User login
Buttocks Injection Dangers Exposed
Injections into the buttocks is a popular and dangerous trend in Hispanic communities that can cause disfiguration, kidney failure, and even death.
Dr. Franco Reyes Jácome performs a complex reconstructive surgery to extract the substance once it has hardened. Dermatologists can extract the substance using liposuction if it is still in liquid form.
Markette Smith interviewed Dr. Jácome at the annual meeting of The American Society for Aesthetic Plastic Surgery.
Injections into the buttocks is a popular and dangerous trend in Hispanic communities that can cause disfiguration, kidney failure, and even death.
Dr. Franco Reyes Jácome performs a complex reconstructive surgery to extract the substance once it has hardened. Dermatologists can extract the substance using liposuction if it is still in liquid form.
Markette Smith interviewed Dr. Jácome at the annual meeting of The American Society for Aesthetic Plastic Surgery.
Injections into the buttocks is a popular and dangerous trend in Hispanic communities that can cause disfiguration, kidney failure, and even death.
Dr. Franco Reyes Jácome performs a complex reconstructive surgery to extract the substance once it has hardened. Dermatologists can extract the substance using liposuction if it is still in liquid form.
Markette Smith interviewed Dr. Jácome at the annual meeting of The American Society for Aesthetic Plastic Surgery.
Novel Device Uses Ultrasound to Treat Acne
PHOENIX – An investigational intense-therapy ultrasound device safely and effectively treated mild to moderate acne in a preliminary study.
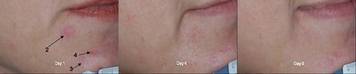
The device, manufactured by Xthetix Inc., was used to treat 5-15 active acne lesions on one side of the face for 5 consecutive days in 18 women and 7 men with a mean age of 26 years. Of the patients, about 84% showed significant improvement after five treatment sessions.
According to a poster presented during the annual meeting of the American Society for Laser Medicine and Surgery, energy generated by the device is delivered to the level of the sebaceous gland, "raising the temperature 5-15 degrees Celsius above ambient skin temperature. It is designed not to cause thermal coagulation, but to increase the tissue temperature for a period of time sufficient to produce a therapeutic effect."
In an interview, lead investigator Dr. Bill Halmi said that although there are a few devices currently on the market that use heat to reduce the duration of an inflammatory acne papule, the machine uses ultrasound to heat the targeted area.
"Putting the energy intradermally into the pilosebaceous unit is the unique aspect of the device," he said. "It changes the inner workings of the gland, kills bacteria, [and] peaks the inflammatory process, among other things."
Each treatment session lasted about 15 minutes. The contralateral side of the face did not receive any ultrasound treatment and served as the control.
The researchers took photographs on all visit days and a masked reviewer conducted posttreatment and facial acne assessments at every visit. Each patient completed daily pain and acne assessments.
Dr. Halmi, who practices dermatology in Phoenix, reported that the greatest percentage of lesion clearance (30%) occurred on day 4 of treatment. "This differs from 'blue light' devices that expect to see improvements after at least 1 week of treatment," he said. "Going into the study we really weren't certain that we would see an immediate effect from the device. We were certainly pleased to discover that this ultrasound device measurably reduced the duration of an acne lesion."
A majority of patients (84%) reported moderate to significant improvement of their treated sides during the course of treatment, while 40% experienced mild transient erythema that lasted less than 30 minutes. The average pain score was 3 on a scale of 1-10, with 10 being the most severe.
The findings suggest that "there is a role for heat in reducing the duration of an acne lesion," Dr. Halmi said. "The advantage ultrasound has is that it can target that heat to the depth desired."
He cautioned that the study is preliminary and that, while encouraging, "repeated studies using more patients will help confirm our findings. Additionally, the role of ultrasound in the prophylactic treatment of acne remains to be revealed."
Dr. Halmi disclosed that he is a paid consultant for Xthetix.
PHOENIX – An investigational intense-therapy ultrasound device safely and effectively treated mild to moderate acne in a preliminary study.
The device, manufactured by Xthetix Inc., was used to treat 5-15 active acne lesions on one side of the face for 5 consecutive days in 18 women and 7 men with a mean age of 26 years. Of the patients, about 84% showed significant improvement after five treatment sessions.
According to a poster presented during the annual meeting of the American Society for Laser Medicine and Surgery, energy generated by the device is delivered to the level of the sebaceous gland, "raising the temperature 5-15 degrees Celsius above ambient skin temperature. It is designed not to cause thermal coagulation, but to increase the tissue temperature for a period of time sufficient to produce a therapeutic effect."
In an interview, lead investigator Dr. Bill Halmi said that although there are a few devices currently on the market that use heat to reduce the duration of an inflammatory acne papule, the machine uses ultrasound to heat the targeted area.
"Putting the energy intradermally into the pilosebaceous unit is the unique aspect of the device," he said. "It changes the inner workings of the gland, kills bacteria, [and] peaks the inflammatory process, among other things."
Each treatment session lasted about 15 minutes. The contralateral side of the face did not receive any ultrasound treatment and served as the control.
The researchers took photographs on all visit days and a masked reviewer conducted posttreatment and facial acne assessments at every visit. Each patient completed daily pain and acne assessments.
Dr. Halmi, who practices dermatology in Phoenix, reported that the greatest percentage of lesion clearance (30%) occurred on day 4 of treatment. "This differs from 'blue light' devices that expect to see improvements after at least 1 week of treatment," he said. "Going into the study we really weren't certain that we would see an immediate effect from the device. We were certainly pleased to discover that this ultrasound device measurably reduced the duration of an acne lesion."
A majority of patients (84%) reported moderate to significant improvement of their treated sides during the course of treatment, while 40% experienced mild transient erythema that lasted less than 30 minutes. The average pain score was 3 on a scale of 1-10, with 10 being the most severe.
The findings suggest that "there is a role for heat in reducing the duration of an acne lesion," Dr. Halmi said. "The advantage ultrasound has is that it can target that heat to the depth desired."
He cautioned that the study is preliminary and that, while encouraging, "repeated studies using more patients will help confirm our findings. Additionally, the role of ultrasound in the prophylactic treatment of acne remains to be revealed."
Dr. Halmi disclosed that he is a paid consultant for Xthetix.
PHOENIX – An investigational intense-therapy ultrasound device safely and effectively treated mild to moderate acne in a preliminary study.
The device, manufactured by Xthetix Inc., was used to treat 5-15 active acne lesions on one side of the face for 5 consecutive days in 18 women and 7 men with a mean age of 26 years. Of the patients, about 84% showed significant improvement after five treatment sessions.
According to a poster presented during the annual meeting of the American Society for Laser Medicine and Surgery, energy generated by the device is delivered to the level of the sebaceous gland, "raising the temperature 5-15 degrees Celsius above ambient skin temperature. It is designed not to cause thermal coagulation, but to increase the tissue temperature for a period of time sufficient to produce a therapeutic effect."
In an interview, lead investigator Dr. Bill Halmi said that although there are a few devices currently on the market that use heat to reduce the duration of an inflammatory acne papule, the machine uses ultrasound to heat the targeted area.
"Putting the energy intradermally into the pilosebaceous unit is the unique aspect of the device," he said. "It changes the inner workings of the gland, kills bacteria, [and] peaks the inflammatory process, among other things."
Each treatment session lasted about 15 minutes. The contralateral side of the face did not receive any ultrasound treatment and served as the control.
The researchers took photographs on all visit days and a masked reviewer conducted posttreatment and facial acne assessments at every visit. Each patient completed daily pain and acne assessments.
Dr. Halmi, who practices dermatology in Phoenix, reported that the greatest percentage of lesion clearance (30%) occurred on day 4 of treatment. "This differs from 'blue light' devices that expect to see improvements after at least 1 week of treatment," he said. "Going into the study we really weren't certain that we would see an immediate effect from the device. We were certainly pleased to discover that this ultrasound device measurably reduced the duration of an acne lesion."
A majority of patients (84%) reported moderate to significant improvement of their treated sides during the course of treatment, while 40% experienced mild transient erythema that lasted less than 30 minutes. The average pain score was 3 on a scale of 1-10, with 10 being the most severe.
The findings suggest that "there is a role for heat in reducing the duration of an acne lesion," Dr. Halmi said. "The advantage ultrasound has is that it can target that heat to the depth desired."
He cautioned that the study is preliminary and that, while encouraging, "repeated studies using more patients will help confirm our findings. Additionally, the role of ultrasound in the prophylactic treatment of acne remains to be revealed."
Dr. Halmi disclosed that he is a paid consultant for Xthetix.
Botox Comparable to Amitriptyline for Migraine Prophylaxis
Botulinum toxin type A, celebrated by seekers of eternal youthfulness for its ability to temporarily smooth wrinkles, also might provide relief of chronic daily migraines, Brazilian investigators suggest.
