User login
Lifesaving future seen for electronic cigarettes
A switch from cigarettes to e-cigarettes has the potential to prevent almost 90,000 premature deaths in the United States in the year 2026, according to a study examining e-cigarette substitution scenarios.
The investigators’ “optimistic scenario” – in which new smokers use e-cigarettes instead of cigarettes, smoking prevalence falls to 5% over a 10-year period, and e-cigarettes have a 5% excess risk over regular cigarettes – projects 380,832 premature deaths from smoking in the year 2026. Under a “status quo scenario,” which projected current cigarette initiation and cessation rates and did not include e-cigarettes or other tobacco products, there would be 470,743 deaths, reported David T. Levy, PhD, and his associates (Tob Control. 2017 Oct 2. doi: 10.1136/tobaccocontrol-2017-053759).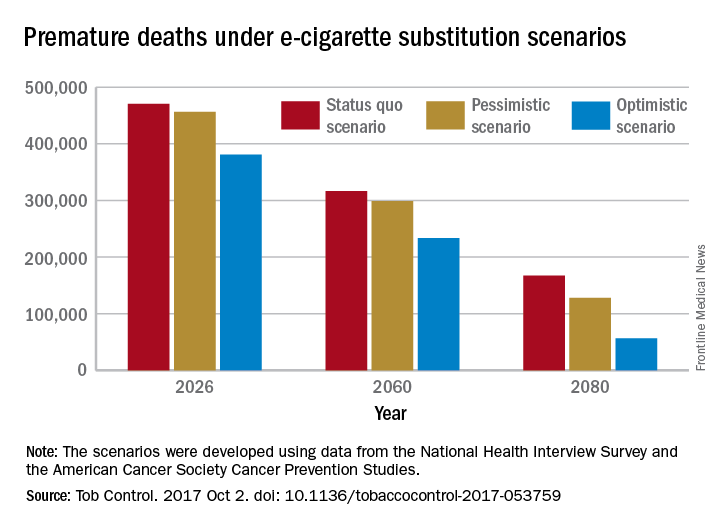
Further projections suggest that the optimistic scenario could result in almost 6.6 million fewer premature deaths and 86.7 million years of life gained by the year 2100, compared with the status quo scenario, while the pessimistic scenario would prevent 1.6 million deaths and add an extra 20.8 million years of life, they noted.
Since “a strategy of replacing cigarette by e-cigarette use can yield substantial gains, even with conservative assumptions about related risks … an endgame scenario for cigarettes might well be within reach, if new technologies for delivering nicotine with substantially less harm, but sufficient satisfaction, are harnessed with sufficient passion and political will to aggressively phase out tobacco cigarettes,” Dr. Levy and his associates wrote.
The study was funded by grants from the National Institute on Drug Abuse and the National Cancer Institute. One investigator received a research grant from Pfizer and served as an advisory board member to Johnson & Johnson, which manufactures smoking cessation medications. No other conflicts of interest were declared.

A switch from cigarettes to e-cigarettes has the potential to prevent almost 90,000 premature deaths in the United States in the year 2026, according to a study examining e-cigarette substitution scenarios.
The investigators’ “optimistic scenario” – in which new smokers use e-cigarettes instead of cigarettes, smoking prevalence falls to 5% over a 10-year period, and e-cigarettes have a 5% excess risk over regular cigarettes – projects 380,832 premature deaths from smoking in the year 2026. Under a “status quo scenario,” which projected current cigarette initiation and cessation rates and did not include e-cigarettes or other tobacco products, there would be 470,743 deaths, reported David T. Levy, PhD, and his associates (Tob Control. 2017 Oct 2. doi: 10.1136/tobaccocontrol-2017-053759).
Further projections suggest that the optimistic scenario could result in almost 6.6 million fewer premature deaths and 86.7 million years of life gained by the year 2100, compared with the status quo scenario, while the pessimistic scenario would prevent 1.6 million deaths and add an extra 20.8 million years of life, they noted.
Since “a strategy of replacing cigarette by e-cigarette use can yield substantial gains, even with conservative assumptions about related risks … an endgame scenario for cigarettes might well be within reach, if new technologies for delivering nicotine with substantially less harm, but sufficient satisfaction, are harnessed with sufficient passion and political will to aggressively phase out tobacco cigarettes,” Dr. Levy and his associates wrote.
The study was funded by grants from the National Institute on Drug Abuse and the National Cancer Institute. One investigator received a research grant from Pfizer and served as an advisory board member to Johnson & Johnson, which manufactures smoking cessation medications. No other conflicts of interest were declared.
A switch from cigarettes to e-cigarettes has the potential to prevent almost 90,000 premature deaths in the United States in the year 2026, according to a study examining e-cigarette substitution scenarios.
The investigators’ “optimistic scenario” – in which new smokers use e-cigarettes instead of cigarettes, smoking prevalence falls to 5% over a 10-year period, and e-cigarettes have a 5% excess risk over regular cigarettes – projects 380,832 premature deaths from smoking in the year 2026. Under a “status quo scenario,” which projected current cigarette initiation and cessation rates and did not include e-cigarettes or other tobacco products, there would be 470,743 deaths, reported David T. Levy, PhD, and his associates (Tob Control. 2017 Oct 2. doi: 10.1136/tobaccocontrol-2017-053759).
Further projections suggest that the optimistic scenario could result in almost 6.6 million fewer premature deaths and 86.7 million years of life gained by the year 2100, compared with the status quo scenario, while the pessimistic scenario would prevent 1.6 million deaths and add an extra 20.8 million years of life, they noted.
Since “a strategy of replacing cigarette by e-cigarette use can yield substantial gains, even with conservative assumptions about related risks … an endgame scenario for cigarettes might well be within reach, if new technologies for delivering nicotine with substantially less harm, but sufficient satisfaction, are harnessed with sufficient passion and political will to aggressively phase out tobacco cigarettes,” Dr. Levy and his associates wrote.
The study was funded by grants from the National Institute on Drug Abuse and the National Cancer Institute. One investigator received a research grant from Pfizer and served as an advisory board member to Johnson & Johnson, which manufactures smoking cessation medications. No other conflicts of interest were declared.
FROM TOBACCO CONTROL
Maternal antepartum depression creates bevy of long-term risks in offspring
PARIS – Maternal depression during pregnancy is a common occurrence that can have far-reaching effects in the offspring, according to Tiina Taka-Eilola, MD, of the University of Oulu (Finland).
Indeed, maternal antepartum depression may best be thought of as an adverse environmental factor that exacerbates the impact of any underlying genetic vulnerability to severe mental disorder that may be present in the offspring, she said at the annual congress of the European College of Neuropsychopharmacology.

At midgestation, back in the mid-1960s, 13.9% of the mothers of the Northern Finland Birth Cohort acknowledged feeling “depressed” or “very depressed,” rates consistent with those reported in other studies using standardized depression assessment instruments. Their offspring, by age 43 years, were 1.6-fold more likely to have a history of a current or past nonpsychotic mood disorder and 2-fold more likely to have had a psychotic mood disorder than did the offspring of mothers free of antepartum depression.
These risks were greatly amplified if either parent experienced a hospital-treated severe mental disorder before, during, or up to 18 years after the pregnancy. Offspring who had both a mother who experienced antepartum depression and a parent with a severe, hospital-treated mental disorder were at 3.9-fold increased risk for being diagnosed with nonpsychotic depression by age 43 years in an analysis adjusted for sex, perinatal complications, and other potential confounders. They also were at 5.6-fold increased risk for psychotic depression and a whopping 7.8-fold greater risk of bipolar disorder than offspring with neither risk factor.
Moreover, in an earlier study, among men in the Northern Finland cohort who were assessed at age 33 years, investigators found that maternal depression during pregnancy was associated with an adjusted 1.4-fold increased likelihood of having a criminal record for a nonviolent offense, a 1.6-fold increased risk of violent crime, and a 1.7-fold increase in violent recidivism. In contrast, women whose mothers were depressed during pregnancy didn’t have a significantly higher rate of criminality, compared with those whose mothers weren’t depressed (J Affect Disord. 2003 May;74[3]:273-8).
In another earlier analysis, Dr. Taka-Eilola’s senior coinvestigators demonstrated that the risk of schizophrenia in the Northern Finland offspring was 2.6-fold greater if there was parental psychosis but no maternal antepartum depression than if neither was present, while the risk was 9.4-fold higher when both risk factors were present (Am J Psychiatry. 2010 Jan;167[1]:70-7).
Dr. Taka-Eilola, a primary care physician, said that postpartum depression garners news headlines and is far more extensively researched than is antepartum depression, but as the Finnish data show, antepartum depression is at least as common and deserves to be taken seriously. It’s important to screen for it and to treat it in an effort to prevent adverse effects in the offspring, as well as out of concern for the mother’s well-being, she emphasized. She believes this is now more likely to happen as a consequence of a recent World Psychiatric Association report calling for greater clinician attention to perinatal mental health.
Dr. Taka-Eilola reported having no financial conflicts of interest regarding the Northern Finland Birth Cohort Study, which is supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit foundations.
PARIS – Maternal depression during pregnancy is a common occurrence that can have far-reaching effects in the offspring, according to Tiina Taka-Eilola, MD, of the University of Oulu (Finland).
Indeed, maternal antepartum depression may best be thought of as an adverse environmental factor that exacerbates the impact of any underlying genetic vulnerability to severe mental disorder that may be present in the offspring, she said at the annual congress of the European College of Neuropsychopharmacology.
At midgestation, back in the mid-1960s, 13.9% of the mothers of the Northern Finland Birth Cohort acknowledged feeling “depressed” or “very depressed,” rates consistent with those reported in other studies using standardized depression assessment instruments. Their offspring, by age 43 years, were 1.6-fold more likely to have a history of a current or past nonpsychotic mood disorder and 2-fold more likely to have had a psychotic mood disorder than did the offspring of mothers free of antepartum depression.
These risks were greatly amplified if either parent experienced a hospital-treated severe mental disorder before, during, or up to 18 years after the pregnancy. Offspring who had both a mother who experienced antepartum depression and a parent with a severe, hospital-treated mental disorder were at 3.9-fold increased risk for being diagnosed with nonpsychotic depression by age 43 years in an analysis adjusted for sex, perinatal complications, and other potential confounders. They also were at 5.6-fold increased risk for psychotic depression and a whopping 7.8-fold greater risk of bipolar disorder than offspring with neither risk factor.
Moreover, in an earlier study, among men in the Northern Finland cohort who were assessed at age 33 years, investigators found that maternal depression during pregnancy was associated with an adjusted 1.4-fold increased likelihood of having a criminal record for a nonviolent offense, a 1.6-fold increased risk of violent crime, and a 1.7-fold increase in violent recidivism. In contrast, women whose mothers were depressed during pregnancy didn’t have a significantly higher rate of criminality, compared with those whose mothers weren’t depressed (J Affect Disord. 2003 May;74[3]:273-8).
