User login
Sliding-Scale Insulin Does Not Improve Blood Glucose Control in Hospitalized Patients
Clinical question: Does the use of sliding-scale insulin improve blood glucose control in hospitalized patients?
Bottom line: Sliding-scale insulin is commonly used to manage hyperglycemia in hospitalized patients. The evidence suggests that this regimen does not result in better blood glucose control. (LOE = 1a-)
Reference: Lee Y, Lin Y, Leu W et al. Sliding-scale insulin used for blood glucose control: a meta-analysis of randomized controlled trials. Metabolism 2015;64:1183-1192.
Study design: Meta-analysis (randomized controlled trials)
Funding source: Government
Allocation: Uncertain
Setting: Inpatient (any location)
Synopsis: These investigators searched multiple databases including PubMed, EMBASE, and the Cochrane Library to find randomized controlled trials that evaluated the efficacy of sliding-scale insulin to manage hyperglycemia in hospitalized patients. Two authors independently evaluated the studies for inclusion, extracted the data, and performed quality assessments.
Eight of the 11 included studies compared regular insulin sliding scale (RISS) regimens with non–sliding-scale regimens. All RISS regimens consisted of subcutaneous regular insulin injections according to patients' blood glucose levels. Non–sliding-scale regimens consisted of basal-bolus or basal insulin regimens, continuous intravenous insulin infusions, and closed-loop artificial pancreas systems. Target blood glucose levels for individual studies varied greatly and included a range of 100 mg/dL to 150 mg/dL, a goal of less than 140 mg/dL, and a goal of less than 180 mg/dL. Hypoglycemia was generally defined as a glucose level of less than 70 mg/dL, though three of the studies had an even lower cut-off.
In the two studies that evaluated hyperglycemia, one defined it as a glucose level greater than 180 mg/dL while the other defined it as greater than 240 mg/dL. A meta-analysis of relevant data showed no significant difference in the percentage of patients who achieved an average blood glucose level in the target range when comparing RISS with non–sliding-scale regimens. The trend, however, favored the non–sliding-scale group and the difference became significant (relative risk 1.48, 95% CI 1.09-2.02) after one study with a very wide confidence interval was removed. Furthermore, the incidence of hyperglycemia and the mean blood glucose levels were significantly higher in the RISS group.
Although overall hypoglycemic episodes occurred more frequently in the non–sliding-scale group, there was no significant difference detected in the incidence of severe or symptomatic hypoglycemia. Length of hospital stay was also similar in both groups. Finally, one study compared the use of routine diabetes medications plus RISS with routine diabetes medications alone and found no difference in the number of hypoglycemic or hyperglycemic events.
Significant heterogeneity was detected in the results of this meta-analysis and can be attributed to the differing patient populations, insulin regimens, and working definitions in the individual studies as noted above.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of sliding-scale insulin improve blood glucose control in hospitalized patients?
Bottom line: Sliding-scale insulin is commonly used to manage hyperglycemia in hospitalized patients. The evidence suggests that this regimen does not result in better blood glucose control. (LOE = 1a-)
Reference: Lee Y, Lin Y, Leu W et al. Sliding-scale insulin used for blood glucose control: a meta-analysis of randomized controlled trials. Metabolism 2015;64:1183-1192.
Study design: Meta-analysis (randomized controlled trials)
Funding source: Government
Allocation: Uncertain
Setting: Inpatient (any location)
Synopsis: These investigators searched multiple databases including PubMed, EMBASE, and the Cochrane Library to find randomized controlled trials that evaluated the efficacy of sliding-scale insulin to manage hyperglycemia in hospitalized patients. Two authors independently evaluated the studies for inclusion, extracted the data, and performed quality assessments.
Eight of the 11 included studies compared regular insulin sliding scale (RISS) regimens with non–sliding-scale regimens. All RISS regimens consisted of subcutaneous regular insulin injections according to patients' blood glucose levels. Non–sliding-scale regimens consisted of basal-bolus or basal insulin regimens, continuous intravenous insulin infusions, and closed-loop artificial pancreas systems. Target blood glucose levels for individual studies varied greatly and included a range of 100 mg/dL to 150 mg/dL, a goal of less than 140 mg/dL, and a goal of less than 180 mg/dL. Hypoglycemia was generally defined as a glucose level of less than 70 mg/dL, though three of the studies had an even lower cut-off.
In the two studies that evaluated hyperglycemia, one defined it as a glucose level greater than 180 mg/dL while the other defined it as greater than 240 mg/dL. A meta-analysis of relevant data showed no significant difference in the percentage of patients who achieved an average blood glucose level in the target range when comparing RISS with non–sliding-scale regimens. The trend, however, favored the non–sliding-scale group and the difference became significant (relative risk 1.48, 95% CI 1.09-2.02) after one study with a very wide confidence interval was removed. Furthermore, the incidence of hyperglycemia and the mean blood glucose levels were significantly higher in the RISS group.
Although overall hypoglycemic episodes occurred more frequently in the non–sliding-scale group, there was no significant difference detected in the incidence of severe or symptomatic hypoglycemia. Length of hospital stay was also similar in both groups. Finally, one study compared the use of routine diabetes medications plus RISS with routine diabetes medications alone and found no difference in the number of hypoglycemic or hyperglycemic events.
Significant heterogeneity was detected in the results of this meta-analysis and can be attributed to the differing patient populations, insulin regimens, and working definitions in the individual studies as noted above.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Does the use of sliding-scale insulin improve blood glucose control in hospitalized patients?
Bottom line: Sliding-scale insulin is commonly used to manage hyperglycemia in hospitalized patients. The evidence suggests that this regimen does not result in better blood glucose control. (LOE = 1a-)
Reference: Lee Y, Lin Y, Leu W et al. Sliding-scale insulin used for blood glucose control: a meta-analysis of randomized controlled trials. Metabolism 2015;64:1183-1192.
Study design: Meta-analysis (randomized controlled trials)
Funding source: Government
Allocation: Uncertain
Setting: Inpatient (any location)
Synopsis: These investigators searched multiple databases including PubMed, EMBASE, and the Cochrane Library to find randomized controlled trials that evaluated the efficacy of sliding-scale insulin to manage hyperglycemia in hospitalized patients. Two authors independently evaluated the studies for inclusion, extracted the data, and performed quality assessments.
Eight of the 11 included studies compared regular insulin sliding scale (RISS) regimens with non–sliding-scale regimens. All RISS regimens consisted of subcutaneous regular insulin injections according to patients' blood glucose levels. Non–sliding-scale regimens consisted of basal-bolus or basal insulin regimens, continuous intravenous insulin infusions, and closed-loop artificial pancreas systems. Target blood glucose levels for individual studies varied greatly and included a range of 100 mg/dL to 150 mg/dL, a goal of less than 140 mg/dL, and a goal of less than 180 mg/dL. Hypoglycemia was generally defined as a glucose level of less than 70 mg/dL, though three of the studies had an even lower cut-off.
In the two studies that evaluated hyperglycemia, one defined it as a glucose level greater than 180 mg/dL while the other defined it as greater than 240 mg/dL. A meta-analysis of relevant data showed no significant difference in the percentage of patients who achieved an average blood glucose level in the target range when comparing RISS with non–sliding-scale regimens. The trend, however, favored the non–sliding-scale group and the difference became significant (relative risk 1.48, 95% CI 1.09-2.02) after one study with a very wide confidence interval was removed. Furthermore, the incidence of hyperglycemia and the mean blood glucose levels were significantly higher in the RISS group.
Although overall hypoglycemic episodes occurred more frequently in the non–sliding-scale group, there was no significant difference detected in the incidence of severe or symptomatic hypoglycemia. Length of hospital stay was also similar in both groups. Finally, one study compared the use of routine diabetes medications plus RISS with routine diabetes medications alone and found no difference in the number of hypoglycemic or hyperglycemic events.
Significant heterogeneity was detected in the results of this meta-analysis and can be attributed to the differing patient populations, insulin regimens, and working definitions in the individual studies as noted above.
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Subclavian Central Lines Have Fewer Infections, Clots; Increased Risk of Pneumothorax
Clinical question: Which insertion site for central venous catheterization results in fewer complications?
Bottom line: Central venous catheterization via a subclavian insertion site, as compared with femoral and jugular sites, decreases the risk of bloodstream infections and symptomatic deep vein thromboses (DVTs), but results in more pneumothoraces. This risk could potentially be mitigated with the use of ultrasound guidance during catheter insertion. ((LOE = 1b)
Reference: Parienti JJ, Mongardon N, Mégarbane B, et al. Intravascular complications of central venous catheterization by insertion site. N Engl J Med 2015;373(13):1220-1229.
Study design: Randomized controlled trial (nonblinded)
Funding source: Government
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis
These investigators randomized 3027 patients in the intensive care unit who required nontunneled central venous access to receive 3471 intravenous catheters at one of three insertion sites: subclavian, jugular, or femoral. The catheters were placed by residents or staff physicians who had prior experience in the procedure. All patients had peripheral blood cultures and catheter tip cultures sent at the time of catheter removal. Patients also underwent compression ultrasonography at the insertion site within two days of catheter removal to assess for DVT. The three groups were well-balanced at baseline and the median duration of catheter use was five days. Analysis was by intention to treat.
The primary composite endpoint of catheter-related bloodstream infections and symptomatic DVTs occurred less frequently in the subclavian group than in the other two groups (1.5 events per 1000 catheter-days in the subclavian group, 3.6 in the jugular group, 4.6 in the femoral group). The risk of this outcome was greater in both the femoral and jugular groups when compared directly with the subclavian group (femoral vs subclavian: hazard ratio [HR] = 3.5; 95% CI 1.5-7.8; P = .003; femoral vs jugular: HR = 2.1; 1.0-4.3; P = .04). The subclavian group, however, did have the highest risk of mechanical complications, mainly pneumothoraces.