A single treatment session consisting of botulinum toxin type A (OnabotulinumtoxinA, BTX-A) injections to 15 sites on the head was comparable to daily oral dosing of the tricyclic antidepressant (TCA) amitriptyline for preventing chronic daily migraine over 90 days, reported Elza Magalhães and her colleagues from the Federal University of Bahia, Brazil (Clin. Neurol. Neurosurg. 2010 April 18; [doi:10.1016/j.clineuro.2010.02.004]).
Both BTX-A injections and amitriptyline reduced the number of pain days by at least 50% in more than two-thirds of patients with chronic daily migraine, and each treatment cut the intensity of patient-rated pain approximately in half, according to the investigators.
“Considering the clinical benefits and the lack of undesirable side effects, such as weight gain and constipation, we argue that BTX-A should be considered for use in patients with chronic headaches as an alternative therapy or should be considered for use in patients who have contraindications for the use of other classes of drugs,” Ms. Magalhães and her coauthors wrote.
They enrolled 72 adults (aged 18 to 56 years) with chronic daily migraine according to International Classification of Headache Disorders-II criteria, and randomly assigned them to receive either BTX-A in a total dose of 250 units (35 patients), or 25 mg or 50 mg of amitriptyline daily (37 patients). Patients on the oral drug initially were given the 25-mg dose, and were titrated upward to the 50 mg dose if they did not have remission of symptoms from the lower dose at 30 days.
Patients assigned to BTX-A received 15 injections into pre-determined sites around the head. The injection sites included areas over sensitive innervations, including the trigeminal, C2, and C3 nerves.
Patients in both treatment groups were evaluated monthly for pain intensity, number of pain days, number of drug doses for pain, and side effects.
In all, 72% of patients treated with amitriptyline had a 50% or greater reduction in pain days, compared with 68% of the patients treated with BTX-A. The mean reported reduction in pain intensity by visual analog scale over baseline was 56% for patients on the oral drug vs. 50% for patients who received the injections. Similar percentages of patients reduced their use of pain drugs in the amitriptyline (77%) and BTX-A groups (71%).
There were no significant between-group differences in either patient or physician assessment of improvement at 90 days, with 88% of patients on the oral medication and 84% of patients on the injections reporting improvement at study end. The investigators determined that 87% of patients improved while taking the antidepressant and 88% of patients improved after receiving the toxin.
Adverse events generally were higher in the amitriptyline group, including the side effects of weight gain (58% for the oral drug vs. 12% for BTX-A), somnolence (53% vs. 4%), dry mouth (44% vs. 14%), and constipation (39% vs. 0%).
The investigators acknowledged that BTX-A is both more expensive and more invasive than oral medications, and suggested additional research to determine which subgroups of migraine sufferers might benefit from the injections compared with other means of migraine prevention.
The study is part of the doctorate of Ms. Magalhães, who received a grant from the Brazilian Federal Agency for the Support and Evaluation of Graduate Education. A coauthor received a research grant from Brazil’s National Council for Scientific and Technological Development. The authors did not report conflicts of interest.
Botulinum toxin type A, celebrated by seekers of eternal youthfulness for its ability to temporarily smooth wrinkles, also might provide relief of chronic daily migraines, Brazilian investigators suggest.
A single treatment session consisting of botulinum toxin type A (OnabotulinumtoxinA, BTX-A) injections to 15 sites on the head was comparable to daily oral dosing of the tricyclic antidepressant (TCA) amitriptyline for preventing chronic daily migraine over 90 days, reported Elza Magalhães and her colleagues from the Federal University of Bahia, Brazil (Clin. Neurol. Neurosurg. 2010 April 18; [doi:10.1016/j.clineuro.2010.02.004]).
Both BTX-A injections and amitriptyline reduced the number of pain days by at least 50% in more than two-thirds of patients with chronic daily migraine, and each treatment cut the intensity of patient-rated pain approximately in half, according to the investigators.
“Considering the clinical benefits and the lack of undesirable side effects, such as weight gain and constipation, we argue that BTX-A should be considered for use in patients with chronic headaches as an alternative therapy or should be considered for use in patients who have contraindications for the use of other classes of drugs,” Ms. Magalhães and her coauthors wrote.
They enrolled 72 adults (aged 18 to 56 years) with chronic daily migraine according to International Classification of Headache Disorders-II criteria, and randomly assigned them to receive either BTX-A in a total dose of 250 units (35 patients), or 25 mg or 50 mg of amitriptyline daily (37 patients). Patients on the oral drug initially were given the 25-mg dose, and were titrated upward to the 50 mg dose if they did not have remission of symptoms from the lower dose at 30 days.
Patients assigned to BTX-A received 15 injections into pre-determined sites around the head. The injection sites included areas over sensitive innervations, including the trigeminal, C2, and C3 nerves.
Patients in both treatment groups were evaluated monthly for pain intensity, number of pain days, number of drug doses for pain, and side effects.
In all, 72% of patients treated with amitriptyline had a 50% or greater reduction in pain days, compared with 68% of the patients treated with BTX-A. The mean reported reduction in pain intensity by visual analog scale over baseline was 56% for patients on the oral drug vs. 50% for patients who received the injections. Similar percentages of patients reduced their use of pain drugs in the amitriptyline (77%) and BTX-A groups (71%).
There were no significant between-group differences in either patient or physician assessment of improvement at 90 days, with 88% of patients on the oral medication and 84% of patients on the injections reporting improvement at study end. The investigators determined that 87% of patients improved while taking the antidepressant and 88% of patients improved after receiving the toxin.
Adverse events generally were higher in the amitriptyline group, including the side effects of weight gain (58% for the oral drug vs. 12% for BTX-A), somnolence (53% vs. 4%), dry mouth (44% vs. 14%), and constipation (39% vs. 0%).
The investigators acknowledged that BTX-A is both more expensive and more invasive than oral medications, and suggested additional research to determine which subgroups of migraine sufferers might benefit from the injections compared with other means of migraine prevention.
The study is part of the doctorate of Ms. Magalhães, who received a grant from the Brazilian Federal Agency for the Support and Evaluation of Graduate Education. A coauthor received a research grant from Brazil’s National Council for Scientific and Technological Development. The authors did not report conflicts of interest.
Botulinum toxin type A, celebrated by seekers of eternal youthfulness for its ability to temporarily smooth wrinkles, also might provide relief of chronic daily migraines, Brazilian investigators suggest.
A single treatment session consisting of botulinum toxin type A (OnabotulinumtoxinA, BTX-A) injections to 15 sites on the head was comparable to daily oral dosing of the tricyclic antidepressant (TCA) amitriptyline for preventing chronic daily migraine over 90 days, reported Elza Magalhães and her colleagues from the Federal University of Bahia, Brazil (Clin. Neurol. Neurosurg. 2010 April 18; [doi:10.1016/j.clineuro.2010.02.004]).
Both BTX-A injections and amitriptyline reduced the number of pain days by at least 50% in more than two-thirds of patients with chronic daily migraine, and each treatment cut the intensity of patient-rated pain approximately in half, according to the investigators.
“Considering the clinical benefits and the lack of undesirable side effects, such as weight gain and constipation, we argue that BTX-A should be considered for use in patients with chronic headaches as an alternative therapy or should be considered for use in patients who have contraindications for the use of other classes of drugs,” Ms. Magalhães and her coauthors wrote.
They enrolled 72 adults (aged 18 to 56 years) with chronic daily migraine according to International Classification of Headache Disorders-II criteria, and randomly assigned them to receive either BTX-A in a total dose of 250 units (35 patients), or 25 mg or 50 mg of amitriptyline daily (37 patients). Patients on the oral drug initially were given the 25-mg dose, and were titrated upward to the 50 mg dose if they did not have remission of symptoms from the lower dose at 30 days.
Patients assigned to BTX-A received 15 injections into pre-determined sites around the head. The injection sites included areas over sensitive innervations, including the trigeminal, C2, and C3 nerves.
Patients in both treatment groups were evaluated monthly for pain intensity, number of pain days, number of drug doses for pain, and side effects.
In all, 72% of patients treated with amitriptyline had a 50% or greater reduction in pain days, compared with 68% of the patients treated with BTX-A. The mean reported reduction in pain intensity by visual analog scale over baseline was 56% for patients on the oral drug vs. 50% for patients who received the injections. Similar percentages of patients reduced their use of pain drugs in the amitriptyline (77%) and BTX-A groups (71%).
There were no significant between-group differences in either patient or physician assessment of improvement at 90 days, with 88% of patients on the oral medication and 84% of patients on the injections reporting improvement at study end. The investigators determined that 87% of patients improved while taking the antidepressant and 88% of patients improved after receiving the toxin.
