User login
Device improves physical exam completion rates in serious mental illness
Using a simple point-of-care (POC) finger prick device to measure blood glucose and lipid levels significantly increases rates of physical health checkups for patients with severe mental illness, new research shows.
In a UK pilot study, use of the Afinion 2 device (Abbott) was associated with a doubling of completed physical health checkups.
However, the effect only occurred in early-intervention services, in which clinicians may feel physical health checkups are most beneficial. This underlines the importance of staff training and payment incentives, the researchers note.
“Clearly, convenience is a great thing about these devices” for both the patient and the mental health clinician, Joseph Butler, MD, a psychiatry trainee at the University of Oxford, United Kingdom, told Medscape Medical News.
He noted that blood test results are rapid, which facilitates immediate discussion of a health management plan.
These tests are “independent from the lab, they’re independent from the general practitioner, and so in terms of convenience, we think it wins on both fronts,” Butler said.
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Poor heart health
Previous research has shown that life expectancy of patients with severe mental illness is 15 to 20 years less than that of the general population, mostly because of complications from poor cardiovascular health.
In the United Kingdom, physical healthcare for patients with serious mental illness is provided by primary care clinicians and community mental health teams (CMHTs). The National Institute for Health and Care Excellence recommends an annual physical examination.
However, a recent audit in the south of England indicated that only 38% of patients with severe mental illness underwent complete physical examinations, primarily because blood glucose and lipid test panels had been omitted.
The researchers note that patients are typically advised to visit their general practitioner for blood tests, “which can be a challenge” for those with severe mental illness.
The Cardiovascular Monitoring in Mental Health (CARMEN) project involved distributing the Afinion 2 device for use in two CMHTs in Oxfordshire, United Kingdom, for 6 months. One CMHT was an early-intervention service, and the other was an adult mental health service.
Care coordinators received training on how to use the device as well as ongoing support to facilitate engagement with the device.
Rates of completion of blood testing and full physical examinations were compared between the intervention CMHTs and two matched control services – an early-intervention group, and an adult metal health services group in Buckinghamshire, a neighboring county.
Better completion rates
The investigators found that .
In contrast, the percentage of physical examinations that were completed remained low in the control CMHT early-intervention service, at just 7.8%.
Direct comparison between the two services showed that use of the POC device was associated with a significant increase in the number of complete physical examinations, at a relative rate of 5.18 (P < .001).
Results were similar when the investigators examined rates at which A1c and lipid panels were completed.
However, there was no difference in completion of physical examinations in the adult mental health service group, for which rates were comparable to those in the control service.
Butler speculated that the way health checkups are funded in the United Kingdom might have contributed to the poor results with the device in the adult mental health service.
In early-intervention services, there is increased awareness of the importance of physical examinations, and funding is contingent on whether clinicians persuade patients to have the examinations.
Overall, the findings show that use of a POC device for physical examinations is acceptable to patients who have severe mental illness as well as to mental health care clinicians, the investigators note.
“In teams where it is well adopted, POC testing can improve physical health check completion...although our qualitative findings highlight important considerations for maximizing clinician engagement,” they add.
The researchers plan to repeat the study across the whole of the south of England, with early-intervention services in the west equipped with POC devices and those in the east serving as controls.
Similar findings
Commenting on the findings for Medscape Medical News, Joe Parks, MD, vice president and practice improvement and medical director at the National Council for Behavioral Health, Washington, DC, noted that he and his colleagues conducted a similar study in the mid-2000s.
Starting in 2004, they distributed a POC finger prick test device for use by community mental health teams to measure blood glucose and lipid levels.
“We required as a condition of payment that the providers get these lab results for everybody they served and report them centrally. Then, we databased them and benchmarked them, and we were able to show significant reductions in HbA1c’s over time,” said Parks, who was not involved with the current research.
Moreover, that program achieved corresponding savings of $23 to $24 million, he noted.
Although his study and the current study show that POC devices work, he emphasized that it’s not enough to make the devices available to clinicians.
“You also have to ensure the providers put it in their clinic workflows and use it with everybody. To do that, it really helps if you have the providers report the results, then give them report cards so they can see who’s doing it and who isn’t,” Parks said.
It wasn’t surprising that in the current study, the introduction of the POC device made less of an impact in the adult community services, he noted.
Although weight reduction is much slower in that setting, “you can still get better control of their lipids and HbA1c›s, and you get at their weight over time. You just have to program for that, too,» said Parks.
He added that it’s hard to achieve weight reduction of more than 5% or 10%, but many of these patients need a 25% to 30% reduction. “The only thing that’s going to get that is bariatric surgery,” he noted.
POC devices are not widely used in the United States.
“The payer paying for the care basically has to insist that [it] be used and then provide the machine and train the staff to use it,” Parks said.
It requires payers “to get actually involved in how providers organize and manage care, which they tend to not like to do. It’s silly because the only way any payer has to make anybody better is through the provider,” he noted.
Parks added that to increase uptake beyond the “motivated few” requires that it be made part of the workflow and not left up to clinician discretion.
The study was funded by the National Institute for Health Research. Butler and Parks have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Using a simple point-of-care (POC) finger prick device to measure blood glucose and lipid levels significantly increases rates of physical health checkups for patients with severe mental illness, new research shows.
In a UK pilot study, use of the Afinion 2 device (Abbott) was associated with a doubling of completed physical health checkups.
However, the effect only occurred in early-intervention services, in which clinicians may feel physical health checkups are most beneficial. This underlines the importance of staff training and payment incentives, the researchers note.
“Clearly, convenience is a great thing about these devices” for both the patient and the mental health clinician, Joseph Butler, MD, a psychiatry trainee at the University of Oxford, United Kingdom, told Medscape Medical News.
He noted that blood test results are rapid, which facilitates immediate discussion of a health management plan.
These tests are “independent from the lab, they’re independent from the general practitioner, and so in terms of convenience, we think it wins on both fronts,” Butler said.
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Poor heart health
Previous research has shown that life expectancy of patients with severe mental illness is 15 to 20 years less than that of the general population, mostly because of complications from poor cardiovascular health.
In the United Kingdom, physical healthcare for patients with serious mental illness is provided by primary care clinicians and community mental health teams (CMHTs). The National Institute for Health and Care Excellence recommends an annual physical examination.
However, a recent audit in the south of England indicated that only 38% of patients with severe mental illness underwent complete physical examinations, primarily because blood glucose and lipid test panels had been omitted.
The researchers note that patients are typically advised to visit their general practitioner for blood tests, “which can be a challenge” for those with severe mental illness.
The Cardiovascular Monitoring in Mental Health (CARMEN) project involved distributing the Afinion 2 device for use in two CMHTs in Oxfordshire, United Kingdom, for 6 months. One CMHT was an early-intervention service, and the other was an adult mental health service.
Care coordinators received training on how to use the device as well as ongoing support to facilitate engagement with the device.
Rates of completion of blood testing and full physical examinations were compared between the intervention CMHTs and two matched control services – an early-intervention group, and an adult metal health services group in Buckinghamshire, a neighboring county.
Better completion rates
The investigators found that .
In contrast, the percentage of physical examinations that were completed remained low in the control CMHT early-intervention service, at just 7.8%.
Direct comparison between the two services showed that use of the POC device was associated with a significant increase in the number of complete physical examinations, at a relative rate of 5.18 (P < .001).
Results were similar when the investigators examined rates at which A1c and lipid panels were completed.
However, there was no difference in completion of physical examinations in the adult mental health service group, for which rates were comparable to those in the control service.
Butler speculated that the way health checkups are funded in the United Kingdom might have contributed to the poor results with the device in the adult mental health service.
In early-intervention services, there is increased awareness of the importance of physical examinations, and funding is contingent on whether clinicians persuade patients to have the examinations.
Overall, the findings show that use of a POC device for physical examinations is acceptable to patients who have severe mental illness as well as to mental health care clinicians, the investigators note.
“In teams where it is well adopted, POC testing can improve physical health check completion...although our qualitative findings highlight important considerations for maximizing clinician engagement,” they add.
The researchers plan to repeat the study across the whole of the south of England, with early-intervention services in the west equipped with POC devices and those in the east serving as controls.
Similar findings
Commenting on the findings for Medscape Medical News, Joe Parks, MD, vice president and practice improvement and medical director at the National Council for Behavioral Health, Washington, DC, noted that he and his colleagues conducted a similar study in the mid-2000s.
Starting in 2004, they distributed a POC finger prick test device for use by community mental health teams to measure blood glucose and lipid levels.
“We required as a condition of payment that the providers get these lab results for everybody they served and report them centrally. Then, we databased them and benchmarked them, and we were able to show significant reductions in HbA1c’s over time,” said Parks, who was not involved with the current research.
Moreover, that program achieved corresponding savings of $23 to $24 million, he noted.
Although his study and the current study show that POC devices work, he emphasized that it’s not enough to make the devices available to clinicians.
“You also have to ensure the providers put it in their clinic workflows and use it with everybody. To do that, it really helps if you have the providers report the results, then give them report cards so they can see who’s doing it and who isn’t,” Parks said.
It wasn’t surprising that in the current study, the introduction of the POC device made less of an impact in the adult community services, he noted.
Although weight reduction is much slower in that setting, “you can still get better control of their lipids and HbA1c›s, and you get at their weight over time. You just have to program for that, too,» said Parks.
He added that it’s hard to achieve weight reduction of more than 5% or 10%, but many of these patients need a 25% to 30% reduction. “The only thing that’s going to get that is bariatric surgery,” he noted.
POC devices are not widely used in the United States.
“The payer paying for the care basically has to insist that [it] be used and then provide the machine and train the staff to use it,” Parks said.
It requires payers “to get actually involved in how providers organize and manage care, which they tend to not like to do. It’s silly because the only way any payer has to make anybody better is through the provider,” he noted.
Parks added that to increase uptake beyond the “motivated few” requires that it be made part of the workflow and not left up to clinician discretion.
The study was funded by the National Institute for Health Research. Butler and Parks have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Using a simple point-of-care (POC) finger prick device to measure blood glucose and lipid levels significantly increases rates of physical health checkups for patients with severe mental illness, new research shows.
In a UK pilot study, use of the Afinion 2 device (Abbott) was associated with a doubling of completed physical health checkups.
However, the effect only occurred in early-intervention services, in which clinicians may feel physical health checkups are most beneficial. This underlines the importance of staff training and payment incentives, the researchers note.
“Clearly, convenience is a great thing about these devices” for both the patient and the mental health clinician, Joseph Butler, MD, a psychiatry trainee at the University of Oxford, United Kingdom, told Medscape Medical News.
He noted that blood test results are rapid, which facilitates immediate discussion of a health management plan.
These tests are “independent from the lab, they’re independent from the general practitioner, and so in terms of convenience, we think it wins on both fronts,” Butler said.
The findings were scheduled to be presented at the Congress of the Schizophrenia International Research Society (SIRS) 2020, but the meeting was canceled because of the coronavirus pandemic.
Poor heart health
Previous research has shown that life expectancy of patients with severe mental illness is 15 to 20 years less than that of the general population, mostly because of complications from poor cardiovascular health.
In the United Kingdom, physical healthcare for patients with serious mental illness is provided by primary care clinicians and community mental health teams (CMHTs). The National Institute for Health and Care Excellence recommends an annual physical examination.
However, a recent audit in the south of England indicated that only 38% of patients with severe mental illness underwent complete physical examinations, primarily because blood glucose and lipid test panels had been omitted.
The researchers note that patients are typically advised to visit their general practitioner for blood tests, “which can be a challenge” for those with severe mental illness.
The Cardiovascular Monitoring in Mental Health (CARMEN) project involved distributing the Afinion 2 device for use in two CMHTs in Oxfordshire, United Kingdom, for 6 months. One CMHT was an early-intervention service, and the other was an adult mental health service.
Care coordinators received training on how to use the device as well as ongoing support to facilitate engagement with the device.
Rates of completion of blood testing and full physical examinations were compared between the intervention CMHTs and two matched control services – an early-intervention group, and an adult metal health services group in Buckinghamshire, a neighboring county.
Better completion rates
The investigators found that .
In contrast, the percentage of physical examinations that were completed remained low in the control CMHT early-intervention service, at just 7.8%.
Direct comparison between the two services showed that use of the POC device was associated with a significant increase in the number of complete physical examinations, at a relative rate of 5.18 (P < .001).
Results were similar when the investigators examined rates at which A1c and lipid panels were completed.
However, there was no difference in completion of physical examinations in the adult mental health service group, for which rates were comparable to those in the control service.
Butler speculated that the way health checkups are funded in the United Kingdom might have contributed to the poor results with the device in the adult mental health service.
In early-intervention services, there is increased awareness of the importance of physical examinations, and funding is contingent on whether clinicians persuade patients to have the examinations.
Overall, the findings show that use of a POC device for physical examinations is acceptable to patients who have severe mental illness as well as to mental health care clinicians, the investigators note.
“In teams where it is well adopted, POC testing can improve physical health check completion...although our qualitative findings highlight important considerations for maximizing clinician engagement,” they add.
The researchers plan to repeat the study across the whole of the south of England, with early-intervention services in the west equipped with POC devices and those in the east serving as controls.
Similar findings
Commenting on the findings for Medscape Medical News, Joe Parks, MD, vice president and practice improvement and medical director at the National Council for Behavioral Health, Washington, DC, noted that he and his colleagues conducted a similar study in the mid-2000s.
Starting in 2004, they distributed a POC finger prick test device for use by community mental health teams to measure blood glucose and lipid levels.
“We required as a condition of payment that the providers get these lab results for everybody they served and report them centrally. Then, we databased them and benchmarked them, and we were able to show significant reductions in HbA1c’s over time,” said Parks, who was not involved with the current research.
Moreover, that program achieved corresponding savings of $23 to $24 million, he noted.
Although his study and the current study show that POC devices work, he emphasized that it’s not enough to make the devices available to clinicians.
“You also have to ensure the providers put it in their clinic workflows and use it with everybody. To do that, it really helps if you have the providers report the results, then give them report cards so they can see who’s doing it and who isn’t,” Parks said.
It wasn’t surprising that in the current study, the introduction of the POC device made less of an impact in the adult community services, he noted.
Although weight reduction is much slower in that setting, “you can still get better control of their lipids and HbA1c›s, and you get at their weight over time. You just have to program for that, too,» said Parks.
He added that it’s hard to achieve weight reduction of more than 5% or 10%, but many of these patients need a 25% to 30% reduction. “The only thing that’s going to get that is bariatric surgery,” he noted.
POC devices are not widely used in the United States.
“The payer paying for the care basically has to insist that [it] be used and then provide the machine and train the staff to use it,” Parks said.
It requires payers “to get actually involved in how providers organize and manage care, which they tend to not like to do. It’s silly because the only way any payer has to make anybody better is through the provider,” he noted.
Parks added that to increase uptake beyond the “motivated few” requires that it be made part of the workflow and not left up to clinician discretion.
The study was funded by the National Institute for Health Research. Butler and Parks have reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM SIRS 2020
Racial differences in rates of atopic dermatitis observed early in life
, results from a single-center retrospective study found.

“Atopic dermatitis is a very common pediatric skin condition with significant morbidity for patients and their families,” lead study author Reesa L. Monir, MD, said during the virtual annual meeting of the Society for Pediatric Dermatology. “Existing studies show increased disease prevalence in Black and Asian children relative to White children, with conflicting data for Hispanic children. The methodology behind many of these existing studies, however, is somewhat questionable. Many were survey-based studies asking parents to remember a diagnosis of eczema or even asking parents to just report an itchy rash and using that as a diagnosis.”
For the current study, Dr. Monir and colleagues reviewed the records of 4,016 infants born between June 1, 2011, and April 30, 2017, who were followed in the University of Florida’s health care system. The researchers defined this as having two or more well-child visits after birth and at least one visit at 300 days of life or later, and the used documentation of specific ICD-9 or ICD-10 codes to capture an objective diagnosis of atopic dermatitis (AD). Of the 4,016 patients, 39.2% were Black, 38.5% were White, 7.1% were Hispanic, 5.3% were Asian, 6.5% were from other racial backgrounds, and 3.4% were multiracial.
Dr. Monir, who is a resident in the department of dermatology at the University of Florida, Gainesville, reported that Black infants had the highest prevalence of AD at 37%, followed by Asian infants (25.8%), Hispanic infants (24.1%), multiracial infants (23%), infants from other racial backgrounds (19.1%), and non-Hispanic White infants (17.9%). Compared with White infants, the odds ratio estimates for AD was highest for Black infants (OR, 2.62), followed by Asian infants (OR, 1.55), multiracial infants (OR, 1.42), Hispanic infants (OR, 1.41), and infants from other racial backgrounds (OR, .97).
On unadjusted analysis, the following factors were significantly associated with race: delivery mode (P = .006), insurance type (P less than .001), NICU stay (P less than .001), and gestational age (P less than .0001). However, on multivariate logistic regression, only two factors were significantly associated with the diagnosis of AD: race (P less than .0001) and NICU stay (P = .0385).
“When we looked at the early childhood period specifically, we found striking racial differences in the rates of AD arising early in life,” Dr. Monir concluded. “The diagnosis was independently associated with race and NICU stay. We suggest that further investigation into these disparities and ways we can mitigate them should focus on this early childhood period.”
The researchers reported having no relevant financial disclosures.
, results from a single-center retrospective study found.
“Atopic dermatitis is a very common pediatric skin condition with significant morbidity for patients and their families,” lead study author Reesa L. Monir, MD, said during the virtual annual meeting of the Society for Pediatric Dermatology. “Existing studies show increased disease prevalence in Black and Asian children relative to White children, with conflicting data for Hispanic children. The methodology behind many of these existing studies, however, is somewhat questionable. Many were survey-based studies asking parents to remember a diagnosis of eczema or even asking parents to just report an itchy rash and using that as a diagnosis.”
For the current study, Dr. Monir and colleagues reviewed the records of 4,016 infants born between June 1, 2011, and April 30, 2017, who were followed in the University of Florida’s health care system. The researchers defined this as having two or more well-child visits after birth and at least one visit at 300 days of life or later, and the used documentation of specific ICD-9 or ICD-10 codes to capture an objective diagnosis of atopic dermatitis (AD). Of the 4,016 patients, 39.2% were Black, 38.5% were White, 7.1% were Hispanic, 5.3% were Asian, 6.5% were from other racial backgrounds, and 3.4% were multiracial.
Dr. Monir, who is a resident in the department of dermatology at the University of Florida, Gainesville, reported that Black infants had the highest prevalence of AD at 37%, followed by Asian infants (25.8%), Hispanic infants (24.1%), multiracial infants (23%), infants from other racial backgrounds (19.1%), and non-Hispanic White infants (17.9%). Compared with White infants, the odds ratio estimates for AD was highest for Black infants (OR, 2.62), followed by Asian infants (OR, 1.55), multiracial infants (OR, 1.42), Hispanic infants (OR, 1.41), and infants from other racial backgrounds (OR, .97).
