User login
Doctor faces apparent retaliation after alleging data manipulation in published trial
A rheumatologist was suspended from a professional society and his license to practice medicine was threatened after he raised concerns about data manipulation in a published study for which he recruited patients, according to documents seen by Retraction Watch.
The study, “Added Value of Anti-CD74 Autoantibodies in Axial SpondyloArthritis in a Population With Low HLA-B27 Prevalence,” was published in Frontiers in Immunology in 2019 and has been cited 13 times, according to Clarivate’s Web of Science. In its acknowledgments, it listed Fouad Fayad, PhD, a rheumatologist at the University of Saint Joseph and Hotel-Dieu de France University Medical Center in Beirut, as one of the researchers who recruited patients for the trial.
Dr. Fayad alleged that the researchers tested patient samples multiple times and used a mix of old and new values in their analysis. After he reported his concerns to the journal and then the university, which both concluded that they could not confirm or refute his allegations, he has faced apparent retaliation, including the suspension of his membership in the Lebanese Society of Rheumatology.
In comments to Retraction Watch, the corresponding author for the study noted that the two investigations did not find data manipulation, and said the issue was “based on a background of personal and professional conflicts.”
In an April video recorded with Nassim Nicholas Taleb, PhD, a former quant trader and retired distinguished professor of finance and risk engineering at New York University’s Tandon School of Engineering, Dr. Fayad explained that he was originally an author on the paper, but after expressing concerns about the methodology to the other authors, they didn’t respond to him and his name was dropped from the author list without warning or explanation.
Dr. Taleb also detailed the issues with the study, showing graphs that indicate “very poor correlation” between the old and new test results from participant samples.
In October 2019, Dr. Fayad contacted Frontiers in Immunology with his concerns. But the journal’s investigation was inconclusive, and a staffer on the research integrity team told him in July 2020 to contact his institution to investigate, according to emails seen by Retraction Watch.
Dr. Fayad did so, but the University of Saint Joseph “rushed an incomplete investigation,” he said. It began in September of 2021 and concluded 2 months later that the investigation committee could not confirm or disprove Dr. Fayad’s allegations of data manipulation, according to a copy of the report seen by Retraction Watch. He said that their statistical reviewer did not receive all of the relevant documents, although he had provided them to the university.
A university official sent the findings from the investigation to the Lebanese Order of Physicians – Beirut, which decided to suspend Dr. Fayad’s membership in the Lebanese Society of Rheumatology. It’s “needless to explain the damage resulting from this suspension,” Dr. Fayad said.
The Beirut organization wrote to the Lebanese Order of Physicians – Tripoli, the body with which Dr. Fayad’s license is registered, informing them of the decision. In a copy of the letter seen by Retraction Watch, the Beirut organization cited the university investigation finding Dr. Fayad’s allegations to be invalid, as well as a letter in which he alleged mismanagement of the rheumatology society, as reasons for the decision, and referred the matter to the Tripoli organization for further investigation.
Dr. Fayad told us that the letter asking the Tripoli organization to investigate him could have led to the suspension of his license to practice medicine:
“My license is registered with the Lebanese Order of Physicians – Tripoli. So legally speaking, it is only Tripoli organization that can suspend my license/permit to practice. Beirut Organization has tried to summon me to their investigation committee, but my license (being registered in Tripoli Organization) does not fall under Beirut’s jurisdiction; in other words Beirut Organization violated the law; they can not approach me directly, they have to go through the Tripoli Organization.
“As such, and since Beirut organization could not suspend my license (as they did for my membership in the Lebanese Society of Rheumatology) they sent the letter to Tripoli organization asking them to investigate the matter and take necessary disciplinary action. This was a threat to suspending my license to practice medicine. Should Tripoli Organization have used the [University of Saint Joseph] letter and investigation report without conducting their own international investigation, my permit to practice would have been suspended.”
The Lebanese Order of Physicians – Tripoli conducted its own investigation and confirmed “the existence of manipulation in the study data and failure to respect the data integrity,” according to an official translation of the investigation report seen by Retraction Watch. The Lebanese Order of Physicians – Tripoli decided after its investigation that Dr. Fayad’s suspension from the rheumatology society was invalid.
The lead author of the study in question, Nelly R. Ziade of Saint Joseph University and Hotel-Dieu de France Hospital in Beirut, told Retraction Watch that the investigation by the Lebanese Order of Physicians – Tripoli “cannot be considered as final or official” and that she was “never approached, interviewed, or asked to provide any documents related to this complaint.”
She continued: “I will always be available to give any scientific clarification requested by the Order of Physicians in Beirut where a serious investigation giving equal voice to both parties is currently conducted.
“Kindly note that the concerned journal has already conducted an internal investigation where both parties provided all documents and it was concluded that there was no scientific foundation for the accusations.
“Again, a similar investigation was conducted by the Saint-Joseph University in Beirut (where myself and the other party work). Both parties presented study documents to a committee including the president of the IRB, the vice president of the University, the medical director of the University Hospital, experts in musculoskeletal system and biostatistics. In brief, the case against the authors was dismissed, no data manipulation was found and the colleague from Tripoli also was submitted to University sanctions. The report of the University can be shared with you should you need it.
“I’m afraid that this issue is based on a background of personal and professional conflicts.”
Dr. Fayad added: “The beauty of science is that the truth will always prevail and cannot be obscured for long time.”
A version of this article first appeared on RetractionWatch.com.
A rheumatologist was suspended from a professional society and his license to practice medicine was threatened after he raised concerns about data manipulation in a published study for which he recruited patients, according to documents seen by Retraction Watch.
The study, “Added Value of Anti-CD74 Autoantibodies in Axial SpondyloArthritis in a Population With Low HLA-B27 Prevalence,” was published in Frontiers in Immunology in 2019 and has been cited 13 times, according to Clarivate’s Web of Science. In its acknowledgments, it listed Fouad Fayad, PhD, a rheumatologist at the University of Saint Joseph and Hotel-Dieu de France University Medical Center in Beirut, as one of the researchers who recruited patients for the trial.
Dr. Fayad alleged that the researchers tested patient samples multiple times and used a mix of old and new values in their analysis. After he reported his concerns to the journal and then the university, which both concluded that they could not confirm or refute his allegations, he has faced apparent retaliation, including the suspension of his membership in the Lebanese Society of Rheumatology.
In comments to Retraction Watch, the corresponding author for the study noted that the two investigations did not find data manipulation, and said the issue was “based on a background of personal and professional conflicts.”
In an April video recorded with Nassim Nicholas Taleb, PhD, a former quant trader and retired distinguished professor of finance and risk engineering at New York University’s Tandon School of Engineering, Dr. Fayad explained that he was originally an author on the paper, but after expressing concerns about the methodology to the other authors, they didn’t respond to him and his name was dropped from the author list without warning or explanation.
Dr. Taleb also detailed the issues with the study, showing graphs that indicate “very poor correlation” between the old and new test results from participant samples.
In October 2019, Dr. Fayad contacted Frontiers in Immunology with his concerns. But the journal’s investigation was inconclusive, and a staffer on the research integrity team told him in July 2020 to contact his institution to investigate, according to emails seen by Retraction Watch.
Dr. Fayad did so, but the University of Saint Joseph “rushed an incomplete investigation,” he said. It began in September of 2021 and concluded 2 months later that the investigation committee could not confirm or disprove Dr. Fayad’s allegations of data manipulation, according to a copy of the report seen by Retraction Watch. He said that their statistical reviewer did not receive all of the relevant documents, although he had provided them to the university.
A university official sent the findings from the investigation to the Lebanese Order of Physicians – Beirut, which decided to suspend Dr. Fayad’s membership in the Lebanese Society of Rheumatology. It’s “needless to explain the damage resulting from this suspension,” Dr. Fayad said.
The Beirut organization wrote to the Lebanese Order of Physicians – Tripoli, the body with which Dr. Fayad’s license is registered, informing them of the decision. In a copy of the letter seen by Retraction Watch, the Beirut organization cited the university investigation finding Dr. Fayad’s allegations to be invalid, as well as a letter in which he alleged mismanagement of the rheumatology society, as reasons for the decision, and referred the matter to the Tripoli organization for further investigation.
Dr. Fayad told us that the letter asking the Tripoli organization to investigate him could have led to the suspension of his license to practice medicine:
“My license is registered with the Lebanese Order of Physicians – Tripoli. So legally speaking, it is only Tripoli organization that can suspend my license/permit to practice. Beirut Organization has tried to summon me to their investigation committee, but my license (being registered in Tripoli Organization) does not fall under Beirut’s jurisdiction; in other words Beirut Organization violated the law; they can not approach me directly, they have to go through the Tripoli Organization.
“As such, and since Beirut organization could not suspend my license (as they did for my membership in the Lebanese Society of Rheumatology) they sent the letter to Tripoli organization asking them to investigate the matter and take necessary disciplinary action. This was a threat to suspending my license to practice medicine. Should Tripoli Organization have used the [University of Saint Joseph] letter and investigation report without conducting their own international investigation, my permit to practice would have been suspended.”
The Lebanese Order of Physicians – Tripoli conducted its own investigation and confirmed “the existence of manipulation in the study data and failure to respect the data integrity,” according to an official translation of the investigation report seen by Retraction Watch. The Lebanese Order of Physicians – Tripoli decided after its investigation that Dr. Fayad’s suspension from the rheumatology society was invalid.
The lead author of the study in question, Nelly R. Ziade of Saint Joseph University and Hotel-Dieu de France Hospital in Beirut, told Retraction Watch that the investigation by the Lebanese Order of Physicians – Tripoli “cannot be considered as final or official” and that she was “never approached, interviewed, or asked to provide any documents related to this complaint.”
She continued: “I will always be available to give any scientific clarification requested by the Order of Physicians in Beirut where a serious investigation giving equal voice to both parties is currently conducted.
“Kindly note that the concerned journal has already conducted an internal investigation where both parties provided all documents and it was concluded that there was no scientific foundation for the accusations.
“Again, a similar investigation was conducted by the Saint-Joseph University in Beirut (where myself and the other party work). Both parties presented study documents to a committee including the president of the IRB, the vice president of the University, the medical director of the University Hospital, experts in musculoskeletal system and biostatistics. In brief, the case against the authors was dismissed, no data manipulation was found and the colleague from Tripoli also was submitted to University sanctions. The report of the University can be shared with you should you need it.
“I’m afraid that this issue is based on a background of personal and professional conflicts.”
Dr. Fayad added: “The beauty of science is that the truth will always prevail and cannot be obscured for long time.”
A version of this article first appeared on RetractionWatch.com.
A rheumatologist was suspended from a professional society and his license to practice medicine was threatened after he raised concerns about data manipulation in a published study for which he recruited patients, according to documents seen by Retraction Watch.
The study, “Added Value of Anti-CD74 Autoantibodies in Axial SpondyloArthritis in a Population With Low HLA-B27 Prevalence,” was published in Frontiers in Immunology in 2019 and has been cited 13 times, according to Clarivate’s Web of Science. In its acknowledgments, it listed Fouad Fayad, PhD, a rheumatologist at the University of Saint Joseph and Hotel-Dieu de France University Medical Center in Beirut, as one of the researchers who recruited patients for the trial.
Dr. Fayad alleged that the researchers tested patient samples multiple times and used a mix of old and new values in their analysis. After he reported his concerns to the journal and then the university, which both concluded that they could not confirm or refute his allegations, he has faced apparent retaliation, including the suspension of his membership in the Lebanese Society of Rheumatology.
In comments to Retraction Watch, the corresponding author for the study noted that the two investigations did not find data manipulation, and said the issue was “based on a background of personal and professional conflicts.”
In an April video recorded with Nassim Nicholas Taleb, PhD, a former quant trader and retired distinguished professor of finance and risk engineering at New York University’s Tandon School of Engineering, Dr. Fayad explained that he was originally an author on the paper, but after expressing concerns about the methodology to the other authors, they didn’t respond to him and his name was dropped from the author list without warning or explanation.
Dr. Taleb also detailed the issues with the study, showing graphs that indicate “very poor correlation” between the old and new test results from participant samples.
In October 2019, Dr. Fayad contacted Frontiers in Immunology with his concerns. But the journal’s investigation was inconclusive, and a staffer on the research integrity team told him in July 2020 to contact his institution to investigate, according to emails seen by Retraction Watch.
Dr. Fayad did so, but the University of Saint Joseph “rushed an incomplete investigation,” he said. It began in September of 2021 and concluded 2 months later that the investigation committee could not confirm or disprove Dr. Fayad’s allegations of data manipulation, according to a copy of the report seen by Retraction Watch. He said that their statistical reviewer did not receive all of the relevant documents, although he had provided them to the university.
A university official sent the findings from the investigation to the Lebanese Order of Physicians – Beirut, which decided to suspend Dr. Fayad’s membership in the Lebanese Society of Rheumatology. It’s “needless to explain the damage resulting from this suspension,” Dr. Fayad said.
The Beirut organization wrote to the Lebanese Order of Physicians – Tripoli, the body with which Dr. Fayad’s license is registered, informing them of the decision. In a copy of the letter seen by Retraction Watch, the Beirut organization cited the university investigation finding Dr. Fayad’s allegations to be invalid, as well as a letter in which he alleged mismanagement of the rheumatology society, as reasons for the decision, and referred the matter to the Tripoli organization for further investigation.
Dr. Fayad told us that the letter asking the Tripoli organization to investigate him could have led to the suspension of his license to practice medicine:
“My license is registered with the Lebanese Order of Physicians – Tripoli. So legally speaking, it is only Tripoli organization that can suspend my license/permit to practice. Beirut Organization has tried to summon me to their investigation committee, but my license (being registered in Tripoli Organization) does not fall under Beirut’s jurisdiction; in other words Beirut Organization violated the law; they can not approach me directly, they have to go through the Tripoli Organization.
“As such, and since Beirut organization could not suspend my license (as they did for my membership in the Lebanese Society of Rheumatology) they sent the letter to Tripoli organization asking them to investigate the matter and take necessary disciplinary action. This was a threat to suspending my license to practice medicine. Should Tripoli Organization have used the [University of Saint Joseph] letter and investigation report without conducting their own international investigation, my permit to practice would have been suspended.”
The Lebanese Order of Physicians – Tripoli conducted its own investigation and confirmed “the existence of manipulation in the study data and failure to respect the data integrity,” according to an official translation of the investigation report seen by Retraction Watch. The Lebanese Order of Physicians – Tripoli decided after its investigation that Dr. Fayad’s suspension from the rheumatology society was invalid.
The lead author of the study in question, Nelly R. Ziade of Saint Joseph University and Hotel-Dieu de France Hospital in Beirut, told Retraction Watch that the investigation by the Lebanese Order of Physicians – Tripoli “cannot be considered as final or official” and that she was “never approached, interviewed, or asked to provide any documents related to this complaint.”
She continued: “I will always be available to give any scientific clarification requested by the Order of Physicians in Beirut where a serious investigation giving equal voice to both parties is currently conducted.
“Kindly note that the concerned journal has already conducted an internal investigation where both parties provided all documents and it was concluded that there was no scientific foundation for the accusations.
“Again, a similar investigation was conducted by the Saint-Joseph University in Beirut (where myself and the other party work). Both parties presented study documents to a committee including the president of the IRB, the vice president of the University, the medical director of the University Hospital, experts in musculoskeletal system and biostatistics. In brief, the case against the authors was dismissed, no data manipulation was found and the colleague from Tripoli also was submitted to University sanctions. The report of the University can be shared with you should you need it.
“I’m afraid that this issue is based on a background of personal and professional conflicts.”
Dr. Fayad added: “The beauty of science is that the truth will always prevail and cannot be obscured for long time.”
A version of this article first appeared on RetractionWatch.com.
Sleep Medicine Network
Home-based Mechanical Ventilation and Neuromuscular Disease Section
Navigating the latest device supply chain challenge: Mechanical airway clearance
(distal airways). Cough augmentation techniques provide lung volume recruitment on the insufflation phase, in addition to mobilization of secretions with augmentation of the peak expiratory flow rate to >160 L/min on the exhalation phase.
A mechanical insufflation-exsufflation (MI-E) device (T70 Cough Assist - Phillips) is now on indefinite backorder. This creates a dangerous situation for our patients requiring cough augmentation for survival. Alternative options that provide both MI-E and high frequency oscillation include two systems (Synclara Cough System – Hill-rom and the Biwaze Cough System-ABM Respiratory Care).
