User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Endometriosis: Disease burden and the problem of missed or delayed diagnosis

What is the incidence of endometriosis in women, and does the condition affect certain patient populations more often than others?
Dr. Taylor: Endometriosis occurs in about 5% to 10% of reproductive-aged women, and it is underdiagnosed. Many women have subtle endometriosis or asymptomatic endometriosis that may be missed or may take a long time to diagnose, and the incidence may be somewhat higher. It is much more common in women with pelvic pain, as these women have a greater than 50% incidence of endometriosis, and those with infertility similarly have roughly a 50% incidence of endometriosis. Endometriosis is a very common disease, most common in the reproductive age range, particularly more common in the most fertile years. The typical course of the disease is that it begins in teenagers or in the early 20s, progresses through the 20s and 30s, but starts to wane in the 40s, and goes away at the time of menopause in the early 50s. Those particularly susceptible to the disease are those with early menarche or frequent or heavy periods. Recurrent periods lead to more retrograde menstruation, which is menstrual flow through the fallopian tubes. It then starts to implant in the abdomen, specifically in the peritoneal cavity.
What are some of the reasons for missed or delayed diagnosis?
Dr. Taylor: There are many reasons why diagnosis may be missed or delayed. One of the most common reasons for delayed diagnosis is that the patient does not know that painful periods are not normal and may not report them to her clinician. Dysmenorrhea, or menstrual pain, is the only pain that we consider normal. It is the only experience we go through that is expected to hurt. It is also a very subjective issue. How do you know if your menstrual cramps are worse than someone else’s? Often, the first thing that happens when someone complains about severe dysmenorrhea is that their friends or family members will say to them, “We all get menstrual cramps. Just toughen up and bear with it.” But, of course, sometimes these menstrual cramps, or dysmenorrhea, get so bad that they become disabling. When people miss school or work, or they cannot participate in normal social or athletic activities, that is when they first get attention. Often, the disease has been bothering someone for a long time before it is diagnosed.
Another reason that diagnosis may be delayed is because of the social stigma surrounding discussing these types of issues. It is difficult sometimes, especially for a teenager, to talk about issues such as painful periods, pain with bowel movements or urination, or pain with intercourse. A generation ago, people did not talk about such topics so openly and publicly. Thankfully, it is becoming easier, and I think this generation is more open to talking about these issues, but it is still difficult for some who are hesitant to discuss it. Parents can also have a difficult time discussing these issues with their children, and they may dismiss it. Even physicians who are not familiar with this issue may not be comfortable discussing these matters.
Other times, it is truly asymptomatic. Someone can have significant endometriosis that does not show up until it is found on ultrasonography or until someone tries to get pregnant but experiences infertility, and then it is recognized. Typically, people with endometriosis do present with painful menses. If we are more attuned to listening for those symptoms and open to talking about these symptoms, I think we can catch this disease much earlier.
Another barrier to diagnosis is that for too long the gold standard has been surgery, a laparoscopy, to look for endometriosis. If that is a clinician’s method of determining if somebody has endometriosis, it creates quite a barrier to diagnosis. In the near future, I believe we will have noninvasive tests that will help us determine if somebody has endometriosis without surgery. Even now a clinical history can be very helpful in deciding who has endometriosis. I am also of the opinion that people are becoming much more confident about making a clinical diagnosis of endometriosis.
Diagnosing endometriosis relies on identifying flags in the patient’s history and through physical exams. How can clinicians better their chances for having the flags converge for successful diagnosis?
Dr. Taylor: I think it is important to keep the focus on some of the main symptoms of endometriosis. Most women with endometriosis start by having dysmenorrhea, which progresses over time. Some women with painful periods from menarche may not have endometriosis. Their primary dysmenorrhea may be due to other etiologies. If someone has relatively normal menses initially and then goes on to have progressively increasing dysmenorrhea, most often that is endometriosis. Eventually, the pain can spread to other times in the cycle, beyond just dysmenorrhea. Pain can start in the pelvis, but, as endometriosis causes side effects outside of the reproductive organs, it can start to affect other organs and start to cause pain outside of the pelvis. Endometriosis can also inflame the pelvis and affect the bowel, the bladder, and many other surrounding organs. If somebody has bowel symptoms or bladder symptoms that are cyclic and accompanied by dysmenorrhea or cyclic pelvic pain, endometriosis should be thought of first, rather than a primary bowel or bladder problem. Too often medical professionals can be misled by these other false clues. I have seen many patients who come to me after a very thorough workup for a gastrointestinal issue, including a colonoscopy, or a bladder issue, including a cystoscopy, when the underlying problem really was endometriosis. It is important not to be misled by these “red herrings,” and to focus on progressive cyclic pelvic pain. Endometriosis is always at least initially cyclic in character.
We also know that endometriosis can have effects far beyond the pelvis. Conditions such as anxiety and depression are more common in patients with endometriosis. Women with endometriosis tend to be thinner. There are many other manifestations of this disease. Although it is complex, and can affect almost any organ system, we need to focus on the primary problem, which is cyclic pelvic pain that is progressive in nature. A woman who has dysmenorrhea that may progress to cyclic pain that gets worse over time, more than likely has endometriosis. We can rule out other etiologies, such as masses, fibroids, and cysts, with a simple physical exam and/or an ultrasound. In general, from a good history focusing on the cyclic progressive pelvic pain and a good physical exam to rule out other etiologies for that pain, we can rapidly narrow in on the diagnosis of endometriosis. We can make the diagnosis very straightforward. Cyclic progressive pelvic pain is essentially synonymous with endometriosis.
With a current medical lens focused on addressing racial disparities and inequities in medicine, do you feel that there are gaps in endometriosis study enrollment, diagnosis, and management that need to be addressed?
Dr. Taylor: Traditionally, there have been disparities in diagnosing endometriosis. There was a time when it was presumed that White women had endometriosis and Black women were more likely to have an infectious etiology for their pelvic pain—which is not true. The incidence is slightly higher in Asian and White women compared with Black women, but this is very likely because of bias and access to care. When examining women who have been diagnosed and are being evaluated and treated for infertility, those racial differences disappear. When access to care is available, when patients are seen by a physician, when they are under medical care for another reason, the racial disparities are not seen in endometriosis; it occurs equally. I think there clearly are disparities in access and bias in how we diagnose endometriosis; we should be cognizant of that and realize that endometriosis is very similar in its frequency in all ethnic groups.
What is the incidence of endometriosis in women, and does the condition affect certain patient populations more often than others?
Dr. Taylor: Endometriosis occurs in about 5% to 10% of reproductive-aged women, and it is underdiagnosed. Many women have subtle endometriosis or asymptomatic endometriosis that may be missed or may take a long time to diagnose, and the incidence may be somewhat higher. It is much more common in women with pelvic pain, as these women have a greater than 50% incidence of endometriosis, and those with infertility similarly have roughly a 50% incidence of endometriosis. Endometriosis is a very common disease, most common in the reproductive age range, particularly more common in the most fertile years. The typical course of the disease is that it begins in teenagers or in the early 20s, progresses through the 20s and 30s, but starts to wane in the 40s, and goes away at the time of menopause in the early 50s. Those particularly susceptible to the disease are those with early menarche or frequent or heavy periods. Recurrent periods lead to more retrograde menstruation, which is menstrual flow through the fallopian tubes. It then starts to implant in the abdomen, specifically in the peritoneal cavity.
What are some of the reasons for missed or delayed diagnosis?
Dr. Taylor: There are many reasons why diagnosis may be missed or delayed. One of the most common reasons for delayed diagnosis is that the patient does not know that painful periods are not normal and may not report them to her clinician. Dysmenorrhea, or menstrual pain, is the only pain that we consider normal. It is the only experience we go through that is expected to hurt. It is also a very subjective issue. How do you know if your menstrual cramps are worse than someone else’s? Often, the first thing that happens when someone complains about severe dysmenorrhea is that their friends or family members will say to them, “We all get menstrual cramps. Just toughen up and bear with it.” But, of course, sometimes these menstrual cramps, or dysmenorrhea, get so bad that they become disabling. When people miss school or work, or they cannot participate in normal social or athletic activities, that is when they first get attention. Often, the disease has been bothering someone for a long time before it is diagnosed.
Another reason that diagnosis may be delayed is because of the social stigma surrounding discussing these types of issues. It is difficult sometimes, especially for a teenager, to talk about issues such as painful periods, pain with bowel movements or urination, or pain with intercourse. A generation ago, people did not talk about such topics so openly and publicly. Thankfully, it is becoming easier, and I think this generation is more open to talking about these issues, but it is still difficult for some who are hesitant to discuss it. Parents can also have a difficult time discussing these issues with their children, and they may dismiss it. Even physicians who are not familiar with this issue may not be comfortable discussing these matters.
Other times, it is truly asymptomatic. Someone can have significant endometriosis that does not show up until it is found on ultrasonography or until someone tries to get pregnant but experiences infertility, and then it is recognized. Typically, people with endometriosis do present with painful menses. If we are more attuned to listening for those symptoms and open to talking about these symptoms, I think we can catch this disease much earlier.
Another barrier to diagnosis is that for too long the gold standard has been surgery, a laparoscopy, to look for endometriosis. If that is a clinician’s method of determining if somebody has endometriosis, it creates quite a barrier to diagnosis. In the near future, I believe we will have noninvasive tests that will help us determine if somebody has endometriosis without surgery. Even now a clinical history can be very helpful in deciding who has endometriosis. I am also of the opinion that people are becoming much more confident about making a clinical diagnosis of endometriosis.
Diagnosing endometriosis relies on identifying flags in the patient’s history and through physical exams. How can clinicians better their chances for having the flags converge for successful diagnosis?
Dr. Taylor: I think it is important to keep the focus on some of the main symptoms of endometriosis. Most women with endometriosis start by having dysmenorrhea, which progresses over time. Some women with painful periods from menarche may not have endometriosis. Their primary dysmenorrhea may be due to other etiologies. If someone has relatively normal menses initially and then goes on to have progressively increasing dysmenorrhea, most often that is endometriosis. Eventually, the pain can spread to other times in the cycle, beyond just dysmenorrhea. Pain can start in the pelvis, but, as endometriosis causes side effects outside of the reproductive organs, it can start to affect other organs and start to cause pain outside of the pelvis. Endometriosis can also inflame the pelvis and affect the bowel, the bladder, and many other surrounding organs. If somebody has bowel symptoms or bladder symptoms that are cyclic and accompanied by dysmenorrhea or cyclic pelvic pain, endometriosis should be thought of first, rather than a primary bowel or bladder problem. Too often medical professionals can be misled by these other false clues. I have seen many patients who come to me after a very thorough workup for a gastrointestinal issue, including a colonoscopy, or a bladder issue, including a cystoscopy, when the underlying problem really was endometriosis. It is important not to be misled by these “red herrings,” and to focus on progressive cyclic pelvic pain. Endometriosis is always at least initially cyclic in character.
We also know that endometriosis can have effects far beyond the pelvis. Conditions such as anxiety and depression are more common in patients with endometriosis. Women with endometriosis tend to be thinner. There are many other manifestations of this disease. Although it is complex, and can affect almost any organ system, we need to focus on the primary problem, which is cyclic pelvic pain that is progressive in nature. A woman who has dysmenorrhea that may progress to cyclic pain that gets worse over time, more than likely has endometriosis. We can rule out other etiologies, such as masses, fibroids, and cysts, with a simple physical exam and/or an ultrasound. In general, from a good history focusing on the cyclic progressive pelvic pain and a good physical exam to rule out other etiologies for that pain, we can rapidly narrow in on the diagnosis of endometriosis. We can make the diagnosis very straightforward. Cyclic progressive pelvic pain is essentially synonymous with endometriosis.
With a current medical lens focused on addressing racial disparities and inequities in medicine, do you feel that there are gaps in endometriosis study enrollment, diagnosis, and management that need to be addressed?
Dr. Taylor: Traditionally, there have been disparities in diagnosing endometriosis. There was a time when it was presumed that White women had endometriosis and Black women were more likely to have an infectious etiology for their pelvic pain—which is not true. The incidence is slightly higher in Asian and White women compared with Black women, but this is very likely because of bias and access to care. When examining women who have been diagnosed and are being evaluated and treated for infertility, those racial differences disappear. When access to care is available, when patients are seen by a physician, when they are under medical care for another reason, the racial disparities are not seen in endometriosis; it occurs equally. I think there clearly are disparities in access and bias in how we diagnose endometriosis; we should be cognizant of that and realize that endometriosis is very similar in its frequency in all ethnic groups.
What is the incidence of endometriosis in women, and does the condition affect certain patient populations more often than others?
Dr. Taylor: Endometriosis occurs in about 5% to 10% of reproductive-aged women, and it is underdiagnosed. Many women have subtle endometriosis or asymptomatic endometriosis that may be missed or may take a long time to diagnose, and the incidence may be somewhat higher. It is much more common in women with pelvic pain, as these women have a greater than 50% incidence of endometriosis, and those with infertility similarly have roughly a 50% incidence of endometriosis. Endometriosis is a very common disease, most common in the reproductive age range, particularly more common in the most fertile years. The typical course of the disease is that it begins in teenagers or in the early 20s, progresses through the 20s and 30s, but starts to wane in the 40s, and goes away at the time of menopause in the early 50s. Those particularly susceptible to the disease are those with early menarche or frequent or heavy periods. Recurrent periods lead to more retrograde menstruation, which is menstrual flow through the fallopian tubes. It then starts to implant in the abdomen, specifically in the peritoneal cavity.
What are some of the reasons for missed or delayed diagnosis?
Dr. Taylor: There are many reasons why diagnosis may be missed or delayed. One of the most common reasons for delayed diagnosis is that the patient does not know that painful periods are not normal and may not report them to her clinician. Dysmenorrhea, or menstrual pain, is the only pain that we consider normal. It is the only experience we go through that is expected to hurt. It is also a very subjective issue. How do you know if your menstrual cramps are worse than someone else’s? Often, the first thing that happens when someone complains about severe dysmenorrhea is that their friends or family members will say to them, “We all get menstrual cramps. Just toughen up and bear with it.” But, of course, sometimes these menstrual cramps, or dysmenorrhea, get so bad that they become disabling. When people miss school or work, or they cannot participate in normal social or athletic activities, that is when they first get attention. Often, the disease has been bothering someone for a long time before it is diagnosed.
Another reason that diagnosis may be delayed is because of the social stigma surrounding discussing these types of issues. It is difficult sometimes, especially for a teenager, to talk about issues such as painful periods, pain with bowel movements or urination, or pain with intercourse. A generation ago, people did not talk about such topics so openly and publicly. Thankfully, it is becoming easier, and I think this generation is more open to talking about these issues, but it is still difficult for some who are hesitant to discuss it. Parents can also have a difficult time discussing these issues with their children, and they may dismiss it. Even physicians who are not familiar with this issue may not be comfortable discussing these matters.
Other times, it is truly asymptomatic. Someone can have significant endometriosis that does not show up until it is found on ultrasonography or until someone tries to get pregnant but experiences infertility, and then it is recognized. Typically, people with endometriosis do present with painful menses. If we are more attuned to listening for those symptoms and open to talking about these symptoms, I think we can catch this disease much earlier.
Another barrier to diagnosis is that for too long the gold standard has been surgery, a laparoscopy, to look for endometriosis. If that is a clinician’s method of determining if somebody has endometriosis, it creates quite a barrier to diagnosis. In the near future, I believe we will have noninvasive tests that will help us determine if somebody has endometriosis without surgery. Even now a clinical history can be very helpful in deciding who has endometriosis. I am also of the opinion that people are becoming much more confident about making a clinical diagnosis of endometriosis.
Diagnosing endometriosis relies on identifying flags in the patient’s history and through physical exams. How can clinicians better their chances for having the flags converge for successful diagnosis?
Dr. Taylor: I think it is important to keep the focus on some of the main symptoms of endometriosis. Most women with endometriosis start by having dysmenorrhea, which progresses over time. Some women with painful periods from menarche may not have endometriosis. Their primary dysmenorrhea may be due to other etiologies. If someone has relatively normal menses initially and then goes on to have progressively increasing dysmenorrhea, most often that is endometriosis. Eventually, the pain can spread to other times in the cycle, beyond just dysmenorrhea. Pain can start in the pelvis, but, as endometriosis causes side effects outside of the reproductive organs, it can start to affect other organs and start to cause pain outside of the pelvis. Endometriosis can also inflame the pelvis and affect the bowel, the bladder, and many other surrounding organs. If somebody has bowel symptoms or bladder symptoms that are cyclic and accompanied by dysmenorrhea or cyclic pelvic pain, endometriosis should be thought of first, rather than a primary bowel or bladder problem. Too often medical professionals can be misled by these other false clues. I have seen many patients who come to me after a very thorough workup for a gastrointestinal issue, including a colonoscopy, or a bladder issue, including a cystoscopy, when the underlying problem really was endometriosis. It is important not to be misled by these “red herrings,” and to focus on progressive cyclic pelvic pain. Endometriosis is always at least initially cyclic in character.
We also know that endometriosis can have effects far beyond the pelvis. Conditions such as anxiety and depression are more common in patients with endometriosis. Women with endometriosis tend to be thinner. There are many other manifestations of this disease. Although it is complex, and can affect almost any organ system, we need to focus on the primary problem, which is cyclic pelvic pain that is progressive in nature. A woman who has dysmenorrhea that may progress to cyclic pain that gets worse over time, more than likely has endometriosis. We can rule out other etiologies, such as masses, fibroids, and cysts, with a simple physical exam and/or an ultrasound. In general, from a good history focusing on the cyclic progressive pelvic pain and a good physical exam to rule out other etiologies for that pain, we can rapidly narrow in on the diagnosis of endometriosis. We can make the diagnosis very straightforward. Cyclic progressive pelvic pain is essentially synonymous with endometriosis.
With a current medical lens focused on addressing racial disparities and inequities in medicine, do you feel that there are gaps in endometriosis study enrollment, diagnosis, and management that need to be addressed?
Dr. Taylor: Traditionally, there have been disparities in diagnosing endometriosis. There was a time when it was presumed that White women had endometriosis and Black women were more likely to have an infectious etiology for their pelvic pain—which is not true. The incidence is slightly higher in Asian and White women compared with Black women, but this is very likely because of bias and access to care. When examining women who have been diagnosed and are being evaluated and treated for infertility, those racial differences disappear. When access to care is available, when patients are seen by a physician, when they are under medical care for another reason, the racial disparities are not seen in endometriosis; it occurs equally. I think there clearly are disparities in access and bias in how we diagnose endometriosis; we should be cognizant of that and realize that endometriosis is very similar in its frequency in all ethnic groups.

CDC adds new medical conditions to COVID-19 high-risk list
The Centers for Disease Control and Prevention has added several new medical conditions to its list of those that predispose adults to more severe COVID-19 illness.