On unadjusted analysis, the following factors were significantly associated with race: delivery mode (P = .006), insurance type (P less than .001), NICU stay (P less than .001), and gestational age (P less than .0001). However, on multivariate logistic regression, only two factors were significantly associated with the diagnosis of AD: race (P less than .0001) and NICU stay (P = .0385).
“When we looked at the early childhood period specifically, we found striking racial differences in the rates of AD arising early in life,” Dr. Monir concluded. “The diagnosis was independently associated with race and NICU stay. We suggest that further investigation into these disparities and ways we can mitigate them should focus on this early childhood period.”
The researchers reported having no relevant financial disclosures.
, results from a single-center retrospective study found.
“Atopic dermatitis is a very common pediatric skin condition with significant morbidity for patients and their families,” lead study author Reesa L. Monir, MD, said during the virtual annual meeting of the Society for Pediatric Dermatology. “Existing studies show increased disease prevalence in Black and Asian children relative to White children, with conflicting data for Hispanic children. The methodology behind many of these existing studies, however, is somewhat questionable. Many were survey-based studies asking parents to remember a diagnosis of eczema or even asking parents to just report an itchy rash and using that as a diagnosis.”
For the current study, Dr. Monir and colleagues reviewed the records of 4,016 infants born between June 1, 2011, and April 30, 2017, who were followed in the University of Florida’s health care system. The researchers defined this as having two or more well-child visits after birth and at least one visit at 300 days of life or later, and the used documentation of specific ICD-9 or ICD-10 codes to capture an objective diagnosis of atopic dermatitis (AD). Of the 4,016 patients, 39.2% were Black, 38.5% were White, 7.1% were Hispanic, 5.3% were Asian, 6.5% were from other racial backgrounds, and 3.4% were multiracial.
Dr. Monir, who is a resident in the department of dermatology at the University of Florida, Gainesville, reported that Black infants had the highest prevalence of AD at 37%, followed by Asian infants (25.8%), Hispanic infants (24.1%), multiracial infants (23%), infants from other racial backgrounds (19.1%), and non-Hispanic White infants (17.9%). Compared with White infants, the odds ratio estimates for AD was highest for Black infants (OR, 2.62), followed by Asian infants (OR, 1.55), multiracial infants (OR, 1.42), Hispanic infants (OR, 1.41), and infants from other racial backgrounds (OR, .97).
On unadjusted analysis, the following factors were significantly associated with race: delivery mode (P = .006), insurance type (P less than .001), NICU stay (P less than .001), and gestational age (P less than .0001). However, on multivariate logistic regression, only two factors were significantly associated with the diagnosis of AD: race (P less than .0001) and NICU stay (P = .0385).
“When we looked at the early childhood period specifically, we found striking racial differences in the rates of AD arising early in life,” Dr. Monir concluded. “The diagnosis was independently associated with race and NICU stay. We suggest that further investigation into these disparities and ways we can mitigate them should focus on this early childhood period.”
The researchers reported having no relevant financial disclosures.
FROM SPD 2020

August 2020 – ICYMI
Gastroenterology
May 2020
Mechanisms of fibrosis development in nonalcoholic steatohepatitis. Robert F. Schwabe et al. 2020 May;158(7):1913-28. doi: 10.1053/j.gastro.2019.11.311
June 2020
Cognitive deficit and white matter changes in persons with celiac disease: A population-based study. Iain D. Croall et al. 2020 Jun;158(8):2112-22. doi: 10.1053/j.gastro.2020.02.028
Efficacy and safety of upadacitinib in a randomized trial of patients with Crohn’s disease. William J. Sandborn et al. 2020 Jun;158(8):2123-38.e8. doi: 10.1053/j.gastro.2020.01.047
The path to gastroenterology leadership: The preparation, the process, and achieving success. Joseph Ahn et al. 2020 Jun;158(8):2033-6.e4. doi: 10.1053/j.gastro.2020.01.054
Clinical Gastroenterology and Hepatology
May 2020
A user’s guide to de-escalating immunomodulator and biologic therapy in inflammatory bowel disease. Robert P. Hirten et al. 2020 May;18(6);1336-45. doi: 10.1016/j.cgh.2019.12.019
Dietary guidance from the International Organization for the Study of Inflammatory Bowel Diseases. Arie Levine et al. 2020 May;18(6):1381-92. doi: 10.1016/j.cgh.2020.01.046
Management of patients with immune checkpoint inhibitor-induced enterocolitis: A systematic review. Michael Collins et al. 2020 May;18(6):1393-403.e1. doi: 10.1016/j.cgh.2020.01.033
June 2020
Worldwide variations in demographics, management, and outcomes of acute pancreatitis. Bassem Matta et al. 2020 Jun;18(7):1567-75.e2. doi: 10.1016/j.cgh.2019.11.017
Rapid recurrence of eosinophilic esophagitis activity after successful treatment in the observation phase of a randomized, double-blind, double-dummy trial. Evan S. Dellon et al. 2020 Jun;18(7):1483-92.e2. doi: 10.1016/j.cgh.2019.08.050
July 2020
Disparities in colorectal cancer screening in the United States before and after implementation of the Affordable Care Act. Folasade P. May et al. 2020 Jul;18(8):1796-804.e2. doi: 10.1016/j.cgh.2019.09.008
Cost-effectiveness of telemedicine-directed specialized vs. standard care for patients with inflammatory bowel diseases in a randomized trial. Marin J. de Jong et al. 2020 Jul;18(8):1744-52. doi: 10.1016/j.cgh.2020.04.038
Artificial intelligence-assisted system improves endoscopic identification of colorectal neoplasms. Shin-ei Kudo et al. 2020 Jul;18(8):1874-81.e2. doi: 10.1016/j.cgh.2019.09.009
Gastroenterology
May 2020
Mechanisms of fibrosis development in nonalcoholic steatohepatitis. Robert F. Schwabe et al. 2020 May;158(7):1913-28. doi: 10.1053/j.gastro.2019.11.311
June 2020
Cognitive deficit and white matter changes in persons with celiac disease: A population-based study. Iain D. Croall et al. 2020 Jun;158(8):2112-22. doi: 10.1053/j.gastro.2020.02.028
Efficacy and safety of upadacitinib in a randomized trial of patients with Crohn’s disease. William J. Sandborn et al. 2020 Jun;158(8):2123-38.e8. doi: 10.1053/j.gastro.2020.01.047
The path to gastroenterology leadership: The preparation, the process, and achieving success. Joseph Ahn et al. 2020 Jun;158(8):2033-6.e4. doi: 10.1053/j.gastro.2020.01.054
Clinical Gastroenterology and Hepatology
May 2020
A user’s guide to de-escalating immunomodulator and biologic therapy in inflammatory bowel disease. Robert P. Hirten et al. 2020 May;18(6);1336-45. doi: 10.1016/j.cgh.2019.12.019
Dietary guidance from the International Organization for the Study of Inflammatory Bowel Diseases. Arie Levine et al. 2020 May;18(6):1381-92. doi: 10.1016/j.cgh.2020.01.046
Management of patients with immune checkpoint inhibitor-induced enterocolitis: A systematic review. Michael Collins et al. 2020 May;18(6):1393-403.e1. doi: 10.1016/j.cgh.2020.01.033
June 2020
Worldwide variations in demographics, management, and outcomes of acute pancreatitis. Bassem Matta et al. 2020 Jun;18(7):1567-75.e2. doi: 10.1016/j.cgh.2019.11.017
Rapid recurrence of eosinophilic esophagitis activity after successful treatment in the observation phase of a randomized, double-blind, double-dummy trial. Evan S. Dellon et al. 2020 Jun;18(7):1483-92.e2. doi: 10.1016/j.cgh.2019.08.050
July 2020
Disparities in colorectal cancer screening in the United States before and after implementation of the Affordable Care Act. Folasade P. May et al. 2020 Jul;18(8):1796-804.e2. doi: 10.1016/j.cgh.2019.09.008
Cost-effectiveness of telemedicine-directed specialized vs. standard care for patients with inflammatory bowel diseases in a randomized trial. Marin J. de Jong et al. 2020 Jul;18(8):1744-52. doi: 10.1016/j.cgh.2020.04.038
Artificial intelligence-assisted system improves endoscopic identification of colorectal neoplasms. Shin-ei Kudo et al. 2020 Jul;18(8):1874-81.e2. doi: 10.1016/j.cgh.2019.09.009
Gastroenterology
May 2020
Mechanisms of fibrosis development in nonalcoholic steatohepatitis. Robert F. Schwabe et al. 2020 May;158(7):1913-28. doi: 10.1053/j.gastro.2019.11.311
June 2020
Cognitive deficit and white matter changes in persons with celiac disease: A population-based study. Iain D. Croall et al. 2020 Jun;158(8):2112-22. doi: 10.1053/j.gastro.2020.02.028
Efficacy and safety of upadacitinib in a randomized trial of patients with Crohn’s disease. William J. Sandborn et al. 2020 Jun;158(8):2123-38.e8. doi: 10.1053/j.gastro.2020.01.047
The path to gastroenterology leadership: The preparation, the process, and achieving success. Joseph Ahn et al. 2020 Jun;158(8):2033-6.e4. doi: 10.1053/j.gastro.2020.01.054
Clinical Gastroenterology and Hepatology
May 2020
A user’s guide to de-escalating immunomodulator and biologic therapy in inflammatory bowel disease. Robert P. Hirten et al. 2020 May;18(6);1336-45. doi: 10.1016/j.cgh.2019.12.019
Dietary guidance from the International Organization for the Study of Inflammatory Bowel Diseases. Arie Levine et al. 2020 May;18(6):1381-92. doi: 10.1016/j.cgh.2020.01.046
Management of patients with immune checkpoint inhibitor-induced enterocolitis: A systematic review. Michael Collins et al. 2020 May;18(6):1393-403.e1. doi: 10.1016/j.cgh.2020.01.033
June 2020
Worldwide variations in demographics, management, and outcomes of acute pancreatitis. Bassem Matta et al. 2020 Jun;18(7):1567-75.e2. doi: 10.1016/j.cgh.2019.11.017
Rapid recurrence of eosinophilic esophagitis activity after successful treatment in the observation phase of a randomized, double-blind, double-dummy trial. Evan S. Dellon et al. 2020 Jun;18(7):1483-92.e2. doi: 10.1016/j.cgh.2019.08.050
July 2020
Disparities in colorectal cancer screening in the United States before and after implementation of the Affordable Care Act. Folasade P. May et al. 2020 Jul;18(8):1796-804.e2. doi: 10.1016/j.cgh.2019.09.008
Cost-effectiveness of telemedicine-directed specialized vs. standard care for patients with inflammatory bowel diseases in a randomized trial. Marin J. de Jong et al. 2020 Jul;18(8):1744-52. doi: 10.1016/j.cgh.2020.04.038
Artificial intelligence-assisted system improves endoscopic identification of colorectal neoplasms. Shin-ei Kudo et al. 2020 Jul;18(8):1874-81.e2. doi: 10.1016/j.cgh.2019.09.009
Why doctors keep monitoring kids who recover from mysterious COVID-linked illness
He’s a 5-year-old boy and would much rather talk about cartoons or the ideas for inventions that constantly pop into his head.
“Hold your horses, I think I know what I’m gonna make,” he said, holding up a finger in the middle of a conversation. “I’m gonna make something that lights up and attaches to things with glue, so if you don’t have a flashlight, you can just use it!”
In New York, at least 237 kids, including Israel, appear to have Multisystem Inflammatory Syndrome in Children (MIS-C). And state officials continue to track the syndrome, but the Centers for Disease Control and Prevention did not respond to repeated requests for information on how many children nationwide have been diagnosed so far with MIS-C.
A study published June 29 in the New England Journal of Medicine reported on 186 patients in 26 states who had been diagnosed with MIS-C. A researcher writing in the same issue added reports from other countries, finding that about 1,000 children worldwide have been diagnosed with MIS-C.
Tracking the long-term health effects of MIS-C
Israel is friendly and energetic, but he’s also really good at sitting still. During a recent checkup at the Children’s Hospital at Montefiore, New York, he had no complaints about all the stickers and wires a health aide attached to him for an EKG. And when Marc Foca, MD, an infectious disease specialist, came by to listen to his heart and lungs, and prod his abdomen, Israel barely seemed to notice.
There were still some tests pending, but overall, Dr. Foca said, “Israel looks like a totally healthy 5-year-old.”
“Stay safe!” Israel called out, as Dr. Foca left. It’s his new sign-off, instead of goodbye. His mother, Janelle Moholland, explained Israel came up with it himself. And she’s also hoping that, after a harrowing couple of weeks in early May, Israel himself will “stay safe.”
That’s why they’ve been returning to Montefiore for the periodic checkups, even though Israel seems to have recovered fully from both COVID-19 and MIS-C.
MIS-C is relatively rare, and it apparently responds well to treatment, but it is new enough – and mysterious enough – that doctors here want to make sure the children who recover don’t experience any related health complications in the future.
“We’ve seen these kids get really sick, and get better and recover and go home, yet we don’t know what the long-term outcomes are,” said Nadine Choueiter, MD, a pediatric cardiologist at Montefiore. “So that’s why we will be seeing them.”
When Israel first got sick at the end of April, his illness didn’t exactly look like COVID-19. He had persistent high fevers, with his temperature reaching 104° F – but no problems breathing. He wasn’t eating. He was barely drinking. He wasn’t using the bathroom. He had abdominal pains. His eyes were red.
They went to the ED a couple of times and visited an urgent care center, but the doctors sent them home without testing him for the coronavirus. Ms. Moholland, 29, said she felt powerless.
“There was nothing I could do but make him comfortable,” she said. “I literally had to just trust in a higher power and just hope that He would come through for us. It taught me a lot about patience and faith.”
As Israel grew sicker, and they still had no answers, Ms. Moholland grew frustrated. “I wish his pediatrician and [the ED and urgent care staff] had done what they were supposed to do and given him a test” when Israel first got sick, Ms. Moholland said. “What harm would it have done? He suffered for about 10 or 11 days that could have been avoided.”
In a later interview, she talked with NPR about how COVID-19 has disproportionately affected the African American community because of a combination of underlying health conditions and lack of access to good health care. She said she felt she, too, had fallen victim to those disparities.
“It affects me, personally, because I am African American, but you just never know,” she said. “It’s hard. We’re living in uncertain times – very uncertain times.”
Finally, the Children’s Hospital at Montefiore admitted Israel – and the test she’d been trying to get for days confirmed he had the virus.
“I was literally in tears, like begging them not to discharge me because I knew he was not fine,” she recalled.
Israel was in shock, and by the time he got to the hospital, doctors were on the lookout for MIS-C, so they recognized his symptoms – which were distinct from most people with COVID-19.
Doctors gave Israel fluids and intravenous immunoglobulin, a substance obtained from donated human plasma, which is used to treat deficiencies in the immune system.
Immunoglobulin has been effective in children like Israel because MIS-C appears to be caused by an immune overreaction to the initial coronavirus infection, according to Dr. Choueiter.
“The immune system starts attacking the body itself, including the arteries of the heart,” she said.
In some MIS-C cases – though not Israel’s – the attack occurs in the coronary arteries, inflaming and dilating them. That also happens in a different syndrome affecting children, Kawasaki disease. About 5% of Kawasaki patients experience aneurysms – which can fatally rupture blood vessels – after the initial condition subsides.
Dr. Choueiter and colleagues want to make sure MIS-C patients don’t face similar risks. So far, they’re cautiously optimistic.
“We have not seen any new decrease in heart function or any new coronary artery dilations,” she said. “When we check their blood, their inflammatory markers are back to normal. For the parents, the child is back to baseline, and it’s as if this illness is a nightmare that’s long gone.”
For a Pennsylvania teen, the MIS-C diagnosis came much later
Not every child who develops MIS-C tests positive for the coronavirus, though many will test positive for antibodies to the coronavirus, indicating they had been infected previously. That was the case with Andrew Lis, a boy from Pennsylvania who was the first MIS-C patient seen at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Andrew had been a healthy 14-year-old boy before he got sick. He and his twin brother love sports and video games. He said the first symptom was a bad headache. He developed a fever the next day, then constipation and intense stomach pain.
“It was terrible,” Andrew said. “It was unbearable. I couldn’t really move a lot.”
His mother, Ingrid Lis, said they were thinking appendicitis, not coronavirus, at first. In fact, she hesitated to take Andrew to the hospital, for fear of exposing him to the virus. But after Andrew stopped eating because of his headache and stomach discomfort, “I knew I couldn’t keep him home anymore,” Mrs. Lis said.
Andrew was admitted to the hospital April 12, but that was before reports of the mysterious syndrome had started trickling out of Europe.
Over about 5 days in the pediatric ICU, Andrew’s condition deteriorated rapidly, as doctors struggled to figure out what was wrong. Puzzled, they tried treatments for scarlet fever, strep throat, and toxic shock syndrome. Andrew’s body broke out in rashes, then his heart began failing and he was put on a ventilator. Andrew’s father, Ed Lis, said doctors told the family to brace for the worst: “We’ve got a healthy kid who a few days ago was just having these sort of strange symptoms. And now they’re telling us that we could lose him.”
Though Andrew’s symptoms were atypical for Kawasaki disease, doctors decided to give him the standard treatment for that condition – administering intravenous immunoglobulin, the same treatment Israel Shippy received.
“Within the 24 hours of the infusion, he was a different person,” Mrs. Lis said. Andrew was removed from the ventilator, and his appetite eventually returned. “That’s when we knew that we had turned that corner.”
It wasn’t until after Andrew’s discharge that his doctors learned about MIS-C from colleagues in Europe. They recommended the whole family be tested for antibodies to the coronavirus. Although Andrew tested positive, the rest of the family – both parents, Andrew’s twin brother and two older siblings – all tested negative. Andrew’s mother is still not sure how he was exposed since the family had been observing a strict lockdown since mid-March. Both she and her husband were working remotely from home, and she says they all wore masks and were conscientious about hand-washing when they ventured out for groceries. She thinks Andrew must have been exposed at least a month before his illness began.
And she’s puzzled why the rest of her close-knit family wasn’t infected as well. “We are a Latino family,” Mrs. Lis said. “We are very used to being together, clustering in the same room.” Even when Andrew was sick, she says, all six of them huddled in his bedroom to comfort him.
Meanwhile, Andrew has made a quick recovery. Not long after his discharge in April, he turned 15 and resumed an exercise routine involving running, push-ups, and sit-ups. A few weeks later, an ECG showed Andrew’s heart was “perfect,” Mr. Lis said. Still, doctors have asked Andrew to follow up with a cardiologist every 3 months.
An eye on the long-term effects
The medical team at Montefiore is tracking the 40 children they have already treated and discharged. With kids showing few symptoms in the immediate aftermath, Dr. Choueiter hopes the long-term trajectory after MIS-C will be similar to what happens after Kawasaki disease.
“Usually children who have had coronary artery dilations [from Kawasaki disease] that have resolved within the first 6 weeks of the illness do well long-term,” said Dr. Choueiter, who runs the Kawasaki disease program at Montefiore.
