User login
DMARDs may hamper pneumococcal vaccine response in systemic sclerosis patients
Patients taking disease-modifying antirheumatic medications for systemic sclerosis appear to have a decreased response to pneumococcal vaccines, a Swedish study has determined.
Those not taking disease-modifying antirheumatic medications (DMARDs), however, had a normal immune response, suggesting that it’s the immunomodulating medications, not the disease itself, that is affecting antibody levels, Roger Hesselstrand, MD, of Lund (Sweden) University and his colleagues reported online in Rheumatology.
“The currently recommended prime-boost vaccination strategy using a dose of PCV13 [13-valent pneumococcal conjugate vaccine] followed by a dose of PPV23 [23-valent pneumococcal polysaccharide vaccine] might be a possible way of enhancing the vaccine immunogenicity in immunosuppressed patients,” Dr. Hesselstrand and his coauthors wrote.
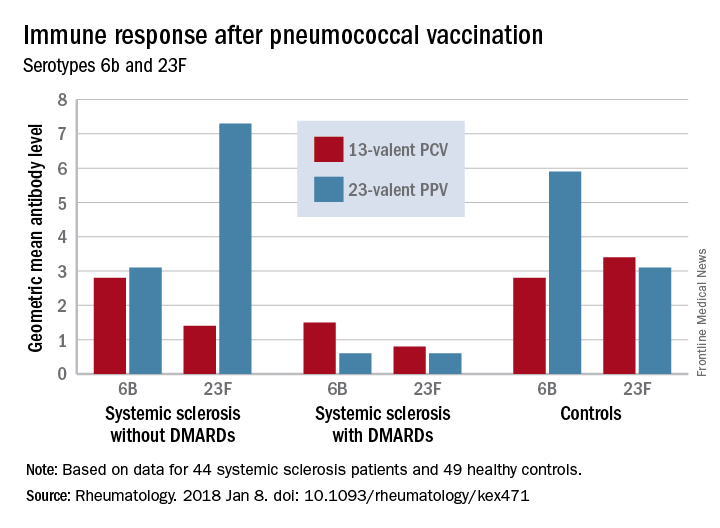
The study comprised 44 subjects with systemic sclerosis, 12 of whom were taking a DMARD (mycophenolate mofetil, azathioprine, or hydroxychloroquine), and 49 healthy controls; all underwent pneumococcal vaccination. The first 13 got a single dose of PPV23 intramuscularly. PCV13 was then licensed for adults in Sweden, and the remaining 31 patients received this vaccine. The primary outcome was 6-week change from baseline in the level of pneumococcal IgG to Streptococcus pneumoniae serotypes 23F and 6B.
Both vaccines were safe and well-tolerated by all patients, including those taking a DMARD.
Before vaccination, antibody levels to both serotypes were similar between the groups. After vaccination, antibody levels for both serotypes increased significantly in systemic sclerosis patients not taking a DMARD and in controls. However, patients taking a DMARD mounted only an adequate response to serotype 6B.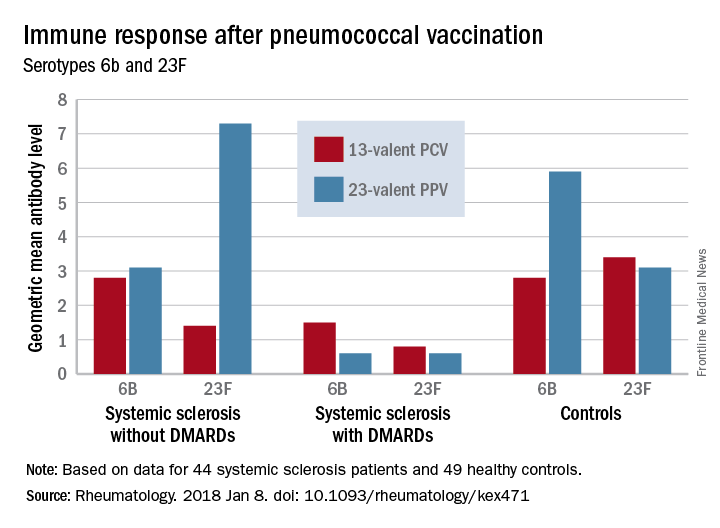
There were fewer responders among those taking DMARDs, whether they received the PCV13 or the PPV23 vaccine. An increase from prevaccination antibody levels of at least twofold occurred in fewer patients taking DMARDs than did in patients not taking DMARDs and in controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
“We demonstrated that the antibody response ... as well as functionality of antibodies in [systemic sclerosis] patients not receiving DMARDs was as good as in controls regardless of vaccine type,” the investigators concluded. “Systemic sclerosis patients treated with DMARDs, however, had lower proportion of patients with positive antibody response, although the functionality of the antibodies was preserved. These results suggest that immunomodulating drugs but not systemic sclerosis itself and/or immunological disturbance as a part of this disease affect the ability to produce a sufficient amount of vaccine-specific antibodies, but not their function.”
None of the authors had conflicts of interest to disclose.
SOURCE: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471.
Patients taking disease-modifying antirheumatic medications for systemic sclerosis appear to have a decreased response to pneumococcal vaccines, a Swedish study has determined.
Those not taking disease-modifying antirheumatic medications (DMARDs), however, had a normal immune response, suggesting that it’s the immunomodulating medications, not the disease itself, that is affecting antibody levels, Roger Hesselstrand, MD, of Lund (Sweden) University and his colleagues reported online in Rheumatology.
“The currently recommended prime-boost vaccination strategy using a dose of PCV13 [13-valent pneumococcal conjugate vaccine] followed by a dose of PPV23 [23-valent pneumococcal polysaccharide vaccine] might be a possible way of enhancing the vaccine immunogenicity in immunosuppressed patients,” Dr. Hesselstrand and his coauthors wrote.
The study comprised 44 subjects with systemic sclerosis, 12 of whom were taking a DMARD (mycophenolate mofetil, azathioprine, or hydroxychloroquine), and 49 healthy controls; all underwent pneumococcal vaccination. The first 13 got a single dose of PPV23 intramuscularly. PCV13 was then licensed for adults in Sweden, and the remaining 31 patients received this vaccine. The primary outcome was 6-week change from baseline in the level of pneumococcal IgG to Streptococcus pneumoniae serotypes 23F and 6B.
Both vaccines were safe and well-tolerated by all patients, including those taking a DMARD.
Before vaccination, antibody levels to both serotypes were similar between the groups. After vaccination, antibody levels for both serotypes increased significantly in systemic sclerosis patients not taking a DMARD and in controls. However, patients taking a DMARD mounted only an adequate response to serotype 6B.
There were fewer responders among those taking DMARDs, whether they received the PCV13 or the PPV23 vaccine. An increase from prevaccination antibody levels of at least twofold occurred in fewer patients taking DMARDs than did in patients not taking DMARDs and in controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
“We demonstrated that the antibody response ... as well as functionality of antibodies in [systemic sclerosis] patients not receiving DMARDs was as good as in controls regardless of vaccine type,” the investigators concluded. “Systemic sclerosis patients treated with DMARDs, however, had lower proportion of patients with positive antibody response, although the functionality of the antibodies was preserved. These results suggest that immunomodulating drugs but not systemic sclerosis itself and/or immunological disturbance as a part of this disease affect the ability to produce a sufficient amount of vaccine-specific antibodies, but not their function.”
None of the authors had conflicts of interest to disclose.
SOURCE: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471.
Patients taking disease-modifying antirheumatic medications for systemic sclerosis appear to have a decreased response to pneumococcal vaccines, a Swedish study has determined.
Those not taking disease-modifying antirheumatic medications (DMARDs), however, had a normal immune response, suggesting that it’s the immunomodulating medications, not the disease itself, that is affecting antibody levels, Roger Hesselstrand, MD, of Lund (Sweden) University and his colleagues reported online in Rheumatology.
“The currently recommended prime-boost vaccination strategy using a dose of PCV13 [13-valent pneumococcal conjugate vaccine] followed by a dose of PPV23 [23-valent pneumococcal polysaccharide vaccine] might be a possible way of enhancing the vaccine immunogenicity in immunosuppressed patients,” Dr. Hesselstrand and his coauthors wrote.
The study comprised 44 subjects with systemic sclerosis, 12 of whom were taking a DMARD (mycophenolate mofetil, azathioprine, or hydroxychloroquine), and 49 healthy controls; all underwent pneumococcal vaccination. The first 13 got a single dose of PPV23 intramuscularly. PCV13 was then licensed for adults in Sweden, and the remaining 31 patients received this vaccine. The primary outcome was 6-week change from baseline in the level of pneumococcal IgG to Streptococcus pneumoniae serotypes 23F and 6B.
Both vaccines were safe and well-tolerated by all patients, including those taking a DMARD.
Before vaccination, antibody levels to both serotypes were similar between the groups. After vaccination, antibody levels for both serotypes increased significantly in systemic sclerosis patients not taking a DMARD and in controls. However, patients taking a DMARD mounted only an adequate response to serotype 6B.
There were fewer responders among those taking DMARDs, whether they received the PCV13 or the PPV23 vaccine. An increase from prevaccination antibody levels of at least twofold occurred in fewer patients taking DMARDs than did in patients not taking DMARDs and in controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
“We demonstrated that the antibody response ... as well as functionality of antibodies in [systemic sclerosis] patients not receiving DMARDs was as good as in controls regardless of vaccine type,” the investigators concluded. “Systemic sclerosis patients treated with DMARDs, however, had lower proportion of patients with positive antibody response, although the functionality of the antibodies was preserved. These results suggest that immunomodulating drugs but not systemic sclerosis itself and/or immunological disturbance as a part of this disease affect the ability to produce a sufficient amount of vaccine-specific antibodies, but not their function.”
None of the authors had conflicts of interest to disclose.
SOURCE: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471.
FROM RHEUMATOLOGY
Key clinical point:
Major finding: An increase in prevaccination antibody levels of at least twofold occurred in significantly fewer patients taking DMARDs than in patients not taking DMARDs and controls, regardless of vaccine type (PPV23, 50% vs. about 55% and 50%, respectively; PCV13, about 17% vs. 57% and 100%, respectively).
Study details: The prospective study comprised 44 systemic sclerosis patients and 49 healthy controls.
Disclosures: None of the authors had conflicts of interest to disclose.
Source: Hesselstrand R et al. Rheumatology [Oxford]. 2018 Jan 8. doi: 10.1093/rheumatology/kex471
Immune-modified RECIST can help identify survival benefit from cancer immunotherapy
Cancer immunotherapy-specific response criteria not only provide improved estimates of treatment response versus standard criteria, but may also better identify patients who achieve an overall survival benefit from therapy.
Compared to standard Response Evaluation Criteria In Solid Tumors (RECIST) v1.1, the immune-modified RECIST provided a 1%-2% greater overall response and an 8%-13% greater rate of disease control, and added 0.5-1.5 months to median progression-free survival among patients treated with the PD-L1 inhibitor atezolizumab, according to analyses of different phase 1 and 2 trials.
In addition, overall survival (OS) benefit in some of the trials could be better delineated using the immune-modified criteria, which account for unique patterns of progression sometimes experienced by patients on cancer immunotherapy, noted the study authors. The report was published in the Journal of Clinical Oncology.
Using immune-specific criteria to evaluate response to cancer immunotherapy is not a new concept. However, there are only limited data on how those criteria might apply to predictions of OS, according to lead author F. Stephen Hodi, MD, of Dana-Farber Cancer Institute, Boston, and his coauthors.
“These analyses reveal aspects of immune-modified RECIST that seem to predict OS better than RECIST v1.1, and aspects needing refinement to improve the ability to predict clinical benefit,” wrote Dr. Hodi and his colleagues.
Typical response criteria may not adequately predict the potential OS benefit of cancer immunotherapy, since patients receiving cancer immunotherapy may exhibit response patterns outside of the “classic response patterns” seen with other anticancer treatments, they noted.
In particular, some patients may experience an initial transient increase in tumor burden before responding, while in other cases, patients with responding baseline lesions might develop new lesions.
Immune-modified criteria have been developed to account for those “other patterns” that can manifest with cancer immunotherapy, the authors said.
