User login
Neurology Reviews covers innovative and emerging news in neurology and neuroscience every month, with a focus on practical approaches to treating Parkinson's disease, epilepsy, headache, stroke, multiple sclerosis, Alzheimer's disease, and other neurologic disorders.
PML
Progressive multifocal leukoencephalopathy
Rituxan
The leading independent newspaper covering neurology news and commentary.
More evidence hydroxychloroquine is ineffective, harmful in COVID-19
Hydroxychloroquine and chloroquine, with or without azithromycin or clarithromycin, offer no benefit in treating patients with COVID-19 and, instead, are associated with ventricular arrhythmias and higher rates of mortality, according to a major new international study.

In the largest observational study of its kind, including close to 100,000 people in 671 hospitals on six continents, investigators compared outcomes in 15,000 patients with COVID-19 treated with hydroxychloroquine and chloroquine alone or in combination with a macrolide with 80,000 control patients with COVID-19 not receiving these agents.
Treatment with any of these medications, either alone or in combination, was associated with increased death during hospitalization; compared with about 10% in control group patients, mortality rates ranged from more than 16% to almost 24% in the treated groups.
Patients treated with hydroxychloroquine plus a macrolide showed the highest rates of serious cardiac arrhythmias, and, even after accounting for demographic factors and comorbidities, this combination was found to be associated with a more than 5-fold increase in the risk of developing a serious arrhythmia while in the hospital.
“In this real-world study, the biggest yet, we looked at 100,000 patients [with COVID-19] across six continents and found not the slightest hint of benefits and only risks, and the data is pretty straightforward,” study coauthor Frank Ruschitzka, MD, director of the Heart Center at University Hospital, Zürich, said in an interview. The study was published online May 22 in The Lancet.
‘Inconclusive’ evidence
The absence of an effective treatment for COVID-19 has led to the “repurposing” of the antimalarial drug chloroquine and its analogue hydroxychloroquine, which is used for treating autoimmune disease, but this approach is based on anecdotal evidence or open-label randomized trials that have been “largely inconclusive,” the authors wrote.
Additional agents used to treat COVID-19 are second-generation macrolides (azithromycin or clarithromycin), in combination with chloroquine or hydroxychloroquine, “despite limited evidence” and the risk for ventricular arrhythmias, the authors noted.
“Our primary question was whether there was any associated benefits of the use of hydroxychloroquine, chloroquine, or a combined regimen with macrolides in treating COVID-19, and — if there was no benefit — would there be harm?” lead author Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine, Brigham and Women’s Hospital, Boston, said in an interview.
The investigators used data from a multinational registry comprising 671 hospitals that included patients (n = 96,032; mean age 53.8 years; 46.3% female) who had been hospitalized between Dec. 20, 2019, and April 14, 2020, with confirmed COVID-19 infection.
They also collected data about demographics, underlying comorbidities, and medical history, and medications that patients were taking at baseline.
Patients receiving treatment (n = 14,888) were divided into four groups: those receiving chloroquine alone (n = 1,868), those receiving chloroquine with a macrolide (n = 3,783), those receiving hydroxychloroquine alone (n = 3,016) and those receiving hydroxychloroquine with a macrolide (n = 6,221).
The remaining patients not treated with these regimens (n = 81,144) were regarded as the control group.
Most patients (65.9%) came from North America, followed by Europe (17.39%), Asia (7.9%), Africa (4.6%), South America (3.7%), and Australia (0.6%). Most (66.9%) were white, followed by patients of Asian origin (14.1%), black patients (9.4%), and Hispanic patients (6.2%).
Comorbidities and underlying conditions included obesity, hyperlipidemia, and hypertension in about 30%.
Comorbidities and underlying conditions
The investigators conducted multiple analyses to control for confounding variables, including Cox proportional hazards regression and propensity score matching analyses.
“In an observational study, there is always a chance of residual confounding, which is why we did propensity score based matched analyses,” Dr. Ruschitzka explained.
No significant differences were found in distribution of demographics and comorbidities between the groups.
As good as it gets
“We found no benefit in any of the four treatment regimens for hospitalized patients with COVID-19, but we did notice higher rates of death and serious ventricular arrhythmias in these patients, compared to the controls,” Dr. Mehra reported.
Of the patients in the control group, roughly 9.3% died during their hospitalization, compared with 16.4% of patients treated with chloroquine alone, 18.0% of those treated with hydroxychloroquine alone, 22.2% of those treated with chloroquine and a macrolide, and 23.8% of those treated with hydroxychloroquine and a macrolide.
After accounting for confounding variables, the researchers estimated that the excess mortality risk attributable to use of the drug regimen ranged from 34% to 45%.
Patients treated with any of the four regimens sustained more serious arrhythmias, compared with those in the control group (0.35), with the biggest increase seen in the group treated with the combination of hydroxychloroquine plus a macrolide (8.1%), followed by chloroquine with a macrolide (6.5%), hydroxychloroquine alone (6.1%), and chloroquine alone (4.3%).
“We were fairly reassured that, although the study was observational, the signals were robust and consistent across all regions of the world in diverse populations, and we did not see any muting of that signal, depending on region,” Dr. Mehra said.
“Two months ago, we were all scratching our heads about how to treat patients with COVID-19, and then came a drug [hydroxychloroquine] with some anecdotal evidence, but now we have 2 months more experience, and we looked to science to provide some answer,” Dr. Ruschitzka said.
“Although this was not a randomized, controlled trial, so we do not have a definite answer, the data provided in this [large, multinational] real-world study is as good as it gets and the best data we have,” he concluded.
“Let the science speak for itself”
Commenting on the study in an interview, Christian Funck-Brentano, MD, from the Hospital Pitié-Salpêtrière and Sorbonne University, both in Paris, said that, although the study is observational and therefore not as reliable as a randomized controlled trial, it is “nevertheless well-documented, studied a huge amount of people, and utilized several sensitivity methods, all of which showed the same results.”
Dr. Funck-Brentano, who is the coauthor of an accompanying editorial in The Lancet and was not involved with the study, said that “we now have no evidence that hydroxychloroquine and chloroquine alone or in combination with a macrolide do any good and we have potential evidence that they do harm and kill people.”
Also commenting on the study in an interview, David Holtgrave, PhD, dean of the School of Public Health at the State University of New York at Albany, said that, “while no one observational study alone would lead to a firm clinical recommendation, I think it is helpful for physicians and public health officials to be aware of the findings of the peer-reviewed observational studies to date and the National Institutes of Health COVID-19 treatment guidelines and the Food and Drug Administration’s statement of drug safety concern about hydroxychloroquine to inform their decision-making as we await the results of randomized clinical trials of these drugs for the treatment of COVID-19,” said Dr. Holtgrave, who was not involved with the study.
He added that, to his knowledge, there are “still no published studies of prophylactic use of these drugs to prevent COVID-19.”
Dr. Mehra emphasized that a cardinal principle of practicing medicine is “first do no harm” and “even in situations where you believe a desperate disease calls for desperate measures, responsible physicians should take a step back and ask if we are doing harm, and until we can say we aren’t, I don’t think it’s wise to push something like this in the absence of good efficacy data.”
Dr. Ruschitzka added that those who are encouraging the use of these agents “should review their decision based on today’s data and let the science speak for itself.”
The study was supported by the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston. Dr. Mehra reported personal fees from Abbott, Medtronic, Janssen, Mesoblast, Portola, Bayer, Baim Institute for Clinical Research, NuPulseCV, FineHeart, Leviticus, Roivant, and Triple Gene. Dr. Ruschitzka was paid for time spent as a committee member for clinical trials, advisory boards, other forms of consulting, and lectures or presentations; these payments were made directly to the University of Zürich and no personal payments were received in relation to these trials or other activities. Dr. Funck-Brentano, his coauthor, and Dr. Holtgrave declared no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Hydroxychloroquine and chloroquine, with or without azithromycin or clarithromycin, offer no benefit in treating patients with COVID-19 and, instead, are associated with ventricular arrhythmias and higher rates of mortality, according to a major new international study.
In the largest observational study of its kind, including close to 100,000 people in 671 hospitals on six continents, investigators compared outcomes in 15,000 patients with COVID-19 treated with hydroxychloroquine and chloroquine alone or in combination with a macrolide with 80,000 control patients with COVID-19 not receiving these agents.
Treatment with any of these medications, either alone or in combination, was associated with increased death during hospitalization; compared with about 10% in control group patients, mortality rates ranged from more than 16% to almost 24% in the treated groups.
Patients treated with hydroxychloroquine plus a macrolide showed the highest rates of serious cardiac arrhythmias, and, even after accounting for demographic factors and comorbidities, this combination was found to be associated with a more than 5-fold increase in the risk of developing a serious arrhythmia while in the hospital.
“In this real-world study, the biggest yet, we looked at 100,000 patients [with COVID-19] across six continents and found not the slightest hint of benefits and only risks, and the data is pretty straightforward,” study coauthor Frank Ruschitzka, MD, director of the Heart Center at University Hospital, Zürich, said in an interview. The study was published online May 22 in The Lancet.
‘Inconclusive’ evidence
The absence of an effective treatment for COVID-19 has led to the “repurposing” of the antimalarial drug chloroquine and its analogue hydroxychloroquine, which is used for treating autoimmune disease, but this approach is based on anecdotal evidence or open-label randomized trials that have been “largely inconclusive,” the authors wrote.
Additional agents used to treat COVID-19 are second-generation macrolides (azithromycin or clarithromycin), in combination with chloroquine or hydroxychloroquine, “despite limited evidence” and the risk for ventricular arrhythmias, the authors noted.
“Our primary question was whether there was any associated benefits of the use of hydroxychloroquine, chloroquine, or a combined regimen with macrolides in treating COVID-19, and — if there was no benefit — would there be harm?” lead author Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine, Brigham and Women’s Hospital, Boston, said in an interview.
The investigators used data from a multinational registry comprising 671 hospitals that included patients (n = 96,032; mean age 53.8 years; 46.3% female) who had been hospitalized between Dec. 20, 2019, and April 14, 2020, with confirmed COVID-19 infection.
They also collected data about demographics, underlying comorbidities, and medical history, and medications that patients were taking at baseline.
Patients receiving treatment (n = 14,888) were divided into four groups: those receiving chloroquine alone (n = 1,868), those receiving chloroquine with a macrolide (n = 3,783), those receiving hydroxychloroquine alone (n = 3,016) and those receiving hydroxychloroquine with a macrolide (n = 6,221).
The remaining patients not treated with these regimens (n = 81,144) were regarded as the control group.
Most patients (65.9%) came from North America, followed by Europe (17.39%), Asia (7.9%), Africa (4.6%), South America (3.7%), and Australia (0.6%). Most (66.9%) were white, followed by patients of Asian origin (14.1%), black patients (9.4%), and Hispanic patients (6.2%).
Comorbidities and underlying conditions included obesity, hyperlipidemia, and hypertension in about 30%.
Comorbidities and underlying conditions
The investigators conducted multiple analyses to control for confounding variables, including Cox proportional hazards regression and propensity score matching analyses.
“In an observational study, there is always a chance of residual confounding, which is why we did propensity score based matched analyses,” Dr. Ruschitzka explained.
No significant differences were found in distribution of demographics and comorbidities between the groups.
As good as it gets
“We found no benefit in any of the four treatment regimens for hospitalized patients with COVID-19, but we did notice higher rates of death and serious ventricular arrhythmias in these patients, compared to the controls,” Dr. Mehra reported.
Of the patients in the control group, roughly 9.3% died during their hospitalization, compared with 16.4% of patients treated with chloroquine alone, 18.0% of those treated with hydroxychloroquine alone, 22.2% of those treated with chloroquine and a macrolide, and 23.8% of those treated with hydroxychloroquine and a macrolide.
After accounting for confounding variables, the researchers estimated that the excess mortality risk attributable to use of the drug regimen ranged from 34% to 45%.
Patients treated with any of the four regimens sustained more serious arrhythmias, compared with those in the control group (0.35), with the biggest increase seen in the group treated with the combination of hydroxychloroquine plus a macrolide (8.1%), followed by chloroquine with a macrolide (6.5%), hydroxychloroquine alone (6.1%), and chloroquine alone (4.3%).
“We were fairly reassured that, although the study was observational, the signals were robust and consistent across all regions of the world in diverse populations, and we did not see any muting of that signal, depending on region,” Dr. Mehra said.
“Two months ago, we were all scratching our heads about how to treat patients with COVID-19, and then came a drug [hydroxychloroquine] with some anecdotal evidence, but now we have 2 months more experience, and we looked to science to provide some answer,” Dr. Ruschitzka said.
“Although this was not a randomized, controlled trial, so we do not have a definite answer, the data provided in this [large, multinational] real-world study is as good as it gets and the best data we have,” he concluded.
“Let the science speak for itself”
Commenting on the study in an interview, Christian Funck-Brentano, MD, from the Hospital Pitié-Salpêtrière and Sorbonne University, both in Paris, said that, although the study is observational and therefore not as reliable as a randomized controlled trial, it is “nevertheless well-documented, studied a huge amount of people, and utilized several sensitivity methods, all of which showed the same results.”
Dr. Funck-Brentano, who is the coauthor of an accompanying editorial in The Lancet and was not involved with the study, said that “we now have no evidence that hydroxychloroquine and chloroquine alone or in combination with a macrolide do any good and we have potential evidence that they do harm and kill people.”
Also commenting on the study in an interview, David Holtgrave, PhD, dean of the School of Public Health at the State University of New York at Albany, said that, “while no one observational study alone would lead to a firm clinical recommendation, I think it is helpful for physicians and public health officials to be aware of the findings of the peer-reviewed observational studies to date and the National Institutes of Health COVID-19 treatment guidelines and the Food and Drug Administration’s statement of drug safety concern about hydroxychloroquine to inform their decision-making as we await the results of randomized clinical trials of these drugs for the treatment of COVID-19,” said Dr. Holtgrave, who was not involved with the study.
He added that, to his knowledge, there are “still no published studies of prophylactic use of these drugs to prevent COVID-19.”
Dr. Mehra emphasized that a cardinal principle of practicing medicine is “first do no harm” and “even in situations where you believe a desperate disease calls for desperate measures, responsible physicians should take a step back and ask if we are doing harm, and until we can say we aren’t, I don’t think it’s wise to push something like this in the absence of good efficacy data.”
Dr. Ruschitzka added that those who are encouraging the use of these agents “should review their decision based on today’s data and let the science speak for itself.”
The study was supported by the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston. Dr. Mehra reported personal fees from Abbott, Medtronic, Janssen, Mesoblast, Portola, Bayer, Baim Institute for Clinical Research, NuPulseCV, FineHeart, Leviticus, Roivant, and Triple Gene. Dr. Ruschitzka was paid for time spent as a committee member for clinical trials, advisory boards, other forms of consulting, and lectures or presentations; these payments were made directly to the University of Zürich and no personal payments were received in relation to these trials or other activities. Dr. Funck-Brentano, his coauthor, and Dr. Holtgrave declared no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Hydroxychloroquine and chloroquine, with or without azithromycin or clarithromycin, offer no benefit in treating patients with COVID-19 and, instead, are associated with ventricular arrhythmias and higher rates of mortality, according to a major new international study.
In the largest observational study of its kind, including close to 100,000 people in 671 hospitals on six continents, investigators compared outcomes in 15,000 patients with COVID-19 treated with hydroxychloroquine and chloroquine alone or in combination with a macrolide with 80,000 control patients with COVID-19 not receiving these agents.
Treatment with any of these medications, either alone or in combination, was associated with increased death during hospitalization; compared with about 10% in control group patients, mortality rates ranged from more than 16% to almost 24% in the treated groups.
Patients treated with hydroxychloroquine plus a macrolide showed the highest rates of serious cardiac arrhythmias, and, even after accounting for demographic factors and comorbidities, this combination was found to be associated with a more than 5-fold increase in the risk of developing a serious arrhythmia while in the hospital.
“In this real-world study, the biggest yet, we looked at 100,000 patients [with COVID-19] across six continents and found not the slightest hint of benefits and only risks, and the data is pretty straightforward,” study coauthor Frank Ruschitzka, MD, director of the Heart Center at University Hospital, Zürich, said in an interview. The study was published online May 22 in The Lancet.
‘Inconclusive’ evidence
The absence of an effective treatment for COVID-19 has led to the “repurposing” of the antimalarial drug chloroquine and its analogue hydroxychloroquine, which is used for treating autoimmune disease, but this approach is based on anecdotal evidence or open-label randomized trials that have been “largely inconclusive,” the authors wrote.
Additional agents used to treat COVID-19 are second-generation macrolides (azithromycin or clarithromycin), in combination with chloroquine or hydroxychloroquine, “despite limited evidence” and the risk for ventricular arrhythmias, the authors noted.
“Our primary question was whether there was any associated benefits of the use of hydroxychloroquine, chloroquine, or a combined regimen with macrolides in treating COVID-19, and — if there was no benefit — would there be harm?” lead author Mandeep R. Mehra, MD, MSc, William Harvey Distinguished Chair in Advanced Cardiovascular Medicine, Brigham and Women’s Hospital, Boston, said in an interview.
The investigators used data from a multinational registry comprising 671 hospitals that included patients (n = 96,032; mean age 53.8 years; 46.3% female) who had been hospitalized between Dec. 20, 2019, and April 14, 2020, with confirmed COVID-19 infection.