The Montefiore team is asking patients affected by MIS-C to return for a checkup 1 week after discharge, then after 1 month, 3 months, 6 months, and a year. They will be evaluated by pediatric cardiologists, hematologists, rheumatologists and infectious disease specialists.
Montefiore and other children’s hospitals around the country are sharing information. Dr. Choueiter wants to establish an even longer-term monitoring program for MIS-C, comparable with registries that exist for other diseases.
Ms. Moholland is glad the hospital is being vigilant.
“The uncertainty of not knowing whether it could come back in his future is a little unsettling,” she said. “But I am hopeful.”
This story is part of a partnership that includes WNYC, NPR, and Kaiser Health News. A version of this article originally appeared on Kaiser Health News.
He’s a 5-year-old boy and would much rather talk about cartoons or the ideas for inventions that constantly pop into his head.
“Hold your horses, I think I know what I’m gonna make,” he said, holding up a finger in the middle of a conversation. “I’m gonna make something that lights up and attaches to things with glue, so if you don’t have a flashlight, you can just use it!”
In New York, at least 237 kids, including Israel, appear to have Multisystem Inflammatory Syndrome in Children (MIS-C). And state officials continue to track the syndrome, but the Centers for Disease Control and Prevention did not respond to repeated requests for information on how many children nationwide have been diagnosed so far with MIS-C.
A study published June 29 in the New England Journal of Medicine reported on 186 patients in 26 states who had been diagnosed with MIS-C. A researcher writing in the same issue added reports from other countries, finding that about 1,000 children worldwide have been diagnosed with MIS-C.
Tracking the long-term health effects of MIS-C
Israel is friendly and energetic, but he’s also really good at sitting still. During a recent checkup at the Children’s Hospital at Montefiore, New York, he had no complaints about all the stickers and wires a health aide attached to him for an EKG. And when Marc Foca, MD, an infectious disease specialist, came by to listen to his heart and lungs, and prod his abdomen, Israel barely seemed to notice.
There were still some tests pending, but overall, Dr. Foca said, “Israel looks like a totally healthy 5-year-old.”
“Stay safe!” Israel called out, as Dr. Foca left. It’s his new sign-off, instead of goodbye. His mother, Janelle Moholland, explained Israel came up with it himself. And she’s also hoping that, after a harrowing couple of weeks in early May, Israel himself will “stay safe.”
That’s why they’ve been returning to Montefiore for the periodic checkups, even though Israel seems to have recovered fully from both COVID-19 and MIS-C.
MIS-C is relatively rare, and it apparently responds well to treatment, but it is new enough – and mysterious enough – that doctors here want to make sure the children who recover don’t experience any related health complications in the future.
“We’ve seen these kids get really sick, and get better and recover and go home, yet we don’t know what the long-term outcomes are,” said Nadine Choueiter, MD, a pediatric cardiologist at Montefiore. “So that’s why we will be seeing them.”
When Israel first got sick at the end of April, his illness didn’t exactly look like COVID-19. He had persistent high fevers, with his temperature reaching 104° F – but no problems breathing. He wasn’t eating. He was barely drinking. He wasn’t using the bathroom. He had abdominal pains. His eyes were red.
They went to the ED a couple of times and visited an urgent care center, but the doctors sent them home without testing him for the coronavirus. Ms. Moholland, 29, said she felt powerless.
“There was nothing I could do but make him comfortable,” she said. “I literally had to just trust in a higher power and just hope that He would come through for us. It taught me a lot about patience and faith.”
As Israel grew sicker, and they still had no answers, Ms. Moholland grew frustrated. “I wish his pediatrician and [the ED and urgent care staff] had done what they were supposed to do and given him a test” when Israel first got sick, Ms. Moholland said. “What harm would it have done? He suffered for about 10 or 11 days that could have been avoided.”
In a later interview, she talked with NPR about how COVID-19 has disproportionately affected the African American community because of a combination of underlying health conditions and lack of access to good health care. She said she felt she, too, had fallen victim to those disparities.
“It affects me, personally, because I am African American, but you just never know,” she said. “It’s hard. We’re living in uncertain times – very uncertain times.”
Finally, the Children’s Hospital at Montefiore admitted Israel – and the test she’d been trying to get for days confirmed he had the virus.
“I was literally in tears, like begging them not to discharge me because I knew he was not fine,” she recalled.
Israel was in shock, and by the time he got to the hospital, doctors were on the lookout for MIS-C, so they recognized his symptoms – which were distinct from most people with COVID-19.
Doctors gave Israel fluids and intravenous immunoglobulin, a substance obtained from donated human plasma, which is used to treat deficiencies in the immune system.
Immunoglobulin has been effective in children like Israel because MIS-C appears to be caused by an immune overreaction to the initial coronavirus infection, according to Dr. Choueiter.
“The immune system starts attacking the body itself, including the arteries of the heart,” she said.
In some MIS-C cases – though not Israel’s – the attack occurs in the coronary arteries, inflaming and dilating them. That also happens in a different syndrome affecting children, Kawasaki disease. About 5% of Kawasaki patients experience aneurysms – which can fatally rupture blood vessels – after the initial condition subsides.
Dr. Choueiter and colleagues want to make sure MIS-C patients don’t face similar risks. So far, they’re cautiously optimistic.
“We have not seen any new decrease in heart function or any new coronary artery dilations,” she said. “When we check their blood, their inflammatory markers are back to normal. For the parents, the child is back to baseline, and it’s as if this illness is a nightmare that’s long gone.”
For a Pennsylvania teen, the MIS-C diagnosis came much later
Not every child who develops MIS-C tests positive for the coronavirus, though many will test positive for antibodies to the coronavirus, indicating they had been infected previously. That was the case with Andrew Lis, a boy from Pennsylvania who was the first MIS-C patient seen at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Andrew had been a healthy 14-year-old boy before he got sick. He and his twin brother love sports and video games. He said the first symptom was a bad headache. He developed a fever the next day, then constipation and intense stomach pain.
“It was terrible,” Andrew said. “It was unbearable. I couldn’t really move a lot.”
His mother, Ingrid Lis, said they were thinking appendicitis, not coronavirus, at first. In fact, she hesitated to take Andrew to the hospital, for fear of exposing him to the virus. But after Andrew stopped eating because of his headache and stomach discomfort, “I knew I couldn’t keep him home anymore,” Mrs. Lis said.
Andrew was admitted to the hospital April 12, but that was before reports of the mysterious syndrome had started trickling out of Europe.
Over about 5 days in the pediatric ICU, Andrew’s condition deteriorated rapidly, as doctors struggled to figure out what was wrong. Puzzled, they tried treatments for scarlet fever, strep throat, and toxic shock syndrome. Andrew’s body broke out in rashes, then his heart began failing and he was put on a ventilator. Andrew’s father, Ed Lis, said doctors told the family to brace for the worst: “We’ve got a healthy kid who a few days ago was just having these sort of strange symptoms. And now they’re telling us that we could lose him.”
Though Andrew’s symptoms were atypical for Kawasaki disease, doctors decided to give him the standard treatment for that condition – administering intravenous immunoglobulin, the same treatment Israel Shippy received.
“Within the 24 hours of the infusion, he was a different person,” Mrs. Lis said. Andrew was removed from the ventilator, and his appetite eventually returned. “That’s when we knew that we had turned that corner.”
It wasn’t until after Andrew’s discharge that his doctors learned about MIS-C from colleagues in Europe. They recommended the whole family be tested for antibodies to the coronavirus. Although Andrew tested positive, the rest of the family – both parents, Andrew’s twin brother and two older siblings – all tested negative. Andrew’s mother is still not sure how he was exposed since the family had been observing a strict lockdown since mid-March. Both she and her husband were working remotely from home, and she says they all wore masks and were conscientious about hand-washing when they ventured out for groceries. She thinks Andrew must have been exposed at least a month before his illness began.
And she’s puzzled why the rest of her close-knit family wasn’t infected as well. “We are a Latino family,” Mrs. Lis said. “We are very used to being together, clustering in the same room.” Even when Andrew was sick, she says, all six of them huddled in his bedroom to comfort him.
Meanwhile, Andrew has made a quick recovery. Not long after his discharge in April, he turned 15 and resumed an exercise routine involving running, push-ups, and sit-ups. A few weeks later, an ECG showed Andrew’s heart was “perfect,” Mr. Lis said. Still, doctors have asked Andrew to follow up with a cardiologist every 3 months.
An eye on the long-term effects
The medical team at Montefiore is tracking the 40 children they have already treated and discharged. With kids showing few symptoms in the immediate aftermath, Dr. Choueiter hopes the long-term trajectory after MIS-C will be similar to what happens after Kawasaki disease.
“Usually children who have had coronary artery dilations [from Kawasaki disease] that have resolved within the first 6 weeks of the illness do well long-term,” said Dr. Choueiter, who runs the Kawasaki disease program at Montefiore.
The Montefiore team is asking patients affected by MIS-C to return for a checkup 1 week after discharge, then after 1 month, 3 months, 6 months, and a year. They will be evaluated by pediatric cardiologists, hematologists, rheumatologists and infectious disease specialists.
Montefiore and other children’s hospitals around the country are sharing information. Dr. Choueiter wants to establish an even longer-term monitoring program for MIS-C, comparable with registries that exist for other diseases.
Ms. Moholland is glad the hospital is being vigilant.
“The uncertainty of not knowing whether it could come back in his future is a little unsettling,” she said. “But I am hopeful.”
This story is part of a partnership that includes WNYC, NPR, and Kaiser Health News. A version of this article originally appeared on Kaiser Health News.
He’s a 5-year-old boy and would much rather talk about cartoons or the ideas for inventions that constantly pop into his head.
“Hold your horses, I think I know what I’m gonna make,” he said, holding up a finger in the middle of a conversation. “I’m gonna make something that lights up and attaches to things with glue, so if you don’t have a flashlight, you can just use it!”
In New York, at least 237 kids, including Israel, appear to have Multisystem Inflammatory Syndrome in Children (MIS-C). And state officials continue to track the syndrome, but the Centers for Disease Control and Prevention did not respond to repeated requests for information on how many children nationwide have been diagnosed so far with MIS-C.
A study published June 29 in the New England Journal of Medicine reported on 186 patients in 26 states who had been diagnosed with MIS-C. A researcher writing in the same issue added reports from other countries, finding that about 1,000 children worldwide have been diagnosed with MIS-C.
Tracking the long-term health effects of MIS-C
Israel is friendly and energetic, but he’s also really good at sitting still. During a recent checkup at the Children’s Hospital at Montefiore, New York, he had no complaints about all the stickers and wires a health aide attached to him for an EKG. And when Marc Foca, MD, an infectious disease specialist, came by to listen to his heart and lungs, and prod his abdomen, Israel barely seemed to notice.
There were still some tests pending, but overall, Dr. Foca said, “Israel looks like a totally healthy 5-year-old.”
“Stay safe!” Israel called out, as Dr. Foca left. It’s his new sign-off, instead of goodbye. His mother, Janelle Moholland, explained Israel came up with it himself. And she’s also hoping that, after a harrowing couple of weeks in early May, Israel himself will “stay safe.”
That’s why they’ve been returning to Montefiore for the periodic checkups, even though Israel seems to have recovered fully from both COVID-19 and MIS-C.
MIS-C is relatively rare, and it apparently responds well to treatment, but it is new enough – and mysterious enough – that doctors here want to make sure the children who recover don’t experience any related health complications in the future.
“We’ve seen these kids get really sick, and get better and recover and go home, yet we don’t know what the long-term outcomes are,” said Nadine Choueiter, MD, a pediatric cardiologist at Montefiore. “So that’s why we will be seeing them.”
When Israel first got sick at the end of April, his illness didn’t exactly look like COVID-19. He had persistent high fevers, with his temperature reaching 104° F – but no problems breathing. He wasn’t eating. He was barely drinking. He wasn’t using the bathroom. He had abdominal pains. His eyes were red.
They went to the ED a couple of times and visited an urgent care center, but the doctors sent them home without testing him for the coronavirus. Ms. Moholland, 29, said she felt powerless.
“There was nothing I could do but make him comfortable,” she said. “I literally had to just trust in a higher power and just hope that He would come through for us. It taught me a lot about patience and faith.”
As Israel grew sicker, and they still had no answers, Ms. Moholland grew frustrated. “I wish his pediatrician and [the ED and urgent care staff] had done what they were supposed to do and given him a test” when Israel first got sick, Ms. Moholland said. “What harm would it have done? He suffered for about 10 or 11 days that could have been avoided.”
In a later interview, she talked with NPR about how COVID-19 has disproportionately affected the African American community because of a combination of underlying health conditions and lack of access to good health care. She said she felt she, too, had fallen victim to those disparities.
“It affects me, personally, because I am African American, but you just never know,” she said. “It’s hard. We’re living in uncertain times – very uncertain times.”
Finally, the Children’s Hospital at Montefiore admitted Israel – and the test she’d been trying to get for days confirmed he had the virus.
“I was literally in tears, like begging them not to discharge me because I knew he was not fine,” she recalled.
Israel was in shock, and by the time he got to the hospital, doctors were on the lookout for MIS-C, so they recognized his symptoms – which were distinct from most people with COVID-19.
Doctors gave Israel fluids and intravenous immunoglobulin, a substance obtained from donated human plasma, which is used to treat deficiencies in the immune system.
Immunoglobulin has been effective in children like Israel because MIS-C appears to be caused by an immune overreaction to the initial coronavirus infection, according to Dr. Choueiter.
“The immune system starts attacking the body itself, including the arteries of the heart,” she said.
In some MIS-C cases – though not Israel’s – the attack occurs in the coronary arteries, inflaming and dilating them. That also happens in a different syndrome affecting children, Kawasaki disease. About 5% of Kawasaki patients experience aneurysms – which can fatally rupture blood vessels – after the initial condition subsides.
Dr. Choueiter and colleagues want to make sure MIS-C patients don’t face similar risks. So far, they’re cautiously optimistic.
“We have not seen any new decrease in heart function or any new coronary artery dilations,” she said. “When we check their blood, their inflammatory markers are back to normal. For the parents, the child is back to baseline, and it’s as if this illness is a nightmare that’s long gone.”
For a Pennsylvania teen, the MIS-C diagnosis came much later
Not every child who develops MIS-C tests positive for the coronavirus, though many will test positive for antibodies to the coronavirus, indicating they had been infected previously. That was the case with Andrew Lis, a boy from Pennsylvania who was the first MIS-C patient seen at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Andrew had been a healthy 14-year-old boy before he got sick. He and his twin brother love sports and video games. He said the first symptom was a bad headache. He developed a fever the next day, then constipation and intense stomach pain.
“It was terrible,” Andrew said. “It was unbearable. I couldn’t really move a lot.”
His mother, Ingrid Lis, said they were thinking appendicitis, not coronavirus, at first. In fact, she hesitated to take Andrew to the hospital, for fear of exposing him to the virus. But after Andrew stopped eating because of his headache and stomach discomfort, “I knew I couldn’t keep him home anymore,” Mrs. Lis said.
Andrew was admitted to the hospital April 12, but that was before reports of the mysterious syndrome had started trickling out of Europe.
Over about 5 days in the pediatric ICU, Andrew’s condition deteriorated rapidly, as doctors struggled to figure out what was wrong. Puzzled, they tried treatments for scarlet fever, strep throat, and toxic shock syndrome. Andrew’s body broke out in rashes, then his heart began failing and he was put on a ventilator. Andrew’s father, Ed Lis, said doctors told the family to brace for the worst: “We’ve got a healthy kid who a few days ago was just having these sort of strange symptoms. And now they’re telling us that we could lose him.”
Though Andrew’s symptoms were atypical for Kawasaki disease, doctors decided to give him the standard treatment for that condition – administering intravenous immunoglobulin, the same treatment Israel Shippy received.
“Within the 24 hours of the infusion, he was a different person,” Mrs. Lis said. Andrew was removed from the ventilator, and his appetite eventually returned. “That’s when we knew that we had turned that corner.”
It wasn’t until after Andrew’s discharge that his doctors learned about MIS-C from colleagues in Europe. They recommended the whole family be tested for antibodies to the coronavirus. Although Andrew tested positive, the rest of the family – both parents, Andrew’s twin brother and two older siblings – all tested negative. Andrew’s mother is still not sure how he was exposed since the family had been observing a strict lockdown since mid-March. Both she and her husband were working remotely from home, and she says they all wore masks and were conscientious about hand-washing when they ventured out for groceries. She thinks Andrew must have been exposed at least a month before his illness began.
And she’s puzzled why the rest of her close-knit family wasn’t infected as well. “We are a Latino family,” Mrs. Lis said. “We are very used to being together, clustering in the same room.” Even when Andrew was sick, she says, all six of them huddled in his bedroom to comfort him.
Meanwhile, Andrew has made a quick recovery. Not long after his discharge in April, he turned 15 and resumed an exercise routine involving running, push-ups, and sit-ups. A few weeks later, an ECG showed Andrew’s heart was “perfect,” Mr. Lis said. Still, doctors have asked Andrew to follow up with a cardiologist every 3 months.
An eye on the long-term effects
The medical team at Montefiore is tracking the 40 children they have already treated and discharged. With kids showing few symptoms in the immediate aftermath, Dr. Choueiter hopes the long-term trajectory after MIS-C will be similar to what happens after Kawasaki disease.
“Usually children who have had coronary artery dilations [from Kawasaki disease] that have resolved within the first 6 weeks of the illness do well long-term,” said Dr. Choueiter, who runs the Kawasaki disease program at Montefiore.
The Montefiore team is asking patients affected by MIS-C to return for a checkup 1 week after discharge, then after 1 month, 3 months, 6 months, and a year. They will be evaluated by pediatric cardiologists, hematologists, rheumatologists and infectious disease specialists.
Montefiore and other children’s hospitals around the country are sharing information. Dr. Choueiter wants to establish an even longer-term monitoring program for MIS-C, comparable with registries that exist for other diseases.
Ms. Moholland is glad the hospital is being vigilant.
“The uncertainty of not knowing whether it could come back in his future is a little unsettling,” she said. “But I am hopeful.”
This story is part of a partnership that includes WNYC, NPR, and Kaiser Health News. A version of this article originally appeared on Kaiser Health News.
Cerclage in twin pregnancies reduces perinatal mortality in randomized trial
according to a randomized controlled trial. The trial, which was published in the American Journal of Obstetrics and Gynecology, included 30 patients at 8 centers. The investigators stopped the trial early because perinatal mortality occurred more often in the group that did not receive the intervention.

The research suggests that a combination of physical exam–indicated cerclage, indomethacin, and antibiotics decreased the incidence of spontaneous preterm birth and prolonged the period from diagnosis to delivery by an average of 5.6 weeks, compared with no cerclage.
“We’ve already incorporated this cerclage into our practice and have been able to offer this to pregnant mothers with twins with great success,” senior author Vincenzo Berghella, MD, said in a news release.
“These results have the potential to change practice and help many more women have healthy twin babies,” said Dr. Berghella, director of the division of maternal fetal medicine at Thomas Jefferson University in Philadelphia.
