User login
Clinical Edge Journal Scan Commentary: Breast Cancer May 2022

A meta-analysis including over 5000 patients with metastatic hormone receptor–positive (HR+) and HER2- breast cancer showed a significant overall survival (OS) benefit with the addition of cyclin-dependent kinase (CDK) 4/6 inhibitors to endocrine therapy (hazard ratio 1.33; P < .001), albeit with higher rates of toxicities, including neutropenia, leukopenia, and diarrhea.3 The MONALEESA-2 study randomly assigned 668 postmenopausal women with metastatic HR+/HER2- breast cancer, treatment-naive in the advanced setting, to either ribociclib or placebo plus letrozole. Updated results with a median follow-up of 6.6 years demonstrated a significant OS benefit with ribociclib + letrozole compared with placebo + letrozole (median OS 63.9 months vs 51.4 months; hazard ratio 0.76; P = .008) (Hortobagyi and colleagues). An OS > 5 years with ribociclib plus endocrine therapy is certainly impressive, and efficacy as well as respective toxicities of the various CDK 4/6 inhibitors are factors taken into consideration when choosing the appropriate therapy for an individual patient.
The optimization of adjuvant endocrine therapy (ET) for HR+ early breast cancer, including use of ovarian suppression and extended adjuvant therapy, has improved outcomes for these women. However, there is a high-risk subset for whom the risk for distant recurrence persists. The phase 3 monarchE trial, which included 5637 patients with high-risk early breast cancer (≥ 4 positive nodes, or 1-3 nodes and either tumor size ≥ 5 cm, histologic grade 3, or central Ki-67 ≥ 20%), demonstrated benefits in invasive disease-free and distant-relapse-free survival with the addition of abemaciclib for 2 years to ET. A safety analysis of the monarchE study among patients who had received at least one dose of the study drug (n = 5591) demonstrated an overall manageable side-effect profile, with the majority of these toxicities addressed via dose holds/reductions or supportive medications (Rugo and colleagues). Abemaciclib + ET led to higher incidence of grade ≥ 3 adverse events vs ET alone (49.7% vs 16.3%), with neutropenia being the most frequent (grade 3 = 19.6%) although without significant clinical implications. Diarrhea was common (83.5%), although the majority was low grade (grade 1/2 = 75.7%), with grade 2/3 events characterized by early onset and short duration. Discontinuation of abemaciclib occurred in 18.5%, with two thirds due to grade 1/2 events and in over half without dose reduction.4 These findings show an acceptable safety profile with abemaciclib in the curative setting and highlight the importance of education, recognition, and early management of side effects to maintain patients on treatment.
The heterogeneity of tumor biology within the HR+ breast cancer subtype indicates the need to refine treatment regimens for an individual patient. Genomic assays (70-gene signature and 21-gene recurrence score) have helped tailor adjuvant systemic therapy and in many cases have identified women for whom chemotherapy can be omitted. CDK 4/6 inhibitors have shown impressive activity in the metastatic/advanced setting, although results from trials in the adjuvant setting have produced mixed results. The phase 2 NEOPAL trial evaluated the combination of letrozole + palbociclib vs chemotherapy (sequential anthracycline-taxane) among 106 postmenopausal women with high-risk, HR+/HER2- early breast cancer (luminal B or luminal A with nodal involvement). At a median follow-up of 40.4 months, 3-year PFS (hazard ratio 1.01; P = .98) and invasive disease-free survival (hazard ratio 0.83; P = .71) were similar in the letrozole + palbociclib and chemotherapy arms (Delaloge and colleagues). The phase 2 CORALLEEN trial,5 which investigated neoadjuvant letrozole + ribociclib vs chemotherapy in HR+/HER2- luminal B early breast cancer, demonstrated similar percentages of patients achieving downstaging via molecular assessment at the time of surgery. The neoadjuvant space represents a valuable setting to further study CDK 4/6 inhibitors as well as other novel therapies; endpoints including pathologic complete response and residual cancer burden correlating with long-term outcomes can provide a more rapid means to identify effective therapies. Translational biomarkers can be gathered and adjuvant strategies can be tailored based on response.
Additional References
- Modi S, Saura C, Yamashita T, et al; DESTINY-Breast01 Investigators. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020;382:610-621. Doi: 10.1056/NEJMoa1914510 Source
- Hurvitz S, Kim S-B, Chung W-P, et al. Trastuzumab deruxtecan (T-DXd; DS-8201a) versus trastuzumab emtansine (T-DM1) in patients (pts) with HER2+ metastatic breast cancer (mBC): Subgroup analyses from the randomized phase 3 study DESTINY-Breast03. Presented at 2021 San Antonio Breast Cancer Symposium; December 7-10, 2021;General Session, GS3-01. Source
- Li J, Huo X, Zhao F, et al. Association of cyclin-dependent kinases 4 and 6 inhibitors with survival in patients with hormone receptor-positive metastatic breast cancer: A systematic review and meta-analysis. JAMA Netw Open. 2020;3:e2020312. Doi: 10.1001/jamanetworkopen.2020.20312 Source
- Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: Updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol. 2021;32:1571-1581. Doi: 10.1016/j.annonc.2021.09.015 Source
- Prat A, Saura C, Pascual T, et al. Ribociclib plus letrozole versus chemotherapy for postmenopausal women with hormone receptor-positive, HER2- negative, luminal B breast cancer (CORALLEEN): An open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2020;21:33-43. Doi: 10.1016/S1470-2045(19)30786-7 Source
A meta-analysis including over 5000 patients with metastatic hormone receptor–positive (HR+) and HER2- breast cancer showed a significant overall survival (OS) benefit with the addition of cyclin-dependent kinase (CDK) 4/6 inhibitors to endocrine therapy (hazard ratio 1.33; P < .001), albeit with higher rates of toxicities, including neutropenia, leukopenia, and diarrhea.3 The MONALEESA-2 study randomly assigned 668 postmenopausal women with metastatic HR+/HER2- breast cancer, treatment-naive in the advanced setting, to either ribociclib or placebo plus letrozole. Updated results with a median follow-up of 6.6 years demonstrated a significant OS benefit with ribociclib + letrozole compared with placebo + letrozole (median OS 63.9 months vs 51.4 months; hazard ratio 0.76; P = .008) (Hortobagyi and colleagues). An OS > 5 years with ribociclib plus endocrine therapy is certainly impressive, and efficacy as well as respective toxicities of the various CDK 4/6 inhibitors are factors taken into consideration when choosing the appropriate therapy for an individual patient.
The optimization of adjuvant endocrine therapy (ET) for HR+ early breast cancer, including use of ovarian suppression and extended adjuvant therapy, has improved outcomes for these women. However, there is a high-risk subset for whom the risk for distant recurrence persists. The phase 3 monarchE trial, which included 5637 patients with high-risk early breast cancer (≥ 4 positive nodes, or 1-3 nodes and either tumor size ≥ 5 cm, histologic grade 3, or central Ki-67 ≥ 20%), demonstrated benefits in invasive disease-free and distant-relapse-free survival with the addition of abemaciclib for 2 years to ET. A safety analysis of the monarchE study among patients who had received at least one dose of the study drug (n = 5591) demonstrated an overall manageable side-effect profile, with the majority of these toxicities addressed via dose holds/reductions or supportive medications (Rugo and colleagues). Abemaciclib + ET led to higher incidence of grade ≥ 3 adverse events vs ET alone (49.7% vs 16.3%), with neutropenia being the most frequent (grade 3 = 19.6%) although without significant clinical implications. Diarrhea was common (83.5%), although the majority was low grade (grade 1/2 = 75.7%), with grade 2/3 events characterized by early onset and short duration. Discontinuation of abemaciclib occurred in 18.5%, with two thirds due to grade 1/2 events and in over half without dose reduction.4 These findings show an acceptable safety profile with abemaciclib in the curative setting and highlight the importance of education, recognition, and early management of side effects to maintain patients on treatment.
The heterogeneity of tumor biology within the HR+ breast cancer subtype indicates the need to refine treatment regimens for an individual patient. Genomic assays (70-gene signature and 21-gene recurrence score) have helped tailor adjuvant systemic therapy and in many cases have identified women for whom chemotherapy can be omitted. CDK 4/6 inhibitors have shown impressive activity in the metastatic/advanced setting, although results from trials in the adjuvant setting have produced mixed results. The phase 2 NEOPAL trial evaluated the combination of letrozole + palbociclib vs chemotherapy (sequential anthracycline-taxane) among 106 postmenopausal women with high-risk, HR+/HER2- early breast cancer (luminal B or luminal A with nodal involvement). At a median follow-up of 40.4 months, 3-year PFS (hazard ratio 1.01; P = .98) and invasive disease-free survival (hazard ratio 0.83; P = .71) were similar in the letrozole + palbociclib and chemotherapy arms (Delaloge and colleagues). The phase 2 CORALLEEN trial,5 which investigated neoadjuvant letrozole + ribociclib vs chemotherapy in HR+/HER2- luminal B early breast cancer, demonstrated similar percentages of patients achieving downstaging via molecular assessment at the time of surgery. The neoadjuvant space represents a valuable setting to further study CDK 4/6 inhibitors as well as other novel therapies; endpoints including pathologic complete response and residual cancer burden correlating with long-term outcomes can provide a more rapid means to identify effective therapies. Translational biomarkers can be gathered and adjuvant strategies can be tailored based on response.
Additional References
- Modi S, Saura C, Yamashita T, et al; DESTINY-Breast01 Investigators. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020;382:610-621. Doi: 10.1056/NEJMoa1914510 Source
- Hurvitz S, Kim S-B, Chung W-P, et al. Trastuzumab deruxtecan (T-DXd; DS-8201a) versus trastuzumab emtansine (T-DM1) in patients (pts) with HER2+ metastatic breast cancer (mBC): Subgroup analyses from the randomized phase 3 study DESTINY-Breast03. Presented at 2021 San Antonio Breast Cancer Symposium; December 7-10, 2021;General Session, GS3-01. Source
- Li J, Huo X, Zhao F, et al. Association of cyclin-dependent kinases 4 and 6 inhibitors with survival in patients with hormone receptor-positive metastatic breast cancer: A systematic review and meta-analysis. JAMA Netw Open. 2020;3:e2020312. Doi: 10.1001/jamanetworkopen.2020.20312 Source
- Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: Updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol. 2021;32:1571-1581. Doi: 10.1016/j.annonc.2021.09.015 Source
- Prat A, Saura C, Pascual T, et al. Ribociclib plus letrozole versus chemotherapy for postmenopausal women with hormone receptor-positive, HER2- negative, luminal B breast cancer (CORALLEEN): An open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2020;21:33-43. Doi: 10.1016/S1470-2045(19)30786-7 Source
A meta-analysis including over 5000 patients with metastatic hormone receptor–positive (HR+) and HER2- breast cancer showed a significant overall survival (OS) benefit with the addition of cyclin-dependent kinase (CDK) 4/6 inhibitors to endocrine therapy (hazard ratio 1.33; P < .001), albeit with higher rates of toxicities, including neutropenia, leukopenia, and diarrhea.3 The MONALEESA-2 study randomly assigned 668 postmenopausal women with metastatic HR+/HER2- breast cancer, treatment-naive in the advanced setting, to either ribociclib or placebo plus letrozole. Updated results with a median follow-up of 6.6 years demonstrated a significant OS benefit with ribociclib + letrozole compared with placebo + letrozole (median OS 63.9 months vs 51.4 months; hazard ratio 0.76; P = .008) (Hortobagyi and colleagues). An OS > 5 years with ribociclib plus endocrine therapy is certainly impressive, and efficacy as well as respective toxicities of the various CDK 4/6 inhibitors are factors taken into consideration when choosing the appropriate therapy for an individual patient.
The optimization of adjuvant endocrine therapy (ET) for HR+ early breast cancer, including use of ovarian suppression and extended adjuvant therapy, has improved outcomes for these women. However, there is a high-risk subset for whom the risk for distant recurrence persists. The phase 3 monarchE trial, which included 5637 patients with high-risk early breast cancer (≥ 4 positive nodes, or 1-3 nodes and either tumor size ≥ 5 cm, histologic grade 3, or central Ki-67 ≥ 20%), demonstrated benefits in invasive disease-free and distant-relapse-free survival with the addition of abemaciclib for 2 years to ET. A safety analysis of the monarchE study among patients who had received at least one dose of the study drug (n = 5591) demonstrated an overall manageable side-effect profile, with the majority of these toxicities addressed via dose holds/reductions or supportive medications (Rugo and colleagues). Abemaciclib + ET led to higher incidence of grade ≥ 3 adverse events vs ET alone (49.7% vs 16.3%), with neutropenia being the most frequent (grade 3 = 19.6%) although without significant clinical implications. Diarrhea was common (83.5%), although the majority was low grade (grade 1/2 = 75.7%), with grade 2/3 events characterized by early onset and short duration. Discontinuation of abemaciclib occurred in 18.5%, with two thirds due to grade 1/2 events and in over half without dose reduction.4 These findings show an acceptable safety profile with abemaciclib in the curative setting and highlight the importance of education, recognition, and early management of side effects to maintain patients on treatment.
The heterogeneity of tumor biology within the HR+ breast cancer subtype indicates the need to refine treatment regimens for an individual patient. Genomic assays (70-gene signature and 21-gene recurrence score) have helped tailor adjuvant systemic therapy and in many cases have identified women for whom chemotherapy can be omitted. CDK 4/6 inhibitors have shown impressive activity in the metastatic/advanced setting, although results from trials in the adjuvant setting have produced mixed results. The phase 2 NEOPAL trial evaluated the combination of letrozole + palbociclib vs chemotherapy (sequential anthracycline-taxane) among 106 postmenopausal women with high-risk, HR+/HER2- early breast cancer (luminal B or luminal A with nodal involvement). At a median follow-up of 40.4 months, 3-year PFS (hazard ratio 1.01; P = .98) and invasive disease-free survival (hazard ratio 0.83; P = .71) were similar in the letrozole + palbociclib and chemotherapy arms (Delaloge and colleagues). The phase 2 CORALLEEN trial,5 which investigated neoadjuvant letrozole + ribociclib vs chemotherapy in HR+/HER2- luminal B early breast cancer, demonstrated similar percentages of patients achieving downstaging via molecular assessment at the time of surgery. The neoadjuvant space represents a valuable setting to further study CDK 4/6 inhibitors as well as other novel therapies; endpoints including pathologic complete response and residual cancer burden correlating with long-term outcomes can provide a more rapid means to identify effective therapies. Translational biomarkers can be gathered and adjuvant strategies can be tailored based on response.
