User login
What's your diagnosis?
Pancreatic adenocarcinoma arising from main duct intraductal papillary mucinous neoplasm with inadvertent main pancreatic duct stenting.
The FNA was positive for carcinoma with abundant mucin, which, taken together with the imaging findings, was indicative of pancreatic adenocarcinoma arising from main duct intraductal papillary mucinous neoplasm (M-IPMN).
The post-endoscopic retrograde cholangiopancreatography (ERCP) CT revealed inadvertent placement of the fully covered self-expanding metallic stent (fcSEMS) within the main pancreatic duct (MPD) stricture and persistent common bile duct (CBD) obstruction. On post hoc review of the fluoroscopic and cross-sectional imaging, it became evident that the massively dilated MPD was mistaken during ERCP for the CBD and left hepatic duct (Figure F). In addition, the patient also had several cysts within the liver (compatible with incidental polycystic liver disease), which further complicated real-time image interpretation.
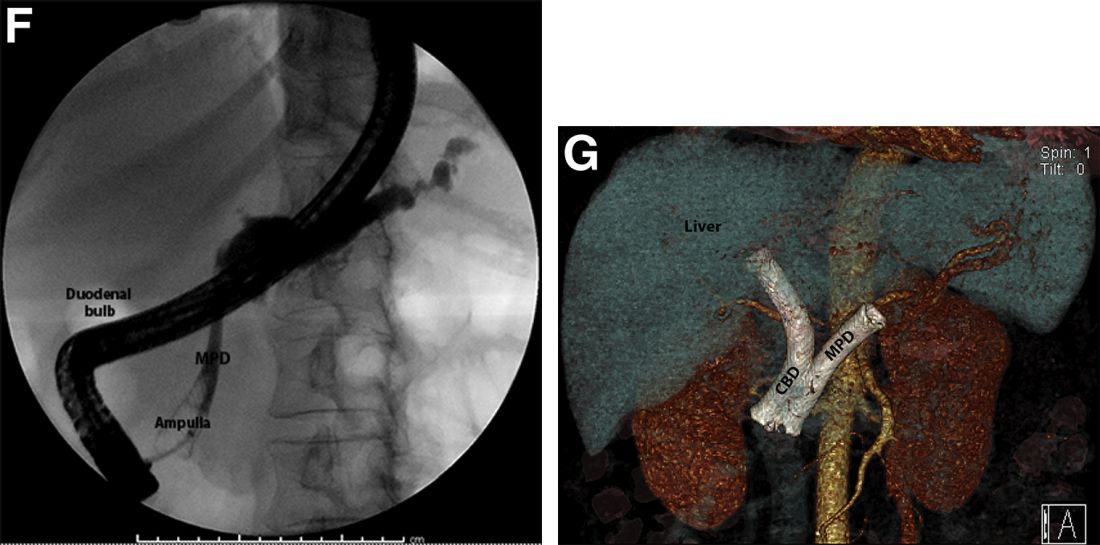
Based on multidisciplinary discussion, the precedent of a prior series of successful palliative MPD stenting in the setting of adenocarcinoma,1 and the notable improvement in the patient's steatorrhea and abdominal pain, the initially placed fcSEMS was left in situ across the MPD stricture, and a second fcSEMS was successfully deployed across the CBD stricture (Figure G), resulting in prompt improvement in serum liver tests. The patient was thereafter initiated on palliative chemotherapy with gemcitabine and abraxane and has maintained clinically stable disease for the last 9 months.
M-IPMN is a premalignant condition in which endoscopy plays an important role. In our patient, because of anatomic and morphologic abnormalities, including the massive dilation of the MPD and severe distal biliary compression in the context of an obstructing pancreatic head mass arising from M-IPMN, initial deployment of the fcSEMS occurred unwittingly into the MPD. Little is known about the impact of fcSEMS in the MPD in patients with pancreatic adenocarcinoma, although in select cases, alleviation of pain caused by MPD obstruction and improvement in quality of life have been reported.2,3 In the case of our patient, fcSEMS placement in the MPD indeed led to symptomatic relief as manifested by a decrease in both diarrhea and pain and an increase in appetite; the addition of a fcSEMS in the CBD led to serum liver test normalization and permitted the initiation of chemotherapy. Further studies are needed to examine the outcomes of palliative MPD stenting in patients with obstructing pancreatic malignancies as well as the epidemiology and biology of M-IPMN and associated pancreatic adenocarcinoma in minority populations.
References
1. Tham TC et al. Am J Gastroenterol. 2000 Apr;95(4):956-60.
2. Grimm IS, Baron TH. Gastroenterology. 2015 Jul;149(1):20-2.
3. Wehrmann T et al. Eur J Gastroenterol Hepatol. 2005 Dec;17(12):1395-400.
Pancreatic adenocarcinoma arising from main duct intraductal papillary mucinous neoplasm with inadvertent main pancreatic duct stenting.
The FNA was positive for carcinoma with abundant mucin, which, taken together with the imaging findings, was indicative of pancreatic adenocarcinoma arising from main duct intraductal papillary mucinous neoplasm (M-IPMN).
The post-endoscopic retrograde cholangiopancreatography (ERCP) CT revealed inadvertent placement of the fully covered self-expanding metallic stent (fcSEMS) within the main pancreatic duct (MPD) stricture and persistent common bile duct (CBD) obstruction. On post hoc review of the fluoroscopic and cross-sectional imaging, it became evident that the massively dilated MPD was mistaken during ERCP for the CBD and left hepatic duct (Figure F). In addition, the patient also had several cysts within the liver (compatible with incidental polycystic liver disease), which further complicated real-time image interpretation.
Based on multidisciplinary discussion, the precedent of a prior series of successful palliative MPD stenting in the setting of adenocarcinoma,1 and the notable improvement in the patient's steatorrhea and abdominal pain, the initially placed fcSEMS was left in situ across the MPD stricture, and a second fcSEMS was successfully deployed across the CBD stricture (Figure G), resulting in prompt improvement in serum liver tests. The patient was thereafter initiated on palliative chemotherapy with gemcitabine and abraxane and has maintained clinically stable disease for the last 9 months.
M-IPMN is a premalignant condition in which endoscopy plays an important role. In our patient, because of anatomic and morphologic abnormalities, including the massive dilation of the MPD and severe distal biliary compression in the context of an obstructing pancreatic head mass arising from M-IPMN, initial deployment of the fcSEMS occurred unwittingly into the MPD. Little is known about the impact of fcSEMS in the MPD in patients with pancreatic adenocarcinoma, although in select cases, alleviation of pain caused by MPD obstruction and improvement in quality of life have been reported.2,3 In the case of our patient, fcSEMS placement in the MPD indeed led to symptomatic relief as manifested by a decrease in both diarrhea and pain and an increase in appetite; the addition of a fcSEMS in the CBD led to serum liver test normalization and permitted the initiation of chemotherapy. Further studies are needed to examine the outcomes of palliative MPD stenting in patients with obstructing pancreatic malignancies as well as the epidemiology and biology of M-IPMN and associated pancreatic adenocarcinoma in minority populations.
References
1. Tham TC et al. Am J Gastroenterol. 2000 Apr;95(4):956-60.
2. Grimm IS, Baron TH. Gastroenterology. 2015 Jul;149(1):20-2.
3. Wehrmann T et al. Eur J Gastroenterol Hepatol. 2005 Dec;17(12):1395-400.
Pancreatic adenocarcinoma arising from main duct intraductal papillary mucinous neoplasm with inadvertent main pancreatic duct stenting.
The FNA was positive for carcinoma with abundant mucin, which, taken together with the imaging findings, was indicative of pancreatic adenocarcinoma arising from main duct intraductal papillary mucinous neoplasm (M-IPMN).
The post-endoscopic retrograde cholangiopancreatography (ERCP) CT revealed inadvertent placement of the fully covered self-expanding metallic stent (fcSEMS) within the main pancreatic duct (MPD) stricture and persistent common bile duct (CBD) obstruction. On post hoc review of the fluoroscopic and cross-sectional imaging, it became evident that the massively dilated MPD was mistaken during ERCP for the CBD and left hepatic duct (Figure F). In addition, the patient also had several cysts within the liver (compatible with incidental polycystic liver disease), which further complicated real-time image interpretation.
Based on multidisciplinary discussion, the precedent of a prior series of successful palliative MPD stenting in the setting of adenocarcinoma,1 and the notable improvement in the patient's steatorrhea and abdominal pain, the initially placed fcSEMS was left in situ across the MPD stricture, and a second fcSEMS was successfully deployed across the CBD stricture (Figure G), resulting in prompt improvement in serum liver tests. The patient was thereafter initiated on palliative chemotherapy with gemcitabine and abraxane and has maintained clinically stable disease for the last 9 months.
M-IPMN is a premalignant condition in which endoscopy plays an important role. In our patient, because of anatomic and morphologic abnormalities, including the massive dilation of the MPD and severe distal biliary compression in the context of an obstructing pancreatic head mass arising from M-IPMN, initial deployment of the fcSEMS occurred unwittingly into the MPD. Little is known about the impact of fcSEMS in the MPD in patients with pancreatic adenocarcinoma, although in select cases, alleviation of pain caused by MPD obstruction and improvement in quality of life have been reported.2,3 In the case of our patient, fcSEMS placement in the MPD indeed led to symptomatic relief as manifested by a decrease in both diarrhea and pain and an increase in appetite; the addition of a fcSEMS in the CBD led to serum liver test normalization and permitted the initiation of chemotherapy. Further studies are needed to examine the outcomes of palliative MPD stenting in patients with obstructing pancreatic malignancies as well as the epidemiology and biology of M-IPMN and associated pancreatic adenocarcinoma in minority populations.
References
1. Tham TC et al. Am J Gastroenterol. 2000 Apr;95(4):956-60.
2. Grimm IS, Baron TH. Gastroenterology. 2015 Jul;149(1):20-2.
3. Wehrmann T et al. Eur J Gastroenterol Hepatol. 2005 Dec;17(12):1395-400.
A 69-year-old Filipino American woman presented with increasing epigastralgia, worsening appetite, jaundice, and oily diarrhea over the course of 3 months. Her past medical history consisted of diabetes, hypertension, hyperlipidemia, and osteopenia being managed with metformin, losartan, and atorvastatin, respectively.
Physical examination revealed she was thin (body mass index, 22 kg/m2) and jaundiced with moderate tenderness to epigastric palpation and 1+ peripheral pitting edema. Laboratory tests were significant for normal complete blood count and elevated alanine aminotransferase (113 U/L), alkaline phosphatase (235 U/L), bilirubin (7.3 mg/dL), international normalized ratio (1.3), and carbohydrate antigen 19-9 (7886 U/L). A CT scan of the abdomen revealed severe extrahepatic and intrahepatic ductal dilation, with a common bile duct (CBD) and main pancreatic duct (MPD) diameter of 2.5 and 1.7 cm, respectively, as well an infiltrating, malignant-appearing, 4.5-cm spheroid mass in the head of the pancreas (Figure A). The mass involved the superior mesenteric vein at the portal confluence and encased >50% of the superior mesenteric artery.

To further characterize these findings, magnetic resonance cholangiopancreatography was performed, which additionally revealed multifocal cysts throughout the liver ranging from 0.5 to 5.0 cm in greatest diameter, as seen on maximal intensity projection algorithm (Figure B).
The patient was referred for same-session endoscopic ultrasound examination with fine needle aspiration (FNA) and endoscopic retrograde cholangiopancreatography (ERCP) for further diagnosis and treatment. Endoscopic ultrasound demonstrated a large, hypoechoic mass in the pancreatic head with severe CBD and MPD dilation proximally, corresponding with the cross-sectional imaging findings; FNA was performed. ERCP demonstrated a long, distal CBD stricture and what appeared to be nonopacification of the right hepatic ductal system; a 10 × 60-mm fully covered self-expanding metallic stent (fcSEMS) was placed across the stricture (Figure C, D). Over the subsequent 3 days, the patient's diarrhea resolved and epigastralgia improved; however, serum liver tests did not downtrend, thus prompting repeat imaging (Figure E).
Based on the patient's clinical history, cross-sectional imaging findings, and only partial response to therapeutic ERCP, what are the patient's likely diagnoses?
Commentary: Looking at Therapies for Patients With HER2-low Breast Cancer, August 2022

DESTINY-Breast04 is the first randomized clinical trial to show that targeting HER2 provides clinically meaningful benefit for patients with HER2-low metastatic breast cancer. This phase 3 study by Modi and colleagues enrolled 557 patients with hormone receptor (HR)–negative or HR-positive breast cancer and centrally confirmed HER2 low expression in those who had been previously treated with one or two prior lines of chemotherapy for metastatic breast cancer. Patients with HR-positive breast cancer were required to have endocrine therapy–refractory disease. Patients were randomized in a 2:1 ratio to receive either an antibody-drug conjugate, trastuzumab deruxtecan (T-DXd), or the physician's choice of standard chemotherapy (capecitabine, eribulin, gemcitabine, paclitaxel, or nanoparticle albumin–bound paclitaxel [nab-paclitaxel]). Among all 557 patients, T-DXd improved median progression-free survival (PFS) by 4.8 months (9.9 vs 5.1 months; hazard ratio [HR] 0.50; P < .001) and median overall survival (OS) by 6.6 months (23.4 vs 16.8 months; HR 0.64; P = .0010) compared with standard single-agent chemotherapy. Among the 494 (88.7%) HR-positive patients, the median PFS was 10.1 months in the T-DXd group and 5.4 months in the chemotherapy group (HR 0.51; P < .001). Median OS was 23.9 months and 17.5 months, respectively (HR 0.64; P = .003). The rates of grade 3 or higher adverse events were lower with T-DXd than with standard chemotherapy (52.6% vs 67.4%, respectively), although higher rates of drug-related interstitial lung disease or pneumonitis were noted in the T-DXd arm (12.1% vs 0.1%). Lung toxicity continues to be an important safety concern with T-DXd. These practice-changing results open the door to a new treatment option for a substantial group of patients with HER2-low disease and support the need to reclassify HER2-low as a new targetable subset of breast cancer, distinct from HER-negative (HER2-0), and to acquire an understanding of the clinical characteristics of and prognosis for these patients.
Tarantino and colleagues evaluated the biologic and prognostic significance of HER2-low expression in breast cancer and investigated the association between HR status and HER2-low expression. Among 5235 patients with HER2-0 invasive breast cancer, HR expression was significantly more common among HER2-low tumors than among HER2-0 tumors (90.6% vs 81.8%; P < .001). The rate of HER2-low tumors increased progressively as estrogen receptor (ER) expression increased (40.1% of ER-negative, 46.3% of ER-low, 55.2% of ER-moderate, 57.8% of ER-high, and 62.1% of ER-very high [ie, ER > 95%] tumors; P < .001). Among 675 patients receiving neoadjuvant chemotherapy, higher pathologic complete response (pCR) rates were seen among those with HER2-0 tumors (26.8% vs 16.6%; P = .002), although no statistically significant differences in pCR rates were noted between HER2-low and HER2-0 tumors when analyzed by HR and ER status. In contrast to the findings of Modi and colleagues, this analysis saw no prognostic significance in terms of survival outcomes for HER2-low expression among patients who had HR-positive or HER2-0 tumors, suggesting that HER2-low breast cancer may not be a distinct biologic subtype. Further studies are needed to clarify whether HER2-low breast cancer needs to be considered separately in practice.
Immunotherapy, particular checkpoint inhibitors, has revolutionized the treatment of many solid tumors. However, their role in HER2-positive breast cancer remains unclear. IMpassion050 is a double-blind, randomized, phase 3 study evaluating the efficacy and safety of adding atezolizumab, an anti–programmed death-ligand 1 (PD-L1) antibody, to neoadjuvant standard of care (chemotherapy + pertuzumab + trastuzumab [PH]) for high-risk, HER2-positive early breast cancer (EBC). In the study by Huober and colleagues, 454 patients with a primary tumor > 2 cm and histologically confirmed positive lymph node status (N1-3) were randomly assigned in a 1:1 ratio to the atezolizumab or placebo group with dose-dense doxorubicin or cyclophosphamide, followed by paclitaxel and PH. In the adjuvant setting, patients continued atezolizumab or placebo and PH to complete 1 year of HER2-targeted therapy; those with residual disease could switch to trastuzumab emtansine with atezolizumab or placebo. At clinical cutoff (February 5, 2021), rates of pCR in the atezolizumab group vs placebo group were similar among all patients in the study (62.4% vs 62.7%; P = .9551) and in the PD-L1–positive population (64.2% vs 72.5%; P = .1846). Treatment-related grade 3-4 adverse events occurred more frequently in the atezolizumab group compared with the placebo group, both during the neoadjuvant treatment phase (47.3% vs 42.2%) and the adjuvant treatment phase (13.4% vs 9.8%).