In another earlier analysis, Dr. Taka-Eilola’s senior coinvestigators demonstrated that the risk of schizophrenia in the Northern Finland offspring was 2.6-fold greater if there was parental psychosis but no maternal antepartum depression than if neither was present, while the risk was 9.4-fold higher when both risk factors were present (Am J Psychiatry. 2010 Jan;167[1]:70-7).
Dr. Taka-Eilola, a primary care physician, said that postpartum depression garners news headlines and is far more extensively researched than is antepartum depression, but as the Finnish data show, antepartum depression is at least as common and deserves to be taken seriously. It’s important to screen for it and to treat it in an effort to prevent adverse effects in the offspring, as well as out of concern for the mother’s well-being, she emphasized. She believes this is now more likely to happen as a consequence of a recent World Psychiatric Association report calling for greater clinician attention to perinatal mental health.
Dr. Taka-Eilola reported having no financial conflicts of interest regarding the Northern Finland Birth Cohort Study, which is supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit foundations.
PARIS – Maternal depression during pregnancy is a common occurrence that can have far-reaching effects in the offspring, according to Tiina Taka-Eilola, MD, of the University of Oulu (Finland).
Indeed, maternal antepartum depression may best be thought of as an adverse environmental factor that exacerbates the impact of any underlying genetic vulnerability to severe mental disorder that may be present in the offspring, she said at the annual congress of the European College of Neuropsychopharmacology.
At midgestation, back in the mid-1960s, 13.9% of the mothers of the Northern Finland Birth Cohort acknowledged feeling “depressed” or “very depressed,” rates consistent with those reported in other studies using standardized depression assessment instruments. Their offspring, by age 43 years, were 1.6-fold more likely to have a history of a current or past nonpsychotic mood disorder and 2-fold more likely to have had a psychotic mood disorder than did the offspring of mothers free of antepartum depression.
These risks were greatly amplified if either parent experienced a hospital-treated severe mental disorder before, during, or up to 18 years after the pregnancy. Offspring who had both a mother who experienced antepartum depression and a parent with a severe, hospital-treated mental disorder were at 3.9-fold increased risk for being diagnosed with nonpsychotic depression by age 43 years in an analysis adjusted for sex, perinatal complications, and other potential confounders. They also were at 5.6-fold increased risk for psychotic depression and a whopping 7.8-fold greater risk of bipolar disorder than offspring with neither risk factor.
Moreover, in an earlier study, among men in the Northern Finland cohort who were assessed at age 33 years, investigators found that maternal depression during pregnancy was associated with an adjusted 1.4-fold increased likelihood of having a criminal record for a nonviolent offense, a 1.6-fold increased risk of violent crime, and a 1.7-fold increase in violent recidivism. In contrast, women whose mothers were depressed during pregnancy didn’t have a significantly higher rate of criminality, compared with those whose mothers weren’t depressed (J Affect Disord. 2003 May;74[3]:273-8).
In another earlier analysis, Dr. Taka-Eilola’s senior coinvestigators demonstrated that the risk of schizophrenia in the Northern Finland offspring was 2.6-fold greater if there was parental psychosis but no maternal antepartum depression than if neither was present, while the risk was 9.4-fold higher when both risk factors were present (Am J Psychiatry. 2010 Jan;167[1]:70-7).
Dr. Taka-Eilola, a primary care physician, said that postpartum depression garners news headlines and is far more extensively researched than is antepartum depression, but as the Finnish data show, antepartum depression is at least as common and deserves to be taken seriously. It’s important to screen for it and to treat it in an effort to prevent adverse effects in the offspring, as well as out of concern for the mother’s well-being, she emphasized. She believes this is now more likely to happen as a consequence of a recent World Psychiatric Association report calling for greater clinician attention to perinatal mental health.
Dr. Taka-Eilola reported having no financial conflicts of interest regarding the Northern Finland Birth Cohort Study, which is supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit foundations.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: By midlife, offspring of an mother who had antepartum depression and a parent with a severe, hospital-treated mental disorder were at an adjusted 5.6-fold increased risk for psychotic depression and 7.8-fold greater risk of bipolar disorder than the offspring with neither risk factor.
Data source: The Northern Finland Birth Cohort 1966 is an ongoing, observational, prospective, general population-based study of the 12,058 individuals born in the two northernmost provinces of Finland during 1966.
Disclosures: The presenter reported having no financial conflicts of interest regarding the study, which is supported by the Academy of Finland, the Finnish Cultural Foundation Lapland Regional Fund, and grants from various nonprofit foundations.
Evenamide impresses for schizophrenia
PARIS – The oral selective glutamate inhibitor evenamide is moving on to advanced clinical trials on the strength of positive results in a phase 2 study, Ravi Anand, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Evenamide is a highly selective inhibitor of voltage-gated sodium channels that also attenuates glutamate release by hyperexcited neurons, explained Dr. Anand, chief medical officer at Newron Pharmaceuticals, a company based in Bresso, Italy, that is developing this novel antipsychotic agent.
The 4-week, randomized, double-blind, placebo-controlled, multicenter study included 89 patients with schizophrenia of a mean 18 years’ duration. All participants showed baseline evidence of breakthrough psychosis despite being on stable therapeutic doses of previously effective risperidone or aripiprazole. They were randomized either to add-on oral evenamide at a starting dose of 15 mg twice daily titrated to 20 or 25 mg twice daily or to placebo.
As a phase 2 study, the primary focus was on safety and tolerability. Evenamide showed no dose-limiting toxicities. Nor did those in the evenamide group experience any of the common dopaminergic side effects seen with currently available antipsychotics, such as sedation, weight gain, sexual dysfunction, cardiac abnormalities, or extrapyramidal symptoms.
The only adverse events more common in the evenamide-treated group than in placebo-treated controls were insomnia and headache, which occurred in 5 and 3 of the 50 patients on evenamide, respectively.
In terms of efficacy, 75% of the evenamide group showed improvement over baseline in terms of the Positive and Negative Syndrome Scale, compared with 44% of controls. From a mean baseline total PANSS score of 62.7, the evenamide group experienced a 5.1-point reduction at day 28, compared with a 3.7-point improvement in controls. The difference between the two study arms was already significant at the first assessment, which took place on day 8.
Furthermore, 55% of patients in the evenamide group showed significant improvement on the Clinical Global Impression Severity score, compared with 36% of controls.
Because evenamide’s efficacy was greater in younger patients, the next round of larger, longer clinical trials will focus on younger patients with more severe symptoms, Dr. Anand said.
PARIS – The oral selective glutamate inhibitor evenamide is moving on to advanced clinical trials on the strength of positive results in a phase 2 study, Ravi Anand, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Evenamide is a highly selective inhibitor of voltage-gated sodium channels that also attenuates glutamate release by hyperexcited neurons, explained Dr. Anand, chief medical officer at Newron Pharmaceuticals, a company based in Bresso, Italy, that is developing this novel antipsychotic agent.
The 4-week, randomized, double-blind, placebo-controlled, multicenter study included 89 patients with schizophrenia of a mean 18 years’ duration. All participants showed baseline evidence of breakthrough psychosis despite being on stable therapeutic doses of previously effective risperidone or aripiprazole. They were randomized either to add-on oral evenamide at a starting dose of 15 mg twice daily titrated to 20 or 25 mg twice daily or to placebo.
As a phase 2 study, the primary focus was on safety and tolerability. Evenamide showed no dose-limiting toxicities. Nor did those in the evenamide group experience any of the common dopaminergic side effects seen with currently available antipsychotics, such as sedation, weight gain, sexual dysfunction, cardiac abnormalities, or extrapyramidal symptoms.
The only adverse events more common in the evenamide-treated group than in placebo-treated controls were insomnia and headache, which occurred in 5 and 3 of the 50 patients on evenamide, respectively.
In terms of efficacy, 75% of the evenamide group showed improvement over baseline in terms of the Positive and Negative Syndrome Scale, compared with 44% of controls. From a mean baseline total PANSS score of 62.7, the evenamide group experienced a 5.1-point reduction at day 28, compared with a 3.7-point improvement in controls. The difference between the two study arms was already significant at the first assessment, which took place on day 8.
Furthermore, 55% of patients in the evenamide group showed significant improvement on the Clinical Global Impression Severity score, compared with 36% of controls.
Because evenamide’s efficacy was greater in younger patients, the next round of larger, longer clinical trials will focus on younger patients with more severe symptoms, Dr. Anand said.
PARIS – The oral selective glutamate inhibitor evenamide is moving on to advanced clinical trials on the strength of positive results in a phase 2 study, Ravi Anand, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
Evenamide is a highly selective inhibitor of voltage-gated sodium channels that also attenuates glutamate release by hyperexcited neurons, explained Dr. Anand, chief medical officer at Newron Pharmaceuticals, a company based in Bresso, Italy, that is developing this novel antipsychotic agent.
The 4-week, randomized, double-blind, placebo-controlled, multicenter study included 89 patients with schizophrenia of a mean 18 years’ duration. All participants showed baseline evidence of breakthrough psychosis despite being on stable therapeutic doses of previously effective risperidone or aripiprazole. They were randomized either to add-on oral evenamide at a starting dose of 15 mg twice daily titrated to 20 or 25 mg twice daily or to placebo.
As a phase 2 study, the primary focus was on safety and tolerability. Evenamide showed no dose-limiting toxicities. Nor did those in the evenamide group experience any of the common dopaminergic side effects seen with currently available antipsychotics, such as sedation, weight gain, sexual dysfunction, cardiac abnormalities, or extrapyramidal symptoms.
The only adverse events more common in the evenamide-treated group than in placebo-treated controls were insomnia and headache, which occurred in 5 and 3 of the 50 patients on evenamide, respectively.
In terms of efficacy, 75% of the evenamide group showed improvement over baseline in terms of the Positive and Negative Syndrome Scale, compared with 44% of controls. From a mean baseline total PANSS score of 62.7, the evenamide group experienced a 5.1-point reduction at day 28, compared with a 3.7-point improvement in controls. The difference between the two study arms was already significant at the first assessment, which took place on day 8.
Furthermore, 55% of patients in the evenamide group showed significant improvement on the Clinical Global Impression Severity score, compared with 36% of controls.
Because evenamide’s efficacy was greater in younger patients, the next round of larger, longer clinical trials will focus on younger patients with more severe symptoms, Dr. Anand said.
AT THE ECNP CONGRESS
Key clinical point:
Major finding: Three-quarters of schizophrenia patients on the oral glutamate modulator evenamide showed improvement over baseline in terms of the Positive and Negative Syndrome Scale, compared with 44% of controls.
Data source: This 4-week, randomized, double-blind, placebo-controlled, multicenter study included 89 patients with schizophrenia.
Disclosures: The study presenter is the chief medical officer at Newron Pharmaceuticals, which is developing the novel antipsychotic.