Conditions that had previously been categorized as “might be” placing individuals at increased risk – but now are listed as high risk – include type 1 diabetes (in addition to type 2), moderate-to-severe asthma, liver disease, dementia or other neurologic conditions, stroke/cerebrovascular disease, HIV infection, cystic fibrosis, and overweight (in addition to obesity).
Substance use disorders, which hadn’t been previously listed, are now also considered high risk.
The new list groups together certain categories, such as chronic lung diseases (chronic obstructive pulmonary disease, asthma, cystic fibrosis, etc) and heart conditions (heart failure, coronary artery disease, hypertension, etc).
Both diabetes types are now grouped under “diabetes.”
The added medical conditions were posted on the CDC website’s COVID-19 page on March 29.
Type 1 diabetes and other conditions now priority for vaccination
The CDC refers to the medical conditions list as phase 1c in regard to COVID-19 vaccine prioritization, which means that anyone with any of these conditions can now be prioritized for vaccination, following those in groups 1a (frontline essential workers and those in long-term care facilities) and 1b (people aged 65-74 years; other essential workers; and people aged 16-64 years with underlying conditions that increase the risk of serious, life-threatening complications from COVID-19).
But in many cases, multiple states have already either fully opened up vaccine eligibility to all adults or have created their own lists of underlying high-risk medical conditions, CDC spokeswoman Kristen Nordlund told this news organization.
No conditions have been removed from the list.
In January, the American Diabetes Association and 18 other organizations sent a letter to the CDC requesting that type 1 diabetes be prioritized along with type 2, based on data from studies showing people with both types to be at high risk for severe COVID-19 illness.
Now, ADA says, “this updated guidance will help to address the fact that in many states, millions of people with type 1 diabetes have not been prioritized equally, slowing their access to critical vaccines.”
While awaiting this latest CDC move, ADA had been urging state governors to prioritize type 1 and type 2 diabetes equally. As of now, 38 states and the District of Columbia had either done so or announced that they would.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has added several new medical conditions to its list of those that predispose adults to more severe COVID-19 illness.
Conditions that had previously been categorized as “might be” placing individuals at increased risk – but now are listed as high risk – include type 1 diabetes (in addition to type 2), moderate-to-severe asthma, liver disease, dementia or other neurologic conditions, stroke/cerebrovascular disease, HIV infection, cystic fibrosis, and overweight (in addition to obesity).
Substance use disorders, which hadn’t been previously listed, are now also considered high risk.
The new list groups together certain categories, such as chronic lung diseases (chronic obstructive pulmonary disease, asthma, cystic fibrosis, etc) and heart conditions (heart failure, coronary artery disease, hypertension, etc).
Both diabetes types are now grouped under “diabetes.”
The added medical conditions were posted on the CDC website’s COVID-19 page on March 29.
Type 1 diabetes and other conditions now priority for vaccination
The CDC refers to the medical conditions list as phase 1c in regard to COVID-19 vaccine prioritization, which means that anyone with any of these conditions can now be prioritized for vaccination, following those in groups 1a (frontline essential workers and those in long-term care facilities) and 1b (people aged 65-74 years; other essential workers; and people aged 16-64 years with underlying conditions that increase the risk of serious, life-threatening complications from COVID-19).
But in many cases, multiple states have already either fully opened up vaccine eligibility to all adults or have created their own lists of underlying high-risk medical conditions, CDC spokeswoman Kristen Nordlund told this news organization.
No conditions have been removed from the list.
In January, the American Diabetes Association and 18 other organizations sent a letter to the CDC requesting that type 1 diabetes be prioritized along with type 2, based on data from studies showing people with both types to be at high risk for severe COVID-19 illness.
Now, ADA says, “this updated guidance will help to address the fact that in many states, millions of people with type 1 diabetes have not been prioritized equally, slowing their access to critical vaccines.”
While awaiting this latest CDC move, ADA had been urging state governors to prioritize type 1 and type 2 diabetes equally. As of now, 38 states and the District of Columbia had either done so or announced that they would.
A version of this article first appeared on Medscape.com.
The Centers for Disease Control and Prevention has added several new medical conditions to its list of those that predispose adults to more severe COVID-19 illness.
Conditions that had previously been categorized as “might be” placing individuals at increased risk – but now are listed as high risk – include type 1 diabetes (in addition to type 2), moderate-to-severe asthma, liver disease, dementia or other neurologic conditions, stroke/cerebrovascular disease, HIV infection, cystic fibrosis, and overweight (in addition to obesity).
Substance use disorders, which hadn’t been previously listed, are now also considered high risk.
The new list groups together certain categories, such as chronic lung diseases (chronic obstructive pulmonary disease, asthma, cystic fibrosis, etc) and heart conditions (heart failure, coronary artery disease, hypertension, etc).
Both diabetes types are now grouped under “diabetes.”
The added medical conditions were posted on the CDC website’s COVID-19 page on March 29.
Type 1 diabetes and other conditions now priority for vaccination
The CDC refers to the medical conditions list as phase 1c in regard to COVID-19 vaccine prioritization, which means that anyone with any of these conditions can now be prioritized for vaccination, following those in groups 1a (frontline essential workers and those in long-term care facilities) and 1b (people aged 65-74 years; other essential workers; and people aged 16-64 years with underlying conditions that increase the risk of serious, life-threatening complications from COVID-19).
But in many cases, multiple states have already either fully opened up vaccine eligibility to all adults or have created their own lists of underlying high-risk medical conditions, CDC spokeswoman Kristen Nordlund told this news organization.
No conditions have been removed from the list.
In January, the American Diabetes Association and 18 other organizations sent a letter to the CDC requesting that type 1 diabetes be prioritized along with type 2, based on data from studies showing people with both types to be at high risk for severe COVID-19 illness.
Now, ADA says, “this updated guidance will help to address the fact that in many states, millions of people with type 1 diabetes have not been prioritized equally, slowing their access to critical vaccines.”
While awaiting this latest CDC move, ADA had been urging state governors to prioritize type 1 and type 2 diabetes equally. As of now, 38 states and the District of Columbia had either done so or announced that they would.
A version of this article first appeared on Medscape.com.
Vaccine mismatch: What to do after dose 1 when plans change
Ideally, Americans receiving their Pfizer/BioNTech or Moderna COVID-19 vaccines will get both doses from the same manufacturer, said Gregory Poland, MD, a vaccinologist at the Mayo Clinic in Rochester, Minn.

After all, that’s how they were tested for efficacy and safety, and it was results from those studies that led to emergency use authorization (EUA) being granted by the Food and Drug Administration.
But states and countries have struggled to keep up with the demand for vaccine, and more flexible vaccination schedules could help.
So researchers are exploring whether it is safe and effective to get the first and second doses from different manufacturers. And they are even wondering whether mixing doses from different manufacturers could increase effectiveness, particularly in light of emerging variants.
It’s called the “interchangeability issue,” said Dr. Poland, who has gotten a steady stream of questions about it.
For example, a patient recently asked about options for his father, who had gotten his first dose of the AstraZeneca vaccine in Ecuador, but had since moved to the United States, where that product has not been approved for use.
Dr. Poland said in an interview that he prefaces each answer with: “I’ve got no science for what I’m about to tell you.”
In this particular case, he recommended that the man’s father talk with his doctor about his level of COVID-19 risk and consider whether he should gamble on the AstraZeneca vaccine getting approved in the United States soon, or whether he should ask for a second dose from one of the three vaccines currently approved.
On March 22, 2021, AstraZeneca released positive results from its phase 3 trial, which will likely speed its path toward use in the United States.
Although clinical trials have started to test combinations and boosters, there’s currently no definitive evidence from human trials on mixing COVID vaccines, Dr. Poland pointed out.
But a study of a mixed-vaccine regimen is currently underway in the United Kingdom.
Participants in that 13-month trial will be given the Oxford/AstraZeneca and Pfizer/BioNTech vaccines in different combinations and at different intervals. The first results from that trial are expected this summer.
And interim results from a trial combining Russia’s Sputnik V and the AstraZeneca vaccines are expected in 2 months, according to a Reuters report.
Mix only in ‘exceptional situations’
The Centers for Disease Control and Prevention has been hesitant to open the door to mixing Pfizer and Moderna vaccinations, noting that the two “are not interchangeable.” But CDC guidance has changed slightly. Now, instead of saying the two vaccines should not be mixed, CDC guidance says they can be mixed in “exceptional situations,” and that the second dose can be administered up to 6 weeks after the first dose.
It is reasonable to assume that mixing COVID-19 vaccines that use the same platform – such as the mRNA platform used by both the Pfizer and Moderna vaccines – will be acceptable, Dr. Poland said, although human trials have not proven that.
However, it is unclear whether vaccines that use different platforms can be mixed. Can the first dose of an mRNA vaccine be followed by an adenovirus-based vaccine, like the Johnson & Johnson product or Novavax, if that vaccine is granted an EUA?
Ross Kedl, PhD, a vaccine researcher and professor of immunology at the University of Colorado at Denver, Aurora, said matching vaccine platforms might not be the preferred vaccination strategy.
He disagreed that there’s a lack of science surrounding the issue, and said all signs point to mixing as not only a good option, but probably a better one.
Researcher says science backs mixing
A mix of two different vaccine platforms likely enhances immunity, Dr. Kedl said. The heterologous prime-boost strategy has been used in animal studies for decades, “and it is well known that this promotes a much better immune response than when immunizing with the same vaccine twice.
“If you think about it in a Venn diagram sort of way, it makes sense,” he said in an interview. “Each vaccine has a number of components in it that influence immunity in various ways, but between the two of them, they only have one component that is similar. In the case of the coronavirus vaccines, the one thing both have in common is the spike protein from SARS-CoV-2. In essence, this gives you two shots at generating immunity against the one thing in each vaccine you care most about, but only one shot for the other vaccine components in each platform, resulting in an amplified response against the common target.”
In fact, the heterologous prime-boost vaccination strategy has proven to be effective in humans in early studies.
For example, an Ebola regimen that consisted of an adenovirus vector, similar to the AstraZeneca COVID vaccine, and a modified vaccinia virus vector showed promise in a phase 1 study. And an HIV regimen that consisted of the combination of a DNA vaccine, similar to the Pfizer and Moderna mRNA vaccines, and another viral vector showed encouraging results in a proof-of-concept study.
In both these cases, the heterologous prime-boost strategy was far better than single-vaccine prime-boost regimens, Dr. Kedl pointed out. And neither study reported any safety issues with the combinations.
For now, it’s best to stick with the same manufacturer for both shots, as the CDC guidance suggests, he said, agreeing with Dr. Poland.
But “I would be very surprised if we didn’t move to a mixing of vaccine platforms for the population,” Dr. Kedl said.
A version of this article first appeared on Medscape.com.
Ideally, Americans receiving their Pfizer/BioNTech or Moderna COVID-19 vaccines will get both doses from the same manufacturer, said Gregory Poland, MD, a vaccinologist at the Mayo Clinic in Rochester, Minn.
After all, that’s how they were tested for efficacy and safety, and it was results from those studies that led to emergency use authorization (EUA) being granted by the Food and Drug Administration.
But states and countries have struggled to keep up with the demand for vaccine, and more flexible vaccination schedules could help.
So researchers are exploring whether it is safe and effective to get the first and second doses from different manufacturers. And they are even wondering whether mixing doses from different manufacturers could increase effectiveness, particularly in light of emerging variants.
It’s called the “interchangeability issue,” said Dr. Poland, who has gotten a steady stream of questions about it.
For example, a patient recently asked about options for his father, who had gotten his first dose of the AstraZeneca vaccine in Ecuador, but had since moved to the United States, where that product has not been approved for use.
Dr. Poland said in an interview that he prefaces each answer with: “I’ve got no science for what I’m about to tell you.”
In this particular case, he recommended that the man’s father talk with his doctor about his level of COVID-19 risk and consider whether he should gamble on the AstraZeneca vaccine getting approved in the United States soon, or whether he should ask for a second dose from one of the three vaccines currently approved.
On March 22, 2021, AstraZeneca released positive results from its phase 3 trial, which will likely speed its path toward use in the United States.
Although clinical trials have started to test combinations and boosters, there’s currently no definitive evidence from human trials on mixing COVID vaccines, Dr. Poland pointed out.
But a study of a mixed-vaccine regimen is currently underway in the United Kingdom.
Participants in that 13-month trial will be given the Oxford/AstraZeneca and Pfizer/BioNTech vaccines in different combinations and at different intervals. The first results from that trial are expected this summer.
And interim results from a trial combining Russia’s Sputnik V and the AstraZeneca vaccines are expected in 2 months, according to a Reuters report.
Mix only in ‘exceptional situations’
The Centers for Disease Control and Prevention has been hesitant to open the door to mixing Pfizer and Moderna vaccinations, noting that the two “are not interchangeable.” But CDC guidance has changed slightly. Now, instead of saying the two vaccines should not be mixed, CDC guidance says they can be mixed in “exceptional situations,” and that the second dose can be administered up to 6 weeks after the first dose.
It is reasonable to assume that mixing COVID-19 vaccines that use the same platform – such as the mRNA platform used by both the Pfizer and Moderna vaccines – will be acceptable, Dr. Poland said, although human trials have not proven that.
However, it is unclear whether vaccines that use different platforms can be mixed. Can the first dose of an mRNA vaccine be followed by an adenovirus-based vaccine, like the Johnson & Johnson product or Novavax, if that vaccine is granted an EUA?
Ross Kedl, PhD, a vaccine researcher and professor of immunology at the University of Colorado at Denver, Aurora, said matching vaccine platforms might not be the preferred vaccination strategy.
He disagreed that there’s a lack of science surrounding the issue, and said all signs point to mixing as not only a good option, but probably a better one.
Researcher says science backs mixing
A mix of two different vaccine platforms likely enhances immunity, Dr. Kedl said. The heterologous prime-boost strategy has been used in animal studies for decades, “and it is well known that this promotes a much better immune response than when immunizing with the same vaccine twice.
“If you think about it in a Venn diagram sort of way, it makes sense,” he said in an interview. “Each vaccine has a number of components in it that influence immunity in various ways, but between the two of them, they only have one component that is similar. In the case of the coronavirus vaccines, the one thing both have in common is the spike protein from SARS-CoV-2. In essence, this gives you two shots at generating immunity against the one thing in each vaccine you care most about, but only one shot for the other vaccine components in each platform, resulting in an amplified response against the common target.”
In fact, the heterologous prime-boost vaccination strategy has proven to be effective in humans in early studies.
For example, an Ebola regimen that consisted of an adenovirus vector, similar to the AstraZeneca COVID vaccine, and a modified vaccinia virus vector showed promise in a phase 1 study. And an HIV regimen that consisted of the combination of a DNA vaccine, similar to the Pfizer and Moderna mRNA vaccines, and another viral vector showed encouraging results in a proof-of-concept study.
In both these cases, the heterologous prime-boost strategy was far better than single-vaccine prime-boost regimens, Dr. Kedl pointed out. And neither study reported any safety issues with the combinations.
For now, it’s best to stick with the same manufacturer for both shots, as the CDC guidance suggests, he said, agreeing with Dr. Poland.
But “I would be very surprised if we didn’t move to a mixing of vaccine platforms for the population,” Dr. Kedl said.
A version of this article first appeared on Medscape.com.
Ideally, Americans receiving their Pfizer/BioNTech or Moderna COVID-19 vaccines will get both doses from the same manufacturer, said Gregory Poland, MD, a vaccinologist at the Mayo Clinic in Rochester, Minn.
After all, that’s how they were tested for efficacy and safety, and it was results from those studies that led to emergency use authorization (EUA) being granted by the Food and Drug Administration.
But states and countries have struggled to keep up with the demand for vaccine, and more flexible vaccination schedules could help.
So researchers are exploring whether it is safe and effective to get the first and second doses from different manufacturers. And they are even wondering whether mixing doses from different manufacturers could increase effectiveness, particularly in light of emerging variants.
It’s called the “interchangeability issue,” said Dr. Poland, who has gotten a steady stream of questions about it.
For example, a patient recently asked about options for his father, who had gotten his first dose of the AstraZeneca vaccine in Ecuador, but had since moved to the United States, where that product has not been approved for use.
Dr. Poland said in an interview that he prefaces each answer with: “I’ve got no science for what I’m about to tell you.”
In this particular case, he recommended that the man’s father talk with his doctor about his level of COVID-19 risk and consider whether he should gamble on the AstraZeneca vaccine getting approved in the United States soon, or whether he should ask for a second dose from one of the three vaccines currently approved.
On March 22, 2021, AstraZeneca released positive results from its phase 3 trial, which will likely speed its path toward use in the United States.
Although clinical trials have started to test combinations and boosters, there’s currently no definitive evidence from human trials on mixing COVID vaccines, Dr. Poland pointed out.
But a study of a mixed-vaccine regimen is currently underway in the United Kingdom.
Participants in that 13-month trial will be given the Oxford/AstraZeneca and Pfizer/BioNTech vaccines in different combinations and at different intervals. The first results from that trial are expected this summer.
And interim results from a trial combining Russia’s Sputnik V and the AstraZeneca vaccines are expected in 2 months, according to a Reuters report.
Mix only in ‘exceptional situations’
The Centers for Disease Control and Prevention has been hesitant to open the door to mixing Pfizer and Moderna vaccinations, noting that the two “are not interchangeable.” But CDC guidance has changed slightly. Now, instead of saying the two vaccines should not be mixed, CDC guidance says they can be mixed in “exceptional situations,” and that the second dose can be administered up to 6 weeks after the first dose.
It is reasonable to assume that mixing COVID-19 vaccines that use the same platform – such as the mRNA platform used by both the Pfizer and Moderna vaccines – will be acceptable, Dr. Poland said, although human trials have not proven that.
However, it is unclear whether vaccines that use different platforms can be mixed. Can the first dose of an mRNA vaccine be followed by an adenovirus-based vaccine, like the Johnson & Johnson product or Novavax, if that vaccine is granted an EUA?
Ross Kedl, PhD, a vaccine researcher and professor of immunology at the University of Colorado at Denver, Aurora, said matching vaccine platforms might not be the preferred vaccination strategy.
He disagreed that there’s a lack of science surrounding the issue, and said all signs point to mixing as not only a good option, but probably a better one.
Researcher says science backs mixing
A mix of two different vaccine platforms likely enhances immunity, Dr. Kedl said. The heterologous prime-boost strategy has been used in animal studies for decades, “and it is well known that this promotes a much better immune response than when immunizing with the same vaccine twice.
“If you think about it in a Venn diagram sort of way, it makes sense,” he said in an interview. “Each vaccine has a number of components in it that influence immunity in various ways, but between the two of them, they only have one component that is similar. In the case of the coronavirus vaccines, the one thing both have in common is the spike protein from SARS-CoV-2. In essence, this gives you two shots at generating immunity against the one thing in each vaccine you care most about, but only one shot for the other vaccine components in each platform, resulting in an amplified response against the common target.”