Adverse events generally were higher in the amitriptyline group, including the side effects of weight gain (58% for the oral drug vs. 12% for BTX-A), somnolence (53% vs. 4%), dry mouth (44% vs. 14%), and constipation (39% vs. 0%).
The investigators acknowledged that BTX-A is both more expensive and more invasive than oral medications, and suggested additional research to determine which subgroups of migraine sufferers might benefit from the injections compared with other means of migraine prevention.
The study is part of the doctorate of Ms. Magalhães, who received a grant from the Brazilian Federal Agency for the Support and Evaluation of Graduate Education. A coauthor received a research grant from Brazil’s National Council for Scientific and Technological Development. The authors did not report conflicts of interest.
Unsupervised Physician Extenders Called Key Malpractice Concern
Improper use of "physician extenders," a lack of informed consent, and patient dissatisfaction are some of the top reasons why patients sue, and all are easily preventable, according to Dr. David J. Goldberg.
The first - the use of unsupervised or improperly trained physician assistants, nurse practitioners, or other physician extenders - hits home for many dermatologists. According to the American Academy of Dermatology, in 2010, 36% of physicians will use NPs and PAs in their practice, up from 30% in 2007 and 20% in 2002, Dr. Goldberg said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.

"NPs and PAs who work for core physicians are clearly the most qualified nonphysicians to perform these procedures," said Dr. Goldberg, director of dermatologic laser research at Mount Sinai School of Medicine, New York. Many have received cosmetic training through the Aesthetic Extender Symposium (www.aestheticextendersymposium.com), he said.
However, there are still risks. A 2006 American Society for Dermatologic Surgery survey found that 51% of ASDS members reported seeing nonphysician, nonsupervised physician-extender complications in their practice, with the two most common being misdiagnosed skin cancer and scarring following dermatologic procedures.
"If the [physician extender] is sued, so will be the provider who is affiliated with the PE," said Dr. Goldberg, who also is on the faculty of Fordham University School of Law in New York.
Poorly informed or uninformed consent is another moneymaker for medical malpractice lawyers in the field of dermatology, according to Dr. Goldberg. "Because dermatologists tend to see large numbers of patients, there is a tendency to be overwhelmed by the paperwork associated with quality informed consent," he said.
One procedure to be especially careful about is botulinum toxin type A injections - there were 2,464,123 in 2008, according to the American Society for Aesthetic Plastic Surgery. The black box warning on Botox reads "swallowing and breathing difficulties can be life threatening and there have been reports of death."
Dr. Goldberg encouraged physicians to instruct patients to read the warning on botulinum toxin "each and every time" they receive it. He also encouraged discussion about these risks and the procedure's other rare but potential side effects, including generalized muscle weakness, diplopia, ptosis, dysphagia, dysphonia, dysarthria, and urinary incontinence.
He noted that many of these potential complications have never been reported with the cosmetic use of botulinum toxin.
Finally, Dr. Goldberg said that dermatologists can keep legal troubles at bay simply by keeping patients happy. He cited a 2006 retrospective chart study of all patients who received botulinum toxin injections over a 2-year period at a private dermatology clinic. The retention rate was 55%. However, the "institution of a 2-week posttreatment evaluation increased the retention rate from 55% to 67%," said Dr. Goldberg (Dermatol. Surg. 2006;32:212-5).
"Probably more important in keeping patients happy - and keeping them coming back - is to communicate with patients," he advised. "Treat each patient as if they are special. Pay total attention to their concerns. They will appreciate your one-on-one interaction with them."
Dr. Goldberg is a founding director of the Aesthetic Extended Symposium. SDEF and this news organization are owned by Elsevier.
Improper use of "physician extenders," a lack of informed consent, and patient dissatisfaction are some of the top reasons why patients sue, and all are easily preventable, according to Dr. David J. Goldberg.
The first - the use of unsupervised or improperly trained physician assistants, nurse practitioners, or other physician extenders - hits home for many dermatologists. According to the American Academy of Dermatology, in 2010, 36% of physicians will use NPs and PAs in their practice, up from 30% in 2007 and 20% in 2002, Dr. Goldberg said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
"NPs and PAs who work for core physicians are clearly the most qualified nonphysicians to perform these procedures," said Dr. Goldberg, director of dermatologic laser research at Mount Sinai School of Medicine, New York. Many have received cosmetic training through the Aesthetic Extender Symposium (www.aestheticextendersymposium.com), he said.
However, there are still risks. A 2006 American Society for Dermatologic Surgery survey found that 51% of ASDS members reported seeing nonphysician, nonsupervised physician-extender complications in their practice, with the two most common being misdiagnosed skin cancer and scarring following dermatologic procedures.
"If the [physician extender] is sued, so will be the provider who is affiliated with the PE," said Dr. Goldberg, who also is on the faculty of Fordham University School of Law in New York.
Poorly informed or uninformed consent is another moneymaker for medical malpractice lawyers in the field of dermatology, according to Dr. Goldberg. "Because dermatologists tend to see large numbers of patients, there is a tendency to be overwhelmed by the paperwork associated with quality informed consent," he said.
One procedure to be especially careful about is botulinum toxin type A injections - there were 2,464,123 in 2008, according to the American Society for Aesthetic Plastic Surgery. The black box warning on Botox reads "swallowing and breathing difficulties can be life threatening and there have been reports of death."
Dr. Goldberg encouraged physicians to instruct patients to read the warning on botulinum toxin "each and every time" they receive it. He also encouraged discussion about these risks and the procedure's other rare but potential side effects, including generalized muscle weakness, diplopia, ptosis, dysphagia, dysphonia, dysarthria, and urinary incontinence.
He noted that many of these potential complications have never been reported with the cosmetic use of botulinum toxin.
Finally, Dr. Goldberg said that dermatologists can keep legal troubles at bay simply by keeping patients happy. He cited a 2006 retrospective chart study of all patients who received botulinum toxin injections over a 2-year period at a private dermatology clinic. The retention rate was 55%. However, the "institution of a 2-week posttreatment evaluation increased the retention rate from 55% to 67%," said Dr. Goldberg (Dermatol. Surg. 2006;32:212-5).
"Probably more important in keeping patients happy - and keeping them coming back - is to communicate with patients," he advised. "Treat each patient as if they are special. Pay total attention to their concerns. They will appreciate your one-on-one interaction with them."
Dr. Goldberg is a founding director of the Aesthetic Extended Symposium. SDEF and this news organization are owned by Elsevier.
Improper use of "physician extenders," a lack of informed consent, and patient dissatisfaction are some of the top reasons why patients sue, and all are easily preventable, according to Dr. David J. Goldberg.
The first - the use of unsupervised or improperly trained physician assistants, nurse practitioners, or other physician extenders - hits home for many dermatologists. According to the American Academy of Dermatology, in 2010, 36% of physicians will use NPs and PAs in their practice, up from 30% in 2007 and 20% in 2002, Dr. Goldberg said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
"NPs and PAs who work for core physicians are clearly the most qualified nonphysicians to perform these procedures," said Dr. Goldberg, director of dermatologic laser research at Mount Sinai School of Medicine, New York. Many have received cosmetic training through the Aesthetic Extender Symposium (www.aestheticextendersymposium.com), he said.
However, there are still risks. A 2006 American Society for Dermatologic Surgery survey found that 51% of ASDS members reported seeing nonphysician, nonsupervised physician-extender complications in their practice, with the two most common being misdiagnosed skin cancer and scarring following dermatologic procedures.
"If the [physician extender] is sued, so will be the provider who is affiliated with the PE," said Dr. Goldberg, who also is on the faculty of Fordham University School of Law in New York.
Poorly informed or uninformed consent is another moneymaker for medical malpractice lawyers in the field of dermatology, according to Dr. Goldberg. "Because dermatologists tend to see large numbers of patients, there is a tendency to be overwhelmed by the paperwork associated with quality informed consent," he said.
One procedure to be especially careful about is botulinum toxin type A injections - there were 2,464,123 in 2008, according to the American Society for Aesthetic Plastic Surgery. The black box warning on Botox reads "swallowing and breathing difficulties can be life threatening and there have been reports of death."
Dr. Goldberg encouraged physicians to instruct patients to read the warning on botulinum toxin "each and every time" they receive it. He also encouraged discussion about these risks and the procedure's other rare but potential side effects, including generalized muscle weakness, diplopia, ptosis, dysphagia, dysphonia, dysarthria, and urinary incontinence.
He noted that many of these potential complications have never been reported with the cosmetic use of botulinum toxin.
Finally, Dr. Goldberg said that dermatologists can keep legal troubles at bay simply by keeping patients happy. He cited a 2006 retrospective chart study of all patients who received botulinum toxin injections over a 2-year period at a private dermatology clinic. The retention rate was 55%. However, the "institution of a 2-week posttreatment evaluation increased the retention rate from 55% to 67%," said Dr. Goldberg (Dermatol. Surg. 2006;32:212-5).
