User login
VIDEO: Improved QOL an added benefit of pembrolizumab for NSCLC patients
VIENNA – Patients with metastatic non–small-cell lung cancer with high levels of PD-L1 who received first-line pembrolizumab treatment had clinically meaningful improvement in their quality of life, compared with patients randomized to chemotherapy, in a prespecified secondary analysis of data from the drug’s pivotal trial.
This boost in quality of life as well as other measures of health status add to the pivotal trial’s primary finding of significantly increased progression-free survival compared with chemotherapy, as well as previously-reported secondary findings of superior overall survival, objective response rate, and safety with pembrolizumab compared with chemotherapy (N Engl J Med. 2016 Nov 10;375[19]:1823-33), Julie R. Brahmer, MD, said at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The primary endpoint of the Study of Pembrolizumab Compared to Platinum-Based Chemotherapies in Participants With Metastatic Non–Small Cell Lung Cancer (KEYNOTE-024) showed an average 4.3-month increase in progression-free survival with pembrolizumab immunotherapy, compared with a standard chemotherapy regimen.
Improved quality of life on top of improved efficacy and safety is an important added benefit from pembrolizumab that should further spur its widespread adoption as first-line treatment for approved patients, Dr. Brahmer said in a video interview.
“When you talk about improving efficacy by months, patients and physicians want to also see improved quality of life,” said Dr. Brahmer, director of thoracic oncology at the Johns Hopkins Kimmel Cancer Center in Baltimore. “If symptoms are not improved or there are a ton of side effects with the treatment then use might be low.”
Based on its performance in KEYNOTE-024, pembrolizumab (Keytruda) received Food and Drug Administration approval on Oct. 24, 2016, as first-line treatment for patients with metastatic non–small-cell lung cancer that has a tumor proportion score of at least 50% for programmed death ligand 1 (PD-L1). Pembrolizumab is a monoclonal antibody that binds and blocks PD-1, the immune-cell receptor that tumor-cell PD-L1 binds to make immune cells less active. Other new immune checkpoint inhibitor drugs that act by blocking PD-1 or PD-L1 have shown similar quality of life benefits, she noted.
Routine availability of pembrolizumab as initial treatment for patients who have tumors with this level of PD-L1 expression (and also have no EGFR or ALK genomic aberrations) is shifting practice, Dr. Brahmer said.
“It’s catching on. The limitation right now is making sure patients get tested” for their PD-L1 tumor proportion score at the time they are first diagnosed. “Medical oncologists need to educate pathologists that we need this testing automatically, upfront. It’s not there yet,” she said.
Patients also are enthused. “There is a lot of chemo-exhaustion among patients. They are looking for something different, and something that uses their immune system makes sense.” But only about one quarter of patients have tumors with this level of PD-L1 expression; the others must start chemotherapy first before trying immunotherapy, unless they have an EGFR mutation. Out-of-pocket cost for pembrolizumab is also a major issues for many patients, she said.
KEYNOTE-024 randomized 305 patients at 102 international sites and followed patients for a median of 11 months. Dr. Brahmer and her associates made two primary analyses of patient-reported outcomes. One was measurement of global health status at 15 weeks after the start of treatment using the European Organization for the Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire designed to assess quality of life. Weighted averaging of the EORTC QCQ-C30 scores showed a mean improvement of 7.8 points (P = .002) in the pembrolizumab patients compared with the chemotherapy patients, a difference Dr. Brahmer called “clinically meaningful” as well as statistically significant.
A second analysis of patient-reported outcomes used a second EORTC instrument, the QLC-LC13, which combines assessment of cough, chest pain, and dyspnea. Treatment with pembrolizumab significantly reduced the time to deterioration as measured by this questionnaire by a relative 34%, (P = .029).
A third analysis looked at 15 individual function or symptom domains that make up the QLQ-C30. In general, these showed more improvements with pembrolizumab than with chemotherapy. One notable subcategory was fatigue, which showed significant improvement with pembrolizumab compared with a small worsening with chemotherapy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
This is a very nice analysis using a well-validated group of instruments to assess quality of life. The researchers also achieved a high level of compliance, with 79%-85% of patients completing the quality-of life questionnaire at 15 weeks, when the primary measure of health status occurred.
The mean difference of the weighted global health status score of 7.8 points between the pembrolizumab and chemotherapy patients was a little less than a minimally important difference, but in the context of a randomized, controlled trial this difference probably tells us that there is health status improvement in the pembrolizumab patients. In addition, the individual symptom and function domains showed that in general pembrolizumab performed better than chemotherapy.

Michael Boyer, MD , is professor of medicine at the University of Sydney and a thoracic oncologist and chief clinical officer of the Chris O’Brien Lifehouse in Sydney. He has received research support from Merck and from Pfizer, Roche, Eli Lilly, BMS, AstraZeneca, and Clovis. He made these comments as designated discussant for the report.
This is a very nice analysis using a well-validated group of instruments to assess quality of life. The researchers also achieved a high level of compliance, with 79%-85% of patients completing the quality-of life questionnaire at 15 weeks, when the primary measure of health status occurred.
The mean difference of the weighted global health status score of 7.8 points between the pembrolizumab and chemotherapy patients was a little less than a minimally important difference, but in the context of a randomized, controlled trial this difference probably tells us that there is health status improvement in the pembrolizumab patients. In addition, the individual symptom and function domains showed that in general pembrolizumab performed better than chemotherapy.
Michael Boyer, MD , is professor of medicine at the University of Sydney and a thoracic oncologist and chief clinical officer of the Chris O’Brien Lifehouse in Sydney. He has received research support from Merck and from Pfizer, Roche, Eli Lilly, BMS, AstraZeneca, and Clovis. He made these comments as designated discussant for the report.
This is a very nice analysis using a well-validated group of instruments to assess quality of life. The researchers also achieved a high level of compliance, with 79%-85% of patients completing the quality-of life questionnaire at 15 weeks, when the primary measure of health status occurred.
The mean difference of the weighted global health status score of 7.8 points between the pembrolizumab and chemotherapy patients was a little less than a minimally important difference, but in the context of a randomized, controlled trial this difference probably tells us that there is health status improvement in the pembrolizumab patients. In addition, the individual symptom and function domains showed that in general pembrolizumab performed better than chemotherapy.
Michael Boyer, MD , is professor of medicine at the University of Sydney and a thoracic oncologist and chief clinical officer of the Chris O’Brien Lifehouse in Sydney. He has received research support from Merck and from Pfizer, Roche, Eli Lilly, BMS, AstraZeneca, and Clovis. He made these comments as designated discussant for the report.
VIENNA – Patients with metastatic non–small-cell lung cancer with high levels of PD-L1 who received first-line pembrolizumab treatment had clinically meaningful improvement in their quality of life, compared with patients randomized to chemotherapy, in a prespecified secondary analysis of data from the drug’s pivotal trial.
This boost in quality of life as well as other measures of health status add to the pivotal trial’s primary finding of significantly increased progression-free survival compared with chemotherapy, as well as previously-reported secondary findings of superior overall survival, objective response rate, and safety with pembrolizumab compared with chemotherapy (N Engl J Med. 2016 Nov 10;375[19]:1823-33), Julie R. Brahmer, MD, said at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The primary endpoint of the Study of Pembrolizumab Compared to Platinum-Based Chemotherapies in Participants With Metastatic Non–Small Cell Lung Cancer (KEYNOTE-024) showed an average 4.3-month increase in progression-free survival with pembrolizumab immunotherapy, compared with a standard chemotherapy regimen.
Improved quality of life on top of improved efficacy and safety is an important added benefit from pembrolizumab that should further spur its widespread adoption as first-line treatment for approved patients, Dr. Brahmer said in a video interview.
“When you talk about improving efficacy by months, patients and physicians want to also see improved quality of life,” said Dr. Brahmer, director of thoracic oncology at the Johns Hopkins Kimmel Cancer Center in Baltimore. “If symptoms are not improved or there are a ton of side effects with the treatment then use might be low.”
Based on its performance in KEYNOTE-024, pembrolizumab (Keytruda) received Food and Drug Administration approval on Oct. 24, 2016, as first-line treatment for patients with metastatic non–small-cell lung cancer that has a tumor proportion score of at least 50% for programmed death ligand 1 (PD-L1). Pembrolizumab is a monoclonal antibody that binds and blocks PD-1, the immune-cell receptor that tumor-cell PD-L1 binds to make immune cells less active. Other new immune checkpoint inhibitor drugs that act by blocking PD-1 or PD-L1 have shown similar quality of life benefits, she noted.
Routine availability of pembrolizumab as initial treatment for patients who have tumors with this level of PD-L1 expression (and also have no EGFR or ALK genomic aberrations) is shifting practice, Dr. Brahmer said.
“It’s catching on. The limitation right now is making sure patients get tested” for their PD-L1 tumor proportion score at the time they are first diagnosed. “Medical oncologists need to educate pathologists that we need this testing automatically, upfront. It’s not there yet,” she said.
Patients also are enthused. “There is a lot of chemo-exhaustion among patients. They are looking for something different, and something that uses their immune system makes sense.” But only about one quarter of patients have tumors with this level of PD-L1 expression; the others must start chemotherapy first before trying immunotherapy, unless they have an EGFR mutation. Out-of-pocket cost for pembrolizumab is also a major issues for many patients, she said.
KEYNOTE-024 randomized 305 patients at 102 international sites and followed patients for a median of 11 months. Dr. Brahmer and her associates made two primary analyses of patient-reported outcomes. One was measurement of global health status at 15 weeks after the start of treatment using the European Organization for the Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire designed to assess quality of life. Weighted averaging of the EORTC QCQ-C30 scores showed a mean improvement of 7.8 points (P = .002) in the pembrolizumab patients compared with the chemotherapy patients, a difference Dr. Brahmer called “clinically meaningful” as well as statistically significant.
A second analysis of patient-reported outcomes used a second EORTC instrument, the QLC-LC13, which combines assessment of cough, chest pain, and dyspnea. Treatment with pembrolizumab significantly reduced the time to deterioration as measured by this questionnaire by a relative 34%, (P = .029).
A third analysis looked at 15 individual function or symptom domains that make up the QLQ-C30. In general, these showed more improvements with pembrolizumab than with chemotherapy. One notable subcategory was fatigue, which showed significant improvement with pembrolizumab compared with a small worsening with chemotherapy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
VIENNA – Patients with metastatic non–small-cell lung cancer with high levels of PD-L1 who received first-line pembrolizumab treatment had clinically meaningful improvement in their quality of life, compared with patients randomized to chemotherapy, in a prespecified secondary analysis of data from the drug’s pivotal trial.
This boost in quality of life as well as other measures of health status add to the pivotal trial’s primary finding of significantly increased progression-free survival compared with chemotherapy, as well as previously-reported secondary findings of superior overall survival, objective response rate, and safety with pembrolizumab compared with chemotherapy (N Engl J Med. 2016 Nov 10;375[19]:1823-33), Julie R. Brahmer, MD, said at the World Conference on Lung Cancer, sponsored by the International Association for the Study of Lung Cancer.
The primary endpoint of the Study of Pembrolizumab Compared to Platinum-Based Chemotherapies in Participants With Metastatic Non–Small Cell Lung Cancer (KEYNOTE-024) showed an average 4.3-month increase in progression-free survival with pembrolizumab immunotherapy, compared with a standard chemotherapy regimen.
Improved quality of life on top of improved efficacy and safety is an important added benefit from pembrolizumab that should further spur its widespread adoption as first-line treatment for approved patients, Dr. Brahmer said in a video interview.
“When you talk about improving efficacy by months, patients and physicians want to also see improved quality of life,” said Dr. Brahmer, director of thoracic oncology at the Johns Hopkins Kimmel Cancer Center in Baltimore. “If symptoms are not improved or there are a ton of side effects with the treatment then use might be low.”
Based on its performance in KEYNOTE-024, pembrolizumab (Keytruda) received Food and Drug Administration approval on Oct. 24, 2016, as first-line treatment for patients with metastatic non–small-cell lung cancer that has a tumor proportion score of at least 50% for programmed death ligand 1 (PD-L1). Pembrolizumab is a monoclonal antibody that binds and blocks PD-1, the immune-cell receptor that tumor-cell PD-L1 binds to make immune cells less active. Other new immune checkpoint inhibitor drugs that act by blocking PD-1 or PD-L1 have shown similar quality of life benefits, she noted.
Routine availability of pembrolizumab as initial treatment for patients who have tumors with this level of PD-L1 expression (and also have no EGFR or ALK genomic aberrations) is shifting practice, Dr. Brahmer said.
“It’s catching on. The limitation right now is making sure patients get tested” for their PD-L1 tumor proportion score at the time they are first diagnosed. “Medical oncologists need to educate pathologists that we need this testing automatically, upfront. It’s not there yet,” she said.
Patients also are enthused. “There is a lot of chemo-exhaustion among patients. They are looking for something different, and something that uses their immune system makes sense.” But only about one quarter of patients have tumors with this level of PD-L1 expression; the others must start chemotherapy first before trying immunotherapy, unless they have an EGFR mutation. Out-of-pocket cost for pembrolizumab is also a major issues for many patients, she said.
KEYNOTE-024 randomized 305 patients at 102 international sites and followed patients for a median of 11 months. Dr. Brahmer and her associates made two primary analyses of patient-reported outcomes. One was measurement of global health status at 15 weeks after the start of treatment using the European Organization for the Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire designed to assess quality of life. Weighted averaging of the EORTC QCQ-C30 scores showed a mean improvement of 7.8 points (P = .002) in the pembrolizumab patients compared with the chemotherapy patients, a difference Dr. Brahmer called “clinically meaningful” as well as statistically significant.
A second analysis of patient-reported outcomes used a second EORTC instrument, the QLC-LC13, which combines assessment of cough, chest pain, and dyspnea. Treatment with pembrolizumab significantly reduced the time to deterioration as measured by this questionnaire by a relative 34%, (P = .029).
A third analysis looked at 15 individual function or symptom domains that make up the QLQ-C30. In general, these showed more improvements with pembrolizumab than with chemotherapy. One notable subcategory was fatigue, which showed significant improvement with pembrolizumab compared with a small worsening with chemotherapy.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT WCLC 2016
Key clinical point:
Major finding: The weighted average change from baseline in QLQ-C30 was 7.8 points higher in pembrolizumab patients compared with chemotherapy patients.
Data source: KEYNOTE-024, a multicenter, international randomized trial comprising 305 patients.
Disclosures: Merck, which markets pembrolizumab (Keytruda), sponsored KEYNOTE-024. Dr. Brahmer has served on an advisory board for Merck.
Biomechanics of Polyhydroxyalkanoate Mesh–Augmented Single-Row Rotator Cuff Repairs
Healing after rotator cuff repair (RCR) can be challenging, especially in cases of large and massive tears, revision repairs, and tendons with poor tissue quality.1-3 Poor tissue quality is associated with increased risk for recurrent tears, independent of age and tear size.3 Various techniques have been used to improve tendon fixation strength in these difficult situations, including augmented suture configurations (eg, massive cuff stitches, rip-stop stitches) and tissue grafts (eg, acellular dermal matrix).4-9 Clinical studies have found improved healing rates for larger tears and revision repairs using acellular dermal matrix grafts.6,10 Synthetic patches are another option for RCR augmentation, but limited clinical data and biomechanical evidence support use of synthetic grafts as an augment for RCRs.11-13
Polyhydroxyalkanoates (PHAs) are a class of biodegradable polymers that have been used as orthopedic devices, tissue scaffolds, patches, and other applications with increasing frequency over the past decade.14 In the laboratory, these implanted materials have been shown to support cell migration and growth.15 The PHA family of polymers typically degrades by hydrolytic and bacterial depolymerase mechanisms over 52-plus weeks in vivo.14PHA grafts have been studied in the setting of RCR. An expanded polytetrafluoroethylene scaffold was shown to improve repair mechanics when used as a bursal side graft in an in vitro ovine model.11 The graft increased tendon footprint contact pressure and failure loads by almost 180 N. In clinical studies, poly-L-lactic acid augmentations have been used to reinforce massive RCRs. Lenart and colleagues16 found that 38% of 16 patients with such tears had an intact rotator cuff at 1.2-year follow-up, and improvement in clinical scores. Proctor13 reported on use of a poly-L-lactic acid retrograde patch for reinforcement of massive tears with both single- and double-row repairs in 18 patients. The cohort had more favorable rates of intact cuffs at 12 months (83%) and 42 months (78%), and ASES (American Shoulder and Elbow Surgeons) scores improved from 25 before surgery to 82 at latest follow-up after surgery.
RCR augmentation traditionally has been performed with an open or mini-open technique.6 Recently, several authors have reported on arthroscopic techniques for augmentation with either acellular dermal matrix or synthetic grafts.13,17,18 Most techniques have involved “bridging” with a graft or patch used to stress-shield a single-row repair.8,9,13 This bridging typically involves placing several sutures medial to where the anchor repair stitches pass through the tendon. An alternative is to pass the repair stitches through both the tendon and the graft.17-19 The overall volume of tissue incorporated into the repair stitches (rotator cuff plus graft) is increased with the augmented technique relative to the bridging technique. Both can be technically challenging, but the augmented technique may be easier to perform arthroscopically.9,19 Regardless, these techniques are complicated and require a higher level of arthroscopic skills compared with those required in arthroscopic RCR without a graft. Simplifying arthroscopic graft augmentation likely will increase its utility because, even for skilled surgeons, adding a graft can increase operative time by 20 to 30 minutes. Simplification will also extend use of the technique to surgeons with less experience and proficiency with arthroscopic repair.
We developed a simple method for augmenting single-row RCR with a strip of bioresorbable soft-tissue scaffold. We also conducted a study to evaluate the initial biomechanical properties of single-row RCR in cadaveric shoulder specimens augmented with PHA mesh (BioFiber; Tornier) graft as compared with single-row RCR without augmentation. Both cyclic gap formation and ultimate failure loads and displacement were quantified. We hypothesized that the augmented RCRs would have decreased gap formation and increased ultimate failure loads compared with nonaugmented RCRs. This study was exempt from having to obtain Institutional Review B
Methods
Eight pairs of fresh-frozen cadaver humeri (6 male, 2 female; mean [SD] age, 61 [9] years) were dissected of all soft tissue (except rotator cuff) by Dr. Tashjian, a board-certified, fellowship-trained orthopedic surgeon. There were no qualitative differences in tendon condition between tendons within a pair. The supraspinatus muscle and tendon were separated from the other rotator cuff muscles. The infraspinatus, subscapularis, and teres minor were removed from the humerus. Last, the supraspinatus was resected at its insertion. Humeral pairs were then randomized into augmented and nonaugmented RCRs within each pair.
In the nonaugmented group, the supraspinatus was reattached to its insertion in a single-row RCR with 2 triple-loaded suture anchors (5.5-mm Insite FT Ti, No. 2 Force Fiber suture; Tornier) and 6 simple stitches (Figure 1A). Anchors were placed midway between the articular margin and the lateral edge of the greater tuberosity at about 45° to the bone surface. 
In the contralateral shoulders, augmented RCRs were performed. Specimens were prepared exactly as they were for the nonaugmented RCRs, including anchor placement and suture passage. Before knot tying, RCRs were augmented with 2 strips of 13-mm × 23-mm PHA mesh (BioFiber) (Figure 1B). One strip was used to augment the 3 sutures of each anchor, overlying the residual tendon, to reinforce the tendon–knot interface. After each suture was passed through the supraspinatus tendon from the intra-articular surface, the stitch was passed through the strip of PHA mesh. Stitches were separated by 5 mm in each mesh strip. All 6 sutures were then tied with a Revo knot between the free end of each suture leg and the leg that passed through the tendon and mesh.
Each humerus was transected at the midshaft and potted and mounted in an Instron 1331 load frame with Model 8800 controller (Instron). A cryoclamp was used to grasp the supraspinatus muscle belly above the musculotendinous junction (Figure 2). 
Three rows of 2-mm fiducial markers were affixed to the bone, tendon, and muscle belly with cyanoacrylate for tracking with a digital video system (DMAS Version 6.5; Spicatek) (Figure 3).21 
A 0.1-MPa pre-stress (applied force/tendon cross-sectional area) was applied to each construct to determine the starting position for the deformation profile. Each repair underwent 1000 cycles of uniaxial load-controlled displacement between 0.1 and 1.0 MPa of effective stress at 1 Hz. Effective stress was determined as the ratio of applied force to cross-sectional area of the tendon at harvest to normalize the applied loads between tendons of varying size. During cyclic testing, gapping of more than 5 mm was defined as construct failure.22 After cyclic loading, each construct was loaded to failure at 1.0 mm/s. Ultimate failure load was defined as the highest load achieved at the maximum displacement before rapid decline in load supported by the construct.
Statistical Analysis
Paired t tests were used to compare the matched pairs of constructs. For all tests, significance was set at P ≤ .05. Post hoc power was calculated for significant results using G*Power Version 3.1.6.23 All data are presented as means (SDs).
