User login
In Case You Missed It: COVID
Psoriasis Therapy During the COVID-19 Pandemic: Should Patients Continue Biologics?
Amid hydroxychloroquine hopes, lupus patients face shortages
For almost a quarter century, Julie Powers, a 48-year-old non-profit professional from Maryland, has been taking the same medication for her lupus — and until recently, she never worried that her supply would run out. Now she’s terrified that she might lose access to a drug that prevents her immune system from attacking her heart, lungs, and skin. She describes a feeling akin to being underwater, near drowning: “That’s what my life would be like,” she said. “I’ll suffocate.”
Powers’ concerns began roughly a week ago when she learned that her lupus drug, hydroxychloroquine (hi-DROCK-see-KLORA-quin), may be helpful in the treatment of Covid-19, the illness caused by the SARS-CoV-2 virus now racing across the planet. The medication was already being used around world to treat Covid-19 patients, but evidence of its effectiveness was largely anecdotal. Then, on March 16, a renowned infectious disease specialist, Didier Raoult, announced the results of a small clinical trial in France showing that patients receiving a combination of hydroxychloroquine and the common antibiotic azithromycin had notably lower levels of the virus in their bloodstream than those who did not receive the medication.
In the last week, this once obscure drug has been thrust into the national spotlight with everyone from doctors, to laypeople, to the U.S. president weighing in. The attention has so dramatically driven up demand that pharmacists are reporting depleted stocks of the drug, leaving many of the roughly 1.5 million lupus patients across the country unable to get their prescriptions filled. They now face an uncertain future as the public clings to one of the first signs of hope to appear since the coronavirus began sweeping across the U.S.
But scientists and physicians caution that this hope is based on studies that have been conducted outside of traditional scientific timelines. “The paper is interesting and certainly would warrant future more definitive studies,” Jeff Sparks, a rheumatologist and researcher at Harvard Medical School, said of the French study. “It might even be enough data to use the regimen off-label for sick and hospitalized patients.
“However,” he added, “it does not prove that the regimen actually works.”
Despite efforts to pin blame for the shortages on Trump alone, however, hydroxychloroquine scarcity was already setting in weeks ago, as doctors began responding on their own to percolating and preliminary research. Some evidence suggests that many doctors are now writing prescriptions prophylactically for patients with no known illness — as well as for themselves and family members — prompting at least one state pharmacy board to call an emergency meeting, scheduled for Sunday morning. The board planned to bar pharmacists from dispensing chloroquine or hydroxychloroquine for anyone other than confirmed Covid-19 patients without approval of the board's director.
A prolonged shortfall in supplies would likely have grave implications for people who depend on it — including Powers, who believes that she would not be alive today without the drug. “I guarantee you, it has saved my life,” she said. “It’s the only thing that’s protecting my organs. There’s nothing else.” Like others, she hopes that pharmaceutical companies that manufacture versions of the drug will be able to quickly ramp up production — something several have already promised to do. In the meantime, Powers has a message for the American public — one echoed by most lupus doctors: When it comes to hydroxychloroquine: “If you don’t need it, don’t get it.”
The origins of hydroxychloroquine can be traced back hundreds of years to South America, where the bark of the cinchona tree appears to have been used by Andean populations to treat shivering. European missionaries eventually brought the bark to Europe, where it was used to treat malaria. In 1820, French researchers isolated the substance in the bark responsible for its beneficial effects. They named it “quinine.” When the supply from South America began to dry up, the British and Dutch decided to grow the tree on plantations.
Over time, synthetic versions were developed, including a drug called chloroquine, which was created in the midst of World War II in an effort to spare overseas American troops from malaria. As it turned out, troops with rashes and arthritis saw an improvement in symptoms after using this anti-malarial medication. After the war, a related drug was created, one with fewer side-effects when taken long-term: hydroxychloroquine. It went on to be used to treat many types of autoimmune diseases, including rheumatoid arthritis and lupus. The latter, which disproportionately affects women, used to cut lives short — typically from failure of the kidneys. Those numbers have been reduced with strict management of the disease, but the Lupus Foundation of America estimates that 10 to 15 percent of patients die prematurely due to complications of the disease.
Jinoos Yazdany, a researcher and chief of the Division of Rheumatology at Zuckerberg San Francisco General Hospital, added that there is strong clinical trial data demonstrating that taking a group of lupus patients off of hydroxychloroquine results in lupus flares. “I am less concerned about a short interruption of a few weeks,” she said in an email message, “but anything longer than a month puts patients at risk.”
Whether or not that will happen is unclear, but Sparks said he has been receiving a raft queries from both lupus and non-lupus patients eager to know more about — and access — hydroxychloroquine: “Can I use this? Should I stockpile it? Can I get refills?” Sparks compares the current medication shortage to the ventilator shortage, where manufacturers make just enough of a certain supply to meet the demand. “We don’t have stockpiles of hydroxychloroquine sitting around,” he said.
Blazer understands that people are scared and says it’s natural that they would want to protect themselves. But she said, the medicine is a limited resource and should be reserved for people with a rheumatological disease or active Covid-19 infection. In order to minimize fallout from the pandemic, she says, “we all have to function as a community.”
As it turns out, there is an extreme paucity of data when it comes to hydroxychloroquine and Covid-19. On March 10, the Journal of Critical Care published online a systematic review of the safety and the effectiveness of hydroxychloroquine and chloroquine in treating Covid-19. The authors’ goal was to identify and summarize all available scientific evidence as of March 1 by searching scientific databases. They found six articles. (In contrast, a search of the database PubMed for hydroxychloroquine and lupus yields 1,654 results.)
“The articles themselves were kind of a menagerie of things that you don’t want to get data from,” said Michael Putman, a rheumatologist at Northwestern University, McGaw Medical Center, in his rheumatology podcast. The study authors found one narrative letter, one test tube study, one editorial, two national guidelines, and one expert consensus paper from China. Conspicuously missing were randomized controlled trials, which randomly assign human participants to an experimental group or a control group, with the experimental group receiving the treatment in question.
“It is kind of scary that that is all the data we had until March 1, for a drug that we are currently talking about rolling out en masse to the world,” said Putman.
Shortly after the systematic review appeared online, Didier Raoult announced the results of his team’s clinical trial. (The paper is now available online.) At first blush, the results are striking. Six days into the study, 70 percent of patients who received hydroxychloroquine were “virologically cured,” as evidenced from samples taken from the back of each patient’s nose. In contrast, just 12.5 percent of the control group, which did not receive the drug cocktail, were free of the virus.
A second potential issue: Patients who refused the treatment or had exclusion criteria served as controls. “It’s hard for me to describe just how problematic this is,” said Putman in his podcast. Ideally patients would be randomly assigned to one of the two treatment groups, said Putman. Patients with exclusion criteria — those unable to take the medication — are not the same as patients who are able to take it, he says. And the same is true for patients who refuse a drug vs. those who don’t.
Whether these and other potential problems with the research will prove salient in coming weeks and months is impossible to know — and most researchers concede that even amid lingering uncertainties, time is of the essence in the frantic hunt to find ways to slow the fast-moving Covid-19 pandemic. “A lot of this,” Kim said, “is the rush of trying to get something out.” On Friday, the University of Minnesota announced the launch of a 1,500-person trial aimed at further exploring the efficacy of hydroxychloroquine against SARS-CoV-2. And drug makers Novartis, Mylan, and Teva announced last week that they were fast-tracking production, with additional plans to donate hundreds of millions of tablets to hospitals around the country to help combat Covid-19 infections.
Still, reports of shortages are mounting. “It’s gone. It’s not in the pharmacy now,'' a physician in Queens told The Washington Post on Friday. The doctor admitted taking the drug himself in the hope of staving off infection, and that he’d prescribed it to 30 patients as a prophylactic.
These sorts of fast-multiplying, ad hoc transactions, are what worry lupus patients like Julie Powers. For now, she says she has enough hydroxychloroquine to last 90 days, and she added that her pharmacist in the Washington, D.C. area is currently hiding the medicine to be sure her regular lupus patients can get their prescriptions refilled.
Powers sounds almost amazed when she describes what that means to her: “I can walk outside,” she said, “and I can live.”
Sara Talpos is a senior editor at Undark and a freelance writer whose recent work has been published in Science, Mosaic, and the Kenyon Review’s special issue on science writing.
Disclosure: The author’s spouse is a rheumatologist at Michigan Medicine.
UPDATES: This story has been updated to clarify Alfred Kim's view on several patients who dropped out of a small French study on the efficacy of using hydroxychloroquine to treat Covid-19 cases. The piece was also edited to include information noting that one state pharmacy board is now taking steps to curtail prescriptions of hydroxychloroquine and chloroquine for Covid-19 prophylaxis.
This article was originally published on Undark. Read the original article.

For almost a quarter century, Julie Powers, a 48-year-old non-profit professional from Maryland, has been taking the same medication for her lupus — and until recently, she never worried that her supply would run out. Now she’s terrified that she might lose access to a drug that prevents her immune system from attacking her heart, lungs, and skin. She describes a feeling akin to being underwater, near drowning: “That’s what my life would be like,” she said. “I’ll suffocate.”
Powers’ concerns began roughly a week ago when she learned that her lupus drug, hydroxychloroquine (hi-DROCK-see-KLORA-quin), may be helpful in the treatment of Covid-19, the illness caused by the SARS-CoV-2 virus now racing across the planet. The medication was already being used around world to treat Covid-19 patients, but evidence of its effectiveness was largely anecdotal. Then, on March 16, a renowned infectious disease specialist, Didier Raoult, announced the results of a small clinical trial in France showing that patients receiving a combination of hydroxychloroquine and the common antibiotic azithromycin had notably lower levels of the virus in their bloodstream than those who did not receive the medication.
In the last week, this once obscure drug has been thrust into the national spotlight with everyone from doctors, to laypeople, to the U.S. president weighing in. The attention has so dramatically driven up demand that pharmacists are reporting depleted stocks of the drug, leaving many of the roughly 1.5 million lupus patients across the country unable to get their prescriptions filled. They now face an uncertain future as the public clings to one of the first signs of hope to appear since the coronavirus began sweeping across the U.S.
But scientists and physicians caution that this hope is based on studies that have been conducted outside of traditional scientific timelines. “The paper is interesting and certainly would warrant future more definitive studies,” Jeff Sparks, a rheumatologist and researcher at Harvard Medical School, said of the French study. “It might even be enough data to use the regimen off-label for sick and hospitalized patients.
“However,” he added, “it does not prove that the regimen actually works.”
Despite efforts to pin blame for the shortages on Trump alone, however, hydroxychloroquine scarcity was already setting in weeks ago, as doctors began responding on their own to percolating and preliminary research. Some evidence suggests that many doctors are now writing prescriptions prophylactically for patients with no known illness — as well as for themselves and family members — prompting at least one state pharmacy board to call an emergency meeting, scheduled for Sunday morning. The board planned to bar pharmacists from dispensing chloroquine or hydroxychloroquine for anyone other than confirmed Covid-19 patients without approval of the board's director.
A prolonged shortfall in supplies would likely have grave implications for people who depend on it — including Powers, who believes that she would not be alive today without the drug. “I guarantee you, it has saved my life,” she said. “It’s the only thing that’s protecting my organs. There’s nothing else.” Like others, she hopes that pharmaceutical companies that manufacture versions of the drug will be able to quickly ramp up production — something several have already promised to do. In the meantime, Powers has a message for the American public — one echoed by most lupus doctors: When it comes to hydroxychloroquine: “If you don’t need it, don’t get it.”
The origins of hydroxychloroquine can be traced back hundreds of years to South America, where the bark of the cinchona tree appears to have been used by Andean populations to treat shivering. European missionaries eventually brought the bark to Europe, where it was used to treat malaria. In 1820, French researchers isolated the substance in the bark responsible for its beneficial effects. They named it “quinine.” When the supply from South America began to dry up, the British and Dutch decided to grow the tree on plantations.
