high burden of SCFIs among outpatient visits in the United States and an increasing trend in their prevalence,” the authors wrote. These results, they added, “highlight the importance of healthcare providers being able to identify, treat, and, when necessary, refer patients with SCFIs, as a high burden of disease is associated with a significant negative impact on the individual and population levels.”
SOURCE:
The study was co-led by Sarah L. Spaulding, BS, and A. Mitchel Wride, BA, from the Yale School of Medicine, New Haven, Connecticut, and was published online October 30 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The authors did not list any study limitations.
DISCLOSURES:
The lead authors were supported by Yale School of Medicine Medical Student Research Fellowships. Two other authors declared receiving consulting fees, research funding, and licensing fees outside the submitted work and also served on a data and safety monitoring board for Advarra Inc.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
IBS: Understanding a Common Yet Misunderstood Condition
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
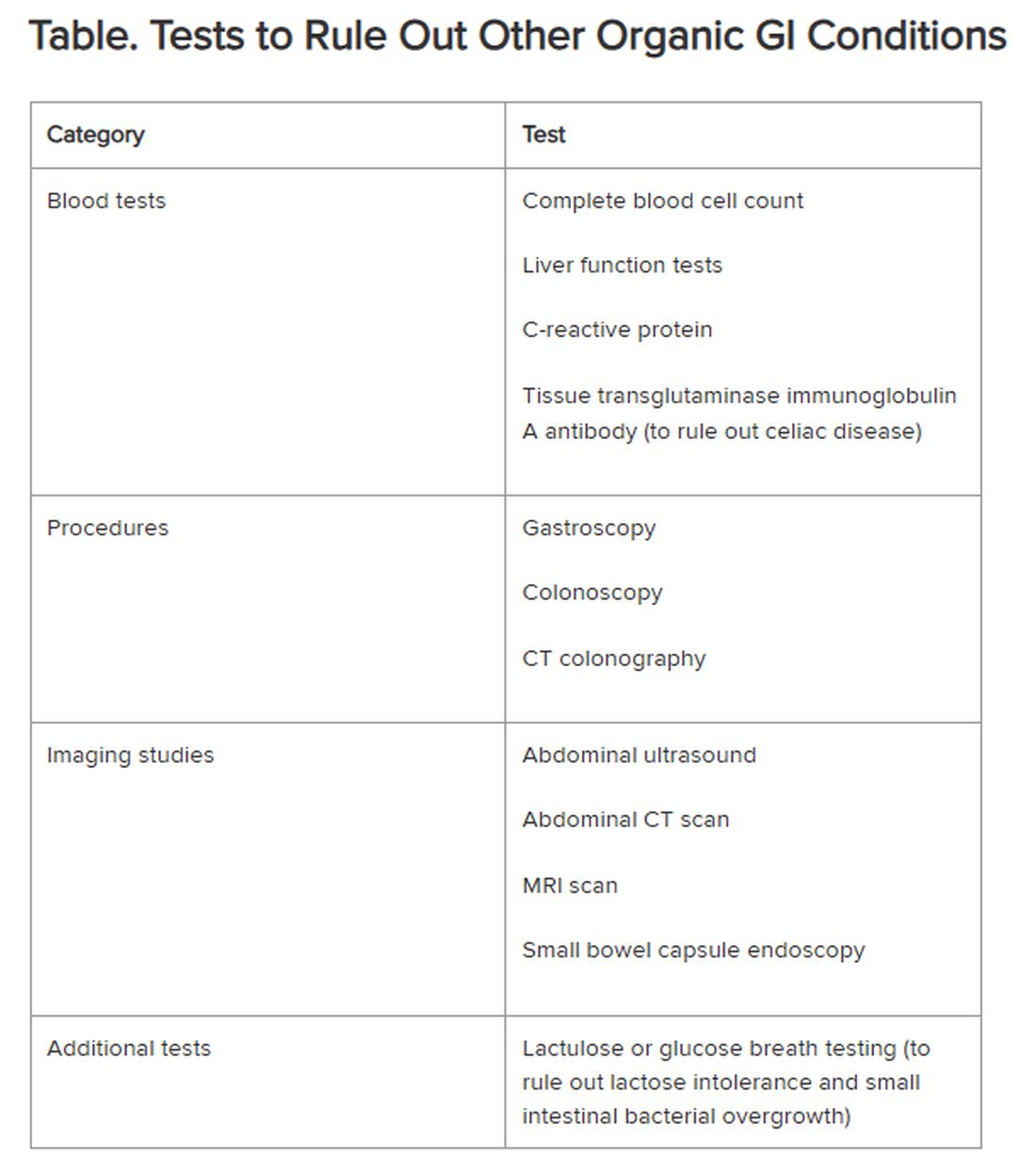
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.