In fact, the heterologous prime-boost vaccination strategy has proven to be effective in humans in early studies.
For example, an Ebola regimen that consisted of an adenovirus vector, similar to the AstraZeneca COVID vaccine, and a modified vaccinia virus vector showed promise in a phase 1 study. And an HIV regimen that consisted of the combination of a DNA vaccine, similar to the Pfizer and Moderna mRNA vaccines, and another viral vector showed encouraging results in a proof-of-concept study.
In both these cases, the heterologous prime-boost strategy was far better than single-vaccine prime-boost regimens, Dr. Kedl pointed out. And neither study reported any safety issues with the combinations.
For now, it’s best to stick with the same manufacturer for both shots, as the CDC guidance suggests, he said, agreeing with Dr. Poland.
But “I would be very surprised if we didn’t move to a mixing of vaccine platforms for the population,” Dr. Kedl said.
A version of this article first appeared on Medscape.com.
COVID vaccines could lose their punch within a year, experts say

In a survey of 77 epidemiologists from 28 countries by the People’s Vaccine Alliance, 66.2% predicted that the world has a year or less before variants make current vaccines ineffective. The People’s Vaccine Alliance is a coalition of more than 50 organizations, including the African Alliance, Oxfam, Public Citizen, and UNAIDS (the Joint United Nations Programme on HIV/AIDS).
Almost a third (32.5%) of those surveyed said ineffectiveness would happen in 9 months or less; 18.2% said 6 months or less.
Paul A. Offit, MD, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, said in an interview that, while it’s hard to say whether vaccines could become ineffective in that time frame, “It’s perfectly reasonable to think it could happen.”
The good news, said Dr. Offit, who was not involved with the survey, is that SARS-CoV-2 mutates slowly, compared with other viruses such as influenza.
“To date,” he said, “the mutations that have occurred are not far enough away from the immunity induced by your natural infection or immunization such that one isn’t protected at least against severe and critical disease.”
That’s the goal of vaccines, he noted: “to keep people from suffering mightily.”
A line may be crossed
“And so far that’s happening, even with the variants,” Dr. Offit said. “That line has not been crossed. But I think we should assume that it might be.”
Dr. Offit said it will be critical to monitor anyone who gets hospitalized who is known to have been infected or fully vaccinated. Then countries need to get really good at sequencing those viruses.
The great majority of those surveyed (88%) said that persistently low vaccine coverage in many countries would make it more likely that vaccine-resistant mutations will appear.
Coverage comparisons between countries are stark.
Many countries haven’t given a single vaccine dose
While rich countries are giving COVID-19 vaccinations at the rate of a person a second, many of the poorest countries have given hardly any vaccines, the People’s Vaccine Alliance says.
Additionally, according to researchers at the Global Health Innovation Center at Duke University, Durham, N.C., high- and upper-middle–income countries, which represent one-fifth of the world’s population, have bought about 6 billion doses. But low- and lower-middle–income countries, which make up four-fifths of the population, have bought only about 2.6 billion, an article in Nature reports.
“You’re only as strong as your weakest country,” Dr. Offit said. “If we haven’t learned that what happens in other countries can [affect the global population], we haven’t been paying attention.”
Gregg Gonsalves, PhD, associate professor of epidemiology at Yale University, New Haven, Conn., one of the academic centers surveyed, didn’t specify a timeline for when vaccines would become ineffective, but said in a press release that the urgency for widespread global vaccination is real.
“Unless we vaccinate the world,” he said, “we leave the playing field open to more and more mutations, which could churn out variants that could evade our current vaccines and require booster shots to deal with them.”
“Dire, but not surprising”
Panagis Galiatsatos, MD, MHS, a pulmonologist at John Hopkins University, Baltimore, whose research focuses on health care disparities, said the survey findings were “dire, but not surprising.”
Johns Hopkins was another of the centers surveyed, but Dr. Galiatsatos wasn’t personally involved with the survey.
COVID-19, Dr. Galiatsatos pointed out, has laid bare disparities, both in who gets the vaccine and who’s involved in trials to develop the vaccines.
“It’s morally concerning and an ethical reckoning,” he said in an interview.
Recognition of the borderless swath of destruction the virus is exacting is critical, he said.
The United States “has to realize this can’t be a U.S.-centric issue,” he said. “We’re going to be back to the beginning if we don’t make sure that every country is doing well. We haven’t seen that level of uniform approach.”
He noted that scientists have always known that viruses mutate, but now the race is on to find the parts of SARS-CoV-2 that don’t mutate as much.
“My suspicion is we’ll probably need boosters instead of a whole different vaccine,” Dr. Galiatsatos said.
Among the strategies sought by the People’s Vaccine Alliance is for all pharmaceutical companies working on COVID-19 vaccines to openly share technology and intellectual property through the World Health Organization COVID-19 Technology Access Pool, to speed production and rollout of vaccines to all countries.
In the survey, 74% said that open sharing of technology and intellectual property could boost global vaccine coverage; 23% said maybe and 3% said it wouldn’t help.
The survey was carried out between Feb. 17 and March 25, 2021. Respondents included epidemiologists, virologists, and infection disease specialists from the following countries: Algeria, Argentina, Australia, Belgium, Bolivia, Canada, Denmark, Ethiopia, France, Guatemala, India, Italy, Kenya, Lebanon, Norway, Philippines, Senegal, Somalia, South Africa, South Sudan, Spain, United Arab Emirates, Uganda, United Kingdom, United States, Vietnam, Zambia, and Zimbabwe.
Dr. Offit and Dr. Galiatsatos reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a survey of 77 epidemiologists from 28 countries by the People’s Vaccine Alliance, 66.2% predicted that the world has a year or less before variants make current vaccines ineffective. The People’s Vaccine Alliance is a coalition of more than 50 organizations, including the African Alliance, Oxfam, Public Citizen, and UNAIDS (the Joint United Nations Programme on HIV/AIDS).
Almost a third (32.5%) of those surveyed said ineffectiveness would happen in 9 months or less; 18.2% said 6 months or less.
Paul A. Offit, MD, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, said in an interview that, while it’s hard to say whether vaccines could become ineffective in that time frame, “It’s perfectly reasonable to think it could happen.”
The good news, said Dr. Offit, who was not involved with the survey, is that SARS-CoV-2 mutates slowly, compared with other viruses such as influenza.
“To date,” he said, “the mutations that have occurred are not far enough away from the immunity induced by your natural infection or immunization such that one isn’t protected at least against severe and critical disease.”
That’s the goal of vaccines, he noted: “to keep people from suffering mightily.”
A line may be crossed
“And so far that’s happening, even with the variants,” Dr. Offit said. “That line has not been crossed. But I think we should assume that it might be.”
Dr. Offit said it will be critical to monitor anyone who gets hospitalized who is known to have been infected or fully vaccinated. Then countries need to get really good at sequencing those viruses.
The great majority of those surveyed (88%) said that persistently low vaccine coverage in many countries would make it more likely that vaccine-resistant mutations will appear.
Coverage comparisons between countries are stark.
Many countries haven’t given a single vaccine dose
While rich countries are giving COVID-19 vaccinations at the rate of a person a second, many of the poorest countries have given hardly any vaccines, the People’s Vaccine Alliance says.
Additionally, according to researchers at the Global Health Innovation Center at Duke University, Durham, N.C., high- and upper-middle–income countries, which represent one-fifth of the world’s population, have bought about 6 billion doses. But low- and lower-middle–income countries, which make up four-fifths of the population, have bought only about 2.6 billion, an article in Nature reports.
“You’re only as strong as your weakest country,” Dr. Offit said. “If we haven’t learned that what happens in other countries can [affect the global population], we haven’t been paying attention.”
Gregg Gonsalves, PhD, associate professor of epidemiology at Yale University, New Haven, Conn., one of the academic centers surveyed, didn’t specify a timeline for when vaccines would become ineffective, but said in a press release that the urgency for widespread global vaccination is real.
“Unless we vaccinate the world,” he said, “we leave the playing field open to more and more mutations, which could churn out variants that could evade our current vaccines and require booster shots to deal with them.”
“Dire, but not surprising”
Panagis Galiatsatos, MD, MHS, a pulmonologist at John Hopkins University, Baltimore, whose research focuses on health care disparities, said the survey findings were “dire, but not surprising.”
Johns Hopkins was another of the centers surveyed, but Dr. Galiatsatos wasn’t personally involved with the survey.
COVID-19, Dr. Galiatsatos pointed out, has laid bare disparities, both in who gets the vaccine and who’s involved in trials to develop the vaccines.
“It’s morally concerning and an ethical reckoning,” he said in an interview.
Recognition of the borderless swath of destruction the virus is exacting is critical, he said.
The United States “has to realize this can’t be a U.S.-centric issue,” he said. “We’re going to be back to the beginning if we don’t make sure that every country is doing well. We haven’t seen that level of uniform approach.”
He noted that scientists have always known that viruses mutate, but now the race is on to find the parts of SARS-CoV-2 that don’t mutate as much.
“My suspicion is we’ll probably need boosters instead of a whole different vaccine,” Dr. Galiatsatos said.
Among the strategies sought by the People’s Vaccine Alliance is for all pharmaceutical companies working on COVID-19 vaccines to openly share technology and intellectual property through the World Health Organization COVID-19 Technology Access Pool, to speed production and rollout of vaccines to all countries.
In the survey, 74% said that open sharing of technology and intellectual property could boost global vaccine coverage; 23% said maybe and 3% said it wouldn’t help.
The survey was carried out between Feb. 17 and March 25, 2021. Respondents included epidemiologists, virologists, and infection disease specialists from the following countries: Algeria, Argentina, Australia, Belgium, Bolivia, Canada, Denmark, Ethiopia, France, Guatemala, India, Italy, Kenya, Lebanon, Norway, Philippines, Senegal, Somalia, South Africa, South Sudan, Spain, United Arab Emirates, Uganda, United Kingdom, United States, Vietnam, Zambia, and Zimbabwe.
Dr. Offit and Dr. Galiatsatos reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a survey of 77 epidemiologists from 28 countries by the People’s Vaccine Alliance, 66.2% predicted that the world has a year or less before variants make current vaccines ineffective. The People’s Vaccine Alliance is a coalition of more than 50 organizations, including the African Alliance, Oxfam, Public Citizen, and UNAIDS (the Joint United Nations Programme on HIV/AIDS).
Almost a third (32.5%) of those surveyed said ineffectiveness would happen in 9 months or less; 18.2% said 6 months or less.
Paul A. Offit, MD, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, said in an interview that, while it’s hard to say whether vaccines could become ineffective in that time frame, “It’s perfectly reasonable to think it could happen.”
The good news, said Dr. Offit, who was not involved with the survey, is that SARS-CoV-2 mutates slowly, compared with other viruses such as influenza.
“To date,” he said, “the mutations that have occurred are not far enough away from the immunity induced by your natural infection or immunization such that one isn’t protected at least against severe and critical disease.”
That’s the goal of vaccines, he noted: “to keep people from suffering mightily.”
A line may be crossed
“And so far that’s happening, even with the variants,” Dr. Offit said. “That line has not been crossed. But I think we should assume that it might be.”
Dr. Offit said it will be critical to monitor anyone who gets hospitalized who is known to have been infected or fully vaccinated. Then countries need to get really good at sequencing those viruses.
The great majority of those surveyed (88%) said that persistently low vaccine coverage in many countries would make it more likely that vaccine-resistant mutations will appear.
Coverage comparisons between countries are stark.
Many countries haven’t given a single vaccine dose
While rich countries are giving COVID-19 vaccinations at the rate of a person a second, many of the poorest countries have given hardly any vaccines, the People’s Vaccine Alliance says.
Additionally, according to researchers at the Global Health Innovation Center at Duke University, Durham, N.C., high- and upper-middle–income countries, which represent one-fifth of the world’s population, have bought about 6 billion doses. But low- and lower-middle–income countries, which make up four-fifths of the population, have bought only about 2.6 billion, an article in Nature reports.
“You’re only as strong as your weakest country,” Dr. Offit said. “If we haven’t learned that what happens in other countries can [affect the global population], we haven’t been paying attention.”
Gregg Gonsalves, PhD, associate professor of epidemiology at Yale University, New Haven, Conn., one of the academic centers surveyed, didn’t specify a timeline for when vaccines would become ineffective, but said in a press release that the urgency for widespread global vaccination is real.
“Unless we vaccinate the world,” he said, “we leave the playing field open to more and more mutations, which could churn out variants that could evade our current vaccines and require booster shots to deal with them.”
“Dire, but not surprising”
Panagis Galiatsatos, MD, MHS, a pulmonologist at John Hopkins University, Baltimore, whose research focuses on health care disparities, said the survey findings were “dire, but not surprising.”
Johns Hopkins was another of the centers surveyed, but Dr. Galiatsatos wasn’t personally involved with the survey.
COVID-19, Dr. Galiatsatos pointed out, has laid bare disparities, both in who gets the vaccine and who’s involved in trials to develop the vaccines.
“It’s morally concerning and an ethical reckoning,” he said in an interview.
Recognition of the borderless swath of destruction the virus is exacting is critical, he said.
The United States “has to realize this can’t be a U.S.-centric issue,” he said. “We’re going to be back to the beginning if we don’t make sure that every country is doing well. We haven’t seen that level of uniform approach.”
He noted that scientists have always known that viruses mutate, but now the race is on to find the parts of SARS-CoV-2 that don’t mutate as much.
“My suspicion is we’ll probably need boosters instead of a whole different vaccine,” Dr. Galiatsatos said.
Among the strategies sought by the People’s Vaccine Alliance is for all pharmaceutical companies working on COVID-19 vaccines to openly share technology and intellectual property through the World Health Organization COVID-19 Technology Access Pool, to speed production and rollout of vaccines to all countries.
In the survey, 74% said that open sharing of technology and intellectual property could boost global vaccine coverage; 23% said maybe and 3% said it wouldn’t help.
The survey was carried out between Feb. 17 and March 25, 2021. Respondents included epidemiologists, virologists, and infection disease specialists from the following countries: Algeria, Argentina, Australia, Belgium, Bolivia, Canada, Denmark, Ethiopia, France, Guatemala, India, Italy, Kenya, Lebanon, Norway, Philippines, Senegal, Somalia, South Africa, South Sudan, Spain, United Arab Emirates, Uganda, United Kingdom, United States, Vietnam, Zambia, and Zimbabwe.
Dr. Offit and Dr. Galiatsatos reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
National Psoriasis Foundation recommends some stop methotrexate for 2 weeks after J&J vaccine
The , Joel M. Gelfand, MD, said at Innovations in Dermatology: Virtual Spring Conference 2021.

The new guidance states: “Patients 60 or older who have at least one comorbidity associated with an increased risk for poor COVID-19 outcomes, and who are taking methotrexate with well-controlled psoriatic disease, may, in consultation with their prescriber, consider holding it for 2 weeks after receiving the Ad26.COV2.S [Johnson & Johnson] vaccine in order to potentially improve vaccine response.”
The key word here is “potentially.” There is no hard evidence that a 2-week hold on methotrexate after receiving the killed adenovirus vaccine will actually provide a clinically meaningful benefit. But it’s a hypothetical possibility. The rationale stems from a small randomized trial conducted in South Korea several years ago in which patients with rheumatoid arthritis were assigned to hold or continue their methotrexate for the first 2 weeks after receiving an inactivated-virus influenza vaccine. The antibody response to the vaccine was better in those who temporarily halted their methotrexate, explained Dr. Gelfand, cochair of the NPF COVID-19 Task Force and professor of dermatology and of epidemiology at the University of Pennsylvania, Philadelphia.
“If you have a patient on methotrexate who’s 60 or older and whose psoriasis is completely controlled and quiescent and the patient is concerned about how well the vaccine is going to work, this is a reasonable thing to consider in someone who’s at higher risk for poor outcomes if they get infected,” he said.
If the informed patient wants to continue on methotrexate without interruption, that’s fine, too, in light of the lack of compelling evidence on this issue, the dermatologist added at the conference, sponsored by MedscapeLIVE! and the producers of the Hawaii Dermatology Seminar and Caribbean Dermatology Symposium.
The NPF task force does not extend the recommendation to consider holding methotrexate in recipients of the mRNA-based Moderna and Pfizer vaccines because of their very different mechanisms of action. Nor is it recommended to hold biologic agents after receiving any of the available COVID-19 vaccines. Studies have shown no altered immunologic response to influenza or pneumococcal vaccines in patients who continued on tumor necrosis factor inhibitors or interleukin-17 inhibitors. The interleukin-23 inhibitors haven’t been studied in this regard.
The task force recommends that most psoriasis patients should continue on treatment throughout the pandemic, and newly diagnosed patients should commence appropriate therapy as if there was no pandemic.
“We’ve learned that many patients who stopped their treatment for psoriatic disease early in the pandemic came to regret that decision because their psoriasis flared and got worse and required reinstitution of therapy,” Dr. Gelfand said. “The current data is largely reassuring that if there is an effect of our therapies on the risk of COVID, it must be rather small and therefore unlikely to be clinically meaningful for our patients.”
Dr. Gelfand reported serving as a consultant to and recipient of institutional research grants from Pfizer and numerous other pharmaceutical companies.
MedscapeLIVE and this news organization are owned by the same parent company.
The , Joel M. Gelfand, MD, said at Innovations in Dermatology: Virtual Spring Conference 2021.
The new guidance states: “Patients 60 or older who have at least one comorbidity associated with an increased risk for poor COVID-19 outcomes, and who are taking methotrexate with well-controlled psoriatic disease, may, in consultation with their prescriber, consider holding it for 2 weeks after receiving the Ad26.COV2.S [Johnson & Johnson] vaccine in order to potentially improve vaccine response.”
The key word here is “potentially.” There is no hard evidence that a 2-week hold on methotrexate after receiving the killed adenovirus vaccine will actually provide a clinically meaningful benefit. But it’s a hypothetical possibility. The rationale stems from a small randomized trial conducted in South Korea several years ago in which patients with rheumatoid arthritis were assigned to hold or continue their methotrexate for the first 2 weeks after receiving an inactivated-virus influenza vaccine. The antibody response to the vaccine was better in those who temporarily halted their methotrexate, explained Dr. Gelfand, cochair of the NPF COVID-19 Task Force and professor of dermatology and of epidemiology at the University of Pennsylvania, Philadelphia.
“If you have a patient on methotrexate who’s 60 or older and whose psoriasis is completely controlled and quiescent and the patient is concerned about how well the vaccine is going to work, this is a reasonable thing to consider in someone who’s at higher risk for poor outcomes if they get infected,” he said.