When all three bad outcomes (infections, DVTs, mechanical complications) are pooled together, the differences between the three groups are not as compelling (percentage of catheters with overall complications: 3.1% subclavian, 3.7% jugular, 3.4% femoral).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Which insertion site for central venous catheterization results in fewer complications?
Bottom line: Central venous catheterization via a subclavian insertion site, as compared with femoral and jugular sites, decreases the risk of bloodstream infections and symptomatic deep vein thromboses (DVTs), but results in more pneumothoraces. This risk could potentially be mitigated with the use of ultrasound guidance during catheter insertion. ((LOE = 1b)
Reference: Parienti JJ, Mongardon N, Mégarbane B, et al. Intravascular complications of central venous catheterization by insertion site. N Engl J Med 2015;373(13):1220-1229.
Study design: Randomized controlled trial (nonblinded)
Funding source: Government
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis
These investigators randomized 3027 patients in the intensive care unit who required nontunneled central venous access to receive 3471 intravenous catheters at one of three insertion sites: subclavian, jugular, or femoral. The catheters were placed by residents or staff physicians who had prior experience in the procedure. All patients had peripheral blood cultures and catheter tip cultures sent at the time of catheter removal. Patients also underwent compression ultrasonography at the insertion site within two days of catheter removal to assess for DVT. The three groups were well-balanced at baseline and the median duration of catheter use was five days. Analysis was by intention to treat.
The primary composite endpoint of catheter-related bloodstream infections and symptomatic DVTs occurred less frequently in the subclavian group than in the other two groups (1.5 events per 1000 catheter-days in the subclavian group, 3.6 in the jugular group, 4.6 in the femoral group). The risk of this outcome was greater in both the femoral and jugular groups when compared directly with the subclavian group (femoral vs subclavian: hazard ratio [HR] = 3.5; 95% CI 1.5-7.8; P = .003; femoral vs jugular: HR = 2.1; 1.0-4.3; P = .04). The subclavian group, however, did have the highest risk of mechanical complications, mainly pneumothoraces.
When all three bad outcomes (infections, DVTs, mechanical complications) are pooled together, the differences between the three groups are not as compelling (percentage of catheters with overall complications: 3.1% subclavian, 3.7% jugular, 3.4% femoral).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Clinical question: Which insertion site for central venous catheterization results in fewer complications?
Bottom line: Central venous catheterization via a subclavian insertion site, as compared with femoral and jugular sites, decreases the risk of bloodstream infections and symptomatic deep vein thromboses (DVTs), but results in more pneumothoraces. This risk could potentially be mitigated with the use of ultrasound guidance during catheter insertion. ((LOE = 1b)
Reference: Parienti JJ, Mongardon N, Mégarbane B, et al. Intravascular complications of central venous catheterization by insertion site. N Engl J Med 2015;373(13):1220-1229.
Study design: Randomized controlled trial (nonblinded)
Funding source: Government
Allocation: Concealed
Setting: Inpatient (ICU only)
Synopsis
These investigators randomized 3027 patients in the intensive care unit who required nontunneled central venous access to receive 3471 intravenous catheters at one of three insertion sites: subclavian, jugular, or femoral. The catheters were placed by residents or staff physicians who had prior experience in the procedure. All patients had peripheral blood cultures and catheter tip cultures sent at the time of catheter removal. Patients also underwent compression ultrasonography at the insertion site within two days of catheter removal to assess for DVT. The three groups were well-balanced at baseline and the median duration of catheter use was five days. Analysis was by intention to treat.
The primary composite endpoint of catheter-related bloodstream infections and symptomatic DVTs occurred less frequently in the subclavian group than in the other two groups (1.5 events per 1000 catheter-days in the subclavian group, 3.6 in the jugular group, 4.6 in the femoral group). The risk of this outcome was greater in both the femoral and jugular groups when compared directly with the subclavian group (femoral vs subclavian: hazard ratio [HR] = 3.5; 95% CI 1.5-7.8; P = .003; femoral vs jugular: HR = 2.1; 1.0-4.3; P = .04). The subclavian group, however, did have the highest risk of mechanical complications, mainly pneumothoraces.
When all three bad outcomes (infections, DVTs, mechanical complications) are pooled together, the differences between the three groups are not as compelling (percentage of catheters with overall complications: 3.1% subclavian, 3.7% jugular, 3.4% femoral).
Dr. Kulkarni is an assistant professor of hospital medicine at Northwestern University in Chicago.
Depression and Psoriasis
While psoriasis is a known risk factor for depression, depression can also exacerbate or trigger psoriasis. This relationship between depression and psoriasis, however, remains to be fully explored.
In an article published online on September 30 in JAMA Dermatology , Cohen et al examined the association between psoriasis and major depression in the US population. The authors conducted a population-based study that utilized individuals who were participating in the National Health and Nutrition Examination Survey from 2009 through 2012.
The authors identified 351 (2.8%) cases of psoriasis and 968 (7.8%) cases of major depression in the 12,382 participants included in the study. Of the patients with psoriasis, 58 (16.5%) met criteria for major depression. The mean (standard deviation) Patient Health Questionnaire-9 score was significantly higher among patients with a history of psoriasis than those without psoriasis (4.54 [5.7] vs 3.22 [4.3], P<.001). After adjustment for sex, age, race, body mass index, physical activity level, smoking history, alcohol use, history of myocardial infarction, history of stroke, and history of diabetes mellitus (odds ratio, 2.09 [95% confidence interval, 1.41–3.11], P<.001), psoriasis was significantly associated with major depression. Having a history of cardiovascular events did not modify the risk of major depression for patients with psoriasis. The investigators also found that the risk of major depression was not significantly different between patients with limited vs extensive psoriasis (odds ratio, 0.66 [95% confidence interval, 0.18–2.44], P=.53).
What’s the Issue?
We know that psoriasis is associated with depression. This study, however, has some surprising findings. The severity of psoriasis was unrelated to the risk of major depression. Additionally, cardiovascular events did not seem to impact major depression in participants with psoriasis. Therefore, all patients with psoriasis, regardless of severity, may be at risk for major depression. Will these findings impact your evaluation of psychological issues in individuals with psoriasis?
While psoriasis is a known risk factor for depression, depression can also exacerbate or trigger psoriasis. This relationship between depression and psoriasis, however, remains to be fully explored.
In an article published online on September 30 in JAMA Dermatology , Cohen et al examined the association between psoriasis and major depression in the US population. The authors conducted a population-based study that utilized individuals who were participating in the National Health and Nutrition Examination Survey from 2009 through 2012.
The authors identified 351 (2.8%) cases of psoriasis and 968 (7.8%) cases of major depression in the 12,382 participants included in the study. Of the patients with psoriasis, 58 (16.5%) met criteria for major depression. The mean (standard deviation) Patient Health Questionnaire-9 score was significantly higher among patients with a history of psoriasis than those without psoriasis (4.54 [5.7] vs 3.22 [4.3], P<.001). After adjustment for sex, age, race, body mass index, physical activity level, smoking history, alcohol use, history of myocardial infarction, history of stroke, and history of diabetes mellitus (odds ratio, 2.09 [95% confidence interval, 1.41–3.11], P<.001), psoriasis was significantly associated with major depression. Having a history of cardiovascular events did not modify the risk of major depression for patients with psoriasis. The investigators also found that the risk of major depression was not significantly different between patients with limited vs extensive psoriasis (odds ratio, 0.66 [95% confidence interval, 0.18–2.44], P=.53).
What’s the Issue?
We know that psoriasis is associated with depression. This study, however, has some surprising findings. The severity of psoriasis was unrelated to the risk of major depression. Additionally, cardiovascular events did not seem to impact major depression in participants with psoriasis. Therefore, all patients with psoriasis, regardless of severity, may be at risk for major depression. Will these findings impact your evaluation of psychological issues in individuals with psoriasis?
While psoriasis is a known risk factor for depression, depression can also exacerbate or trigger psoriasis. This relationship between depression and psoriasis, however, remains to be fully explored.
In an article published online on September 30 in JAMA Dermatology , Cohen et al examined the association between psoriasis and major depression in the US population. The authors conducted a population-based study that utilized individuals who were participating in the National Health and Nutrition Examination Survey from 2009 through 2012.
The authors identified 351 (2.8%) cases of psoriasis and 968 (7.8%) cases of major depression in the 12,382 participants included in the study. Of the patients with psoriasis, 58 (16.5%) met criteria for major depression. The mean (standard deviation) Patient Health Questionnaire-9 score was significantly higher among patients with a history of psoriasis than those without psoriasis (4.54 [5.7] vs 3.22 [4.3], P<.001). After adjustment for sex, age, race, body mass index, physical activity level, smoking history, alcohol use, history of myocardial infarction, history of stroke, and history of diabetes mellitus (odds ratio, 2.09 [95% confidence interval, 1.41–3.11], P<.001), psoriasis was significantly associated with major depression. Having a history of cardiovascular events did not modify the risk of major depression for patients with psoriasis. The investigators also found that the risk of major depression was not significantly different between patients with limited vs extensive psoriasis (odds ratio, 0.66 [95% confidence interval, 0.18–2.44], P=.53).
What’s the Issue?
