User login
With life in the balance, a pediatric palliative care program expands its work to adults
In late March of 2020, when it became clear that hospitals in the greater New York City area would face a capacity crisis in caring for seriously ill patients with COVID-19, members of the leadership team at the Children’s Hospital at Montefiore (CHAM) in the Bronx, N.Y., convened to draft a response plan.

The recommendations put into action that day included moving the hospital’s emergency department from the lower level to the fourth floor, increasing the age limit for patients seen in the ED from 21 years of age to 30 and freeing up an entire hospital floor and a half to accommodate the anticipated surge of patients with COVID-19 admitted to Montefiore’s interconnected adult hospital, according to Sarah E. Norris, MD.
“We made multiple moves all at once,” said Dr. Norris, director of pediatric palliative care at CHAM. “It struck everyone as logical that palliative care had to be expanded, because all of the news we had received as the surge came to New York from around the world was full of death and uncertainty, and would require thoughtful conversations about end-of-life wishes at critical times and how to really respect the person and understand their values.”

When Dr. Norris left the leadership team meeting, she returned to her office, put her face in her hands, and sobbed as she began to process the gravity of what was ahead. “I cried because I knew that so many families were going to suffer a heartbreak, no matter how much we could do,” she said.
Stitching the QUILT
Over the next few days, Dr. Norris began recruiting colleagues from the large Montefiore Health System – most of whom she did not know – who met criteria for work deployment to expand CHAM’s palliative care program of clinician to 27 clinicians consisting of pediatricians, nurse practitioners, and psychologists, to meet the projected needs of COVID-19 patients and their families.
Some candidates for the effort, known as the Quality in Life Team (QUILT), were 65 years of age or older, considered at high risk for developing COVID-19-related complications themselves. Others were immunocompromised or had medical conditions that would not allow them to have direct contact with COVID-19 patients. “There were also clinicians in other parts of our health system whose practice hours were going to be severely reduced,” said Dr. Norris, who is board-certified in general pediatrics and in hospice and palliative care medicine.
Once she assembled QUILT, members participated in a 1-day rapid training webinar covering the basics of palliative care and grief, and readied themselves for one of three roles: physicians to provide face-to-face palliative care in CHAM; supportive callers to provide support to patients with COVID-19 and their families between 12:00-8:00 p.m. each day; and bereavement callers to reach out to families who lost loved ones to COVID-19 and provide grief counseling for 3 weeks.
“This allows families to have at least two contacts a day from the hospital: one from the medical team that’s giving them technical, medical information, and another from members of the QUILT team,” Dr. Norris said. “We provide support for the worry, anxiety, and fear that we know creeps in when you’re separated from your family member, especially during a pandemic when you watch TV and there’s a death count rising.”
During her early meetings with QUILT members via Zoom or on the phone, Dr. Norris encouraged them to stretch their skill sets and mindsets as they shifted from caring for children and adolescents to mostly adults. “Pediatricians are all about family; that’s why we get into this,” she said. “We’re used to treating your kids, but then, suddenly, the parent becomes our patient, like in COVID-19, or the grandparent becomes our patient. We treat you all the same; you’re part of our family. There has been no adult who has died ‘within our house’ that has died alone. There has either been a staff member at their bedside, or when possible, a family member. We are witnessing life until the last breath here.”
‘They have no loved ones with them’
One day, members of CHAM’s medical team contacted Dr. Norris about a patient with COVID-19 who’d been cared for by Montefiore clinicians all of his young life. The boy’s mother, who did not speak English, was at his bedside in the ICU, and the clinicians asked Dr. Norris to speak with her by cell phone while they prepared him for intubation.
“We were looking at each other through a glass window wall in our ICU,” Dr. Norris recalled. “I talked to her the entire time the team worked to put him on the breathing machine, through an interpreter. I asked her to tell me about her son and about her family, and she did. We developed a warm relationship. After that, every day I would see her son through the glass window wall. Every couple of days, I would have the privilege of talking to his mother by phone. At one point, she asked me, ‘Dr. Norris, do you think his lungs will heal?’ I had to tell her no. Almost selfishly, I was relieved we were on the phone, because she cried, and so did I. When he died, she was able to be by his side.”
Frederick J. Kaskel, MD, PhD, joined QUILT as a supportive caller after being asked to go home during his on-call shift on St. Patrick’s Day at CHAM, where he serves as chief emeritus of nephrology. “I was told that I was deemed to be at high risk because of my age,” the 75-year-old said. “The next day, a junior person took over for me, and 2 days later she got sick with COVID-19. She’s fine but she was home for 3 weeks sick as a dog. It was scary.”

In his role as a supportive caller, Dr. Kaskel found himself engaged in his share of detective work, trying to find phone numbers of next of kin for patients hospitalized with COVID-19. “When they come into the ER, they may not have been with a loved one or a family member; they may have been brought in by an EMT,” he said. “Some of them speak little English and others have little documentation with them. It takes a lot of work to get phone numbers.”
Once Dr. Kaskel reaches a loved one by phone, he introduces himself as a member of the QUILT team. “I tell them I’m not calling to update the medical status but just to talk to them about their loved one,” he said. “Then I usually ask, ‘So, how are you doing with this? The stress is enormous, the uncertainties.’ Then they open up and express their fears. I’ve had a lot of people say, ‘we have no money, and I don’t know how we’re going to pay rent for the apartment. We have to line up for food.’ I also ask what they do to alleviate stress. One guy said, ‘I drink a lot, but I’m careful.’ ”
Dr. Kaskel, who is also a past president of the American Society of Pediatric Nephrology, applies that same personable approach in daily conversations with adult patients hospitalized at CHAM with COVID-19, the majority of whom are African Americans in their 30s, 40s, and 50s. “Invariably, they ask, ‘Has my loved one been updated as to my status?’ ” he said. “The second thing they often say is, ‘I’m worried about infecting other people, but I also worry if I’m going to get through this. I’m really afraid I’m going to die.’ I say, ‘You have a wonderful team keeping track of you. They’re seeing you all the time and making changes to your medicines.’ ”
When patients express their fear of dying from the virus, Dr. Kaskel asks them how they’re coping with that fear. Most tell him that they pray.
“If they don’t answer, I ask if they have any hobbies, like ‘Are you watching TV? Are you reading? Do you have your cell phone?’ ” he said. “Then they open up and say things like, ‘I’m listening to music on the cell phone,’ or ‘I’m FaceTiming with my loved ones.’ The use of FaceTime is crucial, because they are in a hospital, critically ill, potentially dying alone with strangers. This really hit me on the first day [of this work]. They have no loved ones with them. They have strangers: the CHAM nurses, the medical residents, the social workers, and the doctors.”
No hospital cheeseburgers
QUILT began its work on April 6, and at one time provided palliative care services for a peak of 92 mostly adult patients with COVID-19. The supportive callers made 249 individual connections with patients and family members by phone from April 6-13, 162 connections from April 13-19, and 130 connections from April 20-26, according to Dr. Norris. As of April 28, the CHAM inpatient census of patients aged 18 years and over with COVID-19 was 42, “and we’re making 130 connections by phone to patients and family members each day,” she said.
QUILT bereavement callers are following 30 families, providing 3 weeks of acute grief counseling from the date of death. “A sad truth is that, here in New York, our entire funeral, burial, cremation system is overwhelmed in volume,” Dr. Norris said. “Only half of the patients we’re following 3 weeks out have been able to have their family member buried or cremated; many are still waiting. What strikes me here is that pediatricians are often partners in care. With time, we’re partners in care in heartbreak, and in the occasional victory. We mourn patients who have died. We’ve had colleagues who died from COVID-19 right here at our hospital. But we stand together like a family.”

Dr. Norris recalled an older woman who came into CHAM’s ICU on a ventilator, critically ill from COVID-19. She called her husband at home every day with updates. “I got to know her husband, and I got to know her through him,” Dr. Norris said. “We talked every single day and she was able to graduate off of the breathing tube and out of the ICU, which was amazing.” The woman was moved to a floor in the adult hospital, but Dr. Norris continues to visit her and to provide her husband with updates, “because I’m devoted to them,” she said.
Recently, physicians in the adult hospital consulted with Dr. Norris about the woman. “They were trying to figure out what to do with her next,” she said. “Could she go home, or did she need rehab? They said, ‘We called you, Dr. Norris, because her husband thinks he can take her home.’ We know that COVID-19 really weakens people, so I went over to see her myself. I thought, ‘No single person could take care of an adult so weak at home.’ So, I called her husband and said, ‘I’m here with your wife, and I have to tell you; if she were my mother, I couldn’t take her home today. I need you to trust me.’ He said, ‘OK. We trust you and know that you have her best interest at heart.’ ”
Dr. Kaskel relayed the story of an older patient who was slowly recovering from COVID-19. During a phone call, he asked the man if there was anything he wanted at that moment.
“He said, ‘I’d love to see my wife and my children and my grandkids. I know I’m going to see them again, but right now, doc, if you could get me a cheeseburger with lettuce and tomato and ketchup and French fries from outside of the hospital, I’d be the happiest man in the world.’
I said, ‘What’s the matter with the cheeseburger made at the hospital?’
He said, ‘No! They can’t make the cheeseburger I want.’
I promised him I’d relay that message to the social worker responsible for the patient. I told her please, if you buy this for him, I’ll pay you back.”
Self-care and the next chapter
Twice each week, QUILT members gather in front of their computer monitors for mandatory Zoom meetings facilitated by two psychologists to share challenges, best practices, and to discuss the difficult work they’re doing. “We meet, because you cannot help someone if you cannot help yourself,” Dr. Norris said. “We have been encouraged each and every meeting to practice self-compassion, and to recognize that things happen during a pandemic – some will be the best you can do.”
She described organizing and serving on QUILT as a grounding experience with important lessons for the delivery of health care after the pandemic subsides and the team members return to their respective practices. “I think we’ve all gained a greater sense of humility, and we understand that the badge I wear every day does not protect me from becoming a patient, or from having my own family fall ill,” she said. “Here, we think about it very simply: ‘I’m going to treat you like you’re part of my own family.’ ”
Dr. Kaskel said that serving on QUILT as a supportive caller is an experience he won’t soon forget.
“The human bond is so accessible if you accept it,” he said. “If someone is an introvert that might not be able to draw out a stranger on the phone, then [he or she] shouldn’t do this [work]. But the fact that you can make a bond with someone that you’re not even seeing in person and know that both sides of this phone call are getting good vibes, that’s a remarkable feeling that I never really knew before, because I’ve never really had to do that before. It brings up feelings like I had after 9/11 – a unified approach to surviving this as people, as a community, the idea that ‘we will get through this,’ even though it’s totally different than anything before. The idea that there’s still hope. Those are things you can’t put a price on.”
An article about how CHAM transformed to provide care to adult COVID-19 patients was published online May 4, 2020, in the Journal of Pediatrics: doi: 10.1016/j.jpeds.2020.04.060.
In late March of 2020, when it became clear that hospitals in the greater New York City area would face a capacity crisis in caring for seriously ill patients with COVID-19, members of the leadership team at the Children’s Hospital at Montefiore (CHAM) in the Bronx, N.Y., convened to draft a response plan.
The recommendations put into action that day included moving the hospital’s emergency department from the lower level to the fourth floor, increasing the age limit for patients seen in the ED from 21 years of age to 30 and freeing up an entire hospital floor and a half to accommodate the anticipated surge of patients with COVID-19 admitted to Montefiore’s interconnected adult hospital, according to Sarah E. Norris, MD.
“We made multiple moves all at once,” said Dr. Norris, director of pediatric palliative care at CHAM. “It struck everyone as logical that palliative care had to be expanded, because all of the news we had received as the surge came to New York from around the world was full of death and uncertainty, and would require thoughtful conversations about end-of-life wishes at critical times and how to really respect the person and understand their values.”
When Dr. Norris left the leadership team meeting, she returned to her office, put her face in her hands, and sobbed as she began to process the gravity of what was ahead. “I cried because I knew that so many families were going to suffer a heartbreak, no matter how much we could do,” she said.
Stitching the QUILT
Over the next few days, Dr. Norris began recruiting colleagues from the large Montefiore Health System – most of whom she did not know – who met criteria for work deployment to expand CHAM’s palliative care program of clinician to 27 clinicians consisting of pediatricians, nurse practitioners, and psychologists, to meet the projected needs of COVID-19 patients and their families.
Some candidates for the effort, known as the Quality in Life Team (QUILT), were 65 years of age or older, considered at high risk for developing COVID-19-related complications themselves. Others were immunocompromised or had medical conditions that would not allow them to have direct contact with COVID-19 patients. “There were also clinicians in other parts of our health system whose practice hours were going to be severely reduced,” said Dr. Norris, who is board-certified in general pediatrics and in hospice and palliative care medicine.
Once she assembled QUILT, members participated in a 1-day rapid training webinar covering the basics of palliative care and grief, and readied themselves for one of three roles: physicians to provide face-to-face palliative care in CHAM; supportive callers to provide support to patients with COVID-19 and their families between 12:00-8:00 p.m. each day; and bereavement callers to reach out to families who lost loved ones to COVID-19 and provide grief counseling for 3 weeks.
“This allows families to have at least two contacts a day from the hospital: one from the medical team that’s giving them technical, medical information, and another from members of the QUILT team,” Dr. Norris said. “We provide support for the worry, anxiety, and fear that we know creeps in when you’re separated from your family member, especially during a pandemic when you watch TV and there’s a death count rising.”
During her early meetings with QUILT members via Zoom or on the phone, Dr. Norris encouraged them to stretch their skill sets and mindsets as they shifted from caring for children and adolescents to mostly adults. “Pediatricians are all about family; that’s why we get into this,” she said. “We’re used to treating your kids, but then, suddenly, the parent becomes our patient, like in COVID-19, or the grandparent becomes our patient. We treat you all the same; you’re part of our family. There has been no adult who has died ‘within our house’ that has died alone. There has either been a staff member at their bedside, or when possible, a family member. We are witnessing life until the last breath here.”
‘They have no loved ones with them’
One day, members of CHAM’s medical team contacted Dr. Norris about a patient with COVID-19 who’d been cared for by Montefiore clinicians all of his young life. The boy’s mother, who did not speak English, was at his bedside in the ICU, and the clinicians asked Dr. Norris to speak with her by cell phone while they prepared him for intubation.
“We were looking at each other through a glass window wall in our ICU,” Dr. Norris recalled. “I talked to her the entire time the team worked to put him on the breathing machine, through an interpreter. I asked her to tell me about her son and about her family, and she did. We developed a warm relationship. After that, every day I would see her son through the glass window wall. Every couple of days, I would have the privilege of talking to his mother by phone. At one point, she asked me, ‘Dr. Norris, do you think his lungs will heal?’ I had to tell her no. Almost selfishly, I was relieved we were on the phone, because she cried, and so did I. When he died, she was able to be by his side.”
Frederick J. Kaskel, MD, PhD, joined QUILT as a supportive caller after being asked to go home during his on-call shift on St. Patrick’s Day at CHAM, where he serves as chief emeritus of nephrology. “I was told that I was deemed to be at high risk because of my age,” the 75-year-old said. “The next day, a junior person took over for me, and 2 days later she got sick with COVID-19. She’s fine but she was home for 3 weeks sick as a dog. It was scary.”
In his role as a supportive caller, Dr. Kaskel found himself engaged in his share of detective work, trying to find phone numbers of next of kin for patients hospitalized with COVID-19. “When they come into the ER, they may not have been with a loved one or a family member; they may have been brought in by an EMT,” he said. “Some of them speak little English and others have little documentation with them. It takes a lot of work to get phone numbers.”