Additional References
- Modi S, Saura C, Yamashita T, et al; DESTINY-Breast01 Investigators. Trastuzumab deruxtecan in previously treated HER2-positive breast cancer. N Engl J Med. 2020;382:610-621. Doi: 10.1056/NEJMoa1914510 Source
- Hurvitz S, Kim S-B, Chung W-P, et al. Trastuzumab deruxtecan (T-DXd; DS-8201a) versus trastuzumab emtansine (T-DM1) in patients (pts) with HER2+ metastatic breast cancer (mBC): Subgroup analyses from the randomized phase 3 study DESTINY-Breast03. Presented at 2021 San Antonio Breast Cancer Symposium; December 7-10, 2021;General Session, GS3-01. Source
- Li J, Huo X, Zhao F, et al. Association of cyclin-dependent kinases 4 and 6 inhibitors with survival in patients with hormone receptor-positive metastatic breast cancer: A systematic review and meta-analysis. JAMA Netw Open. 2020;3:e2020312. Doi: 10.1001/jamanetworkopen.2020.20312 Source
- Harbeck N, Rastogi P, Martin M, et al. Adjuvant abemaciclib combined with endocrine therapy for high-risk early breast cancer: Updated efficacy and Ki-67 analysis from the monarchE study. Ann Oncol. 2021;32:1571-1581. Doi: 10.1016/j.annonc.2021.09.015 Source
- Prat A, Saura C, Pascual T, et al. Ribociclib plus letrozole versus chemotherapy for postmenopausal women with hormone receptor-positive, HER2- negative, luminal B breast cancer (CORALLEEN): An open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2020;21:33-43. Doi: 10.1016/S1470-2045(19)30786-7 Source
What's your diagnosis?
Answer: Colonic Malakoplakia.
Histopathologic examination of the biopsy specimens revealed nodular mixed inflammatory cells and infiltration of the epithelioid histiocytes in lamina propria (Figure D; stain: hematoxylin and eosin; original magnification 40×). The histiocytes showed foamy and eosinophilic cytoplasm (Figure E, arrow) and some of them had a targetoid appearance (Figure E, arrow head; stain: hematoxylin and eosin; original magnification 200×). Von Kossa stains highlighted the targetoid structures in the histiocytes (Figure F, Michaelis-Gutmann bodies). The granular cytoplasm of the histiocytes was positive on periodic acid-Schiff stain (Figure G). Based on these findings, the patient was diagnosed with colonic malakoplakia.
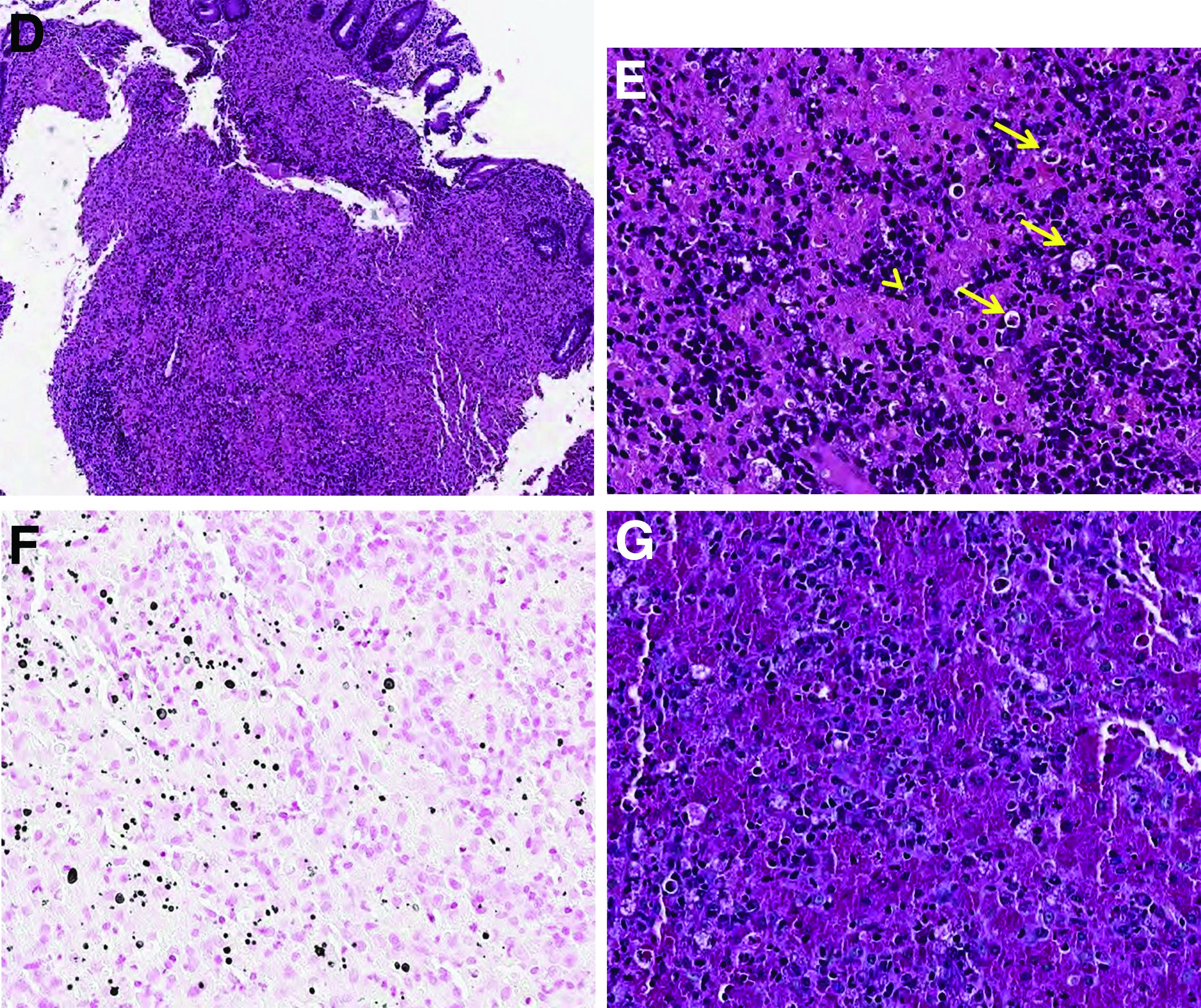
Malakoplakia is an uncommon, chronic, granulomatous inflammatory disease. It most commonly affects the urinary tract and gastrointestinal tract, but may occur at any anatomic site. Malakoplakia of the gastrointestinal tract are seen most frequently in the rectum, sigmoid, and right colon.1 It is diagnosed by the characteristic histologic feature of accumulated histiocytes with abundant eosinophilic granular cytoplasm containing basophilic inclusions, consistent with Michaelis-Gutmann bodies. Although the exact etiology and pathogenesis of malakoplakia are unclear, it seems to originate from an acquired defect in the intracellular destruction of phagocytosed bacteria, usually associated with Escherichia coli, Klebsiella, and Mycobacterium.2 It can have various causes, such as immunosuppression, malignant neoplasms, systemic diseases, and genetic diseases. Clinical manifestation of colonic malakoplakia is diverse, ranging from asymptomatic to malaise, fever, abdominal pain, diarrhea, hematochezia, and intestinal obstruction. Granulomatous reaction of malakoplakia generates the endoscopic appearance of lesions, which ranges from plaques to nodules and yellow-brown masses. In the early stage, malakoplakia commonly presents as soft yellow to tan mucosal plaques endoscopically, as seen in our case (Figure A). As the disease progresses in the later stage, malakoplakia presents as raised, grey to tan polypoid lesions of various sizes with peripheral hyperemia and a central depressed area, as seen in our case (Figure B).3 Owing to this endoscopic morphology, colonic malakoplakia may be misdiagnosed as atypical lymphoma, familial adenomatous polyposis, and metastatic carcinoma. To date, the natural course of malakoplakia of the colon is unclear, and no guidelines for treatment, treatment methods, duration of treatment, or surveillance are currently available. However, treatment of malakoplakia is essential to reduce immunosuppression and includes antibiotics with intracellular action and choline agonists that replenish the decreased cyclic 3’, 5’-guanosine monophosphate levels. In summary, although malakoplakia of the colon is very rare, it should be considered in the differential diagnosis of polypoid colonic lesions, especially in immunocompromised or malnourished patients.
References
1. Cipolletta L et al. Gastrointest Endosc. 1995 Mar;41(3):255-8.
2. Berney T et al. Transpl Int. 1999;12(4):293-6.
3. Weinrach DM et al. Arch Pathol Lab Med. 2004 Oct;128(10):e133-4.
Answer: Colonic Malakoplakia.
Histopathologic examination of the biopsy specimens revealed nodular mixed inflammatory cells and infiltration of the epithelioid histiocytes in lamina propria (Figure D; stain: hematoxylin and eosin; original magnification 40×). The histiocytes showed foamy and eosinophilic cytoplasm (Figure E, arrow) and some of them had a targetoid appearance (Figure E, arrow head; stain: hematoxylin and eosin; original magnification 200×). Von Kossa stains highlighted the targetoid structures in the histiocytes (Figure F, Michaelis-Gutmann bodies). The granular cytoplasm of the histiocytes was positive on periodic acid-Schiff stain (Figure G). Based on these findings, the patient was diagnosed with colonic malakoplakia.
Malakoplakia is an uncommon, chronic, granulomatous inflammatory disease. It most commonly affects the urinary tract and gastrointestinal tract, but may occur at any anatomic site. Malakoplakia of the gastrointestinal tract are seen most frequently in the rectum, sigmoid, and right colon.1 It is diagnosed by the characteristic histologic feature of accumulated histiocytes with abundant eosinophilic granular cytoplasm containing basophilic inclusions, consistent with Michaelis-Gutmann bodies. Although the exact etiology and pathogenesis of malakoplakia are unclear, it seems to originate from an acquired defect in the intracellular destruction of phagocytosed bacteria, usually associated with Escherichia coli, Klebsiella, and Mycobacterium.2 It can have various causes, such as immunosuppression, malignant neoplasms, systemic diseases, and genetic diseases. Clinical manifestation of colonic malakoplakia is diverse, ranging from asymptomatic to malaise, fever, abdominal pain, diarrhea, hematochezia, and intestinal obstruction. Granulomatous reaction of malakoplakia generates the endoscopic appearance of lesions, which ranges from plaques to nodules and yellow-brown masses. In the early stage, malakoplakia commonly presents as soft yellow to tan mucosal plaques endoscopically, as seen in our case (Figure A). As the disease progresses in the later stage, malakoplakia presents as raised, grey to tan polypoid lesions of various sizes with peripheral hyperemia and a central depressed area, as seen in our case (Figure B).3 Owing to this endoscopic morphology, colonic malakoplakia may be misdiagnosed as atypical lymphoma, familial adenomatous polyposis, and metastatic carcinoma. To date, the natural course of malakoplakia of the colon is unclear, and no guidelines for treatment, treatment methods, duration of treatment, or surveillance are currently available. However, treatment of malakoplakia is essential to reduce immunosuppression and includes antibiotics with intracellular action and choline agonists that replenish the decreased cyclic 3’, 5’-guanosine monophosphate levels. In summary, although malakoplakia of the colon is very rare, it should be considered in the differential diagnosis of polypoid colonic lesions, especially in immunocompromised or malnourished patients.
References
1. Cipolletta L et al. Gastrointest Endosc. 1995 Mar;41(3):255-8.
2. Berney T et al. Transpl Int. 1999;12(4):293-6.
3. Weinrach DM et al. Arch Pathol Lab Med. 2004 Oct;128(10):e133-4.
Answer: Colonic Malakoplakia.
Histopathologic examination of the biopsy specimens revealed nodular mixed inflammatory cells and infiltration of the epithelioid histiocytes in lamina propria (Figure D; stain: hematoxylin and eosin; original magnification 40×). The histiocytes showed foamy and eosinophilic cytoplasm (Figure E, arrow) and some of them had a targetoid appearance (Figure E, arrow head; stain: hematoxylin and eosin; original magnification 200×). Von Kossa stains highlighted the targetoid structures in the histiocytes (Figure F, Michaelis-Gutmann bodies). The granular cytoplasm of the histiocytes was positive on periodic acid-Schiff stain (Figure G). Based on these findings, the patient was diagnosed with colonic malakoplakia.
Malakoplakia is an uncommon, chronic, granulomatous inflammatory disease. It most commonly affects the urinary tract and gastrointestinal tract, but may occur at any anatomic site. Malakoplakia of the gastrointestinal tract are seen most frequently in the rectum, sigmoid, and right colon.1 It is diagnosed by the characteristic histologic feature of accumulated histiocytes with abundant eosinophilic granular cytoplasm containing basophilic inclusions, consistent with Michaelis-Gutmann bodies. Although the exact etiology and pathogenesis of malakoplakia are unclear, it seems to originate from an acquired defect in the intracellular destruction of phagocytosed bacteria, usually associated with Escherichia coli, Klebsiella, and Mycobacterium.2 It can have various causes, such as immunosuppression, malignant neoplasms, systemic diseases, and genetic diseases. Clinical manifestation of colonic malakoplakia is diverse, ranging from asymptomatic to malaise, fever, abdominal pain, diarrhea, hematochezia, and intestinal obstruction. Granulomatous reaction of malakoplakia generates the endoscopic appearance of lesions, which ranges from plaques to nodules and yellow-brown masses. In the early stage, malakoplakia commonly presents as soft yellow to tan mucosal plaques endoscopically, as seen in our case (Figure A). As the disease progresses in the later stage, malakoplakia presents as raised, grey to tan polypoid lesions of various sizes with peripheral hyperemia and a central depressed area, as seen in our case (Figure B).3 Owing to this endoscopic morphology, colonic malakoplakia may be misdiagnosed as atypical lymphoma, familial adenomatous polyposis, and metastatic carcinoma. To date, the natural course of malakoplakia of the colon is unclear, and no guidelines for treatment, treatment methods, duration of treatment, or surveillance are currently available. However, treatment of malakoplakia is essential to reduce immunosuppression and includes antibiotics with intracellular action and choline agonists that replenish the decreased cyclic 3’, 5’-guanosine monophosphate levels. In summary, although malakoplakia of the colon is very rare, it should be considered in the differential diagnosis of polypoid colonic lesions, especially in immunocompromised or malnourished patients.
References
1. Cipolletta L et al. Gastrointest Endosc. 1995 Mar;41(3):255-8.
2. Berney T et al. Transpl Int. 1999;12(4):293-6.
3. Weinrach DM et al. Arch Pathol Lab Med. 2004 Oct;128(10):e133-4.
A 60-year-old man with C3 tetraplegia was referred to our department for evaluation of abdominal pain and hematochezia. He was diagnosed with adrenal insufficiency 5 years prior and has been taking low-dose prednisolone (7.5 mg) once a day. One year before presentation, he complained of intermittent loose, mucoid stool and abdominal pain. Sigmoidoscopy revealed multiple small yellowish plaques in the sigmoid colon (Figure A). However, symptoms improved without any treatment, and he was discharged from the rehabilitation department. He was readmitted for respiratory rehabilitation owing to dyspnea. On hospital day 4, he complained of abdominal pain and passing loose stool with foul odor 4-5 times a day. On hospital day 7, the abdominal pain worsened, and hematochezia occurred.
