User login
In Case You Missed It: COVID
COVID-associated pancreatitis may disproportionately affect young, overweight men
Patients with COVID-19 develop a distinct subset of pancreatitis hallmarked by duodenal and periduodenal inflammation, according to a recent case series.
Although all five patients presented with multiple predictive markers of severe pancreatitis, the subsequent clinical pathway “was much more benign than anticipated,” reported lead author Peter Szatmary, MB, BChir, PhD, of the University of Liverpool (England) and colleagues. Still, they noted prolonged hospital stays because of persistent inflammation and poor diabetic control.
“As the global pandemic of SARS-CoV-2 continues, nuances of the disease it precipitates in humans continue to emerge,” the investigators wrote in Gastroenterology. “[A] group from Wuhan reported a series of 9 patients with purported pancreatic injury in the context of SARS-CoV-2 infection, but did not provide robust evidence for pancreatitis relying on mild hyperamylasemia alone.”
For the present series, Dr. Szatmary and colleagues restricted diagnosis of pancreatitis to international consensus guidelines, which require “abdominal pain consistent with pancreatitis, serum amylase/lipase greater than three times the upper limit of normal, and characteristic findings on cross-sectional imaging.”
From middle of March to late April, the investigators identified 35 patients with acute pancreatitis at Royal Liverpool (England) University Hospital, 25 of whom tested negative for SARS-CoV-2, which resulted in study exclusion. An additional five patients were excluded from the series as another etiology for pancreatitis was clearly present, such as gallstones.
“The remaining 5 patients, all with SARS-CoV-2, presented atypically yet homogenously with a distinct metabolic-pancreatitis phenotype,” the investigators wrote.
All five patients were obese or overweight young men with a median body mass index of 30 kg/m2 and age of 42 years. On presentation, all patients had elevated, but nondiagnostic, levels of amylase (median, 149 U/L). Contrast-enhanced abdominal CT revealed moderate to severe hepatic steatosis (less than 104 HU), which rapidly regressed within a week among patients who underwent repeat imaging.
“The pattern of pancreatic inflammation was similarly unusual in these patients,” the investigators wrote, going on to describe “mild pancreatic edema without significant pancreatic or peripancreatic necrosis, with distinct duodenal/periduodenal inflammation involving the second and third part of the duodenum.”
According to Dr. Szatmary and colleagues, these findings were “accompanied by a profound systemic inflammatory response,” including 1-2 criteria for systemic inflammatory response syndrome that increased to 2-4 criteria within 48 hours. During hospitalization, patients also exhibited a “dramatic elevation” of C-reactive protein, from a median of 31 mg/L upon admission to 485 mg/L within 48 hours.
Although these markers predicted severe disease, all cases followed a clinical course similar to “a typical attack of moderate pancreatitis,” the investigators wrote.
All patients were treated with IV fluids, four out of five received broad-spectrum IV antibiotics for pneumonitis, three out of five received fibrate and/or insulin therapy, and two out of five received pancreatic enzyme replacement therapy. No patients required corticosteroids, organ support, or respiratory support beyond low-flow oxygen. Median hospital stay was 14 days.
“We ... propose the combination of male sex, abdominal pain, metabolic stress, and CT-findings of predominantly pancreatico-duodenal inflammation with steatosis represent a distinct subset of pancreatitis in patients infected with SARS-CoV-2,” the investigators wrote.
They suggested that the endocrine pancreas may be “particularly vulnerable to this infection,” citing prolonged hospital stays because of poor diabetic control.
“[T]ransient dyslipidemias and impaired glucose tolerance may be common in SARS-CoV-2 patients and warrant further investigation,” they concluded.
Oscar J. Hines, MD, chief of the division of general surgery at UCLA Medical Center and leader in the field of pancreatitis management, said that the case series has a limited impact.
“The findings are unlikely to change practice and only call attention for physicians to the possibility of pancreatitis in COVID-positive patients,” Dr. Hines said.
The investigators reported grants from NIHR, Wellcome Trust, Mylan, and others.
SOURCE: Szatmary P et al. Gastroenterology. 2020 Jun 1. doi: 10.1053/j.gastro.2020.05.069.
Patients with COVID-19 develop a distinct subset of pancreatitis hallmarked by duodenal and periduodenal inflammation, according to a recent case series.
Although all five patients presented with multiple predictive markers of severe pancreatitis, the subsequent clinical pathway “was much more benign than anticipated,” reported lead author Peter Szatmary, MB, BChir, PhD, of the University of Liverpool (England) and colleagues. Still, they noted prolonged hospital stays because of persistent inflammation and poor diabetic control.
“As the global pandemic of SARS-CoV-2 continues, nuances of the disease it precipitates in humans continue to emerge,” the investigators wrote in Gastroenterology. “[A] group from Wuhan reported a series of 9 patients with purported pancreatic injury in the context of SARS-CoV-2 infection, but did not provide robust evidence for pancreatitis relying on mild hyperamylasemia alone.”
For the present series, Dr. Szatmary and colleagues restricted diagnosis of pancreatitis to international consensus guidelines, which require “abdominal pain consistent with pancreatitis, serum amylase/lipase greater than three times the upper limit of normal, and characteristic findings on cross-sectional imaging.”
From middle of March to late April, the investigators identified 35 patients with acute pancreatitis at Royal Liverpool (England) University Hospital, 25 of whom tested negative for SARS-CoV-2, which resulted in study exclusion. An additional five patients were excluded from the series as another etiology for pancreatitis was clearly present, such as gallstones.
“The remaining 5 patients, all with SARS-CoV-2, presented atypically yet homogenously with a distinct metabolic-pancreatitis phenotype,” the investigators wrote.
All five patients were obese or overweight young men with a median body mass index of 30 kg/m2 and age of 42 years. On presentation, all patients had elevated, but nondiagnostic, levels of amylase (median, 149 U/L). Contrast-enhanced abdominal CT revealed moderate to severe hepatic steatosis (less than 104 HU), which rapidly regressed within a week among patients who underwent repeat imaging.
“The pattern of pancreatic inflammation was similarly unusual in these patients,” the investigators wrote, going on to describe “mild pancreatic edema without significant pancreatic or peripancreatic necrosis, with distinct duodenal/periduodenal inflammation involving the second and third part of the duodenum.”
According to Dr. Szatmary and colleagues, these findings were “accompanied by a profound systemic inflammatory response,” including 1-2 criteria for systemic inflammatory response syndrome that increased to 2-4 criteria within 48 hours. During hospitalization, patients also exhibited a “dramatic elevation” of C-reactive protein, from a median of 31 mg/L upon admission to 485 mg/L within 48 hours.
Although these markers predicted severe disease, all cases followed a clinical course similar to “a typical attack of moderate pancreatitis,” the investigators wrote.
All patients were treated with IV fluids, four out of five received broad-spectrum IV antibiotics for pneumonitis, three out of five received fibrate and/or insulin therapy, and two out of five received pancreatic enzyme replacement therapy. No patients required corticosteroids, organ support, or respiratory support beyond low-flow oxygen. Median hospital stay was 14 days.
“We ... propose the combination of male sex, abdominal pain, metabolic stress, and CT-findings of predominantly pancreatico-duodenal inflammation with steatosis represent a distinct subset of pancreatitis in patients infected with SARS-CoV-2,” the investigators wrote.
They suggested that the endocrine pancreas may be “particularly vulnerable to this infection,” citing prolonged hospital stays because of poor diabetic control.
“[T]ransient dyslipidemias and impaired glucose tolerance may be common in SARS-CoV-2 patients and warrant further investigation,” they concluded.
Oscar J. Hines, MD, chief of the division of general surgery at UCLA Medical Center and leader in the field of pancreatitis management, said that the case series has a limited impact.
“The findings are unlikely to change practice and only call attention for physicians to the possibility of pancreatitis in COVID-positive patients,” Dr. Hines said.
The investigators reported grants from NIHR, Wellcome Trust, Mylan, and others.
SOURCE: Szatmary P et al. Gastroenterology. 2020 Jun 1. doi: 10.1053/j.gastro.2020.05.069.
Patients with COVID-19 develop a distinct subset of pancreatitis hallmarked by duodenal and periduodenal inflammation, according to a recent case series.
Although all five patients presented with multiple predictive markers of severe pancreatitis, the subsequent clinical pathway “was much more benign than anticipated,” reported lead author Peter Szatmary, MB, BChir, PhD, of the University of Liverpool (England) and colleagues. Still, they noted prolonged hospital stays because of persistent inflammation and poor diabetic control.
“As the global pandemic of SARS-CoV-2 continues, nuances of the disease it precipitates in humans continue to emerge,” the investigators wrote in Gastroenterology. “[A] group from Wuhan reported a series of 9 patients with purported pancreatic injury in the context of SARS-CoV-2 infection, but did not provide robust evidence for pancreatitis relying on mild hyperamylasemia alone.”
For the present series, Dr. Szatmary and colleagues restricted diagnosis of pancreatitis to international consensus guidelines, which require “abdominal pain consistent with pancreatitis, serum amylase/lipase greater than three times the upper limit of normal, and characteristic findings on cross-sectional imaging.”
From middle of March to late April, the investigators identified 35 patients with acute pancreatitis at Royal Liverpool (England) University Hospital, 25 of whom tested negative for SARS-CoV-2, which resulted in study exclusion. An additional five patients were excluded from the series as another etiology for pancreatitis was clearly present, such as gallstones.
“The remaining 5 patients, all with SARS-CoV-2, presented atypically yet homogenously with a distinct metabolic-pancreatitis phenotype,” the investigators wrote.
All five patients were obese or overweight young men with a median body mass index of 30 kg/m2 and age of 42 years. On presentation, all patients had elevated, but nondiagnostic, levels of amylase (median, 149 U/L). Contrast-enhanced abdominal CT revealed moderate to severe hepatic steatosis (less than 104 HU), which rapidly regressed within a week among patients who underwent repeat imaging.
“The pattern of pancreatic inflammation was similarly unusual in these patients,” the investigators wrote, going on to describe “mild pancreatic edema without significant pancreatic or peripancreatic necrosis, with distinct duodenal/periduodenal inflammation involving the second and third part of the duodenum.”
According to Dr. Szatmary and colleagues, these findings were “accompanied by a profound systemic inflammatory response,” including 1-2 criteria for systemic inflammatory response syndrome that increased to 2-4 criteria within 48 hours. During hospitalization, patients also exhibited a “dramatic elevation” of C-reactive protein, from a median of 31 mg/L upon admission to 485 mg/L within 48 hours.
Although these markers predicted severe disease, all cases followed a clinical course similar to “a typical attack of moderate pancreatitis,” the investigators wrote.
All patients were treated with IV fluids, four out of five received broad-spectrum IV antibiotics for pneumonitis, three out of five received fibrate and/or insulin therapy, and two out of five received pancreatic enzyme replacement therapy. No patients required corticosteroids, organ support, or respiratory support beyond low-flow oxygen. Median hospital stay was 14 days.
“We ... propose the combination of male sex, abdominal pain, metabolic stress, and CT-findings of predominantly pancreatico-duodenal inflammation with steatosis represent a distinct subset of pancreatitis in patients infected with SARS-CoV-2,” the investigators wrote.
They suggested that the endocrine pancreas may be “particularly vulnerable to this infection,” citing prolonged hospital stays because of poor diabetic control.
“[T]ransient dyslipidemias and impaired glucose tolerance may be common in SARS-CoV-2 patients and warrant further investigation,” they concluded.
Oscar J. Hines, MD, chief of the division of general surgery at UCLA Medical Center and leader in the field of pancreatitis management, said that the case series has a limited impact.
“The findings are unlikely to change practice and only call attention for physicians to the possibility of pancreatitis in COVID-positive patients,” Dr. Hines said.
The investigators reported grants from NIHR, Wellcome Trust, Mylan, and others.
SOURCE: Szatmary P et al. Gastroenterology. 2020 Jun 1. doi: 10.1053/j.gastro.2020.05.069.
