User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Nulliparity, not ART, likely raises risk of ovarian cancer
Women who receive ovarian stimulation for assisted reproductive technology (ART) procedures don’t have an increased risk of developing ovarian cancer when compared to subfertile women who don’t undergo ART, according to a new study.
The results suggest that nulliparity is likely responsible for the increased risk of ovarian cancer observed in patients treated with ART, the researchers said.
Earlier, shorter studies had only compared ART-treated women with women from the general population.
“Subfertile women differ from women in the general population according to several ovarian cancer risk factors. Therefore, to estimate the risk of ovarian cancer associated with ART, it was important to include a comparison group of women who were subfertile and not treated with ART,” said senior study author Flora E. van Leeuwen, PhD, of Netherlands Cancer Institute in Amsterdam.
She and her colleagues conducted a nationwide cohort study of 30,625 women who received ovarian stimulation for ART during 1983-2000 and 9,988 women who received fertility treatments other than ART.
Incident invasive and borderline ovarian tumors were ascertained through linkage with the Netherlands Cancer Registry and the Dutch Pathology Registry. Ovarian tumor risk in ART-treated women was compared with risks in the general population and the subfertile non-ART group.
The researchers reported the results in the Journal of the National Cancer Institute.
Risk of ovarian cancer
Women treated with ART were no more likely to develop ovarian cancer than subfertile women not treated with ART (adjusted hazard ratio, 1.02), but the ART group did have an increased risk of ovarian cancer when compared to the general population (standardized incidence ratio, 1.43).
“This, however, turned out to be due to the fact that the women who had received ART were less likely to have children. Not having children is a known risk factor for ovarian cancer,” Dr. van Leeuwen said.
Women with more ART procedures that resulted in the birth of a child were at lower risk of developing ovarian cancer, compared with women without any successful cycle (Ptrend = .001). However, women who had only cycles not resulting in a birth were not at higher risk of ovarian cancer when they had a greater number of cycles.
“These results indicate that parity decreases the risk of ovarian cancer, also in ART-treated women. But more unsuccessful ART cycles do not increase the risk of ovarian cancer,” Dr. van Leeuwen said.
Risk of borderline ovarian tumors
The risk of developing borderline ovarian tumors was roughly twice as high in women who had received ART, both compared with women who had received other fertility treatments (hazard ratio, 1.84) and women from the general population (standardized incidence ratio, 2.20).
However, the risk of developing borderline ovarian tumors did not increase in women who had received multiple ART procedures.
“If there was a causal association between ART and increased risk of borderline ovarian tumors, we would expect to see this risk increase with a greater number of ART procedures from more hormones and more stimulation of the ovaries. This makes the direct link between ART and increased risk of borderline tumors a bit uncertain. It might be caused by other factors, such as the severity of infertility,” Dr. van Leeuwen said.
Borderline ovarian tumors are rare in the general population in the Netherlands, and women who develop these tumors generally have a good prognosis, she said.
The risk of developing a borderline tumor before the age of 55 for women in the Netherlands is approximately 0.2%. After ART, the study found a risk of approximately 0.3%.
Causal associations with ART 'unlikely'
“Women who develop cancer and have undergone ART procedures in the past may wonder whether their cancer may be caused by ART. Based on the results from our study, that seems unlikely, and that is a very reassuring message from practicing oncologists to women diagnosed with ovarian cancer. Another important message is that, in ART-treated women, increasing parity reduces the risk of ovarian cancer,” Dr. van Leeuwen said.
She added that the risk of borderline ovarian tumors did not increase in women who received multiple ART procedures, “which makes it somewhat less likely that ART would have caused their borderline ovarian tumor.”
The study does not exclude the possibility that ART might increase the risk of ovarian tumors after age 60.
“Despite our long follow-up, the age of the women at the end of our study was still relatively young [average 56 years]. Because the incidence of ovarian cancer increases with older age, it is vital to continue to follow these women. Only then can we be sure that ART does not increase the risk of ovarian tumors in the very long run,” Dr. van Leeuwen said.
“This study offers confirmation of several previous studies and provides reassurance about the risk of ovarian cancer after ART procedures,” said Daniel Kenigsberg, MD, of RMA Long Island IVF in New York. Dr. Kenigsberg was not involved in this study but has performed more than 30,000 ART procedures over the past 32 years.
“Researchers have looked at whether fertility drugs cause ovarian cancer in different ways and in different countries, and there is no cause-and-effect relationship. There was no dose-response relationship between ART and ovarian tumors in this study. It’s more likely there is something wrong with the women’s ovaries that lead to borderline tumors and infertility more than any treatment,” Dr. Kenigsberg added.
“Perhaps both fertility and cancer relate to an underlying ovarian issue, but this would not explain the increased cancer incidence in those who never attempted pregnancy, that is, women who are voluntarily childless. Pregnancy is statistically protective: more pregnancies lead to less ovarian cancer, but this is far from absolute,” he explained.
Dr. Kenigsberg suggested that oncologists should be aware of a patient’s obstetrical history and fertility history as well as any related medical interventions.
“Borderline tumors look like cancer and have histologic features of cancer but do not meet the criteria for a cancer diagnosis,” he said. “They require close surveillance because their relationship to the development of full-fledged cancer is uncertain.”
This research was supported by grants from the Dutch Cancer Society. The authors and Dr. Kenigsberg have no conflicts of interest.
Women who receive ovarian stimulation for assisted reproductive technology (ART) procedures don’t have an increased risk of developing ovarian cancer when compared to subfertile women who don’t undergo ART, according to a new study.
The results suggest that nulliparity is likely responsible for the increased risk of ovarian cancer observed in patients treated with ART, the researchers said.
Earlier, shorter studies had only compared ART-treated women with women from the general population.
“Subfertile women differ from women in the general population according to several ovarian cancer risk factors. Therefore, to estimate the risk of ovarian cancer associated with ART, it was important to include a comparison group of women who were subfertile and not treated with ART,” said senior study author Flora E. van Leeuwen, PhD, of Netherlands Cancer Institute in Amsterdam.
She and her colleagues conducted a nationwide cohort study of 30,625 women who received ovarian stimulation for ART during 1983-2000 and 9,988 women who received fertility treatments other than ART.
Incident invasive and borderline ovarian tumors were ascertained through linkage with the Netherlands Cancer Registry and the Dutch Pathology Registry. Ovarian tumor risk in ART-treated women was compared with risks in the general population and the subfertile non-ART group.
The researchers reported the results in the Journal of the National Cancer Institute.
Risk of ovarian cancer
Women treated with ART were no more likely to develop ovarian cancer than subfertile women not treated with ART (adjusted hazard ratio, 1.02), but the ART group did have an increased risk of ovarian cancer when compared to the general population (standardized incidence ratio, 1.43).
“This, however, turned out to be due to the fact that the women who had received ART were less likely to have children. Not having children is a known risk factor for ovarian cancer,” Dr. van Leeuwen said.
Women with more ART procedures that resulted in the birth of a child were at lower risk of developing ovarian cancer, compared with women without any successful cycle (Ptrend = .001). However, women who had only cycles not resulting in a birth were not at higher risk of ovarian cancer when they had a greater number of cycles.
“These results indicate that parity decreases the risk of ovarian cancer, also in ART-treated women. But more unsuccessful ART cycles do not increase the risk of ovarian cancer,” Dr. van Leeuwen said.
Risk of borderline ovarian tumors
The risk of developing borderline ovarian tumors was roughly twice as high in women who had received ART, both compared with women who had received other fertility treatments (hazard ratio, 1.84) and women from the general population (standardized incidence ratio, 2.20).
However, the risk of developing borderline ovarian tumors did not increase in women who had received multiple ART procedures.
“If there was a causal association between ART and increased risk of borderline ovarian tumors, we would expect to see this risk increase with a greater number of ART procedures from more hormones and more stimulation of the ovaries. This makes the direct link between ART and increased risk of borderline tumors a bit uncertain. It might be caused by other factors, such as the severity of infertility,” Dr. van Leeuwen said.
Borderline ovarian tumors are rare in the general population in the Netherlands, and women who develop these tumors generally have a good prognosis, she said.
The risk of developing a borderline tumor before the age of 55 for women in the Netherlands is approximately 0.2%. After ART, the study found a risk of approximately 0.3%.
Causal associations with ART 'unlikely'
“Women who develop cancer and have undergone ART procedures in the past may wonder whether their cancer may be caused by ART. Based on the results from our study, that seems unlikely, and that is a very reassuring message from practicing oncologists to women diagnosed with ovarian cancer. Another important message is that, in ART-treated women, increasing parity reduces the risk of ovarian cancer,” Dr. van Leeuwen said.
She added that the risk of borderline ovarian tumors did not increase in women who received multiple ART procedures, “which makes it somewhat less likely that ART would have caused their borderline ovarian tumor.”
The study does not exclude the possibility that ART might increase the risk of ovarian tumors after age 60.
“Despite our long follow-up, the age of the women at the end of our study was still relatively young [average 56 years]. Because the incidence of ovarian cancer increases with older age, it is vital to continue to follow these women. Only then can we be sure that ART does not increase the risk of ovarian tumors in the very long run,” Dr. van Leeuwen said.
“This study offers confirmation of several previous studies and provides reassurance about the risk of ovarian cancer after ART procedures,” said Daniel Kenigsberg, MD, of RMA Long Island IVF in New York. Dr. Kenigsberg was not involved in this study but has performed more than 30,000 ART procedures over the past 32 years.
“Researchers have looked at whether fertility drugs cause ovarian cancer in different ways and in different countries, and there is no cause-and-effect relationship. There was no dose-response relationship between ART and ovarian tumors in this study. It’s more likely there is something wrong with the women’s ovaries that lead to borderline tumors and infertility more than any treatment,” Dr. Kenigsberg added.
“Perhaps both fertility and cancer relate to an underlying ovarian issue, but this would not explain the increased cancer incidence in those who never attempted pregnancy, that is, women who are voluntarily childless. Pregnancy is statistically protective: more pregnancies lead to less ovarian cancer, but this is far from absolute,” he explained.
Dr. Kenigsberg suggested that oncologists should be aware of a patient’s obstetrical history and fertility history as well as any related medical interventions.
“Borderline tumors look like cancer and have histologic features of cancer but do not meet the criteria for a cancer diagnosis,” he said. “They require close surveillance because their relationship to the development of full-fledged cancer is uncertain.”
This research was supported by grants from the Dutch Cancer Society. The authors and Dr. Kenigsberg have no conflicts of interest.
Women who receive ovarian stimulation for assisted reproductive technology (ART) procedures don’t have an increased risk of developing ovarian cancer when compared to subfertile women who don’t undergo ART, according to a new study.
The results suggest that nulliparity is likely responsible for the increased risk of ovarian cancer observed in patients treated with ART, the researchers said.
Earlier, shorter studies had only compared ART-treated women with women from the general population.
“Subfertile women differ from women in the general population according to several ovarian cancer risk factors. Therefore, to estimate the risk of ovarian cancer associated with ART, it was important to include a comparison group of women who were subfertile and not treated with ART,” said senior study author Flora E. van Leeuwen, PhD, of Netherlands Cancer Institute in Amsterdam.
She and her colleagues conducted a nationwide cohort study of 30,625 women who received ovarian stimulation for ART during 1983-2000 and 9,988 women who received fertility treatments other than ART.
Incident invasive and borderline ovarian tumors were ascertained through linkage with the Netherlands Cancer Registry and the Dutch Pathology Registry. Ovarian tumor risk in ART-treated women was compared with risks in the general population and the subfertile non-ART group.
The researchers reported the results in the Journal of the National Cancer Institute.
Risk of ovarian cancer
Women treated with ART were no more likely to develop ovarian cancer than subfertile women not treated with ART (adjusted hazard ratio, 1.02), but the ART group did have an increased risk of ovarian cancer when compared to the general population (standardized incidence ratio, 1.43).
“This, however, turned out to be due to the fact that the women who had received ART were less likely to have children. Not having children is a known risk factor for ovarian cancer,” Dr. van Leeuwen said.
Women with more ART procedures that resulted in the birth of a child were at lower risk of developing ovarian cancer, compared with women without any successful cycle (Ptrend = .001). However, women who had only cycles not resulting in a birth were not at higher risk of ovarian cancer when they had a greater number of cycles.
“These results indicate that parity decreases the risk of ovarian cancer, also in ART-treated women. But more unsuccessful ART cycles do not increase the risk of ovarian cancer,” Dr. van Leeuwen said.
Risk of borderline ovarian tumors
The risk of developing borderline ovarian tumors was roughly twice as high in women who had received ART, both compared with women who had received other fertility treatments (hazard ratio, 1.84) and women from the general population (standardized incidence ratio, 2.20).
However, the risk of developing borderline ovarian tumors did not increase in women who had received multiple ART procedures.
“If there was a causal association between ART and increased risk of borderline ovarian tumors, we would expect to see this risk increase with a greater number of ART procedures from more hormones and more stimulation of the ovaries. This makes the direct link between ART and increased risk of borderline tumors a bit uncertain. It might be caused by other factors, such as the severity of infertility,” Dr. van Leeuwen said.
Borderline ovarian tumors are rare in the general population in the Netherlands, and women who develop these tumors generally have a good prognosis, she said.
The risk of developing a borderline tumor before the age of 55 for women in the Netherlands is approximately 0.2%. After ART, the study found a risk of approximately 0.3%.
Causal associations with ART 'unlikely'
“Women who develop cancer and have undergone ART procedures in the past may wonder whether their cancer may be caused by ART. Based on the results from our study, that seems unlikely, and that is a very reassuring message from practicing oncologists to women diagnosed with ovarian cancer. Another important message is that, in ART-treated women, increasing parity reduces the risk of ovarian cancer,” Dr. van Leeuwen said.
She added that the risk of borderline ovarian tumors did not increase in women who received multiple ART procedures, “which makes it somewhat less likely that ART would have caused their borderline ovarian tumor.”
The study does not exclude the possibility that ART might increase the risk of ovarian tumors after age 60.
“Despite our long follow-up, the age of the women at the end of our study was still relatively young [average 56 years]. Because the incidence of ovarian cancer increases with older age, it is vital to continue to follow these women. Only then can we be sure that ART does not increase the risk of ovarian tumors in the very long run,” Dr. van Leeuwen said.
“This study offers confirmation of several previous studies and provides reassurance about the risk of ovarian cancer after ART procedures,” said Daniel Kenigsberg, MD, of RMA Long Island IVF in New York. Dr. Kenigsberg was not involved in this study but has performed more than 30,000 ART procedures over the past 32 years.
“Researchers have looked at whether fertility drugs cause ovarian cancer in different ways and in different countries, and there is no cause-and-effect relationship. There was no dose-response relationship between ART and ovarian tumors in this study. It’s more likely there is something wrong with the women’s ovaries that lead to borderline tumors and infertility more than any treatment,” Dr. Kenigsberg added.
“Perhaps both fertility and cancer relate to an underlying ovarian issue, but this would not explain the increased cancer incidence in those who never attempted pregnancy, that is, women who are voluntarily childless. Pregnancy is statistically protective: more pregnancies lead to less ovarian cancer, but this is far from absolute,” he explained.
Dr. Kenigsberg suggested that oncologists should be aware of a patient’s obstetrical history and fertility history as well as any related medical interventions.
“Borderline tumors look like cancer and have histologic features of cancer but do not meet the criteria for a cancer diagnosis,” he said. “They require close surveillance because their relationship to the development of full-fledged cancer is uncertain.”
This research was supported by grants from the Dutch Cancer Society. The authors and Dr. Kenigsberg have no conflicts of interest.
FROM JOURNAL OF THE NATIONAL CANCER INSTITUTE
Case study: Maternal cervical cancer linked to neonate lung cancer
That’s the conclusion of two ground-breaking cases from Japan in which investigators describe lung cancer in two boys that “probably developed” from their respective mothers via vaginal transmission during birth.
“Transmission of maternal cancer to offspring is extremely rare and is estimated to occur in approximately 1 infant per every 500,000 mothers with cancer,” wrote Ayumu Arakawa, MD, of the National Cancer Center Hospital in Japan, and colleagues, in a paper published Jan. 7 in The New England Journal of Medicine.
Previous cases, of which only 18 have been recorded, have been presumed to occur via transplacental transmission, they said.
In the two new cases, genetic analyses and other evidence suggest that both boys’ lung cancers developed after aspirating uterine cervical cancer tumor cells into their lungs during passage through the birth canal.
Tragically, both mothers, each of whom was diagnosed with cervical cancer after the births, died while their boys were still infants.
“Most of the maternal-to-infant cases reported have been leukemia or melanoma,” said Mel Greaves, PhD, of the Institute of Cancer Research, London, who was asked for comment. In 2009, Dr. Greaves and colleagues published a case study of maternal-to-infant cancer transmission (presumably via the placenta). “It attracted an enormous amount of publicity and no doubt some alarm,” he said in an interview. He emphasized that the phenomenon is “incredibly rare.”
Dr. Greaves explains why such transmission is so rare. “We suspect that cancer cells do transit from mum to unborn child more often, but the foreign (aka paternal) antigens (HLA) on the tumor cells prompt immunological rejection. The extremely rare cases of successful transmission probably do depend on the fortuitous loss of paternal HLA.”
Advances in genetic technology may allow such cases, which have been recorded since 1950, to be rapidly identified now, he said.
“Where there is an adult-type cancer in an infant or child whose mother carried cancer when pregnant, then whole-genome sequencing should quickly tell if the infant’s tumor was of maternal origin,” Dr. Greaves explained.
“I think we will be seeing more reports like this in the future, now that this phenomenon has been described and next-generation sequencing is more readily available,” added Mae Zakhour, MD, of the University of California, Los Angeles, Jonsson Comprehensive Cancer Center, when asked for comment.
In the case of the Japanese boys, both cases were discovered incidentally during an analysis of the results of routine next-generation sequencing testing in a prospective gene-profiling trial in cancer patients, known as TOP-GEAR.
How do the investigators know that the spread happened vaginally and not via the placenta?
They explained that, in other cases of mother-to-fetus transmission, the offspring presented with multiple metastases in the brain, bones, liver, lungs, and soft tissues, which were “consistent with presumed hematogenous spread from the placenta.” However, in the two boys, tumors were observed only in the lungs and were localized along the bronchi.
That peribronchial pattern of tumor growth “suggested that the tumors arose from mother-to-infant vaginal transmission through aspiration of tumor-contaminated vaginal fluids during birth.”
In addition, the tumors in both boys lacked the Y chromosome and shared multiple somatic mutations, an HPV genome, and SNP alleles with tumors from the mothers.
“The identical molecular profiles of maternal and pediatric tumors demonstrated by next-generation sequencing, as well as the location of the tumors in the children, provides strong evidence for cancer transmission during delivery,” Dr. Zakhour summarized.
C-section question
The first of the cases reported by the Japanese team was a toddler (23 months) who presented to a local hospital with a 2-week history of a productive cough. Computed tomography revealed multiple masses scattered along the bronchi in both lungs, and a biopsy revealed neuroendocrine carcinoma of the lung.
Notably, the mother’s cervical cancer was not diagnosed during her pregnancy. A cervical cytologic test performed in the mother 7 months before the birth was negative. The infant was delivered transvaginally at 39 weeks of gestation.
It was only 3 months after the birth that the 35-year-old mother received a diagnosis of squamous cell carcinoma of the cervix. She then underwent radical hysterectomy with pelvic lymphadenectomy, followed by chemotherapy.