They also collected data about demographics, underlying comorbidities, and medical history, and medications that patients were taking at baseline.
Patients receiving treatment (n = 14,888) were divided into four groups: those receiving chloroquine alone (n = 1,868), those receiving chloroquine with a macrolide (n = 3,783), those receiving hydroxychloroquine alone (n = 3,016) and those receiving hydroxychloroquine with a macrolide (n = 6,221).
The remaining patients not treated with these regimens (n = 81,144) were regarded as the control group.
Most patients (65.9%) came from North America, followed by Europe (17.39%), Asia (7.9%), Africa (4.6%), South America (3.7%), and Australia (0.6%). Most (66.9%) were white, followed by patients of Asian origin (14.1%), black patients (9.4%), and Hispanic patients (6.2%).
Comorbidities and underlying conditions included obesity, hyperlipidemia, and hypertension in about 30%.
Comorbidities and underlying conditions
The investigators conducted multiple analyses to control for confounding variables, including Cox proportional hazards regression and propensity score matching analyses.
“In an observational study, there is always a chance of residual confounding, which is why we did propensity score based matched analyses,” Dr. Ruschitzka explained.
No significant differences were found in distribution of demographics and comorbidities between the groups.
As good as it gets
“We found no benefit in any of the four treatment regimens for hospitalized patients with COVID-19, but we did notice higher rates of death and serious ventricular arrhythmias in these patients, compared to the controls,” Dr. Mehra reported.
Of the patients in the control group, roughly 9.3% died during their hospitalization, compared with 16.4% of patients treated with chloroquine alone, 18.0% of those treated with hydroxychloroquine alone, 22.2% of those treated with chloroquine and a macrolide, and 23.8% of those treated with hydroxychloroquine and a macrolide.
After accounting for confounding variables, the researchers estimated that the excess mortality risk attributable to use of the drug regimen ranged from 34% to 45%.
Patients treated with any of the four regimens sustained more serious arrhythmias, compared with those in the control group (0.35), with the biggest increase seen in the group treated with the combination of hydroxychloroquine plus a macrolide (8.1%), followed by chloroquine with a macrolide (6.5%), hydroxychloroquine alone (6.1%), and chloroquine alone (4.3%).
“We were fairly reassured that, although the study was observational, the signals were robust and consistent across all regions of the world in diverse populations, and we did not see any muting of that signal, depending on region,” Dr. Mehra said.
“Two months ago, we were all scratching our heads about how to treat patients with COVID-19, and then came a drug [hydroxychloroquine] with some anecdotal evidence, but now we have 2 months more experience, and we looked to science to provide some answer,” Dr. Ruschitzka said.
“Although this was not a randomized, controlled trial, so we do not have a definite answer, the data provided in this [large, multinational] real-world study is as good as it gets and the best data we have,” he concluded.
“Let the science speak for itself”
Commenting on the study in an interview, Christian Funck-Brentano, MD, from the Hospital Pitié-Salpêtrière and Sorbonne University, both in Paris, said that, although the study is observational and therefore not as reliable as a randomized controlled trial, it is “nevertheless well-documented, studied a huge amount of people, and utilized several sensitivity methods, all of which showed the same results.”
Dr. Funck-Brentano, who is the coauthor of an accompanying editorial in The Lancet and was not involved with the study, said that “we now have no evidence that hydroxychloroquine and chloroquine alone or in combination with a macrolide do any good and we have potential evidence that they do harm and kill people.”
Also commenting on the study in an interview, David Holtgrave, PhD, dean of the School of Public Health at the State University of New York at Albany, said that, “while no one observational study alone would lead to a firm clinical recommendation, I think it is helpful for physicians and public health officials to be aware of the findings of the peer-reviewed observational studies to date and the National Institutes of Health COVID-19 treatment guidelines and the Food and Drug Administration’s statement of drug safety concern about hydroxychloroquine to inform their decision-making as we await the results of randomized clinical trials of these drugs for the treatment of COVID-19,” said Dr. Holtgrave, who was not involved with the study.
He added that, to his knowledge, there are “still no published studies of prophylactic use of these drugs to prevent COVID-19.”
Dr. Mehra emphasized that a cardinal principle of practicing medicine is “first do no harm” and “even in situations where you believe a desperate disease calls for desperate measures, responsible physicians should take a step back and ask if we are doing harm, and until we can say we aren’t, I don’t think it’s wise to push something like this in the absence of good efficacy data.”
Dr. Ruschitzka added that those who are encouraging the use of these agents “should review their decision based on today’s data and let the science speak for itself.”
The study was supported by the William Harvey Distinguished Chair in Advanced Cardiovascular Medicine at Brigham and Women’s Hospital, Boston. Dr. Mehra reported personal fees from Abbott, Medtronic, Janssen, Mesoblast, Portola, Bayer, Baim Institute for Clinical Research, NuPulseCV, FineHeart, Leviticus, Roivant, and Triple Gene. Dr. Ruschitzka was paid for time spent as a committee member for clinical trials, advisory boards, other forms of consulting, and lectures or presentations; these payments were made directly to the University of Zürich and no personal payments were received in relation to these trials or other activities. Dr. Funck-Brentano, his coauthor, and Dr. Holtgrave declared no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Immunotherapy, steroids had positive outcomes in COVID-19–associated multisystem inflammatory syndrome
According to study of a cluster of patients in France and Switzerland, children may experience an acute cardiac decompensation from the severe inflammatory state following SARS-CoV-2 infection, termed multisystem inflammatory syndrome in children (MIS-C). Treatment with immunoglobulin appears to be associated with recovery of left ventricular systolic function.
“The pediatric and cardiology communities should be acutely aware of this new disease probably related to SARS-CoV-2 infection (MIS-C), that shares similarities with Kawasaki disease but has specificities in its presentation,” researchers led by Zahra Belhadjer, MD, of Necker-Enfants Malades Hospital in Paris, wrote in a cases series report published online in Circulation “Early diagnosis and management appear to lead to favorable outcome using classical therapies. Elucidating the immune mechanisms of this disease will afford further insights for treatment and potential global prevention of severe forms.”
Over a 2-month period that coincided with the SARS-CoV-2 pandemic in France and Switzerland, the researchers retrospectively collected clinical, biological, therapeutic, and early-outcomes data in 35 children who were admitted to pediatric ICUs in 14 centers for cardiogenic shock, left ventricular dysfunction, and severe inflammatory state. Their median age was 10 years, all presented with a fever, 80% had gastrointestinal symptoms of abdominal pain, vomiting, or diarrhea, and 28% had comorbidities that included body mass index of greater than 25 kg/m2 (17%), asthma (9%), and lupus (3%), and overweight. Only 17% presented with chest pain. The researchers observed that left ventricular ejection fraction was less than 30% in 28% of patients, and 80% required inotropic support with 28% treated with extracorporeal membrane oxygenation (ECMO). All patients presented with a severe inflammatory state evidenced by elevated C-reactive protein and d-dimer. Interleukin 6 was elevated to a median of 135 pg/mL in 13 of the patients. Elevation of troponin I was constant but mild to moderate, and NT-proBNP or BNP elevation was present in all children.
Nearly all patients 35 (88%) patients tested positive for SARS-CoV-2 infection by polymerase chain reaction of nasopharyngeal swab or serology. Most patients (80%) received IV inotropic support, 71% received first-line IV immunoglobulin, 65% received anticoagulation with heparin, 34% received IV steroids having been considered high-risk patients with symptoms similar to an incomplete form of Kawasaki disease, and 8% received treatment with an interleukin-1 receptor antagonist because of a persistent severe inflammatory state. Left ventricular function was restored in 71% of those discharged from the intensive care unit. No patient died, and all patients treated with ECMO were successfully weaned after a median of 4.5 days.
“Some aspects of this emerging pediatric disease (MIS-C) are similar to those of Kawasaki disease: prolonged fever, multisystem inflammation with skin rash, lymphadenopathy, diarrhea, meningism, and high levels of inflammatory biomarkers,” the researchers wrote. “But differences are important and raise the question as to whether this syndrome is Kawasaki disease with SARS-CoV-2 as the triggering agent, or represents a different syndrome (MIS-C). Kawasaki disease predominantly affects young children younger than 5 years, whereas the median age in our series is 10 years. Incomplete forms of Kawasaki disease occur in infants who may have fever as the sole clinical finding, whereas older patients are more prone to exhibit the complete form.”
They went on to note that the overlapping features between MIS-C and Kawasaki disease “may be due to similar pathophysiology. The etiologic agent of Kawasaki disease is unknown but likely to be ubiquitous, causing asymptomatic childhood infection but triggering the immunologic cascade of Kawasaki disease in genetically susceptible individuals. Please note that infection with a novel RNA virus that enters through the upper respiratory tract has been proposed to be the cause of the disease (see PLoS One. 2008 Feb 13;3:e1582 and J Infect Dis. 2011 Apr 1;203:1021-30).”
Based on the work of authors, it appears that a high index of suspicion for MIS-C is important for children who develop Kawasaki-like symptoms, David J. Goldberg, MD, said in an interview. “Although children have largely been spared from the acute respiratory presentation of the SARS-CoV-2 pandemic, the recognition and understanding of what appears to be a postviral inflammatory response is a critical first step in developing treatment algorithms for this disease process,” said Dr. Goldberg, a board-certified attending cardiologist in the cardiac center and fetal heart program at Children’s Hospital of Philadelphia. “If inflammatory markers are elevated, particularly if there are accompanying gastrointestinal symptoms, the possibility of cardiac involvement suggests the utility of screening echocardiography. Given the potential need for inotropic or mechanical circulatory support, the presence of myocardial dysfunction dictates care in an intensive care unit capable of providing advanced therapies. While the evidence from Dr. Belhadjer’s cohort suggests that full recovery is probable, there is still much to be learned about this unique inflammatory syndrome and the alarm has rightly been sounded.”
The researchers and Dr. Goldberg reported having no disclosures.
SOURCE: Belhadjer Z et al. Circulation 2020 May 17; doi: 10.1161/circulationaha.120.048360.
According to study of a cluster of patients in France and Switzerland, children may experience an acute cardiac decompensation from the severe inflammatory state following SARS-CoV-2 infection, termed multisystem inflammatory syndrome in children (MIS-C). Treatment with immunoglobulin appears to be associated with recovery of left ventricular systolic function.
“The pediatric and cardiology communities should be acutely aware of this new disease probably related to SARS-CoV-2 infection (MIS-C), that shares similarities with Kawasaki disease but has specificities in its presentation,” researchers led by Zahra Belhadjer, MD, of Necker-Enfants Malades Hospital in Paris, wrote in a cases series report published online in Circulation “Early diagnosis and management appear to lead to favorable outcome using classical therapies. Elucidating the immune mechanisms of this disease will afford further insights for treatment and potential global prevention of severe forms.”
Over a 2-month period that coincided with the SARS-CoV-2 pandemic in France and Switzerland, the researchers retrospectively collected clinical, biological, therapeutic, and early-outcomes data in 35 children who were admitted to pediatric ICUs in 14 centers for cardiogenic shock, left ventricular dysfunction, and severe inflammatory state. Their median age was 10 years, all presented with a fever, 80% had gastrointestinal symptoms of abdominal pain, vomiting, or diarrhea, and 28% had comorbidities that included body mass index of greater than 25 kg/m2 (17%), asthma (9%), and lupus (3%), and overweight. Only 17% presented with chest pain. The researchers observed that left ventricular ejection fraction was less than 30% in 28% of patients, and 80% required inotropic support with 28% treated with extracorporeal membrane oxygenation (ECMO). All patients presented with a severe inflammatory state evidenced by elevated C-reactive protein and d-dimer. Interleukin 6 was elevated to a median of 135 pg/mL in 13 of the patients. Elevation of troponin I was constant but mild to moderate, and NT-proBNP or BNP elevation was present in all children.
Nearly all patients 35 (88%) patients tested positive for SARS-CoV-2 infection by polymerase chain reaction of nasopharyngeal swab or serology. Most patients (80%) received IV inotropic support, 71% received first-line IV immunoglobulin, 65% received anticoagulation with heparin, 34% received IV steroids having been considered high-risk patients with symptoms similar to an incomplete form of Kawasaki disease, and 8% received treatment with an interleukin-1 receptor antagonist because of a persistent severe inflammatory state. Left ventricular function was restored in 71% of those discharged from the intensive care unit. No patient died, and all patients treated with ECMO were successfully weaned after a median of 4.5 days.
“Some aspects of this emerging pediatric disease (MIS-C) are similar to those of Kawasaki disease: prolonged fever, multisystem inflammation with skin rash, lymphadenopathy, diarrhea, meningism, and high levels of inflammatory biomarkers,” the researchers wrote. “But differences are important and raise the question as to whether this syndrome is Kawasaki disease with SARS-CoV-2 as the triggering agent, or represents a different syndrome (MIS-C). Kawasaki disease predominantly affects young children younger than 5 years, whereas the median age in our series is 10 years. Incomplete forms of Kawasaki disease occur in infants who may have fever as the sole clinical finding, whereas older patients are more prone to exhibit the complete form.”
They went on to note that the overlapping features between MIS-C and Kawasaki disease “may be due to similar pathophysiology. The etiologic agent of Kawasaki disease is unknown but likely to be ubiquitous, causing asymptomatic childhood infection but triggering the immunologic cascade of Kawasaki disease in genetically susceptible individuals. Please note that infection with a novel RNA virus that enters through the upper respiratory tract has been proposed to be the cause of the disease (see PLoS One. 2008 Feb 13;3:e1582 and J Infect Dis. 2011 Apr 1;203:1021-30).”
Based on the work of authors, it appears that a high index of suspicion for MIS-C is important for children who develop Kawasaki-like symptoms, David J. Goldberg, MD, said in an interview. “Although children have largely been spared from the acute respiratory presentation of the SARS-CoV-2 pandemic, the recognition and understanding of what appears to be a postviral inflammatory response is a critical first step in developing treatment algorithms for this disease process,” said Dr. Goldberg, a board-certified attending cardiologist in the cardiac center and fetal heart program at Children’s Hospital of Philadelphia. “If inflammatory markers are elevated, particularly if there are accompanying gastrointestinal symptoms, the possibility of cardiac involvement suggests the utility of screening echocardiography. Given the potential need for inotropic or mechanical circulatory support, the presence of myocardial dysfunction dictates care in an intensive care unit capable of providing advanced therapies. While the evidence from Dr. Belhadjer’s cohort suggests that full recovery is probable, there is still much to be learned about this unique inflammatory syndrome and the alarm has rightly been sounded.”
The researchers and Dr. Goldberg reported having no disclosures.
SOURCE: Belhadjer Z et al. Circulation 2020 May 17; doi: 10.1161/circulationaha.120.048360.
According to study of a cluster of patients in France and Switzerland, children may experience an acute cardiac decompensation from the severe inflammatory state following SARS-CoV-2 infection, termed multisystem inflammatory syndrome in children (MIS-C). Treatment with immunoglobulin appears to be associated with recovery of left ventricular systolic function.
“The pediatric and cardiology communities should be acutely aware of this new disease probably related to SARS-CoV-2 infection (MIS-C), that shares similarities with Kawasaki disease but has specificities in its presentation,” researchers led by Zahra Belhadjer, MD, of Necker-Enfants Malades Hospital in Paris, wrote in a cases series report published online in Circulation “Early diagnosis and management appear to lead to favorable outcome using classical therapies. Elucidating the immune mechanisms of this disease will afford further insights for treatment and potential global prevention of severe forms.”
Over a 2-month period that coincided with the SARS-CoV-2 pandemic in France and Switzerland, the researchers retrospectively collected clinical, biological, therapeutic, and early-outcomes data in 35 children who were admitted to pediatric ICUs in 14 centers for cardiogenic shock, left ventricular dysfunction, and severe inflammatory state. Their median age was 10 years, all presented with a fever, 80% had gastrointestinal symptoms of abdominal pain, vomiting, or diarrhea, and 28% had comorbidities that included body mass index of greater than 25 kg/m2 (17%), asthma (9%), and lupus (3%), and overweight. Only 17% presented with chest pain. The researchers observed that left ventricular ejection fraction was less than 30% in 28% of patients, and 80% required inotropic support with 28% treated with extracorporeal membrane oxygenation (ECMO). All patients presented with a severe inflammatory state evidenced by elevated C-reactive protein and d-dimer. Interleukin 6 was elevated to a median of 135 pg/mL in 13 of the patients. Elevation of troponin I was constant but mild to moderate, and NT-proBNP or BNP elevation was present in all children.
Nearly all patients 35 (88%) patients tested positive for SARS-CoV-2 infection by polymerase chain reaction of nasopharyngeal swab or serology. Most patients (80%) received IV inotropic support, 71% received first-line IV immunoglobulin, 65% received anticoagulation with heparin, 34% received IV steroids having been considered high-risk patients with symptoms similar to an incomplete form of Kawasaki disease, and 8% received treatment with an interleukin-1 receptor antagonist because of a persistent severe inflammatory state. Left ventricular function was restored in 71% of those discharged from the intensive care unit. No patient died, and all patients treated with ECMO were successfully weaned after a median of 4.5 days.