On physical examination, he was hemodynamically stable and afebrile. The abdomen was soft with mild tenderness on palpation in the periumbilical area without peritoneal signs. Laboratory studies were notable with a hemoglobin level of 10.7 g/dL, total protein of 4.09 g/dL, and albumin of 2.21 g/dL. Inflammatory marker (C-reactive protein) was mildly elevated to 1.83 mg/dL. Serology for human immunodeficiency virus was negative. Tumor markers, such as carcinoembryonic antigen, carbohydrate antigenic determinant, and alpha-fetoprotein, were within the normal range. Antineutrophil cytoplasmic antibody was negative, and rheumatic factor was within the normal range. Findings from stool for acid-fast bacillus and Clostridioides difficile toxin were negative; no pathogens were cultured, and no parasites were identified.
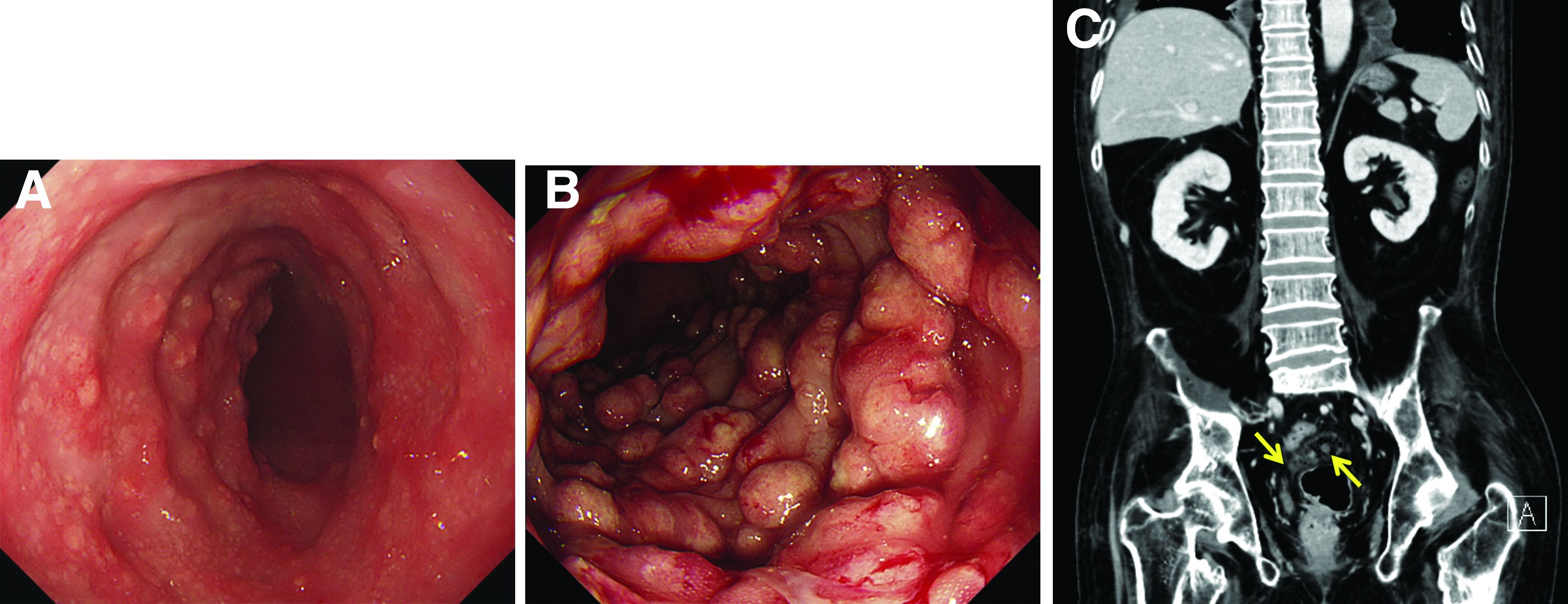
Sigmoidoscopy revealed diverse, multiple polypoid lesions (3-10 mm) with erythema, edema, and friability surrounding the entire lumen on the sigmoid colon (Figure B). The number and size of the polypoid lesions increased compared with the endoscopic findings obtained 1 year prior. The lesions easily bled on contact. Multiple biopsies of different sites were taken. An abdominal computed tomography scan showed multiple polyps of <1 cm that were confined to the sigmoid colon (Figure C, arrow).
Based on this information, what is the most likely diagnosis?
Previously published in Gastroenterology (2020 Feb;158[3]:482-4).
Undertreated hypothyroidism may worsen hospital outcomes
Suboptimal treatment of primary hypothyroidism may increase the risk of worse hospital outcomes, new research suggests.
The risks, including longer length of stay (LOS) and higher readmission rates, were no longer present in patients with adequately treated hypothyroidism, and in fact, appeared better than among those without hypothyroidism.
“Unfortunately, suboptimal treatment is common amongst the patient population with hypothyroidism,” wrote Matthew D. Ettleson, MD, of the Section of Endocrinology, Diabetes, and Metabolism at the University of Chicago, and colleagues.
“It is important for both patients and physicians to know that maintaining optimal thyroid hormone replacement is important to minimize length of hospital stays and hospital readmission. It is particularly important for planned admissions where thyroid hormone replacement can be adjusted if needed prior to admission,” said Dr. Ettleson in a press release from the Endocrine Society.
More evidence of adverse effects of suboptimal treatment
The findings, from a large U.S. claims database, “add to the growing body of evidence demonstrating the serious adverse short- and long-term health effects associated with suboptimal treatment of hypothyroidism,” the authors write in their article, published online in the Journal of Clinical Endocrinology and Metabolism. Dr. Ettleson will also present the data on June 11 at the ENDO 2022 meeting.
Thyroid hormone replacement therapy – generally levothyroxine – is given for primary hypothyroidism with the aim of maintaining serum thyroid-stimulating hormone (TSH) within the normal reference range.
TSH is inversely related to the level of circulating thyroid hormone, so low levels of TSH indicate overtreatment of thyroid disease and high levels indicate undertreatment.
Worse hospital outcomes associated with high TSH
In their study, Dr. Ettleson and colleagues retrospectively examined IBM MarketScan claims for 43,478 privately insured patients younger than age 65 years and hospitalized for medical or surgical reasons in 2008-2015.
Of those, 8,873 met the criteria for primary hypothyroidism based on a pre-admission prescription claim for levothyroxine, TSH > 10.00 mIU/L, confirmed diagnosis of hypothyroidism during hospitalization, or chronic lymphocytic thyroiditis. Of those, 4,770 (53.8%) had a prescription claim for levothyroxine.
Patients who met the clinical criteria for hypothyroidism were divided into four subgroups based on prehospitalization TSH level: low (< 0.40 mIU/L), normal (0.40-4.50 mIU/L), intermediate (4.51-10.00 mIU/L), and high (> 10.00 mIU/L).
The median length of time between TSH collection and hospital admission was 56 days in the hypothyroidism group and 63 days in the control group.
There were no differences in hospital outcomes between those with and without hypothyroidism among those who had low or intermediate TSH levels, in a multivariate analysis that used propensity-score matching.
In those with normal TSH levels, those with hypothyroidism actually had a lower risk of in-hospital death (risk ratio, 0.46; P = .004) and 90-day readmission rate (RR, 0.92; P = .02) than controls.
And those in the high TSH level subgroup had longer length of stay (+1.2 days; P = .003) and higher risk of 30-day readmission (RR, 1.49; P < .001) and 90-day readmission (RR, 1.43; P < .001), compared with balanced controls.
Public health effort needed to improve quality of care
There are multiple reasons why those with undertreated or undiagnosed hypothyroidism might have worse hospital outcomes, the authors say.
A bit more puzzling is why those with well-controlled hypothyroidism appeared to do better than those without hypothyroidism, given that thyroid hormone replacement isn’t likely to provide an advantage over normal, endogenous thyroid hormone production.
Dr. Ettleson and colleagues speculate that in-range TSH values may be a surrogate for regular health care and adherence to medical therapy, which likely leads to better hospital outcomes.
“The long- and short-term adverse health effects associated with off-target treatment of hypothyroidism, coupled with the high frequency of off-target treatment amongst the millions of patients in the United States on thyroid hormone, suggest that a public health effort to improve the quality of care of hypothyroidism is necessary,” Dr. Ettleson and colleagues write.
However, they note that there is currently no quality measure regarding appropriate treatment of hypothyroidism within the Merit-Based Incentive Payment System of the Centers for Medicare & Medicaid Services.
“The presence of guidelines alone may not be sufficient, as demonstrated by the inadequate application of guidelines for the use of levothyroxine in the treatment of thyroid cancer, a serious but much less common disease than clinical hypothyroidism,” the authors add.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health. Dr. Ettleson has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Suboptimal treatment of primary hypothyroidism may increase the risk of worse hospital outcomes, new research suggests.
The risks, including longer length of stay (LOS) and higher readmission rates, were no longer present in patients with adequately treated hypothyroidism, and in fact, appeared better than among those without hypothyroidism.
“Unfortunately, suboptimal treatment is common amongst the patient population with hypothyroidism,” wrote Matthew D. Ettleson, MD, of the Section of Endocrinology, Diabetes, and Metabolism at the University of Chicago, and colleagues.
“It is important for both patients and physicians to know that maintaining optimal thyroid hormone replacement is important to minimize length of hospital stays and hospital readmission. It is particularly important for planned admissions where thyroid hormone replacement can be adjusted if needed prior to admission,” said Dr. Ettleson in a press release from the Endocrine Society.
More evidence of adverse effects of suboptimal treatment
The findings, from a large U.S. claims database, “add to the growing body of evidence demonstrating the serious adverse short- and long-term health effects associated with suboptimal treatment of hypothyroidism,” the authors write in their article, published online in the Journal of Clinical Endocrinology and Metabolism. Dr. Ettleson will also present the data on June 11 at the ENDO 2022 meeting.
Thyroid hormone replacement therapy – generally levothyroxine – is given for primary hypothyroidism with the aim of maintaining serum thyroid-stimulating hormone (TSH) within the normal reference range.
TSH is inversely related to the level of circulating thyroid hormone, so low levels of TSH indicate overtreatment of thyroid disease and high levels indicate undertreatment.
Worse hospital outcomes associated with high TSH
In their study, Dr. Ettleson and colleagues retrospectively examined IBM MarketScan claims for 43,478 privately insured patients younger than age 65 years and hospitalized for medical or surgical reasons in 2008-2015.
Of those, 8,873 met the criteria for primary hypothyroidism based on a pre-admission prescription claim for levothyroxine, TSH > 10.00 mIU/L, confirmed diagnosis of hypothyroidism during hospitalization, or chronic lymphocytic thyroiditis. Of those, 4,770 (53.8%) had a prescription claim for levothyroxine.
Patients who met the clinical criteria for hypothyroidism were divided into four subgroups based on prehospitalization TSH level: low (< 0.40 mIU/L), normal (0.40-4.50 mIU/L), intermediate (4.51-10.00 mIU/L), and high (> 10.00 mIU/L).
The median length of time between TSH collection and hospital admission was 56 days in the hypothyroidism group and 63 days in the control group.
There were no differences in hospital outcomes between those with and without hypothyroidism among those who had low or intermediate TSH levels, in a multivariate analysis that used propensity-score matching.
In those with normal TSH levels, those with hypothyroidism actually had a lower risk of in-hospital death (risk ratio, 0.46; P = .004) and 90-day readmission rate (RR, 0.92; P = .02) than controls.
And those in the high TSH level subgroup had longer length of stay (+1.2 days; P = .003) and higher risk of 30-day readmission (RR, 1.49; P < .001) and 90-day readmission (RR, 1.43; P < .001), compared with balanced controls.
Public health effort needed to improve quality of care
There are multiple reasons why those with undertreated or undiagnosed hypothyroidism might have worse hospital outcomes, the authors say.
A bit more puzzling is why those with well-controlled hypothyroidism appeared to do better than those without hypothyroidism, given that thyroid hormone replacement isn’t likely to provide an advantage over normal, endogenous thyroid hormone production.
Dr. Ettleson and colleagues speculate that in-range TSH values may be a surrogate for regular health care and adherence to medical therapy, which likely leads to better hospital outcomes.
“The long- and short-term adverse health effects associated with off-target treatment of hypothyroidism, coupled with the high frequency of off-target treatment amongst the millions of patients in the United States on thyroid hormone, suggest that a public health effort to improve the quality of care of hypothyroidism is necessary,” Dr. Ettleson and colleagues write.
However, they note that there is currently no quality measure regarding appropriate treatment of hypothyroidism within the Merit-Based Incentive Payment System of the Centers for Medicare & Medicaid Services.
“The presence of guidelines alone may not be sufficient, as demonstrated by the inadequate application of guidelines for the use of levothyroxine in the treatment of thyroid cancer, a serious but much less common disease than clinical hypothyroidism,” the authors add.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health. Dr. Ettleson has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Suboptimal treatment of primary hypothyroidism may increase the risk of worse hospital outcomes, new research suggests.
The risks, including longer length of stay (LOS) and higher readmission rates, were no longer present in patients with adequately treated hypothyroidism, and in fact, appeared better than among those without hypothyroidism.
“Unfortunately, suboptimal treatment is common amongst the patient population with hypothyroidism,” wrote Matthew D. Ettleson, MD, of the Section of Endocrinology, Diabetes, and Metabolism at the University of Chicago, and colleagues.
“It is important for both patients and physicians to know that maintaining optimal thyroid hormone replacement is important to minimize length of hospital stays and hospital readmission. It is particularly important for planned admissions where thyroid hormone replacement can be adjusted if needed prior to admission,” said Dr. Ettleson in a press release from the Endocrine Society.
More evidence of adverse effects of suboptimal treatment
The findings, from a large U.S. claims database, “add to the growing body of evidence demonstrating the serious adverse short- and long-term health effects associated with suboptimal treatment of hypothyroidism,” the authors write in their article, published online in the Journal of Clinical Endocrinology and Metabolism. Dr. Ettleson will also present the data on June 11 at the ENDO 2022 meeting.
Thyroid hormone replacement therapy – generally levothyroxine – is given for primary hypothyroidism with the aim of maintaining serum thyroid-stimulating hormone (TSH) within the normal reference range.
TSH is inversely related to the level of circulating thyroid hormone, so low levels of TSH indicate overtreatment of thyroid disease and high levels indicate undertreatment.
Worse hospital outcomes associated with high TSH
In their study, Dr. Ettleson and colleagues retrospectively examined IBM MarketScan claims for 43,478 privately insured patients younger than age 65 years and hospitalized for medical or surgical reasons in 2008-2015.
Of those, 8,873 met the criteria for primary hypothyroidism based on a pre-admission prescription claim for levothyroxine, TSH > 10.00 mIU/L, confirmed diagnosis of hypothyroidism during hospitalization, or chronic lymphocytic thyroiditis. Of those, 4,770 (53.8%) had a prescription claim for levothyroxine.