If the informed patient wants to continue on methotrexate without interruption, that’s fine, too, in light of the lack of compelling evidence on this issue, the dermatologist added at the conference, sponsored by MedscapeLIVE! and the producers of the Hawaii Dermatology Seminar and Caribbean Dermatology Symposium.
The NPF task force does not extend the recommendation to consider holding methotrexate in recipients of the mRNA-based Moderna and Pfizer vaccines because of their very different mechanisms of action. Nor is it recommended to hold biologic agents after receiving any of the available COVID-19 vaccines. Studies have shown no altered immunologic response to influenza or pneumococcal vaccines in patients who continued on tumor necrosis factor inhibitors or interleukin-17 inhibitors. The interleukin-23 inhibitors haven’t been studied in this regard.
The task force recommends that most psoriasis patients should continue on treatment throughout the pandemic, and newly diagnosed patients should commence appropriate therapy as if there was no pandemic.
“We’ve learned that many patients who stopped their treatment for psoriatic disease early in the pandemic came to regret that decision because their psoriasis flared and got worse and required reinstitution of therapy,” Dr. Gelfand said. “The current data is largely reassuring that if there is an effect of our therapies on the risk of COVID, it must be rather small and therefore unlikely to be clinically meaningful for our patients.”
Dr. Gelfand reported serving as a consultant to and recipient of institutional research grants from Pfizer and numerous other pharmaceutical companies.
MedscapeLIVE and this news organization are owned by the same parent company.
The , Joel M. Gelfand, MD, said at Innovations in Dermatology: Virtual Spring Conference 2021.
The new guidance states: “Patients 60 or older who have at least one comorbidity associated with an increased risk for poor COVID-19 outcomes, and who are taking methotrexate with well-controlled psoriatic disease, may, in consultation with their prescriber, consider holding it for 2 weeks after receiving the Ad26.COV2.S [Johnson & Johnson] vaccine in order to potentially improve vaccine response.”
The key word here is “potentially.” There is no hard evidence that a 2-week hold on methotrexate after receiving the killed adenovirus vaccine will actually provide a clinically meaningful benefit. But it’s a hypothetical possibility. The rationale stems from a small randomized trial conducted in South Korea several years ago in which patients with rheumatoid arthritis were assigned to hold or continue their methotrexate for the first 2 weeks after receiving an inactivated-virus influenza vaccine. The antibody response to the vaccine was better in those who temporarily halted their methotrexate, explained Dr. Gelfand, cochair of the NPF COVID-19 Task Force and professor of dermatology and of epidemiology at the University of Pennsylvania, Philadelphia.
“If you have a patient on methotrexate who’s 60 or older and whose psoriasis is completely controlled and quiescent and the patient is concerned about how well the vaccine is going to work, this is a reasonable thing to consider in someone who’s at higher risk for poor outcomes if they get infected,” he said.
If the informed patient wants to continue on methotrexate without interruption, that’s fine, too, in light of the lack of compelling evidence on this issue, the dermatologist added at the conference, sponsored by MedscapeLIVE! and the producers of the Hawaii Dermatology Seminar and Caribbean Dermatology Symposium.
The NPF task force does not extend the recommendation to consider holding methotrexate in recipients of the mRNA-based Moderna and Pfizer vaccines because of their very different mechanisms of action. Nor is it recommended to hold biologic agents after receiving any of the available COVID-19 vaccines. Studies have shown no altered immunologic response to influenza or pneumococcal vaccines in patients who continued on tumor necrosis factor inhibitors or interleukin-17 inhibitors. The interleukin-23 inhibitors haven’t been studied in this regard.
The task force recommends that most psoriasis patients should continue on treatment throughout the pandemic, and newly diagnosed patients should commence appropriate therapy as if there was no pandemic.
“We’ve learned that many patients who stopped their treatment for psoriatic disease early in the pandemic came to regret that decision because their psoriasis flared and got worse and required reinstitution of therapy,” Dr. Gelfand said. “The current data is largely reassuring that if there is an effect of our therapies on the risk of COVID, it must be rather small and therefore unlikely to be clinically meaningful for our patients.”
Dr. Gelfand reported serving as a consultant to and recipient of institutional research grants from Pfizer and numerous other pharmaceutical companies.
MedscapeLIVE and this news organization are owned by the same parent company.
FROM INNOVATIONS IN DERMATOLOGY
Many unknowns on fertility preservation in transgender patients
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Unknowns around the long-term effects of gender-affirming hormonal treatment on fertility in transgender individuals, especially adolescents, and what this means for fertility preservation, should be red flags for clinicians, according to one expert addressing the issue at the recent virtual ENDO 2021 meeting.
“One of the main concerns regarding fertility preservation in this population is that the decision to seek gender-affirming therapy is often made early in the reproductive lifespan, and for many patients this is well before the consideration of … child-bearing,” remarked Marie Menke, MD, an ob/gyn from University of Michigan, Ann Arbor, presenting in a session dedicated to state-of-the-art approaches to gamete preservation.
“These patients need to consider simultaneously their desire for gender-affirming therapy and their desire for child-bearing,” she added, explaining that gender-affirming therapy typically requires suppression of the hormonal axis that supports reproduction.
“This level of shared decision-making requires time and multidisciplinary involvement in the face of … limited data, and even with the best of counseling it can be quite overwhelming,” Dr. Menke stressed.
Specifically, the effects of gender-affirming therapy on both fertility and fertility preservation options in transgender individuals in comparison to the general population are areas that require much more research, she emphasized.
On the topic of adolescents specifically, she said they are “a special population,” as many seeking medical therapy for gender dysphoria have never considered long-term fertility goals or desires. Reports of such discussions during pediatric gender care vary greatly depending on the age of the patient and their geographic location.
And where such conversations have happened, “often there is no recollection by patients of such discussion prior to referral to endocrinology,” she emphasized.
Session co-moderator Irene Su, MD, a reproductive endocrinologist at the University of California, San Diego, said shared decisions with patients have to be made every day, even though data are limited.
“Little is known about both the adverse medical impact of gender-affirming hormonal therapy on fertility potential, as well as the psychosocial impact of interrupting/reversing gender-affirming hormonal therapy in the future to attempt fertility,” she told this news organization.
However, “because there are reasons to be concerned about an adverse impact on fertility, transgender individuals need access to fertility risk and preservation counseling,” she stressed.
Dr. Su has a special interest in improving reproductive health in young cancer survivors, and this involves similar discussions around fertility preservation – a medical subspecialty known as “oncofertility.”
There is a greater pool of knowledge in this field compared with fertility preservation and family planning in transgender patients, Dr. Su noted.
“While we need similar data in transgender individuals, what we’ve learned from the cancer survivor population is that they and their families want to know about known and unknown fertility risks and options, even if they ultimately do not choose to undertake fertility preservation procedures,” she explains.
Desire for future kids, but <10% currently preserve fertility
Dr. Menke said the estimated prevalence of individuals who identify as transgender is around 0.7% of the U.S. population, and she observed that, “by and large, fertility management involves tissue cryopreservation.”
She presented survey data showing that between 33%-54% of transgender and nonbinary individuals report a desire to have biological children currently, or in the future, and 94.6% are also strongly in support of transgender people having access to fertility preservation procedures.
Likewise, an online cross-sectional survey of over 1,100 people in the general population found that 76.2% agree that transgender individuals should be offered fertility preservation, and 60% support fertility preservation in minors.
Multiple professional societies support counseling in regard to options for fertility preservation and recommend that it should be offered to transgender individuals.
The American Society for Reproductive Medicine (ASRM), the American College of Obstetricians and Gynecologists (ACOG), the World Professional Association for Transgender Health (WPATH), and the Endocrine Society all advocate that individuals seeking gender-affirming medical treatment should receive multidisciplinary counseling regarding fertility preservation prior to puberty suppression in adolescents, and prior to cross-sex hormone treatment in both adolescents and adults.
But despite all of these recommendations and the survey findings, fertility preservation rates in transgender patients are low, “at less than 10%,” reported Dr. Menke.
Fertility preservation counseling and management ideally needs to begin prior to initiation of hormone therapy, stressed Dr. Menke.
Given the limited data on the long-term effects of gender-affirming therapy on fertility and its preservation, such counseling often leads to a myriad of questions, she further explained.
“Patients ask ‘What are the chances of having biological children if I don’t pursue fertility preservation?’, and ‘How likely am I to have a biological child if I do pursue fertility preservation?’, as well as issues around access to care, with patients asking, ‘Will I be able to pursue this option [of fertility preservation]?’”
“The chance of having a biological child if fertility preservation is pursued is similar to those [patients with cancer] who receive ‘oncofertility’ care, which has a good prognosis,” she explained.
However, issues around access to care, and the cost of it, can be barriers.
What does a transgender male, born female, need to do?
For transgender males, options for fertility preservation include the recommended option of cryopreservation of the eggs (oocytes), although freezing of embryos and/or ovarian tissue are also possible.
The latter would be required in a prepubertal individual if they wanted to start puberty blockers and then go straight onto cross-sex hormones, Dr. Menke noted, although she said it’s not definitively known if prepubertal ovarian tissue is capable of being stimulated in the future to produce viable mature oocytes.
In someone who has gone through puberty, the ideal time to freeze eggs is before beginning gender-affirming hormone therapy, Dr. Menke explained. This is because it is not known whether testosterone has any adverse impact on oocyte development.
“We just don’t have definitive data that long-term testosterone isn’t gonadotoxic,” she said in response to a question about this after her talk.
Assessment of the reproductive consequences of gender-affirming therapy in transgender males can also be complicated by coexisting conditions, Dr. Menke explained.
For example, up to 58% of transgender males have polycystic ovary syndrome (PCOS) prior to transitioning, she noted. PCOS itself, and/or the gender-affirming therapy, may cause histologic changes of the ovarian tissue – for example, hyperplasia of ovarian stroma – and it’s not yet known to what extent this may impact future fertility, if present, she noted.
For oocyte preservation in female-to-male transgender individuals, stimulation with gonadotropins for 2-3 weeks is needed, and the procedure is invasive, requiring repeated vaginal ultrasounds. During this period, estradiol levels are supraphysiologic, and there is potential for breast development and vaginal bleeding post-retrieval, which individuals will need to be counseled about, Dr. Menke noted.
The cost of this also needs to be factored into the equation. Depending on insurance coverage, costs may be covered – and where there is no precedent, individuals can try referring their insurance companies to the ‘oncofertility consortium access-to-care model’, Dr. Menke advised.
If there is no coverage, the average cost for one egg-freezing cycle ranges from $10,000-$17,000 in the U.S., and often two to three cycles are needed to generate sufficient oocytes to be sure of a pregnancy. In addition, there are storage costs. Plus, there will be the cost of any future intervention to achieve a pregnancy, she stressed.
How long frozen oocytes remain viable is also still a matter of scientific debate, although “as the technology changes from slow-freeze to vitrification,” this time period should lengthen, Dr. Menke said.
In transgender males who have not preserved oocytes or embryos prior to transitioning, it’s necessary to stop testosterone to have the best chance of harvesting viable gametes, Dr. Menke said. Furthermore, individuals undertaking this procedure need to take into account all of the above-mentioned side effects of egg harvesting.
Although there have been reports of successful pregnancies with eggs retrieved from transgender males who have temporarily stopped testosterone, fertilization and embryo development following discontinuation of testosterone still require “additional investigation,” she observed.
Furthermore, “there are case reports of oocyte stimulation and retrieval of mature oocytes while patients continue testosterone therapy, and this may be an option in the future,” she noted, again stressing that it’s not known if excess testosterone is gonadotoxic.
Other options for fertility preservation in the transgender male include embryo cryopreservation, but this still involves hormonal stimulation and invasive procedures and would require the use of a sperm donor in a person who doesn’t currently have a partner (or who has one, but not necessarily one with whom they want to create a child).
For transgender males there is also the possibility of using a surrogate mother for the pregnancy, she noted.
What about transgender women, assigned male at birth?
For those assigned male at birth who wish to take puberty blockers, fertility preservation would require cryopreservation of testicular tissue, although Dr. Menke stressed that this is still considered “experimental.”
In the postpubertal period, the simplest option is to cryopreserve semen, with this ideally being performed prior to the individual commencing gender-affirming hormone therapy, Dr. Menke said.
If this is not done prior to beginning hormonal treatment, estrogen will need to be discontinued for fertility preservation, she noted.
Return of sperm function following cessation of estrogen may be limited – “expect at least 3 months before return of reproductive function,” Dr. Menke said. And even this may not be sufficient to restore normal spermatogenesis, she cautioned. “Absent or reduced spermatogenesis or morphological changes to Sertoli cells [have been reported in transgender women].”
Also, “there are needs for multiple attempts at ejaculation and storage requirements” for this approach. Cost for freezing sperm in the U.S., if not covered by insurance, is around $400, she noted, with storage costs ranging from $100 to up to $800 a year.
“Case reports using cryopreserved sperm [in transgender individuals] are promising overall … with clinical pregnancy rates following [in vitro fertilization] (IVF) with cryopreserved sperm … equivalent to patients without evidence of male factor fertility,” Dr. Menke reported.
However, she emphasized the fact that IVF, or intracytoplasmic sperm injection (ICSI), will still be necessary for conception, with potential additional costs.
Some individuals may also need to undergo surgical removal of sperm postpuberty; this is typically performed where there is evidence of male factor infertility, for example.
Embryo cryopreservation requires a partner or use of donor oocytes and, again, will have cost implications.
In conclusion, Dr. Menke reiterated that the use of fertility preservation techniques among transgender people is low, and it is more frequently accessed by transgender females. Among the identified barriers to fertility preservation are cost, lack of information, invasiveness of procedures, and desire not to delay medical transition.
Dr. Menke has disclosed no relevant financial relationships. Dr. Su has received a speaker honorarium from Ferring Pharmaceuticals.
A version of this article first appeared on Medscape.com.
Changes required for gynecologic surgeons to achieve greater pay equity
In a recent commentary published in Obstetrics & Gynecology, Katie L. Watson, JD, and Louise P. King, MD, JD, describe the issue of “double discrimination” in gynecologic surgery. The authors outlined how lower pay in a specialty where a majority of the surgeons and all of the patients are women may impact quality of care.
The commentary raises a number of concerns in gynecologic surgery that are important to discuss. Ob.gyn. as a whole is underpaid, as are many nonprocedural specialties such as family medicine and internal medicine. When ob.gyns. were predominantly men, the same situation existed – ob.gyns. were paid less than many other procedural specialties. While we’ve come a long way from the relative value unit (RVU) originally determined from the Harvard studies 30 years ago, there is room for additional improvement.
Several rationales were proposed by the authors to explain the disparities in pay between gynecologic surgery and those in urology: patient gender, surgeon gender, and length of training for gynecologic surgeons. The authors cited comparisons between urology and gynecology regarding “anatomically similar, sex-specific procedures” which require closer examination. Many of the code pairs selected were not actually comparable services. For example, management of Peyronie’s disease is a highly complex treatment performed by urologists that is not comparable with vaginectomy, yet this is an example of two codes used in the reference cited by the authors to conclude that surgeries on women are undervalued.
The overall RVUs for a procedure are also dependent upon the global period. The Centers for Medicare & Medicaid Services designated RVUs as the total amount of work before, during, and after a procedure. If a surgery has a 90-day global period, all the work for 90 days thereafter is bundled into the value, whereas if something is a zero-day global, only that day’s work is counted. A gynecologic surgeon who sees a patient back two or three times is coding and billing for those encounters in addition to that initial procedure.
Many of the code comparisons used in the analysis of gender in RVUs compared services with different global periods. Finally, some of the services that were compared had vastly different utilization. Some of the services and codes that were compared are performed extremely rarely and for that reason have not had their values reassessed over the years. There may be inequities in the RVUs for these services, but they will account for extremely little in overall compensation.
As a former chair of the American Medical Association’s RVS Update Committee (RUC), I spent years attempting to revalue ob.gyn. procedures. CMS assigns work RVUs based on physician work, practice expense, and professional liability insurance. The work is calculated using total physician time and intensity based on surveys completed by the specialty. The American College of Obstetrician and Gynecologist’s Committee on Health Economics and Coding, and the AMA RUC have worked diligently over many years to reassess potentially misvalued services. The ultimate RVUs assigned by CMS for gynecologic surgery are determined by the surveys completed by ACOG members. One issue we encountered with reexamining some procedures under RBRVS is that they have become so low volume that it has been difficult to justify the cost and effort to revalue them.
Lack of ob.gyn. training isn’t the full story
On average, ob.gyns. have between 18 and 24 months of surgical training, which is significantly less than other specialties. Lack of training in gynecologic surgery was proposed as another explanation for reduced compensation among female gynecologic surgeons. This is a complex issue not adequately explained by training time for gynecologic surgeons alone. While the number of trained ob.gyns. has increased in recent decades, the surgical volume has diminished and the workload of gynecologic surgery is far lower than it used to be. Surgical volume during and after training was much higher 35 years ago, prior to the advancements of procedures like endometrial ablation or tubal ligation. Women who had finished childbearing often underwent vaginal hysterectomies to manage contraception along with various other conditions.
With the advent of minimally invasive surgery, laparoscopic sterilization became possible, which has reduced the number of hysterectomies performed. Endometrial ablation is an office-based, noninvasive procedure. The development of the levonorgestrel IUD has helped manage abnormal bleeding, further reducing the need for hysterectomy.
This reduction in surgical volume does have an impact on quality of care. The model of tracking surgical outcomes at Kaiser Health System, as mentioned by the authors, could work well in some, but not all centers. A more approachable solution to address surgical volume for the average ob.gyn. would be to implement a mentoring and coaching process whereby recently trained ob.gyns. assist their senior partner(s) in surgery. This was the model years ago: I was trained by an ob.gyn. who was trained as a general surgeon. It was through the experience of assisting on each one of his cases – and him assisting on each one of my cases – that I received incredibly thorough surgical training.
These changes in practice, however, do not impact reimbursement. Rather than discrimination based on the gender of the surgeon, lower salaries in ob.gyn. are more likely to be the result of these and other factors.
The wage and quality gap in ob.gyn.
As a predominantly female surgical specialty, some of the disparity between gynecology and urology could be explained by how each specialty values its work. Here, gender plays a role in that when ob.gyns. are surveyed during the RUC process they may undervalue their work by reporting they can perform a procedure (and the before and after care) faster than what a urologist reports. The survey results may then result in lower RVUs.
Ob.gyn. is an overpopulated specialty for the number of surgeons needed to manage the volume of gynecologic surgery. When a health system wants to hire a general ob.gyn., it doesn’t have trouble finding one, while urologists are more challenging to recruit. This is not because of the structure of resource-based relative value scale (RBRVS) – despite the overall RVUs for gynecologic surgery, gynecologic oncologists are often paid well because health systems need them – but rather to the market economy of hiring physicians in specialty areas where there is demand.