The Synclara can only be obtained in a direct-to-patient model, contracting with individual respiratory therapists, outside of the standard durable medical equipment model. The final MI-E model option is the VOCSYN multifunctional ventilator (ventilator, cough assist, nebulizer, oxygen concentrator, suction). This multifunction ventilator has had variable acceptance with HCPCS code E0467. If the VOCSYN is chosen, the patient cannot have been issued any component devices or have reached the 36-month cap for oxygen equipment (CR 10854 special payment rule, 42 CFR414.222).
As the supply of devices is exhausted, we will need to shift to evidence-based manual options. Manual cough augmentation can be done effectively with a bag-valve mask, using breath stacking to achieve maximal lung insufflation, optimizing the length tension relationship of elastic recoil on exhalation to increase peak cough flow (PCF).
This can be done alone but is more effective when combined with manually assisted cough (Bach JR. Chest. 1993;104[5]:1553-62). These interventions require training of the caregivers, using resources such as those found at www.canventottawa.ca.
With continued supply chain instability, manual airway clearance techniques should be considered in patients with less advanced cough impairment (PCF 160-270 L/min), to save the remaining devices for those with PCF of <160 L/min.
Jeanette Brown, MD, PhD
Karin Provost, DO, PhD
Members-at-Large
Home-based Mechanical Ventilation and Neuromuscular Disease Section
Navigating the latest device supply chain challenge: Mechanical airway clearance
(distal airways). Cough augmentation techniques provide lung volume recruitment on the insufflation phase, in addition to mobilization of secretions with augmentation of the peak expiratory flow rate to >160 L/min on the exhalation phase.
A mechanical insufflation-exsufflation (MI-E) device (T70 Cough Assist - Phillips) is now on indefinite backorder. This creates a dangerous situation for our patients requiring cough augmentation for survival. Alternative options that provide both MI-E and high frequency oscillation include two systems (Synclara Cough System – Hill-rom and the Biwaze Cough System-ABM Respiratory Care).
The Synclara can only be obtained in a direct-to-patient model, contracting with individual respiratory therapists, outside of the standard durable medical equipment model. The final MI-E model option is the VOCSYN multifunctional ventilator (ventilator, cough assist, nebulizer, oxygen concentrator, suction). This multifunction ventilator has had variable acceptance with HCPCS code E0467. If the VOCSYN is chosen, the patient cannot have been issued any component devices or have reached the 36-month cap for oxygen equipment (CR 10854 special payment rule, 42 CFR414.222).
As the supply of devices is exhausted, we will need to shift to evidence-based manual options. Manual cough augmentation can be done effectively with a bag-valve mask, using breath stacking to achieve maximal lung insufflation, optimizing the length tension relationship of elastic recoil on exhalation to increase peak cough flow (PCF).
This can be done alone but is more effective when combined with manually assisted cough (Bach JR. Chest. 1993;104[5]:1553-62). These interventions require training of the caregivers, using resources such as those found at www.canventottawa.ca.
With continued supply chain instability, manual airway clearance techniques should be considered in patients with less advanced cough impairment (PCF 160-270 L/min), to save the remaining devices for those with PCF of <160 L/min.
Jeanette Brown, MD, PhD
Karin Provost, DO, PhD
Members-at-Large
Home-based Mechanical Ventilation and Neuromuscular Disease Section
Navigating the latest device supply chain challenge: Mechanical airway clearance
(distal airways). Cough augmentation techniques provide lung volume recruitment on the insufflation phase, in addition to mobilization of secretions with augmentation of the peak expiratory flow rate to >160 L/min on the exhalation phase.
A mechanical insufflation-exsufflation (MI-E) device (T70 Cough Assist - Phillips) is now on indefinite backorder. This creates a dangerous situation for our patients requiring cough augmentation for survival. Alternative options that provide both MI-E and high frequency oscillation include two systems (Synclara Cough System – Hill-rom and the Biwaze Cough System-ABM Respiratory Care).
The Synclara can only be obtained in a direct-to-patient model, contracting with individual respiratory therapists, outside of the standard durable medical equipment model. The final MI-E model option is the VOCSYN multifunctional ventilator (ventilator, cough assist, nebulizer, oxygen concentrator, suction). This multifunction ventilator has had variable acceptance with HCPCS code E0467. If the VOCSYN is chosen, the patient cannot have been issued any component devices or have reached the 36-month cap for oxygen equipment (CR 10854 special payment rule, 42 CFR414.222).
As the supply of devices is exhausted, we will need to shift to evidence-based manual options. Manual cough augmentation can be done effectively with a bag-valve mask, using breath stacking to achieve maximal lung insufflation, optimizing the length tension relationship of elastic recoil on exhalation to increase peak cough flow (PCF).
This can be done alone but is more effective when combined with manually assisted cough (Bach JR. Chest. 1993;104[5]:1553-62). These interventions require training of the caregivers, using resources such as those found at www.canventottawa.ca.
With continued supply chain instability, manual airway clearance techniques should be considered in patients with less advanced cough impairment (PCF 160-270 L/min), to save the remaining devices for those with PCF of <160 L/min.
Jeanette Brown, MD, PhD
Karin Provost, DO, PhD
Members-at-Large
Airways Disorders Network
Asthma and COPD Section
Go TEAM! Shared decision-making tool for patient-clinician collaboration in severe asthma

Shared decision-making is associated with improved medication adherence in adults (Wilson, et al. Am J Respir Crit Care Med. 2010;181[6]:566-77) and quality of life and asthma control in children (Taylor, et al. J Asthma. 2018;55[6]:675-83). The Global Initiative for Asthma committee recommends a patient-clinician partnership. Activated and engaged patients play a major role in their asthma management (https://ginasthma.org/gina-reports). Shared decision-making discussions should include potential benefits and harms of the therapeutic options, patient’s values and lifestyle preferences, and addressing concerns.
The CHEST Foundation, the Allergy and Asthma Network, and the American College of Allergy, Asthma, and Immunology developed an online shared decision- making tool for severe asthma (https://asthma.chestnet.org/sdm-tool).
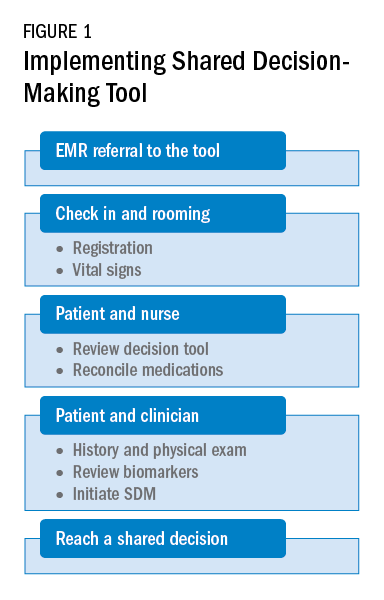
This tool utilizes patient’s values, specifics about triggers, asthma control, medication side effects, and lifestyle preferences to identify personalized management options. The tool provides information about recommended therapeutic options in simple terms, including potential benefits, possible side effects, expected treatment frequency and duration, and financial aid information. The treatment options currently explained in this tool include anti-immunoglobulin E, anti-interleukin-5, anti-interleukin-4/13, bronchial thermoplasty, long-acting muscarinic antagonist, macrolides, oral corticosteroids, and standard of care.

As a team, the patient and the health care professional can use this tool during office visits to help guide management. Figure 1 shows a suggested workflow to utilize the tool in clinical practice.
Potential barriers include excess time and increased human resources. Barrier mitigation may include reviewing the tool and reconciling the medications before the clinician enters the room. With these interventions, many clinician encounters may be completed in 10 to 15 minutes.
Farrukh Abbas, MBBS
Fellow-in-Training
Asthma and COPD Section
Go TEAM! Shared decision-making tool for patient-clinician collaboration in severe asthma
Shared decision-making is associated with improved medication adherence in adults (Wilson, et al. Am J Respir Crit Care Med. 2010;181[6]:566-77) and quality of life and asthma control in children (Taylor, et al. J Asthma. 2018;55[6]:675-83). The Global Initiative for Asthma committee recommends a patient-clinician partnership. Activated and engaged patients play a major role in their asthma management (https://ginasthma.org/gina-reports). Shared decision-making discussions should include potential benefits and harms of the therapeutic options, patient’s values and lifestyle preferences, and addressing concerns.
The CHEST Foundation, the Allergy and Asthma Network, and the American College of Allergy, Asthma, and Immunology developed an online shared decision- making tool for severe asthma (https://asthma.chestnet.org/sdm-tool).
This tool utilizes patient’s values, specifics about triggers, asthma control, medication side effects, and lifestyle preferences to identify personalized management options. The tool provides information about recommended therapeutic options in simple terms, including potential benefits, possible side effects, expected treatment frequency and duration, and financial aid information. The treatment options currently explained in this tool include anti-immunoglobulin E, anti-interleukin-5, anti-interleukin-4/13, bronchial thermoplasty, long-acting muscarinic antagonist, macrolides, oral corticosteroids, and standard of care.
As a team, the patient and the health care professional can use this tool during office visits to help guide management. Figure 1 shows a suggested workflow to utilize the tool in clinical practice.
Potential barriers include excess time and increased human resources. Barrier mitigation may include reviewing the tool and reconciling the medications before the clinician enters the room. With these interventions, many clinician encounters may be completed in 10 to 15 minutes.
Farrukh Abbas, MBBS
Fellow-in-Training
Asthma and COPD Section
Go TEAM! Shared decision-making tool for patient-clinician collaboration in severe asthma
Shared decision-making is associated with improved medication adherence in adults (Wilson, et al. Am J Respir Crit Care Med. 2010;181[6]:566-77) and quality of life and asthma control in children (Taylor, et al. J Asthma. 2018;55[6]:675-83). The Global Initiative for Asthma committee recommends a patient-clinician partnership. Activated and engaged patients play a major role in their asthma management (https://ginasthma.org/gina-reports). Shared decision-making discussions should include potential benefits and harms of the therapeutic options, patient’s values and lifestyle preferences, and addressing concerns.
The CHEST Foundation, the Allergy and Asthma Network, and the American College of Allergy, Asthma, and Immunology developed an online shared decision- making tool for severe asthma (https://asthma.chestnet.org/sdm-tool).
This tool utilizes patient’s values, specifics about triggers, asthma control, medication side effects, and lifestyle preferences to identify personalized management options. The tool provides information about recommended therapeutic options in simple terms, including potential benefits, possible side effects, expected treatment frequency and duration, and financial aid information. The treatment options currently explained in this tool include anti-immunoglobulin E, anti-interleukin-5, anti-interleukin-4/13, bronchial thermoplasty, long-acting muscarinic antagonist, macrolides, oral corticosteroids, and standard of care.
As a team, the patient and the health care professional can use this tool during office visits to help guide management. Figure 1 shows a suggested workflow to utilize the tool in clinical practice.
Potential barriers include excess time and increased human resources. Barrier mitigation may include reviewing the tool and reconciling the medications before the clinician enters the room. With these interventions, many clinician encounters may be completed in 10 to 15 minutes.
Farrukh Abbas, MBBS
Fellow-in-Training
Long COVID doubles risk of some serious outcomes in children, teens
Researchers from the Centers for Disease Control and Prevention report that
Heart inflammation; a blood clot in the lung; or a blood clot in the lower leg, thigh, or pelvis were the most common bad outcomes in a new study. Even though the risk was higher for these and some other serious events, the overall numbers were small.
“Many of these conditions were rare or uncommon among children in this analysis, but even a small increase in these conditions is notable,” a CDC new release stated.
The investigators said their findings stress the importance of COVID-19 vaccination in Americans under the age of 18.
The study was published online in the CDC’s Morbidity and Mortality Weekly Report.
Less is known about long COVID in children
Lyudmyla Kompaniyets, PhD, and colleagues noted that most research on long COVID to date has been done in adults, so little information is available about the risks to Americans ages 17 and younger.
To learn more, they compared post–COVID-19 symptoms and conditions between 781,419 children and teenagers with confirmed COVID-19 to another 2,344,257 without COVID-19. They looked at medical claims and laboratory data for these children and teenagers from March 1, 2020, through Jan. 31, 2022, to see who got any of 15 specific outcomes linked to long COVID-19.
Long COVID was defined as a condition where symptoms that last for or begin at least 4 weeks after a COVID-19 diagnosis.
Compared to children with no history of a COVID-19 diagnosis, the long COVID-19 group was 101% more likely to have an acute pulmonary embolism, 99% more likely to have myocarditis or cardiomyopathy, 87% more likely to have a venous thromboembolic event, 32% more likely to have acute and unspecified renal failure, and 23% more likely to have type 1 diabetes.
“This report points to the fact that the risks of COVID infection itself, both in terms of the acute effects, MIS-C [multisystem inflammatory syndrome in children], as well as the long-term effects, are real, are concerning, and are potentially very serious,” said Stuart Berger, MD, chair of the American Academy of Pediatrics Section on Cardiology and Cardiac Surgery.
“The message that we should take away from this is that we should be very keen on all the methods of prevention for COVID, especially the vaccine,” said Dr. Berger, chief of cardiology in the department of pediatrics at Northwestern University in Chicago.
A ‘wake-up call’
The study findings are “sobering” and are “a reminder of the seriousness of COVID infection,” says Gregory Poland, MD, an infectious disease expert at the Mayo Clinic in Rochester, Minn.
“When you look in particular at the more serious complications from COVID in this young age group, those are life-altering complications that will have consequences and ramifications throughout their lives,” he said.
“I would take this as a serious wake-up call to parents [at a time when] the immunization rates in younger children are so pitifully low,” Dr. Poland said.
Still early days
The study is suggestive but not definitive, said Peter Katona, MD, professor of medicine and infectious diseases expert at the UCLA Fielding School of Public Health.
It’s still too early to draw conclusions about long COVID, including in children, because many questions remain, he said: Should long COVID be defined as symptoms at 1 month or 3 months after infection? How do you define brain fog?
Dr. Katona and colleagues are studying long COVID intervention among students at UCLA to answer some of these questions, including the incidence and effect of early intervention.
The study had “at least seven limitations,” the researchers noted. Among them was the use of medical claims data that noted long COVID outcomes but not how severe they were; some people in the no COVID group might have had the illness but not been diagnosed; and the researchers did not adjust for vaccination status.
Dr. Poland noted that the study was done during surges in COVID variants including Delta and Omicron. In other words, any long COVID effects linked to more recent variants such as BA.5 or BA.2.75 are unknown.
A version of this article first appeared on WebMD.com.
Researchers from the Centers for Disease Control and Prevention report that
Heart inflammation; a blood clot in the lung; or a blood clot in the lower leg, thigh, or pelvis were the most common bad outcomes in a new study. Even though the risk was higher for these and some other serious events, the overall numbers were small.
“Many of these conditions were rare or uncommon among children in this analysis, but even a small increase in these conditions is notable,” a CDC new release stated.
The investigators said their findings stress the importance of COVID-19 vaccination in Americans under the age of 18.
The study was published online in the CDC’s Morbidity and Mortality Weekly Report.
Less is known about long COVID in children
Lyudmyla Kompaniyets, PhD, and colleagues noted that most research on long COVID to date has been done in adults, so little information is available about the risks to Americans ages 17 and younger.
To learn more, they compared post–COVID-19 symptoms and conditions between 781,419 children and teenagers with confirmed COVID-19 to another 2,344,257 without COVID-19. They looked at medical claims and laboratory data for these children and teenagers from March 1, 2020, through Jan. 31, 2022, to see who got any of 15 specific outcomes linked to long COVID-19.
Long COVID was defined as a condition where symptoms that last for or begin at least 4 weeks after a COVID-19 diagnosis.
Compared to children with no history of a COVID-19 diagnosis, the long COVID-19 group was 101% more likely to have an acute pulmonary embolism, 99% more likely to have myocarditis or cardiomyopathy, 87% more likely to have a venous thromboembolic event, 32% more likely to have acute and unspecified renal failure, and 23% more likely to have type 1 diabetes.
“This report points to the fact that the risks of COVID infection itself, both in terms of the acute effects, MIS-C [multisystem inflammatory syndrome in children], as well as the long-term effects, are real, are concerning, and are potentially very serious,” said Stuart Berger, MD, chair of the American Academy of Pediatrics Section on Cardiology and Cardiac Surgery.
“The message that we should take away from this is that we should be very keen on all the methods of prevention for COVID, especially the vaccine,” said Dr. Berger, chief of cardiology in the department of pediatrics at Northwestern University in Chicago.