Results
After 1000 cycles of displacement, mean (SD) gapping was 3.8 (0.9) mm for the nonaugmented repairs and 3.9 (1.1) mm for the PHA mesh–augmented repairs (P = .879) (Figure 4). 
For the nonaugmented repairs, mean (SD) failure displacement was 6.3 (1.7) mm, and mean (SD) ultimate failure load was 472.1 (120.3) N. For the PHA-augmented repairs, failure displacement was 5.5 (1.9) mm, and ultimate failure load was 571.2 (173.0) N. There was no difference in failure displacement (P = .393), but there was a difference in ultimate failure load (P = .042; power = 0.57). During failure testing, mean (SD) tissue deformation was higher (P = .012; power = 0.83) for the PHA-augmented repairs, 1.2 (0.7) mm, than for the nonaugmented repairs, 0.8 (0.5) mm. Failures, which were consistent within pairs, were caused by tissue failure, with sutures pulling through the tissue (4 pairs) or single anchor pullout before ultimate tissue failure (4 pairs). Of the 4 failures with anchor pullout, 3 had anterior anchor pullout, and 1 had posterior anchor pullout. In all specimens with anchor pullout, the second anchor remained stable, and ultimate failure occurred with tissue tearing at the suture interface. There were no significant differences in any metrics between specimens that failed with intact anchors and specimens with single anchor pullout (P ≥ .122). Therefore, both groups were pooled for the failure analysis.
Discussion
RCR augmentation with a synthetic graft is a viable option for improving fixation strength of supraspinatus repairs, as shown in otherwise healthy tendon in the present study. Our hypothesis that there would be decreased gap formation with graft augmentation was not supported, whereas the hypothesis of increased failure loads with graft augmentation was supported. These findings may also be applicable in cases of large tears, revisions, and tendons with poor tissue quality. Simplification of graft application techniques will allow quick and easy arthroscopic augmentation.
Studies of RCRs for large or massive tears have reported retear rates of 25% to 79%.24-26 Latissimus dorsi tendon transfers also show promise in posterosuperior RCRs, with failure rates near 10%.27,28 Although use of PHA patches in RCR augmentation is relatively new, short-term and midterm failure rates are in the range of 20% to 60% in the few small cohorts currently being studied.13,16 It is possible that these rates may improve as indications, surgical experience, and techniques for use of PHA patches are further refined. Regardless, with PHA currently being used in practice, it is important to quantify the biomechanics of the augmentation as a baseline for its performance in reinforcing the tendon–suture interface.
We determined that the initial fixation strength of single-row repairs was higher with the addition of PHA synthetic grafts using a very simple technique. Single-row triple-loaded anchor repairs already provide high initial mechanical strength, and our results are similar to those of another study of this technique.29 Despite the already high mechanical strength of a triple-loaded anchor repair, PHA mesh increased ultimate strength by about 100 N (~25%). Of note, tissue elongation during failure was higher (P = .012; power = 0.83) in the PHA-augmented group (1.2 mm) than in the nonaugmented group (0.8 mm). This was not surprising—failure loads were almost 100 N higher in the PHA-augmented group than in the nonaugmented group. Consequently, much higher forces were placed on the muscle belly, likely resulting in additional elongation of the intact tissue medial to the repair construct.
The ultimate failure loads in our study compare favorably with the biomechanical strength of augmented repairs reported by others.8,9,18 Barber and colleagues18 evaluated an augmented single-row repair with 2 double-loaded suture anchors and an acellular dermal matrix graft. The ultimate failure load of the augmented repairs was 325 N. In contrast, Omae and colleagues8 tested a bridging single-row repair using 2 double-loaded suture anchors and an acellular dermal matrix graft. Ultimate failure load of the augmented repairs was 560 N, similar to our finding. Last, Shea and colleagues9 evaluated a bridging single-row repair using 2 double-loaded suture anchors and an acellular dermal matrix graft, with ultimate failure load of 429 N. The techniques in all 3 studies can be performed arthroscopically but are challenging and require multiple extra sutures and anchors that need management and tying. Our technique provides similar initial fixation strength, has no requirement for extra sutures or anchors, and is very simple to perform.
The supraspinatus tendon is estimated to fail between 800 N and 1000 N.30,31 Biomechanical shoulder simulators use supraspinatus forces in the range of 20 N to 200 N for scapular plane abduction.32-36 Therefore, the single-row repair failures in our study fell between functional and full-thickness failure loads. Studies on the mechanics of degenerated human supraspinatus tendon are limited, but there is evidence the mechanical properties of these tissues are inferior to those of healthy tendon.37 A 100-N increase in failure loads with PHA augmentation may prove highly significant in reinforcing the suture–tendon interface in degenerated tendons.
Adding the mesh did not have any effect on gapping at the repair site after cyclic loading. This finding suggests that construct gapping under cyclic loading is not a function of a reinforced knot–tendon interface but is instead caused by microtearing and cinching of the suture constructs in relation to the underlying bone. Tissue elongation likely was not a strong contributor to overall cyclic gapping, as elongation did not differ between the nonaugmented and augmented repairs (0.5 mm vs 0.7 mm; P = .276) and was small relative to the nearly 4 mm of construct gapping. Gapping may be affected by healing and integration of the mesh into the repaired tendon over time, but this effect could not be captured in the present study. Patients are initially immobilized and passive shoulder motion gradually introduced, in stark contrast to the immediate loading protocol in the present study. Regardless, the 25% increase in overall strength may be clinically important, especially in cases of difficult repair or poor tissue quality.
Our technique simplifies arthroscopic augmentation—stitches are passed through the rotator cuff in simple fashion. Before being tied, the limbs that were passed through the rotator cuff are removed through a cannula and then passed through the synthetic graft. 
Study Limitations
This study had several limitations. First, it was a cadaveric biomechanical study that evaluated only time-zero biomechanical properties. Loads were normalized to tendon size, specimens were randomized between sides, and paired specimens were used to minimize the effects of tendon and bone quality on outcome metrics. In addition, donor tendons were representative of otherwise healthy tissue. Chronic tears and associated resorption/atrophy could have affected the magnitude of forces and gapping detected in this study. Theoretically, over time the tendon tissue will adhere to and grow into the mesh, which could minimize potential differences. Studies are needed to determine the effects of healing on long-term repair strength in affected patients. Last, all constructs were performed in open fashion to improve repeatability of construct placement and provide accessibility for Instron testing. Our technique did not directly replicate the arthroscopic approach, but, unlike other augmentation techniques, it is so simple that transition to all-arthroscopic augmentation is realistic.
Patch augmentation increases the cost of materials and operative time and should be considered a limitation of its utility. We do not recommend augmentation in all RCRs, as it likely is cost-ineffective. Instead, we recommend augmentation in cases of poor tissue quality, which could lead to healing failure, revision surgery, and higher overall patient costs beyond the cost of adding augmentation. Similarly, we recommend augmentation for revision cases in which tendon healing has failed and tissue quality is poor. The goal is to prevent another failure.
Conclusion
PHA graft augmentation of single-row triple-loaded anchor repairs of the supraspinatus tendon improves the overall ultimate load to failure by 25%. There was no difference in gap formation after cyclic loading between augmented and nonaugmented repairs. This technique for arthroscopic augmentation can be used to improve initial biomechanical repair strength in tears at risk for failure.
Am J Orthop. 2016;45(7):E527-E533. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86(2):219-224.
2. Keener JD, Wei AS, Kim HM, et al. Revision arthroscopic rotator cuff repair: repair integrity and clinical outcome. J Bone Joint Surg Am. 2010;92(3):590-598.
3. Nho SJ, Brown BS, Lyman S, Adler RS, Altchek DW, MacGillivray JD. Prospective analysis of arthroscopic rotator cuff repair: prognostic factors affecting clinical and ultrasound outcome. J Shoulder Elbow Surg. 2009;18(1):13-20.
4. Barber FA, Herbert MA, Schroeder FA, Aziz-Jacobo J, Mays MM, Rapley JH. Biomechanical advantages of triple-loaded suture anchors compared with double-row rotator cuff repairs. Arthroscopy. 2010;26(3):316-323.
5. Burkhart SS, Denard PJ, Konicek J, Hanypsiak BT. Biomechanical validation of load-sharing rip-stop fixation for the repair of tissue-deficient rotator cuff tears. Am J Sports Med. 2014;42(2):457-462.
6. Gupta AK, Hug K, Boggess B, Gavigan M, Toth AP. Massive or 2-tendon rotator cuff tears in active patients with minimal glenohumeral arthritis: clinical and radiographic outcomes of reconstruction using dermal tissue matrix xenograft. Am J Sports Med. 2013;41(4):872-879.
7. Ma CB, MacGillivray JD, Clabeaux J, Lee S, Otis JC. Biomechanical evaluation of arthroscopic rotator cuff stitches. J Bone Joint Surg Am. 2004;86(6):1211-1216.
8. Omae H, Steinmann SP, Zhao C, et al. Biomechanical effect of rotator cuff augmentation with an acellular dermal matrix graft: a cadaver study. Clin Biomech. 2012;27(8):789-792.
9. Shea KP, Obopilwe E, Sperling JW, Iannotti JP. A biomechanical analysis of gap formation and failure mechanics of a xenograft-reinforced rotator cuff repair in a cadaveric model. J Shoulder Elbow Surg. 2012;21(8):1072-1079.
10. Agrawal V. Healing rates for challenging rotator cuff tears utilizing an acellular human dermal reinforcement graft. Int J Shoulder Surg. 2012;6(2):36-44.
11. Beimers L, Lam PH, Murrell GA. The biomechanical effects of polytetrafluoroethylene suture augmentations in lateral-row rotator cuff repairs in an ovine model. J Shoulder Elbow Surg. 2014;23(10):1545-1552.
12. McCarron JA, Milks RA, Chen X, Iannotti JP, Derwin KA. Improved time-zero biomechanical properties using poly-L-lactic acid graft augmentation in a cadaveric rotator cuff repair model. J Shoulder Elbow Surg. 2010;19(5):688-696.
13. Proctor CS. Long-term successful arthroscopic repair of large and massive rotator cuff tears with a functional and degradable reinforcement device. J Shoulder Elbow Surg. 2014;23(10):1508-1513.
14. Misra SK, Valappil SP, Roy I, Boccaccini AR. Polyhydroxyalkanoate (PHA)/inorganic phase composites for tissue engineering applications. Biomacromolecules. 2006;7(8):2249-2258.
15. Ellis G, Cano P, Jadraque M, et al. Laser microperforated biodegradable microbial polyhydroxyalkanoate substrates for tissue repair strategies: an infrared microspectroscopy study. Anal Bioanal Chem. 2011;399(7):2379-2388.
16. Lenart BA, Martens KA, Kearns KA, Gillespie RJ, Zoga AC, Williams GR. Treatment of massive and recurrent rotator cuff tears augmented with a poly-l-lactide graft, a preliminary study. J Shoulder Elbow Surg. 2015;24(6):915-921.
17. Barber FA, Burns JP, Deutsch A, Labbé MR, Litchfield RB. A prospective, randomized evaluation of acellular human dermal matrix augmentation for arthroscopic rotator cuff repair. Arthroscopy. 2012;28(1):8-15.
18. Barber FA, Herbert MA, Boothby MH. Ultimate tensile failure loads of a human dermal allograft rotator cuff augmentation. Arthroscopy. 2008;24(1):20-24.
19. Gilot GJ, Attia AK, Alvarez AM. Arthroscopic repair of rotator cuff tears using extracellular matrix graft. Arthrosc Tech. 2014;3(4):e487-e489.
20. Barber FA, Coons DA, Ruiz-Suarez M. Cyclic load testing of biodegradable suture anchors containing 2 high-strength sutures. Arthroscopy. 2007;23(4):355-360.
21. Kullar RS, Reagan JM, Kolz CW, Burks RT, Henninger HB. Suture placement near the musculotendinous junction in the supraspinatus: implications for rotator cuff repair. Am J Sports Med. 2015;43(1):57-62.
22. Burkhart SS, Diaz Pagàn JL, Wirth MA, Athanasiou KA. Cyclic loading of anchor-based rotator cuff repairs: confirmation of the tension overload phenomenon and comparison of suture anchor fixation with transosseous fixation. Arthroscopy. 1997;13(6):720-724.
23. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191.
24. Greenspoon JA, Petri M, Warth RJ, Millett PJ. Massive rotator cuff tears: pathomechanics, current treatment options, and clinical outcomes. J Shoulder Elbow Surg. 2015;24(9):1493-1505.
25. Hein J, Reilly JM, Chae J, Maerz T, Anderson K. Retear rates after arthroscopic single-row, double-row, and suture bridge rotator cuff repair at a minimum of 1 year of imaging follow-up: a systematic review. Arthroscopy. 2015;31(11):2274-2281.
26. Henry P, Wasserstein D, Park S, et al. Arthroscopic repair for chronic massive rotator cuff tears: a systematic review. Arthroscopy. 2015;31(12):2472-2480.
27. El-Azab HM, Rott O, Irlenbusch U. Long-term follow-up after latissimus dorsi transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am. 2015;97(6):462-469.
28. Gerber C, Rahm SA, Catanzaro S, Farshad M, Moor BK. Latissimus dorsi tendon transfer for treatment of irreparable posterosuperior rotator cuff tears: long-term results at a minimum follow-up of ten years. J Bone Joint Surg Am. 2013;95(21):1920-1926.
29. Coons DA, Barber FA, Herbert MA. Triple-loaded single-anchor stitch configurations: an analysis of cyclically loaded suture–tendon interface security. Arthroscopy. 2006;22(11):1154-1158.
30. Itoi E, Berglund LJ, Grabowski JJ, et al. Tensile properties of the supraspinatus tendon. J Orthop Res. 1995;13(4):578-584.
31. Matsuhashi T, Hooke AW, Zhao KD, et al. Tensile properties of a morphologically split supraspinatus tendon. Clin Anat. 2014;27(5):702-706.
32. Apreleva M, Parsons IM 4th, Warner JJ, Fu FH, Woo SL. Experimental investigation of reaction forces at the glenohumeral joint during active abduction. J Shoulder Elbow Surg. 2000;9(5):409-417.
33. Giles JW, Ferreira LM, Athwal GS, Johnson JA. Development and performance evaluation of a multi-PID muscle loading driven in vitro active-motion shoulder simulator and application to assessing reverse total shoulder arthroplasty. J Biomech Eng. 2014;136(12):121007.
34. Hansen ML, Otis JC, Johnson JS, Cordasco FA, Craig EV, Warren RF. Biomechanics of massive rotator cuff tears: implications for treatment. J Bone Joint Surg Am. 2008;90(2):316-325.
35. Henninger HB, Barg A, Anderson AE, Bachus KN, Tashjian RZ, Burks RT. Effect of deltoid tension and humeral version in reverse total shoulder arthroplasty: a biomechanical study. J Shoulder Elbow Surg. 2012;21(4):483-490.
36. Mihata T, Gates J, McGarry MH, Lee J, Kinoshita M, Lee TQ. Effect of rotator cuff muscle imbalance on forceful internal impingement and peel-back of the superior labrum: a cadaveric study. Am J Sports Med. 2009;37(11):2222-2227.
37. Sano H, Ishii H, Yeadon A, Backman DS, Brunet JA, Uhthoff HK. Degeneration at the insertion weakens the tensile strength of the supraspinatus tendon: a comparative mechanical and histologic study of the bone–tendon complex. J Orthop Res. 1997;15(5):719-726.
Healing after rotator cuff repair (RCR) can be challenging, especially in cases of large and massive tears, revision repairs, and tendons with poor tissue quality.1-3 Poor tissue quality is associated with increased risk for recurrent tears, independent of age and tear size.3 Various techniques have been used to improve tendon fixation strength in these difficult situations, including augmented suture configurations (eg, massive cuff stitches, rip-stop stitches) and tissue grafts (eg, acellular dermal matrix).4-9 Clinical studies have found improved healing rates for larger tears and revision repairs using acellular dermal matrix grafts.6,10 Synthetic patches are another option for RCR augmentation, but limited clinical data and biomechanical evidence support use of synthetic grafts as an augment for RCRs.11-13
Polyhydroxyalkanoates (PHAs) are a class of biodegradable polymers that have been used as orthopedic devices, tissue scaffolds, patches, and other applications with increasing frequency over the past decade.14 In the laboratory, these implanted materials have been shown to support cell migration and growth.15 The PHA family of polymers typically degrades by hydrolytic and bacterial depolymerase mechanisms over 52-plus weeks in vivo.14PHA grafts have been studied in the setting of RCR. An expanded polytetrafluoroethylene scaffold was shown to improve repair mechanics when used as a bursal side graft in an in vitro ovine model.11 The graft increased tendon footprint contact pressure and failure loads by almost 180 N. In clinical studies, poly-L-lactic acid augmentations have been used to reinforce massive RCRs. Lenart and colleagues16 found that 38% of 16 patients with such tears had an intact rotator cuff at 1.2-year follow-up, and improvement in clinical scores. Proctor13 reported on use of a poly-L-lactic acid retrograde patch for reinforcement of massive tears with both single- and double-row repairs in 18 patients. The cohort had more favorable rates of intact cuffs at 12 months (83%) and 42 months (78%), and ASES (American Shoulder and Elbow Surgeons) scores improved from 25 before surgery to 82 at latest follow-up after surgery.
RCR augmentation traditionally has been performed with an open or mini-open technique.6 Recently, several authors have reported on arthroscopic techniques for augmentation with either acellular dermal matrix or synthetic grafts.13,17,18 Most techniques have involved “bridging” with a graft or patch used to stress-shield a single-row repair.8,9,13 This bridging typically involves placing several sutures medial to where the anchor repair stitches pass through the tendon. An alternative is to pass the repair stitches through both the tendon and the graft.17-19 The overall volume of tissue incorporated into the repair stitches (rotator cuff plus graft) is increased with the augmented technique relative to the bridging technique. Both can be technically challenging, but the augmented technique may be easier to perform arthroscopically.9,19 Regardless, these techniques are complicated and require a higher level of arthroscopic skills compared with those required in arthroscopic RCR without a graft. Simplifying arthroscopic graft augmentation likely will increase its utility because, even for skilled surgeons, adding a graft can increase operative time by 20 to 30 minutes. Simplification will also extend use of the technique to surgeons with less experience and proficiency with arthroscopic repair.
We developed a simple method for augmenting single-row RCR with a strip of bioresorbable soft-tissue scaffold. We also conducted a study to evaluate the initial biomechanical properties of single-row RCR in cadaveric shoulder specimens augmented with PHA mesh (BioFiber; Tornier) graft as compared with single-row RCR without augmentation. Both cyclic gap formation and ultimate failure loads and displacement were quantified. We hypothesized that the augmented RCRs would have decreased gap formation and increased ultimate failure loads compared with nonaugmented RCRs. This study was exempt from having to obtain Institutional Review B
Methods
Eight pairs of fresh-frozen cadaver humeri (6 male, 2 female; mean [SD] age, 61 [9] years) were dissected of all soft tissue (except rotator cuff) by Dr. Tashjian, a board-certified, fellowship-trained orthopedic surgeon. There were no qualitative differences in tendon condition between tendons within a pair. The supraspinatus muscle and tendon were separated from the other rotator cuff muscles. The infraspinatus, subscapularis, and teres minor were removed from the humerus. Last, the supraspinatus was resected at its insertion. Humeral pairs were then randomized into augmented and nonaugmented RCRs within each pair.
In the nonaugmented group, the supraspinatus was reattached to its insertion in a single-row RCR with 2 triple-loaded suture anchors (5.5-mm Insite FT Ti, No. 2 Force Fiber suture; Tornier) and 6 simple stitches (Figure 1A). Anchors were placed midway between the articular margin and the lateral edge of the greater tuberosity at about 45° to the bone surface.
In the contralateral shoulders, augmented RCRs were performed. Specimens were prepared exactly as they were for the nonaugmented RCRs, including anchor placement and suture passage. Before knot tying, RCRs were augmented with 2 strips of 13-mm × 23-mm PHA mesh (BioFiber) (Figure 1B). One strip was used to augment the 3 sutures of each anchor, overlying the residual tendon, to reinforce the tendon–knot interface. After each suture was passed through the supraspinatus tendon from the intra-articular surface, the stitch was passed through the strip of PHA mesh. Stitches were separated by 5 mm in each mesh strip. All 6 sutures were then tied with a Revo knot between the free end of each suture leg and the leg that passed through the tendon and mesh.
Each humerus was transected at the midshaft and potted and mounted in an Instron 1331 load frame with Model 8800 controller (Instron). A cryoclamp was used to grasp the supraspinatus muscle belly above the musculotendinous junction (Figure 2).