A shift in perspective
More research is needed to establish a standardized approach, but the trial should “open physicians’ perspectives to think about how, in selected cases and with the proper approach, cerclage can work well,” said Ozhan M. Turan, MD, PhD, director of the division of maternal and fetal medicine and director of fetal therapy and complex obstetric surgery at University of Maryland in Baltimore.
Although many physicians use cerclage for twin pregnancies in select situations, the practice is not well established. “If you look at the guidelines or books, mostly everyone thinks that doing a cerclage in twins is not a good idea,” Dr. Turan said in an interview.
In the present trial, the researchers controlled for many factors and carefully selected patients with no signs of preterm labor or infection. It is not simply a matter of saying, “Do the stitch,” he said. “But it is proven: if you select patients well and use the appropriate approach, then you could improve the outcome.”
The study is the first randomized controlled trial of physical exam–indicated cerclage focused on twins, according to its authors. It enrolled patients between July 2015 and July 2019. In the end, the researchers analyzed data from 30 pregnancies, rather than the originally intended 52. They stopped the trial after a data and safety monitoring board considered it “unethical to continue the study due to the considerable perinatal mortality in one of the arms ... and requested to unmask the arms of the study,” the researchers said.
Perinatal mortality occurred in 18% of neonates in the cerclage group (6 of 34), compared with 77% in the group without cerclage (20 of 26). All perinatal mortality cases were associated with delivery before 24 weeks.
“The small number of participants reflects how rare this condition is among all pregnancies,” first author Amanda Roman, MD, of the division of maternal fetal medicine at Thomas Jefferson University, Philadelphia, said in the news release. “But because women were randomized to treatment and nontreatment groups, the results are strong, as confirmed by the independent data and safety monitoring board.”
The researchers enrolled women with twin pregnancies and asymptomatic cervical dilation from 1 to 4 cm before 24 weeks. Exclusion criteria included monochorionic-monoamniotic pregnancy, selective fetal growth restriction, twin-twin transfusion syndrome, major fetal malformation, known genetic anomaly, placenta previa, signs of labor, or clinical chorioamnionitis.
In all, 17 women were randomized to cerclage and 13 to the no-cerclage group. Both groups had similar patient characteristics. About 93% of the twin gestations were diamniotic-dichorionic. Assisted reproductive technology was used by about 36% of the participants, and 20% had a history of singleton preterm birth. Four women assigned to cerclage did not undergo the procedure but were included in the intention-to-treat analysis. Two of the four patients had contraindications that occurred soon after randomization (rupture of amniotic membranes and vaginal bleeding), one had a friable cervix, and one declined cerclage after being randomized.
Spontaneous preterm birth before 34 weeks of gestation, the primary outcome, occurred in 12 of 17 women in the cerclage group and in all 13 women in the no-cerclage group (70% vs. 100%).
Trial to assess ultrasound indicated cerclage
“Expectant management with no cerclage is the current standard of care for these women,” Dr. Roman and coauthors wrote. “Despite small sample size, we were able to show a significant benefit to physical exam–indicated cerclage.”
Inability to place the cerclage in one patient due to friable cervix was the only intraoperative complication. “Larger cohorts in singleton pregnancies have informed a 10%-20% risk of intraoperative rupture of the membranes, cervical laceration, and bleeding during the procedure,” the researchers noted.
All women who received cerclage also received indomethacin and antibiotics, although these elements of management were not prespecified. Given the relatively small sample size, it is unclear what role factors such as indomethacin, which was administered to 82% of the cerclage group versus 31% of the no-cerclage group, and antibiotics may have played, said Dr. Turan.
Prospective studies may help clarify how the degree of cervical dilation, gestational age, use of progesterone, or surgical techniques may influence outcomes. In addition, the researchers are enrolling patients in another trial. That study aims to assess whether cerclage reduces the incidence of spontaneous preterm birth in asymptomatic women with twin gestations and cervical length of 15 mm or less diagnosed by transvaginal ultrasound between 16 and 24 weeks of gestation.
The study had no external financial support. The authors had no conflicts of interest. Dr. Turan said he had no relevant financial disclosures.
SOURCE: Roman A et al. Am J Obstet Gynecol. 2020 Jun. doi: 10.1016/j.ajog.2020.06.047.
according to a randomized controlled trial. The trial, which was published in the American Journal of Obstetrics and Gynecology, included 30 patients at 8 centers. The investigators stopped the trial early because perinatal mortality occurred more often in the group that did not receive the intervention.
The research suggests that a combination of physical exam–indicated cerclage, indomethacin, and antibiotics decreased the incidence of spontaneous preterm birth and prolonged the period from diagnosis to delivery by an average of 5.6 weeks, compared with no cerclage.
“We’ve already incorporated this cerclage into our practice and have been able to offer this to pregnant mothers with twins with great success,” senior author Vincenzo Berghella, MD, said in a news release.
“These results have the potential to change practice and help many more women have healthy twin babies,” said Dr. Berghella, director of the division of maternal fetal medicine at Thomas Jefferson University in Philadelphia.
A shift in perspective
More research is needed to establish a standardized approach, but the trial should “open physicians’ perspectives to think about how, in selected cases and with the proper approach, cerclage can work well,” said Ozhan M. Turan, MD, PhD, director of the division of maternal and fetal medicine and director of fetal therapy and complex obstetric surgery at University of Maryland in Baltimore.
Although many physicians use cerclage for twin pregnancies in select situations, the practice is not well established. “If you look at the guidelines or books, mostly everyone thinks that doing a cerclage in twins is not a good idea,” Dr. Turan said in an interview.
In the present trial, the researchers controlled for many factors and carefully selected patients with no signs of preterm labor or infection. It is not simply a matter of saying, “Do the stitch,” he said. “But it is proven: if you select patients well and use the appropriate approach, then you could improve the outcome.”
The study is the first randomized controlled trial of physical exam–indicated cerclage focused on twins, according to its authors. It enrolled patients between July 2015 and July 2019. In the end, the researchers analyzed data from 30 pregnancies, rather than the originally intended 52. They stopped the trial after a data and safety monitoring board considered it “unethical to continue the study due to the considerable perinatal mortality in one of the arms ... and requested to unmask the arms of the study,” the researchers said.
Perinatal mortality occurred in 18% of neonates in the cerclage group (6 of 34), compared with 77% in the group without cerclage (20 of 26). All perinatal mortality cases were associated with delivery before 24 weeks.
“The small number of participants reflects how rare this condition is among all pregnancies,” first author Amanda Roman, MD, of the division of maternal fetal medicine at Thomas Jefferson University, Philadelphia, said in the news release. “But because women were randomized to treatment and nontreatment groups, the results are strong, as confirmed by the independent data and safety monitoring board.”
The researchers enrolled women with twin pregnancies and asymptomatic cervical dilation from 1 to 4 cm before 24 weeks. Exclusion criteria included monochorionic-monoamniotic pregnancy, selective fetal growth restriction, twin-twin transfusion syndrome, major fetal malformation, known genetic anomaly, placenta previa, signs of labor, or clinical chorioamnionitis.
In all, 17 women were randomized to cerclage and 13 to the no-cerclage group. Both groups had similar patient characteristics. About 93% of the twin gestations were diamniotic-dichorionic. Assisted reproductive technology was used by about 36% of the participants, and 20% had a history of singleton preterm birth. Four women assigned to cerclage did not undergo the procedure but were included in the intention-to-treat analysis. Two of the four patients had contraindications that occurred soon after randomization (rupture of amniotic membranes and vaginal bleeding), one had a friable cervix, and one declined cerclage after being randomized.
Spontaneous preterm birth before 34 weeks of gestation, the primary outcome, occurred in 12 of 17 women in the cerclage group and in all 13 women in the no-cerclage group (70% vs. 100%).
Trial to assess ultrasound indicated cerclage
“Expectant management with no cerclage is the current standard of care for these women,” Dr. Roman and coauthors wrote. “Despite small sample size, we were able to show a significant benefit to physical exam–indicated cerclage.”
Inability to place the cerclage in one patient due to friable cervix was the only intraoperative complication. “Larger cohorts in singleton pregnancies have informed a 10%-20% risk of intraoperative rupture of the membranes, cervical laceration, and bleeding during the procedure,” the researchers noted.
All women who received cerclage also received indomethacin and antibiotics, although these elements of management were not prespecified. Given the relatively small sample size, it is unclear what role factors such as indomethacin, which was administered to 82% of the cerclage group versus 31% of the no-cerclage group, and antibiotics may have played, said Dr. Turan.
Prospective studies may help clarify how the degree of cervical dilation, gestational age, use of progesterone, or surgical techniques may influence outcomes. In addition, the researchers are enrolling patients in another trial. That study aims to assess whether cerclage reduces the incidence of spontaneous preterm birth in asymptomatic women with twin gestations and cervical length of 15 mm or less diagnosed by transvaginal ultrasound between 16 and 24 weeks of gestation.
The study had no external financial support. The authors had no conflicts of interest. Dr. Turan said he had no relevant financial disclosures.
SOURCE: Roman A et al. Am J Obstet Gynecol. 2020 Jun. doi: 10.1016/j.ajog.2020.06.047.
according to a randomized controlled trial. The trial, which was published in the American Journal of Obstetrics and Gynecology, included 30 patients at 8 centers. The investigators stopped the trial early because perinatal mortality occurred more often in the group that did not receive the intervention.
The research suggests that a combination of physical exam–indicated cerclage, indomethacin, and antibiotics decreased the incidence of spontaneous preterm birth and prolonged the period from diagnosis to delivery by an average of 5.6 weeks, compared with no cerclage.
“We’ve already incorporated this cerclage into our practice and have been able to offer this to pregnant mothers with twins with great success,” senior author Vincenzo Berghella, MD, said in a news release.
“These results have the potential to change practice and help many more women have healthy twin babies,” said Dr. Berghella, director of the division of maternal fetal medicine at Thomas Jefferson University in Philadelphia.
A shift in perspective
More research is needed to establish a standardized approach, but the trial should “open physicians’ perspectives to think about how, in selected cases and with the proper approach, cerclage can work well,” said Ozhan M. Turan, MD, PhD, director of the division of maternal and fetal medicine and director of fetal therapy and complex obstetric surgery at University of Maryland in Baltimore.
Although many physicians use cerclage for twin pregnancies in select situations, the practice is not well established. “If you look at the guidelines or books, mostly everyone thinks that doing a cerclage in twins is not a good idea,” Dr. Turan said in an interview.
In the present trial, the researchers controlled for many factors and carefully selected patients with no signs of preterm labor or infection. It is not simply a matter of saying, “Do the stitch,” he said. “But it is proven: if you select patients well and use the appropriate approach, then you could improve the outcome.”
The study is the first randomized controlled trial of physical exam–indicated cerclage focused on twins, according to its authors. It enrolled patients between July 2015 and July 2019. In the end, the researchers analyzed data from 30 pregnancies, rather than the originally intended 52. They stopped the trial after a data and safety monitoring board considered it “unethical to continue the study due to the considerable perinatal mortality in one of the arms ... and requested to unmask the arms of the study,” the researchers said.
Perinatal mortality occurred in 18% of neonates in the cerclage group (6 of 34), compared with 77% in the group without cerclage (20 of 26). All perinatal mortality cases were associated with delivery before 24 weeks.
“The small number of participants reflects how rare this condition is among all pregnancies,” first author Amanda Roman, MD, of the division of maternal fetal medicine at Thomas Jefferson University, Philadelphia, said in the news release. “But because women were randomized to treatment and nontreatment groups, the results are strong, as confirmed by the independent data and safety monitoring board.”
The researchers enrolled women with twin pregnancies and asymptomatic cervical dilation from 1 to 4 cm before 24 weeks. Exclusion criteria included monochorionic-monoamniotic pregnancy, selective fetal growth restriction, twin-twin transfusion syndrome, major fetal malformation, known genetic anomaly, placenta previa, signs of labor, or clinical chorioamnionitis.
In all, 17 women were randomized to cerclage and 13 to the no-cerclage group. Both groups had similar patient characteristics. About 93% of the twin gestations were diamniotic-dichorionic. Assisted reproductive technology was used by about 36% of the participants, and 20% had a history of singleton preterm birth. Four women assigned to cerclage did not undergo the procedure but were included in the intention-to-treat analysis. Two of the four patients had contraindications that occurred soon after randomization (rupture of amniotic membranes and vaginal bleeding), one had a friable cervix, and one declined cerclage after being randomized.
Spontaneous preterm birth before 34 weeks of gestation, the primary outcome, occurred in 12 of 17 women in the cerclage group and in all 13 women in the no-cerclage group (70% vs. 100%).
Trial to assess ultrasound indicated cerclage
“Expectant management with no cerclage is the current standard of care for these women,” Dr. Roman and coauthors wrote. “Despite small sample size, we were able to show a significant benefit to physical exam–indicated cerclage.”
Inability to place the cerclage in one patient due to friable cervix was the only intraoperative complication. “Larger cohorts in singleton pregnancies have informed a 10%-20% risk of intraoperative rupture of the membranes, cervical laceration, and bleeding during the procedure,” the researchers noted.
All women who received cerclage also received indomethacin and antibiotics, although these elements of management were not prespecified. Given the relatively small sample size, it is unclear what role factors such as indomethacin, which was administered to 82% of the cerclage group versus 31% of the no-cerclage group, and antibiotics may have played, said Dr. Turan.
Prospective studies may help clarify how the degree of cervical dilation, gestational age, use of progesterone, or surgical techniques may influence outcomes. In addition, the researchers are enrolling patients in another trial. That study aims to assess whether cerclage reduces the incidence of spontaneous preterm birth in asymptomatic women with twin gestations and cervical length of 15 mm or less diagnosed by transvaginal ultrasound between 16 and 24 weeks of gestation.
The study had no external financial support. The authors had no conflicts of interest. Dr. Turan said he had no relevant financial disclosures.
SOURCE: Roman A et al. Am J Obstet Gynecol. 2020 Jun. doi: 10.1016/j.ajog.2020.06.047.
FROM THE AMERICAN JOURNAL OF OBSTETRICS AND GYNECOLOGY
Stillbirth incidence increases during COVID-19 pandemic
The incidence of stillbirth has increased since the COVID-19 pandemic began, according to a comparative study of pregnancy outcomes in a London hospital.
“The increase in stillbirths may have resulted from indirect effects such as reluctance to attend hospital when needed (e.g., with reduced fetal movements), fear of contracting infection, or not wanting to add to the National Health Service burden,” Asma Khalil, MD, of St George’s University of London and coauthors reported in JAMA.
To further assess reported changes in stillbirth and preterm delivery rates during the pandemic, the researchers began a retrospective study of pregnancy outcomes at St George’s University Hospital in London. They compared two periods: from Oct. 1, 2019, to Jan. 31, 2020 as the pre–COVID-19 period and from Feb. 1, 2020, to June 14, 2020 as the pandemic period. The median age of the mother at time of birth in both periods was 33 years. The prepandemic period had 1,681 births, and the pandemic period had 1,718 births.
Although there were found to be fewer nulliparous women and fewer women with hypertension in the pandemic period, the incidence of stillbirth in that period was significantly higher (n = 16 [9 per 1,000 births]) than in the prepandemic period (n = 4 [2 per 1,000 births]) (difference, 7 per 1,000 births; 95% confidence interval, 1.83-12.0; P = .01). The pandemic rate remained higher when late terminations for fetal abnormality were excluded (difference 6 per 1,000 births; 95% CI 1.54-10.1; P = .01).
None of the pregnant women who experienced stillbirth had COVID-19 symptoms, and none of the postmortems or placental exams indicated infection. There were no significant differences between the two periods in regard to births before 37 weeks’ gestation, births after 34 weeks’ gestation, neonatal unit admission, or cesarean delivery.
“It’s very important to highlight the effects of the pandemic on pregnant patients, even if they’re not infected with COVID-19,” Shannon Clark, MD, of the University of Texas Medical Branch in Galveston said in an interview.
She noted several COVID-related considerations that could have contributed to this increase: the reluctance of both low-risk and high-risk patients to enter a hospital setting during a pandemic, along with safety-centered changes made in antenatal services and care, which includes a reduced number of ultrasounds and screening exams.
“Checking a patient’s blood pressure, checking their weight changes, checking how the baby is growing,” she said. “They’re all simple things that just can’t be done via telemedicine.”
“We’ve thought a lot about the potential effects of getting COVID in pregnancy,” she added, “but it’s just as important to think about what might happen to those who don’t have it and are considered low risk otherwise.”
The study authors noted its limitations, including it being retrospective, analyzing a short time frame, and focusing on a single medical center. It also didn’t factor in the causes of the stillbirths, nor were the time periods precisely comparable, although they did add that “there is no seasonality to stillbirths in the UK.”
One doctor reported receiving grants outside of the submitted work. No other potential conflicts of interest were noted. Dr. Clark said she had no relevant financial disclosures.
SOURCE: Khalil A et al. JAMA. 2020 Jul. doi: 10.1001/jama.2020.12746.
The incidence of stillbirth has increased since the COVID-19 pandemic began, according to a comparative study of pregnancy outcomes in a London hospital.
“The increase in stillbirths may have resulted from indirect effects such as reluctance to attend hospital when needed (e.g., with reduced fetal movements), fear of contracting infection, or not wanting to add to the National Health Service burden,” Asma Khalil, MD, of St George’s University of London and coauthors reported in JAMA.
To further assess reported changes in stillbirth and preterm delivery rates during the pandemic, the researchers began a retrospective study of pregnancy outcomes at St George’s University Hospital in London. They compared two periods: from Oct. 1, 2019, to Jan. 31, 2020 as the pre–COVID-19 period and from Feb. 1, 2020, to June 14, 2020 as the pandemic period. The median age of the mother at time of birth in both periods was 33 years. The prepandemic period had 1,681 births, and the pandemic period had 1,718 births.
Although there were found to be fewer nulliparous women and fewer women with hypertension in the pandemic period, the incidence of stillbirth in that period was significantly higher (n = 16 [9 per 1,000 births]) than in the prepandemic period (n = 4 [2 per 1,000 births]) (difference, 7 per 1,000 births; 95% confidence interval, 1.83-12.0; P = .01). The pandemic rate remained higher when late terminations for fetal abnormality were excluded (difference 6 per 1,000 births; 95% CI 1.54-10.1; P = .01).
None of the pregnant women who experienced stillbirth had COVID-19 symptoms, and none of the postmortems or placental exams indicated infection. There were no significant differences between the two periods in regard to births before 37 weeks’ gestation, births after 34 weeks’ gestation, neonatal unit admission, or cesarean delivery.
“It’s very important to highlight the effects of the pandemic on pregnant patients, even if they’re not infected with COVID-19,” Shannon Clark, MD, of the University of Texas Medical Branch in Galveston said in an interview.
She noted several COVID-related considerations that could have contributed to this increase: the reluctance of both low-risk and high-risk patients to enter a hospital setting during a pandemic, along with safety-centered changes made in antenatal services and care, which includes a reduced number of ultrasounds and screening exams.
“Checking a patient’s blood pressure, checking their weight changes, checking how the baby is growing,” she said. “They’re all simple things that just can’t be done via telemedicine.”