A ‘wake-up call’
The study findings are “sobering” and are “a reminder of the seriousness of COVID infection,” says Gregory Poland, MD, an infectious disease expert at the Mayo Clinic in Rochester, Minn.
“When you look in particular at the more serious complications from COVID in this young age group, those are life-altering complications that will have consequences and ramifications throughout their lives,” he said.
“I would take this as a serious wake-up call to parents [at a time when] the immunization rates in younger children are so pitifully low,” Dr. Poland said.
Still early days
The study is suggestive but not definitive, said Peter Katona, MD, professor of medicine and infectious diseases expert at the UCLA Fielding School of Public Health.
It’s still too early to draw conclusions about long COVID, including in children, because many questions remain, he said: Should long COVID be defined as symptoms at 1 month or 3 months after infection? How do you define brain fog?
Dr. Katona and colleagues are studying long COVID intervention among students at UCLA to answer some of these questions, including the incidence and effect of early intervention.
The study had “at least seven limitations,” the researchers noted. Among them was the use of medical claims data that noted long COVID outcomes but not how severe they were; some people in the no COVID group might have had the illness but not been diagnosed; and the researchers did not adjust for vaccination status.
Dr. Poland noted that the study was done during surges in COVID variants including Delta and Omicron. In other words, any long COVID effects linked to more recent variants such as BA.5 or BA.2.75 are unknown.
A version of this article first appeared on WebMD.com.
Researchers from the Centers for Disease Control and Prevention report that
Heart inflammation; a blood clot in the lung; or a blood clot in the lower leg, thigh, or pelvis were the most common bad outcomes in a new study. Even though the risk was higher for these and some other serious events, the overall numbers were small.
“Many of these conditions were rare or uncommon among children in this analysis, but even a small increase in these conditions is notable,” a CDC new release stated.
The investigators said their findings stress the importance of COVID-19 vaccination in Americans under the age of 18.
The study was published online in the CDC’s Morbidity and Mortality Weekly Report.
Less is known about long COVID in children
Lyudmyla Kompaniyets, PhD, and colleagues noted that most research on long COVID to date has been done in adults, so little information is available about the risks to Americans ages 17 and younger.
To learn more, they compared post–COVID-19 symptoms and conditions between 781,419 children and teenagers with confirmed COVID-19 to another 2,344,257 without COVID-19. They looked at medical claims and laboratory data for these children and teenagers from March 1, 2020, through Jan. 31, 2022, to see who got any of 15 specific outcomes linked to long COVID-19.
Long COVID was defined as a condition where symptoms that last for or begin at least 4 weeks after a COVID-19 diagnosis.
Compared to children with no history of a COVID-19 diagnosis, the long COVID-19 group was 101% more likely to have an acute pulmonary embolism, 99% more likely to have myocarditis or cardiomyopathy, 87% more likely to have a venous thromboembolic event, 32% more likely to have acute and unspecified renal failure, and 23% more likely to have type 1 diabetes.
“This report points to the fact that the risks of COVID infection itself, both in terms of the acute effects, MIS-C [multisystem inflammatory syndrome in children], as well as the long-term effects, are real, are concerning, and are potentially very serious,” said Stuart Berger, MD, chair of the American Academy of Pediatrics Section on Cardiology and Cardiac Surgery.
“The message that we should take away from this is that we should be very keen on all the methods of prevention for COVID, especially the vaccine,” said Dr. Berger, chief of cardiology in the department of pediatrics at Northwestern University in Chicago.
A ‘wake-up call’
The study findings are “sobering” and are “a reminder of the seriousness of COVID infection,” says Gregory Poland, MD, an infectious disease expert at the Mayo Clinic in Rochester, Minn.
“When you look in particular at the more serious complications from COVID in this young age group, those are life-altering complications that will have consequences and ramifications throughout their lives,” he said.
“I would take this as a serious wake-up call to parents [at a time when] the immunization rates in younger children are so pitifully low,” Dr. Poland said.
Still early days
The study is suggestive but not definitive, said Peter Katona, MD, professor of medicine and infectious diseases expert at the UCLA Fielding School of Public Health.
It’s still too early to draw conclusions about long COVID, including in children, because many questions remain, he said: Should long COVID be defined as symptoms at 1 month or 3 months after infection? How do you define brain fog?
Dr. Katona and colleagues are studying long COVID intervention among students at UCLA to answer some of these questions, including the incidence and effect of early intervention.
The study had “at least seven limitations,” the researchers noted. Among them was the use of medical claims data that noted long COVID outcomes but not how severe they were; some people in the no COVID group might have had the illness but not been diagnosed; and the researchers did not adjust for vaccination status.
Dr. Poland noted that the study was done during surges in COVID variants including Delta and Omicron. In other words, any long COVID effects linked to more recent variants such as BA.5 or BA.2.75 are unknown.
A version of this article first appeared on WebMD.com.
FROM THE MMWR
‘Children are not little adults’ and need special protection during heat waves
After more than a week of record-breaking temperatures across much of the country, public health experts are cautioning that children are more susceptible to heat illness than adults are – even more so when they’re on the athletic field, living without air conditioning, or waiting in a parked car.
Cases of heat-related illness are rising with average air temperatures, and experts say almost half of those getting sick are children. The reason is twofold: Children’s bodies have more trouble regulating temperature than do those of adults, and they rely on adults to help protect them from overheating.
Parents, coaches, and other caretakers, who can experience the same heat very differently from the way children do, may struggle to identify a dangerous situation or catch the early symptoms of heat-related illness in children.
“Children are not little adults,” said Dr. Aaron Bernstein, a pediatric hospitalist at Boston Children’s Hospital.
Jan Null, a meteorologist in California, recalled being surprised at the effect of heat in a car. It was 86 degrees on a July afternoon more than 2 decades ago when an infant in San Jose was forgotten in a parked car and died of heatstroke.
Mr. Null said a reporter asked him after the death, “How hot could it have gotten in that car?”
Mr. Null’s research with two emergency doctors at Stanford University eventually produced a startling answer. Within an hour, the temperature in that car could have exceeded 120 degrees Fahrenheit. Their work revealed that a quick errand can be dangerous for a child left behind in the car – even for less than 15 minutes, even with the windows cracked, and even on a mild day.
As record heat becomes more frequent, posing serious risks even to healthy adults, the number of cases of heat-related illnesses has gone up, including among children. Those most at risk are young children in parked vehicles and adolescents returning to school and participating in sports during the hottest days of the year.
More than 9,000 high school athletes are treated for heat-related illnesses every year.
Heat-related illnesses occur when exposure to high temperatures and humidity, which can be intensified by physical exertion, overwhelms the body’s ability to cool itself. Cases range from mild, like benign heat rashes in infants, to more serious, when the body’s core temperature increases. That can lead to life-threatening instances of heatstroke, diagnosed once the body temperature rises above 104 degrees, potentially causing organ failure.
Prevention is key. Experts emphasize that drinking plenty of water, avoiding the outdoors during the hot midday and afternoon hours, and taking it slow when adjusting to exercise are the most effective ways to avoid getting sick.
Children’s bodies take longer to increase sweat production and otherwise acclimatize in a warm environment than adults’ do, research shows. Young children are more susceptible to dehydration because a larger percentage of their body weight is water.
Infants and younger children have more trouble regulating their body temperature, in part because they often don’t recognize when they should drink more water or remove clothing to cool down. A 1995 study showed that young children who spent 30 minutes in a 95-degree room saw their core temperatures rise significantly higher and faster than their mothers’ – even though they sweat more than adults do relative to their size.
Pediatricians advise caretakers to monitor how much water children consume and encourage them to drink before they ask for it. Thirst indicates the body is already dehydrated.
They should dress children in light-colored, lightweight clothes; limit outdoor time during the hottest hours; and look for ways to cool down, such as by visiting an air-conditioned place like a library, taking a cool bath, or going for a swim.
To address the risks to student athletes, the National Athletic Trainers’ Association recommends that high school athletes acclimatize by gradually building their activity over the course of 2 weeks when returning to their sport for a new season – including by slowly stepping up the amount of any protective equipment they wear.
“You’re gradually increasing that intensity over a week to 2 weeks so your body can get used to the heat,” said Kathy Dieringer, president of NATA.
Warning signs and solutions
Experts note a flushed face, fatigue, muscle cramps, headache, dizziness, vomiting, and a lot of sweating are among the symptoms of heat exhaustion, which can develop into heatstroke if untreated. A doctor should be notified if symptoms worsen, such as if the child seems disoriented or cannot drink.
Taking immediate steps to cool a child experiencing heat exhaustion or heatstroke is critical. The child should be taken to a shaded or cool area; be given cool fluids with salt, like sports drinks; and have any sweaty or heavy garments removed.
For adolescents, being submerged in an ice bath is the most effective way to cool the body, while younger children can be wrapped in cold, wet towels or misted with lukewarm water and placed in front of a fan.
Although children’s deaths in parked cars have been well documented, the tragic incidents continue to occur. According to federal statistics, 23 children died of vehicular heatstroke in 2021. Mr. Null, who collects his own data, said 13 children have died so far this year.
Caretakers should never leave children alone in a parked car, Mr. Null said. Take steps to prevent young children from entering the car themselves and becoming trapped, including locking the car while it’s parked at home.
More than half of cases of vehicular pediatric heatstroke occur because a caretaker accidentally left a child behind, he said. While in-car technology reminding adults to check their back seats has become more common, only a fraction of vehicles have it, requiring parents to come up with their own methods, like leaving a stuffed animal in the front seat.
The good news, Mr. Null said, is that simple behavioral changes can protect youngsters. “This is preventable in 100% of the cases,” he said.
A lopsided risk
People living in low-income areas fare worse when temperatures climb. Access to air conditioning, which includes the ability to afford the electricity bill, is a serious health concern.
A study of heat in urban areas released last year showed that low-income neighborhoods and communities of color experience much higher temperatures than those of wealthier, White residents. In more impoverished areas during the summer, temperatures can be as much as 7 degrees Fahrenheit warmer.
The study’s authors said their findings in the United States reflect that “the legacy of redlining looms large,” referring to a federal housing policy that refused to insure mortgages in or near predominantly Black neighborhoods.
“These areas have less tree canopy, more streets, and higher building densities, meaning that in addition to their other racist outcomes, redlining policies directly codified into law existing disparity in urban land use and reinforced urban design choices that magnify urban heating into the present,” they concluded.
Dr. Bernstein, who leads Harvard’s Center for Climate, Health, and the Global Environment, coauthored a commentary in JAMA arguing that advancing health equity is critical to action on climate change.
The center works with front-line health clinics to help their predominantly low-income patients respond to the health impacts of climate change. Federally backed clinics alone provide care to about 30 million Americans, including many children, he said.
Dr. Bernstein also recently led a nationwide study that found that from May through September, days with higher temperatures are associated with more visits to children’s hospital emergency rooms. Many visits were more directly linked to heat, although the study also pointed to how high temperatures can exacerbate existing health conditions such as neurological disorders.
“Children are more vulnerable to climate change through how these climate shocks reshape the world in which they grow up,” Dr. Bernstein said.
Helping people better understand the health risks of extreme heat and how to protect themselves and their families are among the public health system’s major challenges, experts said.
The National Weather Service’s heat alert system is mainly based on the heat index, a measure of how hot it feels when relative humidity is factored in with air temperature.
But the alerts are not related to effects on health, said Kathy Baughman McLeod, director of the Adrienne Arsht-Rockefeller Foundation Resilience Center. By the time temperatures rise to the level that a weather alert is issued, many vulnerable people – like children, pregnant women, and the elderly – may already be experiencing heat exhaustion or heatstroke.
The center developed a new heat alert system, which is being tested in Seville, Spain, historically one of the hottest cities in Europe.
The system marries metrics such as air temperature and humidity with public health data to categorize heat waves and, when they are serious enough, give them names – making it easier for people to understand heat as an environmental threat that requires prevention measures.
The categories are determined through a metric known as excess deaths, which compares how many people died on a day with the forecast temperature versus an average day. That may help health officials understand how severe a heat wave is expected to be and make informed recommendations to the public based on risk factors such as age or medical history.
The health-based alert system would also allow officials to target caretakers of children and seniors through school systems, preschools, and senior centers, Ms. Baughman McLeod said.
Giving people better ways to conceptualize heat is critical, she said.
“It’s not dramatic. It doesn’t rip the roof off of your house,” Ms. Baughman McLeod said. “It’s silent and invisible.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
After more than a week of record-breaking temperatures across much of the country, public health experts are cautioning that children are more susceptible to heat illness than adults are – even more so when they’re on the athletic field, living without air conditioning, or waiting in a parked car.
Cases of heat-related illness are rising with average air temperatures, and experts say almost half of those getting sick are children. The reason is twofold: Children’s bodies have more trouble regulating temperature than do those of adults, and they rely on adults to help protect them from overheating.
Parents, coaches, and other caretakers, who can experience the same heat very differently from the way children do, may struggle to identify a dangerous situation or catch the early symptoms of heat-related illness in children.
“Children are not little adults,” said Dr. Aaron Bernstein, a pediatric hospitalist at Boston Children’s Hospital.
Jan Null, a meteorologist in California, recalled being surprised at the effect of heat in a car. It was 86 degrees on a July afternoon more than 2 decades ago when an infant in San Jose was forgotten in a parked car and died of heatstroke.
Mr. Null said a reporter asked him after the death, “How hot could it have gotten in that car?”
Mr. Null’s research with two emergency doctors at Stanford University eventually produced a startling answer. Within an hour, the temperature in that car could have exceeded 120 degrees Fahrenheit. Their work revealed that a quick errand can be dangerous for a child left behind in the car – even for less than 15 minutes, even with the windows cracked, and even on a mild day.
As record heat becomes more frequent, posing serious risks even to healthy adults, the number of cases of heat-related illnesses has gone up, including among children. Those most at risk are young children in parked vehicles and adolescents returning to school and participating in sports during the hottest days of the year.
More than 9,000 high school athletes are treated for heat-related illnesses every year.
Heat-related illnesses occur when exposure to high temperatures and humidity, which can be intensified by physical exertion, overwhelms the body’s ability to cool itself. Cases range from mild, like benign heat rashes in infants, to more serious, when the body’s core temperature increases. That can lead to life-threatening instances of heatstroke, diagnosed once the body temperature rises above 104 degrees, potentially causing organ failure.
Prevention is key. Experts emphasize that drinking plenty of water, avoiding the outdoors during the hot midday and afternoon hours, and taking it slow when adjusting to exercise are the most effective ways to avoid getting sick.
Children’s bodies take longer to increase sweat production and otherwise acclimatize in a warm environment than adults’ do, research shows. Young children are more susceptible to dehydration because a larger percentage of their body weight is water.
Infants and younger children have more trouble regulating their body temperature, in part because they often don’t recognize when they should drink more water or remove clothing to cool down. A 1995 study showed that young children who spent 30 minutes in a 95-degree room saw their core temperatures rise significantly higher and faster than their mothers’ – even though they sweat more than adults do relative to their size.
Pediatricians advise caretakers to monitor how much water children consume and encourage them to drink before they ask for it. Thirst indicates the body is already dehydrated.
They should dress children in light-colored, lightweight clothes; limit outdoor time during the hottest hours; and look for ways to cool down, such as by visiting an air-conditioned place like a library, taking a cool bath, or going for a swim.
To address the risks to student athletes, the National Athletic Trainers’ Association recommends that high school athletes acclimatize by gradually building their activity over the course of 2 weeks when returning to their sport for a new season – including by slowly stepping up the amount of any protective equipment they wear.
“You’re gradually increasing that intensity over a week to 2 weeks so your body can get used to the heat,” said Kathy Dieringer, president of NATA.
Warning signs and solutions
Experts note a flushed face, fatigue, muscle cramps, headache, dizziness, vomiting, and a lot of sweating are among the symptoms of heat exhaustion, which can develop into heatstroke if untreated. A doctor should be notified if symptoms worsen, such as if the child seems disoriented or cannot drink.
Taking immediate steps to cool a child experiencing heat exhaustion or heatstroke is critical. The child should be taken to a shaded or cool area; be given cool fluids with salt, like sports drinks; and have any sweaty or heavy garments removed.
For adolescents, being submerged in an ice bath is the most effective way to cool the body, while younger children can be wrapped in cold, wet towels or misted with lukewarm water and placed in front of a fan.