Once Dr. Kaskel reaches a loved one by phone, he introduces himself as a member of the QUILT team. “I tell them I’m not calling to update the medical status but just to talk to them about their loved one,” he said. “Then I usually ask, ‘So, how are you doing with this? The stress is enormous, the uncertainties.’ Then they open up and express their fears. I’ve had a lot of people say, ‘we have no money, and I don’t know how we’re going to pay rent for the apartment. We have to line up for food.’ I also ask what they do to alleviate stress. One guy said, ‘I drink a lot, but I’m careful.’ ”
Dr. Kaskel, who is also a past president of the American Society of Pediatric Nephrology, applies that same personable approach in daily conversations with adult patients hospitalized at CHAM with COVID-19, the majority of whom are African Americans in their 30s, 40s, and 50s. “Invariably, they ask, ‘Has my loved one been updated as to my status?’ ” he said. “The second thing they often say is, ‘I’m worried about infecting other people, but I also worry if I’m going to get through this. I’m really afraid I’m going to die.’ I say, ‘You have a wonderful team keeping track of you. They’re seeing you all the time and making changes to your medicines.’ ”
When patients express their fear of dying from the virus, Dr. Kaskel asks them how they’re coping with that fear. Most tell him that they pray.
“If they don’t answer, I ask if they have any hobbies, like ‘Are you watching TV? Are you reading? Do you have your cell phone?’ ” he said. “Then they open up and say things like, ‘I’m listening to music on the cell phone,’ or ‘I’m FaceTiming with my loved ones.’ The use of FaceTime is crucial, because they are in a hospital, critically ill, potentially dying alone with strangers. This really hit me on the first day [of this work]. They have no loved ones with them. They have strangers: the CHAM nurses, the medical residents, the social workers, and the doctors.”
No hospital cheeseburgers
QUILT began its work on April 6, and at one time provided palliative care services for a peak of 92 mostly adult patients with COVID-19. The supportive callers made 249 individual connections with patients and family members by phone from April 6-13, 162 connections from April 13-19, and 130 connections from April 20-26, according to Dr. Norris. As of April 28, the CHAM inpatient census of patients aged 18 years and over with COVID-19 was 42, “and we’re making 130 connections by phone to patients and family members each day,” she said.
QUILT bereavement callers are following 30 families, providing 3 weeks of acute grief counseling from the date of death. “A sad truth is that, here in New York, our entire funeral, burial, cremation system is overwhelmed in volume,” Dr. Norris said. “Only half of the patients we’re following 3 weeks out have been able to have their family member buried or cremated; many are still waiting. What strikes me here is that pediatricians are often partners in care. With time, we’re partners in care in heartbreak, and in the occasional victory. We mourn patients who have died. We’ve had colleagues who died from COVID-19 right here at our hospital. But we stand together like a family.”
Dr. Norris recalled an older woman who came into CHAM’s ICU on a ventilator, critically ill from COVID-19. She called her husband at home every day with updates. “I got to know her husband, and I got to know her through him,” Dr. Norris said. “We talked every single day and she was able to graduate off of the breathing tube and out of the ICU, which was amazing.” The woman was moved to a floor in the adult hospital, but Dr. Norris continues to visit her and to provide her husband with updates, “because I’m devoted to them,” she said.
Recently, physicians in the adult hospital consulted with Dr. Norris about the woman. “They were trying to figure out what to do with her next,” she said. “Could she go home, or did she need rehab? They said, ‘We called you, Dr. Norris, because her husband thinks he can take her home.’ We know that COVID-19 really weakens people, so I went over to see her myself. I thought, ‘No single person could take care of an adult so weak at home.’ So, I called her husband and said, ‘I’m here with your wife, and I have to tell you; if she were my mother, I couldn’t take her home today. I need you to trust me.’ He said, ‘OK. We trust you and know that you have her best interest at heart.’ ”
Dr. Kaskel relayed the story of an older patient who was slowly recovering from COVID-19. During a phone call, he asked the man if there was anything he wanted at that moment.
“He said, ‘I’d love to see my wife and my children and my grandkids. I know I’m going to see them again, but right now, doc, if you could get me a cheeseburger with lettuce and tomato and ketchup and French fries from outside of the hospital, I’d be the happiest man in the world.’
I said, ‘What’s the matter with the cheeseburger made at the hospital?’
He said, ‘No! They can’t make the cheeseburger I want.’
I promised him I’d relay that message to the social worker responsible for the patient. I told her please, if you buy this for him, I’ll pay you back.”
Self-care and the next chapter
Twice each week, QUILT members gather in front of their computer monitors for mandatory Zoom meetings facilitated by two psychologists to share challenges, best practices, and to discuss the difficult work they’re doing. “We meet, because you cannot help someone if you cannot help yourself,” Dr. Norris said. “We have been encouraged each and every meeting to practice self-compassion, and to recognize that things happen during a pandemic – some will be the best you can do.”
She described organizing and serving on QUILT as a grounding experience with important lessons for the delivery of health care after the pandemic subsides and the team members return to their respective practices. “I think we’ve all gained a greater sense of humility, and we understand that the badge I wear every day does not protect me from becoming a patient, or from having my own family fall ill,” she said. “Here, we think about it very simply: ‘I’m going to treat you like you’re part of my own family.’ ”
Dr. Kaskel said that serving on QUILT as a supportive caller is an experience he won’t soon forget.
“The human bond is so accessible if you accept it,” he said. “If someone is an introvert that might not be able to draw out a stranger on the phone, then [he or she] shouldn’t do this [work]. But the fact that you can make a bond with someone that you’re not even seeing in person and know that both sides of this phone call are getting good vibes, that’s a remarkable feeling that I never really knew before, because I’ve never really had to do that before. It brings up feelings like I had after 9/11 – a unified approach to surviving this as people, as a community, the idea that ‘we will get through this,’ even though it’s totally different than anything before. The idea that there’s still hope. Those are things you can’t put a price on.”
An article about how CHAM transformed to provide care to adult COVID-19 patients was published online May 4, 2020, in the Journal of Pediatrics: doi: 10.1016/j.jpeds.2020.04.060.
In late March of 2020, when it became clear that hospitals in the greater New York City area would face a capacity crisis in caring for seriously ill patients with COVID-19, members of the leadership team at the Children’s Hospital at Montefiore (CHAM) in the Bronx, N.Y., convened to draft a response plan.
The recommendations put into action that day included moving the hospital’s emergency department from the lower level to the fourth floor, increasing the age limit for patients seen in the ED from 21 years of age to 30 and freeing up an entire hospital floor and a half to accommodate the anticipated surge of patients with COVID-19 admitted to Montefiore’s interconnected adult hospital, according to Sarah E. Norris, MD.
“We made multiple moves all at once,” said Dr. Norris, director of pediatric palliative care at CHAM. “It struck everyone as logical that palliative care had to be expanded, because all of the news we had received as the surge came to New York from around the world was full of death and uncertainty, and would require thoughtful conversations about end-of-life wishes at critical times and how to really respect the person and understand their values.”
When Dr. Norris left the leadership team meeting, she returned to her office, put her face in her hands, and sobbed as she began to process the gravity of what was ahead. “I cried because I knew that so many families were going to suffer a heartbreak, no matter how much we could do,” she said.
Stitching the QUILT
Over the next few days, Dr. Norris began recruiting colleagues from the large Montefiore Health System – most of whom she did not know – who met criteria for work deployment to expand CHAM’s palliative care program of clinician to 27 clinicians consisting of pediatricians, nurse practitioners, and psychologists, to meet the projected needs of COVID-19 patients and their families.
Some candidates for the effort, known as the Quality in Life Team (QUILT), were 65 years of age or older, considered at high risk for developing COVID-19-related complications themselves. Others were immunocompromised or had medical conditions that would not allow them to have direct contact with COVID-19 patients. “There were also clinicians in other parts of our health system whose practice hours were going to be severely reduced,” said Dr. Norris, who is board-certified in general pediatrics and in hospice and palliative care medicine.
Once she assembled QUILT, members participated in a 1-day rapid training webinar covering the basics of palliative care and grief, and readied themselves for one of three roles: physicians to provide face-to-face palliative care in CHAM; supportive callers to provide support to patients with COVID-19 and their families between 12:00-8:00 p.m. each day; and bereavement callers to reach out to families who lost loved ones to COVID-19 and provide grief counseling for 3 weeks.
“This allows families to have at least two contacts a day from the hospital: one from the medical team that’s giving them technical, medical information, and another from members of the QUILT team,” Dr. Norris said. “We provide support for the worry, anxiety, and fear that we know creeps in when you’re separated from your family member, especially during a pandemic when you watch TV and there’s a death count rising.”
During her early meetings with QUILT members via Zoom or on the phone, Dr. Norris encouraged them to stretch their skill sets and mindsets as they shifted from caring for children and adolescents to mostly adults. “Pediatricians are all about family; that’s why we get into this,” she said. “We’re used to treating your kids, but then, suddenly, the parent becomes our patient, like in COVID-19, or the grandparent becomes our patient. We treat you all the same; you’re part of our family. There has been no adult who has died ‘within our house’ that has died alone. There has either been a staff member at their bedside, or when possible, a family member. We are witnessing life until the last breath here.”
‘They have no loved ones with them’
One day, members of CHAM’s medical team contacted Dr. Norris about a patient with COVID-19 who’d been cared for by Montefiore clinicians all of his young life. The boy’s mother, who did not speak English, was at his bedside in the ICU, and the clinicians asked Dr. Norris to speak with her by cell phone while they prepared him for intubation.
“We were looking at each other through a glass window wall in our ICU,” Dr. Norris recalled. “I talked to her the entire time the team worked to put him on the breathing machine, through an interpreter. I asked her to tell me about her son and about her family, and she did. We developed a warm relationship. After that, every day I would see her son through the glass window wall. Every couple of days, I would have the privilege of talking to his mother by phone. At one point, she asked me, ‘Dr. Norris, do you think his lungs will heal?’ I had to tell her no. Almost selfishly, I was relieved we were on the phone, because she cried, and so did I. When he died, she was able to be by his side.”
Frederick J. Kaskel, MD, PhD, joined QUILT as a supportive caller after being asked to go home during his on-call shift on St. Patrick’s Day at CHAM, where he serves as chief emeritus of nephrology. “I was told that I was deemed to be at high risk because of my age,” the 75-year-old said. “The next day, a junior person took over for me, and 2 days later she got sick with COVID-19. She’s fine but she was home for 3 weeks sick as a dog. It was scary.”
In his role as a supportive caller, Dr. Kaskel found himself engaged in his share of detective work, trying to find phone numbers of next of kin for patients hospitalized with COVID-19. “When they come into the ER, they may not have been with a loved one or a family member; they may have been brought in by an EMT,” he said. “Some of them speak little English and others have little documentation with them. It takes a lot of work to get phone numbers.”
Once Dr. Kaskel reaches a loved one by phone, he introduces himself as a member of the QUILT team. “I tell them I’m not calling to update the medical status but just to talk to them about their loved one,” he said. “Then I usually ask, ‘So, how are you doing with this? The stress is enormous, the uncertainties.’ Then they open up and express their fears. I’ve had a lot of people say, ‘we have no money, and I don’t know how we’re going to pay rent for the apartment. We have to line up for food.’ I also ask what they do to alleviate stress. One guy said, ‘I drink a lot, but I’m careful.’ ”
Dr. Kaskel, who is also a past president of the American Society of Pediatric Nephrology, applies that same personable approach in daily conversations with adult patients hospitalized at CHAM with COVID-19, the majority of whom are African Americans in their 30s, 40s, and 50s. “Invariably, they ask, ‘Has my loved one been updated as to my status?’ ” he said. “The second thing they often say is, ‘I’m worried about infecting other people, but I also worry if I’m going to get through this. I’m really afraid I’m going to die.’ I say, ‘You have a wonderful team keeping track of you. They’re seeing you all the time and making changes to your medicines.’ ”
When patients express their fear of dying from the virus, Dr. Kaskel asks them how they’re coping with that fear. Most tell him that they pray.
“If they don’t answer, I ask if they have any hobbies, like ‘Are you watching TV? Are you reading? Do you have your cell phone?’ ” he said. “Then they open up and say things like, ‘I’m listening to music on the cell phone,’ or ‘I’m FaceTiming with my loved ones.’ The use of FaceTime is crucial, because they are in a hospital, critically ill, potentially dying alone with strangers. This really hit me on the first day [of this work]. They have no loved ones with them. They have strangers: the CHAM nurses, the medical residents, the social workers, and the doctors.”
No hospital cheeseburgers
QUILT began its work on April 6, and at one time provided palliative care services for a peak of 92 mostly adult patients with COVID-19. The supportive callers made 249 individual connections with patients and family members by phone from April 6-13, 162 connections from April 13-19, and 130 connections from April 20-26, according to Dr. Norris. As of April 28, the CHAM inpatient census of patients aged 18 years and over with COVID-19 was 42, “and we’re making 130 connections by phone to patients and family members each day,” she said.
QUILT bereavement callers are following 30 families, providing 3 weeks of acute grief counseling from the date of death. “A sad truth is that, here in New York, our entire funeral, burial, cremation system is overwhelmed in volume,” Dr. Norris said. “Only half of the patients we’re following 3 weeks out have been able to have their family member buried or cremated; many are still waiting. What strikes me here is that pediatricians are often partners in care. With time, we’re partners in care in heartbreak, and in the occasional victory. We mourn patients who have died. We’ve had colleagues who died from COVID-19 right here at our hospital. But we stand together like a family.”
Dr. Norris recalled an older woman who came into CHAM’s ICU on a ventilator, critically ill from COVID-19. She called her husband at home every day with updates. “I got to know her husband, and I got to know her through him,” Dr. Norris said. “We talked every single day and she was able to graduate off of the breathing tube and out of the ICU, which was amazing.” The woman was moved to a floor in the adult hospital, but Dr. Norris continues to visit her and to provide her husband with updates, “because I’m devoted to them,” she said.
Recently, physicians in the adult hospital consulted with Dr. Norris about the woman. “They were trying to figure out what to do with her next,” she said. “Could she go home, or did she need rehab? They said, ‘We called you, Dr. Norris, because her husband thinks he can take her home.’ We know that COVID-19 really weakens people, so I went over to see her myself. I thought, ‘No single person could take care of an adult so weak at home.’ So, I called her husband and said, ‘I’m here with your wife, and I have to tell you; if she were my mother, I couldn’t take her home today. I need you to trust me.’ He said, ‘OK. We trust you and know that you have her best interest at heart.’ ”
Dr. Kaskel relayed the story of an older patient who was slowly recovering from COVID-19. During a phone call, he asked the man if there was anything he wanted at that moment.
“He said, ‘I’d love to see my wife and my children and my grandkids. I know I’m going to see them again, but right now, doc, if you could get me a cheeseburger with lettuce and tomato and ketchup and French fries from outside of the hospital, I’d be the happiest man in the world.’
I said, ‘What’s the matter with the cheeseburger made at the hospital?’
He said, ‘No! They can’t make the cheeseburger I want.’
I promised him I’d relay that message to the social worker responsible for the patient. I told her please, if you buy this for him, I’ll pay you back.”
Self-care and the next chapter
Twice each week, QUILT members gather in front of their computer monitors for mandatory Zoom meetings facilitated by two psychologists to share challenges, best practices, and to discuss the difficult work they’re doing. “We meet, because you cannot help someone if you cannot help yourself,” Dr. Norris said. “We have been encouraged each and every meeting to practice self-compassion, and to recognize that things happen during a pandemic – some will be the best you can do.”
She described organizing and serving on QUILT as a grounding experience with important lessons for the delivery of health care after the pandemic subsides and the team members return to their respective practices. “I think we’ve all gained a greater sense of humility, and we understand that the badge I wear every day does not protect me from becoming a patient, or from having my own family fall ill,” she said. “Here, we think about it very simply: ‘I’m going to treat you like you’re part of my own family.’ ”
Dr. Kaskel said that serving on QUILT as a supportive caller is an experience he won’t soon forget.
“The human bond is so accessible if you accept it,” he said. “If someone is an introvert that might not be able to draw out a stranger on the phone, then [he or she] shouldn’t do this [work]. But the fact that you can make a bond with someone that you’re not even seeing in person and know that both sides of this phone call are getting good vibes, that’s a remarkable feeling that I never really knew before, because I’ve never really had to do that before. It brings up feelings like I had after 9/11 – a unified approach to surviving this as people, as a community, the idea that ‘we will get through this,’ even though it’s totally different than anything before. The idea that there’s still hope. Those are things you can’t put a price on.”