Dr. Hodi and his colleagues sought to evaluate outcomes by RECIST vs. immune-related RECIST criteria among patients treated with atezolizumab in studies of non–small-cell lung cancer (NSCLC) and metastatic urothelial carcinoma.
In the phase 2 BIRCH study of first-line atezolizumab for NSCLC, they found that immune-related RECIST criteria appeared to predict OS better than RECIST. Median overall survival was 4.0 months longer among patients who had progressive disease (PD) by RECIST criteria within 90 days of study enrollment, versus patients who had PD by both RECIST and immune-modified RECIST at that time point, Dr. Hodi and his colleagues reported.
In the POPLAR trial of atezolizumab in NSCLC, median overall survival was 1.4 months longer for patients with PD by RECIST vs. patients with PD by both RECIST and immune-modified RECIST at 90 days, they reported.
For patients with metastatic urothelial bladder cancer treated with atezolizumab in the IMvigor210 study, median overall survival was 4.4 months longer for patients with PD by RECIST only vs. PD by both RECIST and immune-related RECIST within 180 days of enrollment, the researchers noted.
An international effort is underway to compare data sets from larger trial sets and multiple cancer immunotherapy agents, they wrote.
SOURCE: Hodi FS et al., J Clin Oncol. 2018 Jan 17. doi: 10.1200/JCO.2017.75.1644
Cancer immunotherapy-specific response criteria not only provide improved estimates of treatment response versus standard criteria, but may also better identify patients who achieve an overall survival benefit from therapy.
Compared to standard Response Evaluation Criteria In Solid Tumors (RECIST) v1.1, the immune-modified RECIST provided a 1%-2% greater overall response and an 8%-13% greater rate of disease control, and added 0.5-1.5 months to median progression-free survival among patients treated with the PD-L1 inhibitor atezolizumab, according to analyses of different phase 1 and 2 trials.
In addition, overall survival (OS) benefit in some of the trials could be better delineated using the immune-modified criteria, which account for unique patterns of progression sometimes experienced by patients on cancer immunotherapy, noted the study authors. The report was published in the Journal of Clinical Oncology.
Using immune-specific criteria to evaluate response to cancer immunotherapy is not a new concept. However, there are only limited data on how those criteria might apply to predictions of OS, according to lead author F. Stephen Hodi, MD, of Dana-Farber Cancer Institute, Boston, and his coauthors.
“These analyses reveal aspects of immune-modified RECIST that seem to predict OS better than RECIST v1.1, and aspects needing refinement to improve the ability to predict clinical benefit,” wrote Dr. Hodi and his colleagues.
Typical response criteria may not adequately predict the potential OS benefit of cancer immunotherapy, since patients receiving cancer immunotherapy may exhibit response patterns outside of the “classic response patterns” seen with other anticancer treatments, they noted.
In particular, some patients may experience an initial transient increase in tumor burden before responding, while in other cases, patients with responding baseline lesions might develop new lesions.
Immune-modified criteria have been developed to account for those “other patterns” that can manifest with cancer immunotherapy, the authors said.
Dr. Hodi and his colleagues sought to evaluate outcomes by RECIST vs. immune-related RECIST criteria among patients treated with atezolizumab in studies of non–small-cell lung cancer (NSCLC) and metastatic urothelial carcinoma.
In the phase 2 BIRCH study of first-line atezolizumab for NSCLC, they found that immune-related RECIST criteria appeared to predict OS better than RECIST. Median overall survival was 4.0 months longer among patients who had progressive disease (PD) by RECIST criteria within 90 days of study enrollment, versus patients who had PD by both RECIST and immune-modified RECIST at that time point, Dr. Hodi and his colleagues reported.
In the POPLAR trial of atezolizumab in NSCLC, median overall survival was 1.4 months longer for patients with PD by RECIST vs. patients with PD by both RECIST and immune-modified RECIST at 90 days, they reported.
For patients with metastatic urothelial bladder cancer treated with atezolizumab in the IMvigor210 study, median overall survival was 4.4 months longer for patients with PD by RECIST only vs. PD by both RECIST and immune-related RECIST within 180 days of enrollment, the researchers noted.
An international effort is underway to compare data sets from larger trial sets and multiple cancer immunotherapy agents, they wrote.
SOURCE: Hodi FS et al., J Clin Oncol. 2018 Jan 17. doi: 10.1200/JCO.2017.75.1644
Cancer immunotherapy-specific response criteria not only provide improved estimates of treatment response versus standard criteria, but may also better identify patients who achieve an overall survival benefit from therapy.
Compared to standard Response Evaluation Criteria In Solid Tumors (RECIST) v1.1, the immune-modified RECIST provided a 1%-2% greater overall response and an 8%-13% greater rate of disease control, and added 0.5-1.5 months to median progression-free survival among patients treated with the PD-L1 inhibitor atezolizumab, according to analyses of different phase 1 and 2 trials.
In addition, overall survival (OS) benefit in some of the trials could be better delineated using the immune-modified criteria, which account for unique patterns of progression sometimes experienced by patients on cancer immunotherapy, noted the study authors. The report was published in the Journal of Clinical Oncology.
Using immune-specific criteria to evaluate response to cancer immunotherapy is not a new concept. However, there are only limited data on how those criteria might apply to predictions of OS, according to lead author F. Stephen Hodi, MD, of Dana-Farber Cancer Institute, Boston, and his coauthors.
“These analyses reveal aspects of immune-modified RECIST that seem to predict OS better than RECIST v1.1, and aspects needing refinement to improve the ability to predict clinical benefit,” wrote Dr. Hodi and his colleagues.
Typical response criteria may not adequately predict the potential OS benefit of cancer immunotherapy, since patients receiving cancer immunotherapy may exhibit response patterns outside of the “classic response patterns” seen with other anticancer treatments, they noted.
In particular, some patients may experience an initial transient increase in tumor burden before responding, while in other cases, patients with responding baseline lesions might develop new lesions.
Immune-modified criteria have been developed to account for those “other patterns” that can manifest with cancer immunotherapy, the authors said.
Dr. Hodi and his colleagues sought to evaluate outcomes by RECIST vs. immune-related RECIST criteria among patients treated with atezolizumab in studies of non–small-cell lung cancer (NSCLC) and metastatic urothelial carcinoma.
In the phase 2 BIRCH study of first-line atezolizumab for NSCLC, they found that immune-related RECIST criteria appeared to predict OS better than RECIST. Median overall survival was 4.0 months longer among patients who had progressive disease (PD) by RECIST criteria within 90 days of study enrollment, versus patients who had PD by both RECIST and immune-modified RECIST at that time point, Dr. Hodi and his colleagues reported.
In the POPLAR trial of atezolizumab in NSCLC, median overall survival was 1.4 months longer for patients with PD by RECIST vs. patients with PD by both RECIST and immune-modified RECIST at 90 days, they reported.
For patients with metastatic urothelial bladder cancer treated with atezolizumab in the IMvigor210 study, median overall survival was 4.4 months longer for patients with PD by RECIST only vs. PD by both RECIST and immune-related RECIST within 180 days of enrollment, the researchers noted.
An international effort is underway to compare data sets from larger trial sets and multiple cancer immunotherapy agents, they wrote.
SOURCE: Hodi FS et al., J Clin Oncol. 2018 Jan 17. doi: 10.1200/JCO.2017.75.1644
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Compared to standard criteria for response evaluation, criteria developed specifically to evaluate response to cancer immunotherapy better identified patients with an overall survival (OS) benefit.
Major finding: Median OS was 4.0 and 1.4 months longer, respectively, in the BIRCH and POPLAR non–small-cell lung cancer trial among patients who had progressive disease (PD) by standard criteria only, as opposed to patients who also had PD according to the immunotherapy-specific response criteria.
Data source: Analysis of patients treated with single-agent atezolizumab in phase 1 and 2 clinical trials.
Disclosures: The study was supported by F. Hoffmann-La Roche. Authors reported disclosures related to Merck Sharp & Dohme, Novartis, Genentech/Roche, Bristol-Myers Squibb, and others.
Source: Hodi FS et al., J Clin Oncol. 2018 Jan 17. doi: 10.1200/JCO.2017.75.1644.
Papules below eyes

The FP looked at the small papules closely and recognized them as white milia cysts and flesh-colored syringomas. He explained to the patient that both conditions were benign and discussed treatment options.
Milia cysts, which appear as shiny white papules, can be extracted. This procedure is performed without local anesthesia, and the most uncomfortable part is when pressure is applied with the comedone extractor against the infraorbital bone. (The billing code for this procedure is the same as the one used for acne surgery.)
Syringomas, however, are not easily treated. New lesions can form even if some resolve. Treatment options for syringomas include topical trichloroacetic acid, cryosurgery, and electrosurgery. Because this patient’s lesions were on the eyelids, as they often are, there are risks involved.
The patient agreed to extraction of the milia cysts, so the FP removed a number of them using the tip of a Number 11 scalpel blade and a comedone extractor. The patient was happy to have them removed and said that he would think about the options for syringoma treatment at a future date.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Sebaceous hyperplasia. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 931-934.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP looked at the small papules closely and recognized them as white milia cysts and flesh-colored syringomas. He explained to the patient that both conditions were benign and discussed treatment options.
Milia cysts, which appear as shiny white papules, can be extracted. This procedure is performed without local anesthesia, and the most uncomfortable part is when pressure is applied with the comedone extractor against the infraorbital bone. (The billing code for this procedure is the same as the one used for acne surgery.)
Syringomas, however, are not easily treated. New lesions can form even if some resolve. Treatment options for syringomas include topical trichloroacetic acid, cryosurgery, and electrosurgery. Because this patient’s lesions were on the eyelids, as they often are, there are risks involved.
The patient agreed to extraction of the milia cysts, so the FP removed a number of them using the tip of a Number 11 scalpel blade and a comedone extractor. The patient was happy to have them removed and said that he would think about the options for syringoma treatment at a future date.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Sebaceous hyperplasia. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 931-934.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
The FP looked at the small papules closely and recognized them as white milia cysts and flesh-colored syringomas. He explained to the patient that both conditions were benign and discussed treatment options.
Milia cysts, which appear as shiny white papules, can be extracted. This procedure is performed without local anesthesia, and the most uncomfortable part is when pressure is applied with the comedone extractor against the infraorbital bone. (The billing code for this procedure is the same as the one used for acne surgery.)
Syringomas, however, are not easily treated. New lesions can form even if some resolve. Treatment options for syringomas include topical trichloroacetic acid, cryosurgery, and electrosurgery. Because this patient’s lesions were on the eyelids, as they often are, there are risks involved.
The patient agreed to extraction of the milia cysts, so the FP removed a number of them using the tip of a Number 11 scalpel blade and a comedone extractor. The patient was happy to have them removed and said that he would think about the options for syringoma treatment at a future date.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Sebaceous hyperplasia. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 931-934.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

Ixekizumab beats ustekinumab for fingernail psoriasis, hands down
GENEVA – Ixekizumab improved fingernail psoriasis significantly faster and with a higher complete nail clearance rate by week 24 compared with ustekinumab in a head-to-head phase 3b randomized trial, Yves Dutronc, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
This is a clinically important finding because – as dermatologists and psoriasis patients well know – nail and skin psoriasis are two different animals.

He presented a prespecified secondary analysis of the randomized, phase 3b, multicenter IXORA-S trial. The study pit the interleukin-17A inhibitor ixekizumab (Taltz) head-to-head against the interleukin 12/23 inhibitor ustekinumab (Stelara). The primary endpoint, which was the PASI 90 improvement rate, has previously been reported: 73% in the ixekizumab group versus 42% in the ustekinumab group at week 12, and 83% versus 59% at week 24. And ixekizumab’s superior efficacy was achieved with a safety profile similar to that of ustekinumab (Br J Dermatol. 2017 Oct;177[4]:1014-23).
However, change in PASI score or Investigator’s Global Assessment isn’t informative regarding a patient’s change in nail psoriasis status. This was the impetus for the secondary analysis focused on the IXORA-S subgroup with baseline fingernail psoriasis. For this purpose, Dr. Dutronc and his coinvestigators used as their metric the change over time in the Nail Psoriasis Severity Index (NAPSI) total score, which entails a quadrant-by-quadrant assessment of every fingernail.