Over time, synthetic versions were developed, including a drug called chloroquine, which was created in the midst of World War II in an effort to spare overseas American troops from malaria. As it turned out, troops with rashes and arthritis saw an improvement in symptoms after using this anti-malarial medication. After the war, a related drug was created, one with fewer side-effects when taken long-term: hydroxychloroquine. It went on to be used to treat many types of autoimmune diseases, including rheumatoid arthritis and lupus. The latter, which disproportionately affects women, used to cut lives short — typically from failure of the kidneys. Those numbers have been reduced with strict management of the disease, but the Lupus Foundation of America estimates that 10 to 15 percent of patients die prematurely due to complications of the disease.
Jinoos Yazdany, a researcher and chief of the Division of Rheumatology at Zuckerberg San Francisco General Hospital, added that there is strong clinical trial data demonstrating that taking a group of lupus patients off of hydroxychloroquine results in lupus flares. “I am less concerned about a short interruption of a few weeks,” she said in an email message, “but anything longer than a month puts patients at risk.”
Whether or not that will happen is unclear, but Sparks said he has been receiving a raft queries from both lupus and non-lupus patients eager to know more about — and access — hydroxychloroquine: “Can I use this? Should I stockpile it? Can I get refills?” Sparks compares the current medication shortage to the ventilator shortage, where manufacturers make just enough of a certain supply to meet the demand. “We don’t have stockpiles of hydroxychloroquine sitting around,” he said.
Blazer understands that people are scared and says it’s natural that they would want to protect themselves. But she said, the medicine is a limited resource and should be reserved for people with a rheumatological disease or active Covid-19 infection. In order to minimize fallout from the pandemic, she says, “we all have to function as a community.”
As it turns out, there is an extreme paucity of data when it comes to hydroxychloroquine and Covid-19. On March 10, the Journal of Critical Care published online a systematic review of the safety and the effectiveness of hydroxychloroquine and chloroquine in treating Covid-19. The authors’ goal was to identify and summarize all available scientific evidence as of March 1 by searching scientific databases. They found six articles. (In contrast, a search of the database PubMed for hydroxychloroquine and lupus yields 1,654 results.)
“The articles themselves were kind of a menagerie of things that you don’t want to get data from,” said Michael Putman, a rheumatologist at Northwestern University, McGaw Medical Center, in his rheumatology podcast. The study authors found one narrative letter, one test tube study, one editorial, two national guidelines, and one expert consensus paper from China. Conspicuously missing were randomized controlled trials, which randomly assign human participants to an experimental group or a control group, with the experimental group receiving the treatment in question.
“It is kind of scary that that is all the data we had until March 1, for a drug that we are currently talking about rolling out en masse to the world,” said Putman.
Shortly after the systematic review appeared online, Didier Raoult announced the results of his team’s clinical trial. (The paper is now available online.) At first blush, the results are striking. Six days into the study, 70 percent of patients who received hydroxychloroquine were “virologically cured,” as evidenced from samples taken from the back of each patient’s nose. In contrast, just 12.5 percent of the control group, which did not receive the drug cocktail, were free of the virus.
A second potential issue: Patients who refused the treatment or had exclusion criteria served as controls. “It’s hard for me to describe just how problematic this is,” said Putman in his podcast. Ideally patients would be randomly assigned to one of the two treatment groups, said Putman. Patients with exclusion criteria — those unable to take the medication — are not the same as patients who are able to take it, he says. And the same is true for patients who refuse a drug vs. those who don’t.
Whether these and other potential problems with the research will prove salient in coming weeks and months is impossible to know — and most researchers concede that even amid lingering uncertainties, time is of the essence in the frantic hunt to find ways to slow the fast-moving Covid-19 pandemic. “A lot of this,” Kim said, “is the rush of trying to get something out.” On Friday, the University of Minnesota announced the launch of a 1,500-person trial aimed at further exploring the efficacy of hydroxychloroquine against SARS-CoV-2. And drug makers Novartis, Mylan, and Teva announced last week that they were fast-tracking production, with additional plans to donate hundreds of millions of tablets to hospitals around the country to help combat Covid-19 infections.
Still, reports of shortages are mounting. “It’s gone. It’s not in the pharmacy now,'' a physician in Queens told The Washington Post on Friday. The doctor admitted taking the drug himself in the hope of staving off infection, and that he’d prescribed it to 30 patients as a prophylactic.
These sorts of fast-multiplying, ad hoc transactions, are what worry lupus patients like Julie Powers. For now, she says she has enough hydroxychloroquine to last 90 days, and she added that her pharmacist in the Washington, D.C. area is currently hiding the medicine to be sure her regular lupus patients can get their prescriptions refilled.
Powers sounds almost amazed when she describes what that means to her: “I can walk outside,” she said, “and I can live.”
Sara Talpos is a senior editor at Undark and a freelance writer whose recent work has been published in Science, Mosaic, and the Kenyon Review’s special issue on science writing.
Disclosure: The author’s spouse is a rheumatologist at Michigan Medicine.
UPDATES: This story has been updated to clarify Alfred Kim's view on several patients who dropped out of a small French study on the efficacy of using hydroxychloroquine to treat Covid-19 cases. The piece was also edited to include information noting that one state pharmacy board is now taking steps to curtail prescriptions of hydroxychloroquine and chloroquine for Covid-19 prophylaxis.
This article was originally published on Undark. Read the original article.
For almost a quarter century, Julie Powers, a 48-year-old non-profit professional from Maryland, has been taking the same medication for her lupus — and until recently, she never worried that her supply would run out. Now she’s terrified that she might lose access to a drug that prevents her immune system from attacking her heart, lungs, and skin. She describes a feeling akin to being underwater, near drowning: “That’s what my life would be like,” she said. “I’ll suffocate.”
Powers’ concerns began roughly a week ago when she learned that her lupus drug, hydroxychloroquine (hi-DROCK-see-KLORA-quin), may be helpful in the treatment of Covid-19, the illness caused by the SARS-CoV-2 virus now racing across the planet. The medication was already being used around world to treat Covid-19 patients, but evidence of its effectiveness was largely anecdotal. Then, on March 16, a renowned infectious disease specialist, Didier Raoult, announced the results of a small clinical trial in France showing that patients receiving a combination of hydroxychloroquine and the common antibiotic azithromycin had notably lower levels of the virus in their bloodstream than those who did not receive the medication.
In the last week, this once obscure drug has been thrust into the national spotlight with everyone from doctors, to laypeople, to the U.S. president weighing in. The attention has so dramatically driven up demand that pharmacists are reporting depleted stocks of the drug, leaving many of the roughly 1.5 million lupus patients across the country unable to get their prescriptions filled. They now face an uncertain future as the public clings to one of the first signs of hope to appear since the coronavirus began sweeping across the U.S.
But scientists and physicians caution that this hope is based on studies that have been conducted outside of traditional scientific timelines. “The paper is interesting and certainly would warrant future more definitive studies,” Jeff Sparks, a rheumatologist and researcher at Harvard Medical School, said of the French study. “It might even be enough data to use the regimen off-label for sick and hospitalized patients.
“However,” he added, “it does not prove that the regimen actually works.”
Despite efforts to pin blame for the shortages on Trump alone, however, hydroxychloroquine scarcity was already setting in weeks ago, as doctors began responding on their own to percolating and preliminary research. Some evidence suggests that many doctors are now writing prescriptions prophylactically for patients with no known illness — as well as for themselves and family members — prompting at least one state pharmacy board to call an emergency meeting, scheduled for Sunday morning. The board planned to bar pharmacists from dispensing chloroquine or hydroxychloroquine for anyone other than confirmed Covid-19 patients without approval of the board's director.
A prolonged shortfall in supplies would likely have grave implications for people who depend on it — including Powers, who believes that she would not be alive today without the drug. “I guarantee you, it has saved my life,” she said. “It’s the only thing that’s protecting my organs. There’s nothing else.” Like others, she hopes that pharmaceutical companies that manufacture versions of the drug will be able to quickly ramp up production — something several have already promised to do. In the meantime, Powers has a message for the American public — one echoed by most lupus doctors: When it comes to hydroxychloroquine: “If you don’t need it, don’t get it.”
The origins of hydroxychloroquine can be traced back hundreds of years to South America, where the bark of the cinchona tree appears to have been used by Andean populations to treat shivering. European missionaries eventually brought the bark to Europe, where it was used to treat malaria. In 1820, French researchers isolated the substance in the bark responsible for its beneficial effects. They named it “quinine.” When the supply from South America began to dry up, the British and Dutch decided to grow the tree on plantations.
Over time, synthetic versions were developed, including a drug called chloroquine, which was created in the midst of World War II in an effort to spare overseas American troops from malaria. As it turned out, troops with rashes and arthritis saw an improvement in symptoms after using this anti-malarial medication. After the war, a related drug was created, one with fewer side-effects when taken long-term: hydroxychloroquine. It went on to be used to treat many types of autoimmune diseases, including rheumatoid arthritis and lupus. The latter, which disproportionately affects women, used to cut lives short — typically from failure of the kidneys. Those numbers have been reduced with strict management of the disease, but the Lupus Foundation of America estimates that 10 to 15 percent of patients die prematurely due to complications of the disease.
Jinoos Yazdany, a researcher and chief of the Division of Rheumatology at Zuckerberg San Francisco General Hospital, added that there is strong clinical trial data demonstrating that taking a group of lupus patients off of hydroxychloroquine results in lupus flares. “I am less concerned about a short interruption of a few weeks,” she said in an email message, “but anything longer than a month puts patients at risk.”
Whether or not that will happen is unclear, but Sparks said he has been receiving a raft queries from both lupus and non-lupus patients eager to know more about — and access — hydroxychloroquine: “Can I use this? Should I stockpile it? Can I get refills?” Sparks compares the current medication shortage to the ventilator shortage, where manufacturers make just enough of a certain supply to meet the demand. “We don’t have stockpiles of hydroxychloroquine sitting around,” he said.
Blazer understands that people are scared and says it’s natural that they would want to protect themselves. But she said, the medicine is a limited resource and should be reserved for people with a rheumatological disease or active Covid-19 infection. In order to minimize fallout from the pandemic, she says, “we all have to function as a community.”
As it turns out, there is an extreme paucity of data when it comes to hydroxychloroquine and Covid-19. On March 10, the Journal of Critical Care published online a systematic review of the safety and the effectiveness of hydroxychloroquine and chloroquine in treating Covid-19. The authors’ goal was to identify and summarize all available scientific evidence as of March 1 by searching scientific databases. They found six articles. (In contrast, a search of the database PubMed for hydroxychloroquine and lupus yields 1,654 results.)
“The articles themselves were kind of a menagerie of things that you don’t want to get data from,” said Michael Putman, a rheumatologist at Northwestern University, McGaw Medical Center, in his rheumatology podcast. The study authors found one narrative letter, one test tube study, one editorial, two national guidelines, and one expert consensus paper from China. Conspicuously missing were randomized controlled trials, which randomly assign human participants to an experimental group or a control group, with the experimental group receiving the treatment in question.
“It is kind of scary that that is all the data we had until March 1, for a drug that we are currently talking about rolling out en masse to the world,” said Putman.
Shortly after the systematic review appeared online, Didier Raoult announced the results of his team’s clinical trial. (The paper is now available online.) At first blush, the results are striking. Six days into the study, 70 percent of patients who received hydroxychloroquine were “virologically cured,” as evidenced from samples taken from the back of each patient’s nose. In contrast, just 12.5 percent of the control group, which did not receive the drug cocktail, were free of the virus.
A second potential issue: Patients who refused the treatment or had exclusion criteria served as controls. “It’s hard for me to describe just how problematic this is,” said Putman in his podcast. Ideally patients would be randomly assigned to one of the two treatment groups, said Putman. Patients with exclusion criteria — those unable to take the medication — are not the same as patients who are able to take it, he says. And the same is true for patients who refuse a drug vs. those who don’t.