“Some aspects of this emerging pediatric disease (MIS-C) are similar to those of Kawasaki disease: prolonged fever, multisystem inflammation with skin rash, lymphadenopathy, diarrhea, meningism, and high levels of inflammatory biomarkers,” the researchers wrote. “But differences are important and raise the question as to whether this syndrome is Kawasaki disease with SARS-CoV-2 as the triggering agent, or represents a different syndrome (MIS-C). Kawasaki disease predominantly affects young children younger than 5 years, whereas the median age in our series is 10 years. Incomplete forms of Kawasaki disease occur in infants who may have fever as the sole clinical finding, whereas older patients are more prone to exhibit the complete form.”
They went on to note that the overlapping features between MIS-C and Kawasaki disease “may be due to similar pathophysiology. The etiologic agent of Kawasaki disease is unknown but likely to be ubiquitous, causing asymptomatic childhood infection but triggering the immunologic cascade of Kawasaki disease in genetically susceptible individuals. Please note that infection with a novel RNA virus that enters through the upper respiratory tract has been proposed to be the cause of the disease (see PLoS One. 2008 Feb 13;3:e1582 and J Infect Dis. 2011 Apr 1;203:1021-30).”
Based on the work of authors, it appears that a high index of suspicion for MIS-C is important for children who develop Kawasaki-like symptoms, David J. Goldberg, MD, said in an interview. “Although children have largely been spared from the acute respiratory presentation of the SARS-CoV-2 pandemic, the recognition and understanding of what appears to be a postviral inflammatory response is a critical first step in developing treatment algorithms for this disease process,” said Dr. Goldberg, a board-certified attending cardiologist in the cardiac center and fetal heart program at Children’s Hospital of Philadelphia. “If inflammatory markers are elevated, particularly if there are accompanying gastrointestinal symptoms, the possibility of cardiac involvement suggests the utility of screening echocardiography. Given the potential need for inotropic or mechanical circulatory support, the presence of myocardial dysfunction dictates care in an intensive care unit capable of providing advanced therapies. While the evidence from Dr. Belhadjer’s cohort suggests that full recovery is probable, there is still much to be learned about this unique inflammatory syndrome and the alarm has rightly been sounded.”
The researchers and Dr. Goldberg reported having no disclosures.
SOURCE: Belhadjer Z et al. Circulation 2020 May 17; doi: 10.1161/circulationaha.120.048360.
FROM CIRCULATION
Today’s top news highlights: Remdesivir data dive, FDA approves contraceptive gel
:
Remdesivir trial data published
Weeks after topline remdesivir data appeared in the press, investigators published their full experience using the drug to treat COVID-19 patients. The study, published in the New England Journal of Medicine, showed the drug reduced recovery time from 15 to 11 days, compared with placebo. Patients receiving oxygen seemed to fare best from treatment with remdesivir. “There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.” READ MORE.
FDA approves contraceptive gel
The Food and Drug Administration approved Phexxi (lactic acid, citric acid, and potassium bitartrate) vaginal gel to prevent pregnancy in women of reproductive potential. It’s the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5. READ MORE.
COVID-19 lessons from one cancer center
Physicians at Levine Cancer Institute in Charlotte, N.C., largely have been able to keep hematologic oncology patients on their treatment regimens and continue to care for inpatients during the early months of the COVID-19 pandemic. How have they kept the situation managable? Strict infection control, liberal testing, and a proactive plan to defer and temporarily replace infusion care when medically appropriate were all part of the strategy. “My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious, even before the coronavirus, using distancing, masking, and meticulous hand hygiene,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in Levine Cancer Institute’s Department of Hematologic Oncology and Blood Disorders. READ MORE.
Convalescent plasma: Hope or hype?
There are currently more than two dozen trials of convalescent plasma in the United States and elsewhere but most are single-arm trials to determine if one infusion can decrease the need for intubation or help patients on a ventilator to improve. Others researchers are investigating whether convalescent plasma might be used before severe disease sets in. Meanwhile, about 2,200 hospitals are participating in an expanded access program being led by the Mayo Clinic nationwide. The National Institutes of Health recently said that “there are insufficient clinical data to recommend either for or against” its use for COVID-19. READ MORE.
New rosacea treatment guidelines
Patients with rosacea should receive treatments based on their phenotype and specific symptoms, rather than being assigned into distinct subtype categories, according to updated guidance published in the Journal of the American Academy of Dermatology. The update comes from the National Rosacea Society Expert Committee and is based on a review of the evidence. Patients “shouldn’t be classified as having a certain subtype of rosacea” since “many patients have features that overlap more than one subtype,” said Diane Thiboutot, MD, lead author of the update and a professor of dermatology and associate dean of clinical and translational research education at Penn State University, Hershey. READ MORE.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
:
Remdesivir trial data published
Weeks after topline remdesivir data appeared in the press, investigators published their full experience using the drug to treat COVID-19 patients. The study, published in the New England Journal of Medicine, showed the drug reduced recovery time from 15 to 11 days, compared with placebo. Patients receiving oxygen seemed to fare best from treatment with remdesivir. “There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.” READ MORE.
FDA approves contraceptive gel
The Food and Drug Administration approved Phexxi (lactic acid, citric acid, and potassium bitartrate) vaginal gel to prevent pregnancy in women of reproductive potential. It’s the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5. READ MORE.
COVID-19 lessons from one cancer center
Physicians at Levine Cancer Institute in Charlotte, N.C., largely have been able to keep hematologic oncology patients on their treatment regimens and continue to care for inpatients during the early months of the COVID-19 pandemic. How have they kept the situation managable? Strict infection control, liberal testing, and a proactive plan to defer and temporarily replace infusion care when medically appropriate were all part of the strategy. “My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious, even before the coronavirus, using distancing, masking, and meticulous hand hygiene,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in Levine Cancer Institute’s Department of Hematologic Oncology and Blood Disorders. READ MORE.
Convalescent plasma: Hope or hype?
There are currently more than two dozen trials of convalescent plasma in the United States and elsewhere but most are single-arm trials to determine if one infusion can decrease the need for intubation or help patients on a ventilator to improve. Others researchers are investigating whether convalescent plasma might be used before severe disease sets in. Meanwhile, about 2,200 hospitals are participating in an expanded access program being led by the Mayo Clinic nationwide. The National Institutes of Health recently said that “there are insufficient clinical data to recommend either for or against” its use for COVID-19. READ MORE.
New rosacea treatment guidelines
Patients with rosacea should receive treatments based on their phenotype and specific symptoms, rather than being assigned into distinct subtype categories, according to updated guidance published in the Journal of the American Academy of Dermatology. The update comes from the National Rosacea Society Expert Committee and is based on a review of the evidence. Patients “shouldn’t be classified as having a certain subtype of rosacea” since “many patients have features that overlap more than one subtype,” said Diane Thiboutot, MD, lead author of the update and a professor of dermatology and associate dean of clinical and translational research education at Penn State University, Hershey. READ MORE.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
:
Remdesivir trial data published
Weeks after topline remdesivir data appeared in the press, investigators published their full experience using the drug to treat COVID-19 patients. The study, published in the New England Journal of Medicine, showed the drug reduced recovery time from 15 to 11 days, compared with placebo. Patients receiving oxygen seemed to fare best from treatment with remdesivir. “There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.” READ MORE.
FDA approves contraceptive gel
The Food and Drug Administration approved Phexxi (lactic acid, citric acid, and potassium bitartrate) vaginal gel to prevent pregnancy in women of reproductive potential. It’s the first nonhormonal, on-demand, vaginal pH regulator contraceptive designed to maintain vaginal pH within the range of 3.5-4.5. READ MORE.
COVID-19 lessons from one cancer center
Physicians at Levine Cancer Institute in Charlotte, N.C., largely have been able to keep hematologic oncology patients on their treatment regimens and continue to care for inpatients during the early months of the COVID-19 pandemic. How have they kept the situation managable? Strict infection control, liberal testing, and a proactive plan to defer and temporarily replace infusion care when medically appropriate were all part of the strategy. “My impression is that the incidence has been low partly because our patients, especially those with hematologic malignancies including those on active chemotherapy, were already getting warned to be cautious, even before the coronavirus, using distancing, masking, and meticulous hand hygiene,” said Peter Voorhees, MD, professor of medicine and director of Medical Operations and Outreach Services in Levine Cancer Institute’s Department of Hematologic Oncology and Blood Disorders. READ MORE.
Convalescent plasma: Hope or hype?
There are currently more than two dozen trials of convalescent plasma in the United States and elsewhere but most are single-arm trials to determine if one infusion can decrease the need for intubation or help patients on a ventilator to improve. Others researchers are investigating whether convalescent plasma might be used before severe disease sets in. Meanwhile, about 2,200 hospitals are participating in an expanded access program being led by the Mayo Clinic nationwide. The National Institutes of Health recently said that “there are insufficient clinical data to recommend either for or against” its use for COVID-19. READ MORE.
New rosacea treatment guidelines
Patients with rosacea should receive treatments based on their phenotype and specific symptoms, rather than being assigned into distinct subtype categories, according to updated guidance published in the Journal of the American Academy of Dermatology. The update comes from the National Rosacea Society Expert Committee and is based on a review of the evidence. Patients “shouldn’t be classified as having a certain subtype of rosacea” since “many patients have features that overlap more than one subtype,” said Diane Thiboutot, MD, lead author of the update and a professor of dermatology and associate dean of clinical and translational research education at Penn State University, Hershey. READ MORE.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
The limitations of telemedicine
I am SO done with telemedicine.

In mid-March, as quarantine restrictions began, I embraced it. I frantically learned which insurances would and wouldn’t allow it, what billing codes had to be used (which varied wildly between plans), and what communication systems were and weren’t allowed.
For most of us it was a way to continue caring for patients and at least keep a trickle of revenue coming in. We could still go over test results face to face, see how a treatment plan was working, and check in with established patients before sending in refills. It seemed like a great solution. For the first 2-3 weeks I was thinking this was the way to go even after the pandemic calmed down.
Then it became increasingly problematic. New patients wanted to be seen remotely. No, I wasn’t doing that. It upset some, but I didn’t care. A neurologic exam is still a critical part of me assessing someone for the first time.
The next problem that came up was in routine check-ins with established patients. Headaches had recently gotten worse, but now I couldn’t do a fundoscopic exam. A stable seizure patient mentioned he’d had a month of worsening lumbar pain and right-leg weakness, but I can’t really check strength, reflexes, or sensation remotely. A lady I saw last year for a diabetic neuropathy is now being referred back to me for possible Parkinson’s disease. While hypomimia or shuffling gait can be seen on camera, you can’t check for rigidity and cogwheeling that way.
So my use of telemedicine has begun to decrease, and as the pandemic fades will hopefully stop entirely. Currently I’m only using it for recently seen patients to review test results or for established patients doing routine check-ins for stable issues. My secretary asks if they have any new issues to discuss with me when she sets up the appointment, and if they say yes she tells them it has to be in person.
This isn’t, as some will claim, a matter of my trying to increase revenue. It’s about practicing good medicine.
Neurology is a contact sport. We spend years learning to recognize minutiae from the moment we first see a patient. The way they speak, and walk, and move. The details of the exam. These are not, for the most part, things you can do with a camera. Other specialties may be less exam dependent, but not mine, and definitely not me. I’d be practicing substandard care if I did otherwise.
Not only that, but it becomes a liability issue. In a legal action you won’t get a pass if you miss something via remote appointment because it was a pandemic. The daily practice of medicine is full of minefields as it is. I don’t want to add another one.
When things return to normal – whatever the new normal is – I’m hoping to put my webcam away for good. It seemed like a good idea at the time, but in reality is only useful in a handful of cases. For all others, my patients deserve better neurologic care than it lets me provide.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I am SO done with telemedicine.
In mid-March, as quarantine restrictions began, I embraced it. I frantically learned which insurances would and wouldn’t allow it, what billing codes had to be used (which varied wildly between plans), and what communication systems were and weren’t allowed.
For most of us it was a way to continue caring for patients and at least keep a trickle of revenue coming in. We could still go over test results face to face, see how a treatment plan was working, and check in with established patients before sending in refills. It seemed like a great solution. For the first 2-3 weeks I was thinking this was the way to go even after the pandemic calmed down.
Then it became increasingly problematic. New patients wanted to be seen remotely. No, I wasn’t doing that. It upset some, but I didn’t care. A neurologic exam is still a critical part of me assessing someone for the first time.
The next problem that came up was in routine check-ins with established patients. Headaches had recently gotten worse, but now I couldn’t do a fundoscopic exam. A stable seizure patient mentioned he’d had a month of worsening lumbar pain and right-leg weakness, but I can’t really check strength, reflexes, or sensation remotely. A lady I saw last year for a diabetic neuropathy is now being referred back to me for possible Parkinson’s disease. While hypomimia or shuffling gait can be seen on camera, you can’t check for rigidity and cogwheeling that way.
So my use of telemedicine has begun to decrease, and as the pandemic fades will hopefully stop entirely. Currently I’m only using it for recently seen patients to review test results or for established patients doing routine check-ins for stable issues. My secretary asks if they have any new issues to discuss with me when she sets up the appointment, and if they say yes she tells them it has to be in person.
This isn’t, as some will claim, a matter of my trying to increase revenue. It’s about practicing good medicine.
Neurology is a contact sport. We spend years learning to recognize minutiae from the moment we first see a patient. The way they speak, and walk, and move. The details of the exam. These are not, for the most part, things you can do with a camera. Other specialties may be less exam dependent, but not mine, and definitely not me. I’d be practicing substandard care if I did otherwise.
Not only that, but it becomes a liability issue. In a legal action you won’t get a pass if you miss something via remote appointment because it was a pandemic. The daily practice of medicine is full of minefields as it is. I don’t want to add another one.
When things return to normal – whatever the new normal is – I’m hoping to put my webcam away for good. It seemed like a good idea at the time, but in reality is only useful in a handful of cases. For all others, my patients deserve better neurologic care than it lets me provide.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I am SO done with telemedicine.
In mid-March, as quarantine restrictions began, I embraced it. I frantically learned which insurances would and wouldn’t allow it, what billing codes had to be used (which varied wildly between plans), and what communication systems were and weren’t allowed.
For most of us it was a way to continue caring for patients and at least keep a trickle of revenue coming in. We could still go over test results face to face, see how a treatment plan was working, and check in with established patients before sending in refills. It seemed like a great solution. For the first 2-3 weeks I was thinking this was the way to go even after the pandemic calmed down.
Then it became increasingly problematic. New patients wanted to be seen remotely. No, I wasn’t doing that. It upset some, but I didn’t care. A neurologic exam is still a critical part of me assessing someone for the first time.
The next problem that came up was in routine check-ins with established patients. Headaches had recently gotten worse, but now I couldn’t do a fundoscopic exam. A stable seizure patient mentioned he’d had a month of worsening lumbar pain and right-leg weakness, but I can’t really check strength, reflexes, or sensation remotely. A lady I saw last year for a diabetic neuropathy is now being referred back to me for possible Parkinson’s disease. While hypomimia or shuffling gait can be seen on camera, you can’t check for rigidity and cogwheeling that way.
So my use of telemedicine has begun to decrease, and as the pandemic fades will hopefully stop entirely. Currently I’m only using it for recently seen patients to review test results or for established patients doing routine check-ins for stable issues. My secretary asks if they have any new issues to discuss with me when she sets up the appointment, and if they say yes she tells them it has to be in person.
This isn’t, as some will claim, a matter of my trying to increase revenue. It’s about practicing good medicine.
Neurology is a contact sport. We spend years learning to recognize minutiae from the moment we first see a patient. The way they speak, and walk, and move. The details of the exam. These are not, for the most part, things you can do with a camera. Other specialties may be less exam dependent, but not mine, and definitely not me. I’d be practicing substandard care if I did otherwise.
Not only that, but it becomes a liability issue. In a legal action you won’t get a pass if you miss something via remote appointment because it was a pandemic. The daily practice of medicine is full of minefields as it is. I don’t want to add another one.
When things return to normal – whatever the new normal is – I’m hoping to put my webcam away for good. It seemed like a good idea at the time, but in reality is only useful in a handful of cases. For all others, my patients deserve better neurologic care than it lets me provide.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Reimbursement for telemedicine services: A billing code disaster
In December 1917, a large part of Halifax was destroyed when an ammunition ship exploded.
In the wake of the explosion large parts of the city were burning. Surrounding communities’ fire departments raced to the scene, only to find their efforts thwarted by a lack of uniform standards for hydrant-hose-nozzle connectors. With no way to tap into Halifax’s water supply, their hoses were worthless.
In the aftermath of WWI, this led to a standardization of fire hose connectors across multiple countries, to ensure it wouldn’t happen again. Sometimes it takes a disaster to bring such problems to the forefront so they can be fixed.
One issue that has come up repeatedly in talking to other physicians is the complete lack of uniformity in telemedicine billing codes. While not a new issue, the coronavirus pandemic has brought it into focus here, and it’s time to fix it.
Here’s an example of information I’ve found about telemedicine billing codes (Note: I have no idea if any of this is correct, so don’t rely on it in your own billing).
- Aetna: Point of service 02
- Cigna: Point of service 02 with modifier 95.
- BCBS Anthem Point of Service 02 with modifier GT.
- Medicare: Point of service 02 OR Point of service 11 with modifier 95 (I’ve seen conflicting reports).
And that’s just a sample. BCBS, for example, seems to vary by state and sub-network.
This is ridiculous. Even with different plans, the CPT and ICD10 codes are standardized, so why not things such as POS codes and modifiers? The only ones benefiting from this are insurance companies, who get to deny claims on grounds that they weren’t billed correctly.