MIPS: It’s time to get started
David O. Barbe, MD, is urging physicians to participate in the Medicare Quality Payment Program, even if the business case isn’t quite there.
QPP is the value-based payment system created by the Medicare Access and CHIP Reauthorization Act (MACRA). It promotes high-value care through Medicare payment increases. But for some practices, the investment in personnel and technology needed to earn those increases may be more than the increases themselves, leading doctors to do just enough to avoid being penalized.
“I think that many physicians don’t feel they are ever going to get a bonus but sure would like to avoid a penalty,” Dr. Barbe, president of the American Medical Association, said in an exclusive interview. “I am afraid many will simply perform at the lowest level that keeps them out of the penalty. Because many of them find that making the investment it takes to perform highly, there is not a business case for that.”
Full participation in QPP’s Merit-based Incentive Payment System (MIPS) could run small practices an additional $10,000 to $30,000 a year, he said. “If you’ve got $200,000 in Medicare receipts, if you get adjusted even the maximum of 4%, that is $8,000. You can’t cover $20,000 with $8,000. The math doesn’t work. There is not a business case there for it.”
That said, Dr. Barbe still spoke in favor of QPP and noted that the AMA is working with the Centers for Medicare & Medicaid Services as well as Congress to make the program more valuable and meaningful for physicians.
“We understand where we need to go as a profession, as an industry,” he said. “How we get there is the key, it’s the challenge and it requires flexibility. ... CMS has been accommodating but there are limits to how long they can go.”
The AMA is urging doctors who have missed the 90-day window for full participation – which effectively closed for most on Oct. 2 – to consider the Pick Your Pace option offered by the CMS.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Pick Your Pace allows physicians and practices to submit data on one measure for one patient to avoid a reduction in Medicare pay, even though they would not be eligible for a bonus.
“AMA has put out a lot of tools to help physicians assess their readiness, assess the gap between what they are able to do in their practice now and what they need to do to be successful under [the MIPS] primarily down to and including a video that would walk a physician step-by-step through the one patient, one measure, no penalty,” Dr. Barbe said.
He also encouraged doctors to pick a measure that is meaningful to their practice if only to get the ball rolling and get their feet wet in the QPP pool.
“What I tell physicians is pick something that is relevant for your practice,” he said.”If I see a lot of diabetes patients in my practice but I don’t see many people on anticoagulants, it doesn’t make sense for me to pick an anticoagulant measure.”
And if all a practice can do this year is one patient, one measure, Dr. Barbe urged physicians to look toward the next reporting year with an eye to do more, as that will ultimately lead to better quality of care delivered.
“Report on one patient and one measure this year ... but look at next year to say ‘that’s going to be a 90-day project for me,’ and get in on that. There is a pretty long laundry list of conditions and metrics that you can report on.”
And if practices start capturing relevant data, it opens the door to improving their practice if they also take the time to analyze what they are collecting.
“That is the purpose,” Dr. Barbe said. “As you measure yourself along the way, if the threshold for performance is here, and you find yourself working at this [lower] level for the first 30 days or whatever, then you stop and take stock of that” and react accordingly, whether its providing patients with a little more information about their condition or perhaps being more diligent in terms of monitoring high risk patients.
David O. Barbe, MD, is urging physicians to participate in the Medicare Quality Payment Program, even if the business case isn’t quite there.
QPP is the value-based payment system created by the Medicare Access and CHIP Reauthorization Act (MACRA). It promotes high-value care through Medicare payment increases. But for some practices, the investment in personnel and technology needed to earn those increases may be more than the increases themselves, leading doctors to do just enough to avoid being penalized.
“I think that many physicians don’t feel they are ever going to get a bonus but sure would like to avoid a penalty,” Dr. Barbe, president of the American Medical Association, said in an exclusive interview. “I am afraid many will simply perform at the lowest level that keeps them out of the penalty. Because many of them find that making the investment it takes to perform highly, there is not a business case for that.”
Full participation in QPP’s Merit-based Incentive Payment System (MIPS) could run small practices an additional $10,000 to $30,000 a year, he said. “If you’ve got $200,000 in Medicare receipts, if you get adjusted even the maximum of 4%, that is $8,000. You can’t cover $20,000 with $8,000. The math doesn’t work. There is not a business case there for it.”
That said, Dr. Barbe still spoke in favor of QPP and noted that the AMA is working with the Centers for Medicare & Medicaid Services as well as Congress to make the program more valuable and meaningful for physicians.
“We understand where we need to go as a profession, as an industry,” he said. “How we get there is the key, it’s the challenge and it requires flexibility. ... CMS has been accommodating but there are limits to how long they can go.”
The AMA is urging doctors who have missed the 90-day window for full participation – which effectively closed for most on Oct. 2 – to consider the Pick Your Pace option offered by the CMS.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Pick Your Pace allows physicians and practices to submit data on one measure for one patient to avoid a reduction in Medicare pay, even though they would not be eligible for a bonus.
“AMA has put out a lot of tools to help physicians assess their readiness, assess the gap between what they are able to do in their practice now and what they need to do to be successful under [the MIPS] primarily down to and including a video that would walk a physician step-by-step through the one patient, one measure, no penalty,” Dr. Barbe said.
He also encouraged doctors to pick a measure that is meaningful to their practice if only to get the ball rolling and get their feet wet in the QPP pool.
“What I tell physicians is pick something that is relevant for your practice,” he said.”If I see a lot of diabetes patients in my practice but I don’t see many people on anticoagulants, it doesn’t make sense for me to pick an anticoagulant measure.”
And if all a practice can do this year is one patient, one measure, Dr. Barbe urged physicians to look toward the next reporting year with an eye to do more, as that will ultimately lead to better quality of care delivered.
“Report on one patient and one measure this year ... but look at next year to say ‘that’s going to be a 90-day project for me,’ and get in on that. There is a pretty long laundry list of conditions and metrics that you can report on.”
And if practices start capturing relevant data, it opens the door to improving their practice if they also take the time to analyze what they are collecting.
“That is the purpose,” Dr. Barbe said. “As you measure yourself along the way, if the threshold for performance is here, and you find yourself working at this [lower] level for the first 30 days or whatever, then you stop and take stock of that” and react accordingly, whether its providing patients with a little more information about their condition or perhaps being more diligent in terms of monitoring high risk patients.
David O. Barbe, MD, is urging physicians to participate in the Medicare Quality Payment Program, even if the business case isn’t quite there.
QPP is the value-based payment system created by the Medicare Access and CHIP Reauthorization Act (MACRA). It promotes high-value care through Medicare payment increases. But for some practices, the investment in personnel and technology needed to earn those increases may be more than the increases themselves, leading doctors to do just enough to avoid being penalized.
“I think that many physicians don’t feel they are ever going to get a bonus but sure would like to avoid a penalty,” Dr. Barbe, president of the American Medical Association, said in an exclusive interview. “I am afraid many will simply perform at the lowest level that keeps them out of the penalty. Because many of them find that making the investment it takes to perform highly, there is not a business case for that.”
Full participation in QPP’s Merit-based Incentive Payment System (MIPS) could run small practices an additional $10,000 to $30,000 a year, he said. “If you’ve got $200,000 in Medicare receipts, if you get adjusted even the maximum of 4%, that is $8,000. You can’t cover $20,000 with $8,000. The math doesn’t work. There is not a business case there for it.”
That said, Dr. Barbe still spoke in favor of QPP and noted that the AMA is working with the Centers for Medicare & Medicaid Services as well as Congress to make the program more valuable and meaningful for physicians.
“We understand where we need to go as a profession, as an industry,” he said. “How we get there is the key, it’s the challenge and it requires flexibility. ... CMS has been accommodating but there are limits to how long they can go.”
The AMA is urging doctors who have missed the 90-day window for full participation – which effectively closed for most on Oct. 2 – to consider the Pick Your Pace option offered by the CMS.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Pick Your Pace allows physicians and practices to submit data on one measure for one patient to avoid a reduction in Medicare pay, even though they would not be eligible for a bonus.
“AMA has put out a lot of tools to help physicians assess their readiness, assess the gap between what they are able to do in their practice now and what they need to do to be successful under [the MIPS] primarily down to and including a video that would walk a physician step-by-step through the one patient, one measure, no penalty,” Dr. Barbe said.
He also encouraged doctors to pick a measure that is meaningful to their practice if only to get the ball rolling and get their feet wet in the QPP pool.
“What I tell physicians is pick something that is relevant for your practice,” he said.”If I see a lot of diabetes patients in my practice but I don’t see many people on anticoagulants, it doesn’t make sense for me to pick an anticoagulant measure.”
And if all a practice can do this year is one patient, one measure, Dr. Barbe urged physicians to look toward the next reporting year with an eye to do more, as that will ultimately lead to better quality of care delivered.
“Report on one patient and one measure this year ... but look at next year to say ‘that’s going to be a 90-day project for me,’ and get in on that. There is a pretty long laundry list of conditions and metrics that you can report on.”
And if practices start capturing relevant data, it opens the door to improving their practice if they also take the time to analyze what they are collecting.
“That is the purpose,” Dr. Barbe said. “As you measure yourself along the way, if the threshold for performance is here, and you find yourself working at this [lower] level for the first 30 days or whatever, then you stop and take stock of that” and react accordingly, whether its providing patients with a little more information about their condition or perhaps being more diligent in terms of monitoring high risk patients.
ANA 2017 offers career development sessions at all levels
Professional developments courses that will take place each morning during the annual meeting of the American Neurological Association in San Diego offer special opportunities to learn about the rewards and challenges of different career options for neurologists and researchers in academic neurology from those who have gone down a variety of careers paths themselves. Three courses each morning are geared specifically for students, residents, post-docs, and fellows, as well as for professionals at early-, mid-, and university-chair career levels.
For students, residents, post-docs, and fellows
On Oct. 15, young neurology scholars will begin the course with a discussion on the transition from neurology resident to fellow, and then career pathways as a basic scientist, a clinical scientist/researcher, and clinician-administrator. Last year’s recipients of the Derek Denny-Brown Young Neurological Scholar Award also will provide insights on successful early careers in academic neurology.
Global Health has many opportunities for individuals who are looking at potential career paths in neurology to conduct research, clinical care, or educate others in low- to middle-income countries. Speakers on Oct. 16 will share their experiences and discuss emerging trends in global health in neurology and ways in which individuals might pursue careers or opportunities that complement pursuits in academic neurology.
A workshop on Oct. 17 will focus on the essential skills needed for a successful job-seeking experience in academic neurology. There will be opportunities to practice interviewing and negotiating skills, as well as to learn how to market your research and abilities when the opportunity strikes and time is limited.
For early- to mid-career levels
Finding a niche and a successful career trajectory takes a good deal of planning and taking opportunities when the time is right. On Oct. 15, several mid-career level academic neurologists will share their career trajectories and alternative methods they have used for obtaining support and funding for their clinical research, educational enterprises, and curricular development.