Whether these and other potential problems with the research will prove salient in coming weeks and months is impossible to know — and most researchers concede that even amid lingering uncertainties, time is of the essence in the frantic hunt to find ways to slow the fast-moving Covid-19 pandemic. “A lot of this,” Kim said, “is the rush of trying to get something out.” On Friday, the University of Minnesota announced the launch of a 1,500-person trial aimed at further exploring the efficacy of hydroxychloroquine against SARS-CoV-2. And drug makers Novartis, Mylan, and Teva announced last week that they were fast-tracking production, with additional plans to donate hundreds of millions of tablets to hospitals around the country to help combat Covid-19 infections.
Still, reports of shortages are mounting. “It’s gone. It’s not in the pharmacy now,'' a physician in Queens told The Washington Post on Friday. The doctor admitted taking the drug himself in the hope of staving off infection, and that he’d prescribed it to 30 patients as a prophylactic.
These sorts of fast-multiplying, ad hoc transactions, are what worry lupus patients like Julie Powers. For now, she says she has enough hydroxychloroquine to last 90 days, and she added that her pharmacist in the Washington, D.C. area is currently hiding the medicine to be sure her regular lupus patients can get their prescriptions refilled.
Powers sounds almost amazed when she describes what that means to her: “I can walk outside,” she said, “and I can live.”
Sara Talpos is a senior editor at Undark and a freelance writer whose recent work has been published in Science, Mosaic, and the Kenyon Review’s special issue on science writing.
Disclosure: The author’s spouse is a rheumatologist at Michigan Medicine.
UPDATES: This story has been updated to clarify Alfred Kim's view on several patients who dropped out of a small French study on the efficacy of using hydroxychloroquine to treat Covid-19 cases. The piece was also edited to include information noting that one state pharmacy board is now taking steps to curtail prescriptions of hydroxychloroquine and chloroquine for Covid-19 prophylaxis.
This article was originally published on Undark. Read the original article.
Webinar confronts unique issues for the bleeding disorders community facing COVID-19
In a webinar conducted on March 20, Leonard Valentino, MD, president and CEO of the National Hemophilia Foundation (NHF), provided
Overall, the risk of comorbidities is no different in the bleeding disorders population than in the general population, and similar precautions should be maintained, Dr. Valentino stated. He listed some of the at-risk populations as designated by the Centers for Disease Control and Prevention.
In particular, he pointed out that, when the CDC referred to a greater risk of COVID-19 to individuals with bleeding disorders, the organization was referring to patients with HIV and sickle cell disease. The CDC was not referring to patients with other forms of bleeding disorders, such as hemophilia, Dr. Valentino stated.
All individuals should be following CDC and state and federal recommendations with regard to social distancing and hygiene. However, with regard to immunocompromised individuals, “the two populations we [in the bleeding disorders community] have to be concerned about are those in gene therapy clinical trials and those with inhibitors,” said Dr. Valentino.
Patients in a gene therapy clinical trial should exercise additional precautions because the use of steroids, common in these trials. “Steroids are an immunosuppressive drug, and this would increase one’s risk of infection, including COVID-19,” according to Dr. Valentino.
In addition, “I will say, if you have hemophilia and an inhibitor [an antibody to clotting factor treatment], that may alter the immune system, and we don’t know what the implication of that is in terms of coronavirus infection and COVID-19 disease. So people with an inhibitor should take special precautions to limit their exposures.”
Patients with a port should not need to have extra concerns regarding COVID-19, but they should continue to exercise the good hygiene that has always been essential, according to Dr. Valentino.
Dr. Valentino asked: Are patients with a bleeding disorder who become infected with COVID-19 more susceptible to a bleed? “You shouldn’t be more susceptible to bleeding except if you have severe cough, and that cough could result in bleeding to the head,” he answered.
If a patient needs to go to the emergency department for a bleed or possible COVID-19 infection, they should wear a face mask if they are sick to prevent spreading of disease. “This is really the only instance where a face mask may be beneficial” in that it limits other people’s exposure to your infection. It is especially important to call ahead before visiting the doctor or going to the emergency department. “Make sure that they’re aware that you’re coming.”
Of particular concern to patients is the amount of factor product they should have on hand. The current CDC recommendation is a 30-day supply of medicines, but that is misleading, because it refers to general medications, such as high-blood pressure medicine, and not factor products. “The current MASAC [NHF’s Medical and Scientific Advisory Council] recommendation is to have a 14-day supply of factor products available to you,” said Dr. Valentino, “and one should reorder when you have a 1-week supply.”
MASAC has issued a letter on the crisis on the NHF website.
These recommendations should not be exceeded in order to ensure that there is enough factor available to all patients, he added. Hoarding is discouraged, and there are no concerns as yet of factor running out. “We have had conversations with manufacturers and … the supply chain is robust.” The greater concern is with regard to ancillary supplies in the hospital that a hemophilia patient may require during treatment.
Patients and practitioners should consult the COVID-19 pages of both the NHF and Hemophilia Federation of America (HFA) websites. This includes a Health and Wellness update by Dr. Valentino.
With regard to financial issues, he and Sharon Meyers, CEO and president of the HFA, spoke, stating that both NHF and HFA have advocacy for patients seeking to deal with insurance issues or in paying for their products, urging people to go to the organizational websites and to also use their emails: advocate@hemophilia.org and advocacy@hemophiliafed.org.
She also announced that the annual meeting of the HFA was being postponed to Aug. 24-26 at the Hilton Inner Harbor Baltimore, Md.
Dr. Valentino and Ms. Meyers did not provide any disclosure information.
In a webinar conducted on March 20, Leonard Valentino, MD, president and CEO of the National Hemophilia Foundation (NHF), provided
Overall, the risk of comorbidities is no different in the bleeding disorders population than in the general population, and similar precautions should be maintained, Dr. Valentino stated. He listed some of the at-risk populations as designated by the Centers for Disease Control and Prevention.
In particular, he pointed out that, when the CDC referred to a greater risk of COVID-19 to individuals with bleeding disorders, the organization was referring to patients with HIV and sickle cell disease. The CDC was not referring to patients with other forms of bleeding disorders, such as hemophilia, Dr. Valentino stated.
All individuals should be following CDC and state and federal recommendations with regard to social distancing and hygiene. However, with regard to immunocompromised individuals, “the two populations we [in the bleeding disorders community] have to be concerned about are those in gene therapy clinical trials and those with inhibitors,” said Dr. Valentino.
Patients in a gene therapy clinical trial should exercise additional precautions because the use of steroids, common in these trials. “Steroids are an immunosuppressive drug, and this would increase one’s risk of infection, including COVID-19,” according to Dr. Valentino.
In addition, “I will say, if you have hemophilia and an inhibitor [an antibody to clotting factor treatment], that may alter the immune system, and we don’t know what the implication of that is in terms of coronavirus infection and COVID-19 disease. So people with an inhibitor should take special precautions to limit their exposures.”
Patients with a port should not need to have extra concerns regarding COVID-19, but they should continue to exercise the good hygiene that has always been essential, according to Dr. Valentino.
Dr. Valentino asked: Are patients with a bleeding disorder who become infected with COVID-19 more susceptible to a bleed? “You shouldn’t be more susceptible to bleeding except if you have severe cough, and that cough could result in bleeding to the head,” he answered.
If a patient needs to go to the emergency department for a bleed or possible COVID-19 infection, they should wear a face mask if they are sick to prevent spreading of disease. “This is really the only instance where a face mask may be beneficial” in that it limits other people’s exposure to your infection. It is especially important to call ahead before visiting the doctor or going to the emergency department. “Make sure that they’re aware that you’re coming.”
Of particular concern to patients is the amount of factor product they should have on hand. The current CDC recommendation is a 30-day supply of medicines, but that is misleading, because it refers to general medications, such as high-blood pressure medicine, and not factor products. “The current MASAC [NHF’s Medical and Scientific Advisory Council] recommendation is to have a 14-day supply of factor products available to you,” said Dr. Valentino, “and one should reorder when you have a 1-week supply.”
MASAC has issued a letter on the crisis on the NHF website.
These recommendations should not be exceeded in order to ensure that there is enough factor available to all patients, he added. Hoarding is discouraged, and there are no concerns as yet of factor running out. “We have had conversations with manufacturers and … the supply chain is robust.” The greater concern is with regard to ancillary supplies in the hospital that a hemophilia patient may require during treatment.
Patients and practitioners should consult the COVID-19 pages of both the NHF and Hemophilia Federation of America (HFA) websites. This includes a Health and Wellness update by Dr. Valentino.
With regard to financial issues, he and Sharon Meyers, CEO and president of the HFA, spoke, stating that both NHF and HFA have advocacy for patients seeking to deal with insurance issues or in paying for their products, urging people to go to the organizational websites and to also use their emails: advocate@hemophilia.org and advocacy@hemophiliafed.org.
She also announced that the annual meeting of the HFA was being postponed to Aug. 24-26 at the Hilton Inner Harbor Baltimore, Md.
Dr. Valentino and Ms. Meyers did not provide any disclosure information.
In a webinar conducted on March 20, Leonard Valentino, MD, president and CEO of the National Hemophilia Foundation (NHF), provided
Overall, the risk of comorbidities is no different in the bleeding disorders population than in the general population, and similar precautions should be maintained, Dr. Valentino stated. He listed some of the at-risk populations as designated by the Centers for Disease Control and Prevention.
In particular, he pointed out that, when the CDC referred to a greater risk of COVID-19 to individuals with bleeding disorders, the organization was referring to patients with HIV and sickle cell disease. The CDC was not referring to patients with other forms of bleeding disorders, such as hemophilia, Dr. Valentino stated.
All individuals should be following CDC and state and federal recommendations with regard to social distancing and hygiene. However, with regard to immunocompromised individuals, “the two populations we [in the bleeding disorders community] have to be concerned about are those in gene therapy clinical trials and those with inhibitors,” said Dr. Valentino.
Patients in a gene therapy clinical trial should exercise additional precautions because the use of steroids, common in these trials. “Steroids are an immunosuppressive drug, and this would increase one’s risk of infection, including COVID-19,” according to Dr. Valentino.
In addition, “I will say, if you have hemophilia and an inhibitor [an antibody to clotting factor treatment], that may alter the immune system, and we don’t know what the implication of that is in terms of coronavirus infection and COVID-19 disease. So people with an inhibitor should take special precautions to limit their exposures.”
Patients with a port should not need to have extra concerns regarding COVID-19, but they should continue to exercise the good hygiene that has always been essential, according to Dr. Valentino.
Dr. Valentino asked: Are patients with a bleeding disorder who become infected with COVID-19 more susceptible to a bleed? “You shouldn’t be more susceptible to bleeding except if you have severe cough, and that cough could result in bleeding to the head,” he answered.
If a patient needs to go to the emergency department for a bleed or possible COVID-19 infection, they should wear a face mask if they are sick to prevent spreading of disease. “This is really the only instance where a face mask may be beneficial” in that it limits other people’s exposure to your infection. It is especially important to call ahead before visiting the doctor or going to the emergency department. “Make sure that they’re aware that you’re coming.”
Of particular concern to patients is the amount of factor product they should have on hand. The current CDC recommendation is a 30-day supply of medicines, but that is misleading, because it refers to general medications, such as high-blood pressure medicine, and not factor products. “The current MASAC [NHF’s Medical and Scientific Advisory Council] recommendation is to have a 14-day supply of factor products available to you,” said Dr. Valentino, “and one should reorder when you have a 1-week supply.”
MASAC has issued a letter on the crisis on the NHF website.
These recommendations should not be exceeded in order to ensure that there is enough factor available to all patients, he added. Hoarding is discouraged, and there are no concerns as yet of factor running out. “We have had conversations with manufacturers and … the supply chain is robust.” The greater concern is with regard to ancillary supplies in the hospital that a hemophilia patient may require during treatment.