Patients who met the clinical criteria for hypothyroidism were divided into four subgroups based on prehospitalization TSH level: low (< 0.40 mIU/L), normal (0.40-4.50 mIU/L), intermediate (4.51-10.00 mIU/L), and high (> 10.00 mIU/L).
The median length of time between TSH collection and hospital admission was 56 days in the hypothyroidism group and 63 days in the control group.
There were no differences in hospital outcomes between those with and without hypothyroidism among those who had low or intermediate TSH levels, in a multivariate analysis that used propensity-score matching.
In those with normal TSH levels, those with hypothyroidism actually had a lower risk of in-hospital death (risk ratio, 0.46; P = .004) and 90-day readmission rate (RR, 0.92; P = .02) than controls.
And those in the high TSH level subgroup had longer length of stay (+1.2 days; P = .003) and higher risk of 30-day readmission (RR, 1.49; P < .001) and 90-day readmission (RR, 1.43; P < .001), compared with balanced controls.
Public health effort needed to improve quality of care
There are multiple reasons why those with undertreated or undiagnosed hypothyroidism might have worse hospital outcomes, the authors say.
A bit more puzzling is why those with well-controlled hypothyroidism appeared to do better than those without hypothyroidism, given that thyroid hormone replacement isn’t likely to provide an advantage over normal, endogenous thyroid hormone production.
Dr. Ettleson and colleagues speculate that in-range TSH values may be a surrogate for regular health care and adherence to medical therapy, which likely leads to better hospital outcomes.
“The long- and short-term adverse health effects associated with off-target treatment of hypothyroidism, coupled with the high frequency of off-target treatment amongst the millions of patients in the United States on thyroid hormone, suggest that a public health effort to improve the quality of care of hypothyroidism is necessary,” Dr. Ettleson and colleagues write.
However, they note that there is currently no quality measure regarding appropriate treatment of hypothyroidism within the Merit-Based Incentive Payment System of the Centers for Medicare & Medicaid Services.
“The presence of guidelines alone may not be sufficient, as demonstrated by the inadequate application of guidelines for the use of levothyroxine in the treatment of thyroid cancer, a serious but much less common disease than clinical hypothyroidism,” the authors add.
The study was supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health. Dr. Ettleson has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Clinical Edge Journal Scan Commentary: HCC May 2022

Clinical trials for unresectable HCC (uHCC) have mandated excellent underlying liver function. Patients with Child-Pugh (CP) A cirrhosis do not have cirrhosis as their most life-limiting disease. In clinical practice, there are many patients with uHCC who are functionally well yet have CP-B cirrhosis. D'Alessio and colleagues undertook a retrospective evaluation of 202 patients with either CP-A or CP-B cirrhosis who received atezolizumab and bevacizumab as first-line treatment of uHCC. The majority, 154 patients (76%), had CP-A cirrhosis, whereas 48 (24%) had CP-B, including 21 B7, 21 B8, and 6 B9. The authors found that in the overall population, median overall survival (mOS) was 14.9 months (95% CI 13.6-16.3), with patients with CP-A mOS of 16.8 months (95% CI 14.1-23.9), and CP-B mOS of 6.7 months (95% CI 4.3-15.6; P = .0003). Overall response rates (ORR) were comparable, with an ORR of 26% in CP-A and 21% in CP-B, not influenced by Barcelona Clinic Liver Cancer (BCLC) stage, performance status, etiology (viral vs nonviral), portal vein thrombosis (PVT), or extrahepatic spread (P > .05 for all associations). The investigators concluded that atezolizumab and bevacizumab in patients with CP-B was well tolerated, with no relevant difference in terms of clinically significant treatment-related adverse events compared with patients with CP-A.
Shi and colleagues reported a randomized controlled trial of patients with HCC and microvascular invasion (MVI) who underwent suboptimal resection (distance from tumor edge to the cut surface < 1 mm), followed by either stereotactic body radiotherapy (SBRT) or observation. From August 2015 to December 2016, 76 patients with BCLC stage 0/A liver disease, MVI, and no macroscopic vascular invasion were randomized after partial hepatectomy to either observation or SBRT (35 Gy delivered in a week). The 1-, 3-, and 5-year disease free survival (DFS) rates were 92.1%, 65.8%, and 56.1% in the SBRT group vs 76.3%, 36.8%, and 26.3% in the surgery alone group, respectively (P = .005). The 1-, 3-, and 5-year overall survival (OS) rates were 100%, 89.5%, and 75.0% in SBRT group vs 100.0%, 68.4%, and 53.7% in the surgery alone group, respectively (P = .053). The authors concluded that SBRT eradicates residual tumor cells present at the margin and improves surgical outcomes.
Roth and colleagues evaluated the safety and efficacy of transarterial chemoembolization (TACE) in older (> 70 years) patients with intermediate HCC. Out of 271 patients evaluated, 88 were older patients. 20.5% of older patients experienced serious adverse events vs 21.3% of younger patients (P = .87). The predictive factors of serious adverse events were CP stage ≥ B7 (P < .0001), Eastern Cooperative Oncology Group (ECOG) scale ≥ 1 (P = .0019), and Model for End-stage Liver Disease (MELD) score ≥ 9 (P = .0415). The serious adverse event rate was not increased with age (P = .87). The authors concluded that age should not be an exclusionary factor when considering TACE.
Clinical trials for unresectable HCC (uHCC) have mandated excellent underlying liver function. Patients with Child-Pugh (CP) A cirrhosis do not have cirrhosis as their most life-limiting disease. In clinical practice, there are many patients with uHCC who are functionally well yet have CP-B cirrhosis. D'Alessio and colleagues undertook a retrospective evaluation of 202 patients with either CP-A or CP-B cirrhosis who received atezolizumab and bevacizumab as first-line treatment of uHCC. The majority, 154 patients (76%), had CP-A cirrhosis, whereas 48 (24%) had CP-B, including 21 B7, 21 B8, and 6 B9. The authors found that in the overall population, median overall survival (mOS) was 14.9 months (95% CI 13.6-16.3), with patients with CP-A mOS of 16.8 months (95% CI 14.1-23.9), and CP-B mOS of 6.7 months (95% CI 4.3-15.6; P = .0003). Overall response rates (ORR) were comparable, with an ORR of 26% in CP-A and 21% in CP-B, not influenced by Barcelona Clinic Liver Cancer (BCLC) stage, performance status, etiology (viral vs nonviral), portal vein thrombosis (PVT), or extrahepatic spread (P > .05 for all associations). The investigators concluded that atezolizumab and bevacizumab in patients with CP-B was well tolerated, with no relevant difference in terms of clinically significant treatment-related adverse events compared with patients with CP-A.
Shi and colleagues reported a randomized controlled trial of patients with HCC and microvascular invasion (MVI) who underwent suboptimal resection (distance from tumor edge to the cut surface < 1 mm), followed by either stereotactic body radiotherapy (SBRT) or observation. From August 2015 to December 2016, 76 patients with BCLC stage 0/A liver disease, MVI, and no macroscopic vascular invasion were randomized after partial hepatectomy to either observation or SBRT (35 Gy delivered in a week). The 1-, 3-, and 5-year disease free survival (DFS) rates were 92.1%, 65.8%, and 56.1% in the SBRT group vs 76.3%, 36.8%, and 26.3% in the surgery alone group, respectively (P = .005). The 1-, 3-, and 5-year overall survival (OS) rates were 100%, 89.5%, and 75.0% in SBRT group vs 100.0%, 68.4%, and 53.7% in the surgery alone group, respectively (P = .053). The authors concluded that SBRT eradicates residual tumor cells present at the margin and improves surgical outcomes.
Roth and colleagues evaluated the safety and efficacy of transarterial chemoembolization (TACE) in older (> 70 years) patients with intermediate HCC. Out of 271 patients evaluated, 88 were older patients. 20.5% of older patients experienced serious adverse events vs 21.3% of younger patients (P = .87). The predictive factors of serious adverse events were CP stage ≥ B7 (P < .0001), Eastern Cooperative Oncology Group (ECOG) scale ≥ 1 (P = .0019), and Model for End-stage Liver Disease (MELD) score ≥ 9 (P = .0415). The serious adverse event rate was not increased with age (P = .87). The authors concluded that age should not be an exclusionary factor when considering TACE.
Clinical trials for unresectable HCC (uHCC) have mandated excellent underlying liver function. Patients with Child-Pugh (CP) A cirrhosis do not have cirrhosis as their most life-limiting disease. In clinical practice, there are many patients with uHCC who are functionally well yet have CP-B cirrhosis. D'Alessio and colleagues undertook a retrospective evaluation of 202 patients with either CP-A or CP-B cirrhosis who received atezolizumab and bevacizumab as first-line treatment of uHCC. The majority, 154 patients (76%), had CP-A cirrhosis, whereas 48 (24%) had CP-B, including 21 B7, 21 B8, and 6 B9. The authors found that in the overall population, median overall survival (mOS) was 14.9 months (95% CI 13.6-16.3), with patients with CP-A mOS of 16.8 months (95% CI 14.1-23.9), and CP-B mOS of 6.7 months (95% CI 4.3-15.6; P = .0003). Overall response rates (ORR) were comparable, with an ORR of 26% in CP-A and 21% in CP-B, not influenced by Barcelona Clinic Liver Cancer (BCLC) stage, performance status, etiology (viral vs nonviral), portal vein thrombosis (PVT), or extrahepatic spread (P > .05 for all associations). The investigators concluded that atezolizumab and bevacizumab in patients with CP-B was well tolerated, with no relevant difference in terms of clinically significant treatment-related adverse events compared with patients with CP-A.
Shi and colleagues reported a randomized controlled trial of patients with HCC and microvascular invasion (MVI) who underwent suboptimal resection (distance from tumor edge to the cut surface < 1 mm), followed by either stereotactic body radiotherapy (SBRT) or observation. From August 2015 to December 2016, 76 patients with BCLC stage 0/A liver disease, MVI, and no macroscopic vascular invasion were randomized after partial hepatectomy to either observation or SBRT (35 Gy delivered in a week). The 1-, 3-, and 5-year disease free survival (DFS) rates were 92.1%, 65.8%, and 56.1% in the SBRT group vs 76.3%, 36.8%, and 26.3% in the surgery alone group, respectively (P = .005). The 1-, 3-, and 5-year overall survival (OS) rates were 100%, 89.5%, and 75.0% in SBRT group vs 100.0%, 68.4%, and 53.7% in the surgery alone group, respectively (P = .053). The authors concluded that SBRT eradicates residual tumor cells present at the margin and improves surgical outcomes.
Roth and colleagues evaluated the safety and efficacy of transarterial chemoembolization (TACE) in older (> 70 years) patients with intermediate HCC. Out of 271 patients evaluated, 88 were older patients. 20.5% of older patients experienced serious adverse events vs 21.3% of younger patients (P = .87). The predictive factors of serious adverse events were CP stage ≥ B7 (P < .0001), Eastern Cooperative Oncology Group (ECOG) scale ≥ 1 (P = .0019), and Model for End-stage Liver Disease (MELD) score ≥ 9 (P = .0415). The serious adverse event rate was not increased with age (P = .87). The authors concluded that age should not be an exclusionary factor when considering TACE.
Clinical Edge Journal Scan Commentary: HCC May 2022

Clinical trials for unresectable HCC (uHCC) have mandated excellent underlying liver function. Patients with Child-Pugh (CP) A cirrhosis do not have cirrhosis as their most life-limiting disease. In clinical practice, there are many patients with uHCC who are functionally well yet have CP-B cirrhosis. D'Alessio and colleagues undertook a retrospective evaluation of 202 patients with either CP-A or CP-B cirrhosis who received atezolizumab and bevacizumab as first-line treatment of uHCC. The majority, 154 patients (76%), had CP-A cirrhosis, whereas 48 (24%) had CP-B, including 21 B7, 21 B8, and 6 B9. The authors found that in the overall population, median overall survival (mOS) was 14.9 months (95% CI 13.6-16.3), with patients with CP-A mOS of 16.8 months (95% CI 14.1-23.9), and CP-B mOS of 6.7 months (95% CI 4.3-15.6; P = .0003). Overall response rates (ORR) were comparable, with an ORR of 26% in CP-A and 21% in CP-B, not influenced by Barcelona Clinic Liver Cancer (BCLC) stage, performance status, etiology (viral vs nonviral), portal vein thrombosis (PVT), or extrahepatic spread (P > .05 for all associations). The investigators concluded that atezolizumab and bevacizumab in patients with CP-B was well tolerated, with no relevant difference in terms of clinically significant treatment-related adverse events compared with patients with CP-A.
Shi and colleagues reported a randomized controlled trial of patients with HCC and microvascular invasion (MVI) who underwent suboptimal resection (distance from tumor edge to the cut surface < 1 mm), followed by either stereotactic body radiotherapy (SBRT) or observation. From August 2015 to December 2016, 76 patients with BCLC stage 0/A liver disease, MVI, and no macroscopic vascular invasion were randomized after partial hepatectomy to either observation or SBRT (35 Gy delivered in a week). The 1-, 3-, and 5-year disease free survival (DFS) rates were 92.1%, 65.8%, and 56.1% in the SBRT group vs 76.3%, 36.8%, and 26.3% in the surgery alone group, respectively (P = .005). The 1-, 3-, and 5-year overall survival (OS) rates were 100%, 89.5%, and 75.0% in SBRT group vs 100.0%, 68.4%, and 53.7% in the surgery alone group, respectively (P = .053). The authors concluded that SBRT eradicates residual tumor cells present at the margin and improves surgical outcomes.
Roth and colleagues evaluated the safety and efficacy of transarterial chemoembolization (TACE) in older (> 70 years) patients with intermediate HCC. Out of 271 patients evaluated, 88 were older patients. 20.5% of older patients experienced serious adverse events vs 21.3% of younger patients (P = .87). The predictive factors of serious adverse events were CP stage ≥ B7 (P < .0001), Eastern Cooperative Oncology Group (ECOG) scale ≥ 1 (P = .0019), and Model for End-stage Liver Disease (MELD) score ≥ 9 (P = .0415). The serious adverse event rate was not increased with age (P = .87). The authors concluded that age should not be an exclusionary factor when considering TACE.