Women are also chronically undervalued for the hours that we spend with patients. Data show that we spend more time with patients, which does not generate as many RVUs, but it generates better outcomes for patients. Evidence shows that women doctors in internal medicine and family medicine have better outcomes than doctors who are men.
On Jan. 1, 2021, Medicare and other payers implemented a new structure to reporting the level of office visit based on either medical decision-making or time spent on the date of encounter. Time spent with patients will now be rewarded – increased RVUs for increased time.
Part of the solution is value-based medicine and moving away from counting RVUs. This is also an opportunity to look at where time is spent in general ob.gyn. training and redistribute it, focusing on what trainees need for their education and not what hospitals need to service labor and delivery. We should step back and look creatively at optimizing the education and the training of ob.gyns., and where possible utilize other health care professionals such as nurse practitioners and midwives to address the uncomplicated obstetric needs of the hospital which could free up ob.gyn. trainees to obtain further surgical education.
To be clear, gender discrimination in compensation is prevalent and a persistent problem in medicine – ob.gyn. is no exception. Many ob.gyns. are employed by large health systems with payment structures and incentives that don’t align with those of the physician or the patient. There is definite misalignment in the way salaries are determined. Transparency on salaries is a critical component of addressing the pay gap that exists between women and men in medicine and in other industries.
The pay gap as it relates to reimbursement for gynecologic surgery, however, is a more complex matter that relates to how the RBRVS system was developed nearly 30 years ago when gynecologic surgery was not predominantly performed by women.
Dr. Levy is a voluntary clinical professor in the department of obstetrics, gynecology, and reproductive sciences at University of California San Diego Health, the former vice president of health policy at ACOG, past chair of the AMA/RUC, and current voting member of the AMA CPT editorial panel. She reported no relevant financial disclosures.
In a recent commentary published in Obstetrics & Gynecology, Katie L. Watson, JD, and Louise P. King, MD, JD, describe the issue of “double discrimination” in gynecologic surgery. The authors outlined how lower pay in a specialty where a majority of the surgeons and all of the patients are women may impact quality of care.
The commentary raises a number of concerns in gynecologic surgery that are important to discuss. Ob.gyn. as a whole is underpaid, as are many nonprocedural specialties such as family medicine and internal medicine. When ob.gyns. were predominantly men, the same situation existed – ob.gyns. were paid less than many other procedural specialties. While we’ve come a long way from the relative value unit (RVU) originally determined from the Harvard studies 30 years ago, there is room for additional improvement.
Several rationales were proposed by the authors to explain the disparities in pay between gynecologic surgery and those in urology: patient gender, surgeon gender, and length of training for gynecologic surgeons. The authors cited comparisons between urology and gynecology regarding “anatomically similar, sex-specific procedures” which require closer examination. Many of the code pairs selected were not actually comparable services. For example, management of Peyronie’s disease is a highly complex treatment performed by urologists that is not comparable with vaginectomy, yet this is an example of two codes used in the reference cited by the authors to conclude that surgeries on women are undervalued.
The overall RVUs for a procedure are also dependent upon the global period. The Centers for Medicare & Medicaid Services designated RVUs as the total amount of work before, during, and after a procedure. If a surgery has a 90-day global period, all the work for 90 days thereafter is bundled into the value, whereas if something is a zero-day global, only that day’s work is counted. A gynecologic surgeon who sees a patient back two or three times is coding and billing for those encounters in addition to that initial procedure.
Many of the code comparisons used in the analysis of gender in RVUs compared services with different global periods. Finally, some of the services that were compared had vastly different utilization. Some of the services and codes that were compared are performed extremely rarely and for that reason have not had their values reassessed over the years. There may be inequities in the RVUs for these services, but they will account for extremely little in overall compensation.
As a former chair of the American Medical Association’s RVS Update Committee (RUC), I spent years attempting to revalue ob.gyn. procedures. CMS assigns work RVUs based on physician work, practice expense, and professional liability insurance. The work is calculated using total physician time and intensity based on surveys completed by the specialty. The American College of Obstetrician and Gynecologist’s Committee on Health Economics and Coding, and the AMA RUC have worked diligently over many years to reassess potentially misvalued services. The ultimate RVUs assigned by CMS for gynecologic surgery are determined by the surveys completed by ACOG members. One issue we encountered with reexamining some procedures under RBRVS is that they have become so low volume that it has been difficult to justify the cost and effort to revalue them.
Lack of ob.gyn. training isn’t the full story
On average, ob.gyns. have between 18 and 24 months of surgical training, which is significantly less than other specialties. Lack of training in gynecologic surgery was proposed as another explanation for reduced compensation among female gynecologic surgeons. This is a complex issue not adequately explained by training time for gynecologic surgeons alone. While the number of trained ob.gyns. has increased in recent decades, the surgical volume has diminished and the workload of gynecologic surgery is far lower than it used to be. Surgical volume during and after training was much higher 35 years ago, prior to the advancements of procedures like endometrial ablation or tubal ligation. Women who had finished childbearing often underwent vaginal hysterectomies to manage contraception along with various other conditions.
With the advent of minimally invasive surgery, laparoscopic sterilization became possible, which has reduced the number of hysterectomies performed. Endometrial ablation is an office-based, noninvasive procedure. The development of the levonorgestrel IUD has helped manage abnormal bleeding, further reducing the need for hysterectomy.
This reduction in surgical volume does have an impact on quality of care. The model of tracking surgical outcomes at Kaiser Health System, as mentioned by the authors, could work well in some, but not all centers. A more approachable solution to address surgical volume for the average ob.gyn. would be to implement a mentoring and coaching process whereby recently trained ob.gyns. assist their senior partner(s) in surgery. This was the model years ago: I was trained by an ob.gyn. who was trained as a general surgeon. It was through the experience of assisting on each one of his cases – and him assisting on each one of my cases – that I received incredibly thorough surgical training.
These changes in practice, however, do not impact reimbursement. Rather than discrimination based on the gender of the surgeon, lower salaries in ob.gyn. are more likely to be the result of these and other factors.
The wage and quality gap in ob.gyn.
As a predominantly female surgical specialty, some of the disparity between gynecology and urology could be explained by how each specialty values its work. Here, gender plays a role in that when ob.gyns. are surveyed during the RUC process they may undervalue their work by reporting they can perform a procedure (and the before and after care) faster than what a urologist reports. The survey results may then result in lower RVUs.
Ob.gyn. is an overpopulated specialty for the number of surgeons needed to manage the volume of gynecologic surgery. When a health system wants to hire a general ob.gyn., it doesn’t have trouble finding one, while urologists are more challenging to recruit. This is not because of the structure of resource-based relative value scale (RBRVS) – despite the overall RVUs for gynecologic surgery, gynecologic oncologists are often paid well because health systems need them – but rather to the market economy of hiring physicians in specialty areas where there is demand.
Women are also chronically undervalued for the hours that we spend with patients. Data show that we spend more time with patients, which does not generate as many RVUs, but it generates better outcomes for patients. Evidence shows that women doctors in internal medicine and family medicine have better outcomes than doctors who are men.
On Jan. 1, 2021, Medicare and other payers implemented a new structure to reporting the level of office visit based on either medical decision-making or time spent on the date of encounter. Time spent with patients will now be rewarded – increased RVUs for increased time.
Part of the solution is value-based medicine and moving away from counting RVUs. This is also an opportunity to look at where time is spent in general ob.gyn. training and redistribute it, focusing on what trainees need for their education and not what hospitals need to service labor and delivery. We should step back and look creatively at optimizing the education and the training of ob.gyns., and where possible utilize other health care professionals such as nurse practitioners and midwives to address the uncomplicated obstetric needs of the hospital which could free up ob.gyn. trainees to obtain further surgical education.
To be clear, gender discrimination in compensation is prevalent and a persistent problem in medicine – ob.gyn. is no exception. Many ob.gyns. are employed by large health systems with payment structures and incentives that don’t align with those of the physician or the patient. There is definite misalignment in the way salaries are determined. Transparency on salaries is a critical component of addressing the pay gap that exists between women and men in medicine and in other industries.
The pay gap as it relates to reimbursement for gynecologic surgery, however, is a more complex matter that relates to how the RBRVS system was developed nearly 30 years ago when gynecologic surgery was not predominantly performed by women.
Dr. Levy is a voluntary clinical professor in the department of obstetrics, gynecology, and reproductive sciences at University of California San Diego Health, the former vice president of health policy at ACOG, past chair of the AMA/RUC, and current voting member of the AMA CPT editorial panel. She reported no relevant financial disclosures.
In a recent commentary published in Obstetrics & Gynecology, Katie L. Watson, JD, and Louise P. King, MD, JD, describe the issue of “double discrimination” in gynecologic surgery. The authors outlined how lower pay in a specialty where a majority of the surgeons and all of the patients are women may impact quality of care.
The commentary raises a number of concerns in gynecologic surgery that are important to discuss. Ob.gyn. as a whole is underpaid, as are many nonprocedural specialties such as family medicine and internal medicine. When ob.gyns. were predominantly men, the same situation existed – ob.gyns. were paid less than many other procedural specialties. While we’ve come a long way from the relative value unit (RVU) originally determined from the Harvard studies 30 years ago, there is room for additional improvement.
Several rationales were proposed by the authors to explain the disparities in pay between gynecologic surgery and those in urology: patient gender, surgeon gender, and length of training for gynecologic surgeons. The authors cited comparisons between urology and gynecology regarding “anatomically similar, sex-specific procedures” which require closer examination. Many of the code pairs selected were not actually comparable services. For example, management of Peyronie’s disease is a highly complex treatment performed by urologists that is not comparable with vaginectomy, yet this is an example of two codes used in the reference cited by the authors to conclude that surgeries on women are undervalued.
The overall RVUs for a procedure are also dependent upon the global period. The Centers for Medicare & Medicaid Services designated RVUs as the total amount of work before, during, and after a procedure. If a surgery has a 90-day global period, all the work for 90 days thereafter is bundled into the value, whereas if something is a zero-day global, only that day’s work is counted. A gynecologic surgeon who sees a patient back two or three times is coding and billing for those encounters in addition to that initial procedure.
Many of the code comparisons used in the analysis of gender in RVUs compared services with different global periods. Finally, some of the services that were compared had vastly different utilization. Some of the services and codes that were compared are performed extremely rarely and for that reason have not had their values reassessed over the years. There may be inequities in the RVUs for these services, but they will account for extremely little in overall compensation.
As a former chair of the American Medical Association’s RVS Update Committee (RUC), I spent years attempting to revalue ob.gyn. procedures. CMS assigns work RVUs based on physician work, practice expense, and professional liability insurance. The work is calculated using total physician time and intensity based on surveys completed by the specialty. The American College of Obstetrician and Gynecologist’s Committee on Health Economics and Coding, and the AMA RUC have worked diligently over many years to reassess potentially misvalued services. The ultimate RVUs assigned by CMS for gynecologic surgery are determined by the surveys completed by ACOG members. One issue we encountered with reexamining some procedures under RBRVS is that they have become so low volume that it has been difficult to justify the cost and effort to revalue them.
Lack of ob.gyn. training isn’t the full story
On average, ob.gyns. have between 18 and 24 months of surgical training, which is significantly less than other specialties. Lack of training in gynecologic surgery was proposed as another explanation for reduced compensation among female gynecologic surgeons. This is a complex issue not adequately explained by training time for gynecologic surgeons alone. While the number of trained ob.gyns. has increased in recent decades, the surgical volume has diminished and the workload of gynecologic surgery is far lower than it used to be. Surgical volume during and after training was much higher 35 years ago, prior to the advancements of procedures like endometrial ablation or tubal ligation. Women who had finished childbearing often underwent vaginal hysterectomies to manage contraception along with various other conditions.
With the advent of minimally invasive surgery, laparoscopic sterilization became possible, which has reduced the number of hysterectomies performed. Endometrial ablation is an office-based, noninvasive procedure. The development of the levonorgestrel IUD has helped manage abnormal bleeding, further reducing the need for hysterectomy.
This reduction in surgical volume does have an impact on quality of care. The model of tracking surgical outcomes at Kaiser Health System, as mentioned by the authors, could work well in some, but not all centers. A more approachable solution to address surgical volume for the average ob.gyn. would be to implement a mentoring and coaching process whereby recently trained ob.gyns. assist their senior partner(s) in surgery. This was the model years ago: I was trained by an ob.gyn. who was trained as a general surgeon. It was through the experience of assisting on each one of his cases – and him assisting on each one of my cases – that I received incredibly thorough surgical training.
These changes in practice, however, do not impact reimbursement. Rather than discrimination based on the gender of the surgeon, lower salaries in ob.gyn. are more likely to be the result of these and other factors.
The wage and quality gap in ob.gyn.
As a predominantly female surgical specialty, some of the disparity between gynecology and urology could be explained by how each specialty values its work. Here, gender plays a role in that when ob.gyns. are surveyed during the RUC process they may undervalue their work by reporting they can perform a procedure (and the before and after care) faster than what a urologist reports. The survey results may then result in lower RVUs.
Ob.gyn. is an overpopulated specialty for the number of surgeons needed to manage the volume of gynecologic surgery. When a health system wants to hire a general ob.gyn., it doesn’t have trouble finding one, while urologists are more challenging to recruit. This is not because of the structure of resource-based relative value scale (RBRVS) – despite the overall RVUs for gynecologic surgery, gynecologic oncologists are often paid well because health systems need them – but rather to the market economy of hiring physicians in specialty areas where there is demand.
Women are also chronically undervalued for the hours that we spend with patients. Data show that we spend more time with patients, which does not generate as many RVUs, but it generates better outcomes for patients. Evidence shows that women doctors in internal medicine and family medicine have better outcomes than doctors who are men.
On Jan. 1, 2021, Medicare and other payers implemented a new structure to reporting the level of office visit based on either medical decision-making or time spent on the date of encounter. Time spent with patients will now be rewarded – increased RVUs for increased time.
Part of the solution is value-based medicine and moving away from counting RVUs. This is also an opportunity to look at where time is spent in general ob.gyn. training and redistribute it, focusing on what trainees need for their education and not what hospitals need to service labor and delivery. We should step back and look creatively at optimizing the education and the training of ob.gyns., and where possible utilize other health care professionals such as nurse practitioners and midwives to address the uncomplicated obstetric needs of the hospital which could free up ob.gyn. trainees to obtain further surgical education.
To be clear, gender discrimination in compensation is prevalent and a persistent problem in medicine – ob.gyn. is no exception. Many ob.gyns. are employed by large health systems with payment structures and incentives that don’t align with those of the physician or the patient. There is definite misalignment in the way salaries are determined. Transparency on salaries is a critical component of addressing the pay gap that exists between women and men in medicine and in other industries.
The pay gap as it relates to reimbursement for gynecologic surgery, however, is a more complex matter that relates to how the RBRVS system was developed nearly 30 years ago when gynecologic surgery was not predominantly performed by women.
Dr. Levy is a voluntary clinical professor in the department of obstetrics, gynecology, and reproductive sciences at University of California San Diego Health, the former vice president of health policy at ACOG, past chair of the AMA/RUC, and current voting member of the AMA CPT editorial panel. She reported no relevant financial disclosures.
Long-haul COVID-19 brings welcome attention to POTS
Before COVID-19, postural orthostatic tachycardia syndrome (POTS) was one of those diseases that many people, including physicians, dismissed.
“They thought it was just anxious, crazy young women,” said Pam R. Taub, MD, who runs the cardiac rehabilitation program at the University of California, San Diego.
The cryptic autonomic condition was estimated to affect 1-3 million Americans before the pandemic hit. Now case reports confirm that it is a manifestation of postacute sequelae of SARS-CoV-2 infection (PASC), or so-called long-haul COVID-19.
“I’m excited that this condition that has been so often the ugly stepchild of both cardiology and neurology is getting some attention,” said Dr. Taub. She said she is hopeful that the National Institutes of Health’s commitment to PASC research will benefit patients affected by the cardiovascular dysautonomia characterized by orthostatic intolerance in the absence of orthostatic hypotension.
Postinfection POTS is not exclusive to SARS-CoV-2. It has been reported after Lyme disease and Epstein-Barr virus infections, for example. One theory is that some of the antibodies generated against the virus cross react and damage the autonomic nervous system, which regulates heart rate and blood pressure, Dr. Taub explained.
It is not known whether COVID-19 is more likely to trigger POTS than are other infections or whether the rise in cases merely reflects the fact that more than 115 million people worldwide have been infected with the novel coronavirus.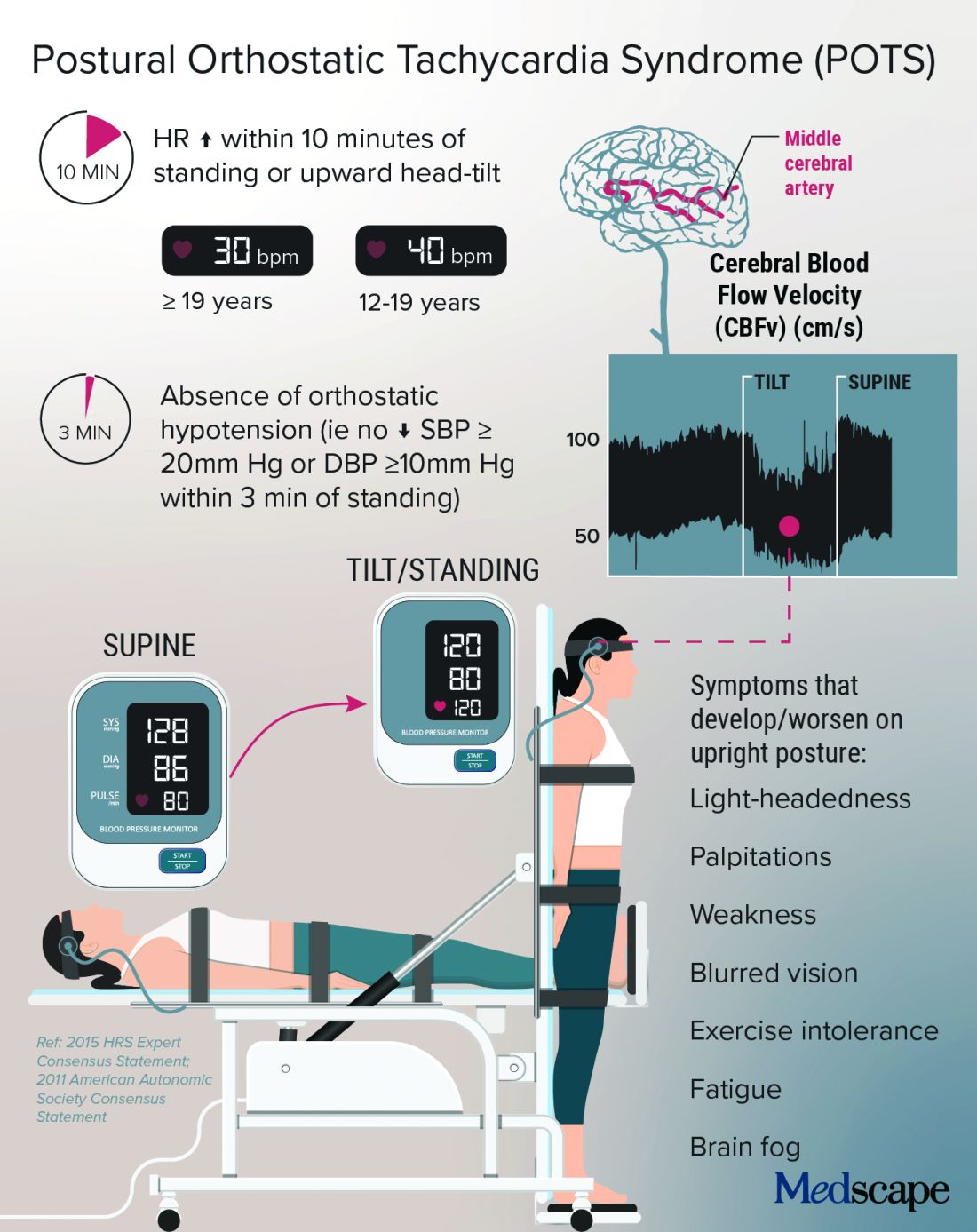
Low blood volume, dysregulation of the autonomic nervous system, and autoimmunity may all play a role in POTS, perhaps leading to distinct subtypes, according to a State of the Science document from the NIH; the National Heart, Lung, and Blood Institute; and the National Institute of Neurological Disorders and Stroke.