Three rows of 2-mm fiducial markers were affixed to the bone, tendon, and muscle belly with cyanoacrylate for tracking with a digital video system (DMAS Version 6.5; Spicatek) (Figure 3).21
A 0.1-MPa pre-stress (applied force/tendon cross-sectional area) was applied to each construct to determine the starting position for the deformation profile. Each repair underwent 1000 cycles of uniaxial load-controlled displacement between 0.1 and 1.0 MPa of effective stress at 1 Hz. Effective stress was determined as the ratio of applied force to cross-sectional area of the tendon at harvest to normalize the applied loads between tendons of varying size. During cyclic testing, gapping of more than 5 mm was defined as construct failure.22 After cyclic loading, each construct was loaded to failure at 1.0 mm/s. Ultimate failure load was defined as the highest load achieved at the maximum displacement before rapid decline in load supported by the construct.
Statistical Analysis
Paired t tests were used to compare the matched pairs of constructs. For all tests, significance was set at P ≤ .05. Post hoc power was calculated for significant results using G*Power Version 3.1.6.23 All data are presented as means (SDs).
Results
After 1000 cycles of displacement, mean (SD) gapping was 3.8 (0.9) mm for the nonaugmented repairs and 3.9 (1.1) mm for the PHA mesh–augmented repairs (P = .879) (Figure 4).
For the nonaugmented repairs, mean (SD) failure displacement was 6.3 (1.7) mm, and mean (SD) ultimate failure load was 472.1 (120.3) N. For the PHA-augmented repairs, failure displacement was 5.5 (1.9) mm, and ultimate failure load was 571.2 (173.0) N. There was no difference in failure displacement (P = .393), but there was a difference in ultimate failure load (P = .042; power = 0.57). During failure testing, mean (SD) tissue deformation was higher (P = .012; power = 0.83) for the PHA-augmented repairs, 1.2 (0.7) mm, than for the nonaugmented repairs, 0.8 (0.5) mm. Failures, which were consistent within pairs, were caused by tissue failure, with sutures pulling through the tissue (4 pairs) or single anchor pullout before ultimate tissue failure (4 pairs). Of the 4 failures with anchor pullout, 3 had anterior anchor pullout, and 1 had posterior anchor pullout. In all specimens with anchor pullout, the second anchor remained stable, and ultimate failure occurred with tissue tearing at the suture interface. There were no significant differences in any metrics between specimens that failed with intact anchors and specimens with single anchor pullout (P ≥ .122). Therefore, both groups were pooled for the failure analysis.
Discussion
RCR augmentation with a synthetic graft is a viable option for improving fixation strength of supraspinatus repairs, as shown in otherwise healthy tendon in the present study. Our hypothesis that there would be decreased gap formation with graft augmentation was not supported, whereas the hypothesis of increased failure loads with graft augmentation was supported. These findings may also be applicable in cases of large tears, revisions, and tendons with poor tissue quality. Simplification of graft application techniques will allow quick and easy arthroscopic augmentation.
Studies of RCRs for large or massive tears have reported retear rates of 25% to 79%.24-26 Latissimus dorsi tendon transfers also show promise in posterosuperior RCRs, with failure rates near 10%.27,28 Although use of PHA patches in RCR augmentation is relatively new, short-term and midterm failure rates are in the range of 20% to 60% in the few small cohorts currently being studied.13,16 It is possible that these rates may improve as indications, surgical experience, and techniques for use of PHA patches are further refined. Regardless, with PHA currently being used in practice, it is important to quantify the biomechanics of the augmentation as a baseline for its performance in reinforcing the tendon–suture interface.
We determined that the initial fixation strength of single-row repairs was higher with the addition of PHA synthetic grafts using a very simple technique. Single-row triple-loaded anchor repairs already provide high initial mechanical strength, and our results are similar to those of another study of this technique.29 Despite the already high mechanical strength of a triple-loaded anchor repair, PHA mesh increased ultimate strength by about 100 N (~25%). Of note, tissue elongation during failure was higher (P = .012; power = 0.83) in the PHA-augmented group (1.2 mm) than in the nonaugmented group (0.8 mm). This was not surprising—failure loads were almost 100 N higher in the PHA-augmented group than in the nonaugmented group. Consequently, much higher forces were placed on the muscle belly, likely resulting in additional elongation of the intact tissue medial to the repair construct.
The ultimate failure loads in our study compare favorably with the biomechanical strength of augmented repairs reported by others.8,9,18 Barber and colleagues18 evaluated an augmented single-row repair with 2 double-loaded suture anchors and an acellular dermal matrix graft. The ultimate failure load of the augmented repairs was 325 N. In contrast, Omae and colleagues8 tested a bridging single-row repair using 2 double-loaded suture anchors and an acellular dermal matrix graft. Ultimate failure load of the augmented repairs was 560 N, similar to our finding. Last, Shea and colleagues9 evaluated a bridging single-row repair using 2 double-loaded suture anchors and an acellular dermal matrix graft, with ultimate failure load of 429 N. The techniques in all 3 studies can be performed arthroscopically but are challenging and require multiple extra sutures and anchors that need management and tying. Our technique provides similar initial fixation strength, has no requirement for extra sutures or anchors, and is very simple to perform.
The supraspinatus tendon is estimated to fail between 800 N and 1000 N.30,31 Biomechanical shoulder simulators use supraspinatus forces in the range of 20 N to 200 N for scapular plane abduction.32-36 Therefore, the single-row repair failures in our study fell between functional and full-thickness failure loads. Studies on the mechanics of degenerated human supraspinatus tendon are limited, but there is evidence the mechanical properties of these tissues are inferior to those of healthy tendon.37 A 100-N increase in failure loads with PHA augmentation may prove highly significant in reinforcing the suture–tendon interface in degenerated tendons.
Adding the mesh did not have any effect on gapping at the repair site after cyclic loading. This finding suggests that construct gapping under cyclic loading is not a function of a reinforced knot–tendon interface but is instead caused by microtearing and cinching of the suture constructs in relation to the underlying bone. Tissue elongation likely was not a strong contributor to overall cyclic gapping, as elongation did not differ between the nonaugmented and augmented repairs (0.5 mm vs 0.7 mm; P = .276) and was small relative to the nearly 4 mm of construct gapping. Gapping may be affected by healing and integration of the mesh into the repaired tendon over time, but this effect could not be captured in the present study. Patients are initially immobilized and passive shoulder motion gradually introduced, in stark contrast to the immediate loading protocol in the present study. Regardless, the 25% increase in overall strength may be clinically important, especially in cases of difficult repair or poor tissue quality.
Our technique simplifies arthroscopic augmentation—stitches are passed through the rotator cuff in simple fashion. Before being tied, the limbs that were passed through the rotator cuff are removed through a cannula and then passed through the synthetic graft.
Study Limitations
This study had several limitations. First, it was a cadaveric biomechanical study that evaluated only time-zero biomechanical properties. Loads were normalized to tendon size, specimens were randomized between sides, and paired specimens were used to minimize the effects of tendon and bone quality on outcome metrics. In addition, donor tendons were representative of otherwise healthy tissue. Chronic tears and associated resorption/atrophy could have affected the magnitude of forces and gapping detected in this study. Theoretically, over time the tendon tissue will adhere to and grow into the mesh, which could minimize potential differences. Studies are needed to determine the effects of healing on long-term repair strength in affected patients. Last, all constructs were performed in open fashion to improve repeatability of construct placement and provide accessibility for Instron testing. Our technique did not directly replicate the arthroscopic approach, but, unlike other augmentation techniques, it is so simple that transition to all-arthroscopic augmentation is realistic.
Patch augmentation increases the cost of materials and operative time and should be considered a limitation of its utility. We do not recommend augmentation in all RCRs, as it likely is cost-ineffective. Instead, we recommend augmentation in cases of poor tissue quality, which could lead to healing failure, revision surgery, and higher overall patient costs beyond the cost of adding augmentation. Similarly, we recommend augmentation for revision cases in which tendon healing has failed and tissue quality is poor. The goal is to prevent another failure.
Conclusion
PHA graft augmentation of single-row triple-loaded anchor repairs of the supraspinatus tendon improves the overall ultimate load to failure by 25%. There was no difference in gap formation after cyclic loading between augmented and nonaugmented repairs. This technique for arthroscopic augmentation can be used to improve initial biomechanical repair strength in tears at risk for failure.
Am J Orthop. 2016;45(7):E527-E533. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
Healing after rotator cuff repair (RCR) can be challenging, especially in cases of large and massive tears, revision repairs, and tendons with poor tissue quality.1-3 Poor tissue quality is associated with increased risk for recurrent tears, independent of age and tear size.3 Various techniques have been used to improve tendon fixation strength in these difficult situations, including augmented suture configurations (eg, massive cuff stitches, rip-stop stitches) and tissue grafts (eg, acellular dermal matrix).4-9 Clinical studies have found improved healing rates for larger tears and revision repairs using acellular dermal matrix grafts.6,10 Synthetic patches are another option for RCR augmentation, but limited clinical data and biomechanical evidence support use of synthetic grafts as an augment for RCRs.11-13
Polyhydroxyalkanoates (PHAs) are a class of biodegradable polymers that have been used as orthopedic devices, tissue scaffolds, patches, and other applications with increasing frequency over the past decade.14 In the laboratory, these implanted materials have been shown to support cell migration and growth.15 The PHA family of polymers typically degrades by hydrolytic and bacterial depolymerase mechanisms over 52-plus weeks in vivo.14PHA grafts have been studied in the setting of RCR. An expanded polytetrafluoroethylene scaffold was shown to improve repair mechanics when used as a bursal side graft in an in vitro ovine model.11 The graft increased tendon footprint contact pressure and failure loads by almost 180 N. In clinical studies, poly-L-lactic acid augmentations have been used to reinforce massive RCRs. Lenart and colleagues16 found that 38% of 16 patients with such tears had an intact rotator cuff at 1.2-year follow-up, and improvement in clinical scores. Proctor13 reported on use of a poly-L-lactic acid retrograde patch for reinforcement of massive tears with both single- and double-row repairs in 18 patients. The cohort had more favorable rates of intact cuffs at 12 months (83%) and 42 months (78%), and ASES (American Shoulder and Elbow Surgeons) scores improved from 25 before surgery to 82 at latest follow-up after surgery.
RCR augmentation traditionally has been performed with an open or mini-open technique.6 Recently, several authors have reported on arthroscopic techniques for augmentation with either acellular dermal matrix or synthetic grafts.13,17,18 Most techniques have involved “bridging” with a graft or patch used to stress-shield a single-row repair.8,9,13 This bridging typically involves placing several sutures medial to where the anchor repair stitches pass through the tendon. An alternative is to pass the repair stitches through both the tendon and the graft.17-19 The overall volume of tissue incorporated into the repair stitches (rotator cuff plus graft) is increased with the augmented technique relative to the bridging technique. Both can be technically challenging, but the augmented technique may be easier to perform arthroscopically.9,19 Regardless, these techniques are complicated and require a higher level of arthroscopic skills compared with those required in arthroscopic RCR without a graft. Simplifying arthroscopic graft augmentation likely will increase its utility because, even for skilled surgeons, adding a graft can increase operative time by 20 to 30 minutes. Simplification will also extend use of the technique to surgeons with less experience and proficiency with arthroscopic repair.
We developed a simple method for augmenting single-row RCR with a strip of bioresorbable soft-tissue scaffold. We also conducted a study to evaluate the initial biomechanical properties of single-row RCR in cadaveric shoulder specimens augmented with PHA mesh (BioFiber; Tornier) graft as compared with single-row RCR without augmentation. Both cyclic gap formation and ultimate failure loads and displacement were quantified. We hypothesized that the augmented RCRs would have decreased gap formation and increased ultimate failure loads compared with nonaugmented RCRs. This study was exempt from having to obtain Institutional Review B
Methods
Eight pairs of fresh-frozen cadaver humeri (6 male, 2 female; mean [SD] age, 61 [9] years) were dissected of all soft tissue (except rotator cuff) by Dr. Tashjian, a board-certified, fellowship-trained orthopedic surgeon. There were no qualitative differences in tendon condition between tendons within a pair. The supraspinatus muscle and tendon were separated from the other rotator cuff muscles. The infraspinatus, subscapularis, and teres minor were removed from the humerus. Last, the supraspinatus was resected at its insertion. Humeral pairs were then randomized into augmented and nonaugmented RCRs within each pair.
In the nonaugmented group, the supraspinatus was reattached to its insertion in a single-row RCR with 2 triple-loaded suture anchors (5.5-mm Insite FT Ti, No. 2 Force Fiber suture; Tornier) and 6 simple stitches (Figure 1A). Anchors were placed midway between the articular margin and the lateral edge of the greater tuberosity at about 45° to the bone surface.
In the contralateral shoulders, augmented RCRs were performed. Specimens were prepared exactly as they were for the nonaugmented RCRs, including anchor placement and suture passage. Before knot tying, RCRs were augmented with 2 strips of 13-mm × 23-mm PHA mesh (BioFiber) (Figure 1B). One strip was used to augment the 3 sutures of each anchor, overlying the residual tendon, to reinforce the tendon–knot interface. After each suture was passed through the supraspinatus tendon from the intra-articular surface, the stitch was passed through the strip of PHA mesh. Stitches were separated by 5 mm in each mesh strip. All 6 sutures were then tied with a Revo knot between the free end of each suture leg and the leg that passed through the tendon and mesh.
Each humerus was transected at the midshaft and potted and mounted in an Instron 1331 load frame with Model 8800 controller (Instron). A cryoclamp was used to grasp the supraspinatus muscle belly above the musculotendinous junction (Figure 2).
Three rows of 2-mm fiducial markers were affixed to the bone, tendon, and muscle belly with cyanoacrylate for tracking with a digital video system (DMAS Version 6.5; Spicatek) (Figure 3).21
A 0.1-MPa pre-stress (applied force/tendon cross-sectional area) was applied to each construct to determine the starting position for the deformation profile. Each repair underwent 1000 cycles of uniaxial load-controlled displacement between 0.1 and 1.0 MPa of effective stress at 1 Hz. Effective stress was determined as the ratio of applied force to cross-sectional area of the tendon at harvest to normalize the applied loads between tendons of varying size. During cyclic testing, gapping of more than 5 mm was defined as construct failure.22 After cyclic loading, each construct was loaded to failure at 1.0 mm/s. Ultimate failure load was defined as the highest load achieved at the maximum displacement before rapid decline in load supported by the construct.
Statistical Analysis
Paired t tests were used to compare the matched pairs of constructs. For all tests, significance was set at P ≤ .05. Post hoc power was calculated for significant results using G*Power Version 3.1.6.23 All data are presented as means (SDs).
Results
After 1000 cycles of displacement, mean (SD) gapping was 3.8 (0.9) mm for the nonaugmented repairs and 3.9 (1.1) mm for the PHA mesh–augmented repairs (P = .879) (Figure 4).
For the nonaugmented repairs, mean (SD) failure displacement was 6.3 (1.7) mm, and mean (SD) ultimate failure load was 472.1 (120.3) N. For the PHA-augmented repairs, failure displacement was 5.5 (1.9) mm, and ultimate failure load was 571.2 (173.0) N. There was no difference in failure displacement (P = .393), but there was a difference in ultimate failure load (P = .042; power = 0.57). During failure testing, mean (SD) tissue deformation was higher (P = .012; power = 0.83) for the PHA-augmented repairs, 1.2 (0.7) mm, than for the nonaugmented repairs, 0.8 (0.5) mm. Failures, which were consistent within pairs, were caused by tissue failure, with sutures pulling through the tissue (4 pairs) or single anchor pullout before ultimate tissue failure (4 pairs). Of the 4 failures with anchor pullout, 3 had anterior anchor pullout, and 1 had posterior anchor pullout. In all specimens with anchor pullout, the second anchor remained stable, and ultimate failure occurred with tissue tearing at the suture interface. There were no significant differences in any metrics between specimens that failed with intact anchors and specimens with single anchor pullout (P ≥ .122). Therefore, both groups were pooled for the failure analysis.
Discussion
RCR augmentation with a synthetic graft is a viable option for improving fixation strength of supraspinatus repairs, as shown in otherwise healthy tendon in the present study. Our hypothesis that there would be decreased gap formation with graft augmentation was not supported, whereas the hypothesis of increased failure loads with graft augmentation was supported. These findings may also be applicable in cases of large tears, revisions, and tendons with poor tissue quality. Simplification of graft application techniques will allow quick and easy arthroscopic augmentation.
Studies of RCRs for large or massive tears have reported retear rates of 25% to 79%.24-26 Latissimus dorsi tendon transfers also show promise in posterosuperior RCRs, with failure rates near 10%.27,28 Although use of PHA patches in RCR augmentation is relatively new, short-term and midterm failure rates are in the range of 20% to 60% in the few small cohorts currently being studied.13,16 It is possible that these rates may improve as indications, surgical experience, and techniques for use of PHA patches are further refined. Regardless, with PHA currently being used in practice, it is important to quantify the biomechanics of the augmentation as a baseline for its performance in reinforcing the tendon–suture interface.
We determined that the initial fixation strength of single-row repairs was higher with the addition of PHA synthetic grafts using a very simple technique. Single-row triple-loaded anchor repairs already provide high initial mechanical strength, and our results are similar to those of another study of this technique.29 Despite the already high mechanical strength of a triple-loaded anchor repair, PHA mesh increased ultimate strength by about 100 N (~25%). Of note, tissue elongation during failure was higher (P = .012; power = 0.83) in the PHA-augmented group (1.2 mm) than in the nonaugmented group (0.8 mm). This was not surprising—failure loads were almost 100 N higher in the PHA-augmented group than in the nonaugmented group. Consequently, much higher forces were placed on the muscle belly, likely resulting in additional elongation of the intact tissue medial to the repair construct.
The ultimate failure loads in our study compare favorably with the biomechanical strength of augmented repairs reported by others.8,9,18 Barber and colleagues18 evaluated an augmented single-row repair with 2 double-loaded suture anchors and an acellular dermal matrix graft. The ultimate failure load of the augmented repairs was 325 N. In contrast, Omae and colleagues8 tested a bridging single-row repair using 2 double-loaded suture anchors and an acellular dermal matrix graft. Ultimate failure load of the augmented repairs was 560 N, similar to our finding. Last, Shea and colleagues9 evaluated a bridging single-row repair using 2 double-loaded suture anchors and an acellular dermal matrix graft, with ultimate failure load of 429 N. The techniques in all 3 studies can be performed arthroscopically but are challenging and require multiple extra sutures and anchors that need management and tying. Our technique provides similar initial fixation strength, has no requirement for extra sutures or anchors, and is very simple to perform.
The supraspinatus tendon is estimated to fail between 800 N and 1000 N.30,31 Biomechanical shoulder simulators use supraspinatus forces in the range of 20 N to 200 N for scapular plane abduction.32-36 Therefore, the single-row repair failures in our study fell between functional and full-thickness failure loads. Studies on the mechanics of degenerated human supraspinatus tendon are limited, but there is evidence the mechanical properties of these tissues are inferior to those of healthy tendon.37 A 100-N increase in failure loads with PHA augmentation may prove highly significant in reinforcing the suture–tendon interface in degenerated tendons.
Adding the mesh did not have any effect on gapping at the repair site after cyclic loading. This finding suggests that construct gapping under cyclic loading is not a function of a reinforced knot–tendon interface but is instead caused by microtearing and cinching of the suture constructs in relation to the underlying bone. Tissue elongation likely was not a strong contributor to overall cyclic gapping, as elongation did not differ between the nonaugmented and augmented repairs (0.5 mm vs 0.7 mm; P = .276) and was small relative to the nearly 4 mm of construct gapping. Gapping may be affected by healing and integration of the mesh into the repaired tendon over time, but this effect could not be captured in the present study. Patients are initially immobilized and passive shoulder motion gradually introduced, in stark contrast to the immediate loading protocol in the present study. Regardless, the 25% increase in overall strength may be clinically important, especially in cases of difficult repair or poor tissue quality.
Our technique simplifies arthroscopic augmentation—stitches are passed through the rotator cuff in simple fashion. Before being tied, the limbs that were passed through the rotator cuff are removed through a cannula and then passed through the synthetic graft.
Study Limitations
This study had several limitations. First, it was a cadaveric biomechanical study that evaluated only time-zero biomechanical properties. Loads were normalized to tendon size, specimens were randomized between sides, and paired specimens were used to minimize the effects of tendon and bone quality on outcome metrics. In addition, donor tendons were representative of otherwise healthy tissue. Chronic tears and associated resorption/atrophy could have affected the magnitude of forces and gapping detected in this study. Theoretically, over time the tendon tissue will adhere to and grow into the mesh, which could minimize potential differences. Studies are needed to determine the effects of healing on long-term repair strength in affected patients. Last, all constructs were performed in open fashion to improve repeatability of construct placement and provide accessibility for Instron testing. Our technique did not directly replicate the arthroscopic approach, but, unlike other augmentation techniques, it is so simple that transition to all-arthroscopic augmentation is realistic.