By play of chance, the 84 patients randomized to ixekizumab had slightly more severe nail psoriasis at baseline than that of the 105 ustekinumab patients. Their mean baseline NAPSI total score was 28.3, compared with 24.8 for the ustekinumab group. More than one-quarter of patients in the ixekizumab arm had a baseline NAPSI score greater than 43, whereas the top quartile of nail psoriasis severity in the ustekinumab group began with a NAPSI score above 34.
Not surprisingly, not much happened in terms of improvement in nail appearance in the first 12 weeks, since new nail grows slowly. But by week 8 the between-group difference in improvement in NAPSI score had become significant in favor of ixekizumab, with a mean 12.9-point reduction from baseline versus a 5.6-point drop in the ustekinumab group. This difference continued to grow over time, such that at week 24 the ixekizumab had a mean 19.9-point reduction, compared with a 13.2-point decrease for the ustekinumab group.
At week 12, 15.5% of the ixekizumab group and 11.3% of the ustekinumab group had reached complete clearance of their fingernail psoriasis. At week 24, complete clearance had been achieved in 48.8% of the ixekizumab group and 22.9% of patients on ustekinumab.
This is an interim analysis. Final results of the IXORA-S nail psoriasis substudy will be reported at 52 weeks of follow-up.
SOURCE: Dutronc Y. https://eadvgeneva2017.org/
GENEVA – Ixekizumab improved fingernail psoriasis significantly faster and with a higher complete nail clearance rate by week 24 compared with ustekinumab in a head-to-head phase 3b randomized trial, Yves Dutronc, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
This is a clinically important finding because – as dermatologists and psoriasis patients well know – nail and skin psoriasis are two different animals.
He presented a prespecified secondary analysis of the randomized, phase 3b, multicenter IXORA-S trial. The study pit the interleukin-17A inhibitor ixekizumab (Taltz) head-to-head against the interleukin 12/23 inhibitor ustekinumab (Stelara). The primary endpoint, which was the PASI 90 improvement rate, has previously been reported: 73% in the ixekizumab group versus 42% in the ustekinumab group at week 12, and 83% versus 59% at week 24. And ixekizumab’s superior efficacy was achieved with a safety profile similar to that of ustekinumab (Br J Dermatol. 2017 Oct;177[4]:1014-23).
However, change in PASI score or Investigator’s Global Assessment isn’t informative regarding a patient’s change in nail psoriasis status. This was the impetus for the secondary analysis focused on the IXORA-S subgroup with baseline fingernail psoriasis. For this purpose, Dr. Dutronc and his coinvestigators used as their metric the change over time in the Nail Psoriasis Severity Index (NAPSI) total score, which entails a quadrant-by-quadrant assessment of every fingernail.
By play of chance, the 84 patients randomized to ixekizumab had slightly more severe nail psoriasis at baseline than that of the 105 ustekinumab patients. Their mean baseline NAPSI total score was 28.3, compared with 24.8 for the ustekinumab group. More than one-quarter of patients in the ixekizumab arm had a baseline NAPSI score greater than 43, whereas the top quartile of nail psoriasis severity in the ustekinumab group began with a NAPSI score above 34.
Not surprisingly, not much happened in terms of improvement in nail appearance in the first 12 weeks, since new nail grows slowly. But by week 8 the between-group difference in improvement in NAPSI score had become significant in favor of ixekizumab, with a mean 12.9-point reduction from baseline versus a 5.6-point drop in the ustekinumab group. This difference continued to grow over time, such that at week 24 the ixekizumab had a mean 19.9-point reduction, compared with a 13.2-point decrease for the ustekinumab group.
At week 12, 15.5% of the ixekizumab group and 11.3% of the ustekinumab group had reached complete clearance of their fingernail psoriasis. At week 24, complete clearance had been achieved in 48.8% of the ixekizumab group and 22.9% of patients on ustekinumab.
This is an interim analysis. Final results of the IXORA-S nail psoriasis substudy will be reported at 52 weeks of follow-up.
SOURCE: Dutronc Y. https://eadvgeneva2017.org/
GENEVA – Ixekizumab improved fingernail psoriasis significantly faster and with a higher complete nail clearance rate by week 24 compared with ustekinumab in a head-to-head phase 3b randomized trial, Yves Dutronc, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
This is a clinically important finding because – as dermatologists and psoriasis patients well know – nail and skin psoriasis are two different animals.
He presented a prespecified secondary analysis of the randomized, phase 3b, multicenter IXORA-S trial. The study pit the interleukin-17A inhibitor ixekizumab (Taltz) head-to-head against the interleukin 12/23 inhibitor ustekinumab (Stelara). The primary endpoint, which was the PASI 90 improvement rate, has previously been reported: 73% in the ixekizumab group versus 42% in the ustekinumab group at week 12, and 83% versus 59% at week 24. And ixekizumab’s superior efficacy was achieved with a safety profile similar to that of ustekinumab (Br J Dermatol. 2017 Oct;177[4]:1014-23).
However, change in PASI score or Investigator’s Global Assessment isn’t informative regarding a patient’s change in nail psoriasis status. This was the impetus for the secondary analysis focused on the IXORA-S subgroup with baseline fingernail psoriasis. For this purpose, Dr. Dutronc and his coinvestigators used as their metric the change over time in the Nail Psoriasis Severity Index (NAPSI) total score, which entails a quadrant-by-quadrant assessment of every fingernail.
By play of chance, the 84 patients randomized to ixekizumab had slightly more severe nail psoriasis at baseline than that of the 105 ustekinumab patients. Their mean baseline NAPSI total score was 28.3, compared with 24.8 for the ustekinumab group. More than one-quarter of patients in the ixekizumab arm had a baseline NAPSI score greater than 43, whereas the top quartile of nail psoriasis severity in the ustekinumab group began with a NAPSI score above 34.
Not surprisingly, not much happened in terms of improvement in nail appearance in the first 12 weeks, since new nail grows slowly. But by week 8 the between-group difference in improvement in NAPSI score had become significant in favor of ixekizumab, with a mean 12.9-point reduction from baseline versus a 5.6-point drop in the ustekinumab group. This difference continued to grow over time, such that at week 24 the ixekizumab had a mean 19.9-point reduction, compared with a 13.2-point decrease for the ustekinumab group.
At week 12, 15.5% of the ixekizumab group and 11.3% of the ustekinumab group had reached complete clearance of their fingernail psoriasis. At week 24, complete clearance had been achieved in 48.8% of the ixekizumab group and 22.9% of patients on ustekinumab.
This is an interim analysis. Final results of the IXORA-S nail psoriasis substudy will be reported at 52 weeks of follow-up.
SOURCE: Dutronc Y. https://eadvgeneva2017.org/
REPORTING FROM THE EADV CONGRESS
Key clinical point:
Major finding: At week 24, complete clearance of fingernail psoriasis was documented in 49% of patients on ixekizumab and 23% on ustekinumab.
Study details: This secondary analysis of the randomized, multicenter, prospective, phase 3b IXORA-S trial included 189 patients with moderate to severe plaque psoriasis with fingernail involvement.
Disclosures: The study was sponsored by Eli Lilly and presented by a company employee.
Source: Dutronc Y. https://eadvgeneva2017.org
Hospitalist leader: Are you burned out? Are you resilient?
I had the privilege of teaching two seminars at the recent Society of Hospital Medicine Leadership Academy in Scottsdale, Ariz. The theme of my second seminar was “Swarm Leadership,” the topic of my September column. There seemed to be enthusiasm and interest in the topic. Participants were intrigued at the notion of leveraging instinctual responses to encourage team spirit and collective outcomes.
The key principles of these swarm-like behaviors are: 1) unity of mission, 2) generosity of spirit, 3) staying in lanes and helping others succeed in theirs, 4) no ego/no blame, and 5) a foundation of trust among those working together. Leaders create the conditions in which these behaviors are more likely to emerge. The resulting team spirit and productivity raise morale and increase the sense of work-related purpose and mission.

People expressed their sense of being burned out and overworked, even to the extent of being exploited. I was stunned at the prevalence of this sensation in the room. Not everyone spoke though many people identified with the theme.
What I heard was enough to raise the question here: For hospitalist leaders, to what extent is burnout significant enough to give it serious attention? (I want to be abundantly clear: I report observations as anecdotal and impressionistic. There is no implied critique of hospitalists on the whole nor any individual or groups.)
Burnout includes sensations of being exhausted, overburdened, underappreciated, undercompensated, cynical, and depressed. These phenomena together can affect your productivity, the quality of your work, and your endurance when the workload gets tough.
By contrast, the opposite of burnout is balance, including sensations of being engaged, enthusiastic, energetic, absorbed, challenged, and dedicated. Work is part of the equilibrium you establish in your life, which includes a variety of fulfilling and motivating experiences and accomplishments.
Ideal balance would have all the different parts of your life – from family to hobbies to work – in perfect synergy with one another. Complete burnout would have all parts of your life imploding on one another, with little room for joy, personal contentment, and professional satisfaction.
How do you assess the differences between burnout and balance? First, this is a very individual metric. What one person might consider challenging and engaging another would experience as overwhelming and alienating. When you assess a group of people, these differences are important and could inform how work assignments and heavy lifting are assigned.
During the SHM session and in private comments, people described this rise in burnout not as a personal phenomena. Rather, it results from the health system expecting more of hospitalists than they can reasonably and reliably produce. People described hospitalists getting to the breaking point with no relief in sight. What can be done about this phenomenon?
First, hold a mirror up to yourself. You cannot help others as a leader if you are not clear with your own state of burnout and balance. The questions for you – a leader of other hospitalists – include: To what extent are you burned out? If so, why? If not, why not? If you were to draw a continuum between burned out and balanced, where on that range would you place yourself? Where would others in your group or department pinpoint themselves, relative to one another, on this continuum?
How might burnout develop for hospitalist leaders? Like a car, even a high performance vehicle, you can only go so fast and so far. Push too hard on the accelerator and the vehicle begins to shake as performance declines. If your system is expecting the pace and productivity to outstrip what you consider reasonable, your performance, job satisfaction and morale drops. Impose those demands upon a group of people and the unhappiness can become infectious.
With a decline in performance comes a decline in confidence. You and your colleagues strive for top-rate outcomes. Fatigue, pressure, and unreasonable expectations challenge your ability to feel good about what you are doing. That satisfaction is part of why you chose hospital medicine and without it, you wonder about what you are doing and why you are doing it.
When you and your colleagues sense that you are unappreciated, it can spark a profound sense of disappointment. That realization could express itself in many forms, including unhappiness about pay and workload to dissatisfaction with professional support or acknowledgment. When the system on the whole is driving so fast that it cannot stop to ensure and reward good work, the rattling can have a stunting effect on performance.
When I first began teaching at SHM conferences and had hospitalists in my classes at the Harvard School of Public Health – way back when – the field was novel, revolutionary, and striving to establish a newly effective and efficient way to provide patient services. It is useful to keep these roots in perspective – hospital medicine over the arc of time – from what WAS, to what IS and eventually what WILL BE. The cleverness of hospitalist leaders has been their capacity to understand this evolution and work with it. Hospitalist medicine built opportunities in response to high costs, the lack of continuity of care, and problems of communication. It was a solution.
How might you diagnose your burnout – and that of others with whom you work – in order to build solutions? Is it a phenomenon that involves just several individuals or is it characteristic of your group as a whole? What are the causes? What are the symptoms and what are the core issues? Some are system problems in which expectations for performance – and the resources to meet those objectives – are not reasonably aligned. There is a cost for trying to reduce costs on the backs of overworked clinicians.
If this is more than an individual problem, systematically ask the question and seek systematic answers. The better you document root causes and implications, the better are you able to make a data-driven case for change. Interview, survey, and with all this, you demonstrate your concern for staff, their work, and their work experience.