"Probably more important in keeping patients happy - and keeping them coming back - is to communicate with patients," he advised. "Treat each patient as if they are special. Pay total attention to their concerns. They will appreciate your one-on-one interaction with them."
Dr. Goldberg is a founding director of the Aesthetic Extended Symposium. SDEF and this news organization are owned by Elsevier.
Frequent, Lower Botox Dosing Best for Some Areas
Lower doses of botulinum toxin type A delivered more frequently yield better results in certain areas of the face, according to Dr. Joel L. Cohen.
While crow's feet and the glabella still do better with a higher dose and a 3- to 4-month dosing interval, there are several areas that do better with half the typical dose and half the dosing interval.

The forehead is one such area. "We use lighter doses in the forehead because we really want things to be more natural in terms of still having movement," Dr. Cohen said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif. "Sometimes these patients need to be dosed in the forehead every 8-10 weeks, whereas in the glabella and the crow's feet, if you're using regular doses, you might only need to inject them every 3.5 or 4 months. Sometimes they're in a cycle where they come in for Botox or Dysport in the forehead every 8 or 10 weeks and every 16 weeks or 18 weeks for the glabella and the crow's feet."
Brow lifts also do better with lower doses at shorter intervals. But Dr. Cohen, director of AboutSkin Dermatology and DermSurgery, Englewood, Colo., cautioned that brow lifts with botulinum toxin should not be attempted in patients who have a lot of sagging in the lateral brow. These patients require surgery; botulinum toxin should be reserved for patients with mild redundancy between the brow and the eyelid. Occasionally, patients with moderate sagging can benefit as well.
Around the mouth, Dr. Cohen uses 5-7 units of botulinum toxin to treat the vertical muscle columns of the upper lip and to prevent etched-in lines. At the same time, he uses 2-3 units in the lower lip, "so it doesn't feel funny." Once again, this needs to be repeated every 8-10 weeks, he said.
There is another class of patients in which low doses of perioral botulinum toxin may be beneficial. Studies have shown that healing after resurfacing procedures tends to be better after the area has previously been immobilized with botulinum toxin.
"There's decreasing contraction across the wound, so you're not imprinting lines where you already have lines," Dr. Cohen said. "And the second thing is there is decreased inflammation because there's less mobility of the area."
For one-time erbium or CO2 laser resurfacing, Dr. Cohen recommends the patient be treated with botulinum toxin a week to 10 days before. "Or you can do pretreatment a week or two before you do a fractionated ablative laser where the plan is to do three, four, or five treatments. By treating the patient with the fractionated laser every 3 weeks, you may really be able to get a session of three treatments in for every one pretreatment with Botox. The overall goal is less movement across what you're trying to heal."
Dr. Cohen acknowledged participating in clinical trials and serving as a consultant for Allergan, Medicis, Johnson and Johnson/Mentor, and Merz. SDEF and this news organization are owned by Elsevier.
Lower doses of botulinum toxin type A delivered more frequently yield better results in certain areas of the face, according to Dr. Joel L. Cohen.
While crow's feet and the glabella still do better with a higher dose and a 3- to 4-month dosing interval, there are several areas that do better with half the typical dose and half the dosing interval.
The forehead is one such area. "We use lighter doses in the forehead because we really want things to be more natural in terms of still having movement," Dr. Cohen said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif. "Sometimes these patients need to be dosed in the forehead every 8-10 weeks, whereas in the glabella and the crow's feet, if you're using regular doses, you might only need to inject them every 3.5 or 4 months. Sometimes they're in a cycle where they come in for Botox or Dysport in the forehead every 8 or 10 weeks and every 16 weeks or 18 weeks for the glabella and the crow's feet."
Brow lifts also do better with lower doses at shorter intervals. But Dr. Cohen, director of AboutSkin Dermatology and DermSurgery, Englewood, Colo., cautioned that brow lifts with botulinum toxin should not be attempted in patients who have a lot of sagging in the lateral brow. These patients require surgery; botulinum toxin should be reserved for patients with mild redundancy between the brow and the eyelid. Occasionally, patients with moderate sagging can benefit as well.
Around the mouth, Dr. Cohen uses 5-7 units of botulinum toxin to treat the vertical muscle columns of the upper lip and to prevent etched-in lines. At the same time, he uses 2-3 units in the lower lip, "so it doesn't feel funny." Once again, this needs to be repeated every 8-10 weeks, he said.
There is another class of patients in which low doses of perioral botulinum toxin may be beneficial. Studies have shown that healing after resurfacing procedures tends to be better after the area has previously been immobilized with botulinum toxin.
"There's decreasing contraction across the wound, so you're not imprinting lines where you already have lines," Dr. Cohen said. "And the second thing is there is decreased inflammation because there's less mobility of the area."
For one-time erbium or CO2 laser resurfacing, Dr. Cohen recommends the patient be treated with botulinum toxin a week to 10 days before. "Or you can do pretreatment a week or two before you do a fractionated ablative laser where the plan is to do three, four, or five treatments. By treating the patient with the fractionated laser every 3 weeks, you may really be able to get a session of three treatments in for every one pretreatment with Botox. The overall goal is less movement across what you're trying to heal."
Dr. Cohen acknowledged participating in clinical trials and serving as a consultant for Allergan, Medicis, Johnson and Johnson/Mentor, and Merz. SDEF and this news organization are owned by Elsevier.
Lower doses of botulinum toxin type A delivered more frequently yield better results in certain areas of the face, according to Dr. Joel L. Cohen.
While crow's feet and the glabella still do better with a higher dose and a 3- to 4-month dosing interval, there are several areas that do better with half the typical dose and half the dosing interval.
The forehead is one such area. "We use lighter doses in the forehead because we really want things to be more natural in terms of still having movement," Dr. Cohen said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif. "Sometimes these patients need to be dosed in the forehead every 8-10 weeks, whereas in the glabella and the crow's feet, if you're using regular doses, you might only need to inject them every 3.5 or 4 months. Sometimes they're in a cycle where they come in for Botox or Dysport in the forehead every 8 or 10 weeks and every 16 weeks or 18 weeks for the glabella and the crow's feet."
Brow lifts also do better with lower doses at shorter intervals. But Dr. Cohen, director of AboutSkin Dermatology and DermSurgery, Englewood, Colo., cautioned that brow lifts with botulinum toxin should not be attempted in patients who have a lot of sagging in the lateral brow. These patients require surgery; botulinum toxin should be reserved for patients with mild redundancy between the brow and the eyelid. Occasionally, patients with moderate sagging can benefit as well.
Around the mouth, Dr. Cohen uses 5-7 units of botulinum toxin to treat the vertical muscle columns of the upper lip and to prevent etched-in lines. At the same time, he uses 2-3 units in the lower lip, "so it doesn't feel funny." Once again, this needs to be repeated every 8-10 weeks, he said.
There is another class of patients in which low doses of perioral botulinum toxin may be beneficial. Studies have shown that healing after resurfacing procedures tends to be better after the area has previously been immobilized with botulinum toxin.
"There's decreasing contraction across the wound, so you're not imprinting lines where you already have lines," Dr. Cohen said. "And the second thing is there is decreased inflammation because there's less mobility of the area."
For one-time erbium or CO2 laser resurfacing, Dr. Cohen recommends the patient be treated with botulinum toxin a week to 10 days before. "Or you can do pretreatment a week or two before you do a fractionated ablative laser where the plan is to do three, four, or five treatments. By treating the patient with the fractionated laser every 3 weeks, you may really be able to get a session of three treatments in for every one pretreatment with Botox. The overall goal is less movement across what you're trying to heal."
Dr. Cohen acknowledged participating in clinical trials and serving as a consultant for Allergan, Medicis, Johnson and Johnson/Mentor, and Merz. SDEF and this news organization are owned by Elsevier.
Treatments Minimize Infantile Hemangiomas
New medical and surgical treatments can minimize infantile hemangiomas in their proliferative phase and decrease residual scarring after they involute, according to Dr. Brandie J. Metz.
The first decision in treating a hemangioma is whether to use a surgical or medical approach, Dr. Metz said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.

Medical treatment is usually a first-line choice, although surgery may be considered when the patient presents with severe refractory pain from ulceration or when residua after involution would likely require surgical treatment. "In that case, why wait?" said Dr. Metz, the director of pediatric dermatology at the University of California, Irvine.
In the past 2 years, propranolol has gained acceptance as an effective medical therapy. Its use was first noted in a case series published in 2008 (N. Engl. J. Med. 2008;358:2649-51). In this French report, 11 infants received propranolol for varying treatment periods. Within 24 hours, all of the hemangiomas responded with softening and a change in color from red to purple, indicating decreased vascularity.