In Dr. Taub’s experience, “The truth is that patients actually have a mix of the subtypes.”
Kamal Shouman, MD, an autonomic neurologist at Mayo Clinic, Rochester, Minn., said in an interview that he has seen patients present with post–COVID-19 POTS in “all flavors,” including “neuropathic POTS, which is thought of as the classic postinfectious phenomenon.”

Why does it mostly affect athletic women?
The condition, which can be the result of dehydration or prolonged bed rest, leading to deconditioning, affects women disproportionately.
According to Manesh Patel, MD, if a patient with POTS who is not a young woman is presented on medical rounds, the response is, “Tell me again why you think this patient has POTS.”

Dr. Patel, chief of the division of cardiology at Duke University, Durham, N.C., has a theory for why many of the women who have POTS are athletes or are highly active: They likely have an underlying predisposition, compounded by a smaller body volume, leaving less margin for error. “If they decondition and lose 500 cc’s, it makes a bigger difference to them than, say, a 300-pound offensive lineman,” Dr. Patel explained.
That hypothesis makes sense to Dr. Taub, who added, “There are just some people metabolically that are more hyperadrenergic,” and it may be that “all their activity really helps tone down that sympathetic output,” but the infection affects these regulatory processes, and deconditioning disrupts things further.
Women also have more autoimmune disorders than do men. The driving force of the dysregulation of the autonomic nervous system is thought to be “immune mediated; we think it’s triggered by a response to a virus,” she said.
Dr. Shouman said the underlying susceptibility may predispose toward orthostatic intolerance. For example, patients will tell him, “Well, many years ago, I was prone to fainting.” He emphasized that POTS is not exclusive to women – he sees men with POTS, and one of the three recent case reports of post–COVID-19 POTS involved a 37-year-old man. So far, the male POTS patients that Dr. Patel has encountered have been deconditioned athletes.
Poor (wo)man’s tilt test and treatment options
POTS is typically diagnosed with a tilt test and transcranial Doppler. Dr. Taub described her “poor man’s tilt test” of asking the patient to lie down for 5-10 minutes and then having the patient stand up.
She likes the fact that transcranial Doppler helps validate the brain fog that patients report, which can be dismissed as “just your excuse for not wanting to work.” If blood perfusion to the brain is cut by 40%-50%, “how are you going to think clearly?” she said.
Dr. Shouman noted that overall volume expansion with salt water, compression garments, and a graduated exercise program play a major role in the rehabilitation of all POTS patients.
He likes to tailor treatments to the most likely underlying cause. But patients should first undergo a medical assessment by their internists to make sure there isn’t a primary lung or heart problem.
“Once the decision is made for them to be evaluated in the autonomic practice and [a] POTS diagnosis is made, I think it is very useful to determine what type of POTS,” he said.
With hyperadrenergic POTS, “you are looking at a standing norepinephrine level of over 600 pg/mL or so.” For these patients, drugs such as ivabradine or beta-blockers can help, he noted.
Dr. Taub recently conducted a small study that showed a benefit with the selective If channel blocker ivabradine for patients with hyperadrenergic POTS unrelated to COVID-19. She tends to favor ivabradine over beta-blockers because it lowers heart rate but not blood pressure. In addition, beta-blockers can exacerbate fatigue and brain fog.
A small crossover study will compare propranolol and ivabradine in POTS. For someone who is very hypovolemic, “you might try a salt tablet or a prescription drug like fludrocortisone,” Dr. Taub explained.
Another problem that patients with POTS experience is an inability to exercise because of orthostatic intolerance. Recumbent exercise targets deconditioning and can tamp down the hyperadrenergic effect. Dr. Shouman’s approach is to start gradually with swimming or the use of a recumbent bike or a rowing machine.
Dr. Taub recommends wearables to patients because POTS is “a very dynamic condition” that is easy to overmedicate or undermedicate. If it’s a good day, the patients are well hydrated, and the standing heart rate is only 80 bpm, she tells them they could titrate down their second dose of ivabradine, for example. The feedback from wearables also helps patients manage their exercise response.
For Dr. Shouman, wearables are not always as accurate as he would like. He tells his patients that it’s okay to use one as long as it doesn’t become a source of anxiety such that they’re constantly checking it.
POTS hope: A COVID-19 silver lining?
With increasing attention being paid to long-haul COVID-19, are there any concerns that POTS will get lost among the myriad symptoms connected to PASC?
Dr. Shouman cautioned, “Not all long COVID is POTS,” and said that clinicians at long-haul clinics should be able to recognize the different conditions “when POTS is suspected. I think it is useful for those providers to make the appropriate referral for POTS clinic autonomic assessment.”
He and his colleagues at Mayo have seen quite a few patients who have post–COVID-19 autonomic dysfunction, such as vasodepressor syncope, not just POTS. They plan to write about this soon.
“Of all the things I treat in cardiology, this is the most complex, because there’s so many different systems involved,” said Dr. Taub, who has seen patients recover fully from POTS. “There’s a spectrum, and there’s people that are definitely on one end of the spectrum where they have very severe diseases.”
For her, the important message is, “No matter where you are on the spectrum, there are things we can do to make your symptoms better.” And with grant funding for PASC research, “hopefully we will address the mechanisms of disease, and we’ll be able to cure this,” she said.
Dr. Patel has served as a consultant for Bayer, Janssen, AstraZeneca, and Heartflow and has received research grants from Bayer, Janssen, AstraZeneca, and the National Heart, Lung, and Blood Institute. Dr. Shouman reports no relevant financial relationships. Dr. Taub has served as a consultant for Amgen, Bayer, Esperion, Boehringer Ingelheim, Novo Nordisk, and Sanofi; is a shareholder in Epirium Bio; and has received research grants from the National Institutes of Health, the American Heart Association, and the Department of Homeland Security/FEMA.
A version of this article first appeared on Medscape.com.
Before COVID-19, postural orthostatic tachycardia syndrome (POTS) was one of those diseases that many people, including physicians, dismissed.
“They thought it was just anxious, crazy young women,” said Pam R. Taub, MD, who runs the cardiac rehabilitation program at the University of California, San Diego.
The cryptic autonomic condition was estimated to affect 1-3 million Americans before the pandemic hit. Now case reports confirm that it is a manifestation of postacute sequelae of SARS-CoV-2 infection (PASC), or so-called long-haul COVID-19.
“I’m excited that this condition that has been so often the ugly stepchild of both cardiology and neurology is getting some attention,” said Dr. Taub. She said she is hopeful that the National Institutes of Health’s commitment to PASC research will benefit patients affected by the cardiovascular dysautonomia characterized by orthostatic intolerance in the absence of orthostatic hypotension.
Postinfection POTS is not exclusive to SARS-CoV-2. It has been reported after Lyme disease and Epstein-Barr virus infections, for example. One theory is that some of the antibodies generated against the virus cross react and damage the autonomic nervous system, which regulates heart rate and blood pressure, Dr. Taub explained.
It is not known whether COVID-19 is more likely to trigger POTS than are other infections or whether the rise in cases merely reflects the fact that more than 115 million people worldwide have been infected with the novel coronavirus.
Low blood volume, dysregulation of the autonomic nervous system, and autoimmunity may all play a role in POTS, perhaps leading to distinct subtypes, according to a State of the Science document from the NIH; the National Heart, Lung, and Blood Institute; and the National Institute of Neurological Disorders and Stroke.
In Dr. Taub’s experience, “The truth is that patients actually have a mix of the subtypes.”
Kamal Shouman, MD, an autonomic neurologist at Mayo Clinic, Rochester, Minn., said in an interview that he has seen patients present with post–COVID-19 POTS in “all flavors,” including “neuropathic POTS, which is thought of as the classic postinfectious phenomenon.”
Why does it mostly affect athletic women?
The condition, which can be the result of dehydration or prolonged bed rest, leading to deconditioning, affects women disproportionately.
According to Manesh Patel, MD, if a patient with POTS who is not a young woman is presented on medical rounds, the response is, “Tell me again why you think this patient has POTS.”
Dr. Patel, chief of the division of cardiology at Duke University, Durham, N.C., has a theory for why many of the women who have POTS are athletes or are highly active: They likely have an underlying predisposition, compounded by a smaller body volume, leaving less margin for error. “If they decondition and lose 500 cc’s, it makes a bigger difference to them than, say, a 300-pound offensive lineman,” Dr. Patel explained.
That hypothesis makes sense to Dr. Taub, who added, “There are just some people metabolically that are more hyperadrenergic,” and it may be that “all their activity really helps tone down that sympathetic output,” but the infection affects these regulatory processes, and deconditioning disrupts things further.
Women also have more autoimmune disorders than do men. The driving force of the dysregulation of the autonomic nervous system is thought to be “immune mediated; we think it’s triggered by a response to a virus,” she said.
Dr. Shouman said the underlying susceptibility may predispose toward orthostatic intolerance. For example, patients will tell him, “Well, many years ago, I was prone to fainting.” He emphasized that POTS is not exclusive to women – he sees men with POTS, and one of the three recent case reports of post–COVID-19 POTS involved a 37-year-old man. So far, the male POTS patients that Dr. Patel has encountered have been deconditioned athletes.
Poor (wo)man’s tilt test and treatment options
POTS is typically diagnosed with a tilt test and transcranial Doppler. Dr. Taub described her “poor man’s tilt test” of asking the patient to lie down for 5-10 minutes and then having the patient stand up.
She likes the fact that transcranial Doppler helps validate the brain fog that patients report, which can be dismissed as “just your excuse for not wanting to work.” If blood perfusion to the brain is cut by 40%-50%, “how are you going to think clearly?” she said.
Dr. Shouman noted that overall volume expansion with salt water, compression garments, and a graduated exercise program play a major role in the rehabilitation of all POTS patients.
He likes to tailor treatments to the most likely underlying cause. But patients should first undergo a medical assessment by their internists to make sure there isn’t a primary lung or heart problem.
“Once the decision is made for them to be evaluated in the autonomic practice and [a] POTS diagnosis is made, I think it is very useful to determine what type of POTS,” he said.
With hyperadrenergic POTS, “you are looking at a standing norepinephrine level of over 600 pg/mL or so.” For these patients, drugs such as ivabradine or beta-blockers can help, he noted.
Dr. Taub recently conducted a small study that showed a benefit with the selective If channel blocker ivabradine for patients with hyperadrenergic POTS unrelated to COVID-19. She tends to favor ivabradine over beta-blockers because it lowers heart rate but not blood pressure. In addition, beta-blockers can exacerbate fatigue and brain fog.
A small crossover study will compare propranolol and ivabradine in POTS. For someone who is very hypovolemic, “you might try a salt tablet or a prescription drug like fludrocortisone,” Dr. Taub explained.
Another problem that patients with POTS experience is an inability to exercise because of orthostatic intolerance. Recumbent exercise targets deconditioning and can tamp down the hyperadrenergic effect. Dr. Shouman’s approach is to start gradually with swimming or the use of a recumbent bike or a rowing machine.
Dr. Taub recommends wearables to patients because POTS is “a very dynamic condition” that is easy to overmedicate or undermedicate. If it’s a good day, the patients are well hydrated, and the standing heart rate is only 80 bpm, she tells them they could titrate down their second dose of ivabradine, for example. The feedback from wearables also helps patients manage their exercise response.
For Dr. Shouman, wearables are not always as accurate as he would like. He tells his patients that it’s okay to use one as long as it doesn’t become a source of anxiety such that they’re constantly checking it.
POTS hope: A COVID-19 silver lining?
With increasing attention being paid to long-haul COVID-19, are there any concerns that POTS will get lost among the myriad symptoms connected to PASC?
Dr. Shouman cautioned, “Not all long COVID is POTS,” and said that clinicians at long-haul clinics should be able to recognize the different conditions “when POTS is suspected. I think it is useful for those providers to make the appropriate referral for POTS clinic autonomic assessment.”
He and his colleagues at Mayo have seen quite a few patients who have post–COVID-19 autonomic dysfunction, such as vasodepressor syncope, not just POTS. They plan to write about this soon.
“Of all the things I treat in cardiology, this is the most complex, because there’s so many different systems involved,” said Dr. Taub, who has seen patients recover fully from POTS. “There’s a spectrum, and there’s people that are definitely on one end of the spectrum where they have very severe diseases.”
For her, the important message is, “No matter where you are on the spectrum, there are things we can do to make your symptoms better.” And with grant funding for PASC research, “hopefully we will address the mechanisms of disease, and we’ll be able to cure this,” she said.
Dr. Patel has served as a consultant for Bayer, Janssen, AstraZeneca, and Heartflow and has received research grants from Bayer, Janssen, AstraZeneca, and the National Heart, Lung, and Blood Institute. Dr. Shouman reports no relevant financial relationships. Dr. Taub has served as a consultant for Amgen, Bayer, Esperion, Boehringer Ingelheim, Novo Nordisk, and Sanofi; is a shareholder in Epirium Bio; and has received research grants from the National Institutes of Health, the American Heart Association, and the Department of Homeland Security/FEMA.
A version of this article first appeared on Medscape.com.
Before COVID-19, postural orthostatic tachycardia syndrome (POTS) was one of those diseases that many people, including physicians, dismissed.
“They thought it was just anxious, crazy young women,” said Pam R. Taub, MD, who runs the cardiac rehabilitation program at the University of California, San Diego.
The cryptic autonomic condition was estimated to affect 1-3 million Americans before the pandemic hit. Now case reports confirm that it is a manifestation of postacute sequelae of SARS-CoV-2 infection (PASC), or so-called long-haul COVID-19.
“I’m excited that this condition that has been so often the ugly stepchild of both cardiology and neurology is getting some attention,” said Dr. Taub. She said she is hopeful that the National Institutes of Health’s commitment to PASC research will benefit patients affected by the cardiovascular dysautonomia characterized by orthostatic intolerance in the absence of orthostatic hypotension.
Postinfection POTS is not exclusive to SARS-CoV-2. It has been reported after Lyme disease and Epstein-Barr virus infections, for example. One theory is that some of the antibodies generated against the virus cross react and damage the autonomic nervous system, which regulates heart rate and blood pressure, Dr. Taub explained.
It is not known whether COVID-19 is more likely to trigger POTS than are other infections or whether the rise in cases merely reflects the fact that more than 115 million people worldwide have been infected with the novel coronavirus.
Low blood volume, dysregulation of the autonomic nervous system, and autoimmunity may all play a role in POTS, perhaps leading to distinct subtypes, according to a State of the Science document from the NIH; the National Heart, Lung, and Blood Institute; and the National Institute of Neurological Disorders and Stroke.
In Dr. Taub’s experience, “The truth is that patients actually have a mix of the subtypes.”
Kamal Shouman, MD, an autonomic neurologist at Mayo Clinic, Rochester, Minn., said in an interview that he has seen patients present with post–COVID-19 POTS in “all flavors,” including “neuropathic POTS, which is thought of as the classic postinfectious phenomenon.”
Why does it mostly affect athletic women?
The condition, which can be the result of dehydration or prolonged bed rest, leading to deconditioning, affects women disproportionately.
According to Manesh Patel, MD, if a patient with POTS who is not a young woman is presented on medical rounds, the response is, “Tell me again why you think this patient has POTS.”
Dr. Patel, chief of the division of cardiology at Duke University, Durham, N.C., has a theory for why many of the women who have POTS are athletes or are highly active: They likely have an underlying predisposition, compounded by a smaller body volume, leaving less margin for error. “If they decondition and lose 500 cc’s, it makes a bigger difference to them than, say, a 300-pound offensive lineman,” Dr. Patel explained.
That hypothesis makes sense to Dr. Taub, who added, “There are just some people metabolically that are more hyperadrenergic,” and it may be that “all their activity really helps tone down that sympathetic output,” but the infection affects these regulatory processes, and deconditioning disrupts things further.
Women also have more autoimmune disorders than do men. The driving force of the dysregulation of the autonomic nervous system is thought to be “immune mediated; we think it’s triggered by a response to a virus,” she said.
Dr. Shouman said the underlying susceptibility may predispose toward orthostatic intolerance. For example, patients will tell him, “Well, many years ago, I was prone to fainting.” He emphasized that POTS is not exclusive to women – he sees men with POTS, and one of the three recent case reports of post–COVID-19 POTS involved a 37-year-old man. So far, the male POTS patients that Dr. Patel has encountered have been deconditioned athletes.
Poor (wo)man’s tilt test and treatment options
POTS is typically diagnosed with a tilt test and transcranial Doppler. Dr. Taub described her “poor man’s tilt test” of asking the patient to lie down for 5-10 minutes and then having the patient stand up.
She likes the fact that transcranial Doppler helps validate the brain fog that patients report, which can be dismissed as “just your excuse for not wanting to work.” If blood perfusion to the brain is cut by 40%-50%, “how are you going to think clearly?” she said.
Dr. Shouman noted that overall volume expansion with salt water, compression garments, and a graduated exercise program play a major role in the rehabilitation of all POTS patients.
He likes to tailor treatments to the most likely underlying cause. But patients should first undergo a medical assessment by their internists to make sure there isn’t a primary lung or heart problem.