In summary, the phase 3 IMpassion050 trial showed no significant improvement in pCR with the addition of atezolizumab to neoadjuvant therapy in patients with high-risk, HER2-positive EBC, including those with PD-L1–positive tumors. At this time, PH and chemotherapy remain the standard of care in this patient population. Longer follow-up is needed in respect to the long-term effect of atezolizumab in this setting.
DESTINY-Breast04 is the first randomized clinical trial to show that targeting HER2 provides clinically meaningful benefit for patients with HER2-low metastatic breast cancer. This phase 3 study by Modi and colleagues enrolled 557 patients with hormone receptor (HR)–negative or HR-positive breast cancer and centrally confirmed HER2 low expression in those who had been previously treated with one or two prior lines of chemotherapy for metastatic breast cancer. Patients with HR-positive breast cancer were required to have endocrine therapy–refractory disease. Patients were randomized in a 2:1 ratio to receive either an antibody-drug conjugate, trastuzumab deruxtecan (T-DXd), or the physician's choice of standard chemotherapy (capecitabine, eribulin, gemcitabine, paclitaxel, or nanoparticle albumin–bound paclitaxel [nab-paclitaxel]). Among all 557 patients, T-DXd improved median progression-free survival (PFS) by 4.8 months (9.9 vs 5.1 months; hazard ratio [HR] 0.50; P < .001) and median overall survival (OS) by 6.6 months (23.4 vs 16.8 months; HR 0.64; P = .0010) compared with standard single-agent chemotherapy. Among the 494 (88.7%) HR-positive patients, the median PFS was 10.1 months in the T-DXd group and 5.4 months in the chemotherapy group (HR 0.51; P < .001). Median OS was 23.9 months and 17.5 months, respectively (HR 0.64; P = .003). The rates of grade 3 or higher adverse events were lower with T-DXd than with standard chemotherapy (52.6% vs 67.4%, respectively), although higher rates of drug-related interstitial lung disease or pneumonitis were noted in the T-DXd arm (12.1% vs 0.1%). Lung toxicity continues to be an important safety concern with T-DXd. These practice-changing results open the door to a new treatment option for a substantial group of patients with HER2-low disease and support the need to reclassify HER2-low as a new targetable subset of breast cancer, distinct from HER-negative (HER2-0), and to acquire an understanding of the clinical characteristics of and prognosis for these patients.
Tarantino and colleagues evaluated the biologic and prognostic significance of HER2-low expression in breast cancer and investigated the association between HR status and HER2-low expression. Among 5235 patients with HER2-0 invasive breast cancer, HR expression was significantly more common among HER2-low tumors than among HER2-0 tumors (90.6% vs 81.8%; P < .001). The rate of HER2-low tumors increased progressively as estrogen receptor (ER) expression increased (40.1% of ER-negative, 46.3% of ER-low, 55.2% of ER-moderate, 57.8% of ER-high, and 62.1% of ER-very high [ie, ER > 95%] tumors; P < .001). Among 675 patients receiving neoadjuvant chemotherapy, higher pathologic complete response (pCR) rates were seen among those with HER2-0 tumors (26.8% vs 16.6%; P = .002), although no statistically significant differences in pCR rates were noted between HER2-low and HER2-0 tumors when analyzed by HR and ER status. In contrast to the findings of Modi and colleagues, this analysis saw no prognostic significance in terms of survival outcomes for HER2-low expression among patients who had HR-positive or HER2-0 tumors, suggesting that HER2-low breast cancer may not be a distinct biologic subtype. Further studies are needed to clarify whether HER2-low breast cancer needs to be considered separately in practice.
Immunotherapy, particular checkpoint inhibitors, has revolutionized the treatment of many solid tumors. However, their role in HER2-positive breast cancer remains unclear. IMpassion050 is a double-blind, randomized, phase 3 study evaluating the efficacy and safety of adding atezolizumab, an anti–programmed death-ligand 1 (PD-L1) antibody, to neoadjuvant standard of care (chemotherapy + pertuzumab + trastuzumab [PH]) for high-risk, HER2-positive early breast cancer (EBC). In the study by Huober and colleagues, 454 patients with a primary tumor > 2 cm and histologically confirmed positive lymph node status (N1-3) were randomly assigned in a 1:1 ratio to the atezolizumab or placebo group with dose-dense doxorubicin or cyclophosphamide, followed by paclitaxel and PH. In the adjuvant setting, patients continued atezolizumab or placebo and PH to complete 1 year of HER2-targeted therapy; those with residual disease could switch to trastuzumab emtansine with atezolizumab or placebo. At clinical cutoff (February 5, 2021), rates of pCR in the atezolizumab group vs placebo group were similar among all patients in the study (62.4% vs 62.7%; P = .9551) and in the PD-L1–positive population (64.2% vs 72.5%; P = .1846). Treatment-related grade 3-4 adverse events occurred more frequently in the atezolizumab group compared with the placebo group, both during the neoadjuvant treatment phase (47.3% vs 42.2%) and the adjuvant treatment phase (13.4% vs 9.8%).
In summary, the phase 3 IMpassion050 trial showed no significant improvement in pCR with the addition of atezolizumab to neoadjuvant therapy in patients with high-risk, HER2-positive EBC, including those with PD-L1–positive tumors. At this time, PH and chemotherapy remain the standard of care in this patient population. Longer follow-up is needed in respect to the long-term effect of atezolizumab in this setting.
DESTINY-Breast04 is the first randomized clinical trial to show that targeting HER2 provides clinically meaningful benefit for patients with HER2-low metastatic breast cancer. This phase 3 study by Modi and colleagues enrolled 557 patients with hormone receptor (HR)–negative or HR-positive breast cancer and centrally confirmed HER2 low expression in those who had been previously treated with one or two prior lines of chemotherapy for metastatic breast cancer. Patients with HR-positive breast cancer were required to have endocrine therapy–refractory disease. Patients were randomized in a 2:1 ratio to receive either an antibody-drug conjugate, trastuzumab deruxtecan (T-DXd), or the physician's choice of standard chemotherapy (capecitabine, eribulin, gemcitabine, paclitaxel, or nanoparticle albumin–bound paclitaxel [nab-paclitaxel]). Among all 557 patients, T-DXd improved median progression-free survival (PFS) by 4.8 months (9.9 vs 5.1 months; hazard ratio [HR] 0.50; P < .001) and median overall survival (OS) by 6.6 months (23.4 vs 16.8 months; HR 0.64; P = .0010) compared with standard single-agent chemotherapy. Among the 494 (88.7%) HR-positive patients, the median PFS was 10.1 months in the T-DXd group and 5.4 months in the chemotherapy group (HR 0.51; P < .001). Median OS was 23.9 months and 17.5 months, respectively (HR 0.64; P = .003). The rates of grade 3 or higher adverse events were lower with T-DXd than with standard chemotherapy (52.6% vs 67.4%, respectively), although higher rates of drug-related interstitial lung disease or pneumonitis were noted in the T-DXd arm (12.1% vs 0.1%). Lung toxicity continues to be an important safety concern with T-DXd. These practice-changing results open the door to a new treatment option for a substantial group of patients with HER2-low disease and support the need to reclassify HER2-low as a new targetable subset of breast cancer, distinct from HER-negative (HER2-0), and to acquire an understanding of the clinical characteristics of and prognosis for these patients.
Tarantino and colleagues evaluated the biologic and prognostic significance of HER2-low expression in breast cancer and investigated the association between HR status and HER2-low expression. Among 5235 patients with HER2-0 invasive breast cancer, HR expression was significantly more common among HER2-low tumors than among HER2-0 tumors (90.6% vs 81.8%; P < .001). The rate of HER2-low tumors increased progressively as estrogen receptor (ER) expression increased (40.1% of ER-negative, 46.3% of ER-low, 55.2% of ER-moderate, 57.8% of ER-high, and 62.1% of ER-very high [ie, ER > 95%] tumors; P < .001). Among 675 patients receiving neoadjuvant chemotherapy, higher pathologic complete response (pCR) rates were seen among those with HER2-0 tumors (26.8% vs 16.6%; P = .002), although no statistically significant differences in pCR rates were noted between HER2-low and HER2-0 tumors when analyzed by HR and ER status. In contrast to the findings of Modi and colleagues, this analysis saw no prognostic significance in terms of survival outcomes for HER2-low expression among patients who had HR-positive or HER2-0 tumors, suggesting that HER2-low breast cancer may not be a distinct biologic subtype. Further studies are needed to clarify whether HER2-low breast cancer needs to be considered separately in practice.
Immunotherapy, particular checkpoint inhibitors, has revolutionized the treatment of many solid tumors. However, their role in HER2-positive breast cancer remains unclear. IMpassion050 is a double-blind, randomized, phase 3 study evaluating the efficacy and safety of adding atezolizumab, an anti–programmed death-ligand 1 (PD-L1) antibody, to neoadjuvant standard of care (chemotherapy + pertuzumab + trastuzumab [PH]) for high-risk, HER2-positive early breast cancer (EBC). In the study by Huober and colleagues, 454 patients with a primary tumor > 2 cm and histologically confirmed positive lymph node status (N1-3) were randomly assigned in a 1:1 ratio to the atezolizumab or placebo group with dose-dense doxorubicin or cyclophosphamide, followed by paclitaxel and PH. In the adjuvant setting, patients continued atezolizumab or placebo and PH to complete 1 year of HER2-targeted therapy; those with residual disease could switch to trastuzumab emtansine with atezolizumab or placebo. At clinical cutoff (February 5, 2021), rates of pCR in the atezolizumab group vs placebo group were similar among all patients in the study (62.4% vs 62.7%; P = .9551) and in the PD-L1–positive population (64.2% vs 72.5%; P = .1846). Treatment-related grade 3-4 adverse events occurred more frequently in the atezolizumab group compared with the placebo group, both during the neoadjuvant treatment phase (47.3% vs 42.2%) and the adjuvant treatment phase (13.4% vs 9.8%).
In summary, the phase 3 IMpassion050 trial showed no significant improvement in pCR with the addition of atezolizumab to neoadjuvant therapy in patients with high-risk, HER2-positive EBC, including those with PD-L1–positive tumors. At this time, PH and chemotherapy remain the standard of care in this patient population. Longer follow-up is needed in respect to the long-term effect of atezolizumab in this setting.
Aesthetics abound for the aging face
At the MedscapeLive’s Women’s and Pediatric Dermatology Seminar, Jacqueline Watchmaker, MD, a dermatologist in Scottsdale, Ariz., provided an overview of current options, along with advice on how to keep patients’ expectations realistic and how to properly choose the best candidates for the best procedures.
“One of the most common concerns patients come to me with are wrinkles on the upper face,” but this is far from their only concern, Dr. Watchmaker said. Wrinkles and sagging of the lower face, areas under the eyes, nasolabial folds, marionette lines, and the neck also draw concern. Uneven coloration is another common concern, she said.
“So, what can we do for all of this?” she asked. The options are plentiful. Wrinkles of the upper face are easy to address with neuromodulators, she said, and soft-tissue fillers help the jawline and cheek areas.
“For the lower face, skin tightening devices really shine,” she added. And lasers can help correct uneven coloration. Surgery, of course, can also produce good results, but many patients want to stick with noninvasive or minimally invasive procedures.
Case: 83-year-old woman
Dr. Watchmaker discussed an 83-year old patient, who had malar mounds and accentuation of the infraorbital hollowness resulting from changes in subcutaneous fat and ligament laxity. She also had uneven coloration from photo damage, wrinkles on the upper face, linear appearance of zygoma related to underlying bony changes and fat compartment descent, and nasolabial folds and jowls related to decreased bony compartments, ligament laxity, and shifting of fat. She was naive to any cosmetic procedure.
Despite her age, this patient had no wrinkling on the upper forehead. Dr. Watchmaker did not inject neuromodulator in the upper forehead, as this patient also had a slightly heavy eyelid. “If you inject too much, it can cause some drooping of the eyelid and eyebrow,” she said.
For filler, she used a combination of high G (firmness, support) hyaluronic acid filler, a medium G acid filler, and a low G filler. The result: The woman’s face became more balanced, the mid-face volumization lifted the lower face, and the glabellar and periocular lines were softer, although still present. “It’s important to counsel patients that neuromodulators won’t make the lines go away the first time, but they will be softened.”
Practice tips
It’s important to titrate neuromodulators to fit the patient, Dr. Watchmaker said. Ask: What are their goals: Reversal of static lines? Softening wrinkles? Maintaining current status? “There’s not one dosing regimen,” and both dosing and frequency of neuromodulators can be titrated to fit each patient’s aesthetic goals, she said. For older patients who want to soften or maintain appearance, she suggested treatment every 4-6 months. And some patients just want to maintain the status quo, she noted.
Ideal candidates
For neuromodulators and fillers, who is an ideal candidate? “I think it’s anyone who has realistic expectations,” she said. Patients need to know how many treatments are needed and how much it will cost. For patients with extensive wrinkling and sagging, she said, she does extensive counseling about what results to expect “because I don’t want them to feel like they wasted their time or their money.”
She also suggests a surgical consult, as some may opt for that route after learning about the options and expected results.
Skin tightening
Both radiofrequency and microfocused ultrasound are noninvasive and additional options. Radiofrequency uses radio waves, with electromagnetic energy to stimulate heat. Ultrasound uses ultrasound waves to stimulate heat. Both approaches cause collagen contraction, neocollagenesis, and skin tightening.
These procedures do well for the lower face, Dr. Watchmaker said, but “I am relatively unimpressed for how well they do for the upper face.” Ideal candidates have mild to moderate skin laxity and want to avoid surgery. She also tells patients that collagen isn’t made overnight. “You won’t see much for 3-6 months after.” The good news? Usually the treatments need to be repeated only every 1.5-2 years, she said.
Lasers
“There are so many lasers out there,” said Dr. Watchmaker, who groups them into three categories: those used for wrinkles, dyschromia, and erythema. Her picks: ablative lasers (CO2 and erbium) and erbium-doped YAG 1550 nm laser for rhytids. Thulium 1927 and QS and picosecond lasers are her picks for dyschromia, and for erythema, pulsed dye and KTP lasers.
Some laser treatments are not a “walk in the park,” as she warns patients. For example, after treatment with ablative lasers, there is pain, post-procedure redness, and crusting.
Take-home points
A combination of noninvasive and minimally invasive procedures can produce appearance-improving results. That’s more likely if dermatologists choose ideal candidates, personalize the treatment, and set realistic expectations. “We have a finite number of tools,” she said, but they can be used in a variety of ways.
At the interactive panel discussion following her presentation, Dr. Watchmaker was asked what she tells patients about sun protection. “I talk a lot about sunscreens,’’ she said, always urging patients to use them. While the options for rejuvenation are numerous, taking care of the skin is still crucial.
Dr. Watchmaker had no disclosures. MedscapeLive and this news organization are owned by the same parent company.
At the MedscapeLive’s Women’s and Pediatric Dermatology Seminar, Jacqueline Watchmaker, MD, a dermatologist in Scottsdale, Ariz., provided an overview of current options, along with advice on how to keep patients’ expectations realistic and how to properly choose the best candidates for the best procedures.
“One of the most common concerns patients come to me with are wrinkles on the upper face,” but this is far from their only concern, Dr. Watchmaker said. Wrinkles and sagging of the lower face, areas under the eyes, nasolabial folds, marionette lines, and the neck also draw concern. Uneven coloration is another common concern, she said.
“So, what can we do for all of this?” she asked. The options are plentiful. Wrinkles of the upper face are easy to address with neuromodulators, she said, and soft-tissue fillers help the jawline and cheek areas.