This is, allegedly, the Internet age. Medical bills are submitted electronically, and often paid the same way. If such a complicated system can be made to work in so many other ways, it should be standardized to benefit all involved. Including those doing our best to care for patients in this challenging time – and at all times.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In December 1917, a large part of Halifax was destroyed when an ammunition ship exploded.
In the wake of the explosion large parts of the city were burning. Surrounding communities’ fire departments raced to the scene, only to find their efforts thwarted by a lack of uniform standards for hydrant-hose-nozzle connectors. With no way to tap into Halifax’s water supply, their hoses were worthless.
In the aftermath of WWI, this led to a standardization of fire hose connectors across multiple countries, to ensure it wouldn’t happen again. Sometimes it takes a disaster to bring such problems to the forefront so they can be fixed.
One issue that has come up repeatedly in talking to other physicians is the complete lack of uniformity in telemedicine billing codes. While not a new issue, the coronavirus pandemic has brought it into focus here, and it’s time to fix it.
Here’s an example of information I’ve found about telemedicine billing codes (Note: I have no idea if any of this is correct, so don’t rely on it in your own billing).
- Aetna: Point of service 02
- Cigna: Point of service 02 with modifier 95.
- BCBS Anthem Point of Service 02 with modifier GT.
- Medicare: Point of service 02 OR Point of service 11 with modifier 95 (I’ve seen conflicting reports).
And that’s just a sample. BCBS, for example, seems to vary by state and sub-network.
This is ridiculous. Even with different plans, the CPT and ICD10 codes are standardized, so why not things such as POS codes and modifiers? The only ones benefiting from this are insurance companies, who get to deny claims on grounds that they weren’t billed correctly.
This is, allegedly, the Internet age. Medical bills are submitted electronically, and often paid the same way. If such a complicated system can be made to work in so many other ways, it should be standardized to benefit all involved. Including those doing our best to care for patients in this challenging time – and at all times.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In December 1917, a large part of Halifax was destroyed when an ammunition ship exploded.
In the wake of the explosion large parts of the city were burning. Surrounding communities’ fire departments raced to the scene, only to find their efforts thwarted by a lack of uniform standards for hydrant-hose-nozzle connectors. With no way to tap into Halifax’s water supply, their hoses were worthless.
In the aftermath of WWI, this led to a standardization of fire hose connectors across multiple countries, to ensure it wouldn’t happen again. Sometimes it takes a disaster to bring such problems to the forefront so they can be fixed.
One issue that has come up repeatedly in talking to other physicians is the complete lack of uniformity in telemedicine billing codes. While not a new issue, the coronavirus pandemic has brought it into focus here, and it’s time to fix it.
Here’s an example of information I’ve found about telemedicine billing codes (Note: I have no idea if any of this is correct, so don’t rely on it in your own billing).
- Aetna: Point of service 02
- Cigna: Point of service 02 with modifier 95.
- BCBS Anthem Point of Service 02 with modifier GT.
- Medicare: Point of service 02 OR Point of service 11 with modifier 95 (I’ve seen conflicting reports).
And that’s just a sample. BCBS, for example, seems to vary by state and sub-network.
This is ridiculous. Even with different plans, the CPT and ICD10 codes are standardized, so why not things such as POS codes and modifiers? The only ones benefiting from this are insurance companies, who get to deny claims on grounds that they weren’t billed correctly.
This is, allegedly, the Internet age. Medical bills are submitted electronically, and often paid the same way. If such a complicated system can be made to work in so many other ways, it should be standardized to benefit all involved. Including those doing our best to care for patients in this challenging time – and at all times.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Convalescent plasma: ‘Flavor of the month’ or valid COVID-19 treatment?
On March 31, soon after the Food and Drug Administration authorized emergency use of antibody-packed plasma from recovered patients with COVID-19, Marisa Leuzzi became the first donor at an American Red Cross center. She hoped it could help her aunt, Renee Bannister, who was failing after 3 weeks on a ventilator at Virtua Hospital in Voorhees, N.J.
It may have worked; 11 days after receiving the plasma, Ms. Bannister was weaned off the ventilator and she is now awake and speaking, said Red Cross spokesperson Stephanie Rendon.
This kind of anecdote is fueling demand for the therapy, which can be provided through an expanded access program led by the Mayo Clinic, backed by the FDA, and the plasma paid for by the U.S. Department of Health & Human Services. But while this program is collecting safety and outcomes data, it’s not a randomized, controlled trial.
Others, however, are pursuing that data.
“One of the things I don’t want this to be is the flavor of the month,” Shmuel Shoham, MD, associate professor of medicine at Johns Hopkins University, said in an interview.
Dr. Shoham, principal investigator for a study evaluating convalescent plasma to prevent the infection in high-risk individuals, said some clinicians, desperate for any treatment, have tried potential therapies such as hydroxychloroquine and remdesivir without evidence of safety or efficacy in COVID-19.
The National Institutes of Health recently said something similar for convalescent plasma, that “there are insufficient clinical data to recommend either for or against” its use for COVID-19.
But plasma has promise, according to a Johns Hopkins School of Medicine’s Bloomberg Distinguished Professor, Arturo Casadevall, MD, PhD, in Baltimore, and Liise-anne Pirofski, MD, a professor at Albert Einstein College of Medicine, New York. They lay out the case for convalescent plasma in an article published online March 13 in the Journal of Clinical Investigation. Passive antibody therapy, they wrote, has been used to stem polio, measles, mumps, and influenza, and more recently has shown some success against SARS-CoV-1 and Middle East respiratory syndrome (MERS).
“The special attraction of this modality of treatment is that, unlike vaccines or newly developed drugs, it could, in principle, be made available very rapidly,” said researchers with the National COVID-19 Convalescent Plasma Project, which includes physicians and scientists from 57 institutions in 46 states. But where principle veers from reality is in availability of the plasma itself, and donors are in short supply.
Aiming to prevent infection
So far, the FDA has approved 12 plasma trials – including Dr. Shoham’s – and the NIH’s clinicaltrials.gov lists more than two dozen convalescent plasma studies in the United States and elsewhere.
Most are single-arm trials to determine if one infusion can decrease the need for intubation or help those on a ventilator improve. Two others, one at Johns Hopkins and one at Stanford (Calif.) Hospital are investigating whether convalescent plasma might be used before severe disease sets in.
“A general principle of passive antibody therapy is that it is more effective when used for prophylaxis than for treatment of disease,” Dr. Casadevall and Dr. Pirofski wrote.
Stanford’s randomized, double-blind study will evaluate regular versus convalescent plasma in ED patients who are not sick enough to require hospitalization.
The Johns Hopkins trial, which aims to protect against infection in the first place, will begin at Johns Hopkins, Baltimore, and at Hopkins-affiliated hospitals throughout Maryland, Dr. Shoham said. He hopes it will expand nationwide eventually, and said that they expect to enroll the first patients soon.
To start, the prevention study will enroll only 150 patients, each of whom must have had close contact with someone who has COVID-19 within the previous 120 hours and be asymptomatic. The number of subjects is small, compared with the trial size of other potential therapies, and an issue, Shoham said, “that keeps me up at night.” But finding thousands of enrollees for plasma studies is hard, in part because it’s so difficult to recruit donors.
Participants will receive normal plasma (which will act as a placebo) or convalescent plasma.
The primary endpoint is cumulative incidence of COVID-19, defined as symptoms and a polymerase chain reaction–positive test; participants will be tracked for 90 days. Hospitals and health care workers could then decide if they want to use the therapy, he said.
The study will not answer whether participants will continue to have antibodies beyond the 90 days. Convalescent plasma is given as a rapid response to an emergent pathogen – a short-term boost of immunity rather than a long-term therapeutic.
What can we learn from expanded access?
Meanwhile, some 2,200 hospitals are participating in the expanded access program being led by the Mayo Clinic nationwide; more than 9,000 patients had received infusions at press time.
One participant is Northwell Health, a 23-hospital system that sprawls across the U.S. COVID epicenter: four of the five boroughs of New York City and Long Island.
Convalescent plasma is an in-demand therapy, said Christina Brennan, MD, vice president of clinical research at Northwell. “We get patients, family members, they say my family member is at X hospital – if it’s not being offered there, can you have them transferred?” she said in an interview.
When Northwell – through the New York Blood Bank – opened up donor registration, 800 people signed up in the first 24 hours, Dr. Brennan said. As of mid-May, 527 patients had received a transfusion.
Who’s the best donor and when should donation occur?
The Red Cross, hospitals, and independent blood banks are all soliciting donors, who can sign up at the Red Cross website. The FDA recommends that donors have a history of COVID-19 as confirmed by molecular or antibody testing, be symptom free for 14 days, have a negative follow-up molecular test, and be virus free at the time of collection. The FDA also suggests measuring a donor’s SARS-CoV-2 neutralizing antibody titers, if available, with a recommendation of at least 1:160.
But questions remain, such as whether there is a theoretical risk for antibody-dependent enhancement (ADE) of infection with SARS-CoV-2. “Antibodies to one type of coronavirus could enhance infection to another viral strain,” of coronavirus, Dr. Casadevall wrote. ADE has been observed in both severe acute respiratory syndrome (SARS) and MERS.
The other risk is that donors may still be shedding active virus. While the FDA suggests that donors are unlikely to still be infectious 14 days after infection, that is as of yet unproven. Both COVID-19 diagnostics and antibody tests have high rates of false negatives, which raises the specter that infection could be spread via the plasma donation.
Daniele Focosi, MD, PhD, from Pisa (Italy) University Hospital and colleagues raise that concern in a preprint review on convalescent plasma in COVID-19. “Although the recipient is already infected, theoretically transmission of more infectious particles could worsen clinical conditions,” they wrote, noting that “such a concern can be somewhat reduced by treatment with modern pathogen inactivation techniques.”
No evidence exists that SARS-CoV-2 can be transmitted through blood, but “we don’t know for sure,” Dr. Shoham said in an interview. A reassuring point: Even those with severe infection do not have viral RNA in their blood, he said, adding, “We don’t think there’s going to be viral transmission of this particular virus with transfusion.”
For another highly infectious pathogen, the Ebola virus, the World Health Organization recommended in 2014 that potential plasma donors wait at least 28 days after infection.
It’s also not known how long SARS-CoV-2 antibodies persist in the blood; longer viability could mean a longer donation window. Dr. Focosi noted that a previous Chinese study had shown that SARS-specific antibodies in people infected with the first SARS virus, SARS-CoV-1, persisted for 2 years.
Dr. Casadevall and Dr. Pirofski have disclosed no relevant financial relationships. Shoham has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
On March 31, soon after the Food and Drug Administration authorized emergency use of antibody-packed plasma from recovered patients with COVID-19, Marisa Leuzzi became the first donor at an American Red Cross center. She hoped it could help her aunt, Renee Bannister, who was failing after 3 weeks on a ventilator at Virtua Hospital in Voorhees, N.J.
It may have worked; 11 days after receiving the plasma, Ms. Bannister was weaned off the ventilator and she is now awake and speaking, said Red Cross spokesperson Stephanie Rendon.
This kind of anecdote is fueling demand for the therapy, which can be provided through an expanded access program led by the Mayo Clinic, backed by the FDA, and the plasma paid for by the U.S. Department of Health & Human Services. But while this program is collecting safety and outcomes data, it’s not a randomized, controlled trial.
Others, however, are pursuing that data.
“One of the things I don’t want this to be is the flavor of the month,” Shmuel Shoham, MD, associate professor of medicine at Johns Hopkins University, said in an interview.
Dr. Shoham, principal investigator for a study evaluating convalescent plasma to prevent the infection in high-risk individuals, said some clinicians, desperate for any treatment, have tried potential therapies such as hydroxychloroquine and remdesivir without evidence of safety or efficacy in COVID-19.
The National Institutes of Health recently said something similar for convalescent plasma, that “there are insufficient clinical data to recommend either for or against” its use for COVID-19.
But plasma has promise, according to a Johns Hopkins School of Medicine’s Bloomberg Distinguished Professor, Arturo Casadevall, MD, PhD, in Baltimore, and Liise-anne Pirofski, MD, a professor at Albert Einstein College of Medicine, New York. They lay out the case for convalescent plasma in an article published online March 13 in the Journal of Clinical Investigation. Passive antibody therapy, they wrote, has been used to stem polio, measles, mumps, and influenza, and more recently has shown some success against SARS-CoV-1 and Middle East respiratory syndrome (MERS).
“The special attraction of this modality of treatment is that, unlike vaccines or newly developed drugs, it could, in principle, be made available very rapidly,” said researchers with the National COVID-19 Convalescent Plasma Project, which includes physicians and scientists from 57 institutions in 46 states. But where principle veers from reality is in availability of the plasma itself, and donors are in short supply.
Aiming to prevent infection
So far, the FDA has approved 12 plasma trials – including Dr. Shoham’s – and the NIH’s clinicaltrials.gov lists more than two dozen convalescent plasma studies in the United States and elsewhere.
Most are single-arm trials to determine if one infusion can decrease the need for intubation or help those on a ventilator improve. Two others, one at Johns Hopkins and one at Stanford (Calif.) Hospital are investigating whether convalescent plasma might be used before severe disease sets in.
“A general principle of passive antibody therapy is that it is more effective when used for prophylaxis than for treatment of disease,” Dr. Casadevall and Dr. Pirofski wrote.
Stanford’s randomized, double-blind study will evaluate regular versus convalescent plasma in ED patients who are not sick enough to require hospitalization.
The Johns Hopkins trial, which aims to protect against infection in the first place, will begin at Johns Hopkins, Baltimore, and at Hopkins-affiliated hospitals throughout Maryland, Dr. Shoham said. He hopes it will expand nationwide eventually, and said that they expect to enroll the first patients soon.
To start, the prevention study will enroll only 150 patients, each of whom must have had close contact with someone who has COVID-19 within the previous 120 hours and be asymptomatic. The number of subjects is small, compared with the trial size of other potential therapies, and an issue, Shoham said, “that keeps me up at night.” But finding thousands of enrollees for plasma studies is hard, in part because it’s so difficult to recruit donors.
Participants will receive normal plasma (which will act as a placebo) or convalescent plasma.
The primary endpoint is cumulative incidence of COVID-19, defined as symptoms and a polymerase chain reaction–positive test; participants will be tracked for 90 days. Hospitals and health care workers could then decide if they want to use the therapy, he said.
The study will not answer whether participants will continue to have antibodies beyond the 90 days. Convalescent plasma is given as a rapid response to an emergent pathogen – a short-term boost of immunity rather than a long-term therapeutic.
What can we learn from expanded access?
Meanwhile, some 2,200 hospitals are participating in the expanded access program being led by the Mayo Clinic nationwide; more than 9,000 patients had received infusions at press time.
One participant is Northwell Health, a 23-hospital system that sprawls across the U.S. COVID epicenter: four of the five boroughs of New York City and Long Island.
Convalescent plasma is an in-demand therapy, said Christina Brennan, MD, vice president of clinical research at Northwell. “We get patients, family members, they say my family member is at X hospital – if it’s not being offered there, can you have them transferred?” she said in an interview.
When Northwell – through the New York Blood Bank – opened up donor registration, 800 people signed up in the first 24 hours, Dr. Brennan said. As of mid-May, 527 patients had received a transfusion.
Who’s the best donor and when should donation occur?
The Red Cross, hospitals, and independent blood banks are all soliciting donors, who can sign up at the Red Cross website. The FDA recommends that donors have a history of COVID-19 as confirmed by molecular or antibody testing, be symptom free for 14 days, have a negative follow-up molecular test, and be virus free at the time of collection. The FDA also suggests measuring a donor’s SARS-CoV-2 neutralizing antibody titers, if available, with a recommendation of at least 1:160.
But questions remain, such as whether there is a theoretical risk for antibody-dependent enhancement (ADE) of infection with SARS-CoV-2. “Antibodies to one type of coronavirus could enhance infection to another viral strain,” of coronavirus, Dr. Casadevall wrote. ADE has been observed in both severe acute respiratory syndrome (SARS) and MERS.
The other risk is that donors may still be shedding active virus. While the FDA suggests that donors are unlikely to still be infectious 14 days after infection, that is as of yet unproven. Both COVID-19 diagnostics and antibody tests have high rates of false negatives, which raises the specter that infection could be spread via the plasma donation.
Daniele Focosi, MD, PhD, from Pisa (Italy) University Hospital and colleagues raise that concern in a preprint review on convalescent plasma in COVID-19. “Although the recipient is already infected, theoretically transmission of more infectious particles could worsen clinical conditions,” they wrote, noting that “such a concern can be somewhat reduced by treatment with modern pathogen inactivation techniques.”
No evidence exists that SARS-CoV-2 can be transmitted through blood, but “we don’t know for sure,” Dr. Shoham said in an interview. A reassuring point: Even those with severe infection do not have viral RNA in their blood, he said, adding, “We don’t think there’s going to be viral transmission of this particular virus with transfusion.”
For another highly infectious pathogen, the Ebola virus, the World Health Organization recommended in 2014 that potential plasma donors wait at least 28 days after infection.
It’s also not known how long SARS-CoV-2 antibodies persist in the blood; longer viability could mean a longer donation window. Dr. Focosi noted that a previous Chinese study had shown that SARS-specific antibodies in people infected with the first SARS virus, SARS-CoV-1, persisted for 2 years.