Patch augmentation increases the cost of materials and operative time and should be considered a limitation of its utility. We do not recommend augmentation in all RCRs, as it likely is cost-ineffective. Instead, we recommend augmentation in cases of poor tissue quality, which could lead to healing failure, revision surgery, and higher overall patient costs beyond the cost of adding augmentation. Similarly, we recommend augmentation for revision cases in which tendon healing has failed and tissue quality is poor. The goal is to prevent another failure.
Conclusion
PHA graft augmentation of single-row triple-loaded anchor repairs of the supraspinatus tendon improves the overall ultimate load to failure by 25%. There was no difference in gap formation after cyclic loading between augmented and nonaugmented repairs. This technique for arthroscopic augmentation can be used to improve initial biomechanical repair strength in tears at risk for failure.
Am J Orthop. 2016;45(7):E527-E533. Copyright Frontline Medical Communications Inc. 2016. All rights reserved.
1. Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86(2):219-224.
2. Keener JD, Wei AS, Kim HM, et al. Revision arthroscopic rotator cuff repair: repair integrity and clinical outcome. J Bone Joint Surg Am. 2010;92(3):590-598.
3. Nho SJ, Brown BS, Lyman S, Adler RS, Altchek DW, MacGillivray JD. Prospective analysis of arthroscopic rotator cuff repair: prognostic factors affecting clinical and ultrasound outcome. J Shoulder Elbow Surg. 2009;18(1):13-20.
4. Barber FA, Herbert MA, Schroeder FA, Aziz-Jacobo J, Mays MM, Rapley JH. Biomechanical advantages of triple-loaded suture anchors compared with double-row rotator cuff repairs. Arthroscopy. 2010;26(3):316-323.
5. Burkhart SS, Denard PJ, Konicek J, Hanypsiak BT. Biomechanical validation of load-sharing rip-stop fixation for the repair of tissue-deficient rotator cuff tears. Am J Sports Med. 2014;42(2):457-462.
6. Gupta AK, Hug K, Boggess B, Gavigan M, Toth AP. Massive or 2-tendon rotator cuff tears in active patients with minimal glenohumeral arthritis: clinical and radiographic outcomes of reconstruction using dermal tissue matrix xenograft. Am J Sports Med. 2013;41(4):872-879.
7. Ma CB, MacGillivray JD, Clabeaux J, Lee S, Otis JC. Biomechanical evaluation of arthroscopic rotator cuff stitches. J Bone Joint Surg Am. 2004;86(6):1211-1216.
8. Omae H, Steinmann SP, Zhao C, et al. Biomechanical effect of rotator cuff augmentation with an acellular dermal matrix graft: a cadaver study. Clin Biomech. 2012;27(8):789-792.
9. Shea KP, Obopilwe E, Sperling JW, Iannotti JP. A biomechanical analysis of gap formation and failure mechanics of a xenograft-reinforced rotator cuff repair in a cadaveric model. J Shoulder Elbow Surg. 2012;21(8):1072-1079.
10. Agrawal V. Healing rates for challenging rotator cuff tears utilizing an acellular human dermal reinforcement graft. Int J Shoulder Surg. 2012;6(2):36-44.
11. Beimers L, Lam PH, Murrell GA. The biomechanical effects of polytetrafluoroethylene suture augmentations in lateral-row rotator cuff repairs in an ovine model. J Shoulder Elbow Surg. 2014;23(10):1545-1552.
12. McCarron JA, Milks RA, Chen X, Iannotti JP, Derwin KA. Improved time-zero biomechanical properties using poly-L-lactic acid graft augmentation in a cadaveric rotator cuff repair model. J Shoulder Elbow Surg. 2010;19(5):688-696.
13. Proctor CS. Long-term successful arthroscopic repair of large and massive rotator cuff tears with a functional and degradable reinforcement device. J Shoulder Elbow Surg. 2014;23(10):1508-1513.
14. Misra SK, Valappil SP, Roy I, Boccaccini AR. Polyhydroxyalkanoate (PHA)/inorganic phase composites for tissue engineering applications. Biomacromolecules. 2006;7(8):2249-2258.
15. Ellis G, Cano P, Jadraque M, et al. Laser microperforated biodegradable microbial polyhydroxyalkanoate substrates for tissue repair strategies: an infrared microspectroscopy study. Anal Bioanal Chem. 2011;399(7):2379-2388.
16. Lenart BA, Martens KA, Kearns KA, Gillespie RJ, Zoga AC, Williams GR. Treatment of massive and recurrent rotator cuff tears augmented with a poly-l-lactide graft, a preliminary study. J Shoulder Elbow Surg. 2015;24(6):915-921.
17. Barber FA, Burns JP, Deutsch A, Labbé MR, Litchfield RB. A prospective, randomized evaluation of acellular human dermal matrix augmentation for arthroscopic rotator cuff repair. Arthroscopy. 2012;28(1):8-15.
18. Barber FA, Herbert MA, Boothby MH. Ultimate tensile failure loads of a human dermal allograft rotator cuff augmentation. Arthroscopy. 2008;24(1):20-24.
19. Gilot GJ, Attia AK, Alvarez AM. Arthroscopic repair of rotator cuff tears using extracellular matrix graft. Arthrosc Tech. 2014;3(4):e487-e489.
20. Barber FA, Coons DA, Ruiz-Suarez M. Cyclic load testing of biodegradable suture anchors containing 2 high-strength sutures. Arthroscopy. 2007;23(4):355-360.
21. Kullar RS, Reagan JM, Kolz CW, Burks RT, Henninger HB. Suture placement near the musculotendinous junction in the supraspinatus: implications for rotator cuff repair. Am J Sports Med. 2015;43(1):57-62.
22. Burkhart SS, Diaz Pagàn JL, Wirth MA, Athanasiou KA. Cyclic loading of anchor-based rotator cuff repairs: confirmation of the tension overload phenomenon and comparison of suture anchor fixation with transosseous fixation. Arthroscopy. 1997;13(6):720-724.
23. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191.
24. Greenspoon JA, Petri M, Warth RJ, Millett PJ. Massive rotator cuff tears: pathomechanics, current treatment options, and clinical outcomes. J Shoulder Elbow Surg. 2015;24(9):1493-1505.
25. Hein J, Reilly JM, Chae J, Maerz T, Anderson K. Retear rates after arthroscopic single-row, double-row, and suture bridge rotator cuff repair at a minimum of 1 year of imaging follow-up: a systematic review. Arthroscopy. 2015;31(11):2274-2281.
26. Henry P, Wasserstein D, Park S, et al. Arthroscopic repair for chronic massive rotator cuff tears: a systematic review. Arthroscopy. 2015;31(12):2472-2480.
27. El-Azab HM, Rott O, Irlenbusch U. Long-term follow-up after latissimus dorsi transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am. 2015;97(6):462-469.
28. Gerber C, Rahm SA, Catanzaro S, Farshad M, Moor BK. Latissimus dorsi tendon transfer for treatment of irreparable posterosuperior rotator cuff tears: long-term results at a minimum follow-up of ten years. J Bone Joint Surg Am. 2013;95(21):1920-1926.
29. Coons DA, Barber FA, Herbert MA. Triple-loaded single-anchor stitch configurations: an analysis of cyclically loaded suture–tendon interface security. Arthroscopy. 2006;22(11):1154-1158.
30. Itoi E, Berglund LJ, Grabowski JJ, et al. Tensile properties of the supraspinatus tendon. J Orthop Res. 1995;13(4):578-584.
31. Matsuhashi T, Hooke AW, Zhao KD, et al. Tensile properties of a morphologically split supraspinatus tendon. Clin Anat. 2014;27(5):702-706.
32. Apreleva M, Parsons IM 4th, Warner JJ, Fu FH, Woo SL. Experimental investigation of reaction forces at the glenohumeral joint during active abduction. J Shoulder Elbow Surg. 2000;9(5):409-417.
33. Giles JW, Ferreira LM, Athwal GS, Johnson JA. Development and performance evaluation of a multi-PID muscle loading driven in vitro active-motion shoulder simulator and application to assessing reverse total shoulder arthroplasty. J Biomech Eng. 2014;136(12):121007.
34. Hansen ML, Otis JC, Johnson JS, Cordasco FA, Craig EV, Warren RF. Biomechanics of massive rotator cuff tears: implications for treatment. J Bone Joint Surg Am. 2008;90(2):316-325.
35. Henninger HB, Barg A, Anderson AE, Bachus KN, Tashjian RZ, Burks RT. Effect of deltoid tension and humeral version in reverse total shoulder arthroplasty: a biomechanical study. J Shoulder Elbow Surg. 2012;21(4):483-490.
36. Mihata T, Gates J, McGarry MH, Lee J, Kinoshita M, Lee TQ. Effect of rotator cuff muscle imbalance on forceful internal impingement and peel-back of the superior labrum: a cadaveric study. Am J Sports Med. 2009;37(11):2222-2227.
37. Sano H, Ishii H, Yeadon A, Backman DS, Brunet JA, Uhthoff HK. Degeneration at the insertion weakens the tensile strength of the supraspinatus tendon: a comparative mechanical and histologic study of the bone–tendon complex. J Orthop Res. 1997;15(5):719-726.
1. Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86(2):219-224.
2. Keener JD, Wei AS, Kim HM, et al. Revision arthroscopic rotator cuff repair: repair integrity and clinical outcome. J Bone Joint Surg Am. 2010;92(3):590-598.
3. Nho SJ, Brown BS, Lyman S, Adler RS, Altchek DW, MacGillivray JD. Prospective analysis of arthroscopic rotator cuff repair: prognostic factors affecting clinical and ultrasound outcome. J Shoulder Elbow Surg. 2009;18(1):13-20.
4. Barber FA, Herbert MA, Schroeder FA, Aziz-Jacobo J, Mays MM, Rapley JH. Biomechanical advantages of triple-loaded suture anchors compared with double-row rotator cuff repairs. Arthroscopy. 2010;26(3):316-323.
5. Burkhart SS, Denard PJ, Konicek J, Hanypsiak BT. Biomechanical validation of load-sharing rip-stop fixation for the repair of tissue-deficient rotator cuff tears. Am J Sports Med. 2014;42(2):457-462.
6. Gupta AK, Hug K, Boggess B, Gavigan M, Toth AP. Massive or 2-tendon rotator cuff tears in active patients with minimal glenohumeral arthritis: clinical and radiographic outcomes of reconstruction using dermal tissue matrix xenograft. Am J Sports Med. 2013;41(4):872-879.
7. Ma CB, MacGillivray JD, Clabeaux J, Lee S, Otis JC. Biomechanical evaluation of arthroscopic rotator cuff stitches. J Bone Joint Surg Am. 2004;86(6):1211-1216.
8. Omae H, Steinmann SP, Zhao C, et al. Biomechanical effect of rotator cuff augmentation with an acellular dermal matrix graft: a cadaver study. Clin Biomech. 2012;27(8):789-792.
9. Shea KP, Obopilwe E, Sperling JW, Iannotti JP. A biomechanical analysis of gap formation and failure mechanics of a xenograft-reinforced rotator cuff repair in a cadaveric model. J Shoulder Elbow Surg. 2012;21(8):1072-1079.
10. Agrawal V. Healing rates for challenging rotator cuff tears utilizing an acellular human dermal reinforcement graft. Int J Shoulder Surg. 2012;6(2):36-44.
11. Beimers L, Lam PH, Murrell GA. The biomechanical effects of polytetrafluoroethylene suture augmentations in lateral-row rotator cuff repairs in an ovine model. J Shoulder Elbow Surg. 2014;23(10):1545-1552.
12. McCarron JA, Milks RA, Chen X, Iannotti JP, Derwin KA. Improved time-zero biomechanical properties using poly-L-lactic acid graft augmentation in a cadaveric rotator cuff repair model. J Shoulder Elbow Surg. 2010;19(5):688-696.
13. Proctor CS. Long-term successful arthroscopic repair of large and massive rotator cuff tears with a functional and degradable reinforcement device. J Shoulder Elbow Surg. 2014;23(10):1508-1513.
14. Misra SK, Valappil SP, Roy I, Boccaccini AR. Polyhydroxyalkanoate (PHA)/inorganic phase composites for tissue engineering applications. Biomacromolecules. 2006;7(8):2249-2258.
15. Ellis G, Cano P, Jadraque M, et al. Laser microperforated biodegradable microbial polyhydroxyalkanoate substrates for tissue repair strategies: an infrared microspectroscopy study. Anal Bioanal Chem. 2011;399(7):2379-2388.
16. Lenart BA, Martens KA, Kearns KA, Gillespie RJ, Zoga AC, Williams GR. Treatment of massive and recurrent rotator cuff tears augmented with a poly-l-lactide graft, a preliminary study. J Shoulder Elbow Surg. 2015;24(6):915-921.
17. Barber FA, Burns JP, Deutsch A, Labbé MR, Litchfield RB. A prospective, randomized evaluation of acellular human dermal matrix augmentation for arthroscopic rotator cuff repair. Arthroscopy. 2012;28(1):8-15.
18. Barber FA, Herbert MA, Boothby MH. Ultimate tensile failure loads of a human dermal allograft rotator cuff augmentation. Arthroscopy. 2008;24(1):20-24.
19. Gilot GJ, Attia AK, Alvarez AM. Arthroscopic repair of rotator cuff tears using extracellular matrix graft. Arthrosc Tech. 2014;3(4):e487-e489.
20. Barber FA, Coons DA, Ruiz-Suarez M. Cyclic load testing of biodegradable suture anchors containing 2 high-strength sutures. Arthroscopy. 2007;23(4):355-360.
21. Kullar RS, Reagan JM, Kolz CW, Burks RT, Henninger HB. Suture placement near the musculotendinous junction in the supraspinatus: implications for rotator cuff repair. Am J Sports Med. 2015;43(1):57-62.
22. Burkhart SS, Diaz Pagàn JL, Wirth MA, Athanasiou KA. Cyclic loading of anchor-based rotator cuff repairs: confirmation of the tension overload phenomenon and comparison of suture anchor fixation with transosseous fixation. Arthroscopy. 1997;13(6):720-724.
23. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191.
24. Greenspoon JA, Petri M, Warth RJ, Millett PJ. Massive rotator cuff tears: pathomechanics, current treatment options, and clinical outcomes. J Shoulder Elbow Surg. 2015;24(9):1493-1505.
25. Hein J, Reilly JM, Chae J, Maerz T, Anderson K. Retear rates after arthroscopic single-row, double-row, and suture bridge rotator cuff repair at a minimum of 1 year of imaging follow-up: a systematic review. Arthroscopy. 2015;31(11):2274-2281.
26. Henry P, Wasserstein D, Park S, et al. Arthroscopic repair for chronic massive rotator cuff tears: a systematic review. Arthroscopy. 2015;31(12):2472-2480.
27. El-Azab HM, Rott O, Irlenbusch U. Long-term follow-up after latissimus dorsi transfer for irreparable posterosuperior rotator cuff tears. J Bone Joint Surg Am. 2015;97(6):462-469.
28. Gerber C, Rahm SA, Catanzaro S, Farshad M, Moor BK. Latissimus dorsi tendon transfer for treatment of irreparable posterosuperior rotator cuff tears: long-term results at a minimum follow-up of ten years. J Bone Joint Surg Am. 2013;95(21):1920-1926.
29. Coons DA, Barber FA, Herbert MA. Triple-loaded single-anchor stitch configurations: an analysis of cyclically loaded suture–tendon interface security. Arthroscopy. 2006;22(11):1154-1158.
30. Itoi E, Berglund LJ, Grabowski JJ, et al. Tensile properties of the supraspinatus tendon. J Orthop Res. 1995;13(4):578-584.
31. Matsuhashi T, Hooke AW, Zhao KD, et al. Tensile properties of a morphologically split supraspinatus tendon. Clin Anat. 2014;27(5):702-706.
32. Apreleva M, Parsons IM 4th, Warner JJ, Fu FH, Woo SL. Experimental investigation of reaction forces at the glenohumeral joint during active abduction. J Shoulder Elbow Surg. 2000;9(5):409-417.
33. Giles JW, Ferreira LM, Athwal GS, Johnson JA. Development and performance evaluation of a multi-PID muscle loading driven in vitro active-motion shoulder simulator and application to assessing reverse total shoulder arthroplasty. J Biomech Eng. 2014;136(12):121007.
34. Hansen ML, Otis JC, Johnson JS, Cordasco FA, Craig EV, Warren RF. Biomechanics of massive rotator cuff tears: implications for treatment. J Bone Joint Surg Am. 2008;90(2):316-325.
35. Henninger HB, Barg A, Anderson AE, Bachus KN, Tashjian RZ, Burks RT. Effect of deltoid tension and humeral version in reverse total shoulder arthroplasty: a biomechanical study. J Shoulder Elbow Surg. 2012;21(4):483-490.
36. Mihata T, Gates J, McGarry MH, Lee J, Kinoshita M, Lee TQ. Effect of rotator cuff muscle imbalance on forceful internal impingement and peel-back of the superior labrum: a cadaveric study. Am J Sports Med. 2009;37(11):2222-2227.
37. Sano H, Ishii H, Yeadon A, Backman DS, Brunet JA, Uhthoff HK. Degeneration at the insertion weakens the tensile strength of the supraspinatus tendon: a comparative mechanical and histologic study of the bone–tendon complex. J Orthop Res. 1997;15(5):719-726.
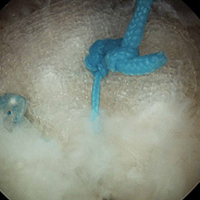
Telephone calls improve long-term follow-up after hernia repair
Follow-up telephone calls can significantly improve the collection of long-term patient-reported outcomes following ventral hernia repair, according to a study published online in the Oct. 20 edition of the Journal of the American College of Surgeons.
Nishant Ganesh Kumar, a medical student, and his colleagues at Vanderbilt University, Nashville, Tenn., wrote that while ventral hernia repair is one of the most common surgical procedures in the world, reliable long-term, prospective data on outcomes has been extremely difficult to collect.
In this Plan-Do-Study-Act (PDSA) prospective study, 99 patients who had undergone ventral hernia repair were followed up by telephone, in addition to the usual email communication, 1 year after their procedure. The calls were initially made between 1:00 p.m. and 3:00 p.m. in the first phase of the study, then changed to after 3:00 p.m. in the second phase.
Compared to the long-term completion rate of 16.3% prior to the intervention – where follow-up was largely through physical clinical visits – researchers saw a completion rate of 35.7% with the telephone calls between 1:00 p.m. and 3:00 p.m., and a 55.1% completion rate after changing the call time to after 3:00 p.m. The mean participation rate was 45.4%.
Once contact was made, all the patients completed the full patient-reported outcomes assessment, although the researchers did note that some seem to experience fatigue during questioning that required the interviewers to gently steer them back to the questions.
“The advantage of making phone calls was severalfold, including clarification of survey questions to help patients with providing more insightful responses, allaying concerns of patients, and personalizing long-term follow-up, a crucial aspect missing through automated surveys,” the authors wrote.
In addition to changing the time in which the calls were made, the researchers also changed how the survey was introduced to the patients, such as referring to the survey as “follow-up,” which seemed to improve patient participation.
“Further, it was observed that during conversations with the patient, highlighting relevant features of their medical and surgical history, such as the date of the surgery, the surgeon who operated on them, and their disease progression since surgery helped in developing a rapport with the patient and increased the chances of their participation,” they reported. “With these approaches, the participation rate after the second PDSA cycle increased to 55.1%.”
The data analyses in the study were supported by the Americas Hernia Society Quality Collaborative. There were no disclosures relevant to the study.
Follow-up telephone calls can significantly improve the collection of long-term patient-reported outcomes following ventral hernia repair, according to a study published online in the Oct. 20 edition of the Journal of the American College of Surgeons.
Nishant Ganesh Kumar, a medical student, and his colleagues at Vanderbilt University, Nashville, Tenn., wrote that while ventral hernia repair is one of the most common surgical procedures in the world, reliable long-term, prospective data on outcomes has been extremely difficult to collect.
In this Plan-Do-Study-Act (PDSA) prospective study, 99 patients who had undergone ventral hernia repair were followed up by telephone, in addition to the usual email communication, 1 year after their procedure. The calls were initially made between 1:00 p.m. and 3:00 p.m. in the first phase of the study, then changed to after 3:00 p.m. in the second phase.
Compared to the long-term completion rate of 16.3% prior to the intervention – where follow-up was largely through physical clinical visits – researchers saw a completion rate of 35.7% with the telephone calls between 1:00 p.m. and 3:00 p.m., and a 55.1% completion rate after changing the call time to after 3:00 p.m. The mean participation rate was 45.4%.
Once contact was made, all the patients completed the full patient-reported outcomes assessment, although the researchers did note that some seem to experience fatigue during questioning that required the interviewers to gently steer them back to the questions.