Had it been known that she had cervical cancer, she may have been advised to have a cesarean section.
The study authors propose, on the basis of their paper, that all women with cervical cancer should have a cesarean section.
But a U.S. expert questioned this, and said the situation is “a bit nuanced.”
William Grobman, MD, of Northwestern University in Chicago, said the current standard recommendation for many pregnant women known to have cervical cancer is to have a cesarean section and that “the strength of the recommendation is dependent on factors such as stage and size.”
However, in an interview, he added that “it may be premature to make a blanket recommendation for all people based on two reports without any idea of the frequency of this event, and with such uncertainty, it seems that disclosure of all information and shared decision-making would be a key approach.”
In this case report, the authors also noted that the cancer found in the toddler looked similar to the cancer in the mother.
“Histologic similarities between the tumor samples from the mother and child prompted us to compare the results of their next-generation sequencing tests,” they said.
The result? “The comparison of the gene profiles in the samples of tumor and normal tissue confirmed that transmission of maternal tumor to the child had occurred.”
The lung cancer in the toddler progressed despite two chemotherapy regimens, so he was enrolled in a clinical trial of nivolumab therapy. He had a response that continued for 7 months, with no appearance of new lesions. Lobectomy was performed to resect a single remaining nodule. The boy had no evidence of disease recurrence at 12 months after lobectomy.
His mother was also enrolled in a nivolumab trial, but her cervical cancer had spread, and she died 5 months after disease progression.
Second case
In the second reported case, a 6-year-old boy presented to a local hospital with chest pain on the left side. Computed tomography revealed a mass in the left lung, and mucinous adenocarcinoma was eventually diagnosed.
In this case, the mother had a cervical polypoid tumor detected during pregnancy. But, as in the other case, cervical cytologic analysis was negative. Because the tumor was stable without any intervention, the mother delivered the boy vaginally at 38 weeks of gestation.
However, after the delivery, biopsy of the cervical lesion revealed adenocarcinoma. The mother underwent radical hysterectomy and bilateral salpingo-oophorectomy 3 months after delivery. She died of the disease 2 years after the surgery.
The boy received chemotherapy and had a partial response, with a reduction in levels of the tumor marker CA19-9 to normal levels. But 3 months later, the disease recurred in the left lung. After more chemotherapy, he underwent total left pneumonectomy and was subsequently free of disease.
The study authors said that they did not suspect maternal transmission of the cancer when her child received a diagnosis at 6 years of age. They explained that metastatic cervical cancer is typically a fast-growing tumor and the slow growth in the child seemed inconsistent with the idea that the cancer had been transmitted to him.
However, the pathology exam showed that the boy had mucinous adenocarcinoma, “which is an unusual morphologic finding for a primary lung tumor, but it was similar to the uterine cervical tumor in the mother,” the authors reported.
Samples of the cervical tumor from the mother and from the lung tumor of the child were submitted for next-generation sequencing tests and, said the authors, indicated mother-to-infant transmission.
The study was supported by grants from the Japan Agency for Medical Research and Development; the National Cancer Center Research and Development Fund; and the Ministry of Education, Culture, Sports, Science and Technology; and funding from Ono Pharmaceutical.
A version of this article first appeared on Medscape.com.
That’s the conclusion of two ground-breaking cases from Japan in which investigators describe lung cancer in two boys that “probably developed” from their respective mothers via vaginal transmission during birth.
“Transmission of maternal cancer to offspring is extremely rare and is estimated to occur in approximately 1 infant per every 500,000 mothers with cancer,” wrote Ayumu Arakawa, MD, of the National Cancer Center Hospital in Japan, and colleagues, in a paper published Jan. 7 in The New England Journal of Medicine.
Previous cases, of which only 18 have been recorded, have been presumed to occur via transplacental transmission, they said.
In the two new cases, genetic analyses and other evidence suggest that both boys’ lung cancers developed after aspirating uterine cervical cancer tumor cells into their lungs during passage through the birth canal.
Tragically, both mothers, each of whom was diagnosed with cervical cancer after the births, died while their boys were still infants.
“Most of the maternal-to-infant cases reported have been leukemia or melanoma,” said Mel Greaves, PhD, of the Institute of Cancer Research, London, who was asked for comment. In 2009, Dr. Greaves and colleagues published a case study of maternal-to-infant cancer transmission (presumably via the placenta). “It attracted an enormous amount of publicity and no doubt some alarm,” he said in an interview. He emphasized that the phenomenon is “incredibly rare.”
Dr. Greaves explains why such transmission is so rare. “We suspect that cancer cells do transit from mum to unborn child more often, but the foreign (aka paternal) antigens (HLA) on the tumor cells prompt immunological rejection. The extremely rare cases of successful transmission probably do depend on the fortuitous loss of paternal HLA.”
Advances in genetic technology may allow such cases, which have been recorded since 1950, to be rapidly identified now, he said.
“Where there is an adult-type cancer in an infant or child whose mother carried cancer when pregnant, then whole-genome sequencing should quickly tell if the infant’s tumor was of maternal origin,” Dr. Greaves explained.
“I think we will be seeing more reports like this in the future, now that this phenomenon has been described and next-generation sequencing is more readily available,” added Mae Zakhour, MD, of the University of California, Los Angeles, Jonsson Comprehensive Cancer Center, when asked for comment.
In the case of the Japanese boys, both cases were discovered incidentally during an analysis of the results of routine next-generation sequencing testing in a prospective gene-profiling trial in cancer patients, known as TOP-GEAR.
How do the investigators know that the spread happened vaginally and not via the placenta?
They explained that, in other cases of mother-to-fetus transmission, the offspring presented with multiple metastases in the brain, bones, liver, lungs, and soft tissues, which were “consistent with presumed hematogenous spread from the placenta.” However, in the two boys, tumors were observed only in the lungs and were localized along the bronchi.
That peribronchial pattern of tumor growth “suggested that the tumors arose from mother-to-infant vaginal transmission through aspiration of tumor-contaminated vaginal fluids during birth.”
In addition, the tumors in both boys lacked the Y chromosome and shared multiple somatic mutations, an HPV genome, and SNP alleles with tumors from the mothers.
“The identical molecular profiles of maternal and pediatric tumors demonstrated by next-generation sequencing, as well as the location of the tumors in the children, provides strong evidence for cancer transmission during delivery,” Dr. Zakhour summarized.
C-section question
The first of the cases reported by the Japanese team was a toddler (23 months) who presented to a local hospital with a 2-week history of a productive cough. Computed tomography revealed multiple masses scattered along the bronchi in both lungs, and a biopsy revealed neuroendocrine carcinoma of the lung.
Notably, the mother’s cervical cancer was not diagnosed during her pregnancy. A cervical cytologic test performed in the mother 7 months before the birth was negative. The infant was delivered transvaginally at 39 weeks of gestation.
It was only 3 months after the birth that the 35-year-old mother received a diagnosis of squamous cell carcinoma of the cervix. She then underwent radical hysterectomy with pelvic lymphadenectomy, followed by chemotherapy.
Had it been known that she had cervical cancer, she may have been advised to have a cesarean section.
The study authors propose, on the basis of their paper, that all women with cervical cancer should have a cesarean section.
But a U.S. expert questioned this, and said the situation is “a bit nuanced.”
William Grobman, MD, of Northwestern University in Chicago, said the current standard recommendation for many pregnant women known to have cervical cancer is to have a cesarean section and that “the strength of the recommendation is dependent on factors such as stage and size.”
However, in an interview, he added that “it may be premature to make a blanket recommendation for all people based on two reports without any idea of the frequency of this event, and with such uncertainty, it seems that disclosure of all information and shared decision-making would be a key approach.”
In this case report, the authors also noted that the cancer found in the toddler looked similar to the cancer in the mother.
“Histologic similarities between the tumor samples from the mother and child prompted us to compare the results of their next-generation sequencing tests,” they said.
The result? “The comparison of the gene profiles in the samples of tumor and normal tissue confirmed that transmission of maternal tumor to the child had occurred.”
The lung cancer in the toddler progressed despite two chemotherapy regimens, so he was enrolled in a clinical trial of nivolumab therapy. He had a response that continued for 7 months, with no appearance of new lesions. Lobectomy was performed to resect a single remaining nodule. The boy had no evidence of disease recurrence at 12 months after lobectomy.
His mother was also enrolled in a nivolumab trial, but her cervical cancer had spread, and she died 5 months after disease progression.
Second case
In the second reported case, a 6-year-old boy presented to a local hospital with chest pain on the left side. Computed tomography revealed a mass in the left lung, and mucinous adenocarcinoma was eventually diagnosed.
In this case, the mother had a cervical polypoid tumor detected during pregnancy. But, as in the other case, cervical cytologic analysis was negative. Because the tumor was stable without any intervention, the mother delivered the boy vaginally at 38 weeks of gestation.
However, after the delivery, biopsy of the cervical lesion revealed adenocarcinoma. The mother underwent radical hysterectomy and bilateral salpingo-oophorectomy 3 months after delivery. She died of the disease 2 years after the surgery.
The boy received chemotherapy and had a partial response, with a reduction in levels of the tumor marker CA19-9 to normal levels. But 3 months later, the disease recurred in the left lung. After more chemotherapy, he underwent total left pneumonectomy and was subsequently free of disease.
The study authors said that they did not suspect maternal transmission of the cancer when her child received a diagnosis at 6 years of age. They explained that metastatic cervical cancer is typically a fast-growing tumor and the slow growth in the child seemed inconsistent with the idea that the cancer had been transmitted to him.
However, the pathology exam showed that the boy had mucinous adenocarcinoma, “which is an unusual morphologic finding for a primary lung tumor, but it was similar to the uterine cervical tumor in the mother,” the authors reported.
Samples of the cervical tumor from the mother and from the lung tumor of the child were submitted for next-generation sequencing tests and, said the authors, indicated mother-to-infant transmission.
The study was supported by grants from the Japan Agency for Medical Research and Development; the National Cancer Center Research and Development Fund; and the Ministry of Education, Culture, Sports, Science and Technology; and funding from Ono Pharmaceutical.
A version of this article first appeared on Medscape.com.
That’s the conclusion of two ground-breaking cases from Japan in which investigators describe lung cancer in two boys that “probably developed” from their respective mothers via vaginal transmission during birth.
“Transmission of maternal cancer to offspring is extremely rare and is estimated to occur in approximately 1 infant per every 500,000 mothers with cancer,” wrote Ayumu Arakawa, MD, of the National Cancer Center Hospital in Japan, and colleagues, in a paper published Jan. 7 in The New England Journal of Medicine.
Previous cases, of which only 18 have been recorded, have been presumed to occur via transplacental transmission, they said.
In the two new cases, genetic analyses and other evidence suggest that both boys’ lung cancers developed after aspirating uterine cervical cancer tumor cells into their lungs during passage through the birth canal.
Tragically, both mothers, each of whom was diagnosed with cervical cancer after the births, died while their boys were still infants.
“Most of the maternal-to-infant cases reported have been leukemia or melanoma,” said Mel Greaves, PhD, of the Institute of Cancer Research, London, who was asked for comment. In 2009, Dr. Greaves and colleagues published a case study of maternal-to-infant cancer transmission (presumably via the placenta). “It attracted an enormous amount of publicity and no doubt some alarm,” he said in an interview. He emphasized that the phenomenon is “incredibly rare.”
Dr. Greaves explains why such transmission is so rare. “We suspect that cancer cells do transit from mum to unborn child more often, but the foreign (aka paternal) antigens (HLA) on the tumor cells prompt immunological rejection. The extremely rare cases of successful transmission probably do depend on the fortuitous loss of paternal HLA.”
Advances in genetic technology may allow such cases, which have been recorded since 1950, to be rapidly identified now, he said.
“Where there is an adult-type cancer in an infant or child whose mother carried cancer when pregnant, then whole-genome sequencing should quickly tell if the infant’s tumor was of maternal origin,” Dr. Greaves explained.
“I think we will be seeing more reports like this in the future, now that this phenomenon has been described and next-generation sequencing is more readily available,” added Mae Zakhour, MD, of the University of California, Los Angeles, Jonsson Comprehensive Cancer Center, when asked for comment.
In the case of the Japanese boys, both cases were discovered incidentally during an analysis of the results of routine next-generation sequencing testing in a prospective gene-profiling trial in cancer patients, known as TOP-GEAR.
How do the investigators know that the spread happened vaginally and not via the placenta?
They explained that, in other cases of mother-to-fetus transmission, the offspring presented with multiple metastases in the brain, bones, liver, lungs, and soft tissues, which were “consistent with presumed hematogenous spread from the placenta.” However, in the two boys, tumors were observed only in the lungs and were localized along the bronchi.
That peribronchial pattern of tumor growth “suggested that the tumors arose from mother-to-infant vaginal transmission through aspiration of tumor-contaminated vaginal fluids during birth.”
In addition, the tumors in both boys lacked the Y chromosome and shared multiple somatic mutations, an HPV genome, and SNP alleles with tumors from the mothers.
“The identical molecular profiles of maternal and pediatric tumors demonstrated by next-generation sequencing, as well as the location of the tumors in the children, provides strong evidence for cancer transmission during delivery,” Dr. Zakhour summarized.
C-section question
The first of the cases reported by the Japanese team was a toddler (23 months) who presented to a local hospital with a 2-week history of a productive cough. Computed tomography revealed multiple masses scattered along the bronchi in both lungs, and a biopsy revealed neuroendocrine carcinoma of the lung.
Notably, the mother’s cervical cancer was not diagnosed during her pregnancy. A cervical cytologic test performed in the mother 7 months before the birth was negative. The infant was delivered transvaginally at 39 weeks of gestation.
It was only 3 months after the birth that the 35-year-old mother received a diagnosis of squamous cell carcinoma of the cervix. She then underwent radical hysterectomy with pelvic lymphadenectomy, followed by chemotherapy.
Had it been known that she had cervical cancer, she may have been advised to have a cesarean section.
The study authors propose, on the basis of their paper, that all women with cervical cancer should have a cesarean section.
But a U.S. expert questioned this, and said the situation is “a bit nuanced.”
William Grobman, MD, of Northwestern University in Chicago, said the current standard recommendation for many pregnant women known to have cervical cancer is to have a cesarean section and that “the strength of the recommendation is dependent on factors such as stage and size.”
However, in an interview, he added that “it may be premature to make a blanket recommendation for all people based on two reports without any idea of the frequency of this event, and with such uncertainty, it seems that disclosure of all information and shared decision-making would be a key approach.”
In this case report, the authors also noted that the cancer found in the toddler looked similar to the cancer in the mother.
“Histologic similarities between the tumor samples from the mother and child prompted us to compare the results of their next-generation sequencing tests,” they said.
The result? “The comparison of the gene profiles in the samples of tumor and normal tissue confirmed that transmission of maternal tumor to the child had occurred.”
The lung cancer in the toddler progressed despite two chemotherapy regimens, so he was enrolled in a clinical trial of nivolumab therapy. He had a response that continued for 7 months, with no appearance of new lesions. Lobectomy was performed to resect a single remaining nodule. The boy had no evidence of disease recurrence at 12 months after lobectomy.
His mother was also enrolled in a nivolumab trial, but her cervical cancer had spread, and she died 5 months after disease progression.
Second case
In the second reported case, a 6-year-old boy presented to a local hospital with chest pain on the left side. Computed tomography revealed a mass in the left lung, and mucinous adenocarcinoma was eventually diagnosed.
In this case, the mother had a cervical polypoid tumor detected during pregnancy. But, as in the other case, cervical cytologic analysis was negative. Because the tumor was stable without any intervention, the mother delivered the boy vaginally at 38 weeks of gestation.
However, after the delivery, biopsy of the cervical lesion revealed adenocarcinoma. The mother underwent radical hysterectomy and bilateral salpingo-oophorectomy 3 months after delivery. She died of the disease 2 years after the surgery.
The boy received chemotherapy and had a partial response, with a reduction in levels of the tumor marker CA19-9 to normal levels. But 3 months later, the disease recurred in the left lung. After more chemotherapy, he underwent total left pneumonectomy and was subsequently free of disease.
The study authors said that they did not suspect maternal transmission of the cancer when her child received a diagnosis at 6 years of age. They explained that metastatic cervical cancer is typically a fast-growing tumor and the slow growth in the child seemed inconsistent with the idea that the cancer had been transmitted to him.
However, the pathology exam showed that the boy had mucinous adenocarcinoma, “which is an unusual morphologic finding for a primary lung tumor, but it was similar to the uterine cervical tumor in the mother,” the authors reported.
Samples of the cervical tumor from the mother and from the lung tumor of the child were submitted for next-generation sequencing tests and, said the authors, indicated mother-to-infant transmission.
The study was supported by grants from the Japan Agency for Medical Research and Development; the National Cancer Center Research and Development Fund; and the Ministry of Education, Culture, Sports, Science and Technology; and funding from Ono Pharmaceutical.
A version of this article first appeared on Medscape.com.
An introduction to Naikan
The list of things to be ungrateful for last year is long. You’re not supposed to make this list, though. The best practice is to list what you’re grateful for, even when living in trying times. That’s a long list too, but I find making it similarly unfruitful.
Of course, I’m grateful I don’t have COVID-19, thankful my practice hasn’t been significantly impacted, grateful I got the vaccine. But simply repeating these gratitudes daily seems ineffective. I’ve learned a different “gratefulness practice” that perhaps works better.

It’s a Japanese method called Naikan (pronounced “nye-kan”). The word means introspection and the practice is one of self-reflection. But . Yoshimoto Ishin developed Naikan in the 1940s. He was a Japanese businessman and devout Buddhist who wanted to make a difficult form of meditation more accessible. He removed the ascetic bits like sleep deprivation and refined the exercises such that they better see how others see us. The result is a way to reframe your life experiences and help you understand how much others do for us and how our actions and attitudes impact others. It can be done alone or with a partner. You can do it at the beginning or end of your day.
The method is simple. You ask three questions:
What have I received today from ___________?
What have I given today to ___________?
What difficulty or trouble have I caused to ___________?
The first question is similar to most gratitude practices. For example, you might ask, “What have I received from (my husband or nurse or friend, etc.)? Today, I received a beautifully tidied-up office from my wife who spent time last night sorting things. This made it easy for me to sit down and start writing this piece.

The second question is better. What have I given today to (my wife, or patient, or mom, etc.)? It can be simple as: Today, I slowed down to let everyone who was in the closed highway lane back into traffic (even though some were clearly undeserving of my generosity). Or last night, I worked to coordinate with anesthesia and scheduling to help a little girl who would benefit from conscious sedation for her procedure.
Combined, these two questions pull you 180 degrees from our default mode, which is complaining. We are wired to find, and talk about, all the inconveniences in our lives: Roadway construction caused a traffic backup that led to running late for clinic. First patient was peeved and had a list of complaints, the last of which was hair loss. Isn’t it much better to rave about how our dermatology nurse volunteered to work the hospital COVID-19 unit to give her colleagues a break? Or how my 10:15 patient came early to be sure she was on time? (It happens.)
The last question is the best. We all spend time thinking about what others think of us. We should spend time thinking about what impact we’ve had on them. Like a cold shower, it’s both briskly awakening and easy to do. Go back through your day and reflect on what you did that made things difficult for others. It can be as simple as I started whining about how a patient waylaid me with her silly complaints. That led to my colleague’s joining in about difficult patients. Or I was late turning in my article, which made my editor have to work harder to get it completed in time.
There’s plenty of things we should be grateful for. In doing these exercises you’ll learn just how much others have cared for you and, I hope, how you might do things to make them grateful for you.