Showing that you care about the professional and personal well-being and balance of your workforce, in and of itself, is the beginning of an intervention. Be honest with yourself about your own experience. And then be open to the experiences of others. As a leader, your colleagues may suggest changes you make in your own leadership that could ameliorate some of that burnout. Better communication? Improved organization? Enhanced flexibility as appropriate? These are problems you can fix.
Other solutions must be negotiated with others on the systems level. With documentation in hand, build your case for the necessary changes, whatever that might entail. Hospitalist leaders negotiated their way into respected and productive positions in the health care system. Similarly, they must negotiate the right balance now to ensure the quality, morale, and reasonable productivity of their departments and workforce.
As a hospitalist leader, you know that each day will bring its complexities, challenges, and at times, its burdens. Your objective is to encourage – for yourself, for your colleagues, and for your system – resilience that is both personal and organizational. That resilience – the ability to take a hit and bounce back – is an encouraging signal of hope and recovery, for your workforce as well as the people for whom you care. The principles of swarm leadership – reinvigorated for your group – could very well provide signposts on that everyday quest for personal and group resilience.
Leonard J. Marcus, PhD, is coauthor of “Renegotiating Health Care: Resolving Conflict to Build Collaboration,” Second Edition (San Francisco: Jossey-Bass Publishers, 2011) and is director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard T.H. Chan School of Public Health. Dr. Marcus teaches regularly in the SHM Leadership Academy. He can be reached at ljmarcus@hsph.harvard.edu.
I had the privilege of teaching two seminars at the recent Society of Hospital Medicine Leadership Academy in Scottsdale, Ariz. The theme of my second seminar was “Swarm Leadership,” the topic of my September column. There seemed to be enthusiasm and interest in the topic. Participants were intrigued at the notion of leveraging instinctual responses to encourage team spirit and collective outcomes.
The key principles of these swarm-like behaviors are: 1) unity of mission, 2) generosity of spirit, 3) staying in lanes and helping others succeed in theirs, 4) no ego/no blame, and 5) a foundation of trust among those working together. Leaders create the conditions in which these behaviors are more likely to emerge. The resulting team spirit and productivity raise morale and increase the sense of work-related purpose and mission.
People expressed their sense of being burned out and overworked, even to the extent of being exploited. I was stunned at the prevalence of this sensation in the room. Not everyone spoke though many people identified with the theme.
What I heard was enough to raise the question here: For hospitalist leaders, to what extent is burnout significant enough to give it serious attention? (I want to be abundantly clear: I report observations as anecdotal and impressionistic. There is no implied critique of hospitalists on the whole nor any individual or groups.)
Burnout includes sensations of being exhausted, overburdened, underappreciated, undercompensated, cynical, and depressed. These phenomena together can affect your productivity, the quality of your work, and your endurance when the workload gets tough.
By contrast, the opposite of burnout is balance, including sensations of being engaged, enthusiastic, energetic, absorbed, challenged, and dedicated. Work is part of the equilibrium you establish in your life, which includes a variety of fulfilling and motivating experiences and accomplishments.
Ideal balance would have all the different parts of your life – from family to hobbies to work – in perfect synergy with one another. Complete burnout would have all parts of your life imploding on one another, with little room for joy, personal contentment, and professional satisfaction.
How do you assess the differences between burnout and balance? First, this is a very individual metric. What one person might consider challenging and engaging another would experience as overwhelming and alienating. When you assess a group of people, these differences are important and could inform how work assignments and heavy lifting are assigned.
During the SHM session and in private comments, people described this rise in burnout not as a personal phenomena. Rather, it results from the health system expecting more of hospitalists than they can reasonably and reliably produce. People described hospitalists getting to the breaking point with no relief in sight. What can be done about this phenomenon?
First, hold a mirror up to yourself. You cannot help others as a leader if you are not clear with your own state of burnout and balance. The questions for you – a leader of other hospitalists – include: To what extent are you burned out? If so, why? If not, why not? If you were to draw a continuum between burned out and balanced, where on that range would you place yourself? Where would others in your group or department pinpoint themselves, relative to one another, on this continuum?
How might burnout develop for hospitalist leaders? Like a car, even a high performance vehicle, you can only go so fast and so far. Push too hard on the accelerator and the vehicle begins to shake as performance declines. If your system is expecting the pace and productivity to outstrip what you consider reasonable, your performance, job satisfaction and morale drops. Impose those demands upon a group of people and the unhappiness can become infectious.
With a decline in performance comes a decline in confidence. You and your colleagues strive for top-rate outcomes. Fatigue, pressure, and unreasonable expectations challenge your ability to feel good about what you are doing. That satisfaction is part of why you chose hospital medicine and without it, you wonder about what you are doing and why you are doing it.
When you and your colleagues sense that you are unappreciated, it can spark a profound sense of disappointment. That realization could express itself in many forms, including unhappiness about pay and workload to dissatisfaction with professional support or acknowledgment. When the system on the whole is driving so fast that it cannot stop to ensure and reward good work, the rattling can have a stunting effect on performance.
When I first began teaching at SHM conferences and had hospitalists in my classes at the Harvard School of Public Health – way back when – the field was novel, revolutionary, and striving to establish a newly effective and efficient way to provide patient services. It is useful to keep these roots in perspective – hospital medicine over the arc of time – from what WAS, to what IS and eventually what WILL BE. The cleverness of hospitalist leaders has been their capacity to understand this evolution and work with it. Hospitalist medicine built opportunities in response to high costs, the lack of continuity of care, and problems of communication. It was a solution.
How might you diagnose your burnout – and that of others with whom you work – in order to build solutions? Is it a phenomenon that involves just several individuals or is it characteristic of your group as a whole? What are the causes? What are the symptoms and what are the core issues? Some are system problems in which expectations for performance – and the resources to meet those objectives – are not reasonably aligned. There is a cost for trying to reduce costs on the backs of overworked clinicians.
If this is more than an individual problem, systematically ask the question and seek systematic answers. The better you document root causes and implications, the better are you able to make a data-driven case for change. Interview, survey, and with all this, you demonstrate your concern for staff, their work, and their work experience.
Showing that you care about the professional and personal well-being and balance of your workforce, in and of itself, is the beginning of an intervention. Be honest with yourself about your own experience. And then be open to the experiences of others. As a leader, your colleagues may suggest changes you make in your own leadership that could ameliorate some of that burnout. Better communication? Improved organization? Enhanced flexibility as appropriate? These are problems you can fix.
Other solutions must be negotiated with others on the systems level. With documentation in hand, build your case for the necessary changes, whatever that might entail. Hospitalist leaders negotiated their way into respected and productive positions in the health care system. Similarly, they must negotiate the right balance now to ensure the quality, morale, and reasonable productivity of their departments and workforce.
As a hospitalist leader, you know that each day will bring its complexities, challenges, and at times, its burdens. Your objective is to encourage – for yourself, for your colleagues, and for your system – resilience that is both personal and organizational. That resilience – the ability to take a hit and bounce back – is an encouraging signal of hope and recovery, for your workforce as well as the people for whom you care. The principles of swarm leadership – reinvigorated for your group – could very well provide signposts on that everyday quest for personal and group resilience.
Leonard J. Marcus, PhD, is coauthor of “Renegotiating Health Care: Resolving Conflict to Build Collaboration,” Second Edition (San Francisco: Jossey-Bass Publishers, 2011) and is director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard T.H. Chan School of Public Health. Dr. Marcus teaches regularly in the SHM Leadership Academy. He can be reached at ljmarcus@hsph.harvard.edu.
I had the privilege of teaching two seminars at the recent Society of Hospital Medicine Leadership Academy in Scottsdale, Ariz. The theme of my second seminar was “Swarm Leadership,” the topic of my September column. There seemed to be enthusiasm and interest in the topic. Participants were intrigued at the notion of leveraging instinctual responses to encourage team spirit and collective outcomes.
The key principles of these swarm-like behaviors are: 1) unity of mission, 2) generosity of spirit, 3) staying in lanes and helping others succeed in theirs, 4) no ego/no blame, and 5) a foundation of trust among those working together. Leaders create the conditions in which these behaviors are more likely to emerge. The resulting team spirit and productivity raise morale and increase the sense of work-related purpose and mission.
People expressed their sense of being burned out and overworked, even to the extent of being exploited. I was stunned at the prevalence of this sensation in the room. Not everyone spoke though many people identified with the theme.
What I heard was enough to raise the question here: For hospitalist leaders, to what extent is burnout significant enough to give it serious attention? (I want to be abundantly clear: I report observations as anecdotal and impressionistic. There is no implied critique of hospitalists on the whole nor any individual or groups.)
Burnout includes sensations of being exhausted, overburdened, underappreciated, undercompensated, cynical, and depressed. These phenomena together can affect your productivity, the quality of your work, and your endurance when the workload gets tough.
By contrast, the opposite of burnout is balance, including sensations of being engaged, enthusiastic, energetic, absorbed, challenged, and dedicated. Work is part of the equilibrium you establish in your life, which includes a variety of fulfilling and motivating experiences and accomplishments.
Ideal balance would have all the different parts of your life – from family to hobbies to work – in perfect synergy with one another. Complete burnout would have all parts of your life imploding on one another, with little room for joy, personal contentment, and professional satisfaction.
How do you assess the differences between burnout and balance? First, this is a very individual metric. What one person might consider challenging and engaging another would experience as overwhelming and alienating. When you assess a group of people, these differences are important and could inform how work assignments and heavy lifting are assigned.
During the SHM session and in private comments, people described this rise in burnout not as a personal phenomena. Rather, it results from the health system expecting more of hospitalists than they can reasonably and reliably produce. People described hospitalists getting to the breaking point with no relief in sight. What can be done about this phenomenon?
First, hold a mirror up to yourself. You cannot help others as a leader if you are not clear with your own state of burnout and balance. The questions for you – a leader of other hospitalists – include: To what extent are you burned out? If so, why? If not, why not? If you were to draw a continuum between burned out and balanced, where on that range would you place yourself? Where would others in your group or department pinpoint themselves, relative to one another, on this continuum?
How might burnout develop for hospitalist leaders? Like a car, even a high performance vehicle, you can only go so fast and so far. Push too hard on the accelerator and the vehicle begins to shake as performance declines. If your system is expecting the pace and productivity to outstrip what you consider reasonable, your performance, job satisfaction and morale drops. Impose those demands upon a group of people and the unhappiness can become infectious.
With a decline in performance comes a decline in confidence. You and your colleagues strive for top-rate outcomes. Fatigue, pressure, and unreasonable expectations challenge your ability to feel good about what you are doing. That satisfaction is part of why you chose hospital medicine and without it, you wonder about what you are doing and why you are doing it.
When you and your colleagues sense that you are unappreciated, it can spark a profound sense of disappointment. That realization could express itself in many forms, including unhappiness about pay and workload to dissatisfaction with professional support or acknowledgment. When the system on the whole is driving so fast that it cannot stop to ensure and reward good work, the rattling can have a stunting effect on performance.
When I first began teaching at SHM conferences and had hospitalists in my classes at the Harvard School of Public Health – way back when – the field was novel, revolutionary, and striving to establish a newly effective and efficient way to provide patient services. It is useful to keep these roots in perspective – hospital medicine over the arc of time – from what WAS, to what IS and eventually what WILL BE. The cleverness of hospitalist leaders has been their capacity to understand this evolution and work with it. Hospitalist medicine built opportunities in response to high costs, the lack of continuity of care, and problems of communication. It was a solution.
How might you diagnose your burnout – and that of others with whom you work – in order to build solutions? Is it a phenomenon that involves just several individuals or is it characteristic of your group as a whole? What are the causes? What are the symptoms and what are the core issues? Some are system problems in which expectations for performance – and the resources to meet those objectives – are not reasonably aligned. There is a cost for trying to reduce costs on the backs of overworked clinicians.
If this is more than an individual problem, systematically ask the question and seek systematic answers. The better you document root causes and implications, the better are you able to make a data-driven case for change. Interview, survey, and with all this, you demonstrate your concern for staff, their work, and their work experience.
Showing that you care about the professional and personal well-being and balance of your workforce, in and of itself, is the beginning of an intervention. Be honest with yourself about your own experience. And then be open to the experiences of others. As a leader, your colleagues may suggest changes you make in your own leadership that could ameliorate some of that burnout. Better communication? Improved organization? Enhanced flexibility as appropriate? These are problems you can fix.