The Oct. 16 career development course will outline methods for setting milestones for career development and finding the resources and mentoring individuals you will need for career advancement.
To learn skills and discover tools that will help to write successful grant proposals, particularly for the National Institutes of Health, come to the session on Oct. 17. You can learn how to develop your grant application, respond to critiques of your application, and hear about a variety of sources of funding.
For university chairs of neurology
At a time in which funding for salaries is hampered by many factors, salary disparities are changing across subspecialties as well as in different faculty positions, with some disparities widening and others shrinking. Come to the career development course on Oct. 15 to learn about novel revenue sources and ways in which you can best subsidize the salaries of faculties in your department as well as offer nonmonetary compensation.
Given the current uncertainties of the fates of Affordable Care Act, Medicare, and other major systems supporting health care, it is important to know the best approach to take in advocating for academic neurology and your department’s needs. At the course on Oct. 16, come learn about current health policy issues and the political climate and determine how and when to be politically active.
To understand the impact that the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) requirements will have on academic neurology, come to the session on Oct. 17. You’ll learn how population health measures and value-based care can be brought into an academic neurology practice, how to report on quality measures in the Merit-based Incentive Payment System, and how to participate in Advanced Alternative Payment Models.
Professional developments courses that will take place each morning during the annual meeting of the American Neurological Association in San Diego offer special opportunities to learn about the rewards and challenges of different career options for neurologists and researchers in academic neurology from those who have gone down a variety of careers paths themselves. Three courses each morning are geared specifically for students, residents, post-docs, and fellows, as well as for professionals at early-, mid-, and university-chair career levels.
For students, residents, post-docs, and fellows
On Oct. 15, young neurology scholars will begin the course with a discussion on the transition from neurology resident to fellow, and then career pathways as a basic scientist, a clinical scientist/researcher, and clinician-administrator. Last year’s recipients of the Derek Denny-Brown Young Neurological Scholar Award also will provide insights on successful early careers in academic neurology.
Global Health has many opportunities for individuals who are looking at potential career paths in neurology to conduct research, clinical care, or educate others in low- to middle-income countries. Speakers on Oct. 16 will share their experiences and discuss emerging trends in global health in neurology and ways in which individuals might pursue careers or opportunities that complement pursuits in academic neurology.
A workshop on Oct. 17 will focus on the essential skills needed for a successful job-seeking experience in academic neurology. There will be opportunities to practice interviewing and negotiating skills, as well as to learn how to market your research and abilities when the opportunity strikes and time is limited.
For early- to mid-career levels
Finding a niche and a successful career trajectory takes a good deal of planning and taking opportunities when the time is right. On Oct. 15, several mid-career level academic neurologists will share their career trajectories and alternative methods they have used for obtaining support and funding for their clinical research, educational enterprises, and curricular development.
The Oct. 16 career development course will outline methods for setting milestones for career development and finding the resources and mentoring individuals you will need for career advancement.
To learn skills and discover tools that will help to write successful grant proposals, particularly for the National Institutes of Health, come to the session on Oct. 17. You can learn how to develop your grant application, respond to critiques of your application, and hear about a variety of sources of funding.
For university chairs of neurology
At a time in which funding for salaries is hampered by many factors, salary disparities are changing across subspecialties as well as in different faculty positions, with some disparities widening and others shrinking. Come to the career development course on Oct. 15 to learn about novel revenue sources and ways in which you can best subsidize the salaries of faculties in your department as well as offer nonmonetary compensation.
Given the current uncertainties of the fates of Affordable Care Act, Medicare, and other major systems supporting health care, it is important to know the best approach to take in advocating for academic neurology and your department’s needs. At the course on Oct. 16, come learn about current health policy issues and the political climate and determine how and when to be politically active.
To understand the impact that the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) requirements will have on academic neurology, come to the session on Oct. 17. You’ll learn how population health measures and value-based care can be brought into an academic neurology practice, how to report on quality measures in the Merit-based Incentive Payment System, and how to participate in Advanced Alternative Payment Models.
Professional developments courses that will take place each morning during the annual meeting of the American Neurological Association in San Diego offer special opportunities to learn about the rewards and challenges of different career options for neurologists and researchers in academic neurology from those who have gone down a variety of careers paths themselves. Three courses each morning are geared specifically for students, residents, post-docs, and fellows, as well as for professionals at early-, mid-, and university-chair career levels.
For students, residents, post-docs, and fellows
On Oct. 15, young neurology scholars will begin the course with a discussion on the transition from neurology resident to fellow, and then career pathways as a basic scientist, a clinical scientist/researcher, and clinician-administrator. Last year’s recipients of the Derek Denny-Brown Young Neurological Scholar Award also will provide insights on successful early careers in academic neurology.
Global Health has many opportunities for individuals who are looking at potential career paths in neurology to conduct research, clinical care, or educate others in low- to middle-income countries. Speakers on Oct. 16 will share their experiences and discuss emerging trends in global health in neurology and ways in which individuals might pursue careers or opportunities that complement pursuits in academic neurology.
A workshop on Oct. 17 will focus on the essential skills needed for a successful job-seeking experience in academic neurology. There will be opportunities to practice interviewing and negotiating skills, as well as to learn how to market your research and abilities when the opportunity strikes and time is limited.
For early- to mid-career levels
Finding a niche and a successful career trajectory takes a good deal of planning and taking opportunities when the time is right. On Oct. 15, several mid-career level academic neurologists will share their career trajectories and alternative methods they have used for obtaining support and funding for their clinical research, educational enterprises, and curricular development.
The Oct. 16 career development course will outline methods for setting milestones for career development and finding the resources and mentoring individuals you will need for career advancement.
To learn skills and discover tools that will help to write successful grant proposals, particularly for the National Institutes of Health, come to the session on Oct. 17. You can learn how to develop your grant application, respond to critiques of your application, and hear about a variety of sources of funding.
For university chairs of neurology
At a time in which funding for salaries is hampered by many factors, salary disparities are changing across subspecialties as well as in different faculty positions, with some disparities widening and others shrinking. Come to the career development course on Oct. 15 to learn about novel revenue sources and ways in which you can best subsidize the salaries of faculties in your department as well as offer nonmonetary compensation.
Given the current uncertainties of the fates of Affordable Care Act, Medicare, and other major systems supporting health care, it is important to know the best approach to take in advocating for academic neurology and your department’s needs. At the course on Oct. 16, come learn about current health policy issues and the political climate and determine how and when to be politically active.
To understand the impact that the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) requirements will have on academic neurology, come to the session on Oct. 17. You’ll learn how population health measures and value-based care can be brought into an academic neurology practice, how to report on quality measures in the Merit-based Incentive Payment System, and how to participate in Advanced Alternative Payment Models.
Here’s what’s trending at SHM – Oct. 2017
Don’t miss pre-courses at HM18
Enrich your educational experience and earn additional CME credit and MOC points with pre-courses at Hospital Medicine 2018 (HM18), to be held from April 8-11, 2018, at the Orlando (Fla.) World Center Marriott.
Broaden your skills, fine-tune your practice, and immerse yourself in a day of learning by enrolling in one of the following:
• Bedside procedures for the hospitalist
• Essentials of perioperative medicine and comanagement for the hospitalist
• Hospitalist practice management: How to thrive in a time of intense change
• Sepsis: New insights into detection and management
• Keep your finger on the pulse – cardiology update for the hospitalist
• Maintenance of certification and board prep
• Point-of-care ultrasound for the hospitalist
Pre-course day is Sunday, April 8, 2018. Learn more and register at shmannualconference.org/precourse.
Improve quality at your institution with SHM
The National Association for Healthcare Quality’s (NAHQ) Healthcare Quality Week is Oct. 15-21, 2017, a week dedicated to celebrating the contributions professionals have made in the field and bringing awareness to the profession of health care quality. SHM’s Center for Quality Improvement provides a variety of resources, tools, and programs to address quality and patient safety issues at your institution. Learn more at hospitalmedicine.org/QI.
Distinguish yourself as a Class of 2018 Fellow in Hospital Medicine
SHM’s Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently over 2,000 hospitalists who have earned the Fellow in Hospital Medicine (FHM) or Senior Fellow in Hospital Medicine (SFHM) designation by demonstrating the core values of leadership, teamwork, and quality improvement.
Apply now and learn how you can join this prestigious group of hospitalists at hospitalmedicine.org/fellows. Applications officially close on Nov. 30, 2017.
Critical care for the hospitalist: Now on the SHM Learning Portal
Many hospitalists provide critical care services without adequate support or training, putting patients at risk and exposing hospitalists to medical liability. Don’t miss the newest SHM Learning Portal series, Critical Care for the Hospitalist. The four courses in this educational series cover common or high-risk clinical scenarios that hospitalists encounter in and out of the intensive care unit, including:
1. Airway management for the hospitalist
2. Noninvasive positive pressure ventilation for the hospitalist
3. Arrhythmias
4. High-risk pulmonary embolism
This series is free for SHM members and $45 per module for nonmembers. Earn 0.75 AMA PRA Category 1 Credit™ and ABIM MOC points per each module. Visit shmlearningportal.org to get started today.
Connect with SHM locally at a chapter meeting near you
Attend a chapter meeting to experience SHM at the local level. Chapter meetings provide focused educational topics through keynote speakers, presentations, and opportunities to network with other hospitalists in your area. Find a chapter meeting close to you at hospitalmedicine.org/chapters.
Stay on top of trending topics in practice management
SHM recently released white papers on trending topics in practice management: Hospitalist Perspectives on EMRs, Telemedicine in Hospital Medicine, and the Evolution of Co-Management in Hospital Medicine. These resources are free to download to members and can be found at hospitalmedicine.org under the Practice Management tab.
Enhance your coding skills and earn CME
SHM’s Clinical Documentation & Coding for Hospitalists (formerly CODE-H) recently launched an updated program with all-new content that offers hospitalists the latest information on best practices in coding, documentation, and compliance from national experts. It provides eight recorded webinar sessions presented by expert faculty, downloadable resources, and an interactive discussion forum on SHM’s online community.
CME credits are offered through an evaluation following the webinars. Each participant is eligible for CME credits for completion of the series.
To learn more, visit hospitalmedicine.org/CODEH. If you have questions on the new program, please contact education@hospitalmedicine.org.
Mr. Radler is marketing communications manager at the Society of Hospital Medicine.
Don’t miss pre-courses at HM18
Enrich your educational experience and earn additional CME credit and MOC points with pre-courses at Hospital Medicine 2018 (HM18), to be held from April 8-11, 2018, at the Orlando (Fla.) World Center Marriott.
Broaden your skills, fine-tune your practice, and immerse yourself in a day of learning by enrolling in one of the following:
• Bedside procedures for the hospitalist
• Essentials of perioperative medicine and comanagement for the hospitalist
• Hospitalist practice management: How to thrive in a time of intense change
• Sepsis: New insights into detection and management
• Keep your finger on the pulse – cardiology update for the hospitalist
• Maintenance of certification and board prep
• Point-of-care ultrasound for the hospitalist
Pre-course day is Sunday, April 8, 2018. Learn more and register at shmannualconference.org/precourse.