The treatment is not without risks, Dr. Metz noted. "Possible side effects are bradycardia, hypotension, hypoglycemia, and bronchospasm. A gradual dose escalation with close monitoring is the best way to go."
She is an investigator for a large, double-blind, placebo-controlled trial of propranolol that is currently underway. Patients receive either placebo or propranolol at 3 mg/kg for 15 days, followed by another 15 days at 4 mg/kg. The primary outcome will be hemangioma thickness variation measured by ultrasonography from baseline to 1 month.
When a lesion is easily resectable and a patient has failed medical therapy, or if ulceration and pain are present, surgery can be considered. Generally, thin plaques with a gradual slope have a better surgical prognosis. A circular incision around the lesion, with purse string closure, is the usual technique. A 2002 study of 25 patients found that this method reduced hemangiomas by a mean of 73% in width and 45% in length (Plast. Reconstr. Surg. 2002;109:1544-54).
Lasers can treat superficial proliferating hemangiomas, as well as the residua left after involution, Dr. Metz said. The pulsed dye laser is one option. Short pulses of 0.45-1.5 millisecond are used at either a 585- or 595-nm wavelength. The concomitant use of a dynamic cooling device makes the treatment less painful and can allow the use of a higher fluence.
Several studies attest to the success of pulsed dye lasers for hemangiomas. A 2009 study of 90 patients with 105 hemangiomas reported complete or near-complete clearance of color for 81% and thickness for 64%. Although there was no scarring or atrophy, one patient did develop an ulceration that resolved. Hyperpigmentation occurred in 4% and hypopigmentation in 14% (Derm. Surg. 2009;35:1947-54).
A 2006 study noted complications related to pulsed dye laser treatment. Of 12 patients with segmental facial hemangiomas, there were 8 ulcerations and 4 with atrophic scarring (Lasers Surg. Med. 2006;38:116-23).
Two published reports detail the use of fractionated laser for residua. A 2008 report found that the laser effectively decreased fibrofatty tissue and redundant skin that resulted from an extensive mixed facial hemangioma (Derm. Surg. 2008;34:1112-4). A 2009 report found similar results on residua from another facial hemangioma (Arch. Dermatol. 2009;145:748-50).
Dr. Metz disclosed that she is an investigator on the current propranolol trial, sponsored by University Hospital, Bordeaux, France.
SDEF and this news organization are owned by Elsevier.
New medical and surgical treatments can minimize infantile hemangiomas in their proliferative phase and decrease residual scarring after they involute, according to Dr. Brandie J. Metz.
The first decision in treating a hemangioma is whether to use a surgical or medical approach, Dr. Metz said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
Medical treatment is usually a first-line choice, although surgery may be considered when the patient presents with severe refractory pain from ulceration or when residua after involution would likely require surgical treatment. "In that case, why wait?" said Dr. Metz, the director of pediatric dermatology at the University of California, Irvine.
In the past 2 years, propranolol has gained acceptance as an effective medical therapy. Its use was first noted in a case series published in 2008 (N. Engl. J. Med. 2008;358:2649-51). In this French report, 11 infants received propranolol for varying treatment periods. Within 24 hours, all of the hemangiomas responded with softening and a change in color from red to purple, indicating decreased vascularity.
The treatment is not without risks, Dr. Metz noted. "Possible side effects are bradycardia, hypotension, hypoglycemia, and bronchospasm. A gradual dose escalation with close monitoring is the best way to go."
She is an investigator for a large, double-blind, placebo-controlled trial of propranolol that is currently underway. Patients receive either placebo or propranolol at 3 mg/kg for 15 days, followed by another 15 days at 4 mg/kg. The primary outcome will be hemangioma thickness variation measured by ultrasonography from baseline to 1 month.
When a lesion is easily resectable and a patient has failed medical therapy, or if ulceration and pain are present, surgery can be considered. Generally, thin plaques with a gradual slope have a better surgical prognosis. A circular incision around the lesion, with purse string closure, is the usual technique. A 2002 study of 25 patients found that this method reduced hemangiomas by a mean of 73% in width and 45% in length (Plast. Reconstr. Surg. 2002;109:1544-54).
Lasers can treat superficial proliferating hemangiomas, as well as the residua left after involution, Dr. Metz said. The pulsed dye laser is one option. Short pulses of 0.45-1.5 millisecond are used at either a 585- or 595-nm wavelength. The concomitant use of a dynamic cooling device makes the treatment less painful and can allow the use of a higher fluence.
Several studies attest to the success of pulsed dye lasers for hemangiomas. A 2009 study of 90 patients with 105 hemangiomas reported complete or near-complete clearance of color for 81% and thickness for 64%. Although there was no scarring or atrophy, one patient did develop an ulceration that resolved. Hyperpigmentation occurred in 4% and hypopigmentation in 14% (Derm. Surg. 2009;35:1947-54).
A 2006 study noted complications related to pulsed dye laser treatment. Of 12 patients with segmental facial hemangiomas, there were 8 ulcerations and 4 with atrophic scarring (Lasers Surg. Med. 2006;38:116-23).
Two published reports detail the use of fractionated laser for residua. A 2008 report found that the laser effectively decreased fibrofatty tissue and redundant skin that resulted from an extensive mixed facial hemangioma (Derm. Surg. 2008;34:1112-4). A 2009 report found similar results on residua from another facial hemangioma (Arch. Dermatol. 2009;145:748-50).
Dr. Metz disclosed that she is an investigator on the current propranolol trial, sponsored by University Hospital, Bordeaux, France.
SDEF and this news organization are owned by Elsevier.
New medical and surgical treatments can minimize infantile hemangiomas in their proliferative phase and decrease residual scarring after they involute, according to Dr. Brandie J. Metz.
The first decision in treating a hemangioma is whether to use a surgical or medical approach, Dr. Metz said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
Medical treatment is usually a first-line choice, although surgery may be considered when the patient presents with severe refractory pain from ulceration or when residua after involution would likely require surgical treatment. "In that case, why wait?" said Dr. Metz, the director of pediatric dermatology at the University of California, Irvine.
In the past 2 years, propranolol has gained acceptance as an effective medical therapy. Its use was first noted in a case series published in 2008 (N. Engl. J. Med. 2008;358:2649-51). In this French report, 11 infants received propranolol for varying treatment periods. Within 24 hours, all of the hemangiomas responded with softening and a change in color from red to purple, indicating decreased vascularity.
The treatment is not without risks, Dr. Metz noted. "Possible side effects are bradycardia, hypotension, hypoglycemia, and bronchospasm. A gradual dose escalation with close monitoring is the best way to go."
She is an investigator for a large, double-blind, placebo-controlled trial of propranolol that is currently underway. Patients receive either placebo or propranolol at 3 mg/kg for 15 days, followed by another 15 days at 4 mg/kg. The primary outcome will be hemangioma thickness variation measured by ultrasonography from baseline to 1 month.
When a lesion is easily resectable and a patient has failed medical therapy, or if ulceration and pain are present, surgery can be considered. Generally, thin plaques with a gradual slope have a better surgical prognosis. A circular incision around the lesion, with purse string closure, is the usual technique. A 2002 study of 25 patients found that this method reduced hemangiomas by a mean of 73% in width and 45% in length (Plast. Reconstr. Surg. 2002;109:1544-54).
Lasers can treat superficial proliferating hemangiomas, as well as the residua left after involution, Dr. Metz said. The pulsed dye laser is one option. Short pulses of 0.45-1.5 millisecond are used at either a 585- or 595-nm wavelength. The concomitant use of a dynamic cooling device makes the treatment less painful and can allow the use of a higher fluence.
Several studies attest to the success of pulsed dye lasers for hemangiomas. A 2009 study of 90 patients with 105 hemangiomas reported complete or near-complete clearance of color for 81% and thickness for 64%. Although there was no scarring or atrophy, one patient did develop an ulceration that resolved. Hyperpigmentation occurred in 4% and hypopigmentation in 14% (Derm. Surg. 2009;35:1947-54).
A 2006 study noted complications related to pulsed dye laser treatment. Of 12 patients with segmental facial hemangiomas, there were 8 ulcerations and 4 with atrophic scarring (Lasers Surg. Med. 2006;38:116-23).
Two published reports detail the use of fractionated laser for residua. A 2008 report found that the laser effectively decreased fibrofatty tissue and redundant skin that resulted from an extensive mixed facial hemangioma (Derm. Surg. 2008;34:1112-4). A 2009 report found similar results on residua from another facial hemangioma (Arch. Dermatol. 2009;145:748-50).
Dr. Metz disclosed that she is an investigator on the current propranolol trial, sponsored by University Hospital, Bordeaux, France.
SDEF and this news organization are owned by Elsevier.