An article about how CHAM transformed to provide care to adult COVID-19 patients was published online May 4, 2020, in the Journal of Pediatrics: doi: 10.1016/j.jpeds.2020.04.060.
L-thyroxine no help for older patients with symptomatic SCH
A new analysis of the large, randomized TRUST trial shows that L-thyroxine does not improve pronounced symptoms in older people with subclinical hypothyroidism.
The original trial established that the synthetic hormone did not improve symptoms in the overall trial population, a finding that called into question the routine prescribing of thyroid medication for this patient group.
But questions lingered as to whether patients with a higher burden of symptoms might still benefit from treatment with L-thyroxine.
For their research, published in Annals of Internal Medicine, Maria de Montmollin, MD, of the University of Bern (Switzerland), looked at results for 638 subjects randomized to L-thyroxine treatment (50 mcg daily for most patients) or placebo and followed for at least 1 year in the Thyroid Hormone Therapy for Older Adults With Subclinical Hypothyroidism (TRUST) trial (N Engl J Med. 2017;376:2534-2544). All were 65 years or older and met the criteria for subclinical hypothyroidism, defined as persistent elevated TSH levels (4.60-19.99 mIU/L) in combination with a normal free-thyroxine level.
Dr. de Montmollin and her colleagues identified 132 participants with high hypothyroid symptom burden at baseline and 133 patients with high scores for tiredness, using the Thyroid-Related Quality-of-Life Patient-Reported Outcome Questionnaire. Cutoffs were a baseline symptoms score of higher than 30 (on a 1-100 scale), or a tiredness score of over 40.
At 1 year, researchers saw no statistically significant improvements in either measure for the L-thyroxine treated patients, compared with placebo.
Among the patients with high symptom burden, those on L-thyroxine saw a score improvement of –12.3 points, compared with –10.4 for those on placebo, for an adjusted between-group difference of –2.0 (95% confidence interval, –5.5 to 1.5; P = 0.27). Tiredness scores also improved similarly, dropping 8.9 points for L-thyroxine–treated patients, compared with –10.9 for those receiving placebo, for an adjusted between-group difference of 0.0 (95% CI, –4.1 to 4.0; P = 0.99).
Dr. de Montmollin and colleagues also noted no significant between-group differences in two secondary measures they looked at in the study: patient self-reported quality of life and handgrip strength, an objective measure of weakness.
The results “do not support the hypothesis that the subgroup of adults with SCH [subclinical hypothyroidism] and high symptom burden before treatment benefit from L-thyroxine therapy,” the investigators wrote in their analysis. “This may be because of regression to the mean, the natural history of SCH, or the placebo effect and may explain why many persons with symptomatic SCH and their treating physicians are convinced that L-thyroxine is beneficial,” they added.
In an interview, Dr. de Montmollin commented that treating physicians “should reconsider prescribing or offering L-thyroxine to older adults with SCH, even those with consistent symptoms, because there is no clear evidence for its benefit in treating SCH to date and a risk of harm related to overtreatment is still possible. In addition, it is associated with unnecessary costs for the patient and for the health system.”
The investigators mentioned several limitations to their study, including its post hoc design and a small sample size. Additionally, they wrote, the findings “cannot exclude the possibility that a rare subgroup with greater symptom burden would benefit from L-thyroxine therapy” or that more aggressive treatment leading to lower TSH levels would confer benefit.
The study was sponsored by the National Health Service Greater Glasgow and Clyde Health Board, while the TRUST trial was sponsored by the European Union and with medication donated by Merck. Dr. de Montmollin and her coauthors disclosed no financial ties to industry.
SOURCE: De Montmollin et al. Ann Intern Med 2020 May 5. doi: 10.7326/M19-3193.
A new analysis of the large, randomized TRUST trial shows that L-thyroxine does not improve pronounced symptoms in older people with subclinical hypothyroidism.
The original trial established that the synthetic hormone did not improve symptoms in the overall trial population, a finding that called into question the routine prescribing of thyroid medication for this patient group.
But questions lingered as to whether patients with a higher burden of symptoms might still benefit from treatment with L-thyroxine.
For their research, published in Annals of Internal Medicine, Maria de Montmollin, MD, of the University of Bern (Switzerland), looked at results for 638 subjects randomized to L-thyroxine treatment (50 mcg daily for most patients) or placebo and followed for at least 1 year in the Thyroid Hormone Therapy for Older Adults With Subclinical Hypothyroidism (TRUST) trial (N Engl J Med. 2017;376:2534-2544). All were 65 years or older and met the criteria for subclinical hypothyroidism, defined as persistent elevated TSH levels (4.60-19.99 mIU/L) in combination with a normal free-thyroxine level.
Dr. de Montmollin and her colleagues identified 132 participants with high hypothyroid symptom burden at baseline and 133 patients with high scores for tiredness, using the Thyroid-Related Quality-of-Life Patient-Reported Outcome Questionnaire. Cutoffs were a baseline symptoms score of higher than 30 (on a 1-100 scale), or a tiredness score of over 40.
At 1 year, researchers saw no statistically significant improvements in either measure for the L-thyroxine treated patients, compared with placebo.
Among the patients with high symptom burden, those on L-thyroxine saw a score improvement of –12.3 points, compared with –10.4 for those on placebo, for an adjusted between-group difference of –2.0 (95% confidence interval, –5.5 to 1.5; P = 0.27). Tiredness scores also improved similarly, dropping 8.9 points for L-thyroxine–treated patients, compared with –10.9 for those receiving placebo, for an adjusted between-group difference of 0.0 (95% CI, –4.1 to 4.0; P = 0.99).
Dr. de Montmollin and colleagues also noted no significant between-group differences in two secondary measures they looked at in the study: patient self-reported quality of life and handgrip strength, an objective measure of weakness.
The results “do not support the hypothesis that the subgroup of adults with SCH [subclinical hypothyroidism] and high symptom burden before treatment benefit from L-thyroxine therapy,” the investigators wrote in their analysis. “This may be because of regression to the mean, the natural history of SCH, or the placebo effect and may explain why many persons with symptomatic SCH and their treating physicians are convinced that L-thyroxine is beneficial,” they added.
In an interview, Dr. de Montmollin commented that treating physicians “should reconsider prescribing or offering L-thyroxine to older adults with SCH, even those with consistent symptoms, because there is no clear evidence for its benefit in treating SCH to date and a risk of harm related to overtreatment is still possible. In addition, it is associated with unnecessary costs for the patient and for the health system.”
The investigators mentioned several limitations to their study, including its post hoc design and a small sample size. Additionally, they wrote, the findings “cannot exclude the possibility that a rare subgroup with greater symptom burden would benefit from L-thyroxine therapy” or that more aggressive treatment leading to lower TSH levels would confer benefit.
The study was sponsored by the National Health Service Greater Glasgow and Clyde Health Board, while the TRUST trial was sponsored by the European Union and with medication donated by Merck. Dr. de Montmollin and her coauthors disclosed no financial ties to industry.
SOURCE: De Montmollin et al. Ann Intern Med 2020 May 5. doi: 10.7326/M19-3193.
A new analysis of the large, randomized TRUST trial shows that L-thyroxine does not improve pronounced symptoms in older people with subclinical hypothyroidism.
The original trial established that the synthetic hormone did not improve symptoms in the overall trial population, a finding that called into question the routine prescribing of thyroid medication for this patient group.
But questions lingered as to whether patients with a higher burden of symptoms might still benefit from treatment with L-thyroxine.
For their research, published in Annals of Internal Medicine, Maria de Montmollin, MD, of the University of Bern (Switzerland), looked at results for 638 subjects randomized to L-thyroxine treatment (50 mcg daily for most patients) or placebo and followed for at least 1 year in the Thyroid Hormone Therapy for Older Adults With Subclinical Hypothyroidism (TRUST) trial (N Engl J Med. 2017;376:2534-2544). All were 65 years or older and met the criteria for subclinical hypothyroidism, defined as persistent elevated TSH levels (4.60-19.99 mIU/L) in combination with a normal free-thyroxine level.
Dr. de Montmollin and her colleagues identified 132 participants with high hypothyroid symptom burden at baseline and 133 patients with high scores for tiredness, using the Thyroid-Related Quality-of-Life Patient-Reported Outcome Questionnaire. Cutoffs were a baseline symptoms score of higher than 30 (on a 1-100 scale), or a tiredness score of over 40.
At 1 year, researchers saw no statistically significant improvements in either measure for the L-thyroxine treated patients, compared with placebo.
Among the patients with high symptom burden, those on L-thyroxine saw a score improvement of –12.3 points, compared with –10.4 for those on placebo, for an adjusted between-group difference of –2.0 (95% confidence interval, –5.5 to 1.5; P = 0.27). Tiredness scores also improved similarly, dropping 8.9 points for L-thyroxine–treated patients, compared with –10.9 for those receiving placebo, for an adjusted between-group difference of 0.0 (95% CI, –4.1 to 4.0; P = 0.99).
Dr. de Montmollin and colleagues also noted no significant between-group differences in two secondary measures they looked at in the study: patient self-reported quality of life and handgrip strength, an objective measure of weakness.
The results “do not support the hypothesis that the subgroup of adults with SCH [subclinical hypothyroidism] and high symptom burden before treatment benefit from L-thyroxine therapy,” the investigators wrote in their analysis. “This may be because of regression to the mean, the natural history of SCH, or the placebo effect and may explain why many persons with symptomatic SCH and their treating physicians are convinced that L-thyroxine is beneficial,” they added.
In an interview, Dr. de Montmollin commented that treating physicians “should reconsider prescribing or offering L-thyroxine to older adults with SCH, even those with consistent symptoms, because there is no clear evidence for its benefit in treating SCH to date and a risk of harm related to overtreatment is still possible. In addition, it is associated with unnecessary costs for the patient and for the health system.”
The investigators mentioned several limitations to their study, including its post hoc design and a small sample size. Additionally, they wrote, the findings “cannot exclude the possibility that a rare subgroup with greater symptom burden would benefit from L-thyroxine therapy” or that more aggressive treatment leading to lower TSH levels would confer benefit.
The study was sponsored by the National Health Service Greater Glasgow and Clyde Health Board, while the TRUST trial was sponsored by the European Union and with medication donated by Merck. Dr. de Montmollin and her coauthors disclosed no financial ties to industry.
SOURCE: De Montmollin et al. Ann Intern Med 2020 May 5. doi: 10.7326/M19-3193.
FROM ANNALS OF INTERNAL MEDICINE
Evidence builds linking anticoagulation to COVID-19 survival
, a large study from the epicenter of the U.S. outbreak suggests.

Among nearly 3,000 patients with COVID-19 admitted to New York City’s Mount Sinai Health System beginning in mid-March, median survival increased from 14 days to 21 days with the addition of anticoagulation.
The results were particularly striking among sicker patients who required mechanical ventilation, in whom in-hospital mortality fell from 62.7% to 29.1% and median survival jumped from 9 days to 21 days.
Interestingly, the association with anticoagulation and improved survival remained even after adjusting for mechanical ventilation, the authors reported May 6 in the Journal of the American College of Cardiology.
“It’s important for the community to know, first of all, how this should be approached and, second, it’s really opening a door to a new reality,” senior corresponding author Valentin Fuster, MD, PhD, director of Mount Sinai’s Zena and Michael A. Wiener Cardiovascular Institute and JACC editor-in-chief.
“I can tell you any family of mine who will have this disease absolutely will be on antithrombotic therapy and, actually, so are all of the patients at Mount Sinai now,” he said in an interview. COVID-19 is thought to promote thrombosis but the exact role of anticoagulation in the management of COVID-19 and optimal regimen are unknown.
In late March, the International Society on Thrombosis and Haemostasis recommended that all hospitalized COVID-19 patients, even those not in the ICU, should receive prophylactic-dose low-molecular-weight heparin (LMWH), unless they have contraindications.
Last month, international consensus-based recommendations were published for the diagnosis and management of thrombotic disease in patients with COVID-19.
In early March, however, data were scare and only a minimal number of patients were receiving anticoagulants at Mount Sinai.
“But after a few weeks, we reached an intuitive feeling that anticoagulation was of benefit and, at the same time, the literature was beginning to say clots were important in this disease,” Dr. Fuster said. “So we took a very straightforward approach and set up a policy in our institution that all COVID-19 patients should be on antithrombotic therapy. It was a decision made without data, but it was a feeling.”
For the present study, the researchers examined mortality and bleeding among 2,773 patients hospitalized at Mount Sinai with confirmed COVID-19 between March 14 and April 11.
Of these, 786 (28%) received systemic anticoagulation including subcutaneous heparin, LMWH, fractionated heparin, and the novel oral anticoagulants apixaban and dabigatran, for a median of 3 days (range, 2-7 days). Tissue plasminogen activator was also used in some ICU cases.
Major bleeding was defined as hemoglobin less than 7 g/dL and any red blood cell transfusion; at least two units of red blood cell transfusion within 48 hours; or a diagnosis code for major bleeding, notably including intracranial hemorrhage.
Patients treated with anticoagulation were more likely to require invasive mechanical ventilation (29.8% vs. 8.1%) and to have significantly increased prothrombin time, activated partial thromboplastin time, lactate dehydrogenase, ferritin, C-reactive protein, and d-dimer values. In-hospital mortality was 22.5% with anticoagulation and 22.8% without anticoagulation (median survival, 14 days vs. 21 days).
In multivariate analysis, longer anticoagulation duration was associated with a 14% lower adjusted risk of in-hospital death (hazard ratio, 0.86 per day; 95% confidence interval, 0.82-0.89; P < .001).
The model adjusted for several potential confounders such as age, ethnicity, body mass index, and prehospital anticoagulation use. To adjust for differential length of stay and anticoagulation initiation, anticoagulation duration was used as a covariate and intubation was treated as a time-dependent variable.
Bleeding events were similar in patients treated with and without anticoagulation (3% vs. 1.9%; P = .2) but were more common among the 375 intubated patients than among nonintubated patients (7.5% vs. 1.35%; P value not given). “The most important thing was there was no increase in bleeding,” said Dr. Fuster.
Additional support for a possible survival benefit was published April 27 and included 449 patients with severe COVID-19 treated with heparin (mostly LMWH) for at least 7 days in Hunan, China. Overall, 28-day mortality was similar between heparin users and nonusers (30.3% vs. 29.7%) but was significantly lower among heparin users who had a Sepsis-Induced Coagulopathy score of at least 4 (40% vs. 64.2%; P = .02) or d-dimer greater than sixfold the upper limit of normal (32.8% vs. 52.4%; P = .01).
In multivariate analysis, d-dimer, prothrombin time, and age were positively correlated with 28-day mortality, and platelet count was negatively correlated with 28-day mortality.
Victor F. Tapson, MD, who directs the pulmonary embolism response team at Cedars-Sinai Medical Center in Los Angeles and was not involved with the study, said, “The Chinese data were not enough for me to anticoagulate patients therapeutically” but the Mount Sinai data strengthen the case.
“They’re wise to call this a ‘suggestion of improved outcomes,’ but it’s pretty compelling that those patients who were on anticoagulation had improved survival after adjusting for mechanical ventilation,” he said in an interview. “These are sicker patients and sicker patients may get anticoagulated more, but they may bleed more. The bleed risks were a little different but they didn’t seem too concerning.”
“I think this helps move us forward some that we should consider anticoagulating with therapeutic anticoagulation certain patients that meet certain criteria,” Dr. Tapson said. “An easy example is a patient who comes to the hospital, has active cancer and is on a DOAC [direct oral anticoagulant], and comes up with COVID.”