Improve quality at your institution with SHM
The National Association for Healthcare Quality’s (NAHQ) Healthcare Quality Week is Oct. 15-21, 2017, a week dedicated to celebrating the contributions professionals have made in the field and bringing awareness to the profession of health care quality. SHM’s Center for Quality Improvement provides a variety of resources, tools, and programs to address quality and patient safety issues at your institution. Learn more at hospitalmedicine.org/QI.
Distinguish yourself as a Class of 2018 Fellow in Hospital Medicine
SHM’s Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently over 2,000 hospitalists who have earned the Fellow in Hospital Medicine (FHM) or Senior Fellow in Hospital Medicine (SFHM) designation by demonstrating the core values of leadership, teamwork, and quality improvement.
Apply now and learn how you can join this prestigious group of hospitalists at hospitalmedicine.org/fellows. Applications officially close on Nov. 30, 2017.
Critical care for the hospitalist: Now on the SHM Learning Portal
Many hospitalists provide critical care services without adequate support or training, putting patients at risk and exposing hospitalists to medical liability. Don’t miss the newest SHM Learning Portal series, Critical Care for the Hospitalist. The four courses in this educational series cover common or high-risk clinical scenarios that hospitalists encounter in and out of the intensive care unit, including:
1. Airway management for the hospitalist
2. Noninvasive positive pressure ventilation for the hospitalist
3. Arrhythmias
4. High-risk pulmonary embolism
This series is free for SHM members and $45 per module for nonmembers. Earn 0.75 AMA PRA Category 1 Credit™ and ABIM MOC points per each module. Visit shmlearningportal.org to get started today.
Connect with SHM locally at a chapter meeting near you
Attend a chapter meeting to experience SHM at the local level. Chapter meetings provide focused educational topics through keynote speakers, presentations, and opportunities to network with other hospitalists in your area. Find a chapter meeting close to you at hospitalmedicine.org/chapters.
Stay on top of trending topics in practice management
SHM recently released white papers on trending topics in practice management: Hospitalist Perspectives on EMRs, Telemedicine in Hospital Medicine, and the Evolution of Co-Management in Hospital Medicine. These resources are free to download to members and can be found at hospitalmedicine.org under the Practice Management tab.
Enhance your coding skills and earn CME
SHM’s Clinical Documentation & Coding for Hospitalists (formerly CODE-H) recently launched an updated program with all-new content that offers hospitalists the latest information on best practices in coding, documentation, and compliance from national experts. It provides eight recorded webinar sessions presented by expert faculty, downloadable resources, and an interactive discussion forum on SHM’s online community.
CME credits are offered through an evaluation following the webinars. Each participant is eligible for CME credits for completion of the series.
To learn more, visit hospitalmedicine.org/CODEH. If you have questions on the new program, please contact education@hospitalmedicine.org.
Mr. Radler is marketing communications manager at the Society of Hospital Medicine.
Don’t miss pre-courses at HM18
Enrich your educational experience and earn additional CME credit and MOC points with pre-courses at Hospital Medicine 2018 (HM18), to be held from April 8-11, 2018, at the Orlando (Fla.) World Center Marriott.
Broaden your skills, fine-tune your practice, and immerse yourself in a day of learning by enrolling in one of the following:
• Bedside procedures for the hospitalist
• Essentials of perioperative medicine and comanagement for the hospitalist
• Hospitalist practice management: How to thrive in a time of intense change
• Sepsis: New insights into detection and management
• Keep your finger on the pulse – cardiology update for the hospitalist
• Maintenance of certification and board prep
• Point-of-care ultrasound for the hospitalist
Pre-course day is Sunday, April 8, 2018. Learn more and register at shmannualconference.org/precourse.
Improve quality at your institution with SHM
The National Association for Healthcare Quality’s (NAHQ) Healthcare Quality Week is Oct. 15-21, 2017, a week dedicated to celebrating the contributions professionals have made in the field and bringing awareness to the profession of health care quality. SHM’s Center for Quality Improvement provides a variety of resources, tools, and programs to address quality and patient safety issues at your institution. Learn more at hospitalmedicine.org/QI.
Distinguish yourself as a Class of 2018 Fellow in Hospital Medicine
SHM’s Fellows designation is a prestigious way to differentiate yourself in the rapidly growing profession of hospital medicine. There are currently over 2,000 hospitalists who have earned the Fellow in Hospital Medicine (FHM) or Senior Fellow in Hospital Medicine (SFHM) designation by demonstrating the core values of leadership, teamwork, and quality improvement.
Apply now and learn how you can join this prestigious group of hospitalists at hospitalmedicine.org/fellows. Applications officially close on Nov. 30, 2017.
Critical care for the hospitalist: Now on the SHM Learning Portal
Many hospitalists provide critical care services without adequate support or training, putting patients at risk and exposing hospitalists to medical liability. Don’t miss the newest SHM Learning Portal series, Critical Care for the Hospitalist. The four courses in this educational series cover common or high-risk clinical scenarios that hospitalists encounter in and out of the intensive care unit, including:
1. Airway management for the hospitalist
2. Noninvasive positive pressure ventilation for the hospitalist
3. Arrhythmias
4. High-risk pulmonary embolism
This series is free for SHM members and $45 per module for nonmembers. Earn 0.75 AMA PRA Category 1 Credit™ and ABIM MOC points per each module. Visit shmlearningportal.org to get started today.
Connect with SHM locally at a chapter meeting near you
Attend a chapter meeting to experience SHM at the local level. Chapter meetings provide focused educational topics through keynote speakers, presentations, and opportunities to network with other hospitalists in your area. Find a chapter meeting close to you at hospitalmedicine.org/chapters.
Stay on top of trending topics in practice management
SHM recently released white papers on trending topics in practice management: Hospitalist Perspectives on EMRs, Telemedicine in Hospital Medicine, and the Evolution of Co-Management in Hospital Medicine. These resources are free to download to members and can be found at hospitalmedicine.org under the Practice Management tab.
Enhance your coding skills and earn CME
SHM’s Clinical Documentation & Coding for Hospitalists (formerly CODE-H) recently launched an updated program with all-new content that offers hospitalists the latest information on best practices in coding, documentation, and compliance from national experts. It provides eight recorded webinar sessions presented by expert faculty, downloadable resources, and an interactive discussion forum on SHM’s online community.
CME credits are offered through an evaluation following the webinars. Each participant is eligible for CME credits for completion of the series.
To learn more, visit hospitalmedicine.org/CODEH. If you have questions on the new program, please contact education@hospitalmedicine.org.
Mr. Radler is marketing communications manager at the Society of Hospital Medicine.
Blood donation intervals of 8 weeks safe for most donors
Reducing the interval between blood donations from every 12 weeks to every 8 weeks increases blood units collected with little ill effects on donor quality of life other than symptoms related to iron deficiency, based on results reported by the INTERVAL Trial Group.
In the United States, men and women can donate blood every 8 weeks; the Food and Drug Administration and the AABB (formerly the American Association of Blood Banks) have considered lengthening the 8-week minimum inter-donation interval to reduce the risk of iron deficiency. The current practice in the United Kingdom is to allow men to donate every 12 weeks and women every 16 weeks, the authors noted.
The INTERVAL study examined hemoglobin levels, ferritin levels, and self-reported symptoms as well as the number of blood donations over a 2-year period among 22,466 men randomly assigned to either 8-, 10-, or 12-week blood donation intervals and 22,797 women randomly assigned to donation intervals of 12, 14, and 16 weeks.
Men in the 8-week interval group donated significantly more blood on a per-donor basis, contributing 1.69 and 7.9 units more than the men in the 10- and 12-week interval groups, respectively. Similarly, women in the 12-week interval group contributed approximately 0.84 and 0.46 units more than did women in the 14- and 16-week interval groups.
Hemoglobin and ferritin concentrations stayed relatively stable throughout the study in men and women in all donation interval groups. The baseline hemoglobin and ferritin averages were 149.7 g/L and 44.9 mcg/L in men, and 133.9 g/L and 24.6 mcg/L in women, respectively. Ultimately, mean hemoglobin level decreased by 1%-2%. Ferritin level decreased by 15%-30%, indicating that it is a more accurate marker of iron depletion, the study authors wrote. The report was published online in The Lancet.
The researchers also analyzed self-reported symptoms associated with blood donations derived from donor follow-up surveys sent at 6-, 12-, and 18-month intervals. At the end of the 2-year study, donors underwent a series of cognitive function tests and answered a physical activity questionnaire. Increased donation rates correlated with increased symptoms of iron deficiency such as tiredness, restless legs, and dizziness. This effect was reported more strongly in men.
About 10% of participants were allowed to donate despite having baseline hemoglobin concentrations below the minimum regulatory threshold, said the authors, who said that the screening method used in the United Kingdom to test eligibility to donate needs to be reviewed.
“In response to these findings, we have started the COMPARE study (ISRCTN90871183) to provide a systematic, within-person comparison of the relative merits of different haemoglobin screening methods,” they wrote
The study was funded by National Health Service Blood and Transplant and the National Institute for Health Research Blood and Transplant Research Unit in Donor Health and Genomics (NIHR BTRU-2014-10024).
Donating blood serves an important function in medicine, but the practices associated with blood donations do not consider the effect it has on the donors. The amount of blood that most donors give is around 500 mL, or about 10% of total blood volume. The ratio of iron to blood is 1:1, meaning that for each milligram of blood drawn, one milligram of iron is lost. Considering that women only have 250 mg of iron reserves and men have 1,000 mg of reserves, many frequent donors are at risk of developing iron deficiency.
This study found that the total units of blood collected increased with shorter inter-donation intervals, while secondary safety outcomes of hemoglobin and ferritin levels remained similar between short and long inter-donation interval groups. While overall health did not decline, short inter-donation donors reported symptoms consistent with iron deficiency, including dizziness, tiredness, and restless legs. Researchers found that “about 25% of men and women at the most frequent inter-donation interval had iron deficiency and a third had at least one deferral for low hemoglobin.”
Iron deficiency can be mitigated by iron supplements or by lengthening the time between donations, but this does not fully correct the issue. Some blood centers have already introduced ferritin screening and lengthened the inter-donation interval for donors found to have low ferritin concentrations. Given the advances in automated laboratory testing, information technology, and the high compliance of blood donors, individualized approaches for prevention of iron deficiency could be feasible.
Alan E. Mast, MD , is the medical director for the Blood Center of Wisconsin, and an associate professor of pathology and cell biology at the Medical College of Wisconsin, Milwaukee. Edward L. Murphy, MD , is resident professor of laboratory medicine at University of California, San Francisco, and an affiliate of the Blood Systems Research Institute. They made their comments in an editorial that accompanied the study.