If you’re interested in learning more about Naikan, I discovered this from Brett McKay’s The Art of Manliness podcast and the teaching of Gregg Krech, summarized in his book, “Naikan: Gratitude, Grace, and the Japanese Art of Self-Reflection.”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com .
The list of things to be ungrateful for last year is long. You’re not supposed to make this list, though. The best practice is to list what you’re grateful for, even when living in trying times. That’s a long list too, but I find making it similarly unfruitful.
Of course, I’m grateful I don’t have COVID-19, thankful my practice hasn’t been significantly impacted, grateful I got the vaccine. But simply repeating these gratitudes daily seems ineffective. I’ve learned a different “gratefulness practice” that perhaps works better.
It’s a Japanese method called Naikan (pronounced “nye-kan”). The word means introspection and the practice is one of self-reflection. But . Yoshimoto Ishin developed Naikan in the 1940s. He was a Japanese businessman and devout Buddhist who wanted to make a difficult form of meditation more accessible. He removed the ascetic bits like sleep deprivation and refined the exercises such that they better see how others see us. The result is a way to reframe your life experiences and help you understand how much others do for us and how our actions and attitudes impact others. It can be done alone or with a partner. You can do it at the beginning or end of your day.
The method is simple. You ask three questions:
What have I received today from ___________?
What have I given today to ___________?
What difficulty or trouble have I caused to ___________?
The first question is similar to most gratitude practices. For example, you might ask, “What have I received from (my husband or nurse or friend, etc.)? Today, I received a beautifully tidied-up office from my wife who spent time last night sorting things. This made it easy for me to sit down and start writing this piece.
The second question is better. What have I given today to (my wife, or patient, or mom, etc.)? It can be simple as: Today, I slowed down to let everyone who was in the closed highway lane back into traffic (even though some were clearly undeserving of my generosity). Or last night, I worked to coordinate with anesthesia and scheduling to help a little girl who would benefit from conscious sedation for her procedure.
Combined, these two questions pull you 180 degrees from our default mode, which is complaining. We are wired to find, and talk about, all the inconveniences in our lives: Roadway construction caused a traffic backup that led to running late for clinic. First patient was peeved and had a list of complaints, the last of which was hair loss. Isn’t it much better to rave about how our dermatology nurse volunteered to work the hospital COVID-19 unit to give her colleagues a break? Or how my 10:15 patient came early to be sure she was on time? (It happens.)
The last question is the best. We all spend time thinking about what others think of us. We should spend time thinking about what impact we’ve had on them. Like a cold shower, it’s both briskly awakening and easy to do. Go back through your day and reflect on what you did that made things difficult for others. It can be as simple as I started whining about how a patient waylaid me with her silly complaints. That led to my colleague’s joining in about difficult patients. Or I was late turning in my article, which made my editor have to work harder to get it completed in time.
There’s plenty of things we should be grateful for. In doing these exercises you’ll learn just how much others have cared for you and, I hope, how you might do things to make them grateful for you.
If you’re interested in learning more about Naikan, I discovered this from Brett McKay’s The Art of Manliness podcast and the teaching of Gregg Krech, summarized in his book, “Naikan: Gratitude, Grace, and the Japanese Art of Self-Reflection.”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com .
The list of things to be ungrateful for last year is long. You’re not supposed to make this list, though. The best practice is to list what you’re grateful for, even when living in trying times. That’s a long list too, but I find making it similarly unfruitful.
Of course, I’m grateful I don’t have COVID-19, thankful my practice hasn’t been significantly impacted, grateful I got the vaccine. But simply repeating these gratitudes daily seems ineffective. I’ve learned a different “gratefulness practice” that perhaps works better.
It’s a Japanese method called Naikan (pronounced “nye-kan”). The word means introspection and the practice is one of self-reflection. But . Yoshimoto Ishin developed Naikan in the 1940s. He was a Japanese businessman and devout Buddhist who wanted to make a difficult form of meditation more accessible. He removed the ascetic bits like sleep deprivation and refined the exercises such that they better see how others see us. The result is a way to reframe your life experiences and help you understand how much others do for us and how our actions and attitudes impact others. It can be done alone or with a partner. You can do it at the beginning or end of your day.
The method is simple. You ask three questions:
What have I received today from ___________?
What have I given today to ___________?
What difficulty or trouble have I caused to ___________?
The first question is similar to most gratitude practices. For example, you might ask, “What have I received from (my husband or nurse or friend, etc.)? Today, I received a beautifully tidied-up office from my wife who spent time last night sorting things. This made it easy for me to sit down and start writing this piece.
The second question is better. What have I given today to (my wife, or patient, or mom, etc.)? It can be simple as: Today, I slowed down to let everyone who was in the closed highway lane back into traffic (even though some were clearly undeserving of my generosity). Or last night, I worked to coordinate with anesthesia and scheduling to help a little girl who would benefit from conscious sedation for her procedure.
Combined, these two questions pull you 180 degrees from our default mode, which is complaining. We are wired to find, and talk about, all the inconveniences in our lives: Roadway construction caused a traffic backup that led to running late for clinic. First patient was peeved and had a list of complaints, the last of which was hair loss. Isn’t it much better to rave about how our dermatology nurse volunteered to work the hospital COVID-19 unit to give her colleagues a break? Or how my 10:15 patient came early to be sure she was on time? (It happens.)
The last question is the best. We all spend time thinking about what others think of us. We should spend time thinking about what impact we’ve had on them. Like a cold shower, it’s both briskly awakening and easy to do. Go back through your day and reflect on what you did that made things difficult for others. It can be as simple as I started whining about how a patient waylaid me with her silly complaints. That led to my colleague’s joining in about difficult patients. Or I was late turning in my article, which made my editor have to work harder to get it completed in time.
There’s plenty of things we should be grateful for. In doing these exercises you’ll learn just how much others have cared for you and, I hope, how you might do things to make them grateful for you.
If you’re interested in learning more about Naikan, I discovered this from Brett McKay’s The Art of Manliness podcast and the teaching of Gregg Krech, summarized in his book, “Naikan: Gratitude, Grace, and the Japanese Art of Self-Reflection.”
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com .
The next likely COVID-19 vaccine has its advantages
Among the multiple vaccine candidates around the globe, next up in the arsenal against COVID-19 is likely the single-dose Ad26.COV2.S vaccine in development from Johnson & Johnson/Janssen, infectious disease experts predict.
And it got closer with promising interim phase 1/2a trial results, published online Jan. 13 in The New England Journal of Medicine.
A single Ad26.COV2.S dose was associated with S-binding and neutralizing antibodies in more than 90% of the participants. The finding was observed in both adults aged 18-55 years and participants 65 and older, as well as for participants given low-dose or high-dose vaccinations.
The results also suggest a durable vaccine response. “The take-home message [includes] a high neutralizing antibody responder rate to a single dose of our Ad26.COV2.S COVID-19 vaccine candidate. In addition, we see that these responses and antibody titers are stable for at least 71 days,” senior study author Hanneke Schuitemaker, PhD, global head of viral vaccine discovery and translational medicine at Johnson & Johnson in Leiden, the Netherlands, said in an interview.
If the single-dose Johnson & Johnson product gains Food and Drug Administration emergency use authorization (EUA), it could significantly boost the number of overall immunizations available. Less stringent storage requirements – only regular refrigeration vs. a need to freeze the Pfizer/BioNTech and Moderna COVID-19 vaccines – is another potential advantage. The Ad26.COV2.S vaccine can be refrigerated for up to 3 months at 36°-46 °F (2°-8 °C).
“Phase 1-2 trial data on the J&J vaccine: If it works as well as the mRNA options, it will have substantial advantages,” Jeremy Faust, MD, an emergency room physician affiliated with Brigham & Women’s Hospital and Harvard Medical School, Boston, tweeted on Jan. 13.
Unlike the Pfizer/BioNTech and Moderna messenger RNA vaccines, the Johnson & Johnson product is a recombinant, replication-incompetent adenovirus serotype 26 (Ad26) vector encoding a full-length and stabilized SARS-CoV-2 spike (S) protein.
Phase 3 efficacy/safety results pending
Under normal circumstances, phase 3 trial results would not be anticipated within weeks of phase 1/2a trial findings. However, the urgency of the COVID-19 pandemic accelerated the vaccine development process, so preclinical trials were conducted simultaneously and not sequentially. For this reason, phase 3 interim results for the Johnson & Johnson vaccine are expected within weeks, and a company executive told Reuters that the rollout is on track for March.
“We hope to report data from our first phase 3 study, ENSEMBLE, in which we are testing the protective efficacy of a single dose of Ad26.COV2.S, by the end of this month or early February,” Dr. Schuitemaker said.
In the meantime, the phase 1/2a ongoing, multicenter, randomized, double-blind, and placebo-controlled trial interim results have drawn positive reactions.
“Data is highly encouraging and supports the single inoculation approach that makes this vaccine unique,” Carlos del Rio, executive associate dean for Emory University at Grady in Atlanta, wrote in a tweet on Jan. 13.
“Encouraging COVID vaccine data from J&J published [Jan. 13]. Solid antibody, CD4 T cell, and CD8 T cell responses – a nice trifecta of vaccine immune responses to see! And safe!” tweeted Shane Crotty, PhD, vaccine scientist and professor at the La Jolla (Calif.) Institute for Immunology.
First results in 800+ participants
At baseline for the phase 1/2a trial, 2% of the younger group and 1% of the 65+ group were seropositive for SARS-CoV-2 S-specific antibodies.
A total of 402 people in the younger age cohort and 403 in the 65 and older group received a first dose of the Johnson & Johnson vaccine. Many participants also received a second dose 56 days later for a separate trial, ENSEMBLE2, designed to compare safety and efficacy between single- and double-dose regimens. Results of that trial are still pending.
Safety profile
A single dose was associated with a higher incidence of solicited systemic adverse events in the higher vaccine dose group. They also found that grade 3 adverse events decreased with increasing age.
Injection site pain on the day of immunization or the next day was the most common local reaction. The pain generally resolved within 24 hours. Fever was reported by 15% of the low-dose vaccine group and 39% of the high-dose cohort. Fatigue, headache, and myalgia were the most common grade 1 or 2 solicited systemic adverse events reported.
Five serious adverse events were reported, including four that investigators deemed unrelated to vaccination: hypotension, bilateral nephrolithiasis, legionella pneumonia, and one case of worsening of multiple sclerosis. The vaccine-related serious adverse event was a fever that resulted in hospitalization because of suspicion of COVID-19. The patient recovered within 12 hours.
“These data confirm our previous experience with vaccine candidates based on our Ad26 viral vector platform in the younger age group. The almost similar performance in older adults is promising,” Dr. Schuitemaker said.
A potential limitation of the phase 1/2a trial is “the lack of representation of minority groups,” the researchers noted. Johnson & Johnson is working on improving the diversity of study participants “with respect to groups that seem to be affected most by the COVID-19 pandemic.”
AstraZeneca/Oxford vaccine status
The AstraZeneca/Oxford AZD1222 vaccine in development received approval for use in the United Kingdom on Dec. 30. The approval came after Public Health England said the country was facing “unprecedented” levels of infections, the BBC reported. AstraZeneca applied for European Medical Agency approval earlier in the week of Jan. 10, which could lead to more widespread use across Europe.
The status of the vaccine remains uncertain in the United States. A phase 3 trial that started in August was paused for about 6 weeks in September and October after an adverse event in a British volunteer halted studies worldwide. On Oct. 23, the FDA permitted researchers to continue the trial with approximately 40,000 participants.
There was some suggestion in the clinical trials that a half dose of the AstraZeneca vaccine was more effective than a full dose, 90% vs. 62%, but some irregularities in the research require further investigation.
Although the AstraZeneca vaccine is delivered to cells by an adenovirus – as with the Johnson & Johnson product – it is designed to be delivered in two doses 28 days apart, like the administration schedule of the Moderna mRNA vaccine.
A need for speed, and more doses
Regardless of which vaccine product is next to gain an EUA in the United States, many experts agree the COVID-19 vaccine rollouts so far have been problematic, at a time when cases are climbing to record-breaking levels, and likely more related to logistics over administration of the vaccine than production of the doses.
“Lots of doses being manufactured. In December 20 million, January 40 million, February 80 million and J&J hopefully soon to add to the count. The shortage is the number arms not getting vaccinated. Freezers do not get COVID. They do not need all those vaccines,” Daniel Griffin, MD, PhD, an infectious disease expert in Port Washington, N.Y., tweeted on Jan. 12.
“Unfortunately, the rollout has not gone smoothly, partly due to a lack of resources for this distribution phase we’re in,” Andrew T. Pavia, MD, chief of the division of pediatric infectious diseases at the University of Utah, Salt Lake City, said during a media briefing Jan. 14 sponsored by the Infectious Diseases Society of America (IDSA).
“We’re concerned about the mismatch between the number of people who are being told they are eligible and the amount of vaccine that is being distributed,” he said.
Complicating the rollout is a directive from U.S. Health and Human Services Secretary Alex Azar that states should start vaccinating everyone 65 and older as well as those with underlying conditions.
Expanding distribution to the 15% of Americans in just this age group is a big challenge, Dr. Pavia said. “We have enough vaccine maybe to vaccinate 40 million by the end of this month. There is a huge disconnect, and that creates a lot of problems.”
“One of the biggest problems is we are trying to do this mass vaccination program in the middle of the biggest surge we’ve ever seen,” Julie Vaishampayan, MD, MPH, chair of the IDSA Public Health Committee, said during the briefing. Without sufficient time for public health officials to plan for vaccinating a larger population, “people will come and stand in extremely long lines.”
Trying to expand immunization access without a proportionate increase in available doses prompted Dr. Vaishampayan to share an analogy from a colleague: “We are trying to fill a lake with a garden hose. Rather than making the lake bigger, what we really need is more water.”
Dr. Pavia emphasized that infectious disease experts “know the measures that work.” Not using masks, physical distancing, and hand hygiene, he said, “is a bit like knowing that really good shark repellents will be available in summer, so I’m going to jump into the ocean covered in blood while the great whites are swimming around.”
An official at the World Health Organization agreed. “Vaccines are coming online and I do believe vaccines will make a huge difference. But they are not here yet in enough quantities and in enough people to make that difference,” Michael Ryan, MB, WHO executive director of health emergencies, said during an online media briefing Jan. 13, held in conjunction with Emory University.
Dr. Ryan predicted that “we’ve got weeks if not months ahead of us in which our weapon is our knowledge ... what we know about this virus, its transmission, and stopping that transmission.
“And as the vaccines roll in, we can hopefully end this horrific pandemic.”
Dr. Schuitemaker reports grants from BARDA during the conduct of the study; personal fees and other from Janssen Vaccines and Prevention, a J&J company, outside the submitted work. Johnson & Johnson and the Biomedical Advanced Research and Development Authority of the Department of Health and Human Services funded the phase 1/2a study.
A version of this article first appeared on Medscape.com.
Among the multiple vaccine candidates around the globe, next up in the arsenal against COVID-19 is likely the single-dose Ad26.COV2.S vaccine in development from Johnson & Johnson/Janssen, infectious disease experts predict.
And it got closer with promising interim phase 1/2a trial results, published online Jan. 13 in The New England Journal of Medicine.
A single Ad26.COV2.S dose was associated with S-binding and neutralizing antibodies in more than 90% of the participants. The finding was observed in both adults aged 18-55 years and participants 65 and older, as well as for participants given low-dose or high-dose vaccinations.
The results also suggest a durable vaccine response. “The take-home message [includes] a high neutralizing antibody responder rate to a single dose of our Ad26.COV2.S COVID-19 vaccine candidate. In addition, we see that these responses and antibody titers are stable for at least 71 days,” senior study author Hanneke Schuitemaker, PhD, global head of viral vaccine discovery and translational medicine at Johnson & Johnson in Leiden, the Netherlands, said in an interview.
If the single-dose Johnson & Johnson product gains Food and Drug Administration emergency use authorization (EUA), it could significantly boost the number of overall immunizations available. Less stringent storage requirements – only regular refrigeration vs. a need to freeze the Pfizer/BioNTech and Moderna COVID-19 vaccines – is another potential advantage. The Ad26.COV2.S vaccine can be refrigerated for up to 3 months at 36°-46 °F (2°-8 °C).
“Phase 1-2 trial data on the J&J vaccine: If it works as well as the mRNA options, it will have substantial advantages,” Jeremy Faust, MD, an emergency room physician affiliated with Brigham & Women’s Hospital and Harvard Medical School, Boston, tweeted on Jan. 13.
Unlike the Pfizer/BioNTech and Moderna messenger RNA vaccines, the Johnson & Johnson product is a recombinant, replication-incompetent adenovirus serotype 26 (Ad26) vector encoding a full-length and stabilized SARS-CoV-2 spike (S) protein.
Phase 3 efficacy/safety results pending
Under normal circumstances, phase 3 trial results would not be anticipated within weeks of phase 1/2a trial findings. However, the urgency of the COVID-19 pandemic accelerated the vaccine development process, so preclinical trials were conducted simultaneously and not sequentially. For this reason, phase 3 interim results for the Johnson & Johnson vaccine are expected within weeks, and a company executive told Reuters that the rollout is on track for March.
“We hope to report data from our first phase 3 study, ENSEMBLE, in which we are testing the protective efficacy of a single dose of Ad26.COV2.S, by the end of this month or early February,” Dr. Schuitemaker said.
In the meantime, the phase 1/2a ongoing, multicenter, randomized, double-blind, and placebo-controlled trial interim results have drawn positive reactions.
“Data is highly encouraging and supports the single inoculation approach that makes this vaccine unique,” Carlos del Rio, executive associate dean for Emory University at Grady in Atlanta, wrote in a tweet on Jan. 13.
“Encouraging COVID vaccine data from J&J published [Jan. 13]. Solid antibody, CD4 T cell, and CD8 T cell responses – a nice trifecta of vaccine immune responses to see! And safe!” tweeted Shane Crotty, PhD, vaccine scientist and professor at the La Jolla (Calif.) Institute for Immunology.
First results in 800+ participants
At baseline for the phase 1/2a trial, 2% of the younger group and 1% of the 65+ group were seropositive for SARS-CoV-2 S-specific antibodies.
A total of 402 people in the younger age cohort and 403 in the 65 and older group received a first dose of the Johnson & Johnson vaccine. Many participants also received a second dose 56 days later for a separate trial, ENSEMBLE2, designed to compare safety and efficacy between single- and double-dose regimens. Results of that trial are still pending.
Safety profile
A single dose was associated with a higher incidence of solicited systemic adverse events in the higher vaccine dose group. They also found that grade 3 adverse events decreased with increasing age.
Injection site pain on the day of immunization or the next day was the most common local reaction. The pain generally resolved within 24 hours. Fever was reported by 15% of the low-dose vaccine group and 39% of the high-dose cohort. Fatigue, headache, and myalgia were the most common grade 1 or 2 solicited systemic adverse events reported.
Five serious adverse events were reported, including four that investigators deemed unrelated to vaccination: hypotension, bilateral nephrolithiasis, legionella pneumonia, and one case of worsening of multiple sclerosis. The vaccine-related serious adverse event was a fever that resulted in hospitalization because of suspicion of COVID-19. The patient recovered within 12 hours.
“These data confirm our previous experience with vaccine candidates based on our Ad26 viral vector platform in the younger age group. The almost similar performance in older adults is promising,” Dr. Schuitemaker said.