Dr. Casadevall and Dr. Pirofski have disclosed no relevant financial relationships. Shoham has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
On March 31, soon after the Food and Drug Administration authorized emergency use of antibody-packed plasma from recovered patients with COVID-19, Marisa Leuzzi became the first donor at an American Red Cross center. She hoped it could help her aunt, Renee Bannister, who was failing after 3 weeks on a ventilator at Virtua Hospital in Voorhees, N.J.
It may have worked; 11 days after receiving the plasma, Ms. Bannister was weaned off the ventilator and she is now awake and speaking, said Red Cross spokesperson Stephanie Rendon.
This kind of anecdote is fueling demand for the therapy, which can be provided through an expanded access program led by the Mayo Clinic, backed by the FDA, and the plasma paid for by the U.S. Department of Health & Human Services. But while this program is collecting safety and outcomes data, it’s not a randomized, controlled trial.
Others, however, are pursuing that data.
“One of the things I don’t want this to be is the flavor of the month,” Shmuel Shoham, MD, associate professor of medicine at Johns Hopkins University, said in an interview.
Dr. Shoham, principal investigator for a study evaluating convalescent plasma to prevent the infection in high-risk individuals, said some clinicians, desperate for any treatment, have tried potential therapies such as hydroxychloroquine and remdesivir without evidence of safety or efficacy in COVID-19.
The National Institutes of Health recently said something similar for convalescent plasma, that “there are insufficient clinical data to recommend either for or against” its use for COVID-19.
But plasma has promise, according to a Johns Hopkins School of Medicine’s Bloomberg Distinguished Professor, Arturo Casadevall, MD, PhD, in Baltimore, and Liise-anne Pirofski, MD, a professor at Albert Einstein College of Medicine, New York. They lay out the case for convalescent plasma in an article published online March 13 in the Journal of Clinical Investigation. Passive antibody therapy, they wrote, has been used to stem polio, measles, mumps, and influenza, and more recently has shown some success against SARS-CoV-1 and Middle East respiratory syndrome (MERS).
“The special attraction of this modality of treatment is that, unlike vaccines or newly developed drugs, it could, in principle, be made available very rapidly,” said researchers with the National COVID-19 Convalescent Plasma Project, which includes physicians and scientists from 57 institutions in 46 states. But where principle veers from reality is in availability of the plasma itself, and donors are in short supply.
Aiming to prevent infection
So far, the FDA has approved 12 plasma trials – including Dr. Shoham’s – and the NIH’s clinicaltrials.gov lists more than two dozen convalescent plasma studies in the United States and elsewhere.
Most are single-arm trials to determine if one infusion can decrease the need for intubation or help those on a ventilator improve. Two others, one at Johns Hopkins and one at Stanford (Calif.) Hospital are investigating whether convalescent plasma might be used before severe disease sets in.
“A general principle of passive antibody therapy is that it is more effective when used for prophylaxis than for treatment of disease,” Dr. Casadevall and Dr. Pirofski wrote.
Stanford’s randomized, double-blind study will evaluate regular versus convalescent plasma in ED patients who are not sick enough to require hospitalization.
The Johns Hopkins trial, which aims to protect against infection in the first place, will begin at Johns Hopkins, Baltimore, and at Hopkins-affiliated hospitals throughout Maryland, Dr. Shoham said. He hopes it will expand nationwide eventually, and said that they expect to enroll the first patients soon.
To start, the prevention study will enroll only 150 patients, each of whom must have had close contact with someone who has COVID-19 within the previous 120 hours and be asymptomatic. The number of subjects is small, compared with the trial size of other potential therapies, and an issue, Shoham said, “that keeps me up at night.” But finding thousands of enrollees for plasma studies is hard, in part because it’s so difficult to recruit donors.
Participants will receive normal plasma (which will act as a placebo) or convalescent plasma.
The primary endpoint is cumulative incidence of COVID-19, defined as symptoms and a polymerase chain reaction–positive test; participants will be tracked for 90 days. Hospitals and health care workers could then decide if they want to use the therapy, he said.
The study will not answer whether participants will continue to have antibodies beyond the 90 days. Convalescent plasma is given as a rapid response to an emergent pathogen – a short-term boost of immunity rather than a long-term therapeutic.
What can we learn from expanded access?
Meanwhile, some 2,200 hospitals are participating in the expanded access program being led by the Mayo Clinic nationwide; more than 9,000 patients had received infusions at press time.
One participant is Northwell Health, a 23-hospital system that sprawls across the U.S. COVID epicenter: four of the five boroughs of New York City and Long Island.
Convalescent plasma is an in-demand therapy, said Christina Brennan, MD, vice president of clinical research at Northwell. “We get patients, family members, they say my family member is at X hospital – if it’s not being offered there, can you have them transferred?” she said in an interview.
When Northwell – through the New York Blood Bank – opened up donor registration, 800 people signed up in the first 24 hours, Dr. Brennan said. As of mid-May, 527 patients had received a transfusion.
Who’s the best donor and when should donation occur?
The Red Cross, hospitals, and independent blood banks are all soliciting donors, who can sign up at the Red Cross website. The FDA recommends that donors have a history of COVID-19 as confirmed by molecular or antibody testing, be symptom free for 14 days, have a negative follow-up molecular test, and be virus free at the time of collection. The FDA also suggests measuring a donor’s SARS-CoV-2 neutralizing antibody titers, if available, with a recommendation of at least 1:160.
But questions remain, such as whether there is a theoretical risk for antibody-dependent enhancement (ADE) of infection with SARS-CoV-2. “Antibodies to one type of coronavirus could enhance infection to another viral strain,” of coronavirus, Dr. Casadevall wrote. ADE has been observed in both severe acute respiratory syndrome (SARS) and MERS.
The other risk is that donors may still be shedding active virus. While the FDA suggests that donors are unlikely to still be infectious 14 days after infection, that is as of yet unproven. Both COVID-19 diagnostics and antibody tests have high rates of false negatives, which raises the specter that infection could be spread via the plasma donation.
Daniele Focosi, MD, PhD, from Pisa (Italy) University Hospital and colleagues raise that concern in a preprint review on convalescent plasma in COVID-19. “Although the recipient is already infected, theoretically transmission of more infectious particles could worsen clinical conditions,” they wrote, noting that “such a concern can be somewhat reduced by treatment with modern pathogen inactivation techniques.”
No evidence exists that SARS-CoV-2 can be transmitted through blood, but “we don’t know for sure,” Dr. Shoham said in an interview. A reassuring point: Even those with severe infection do not have viral RNA in their blood, he said, adding, “We don’t think there’s going to be viral transmission of this particular virus with transfusion.”
For another highly infectious pathogen, the Ebola virus, the World Health Organization recommended in 2014 that potential plasma donors wait at least 28 days after infection.
It’s also not known how long SARS-CoV-2 antibodies persist in the blood; longer viability could mean a longer donation window. Dr. Focosi noted that a previous Chinese study had shown that SARS-specific antibodies in people infected with the first SARS virus, SARS-CoV-1, persisted for 2 years.
Dr. Casadevall and Dr. Pirofski have disclosed no relevant financial relationships. Shoham has disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Remdesivir shortens COVID-19 time to recovery in published study
Much-anticipated results from the National Institute of Allergy and Infectious Diseases’ clinical trial of remdesivir in COVID-19 patients published in the New England Journal of Medicine suggest remdesivir shortens the disease course for hospitalized COVID-19 patients.
The agency reported initial promising results from the study earlier this month, which prompted the Food and Drug Administration to issue an emergency use authorization (EUA) for the drug, but the full data and results have not been widely available until now.
The findings also suggest remdesivir should be started, if possible, before patients have such severe pulmonary disease that they require mechanical ventilation, according to the study authors.
The published results are “completely consistent” with the NIAID’s earlier announcement, H. Clifford Lane, MD, deputy director for clinical research and special projects at the NIAID, said in an interview. “The benefit appeared to be the greatest for the patients who are hospitalized with severe disease who require supplemental oxygen.”
Given the limited supply of remdesivir, physicians have been eager to see the full data to ensure they use the drug most effectively, Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said in an interview. Hospitals in states across the country, including New York, Michigan, and Washington, have received limited supplies of the drug in the last couple of weeks since the FDA’s authorization.
“I am losing my patience waiting for #remdesivir data. I was willing to give them a week to verify the numbers, triple proof the tables, cautiously frame conclusions. But it’s gone on too long. We are rationing with no rationale. We are floating on whisps [sic] of data, adrift,” Kate Stephenson, MD, an infectious diseases specialist at the Center for Virology and Vaccine Research at Harvard Medical School, Boston, wrote on Twitter May 18. After reading the paper, she tweeted Friday evening that she was “relieved to see convincing benefit – I was starting to worry!”
In the midst of a public health crisis, however, it is not unusual to make an announcement about trial results before the full dataset has been analyzed, said Dr. Lane. The NIAID followed a similar playbook for the PALM trial evaluating possible Ebola treatments in the Democratic Republic of Congo, with the independent monitoring board recommending the trial be terminated early in response to positive results from two of the four candidate drugs.
“When you have a result you think is of public health importance, you don’t wait for it to be published in a peer-reviewed journal,” said Dr. Lane, a coauthor of the study. The lag time from announcement to study publication was a result of the time it took to write up the paper for publication and go through peer review, Dr. Lane added. He also noted that the FDA had access to the data when the agency wrote its guidance for physicians administering the drug to patients under the EUA.
The authors opted not to publish the initial findings on a preprint server because they felt it was important to undergo peer review, said Dr. Lane. “The last thing you want for something this critical is for incomplete data to be out there, or you don’t have everything audited to the level that you want.”
Trial details
In the ACTT-1 randomized, placebo-controlled, double-blinded trial, researchers enrolled 1,063 patients from Feb. 21 to April 19, 2020, at 60 trial sites and 13 subsites worldwide (45 sites in the United States). The remdesivir group had 541 patients, and the placebo group had 522. A small number of patients (49 in the remdesivir group and 53 in the placebo group) discontinued treatment before day 10 because of an adverse event or withdrawn consent. When data collection for this preliminary analysis ended in late April, 301 patients had not recovered and had not completed their final follow-up visit.
Most of the patients had one (27%) or more (52.1%) preexisting conditions, including hypertension (49.6%), obesity (37%), and type 2 diabetes mellitus (29.7%). Mean patient age was 58.9 years, and the majority of patients were men (64.3%). The median number of days from symptom onset to randomization was 9, and 53.6% of the patients were white, 20.6% were black, 12.6% were Asian, 23.4% were Hispanic or Latino, and the ethnicity of 13.6% were not reported or reported as other.
Patients received one 200-mg loading dose on the first day of the trial, and then one 100-mg maintenance dose every day for days 2 through 10, or until discharge or death. Patients in the control group of the study received a matching placebo on the same schedule and volume. The clinical status of each patient was assessed every day, from day 1 through day 29 of his or her hospital stay, according to an eight-category ordinal scale.
Time to recovery was defined as the first day during the 28-day enrollment period that a patient’s clinical status met a 1 (not hospitalization, no activity limitations), 2 (not hospitalized, activity limitation, oxygen requirement or both), or 3 (hospitalized, not requiring supplemental oxygen or medical care if hospitalization was extended for infection-control reasons) on the eight-category scale. A score of 4 indicated a patient was hospitalized and needed ongoing medical care, but did not require supplemental oxygen; a score of 8 signified death.
The analysis found remdesivir patients had a median time to recovery of 11 days, compared with the median 15 days for patients on the placebo (rate ratio for recovery, 1.32; 95% confidence interval, 1.12-1.55; P < .001). Mortality was also lower in the remdesivir group (hazard ratio for death, 0.70; 95% CI, 0.47-1.04), but the result was not statistically significant. By 14 days, the Kaplan-Meier estimate of mortality was 7.1 % in the remdesivir group and 11.9% in the placebo group.
Patients receiving oxygen, but not yet requiring high-flow oxygen, mechanical ventilation, or extracorporeal membrane oxygenation, seemed to fare best from treatment with remdesivir (these patients had a baseline ordinal score of 5). That may be a result of the larger sample size of these patients, the researchers note in the study. The study authors were unable to estimate the recovery time for the most severely ill patients (category 7), possibly because the follow-up time was too short to fully evaluate this subgroup.
“There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Dr. Kaul, who was not involved in the study, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.”
Dr. Kaul said there is still the possibility that remdesivir could benefit patients on mechanical ventilation, but “clinicians will have to determine if the evidence suggesting no benefit in those who are intubated is strong enough to justify using this currently scarce resource in that population versus limiting use to those requiring oxygen but not on mechanical ventilation.”
Site investigators estimated that just four serious adverse events (two in each group) in enrolled patients were related to remdesivir or placebo. No deaths were attributed to the treatments, although acute respiratory failure, hypotension, acute kidney injury, and viral pneumonia were slightly more common in patients receiving the placebo than those receiving remdesivir.
The researchers plan to publish a follow-up study in the coming weeks or months, after the full cohort has completed 28 days of follow-up, Dr. Lane said. In future studies, the agency will likely focus on comparing remdesivir with combinations of remdesivir with other treatments, like the anti-inflammatory baricitinib.
A version of this article originally appeared on Medscape.com.
Much-anticipated results from the National Institute of Allergy and Infectious Diseases’ clinical trial of remdesivir in COVID-19 patients published in the New England Journal of Medicine suggest remdesivir shortens the disease course for hospitalized COVID-19 patients.
The agency reported initial promising results from the study earlier this month, which prompted the Food and Drug Administration to issue an emergency use authorization (EUA) for the drug, but the full data and results have not been widely available until now.
The findings also suggest remdesivir should be started, if possible, before patients have such severe pulmonary disease that they require mechanical ventilation, according to the study authors.
The published results are “completely consistent” with the NIAID’s earlier announcement, H. Clifford Lane, MD, deputy director for clinical research and special projects at the NIAID, said in an interview. “The benefit appeared to be the greatest for the patients who are hospitalized with severe disease who require supplemental oxygen.”
Given the limited supply of remdesivir, physicians have been eager to see the full data to ensure they use the drug most effectively, Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said in an interview. Hospitals in states across the country, including New York, Michigan, and Washington, have received limited supplies of the drug in the last couple of weeks since the FDA’s authorization.
“I am losing my patience waiting for #remdesivir data. I was willing to give them a week to verify the numbers, triple proof the tables, cautiously frame conclusions. But it’s gone on too long. We are rationing with no rationale. We are floating on whisps [sic] of data, adrift,” Kate Stephenson, MD, an infectious diseases specialist at the Center for Virology and Vaccine Research at Harvard Medical School, Boston, wrote on Twitter May 18. After reading the paper, she tweeted Friday evening that she was “relieved to see convincing benefit – I was starting to worry!”
In the midst of a public health crisis, however, it is not unusual to make an announcement about trial results before the full dataset has been analyzed, said Dr. Lane. The NIAID followed a similar playbook for the PALM trial evaluating possible Ebola treatments in the Democratic Republic of Congo, with the independent monitoring board recommending the trial be terminated early in response to positive results from two of the four candidate drugs.
“When you have a result you think is of public health importance, you don’t wait for it to be published in a peer-reviewed journal,” said Dr. Lane, a coauthor of the study. The lag time from announcement to study publication was a result of the time it took to write up the paper for publication and go through peer review, Dr. Lane added. He also noted that the FDA had access to the data when the agency wrote its guidance for physicians administering the drug to patients under the EUA.
The authors opted not to publish the initial findings on a preprint server because they felt it was important to undergo peer review, said Dr. Lane. “The last thing you want for something this critical is for incomplete data to be out there, or you don’t have everything audited to the level that you want.”
Trial details
In the ACTT-1 randomized, placebo-controlled, double-blinded trial, researchers enrolled 1,063 patients from Feb. 21 to April 19, 2020, at 60 trial sites and 13 subsites worldwide (45 sites in the United States). The remdesivir group had 541 patients, and the placebo group had 522. A small number of patients (49 in the remdesivir group and 53 in the placebo group) discontinued treatment before day 10 because of an adverse event or withdrawn consent. When data collection for this preliminary analysis ended in late April, 301 patients had not recovered and had not completed their final follow-up visit.
Most of the patients had one (27%) or more (52.1%) preexisting conditions, including hypertension (49.6%), obesity (37%), and type 2 diabetes mellitus (29.7%). Mean patient age was 58.9 years, and the majority of patients were men (64.3%). The median number of days from symptom onset to randomization was 9, and 53.6% of the patients were white, 20.6% were black, 12.6% were Asian, 23.4% were Hispanic or Latino, and the ethnicity of 13.6% were not reported or reported as other.
Patients received one 200-mg loading dose on the first day of the trial, and then one 100-mg maintenance dose every day for days 2 through 10, or until discharge or death. Patients in the control group of the study received a matching placebo on the same schedule and volume. The clinical status of each patient was assessed every day, from day 1 through day 29 of his or her hospital stay, according to an eight-category ordinal scale.
Time to recovery was defined as the first day during the 28-day enrollment period that a patient’s clinical status met a 1 (not hospitalization, no activity limitations), 2 (not hospitalized, activity limitation, oxygen requirement or both), or 3 (hospitalized, not requiring supplemental oxygen or medical care if hospitalization was extended for infection-control reasons) on the eight-category scale. A score of 4 indicated a patient was hospitalized and needed ongoing medical care, but did not require supplemental oxygen; a score of 8 signified death.