Donating blood serves an important function in medicine, but the practices associated with blood donations do not consider the effect it has on the donors. The amount of blood that most donors give is around 500 mL, or about 10% of total blood volume. The ratio of iron to blood is 1:1, meaning that for each milligram of blood drawn, one milligram of iron is lost. Considering that women only have 250 mg of iron reserves and men have 1,000 mg of reserves, many frequent donors are at risk of developing iron deficiency.
This study found that the total units of blood collected increased with shorter inter-donation intervals, while secondary safety outcomes of hemoglobin and ferritin levels remained similar between short and long inter-donation interval groups. While overall health did not decline, short inter-donation donors reported symptoms consistent with iron deficiency, including dizziness, tiredness, and restless legs. Researchers found that “about 25% of men and women at the most frequent inter-donation interval had iron deficiency and a third had at least one deferral for low hemoglobin.”
Iron deficiency can be mitigated by iron supplements or by lengthening the time between donations, but this does not fully correct the issue. Some blood centers have already introduced ferritin screening and lengthened the inter-donation interval for donors found to have low ferritin concentrations. Given the advances in automated laboratory testing, information technology, and the high compliance of blood donors, individualized approaches for prevention of iron deficiency could be feasible.
Alan E. Mast, MD , is the medical director for the Blood Center of Wisconsin, and an associate professor of pathology and cell biology at the Medical College of Wisconsin, Milwaukee. Edward L. Murphy, MD , is resident professor of laboratory medicine at University of California, San Francisco, and an affiliate of the Blood Systems Research Institute. They made their comments in an editorial that accompanied the study.
Donating blood serves an important function in medicine, but the practices associated with blood donations do not consider the effect it has on the donors. The amount of blood that most donors give is around 500 mL, or about 10% of total blood volume. The ratio of iron to blood is 1:1, meaning that for each milligram of blood drawn, one milligram of iron is lost. Considering that women only have 250 mg of iron reserves and men have 1,000 mg of reserves, many frequent donors are at risk of developing iron deficiency.
This study found that the total units of blood collected increased with shorter inter-donation intervals, while secondary safety outcomes of hemoglobin and ferritin levels remained similar between short and long inter-donation interval groups. While overall health did not decline, short inter-donation donors reported symptoms consistent with iron deficiency, including dizziness, tiredness, and restless legs. Researchers found that “about 25% of men and women at the most frequent inter-donation interval had iron deficiency and a third had at least one deferral for low hemoglobin.”
Iron deficiency can be mitigated by iron supplements or by lengthening the time between donations, but this does not fully correct the issue. Some blood centers have already introduced ferritin screening and lengthened the inter-donation interval for donors found to have low ferritin concentrations. Given the advances in automated laboratory testing, information technology, and the high compliance of blood donors, individualized approaches for prevention of iron deficiency could be feasible.
Alan E. Mast, MD , is the medical director for the Blood Center of Wisconsin, and an associate professor of pathology and cell biology at the Medical College of Wisconsin, Milwaukee. Edward L. Murphy, MD , is resident professor of laboratory medicine at University of California, San Francisco, and an affiliate of the Blood Systems Research Institute. They made their comments in an editorial that accompanied the study.
Reducing the interval between blood donations from every 12 weeks to every 8 weeks increases blood units collected with little ill effects on donor quality of life other than symptoms related to iron deficiency, based on results reported by the INTERVAL Trial Group.
In the United States, men and women can donate blood every 8 weeks; the Food and Drug Administration and the AABB (formerly the American Association of Blood Banks) have considered lengthening the 8-week minimum inter-donation interval to reduce the risk of iron deficiency. The current practice in the United Kingdom is to allow men to donate every 12 weeks and women every 16 weeks, the authors noted.
The INTERVAL study examined hemoglobin levels, ferritin levels, and self-reported symptoms as well as the number of blood donations over a 2-year period among 22,466 men randomly assigned to either 8-, 10-, or 12-week blood donation intervals and 22,797 women randomly assigned to donation intervals of 12, 14, and 16 weeks.
Men in the 8-week interval group donated significantly more blood on a per-donor basis, contributing 1.69 and 7.9 units more than the men in the 10- and 12-week interval groups, respectively. Similarly, women in the 12-week interval group contributed approximately 0.84 and 0.46 units more than did women in the 14- and 16-week interval groups.
Hemoglobin and ferritin concentrations stayed relatively stable throughout the study in men and women in all donation interval groups. The baseline hemoglobin and ferritin averages were 149.7 g/L and 44.9 mcg/L in men, and 133.9 g/L and 24.6 mcg/L in women, respectively. Ultimately, mean hemoglobin level decreased by 1%-2%. Ferritin level decreased by 15%-30%, indicating that it is a more accurate marker of iron depletion, the study authors wrote. The report was published online in The Lancet.
The researchers also analyzed self-reported symptoms associated with blood donations derived from donor follow-up surveys sent at 6-, 12-, and 18-month intervals. At the end of the 2-year study, donors underwent a series of cognitive function tests and answered a physical activity questionnaire. Increased donation rates correlated with increased symptoms of iron deficiency such as tiredness, restless legs, and dizziness. This effect was reported more strongly in men.
About 10% of participants were allowed to donate despite having baseline hemoglobin concentrations below the minimum regulatory threshold, said the authors, who said that the screening method used in the United Kingdom to test eligibility to donate needs to be reviewed.
“In response to these findings, we have started the COMPARE study (ISRCTN90871183) to provide a systematic, within-person comparison of the relative merits of different haemoglobin screening methods,” they wrote
The study was funded by National Health Service Blood and Transplant and the National Institute for Health Research Blood and Transplant Research Unit in Donor Health and Genomics (NIHR BTRU-2014-10024).
Reducing the interval between blood donations from every 12 weeks to every 8 weeks increases blood units collected with little ill effects on donor quality of life other than symptoms related to iron deficiency, based on results reported by the INTERVAL Trial Group.
In the United States, men and women can donate blood every 8 weeks; the Food and Drug Administration and the AABB (formerly the American Association of Blood Banks) have considered lengthening the 8-week minimum inter-donation interval to reduce the risk of iron deficiency. The current practice in the United Kingdom is to allow men to donate every 12 weeks and women every 16 weeks, the authors noted.
The INTERVAL study examined hemoglobin levels, ferritin levels, and self-reported symptoms as well as the number of blood donations over a 2-year period among 22,466 men randomly assigned to either 8-, 10-, or 12-week blood donation intervals and 22,797 women randomly assigned to donation intervals of 12, 14, and 16 weeks.
Men in the 8-week interval group donated significantly more blood on a per-donor basis, contributing 1.69 and 7.9 units more than the men in the 10- and 12-week interval groups, respectively. Similarly, women in the 12-week interval group contributed approximately 0.84 and 0.46 units more than did women in the 14- and 16-week interval groups.
Hemoglobin and ferritin concentrations stayed relatively stable throughout the study in men and women in all donation interval groups. The baseline hemoglobin and ferritin averages were 149.7 g/L and 44.9 mcg/L in men, and 133.9 g/L and 24.6 mcg/L in women, respectively. Ultimately, mean hemoglobin level decreased by 1%-2%. Ferritin level decreased by 15%-30%, indicating that it is a more accurate marker of iron depletion, the study authors wrote. The report was published online in The Lancet.
The researchers also analyzed self-reported symptoms associated with blood donations derived from donor follow-up surveys sent at 6-, 12-, and 18-month intervals. At the end of the 2-year study, donors underwent a series of cognitive function tests and answered a physical activity questionnaire. Increased donation rates correlated with increased symptoms of iron deficiency such as tiredness, restless legs, and dizziness. This effect was reported more strongly in men.
About 10% of participants were allowed to donate despite having baseline hemoglobin concentrations below the minimum regulatory threshold, said the authors, who said that the screening method used in the United Kingdom to test eligibility to donate needs to be reviewed.
“In response to these findings, we have started the COMPARE study (ISRCTN90871183) to provide a systematic, within-person comparison of the relative merits of different haemoglobin screening methods,” they wrote
The study was funded by National Health Service Blood and Transplant and the National Institute for Health Research Blood and Transplant Research Unit in Donor Health and Genomics (NIHR BTRU-2014-10024).
FROM THE LANCET
Key clinical point:
Major finding: Reducing inter-donation intervals increases blood collections by 33% in men and 24% in women.
Data source: Parallel group, pragmatic, randomized trial of 22,466 men and 22,797 women from the 25 donor centers of National Health Service Blood and Transplant.
Disclosures: The study was funded by National Health Service Blood and Transplant and the National Institute for Health Research Blood and Transplant Research Unit in Donor Health and Genomics.
Oral anticoagulation ‘reasonable’ in advanced kidney disease with A-fib
BARCELONA – Oral anticoagulation had a net overall benefit for patients with atrial fibrillation and advanced chronic kidney disease, based on results of a large observational study reported at the annual congress of the European Society of Cardiology.
The novel direct-acting oral anticoagulants (NOACs) and warfarin were all similarly effective in this study of 39,241 patients who had stage 4 or 5 chronic kidney disease (CKD), atrial fibrillation, and were not on dialysis. Compared with no oral anticoagulation, the drugs cut in half the risk of stroke or systemic embolism, with no increased risk of major bleeding.
“In patients with advanced CKD, it appears that OACs [oral anticoagulants] are reasonable,” concluded Peter A. Noseworthy, MD, of the Mayo Clinic in Rochester, Minn.

This is a potentially practice-changing finding given the “striking underutilization” of OACs in advanced CKD, he noted. Indeed, only one-third of the patients in this study were prescribed an OAC and picked up their prescriptions. And while the study has the limitations inherent to an observational study reliant upon data from a large U.S. administrative database – chiefly, the potential for residual confounding because of factors that couldn’t be adjusted for statistically – these real-world data may be as good as it gets, since patients with advanced CKD were excluded from the pivotal trials of the NOACs.
Apixaban (Eliquis) was the winner in this study: It separated itself from the pack by reducing the major bleeding risk by 57%, compared with warfarin, although it wasn’t significantly more effective than the other drugs in terms of stroke prevention. In contrast, the major bleeding rates for dabigatran (Pradaxa) and rivaroxaban (Xarelto) weren’t significantly different from warfarin in this challenging patient population.
In a related analysis of 10,712 patients with atrial fibrillation and advanced CKD who were on dialysis, use of an OAC was once again a winning strategy: It resulted not only in an impressive 58% reduction in the risk of stroke or systemic embolism, but also a 26% reduction in the risk of major bleeding, compared with no OAC.
Here again, apixaban was arguably the drug of choice. None of the 125 dialysis patients on apixaban experienced a stroke or systemic embolism. In contrast, dabigatran and rivaroxaban were associated with greater than threefold higher stroke rates than in patients on warfarin, although these differences didn’t achieve statistical significance because of small numbers, just 36 patients on dabigatran and 56 on rivaroxaban, the cardiologist continued.