At the same time, some clinicians want to increase prophylactic anticoagulation “using enoxaparin 40 mg once a day and maybe go to twice a day – not quite therapeutic doses but increased prophylaxis,” he observed. Anticoagulation was given at “relatively low doses” in the Mount Sinai study but that is evolving in light of the reassuring bleeding data, Dr. Fuster said. They now have three enoxaparin regimens and, for example, give patients who don’t require intensive care enoxaparin 30 mg twice a day, up from 40 mg a day initially.
Patients are also stratified by factors such as renal failure and obesity, creating an intermediate group between those not initially needing intensive care and ICU cases.
In the coming weeks, the researchers will evaluate anticoagulation regimens and a broader array of outcomes among 5,000 patients, two-thirds of whom received anticoagulation after Mount Sinai enacted its anticoagulation policy. “We’re now going to look at the difference between all these [regimens],” Dr. Fuster said. “My personal feeling and, for feasibility issues, I hope the winner is subcutaneous heparin.”
Three randomized trials are also planned. “Three questions we really want to ask are: what to give in the hospital, what to give those who go home after the hospital, and what to give those who are not hospitalized,” he said.
The work was supported by U54 TR001433-05, National Center for Advancing Translational Sciences, National Institutes of Health. Dr. Fuster has disclosed no relevant financial relationships. Dr. Tapson reported consulting and clinical trial work for BMS, Janssen, Daiichi Medical, ECOS/BTG, Inari, and Penumbra.
A version of this article originally appeared on Medscape.com.
, a large study from the epicenter of the U.S. outbreak suggests.
Among nearly 3,000 patients with COVID-19 admitted to New York City’s Mount Sinai Health System beginning in mid-March, median survival increased from 14 days to 21 days with the addition of anticoagulation.
The results were particularly striking among sicker patients who required mechanical ventilation, in whom in-hospital mortality fell from 62.7% to 29.1% and median survival jumped from 9 days to 21 days.
Interestingly, the association with anticoagulation and improved survival remained even after adjusting for mechanical ventilation, the authors reported May 6 in the Journal of the American College of Cardiology.
“It’s important for the community to know, first of all, how this should be approached and, second, it’s really opening a door to a new reality,” senior corresponding author Valentin Fuster, MD, PhD, director of Mount Sinai’s Zena and Michael A. Wiener Cardiovascular Institute and JACC editor-in-chief.
“I can tell you any family of mine who will have this disease absolutely will be on antithrombotic therapy and, actually, so are all of the patients at Mount Sinai now,” he said in an interview. COVID-19 is thought to promote thrombosis but the exact role of anticoagulation in the management of COVID-19 and optimal regimen are unknown.
In late March, the International Society on Thrombosis and Haemostasis recommended that all hospitalized COVID-19 patients, even those not in the ICU, should receive prophylactic-dose low-molecular-weight heparin (LMWH), unless they have contraindications.
Last month, international consensus-based recommendations were published for the diagnosis and management of thrombotic disease in patients with COVID-19.
In early March, however, data were scare and only a minimal number of patients were receiving anticoagulants at Mount Sinai.
“But after a few weeks, we reached an intuitive feeling that anticoagulation was of benefit and, at the same time, the literature was beginning to say clots were important in this disease,” Dr. Fuster said. “So we took a very straightforward approach and set up a policy in our institution that all COVID-19 patients should be on antithrombotic therapy. It was a decision made without data, but it was a feeling.”
For the present study, the researchers examined mortality and bleeding among 2,773 patients hospitalized at Mount Sinai with confirmed COVID-19 between March 14 and April 11.
Of these, 786 (28%) received systemic anticoagulation including subcutaneous heparin, LMWH, fractionated heparin, and the novel oral anticoagulants apixaban and dabigatran, for a median of 3 days (range, 2-7 days). Tissue plasminogen activator was also used in some ICU cases.
Major bleeding was defined as hemoglobin less than 7 g/dL and any red blood cell transfusion; at least two units of red blood cell transfusion within 48 hours; or a diagnosis code for major bleeding, notably including intracranial hemorrhage.
Patients treated with anticoagulation were more likely to require invasive mechanical ventilation (29.8% vs. 8.1%) and to have significantly increased prothrombin time, activated partial thromboplastin time, lactate dehydrogenase, ferritin, C-reactive protein, and d-dimer values. In-hospital mortality was 22.5% with anticoagulation and 22.8% without anticoagulation (median survival, 14 days vs. 21 days).
In multivariate analysis, longer anticoagulation duration was associated with a 14% lower adjusted risk of in-hospital death (hazard ratio, 0.86 per day; 95% confidence interval, 0.82-0.89; P < .001).
The model adjusted for several potential confounders such as age, ethnicity, body mass index, and prehospital anticoagulation use. To adjust for differential length of stay and anticoagulation initiation, anticoagulation duration was used as a covariate and intubation was treated as a time-dependent variable.
Bleeding events were similar in patients treated with and without anticoagulation (3% vs. 1.9%; P = .2) but were more common among the 375 intubated patients than among nonintubated patients (7.5% vs. 1.35%; P value not given). “The most important thing was there was no increase in bleeding,” said Dr. Fuster.
Additional support for a possible survival benefit was published April 27 and included 449 patients with severe COVID-19 treated with heparin (mostly LMWH) for at least 7 days in Hunan, China. Overall, 28-day mortality was similar between heparin users and nonusers (30.3% vs. 29.7%) but was significantly lower among heparin users who had a Sepsis-Induced Coagulopathy score of at least 4 (40% vs. 64.2%; P = .02) or d-dimer greater than sixfold the upper limit of normal (32.8% vs. 52.4%; P = .01).
In multivariate analysis, d-dimer, prothrombin time, and age were positively correlated with 28-day mortality, and platelet count was negatively correlated with 28-day mortality.
Victor F. Tapson, MD, who directs the pulmonary embolism response team at Cedars-Sinai Medical Center in Los Angeles and was not involved with the study, said, “The Chinese data were not enough for me to anticoagulate patients therapeutically” but the Mount Sinai data strengthen the case.
“They’re wise to call this a ‘suggestion of improved outcomes,’ but it’s pretty compelling that those patients who were on anticoagulation had improved survival after adjusting for mechanical ventilation,” he said in an interview. “These are sicker patients and sicker patients may get anticoagulated more, but they may bleed more. The bleed risks were a little different but they didn’t seem too concerning.”
“I think this helps move us forward some that we should consider anticoagulating with therapeutic anticoagulation certain patients that meet certain criteria,” Dr. Tapson said. “An easy example is a patient who comes to the hospital, has active cancer and is on a DOAC [direct oral anticoagulant], and comes up with COVID.”
At the same time, some clinicians want to increase prophylactic anticoagulation “using enoxaparin 40 mg once a day and maybe go to twice a day – not quite therapeutic doses but increased prophylaxis,” he observed. Anticoagulation was given at “relatively low doses” in the Mount Sinai study but that is evolving in light of the reassuring bleeding data, Dr. Fuster said. They now have three enoxaparin regimens and, for example, give patients who don’t require intensive care enoxaparin 30 mg twice a day, up from 40 mg a day initially.
Patients are also stratified by factors such as renal failure and obesity, creating an intermediate group between those not initially needing intensive care and ICU cases.
In the coming weeks, the researchers will evaluate anticoagulation regimens and a broader array of outcomes among 5,000 patients, two-thirds of whom received anticoagulation after Mount Sinai enacted its anticoagulation policy. “We’re now going to look at the difference between all these [regimens],” Dr. Fuster said. “My personal feeling and, for feasibility issues, I hope the winner is subcutaneous heparin.”
Three randomized trials are also planned. “Three questions we really want to ask are: what to give in the hospital, what to give those who go home after the hospital, and what to give those who are not hospitalized,” he said.
The work was supported by U54 TR001433-05, National Center for Advancing Translational Sciences, National Institutes of Health. Dr. Fuster has disclosed no relevant financial relationships. Dr. Tapson reported consulting and clinical trial work for BMS, Janssen, Daiichi Medical, ECOS/BTG, Inari, and Penumbra.
A version of this article originally appeared on Medscape.com.
, a large study from the epicenter of the U.S. outbreak suggests.
Among nearly 3,000 patients with COVID-19 admitted to New York City’s Mount Sinai Health System beginning in mid-March, median survival increased from 14 days to 21 days with the addition of anticoagulation.
The results were particularly striking among sicker patients who required mechanical ventilation, in whom in-hospital mortality fell from 62.7% to 29.1% and median survival jumped from 9 days to 21 days.
Interestingly, the association with anticoagulation and improved survival remained even after adjusting for mechanical ventilation, the authors reported May 6 in the Journal of the American College of Cardiology.
“It’s important for the community to know, first of all, how this should be approached and, second, it’s really opening a door to a new reality,” senior corresponding author Valentin Fuster, MD, PhD, director of Mount Sinai’s Zena and Michael A. Wiener Cardiovascular Institute and JACC editor-in-chief.
“I can tell you any family of mine who will have this disease absolutely will be on antithrombotic therapy and, actually, so are all of the patients at Mount Sinai now,” he said in an interview. COVID-19 is thought to promote thrombosis but the exact role of anticoagulation in the management of COVID-19 and optimal regimen are unknown.
In late March, the International Society on Thrombosis and Haemostasis recommended that all hospitalized COVID-19 patients, even those not in the ICU, should receive prophylactic-dose low-molecular-weight heparin (LMWH), unless they have contraindications.
Last month, international consensus-based recommendations were published for the diagnosis and management of thrombotic disease in patients with COVID-19.
In early March, however, data were scare and only a minimal number of patients were receiving anticoagulants at Mount Sinai.
“But after a few weeks, we reached an intuitive feeling that anticoagulation was of benefit and, at the same time, the literature was beginning to say clots were important in this disease,” Dr. Fuster said. “So we took a very straightforward approach and set up a policy in our institution that all COVID-19 patients should be on antithrombotic therapy. It was a decision made without data, but it was a feeling.”
For the present study, the researchers examined mortality and bleeding among 2,773 patients hospitalized at Mount Sinai with confirmed COVID-19 between March 14 and April 11.
Of these, 786 (28%) received systemic anticoagulation including subcutaneous heparin, LMWH, fractionated heparin, and the novel oral anticoagulants apixaban and dabigatran, for a median of 3 days (range, 2-7 days). Tissue plasminogen activator was also used in some ICU cases.
Major bleeding was defined as hemoglobin less than 7 g/dL and any red blood cell transfusion; at least two units of red blood cell transfusion within 48 hours; or a diagnosis code for major bleeding, notably including intracranial hemorrhage.
Patients treated with anticoagulation were more likely to require invasive mechanical ventilation (29.8% vs. 8.1%) and to have significantly increased prothrombin time, activated partial thromboplastin time, lactate dehydrogenase, ferritin, C-reactive protein, and d-dimer values. In-hospital mortality was 22.5% with anticoagulation and 22.8% without anticoagulation (median survival, 14 days vs. 21 days).
In multivariate analysis, longer anticoagulation duration was associated with a 14% lower adjusted risk of in-hospital death (hazard ratio, 0.86 per day; 95% confidence interval, 0.82-0.89; P < .001).
The model adjusted for several potential confounders such as age, ethnicity, body mass index, and prehospital anticoagulation use. To adjust for differential length of stay and anticoagulation initiation, anticoagulation duration was used as a covariate and intubation was treated as a time-dependent variable.
Bleeding events were similar in patients treated with and without anticoagulation (3% vs. 1.9%; P = .2) but were more common among the 375 intubated patients than among nonintubated patients (7.5% vs. 1.35%; P value not given). “The most important thing was there was no increase in bleeding,” said Dr. Fuster.
Additional support for a possible survival benefit was published April 27 and included 449 patients with severe COVID-19 treated with heparin (mostly LMWH) for at least 7 days in Hunan, China. Overall, 28-day mortality was similar between heparin users and nonusers (30.3% vs. 29.7%) but was significantly lower among heparin users who had a Sepsis-Induced Coagulopathy score of at least 4 (40% vs. 64.2%; P = .02) or d-dimer greater than sixfold the upper limit of normal (32.8% vs. 52.4%; P = .01).
In multivariate analysis, d-dimer, prothrombin time, and age were positively correlated with 28-day mortality, and platelet count was negatively correlated with 28-day mortality.
Victor F. Tapson, MD, who directs the pulmonary embolism response team at Cedars-Sinai Medical Center in Los Angeles and was not involved with the study, said, “The Chinese data were not enough for me to anticoagulate patients therapeutically” but the Mount Sinai data strengthen the case.
“They’re wise to call this a ‘suggestion of improved outcomes,’ but it’s pretty compelling that those patients who were on anticoagulation had improved survival after adjusting for mechanical ventilation,” he said in an interview. “These are sicker patients and sicker patients may get anticoagulated more, but they may bleed more. The bleed risks were a little different but they didn’t seem too concerning.”
“I think this helps move us forward some that we should consider anticoagulating with therapeutic anticoagulation certain patients that meet certain criteria,” Dr. Tapson said. “An easy example is a patient who comes to the hospital, has active cancer and is on a DOAC [direct oral anticoagulant], and comes up with COVID.”
At the same time, some clinicians want to increase prophylactic anticoagulation “using enoxaparin 40 mg once a day and maybe go to twice a day – not quite therapeutic doses but increased prophylaxis,” he observed. Anticoagulation was given at “relatively low doses” in the Mount Sinai study but that is evolving in light of the reassuring bleeding data, Dr. Fuster said. They now have three enoxaparin regimens and, for example, give patients who don’t require intensive care enoxaparin 30 mg twice a day, up from 40 mg a day initially.
Patients are also stratified by factors such as renal failure and obesity, creating an intermediate group between those not initially needing intensive care and ICU cases.
In the coming weeks, the researchers will evaluate anticoagulation regimens and a broader array of outcomes among 5,000 patients, two-thirds of whom received anticoagulation after Mount Sinai enacted its anticoagulation policy. “We’re now going to look at the difference between all these [regimens],” Dr. Fuster said. “My personal feeling and, for feasibility issues, I hope the winner is subcutaneous heparin.”
Three randomized trials are also planned. “Three questions we really want to ask are: what to give in the hospital, what to give those who go home after the hospital, and what to give those who are not hospitalized,” he said.
The work was supported by U54 TR001433-05, National Center for Advancing Translational Sciences, National Institutes of Health. Dr. Fuster has disclosed no relevant financial relationships. Dr. Tapson reported consulting and clinical trial work for BMS, Janssen, Daiichi Medical, ECOS/BTG, Inari, and Penumbra.
A version of this article originally appeared on Medscape.com.
Operation Quack Hack: FDA moves to stop fraudulent COVID-19 products
No form of human misery can be allowed to go unexploited, and the pandemic, it seems, is no exception.
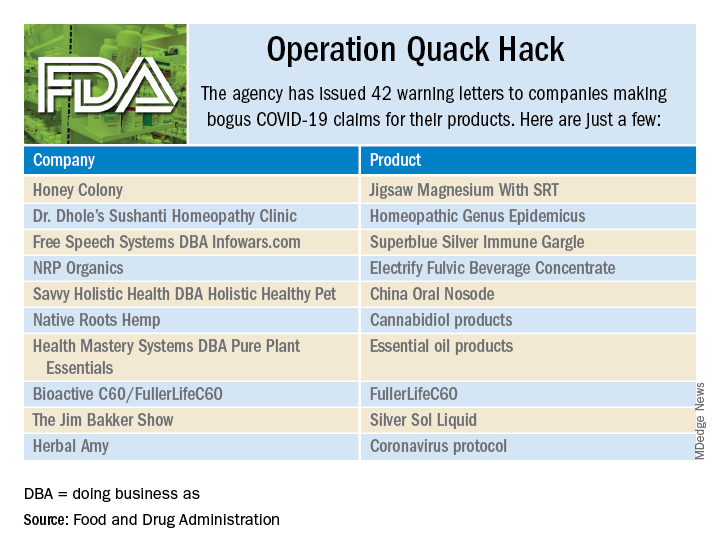
As part of Operation Quack Hack, the Food and Drug Administration has stepped up its investigation and enforcement efforts against companies and individuals that are “taking advantage of widespread fear among consumers during the COVID-19 pandemic” by selling fake products and treatments for coronavirus.