FROM GASTROENTEROLOGY
First reported U.S. case of COVID-19 linked to Guillain-Barré syndrome
further supporting a link between the virus and neurologic complications, including GBS.
Physicians in China reported the first case of COVID-19 that initially presented as acute GBS. The patient was a 61-year-old woman returning home from Wuhan during the pandemic.
Subsequently, physicians in Italy reported five cases of GBS in association with COVID-19.
The first U.S. case is described in the June issue of the Journal of Clinical Neuromuscular Disease.
Like cases from China and Italy, the U.S. patient’s symptoms of GBS reportedly occurred within days of being infected with SARS-CoV-2. “This onset is similar to a case report of acute Zika virus infection with concurrent GBS suggesting a parainfectious complication,” first author Sandeep Rana, MD, and colleagues noted.
The 54-year-old man was transferred to Allegheny General Hospital after developing ascending limb weakness and numbness that followed symptoms of a respiratory infection. Two weeks earlier, he initially developed rhinorrhea, odynophagia, fevers, chills, and night sweats. The man reported that his wife had tested positive for COVID-19 and that his symptoms started soon after her illness. The man also tested positive for COVID-19.
His deficits were characterized by quadriparesis and areflexia, burning dysesthesias, mild ophthalmoparesis, and dysautonomia. He did not have the loss of smell and taste documented in other COVID-19 patients. He briefly required mechanical ventilation and was successfully weaned after receiving a course of intravenous immunoglobulin.
Compared with other cases reported in the literature, the unique clinical features in the U.S. case are urinary retention secondary to dysautonomia and ocular symptoms of diplopia. These highlight the variability in the clinical presentation of GBS associated with COVID-19, the researchers noted.
They added that, with the Pittsburgh patient, electrophysiological findings were typical of demyelinating polyneuropathy seen in patients with GBS. The case series from Italy suggests that axonal variants could be as common in COVID-19–associated GBS.
“Although the number of documented cases internationally is notably small to date, it’s not completely surprising that a COVID-19 diagnosis may lead to a patient developing GBS. The increase of inflammation and inflammatory cells caused by the infection may trigger an irregular immune response that leads to the hallmark symptoms of this neurological disorder,” Dr. Rana said in a news release.
“Since GBS can significantly affect the respiratory system and other vital organs being pushed into overdrive during a COVID-19 immune response, it will be critically important to further investigate and understand this potential connection,” he added.
A version of this article originally appeared on Medscape.com.
further supporting a link between the virus and neurologic complications, including GBS.
Physicians in China reported the first case of COVID-19 that initially presented as acute GBS. The patient was a 61-year-old woman returning home from Wuhan during the pandemic.
Subsequently, physicians in Italy reported five cases of GBS in association with COVID-19.
The first U.S. case is described in the June issue of the Journal of Clinical Neuromuscular Disease.
Like cases from China and Italy, the U.S. patient’s symptoms of GBS reportedly occurred within days of being infected with SARS-CoV-2. “This onset is similar to a case report of acute Zika virus infection with concurrent GBS suggesting a parainfectious complication,” first author Sandeep Rana, MD, and colleagues noted.
The 54-year-old man was transferred to Allegheny General Hospital after developing ascending limb weakness and numbness that followed symptoms of a respiratory infection. Two weeks earlier, he initially developed rhinorrhea, odynophagia, fevers, chills, and night sweats. The man reported that his wife had tested positive for COVID-19 and that his symptoms started soon after her illness. The man also tested positive for COVID-19.
His deficits were characterized by quadriparesis and areflexia, burning dysesthesias, mild ophthalmoparesis, and dysautonomia. He did not have the loss of smell and taste documented in other COVID-19 patients. He briefly required mechanical ventilation and was successfully weaned after receiving a course of intravenous immunoglobulin.
Compared with other cases reported in the literature, the unique clinical features in the U.S. case are urinary retention secondary to dysautonomia and ocular symptoms of diplopia. These highlight the variability in the clinical presentation of GBS associated with COVID-19, the researchers noted.
They added that, with the Pittsburgh patient, electrophysiological findings were typical of demyelinating polyneuropathy seen in patients with GBS. The case series from Italy suggests that axonal variants could be as common in COVID-19–associated GBS.
“Although the number of documented cases internationally is notably small to date, it’s not completely surprising that a COVID-19 diagnosis may lead to a patient developing GBS. The increase of inflammation and inflammatory cells caused by the infection may trigger an irregular immune response that leads to the hallmark symptoms of this neurological disorder,” Dr. Rana said in a news release.
“Since GBS can significantly affect the respiratory system and other vital organs being pushed into overdrive during a COVID-19 immune response, it will be critically important to further investigate and understand this potential connection,” he added.
A version of this article originally appeared on Medscape.com.
further supporting a link between the virus and neurologic complications, including GBS.
Physicians in China reported the first case of COVID-19 that initially presented as acute GBS. The patient was a 61-year-old woman returning home from Wuhan during the pandemic.
Subsequently, physicians in Italy reported five cases of GBS in association with COVID-19.
The first U.S. case is described in the June issue of the Journal of Clinical Neuromuscular Disease.
Like cases from China and Italy, the U.S. patient’s symptoms of GBS reportedly occurred within days of being infected with SARS-CoV-2. “This onset is similar to a case report of acute Zika virus infection with concurrent GBS suggesting a parainfectious complication,” first author Sandeep Rana, MD, and colleagues noted.
The 54-year-old man was transferred to Allegheny General Hospital after developing ascending limb weakness and numbness that followed symptoms of a respiratory infection. Two weeks earlier, he initially developed rhinorrhea, odynophagia, fevers, chills, and night sweats. The man reported that his wife had tested positive for COVID-19 and that his symptoms started soon after her illness. The man also tested positive for COVID-19.
His deficits were characterized by quadriparesis and areflexia, burning dysesthesias, mild ophthalmoparesis, and dysautonomia. He did not have the loss of smell and taste documented in other COVID-19 patients. He briefly required mechanical ventilation and was successfully weaned after receiving a course of intravenous immunoglobulin.
Compared with other cases reported in the literature, the unique clinical features in the U.S. case are urinary retention secondary to dysautonomia and ocular symptoms of diplopia. These highlight the variability in the clinical presentation of GBS associated with COVID-19, the researchers noted.
They added that, with the Pittsburgh patient, electrophysiological findings were typical of demyelinating polyneuropathy seen in patients with GBS. The case series from Italy suggests that axonal variants could be as common in COVID-19–associated GBS.
“Although the number of documented cases internationally is notably small to date, it’s not completely surprising that a COVID-19 diagnosis may lead to a patient developing GBS. The increase of inflammation and inflammatory cells caused by the infection may trigger an irregular immune response that leads to the hallmark symptoms of this neurological disorder,” Dr. Rana said in a news release.
“Since GBS can significantly affect the respiratory system and other vital organs being pushed into overdrive during a COVID-19 immune response, it will be critically important to further investigate and understand this potential connection,” he added.
A version of this article originally appeared on Medscape.com.
The merger of personal and professional: A psychologist’s experience with the effects of COVID-19
The concepts of days, weeks, and months have all but lost their meaning during the times of coronavirus. This became all too clear when I found myself weeks into June before realizing that we were in the second half of 2020. The world has been in the grips of COVID-19 (the disease caused by SARS-CoV-2) for over half a year, and the end is still not in sight. Even more chilling is the fact that the virus’s effects will continue to be felt by humanity for years to come.

By now, most of us have been affected by COVID-19, whether directly or indirectly. Consequently, we’ve seen that the psychological toll the pandemic takes is as wide ranging as the disease caused by the novel coronavirus itself. Confusion, denial, fear, anxiety, depression/sadness, and emotional dysregulation have become all too common an experience. Many mental health experts have even likened our psychological response to COVID-19 to that of trauma survivors.
In early 2020, triggered by two separate but related threats. In addition to concerns regarding COVID-19, we also began to experience fear for our physical safety as anti-Chinese sentiment began to rise across the country and the world. Discrimination and acts of violence toward Chinese people worldwide began to spread almost as rapidly as the virus itself. Anxiety and fear became a common daily experience of countless people, myself included.
In late March, amid coping with existing stressors, my situation became significantly worse when my brother, a New York City firefighter, contracted COVID-19 while working on the front lines. Shortly thereafter, my parents, both aged 60 years and older, with whom my brother shares a home, contracted the virus as well. My anxiety triggers related to the spread of the virus and xenophobia suddenly became a distant memory. I now found myself grappling with the much greater fear of losing my entire family.
At the time, the availability of testing was very limited, even for those working on the front lines. Although not without a short delay, my brother was able to access testing through Fire Department of New York connections. After about 3 weeks in self-isolation at home and with the use of over the counter pain relievers, he made a full recovery and returned to work. My parents, on the other hand, were placed at the end of a weeks-long line for testing, during which time their conditions deteriorated. Nine days following the onset of my mother’s symptoms, her condition had gotten so bad, she required hospitalization. Six days later, my father followed suit.
Being in the epicenter of the COVID-19 outbreak, New York hospitals were severely overwhelmed. Upon admission, my mother was held in the ED and other temporary open spaces in the hospital for nearly 24 hours because there was a lack of available patient rooms. During this time, she was packed into small spaces with dozens of other patients afflicted with the same disease. Four days later, she was transferred to a different hospital 10 miles away to make room for new patients. Decisions needed to be made rapidly and often with limited communication, which made for a roller coaster of emotions that would not relent.
Confusion. One of the few things we know with certainty about coronavirus is how much we don’t know. The Centers for Disease Control and Prevention data indicate that older adults with underlying health conditions have worse outcomes. Yet my mother, who is younger and in better physical health than my father, became much sicker in a drastically shorter period of time. Furthermore, my parents’ symptoms were completely inconsistent with one another’s. Based on their symptoms alone, it appeared as though they were suffering with different conditions entirely. My mother experienced body aches and gastrointestinal symptoms, whereas my father developed the typical cough and fever associated with COVID-19. In addition to confusion regarding their symptoms and, therefore, in determining the best at-home supportive care prior to their hospitalizations, the lack of available testing made the very question of whether they even had COVID-19 an uncertainty.
Denial. When my family members first became symptomatic, I found myself in a state of denial not unlike that of individuals experiencing grief. I frequently engaged in both internal and external dialogues in which I would attempt to convince myself of the reasons why my family did not have COVID-19.
“My brother wears PPE while at work.”
“My father’s cough was mild.”
“My mother does not have a cough or a fever.”
Despite knowing better, I was initially unable to accept that everyone in my family had contracted a disease that had already claimed the lives of tens of thousands globally.
Fear. In order to prevent the spread of infection, many hospitals made changes to their visitor policies, placing greater restrictions on who can come and go. This has meant hospital patients who have died from COVID-19 complications have done so separated from their loved ones. After transporting my mother to the hospital ED, I was politely but firmly asked to leave per the new visitor policy. I felt as though there were cinder blocks attached to my feet as I reluctantly walked away, not knowing if it would be the last time I would see her. I experienced a fear and sadness so intense, it continues to elicit an emotional response today as I think back on that moment.
Anxiety. The difference between fear and anxiety is fear is an emotional response to a known threat or danger, and anxiety is a response to an unknown threat or danger. The days that followed my parents’ hospitalizations were riddled with anxiety that would come in waves. How were they doing? Could they breathe? Do the overwhelmed hospital staff have time to take care of them? What can I do to help? Is there anything I can do to help? The worrisome thoughts and unanswerable questions were incessant and seemed unresponsive to my efforts to quell them.
Sadness. To feel sadness is to be human. In my work as a psychologist, I emphasize the value in experiencing this emotion when therapeutically beneficial. This technique is used as part of acceptance and commitment therapy (ACT), which emphasizes the value of being present or in touch with one’s thoughts and emotions, instead of working to eliminate them. During these scary times, I leaned into this notion more than ever. I gave myself permission to not feel okay, to cry more than I had in a long time, and to be unapologetically sad. I flip-flopped between states of near-despair and hopeful, with the switch usually following a call from a member of the hospital care team with updates on my parents’ conditions.