Although children’s deaths in parked cars have been well documented, the tragic incidents continue to occur. According to federal statistics, 23 children died of vehicular heatstroke in 2021. Mr. Null, who collects his own data, said 13 children have died so far this year.
Caretakers should never leave children alone in a parked car, Mr. Null said. Take steps to prevent young children from entering the car themselves and becoming trapped, including locking the car while it’s parked at home.
More than half of cases of vehicular pediatric heatstroke occur because a caretaker accidentally left a child behind, he said. While in-car technology reminding adults to check their back seats has become more common, only a fraction of vehicles have it, requiring parents to come up with their own methods, like leaving a stuffed animal in the front seat.
The good news, Mr. Null said, is that simple behavioral changes can protect youngsters. “This is preventable in 100% of the cases,” he said.
A lopsided risk
People living in low-income areas fare worse when temperatures climb. Access to air conditioning, which includes the ability to afford the electricity bill, is a serious health concern.
A study of heat in urban areas released last year showed that low-income neighborhoods and communities of color experience much higher temperatures than those of wealthier, White residents. In more impoverished areas during the summer, temperatures can be as much as 7 degrees Fahrenheit warmer.
The study’s authors said their findings in the United States reflect that “the legacy of redlining looms large,” referring to a federal housing policy that refused to insure mortgages in or near predominantly Black neighborhoods.
“These areas have less tree canopy, more streets, and higher building densities, meaning that in addition to their other racist outcomes, redlining policies directly codified into law existing disparity in urban land use and reinforced urban design choices that magnify urban heating into the present,” they concluded.
Dr. Bernstein, who leads Harvard’s Center for Climate, Health, and the Global Environment, coauthored a commentary in JAMA arguing that advancing health equity is critical to action on climate change.
The center works with front-line health clinics to help their predominantly low-income patients respond to the health impacts of climate change. Federally backed clinics alone provide care to about 30 million Americans, including many children, he said.
Dr. Bernstein also recently led a nationwide study that found that from May through September, days with higher temperatures are associated with more visits to children’s hospital emergency rooms. Many visits were more directly linked to heat, although the study also pointed to how high temperatures can exacerbate existing health conditions such as neurological disorders.
“Children are more vulnerable to climate change through how these climate shocks reshape the world in which they grow up,” Dr. Bernstein said.
Helping people better understand the health risks of extreme heat and how to protect themselves and their families are among the public health system’s major challenges, experts said.
The National Weather Service’s heat alert system is mainly based on the heat index, a measure of how hot it feels when relative humidity is factored in with air temperature.
But the alerts are not related to effects on health, said Kathy Baughman McLeod, director of the Adrienne Arsht-Rockefeller Foundation Resilience Center. By the time temperatures rise to the level that a weather alert is issued, many vulnerable people – like children, pregnant women, and the elderly – may already be experiencing heat exhaustion or heatstroke.
The center developed a new heat alert system, which is being tested in Seville, Spain, historically one of the hottest cities in Europe.
The system marries metrics such as air temperature and humidity with public health data to categorize heat waves and, when they are serious enough, give them names – making it easier for people to understand heat as an environmental threat that requires prevention measures.
The categories are determined through a metric known as excess deaths, which compares how many people died on a day with the forecast temperature versus an average day. That may help health officials understand how severe a heat wave is expected to be and make informed recommendations to the public based on risk factors such as age or medical history.
The health-based alert system would also allow officials to target caretakers of children and seniors through school systems, preschools, and senior centers, Ms. Baughman McLeod said.
Giving people better ways to conceptualize heat is critical, she said.
“It’s not dramatic. It doesn’t rip the roof off of your house,” Ms. Baughman McLeod said. “It’s silent and invisible.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
After more than a week of record-breaking temperatures across much of the country, public health experts are cautioning that children are more susceptible to heat illness than adults are – even more so when they’re on the athletic field, living without air conditioning, or waiting in a parked car.
Cases of heat-related illness are rising with average air temperatures, and experts say almost half of those getting sick are children. The reason is twofold: Children’s bodies have more trouble regulating temperature than do those of adults, and they rely on adults to help protect them from overheating.
Parents, coaches, and other caretakers, who can experience the same heat very differently from the way children do, may struggle to identify a dangerous situation or catch the early symptoms of heat-related illness in children.
“Children are not little adults,” said Dr. Aaron Bernstein, a pediatric hospitalist at Boston Children’s Hospital.
Jan Null, a meteorologist in California, recalled being surprised at the effect of heat in a car. It was 86 degrees on a July afternoon more than 2 decades ago when an infant in San Jose was forgotten in a parked car and died of heatstroke.
Mr. Null said a reporter asked him after the death, “How hot could it have gotten in that car?”
Mr. Null’s research with two emergency doctors at Stanford University eventually produced a startling answer. Within an hour, the temperature in that car could have exceeded 120 degrees Fahrenheit. Their work revealed that a quick errand can be dangerous for a child left behind in the car – even for less than 15 minutes, even with the windows cracked, and even on a mild day.
As record heat becomes more frequent, posing serious risks even to healthy adults, the number of cases of heat-related illnesses has gone up, including among children. Those most at risk are young children in parked vehicles and adolescents returning to school and participating in sports during the hottest days of the year.
More than 9,000 high school athletes are treated for heat-related illnesses every year.
Heat-related illnesses occur when exposure to high temperatures and humidity, which can be intensified by physical exertion, overwhelms the body’s ability to cool itself. Cases range from mild, like benign heat rashes in infants, to more serious, when the body’s core temperature increases. That can lead to life-threatening instances of heatstroke, diagnosed once the body temperature rises above 104 degrees, potentially causing organ failure.
Prevention is key. Experts emphasize that drinking plenty of water, avoiding the outdoors during the hot midday and afternoon hours, and taking it slow when adjusting to exercise are the most effective ways to avoid getting sick.
Children’s bodies take longer to increase sweat production and otherwise acclimatize in a warm environment than adults’ do, research shows. Young children are more susceptible to dehydration because a larger percentage of their body weight is water.
Infants and younger children have more trouble regulating their body temperature, in part because they often don’t recognize when they should drink more water or remove clothing to cool down. A 1995 study showed that young children who spent 30 minutes in a 95-degree room saw their core temperatures rise significantly higher and faster than their mothers’ – even though they sweat more than adults do relative to their size.
Pediatricians advise caretakers to monitor how much water children consume and encourage them to drink before they ask for it. Thirst indicates the body is already dehydrated.
They should dress children in light-colored, lightweight clothes; limit outdoor time during the hottest hours; and look for ways to cool down, such as by visiting an air-conditioned place like a library, taking a cool bath, or going for a swim.
To address the risks to student athletes, the National Athletic Trainers’ Association recommends that high school athletes acclimatize by gradually building their activity over the course of 2 weeks when returning to their sport for a new season – including by slowly stepping up the amount of any protective equipment they wear.
“You’re gradually increasing that intensity over a week to 2 weeks so your body can get used to the heat,” said Kathy Dieringer, president of NATA.
Warning signs and solutions
Experts note a flushed face, fatigue, muscle cramps, headache, dizziness, vomiting, and a lot of sweating are among the symptoms of heat exhaustion, which can develop into heatstroke if untreated. A doctor should be notified if symptoms worsen, such as if the child seems disoriented or cannot drink.
Taking immediate steps to cool a child experiencing heat exhaustion or heatstroke is critical. The child should be taken to a shaded or cool area; be given cool fluids with salt, like sports drinks; and have any sweaty or heavy garments removed.
For adolescents, being submerged in an ice bath is the most effective way to cool the body, while younger children can be wrapped in cold, wet towels or misted with lukewarm water and placed in front of a fan.
Although children’s deaths in parked cars have been well documented, the tragic incidents continue to occur. According to federal statistics, 23 children died of vehicular heatstroke in 2021. Mr. Null, who collects his own data, said 13 children have died so far this year.
Caretakers should never leave children alone in a parked car, Mr. Null said. Take steps to prevent young children from entering the car themselves and becoming trapped, including locking the car while it’s parked at home.
More than half of cases of vehicular pediatric heatstroke occur because a caretaker accidentally left a child behind, he said. While in-car technology reminding adults to check their back seats has become more common, only a fraction of vehicles have it, requiring parents to come up with their own methods, like leaving a stuffed animal in the front seat.
The good news, Mr. Null said, is that simple behavioral changes can protect youngsters. “This is preventable in 100% of the cases,” he said.
A lopsided risk
People living in low-income areas fare worse when temperatures climb. Access to air conditioning, which includes the ability to afford the electricity bill, is a serious health concern.
A study of heat in urban areas released last year showed that low-income neighborhoods and communities of color experience much higher temperatures than those of wealthier, White residents. In more impoverished areas during the summer, temperatures can be as much as 7 degrees Fahrenheit warmer.
The study’s authors said their findings in the United States reflect that “the legacy of redlining looms large,” referring to a federal housing policy that refused to insure mortgages in or near predominantly Black neighborhoods.
“These areas have less tree canopy, more streets, and higher building densities, meaning that in addition to their other racist outcomes, redlining policies directly codified into law existing disparity in urban land use and reinforced urban design choices that magnify urban heating into the present,” they concluded.
Dr. Bernstein, who leads Harvard’s Center for Climate, Health, and the Global Environment, coauthored a commentary in JAMA arguing that advancing health equity is critical to action on climate change.
The center works with front-line health clinics to help their predominantly low-income patients respond to the health impacts of climate change. Federally backed clinics alone provide care to about 30 million Americans, including many children, he said.
Dr. Bernstein also recently led a nationwide study that found that from May through September, days with higher temperatures are associated with more visits to children’s hospital emergency rooms. Many visits were more directly linked to heat, although the study also pointed to how high temperatures can exacerbate existing health conditions such as neurological disorders.
“Children are more vulnerable to climate change through how these climate shocks reshape the world in which they grow up,” Dr. Bernstein said.
Helping people better understand the health risks of extreme heat and how to protect themselves and their families are among the public health system’s major challenges, experts said.
The National Weather Service’s heat alert system is mainly based on the heat index, a measure of how hot it feels when relative humidity is factored in with air temperature.
But the alerts are not related to effects on health, said Kathy Baughman McLeod, director of the Adrienne Arsht-Rockefeller Foundation Resilience Center. By the time temperatures rise to the level that a weather alert is issued, many vulnerable people – like children, pregnant women, and the elderly – may already be experiencing heat exhaustion or heatstroke.
The center developed a new heat alert system, which is being tested in Seville, Spain, historically one of the hottest cities in Europe.
The system marries metrics such as air temperature and humidity with public health data to categorize heat waves and, when they are serious enough, give them names – making it easier for people to understand heat as an environmental threat that requires prevention measures.
The categories are determined through a metric known as excess deaths, which compares how many people died on a day with the forecast temperature versus an average day. That may help health officials understand how severe a heat wave is expected to be and make informed recommendations to the public based on risk factors such as age or medical history.
The health-based alert system would also allow officials to target caretakers of children and seniors through school systems, preschools, and senior centers, Ms. Baughman McLeod said.
Giving people better ways to conceptualize heat is critical, she said.
“It’s not dramatic. It doesn’t rip the roof off of your house,” Ms. Baughman McLeod said. “It’s silent and invisible.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
‘Go Ask Alice’: A fake view of teen mental health
If you grew up in the 1970s and 1980s, chances are high you’re familiar with “Go Ask Alice.”
What was then said to be the real diary of a 15-year-old promising teen turned drug addict was released in 1971 as a cautionary tale and has since sold over 5 million copies. The diary was harrowing against the backdrop of the war on drugs and soon became both acclaimed and banned from classrooms across the country.
Schools citied “inappropriate” language that “borders on pornography” as grounds to prohibit teenagers from reading Alice’s story. But as much as the book’s vivid writing offended readers, it drew millions in with its profanity and graphic descriptions of sex, drugs, and mental health struggles.
At the time, The New York Times reviewed the book as “a strong, painfully honest, nakedly candid and true story ... a document of horrifying reality,” but the popular diary was later found to be a ploy – a fake story written by a 54-year-old Mormon youth counselor named Beatrice Sparks.
Now, Ms. Sparks, who died in 2012, has been further exposed in radio personality Rick Emerson’s new book, “Unmask Alice: LSD, Satanic Panic, and the Imposter Behind the World’s Most Notorious Diaries.” Mr. Emerson published the exposé in July, years after he had the idea to investigate Ms. Sparks’s work in 2015. The book details Ms. Sparks’s background, her journey in creating Alice, and her quest to be recognized for the teen diary she had published as “Anonymous.”
“After 30 years of trying, Beatrice Sparks had changed the world. And nobody knew it,” Mr. Emerson told the New York Post.In his work, Mr. Emerson also dives into the profound impact of the diary at a time when not as much research existed on teen mental health.
When the teenager whose diary inspired Ms. Sparks’s writing “died in March 1971, the very first true study of adolescent psychology had just barely come out,” Mr. Emerson said to Rolling Stone. “Mental health, especially for young people, was still very much on training wheels.”
According to Mr. Emerson, a lack of insight into mental health issues allowed Ms. Sparks’s description to go relatively unchallenged and for the book’s influence to spread despite its misinformation.
“It’s indisputable that large sections of ‘Go Ask Alice’ are just embellished and/or false,” he told the Post.
Then versus now
This landscape is in stark contrast to today, where thousands of studies on the topic have been done, compared with the mere dozens in the 1970s.
Anxiety and depression in minors have increased over time, a trend worsened by the COVID-19 pandemic, according to the CDC. Studies have shown that reported drug use in teens has decreased over time, proving significant during the pandemic, according to the National Institutes of Health.
While Alice from “Go Ask Alice” has not existed in either, comparing the two periods can offer insight into teen struggles in the 1970s versus today and sheds light on how literature – fiction or even faked nonfiction – can transform a nation.
A version of this article first appeared on WebMD.com.
If you grew up in the 1970s and 1980s, chances are high you’re familiar with “Go Ask Alice.”
What was then said to be the real diary of a 15-year-old promising teen turned drug addict was released in 1971 as a cautionary tale and has since sold over 5 million copies. The diary was harrowing against the backdrop of the war on drugs and soon became both acclaimed and banned from classrooms across the country.
Schools citied “inappropriate” language that “borders on pornography” as grounds to prohibit teenagers from reading Alice’s story. But as much as the book’s vivid writing offended readers, it drew millions in with its profanity and graphic descriptions of sex, drugs, and mental health struggles.
At the time, The New York Times reviewed the book as “a strong, painfully honest, nakedly candid and true story ... a document of horrifying reality,” but the popular diary was later found to be a ploy – a fake story written by a 54-year-old Mormon youth counselor named Beatrice Sparks.
Now, Ms. Sparks, who died in 2012, has been further exposed in radio personality Rick Emerson’s new book, “Unmask Alice: LSD, Satanic Panic, and the Imposter Behind the World’s Most Notorious Diaries.” Mr. Emerson published the exposé in July, years after he had the idea to investigate Ms. Sparks’s work in 2015. The book details Ms. Sparks’s background, her journey in creating Alice, and her quest to be recognized for the teen diary she had published as “Anonymous.”
“After 30 years of trying, Beatrice Sparks had changed the world. And nobody knew it,” Mr. Emerson told the New York Post.In his work, Mr. Emerson also dives into the profound impact of the diary at a time when not as much research existed on teen mental health.
When the teenager whose diary inspired Ms. Sparks’s writing “died in March 1971, the very first true study of adolescent psychology had just barely come out,” Mr. Emerson said to Rolling Stone. “Mental health, especially for young people, was still very much on training wheels.”
According to Mr. Emerson, a lack of insight into mental health issues allowed Ms. Sparks’s description to go relatively unchallenged and for the book’s influence to spread despite its misinformation.
“It’s indisputable that large sections of ‘Go Ask Alice’ are just embellished and/or false,” he told the Post.
Then versus now
This landscape is in stark contrast to today, where thousands of studies on the topic have been done, compared with the mere dozens in the 1970s.
Anxiety and depression in minors have increased over time, a trend worsened by the COVID-19 pandemic, according to the CDC. Studies have shown that reported drug use in teens has decreased over time, proving significant during the pandemic, according to the National Institutes of Health.
While Alice from “Go Ask Alice” has not existed in either, comparing the two periods can offer insight into teen struggles in the 1970s versus today and sheds light on how literature – fiction or even faked nonfiction – can transform a nation.
A version of this article first appeared on WebMD.com.