As of May 7, 2020, the agency had issued 42 warning letters to companies that were “selling unapproved products that fraudulently claim to mitigate, prevent, treat, diagnose or cure COVID-19,” the FDA announced in a written statement. Of those 42 products, 29 are no longer being sold with any sort of COVID-19 claim.
Since the beginning of the pandemic, Operation Quack Hack has uncovered hundreds of such products – drugs, testing kits, and personal protective equipment – being sold online, and complaints were sent to domain-name registrars and Internet marketplaces that have, in most cases, removed the postings, the FDA said.
“We will continue to monitor the online ecosystem for fraudulent products peddled by bad actors seeking to profit from this global pandemic. We encourage anyone aware of suspected fraudulent medical products for COVID-19 to report them to the FDA,” the statement said.
No form of human misery can be allowed to go unexploited, and the pandemic, it seems, is no exception.
As part of Operation Quack Hack, the Food and Drug Administration has stepped up its investigation and enforcement efforts against companies and individuals that are “taking advantage of widespread fear among consumers during the COVID-19 pandemic” by selling fake products and treatments for coronavirus.
As of May 7, 2020, the agency had issued 42 warning letters to companies that were “selling unapproved products that fraudulently claim to mitigate, prevent, treat, diagnose or cure COVID-19,” the FDA announced in a written statement. Of those 42 products, 29 are no longer being sold with any sort of COVID-19 claim.
Since the beginning of the pandemic, Operation Quack Hack has uncovered hundreds of such products – drugs, testing kits, and personal protective equipment – being sold online, and complaints were sent to domain-name registrars and Internet marketplaces that have, in most cases, removed the postings, the FDA said.
“We will continue to monitor the online ecosystem for fraudulent products peddled by bad actors seeking to profit from this global pandemic. We encourage anyone aware of suspected fraudulent medical products for COVID-19 to report them to the FDA,” the statement said.
No form of human misery can be allowed to go unexploited, and the pandemic, it seems, is no exception.
As part of Operation Quack Hack, the Food and Drug Administration has stepped up its investigation and enforcement efforts against companies and individuals that are “taking advantage of widespread fear among consumers during the COVID-19 pandemic” by selling fake products and treatments for coronavirus.
As of May 7, 2020, the agency had issued 42 warning letters to companies that were “selling unapproved products that fraudulently claim to mitigate, prevent, treat, diagnose or cure COVID-19,” the FDA announced in a written statement. Of those 42 products, 29 are no longer being sold with any sort of COVID-19 claim.
Since the beginning of the pandemic, Operation Quack Hack has uncovered hundreds of such products – drugs, testing kits, and personal protective equipment – being sold online, and complaints were sent to domain-name registrars and Internet marketplaces that have, in most cases, removed the postings, the FDA said.
“We will continue to monitor the online ecosystem for fraudulent products peddled by bad actors seeking to profit from this global pandemic. We encourage anyone aware of suspected fraudulent medical products for COVID-19 to report them to the FDA,” the statement said.
COVID-19 & Mental Health
On Thursday, April 23, 2020, MDedge Psychiatry hosted a Twitter conversation at #MDedgeChats on COVID-19 and mental health.
Two psychiatrists affiliated with Johns Hopkins University, Dinah Miller, MD (@shrinkrapdinah), and Elizabeth Ryznar, MD (@RyznarMD), hosted the conversation. Throughout the conversation several themes emerged. One is that COVID-19 illustrates the connections between housing and health, and another is that stigma tied to being COVID positive is leading to suicidality, particularly in Haiti. The discussants also talked about the importance of self-care.
Questions asked during the Twitter chat:
- How are your pre-pandemic patients doing during this crisis?
- How has COVID-19 affected inpatient and outpatient care for you?
- How are our most vulnerable populations being affected by COVID-19?
- How are you doing personally and professionally as medical professionals during the pandemic?
- What psychiatric manifestations are you seeing in your patients who have had COVID-19?
The following is an edited version of the discussion. For the full experience, visit our Twitter archive, you can still join the conversation.













Some experts are predicting that the magnitude of the mental health fallout from the COVID-19 pandemic will be profound. They also have concerns that physical distancing and increased unemployment forced by the pandemic will lead to a rise in suicide risk, particularly for at-risk populations.1
For psychiatric patients, COVID-19 is expected to leave behind higher levels of anxiety, depression, and insomnia.2
And for health care workers on the front lines, the mental health toll could lead to stress, burnout, and worse.
Clinicians are also dealing with shortages of PPE and medical equipment, worrying about their safety and that of their families, while trying to save lives amid great uncertainty about SARS-CoV-2, the coronavirus that causes COVID-19.
Most recently an emergency department physician in New York who was recovering from COVID-19 herself reportedly recently ended her own life, according to her father, who is a physician.
As Dr. Sarah Candler said in a previous twitter chat with MDedge Internal Medicine, “Good doctors take care of themselves, too.” Be kind to yourself during this global crisis.
The National Suicide Prevention Lifeline is always available at 1-800-273-TALK (8255).
Resources
- Mental health and the COVID-19 pandemic
- Brief examines the COVID-19 crisis’ implications for Americans’ mental health
- COVID-19: Helping health care workers on the front lines
- Overcoming COVID-related stress
- Confessions of an outpatient psychiatrist during the pandemic
- Psychiatric patients may be among the hardest hit
- Experts hasten to head off mental health crisis
- Podcast: Physician Suicide
1Lancet Psychiatry. 2020 Apr 21. doi: 10.1016/S2215-0366(20):30171-1.
2Brain, Behav Immun. 2020 Apr 27. doi: 10.10116/j.bbi.2020.04.069).
On Thursday, April 23, 2020, MDedge Psychiatry hosted a Twitter conversation at #MDedgeChats on COVID-19 and mental health.
Two psychiatrists affiliated with Johns Hopkins University, Dinah Miller, MD (@shrinkrapdinah), and Elizabeth Ryznar, MD (@RyznarMD), hosted the conversation. Throughout the conversation several themes emerged. One is that COVID-19 illustrates the connections between housing and health, and another is that stigma tied to being COVID positive is leading to suicidality, particularly in Haiti. The discussants also talked about the importance of self-care.
Questions asked during the Twitter chat:
- How are your pre-pandemic patients doing during this crisis?
- How has COVID-19 affected inpatient and outpatient care for you?
- How are our most vulnerable populations being affected by COVID-19?
- How are you doing personally and professionally as medical professionals during the pandemic?
- What psychiatric manifestations are you seeing in your patients who have had COVID-19?
The following is an edited version of the discussion. For the full experience, visit our Twitter archive, you can still join the conversation.
Some experts are predicting that the magnitude of the mental health fallout from the COVID-19 pandemic will be profound. They also have concerns that physical distancing and increased unemployment forced by the pandemic will lead to a rise in suicide risk, particularly for at-risk populations.1
For psychiatric patients, COVID-19 is expected to leave behind higher levels of anxiety, depression, and insomnia.2
And for health care workers on the front lines, the mental health toll could lead to stress, burnout, and worse.
Clinicians are also dealing with shortages of PPE and medical equipment, worrying about their safety and that of their families, while trying to save lives amid great uncertainty about SARS-CoV-2, the coronavirus that causes COVID-19.
Most recently an emergency department physician in New York who was recovering from COVID-19 herself reportedly recently ended her own life, according to her father, who is a physician.
As Dr. Sarah Candler said in a previous twitter chat with MDedge Internal Medicine, “Good doctors take care of themselves, too.” Be kind to yourself during this global crisis.
The National Suicide Prevention Lifeline is always available at 1-800-273-TALK (8255).
Resources
- Mental health and the COVID-19 pandemic
- Brief examines the COVID-19 crisis’ implications for Americans’ mental health
- COVID-19: Helping health care workers on the front lines
- Overcoming COVID-related stress
- Confessions of an outpatient psychiatrist during the pandemic
- Psychiatric patients may be among the hardest hit
- Experts hasten to head off mental health crisis
- Podcast: Physician Suicide
1Lancet Psychiatry. 2020 Apr 21. doi: 10.1016/S2215-0366(20):30171-1.
2Brain, Behav Immun. 2020 Apr 27. doi: 10.10116/j.bbi.2020.04.069).
On Thursday, April 23, 2020, MDedge Psychiatry hosted a Twitter conversation at #MDedgeChats on COVID-19 and mental health.
Two psychiatrists affiliated with Johns Hopkins University, Dinah Miller, MD (@shrinkrapdinah), and Elizabeth Ryznar, MD (@RyznarMD), hosted the conversation. Throughout the conversation several themes emerged. One is that COVID-19 illustrates the connections between housing and health, and another is that stigma tied to being COVID positive is leading to suicidality, particularly in Haiti. The discussants also talked about the importance of self-care.
Questions asked during the Twitter chat:
- How are your pre-pandemic patients doing during this crisis?
- How has COVID-19 affected inpatient and outpatient care for you?
- How are our most vulnerable populations being affected by COVID-19?
- How are you doing personally and professionally as medical professionals during the pandemic?
- What psychiatric manifestations are you seeing in your patients who have had COVID-19?
The following is an edited version of the discussion. For the full experience, visit our Twitter archive, you can still join the conversation.
Some experts are predicting that the magnitude of the mental health fallout from the COVID-19 pandemic will be profound. They also have concerns that physical distancing and increased unemployment forced by the pandemic will lead to a rise in suicide risk, particularly for at-risk populations.1
For psychiatric patients, COVID-19 is expected to leave behind higher levels of anxiety, depression, and insomnia.2
And for health care workers on the front lines, the mental health toll could lead to stress, burnout, and worse.
Clinicians are also dealing with shortages of PPE and medical equipment, worrying about their safety and that of their families, while trying to save lives amid great uncertainty about SARS-CoV-2, the coronavirus that causes COVID-19.
Most recently an emergency department physician in New York who was recovering from COVID-19 herself reportedly recently ended her own life, according to her father, who is a physician.
As Dr. Sarah Candler said in a previous twitter chat with MDedge Internal Medicine, “Good doctors take care of themselves, too.” Be kind to yourself during this global crisis.
The National Suicide Prevention Lifeline is always available at 1-800-273-TALK (8255).
Resources
- Mental health and the COVID-19 pandemic
- Brief examines the COVID-19 crisis’ implications for Americans’ mental health
- COVID-19: Helping health care workers on the front lines
- Overcoming COVID-related stress
- Confessions of an outpatient psychiatrist during the pandemic
- Psychiatric patients may be among the hardest hit
- Experts hasten to head off mental health crisis
- Podcast: Physician Suicide
1Lancet Psychiatry. 2020 Apr 21. doi: 10.1016/S2215-0366(20):30171-1.
2Brain, Behav Immun. 2020 Apr 27. doi: 10.10116/j.bbi.2020.04.069).
Coronary CT angiography gives superior MI risk prediction
In patients with stable chest pain, the burden of low-attenuation noncalcified plaque on coronary CT angiography is a better predictor of future myocardial infarction risk than a cardiovascular risk score, an Agatson coronary artery calcium score, or angiographic severity of coronary stenoses, Michelle C. Williams, MBChB, PhD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.

These findings from a post hoc analysis of the large multicenter SCOT-HEART trial challenge current concepts regarding the supposed superiority of the classic tools for MI risk prediction, noted Dr. Williams, a senior clinical research fellow at the University of Edinburgh.
Indeed, it’s likely that the current established predictors of risk – that is, coronary artery calcium, severity of stenosis, and cardiovascular risk score – are associated with clinical events only indirectly through their correlation with low-attenuated calcified plaque burden, which is the real driver of future MI, she continued.
Histologically, low-attenuated noncalcified plaque on coronary CT angiography (CCTA) is defined by a thin fibrous cap, a large, inflamed, lipid-rich necrotic core, and microcalcification. Previously, Dr. Williams and her coinvestigators demonstrated that visual identification of this unstable plaque subtype is of benefit in predicting future risk of MI (J Am Coll Cardiol. 2019 Jan 29;73[3]:291-301).
But visual identification of plaque subtypes is a crude and laborious process. In her current study, she and her coworkers have taken things a giant step further, using commercially available CCTA software to semiautomatically quantify the burden of this highest-risk plaque subtype as well as all the other subtypes.
This post hoc analysis of the previously reported main SCOT-HEART trial (N Engl J Med. 2018 Sep 6;379[10]:924-933) included 1,769 patients with stable chest pain randomized to standard care with or without CCTA guidance and followed for a median of 4.7 years, during which 41 patients had a fatal or nonfatal MI. At enrollment, 37% of participants had normal coronary arteries, 38% had nonobstructive coronary artery disease (CAD), and the remainder had obstructive CAD.
In a multivariate analysis, low-attenuation noncalcified plaque burden was the strongest predictor of future MI, with an adjusted hazard ratio of 1.6 per doubling. This metric was strongly correlated with coronary artery calcium score, underscoring the limited value of doing noncontrast CT in order to determine a coronary artery calcium score when CCTA is performed.
Low-attenuation plaque burden correlated very strongly with angiographic severity of stenosis, and only weakly with cardiovascular risk score, perhaps explaining the poor prognostic performance of cardiovascular risk scores in SCOT-HEART and other studies, according to Dr. Williams.
Patients with a low-attenuation noncalcified plaque burden greater than 4% in their coronary tree were 4.7 times more likely to have a subsequent MI than were those with a lesser burden. The predictive power was even greater in patients with nonobstructive CAD, where a low-attenuation noncalcified plaque burden in excess of 4% conferred a 6.6-fold greater likelihood of fatal or nonfatal MI, she observed.
Two things need to happen before measurement of low-attenuation noncalcified plaque via CCTA to predict MI risk is ready to be adopted in routine clinical practice, according to Dr. Williams. These SCOT-HEART results need to be validated in other cohorts, a process now underway in the SCOT-HEART 2 trial and other studies. Also, improved software incorporating machine learning is needed in order to speed up the semiautomated analysis of plaque subtypes, which now takes 20-30 minutes.
Dr. Williams reported having no financial conflicts regarding her study, funded by the National Health Service.
In conjunction with her virtual presentation at ACC 2020, the SCOT-HEART study results were published online (Circulation. 2020 Mar 16. doi: 10.1161/CIRCULATIONAHA.119.044720. [Epub ahead of print]).
SOURCE: Williams MC et al. ACC 2020, Abstract 909-06.
In patients with stable chest pain, the burden of low-attenuation noncalcified plaque on coronary CT angiography is a better predictor of future myocardial infarction risk than a cardiovascular risk score, an Agatson coronary artery calcium score, or angiographic severity of coronary stenoses, Michelle C. Williams, MBChB, PhD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.
These findings from a post hoc analysis of the large multicenter SCOT-HEART trial challenge current concepts regarding the supposed superiority of the classic tools for MI risk prediction, noted Dr. Williams, a senior clinical research fellow at the University of Edinburgh.
Indeed, it’s likely that the current established predictors of risk – that is, coronary artery calcium, severity of stenosis, and cardiovascular risk score – are associated with clinical events only indirectly through their correlation with low-attenuated calcified plaque burden, which is the real driver of future MI, she continued.
Histologically, low-attenuated noncalcified plaque on coronary CT angiography (CCTA) is defined by a thin fibrous cap, a large, inflamed, lipid-rich necrotic core, and microcalcification. Previously, Dr. Williams and her coinvestigators demonstrated that visual identification of this unstable plaque subtype is of benefit in predicting future risk of MI (J Am Coll Cardiol. 2019 Jan 29;73[3]:291-301).
But visual identification of plaque subtypes is a crude and laborious process. In her current study, she and her coworkers have taken things a giant step further, using commercially available CCTA software to semiautomatically quantify the burden of this highest-risk plaque subtype as well as all the other subtypes.