Irritable bowel syndrome (IBS) is one of the most common conditions encountered by both primary care providers and gastroenterologists, with a pooled global prevalence of 11.2%. This functional bowel disorder is characterized by abdominal pain or discomfort, diarrhea and/or constipation, and bloating.
Unfortunately, , according to Alan Desmond, MB, consultant in gastroenterology and general internal medicine, Torbay Hospital, UK National Health Service.
Desmond regularly sees patients who either haven’t been accurately diagnosed or have been told, “Don’t worry, it’s ‘just’ irritable bowel syndrome,” he said at the recent International Conference on Nutrition in Medicine.
A 2017 study involving nearly 2000 patients with a history of gastrointestinal (GI) symptoms found that 43.1% of those who met the criteria for IBS were undiagnosed, and among those who were diagnosed, 26% were not receiving treatment.
“Many clinicians vastly underestimate the impact functional GI symptoms have on our patients in lack of productivity, becoming homebound or losing employment, the inability to enjoy a meal with friends or family, and always needing to know where the nearest bathroom is, for example,” Desmond said in an interview.
IBS can profoundly affect patients’ mental health. One study found that 38% of patients with IBS attending a tertiary care clinic contemplated suicide because they felt hopeless about ever achieving symptom relief.
Today, several dietary, pharmacologic, and psychological/behavioral approaches are available to treat patients with IBS, noted William D. Chey, MD, AGAF, chief of the Division of Gastroenterology and Hepatology, University of Michigan, Ann Arbor, Michigan.
“Each individual patient may need a different combination of these foundational treatments,” he said. “One size doesn’t fit all.”
Diagnostic Pathway
One reason IBS is so hard to diagnose is that it’s a “symptom-based disorder, with identification of the condition predicated upon certain key characteristics that are heterogeneous,” Chey said in an interview. “IBS in patient ‘A’ may not present the same way as IBS in patient ‘B,’ although there are certain foundational common characteristics.”
IBS involves “abnormalities in the motility and contractility of the GI tract,” he said. It can present with diarrhea (IBS-D), constipation (IBS-C), or a mixture or alternation of diarrhea and constipation (IBS-M).
Patients with IBS-D often have an exaggerated gastro-colonic response, while those with IBS-C often have a blunted response.
Beyond stool abnormalities and abdominal pain/discomfort, patients often report bloating/distension, low backache, lethargy, nausea, thigh pain, and urinary and gynecologic symptoms.
Historically, IBS has been regarded as a “diagnosis of exclusion” because classic diagnostic tests typically yield no concrete findings. Desmond noted that several blood tests, procedures, imaging studies, and other tests are available to rule out other organic GI conditions, as outlined in the Table.
If the patient comes from a geographical region where giardia is endemic, clinicians also should consider testing for the parasite, Chey said.
New Understanding of IBS Etiology
Now, advances in the understanding of IBS are changing the approach to the disease.
“The field is moving away from seeing IBS as a ‘wastebasket diagnosis,’ recognizing that there are other causes of a patient’s symptoms,” Mark Pimentel, MD, associate professor of medicine and gastroenterology, Cedars-Sinai, Los Angeles, said in an interview. “What’s made IBS so difficult to diagnose has been the absence of biological markers and hallmark findings on endoscopy.”
Recent research points to novel bacterial causes as culprits in the development of IBS. In particular, altered small bowel microbiota can be triggered by acute gastroenteritis.