Other solutions must be negotiated with others on the systems level. With documentation in hand, build your case for the necessary changes, whatever that might entail. Hospitalist leaders negotiated their way into respected and productive positions in the health care system. Similarly, they must negotiate the right balance now to ensure the quality, morale, and reasonable productivity of their departments and workforce.
As a hospitalist leader, you know that each day will bring its complexities, challenges, and at times, its burdens. Your objective is to encourage – for yourself, for your colleagues, and for your system – resilience that is both personal and organizational. That resilience – the ability to take a hit and bounce back – is an encouraging signal of hope and recovery, for your workforce as well as the people for whom you care. The principles of swarm leadership – reinvigorated for your group – could very well provide signposts on that everyday quest for personal and group resilience.
Leonard J. Marcus, PhD, is coauthor of “Renegotiating Health Care: Resolving Conflict to Build Collaboration,” Second Edition (San Francisco: Jossey-Bass Publishers, 2011) and is director of the Program for Health Care Negotiation and Conflict Resolution at the Harvard T.H. Chan School of Public Health. Dr. Marcus teaches regularly in the SHM Leadership Academy. He can be reached at ljmarcus@hsph.harvard.edu.
Proinflammatory diet may increase colorectal cancer risk
by increasing inflammation, new research suggests.
In the Jan. 18 online edition of JAMA Oncology, Fred K. Tabung, PhD, from the department of nutrition at the Harvard T.H. Chan School of Public Health, Boston, and coauthors presented analysis of data from 46,804 men in the Health Professionals Follow-up Study and 74,246 women in the Nurses’ Health Study, examining the relationship between proinflammatory diets and colorectal cancer.
The effect was more pronounced in men with highly inflammatory diets, who had a 44% higher risk of colorectal cancer, compared with those whose diets had low inflammatory potential (95% CI, 1.19-1.74; P less than .001). Women in the highest quintile had a 22% higher risk of colorectal cancer, compared with those in lowest quintile (95% CI, 1.02-1.45; P = .007). These increases in risk were seen even after adjusting for potential confounders such as age, family history of cancer, physical activity, smoking, NSAID use, and menopause status (JAMA Oncology. 2018 Jan 18. doi: 10.1001/jamaoncol.2017.4844).
Overall, there were 2,699 cases of incident colorectal cancer over 2,571,831 person-years of follow-up. Researchers noted 38 more incidents of colorectal cancer per 100,000 person-years among men in the highest quintile, and 12 more among women in the highest quintile, compared with men and women in the lowest quintiles.
The score used in the study looks at intake of foods such as processed, red, and organ meat; fish, vegetables other than green leafy or dark yellow vegetables, refined grains, high-energy and low-energy drinks, and tomatoes, which are all positively related to concentrations of the inflammatory markers. Foods linked to low concentrations of inflammatory markers include beer, wine, tea, coffee, dark yellow vegetables, green leafy vegetables, snacks, fruit juice, and pizza.
The association between proinflammatory diet and colorectal cancer risk was found in all anatomic locations, including the proximal and distal colon. The only exception was for rectal cancer in women, where dietary inflammatory potential did not significantly change cancer risk.
“It is not entirely clear why associations for rectal cancer were stronger in men than in women but are unlikely to be due to chance given the large significant heterogeneity by sex,” wrote Dr. Tabung and coauthors. They suggested the difference in risk pattern for rectal cancer may relate to broader differences in risk patterns between sexes.
“For example, higher body weight strongly predisposes men to higher risk of proximal colon cancer, distal colon cancer, and rectal cancer, and predisposes women to mainly higher risk of distal colon cancer but not rectal cancer.”
This was also evident when the authors looked at subgroup effects based on body mass index and alcohol intake. Men who were overweight or obese and who were on the most proinflammatory diet had a significant, 48% higher risk of colorectal cancer, compared with the lowest quintile. The same effect was not seen in overweight or obese women.
When alcohol intake was examined, researchers saw a significant 62% higher risk of colorectal cancer among men who were in the highest quintile for dietary inflammatory potential, but who did not drink alcohol, compared with teetotalers in the lowest quintile. In women, there was a 33% higher risk in the highest quintile, compared with the lowest in those who did not drink.
A similar trend was evident in individuals who drank up to one alcoholic drink a day, but it was only borderline significant, and there was no significant effect seen in individuals who drank more than one alcoholic drink a day, despite the fact that a high intake of alcohol has been associated with cancer risk in both men and women.
“It is possible that the adverse effects of alcohol intake through other mechanisms may be more dominant than those of its effect on the EDIP and may partially explain the stronger associations among men and women not consuming alcohol than among alcohol consumers.”
The Health Professionals Follow-up Study and Nurses’ Health Study are supported by the National Institutes of Health. Three authors were also supported by grants from the National Institutes of Health, and one also received support from the Friends of the Dana-Farber Cancer Institute and the Dana-Farber Harvard Cancer Center. No conflicts of interest were declared.
SOURCE: Tabung FK et al. JAMA Oncology. 2018 Jan 18. doi: 10.1001/jamaoncol.2017.4844
by increasing inflammation, new research suggests.
In the Jan. 18 online edition of JAMA Oncology, Fred K. Tabung, PhD, from the department of nutrition at the Harvard T.H. Chan School of Public Health, Boston, and coauthors presented analysis of data from 46,804 men in the Health Professionals Follow-up Study and 74,246 women in the Nurses’ Health Study, examining the relationship between proinflammatory diets and colorectal cancer.
The effect was more pronounced in men with highly inflammatory diets, who had a 44% higher risk of colorectal cancer, compared with those whose diets had low inflammatory potential (95% CI, 1.19-1.74; P less than .001). Women in the highest quintile had a 22% higher risk of colorectal cancer, compared with those in lowest quintile (95% CI, 1.02-1.45; P = .007). These increases in risk were seen even after adjusting for potential confounders such as age, family history of cancer, physical activity, smoking, NSAID use, and menopause status (JAMA Oncology. 2018 Jan 18. doi: 10.1001/jamaoncol.2017.4844).
Overall, there were 2,699 cases of incident colorectal cancer over 2,571,831 person-years of follow-up. Researchers noted 38 more incidents of colorectal cancer per 100,000 person-years among men in the highest quintile, and 12 more among women in the highest quintile, compared with men and women in the lowest quintiles.
The score used in the study looks at intake of foods such as processed, red, and organ meat; fish, vegetables other than green leafy or dark yellow vegetables, refined grains, high-energy and low-energy drinks, and tomatoes, which are all positively related to concentrations of the inflammatory markers. Foods linked to low concentrations of inflammatory markers include beer, wine, tea, coffee, dark yellow vegetables, green leafy vegetables, snacks, fruit juice, and pizza.
The association between proinflammatory diet and colorectal cancer risk was found in all anatomic locations, including the proximal and distal colon. The only exception was for rectal cancer in women, where dietary inflammatory potential did not significantly change cancer risk.
“It is not entirely clear why associations for rectal cancer were stronger in men than in women but are unlikely to be due to chance given the large significant heterogeneity by sex,” wrote Dr. Tabung and coauthors. They suggested the difference in risk pattern for rectal cancer may relate to broader differences in risk patterns between sexes.
“For example, higher body weight strongly predisposes men to higher risk of proximal colon cancer, distal colon cancer, and rectal cancer, and predisposes women to mainly higher risk of distal colon cancer but not rectal cancer.”
This was also evident when the authors looked at subgroup effects based on body mass index and alcohol intake. Men who were overweight or obese and who were on the most proinflammatory diet had a significant, 48% higher risk of colorectal cancer, compared with the lowest quintile. The same effect was not seen in overweight or obese women.
When alcohol intake was examined, researchers saw a significant 62% higher risk of colorectal cancer among men who were in the highest quintile for dietary inflammatory potential, but who did not drink alcohol, compared with teetotalers in the lowest quintile. In women, there was a 33% higher risk in the highest quintile, compared with the lowest in those who did not drink.
A similar trend was evident in individuals who drank up to one alcoholic drink a day, but it was only borderline significant, and there was no significant effect seen in individuals who drank more than one alcoholic drink a day, despite the fact that a high intake of alcohol has been associated with cancer risk in both men and women.
“It is possible that the adverse effects of alcohol intake through other mechanisms may be more dominant than those of its effect on the EDIP and may partially explain the stronger associations among men and women not consuming alcohol than among alcohol consumers.”
The Health Professionals Follow-up Study and Nurses’ Health Study are supported by the National Institutes of Health. Three authors were also supported by grants from the National Institutes of Health, and one also received support from the Friends of the Dana-Farber Cancer Institute and the Dana-Farber Harvard Cancer Center. No conflicts of interest were declared.
SOURCE: Tabung FK et al. JAMA Oncology. 2018 Jan 18. doi: 10.1001/jamaoncol.2017.4844
by increasing inflammation, new research suggests.
In the Jan. 18 online edition of JAMA Oncology, Fred K. Tabung, PhD, from the department of nutrition at the Harvard T.H. Chan School of Public Health, Boston, and coauthors presented analysis of data from 46,804 men in the Health Professionals Follow-up Study and 74,246 women in the Nurses’ Health Study, examining the relationship between proinflammatory diets and colorectal cancer.
The effect was more pronounced in men with highly inflammatory diets, who had a 44% higher risk of colorectal cancer, compared with those whose diets had low inflammatory potential (95% CI, 1.19-1.74; P less than .001). Women in the highest quintile had a 22% higher risk of colorectal cancer, compared with those in lowest quintile (95% CI, 1.02-1.45; P = .007). These increases in risk were seen even after adjusting for potential confounders such as age, family history of cancer, physical activity, smoking, NSAID use, and menopause status (JAMA Oncology. 2018 Jan 18. doi: 10.1001/jamaoncol.2017.4844).
Overall, there were 2,699 cases of incident colorectal cancer over 2,571,831 person-years of follow-up. Researchers noted 38 more incidents of colorectal cancer per 100,000 person-years among men in the highest quintile, and 12 more among women in the highest quintile, compared with men and women in the lowest quintiles.
The score used in the study looks at intake of foods such as processed, red, and organ meat; fish, vegetables other than green leafy or dark yellow vegetables, refined grains, high-energy and low-energy drinks, and tomatoes, which are all positively related to concentrations of the inflammatory markers. Foods linked to low concentrations of inflammatory markers include beer, wine, tea, coffee, dark yellow vegetables, green leafy vegetables, snacks, fruit juice, and pizza.
The association between proinflammatory diet and colorectal cancer risk was found in all anatomic locations, including the proximal and distal colon. The only exception was for rectal cancer in women, where dietary inflammatory potential did not significantly change cancer risk.
“It is not entirely clear why associations for rectal cancer were stronger in men than in women but are unlikely to be due to chance given the large significant heterogeneity by sex,” wrote Dr. Tabung and coauthors. They suggested the difference in risk pattern for rectal cancer may relate to broader differences in risk patterns between sexes.
“For example, higher body weight strongly predisposes men to higher risk of proximal colon cancer, distal colon cancer, and rectal cancer, and predisposes women to mainly higher risk of distal colon cancer but not rectal cancer.”
This was also evident when the authors looked at subgroup effects based on body mass index and alcohol intake. Men who were overweight or obese and who were on the most proinflammatory diet had a significant, 48% higher risk of colorectal cancer, compared with the lowest quintile. The same effect was not seen in overweight or obese women.
When alcohol intake was examined, researchers saw a significant 62% higher risk of colorectal cancer among men who were in the highest quintile for dietary inflammatory potential, but who did not drink alcohol, compared with teetotalers in the lowest quintile. In women, there was a 33% higher risk in the highest quintile, compared with the lowest in those who did not drink.
A similar trend was evident in individuals who drank up to one alcoholic drink a day, but it was only borderline significant, and there was no significant effect seen in individuals who drank more than one alcoholic drink a day, despite the fact that a high intake of alcohol has been associated with cancer risk in both men and women.
“It is possible that the adverse effects of alcohol intake through other mechanisms may be more dominant than those of its effect on the EDIP and may partially explain the stronger associations among men and women not consuming alcohol than among alcohol consumers.”