My parents’ road to recovery extended far beyond their discharge from the hospital and was not without incident, but with support and appropriate follow-up care, they have since made full recoveries from COVID-19. Although the relief and happiness this brings me is immeasurable, the experience has left a lasting impression on me as both a person and a psychologist. Speaking as a person, I cannot overstate the value of relying on one’s social support network while coping with stressors related to COVID-19. Whether you are directly or indirectly affected by the disease, the emotional effects can feel equally intense. As in times of happiness and celebration, times of sadness can and should be shared by those who are equipped to provide support. This can be tricky in an era during which isolation is prescribed for our safety, but we have more options today for connecting virtually with others than ever before, including video conferencing, email, and that old friend, the telephone. Furthermore, identify and assert your boundaries. Sometimes, saying no to others is the best way to say yes to yourself. Certain work, chores, and social obligations that can wait, should wait.
As a psychologist, my experience has given me a renewed appreciation for the power of the therapeutic use of self in psychotherapy. The factor with the greatest effects on psychotherapy outcomes is the quality of the therapeutic alliance, a concept introduced by Sigmund Freud in 1912. I believe a therapist’s willingness to show that we, too, experience life’s ups and downs strengthens our ability to demonstrate empathy and further promote a sense of alliance. Therapists are not immune to the effects of COVID-19, and to acknowledge this fact allows us to relate to our patients on a basic human level, which is more important now than ever.
Dr. Tseng, a licensed clinical psychologist, is in private practice in New York. She disclosed no relevant financial relationships.
The concepts of days, weeks, and months have all but lost their meaning during the times of coronavirus. This became all too clear when I found myself weeks into June before realizing that we were in the second half of 2020. The world has been in the grips of COVID-19 (the disease caused by SARS-CoV-2) for over half a year, and the end is still not in sight. Even more chilling is the fact that the virus’s effects will continue to be felt by humanity for years to come.
By now, most of us have been affected by COVID-19, whether directly or indirectly. Consequently, we’ve seen that the psychological toll the pandemic takes is as wide ranging as the disease caused by the novel coronavirus itself. Confusion, denial, fear, anxiety, depression/sadness, and emotional dysregulation have become all too common an experience. Many mental health experts have even likened our psychological response to COVID-19 to that of trauma survivors.
In early 2020, triggered by two separate but related threats. In addition to concerns regarding COVID-19, we also began to experience fear for our physical safety as anti-Chinese sentiment began to rise across the country and the world. Discrimination and acts of violence toward Chinese people worldwide began to spread almost as rapidly as the virus itself. Anxiety and fear became a common daily experience of countless people, myself included.
In late March, amid coping with existing stressors, my situation became significantly worse when my brother, a New York City firefighter, contracted COVID-19 while working on the front lines. Shortly thereafter, my parents, both aged 60 years and older, with whom my brother shares a home, contracted the virus as well. My anxiety triggers related to the spread of the virus and xenophobia suddenly became a distant memory. I now found myself grappling with the much greater fear of losing my entire family.
At the time, the availability of testing was very limited, even for those working on the front lines. Although not without a short delay, my brother was able to access testing through Fire Department of New York connections. After about 3 weeks in self-isolation at home and with the use of over the counter pain relievers, he made a full recovery and returned to work. My parents, on the other hand, were placed at the end of a weeks-long line for testing, during which time their conditions deteriorated. Nine days following the onset of my mother’s symptoms, her condition had gotten so bad, she required hospitalization. Six days later, my father followed suit.
Being in the epicenter of the COVID-19 outbreak, New York hospitals were severely overwhelmed. Upon admission, my mother was held in the ED and other temporary open spaces in the hospital for nearly 24 hours because there was a lack of available patient rooms. During this time, she was packed into small spaces with dozens of other patients afflicted with the same disease. Four days later, she was transferred to a different hospital 10 miles away to make room for new patients. Decisions needed to be made rapidly and often with limited communication, which made for a roller coaster of emotions that would not relent.
Confusion. One of the few things we know with certainty about coronavirus is how much we don’t know. The Centers for Disease Control and Prevention data indicate that older adults with underlying health conditions have worse outcomes. Yet my mother, who is younger and in better physical health than my father, became much sicker in a drastically shorter period of time. Furthermore, my parents’ symptoms were completely inconsistent with one another’s. Based on their symptoms alone, it appeared as though they were suffering with different conditions entirely. My mother experienced body aches and gastrointestinal symptoms, whereas my father developed the typical cough and fever associated with COVID-19. In addition to confusion regarding their symptoms and, therefore, in determining the best at-home supportive care prior to their hospitalizations, the lack of available testing made the very question of whether they even had COVID-19 an uncertainty.
Denial. When my family members first became symptomatic, I found myself in a state of denial not unlike that of individuals experiencing grief. I frequently engaged in both internal and external dialogues in which I would attempt to convince myself of the reasons why my family did not have COVID-19.
“My brother wears PPE while at work.”
“My father’s cough was mild.”
“My mother does not have a cough or a fever.”
Despite knowing better, I was initially unable to accept that everyone in my family had contracted a disease that had already claimed the lives of tens of thousands globally.
Fear. In order to prevent the spread of infection, many hospitals made changes to their visitor policies, placing greater restrictions on who can come and go. This has meant hospital patients who have died from COVID-19 complications have done so separated from their loved ones. After transporting my mother to the hospital ED, I was politely but firmly asked to leave per the new visitor policy. I felt as though there were cinder blocks attached to my feet as I reluctantly walked away, not knowing if it would be the last time I would see her. I experienced a fear and sadness so intense, it continues to elicit an emotional response today as I think back on that moment.
Anxiety. The difference between fear and anxiety is fear is an emotional response to a known threat or danger, and anxiety is a response to an unknown threat or danger. The days that followed my parents’ hospitalizations were riddled with anxiety that would come in waves. How were they doing? Could they breathe? Do the overwhelmed hospital staff have time to take care of them? What can I do to help? Is there anything I can do to help? The worrisome thoughts and unanswerable questions were incessant and seemed unresponsive to my efforts to quell them.
Sadness. To feel sadness is to be human. In my work as a psychologist, I emphasize the value in experiencing this emotion when therapeutically beneficial. This technique is used as part of acceptance and commitment therapy (ACT), which emphasizes the value of being present or in touch with one’s thoughts and emotions, instead of working to eliminate them. During these scary times, I leaned into this notion more than ever. I gave myself permission to not feel okay, to cry more than I had in a long time, and to be unapologetically sad. I flip-flopped between states of near-despair and hopeful, with the switch usually following a call from a member of the hospital care team with updates on my parents’ conditions.
My parents’ road to recovery extended far beyond their discharge from the hospital and was not without incident, but with support and appropriate follow-up care, they have since made full recoveries from COVID-19. Although the relief and happiness this brings me is immeasurable, the experience has left a lasting impression on me as both a person and a psychologist. Speaking as a person, I cannot overstate the value of relying on one’s social support network while coping with stressors related to COVID-19. Whether you are directly or indirectly affected by the disease, the emotional effects can feel equally intense. As in times of happiness and celebration, times of sadness can and should be shared by those who are equipped to provide support. This can be tricky in an era during which isolation is prescribed for our safety, but we have more options today for connecting virtually with others than ever before, including video conferencing, email, and that old friend, the telephone. Furthermore, identify and assert your boundaries. Sometimes, saying no to others is the best way to say yes to yourself. Certain work, chores, and social obligations that can wait, should wait.
As a psychologist, my experience has given me a renewed appreciation for the power of the therapeutic use of self in psychotherapy. The factor with the greatest effects on psychotherapy outcomes is the quality of the therapeutic alliance, a concept introduced by Sigmund Freud in 1912. I believe a therapist’s willingness to show that we, too, experience life’s ups and downs strengthens our ability to demonstrate empathy and further promote a sense of alliance. Therapists are not immune to the effects of COVID-19, and to acknowledge this fact allows us to relate to our patients on a basic human level, which is more important now than ever.
Dr. Tseng, a licensed clinical psychologist, is in private practice in New York. She disclosed no relevant financial relationships.
The concepts of days, weeks, and months have all but lost their meaning during the times of coronavirus. This became all too clear when I found myself weeks into June before realizing that we were in the second half of 2020. The world has been in the grips of COVID-19 (the disease caused by SARS-CoV-2) for over half a year, and the end is still not in sight. Even more chilling is the fact that the virus’s effects will continue to be felt by humanity for years to come.
By now, most of us have been affected by COVID-19, whether directly or indirectly. Consequently, we’ve seen that the psychological toll the pandemic takes is as wide ranging as the disease caused by the novel coronavirus itself. Confusion, denial, fear, anxiety, depression/sadness, and emotional dysregulation have become all too common an experience. Many mental health experts have even likened our psychological response to COVID-19 to that of trauma survivors.
In early 2020, triggered by two separate but related threats. In addition to concerns regarding COVID-19, we also began to experience fear for our physical safety as anti-Chinese sentiment began to rise across the country and the world. Discrimination and acts of violence toward Chinese people worldwide began to spread almost as rapidly as the virus itself. Anxiety and fear became a common daily experience of countless people, myself included.
In late March, amid coping with existing stressors, my situation became significantly worse when my brother, a New York City firefighter, contracted COVID-19 while working on the front lines. Shortly thereafter, my parents, both aged 60 years and older, with whom my brother shares a home, contracted the virus as well. My anxiety triggers related to the spread of the virus and xenophobia suddenly became a distant memory. I now found myself grappling with the much greater fear of losing my entire family.
At the time, the availability of testing was very limited, even for those working on the front lines. Although not without a short delay, my brother was able to access testing through Fire Department of New York connections. After about 3 weeks in self-isolation at home and with the use of over the counter pain relievers, he made a full recovery and returned to work. My parents, on the other hand, were placed at the end of a weeks-long line for testing, during which time their conditions deteriorated. Nine days following the onset of my mother’s symptoms, her condition had gotten so bad, she required hospitalization. Six days later, my father followed suit.
Being in the epicenter of the COVID-19 outbreak, New York hospitals were severely overwhelmed. Upon admission, my mother was held in the ED and other temporary open spaces in the hospital for nearly 24 hours because there was a lack of available patient rooms. During this time, she was packed into small spaces with dozens of other patients afflicted with the same disease. Four days later, she was transferred to a different hospital 10 miles away to make room for new patients. Decisions needed to be made rapidly and often with limited communication, which made for a roller coaster of emotions that would not relent.
Confusion. One of the few things we know with certainty about coronavirus is how much we don’t know. The Centers for Disease Control and Prevention data indicate that older adults with underlying health conditions have worse outcomes. Yet my mother, who is younger and in better physical health than my father, became much sicker in a drastically shorter period of time. Furthermore, my parents’ symptoms were completely inconsistent with one another’s. Based on their symptoms alone, it appeared as though they were suffering with different conditions entirely. My mother experienced body aches and gastrointestinal symptoms, whereas my father developed the typical cough and fever associated with COVID-19. In addition to confusion regarding their symptoms and, therefore, in determining the best at-home supportive care prior to their hospitalizations, the lack of available testing made the very question of whether they even had COVID-19 an uncertainty.
Denial. When my family members first became symptomatic, I found myself in a state of denial not unlike that of individuals experiencing grief. I frequently engaged in both internal and external dialogues in which I would attempt to convince myself of the reasons why my family did not have COVID-19.
“My brother wears PPE while at work.”
“My father’s cough was mild.”
“My mother does not have a cough or a fever.”
Despite knowing better, I was initially unable to accept that everyone in my family had contracted a disease that had already claimed the lives of tens of thousands globally.