Ultrasound Offers Noninvasive Skin Tightening Alternatives
Ultrasound and related radiofrequency technologies are relatively novel, effective, and noninvasive methods for body contouring and localized skin tightening, according to Dr. David J. Goldberg.
The only cosmetic ultrasound therapy currently approved by the Food and Drug Administration is the Ulthera System for skin tightening, Dr. Goldberg said at a cosmetic dermatology seminar sponsored by the Skin Disease Education Foundation in Santa Monica, Calif. The device non-specifically heats deep dermal collagen, which is thought to tighten cellulite.

In a 2008 study led by Dr. Goldberg, director of dermatologic laser research at Mount Sinai School of Medicine, New York, 30 female patients underwent six treatments with a unipolar radiofrequency device directed at cellulite on their upper thighs.
Following treatment, 27 of 30 patients had clinical improvements, with a mean decrease in thigh circumference of 2.45 cm (Dermatol. Surg. 2008;34:204-9).
The treatment was "fairly painless," he said. Side effects included post treatment erythema, which lasted for about 30-120 minutes; there were no blisters, scars, or pigmentary changes.
Another technology, known as UltraShape, delivers focused ultrasound to dissolve unwanted fat. In a recent multi-center, single-treatment, controlled study, 82% of 162 patients had measurable reductions in the circumference of their thighs, abdomens, and flanks. The decreases averaged 2 cm at 28 days, and were maintained at 84 days post treatment.
In the study, presented at the 2009 International Masters Course on Aging Skin in Paris, 76% of patients reported being satisfied with a single treatment, and 92% reported having no pain or discomfort.
According to Dr. Goldberg, UltraShape is currently used in over 57 countries. Approval has not yet been granted in the United States.
Dr. Goldberg disclosed receiving research grants from Alma Lasers, Thermage, Cynosure, UltraShape and Zeltiq, all makers of laser, ultrasound and radiofrequency skin-tightening and body-contouring technologies. SDEF and this news organization are owned by Elsevier.
Ultrasound and related radiofrequency technologies are relatively novel, effective, and noninvasive methods for body contouring and localized skin tightening, according to Dr. David J. Goldberg.
The only cosmetic ultrasound therapy currently approved by the Food and Drug Administration is the Ulthera System for skin tightening, Dr. Goldberg said at a cosmetic dermatology seminar sponsored by the Skin Disease Education Foundation in Santa Monica, Calif. The device non-specifically heats deep dermal collagen, which is thought to tighten cellulite.
In a 2008 study led by Dr. Goldberg, director of dermatologic laser research at Mount Sinai School of Medicine, New York, 30 female patients underwent six treatments with a unipolar radiofrequency device directed at cellulite on their upper thighs.
Following treatment, 27 of 30 patients had clinical improvements, with a mean decrease in thigh circumference of 2.45 cm (Dermatol. Surg. 2008;34:204-9).
The treatment was "fairly painless," he said. Side effects included post treatment erythema, which lasted for about 30-120 minutes; there were no blisters, scars, or pigmentary changes.
Another technology, known as UltraShape, delivers focused ultrasound to dissolve unwanted fat. In a recent multi-center, single-treatment, controlled study, 82% of 162 patients had measurable reductions in the circumference of their thighs, abdomens, and flanks. The decreases averaged 2 cm at 28 days, and were maintained at 84 days post treatment.
In the study, presented at the 2009 International Masters Course on Aging Skin in Paris, 76% of patients reported being satisfied with a single treatment, and 92% reported having no pain or discomfort.
According to Dr. Goldberg, UltraShape is currently used in over 57 countries. Approval has not yet been granted in the United States.
Dr. Goldberg disclosed receiving research grants from Alma Lasers, Thermage, Cynosure, UltraShape and Zeltiq, all makers of laser, ultrasound and radiofrequency skin-tightening and body-contouring technologies. SDEF and this news organization are owned by Elsevier.
Ultrasound and related radiofrequency technologies are relatively novel, effective, and noninvasive methods for body contouring and localized skin tightening, according to Dr. David J. Goldberg.
The only cosmetic ultrasound therapy currently approved by the Food and Drug Administration is the Ulthera System for skin tightening, Dr. Goldberg said at a cosmetic dermatology seminar sponsored by the Skin Disease Education Foundation in Santa Monica, Calif. The device non-specifically heats deep dermal collagen, which is thought to tighten cellulite.
In a 2008 study led by Dr. Goldberg, director of dermatologic laser research at Mount Sinai School of Medicine, New York, 30 female patients underwent six treatments with a unipolar radiofrequency device directed at cellulite on their upper thighs.
Following treatment, 27 of 30 patients had clinical improvements, with a mean decrease in thigh circumference of 2.45 cm (Dermatol. Surg. 2008;34:204-9).
The treatment was "fairly painless," he said. Side effects included post treatment erythema, which lasted for about 30-120 minutes; there were no blisters, scars, or pigmentary changes.
Another technology, known as UltraShape, delivers focused ultrasound to dissolve unwanted fat. In a recent multi-center, single-treatment, controlled study, 82% of 162 patients had measurable reductions in the circumference of their thighs, abdomens, and flanks. The decreases averaged 2 cm at 28 days, and were maintained at 84 days post treatment.
In the study, presented at the 2009 International Masters Course on Aging Skin in Paris, 76% of patients reported being satisfied with a single treatment, and 92% reported having no pain or discomfort.
According to Dr. Goldberg, UltraShape is currently used in over 57 countries. Approval has not yet been granted in the United States.
Dr. Goldberg disclosed receiving research grants from Alma Lasers, Thermage, Cynosure, UltraShape and Zeltiq, all makers of laser, ultrasound and radiofrequency skin-tightening and body-contouring technologies. SDEF and this news organization are owned by Elsevier.
Laser Treatment Research for Port Wine Stains Continues
Improving the appearance of port wine stains usually requires multiple laser treatments, and research is ongoing to improve results, according to Dr. Kristen Kelly.
Port wine stains (PWS) are the most common vascular malformations treated by dermatologists. About 0.3% of newborns have a PWS birthmark, which does not proliferate rapidly, but "may thicken, darken and develop nodules over time," Dr. Kelly said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
Historically, treatments for PWS have included tattoos or radiation, but for almost 30 years laser therapy has been the mainstay of treatment. Although these devices have improved, 2-15 or more laser applications are needed at approximately 4-week intervals for successful treatment of these lesions, said Dr. Kelly of the University of California, Irvine, and the Beckman Laser Institute and Medical Clinic.
The pulsed dye laser is the standard of care for PWS treatment and is the laser that she and her associates use most often. However, "we use different lasers and settings over a course of treatment to try to improve our results," Dr. Kelly said in an interview. The other lasers they use include the 755-nm alexandrite laser and combined 1,064:595-nm laser system, as well as intense pulsed light.
For some patients undergoing treatment of a PWS, preparation may include use of a bleaching cream for several weeks before treatment. Sun protection of the area to be treated is recommended for all patients. She and her associates use general anesthesia for patients with large lesions and for children and infants, although this is not a universal practice among dermatologists, she pointed out.
Eye protection with a corneal shield is very important for patients if treatment involves the periorbital or eyelid area, Dr. Kelly said, noting that proper eye protection is also important for those treating the patient.
During treatment, she recommends using a 585-nm or 595-nm wavelength and 0.45-3 millisecond pulse duration--varying pulse duration and wavelength over time to achieve optimal results. Placing patients in the Trendelenburg position can increase blood flow to the area of the PWS, according to Dr. Kelly, who is also with the university's Vascular Birthmarks and Malformations Diagnostic Treatment Center.
Postoperatively, ice should be applied to the treated area, which should be elevated for the first 1-2 postoperative days. A mild analgesic like acetaminophen should be used for discomfort, she said. An emollient should be applied to the treated area, and patients should protect the treated area from sun exposure. A bleaching cream such as hydroquinone may be started 2-3 weeks after treatment for some patients.
Dr. Kelly said that most PWS birthmarks get lighter but require multiple treatments. Some lesions, however, are resistant to treatment, and complete removal is uncommon.
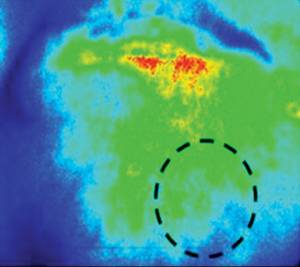
Research on improving results of PWS - to achieve more complete clearance over a shorter period of time - includes studies of imaging methods like laser speckle imaging (LSI), which is used intraoperatively to evaluate the impact of laser treatment on blood flow to determine if flow to the lesional blood vessel is decreased dramatically or shut down.
"Presumably, a greater reduction in flow is associated with greater damage to the blood vessels," said Dr. Kelly, who, with her associates, is studying whether a greater reduction in blood flow during treatment ultimately leads to better results. "We think it does, but we don't know that for sure yet," she said.