We know that psoriasis is associated with depression. This study, however, has some surprising findings. The severity of psoriasis was unrelated to the risk of major depression. Additionally, cardiovascular events did not seem to impact major depression in participants with psoriasis. Therefore, all patients with psoriasis, regardless of severity, may be at risk for major depression. Will these findings impact your evaluation of psychological issues in individuals with psoriasis?

Adjuvant imatinib for 3 years better than 1 year in high-risk GIST
After surgery for high-risk gastrointestinal stromal tumor (GIST), patients who received adjuvant imatinib for 3 years achieved longer relapse-free survival (RFS) and overall survival (OS) compared with those treated for 1 year, according to a study published online in Journal of Clinical Oncology.
With a median follow up of 7.5 years, the 5-year survival rates of greater than 90% represent the highest reported to date in high-risk GIST.
“We speculate that, other than adjuvant imatinib, two procedures were crucially important for achieving the high overall survival rates: longitudinal monitoring of the abdomen with CT to detect GIST recurrence early when the tumor bulk was still small and restarting of imatinib after recurrence was detected,” wrote Dr. Heikki Joensuu of the Comprehensive Cancer Center Helsinki and University of Helsinki, Finland, and colleagues.
Five-year RFS rates for 3- and 1-year treatment durations were 71.1% and 52.3%, respectively (hazard ratio, 0.60; 95% CI, 0.44-0.81; P less than .001); 5-year OS rates were 91.9% and 85.3%, respectively (HR, 0.60; 95% CI, 0.37-0.97; P = .036), the investigators reported (J Clin Oncol. 2015 Nov. 2. doi: 10.1200/JCO.2015.62.9170).
After a median follow up of 90 months, the second planned analysis of the open-label Scandinavian Sarcoma Group XVIII/AIO study evaluated outcomes of 358 patients, 181 in the 12-month group and 177 in the 36-month group. Earlier results from the SSGXVIII/AIO trial (after a 4.5-year follow up) showed significantly longer survival in patients who received imatinib for 3 years versus 1 year, and these results have informed treatment guidelines.
However, two other large randomized trials evaluated adjuvant imatinib for durations less than 3 years in patients with lower-risk GIST, and neither study found a survival benefit. The investigators point out that because low- or intermediate-risk GIST is cured with surgery alone in the great majority of patients, most do not benefit from adjuvant imatinib.
“Hypothetically, these results suggest that obtaining overall survival benefit may require durable administrations of imatinib and that the patients at high risk for recurrence are the optimal target population,” they wrote.
All but two patients reported at least one adverse event, but most events were mild. Previous reports have suggested cardiac toxicity of imatinib, but only one patient had cardiac failure, perhaps due to the low 400 mg adjuvant daily dosage.
Dr. Joensuu reported consulting or advisory roles with Blueprint Medicines, ARIAD Pharmaceuticals, and Orion Pharma. Several of his coauthors reported ties to industry sources.
After surgery for high-risk gastrointestinal stromal tumor (GIST), patients who received adjuvant imatinib for 3 years achieved longer relapse-free survival (RFS) and overall survival (OS) compared with those treated for 1 year, according to a study published online in Journal of Clinical Oncology.
With a median follow up of 7.5 years, the 5-year survival rates of greater than 90% represent the highest reported to date in high-risk GIST.
“We speculate that, other than adjuvant imatinib, two procedures were crucially important for achieving the high overall survival rates: longitudinal monitoring of the abdomen with CT to detect GIST recurrence early when the tumor bulk was still small and restarting of imatinib after recurrence was detected,” wrote Dr. Heikki Joensuu of the Comprehensive Cancer Center Helsinki and University of Helsinki, Finland, and colleagues.
Five-year RFS rates for 3- and 1-year treatment durations were 71.1% and 52.3%, respectively (hazard ratio, 0.60; 95% CI, 0.44-0.81; P less than .001); 5-year OS rates were 91.9% and 85.3%, respectively (HR, 0.60; 95% CI, 0.37-0.97; P = .036), the investigators reported (J Clin Oncol. 2015 Nov. 2. doi: 10.1200/JCO.2015.62.9170).
After a median follow up of 90 months, the second planned analysis of the open-label Scandinavian Sarcoma Group XVIII/AIO study evaluated outcomes of 358 patients, 181 in the 12-month group and 177 in the 36-month group. Earlier results from the SSGXVIII/AIO trial (after a 4.5-year follow up) showed significantly longer survival in patients who received imatinib for 3 years versus 1 year, and these results have informed treatment guidelines.
However, two other large randomized trials evaluated adjuvant imatinib for durations less than 3 years in patients with lower-risk GIST, and neither study found a survival benefit. The investigators point out that because low- or intermediate-risk GIST is cured with surgery alone in the great majority of patients, most do not benefit from adjuvant imatinib.
“Hypothetically, these results suggest that obtaining overall survival benefit may require durable administrations of imatinib and that the patients at high risk for recurrence are the optimal target population,” they wrote.
All but two patients reported at least one adverse event, but most events were mild. Previous reports have suggested cardiac toxicity of imatinib, but only one patient had cardiac failure, perhaps due to the low 400 mg adjuvant daily dosage.
Dr. Joensuu reported consulting or advisory roles with Blueprint Medicines, ARIAD Pharmaceuticals, and Orion Pharma. Several of his coauthors reported ties to industry sources.
After surgery for high-risk gastrointestinal stromal tumor (GIST), patients who received adjuvant imatinib for 3 years achieved longer relapse-free survival (RFS) and overall survival (OS) compared with those treated for 1 year, according to a study published online in Journal of Clinical Oncology.
With a median follow up of 7.5 years, the 5-year survival rates of greater than 90% represent the highest reported to date in high-risk GIST.
“We speculate that, other than adjuvant imatinib, two procedures were crucially important for achieving the high overall survival rates: longitudinal monitoring of the abdomen with CT to detect GIST recurrence early when the tumor bulk was still small and restarting of imatinib after recurrence was detected,” wrote Dr. Heikki Joensuu of the Comprehensive Cancer Center Helsinki and University of Helsinki, Finland, and colleagues.
Five-year RFS rates for 3- and 1-year treatment durations were 71.1% and 52.3%, respectively (hazard ratio, 0.60; 95% CI, 0.44-0.81; P less than .001); 5-year OS rates were 91.9% and 85.3%, respectively (HR, 0.60; 95% CI, 0.37-0.97; P = .036), the investigators reported (J Clin Oncol. 2015 Nov. 2. doi: 10.1200/JCO.2015.62.9170).
After a median follow up of 90 months, the second planned analysis of the open-label Scandinavian Sarcoma Group XVIII/AIO study evaluated outcomes of 358 patients, 181 in the 12-month group and 177 in the 36-month group. Earlier results from the SSGXVIII/AIO trial (after a 4.5-year follow up) showed significantly longer survival in patients who received imatinib for 3 years versus 1 year, and these results have informed treatment guidelines.
However, two other large randomized trials evaluated adjuvant imatinib for durations less than 3 years in patients with lower-risk GIST, and neither study found a survival benefit. The investigators point out that because low- or intermediate-risk GIST is cured with surgery alone in the great majority of patients, most do not benefit from adjuvant imatinib.
“Hypothetically, these results suggest that obtaining overall survival benefit may require durable administrations of imatinib and that the patients at high risk for recurrence are the optimal target population,” they wrote.
All but two patients reported at least one adverse event, but most events were mild. Previous reports have suggested cardiac toxicity of imatinib, but only one patient had cardiac failure, perhaps due to the low 400 mg adjuvant daily dosage.
Dr. Joensuu reported consulting or advisory roles with Blueprint Medicines, ARIAD Pharmaceuticals, and Orion Pharma. Several of his coauthors reported ties to industry sources.
Key clinical point: Patients with high-risk GIST treated with adjuvant imatinib for 3 years had longer relapse-free survival (RFS) and overall survival (OS) than did those treated for 1 year.
Major finding: Five-year RFS rates for 3- and 1-year treatment durations were 71.1% and 52.3%, respectively (hazard ratio, 0.60; 95% CI, 0.44-0.81; P less than .001); 5-year OS rates were 91.9% and 85.3%, respectively (HR, 0.60; 95% CI, 0.37-0.97; P = .036).
Data source: After a median follow up of 90 months, a second planned analysis of the open-label SSGXVIII/AIO study evaluated outcomes of 358 patients, 181 in the 12-month group and 177 in the 36-month group.
Disclosures: Dr. Joensuu reported consulting or advisory roles with Blueprint Medicines, ARIAD Pharmaceuticals, and Orion Pharma. Several of his coauthors reported ties to industry sources.
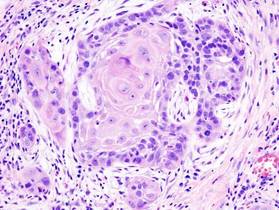
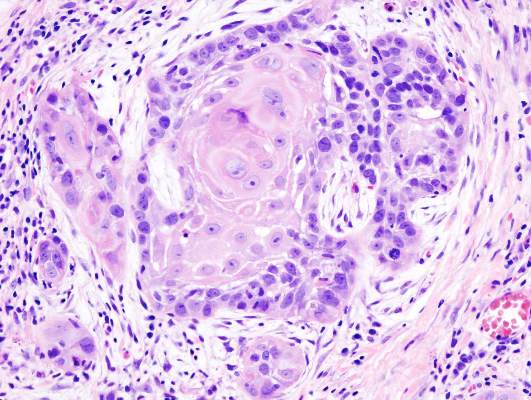
Adjuvant lapatinib added no benefit against head and neck squamous cell carcinoma
Lapatinib in combination with platinum-based chemoradiotherapy and as long-term maintenance therapy showed no benefit in patients with surgically treated high-risk squamous cell carcinoma of the head and neck (SCCHN).