This post hoc analysis of the previously reported main SCOT-HEART trial (N Engl J Med. 2018 Sep 6;379[10]:924-933) included 1,769 patients with stable chest pain randomized to standard care with or without CCTA guidance and followed for a median of 4.7 years, during which 41 patients had a fatal or nonfatal MI. At enrollment, 37% of participants had normal coronary arteries, 38% had nonobstructive coronary artery disease (CAD), and the remainder had obstructive CAD.
In a multivariate analysis, low-attenuation noncalcified plaque burden was the strongest predictor of future MI, with an adjusted hazard ratio of 1.6 per doubling. This metric was strongly correlated with coronary artery calcium score, underscoring the limited value of doing noncontrast CT in order to determine a coronary artery calcium score when CCTA is performed.
Low-attenuation plaque burden correlated very strongly with angiographic severity of stenosis, and only weakly with cardiovascular risk score, perhaps explaining the poor prognostic performance of cardiovascular risk scores in SCOT-HEART and other studies, according to Dr. Williams.
Patients with a low-attenuation noncalcified plaque burden greater than 4% in their coronary tree were 4.7 times more likely to have a subsequent MI than were those with a lesser burden. The predictive power was even greater in patients with nonobstructive CAD, where a low-attenuation noncalcified plaque burden in excess of 4% conferred a 6.6-fold greater likelihood of fatal or nonfatal MI, she observed.
Two things need to happen before measurement of low-attenuation noncalcified plaque via CCTA to predict MI risk is ready to be adopted in routine clinical practice, according to Dr. Williams. These SCOT-HEART results need to be validated in other cohorts, a process now underway in the SCOT-HEART 2 trial and other studies. Also, improved software incorporating machine learning is needed in order to speed up the semiautomated analysis of plaque subtypes, which now takes 20-30 minutes.
Dr. Williams reported having no financial conflicts regarding her study, funded by the National Health Service.
In conjunction with her virtual presentation at ACC 2020, the SCOT-HEART study results were published online (Circulation. 2020 Mar 16. doi: 10.1161/CIRCULATIONAHA.119.044720. [Epub ahead of print]).
SOURCE: Williams MC et al. ACC 2020, Abstract 909-06.
In patients with stable chest pain, the burden of low-attenuation noncalcified plaque on coronary CT angiography is a better predictor of future myocardial infarction risk than a cardiovascular risk score, an Agatson coronary artery calcium score, or angiographic severity of coronary stenoses, Michelle C. Williams, MBChB, PhD, reported at the joint scientific sessions of the American College of Cardiology and the World Heart Federation. The meeting was conducted online after its cancellation because of the COVID-19 pandemic.
These findings from a post hoc analysis of the large multicenter SCOT-HEART trial challenge current concepts regarding the supposed superiority of the classic tools for MI risk prediction, noted Dr. Williams, a senior clinical research fellow at the University of Edinburgh.
Indeed, it’s likely that the current established predictors of risk – that is, coronary artery calcium, severity of stenosis, and cardiovascular risk score – are associated with clinical events only indirectly through their correlation with low-attenuated calcified plaque burden, which is the real driver of future MI, she continued.
Histologically, low-attenuated noncalcified plaque on coronary CT angiography (CCTA) is defined by a thin fibrous cap, a large, inflamed, lipid-rich necrotic core, and microcalcification. Previously, Dr. Williams and her coinvestigators demonstrated that visual identification of this unstable plaque subtype is of benefit in predicting future risk of MI (J Am Coll Cardiol. 2019 Jan 29;73[3]:291-301).
But visual identification of plaque subtypes is a crude and laborious process. In her current study, she and her coworkers have taken things a giant step further, using commercially available CCTA software to semiautomatically quantify the burden of this highest-risk plaque subtype as well as all the other subtypes.
This post hoc analysis of the previously reported main SCOT-HEART trial (N Engl J Med. 2018 Sep 6;379[10]:924-933) included 1,769 patients with stable chest pain randomized to standard care with or without CCTA guidance and followed for a median of 4.7 years, during which 41 patients had a fatal or nonfatal MI. At enrollment, 37% of participants had normal coronary arteries, 38% had nonobstructive coronary artery disease (CAD), and the remainder had obstructive CAD.
In a multivariate analysis, low-attenuation noncalcified plaque burden was the strongest predictor of future MI, with an adjusted hazard ratio of 1.6 per doubling. This metric was strongly correlated with coronary artery calcium score, underscoring the limited value of doing noncontrast CT in order to determine a coronary artery calcium score when CCTA is performed.
Low-attenuation plaque burden correlated very strongly with angiographic severity of stenosis, and only weakly with cardiovascular risk score, perhaps explaining the poor prognostic performance of cardiovascular risk scores in SCOT-HEART and other studies, according to Dr. Williams.
Patients with a low-attenuation noncalcified plaque burden greater than 4% in their coronary tree were 4.7 times more likely to have a subsequent MI than were those with a lesser burden. The predictive power was even greater in patients with nonobstructive CAD, where a low-attenuation noncalcified plaque burden in excess of 4% conferred a 6.6-fold greater likelihood of fatal or nonfatal MI, she observed.
Two things need to happen before measurement of low-attenuation noncalcified plaque via CCTA to predict MI risk is ready to be adopted in routine clinical practice, according to Dr. Williams. These SCOT-HEART results need to be validated in other cohorts, a process now underway in the SCOT-HEART 2 trial and other studies. Also, improved software incorporating machine learning is needed in order to speed up the semiautomated analysis of plaque subtypes, which now takes 20-30 minutes.
Dr. Williams reported having no financial conflicts regarding her study, funded by the National Health Service.
In conjunction with her virtual presentation at ACC 2020, the SCOT-HEART study results were published online (Circulation. 2020 Mar 16. doi: 10.1161/CIRCULATIONAHA.119.044720. [Epub ahead of print]).
SOURCE: Williams MC et al. ACC 2020, Abstract 909-06.
FROM ACC 2020
U.S. ‘deaths of despair’ from COVID-19 could top 75,000, experts warn
The number of “deaths of despair” could be even higher if the country fails to take bold action to address the mental health toll of unemployment, isolation, and uncertainty, according to the report from the Well Being Trust (WBT) and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care.
“If nothing happens and nothing improves – ie, the worst-case scenario – we could be looking at an additional 150,000 people who died who didn’t have to,” Benjamin Miller, PsyD, WBT chief strategy officer, told Medscape Medical News.
“We can prevent these deaths. We know how and have a bevy of evidence-based solutions. We lack the resources to really stand this up in a way that can most positively impact communities,” Miller added.
Slow recovery, quick recovery scenarios
For the analysis, Miller and colleagues combined information on the number of deaths from suicide, alcohol, and drugs from 2018 as a baseline (n = 181,686). They projected levels of unemployment from 2020 to 2029 and then used economic modeling to estimate the additional annual number of deaths.
Across nine different scenarios, the number of additional deaths of despair range from 27,644 (quick recovery, smallest impact of unemployment on suicide, alcohol-, and drug-related deaths) to 154,037 (slow recovery, greatest impact of unemployment on these deaths), with 75,000 being the most likely.
The report offers several policy solutions to prevent a surge in “avoidable” deaths. They include finding ways to ameliorate the effects of unemployment and provide meaningful work to those who are out of work. Making access to care easier and fully integrating mental health and addiction care into primary and clinical care as well as community settings are also essential.
These solutions should also serve to prevent drug and alcohol misuse and suicide in normal times, the researchers say.
Miller believes it’s time for the federal government to fully support a framework of excellence in mental health and well-being and to invest in mental health now.
“In the short term, we need at least $48 billion to keep the lights on in the current system,” he said.
“This is because 92.6% of mental health organizations have had to reduce their operations in some capacity, 61.8% have had to completely close at least one program, and 31.0% have had to turn away patients. This scenario is not optimal for people who will need a system to help them right now during a crisis,” he added.
In the long term, $150 billion is needed for a “massive structural redesign” of the US mental health system, Miller said.
“This means bringing mental health fully into all facets of our healthcare system, of our community. It will take robust investment in creating new mechanisms for care ― those that are team-based, create a new type of workforce to deliver that care, and one that is seamless across clinical and community settings,” said Miller.
A version of this article first appeared on Medscape.com.
The number of “deaths of despair” could be even higher if the country fails to take bold action to address the mental health toll of unemployment, isolation, and uncertainty, according to the report from the Well Being Trust (WBT) and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care.
“If nothing happens and nothing improves – ie, the worst-case scenario – we could be looking at an additional 150,000 people who died who didn’t have to,” Benjamin Miller, PsyD, WBT chief strategy officer, told Medscape Medical News.
“We can prevent these deaths. We know how and have a bevy of evidence-based solutions. We lack the resources to really stand this up in a way that can most positively impact communities,” Miller added.
Slow recovery, quick recovery scenarios
For the analysis, Miller and colleagues combined information on the number of deaths from suicide, alcohol, and drugs from 2018 as a baseline (n = 181,686). They projected levels of unemployment from 2020 to 2029 and then used economic modeling to estimate the additional annual number of deaths.
Across nine different scenarios, the number of additional deaths of despair range from 27,644 (quick recovery, smallest impact of unemployment on suicide, alcohol-, and drug-related deaths) to 154,037 (slow recovery, greatest impact of unemployment on these deaths), with 75,000 being the most likely.
The report offers several policy solutions to prevent a surge in “avoidable” deaths. They include finding ways to ameliorate the effects of unemployment and provide meaningful work to those who are out of work. Making access to care easier and fully integrating mental health and addiction care into primary and clinical care as well as community settings are also essential.
These solutions should also serve to prevent drug and alcohol misuse and suicide in normal times, the researchers say.
Miller believes it’s time for the federal government to fully support a framework of excellence in mental health and well-being and to invest in mental health now.
“In the short term, we need at least $48 billion to keep the lights on in the current system,” he said.
“This is because 92.6% of mental health organizations have had to reduce their operations in some capacity, 61.8% have had to completely close at least one program, and 31.0% have had to turn away patients. This scenario is not optimal for people who will need a system to help them right now during a crisis,” he added.
In the long term, $150 billion is needed for a “massive structural redesign” of the US mental health system, Miller said.
“This means bringing mental health fully into all facets of our healthcare system, of our community. It will take robust investment in creating new mechanisms for care ― those that are team-based, create a new type of workforce to deliver that care, and one that is seamless across clinical and community settings,” said Miller.
A version of this article first appeared on Medscape.com.
The number of “deaths of despair” could be even higher if the country fails to take bold action to address the mental health toll of unemployment, isolation, and uncertainty, according to the report from the Well Being Trust (WBT) and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care.
“If nothing happens and nothing improves – ie, the worst-case scenario – we could be looking at an additional 150,000 people who died who didn’t have to,” Benjamin Miller, PsyD, WBT chief strategy officer, told Medscape Medical News.
“We can prevent these deaths. We know how and have a bevy of evidence-based solutions. We lack the resources to really stand this up in a way that can most positively impact communities,” Miller added.
Slow recovery, quick recovery scenarios
For the analysis, Miller and colleagues combined information on the number of deaths from suicide, alcohol, and drugs from 2018 as a baseline (n = 181,686). They projected levels of unemployment from 2020 to 2029 and then used economic modeling to estimate the additional annual number of deaths.
Across nine different scenarios, the number of additional deaths of despair range from 27,644 (quick recovery, smallest impact of unemployment on suicide, alcohol-, and drug-related deaths) to 154,037 (slow recovery, greatest impact of unemployment on these deaths), with 75,000 being the most likely.
The report offers several policy solutions to prevent a surge in “avoidable” deaths. They include finding ways to ameliorate the effects of unemployment and provide meaningful work to those who are out of work. Making access to care easier and fully integrating mental health and addiction care into primary and clinical care as well as community settings are also essential.
These solutions should also serve to prevent drug and alcohol misuse and suicide in normal times, the researchers say.
Miller believes it’s time for the federal government to fully support a framework of excellence in mental health and well-being and to invest in mental health now.
“In the short term, we need at least $48 billion to keep the lights on in the current system,” he said.
“This is because 92.6% of mental health organizations have had to reduce their operations in some capacity, 61.8% have had to completely close at least one program, and 31.0% have had to turn away patients. This scenario is not optimal for people who will need a system to help them right now during a crisis,” he added.
In the long term, $150 billion is needed for a “massive structural redesign” of the US mental health system, Miller said.
“This means bringing mental health fully into all facets of our healthcare system, of our community. It will take robust investment in creating new mechanisms for care ― those that are team-based, create a new type of workforce to deliver that care, and one that is seamless across clinical and community settings,” said Miller.
A version of this article first appeared on Medscape.com.
Fewer than 20% of eligible children received the recommended two doses of flu vaccine
A second booster dose of the influenza vaccine in vaccine-naive children may significantly reduce their likelihood of getting the disease, new research suggests.

Writing for JAMA Pediatrics, researchers reported on a case-control study of 7,533 children presenting to outpatient clinics – all in the U.S. Influenza Vaccine Effectiveness Network – with acute respiratory tract illnesses from 2014 to 2018. The study looked at the effectiveness of vaccination against laboratory-confirmed influenza.
Current U.S. guidelines recommend that children aged 6 months to 8 years receive two doses of the influenza vaccine initially – a priming dose and a booster dose – while those aged 9 years or older are considered to be ‘immunologically primed’ and therefore only require one annual dose.
The study found that 60% of the children had received two doses of the influenza vaccine during their first vaccination season, and 68% were first vaccinated before the current influenza season. Of those who had been vaccinated, 89% had received their first influenza vaccine dose when they were younger than 2 years.
Among the 2,140 children who were unvaccinated before the current influenza season, the 436 children who received two doses of the influenza vaccine had 43% lower odds of influenza compared with the 466 children who received one dose. The overall vaccine effectiveness among this vaccine-naive group aged under 2 years was 38%; for those who received two doses it was 53%, and for those who received one dose it was 23%.
“The higher risk of infection resulting from underdeveloped immune and respiratory tract systems provides a reason to identify vaccination strategies focusing on this vulnerable population of younger children,” wrote Jessie R. Chung, MPH, of the Influenza Division of the Centers for Disease Control and Prevention, and coauthors. “Promoting efforts to improve influenza vaccine coverage—particularly with 2 doses in the first vaccination season – may reduce the burden of influenza illness among young children, who are particularly vulnerable to complications and death from influenza infection.”
Overall 52% of children were unvaccinated for the current influenza season and 9% were partially vaccinated. Of those who were fully vaccinated for the current season, 83% had received one dose in the current season, and 17% had received two doses.
The authors found that full vaccination against any influenza was associated with a 22% lower odds of influenza compared with partial vaccination (95% confidence interval, 0.61-1.01), with partial vaccination defined as anything less than two doses of vaccine in the current season – at least 4 weeks apart – or two or more doses before the current season and one or more doses in the current season. However, even children who were only partially vaccinated still showed statistically significant vaccine effectiveness, except for those who received one dose of vaccine in the current season and were aged under 2 years.
“Compared with older children, young children, even if healthy, are at an elevated risk of influenza infection and influenza-associated complications, such as hospitalization,” the authors wrote. “One recent simulation study reported that even small improvements in either vaccine coverage or VE [vaccine effectiveness], and ideally both, may avert substantial amounts of influenza-associated illnesses, medical visits, and hospitalizations.”
The study also noted that children who had received only a single previous vaccine dose rarely received two doses in the current season.
In an accompanying editorial, Claire Abraham, MD, and Melissa S. Stockwell, MD, of Columbia University Medical Center, New York, wrote that modeling suggested that in the 2017-2018 influenza season, vaccination prevented 1.3 million cases of infection, 895,000 medical visits, 10,500 hospitalizations and 111 deaths in children aged under 5 years.
“This study highlights the importance of administering 2 doses of the influenza vaccine to children younger than 9 years for whom 2 doses are needed, and especially to vaccine naive children younger than 2 years,” they wrote.
But despite many studies showing the impact and importance of influenza vaccination, uptake of this vaccine remained lower than for other pediatric vaccines.