For these analyses of the relationship between OAC exposure and stroke and bleeding outcomes, Dr. Noseworthy and his coinvestigators used propensity scores based upon 59 clinical and sociodemographic characteristics.
Asked why rates of utilization of OACs are so low in patients with advanced CKD, Dr. Noseworthy replied that he didn’t find that particularly surprising.
“Even if you look only at patients without renal dysfunction, there is incredible undertreatment of atrial fibrillation with OACs. And adherence is very poor,” he observed.
Moreover, in talking with nephrologists, he finds many of them have legitimate reservations about prescribing OACs for patients with end-stage renal disease on hemodialysis.
“They’re undergoing a lot of procedures. They’re having a ton of lines placed; they’re having fistulas revised; and they have very high rates of GI bleeding. In some studies the annual risk of bleeding is 20%-40% in this population. And they’re a frail population with frequent falls,” Dr. Noseworthy said.
He reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
BARCELONA – Oral anticoagulation had a net overall benefit for patients with atrial fibrillation and advanced chronic kidney disease, based on results of a large observational study reported at the annual congress of the European Society of Cardiology.
The novel direct-acting oral anticoagulants (NOACs) and warfarin were all similarly effective in this study of 39,241 patients who had stage 4 or 5 chronic kidney disease (CKD), atrial fibrillation, and were not on dialysis. Compared with no oral anticoagulation, the drugs cut in half the risk of stroke or systemic embolism, with no increased risk of major bleeding.
“In patients with advanced CKD, it appears that OACs [oral anticoagulants] are reasonable,” concluded Peter A. Noseworthy, MD, of the Mayo Clinic in Rochester, Minn.
This is a potentially practice-changing finding given the “striking underutilization” of OACs in advanced CKD, he noted. Indeed, only one-third of the patients in this study were prescribed an OAC and picked up their prescriptions. And while the study has the limitations inherent to an observational study reliant upon data from a large U.S. administrative database – chiefly, the potential for residual confounding because of factors that couldn’t be adjusted for statistically – these real-world data may be as good as it gets, since patients with advanced CKD were excluded from the pivotal trials of the NOACs.
Apixaban (Eliquis) was the winner in this study: It separated itself from the pack by reducing the major bleeding risk by 57%, compared with warfarin, although it wasn’t significantly more effective than the other drugs in terms of stroke prevention. In contrast, the major bleeding rates for dabigatran (Pradaxa) and rivaroxaban (Xarelto) weren’t significantly different from warfarin in this challenging patient population.
In a related analysis of 10,712 patients with atrial fibrillation and advanced CKD who were on dialysis, use of an OAC was once again a winning strategy: It resulted not only in an impressive 58% reduction in the risk of stroke or systemic embolism, but also a 26% reduction in the risk of major bleeding, compared with no OAC.
Here again, apixaban was arguably the drug of choice. None of the 125 dialysis patients on apixaban experienced a stroke or systemic embolism. In contrast, dabigatran and rivaroxaban were associated with greater than threefold higher stroke rates than in patients on warfarin, although these differences didn’t achieve statistical significance because of small numbers, just 36 patients on dabigatran and 56 on rivaroxaban, the cardiologist continued.
For these analyses of the relationship between OAC exposure and stroke and bleeding outcomes, Dr. Noseworthy and his coinvestigators used propensity scores based upon 59 clinical and sociodemographic characteristics.
Asked why rates of utilization of OACs are so low in patients with advanced CKD, Dr. Noseworthy replied that he didn’t find that particularly surprising.
“Even if you look only at patients without renal dysfunction, there is incredible undertreatment of atrial fibrillation with OACs. And adherence is very poor,” he observed.
Moreover, in talking with nephrologists, he finds many of them have legitimate reservations about prescribing OACs for patients with end-stage renal disease on hemodialysis.
“They’re undergoing a lot of procedures. They’re having a ton of lines placed; they’re having fistulas revised; and they have very high rates of GI bleeding. In some studies the annual risk of bleeding is 20%-40% in this population. And they’re a frail population with frequent falls,” Dr. Noseworthy said.
He reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
BARCELONA – Oral anticoagulation had a net overall benefit for patients with atrial fibrillation and advanced chronic kidney disease, based on results of a large observational study reported at the annual congress of the European Society of Cardiology.
The novel direct-acting oral anticoagulants (NOACs) and warfarin were all similarly effective in this study of 39,241 patients who had stage 4 or 5 chronic kidney disease (CKD), atrial fibrillation, and were not on dialysis. Compared with no oral anticoagulation, the drugs cut in half the risk of stroke or systemic embolism, with no increased risk of major bleeding.
“In patients with advanced CKD, it appears that OACs [oral anticoagulants] are reasonable,” concluded Peter A. Noseworthy, MD, of the Mayo Clinic in Rochester, Minn.
This is a potentially practice-changing finding given the “striking underutilization” of OACs in advanced CKD, he noted. Indeed, only one-third of the patients in this study were prescribed an OAC and picked up their prescriptions. And while the study has the limitations inherent to an observational study reliant upon data from a large U.S. administrative database – chiefly, the potential for residual confounding because of factors that couldn’t be adjusted for statistically – these real-world data may be as good as it gets, since patients with advanced CKD were excluded from the pivotal trials of the NOACs.
Apixaban (Eliquis) was the winner in this study: It separated itself from the pack by reducing the major bleeding risk by 57%, compared with warfarin, although it wasn’t significantly more effective than the other drugs in terms of stroke prevention. In contrast, the major bleeding rates for dabigatran (Pradaxa) and rivaroxaban (Xarelto) weren’t significantly different from warfarin in this challenging patient population.
In a related analysis of 10,712 patients with atrial fibrillation and advanced CKD who were on dialysis, use of an OAC was once again a winning strategy: It resulted not only in an impressive 58% reduction in the risk of stroke or systemic embolism, but also a 26% reduction in the risk of major bleeding, compared with no OAC.
Here again, apixaban was arguably the drug of choice. None of the 125 dialysis patients on apixaban experienced a stroke or systemic embolism. In contrast, dabigatran and rivaroxaban were associated with greater than threefold higher stroke rates than in patients on warfarin, although these differences didn’t achieve statistical significance because of small numbers, just 36 patients on dabigatran and 56 on rivaroxaban, the cardiologist continued.
For these analyses of the relationship between OAC exposure and stroke and bleeding outcomes, Dr. Noseworthy and his coinvestigators used propensity scores based upon 59 clinical and sociodemographic characteristics.
Asked why rates of utilization of OACs are so low in patients with advanced CKD, Dr. Noseworthy replied that he didn’t find that particularly surprising.
“Even if you look only at patients without renal dysfunction, there is incredible undertreatment of atrial fibrillation with OACs. And adherence is very poor,” he observed.
Moreover, in talking with nephrologists, he finds many of them have legitimate reservations about prescribing OACs for patients with end-stage renal disease on hemodialysis.
“They’re undergoing a lot of procedures. They’re having a ton of lines placed; they’re having fistulas revised; and they have very high rates of GI bleeding. In some studies the annual risk of bleeding is 20%-40% in this population. And they’re a frail population with frequent falls,” Dr. Noseworthy said.
He reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
AT THE ESC CONGRESS 2017
Key clinical point:
Major finding: The risk of stroke/systemic embolism in patients with advanced chronic kidney disease who were on oral anticoagulation was reduced by 49% among those not on hemodialysis and by 58% in those who were, compared with similar patients not on oral anticoagulation.
Data source: This was an observational study of nearly 50,000 patients with atrial fibrillation and stage 4 or 5 chronic kidney disease in a large U.S. administrative database.
Disclosures: The presenter reported having no financial conflicts of interest regarding his study, which was conducted free of commercial support.
Hospital mortality for emergency bowel resection linked to failure to rescue
BALTIMORE – The variation among hospitals in mortality for emergent bowel resection may be explained in part by failure-to-rescue (FTR) rates, according to a study presented at the American Association for Surgery of Trauma annual meeting.
Ambar Mehta, a medical student at Johns Hopkins University School of Medicine in Baltimore, and a team of colleagues reviewed case data on 105,925 bowel resections that occurred between 2010 and 2013 using the Agency for Healthcare Research and Quality Nationwide Inpatient Sample.
Hospitals included were ranked by mortality for emergency bowel resection with the top quintile representing lowest mortality (1.5%) and bottom quintile representing the highest (14.9%).
Failure to rescue was defined as death after a major postoperative complication, according to Mr. Mehta. Overall failure-to-rescue rates were 9.8-fold higher in the bottom quintile hospitals, compared with those in the top quintile (33.4% vs. 3.4%). Patients studied were majority white (78.9%), female (53.9%), and younger than 65 years (52%).
Although FTR rates were significantly higher in the bottom quintile hospitals, complication rates were comparable (41.6% for bottom vs. 33.3% for top), suggesting that it was not complications per se that drove mortality but other postop factors.
Complications measured were acute renal failure, pulmonary failure, pneumonia, hemorrhage, gastrointestinal bleeding, pulmonary embolism, surgical site infections, and myocardial infarction.
Risk ratios for failure to rescue showed a similar increasing trend in correlation with mortality, with the hospitals in the lowest quintile showing a risk of 13 (P less than .01), compared with a risk of 3.2 (P less than .01) among hospitals in the highest quintile.
Correlation between failure to rescue and mortality was still evident when investigators adjusted analysis to compare hospitals that conducted more than 10 resections annually, causing investigators to suggest a need for changes in resection procedures.
“Our data suggest rates of failure to rescue correlate to rates of hospital mortality and we believe that system-level initiatives such as focusing on teamwork and team culture can reduce nationwide variations in mortality,” said Mr. Mehta.
Discussant Andrew Peitzman, MD, FACS, vice president for Trauma and Surgical Services at the University of Pittsburgh, acknowledged the link between mortality and failure to rescue among bowel resection patients and brought up the question of how to avoid such issues in the first place.
“This study validates the principle that a patient will generally tolerate an operation but not the first complication,” said Dr. Peitzman. “How do we avoid the first complication [and] what do you recommend in our acute care surgery practices and hospital structures to rescue our patients?”
Understanding why the complications happen at all is the first step to preventing them, Mr. Mehta said. Emergency general surgery–specific programs or mentorship programs may be a good start to cutting down on the inherent risk increase of emergent procedures.
Having greater than 20 beds designated to the intensive care unit and having a greater ratio of nursing staff to patients may be other viable solutions, according to a study Mr. Mehta cited; however, he asserted, focusing on team protocols seems to be the most successful course.
When asked by audience members about the idea of regionalizing care, Dr. Mehta said more data would be needed. “Regionalization has definitely shown benefits in a trauma setting,” said Mr. Mehta. “Copying a model of that idea for nontrauma [emergency general surgery] procedures may work, but it would require studies in a multicenter program.”