If you grew up in the 1970s and 1980s, chances are high you’re familiar with “Go Ask Alice.”
What was then said to be the real diary of a 15-year-old promising teen turned drug addict was released in 1971 as a cautionary tale and has since sold over 5 million copies. The diary was harrowing against the backdrop of the war on drugs and soon became both acclaimed and banned from classrooms across the country.
Schools citied “inappropriate” language that “borders on pornography” as grounds to prohibit teenagers from reading Alice’s story. But as much as the book’s vivid writing offended readers, it drew millions in with its profanity and graphic descriptions of sex, drugs, and mental health struggles.
At the time, The New York Times reviewed the book as “a strong, painfully honest, nakedly candid and true story ... a document of horrifying reality,” but the popular diary was later found to be a ploy – a fake story written by a 54-year-old Mormon youth counselor named Beatrice Sparks.
Now, Ms. Sparks, who died in 2012, has been further exposed in radio personality Rick Emerson’s new book, “Unmask Alice: LSD, Satanic Panic, and the Imposter Behind the World’s Most Notorious Diaries.” Mr. Emerson published the exposé in July, years after he had the idea to investigate Ms. Sparks’s work in 2015. The book details Ms. Sparks’s background, her journey in creating Alice, and her quest to be recognized for the teen diary she had published as “Anonymous.”
“After 30 years of trying, Beatrice Sparks had changed the world. And nobody knew it,” Mr. Emerson told the New York Post.In his work, Mr. Emerson also dives into the profound impact of the diary at a time when not as much research existed on teen mental health.
When the teenager whose diary inspired Ms. Sparks’s writing “died in March 1971, the very first true study of adolescent psychology had just barely come out,” Mr. Emerson said to Rolling Stone. “Mental health, especially for young people, was still very much on training wheels.”
According to Mr. Emerson, a lack of insight into mental health issues allowed Ms. Sparks’s description to go relatively unchallenged and for the book’s influence to spread despite its misinformation.
“It’s indisputable that large sections of ‘Go Ask Alice’ are just embellished and/or false,” he told the Post.
Then versus now
This landscape is in stark contrast to today, where thousands of studies on the topic have been done, compared with the mere dozens in the 1970s.
Anxiety and depression in minors have increased over time, a trend worsened by the COVID-19 pandemic, according to the CDC. Studies have shown that reported drug use in teens has decreased over time, proving significant during the pandemic, according to the National Institutes of Health.
While Alice from “Go Ask Alice” has not existed in either, comparing the two periods can offer insight into teen struggles in the 1970s versus today and sheds light on how literature – fiction or even faked nonfiction – can transform a nation.
A version of this article first appeared on WebMD.com.
AAP updates hyperbilirubinemia guideline
Raising phototherapy thresholds and revising risk assessment are among the key changes in the American Academy of Pediatrics’ updated guidelines for managing hyperbilirubinemia in infants 35 weeks’ gestation and older.
“More than 80% of newborn infants will have some degree of jaundice,” Alex R. Kemper, MD, of Nationwide Children’s Hospital, Columbus, Ohio, and coauthors wrote. Careful monitoring is needed manage high bilirubin concentrations and avoid acute bilirubin encephalopathy (ABE) and kernicterus, a disabling neurologic condition.
The current revision, published in Pediatrics, updates and replaces the 2004 AAP clinical practice guidelines for the management and prevention of hyperbilirubinemia in newborns of at least 35 weeks’ gestation.
The guideline committee reviewed evidence published since the previous guidelines were issued in 2004, and addressed similar issues of prevention, risk assessment, monitoring, and treatment.
A notable change from 2004 was the inclusion of a 2009 recommendation update for “universal predischarge bilirubin screening with measures of total serum bilirubin (TSB) or transcutaneous bilirubin (TcB) linked to specific recommendations for follow-up,” the authors wrote.
In terms of prevention, recommendations include a direct antiglobulin test (DAT) for infants whose mother’s antibody screen was positive or unknown. In addition, exclusive breastfeeding is known to be associated with hyperbilirubinemia, but clinicians should support breastfeeding while monitoring for signs of hyperbilirubinemia because of suboptimal feeding, the authors noted. However, the guidelines recommend against oral supplementation with water or dextrose water to prevent hyperbilirubinemia.
For assessment and monitoring, the guidelines advise the use of total serum bilirubin (TSB) as the definitive test for hyperbilirubinemia to guide phototherapy and escalation of care, including exchange transfusion. “The presence of hyperbilirubinemia neurotoxicity risk factors lowers the threshold for treatment with phototherapy and the level at which care should be escalated,” the authors wrote. They also emphasized the need to consider glucose-6-phosphate dehydrogenase deficiency, a genetic condition that decreases protection against oxidative stress and has been identified as a leading cause of hazardous hyperbilirubinemia worldwide.
The guidelines recommend assessing all infants for jaundice at least every 12 hours after delivery until discharge, with TSB or TcB measured as soon as possible for those with suspected jaundice. The complete guidelines include charts for TSB levels to guide escalation of care. “Blood for TSB can be obtained at the time it is collected for newborn screening tests to avoid an additional heel stick,” the authors noted.
The rate of increase in TSB or TcB, if more than one measure is available, may identify infants at higher risk of hyperbilirubinemia, according to the guidelines, and a possible delay of hospital discharge may be needed for infants if appropriate follow-up is not feasible.
In terms of treatment, new evidence that bilirubin neurotoxicity does not occur until concentrations well above those given in the 2004 guidelines justified raising the treatment thresholds, although by a narrow range. “With the increased phototherapy thresholds, appropriately following the current guidelines including bilirubin screening during the birth hospitalization and timely postdischarge follow-up is important,” the authors wrote. The new thresholds, outlined in the complete guidelines, are based on gestational age, hyperbilirubinemia neurotoxicity risk factors, and the age of the infant in hours. However, infants may be treated at lower levels, based on individual circumstances, family preferences, and shared decision-making with clinicians. Home-based phototherapy may be used in some infants, but should not be used if there is a question about the device quality, delivery time, and ability of caregivers to use the device correctly.
“Discontinuing phototherapy is an option when the TSB has decreased by at least 2 mg/dL below the hour-specific threshold at the initiation of phototherapy,” and follow-up should be based on risk of rebound hyperbilirubinemia, according to the guidelines.
“This clinical practice guideline provides indications and approaches for phototherapy and escalation of care and when treatment and monitoring can be safely discontinued,” However, clinicians should understand the rationale for the recommendations and combine them with their clinical judgment, including shared decision-making when appropriate, the authors concluded.
Updated evidence supports escalating care
The take-home message for pediatricians is that neonatal hyperbilirubinemia is a very common finding, and complications are rare, but the condition can result in devastating life-long results, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., said in an interview.
“Previous guidelines published in 2004 and updated in 2009 included evidence-based recommendations, but additional research was still needed to provide guidance for providers to prevent complications of hyperbilirubinemia,” said Dr. Haut, who was not involved in producing the guidelines.
“New data documenting additional risk factors, the importance of ongoing breastfeeding support, and addressing hyperbilirubinemia as an urgent problem” are additions to prevention methods in the latest published guidelines, she said.
“Acute encephalopathy and kernicterus can result from hyperbilirubinemia with severe and devastating neurologic effects, but are preventable by early identification and treatment,” said Dr. Haut. Therefore, “it is not surprising that the AAP utilized continuing and more recent evidence to support new recommendations. Both maternal and neonatal risk factors have long been considered in the development of neonatal hyperbilirubinemia, but recent recommendations incorporate additional risk factor evaluation and urgency in time to appropriate care. Detailed thresholds for phototherapy and exchange transfusion will benefit the families of full-term infants without other risk factors and escalate care for those neonates with risk factors.”
However, potential barriers to following the guidelines persist, Dr. Haut noted.
“Frequent infant follow-up can be challenging for busy primary care offices with outpatient laboratory results often taking much longer to obtain than in a hospital setting,” she said.
Also, “taking a newborn to the emergency department or an inpatient laboratory can be frightening for families with the risk of illness exposure. Frequent monitoring of serum bilirubin levels is disturbing for parents and inconvenient immediately postpartum,” Dr. Haut explained. “Few practices utilize transcutaneous bilirubin monitoring which may be one method of added screening.”
In addition, “despite the importance of breastfeeding, ongoing support is not readily available for mothers after hospital discharge. A lactation specialist in the office setting can take the burden off providers and add opportunity for family education.”
As for additional research, “continued evaluation of the comparison of transcutaneous bilirubin monitoring and serum levels along with the use of transcutaneous monitoring in facilities outside the hospital setting may be warranted,” Dr. Haut said. “Data collection on incidence and accompanying risk factors of neonates who develop acute hyperbilirubinemia encephalopathy and kernicterus is a long-term study opportunity.”
The guidelines received no external funding. Lead author Dr. Kemper had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Raising phototherapy thresholds and revising risk assessment are among the key changes in the American Academy of Pediatrics’ updated guidelines for managing hyperbilirubinemia in infants 35 weeks’ gestation and older.
“More than 80% of newborn infants will have some degree of jaundice,” Alex R. Kemper, MD, of Nationwide Children’s Hospital, Columbus, Ohio, and coauthors wrote. Careful monitoring is needed manage high bilirubin concentrations and avoid acute bilirubin encephalopathy (ABE) and kernicterus, a disabling neurologic condition.
The current revision, published in Pediatrics, updates and replaces the 2004 AAP clinical practice guidelines for the management and prevention of hyperbilirubinemia in newborns of at least 35 weeks’ gestation.
The guideline committee reviewed evidence published since the previous guidelines were issued in 2004, and addressed similar issues of prevention, risk assessment, monitoring, and treatment.
A notable change from 2004 was the inclusion of a 2009 recommendation update for “universal predischarge bilirubin screening with measures of total serum bilirubin (TSB) or transcutaneous bilirubin (TcB) linked to specific recommendations for follow-up,” the authors wrote.
In terms of prevention, recommendations include a direct antiglobulin test (DAT) for infants whose mother’s antibody screen was positive or unknown. In addition, exclusive breastfeeding is known to be associated with hyperbilirubinemia, but clinicians should support breastfeeding while monitoring for signs of hyperbilirubinemia because of suboptimal feeding, the authors noted. However, the guidelines recommend against oral supplementation with water or dextrose water to prevent hyperbilirubinemia.
For assessment and monitoring, the guidelines advise the use of total serum bilirubin (TSB) as the definitive test for hyperbilirubinemia to guide phototherapy and escalation of care, including exchange transfusion. “The presence of hyperbilirubinemia neurotoxicity risk factors lowers the threshold for treatment with phototherapy and the level at which care should be escalated,” the authors wrote. They also emphasized the need to consider glucose-6-phosphate dehydrogenase deficiency, a genetic condition that decreases protection against oxidative stress and has been identified as a leading cause of hazardous hyperbilirubinemia worldwide.
The guidelines recommend assessing all infants for jaundice at least every 12 hours after delivery until discharge, with TSB or TcB measured as soon as possible for those with suspected jaundice. The complete guidelines include charts for TSB levels to guide escalation of care. “Blood for TSB can be obtained at the time it is collected for newborn screening tests to avoid an additional heel stick,” the authors noted.
The rate of increase in TSB or TcB, if more than one measure is available, may identify infants at higher risk of hyperbilirubinemia, according to the guidelines, and a possible delay of hospital discharge may be needed for infants if appropriate follow-up is not feasible.
In terms of treatment, new evidence that bilirubin neurotoxicity does not occur until concentrations well above those given in the 2004 guidelines justified raising the treatment thresholds, although by a narrow range. “With the increased phototherapy thresholds, appropriately following the current guidelines including bilirubin screening during the birth hospitalization and timely postdischarge follow-up is important,” the authors wrote. The new thresholds, outlined in the complete guidelines, are based on gestational age, hyperbilirubinemia neurotoxicity risk factors, and the age of the infant in hours. However, infants may be treated at lower levels, based on individual circumstances, family preferences, and shared decision-making with clinicians. Home-based phototherapy may be used in some infants, but should not be used if there is a question about the device quality, delivery time, and ability of caregivers to use the device correctly.
“Discontinuing phototherapy is an option when the TSB has decreased by at least 2 mg/dL below the hour-specific threshold at the initiation of phototherapy,” and follow-up should be based on risk of rebound hyperbilirubinemia, according to the guidelines.
“This clinical practice guideline provides indications and approaches for phototherapy and escalation of care and when treatment and monitoring can be safely discontinued,” However, clinicians should understand the rationale for the recommendations and combine them with their clinical judgment, including shared decision-making when appropriate, the authors concluded.
Updated evidence supports escalating care
The take-home message for pediatricians is that neonatal hyperbilirubinemia is a very common finding, and complications are rare, but the condition can result in devastating life-long results, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., said in an interview.
“Previous guidelines published in 2004 and updated in 2009 included evidence-based recommendations, but additional research was still needed to provide guidance for providers to prevent complications of hyperbilirubinemia,” said Dr. Haut, who was not involved in producing the guidelines.
“New data documenting additional risk factors, the importance of ongoing breastfeeding support, and addressing hyperbilirubinemia as an urgent problem” are additions to prevention methods in the latest published guidelines, she said.
“Acute encephalopathy and kernicterus can result from hyperbilirubinemia with severe and devastating neurologic effects, but are preventable by early identification and treatment,” said Dr. Haut. Therefore, “it is not surprising that the AAP utilized continuing and more recent evidence to support new recommendations. Both maternal and neonatal risk factors have long been considered in the development of neonatal hyperbilirubinemia, but recent recommendations incorporate additional risk factor evaluation and urgency in time to appropriate care. Detailed thresholds for phototherapy and exchange transfusion will benefit the families of full-term infants without other risk factors and escalate care for those neonates with risk factors.”
However, potential barriers to following the guidelines persist, Dr. Haut noted.
“Frequent infant follow-up can be challenging for busy primary care offices with outpatient laboratory results often taking much longer to obtain than in a hospital setting,” she said.
Also, “taking a newborn to the emergency department or an inpatient laboratory can be frightening for families with the risk of illness exposure. Frequent monitoring of serum bilirubin levels is disturbing for parents and inconvenient immediately postpartum,” Dr. Haut explained. “Few practices utilize transcutaneous bilirubin monitoring which may be one method of added screening.”
In addition, “despite the importance of breastfeeding, ongoing support is not readily available for mothers after hospital discharge. A lactation specialist in the office setting can take the burden off providers and add opportunity for family education.”
As for additional research, “continued evaluation of the comparison of transcutaneous bilirubin monitoring and serum levels along with the use of transcutaneous monitoring in facilities outside the hospital setting may be warranted,” Dr. Haut said. “Data collection on incidence and accompanying risk factors of neonates who develop acute hyperbilirubinemia encephalopathy and kernicterus is a long-term study opportunity.”
The guidelines received no external funding. Lead author Dr. Kemper had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
Raising phototherapy thresholds and revising risk assessment are among the key changes in the American Academy of Pediatrics’ updated guidelines for managing hyperbilirubinemia in infants 35 weeks’ gestation and older.
“More than 80% of newborn infants will have some degree of jaundice,” Alex R. Kemper, MD, of Nationwide Children’s Hospital, Columbus, Ohio, and coauthors wrote. Careful monitoring is needed manage high bilirubin concentrations and avoid acute bilirubin encephalopathy (ABE) and kernicterus, a disabling neurologic condition.
The current revision, published in Pediatrics, updates and replaces the 2004 AAP clinical practice guidelines for the management and prevention of hyperbilirubinemia in newborns of at least 35 weeks’ gestation.
The guideline committee reviewed evidence published since the previous guidelines were issued in 2004, and addressed similar issues of prevention, risk assessment, monitoring, and treatment.
A notable change from 2004 was the inclusion of a 2009 recommendation update for “universal predischarge bilirubin screening with measures of total serum bilirubin (TSB) or transcutaneous bilirubin (TcB) linked to specific recommendations for follow-up,” the authors wrote.
In terms of prevention, recommendations include a direct antiglobulin test (DAT) for infants whose mother’s antibody screen was positive or unknown. In addition, exclusive breastfeeding is known to be associated with hyperbilirubinemia, but clinicians should support breastfeeding while monitoring for signs of hyperbilirubinemia because of suboptimal feeding, the authors noted. However, the guidelines recommend against oral supplementation with water or dextrose water to prevent hyperbilirubinemia.