“This present study reemphasizes the need for further research exploring why families who are seemingly willing to vaccinate their children against influenza, as indicated by their receiving the first needed dose of influenza vaccine, find barriers to receiving all of the needed doses, placing their children at higher risk for contracting a potentially devastating virus.”
The U.S. Influenza Vaccine Effectiveness Network is funded by the CDC, and this project also received support from the National Institutes of Health. Eight authors declared grants from the CDC during the conduct of the study, and five declared grants and other funding from private industry outside the study.
SOURCE: Chung J et al. JAMA Pediatrics 2020 May 4. doi: 10.1001/jamapediatrics.2020.0372.
A second booster dose of the influenza vaccine in vaccine-naive children may significantly reduce their likelihood of getting the disease, new research suggests.
Writing for JAMA Pediatrics, researchers reported on a case-control study of 7,533 children presenting to outpatient clinics – all in the U.S. Influenza Vaccine Effectiveness Network – with acute respiratory tract illnesses from 2014 to 2018. The study looked at the effectiveness of vaccination against laboratory-confirmed influenza.
Current U.S. guidelines recommend that children aged 6 months to 8 years receive two doses of the influenza vaccine initially – a priming dose and a booster dose – while those aged 9 years or older are considered to be ‘immunologically primed’ and therefore only require one annual dose.
The study found that 60% of the children had received two doses of the influenza vaccine during their first vaccination season, and 68% were first vaccinated before the current influenza season. Of those who had been vaccinated, 89% had received their first influenza vaccine dose when they were younger than 2 years.
Among the 2,140 children who were unvaccinated before the current influenza season, the 436 children who received two doses of the influenza vaccine had 43% lower odds of influenza compared with the 466 children who received one dose. The overall vaccine effectiveness among this vaccine-naive group aged under 2 years was 38%; for those who received two doses it was 53%, and for those who received one dose it was 23%.
“The higher risk of infection resulting from underdeveloped immune and respiratory tract systems provides a reason to identify vaccination strategies focusing on this vulnerable population of younger children,” wrote Jessie R. Chung, MPH, of the Influenza Division of the Centers for Disease Control and Prevention, and coauthors. “Promoting efforts to improve influenza vaccine coverage—particularly with 2 doses in the first vaccination season – may reduce the burden of influenza illness among young children, who are particularly vulnerable to complications and death from influenza infection.”
Overall 52% of children were unvaccinated for the current influenza season and 9% were partially vaccinated. Of those who were fully vaccinated for the current season, 83% had received one dose in the current season, and 17% had received two doses.
The authors found that full vaccination against any influenza was associated with a 22% lower odds of influenza compared with partial vaccination (95% confidence interval, 0.61-1.01), with partial vaccination defined as anything less than two doses of vaccine in the current season – at least 4 weeks apart – or two or more doses before the current season and one or more doses in the current season. However, even children who were only partially vaccinated still showed statistically significant vaccine effectiveness, except for those who received one dose of vaccine in the current season and were aged under 2 years.
“Compared with older children, young children, even if healthy, are at an elevated risk of influenza infection and influenza-associated complications, such as hospitalization,” the authors wrote. “One recent simulation study reported that even small improvements in either vaccine coverage or VE [vaccine effectiveness], and ideally both, may avert substantial amounts of influenza-associated illnesses, medical visits, and hospitalizations.”
The study also noted that children who had received only a single previous vaccine dose rarely received two doses in the current season.
In an accompanying editorial, Claire Abraham, MD, and Melissa S. Stockwell, MD, of Columbia University Medical Center, New York, wrote that modeling suggested that in the 2017-2018 influenza season, vaccination prevented 1.3 million cases of infection, 895,000 medical visits, 10,500 hospitalizations and 111 deaths in children aged under 5 years.
“This study highlights the importance of administering 2 doses of the influenza vaccine to children younger than 9 years for whom 2 doses are needed, and especially to vaccine naive children younger than 2 years,” they wrote.
But despite many studies showing the impact and importance of influenza vaccination, uptake of this vaccine remained lower than for other pediatric vaccines.
“This present study reemphasizes the need for further research exploring why families who are seemingly willing to vaccinate their children against influenza, as indicated by their receiving the first needed dose of influenza vaccine, find barriers to receiving all of the needed doses, placing their children at higher risk for contracting a potentially devastating virus.”
The U.S. Influenza Vaccine Effectiveness Network is funded by the CDC, and this project also received support from the National Institutes of Health. Eight authors declared grants from the CDC during the conduct of the study, and five declared grants and other funding from private industry outside the study.
SOURCE: Chung J et al. JAMA Pediatrics 2020 May 4. doi: 10.1001/jamapediatrics.2020.0372.
A second booster dose of the influenza vaccine in vaccine-naive children may significantly reduce their likelihood of getting the disease, new research suggests.
Writing for JAMA Pediatrics, researchers reported on a case-control study of 7,533 children presenting to outpatient clinics – all in the U.S. Influenza Vaccine Effectiveness Network – with acute respiratory tract illnesses from 2014 to 2018. The study looked at the effectiveness of vaccination against laboratory-confirmed influenza.
Current U.S. guidelines recommend that children aged 6 months to 8 years receive two doses of the influenza vaccine initially – a priming dose and a booster dose – while those aged 9 years or older are considered to be ‘immunologically primed’ and therefore only require one annual dose.
The study found that 60% of the children had received two doses of the influenza vaccine during their first vaccination season, and 68% were first vaccinated before the current influenza season. Of those who had been vaccinated, 89% had received their first influenza vaccine dose when they were younger than 2 years.
Among the 2,140 children who were unvaccinated before the current influenza season, the 436 children who received two doses of the influenza vaccine had 43% lower odds of influenza compared with the 466 children who received one dose. The overall vaccine effectiveness among this vaccine-naive group aged under 2 years was 38%; for those who received two doses it was 53%, and for those who received one dose it was 23%.
“The higher risk of infection resulting from underdeveloped immune and respiratory tract systems provides a reason to identify vaccination strategies focusing on this vulnerable population of younger children,” wrote Jessie R. Chung, MPH, of the Influenza Division of the Centers for Disease Control and Prevention, and coauthors. “Promoting efforts to improve influenza vaccine coverage—particularly with 2 doses in the first vaccination season – may reduce the burden of influenza illness among young children, who are particularly vulnerable to complications and death from influenza infection.”
Overall 52% of children were unvaccinated for the current influenza season and 9% were partially vaccinated. Of those who were fully vaccinated for the current season, 83% had received one dose in the current season, and 17% had received two doses.
The authors found that full vaccination against any influenza was associated with a 22% lower odds of influenza compared with partial vaccination (95% confidence interval, 0.61-1.01), with partial vaccination defined as anything less than two doses of vaccine in the current season – at least 4 weeks apart – or two or more doses before the current season and one or more doses in the current season. However, even children who were only partially vaccinated still showed statistically significant vaccine effectiveness, except for those who received one dose of vaccine in the current season and were aged under 2 years.
“Compared with older children, young children, even if healthy, are at an elevated risk of influenza infection and influenza-associated complications, such as hospitalization,” the authors wrote. “One recent simulation study reported that even small improvements in either vaccine coverage or VE [vaccine effectiveness], and ideally both, may avert substantial amounts of influenza-associated illnesses, medical visits, and hospitalizations.”
The study also noted that children who had received only a single previous vaccine dose rarely received two doses in the current season.
In an accompanying editorial, Claire Abraham, MD, and Melissa S. Stockwell, MD, of Columbia University Medical Center, New York, wrote that modeling suggested that in the 2017-2018 influenza season, vaccination prevented 1.3 million cases of infection, 895,000 medical visits, 10,500 hospitalizations and 111 deaths in children aged under 5 years.
“This study highlights the importance of administering 2 doses of the influenza vaccine to children younger than 9 years for whom 2 doses are needed, and especially to vaccine naive children younger than 2 years,” they wrote.
But despite many studies showing the impact and importance of influenza vaccination, uptake of this vaccine remained lower than for other pediatric vaccines.
“This present study reemphasizes the need for further research exploring why families who are seemingly willing to vaccinate their children against influenza, as indicated by their receiving the first needed dose of influenza vaccine, find barriers to receiving all of the needed doses, placing their children at higher risk for contracting a potentially devastating virus.”
The U.S. Influenza Vaccine Effectiveness Network is funded by the CDC, and this project also received support from the National Institutes of Health. Eight authors declared grants from the CDC during the conduct of the study, and five declared grants and other funding from private industry outside the study.
SOURCE: Chung J et al. JAMA Pediatrics 2020 May 4. doi: 10.1001/jamapediatrics.2020.0372.
FROM JAMA PEDIATRICS
Andexanet alfa reverses factor Xa inhibitors
Background: Factor Xa inhibitors have become increasingly popular in the treatment and prevention of thrombotic events, but the lack of specific reversal agents in the event of life-threatening or uncontrolled bleeding may limit their use. Andexanet alfa is a new Food and Drug Administration–approved reversal agent which rapidly reduces anti–factor Xa activity, thereby reversing the anticoagulation effects of factor Xa inhibitors.

Study design: A prospective, open-label, single-group cohort study.
Setting: An industry-sponsored, multicenter study.
Synopsis: The study evaluated 352 adult patients who had acute major bleeding (such as intracranial hemorrhage [64%] or GI bleeding [26%] within 18 hours after administration of a factor Xa inhibitor, including apixaban, rivaroxaban, or edoxaban). Efficacy was assessed in 254 patients who met criteria for severe bleeding and elevated baseline anti–factor Xa activity. Patients were administered a bolus dose of andexanet alfa followed by a 2-hour infusion. The median anti–factor Xa activity reduced by 92% each among patients receiving apixaban or rivaroxaban. The majority (82%) of evaluable patients achieved excellent or good hemostasis at 12 hours after andexanet alfa administration, which compares favorably with the hemostatic efficacy of 72% observed with prothrombin complex concentrate used to reverse anticoagulation in patients treated with vitamin K antagonists. Of patients in the study, 10% experienced a thrombotic event during the 30-day follow-up period, and 14% died.
Limitations of the study include lack of a control group and absence of a significant relationship between a reduction in anti–factor Xa activity and hemostasis. The sponsor is planning to conduct a randomized trial with FDA guidance in the near future.
Bottom line: Andexanet alfa is an FDA-approved agent and appears effective in achieving hemostasis in patients with a factor Xa inhibitor–associated major acute bleeding.
Citation: Connolly SJ et al. Full study report of andexanet alfa for bleeding associated with factor Xa inhibitors. N Eng J Med. 2019 Feb 7. doi: 10.1056/NEJMoa1814051.
Dr. Vedamurthy is a hospitalist at Massachusetts General Hospital.
Background: Factor Xa inhibitors have become increasingly popular in the treatment and prevention of thrombotic events, but the lack of specific reversal agents in the event of life-threatening or uncontrolled bleeding may limit their use. Andexanet alfa is a new Food and Drug Administration–approved reversal agent which rapidly reduces anti–factor Xa activity, thereby reversing the anticoagulation effects of factor Xa inhibitors.
Study design: A prospective, open-label, single-group cohort study.
Setting: An industry-sponsored, multicenter study.
Synopsis: The study evaluated 352 adult patients who had acute major bleeding (such as intracranial hemorrhage [64%] or GI bleeding [26%] within 18 hours after administration of a factor Xa inhibitor, including apixaban, rivaroxaban, or edoxaban). Efficacy was assessed in 254 patients who met criteria for severe bleeding and elevated baseline anti–factor Xa activity. Patients were administered a bolus dose of andexanet alfa followed by a 2-hour infusion. The median anti–factor Xa activity reduced by 92% each among patients receiving apixaban or rivaroxaban. The majority (82%) of evaluable patients achieved excellent or good hemostasis at 12 hours after andexanet alfa administration, which compares favorably with the hemostatic efficacy of 72% observed with prothrombin complex concentrate used to reverse anticoagulation in patients treated with vitamin K antagonists. Of patients in the study, 10% experienced a thrombotic event during the 30-day follow-up period, and 14% died.
Limitations of the study include lack of a control group and absence of a significant relationship between a reduction in anti–factor Xa activity and hemostasis. The sponsor is planning to conduct a randomized trial with FDA guidance in the near future.
Bottom line: Andexanet alfa is an FDA-approved agent and appears effective in achieving hemostasis in patients with a factor Xa inhibitor–associated major acute bleeding.
Citation: Connolly SJ et al. Full study report of andexanet alfa for bleeding associated with factor Xa inhibitors. N Eng J Med. 2019 Feb 7. doi: 10.1056/NEJMoa1814051.
Dr. Vedamurthy is a hospitalist at Massachusetts General Hospital.
Background: Factor Xa inhibitors have become increasingly popular in the treatment and prevention of thrombotic events, but the lack of specific reversal agents in the event of life-threatening or uncontrolled bleeding may limit their use. Andexanet alfa is a new Food and Drug Administration–approved reversal agent which rapidly reduces anti–factor Xa activity, thereby reversing the anticoagulation effects of factor Xa inhibitors.
Study design: A prospective, open-label, single-group cohort study.
Setting: An industry-sponsored, multicenter study.
Synopsis: The study evaluated 352 adult patients who had acute major bleeding (such as intracranial hemorrhage [64%] or GI bleeding [26%] within 18 hours after administration of a factor Xa inhibitor, including apixaban, rivaroxaban, or edoxaban). Efficacy was assessed in 254 patients who met criteria for severe bleeding and elevated baseline anti–factor Xa activity. Patients were administered a bolus dose of andexanet alfa followed by a 2-hour infusion. The median anti–factor Xa activity reduced by 92% each among patients receiving apixaban or rivaroxaban. The majority (82%) of evaluable patients achieved excellent or good hemostasis at 12 hours after andexanet alfa administration, which compares favorably with the hemostatic efficacy of 72% observed with prothrombin complex concentrate used to reverse anticoagulation in patients treated with vitamin K antagonists. Of patients in the study, 10% experienced a thrombotic event during the 30-day follow-up period, and 14% died.
Limitations of the study include lack of a control group and absence of a significant relationship between a reduction in anti–factor Xa activity and hemostasis. The sponsor is planning to conduct a randomized trial with FDA guidance in the near future.
Bottom line: Andexanet alfa is an FDA-approved agent and appears effective in achieving hemostasis in patients with a factor Xa inhibitor–associated major acute bleeding.
Citation: Connolly SJ et al. Full study report of andexanet alfa for bleeding associated with factor Xa inhibitors. N Eng J Med. 2019 Feb 7. doi: 10.1056/NEJMoa1814051.
Dr. Vedamurthy is a hospitalist at Massachusetts General Hospital.
Neoadjuvant nivolumab ‘promising’ in Merkel cell carcinoma
Neoadjuvant nivolumab (Opdivo, Bristol-Myers Squibb) could improve outcomes for patients with high-risk resectable Merkel cell carcinoma (MCC), say researchers reporting the first trial in this patient population.
The results come from a cohort of 39 patients with stage IIA-IV disease, all of whom received nivolumab 240 mg intravenously on days 1 and 15, with surgery planned for day 29. About half achieved a pathologic complete response (pCR) and/or a radiographic response. Recurrence-free survival was also prolonged among responders, and no relapses were observed at a median follow-up of 19.3 months.
“Additional investigation of these promising findings is warranted,” say the investigators.
“To our knowledge, this is the first study to examine neoadjuvant anti-PD-1 therapy in MCC,” said lead author Suzanne Topalian, MD, professor of surgery at the Bloomberg-Kimmel Institute for Cancer Immunotherapy at Johns Hopkins Medicine, Baltimore, Maryland. “While the results seem encouraging, I think that clinical trial experience with a greater number of patients and follow-up for a longer time period will be needed to assess whether this treatment approach should become standard for high-risk resectable MCC.”
The study was published online April 23 in the Journal of Clinical Oncology.
Rare and Aggressive Skin Cancer
MCC is a rare and aggressive neuroendocrine skin cancer that is diagnosed in approximately 1600 people each year in the United States, note the authors.
The annual incidence of new MCC cases rose by 95% between 2000 and 2013, as previously reported by Medscape Medical News.