They also are studying whether the use of adjunctive agents after laser treatment improves results. These agents include antiangiogenic agents applied topically or administered orally or intravenously. An early study of imiquimod, an immune modulator with antiangiogenic effects, is underway, she noted.
Dr. Kelly disclosed that she has received research grants from Candela Corp. and Graceway Pharmaceuticals, and has served as a consultant to Lumenis. In addition, Graceway and Genentech have donated products for studies she is conducting.
SDEF and this news organization are both owned by Elsevier.
Improving the appearance of port wine stains usually requires multiple laser treatments, and research is ongoing to improve results, according to Dr. Kristen Kelly.
Port wine stains (PWS) are the most common vascular malformations treated by dermatologists. About 0.3% of newborns have a PWS birthmark, which does not proliferate rapidly, but "may thicken, darken and develop nodules over time," Dr. Kelly said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
Historically, treatments for PWS have included tattoos or radiation, but for almost 30 years laser therapy has been the mainstay of treatment. Although these devices have improved, 2-15 or more laser applications are needed at approximately 4-week intervals for successful treatment of these lesions, said Dr. Kelly of the University of California, Irvine, and the Beckman Laser Institute and Medical Clinic.
The pulsed dye laser is the standard of care for PWS treatment and is the laser that she and her associates use most often. However, "we use different lasers and settings over a course of treatment to try to improve our results," Dr. Kelly said in an interview. The other lasers they use include the 755-nm alexandrite laser and combined 1,064:595-nm laser system, as well as intense pulsed light.
For some patients undergoing treatment of a PWS, preparation may include use of a bleaching cream for several weeks before treatment. Sun protection of the area to be treated is recommended for all patients. She and her associates use general anesthesia for patients with large lesions and for children and infants, although this is not a universal practice among dermatologists, she pointed out.
Eye protection with a corneal shield is very important for patients if treatment involves the periorbital or eyelid area, Dr. Kelly said, noting that proper eye protection is also important for those treating the patient.
During treatment, she recommends using a 585-nm or 595-nm wavelength and 0.45-3 millisecond pulse duration--varying pulse duration and wavelength over time to achieve optimal results. Placing patients in the Trendelenburg position can increase blood flow to the area of the PWS, according to Dr. Kelly, who is also with the university's Vascular Birthmarks and Malformations Diagnostic Treatment Center.
Postoperatively, ice should be applied to the treated area, which should be elevated for the first 1-2 postoperative days. A mild analgesic like acetaminophen should be used for discomfort, she said. An emollient should be applied to the treated area, and patients should protect the treated area from sun exposure. A bleaching cream such as hydroquinone may be started 2-3 weeks after treatment for some patients.
Dr. Kelly said that most PWS birthmarks get lighter but require multiple treatments. Some lesions, however, are resistant to treatment, and complete removal is uncommon.
Research on improving results of PWS - to achieve more complete clearance over a shorter period of time - includes studies of imaging methods like laser speckle imaging (LSI), which is used intraoperatively to evaluate the impact of laser treatment on blood flow to determine if flow to the lesional blood vessel is decreased dramatically or shut down.
"Presumably, a greater reduction in flow is associated with greater damage to the blood vessels," said Dr. Kelly, who, with her associates, is studying whether a greater reduction in blood flow during treatment ultimately leads to better results. "We think it does, but we don't know that for sure yet," she said.
They also are studying whether the use of adjunctive agents after laser treatment improves results. These agents include antiangiogenic agents applied topically or administered orally or intravenously. An early study of imiquimod, an immune modulator with antiangiogenic effects, is underway, she noted.
Dr. Kelly disclosed that she has received research grants from Candela Corp. and Graceway Pharmaceuticals, and has served as a consultant to Lumenis. In addition, Graceway and Genentech have donated products for studies she is conducting.
SDEF and this news organization are both owned by Elsevier.
Improving the appearance of port wine stains usually requires multiple laser treatments, and research is ongoing to improve results, according to Dr. Kristen Kelly.
Port wine stains (PWS) are the most common vascular malformations treated by dermatologists. About 0.3% of newborns have a PWS birthmark, which does not proliferate rapidly, but "may thicken, darken and develop nodules over time," Dr. Kelly said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
Historically, treatments for PWS have included tattoos or radiation, but for almost 30 years laser therapy has been the mainstay of treatment. Although these devices have improved, 2-15 or more laser applications are needed at approximately 4-week intervals for successful treatment of these lesions, said Dr. Kelly of the University of California, Irvine, and the Beckman Laser Institute and Medical Clinic.
The pulsed dye laser is the standard of care for PWS treatment and is the laser that she and her associates use most often. However, "we use different lasers and settings over a course of treatment to try to improve our results," Dr. Kelly said in an interview. The other lasers they use include the 755-nm alexandrite laser and combined 1,064:595-nm laser system, as well as intense pulsed light.
For some patients undergoing treatment of a PWS, preparation may include use of a bleaching cream for several weeks before treatment. Sun protection of the area to be treated is recommended for all patients. She and her associates use general anesthesia for patients with large lesions and for children and infants, although this is not a universal practice among dermatologists, she pointed out.
Eye protection with a corneal shield is very important for patients if treatment involves the periorbital or eyelid area, Dr. Kelly said, noting that proper eye protection is also important for those treating the patient.
During treatment, she recommends using a 585-nm or 595-nm wavelength and 0.45-3 millisecond pulse duration--varying pulse duration and wavelength over time to achieve optimal results. Placing patients in the Trendelenburg position can increase blood flow to the area of the PWS, according to Dr. Kelly, who is also with the university's Vascular Birthmarks and Malformations Diagnostic Treatment Center.
Postoperatively, ice should be applied to the treated area, which should be elevated for the first 1-2 postoperative days. A mild analgesic like acetaminophen should be used for discomfort, she said. An emollient should be applied to the treated area, and patients should protect the treated area from sun exposure. A bleaching cream such as hydroquinone may be started 2-3 weeks after treatment for some patients.
Dr. Kelly said that most PWS birthmarks get lighter but require multiple treatments. Some lesions, however, are resistant to treatment, and complete removal is uncommon.
Research on improving results of PWS - to achieve more complete clearance over a shorter period of time - includes studies of imaging methods like laser speckle imaging (LSI), which is used intraoperatively to evaluate the impact of laser treatment on blood flow to determine if flow to the lesional blood vessel is decreased dramatically or shut down.
"Presumably, a greater reduction in flow is associated with greater damage to the blood vessels," said Dr. Kelly, who, with her associates, is studying whether a greater reduction in blood flow during treatment ultimately leads to better results. "We think it does, but we don't know that for sure yet," she said.
They also are studying whether the use of adjunctive agents after laser treatment improves results. These agents include antiangiogenic agents applied topically or administered orally or intravenously. An early study of imiquimod, an immune modulator with antiangiogenic effects, is underway, she noted.
Dr. Kelly disclosed that she has received research grants from Candela Corp. and Graceway Pharmaceuticals, and has served as a consultant to Lumenis. In addition, Graceway and Genentech have donated products for studies she is conducting.
SDEF and this news organization are both owned by Elsevier.
Pearls for Avoiding Filler Injection Danger Zones
Most dermatologists are well aware of the danger of damaging nerves during cold-steel surgery, but may be less aware of the danger zones involved in filler injection, said Dr. Howard K. Steinman at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
"Unlike the risk with a scalpel, where you're going to damage a nerve, the risk with fillers is that you may compress or occlude an artery," Dr. Steinman said in an interview. "You will get necrosis and scarring and disfigurement."

Dr. Steinman, director of dermatologic and skin cancer surgery at Texas A&M College of Medicine in College Station, offered some tips for avoiding the problem and suggestions on what to do if an occlusion occurs.
"The one everybody knows about from all the way back to the days of collagen is in the glabella," he said. If collagen is injected into the frown line, it is possible to damage the supratrochlear artery. If compressed or occluded, this artery can get a band-like area of damage extending up the forehead.
A second danger zone is at the nasolabial fold, where the angular artery runs close to the surface. Interrupting the blood flow here can cause damage to skin at the nasolabial fold and the side and tip of the nose. Although this is a relatively rare complication, the nasolabial fold is a popular site for filler injections, and physicians need to be mindful of this side effect, Dr. Steinman noted.
The third danger zone comes at the lips, where injections can interrupt flow in the labial artery.
In all cases, the symptoms are similar: There will be blanching, erythema, or edema, followed by necrosis unless the occlusion is treated promptly.
To avoid occlusion, he recommended injecting the filler perpendicular to the direction of the artery and remaining superficial but also pointed out that an artery can be indirectly occluded. According to one theory, simply injecting too much filler can compress the artery to the point of interrupting the flow.
Occlusions and compressions should be treated as soon as detected. The first step is an aggressive tapping and massaging of the area to try to break up the mass, Dr. Steinman said.