A potential limitation of the phase 1/2a trial is “the lack of representation of minority groups,” the researchers noted. Johnson & Johnson is working on improving the diversity of study participants “with respect to groups that seem to be affected most by the COVID-19 pandemic.”
AstraZeneca/Oxford vaccine status
The AstraZeneca/Oxford AZD1222 vaccine in development received approval for use in the United Kingdom on Dec. 30. The approval came after Public Health England said the country was facing “unprecedented” levels of infections, the BBC reported. AstraZeneca applied for European Medical Agency approval earlier in the week of Jan. 10, which could lead to more widespread use across Europe.
The status of the vaccine remains uncertain in the United States. A phase 3 trial that started in August was paused for about 6 weeks in September and October after an adverse event in a British volunteer halted studies worldwide. On Oct. 23, the FDA permitted researchers to continue the trial with approximately 40,000 participants.
There was some suggestion in the clinical trials that a half dose of the AstraZeneca vaccine was more effective than a full dose, 90% vs. 62%, but some irregularities in the research require further investigation.
Although the AstraZeneca vaccine is delivered to cells by an adenovirus – as with the Johnson & Johnson product – it is designed to be delivered in two doses 28 days apart, like the administration schedule of the Moderna mRNA vaccine.
A need for speed, and more doses
Regardless of which vaccine product is next to gain an EUA in the United States, many experts agree the COVID-19 vaccine rollouts so far have been problematic, at a time when cases are climbing to record-breaking levels, and likely more related to logistics over administration of the vaccine than production of the doses.
“Lots of doses being manufactured. In December 20 million, January 40 million, February 80 million and J&J hopefully soon to add to the count. The shortage is the number arms not getting vaccinated. Freezers do not get COVID. They do not need all those vaccines,” Daniel Griffin, MD, PhD, an infectious disease expert in Port Washington, N.Y., tweeted on Jan. 12.
“Unfortunately, the rollout has not gone smoothly, partly due to a lack of resources for this distribution phase we’re in,” Andrew T. Pavia, MD, chief of the division of pediatric infectious diseases at the University of Utah, Salt Lake City, said during a media briefing Jan. 14 sponsored by the Infectious Diseases Society of America (IDSA).
“We’re concerned about the mismatch between the number of people who are being told they are eligible and the amount of vaccine that is being distributed,” he said.
Complicating the rollout is a directive from U.S. Health and Human Services Secretary Alex Azar that states should start vaccinating everyone 65 and older as well as those with underlying conditions.
Expanding distribution to the 15% of Americans in just this age group is a big challenge, Dr. Pavia said. “We have enough vaccine maybe to vaccinate 40 million by the end of this month. There is a huge disconnect, and that creates a lot of problems.”
“One of the biggest problems is we are trying to do this mass vaccination program in the middle of the biggest surge we’ve ever seen,” Julie Vaishampayan, MD, MPH, chair of the IDSA Public Health Committee, said during the briefing. Without sufficient time for public health officials to plan for vaccinating a larger population, “people will come and stand in extremely long lines.”
Trying to expand immunization access without a proportionate increase in available doses prompted Dr. Vaishampayan to share an analogy from a colleague: “We are trying to fill a lake with a garden hose. Rather than making the lake bigger, what we really need is more water.”
Dr. Pavia emphasized that infectious disease experts “know the measures that work.” Not using masks, physical distancing, and hand hygiene, he said, “is a bit like knowing that really good shark repellents will be available in summer, so I’m going to jump into the ocean covered in blood while the great whites are swimming around.”
An official at the World Health Organization agreed. “Vaccines are coming online and I do believe vaccines will make a huge difference. But they are not here yet in enough quantities and in enough people to make that difference,” Michael Ryan, MB, WHO executive director of health emergencies, said during an online media briefing Jan. 13, held in conjunction with Emory University.
Dr. Ryan predicted that “we’ve got weeks if not months ahead of us in which our weapon is our knowledge ... what we know about this virus, its transmission, and stopping that transmission.
“And as the vaccines roll in, we can hopefully end this horrific pandemic.”
Dr. Schuitemaker reports grants from BARDA during the conduct of the study; personal fees and other from Janssen Vaccines and Prevention, a J&J company, outside the submitted work. Johnson & Johnson and the Biomedical Advanced Research and Development Authority of the Department of Health and Human Services funded the phase 1/2a study.
A version of this article first appeared on Medscape.com.
Among the multiple vaccine candidates around the globe, next up in the arsenal against COVID-19 is likely the single-dose Ad26.COV2.S vaccine in development from Johnson & Johnson/Janssen, infectious disease experts predict.
And it got closer with promising interim phase 1/2a trial results, published online Jan. 13 in The New England Journal of Medicine.
A single Ad26.COV2.S dose was associated with S-binding and neutralizing antibodies in more than 90% of the participants. The finding was observed in both adults aged 18-55 years and participants 65 and older, as well as for participants given low-dose or high-dose vaccinations.
The results also suggest a durable vaccine response. “The take-home message [includes] a high neutralizing antibody responder rate to a single dose of our Ad26.COV2.S COVID-19 vaccine candidate. In addition, we see that these responses and antibody titers are stable for at least 71 days,” senior study author Hanneke Schuitemaker, PhD, global head of viral vaccine discovery and translational medicine at Johnson & Johnson in Leiden, the Netherlands, said in an interview.
If the single-dose Johnson & Johnson product gains Food and Drug Administration emergency use authorization (EUA), it could significantly boost the number of overall immunizations available. Less stringent storage requirements – only regular refrigeration vs. a need to freeze the Pfizer/BioNTech and Moderna COVID-19 vaccines – is another potential advantage. The Ad26.COV2.S vaccine can be refrigerated for up to 3 months at 36°-46 °F (2°-8 °C).
“Phase 1-2 trial data on the J&J vaccine: If it works as well as the mRNA options, it will have substantial advantages,” Jeremy Faust, MD, an emergency room physician affiliated with Brigham & Women’s Hospital and Harvard Medical School, Boston, tweeted on Jan. 13.
Unlike the Pfizer/BioNTech and Moderna messenger RNA vaccines, the Johnson & Johnson product is a recombinant, replication-incompetent adenovirus serotype 26 (Ad26) vector encoding a full-length and stabilized SARS-CoV-2 spike (S) protein.
Phase 3 efficacy/safety results pending
Under normal circumstances, phase 3 trial results would not be anticipated within weeks of phase 1/2a trial findings. However, the urgency of the COVID-19 pandemic accelerated the vaccine development process, so preclinical trials were conducted simultaneously and not sequentially. For this reason, phase 3 interim results for the Johnson & Johnson vaccine are expected within weeks, and a company executive told Reuters that the rollout is on track for March.
“We hope to report data from our first phase 3 study, ENSEMBLE, in which we are testing the protective efficacy of a single dose of Ad26.COV2.S, by the end of this month or early February,” Dr. Schuitemaker said.
In the meantime, the phase 1/2a ongoing, multicenter, randomized, double-blind, and placebo-controlled trial interim results have drawn positive reactions.
“Data is highly encouraging and supports the single inoculation approach that makes this vaccine unique,” Carlos del Rio, executive associate dean for Emory University at Grady in Atlanta, wrote in a tweet on Jan. 13.
“Encouraging COVID vaccine data from J&J published [Jan. 13]. Solid antibody, CD4 T cell, and CD8 T cell responses – a nice trifecta of vaccine immune responses to see! And safe!” tweeted Shane Crotty, PhD, vaccine scientist and professor at the La Jolla (Calif.) Institute for Immunology.
First results in 800+ participants
At baseline for the phase 1/2a trial, 2% of the younger group and 1% of the 65+ group were seropositive for SARS-CoV-2 S-specific antibodies.
A total of 402 people in the younger age cohort and 403 in the 65 and older group received a first dose of the Johnson & Johnson vaccine. Many participants also received a second dose 56 days later for a separate trial, ENSEMBLE2, designed to compare safety and efficacy between single- and double-dose regimens. Results of that trial are still pending.
Safety profile
A single dose was associated with a higher incidence of solicited systemic adverse events in the higher vaccine dose group. They also found that grade 3 adverse events decreased with increasing age.
Injection site pain on the day of immunization or the next day was the most common local reaction. The pain generally resolved within 24 hours. Fever was reported by 15% of the low-dose vaccine group and 39% of the high-dose cohort. Fatigue, headache, and myalgia were the most common grade 1 or 2 solicited systemic adverse events reported.
Five serious adverse events were reported, including four that investigators deemed unrelated to vaccination: hypotension, bilateral nephrolithiasis, legionella pneumonia, and one case of worsening of multiple sclerosis. The vaccine-related serious adverse event was a fever that resulted in hospitalization because of suspicion of COVID-19. The patient recovered within 12 hours.
“These data confirm our previous experience with vaccine candidates based on our Ad26 viral vector platform in the younger age group. The almost similar performance in older adults is promising,” Dr. Schuitemaker said.
A potential limitation of the phase 1/2a trial is “the lack of representation of minority groups,” the researchers noted. Johnson & Johnson is working on improving the diversity of study participants “with respect to groups that seem to be affected most by the COVID-19 pandemic.”
AstraZeneca/Oxford vaccine status
The AstraZeneca/Oxford AZD1222 vaccine in development received approval for use in the United Kingdom on Dec. 30. The approval came after Public Health England said the country was facing “unprecedented” levels of infections, the BBC reported. AstraZeneca applied for European Medical Agency approval earlier in the week of Jan. 10, which could lead to more widespread use across Europe.
The status of the vaccine remains uncertain in the United States. A phase 3 trial that started in August was paused for about 6 weeks in September and October after an adverse event in a British volunteer halted studies worldwide. On Oct. 23, the FDA permitted researchers to continue the trial with approximately 40,000 participants.
There was some suggestion in the clinical trials that a half dose of the AstraZeneca vaccine was more effective than a full dose, 90% vs. 62%, but some irregularities in the research require further investigation.
Although the AstraZeneca vaccine is delivered to cells by an adenovirus – as with the Johnson & Johnson product – it is designed to be delivered in two doses 28 days apart, like the administration schedule of the Moderna mRNA vaccine.
A need for speed, and more doses
Regardless of which vaccine product is next to gain an EUA in the United States, many experts agree the COVID-19 vaccine rollouts so far have been problematic, at a time when cases are climbing to record-breaking levels, and likely more related to logistics over administration of the vaccine than production of the doses.
“Lots of doses being manufactured. In December 20 million, January 40 million, February 80 million and J&J hopefully soon to add to the count. The shortage is the number arms not getting vaccinated. Freezers do not get COVID. They do not need all those vaccines,” Daniel Griffin, MD, PhD, an infectious disease expert in Port Washington, N.Y., tweeted on Jan. 12.
“Unfortunately, the rollout has not gone smoothly, partly due to a lack of resources for this distribution phase we’re in,” Andrew T. Pavia, MD, chief of the division of pediatric infectious diseases at the University of Utah, Salt Lake City, said during a media briefing Jan. 14 sponsored by the Infectious Diseases Society of America (IDSA).
“We’re concerned about the mismatch between the number of people who are being told they are eligible and the amount of vaccine that is being distributed,” he said.
Complicating the rollout is a directive from U.S. Health and Human Services Secretary Alex Azar that states should start vaccinating everyone 65 and older as well as those with underlying conditions.
Expanding distribution to the 15% of Americans in just this age group is a big challenge, Dr. Pavia said. “We have enough vaccine maybe to vaccinate 40 million by the end of this month. There is a huge disconnect, and that creates a lot of problems.”
“One of the biggest problems is we are trying to do this mass vaccination program in the middle of the biggest surge we’ve ever seen,” Julie Vaishampayan, MD, MPH, chair of the IDSA Public Health Committee, said during the briefing. Without sufficient time for public health officials to plan for vaccinating a larger population, “people will come and stand in extremely long lines.”
Trying to expand immunization access without a proportionate increase in available doses prompted Dr. Vaishampayan to share an analogy from a colleague: “We are trying to fill a lake with a garden hose. Rather than making the lake bigger, what we really need is more water.”
Dr. Pavia emphasized that infectious disease experts “know the measures that work.” Not using masks, physical distancing, and hand hygiene, he said, “is a bit like knowing that really good shark repellents will be available in summer, so I’m going to jump into the ocean covered in blood while the great whites are swimming around.”
An official at the World Health Organization agreed. “Vaccines are coming online and I do believe vaccines will make a huge difference. But they are not here yet in enough quantities and in enough people to make that difference,” Michael Ryan, MB, WHO executive director of health emergencies, said during an online media briefing Jan. 13, held in conjunction with Emory University.
Dr. Ryan predicted that “we’ve got weeks if not months ahead of us in which our weapon is our knowledge ... what we know about this virus, its transmission, and stopping that transmission.
“And as the vaccines roll in, we can hopefully end this horrific pandemic.”
Dr. Schuitemaker reports grants from BARDA during the conduct of the study; personal fees and other from Janssen Vaccines and Prevention, a J&J company, outside the submitted work. Johnson & Johnson and the Biomedical Advanced Research and Development Authority of the Department of Health and Human Services funded the phase 1/2a study.
A version of this article first appeared on Medscape.com.
Pityriasis rosea carries few risks for pregnant women
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
according to a review of 33 patients.
“Though generally considered benign, PR may be associated with an increased risk of birth complications if acquired during pregnancy,” and previous studies have shown increased rates of complications including miscarriage and neonatal hypotonia in these patients, wrote Julian Stashower of the University of Virginia, Charlottesville, and colleagues.
In a retrospective study published in the Journal of the American Academy of Dermatology, the researchers assessed pregnancy outcomes in women who developed PR during pregnancy. They were identified from medical records at three institutions between September 2010 and June 2020. Diagnosis of PR, a papulosquamous skin eruption associated with human herpesvirus (HHV)–6/7 reactivation, was based on history and physical examination.
Overall, 8 of the 33 women (24%) had birth complications; the rates of preterm delivery, spontaneous pregnancy loss in clinically detectable pregnancies, and oligohydramnios were 6%, 0%, and 3%, respectively. The average onset of PR during pregnancy was earlier among women with complications, compared with those without complications (10.75 weeks’ gestation vs. 15.21 weeks’ gestation), but the difference was not statistically significant.
The researchers noted that their findings differed from the most recent study of PR in pregnancy, which included 60 patients and found a notably higher incidence of overall birth complications (50%), as well as higher incidence of neonatal hypotonia (25%), and miscarriage (13%).
The previous study also showed an increased risk of birth complications when PR onset occurred prior to 15 weeks’ gestation, but the current study did not reflect that finding, they wrote.
The current study findings were limited by several factors including the small sample size, retrospective design, and lack of confirmation of PR with HHV-6/7 testing, as well as lack of exclusion of atypical PR cases, the researchers noted. However, the results suggest that birth complications associated with PR may be lower than previously reported. “Further research is needed to guide future care and fully elucidate this possible association, which has important implications for both pregnant women with PR and their providers.”
The study received no outside funding. The researchers had no financial conflict to disclose.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Consensus bundle has potential to affect postpartum morbidity, mortality
Health care professionals miss an important opportunity if they do not use a holistic patient-centered approach in providing support to their postpartum patients, advised Alison M. Stuebe, MD, MSc, of the division of maternal-fetal medicine at the University of North Carolina at Chapel Hill, and colleagues.
Too often, the emphasis for health care professionals is on less common, highly morbid complications, while their patients’ needs are focused more on daily functioning.
More than half of maternal deaths occur not during delivery, but in the days, weeks, and months following birth. Many serious complications and management of less-emergent conditions such as flu-like symptoms go unnoticed or result in treatment delays. Routinely asking women who present for care whether they have been pregnant during the past year could go a long way in helping clinicians connect the dots for conditions they might not otherwise consider, suggested Dr. Stuebe and colleagues.
In response to what is becoming a growing burden of postpartum maternal morbidity and mortality in the United States, Dr. Stuebe and associates, in coordination with the Alliance of Innovation in Maternal Health, prepared a comprehensive consensus statement on postpartum care basics. The work came out of a day-long planning meeting of an interdisciplinary work group funded by AIMH to develop the maternal safety bundle, which established 28 goals across four phases – readiness, recognition and prevention, response, and reporting. Each phase is intended to occur as part of a coordinated effort between women experiencing pregnancy and their health care providers, with involvement from multiple clinical settings and health systems.
America needs to change the way it treats its new mothers
In a separate interview, Dr. Stuebe shared additional insights into the development of the consensus statement: “This article is part of a broader movement to change the way America treats new mothers. For too long, we’ve lavished attention on women in the weeks before birth and then left them alone to manage recovery, plunging hormones, sleepless nights, and new baby care. The goal of this article is to set out the ways that we can better support women in this critical transition period.
“We need to start during pregnancy, by working with women to plan for the fourth trimester and identify a care team that will support her and her baby. After birth, we need to adapt those plans and make sure she has the emotional and material support she needs to navigate the coming months. Many of these decisions are deeply personal, and we need to center the values and preferences of the woman and her family.”
Dr. Stuebe also spotlighted a new University of North Carolina–based program designed to support shared decision-making. Their Trimester Project team partnered with mothers to design NewMomHealth.com, the first national postpartum resource designed by and for new mothers, which is in the process of launching a culturally adapted Spanish-language site, saludmadre.com, in partnership with Urban Strategies.
Readiness prepares mothers, HCPs, and clinical settings for the fourth trimester
In the first phase, Readiness, there are three key parties involved: the woman experiencing pregnancy, the health care providers (HCPs) supporting her, and the clinical settings involved in her care. Each player has specific goals to achieve in this phase, women are responsible for four goals, health care providers have two goals, and clinical settings have five.
Prenatally, every woman should work with health care providers to develop a comprehensive, individualized postpartum care plan that designates a postpartum clinical “home” for addressing any care needed between birth and the “comprehensive postpartum visit.” The plan encourages the patient and her health care team give attention to social support, birth recovery, infant care and feeding plans, thoughts concerning future pregnancies, and specifically use of contraception, as well as any chronic health concerns and overall emotional well-being.
The plan should consist of a postpartum care team that includes friends and family and ensures that medical, material, and social support are available in the weeks following birth for both mother and baby.
The authors emphasized the importance for clinicians to develop a keen awareness of “reproductive justice,” which respects a woman’s right “to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.” They encouraged adopting a sensitivity to concerns deeply rooted in the history of family planning, which is perceived to have been “fraught by coercive tactics to incentivize sterilization and contraceptive implants among marginalized groups.” With this in mind, they urged clinicians to respectfully ask about the patient’s intentions before making any suggestions concerning future births and family planning preferences.
HCP readiness ensures that each woman “has a documented postpartum care plan and care team identified in the prenatal period.” HCPs are also responsible for developing and maintaining “a working knowledge of evidence-based evaluation and management of common issues facing the mother-infant dyad.”
Clinical setting readiness ensures that woman-centered postpartum care and education have been developed and optimized using adult learning principles whenever possible. Diversity of family structures, cultural traditions, and parenting practices are fully embraced. Dr. Stuebe and colleagues emphasized that traditional top-down teaching methods are ineffective and should be avoided.
Clinical setting readiness also ensures that systems are developed to pair families with community-based resources that provide medical follow-up as well as social and material support. Clinical protocols and reimbursement options should be available that give women easy access to preferred contraception. Systems should be in place that facilitate prompt, pertinent communication between in- and outpatient providers. Lastly, and perhaps most importantly, clinical setting readiness demands the development of protocols to screen and treat key postpartum concerns, such as depression, substance use disorders, family violence, and even incontinence in coordination with locally identified specialists.