Patients and practitioners should consult the COVID-19 pages of both the NHF and Hemophilia Federation of America (HFA) websites. This includes a Health and Wellness update by Dr. Valentino.
With regard to financial issues, he and Sharon Meyers, CEO and president of the HFA, spoke, stating that both NHF and HFA have advocacy for patients seeking to deal with insurance issues or in paying for their products, urging people to go to the organizational websites and to also use their emails: advocate@hemophilia.org and advocacy@hemophiliafed.org.
She also announced that the annual meeting of the HFA was being postponed to Aug. 24-26 at the Hilton Inner Harbor Baltimore, Md.
Dr. Valentino and Ms. Meyers did not provide any disclosure information.
SECURE-IBD registry traces COVID-19 in patients with Crohn’s, colitis
Gastroenterologists and other clinicians caring for patients with inflammatory bowel disease are being encouraged to report outcomes for pediatric and adult patients with IBD and COVID-19 infections to a new international registry.
The Surveillance Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD) registry is a repository for data on all cases of COVID-19 in patients with IBD, including those who are asymptomatic and detected only through public health screening.
The idea for the registry came from gastroenterologists at the University of North Carolina at Chapel Hill and at the Icahn School of Medicine at Mount Sinai, New York.
It was developed out of the recognition that, “with the emergence of this international health crisis, it would make sense to develop a registry to allow clinicians taking care of patients with inflammatory bowel disease to report on the specifics of their cases, so that we could then quickly define what the impact is of this disease on our patients, and determine how disease severity, medication, and specific demographics impact COVID-related outcomes in our population,” said registry cofounder Erica Brenner, MD, a pediatric gastroenterology fellow at UNC.
As of March 19, 2020, 14 cases of COVID-19 infections in patients with IBD had been reported to the registry: 6 from the United States, 3 from Spain, and 1 each from the United Kingdom, Switzerland, Ireland, Italy and the Netherlands. There were no patient deaths, and only two required hospitalization. Neither of the hospitalized patients required intensive care or ventilator support.
Dr. Brenner noted that it’s still early days, and that a clearer picture of the pandemic will begin to emerge as more cases are reported.
“We are planning at least weekly to update our ‘Updates and Data’ tab on the registry with summary data and aggregate information,” she said in an interview.
All data in the registry are deidentified in accordance with HIPAA Safe Harbor standards. The UNC–Chapel Hill Office for Human Research Ethics has determined that storage and analysis of deidentified data is exempt from institutional review board requirement because it does not constitute human subjects research as defined under federal regulations.
SECURE-IBD was the inspiration for a similarly designed COVID-19 registry for clinicians who treat patients with rheumatologic disorders, who often are treated with immunosuppressive agents familiar to the rheumatology community, such as infliximab (Remicade and biosimilars), adalimumab (Humira and biosimilars), and methotrexate.
“We’re in the process of talking to different leaders across specialties to leverage our blueprint to implement registries in all sorts of disease states, including cirrhosis, psoriasis, lupus, and sickle cell disease,” Dr. Brenner said.
The data entry process is estimated to take 5 minutes. Participating clinicians are requested to reported on confirmed COVID-19 cases only “after sufficient time has passed to observe the disease course through resolution of acute illness and/or death.”
“The success of this registry depends on international collaboration and buy-in from clinicians around the world, so we really encourage all clinicians who take care of patients with inflammatory bowel disease to go to our website and report a case,” Dr. Brenner said.
Gastroenterologists and other clinicians caring for patients with inflammatory bowel disease are being encouraged to report outcomes for pediatric and adult patients with IBD and COVID-19 infections to a new international registry.
The Surveillance Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD) registry is a repository for data on all cases of COVID-19 in patients with IBD, including those who are asymptomatic and detected only through public health screening.
The idea for the registry came from gastroenterologists at the University of North Carolina at Chapel Hill and at the Icahn School of Medicine at Mount Sinai, New York.
It was developed out of the recognition that, “with the emergence of this international health crisis, it would make sense to develop a registry to allow clinicians taking care of patients with inflammatory bowel disease to report on the specifics of their cases, so that we could then quickly define what the impact is of this disease on our patients, and determine how disease severity, medication, and specific demographics impact COVID-related outcomes in our population,” said registry cofounder Erica Brenner, MD, a pediatric gastroenterology fellow at UNC.
As of March 19, 2020, 14 cases of COVID-19 infections in patients with IBD had been reported to the registry: 6 from the United States, 3 from Spain, and 1 each from the United Kingdom, Switzerland, Ireland, Italy and the Netherlands. There were no patient deaths, and only two required hospitalization. Neither of the hospitalized patients required intensive care or ventilator support.
Dr. Brenner noted that it’s still early days, and that a clearer picture of the pandemic will begin to emerge as more cases are reported.
“We are planning at least weekly to update our ‘Updates and Data’ tab on the registry with summary data and aggregate information,” she said in an interview.
All data in the registry are deidentified in accordance with HIPAA Safe Harbor standards. The UNC–Chapel Hill Office for Human Research Ethics has determined that storage and analysis of deidentified data is exempt from institutional review board requirement because it does not constitute human subjects research as defined under federal regulations.
SECURE-IBD was the inspiration for a similarly designed COVID-19 registry for clinicians who treat patients with rheumatologic disorders, who often are treated with immunosuppressive agents familiar to the rheumatology community, such as infliximab (Remicade and biosimilars), adalimumab (Humira and biosimilars), and methotrexate.
“We’re in the process of talking to different leaders across specialties to leverage our blueprint to implement registries in all sorts of disease states, including cirrhosis, psoriasis, lupus, and sickle cell disease,” Dr. Brenner said.
The data entry process is estimated to take 5 minutes. Participating clinicians are requested to reported on confirmed COVID-19 cases only “after sufficient time has passed to observe the disease course through resolution of acute illness and/or death.”
“The success of this registry depends on international collaboration and buy-in from clinicians around the world, so we really encourage all clinicians who take care of patients with inflammatory bowel disease to go to our website and report a case,” Dr. Brenner said.
Gastroenterologists and other clinicians caring for patients with inflammatory bowel disease are being encouraged to report outcomes for pediatric and adult patients with IBD and COVID-19 infections to a new international registry.
The Surveillance Epidemiology of Coronavirus Under Research Exclusion (SECURE-IBD) registry is a repository for data on all cases of COVID-19 in patients with IBD, including those who are asymptomatic and detected only through public health screening.
The idea for the registry came from gastroenterologists at the University of North Carolina at Chapel Hill and at the Icahn School of Medicine at Mount Sinai, New York.
It was developed out of the recognition that, “with the emergence of this international health crisis, it would make sense to develop a registry to allow clinicians taking care of patients with inflammatory bowel disease to report on the specifics of their cases, so that we could then quickly define what the impact is of this disease on our patients, and determine how disease severity, medication, and specific demographics impact COVID-related outcomes in our population,” said registry cofounder Erica Brenner, MD, a pediatric gastroenterology fellow at UNC.
As of March 19, 2020, 14 cases of COVID-19 infections in patients with IBD had been reported to the registry: 6 from the United States, 3 from Spain, and 1 each from the United Kingdom, Switzerland, Ireland, Italy and the Netherlands. There were no patient deaths, and only two required hospitalization. Neither of the hospitalized patients required intensive care or ventilator support.
Dr. Brenner noted that it’s still early days, and that a clearer picture of the pandemic will begin to emerge as more cases are reported.
“We are planning at least weekly to update our ‘Updates and Data’ tab on the registry with summary data and aggregate information,” she said in an interview.
All data in the registry are deidentified in accordance with HIPAA Safe Harbor standards. The UNC–Chapel Hill Office for Human Research Ethics has determined that storage and analysis of deidentified data is exempt from institutional review board requirement because it does not constitute human subjects research as defined under federal regulations.
SECURE-IBD was the inspiration for a similarly designed COVID-19 registry for clinicians who treat patients with rheumatologic disorders, who often are treated with immunosuppressive agents familiar to the rheumatology community, such as infliximab (Remicade and biosimilars), adalimumab (Humira and biosimilars), and methotrexate.
“We’re in the process of talking to different leaders across specialties to leverage our blueprint to implement registries in all sorts of disease states, including cirrhosis, psoriasis, lupus, and sickle cell disease,” Dr. Brenner said.
The data entry process is estimated to take 5 minutes. Participating clinicians are requested to reported on confirmed COVID-19 cases only “after sufficient time has passed to observe the disease course through resolution of acute illness and/or death.”
“The success of this registry depends on international collaboration and buy-in from clinicians around the world, so we really encourage all clinicians who take care of patients with inflammatory bowel disease to go to our website and report a case,” Dr. Brenner said.
Should patients with COVID-19 avoid ibuprofen or RAAS antagonists?
Researchers have hypothesized that treatments that increase angiotensin-converting enzyme 2 (ACE2) may also increase the risk of novel coronavirus disease (COVID-19). This speculation and other concerns have led some officials and organizations to question whether ibuprofen or other drugs such as renin angiotensin aldosterone system (RAAS) antagonists should be avoided as treatments in patients with COVID-19. Health agencies and professional organizations have said they are not recommending against these medications.
The Food and Drug Administration on March 19 advised patients that it was “not aware of scientific evidence connecting” nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen “with worsening COVID-19 symptoms.”
“The agency is investigating this issue further and will communicate publicly when more information is available,” the FDA said. “However, all prescription NSAID labels warn that ‘the pharmacological activity of NSAIDs in reducing inflammation, and possibly fever, may diminish the utility of diagnostic signs in detecting infections.’ ” The FDA also noted that other over-the-counter and prescription medications are available for pain relief and fever reduction, and patients who “are concerned about taking NSAIDs and rely on these medications to treat chronic diseases” should talk to a health care provider.
A World Health Organization spokesperson said during a press conference on March 17 that the organization was looking into concerns about ibuprofen use in patients with COVID-19 and suggested that in the meantime patients take acetaminophen for fever instead. On March 18, the WHO said that it was not recommending against the use of ibuprofen.
“At present, based on currently available information, WHO does not recommend against the use of ibuprofen,” the organization said. “We are also consulting with physicians treating COVID-19 patients and are not aware of reports of any negative effects of ibuprofen, beyond the usual known side effects that limit its use in certain populations. WHO is not aware of published clinical or population-based data on this topic.”
A spokesperson for the National Institute of Allergy and Infectious Diseases said on March 18, “More research is needed to evaluate reports that ibruprofen and other over-the-counter anti-inflammatory drugs may affect the course of COVID-19. Currently, there is no conclusive evidence that ibuprofen and other over-the-counter anti-inflammatory drugs increase the risk of serious complications or of acquiring the virus that causes COVID-19. There is also no conclusive evidence that taking over-the-counter anti-inflammatory drugs is harmful for other respiratory infections.”
The European Medicines Agency (EMA) on March 18 said, “There is currently no scientific evidence establishing a link between ibuprofen and worsening of COVID‑19. EMA is monitoring the situation closely and will review any new information that becomes available on this issue in the context of the pandemic.”
In correspondence published March 11 in the Lancet Respiratory Medicine, Lei Fang, MD, of the department of biomedicine at University Hospital Basel (Switzerland), and colleagues suggested that patients with hypertension and diabetes mellitus may be at increased risk of COVID-19 because these comorbidities “are often treated with angiotensin converting enzyme (ACE) inhibitors.” In addition, “ACE2 polymorphisms that have been linked to diabetes mellitus, cerebral stroke, and hypertension” also may play a role, the researchers said (Lancet Respir Med. 2020 Mar 11. https://doi.org/10.1016/S2213-2600(20)30116-8).