The analysis found remdesivir patients had a median time to recovery of 11 days, compared with the median 15 days for patients on the placebo (rate ratio for recovery, 1.32; 95% confidence interval, 1.12-1.55; P < .001). Mortality was also lower in the remdesivir group (hazard ratio for death, 0.70; 95% CI, 0.47-1.04), but the result was not statistically significant. By 14 days, the Kaplan-Meier estimate of mortality was 7.1 % in the remdesivir group and 11.9% in the placebo group.
Patients receiving oxygen, but not yet requiring high-flow oxygen, mechanical ventilation, or extracorporeal membrane oxygenation, seemed to fare best from treatment with remdesivir (these patients had a baseline ordinal score of 5). That may be a result of the larger sample size of these patients, the researchers note in the study. The study authors were unable to estimate the recovery time for the most severely ill patients (category 7), possibly because the follow-up time was too short to fully evaluate this subgroup.
“There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Dr. Kaul, who was not involved in the study, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.”
Dr. Kaul said there is still the possibility that remdesivir could benefit patients on mechanical ventilation, but “clinicians will have to determine if the evidence suggesting no benefit in those who are intubated is strong enough to justify using this currently scarce resource in that population versus limiting use to those requiring oxygen but not on mechanical ventilation.”
Site investigators estimated that just four serious adverse events (two in each group) in enrolled patients were related to remdesivir or placebo. No deaths were attributed to the treatments, although acute respiratory failure, hypotension, acute kidney injury, and viral pneumonia were slightly more common in patients receiving the placebo than those receiving remdesivir.
The researchers plan to publish a follow-up study in the coming weeks or months, after the full cohort has completed 28 days of follow-up, Dr. Lane said. In future studies, the agency will likely focus on comparing remdesivir with combinations of remdesivir with other treatments, like the anti-inflammatory baricitinib.
A version of this article originally appeared on Medscape.com.
Much-anticipated results from the National Institute of Allergy and Infectious Diseases’ clinical trial of remdesivir in COVID-19 patients published in the New England Journal of Medicine suggest remdesivir shortens the disease course for hospitalized COVID-19 patients.
The agency reported initial promising results from the study earlier this month, which prompted the Food and Drug Administration to issue an emergency use authorization (EUA) for the drug, but the full data and results have not been widely available until now.
The findings also suggest remdesivir should be started, if possible, before patients have such severe pulmonary disease that they require mechanical ventilation, according to the study authors.
The published results are “completely consistent” with the NIAID’s earlier announcement, H. Clifford Lane, MD, deputy director for clinical research and special projects at the NIAID, said in an interview. “The benefit appeared to be the greatest for the patients who are hospitalized with severe disease who require supplemental oxygen.”
Given the limited supply of remdesivir, physicians have been eager to see the full data to ensure they use the drug most effectively, Daniel Kaul, MD, a professor of infectious diseases at the University of Michigan, Ann Arbor, said in an interview. Hospitals in states across the country, including New York, Michigan, and Washington, have received limited supplies of the drug in the last couple of weeks since the FDA’s authorization.
“I am losing my patience waiting for #remdesivir data. I was willing to give them a week to verify the numbers, triple proof the tables, cautiously frame conclusions. But it’s gone on too long. We are rationing with no rationale. We are floating on whisps [sic] of data, adrift,” Kate Stephenson, MD, an infectious diseases specialist at the Center for Virology and Vaccine Research at Harvard Medical School, Boston, wrote on Twitter May 18. After reading the paper, she tweeted Friday evening that she was “relieved to see convincing benefit – I was starting to worry!”
In the midst of a public health crisis, however, it is not unusual to make an announcement about trial results before the full dataset has been analyzed, said Dr. Lane. The NIAID followed a similar playbook for the PALM trial evaluating possible Ebola treatments in the Democratic Republic of Congo, with the independent monitoring board recommending the trial be terminated early in response to positive results from two of the four candidate drugs.
“When you have a result you think is of public health importance, you don’t wait for it to be published in a peer-reviewed journal,” said Dr. Lane, a coauthor of the study. The lag time from announcement to study publication was a result of the time it took to write up the paper for publication and go through peer review, Dr. Lane added. He also noted that the FDA had access to the data when the agency wrote its guidance for physicians administering the drug to patients under the EUA.
The authors opted not to publish the initial findings on a preprint server because they felt it was important to undergo peer review, said Dr. Lane. “The last thing you want for something this critical is for incomplete data to be out there, or you don’t have everything audited to the level that you want.”
Trial details
In the ACTT-1 randomized, placebo-controlled, double-blinded trial, researchers enrolled 1,063 patients from Feb. 21 to April 19, 2020, at 60 trial sites and 13 subsites worldwide (45 sites in the United States). The remdesivir group had 541 patients, and the placebo group had 522. A small number of patients (49 in the remdesivir group and 53 in the placebo group) discontinued treatment before day 10 because of an adverse event or withdrawn consent. When data collection for this preliminary analysis ended in late April, 301 patients had not recovered and had not completed their final follow-up visit.
Most of the patients had one (27%) or more (52.1%) preexisting conditions, including hypertension (49.6%), obesity (37%), and type 2 diabetes mellitus (29.7%). Mean patient age was 58.9 years, and the majority of patients were men (64.3%). The median number of days from symptom onset to randomization was 9, and 53.6% of the patients were white, 20.6% were black, 12.6% were Asian, 23.4% were Hispanic or Latino, and the ethnicity of 13.6% were not reported or reported as other.
Patients received one 200-mg loading dose on the first day of the trial, and then one 100-mg maintenance dose every day for days 2 through 10, or until discharge or death. Patients in the control group of the study received a matching placebo on the same schedule and volume. The clinical status of each patient was assessed every day, from day 1 through day 29 of his or her hospital stay, according to an eight-category ordinal scale.
Time to recovery was defined as the first day during the 28-day enrollment period that a patient’s clinical status met a 1 (not hospitalization, no activity limitations), 2 (not hospitalized, activity limitation, oxygen requirement or both), or 3 (hospitalized, not requiring supplemental oxygen or medical care if hospitalization was extended for infection-control reasons) on the eight-category scale. A score of 4 indicated a patient was hospitalized and needed ongoing medical care, but did not require supplemental oxygen; a score of 8 signified death.
The analysis found remdesivir patients had a median time to recovery of 11 days, compared with the median 15 days for patients on the placebo (rate ratio for recovery, 1.32; 95% confidence interval, 1.12-1.55; P < .001). Mortality was also lower in the remdesivir group (hazard ratio for death, 0.70; 95% CI, 0.47-1.04), but the result was not statistically significant. By 14 days, the Kaplan-Meier estimate of mortality was 7.1 % in the remdesivir group and 11.9% in the placebo group.
Patients receiving oxygen, but not yet requiring high-flow oxygen, mechanical ventilation, or extracorporeal membrane oxygenation, seemed to fare best from treatment with remdesivir (these patients had a baseline ordinal score of 5). That may be a result of the larger sample size of these patients, the researchers note in the study. The study authors were unable to estimate the recovery time for the most severely ill patients (category 7), possibly because the follow-up time was too short to fully evaluate this subgroup.
“There is clear and consistent evidence of clinically significant benefit for those hospitalized on oxygen but not yet requiring mechanical ventilation,” Dr. Kaul, who was not involved in the study, said after seeing the published results. “Surprisingly, early dosing as measured from time to onset of symptoms did not seem to make a difference.”
Dr. Kaul said there is still the possibility that remdesivir could benefit patients on mechanical ventilation, but “clinicians will have to determine if the evidence suggesting no benefit in those who are intubated is strong enough to justify using this currently scarce resource in that population versus limiting use to those requiring oxygen but not on mechanical ventilation.”
Site investigators estimated that just four serious adverse events (two in each group) in enrolled patients were related to remdesivir or placebo. No deaths were attributed to the treatments, although acute respiratory failure, hypotension, acute kidney injury, and viral pneumonia were slightly more common in patients receiving the placebo than those receiving remdesivir.
The researchers plan to publish a follow-up study in the coming weeks or months, after the full cohort has completed 28 days of follow-up, Dr. Lane said. In future studies, the agency will likely focus on comparing remdesivir with combinations of remdesivir with other treatments, like the anti-inflammatory baricitinib.
A version of this article originally appeared on Medscape.com.
COVID-19 and Mental Health Awareness Month
#howareyoureally challenge seeks to increase access to care
We are months into the COVID-19 crisis, and mental health issues are proving to be rampant. In every crisis, there is opportunity, and this one is no different. The opportunity is clear. For Mental Health Awareness Month and beyond, we must convey a powerful message that mental health is key to our well-being and must be actively addressed. Because almost everyone has felt excess anxiety these last months, we have a unique chance to engage a wider audience.

To address the urgent need, the Mental Health Coalition was formed with the understanding that the mental health crisis is fueled by a pervasive and devastating stigma, preventing millions of individuals from being able to seek the critical treatment they need. Spearheaded by social activist and fashion designer, Kenneth Cole, it is a coalition of leading mental health organizations, brands, celebrities, and advocates who have joined forces to end the stigma surrounding mental health and to change the way people talk about, and care for, mental illness. The group’s mission listed on its website states: “We must increase the conversation around mental health. We must act to end silence, reduce stigma, and engage our community to inspire hope at this essential moment.”
As most of the United States has been under stay-at-home orders, our traditional relationships have been radically disrupted. New types of relationships are forming as we are relying even more on technology to connect us. Social media seems to be on the only “social” we can now safely engage in.
The coalition’s campaign, “#howareyoureally?” is harnessing the power of social media and creating a storytelling platform to allow users to more genuinely share their feelings in these unprecedented times. Celebrities include Whoopi Goldberg, Kendall Jenner, Chris Cuomo, Deepak Chopra, Kesha, and many more have already shared their stories.
“How Are You, Really?” challenges people to answer this question using social media in an open and honest fashion while still providing hope.
The second component of the initiative is to increase access to care, and they have a long list of collaborators, including leading mental health organizations such as the American Foundation for Suicide Prevention, Anxiety and Depression Association of America, Child Mind Institute, Depression and Bipolar Support Alliance, Didi Hirsch Mental Health Services, National Alliance on Mental Illness, and many more.
We have a unique opportunity this Mental Health Awareness Month, and As a community, we must be prepared to meet the escalating needs of our population.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach, Fla. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
#howareyoureally challenge seeks to increase access to care
#howareyoureally challenge seeks to increase access to care
We are months into the COVID-19 crisis, and mental health issues are proving to be rampant. In every crisis, there is opportunity, and this one is no different. The opportunity is clear. For Mental Health Awareness Month and beyond, we must convey a powerful message that mental health is key to our well-being and must be actively addressed. Because almost everyone has felt excess anxiety these last months, we have a unique chance to engage a wider audience.
To address the urgent need, the Mental Health Coalition was formed with the understanding that the mental health crisis is fueled by a pervasive and devastating stigma, preventing millions of individuals from being able to seek the critical treatment they need. Spearheaded by social activist and fashion designer, Kenneth Cole, it is a coalition of leading mental health organizations, brands, celebrities, and advocates who have joined forces to end the stigma surrounding mental health and to change the way people talk about, and care for, mental illness. The group’s mission listed on its website states: “We must increase the conversation around mental health. We must act to end silence, reduce stigma, and engage our community to inspire hope at this essential moment.”
As most of the United States has been under stay-at-home orders, our traditional relationships have been radically disrupted. New types of relationships are forming as we are relying even more on technology to connect us. Social media seems to be on the only “social” we can now safely engage in.
The coalition’s campaign, “#howareyoureally?” is harnessing the power of social media and creating a storytelling platform to allow users to more genuinely share their feelings in these unprecedented times. Celebrities include Whoopi Goldberg, Kendall Jenner, Chris Cuomo, Deepak Chopra, Kesha, and many more have already shared their stories.
“How Are You, Really?” challenges people to answer this question using social media in an open and honest fashion while still providing hope.
The second component of the initiative is to increase access to care, and they have a long list of collaborators, including leading mental health organizations such as the American Foundation for Suicide Prevention, Anxiety and Depression Association of America, Child Mind Institute, Depression and Bipolar Support Alliance, Didi Hirsch Mental Health Services, National Alliance on Mental Illness, and many more.
We have a unique opportunity this Mental Health Awareness Month, and As a community, we must be prepared to meet the escalating needs of our population.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach, Fla. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
We are months into the COVID-19 crisis, and mental health issues are proving to be rampant. In every crisis, there is opportunity, and this one is no different. The opportunity is clear. For Mental Health Awareness Month and beyond, we must convey a powerful message that mental health is key to our well-being and must be actively addressed. Because almost everyone has felt excess anxiety these last months, we have a unique chance to engage a wider audience.
To address the urgent need, the Mental Health Coalition was formed with the understanding that the mental health crisis is fueled by a pervasive and devastating stigma, preventing millions of individuals from being able to seek the critical treatment they need. Spearheaded by social activist and fashion designer, Kenneth Cole, it is a coalition of leading mental health organizations, brands, celebrities, and advocates who have joined forces to end the stigma surrounding mental health and to change the way people talk about, and care for, mental illness. The group’s mission listed on its website states: “We must increase the conversation around mental health. We must act to end silence, reduce stigma, and engage our community to inspire hope at this essential moment.”
As most of the United States has been under stay-at-home orders, our traditional relationships have been radically disrupted. New types of relationships are forming as we are relying even more on technology to connect us. Social media seems to be on the only “social” we can now safely engage in.
The coalition’s campaign, “#howareyoureally?” is harnessing the power of social media and creating a storytelling platform to allow users to more genuinely share their feelings in these unprecedented times. Celebrities include Whoopi Goldberg, Kendall Jenner, Chris Cuomo, Deepak Chopra, Kesha, and many more have already shared their stories.
“How Are You, Really?” challenges people to answer this question using social media in an open and honest fashion while still providing hope.
The second component of the initiative is to increase access to care, and they have a long list of collaborators, including leading mental health organizations such as the American Foundation for Suicide Prevention, Anxiety and Depression Association of America, Child Mind Institute, Depression and Bipolar Support Alliance, Didi Hirsch Mental Health Services, National Alliance on Mental Illness, and many more.
We have a unique opportunity this Mental Health Awareness Month, and As a community, we must be prepared to meet the escalating needs of our population.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach, Fla. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
Neurologists’ pay gets a boost, most happy with career choice
findings from the newly released Medscape Neurologist Compensation Report 2020 show.
Neurologists’ average annual income this year rose to $280,000, up from $267,000 last year. More than half of neurologists (53%) feel fairly compensated, similar to last year’s percentage.
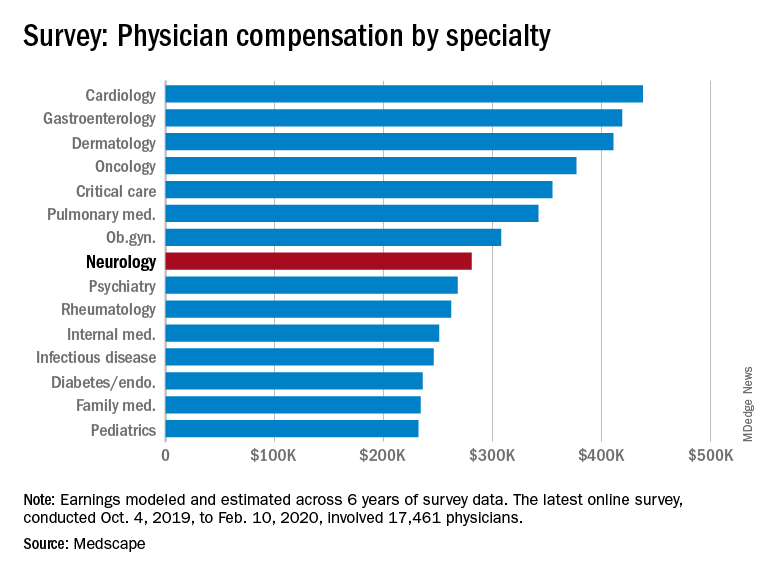
Neurologists are below the middle earners of all physician specialties. At $280,000 in annual compensation for patient care, neurologists rank ninth from the bottom, just below allergists/immunologists ($301,000) but ahead of psychiatrists ($268,000), rheumatologists ($262,000), and internists ($251,000).
Orthopedists are the top earners ($511,000 annual pay), followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according the overall Medscape Physician Compensation Report 2020, which covers U.S. physicians as a whole. The survey included more than 17,000 physicians in over 30 specialties.
COVID-19 impact
An important caveat is that the data for this year’s report were collected prior to Feb. 10, 2020, and therefore reflect physician salary and income prior to the COVID-19 crisis, which has had a huge impact on physicians.
For example, data show that since the start of the crisis, physician practices have seen a 55% dip in revenue and a 60% dip in patient volume on average. Hospitals and physician groups nationwide have implemented layoffs, furloughs, and pay cuts.
In March, 43,000 health care workers were laid off; 9% of independent medical practices reported that they had closed their practices, at least temporarily.
There continues to be a gender pay gap in neurology, with male neurologists earning about 26% more than their female peers ($299,000 vs. $237,000). Among all specialists, men earn 31% more than women, similar to last year’s figure of 33%. There continues to be a 25% gender pay gap among primary care physicians.
More than half of all physicians (56%) say they receive an incentive bonus. Neurologists report that they are eligible for an annual incentive bonus of $35,000. Average annual incentive bonuses are highest among orthopedists ($96,000) and lowest among family medicine physicians ($24,000).