The Health Professionals Follow-up Study and Nurses’ Health Study are supported by the National Institutes of Health. Three authors were also supported by grants from the National Institutes of Health, and one also received support from the Friends of the Dana-Farber Cancer Institute and the Dana-Farber Harvard Cancer Center. No conflicts of interest were declared.
SOURCE: Tabung FK et al. JAMA Oncology. 2018 Jan 18. doi: 10.1001/jamaoncol.2017.4844
FROM JAMA ONCOLOGY
Key clinical point: A diet high in foods such as processed meats, refined grains, and soda may increase the risk of colorectal cancer by promoting inflammation.
Major finding: People in the highest quintile of dietary inflammatory score had a 32% higher risk of developing colorectal cancer, compared with those in the lowest quintile.
Data source: Analysis of data from 46,804 men in the Health Professionals Follow-up Study, and 74,246 women in the Nurses’ Health Study.
Disclosures: The Health Professionals Follow-up Study and Nurses’ Health Study are supported by the National Institutes of Health. Three authors were supported by grants from the National Institutes of Health, and one also received support from the Friends of the Dana-Farber Cancer Institute, and the Dana-Farber Harvard Cancer Center. No conflicts of interest were declared.
Source: JAMA Oncology. 2018 Jan 18. doi: 10.1001/jamaoncol.2017.4844
Listen up: Acoustic device useful for diabetic foot ulcers
The Food & Drug Administration has approved the marketing of a device that uses acoustic shock waves to boost wound closure in patients with diabetic foot ulcers (DFUs), an especially stubborn and dangerous condition.
The treatment is experimental, and only limited research into its effectiveness has been published. Still, representatives of its manufacturer say the device, known as dermaPACE, has produced promising results as a secondary treatment in stubborn cases.

A wound care specialist said in an interview that the shock wave technology appears to hold promise.
“A shortcoming in the field of wound care is that providers are typically not trained in a standardized fashion on when and how to a perform meticulous excisional sharp debridement of a wound,” said Bill Tettelbach, MD, systems medical director of Wound Care & Hyperbaric Medicine Services at Intermountain Healthcare in Salt Lake City. “In the majority of cases, the better the debridement, the more rapidly the patient will obtain wound closure.”
This new therapy may provide a benefit as a secondary treatment, especially when the patient cannot tolerate extensive sharp debridement, he said. It also could potentially improve biofilm penetration of antimicrobial topical treatments, he said.
DFUs are believed to affect as many as 1 in 4 people with diabetes over the course of their lifetimes. A 2014 report estimated that care of these wounds costs insurers as much as $13 billion a year in the U.S. alone (Diabetes Care. 2014 Mar;37[3]:651-8).
Treatment options include debridement and, in more extreme cases, hyperbaric oxygen treatment. Amputation can be required if treatment is unsuccessful.
According to Mr. Stegagno, the shock wave device is about the size of a desktop computer from a decade ago. A high-voltage generator box is connected to a handheld therapy head and delivers an acoustic pulse to the patient. The system “is like a spark plug that you see in your automobile,” he said. “It’s pretty much the same technology as lithotripsy, just downsized significantly. The key part is a highly focused, high-energy pulse.”
In a news release, the FDA said it examined the results of two studies of patients with diabetes who received usual DFU care along with either the shock wave therapy or a sham therapy. A total of 336 patients took part in the multicenter, randomized, double-blind studies.
According to the FDA, the studies found a 44% wound closure rate at 24 weeks in patients who had undergone 1-7 shock wave treatments, compared with the 30% wound closure rate in those who received the sham treatment.
Side effects included pain while the device was applied, bruising and numbness, migraines, nausea, fainting, wound infection, fever, and infection beyond the wound such as cellulitis and osteomyelitis.
“There were no meaningful statistical differences in the adverse event rates between the dermaPACE-treated patients and the sham-control group,” Mr. Stegagno said. “There were no issues regarding the tolerability of the treatment, which suggests that a second course of treatment, if needed, is a clinically viable option.”
Mr. Stegagno said the FDA expressed concern about “increased incidences of osteomyelitis at later points in the trials, particularly at the 10-week mark and later.” In response to the agency’s concerns, warning statements were added to labeling, he said.
According to Mr. Stegagno, only one study into the shock wave treatment for DFU has been published, although research has been released through posters and abstracts. The small published study favorably compared shock wave therapy with hyperbaric oxygen therapy. (Diabetes Res Clin Pract. 2011 May;92[2]:187-93)
“Sanuwave will be sponsoring additional studies later this year in the [United States] as follow-on studies to the just-completed DFU trials,” Mr. Stegagno said.
The FDA says the device is intended to be used in adults aged 22 and up with certain types of chronic DFUs. The Sanuwave company says patients should be treated with 4-8 applications over 2-10 weeks.
The shock wave process appears to boost healing through a process that leads to inflammatory responses and oxygenation, Mr. Stegagno said, by first creating an initial compression phase that “squeezes the cell and creates a microtrauma.”
“The cell wakes up and says, ‘Something just punched me,’ ” he said. “This tissue and cellular disruption is believed to initiate the cellular signaling for growth factors and other proteins noted in studies.”
The effects of negative pressure also play a role in stimulation of the wound, he said.
The shock wave therapy will cost an estimated $3,000-$4,000 per protocol of 8 treatments, said Kevin A. Richardson II, the CEO and chairman of the board at Sanuwave, in an interview. The initial plan is for the company to place the devices with doctors while the firm still owns the machines, he said.
The FDA approved the marketing of the device as part of its de novo premarket review pathway, which allows certain new types of devices to be approved when approved similar devices don’t yet exist for the purposes of comparison.
Mr. Stegagno and Mr. Richardson work for Sanuwave. Dr. Tettelbach reported no relevant disclosures.
The Food & Drug Administration has approved the marketing of a device that uses acoustic shock waves to boost wound closure in patients with diabetic foot ulcers (DFUs), an especially stubborn and dangerous condition.
The treatment is experimental, and only limited research into its effectiveness has been published. Still, representatives of its manufacturer say the device, known as dermaPACE, has produced promising results as a secondary treatment in stubborn cases.
A wound care specialist said in an interview that the shock wave technology appears to hold promise.
“A shortcoming in the field of wound care is that providers are typically not trained in a standardized fashion on when and how to a perform meticulous excisional sharp debridement of a wound,” said Bill Tettelbach, MD, systems medical director of Wound Care & Hyperbaric Medicine Services at Intermountain Healthcare in Salt Lake City. “In the majority of cases, the better the debridement, the more rapidly the patient will obtain wound closure.”
This new therapy may provide a benefit as a secondary treatment, especially when the patient cannot tolerate extensive sharp debridement, he said. It also could potentially improve biofilm penetration of antimicrobial topical treatments, he said.
DFUs are believed to affect as many as 1 in 4 people with diabetes over the course of their lifetimes. A 2014 report estimated that care of these wounds costs insurers as much as $13 billion a year in the U.S. alone (Diabetes Care. 2014 Mar;37[3]:651-8).
Treatment options include debridement and, in more extreme cases, hyperbaric oxygen treatment. Amputation can be required if treatment is unsuccessful.
According to Mr. Stegagno, the shock wave device is about the size of a desktop computer from a decade ago. A high-voltage generator box is connected to a handheld therapy head and delivers an acoustic pulse to the patient. The system “is like a spark plug that you see in your automobile,” he said. “It’s pretty much the same technology as lithotripsy, just downsized significantly. The key part is a highly focused, high-energy pulse.”
In a news release, the FDA said it examined the results of two studies of patients with diabetes who received usual DFU care along with either the shock wave therapy or a sham therapy. A total of 336 patients took part in the multicenter, randomized, double-blind studies.
According to the FDA, the studies found a 44% wound closure rate at 24 weeks in patients who had undergone 1-7 shock wave treatments, compared with the 30% wound closure rate in those who received the sham treatment.
Side effects included pain while the device was applied, bruising and numbness, migraines, nausea, fainting, wound infection, fever, and infection beyond the wound such as cellulitis and osteomyelitis.
“There were no meaningful statistical differences in the adverse event rates between the dermaPACE-treated patients and the sham-control group,” Mr. Stegagno said. “There were no issues regarding the tolerability of the treatment, which suggests that a second course of treatment, if needed, is a clinically viable option.”
Mr. Stegagno said the FDA expressed concern about “increased incidences of osteomyelitis at later points in the trials, particularly at the 10-week mark and later.” In response to the agency’s concerns, warning statements were added to labeling, he said.
According to Mr. Stegagno, only one study into the shock wave treatment for DFU has been published, although research has been released through posters and abstracts. The small published study favorably compared shock wave therapy with hyperbaric oxygen therapy. (Diabetes Res Clin Pract. 2011 May;92[2]:187-93)
“Sanuwave will be sponsoring additional studies later this year in the [United States] as follow-on studies to the just-completed DFU trials,” Mr. Stegagno said.
The FDA says the device is intended to be used in adults aged 22 and up with certain types of chronic DFUs. The Sanuwave company says patients should be treated with 4-8 applications over 2-10 weeks.
The shock wave process appears to boost healing through a process that leads to inflammatory responses and oxygenation, Mr. Stegagno said, by first creating an initial compression phase that “squeezes the cell and creates a microtrauma.”
“The cell wakes up and says, ‘Something just punched me,’ ” he said. “This tissue and cellular disruption is believed to initiate the cellular signaling for growth factors and other proteins noted in studies.”
The effects of negative pressure also play a role in stimulation of the wound, he said.
The shock wave therapy will cost an estimated $3,000-$4,000 per protocol of 8 treatments, said Kevin A. Richardson II, the CEO and chairman of the board at Sanuwave, in an interview. The initial plan is for the company to place the devices with doctors while the firm still owns the machines, he said.
The FDA approved the marketing of the device as part of its de novo premarket review pathway, which allows certain new types of devices to be approved when approved similar devices don’t yet exist for the purposes of comparison.
Mr. Stegagno and Mr. Richardson work for Sanuwave. Dr. Tettelbach reported no relevant disclosures.
The Food & Drug Administration has approved the marketing of a device that uses acoustic shock waves to boost wound closure in patients with diabetic foot ulcers (DFUs), an especially stubborn and dangerous condition.
The treatment is experimental, and only limited research into its effectiveness has been published. Still, representatives of its manufacturer say the device, known as dermaPACE, has produced promising results as a secondary treatment in stubborn cases.
A wound care specialist said in an interview that the shock wave technology appears to hold promise.
“A shortcoming in the field of wound care is that providers are typically not trained in a standardized fashion on when and how to a perform meticulous excisional sharp debridement of a wound,” said Bill Tettelbach, MD, systems medical director of Wound Care & Hyperbaric Medicine Services at Intermountain Healthcare in Salt Lake City. “In the majority of cases, the better the debridement, the more rapidly the patient will obtain wound closure.”
This new therapy may provide a benefit as a secondary treatment, especially when the patient cannot tolerate extensive sharp debridement, he said. It also could potentially improve biofilm penetration of antimicrobial topical treatments, he said.
DFUs are believed to affect as many as 1 in 4 people with diabetes over the course of their lifetimes. A 2014 report estimated that care of these wounds costs insurers as much as $13 billion a year in the U.S. alone (Diabetes Care. 2014 Mar;37[3]:651-8).
Treatment options include debridement and, in more extreme cases, hyperbaric oxygen treatment. Amputation can be required if treatment is unsuccessful.
According to Mr. Stegagno, the shock wave device is about the size of a desktop computer from a decade ago. A high-voltage generator box is connected to a handheld therapy head and delivers an acoustic pulse to the patient. The system “is like a spark plug that you see in your automobile,” he said. “It’s pretty much the same technology as lithotripsy, just downsized significantly. The key part is a highly focused, high-energy pulse.”
In a news release, the FDA said it examined the results of two studies of patients with diabetes who received usual DFU care along with either the shock wave therapy or a sham therapy. A total of 336 patients took part in the multicenter, randomized, double-blind studies.