Clinical trials for unresectable HCC (uHCC) have mandated excellent underlying liver function. Patients with Child-Pugh (CP) A cirrhosis do not have cirrhosis as their most life-limiting disease. In clinical practice, there are many patients with uHCC who are functionally well yet have CP-B cirrhosis. D'Alessio and colleagues undertook a retrospective evaluation of 202 patients with either CP-A or CP-B cirrhosis who received atezolizumab and bevacizumab as first-line treatment of uHCC. The majority, 154 patients (76%), had CP-A cirrhosis, whereas 48 (24%) had CP-B, including 21 B7, 21 B8, and 6 B9. The authors found that in the overall population, median overall survival (mOS) was 14.9 months (95% CI 13.6-16.3), with patients with CP-A mOS of 16.8 months (95% CI 14.1-23.9), and CP-B mOS of 6.7 months (95% CI 4.3-15.6; P = .0003). Overall response rates (ORR) were comparable, with an ORR of 26% in CP-A and 21% in CP-B, not influenced by Barcelona Clinic Liver Cancer (BCLC) stage, performance status, etiology (viral vs nonviral), portal vein thrombosis (PVT), or extrahepatic spread (P > .05 for all associations). The investigators concluded that atezolizumab and bevacizumab in patients with CP-B was well tolerated, with no relevant difference in terms of clinically significant treatment-related adverse events compared with patients with CP-A.
Shi and colleagues reported a randomized controlled trial of patients with HCC and microvascular invasion (MVI) who underwent suboptimal resection (distance from tumor edge to the cut surface < 1 mm), followed by either stereotactic body radiotherapy (SBRT) or observation. From August 2015 to December 2016, 76 patients with BCLC stage 0/A liver disease, MVI, and no macroscopic vascular invasion were randomized after partial hepatectomy to either observation or SBRT (35 Gy delivered in a week). The 1-, 3-, and 5-year disease free survival (DFS) rates were 92.1%, 65.8%, and 56.1% in the SBRT group vs 76.3%, 36.8%, and 26.3% in the surgery alone group, respectively (P = .005). The 1-, 3-, and 5-year overall survival (OS) rates were 100%, 89.5%, and 75.0% in SBRT group vs 100.0%, 68.4%, and 53.7% in the surgery alone group, respectively (P = .053). The authors concluded that SBRT eradicates residual tumor cells present at the margin and improves surgical outcomes.
Roth and colleagues evaluated the safety and efficacy of transarterial chemoembolization (TACE) in older (> 70 years) patients with intermediate HCC. Out of 271 patients evaluated, 88 were older patients. 20.5% of older patients experienced serious adverse events vs 21.3% of younger patients (P = .87). The predictive factors of serious adverse events were CP stage ≥ B7 (P < .0001), Eastern Cooperative Oncology Group (ECOG) scale ≥ 1 (P = .0019), and Model for End-stage Liver Disease (MELD) score ≥ 9 (P = .0415). The serious adverse event rate was not increased with age (P = .87). The authors concluded that age should not be an exclusionary factor when considering TACE.
Clinical trials for unresectable HCC (uHCC) have mandated excellent underlying liver function. Patients with Child-Pugh (CP) A cirrhosis do not have cirrhosis as their most life-limiting disease. In clinical practice, there are many patients with uHCC who are functionally well yet have CP-B cirrhosis. D'Alessio and colleagues undertook a retrospective evaluation of 202 patients with either CP-A or CP-B cirrhosis who received atezolizumab and bevacizumab as first-line treatment of uHCC. The majority, 154 patients (76%), had CP-A cirrhosis, whereas 48 (24%) had CP-B, including 21 B7, 21 B8, and 6 B9. The authors found that in the overall population, median overall survival (mOS) was 14.9 months (95% CI 13.6-16.3), with patients with CP-A mOS of 16.8 months (95% CI 14.1-23.9), and CP-B mOS of 6.7 months (95% CI 4.3-15.6; P = .0003). Overall response rates (ORR) were comparable, with an ORR of 26% in CP-A and 21% in CP-B, not influenced by Barcelona Clinic Liver Cancer (BCLC) stage, performance status, etiology (viral vs nonviral), portal vein thrombosis (PVT), or extrahepatic spread (P > .05 for all associations). The investigators concluded that atezolizumab and bevacizumab in patients with CP-B was well tolerated, with no relevant difference in terms of clinically significant treatment-related adverse events compared with patients with CP-A.
Shi and colleagues reported a randomized controlled trial of patients with HCC and microvascular invasion (MVI) who underwent suboptimal resection (distance from tumor edge to the cut surface < 1 mm), followed by either stereotactic body radiotherapy (SBRT) or observation. From August 2015 to December 2016, 76 patients with BCLC stage 0/A liver disease, MVI, and no macroscopic vascular invasion were randomized after partial hepatectomy to either observation or SBRT (35 Gy delivered in a week). The 1-, 3-, and 5-year disease free survival (DFS) rates were 92.1%, 65.8%, and 56.1% in the SBRT group vs 76.3%, 36.8%, and 26.3% in the surgery alone group, respectively (P = .005). The 1-, 3-, and 5-year overall survival (OS) rates were 100%, 89.5%, and 75.0% in SBRT group vs 100.0%, 68.4%, and 53.7% in the surgery alone group, respectively (P = .053). The authors concluded that SBRT eradicates residual tumor cells present at the margin and improves surgical outcomes.
Roth and colleagues evaluated the safety and efficacy of transarterial chemoembolization (TACE) in older (> 70 years) patients with intermediate HCC. Out of 271 patients evaluated, 88 were older patients. 20.5% of older patients experienced serious adverse events vs 21.3% of younger patients (P = .87). The predictive factors of serious adverse events were CP stage ≥ B7 (P < .0001), Eastern Cooperative Oncology Group (ECOG) scale ≥ 1 (P = .0019), and Model for End-stage Liver Disease (MELD) score ≥ 9 (P = .0415). The serious adverse event rate was not increased with age (P = .87). The authors concluded that age should not be an exclusionary factor when considering TACE.
New blood biomarker to detect early dementia?
Investigators found that plasma concentrations of 2-aminoethyl dihydrogen phosphate and taurine could distinguish adults with early-stage Alzheimer’s disease from cognitively normal adults.
“Our biomarker for early-stage Alzheimer’s disease represents new thinking and is unique from the amyloid-beta and p-tau molecules that are currently being investigated to diagnose AD,” Sandra Banack, PhD, senior scientist, Brain Chemistry Labs, Jackson, Wyoming, told this news organization.
If further studies pan out, Dr. Banack said this biomarker could “easily be transformed into a test to aid clinical evaluations for Alzheimer’s disease.”
The study was published online in PLOS ONE.
New drug target?
The researchers measured concentrations of 2-aminoethyl dihydrogen phosphate and taurine in blood plasma samples in 25 patients (21 men; mean age, 71) with a clinical diagnosis of early-stage Alzheimer’s based on a Clinical Dementia Rating (CDR) score of 0.5, suggesting very mild cognitive impairment, and 25 healthy controls (20 men; mean age, 39).
The concentration of 2-aminoethyl dihydrogen phosphate, normalized by the concentration of taurine, reliably distinguished blood samples of early-stage Alzheimer’s patients from controls in a blinded analysis.
This biomarker “could lead to new understanding of [AD] and lead to new drug candidates,” Dr. Banack told this news organization.
The researchers note that 2-aminoethyl dihydrogen phosphate plays an important role in the structure and function of cellular membranes.
Physiologic effects of increased 2-aminoethyl dihydrogen phosphate concentrations in the blood are not known. However, in one study, concentrations of this molecule were found to be significantly lower in the temporal cortex, frontal cortex, and hippocampus (40%) in patients with Alzheimer’s disease, compared with controls.
“New biomarkers take time before they can be implemented in the clinic. The next step will be to repeat the experiments using a large sample size of AD patient blood samples,” Dr. Banack told this news organization.
The study team is looking to source a larger sample size of AD blood samples to replicate these findings. They are also examining this biomarker relative to other neurodegenerative diseases.
“If verified with larger sample sizes, the quantification of 2-aminoethyl dihydrogen phosphate could potentially assist in the diagnosis of early-stage Alzheimer’s disease when used in conjunction with the patient’s CDR score and other potential AD biomarkers,” Dr. Banack and colleagues say.
Caveats, cautionary notes
Commenting on the findings, Rebecca M. Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, said the study is “interesting, though very small-scale and very preliminary.”

Dr. Edelmayer said one “major limitation” is that participants did not have their Alzheimer’s diagnosis confirmed with “gold standard biomarkers. They have been diagnosed based only on their cognitive and behavioral symptoms.”
She also cautioned that the study population is not representative – either of the general public or people living with Alzheimer’s disease.
For example, 41 out of all 50 samples are from men, “though we know women are disproportionately impacted by Alzheimer’s.”
“There is a mismatch in the age of the study groups,” Dr. Edelmayer noted. The mean age of controls in the study was 39 and the mean age of people with dementia was 71. Race or ethnicity and other demographic information is also unclear from the article.
“There is an urgent need for simple, inexpensive, noninvasive and easily available diagnostic tools for Alzheimer’s, such as a blood test. A simple blood test for Alzheimer’s would be a great advance for individuals with – and at risk for – the disease, families, doctors, and researchers,” Dr. Edelmayer said.
“Bottom line,” Dr. Edelmayer continued, “these results need to be further tested and verified in long-term, large-scale studies with diverse populations that are representative of those living with Alzheimer’s disease.”
This research was supported by the William Stamps Farish Fund and the Josephine P. & John J. Louis Foundation. Brain Chemistry Labs has applied for a patent related to this research. Dr. Edelmayer has no relevant disclosures.
A version of this article first appeared on Medscape.com.
Investigators found that plasma concentrations of 2-aminoethyl dihydrogen phosphate and taurine could distinguish adults with early-stage Alzheimer’s disease from cognitively normal adults.
“Our biomarker for early-stage Alzheimer’s disease represents new thinking and is unique from the amyloid-beta and p-tau molecules that are currently being investigated to diagnose AD,” Sandra Banack, PhD, senior scientist, Brain Chemistry Labs, Jackson, Wyoming, told this news organization.
If further studies pan out, Dr. Banack said this biomarker could “easily be transformed into a test to aid clinical evaluations for Alzheimer’s disease.”
The study was published online in PLOS ONE.
New drug target?
The researchers measured concentrations of 2-aminoethyl dihydrogen phosphate and taurine in blood plasma samples in 25 patients (21 men; mean age, 71) with a clinical diagnosis of early-stage Alzheimer’s based on a Clinical Dementia Rating (CDR) score of 0.5, suggesting very mild cognitive impairment, and 25 healthy controls (20 men; mean age, 39).
The concentration of 2-aminoethyl dihydrogen phosphate, normalized by the concentration of taurine, reliably distinguished blood samples of early-stage Alzheimer’s patients from controls in a blinded analysis.
This biomarker “could lead to new understanding of [AD] and lead to new drug candidates,” Dr. Banack told this news organization.
The researchers note that 2-aminoethyl dihydrogen phosphate plays an important role in the structure and function of cellular membranes.
Physiologic effects of increased 2-aminoethyl dihydrogen phosphate concentrations in the blood are not known. However, in one study, concentrations of this molecule were found to be significantly lower in the temporal cortex, frontal cortex, and hippocampus (40%) in patients with Alzheimer’s disease, compared with controls.
“New biomarkers take time before they can be implemented in the clinic. The next step will be to repeat the experiments using a large sample size of AD patient blood samples,” Dr. Banack told this news organization.
The study team is looking to source a larger sample size of AD blood samples to replicate these findings. They are also examining this biomarker relative to other neurodegenerative diseases.
“If verified with larger sample sizes, the quantification of 2-aminoethyl dihydrogen phosphate could potentially assist in the diagnosis of early-stage Alzheimer’s disease when used in conjunction with the patient’s CDR score and other potential AD biomarkers,” Dr. Banack and colleagues say.
Caveats, cautionary notes
Commenting on the findings, Rebecca M. Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, said the study is “interesting, though very small-scale and very preliminary.”
Dr. Edelmayer said one “major limitation” is that participants did not have their Alzheimer’s diagnosis confirmed with “gold standard biomarkers. They have been diagnosed based only on their cognitive and behavioral symptoms.”
She also cautioned that the study population is not representative – either of the general public or people living with Alzheimer’s disease.
For example, 41 out of all 50 samples are from men, “though we know women are disproportionately impacted by Alzheimer’s.”
“There is a mismatch in the age of the study groups,” Dr. Edelmayer noted. The mean age of controls in the study was 39 and the mean age of people with dementia was 71. Race or ethnicity and other demographic information is also unclear from the article.
“There is an urgent need for simple, inexpensive, noninvasive and easily available diagnostic tools for Alzheimer’s, such as a blood test. A simple blood test for Alzheimer’s would be a great advance for individuals with – and at risk for – the disease, families, doctors, and researchers,” Dr. Edelmayer said.
“Bottom line,” Dr. Edelmayer continued, “these results need to be further tested and verified in long-term, large-scale studies with diverse populations that are representative of those living with Alzheimer’s disease.”
This research was supported by the William Stamps Farish Fund and the Josephine P. & John J. Louis Foundation. Brain Chemistry Labs has applied for a patent related to this research. Dr. Edelmayer has no relevant disclosures.
A version of this article first appeared on Medscape.com.
Investigators found that plasma concentrations of 2-aminoethyl dihydrogen phosphate and taurine could distinguish adults with early-stage Alzheimer’s disease from cognitively normal adults.
“Our biomarker for early-stage Alzheimer’s disease represents new thinking and is unique from the amyloid-beta and p-tau molecules that are currently being investigated to diagnose AD,” Sandra Banack, PhD, senior scientist, Brain Chemistry Labs, Jackson, Wyoming, told this news organization.
If further studies pan out, Dr. Banack said this biomarker could “easily be transformed into a test to aid clinical evaluations for Alzheimer’s disease.”
The study was published online in PLOS ONE.
New drug target?
The researchers measured concentrations of 2-aminoethyl dihydrogen phosphate and taurine in blood plasma samples in 25 patients (21 men; mean age, 71) with a clinical diagnosis of early-stage Alzheimer’s based on a Clinical Dementia Rating (CDR) score of 0.5, suggesting very mild cognitive impairment, and 25 healthy controls (20 men; mean age, 39).
The concentration of 2-aminoethyl dihydrogen phosphate, normalized by the concentration of taurine, reliably distinguished blood samples of early-stage Alzheimer’s patients from controls in a blinded analysis.
This biomarker “could lead to new understanding of [AD] and lead to new drug candidates,” Dr. Banack told this news organization.
The researchers note that 2-aminoethyl dihydrogen phosphate plays an important role in the structure and function of cellular membranes.
Physiologic effects of increased 2-aminoethyl dihydrogen phosphate concentrations in the blood are not known. However, in one study, concentrations of this molecule were found to be significantly lower in the temporal cortex, frontal cortex, and hippocampus (40%) in patients with Alzheimer’s disease, compared with controls.
“New biomarkers take time before they can be implemented in the clinic. The next step will be to repeat the experiments using a large sample size of AD patient blood samples,” Dr. Banack told this news organization.
The study team is looking to source a larger sample size of AD blood samples to replicate these findings. They are also examining this biomarker relative to other neurodegenerative diseases.
“If verified with larger sample sizes, the quantification of 2-aminoethyl dihydrogen phosphate could potentially assist in the diagnosis of early-stage Alzheimer’s disease when used in conjunction with the patient’s CDR score and other potential AD biomarkers,” Dr. Banack and colleagues say.