“For the lower face, skin tightening devices really shine,” she added. And lasers can help correct uneven coloration. Surgery, of course, can also produce good results, but many patients want to stick with noninvasive or minimally invasive procedures.
Case: 83-year-old woman
Dr. Watchmaker discussed an 83-year old patient, who had malar mounds and accentuation of the infraorbital hollowness resulting from changes in subcutaneous fat and ligament laxity. She also had uneven coloration from photo damage, wrinkles on the upper face, linear appearance of zygoma related to underlying bony changes and fat compartment descent, and nasolabial folds and jowls related to decreased bony compartments, ligament laxity, and shifting of fat. She was naive to any cosmetic procedure.
Despite her age, this patient had no wrinkling on the upper forehead. Dr. Watchmaker did not inject neuromodulator in the upper forehead, as this patient also had a slightly heavy eyelid. “If you inject too much, it can cause some drooping of the eyelid and eyebrow,” she said.
For filler, she used a combination of high G (firmness, support) hyaluronic acid filler, a medium G acid filler, and a low G filler. The result: The woman’s face became more balanced, the mid-face volumization lifted the lower face, and the glabellar and periocular lines were softer, although still present. “It’s important to counsel patients that neuromodulators won’t make the lines go away the first time, but they will be softened.”
Practice tips
It’s important to titrate neuromodulators to fit the patient, Dr. Watchmaker said. Ask: What are their goals: Reversal of static lines? Softening wrinkles? Maintaining current status? “There’s not one dosing regimen,” and both dosing and frequency of neuromodulators can be titrated to fit each patient’s aesthetic goals, she said. For older patients who want to soften or maintain appearance, she suggested treatment every 4-6 months. And some patients just want to maintain the status quo, she noted.
Ideal candidates
For neuromodulators and fillers, who is an ideal candidate? “I think it’s anyone who has realistic expectations,” she said. Patients need to know how many treatments are needed and how much it will cost. For patients with extensive wrinkling and sagging, she said, she does extensive counseling about what results to expect “because I don’t want them to feel like they wasted their time or their money.”
She also suggests a surgical consult, as some may opt for that route after learning about the options and expected results.
Skin tightening
Both radiofrequency and microfocused ultrasound are noninvasive and additional options. Radiofrequency uses radio waves, with electromagnetic energy to stimulate heat. Ultrasound uses ultrasound waves to stimulate heat. Both approaches cause collagen contraction, neocollagenesis, and skin tightening.
These procedures do well for the lower face, Dr. Watchmaker said, but “I am relatively unimpressed for how well they do for the upper face.” Ideal candidates have mild to moderate skin laxity and want to avoid surgery. She also tells patients that collagen isn’t made overnight. “You won’t see much for 3-6 months after.” The good news? Usually the treatments need to be repeated only every 1.5-2 years, she said.
Lasers
“There are so many lasers out there,” said Dr. Watchmaker, who groups them into three categories: those used for wrinkles, dyschromia, and erythema. Her picks: ablative lasers (CO2 and erbium) and erbium-doped YAG 1550 nm laser for rhytids. Thulium 1927 and QS and picosecond lasers are her picks for dyschromia, and for erythema, pulsed dye and KTP lasers.
Some laser treatments are not a “walk in the park,” as she warns patients. For example, after treatment with ablative lasers, there is pain, post-procedure redness, and crusting.
Take-home points
A combination of noninvasive and minimally invasive procedures can produce appearance-improving results. That’s more likely if dermatologists choose ideal candidates, personalize the treatment, and set realistic expectations. “We have a finite number of tools,” she said, but they can be used in a variety of ways.
At the interactive panel discussion following her presentation, Dr. Watchmaker was asked what she tells patients about sun protection. “I talk a lot about sunscreens,’’ she said, always urging patients to use them. While the options for rejuvenation are numerous, taking care of the skin is still crucial.
Dr. Watchmaker had no disclosures. MedscapeLive and this news organization are owned by the same parent company.
At the MedscapeLive’s Women’s and Pediatric Dermatology Seminar, Jacqueline Watchmaker, MD, a dermatologist in Scottsdale, Ariz., provided an overview of current options, along with advice on how to keep patients’ expectations realistic and how to properly choose the best candidates for the best procedures.
“One of the most common concerns patients come to me with are wrinkles on the upper face,” but this is far from their only concern, Dr. Watchmaker said. Wrinkles and sagging of the lower face, areas under the eyes, nasolabial folds, marionette lines, and the neck also draw concern. Uneven coloration is another common concern, she said.
“So, what can we do for all of this?” she asked. The options are plentiful. Wrinkles of the upper face are easy to address with neuromodulators, she said, and soft-tissue fillers help the jawline and cheek areas.
“For the lower face, skin tightening devices really shine,” she added. And lasers can help correct uneven coloration. Surgery, of course, can also produce good results, but many patients want to stick with noninvasive or minimally invasive procedures.
Case: 83-year-old woman
Dr. Watchmaker discussed an 83-year old patient, who had malar mounds and accentuation of the infraorbital hollowness resulting from changes in subcutaneous fat and ligament laxity. She also had uneven coloration from photo damage, wrinkles on the upper face, linear appearance of zygoma related to underlying bony changes and fat compartment descent, and nasolabial folds and jowls related to decreased bony compartments, ligament laxity, and shifting of fat. She was naive to any cosmetic procedure.
Despite her age, this patient had no wrinkling on the upper forehead. Dr. Watchmaker did not inject neuromodulator in the upper forehead, as this patient also had a slightly heavy eyelid. “If you inject too much, it can cause some drooping of the eyelid and eyebrow,” she said.
For filler, she used a combination of high G (firmness, support) hyaluronic acid filler, a medium G acid filler, and a low G filler. The result: The woman’s face became more balanced, the mid-face volumization lifted the lower face, and the glabellar and periocular lines were softer, although still present. “It’s important to counsel patients that neuromodulators won’t make the lines go away the first time, but they will be softened.”
Practice tips
It’s important to titrate neuromodulators to fit the patient, Dr. Watchmaker said. Ask: What are their goals: Reversal of static lines? Softening wrinkles? Maintaining current status? “There’s not one dosing regimen,” and both dosing and frequency of neuromodulators can be titrated to fit each patient’s aesthetic goals, she said. For older patients who want to soften or maintain appearance, she suggested treatment every 4-6 months. And some patients just want to maintain the status quo, she noted.
Ideal candidates
For neuromodulators and fillers, who is an ideal candidate? “I think it’s anyone who has realistic expectations,” she said. Patients need to know how many treatments are needed and how much it will cost. For patients with extensive wrinkling and sagging, she said, she does extensive counseling about what results to expect “because I don’t want them to feel like they wasted their time or their money.”
She also suggests a surgical consult, as some may opt for that route after learning about the options and expected results.
Skin tightening
Both radiofrequency and microfocused ultrasound are noninvasive and additional options. Radiofrequency uses radio waves, with electromagnetic energy to stimulate heat. Ultrasound uses ultrasound waves to stimulate heat. Both approaches cause collagen contraction, neocollagenesis, and skin tightening.
These procedures do well for the lower face, Dr. Watchmaker said, but “I am relatively unimpressed for how well they do for the upper face.” Ideal candidates have mild to moderate skin laxity and want to avoid surgery. She also tells patients that collagen isn’t made overnight. “You won’t see much for 3-6 months after.” The good news? Usually the treatments need to be repeated only every 1.5-2 years, she said.
Lasers
“There are so many lasers out there,” said Dr. Watchmaker, who groups them into three categories: those used for wrinkles, dyschromia, and erythema. Her picks: ablative lasers (CO2 and erbium) and erbium-doped YAG 1550 nm laser for rhytids. Thulium 1927 and QS and picosecond lasers are her picks for dyschromia, and for erythema, pulsed dye and KTP lasers.
Some laser treatments are not a “walk in the park,” as she warns patients. For example, after treatment with ablative lasers, there is pain, post-procedure redness, and crusting.
Take-home points
A combination of noninvasive and minimally invasive procedures can produce appearance-improving results. That’s more likely if dermatologists choose ideal candidates, personalize the treatment, and set realistic expectations. “We have a finite number of tools,” she said, but they can be used in a variety of ways.
At the interactive panel discussion following her presentation, Dr. Watchmaker was asked what she tells patients about sun protection. “I talk a lot about sunscreens,’’ she said, always urging patients to use them. While the options for rejuvenation are numerous, taking care of the skin is still crucial.
Dr. Watchmaker had no disclosures. MedscapeLive and this news organization are owned by the same parent company.
FROM MEDSCAPELIVE WOMEN’S & PEDIATRIC DERMATOLOGY SEMINAR
Doxycycline cuts STI risk in men and trans women having sex with men
MONTREAL – (PrEP). The results of the open-label DoxyPEP trial were reported at a press conference at a meeting of the International AIDS Society.
“It is time to take action on the data that we have and really think about incorporating it into guidelines and rolling this out in a safe and thoughtful way,” said co-principal investigator Annie Luetkemeyer, MD, of Zuckerberg San Francisco General Hospital, and professor of medicine at the University of California, San Francisco (UCSF).
The open-label trial, conducted in Seattle and San Francisco, randomized MSM/TGW living with HIV or on PrEP, and with a history of N. gonorrhoeae (GC), C. trachomatis (CT), or early syphilis in the past year, to either doxycycline or none within 72 hours of having condomless sex. It was stopped early in May when a planned interim analysis showed those randomized to take doxycycline had substantially fewer STIs than participants assigned to the control group.
The intent-to-treat analysis included 501 patients with at least one quarter of follow-up: 327 taking PrEP and 174 living with HIV. Among those taking PrEP, new STIs (GC, CT or syphilis) occurred in 31.9% of control participants vs. 10.7% of those taking doxycycline – a reduction of 66% per quarter (P < .001). Among participants living with HIV, new STIs occurred in 30.5% of controls vs. 11.8% taking doxycycline, for a 62% reduction in STIs per quarter (P < .0001).
“Participants reported taking doxycycline 87% of the time after having condomless sex, about half of participants took fewer than 10 doses per month, 30% took 10-20 doses per month, and 16% took more than 20 doses of doxycycline per month,” said Dr. Luetkemeyer, adding that there were no serious – grade 2 or greater – adverse events, and “the majority of participants reported that taking doxy was acceptable or very acceptable.”
Asked how broadly doxycycline prophylaxis could be used in other populations, Dr. Luetkemeyer was cautious. “Our study participants had a very high rate of new STIs – a 30% incidence per quarter and using doxyPEP was well tolerated and very effective to reduce new STIs. However, this is a fairly limited population,” she said. “Whether doxyPEP should be considered for other groups, such as women on PrEP or with an elevated risk for STIs, will need more data which will be forthcoming from ongoing studies.”
Dr. Luetkemeyer said her group is looking at three possible risks of antibiotic resistance with the doxyPEP regimen: the risk to bystander bacteria such as Staphylococcus aureus or commensal neisseria; the impact on the gut; and the risk of resistance to antibiotic treatments for STI.
For the latter, “we don’t really think this is going to be an issue in chlamydia and syphilis, and we’re looking carefully at gonorrhea,” she said, adding that it will be challenging to get definitive data from this particular study because of its short follow-up.
“Available culture data from those who had gonorrhea infections during the study demonstrated a relatively low rate of tetracycline resistance, which is a proxy for doxycycline resistance, at 20%. ... However, larger studies and population-based surveillance of those taking doxycycline as PEP are needed to understand if doxycycline use could drive the element of tetracycline resistance in gonorrhea,” she said, emphasizing that doxycycline is not used to treat active gonorrhea infections.
Calling the doxyPEP regimen a “game-changing strategy,” Sharon Lewin, AO, PhD, president-elect of the International AIDS Society, said many physicians are already prescribing it off label based on the IPERGAY study (N Engl J Med. 2015; 373:2237-46) “but there’s a clear need for more evidence to guide the use of this intervention.”
“This study has huge implications for clinical care,” said Monica Gandhi, MD, MPH, an infectious diseases doctor, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at UCSF. “Although the data on drug resistance is very important to evaluate, we should certainly consider at this point using doxycycline PEP within 72 hours of condomless sex for our patients for STI prevention,” she said in an interview.
“In our practice, we are very excited about the possibility of a simple one-pill postexposure prophylactic agent (doxycycline 200 mg) to reduce the risk of a number of STIs. We have used PEP for HIV infection for a number of years and are very familiar with the concept of preventing infections after an exposure,” said Dr. Gandhi, director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “We are planning to institute doxycycline as PEP at my clinic after the release of these findings and will follow the remainder of the study findings closely.”
The trial was funded by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, through grant R01AI143439. It was conducted at the HIV clinic at Zuckerberg San Francisco General Hospital and the San Francisco City Clinic, both part of the San Francisco Department of Public Health, and the Madison Clinic and the Sexual Health Clinic at Harborview Medical Center, both at the University of Washington. Medications were provided by Mayne Pharmaceuticals, and lab support by Hologic & Cepheid.
Dr. Lewin has the following disclosures: investigator-initiated, industry-funded research for Gilead, Viiv, Merck; scientific advisory board (honoraria paid to her personally) for Gilead, Merck, Viiv, Esfam, Immunocore, Vaxxinity; collaborative research (nonfunded) for AbbVie, Genentech, BMS. Dr. Luetkemeyer and Dr. Gandhi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – (PrEP). The results of the open-label DoxyPEP trial were reported at a press conference at a meeting of the International AIDS Society.
“It is time to take action on the data that we have and really think about incorporating it into guidelines and rolling this out in a safe and thoughtful way,” said co-principal investigator Annie Luetkemeyer, MD, of Zuckerberg San Francisco General Hospital, and professor of medicine at the University of California, San Francisco (UCSF).
The open-label trial, conducted in Seattle and San Francisco, randomized MSM/TGW living with HIV or on PrEP, and with a history of N. gonorrhoeae (GC), C. trachomatis (CT), or early syphilis in the past year, to either doxycycline or none within 72 hours of having condomless sex. It was stopped early in May when a planned interim analysis showed those randomized to take doxycycline had substantially fewer STIs than participants assigned to the control group.
The intent-to-treat analysis included 501 patients with at least one quarter of follow-up: 327 taking PrEP and 174 living with HIV. Among those taking PrEP, new STIs (GC, CT or syphilis) occurred in 31.9% of control participants vs. 10.7% of those taking doxycycline – a reduction of 66% per quarter (P < .001). Among participants living with HIV, new STIs occurred in 30.5% of controls vs. 11.8% taking doxycycline, for a 62% reduction in STIs per quarter (P < .0001).
“Participants reported taking doxycycline 87% of the time after having condomless sex, about half of participants took fewer than 10 doses per month, 30% took 10-20 doses per month, and 16% took more than 20 doses of doxycycline per month,” said Dr. Luetkemeyer, adding that there were no serious – grade 2 or greater – adverse events, and “the majority of participants reported that taking doxy was acceptable or very acceptable.”
Asked how broadly doxycycline prophylaxis could be used in other populations, Dr. Luetkemeyer was cautious. “Our study participants had a very high rate of new STIs – a 30% incidence per quarter and using doxyPEP was well tolerated and very effective to reduce new STIs. However, this is a fairly limited population,” she said. “Whether doxyPEP should be considered for other groups, such as women on PrEP or with an elevated risk for STIs, will need more data which will be forthcoming from ongoing studies.”
Dr. Luetkemeyer said her group is looking at three possible risks of antibiotic resistance with the doxyPEP regimen: the risk to bystander bacteria such as Staphylococcus aureus or commensal neisseria; the impact on the gut; and the risk of resistance to antibiotic treatments for STI.
For the latter, “we don’t really think this is going to be an issue in chlamydia and syphilis, and we’re looking carefully at gonorrhea,” she said, adding that it will be challenging to get definitive data from this particular study because of its short follow-up.
“Available culture data from those who had gonorrhea infections during the study demonstrated a relatively low rate of tetracycline resistance, which is a proxy for doxycycline resistance, at 20%. ... However, larger studies and population-based surveillance of those taking doxycycline as PEP are needed to understand if doxycycline use could drive the element of tetracycline resistance in gonorrhea,” she said, emphasizing that doxycycline is not used to treat active gonorrhea infections.