“ACE2 is substantially increased in patients with type 1 or type 2 diabetes, who are treated with ACE inhibitors and angiotensin II type-I receptor blockers (ARBs). Hypertension is also treated with ACE inhibitors and ARBs, which results in an upregulation of ACE2. ACE2 can also be increased by thiazolidinediones and ibuprofen.”
A March 16 statement from the Heart Failure Society of America (HSFC), American College of Cardiology (ACC), and American Heart Association (AHA) addressed concerns about using RAAS antagonists in COVID-19.
“Patients with underlying cardiovascular diseases appear to have an increased risk for adverse outcomes with [COVID-19],” the organizations said. “Although the clinical manifestations of COVID-19 are dominated by respiratory symptoms, some patients also may have severe cardiovascular damage. [ACE2] receptors have been shown to be the entry point into human cells for SARS-CoV-2, the virus that causes COVID-19. In a few experimental studies with animal models, both [ACE] inhibitors and angiotensin receptor blockers (ARBs) have been shown to upregulate ACE2 expression in the heart. Though these have not been shown in human studies, or in the setting of COVID-19, such potential upregulation of ACE2 by ACE inhibitors or ARBs has resulted in a speculation of potential increased risk for COVID-19 infection in patients with background treatment of these medications.”
ACE2, ACE, angiotensin II, and other RAAS system interactions “are quite complex, and at times, paradoxical,” the statement says. “In experimental studies, both ACE inhibitors and ARBs have been shown to reduce severe lung injury in certain viral pneumonias, and it has been speculated that these agents could be beneficial in COVID-19.
“Currently there are no experimental or clinical data demonstrating beneficial or adverse outcomes with background use of ACE inhibitors, ARBs or other RAAS antagonists in COVID-19 or among COVID-19 patients with a history of cardiovascular disease treated with such agents. The HFSA, ACC, and AHA recommend continuation of RAAS antagonists for those patients who are currently prescribed such agents for indications for which these agents are known to be beneficial, such as heart failure, hypertension, or ischemic heart disease. In the event patients with cardiovascular disease are diagnosed with COVID-19, individualized treatment decisions should be made according to each patient’s hemodynamic status and clinical presentation. Therefore, be advised not to add or remove any RAAS-related treatments, beyond actions based on standard clinical practice.
“These theoretical concerns and findings of cardiovascular involvement with COVID-19 deserve much more detailed research, and quickly. As further research and developments related to this issue evolve, we will update these recommendations as needed.”
Dr. Fang and colleagues had no competing interests.
SOURCE: Fang L et al. Lancet Respir Med. 2020 Mar 11. doi: 10.1016/S2213-2600(20)30116-8.
Researchers have hypothesized that treatments that increase angiotensin-converting enzyme 2 (ACE2) may also increase the risk of novel coronavirus disease (COVID-19). This speculation and other concerns have led some officials and organizations to question whether ibuprofen or other drugs such as renin angiotensin aldosterone system (RAAS) antagonists should be avoided as treatments in patients with COVID-19. Health agencies and professional organizations have said they are not recommending against these medications.
The Food and Drug Administration on March 19 advised patients that it was “not aware of scientific evidence connecting” nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen “with worsening COVID-19 symptoms.”
“The agency is investigating this issue further and will communicate publicly when more information is available,” the FDA said. “However, all prescription NSAID labels warn that ‘the pharmacological activity of NSAIDs in reducing inflammation, and possibly fever, may diminish the utility of diagnostic signs in detecting infections.’ ” The FDA also noted that other over-the-counter and prescription medications are available for pain relief and fever reduction, and patients who “are concerned about taking NSAIDs and rely on these medications to treat chronic diseases” should talk to a health care provider.
A World Health Organization spokesperson said during a press conference on March 17 that the organization was looking into concerns about ibuprofen use in patients with COVID-19 and suggested that in the meantime patients take acetaminophen for fever instead. On March 18, the WHO said that it was not recommending against the use of ibuprofen.
“At present, based on currently available information, WHO does not recommend against the use of ibuprofen,” the organization said. “We are also consulting with physicians treating COVID-19 patients and are not aware of reports of any negative effects of ibuprofen, beyond the usual known side effects that limit its use in certain populations. WHO is not aware of published clinical or population-based data on this topic.”
A spokesperson for the National Institute of Allergy and Infectious Diseases said on March 18, “More research is needed to evaluate reports that ibruprofen and other over-the-counter anti-inflammatory drugs may affect the course of COVID-19. Currently, there is no conclusive evidence that ibuprofen and other over-the-counter anti-inflammatory drugs increase the risk of serious complications or of acquiring the virus that causes COVID-19. There is also no conclusive evidence that taking over-the-counter anti-inflammatory drugs is harmful for other respiratory infections.”
The European Medicines Agency (EMA) on March 18 said, “There is currently no scientific evidence establishing a link between ibuprofen and worsening of COVID‑19. EMA is monitoring the situation closely and will review any new information that becomes available on this issue in the context of the pandemic.”
In correspondence published March 11 in the Lancet Respiratory Medicine, Lei Fang, MD, of the department of biomedicine at University Hospital Basel (Switzerland), and colleagues suggested that patients with hypertension and diabetes mellitus may be at increased risk of COVID-19 because these comorbidities “are often treated with angiotensin converting enzyme (ACE) inhibitors.” In addition, “ACE2 polymorphisms that have been linked to diabetes mellitus, cerebral stroke, and hypertension” also may play a role, the researchers said (Lancet Respir Med. 2020 Mar 11. https://doi.org/10.1016/S2213-2600(20)30116-8).
“ACE2 is substantially increased in patients with type 1 or type 2 diabetes, who are treated with ACE inhibitors and angiotensin II type-I receptor blockers (ARBs). Hypertension is also treated with ACE inhibitors and ARBs, which results in an upregulation of ACE2. ACE2 can also be increased by thiazolidinediones and ibuprofen.”
A March 16 statement from the Heart Failure Society of America (HSFC), American College of Cardiology (ACC), and American Heart Association (AHA) addressed concerns about using RAAS antagonists in COVID-19.
“Patients with underlying cardiovascular diseases appear to have an increased risk for adverse outcomes with [COVID-19],” the organizations said. “Although the clinical manifestations of COVID-19 are dominated by respiratory symptoms, some patients also may have severe cardiovascular damage. [ACE2] receptors have been shown to be the entry point into human cells for SARS-CoV-2, the virus that causes COVID-19. In a few experimental studies with animal models, both [ACE] inhibitors and angiotensin receptor blockers (ARBs) have been shown to upregulate ACE2 expression in the heart. Though these have not been shown in human studies, or in the setting of COVID-19, such potential upregulation of ACE2 by ACE inhibitors or ARBs has resulted in a speculation of potential increased risk for COVID-19 infection in patients with background treatment of these medications.”
ACE2, ACE, angiotensin II, and other RAAS system interactions “are quite complex, and at times, paradoxical,” the statement says. “In experimental studies, both ACE inhibitors and ARBs have been shown to reduce severe lung injury in certain viral pneumonias, and it has been speculated that these agents could be beneficial in COVID-19.
“Currently there are no experimental or clinical data demonstrating beneficial or adverse outcomes with background use of ACE inhibitors, ARBs or other RAAS antagonists in COVID-19 or among COVID-19 patients with a history of cardiovascular disease treated with such agents. The HFSA, ACC, and AHA recommend continuation of RAAS antagonists for those patients who are currently prescribed such agents for indications for which these agents are known to be beneficial, such as heart failure, hypertension, or ischemic heart disease. In the event patients with cardiovascular disease are diagnosed with COVID-19, individualized treatment decisions should be made according to each patient’s hemodynamic status and clinical presentation. Therefore, be advised not to add or remove any RAAS-related treatments, beyond actions based on standard clinical practice.
“These theoretical concerns and findings of cardiovascular involvement with COVID-19 deserve much more detailed research, and quickly. As further research and developments related to this issue evolve, we will update these recommendations as needed.”
Dr. Fang and colleagues had no competing interests.
SOURCE: Fang L et al. Lancet Respir Med. 2020 Mar 11. doi: 10.1016/S2213-2600(20)30116-8.
Researchers have hypothesized that treatments that increase angiotensin-converting enzyme 2 (ACE2) may also increase the risk of novel coronavirus disease (COVID-19). This speculation and other concerns have led some officials and organizations to question whether ibuprofen or other drugs such as renin angiotensin aldosterone system (RAAS) antagonists should be avoided as treatments in patients with COVID-19. Health agencies and professional organizations have said they are not recommending against these medications.
The Food and Drug Administration on March 19 advised patients that it was “not aware of scientific evidence connecting” nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen “with worsening COVID-19 symptoms.”
“The agency is investigating this issue further and will communicate publicly when more information is available,” the FDA said. “However, all prescription NSAID labels warn that ‘the pharmacological activity of NSAIDs in reducing inflammation, and possibly fever, may diminish the utility of diagnostic signs in detecting infections.’ ” The FDA also noted that other over-the-counter and prescription medications are available for pain relief and fever reduction, and patients who “are concerned about taking NSAIDs and rely on these medications to treat chronic diseases” should talk to a health care provider.
A World Health Organization spokesperson said during a press conference on March 17 that the organization was looking into concerns about ibuprofen use in patients with COVID-19 and suggested that in the meantime patients take acetaminophen for fever instead. On March 18, the WHO said that it was not recommending against the use of ibuprofen.
“At present, based on currently available information, WHO does not recommend against the use of ibuprofen,” the organization said. “We are also consulting with physicians treating COVID-19 patients and are not aware of reports of any negative effects of ibuprofen, beyond the usual known side effects that limit its use in certain populations. WHO is not aware of published clinical or population-based data on this topic.”
A spokesperson for the National Institute of Allergy and Infectious Diseases said on March 18, “More research is needed to evaluate reports that ibruprofen and other over-the-counter anti-inflammatory drugs may affect the course of COVID-19. Currently, there is no conclusive evidence that ibuprofen and other over-the-counter anti-inflammatory drugs increase the risk of serious complications or of acquiring the virus that causes COVID-19. There is also no conclusive evidence that taking over-the-counter anti-inflammatory drugs is harmful for other respiratory infections.”
The European Medicines Agency (EMA) on March 18 said, “There is currently no scientific evidence establishing a link between ibuprofen and worsening of COVID‑19. EMA is monitoring the situation closely and will review any new information that becomes available on this issue in the context of the pandemic.”
In correspondence published March 11 in the Lancet Respiratory Medicine, Lei Fang, MD, of the department of biomedicine at University Hospital Basel (Switzerland), and colleagues suggested that patients with hypertension and diabetes mellitus may be at increased risk of COVID-19 because these comorbidities “are often treated with angiotensin converting enzyme (ACE) inhibitors.” In addition, “ACE2 polymorphisms that have been linked to diabetes mellitus, cerebral stroke, and hypertension” also may play a role, the researchers said (Lancet Respir Med. 2020 Mar 11. https://doi.org/10.1016/S2213-2600(20)30116-8).
“ACE2 is substantially increased in patients with type 1 or type 2 diabetes, who are treated with ACE inhibitors and angiotensin II type-I receptor blockers (ARBs). Hypertension is also treated with ACE inhibitors and ARBs, which results in an upregulation of ACE2. ACE2 can also be increased by thiazolidinediones and ibuprofen.”
A March 16 statement from the Heart Failure Society of America (HSFC), American College of Cardiology (ACC), and American Heart Association (AHA) addressed concerns about using RAAS antagonists in COVID-19.
“Patients with underlying cardiovascular diseases appear to have an increased risk for adverse outcomes with [COVID-19],” the organizations said. “Although the clinical manifestations of COVID-19 are dominated by respiratory symptoms, some patients also may have severe cardiovascular damage. [ACE2] receptors have been shown to be the entry point into human cells for SARS-CoV-2, the virus that causes COVID-19. In a few experimental studies with animal models, both [ACE] inhibitors and angiotensin receptor blockers (ARBs) have been shown to upregulate ACE2 expression in the heart. Though these have not been shown in human studies, or in the setting of COVID-19, such potential upregulation of ACE2 by ACE inhibitors or ARBs has resulted in a speculation of potential increased risk for COVID-19 infection in patients with background treatment of these medications.”