“We’ve thought a lot about the potential effects of getting COVID in pregnancy,” she added, “but it’s just as important to think about what might happen to those who don’t have it and are considered low risk otherwise.”
The study authors noted its limitations, including it being retrospective, analyzing a short time frame, and focusing on a single medical center. It also didn’t factor in the causes of the stillbirths, nor were the time periods precisely comparable, although they did add that “there is no seasonality to stillbirths in the UK.”
One doctor reported receiving grants outside of the submitted work. No other potential conflicts of interest were noted. Dr. Clark said she had no relevant financial disclosures.
SOURCE: Khalil A et al. JAMA. 2020 Jul. doi: 10.1001/jama.2020.12746.
The incidence of stillbirth has increased since the COVID-19 pandemic began, according to a comparative study of pregnancy outcomes in a London hospital.
“The increase in stillbirths may have resulted from indirect effects such as reluctance to attend hospital when needed (e.g., with reduced fetal movements), fear of contracting infection, or not wanting to add to the National Health Service burden,” Asma Khalil, MD, of St George’s University of London and coauthors reported in JAMA.
To further assess reported changes in stillbirth and preterm delivery rates during the pandemic, the researchers began a retrospective study of pregnancy outcomes at St George’s University Hospital in London. They compared two periods: from Oct. 1, 2019, to Jan. 31, 2020 as the pre–COVID-19 period and from Feb. 1, 2020, to June 14, 2020 as the pandemic period. The median age of the mother at time of birth in both periods was 33 years. The prepandemic period had 1,681 births, and the pandemic period had 1,718 births.
Although there were found to be fewer nulliparous women and fewer women with hypertension in the pandemic period, the incidence of stillbirth in that period was significantly higher (n = 16 [9 per 1,000 births]) than in the prepandemic period (n = 4 [2 per 1,000 births]) (difference, 7 per 1,000 births; 95% confidence interval, 1.83-12.0; P = .01). The pandemic rate remained higher when late terminations for fetal abnormality were excluded (difference 6 per 1,000 births; 95% CI 1.54-10.1; P = .01).
None of the pregnant women who experienced stillbirth had COVID-19 symptoms, and none of the postmortems or placental exams indicated infection. There were no significant differences between the two periods in regard to births before 37 weeks’ gestation, births after 34 weeks’ gestation, neonatal unit admission, or cesarean delivery.
“It’s very important to highlight the effects of the pandemic on pregnant patients, even if they’re not infected with COVID-19,” Shannon Clark, MD, of the University of Texas Medical Branch in Galveston said in an interview.
She noted several COVID-related considerations that could have contributed to this increase: the reluctance of both low-risk and high-risk patients to enter a hospital setting during a pandemic, along with safety-centered changes made in antenatal services and care, which includes a reduced number of ultrasounds and screening exams.
“Checking a patient’s blood pressure, checking their weight changes, checking how the baby is growing,” she said. “They’re all simple things that just can’t be done via telemedicine.”
“We’ve thought a lot about the potential effects of getting COVID in pregnancy,” she added, “but it’s just as important to think about what might happen to those who don’t have it and are considered low risk otherwise.”
The study authors noted its limitations, including it being retrospective, analyzing a short time frame, and focusing on a single medical center. It also didn’t factor in the causes of the stillbirths, nor were the time periods precisely comparable, although they did add that “there is no seasonality to stillbirths in the UK.”
One doctor reported receiving grants outside of the submitted work. No other potential conflicts of interest were noted. Dr. Clark said she had no relevant financial disclosures.
SOURCE: Khalil A et al. JAMA. 2020 Jul. doi: 10.1001/jama.2020.12746.
FROM JAMA
Exposing hospital gowns
Bare bottoms, bare minimum
“Don’t let the gown get you down,” was the advice a 26-year-old gentleman with leukemia offered in a study investigating the psychosocial impact of hospital gowns on patients and providers.1 Patients were found to be resigned to their “uncomfortable,” “expos[ing],” “nightmare-[ish]” “uniform,” afraid to even ask to wear more dignifying attire for fear of seeming difficult to providers and potentially harming the therapeutic relationship; one 64-year-old woman with terminal cancer detailed, “I have my own pajamas at home, but I don’t bring them because you can’t wear them here … [wearing a gown] is really not fun, but hey, this is what [providers] have to do, so it’s what you have to do.”1-3

Research has consistently shown that patients are vulnerable to dehumanization and loss of identity in the hospital, often exacerbated by wearing the standard hospital gown.3-8 Case in point, a mixed-methods study revealed that hospital gowns may lead to an increased sense of exposure, discomfort, disempowerment, and embarrassment for patients during a period of potential vulnerability while undergoing medical intervention.8
Hospital gowns strip autonomy from individuals humbly coming to the hospital for help. The gown has become a linchpin of change, initiating the dehumanizing process of “person” to “patient.” One of the main problems with the hospital gown is its exposing nature, often made light of on the wards with the joke, “Do you know who invented the hospital gown?…See-more Hiney!” The joke continued in two Super Bowl LIII commercials for a large academic health care system and insurance provider in Pennsylvania, depicting a construction worker and businessman clad in hospital gowns, mooning their less-than-pleased coworkers, to inform patients of expanded insurance coverage, i.e., “completely covered.” Hospital gowns are also a source of comedic fodder on sitcoms, including “It’s Always Sunny in Philadelphia,” “Man with a Plan,” and “Carol’s Second Act.”
It is common knowledge that hospital gowns are flawed, but very little has been done to change them. Little is known about the origin of hospital gowns, and like their design, their history has many gaps. PubMed, Google, and Wikipedia yield no fruitful insight into the evolution of the hospital gown, and perhaps the best way to understand the hospital gown over time is to watch depictions of patients in television sitcoms, dramas, and movies, ranging from the days of black-and-white into the modern era, and view artistic depictions of hospitals across eras. Case in point, depictions of fourteenth century hospital wards in art show that all patients wore night shirts, under which they also wore some type of underclothing.9 By the end of the 1800s and beginning of the 1900s, pajamas for men became more common as hospital attire.9 Although it is not known who originally invented the traditional hospital gown, the original gown was designed around a century ago with an open back for use on patients admitted the night prior to surgery, who were sedated prior to transfer to the anesthetic room while half-asleep.10
In general, the most common reason that hospitals began to provide, require, or offer clothing to patients was to reduce infection and improve hygiene, as clothing can be ruined by leakage of bodily fluids from various examinations, treatments, and procedures.9 In addition, in certain settings, lifesaving measures require access to the naked body to allow equipment, like a defibrillator, to be connected to the patient; a gown can theoretically be removed quickly.9 For some reason along the way, the simple, open-backed “johnny” gown of the early 20th century became standard of care with minimal meaningful modifications in the last hundred years. One possible explanation for the persistence of the “johnny” gown is that in past eras of medicine, patients in gowns were expected to be bedbound for recovery, keeping their bare bottom under wraps, and this norm became the status quo. Today, ambulation is encouraged in patients as part of venous thromboembolism (VTE) prophylaxis but the gown design has fallen behind.

Modern medicine emphasizes, values, and even advertises evidence-based medicine, patient-centered care, and high-quality care, yet the hospital gown stands as a stark contrast to this pledge to move forward as beacons of change. Hospital gowns have fallen outside of the scope of evidence-based research.11 One may ask why the gown remains decades behind modern medicine, and it appears that this apathy stems from (1) accepting “medical tradition” and choosing to overlook the flaws of the current hospital gown, and (2) believing that changing the hospital gown would cost money, affronting an institution’s almighty bottom-line. Still, several institutions have attempted change, including Hackensack University Medical Center partnering with Cynthia Rowley and Nicole Miller (1999), Cleveland Clinic partnering with Diane von Furstenberg (2010), and Henry Ford Health System of Detroit’s “Model G” gown (2016).12-15
In spite of these efforts to revamp the hospital gown at academic medical centers, change has been neither long lasting nor widely disseminated. Traci Lamar, a professor at the North Carolina State University College of Textiles reasoned that, “There are number of pressures in the hospital environment that influence what they purchase and when they purchase. Cost management, inventory management, storage space. ... There’s more value coming with the apparel item if it also becomes something that replaces or enhances other equipment that’s used in the hospital environment. Like a gown that can also keep an eye on your blood pressure or measure your heart rate.”15
The hospital gown remains a poor attempt at proper attire for human beings, with the most similar evolutionary relative being a hairdresser’s cape. Taken a step further, functionally the hospital gown is most similar to a prison uniform. Although this may seem bold and sensational, one must stop and think about it, considering the parallels. When individuals are admitted to the hospital, they exchange their clothing for a hospital gown, so that they can be easily identified as a “patient” and remain safe in the hospital. When individuals are sentenced to prison, they exchange their clothing for a uniform, so that they can be easily identified as a “prisoner” and remain safe in jail. The problem is, more time, money, and effort has gone into designing prisoners’ garments, who expect a loss of autonomy, than designing patients’ garments, who should never expect a loss of autonomy.
Prison uniforms are designed with safety in mind, ensuring the absence of potential ligatures or improvised weapons. The United Nations even passed an amendment to its Standard Minimum Rules for the Treatment of Prisoners in 2015, prohibiting humiliating clothing and requiring every prisoner who is “not allowed to wear his or her own clothing” to “be provided with an outfit of clothing suitable for the climate and adequate to keep him or her in good health.”16 They also stipulated that prisoners’ clothing could not be degrading or humiliating and was mandated to “be clean and kept in proper condition”.16 Even more compelling, a physician was bequeathed the task of inspecting, and advising the prison director on “the suitability and cleanliness of the prisoners’ clothing and bedding.”16 However, there are no standard minimum rules for hospital patients’ clothing. Hospital gowns have been described as “threadbare,” “one-size-fits-none,” “stained,” and “drafty,” antithetical to both hygiene and the hospital climate – far from “proper condition” (See Figure 1).1
Where are the standard minimum rules for hospital gowns? Patients have admittedly wondered, “What happened to the person who wore this gown before I did?” or worse, “Who died in this gown?” Even more, the current hospital gown can unintentionally put a patient in harms’ way, posing a fall risk for patients with petite frames overwhelmed by the bulk of the gown and also inhibiting fast access to the chest for placement of defibrillation pads in a code. Ironically, prison uniforms have the main things patients have requested: bottoms, modesty, multiple sizes, and … color!1-3
Although jailhouse orange or stripes are unlikely to be high fashion in the hospital, it is important to consider that, through indifference about the current hospital gown, institutions are teaching that it is acceptable for patients to wear this dehumanizing garment analogous to a prison uniform, except less colorful and more exposing. The hospital gown has persisted under the myth of medical tradition, masking the fact that there is neither evidence for the current hospital gown design nor data to support its functional success for patients or providers.3,12,14 Silence speaks volumes, and patients are taught to expect and accept a loss of dignity without questioning this archaic aspect of medical culture. Patients, nurses, and physicians do not challenge the status quo because the hospital gown “is the way it has always been done.” Perceived added-cost and medical tradition have further perpetuated the current open-backed hospital gown because meaningful change would require money.

With that said, “double gowning,” the method hospitals have used to combat lunar eclipses in the hallways and provide a semblance of dignity to patients, is already costing hospitals more money, costs that can be reduced by creating an evidence-based, patient-guided, provider-approved design. As Mike Forbes, the product designer and licensing associate for the Model G gown, argued, “By using two, you’re purchasing two gowns because one doesn’t do the job, which costs money. … If you’re washing twice as many gowns as you need, you’re spending twice as much money as you need on laundry.”17
Thus, improvements can be made without breaking the bank and may even save hospitals money in the long run. For instance, a hospital administrator can order more colors or styles of hospital gowns and bottoms to give patients a choice of what they would prefer to wear: a small piece of autonomy in an environment where minimal autonomy exists. A physician or nurse can not only permit, but also encourage, a patient to wear his or her own attire within reason, for example, a loose-fitting t-shirt and sweatpants from home or pajama pants under a hospital gown. More complex solutions could include a community design contest for a medical center’s new hospital gown print, or even bolder, a community design contest for a medical center’s new inpatient attire. Above all, patients need to know that hospitals and providers care about what patients wear in the hospital. As a terminally ill patient suggested, “maybe all administrators and office staff should have to spend one day in a gown. …They advertise this: ‘We always put the patient first.’ Okay, so then I guess you have to put your money where your mouth is.”3
This new decade offers the opportunity to give patients a sense of dignity back and make concerted, evidence-based efforts towards meaningful and sustainable change in patient attire, be it purchasing more colorful and modest gown options in the present or total redesign in the future. The financial cost may seem burdensome, but the reward would be immensely bountiful. It is time to stop making hospital gown–clad patients’ exposed bottoms the butt of the joke, and the only way to change the punchline is to change the hospital gown. Patients deserve more than the bare minimum and a bare bottom, so hospitals must consider putting their money where their mouth is.
Dr. Lucas is based in the department of pediatrics, University of Pittsburgh Medical Center Children’s Hospital of Pittsburgh. She has a provisional utility patent pending for a novel patient gown. You can contact her at clucas3@alumni.nd.edu. Dr. Dellasega is based in the department of humanities, Penn State University, Hershey.
References
1. Lucas C et al. “Don’t let the gown get you down: How patients and providers perceive hospital gowns.” Abstract published at Hospital Medicine 2019, Mar 24-27, National Harbor, Md., Abstract 322.
2. Lucas C and Dellasega C. “You don’t have to be dying to do comfort measures: Patients’ and physicians’ perceptions of inpatient attire.” Abstract published at ACP Internal Medicine 2019, Apr 11-13, Philadelphia, Abstract.
3. Lucas C and Dellasega C. Finding common threads: How patients, physicians, and nurses perceive the patient gown. Patient Exp J. 2020;7(1):51-64.
4. Detsky A and Krumholtz H. Reducing the trauma of hospitalization. JAMA. 2014;311(21):2169-70.
5. Krumholz H. Post-hospital syndrome – an acquired, transient condition of generalized risk. N Engl J Med. 2013;368(2):100-2.
6. Wellbery C and Chan M. White coat, patient gown. Med Humanit. 2014;40(2):90-6.
7. McDonald E et al. Inpatient attire: An opportunity to improve the patient experience. JAMA Intern Med. 2014;174(11):1865-67.
8. Cogan N et al. Mixed methods study exploring the impact of the hospital gown on recovery and wellbeing: Implications for policy and practice. Lancet. 2019. doi: 10.1016/S0140-6736(19)32829-6.
9. Bergbom I, Pettersson M, and Mattsson E. Patient clothing – practical solution or means of imposing anonymity? J Hosp Med Manage. 2017;3(22):1-6.
10. Who invented the hospital gown? Interweave Healthcare. Accessed Mar 30, 2020.
11. Gordon L and Guttmann S. A user-centered approach to the redesign of the patient hospital gown. Fashion Practice. 2013;5(1):137-51. doi: 10.2752/175693813X13559997788961.
12. Limbong A. “Can a Patient Gown Makeover Move Hospitals to Embrace Change?” NPR. 2018 Feb 11. Accessed Mar 26, 2020.
13. Schiro A. “Patterns: Hospital Style.” New York Times. 1999 June 29. Accessed Mar 26, 2020.
14. Luthra S. “Hospital Gowns Get a Makeover.” The Atlantic. 2015 Apr 4. Accessed Mar 26, 2020.
15. Tien E. “Hospital Gowns Get a Life.” New York Times. 1998 Oct 18. Accessed Mar 26, 2020.
16. McCall-Smith K. United Nations Standard Minimum Rules for the Treatment of Prisoners (Nelson Mandela Rules). Int Leg Materials. 2016;55(6),1180-205.
17. Green C. “Updated hospital gowns a good investment, execs say, restore ‘dignity.’ ” Healthcare Finance. 2015 Aug 3. Accessed Apr 1, 2020.
Bare bottoms, bare minimum
Bare bottoms, bare minimum
“Don’t let the gown get you down,” was the advice a 26-year-old gentleman with leukemia offered in a study investigating the psychosocial impact of hospital gowns on patients and providers.1 Patients were found to be resigned to their “uncomfortable,” “expos[ing],” “nightmare-[ish]” “uniform,” afraid to even ask to wear more dignifying attire for fear of seeming difficult to providers and potentially harming the therapeutic relationship; one 64-year-old woman with terminal cancer detailed, “I have my own pajamas at home, but I don’t bring them because you can’t wear them here … [wearing a gown] is really not fun, but hey, this is what [providers] have to do, so it’s what you have to do.”1-3
Research has consistently shown that patients are vulnerable to dehumanization and loss of identity in the hospital, often exacerbated by wearing the standard hospital gown.3-8 Case in point, a mixed-methods study revealed that hospital gowns may lead to an increased sense of exposure, discomfort, disempowerment, and embarrassment for patients during a period of potential vulnerability while undergoing medical intervention.8
Hospital gowns strip autonomy from individuals humbly coming to the hospital for help. The gown has become a linchpin of change, initiating the dehumanizing process of “person” to “patient.” One of the main problems with the hospital gown is its exposing nature, often made light of on the wards with the joke, “Do you know who invented the hospital gown?…See-more Hiney!” The joke continued in two Super Bowl LIII commercials for a large academic health care system and insurance provider in Pennsylvania, depicting a construction worker and businessman clad in hospital gowns, mooning their less-than-pleased coworkers, to inform patients of expanded insurance coverage, i.e., “completely covered.” Hospital gowns are also a source of comedic fodder on sitcoms, including “It’s Always Sunny in Philadelphia,” “Man with a Plan,” and “Carol’s Second Act.”
It is common knowledge that hospital gowns are flawed, but very little has been done to change them. Little is known about the origin of hospital gowns, and like their design, their history has many gaps. PubMed, Google, and Wikipedia yield no fruitful insight into the evolution of the hospital gown, and perhaps the best way to understand the hospital gown over time is to watch depictions of patients in television sitcoms, dramas, and movies, ranging from the days of black-and-white into the modern era, and view artistic depictions of hospitals across eras. Case in point, depictions of fourteenth century hospital wards in art show that all patients wore night shirts, under which they also wore some type of underclothing.9 By the end of the 1800s and beginning of the 1900s, pajamas for men became more common as hospital attire.9 Although it is not known who originally invented the traditional hospital gown, the original gown was designed around a century ago with an open back for use on patients admitted the night prior to surgery, who were sedated prior to transfer to the anesthetic room while half-asleep.10
In general, the most common reason that hospitals began to provide, require, or offer clothing to patients was to reduce infection and improve hygiene, as clothing can be ruined by leakage of bodily fluids from various examinations, treatments, and procedures.9 In addition, in certain settings, lifesaving measures require access to the naked body to allow equipment, like a defibrillator, to be connected to the patient; a gown can theoretically be removed quickly.9 For some reason along the way, the simple, open-backed “johnny” gown of the early 20th century became standard of care with minimal meaningful modifications in the last hundred years. One possible explanation for the persistence of the “johnny” gown is that in past eras of medicine, patients in gowns were expected to be bedbound for recovery, keeping their bare bottom under wraps, and this norm became the status quo. Today, ambulation is encouraged in patients as part of venous thromboembolism (VTE) prophylaxis but the gown design has fallen behind.