Calling the doxyPEP regimen a “game-changing strategy,” Sharon Lewin, AO, PhD, president-elect of the International AIDS Society, said many physicians are already prescribing it off label based on the IPERGAY study (N Engl J Med. 2015; 373:2237-46) “but there’s a clear need for more evidence to guide the use of this intervention.”
“This study has huge implications for clinical care,” said Monica Gandhi, MD, MPH, an infectious diseases doctor, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at UCSF. “Although the data on drug resistance is very important to evaluate, we should certainly consider at this point using doxycycline PEP within 72 hours of condomless sex for our patients for STI prevention,” she said in an interview.
“In our practice, we are very excited about the possibility of a simple one-pill postexposure prophylactic agent (doxycycline 200 mg) to reduce the risk of a number of STIs. We have used PEP for HIV infection for a number of years and are very familiar with the concept of preventing infections after an exposure,” said Dr. Gandhi, director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “We are planning to institute doxycycline as PEP at my clinic after the release of these findings and will follow the remainder of the study findings closely.”
The trial was funded by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, through grant R01AI143439. It was conducted at the HIV clinic at Zuckerberg San Francisco General Hospital and the San Francisco City Clinic, both part of the San Francisco Department of Public Health, and the Madison Clinic and the Sexual Health Clinic at Harborview Medical Center, both at the University of Washington. Medications were provided by Mayne Pharmaceuticals, and lab support by Hologic & Cepheid.
Dr. Lewin has the following disclosures: investigator-initiated, industry-funded research for Gilead, Viiv, Merck; scientific advisory board (honoraria paid to her personally) for Gilead, Merck, Viiv, Esfam, Immunocore, Vaxxinity; collaborative research (nonfunded) for AbbVie, Genentech, BMS. Dr. Luetkemeyer and Dr. Gandhi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MONTREAL – (PrEP). The results of the open-label DoxyPEP trial were reported at a press conference at a meeting of the International AIDS Society.
“It is time to take action on the data that we have and really think about incorporating it into guidelines and rolling this out in a safe and thoughtful way,” said co-principal investigator Annie Luetkemeyer, MD, of Zuckerberg San Francisco General Hospital, and professor of medicine at the University of California, San Francisco (UCSF).
The open-label trial, conducted in Seattle and San Francisco, randomized MSM/TGW living with HIV or on PrEP, and with a history of N. gonorrhoeae (GC), C. trachomatis (CT), or early syphilis in the past year, to either doxycycline or none within 72 hours of having condomless sex. It was stopped early in May when a planned interim analysis showed those randomized to take doxycycline had substantially fewer STIs than participants assigned to the control group.
The intent-to-treat analysis included 501 patients with at least one quarter of follow-up: 327 taking PrEP and 174 living with HIV. Among those taking PrEP, new STIs (GC, CT or syphilis) occurred in 31.9% of control participants vs. 10.7% of those taking doxycycline – a reduction of 66% per quarter (P < .001). Among participants living with HIV, new STIs occurred in 30.5% of controls vs. 11.8% taking doxycycline, for a 62% reduction in STIs per quarter (P < .0001).
“Participants reported taking doxycycline 87% of the time after having condomless sex, about half of participants took fewer than 10 doses per month, 30% took 10-20 doses per month, and 16% took more than 20 doses of doxycycline per month,” said Dr. Luetkemeyer, adding that there were no serious – grade 2 or greater – adverse events, and “the majority of participants reported that taking doxy was acceptable or very acceptable.”
Asked how broadly doxycycline prophylaxis could be used in other populations, Dr. Luetkemeyer was cautious. “Our study participants had a very high rate of new STIs – a 30% incidence per quarter and using doxyPEP was well tolerated and very effective to reduce new STIs. However, this is a fairly limited population,” she said. “Whether doxyPEP should be considered for other groups, such as women on PrEP or with an elevated risk for STIs, will need more data which will be forthcoming from ongoing studies.”
Dr. Luetkemeyer said her group is looking at three possible risks of antibiotic resistance with the doxyPEP regimen: the risk to bystander bacteria such as Staphylococcus aureus or commensal neisseria; the impact on the gut; and the risk of resistance to antibiotic treatments for STI.
For the latter, “we don’t really think this is going to be an issue in chlamydia and syphilis, and we’re looking carefully at gonorrhea,” she said, adding that it will be challenging to get definitive data from this particular study because of its short follow-up.
“Available culture data from those who had gonorrhea infections during the study demonstrated a relatively low rate of tetracycline resistance, which is a proxy for doxycycline resistance, at 20%. ... However, larger studies and population-based surveillance of those taking doxycycline as PEP are needed to understand if doxycycline use could drive the element of tetracycline resistance in gonorrhea,” she said, emphasizing that doxycycline is not used to treat active gonorrhea infections.
Calling the doxyPEP regimen a “game-changing strategy,” Sharon Lewin, AO, PhD, president-elect of the International AIDS Society, said many physicians are already prescribing it off label based on the IPERGAY study (N Engl J Med. 2015; 373:2237-46) “but there’s a clear need for more evidence to guide the use of this intervention.”
“This study has huge implications for clinical care,” said Monica Gandhi, MD, MPH, an infectious diseases doctor, professor of medicine, and associate chief in the division of HIV, infectious diseases, and global medicine at UCSF. “Although the data on drug resistance is very important to evaluate, we should certainly consider at this point using doxycycline PEP within 72 hours of condomless sex for our patients for STI prevention,” she said in an interview.
“In our practice, we are very excited about the possibility of a simple one-pill postexposure prophylactic agent (doxycycline 200 mg) to reduce the risk of a number of STIs. We have used PEP for HIV infection for a number of years and are very familiar with the concept of preventing infections after an exposure,” said Dr. Gandhi, director of the UCSF Center for AIDS Research and medical director of the HIV Clinic (“Ward 86”) at San Francisco General Hospital. “We are planning to institute doxycycline as PEP at my clinic after the release of these findings and will follow the remainder of the study findings closely.”
The trial was funded by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, through grant R01AI143439. It was conducted at the HIV clinic at Zuckerberg San Francisco General Hospital and the San Francisco City Clinic, both part of the San Francisco Department of Public Health, and the Madison Clinic and the Sexual Health Clinic at Harborview Medical Center, both at the University of Washington. Medications were provided by Mayne Pharmaceuticals, and lab support by Hologic & Cepheid.
Dr. Lewin has the following disclosures: investigator-initiated, industry-funded research for Gilead, Viiv, Merck; scientific advisory board (honoraria paid to her personally) for Gilead, Merck, Viiv, Esfam, Immunocore, Vaxxinity; collaborative research (nonfunded) for AbbVie, Genentech, BMS. Dr. Luetkemeyer and Dr. Gandhi reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT AIDS 2022
U.S. clears 786,000 monkeypox vaccine doses for distribution
More than 780,000 doses of the JYNNEOS monkeypox vaccine will be available in the United States beginning July 29, the Department of Health & Human Services announced on July 28 in a press call.
HHS Secretary Xavier Becerra urged local and state public health departments to use these doses for preventive vaccination efforts to stay ahead of the virus and end the outbreak, noting that the HHS and Centers for Disease Control and Prevention do not control how vaccines are distributed at state and local levels. “We don’t have the authority to tell them what to do,” he said during the call. “We need them to work with us.”
As of July 28, there were 4,907 reported cases of monkeypox in the United States and officials expect cases will continue to rise in the coming weeks.
The vaccine is manufactured by the small Danish company Bavarian Nordic. These additional 786,000 doses were previously stored at a plant in Denmark, awaiting the completion of an inspection and authorization of the vaccine plant by the Food and Drug Administration. The agency announced on July 27 that both the vaccine doses and the manufacturing plant met standards.
With the announcement of these additional doses, the vaccine allocation plan is also being updated to take into account two important factors: the number of people at high risk in a jurisdiction and the number of new cases reported since the last vaccine allocation.
“This update gives greater weight to prioritizing vaccines to areas with the greatest number of people at risk, which includes men who have sex with men who have HIV or who are eligible for HIV pre-exposure prophylaxis, while still considering where we are seeing cases increase,” said Capt. Jennifer McQuiston, DVM, deputy director of the division of high consequence pathogens and pathology at the CDC.
Capt.McQuiston also provided additional demographic information on the U.S. outbreak. The median age of people with confirmed cases is 35 years old, with a range from 17 to 76. (This does not include the two cases in children reported on July 22.) Of the cases where sex at birth was provided, 99% were individuals assigned male sex at birth. In cases with reported ethnicity and race, 37% were non-Hispanic White people, 31% were Hispanic/Latino, 27% were Black or African American, and 4% were of Asian descent. The most common symptoms were rash – present in 99% of cases – malaise, fever, and swollen lymph nodes.
HHS and CDC did not have data on how many people have received at least one dose of the monkeypox vaccine. When asked how many people need to be fully vaccinated against monkeypox to contain the outbreak, Mr. Becerra did not provide an estimate but implied that preventive vaccination could help limit the number of vaccines needed and expressed optimism about quelling the outbreak in the United States. “We believe that we have done everything we can at the federal level to work with our state and local partners and communities affected to make sure we can stay ahead of this and end this outbreak,” he said, “but everybody’s got to do their part.”
A version of this article first appeared on Medscape.com.
More than 780,000 doses of the JYNNEOS monkeypox vaccine will be available in the United States beginning July 29, the Department of Health & Human Services announced on July 28 in a press call.
HHS Secretary Xavier Becerra urged local and state public health departments to use these doses for preventive vaccination efforts to stay ahead of the virus and end the outbreak, noting that the HHS and Centers for Disease Control and Prevention do not control how vaccines are distributed at state and local levels. “We don’t have the authority to tell them what to do,” he said during the call. “We need them to work with us.”
As of July 28, there were 4,907 reported cases of monkeypox in the United States and officials expect cases will continue to rise in the coming weeks.
The vaccine is manufactured by the small Danish company Bavarian Nordic. These additional 786,000 doses were previously stored at a plant in Denmark, awaiting the completion of an inspection and authorization of the vaccine plant by the Food and Drug Administration. The agency announced on July 27 that both the vaccine doses and the manufacturing plant met standards.
With the announcement of these additional doses, the vaccine allocation plan is also being updated to take into account two important factors: the number of people at high risk in a jurisdiction and the number of new cases reported since the last vaccine allocation.
“This update gives greater weight to prioritizing vaccines to areas with the greatest number of people at risk, which includes men who have sex with men who have HIV or who are eligible for HIV pre-exposure prophylaxis, while still considering where we are seeing cases increase,” said Capt. Jennifer McQuiston, DVM, deputy director of the division of high consequence pathogens and pathology at the CDC.
Capt.McQuiston also provided additional demographic information on the U.S. outbreak. The median age of people with confirmed cases is 35 years old, with a range from 17 to 76. (This does not include the two cases in children reported on July 22.) Of the cases where sex at birth was provided, 99% were individuals assigned male sex at birth. In cases with reported ethnicity and race, 37% were non-Hispanic White people, 31% were Hispanic/Latino, 27% were Black or African American, and 4% were of Asian descent. The most common symptoms were rash – present in 99% of cases – malaise, fever, and swollen lymph nodes.
HHS and CDC did not have data on how many people have received at least one dose of the monkeypox vaccine. When asked how many people need to be fully vaccinated against monkeypox to contain the outbreak, Mr. Becerra did not provide an estimate but implied that preventive vaccination could help limit the number of vaccines needed and expressed optimism about quelling the outbreak in the United States. “We believe that we have done everything we can at the federal level to work with our state and local partners and communities affected to make sure we can stay ahead of this and end this outbreak,” he said, “but everybody’s got to do their part.”
A version of this article first appeared on Medscape.com.
More than 780,000 doses of the JYNNEOS monkeypox vaccine will be available in the United States beginning July 29, the Department of Health & Human Services announced on July 28 in a press call.
HHS Secretary Xavier Becerra urged local and state public health departments to use these doses for preventive vaccination efforts to stay ahead of the virus and end the outbreak, noting that the HHS and Centers for Disease Control and Prevention do not control how vaccines are distributed at state and local levels. “We don’t have the authority to tell them what to do,” he said during the call. “We need them to work with us.”
As of July 28, there were 4,907 reported cases of monkeypox in the United States and officials expect cases will continue to rise in the coming weeks.
The vaccine is manufactured by the small Danish company Bavarian Nordic. These additional 786,000 doses were previously stored at a plant in Denmark, awaiting the completion of an inspection and authorization of the vaccine plant by the Food and Drug Administration. The agency announced on July 27 that both the vaccine doses and the manufacturing plant met standards.
With the announcement of these additional doses, the vaccine allocation plan is also being updated to take into account two important factors: the number of people at high risk in a jurisdiction and the number of new cases reported since the last vaccine allocation.
“This update gives greater weight to prioritizing vaccines to areas with the greatest number of people at risk, which includes men who have sex with men who have HIV or who are eligible for HIV pre-exposure prophylaxis, while still considering where we are seeing cases increase,” said Capt. Jennifer McQuiston, DVM, deputy director of the division of high consequence pathogens and pathology at the CDC.
Capt.McQuiston also provided additional demographic information on the U.S. outbreak. The median age of people with confirmed cases is 35 years old, with a range from 17 to 76. (This does not include the two cases in children reported on July 22.) Of the cases where sex at birth was provided, 99% were individuals assigned male sex at birth. In cases with reported ethnicity and race, 37% were non-Hispanic White people, 31% were Hispanic/Latino, 27% were Black or African American, and 4% were of Asian descent. The most common symptoms were rash – present in 99% of cases – malaise, fever, and swollen lymph nodes.
HHS and CDC did not have data on how many people have received at least one dose of the monkeypox vaccine. When asked how many people need to be fully vaccinated against monkeypox to contain the outbreak, Mr. Becerra did not provide an estimate but implied that preventive vaccination could help limit the number of vaccines needed and expressed optimism about quelling the outbreak in the United States. “We believe that we have done everything we can at the federal level to work with our state and local partners and communities affected to make sure we can stay ahead of this and end this outbreak,” he said, “but everybody’s got to do their part.”
A version of this article first appeared on Medscape.com.
Prolonged remission in patient with HIV may open new avenues to functional cure
MONTREAL – The case of a patient in an HIV study whose viral load dropped to undetectable levels and whose immune cells soared has captured the attention of organizers at a meeting of the International AIDS Society.
Although the 59-year-old woman is one of many who are known as posttreatment controllers (PTCs) – having been in remission for more than 15 years after stopping antiretroviral therapy (ART) –
“This case opens new avenues in the HIV functional-cure field,” lead investigator Núria Climent, PhD, of the HIV unit at Hospital Clinic-IDIBAPS/University of Barcelona, told this news organization.
“As far as we know, this is the first time that the gamma-delta T cells have been identified in a PTC, and concerning the memory-like NK cells, there are very few published data and only sparse information presented in several congresses,” she said, explaining that these cells “have a high capacity to inhibit the replication of the virus in vitro. For that reason, we think that this PTC has cells able to dramatically reduce the virus amount. We think that the potential capacity to increase these cells in this PTC woman could be not only mediated by especial genetic factors ... but also mediated by early ART treatment and might be by the immunomediated treatment.”
The findings suggest the potential for “increasing the amount of those memory-like NK cells and gamma-delta T cells in order to translate this potent antiviral activity in new therapies to achieve an HIV functional cure,” she said, adding: “As far as we know, aiming to increase these specific cells has never been done before in people living with HIV.”
In a press conference during the meeting, Dr. Climent explained that the patient was enrolled in a study in which she received a combination of ART and immunomodulatory therapy. This involved a combination of cyclosporine A, low-dose interleukin 2, granulocyte macrophage colony-stimulating factor, and pegylated interferon alfa-2b.
“None of the other 19 patients included in the trial controlled viral replication,” senior investigator Jose Miro, MD, PhD, also from the HIV unit at Hospital Clinic-IDIBAPS/University of Barcelona, told this news organization.
Sharon Lewin, MD, president-elect of the International AIDS Society, which runs the conference, said in an interview that although the significance of the case is unclear, the IAS selected it as a highlight for the meeting. “It is important for clinicians to understand the complexities in interpreting these case reports. Their patients are probably likely to ask them about the report, and it’s important [that] they can explain it to them.”