If that does not work, and the filler being used is hyaluronic acid-based, the next step is an injection of hyaluronidase, an enzyme that dissolves hyaluronic acid.
A third possibility is to apply nitroglycerin paste to the skin directly above the affected area. Typically used to keep the arteries dilated, the paste can improve flow in the case of occlusion or compression.
Unfortunately, the symptoms of an occluded artery do not always become evident immediately. "In some cases the patient won't notice this for hours after you have done the procedure," Dr. Steinman said. "They'll call you and they'll say, 'I'm having a problem.' You can certainly have them tap and massage as soon as possible, but you should meet them, even if it's at night, and start this protocol as soon as practical. It's not something you want to ignore. 'I'll see you in the morning,' is not the correct option for this."
Dr. Steinman stated that he had no conflicts of interest to disclose. SDEF and this news organization are owned by Elsevier.
Most dermatologists are well aware of the danger of damaging nerves during cold-steel surgery, but may be less aware of the danger zones involved in filler injection, said Dr. Howard K. Steinman at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
"Unlike the risk with a scalpel, where you're going to damage a nerve, the risk with fillers is that you may compress or occlude an artery," Dr. Steinman said in an interview. "You will get necrosis and scarring and disfigurement."
Dr. Steinman, director of dermatologic and skin cancer surgery at Texas A&M College of Medicine in College Station, offered some tips for avoiding the problem and suggestions on what to do if an occlusion occurs.
"The one everybody knows about from all the way back to the days of collagen is in the glabella," he said. If collagen is injected into the frown line, it is possible to damage the supratrochlear artery. If compressed or occluded, this artery can get a band-like area of damage extending up the forehead.
A second danger zone is at the nasolabial fold, where the angular artery runs close to the surface. Interrupting the blood flow here can cause damage to skin at the nasolabial fold and the side and tip of the nose. Although this is a relatively rare complication, the nasolabial fold is a popular site for filler injections, and physicians need to be mindful of this side effect, Dr. Steinman noted.
The third danger zone comes at the lips, where injections can interrupt flow in the labial artery.
In all cases, the symptoms are similar: There will be blanching, erythema, or edema, followed by necrosis unless the occlusion is treated promptly.
To avoid occlusion, he recommended injecting the filler perpendicular to the direction of the artery and remaining superficial but also pointed out that an artery can be indirectly occluded. According to one theory, simply injecting too much filler can compress the artery to the point of interrupting the flow.
Occlusions and compressions should be treated as soon as detected. The first step is an aggressive tapping and massaging of the area to try to break up the mass, Dr. Steinman said.
If that does not work, and the filler being used is hyaluronic acid-based, the next step is an injection of hyaluronidase, an enzyme that dissolves hyaluronic acid.
A third possibility is to apply nitroglycerin paste to the skin directly above the affected area. Typically used to keep the arteries dilated, the paste can improve flow in the case of occlusion or compression.
Unfortunately, the symptoms of an occluded artery do not always become evident immediately. "In some cases the patient won't notice this for hours after you have done the procedure," Dr. Steinman said. "They'll call you and they'll say, 'I'm having a problem.' You can certainly have them tap and massage as soon as possible, but you should meet them, even if it's at night, and start this protocol as soon as practical. It's not something you want to ignore. 'I'll see you in the morning,' is not the correct option for this."
Dr. Steinman stated that he had no conflicts of interest to disclose. SDEF and this news organization are owned by Elsevier.
Most dermatologists are well aware of the danger of damaging nerves during cold-steel surgery, but may be less aware of the danger zones involved in filler injection, said Dr. Howard K. Steinman at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
"Unlike the risk with a scalpel, where you're going to damage a nerve, the risk with fillers is that you may compress or occlude an artery," Dr. Steinman said in an interview. "You will get necrosis and scarring and disfigurement."
Dr. Steinman, director of dermatologic and skin cancer surgery at Texas A&M College of Medicine in College Station, offered some tips for avoiding the problem and suggestions on what to do if an occlusion occurs.
"The one everybody knows about from all the way back to the days of collagen is in the glabella," he said. If collagen is injected into the frown line, it is possible to damage the supratrochlear artery. If compressed or occluded, this artery can get a band-like area of damage extending up the forehead.
A second danger zone is at the nasolabial fold, where the angular artery runs close to the surface. Interrupting the blood flow here can cause damage to skin at the nasolabial fold and the side and tip of the nose. Although this is a relatively rare complication, the nasolabial fold is a popular site for filler injections, and physicians need to be mindful of this side effect, Dr. Steinman noted.
The third danger zone comes at the lips, where injections can interrupt flow in the labial artery.
In all cases, the symptoms are similar: There will be blanching, erythema, or edema, followed by necrosis unless the occlusion is treated promptly.
To avoid occlusion, he recommended injecting the filler perpendicular to the direction of the artery and remaining superficial but also pointed out that an artery can be indirectly occluded. According to one theory, simply injecting too much filler can compress the artery to the point of interrupting the flow.
Occlusions and compressions should be treated as soon as detected. The first step is an aggressive tapping and massaging of the area to try to break up the mass, Dr. Steinman said.
If that does not work, and the filler being used is hyaluronic acid-based, the next step is an injection of hyaluronidase, an enzyme that dissolves hyaluronic acid.
A third possibility is to apply nitroglycerin paste to the skin directly above the affected area. Typically used to keep the arteries dilated, the paste can improve flow in the case of occlusion or compression.
Unfortunately, the symptoms of an occluded artery do not always become evident immediately. "In some cases the patient won't notice this for hours after you have done the procedure," Dr. Steinman said. "They'll call you and they'll say, 'I'm having a problem.' You can certainly have them tap and massage as soon as possible, but you should meet them, even if it's at night, and start this protocol as soon as practical. It's not something you want to ignore. 'I'll see you in the morning,' is not the correct option for this."
Dr. Steinman stated that he had no conflicts of interest to disclose. SDEF and this news organization are owned by Elsevier.
Two Lasers May Be Better Than One for Hair Removal
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
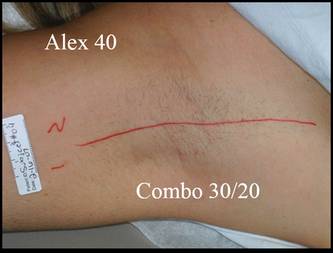
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.
Recent advances in laser hair removal include using combination wavelengths, longer pulses, and larger spot sizes for all skin types, and using longer wavelengths for darker skin, according to Dr. E. Victor Ross.
Better pain control and cooling techniques also can make device-based hair removal a more comfortable option for patients, Dr. Ross said at a cosmetic dermatology seminar sponsored by Skin Disease Education Foundation in Santa Monica, Calif.
When using lasers for hair removal, cooling the skin before and after treatment can reduce pain and swelling, and cooling the skin during laser exposure "tends to minimize the dermal epidermal temperature," said Dr. Ross, director of the Scripps Clinic Laser and Cosmetic Dermatology Center in Carmel Valley, Calif.
Historically, fair-skinned patients have been treated with a 755-nm alexandrite laser for hair removal. For dark or tanned skin, or coarser hair, a 1064-nm Nd:YAG might be more effective, but it can be more painful for patients, Dr. Ross noted.
In his experience, a blended treatment including both the 755-nm and 1064-nm lasers can be more effective for removing fine hair on the legs than either laser alone, he said, adding that some patients still prefer the 755-nm alexandrite laser because the combination therapy is more painful than the 755 nm, although it is less painful than the 1064 nm alone.
New hair removal technologies include ultrasound and microwave radiation, as well as lower-fluence intense pulsed light and diode options with suction.
Approaches using high repetition with low fluence have been applied in some settings. The advantage is less pain, but more research is needed to determine whether lower fluences at high rates of repetition are effective, and what types of treatments are effective for white hair, said Dr. Ross.
Suction devices are an option to assist with permanent hair reduction over larger areas. A larger spot size allows more photons to remain in the target area, while vacuum-assisted suction concentrates more cumulative energy at any given depth and allows for effective treatment at a lower fluence.
Dr. Ross also addressed laser-diode hair removal devices being marketed for home use. The key issues to consider when evaluating at-home devices are safety for all skin types; safety with open or closed eyes; effectiveness in removing fine, gray, or white hair; and, of course, cost.
The TRIA hair removal device from TRIA Beauty Inc. is approved by the Food and Drug Administration for home use. The device packs an 800-nm wavelength and fluences of 7, 12, or 20 J/cm2, and efficacy data on this product are promising, Dr. Ross said.
Dr. Ross disclosed that he is a researcher for and receives funding from multiple laser companies, including Candela, Cutera, Lumenis, Sciton, and Syneron. SDEF and this news organization are both owned by Elsevier.