Close to one third of physicians overall who receive incentive bonuses say the prospect of receiving the bonus has encouraged them to work longer hours. A higher percentage of neurologists (41%) say their potential bonus influenced them to increase their work hours.
Fifty-eight percent of neurologists achieve more than three quarters of their potential annual incentive bonus. On average, neurologists achieve about two thirds of their potential bonus, the same proportion as for physicians overall.
However, COVID-19 may change that. Experts who were interviewed recently by Medscape noted that productivity benchmarks for physicians are likely to be lowered in light of plunging patient numbers from COVID-19, and bonuses are expected to take a hit.
Happy at work
On average, male neurologists spend 37.7 hours per week seeing patients, somewhat more hours per week than female neurologists (36.1 hours); the average for all physicians is 37.9 hours per week.
Bureaucratic tasks continue to be a burden for physicians in all specialties. On average, neurologists spend 16.9 hours per week on paperwork and administration, about the same as physicians overall (15.6 hours).
Intensivists top the list regarding such tasks (19.1 hours), followed by internists (18.5), infectious disease physicians (18.5), and psychiatrists (18.3). Anesthesiologists and ophthalmologists spend the least amount of time on paperwork/administration (10.0 and 9.8 hours per week, respectively).
What is most rewarding about being a neurologist? Being good at what they do/finding answers, diagnoses tops the list (33%), followed by making the world a better place/helping others (26%), relationships with and gratitude from patients (18%), and making good money at a job they like (11%). A few cited teaching (5%) and pride in their profession (4%).
The most challenging part of practicing neurology is having to follow so many rules and regulations (26%). Other challenges include having to work long hours (18%), dealing with difficult patients (17%), trouble getting fair reimbursement (13%), and working with electronic health records (10%).
Despite the challenges, if they had to do it all over again, 73% of neurologists would still choose medicine as a career, and 86% would again choose neurology.
Other key findings in the latest report regarding neurologists include the following:
- At 18%, neurologists rank near the middle among physicians with regard to losing money on denied or resubmitted claims. Plastic surgery and emergency medicine have the highest percentage of claims denied or resubmitted (28% and 22%, respectively). One study found that, on average, 63% of denied claims are recoverable, but healthcare professionals spend about $118 per claim on appeals.
- 29% of neurologists say they use physician assistants (PAs) to treat patients in their practices, and 53% use nurse practitioners (NPs); 38% use neither for patient care. Of neurologists who work with PAs and NPs in their offices, 49% say these employees have helped boost profitability.
- Two-thirds of neurologists say they will continue taking new and current Medicare/Medicaid patients; none say they will not take new Medicare patients; and 26% are undecided.
- Neurologists participate in various payment methods; 78% are reimbursed via insurance, 35% have fee-for-service arrangements, and 28% are in accountable care organizations.
- Nearly 40% of neurologists expect to participate in the merit-based incentive payment system option, and 10% expect to participate in alternative payment models.
This article first appeared on Medscape.com.
findings from the newly released Medscape Neurologist Compensation Report 2020 show.
Neurologists’ average annual income this year rose to $280,000, up from $267,000 last year. More than half of neurologists (53%) feel fairly compensated, similar to last year’s percentage.
Neurologists are below the middle earners of all physician specialties. At $280,000 in annual compensation for patient care, neurologists rank ninth from the bottom, just below allergists/immunologists ($301,000) but ahead of psychiatrists ($268,000), rheumatologists ($262,000), and internists ($251,000).
Orthopedists are the top earners ($511,000 annual pay), followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according the overall Medscape Physician Compensation Report 2020, which covers U.S. physicians as a whole. The survey included more than 17,000 physicians in over 30 specialties.
COVID-19 impact
An important caveat is that the data for this year’s report were collected prior to Feb. 10, 2020, and therefore reflect physician salary and income prior to the COVID-19 crisis, which has had a huge impact on physicians.
For example, data show that since the start of the crisis, physician practices have seen a 55% dip in revenue and a 60% dip in patient volume on average. Hospitals and physician groups nationwide have implemented layoffs, furloughs, and pay cuts.
In March, 43,000 health care workers were laid off; 9% of independent medical practices reported that they had closed their practices, at least temporarily.
There continues to be a gender pay gap in neurology, with male neurologists earning about 26% more than their female peers ($299,000 vs. $237,000). Among all specialists, men earn 31% more than women, similar to last year’s figure of 33%. There continues to be a 25% gender pay gap among primary care physicians.
More than half of all physicians (56%) say they receive an incentive bonus. Neurologists report that they are eligible for an annual incentive bonus of $35,000. Average annual incentive bonuses are highest among orthopedists ($96,000) and lowest among family medicine physicians ($24,000).
Close to one third of physicians overall who receive incentive bonuses say the prospect of receiving the bonus has encouraged them to work longer hours. A higher percentage of neurologists (41%) say their potential bonus influenced them to increase their work hours.
Fifty-eight percent of neurologists achieve more than three quarters of their potential annual incentive bonus. On average, neurologists achieve about two thirds of their potential bonus, the same proportion as for physicians overall.
However, COVID-19 may change that. Experts who were interviewed recently by Medscape noted that productivity benchmarks for physicians are likely to be lowered in light of plunging patient numbers from COVID-19, and bonuses are expected to take a hit.
Happy at work
On average, male neurologists spend 37.7 hours per week seeing patients, somewhat more hours per week than female neurologists (36.1 hours); the average for all physicians is 37.9 hours per week.
Bureaucratic tasks continue to be a burden for physicians in all specialties. On average, neurologists spend 16.9 hours per week on paperwork and administration, about the same as physicians overall (15.6 hours).
Intensivists top the list regarding such tasks (19.1 hours), followed by internists (18.5), infectious disease physicians (18.5), and psychiatrists (18.3). Anesthesiologists and ophthalmologists spend the least amount of time on paperwork/administration (10.0 and 9.8 hours per week, respectively).
What is most rewarding about being a neurologist? Being good at what they do/finding answers, diagnoses tops the list (33%), followed by making the world a better place/helping others (26%), relationships with and gratitude from patients (18%), and making good money at a job they like (11%). A few cited teaching (5%) and pride in their profession (4%).
The most challenging part of practicing neurology is having to follow so many rules and regulations (26%). Other challenges include having to work long hours (18%), dealing with difficult patients (17%), trouble getting fair reimbursement (13%), and working with electronic health records (10%).
Despite the challenges, if they had to do it all over again, 73% of neurologists would still choose medicine as a career, and 86% would again choose neurology.
Other key findings in the latest report regarding neurologists include the following:
- At 18%, neurologists rank near the middle among physicians with regard to losing money on denied or resubmitted claims. Plastic surgery and emergency medicine have the highest percentage of claims denied or resubmitted (28% and 22%, respectively). One study found that, on average, 63% of denied claims are recoverable, but healthcare professionals spend about $118 per claim on appeals.
- 29% of neurologists say they use physician assistants (PAs) to treat patients in their practices, and 53% use nurse practitioners (NPs); 38% use neither for patient care. Of neurologists who work with PAs and NPs in their offices, 49% say these employees have helped boost profitability.
- Two-thirds of neurologists say they will continue taking new and current Medicare/Medicaid patients; none say they will not take new Medicare patients; and 26% are undecided.
- Neurologists participate in various payment methods; 78% are reimbursed via insurance, 35% have fee-for-service arrangements, and 28% are in accountable care organizations.
- Nearly 40% of neurologists expect to participate in the merit-based incentive payment system option, and 10% expect to participate in alternative payment models.
This article first appeared on Medscape.com.
findings from the newly released Medscape Neurologist Compensation Report 2020 show.
Neurologists’ average annual income this year rose to $280,000, up from $267,000 last year. More than half of neurologists (53%) feel fairly compensated, similar to last year’s percentage.
Neurologists are below the middle earners of all physician specialties. At $280,000 in annual compensation for patient care, neurologists rank ninth from the bottom, just below allergists/immunologists ($301,000) but ahead of psychiatrists ($268,000), rheumatologists ($262,000), and internists ($251,000).
Orthopedists are the top earners ($511,000 annual pay), followed by plastic surgeons ($479,000), otolaryngologists ($455,000), and cardiologists ($438,000), according the overall Medscape Physician Compensation Report 2020, which covers U.S. physicians as a whole. The survey included more than 17,000 physicians in over 30 specialties.
COVID-19 impact
An important caveat is that the data for this year’s report were collected prior to Feb. 10, 2020, and therefore reflect physician salary and income prior to the COVID-19 crisis, which has had a huge impact on physicians.
For example, data show that since the start of the crisis, physician practices have seen a 55% dip in revenue and a 60% dip in patient volume on average. Hospitals and physician groups nationwide have implemented layoffs, furloughs, and pay cuts.
In March, 43,000 health care workers were laid off; 9% of independent medical practices reported that they had closed their practices, at least temporarily.
There continues to be a gender pay gap in neurology, with male neurologists earning about 26% more than their female peers ($299,000 vs. $237,000). Among all specialists, men earn 31% more than women, similar to last year’s figure of 33%. There continues to be a 25% gender pay gap among primary care physicians.
More than half of all physicians (56%) say they receive an incentive bonus. Neurologists report that they are eligible for an annual incentive bonus of $35,000. Average annual incentive bonuses are highest among orthopedists ($96,000) and lowest among family medicine physicians ($24,000).
Close to one third of physicians overall who receive incentive bonuses say the prospect of receiving the bonus has encouraged them to work longer hours. A higher percentage of neurologists (41%) say their potential bonus influenced them to increase their work hours.
Fifty-eight percent of neurologists achieve more than three quarters of their potential annual incentive bonus. On average, neurologists achieve about two thirds of their potential bonus, the same proportion as for physicians overall.
However, COVID-19 may change that. Experts who were interviewed recently by Medscape noted that productivity benchmarks for physicians are likely to be lowered in light of plunging patient numbers from COVID-19, and bonuses are expected to take a hit.
Happy at work
On average, male neurologists spend 37.7 hours per week seeing patients, somewhat more hours per week than female neurologists (36.1 hours); the average for all physicians is 37.9 hours per week.
Bureaucratic tasks continue to be a burden for physicians in all specialties. On average, neurologists spend 16.9 hours per week on paperwork and administration, about the same as physicians overall (15.6 hours).
Intensivists top the list regarding such tasks (19.1 hours), followed by internists (18.5), infectious disease physicians (18.5), and psychiatrists (18.3). Anesthesiologists and ophthalmologists spend the least amount of time on paperwork/administration (10.0 and 9.8 hours per week, respectively).
What is most rewarding about being a neurologist? Being good at what they do/finding answers, diagnoses tops the list (33%), followed by making the world a better place/helping others (26%), relationships with and gratitude from patients (18%), and making good money at a job they like (11%). A few cited teaching (5%) and pride in their profession (4%).
The most challenging part of practicing neurology is having to follow so many rules and regulations (26%). Other challenges include having to work long hours (18%), dealing with difficult patients (17%), trouble getting fair reimbursement (13%), and working with electronic health records (10%).
Despite the challenges, if they had to do it all over again, 73% of neurologists would still choose medicine as a career, and 86% would again choose neurology.
Other key findings in the latest report regarding neurologists include the following:
- At 18%, neurologists rank near the middle among physicians with regard to losing money on denied or resubmitted claims. Plastic surgery and emergency medicine have the highest percentage of claims denied or resubmitted (28% and 22%, respectively). One study found that, on average, 63% of denied claims are recoverable, but healthcare professionals spend about $118 per claim on appeals.
- 29% of neurologists say they use physician assistants (PAs) to treat patients in their practices, and 53% use nurse practitioners (NPs); 38% use neither for patient care. Of neurologists who work with PAs and NPs in their offices, 49% say these employees have helped boost profitability.
- Two-thirds of neurologists say they will continue taking new and current Medicare/Medicaid patients; none say they will not take new Medicare patients; and 26% are undecided.
- Neurologists participate in various payment methods; 78% are reimbursed via insurance, 35% have fee-for-service arrangements, and 28% are in accountable care organizations.
- Nearly 40% of neurologists expect to participate in the merit-based incentive payment system option, and 10% expect to participate in alternative payment models.
This article first appeared on Medscape.com.
ACE inhibitors and severe COVID-19: Protective in older patients?
.
In addition, a new meta-analysis of all the available data on the use of ACE inhibitors and angiotensin-receptor blockers (ARBs) in COVID-19–infected patients has concluded that these drugs are not associated with more severe disease and do not increase susceptibility to infection.
The observational study, which was published on the MedRxiv preprint server on May 19 and has not yet been peer reviewed, was conducted by the health insurance company United Heath Group and by Yale University, New Haven, Conn.
The investigators analyzed data from 10,000 patients from across the United States who had tested positive for COVID-19, who were enrolled in Medicare Advantage insurance plans or were commercially insured, and who had received a prescription for one or more antihypertensive medications.
Results showed that the use of ACE inhibitors was associated with an almost 40% lower risk for COVID-19 hospitalization for older people enrolled in Medicare Advantage plans. No such benefit was seen in the younger commercially insured patients or in either group with ARBs.

At a telephone media briefing on the study, senior investigator Harlan M. Krumholz, MD, said: “We don’t believe this is enough info to change practice, but we do think this is an interesting and intriguing result.
“These findings merit a clinical trial to formally test whether ACE inhibitors – which are cheap, widely available, and well-tolerated drugs – can reduce hospitalization of patients infected with COVID-19,” added Dr. Krumholz, professor of medicine at Yale and director of the Yale New Haven Hospital Center for Outcomes Research.
A pragmatic clinical trial is now being planned. In this trial, 10,000 older people who test positive for COVID-19 will be randomly assigned to receive either a low dose of an ACE inhibitor or placebo. It is hoped that recruitment for the trial will begin in June of 2020. It is open to all eligible Americans who are older than 50 years, who test negative for COVID-19, and who are not taking medications for hypertension. Prospective patients can sign up at a dedicated website.
The randomized trial, also conducted by United Health Group and Yale, is said to be “one of the first virtual COVID-19 clinical trials to be launched at scale.”
For the observational study, the researchers identified 2,263 people who were receiving medication for hypertension and who tested positive for COVID-19. Of these, approximately two-thirds were older, Medicare Advantage enrollees; one-third were younger, commercially insured individuals.
In a propensity score–matched analysis, the investigators matched 441 patients who were taking ACE inhibitors to 441 patients who were taking other antihypertensive agents; and 412 patients who were receiving an ARB to 412 patients who were receiving other antihypertensive agents.
Results showed that during a median of 30 days after testing positive, 12.7% of the cohort were hospitalized for COVID-19. In propensity score–matched analyses, neither ACE inhibitors (hazard ratio [HR], 0.77; P = .18) nor ARBs (HR, 0.88; P =.48) were significantly associated with risk for hospitalization.
However, in analyses stratified by the insurance group, ACE inhibitors (but not ARBs) were associated with a significant lower risk for hospitalization among the Medicare group (HR, 0.61; P = .02) but not among the commercially insured group (HR, 2.14; P = .12).
A second study examined outcomes of 7,933 individuals with hypertension who were hospitalized with COVID-19 (92% of these patients were Medicare Advantage enrollees). Of these, 14.2% died, 59.5% survived to discharge, and 26.3% underwent ongoing hospitalization. In propensity score–matched analyses, use of neither an ACE inhibitor (HR, 0.97; P = .74) nor an ARB (HR, 1.15; P = .15) was associated with risk of in-hospital mortality.
The researchers said their findings are consistent with prior evidence from randomized clinical trials suggesting a reduced risk for pneumonia with ACE inhibitors that is not observed with ARBs.
They also cited some preclinical evidence that they said suggests a possible protective role for ACE inhibitors in COVID-19: that ACE inhibitors, but not ARBs, are associated with the upregulation of ACE2 receptors, which modulate the local interactions of the renin-angiotensin-aldosterone system in the lung tissue.
“The presence of ACE2 receptors, therefore, exerts a protective effect against the development of acute lung injury in infections with SARS coronaviruses, which lead to dysregulation of these mechanisms and endothelial damage,” they added. “Further, our observations do not support theoretical concerns of adverse outcomes due to enhanced virulence of SARS coronaviruses due to overexpression of ACE2 receptors in cell cultures – an indirect binding site for these viruses.”
The authors also noted that their findings have “important implications” for four ongoing randomized trials of ACE inhibitors/ARBs in COVID-19, “as none of them align with the observations of our study.”
They pointed out that of the four ongoing trials, three are testing the use of ACE inhibitors or ARBs in the treatment of hospitalized COVID-19 patients, and one is testing the use of a 10-day course of ARBs after a positive SARS-CoV-2 test to prevent hospitalization.
Experts cautious
However, two cardiovascular experts who were asked to comment on this latest study were not overly optimistic about the data.
Michael A. Weber, MD, professor of medicine at the State University of New York, Brooklyn, said: “This report adds to the growing number of observational studies that show varying effects of ACE inhibitors and ARBs in increasing or decreasing hospitalizations for COVID-19 and the likelihood of in-hospital mortality. Overall, this new report differs from others in the remarkable effects of insurance coverage: In particular, for ACE inhibitors, there was a 40% reduction in fatal events in Medicare patients but a twofold increase in patients using commercial insurance – albeit the test for heterogeneity when comparing the two groups did not quite reach statistical significance.