For assessment and monitoring, the guidelines advise the use of total serum bilirubin (TSB) as the definitive test for hyperbilirubinemia to guide phototherapy and escalation of care, including exchange transfusion. “The presence of hyperbilirubinemia neurotoxicity risk factors lowers the threshold for treatment with phototherapy and the level at which care should be escalated,” the authors wrote. They also emphasized the need to consider glucose-6-phosphate dehydrogenase deficiency, a genetic condition that decreases protection against oxidative stress and has been identified as a leading cause of hazardous hyperbilirubinemia worldwide.
The guidelines recommend assessing all infants for jaundice at least every 12 hours after delivery until discharge, with TSB or TcB measured as soon as possible for those with suspected jaundice. The complete guidelines include charts for TSB levels to guide escalation of care. “Blood for TSB can be obtained at the time it is collected for newborn screening tests to avoid an additional heel stick,” the authors noted.
The rate of increase in TSB or TcB, if more than one measure is available, may identify infants at higher risk of hyperbilirubinemia, according to the guidelines, and a possible delay of hospital discharge may be needed for infants if appropriate follow-up is not feasible.
In terms of treatment, new evidence that bilirubin neurotoxicity does not occur until concentrations well above those given in the 2004 guidelines justified raising the treatment thresholds, although by a narrow range. “With the increased phototherapy thresholds, appropriately following the current guidelines including bilirubin screening during the birth hospitalization and timely postdischarge follow-up is important,” the authors wrote. The new thresholds, outlined in the complete guidelines, are based on gestational age, hyperbilirubinemia neurotoxicity risk factors, and the age of the infant in hours. However, infants may be treated at lower levels, based on individual circumstances, family preferences, and shared decision-making with clinicians. Home-based phototherapy may be used in some infants, but should not be used if there is a question about the device quality, delivery time, and ability of caregivers to use the device correctly.
“Discontinuing phototherapy is an option when the TSB has decreased by at least 2 mg/dL below the hour-specific threshold at the initiation of phototherapy,” and follow-up should be based on risk of rebound hyperbilirubinemia, according to the guidelines.
“This clinical practice guideline provides indications and approaches for phototherapy and escalation of care and when treatment and monitoring can be safely discontinued,” However, clinicians should understand the rationale for the recommendations and combine them with their clinical judgment, including shared decision-making when appropriate, the authors concluded.
Updated evidence supports escalating care
The take-home message for pediatricians is that neonatal hyperbilirubinemia is a very common finding, and complications are rare, but the condition can result in devastating life-long results, Cathy Haut, DNP, CPNP-AC, CPNP-PC, a pediatric nurse practitioner in Rehoboth Beach, Del., said in an interview.
“Previous guidelines published in 2004 and updated in 2009 included evidence-based recommendations, but additional research was still needed to provide guidance for providers to prevent complications of hyperbilirubinemia,” said Dr. Haut, who was not involved in producing the guidelines.
“New data documenting additional risk factors, the importance of ongoing breastfeeding support, and addressing hyperbilirubinemia as an urgent problem” are additions to prevention methods in the latest published guidelines, she said.
“Acute encephalopathy and kernicterus can result from hyperbilirubinemia with severe and devastating neurologic effects, but are preventable by early identification and treatment,” said Dr. Haut. Therefore, “it is not surprising that the AAP utilized continuing and more recent evidence to support new recommendations. Both maternal and neonatal risk factors have long been considered in the development of neonatal hyperbilirubinemia, but recent recommendations incorporate additional risk factor evaluation and urgency in time to appropriate care. Detailed thresholds for phototherapy and exchange transfusion will benefit the families of full-term infants without other risk factors and escalate care for those neonates with risk factors.”
However, potential barriers to following the guidelines persist, Dr. Haut noted.
“Frequent infant follow-up can be challenging for busy primary care offices with outpatient laboratory results often taking much longer to obtain than in a hospital setting,” she said.
Also, “taking a newborn to the emergency department or an inpatient laboratory can be frightening for families with the risk of illness exposure. Frequent monitoring of serum bilirubin levels is disturbing for parents and inconvenient immediately postpartum,” Dr. Haut explained. “Few practices utilize transcutaneous bilirubin monitoring which may be one method of added screening.”
In addition, “despite the importance of breastfeeding, ongoing support is not readily available for mothers after hospital discharge. A lactation specialist in the office setting can take the burden off providers and add opportunity for family education.”
As for additional research, “continued evaluation of the comparison of transcutaneous bilirubin monitoring and serum levels along with the use of transcutaneous monitoring in facilities outside the hospital setting may be warranted,” Dr. Haut said. “Data collection on incidence and accompanying risk factors of neonates who develop acute hyperbilirubinemia encephalopathy and kernicterus is a long-term study opportunity.”
The guidelines received no external funding. Lead author Dr. Kemper had no financial conflicts to disclose. Dr. Haut had no financial conflicts to disclose and serves on the editorial advisory board of Pediatric News.
FROM PEDIATRICS
Patient CRC screening preferences don’t match what they’re being offered
Patients said they’d prefer fecal immunochemical test (FIT)–fecal DNA tests over any of the other colorectal cancer screening (CRC) modalities currently recommended by the U.S. Multi-Society Task Force, according to a study published in Clinical Gastroenterology and Hepatology.
Just over a third of American adults aged 40 and older who hadn’t yet been screened for CRC preferred the FIT–fecal DNA test every 3 years, whereas just one in seven respondents preferred a colonoscopy – considered the gold standard in colorectal cancer screening – every 10 years.
”When you talk to patients and to your friends and family members, people tend to think colonoscopy is synonymous with colon cancer screening, but we have lots of different tests,” senior author Christopher V. Almario, MD, MSHPM, of the department of medicine at the Karsh division of gastroenterology and hepatology, Cedars-Sinai Medical Center, Los Angeles, said in an interview.
“Most people in general tend to prefer noninvasive stool tests, and when we try to predict who would prefer what, we actually couldn’t, so this is a very personal decision,” Dr. Almario said. “It’s important for clinicians to offer multiple choices to their patients, not to mention just colonoscopy. We have data from observing clinician-patient interactions showing that, a lot of times, colonoscopy is the only test that’s offered, despite there being multiple options.”
At the very least, Dr. Almario said, providers should offer patients a colonoscopy along with a noninvasive test, particularly a stool test, and discuss the two options, getting the patient’s input in terms of what they prefer. “The best test is the test that actually gets done,” he said.
Offering patients options
Reid M. Ness, MD, MPH, an associate professor of medicine in the division of gastroenterology, hepatology and nutrition at Vanderbilt University Medical Center in Nashville, was not involved with the study but wasn’t surprised at the findings since “most people wisely prefer to avoid invasive procedures,” he said in an interview. He agreed that many patients aren’t necessarily informed of all their options for screening.
“Many people who are now being offered colonoscopy as their only screening option may prefer a noninvasive option, such as FIT or multitarget stool DNA testing,” Dr. Ness said. “Also, people now refusing colonoscopy for colorectal cancer screening may instead accept FIT or multitarget stool DNA testing. It is difficult to know how many people now refusing colorectal cancer screening may have accepted screening if it had been offered differently.”
That’s precisely what Dr. Almario and his colleagues wanted to find out. They surveyed 1,000 people aged 40 and older who were at average risk for colorectal cancer to find out their preferences for different screening modalities and what features of different screening types they most valued. The researchers asked about the following screening tests recommended by the U.S. Multi-Society Task Force:
- FIT every year.
- FIT–fecal DNA every 3 years.
- Colon video capsule every 5 years.
- CT colonography every 5 years.
- Colonoscopy every 10 years.
The respondents who completed the online survey were recruited from a sample of more than 20 million people across the United States who have agreed to receive survey invitations. Respondents were excluded if they had a first-degree relative with colorectal cancer, had already undergone colorectal cancer screening or had been diagnosed with colon polyps, Crohn’s disease, or ulcerative colitis.
The respondents were split into those aged 40-49 (61% of the sample) who had not yet discussed colorectal cancer screening with their providers and those aged 50 and older, who might have already discussed it and declined. Eighty percent of the respondents were White, 6% were Black, 6% were Hispanic, 4% were Asian, and 3% reported another race/ethnicity. Just over half (52%) had at least two comorbidities. A quarter (25%) reported one comorbidity, and 22% reported none.
In thinking about the decision to get screened, respondents ranked the test type as the most important consideration, followed by the reduction in their chance of developing colorectal cancer and then frequency of the test. Lower priority on the list of considerations were their chances of a complication, bowel prep before the test, and required diet changes before the test.
The test preferred by the highest proportion of respondents was the FIT–fecal DNA test every 3 years, preferred by 35% of respondents, followed by the colon capsule video test every 5 years (28%). About one in seven respondents (14%) preferred a colonoscopy every 10 years, followed by the annual FIT (12%) and CT colonography every 5 years (11%). When limited only to the two tier 1–option tests – the annual FIT or a colonoscopy every 10 years – a substantial majority of the younger (69%) and older (77%) groups preferred the annual FIT.
”This finding is discordant with current CRC screening utilization in the United States where colonoscopy is the most commonly performed test, and this may partially explain our suboptimal screening rates,” the authors wrote. “Our findings suggest that screening programs should strongly consider a sequential-based strategy where FIT is offered first, and if declined then colonoscopy.”
Underlying factors
Dr. Ness said that many primary care providers might prefer to offer colonoscopies instead of annual FIT tests because it’s easier to track a test given every 10 years instead of every year or every 3 years.
“Providers across most of the U.S. are incentivized to recommend colonoscopy as the primary screening modality because the burden of follow-up on them is less,” Dr. Ness said. “They are able to justify this choice given colonoscopy remains the most accurate screening modality.”
Dr. Ness pointed to the programmatic screening program at Kaiser Permanente of Northern California health care system as a model for a program that utilizes FIT tests more often.
“The only way to accomplish an efficient and equitable colorectal cancer screening program is within the context of a national health service or plan,” Dr. Ness added. “Otherwise, the uninsured and underinsured will remain excluded from the benefits of colorectal cancer screening.”
Preferences did not differ a great deal between the age groups, with 35% of the younger group and 37% of the older group both preferring the FIT–fecal DNA tests every 3 years. Slightly more people in the 50+ age group preferred an annual fit (19% vs. 12%) as opposed to the colon capsule video every 5 years (28% of younger group vs. 23%) or colon CT scan every 5 years (11% of younger group vs. 8%), but the differences were statistically significant (P = .019).
In fact, “sociodemographic, clinical characteristics, and colorectal cancer screening knowledge, attitudes, and beliefs were not predictive of selecting FIT or colonoscopy,” the authors found. ”This demonstrates the individualized nature of decision making on colorectal cancer screening tests. Moreover, as most individuals preferred FIT, it again emphasizes the importance of sequential or choice-based strategies for colorectal cancer screening.”
However, one of the study’s notable limitations was its high proportion of White patients relative to other racial/ethnic groups, so additional research may illuminate whether different sociodemographic groups do have slight preferences for one test over another, Dr. Almario said. The advantage to colonoscopies, he noted, is that they only occur every 10 years and if polyps are discovered, they can be taken care of right away.
”You don’t have to think about it for a decade, which is certainly a pro for the colonoscopy,” Dr. Almario said. “The FIT test is obviously less invasive, but you have to do it every year for it to be an effective screening test.” He noted that some data have shown a drop-off in compliance over multiple years. “We certainly need more systems in place to remind patients and providers to do it annually so that we can see the ultimate screening benefit from doing that test specifically.”
“The most important point from the clinical perspective is, when we’re talking to patients about colon cancer screening, make sure to give them a choice,” Dr. Almario said. “We just can’t look at someone’s chart, their clinical characteristics or demographics, and predict what tests they would prefer. We need to ask them. We need to present them with the options, go over the pros and cons of colonoscopy, the pros and cons of the stool test, and ask the patient what they would prefer to do.”
The research was funded by the National Cancer Institute and the National Institutes of Health. One author served on an advisory board with Exact Sciences. The other authors and Dr. Ness had no disclosures.
Patients said they’d prefer fecal immunochemical test (FIT)–fecal DNA tests over any of the other colorectal cancer screening (CRC) modalities currently recommended by the U.S. Multi-Society Task Force, according to a study published in Clinical Gastroenterology and Hepatology.
Just over a third of American adults aged 40 and older who hadn’t yet been screened for CRC preferred the FIT–fecal DNA test every 3 years, whereas just one in seven respondents preferred a colonoscopy – considered the gold standard in colorectal cancer screening – every 10 years.
”When you talk to patients and to your friends and family members, people tend to think colonoscopy is synonymous with colon cancer screening, but we have lots of different tests,” senior author Christopher V. Almario, MD, MSHPM, of the department of medicine at the Karsh division of gastroenterology and hepatology, Cedars-Sinai Medical Center, Los Angeles, said in an interview.
“Most people in general tend to prefer noninvasive stool tests, and when we try to predict who would prefer what, we actually couldn’t, so this is a very personal decision,” Dr. Almario said. “It’s important for clinicians to offer multiple choices to their patients, not to mention just colonoscopy. We have data from observing clinician-patient interactions showing that, a lot of times, colonoscopy is the only test that’s offered, despite there being multiple options.”
At the very least, Dr. Almario said, providers should offer patients a colonoscopy along with a noninvasive test, particularly a stool test, and discuss the two options, getting the patient’s input in terms of what they prefer. “The best test is the test that actually gets done,” he said.
Offering patients options
Reid M. Ness, MD, MPH, an associate professor of medicine in the division of gastroenterology, hepatology and nutrition at Vanderbilt University Medical Center in Nashville, was not involved with the study but wasn’t surprised at the findings since “most people wisely prefer to avoid invasive procedures,” he said in an interview. He agreed that many patients aren’t necessarily informed of all their options for screening.
“Many people who are now being offered colonoscopy as their only screening option may prefer a noninvasive option, such as FIT or multitarget stool DNA testing,” Dr. Ness said. “Also, people now refusing colonoscopy for colorectal cancer screening may instead accept FIT or multitarget stool DNA testing. It is difficult to know how many people now refusing colorectal cancer screening may have accepted screening if it had been offered differently.”
That’s precisely what Dr. Almario and his colleagues wanted to find out. They surveyed 1,000 people aged 40 and older who were at average risk for colorectal cancer to find out their preferences for different screening modalities and what features of different screening types they most valued. The researchers asked about the following screening tests recommended by the U.S. Multi-Society Task Force:
- FIT every year.
- FIT–fecal DNA every 3 years.
- Colon video capsule every 5 years.
- CT colonography every 5 years.
- Colonoscopy every 10 years.
The respondents who completed the online survey were recruited from a sample of more than 20 million people across the United States who have agreed to receive survey invitations. Respondents were excluded if they had a first-degree relative with colorectal cancer, had already undergone colorectal cancer screening or had been diagnosed with colon polyps, Crohn’s disease, or ulcerative colitis.
The respondents were split into those aged 40-49 (61% of the sample) who had not yet discussed colorectal cancer screening with their providers and those aged 50 and older, who might have already discussed it and declined. Eighty percent of the respondents were White, 6% were Black, 6% were Hispanic, 4% were Asian, and 3% reported another race/ethnicity. Just over half (52%) had at least two comorbidities. A quarter (25%) reported one comorbidity, and 22% reported none.
In thinking about the decision to get screened, respondents ranked the test type as the most important consideration, followed by the reduction in their chance of developing colorectal cancer and then frequency of the test. Lower priority on the list of considerations were their chances of a complication, bowel prep before the test, and required diet changes before the test.
The test preferred by the highest proportion of respondents was the FIT–fecal DNA test every 3 years, preferred by 35% of respondents, followed by the colon capsule video test every 5 years (28%). About one in seven respondents (14%) preferred a colonoscopy every 10 years, followed by the annual FIT (12%) and CT colonography every 5 years (11%). When limited only to the two tier 1–option tests – the annual FIT or a colonoscopy every 10 years – a substantial majority of the younger (69%) and older (77%) groups preferred the annual FIT.
”This finding is discordant with current CRC screening utilization in the United States where colonoscopy is the most commonly performed test, and this may partially explain our suboptimal screening rates,” the authors wrote. “Our findings suggest that screening programs should strongly consider a sequential-based strategy where FIT is offered first, and if declined then colonoscopy.”
Underlying factors
Dr. Ness said that many primary care providers might prefer to offer colonoscopies instead of annual FIT tests because it’s easier to track a test given every 10 years instead of every year or every 3 years.