“The advantage of making phone calls was severalfold, including clarification of survey questions to help patients with providing more insightful responses, allaying concerns of patients, and personalizing long-term follow-up, a crucial aspect missing through automated surveys,” the authors wrote.
In addition to changing the time in which the calls were made, the researchers also changed how the survey was introduced to the patients, such as referring to the survey as “follow-up,” which seemed to improve patient participation.
“Further, it was observed that during conversations with the patient, highlighting relevant features of their medical and surgical history, such as the date of the surgery, the surgeon who operated on them, and their disease progression since surgery helped in developing a rapport with the patient and increased the chances of their participation,” they reported. “With these approaches, the participation rate after the second PDSA cycle increased to 55.1%.”
The data analyses in the study were supported by the Americas Hernia Society Quality Collaborative. There were no disclosures relevant to the study.
Follow-up telephone calls can significantly improve the collection of long-term patient-reported outcomes following ventral hernia repair, according to a study published online in the Oct. 20 edition of the Journal of the American College of Surgeons.
Nishant Ganesh Kumar, a medical student, and his colleagues at Vanderbilt University, Nashville, Tenn., wrote that while ventral hernia repair is one of the most common surgical procedures in the world, reliable long-term, prospective data on outcomes has been extremely difficult to collect.
In this Plan-Do-Study-Act (PDSA) prospective study, 99 patients who had undergone ventral hernia repair were followed up by telephone, in addition to the usual email communication, 1 year after their procedure. The calls were initially made between 1:00 p.m. and 3:00 p.m. in the first phase of the study, then changed to after 3:00 p.m. in the second phase.
Compared to the long-term completion rate of 16.3% prior to the intervention – where follow-up was largely through physical clinical visits – researchers saw a completion rate of 35.7% with the telephone calls between 1:00 p.m. and 3:00 p.m., and a 55.1% completion rate after changing the call time to after 3:00 p.m. The mean participation rate was 45.4%.
Once contact was made, all the patients completed the full patient-reported outcomes assessment, although the researchers did note that some seem to experience fatigue during questioning that required the interviewers to gently steer them back to the questions.
“The advantage of making phone calls was severalfold, including clarification of survey questions to help patients with providing more insightful responses, allaying concerns of patients, and personalizing long-term follow-up, a crucial aspect missing through automated surveys,” the authors wrote.
In addition to changing the time in which the calls were made, the researchers also changed how the survey was introduced to the patients, such as referring to the survey as “follow-up,” which seemed to improve patient participation.
“Further, it was observed that during conversations with the patient, highlighting relevant features of their medical and surgical history, such as the date of the surgery, the surgeon who operated on them, and their disease progression since surgery helped in developing a rapport with the patient and increased the chances of their participation,” they reported. “With these approaches, the participation rate after the second PDSA cycle increased to 55.1%.”
The data analyses in the study were supported by the Americas Hernia Society Quality Collaborative. There were no disclosures relevant to the study.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF SURGEONS
Key clinical point: Follow-up telephone calls can significantly improve the collection of long-term patient-reported outcomes following ventral hernia repair.
Major finding: Compared to the long-term completion rate of 16.3% prior to the intervention, a telephone call follow-up increased the mean participation rate to 45.4%.
Data source: Prospective cohort study of 99 patients who underwent ventral hernia repair.
Disclosures: The data analyses in the study were supported by the Americas Hernia Society Quality Collaborative. There were no disclosures relevant to the study.
Lenalidomide improves PFS after 1st and 2nd line CLL therapy
SAN DIEGO – Lenalidomide, a mainstay of maintenance therapy for multiple myeloma, is now making inroads into maintenance therapy following first- and second-line therapy for chronic lymphocytic leukemia (CLL), investigators reported in two phase III studies.
Among patients with previously untreated CLL who were at high risk for early disease progression following standard chemotherapy, lenalidomide (Revlimid) maintenance therapy was associated with an 80% reduction in the relative risk for disease progression compared with placebo, reported Anna Fink, MD, of the University of Cologne, Germany, and her colleagues in the German CLL Study Group.
Similarly, lenalidomide maintenance significantly improved progression-free survival (PFS) compared with placebo among patients with CLL who had at least partial responses to second-line therapy, reported Anna Schuh, MD, of the University of Oxford, England, and her colleagues in the CONTINUUM trial.
“Lenalidomide maintenance therapy significantly improved progression-free survival, from just about 9 months to almost 40 months when given to patients with CLL who responded to second-line therapy,” Dr. Schuh said at the American Society of Hematology annual meeting.
Both studies were unblinded because of the superiority of lenalidomide after prespecified analyses, on the recommendation of the respective data safety monitoring boards (DSMBs).
The PFS advantage with lenalidomide seen in each study did not translate into differences in overall survival in either study, however.
Maintenance after first-line therapy
In the CLLM1 trial, Dr. Fink and her colleagues enrolled physically fit, previously untreated patients with CLL and delivered chemoimmunotherapy at the investigator’s choice: either FCR (fludarabine, cyclophosphamide, and rituximab), FR (fludarabine and rituximab), FC (fludarabine and cyclophosphamide), or BR (bendamustine and rituximab).
Patients who had at least a partial response after a minimum of four cycles were identified as being at high risk for progression if they had minimal residual disease (MRD) levels of at least 10-2 cells, or MRD levels from 10-4 to less than 10-2 combined with either an unmutated IGHV gene status, del(17p) or TP53 mutation at baseline.
Of 468 screened patients, 89 were deemed to have high risk disease, and these patients were randomly assigned on a 2:1 basis to maintenance with lenalidomide given 5 mg orally for the first cycle and escalated to a target dose of 15 mg by the seventh cycle, or to placebo.
Additional dose escalations could be performed based on MRD assessments every 6 months, with the drug continued until progression or unacceptable toxicity. Patients also were assigned to daily low-dose aspirin or to an anticoagulation agent depending on their individual risk for thromboembolic events.
The study was stopped and unblinded after a planned interim analysis showed that the difference in PFS met the stopping boundary for efficacy.
Ultimately, 56 patients assigned to lenalidomide received study treatment, as did 29 assigned to placebo.
At a median follow-up of 17.5 months, the median PFS according to independent review was not reached for lenalidomide, vs. 13.3 months for placebo. Lenalidomide was associated with a hazard ratio (HR) for progression of 0.148 (P less than .00001), and a relative risk reduction of 80%.
Lenalidomide was also significantly better for PFS in analysis by MRD at baseline, with a PFS of 19.4 months for placebo vs. not reached among patients with less than 10-2 but more than 10-4 cells (HR, 0.125) and 3.7 vs. 32.3 months, respectively, for patients with MRD greater than 10-2 (HR 0.165).
There were three deaths (two in patients on placebo), and at the last analysis there was no difference in overall survival. In all, 42.9% of patients on lenalidomide discontinued because of adverse events, compared with 72.4% of those on placebo.
Maintenance after second-line therapy
In CONTINUUM, patients with at least a partial response after two prior lines of therapy and an Eastern Cooperative Oncology Group performance score of 0-2 were enrolled and randomized to receive either lenalidomide (160 patients) at a starting dose of 2.5 mg/day for the first 28-day cycle, 5 mg/day from cycle 2, and, if well tolerated, up to 10 mg/day from cycle 7 on, or to placebo (154 patients).
This study, as noted before, was also unblinded at the time of the primary analysis as recommended by the DSMB, after a prespecified number of events had occurred.
At a median follow-up of 31.5 months, the median PFS, a co-primary endpoint with OS, was 33.9 months in the lenalidomide arm, compared with 9.2 months in the placebo arm, translating into a HR for lenalidomide of 0.40 (P less than .001).
The lenalidomide advantage also was seen in a subgroup analysis by age, prior response to chemotherapy, and number of factors for poor prognosis. Of note, among patients older than age 70, the PFS with lenalidomide was 52.5 months, compared with 7.3 months for placebo (HR 0.34, P = .005).
In a second PFS analysis conducted after 71 months of follow-up, lenalidomide remained superior, with a median PFS of 57.5 months vs. 32.7 months in the placebo arm. As noted, there was no difference in overall survival in this study.
Grade 3 or greater adverse events occurring more frequently with lenalidomide were neutropenia, thrombocytopenia, diarrhea, pneumonia, fatigue, hypokalemia, pulmonary embolism, and sepsis. There was no difference in the incidence of second primary malignancies, however.
CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from the company, and travel grants and honoraria from others. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
SAN DIEGO – Lenalidomide, a mainstay of maintenance therapy for multiple myeloma, is now making inroads into maintenance therapy following first- and second-line therapy for chronic lymphocytic leukemia (CLL), investigators reported in two phase III studies.
Among patients with previously untreated CLL who were at high risk for early disease progression following standard chemotherapy, lenalidomide (Revlimid) maintenance therapy was associated with an 80% reduction in the relative risk for disease progression compared with placebo, reported Anna Fink, MD, of the University of Cologne, Germany, and her colleagues in the German CLL Study Group.
Similarly, lenalidomide maintenance significantly improved progression-free survival (PFS) compared with placebo among patients with CLL who had at least partial responses to second-line therapy, reported Anna Schuh, MD, of the University of Oxford, England, and her colleagues in the CONTINUUM trial.
“Lenalidomide maintenance therapy significantly improved progression-free survival, from just about 9 months to almost 40 months when given to patients with CLL who responded to second-line therapy,” Dr. Schuh said at the American Society of Hematology annual meeting.
Both studies were unblinded because of the superiority of lenalidomide after prespecified analyses, on the recommendation of the respective data safety monitoring boards (DSMBs).
The PFS advantage with lenalidomide seen in each study did not translate into differences in overall survival in either study, however.
Maintenance after first-line therapy
In the CLLM1 trial, Dr. Fink and her colleagues enrolled physically fit, previously untreated patients with CLL and delivered chemoimmunotherapy at the investigator’s choice: either FCR (fludarabine, cyclophosphamide, and rituximab), FR (fludarabine and rituximab), FC (fludarabine and cyclophosphamide), or BR (bendamustine and rituximab).
Patients who had at least a partial response after a minimum of four cycles were identified as being at high risk for progression if they had minimal residual disease (MRD) levels of at least 10-2 cells, or MRD levels from 10-4 to less than 10-2 combined with either an unmutated IGHV gene status, del(17p) or TP53 mutation at baseline.
Of 468 screened patients, 89 were deemed to have high risk disease, and these patients were randomly assigned on a 2:1 basis to maintenance with lenalidomide given 5 mg orally for the first cycle and escalated to a target dose of 15 mg by the seventh cycle, or to placebo.
Additional dose escalations could be performed based on MRD assessments every 6 months, with the drug continued until progression or unacceptable toxicity. Patients also were assigned to daily low-dose aspirin or to an anticoagulation agent depending on their individual risk for thromboembolic events.
The study was stopped and unblinded after a planned interim analysis showed that the difference in PFS met the stopping boundary for efficacy.
Ultimately, 56 patients assigned to lenalidomide received study treatment, as did 29 assigned to placebo.
At a median follow-up of 17.5 months, the median PFS according to independent review was not reached for lenalidomide, vs. 13.3 months for placebo. Lenalidomide was associated with a hazard ratio (HR) for progression of 0.148 (P less than .00001), and a relative risk reduction of 80%.
Lenalidomide was also significantly better for PFS in analysis by MRD at baseline, with a PFS of 19.4 months for placebo vs. not reached among patients with less than 10-2 but more than 10-4 cells (HR, 0.125) and 3.7 vs. 32.3 months, respectively, for patients with MRD greater than 10-2 (HR 0.165).
There were three deaths (two in patients on placebo), and at the last analysis there was no difference in overall survival. In all, 42.9% of patients on lenalidomide discontinued because of adverse events, compared with 72.4% of those on placebo.
Maintenance after second-line therapy
In CONTINUUM, patients with at least a partial response after two prior lines of therapy and an Eastern Cooperative Oncology Group performance score of 0-2 were enrolled and randomized to receive either lenalidomide (160 patients) at a starting dose of 2.5 mg/day for the first 28-day cycle, 5 mg/day from cycle 2, and, if well tolerated, up to 10 mg/day from cycle 7 on, or to placebo (154 patients).
This study, as noted before, was also unblinded at the time of the primary analysis as recommended by the DSMB, after a prespecified number of events had occurred.
At a median follow-up of 31.5 months, the median PFS, a co-primary endpoint with OS, was 33.9 months in the lenalidomide arm, compared with 9.2 months in the placebo arm, translating into a HR for lenalidomide of 0.40 (P less than .001).
The lenalidomide advantage also was seen in a subgroup analysis by age, prior response to chemotherapy, and number of factors for poor prognosis. Of note, among patients older than age 70, the PFS with lenalidomide was 52.5 months, compared with 7.3 months for placebo (HR 0.34, P = .005).
In a second PFS analysis conducted after 71 months of follow-up, lenalidomide remained superior, with a median PFS of 57.5 months vs. 32.7 months in the placebo arm. As noted, there was no difference in overall survival in this study.
Grade 3 or greater adverse events occurring more frequently with lenalidomide were neutropenia, thrombocytopenia, diarrhea, pneumonia, fatigue, hypokalemia, pulmonary embolism, and sepsis. There was no difference in the incidence of second primary malignancies, however.
CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from the company, and travel grants and honoraria from others. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
SAN DIEGO – Lenalidomide, a mainstay of maintenance therapy for multiple myeloma, is now making inroads into maintenance therapy following first- and second-line therapy for chronic lymphocytic leukemia (CLL), investigators reported in two phase III studies.
Among patients with previously untreated CLL who were at high risk for early disease progression following standard chemotherapy, lenalidomide (Revlimid) maintenance therapy was associated with an 80% reduction in the relative risk for disease progression compared with placebo, reported Anna Fink, MD, of the University of Cologne, Germany, and her colleagues in the German CLL Study Group.
Similarly, lenalidomide maintenance significantly improved progression-free survival (PFS) compared with placebo among patients with CLL who had at least partial responses to second-line therapy, reported Anna Schuh, MD, of the University of Oxford, England, and her colleagues in the CONTINUUM trial.
“Lenalidomide maintenance therapy significantly improved progression-free survival, from just about 9 months to almost 40 months when given to patients with CLL who responded to second-line therapy,” Dr. Schuh said at the American Society of Hematology annual meeting.
Both studies were unblinded because of the superiority of lenalidomide after prespecified analyses, on the recommendation of the respective data safety monitoring boards (DSMBs).
The PFS advantage with lenalidomide seen in each study did not translate into differences in overall survival in either study, however.
Maintenance after first-line therapy
In the CLLM1 trial, Dr. Fink and her colleagues enrolled physically fit, previously untreated patients with CLL and delivered chemoimmunotherapy at the investigator’s choice: either FCR (fludarabine, cyclophosphamide, and rituximab), FR (fludarabine and rituximab), FC (fludarabine and cyclophosphamide), or BR (bendamustine and rituximab).
Patients who had at least a partial response after a minimum of four cycles were identified as being at high risk for progression if they had minimal residual disease (MRD) levels of at least 10-2 cells, or MRD levels from 10-4 to less than 10-2 combined with either an unmutated IGHV gene status, del(17p) or TP53 mutation at baseline.
Of 468 screened patients, 89 were deemed to have high risk disease, and these patients were randomly assigned on a 2:1 basis to maintenance with lenalidomide given 5 mg orally for the first cycle and escalated to a target dose of 15 mg by the seventh cycle, or to placebo.
Additional dose escalations could be performed based on MRD assessments every 6 months, with the drug continued until progression or unacceptable toxicity. Patients also were assigned to daily low-dose aspirin or to an anticoagulation agent depending on their individual risk for thromboembolic events.
The study was stopped and unblinded after a planned interim analysis showed that the difference in PFS met the stopping boundary for efficacy.
Ultimately, 56 patients assigned to lenalidomide received study treatment, as did 29 assigned to placebo.
At a median follow-up of 17.5 months, the median PFS according to independent review was not reached for lenalidomide, vs. 13.3 months for placebo. Lenalidomide was associated with a hazard ratio (HR) for progression of 0.148 (P less than .00001), and a relative risk reduction of 80%.
Lenalidomide was also significantly better for PFS in analysis by MRD at baseline, with a PFS of 19.4 months for placebo vs. not reached among patients with less than 10-2 but more than 10-4 cells (HR, 0.125) and 3.7 vs. 32.3 months, respectively, for patients with MRD greater than 10-2 (HR 0.165).
There were three deaths (two in patients on placebo), and at the last analysis there was no difference in overall survival. In all, 42.9% of patients on lenalidomide discontinued because of adverse events, compared with 72.4% of those on placebo.
Maintenance after second-line therapy
In CONTINUUM, patients with at least a partial response after two prior lines of therapy and an Eastern Cooperative Oncology Group performance score of 0-2 were enrolled and randomized to receive either lenalidomide (160 patients) at a starting dose of 2.5 mg/day for the first 28-day cycle, 5 mg/day from cycle 2, and, if well tolerated, up to 10 mg/day from cycle 7 on, or to placebo (154 patients).
This study, as noted before, was also unblinded at the time of the primary analysis as recommended by the DSMB, after a prespecified number of events had occurred.
At a median follow-up of 31.5 months, the median PFS, a co-primary endpoint with OS, was 33.9 months in the lenalidomide arm, compared with 9.2 months in the placebo arm, translating into a HR for lenalidomide of 0.40 (P less than .001).
The lenalidomide advantage also was seen in a subgroup analysis by age, prior response to chemotherapy, and number of factors for poor prognosis. Of note, among patients older than age 70, the PFS with lenalidomide was 52.5 months, compared with 7.3 months for placebo (HR 0.34, P = .005).
In a second PFS analysis conducted after 71 months of follow-up, lenalidomide remained superior, with a median PFS of 57.5 months vs. 32.7 months in the placebo arm. As noted, there was no difference in overall survival in this study.
Grade 3 or greater adverse events occurring more frequently with lenalidomide were neutropenia, thrombocytopenia, diarrhea, pneumonia, fatigue, hypokalemia, pulmonary embolism, and sepsis. There was no difference in the incidence of second primary malignancies, however.
CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from the company, and travel grants and honoraria from others. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
AT ASH 2016
Key clinical point: Lenalidomide (Revlimid) maintenance improves progression free survival following first- and second-line therapies for chronic lymphocytic leukemia.
Major finding: Median PFS vs. placebo was not reached vs. 13.3 months in CLLM1, and 33.9 vs. 9.2 months in CONTINUUM.
Data source: Phase III randomized studies of lenalidomide maintenance following first-line therapy (CLLM1) and second-line therapy (CONTINUUM).
Disclosures: CLLM1 was sponsored by the German CLL Study Group with support from Celgene. CONTINUUM was supported by Celgene. Dr. Fink disclosed research funding from Celgene, and travel grants and honoraria from other drug companies. Dr. Schuh disclosed honoraria from and consulting with Celgene and other companies.
Adding respiratory rate to triage criteria improves accurate staging of chest trauma patients
WASHINGTON – Adding respiratory rate and suspected blunt chest injury to a trauma assessment in the field significantly improved the appropriate triaging of level III trauma patients.
When the assessment specifically evaluated for tachypnea in the setting of blunt chest injury, undertriaging improved by 1.2%, John Yonge, MD, said at the annual clinical congress of the American College of Surgeons.
“When we applied this new criteria to our 10-year study, we identified 661 patients who should have been activated as a level I or level II,” but instead were assessed as less critically injured, Dr. Yonge said in an interview. This initial misstep significantly extended the time before patients could have critical surgical procedures and was related to higher mortality among them.
Dr. Yonge, a surgical fellow at Oregon Health & Science University, Portland, and his mentor Martin Schreiber, MD, conducted the retrospective study of 7,880 trauma patients admitted at level III activation from 2004 to 2014. The OHSU trauma system has three activation levels.
• Level I activations are reserved for the most critically injured patients; attending trauma surgeon and anesthesiologist presence is mandatory.
• Level II activations capture moderate to severe injuries; trauma surgeon and respiratory therapist presence is mandated.
• Level III activations are designed to capture patients who do not require an immediate lifesaving intervention; the presence of the trauma surgery chief resident and attending emergency medicine physician is mandatory.
Patients were considered undertriaged if they were admitted as level III activations, but then required a critical intervention (chest tube placement, intubation, needle thoracostomy, or intracranial pressure monitoring) in the emergency department or ultimately met level I or II activation criteria.
Among all the level III patients, 466 (6%) were undertriaged: 390 were undertriaged based on the existing level I or II activation criteria, and 76 were considered undertriaged based on the need for a critical intervention.
Most of the undertriaged patients (65%) met criteria for level I activation; the rest should have been triaged as level II patients. Compared with appropriately staged level III patients, mortality among the undertriaged patients was significantly higher (3.2% vs. 0.6%). Undertriaged patients also experienced longer delays before initiation of major emergency surgery: a mean of 147 minutes, compared with 106 minutes for appropriately triaged level I patients and 62 minutes for appropriately triaged level II patients.