Modern medicine emphasizes, values, and even advertises evidence-based medicine, patient-centered care, and high-quality care, yet the hospital gown stands as a stark contrast to this pledge to move forward as beacons of change. Hospital gowns have fallen outside of the scope of evidence-based research.11 One may ask why the gown remains decades behind modern medicine, and it appears that this apathy stems from (1) accepting “medical tradition” and choosing to overlook the flaws of the current hospital gown, and (2) believing that changing the hospital gown would cost money, affronting an institution’s almighty bottom-line. Still, several institutions have attempted change, including Hackensack University Medical Center partnering with Cynthia Rowley and Nicole Miller (1999), Cleveland Clinic partnering with Diane von Furstenberg (2010), and Henry Ford Health System of Detroit’s “Model G” gown (2016).12-15
In spite of these efforts to revamp the hospital gown at academic medical centers, change has been neither long lasting nor widely disseminated. Traci Lamar, a professor at the North Carolina State University College of Textiles reasoned that, “There are number of pressures in the hospital environment that influence what they purchase and when they purchase. Cost management, inventory management, storage space. ... There’s more value coming with the apparel item if it also becomes something that replaces or enhances other equipment that’s used in the hospital environment. Like a gown that can also keep an eye on your blood pressure or measure your heart rate.”15
The hospital gown remains a poor attempt at proper attire for human beings, with the most similar evolutionary relative being a hairdresser’s cape. Taken a step further, functionally the hospital gown is most similar to a prison uniform. Although this may seem bold and sensational, one must stop and think about it, considering the parallels. When individuals are admitted to the hospital, they exchange their clothing for a hospital gown, so that they can be easily identified as a “patient” and remain safe in the hospital. When individuals are sentenced to prison, they exchange their clothing for a uniform, so that they can be easily identified as a “prisoner” and remain safe in jail. The problem is, more time, money, and effort has gone into designing prisoners’ garments, who expect a loss of autonomy, than designing patients’ garments, who should never expect a loss of autonomy.
Prison uniforms are designed with safety in mind, ensuring the absence of potential ligatures or improvised weapons. The United Nations even passed an amendment to its Standard Minimum Rules for the Treatment of Prisoners in 2015, prohibiting humiliating clothing and requiring every prisoner who is “not allowed to wear his or her own clothing” to “be provided with an outfit of clothing suitable for the climate and adequate to keep him or her in good health.”16 They also stipulated that prisoners’ clothing could not be degrading or humiliating and was mandated to “be clean and kept in proper condition”.16 Even more compelling, a physician was bequeathed the task of inspecting, and advising the prison director on “the suitability and cleanliness of the prisoners’ clothing and bedding.”16 However, there are no standard minimum rules for hospital patients’ clothing. Hospital gowns have been described as “threadbare,” “one-size-fits-none,” “stained,” and “drafty,” antithetical to both hygiene and the hospital climate – far from “proper condition” (See Figure 1).1
Where are the standard minimum rules for hospital gowns? Patients have admittedly wondered, “What happened to the person who wore this gown before I did?” or worse, “Who died in this gown?” Even more, the current hospital gown can unintentionally put a patient in harms’ way, posing a fall risk for patients with petite frames overwhelmed by the bulk of the gown and also inhibiting fast access to the chest for placement of defibrillation pads in a code. Ironically, prison uniforms have the main things patients have requested: bottoms, modesty, multiple sizes, and … color!1-3
Although jailhouse orange or stripes are unlikely to be high fashion in the hospital, it is important to consider that, through indifference about the current hospital gown, institutions are teaching that it is acceptable for patients to wear this dehumanizing garment analogous to a prison uniform, except less colorful and more exposing. The hospital gown has persisted under the myth of medical tradition, masking the fact that there is neither evidence for the current hospital gown design nor data to support its functional success for patients or providers.3,12,14 Silence speaks volumes, and patients are taught to expect and accept a loss of dignity without questioning this archaic aspect of medical culture. Patients, nurses, and physicians do not challenge the status quo because the hospital gown “is the way it has always been done.” Perceived added-cost and medical tradition have further perpetuated the current open-backed hospital gown because meaningful change would require money.
With that said, “double gowning,” the method hospitals have used to combat lunar eclipses in the hallways and provide a semblance of dignity to patients, is already costing hospitals more money, costs that can be reduced by creating an evidence-based, patient-guided, provider-approved design. As Mike Forbes, the product designer and licensing associate for the Model G gown, argued, “By using two, you’re purchasing two gowns because one doesn’t do the job, which costs money. … If you’re washing twice as many gowns as you need, you’re spending twice as much money as you need on laundry.”17
Thus, improvements can be made without breaking the bank and may even save hospitals money in the long run. For instance, a hospital administrator can order more colors or styles of hospital gowns and bottoms to give patients a choice of what they would prefer to wear: a small piece of autonomy in an environment where minimal autonomy exists. A physician or nurse can not only permit, but also encourage, a patient to wear his or her own attire within reason, for example, a loose-fitting t-shirt and sweatpants from home or pajama pants under a hospital gown. More complex solutions could include a community design contest for a medical center’s new hospital gown print, or even bolder, a community design contest for a medical center’s new inpatient attire. Above all, patients need to know that hospitals and providers care about what patients wear in the hospital. As a terminally ill patient suggested, “maybe all administrators and office staff should have to spend one day in a gown. …They advertise this: ‘We always put the patient first.’ Okay, so then I guess you have to put your money where your mouth is.”3
This new decade offers the opportunity to give patients a sense of dignity back and make concerted, evidence-based efforts towards meaningful and sustainable change in patient attire, be it purchasing more colorful and modest gown options in the present or total redesign in the future. The financial cost may seem burdensome, but the reward would be immensely bountiful. It is time to stop making hospital gown–clad patients’ exposed bottoms the butt of the joke, and the only way to change the punchline is to change the hospital gown. Patients deserve more than the bare minimum and a bare bottom, so hospitals must consider putting their money where their mouth is.
Dr. Lucas is based in the department of pediatrics, University of Pittsburgh Medical Center Children’s Hospital of Pittsburgh. She has a provisional utility patent pending for a novel patient gown. You can contact her at clucas3@alumni.nd.edu. Dr. Dellasega is based in the department of humanities, Penn State University, Hershey.
References
1. Lucas C et al. “Don’t let the gown get you down: How patients and providers perceive hospital gowns.” Abstract published at Hospital Medicine 2019, Mar 24-27, National Harbor, Md., Abstract 322.
2. Lucas C and Dellasega C. “You don’t have to be dying to do comfort measures: Patients’ and physicians’ perceptions of inpatient attire.” Abstract published at ACP Internal Medicine 2019, Apr 11-13, Philadelphia, Abstract.
3. Lucas C and Dellasega C. Finding common threads: How patients, physicians, and nurses perceive the patient gown. Patient Exp J. 2020;7(1):51-64.
4. Detsky A and Krumholtz H. Reducing the trauma of hospitalization. JAMA. 2014;311(21):2169-70.
5. Krumholz H. Post-hospital syndrome – an acquired, transient condition of generalized risk. N Engl J Med. 2013;368(2):100-2.
6. Wellbery C and Chan M. White coat, patient gown. Med Humanit. 2014;40(2):90-6.
7. McDonald E et al. Inpatient attire: An opportunity to improve the patient experience. JAMA Intern Med. 2014;174(11):1865-67.
8. Cogan N et al. Mixed methods study exploring the impact of the hospital gown on recovery and wellbeing: Implications for policy and practice. Lancet. 2019. doi: 10.1016/S0140-6736(19)32829-6.
9. Bergbom I, Pettersson M, and Mattsson E. Patient clothing – practical solution or means of imposing anonymity? J Hosp Med Manage. 2017;3(22):1-6.
10. Who invented the hospital gown? Interweave Healthcare. Accessed Mar 30, 2020.
11. Gordon L and Guttmann S. A user-centered approach to the redesign of the patient hospital gown. Fashion Practice. 2013;5(1):137-51. doi: 10.2752/175693813X13559997788961.
12. Limbong A. “Can a Patient Gown Makeover Move Hospitals to Embrace Change?” NPR. 2018 Feb 11. Accessed Mar 26, 2020.
13. Schiro A. “Patterns: Hospital Style.” New York Times. 1999 June 29. Accessed Mar 26, 2020.
14. Luthra S. “Hospital Gowns Get a Makeover.” The Atlantic. 2015 Apr 4. Accessed Mar 26, 2020.
15. Tien E. “Hospital Gowns Get a Life.” New York Times. 1998 Oct 18. Accessed Mar 26, 2020.
16. McCall-Smith K. United Nations Standard Minimum Rules for the Treatment of Prisoners (Nelson Mandela Rules). Int Leg Materials. 2016;55(6),1180-205.
17. Green C. “Updated hospital gowns a good investment, execs say, restore ‘dignity.’ ” Healthcare Finance. 2015 Aug 3. Accessed Apr 1, 2020.
“Don’t let the gown get you down,” was the advice a 26-year-old gentleman with leukemia offered in a study investigating the psychosocial impact of hospital gowns on patients and providers.1 Patients were found to be resigned to their “uncomfortable,” “expos[ing],” “nightmare-[ish]” “uniform,” afraid to even ask to wear more dignifying attire for fear of seeming difficult to providers and potentially harming the therapeutic relationship; one 64-year-old woman with terminal cancer detailed, “I have my own pajamas at home, but I don’t bring them because you can’t wear them here … [wearing a gown] is really not fun, but hey, this is what [providers] have to do, so it’s what you have to do.”1-3
Research has consistently shown that patients are vulnerable to dehumanization and loss of identity in the hospital, often exacerbated by wearing the standard hospital gown.3-8 Case in point, a mixed-methods study revealed that hospital gowns may lead to an increased sense of exposure, discomfort, disempowerment, and embarrassment for patients during a period of potential vulnerability while undergoing medical intervention.8
Hospital gowns strip autonomy from individuals humbly coming to the hospital for help. The gown has become a linchpin of change, initiating the dehumanizing process of “person” to “patient.” One of the main problems with the hospital gown is its exposing nature, often made light of on the wards with the joke, “Do you know who invented the hospital gown?…See-more Hiney!” The joke continued in two Super Bowl LIII commercials for a large academic health care system and insurance provider in Pennsylvania, depicting a construction worker and businessman clad in hospital gowns, mooning their less-than-pleased coworkers, to inform patients of expanded insurance coverage, i.e., “completely covered.” Hospital gowns are also a source of comedic fodder on sitcoms, including “It’s Always Sunny in Philadelphia,” “Man with a Plan,” and “Carol’s Second Act.”
It is common knowledge that hospital gowns are flawed, but very little has been done to change them. Little is known about the origin of hospital gowns, and like their design, their history has many gaps. PubMed, Google, and Wikipedia yield no fruitful insight into the evolution of the hospital gown, and perhaps the best way to understand the hospital gown over time is to watch depictions of patients in television sitcoms, dramas, and movies, ranging from the days of black-and-white into the modern era, and view artistic depictions of hospitals across eras. Case in point, depictions of fourteenth century hospital wards in art show that all patients wore night shirts, under which they also wore some type of underclothing.9 By the end of the 1800s and beginning of the 1900s, pajamas for men became more common as hospital attire.9 Although it is not known who originally invented the traditional hospital gown, the original gown was designed around a century ago with an open back for use on patients admitted the night prior to surgery, who were sedated prior to transfer to the anesthetic room while half-asleep.10
In general, the most common reason that hospitals began to provide, require, or offer clothing to patients was to reduce infection and improve hygiene, as clothing can be ruined by leakage of bodily fluids from various examinations, treatments, and procedures.9 In addition, in certain settings, lifesaving measures require access to the naked body to allow equipment, like a defibrillator, to be connected to the patient; a gown can theoretically be removed quickly.9 For some reason along the way, the simple, open-backed “johnny” gown of the early 20th century became standard of care with minimal meaningful modifications in the last hundred years. One possible explanation for the persistence of the “johnny” gown is that in past eras of medicine, patients in gowns were expected to be bedbound for recovery, keeping their bare bottom under wraps, and this norm became the status quo. Today, ambulation is encouraged in patients as part of venous thromboembolism (VTE) prophylaxis but the gown design has fallen behind.
Modern medicine emphasizes, values, and even advertises evidence-based medicine, patient-centered care, and high-quality care, yet the hospital gown stands as a stark contrast to this pledge to move forward as beacons of change. Hospital gowns have fallen outside of the scope of evidence-based research.11 One may ask why the gown remains decades behind modern medicine, and it appears that this apathy stems from (1) accepting “medical tradition” and choosing to overlook the flaws of the current hospital gown, and (2) believing that changing the hospital gown would cost money, affronting an institution’s almighty bottom-line. Still, several institutions have attempted change, including Hackensack University Medical Center partnering with Cynthia Rowley and Nicole Miller (1999), Cleveland Clinic partnering with Diane von Furstenberg (2010), and Henry Ford Health System of Detroit’s “Model G” gown (2016).12-15
In spite of these efforts to revamp the hospital gown at academic medical centers, change has been neither long lasting nor widely disseminated. Traci Lamar, a professor at the North Carolina State University College of Textiles reasoned that, “There are number of pressures in the hospital environment that influence what they purchase and when they purchase. Cost management, inventory management, storage space. ... There’s more value coming with the apparel item if it also becomes something that replaces or enhances other equipment that’s used in the hospital environment. Like a gown that can also keep an eye on your blood pressure or measure your heart rate.”15
The hospital gown remains a poor attempt at proper attire for human beings, with the most similar evolutionary relative being a hairdresser’s cape. Taken a step further, functionally the hospital gown is most similar to a prison uniform. Although this may seem bold and sensational, one must stop and think about it, considering the parallels. When individuals are admitted to the hospital, they exchange their clothing for a hospital gown, so that they can be easily identified as a “patient” and remain safe in the hospital. When individuals are sentenced to prison, they exchange their clothing for a uniform, so that they can be easily identified as a “prisoner” and remain safe in jail. The problem is, more time, money, and effort has gone into designing prisoners’ garments, who expect a loss of autonomy, than designing patients’ garments, who should never expect a loss of autonomy.
Prison uniforms are designed with safety in mind, ensuring the absence of potential ligatures or improvised weapons. The United Nations even passed an amendment to its Standard Minimum Rules for the Treatment of Prisoners in 2015, prohibiting humiliating clothing and requiring every prisoner who is “not allowed to wear his or her own clothing” to “be provided with an outfit of clothing suitable for the climate and adequate to keep him or her in good health.”16 They also stipulated that prisoners’ clothing could not be degrading or humiliating and was mandated to “be clean and kept in proper condition”.16 Even more compelling, a physician was bequeathed the task of inspecting, and advising the prison director on “the suitability and cleanliness of the prisoners’ clothing and bedding.”16 However, there are no standard minimum rules for hospital patients’ clothing. Hospital gowns have been described as “threadbare,” “one-size-fits-none,” “stained,” and “drafty,” antithetical to both hygiene and the hospital climate – far from “proper condition” (See Figure 1).1
Where are the standard minimum rules for hospital gowns? Patients have admittedly wondered, “What happened to the person who wore this gown before I did?” or worse, “Who died in this gown?” Even more, the current hospital gown can unintentionally put a patient in harms’ way, posing a fall risk for patients with petite frames overwhelmed by the bulk of the gown and also inhibiting fast access to the chest for placement of defibrillation pads in a code. Ironically, prison uniforms have the main things patients have requested: bottoms, modesty, multiple sizes, and … color!1-3
Although jailhouse orange or stripes are unlikely to be high fashion in the hospital, it is important to consider that, through indifference about the current hospital gown, institutions are teaching that it is acceptable for patients to wear this dehumanizing garment analogous to a prison uniform, except less colorful and more exposing. The hospital gown has persisted under the myth of medical tradition, masking the fact that there is neither evidence for the current hospital gown design nor data to support its functional success for patients or providers.3,12,14 Silence speaks volumes, and patients are taught to expect and accept a loss of dignity without questioning this archaic aspect of medical culture. Patients, nurses, and physicians do not challenge the status quo because the hospital gown “is the way it has always been done.” Perceived added-cost and medical tradition have further perpetuated the current open-backed hospital gown because meaningful change would require money.
With that said, “double gowning,” the method hospitals have used to combat lunar eclipses in the hallways and provide a semblance of dignity to patients, is already costing hospitals more money, costs that can be reduced by creating an evidence-based, patient-guided, provider-approved design. As Mike Forbes, the product designer and licensing associate for the Model G gown, argued, “By using two, you’re purchasing two gowns because one doesn’t do the job, which costs money. … If you’re washing twice as many gowns as you need, you’re spending twice as much money as you need on laundry.”17
Thus, improvements can be made without breaking the bank and may even save hospitals money in the long run. For instance, a hospital administrator can order more colors or styles of hospital gowns and bottoms to give patients a choice of what they would prefer to wear: a small piece of autonomy in an environment where minimal autonomy exists. A physician or nurse can not only permit, but also encourage, a patient to wear his or her own attire within reason, for example, a loose-fitting t-shirt and sweatpants from home or pajama pants under a hospital gown. More complex solutions could include a community design contest for a medical center’s new hospital gown print, or even bolder, a community design contest for a medical center’s new inpatient attire. Above all, patients need to know that hospitals and providers care about what patients wear in the hospital. As a terminally ill patient suggested, “maybe all administrators and office staff should have to spend one day in a gown. …They advertise this: ‘We always put the patient first.’ Okay, so then I guess you have to put your money where your mouth is.”3
This new decade offers the opportunity to give patients a sense of dignity back and make concerted, evidence-based efforts towards meaningful and sustainable change in patient attire, be it purchasing more colorful and modest gown options in the present or total redesign in the future. The financial cost may seem burdensome, but the reward would be immensely bountiful. It is time to stop making hospital gown–clad patients’ exposed bottoms the butt of the joke, and the only way to change the punchline is to change the hospital gown. Patients deserve more than the bare minimum and a bare bottom, so hospitals must consider putting their money where their mouth is.
Dr. Lucas is based in the department of pediatrics, University of Pittsburgh Medical Center Children’s Hospital of Pittsburgh. She has a provisional utility patent pending for a novel patient gown. You can contact her at clucas3@alumni.nd.edu. Dr. Dellasega is based in the department of humanities, Penn State University, Hershey.
References
1. Lucas C et al. “Don’t let the gown get you down: How patients and providers perceive hospital gowns.” Abstract published at Hospital Medicine 2019, Mar 24-27, National Harbor, Md., Abstract 322.
2. Lucas C and Dellasega C. “You don’t have to be dying to do comfort measures: Patients’ and physicians’ perceptions of inpatient attire.” Abstract published at ACP Internal Medicine 2019, Apr 11-13, Philadelphia, Abstract.
3. Lucas C and Dellasega C. Finding common threads: How patients, physicians, and nurses perceive the patient gown. Patient Exp J. 2020;7(1):51-64.