The study was limited by the use of administrative claims data, including being unable to determine if deaths were caused by a failure to rescue or whether families determined to end care after an initial complication. Investigators were also unable to identify which surgical diagnoses led to the procedure, nor could they adjust for varying hospital resources.
Investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
BALTIMORE – The variation among hospitals in mortality for emergent bowel resection may be explained in part by failure-to-rescue (FTR) rates, according to a study presented at the American Association for Surgery of Trauma annual meeting.
Ambar Mehta, a medical student at Johns Hopkins University School of Medicine in Baltimore, and a team of colleagues reviewed case data on 105,925 bowel resections that occurred between 2010 and 2013 using the Agency for Healthcare Research and Quality Nationwide Inpatient Sample.
Hospitals included were ranked by mortality for emergency bowel resection with the top quintile representing lowest mortality (1.5%) and bottom quintile representing the highest (14.9%).
Failure to rescue was defined as death after a major postoperative complication, according to Mr. Mehta. Overall failure-to-rescue rates were 9.8-fold higher in the bottom quintile hospitals, compared with those in the top quintile (33.4% vs. 3.4%). Patients studied were majority white (78.9%), female (53.9%), and younger than 65 years (52%).
Although FTR rates were significantly higher in the bottom quintile hospitals, complication rates were comparable (41.6% for bottom vs. 33.3% for top), suggesting that it was not complications per se that drove mortality but other postop factors.
Complications measured were acute renal failure, pulmonary failure, pneumonia, hemorrhage, gastrointestinal bleeding, pulmonary embolism, surgical site infections, and myocardial infarction.
Risk ratios for failure to rescue showed a similar increasing trend in correlation with mortality, with the hospitals in the lowest quintile showing a risk of 13 (P less than .01), compared with a risk of 3.2 (P less than .01) among hospitals in the highest quintile.
Correlation between failure to rescue and mortality was still evident when investigators adjusted analysis to compare hospitals that conducted more than 10 resections annually, causing investigators to suggest a need for changes in resection procedures.
“Our data suggest rates of failure to rescue correlate to rates of hospital mortality and we believe that system-level initiatives such as focusing on teamwork and team culture can reduce nationwide variations in mortality,” said Mr. Mehta.
Discussant Andrew Peitzman, MD, FACS, vice president for Trauma and Surgical Services at the University of Pittsburgh, acknowledged the link between mortality and failure to rescue among bowel resection patients and brought up the question of how to avoid such issues in the first place.
“This study validates the principle that a patient will generally tolerate an operation but not the first complication,” said Dr. Peitzman. “How do we avoid the first complication [and] what do you recommend in our acute care surgery practices and hospital structures to rescue our patients?”
Understanding why the complications happen at all is the first step to preventing them, Mr. Mehta said. Emergency general surgery–specific programs or mentorship programs may be a good start to cutting down on the inherent risk increase of emergent procedures.
Having greater than 20 beds designated to the intensive care unit and having a greater ratio of nursing staff to patients may be other viable solutions, according to a study Mr. Mehta cited; however, he asserted, focusing on team protocols seems to be the most successful course.
When asked by audience members about the idea of regionalizing care, Dr. Mehta said more data would be needed. “Regionalization has definitely shown benefits in a trauma setting,” said Mr. Mehta. “Copying a model of that idea for nontrauma [emergency general surgery] procedures may work, but it would require studies in a multicenter program.”
The study was limited by the use of administrative claims data, including being unable to determine if deaths were caused by a failure to rescue or whether families determined to end care after an initial complication. Investigators were also unable to identify which surgical diagnoses led to the procedure, nor could they adjust for varying hospital resources.
Investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
BALTIMORE – The variation among hospitals in mortality for emergent bowel resection may be explained in part by failure-to-rescue (FTR) rates, according to a study presented at the American Association for Surgery of Trauma annual meeting.
Ambar Mehta, a medical student at Johns Hopkins University School of Medicine in Baltimore, and a team of colleagues reviewed case data on 105,925 bowel resections that occurred between 2010 and 2013 using the Agency for Healthcare Research and Quality Nationwide Inpatient Sample.
Hospitals included were ranked by mortality for emergency bowel resection with the top quintile representing lowest mortality (1.5%) and bottom quintile representing the highest (14.9%).
Failure to rescue was defined as death after a major postoperative complication, according to Mr. Mehta. Overall failure-to-rescue rates were 9.8-fold higher in the bottom quintile hospitals, compared with those in the top quintile (33.4% vs. 3.4%). Patients studied were majority white (78.9%), female (53.9%), and younger than 65 years (52%).
Although FTR rates were significantly higher in the bottom quintile hospitals, complication rates were comparable (41.6% for bottom vs. 33.3% for top), suggesting that it was not complications per se that drove mortality but other postop factors.
Complications measured were acute renal failure, pulmonary failure, pneumonia, hemorrhage, gastrointestinal bleeding, pulmonary embolism, surgical site infections, and myocardial infarction.
Risk ratios for failure to rescue showed a similar increasing trend in correlation with mortality, with the hospitals in the lowest quintile showing a risk of 13 (P less than .01), compared with a risk of 3.2 (P less than .01) among hospitals in the highest quintile.
Correlation between failure to rescue and mortality was still evident when investigators adjusted analysis to compare hospitals that conducted more than 10 resections annually, causing investigators to suggest a need for changes in resection procedures.
“Our data suggest rates of failure to rescue correlate to rates of hospital mortality and we believe that system-level initiatives such as focusing on teamwork and team culture can reduce nationwide variations in mortality,” said Mr. Mehta.
Discussant Andrew Peitzman, MD, FACS, vice president for Trauma and Surgical Services at the University of Pittsburgh, acknowledged the link between mortality and failure to rescue among bowel resection patients and brought up the question of how to avoid such issues in the first place.
“This study validates the principle that a patient will generally tolerate an operation but not the first complication,” said Dr. Peitzman. “How do we avoid the first complication [and] what do you recommend in our acute care surgery practices and hospital structures to rescue our patients?”
Understanding why the complications happen at all is the first step to preventing them, Mr. Mehta said. Emergency general surgery–specific programs or mentorship programs may be a good start to cutting down on the inherent risk increase of emergent procedures.
Having greater than 20 beds designated to the intensive care unit and having a greater ratio of nursing staff to patients may be other viable solutions, according to a study Mr. Mehta cited; however, he asserted, focusing on team protocols seems to be the most successful course.
When asked by audience members about the idea of regionalizing care, Dr. Mehta said more data would be needed. “Regionalization has definitely shown benefits in a trauma setting,” said Mr. Mehta. “Copying a model of that idea for nontrauma [emergency general surgery] procedures may work, but it would require studies in a multicenter program.”
The study was limited by the use of administrative claims data, including being unable to determine if deaths were caused by a failure to rescue or whether families determined to end care after an initial complication. Investigators were also unable to identify which surgical diagnoses led to the procedure, nor could they adjust for varying hospital resources.
Investigators reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
FROM AAST
Key clinical point:
Major finding: Risk-adjusted failure-to-rescue rates were 9.8 times higher in hospitals with the highest mortality than in those with the lowest (33.4% vs. 3.1%).
Data source: Study of 105,925 bowel resections that occurred between 2010 and 2013 collected from the AHRQ Nationwide Inpatient Sample.
Disclosures: Investigators reported no relevant financial disclosures.
Increase in Kids Who Are Getting the HPV Vaccine
The HPV vaccine has led to “dramatic declines” in HPV infections, according to the CDC. Since the first HPV vaccine was introduced 10 years ago, the percentage of infections that cause cancers and genital warts has dropped by 71% among teenage girls and 61% among young women. According to the annual National Immunization Survey-Teen report, 60% of teens aged 13 to 17 years received ≥ 1 doses of HPV vaccine in 2016, up 4 percentage points from 2015.
More boys are getting the vaccine, too. About 56% of boys received their first dose (although that is still less than the 65% seen in girls)—representing a 6% increase from 2015; rates for girls remained stable.
As encouraging as those numbers are, there is more work to do, the CDC says. Although most adolescents have received the first dose, only 43% are up-to-date on all the recommended doses. The CDC recommends that 11- to 12-year-olds get 2 doses of HPV vaccine at least 6 months apart. The CDC updated its HPV vaccine recommendations in 2016 when new evidence showed that 2 doses of the vaccine provided levels of protection similar to those seen for 3 doses in older adolescents and young adults.
Parents can get the vaccine for their child during any doctor’s visit, but the CDC recommends that adolescents get the HPV vaccine during the same visit that they get whooping cough and meningitis vaccine.
The HPV vaccine has led to “dramatic declines” in HPV infections, according to the CDC. Since the first HPV vaccine was introduced 10 years ago, the percentage of infections that cause cancers and genital warts has dropped by 71% among teenage girls and 61% among young women. According to the annual National Immunization Survey-Teen report, 60% of teens aged 13 to 17 years received ≥ 1 doses of HPV vaccine in 2016, up 4 percentage points from 2015.
More boys are getting the vaccine, too. About 56% of boys received their first dose (although that is still less than the 65% seen in girls)—representing a 6% increase from 2015; rates for girls remained stable.
As encouraging as those numbers are, there is more work to do, the CDC says. Although most adolescents have received the first dose, only 43% are up-to-date on all the recommended doses. The CDC recommends that 11- to 12-year-olds get 2 doses of HPV vaccine at least 6 months apart. The CDC updated its HPV vaccine recommendations in 2016 when new evidence showed that 2 doses of the vaccine provided levels of protection similar to those seen for 3 doses in older adolescents and young adults.
Parents can get the vaccine for their child during any doctor’s visit, but the CDC recommends that adolescents get the HPV vaccine during the same visit that they get whooping cough and meningitis vaccine.
The HPV vaccine has led to “dramatic declines” in HPV infections, according to the CDC. Since the first HPV vaccine was introduced 10 years ago, the percentage of infections that cause cancers and genital warts has dropped by 71% among teenage girls and 61% among young women. According to the annual National Immunization Survey-Teen report, 60% of teens aged 13 to 17 years received ≥ 1 doses of HPV vaccine in 2016, up 4 percentage points from 2015.
More boys are getting the vaccine, too. About 56% of boys received their first dose (although that is still less than the 65% seen in girls)—representing a 6% increase from 2015; rates for girls remained stable.
As encouraging as those numbers are, there is more work to do, the CDC says. Although most adolescents have received the first dose, only 43% are up-to-date on all the recommended doses. The CDC recommends that 11- to 12-year-olds get 2 doses of HPV vaccine at least 6 months apart. The CDC updated its HPV vaccine recommendations in 2016 when new evidence showed that 2 doses of the vaccine provided levels of protection similar to those seen for 3 doses in older adolescents and young adults.
Parents can get the vaccine for their child during any doctor’s visit, but the CDC recommends that adolescents get the HPV vaccine during the same visit that they get whooping cough and meningitis vaccine.