Recognition and prevention promotes accountability and establishes key guidelines
Recognition and prevention require coordinated participation between women experiencing pregnancy and the clinical environments supporting their care. In this phase, women are responsible for three goals; clinical environments have four goals.
Women are to be identified and respected as the expert most knowledgeable of their own needs, cautioned the authors. They should also be empowered to trust their instincts, seeking care as early and as often as needed in the weeks after they give birth. Postpartum care needs to be viewed as an ongoing process, not just a singular encounter.
Women also need to take ownership for their postpartum care plan, reviewing and revising it as needed in coordination with their health care providers before maternity discharge is complete. Every plan should include a comprehensive list of warning signs and recommended action plans when faced with life-threatening complications, a list of resources for lactation support, and a “first-call” phone number that identifies the postpartum medical providers available to address breastfeeding issues and for postpartum care visits, including prescheduled dates and times.
Lastly, women are to take responsibility for attending their postpartum visit. Although new guidance suggests that the comprehensive visit take place no later than 12 weeks post partum, it also recognizes multiple visits may be required to address individual needs. All women should have contact with a maternal care provider within 3 weeks post partum, the American College of Obstetricians and Gynecologists recommends.
Responsibility for recognition and prevention in the clinical setting begins with determining guidelines for early postpartum visits, considering chronic conditions such as hypertension, diabetes, or substance abuse disorder and risk for postpartum conditions such as wound complications or postpartum depression, the authors wrote. Ongoing care between inpatient and outpatient settings as well as between maternal and infant care providers is coordinated to ensure health and well-being of both patients. Screening and treatment of common comorbidities such as mental health issues, smoking, and substance use as well as issues related to unstable housing and food insecurities are also addressed in the clinical environment. Lastly, clinicians are tasked with ensuring that every patient has selected a primary care provider for ongoing care.
Response ensures key parties and resources are connected at every step
In the response phase, clinical settings and health care providers are the key participants and they have two goals each.
Every clinical setting is tasked with implementing treatment protocols and providing needed care or facilitating referral in a timely fashion. The importance of a “warm hand-off” and “face-to-face introduction to the specialist to whom the patient is being referred” is encouraged. They are also responsible for keeping an updated inventory of community resources on hand for such unmet needs as 24-hour hotlines, food banks, diaper banks, lactation support groups, and home-visiting programs.
Every health care provider is tasked with developing strategies designed to reach women who do not attend their comprehensive postpartum visit. They are also responsible for assessing the severity of identified needs, and arranging immediate transportation to appropriate facilities in life-threatening circumstances. In nonacute cases, the woman and her care providers work with her to make appropriate decisions.
Reporting gives health systems the opportunity to assess and improve
Sole responsibility in the reporting phase falls to every health system. In this phase, they have a total of six goals.
Health systems are ideally organized to convene strategy-sharing sessions with inpatient as well as outpatient professionals to evaluate successes and opportunities for improvement. They are equally qualified to identify and monitor such quality measures as postpartum emergency department utilization and readmission rates. They are tasked with working toward quality metrics that compare postpartum outcomes and prenatal intentions, including patient receipt of preferred contraception or completion of planned breastfeeding duration.
Health systems are expected to conduct quality improvement measures designed to reduce postpartum morbidity when preventable. They are also the logical choice for maintaining a clearinghouse for resources, in collaboration with the community, that is designed to meet the postpartum needs of women.
Lastly, they play an important role in ensuring that reimbursement policies are structured such that they do not disincentivize postpartum visits.
The consensus bundle encourages change in the way America treats its new mothers
Angela Bianco, MD, maternal and fetal medicine specialist at Mount Sinai Hospital, New York, also interviewed separately, noted: “I think the fact that ACOG has created a postpartum bundle for providers to use for guidance is long overdue. The current prenatal care paradigm focuses on numerous/intensive prenatal visits but only a single postpartum visit. Many women report feeling ill-equipped to navigate the challenges that arise post delivery, including self-care, newborn care, and breastfeeding. In addition, most women experience the impact of dramatic hormonal fluctuations resulting in mood alterations. Add profound sleep deprivation to this and the result is often some degree of postpartum blues and/or depression. The importance of anticipatory guidance for our patients cannot be underestimated. Helping to facilitate potential social support structures be in place prior to the birth is optimal. Providers should reinforce the importance of access to a variety of tools, including digital apps, community support groups, and 24/7 web access services. Moving forward, it should be considered unconscionable to send a new mother home without ensuring the appropriate resources are in place. Postpartum care should be tailored to a woman’s needs and may require multiple visits and/or referrals.”
Dr. Stuebe and colleagues, as well as Dr. Bianco, disclosed receiving honoraria for various projects. Funding for the study was supported by the Alliance for Innovation on Maternal and Child Health, which is funded by a grant from the Health Resources and Services Administration.
Health care professionals miss an important opportunity if they do not use a holistic patient-centered approach in providing support to their postpartum patients, advised Alison M. Stuebe, MD, MSc, of the division of maternal-fetal medicine at the University of North Carolina at Chapel Hill, and colleagues.
Too often, the emphasis for health care professionals is on less common, highly morbid complications, while their patients’ needs are focused more on daily functioning.
More than half of maternal deaths occur not during delivery, but in the days, weeks, and months following birth. Many serious complications and management of less-emergent conditions such as flu-like symptoms go unnoticed or result in treatment delays. Routinely asking women who present for care whether they have been pregnant during the past year could go a long way in helping clinicians connect the dots for conditions they might not otherwise consider, suggested Dr. Stuebe and colleagues.
In response to what is becoming a growing burden of postpartum maternal morbidity and mortality in the United States, Dr. Stuebe and associates, in coordination with the Alliance of Innovation in Maternal Health, prepared a comprehensive consensus statement on postpartum care basics. The work came out of a day-long planning meeting of an interdisciplinary work group funded by AIMH to develop the maternal safety bundle, which established 28 goals across four phases – readiness, recognition and prevention, response, and reporting. Each phase is intended to occur as part of a coordinated effort between women experiencing pregnancy and their health care providers, with involvement from multiple clinical settings and health systems.
America needs to change the way it treats its new mothers
In a separate interview, Dr. Stuebe shared additional insights into the development of the consensus statement: “This article is part of a broader movement to change the way America treats new mothers. For too long, we’ve lavished attention on women in the weeks before birth and then left them alone to manage recovery, plunging hormones, sleepless nights, and new baby care. The goal of this article is to set out the ways that we can better support women in this critical transition period.
“We need to start during pregnancy, by working with women to plan for the fourth trimester and identify a care team that will support her and her baby. After birth, we need to adapt those plans and make sure she has the emotional and material support she needs to navigate the coming months. Many of these decisions are deeply personal, and we need to center the values and preferences of the woman and her family.”
Dr. Stuebe also spotlighted a new University of North Carolina–based program designed to support shared decision-making. Their Trimester Project team partnered with mothers to design NewMomHealth.com, the first national postpartum resource designed by and for new mothers, which is in the process of launching a culturally adapted Spanish-language site, saludmadre.com, in partnership with Urban Strategies.
Readiness prepares mothers, HCPs, and clinical settings for the fourth trimester
In the first phase, Readiness, there are three key parties involved: the woman experiencing pregnancy, the health care providers (HCPs) supporting her, and the clinical settings involved in her care. Each player has specific goals to achieve in this phase, women are responsible for four goals, health care providers have two goals, and clinical settings have five.
Prenatally, every woman should work with health care providers to develop a comprehensive, individualized postpartum care plan that designates a postpartum clinical “home” for addressing any care needed between birth and the “comprehensive postpartum visit.” The plan encourages the patient and her health care team give attention to social support, birth recovery, infant care and feeding plans, thoughts concerning future pregnancies, and specifically use of contraception, as well as any chronic health concerns and overall emotional well-being.
The plan should consist of a postpartum care team that includes friends and family and ensures that medical, material, and social support are available in the weeks following birth for both mother and baby.
The authors emphasized the importance for clinicians to develop a keen awareness of “reproductive justice,” which respects a woman’s right “to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.” They encouraged adopting a sensitivity to concerns deeply rooted in the history of family planning, which is perceived to have been “fraught by coercive tactics to incentivize sterilization and contraceptive implants among marginalized groups.” With this in mind, they urged clinicians to respectfully ask about the patient’s intentions before making any suggestions concerning future births and family planning preferences.
HCP readiness ensures that each woman “has a documented postpartum care plan and care team identified in the prenatal period.” HCPs are also responsible for developing and maintaining “a working knowledge of evidence-based evaluation and management of common issues facing the mother-infant dyad.”
Clinical setting readiness ensures that woman-centered postpartum care and education have been developed and optimized using adult learning principles whenever possible. Diversity of family structures, cultural traditions, and parenting practices are fully embraced. Dr. Stuebe and colleagues emphasized that traditional top-down teaching methods are ineffective and should be avoided.
Clinical setting readiness also ensures that systems are developed to pair families with community-based resources that provide medical follow-up as well as social and material support. Clinical protocols and reimbursement options should be available that give women easy access to preferred contraception. Systems should be in place that facilitate prompt, pertinent communication between in- and outpatient providers. Lastly, and perhaps most importantly, clinical setting readiness demands the development of protocols to screen and treat key postpartum concerns, such as depression, substance use disorders, family violence, and even incontinence in coordination with locally identified specialists.
Recognition and prevention promotes accountability and establishes key guidelines
Recognition and prevention require coordinated participation between women experiencing pregnancy and the clinical environments supporting their care. In this phase, women are responsible for three goals; clinical environments have four goals.
Women are to be identified and respected as the expert most knowledgeable of their own needs, cautioned the authors. They should also be empowered to trust their instincts, seeking care as early and as often as needed in the weeks after they give birth. Postpartum care needs to be viewed as an ongoing process, not just a singular encounter.
Women also need to take ownership for their postpartum care plan, reviewing and revising it as needed in coordination with their health care providers before maternity discharge is complete. Every plan should include a comprehensive list of warning signs and recommended action plans when faced with life-threatening complications, a list of resources for lactation support, and a “first-call” phone number that identifies the postpartum medical providers available to address breastfeeding issues and for postpartum care visits, including prescheduled dates and times.
Lastly, women are to take responsibility for attending their postpartum visit. Although new guidance suggests that the comprehensive visit take place no later than 12 weeks post partum, it also recognizes multiple visits may be required to address individual needs. All women should have contact with a maternal care provider within 3 weeks post partum, the American College of Obstetricians and Gynecologists recommends.
Responsibility for recognition and prevention in the clinical setting begins with determining guidelines for early postpartum visits, considering chronic conditions such as hypertension, diabetes, or substance abuse disorder and risk for postpartum conditions such as wound complications or postpartum depression, the authors wrote. Ongoing care between inpatient and outpatient settings as well as between maternal and infant care providers is coordinated to ensure health and well-being of both patients. Screening and treatment of common comorbidities such as mental health issues, smoking, and substance use as well as issues related to unstable housing and food insecurities are also addressed in the clinical environment. Lastly, clinicians are tasked with ensuring that every patient has selected a primary care provider for ongoing care.
Response ensures key parties and resources are connected at every step
In the response phase, clinical settings and health care providers are the key participants and they have two goals each.
Every clinical setting is tasked with implementing treatment protocols and providing needed care or facilitating referral in a timely fashion. The importance of a “warm hand-off” and “face-to-face introduction to the specialist to whom the patient is being referred” is encouraged. They are also responsible for keeping an updated inventory of community resources on hand for such unmet needs as 24-hour hotlines, food banks, diaper banks, lactation support groups, and home-visiting programs.
Every health care provider is tasked with developing strategies designed to reach women who do not attend their comprehensive postpartum visit. They are also responsible for assessing the severity of identified needs, and arranging immediate transportation to appropriate facilities in life-threatening circumstances. In nonacute cases, the woman and her care providers work with her to make appropriate decisions.
Reporting gives health systems the opportunity to assess and improve
Sole responsibility in the reporting phase falls to every health system. In this phase, they have a total of six goals.
Health systems are ideally organized to convene strategy-sharing sessions with inpatient as well as outpatient professionals to evaluate successes and opportunities for improvement. They are equally qualified to identify and monitor such quality measures as postpartum emergency department utilization and readmission rates. They are tasked with working toward quality metrics that compare postpartum outcomes and prenatal intentions, including patient receipt of preferred contraception or completion of planned breastfeeding duration.
Health systems are expected to conduct quality improvement measures designed to reduce postpartum morbidity when preventable. They are also the logical choice for maintaining a clearinghouse for resources, in collaboration with the community, that is designed to meet the postpartum needs of women.
Lastly, they play an important role in ensuring that reimbursement policies are structured such that they do not disincentivize postpartum visits.
The consensus bundle encourages change in the way America treats its new mothers
Angela Bianco, MD, maternal and fetal medicine specialist at Mount Sinai Hospital, New York, also interviewed separately, noted: “I think the fact that ACOG has created a postpartum bundle for providers to use for guidance is long overdue. The current prenatal care paradigm focuses on numerous/intensive prenatal visits but only a single postpartum visit. Many women report feeling ill-equipped to navigate the challenges that arise post delivery, including self-care, newborn care, and breastfeeding. In addition, most women experience the impact of dramatic hormonal fluctuations resulting in mood alterations. Add profound sleep deprivation to this and the result is often some degree of postpartum blues and/or depression. The importance of anticipatory guidance for our patients cannot be underestimated. Helping to facilitate potential social support structures be in place prior to the birth is optimal. Providers should reinforce the importance of access to a variety of tools, including digital apps, community support groups, and 24/7 web access services. Moving forward, it should be considered unconscionable to send a new mother home without ensuring the appropriate resources are in place. Postpartum care should be tailored to a woman’s needs and may require multiple visits and/or referrals.”
Dr. Stuebe and colleagues, as well as Dr. Bianco, disclosed receiving honoraria for various projects. Funding for the study was supported by the Alliance for Innovation on Maternal and Child Health, which is funded by a grant from the Health Resources and Services Administration.
Health care professionals miss an important opportunity if they do not use a holistic patient-centered approach in providing support to their postpartum patients, advised Alison M. Stuebe, MD, MSc, of the division of maternal-fetal medicine at the University of North Carolina at Chapel Hill, and colleagues.
Too often, the emphasis for health care professionals is on less common, highly morbid complications, while their patients’ needs are focused more on daily functioning.
More than half of maternal deaths occur not during delivery, but in the days, weeks, and months following birth. Many serious complications and management of less-emergent conditions such as flu-like symptoms go unnoticed or result in treatment delays. Routinely asking women who present for care whether they have been pregnant during the past year could go a long way in helping clinicians connect the dots for conditions they might not otherwise consider, suggested Dr. Stuebe and colleagues.
In response to what is becoming a growing burden of postpartum maternal morbidity and mortality in the United States, Dr. Stuebe and associates, in coordination with the Alliance of Innovation in Maternal Health, prepared a comprehensive consensus statement on postpartum care basics. The work came out of a day-long planning meeting of an interdisciplinary work group funded by AIMH to develop the maternal safety bundle, which established 28 goals across four phases – readiness, recognition and prevention, response, and reporting. Each phase is intended to occur as part of a coordinated effort between women experiencing pregnancy and their health care providers, with involvement from multiple clinical settings and health systems.
America needs to change the way it treats its new mothers
In a separate interview, Dr. Stuebe shared additional insights into the development of the consensus statement: “This article is part of a broader movement to change the way America treats new mothers. For too long, we’ve lavished attention on women in the weeks before birth and then left them alone to manage recovery, plunging hormones, sleepless nights, and new baby care. The goal of this article is to set out the ways that we can better support women in this critical transition period.
“We need to start during pregnancy, by working with women to plan for the fourth trimester and identify a care team that will support her and her baby. After birth, we need to adapt those plans and make sure she has the emotional and material support she needs to navigate the coming months. Many of these decisions are deeply personal, and we need to center the values and preferences of the woman and her family.”
Dr. Stuebe also spotlighted a new University of North Carolina–based program designed to support shared decision-making. Their Trimester Project team partnered with mothers to design NewMomHealth.com, the first national postpartum resource designed by and for new mothers, which is in the process of launching a culturally adapted Spanish-language site, saludmadre.com, in partnership with Urban Strategies.
Readiness prepares mothers, HCPs, and clinical settings for the fourth trimester
In the first phase, Readiness, there are three key parties involved: the woman experiencing pregnancy, the health care providers (HCPs) supporting her, and the clinical settings involved in her care. Each player has specific goals to achieve in this phase, women are responsible for four goals, health care providers have two goals, and clinical settings have five.
Prenatally, every woman should work with health care providers to develop a comprehensive, individualized postpartum care plan that designates a postpartum clinical “home” for addressing any care needed between birth and the “comprehensive postpartum visit.” The plan encourages the patient and her health care team give attention to social support, birth recovery, infant care and feeding plans, thoughts concerning future pregnancies, and specifically use of contraception, as well as any chronic health concerns and overall emotional well-being.
The plan should consist of a postpartum care team that includes friends and family and ensures that medical, material, and social support are available in the weeks following birth for both mother and baby.
The authors emphasized the importance for clinicians to develop a keen awareness of “reproductive justice,” which respects a woman’s right “to maintain personal bodily autonomy, have children, not have children, and parent the children we have in safe and sustainable communities.” They encouraged adopting a sensitivity to concerns deeply rooted in the history of family planning, which is perceived to have been “fraught by coercive tactics to incentivize sterilization and contraceptive implants among marginalized groups.” With this in mind, they urged clinicians to respectfully ask about the patient’s intentions before making any suggestions concerning future births and family planning preferences.
HCP readiness ensures that each woman “has a documented postpartum care plan and care team identified in the prenatal period.” HCPs are also responsible for developing and maintaining “a working knowledge of evidence-based evaluation and management of common issues facing the mother-infant dyad.”
Clinical setting readiness ensures that woman-centered postpartum care and education have been developed and optimized using adult learning principles whenever possible. Diversity of family structures, cultural traditions, and parenting practices are fully embraced. Dr. Stuebe and colleagues emphasized that traditional top-down teaching methods are ineffective and should be avoided.
Clinical setting readiness also ensures that systems are developed to pair families with community-based resources that provide medical follow-up as well as social and material support. Clinical protocols and reimbursement options should be available that give women easy access to preferred contraception. Systems should be in place that facilitate prompt, pertinent communication between in- and outpatient providers. Lastly, and perhaps most importantly, clinical setting readiness demands the development of protocols to screen and treat key postpartum concerns, such as depression, substance use disorders, family violence, and even incontinence in coordination with locally identified specialists.
Recognition and prevention promotes accountability and establishes key guidelines
Recognition and prevention require coordinated participation between women experiencing pregnancy and the clinical environments supporting their care. In this phase, women are responsible for three goals; clinical environments have four goals.
Women are to be identified and respected as the expert most knowledgeable of their own needs, cautioned the authors. They should also be empowered to trust their instincts, seeking care as early and as often as needed in the weeks after they give birth. Postpartum care needs to be viewed as an ongoing process, not just a singular encounter.
Women also need to take ownership for their postpartum care plan, reviewing and revising it as needed in coordination with their health care providers before maternity discharge is complete. Every plan should include a comprehensive list of warning signs and recommended action plans when faced with life-threatening complications, a list of resources for lactation support, and a “first-call” phone number that identifies the postpartum medical providers available to address breastfeeding issues and for postpartum care visits, including prescheduled dates and times.