Dr. Lewin, who is professor of medicine at the University of Melbourne and director of the Peter Doherty Institute for Infection and Immunity in Melbourne, added that it is impossible to determine the mechanism of action from a single case report. “We don’t know if the intervention played a role or if this person is a ‘posttreatment controller,’ which has been previously described many times,” she said in an interview. “In this patient, the virus is at very low, but controlled, levels, and virus could be grown out. While it’s still exciting and important, this is really what we would consider a remission. The intense study of a single case such as this is certainly worthwhile and important but can only provide new ideas for research. So, I don’t think we can draw any conclusion on the role of NK cells, et cetera. We need much larger case series or controlled trials to reach any conclusion on the reasons for her remission.”
Dr. Climent disclosed no relevant financial conflicts of interest. Dr. Lewin has disclosed investigator-initiated industry-funded research (Gilead, ViiV, Merck), scientific advisory board honoraria paid to her personally (Gilead, Merck, ViiV, Esfam, Immunocore, Vaxxinity), and nonfunded collaborative research (AbbVie, Genentech, Bristol-Myers Squibb).
A version of this article first appeared on Medscape.com.
MONTREAL – The case of a patient in an HIV study whose viral load dropped to undetectable levels and whose immune cells soared has captured the attention of organizers at a meeting of the International AIDS Society.
Although the 59-year-old woman is one of many who are known as posttreatment controllers (PTCs) – having been in remission for more than 15 years after stopping antiretroviral therapy (ART) –
“This case opens new avenues in the HIV functional-cure field,” lead investigator Núria Climent, PhD, of the HIV unit at Hospital Clinic-IDIBAPS/University of Barcelona, told this news organization.
“As far as we know, this is the first time that the gamma-delta T cells have been identified in a PTC, and concerning the memory-like NK cells, there are very few published data and only sparse information presented in several congresses,” she said, explaining that these cells “have a high capacity to inhibit the replication of the virus in vitro. For that reason, we think that this PTC has cells able to dramatically reduce the virus amount. We think that the potential capacity to increase these cells in this PTC woman could be not only mediated by especial genetic factors ... but also mediated by early ART treatment and might be by the immunomediated treatment.”
The findings suggest the potential for “increasing the amount of those memory-like NK cells and gamma-delta T cells in order to translate this potent antiviral activity in new therapies to achieve an HIV functional cure,” she said, adding: “As far as we know, aiming to increase these specific cells has never been done before in people living with HIV.”
In a press conference during the meeting, Dr. Climent explained that the patient was enrolled in a study in which she received a combination of ART and immunomodulatory therapy. This involved a combination of cyclosporine A, low-dose interleukin 2, granulocyte macrophage colony-stimulating factor, and pegylated interferon alfa-2b.
“None of the other 19 patients included in the trial controlled viral replication,” senior investigator Jose Miro, MD, PhD, also from the HIV unit at Hospital Clinic-IDIBAPS/University of Barcelona, told this news organization.
Sharon Lewin, MD, president-elect of the International AIDS Society, which runs the conference, said in an interview that although the significance of the case is unclear, the IAS selected it as a highlight for the meeting. “It is important for clinicians to understand the complexities in interpreting these case reports. Their patients are probably likely to ask them about the report, and it’s important [that] they can explain it to them.”
Dr. Lewin, who is professor of medicine at the University of Melbourne and director of the Peter Doherty Institute for Infection and Immunity in Melbourne, added that it is impossible to determine the mechanism of action from a single case report. “We don’t know if the intervention played a role or if this person is a ‘posttreatment controller,’ which has been previously described many times,” she said in an interview. “In this patient, the virus is at very low, but controlled, levels, and virus could be grown out. While it’s still exciting and important, this is really what we would consider a remission. The intense study of a single case such as this is certainly worthwhile and important but can only provide new ideas for research. So, I don’t think we can draw any conclusion on the role of NK cells, et cetera. We need much larger case series or controlled trials to reach any conclusion on the reasons for her remission.”
Dr. Climent disclosed no relevant financial conflicts of interest. Dr. Lewin has disclosed investigator-initiated industry-funded research (Gilead, ViiV, Merck), scientific advisory board honoraria paid to her personally (Gilead, Merck, ViiV, Esfam, Immunocore, Vaxxinity), and nonfunded collaborative research (AbbVie, Genentech, Bristol-Myers Squibb).
A version of this article first appeared on Medscape.com.
MONTREAL – The case of a patient in an HIV study whose viral load dropped to undetectable levels and whose immune cells soared has captured the attention of organizers at a meeting of the International AIDS Society.
Although the 59-year-old woman is one of many who are known as posttreatment controllers (PTCs) – having been in remission for more than 15 years after stopping antiretroviral therapy (ART) –
“This case opens new avenues in the HIV functional-cure field,” lead investigator Núria Climent, PhD, of the HIV unit at Hospital Clinic-IDIBAPS/University of Barcelona, told this news organization.
“As far as we know, this is the first time that the gamma-delta T cells have been identified in a PTC, and concerning the memory-like NK cells, there are very few published data and only sparse information presented in several congresses,” she said, explaining that these cells “have a high capacity to inhibit the replication of the virus in vitro. For that reason, we think that this PTC has cells able to dramatically reduce the virus amount. We think that the potential capacity to increase these cells in this PTC woman could be not only mediated by especial genetic factors ... but also mediated by early ART treatment and might be by the immunomediated treatment.”
The findings suggest the potential for “increasing the amount of those memory-like NK cells and gamma-delta T cells in order to translate this potent antiviral activity in new therapies to achieve an HIV functional cure,” she said, adding: “As far as we know, aiming to increase these specific cells has never been done before in people living with HIV.”
In a press conference during the meeting, Dr. Climent explained that the patient was enrolled in a study in which she received a combination of ART and immunomodulatory therapy. This involved a combination of cyclosporine A, low-dose interleukin 2, granulocyte macrophage colony-stimulating factor, and pegylated interferon alfa-2b.
“None of the other 19 patients included in the trial controlled viral replication,” senior investigator Jose Miro, MD, PhD, also from the HIV unit at Hospital Clinic-IDIBAPS/University of Barcelona, told this news organization.
Sharon Lewin, MD, president-elect of the International AIDS Society, which runs the conference, said in an interview that although the significance of the case is unclear, the IAS selected it as a highlight for the meeting. “It is important for clinicians to understand the complexities in interpreting these case reports. Their patients are probably likely to ask them about the report, and it’s important [that] they can explain it to them.”
Dr. Lewin, who is professor of medicine at the University of Melbourne and director of the Peter Doherty Institute for Infection and Immunity in Melbourne, added that it is impossible to determine the mechanism of action from a single case report. “We don’t know if the intervention played a role or if this person is a ‘posttreatment controller,’ which has been previously described many times,” she said in an interview. “In this patient, the virus is at very low, but controlled, levels, and virus could be grown out. While it’s still exciting and important, this is really what we would consider a remission. The intense study of a single case such as this is certainly worthwhile and important but can only provide new ideas for research. So, I don’t think we can draw any conclusion on the role of NK cells, et cetera. We need much larger case series or controlled trials to reach any conclusion on the reasons for her remission.”
Dr. Climent disclosed no relevant financial conflicts of interest. Dr. Lewin has disclosed investigator-initiated industry-funded research (Gilead, ViiV, Merck), scientific advisory board honoraria paid to her personally (Gilead, Merck, ViiV, Esfam, Immunocore, Vaxxinity), and nonfunded collaborative research (AbbVie, Genentech, Bristol-Myers Squibb).
A version of this article first appeared on Medscape.com.
AT AIDS 2022
Potentially deadly bacteria detected in U.S. soil
, according to a new alert from the Centers for Disease Control and Prevention.
The bacteria, Burkholderia pseudomallei, was found along the Gulf Coast region in southern Mississippi. Typically, the bacteria are in tropical and subtropical climates, especially in parts of Southeast Asia, northern Australia, Central America, South America, Puerto Rico, and the U.S. Virgin Islands.
The bacteria can cause melioidosis, a rare and serious infectious disease that spreads to animals and humans through contact with contaminated soil and water via cuts, wounds, mucous membranes, breathing the bacteria in, or eating or drinking it. Worldwide, the disease is fatal in 10%-50% of those who become infected.
CDC and state officials are investigating the samples to find out how widespread the bacteria are within the United States. So far, modeling suggests that the environmental conditions on the Gulf Coast support the growth of B. pseudomallei.
“It is unclear how long the bacteria has been in the environment and where else it might be found in the U.S.,” according to the CDC statement. “CDC is alerting clinicians throughout the country of this discovery through a national health advisory, reminding them to be aware of the signs and symptoms of melioidosis and to consider melioidosis in patients that present with symptoms of the disease.”
Two unrelated people who live near the Gulf Coast region of Mississippi became sick with melioidosis recently – one in July 2020 and one in May 2022. Neither had traveled outside of the United States. The cases led the CDC and the Mississippi State Department of Health to collect environmental samples and test household products at the patients’ homes in June 2022. Three of the samples taken from soil and puddle water in the 2020 case tested positive for the bacteria.
Genomic sequencing revealed that both patients were infected with the same strain of the bacteria from the Western Hemisphere. They were hospitalized with sepsis due to pneumonia and had known risk factors for melioidosis. Both patients recovered after they were treated with antibiotics.
An average of 12 melioidosis cases are diagnosed in the United States each year, with most in people with recent travel to a country where the bacteria is endemic, or regularly found. Cases have also been linked to contaminated products imported from endemic countries. In late 2021, four cases in four states – Georgia, Kansas, Minnesota, and Texas – were linked to a contaminated aromatherapy spray that was imported, and Walmart issued a recall in November of that year, according to a CDC announcement. Two of the four people died.
Given the small number of cases found in the United States, the CDC believes the risk of melioidosis for the general population continues to be “very low,” and the risk of person-to-person spread is considered “extremely low.” But people who live on the Gulf Coast of Mississippi and who have health conditions that may put them at a higher risk, such as diabetes, chronic kidney disease, chronic lung disease, excessive alcohol use, and immunosuppressive conditions, should protect themselves.
The CDC recommends avoiding contact with soil or muddy water, particularly after heavy rains, and protecting open wounds with waterproof bandages. People should also wear waterproof boots when gardening, working in the yard, or doing agricultural work, which can prevent infection through the feet and lower legs, especially after flooding or storms. People should also wear gloves to protect their hands when working directly with soil.
Melioidosis has a wide range of symptoms, including fever, joint pain, headaches, coughing, chest pain, and belly pain. It can also cause conditions such as pneumonia, abscesses, and blood infections. The disease can infect any organ, including the brain. In most cases, symptoms appear within 1-21 days after exposure, with an average of 7 days after exposure.
The CDC’s health advisory for health professionals and public health officials shows that melioidosis is now considered to be locally endemic in areas of the Gulf Coast region in Mississippi.
“Once well-established in the soil, B. pseudomallei cannot feasibly be removed from the soil,” according to the advisory. “Public health efforts should focus primarily on improving identification of cases so that appropriate treatment can be administered.”
A version of this article first appeared on WebMD.com.
, according to a new alert from the Centers for Disease Control and Prevention.
The bacteria, Burkholderia pseudomallei, was found along the Gulf Coast region in southern Mississippi. Typically, the bacteria are in tropical and subtropical climates, especially in parts of Southeast Asia, northern Australia, Central America, South America, Puerto Rico, and the U.S. Virgin Islands.
The bacteria can cause melioidosis, a rare and serious infectious disease that spreads to animals and humans through contact with contaminated soil and water via cuts, wounds, mucous membranes, breathing the bacteria in, or eating or drinking it. Worldwide, the disease is fatal in 10%-50% of those who become infected.
CDC and state officials are investigating the samples to find out how widespread the bacteria are within the United States. So far, modeling suggests that the environmental conditions on the Gulf Coast support the growth of B. pseudomallei.
“It is unclear how long the bacteria has been in the environment and where else it might be found in the U.S.,” according to the CDC statement. “CDC is alerting clinicians throughout the country of this discovery through a national health advisory, reminding them to be aware of the signs and symptoms of melioidosis and to consider melioidosis in patients that present with symptoms of the disease.”
Two unrelated people who live near the Gulf Coast region of Mississippi became sick with melioidosis recently – one in July 2020 and one in May 2022. Neither had traveled outside of the United States. The cases led the CDC and the Mississippi State Department of Health to collect environmental samples and test household products at the patients’ homes in June 2022. Three of the samples taken from soil and puddle water in the 2020 case tested positive for the bacteria.
Genomic sequencing revealed that both patients were infected with the same strain of the bacteria from the Western Hemisphere. They were hospitalized with sepsis due to pneumonia and had known risk factors for melioidosis. Both patients recovered after they were treated with antibiotics.
An average of 12 melioidosis cases are diagnosed in the United States each year, with most in people with recent travel to a country where the bacteria is endemic, or regularly found. Cases have also been linked to contaminated products imported from endemic countries. In late 2021, four cases in four states – Georgia, Kansas, Minnesota, and Texas – were linked to a contaminated aromatherapy spray that was imported, and Walmart issued a recall in November of that year, according to a CDC announcement. Two of the four people died.
Given the small number of cases found in the United States, the CDC believes the risk of melioidosis for the general population continues to be “very low,” and the risk of person-to-person spread is considered “extremely low.” But people who live on the Gulf Coast of Mississippi and who have health conditions that may put them at a higher risk, such as diabetes, chronic kidney disease, chronic lung disease, excessive alcohol use, and immunosuppressive conditions, should protect themselves.
The CDC recommends avoiding contact with soil or muddy water, particularly after heavy rains, and protecting open wounds with waterproof bandages. People should also wear waterproof boots when gardening, working in the yard, or doing agricultural work, which can prevent infection through the feet and lower legs, especially after flooding or storms. People should also wear gloves to protect their hands when working directly with soil.
Melioidosis has a wide range of symptoms, including fever, joint pain, headaches, coughing, chest pain, and belly pain. It can also cause conditions such as pneumonia, abscesses, and blood infections. The disease can infect any organ, including the brain. In most cases, symptoms appear within 1-21 days after exposure, with an average of 7 days after exposure.
The CDC’s health advisory for health professionals and public health officials shows that melioidosis is now considered to be locally endemic in areas of the Gulf Coast region in Mississippi.
“Once well-established in the soil, B. pseudomallei cannot feasibly be removed from the soil,” according to the advisory. “Public health efforts should focus primarily on improving identification of cases so that appropriate treatment can be administered.”
A version of this article first appeared on WebMD.com.
, according to a new alert from the Centers for Disease Control and Prevention.
The bacteria, Burkholderia pseudomallei, was found along the Gulf Coast region in southern Mississippi. Typically, the bacteria are in tropical and subtropical climates, especially in parts of Southeast Asia, northern Australia, Central America, South America, Puerto Rico, and the U.S. Virgin Islands.
The bacteria can cause melioidosis, a rare and serious infectious disease that spreads to animals and humans through contact with contaminated soil and water via cuts, wounds, mucous membranes, breathing the bacteria in, or eating or drinking it. Worldwide, the disease is fatal in 10%-50% of those who become infected.
CDC and state officials are investigating the samples to find out how widespread the bacteria are within the United States. So far, modeling suggests that the environmental conditions on the Gulf Coast support the growth of B. pseudomallei.
“It is unclear how long the bacteria has been in the environment and where else it might be found in the U.S.,” according to the CDC statement. “CDC is alerting clinicians throughout the country of this discovery through a national health advisory, reminding them to be aware of the signs and symptoms of melioidosis and to consider melioidosis in patients that present with symptoms of the disease.”
Two unrelated people who live near the Gulf Coast region of Mississippi became sick with melioidosis recently – one in July 2020 and one in May 2022. Neither had traveled outside of the United States. The cases led the CDC and the Mississippi State Department of Health to collect environmental samples and test household products at the patients’ homes in June 2022. Three of the samples taken from soil and puddle water in the 2020 case tested positive for the bacteria.
Genomic sequencing revealed that both patients were infected with the same strain of the bacteria from the Western Hemisphere. They were hospitalized with sepsis due to pneumonia and had known risk factors for melioidosis. Both patients recovered after they were treated with antibiotics.
An average of 12 melioidosis cases are diagnosed in the United States each year, with most in people with recent travel to a country where the bacteria is endemic, or regularly found. Cases have also been linked to contaminated products imported from endemic countries. In late 2021, four cases in four states – Georgia, Kansas, Minnesota, and Texas – were linked to a contaminated aromatherapy spray that was imported, and Walmart issued a recall in November of that year, according to a CDC announcement. Two of the four people died.