Food poisoning can trigger the onset of IBS — a phenomenon called “postinfectious IBS (PI-IBS),” said Pimentel, who is also executive director of the Medically Associated Science and Technology Program at Cedars-Sinai. PI-IBS almost always takes the form of IBS-D, with up to 60% of patients with IBS-D suffering the long-term sequelae of food poisoning.
The types of bacteria most commonly associated with gastroenteritis are Shigella, Campylobacter, Salmonella, and Escherichia coli, Pimentel said. All of them release cytolethal distending toxin B (CdtB), causing the body to produce antibodies to the toxin.
CdtB resembles vinculin, a naturally occurring protein critical for healthy gut function. “Because of this molecular resemblance, the immune system often mistakes one for the other, producing anti-vinculin,” Pimentel explained.
This autoimmune response leads to disruptions in the gut microbiome, ultimately resulting in PI-IBS. The chain of events “doesn’t necessarily happen immediately,” Pimentel said. “You might have developed food poisoning at a party weeks or months ago.”
Acute gastroenteritis is common, affecting as many as 179 million people in the United States annually. A meta-analysis of 47 studies, incorporating 28,270 patients, found that those who had experienced acute gastroenteritis had a fourfold higher risk of developing IBS compared with nonexposed controls.
“The problem isn’t only the IBS itself, but the fact that people with PI-IBS are four times as likely to contract food poisoning again, which can further exacerbate IBS symptoms,” Pimentel said.
Diarrhea-predominant IBS can be detected through the presence of two blood biomarkers — anti-CdtB and anti-vinculin — in a blood test developed by Pimentel and his group.
“Elevation in either of these biomarkers establishes the diagnosis,” Pimentel said. “This is a breakthrough because it represents the first test that can make IBS a ‘diagnosis of inclusion.’”
The blood test also can identify IBS-M but not IBS-C.
Pimentel said that IBS-C is associated with increased levels of methanogenic archaea, which can be diagnosed by a positive methane breath test. “Methane gas slows intestinal contractility, which might result in constipation,” he said.
Diet as a Treatment Option
Diet is usually the starting point for IBS treatment, Chey said. “The standard dietary recommendations, as defined by the National Institute for Health and Care Excellence Guidance for managing IBS, are reasonable and common sense — eating three meals a day, avoiding carbonated beverages, excess alcohol, and excess caffeine, and avoiding hard-to-digest foods that can be gas producing.”
A diet low in fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs), which are carbohydrates that aren’t completely absorbed in the intestines, has been shown to be effective in alleviating GI distress in as many as 86% of patients with IBS, leading to improvements in overall GI symptoms as well as individual symptoms (eg, abdominal pain, bloating, constipation, diarrhea, and flatulence).
Desmond recommends the low FODMAP program delineated by Monash University in Australia. The diet should be undertaken only under the supervision of a dietitian, he warned. Moreover, following it on a long-term basis can have an adverse impact on dietary quality and the gut microbiome. Therefore, “it’s important to embark on stepwise reintroduction of FODMAPS under supervision to find acceptable thresholds that don’t cause a return of symptoms.”
A growing body of research suggests that following the Mediterranean diet can be helpful in reducing IBS symptoms. Chey said that some patients who tend to over-restrict their eating might benefit from a less restrictive diet than the typical low FODMAPs diet. For them, the Mediterranean diet may be a good option.
Pharmacotherapy for IBS
Nutritional approaches aren’t for everyone, Chey noted. “Some people don’t want to be on a highly restricted diet.” For them, medications addressing symptoms might be a better option.
Antispasmodics — either anticholinergics (hyoscine and dicyclomine) or smooth muscle relaxants (alverine, mebeverine, and peppermint oil) — can be helpful, although they can worsen constipation in a dose-dependent manner. It is advisable to use them on an as-needed rather than long-term basis.
Antidiarrheal agents include loperamide and diphenoxylate.
For constipation, laxatives (eg, senna, bisacodyl, polyethylene glycol, and sodium picosulfate) can be helpful.
Desmond noted that the American Gastroenterological Association does not recommend routine use of probiotics for most GI disorders, including IBS. Exceptions include prevention of Clostridioides difficile, ulcerative colitis, and pouchitis.