Dr. Yonge then looked for clinical measures that would improve triage. Tachypnea (respiratory rate of more than 20 breaths per minute) in the field stood out as a significant factor. Tachypneic patients who had a suspected chest injury were 70% more likely to be undertriaged than were those with a normal respiratory rate. Tachypnea was significantly associated with a diagnosis of flail chest, emergency department intubation, and chest tube placement.
The team then constructed a new triage criterion for patients with suspected chest injury – tachypnea combined with suspected blunt thoracic injury. By applying that model to their study population of level III patients, they determined that the level III undertriage rate would be reduced by 1.2%.
Tying the physiologic marker of tachypnea to a suspected clinical diagnosis is a key factor, Dr. Yonge noted. “Just adding tachypnea doesn’t help us. In fact, it would overwhelm us, because a trauma patient could very well be tachypneic because he’s experiencing panic. But tying it to a suspected clinical diagnosis gives us a meaningful result.”
He confirmed this linkage with an additional analysis. “We looked to see how severely injured these patients were and found that 71% of them had an Abbreviated Injury Score (AIS) to the chest of 3 or more, indicating a severe chest injury. Only 29% had an AIS of 2 or less. So this proves that respiratory rate is a valid triage criterion and can be used to identify patients who need a higher level of trauma care.”
The challenge now, Dr. Yonge said, is incorporating the marker into clinical practice. “It doesn’t matter how many statistics you do, if you can’t educate the prehospital providers in this, it’s useless. They are the crux of the trauma system.”
Although national guidelines do recommend assessing respiratory rate as part of field triage, it often isn’t recorded or is only estimated, Dr. Yonge said. That’s one reason he used the 20-breaths-per-minute cutoff rate. “It doesn’t even take a full minute to assess this, but it can make a big improvement in care.”
Neither he nor Dr. Schreiber had any financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
WASHINGTON – Adding respiratory rate and suspected blunt chest injury to a trauma assessment in the field significantly improved the appropriate triaging of level III trauma patients.
When the assessment specifically evaluated for tachypnea in the setting of blunt chest injury, undertriaging improved by 1.2%, John Yonge, MD, said at the annual clinical congress of the American College of Surgeons.
“When we applied this new criteria to our 10-year study, we identified 661 patients who should have been activated as a level I or level II,” but instead were assessed as less critically injured, Dr. Yonge said in an interview. This initial misstep significantly extended the time before patients could have critical surgical procedures and was related to higher mortality among them.
Dr. Yonge, a surgical fellow at Oregon Health & Science University, Portland, and his mentor Martin Schreiber, MD, conducted the retrospective study of 7,880 trauma patients admitted at level III activation from 2004 to 2014. The OHSU trauma system has three activation levels.
• Level I activations are reserved for the most critically injured patients; attending trauma surgeon and anesthesiologist presence is mandatory.
• Level II activations capture moderate to severe injuries; trauma surgeon and respiratory therapist presence is mandated.
• Level III activations are designed to capture patients who do not require an immediate lifesaving intervention; the presence of the trauma surgery chief resident and attending emergency medicine physician is mandatory.
Patients were considered undertriaged if they were admitted as level III activations, but then required a critical intervention (chest tube placement, intubation, needle thoracostomy, or intracranial pressure monitoring) in the emergency department or ultimately met level I or II activation criteria.
Among all the level III patients, 466 (6%) were undertriaged: 390 were undertriaged based on the existing level I or II activation criteria, and 76 were considered undertriaged based on the need for a critical intervention.
Most of the undertriaged patients (65%) met criteria for level I activation; the rest should have been triaged as level II patients. Compared with appropriately staged level III patients, mortality among the undertriaged patients was significantly higher (3.2% vs. 0.6%). Undertriaged patients also experienced longer delays before initiation of major emergency surgery: a mean of 147 minutes, compared with 106 minutes for appropriately triaged level I patients and 62 minutes for appropriately triaged level II patients.
Dr. Yonge then looked for clinical measures that would improve triage. Tachypnea (respiratory rate of more than 20 breaths per minute) in the field stood out as a significant factor. Tachypneic patients who had a suspected chest injury were 70% more likely to be undertriaged than were those with a normal respiratory rate. Tachypnea was significantly associated with a diagnosis of flail chest, emergency department intubation, and chest tube placement.
The team then constructed a new triage criterion for patients with suspected chest injury – tachypnea combined with suspected blunt thoracic injury. By applying that model to their study population of level III patients, they determined that the level III undertriage rate would be reduced by 1.2%.
Tying the physiologic marker of tachypnea to a suspected clinical diagnosis is a key factor, Dr. Yonge noted. “Just adding tachypnea doesn’t help us. In fact, it would overwhelm us, because a trauma patient could very well be tachypneic because he’s experiencing panic. But tying it to a suspected clinical diagnosis gives us a meaningful result.”
He confirmed this linkage with an additional analysis. “We looked to see how severely injured these patients were and found that 71% of them had an Abbreviated Injury Score (AIS) to the chest of 3 or more, indicating a severe chest injury. Only 29% had an AIS of 2 or less. So this proves that respiratory rate is a valid triage criterion and can be used to identify patients who need a higher level of trauma care.”
The challenge now, Dr. Yonge said, is incorporating the marker into clinical practice. “It doesn’t matter how many statistics you do, if you can’t educate the prehospital providers in this, it’s useless. They are the crux of the trauma system.”
Although national guidelines do recommend assessing respiratory rate as part of field triage, it often isn’t recorded or is only estimated, Dr. Yonge said. That’s one reason he used the 20-breaths-per-minute cutoff rate. “It doesn’t even take a full minute to assess this, but it can make a big improvement in care.”
Neither he nor Dr. Schreiber had any financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
WASHINGTON – Adding respiratory rate and suspected blunt chest injury to a trauma assessment in the field significantly improved the appropriate triaging of level III trauma patients.
When the assessment specifically evaluated for tachypnea in the setting of blunt chest injury, undertriaging improved by 1.2%, John Yonge, MD, said at the annual clinical congress of the American College of Surgeons.
“When we applied this new criteria to our 10-year study, we identified 661 patients who should have been activated as a level I or level II,” but instead were assessed as less critically injured, Dr. Yonge said in an interview. This initial misstep significantly extended the time before patients could have critical surgical procedures and was related to higher mortality among them.
Dr. Yonge, a surgical fellow at Oregon Health & Science University, Portland, and his mentor Martin Schreiber, MD, conducted the retrospective study of 7,880 trauma patients admitted at level III activation from 2004 to 2014. The OHSU trauma system has three activation levels.
• Level I activations are reserved for the most critically injured patients; attending trauma surgeon and anesthesiologist presence is mandatory.
• Level II activations capture moderate to severe injuries; trauma surgeon and respiratory therapist presence is mandated.
• Level III activations are designed to capture patients who do not require an immediate lifesaving intervention; the presence of the trauma surgery chief resident and attending emergency medicine physician is mandatory.
Patients were considered undertriaged if they were admitted as level III activations, but then required a critical intervention (chest tube placement, intubation, needle thoracostomy, or intracranial pressure monitoring) in the emergency department or ultimately met level I or II activation criteria.
Among all the level III patients, 466 (6%) were undertriaged: 390 were undertriaged based on the existing level I or II activation criteria, and 76 were considered undertriaged based on the need for a critical intervention.
Most of the undertriaged patients (65%) met criteria for level I activation; the rest should have been triaged as level II patients. Compared with appropriately staged level III patients, mortality among the undertriaged patients was significantly higher (3.2% vs. 0.6%). Undertriaged patients also experienced longer delays before initiation of major emergency surgery: a mean of 147 minutes, compared with 106 minutes for appropriately triaged level I patients and 62 minutes for appropriately triaged level II patients.
Dr. Yonge then looked for clinical measures that would improve triage. Tachypnea (respiratory rate of more than 20 breaths per minute) in the field stood out as a significant factor. Tachypneic patients who had a suspected chest injury were 70% more likely to be undertriaged than were those with a normal respiratory rate. Tachypnea was significantly associated with a diagnosis of flail chest, emergency department intubation, and chest tube placement.
The team then constructed a new triage criterion for patients with suspected chest injury – tachypnea combined with suspected blunt thoracic injury. By applying that model to their study population of level III patients, they determined that the level III undertriage rate would be reduced by 1.2%.
Tying the physiologic marker of tachypnea to a suspected clinical diagnosis is a key factor, Dr. Yonge noted. “Just adding tachypnea doesn’t help us. In fact, it would overwhelm us, because a trauma patient could very well be tachypneic because he’s experiencing panic. But tying it to a suspected clinical diagnosis gives us a meaningful result.”
He confirmed this linkage with an additional analysis. “We looked to see how severely injured these patients were and found that 71% of them had an Abbreviated Injury Score (AIS) to the chest of 3 or more, indicating a severe chest injury. Only 29% had an AIS of 2 or less. So this proves that respiratory rate is a valid triage criterion and can be used to identify patients who need a higher level of trauma care.”
The challenge now, Dr. Yonge said, is incorporating the marker into clinical practice. “It doesn’t matter how many statistics you do, if you can’t educate the prehospital providers in this, it’s useless. They are the crux of the trauma system.”
Although national guidelines do recommend assessing respiratory rate as part of field triage, it often isn’t recorded or is only estimated, Dr. Yonge said. That’s one reason he used the 20-breaths-per-minute cutoff rate. “It doesn’t even take a full minute to assess this, but it can make a big improvement in care.”
Neither he nor Dr. Schreiber had any financial disclosures.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
AT THE ACS CLINICAL CONGRESS
Key clinical point:
Major finding: Adding a triage assessment criterion of tachypnea plus suspected chest injury improved undertriage of chest trauma patients by 1.2%.
Data source: The retrospective database study comprising 7,880 patients.
Disclosures: Neither Dr. Yonge nor Dr. Schreiber had any financial disclosures.
Impact of Medicaid expansion on inpatient outcomes
The Affordable Care Act (ACA) has greatly increased the number of Medicaid enrollees since it expanded eligibility criteria on Jan. 1, 2014. Nearly 9 million additional U.S. adults now have Medicaid coverage, mostly in the 31 states and Washington, which have opted into Medicaid expansion.
The ACA has also had an important impact on hospital payer mix, mainly by decreasing the amount of uncompensated care in Medicaid-expansion states. Previous studies have shown disparities in the quality of inpatient care based on insurance type. Patients with Medicaid insurance often have longer hospitalizations and higher in-hospital mortality than commercially-insured patients and occasionally even than uninsured patients.
In our study published in the Journal of Hospital Medicine (2016 Dec. doi: 10.1002/jhm.2649), we evaluated the impact of state Medicaid expansion status on payer mix, length of stay, and in-hospital mortality for general medicine patients discharged from U.S. academic medical centers. We considered Jan. 1, 2014, to be the date of ACA implementation for all states except Michigan, New Hampshire, Pennsylvania, and Indiana, which had unique dates of Medicaid expansion.
We were able to identify 3,144,488 discharges from 156 hospitals in 24 Medicaid-expansion states and Washington, and 1,114,464 discharges from 55 hospitals in 14 nonexpansion states between October 2012 and September 2015.

Despite this difference in payer mix trends, state Medicaid expansion status was not associated with differences in overall length of stay or in-hospital mortality in our study. More precisely, we looked at the length of stay and mortality indices, or ratio of observed to expected values, to control for such potential confounders as disease severity and comorbid conditions.
One possible explanation for our findings is that the higher proportion of Medicare and commercially-insured patients overshadowed the contribution of Medicaid patients to the overall length of stay and mortality indices.
To our knowledge, our study is the first to look at the effect of ACA implementation on inpatient outcomes. Early evidence suggests that Medicaid expansion has improved outpatient outcomes. Low-income adults in Medicaid-expansion states have shown greater gains in access to primary care clinics and medications and in the diagnosis of certain chronic health conditions than those in non-expansion states. However, these changes would not necessarily lead to improvements in the length of stay or mortality indices for Medicaid-expansion hospitals, since the measures account for patient acuity on admission.
The take-home message from our study for health policy makers is that state Medicaid expansion status had a neutral effect on both length of stay and mortality indices. This should be reassuring for states considering expansion of their Medicaid programs in the future.
As a next step, it would be useful to see research on the impact of ACA implementation on other inpatient outcomes that may vary with insurance type, such as readmissions or hospital-acquired complications.
The take-home message for hospitalists is that there is more work to be done in reducing disparities in inpatient care based on payer status. Though not a primary focus of our study, we did see variation in the length of stay and mortality indices based on insurance type.
It is unclear whether these differences occurred because of variation in the expertise of inpatient providers, access to invasive procedures or medical therapies, the timeliness of discharge to post-acute care facilities, or other patient- or system-level factors. However, these disparities warrant our improvement efforts moving forward.
Mary Anderson, MD, and Christine Jones, MD, are hospitalists at the University of Colorado (Aurora) Hospital and assistant professors in the department of medicine at the University of Colorado.
The Affordable Care Act (ACA) has greatly increased the number of Medicaid enrollees since it expanded eligibility criteria on Jan. 1, 2014. Nearly 9 million additional U.S. adults now have Medicaid coverage, mostly in the 31 states and Washington, which have opted into Medicaid expansion.
The ACA has also had an important impact on hospital payer mix, mainly by decreasing the amount of uncompensated care in Medicaid-expansion states. Previous studies have shown disparities in the quality of inpatient care based on insurance type. Patients with Medicaid insurance often have longer hospitalizations and higher in-hospital mortality than commercially-insured patients and occasionally even than uninsured patients.
In our study published in the Journal of Hospital Medicine (2016 Dec. doi: 10.1002/jhm.2649), we evaluated the impact of state Medicaid expansion status on payer mix, length of stay, and in-hospital mortality for general medicine patients discharged from U.S. academic medical centers. We considered Jan. 1, 2014, to be the date of ACA implementation for all states except Michigan, New Hampshire, Pennsylvania, and Indiana, which had unique dates of Medicaid expansion.
We were able to identify 3,144,488 discharges from 156 hospitals in 24 Medicaid-expansion states and Washington, and 1,114,464 discharges from 55 hospitals in 14 nonexpansion states between October 2012 and September 2015.
Despite this difference in payer mix trends, state Medicaid expansion status was not associated with differences in overall length of stay or in-hospital mortality in our study. More precisely, we looked at the length of stay and mortality indices, or ratio of observed to expected values, to control for such potential confounders as disease severity and comorbid conditions.
One possible explanation for our findings is that the higher proportion of Medicare and commercially-insured patients overshadowed the contribution of Medicaid patients to the overall length of stay and mortality indices.
To our knowledge, our study is the first to look at the effect of ACA implementation on inpatient outcomes. Early evidence suggests that Medicaid expansion has improved outpatient outcomes. Low-income adults in Medicaid-expansion states have shown greater gains in access to primary care clinics and medications and in the diagnosis of certain chronic health conditions than those in non-expansion states. However, these changes would not necessarily lead to improvements in the length of stay or mortality indices for Medicaid-expansion hospitals, since the measures account for patient acuity on admission.
The take-home message from our study for health policy makers is that state Medicaid expansion status had a neutral effect on both length of stay and mortality indices. This should be reassuring for states considering expansion of their Medicaid programs in the future.
As a next step, it would be useful to see research on the impact of ACA implementation on other inpatient outcomes that may vary with insurance type, such as readmissions or hospital-acquired complications.
The take-home message for hospitalists is that there is more work to be done in reducing disparities in inpatient care based on payer status. Though not a primary focus of our study, we did see variation in the length of stay and mortality indices based on insurance type.
It is unclear whether these differences occurred because of variation in the expertise of inpatient providers, access to invasive procedures or medical therapies, the timeliness of discharge to post-acute care facilities, or other patient- or system-level factors. However, these disparities warrant our improvement efforts moving forward.
Mary Anderson, MD, and Christine Jones, MD, are hospitalists at the University of Colorado (Aurora) Hospital and assistant professors in the department of medicine at the University of Colorado.
The Affordable Care Act (ACA) has greatly increased the number of Medicaid enrollees since it expanded eligibility criteria on Jan. 1, 2014. Nearly 9 million additional U.S. adults now have Medicaid coverage, mostly in the 31 states and Washington, which have opted into Medicaid expansion.
The ACA has also had an important impact on hospital payer mix, mainly by decreasing the amount of uncompensated care in Medicaid-expansion states. Previous studies have shown disparities in the quality of inpatient care based on insurance type. Patients with Medicaid insurance often have longer hospitalizations and higher in-hospital mortality than commercially-insured patients and occasionally even than uninsured patients.
In our study published in the Journal of Hospital Medicine (2016 Dec. doi: 10.1002/jhm.2649), we evaluated the impact of state Medicaid expansion status on payer mix, length of stay, and in-hospital mortality for general medicine patients discharged from U.S. academic medical centers. We considered Jan. 1, 2014, to be the date of ACA implementation for all states except Michigan, New Hampshire, Pennsylvania, and Indiana, which had unique dates of Medicaid expansion.
We were able to identify 3,144,488 discharges from 156 hospitals in 24 Medicaid-expansion states and Washington, and 1,114,464 discharges from 55 hospitals in 14 nonexpansion states between October 2012 and September 2015.
Despite this difference in payer mix trends, state Medicaid expansion status was not associated with differences in overall length of stay or in-hospital mortality in our study. More precisely, we looked at the length of stay and mortality indices, or ratio of observed to expected values, to control for such potential confounders as disease severity and comorbid conditions.
One possible explanation for our findings is that the higher proportion of Medicare and commercially-insured patients overshadowed the contribution of Medicaid patients to the overall length of stay and mortality indices.
To our knowledge, our study is the first to look at the effect of ACA implementation on inpatient outcomes. Early evidence suggests that Medicaid expansion has improved outpatient outcomes. Low-income adults in Medicaid-expansion states have shown greater gains in access to primary care clinics and medications and in the diagnosis of certain chronic health conditions than those in non-expansion states. However, these changes would not necessarily lead to improvements in the length of stay or mortality indices for Medicaid-expansion hospitals, since the measures account for patient acuity on admission.
The take-home message from our study for health policy makers is that state Medicaid expansion status had a neutral effect on both length of stay and mortality indices. This should be reassuring for states considering expansion of their Medicaid programs in the future.
As a next step, it would be useful to see research on the impact of ACA implementation on other inpatient outcomes that may vary with insurance type, such as readmissions or hospital-acquired complications.
The take-home message for hospitalists is that there is more work to be done in reducing disparities in inpatient care based on payer status. Though not a primary focus of our study, we did see variation in the length of stay and mortality indices based on insurance type.
It is unclear whether these differences occurred because of variation in the expertise of inpatient providers, access to invasive procedures or medical therapies, the timeliness of discharge to post-acute care facilities, or other patient- or system-level factors. However, these disparities warrant our improvement efforts moving forward.
Mary Anderson, MD, and Christine Jones, MD, are hospitalists at the University of Colorado (Aurora) Hospital and assistant professors in the department of medicine at the University of Colorado.
VA Confronts Fallout of SAIL Facility Ratings
VA Secretary Robert McDonald minced few words in his reaction to the USA Today story that published VA’s 5-star ratings for VAMCs based on its Strategic Analytics for Improvement and Learning (SAIL) data. “What concerns all of us at VA is that USA Today has a consistent narrative of negativity in their news of VA,” McDonald charged. Specifically, use of the word secret in the headline was an “egregious hyperbole,” he insisted.
Still, within days, a number of VA facilities were using the story as an opportunity to tout their success. VA Central Western Massachusetts Healthcare System in Worcester, for example, used the opportunity to tell local media that it was “in the top 10% of the 152 VA medical centers in the nation for quality of care,” and 1 of 3 5-star facilities in Massachusetts.
Other facilities, however, were forced to explain the relative nature of the 5-star scale. Keith Sullivan, director of the Chillicothe VAMC in Ohio, which received a 3-star rating, responded to reporters by noting that, “Although SAIL is a tool that helps look at areas in need of improvements, we have many other ways to ensure quality care is in place,” he said.
Many VA officials point out that the comparison to other VA facilities may be unfair, especially in underserved locations. The VA Health Care Center at Harlingen in Texas recently improved from 1 to 2 stars. It received this score, in part, because of its difficulty filling open vacancies. “Compared to the nurse retention rates in our local communities we are doing very well, [but] not so much as compared to other VA health care systems in the nation,” a Harlingen customer service manager told a local newspaper.
To allay veterans’ fears, the VA Southern Oregon Rehabilitation Center and Clinics (VA SORCC) sent out a news release to explain the ratings and reassure the public that progress was being made even as it struggles with a shortage of providers. Insisting it had made “absolute performance improvements in wait times for both mental health and specialty care appointments” while acknowledging that the rating also shows “continued frustrations with difficulty in navigating the system and with coordination of care." These frustrations impact Veterans’ experience at the facility, leading to lower scores.” The release pledged that “VA SORCC is currently a 1-star facility but fully expects to move to a 2-star facility in the next quarter.”