Given the small number of cases found in the United States, the CDC believes the risk of melioidosis for the general population continues to be “very low,” and the risk of person-to-person spread is considered “extremely low.” But people who live on the Gulf Coast of Mississippi and who have health conditions that may put them at a higher risk, such as diabetes, chronic kidney disease, chronic lung disease, excessive alcohol use, and immunosuppressive conditions, should protect themselves.
The CDC recommends avoiding contact with soil or muddy water, particularly after heavy rains, and protecting open wounds with waterproof bandages. People should also wear waterproof boots when gardening, working in the yard, or doing agricultural work, which can prevent infection through the feet and lower legs, especially after flooding or storms. People should also wear gloves to protect their hands when working directly with soil.
Melioidosis has a wide range of symptoms, including fever, joint pain, headaches, coughing, chest pain, and belly pain. It can also cause conditions such as pneumonia, abscesses, and blood infections. The disease can infect any organ, including the brain. In most cases, symptoms appear within 1-21 days after exposure, with an average of 7 days after exposure.
The CDC’s health advisory for health professionals and public health officials shows that melioidosis is now considered to be locally endemic in areas of the Gulf Coast region in Mississippi.
“Once well-established in the soil, B. pseudomallei cannot feasibly be removed from the soil,” according to the advisory. “Public health efforts should focus primarily on improving identification of cases so that appropriate treatment can be administered.”
A version of this article first appeared on WebMD.com.
More evidence that COVID-19 started in Wuhan marketplace
The original spread of the virus was a one-two punch, the studies found. Twice, the virus jumped from animals to humans. Virus genetics and outbreak modeling in one study revealed two strains released a few weeks apart in November and December 2019.
“Now I realize it sounds like I just said that a once-in-a-generation event happened twice in short succession, and pandemics are indeed rare,” Joel O. Wertheim, PhD, said at a briefing sponsored by the American Association for the Advancement of Science.
A unique storm of factors had to be present for the outbreak to blow up into a pandemic: Animals carrying a virus that could spread to humans, close human contact with these animals, and a city large enough for the infection to take off before it could be contained are examples.
Unluckily for us humans, this coronavirus – SARS-CoV-2 – is a “generalist virus” capable of infecting many animals, including humans.
“Once all the conditions are in place ... the barriers to spillover have been lowered,” said Dr. Wertheim, a researcher in genetic and molecular networks at the University of California, San Diego. In fact, beyond the two strains of the virus that took hold, there were likely up to two dozen more times where people got the virus but did not spread it far and wide, and it died out.
Overall, the odds were against the virus – 78% of the time, the “introduction” to humans was likely to go extinct, the study showed.
The research revealed the COVID-19 pandemic started small.
“Our model shows that there were likely only a few dozen infections, and only several hospitalizations due to COVID-19, by early December,” said Jonathan Pekar, a graduate student working with Dr. Wertheim.
In Wuhan in late 2019, Mr. Pekar said, there was not a single positive coronavirus sample from thousands of samples from healthy blood donors tested between September and December. Likewise, not one blood sample from patients hospitalized with flu-like illness from October to December 2019 tested positive for SARS-CoV-2.
Mapping the outbreak
A second study published in the journal Science mapped out the earliest COVID-19 cases. This effort showed a tight cluster around the wholesale seafood market inside Wuhan, a city of 11 million residents.
When researchers tried other scenarios – modeling outbreaks in other parts of the city – the pattern did not hold. Again, the Wuhan market appeared to be ground zero for the start of the pandemic.
Michael Worobey, PhD, and colleagues used data from Chinese scientists and the World Health Organization for the study.
“There was this extraordinary pattern where the highest density of cases was both extremely near to and very centered on this market,” said Dr. Worobey, head of ecology and evolutionary biology at the University of Arizona, Tucson.
The highest density of cases, in a city of 8,000 square kilometers, was a “very, very small area of about a third of a kilometer square,” he said.
The outbreak pattern showed the Wuhan market “smack dab in the middle.”
So if it started with infected workers at the market, how did it spread from there? It’s likely the virus got into the community as the vendors at the market went to local shops, infecting people in those stores. Then local community members not linked to the market started getting the virus, Dr. Worobey said.
The investigators also identified which stalls in the market were most likely involved, a sort of internal clustering. “That clustering is very, very specifically in the parts of the market where ... they were selling wildlife, including, for example, raccoon dogs and other animals that we know are susceptible to infection with SARS-CoV-2,” said Kristian Andersen, PhD, director of infectious disease genomics at the Scripps Research Institute in La Jolla, Calif.
What remains unknown is which animal or animals carried the virus, although the raccoon dog – an animal similar to a fox that is native to parts of Asia – remains central to most theories. In addition, many of the farms supplying animals to the market have since been closed, making it challenging for researchers to figure out exactly where infected animals came from.
“We don’t know necessarily, but raccoon dogs were sold at this market all the way up to the beginning of the pandemic,” Dr. Andersen said.
Not ruling out other theories
People who believe SARS-CoV-2 was released from a laboratory in China at first included Dr. Worobey himself. “I’ve in the past been much more open to the lab leak idea,” he said. “And published that in a letter in Science” in November 2021.
The letter was “much more influential than I thought it would be in ways that I think it turned out to be quite damaging,” he said. As more evidence emerged since then, Dr. Worobey said he came around to the Wuhan market source theory.
Dr. Andersen agreed he was more open to the lab-leak theory at first. “I was quite convinced of the lab leak myself until we dove into this very carefully and looked at it much closer,” he said. Newer evidence convinced him “that actually, the data points to this particular market.”
“Have we disproved the lab-leak theory? No,” Dr. Anderson said. “Will we ever be able to? No.” But the Wuhan market origin scenario is more plausible. “I would say these two papers combined present the strongest evidence of that to date.”
Identifying the source of the outbreak that led to the COVID-19 pandemic is based in science, Dr. Andersen said. “What we’re trying to understand is the origin of the pandemic. We’re not trying to place blame.”
Future directions
“With pandemics being pandemics, they affect all of us,” Dr. Andersen said. “We can’t prevent these kinds of events that led to the COVID-19 pandemic. But what we can hope to do is to prevent outbreaks from becoming pandemics.”
Rapid reporting of data and cooperation are needed going forward, Dr. Andersen said. Very strong surveillance systems, including wastewater surveillance, could help monitor for SARS-CoV-2, and other pathogens of potential concern in the future as well.
It should be standard practice for medical professionals to be on alert for unusual respiratory infections too, the researchers said.
“It’s a bloody lucky thing that the doctors at the Shinwa hospital were so on the ball, that they noticed that these cases were something unusual at the end of December,” Dr. Worobey said. “It didn’t have to work out that way.”
A version of this article first appeared on WebMD.com.
The original spread of the virus was a one-two punch, the studies found. Twice, the virus jumped from animals to humans. Virus genetics and outbreak modeling in one study revealed two strains released a few weeks apart in November and December 2019.
“Now I realize it sounds like I just said that a once-in-a-generation event happened twice in short succession, and pandemics are indeed rare,” Joel O. Wertheim, PhD, said at a briefing sponsored by the American Association for the Advancement of Science.
A unique storm of factors had to be present for the outbreak to blow up into a pandemic: Animals carrying a virus that could spread to humans, close human contact with these animals, and a city large enough for the infection to take off before it could be contained are examples.
Unluckily for us humans, this coronavirus – SARS-CoV-2 – is a “generalist virus” capable of infecting many animals, including humans.
“Once all the conditions are in place ... the barriers to spillover have been lowered,” said Dr. Wertheim, a researcher in genetic and molecular networks at the University of California, San Diego. In fact, beyond the two strains of the virus that took hold, there were likely up to two dozen more times where people got the virus but did not spread it far and wide, and it died out.
Overall, the odds were against the virus – 78% of the time, the “introduction” to humans was likely to go extinct, the study showed.
The research revealed the COVID-19 pandemic started small.
“Our model shows that there were likely only a few dozen infections, and only several hospitalizations due to COVID-19, by early December,” said Jonathan Pekar, a graduate student working with Dr. Wertheim.
In Wuhan in late 2019, Mr. Pekar said, there was not a single positive coronavirus sample from thousands of samples from healthy blood donors tested between September and December. Likewise, not one blood sample from patients hospitalized with flu-like illness from October to December 2019 tested positive for SARS-CoV-2.
Mapping the outbreak
A second study published in the journal Science mapped out the earliest COVID-19 cases. This effort showed a tight cluster around the wholesale seafood market inside Wuhan, a city of 11 million residents.
When researchers tried other scenarios – modeling outbreaks in other parts of the city – the pattern did not hold. Again, the Wuhan market appeared to be ground zero for the start of the pandemic.
Michael Worobey, PhD, and colleagues used data from Chinese scientists and the World Health Organization for the study.
“There was this extraordinary pattern where the highest density of cases was both extremely near to and very centered on this market,” said Dr. Worobey, head of ecology and evolutionary biology at the University of Arizona, Tucson.
The highest density of cases, in a city of 8,000 square kilometers, was a “very, very small area of about a third of a kilometer square,” he said.
The outbreak pattern showed the Wuhan market “smack dab in the middle.”
So if it started with infected workers at the market, how did it spread from there? It’s likely the virus got into the community as the vendors at the market went to local shops, infecting people in those stores. Then local community members not linked to the market started getting the virus, Dr. Worobey said.
The investigators also identified which stalls in the market were most likely involved, a sort of internal clustering. “That clustering is very, very specifically in the parts of the market where ... they were selling wildlife, including, for example, raccoon dogs and other animals that we know are susceptible to infection with SARS-CoV-2,” said Kristian Andersen, PhD, director of infectious disease genomics at the Scripps Research Institute in La Jolla, Calif.
What remains unknown is which animal or animals carried the virus, although the raccoon dog – an animal similar to a fox that is native to parts of Asia – remains central to most theories. In addition, many of the farms supplying animals to the market have since been closed, making it challenging for researchers to figure out exactly where infected animals came from.
“We don’t know necessarily, but raccoon dogs were sold at this market all the way up to the beginning of the pandemic,” Dr. Andersen said.
Not ruling out other theories
People who believe SARS-CoV-2 was released from a laboratory in China at first included Dr. Worobey himself. “I’ve in the past been much more open to the lab leak idea,” he said. “And published that in a letter in Science” in November 2021.
The letter was “much more influential than I thought it would be in ways that I think it turned out to be quite damaging,” he said. As more evidence emerged since then, Dr. Worobey said he came around to the Wuhan market source theory.
Dr. Andersen agreed he was more open to the lab-leak theory at first. “I was quite convinced of the lab leak myself until we dove into this very carefully and looked at it much closer,” he said. Newer evidence convinced him “that actually, the data points to this particular market.”
“Have we disproved the lab-leak theory? No,” Dr. Anderson said. “Will we ever be able to? No.” But the Wuhan market origin scenario is more plausible. “I would say these two papers combined present the strongest evidence of that to date.”
Identifying the source of the outbreak that led to the COVID-19 pandemic is based in science, Dr. Andersen said. “What we’re trying to understand is the origin of the pandemic. We’re not trying to place blame.”
Future directions
“With pandemics being pandemics, they affect all of us,” Dr. Andersen said. “We can’t prevent these kinds of events that led to the COVID-19 pandemic. But what we can hope to do is to prevent outbreaks from becoming pandemics.”
Rapid reporting of data and cooperation are needed going forward, Dr. Andersen said. Very strong surveillance systems, including wastewater surveillance, could help monitor for SARS-CoV-2, and other pathogens of potential concern in the future as well.
It should be standard practice for medical professionals to be on alert for unusual respiratory infections too, the researchers said.
“It’s a bloody lucky thing that the doctors at the Shinwa hospital were so on the ball, that they noticed that these cases were something unusual at the end of December,” Dr. Worobey said. “It didn’t have to work out that way.”
A version of this article first appeared on WebMD.com.
The original spread of the virus was a one-two punch, the studies found. Twice, the virus jumped from animals to humans. Virus genetics and outbreak modeling in one study revealed two strains released a few weeks apart in November and December 2019.
“Now I realize it sounds like I just said that a once-in-a-generation event happened twice in short succession, and pandemics are indeed rare,” Joel O. Wertheim, PhD, said at a briefing sponsored by the American Association for the Advancement of Science.
A unique storm of factors had to be present for the outbreak to blow up into a pandemic: Animals carrying a virus that could spread to humans, close human contact with these animals, and a city large enough for the infection to take off before it could be contained are examples.
Unluckily for us humans, this coronavirus – SARS-CoV-2 – is a “generalist virus” capable of infecting many animals, including humans.
“Once all the conditions are in place ... the barriers to spillover have been lowered,” said Dr. Wertheim, a researcher in genetic and molecular networks at the University of California, San Diego. In fact, beyond the two strains of the virus that took hold, there were likely up to two dozen more times where people got the virus but did not spread it far and wide, and it died out.
Overall, the odds were against the virus – 78% of the time, the “introduction” to humans was likely to go extinct, the study showed.
The research revealed the COVID-19 pandemic started small.
“Our model shows that there were likely only a few dozen infections, and only several hospitalizations due to COVID-19, by early December,” said Jonathan Pekar, a graduate student working with Dr. Wertheim.
In Wuhan in late 2019, Mr. Pekar said, there was not a single positive coronavirus sample from thousands of samples from healthy blood donors tested between September and December. Likewise, not one blood sample from patients hospitalized with flu-like illness from October to December 2019 tested positive for SARS-CoV-2.
Mapping the outbreak
A second study published in the journal Science mapped out the earliest COVID-19 cases. This effort showed a tight cluster around the wholesale seafood market inside Wuhan, a city of 11 million residents.
When researchers tried other scenarios – modeling outbreaks in other parts of the city – the pattern did not hold. Again, the Wuhan market appeared to be ground zero for the start of the pandemic.
Michael Worobey, PhD, and colleagues used data from Chinese scientists and the World Health Organization for the study.
“There was this extraordinary pattern where the highest density of cases was both extremely near to and very centered on this market,” said Dr. Worobey, head of ecology and evolutionary biology at the University of Arizona, Tucson.
The highest density of cases, in a city of 8,000 square kilometers, was a “very, very small area of about a third of a kilometer square,” he said.
The outbreak pattern showed the Wuhan market “smack dab in the middle.”
So if it started with infected workers at the market, how did it spread from there? It’s likely the virus got into the community as the vendors at the market went to local shops, infecting people in those stores. Then local community members not linked to the market started getting the virus, Dr. Worobey said.
The investigators also identified which stalls in the market were most likely involved, a sort of internal clustering. “That clustering is very, very specifically in the parts of the market where ... they were selling wildlife, including, for example, raccoon dogs and other animals that we know are susceptible to infection with SARS-CoV-2,” said Kristian Andersen, PhD, director of infectious disease genomics at the Scripps Research Institute in La Jolla, Calif.
What remains unknown is which animal or animals carried the virus, although the raccoon dog – an animal similar to a fox that is native to parts of Asia – remains central to most theories. In addition, many of the farms supplying animals to the market have since been closed, making it challenging for researchers to figure out exactly where infected animals came from.
“We don’t know necessarily, but raccoon dogs were sold at this market all the way up to the beginning of the pandemic,” Dr. Andersen said.
Not ruling out other theories
People who believe SARS-CoV-2 was released from a laboratory in China at first included Dr. Worobey himself. “I’ve in the past been much more open to the lab leak idea,” he said. “And published that in a letter in Science” in November 2021.
The letter was “much more influential than I thought it would be in ways that I think it turned out to be quite damaging,” he said. As more evidence emerged since then, Dr. Worobey said he came around to the Wuhan market source theory.
Dr. Andersen agreed he was more open to the lab-leak theory at first. “I was quite convinced of the lab leak myself until we dove into this very carefully and looked at it much closer,” he said. Newer evidence convinced him “that actually, the data points to this particular market.”
“Have we disproved the lab-leak theory? No,” Dr. Anderson said. “Will we ever be able to? No.” But the Wuhan market origin scenario is more plausible. “I would say these two papers combined present the strongest evidence of that to date.”