“Providers across most of the U.S. are incentivized to recommend colonoscopy as the primary screening modality because the burden of follow-up on them is less,” Dr. Ness said. “They are able to justify this choice given colonoscopy remains the most accurate screening modality.”
Dr. Ness pointed to the programmatic screening program at Kaiser Permanente of Northern California health care system as a model for a program that utilizes FIT tests more often.
“The only way to accomplish an efficient and equitable colorectal cancer screening program is within the context of a national health service or plan,” Dr. Ness added. “Otherwise, the uninsured and underinsured will remain excluded from the benefits of colorectal cancer screening.”
Preferences did not differ a great deal between the age groups, with 35% of the younger group and 37% of the older group both preferring the FIT–fecal DNA tests every 3 years. Slightly more people in the 50+ age group preferred an annual fit (19% vs. 12%) as opposed to the colon capsule video every 5 years (28% of younger group vs. 23%) or colon CT scan every 5 years (11% of younger group vs. 8%), but the differences were statistically significant (P = .019).
In fact, “sociodemographic, clinical characteristics, and colorectal cancer screening knowledge, attitudes, and beliefs were not predictive of selecting FIT or colonoscopy,” the authors found. ”This demonstrates the individualized nature of decision making on colorectal cancer screening tests. Moreover, as most individuals preferred FIT, it again emphasizes the importance of sequential or choice-based strategies for colorectal cancer screening.”
However, one of the study’s notable limitations was its high proportion of White patients relative to other racial/ethnic groups, so additional research may illuminate whether different sociodemographic groups do have slight preferences for one test over another, Dr. Almario said. The advantage to colonoscopies, he noted, is that they only occur every 10 years and if polyps are discovered, they can be taken care of right away.
”You don’t have to think about it for a decade, which is certainly a pro for the colonoscopy,” Dr. Almario said. “The FIT test is obviously less invasive, but you have to do it every year for it to be an effective screening test.” He noted that some data have shown a drop-off in compliance over multiple years. “We certainly need more systems in place to remind patients and providers to do it annually so that we can see the ultimate screening benefit from doing that test specifically.”
“The most important point from the clinical perspective is, when we’re talking to patients about colon cancer screening, make sure to give them a choice,” Dr. Almario said. “We just can’t look at someone’s chart, their clinical characteristics or demographics, and predict what tests they would prefer. We need to ask them. We need to present them with the options, go over the pros and cons of colonoscopy, the pros and cons of the stool test, and ask the patient what they would prefer to do.”
The research was funded by the National Cancer Institute and the National Institutes of Health. One author served on an advisory board with Exact Sciences. The other authors and Dr. Ness had no disclosures.
Patients said they’d prefer fecal immunochemical test (FIT)–fecal DNA tests over any of the other colorectal cancer screening (CRC) modalities currently recommended by the U.S. Multi-Society Task Force, according to a study published in Clinical Gastroenterology and Hepatology.
Just over a third of American adults aged 40 and older who hadn’t yet been screened for CRC preferred the FIT–fecal DNA test every 3 years, whereas just one in seven respondents preferred a colonoscopy – considered the gold standard in colorectal cancer screening – every 10 years.
”When you talk to patients and to your friends and family members, people tend to think colonoscopy is synonymous with colon cancer screening, but we have lots of different tests,” senior author Christopher V. Almario, MD, MSHPM, of the department of medicine at the Karsh division of gastroenterology and hepatology, Cedars-Sinai Medical Center, Los Angeles, said in an interview.
“Most people in general tend to prefer noninvasive stool tests, and when we try to predict who would prefer what, we actually couldn’t, so this is a very personal decision,” Dr. Almario said. “It’s important for clinicians to offer multiple choices to their patients, not to mention just colonoscopy. We have data from observing clinician-patient interactions showing that, a lot of times, colonoscopy is the only test that’s offered, despite there being multiple options.”
At the very least, Dr. Almario said, providers should offer patients a colonoscopy along with a noninvasive test, particularly a stool test, and discuss the two options, getting the patient’s input in terms of what they prefer. “The best test is the test that actually gets done,” he said.
Offering patients options
Reid M. Ness, MD, MPH, an associate professor of medicine in the division of gastroenterology, hepatology and nutrition at Vanderbilt University Medical Center in Nashville, was not involved with the study but wasn’t surprised at the findings since “most people wisely prefer to avoid invasive procedures,” he said in an interview. He agreed that many patients aren’t necessarily informed of all their options for screening.
“Many people who are now being offered colonoscopy as their only screening option may prefer a noninvasive option, such as FIT or multitarget stool DNA testing,” Dr. Ness said. “Also, people now refusing colonoscopy for colorectal cancer screening may instead accept FIT or multitarget stool DNA testing. It is difficult to know how many people now refusing colorectal cancer screening may have accepted screening if it had been offered differently.”
That’s precisely what Dr. Almario and his colleagues wanted to find out. They surveyed 1,000 people aged 40 and older who were at average risk for colorectal cancer to find out their preferences for different screening modalities and what features of different screening types they most valued. The researchers asked about the following screening tests recommended by the U.S. Multi-Society Task Force:
- FIT every year.
- FIT–fecal DNA every 3 years.
- Colon video capsule every 5 years.
- CT colonography every 5 years.
- Colonoscopy every 10 years.
The respondents who completed the online survey were recruited from a sample of more than 20 million people across the United States who have agreed to receive survey invitations. Respondents were excluded if they had a first-degree relative with colorectal cancer, had already undergone colorectal cancer screening or had been diagnosed with colon polyps, Crohn’s disease, or ulcerative colitis.
The respondents were split into those aged 40-49 (61% of the sample) who had not yet discussed colorectal cancer screening with their providers and those aged 50 and older, who might have already discussed it and declined. Eighty percent of the respondents were White, 6% were Black, 6% were Hispanic, 4% were Asian, and 3% reported another race/ethnicity. Just over half (52%) had at least two comorbidities. A quarter (25%) reported one comorbidity, and 22% reported none.
In thinking about the decision to get screened, respondents ranked the test type as the most important consideration, followed by the reduction in their chance of developing colorectal cancer and then frequency of the test. Lower priority on the list of considerations were their chances of a complication, bowel prep before the test, and required diet changes before the test.
The test preferred by the highest proportion of respondents was the FIT–fecal DNA test every 3 years, preferred by 35% of respondents, followed by the colon capsule video test every 5 years (28%). About one in seven respondents (14%) preferred a colonoscopy every 10 years, followed by the annual FIT (12%) and CT colonography every 5 years (11%). When limited only to the two tier 1–option tests – the annual FIT or a colonoscopy every 10 years – a substantial majority of the younger (69%) and older (77%) groups preferred the annual FIT.
”This finding is discordant with current CRC screening utilization in the United States where colonoscopy is the most commonly performed test, and this may partially explain our suboptimal screening rates,” the authors wrote. “Our findings suggest that screening programs should strongly consider a sequential-based strategy where FIT is offered first, and if declined then colonoscopy.”
Underlying factors
Dr. Ness said that many primary care providers might prefer to offer colonoscopies instead of annual FIT tests because it’s easier to track a test given every 10 years instead of every year or every 3 years.
“Providers across most of the U.S. are incentivized to recommend colonoscopy as the primary screening modality because the burden of follow-up on them is less,” Dr. Ness said. “They are able to justify this choice given colonoscopy remains the most accurate screening modality.”
Dr. Ness pointed to the programmatic screening program at Kaiser Permanente of Northern California health care system as a model for a program that utilizes FIT tests more often.
“The only way to accomplish an efficient and equitable colorectal cancer screening program is within the context of a national health service or plan,” Dr. Ness added. “Otherwise, the uninsured and underinsured will remain excluded from the benefits of colorectal cancer screening.”
Preferences did not differ a great deal between the age groups, with 35% of the younger group and 37% of the older group both preferring the FIT–fecal DNA tests every 3 years. Slightly more people in the 50+ age group preferred an annual fit (19% vs. 12%) as opposed to the colon capsule video every 5 years (28% of younger group vs. 23%) or colon CT scan every 5 years (11% of younger group vs. 8%), but the differences were statistically significant (P = .019).
In fact, “sociodemographic, clinical characteristics, and colorectal cancer screening knowledge, attitudes, and beliefs were not predictive of selecting FIT or colonoscopy,” the authors found. ”This demonstrates the individualized nature of decision making on colorectal cancer screening tests. Moreover, as most individuals preferred FIT, it again emphasizes the importance of sequential or choice-based strategies for colorectal cancer screening.”
However, one of the study’s notable limitations was its high proportion of White patients relative to other racial/ethnic groups, so additional research may illuminate whether different sociodemographic groups do have slight preferences for one test over another, Dr. Almario said. The advantage to colonoscopies, he noted, is that they only occur every 10 years and if polyps are discovered, they can be taken care of right away.
”You don’t have to think about it for a decade, which is certainly a pro for the colonoscopy,” Dr. Almario said. “The FIT test is obviously less invasive, but you have to do it every year for it to be an effective screening test.” He noted that some data have shown a drop-off in compliance over multiple years. “We certainly need more systems in place to remind patients and providers to do it annually so that we can see the ultimate screening benefit from doing that test specifically.”
“The most important point from the clinical perspective is, when we’re talking to patients about colon cancer screening, make sure to give them a choice,” Dr. Almario said. “We just can’t look at someone’s chart, their clinical characteristics or demographics, and predict what tests they would prefer. We need to ask them. We need to present them with the options, go over the pros and cons of colonoscopy, the pros and cons of the stool test, and ask the patient what they would prefer to do.”
The research was funded by the National Cancer Institute and the National Institutes of Health. One author served on an advisory board with Exact Sciences. The other authors and Dr. Ness had no disclosures.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
White House declares monkeypox a public health emergency
There have been more than 6,600 reported cases of the disease in the United States, up from less than 5,000 cases reported last week.
“This public health emergency will allow us to explore additional strategies to get vaccines and treatments more quickly out in the affected communities. And it will allow us to get more data from jurisdictions so we can effectively track and attack this outbreak,” Robert Fenton, who was named as the national monkeypox response coordinator this week, said at a news briefing Aug. 4.
Those who catch the virus usually have fever-like symptoms, followed by red lesions on the body that can raise and develop pus. Those at highest risk of monkeypox are gay and bisexual men, as well as men who have sex with other men. There are between 1.6 million and 1.7 million Americans in this high-risk group, Health and Human Services Secretary Xavier Becerra said at the briefing.
The Jynneos vaccine is being distributed to protect against monkeypox and can prevent severe symptoms. It’s mostly going to those with the greatest risk of catching the virus.
Last week, the Biden administration made over 1.1 million doses of the Jynneos vaccine available – of which over 600,000 doses have already been distributed across the country – and have secured over 6.9 million Jynneos doses altogether.
Around 786,000 vaccines have already been allocated, and the first doses were shipped this week. States will be able to order more doses beginning Aug. 15. If a state has used 90% or more of its vaccine supply, it will be eligible to order more doses before Aug. 15, according to Dawn O’Connell, JD, assistant secretary for preparedness and response at the U.S. Department of Health and Human Services.
An additional 150,000 doses will be added to the national stockpile in September, with more doses to come later this year, Ms. O’Connell says.
The administration is also stressing the importance of monkeypox testing and says it can now distribute 80,000 monkeypox tests per week.
An antiviral drug – known as TPOXX – is also available to treat severe cases of monkeypox. Around 1,700,000 doses are available in the Strategic National Stockpile, public health officials say.
“We are prepared to take our response to the next level, and we urge every American to take this seriously and to take responsibility to help us tackle this virus,” Secretary Becerra told reporters.
The White House says it will continue reaching out to doctors, public health partners, LGBTQ advocates, and other impacted communities.
“The public health emergency further raises awareness about monkeypox, which will encourage clinicians to test for it,” Rochelle Walensky, MD, director of the Centers for Disease Control and Prevention, said at the briefing.
This week, President Joe Biden appointed a new White House monkeypox response team. Besides Mr. Fenton as the response coordinator, Demetre Daskalakis, MD, will serve as the White House national monkeypox response deputy coordinator. He is the director of the CDC’s Division of HIV Prevention.
“This virus is moving fast. This is a unique outbreak that is spreading faster than previous outbreaks,” Mr. Fenton told reporters Aug. 4. “That’s why the president asked me to explore everything we can do to combat monkeypox and protect communities at risk.”
This article was updated 8/4/22.
There have been more than 6,600 reported cases of the disease in the United States, up from less than 5,000 cases reported last week.
“This public health emergency will allow us to explore additional strategies to get vaccines and treatments more quickly out in the affected communities. And it will allow us to get more data from jurisdictions so we can effectively track and attack this outbreak,” Robert Fenton, who was named as the national monkeypox response coordinator this week, said at a news briefing Aug. 4.
Those who catch the virus usually have fever-like symptoms, followed by red lesions on the body that can raise and develop pus. Those at highest risk of monkeypox are gay and bisexual men, as well as men who have sex with other men. There are between 1.6 million and 1.7 million Americans in this high-risk group, Health and Human Services Secretary Xavier Becerra said at the briefing.
The Jynneos vaccine is being distributed to protect against monkeypox and can prevent severe symptoms. It’s mostly going to those with the greatest risk of catching the virus.
Last week, the Biden administration made over 1.1 million doses of the Jynneos vaccine available – of which over 600,000 doses have already been distributed across the country – and have secured over 6.9 million Jynneos doses altogether.
Around 786,000 vaccines have already been allocated, and the first doses were shipped this week. States will be able to order more doses beginning Aug. 15. If a state has used 90% or more of its vaccine supply, it will be eligible to order more doses before Aug. 15, according to Dawn O’Connell, JD, assistant secretary for preparedness and response at the U.S. Department of Health and Human Services.
An additional 150,000 doses will be added to the national stockpile in September, with more doses to come later this year, Ms. O’Connell says.
The administration is also stressing the importance of monkeypox testing and says it can now distribute 80,000 monkeypox tests per week.
An antiviral drug – known as TPOXX – is also available to treat severe cases of monkeypox. Around 1,700,000 doses are available in the Strategic National Stockpile, public health officials say.
“We are prepared to take our response to the next level, and we urge every American to take this seriously and to take responsibility to help us tackle this virus,” Secretary Becerra told reporters.
The White House says it will continue reaching out to doctors, public health partners, LGBTQ advocates, and other impacted communities.
“The public health emergency further raises awareness about monkeypox, which will encourage clinicians to test for it,” Rochelle Walensky, MD, director of the Centers for Disease Control and Prevention, said at the briefing.
This week, President Joe Biden appointed a new White House monkeypox response team. Besides Mr. Fenton as the response coordinator, Demetre Daskalakis, MD, will serve as the White House national monkeypox response deputy coordinator. He is the director of the CDC’s Division of HIV Prevention.
“This virus is moving fast. This is a unique outbreak that is spreading faster than previous outbreaks,” Mr. Fenton told reporters Aug. 4. “That’s why the president asked me to explore everything we can do to combat monkeypox and protect communities at risk.”
This article was updated 8/4/22.
There have been more than 6,600 reported cases of the disease in the United States, up from less than 5,000 cases reported last week.
“This public health emergency will allow us to explore additional strategies to get vaccines and treatments more quickly out in the affected communities. And it will allow us to get more data from jurisdictions so we can effectively track and attack this outbreak,” Robert Fenton, who was named as the national monkeypox response coordinator this week, said at a news briefing Aug. 4.
Those who catch the virus usually have fever-like symptoms, followed by red lesions on the body that can raise and develop pus. Those at highest risk of monkeypox are gay and bisexual men, as well as men who have sex with other men. There are between 1.6 million and 1.7 million Americans in this high-risk group, Health and Human Services Secretary Xavier Becerra said at the briefing.
The Jynneos vaccine is being distributed to protect against monkeypox and can prevent severe symptoms. It’s mostly going to those with the greatest risk of catching the virus.
Last week, the Biden administration made over 1.1 million doses of the Jynneos vaccine available – of which over 600,000 doses have already been distributed across the country – and have secured over 6.9 million Jynneos doses altogether.
Around 786,000 vaccines have already been allocated, and the first doses were shipped this week. States will be able to order more doses beginning Aug. 15. If a state has used 90% or more of its vaccine supply, it will be eligible to order more doses before Aug. 15, according to Dawn O’Connell, JD, assistant secretary for preparedness and response at the U.S. Department of Health and Human Services.
An additional 150,000 doses will be added to the national stockpile in September, with more doses to come later this year, Ms. O’Connell says.