Lastly, women are to take responsibility for attending their postpartum visit. Although new guidance suggests that the comprehensive visit take place no later than 12 weeks post partum, it also recognizes multiple visits may be required to address individual needs. All women should have contact with a maternal care provider within 3 weeks post partum, the American College of Obstetricians and Gynecologists recommends.
Responsibility for recognition and prevention in the clinical setting begins with determining guidelines for early postpartum visits, considering chronic conditions such as hypertension, diabetes, or substance abuse disorder and risk for postpartum conditions such as wound complications or postpartum depression, the authors wrote. Ongoing care between inpatient and outpatient settings as well as between maternal and infant care providers is coordinated to ensure health and well-being of both patients. Screening and treatment of common comorbidities such as mental health issues, smoking, and substance use as well as issues related to unstable housing and food insecurities are also addressed in the clinical environment. Lastly, clinicians are tasked with ensuring that every patient has selected a primary care provider for ongoing care.
Response ensures key parties and resources are connected at every step
In the response phase, clinical settings and health care providers are the key participants and they have two goals each.
Every clinical setting is tasked with implementing treatment protocols and providing needed care or facilitating referral in a timely fashion. The importance of a “warm hand-off” and “face-to-face introduction to the specialist to whom the patient is being referred” is encouraged. They are also responsible for keeping an updated inventory of community resources on hand for such unmet needs as 24-hour hotlines, food banks, diaper banks, lactation support groups, and home-visiting programs.
Every health care provider is tasked with developing strategies designed to reach women who do not attend their comprehensive postpartum visit. They are also responsible for assessing the severity of identified needs, and arranging immediate transportation to appropriate facilities in life-threatening circumstances. In nonacute cases, the woman and her care providers work with her to make appropriate decisions.
Reporting gives health systems the opportunity to assess and improve
Sole responsibility in the reporting phase falls to every health system. In this phase, they have a total of six goals.
Health systems are ideally organized to convene strategy-sharing sessions with inpatient as well as outpatient professionals to evaluate successes and opportunities for improvement. They are equally qualified to identify and monitor such quality measures as postpartum emergency department utilization and readmission rates. They are tasked with working toward quality metrics that compare postpartum outcomes and prenatal intentions, including patient receipt of preferred contraception or completion of planned breastfeeding duration.
Health systems are expected to conduct quality improvement measures designed to reduce postpartum morbidity when preventable. They are also the logical choice for maintaining a clearinghouse for resources, in collaboration with the community, that is designed to meet the postpartum needs of women.
Lastly, they play an important role in ensuring that reimbursement policies are structured such that they do not disincentivize postpartum visits.
The consensus bundle encourages change in the way America treats its new mothers
Angela Bianco, MD, maternal and fetal medicine specialist at Mount Sinai Hospital, New York, also interviewed separately, noted: “I think the fact that ACOG has created a postpartum bundle for providers to use for guidance is long overdue. The current prenatal care paradigm focuses on numerous/intensive prenatal visits but only a single postpartum visit. Many women report feeling ill-equipped to navigate the challenges that arise post delivery, including self-care, newborn care, and breastfeeding. In addition, most women experience the impact of dramatic hormonal fluctuations resulting in mood alterations. Add profound sleep deprivation to this and the result is often some degree of postpartum blues and/or depression. The importance of anticipatory guidance for our patients cannot be underestimated. Helping to facilitate potential social support structures be in place prior to the birth is optimal. Providers should reinforce the importance of access to a variety of tools, including digital apps, community support groups, and 24/7 web access services. Moving forward, it should be considered unconscionable to send a new mother home without ensuring the appropriate resources are in place. Postpartum care should be tailored to a woman’s needs and may require multiple visits and/or referrals.”
Dr. Stuebe and colleagues, as well as Dr. Bianco, disclosed receiving honoraria for various projects. Funding for the study was supported by the Alliance for Innovation on Maternal and Child Health, which is funded by a grant from the Health Resources and Services Administration.
FROM OBSTETRICS AND GYNECOLOGY
Family physicians can help achieve national goals on STIs
Among these are the U.S. Department of Health and Human Services’ first “Sexually Transmitted Infections (STIs) National Strategic Plan for the United States,” which has a strong encompassing vision.

“The United States will be a place where sexually transmitted infections are prevented and where every person has high-quality STI prevention care, and treatment while living free from stigma and discrimination. The vision includes all people, regardless of age, sex, gender identity, sexual orientation, race, ethnicity, religion, disability, geographic location, or socioeconomic circumstance,” the new HHS plan states.1
Family physicians can and should play important roles in helping our country meet this plan’s goals particularly by following two important updated clinical guidelines, one from the U.S. Preventive Services Task Force (USPSTF) and another from the Centers for Disease Control and Prevention (CDC).
This strategic plan includes the following five overarching goals with associated objectives:
- Prevent New STIs.
- Improve the health of people by reducing adverse outcomes of STIs.
- Accelerate progress in STI research, technology, and innovation.
- Reduce STI-related health disparities and health inequities.
- Achieve integrated, coordinated efforts that address the STI epidemic.1
In my opinion, family physicians have important roles to play in order for each of these goals to be achieved.Unfortunately, there are approximately 20 million new cases of STIs each year, and the U.S. has seen increases in the rates of STIs in the past decade.
“Sexually transmitted infections are frequently asymptomatic, which may delay diagnosis and treatment and lead persons to unknowingly transmit STIs to others,” according to a new recommendation statement from the USPSTF.2 STIs may lead to serious health consequences for patients, cause harms to a mother and infant during pregnancy, and lead to cases of cancer among other concerning outcomes. As such, following the HHS new national strategic plan is critical for us to address the needs of our communities.
Preventing new STIs
Family physicians can be vital in achieving the first goal of the plan by helping to prevent new STIs. In August 2020, the USPSTF updated its guideline on behavioral counseling interventions to prevent STIs. In my opinion, the USPSTF offers some practical improvements from the earlier version of this guideline.
The task force provides a grade B recommendation that all sexually active adolescents and adults at increased risk for STIs be provided with behavioral counseling to prevent STIs. The guideline indicates that behavioral counseling interventions reduce the likelihood of those at increased risk for acquiring STIs.2
The 2014 guideline had recommended intensive interventions with a minimum of 30 minutes of counseling. Many family physicians may have found this previous recommendation impractical to implement. These updated recommendations now include a variety of interventions, such as those that take less than 30 minutes.
Although interventions with more than 120 minutes of contact time had the most effect, those with less than 30 minutes still demonstrated statistically significant fewer acquisitions of STIs during follow-up. These options include in-person counseling, and providing written materials, websites, videos, and telephone and text support to patients. These interventions can be delivered directly by the family physician, or patients may be referred to other settings or the media interventions.
The task force’s updated recommendation statement refers to a variety of resources that can be used to identify these interventions. Many of the studies reviewed for this guideline were conducted in STI clinics, and the guideline authors recommended further studies in primary care as opportunities for more generalizability.
In addition to behavioral counseling for STI prevention, family physicians can help prevent STIs in their patients through HPV vaccination and HIV pre-exposure prophylaxis (PrEP provision) within their practices. As the first contact for health care for many patients, we have an opportunity to significantly impact this first goal of prevention.
Treating STIs
Within the second goal of the national strategic plan is treatment of STIs, which family physicians should include in their practices as well as the diagnosis of STIs.
In December 2020, an update to the CDC’s treatment guideline for gonococcal infection was released. Prior to the publishing of this updated recommendation, the CDC recommended combination therapy of 250 mg intramuscular (IM) dose of ceftriaxone and either doxycycline or azithromycin. This recommendation has been changed to a single 500-mg IM dose of ceftriaxone for uncomplicated urogenital, anorectal, and pharyngeal gonorrhea. If chlamydia cannot be excluded, then the addition of oral doxycycline 100 mg twice daily for 7 days is recommended for nonpregnant persons, and 1 g oral azithromycin for pregnant persons. The previous treatment was recommended based on a concern for gonococcal resistance.
This updated guideline reflects increasing concerns for antimicrobial stewardship and emerging azithromycin resistance. It does not recommend a test-of-cure for urogenital or rectal gonorrhea, though did recommend a test-of-cure 7-14 days after treatment of pharyngeal gonorrhea. The guideline also recommends testing for reinfection 3-12 months after treatment as the rate of reinfection ranges from 7% to 12% among those previously treated.3
For some offices, the provision of the IM injection may be challenging, though having this medication in stock with the possibility of provision can greatly improve access and ease of treatment for patients. Family physicians can incorporate these updated recommendations along with those for other STIs such as chlamydia and syphilis with standing orders for treatment and testing within their offices.
Accelerating progress in STI research
Family physicians can also support the national strategic plan by participating in studies looking at the impact of behavioral counseling in the primary care office as opposed to in STI clinics. In addition, by following the STI treatment and screening guidelines, family physicians will contribute to the body of knowledge of prevalence, treatment failure, and reinfection rates of STIs. We can also help advance the research by providing feedback on interventions that have success within our practices.
Reducing STI-related health disparities and inequities
Family physicians are also in important places to support the strategic plan’s fourth goal of reducing health disparities and health inequities.
If we continue to ask the questions to identify those at high risk and ensure that we are offering appropriate STI prevention, care, and treatment services within our clinics, we can expand access to all who need services and improve equity. By offering these services within the primary care office, we may be able to decrease the stigma some may feel going to an STI clinic for services.
By incorporating additional screening and counseling in our practices we may identify some patients who were not aware that they were at risk for an STI and offer them preventive services.
Achieving integrated and coordinated efforts
Finally, as many family physicians have integrated practices, we are uniquely poised to support the fifth goal of the strategic plan of achieving integrated and coordinated efforts addressing the STI epidemic. In our practices we can participate in, lead, and refer to programs for substance use disorders, viral hepatitis, STIs, and HIV as part of full scope primary care.
Family physicians and other primary care providers should work to support the entire strategic plan to ensure that we are fully caring for our patients and communities and stopping the past decade’s increase in STIs. We have an opportunity to use this strategy and make a large impact in our communities.
Dr. Wheat is a family physician at Erie Family Health Center in Chicago. She is program director of Northwestern’s McGaw Family Medicine residency program at Humboldt Park, Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
References
1. U.S. Department of Health and Human Services. 2020. Sexually Transmitted Infections National Strategic Plan for the United States: 2021-2025. Washington.
2. U.S. Preventive Services Task Force. Behavioral counseling interventions to prevent sexually transmitted infections: U.S. Preventive Services Task Force Recommendation Statement. JAMA. 2020;324(7):674-81. doi: 10.1001/jama.2020.13095.
3. St. Cyr S et al. Update to CDC’s Treatment Guideline for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep 2020;69:1911-6. doi: 10.15585/mmwr.mm6950a6external_icon.
Among these are the U.S. Department of Health and Human Services’ first “Sexually Transmitted Infections (STIs) National Strategic Plan for the United States,” which has a strong encompassing vision.
“The United States will be a place where sexually transmitted infections are prevented and where every person has high-quality STI prevention care, and treatment while living free from stigma and discrimination. The vision includes all people, regardless of age, sex, gender identity, sexual orientation, race, ethnicity, religion, disability, geographic location, or socioeconomic circumstance,” the new HHS plan states.1
Family physicians can and should play important roles in helping our country meet this plan’s goals particularly by following two important updated clinical guidelines, one from the U.S. Preventive Services Task Force (USPSTF) and another from the Centers for Disease Control and Prevention (CDC).
This strategic plan includes the following five overarching goals with associated objectives:
- Prevent New STIs.
- Improve the health of people by reducing adverse outcomes of STIs.
- Accelerate progress in STI research, technology, and innovation.
- Reduce STI-related health disparities and health inequities.
- Achieve integrated, coordinated efforts that address the STI epidemic.1
In my opinion, family physicians have important roles to play in order for each of these goals to be achieved.Unfortunately, there are approximately 20 million new cases of STIs each year, and the U.S. has seen increases in the rates of STIs in the past decade.
“Sexually transmitted infections are frequently asymptomatic, which may delay diagnosis and treatment and lead persons to unknowingly transmit STIs to others,” according to a new recommendation statement from the USPSTF.2 STIs may lead to serious health consequences for patients, cause harms to a mother and infant during pregnancy, and lead to cases of cancer among other concerning outcomes. As such, following the HHS new national strategic plan is critical for us to address the needs of our communities.
Preventing new STIs
Family physicians can be vital in achieving the first goal of the plan by helping to prevent new STIs. In August 2020, the USPSTF updated its guideline on behavioral counseling interventions to prevent STIs. In my opinion, the USPSTF offers some practical improvements from the earlier version of this guideline.
The task force provides a grade B recommendation that all sexually active adolescents and adults at increased risk for STIs be provided with behavioral counseling to prevent STIs. The guideline indicates that behavioral counseling interventions reduce the likelihood of those at increased risk for acquiring STIs.2
The 2014 guideline had recommended intensive interventions with a minimum of 30 minutes of counseling. Many family physicians may have found this previous recommendation impractical to implement. These updated recommendations now include a variety of interventions, such as those that take less than 30 minutes.
Although interventions with more than 120 minutes of contact time had the most effect, those with less than 30 minutes still demonstrated statistically significant fewer acquisitions of STIs during follow-up. These options include in-person counseling, and providing written materials, websites, videos, and telephone and text support to patients. These interventions can be delivered directly by the family physician, or patients may be referred to other settings or the media interventions.
The task force’s updated recommendation statement refers to a variety of resources that can be used to identify these interventions. Many of the studies reviewed for this guideline were conducted in STI clinics, and the guideline authors recommended further studies in primary care as opportunities for more generalizability.
In addition to behavioral counseling for STI prevention, family physicians can help prevent STIs in their patients through HPV vaccination and HIV pre-exposure prophylaxis (PrEP provision) within their practices. As the first contact for health care for many patients, we have an opportunity to significantly impact this first goal of prevention.
Treating STIs
Within the second goal of the national strategic plan is treatment of STIs, which family physicians should include in their practices as well as the diagnosis of STIs.
In December 2020, an update to the CDC’s treatment guideline for gonococcal infection was released. Prior to the publishing of this updated recommendation, the CDC recommended combination therapy of 250 mg intramuscular (IM) dose of ceftriaxone and either doxycycline or azithromycin. This recommendation has been changed to a single 500-mg IM dose of ceftriaxone for uncomplicated urogenital, anorectal, and pharyngeal gonorrhea. If chlamydia cannot be excluded, then the addition of oral doxycycline 100 mg twice daily for 7 days is recommended for nonpregnant persons, and 1 g oral azithromycin for pregnant persons. The previous treatment was recommended based on a concern for gonococcal resistance.
This updated guideline reflects increasing concerns for antimicrobial stewardship and emerging azithromycin resistance. It does not recommend a test-of-cure for urogenital or rectal gonorrhea, though did recommend a test-of-cure 7-14 days after treatment of pharyngeal gonorrhea. The guideline also recommends testing for reinfection 3-12 months after treatment as the rate of reinfection ranges from 7% to 12% among those previously treated.3
For some offices, the provision of the IM injection may be challenging, though having this medication in stock with the possibility of provision can greatly improve access and ease of treatment for patients. Family physicians can incorporate these updated recommendations along with those for other STIs such as chlamydia and syphilis with standing orders for treatment and testing within their offices.
Accelerating progress in STI research
Family physicians can also support the national strategic plan by participating in studies looking at the impact of behavioral counseling in the primary care office as opposed to in STI clinics. In addition, by following the STI treatment and screening guidelines, family physicians will contribute to the body of knowledge of prevalence, treatment failure, and reinfection rates of STIs. We can also help advance the research by providing feedback on interventions that have success within our practices.
Reducing STI-related health disparities and inequities
Family physicians are also in important places to support the strategic plan’s fourth goal of reducing health disparities and health inequities.
If we continue to ask the questions to identify those at high risk and ensure that we are offering appropriate STI prevention, care, and treatment services within our clinics, we can expand access to all who need services and improve equity. By offering these services within the primary care office, we may be able to decrease the stigma some may feel going to an STI clinic for services.
By incorporating additional screening and counseling in our practices we may identify some patients who were not aware that they were at risk for an STI and offer them preventive services.
Achieving integrated and coordinated efforts
Finally, as many family physicians have integrated practices, we are uniquely poised to support the fifth goal of the strategic plan of achieving integrated and coordinated efforts addressing the STI epidemic. In our practices we can participate in, lead, and refer to programs for substance use disorders, viral hepatitis, STIs, and HIV as part of full scope primary care.
Family physicians and other primary care providers should work to support the entire strategic plan to ensure that we are fully caring for our patients and communities and stopping the past decade’s increase in STIs. We have an opportunity to use this strategy and make a large impact in our communities.
Dr. Wheat is a family physician at Erie Family Health Center in Chicago. She is program director of Northwestern’s McGaw Family Medicine residency program at Humboldt Park, Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
References
1. U.S. Department of Health and Human Services. 2020. Sexually Transmitted Infections National Strategic Plan for the United States: 2021-2025. Washington.
2. U.S. Preventive Services Task Force. Behavioral counseling interventions to prevent sexually transmitted infections: U.S. Preventive Services Task Force Recommendation Statement. JAMA. 2020;324(7):674-81. doi: 10.1001/jama.2020.13095.
3. St. Cyr S et al. Update to CDC’s Treatment Guideline for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep 2020;69:1911-6. doi: 10.15585/mmwr.mm6950a6external_icon.
Among these are the U.S. Department of Health and Human Services’ first “Sexually Transmitted Infections (STIs) National Strategic Plan for the United States,” which has a strong encompassing vision.
“The United States will be a place where sexually transmitted infections are prevented and where every person has high-quality STI prevention care, and treatment while living free from stigma and discrimination. The vision includes all people, regardless of age, sex, gender identity, sexual orientation, race, ethnicity, religion, disability, geographic location, or socioeconomic circumstance,” the new HHS plan states.1
Family physicians can and should play important roles in helping our country meet this plan’s goals particularly by following two important updated clinical guidelines, one from the U.S. Preventive Services Task Force (USPSTF) and another from the Centers for Disease Control and Prevention (CDC).
This strategic plan includes the following five overarching goals with associated objectives:
- Prevent New STIs.
- Improve the health of people by reducing adverse outcomes of STIs.
- Accelerate progress in STI research, technology, and innovation.
- Reduce STI-related health disparities and health inequities.
- Achieve integrated, coordinated efforts that address the STI epidemic.1
In my opinion, family physicians have important roles to play in order for each of these goals to be achieved.Unfortunately, there are approximately 20 million new cases of STIs each year, and the U.S. has seen increases in the rates of STIs in the past decade.
“Sexually transmitted infections are frequently asymptomatic, which may delay diagnosis and treatment and lead persons to unknowingly transmit STIs to others,” according to a new recommendation statement from the USPSTF.2 STIs may lead to serious health consequences for patients, cause harms to a mother and infant during pregnancy, and lead to cases of cancer among other concerning outcomes. As such, following the HHS new national strategic plan is critical for us to address the needs of our communities.
Preventing new STIs
Family physicians can be vital in achieving the first goal of the plan by helping to prevent new STIs. In August 2020, the USPSTF updated its guideline on behavioral counseling interventions to prevent STIs. In my opinion, the USPSTF offers some practical improvements from the earlier version of this guideline.
The task force provides a grade B recommendation that all sexually active adolescents and adults at increased risk for STIs be provided with behavioral counseling to prevent STIs. The guideline indicates that behavioral counseling interventions reduce the likelihood of those at increased risk for acquiring STIs.2
The 2014 guideline had recommended intensive interventions with a minimum of 30 minutes of counseling. Many family physicians may have found this previous recommendation impractical to implement. These updated recommendations now include a variety of interventions, such as those that take less than 30 minutes.