Identifying the source of the outbreak that led to the COVID-19 pandemic is based in science, Dr. Andersen said. “What we’re trying to understand is the origin of the pandemic. We’re not trying to place blame.”
Future directions
“With pandemics being pandemics, they affect all of us,” Dr. Andersen said. “We can’t prevent these kinds of events that led to the COVID-19 pandemic. But what we can hope to do is to prevent outbreaks from becoming pandemics.”
Rapid reporting of data and cooperation are needed going forward, Dr. Andersen said. Very strong surveillance systems, including wastewater surveillance, could help monitor for SARS-CoV-2, and other pathogens of potential concern in the future as well.
It should be standard practice for medical professionals to be on alert for unusual respiratory infections too, the researchers said.
“It’s a bloody lucky thing that the doctors at the Shinwa hospital were so on the ball, that they noticed that these cases were something unusual at the end of December,” Dr. Worobey said. “It didn’t have to work out that way.”
A version of this article first appeared on WebMD.com.
Novel liquid biopsy may identify NASH, fibrosis
A novel liquid biopsy test, which uses two circulating proteins, appears to be effective for diagnosing two major liver conditions, according to a new study published in Gut.
The test could allow clinicians to determine the staging of both liver fibrosis and nonalcoholic steatohepatitis, wrote the researchers led by Giulia Angelini, PhD, a postdoctoral fellow focused on nonalcoholic fatty liver disease pathophysiology at the Catholic University of the Sacred Heart in Rome.
“The diagnosis of nonalcoholic steatohepatitis (NASH) currently relies on invasive liver biopsy,” they wrote. “There is, therefore, an urgent need to find noninvasive biomarkers for NASH diagnosis, disease progression, and intervention response monitoring.”
The research team sought to identify a biomarker and algorithm able to predict the presence and severity of nonalcoholic steatohepatitis (NASH) or liver fibrosis. The study evaluated two proteins found in circulating monocytes, which are a type of white blood cell: PLIN2 as a predictor of histological NASH and RAB14 levels as a predictor of liver fibrosis.
The multicenter study included 250 patients, with 100 subjects in the discovery cohort from the Bariatric Surgery Versus Nonalcoholic Steatohepatitis trial, or BRAVES, and 150 subjects in the validation cohort from the Liquid Biopsy for NASH and Liver Fibrosis trial, or LIBRA. The patients had histologically proven nonalcoholic fatty liver disease or NASH with or without fibrosis.
After careful molecular analysis, the research team used neural network classifiers to predict the presence of NASH and NASH stages. The analysis for the prediction of the presence of NASH produced an accuracy of 93% in the discovery cohort and 92% in the validation cohort. Sensitivity and specificity were 95% and 90% in the discovery group and 88% and 100% in the validation group, respectively. The research team also used a neural network analysis to predict the stages of NASH, which showed an accuracy of 85% in the discovery group and 85.2% in the validation cohort.
RAB14 was used to predict liver fibrosis with a logistic model that included waist circumference, age, plasma glucose, high-density lipoprotein, and alanine aminotransferase. In the discovery group, accuracy was 99.2%, sensitivity was 100%, and specificity was 95.8%. In the validation group, accuracy was 97.6%, sensitivity was 99%, and specificity was 89.6%.
When RAB14 was used as the only variable in the model, the accuracy, sensitivity, and specificity in the discovery cohort were 86.4%, 96%, and 45.8%, respectively. In the validation cohort, they were 92.4%, 96.9%, and 34.5%, respectively. In both cohorts, half of the subjects without fibrosis were erroneously predicted as having fibrosis, but the diagnosis of fibrosis was correctly predicted in nearly all subjects.
A limitation of the study is that only White subjects were enrolled, which limits the generalizability to other racial/ethnic groups, the investigators wrote, although they don’t expect differences would be seen in other groups.
“PLIN2 and RAB14 may permit diagnosis of NASH and/or liver fibrosis with a simple blood test,” they wrote. “Our biomarkers can be used in community and population studies permitting to investigate the real prevalence of NASH and liver fibrosis. Moreover, since it requires only blood sampling, they are potentially valuable tools for population-based and prevention studies in children.”
A step forward
“Obesity is a silent pandemic with an expected prevalence rate that will exceed 50% globally by 2030, of which 25% of the adults have fatty liver and approximately 6.5% with NASH, a progressive form of fatty liver,” said Kalyan Ram Bhamidimarri, MD, chief of hepatology and associate professor of clinical medicine at the University of Miami, who was not involved in the research. “Liver biopsy is the current clinical standard to diagnose NASH, but relying on an invasive procedure like liver biopsy that is fraught with several risks in a consistently growing volume of individuals with obesity is unsustainable.

“So, there is an unmet need to diagnose NASH without invasive procedures such as liver biopsy,” he said. He pointed out that many of the alternatives to liver biopsy, such as liver stiffness measurements and scoring systems, pose their own difficulties.
On the other hand, he noted that “blood-based tests that correlate well with liver biopsy, the so-called wet biomarkers or liquid liver biopsy, are easier to perform, accessed widely, and could be tested frequently to assess efficacy of therapies.”
The study was funded by Elucidating Pathways of Steatohepatitis (EPOS Horizon 2020), Stratification of Obese Phenotypes to Optimize Future Obesity Therapy (SOPHIA IMI), Metadeq Inc., and support from the Transcampus Initiative. The study authors declared various competing interests, including some who serve as an advisor or stock option holder for Metadeq Limited. Dr. Bhamidimarri reported no relevant conflicts of interest.
Help your patients understand their risks for NASH by sharing AGA patient education at www.gastro.org/NASH.
A novel liquid biopsy test, which uses two circulating proteins, appears to be effective for diagnosing two major liver conditions, according to a new study published in Gut.
The test could allow clinicians to determine the staging of both liver fibrosis and nonalcoholic steatohepatitis, wrote the researchers led by Giulia Angelini, PhD, a postdoctoral fellow focused on nonalcoholic fatty liver disease pathophysiology at the Catholic University of the Sacred Heart in Rome.
“The diagnosis of nonalcoholic steatohepatitis (NASH) currently relies on invasive liver biopsy,” they wrote. “There is, therefore, an urgent need to find noninvasive biomarkers for NASH diagnosis, disease progression, and intervention response monitoring.”
The research team sought to identify a biomarker and algorithm able to predict the presence and severity of nonalcoholic steatohepatitis (NASH) or liver fibrosis. The study evaluated two proteins found in circulating monocytes, which are a type of white blood cell: PLIN2 as a predictor of histological NASH and RAB14 levels as a predictor of liver fibrosis.
The multicenter study included 250 patients, with 100 subjects in the discovery cohort from the Bariatric Surgery Versus Nonalcoholic Steatohepatitis trial, or BRAVES, and 150 subjects in the validation cohort from the Liquid Biopsy for NASH and Liver Fibrosis trial, or LIBRA. The patients had histologically proven nonalcoholic fatty liver disease or NASH with or without fibrosis.
After careful molecular analysis, the research team used neural network classifiers to predict the presence of NASH and NASH stages. The analysis for the prediction of the presence of NASH produced an accuracy of 93% in the discovery cohort and 92% in the validation cohort. Sensitivity and specificity were 95% and 90% in the discovery group and 88% and 100% in the validation group, respectively. The research team also used a neural network analysis to predict the stages of NASH, which showed an accuracy of 85% in the discovery group and 85.2% in the validation cohort.
RAB14 was used to predict liver fibrosis with a logistic model that included waist circumference, age, plasma glucose, high-density lipoprotein, and alanine aminotransferase. In the discovery group, accuracy was 99.2%, sensitivity was 100%, and specificity was 95.8%. In the validation group, accuracy was 97.6%, sensitivity was 99%, and specificity was 89.6%.
When RAB14 was used as the only variable in the model, the accuracy, sensitivity, and specificity in the discovery cohort were 86.4%, 96%, and 45.8%, respectively. In the validation cohort, they were 92.4%, 96.9%, and 34.5%, respectively. In both cohorts, half of the subjects without fibrosis were erroneously predicted as having fibrosis, but the diagnosis of fibrosis was correctly predicted in nearly all subjects.
A limitation of the study is that only White subjects were enrolled, which limits the generalizability to other racial/ethnic groups, the investigators wrote, although they don’t expect differences would be seen in other groups.
“PLIN2 and RAB14 may permit diagnosis of NASH and/or liver fibrosis with a simple blood test,” they wrote. “Our biomarkers can be used in community and population studies permitting to investigate the real prevalence of NASH and liver fibrosis. Moreover, since it requires only blood sampling, they are potentially valuable tools for population-based and prevention studies in children.”
A step forward
“Obesity is a silent pandemic with an expected prevalence rate that will exceed 50% globally by 2030, of which 25% of the adults have fatty liver and approximately 6.5% with NASH, a progressive form of fatty liver,” said Kalyan Ram Bhamidimarri, MD, chief of hepatology and associate professor of clinical medicine at the University of Miami, who was not involved in the research. “Liver biopsy is the current clinical standard to diagnose NASH, but relying on an invasive procedure like liver biopsy that is fraught with several risks in a consistently growing volume of individuals with obesity is unsustainable.
“So, there is an unmet need to diagnose NASH without invasive procedures such as liver biopsy,” he said. He pointed out that many of the alternatives to liver biopsy, such as liver stiffness measurements and scoring systems, pose their own difficulties.
On the other hand, he noted that “blood-based tests that correlate well with liver biopsy, the so-called wet biomarkers or liquid liver biopsy, are easier to perform, accessed widely, and could be tested frequently to assess efficacy of therapies.”
The study was funded by Elucidating Pathways of Steatohepatitis (EPOS Horizon 2020), Stratification of Obese Phenotypes to Optimize Future Obesity Therapy (SOPHIA IMI), Metadeq Inc., and support from the Transcampus Initiative. The study authors declared various competing interests, including some who serve as an advisor or stock option holder for Metadeq Limited. Dr. Bhamidimarri reported no relevant conflicts of interest.
Help your patients understand their risks for NASH by sharing AGA patient education at www.gastro.org/NASH.
A novel liquid biopsy test, which uses two circulating proteins, appears to be effective for diagnosing two major liver conditions, according to a new study published in Gut.
The test could allow clinicians to determine the staging of both liver fibrosis and nonalcoholic steatohepatitis, wrote the researchers led by Giulia Angelini, PhD, a postdoctoral fellow focused on nonalcoholic fatty liver disease pathophysiology at the Catholic University of the Sacred Heart in Rome.
“The diagnosis of nonalcoholic steatohepatitis (NASH) currently relies on invasive liver biopsy,” they wrote. “There is, therefore, an urgent need to find noninvasive biomarkers for NASH diagnosis, disease progression, and intervention response monitoring.”
The research team sought to identify a biomarker and algorithm able to predict the presence and severity of nonalcoholic steatohepatitis (NASH) or liver fibrosis. The study evaluated two proteins found in circulating monocytes, which are a type of white blood cell: PLIN2 as a predictor of histological NASH and RAB14 levels as a predictor of liver fibrosis.
The multicenter study included 250 patients, with 100 subjects in the discovery cohort from the Bariatric Surgery Versus Nonalcoholic Steatohepatitis trial, or BRAVES, and 150 subjects in the validation cohort from the Liquid Biopsy for NASH and Liver Fibrosis trial, or LIBRA. The patients had histologically proven nonalcoholic fatty liver disease or NASH with or without fibrosis.
After careful molecular analysis, the research team used neural network classifiers to predict the presence of NASH and NASH stages. The analysis for the prediction of the presence of NASH produced an accuracy of 93% in the discovery cohort and 92% in the validation cohort. Sensitivity and specificity were 95% and 90% in the discovery group and 88% and 100% in the validation group, respectively. The research team also used a neural network analysis to predict the stages of NASH, which showed an accuracy of 85% in the discovery group and 85.2% in the validation cohort.
RAB14 was used to predict liver fibrosis with a logistic model that included waist circumference, age, plasma glucose, high-density lipoprotein, and alanine aminotransferase. In the discovery group, accuracy was 99.2%, sensitivity was 100%, and specificity was 95.8%. In the validation group, accuracy was 97.6%, sensitivity was 99%, and specificity was 89.6%.
When RAB14 was used as the only variable in the model, the accuracy, sensitivity, and specificity in the discovery cohort were 86.4%, 96%, and 45.8%, respectively. In the validation cohort, they were 92.4%, 96.9%, and 34.5%, respectively. In both cohorts, half of the subjects without fibrosis were erroneously predicted as having fibrosis, but the diagnosis of fibrosis was correctly predicted in nearly all subjects.
A limitation of the study is that only White subjects were enrolled, which limits the generalizability to other racial/ethnic groups, the investigators wrote, although they don’t expect differences would be seen in other groups.
“PLIN2 and RAB14 may permit diagnosis of NASH and/or liver fibrosis with a simple blood test,” they wrote. “Our biomarkers can be used in community and population studies permitting to investigate the real prevalence of NASH and liver fibrosis. Moreover, since it requires only blood sampling, they are potentially valuable tools for population-based and prevention studies in children.”
A step forward
“Obesity is a silent pandemic with an expected prevalence rate that will exceed 50% globally by 2030, of which 25% of the adults have fatty liver and approximately 6.5% with NASH, a progressive form of fatty liver,” said Kalyan Ram Bhamidimarri, MD, chief of hepatology and associate professor of clinical medicine at the University of Miami, who was not involved in the research. “Liver biopsy is the current clinical standard to diagnose NASH, but relying on an invasive procedure like liver biopsy that is fraught with several risks in a consistently growing volume of individuals with obesity is unsustainable.
“So, there is an unmet need to diagnose NASH without invasive procedures such as liver biopsy,” he said. He pointed out that many of the alternatives to liver biopsy, such as liver stiffness measurements and scoring systems, pose their own difficulties.
On the other hand, he noted that “blood-based tests that correlate well with liver biopsy, the so-called wet biomarkers or liquid liver biopsy, are easier to perform, accessed widely, and could be tested frequently to assess efficacy of therapies.”
The study was funded by Elucidating Pathways of Steatohepatitis (EPOS Horizon 2020), Stratification of Obese Phenotypes to Optimize Future Obesity Therapy (SOPHIA IMI), Metadeq Inc., and support from the Transcampus Initiative. The study authors declared various competing interests, including some who serve as an advisor or stock option holder for Metadeq Limited. Dr. Bhamidimarri reported no relevant conflicts of interest.
Help your patients understand their risks for NASH by sharing AGA patient education at www.gastro.org/NASH.
FROM GUT
Remnant cholesterol captures residual CV risk in patients with T2D
Adding to a growing body of evidence that elevated remnant cholesterol (remnant-C) provides additional and independent risk prediction for major cardiovascular events (MACE), a new analysis has this shown this biomarker has prognostic value specifically in patients with type 2 diabetes (T2D).
In a post hoc analysis of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, each standard-deviation increase in remnant-C was associated with a 7% increased risk in MACE (P = .004) after adjustment for several risk factors including other cholesterol values.
“In type 2 diabetes, remnant-C levels are associated with MACE regardless of LDL-C,” reported a team of investigators led by Liyao Fu, MD, Second Xiangya Hospital of Central South University, Changsha, China .
Remnant-C is one component of triglyceride-rich lipoproteins. Within triglyceride-rich lipoproteins, remnant-C has become a major focus of efforts to explain cardiovascular (CV) residual risk, according to the investigators.
Residual risk is a term used to explain why cardiovascular events occur after all known modifiable factors, such as LDL cholesterol (LDL-C), are controlled.
“Our primary findings indicate that baseline estimated remnant-C levels were associated with MACE regardless of clinical phenotypes, lifestyle confounders relative to CV risk, and lipid-lowering treatment,” said the authors of the analysis.
In the post hoc analysis of the ACCORD trial, which evaluated the effects of intensive glucose lowering in T2D more than 10 years ago, there were data on remnant-C over a median of 8.8 years of follow-up in 9,650 T2D patients. Over this period, 1,815 (17.8%) developed MACE.
Multiple analyses support prognostic value of remnant-C
In addition to the 7% rise in MACE for each standard-deviation increase in remnant-C when calculated as a continuous variable, other analyses told the same story.