ACE2, ACE, angiotensin II, and other RAAS system interactions “are quite complex, and at times, paradoxical,” the statement says. “In experimental studies, both ACE inhibitors and ARBs have been shown to reduce severe lung injury in certain viral pneumonias, and it has been speculated that these agents could be beneficial in COVID-19.
“Currently there are no experimental or clinical data demonstrating beneficial or adverse outcomes with background use of ACE inhibitors, ARBs or other RAAS antagonists in COVID-19 or among COVID-19 patients with a history of cardiovascular disease treated with such agents. The HFSA, ACC, and AHA recommend continuation of RAAS antagonists for those patients who are currently prescribed such agents for indications for which these agents are known to be beneficial, such as heart failure, hypertension, or ischemic heart disease. In the event patients with cardiovascular disease are diagnosed with COVID-19, individualized treatment decisions should be made according to each patient’s hemodynamic status and clinical presentation. Therefore, be advised not to add or remove any RAAS-related treatments, beyond actions based on standard clinical practice.
“These theoretical concerns and findings of cardiovascular involvement with COVID-19 deserve much more detailed research, and quickly. As further research and developments related to this issue evolve, we will update these recommendations as needed.”
Dr. Fang and colleagues had no competing interests.
SOURCE: Fang L et al. Lancet Respir Med. 2020 Mar 11. doi: 10.1016/S2213-2600(20)30116-8.
Managing the COVID-19 isolation floor at UCSF Medical Center
Robert Wachter, MD, MHM, chair of the department of medicine at UCSF, interviewed Armond Esmaili, MD, a hospitalist and assistant professor of medicine at UCSF, who is the leader of the Respiratory Isolation Unit at UCSF Medical Center, where the institution's COVID-19 and rule-out COVID-19 patients are being cohorted.
Robert Wachter, MD, MHM, chair of the department of medicine at UCSF, interviewed Armond Esmaili, MD, a hospitalist and assistant professor of medicine at UCSF, who is the leader of the Respiratory Isolation Unit at UCSF Medical Center, where the institution's COVID-19 and rule-out COVID-19 patients are being cohorted.
Robert Wachter, MD, MHM, chair of the department of medicine at UCSF, interviewed Armond Esmaili, MD, a hospitalist and assistant professor of medicine at UCSF, who is the leader of the Respiratory Isolation Unit at UCSF Medical Center, where the institution's COVID-19 and rule-out COVID-19 patients are being cohorted.
Flu now riding on COVID-19’s coattails
The viral tsunami that is COVID-19 has hit the United States, and influenza appears to be riding the crest of the wave.
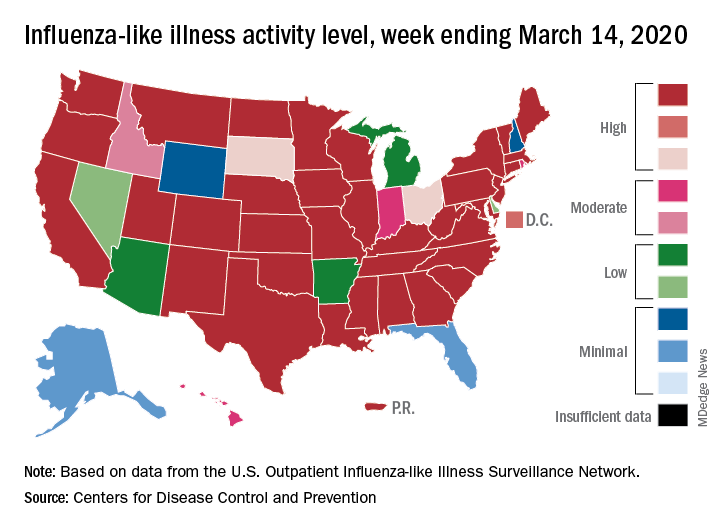
according to the Centers for Disease Control. Flu-related visits went from 5.2% of all outpatient visits the week before to 5.8% during the week ending March 14.
“The COVID-19 outbreak unfolding in the United States may affect healthcare seeking behavior which in turn would impact data from” the U.S. Outpatient Influenza-like Illness Surveillance Network, the CDC explained.
Data from clinical laboratories show that, despite the increased activity, fewer respiratory specimens tested positive for influenza: 15.3% for the week of March 8-14, compared with 21.1% the week before, the CDC’s influenza division said in its latest FluView report.
Influenza activity also increased slightly among the states, with 35 states and Puerto Rico at the highest level on the CDC’s 1-10 scale, versus 34 states and Puerto Rico the previous week. The count was down to 33 for the last week of February, CDC data show.
Severity measures remain mixed as overall hospitalization continues to be moderate but rates for children aged 0-4 years and adults aged 18-49 years are the highest on record and rates for children aged 5-17 years are the highest since the 2009 pandemic, the influenza division said.
Mortality data present a similar picture: The overall death rate is low, but the 149 flu-related deaths reported among children is the most for this point of the season since 2009, the CDC said.
The viral tsunami that is COVID-19 has hit the United States, and influenza appears to be riding the crest of the wave.
according to the Centers for Disease Control. Flu-related visits went from 5.2% of all outpatient visits the week before to 5.8% during the week ending March 14.
“The COVID-19 outbreak unfolding in the United States may affect healthcare seeking behavior which in turn would impact data from” the U.S. Outpatient Influenza-like Illness Surveillance Network, the CDC explained.
Data from clinical laboratories show that, despite the increased activity, fewer respiratory specimens tested positive for influenza: 15.3% for the week of March 8-14, compared with 21.1% the week before, the CDC’s influenza division said in its latest FluView report.
Influenza activity also increased slightly among the states, with 35 states and Puerto Rico at the highest level on the CDC’s 1-10 scale, versus 34 states and Puerto Rico the previous week. The count was down to 33 for the last week of February, CDC data show.
Severity measures remain mixed as overall hospitalization continues to be moderate but rates for children aged 0-4 years and adults aged 18-49 years are the highest on record and rates for children aged 5-17 years are the highest since the 2009 pandemic, the influenza division said.
Mortality data present a similar picture: The overall death rate is low, but the 149 flu-related deaths reported among children is the most for this point of the season since 2009, the CDC said.
The viral tsunami that is COVID-19 has hit the United States, and influenza appears to be riding the crest of the wave.
according to the Centers for Disease Control. Flu-related visits went from 5.2% of all outpatient visits the week before to 5.8% during the week ending March 14.
“The COVID-19 outbreak unfolding in the United States may affect healthcare seeking behavior which in turn would impact data from” the U.S. Outpatient Influenza-like Illness Surveillance Network, the CDC explained.
Data from clinical laboratories show that, despite the increased activity, fewer respiratory specimens tested positive for influenza: 15.3% for the week of March 8-14, compared with 21.1% the week before, the CDC’s influenza division said in its latest FluView report.
Influenza activity also increased slightly among the states, with 35 states and Puerto Rico at the highest level on the CDC’s 1-10 scale, versus 34 states and Puerto Rico the previous week. The count was down to 33 for the last week of February, CDC data show.
Severity measures remain mixed as overall hospitalization continues to be moderate but rates for children aged 0-4 years and adults aged 18-49 years are the highest on record and rates for children aged 5-17 years are the highest since the 2009 pandemic, the influenza division said.
Mortality data present a similar picture: The overall death rate is low, but the 149 flu-related deaths reported among children is the most for this point of the season since 2009, the CDC said.
Preventable diseases could gain a foothold because of COVID-19
There is a highly infectious virus spreading around the world and it is targeting the most vulnerable among us. It is among the most contagious of human diseases, spreading through the air unseen. No, it isn’t the novel coronavirus, COVID-19. It’s measles.

Remember measles? Outbreaks in recent years have brought the disease, which once was declared eliminated in the United States, back into the news and public awareness, but measles never has really gone away. Every year there are millions of cases worldwide – in 2018 alone there were nearly 10 million estimated cases and 142,300 deaths, according to the World Health Organization. The good news is that measles vaccination is highly effective, at about 97% after the recommended two doses. According to the Centers for Disease Control and Prevention, “because of vaccination, more than 21 million lives have been saved and measles deaths have been reduced by 80% since 2000.” This is a tremendous public health success and a cause for celebration. But our work is not done. The recent increases in vaccine hesitancy and refusal in many countries has contributed to the resurgence of measles worldwide.
Influenza still is in full swing with the CDC reporting high activity in 1 states for the week ending April 4th. Seasonal influenza, according to currently available data, has a lower fatality rate than COVID-19, but that doesn’t mean it is harmless. Thus far in the 2019-2020 flu season, there have been at least 24,000 deaths because of influenza in the United States alone, 166 of which were among pediatric patients.*
Like many pediatricians, I have seen firsthand the impact of vaccine-preventable illnesses like influenza, pertussis, and varicella. I have personally cared for an infant with pertussis who had to be intubated and on a ventilator for nearly a week. I have told the family of a child with cancer that they would have to be admitted to the hospital yet again for intravenous antiviral medication because that little rash turned out to be varicella. I have performed CPR on a previously healthy teenager with the flu whose heart was failing despite maximum ventilator support. All these illnesses might have been prevented had these patients or those around them been appropriately vaccinated.
Right now, the United States and governments around the world are taking unprecedented public health measures to prevent the spread of COVID-19, directing the public to stay home, avoid unnecessary contact with other people, practice good hand-washing and infection-control techniques. In order to promote social distancing, many primary care clinics are canceling nonurgent appointments or converting them to virtual visits, including some visits for routine vaccinations for older children, teens, and adults. This is a responsible choice to keep potentially asymptomatic people from spreading COVID-19, but once restrictions begin to lift, we all will need to act to help our patients catch up on these missing vaccinations.
This pandemic has made it more apparent than ever that we all rely upon each other to stay healthy. While this pandemic has disrupted nearly every aspect of daily life, we can’t let it disrupt one of the great successes in health care today: the prevention of serious illnesses. As soon as it is safe to do so, we must help and encourage patients to catch up on missing vaccinations. It’s rare that preventative public health measures and vaccine developments are in the nightly news, so we should use this increased public awareness to ensure patients are well educated and protected from every disease. As part of this, we must continue our efforts to share accurate information on the safety and efficacy of routine vaccination. And when there is a vaccine for COVID-19? Let’s make sure everyone gets that too.
Dr. Leighton is a pediatrician in the ED at Children’s National Hospital and currently is completing her MPH in health policy at George Washington University, both in Washington. She had no relevant financial disclosures.*
* This article was updated 4/10/2020.
There is a highly infectious virus spreading around the world and it is targeting the most vulnerable among us. It is among the most contagious of human diseases, spreading through the air unseen. No, it isn’t the novel coronavirus, COVID-19. It’s measles.
Remember measles? Outbreaks in recent years have brought the disease, which once was declared eliminated in the United States, back into the news and public awareness, but measles never has really gone away. Every year there are millions of cases worldwide – in 2018 alone there were nearly 10 million estimated cases and 142,300 deaths, according to the World Health Organization. The good news is that measles vaccination is highly effective, at about 97% after the recommended two doses. According to the Centers for Disease Control and Prevention, “because of vaccination, more than 21 million lives have been saved and measles deaths have been reduced by 80% since 2000.” This is a tremendous public health success and a cause for celebration. But our work is not done. The recent increases in vaccine hesitancy and refusal in many countries has contributed to the resurgence of measles worldwide.