No difference was observed between treatment arms in the primary endpoint of disease-free survival (DFS) or the secondary endpoints of investigator-assessed DFS and overall survival.
“Certainly, these findings should serve as a note of caution on the risks of initiating large phase III studies (of this and other drugs) with insufficient evidence of single-agent activity,” wrote Dr. Kevin Harrington of the division of radiotherapy and imaging at the Institute of Cancer Research and Royal Marsden Hospital, London, and his colleagues (Journ Clin Onc. 2015 Nov. 2. doi: 10.1200/JCO.2015.61.4370).
The placebo-controlled phase III trial from 84 sites in 21 countries randomized 688 patients with resected SCCHN to receive placebo or lapatinib. The study was halted early because of the apparent plateauing of DFS events at the median follow-up time of 35.3 months, the investigators reported.
DFS events (disease recurrence or death) occurred in 32% of patients who received placebo versus 35% of patients who received lapatinib (HR, 1.10; 95% CI, 0.85-1.43; P = .45). No significant differences in DFS were observed between treatment arms by human papillomavirus or EGFR status.
Lapatinib is a small-molecule inhibitor of epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 2 (HER2) and was postulated to be active in squamous cell carcinoma of the head and neck tumors because many overexpress EGFR. Lapatinib has shown efficacy in HER2-positive metastatic breast cancer, but not in other EGFR-driven cancers.
Compliance was high in both placebo and lapatinib arms, with 83% and 76%, respectively, achieving greater than 80% compliance. Adverse events of grade 3 or higher were observed in 67% of the placebo arm and 75% of the lapatinib arm. The most common grade 3 or 4 adverse events were lymphopenia and mucosal inflammation.
Lapatinib in combination with platinum-based chemoradiotherapy and as long-term maintenance therapy showed no benefit in patients with surgically treated high-risk squamous cell carcinoma of the head and neck (SCCHN).
No difference was observed between treatment arms in the primary endpoint of disease-free survival (DFS) or the secondary endpoints of investigator-assessed DFS and overall survival.
“Certainly, these findings should serve as a note of caution on the risks of initiating large phase III studies (of this and other drugs) with insufficient evidence of single-agent activity,” wrote Dr. Kevin Harrington of the division of radiotherapy and imaging at the Institute of Cancer Research and Royal Marsden Hospital, London, and his colleagues (Journ Clin Onc. 2015 Nov. 2. doi: 10.1200/JCO.2015.61.4370).
The placebo-controlled phase III trial from 84 sites in 21 countries randomized 688 patients with resected SCCHN to receive placebo or lapatinib. The study was halted early because of the apparent plateauing of DFS events at the median follow-up time of 35.3 months, the investigators reported.
DFS events (disease recurrence or death) occurred in 32% of patients who received placebo versus 35% of patients who received lapatinib (HR, 1.10; 95% CI, 0.85-1.43; P = .45). No significant differences in DFS were observed between treatment arms by human papillomavirus or EGFR status.
Lapatinib is a small-molecule inhibitor of epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 2 (HER2) and was postulated to be active in squamous cell carcinoma of the head and neck tumors because many overexpress EGFR. Lapatinib has shown efficacy in HER2-positive metastatic breast cancer, but not in other EGFR-driven cancers.
Compliance was high in both placebo and lapatinib arms, with 83% and 76%, respectively, achieving greater than 80% compliance. Adverse events of grade 3 or higher were observed in 67% of the placebo arm and 75% of the lapatinib arm. The most common grade 3 or 4 adverse events were lymphopenia and mucosal inflammation.
Lapatinib in combination with platinum-based chemoradiotherapy and as long-term maintenance therapy showed no benefit in patients with surgically treated high-risk squamous cell carcinoma of the head and neck (SCCHN).
No difference was observed between treatment arms in the primary endpoint of disease-free survival (DFS) or the secondary endpoints of investigator-assessed DFS and overall survival.
“Certainly, these findings should serve as a note of caution on the risks of initiating large phase III studies (of this and other drugs) with insufficient evidence of single-agent activity,” wrote Dr. Kevin Harrington of the division of radiotherapy and imaging at the Institute of Cancer Research and Royal Marsden Hospital, London, and his colleagues (Journ Clin Onc. 2015 Nov. 2. doi: 10.1200/JCO.2015.61.4370).
The placebo-controlled phase III trial from 84 sites in 21 countries randomized 688 patients with resected SCCHN to receive placebo or lapatinib. The study was halted early because of the apparent plateauing of DFS events at the median follow-up time of 35.3 months, the investigators reported.
DFS events (disease recurrence or death) occurred in 32% of patients who received placebo versus 35% of patients who received lapatinib (HR, 1.10; 95% CI, 0.85-1.43; P = .45). No significant differences in DFS were observed between treatment arms by human papillomavirus or EGFR status.
Lapatinib is a small-molecule inhibitor of epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 2 (HER2) and was postulated to be active in squamous cell carcinoma of the head and neck tumors because many overexpress EGFR. Lapatinib has shown efficacy in HER2-positive metastatic breast cancer, but not in other EGFR-driven cancers.
Compliance was high in both placebo and lapatinib arms, with 83% and 76%, respectively, achieving greater than 80% compliance. Adverse events of grade 3 or higher were observed in 67% of the placebo arm and 75% of the lapatinib arm. The most common grade 3 or 4 adverse events were lymphopenia and mucosal inflammation.
Key clinical point: After surgery for high-risk squamous cell carcinoma of the head and neck, the addition of lapatinib to chemoradiotherapy and as long-term maintenance therapy offered no benefit.
Major finding: Disease-free survival events occurred in 32% of patients who received placebo versus 35% of patients who received lapatinib (HR, 1.10; 95% CI, 0.85-1.43; P = .45).
Data source: A phase III trial from 84 sites in 21 countries randomizing 688 patients with resected SCCHN to receive placebo or lapatinib.
Disclosures: Dr. Harrington reported financial ties to Merck Sharp & Dohme, Oncos Therapeutics, Cellgene, Viralytics, Lytix, Oncolytics Biotech, Genelux, and AstraZeneca. Several of his coauthors reported ties to industry sources.
Severe acne patients stay on antibiotics too long
Patients with severe acne often remained on antibiotics longer than recommended before beginning treatment with isotretinoin, in a retrospective chart review of patients treated for acne at New York University.
The medical records analysis of 137 patients with severe acne who eventually received isotretinoin found that the average duration of antibiotic use in these patients was 331.3 days, far exceeding expert recommendations to limit use to 3 months, reported Dr. Arielle R. Nagler and her associates in the department of dermatology, New York University.

In total, 15.3% of patients in the study were treated with antibiotics for 3 months or less, and 64.2% were treated with antibiotics for 6 months or longer. Almost 34% were treated with antibiotics for 1 year or longer.
The mean time elapsed between the first recorded mention of possible isotretinoin use and actual initiation of treatment was 155.8 days, Dr. Nagler and her colleagues reported. The mean age of initiation of isotretinoin was 19.6 years.
“Prolonged courses of systemic antibiotics are discouraged for several reasons including increasing resistance of P. acnes [Propionibacterium acnes] to antibiotics,” the authors wrote. “Courses 6 months or longer are highly likely to induce resistance.”
Patients who received antibiotic treatment only at the study site took antibiotics for a mean duration of 283.1 days, whereas those treated at multiple institutions had a mean duration of 380.2 days, they added (P = .054).
“Dermatologists should be aware that patients presenting to them who have been cared for by other providers are at particular risk for extended courses of antibiotics,” they said.
To help reduce unnecessary antibiotic use, providers should recognize patients who are not improving after 6-8 weeks, and consider starting isotretinoin therapy “at an earlier time point, especially in those with severe acne,” Dr. Nagler and her coauthors advised.
Read the full report in the Journal of the American Academy of Dermatology.
Patients with severe acne often remained on antibiotics longer than recommended before beginning treatment with isotretinoin, in a retrospective chart review of patients treated for acne at New York University.
The medical records analysis of 137 patients with severe acne who eventually received isotretinoin found that the average duration of antibiotic use in these patients was 331.3 days, far exceeding expert recommendations to limit use to 3 months, reported Dr. Arielle R. Nagler and her associates in the department of dermatology, New York University.
In total, 15.3% of patients in the study were treated with antibiotics for 3 months or less, and 64.2% were treated with antibiotics for 6 months or longer. Almost 34% were treated with antibiotics for 1 year or longer.
The mean time elapsed between the first recorded mention of possible isotretinoin use and actual initiation of treatment was 155.8 days, Dr. Nagler and her colleagues reported. The mean age of initiation of isotretinoin was 19.6 years.
“Prolonged courses of systemic antibiotics are discouraged for several reasons including increasing resistance of P. acnes [Propionibacterium acnes] to antibiotics,” the authors wrote. “Courses 6 months or longer are highly likely to induce resistance.”
Patients who received antibiotic treatment only at the study site took antibiotics for a mean duration of 283.1 days, whereas those treated at multiple institutions had a mean duration of 380.2 days, they added (P = .054).
“Dermatologists should be aware that patients presenting to them who have been cared for by other providers are at particular risk for extended courses of antibiotics,” they said.
To help reduce unnecessary antibiotic use, providers should recognize patients who are not improving after 6-8 weeks, and consider starting isotretinoin therapy “at an earlier time point, especially in those with severe acne,” Dr. Nagler and her coauthors advised.
Read the full report in the Journal of the American Academy of Dermatology.