The worry for many at the VA is that the veterans might avoid 1- and 2-star facilities. “My concern is that veterans are going to see that their hospital is a ‘one’ in our star system, assume that’s bad quality and veterans that need care are not going to get care,” VA Under Secretary of Health David J. Shulkin, MD, told USA Today. “And they’re going to stay away from hospitals and that’s going to hurt people.”
VA Secretary Robert McDonald minced few words in his reaction to the USA Today story that published VA’s 5-star ratings for VAMCs based on its Strategic Analytics for Improvement and Learning (SAIL) data. “What concerns all of us at VA is that USA Today has a consistent narrative of negativity in their news of VA,” McDonald charged. Specifically, use of the word secret in the headline was an “egregious hyperbole,” he insisted.
Still, within days, a number of VA facilities were using the story as an opportunity to tout their success. VA Central Western Massachusetts Healthcare System in Worcester, for example, used the opportunity to tell local media that it was “in the top 10% of the 152 VA medical centers in the nation for quality of care,” and 1 of 3 5-star facilities in Massachusetts.
Other facilities, however, were forced to explain the relative nature of the 5-star scale. Keith Sullivan, director of the Chillicothe VAMC in Ohio, which received a 3-star rating, responded to reporters by noting that, “Although SAIL is a tool that helps look at areas in need of improvements, we have many other ways to ensure quality care is in place,” he said.
Many VA officials point out that the comparison to other VA facilities may be unfair, especially in underserved locations. The VA Health Care Center at Harlingen in Texas recently improved from 1 to 2 stars. It received this score, in part, because of its difficulty filling open vacancies. “Compared to the nurse retention rates in our local communities we are doing very well, [but] not so much as compared to other VA health care systems in the nation,” a Harlingen customer service manager told a local newspaper.
To allay veterans’ fears, the VA Southern Oregon Rehabilitation Center and Clinics (VA SORCC) sent out a news release to explain the ratings and reassure the public that progress was being made even as it struggles with a shortage of providers. Insisting it had made “absolute performance improvements in wait times for both mental health and specialty care appointments” while acknowledging that the rating also shows “continued frustrations with difficulty in navigating the system and with coordination of care." These frustrations impact Veterans’ experience at the facility, leading to lower scores.” The release pledged that “VA SORCC is currently a 1-star facility but fully expects to move to a 2-star facility in the next quarter.”
The worry for many at the VA is that the veterans might avoid 1- and 2-star facilities. “My concern is that veterans are going to see that their hospital is a ‘one’ in our star system, assume that’s bad quality and veterans that need care are not going to get care,” VA Under Secretary of Health David J. Shulkin, MD, told USA Today. “And they’re going to stay away from hospitals and that’s going to hurt people.”
VA Secretary Robert McDonald minced few words in his reaction to the USA Today story that published VA’s 5-star ratings for VAMCs based on its Strategic Analytics for Improvement and Learning (SAIL) data. “What concerns all of us at VA is that USA Today has a consistent narrative of negativity in their news of VA,” McDonald charged. Specifically, use of the word secret in the headline was an “egregious hyperbole,” he insisted.
Still, within days, a number of VA facilities were using the story as an opportunity to tout their success. VA Central Western Massachusetts Healthcare System in Worcester, for example, used the opportunity to tell local media that it was “in the top 10% of the 152 VA medical centers in the nation for quality of care,” and 1 of 3 5-star facilities in Massachusetts.
Other facilities, however, were forced to explain the relative nature of the 5-star scale. Keith Sullivan, director of the Chillicothe VAMC in Ohio, which received a 3-star rating, responded to reporters by noting that, “Although SAIL is a tool that helps look at areas in need of improvements, we have many other ways to ensure quality care is in place,” he said.
Many VA officials point out that the comparison to other VA facilities may be unfair, especially in underserved locations. The VA Health Care Center at Harlingen in Texas recently improved from 1 to 2 stars. It received this score, in part, because of its difficulty filling open vacancies. “Compared to the nurse retention rates in our local communities we are doing very well, [but] not so much as compared to other VA health care systems in the nation,” a Harlingen customer service manager told a local newspaper.
To allay veterans’ fears, the VA Southern Oregon Rehabilitation Center and Clinics (VA SORCC) sent out a news release to explain the ratings and reassure the public that progress was being made even as it struggles with a shortage of providers. Insisting it had made “absolute performance improvements in wait times for both mental health and specialty care appointments” while acknowledging that the rating also shows “continued frustrations with difficulty in navigating the system and with coordination of care." These frustrations impact Veterans’ experience at the facility, leading to lower scores.” The release pledged that “VA SORCC is currently a 1-star facility but fully expects to move to a 2-star facility in the next quarter.”
The worry for many at the VA is that the veterans might avoid 1- and 2-star facilities. “My concern is that veterans are going to see that their hospital is a ‘one’ in our star system, assume that’s bad quality and veterans that need care are not going to get care,” VA Under Secretary of Health David J. Shulkin, MD, told USA Today. “And they’re going to stay away from hospitals and that’s going to hurt people.”
‘Unprecedented’ MRD negativity with daratumumab in MM

© Todd Buchanan 2016
SAN DIEGO—Daratumumab added to standard of care regimens drives deep clinical responses beyond complete response (CR), a magnitude that is “unprecedented” in the relapsed/refractory multiple myeloma (MM) setting, according to a speaker at the 2016 ASH Annual Meeting.
Investigators added daratumumab to lenalidomide/dexamethasone in the POLLUX trial and to bortezomib/dexamethasone in the CASTOR trial.
In both phase 3 trials, the addition of daratumumab resulted in significant improvements in progression-free survival (PFS), overall response rate, and minimal residual disease (MRD) negativity when compared to control groups.
“The magnitude of daratumumab-induced MRD negativity in the relapsed setting is unprecedented and, for me, was not expected,” said Hervé Avet-Loiseau, MD, of Centre Hospitalier Universitaire Rangueil, Unité de Genomique du Myelome in Toulouse, France.
Dr Avet-Loiseau presented the MRD findings from CASTOR and POLLUX at the ASH Annual Meeting as abstract 246.*
He noted that, based on these studies, daratumumab received US Food and Drug Administration approvals for use in combination with standard of care regimens for MM patients who had received 1 or more prior lines of treatment.
Daratumumab had been previously approved as monotherapy for relapsed or refractory MM.
Study designs and findings from the POLLUX and CASTOR trials have been described earlier in Hematology Times.
Dr Avet-Loiseau provided updated PFS figures for the 2 studies.
At 18 months’ follow-up in the POLLUX study, the PFS rate for patients treated with daratumumab/lenalidomide/dexamethasone was 76%, compared to 49% in the lenalidomide/dexamethasone arm (P<0.0001).
At 12 months’ follow-up in the CASTOR study, the PFS with daratumumab was 60%, compared to 22% for bortezomib/dexamethasone (P<0.0001).
MRD criteria
In both studies, MRD assessments were conducted at suspected complete response (CR). Assessments were also conducted at 3 months and 6 months after CR in the POLLUX study and at 6 months and 12 months after the first study dose in the CASTOR study.
For the assessment of MRD, investigators used bone marrow aspirate samples and the ClonoSEQTM NGS-based assay.
Investigators evaluated MRD at 3 sensitivity thresholds: 10-4, 10-5, and 10-6.
And they used a stringent, unbiased evaluation, Dr Avet-Loiseau said. Any patient in the intent-to-treat population who was not assessed to be MRD negative was scored as MRD positive.
And the minimum cell input equivalent to the sensitivity threshold was required to determine MRD negativity.
MRD results
In the POLLUX study, 24.8% of patients achieved MRD negativity at the 10-5 cutoff, and 11.9% achieved MRD negativity at the 10-6 cutoff with the daratumumab combination.
This compared to 5.7% and 2.5% MRD negativity at the 10-5 and 10-6 cutoffs, respectively, without daratumumab (P<0.0001).
In the CASTOR study, the daratumumab-treated patients achieved 10.4% and 4.4% MRD negativity at the 10-5 and 10-6 cutoffs, respectively.
This compared to 2.4% and 0.8% MRD negativity in the control arm at the 10-5 and 10-6 cutoffs (P<0.005 and P<0.05), respectively.
“So, definitely, the addition of daratumumab improved the MRD negativity rate in both studies,” Dr Avet-Loiseau said.
“If you just look at the patients who did achieve CR in the POLLUX study, almost 50% of the patients [treated with daratumumab] achieved CR, and half of them were MRD negative at the cutoff of 10-5.”
In the CASTOR study, 25% of the patients treated with daratumumab achieved a CR. The MRD negativity rate was one-third in these patients.
“So again, we have consistently higher MRD negative rates in patients who achieve CR when they were treated in the daratumumab arms,” Dr Avet-Loiseau said.
“What is interesting, I think, is that the achievement of molecular CR was very rapid. [A]t 3 months, some patients did already achieve MRD negativity, and so we continued to see an improvement. [W]e still continue to see some achievement of MRD negativity.”
Investigators continue to follow the patients annually.
The investigators also analyzed MRD at 10-5 by cytogenetic risk and did not observe any MRD negativity in the control arm in either the POLLUX or CASTOR study.
“In contrast, we did observe some significant MRD negativity in the experimental arm with daratumumab—18% (POLLUX) and 14% (CASTOR) in high-risk patients,” Dr Avet-Loiseau said. “The most important prognostic factor is to achieve MRD negativity.”
However, even for patients who did not achieve MRD negativity, the PFS was much better in the experimental arms than in the control arms, he added.
This study, presented as a “Best of ASH” abstract, was funded by Janssen Research & Development, LLC. ![]()
*Information in the abstract differs from that presented at the meeting.
© Todd Buchanan 2016
SAN DIEGO—Daratumumab added to standard of care regimens drives deep clinical responses beyond complete response (CR), a magnitude that is “unprecedented” in the relapsed/refractory multiple myeloma (MM) setting, according to a speaker at the 2016 ASH Annual Meeting.
Investigators added daratumumab to lenalidomide/dexamethasone in the POLLUX trial and to bortezomib/dexamethasone in the CASTOR trial.
In both phase 3 trials, the addition of daratumumab resulted in significant improvements in progression-free survival (PFS), overall response rate, and minimal residual disease (MRD) negativity when compared to control groups.
“The magnitude of daratumumab-induced MRD negativity in the relapsed setting is unprecedented and, for me, was not expected,” said Hervé Avet-Loiseau, MD, of Centre Hospitalier Universitaire Rangueil, Unité de Genomique du Myelome in Toulouse, France.
Dr Avet-Loiseau presented the MRD findings from CASTOR and POLLUX at the ASH Annual Meeting as abstract 246.*
He noted that, based on these studies, daratumumab received US Food and Drug Administration approvals for use in combination with standard of care regimens for MM patients who had received 1 or more prior lines of treatment.
Daratumumab had been previously approved as monotherapy for relapsed or refractory MM.
Study designs and findings from the POLLUX and CASTOR trials have been described earlier in Hematology Times.
Dr Avet-Loiseau provided updated PFS figures for the 2 studies.
At 18 months’ follow-up in the POLLUX study, the PFS rate for patients treated with daratumumab/lenalidomide/dexamethasone was 76%, compared to 49% in the lenalidomide/dexamethasone arm (P<0.0001).
At 12 months’ follow-up in the CASTOR study, the PFS with daratumumab was 60%, compared to 22% for bortezomib/dexamethasone (P<0.0001).
MRD criteria
In both studies, MRD assessments were conducted at suspected complete response (CR). Assessments were also conducted at 3 months and 6 months after CR in the POLLUX study and at 6 months and 12 months after the first study dose in the CASTOR study.
For the assessment of MRD, investigators used bone marrow aspirate samples and the ClonoSEQTM NGS-based assay.
Investigators evaluated MRD at 3 sensitivity thresholds: 10-4, 10-5, and 10-6.
And they used a stringent, unbiased evaluation, Dr Avet-Loiseau said. Any patient in the intent-to-treat population who was not assessed to be MRD negative was scored as MRD positive.
And the minimum cell input equivalent to the sensitivity threshold was required to determine MRD negativity.
MRD results
In the POLLUX study, 24.8% of patients achieved MRD negativity at the 10-5 cutoff, and 11.9% achieved MRD negativity at the 10-6 cutoff with the daratumumab combination.
This compared to 5.7% and 2.5% MRD negativity at the 10-5 and 10-6 cutoffs, respectively, without daratumumab (P<0.0001).
In the CASTOR study, the daratumumab-treated patients achieved 10.4% and 4.4% MRD negativity at the 10-5 and 10-6 cutoffs, respectively.
This compared to 2.4% and 0.8% MRD negativity in the control arm at the 10-5 and 10-6 cutoffs (P<0.005 and P<0.05), respectively.
“So, definitely, the addition of daratumumab improved the MRD negativity rate in both studies,” Dr Avet-Loiseau said.
“If you just look at the patients who did achieve CR in the POLLUX study, almost 50% of the patients [treated with daratumumab] achieved CR, and half of them were MRD negative at the cutoff of 10-5.”
In the CASTOR study, 25% of the patients treated with daratumumab achieved a CR. The MRD negativity rate was one-third in these patients.
“So again, we have consistently higher MRD negative rates in patients who achieve CR when they were treated in the daratumumab arms,” Dr Avet-Loiseau said.
“What is interesting, I think, is that the achievement of molecular CR was very rapid. [A]t 3 months, some patients did already achieve MRD negativity, and so we continued to see an improvement. [W]e still continue to see some achievement of MRD negativity.”
Investigators continue to follow the patients annually.
The investigators also analyzed MRD at 10-5 by cytogenetic risk and did not observe any MRD negativity in the control arm in either the POLLUX or CASTOR study.
“In contrast, we did observe some significant MRD negativity in the experimental arm with daratumumab—18% (POLLUX) and 14% (CASTOR) in high-risk patients,” Dr Avet-Loiseau said. “The most important prognostic factor is to achieve MRD negativity.”
However, even for patients who did not achieve MRD negativity, the PFS was much better in the experimental arms than in the control arms, he added.
This study, presented as a “Best of ASH” abstract, was funded by Janssen Research & Development, LLC. ![]()
*Information in the abstract differs from that presented at the meeting.
© Todd Buchanan 2016
SAN DIEGO—Daratumumab added to standard of care regimens drives deep clinical responses beyond complete response (CR), a magnitude that is “unprecedented” in the relapsed/refractory multiple myeloma (MM) setting, according to a speaker at the 2016 ASH Annual Meeting.
Investigators added daratumumab to lenalidomide/dexamethasone in the POLLUX trial and to bortezomib/dexamethasone in the CASTOR trial.
In both phase 3 trials, the addition of daratumumab resulted in significant improvements in progression-free survival (PFS), overall response rate, and minimal residual disease (MRD) negativity when compared to control groups.
“The magnitude of daratumumab-induced MRD negativity in the relapsed setting is unprecedented and, for me, was not expected,” said Hervé Avet-Loiseau, MD, of Centre Hospitalier Universitaire Rangueil, Unité de Genomique du Myelome in Toulouse, France.
Dr Avet-Loiseau presented the MRD findings from CASTOR and POLLUX at the ASH Annual Meeting as abstract 246.*
He noted that, based on these studies, daratumumab received US Food and Drug Administration approvals for use in combination with standard of care regimens for MM patients who had received 1 or more prior lines of treatment.
Daratumumab had been previously approved as monotherapy for relapsed or refractory MM.
Study designs and findings from the POLLUX and CASTOR trials have been described earlier in Hematology Times.
Dr Avet-Loiseau provided updated PFS figures for the 2 studies.
At 18 months’ follow-up in the POLLUX study, the PFS rate for patients treated with daratumumab/lenalidomide/dexamethasone was 76%, compared to 49% in the lenalidomide/dexamethasone arm (P<0.0001).
At 12 months’ follow-up in the CASTOR study, the PFS with daratumumab was 60%, compared to 22% for bortezomib/dexamethasone (P<0.0001).
MRD criteria
In both studies, MRD assessments were conducted at suspected complete response (CR). Assessments were also conducted at 3 months and 6 months after CR in the POLLUX study and at 6 months and 12 months after the first study dose in the CASTOR study.
For the assessment of MRD, investigators used bone marrow aspirate samples and the ClonoSEQTM NGS-based assay.
Investigators evaluated MRD at 3 sensitivity thresholds: 10-4, 10-5, and 10-6.
And they used a stringent, unbiased evaluation, Dr Avet-Loiseau said. Any patient in the intent-to-treat population who was not assessed to be MRD negative was scored as MRD positive.
And the minimum cell input equivalent to the sensitivity threshold was required to determine MRD negativity.
MRD results
In the POLLUX study, 24.8% of patients achieved MRD negativity at the 10-5 cutoff, and 11.9% achieved MRD negativity at the 10-6 cutoff with the daratumumab combination.
This compared to 5.7% and 2.5% MRD negativity at the 10-5 and 10-6 cutoffs, respectively, without daratumumab (P<0.0001).
In the CASTOR study, the daratumumab-treated patients achieved 10.4% and 4.4% MRD negativity at the 10-5 and 10-6 cutoffs, respectively.
This compared to 2.4% and 0.8% MRD negativity in the control arm at the 10-5 and 10-6 cutoffs (P<0.005 and P<0.05), respectively.
“So, definitely, the addition of daratumumab improved the MRD negativity rate in both studies,” Dr Avet-Loiseau said.
“If you just look at the patients who did achieve CR in the POLLUX study, almost 50% of the patients [treated with daratumumab] achieved CR, and half of them were MRD negative at the cutoff of 10-5.”
In the CASTOR study, 25% of the patients treated with daratumumab achieved a CR. The MRD negativity rate was one-third in these patients.
“So again, we have consistently higher MRD negative rates in patients who achieve CR when they were treated in the daratumumab arms,” Dr Avet-Loiseau said.
“What is interesting, I think, is that the achievement of molecular CR was very rapid. [A]t 3 months, some patients did already achieve MRD negativity, and so we continued to see an improvement. [W]e still continue to see some achievement of MRD negativity.”
Investigators continue to follow the patients annually.
The investigators also analyzed MRD at 10-5 by cytogenetic risk and did not observe any MRD negativity in the control arm in either the POLLUX or CASTOR study.
“In contrast, we did observe some significant MRD negativity in the experimental arm with daratumumab—18% (POLLUX) and 14% (CASTOR) in high-risk patients,” Dr Avet-Loiseau said. “The most important prognostic factor is to achieve MRD negativity.”
However, even for patients who did not achieve MRD negativity, the PFS was much better in the experimental arms than in the control arms, he added.
This study, presented as a “Best of ASH” abstract, was funded by Janssen Research & Development, LLC. ![]()
*Information in the abstract differs from that presented at the meeting.
How old is too old to be on a kids’ protocol for ALL?

Photo by Bill Branson
SAN DIEGO—In recent years, pediatric or pediatric-inspired protocols have become the preferred treatment approach for younger adults with acute lymphoblastic leukemia (ALL).
These protocols include higher doses of steroids, vincristine, methotrexate, and L-asparaginase.
However, the upper age limit for this strategy has not been defined.
With the GRAALL-2005 study, investigators set out to determine how old is too old to be treated on pediatric protocols.
Their results suggest 55 is likely the upper age limit for patients with Ph-negative ALL.
The investigators also evaluated a hyper-fractionated (hyper-C) versus standard dose (standard-C) of cyclophosphamide during induction and late intensification.
They found that hyper-C did not provide an event-free survival (EFS) benefit in the overall study population, but patients age 55 and older did appear to benefit from hyper-C.
Françoise Huguet, MD, of the Institut Universitaire du Cancer de Toulouse in Toulouse, France, presented these findings at the 2016 ASH Annual Meeting (abstract 762).
GRAALL investigators had previously evaluated a pediatric-inspired protocol for adult patients in the GRAALL-2003 study, which validated the approach.
Study design
Patients with newly diagnosed, Ph-negative ALL were eligible to enroll if they were 18 to 59 years of age.
Treatment comprised a steroid pre-phase, a 5-drug induction, two 3-block dose-dense consolidation phases, a late intensification, a third consolidation phase, CNS irradiation, and a 2-year maintenance phase.
Patients could proceed to allogeneic transplant in first complete remission (CR) if eligible.
During induction and late intensification, patients received cyclophosphamide at 750 mg/m2 on day 1 and were then randomized to hyper-C (300 mg/m2/every 12 hours on days 15 to 17) or standard-C (750 mg/m2 on day 15).
The primary endpoint was EFS.
Patient population
Investigators randomized 787 evaluable patients—398 in the standard-C arm and 389 in the hyper-C arm.
Their median age was 36 years, 67% of patients had B-cell precursor ALL, and 33% had T-ALL.
Most had high-risk ALL, 72% of them receiving standard-C and 66% receiving hyper-C.