Influenza still is in full swing with the CDC reporting high activity in 1 states for the week ending April 4th. Seasonal influenza, according to currently available data, has a lower fatality rate than COVID-19, but that doesn’t mean it is harmless. Thus far in the 2019-2020 flu season, there have been at least 24,000 deaths because of influenza in the United States alone, 166 of which were among pediatric patients.*
Like many pediatricians, I have seen firsthand the impact of vaccine-preventable illnesses like influenza, pertussis, and varicella. I have personally cared for an infant with pertussis who had to be intubated and on a ventilator for nearly a week. I have told the family of a child with cancer that they would have to be admitted to the hospital yet again for intravenous antiviral medication because that little rash turned out to be varicella. I have performed CPR on a previously healthy teenager with the flu whose heart was failing despite maximum ventilator support. All these illnesses might have been prevented had these patients or those around them been appropriately vaccinated.
Right now, the United States and governments around the world are taking unprecedented public health measures to prevent the spread of COVID-19, directing the public to stay home, avoid unnecessary contact with other people, practice good hand-washing and infection-control techniques. In order to promote social distancing, many primary care clinics are canceling nonurgent appointments or converting them to virtual visits, including some visits for routine vaccinations for older children, teens, and adults. This is a responsible choice to keep potentially asymptomatic people from spreading COVID-19, but once restrictions begin to lift, we all will need to act to help our patients catch up on these missing vaccinations.
This pandemic has made it more apparent than ever that we all rely upon each other to stay healthy. While this pandemic has disrupted nearly every aspect of daily life, we can’t let it disrupt one of the great successes in health care today: the prevention of serious illnesses. As soon as it is safe to do so, we must help and encourage patients to catch up on missing vaccinations. It’s rare that preventative public health measures and vaccine developments are in the nightly news, so we should use this increased public awareness to ensure patients are well educated and protected from every disease. As part of this, we must continue our efforts to share accurate information on the safety and efficacy of routine vaccination. And when there is a vaccine for COVID-19? Let’s make sure everyone gets that too.
Dr. Leighton is a pediatrician in the ED at Children’s National Hospital and currently is completing her MPH in health policy at George Washington University, both in Washington. She had no relevant financial disclosures.*
* This article was updated 4/10/2020.
There is a highly infectious virus spreading around the world and it is targeting the most vulnerable among us. It is among the most contagious of human diseases, spreading through the air unseen. No, it isn’t the novel coronavirus, COVID-19. It’s measles.
Remember measles? Outbreaks in recent years have brought the disease, which once was declared eliminated in the United States, back into the news and public awareness, but measles never has really gone away. Every year there are millions of cases worldwide – in 2018 alone there were nearly 10 million estimated cases and 142,300 deaths, according to the World Health Organization. The good news is that measles vaccination is highly effective, at about 97% after the recommended two doses. According to the Centers for Disease Control and Prevention, “because of vaccination, more than 21 million lives have been saved and measles deaths have been reduced by 80% since 2000.” This is a tremendous public health success and a cause for celebration. But our work is not done. The recent increases in vaccine hesitancy and refusal in many countries has contributed to the resurgence of measles worldwide.
Influenza still is in full swing with the CDC reporting high activity in 1 states for the week ending April 4th. Seasonal influenza, according to currently available data, has a lower fatality rate than COVID-19, but that doesn’t mean it is harmless. Thus far in the 2019-2020 flu season, there have been at least 24,000 deaths because of influenza in the United States alone, 166 of which were among pediatric patients.*
Like many pediatricians, I have seen firsthand the impact of vaccine-preventable illnesses like influenza, pertussis, and varicella. I have personally cared for an infant with pertussis who had to be intubated and on a ventilator for nearly a week. I have told the family of a child with cancer that they would have to be admitted to the hospital yet again for intravenous antiviral medication because that little rash turned out to be varicella. I have performed CPR on a previously healthy teenager with the flu whose heart was failing despite maximum ventilator support. All these illnesses might have been prevented had these patients or those around them been appropriately vaccinated.
Right now, the United States and governments around the world are taking unprecedented public health measures to prevent the spread of COVID-19, directing the public to stay home, avoid unnecessary contact with other people, practice good hand-washing and infection-control techniques. In order to promote social distancing, many primary care clinics are canceling nonurgent appointments or converting them to virtual visits, including some visits for routine vaccinations for older children, teens, and adults. This is a responsible choice to keep potentially asymptomatic people from spreading COVID-19, but once restrictions begin to lift, we all will need to act to help our patients catch up on these missing vaccinations.
This pandemic has made it more apparent than ever that we all rely upon each other to stay healthy. While this pandemic has disrupted nearly every aspect of daily life, we can’t let it disrupt one of the great successes in health care today: the prevention of serious illnesses. As soon as it is safe to do so, we must help and encourage patients to catch up on missing vaccinations. It’s rare that preventative public health measures and vaccine developments are in the nightly news, so we should use this increased public awareness to ensure patients are well educated and protected from every disease. As part of this, we must continue our efforts to share accurate information on the safety and efficacy of routine vaccination. And when there is a vaccine for COVID-19? Let’s make sure everyone gets that too.
Dr. Leighton is a pediatrician in the ED at Children’s National Hospital and currently is completing her MPH in health policy at George Washington University, both in Washington. She had no relevant financial disclosures.*
* This article was updated 4/10/2020.
Emergency Rule: Docs can bill for telehealth and COVID-19 tests. Here’s how
Many medical practices have long wanted to use telehealth to perform office visits and other evaluation and management (E/M) services. The technology readily exists and many electronic health records are set up to do telehealth visits. The problem has been getting paid for those visits. Medicare limited telehealth services to patients in underserved areas, and commercial insurances wouldn’t pay. But amid the COVID-19 crisis, things have changed.
On March 17, Congress passed a law allowing Medicare to waive some telehealth restrictions during a government state of emergency only, which we are in now. Specifically, the patient no longer needs to be in a medically underserved area and no longer needs to go to an originating site, such as a hospital. The patient can be located anywhere in the country and be in their own home.
Further, the Centers for Medicare & Medicaid is waiving the requirement that the practitioner use a HIPAA-compliant platform for the telehealth service. The service must still be provided using a real-time audiovisual platform, but that could be via FaceTime or Skype, both of which are readily available via a patient’s smartphone or home computer. Audio alone – that is, phone calls between physician and patient – is still insufficient.
Billing for telemedicine
There are two lists of services that you can bill for telehealth. One of the lists is in Medicare’s telehealth fact sheet and includes both CPT and HCPCS codes. The second is in your CPT book, Appendix P, and lists only CPT codes.
Practices may bill all of the Medicare-covered telehealth services using these new rules. This includes new and established patient visits 99201–99215. It includes inpatient and skilled nursing services, for which CMS uses HCPCS codes in place of CPT codes.
Some notable additional services that you may bill via telehealth are: smoking cessation, transitional care management, advanced care planning, psychiatric diagnostic interviews and psychotherapy, and initial and subsequent Medicare wellness visits. The Welcome to Medicare visit is not on the list.
Report these services to Medicare with the correct CPT code and use place of service 02 (telehealth) on the claim. There is a CPT modifier for telehealth (Modifier -95 Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunications System) but Medicare does not require it.
If you perform an office visit and also do smoking cessation, document those just as you would if you saw the patient in person. Document the history; observational exam, if relevant; and the assessment and plan. Note the additional time spent in smoking cessation counseling. If it was a level three established patient, code 99213-25 and 99406 (smoking and tobacco use cessation counseling visit, intermediate, 3-10 minutes).
The Office of Inspector General is allowing practices to reduce or waive copays and patient due amounts. However, a practice is not required to waive the copay or patient due amount for a telehealth service.
Medicare Advantage plans are required to cover all services that original Medicare covers. State Medicaid plans and Medicaid managed care organizations can set their own rules.
What about commercial payers?
While CMS has issued its Medicare guidelines, commercial insurance companies can also set their own rules about covering telehealth services. Many of them have rushed to update their policies to allow office visits to be billed via telehealth.
Unfortunately, each payer can set its own rules about whether to cover telehealth and if the place of service 02 and/or modifier -95 is needed. UnitedHealthcare is covering telehealth visits for all of its Medicare Advantage, Medicaid, and commercial accounts.
Humana also is covering telemedicine for urgent care needs. Some private insurers are continuing to offer virtual visits with their contracted telehealth provider, not with the patient’s own physician. It is likely that this will change in the days ahead, but it means practices must check their payer policies and pay attention to the emails they receive from the payers. If patient foot traffic is slow, this may be a good time to call each payer to not only find out their telehealth rules, but to also learn what else is being suspended during the COVID-19 pandemic.
This would also be a good job for an employee to do from home versus coming into the practice.
None of the payers are limiting the diagnosis code for telemedicine services. The patient does not need to have a cough or fever to have telemedicine covered. Any diagnosis or condition is eligible to be billed via telehealth.
The waived restrictions by Medicare are in place only as long as the government state of emergency. Commercial payers are also describing these as temporary. However, it may be hard to put the genie back in the bottle. Medical practices and patients may find that these visits are just what the doctor ordered.
COVID-19 testing
Although testing is still not widely available, the American Medical Association has developed a CPT code for the test:
- 87635: Infectious agent detection by nucleic acid (DNA or RNA); severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), amplified probe technique
CMS has also developed codes for testing for this new coronavirus. One (U0001) is specifically for tests done in the CDC lab. The second (U0002) was for other labs, but it seems likely that the CPT code will replace it.
In February, the U.S. Food and Drug Administration issued a new policy for certain labs to develop their own validated COVID-19 diagnostics. This second HCPCS code could be used for such tests when submitting claims to Medicare or other insurers.
The hope by CMS is that having these specific codes will encourage further testing and improve tracking of the virus.
This article first appeared on Medscape.com.
Many medical practices have long wanted to use telehealth to perform office visits and other evaluation and management (E/M) services. The technology readily exists and many electronic health records are set up to do telehealth visits. The problem has been getting paid for those visits. Medicare limited telehealth services to patients in underserved areas, and commercial insurances wouldn’t pay. But amid the COVID-19 crisis, things have changed.
On March 17, Congress passed a law allowing Medicare to waive some telehealth restrictions during a government state of emergency only, which we are in now. Specifically, the patient no longer needs to be in a medically underserved area and no longer needs to go to an originating site, such as a hospital. The patient can be located anywhere in the country and be in their own home.
Further, the Centers for Medicare & Medicaid is waiving the requirement that the practitioner use a HIPAA-compliant platform for the telehealth service. The service must still be provided using a real-time audiovisual platform, but that could be via FaceTime or Skype, both of which are readily available via a patient’s smartphone or home computer. Audio alone – that is, phone calls between physician and patient – is still insufficient.
Billing for telemedicine
There are two lists of services that you can bill for telehealth. One of the lists is in Medicare’s telehealth fact sheet and includes both CPT and HCPCS codes. The second is in your CPT book, Appendix P, and lists only CPT codes.
Practices may bill all of the Medicare-covered telehealth services using these new rules. This includes new and established patient visits 99201–99215. It includes inpatient and skilled nursing services, for which CMS uses HCPCS codes in place of CPT codes.
Some notable additional services that you may bill via telehealth are: smoking cessation, transitional care management, advanced care planning, psychiatric diagnostic interviews and psychotherapy, and initial and subsequent Medicare wellness visits. The Welcome to Medicare visit is not on the list.
Report these services to Medicare with the correct CPT code and use place of service 02 (telehealth) on the claim. There is a CPT modifier for telehealth (Modifier -95 Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunications System) but Medicare does not require it.
If you perform an office visit and also do smoking cessation, document those just as you would if you saw the patient in person. Document the history; observational exam, if relevant; and the assessment and plan. Note the additional time spent in smoking cessation counseling. If it was a level three established patient, code 99213-25 and 99406 (smoking and tobacco use cessation counseling visit, intermediate, 3-10 minutes).
The Office of Inspector General is allowing practices to reduce or waive copays and patient due amounts. However, a practice is not required to waive the copay or patient due amount for a telehealth service.
Medicare Advantage plans are required to cover all services that original Medicare covers. State Medicaid plans and Medicaid managed care organizations can set their own rules.