4. Detsky A and Krumholtz H. Reducing the trauma of hospitalization. JAMA. 2014;311(21):2169-70.
5. Krumholz H. Post-hospital syndrome – an acquired, transient condition of generalized risk. N Engl J Med. 2013;368(2):100-2.
6. Wellbery C and Chan M. White coat, patient gown. Med Humanit. 2014;40(2):90-6.
7. McDonald E et al. Inpatient attire: An opportunity to improve the patient experience. JAMA Intern Med. 2014;174(11):1865-67.
8. Cogan N et al. Mixed methods study exploring the impact of the hospital gown on recovery and wellbeing: Implications for policy and practice. Lancet. 2019. doi: 10.1016/S0140-6736(19)32829-6.
9. Bergbom I, Pettersson M, and Mattsson E. Patient clothing – practical solution or means of imposing anonymity? J Hosp Med Manage. 2017;3(22):1-6.
10. Who invented the hospital gown? Interweave Healthcare. Accessed Mar 30, 2020.
11. Gordon L and Guttmann S. A user-centered approach to the redesign of the patient hospital gown. Fashion Practice. 2013;5(1):137-51. doi: 10.2752/175693813X13559997788961.
12. Limbong A. “Can a Patient Gown Makeover Move Hospitals to Embrace Change?” NPR. 2018 Feb 11. Accessed Mar 26, 2020.
13. Schiro A. “Patterns: Hospital Style.” New York Times. 1999 June 29. Accessed Mar 26, 2020.
14. Luthra S. “Hospital Gowns Get a Makeover.” The Atlantic. 2015 Apr 4. Accessed Mar 26, 2020.
15. Tien E. “Hospital Gowns Get a Life.” New York Times. 1998 Oct 18. Accessed Mar 26, 2020.
16. McCall-Smith K. United Nations Standard Minimum Rules for the Treatment of Prisoners (Nelson Mandela Rules). Int Leg Materials. 2016;55(6),1180-205.
17. Green C. “Updated hospital gowns a good investment, execs say, restore ‘dignity.’ ” Healthcare Finance. 2015 Aug 3. Accessed Apr 1, 2020.
Intraventricular methotrexate may improve survival for medulloblastoma subtypes
according to research published in the Journal of Clinical Oncology.
Investigators conducted a prospective trial of 87 children diagnosed with nonmetastatic medulloblastoma before the age of 4 years who were treated from 2001-2011.
At 5 years after diagnosis, the 42 DMB/MBEN patients had a 93% progression-free survival (PFS) rate, a 100% overall survival (OS) rate, and a 93% craniospinal irradiation (CSI)–free survival rate.
“Our results suggest that ... poor outcomes of patients treated with systemic chemotherapy alone can be improved by the addition of intraventricular [methotrexate],” wrote Martin Mynarek, MD, of the University Medical Center Hamburg-Eppendorf (Germany), and colleagues.
However, it was a different story for the 45 patients with classic medulloblastoma (CMB) or large-cell/anaplastic medulloblastoma (CLA), in which outcomes are historically worse. At 5 years, the PFS was 37%, the OS was 62%, and the CSI-free survival was 39% in these patients.
In 2006, the CMB and CLA patients started receiving local radiotherapy in addition to chemotherapy and intraventricular methotrexate, but the radiotherapy did not seem to help with their disease.
“Because data suggest no effects, or even adverse effects, of local radiotherapy, additional development of this approach does not seem justified,” the investigators wrote.
“Interestingly, almost all patients with CMB/LCA had distant or combined relapses after local radiotherapy,” they added. “One might speculate that local radiotherapy reduced disease burden of the primary tumor and subclinical metastasis in the posterior fossa, leading to a survival advantage of distant subclinical metastasis over local residues.”
Treatment details
The 87 patients were enrolled in the BIS4 arm of the HIT 2000 trial (NCT00303810), which was designed to test six protocols and identify the optimal approach for treating young patients with medulloblastoma, supratentorial primitive neuroectodermal tumor, or ependymoma.
Patients started “HIT-SKK” chemotherapy within 2-4 weeks of surgery. They received three cycles of intravenous cyclophosphamide, vincristine, methotrexate (followed by leucovorin rescue after 42 hours), carboplatin, and etoposide, with concomitant intraventricular methotrexate, for a duration of 6 months (Neuro Oncol. 2011 Jun;13[6]:669-79).
Among patients who achieved a complete remission, treatment was ended after two additional cycles of chemotherapy. For other patients, secondary surgery, radiotherapy, and consolidation chemotherapy were recommended.
Starting in 2006, DMB and MBEN patients without complete remissions, as well as those with CMB or LCA, received 54 Gy of focal radiotherapy to the tumor bed after the first three treatment cycles.
SHH-I vs. SHH-II DMB/MBEN
DNA methylation profiling was available for 50 of the 87 patients in this analysis, 28 of whom had infantile sonic hedgehog (SHH)–activated DMB/MBEN. Data from these 28 patients – and 71 patients in a validation cohort – revealed no significant difference in 5-year PFS or OS based on methylation subtype.
The 5-year PFS was 73% in SHH-I patients and 83% in SHH-II patients (P = .25). The 5-year OS was 88% and 97%, respectively (P = .099).
“This suggests that the higher risk of relapse in the less favorable [SHH-I subtype] can be abrogated by the addition of intraventricular [methotrexate] to systemic chemotherapy,” the investigators wrote.
The results suggest SHH-I patients “markedly benefit” from the addition of intraventricular chemotherapy, according to the authors of a related editorial, Giles Robinson, MD, and Amar Gajjar, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn.
“However, cross-trial comparison of PFS among the SHH-II subtype does not suggest that SHH-II patients derive the same benefit,” the editorialists wrote.
These data divide SHH medulloblastoma into SHH-I, which benefits from chemotherapy with intraventricular methotrexate, and SHH-II, which can be cured without intraventricular methotrexate, high-dose chemotherapy, or focal radiotherapy, according to the editorialists.
This new information might prompt investigation of a risk-adapted approach. SHH-II patients would receive a reduced-intensity regimen with systemic chemotherapy only, and SHH-I patients would receive systemic chemotherapy combined with intraventricular methotrexate. This could avoid exposing young children to “more intensive therapy than necessary,” according to the editorialists.
Non-WNT/non-SHH disease
Patients with non-WNT/non-SHH medulloblastoma (CMB or LCA) were divided into molecularly defined subtypes group 3 (n = 14) and group 4 (n = 6). The patients in group 3 had lower survival rates than patients in group 4. The 5-year PFS rate was 36% and 83%, respectively (P < .001 ). The 5-year OS rate was 49% and 100%, respectively (P < .001).
“This represents the third recent publication to describe a poor PFS for group 3, and it signals a desperate need for better therapy,” the editorialists wrote. As for the “encouraging” survival rate for group 4 patients, there were only six subjects, which makes this finding “worthy of follow-up but not actionable.”
Even so, the investigators noted that “although poor survival has been reported for non-SHH CMB/LCA in almost every series of patients treated with CSI-sparing approaches, again, use of intraventricular [methotrexate] might be associated with slightly higher PFS, compared with conventional chemotherapy alone.”
As expected, IQ was significantly lower in patients who received CSI salvage. The mean IQ was 74 in patients who received CSI and 90 in patients who did not (P = .012). Neurocognitive outcomes were poor in general among CMB/LCA survivors, “which was closely related to use of radiotherapy,” according to the investigators.
“It is important to recognize that these studies were not designed to define outcome on the basis of molecular subgroup or subtype and that the sample size in all these studies is small,” Dr. Robinson and Dr. Gajjar wrote. “Thus, caution should be used when basing any treatment recommendation on these results, and it is our strong-held opinion that any treatment change be done on a well-planned and well-monitored clinical trial.”
This research was supported by the German Childhood Cancer Foundation, Styrian Childhood Cancer Foundation, and other organizations. Dr. Mynarek and colleagues disclosed relationships with Medac, Novartis, Eli Lilly, Bayer, Roche, and numerous other companies. Dr. Robinson disclosed relationships with Eli Lilly, Genentech, and Novartis. Dr. Gajjar reported relationships with Genentech and Kazia Therapeutics.
SOURCE: Mynarek M et al. J Clin Oncol. 2020 Jun 20;38(18):2028-40.
according to research published in the Journal of Clinical Oncology.
Investigators conducted a prospective trial of 87 children diagnosed with nonmetastatic medulloblastoma before the age of 4 years who were treated from 2001-2011.
At 5 years after diagnosis, the 42 DMB/MBEN patients had a 93% progression-free survival (PFS) rate, a 100% overall survival (OS) rate, and a 93% craniospinal irradiation (CSI)–free survival rate.
“Our results suggest that ... poor outcomes of patients treated with systemic chemotherapy alone can be improved by the addition of intraventricular [methotrexate],” wrote Martin Mynarek, MD, of the University Medical Center Hamburg-Eppendorf (Germany), and colleagues.
However, it was a different story for the 45 patients with classic medulloblastoma (CMB) or large-cell/anaplastic medulloblastoma (CLA), in which outcomes are historically worse. At 5 years, the PFS was 37%, the OS was 62%, and the CSI-free survival was 39% in these patients.
In 2006, the CMB and CLA patients started receiving local radiotherapy in addition to chemotherapy and intraventricular methotrexate, but the radiotherapy did not seem to help with their disease.
“Because data suggest no effects, or even adverse effects, of local radiotherapy, additional development of this approach does not seem justified,” the investigators wrote.
“Interestingly, almost all patients with CMB/LCA had distant or combined relapses after local radiotherapy,” they added. “One might speculate that local radiotherapy reduced disease burden of the primary tumor and subclinical metastasis in the posterior fossa, leading to a survival advantage of distant subclinical metastasis over local residues.”
Treatment details
The 87 patients were enrolled in the BIS4 arm of the HIT 2000 trial (NCT00303810), which was designed to test six protocols and identify the optimal approach for treating young patients with medulloblastoma, supratentorial primitive neuroectodermal tumor, or ependymoma.
Patients started “HIT-SKK” chemotherapy within 2-4 weeks of surgery. They received three cycles of intravenous cyclophosphamide, vincristine, methotrexate (followed by leucovorin rescue after 42 hours), carboplatin, and etoposide, with concomitant intraventricular methotrexate, for a duration of 6 months (Neuro Oncol. 2011 Jun;13[6]:669-79).
Among patients who achieved a complete remission, treatment was ended after two additional cycles of chemotherapy. For other patients, secondary surgery, radiotherapy, and consolidation chemotherapy were recommended.
Starting in 2006, DMB and MBEN patients without complete remissions, as well as those with CMB or LCA, received 54 Gy of focal radiotherapy to the tumor bed after the first three treatment cycles.
SHH-I vs. SHH-II DMB/MBEN
DNA methylation profiling was available for 50 of the 87 patients in this analysis, 28 of whom had infantile sonic hedgehog (SHH)–activated DMB/MBEN. Data from these 28 patients – and 71 patients in a validation cohort – revealed no significant difference in 5-year PFS or OS based on methylation subtype.
The 5-year PFS was 73% in SHH-I patients and 83% in SHH-II patients (P = .25). The 5-year OS was 88% and 97%, respectively (P = .099).
“This suggests that the higher risk of relapse in the less favorable [SHH-I subtype] can be abrogated by the addition of intraventricular [methotrexate] to systemic chemotherapy,” the investigators wrote.
The results suggest SHH-I patients “markedly benefit” from the addition of intraventricular chemotherapy, according to the authors of a related editorial, Giles Robinson, MD, and Amar Gajjar, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn.
“However, cross-trial comparison of PFS among the SHH-II subtype does not suggest that SHH-II patients derive the same benefit,” the editorialists wrote.
These data divide SHH medulloblastoma into SHH-I, which benefits from chemotherapy with intraventricular methotrexate, and SHH-II, which can be cured without intraventricular methotrexate, high-dose chemotherapy, or focal radiotherapy, according to the editorialists.
This new information might prompt investigation of a risk-adapted approach. SHH-II patients would receive a reduced-intensity regimen with systemic chemotherapy only, and SHH-I patients would receive systemic chemotherapy combined with intraventricular methotrexate. This could avoid exposing young children to “more intensive therapy than necessary,” according to the editorialists.
Non-WNT/non-SHH disease
Patients with non-WNT/non-SHH medulloblastoma (CMB or LCA) were divided into molecularly defined subtypes group 3 (n = 14) and group 4 (n = 6). The patients in group 3 had lower survival rates than patients in group 4. The 5-year PFS rate was 36% and 83%, respectively (P < .001 ). The 5-year OS rate was 49% and 100%, respectively (P < .001).
“This represents the third recent publication to describe a poor PFS for group 3, and it signals a desperate need for better therapy,” the editorialists wrote. As for the “encouraging” survival rate for group 4 patients, there were only six subjects, which makes this finding “worthy of follow-up but not actionable.”
Even so, the investigators noted that “although poor survival has been reported for non-SHH CMB/LCA in almost every series of patients treated with CSI-sparing approaches, again, use of intraventricular [methotrexate] might be associated with slightly higher PFS, compared with conventional chemotherapy alone.”
As expected, IQ was significantly lower in patients who received CSI salvage. The mean IQ was 74 in patients who received CSI and 90 in patients who did not (P = .012). Neurocognitive outcomes were poor in general among CMB/LCA survivors, “which was closely related to use of radiotherapy,” according to the investigators.
“It is important to recognize that these studies were not designed to define outcome on the basis of molecular subgroup or subtype and that the sample size in all these studies is small,” Dr. Robinson and Dr. Gajjar wrote. “Thus, caution should be used when basing any treatment recommendation on these results, and it is our strong-held opinion that any treatment change be done on a well-planned and well-monitored clinical trial.”
This research was supported by the German Childhood Cancer Foundation, Styrian Childhood Cancer Foundation, and other organizations. Dr. Mynarek and colleagues disclosed relationships with Medac, Novartis, Eli Lilly, Bayer, Roche, and numerous other companies. Dr. Robinson disclosed relationships with Eli Lilly, Genentech, and Novartis. Dr. Gajjar reported relationships with Genentech and Kazia Therapeutics.
SOURCE: Mynarek M et al. J Clin Oncol. 2020 Jun 20;38(18):2028-40.
according to research published in the Journal of Clinical Oncology.
Investigators conducted a prospective trial of 87 children diagnosed with nonmetastatic medulloblastoma before the age of 4 years who were treated from 2001-2011.
At 5 years after diagnosis, the 42 DMB/MBEN patients had a 93% progression-free survival (PFS) rate, a 100% overall survival (OS) rate, and a 93% craniospinal irradiation (CSI)–free survival rate.
“Our results suggest that ... poor outcomes of patients treated with systemic chemotherapy alone can be improved by the addition of intraventricular [methotrexate],” wrote Martin Mynarek, MD, of the University Medical Center Hamburg-Eppendorf (Germany), and colleagues.
However, it was a different story for the 45 patients with classic medulloblastoma (CMB) or large-cell/anaplastic medulloblastoma (CLA), in which outcomes are historically worse. At 5 years, the PFS was 37%, the OS was 62%, and the CSI-free survival was 39% in these patients.
In 2006, the CMB and CLA patients started receiving local radiotherapy in addition to chemotherapy and intraventricular methotrexate, but the radiotherapy did not seem to help with their disease.
“Because data suggest no effects, or even adverse effects, of local radiotherapy, additional development of this approach does not seem justified,” the investigators wrote.
“Interestingly, almost all patients with CMB/LCA had distant or combined relapses after local radiotherapy,” they added. “One might speculate that local radiotherapy reduced disease burden of the primary tumor and subclinical metastasis in the posterior fossa, leading to a survival advantage of distant subclinical metastasis over local residues.”
Treatment details
The 87 patients were enrolled in the BIS4 arm of the HIT 2000 trial (NCT00303810), which was designed to test six protocols and identify the optimal approach for treating young patients with medulloblastoma, supratentorial primitive neuroectodermal tumor, or ependymoma.
Patients started “HIT-SKK” chemotherapy within 2-4 weeks of surgery. They received three cycles of intravenous cyclophosphamide, vincristine, methotrexate (followed by leucovorin rescue after 42 hours), carboplatin, and etoposide, with concomitant intraventricular methotrexate, for a duration of 6 months (Neuro Oncol. 2011 Jun;13[6]:669-79).
Among patients who achieved a complete remission, treatment was ended after two additional cycles of chemotherapy. For other patients, secondary surgery, radiotherapy, and consolidation chemotherapy were recommended.
Starting in 2006, DMB and MBEN patients without complete remissions, as well as those with CMB or LCA, received 54 Gy of focal radiotherapy to the tumor bed after the first three treatment cycles.
SHH-I vs. SHH-II DMB/MBEN
DNA methylation profiling was available for 50 of the 87 patients in this analysis, 28 of whom had infantile sonic hedgehog (SHH)–activated DMB/MBEN. Data from these 28 patients – and 71 patients in a validation cohort – revealed no significant difference in 5-year PFS or OS based on methylation subtype.
The 5-year PFS was 73% in SHH-I patients and 83% in SHH-II patients (P = .25). The 5-year OS was 88% and 97%, respectively (P = .099).
“This suggests that the higher risk of relapse in the less favorable [SHH-I subtype] can be abrogated by the addition of intraventricular [methotrexate] to systemic chemotherapy,” the investigators wrote.
The results suggest SHH-I patients “markedly benefit” from the addition of intraventricular chemotherapy, according to the authors of a related editorial, Giles Robinson, MD, and Amar Gajjar, MD, of St. Jude Children’s Research Hospital in Memphis, Tenn.
“However, cross-trial comparison of PFS among the SHH-II subtype does not suggest that SHH-II patients derive the same benefit,” the editorialists wrote.
These data divide SHH medulloblastoma into SHH-I, which benefits from chemotherapy with intraventricular methotrexate, and SHH-II, which can be cured without intraventricular methotrexate, high-dose chemotherapy, or focal radiotherapy, according to the editorialists.
This new information might prompt investigation of a risk-adapted approach. SHH-II patients would receive a reduced-intensity regimen with systemic chemotherapy only, and SHH-I patients would receive systemic chemotherapy combined with intraventricular methotrexate. This could avoid exposing young children to “more intensive therapy than necessary,” according to the editorialists.
Non-WNT/non-SHH disease
Patients with non-WNT/non-SHH medulloblastoma (CMB or LCA) were divided into molecularly defined subtypes group 3 (n = 14) and group 4 (n = 6). The patients in group 3 had lower survival rates than patients in group 4. The 5-year PFS rate was 36% and 83%, respectively (P < .001 ). The 5-year OS rate was 49% and 100%, respectively (P < .001).
“This represents the third recent publication to describe a poor PFS for group 3, and it signals a desperate need for better therapy,” the editorialists wrote. As for the “encouraging” survival rate for group 4 patients, there were only six subjects, which makes this finding “worthy of follow-up but not actionable.”
Even so, the investigators noted that “although poor survival has been reported for non-SHH CMB/LCA in almost every series of patients treated with CSI-sparing approaches, again, use of intraventricular [methotrexate] might be associated with slightly higher PFS, compared with conventional chemotherapy alone.”