“Once the decision is made for them to be evaluated in the autonomic practice and [a] POTS diagnosis is made, I think it is very useful to determine what type of POTS,” he said.
With hyperadrenergic POTS, “you are looking at a standing norepinephrine level of over 600 pg/mL or so.” For these patients, drugs such as ivabradine or beta-blockers can help, he noted.
Dr. Taub recently conducted a small study that showed a benefit with the selective If channel blocker ivabradine for patients with hyperadrenergic POTS unrelated to COVID-19. She tends to favor ivabradine over beta-blockers because it lowers heart rate but not blood pressure. In addition, beta-blockers can exacerbate fatigue and brain fog.
A small crossover study will compare propranolol and ivabradine in POTS. For someone who is very hypovolemic, “you might try a salt tablet or a prescription drug like fludrocortisone,” Dr. Taub explained.
Another problem that patients with POTS experience is an inability to exercise because of orthostatic intolerance. Recumbent exercise targets deconditioning and can tamp down the hyperadrenergic effect. Dr. Shouman’s approach is to start gradually with swimming or the use of a recumbent bike or a rowing machine.
Dr. Taub recommends wearables to patients because POTS is “a very dynamic condition” that is easy to overmedicate or undermedicate. If it’s a good day, the patients are well hydrated, and the standing heart rate is only 80 bpm, she tells them they could titrate down their second dose of ivabradine, for example. The feedback from wearables also helps patients manage their exercise response.
For Dr. Shouman, wearables are not always as accurate as he would like. He tells his patients that it’s okay to use one as long as it doesn’t become a source of anxiety such that they’re constantly checking it.
POTS hope: A COVID-19 silver lining?
With increasing attention being paid to long-haul COVID-19, are there any concerns that POTS will get lost among the myriad symptoms connected to PASC?
Dr. Shouman cautioned, “Not all long COVID is POTS,” and said that clinicians at long-haul clinics should be able to recognize the different conditions “when POTS is suspected. I think it is useful for those providers to make the appropriate referral for POTS clinic autonomic assessment.”
He and his colleagues at Mayo have seen quite a few patients who have post–COVID-19 autonomic dysfunction, such as vasodepressor syncope, not just POTS. They plan to write about this soon.
“Of all the things I treat in cardiology, this is the most complex, because there’s so many different systems involved,” said Dr. Taub, who has seen patients recover fully from POTS. “There’s a spectrum, and there’s people that are definitely on one end of the spectrum where they have very severe diseases.”
For her, the important message is, “No matter where you are on the spectrum, there are things we can do to make your symptoms better.” And with grant funding for PASC research, “hopefully we will address the mechanisms of disease, and we’ll be able to cure this,” she said.
Dr. Patel has served as a consultant for Bayer, Janssen, AstraZeneca, and Heartflow and has received research grants from Bayer, Janssen, AstraZeneca, and the National Heart, Lung, and Blood Institute. Dr. Shouman reports no relevant financial relationships. Dr. Taub has served as a consultant for Amgen, Bayer, Esperion, Boehringer Ingelheim, Novo Nordisk, and Sanofi; is a shareholder in Epirium Bio; and has received research grants from the National Institutes of Health, the American Heart Association, and the Department of Homeland Security/FEMA.
A version of this article first appeared on Medscape.com.
Call to eradicate all types of HPV cancers, not just cervical
The World Health Organization’s call for the elimination of cervical cancer worldwide is a laudable goal and one that many organizations across the globe have endorsed.
Yet some would say that this goal goes only halfway, and that the real finish line should be to eliminate all vaccine-type HPV infections that cause multiple cancers, in men as well as women.
One proponent of sweeping HPV prevention is Mark Jit, PhD, from the London School of Hygiene & Tropical Medicine.
In the long run, the WHO’s call to eliminate cervical cancer is “insufficiently ambitious” he writes in a special issue of Preventive Medicine.
“The point is, if you are trying to eliminate cervical cancer, you’ve run part of the race,” he said.
“But why not run that extra third and get rid of the virus, then you never have to worry about it again,” Dr. Jit elaborated in an interview.
Winning that race, however, is dependent on a gender-neutral HPV vaccination policy, he pointed out.
At present, the WHO advocates only for female vaccination and screening.
Some countries have already taken the matter into their own hands. As of May 2020, 33 countries and four territories have gender-neutral vaccination schedules.
Others are also calling for gender-neutral HPV vaccination to achieve a far wider public health good.
“I completely agree that our ultimate goal should be the elimination of all HPV-related cancers – but we will require gender-neutral vaccination to do it,” says Anna Giuliano, PhD, professor and director, Center for Immunization and Infection Research in Cancer, Moffitt Cancer Center, Tampa.
“The reason why WHO started with cervical cancer elimination is that it is likely to be the first cancer that we can achieve this with, and if you look internationally, cervical cancer has the highest burden,” Dr. Giuliano told this news organization.
“But it’s important to understand that it’s not just females who are at risk for HPV disease, men have serious consequences from HPV infection, too,” she said.
In fact, rates of HPV-related cancers and mortality in men exceed those for women in countries that have effective cervical cancer screening programs, she points out in an editorial in the same issue of Preventive Medicine.
Rates in men are driven largely by HPV-related oropharyngeal cancer, but not only, Dr. Giuliano noted in an interview.
Rates of anal cancer among men who have sex with men (MSM) are at least as high as rates of cervical cancer among women living in the poorest countries of the world, where 85% of cervical cancer deaths now occur, she noted. If MSM are HIV positive, rates of anal cancer are even higher.
Unethical to leave males out?
Arguments in favor of gender-neutral HPV vaccination abound, but the most compelling among them is that society really should give males an opportunity to receive direct protection against all types of HPV infection, Dr. Giuliano commented.
Indeed, in the U.K., experts argue that it is unethical to leave males out of achieving direct protection against HPV infection, she noted.
With a female-only vaccination strategy, “males are only protected if they stay in a population where there are high female vaccination rates – and very few countries have achieved high rates of vaccine dissemination and have sustained it,” she pointed out. But that applies only to heterosexual men, who develop some herd immunity from exposure to vaccinated females; this is not the case for MSM.
On a pragmatic note, a vaccine program that targets a larger number of people against HPV infection – which would be achieved with gender-neutral vaccination – is going to be more resilient against temporary changes in vaccine uptake, such as what has happened over the past year.
“During the pandemic, people may have had virtual clinic visits, but they haven’t had in-person visits, which is what you need for vaccination,” Dr. Giuliano pointed out. “So over the past year, there has been a major drop in vaccination rates,” she said.
Eliminating cervical cancer
Currently, the WHO plans for eliminating cervical cancer involve a strategy of vaccinating 90% of girls by the age of 15, screening 70% of women with a high performance test by the age of 35 and again at 45, and treating 90% of women with cervical disease – the so-called “90-70-90” strategy.
Dr. Jit agrees that very high levels of vaccine coverage would eradicate the HPV types causing almost all cases of cervical cancer. The same strategy would also sharply reduce the need for preventive measures in the future.
However, as Dr. Jit argues, 90% female-only coverage will not be sufficient to eliminate HPV 16 transmission, although 90% coverage in both males and females – namely a gender-neutral strategy – might. To show this, Dr. Jit and colleagues used the HPV-ADVISE transmission model in India.
Results from this modeling exercise suggest that 90% coverage of both sexes would bring the prevalence of HPV 16 close to elimination, defined as reducing the prevalence of HPV 16 to below 10 per 100,000 in the population.
In addition, because even at this low level, HPV transmission can be sustained in a small group of sex workers and their clients, achieving 95% coverage of 10-year-old girls who might become female sex workers in the future will likely achieve the goal of HPV 16 elimination, as Dr. Jit suggests.
OPSCC elimination
Elimination of another HPV-related cancer, oropharyngeal squamous cell carcinomas (OPSCCs), is discussed in another paper in the same journal.
HPV-related OPSCCs are mostly associated specifically with HPV 16.
There is currently an epidemic of this cancer among middle-aged men in the Nordic countries of Denmark, Finland, Norway, and Sweden; incidence rates have tripled over the past 30 years, note Tuomas Lehtinen, PhD, FICAN-MID, Tampere, Finland and colleagues.
They propose a two-step action plan – gender-neutral vaccination in adolescent boys and girls, and a screening program for adults born in 1995 or earlier.
The first step is already underway, and the recent implementation of school-based HPV vaccination programs in the Nordic countries is predicted to gradually decrease the incidence of HPV-related OPSCCs, they write.
“Even if HPV vaccination does not cure established infections, it can prevent re-infection/recurrence of associated lesions in 45% to 65% of individuals with anal or cervical intraepithelial neoplasia,” the authors write, “and there is high VE (vaccine efficacy) against oropharyngeal HPV infections as well.”
Furthermore, there is a tenfold relative risk of tonsillar and base of tongue cancers in spouses of women diagnosed with invasive anogenital cancer, researchers also point out. “This underlines the importance of breaking genito-oral transmission chains.”
The screening of adults born in 1995 for HPV-related OPSCC is still at a planning stage.
In a proof-of-concept study for the stepwise prevention of OPSCC, the authors suggest that target birth cohorts first be stratified and then randomized into serological HPV 16 E6 antibody screening or no screening. HPV 16 antibody-positive women and their spouses then could be invited for HPV vaccination followed by 2 HPV DNA tests.
Unscreened women and their spouses would serve as population-based controls. “Even if gender-neutral vaccination results in rapid elimination of HPV circulation, the effects of persistent, [prevalent] HPV infections on the most HPV-associated tonsillar cancer will continue for decades after HPV circulation has stopped,” the authors predict.
The Jit study was funded by the Bill & Melinda Gates Foundation and the National Institute for Health. The Lehtinen study was supported by grants from the Finnish Cancer Society and Tampere Tuberculosis Foundation. Dr. Jit and Dr. Lehtinen have disclosed no relevant financial relationships. Dr. Giuliano serves on the advisory board for Merck, which markets the HPV vaccine Gardasil.
A version of this article first appeared on Medscape.com.
The World Health Organization’s call for the elimination of cervical cancer worldwide is a laudable goal and one that many organizations across the globe have endorsed.
Yet some would say that this goal goes only halfway, and that the real finish line should be to eliminate all vaccine-type HPV infections that cause multiple cancers, in men as well as women.
One proponent of sweeping HPV prevention is Mark Jit, PhD, from the London School of Hygiene & Tropical Medicine.
In the long run, the WHO’s call to eliminate cervical cancer is “insufficiently ambitious” he writes in a special issue of Preventive Medicine.
“The point is, if you are trying to eliminate cervical cancer, you’ve run part of the race,” he said.
“But why not run that extra third and get rid of the virus, then you never have to worry about it again,” Dr. Jit elaborated in an interview.
Winning that race, however, is dependent on a gender-neutral HPV vaccination policy, he pointed out.
At present, the WHO advocates only for female vaccination and screening.
Some countries have already taken the matter into their own hands. As of May 2020, 33 countries and four territories have gender-neutral vaccination schedules.
Others are also calling for gender-neutral HPV vaccination to achieve a far wider public health good.
“I completely agree that our ultimate goal should be the elimination of all HPV-related cancers – but we will require gender-neutral vaccination to do it,” says Anna Giuliano, PhD, professor and director, Center for Immunization and Infection Research in Cancer, Moffitt Cancer Center, Tampa.
“The reason why WHO started with cervical cancer elimination is that it is likely to be the first cancer that we can achieve this with, and if you look internationally, cervical cancer has the highest burden,” Dr. Giuliano told this news organization.
“But it’s important to understand that it’s not just females who are at risk for HPV disease, men have serious consequences from HPV infection, too,” she said.
In fact, rates of HPV-related cancers and mortality in men exceed those for women in countries that have effective cervical cancer screening programs, she points out in an editorial in the same issue of Preventive Medicine.
Rates in men are driven largely by HPV-related oropharyngeal cancer, but not only, Dr. Giuliano noted in an interview.
Rates of anal cancer among men who have sex with men (MSM) are at least as high as rates of cervical cancer among women living in the poorest countries of the world, where 85% of cervical cancer deaths now occur, she noted. If MSM are HIV positive, rates of anal cancer are even higher.
Unethical to leave males out?
Arguments in favor of gender-neutral HPV vaccination abound, but the most compelling among them is that society really should give males an opportunity to receive direct protection against all types of HPV infection, Dr. Giuliano commented.
Indeed, in the U.K., experts argue that it is unethical to leave males out of achieving direct protection against HPV infection, she noted.
With a female-only vaccination strategy, “males are only protected if they stay in a population where there are high female vaccination rates – and very few countries have achieved high rates of vaccine dissemination and have sustained it,” she pointed out. But that applies only to heterosexual men, who develop some herd immunity from exposure to vaccinated females; this is not the case for MSM.
On a pragmatic note, a vaccine program that targets a larger number of people against HPV infection – which would be achieved with gender-neutral vaccination – is going to be more resilient against temporary changes in vaccine uptake, such as what has happened over the past year.
“During the pandemic, people may have had virtual clinic visits, but they haven’t had in-person visits, which is what you need for vaccination,” Dr. Giuliano pointed out. “So over the past year, there has been a major drop in vaccination rates,” she said.
Eliminating cervical cancer
Currently, the WHO plans for eliminating cervical cancer involve a strategy of vaccinating 90% of girls by the age of 15, screening 70% of women with a high performance test by the age of 35 and again at 45, and treating 90% of women with cervical disease – the so-called “90-70-90” strategy.
Dr. Jit agrees that very high levels of vaccine coverage would eradicate the HPV types causing almost all cases of cervical cancer. The same strategy would also sharply reduce the need for preventive measures in the future.
However, as Dr. Jit argues, 90% female-only coverage will not be sufficient to eliminate HPV 16 transmission, although 90% coverage in both males and females – namely a gender-neutral strategy – might. To show this, Dr. Jit and colleagues used the HPV-ADVISE transmission model in India.
Results from this modeling exercise suggest that 90% coverage of both sexes would bring the prevalence of HPV 16 close to elimination, defined as reducing the prevalence of HPV 16 to below 10 per 100,000 in the population.
In addition, because even at this low level, HPV transmission can be sustained in a small group of sex workers and their clients, achieving 95% coverage of 10-year-old girls who might become female sex workers in the future will likely achieve the goal of HPV 16 elimination, as Dr. Jit suggests.
OPSCC elimination
Elimination of another HPV-related cancer, oropharyngeal squamous cell carcinomas (OPSCCs), is discussed in another paper in the same journal.
HPV-related OPSCCs are mostly associated specifically with HPV 16.
There is currently an epidemic of this cancer among middle-aged men in the Nordic countries of Denmark, Finland, Norway, and Sweden; incidence rates have tripled over the past 30 years, note Tuomas Lehtinen, PhD, FICAN-MID, Tampere, Finland and colleagues.
They propose a two-step action plan – gender-neutral vaccination in adolescent boys and girls, and a screening program for adults born in 1995 or earlier.
The first step is already underway, and the recent implementation of school-based HPV vaccination programs in the Nordic countries is predicted to gradually decrease the incidence of HPV-related OPSCCs, they write.
“Even if HPV vaccination does not cure established infections, it can prevent re-infection/recurrence of associated lesions in 45% to 65% of individuals with anal or cervical intraepithelial neoplasia,” the authors write, “and there is high VE (vaccine efficacy) against oropharyngeal HPV infections as well.”
Furthermore, there is a tenfold relative risk of tonsillar and base of tongue cancers in spouses of women diagnosed with invasive anogenital cancer, researchers also point out. “This underlines the importance of breaking genito-oral transmission chains.”
The screening of adults born in 1995 for HPV-related OPSCC is still at a planning stage.
In a proof-of-concept study for the stepwise prevention of OPSCC, the authors suggest that target birth cohorts first be stratified and then randomized into serological HPV 16 E6 antibody screening or no screening. HPV 16 antibody-positive women and their spouses then could be invited for HPV vaccination followed by 2 HPV DNA tests.
Unscreened women and their spouses would serve as population-based controls. “Even if gender-neutral vaccination results in rapid elimination of HPV circulation, the effects of persistent, [prevalent] HPV infections on the most HPV-associated tonsillar cancer will continue for decades after HPV circulation has stopped,” the authors predict.
The Jit study was funded by the Bill & Melinda Gates Foundation and the National Institute for Health. The Lehtinen study was supported by grants from the Finnish Cancer Society and Tampere Tuberculosis Foundation. Dr. Jit and Dr. Lehtinen have disclosed no relevant financial relationships. Dr. Giuliano serves on the advisory board for Merck, which markets the HPV vaccine Gardasil.
A version of this article first appeared on Medscape.com.
The World Health Organization’s call for the elimination of cervical cancer worldwide is a laudable goal and one that many organizations across the globe have endorsed.
Yet some would say that this goal goes only halfway, and that the real finish line should be to eliminate all vaccine-type HPV infections that cause multiple cancers, in men as well as women.
One proponent of sweeping HPV prevention is Mark Jit, PhD, from the London School of Hygiene & Tropical Medicine.
In the long run, the WHO’s call to eliminate cervical cancer is “insufficiently ambitious” he writes in a special issue of Preventive Medicine.
“The point is, if you are trying to eliminate cervical cancer, you’ve run part of the race,” he said.
“But why not run that extra third and get rid of the virus, then you never have to worry about it again,” Dr. Jit elaborated in an interview.
Winning that race, however, is dependent on a gender-neutral HPV vaccination policy, he pointed out.
At present, the WHO advocates only for female vaccination and screening.
Some countries have already taken the matter into their own hands. As of May 2020, 33 countries and four territories have gender-neutral vaccination schedules.
Others are also calling for gender-neutral HPV vaccination to achieve a far wider public health good.
“I completely agree that our ultimate goal should be the elimination of all HPV-related cancers – but we will require gender-neutral vaccination to do it,” says Anna Giuliano, PhD, professor and director, Center for Immunization and Infection Research in Cancer, Moffitt Cancer Center, Tampa.
“The reason why WHO started with cervical cancer elimination is that it is likely to be the first cancer that we can achieve this with, and if you look internationally, cervical cancer has the highest burden,” Dr. Giuliano told this news organization.
“But it’s important to understand that it’s not just females who are at risk for HPV disease, men have serious consequences from HPV infection, too,” she said.
In fact, rates of HPV-related cancers and mortality in men exceed those for women in countries that have effective cervical cancer screening programs, she points out in an editorial in the same issue of Preventive Medicine.
Rates in men are driven largely by HPV-related oropharyngeal cancer, but not only, Dr. Giuliano noted in an interview.
Rates of anal cancer among men who have sex with men (MSM) are at least as high as rates of cervical cancer among women living in the poorest countries of the world, where 85% of cervical cancer deaths now occur, she noted. If MSM are HIV positive, rates of anal cancer are even higher.
Unethical to leave males out?
Arguments in favor of gender-neutral HPV vaccination abound, but the most compelling among them is that society really should give males an opportunity to receive direct protection against all types of HPV infection, Dr. Giuliano commented.