Fear. In order to prevent the spread of infection, many hospitals made changes to their visitor policies, placing greater restrictions on who can come and go. This has meant hospital patients who have died from COVID-19 complications have done so separated from their loved ones. After transporting my mother to the hospital ED, I was politely but firmly asked to leave per the new visitor policy. I felt as though there were cinder blocks attached to my feet as I reluctantly walked away, not knowing if it would be the last time I would see her. I experienced a fear and sadness so intense, it continues to elicit an emotional response today as I think back on that moment.
Anxiety. The difference between fear and anxiety is fear is an emotional response to a known threat or danger, and anxiety is a response to an unknown threat or danger. The days that followed my parents’ hospitalizations were riddled with anxiety that would come in waves. How were they doing? Could they breathe? Do the overwhelmed hospital staff have time to take care of them? What can I do to help? Is there anything I can do to help? The worrisome thoughts and unanswerable questions were incessant and seemed unresponsive to my efforts to quell them.
Sadness. To feel sadness is to be human. In my work as a psychologist, I emphasize the value in experiencing this emotion when therapeutically beneficial. This technique is used as part of acceptance and commitment therapy (ACT), which emphasizes the value of being present or in touch with one’s thoughts and emotions, instead of working to eliminate them. During these scary times, I leaned into this notion more than ever. I gave myself permission to not feel okay, to cry more than I had in a long time, and to be unapologetically sad. I flip-flopped between states of near-despair and hopeful, with the switch usually following a call from a member of the hospital care team with updates on my parents’ conditions.
My parents’ road to recovery extended far beyond their discharge from the hospital and was not without incident, but with support and appropriate follow-up care, they have since made full recoveries from COVID-19. Although the relief and happiness this brings me is immeasurable, the experience has left a lasting impression on me as both a person and a psychologist. Speaking as a person, I cannot overstate the value of relying on one’s social support network while coping with stressors related to COVID-19. Whether you are directly or indirectly affected by the disease, the emotional effects can feel equally intense. As in times of happiness and celebration, times of sadness can and should be shared by those who are equipped to provide support. This can be tricky in an era during which isolation is prescribed for our safety, but we have more options today for connecting virtually with others than ever before, including video conferencing, email, and that old friend, the telephone. Furthermore, identify and assert your boundaries. Sometimes, saying no to others is the best way to say yes to yourself. Certain work, chores, and social obligations that can wait, should wait.
As a psychologist, my experience has given me a renewed appreciation for the power of the therapeutic use of self in psychotherapy. The factor with the greatest effects on psychotherapy outcomes is the quality of the therapeutic alliance, a concept introduced by Sigmund Freud in 1912. I believe a therapist’s willingness to show that we, too, experience life’s ups and downs strengthens our ability to demonstrate empathy and further promote a sense of alliance. Therapists are not immune to the effects of COVID-19, and to acknowledge this fact allows us to relate to our patients on a basic human level, which is more important now than ever.
Dr. Tseng, a licensed clinical psychologist, is in private practice in New York. She disclosed no relevant financial relationships.
What COVID-19 has taught us about senior care
Across the globe, there are marked differences in how countries responded to the COVID-19 outbreak, with varying degrees of success in limiting the spread of the virus. Some countries learned important lessons from previous outbreaks, including SARS and MERS, and put policies in place that contributed to lower infection and death rates from COVID-19 in these countries. Others struggled to respond appropriately to the outbreak.

The United States and most of the world was not affected significantly by SARS and MERS. Hence there is a need for different perspectives and observations on lessons that can be learned from this outbreak to help develop effective strategies and policies for the future. It also makes sense to focus intently on the demographic most affected by COVID-19 – the elderly.
Medical care, for the most part, is governed by protocols that clearly detail processes to be followed for the prevention and treatment of disease. Caring for older patients requires going above and beyond the protocols. That is one of the lessons learned from the COVID-19 pandemic – a wake-up call for a more proactive approach for at-risk patients, in this case everyone over the age of 60 years.
In this context, it is important for medical outreach to continue with the senior population long after the pandemic has run its course. Many seniors, particularly those susceptible to other illnesses or exhibiting ongoing issues, would benefit from a consistent and preplanned pattern of contacts by medical professionals and agencies that work with the aging population. These proactive follow-ups can facilitate prevention and treatment and, at the same time, reduce costs that would otherwise increase when health care is reactive.
Lessons in infectious disease containment
As COVID-19 spread globally, there were contrasting responses from individual countries in their efforts to contain the disease. Unfortunately, Italy suffered from its decision to lock down only specific regions of the country initially. The leadership in Italy may have ignored the advice of medical experts and been caught off guard by the intensity of the spread of COVID-19. In fact, they might not have taken strict actions right away because they did not want their responses to be viewed as an overreaction to the disease.
The government decided to shut down areas where the infection rates were high (“red zones”) rather than implement restrictions nationally. This may have inadvertently increased the spread as Italians vacated those “red zones” for other areas of the country not yet affected by COVID-19. Italy’s decentralized health care system also played a part in the effects of the disease, with some regions demonstrating more success in slowing the reach of the disease. According to an article in the Harvard Business Review, the neighboring regions of Lombardy and Veneto applied similar approaches to social distancing and retail closures. Veneto was more proactive, and its response to the outbreak was multipronged, including putting a “strong emphasis on home diagnosis and care” and “specific efforts to monitor and protect health care and other essential workers.” These measures most likely contributed to a slowdown of the spread of the disease in Veneto’s health care facilities, which lessened the load on medical providers.1
Conversely, Taiwan implemented proactive measures swiftly after learning about COVID-19. Taiwan was impacted adversely by the SARS outbreak in 2003 and, afterward, revised their medical policies and procedures to respond quickly to future infectious disease crises. In the beginning, little was known about COVID-19 or how it spread. However, Taiwan’s swift public health response to COVID-19 included early travel restrictions, patient screening, and quarantining of symptomatic patients. The government emphasized education and created real-time digital updates and alerts sent to their citizens, as well as partnering with media to broadcast crucial proactive health information and quickly disproving false information related to COVID-19. They coordinated with organizations throughout the country to increase supplies of personal protective equipment (PPE).2
Although countries and even cities within a country differ in terms of population demographics, health resources, government policies, and cultural practices, initial success stories have some similarities, including the following:
- Early travel restrictions from countries with positive cases, with some circumstances requiring compulsory quarantine periods and testing before entry.
- Extensive testing and proactive tracing of symptomatic cases early. Contacts of people testing positive were also tested, irrespective of being symptomatic or asymptomatic. If testing kits were unavailable, the contacts were self-quarantined.
- Emphasis on avoiding overburdening hospitals by having the public health infrastructure to divert people exhibiting symptoms, including using public health hotlines to send patients to dedicated testing sites and drive-through testing, rather than have patients presenting to emergency rooms and hospitals. This approach protected medical staff from exposure and allowed the focus to remain on treating severe symptomatic patients.

The vastly different response to the COVID-19 outbreak in these two countries illuminates the need for better preparation in the United States. At the onset of this outbreak, emergency room medical professionals, hospitalists, and outpatient primary care providers did not know how to screen for or treat this virus. Additionally, there was limited information on the most effective contact protocols for medical professionals, patients, and visitors. Finally, the lack of PPE and COVID-19 test kits hindered the U.S. response. Once the country is on the road to recovery from COVID-19, it is imperative to set the groundwork to prepare for future outbreaks and create mechanisms to quickly identify vulnerable populations when outbreaks occur.
Senior care in future infectious disease outbreaks
How can medical providers translate lessons learned from this outbreak into improving the quality of care for seniors? The National Institute on Aging (NIA) maintains a website with information about healthy aging. Seniors and their caregivers can use this website to learn more about chronic diseases, lifestyle modifications, disease prevention, and mental health.
In times of a pandemic, this website provides consistent and accurate information and education. One recommendation for reaching the elderly population during future outbreaks is for NIA to develop and implement strategies to increase the use of the website, including adding more audio and visual interfaces and developing a mobile app. Other recommendations for improving the quality of care for seniors include the following:
1. Identify which populations may be most affected when future outbreaks occur.
2. Consider nontraditional platforms, including social media, for communicating with the general population and for medical providers worldwide to learn from each other about new diseases, including the signs, symptoms, and treatment plans. Some medical professionals created specific WhatsApp groups to communicate, and the World Health Organization sent updated information about COVID-19 to anyone who texted them via WhatsApp.3
3. Create a checklist of signs and symptoms related to current infectious diseases and assess every vulnerable patient.
4. Share these guidelines with medical facilities that treat these populations, such as senior care, assisted living and rehabilitation facilities, hospitals, and outpatient treatment centers. Teach the staff at these medical facilities how to screen patients for signs and symptoms of the disease.
5. Implement social isolation strategies, travel and visitor restrictions, and testing and screening as soon as possible at these medical facilities.
6. Recognize that these strategies may affect the psychological and emotional well-being of seniors, increasing their risk for depression and anxiety and negatively affecting their immunity and mental health. Additionally, the use of PPE, either by the medical providers or the patient, may cause anxiety in seniors and those with mild cognitive impairment.
7. Encourage these medical facilities to improve coping strategies with older patients, such as incorporating communication technology that helps seniors stay connected with their families, and participating in physical and mental exercise, as well as religious activities.
8. Ask these medical facilities to create isolation or quarantine rooms for infected seniors.
9. Work with family members to proactively report to medical professionals any symptoms noticed in their senior relatives. Educate seniors to report symptoms earlier.
10. Offer incentives for medical professionals to conduct on-site testing in primary care offices or senior care facilities instead of sending patients to hospital emergency rooms for evaluation. This will only be effective if there are enough test kits available.
11. Urge insurance companies and Medicare to allow additional medical visits for screening vulnerable populations. Encourage the use of telemedicine in place of in-office visits (preferably billed at the same rate as an in-office visit) where appropriate, especially with nonambulatory patients or those with transportation issues. Many insurance companies, including Medicare, approved COVID-19–related coverage of telemedicine in place of office visits to limit the spread of the disease.
12. Provide community health care and integration and better coordination of local, state, and national health care.
13. Hold regular epidemic and pandemic preparedness exercises in every hospital, nursing home, and assisted living facility.
Proactive health care outreach
It is easier to identify the signs and symptoms of already identified infectious diseases as opposed to a novel one like COVID-19. The United States faced a steep learning curve with COVID-19. Hospitalists and other medical professionals were not able to learn about COVID-19 in a journal. At first, they did not know how to screen patients coming into the ER, how to protect staff, or what the treatment plan was for this new disease. As a result, the medical system experienced disorder and confusion. Investing in community health care and better coordination of local, state, and national health care resources is a priority.
The senior citizen population appears to be most vulnerable to this virus and may be just as vulnerable in future outbreaks. Yet the insights gained from this pandemic can lead to a more comprehensive outreach to senior patients and increased screenings for comorbidities and future contagious diseases. An emphasis on proactive health care and outreach for seniors, with a focus on identifying and treating comorbid conditions, improves the medical care system overall and may prevent or slow future community outbreaks.
Dr. Kasarla is a hospitalist with APOGEE Physicians at Wise Surgical at Parkway in Fort Worth, Tex. He did his internal medicine residency at Mercy Hospital & Medical Center, Chicago. Readers can contact him at madhukarreddy.kasarla@apogeephysicians.com. Dr. Devireddy is a family physician at Positive Health Medical Center, Kingston, Jamaica. Contact him at drjaisheel@gmail.com.
References
1. Pisano GP et al. Lessons from Italy’s response to coronavirus. Harvard Business Review. 2020 Mar 27. https://hbr.org/2020/03/lessons-from-italys-response-to-coronavirus.
2. Tu C. Lessons from Taiwan’s experience with COVID-19. New Atlanticist. 2020 Apr 7. https://atlanticcouncil.org/blogs/new-atlanticist/lessons-from-taiwans-experience-with-covid-19/.
3. Newman LH. WhatsApp is at the center of coronavirus response. WIRED. 2020 Mar 20. https://www.wired.com/story/whatsapp-coronavirus-who-information-app/.