“In essence, these authors are saying that ACE inhibitors are highly protective in patients aged 65 or older but bordering on harmful in patients aged below 65. I agree that it’s worthwhile to check this finding in a prospective trial ... but this hypothesis does seem to be a reach.”
Dr. Weber noted that both ACE inhibitors and ARBs increase the level of the ACE2 enzyme to which the COVID-19 virus binds in the lungs.
“The ACE inhibitors do so by inhibiting the enzyme’s action and thus stimulate further enzyme production; the ARBs block the effects of angiotensin II, which results in high angiotensin II levels that also upregulate ACE2 production,” he said. “Perhaps the ACE inhibitors, by binding to the ACE enzyme, can in some way interfere with the enzyme’s uptake of the COVID virus and thus provide some measure of clinical protection. This is possible, but why would this effect be apparent only in older people?”

John McMurray, MD, professor of medical cardiology at the University of Glasgow, Scotland, added: “This looks like a subgroup of a subgroup type analysis based on small numbers of events – I think there were only 77 hospitalizations among the 722 patients treated with an ACE inhibitor, and the Medicare Advantage subgroup was only 581 of those 722 patients.
“The hazard ratio had wide 95% CI [confidence interval] and a modest P value,” Dr. McMurray added. “So yes, interesting and hypothesis-generating, but not definitive.”
New meta-analysis
The new meta-analysis of all data so far available on ACE inhibitor and ARB use for patients with COVID-19 was published online in Annals of Internal Medicine on May 15.
The analysis is a living, systematic review with ongoing literature surveillance and critical appraisal, which will be updated as new data become available. It included 14 observational studies.
The authors, led by Katherine M. Mackey, MD, VA Portland Health Care System, Oregon, concluded: “High-certainty evidence suggests that ACE-inhibitor or ARB use is not associated with more severe COVID-19 disease, and moderate certainty evidence suggested no association between use of these medications and positive SARS-CoV-2 test results among symptomatic patients. Whether these medications increase the risk for mild or asymptomatic disease or are beneficial in COVID-19 treatment remains uncertain.”
In an accompanying editorial, William G. Kussmaul III, MD, Drexel University, Philadelphia, said that initial fears that these drugs may be harmful for patients with COVID-19 now seem to have been unfounded.
“We now have reasonable reassurance that drugs that alter the renin-angiotensin system do not pose substantial threats as either COVID-19 risk factors or severity multipliers,” he wrote.
A version of this article originally appeared on Medscape.com.
.
In addition, a new meta-analysis of all the available data on the use of ACE inhibitors and angiotensin-receptor blockers (ARBs) in COVID-19–infected patients has concluded that these drugs are not associated with more severe disease and do not increase susceptibility to infection.
The observational study, which was published on the MedRxiv preprint server on May 19 and has not yet been peer reviewed, was conducted by the health insurance company United Heath Group and by Yale University, New Haven, Conn.
The investigators analyzed data from 10,000 patients from across the United States who had tested positive for COVID-19, who were enrolled in Medicare Advantage insurance plans or were commercially insured, and who had received a prescription for one or more antihypertensive medications.
Results showed that the use of ACE inhibitors was associated with an almost 40% lower risk for COVID-19 hospitalization for older people enrolled in Medicare Advantage plans. No such benefit was seen in the younger commercially insured patients or in either group with ARBs.
At a telephone media briefing on the study, senior investigator Harlan M. Krumholz, MD, said: “We don’t believe this is enough info to change practice, but we do think this is an interesting and intriguing result.
“These findings merit a clinical trial to formally test whether ACE inhibitors – which are cheap, widely available, and well-tolerated drugs – can reduce hospitalization of patients infected with COVID-19,” added Dr. Krumholz, professor of medicine at Yale and director of the Yale New Haven Hospital Center for Outcomes Research.
A pragmatic clinical trial is now being planned. In this trial, 10,000 older people who test positive for COVID-19 will be randomly assigned to receive either a low dose of an ACE inhibitor or placebo. It is hoped that recruitment for the trial will begin in June of 2020. It is open to all eligible Americans who are older than 50 years, who test negative for COVID-19, and who are not taking medications for hypertension. Prospective patients can sign up at a dedicated website.
The randomized trial, also conducted by United Health Group and Yale, is said to be “one of the first virtual COVID-19 clinical trials to be launched at scale.”
For the observational study, the researchers identified 2,263 people who were receiving medication for hypertension and who tested positive for COVID-19. Of these, approximately two-thirds were older, Medicare Advantage enrollees; one-third were younger, commercially insured individuals.
In a propensity score–matched analysis, the investigators matched 441 patients who were taking ACE inhibitors to 441 patients who were taking other antihypertensive agents; and 412 patients who were receiving an ARB to 412 patients who were receiving other antihypertensive agents.
Results showed that during a median of 30 days after testing positive, 12.7% of the cohort were hospitalized for COVID-19. In propensity score–matched analyses, neither ACE inhibitors (hazard ratio [HR], 0.77; P = .18) nor ARBs (HR, 0.88; P =.48) were significantly associated with risk for hospitalization.
However, in analyses stratified by the insurance group, ACE inhibitors (but not ARBs) were associated with a significant lower risk for hospitalization among the Medicare group (HR, 0.61; P = .02) but not among the commercially insured group (HR, 2.14; P = .12).
A second study examined outcomes of 7,933 individuals with hypertension who were hospitalized with COVID-19 (92% of these patients were Medicare Advantage enrollees). Of these, 14.2% died, 59.5% survived to discharge, and 26.3% underwent ongoing hospitalization. In propensity score–matched analyses, use of neither an ACE inhibitor (HR, 0.97; P = .74) nor an ARB (HR, 1.15; P = .15) was associated with risk of in-hospital mortality.
The researchers said their findings are consistent with prior evidence from randomized clinical trials suggesting a reduced risk for pneumonia with ACE inhibitors that is not observed with ARBs.
They also cited some preclinical evidence that they said suggests a possible protective role for ACE inhibitors in COVID-19: that ACE inhibitors, but not ARBs, are associated with the upregulation of ACE2 receptors, which modulate the local interactions of the renin-angiotensin-aldosterone system in the lung tissue.
“The presence of ACE2 receptors, therefore, exerts a protective effect against the development of acute lung injury in infections with SARS coronaviruses, which lead to dysregulation of these mechanisms and endothelial damage,” they added. “Further, our observations do not support theoretical concerns of adverse outcomes due to enhanced virulence of SARS coronaviruses due to overexpression of ACE2 receptors in cell cultures – an indirect binding site for these viruses.”
The authors also noted that their findings have “important implications” for four ongoing randomized trials of ACE inhibitors/ARBs in COVID-19, “as none of them align with the observations of our study.”
They pointed out that of the four ongoing trials, three are testing the use of ACE inhibitors or ARBs in the treatment of hospitalized COVID-19 patients, and one is testing the use of a 10-day course of ARBs after a positive SARS-CoV-2 test to prevent hospitalization.
Experts cautious
However, two cardiovascular experts who were asked to comment on this latest study were not overly optimistic about the data.
Michael A. Weber, MD, professor of medicine at the State University of New York, Brooklyn, said: “This report adds to the growing number of observational studies that show varying effects of ACE inhibitors and ARBs in increasing or decreasing hospitalizations for COVID-19 and the likelihood of in-hospital mortality. Overall, this new report differs from others in the remarkable effects of insurance coverage: In particular, for ACE inhibitors, there was a 40% reduction in fatal events in Medicare patients but a twofold increase in patients using commercial insurance – albeit the test for heterogeneity when comparing the two groups did not quite reach statistical significance.
“In essence, these authors are saying that ACE inhibitors are highly protective in patients aged 65 or older but bordering on harmful in patients aged below 65. I agree that it’s worthwhile to check this finding in a prospective trial ... but this hypothesis does seem to be a reach.”
Dr. Weber noted that both ACE inhibitors and ARBs increase the level of the ACE2 enzyme to which the COVID-19 virus binds in the lungs.
“The ACE inhibitors do so by inhibiting the enzyme’s action and thus stimulate further enzyme production; the ARBs block the effects of angiotensin II, which results in high angiotensin II levels that also upregulate ACE2 production,” he said. “Perhaps the ACE inhibitors, by binding to the ACE enzyme, can in some way interfere with the enzyme’s uptake of the COVID virus and thus provide some measure of clinical protection. This is possible, but why would this effect be apparent only in older people?”
John McMurray, MD, professor of medical cardiology at the University of Glasgow, Scotland, added: “This looks like a subgroup of a subgroup type analysis based on small numbers of events – I think there were only 77 hospitalizations among the 722 patients treated with an ACE inhibitor, and the Medicare Advantage subgroup was only 581 of those 722 patients.
“The hazard ratio had wide 95% CI [confidence interval] and a modest P value,” Dr. McMurray added. “So yes, interesting and hypothesis-generating, but not definitive.”
New meta-analysis
The new meta-analysis of all data so far available on ACE inhibitor and ARB use for patients with COVID-19 was published online in Annals of Internal Medicine on May 15.
The analysis is a living, systematic review with ongoing literature surveillance and critical appraisal, which will be updated as new data become available. It included 14 observational studies.
The authors, led by Katherine M. Mackey, MD, VA Portland Health Care System, Oregon, concluded: “High-certainty evidence suggests that ACE-inhibitor or ARB use is not associated with more severe COVID-19 disease, and moderate certainty evidence suggested no association between use of these medications and positive SARS-CoV-2 test results among symptomatic patients. Whether these medications increase the risk for mild or asymptomatic disease or are beneficial in COVID-19 treatment remains uncertain.”
In an accompanying editorial, William G. Kussmaul III, MD, Drexel University, Philadelphia, said that initial fears that these drugs may be harmful for patients with COVID-19 now seem to have been unfounded.
“We now have reasonable reassurance that drugs that alter the renin-angiotensin system do not pose substantial threats as either COVID-19 risk factors or severity multipliers,” he wrote.
A version of this article originally appeared on Medscape.com.
.
In addition, a new meta-analysis of all the available data on the use of ACE inhibitors and angiotensin-receptor blockers (ARBs) in COVID-19–infected patients has concluded that these drugs are not associated with more severe disease and do not increase susceptibility to infection.
The observational study, which was published on the MedRxiv preprint server on May 19 and has not yet been peer reviewed, was conducted by the health insurance company United Heath Group and by Yale University, New Haven, Conn.
The investigators analyzed data from 10,000 patients from across the United States who had tested positive for COVID-19, who were enrolled in Medicare Advantage insurance plans or were commercially insured, and who had received a prescription for one or more antihypertensive medications.
Results showed that the use of ACE inhibitors was associated with an almost 40% lower risk for COVID-19 hospitalization for older people enrolled in Medicare Advantage plans. No such benefit was seen in the younger commercially insured patients or in either group with ARBs.
At a telephone media briefing on the study, senior investigator Harlan M. Krumholz, MD, said: “We don’t believe this is enough info to change practice, but we do think this is an interesting and intriguing result.
“These findings merit a clinical trial to formally test whether ACE inhibitors – which are cheap, widely available, and well-tolerated drugs – can reduce hospitalization of patients infected with COVID-19,” added Dr. Krumholz, professor of medicine at Yale and director of the Yale New Haven Hospital Center for Outcomes Research.
A pragmatic clinical trial is now being planned. In this trial, 10,000 older people who test positive for COVID-19 will be randomly assigned to receive either a low dose of an ACE inhibitor or placebo. It is hoped that recruitment for the trial will begin in June of 2020. It is open to all eligible Americans who are older than 50 years, who test negative for COVID-19, and who are not taking medications for hypertension. Prospective patients can sign up at a dedicated website.
The randomized trial, also conducted by United Health Group and Yale, is said to be “one of the first virtual COVID-19 clinical trials to be launched at scale.”
For the observational study, the researchers identified 2,263 people who were receiving medication for hypertension and who tested positive for COVID-19. Of these, approximately two-thirds were older, Medicare Advantage enrollees; one-third were younger, commercially insured individuals.
In a propensity score–matched analysis, the investigators matched 441 patients who were taking ACE inhibitors to 441 patients who were taking other antihypertensive agents; and 412 patients who were receiving an ARB to 412 patients who were receiving other antihypertensive agents.
Results showed that during a median of 30 days after testing positive, 12.7% of the cohort were hospitalized for COVID-19. In propensity score–matched analyses, neither ACE inhibitors (hazard ratio [HR], 0.77; P = .18) nor ARBs (HR, 0.88; P =.48) were significantly associated with risk for hospitalization.
However, in analyses stratified by the insurance group, ACE inhibitors (but not ARBs) were associated with a significant lower risk for hospitalization among the Medicare group (HR, 0.61; P = .02) but not among the commercially insured group (HR, 2.14; P = .12).
A second study examined outcomes of 7,933 individuals with hypertension who were hospitalized with COVID-19 (92% of these patients were Medicare Advantage enrollees). Of these, 14.2% died, 59.5% survived to discharge, and 26.3% underwent ongoing hospitalization. In propensity score–matched analyses, use of neither an ACE inhibitor (HR, 0.97; P = .74) nor an ARB (HR, 1.15; P = .15) was associated with risk of in-hospital mortality.
The researchers said their findings are consistent with prior evidence from randomized clinical trials suggesting a reduced risk for pneumonia with ACE inhibitors that is not observed with ARBs.
They also cited some preclinical evidence that they said suggests a possible protective role for ACE inhibitors in COVID-19: that ACE inhibitors, but not ARBs, are associated with the upregulation of ACE2 receptors, which modulate the local interactions of the renin-angiotensin-aldosterone system in the lung tissue.
“The presence of ACE2 receptors, therefore, exerts a protective effect against the development of acute lung injury in infections with SARS coronaviruses, which lead to dysregulation of these mechanisms and endothelial damage,” they added. “Further, our observations do not support theoretical concerns of adverse outcomes due to enhanced virulence of SARS coronaviruses due to overexpression of ACE2 receptors in cell cultures – an indirect binding site for these viruses.”
The authors also noted that their findings have “important implications” for four ongoing randomized trials of ACE inhibitors/ARBs in COVID-19, “as none of them align with the observations of our study.”
They pointed out that of the four ongoing trials, three are testing the use of ACE inhibitors or ARBs in the treatment of hospitalized COVID-19 patients, and one is testing the use of a 10-day course of ARBs after a positive SARS-CoV-2 test to prevent hospitalization.
Experts cautious
However, two cardiovascular experts who were asked to comment on this latest study were not overly optimistic about the data.
Michael A. Weber, MD, professor of medicine at the State University of New York, Brooklyn, said: “This report adds to the growing number of observational studies that show varying effects of ACE inhibitors and ARBs in increasing or decreasing hospitalizations for COVID-19 and the likelihood of in-hospital mortality. Overall, this new report differs from others in the remarkable effects of insurance coverage: In particular, for ACE inhibitors, there was a 40% reduction in fatal events in Medicare patients but a twofold increase in patients using commercial insurance – albeit the test for heterogeneity when comparing the two groups did not quite reach statistical significance.
“In essence, these authors are saying that ACE inhibitors are highly protective in patients aged 65 or older but bordering on harmful in patients aged below 65. I agree that it’s worthwhile to check this finding in a prospective trial ... but this hypothesis does seem to be a reach.”
Dr. Weber noted that both ACE inhibitors and ARBs increase the level of the ACE2 enzyme to which the COVID-19 virus binds in the lungs.
“The ACE inhibitors do so by inhibiting the enzyme’s action and thus stimulate further enzyme production; the ARBs block the effects of angiotensin II, which results in high angiotensin II levels that also upregulate ACE2 production,” he said. “Perhaps the ACE inhibitors, by binding to the ACE enzyme, can in some way interfere with the enzyme’s uptake of the COVID virus and thus provide some measure of clinical protection. This is possible, but why would this effect be apparent only in older people?”
John McMurray, MD, professor of medical cardiology at the University of Glasgow, Scotland, added: “This looks like a subgroup of a subgroup type analysis based on small numbers of events – I think there were only 77 hospitalizations among the 722 patients treated with an ACE inhibitor, and the Medicare Advantage subgroup was only 581 of those 722 patients.
“The hazard ratio had wide 95% CI [confidence interval] and a modest P value,” Dr. McMurray added. “So yes, interesting and hypothesis-generating, but not definitive.”
New meta-analysis
The new meta-analysis of all data so far available on ACE inhibitor and ARB use for patients with COVID-19 was published online in Annals of Internal Medicine on May 15.
The analysis is a living, systematic review with ongoing literature surveillance and critical appraisal, which will be updated as new data become available. It included 14 observational studies.
The authors, led by Katherine M. Mackey, MD, VA Portland Health Care System, Oregon, concluded: “High-certainty evidence suggests that ACE-inhibitor or ARB use is not associated with more severe COVID-19 disease, and moderate certainty evidence suggested no association between use of these medications and positive SARS-CoV-2 test results among symptomatic patients. Whether these medications increase the risk for mild or asymptomatic disease or are beneficial in COVID-19 treatment remains uncertain.”
In an accompanying editorial, William G. Kussmaul III, MD, Drexel University, Philadelphia, said that initial fears that these drugs may be harmful for patients with COVID-19 now seem to have been unfounded.
“We now have reasonable reassurance that drugs that alter the renin-angiotensin system do not pose substantial threats as either COVID-19 risk factors or severity multipliers,” he wrote.
A version of this article originally appeared on Medscape.com.