Although nearly two thirds of patients present with localized disease, regional and distant metastases often occur. Until recently, cytotoxic chemotherapy was the primary systemic therapy for advanced MCC. Although patients frequently respond to chemotherapy, the duration tends to be very limited, and 95% of patients experience disease progression within 1 year, the authors comment.
Growing evidence supports the hypothesis that MCC is an immunogenic cancer. Clinical trials of PD-L1 inhibitors have demonstrated increased progression-free and overall survival compared with chemotherapy when used either in the first-line or second-line setting, as reported by Medscape Medical News.
“Neoadjuvant anti-PD-1 cancer therapy is still early in development, and there are many aspects deserving careful consideration,” Topalian told Medscape Medical News. “They are centered on balancing patient risk and benefit, finding an optimal presurgical treatment interval, exploring treatment combinations, determining if anti-PD-1 therapy should be continued after surgery, and defining biomarkers to guide treatment strategies for individual patients.”
Study Details
Topian and colleagues investigated neoadjuvant use of nivolumab in the CheckMate 358 study, which involved 39 patients with stage IIA-IV MCC (of whom 36 went on to surgery).
The median age of the patients was 68 years, and at enrollment, most patients (66.7%) had stage III disease. For 35 patients, tumors were evaluable for MCPyV status; 22 (62.9%) were positive. Quantifiable tumor cell PD-L1 expression occurred in 27 patients; expression was 1% or higher for seven of those patients (25.9%).
The primary endpoint for the neoadjuvant cohort was safety and tolerability of nivolumab, as measured by treatment-related adverse events (TRAEs) and surgical delays, defined as the proportion of patients who experienced TRAE-related delays of more than 4 weeks from the planned surgery date.
Exploratory endpoints included pCR, radiographic response, recurrence-free survival, overall survival, association of tumor MCPyV status, and PD-L1 expression with efficacy.
The median follow-up was 20.3 months. TRAEs of any grade were reported in 18 patients (46.2%). Three (7.7%) experienced a grade 3/4 event. TRAEs with potential immunologic causes occurred in six (15.4%) patients (two TRAEs were of grade 3/4).
Among those who underwent surgery, 17 (47.2%) achieved a pCR. Among patients who were radiographically evaluable (n = 33), 29 (87.9%) achieved some degree of radiographic tumor reduction. Within this group, 18 (54.5%) experienced tumor reductions of 30% or greater (the median change in tumor burden from baseline was −32.8%). Responses were observed regardless of tumor MCPyV, PD-L1, or TMB status.
Survival Outcomes
The median relapse-free survival was not reached for any of the patients who underwent surgery. At 12 and 24 months postoperatively, rates were 77.5% and 68.5%, respectively.
Among patients with pCR, relapse-free survival at 12 months was 100.0%, compared with 59.6% among those without pCR. At 24 months, it was 88.9% for those with pCR, vs 52.2% for those without pCR (hazard ratio [HR], 0.12; 95% confidence interval [CI], 0.01 – 0.93]).
Relapse-free survival was also higher for patients with radiographic tumor reduction of ≥30% in comparison with those with reduction of <30% or progression. At 12 months, it was 100.0%, vs 56.5%; at 24 months, it was 90.9%, vs 48.5% (HR, 0.11; 95% CI, 0.01 – 0.87). No substantial difference was noted between patient subgroups with respect to tumor MCPyV status or PD-L1 expression.
Median overall survival was not reached in the entire cohort. At 12 and 24 months following the first dose of nivolumab, rates were 93.2% and 79.4%, respectively. For the patients who underwent surgery and were evaluable for pathologic response or radiographic response, 100.0% and 88.9% of patients with pCR and all patients with radiographic tumor reduction of ≥30% were alive at 12 and 24 months, respectively.
Overall survival rates among patients who underwent surgery were comparable in subgroups with regard to tumor MCPyV status and PD-L1 expression.
The study was supported by Bristol-Myers Squibb and Ono, the Mark Foundation for Cancer Research, and the National Cancer Institute. Topalian reports relationships with Aduro, Potenza, Five Prime, Tizona, DNAtrix, FLX Bio, WindMIL, Dragonfly, ERVAXX, Trieza, Amgen, MedImmune, Merck, Compugen, DNAtrix, FLX Bio, Dynavax, Immunomic, Janssen Oncology, Immunocore, Bristol-Myers Squibb, Compugen Arbor, and NexImmune. Several coauthors have also disclosed relationships with industry.
This article first appeared on Medscape.com.
Neoadjuvant nivolumab (Opdivo, Bristol-Myers Squibb) could improve outcomes for patients with high-risk resectable Merkel cell carcinoma (MCC), say researchers reporting the first trial in this patient population.
The results come from a cohort of 39 patients with stage IIA-IV disease, all of whom received nivolumab 240 mg intravenously on days 1 and 15, with surgery planned for day 29. About half achieved a pathologic complete response (pCR) and/or a radiographic response. Recurrence-free survival was also prolonged among responders, and no relapses were observed at a median follow-up of 19.3 months.
“Additional investigation of these promising findings is warranted,” say the investigators.
“To our knowledge, this is the first study to examine neoadjuvant anti-PD-1 therapy in MCC,” said lead author Suzanne Topalian, MD, professor of surgery at the Bloomberg-Kimmel Institute for Cancer Immunotherapy at Johns Hopkins Medicine, Baltimore, Maryland. “While the results seem encouraging, I think that clinical trial experience with a greater number of patients and follow-up for a longer time period will be needed to assess whether this treatment approach should become standard for high-risk resectable MCC.”
The study was published online April 23 in the Journal of Clinical Oncology.
Rare and Aggressive Skin Cancer
MCC is a rare and aggressive neuroendocrine skin cancer that is diagnosed in approximately 1600 people each year in the United States, note the authors.
The annual incidence of new MCC cases rose by 95% between 2000 and 2013, as previously reported by Medscape Medical News.
Although nearly two thirds of patients present with localized disease, regional and distant metastases often occur. Until recently, cytotoxic chemotherapy was the primary systemic therapy for advanced MCC. Although patients frequently respond to chemotherapy, the duration tends to be very limited, and 95% of patients experience disease progression within 1 year, the authors comment.
Growing evidence supports the hypothesis that MCC is an immunogenic cancer. Clinical trials of PD-L1 inhibitors have demonstrated increased progression-free and overall survival compared with chemotherapy when used either in the first-line or second-line setting, as reported by Medscape Medical News.
“Neoadjuvant anti-PD-1 cancer therapy is still early in development, and there are many aspects deserving careful consideration,” Topalian told Medscape Medical News. “They are centered on balancing patient risk and benefit, finding an optimal presurgical treatment interval, exploring treatment combinations, determining if anti-PD-1 therapy should be continued after surgery, and defining biomarkers to guide treatment strategies for individual patients.”
Study Details
Topian and colleagues investigated neoadjuvant use of nivolumab in the CheckMate 358 study, which involved 39 patients with stage IIA-IV MCC (of whom 36 went on to surgery).
The median age of the patients was 68 years, and at enrollment, most patients (66.7%) had stage III disease. For 35 patients, tumors were evaluable for MCPyV status; 22 (62.9%) were positive. Quantifiable tumor cell PD-L1 expression occurred in 27 patients; expression was 1% or higher for seven of those patients (25.9%).
The primary endpoint for the neoadjuvant cohort was safety and tolerability of nivolumab, as measured by treatment-related adverse events (TRAEs) and surgical delays, defined as the proportion of patients who experienced TRAE-related delays of more than 4 weeks from the planned surgery date.
Exploratory endpoints included pCR, radiographic response, recurrence-free survival, overall survival, association of tumor MCPyV status, and PD-L1 expression with efficacy.
The median follow-up was 20.3 months. TRAEs of any grade were reported in 18 patients (46.2%). Three (7.7%) experienced a grade 3/4 event. TRAEs with potential immunologic causes occurred in six (15.4%) patients (two TRAEs were of grade 3/4).
Among those who underwent surgery, 17 (47.2%) achieved a pCR. Among patients who were radiographically evaluable (n = 33), 29 (87.9%) achieved some degree of radiographic tumor reduction. Within this group, 18 (54.5%) experienced tumor reductions of 30% or greater (the median change in tumor burden from baseline was −32.8%). Responses were observed regardless of tumor MCPyV, PD-L1, or TMB status.
Survival Outcomes
The median relapse-free survival was not reached for any of the patients who underwent surgery. At 12 and 24 months postoperatively, rates were 77.5% and 68.5%, respectively.
Among patients with pCR, relapse-free survival at 12 months was 100.0%, compared with 59.6% among those without pCR. At 24 months, it was 88.9% for those with pCR, vs 52.2% for those without pCR (hazard ratio [HR], 0.12; 95% confidence interval [CI], 0.01 – 0.93]).
Relapse-free survival was also higher for patients with radiographic tumor reduction of ≥30% in comparison with those with reduction of <30% or progression. At 12 months, it was 100.0%, vs 56.5%; at 24 months, it was 90.9%, vs 48.5% (HR, 0.11; 95% CI, 0.01 – 0.87). No substantial difference was noted between patient subgroups with respect to tumor MCPyV status or PD-L1 expression.
Median overall survival was not reached in the entire cohort. At 12 and 24 months following the first dose of nivolumab, rates were 93.2% and 79.4%, respectively. For the patients who underwent surgery and were evaluable for pathologic response or radiographic response, 100.0% and 88.9% of patients with pCR and all patients with radiographic tumor reduction of ≥30% were alive at 12 and 24 months, respectively.
Overall survival rates among patients who underwent surgery were comparable in subgroups with regard to tumor MCPyV status and PD-L1 expression.
The study was supported by Bristol-Myers Squibb and Ono, the Mark Foundation for Cancer Research, and the National Cancer Institute. Topalian reports relationships with Aduro, Potenza, Five Prime, Tizona, DNAtrix, FLX Bio, WindMIL, Dragonfly, ERVAXX, Trieza, Amgen, MedImmune, Merck, Compugen, DNAtrix, FLX Bio, Dynavax, Immunomic, Janssen Oncology, Immunocore, Bristol-Myers Squibb, Compugen Arbor, and NexImmune. Several coauthors have also disclosed relationships with industry.
This article first appeared on Medscape.com.
Neoadjuvant nivolumab (Opdivo, Bristol-Myers Squibb) could improve outcomes for patients with high-risk resectable Merkel cell carcinoma (MCC), say researchers reporting the first trial in this patient population.
The results come from a cohort of 39 patients with stage IIA-IV disease, all of whom received nivolumab 240 mg intravenously on days 1 and 15, with surgery planned for day 29. About half achieved a pathologic complete response (pCR) and/or a radiographic response. Recurrence-free survival was also prolonged among responders, and no relapses were observed at a median follow-up of 19.3 months.
“Additional investigation of these promising findings is warranted,” say the investigators.
“To our knowledge, this is the first study to examine neoadjuvant anti-PD-1 therapy in MCC,” said lead author Suzanne Topalian, MD, professor of surgery at the Bloomberg-Kimmel Institute for Cancer Immunotherapy at Johns Hopkins Medicine, Baltimore, Maryland. “While the results seem encouraging, I think that clinical trial experience with a greater number of patients and follow-up for a longer time period will be needed to assess whether this treatment approach should become standard for high-risk resectable MCC.”
The study was published online April 23 in the Journal of Clinical Oncology.
Rare and Aggressive Skin Cancer
MCC is a rare and aggressive neuroendocrine skin cancer that is diagnosed in approximately 1600 people each year in the United States, note the authors.
The annual incidence of new MCC cases rose by 95% between 2000 and 2013, as previously reported by Medscape Medical News.
Although nearly two thirds of patients present with localized disease, regional and distant metastases often occur. Until recently, cytotoxic chemotherapy was the primary systemic therapy for advanced MCC. Although patients frequently respond to chemotherapy, the duration tends to be very limited, and 95% of patients experience disease progression within 1 year, the authors comment.
Growing evidence supports the hypothesis that MCC is an immunogenic cancer. Clinical trials of PD-L1 inhibitors have demonstrated increased progression-free and overall survival compared with chemotherapy when used either in the first-line or second-line setting, as reported by Medscape Medical News.
“Neoadjuvant anti-PD-1 cancer therapy is still early in development, and there are many aspects deserving careful consideration,” Topalian told Medscape Medical News. “They are centered on balancing patient risk and benefit, finding an optimal presurgical treatment interval, exploring treatment combinations, determining if anti-PD-1 therapy should be continued after surgery, and defining biomarkers to guide treatment strategies for individual patients.”
Study Details
Topian and colleagues investigated neoadjuvant use of nivolumab in the CheckMate 358 study, which involved 39 patients with stage IIA-IV MCC (of whom 36 went on to surgery).
The median age of the patients was 68 years, and at enrollment, most patients (66.7%) had stage III disease. For 35 patients, tumors were evaluable for MCPyV status; 22 (62.9%) were positive. Quantifiable tumor cell PD-L1 expression occurred in 27 patients; expression was 1% or higher for seven of those patients (25.9%).
The primary endpoint for the neoadjuvant cohort was safety and tolerability of nivolumab, as measured by treatment-related adverse events (TRAEs) and surgical delays, defined as the proportion of patients who experienced TRAE-related delays of more than 4 weeks from the planned surgery date.
Exploratory endpoints included pCR, radiographic response, recurrence-free survival, overall survival, association of tumor MCPyV status, and PD-L1 expression with efficacy.
The median follow-up was 20.3 months. TRAEs of any grade were reported in 18 patients (46.2%). Three (7.7%) experienced a grade 3/4 event. TRAEs with potential immunologic causes occurred in six (15.4%) patients (two TRAEs were of grade 3/4).
Among those who underwent surgery, 17 (47.2%) achieved a pCR. Among patients who were radiographically evaluable (n = 33), 29 (87.9%) achieved some degree of radiographic tumor reduction. Within this group, 18 (54.5%) experienced tumor reductions of 30% or greater (the median change in tumor burden from baseline was −32.8%). Responses were observed regardless of tumor MCPyV, PD-L1, or TMB status.
Survival Outcomes
The median relapse-free survival was not reached for any of the patients who underwent surgery. At 12 and 24 months postoperatively, rates were 77.5% and 68.5%, respectively.
Among patients with pCR, relapse-free survival at 12 months was 100.0%, compared with 59.6% among those without pCR. At 24 months, it was 88.9% for those with pCR, vs 52.2% for those without pCR (hazard ratio [HR], 0.12; 95% confidence interval [CI], 0.01 – 0.93]).
Relapse-free survival was also higher for patients with radiographic tumor reduction of ≥30% in comparison with those with reduction of <30% or progression. At 12 months, it was 100.0%, vs 56.5%; at 24 months, it was 90.9%, vs 48.5% (HR, 0.11; 95% CI, 0.01 – 0.87). No substantial difference was noted between patient subgroups with respect to tumor MCPyV status or PD-L1 expression.
Median overall survival was not reached in the entire cohort. At 12 and 24 months following the first dose of nivolumab, rates were 93.2% and 79.4%, respectively. For the patients who underwent surgery and were evaluable for pathologic response or radiographic response, 100.0% and 88.9% of patients with pCR and all patients with radiographic tumor reduction of ≥30% were alive at 12 and 24 months, respectively.
Overall survival rates among patients who underwent surgery were comparable in subgroups with regard to tumor MCPyV status and PD-L1 expression.
The study was supported by Bristol-Myers Squibb and Ono, the Mark Foundation for Cancer Research, and the National Cancer Institute. Topalian reports relationships with Aduro, Potenza, Five Prime, Tizona, DNAtrix, FLX Bio, WindMIL, Dragonfly, ERVAXX, Trieza, Amgen, MedImmune, Merck, Compugen, DNAtrix, FLX Bio, Dynavax, Immunomic, Janssen Oncology, Immunocore, Bristol-Myers Squibb, Compugen Arbor, and NexImmune. Several coauthors have also disclosed relationships with industry.
This article first appeared on Medscape.com.