Across the globe, there are marked differences in how countries responded to the COVID-19 outbreak, with varying degrees of success in limiting the spread of the virus. Some countries learned important lessons from previous outbreaks, including SARS and MERS, and put policies in place that contributed to lower infection and death rates from COVID-19 in these countries. Others struggled to respond appropriately to the outbreak.
The United States and most of the world was not affected significantly by SARS and MERS. Hence there is a need for different perspectives and observations on lessons that can be learned from this outbreak to help develop effective strategies and policies for the future. It also makes sense to focus intently on the demographic most affected by COVID-19 – the elderly.
Medical care, for the most part, is governed by protocols that clearly detail processes to be followed for the prevention and treatment of disease. Caring for older patients requires going above and beyond the protocols. That is one of the lessons learned from the COVID-19 pandemic – a wake-up call for a more proactive approach for at-risk patients, in this case everyone over the age of 60 years.
In this context, it is important for medical outreach to continue with the senior population long after the pandemic has run its course. Many seniors, particularly those susceptible to other illnesses or exhibiting ongoing issues, would benefit from a consistent and preplanned pattern of contacts by medical professionals and agencies that work with the aging population. These proactive follow-ups can facilitate prevention and treatment and, at the same time, reduce costs that would otherwise increase when health care is reactive.
Lessons in infectious disease containment
As COVID-19 spread globally, there were contrasting responses from individual countries in their efforts to contain the disease. Unfortunately, Italy suffered from its decision to lock down only specific regions of the country initially. The leadership in Italy may have ignored the advice of medical experts and been caught off guard by the intensity of the spread of COVID-19. In fact, they might not have taken strict actions right away because they did not want their responses to be viewed as an overreaction to the disease.
The government decided to shut down areas where the infection rates were high (“red zones”) rather than implement restrictions nationally. This may have inadvertently increased the spread as Italians vacated those “red zones” for other areas of the country not yet affected by COVID-19. Italy’s decentralized health care system also played a part in the effects of the disease, with some regions demonstrating more success in slowing the reach of the disease. According to an article in the Harvard Business Review, the neighboring regions of Lombardy and Veneto applied similar approaches to social distancing and retail closures. Veneto was more proactive, and its response to the outbreak was multipronged, including putting a “strong emphasis on home diagnosis and care” and “specific efforts to monitor and protect health care and other essential workers.” These measures most likely contributed to a slowdown of the spread of the disease in Veneto’s health care facilities, which lessened the load on medical providers.1
Conversely, Taiwan implemented proactive measures swiftly after learning about COVID-19. Taiwan was impacted adversely by the SARS outbreak in 2003 and, afterward, revised their medical policies and procedures to respond quickly to future infectious disease crises. In the beginning, little was known about COVID-19 or how it spread. However, Taiwan’s swift public health response to COVID-19 included early travel restrictions, patient screening, and quarantining of symptomatic patients. The government emphasized education and created real-time digital updates and alerts sent to their citizens, as well as partnering with media to broadcast crucial proactive health information and quickly disproving false information related to COVID-19. They coordinated with organizations throughout the country to increase supplies of personal protective equipment (PPE).2
Although countries and even cities within a country differ in terms of population demographics, health resources, government policies, and cultural practices, initial success stories have some similarities, including the following:
- Early travel restrictions from countries with positive cases, with some circumstances requiring compulsory quarantine periods and testing before entry.
- Extensive testing and proactive tracing of symptomatic cases early. Contacts of people testing positive were also tested, irrespective of being symptomatic or asymptomatic. If testing kits were unavailable, the contacts were self-quarantined.
- Emphasis on avoiding overburdening hospitals by having the public health infrastructure to divert people exhibiting symptoms, including using public health hotlines to send patients to dedicated testing sites and drive-through testing, rather than have patients presenting to emergency rooms and hospitals. This approach protected medical staff from exposure and allowed the focus to remain on treating severe symptomatic patients.
The vastly different response to the COVID-19 outbreak in these two countries illuminates the need for better preparation in the United States. At the onset of this outbreak, emergency room medical professionals, hospitalists, and outpatient primary care providers did not know how to screen for or treat this virus. Additionally, there was limited information on the most effective contact protocols for medical professionals, patients, and visitors. Finally, the lack of PPE and COVID-19 test kits hindered the U.S. response. Once the country is on the road to recovery from COVID-19, it is imperative to set the groundwork to prepare for future outbreaks and create mechanisms to quickly identify vulnerable populations when outbreaks occur.
Senior care in future infectious disease outbreaks
How can medical providers translate lessons learned from this outbreak into improving the quality of care for seniors? The National Institute on Aging (NIA) maintains a website with information about healthy aging. Seniors and their caregivers can use this website to learn more about chronic diseases, lifestyle modifications, disease prevention, and mental health.
In times of a pandemic, this website provides consistent and accurate information and education. One recommendation for reaching the elderly population during future outbreaks is for NIA to develop and implement strategies to increase the use of the website, including adding more audio and visual interfaces and developing a mobile app. Other recommendations for improving the quality of care for seniors include the following:
1. Identify which populations may be most affected when future outbreaks occur.
2. Consider nontraditional platforms, including social media, for communicating with the general population and for medical providers worldwide to learn from each other about new diseases, including the signs, symptoms, and treatment plans. Some medical professionals created specific WhatsApp groups to communicate, and the World Health Organization sent updated information about COVID-19 to anyone who texted them via WhatsApp.3
3. Create a checklist of signs and symptoms related to current infectious diseases and assess every vulnerable patient.
4. Share these guidelines with medical facilities that treat these populations, such as senior care, assisted living and rehabilitation facilities, hospitals, and outpatient treatment centers. Teach the staff at these medical facilities how to screen patients for signs and symptoms of the disease.
5. Implement social isolation strategies, travel and visitor restrictions, and testing and screening as soon as possible at these medical facilities.
6. Recognize that these strategies may affect the psychological and emotional well-being of seniors, increasing their risk for depression and anxiety and negatively affecting their immunity and mental health. Additionally, the use of PPE, either by the medical providers or the patient, may cause anxiety in seniors and those with mild cognitive impairment.
7. Encourage these medical facilities to improve coping strategies with older patients, such as incorporating communication technology that helps seniors stay connected with their families, and participating in physical and mental exercise, as well as religious activities.
8. Ask these medical facilities to create isolation or quarantine rooms for infected seniors.
9. Work with family members to proactively report to medical professionals any symptoms noticed in their senior relatives. Educate seniors to report symptoms earlier.
10. Offer incentives for medical professionals to conduct on-site testing in primary care offices or senior care facilities instead of sending patients to hospital emergency rooms for evaluation. This will only be effective if there are enough test kits available.
11. Urge insurance companies and Medicare to allow additional medical visits for screening vulnerable populations. Encourage the use of telemedicine in place of in-office visits (preferably billed at the same rate as an in-office visit) where appropriate, especially with nonambulatory patients or those with transportation issues. Many insurance companies, including Medicare, approved COVID-19–related coverage of telemedicine in place of office visits to limit the spread of the disease.
12. Provide community health care and integration and better coordination of local, state, and national health care.
13. Hold regular epidemic and pandemic preparedness exercises in every hospital, nursing home, and assisted living facility.
Proactive health care outreach
It is easier to identify the signs and symptoms of already identified infectious diseases as opposed to a novel one like COVID-19. The United States faced a steep learning curve with COVID-19. Hospitalists and other medical professionals were not able to learn about COVID-19 in a journal. At first, they did not know how to screen patients coming into the ER, how to protect staff, or what the treatment plan was for this new disease. As a result, the medical system experienced disorder and confusion. Investing in community health care and better coordination of local, state, and national health care resources is a priority.
The senior citizen population appears to be most vulnerable to this virus and may be just as vulnerable in future outbreaks. Yet the insights gained from this pandemic can lead to a more comprehensive outreach to senior patients and increased screenings for comorbidities and future contagious diseases. An emphasis on proactive health care and outreach for seniors, with a focus on identifying and treating comorbid conditions, improves the medical care system overall and may prevent or slow future community outbreaks.
Dr. Kasarla is a hospitalist with APOGEE Physicians at Wise Surgical at Parkway in Fort Worth, Tex. He did his internal medicine residency at Mercy Hospital & Medical Center, Chicago. Readers can contact him at madhukarreddy.kasarla@apogeephysicians.com. Dr. Devireddy is a family physician at Positive Health Medical Center, Kingston, Jamaica. Contact him at drjaisheel@gmail.com.
References
1. Pisano GP et al. Lessons from Italy’s response to coronavirus. Harvard Business Review. 2020 Mar 27. https://hbr.org/2020/03/lessons-from-italys-response-to-coronavirus.
2. Tu C. Lessons from Taiwan’s experience with COVID-19. New Atlanticist. 2020 Apr 7. https://atlanticcouncil.org/blogs/new-atlanticist/lessons-from-taiwans-experience-with-covid-19/.
3. Newman LH. WhatsApp is at the center of coronavirus response. WIRED. 2020 Mar 20. https://www.wired.com/story/whatsapp-coronavirus-who-information-app/.
Across the globe, there are marked differences in how countries responded to the COVID-19 outbreak, with varying degrees of success in limiting the spread of the virus. Some countries learned important lessons from previous outbreaks, including SARS and MERS, and put policies in place that contributed to lower infection and death rates from COVID-19 in these countries. Others struggled to respond appropriately to the outbreak.
The United States and most of the world was not affected significantly by SARS and MERS. Hence there is a need for different perspectives and observations on lessons that can be learned from this outbreak to help develop effective strategies and policies for the future. It also makes sense to focus intently on the demographic most affected by COVID-19 – the elderly.
Medical care, for the most part, is governed by protocols that clearly detail processes to be followed for the prevention and treatment of disease. Caring for older patients requires going above and beyond the protocols. That is one of the lessons learned from the COVID-19 pandemic – a wake-up call for a more proactive approach for at-risk patients, in this case everyone over the age of 60 years.
In this context, it is important for medical outreach to continue with the senior population long after the pandemic has run its course. Many seniors, particularly those susceptible to other illnesses or exhibiting ongoing issues, would benefit from a consistent and preplanned pattern of contacts by medical professionals and agencies that work with the aging population. These proactive follow-ups can facilitate prevention and treatment and, at the same time, reduce costs that would otherwise increase when health care is reactive.
Lessons in infectious disease containment
As COVID-19 spread globally, there were contrasting responses from individual countries in their efforts to contain the disease. Unfortunately, Italy suffered from its decision to lock down only specific regions of the country initially. The leadership in Italy may have ignored the advice of medical experts and been caught off guard by the intensity of the spread of COVID-19. In fact, they might not have taken strict actions right away because they did not want their responses to be viewed as an overreaction to the disease.
The government decided to shut down areas where the infection rates were high (“red zones”) rather than implement restrictions nationally. This may have inadvertently increased the spread as Italians vacated those “red zones” for other areas of the country not yet affected by COVID-19. Italy’s decentralized health care system also played a part in the effects of the disease, with some regions demonstrating more success in slowing the reach of the disease. According to an article in the Harvard Business Review, the neighboring regions of Lombardy and Veneto applied similar approaches to social distancing and retail closures. Veneto was more proactive, and its response to the outbreak was multipronged, including putting a “strong emphasis on home diagnosis and care” and “specific efforts to monitor and protect health care and other essential workers.” These measures most likely contributed to a slowdown of the spread of the disease in Veneto’s health care facilities, which lessened the load on medical providers.1
Conversely, Taiwan implemented proactive measures swiftly after learning about COVID-19. Taiwan was impacted adversely by the SARS outbreak in 2003 and, afterward, revised their medical policies and procedures to respond quickly to future infectious disease crises. In the beginning, little was known about COVID-19 or how it spread. However, Taiwan’s swift public health response to COVID-19 included early travel restrictions, patient screening, and quarantining of symptomatic patients. The government emphasized education and created real-time digital updates and alerts sent to their citizens, as well as partnering with media to broadcast crucial proactive health information and quickly disproving false information related to COVID-19. They coordinated with organizations throughout the country to increase supplies of personal protective equipment (PPE).2
Although countries and even cities within a country differ in terms of population demographics, health resources, government policies, and cultural practices, initial success stories have some similarities, including the following:
- Early travel restrictions from countries with positive cases, with some circumstances requiring compulsory quarantine periods and testing before entry.