The administration is also stressing the importance of monkeypox testing and says it can now distribute 80,000 monkeypox tests per week.
An antiviral drug – known as TPOXX – is also available to treat severe cases of monkeypox. Around 1,700,000 doses are available in the Strategic National Stockpile, public health officials say.
“We are prepared to take our response to the next level, and we urge every American to take this seriously and to take responsibility to help us tackle this virus,” Secretary Becerra told reporters.
The White House says it will continue reaching out to doctors, public health partners, LGBTQ advocates, and other impacted communities.
“The public health emergency further raises awareness about monkeypox, which will encourage clinicians to test for it,” Rochelle Walensky, MD, director of the Centers for Disease Control and Prevention, said at the briefing.
This week, President Joe Biden appointed a new White House monkeypox response team. Besides Mr. Fenton as the response coordinator, Demetre Daskalakis, MD, will serve as the White House national monkeypox response deputy coordinator. He is the director of the CDC’s Division of HIV Prevention.
“This virus is moving fast. This is a unique outbreak that is spreading faster than previous outbreaks,” Mr. Fenton told reporters Aug. 4. “That’s why the president asked me to explore everything we can do to combat monkeypox and protect communities at risk.”
This article was updated 8/4/22.
‘Staggering’ CVD rise projected in U.S., especially in minorities
A new analysis projects steep increases by 2060 in the prevalence of cardiovascular (CV) risk factors and disease that will disproportionately affect non-White populations who have limited access to health care.
The study by Reza Mohebi, MD, Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues was published in the Journal of the American College of Cardiology.
“Even though several assumptions underlie these projections, the importance of this work cannot be overestimated,” Andreas P. Kalogeropoulos, MD, MPH, PhD, and Javed Butler, MD, MPH, MBA, wrote in an accompanying editorial. “The absolute numbers are staggering.”
From 2025 to 2060, the number of people with any one of four CV risk factors – type 2 diabetes, hypertension, dyslipidemia, and obesity – is projected to increase by 15.4 million, to 34.7 million.
And the number of people with of any one of four CV disease types – ischemic heart disease, heart failure, MI, and stroke – is projected to increase by 3.2 million, to 6.8 million.
Although the model predicts that the prevalence of CV risk factors will gradually decrease among White Americans, the highest prevalence of CV risk factors will be among the White population because of its overall size.
Conversely, the projected prevalence of CV risk factors is expected to increase in Black, Hispanic, Asian, and other race/ethnicity populations.
In parallel, the prevalence of CV disease is projected to decrease in the White population and increase among all other race/ethnicities, particularly in the Black and Hispanic populations.

“Our results project a worrisome increase with a particularly ominous increase in risk factors and disease in our most vulnerable patients, including Blacks and Hispanics,” senior author James L. Januzzi Jr., MD, summarized in a video issued by the society.
“The steep rise in CV risk factors and disease reflects the generally higher prevalence in populations projected to increase in the United States, owing to immigration and growth, including Black or Hispanic individuals,” Dr. Januzzi, also from Massachusetts General and Harvard, said in an interview.
“The disproportionate size of the risk is expected in a sense, as minority populations are disproportionately disadvantaged with respect to their health care,” he said. “But whether it is expected or not, the increase in projected prevalence is, nonetheless, concerning and a call to action.”
This study identifies “areas of opportunity for change in the U.S. health care system,” he continued. “Business as usual will result in us encountering a huge number of individuals with CV risk factors and diseases.”
The results from the current analysis assume there will be no modification in health care policies or changes in access to care for at-risk populations, Dr. Mohebi and colleagues noted.
To “stem the rising tide of CV disease in at-risk individuals,” would require strategies such as “emphasis on education regarding CV risk factors, improving access to quality healthcare, and facilitating lower-cost access to effective therapies for treatment of CV risk factors,” according to the researchers.
“Such advances need to be applied in a more equitable way throughout the United States, however,” they cautioned.
Census plus NHANES data
The researchers used 2020 U.S. census data and projected growth and 2013-2018 U.S. National Health and Nutrition Survey data to estimate the number of people with CV risk factors and CV disease from 2025 to 2060.
The estimates are based on a growing population and a fixed frequency.
The projected changes in CV risk factors and disease over time were similar in men and women.
The researchers acknowledge that study limitations include the assumption that the prevalence patterns for CV risk factors and disease will be stable.
“To the extent the frequency of risk factors and disease are not likely to remain static, that assumption may reduce the accuracy of the projections,” Dr. Januzzi said. “However, we would point out that the goals of our analysis were to set general trends, and not to seek to project exact figures.”
Also, they did not take into account the effect of COVID-19. CV diseases were also based on self-report and CV risk factors could have been underestimated in minority populations that do not access health care.
Changing demographic landscape
It is “striking” that the numbers of non-White individuals with CV risk factors is projected to surpass the number of White individuals over time, and the number of non-White individuals with CV disease will be almost as many as White individuals by the year 2060, the editorialists noted.
“From a policy perspective, this means that unless appropriate, targeted action is taken, disparities in the burden of cardiovascular disease are only going to be exacerbated over time,” wrote Dr. Kalogeropoulos, from Stony Brook (N.Y.) University, and Dr. Butler, from Baylor College of Medicine, Dallas.
“On the positive side,” they continued, “the absolute increase in the percent prevalence of cardiovascular risk factors and conditions is projected to lie within a manageable range,” assuming that specific prevention policies are implemented.
“This is an opportunity for professional societies, including the cardiovascular care community, to re-evaluate priorities and strategies, for both training and practice, to best match the growing demands of a changing demographic landscape in the United States,” Dr. Kalogeropoulos and Dr. Butler concluded.
Dr. Mohebi is supported by the Barry Fellowship. Dr. Januzzi is supported by the Hutter Family Professorship; is a Trustee of the American College of Cardiology; is a board member of Imbria Pharmaceuticals; has received grant support from Abbott Diagnostics, Applied Therapeutics, Innolife, and Novartis; has received consulting income from Abbott Diagnostics, Boehringer Ingelheim, Janssen, Novartis, and Roche Diagnostics; and participates in clinical endpoint committees/data safety monitoring boards for AbbVie, Siemens, Takeda, and Vifor. Dr. Kalogeropoulos has received research funding from the National Heart, Lung, and Blood Institute; the American Heart Association; and the Centers for Disease Control and Prevention. Dr. Butler has been a consultant for numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
A new analysis projects steep increases by 2060 in the prevalence of cardiovascular (CV) risk factors and disease that will disproportionately affect non-White populations who have limited access to health care.
The study by Reza Mohebi, MD, Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues was published in the Journal of the American College of Cardiology.
“Even though several assumptions underlie these projections, the importance of this work cannot be overestimated,” Andreas P. Kalogeropoulos, MD, MPH, PhD, and Javed Butler, MD, MPH, MBA, wrote in an accompanying editorial. “The absolute numbers are staggering.”
From 2025 to 2060, the number of people with any one of four CV risk factors – type 2 diabetes, hypertension, dyslipidemia, and obesity – is projected to increase by 15.4 million, to 34.7 million.
And the number of people with of any one of four CV disease types – ischemic heart disease, heart failure, MI, and stroke – is projected to increase by 3.2 million, to 6.8 million.
Although the model predicts that the prevalence of CV risk factors will gradually decrease among White Americans, the highest prevalence of CV risk factors will be among the White population because of its overall size.
Conversely, the projected prevalence of CV risk factors is expected to increase in Black, Hispanic, Asian, and other race/ethnicity populations.
In parallel, the prevalence of CV disease is projected to decrease in the White population and increase among all other race/ethnicities, particularly in the Black and Hispanic populations.
“Our results project a worrisome increase with a particularly ominous increase in risk factors and disease in our most vulnerable patients, including Blacks and Hispanics,” senior author James L. Januzzi Jr., MD, summarized in a video issued by the society.
“The steep rise in CV risk factors and disease reflects the generally higher prevalence in populations projected to increase in the United States, owing to immigration and growth, including Black or Hispanic individuals,” Dr. Januzzi, also from Massachusetts General and Harvard, said in an interview.
“The disproportionate size of the risk is expected in a sense, as minority populations are disproportionately disadvantaged with respect to their health care,” he said. “But whether it is expected or not, the increase in projected prevalence is, nonetheless, concerning and a call to action.”
This study identifies “areas of opportunity for change in the U.S. health care system,” he continued. “Business as usual will result in us encountering a huge number of individuals with CV risk factors and diseases.”
The results from the current analysis assume there will be no modification in health care policies or changes in access to care for at-risk populations, Dr. Mohebi and colleagues noted.
To “stem the rising tide of CV disease in at-risk individuals,” would require strategies such as “emphasis on education regarding CV risk factors, improving access to quality healthcare, and facilitating lower-cost access to effective therapies for treatment of CV risk factors,” according to the researchers.
“Such advances need to be applied in a more equitable way throughout the United States, however,” they cautioned.
Census plus NHANES data
The researchers used 2020 U.S. census data and projected growth and 2013-2018 U.S. National Health and Nutrition Survey data to estimate the number of people with CV risk factors and CV disease from 2025 to 2060.
The estimates are based on a growing population and a fixed frequency.
The projected changes in CV risk factors and disease over time were similar in men and women.
The researchers acknowledge that study limitations include the assumption that the prevalence patterns for CV risk factors and disease will be stable.
“To the extent the frequency of risk factors and disease are not likely to remain static, that assumption may reduce the accuracy of the projections,” Dr. Januzzi said. “However, we would point out that the goals of our analysis were to set general trends, and not to seek to project exact figures.”
Also, they did not take into account the effect of COVID-19. CV diseases were also based on self-report and CV risk factors could have been underestimated in minority populations that do not access health care.
Changing demographic landscape
It is “striking” that the numbers of non-White individuals with CV risk factors is projected to surpass the number of White individuals over time, and the number of non-White individuals with CV disease will be almost as many as White individuals by the year 2060, the editorialists noted.
“From a policy perspective, this means that unless appropriate, targeted action is taken, disparities in the burden of cardiovascular disease are only going to be exacerbated over time,” wrote Dr. Kalogeropoulos, from Stony Brook (N.Y.) University, and Dr. Butler, from Baylor College of Medicine, Dallas.
“On the positive side,” they continued, “the absolute increase in the percent prevalence of cardiovascular risk factors and conditions is projected to lie within a manageable range,” assuming that specific prevention policies are implemented.
“This is an opportunity for professional societies, including the cardiovascular care community, to re-evaluate priorities and strategies, for both training and practice, to best match the growing demands of a changing demographic landscape in the United States,” Dr. Kalogeropoulos and Dr. Butler concluded.
Dr. Mohebi is supported by the Barry Fellowship. Dr. Januzzi is supported by the Hutter Family Professorship; is a Trustee of the American College of Cardiology; is a board member of Imbria Pharmaceuticals; has received grant support from Abbott Diagnostics, Applied Therapeutics, Innolife, and Novartis; has received consulting income from Abbott Diagnostics, Boehringer Ingelheim, Janssen, Novartis, and Roche Diagnostics; and participates in clinical endpoint committees/data safety monitoring boards for AbbVie, Siemens, Takeda, and Vifor. Dr. Kalogeropoulos has received research funding from the National Heart, Lung, and Blood Institute; the American Heart Association; and the Centers for Disease Control and Prevention. Dr. Butler has been a consultant for numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
A new analysis projects steep increases by 2060 in the prevalence of cardiovascular (CV) risk factors and disease that will disproportionately affect non-White populations who have limited access to health care.
The study by Reza Mohebi, MD, Massachusetts General Hospital and Harvard Medical School, both in Boston, and colleagues was published in the Journal of the American College of Cardiology.
“Even though several assumptions underlie these projections, the importance of this work cannot be overestimated,” Andreas P. Kalogeropoulos, MD, MPH, PhD, and Javed Butler, MD, MPH, MBA, wrote in an accompanying editorial. “The absolute numbers are staggering.”
From 2025 to 2060, the number of people with any one of four CV risk factors – type 2 diabetes, hypertension, dyslipidemia, and obesity – is projected to increase by 15.4 million, to 34.7 million.
And the number of people with of any one of four CV disease types – ischemic heart disease, heart failure, MI, and stroke – is projected to increase by 3.2 million, to 6.8 million.
Although the model predicts that the prevalence of CV risk factors will gradually decrease among White Americans, the highest prevalence of CV risk factors will be among the White population because of its overall size.
Conversely, the projected prevalence of CV risk factors is expected to increase in Black, Hispanic, Asian, and other race/ethnicity populations.
In parallel, the prevalence of CV disease is projected to decrease in the White population and increase among all other race/ethnicities, particularly in the Black and Hispanic populations.
“Our results project a worrisome increase with a particularly ominous increase in risk factors and disease in our most vulnerable patients, including Blacks and Hispanics,” senior author James L. Januzzi Jr., MD, summarized in a video issued by the society.
“The steep rise in CV risk factors and disease reflects the generally higher prevalence in populations projected to increase in the United States, owing to immigration and growth, including Black or Hispanic individuals,” Dr. Januzzi, also from Massachusetts General and Harvard, said in an interview.
“The disproportionate size of the risk is expected in a sense, as minority populations are disproportionately disadvantaged with respect to their health care,” he said. “But whether it is expected or not, the increase in projected prevalence is, nonetheless, concerning and a call to action.”
This study identifies “areas of opportunity for change in the U.S. health care system,” he continued. “Business as usual will result in us encountering a huge number of individuals with CV risk factors and diseases.”
The results from the current analysis assume there will be no modification in health care policies or changes in access to care for at-risk populations, Dr. Mohebi and colleagues noted.
To “stem the rising tide of CV disease in at-risk individuals,” would require strategies such as “emphasis on education regarding CV risk factors, improving access to quality healthcare, and facilitating lower-cost access to effective therapies for treatment of CV risk factors,” according to the researchers.
“Such advances need to be applied in a more equitable way throughout the United States, however,” they cautioned.
Census plus NHANES data
The researchers used 2020 U.S. census data and projected growth and 2013-2018 U.S. National Health and Nutrition Survey data to estimate the number of people with CV risk factors and CV disease from 2025 to 2060.
The estimates are based on a growing population and a fixed frequency.
The projected changes in CV risk factors and disease over time were similar in men and women.
The researchers acknowledge that study limitations include the assumption that the prevalence patterns for CV risk factors and disease will be stable.
“To the extent the frequency of risk factors and disease are not likely to remain static, that assumption may reduce the accuracy of the projections,” Dr. Januzzi said. “However, we would point out that the goals of our analysis were to set general trends, and not to seek to project exact figures.”
Also, they did not take into account the effect of COVID-19. CV diseases were also based on self-report and CV risk factors could have been underestimated in minority populations that do not access health care.
Changing demographic landscape
It is “striking” that the numbers of non-White individuals with CV risk factors is projected to surpass the number of White individuals over time, and the number of non-White individuals with CV disease will be almost as many as White individuals by the year 2060, the editorialists noted.
“From a policy perspective, this means that unless appropriate, targeted action is taken, disparities in the burden of cardiovascular disease are only going to be exacerbated over time,” wrote Dr. Kalogeropoulos, from Stony Brook (N.Y.) University, and Dr. Butler, from Baylor College of Medicine, Dallas.
“On the positive side,” they continued, “the absolute increase in the percent prevalence of cardiovascular risk factors and conditions is projected to lie within a manageable range,” assuming that specific prevention policies are implemented.
“This is an opportunity for professional societies, including the cardiovascular care community, to re-evaluate priorities and strategies, for both training and practice, to best match the growing demands of a changing demographic landscape in the United States,” Dr. Kalogeropoulos and Dr. Butler concluded.
Dr. Mohebi is supported by the Barry Fellowship. Dr. Januzzi is supported by the Hutter Family Professorship; is a Trustee of the American College of Cardiology; is a board member of Imbria Pharmaceuticals; has received grant support from Abbott Diagnostics, Applied Therapeutics, Innolife, and Novartis; has received consulting income from Abbott Diagnostics, Boehringer Ingelheim, Janssen, Novartis, and Roche Diagnostics; and participates in clinical endpoint committees/data safety monitoring boards for AbbVie, Siemens, Takeda, and Vifor. Dr. Kalogeropoulos has received research funding from the National Heart, Lung, and Blood Institute; the American Heart Association; and the Centers for Disease Control and Prevention. Dr. Butler has been a consultant for numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF AMERICAN COLLEGE OF CARDIOLOGY