What about commercial payers?
While CMS has issued its Medicare guidelines, commercial insurance companies can also set their own rules about covering telehealth services. Many of them have rushed to update their policies to allow office visits to be billed via telehealth.
Unfortunately, each payer can set its own rules about whether to cover telehealth and if the place of service 02 and/or modifier -95 is needed. UnitedHealthcare is covering telehealth visits for all of its Medicare Advantage, Medicaid, and commercial accounts.
Humana also is covering telemedicine for urgent care needs. Some private insurers are continuing to offer virtual visits with their contracted telehealth provider, not with the patient’s own physician. It is likely that this will change in the days ahead, but it means practices must check their payer policies and pay attention to the emails they receive from the payers. If patient foot traffic is slow, this may be a good time to call each payer to not only find out their telehealth rules, but to also learn what else is being suspended during the COVID-19 pandemic.
This would also be a good job for an employee to do from home versus coming into the practice.
None of the payers are limiting the diagnosis code for telemedicine services. The patient does not need to have a cough or fever to have telemedicine covered. Any diagnosis or condition is eligible to be billed via telehealth.
The waived restrictions by Medicare are in place only as long as the government state of emergency. Commercial payers are also describing these as temporary. However, it may be hard to put the genie back in the bottle. Medical practices and patients may find that these visits are just what the doctor ordered.
COVID-19 testing
Although testing is still not widely available, the American Medical Association has developed a CPT code for the test:
- 87635: Infectious agent detection by nucleic acid (DNA or RNA); severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), amplified probe technique
CMS has also developed codes for testing for this new coronavirus. One (U0001) is specifically for tests done in the CDC lab. The second (U0002) was for other labs, but it seems likely that the CPT code will replace it.
In February, the U.S. Food and Drug Administration issued a new policy for certain labs to develop their own validated COVID-19 diagnostics. This second HCPCS code could be used for such tests when submitting claims to Medicare or other insurers.
The hope by CMS is that having these specific codes will encourage further testing and improve tracking of the virus.
This article first appeared on Medscape.com.
Many medical practices have long wanted to use telehealth to perform office visits and other evaluation and management (E/M) services. The technology readily exists and many electronic health records are set up to do telehealth visits. The problem has been getting paid for those visits. Medicare limited telehealth services to patients in underserved areas, and commercial insurances wouldn’t pay. But amid the COVID-19 crisis, things have changed.
On March 17, Congress passed a law allowing Medicare to waive some telehealth restrictions during a government state of emergency only, which we are in now. Specifically, the patient no longer needs to be in a medically underserved area and no longer needs to go to an originating site, such as a hospital. The patient can be located anywhere in the country and be in their own home.
Further, the Centers for Medicare & Medicaid is waiving the requirement that the practitioner use a HIPAA-compliant platform for the telehealth service. The service must still be provided using a real-time audiovisual platform, but that could be via FaceTime or Skype, both of which are readily available via a patient’s smartphone or home computer. Audio alone – that is, phone calls between physician and patient – is still insufficient.
Billing for telemedicine
There are two lists of services that you can bill for telehealth. One of the lists is in Medicare’s telehealth fact sheet and includes both CPT and HCPCS codes. The second is in your CPT book, Appendix P, and lists only CPT codes.
Practices may bill all of the Medicare-covered telehealth services using these new rules. This includes new and established patient visits 99201–99215. It includes inpatient and skilled nursing services, for which CMS uses HCPCS codes in place of CPT codes.
Some notable additional services that you may bill via telehealth are: smoking cessation, transitional care management, advanced care planning, psychiatric diagnostic interviews and psychotherapy, and initial and subsequent Medicare wellness visits. The Welcome to Medicare visit is not on the list.
Report these services to Medicare with the correct CPT code and use place of service 02 (telehealth) on the claim. There is a CPT modifier for telehealth (Modifier -95 Synchronous Telemedicine Service Rendered Via a Real-Time Interactive Audio and Video Telecommunications System) but Medicare does not require it.
If you perform an office visit and also do smoking cessation, document those just as you would if you saw the patient in person. Document the history; observational exam, if relevant; and the assessment and plan. Note the additional time spent in smoking cessation counseling. If it was a level three established patient, code 99213-25 and 99406 (smoking and tobacco use cessation counseling visit, intermediate, 3-10 minutes).
The Office of Inspector General is allowing practices to reduce or waive copays and patient due amounts. However, a practice is not required to waive the copay or patient due amount for a telehealth service.
Medicare Advantage plans are required to cover all services that original Medicare covers. State Medicaid plans and Medicaid managed care organizations can set their own rules.
What about commercial payers?
While CMS has issued its Medicare guidelines, commercial insurance companies can also set their own rules about covering telehealth services. Many of them have rushed to update their policies to allow office visits to be billed via telehealth.
Unfortunately, each payer can set its own rules about whether to cover telehealth and if the place of service 02 and/or modifier -95 is needed. UnitedHealthcare is covering telehealth visits for all of its Medicare Advantage, Medicaid, and commercial accounts.
Humana also is covering telemedicine for urgent care needs. Some private insurers are continuing to offer virtual visits with their contracted telehealth provider, not with the patient’s own physician. It is likely that this will change in the days ahead, but it means practices must check their payer policies and pay attention to the emails they receive from the payers. If patient foot traffic is slow, this may be a good time to call each payer to not only find out their telehealth rules, but to also learn what else is being suspended during the COVID-19 pandemic.
This would also be a good job for an employee to do from home versus coming into the practice.
None of the payers are limiting the diagnosis code for telemedicine services. The patient does not need to have a cough or fever to have telemedicine covered. Any diagnosis or condition is eligible to be billed via telehealth.
The waived restrictions by Medicare are in place only as long as the government state of emergency. Commercial payers are also describing these as temporary. However, it may be hard to put the genie back in the bottle. Medical practices and patients may find that these visits are just what the doctor ordered.
COVID-19 testing
Although testing is still not widely available, the American Medical Association has developed a CPT code for the test:
- 87635: Infectious agent detection by nucleic acid (DNA or RNA); severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Coronavirus disease [COVID-19]), amplified probe technique
CMS has also developed codes for testing for this new coronavirus. One (U0001) is specifically for tests done in the CDC lab. The second (U0002) was for other labs, but it seems likely that the CPT code will replace it.
In February, the U.S. Food and Drug Administration issued a new policy for certain labs to develop their own validated COVID-19 diagnostics. This second HCPCS code could be used for such tests when submitting claims to Medicare or other insurers.
The hope by CMS is that having these specific codes will encourage further testing and improve tracking of the virus.
This article first appeared on Medscape.com.
New ASAM guideline released amid COVID-19 concerns
Home-based buprenorphine induction deemed safe for OUD
The American Society of Addiction Medicine has released an updated practice guideline for patients with opioid use disorder.
The guideline, called a focused update, advances ASAM’s 2015 National Practice Guidelines for the Treament of Opioid Use Disorder. “During the ongoing COVID-19 pandemic and the associated need for social distancing, it is especially important that clinicians and health care providers across the country take steps to ensure that individuals with OUD can continue to receive evidence-based care,” said Paul H. Earley, MD, president of ASAM, in a press release announcing the new guideline.
The guideline specifies that home-based buprenorphine induction is safe and effective for treatment of opioid use disorder and that no individual entering the criminal justice system should be subjected to opioid withdrawal.
“The research is clear, providing methadone or buprenorphine, even without psychosocial treatment, reduces the patient’s risk of death,” said Kyle Kampman, MD, chair of the group’s Guideline Writing Committee, in the release. “Ultimately, keeping patients with the disease of addiction alive and engaged to become ready for recovery is absolutely critical in the context of the deadly overdose epidemic that has struck communities across our country.”
The society released this focused update to reflect new medications and formulations, published evidence, and clinical guidance related to treatment of OUD. This update includes the addition of 13 new recommendations and major revisions to 35 existing recommendations. One concern the society has is how to help patients being treated for OUD who are limited in their ability to leave their homes. Because of these same concerns, the Substance Abuse and Mental Health Services Administration relaxed regulations on March 16 regarding patient eligibility for take-home medications, such as buprenorphine and methadone, which dovetails with the society’s guidance regarding home-based induction.
, continuing on to pharmacologic treatment even if the patient declines recommended psychosocial treatment, keeping naloxone kits available in correctional facilities, and more. Additional information about this update can be found on ASAM’s website.
Home-based buprenorphine induction deemed safe for OUD
Home-based buprenorphine induction deemed safe for OUD
The American Society of Addiction Medicine has released an updated practice guideline for patients with opioid use disorder.
The guideline, called a focused update, advances ASAM’s 2015 National Practice Guidelines for the Treament of Opioid Use Disorder. “During the ongoing COVID-19 pandemic and the associated need for social distancing, it is especially important that clinicians and health care providers across the country take steps to ensure that individuals with OUD can continue to receive evidence-based care,” said Paul H. Earley, MD, president of ASAM, in a press release announcing the new guideline.
The guideline specifies that home-based buprenorphine induction is safe and effective for treatment of opioid use disorder and that no individual entering the criminal justice system should be subjected to opioid withdrawal.
“The research is clear, providing methadone or buprenorphine, even without psychosocial treatment, reduces the patient’s risk of death,” said Kyle Kampman, MD, chair of the group’s Guideline Writing Committee, in the release. “Ultimately, keeping patients with the disease of addiction alive and engaged to become ready for recovery is absolutely critical in the context of the deadly overdose epidemic that has struck communities across our country.”
The society released this focused update to reflect new medications and formulations, published evidence, and clinical guidance related to treatment of OUD. This update includes the addition of 13 new recommendations and major revisions to 35 existing recommendations. One concern the society has is how to help patients being treated for OUD who are limited in their ability to leave their homes. Because of these same concerns, the Substance Abuse and Mental Health Services Administration relaxed regulations on March 16 regarding patient eligibility for take-home medications, such as buprenorphine and methadone, which dovetails with the society’s guidance regarding home-based induction.
, continuing on to pharmacologic treatment even if the patient declines recommended psychosocial treatment, keeping naloxone kits available in correctional facilities, and more. Additional information about this update can be found on ASAM’s website.
The American Society of Addiction Medicine has released an updated practice guideline for patients with opioid use disorder.
The guideline, called a focused update, advances ASAM’s 2015 National Practice Guidelines for the Treament of Opioid Use Disorder. “During the ongoing COVID-19 pandemic and the associated need for social distancing, it is especially important that clinicians and health care providers across the country take steps to ensure that individuals with OUD can continue to receive evidence-based care,” said Paul H. Earley, MD, president of ASAM, in a press release announcing the new guideline.
The guideline specifies that home-based buprenorphine induction is safe and effective for treatment of opioid use disorder and that no individual entering the criminal justice system should be subjected to opioid withdrawal.
“The research is clear, providing methadone or buprenorphine, even without psychosocial treatment, reduces the patient’s risk of death,” said Kyle Kampman, MD, chair of the group’s Guideline Writing Committee, in the release. “Ultimately, keeping patients with the disease of addiction alive and engaged to become ready for recovery is absolutely critical in the context of the deadly overdose epidemic that has struck communities across our country.”
The society released this focused update to reflect new medications and formulations, published evidence, and clinical guidance related to treatment of OUD. This update includes the addition of 13 new recommendations and major revisions to 35 existing recommendations. One concern the society has is how to help patients being treated for OUD who are limited in their ability to leave their homes. Because of these same concerns, the Substance Abuse and Mental Health Services Administration relaxed regulations on March 16 regarding patient eligibility for take-home medications, such as buprenorphine and methadone, which dovetails with the society’s guidance regarding home-based induction.
, continuing on to pharmacologic treatment even if the patient declines recommended psychosocial treatment, keeping naloxone kits available in correctional facilities, and more. Additional information about this update can be found on ASAM’s website.