- Extensive testing and proactive tracing of symptomatic cases early. Contacts of people testing positive were also tested, irrespective of being symptomatic or asymptomatic. If testing kits were unavailable, the contacts were self-quarantined.
- Emphasis on avoiding overburdening hospitals by having the public health infrastructure to divert people exhibiting symptoms, including using public health hotlines to send patients to dedicated testing sites and drive-through testing, rather than have patients presenting to emergency rooms and hospitals. This approach protected medical staff from exposure and allowed the focus to remain on treating severe symptomatic patients.
The vastly different response to the COVID-19 outbreak in these two countries illuminates the need for better preparation in the United States. At the onset of this outbreak, emergency room medical professionals, hospitalists, and outpatient primary care providers did not know how to screen for or treat this virus. Additionally, there was limited information on the most effective contact protocols for medical professionals, patients, and visitors. Finally, the lack of PPE and COVID-19 test kits hindered the U.S. response. Once the country is on the road to recovery from COVID-19, it is imperative to set the groundwork to prepare for future outbreaks and create mechanisms to quickly identify vulnerable populations when outbreaks occur.
Senior care in future infectious disease outbreaks
How can medical providers translate lessons learned from this outbreak into improving the quality of care for seniors? The National Institute on Aging (NIA) maintains a website with information about healthy aging. Seniors and their caregivers can use this website to learn more about chronic diseases, lifestyle modifications, disease prevention, and mental health.
In times of a pandemic, this website provides consistent and accurate information and education. One recommendation for reaching the elderly population during future outbreaks is for NIA to develop and implement strategies to increase the use of the website, including adding more audio and visual interfaces and developing a mobile app. Other recommendations for improving the quality of care for seniors include the following:
1. Identify which populations may be most affected when future outbreaks occur.
2. Consider nontraditional platforms, including social media, for communicating with the general population and for medical providers worldwide to learn from each other about new diseases, including the signs, symptoms, and treatment plans. Some medical professionals created specific WhatsApp groups to communicate, and the World Health Organization sent updated information about COVID-19 to anyone who texted them via WhatsApp.3
3. Create a checklist of signs and symptoms related to current infectious diseases and assess every vulnerable patient.
4. Share these guidelines with medical facilities that treat these populations, such as senior care, assisted living and rehabilitation facilities, hospitals, and outpatient treatment centers. Teach the staff at these medical facilities how to screen patients for signs and symptoms of the disease.
5. Implement social isolation strategies, travel and visitor restrictions, and testing and screening as soon as possible at these medical facilities.
6. Recognize that these strategies may affect the psychological and emotional well-being of seniors, increasing their risk for depression and anxiety and negatively affecting their immunity and mental health. Additionally, the use of PPE, either by the medical providers or the patient, may cause anxiety in seniors and those with mild cognitive impairment.
7. Encourage these medical facilities to improve coping strategies with older patients, such as incorporating communication technology that helps seniors stay connected with their families, and participating in physical and mental exercise, as well as religious activities.
8. Ask these medical facilities to create isolation or quarantine rooms for infected seniors.
9. Work with family members to proactively report to medical professionals any symptoms noticed in their senior relatives. Educate seniors to report symptoms earlier.
10. Offer incentives for medical professionals to conduct on-site testing in primary care offices or senior care facilities instead of sending patients to hospital emergency rooms for evaluation. This will only be effective if there are enough test kits available.
11. Urge insurance companies and Medicare to allow additional medical visits for screening vulnerable populations. Encourage the use of telemedicine in place of in-office visits (preferably billed at the same rate as an in-office visit) where appropriate, especially with nonambulatory patients or those with transportation issues. Many insurance companies, including Medicare, approved COVID-19–related coverage of telemedicine in place of office visits to limit the spread of the disease.
12. Provide community health care and integration and better coordination of local, state, and national health care.
13. Hold regular epidemic and pandemic preparedness exercises in every hospital, nursing home, and assisted living facility.
Proactive health care outreach
It is easier to identify the signs and symptoms of already identified infectious diseases as opposed to a novel one like COVID-19. The United States faced a steep learning curve with COVID-19. Hospitalists and other medical professionals were not able to learn about COVID-19 in a journal. At first, they did not know how to screen patients coming into the ER, how to protect staff, or what the treatment plan was for this new disease. As a result, the medical system experienced disorder and confusion. Investing in community health care and better coordination of local, state, and national health care resources is a priority.
The senior citizen population appears to be most vulnerable to this virus and may be just as vulnerable in future outbreaks. Yet the insights gained from this pandemic can lead to a more comprehensive outreach to senior patients and increased screenings for comorbidities and future contagious diseases. An emphasis on proactive health care and outreach for seniors, with a focus on identifying and treating comorbid conditions, improves the medical care system overall and may prevent or slow future community outbreaks.
Dr. Kasarla is a hospitalist with APOGEE Physicians at Wise Surgical at Parkway in Fort Worth, Tex. He did his internal medicine residency at Mercy Hospital & Medical Center, Chicago. Readers can contact him at madhukarreddy.kasarla@apogeephysicians.com. Dr. Devireddy is a family physician at Positive Health Medical Center, Kingston, Jamaica. Contact him at drjaisheel@gmail.com.
References
1. Pisano GP et al. Lessons from Italy’s response to coronavirus. Harvard Business Review. 2020 Mar 27. https://hbr.org/2020/03/lessons-from-italys-response-to-coronavirus.
2. Tu C. Lessons from Taiwan’s experience with COVID-19. New Atlanticist. 2020 Apr 7. https://atlanticcouncil.org/blogs/new-atlanticist/lessons-from-taiwans-experience-with-covid-19/.
3. Newman LH. WhatsApp is at the center of coronavirus response. WIRED. 2020 Mar 20. https://www.wired.com/story/whatsapp-coronavirus-who-information-app/.
A tribute to Edward Ross Ritvo, MD, 1930-2020
Reflections on loss amid COVID-19
I sit here on Father’s Day during a global pandemic and can’t help but think of Mark Twain’s quote, “Truth is stranger than fiction.” Isn’t that what calls us to our profession? When friends ask if I have watched a particular movie or TV show, I almost always say no. Why would I? Day after day at “work” I am hearing the most remarkable stories – many unfolding right before my eyes.
My Dad’s story is no less remarkable. As he was a pioneer in our field, I hope you will allow me to share a few recollections.
June 10, just 10 days after turning 90, Dad died peacefully in his home. His obituary, written by James McCracken, MD, says: “He was an internationally known child psychiatrist who, with colleagues, formed the vanguard of UCLA researchers establishing the biomedical basis of autism in the 1960s despite the prevailing psychological theories of the day ... who would later break new ground in identifying the role of genetics, sleep, and neurophysiological differences, perinatal risk factors, and biomarkers relating to autism and autism risk.”
Dad had extensive training in psychoanalysis and worked hard to maintain expertise in both the psychological and biological arenas. While he helped established autism as a neurologic disease and advocated for DSM criteria changes, he continued teaching Psychodynamic Theory of Personality to the UCLA medical students and maintained a clinical practice based in psychotherapeutic techniques. He was practicing biopsychosocial medicine long before the concept was articulated.

He conducted the first epidemiologic survey of autism in the state of Utah. He chose Utah because the Mormons keep perfect genealogical records. He identified multiple families with more than one child affected as well as examining, pre-, peri-, and postnatal factors affecting these families. Being a maverick has its challenges. One paper about parents with mild autism was rejected from publication seven times before a watered-down version of clinical vignettes finally got accepted. In collaboration with his wife, Riva Ariella Ritvo, he developed the Ritvo Autism Asperger Diagnostic Scale–Revised, (RAADS-R) still in use today.
Dad’s career was complicated by medical issues beginning in his 40s when he had a near-fatal heart attack at the top of Mammoth Mountain while skiing. After struggling for 20 years, he ultimately had a heart transplant at Cedars-Sinai Medical Center at 69 years old. Months after the transplant, he was back at work. He was unstoppable and maintained his optimism and great sense of humor throughout this complicated ordeal. He always remembered his commitment to his donor and his new heart, and worked out every day. Living to 90 was against all the odds.
Dad also persevered throughout his youngest son’s 10-year battle with Ewing’s sarcoma. Despite losing Max in 2016, Dad was active in research and clinical practice until the very end. He was doing telepsychiatry with patients in prisons and rehabilitation hospitals the last few years because he was too weak to travel to an office. He continued his research, and his last paper on eye movement responses as a possible biological marker of autism was published in February 2020.
Although Dad did not have COVID-19, the social isolation and stress of the last few months hastened his decline. The last week in the hospital with no visitors was too much for such a social man, and he died days after he was discharged. Always a trailblazer, Dad’s Zoom funeral was watched across the country by his children, grandchildren, extended family, and friends. Choosing to honor his wish to be cautious in this pandemic, we remained sheltering in place.

As Dad was the ultimate professor, I know he would want us to learn from his life and his passing. We are in an accelerated growth phase now as our lives and the lives of our patients are radically altered.
I hope, like Dad, we can choose to feel nourished by our meaningful work as we travel through life’s ups and downs. We must learn new ways to care for ourselves, our families, and our patients during these challenging times. We must find ways to mourn and celebrate those lost during the pandemic.
I know Dad would love synchronicity that I spent Father’s Day writing about him for Clinical Psychiatry News! Thank you for giving me this gift of reflection on this special day.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
Reflections on loss amid COVID-19
Reflections on loss amid COVID-19
I sit here on Father’s Day during a global pandemic and can’t help but think of Mark Twain’s quote, “Truth is stranger than fiction.” Isn’t that what calls us to our profession? When friends ask if I have watched a particular movie or TV show, I almost always say no. Why would I? Day after day at “work” I am hearing the most remarkable stories – many unfolding right before my eyes.
My Dad’s story is no less remarkable. As he was a pioneer in our field, I hope you will allow me to share a few recollections.
June 10, just 10 days after turning 90, Dad died peacefully in his home. His obituary, written by James McCracken, MD, says: “He was an internationally known child psychiatrist who, with colleagues, formed the vanguard of UCLA researchers establishing the biomedical basis of autism in the 1960s despite the prevailing psychological theories of the day ... who would later break new ground in identifying the role of genetics, sleep, and neurophysiological differences, perinatal risk factors, and biomarkers relating to autism and autism risk.”
Dad had extensive training in psychoanalysis and worked hard to maintain expertise in both the psychological and biological arenas. While he helped established autism as a neurologic disease and advocated for DSM criteria changes, he continued teaching Psychodynamic Theory of Personality to the UCLA medical students and maintained a clinical practice based in psychotherapeutic techniques. He was practicing biopsychosocial medicine long before the concept was articulated.
He conducted the first epidemiologic survey of autism in the state of Utah. He chose Utah because the Mormons keep perfect genealogical records. He identified multiple families with more than one child affected as well as examining, pre-, peri-, and postnatal factors affecting these families. Being a maverick has its challenges. One paper about parents with mild autism was rejected from publication seven times before a watered-down version of clinical vignettes finally got accepted. In collaboration with his wife, Riva Ariella Ritvo, he developed the Ritvo Autism Asperger Diagnostic Scale–Revised, (RAADS-R) still in use today.
Dad’s career was complicated by medical issues beginning in his 40s when he had a near-fatal heart attack at the top of Mammoth Mountain while skiing. After struggling for 20 years, he ultimately had a heart transplant at Cedars-Sinai Medical Center at 69 years old. Months after the transplant, he was back at work. He was unstoppable and maintained his optimism and great sense of humor throughout this complicated ordeal. He always remembered his commitment to his donor and his new heart, and worked out every day. Living to 90 was against all the odds.