Patients with severe acne often remained on antibiotics longer than recommended before beginning treatment with isotretinoin, in a retrospective chart review of patients treated for acne at New York University.
The medical records analysis of 137 patients with severe acne who eventually received isotretinoin found that the average duration of antibiotic use in these patients was 331.3 days, far exceeding expert recommendations to limit use to 3 months, reported Dr. Arielle R. Nagler and her associates in the department of dermatology, New York University.
In total, 15.3% of patients in the study were treated with antibiotics for 3 months or less, and 64.2% were treated with antibiotics for 6 months or longer. Almost 34% were treated with antibiotics for 1 year or longer.
The mean time elapsed between the first recorded mention of possible isotretinoin use and actual initiation of treatment was 155.8 days, Dr. Nagler and her colleagues reported. The mean age of initiation of isotretinoin was 19.6 years.
“Prolonged courses of systemic antibiotics are discouraged for several reasons including increasing resistance of P. acnes [Propionibacterium acnes] to antibiotics,” the authors wrote. “Courses 6 months or longer are highly likely to induce resistance.”
Patients who received antibiotic treatment only at the study site took antibiotics for a mean duration of 283.1 days, whereas those treated at multiple institutions had a mean duration of 380.2 days, they added (P = .054).
“Dermatologists should be aware that patients presenting to them who have been cared for by other providers are at particular risk for extended courses of antibiotics,” they said.
To help reduce unnecessary antibiotic use, providers should recognize patients who are not improving after 6-8 weeks, and consider starting isotretinoin therapy “at an earlier time point, especially in those with severe acne,” Dr. Nagler and her coauthors advised.
Read the full report in the Journal of the American Academy of Dermatology.

CMS Releases Updated Two-Midnight Rule for 2016
On November 13, the Centers for Medicare & Medicaid Services (CMS) is scheduled to publish its final OPPS rule for 2016. One of the biggest impacts for hospitalists is the update to the two-midnight rule. Here are six areas of interest to hospitalists:
1. The two-midnight rule became effective just over two years ago, on October 1, 2013. The purpose of the rule is to define which Medicare beneficiary hospital stays are appropriate for Medicare Part A payment.
2. The original rule stated that if the physician (or other practitioner) expects the patient to stay for fewer than two midnights, then the services should be billed as outpatient (Medicare Part B), and not inpatient.
3. In the first two years of this rule, the only exception was for those diagnoses that CMS designates as “inpatient only.”
4. The new rule modifies the exceptions to the two-midnight rule. Under the new rule, the exception can now be determined by the physician (or other practitioner) on a “case-by-case basis.” Every case can still be subjected to medical review.
5. Another change is that short stays will no longer be reviewed by Medicare administrative contractors or recovery audit contractors, which are usually funded on a contingency basis. Under the updated rule, the quality improvement organization contractors will review short inpatient stays. This went into effect on October 1, 2015.
6. Additionally, the new rule does state “we [CMS] continue to expect that stays under 24 hours would rarely qualify for an exception to the two-midnight benchmark.”
On November 13, the Centers for Medicare & Medicaid Services (CMS) is scheduled to publish its final OPPS rule for 2016. One of the biggest impacts for hospitalists is the update to the two-midnight rule. Here are six areas of interest to hospitalists:
1. The two-midnight rule became effective just over two years ago, on October 1, 2013. The purpose of the rule is to define which Medicare beneficiary hospital stays are appropriate for Medicare Part A payment.
2. The original rule stated that if the physician (or other practitioner) expects the patient to stay for fewer than two midnights, then the services should be billed as outpatient (Medicare Part B), and not inpatient.
3. In the first two years of this rule, the only exception was for those diagnoses that CMS designates as “inpatient only.”
4. The new rule modifies the exceptions to the two-midnight rule. Under the new rule, the exception can now be determined by the physician (or other practitioner) on a “case-by-case basis.” Every case can still be subjected to medical review.
5. Another change is that short stays will no longer be reviewed by Medicare administrative contractors or recovery audit contractors, which are usually funded on a contingency basis. Under the updated rule, the quality improvement organization contractors will review short inpatient stays. This went into effect on October 1, 2015.
6. Additionally, the new rule does state “we [CMS] continue to expect that stays under 24 hours would rarely qualify for an exception to the two-midnight benchmark.”
On November 13, the Centers for Medicare & Medicaid Services (CMS) is scheduled to publish its final OPPS rule for 2016. One of the biggest impacts for hospitalists is the update to the two-midnight rule. Here are six areas of interest to hospitalists:
1. The two-midnight rule became effective just over two years ago, on October 1, 2013. The purpose of the rule is to define which Medicare beneficiary hospital stays are appropriate for Medicare Part A payment.
2. The original rule stated that if the physician (or other practitioner) expects the patient to stay for fewer than two midnights, then the services should be billed as outpatient (Medicare Part B), and not inpatient.
3. In the first two years of this rule, the only exception was for those diagnoses that CMS designates as “inpatient only.”
4. The new rule modifies the exceptions to the two-midnight rule. Under the new rule, the exception can now be determined by the physician (or other practitioner) on a “case-by-case basis.” Every case can still be subjected to medical review.
5. Another change is that short stays will no longer be reviewed by Medicare administrative contractors or recovery audit contractors, which are usually funded on a contingency basis. Under the updated rule, the quality improvement organization contractors will review short inpatient stays. This went into effect on October 1, 2015.
6. Additionally, the new rule does state “we [CMS] continue to expect that stays under 24 hours would rarely qualify for an exception to the two-midnight benchmark.”
Even subclinical hypothyroidism ups risk for metabolic syndrome
LAKE BUENA VISTA, FLA. – Patients with low thyroid function may experience a “double whammy” of hypothyroidism and metabolic syndrome.
Even subclinical hypothyroidism affects many metabolic pathways that can contribute to deranged glucose and lipid metabolism, raising the risk of metabolic syndrome, according to Dr. Gabriela Brenta of the department of endocrinology at the Dr. Cesar Milstein Hospital in Buenos Aires. Though some mechanisms are incompletely understood, the association is clear enough to warrant screening all metabolic syndrome patients for hypothyroidism, she said.
Dr. Brenta described the recent work she and others have completed in the field. Basic science work revealed some early clues. For example, those who studied the effects of acute thyroid hormone withdrawal on patients with no thyroid gland found that these patients saw a rapid rise in insulin resistance. It’s known that even subclinical insulin resistance can lead to impaired glucose metabolism, making it logical to follow both normal and deranged metabolic pathways to help sort out the relationship between thyroid dysfunction and impaired glucose metabolism, she reported at the International Thyroid Congress.
Hypothyroidism can affect glucose homeostasis through multiple mechanisms, said Dr. Brenta. Firstly, hypothyroidism can lead to decreased hepatic gluconeogenesis and glycogenolysis. Hypothyroidism also can lead to reduced baseline plasma insulin levels and increased postglucose insulin secretion. In the peripheral tissues, hypothyroidism can interfere with glucose metabolism and disposal. All of these mechanisms can decrease hepatic glucose metabolism and lead to a postabsorptive hyperglycemia state, said Dr. Brenta, noting: “Insulin resistance is in some way the backbone of metabolic syndrome.”
Lipid metabolism is also affected by subclinical hypothyroidism, which can decrease expression of mRNA for LDL-C receptors, leading to LDL-C receptor down-regulation. With fewer receptors available, serum levels of LDL-C increase, with resultant increased susceptibility to oxidative effects and increased foam cell generation.
Dr. Brenta cited her earlier work showing that “triglyceride enrichment of LDL particles correlates with lower hepatic lipase activity” for individuals with subclinical hypothyroidism, with significantly lower hepatic lipase activity and a higher LDL-C to triglyceride ratio for those patients than for controls (Thyroid. 2007 May;17[5]:453-60). Overall, in hypothyroidism, “LDL particles are exposed to more substances that make them more atherogenic with decreased degradation and increased half-life,” said Dr. Brenta.
The increased risk for hypertension in both subclinical and overt hypothyroidism may be related, in part, to the fact that triiodothyronine deficiency can contribute to endothelial dysfunction. The relationship between subclinical hypothyroidism and hypertension was confirmed in a 2011 meta-analysis, said Dr. Brenta (Hypertens Res. 2011 Oct;34[10]:1098-105).
Though many factors contribute to obesity and thyroid function alone does not regulate body weight, a large population-based Danish study found that “even mild elevations of TSH are important for body weight,” said Dr. Brenta. The relationship is complex and bidirectional – a classic “chicken and egg” story – since obesity also may modulate TSH, she said; “however, we must not forget the ample literature on low levels of thyroid hormones reducing resting energy expenditure” (J Clin Endocrinol Metab. 2005 Jul;90[7]:4019-24).
Even though TSH tends to rise naturally through the lifespan, the association between elevated TSH and increased risk of metabolic syndrome held true even for older patients in one study, with “each one unit increase in TSH predicting a 3% increase in the odds of metabolic syndrome,” even after adjustment for age, BMI, and HOMA-IR status, among other variables, said Dr. Brenta (Clin Endocrinol [Oxf]. 2012 Jun;76[6]:911-8).
Advocating for universal screening for hypothyroidism among patients with metabolic syndrome, Dr. Brenta said that “hypothyroid disturbances are associated with an adverse metabolic profile, and even low normal TSH levels are associated with the metabolic traits of metabolic syndrome.”
The meeting was held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society. Dr. Brenta did not identify any conflicts of interest.
On Twitter @karioakes
LAKE BUENA VISTA, FLA. – Patients with low thyroid function may experience a “double whammy” of hypothyroidism and metabolic syndrome.