Caveats, cautionary notes
Commenting on the findings, Rebecca M. Edelmayer, PhD, Alzheimer’s Association senior director of scientific engagement, said the study is “interesting, though very small-scale and very preliminary.”
Dr. Edelmayer said one “major limitation” is that participants did not have their Alzheimer’s diagnosis confirmed with “gold standard biomarkers. They have been diagnosed based only on their cognitive and behavioral symptoms.”
She also cautioned that the study population is not representative – either of the general public or people living with Alzheimer’s disease.
For example, 41 out of all 50 samples are from men, “though we know women are disproportionately impacted by Alzheimer’s.”
“There is a mismatch in the age of the study groups,” Dr. Edelmayer noted. The mean age of controls in the study was 39 and the mean age of people with dementia was 71. Race or ethnicity and other demographic information is also unclear from the article.
“There is an urgent need for simple, inexpensive, noninvasive and easily available diagnostic tools for Alzheimer’s, such as a blood test. A simple blood test for Alzheimer’s would be a great advance for individuals with – and at risk for – the disease, families, doctors, and researchers,” Dr. Edelmayer said.
“Bottom line,” Dr. Edelmayer continued, “these results need to be further tested and verified in long-term, large-scale studies with diverse populations that are representative of those living with Alzheimer’s disease.”
This research was supported by the William Stamps Farish Fund and the Josephine P. & John J. Louis Foundation. Brain Chemistry Labs has applied for a patent related to this research. Dr. Edelmayer has no relevant disclosures.
A version of this article first appeared on Medscape.com.
First-ever best practices for percutaneous axillary access
The Society for Cardiovascular Angiography and Interventions (SCAI) has issued the first statement on best practices for percutaneous axillary arterial access and training.
The position statement helps fill a gap amid increasing use of transaxillary access as an alternative to the femoral route for large-bore transcatheter aortic valve replacement (TAVR), endovascular aortic repair (EVAR), and mechanical circulatory support.
“The need for alternative access has increased as we are using more and more TAVR for our elderly population, and EVAR has also increased,” writing committee chair Arnold H. Seto, MD, Long Beach VA Health Care System (California) said in an interview. “There’s also a set of patients who require balloon pumps for a prolonged period, and people were using balloon pumps from the axillary approach, which were not custom-designed for that purpose.”
He noted that the evidence base leans heavily on case reports and case series, and that they were approached for guidance by a vendor developing a balloon pump specific to axillary access. “So that helped spur all of us to get together and decide to write up something on this topic, which was developing, but was certainly picking up steam rapidly.”
The statement was published in the Journal of the Society for Cardiovascular Angiography and Interventions, and it reflects the consensus of experts in heart failure, interventional cardiology and radiology, and cardiothoracic and vascular surgery. It reviews anatomic considerations and risks for percutaneous axillary access and suggests techniques for insertion, closure, and complication management.
Although the femoral artery is the most frequent access site for percutaneous large-bore procedures, the document notes that this approach may be limited in 13%-20% of patients because of prior surgeries or severe aortoiliac and/or iliofemoral atherosclerotic disease, tortuosity, or calcification.
“Absolutely, the femoral should be the predominant access site,” Dr. Seto said. Whenever there is a compromised femoral artery, “the axillary artery, which is rarely involved with atherosclerosis, makes for the most optimal alternative access. Other forms of alternative access, including transcaval and transcarotid, are possible but have their own issues and difficulties.”
Axillary access has traditionally been done through an open surgical approach, which allows for direct puncture, primary arterial repair, or placement of a sidearm conduit. Percutaneous transaxillary access avoids a surgical incision and general anesthesia and, theoretically, reduces the risk of infection, he said. It also allows for better mobility for patients, for example, who may have a balloon pump in place for weeks or even a month when waiting for a bridge to transplant.
In terms of technique, key recommendations include:
- Gaining access preferably through the left axillary
- Inserting the needle directly through the pectoralis minor into the second segment of the axillary artery
- Using a shallow-needle angle of 25-30 degrees to improve access success and decrease sheath malformation, kinking, bleeding, or vessel perforation
- Using micropuncture needles to minimize trauma to adjacent tissues
- Abducting the patient’s arm to 45-90 degrees to reduce tortuosity
- Using angiographic and ultrasound techniques to optimize vascular access
The latter point was the one area of debate among the writing committee, Dr. Seto observed. “That is one of the controversies: Should we make ultrasound mandatory? ... Everybody agreed that it can be quite useful and was likely to be useful because of its success in every other access area,” he said. “But in the absence of randomized evidence, we couldn’t make it mandatory or a strong recommendation. We just had to make it one of several options for the operator.”
The document highlights the need for familiarity with potential axillary artery complications and their management, noting that the axillary is more fragile than the femoral artery and, thus, potentially more prone to complications during instrumentation.
Data from the ARMS study in 102 patients undergoing transaxillary access for mechanical hemodynamic support reported 17 procedural complications, including 10 minor access site bleeding events, one stroke, and one pseudoaneurysm. A small study of 25 complex EVAR procedures reported a perioperative access complication rate of 8%, including one axillary artery dissection and one stenosis.
“Despite the brachial plexus being around there, there’s actually rare reports of neurologic injury and certainly none that have been permanent,” Dr. Seto said. “Also, stroke risk is probably more related to your device size and type of device rather than the approach itself.”
A significant amount of the paper is also devoted to training and privileging suggestions with an emphasis on a multidisciplinary team. The writing group recommends graduate medical education programs develop training curricula in percutaneous axillary artery access.
Those already in practice should participate in a formal training program that focuses on axillary artery anatomy, training in large bore access and closure devices, and didactic training in imaging modalities as applied to the axillary artery. Training can occur hands-on or using online simulations.
They also recommend outlining the potential need or role for proctoring and call for ongoing formal professional monitoring programs to evaluate operator outcomes using local or registry data.
“From a privileging standpoint, it was important for hospitals to be equally fair, regardless of the specialty that a requesting practitioner came from,” Dr. Seto said. “In other words, treat the vascular surgeons and interventional cardiologists and radiologists equally in terms of who has the privilege to do transaxillary access.”
The SCAI position statement has been endorsed by the American College of Cardiology, the Heart Failure Society of America, the Society of Interventional Radiology, and the Vascular & Endovascular Surgery Society.
Dr. Seto reported receiving honoraria from Getinge prior to initiation of the document. Disclosures for the rest of the writing group are available with the original article.
A version of this article first appeared on Medscape.com.
The Society for Cardiovascular Angiography and Interventions (SCAI) has issued the first statement on best practices for percutaneous axillary arterial access and training.
The position statement helps fill a gap amid increasing use of transaxillary access as an alternative to the femoral route for large-bore transcatheter aortic valve replacement (TAVR), endovascular aortic repair (EVAR), and mechanical circulatory support.
“The need for alternative access has increased as we are using more and more TAVR for our elderly population, and EVAR has also increased,” writing committee chair Arnold H. Seto, MD, Long Beach VA Health Care System (California) said in an interview. “There’s also a set of patients who require balloon pumps for a prolonged period, and people were using balloon pumps from the axillary approach, which were not custom-designed for that purpose.”
He noted that the evidence base leans heavily on case reports and case series, and that they were approached for guidance by a vendor developing a balloon pump specific to axillary access. “So that helped spur all of us to get together and decide to write up something on this topic, which was developing, but was certainly picking up steam rapidly.”
The statement was published in the Journal of the Society for Cardiovascular Angiography and Interventions, and it reflects the consensus of experts in heart failure, interventional cardiology and radiology, and cardiothoracic and vascular surgery. It reviews anatomic considerations and risks for percutaneous axillary access and suggests techniques for insertion, closure, and complication management.
Although the femoral artery is the most frequent access site for percutaneous large-bore procedures, the document notes that this approach may be limited in 13%-20% of patients because of prior surgeries or severe aortoiliac and/or iliofemoral atherosclerotic disease, tortuosity, or calcification.
“Absolutely, the femoral should be the predominant access site,” Dr. Seto said. Whenever there is a compromised femoral artery, “the axillary artery, which is rarely involved with atherosclerosis, makes for the most optimal alternative access. Other forms of alternative access, including transcaval and transcarotid, are possible but have their own issues and difficulties.”
Axillary access has traditionally been done through an open surgical approach, which allows for direct puncture, primary arterial repair, or placement of a sidearm conduit. Percutaneous transaxillary access avoids a surgical incision and general anesthesia and, theoretically, reduces the risk of infection, he said. It also allows for better mobility for patients, for example, who may have a balloon pump in place for weeks or even a month when waiting for a bridge to transplant.
In terms of technique, key recommendations include:
- Gaining access preferably through the left axillary
- Inserting the needle directly through the pectoralis minor into the second segment of the axillary artery
- Using a shallow-needle angle of 25-30 degrees to improve access success and decrease sheath malformation, kinking, bleeding, or vessel perforation
- Using micropuncture needles to minimize trauma to adjacent tissues
- Abducting the patient’s arm to 45-90 degrees to reduce tortuosity
- Using angiographic and ultrasound techniques to optimize vascular access
The latter point was the one area of debate among the writing committee, Dr. Seto observed. “That is one of the controversies: Should we make ultrasound mandatory? ... Everybody agreed that it can be quite useful and was likely to be useful because of its success in every other access area,” he said. “But in the absence of randomized evidence, we couldn’t make it mandatory or a strong recommendation. We just had to make it one of several options for the operator.”
The document highlights the need for familiarity with potential axillary artery complications and their management, noting that the axillary is more fragile than the femoral artery and, thus, potentially more prone to complications during instrumentation.
Data from the ARMS study in 102 patients undergoing transaxillary access for mechanical hemodynamic support reported 17 procedural complications, including 10 minor access site bleeding events, one stroke, and one pseudoaneurysm. A small study of 25 complex EVAR procedures reported a perioperative access complication rate of 8%, including one axillary artery dissection and one stenosis.
“Despite the brachial plexus being around there, there’s actually rare reports of neurologic injury and certainly none that have been permanent,” Dr. Seto said. “Also, stroke risk is probably more related to your device size and type of device rather than the approach itself.”
A significant amount of the paper is also devoted to training and privileging suggestions with an emphasis on a multidisciplinary team. The writing group recommends graduate medical education programs develop training curricula in percutaneous axillary artery access.
Those already in practice should participate in a formal training program that focuses on axillary artery anatomy, training in large bore access and closure devices, and didactic training in imaging modalities as applied to the axillary artery. Training can occur hands-on or using online simulations.
They also recommend outlining the potential need or role for proctoring and call for ongoing formal professional monitoring programs to evaluate operator outcomes using local or registry data.
“From a privileging standpoint, it was important for hospitals to be equally fair, regardless of the specialty that a requesting practitioner came from,” Dr. Seto said. “In other words, treat the vascular surgeons and interventional cardiologists and radiologists equally in terms of who has the privilege to do transaxillary access.”
The SCAI position statement has been endorsed by the American College of Cardiology, the Heart Failure Society of America, the Society of Interventional Radiology, and the Vascular & Endovascular Surgery Society.
Dr. Seto reported receiving honoraria from Getinge prior to initiation of the document. Disclosures for the rest of the writing group are available with the original article.
A version of this article first appeared on Medscape.com.
The Society for Cardiovascular Angiography and Interventions (SCAI) has issued the first statement on best practices for percutaneous axillary arterial access and training.
The position statement helps fill a gap amid increasing use of transaxillary access as an alternative to the femoral route for large-bore transcatheter aortic valve replacement (TAVR), endovascular aortic repair (EVAR), and mechanical circulatory support.
“The need for alternative access has increased as we are using more and more TAVR for our elderly population, and EVAR has also increased,” writing committee chair Arnold H. Seto, MD, Long Beach VA Health Care System (California) said in an interview. “There’s also a set of patients who require balloon pumps for a prolonged period, and people were using balloon pumps from the axillary approach, which were not custom-designed for that purpose.”
He noted that the evidence base leans heavily on case reports and case series, and that they were approached for guidance by a vendor developing a balloon pump specific to axillary access. “So that helped spur all of us to get together and decide to write up something on this topic, which was developing, but was certainly picking up steam rapidly.”
The statement was published in the Journal of the Society for Cardiovascular Angiography and Interventions, and it reflects the consensus of experts in heart failure, interventional cardiology and radiology, and cardiothoracic and vascular surgery. It reviews anatomic considerations and risks for percutaneous axillary access and suggests techniques for insertion, closure, and complication management.
Although the femoral artery is the most frequent access site for percutaneous large-bore procedures, the document notes that this approach may be limited in 13%-20% of patients because of prior surgeries or severe aortoiliac and/or iliofemoral atherosclerotic disease, tortuosity, or calcification.
“Absolutely, the femoral should be the predominant access site,” Dr. Seto said. Whenever there is a compromised femoral artery, “the axillary artery, which is rarely involved with atherosclerosis, makes for the most optimal alternative access. Other forms of alternative access, including transcaval and transcarotid, are possible but have their own issues and difficulties.”
Axillary access has traditionally been done through an open surgical approach, which allows for direct puncture, primary arterial repair, or placement of a sidearm conduit. Percutaneous transaxillary access avoids a surgical incision and general anesthesia and, theoretically, reduces the risk of infection, he said. It also allows for better mobility for patients, for example, who may have a balloon pump in place for weeks or even a month when waiting for a bridge to transplant.
In terms of technique, key recommendations include:
- Gaining access preferably through the left axillary
- Inserting the needle directly through the pectoralis minor into the second segment of the axillary artery
- Using a shallow-needle angle of 25-30 degrees to improve access success and decrease sheath malformation, kinking, bleeding, or vessel perforation
- Using micropuncture needles to minimize trauma to adjacent tissues
- Abducting the patient’s arm to 45-90 degrees to reduce tortuosity
- Using angiographic and ultrasound techniques to optimize vascular access
The latter point was the one area of debate among the writing committee, Dr. Seto observed. “That is one of the controversies: Should we make ultrasound mandatory? ... Everybody agreed that it can be quite useful and was likely to be useful because of its success in every other access area,” he said. “But in the absence of randomized evidence, we couldn’t make it mandatory or a strong recommendation. We just had to make it one of several options for the operator.”
The document highlights the need for familiarity with potential axillary artery complications and their management, noting that the axillary is more fragile than the femoral artery and, thus, potentially more prone to complications during instrumentation.
Data from the ARMS study in 102 patients undergoing transaxillary access for mechanical hemodynamic support reported 17 procedural complications, including 10 minor access site bleeding events, one stroke, and one pseudoaneurysm. A small study of 25 complex EVAR procedures reported a perioperative access complication rate of 8%, including one axillary artery dissection and one stenosis.
“Despite the brachial plexus being around there, there’s actually rare reports of neurologic injury and certainly none that have been permanent,” Dr. Seto said. “Also, stroke risk is probably more related to your device size and type of device rather than the approach itself.”