Dad also persevered throughout his youngest son’s 10-year battle with Ewing’s sarcoma. Despite losing Max in 2016, Dad was active in research and clinical practice until the very end. He was doing telepsychiatry with patients in prisons and rehabilitation hospitals the last few years because he was too weak to travel to an office. He continued his research, and his last paper on eye movement responses as a possible biological marker of autism was published in February 2020.
Although Dad did not have COVID-19, the social isolation and stress of the last few months hastened his decline. The last week in the hospital with no visitors was too much for such a social man, and he died days after he was discharged. Always a trailblazer, Dad’s Zoom funeral was watched across the country by his children, grandchildren, extended family, and friends. Choosing to honor his wish to be cautious in this pandemic, we remained sheltering in place.
As Dad was the ultimate professor, I know he would want us to learn from his life and his passing. We are in an accelerated growth phase now as our lives and the lives of our patients are radically altered.
I hope, like Dad, we can choose to feel nourished by our meaningful work as we travel through life’s ups and downs. We must learn new ways to care for ourselves, our families, and our patients during these challenging times. We must find ways to mourn and celebrate those lost during the pandemic.
I know Dad would love synchronicity that I spent Father’s Day writing about him for Clinical Psychiatry News! Thank you for giving me this gift of reflection on this special day.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
I sit here on Father’s Day during a global pandemic and can’t help but think of Mark Twain’s quote, “Truth is stranger than fiction.” Isn’t that what calls us to our profession? When friends ask if I have watched a particular movie or TV show, I almost always say no. Why would I? Day after day at “work” I am hearing the most remarkable stories – many unfolding right before my eyes.
My Dad’s story is no less remarkable. As he was a pioneer in our field, I hope you will allow me to share a few recollections.
June 10, just 10 days after turning 90, Dad died peacefully in his home. His obituary, written by James McCracken, MD, says: “He was an internationally known child psychiatrist who, with colleagues, formed the vanguard of UCLA researchers establishing the biomedical basis of autism in the 1960s despite the prevailing psychological theories of the day ... who would later break new ground in identifying the role of genetics, sleep, and neurophysiological differences, perinatal risk factors, and biomarkers relating to autism and autism risk.”
Dad had extensive training in psychoanalysis and worked hard to maintain expertise in both the psychological and biological arenas. While he helped established autism as a neurologic disease and advocated for DSM criteria changes, he continued teaching Psychodynamic Theory of Personality to the UCLA medical students and maintained a clinical practice based in psychotherapeutic techniques. He was practicing biopsychosocial medicine long before the concept was articulated.
He conducted the first epidemiologic survey of autism in the state of Utah. He chose Utah because the Mormons keep perfect genealogical records. He identified multiple families with more than one child affected as well as examining, pre-, peri-, and postnatal factors affecting these families. Being a maverick has its challenges. One paper about parents with mild autism was rejected from publication seven times before a watered-down version of clinical vignettes finally got accepted. In collaboration with his wife, Riva Ariella Ritvo, he developed the Ritvo Autism Asperger Diagnostic Scale–Revised, (RAADS-R) still in use today.
Dad’s career was complicated by medical issues beginning in his 40s when he had a near-fatal heart attack at the top of Mammoth Mountain while skiing. After struggling for 20 years, he ultimately had a heart transplant at Cedars-Sinai Medical Center at 69 years old. Months after the transplant, he was back at work. He was unstoppable and maintained his optimism and great sense of humor throughout this complicated ordeal. He always remembered his commitment to his donor and his new heart, and worked out every day. Living to 90 was against all the odds.
Dad also persevered throughout his youngest son’s 10-year battle with Ewing’s sarcoma. Despite losing Max in 2016, Dad was active in research and clinical practice until the very end. He was doing telepsychiatry with patients in prisons and rehabilitation hospitals the last few years because he was too weak to travel to an office. He continued his research, and his last paper on eye movement responses as a possible biological marker of autism was published in February 2020.
Although Dad did not have COVID-19, the social isolation and stress of the last few months hastened his decline. The last week in the hospital with no visitors was too much for such a social man, and he died days after he was discharged. Always a trailblazer, Dad’s Zoom funeral was watched across the country by his children, grandchildren, extended family, and friends. Choosing to honor his wish to be cautious in this pandemic, we remained sheltering in place.
As Dad was the ultimate professor, I know he would want us to learn from his life and his passing. We are in an accelerated growth phase now as our lives and the lives of our patients are radically altered.
I hope, like Dad, we can choose to feel nourished by our meaningful work as we travel through life’s ups and downs. We must learn new ways to care for ourselves, our families, and our patients during these challenging times. We must find ways to mourn and celebrate those lost during the pandemic.
I know Dad would love synchronicity that I spent Father’s Day writing about him for Clinical Psychiatry News! Thank you for giving me this gift of reflection on this special day.
Dr. Ritvo, a psychiatrist with more than 25 years’ experience, practices in Miami Beach. She is the author of “Bekindr – The Transformative Power of Kindness” (Hellertown, Pa.: Momosa Publishing, 2018) and is the founder of the Bekindr Global Initiative, a movement aimed at cultivating kindness in the world. Dr. Ritvo also is the cofounder of the Bold Beauty Project, a nonprofit group that pairs women with disabilities with photographers who create art exhibitions to raise awareness.
School daze
A few weeks ago I was asked by the head of our local parks and recreation department for my opinion on whether the town should open its summer recreation camps program. He had been receiving multiple inquiries from parents who in the past had relied on the day camps for day care. The director already had surveyed health care administrators and other providers in the town and his team had crafted a plan based on what guidelines they could glean from state and federal advisory groups. The feedback he had received from town officials and health care representatives was that they felt opening would be a bad decision. One physician observed that there is just “so much we don’t know about the virus at this point.”
I certainly agreed that we still have much to learn about COVID-19, but I told the director that we know enough that I would feel comfortable with opening the day camps, which have traditionally been held outdoors under open-sided tents. If group sizes were kept small, staff personnel were dedicated to just one group, and temperatures were taken at the beginning and at the midpoint of each daily session, I felt that the risk of triggering an outbreak was small. I told him that in my mind the Achilles heel of the plan was whether the camp staff, who are generally high school and college-age young people, could be trusted to follow rigorous social distancing in their off-work hours.
Eventually the decision was made by the traditionally risk-averse town officials to open the camps. I hope that this step forward will spur the process of reopening the schools in the fall by demonstrating that, at least in an open-air environment, some simple common sense measures could create a safe environment for children to congregate in. Unfortunately, the long delay in formulating the plan and a basic hesitancy on the part of some parents has resulted in disappointing enrollment figures so far.
I suspect that many of you have been asked to participate in the planning and decision-making processes for opening the school systems in your community or at least have some thoughts of your own about how best to begin the reopening process.
I suspect you agree that, if the number of new cases detected each day in your state is still rising and/or your state’s ability to test, track, case find, and quarantine is inadequate, reopening schools is probably just asking for trouble. However, a recent study has found that children and young adults under the age of 20 years were almost half as likely to become infected as those over the age of 20 (Nat Med. 2020 Jun 16. doi: 10.1038/s41591-020-0962-9). We already know that, in general, children are presenting with less severe illness. Although the authors observe that we still need to learn more about the transmissibility of subclinical infections, particularly in children, they suggest that “interventions aimed at children might have relatively little impact on reducing SARS-CoV-2 transmission.” It is sounding like reopening schools will place the children at relatively low risk. However, until we know more about transmissibility we have to assume reopening schools may place the community at an increased risk.

If this new information is confirmed by other studies, how would this change the recommendations you would make to the community about reopening its schools? What about masks? We are learning that they make a difference for adults, but is this true for very young children as well? Masks should probably remain part of the hygiene education program as well for at least the foreseeable future.
Do you think your school system can broaden its focus beyond surface cleaning to air handling and ventilation? Here in Maine, keeping the windows open for more than a few weeks a year is going to present problems that may be expensive to remedy.
There are always more questions than answers, but my hope is that here in Maine our apparent success on a state level will allow us to reopen the schools as long as we remain vigilant for the first signs that we need to return to lock down. How do you feel about your community’s situation?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
A few weeks ago I was asked by the head of our local parks and recreation department for my opinion on whether the town should open its summer recreation camps program. He had been receiving multiple inquiries from parents who in the past had relied on the day camps for day care. The director already had surveyed health care administrators and other providers in the town and his team had crafted a plan based on what guidelines they could glean from state and federal advisory groups. The feedback he had received from town officials and health care representatives was that they felt opening would be a bad decision. One physician observed that there is just “so much we don’t know about the virus at this point.”
I certainly agreed that we still have much to learn about COVID-19, but I told the director that we know enough that I would feel comfortable with opening the day camps, which have traditionally been held outdoors under open-sided tents. If group sizes were kept small, staff personnel were dedicated to just one group, and temperatures were taken at the beginning and at the midpoint of each daily session, I felt that the risk of triggering an outbreak was small. I told him that in my mind the Achilles heel of the plan was whether the camp staff, who are generally high school and college-age young people, could be trusted to follow rigorous social distancing in their off-work hours.
Eventually the decision was made by the traditionally risk-averse town officials to open the camps. I hope that this step forward will spur the process of reopening the schools in the fall by demonstrating that, at least in an open-air environment, some simple common sense measures could create a safe environment for children to congregate in. Unfortunately, the long delay in formulating the plan and a basic hesitancy on the part of some parents has resulted in disappointing enrollment figures so far.
I suspect that many of you have been asked to participate in the planning and decision-making processes for opening the school systems in your community or at least have some thoughts of your own about how best to begin the reopening process.
I suspect you agree that, if the number of new cases detected each day in your state is still rising and/or your state’s ability to test, track, case find, and quarantine is inadequate, reopening schools is probably just asking for trouble. However, a recent study has found that children and young adults under the age of 20 years were almost half as likely to become infected as those over the age of 20 (Nat Med. 2020 Jun 16. doi: 10.1038/s41591-020-0962-9). We already know that, in general, children are presenting with less severe illness. Although the authors observe that we still need to learn more about the transmissibility of subclinical infections, particularly in children, they suggest that “interventions aimed at children might have relatively little impact on reducing SARS-CoV-2 transmission.” It is sounding like reopening schools will place the children at relatively low risk. However, until we know more about transmissibility we have to assume reopening schools may place the community at an increased risk.
If this new information is confirmed by other studies, how would this change the recommendations you would make to the community about reopening its schools? What about masks? We are learning that they make a difference for adults, but is this true for very young children as well? Masks should probably remain part of the hygiene education program as well for at least the foreseeable future.
Do you think your school system can broaden its focus beyond surface cleaning to air handling and ventilation? Here in Maine, keeping the windows open for more than a few weeks a year is going to present problems that may be expensive to remedy.
There are always more questions than answers, but my hope is that here in Maine our apparent success on a state level will allow us to reopen the schools as long as we remain vigilant for the first signs that we need to return to lock down. How do you feel about your community’s situation?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
A few weeks ago I was asked by the head of our local parks and recreation department for my opinion on whether the town should open its summer recreation camps program. He had been receiving multiple inquiries from parents who in the past had relied on the day camps for day care. The director already had surveyed health care administrators and other providers in the town and his team had crafted a plan based on what guidelines they could glean from state and federal advisory groups. The feedback he had received from town officials and health care representatives was that they felt opening would be a bad decision. One physician observed that there is just “so much we don’t know about the virus at this point.”
I certainly agreed that we still have much to learn about COVID-19, but I told the director that we know enough that I would feel comfortable with opening the day camps, which have traditionally been held outdoors under open-sided tents. If group sizes were kept small, staff personnel were dedicated to just one group, and temperatures were taken at the beginning and at the midpoint of each daily session, I felt that the risk of triggering an outbreak was small. I told him that in my mind the Achilles heel of the plan was whether the camp staff, who are generally high school and college-age young people, could be trusted to follow rigorous social distancing in their off-work hours.