Even subclinical hypothyroidism affects many metabolic pathways that can contribute to deranged glucose and lipid metabolism, raising the risk of metabolic syndrome, according to Dr. Gabriela Brenta of the department of endocrinology at the Dr. Cesar Milstein Hospital in Buenos Aires. Though some mechanisms are incompletely understood, the association is clear enough to warrant screening all metabolic syndrome patients for hypothyroidism, she said.
Dr. Brenta described the recent work she and others have completed in the field. Basic science work revealed some early clues. For example, those who studied the effects of acute thyroid hormone withdrawal on patients with no thyroid gland found that these patients saw a rapid rise in insulin resistance. It’s known that even subclinical insulin resistance can lead to impaired glucose metabolism, making it logical to follow both normal and deranged metabolic pathways to help sort out the relationship between thyroid dysfunction and impaired glucose metabolism, she reported at the International Thyroid Congress.
Hypothyroidism can affect glucose homeostasis through multiple mechanisms, said Dr. Brenta. Firstly, hypothyroidism can lead to decreased hepatic gluconeogenesis and glycogenolysis. Hypothyroidism also can lead to reduced baseline plasma insulin levels and increased postglucose insulin secretion. In the peripheral tissues, hypothyroidism can interfere with glucose metabolism and disposal. All of these mechanisms can decrease hepatic glucose metabolism and lead to a postabsorptive hyperglycemia state, said Dr. Brenta, noting: “Insulin resistance is in some way the backbone of metabolic syndrome.”
Lipid metabolism is also affected by subclinical hypothyroidism, which can decrease expression of mRNA for LDL-C receptors, leading to LDL-C receptor down-regulation. With fewer receptors available, serum levels of LDL-C increase, with resultant increased susceptibility to oxidative effects and increased foam cell generation.
Dr. Brenta cited her earlier work showing that “triglyceride enrichment of LDL particles correlates with lower hepatic lipase activity” for individuals with subclinical hypothyroidism, with significantly lower hepatic lipase activity and a higher LDL-C to triglyceride ratio for those patients than for controls (Thyroid. 2007 May;17[5]:453-60). Overall, in hypothyroidism, “LDL particles are exposed to more substances that make them more atherogenic with decreased degradation and increased half-life,” said Dr. Brenta.
The increased risk for hypertension in both subclinical and overt hypothyroidism may be related, in part, to the fact that triiodothyronine deficiency can contribute to endothelial dysfunction. The relationship between subclinical hypothyroidism and hypertension was confirmed in a 2011 meta-analysis, said Dr. Brenta (Hypertens Res. 2011 Oct;34[10]:1098-105).
Though many factors contribute to obesity and thyroid function alone does not regulate body weight, a large population-based Danish study found that “even mild elevations of TSH are important for body weight,” said Dr. Brenta. The relationship is complex and bidirectional – a classic “chicken and egg” story – since obesity also may modulate TSH, she said; “however, we must not forget the ample literature on low levels of thyroid hormones reducing resting energy expenditure” (J Clin Endocrinol Metab. 2005 Jul;90[7]:4019-24).
Even though TSH tends to rise naturally through the lifespan, the association between elevated TSH and increased risk of metabolic syndrome held true even for older patients in one study, with “each one unit increase in TSH predicting a 3% increase in the odds of metabolic syndrome,” even after adjustment for age, BMI, and HOMA-IR status, among other variables, said Dr. Brenta (Clin Endocrinol [Oxf]. 2012 Jun;76[6]:911-8).
Advocating for universal screening for hypothyroidism among patients with metabolic syndrome, Dr. Brenta said that “hypothyroid disturbances are associated with an adverse metabolic profile, and even low normal TSH levels are associated with the metabolic traits of metabolic syndrome.”
The meeting was held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society. Dr. Brenta did not identify any conflicts of interest.
On Twitter @karioakes
LAKE BUENA VISTA, FLA. – Patients with low thyroid function may experience a “double whammy” of hypothyroidism and metabolic syndrome.
Even subclinical hypothyroidism affects many metabolic pathways that can contribute to deranged glucose and lipid metabolism, raising the risk of metabolic syndrome, according to Dr. Gabriela Brenta of the department of endocrinology at the Dr. Cesar Milstein Hospital in Buenos Aires. Though some mechanisms are incompletely understood, the association is clear enough to warrant screening all metabolic syndrome patients for hypothyroidism, she said.
Dr. Brenta described the recent work she and others have completed in the field. Basic science work revealed some early clues. For example, those who studied the effects of acute thyroid hormone withdrawal on patients with no thyroid gland found that these patients saw a rapid rise in insulin resistance. It’s known that even subclinical insulin resistance can lead to impaired glucose metabolism, making it logical to follow both normal and deranged metabolic pathways to help sort out the relationship between thyroid dysfunction and impaired glucose metabolism, she reported at the International Thyroid Congress.
Hypothyroidism can affect glucose homeostasis through multiple mechanisms, said Dr. Brenta. Firstly, hypothyroidism can lead to decreased hepatic gluconeogenesis and glycogenolysis. Hypothyroidism also can lead to reduced baseline plasma insulin levels and increased postglucose insulin secretion. In the peripheral tissues, hypothyroidism can interfere with glucose metabolism and disposal. All of these mechanisms can decrease hepatic glucose metabolism and lead to a postabsorptive hyperglycemia state, said Dr. Brenta, noting: “Insulin resistance is in some way the backbone of metabolic syndrome.”
Lipid metabolism is also affected by subclinical hypothyroidism, which can decrease expression of mRNA for LDL-C receptors, leading to LDL-C receptor down-regulation. With fewer receptors available, serum levels of LDL-C increase, with resultant increased susceptibility to oxidative effects and increased foam cell generation.
Dr. Brenta cited her earlier work showing that “triglyceride enrichment of LDL particles correlates with lower hepatic lipase activity” for individuals with subclinical hypothyroidism, with significantly lower hepatic lipase activity and a higher LDL-C to triglyceride ratio for those patients than for controls (Thyroid. 2007 May;17[5]:453-60). Overall, in hypothyroidism, “LDL particles are exposed to more substances that make them more atherogenic with decreased degradation and increased half-life,” said Dr. Brenta.
The increased risk for hypertension in both subclinical and overt hypothyroidism may be related, in part, to the fact that triiodothyronine deficiency can contribute to endothelial dysfunction. The relationship between subclinical hypothyroidism and hypertension was confirmed in a 2011 meta-analysis, said Dr. Brenta (Hypertens Res. 2011 Oct;34[10]:1098-105).
Though many factors contribute to obesity and thyroid function alone does not regulate body weight, a large population-based Danish study found that “even mild elevations of TSH are important for body weight,” said Dr. Brenta. The relationship is complex and bidirectional – a classic “chicken and egg” story – since obesity also may modulate TSH, she said; “however, we must not forget the ample literature on low levels of thyroid hormones reducing resting energy expenditure” (J Clin Endocrinol Metab. 2005 Jul;90[7]:4019-24).
Even though TSH tends to rise naturally through the lifespan, the association between elevated TSH and increased risk of metabolic syndrome held true even for older patients in one study, with “each one unit increase in TSH predicting a 3% increase in the odds of metabolic syndrome,” even after adjustment for age, BMI, and HOMA-IR status, among other variables, said Dr. Brenta (Clin Endocrinol [Oxf]. 2012 Jun;76[6]:911-8).
Advocating for universal screening for hypothyroidism among patients with metabolic syndrome, Dr. Brenta said that “hypothyroid disturbances are associated with an adverse metabolic profile, and even low normal TSH levels are associated with the metabolic traits of metabolic syndrome.”
The meeting was held by the American Thyroid Association, Asia-Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society. Dr. Brenta did not identify any conflicts of interest.
On Twitter @karioakes
EXPERT ANALYSIS FROM ITC 2015
Gastrointestinal and liver diseases remain substantial public health burden
Diseases such as Clostridium difficile infection, inflammatory bowel disease, and liver cancer continue to cost billions and cause many thousands of deaths in the United States every year, investigators reported in the December issue of Gastroenterology.
“Gastrointestinal and liver diseases are a source of substantial burden and cost,” said Dr. Anne Peery and her associates at the University of North Carolina School of Medicine and the Gillings School of Public Health, both in Chapel Hill. The Affordable Care Act has extended health insurance to more than 16 million Americans, which is “expected to change the landscape of care for GI illnesses” and intensifies the need for their comprehensive study, the researchers added.
They analyzed health care visits, costs, and deaths from GI, pancreatic, and hepatic diseases for 2007 through 2012 by using surveillance data from the Centers for Disease Control and Prevention, the Agency for Healthcare Research and Quality, and the National Cancer Institute. Chronic hepatitis C virus infection was a leading disease burden, they found. Associated emergency department visits rose by 176% between 2006 and 2012, hospital admissions increased by 225% between 2003 and 2012, and in-hospital mortality approached 6%. These trends reflect the aging of baby boomers, who make up three-quarters of infected patients, the investigators noted. As a result, rates of new liver cancers also are rising, and end-stage liver disease is expected to keep increasing until 2030, they added (Gastroenterology. 2015 Aug 20. doi: 10.1053/j.gastro.2015.08.045). Aging boomers are increasingly seeking care for other age-related GI disorders, the investigators reported. Outpatient visits for hemorrhoids are rising, as are emergency department visits for constipation and lower-GI bleeding, and hospitalizations for acute diverticulitis and C. difficile infection. Gastrointestinal hemorrhage was the most common diagnosis at hospitalization, accounting for more than 500,000 discharges and costing almost $5 billion dollars in 2012 alone, the researchers said.