According to the FDA, the studies found a 44% wound closure rate at 24 weeks in patients who had undergone 1-7 shock wave treatments, compared with the 30% wound closure rate in those who received the sham treatment.
Side effects included pain while the device was applied, bruising and numbness, migraines, nausea, fainting, wound infection, fever, and infection beyond the wound such as cellulitis and osteomyelitis.
“There were no meaningful statistical differences in the adverse event rates between the dermaPACE-treated patients and the sham-control group,” Mr. Stegagno said. “There were no issues regarding the tolerability of the treatment, which suggests that a second course of treatment, if needed, is a clinically viable option.”
Mr. Stegagno said the FDA expressed concern about “increased incidences of osteomyelitis at later points in the trials, particularly at the 10-week mark and later.” In response to the agency’s concerns, warning statements were added to labeling, he said.
According to Mr. Stegagno, only one study into the shock wave treatment for DFU has been published, although research has been released through posters and abstracts. The small published study favorably compared shock wave therapy with hyperbaric oxygen therapy. (Diabetes Res Clin Pract. 2011 May;92[2]:187-93)
“Sanuwave will be sponsoring additional studies later this year in the [United States] as follow-on studies to the just-completed DFU trials,” Mr. Stegagno said.
The FDA says the device is intended to be used in adults aged 22 and up with certain types of chronic DFUs. The Sanuwave company says patients should be treated with 4-8 applications over 2-10 weeks.
The shock wave process appears to boost healing through a process that leads to inflammatory responses and oxygenation, Mr. Stegagno said, by first creating an initial compression phase that “squeezes the cell and creates a microtrauma.”
“The cell wakes up and says, ‘Something just punched me,’ ” he said. “This tissue and cellular disruption is believed to initiate the cellular signaling for growth factors and other proteins noted in studies.”
The effects of negative pressure also play a role in stimulation of the wound, he said.
The shock wave therapy will cost an estimated $3,000-$4,000 per protocol of 8 treatments, said Kevin A. Richardson II, the CEO and chairman of the board at Sanuwave, in an interview. The initial plan is for the company to place the devices with doctors while the firm still owns the machines, he said.
The FDA approved the marketing of the device as part of its de novo premarket review pathway, which allows certain new types of devices to be approved when approved similar devices don’t yet exist for the purposes of comparison.
Mr. Stegagno and Mr. Richardson work for Sanuwave. Dr. Tettelbach reported no relevant disclosures.
A Sore Subject
For several years, a 60-year-old woman has had a nonhealing, asymptomatic “sore” on her upper right cheek. The lesion causes no pain or discomfort; it bothers her simply because it will not go away. It does occasionally bleed.
Several attempts at treatment—including antibiotic ointment, peroxide, and topical alcohol— have failed. A dermatologist once treated the lesion with cryotherapy; this initially reduced its size, but the effect didn’t last.
The patient admits to “worshipping the sun” as a youngster, tanning at every opportunity. Several family members, including her sister and mother, have had skin cancer.
EXAMINATION
A 6.5-mm, round, red nodule is located on the mid-upper right cheek, below the eye. On closer inspection, it appears glassy and translucent, with several obvious telangiectasias. It is surprisingly firm on palpation, though not at all tender to touch.

Elsewhere, the patient’s fair skin has abundant evidence of sun damage, including wrinkles, discoloration, and focal telangiectasias. No other lesions are seen. No nodes are palpable in her head or neck.
With the patient’s permission, and after discussion of the indications, procedure, alternatives, and risks, the lesion is removed by curettement. It is quite friable and shallow, allowing complete removal. The area is left to heal by secondary intention, and the specimen is submitted to pathology.
What is the diagnosis?
DISCUSSION
The pathology report confirmed the suspected diagnosis: noduloulcerative basal cell carcinoma (BCC). By far the most common type of skin cancer in the world, noduloulcerative BCCs are caused by overexposure to the sun.
As obvious as this diagnosis seemed to be, biopsy was warranted to confirm it and to rule out several other items in the differential. The latter include squamous cell carcinoma (which has far more harmful potential than BCC), sebaceous carcinoma, Merkel cell carcinoma, and melanoma.
Not all BCCs are created equal—certain clinical and histologic characteristics predict a more aggressive course. While most BCCs require surgical excision, other treatment options do exist. In this patient’s case, the size and location of the lesion lent it to curettement and healing by secondary intention. Other methods could have included immunotherapy with imiquimod, antitumor creams (eg, 5-fluorouracil), or even radiation therapy. Her lesion was small and well-defined enough that Mohs surgery was not indicated—though some might disagree with that assessment.
TAKE-HOME LEARNING POINTS
- Like all basal cell carcinomas (BCCs), ulcerative BCC—the most common type—is caused by overexposure to the sun.
- BCCs are often mistaken for infection or other sore, which delays the diagnosis.
- Nonhealing lesions should be considered cancerous until proven otherwise.
- Though this diagnosis was fairly obvious, biopsy is necessary to rule out other items in the differential—some of which (ie, Merkel cell carcinoma, melanoma) are potentially fatal.
For several years, a 60-year-old woman has had a nonhealing, asymptomatic “sore” on her upper right cheek. The lesion causes no pain or discomfort; it bothers her simply because it will not go away. It does occasionally bleed.
Several attempts at treatment—including antibiotic ointment, peroxide, and topical alcohol— have failed. A dermatologist once treated the lesion with cryotherapy; this initially reduced its size, but the effect didn’t last.
The patient admits to “worshipping the sun” as a youngster, tanning at every opportunity. Several family members, including her sister and mother, have had skin cancer.
EXAMINATION
A 6.5-mm, round, red nodule is located on the mid-upper right cheek, below the eye. On closer inspection, it appears glassy and translucent, with several obvious telangiectasias. It is surprisingly firm on palpation, though not at all tender to touch.
Elsewhere, the patient’s fair skin has abundant evidence of sun damage, including wrinkles, discoloration, and focal telangiectasias. No other lesions are seen. No nodes are palpable in her head or neck.
With the patient’s permission, and after discussion of the indications, procedure, alternatives, and risks, the lesion is removed by curettement. It is quite friable and shallow, allowing complete removal. The area is left to heal by secondary intention, and the specimen is submitted to pathology.
What is the diagnosis?
DISCUSSION
The pathology report confirmed the suspected diagnosis: noduloulcerative basal cell carcinoma (BCC). By far the most common type of skin cancer in the world, noduloulcerative BCCs are caused by overexposure to the sun.
As obvious as this diagnosis seemed to be, biopsy was warranted to confirm it and to rule out several other items in the differential. The latter include squamous cell carcinoma (which has far more harmful potential than BCC), sebaceous carcinoma, Merkel cell carcinoma, and melanoma.
Not all BCCs are created equal—certain clinical and histologic characteristics predict a more aggressive course. While most BCCs require surgical excision, other treatment options do exist. In this patient’s case, the size and location of the lesion lent it to curettement and healing by secondary intention. Other methods could have included immunotherapy with imiquimod, antitumor creams (eg, 5-fluorouracil), or even radiation therapy. Her lesion was small and well-defined enough that Mohs surgery was not indicated—though some might disagree with that assessment.
TAKE-HOME LEARNING POINTS
- Like all basal cell carcinomas (BCCs), ulcerative BCC—the most common type—is caused by overexposure to the sun.
- BCCs are often mistaken for infection or other sore, which delays the diagnosis.
- Nonhealing lesions should be considered cancerous until proven otherwise.
- Though this diagnosis was fairly obvious, biopsy is necessary to rule out other items in the differential—some of which (ie, Merkel cell carcinoma, melanoma) are potentially fatal.
For several years, a 60-year-old woman has had a nonhealing, asymptomatic “sore” on her upper right cheek. The lesion causes no pain or discomfort; it bothers her simply because it will not go away. It does occasionally bleed.
Several attempts at treatment—including antibiotic ointment, peroxide, and topical alcohol— have failed. A dermatologist once treated the lesion with cryotherapy; this initially reduced its size, but the effect didn’t last.
The patient admits to “worshipping the sun” as a youngster, tanning at every opportunity. Several family members, including her sister and mother, have had skin cancer.
EXAMINATION
A 6.5-mm, round, red nodule is located on the mid-upper right cheek, below the eye. On closer inspection, it appears glassy and translucent, with several obvious telangiectasias. It is surprisingly firm on palpation, though not at all tender to touch.
Elsewhere, the patient’s fair skin has abundant evidence of sun damage, including wrinkles, discoloration, and focal telangiectasias. No other lesions are seen. No nodes are palpable in her head or neck.
With the patient’s permission, and after discussion of the indications, procedure, alternatives, and risks, the lesion is removed by curettement. It is quite friable and shallow, allowing complete removal. The area is left to heal by secondary intention, and the specimen is submitted to pathology.
What is the diagnosis?
DISCUSSION
The pathology report confirmed the suspected diagnosis: noduloulcerative basal cell carcinoma (BCC). By far the most common type of skin cancer in the world, noduloulcerative BCCs are caused by overexposure to the sun.
As obvious as this diagnosis seemed to be, biopsy was warranted to confirm it and to rule out several other items in the differential. The latter include squamous cell carcinoma (which has far more harmful potential than BCC), sebaceous carcinoma, Merkel cell carcinoma, and melanoma.
Not all BCCs are created equal—certain clinical and histologic characteristics predict a more aggressive course. While most BCCs require surgical excision, other treatment options do exist. In this patient’s case, the size and location of the lesion lent it to curettement and healing by secondary intention. Other methods could have included immunotherapy with imiquimod, antitumor creams (eg, 5-fluorouracil), or even radiation therapy. Her lesion was small and well-defined enough that Mohs surgery was not indicated—though some might disagree with that assessment.
TAKE-HOME LEARNING POINTS
- Like all basal cell carcinomas (BCCs), ulcerative BCC—the most common type—is caused by overexposure to the sun.
- BCCs are often mistaken for infection or other sore, which delays the diagnosis.
- Nonhealing lesions should be considered cancerous until proven otherwise.
- Though this diagnosis was fairly obvious, biopsy is necessary to rule out other items in the differential—some of which (ie, Merkel cell carcinoma, melanoma) are potentially fatal.
Gastric bypass T2D benefit can fade over time
but the effect diminished over time, according to findings published Jan. 16 in JAMA.
In a randomized study of 113 obese patients with diabetes, about 50% of those who received gastric bypass in addition to lifestyle and medical management achieved the composite endpoint of a hemoglobin A1c (HbA1c) value of less than 7%, an LDL cholesterol level of less than 100 mg/dL, and a systolic blood pressure of less than 130 mm Hg after 1 year, reported Sayeed Ikramuddin, MD, FACS, of the department of surgery at the University of Minnesota, Minneapolis, and his coauthors. For comparison, just 16% in the lifestyle/medical management group achieved the endpoint (difference, 34%; 95% confidence interval, 14%-54%; P = .003) .
At 5 years’ follow-up, about 23% of patients in the gastric bypass group and 4% in the lifestyle/medical management group achieved the composite triple endpoint (difference, 19%; 95% CI, 4%-34%; P = .01), the authors reported.
The study included 120 patients at four sites in the United States and Taiwan, 7 of whom either died or were lost to follow-up before completion of the study. Participants had an HbA1c level of 8% or higher and a body mass index between 30 and 39.9 kg/m2.
Patients were randomized to receive either 2 years of lifestyle and medical management alone or in conjunction with standardized Roux-en-Y gastric bypass. During the first 2 years of intervention, patients were told to record weight, exercise, and food intake and were prescribed 325 minutes of physical activity per week. Participants also met regularly with a trained interventionist and an endocrinologist and were given pharmacologic therapy for hyperglycemia, cholesterol, and hypertension, the authors said. Aside from usual visits with a primary physician, all study interventions ceased after the initial 2-year period.
At baseline, the group that received only lifestyle/medical management had a mean BMI of 34.4 and HbA1c level of 9.6%, compared with a mean BMI of 34.9 and HbA1c level of 9.6% in the gastric bypass group.
Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group, but it remained stable from year 3 through year 5, Dr. Ikramuddin and his coauthors said in the report.