A significant amount of the paper is also devoted to training and privileging suggestions with an emphasis on a multidisciplinary team. The writing group recommends graduate medical education programs develop training curricula in percutaneous axillary artery access.
Those already in practice should participate in a formal training program that focuses on axillary artery anatomy, training in large bore access and closure devices, and didactic training in imaging modalities as applied to the axillary artery. Training can occur hands-on or using online simulations.
They also recommend outlining the potential need or role for proctoring and call for ongoing formal professional monitoring programs to evaluate operator outcomes using local or registry data.
“From a privileging standpoint, it was important for hospitals to be equally fair, regardless of the specialty that a requesting practitioner came from,” Dr. Seto said. “In other words, treat the vascular surgeons and interventional cardiologists and radiologists equally in terms of who has the privilege to do transaxillary access.”
The SCAI position statement has been endorsed by the American College of Cardiology, the Heart Failure Society of America, the Society of Interventional Radiology, and the Vascular & Endovascular Surgery Society.
Dr. Seto reported receiving honoraria from Getinge prior to initiation of the document. Disclosures for the rest of the writing group are available with the original article.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE SOCIETY FOR CARDIOVASCULAR ANGIOGRAPHY AND INTERVENTIONS
FDA clears mavacamten (Camzyos) for obstructive hypertrophic cardiomyopathy
The U.S. Food and Drug Administration has approved mavacamten (Camzyos, Bristol Myers Squibb) to improve functional capacity and symptoms in adults with symptomatic New York Heart Association (NYHA) class II-III obstructive hypertrophic cardiomyopathy (oHCM).
Mavacamten is the first FDA-approved allosteric and reversible inhibitor selective for cardiac myosin that targets the underlying pathophysiology of the genetic disorder. It’s available in 2.5-mg, 5-mg, 10-mg, and 15-mg capsules.
“The approval of Camzyos represents a significant milestone for appropriate symptomatic obstructive HCM patients and their families, who have long awaited a new treatment option for this chronic and progressive disease,” Anjali T. Owens, MD, medical director of the Center for Inherited Cardiac Disease and assistant professor of medicine, University of Pennsylvania, Philadelphia, said in a news release.
‘Revolutionary’ change
The approval of mavacamten was based on data from the pivotal EXPLORER-HCM and EXPLORER-LTE (long-term extension) trial of adults with symptomatic NYHA class II-III oHCM.
In EXPLORER-HCM, treatment with mavacamten over 30 weeks led to significant improvement in exercise capacity, left ventricular outflow tract (LVOT) obstruction, NYHA functional class, and health status, as reported by this news organization.
The safety and efficacy findings seen at the end of the blinded, randomized, initial 30-week phase of EXPLORER-LTE were maintained in patients who continued treatment for a median of about 62 weeks.
Mavacamten represents “an almost revolutionary change” for the treatment of oHCM, Maya E. Guglin, MD, professor of clinical medicine and an advanced heart failure physician at Indiana University, Indianapolis, said during a press briefing earlier this month at the American College of Cardiology 2022 Scientific Session earlier this month.
“Until now, there was no good medical treatment for symptomatic oHCM. This will change the landscape, and without question it will change guidelines for treating oHCM,” Dr. Guglin said.
The product information for mavacamten includes a boxed warning citing a risk for heart failure.
Echocardiogram assessments of left ventricular ejection fraction (LVEF) are required before and during treatment.
Starting mavacamten in patients with LVEF below 55% is not recommended and the drug should be interrupted if LVEF falls below 50% at any visit or if the patient experiences heart failure symptoms or worsening clinical status.
Concomitant use of mavacamten with certain cytochrome P450 inhibitors or discontinuation of certain cytochrome P450 inducers can increase the risk for heart failure attributable to systolic dysfunction. Therefore, its use is contraindicated in patients using moderate to strong CYP2C19 inhibitors or strong CYP3A4 inhibitors, and moderate to strong CYP2C19 inducers or moderate to strong CYP3A4 inducers.
Because of the risk for heart failure attributable to systolic dysfunction, mavacamten is only available through the Camzyos Risk Evaluation and Mitigation Strategy (REMS) Program.
Full prescribing information is available online.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has approved mavacamten (Camzyos, Bristol Myers Squibb) to improve functional capacity and symptoms in adults with symptomatic New York Heart Association (NYHA) class II-III obstructive hypertrophic cardiomyopathy (oHCM).
Mavacamten is the first FDA-approved allosteric and reversible inhibitor selective for cardiac myosin that targets the underlying pathophysiology of the genetic disorder. It’s available in 2.5-mg, 5-mg, 10-mg, and 15-mg capsules.
“The approval of Camzyos represents a significant milestone for appropriate symptomatic obstructive HCM patients and their families, who have long awaited a new treatment option for this chronic and progressive disease,” Anjali T. Owens, MD, medical director of the Center for Inherited Cardiac Disease and assistant professor of medicine, University of Pennsylvania, Philadelphia, said in a news release.
‘Revolutionary’ change
The approval of mavacamten was based on data from the pivotal EXPLORER-HCM and EXPLORER-LTE (long-term extension) trial of adults with symptomatic NYHA class II-III oHCM.
In EXPLORER-HCM, treatment with mavacamten over 30 weeks led to significant improvement in exercise capacity, left ventricular outflow tract (LVOT) obstruction, NYHA functional class, and health status, as reported by this news organization.
The safety and efficacy findings seen at the end of the blinded, randomized, initial 30-week phase of EXPLORER-LTE were maintained in patients who continued treatment for a median of about 62 weeks.
Mavacamten represents “an almost revolutionary change” for the treatment of oHCM, Maya E. Guglin, MD, professor of clinical medicine and an advanced heart failure physician at Indiana University, Indianapolis, said during a press briefing earlier this month at the American College of Cardiology 2022 Scientific Session earlier this month.
“Until now, there was no good medical treatment for symptomatic oHCM. This will change the landscape, and without question it will change guidelines for treating oHCM,” Dr. Guglin said.
The product information for mavacamten includes a boxed warning citing a risk for heart failure.
Echocardiogram assessments of left ventricular ejection fraction (LVEF) are required before and during treatment.
Starting mavacamten in patients with LVEF below 55% is not recommended and the drug should be interrupted if LVEF falls below 50% at any visit or if the patient experiences heart failure symptoms or worsening clinical status.
Concomitant use of mavacamten with certain cytochrome P450 inhibitors or discontinuation of certain cytochrome P450 inducers can increase the risk for heart failure attributable to systolic dysfunction. Therefore, its use is contraindicated in patients using moderate to strong CYP2C19 inhibitors or strong CYP3A4 inhibitors, and moderate to strong CYP2C19 inducers or moderate to strong CYP3A4 inducers.
Because of the risk for heart failure attributable to systolic dysfunction, mavacamten is only available through the Camzyos Risk Evaluation and Mitigation Strategy (REMS) Program.
Full prescribing information is available online.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has approved mavacamten (Camzyos, Bristol Myers Squibb) to improve functional capacity and symptoms in adults with symptomatic New York Heart Association (NYHA) class II-III obstructive hypertrophic cardiomyopathy (oHCM).
Mavacamten is the first FDA-approved allosteric and reversible inhibitor selective for cardiac myosin that targets the underlying pathophysiology of the genetic disorder. It’s available in 2.5-mg, 5-mg, 10-mg, and 15-mg capsules.
“The approval of Camzyos represents a significant milestone for appropriate symptomatic obstructive HCM patients and their families, who have long awaited a new treatment option for this chronic and progressive disease,” Anjali T. Owens, MD, medical director of the Center for Inherited Cardiac Disease and assistant professor of medicine, University of Pennsylvania, Philadelphia, said in a news release.
‘Revolutionary’ change
The approval of mavacamten was based on data from the pivotal EXPLORER-HCM and EXPLORER-LTE (long-term extension) trial of adults with symptomatic NYHA class II-III oHCM.
In EXPLORER-HCM, treatment with mavacamten over 30 weeks led to significant improvement in exercise capacity, left ventricular outflow tract (LVOT) obstruction, NYHA functional class, and health status, as reported by this news organization.
The safety and efficacy findings seen at the end of the blinded, randomized, initial 30-week phase of EXPLORER-LTE were maintained in patients who continued treatment for a median of about 62 weeks.
Mavacamten represents “an almost revolutionary change” for the treatment of oHCM, Maya E. Guglin, MD, professor of clinical medicine and an advanced heart failure physician at Indiana University, Indianapolis, said during a press briefing earlier this month at the American College of Cardiology 2022 Scientific Session earlier this month.
“Until now, there was no good medical treatment for symptomatic oHCM. This will change the landscape, and without question it will change guidelines for treating oHCM,” Dr. Guglin said.
The product information for mavacamten includes a boxed warning citing a risk for heart failure.
Echocardiogram assessments of left ventricular ejection fraction (LVEF) are required before and during treatment.
Starting mavacamten in patients with LVEF below 55% is not recommended and the drug should be interrupted if LVEF falls below 50% at any visit or if the patient experiences heart failure symptoms or worsening clinical status.
Concomitant use of mavacamten with certain cytochrome P450 inhibitors or discontinuation of certain cytochrome P450 inducers can increase the risk for heart failure attributable to systolic dysfunction. Therefore, its use is contraindicated in patients using moderate to strong CYP2C19 inhibitors or strong CYP3A4 inhibitors, and moderate to strong CYP2C19 inducers or moderate to strong CYP3A4 inducers.
Because of the risk for heart failure attributable to systolic dysfunction, mavacamten is only available through the Camzyos Risk Evaluation and Mitigation Strategy (REMS) Program.
Full prescribing information is available online.
A version of this article first appeared on Medscape.com.
FDA warns of pump defect with Medtronic HVAD system
Patients implanted with the Medtronic HeartWare ventricular assist device (HVAD) System who develop pump thrombosis could have a welding defect in the internal pump causing the pump to malfunction, the Food and Drug Administration said in a letter to health care professionals.
Medtronic has sent providers an urgent medical device notice about the pump weld defect and is trying to identify which HVAD pumps are affected.
The Medtronic HVAD System was approved as a bridge to heart transplantation in 2012. Since then, it has been fraught with problems.
This past June, the company announced it was stopping all sales of the device and advised physicians to stop implanting it, as reported by this news organization.
Pump thrombosis
Medtronic has received complaints of suspected pump thrombosis in three patients with the HVAD System.
All three patients presented with one or more of the following signs or symptoms: grinding sound, transient power spikes on log files and high watt alarms, elevated lactate dehydrogenase, and low motor speed resulting in low perfusion or dizziness or lightheadedness.
Inspection of the returned pumps in these three cases identified a malfunction of the internal pump. The pumps were exchanged in all three patients. Two patients died after the pump exchange.
The FDA does not recommend the elective removal of properly functioning systems.
“Decisions about removing or exchanging the Medtronic HVAD System should be made by health care providers and patients on a case-by-case basis, considering the patient’s clinical status and surgical risks,” the agency advised.
Patients who present with one or more of the signs or symptoms of pump thrombosis should be first treated for pump thrombosis.
If symptoms fail to resolve, providers may consider whether the patient is a candidate for pump exchange, heart transplant, or pump explant for recovery, taking into account the patient’s clinical condition and surgical risks.
For patients with any of the signs and symptoms of pump thrombosis, logfiles from the controller should be uploaded to Medtronic.
The FDA is working with Medtronic to monitor for any adverse events related to pump weld defects and ensure patients with the HVAD implant continue to receive appropriate follow-up monitoring.
Problems related to the Medtronic HVAD System should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Patients implanted with the Medtronic HeartWare ventricular assist device (HVAD) System who develop pump thrombosis could have a welding defect in the internal pump causing the pump to malfunction, the Food and Drug Administration said in a letter to health care professionals.
Medtronic has sent providers an urgent medical device notice about the pump weld defect and is trying to identify which HVAD pumps are affected.
The Medtronic HVAD System was approved as a bridge to heart transplantation in 2012. Since then, it has been fraught with problems.
This past June, the company announced it was stopping all sales of the device and advised physicians to stop implanting it, as reported by this news organization.
Pump thrombosis
Medtronic has received complaints of suspected pump thrombosis in three patients with the HVAD System.
All three patients presented with one or more of the following signs or symptoms: grinding sound, transient power spikes on log files and high watt alarms, elevated lactate dehydrogenase, and low motor speed resulting in low perfusion or dizziness or lightheadedness.
Inspection of the returned pumps in these three cases identified a malfunction of the internal pump. The pumps were exchanged in all three patients. Two patients died after the pump exchange.
The FDA does not recommend the elective removal of properly functioning systems.
“Decisions about removing or exchanging the Medtronic HVAD System should be made by health care providers and patients on a case-by-case basis, considering the patient’s clinical status and surgical risks,” the agency advised.
Patients who present with one or more of the signs or symptoms of pump thrombosis should be first treated for pump thrombosis.
If symptoms fail to resolve, providers may consider whether the patient is a candidate for pump exchange, heart transplant, or pump explant for recovery, taking into account the patient’s clinical condition and surgical risks.
For patients with any of the signs and symptoms of pump thrombosis, logfiles from the controller should be uploaded to Medtronic.
The FDA is working with Medtronic to monitor for any adverse events related to pump weld defects and ensure patients with the HVAD implant continue to receive appropriate follow-up monitoring.
Problems related to the Medtronic HVAD System should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Patients implanted with the Medtronic HeartWare ventricular assist device (HVAD) System who develop pump thrombosis could have a welding defect in the internal pump causing the pump to malfunction, the Food and Drug Administration said in a letter to health care professionals.
Medtronic has sent providers an urgent medical device notice about the pump weld defect and is trying to identify which HVAD pumps are affected.
The Medtronic HVAD System was approved as a bridge to heart transplantation in 2012. Since then, it has been fraught with problems.
This past June, the company announced it was stopping all sales of the device and advised physicians to stop implanting it, as reported by this news organization.
Pump thrombosis
Medtronic has received complaints of suspected pump thrombosis in three patients with the HVAD System.
All three patients presented with one or more of the following signs or symptoms: grinding sound, transient power spikes on log files and high watt alarms, elevated lactate dehydrogenase, and low motor speed resulting in low perfusion or dizziness or lightheadedness.
Inspection of the returned pumps in these three cases identified a malfunction of the internal pump. The pumps were exchanged in all three patients. Two patients died after the pump exchange.
The FDA does not recommend the elective removal of properly functioning systems.
“Decisions about removing or exchanging the Medtronic HVAD System should be made by health care providers and patients on a case-by-case basis, considering the patient’s clinical status and surgical risks,” the agency advised.
Patients who present with one or more of the signs or symptoms of pump thrombosis should be first treated for pump thrombosis.
If symptoms fail to resolve, providers may consider whether the patient is a candidate for pump exchange, heart transplant, or pump explant for recovery, taking into account the patient’s clinical condition and surgical risks.