Despite better treatments, hospital admissions for Crohn’s disease and ulcerative colitis also rose from less than 60,000 in 1993 to about 100,000 in 2012, said Dr. Peery and her associates. “This is congruent with earlier trends using the National Hospital Discharge Survey. Emergency department visits [for inflammatory bowel disease] are also rising,” they added.
In contrast, cases and deaths from colorectal cancer continue to drop, partly because of intensified screening efforts, the investigators said. They called the trend “encouraging,” but noted that CRC still tops cancers of the pancreas, liver, and intrahepatic bile ducts as the leading GI cause of mortality in the United States. In 2012, more than 51,000 Americans died from CRC, and screening efforts captured only 58% of those between 50 and 75 years old. Boosting that percentage to 80% by 2018 http://nccrt.org/tools/80-percent-by-2018/ could prevent 280,000 CRC cases and 200,000 deaths within 20 years, Dr. Peery and her associates noted.
The National Institutes of Health helped fund the work. The investigators reported having no conflicts of interest.
Source: American Gastroenterological Association
In the excellent study by Peery and colleagues, statistics on health care utilization in the ambulatory and hospital settings, incidence and mortality from GI cancers, and mortality associated with other GI illnesses from 2007 to 2012 was collected using data from multiple complementary databases. This is the ideal methodology for this type of study because it quantifies utilization data from several complementary national databases. Of course, these data may be limited by systematic errors in ICD coding and costs are estimated using Medicare’s cost-to-charge ratio. Nevertheless, these data provide the best “snap shot” of trends in the burden of gastrointestinal and liver illness as of 2012.
What are the key points? First, the increase in the burden of GI and liver illness probably reflects the aging of the “baby boomer” population. Furthermore, since the Affordable Care Act is expanding access to health care, the burden on gastroenterologists is also likely to expand. Second, although we’re doing a good job with CRC screening, there is also room for improvement. While the incidence of CRC continues to decrease, only 58% of adults aged 50-75 years old had CRC screening in 2010. Third, HCV-associated hospitalizations have doubled from 2003 to 2012. Since HCV-associated cirrhosis is likely to increase until 2030, insurers and public health officials will have to carefully weigh the initial high cost of using new and highly effective regimens of direct-acting antiviral agents versus the downstream costs of managing these individuals after developing decompensated cirrhosis.
Dr. Philip S. Schoenfeld is professor of medicine and director, training program in GI epidemiology, division of gastroenterology, University of Michigan, Ann Arbor. He has no conflicts of interest.
In the excellent study by Peery and colleagues, statistics on health care utilization in the ambulatory and hospital settings, incidence and mortality from GI cancers, and mortality associated with other GI illnesses from 2007 to 2012 was collected using data from multiple complementary databases. This is the ideal methodology for this type of study because it quantifies utilization data from several complementary national databases. Of course, these data may be limited by systematic errors in ICD coding and costs are estimated using Medicare’s cost-to-charge ratio. Nevertheless, these data provide the best “snap shot” of trends in the burden of gastrointestinal and liver illness as of 2012.
What are the key points? First, the increase in the burden of GI and liver illness probably reflects the aging of the “baby boomer” population. Furthermore, since the Affordable Care Act is expanding access to health care, the burden on gastroenterologists is also likely to expand. Second, although we’re doing a good job with CRC screening, there is also room for improvement. While the incidence of CRC continues to decrease, only 58% of adults aged 50-75 years old had CRC screening in 2010. Third, HCV-associated hospitalizations have doubled from 2003 to 2012. Since HCV-associated cirrhosis is likely to increase until 2030, insurers and public health officials will have to carefully weigh the initial high cost of using new and highly effective regimens of direct-acting antiviral agents versus the downstream costs of managing these individuals after developing decompensated cirrhosis.
Dr. Philip S. Schoenfeld is professor of medicine and director, training program in GI epidemiology, division of gastroenterology, University of Michigan, Ann Arbor. He has no conflicts of interest.
In the excellent study by Peery and colleagues, statistics on health care utilization in the ambulatory and hospital settings, incidence and mortality from GI cancers, and mortality associated with other GI illnesses from 2007 to 2012 was collected using data from multiple complementary databases. This is the ideal methodology for this type of study because it quantifies utilization data from several complementary national databases. Of course, these data may be limited by systematic errors in ICD coding and costs are estimated using Medicare’s cost-to-charge ratio. Nevertheless, these data provide the best “snap shot” of trends in the burden of gastrointestinal and liver illness as of 2012.
What are the key points? First, the increase in the burden of GI and liver illness probably reflects the aging of the “baby boomer” population. Furthermore, since the Affordable Care Act is expanding access to health care, the burden on gastroenterologists is also likely to expand. Second, although we’re doing a good job with CRC screening, there is also room for improvement. While the incidence of CRC continues to decrease, only 58% of adults aged 50-75 years old had CRC screening in 2010. Third, HCV-associated hospitalizations have doubled from 2003 to 2012. Since HCV-associated cirrhosis is likely to increase until 2030, insurers and public health officials will have to carefully weigh the initial high cost of using new and highly effective regimens of direct-acting antiviral agents versus the downstream costs of managing these individuals after developing decompensated cirrhosis.
Dr. Philip S. Schoenfeld is professor of medicine and director, training program in GI epidemiology, division of gastroenterology, University of Michigan, Ann Arbor. He has no conflicts of interest.
Diseases such as Clostridium difficile infection, inflammatory bowel disease, and liver cancer continue to cost billions and cause many thousands of deaths in the United States every year, investigators reported in the December issue of Gastroenterology.
“Gastrointestinal and liver diseases are a source of substantial burden and cost,” said Dr. Anne Peery and her associates at the University of North Carolina School of Medicine and the Gillings School of Public Health, both in Chapel Hill. The Affordable Care Act has extended health insurance to more than 16 million Americans, which is “expected to change the landscape of care for GI illnesses” and intensifies the need for their comprehensive study, the researchers added.
They analyzed health care visits, costs, and deaths from GI, pancreatic, and hepatic diseases for 2007 through 2012 by using surveillance data from the Centers for Disease Control and Prevention, the Agency for Healthcare Research and Quality, and the National Cancer Institute. Chronic hepatitis C virus infection was a leading disease burden, they found. Associated emergency department visits rose by 176% between 2006 and 2012, hospital admissions increased by 225% between 2003 and 2012, and in-hospital mortality approached 6%. These trends reflect the aging of baby boomers, who make up three-quarters of infected patients, the investigators noted. As a result, rates of new liver cancers also are rising, and end-stage liver disease is expected to keep increasing until 2030, they added (Gastroenterology. 2015 Aug 20. doi: 10.1053/j.gastro.2015.08.045). Aging boomers are increasingly seeking care for other age-related GI disorders, the investigators reported. Outpatient visits for hemorrhoids are rising, as are emergency department visits for constipation and lower-GI bleeding, and hospitalizations for acute diverticulitis and C. difficile infection. Gastrointestinal hemorrhage was the most common diagnosis at hospitalization, accounting for more than 500,000 discharges and costing almost $5 billion dollars in 2012 alone, the researchers said.
Despite better treatments, hospital admissions for Crohn’s disease and ulcerative colitis also rose from less than 60,000 in 1993 to about 100,000 in 2012, said Dr. Peery and her associates. “This is congruent with earlier trends using the National Hospital Discharge Survey. Emergency department visits [for inflammatory bowel disease] are also rising,” they added.
In contrast, cases and deaths from colorectal cancer continue to drop, partly because of intensified screening efforts, the investigators said. They called the trend “encouraging,” but noted that CRC still tops cancers of the pancreas, liver, and intrahepatic bile ducts as the leading GI cause of mortality in the United States. In 2012, more than 51,000 Americans died from CRC, and screening efforts captured only 58% of those between 50 and 75 years old. Boosting that percentage to 80% by 2018 http://nccrt.org/tools/80-percent-by-2018/ could prevent 280,000 CRC cases and 200,000 deaths within 20 years, Dr. Peery and her associates noted.
The National Institutes of Health helped fund the work. The investigators reported having no conflicts of interest.
Source: American Gastroenterological Association
Diseases such as Clostridium difficile infection, inflammatory bowel disease, and liver cancer continue to cost billions and cause many thousands of deaths in the United States every year, investigators reported in the December issue of Gastroenterology.
“Gastrointestinal and liver diseases are a source of substantial burden and cost,” said Dr. Anne Peery and her associates at the University of North Carolina School of Medicine and the Gillings School of Public Health, both in Chapel Hill. The Affordable Care Act has extended health insurance to more than 16 million Americans, which is “expected to change the landscape of care for GI illnesses” and intensifies the need for their comprehensive study, the researchers added.
They analyzed health care visits, costs, and deaths from GI, pancreatic, and hepatic diseases for 2007 through 2012 by using surveillance data from the Centers for Disease Control and Prevention, the Agency for Healthcare Research and Quality, and the National Cancer Institute. Chronic hepatitis C virus infection was a leading disease burden, they found. Associated emergency department visits rose by 176% between 2006 and 2012, hospital admissions increased by 225% between 2003 and 2012, and in-hospital mortality approached 6%. These trends reflect the aging of baby boomers, who make up three-quarters of infected patients, the investigators noted. As a result, rates of new liver cancers also are rising, and end-stage liver disease is expected to keep increasing until 2030, they added (Gastroenterology. 2015 Aug 20. doi: 10.1053/j.gastro.2015.08.045). Aging boomers are increasingly seeking care for other age-related GI disorders, the investigators reported. Outpatient visits for hemorrhoids are rising, as are emergency department visits for constipation and lower-GI bleeding, and hospitalizations for acute diverticulitis and C. difficile infection. Gastrointestinal hemorrhage was the most common diagnosis at hospitalization, accounting for more than 500,000 discharges and costing almost $5 billion dollars in 2012 alone, the researchers said.