Overall, 26% of patients who had gastric bypass surgery during the first year achieved the triple endpoint at 5 years, compared with 8% of those who did not have surgery (difference, 18%; 95% CI, 6%-32%; P = .04).
The mean weight loss for participants in the gastric bypass group was 21.8% at 5 years, compared with 9.6% in the lifestyle/medical management group (difference, 12.2%; 95% CI, 8.9%-15.5%).
The results suggest that “gastric bypass provides significant benefit but with a smaller and less durable effect size than what is seen in the evaluation of glycemic control alone,” the authors wrote.
“Because the effect size diminished over 5 years, further follow-up is needed to understand the durability of the improvement,” Dr. Ikramuddin and his colleagues concluded.
Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics.
acssurgerynews@frontlinemedcom.com
SOURCE: Ikramuddin S. JAMA. 2018;319(3):266-278.
but the effect diminished over time, according to findings published Jan. 16 in JAMA.
In a randomized study of 113 obese patients with diabetes, about 50% of those who received gastric bypass in addition to lifestyle and medical management achieved the composite endpoint of a hemoglobin A1c (HbA1c) value of less than 7%, an LDL cholesterol level of less than 100 mg/dL, and a systolic blood pressure of less than 130 mm Hg after 1 year, reported Sayeed Ikramuddin, MD, FACS, of the department of surgery at the University of Minnesota, Minneapolis, and his coauthors. For comparison, just 16% in the lifestyle/medical management group achieved the endpoint (difference, 34%; 95% confidence interval, 14%-54%; P = .003) .
At 5 years’ follow-up, about 23% of patients in the gastric bypass group and 4% in the lifestyle/medical management group achieved the composite triple endpoint (difference, 19%; 95% CI, 4%-34%; P = .01), the authors reported.
The study included 120 patients at four sites in the United States and Taiwan, 7 of whom either died or were lost to follow-up before completion of the study. Participants had an HbA1c level of 8% or higher and a body mass index between 30 and 39.9 kg/m2.
Patients were randomized to receive either 2 years of lifestyle and medical management alone or in conjunction with standardized Roux-en-Y gastric bypass. During the first 2 years of intervention, patients were told to record weight, exercise, and food intake and were prescribed 325 minutes of physical activity per week. Participants also met regularly with a trained interventionist and an endocrinologist and were given pharmacologic therapy for hyperglycemia, cholesterol, and hypertension, the authors said. Aside from usual visits with a primary physician, all study interventions ceased after the initial 2-year period.
At baseline, the group that received only lifestyle/medical management had a mean BMI of 34.4 and HbA1c level of 9.6%, compared with a mean BMI of 34.9 and HbA1c level of 9.6% in the gastric bypass group.
Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group, but it remained stable from year 3 through year 5, Dr. Ikramuddin and his coauthors said in the report.
Overall, 26% of patients who had gastric bypass surgery during the first year achieved the triple endpoint at 5 years, compared with 8% of those who did not have surgery (difference, 18%; 95% CI, 6%-32%; P = .04).
The mean weight loss for participants in the gastric bypass group was 21.8% at 5 years, compared with 9.6% in the lifestyle/medical management group (difference, 12.2%; 95% CI, 8.9%-15.5%).
The results suggest that “gastric bypass provides significant benefit but with a smaller and less durable effect size than what is seen in the evaluation of glycemic control alone,” the authors wrote.
“Because the effect size diminished over 5 years, further follow-up is needed to understand the durability of the improvement,” Dr. Ikramuddin and his colleagues concluded.
Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics.
acssurgerynews@frontlinemedcom.com
SOURCE: Ikramuddin S. JAMA. 2018;319(3):266-278.
but the effect diminished over time, according to findings published Jan. 16 in JAMA.
In a randomized study of 113 obese patients with diabetes, about 50% of those who received gastric bypass in addition to lifestyle and medical management achieved the composite endpoint of a hemoglobin A1c (HbA1c) value of less than 7%, an LDL cholesterol level of less than 100 mg/dL, and a systolic blood pressure of less than 130 mm Hg after 1 year, reported Sayeed Ikramuddin, MD, FACS, of the department of surgery at the University of Minnesota, Minneapolis, and his coauthors. For comparison, just 16% in the lifestyle/medical management group achieved the endpoint (difference, 34%; 95% confidence interval, 14%-54%; P = .003) .
At 5 years’ follow-up, about 23% of patients in the gastric bypass group and 4% in the lifestyle/medical management group achieved the composite triple endpoint (difference, 19%; 95% CI, 4%-34%; P = .01), the authors reported.
The study included 120 patients at four sites in the United States and Taiwan, 7 of whom either died or were lost to follow-up before completion of the study. Participants had an HbA1c level of 8% or higher and a body mass index between 30 and 39.9 kg/m2.
Patients were randomized to receive either 2 years of lifestyle and medical management alone or in conjunction with standardized Roux-en-Y gastric bypass. During the first 2 years of intervention, patients were told to record weight, exercise, and food intake and were prescribed 325 minutes of physical activity per week. Participants also met regularly with a trained interventionist and an endocrinologist and were given pharmacologic therapy for hyperglycemia, cholesterol, and hypertension, the authors said. Aside from usual visits with a primary physician, all study interventions ceased after the initial 2-year period.
At baseline, the group that received only lifestyle/medical management had a mean BMI of 34.4 and HbA1c level of 9.6%, compared with a mean BMI of 34.9 and HbA1c level of 9.6% in the gastric bypass group.
Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group, but it remained stable from year 3 through year 5, Dr. Ikramuddin and his coauthors said in the report.
Overall, 26% of patients who had gastric bypass surgery during the first year achieved the triple endpoint at 5 years, compared with 8% of those who did not have surgery (difference, 18%; 95% CI, 6%-32%; P = .04).
The mean weight loss for participants in the gastric bypass group was 21.8% at 5 years, compared with 9.6% in the lifestyle/medical management group (difference, 12.2%; 95% CI, 8.9%-15.5%).
The results suggest that “gastric bypass provides significant benefit but with a smaller and less durable effect size than what is seen in the evaluation of glycemic control alone,” the authors wrote.
“Because the effect size diminished over 5 years, further follow-up is needed to understand the durability of the improvement,” Dr. Ikramuddin and his colleagues concluded.
Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics.
acssurgerynews@frontlinemedcom.com
SOURCE: Ikramuddin S. JAMA. 2018;319(3):266-278.
FROM JAMA
Key clinical point: Adding gastric bypass surgery to lifestyle and medical management improves diabetes outcomes – but with diminished effect over time.
Major finding: Primary endpoint success rates decreased in both groups between years 1 and 3, going from 50% to 23% in the gastric bypass group and from 16% to 4% in the lifestyle/medical management group.
Data source: A randomized study of 113 patients at four sites in the United States and Taiwan with a HbA1c level of 8% or higher and a BMI of 30-39.9 kg/m2.
Disclosures: Dr. Ikramuddin disclosed relationships with Novo Nordisk, USGI Medical, Medica, Metamodix, Medtronic, ReShape Medical, and EnteroMedics
SOURCE: Ikramuddin S et al. JAMA. 2018;319(3):266-278.
Risk-stratification tool predicts severe hypoglycemia
Background: Severe hypoglycemia caused by glucose-lowering medications is a known public health and patient safety issue. Identifying patients with T2D at risk of severe hypoglycemia might facilitate interventions to offset that risk.
Study design: Prospective cohort.
Setting: Kaiser Permanente Northern California (derivation and internal validation cohort); Veterans Affairs Diabetes Epidemiology Cohort and Group Health Cooperative (external validation cohorts).
Synopsis: Through EHR data, 206,435 eligible patients with T2D were randomly split into derivation (80%) and internal validation (20%) samples. EHR data were reviewed for preselected clinical risk factors for hypoglycemia with a primary outcome of ED visit or hospital admission with a primary diagnosis of hypoglycemia over the ensuing year. A predictive tool was built based on six variables: prior hypoglycemia episodes, number of ED encounters for any reason in the prior year, insulin use, sulfonylurea use, presence of severe or end-stage kidney disease, and age. Predicted 12-month risk was categorized as high (greater than 5%), intermediate (1%-5%) or low (less than 1%). In the internal validation sample, 2.0%, 10.7%, and 87.3% of patients were categorized as high, intermediate, and low risk, respectively. Observed 12-month hypoglycemia-related health care utilization rates were 6.7%, 1.4%, and 0.2%, respectively. The external validation cohorts performed similarly.
Bottom line: A simple tool using readily available data can be used to estimate the 12-month risk of severe hypoglycemia in patients with T2D.
Citation: Karter AJ et al. Development and validation of a tool to identify patients with type 2 diabetes at high risk of hypoglycemia-related emergency department or hospital use. JAMA Intern Med. 2017 Oct 1;177(10):1461-70.
Dr. Hoegh is a hospitalist at the University of Colorado School of Medicine.
Background: Severe hypoglycemia caused by glucose-lowering medications is a known public health and patient safety issue. Identifying patients with T2D at risk of severe hypoglycemia might facilitate interventions to offset that risk.
Study design: Prospective cohort.
Setting: Kaiser Permanente Northern California (derivation and internal validation cohort); Veterans Affairs Diabetes Epidemiology Cohort and Group Health Cooperative (external validation cohorts).
Synopsis: Through EHR data, 206,435 eligible patients with T2D were randomly split into derivation (80%) and internal validation (20%) samples. EHR data were reviewed for preselected clinical risk factors for hypoglycemia with a primary outcome of ED visit or hospital admission with a primary diagnosis of hypoglycemia over the ensuing year. A predictive tool was built based on six variables: prior hypoglycemia episodes, number of ED encounters for any reason in the prior year, insulin use, sulfonylurea use, presence of severe or end-stage kidney disease, and age. Predicted 12-month risk was categorized as high (greater than 5%), intermediate (1%-5%) or low (less than 1%). In the internal validation sample, 2.0%, 10.7%, and 87.3% of patients were categorized as high, intermediate, and low risk, respectively. Observed 12-month hypoglycemia-related health care utilization rates were 6.7%, 1.4%, and 0.2%, respectively. The external validation cohorts performed similarly.
Bottom line: A simple tool using readily available data can be used to estimate the 12-month risk of severe hypoglycemia in patients with T2D.
Citation: Karter AJ et al. Development and validation of a tool to identify patients with type 2 diabetes at high risk of hypoglycemia-related emergency department or hospital use. JAMA Intern Med. 2017 Oct 1;177(10):1461-70.
Dr. Hoegh is a hospitalist at the University of Colorado School of Medicine.
Background: Severe hypoglycemia caused by glucose-lowering medications is a known public health and patient safety issue. Identifying patients with T2D at risk of severe hypoglycemia might facilitate interventions to offset that risk.
Study design: Prospective cohort.
Setting: Kaiser Permanente Northern California (derivation and internal validation cohort); Veterans Affairs Diabetes Epidemiology Cohort and Group Health Cooperative (external validation cohorts).
Synopsis: Through EHR data, 206,435 eligible patients with T2D were randomly split into derivation (80%) and internal validation (20%) samples. EHR data were reviewed for preselected clinical risk factors for hypoglycemia with a primary outcome of ED visit or hospital admission with a primary diagnosis of hypoglycemia over the ensuing year. A predictive tool was built based on six variables: prior hypoglycemia episodes, number of ED encounters for any reason in the prior year, insulin use, sulfonylurea use, presence of severe or end-stage kidney disease, and age. Predicted 12-month risk was categorized as high (greater than 5%), intermediate (1%-5%) or low (less than 1%). In the internal validation sample, 2.0%, 10.7%, and 87.3% of patients were categorized as high, intermediate, and low risk, respectively. Observed 12-month hypoglycemia-related health care utilization rates were 6.7%, 1.4%, and 0.2%, respectively. The external validation cohorts performed similarly.
Bottom line: A simple tool using readily available data can be used to estimate the 12-month risk of severe hypoglycemia in patients with T2D.
Citation: Karter AJ et al. Development and validation of a tool to identify patients with type 2 diabetes at high risk of hypoglycemia-related emergency department or hospital use. JAMA Intern Med. 2017 Oct 1;177(10):1461-70.
Dr. Hoegh is a hospitalist at the University of Colorado School of Medicine.