For patients with any of the signs and symptoms of pump thrombosis, logfiles from the controller should be uploaded to Medtronic.
The FDA is working with Medtronic to monitor for any adverse events related to pump weld defects and ensure patients with the HVAD implant continue to receive appropriate follow-up monitoring.
Problems related to the Medtronic HVAD System should be reported to the FDA’s MedWatch program.
A version of this article first appeared on Medscape.com.
Use of bone densitometry to grade hip OA could be boon to diagnosis, prognosis
Bone densitometry scans provide useful information that can be used to classify radiographic hip osteoarthritis more objectively than does currently used methods, UK researchers believe.
Based on detecting osteophytes using high-resolution dual energy x-ray absorptiometry (DEXA), the novel grading system they have developed showed an exponential relationship with worsening clinical outcomes such as hip pain, hospital-diagnosed OA, and total hip replacement (THR).
“Given the low radiation doses involved in DEXA, this could open up opportunities for ascertaining OA in larger population-based cohorts than those available for x-rays,” Ben G. Faber, MBBS, BSc, reported at the annual meeting of the British Society for Rheumatology during the best oral abstracts session.
This not only supports further research into OA but also means that it might be possible to use DEXA scans to help screen for hip OA and assess the risk for hip replacement in the future, added Dr. Faber, a Medical Research Council Clinical Research Fellow at the University of Bristol and rheumatology registrar for the North Bristol NHS Trust in England.
Session chair Tonia Vincent, MBBS, PhD, FRCP, a consultant rheumatologist and director of the Centre for Osteoarthritis Pathogenesis at the Kennedy Institute of Rheumatology at the University of Oxford (England), found the relationship between the DEXA findings and Kellgren and Lawrence (KL) grade and clinical outcomes to be “really striking.”
It highlights “a very important structure-symptom relationship, which people in the textbooks say doesn’t exist for osteoarthritis,” Dr. Vincent observed.
New scanners, new score
DEXA scans are a mainstay of assessing fracture risk in osteoporosis. Although originally developed for assessing bone mineral density, the newer scanners have such high resolution that they can now show radiographic features such as joint space narrowing (JSN) and the presence of osteophytes.
Both are given equal weighting in existing x-ray grading or scoring systems, which are fairly subjective, Dr. Faber said, but recent research conducted by him and his collaborators has suggested that the presence of osteophytes may be a better indicator of hip pain than JSN.
Using more than 40,000 DEXA scans obtained from the UK Biobank, Dr. Faber and associates developed a semi-automated tool that measured both JSN and osteophytes, giving greater weight to the latter. These patients with DEXA scans in the Biobank had a mean age of 63.7 years. Hip pain was present in 8.1%, hospital-diagnosed OA in 1.3%, and total hip replacement occurred in 0.6%.
The tool the researchers developed automatically calculated the minimum joint space width using a machine-learning-based approach, whereas they manually identified osteophytes at three key locations – the lateral acetabulum, the superior lateral femoral head, and the inferior medial femoral head. However, Dr. Faber said, “we’re now very close to fully automating that part of the process.”
Minimum JSN and osteophyte presence at each location was quantified using a scale of 0 (none) to 3 (greatest) to give a total score out of a possible 12; they then used this score to create five ‘grades’ from 0 (least) to 4 (most).
Applying these new radiographic hip OA grades to the Biobank DEXA scans revealed a strong and increasing association between the presences of osteophytes and the clinical outcomes considered.
For instance, when any osteophytes were detected, the odds ratios (ORs) for having hip pain for more than 3 months, a hospital diagnosis of OA, or THR were a respective 2.05, 4.98, and 6.17.
The presence of inferior or superior femoral osteophytes carried higher ORs for the three outcomes than did acetabular osteophytes, with the greatest ORs seen in patients with osteophytes at all three locations (6.95, 20.53, and 21.79, respectively). By comparison, ORs for JSN were 1.37, 3.48, and 3.91.
There were “strong progressive relationships between each grade of OA and the clinical outcomes,” Dr. Faber said, noting that “the headline figure” was that comparing people with grade 4 with grade 0, the risk for needing THR was 58 times higher. This tallies with what would be expected, Dr. Faber said, since “one would expect to see OA on imaging findings before someone had a total hip replacement.”
What might the future hold?
“One of the strengths of this study is that by using a semi-automated approach, we feel that this is a more objective measure of radiographic hip OA, which hopefully will mean that it’s more reproducible in the future when repeating in other cohorts,” Dr. Faber said.
Asked what he thought the future held, Dr. Faber responded: “A grand vision might be that you’re already doing DEXA scans to look at bone health in individuals, and from those same DEXAs you could get information on radiographic hip OA,” he hypothesized.
“We do this with BMD and we feed that into FRAX [Fracture Risk Assessment Tool] to give someone a fracture risk. Could we do the same for total hip replacement to really identify people are high risk of OA in the future?” he wondered. “Then could we intervene to potentially prevent that ... or increase the duration that they’re healthy before they require the operation? There’s still plenty of work needed to get there.”
Dr. Faber and colleagues work was recently published in Rheumatology.
Dr. Faber had no conflicts of interest to disclose. Dr. Vincent had nothing to declare; her research is funded by Versus Arthritis, the Medical Research Council, the European Research Council, FOREUM (Foundation for Research in Rheumatology), the Dunhill Trust, and the Kennedy Trust for Rheumatology Research.
Bone densitometry scans provide useful information that can be used to classify radiographic hip osteoarthritis more objectively than does currently used methods, UK researchers believe.
Based on detecting osteophytes using high-resolution dual energy x-ray absorptiometry (DEXA), the novel grading system they have developed showed an exponential relationship with worsening clinical outcomes such as hip pain, hospital-diagnosed OA, and total hip replacement (THR).
“Given the low radiation doses involved in DEXA, this could open up opportunities for ascertaining OA in larger population-based cohorts than those available for x-rays,” Ben G. Faber, MBBS, BSc, reported at the annual meeting of the British Society for Rheumatology during the best oral abstracts session.
This not only supports further research into OA but also means that it might be possible to use DEXA scans to help screen for hip OA and assess the risk for hip replacement in the future, added Dr. Faber, a Medical Research Council Clinical Research Fellow at the University of Bristol and rheumatology registrar for the North Bristol NHS Trust in England.
Session chair Tonia Vincent, MBBS, PhD, FRCP, a consultant rheumatologist and director of the Centre for Osteoarthritis Pathogenesis at the Kennedy Institute of Rheumatology at the University of Oxford (England), found the relationship between the DEXA findings and Kellgren and Lawrence (KL) grade and clinical outcomes to be “really striking.”
It highlights “a very important structure-symptom relationship, which people in the textbooks say doesn’t exist for osteoarthritis,” Dr. Vincent observed.
New scanners, new score
DEXA scans are a mainstay of assessing fracture risk in osteoporosis. Although originally developed for assessing bone mineral density, the newer scanners have such high resolution that they can now show radiographic features such as joint space narrowing (JSN) and the presence of osteophytes.
Both are given equal weighting in existing x-ray grading or scoring systems, which are fairly subjective, Dr. Faber said, but recent research conducted by him and his collaborators has suggested that the presence of osteophytes may be a better indicator of hip pain than JSN.
Using more than 40,000 DEXA scans obtained from the UK Biobank, Dr. Faber and associates developed a semi-automated tool that measured both JSN and osteophytes, giving greater weight to the latter. These patients with DEXA scans in the Biobank had a mean age of 63.7 years. Hip pain was present in 8.1%, hospital-diagnosed OA in 1.3%, and total hip replacement occurred in 0.6%.
The tool the researchers developed automatically calculated the minimum joint space width using a machine-learning-based approach, whereas they manually identified osteophytes at three key locations – the lateral acetabulum, the superior lateral femoral head, and the inferior medial femoral head. However, Dr. Faber said, “we’re now very close to fully automating that part of the process.”
Minimum JSN and osteophyte presence at each location was quantified using a scale of 0 (none) to 3 (greatest) to give a total score out of a possible 12; they then used this score to create five ‘grades’ from 0 (least) to 4 (most).
Applying these new radiographic hip OA grades to the Biobank DEXA scans revealed a strong and increasing association between the presences of osteophytes and the clinical outcomes considered.
For instance, when any osteophytes were detected, the odds ratios (ORs) for having hip pain for more than 3 months, a hospital diagnosis of OA, or THR were a respective 2.05, 4.98, and 6.17.
The presence of inferior or superior femoral osteophytes carried higher ORs for the three outcomes than did acetabular osteophytes, with the greatest ORs seen in patients with osteophytes at all three locations (6.95, 20.53, and 21.79, respectively). By comparison, ORs for JSN were 1.37, 3.48, and 3.91.
There were “strong progressive relationships between each grade of OA and the clinical outcomes,” Dr. Faber said, noting that “the headline figure” was that comparing people with grade 4 with grade 0, the risk for needing THR was 58 times higher. This tallies with what would be expected, Dr. Faber said, since “one would expect to see OA on imaging findings before someone had a total hip replacement.”
What might the future hold?
“One of the strengths of this study is that by using a semi-automated approach, we feel that this is a more objective measure of radiographic hip OA, which hopefully will mean that it’s more reproducible in the future when repeating in other cohorts,” Dr. Faber said.
Asked what he thought the future held, Dr. Faber responded: “A grand vision might be that you’re already doing DEXA scans to look at bone health in individuals, and from those same DEXAs you could get information on radiographic hip OA,” he hypothesized.
“We do this with BMD and we feed that into FRAX [Fracture Risk Assessment Tool] to give someone a fracture risk. Could we do the same for total hip replacement to really identify people are high risk of OA in the future?” he wondered. “Then could we intervene to potentially prevent that ... or increase the duration that they’re healthy before they require the operation? There’s still plenty of work needed to get there.”
Dr. Faber and colleagues work was recently published in Rheumatology.
Dr. Faber had no conflicts of interest to disclose. Dr. Vincent had nothing to declare; her research is funded by Versus Arthritis, the Medical Research Council, the European Research Council, FOREUM (Foundation for Research in Rheumatology), the Dunhill Trust, and the Kennedy Trust for Rheumatology Research.
Bone densitometry scans provide useful information that can be used to classify radiographic hip osteoarthritis more objectively than does currently used methods, UK researchers believe.
Based on detecting osteophytes using high-resolution dual energy x-ray absorptiometry (DEXA), the novel grading system they have developed showed an exponential relationship with worsening clinical outcomes such as hip pain, hospital-diagnosed OA, and total hip replacement (THR).
“Given the low radiation doses involved in DEXA, this could open up opportunities for ascertaining OA in larger population-based cohorts than those available for x-rays,” Ben G. Faber, MBBS, BSc, reported at the annual meeting of the British Society for Rheumatology during the best oral abstracts session.
This not only supports further research into OA but also means that it might be possible to use DEXA scans to help screen for hip OA and assess the risk for hip replacement in the future, added Dr. Faber, a Medical Research Council Clinical Research Fellow at the University of Bristol and rheumatology registrar for the North Bristol NHS Trust in England.
Session chair Tonia Vincent, MBBS, PhD, FRCP, a consultant rheumatologist and director of the Centre for Osteoarthritis Pathogenesis at the Kennedy Institute of Rheumatology at the University of Oxford (England), found the relationship between the DEXA findings and Kellgren and Lawrence (KL) grade and clinical outcomes to be “really striking.”
It highlights “a very important structure-symptom relationship, which people in the textbooks say doesn’t exist for osteoarthritis,” Dr. Vincent observed.
New scanners, new score
DEXA scans are a mainstay of assessing fracture risk in osteoporosis. Although originally developed for assessing bone mineral density, the newer scanners have such high resolution that they can now show radiographic features such as joint space narrowing (JSN) and the presence of osteophytes.
Both are given equal weighting in existing x-ray grading or scoring systems, which are fairly subjective, Dr. Faber said, but recent research conducted by him and his collaborators has suggested that the presence of osteophytes may be a better indicator of hip pain than JSN.
Using more than 40,000 DEXA scans obtained from the UK Biobank, Dr. Faber and associates developed a semi-automated tool that measured both JSN and osteophytes, giving greater weight to the latter. These patients with DEXA scans in the Biobank had a mean age of 63.7 years. Hip pain was present in 8.1%, hospital-diagnosed OA in 1.3%, and total hip replacement occurred in 0.6%.
The tool the researchers developed automatically calculated the minimum joint space width using a machine-learning-based approach, whereas they manually identified osteophytes at three key locations – the lateral acetabulum, the superior lateral femoral head, and the inferior medial femoral head. However, Dr. Faber said, “we’re now very close to fully automating that part of the process.”
Minimum JSN and osteophyte presence at each location was quantified using a scale of 0 (none) to 3 (greatest) to give a total score out of a possible 12; they then used this score to create five ‘grades’ from 0 (least) to 4 (most).
Applying these new radiographic hip OA grades to the Biobank DEXA scans revealed a strong and increasing association between the presences of osteophytes and the clinical outcomes considered.
For instance, when any osteophytes were detected, the odds ratios (ORs) for having hip pain for more than 3 months, a hospital diagnosis of OA, or THR were a respective 2.05, 4.98, and 6.17.
The presence of inferior or superior femoral osteophytes carried higher ORs for the three outcomes than did acetabular osteophytes, with the greatest ORs seen in patients with osteophytes at all three locations (6.95, 20.53, and 21.79, respectively). By comparison, ORs for JSN were 1.37, 3.48, and 3.91.
There were “strong progressive relationships between each grade of OA and the clinical outcomes,” Dr. Faber said, noting that “the headline figure” was that comparing people with grade 4 with grade 0, the risk for needing THR was 58 times higher. This tallies with what would be expected, Dr. Faber said, since “one would expect to see OA on imaging findings before someone had a total hip replacement.”
What might the future hold?
“One of the strengths of this study is that by using a semi-automated approach, we feel that this is a more objective measure of radiographic hip OA, which hopefully will mean that it’s more reproducible in the future when repeating in other cohorts,” Dr. Faber said.
Asked what he thought the future held, Dr. Faber responded: “A grand vision might be that you’re already doing DEXA scans to look at bone health in individuals, and from those same DEXAs you could get information on radiographic hip OA,” he hypothesized.
“We do this with BMD and we feed that into FRAX [Fracture Risk Assessment Tool] to give someone a fracture risk. Could we do the same for total hip replacement to really identify people are high risk of OA in the future?” he wondered. “Then could we intervene to potentially prevent that ... or increase the duration that they’re healthy before they require the operation? There’s still plenty of work needed to get there.”
Dr. Faber and colleagues work was recently published in Rheumatology.
Dr. Faber had no conflicts of interest to disclose. Dr. Vincent had nothing to declare; her research is funded by Versus Arthritis, the Medical Research Council, the European Research Council, FOREUM (Foundation for Research in Rheumatology), the Dunhill Trust, and the Kennedy Trust for Rheumatology Research.
FROM BSR 2022