Although interventions with more than 120 minutes of contact time had the most effect, those with less than 30 minutes still demonstrated statistically significant fewer acquisitions of STIs during follow-up. These options include in-person counseling, and providing written materials, websites, videos, and telephone and text support to patients. These interventions can be delivered directly by the family physician, or patients may be referred to other settings or the media interventions.
The task force’s updated recommendation statement refers to a variety of resources that can be used to identify these interventions. Many of the studies reviewed for this guideline were conducted in STI clinics, and the guideline authors recommended further studies in primary care as opportunities for more generalizability.
In addition to behavioral counseling for STI prevention, family physicians can help prevent STIs in their patients through HPV vaccination and HIV pre-exposure prophylaxis (PrEP provision) within their practices. As the first contact for health care for many patients, we have an opportunity to significantly impact this first goal of prevention.
Treating STIs
Within the second goal of the national strategic plan is treatment of STIs, which family physicians should include in their practices as well as the diagnosis of STIs.
In December 2020, an update to the CDC’s treatment guideline for gonococcal infection was released. Prior to the publishing of this updated recommendation, the CDC recommended combination therapy of 250 mg intramuscular (IM) dose of ceftriaxone and either doxycycline or azithromycin. This recommendation has been changed to a single 500-mg IM dose of ceftriaxone for uncomplicated urogenital, anorectal, and pharyngeal gonorrhea. If chlamydia cannot be excluded, then the addition of oral doxycycline 100 mg twice daily for 7 days is recommended for nonpregnant persons, and 1 g oral azithromycin for pregnant persons. The previous treatment was recommended based on a concern for gonococcal resistance.
This updated guideline reflects increasing concerns for antimicrobial stewardship and emerging azithromycin resistance. It does not recommend a test-of-cure for urogenital or rectal gonorrhea, though did recommend a test-of-cure 7-14 days after treatment of pharyngeal gonorrhea. The guideline also recommends testing for reinfection 3-12 months after treatment as the rate of reinfection ranges from 7% to 12% among those previously treated.3
For some offices, the provision of the IM injection may be challenging, though having this medication in stock with the possibility of provision can greatly improve access and ease of treatment for patients. Family physicians can incorporate these updated recommendations along with those for other STIs such as chlamydia and syphilis with standing orders for treatment and testing within their offices.
Accelerating progress in STI research
Family physicians can also support the national strategic plan by participating in studies looking at the impact of behavioral counseling in the primary care office as opposed to in STI clinics. In addition, by following the STI treatment and screening guidelines, family physicians will contribute to the body of knowledge of prevalence, treatment failure, and reinfection rates of STIs. We can also help advance the research by providing feedback on interventions that have success within our practices.
Reducing STI-related health disparities and inequities
Family physicians are also in important places to support the strategic plan’s fourth goal of reducing health disparities and health inequities.
If we continue to ask the questions to identify those at high risk and ensure that we are offering appropriate STI prevention, care, and treatment services within our clinics, we can expand access to all who need services and improve equity. By offering these services within the primary care office, we may be able to decrease the stigma some may feel going to an STI clinic for services.
By incorporating additional screening and counseling in our practices we may identify some patients who were not aware that they were at risk for an STI and offer them preventive services.
Achieving integrated and coordinated efforts
Finally, as many family physicians have integrated practices, we are uniquely poised to support the fifth goal of the strategic plan of achieving integrated and coordinated efforts addressing the STI epidemic. In our practices we can participate in, lead, and refer to programs for substance use disorders, viral hepatitis, STIs, and HIV as part of full scope primary care.
Family physicians and other primary care providers should work to support the entire strategic plan to ensure that we are fully caring for our patients and communities and stopping the past decade’s increase in STIs. We have an opportunity to use this strategy and make a large impact in our communities.
Dr. Wheat is a family physician at Erie Family Health Center in Chicago. She is program director of Northwestern’s McGaw Family Medicine residency program at Humboldt Park, Chicago. Dr. Wheat serves on the editorial advisory board of Family Practice News. You can contact her at fpnews@mdedge.com.
References
1. U.S. Department of Health and Human Services. 2020. Sexually Transmitted Infections National Strategic Plan for the United States: 2021-2025. Washington.
2. U.S. Preventive Services Task Force. Behavioral counseling interventions to prevent sexually transmitted infections: U.S. Preventive Services Task Force Recommendation Statement. JAMA. 2020;324(7):674-81. doi: 10.1001/jama.2020.13095.
3. St. Cyr S et al. Update to CDC’s Treatment Guideline for Gonococcal Infection, 2020. MMWR Morb Mortal Wkly Rep 2020;69:1911-6. doi: 10.15585/mmwr.mm6950a6external_icon.
Pressure builds on CDC to prioritize both diabetes types for vaccine
The American Diabetes Association, along with 18 other organizations, has sent a letter to the U.S. Centers for Disease Control and Prevention urging them to rank people with type 1 diabetes as equally high risk for COVID-19 severity, and therefore vaccination, as those with type 2 diabetes.
On Jan. 12, the CDC recommended states vaccinate all Americans over age 65 and those with underlying health conditions that make them more vulnerable to COVID-19.
Currently, type 2 diabetes is listed among 12 conditions that place adults “at increased risk of severe illness from the virus that causes COVID-19,” with the latter defined as “hospitalization, admission to the intensive care unit, intubation or mechanical ventilation, or death.”
On the other hand, the autoimmune condition type 1 diabetes is among 11 conditions the CDC says “might be at increased risk” for COVID-19, but limited data were available at the time of the last update on Dec. 23, 2020.
“States are utilizing the CDC risk classification when designing their vaccine distribution plans. This raises an obvious concern as it could result in the approximately 1.6 million with type 1 diabetes receiving the vaccination later than others with the same risk,” states the ADA letter, sent to the CDC on Jan. 13.
Representatives from the Endocrine Society, American Association of Clinical Endocrinology, Pediatric Endocrine Society, Association of Diabetes Care & Education Specialists, and JDRF, among others, cosigned the letter.
Newer data show those with type 1 diabetes at equally high risk
While acknowledging that “early data did not provide as much clarity about the extent to which those with type 1 diabetes are at high risk,” the ADA says newer evidence has emerged, as previously reported by this news organization, that “convincingly demonstrates that COVID-19 severity is more than tripled in individuals with type 1 diabetes.”
The letter also cites another study showing that people with type 1 diabetes “have a 3.3-fold greater risk of severe illness, are 3.9 times more likely to be hospitalized with COVID-19, and have a 3-fold increase in mortality compared to those without type 1 diabetes.”
Those risks, they note, are comparable to the increased risk established for those with type 2 diabetes, as shown in a third study from Scotland, published last month.
Asked for comment, CDC representative Kirsten Nordlund said in an interview, “This list is a living document that will be periodically updated by CDC, and it could rapidly change as the science evolves.”
In addition, Ms. Nordlund said, “Decisions about transitioning to subsequent phases should depend on supply; demand; equitable vaccine distribution; and local, state, or territorial context.”
“Phased vaccine recommendations are meant to be fluid and not restrictive for jurisdictions. It is not necessary to vaccinate all individuals in one phase before initiating the next phase; phases may overlap,” she noted. More information is available here.
Tennessee gives type 1 and type 2 diabetes equal priority for vaccination
Meanwhile, at least one state, Tennessee, has updated its guidance to include both types of diabetes as being priority for COVID-19 vaccination.
Vanderbilt University pediatric endocrinologist Justin M. Gregory, MD, said in an interview: “I was thrilled when our state modified its guidance on December 30th to include both type 1 and type 2 diabetes in the ‘high-risk category.’ Other states have not modified that guidance though.”
It’s unclear how this might play out on the ground, noted Dr. Gregory, who led one of the three studies demonstrating increased COVID-19 risk for people with type 1 diabetes.
“To tell you the truth, I don’t really know how individual organizations dispensing the vaccination [will handle] people who come to their facility saying they have ‘diabetes.’ Individual states set the vaccine-dispensing guidance and individual county health departments and health care systems mirror that guidance,” he said.
Thus, he added, “Although it’s possible an individual nurse may take the ‘I’ll ask you no questions, and you’ll tell me no lies’ approach if someone with type 1 diabetes says they have ‘diabetes’, websites and health department–recorded telephone messages are going to tell people with type 1 diabetes they have to wait further back in line if that is what their state’s guidance directs.”
A version of this article first appeared on Medscape.com.
The American Diabetes Association, along with 18 other organizations, has sent a letter to the U.S. Centers for Disease Control and Prevention urging them to rank people with type 1 diabetes as equally high risk for COVID-19 severity, and therefore vaccination, as those with type 2 diabetes.
On Jan. 12, the CDC recommended states vaccinate all Americans over age 65 and those with underlying health conditions that make them more vulnerable to COVID-19.
Currently, type 2 diabetes is listed among 12 conditions that place adults “at increased risk of severe illness from the virus that causes COVID-19,” with the latter defined as “hospitalization, admission to the intensive care unit, intubation or mechanical ventilation, or death.”
On the other hand, the autoimmune condition type 1 diabetes is among 11 conditions the CDC says “might be at increased risk” for COVID-19, but limited data were available at the time of the last update on Dec. 23, 2020.
“States are utilizing the CDC risk classification when designing their vaccine distribution plans. This raises an obvious concern as it could result in the approximately 1.6 million with type 1 diabetes receiving the vaccination later than others with the same risk,” states the ADA letter, sent to the CDC on Jan. 13.
Representatives from the Endocrine Society, American Association of Clinical Endocrinology, Pediatric Endocrine Society, Association of Diabetes Care & Education Specialists, and JDRF, among others, cosigned the letter.
Newer data show those with type 1 diabetes at equally high risk
While acknowledging that “early data did not provide as much clarity about the extent to which those with type 1 diabetes are at high risk,” the ADA says newer evidence has emerged, as previously reported by this news organization, that “convincingly demonstrates that COVID-19 severity is more than tripled in individuals with type 1 diabetes.”
The letter also cites another study showing that people with type 1 diabetes “have a 3.3-fold greater risk of severe illness, are 3.9 times more likely to be hospitalized with COVID-19, and have a 3-fold increase in mortality compared to those without type 1 diabetes.”
Those risks, they note, are comparable to the increased risk established for those with type 2 diabetes, as shown in a third study from Scotland, published last month.
Asked for comment, CDC representative Kirsten Nordlund said in an interview, “This list is a living document that will be periodically updated by CDC, and it could rapidly change as the science evolves.”
In addition, Ms. Nordlund said, “Decisions about transitioning to subsequent phases should depend on supply; demand; equitable vaccine distribution; and local, state, or territorial context.”
“Phased vaccine recommendations are meant to be fluid and not restrictive for jurisdictions. It is not necessary to vaccinate all individuals in one phase before initiating the next phase; phases may overlap,” she noted. More information is available here.
Tennessee gives type 1 and type 2 diabetes equal priority for vaccination
Meanwhile, at least one state, Tennessee, has updated its guidance to include both types of diabetes as being priority for COVID-19 vaccination.
Vanderbilt University pediatric endocrinologist Justin M. Gregory, MD, said in an interview: “I was thrilled when our state modified its guidance on December 30th to include both type 1 and type 2 diabetes in the ‘high-risk category.’ Other states have not modified that guidance though.”
It’s unclear how this might play out on the ground, noted Dr. Gregory, who led one of the three studies demonstrating increased COVID-19 risk for people with type 1 diabetes.
“To tell you the truth, I don’t really know how individual organizations dispensing the vaccination [will handle] people who come to their facility saying they have ‘diabetes.’ Individual states set the vaccine-dispensing guidance and individual county health departments and health care systems mirror that guidance,” he said.
Thus, he added, “Although it’s possible an individual nurse may take the ‘I’ll ask you no questions, and you’ll tell me no lies’ approach if someone with type 1 diabetes says they have ‘diabetes’, websites and health department–recorded telephone messages are going to tell people with type 1 diabetes they have to wait further back in line if that is what their state’s guidance directs.”
A version of this article first appeared on Medscape.com.
The American Diabetes Association, along with 18 other organizations, has sent a letter to the U.S. Centers for Disease Control and Prevention urging them to rank people with type 1 diabetes as equally high risk for COVID-19 severity, and therefore vaccination, as those with type 2 diabetes.
On Jan. 12, the CDC recommended states vaccinate all Americans over age 65 and those with underlying health conditions that make them more vulnerable to COVID-19.
Currently, type 2 diabetes is listed among 12 conditions that place adults “at increased risk of severe illness from the virus that causes COVID-19,” with the latter defined as “hospitalization, admission to the intensive care unit, intubation or mechanical ventilation, or death.”
On the other hand, the autoimmune condition type 1 diabetes is among 11 conditions the CDC says “might be at increased risk” for COVID-19, but limited data were available at the time of the last update on Dec. 23, 2020.
“States are utilizing the CDC risk classification when designing their vaccine distribution plans. This raises an obvious concern as it could result in the approximately 1.6 million with type 1 diabetes receiving the vaccination later than others with the same risk,” states the ADA letter, sent to the CDC on Jan. 13.
Representatives from the Endocrine Society, American Association of Clinical Endocrinology, Pediatric Endocrine Society, Association of Diabetes Care & Education Specialists, and JDRF, among others, cosigned the letter.
Newer data show those with type 1 diabetes at equally high risk
While acknowledging that “early data did not provide as much clarity about the extent to which those with type 1 diabetes are at high risk,” the ADA says newer evidence has emerged, as previously reported by this news organization, that “convincingly demonstrates that COVID-19 severity is more than tripled in individuals with type 1 diabetes.”
The letter also cites another study showing that people with type 1 diabetes “have a 3.3-fold greater risk of severe illness, are 3.9 times more likely to be hospitalized with COVID-19, and have a 3-fold increase in mortality compared to those without type 1 diabetes.”
Those risks, they note, are comparable to the increased risk established for those with type 2 diabetes, as shown in a third study from Scotland, published last month.
Asked for comment, CDC representative Kirsten Nordlund said in an interview, “This list is a living document that will be periodically updated by CDC, and it could rapidly change as the science evolves.”
In addition, Ms. Nordlund said, “Decisions about transitioning to subsequent phases should depend on supply; demand; equitable vaccine distribution; and local, state, or territorial context.”
“Phased vaccine recommendations are meant to be fluid and not restrictive for jurisdictions. It is not necessary to vaccinate all individuals in one phase before initiating the next phase; phases may overlap,” she noted. More information is available here.
Tennessee gives type 1 and type 2 diabetes equal priority for vaccination
Meanwhile, at least one state, Tennessee, has updated its guidance to include both types of diabetes as being priority for COVID-19 vaccination.
Vanderbilt University pediatric endocrinologist Justin M. Gregory, MD, said in an interview: “I was thrilled when our state modified its guidance on December 30th to include both type 1 and type 2 diabetes in the ‘high-risk category.’ Other states have not modified that guidance though.”
It’s unclear how this might play out on the ground, noted Dr. Gregory, who led one of the three studies demonstrating increased COVID-19 risk for people with type 1 diabetes.
“To tell you the truth, I don’t really know how individual organizations dispensing the vaccination [will handle] people who come to their facility saying they have ‘diabetes.’ Individual states set the vaccine-dispensing guidance and individual county health departments and health care systems mirror that guidance,” he said.
Thus, he added, “Although it’s possible an individual nurse may take the ‘I’ll ask you no questions, and you’ll tell me no lies’ approach if someone with type 1 diabetes says they have ‘diabetes’, websites and health department–recorded telephone messages are going to tell people with type 1 diabetes they have to wait further back in line if that is what their state’s guidance directs.”
A version of this article first appeared on Medscape.com.
COVID-19 symptoms persist months after acute infection
, according to a follow-up study involving 1,733 patients.
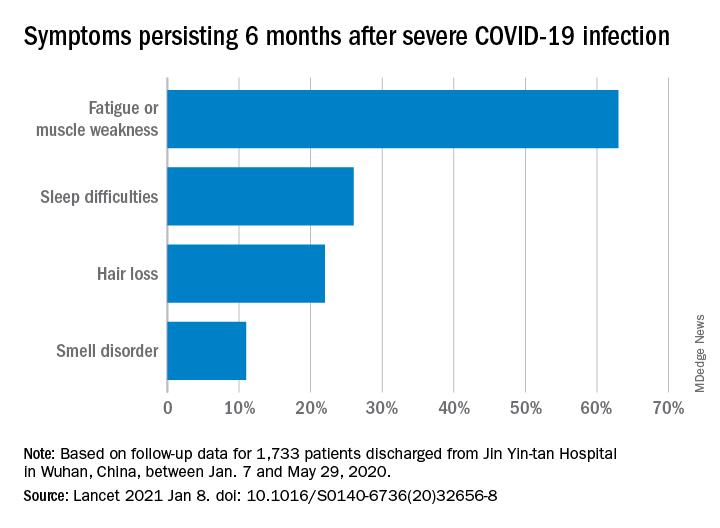
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
, according to a follow-up study involving 1,733 patients.
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
, according to a follow-up study involving 1,733 patients.
“Patients with COVID-19 had symptoms of fatigue or muscle weakness, sleep difficulties, and anxiety or depression,” and those with “more severe illness during their hospital stay had increasingly impaired pulmonary diffusion capacities and abnormal chest imaging manifestations,” Chaolin Huang, MD, of Jin Yin-tan Hospital in Wuhan, China, and associates wrote in the Lancet.
Fatigue or muscle weakness, reported by 63% of patients, was the most common symptom, followed by sleep difficulties, hair loss, and smell disorder. Altogether, 76% of those examined 6 months after discharge from Jin Yin-tan hospital – the first designated for patients with COVID-19 in Wuhan – reported at least one symptom, they said.
Symptoms were more common in women than men: 81% vs. 73% had at least one symptom, and 66% vs. 59% had fatigue or muscle weakness. Women were also more likely than men to report anxiety or depression at follow-up: 28% vs. 18% (23% overall), the investigators said.
Patients with the most severe COVID-19 were 2.4 times as likely to report any symptom later, compared with those who had the least severe levels of infection. Among the 349 participants who completed a lung function test at follow-up, lung diffusion impairment was seen in 56% of those with the most severe illness and 22% of those with the lowest level, Dr. Huang and associates reported.
In a different subset of 94 patients from whom plasma samples were collected, the “seropositivity and median titres of the neutralising antibodies were significantly lower than at the acute phase,” raising concern for reinfection, they said.
The results of the study, the investigators noted, “support that those with severe disease need post-discharge care. Longer follow-up studies in a larger population are necessary to understand the full spectrum of health consequences from COVID-19.”
FROM THE LANCET
CVD deaths rose, imaging declined during pandemic
While the direct toll of the COVID-19 pandemic is being tallied and shared on the nightly news, the indirect effects will undoubtedly take years to fully measure.

In two papers published online Jan. 11 in the Journal of the American College of Cardiology, researchers have started the process of quantifying the impact of the pandemic on the care of patients with cardiovascular disease (CVD).
In the first study, Rishi Wadhera, MD, MPP, MPhil, and colleagues from the Beth Israel Deaconess Medical Center and Harvard Medical School in Boston examined population-level data to determine how deaths from cardiovascular causes changed in the United States in the early months of the pandemic relative to the same periods in 2019.
In a second paper, Andrew J. Einstein, MD, PhD, from Columbia University Irving Medical Center/New York–Presbyterian Hospital and colleagues looked at the pandemic’s international impact on the diagnosis of heart disease.