Despite better treatments, hospital admissions for Crohn’s disease and ulcerative colitis also rose from less than 60,000 in 1993 to about 100,000 in 2012, said Dr. Peery and her associates. “This is congruent with earlier trends using the National Hospital Discharge Survey. Emergency department visits [for inflammatory bowel disease] are also rising,” they added.
In contrast, cases and deaths from colorectal cancer continue to drop, partly because of intensified screening efforts, the investigators said. They called the trend “encouraging,” but noted that CRC still tops cancers of the pancreas, liver, and intrahepatic bile ducts as the leading GI cause of mortality in the United States. In 2012, more than 51,000 Americans died from CRC, and screening efforts captured only 58% of those between 50 and 75 years old. Boosting that percentage to 80% by 2018 http://nccrt.org/tools/80-percent-by-2018/ could prevent 280,000 CRC cases and 200,000 deaths within 20 years, Dr. Peery and her associates noted.
The National Institutes of Health helped fund the work. The investigators reported having no conflicts of interest.
Source: American Gastroenterological Association
FROM GASTROENTEROLOGY
Key clinical point: Gastrointestinal and liver diseases remain a major cause of health care utilization and associated costs in the United States.
Major finding: Hospital admissions and associated costs for Clostridium difficile infection, inflammatory bowel disease, and liver disease all rose substantially between 1993 and 2012.
Data source: Analysis of surveillance data from the Centers for Disease Control and Prevention, Agency for Healthcare Research and Quality, and National Cancer Institute.
Disclosures: The National Institutes of Health helped fund the work. The investigators reported having no conflicts of interest.
Prognostic Disclosures Benefit Cancer Patients
When doctors discuss prognosis with advanced cancer patients, those patients have more realistic views of their life expectancy and don't seem to experience a decrease in emotional wellbeing, according to a new study.
"That the vast majority of cancer patients who are dying say that they want to know their prognosis seems surprisingly courageous," said senior author Holly G. Prigerson of Weill Cornell Medical College in New York City.
Every patient needs to know their prognosis, including life expectancy, and expected outcomes of treatment; for example, they should know that chemotherapy cannot cure incurable cancer, Prigerson said.
"Providers often are reluctant to communicate grim news, as anyone would be," she said.
The study included 590 patients with advanced, metastatic cancer who had been treated with at least one round of palliative chemotherapy, which is meant to improve comfort rather than to cure.
Researchers asked the patients whether their oncologist had ever given them a prognosis with a life expectancy estimate, then asked the patients to estimate their own life expectancy and to complete assessments of emotional distress, whether they had advance directives and their end-of-life care preferences.
The patients also described their relationship with their doctors.
Half of the patients survived for less than six months after the study began.
About 70 percent wanted to be told their life expectancy, but only about 18 percent recalled having this discussion with their oncologist.
Half of the patients were willing to estimate their own life expectancy, and those who remembered having a prognosis conversation with their doctor estimated a life expectancy closer to their actual survival than those who did not.
Less than 10 percent of those who remembered having a conversation with their doctor made estimates that were more than five years longer than their actual survival. That compares with 35 percent of those who did not remember having the conversation who overestimated their life expectancy by more than five years.
Remembering a prognostic discussion with a doctor decreased patient estimated life expectancy by about 17 months, when the researchers accounted for other factors, according to the results in the Journal of Clinical Oncology.
Talking to a doctor about life expectancy was not tied to worse doctor-patient relationship, more sadness or higher anxiety, the surveys found.
"It is encouraging that the patients who reported a prognostic disclosure by their oncologist were more realistic in their life-expectancy estimate, more likely to complete a [Do Not Resuscitate] order and to want comfort care," Prigerson said by email.
"There was no emotional fallout that damaged their relationship with their oncologist - as reported by the patient," she said.
Often these conversations should happen, but they do not, for a multitude of reasons, she said. The patient may not be ready to hear bad news, some patients may reject information they are given because they believe a miracle may happen, and other reasons, she said.
"Some patients are not able to hear and process poor prognoses and more harm than good can be done by forcing the situation," Prigerson said. "However, we have found that over 90 percent of patients benefit from prognostic disclosures and it is a minority of patients for religious or personal or social reasons that do not benefit."
When doctors discuss prognosis with advanced cancer patients, those patients have more realistic views of their life expectancy and don't seem to experience a decrease in emotional wellbeing, according to a new study.
"That the vast majority of cancer patients who are dying say that they want to know their prognosis seems surprisingly courageous," said senior author Holly G. Prigerson of Weill Cornell Medical College in New York City.
Every patient needs to know their prognosis, including life expectancy, and expected outcomes of treatment; for example, they should know that chemotherapy cannot cure incurable cancer, Prigerson said.
"Providers often are reluctant to communicate grim news, as anyone would be," she said.
The study included 590 patients with advanced, metastatic cancer who had been treated with at least one round of palliative chemotherapy, which is meant to improve comfort rather than to cure.
Researchers asked the patients whether their oncologist had ever given them a prognosis with a life expectancy estimate, then asked the patients to estimate their own life expectancy and to complete assessments of emotional distress, whether they had advance directives and their end-of-life care preferences.
The patients also described their relationship with their doctors.
Half of the patients survived for less than six months after the study began.
About 70 percent wanted to be told their life expectancy, but only about 18 percent recalled having this discussion with their oncologist.
Half of the patients were willing to estimate their own life expectancy, and those who remembered having a prognosis conversation with their doctor estimated a life expectancy closer to their actual survival than those who did not.
Less than 10 percent of those who remembered having a conversation with their doctor made estimates that were more than five years longer than their actual survival. That compares with 35 percent of those who did not remember having the conversation who overestimated their life expectancy by more than five years.
Remembering a prognostic discussion with a doctor decreased patient estimated life expectancy by about 17 months, when the researchers accounted for other factors, according to the results in the Journal of Clinical Oncology.
Talking to a doctor about life expectancy was not tied to worse doctor-patient relationship, more sadness or higher anxiety, the surveys found.
"It is encouraging that the patients who reported a prognostic disclosure by their oncologist were more realistic in their life-expectancy estimate, more likely to complete a [Do Not Resuscitate] order and to want comfort care," Prigerson said by email.
"There was no emotional fallout that damaged their relationship with their oncologist - as reported by the patient," she said.
Often these conversations should happen, but they do not, for a multitude of reasons, she said. The patient may not be ready to hear bad news, some patients may reject information they are given because they believe a miracle may happen, and other reasons, she said.
"Some patients are not able to hear and process poor prognoses and more harm than good can be done by forcing the situation," Prigerson said. "However, we have found that over 90 percent of patients benefit from prognostic disclosures and it is a minority of patients for religious or personal or social reasons that do not benefit."
When doctors discuss prognosis with advanced cancer patients, those patients have more realistic views of their life expectancy and don't seem to experience a decrease in emotional wellbeing, according to a new study.
"That the vast majority of cancer patients who are dying say that they want to know their prognosis seems surprisingly courageous," said senior author Holly G. Prigerson of Weill Cornell Medical College in New York City.
Every patient needs to know their prognosis, including life expectancy, and expected outcomes of treatment; for example, they should know that chemotherapy cannot cure incurable cancer, Prigerson said.
"Providers often are reluctant to communicate grim news, as anyone would be," she said.
The study included 590 patients with advanced, metastatic cancer who had been treated with at least one round of palliative chemotherapy, which is meant to improve comfort rather than to cure.
Researchers asked the patients whether their oncologist had ever given them a prognosis with a life expectancy estimate, then asked the patients to estimate their own life expectancy and to complete assessments of emotional distress, whether they had advance directives and their end-of-life care preferences.
The patients also described their relationship with their doctors.
Half of the patients survived for less than six months after the study began.
About 70 percent wanted to be told their life expectancy, but only about 18 percent recalled having this discussion with their oncologist.
Half of the patients were willing to estimate their own life expectancy, and those who remembered having a prognosis conversation with their doctor estimated a life expectancy closer to their actual survival than those who did not.
Less than 10 percent of those who remembered having a conversation with their doctor made estimates that were more than five years longer than their actual survival. That compares with 35 percent of those who did not remember having the conversation who overestimated their life expectancy by more than five years.
Remembering a prognostic discussion with a doctor decreased patient estimated life expectancy by about 17 months, when the researchers accounted for other factors, according to the results in the Journal of Clinical Oncology.
Talking to a doctor about life expectancy was not tied to worse doctor-patient relationship, more sadness or higher anxiety, the surveys found.
"It is encouraging that the patients who reported a prognostic disclosure by their oncologist were more realistic in their life-expectancy estimate, more likely to complete a [Do Not Resuscitate] order and to want comfort care," Prigerson said by email.
"There was no emotional fallout that damaged their relationship with their oncologist - as reported by the patient," she said.
Often these conversations should happen, but they do not, for a multitude of reasons, she said. The patient may not be ready to hear bad news, some patients may reject information they are given because they believe a miracle may happen, and other reasons, she said.
"Some patients are not able to hear and process poor prognoses and more harm than good can be done by forcing the situation," Prigerson said. "However, we have found that over 90 percent of patients benefit from prognostic disclosures and it is a minority of patients for religious or personal or social reasons that do not benefit."