About a third of the patients in each arm proceeded to allogeneic stem cell transplant in first CR.
Results
The CR rate after induction therapy was 90.2% in the standard-C arm and 93.6% in the hyper-C arm, for an overall CR rate of 92%.
Most patients—87.5% in the standard-C arm and 91.8% in the hyper-C arm—achieved a response in 1 course of therapy.
Sixty percent of patients tested in the standard-C arm and 66% of those tested in the hyper-C arm were minimal residual disease negative at less than 10-4.
There were 26 (6.5%) deaths in the standard-C arm and 18 (4.6%) in the hyper-C arm.
The 5-year EFS rate was 52% overall, and hyper-C treatment had no impact on EFS (hazard ratio=0.89 [range, 0.7-1.1]; P=0.26).
Impact of age
Investigators conducted a post-hoc subgroup analysis of 5 age groups—18-24 years (n=200), 25-34 (n=172), 35-44 (n=171), 45-54 (n=151), and 55+ (n=93).
Overall, the CR rate tended to decrease with age. The rates were 98.5% (18-24), 95.3% (25-34), 87.7% (35-44), 89.4% (45-54), and 79.6% (55+).
Induction death rates increased from 0.5% in the youngest group to 18.3% in the oldest, but the rate of cumulative incidences of failure at 5 years was similar among all the age groups.
The cumulative incidence of treatment-related mortality, without censoring for transplant, ranged from 7.6% in the youngest group to 39.7% in the oldest.
And the 5-year EFS for the youngest patients was 60%, while, for the oldest, it was 26%.
“Above 50 years, the increase in age became highly significant,” Dr Huguet emphasized. “There were fewer CRs and lower survival.”
Treatment compliance
In terms of treatment compliance and median dose received in the induction course, patients aged 55-59 received significantly less L-asparaginase than those aged 18-54 (P<0.001).
During all 3 consolidation phases, patients aged 55-59 received significantly lower median doses of all medications—cytarabine, methotrexate, cyclophosphamide—than patients aged 18-54.
And in late intensification, patients aged 55-59 received significantly lower median doses of vincristine, prednisone, daunorubicin, and hyper-C than all other patients. The median doses of L-asparaginase and standard-C received were lower in the older patients but not significantly so.
EFS by age and randomization
The 5-year EFS for patients aged 18-54 was 57% with hyper-C, compared with 55% in the standard-C arm (P=0.66).
However, for older patients, there was a significant advantage for those receiving hyper-C. The 5-year EFS was 38% with hyper-C, compared to 12% with standard-C (P=0.007).
Dr Huguet explained that inferior compliance in patients 55 and older “might explain why a benefit associated with early hyper-C reinforcement became apparent in these older patients only.”
Dr Huguet concluded that the results “suggest that 55 years is likely to be the upper age limit to tolerate a pediatric-like therapy for younger adults with Ph-negative ALL.”
She added that patients over 54 might benefit from alternative front-line strategies.
Accordingly, investigators are planning to use new agents, such as blinatumomab or inotuzumab ozogamicin, in the next European Working Group on Adult ALL studies. ![]()
Photo by Bill Branson
SAN DIEGO—In recent years, pediatric or pediatric-inspired protocols have become the preferred treatment approach for younger adults with acute lymphoblastic leukemia (ALL).
These protocols include higher doses of steroids, vincristine, methotrexate, and L-asparaginase.
However, the upper age limit for this strategy has not been defined.
With the GRAALL-2005 study, investigators set out to determine how old is too old to be treated on pediatric protocols.
Their results suggest 55 is likely the upper age limit for patients with Ph-negative ALL.
The investigators also evaluated a hyper-fractionated (hyper-C) versus standard dose (standard-C) of cyclophosphamide during induction and late intensification.
They found that hyper-C did not provide an event-free survival (EFS) benefit in the overall study population, but patients age 55 and older did appear to benefit from hyper-C.
Françoise Huguet, MD, of the Institut Universitaire du Cancer de Toulouse in Toulouse, France, presented these findings at the 2016 ASH Annual Meeting (abstract 762).
GRAALL investigators had previously evaluated a pediatric-inspired protocol for adult patients in the GRAALL-2003 study, which validated the approach.
Study design
Patients with newly diagnosed, Ph-negative ALL were eligible to enroll if they were 18 to 59 years of age.
Treatment comprised a steroid pre-phase, a 5-drug induction, two 3-block dose-dense consolidation phases, a late intensification, a third consolidation phase, CNS irradiation, and a 2-year maintenance phase.
Patients could proceed to allogeneic transplant in first complete remission (CR) if eligible.
During induction and late intensification, patients received cyclophosphamide at 750 mg/m2 on day 1 and were then randomized to hyper-C (300 mg/m2/every 12 hours on days 15 to 17) or standard-C (750 mg/m2 on day 15).
The primary endpoint was EFS.
Patient population
Investigators randomized 787 evaluable patients—398 in the standard-C arm and 389 in the hyper-C arm.
Their median age was 36 years, 67% of patients had B-cell precursor ALL, and 33% had T-ALL.
Most had high-risk ALL, 72% of them receiving standard-C and 66% receiving hyper-C.
About a third of the patients in each arm proceeded to allogeneic stem cell transplant in first CR.
Results
The CR rate after induction therapy was 90.2% in the standard-C arm and 93.6% in the hyper-C arm, for an overall CR rate of 92%.
Most patients—87.5% in the standard-C arm and 91.8% in the hyper-C arm—achieved a response in 1 course of therapy.
Sixty percent of patients tested in the standard-C arm and 66% of those tested in the hyper-C arm were minimal residual disease negative at less than 10-4.
There were 26 (6.5%) deaths in the standard-C arm and 18 (4.6%) in the hyper-C arm.
The 5-year EFS rate was 52% overall, and hyper-C treatment had no impact on EFS (hazard ratio=0.89 [range, 0.7-1.1]; P=0.26).
Impact of age
Investigators conducted a post-hoc subgroup analysis of 5 age groups—18-24 years (n=200), 25-34 (n=172), 35-44 (n=171), 45-54 (n=151), and 55+ (n=93).
Overall, the CR rate tended to decrease with age. The rates were 98.5% (18-24), 95.3% (25-34), 87.7% (35-44), 89.4% (45-54), and 79.6% (55+).
Induction death rates increased from 0.5% in the youngest group to 18.3% in the oldest, but the rate of cumulative incidences of failure at 5 years was similar among all the age groups.
The cumulative incidence of treatment-related mortality, without censoring for transplant, ranged from 7.6% in the youngest group to 39.7% in the oldest.
And the 5-year EFS for the youngest patients was 60%, while, for the oldest, it was 26%.
“Above 50 years, the increase in age became highly significant,” Dr Huguet emphasized. “There were fewer CRs and lower survival.”
Treatment compliance
In terms of treatment compliance and median dose received in the induction course, patients aged 55-59 received significantly less L-asparaginase than those aged 18-54 (P<0.001).
During all 3 consolidation phases, patients aged 55-59 received significantly lower median doses of all medications—cytarabine, methotrexate, cyclophosphamide—than patients aged 18-54.
And in late intensification, patients aged 55-59 received significantly lower median doses of vincristine, prednisone, daunorubicin, and hyper-C than all other patients. The median doses of L-asparaginase and standard-C received were lower in the older patients but not significantly so.
EFS by age and randomization
The 5-year EFS for patients aged 18-54 was 57% with hyper-C, compared with 55% in the standard-C arm (P=0.66).
However, for older patients, there was a significant advantage for those receiving hyper-C. The 5-year EFS was 38% with hyper-C, compared to 12% with standard-C (P=0.007).
Dr Huguet explained that inferior compliance in patients 55 and older “might explain why a benefit associated with early hyper-C reinforcement became apparent in these older patients only.”
Dr Huguet concluded that the results “suggest that 55 years is likely to be the upper age limit to tolerate a pediatric-like therapy for younger adults with Ph-negative ALL.”
She added that patients over 54 might benefit from alternative front-line strategies.
Accordingly, investigators are planning to use new agents, such as blinatumomab or inotuzumab ozogamicin, in the next European Working Group on Adult ALL studies. ![]()
Photo by Bill Branson
SAN DIEGO—In recent years, pediatric or pediatric-inspired protocols have become the preferred treatment approach for younger adults with acute lymphoblastic leukemia (ALL).
These protocols include higher doses of steroids, vincristine, methotrexate, and L-asparaginase.
However, the upper age limit for this strategy has not been defined.
With the GRAALL-2005 study, investigators set out to determine how old is too old to be treated on pediatric protocols.
Their results suggest 55 is likely the upper age limit for patients with Ph-negative ALL.
The investigators also evaluated a hyper-fractionated (hyper-C) versus standard dose (standard-C) of cyclophosphamide during induction and late intensification.
They found that hyper-C did not provide an event-free survival (EFS) benefit in the overall study population, but patients age 55 and older did appear to benefit from hyper-C.
Françoise Huguet, MD, of the Institut Universitaire du Cancer de Toulouse in Toulouse, France, presented these findings at the 2016 ASH Annual Meeting (abstract 762).
GRAALL investigators had previously evaluated a pediatric-inspired protocol for adult patients in the GRAALL-2003 study, which validated the approach.
Study design
Patients with newly diagnosed, Ph-negative ALL were eligible to enroll if they were 18 to 59 years of age.
Treatment comprised a steroid pre-phase, a 5-drug induction, two 3-block dose-dense consolidation phases, a late intensification, a third consolidation phase, CNS irradiation, and a 2-year maintenance phase.
Patients could proceed to allogeneic transplant in first complete remission (CR) if eligible.
During induction and late intensification, patients received cyclophosphamide at 750 mg/m2 on day 1 and were then randomized to hyper-C (300 mg/m2/every 12 hours on days 15 to 17) or standard-C (750 mg/m2 on day 15).
The primary endpoint was EFS.
Patient population
Investigators randomized 787 evaluable patients—398 in the standard-C arm and 389 in the hyper-C arm.
Their median age was 36 years, 67% of patients had B-cell precursor ALL, and 33% had T-ALL.
Most had high-risk ALL, 72% of them receiving standard-C and 66% receiving hyper-C.
About a third of the patients in each arm proceeded to allogeneic stem cell transplant in first CR.
Results
The CR rate after induction therapy was 90.2% in the standard-C arm and 93.6% in the hyper-C arm, for an overall CR rate of 92%.
Most patients—87.5% in the standard-C arm and 91.8% in the hyper-C arm—achieved a response in 1 course of therapy.
Sixty percent of patients tested in the standard-C arm and 66% of those tested in the hyper-C arm were minimal residual disease negative at less than 10-4.
There were 26 (6.5%) deaths in the standard-C arm and 18 (4.6%) in the hyper-C arm.
The 5-year EFS rate was 52% overall, and hyper-C treatment had no impact on EFS (hazard ratio=0.89 [range, 0.7-1.1]; P=0.26).
Impact of age
Investigators conducted a post-hoc subgroup analysis of 5 age groups—18-24 years (n=200), 25-34 (n=172), 35-44 (n=171), 45-54 (n=151), and 55+ (n=93).
Overall, the CR rate tended to decrease with age. The rates were 98.5% (18-24), 95.3% (25-34), 87.7% (35-44), 89.4% (45-54), and 79.6% (55+).
Induction death rates increased from 0.5% in the youngest group to 18.3% in the oldest, but the rate of cumulative incidences of failure at 5 years was similar among all the age groups.
The cumulative incidence of treatment-related mortality, without censoring for transplant, ranged from 7.6% in the youngest group to 39.7% in the oldest.
And the 5-year EFS for the youngest patients was 60%, while, for the oldest, it was 26%.
“Above 50 years, the increase in age became highly significant,” Dr Huguet emphasized. “There were fewer CRs and lower survival.”
Treatment compliance
In terms of treatment compliance and median dose received in the induction course, patients aged 55-59 received significantly less L-asparaginase than those aged 18-54 (P<0.001).
During all 3 consolidation phases, patients aged 55-59 received significantly lower median doses of all medications—cytarabine, methotrexate, cyclophosphamide—than patients aged 18-54.
And in late intensification, patients aged 55-59 received significantly lower median doses of vincristine, prednisone, daunorubicin, and hyper-C than all other patients. The median doses of L-asparaginase and standard-C received were lower in the older patients but not significantly so.
EFS by age and randomization
The 5-year EFS for patients aged 18-54 was 57% with hyper-C, compared with 55% in the standard-C arm (P=0.66).
However, for older patients, there was a significant advantage for those receiving hyper-C. The 5-year EFS was 38% with hyper-C, compared to 12% with standard-C (P=0.007).
Dr Huguet explained that inferior compliance in patients 55 and older “might explain why a benefit associated with early hyper-C reinforcement became apparent in these older patients only.”
Dr Huguet concluded that the results “suggest that 55 years is likely to be the upper age limit to tolerate a pediatric-like therapy for younger adults with Ph-negative ALL.”
She added that patients over 54 might benefit from alternative front-line strategies.
Accordingly, investigators are planning to use new agents, such as blinatumomab or inotuzumab ozogamicin, in the next European Working Group on Adult ALL studies. ![]()
Two mutations may help drive CBF-AML

2016 ASH Annual Meeting
SAN DIEGO—Researchers have found evidence to suggest that mutations in the CCND1 and CCND2 genes may contribute to the development of core-binding factor acute myeloid leukemia (CBF-AML).
The team noted that CBF-AML is defined by the presence of either t(8;21)(q22;q22)/RUNX1-RUNX1T1 or inv(16)(p13.1q22)/t(16;16)(p13.1;q22)/CBFB-MYH11.
However, the fusion genes alone are not capable of causing CBF-AML.
“The hematology community has long sought to determine what other factors in addition to the fusion genes occur in this special type of leukemia,” said Ann-Kathrin Eisfeld, MD, of The Ohio State University Comprehensive Cancer Center in Columbus.
“We are now the first to describe that mutations in CCND1—and among the first to describe that mutations in the sister gene CCND2—are unique features of CBF-AML with t(8;21). In addition, we have collected the first evidence that mutations in CCND2 lead to more aggressive growth of leukemia cell lines.”
Dr Eisfeld and her colleagues reported these findings in a paper published in Leukemia and in a poster presented at the 2016 ASH Annual Meeting (abstract 2740).
A previous study of genetic mutations in CBF-AML revealed the presence of at least 1 mutation in 85% of patients studied. This meant the remaining 15% of patients harbored other, undiscovered mutations.
For the current study, Dr Eisfeld and her colleagues searched CBF-AML samples for the missing mutations that, together with the fusion genes, might contribute to the leukemia in this subgroup of cases.
The team analyzed pretreatment bone marrow and peripheral blood samples from 177 adult CBF-AML patients who received similar treatment through a clinical trial conducted at multiple centers across the US.
Using a targeted, next-generation sequencing approach, the researchers looked for mutations in 84 leukemia- and/or cancer-associated genes. They also performed tests on blood or bone marrow cells to look for chromosomal irregularities.
The team discovered 2 significant mutations in the CCND1 and CCND2 genes, representing the first dual evidence of these recurrent mutations in patients with t(8;21)-positive CBF-AML.
CCND1 and CCND2 mutations were found in 15% (n=10) of patients with t(8;21)-positive CBF-AML. Two patients had mutations in CCND1, and 8 had mutations in CCND2.
The researchers also found a single CCND2 mutation in 1 (0.9%) patient with inv(16)-positive CBF-AML.
In comparison, the incidence of CCND1 and CCND2 mutations was 0.77% (n=11) in a cohort of 1426 patients with non-CBF-AML.
“This is extremely valuable information that was previously unknown,” Dr Eisfeld said, “and it might help us develop targeted therapies more likely to help patients with [CBF-AML] in the near future.” ![]()
2016 ASH Annual Meeting
SAN DIEGO—Researchers have found evidence to suggest that mutations in the CCND1 and CCND2 genes may contribute to the development of core-binding factor acute myeloid leukemia (CBF-AML).
The team noted that CBF-AML is defined by the presence of either t(8;21)(q22;q22)/RUNX1-RUNX1T1 or inv(16)(p13.1q22)/t(16;16)(p13.1;q22)/CBFB-MYH11.
However, the fusion genes alone are not capable of causing CBF-AML.
“The hematology community has long sought to determine what other factors in addition to the fusion genes occur in this special type of leukemia,” said Ann-Kathrin Eisfeld, MD, of The Ohio State University Comprehensive Cancer Center in Columbus.
“We are now the first to describe that mutations in CCND1—and among the first to describe that mutations in the sister gene CCND2—are unique features of CBF-AML with t(8;21). In addition, we have collected the first evidence that mutations in CCND2 lead to more aggressive growth of leukemia cell lines.”
Dr Eisfeld and her colleagues reported these findings in a paper published in Leukemia and in a poster presented at the 2016 ASH Annual Meeting (abstract 2740).
A previous study of genetic mutations in CBF-AML revealed the presence of at least 1 mutation in 85% of patients studied. This meant the remaining 15% of patients harbored other, undiscovered mutations.
For the current study, Dr Eisfeld and her colleagues searched CBF-AML samples for the missing mutations that, together with the fusion genes, might contribute to the leukemia in this subgroup of cases.
The team analyzed pretreatment bone marrow and peripheral blood samples from 177 adult CBF-AML patients who received similar treatment through a clinical trial conducted at multiple centers across the US.
Using a targeted, next-generation sequencing approach, the researchers looked for mutations in 84 leukemia- and/or cancer-associated genes. They also performed tests on blood or bone marrow cells to look for chromosomal irregularities.
The team discovered 2 significant mutations in the CCND1 and CCND2 genes, representing the first dual evidence of these recurrent mutations in patients with t(8;21)-positive CBF-AML.
CCND1 and CCND2 mutations were found in 15% (n=10) of patients with t(8;21)-positive CBF-AML. Two patients had mutations in CCND1, and 8 had mutations in CCND2.
The researchers also found a single CCND2 mutation in 1 (0.9%) patient with inv(16)-positive CBF-AML.
In comparison, the incidence of CCND1 and CCND2 mutations was 0.77% (n=11) in a cohort of 1426 patients with non-CBF-AML.
“This is extremely valuable information that was previously unknown,” Dr Eisfeld said, “and it might help us develop targeted therapies more likely to help patients with [CBF-AML] in the near future.” ![]()
2016 ASH Annual Meeting
SAN DIEGO—Researchers have found evidence to suggest that mutations in the CCND1 and CCND2 genes may contribute to the development of core-binding factor acute myeloid leukemia (CBF-AML).
The team noted that CBF-AML is defined by the presence of either t(8;21)(q22;q22)/RUNX1-RUNX1T1 or inv(16)(p13.1q22)/t(16;16)(p13.1;q22)/CBFB-MYH11.
However, the fusion genes alone are not capable of causing CBF-AML.
“The hematology community has long sought to determine what other factors in addition to the fusion genes occur in this special type of leukemia,” said Ann-Kathrin Eisfeld, MD, of The Ohio State University Comprehensive Cancer Center in Columbus.
“We are now the first to describe that mutations in CCND1—and among the first to describe that mutations in the sister gene CCND2—are unique features of CBF-AML with t(8;21). In addition, we have collected the first evidence that mutations in CCND2 lead to more aggressive growth of leukemia cell lines.”
Dr Eisfeld and her colleagues reported these findings in a paper published in Leukemia and in a poster presented at the 2016 ASH Annual Meeting (abstract 2740).
A previous study of genetic mutations in CBF-AML revealed the presence of at least 1 mutation in 85% of patients studied. This meant the remaining 15% of patients harbored other, undiscovered mutations.
For the current study, Dr Eisfeld and her colleagues searched CBF-AML samples for the missing mutations that, together with the fusion genes, might contribute to the leukemia in this subgroup of cases.
The team analyzed pretreatment bone marrow and peripheral blood samples from 177 adult CBF-AML patients who received similar treatment through a clinical trial conducted at multiple centers across the US.
Using a targeted, next-generation sequencing approach, the researchers looked for mutations in 84 leukemia- and/or cancer-associated genes. They also performed tests on blood or bone marrow cells to look for chromosomal irregularities.
The team discovered 2 significant mutations in the CCND1 and CCND2 genes, representing the first dual evidence of these recurrent mutations in patients with t(8;21)-positive CBF-AML.
CCND1 and CCND2 mutations were found in 15% (n=10) of patients with t(8;21)-positive CBF-AML. Two patients had mutations in CCND1, and 8 had mutations in CCND2.
The researchers also found a single CCND2 mutation in 1 (0.9%) patient with inv(16)-positive CBF-AML.
In comparison, the incidence of CCND1 and CCND2 mutations was 0.77% (n=11) in a cohort of 1426 patients with non-CBF-AML.
“This is extremely valuable information that was previously unknown,” Dr Eisfeld said, “and it might help us develop targeted therapies more likely to help patients with [CBF-AML] in the near future.” ![]()