Targeting the Gut-Brain Relationship
Stress plays a role in exacerbating symptoms in patients with IBS and is an important target for intervention.
“If patients are living with a level of stress that’s impairing, we won’t be able to solve their gut issues until we resolve their stress issues,” Desmond said. “We need to calm the gut-microbiome-brain axis, which is multidimensional and bidirectional.”
Many people — even those without IBS — experience queasiness or diarrhea prior to a major event they’re nervous about, Chey noted. These events activate the brain, which activates the nervous system, which interacts with the GI tract. Indeed, IBS is now recognized as a disorder of gut-brain interaction, he said.
“We now know that the microbiome in the GI tract influences cognition and emotional function, depression, and anxiety. One might say that the gut is the ‘center of the universe’ to human beings,” Chey said.
Evidence-based psychological approaches for stress reduction in patients with IBS include cognitive behavioral therapy, specifically tailored to helping the patient identify associations between IBS symptoms and thoughts, emotions, and actions, as well as learning new behaviors and engaging in stress management. Psychodynamic (interpersonal) therapy enables patients to understand the connection between GI symptoms and interpersonal conflicts, emotional factors, or relationship difficulties.
Gut-directed hypnotherapy (GDH) is a “proven modality for IBS,” Desmond said. Unlike other forms of hypnotherapy, GDH focuses specifically on controlling and normalizing GI function. Studies have shown a reduction of ≥ 30% in abdominal pain in two thirds of participants, with overall response rates up to 85%. It can be delivered in an individual or group setting or via a smartphone.
Desmond recommends mindfulness-based therapy (MBT) for IBS. MBT focuses on the “cultivation of mindfulness, defined as intentional, nonjudgmental, present-focused awareness.” It has been found effective in reducing flares and the markers of gut inflammation in ulcerative colitis, as well as reducing symptoms of IBS.
Chey noted that an emerging body of literature supports the potential role of acupuncture in treating IBS, and his clinic employs it. “I would like to see further research into other areas of CAM [complementary and alternative medicine], including herbal approaches to IBS symptoms as well as stress.”
Finally, all the experts agree that more research is needed.
“The real tragedy is that the NIH invests next to nothing in IBS, in contrast to inflammatory bowel disease and many other conditions,” Pimentel said. “Yet IBS is 45 times more common than inflammatory bowel disease.”
Pimentel hopes that with enough advocacy and recognition that IBS isn’t “just stress-related,” more resources will be devoted to understanding this debilitating condition.
Desmond is the author of a book on the benefits of a plant-based diet. He has also received honoraria, speaking, and consultancy fees from the European Space Agency, Dyson Institute of Engineering and Technology, Riverford Organic Farmers, Ltd., Salesforce Inc., Sentara Healthcare, Saudi Sports for All Federation, the Physicians Committee for Responsible Medicine, The Plantrician Project, Doctors for Nutrition, and The Happy Pear.
Pimentel is a consultant for Bausch Health, Ferring Pharmaceuticals, and Ardelyx. He holds equity in and is also a consultant for Dieta Health, Salvo Health, Cylinder Health, and Gemelli Biotech. Cedars-Sinai has a licensing agreement with Gemelli Biotech and Hobbs Medical.
Chey is a consultant to AbbVie, Ardelyx, Atmo, Biomerica, Gemelli Biotech, Ironwood Pharmaceuticals, Nestlé, QOL Medical, Phathom Pharmaceuticals, Redhill, Salix/Valeant, Takeda, and Vibrant. He receives grant/research funding from Commonwealth Diagnostics International, Inc., US Food and Drug Administration, National Institutes of Health, QOL Medical, and Salix/Valeant. He holds stock options in Coprata, Dieta Health, Evinature, FoodMarble, Kiwi Biosciences, and ModifyHealth. He is a board or advisory panel member of the American College of Gastroenterology, GI Health Foundation, International Foundation for Gastrointestinal Disorders, Rome. He holds patents on My Nutrition Health, Digital Manometry, and Rectal Expulsion Device.
A version of this article appeared on Medscape.com.