Using data from the National Center for Health Statistics, Dr. Wadhera and colleagues compared death rates from cardiovascular causes in the United States from March 18, 2020, to June 2, 2020, (the first wave of the pandemic) and from Jan. 1, 2020, to March 17, 2020, (the period just before the pandemic started) and compared them to the same periods in 2019. ICD codes were used to identify underlying causes of death.
Relative to 2019, they found a significant increase in deaths from ischemic heart disease nationally (1.11; 95% confidence interval, 1.04-1.18), as well as an increase in deaths caused by hypertensive disease (1.17; 95% CI, 1.09-1.26). There was no apparent increase in deaths from heart failure, cerebrovascular disease, or other diseases of the circulatory system.
When they looked just at New York City, the area hit hardest during the early part of the pandemic, the relative increases in deaths from ischemic heart disease were more pronounced.
Deaths from ischemic heart disease or hypertensive diseases jumped 139% and 164%, respectively, between March 18, 2020, and June 2, 2020.
More modest increases in deaths were seen in the remainder of New York state, New Jersey, Michigan and Illinois, while Massachusetts and Louisiana did not see a change in cardiovascular deaths.
Several studies from different parts of the world have indicated a 40%-50% drop in hospitalization for myocardial infarction in the initial months of the pandemic, said Dr. Wadhera in an interview.
“We wanted to understand where did all the heart attacks go? And we worried that patients with urgent heart conditions were not seeking the medical care they needed. I think our data suggest that this may have been the case,” reported Dr. Wadhera.
“This very much reflects the reality of what we’re seeing on the ground,” he told this news organization. “After the initial surge ended, when hospital volumes began to return to normal, we saw patients come into the hospital who clearly had a heart attack during the surge months – and were now experiencing complications of that event – because they had initially not come into the hospital due to concerns about exposure to the virus.”
A limitation of their data, he stressed, is whether some deaths coded as CVD deaths were really deaths from undiagnosed COVID-19. “It’s possible that some portion of the increased deaths we observed really reflect the cardiovascular complications of undiagnosed COVID-19, because we know that testing was quite limited during the early first surge of cases.”
“I think that basically three factors – patients avoiding the health care system because of fear of getting COVID, health care systems being strained and overwhelmed leading to the deferral of cardiovascular care and semi-elective procedures, and the cardiovascular complications of COVID-19 itself – all probably collectively contributed to the rise in cardiovascular deaths that we observed,” said Dr. Wadhera.
In an accompanying editorial, Michael N. Young, MD, Geisel School of Medicine at Dartmouth, Lebanon, N.H., and colleagues write that these data, taken together with an earlier study showing an increase in out-of-hospital cardiac arrests at the pandemic peak in New York City, “support the notion of excess fatalities due to unattended comorbid illnesses.” That said, attribution of death in the COVID era “remains problematic.”
In the second article, Andrew Einstein, MD, PhD, and the INCAPS COVID Investigators Group took a broader approach and looked at the impact of COVID-19 on cardiac diagnostic procedures in over 100 countries.
The INCAPS (International Atomic Energy Agency Noninvasive Cardiology Protocols Study) group has for the past decade conducted numerous studies addressing the use of best practices and worldwide practice variation in CVD diagnosis.
For this effort, they sent a survey link to INCAPS participants worldwide, ultimately including 909 survey responses from 108 countries in the final analysis.
Compared with March 2019, overall procedure volume decreased 42% in March 2020 and 64% in April 2020.
The greatest decreases were seen in stress testing (78%) and transesophageal echocardiography (76%), both procedures, noted Dr. Einstein, associated with a greater risk of aerosolization.
“Whether as we reset after COVID we return to the same place in terms of the use of cardiovascular diagnostic testing remains to be seen, but it certainly poses an opportunity to improve our utilization of various modes of testing,” said Dr. Einstein.
Using regression analysis, Dr. Einstein and colleagues were able to see that sites located in low-income and lower-middle-income countries saw an additional 22% reduction in cardiac procedures and less availability of personal protective equipment (PPE) and telehealth.
Fifty-two percent of survey respondents reported significant shortages of N95 masks early in the pandemic, with fewer issues in supplies of gloves, gowns, and face shields. Lower-income countries were more likely to face significant PPE shortages and less likely to be able to implement telehealth strategies to make up for reduced in-person care. PPE shortage itself, however, was not related to lower procedural volume on multivariable regression.
“It all really begs the question of whether there is more that the world can do to help out the developing world in terms of managing the pandemic in all its facets,” said Dr. Einstein in an interview, adding he was “shocked” to learn how difficult it was for some lower-income countries to get sufficient PPE.
Did shutdowns go too far?
Calling this a “remarkable study,” an editorial written by Darryl P. Leong, MBBS, PhD, John W. Eikelboom, MBBS, and Salim Yusuf, MBBS, DPhil, all from McMaster University, Hamilton, Ont., suggests that perhaps health systems in some places went too far in closing down during the first wave of the pandemic, naming specifically Canada, Eastern Europe, and Saudi Arabia as examples.
“Although these measures were taken to prepare for the worst, overwhelming numbers of patients with COVID-19 did not materialize during the first wave of the pandemic in these countries. It is possible that delaying so-called nonessential services may have been unnecessary and potentially harmful, because it likely led to delays in providing care for the treatment of serious non–COVID-19 illnesses.”
Since then, more experience and more data have largely allowed hospital systems to “tackle the ebb and flow” of COVID-19 cases in ways that limit shutdowns of important health services, they said.
Given the more pronounced effect in low- and middle-income countries, they stressed the need to focus resources on ways to promote prevention and treatment that do not rely on diagnostic procedures.
“This calls for more emphasis on developing efficient systems of telehealth, especially in poorer countries or in remote settings in all countries,” Dr. Leong and colleagues conclude.
Dr. Wadhera has reported research support from the National Heart, Lung, and Blood Institute, along with fellow senior author Robert W. Yeh, MD, MBA, who has also received personal fees and grants from several companies not related to the submitted work. Dr. Einstein, Dr. Leong, Dr. Eikelboom, and Dr. Yusuf have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
While the direct toll of the COVID-19 pandemic is being tallied and shared on the nightly news, the indirect effects will undoubtedly take years to fully measure.
In two papers published online Jan. 11 in the Journal of the American College of Cardiology, researchers have started the process of quantifying the impact of the pandemic on the care of patients with cardiovascular disease (CVD).
In the first study, Rishi Wadhera, MD, MPP, MPhil, and colleagues from the Beth Israel Deaconess Medical Center and Harvard Medical School in Boston examined population-level data to determine how deaths from cardiovascular causes changed in the United States in the early months of the pandemic relative to the same periods in 2019.
In a second paper, Andrew J. Einstein, MD, PhD, from Columbia University Irving Medical Center/New York–Presbyterian Hospital and colleagues looked at the pandemic’s international impact on the diagnosis of heart disease.
Using data from the National Center for Health Statistics, Dr. Wadhera and colleagues compared death rates from cardiovascular causes in the United States from March 18, 2020, to June 2, 2020, (the first wave of the pandemic) and from Jan. 1, 2020, to March 17, 2020, (the period just before the pandemic started) and compared them to the same periods in 2019. ICD codes were used to identify underlying causes of death.
Relative to 2019, they found a significant increase in deaths from ischemic heart disease nationally (1.11; 95% confidence interval, 1.04-1.18), as well as an increase in deaths caused by hypertensive disease (1.17; 95% CI, 1.09-1.26). There was no apparent increase in deaths from heart failure, cerebrovascular disease, or other diseases of the circulatory system.
When they looked just at New York City, the area hit hardest during the early part of the pandemic, the relative increases in deaths from ischemic heart disease were more pronounced.
Deaths from ischemic heart disease or hypertensive diseases jumped 139% and 164%, respectively, between March 18, 2020, and June 2, 2020.
More modest increases in deaths were seen in the remainder of New York state, New Jersey, Michigan and Illinois, while Massachusetts and Louisiana did not see a change in cardiovascular deaths.
Several studies from different parts of the world have indicated a 40%-50% drop in hospitalization for myocardial infarction in the initial months of the pandemic, said Dr. Wadhera in an interview.
“We wanted to understand where did all the heart attacks go? And we worried that patients with urgent heart conditions were not seeking the medical care they needed. I think our data suggest that this may have been the case,” reported Dr. Wadhera.
“This very much reflects the reality of what we’re seeing on the ground,” he told this news organization. “After the initial surge ended, when hospital volumes began to return to normal, we saw patients come into the hospital who clearly had a heart attack during the surge months – and were now experiencing complications of that event – because they had initially not come into the hospital due to concerns about exposure to the virus.”
A limitation of their data, he stressed, is whether some deaths coded as CVD deaths were really deaths from undiagnosed COVID-19. “It’s possible that some portion of the increased deaths we observed really reflect the cardiovascular complications of undiagnosed COVID-19, because we know that testing was quite limited during the early first surge of cases.”
“I think that basically three factors – patients avoiding the health care system because of fear of getting COVID, health care systems being strained and overwhelmed leading to the deferral of cardiovascular care and semi-elective procedures, and the cardiovascular complications of COVID-19 itself – all probably collectively contributed to the rise in cardiovascular deaths that we observed,” said Dr. Wadhera.
In an accompanying editorial, Michael N. Young, MD, Geisel School of Medicine at Dartmouth, Lebanon, N.H., and colleagues write that these data, taken together with an earlier study showing an increase in out-of-hospital cardiac arrests at the pandemic peak in New York City, “support the notion of excess fatalities due to unattended comorbid illnesses.” That said, attribution of death in the COVID era “remains problematic.”
In the second article, Andrew Einstein, MD, PhD, and the INCAPS COVID Investigators Group took a broader approach and looked at the impact of COVID-19 on cardiac diagnostic procedures in over 100 countries.
The INCAPS (International Atomic Energy Agency Noninvasive Cardiology Protocols Study) group has for the past decade conducted numerous studies addressing the use of best practices and worldwide practice variation in CVD diagnosis.
For this effort, they sent a survey link to INCAPS participants worldwide, ultimately including 909 survey responses from 108 countries in the final analysis.
Compared with March 2019, overall procedure volume decreased 42% in March 2020 and 64% in April 2020.
The greatest decreases were seen in stress testing (78%) and transesophageal echocardiography (76%), both procedures, noted Dr. Einstein, associated with a greater risk of aerosolization.
“Whether as we reset after COVID we return to the same place in terms of the use of cardiovascular diagnostic testing remains to be seen, but it certainly poses an opportunity to improve our utilization of various modes of testing,” said Dr. Einstein.
Using regression analysis, Dr. Einstein and colleagues were able to see that sites located in low-income and lower-middle-income countries saw an additional 22% reduction in cardiac procedures and less availability of personal protective equipment (PPE) and telehealth.
Fifty-two percent of survey respondents reported significant shortages of N95 masks early in the pandemic, with fewer issues in supplies of gloves, gowns, and face shields. Lower-income countries were more likely to face significant PPE shortages and less likely to be able to implement telehealth strategies to make up for reduced in-person care. PPE shortage itself, however, was not related to lower procedural volume on multivariable regression.
“It all really begs the question of whether there is more that the world can do to help out the developing world in terms of managing the pandemic in all its facets,” said Dr. Einstein in an interview, adding he was “shocked” to learn how difficult it was for some lower-income countries to get sufficient PPE.
Did shutdowns go too far?
Calling this a “remarkable study,” an editorial written by Darryl P. Leong, MBBS, PhD, John W. Eikelboom, MBBS, and Salim Yusuf, MBBS, DPhil, all from McMaster University, Hamilton, Ont., suggests that perhaps health systems in some places went too far in closing down during the first wave of the pandemic, naming specifically Canada, Eastern Europe, and Saudi Arabia as examples.
“Although these measures were taken to prepare for the worst, overwhelming numbers of patients with COVID-19 did not materialize during the first wave of the pandemic in these countries. It is possible that delaying so-called nonessential services may have been unnecessary and potentially harmful, because it likely led to delays in providing care for the treatment of serious non–COVID-19 illnesses.”
Since then, more experience and more data have largely allowed hospital systems to “tackle the ebb and flow” of COVID-19 cases in ways that limit shutdowns of important health services, they said.
Given the more pronounced effect in low- and middle-income countries, they stressed the need to focus resources on ways to promote prevention and treatment that do not rely on diagnostic procedures.
“This calls for more emphasis on developing efficient systems of telehealth, especially in poorer countries or in remote settings in all countries,” Dr. Leong and colleagues conclude.
Dr. Wadhera has reported research support from the National Heart, Lung, and Blood Institute, along with fellow senior author Robert W. Yeh, MD, MBA, who has also received personal fees and grants from several companies not related to the submitted work. Dr. Einstein, Dr. Leong, Dr. Eikelboom, and Dr. Yusuf have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
While the direct toll of the COVID-19 pandemic is being tallied and shared on the nightly news, the indirect effects will undoubtedly take years to fully measure.
In two papers published online Jan. 11 in the Journal of the American College of Cardiology, researchers have started the process of quantifying the impact of the pandemic on the care of patients with cardiovascular disease (CVD).
In the first study, Rishi Wadhera, MD, MPP, MPhil, and colleagues from the Beth Israel Deaconess Medical Center and Harvard Medical School in Boston examined population-level data to determine how deaths from cardiovascular causes changed in the United States in the early months of the pandemic relative to the same periods in 2019.
In a second paper, Andrew J. Einstein, MD, PhD, from Columbia University Irving Medical Center/New York–Presbyterian Hospital and colleagues looked at the pandemic’s international impact on the diagnosis of heart disease.
Using data from the National Center for Health Statistics, Dr. Wadhera and colleagues compared death rates from cardiovascular causes in the United States from March 18, 2020, to June 2, 2020, (the first wave of the pandemic) and from Jan. 1, 2020, to March 17, 2020, (the period just before the pandemic started) and compared them to the same periods in 2019. ICD codes were used to identify underlying causes of death.
Relative to 2019, they found a significant increase in deaths from ischemic heart disease nationally (1.11; 95% confidence interval, 1.04-1.18), as well as an increase in deaths caused by hypertensive disease (1.17; 95% CI, 1.09-1.26). There was no apparent increase in deaths from heart failure, cerebrovascular disease, or other diseases of the circulatory system.
When they looked just at New York City, the area hit hardest during the early part of the pandemic, the relative increases in deaths from ischemic heart disease were more pronounced.
Deaths from ischemic heart disease or hypertensive diseases jumped 139% and 164%, respectively, between March 18, 2020, and June 2, 2020.
More modest increases in deaths were seen in the remainder of New York state, New Jersey, Michigan and Illinois, while Massachusetts and Louisiana did not see a change in cardiovascular deaths.
Several studies from different parts of the world have indicated a 40%-50% drop in hospitalization for myocardial infarction in the initial months of the pandemic, said Dr. Wadhera in an interview.
“We wanted to understand where did all the heart attacks go? And we worried that patients with urgent heart conditions were not seeking the medical care they needed. I think our data suggest that this may have been the case,” reported Dr. Wadhera.
“This very much reflects the reality of what we’re seeing on the ground,” he told this news organization. “After the initial surge ended, when hospital volumes began to return to normal, we saw patients come into the hospital who clearly had a heart attack during the surge months – and were now experiencing complications of that event – because they had initially not come into the hospital due to concerns about exposure to the virus.”
A limitation of their data, he stressed, is whether some deaths coded as CVD deaths were really deaths from undiagnosed COVID-19. “It’s possible that some portion of the increased deaths we observed really reflect the cardiovascular complications of undiagnosed COVID-19, because we know that testing was quite limited during the early first surge of cases.”
“I think that basically three factors – patients avoiding the health care system because of fear of getting COVID, health care systems being strained and overwhelmed leading to the deferral of cardiovascular care and semi-elective procedures, and the cardiovascular complications of COVID-19 itself – all probably collectively contributed to the rise in cardiovascular deaths that we observed,” said Dr. Wadhera.
In an accompanying editorial, Michael N. Young, MD, Geisel School of Medicine at Dartmouth, Lebanon, N.H., and colleagues write that these data, taken together with an earlier study showing an increase in out-of-hospital cardiac arrests at the pandemic peak in New York City, “support the notion of excess fatalities due to unattended comorbid illnesses.” That said, attribution of death in the COVID era “remains problematic.”
In the second article, Andrew Einstein, MD, PhD, and the INCAPS COVID Investigators Group took a broader approach and looked at the impact of COVID-19 on cardiac diagnostic procedures in over 100 countries.
The INCAPS (International Atomic Energy Agency Noninvasive Cardiology Protocols Study) group has for the past decade conducted numerous studies addressing the use of best practices and worldwide practice variation in CVD diagnosis.
For this effort, they sent a survey link to INCAPS participants worldwide, ultimately including 909 survey responses from 108 countries in the final analysis.
Compared with March 2019, overall procedure volume decreased 42% in March 2020 and 64% in April 2020.
The greatest decreases were seen in stress testing (78%) and transesophageal echocardiography (76%), both procedures, noted Dr. Einstein, associated with a greater risk of aerosolization.
“Whether as we reset after COVID we return to the same place in terms of the use of cardiovascular diagnostic testing remains to be seen, but it certainly poses an opportunity to improve our utilization of various modes of testing,” said Dr. Einstein.
Using regression analysis, Dr. Einstein and colleagues were able to see that sites located in low-income and lower-middle-income countries saw an additional 22% reduction in cardiac procedures and less availability of personal protective equipment (PPE) and telehealth.
Fifty-two percent of survey respondents reported significant shortages of N95 masks early in the pandemic, with fewer issues in supplies of gloves, gowns, and face shields. Lower-income countries were more likely to face significant PPE shortages and less likely to be able to implement telehealth strategies to make up for reduced in-person care. PPE shortage itself, however, was not related to lower procedural volume on multivariable regression.
“It all really begs the question of whether there is more that the world can do to help out the developing world in terms of managing the pandemic in all its facets,” said Dr. Einstein in an interview, adding he was “shocked” to learn how difficult it was for some lower-income countries to get sufficient PPE.
Did shutdowns go too far?
Calling this a “remarkable study,” an editorial written by Darryl P. Leong, MBBS, PhD, John W. Eikelboom, MBBS, and Salim Yusuf, MBBS, DPhil, all from McMaster University, Hamilton, Ont., suggests that perhaps health systems in some places went too far in closing down during the first wave of the pandemic, naming specifically Canada, Eastern Europe, and Saudi Arabia as examples.
“Although these measures were taken to prepare for the worst, overwhelming numbers of patients with COVID-19 did not materialize during the first wave of the pandemic in these countries. It is possible that delaying so-called nonessential services may have been unnecessary and potentially harmful, because it likely led to delays in providing care for the treatment of serious non–COVID-19 illnesses.”
Since then, more experience and more data have largely allowed hospital systems to “tackle the ebb and flow” of COVID-19 cases in ways that limit shutdowns of important health services, they said.
Given the more pronounced effect in low- and middle-income countries, they stressed the need to focus resources on ways to promote prevention and treatment that do not rely on diagnostic procedures.
“This calls for more emphasis on developing efficient systems of telehealth, especially in poorer countries or in remote settings in all countries,” Dr. Leong and colleagues conclude.
Dr. Wadhera has reported research support from the National Heart, Lung, and Blood Institute, along with fellow senior author Robert W. Yeh, MD, MBA, who has also received personal fees and grants from several companies not related to the submitted work. Dr. Einstein, Dr. Leong, Dr. Eikelboom, and Dr. Yusuf have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.