As expected, IQ was significantly lower in patients who received CSI salvage. The mean IQ was 74 in patients who received CSI and 90 in patients who did not (P = .012). Neurocognitive outcomes were poor in general among CMB/LCA survivors, “which was closely related to use of radiotherapy,” according to the investigators.
“It is important to recognize that these studies were not designed to define outcome on the basis of molecular subgroup or subtype and that the sample size in all these studies is small,” Dr. Robinson and Dr. Gajjar wrote. “Thus, caution should be used when basing any treatment recommendation on these results, and it is our strong-held opinion that any treatment change be done on a well-planned and well-monitored clinical trial.”
This research was supported by the German Childhood Cancer Foundation, Styrian Childhood Cancer Foundation, and other organizations. Dr. Mynarek and colleagues disclosed relationships with Medac, Novartis, Eli Lilly, Bayer, Roche, and numerous other companies. Dr. Robinson disclosed relationships with Eli Lilly, Genentech, and Novartis. Dr. Gajjar reported relationships with Genentech and Kazia Therapeutics.
SOURCE: Mynarek M et al. J Clin Oncol. 2020 Jun 20;38(18):2028-40.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Rilzabrutinib shows positive results in phase 2b for pemphigus
accompanied by markedly reduced need for systemic corticosteroids in the phase 2b BELIEVE-PV trial, Dedee F. Murrell, MD, said at the virtual annual meeting of the American Academy of Dermatology.

Moreover, in sharp contrast to the standard first-line treatments for pemphigus – rituximab (Rituxan) and high-dose corticosteroids – the treatment-emergent adverse events that arose with 6 months of rilzabrutinib in BELIEVE-PV were uniformly mild to moderate and transient, added Dr. Murrell, professor of dermatology at the University of New South Wales and head of the department of dermatology at St. George University Hospital, Sydney.
The phase 2b BELIEVE-PV trial was a small, 24-week, open-label study that included six patients with newly diagnosed pemphigus and nine others with relapsing pemphigus. The primary endpoint was control of disease activity, defined as no new lesions appearing and established lesions beginning to heal. This was achieved in 9 of 15 patients (60%) at 4 weeks and in 13 patients by week 12. Meanwhile, the mean daily dose of prednisone fell from 21 mg at baseline to 6 mg at 24 weeks.
The mean score on the Pemphigus Disease Area Index (PDAI) dropped by 79% from a baseline of 15.5. Ten of 15 subjects improved to a PDAI of 0 or 1 – clear or almost clear skin – by week 24. The complete remission rate, defined as an absence of both new and established lesions while on no or a very low dose of prednisone, was 40% at week 24.
Treatment-emergent adverse events consisted of nausea in four patients, dizziness in two, and abdominal distension in two, all of which were grade 1 or 2.
Based upon these favorable results, the pivotal phase 3, double-blind, international PEGASUS trial is underway, led by Dr. Murrell. The trial will enroll 120 pemphigus patients, randomized to rilzabrutinib at 400 mg twice daily or placebo on top of background steroid tapering.
Rilzabrutinib is also in earlier-stage clinical trials for the treatment of immune thrombocytopenia.
Dr. Murrell reported serving as a consultant to Principia Biopharma, sponsor of the BELIEVE-PV and PEGASUS trials, and has received institutional research grants from numerous pharmaceutical companies.
SOURCE: Murrell DF. AAD 2020 LBCT.
accompanied by markedly reduced need for systemic corticosteroids in the phase 2b BELIEVE-PV trial, Dedee F. Murrell, MD, said at the virtual annual meeting of the American Academy of Dermatology.
Moreover, in sharp contrast to the standard first-line treatments for pemphigus – rituximab (Rituxan) and high-dose corticosteroids – the treatment-emergent adverse events that arose with 6 months of rilzabrutinib in BELIEVE-PV were uniformly mild to moderate and transient, added Dr. Murrell, professor of dermatology at the University of New South Wales and head of the department of dermatology at St. George University Hospital, Sydney.
The phase 2b BELIEVE-PV trial was a small, 24-week, open-label study that included six patients with newly diagnosed pemphigus and nine others with relapsing pemphigus. The primary endpoint was control of disease activity, defined as no new lesions appearing and established lesions beginning to heal. This was achieved in 9 of 15 patients (60%) at 4 weeks and in 13 patients by week 12. Meanwhile, the mean daily dose of prednisone fell from 21 mg at baseline to 6 mg at 24 weeks.
The mean score on the Pemphigus Disease Area Index (PDAI) dropped by 79% from a baseline of 15.5. Ten of 15 subjects improved to a PDAI of 0 or 1 – clear or almost clear skin – by week 24. The complete remission rate, defined as an absence of both new and established lesions while on no or a very low dose of prednisone, was 40% at week 24.
Treatment-emergent adverse events consisted of nausea in four patients, dizziness in two, and abdominal distension in two, all of which were grade 1 or 2.
Based upon these favorable results, the pivotal phase 3, double-blind, international PEGASUS trial is underway, led by Dr. Murrell. The trial will enroll 120 pemphigus patients, randomized to rilzabrutinib at 400 mg twice daily or placebo on top of background steroid tapering.
Rilzabrutinib is also in earlier-stage clinical trials for the treatment of immune thrombocytopenia.
Dr. Murrell reported serving as a consultant to Principia Biopharma, sponsor of the BELIEVE-PV and PEGASUS trials, and has received institutional research grants from numerous pharmaceutical companies.
SOURCE: Murrell DF. AAD 2020 LBCT.
accompanied by markedly reduced need for systemic corticosteroids in the phase 2b BELIEVE-PV trial, Dedee F. Murrell, MD, said at the virtual annual meeting of the American Academy of Dermatology.
Moreover, in sharp contrast to the standard first-line treatments for pemphigus – rituximab (Rituxan) and high-dose corticosteroids – the treatment-emergent adverse events that arose with 6 months of rilzabrutinib in BELIEVE-PV were uniformly mild to moderate and transient, added Dr. Murrell, professor of dermatology at the University of New South Wales and head of the department of dermatology at St. George University Hospital, Sydney.
The phase 2b BELIEVE-PV trial was a small, 24-week, open-label study that included six patients with newly diagnosed pemphigus and nine others with relapsing pemphigus. The primary endpoint was control of disease activity, defined as no new lesions appearing and established lesions beginning to heal. This was achieved in 9 of 15 patients (60%) at 4 weeks and in 13 patients by week 12. Meanwhile, the mean daily dose of prednisone fell from 21 mg at baseline to 6 mg at 24 weeks.
The mean score on the Pemphigus Disease Area Index (PDAI) dropped by 79% from a baseline of 15.5. Ten of 15 subjects improved to a PDAI of 0 or 1 – clear or almost clear skin – by week 24. The complete remission rate, defined as an absence of both new and established lesions while on no or a very low dose of prednisone, was 40% at week 24.
Treatment-emergent adverse events consisted of nausea in four patients, dizziness in two, and abdominal distension in two, all of which were grade 1 or 2.
Based upon these favorable results, the pivotal phase 3, double-blind, international PEGASUS trial is underway, led by Dr. Murrell. The trial will enroll 120 pemphigus patients, randomized to rilzabrutinib at 400 mg twice daily or placebo on top of background steroid tapering.
Rilzabrutinib is also in earlier-stage clinical trials for the treatment of immune thrombocytopenia.
Dr. Murrell reported serving as a consultant to Principia Biopharma, sponsor of the BELIEVE-PV and PEGASUS trials, and has received institutional research grants from numerous pharmaceutical companies.
SOURCE: Murrell DF. AAD 2020 LBCT.
FROM AAD 20
Early data support further study of ivosidenib in mIDH1 glioma
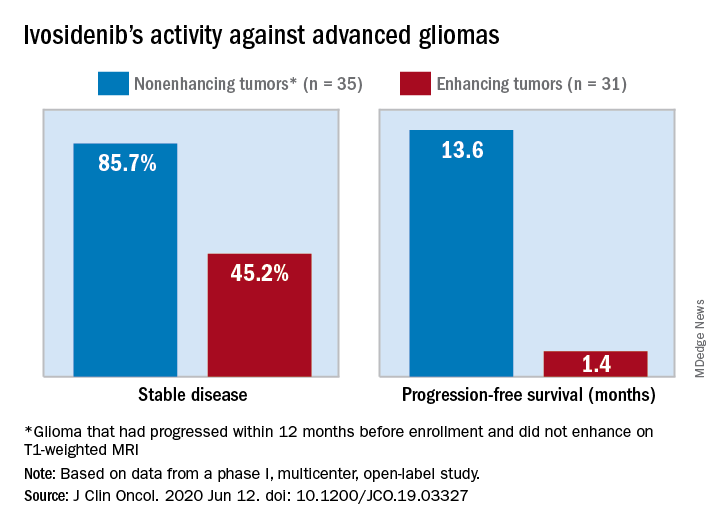
The median progression-free survival was 13.6 months for patients with nonenhancing tumors and 1.4 months for patients with enhancing tumors in a study of 66 adults with mIDH1 advanced glioma.
“On the basis of these data, additional clinical development of mIDH inhibitors for mIDH low-grade gliomas is warranted,” Ingo Mellinghoff, MD, of Memorial Sloan Kettering Cancer Center in New York, and colleagues wrote in the Journal of Clinical Oncology.
“This is not a home run but is of interest to the community,” said Lawrence Recht, MD, of Stanford (Calif.) University, who was not involved in this study. “Other companies are also developing agents like this.”
Considering that the ivosidenib study “is uncontrolled, one cannot say for sure that this wasn’t just the natural history of the disease,” Dr. Recht continued. “This type of tumor can behave very indolently, and patients can survive years without treatment, so this is rather a short interval to make a long-time statement. I think the authors are a bit overenthusiastic.”
The authors tested ivosidenib in 66 adults with mIDH1 glioma – 35 with nonenhancing glioma and 31 with enhancing glioma. Tumors had recurred after, or did not respond to, initial surgery, radiation, or chemotherapy.
The patients’ median age was 41 years (range, 21-71 years), and 25 patients (37.9%) were women. The most common tumor type at screening was oligodendroglioma in 23 patients (34.8%).
Patients received ivosidenib at doses ranging from 100 mg twice a day to 900 mg once a day. A total of 50 patients received the phase 2 recommended dose – 500 mg once a day. There were no dose-limiting toxicities, and there was no maximum-tolerated dose.
Adverse events of grade 3 or higher occurred in 19.7% of patients and included headache, seizure, hyperglycemia, neutropenia, and hypophosphatemia. Grade 3 or higher treatment-related adverse events occurred in two patients.
A total of 30 patients with nonenhancing tumors (85.7%) and 14 with enhancing tumors (45.2%) had a best response of stable disease. There was one partial response in a nonenhancing patient on 500 mg/day. The rest of the subjects had a best response of progressive disease.
The median treatment duration was 18.4 months among patients with nonenhancing tumors and 1.9 months among those with enhancing tumors. Discontinuation was caused byo progression in all but one case.
Among patients with measurable disease, tumor measurements decreased from baseline in 22 nonenhancing tumors (66.7%) and in 9 enhancing tumors (33.3%).
“Despite the heterogeneous patient population in our trial, the nonrandomized design, and the lack of central pathology review, the data from our trial suggest that ivosidenib has greater activity against nonenhancing gliomas than against enhancing gliomas,” the investigators wrote. “This finding may seem surprising because the absence of contrast enhancement is typically associated with impaired drug delivery.
“We hypothesize that ivosidenib may be more effective in nonenhancing gliomas because these tumors represent an earlier disease stage with fewer genetic alterations, reminiscent of the greater antitumor activity of the BCR-ABL inhibitor imatinib in earlier stages of chronic myeloid leukemia,” the investigators wrote.
The team also noted that the median progression-free survival for patients with nonenhancing gliomas in the current study “compares favorably to that reported for temozolomide” in advanced mIDH1 low-grade glioma, which was approximately 7 months.
This research was funded by Agios Pharmaceuticals, the company developing ivosidenib. Dr. Mellinghoff receives travel compensation from and is an adviser to the company. Several other investigators are employees. Dr. Recht disclosed no conflicts of interest.
SOURCE: Mellinghoff I et al. J Clin Oncol. 2020 Jun 12. doi: 10.1200/JCO.19.03327
The median progression-free survival was 13.6 months for patients with nonenhancing tumors and 1.4 months for patients with enhancing tumors in a study of 66 adults with mIDH1 advanced glioma.
“On the basis of these data, additional clinical development of mIDH inhibitors for mIDH low-grade gliomas is warranted,” Ingo Mellinghoff, MD, of Memorial Sloan Kettering Cancer Center in New York, and colleagues wrote in the Journal of Clinical Oncology.
“This is not a home run but is of interest to the community,” said Lawrence Recht, MD, of Stanford (Calif.) University, who was not involved in this study. “Other companies are also developing agents like this.”
Considering that the ivosidenib study “is uncontrolled, one cannot say for sure that this wasn’t just the natural history of the disease,” Dr. Recht continued. “This type of tumor can behave very indolently, and patients can survive years without treatment, so this is rather a short interval to make a long-time statement. I think the authors are a bit overenthusiastic.”
The authors tested ivosidenib in 66 adults with mIDH1 glioma – 35 with nonenhancing glioma and 31 with enhancing glioma. Tumors had recurred after, or did not respond to, initial surgery, radiation, or chemotherapy.
The patients’ median age was 41 years (range, 21-71 years), and 25 patients (37.9%) were women. The most common tumor type at screening was oligodendroglioma in 23 patients (34.8%).
Patients received ivosidenib at doses ranging from 100 mg twice a day to 900 mg once a day. A total of 50 patients received the phase 2 recommended dose – 500 mg once a day. There were no dose-limiting toxicities, and there was no maximum-tolerated dose.
Adverse events of grade 3 or higher occurred in 19.7% of patients and included headache, seizure, hyperglycemia, neutropenia, and hypophosphatemia. Grade 3 or higher treatment-related adverse events occurred in two patients.
A total of 30 patients with nonenhancing tumors (85.7%) and 14 with enhancing tumors (45.2%) had a best response of stable disease. There was one partial response in a nonenhancing patient on 500 mg/day. The rest of the subjects had a best response of progressive disease.
The median treatment duration was 18.4 months among patients with nonenhancing tumors and 1.9 months among those with enhancing tumors. Discontinuation was caused byo progression in all but one case.
Among patients with measurable disease, tumor measurements decreased from baseline in 22 nonenhancing tumors (66.7%) and in 9 enhancing tumors (33.3%).
“Despite the heterogeneous patient population in our trial, the nonrandomized design, and the lack of central pathology review, the data from our trial suggest that ivosidenib has greater activity against nonenhancing gliomas than against enhancing gliomas,” the investigators wrote. “This finding may seem surprising because the absence of contrast enhancement is typically associated with impaired drug delivery.
“We hypothesize that ivosidenib may be more effective in nonenhancing gliomas because these tumors represent an earlier disease stage with fewer genetic alterations, reminiscent of the greater antitumor activity of the BCR-ABL inhibitor imatinib in earlier stages of chronic myeloid leukemia,” the investigators wrote.
The team also noted that the median progression-free survival for patients with nonenhancing gliomas in the current study “compares favorably to that reported for temozolomide” in advanced mIDH1 low-grade glioma, which was approximately 7 months.
This research was funded by Agios Pharmaceuticals, the company developing ivosidenib. Dr. Mellinghoff receives travel compensation from and is an adviser to the company. Several other investigators are employees. Dr. Recht disclosed no conflicts of interest.
SOURCE: Mellinghoff I et al. J Clin Oncol. 2020 Jun 12. doi: 10.1200/JCO.19.03327
The median progression-free survival was 13.6 months for patients with nonenhancing tumors and 1.4 months for patients with enhancing tumors in a study of 66 adults with mIDH1 advanced glioma.
“On the basis of these data, additional clinical development of mIDH inhibitors for mIDH low-grade gliomas is warranted,” Ingo Mellinghoff, MD, of Memorial Sloan Kettering Cancer Center in New York, and colleagues wrote in the Journal of Clinical Oncology.
“This is not a home run but is of interest to the community,” said Lawrence Recht, MD, of Stanford (Calif.) University, who was not involved in this study. “Other companies are also developing agents like this.”
Considering that the ivosidenib study “is uncontrolled, one cannot say for sure that this wasn’t just the natural history of the disease,” Dr. Recht continued. “This type of tumor can behave very indolently, and patients can survive years without treatment, so this is rather a short interval to make a long-time statement. I think the authors are a bit overenthusiastic.”
The authors tested ivosidenib in 66 adults with mIDH1 glioma – 35 with nonenhancing glioma and 31 with enhancing glioma. Tumors had recurred after, or did not respond to, initial surgery, radiation, or chemotherapy.
The patients’ median age was 41 years (range, 21-71 years), and 25 patients (37.9%) were women. The most common tumor type at screening was oligodendroglioma in 23 patients (34.8%).
Patients received ivosidenib at doses ranging from 100 mg twice a day to 900 mg once a day. A total of 50 patients received the phase 2 recommended dose – 500 mg once a day. There were no dose-limiting toxicities, and there was no maximum-tolerated dose.
Adverse events of grade 3 or higher occurred in 19.7% of patients and included headache, seizure, hyperglycemia, neutropenia, and hypophosphatemia. Grade 3 or higher treatment-related adverse events occurred in two patients.
A total of 30 patients with nonenhancing tumors (85.7%) and 14 with enhancing tumors (45.2%) had a best response of stable disease. There was one partial response in a nonenhancing patient on 500 mg/day. The rest of the subjects had a best response of progressive disease.
The median treatment duration was 18.4 months among patients with nonenhancing tumors and 1.9 months among those with enhancing tumors. Discontinuation was caused byo progression in all but one case.
Among patients with measurable disease, tumor measurements decreased from baseline in 22 nonenhancing tumors (66.7%) and in 9 enhancing tumors (33.3%).
“Despite the heterogeneous patient population in our trial, the nonrandomized design, and the lack of central pathology review, the data from our trial suggest that ivosidenib has greater activity against nonenhancing gliomas than against enhancing gliomas,” the investigators wrote. “This finding may seem surprising because the absence of contrast enhancement is typically associated with impaired drug delivery.
“We hypothesize that ivosidenib may be more effective in nonenhancing gliomas because these tumors represent an earlier disease stage with fewer genetic alterations, reminiscent of the greater antitumor activity of the BCR-ABL inhibitor imatinib in earlier stages of chronic myeloid leukemia,” the investigators wrote.
The team also noted that the median progression-free survival for patients with nonenhancing gliomas in the current study “compares favorably to that reported for temozolomide” in advanced mIDH1 low-grade glioma, which was approximately 7 months.
This research was funded by Agios Pharmaceuticals, the company developing ivosidenib. Dr. Mellinghoff receives travel compensation from and is an adviser to the company. Several other investigators are employees. Dr. Recht disclosed no conflicts of interest.
SOURCE: Mellinghoff I et al. J Clin Oncol. 2020 Jun 12. doi: 10.1200/JCO.19.03327
FROM THE JOURNAL OF CLINICAL ONCOLOGY