This included an assessment by remnant-C tertiles. Not only was there a significant trend (P < .001) for greater risk with each higher baseline tertile of remnant-C, those in the highest tertile had a 38% greater risk of MACE relative to those in the lowest tertile (hazard ratio, 1.38; P < .001) after adjustment for confounders.
The same pattern was seen for several components of MACE, such as CV death and nonfatal myocardial infarction, when remnant-C tertiles were compared.
Visit-to-visit variability in remnant-C over the course of follow-up was also associated with greater risk of MACE. In logarithmic calculations, the risk of MACE climbed about 40% across all three models of risk adjustment. These models included adjustments for different sets of confounders, such as sex, age, blood pressure, CV disease history, and glucose levels. On an unadjusted basis, the risk was increased about 50% (HR, 1.52; P < .001).
For visit-to-visit variability in remnant-C, the greatest effect was on risk of nonfatal MI across models. In model 3, for example, which adjusted for the most confounders, the risk was nearly doubled (HR, 1.92; P < .001). In contrast, there did not appear to be a link between visit-to-visit variability and nonfatal stroke.
In a discordant analysis that was conducted to examine the relative risk of remnant-C independent of LDL-C, those who had a remnant-C level of at least 31 mg/dL were found to have a higher risk of MACE regardless of LDL-C level. Yet, the risk was higher if both remnant-C and LDL-C were elevated. For example, the risk was increased 22% for those with LDL-C at or below 100 mg/dL and remnant-C levels of at least 31 mg/dL (HR, 1.22; P = .015) but climbed to 37% for those with LDL-C above 100 mg/dL if remnant-C was at least 31 mg/dL (HR, 1.38; P = .007).
Remnant-C shows prognostic value in other risk groups
Although this study suggests an important prognostic value for remnant-C in T2D, there are numerous studies suggesting that it has prognostic value in other risk groups, such as those with a history of CV disease. This includes a study published earlier this year with 10 years of follow-up in 41,928 patients in Denmark. When combined with other risk factors, remnant-C substantially improved the accuracy of risk of events over time.
The investigators from this previous study, like the new study in patients with T2D, predict that remnant-C will be eventually included in guidelines.
According to Shi Tai, MD, a coauthor of the T2D study, remnant-C “may allow for the development of specific preventive and therapeutic approaches” to CV risk in patients with T2D.
T2D patients “with elevated plasma remnant-C levels represent a special population that deserves more attention regarding residual risk,” said Dr. Tai of the department of cardiovascular medicine at the Hospital of South Central China.
Great interest, but ready for guidelines?
This is an important direction of ongoing research, according to Christie M. Ballantyne, MD, professor of medicine, Baylor College of Medicine, Houston.
“There is a great deal of interest from both clinicians and trialists to find a simple way to identify patients with high residual risk who are on statin therapy,” he said. He thinks remnant-C has promise in this regard.
“Remnant-C is not in current guidelines,” he said in an interview, but he suggested that there is now a substantial body of evidence to suggest that it might be added if validated in further studies.
“Remnant-C is easy to calculate and may be helpful in practice now to identify patients who need more aggressive therapy to reduce risk and may be useful to identify patients for clinical trials who will benefit from new therapies that are in development,” he said.
However, the clinical relevance of therapies addressed at triglyceride-rich lipoproteins in general or their components, including triglycerides or remnant-C, has never been demonstrated, pointed out Peter W.F. Wilson, MD, PhD.
“Higher fasting or nonfasting triglyceride levels or their surrogates have been shown to be associated with increased risk for cardiovascular disease events in observational studies, but the importance of such measurements in persons already treated with very aggressive LDL-C lowering therapy is not known,” commented Dr. Wilson, director of epidemiology and genomic medicine, Emory School of Medicine, Atlanta.
Dr. Wilson was the coauthor of an editorial that accompanied the previously published Danish study of remnant-C. In his editorial, he suggested that remnant-C has promise for better understanding residual risk, but when contacted about these latest data he emphasized a lack of support so far for clinical relevance.
“Unfortunately, clinical trials have generally not shown that triglyceride lowering [to favorably alter remnant-C] in this situation favorably affects the risk of CV disease events,” he said in an interview. This does not preclude remnant-C as a targetable risk factor, but these data are needed.
Dr. Fu, Dr. Tai, and Dr. Wilson report no potential conflicts of interest. Dr. Ballantyne has financial relationships with more than 25 pharmaceutical companies, including several that produce products employed for the treatment of lipid abnormalities.
Adding to a growing body of evidence that elevated remnant cholesterol (remnant-C) provides additional and independent risk prediction for major cardiovascular events (MACE), a new analysis has this shown this biomarker has prognostic value specifically in patients with type 2 diabetes (T2D).
In a post hoc analysis of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, each standard-deviation increase in remnant-C was associated with a 7% increased risk in MACE (P = .004) after adjustment for several risk factors including other cholesterol values.
“In type 2 diabetes, remnant-C levels are associated with MACE regardless of LDL-C,” reported a team of investigators led by Liyao Fu, MD, Second Xiangya Hospital of Central South University, Changsha, China .
Remnant-C is one component of triglyceride-rich lipoproteins. Within triglyceride-rich lipoproteins, remnant-C has become a major focus of efforts to explain cardiovascular (CV) residual risk, according to the investigators.
Residual risk is a term used to explain why cardiovascular events occur after all known modifiable factors, such as LDL cholesterol (LDL-C), are controlled.
“Our primary findings indicate that baseline estimated remnant-C levels were associated with MACE regardless of clinical phenotypes, lifestyle confounders relative to CV risk, and lipid-lowering treatment,” said the authors of the analysis.
In the post hoc analysis of the ACCORD trial, which evaluated the effects of intensive glucose lowering in T2D more than 10 years ago, there were data on remnant-C over a median of 8.8 years of follow-up in 9,650 T2D patients. Over this period, 1,815 (17.8%) developed MACE.
Multiple analyses support prognostic value of remnant-C
In addition to the 7% rise in MACE for each standard-deviation increase in remnant-C when calculated as a continuous variable, other analyses told the same story.
This included an assessment by remnant-C tertiles. Not only was there a significant trend (P < .001) for greater risk with each higher baseline tertile of remnant-C, those in the highest tertile had a 38% greater risk of MACE relative to those in the lowest tertile (hazard ratio, 1.38; P < .001) after adjustment for confounders.
The same pattern was seen for several components of MACE, such as CV death and nonfatal myocardial infarction, when remnant-C tertiles were compared.
Visit-to-visit variability in remnant-C over the course of follow-up was also associated with greater risk of MACE. In logarithmic calculations, the risk of MACE climbed about 40% across all three models of risk adjustment. These models included adjustments for different sets of confounders, such as sex, age, blood pressure, CV disease history, and glucose levels. On an unadjusted basis, the risk was increased about 50% (HR, 1.52; P < .001).
For visit-to-visit variability in remnant-C, the greatest effect was on risk of nonfatal MI across models. In model 3, for example, which adjusted for the most confounders, the risk was nearly doubled (HR, 1.92; P < .001). In contrast, there did not appear to be a link between visit-to-visit variability and nonfatal stroke.
In a discordant analysis that was conducted to examine the relative risk of remnant-C independent of LDL-C, those who had a remnant-C level of at least 31 mg/dL were found to have a higher risk of MACE regardless of LDL-C level. Yet, the risk was higher if both remnant-C and LDL-C were elevated. For example, the risk was increased 22% for those with LDL-C at or below 100 mg/dL and remnant-C levels of at least 31 mg/dL (HR, 1.22; P = .015) but climbed to 37% for those with LDL-C above 100 mg/dL if remnant-C was at least 31 mg/dL (HR, 1.38; P = .007).
Remnant-C shows prognostic value in other risk groups
Although this study suggests an important prognostic value for remnant-C in T2D, there are numerous studies suggesting that it has prognostic value in other risk groups, such as those with a history of CV disease. This includes a study published earlier this year with 10 years of follow-up in 41,928 patients in Denmark. When combined with other risk factors, remnant-C substantially improved the accuracy of risk of events over time.
The investigators from this previous study, like the new study in patients with T2D, predict that remnant-C will be eventually included in guidelines.
According to Shi Tai, MD, a coauthor of the T2D study, remnant-C “may allow for the development of specific preventive and therapeutic approaches” to CV risk in patients with T2D.
T2D patients “with elevated plasma remnant-C levels represent a special population that deserves more attention regarding residual risk,” said Dr. Tai of the department of cardiovascular medicine at the Hospital of South Central China.
Great interest, but ready for guidelines?
This is an important direction of ongoing research, according to Christie M. Ballantyne, MD, professor of medicine, Baylor College of Medicine, Houston.
“There is a great deal of interest from both clinicians and trialists to find a simple way to identify patients with high residual risk who are on statin therapy,” he said. He thinks remnant-C has promise in this regard.
“Remnant-C is not in current guidelines,” he said in an interview, but he suggested that there is now a substantial body of evidence to suggest that it might be added if validated in further studies.
“Remnant-C is easy to calculate and may be helpful in practice now to identify patients who need more aggressive therapy to reduce risk and may be useful to identify patients for clinical trials who will benefit from new therapies that are in development,” he said.
However, the clinical relevance of therapies addressed at triglyceride-rich lipoproteins in general or their components, including triglycerides or remnant-C, has never been demonstrated, pointed out Peter W.F. Wilson, MD, PhD.
“Higher fasting or nonfasting triglyceride levels or their surrogates have been shown to be associated with increased risk for cardiovascular disease events in observational studies, but the importance of such measurements in persons already treated with very aggressive LDL-C lowering therapy is not known,” commented Dr. Wilson, director of epidemiology and genomic medicine, Emory School of Medicine, Atlanta.
Dr. Wilson was the coauthor of an editorial that accompanied the previously published Danish study of remnant-C. In his editorial, he suggested that remnant-C has promise for better understanding residual risk, but when contacted about these latest data he emphasized a lack of support so far for clinical relevance.
“Unfortunately, clinical trials have generally not shown that triglyceride lowering [to favorably alter remnant-C] in this situation favorably affects the risk of CV disease events,” he said in an interview. This does not preclude remnant-C as a targetable risk factor, but these data are needed.
Dr. Fu, Dr. Tai, and Dr. Wilson report no potential conflicts of interest. Dr. Ballantyne has financial relationships with more than 25 pharmaceutical companies, including several that produce products employed for the treatment of lipid abnormalities.
Adding to a growing body of evidence that elevated remnant cholesterol (remnant-C) provides additional and independent risk prediction for major cardiovascular events (MACE), a new analysis has this shown this biomarker has prognostic value specifically in patients with type 2 diabetes (T2D).
In a post hoc analysis of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, each standard-deviation increase in remnant-C was associated with a 7% increased risk in MACE (P = .004) after adjustment for several risk factors including other cholesterol values.
“In type 2 diabetes, remnant-C levels are associated with MACE regardless of LDL-C,” reported a team of investigators led by Liyao Fu, MD, Second Xiangya Hospital of Central South University, Changsha, China .
Remnant-C is one component of triglyceride-rich lipoproteins. Within triglyceride-rich lipoproteins, remnant-C has become a major focus of efforts to explain cardiovascular (CV) residual risk, according to the investigators.
Residual risk is a term used to explain why cardiovascular events occur after all known modifiable factors, such as LDL cholesterol (LDL-C), are controlled.
“Our primary findings indicate that baseline estimated remnant-C levels were associated with MACE regardless of clinical phenotypes, lifestyle confounders relative to CV risk, and lipid-lowering treatment,” said the authors of the analysis.
In the post hoc analysis of the ACCORD trial, which evaluated the effects of intensive glucose lowering in T2D more than 10 years ago, there were data on remnant-C over a median of 8.8 years of follow-up in 9,650 T2D patients. Over this period, 1,815 (17.8%) developed MACE.
Multiple analyses support prognostic value of remnant-C
In addition to the 7% rise in MACE for each standard-deviation increase in remnant-C when calculated as a continuous variable, other analyses told the same story.
This included an assessment by remnant-C tertiles. Not only was there a significant trend (P < .001) for greater risk with each higher baseline tertile of remnant-C, those in the highest tertile had a 38% greater risk of MACE relative to those in the lowest tertile (hazard ratio, 1.38; P < .001) after adjustment for confounders.
The same pattern was seen for several components of MACE, such as CV death and nonfatal myocardial infarction, when remnant-C tertiles were compared.
Visit-to-visit variability in remnant-C over the course of follow-up was also associated with greater risk of MACE. In logarithmic calculations, the risk of MACE climbed about 40% across all three models of risk adjustment. These models included adjustments for different sets of confounders, such as sex, age, blood pressure, CV disease history, and glucose levels. On an unadjusted basis, the risk was increased about 50% (HR, 1.52; P < .001).
For visit-to-visit variability in remnant-C, the greatest effect was on risk of nonfatal MI across models. In model 3, for example, which adjusted for the most confounders, the risk was nearly doubled (HR, 1.92; P < .001). In contrast, there did not appear to be a link between visit-to-visit variability and nonfatal stroke.
In a discordant analysis that was conducted to examine the relative risk of remnant-C independent of LDL-C, those who had a remnant-C level of at least 31 mg/dL were found to have a higher risk of MACE regardless of LDL-C level. Yet, the risk was higher if both remnant-C and LDL-C were elevated. For example, the risk was increased 22% for those with LDL-C at or below 100 mg/dL and remnant-C levels of at least 31 mg/dL (HR, 1.22; P = .015) but climbed to 37% for those with LDL-C above 100 mg/dL if remnant-C was at least 31 mg/dL (HR, 1.38; P = .007).
Remnant-C shows prognostic value in other risk groups
Although this study suggests an important prognostic value for remnant-C in T2D, there are numerous studies suggesting that it has prognostic value in other risk groups, such as those with a history of CV disease. This includes a study published earlier this year with 10 years of follow-up in 41,928 patients in Denmark. When combined with other risk factors, remnant-C substantially improved the accuracy of risk of events over time.
The investigators from this previous study, like the new study in patients with T2D, predict that remnant-C will be eventually included in guidelines.
According to Shi Tai, MD, a coauthor of the T2D study, remnant-C “may allow for the development of specific preventive and therapeutic approaches” to CV risk in patients with T2D.
T2D patients “with elevated plasma remnant-C levels represent a special population that deserves more attention regarding residual risk,” said Dr. Tai of the department of cardiovascular medicine at the Hospital of South Central China.
Great interest, but ready for guidelines?
This is an important direction of ongoing research, according to Christie M. Ballantyne, MD, professor of medicine, Baylor College of Medicine, Houston.
“There is a great deal of interest from both clinicians and trialists to find a simple way to identify patients with high residual risk who are on statin therapy,” he said. He thinks remnant-C has promise in this regard.
“Remnant-C is not in current guidelines,” he said in an interview, but he suggested that there is now a substantial body of evidence to suggest that it might be added if validated in further studies.
“Remnant-C is easy to calculate and may be helpful in practice now to identify patients who need more aggressive therapy to reduce risk and may be useful to identify patients for clinical trials who will benefit from new therapies that are in development,” he said.
However, the clinical relevance of therapies addressed at triglyceride-rich lipoproteins in general or their components, including triglycerides or remnant-C, has never been demonstrated, pointed out Peter W.F. Wilson, MD, PhD.
“Higher fasting or nonfasting triglyceride levels or their surrogates have been shown to be associated with increased risk for cardiovascular disease events in observational studies, but the importance of such measurements in persons already treated with very aggressive LDL-C lowering therapy is not known,” commented Dr. Wilson, director of epidemiology and genomic medicine, Emory School of Medicine, Atlanta.
Dr. Wilson was the coauthor of an editorial that accompanied the previously published Danish study of remnant-C. In his editorial, he suggested that remnant-C has promise for better understanding residual risk, but when contacted about these latest data he emphasized a lack of support so far for clinical relevance.
“Unfortunately, clinical trials have generally not shown that triglyceride lowering [to favorably alter remnant-C] in this situation favorably affects the risk of CV disease events,” he said in an interview. This does not preclude remnant-C as a targetable risk factor, but these data are needed.
Dr. Fu, Dr. Tai, and Dr. Wilson report no potential conflicts of interest. Dr. Ballantyne has financial relationships with more than 25 pharmaceutical companies, including several that produce products employed for the treatment of lipid abnormalities.
FROM DIABETES CARE