Indeed, in the U.K., experts argue that it is unethical to leave males out of achieving direct protection against HPV infection, she noted.
With a female-only vaccination strategy, “males are only protected if they stay in a population where there are high female vaccination rates – and very few countries have achieved high rates of vaccine dissemination and have sustained it,” she pointed out. But that applies only to heterosexual men, who develop some herd immunity from exposure to vaccinated females; this is not the case for MSM.
On a pragmatic note, a vaccine program that targets a larger number of people against HPV infection – which would be achieved with gender-neutral vaccination – is going to be more resilient against temporary changes in vaccine uptake, such as what has happened over the past year.
“During the pandemic, people may have had virtual clinic visits, but they haven’t had in-person visits, which is what you need for vaccination,” Dr. Giuliano pointed out. “So over the past year, there has been a major drop in vaccination rates,” she said.
Eliminating cervical cancer
Currently, the WHO plans for eliminating cervical cancer involve a strategy of vaccinating 90% of girls by the age of 15, screening 70% of women with a high performance test by the age of 35 and again at 45, and treating 90% of women with cervical disease – the so-called “90-70-90” strategy.
Dr. Jit agrees that very high levels of vaccine coverage would eradicate the HPV types causing almost all cases of cervical cancer. The same strategy would also sharply reduce the need for preventive measures in the future.
However, as Dr. Jit argues, 90% female-only coverage will not be sufficient to eliminate HPV 16 transmission, although 90% coverage in both males and females – namely a gender-neutral strategy – might. To show this, Dr. Jit and colleagues used the HPV-ADVISE transmission model in India.
Results from this modeling exercise suggest that 90% coverage of both sexes would bring the prevalence of HPV 16 close to elimination, defined as reducing the prevalence of HPV 16 to below 10 per 100,000 in the population.
In addition, because even at this low level, HPV transmission can be sustained in a small group of sex workers and their clients, achieving 95% coverage of 10-year-old girls who might become female sex workers in the future will likely achieve the goal of HPV 16 elimination, as Dr. Jit suggests.
OPSCC elimination
Elimination of another HPV-related cancer, oropharyngeal squamous cell carcinomas (OPSCCs), is discussed in another paper in the same journal.
HPV-related OPSCCs are mostly associated specifically with HPV 16.
There is currently an epidemic of this cancer among middle-aged men in the Nordic countries of Denmark, Finland, Norway, and Sweden; incidence rates have tripled over the past 30 years, note Tuomas Lehtinen, PhD, FICAN-MID, Tampere, Finland and colleagues.
They propose a two-step action plan – gender-neutral vaccination in adolescent boys and girls, and a screening program for adults born in 1995 or earlier.
The first step is already underway, and the recent implementation of school-based HPV vaccination programs in the Nordic countries is predicted to gradually decrease the incidence of HPV-related OPSCCs, they write.
“Even if HPV vaccination does not cure established infections, it can prevent re-infection/recurrence of associated lesions in 45% to 65% of individuals with anal or cervical intraepithelial neoplasia,” the authors write, “and there is high VE (vaccine efficacy) against oropharyngeal HPV infections as well.”
Furthermore, there is a tenfold relative risk of tonsillar and base of tongue cancers in spouses of women diagnosed with invasive anogenital cancer, researchers also point out. “This underlines the importance of breaking genito-oral transmission chains.”
The screening of adults born in 1995 for HPV-related OPSCC is still at a planning stage.
In a proof-of-concept study for the stepwise prevention of OPSCC, the authors suggest that target birth cohorts first be stratified and then randomized into serological HPV 16 E6 antibody screening or no screening. HPV 16 antibody-positive women and their spouses then could be invited for HPV vaccination followed by 2 HPV DNA tests.
Unscreened women and their spouses would serve as population-based controls. “Even if gender-neutral vaccination results in rapid elimination of HPV circulation, the effects of persistent, [prevalent] HPV infections on the most HPV-associated tonsillar cancer will continue for decades after HPV circulation has stopped,” the authors predict.
The Jit study was funded by the Bill & Melinda Gates Foundation and the National Institute for Health. The Lehtinen study was supported by grants from the Finnish Cancer Society and Tampere Tuberculosis Foundation. Dr. Jit and Dr. Lehtinen have disclosed no relevant financial relationships. Dr. Giuliano serves on the advisory board for Merck, which markets the HPV vaccine Gardasil.
A version of this article first appeared on Medscape.com.
Niraparib maintenance offers continued benefit in some with recurrent ovarian cancer
The final analysis showed a significant difference in second progression-free survival (PFS2) with niraparib versus placebo, but only in patients with germline BRCA mutations.
The overall survival analysis was limited because the study was not powered to detect differences in OS. Still, the investigators found a trend toward better OS with niraparib in patients who had germline BRCA mutations.
These results were presented at the Society of Gynecologic Oncology’s Virtual Annual Meeting on Women’s Cancer (Abstract 11139).
The final analysis of this study was muddied by missing data for many of the 553 patients originally randomized, according to Ursula Matulonis, MD, of the Dana-Farber Cancer Institute in Boston, who presented the study’s results at the meeting.
“Since 2014, approvals of PARP [poly (ADP-ribose) polymerase] inhibitors worldwide in different lines of ovarian cancer therapy have revolutionized the treatment of women with ovarian cancer,” Dr. Matulonis said. “During the time from the initial results of the NOVA study in 2016 to this final analysis, PARP inhibitors have become available commercially globally.”
The wider availability of PARP inhibitors led to premature unblinding and withdrawals from the trial, resulting in missing data for a large proportion of patients.
Initial results
In the primary analysis of the trial, the median PFS was 21 months among patients with germline BRCA mutations who received niraparib and 5.5 months for patients with germline BRCA mutations who received placebo (P < .001).
Among patients with no germline BRCA mutations, the median PFS was 9.3 months for those who received niraparib and 3.9 months for placebo-treated controls (P < .001).
At the time of the primary PFS analysis in 2016, 155 of the 553 patients originally enrolled had left the study for reasons other than death.
In both treatment cohorts, a large number of patients were unblinded as to their treatment assignments by investigators, which required them to withdraw consent from the study under the protocol, resulting in the aforementioned loss of some data on subsequent therapy and survival status.
Final results: PFS2 and OS
At the time of the final data lock on Oct. 1, 2020, the mean follow-up was 67 months (5.6 years).
In all, 64 patients originally assigned to niraparib were still on study (28 in the germline BRCA mutation cohort and 36 in the nonmutated cohort), as were 28 patients originally assigned to placebo (9 and 19, respectively).
For the final analysis, the investigators were able to retrieve survival data on 51% of the patients originally enrolled, either through protocol amendments and obtaining consent again or through national databases.
Although crossover to the niraparib arm was not allowed on study, patients could receive a PARP inhibitor following disease progression or study withdrawal. Because of discontinuations, data on postprogression therapy were missing for 138 of the 553 patients (25%).
The hazard ratio for PFS2 with niraparib versus placebo was 0.67 for patients with germline BRCA mutations (95% confidence interval, 0.479-0.948) and 0.81 for patients without the mutations (95% CI, 0.632-1.050).
In an analysis adjusted for subsequent PARP inhibitor therapy, there was no significant difference in median OS between the niraparib and placebo arms, regardless of mutation status. In the cohort without BRCA mutations, the median OS was 31.3 months with niraparib and 35.9 months with placebo (HR, 0.97; 95% CI, 0.74-1.26).
However, there was a trend toward improved OS with niraparib among patients with germline BRCA mutations. The median OS was 43.8 months with niraparib and 34.1 months with placebo (HR, 0.66; 95% CI, 0.44-0.99).
Safety: MDS/AML
Hematologic treatment-emergent adverse events occurred primarily in the first year of niraparib treatment. The incidence of grade 3 or greater thrombocytopenia decreased from 33.8% at 1 year to 2.8% in years 2-3. The incidence of anemia decreased from 25.6% to 0.7%, and the neutropenia incidence decreased from 19.3% to 2.1%.
At last follow-up, 13 patients in the niraparib arm (3.5%) and 3 in the placebo arm (1.7%) had developed myelodysplastic syndromes (MDS) or acute myeloid leukemia (AML).
The incidence of MDS/AML was 6.6% among patients with germline BRCA mutations who received niraparib, noted invited discussant Deborah K. Armstrong, MD, of the Johns Hopkins Kimmel Cancer Center in Baltimore.
That incidence was nearly as high as the 8% incidence of MDS/AML seen among similar patients in the SOLO-2 trial of olaparib maintenance, she noted.
This observation raises the question “of whether more extensive prior therapy or the longer duration of PARP inhibitor therapy in patients who have recurrent platinum-sensitive disease is the biggest contributor to that,” she said.
Dr. Armstrong commented that it remains to be seen whether the incidence of MDS/AML will increase with longer follow-up, particularly among patients who were more heavily pretreated with chemotherapy prior to PARP inhibitor maintenance, and in patients who remain on a PARP inhibitor until progression in ongoing trials of PARP inhibitors as frontline therapy.
The ENGOT-OV16/NOVA trial was funded by GlaxoSmithKline. Dr. Matulonis reported consulting/advisory fees from Merck, Novartis, and NextCure. Dr. Armstrong disclosed relationships with several companies, not including GlaxoSmithKline.
The final analysis showed a significant difference in second progression-free survival (PFS2) with niraparib versus placebo, but only in patients with germline BRCA mutations.
The overall survival analysis was limited because the study was not powered to detect differences in OS. Still, the investigators found a trend toward better OS with niraparib in patients who had germline BRCA mutations.
These results were presented at the Society of Gynecologic Oncology’s Virtual Annual Meeting on Women’s Cancer (Abstract 11139).
The final analysis of this study was muddied by missing data for many of the 553 patients originally randomized, according to Ursula Matulonis, MD, of the Dana-Farber Cancer Institute in Boston, who presented the study’s results at the meeting.
“Since 2014, approvals of PARP [poly (ADP-ribose) polymerase] inhibitors worldwide in different lines of ovarian cancer therapy have revolutionized the treatment of women with ovarian cancer,” Dr. Matulonis said. “During the time from the initial results of the NOVA study in 2016 to this final analysis, PARP inhibitors have become available commercially globally.”
The wider availability of PARP inhibitors led to premature unblinding and withdrawals from the trial, resulting in missing data for a large proportion of patients.
Initial results
In the primary analysis of the trial, the median PFS was 21 months among patients with germline BRCA mutations who received niraparib and 5.5 months for patients with germline BRCA mutations who received placebo (P < .001).
Among patients with no germline BRCA mutations, the median PFS was 9.3 months for those who received niraparib and 3.9 months for placebo-treated controls (P < .001).
At the time of the primary PFS analysis in 2016, 155 of the 553 patients originally enrolled had left the study for reasons other than death.
In both treatment cohorts, a large number of patients were unblinded as to their treatment assignments by investigators, which required them to withdraw consent from the study under the protocol, resulting in the aforementioned loss of some data on subsequent therapy and survival status.
Final results: PFS2 and OS
At the time of the final data lock on Oct. 1, 2020, the mean follow-up was 67 months (5.6 years).
In all, 64 patients originally assigned to niraparib were still on study (28 in the germline BRCA mutation cohort and 36 in the nonmutated cohort), as were 28 patients originally assigned to placebo (9 and 19, respectively).
For the final analysis, the investigators were able to retrieve survival data on 51% of the patients originally enrolled, either through protocol amendments and obtaining consent again or through national databases.
Although crossover to the niraparib arm was not allowed on study, patients could receive a PARP inhibitor following disease progression or study withdrawal. Because of discontinuations, data on postprogression therapy were missing for 138 of the 553 patients (25%).
The hazard ratio for PFS2 with niraparib versus placebo was 0.67 for patients with germline BRCA mutations (95% confidence interval, 0.479-0.948) and 0.81 for patients without the mutations (95% CI, 0.632-1.050).
In an analysis adjusted for subsequent PARP inhibitor therapy, there was no significant difference in median OS between the niraparib and placebo arms, regardless of mutation status. In the cohort without BRCA mutations, the median OS was 31.3 months with niraparib and 35.9 months with placebo (HR, 0.97; 95% CI, 0.74-1.26).
However, there was a trend toward improved OS with niraparib among patients with germline BRCA mutations. The median OS was 43.8 months with niraparib and 34.1 months with placebo (HR, 0.66; 95% CI, 0.44-0.99).
Safety: MDS/AML
Hematologic treatment-emergent adverse events occurred primarily in the first year of niraparib treatment. The incidence of grade 3 or greater thrombocytopenia decreased from 33.8% at 1 year to 2.8% in years 2-3. The incidence of anemia decreased from 25.6% to 0.7%, and the neutropenia incidence decreased from 19.3% to 2.1%.
At last follow-up, 13 patients in the niraparib arm (3.5%) and 3 in the placebo arm (1.7%) had developed myelodysplastic syndromes (MDS) or acute myeloid leukemia (AML).
The incidence of MDS/AML was 6.6% among patients with germline BRCA mutations who received niraparib, noted invited discussant Deborah K. Armstrong, MD, of the Johns Hopkins Kimmel Cancer Center in Baltimore.
That incidence was nearly as high as the 8% incidence of MDS/AML seen among similar patients in the SOLO-2 trial of olaparib maintenance, she noted.
This observation raises the question “of whether more extensive prior therapy or the longer duration of PARP inhibitor therapy in patients who have recurrent platinum-sensitive disease is the biggest contributor to that,” she said.
Dr. Armstrong commented that it remains to be seen whether the incidence of MDS/AML will increase with longer follow-up, particularly among patients who were more heavily pretreated with chemotherapy prior to PARP inhibitor maintenance, and in patients who remain on a PARP inhibitor until progression in ongoing trials of PARP inhibitors as frontline therapy.
The ENGOT-OV16/NOVA trial was funded by GlaxoSmithKline. Dr. Matulonis reported consulting/advisory fees from Merck, Novartis, and NextCure. Dr. Armstrong disclosed relationships with several companies, not including GlaxoSmithKline.
The final analysis showed a significant difference in second progression-free survival (PFS2) with niraparib versus placebo, but only in patients with germline BRCA mutations.
The overall survival analysis was limited because the study was not powered to detect differences in OS. Still, the investigators found a trend toward better OS with niraparib in patients who had germline BRCA mutations.
These results were presented at the Society of Gynecologic Oncology’s Virtual Annual Meeting on Women’s Cancer (Abstract 11139).
The final analysis of this study was muddied by missing data for many of the 553 patients originally randomized, according to Ursula Matulonis, MD, of the Dana-Farber Cancer Institute in Boston, who presented the study’s results at the meeting.
“Since 2014, approvals of PARP [poly (ADP-ribose) polymerase] inhibitors worldwide in different lines of ovarian cancer therapy have revolutionized the treatment of women with ovarian cancer,” Dr. Matulonis said. “During the time from the initial results of the NOVA study in 2016 to this final analysis, PARP inhibitors have become available commercially globally.”
The wider availability of PARP inhibitors led to premature unblinding and withdrawals from the trial, resulting in missing data for a large proportion of patients.
Initial results
In the primary analysis of the trial, the median PFS was 21 months among patients with germline BRCA mutations who received niraparib and 5.5 months for patients with germline BRCA mutations who received placebo (P < .001).
Among patients with no germline BRCA mutations, the median PFS was 9.3 months for those who received niraparib and 3.9 months for placebo-treated controls (P < .001).
At the time of the primary PFS analysis in 2016, 155 of the 553 patients originally enrolled had left the study for reasons other than death.
In both treatment cohorts, a large number of patients were unblinded as to their treatment assignments by investigators, which required them to withdraw consent from the study under the protocol, resulting in the aforementioned loss of some data on subsequent therapy and survival status.
Final results: PFS2 and OS
At the time of the final data lock on Oct. 1, 2020, the mean follow-up was 67 months (5.6 years).
In all, 64 patients originally assigned to niraparib were still on study (28 in the germline BRCA mutation cohort and 36 in the nonmutated cohort), as were 28 patients originally assigned to placebo (9 and 19, respectively).
For the final analysis, the investigators were able to retrieve survival data on 51% of the patients originally enrolled, either through protocol amendments and obtaining consent again or through national databases.
Although crossover to the niraparib arm was not allowed on study, patients could receive a PARP inhibitor following disease progression or study withdrawal. Because of discontinuations, data on postprogression therapy were missing for 138 of the 553 patients (25%).
The hazard ratio for PFS2 with niraparib versus placebo was 0.67 for patients with germline BRCA mutations (95% confidence interval, 0.479-0.948) and 0.81 for patients without the mutations (95% CI, 0.632-1.050).
In an analysis adjusted for subsequent PARP inhibitor therapy, there was no significant difference in median OS between the niraparib and placebo arms, regardless of mutation status. In the cohort without BRCA mutations, the median OS was 31.3 months with niraparib and 35.9 months with placebo (HR, 0.97; 95% CI, 0.74-1.26).
However, there was a trend toward improved OS with niraparib among patients with germline BRCA mutations. The median OS was 43.8 months with niraparib and 34.1 months with placebo (HR, 0.66; 95% CI, 0.44-0.99).
Safety: MDS/AML
Hematologic treatment-emergent adverse events occurred primarily in the first year of niraparib treatment. The incidence of grade 3 or greater thrombocytopenia decreased from 33.8% at 1 year to 2.8% in years 2-3. The incidence of anemia decreased from 25.6% to 0.7%, and the neutropenia incidence decreased from 19.3% to 2.1%.
At last follow-up, 13 patients in the niraparib arm (3.5%) and 3 in the placebo arm (1.7%) had developed myelodysplastic syndromes (MDS) or acute myeloid leukemia (AML).
The incidence of MDS/AML was 6.6% among patients with germline BRCA mutations who received niraparib, noted invited discussant Deborah K. Armstrong, MD, of the Johns Hopkins Kimmel Cancer Center in Baltimore.
That incidence was nearly as high as the 8% incidence of MDS/AML seen among similar patients in the SOLO-2 trial of olaparib maintenance, she noted.
This observation raises the question “of whether more extensive prior therapy or the longer duration of PARP inhibitor therapy in patients who have recurrent platinum-sensitive disease is the biggest contributor to that,” she said.
Dr. Armstrong commented that it remains to be seen whether the incidence of MDS/AML will increase with longer follow-up, particularly among patients who were more heavily pretreated with chemotherapy prior to PARP inhibitor maintenance, and in patients who remain on a PARP inhibitor until progression in ongoing trials of PARP inhibitors as frontline therapy.
The ENGOT-OV16/NOVA trial was funded by GlaxoSmithKline. Dr. Matulonis reported consulting/advisory fees from Merck, Novartis, and NextCure. Dr. Armstrong disclosed relationships with several companies, not including GlaxoSmithKline.
FROM SGO 2021