Eventually the decision was made by the traditionally risk-averse town officials to open the camps. I hope that this step forward will spur the process of reopening the schools in the fall by demonstrating that, at least in an open-air environment, some simple common sense measures could create a safe environment for children to congregate in. Unfortunately, the long delay in formulating the plan and a basic hesitancy on the part of some parents has resulted in disappointing enrollment figures so far.
I suspect that many of you have been asked to participate in the planning and decision-making processes for opening the school systems in your community or at least have some thoughts of your own about how best to begin the reopening process.
I suspect you agree that, if the number of new cases detected each day in your state is still rising and/or your state’s ability to test, track, case find, and quarantine is inadequate, reopening schools is probably just asking for trouble. However, a recent study has found that children and young adults under the age of 20 years were almost half as likely to become infected as those over the age of 20 (Nat Med. 2020 Jun 16. doi: 10.1038/s41591-020-0962-9). We already know that, in general, children are presenting with less severe illness. Although the authors observe that we still need to learn more about the transmissibility of subclinical infections, particularly in children, they suggest that “interventions aimed at children might have relatively little impact on reducing SARS-CoV-2 transmission.” It is sounding like reopening schools will place the children at relatively low risk. However, until we know more about transmissibility we have to assume reopening schools may place the community at an increased risk.
If this new information is confirmed by other studies, how would this change the recommendations you would make to the community about reopening its schools? What about masks? We are learning that they make a difference for adults, but is this true for very young children as well? Masks should probably remain part of the hygiene education program as well for at least the foreseeable future.
Do you think your school system can broaden its focus beyond surface cleaning to air handling and ventilation? Here in Maine, keeping the windows open for more than a few weeks a year is going to present problems that may be expensive to remedy.
There are always more questions than answers, but my hope is that here in Maine our apparent success on a state level will allow us to reopen the schools as long as we remain vigilant for the first signs that we need to return to lock down. How do you feel about your community’s situation?
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
COVID-19: Medicare data show long hospital stays, disparities
according to a new analysis by the Centers for Medicare & Medicaid Services.
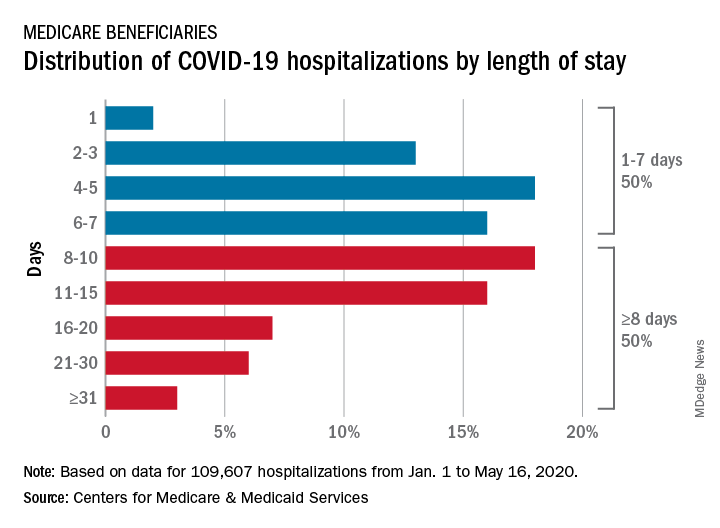
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
according to a new analysis by the Centers for Medicare & Medicaid Services.
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
according to a new analysis by the Centers for Medicare & Medicaid Services.
CMS encounter and claims data show almost 110,000 hospital stays for COVID-19 from Jan. 1 to May 16, 2020. Of the longer admissions, 18% were 8-10 days, 16% were 11-15 days, and another 16% were 16 days or longer, the CMS reported in a preliminary data snapshot released June 22.
The hospitalization rate for the Medicare population was 175 per 100,000 as of May 16, but the CMS data show a number of disparities involving race/ethnicity and other demographic characteristics were uncovered, such as the following:
- Black patients were hospitalized for COVID-19 at a much higher rate, at 465 per 100,000 beneficiaries, than were Hispanics (258), Asians (187), and whites (123).
- Residents of urban/suburban areas had a much higher hospitalization rate than did those living in rural areas: 205 versus 57 per 100,000.
- Beneficiaries enrolled in both Medicare and Medicaid had 473 hospitalizations per 100,000, but the rate for those with Medicare only was 112.
“The disparities in the data reflect longstanding challenges facing minority communities and low-income older adults, many of whom face structural challenges to their health that go far beyond what is traditionally considered ‘medical,’ ” CMS Administrator Seema Verma said in a separate statement.
Inside Mercy’s mission to care for non-COVID patients in Los Angeles
When the hospital ship USNS Mercy departed San Diego’s Naval Station North Island on March 23, 2020, to support the Department of Defense efforts in Los Angeles during the coronavirus outbreak, Commander Erin Blevins remembers the crew’s excitement was palpable.

“We normally do partnerships abroad and respond to tsunamis and earthquakes,” said Cdr. Blevins, MD, a pediatric hematologist-oncologist who served as director of medical services for the mission. “This was a slight change in situation, but still disaster relief in the form of a pandemic. We switched our mindset to putting together the best experts for an infectious disease pandemic versus an earthquake disaster relief.”
A new mission

The 1,000-bed Mercy ship – a converted San Clemente–class oil tanker that was delivered in 1986 – spent nearly 50 days pier side in Los Angeles as a referral hospital for non–COVID-19 patients, so that clinicians at Los Angeles area hospitals could care for an anticipated surge of COVID-19 patients. “We went into it with expectations of, ‘We’ll treat as many patients as you need us to take,” Cdr. Blevins recalled. “I don’t even think Los Angeles [health officials] knew exactly where they were going to peak and what the need was going to be.”
Between March 29 and May 15, about 1,071 medical personnel aboard the Mercy cared for 77 patients with an average age of 53 years who were referred from 11 Los Angeles area hospitals. The physicians, nurses, and other medical support personnel were drawn from military treatment facilities across the country. “We had additional people join us as we scoped the mission to be more medically heavy and surgically light,” said Captain John Rotruck, MD, an anesthesiologist who is commanding officer of Mercy’s medical treatment facility. “We did adjust to make sure that we had the right staffing mix to meet the parameters that we were assigned. That was the crux of the change: a change in flavors of staffing to ensure that we focused on ICU and ward medical care as opposed to very heavy surgical care in support of a combat operation.”

About 10% of the team consisted of reservists who volunteered for the mission. “There’s no way you could have walked around the ship and known who was active duty and who was reservist,” said Capt. Rotruck, who was formerly chief of staff at Walter Reed National Military Medical Center, Bethesda, Md. “They worked together so well, and I think that marriage of active duty who are used to working in a military medical treatment facility – in our case, a Navy medical treatment facility – together with our reservist physician colleagues who work in civilian facilities around the country, was beneficial. It was a synergistic relationship. I think both sides walked away learning quite a bit from each other.”
Start with screening
All crew members underwent a temperature check and completed a health screening questionnaire: once before departing their home of record and again before boarding Mercy. Based on those results, crew members and medical staff were screened for COVID-19 and tested as needed in order to minimize the risk of an outbreak aboard the ship.
Fewer than 1% of crew members developed COVID-19 or tested positive for the virus during the mission, according to Capt. Rotruck. Affected individuals were isolated and quarantined. “All staff have recovered and are doing well,” he said.
Mercy personnel worked with local health officials to ensure that all patients transferred to the ship tested negative for COVID-19. Physicians aboard the Mercy then worked directly with the patients’ civilian physician to ensure a safe and thorough turnover process before the patients were transferred.
From basic medical to trauma care

Care aboard the ship, which consists of open-bay medical wards, ranged from basic medical and surgical care to critical care and trauma. The most common procedures were cholecystectomies and orthopedic procedures, and the average length of stay was 4-5 days, according to Cdr. Blevins. Over the course of the mission, the medical professionals conducted 36 surgeries, 77 x-ray exams, 26 CT scans, and administered hundreds of ancillary studies ranging from routine labs to high-end x-rays and blood transfusion support.
“Within our ICU, we did have some end-of-life patients who ended up dying on our ship in comfort care,” Cdr. Blevins said. “Fortunately, we had a wonderful ICU team who had a great deal of experience with end-of-life care and were able to take care of these patients very comfortably and ensure good communication with family and loved ones during that time. In most instances we tried to make sure that people got to FaceTime or video chat with their loved one before they passed away.”

The Mercy, which includes 12 operating rooms, four x-ray units, and one CAT-scan unit, was not equipped to deliver pediatric or obstetrical care. Other unavailable services included psychiatry, oncology, cardiac and thoracic surgery, nuclear medicine, MRI, mammography, electrophysiology, cardiac catheterization, negative-pressure isolation, speech therapy, and occupational therapy.
Not your typical hospital experience
But for patients who did receive medical care aboard the Mercy – which made three 150-day deployments in recent years for the military-led humanitarian response known as Pacific Partnership in 2015, 2016, and 2018 – it was an experience that they are unlikely to forget.
“Every time a patient left the ship, our team on the ground surveyed them to see how their experience was and see what we could do to improve,” Cdr. Blevins said. “Across the board, they were all very appreciative of the medical care. We had a couple of veterans on board. They got [USNS Mercy] hats on their way out and seemed to very much enjoy a slightly different experience than they would get at a regular hospital.”
Capt. Rotruck added that the enthusiasm crew members had for supporting fellow Americans “really energized our team and really saturated that caring aspect of the people who interacted directly with patients,” he said. “It wasn’t just the physicians and nurses, but it was the staff delivering the food and coming to take blood samples and every other interaction that the patients had with our team. I think they really felt that enthusiasm for being there and supporting our neighbors in LA [Los Angeles].”
Crew life aboard the Mercy
Just as with any hospital on shore, personnel aboard the Mercy practiced preventive hygiene measures recommended by the Centers for Disease Control and Prevention to help prevent the spread of COVID-19, such as wearing cloth face masks, spacing out tables in the dining hall, closing indoor gyms, and devising creative ways to stay physically fit. Popular options included jogging around the perimeter of the ship and practicing yoga and calisthenics on the deck, “making sure you were physically distanced appropriately, and when you were done, putting your mask back on,” Cdr. Blevins said. Others supplemented their workouts with a pull-up bar on the deck. “In addition, we have a series of ramps that run on the starboard side of the ship that we can use for patient movement with litters on wheels or patient beds,” Capt. Rotruck said. “The uphill portion of those ramps represents a good workout opportunity as well.”
Downtime in an era of physical distancing also afforded crew members the opportunity to call or FaceTime with loved ones, watch streamed TV shows and movies, and work on their own professional development. Some continued with coursework for online degree programs offered by colleges and universities they were enrolled in, while some enlisted personnel used the time to complete the Navy Enlisted Warfare Qualification Programs Instruction, which issues the basic overarching requirements for the qualification and designation of all enlisted warfare programs.
“As you can imagine, people spend a lot of time learning how the ship works and how it integrates into larger naval forces and so forth,” Capt. Rotruck said. “Not just our ship but also other ships: their weapons systems and defense mechanisms and navigation systems. We had people spending a significant amount of time working on that. We had people complete their Enlisted Surface Warfare qualification while we were on the mission.”
End of the mission
Mercy returned to its home base in San Diego on May 15, but about 60 medical personnel stayed behind in Los Angeles to support Federal Emergency Management Agency (FEMA), state, and local health care professionals. Some worked at a site where clinicians provided care for COVID-19–positive patients who had been transferred from area skilled nursing facilities.
In addition, a team consisting of one nurse and five corpsmen “would go out to individual skilled nursing facilities and mainly conduct assessments and training, such as training in donning proper PPE [personal protective equipment] and determining what needs they had,” Capt. Rotruck said. “They met those needs if possible or [communicated with California officials] and let them know what the requirements were and what the needs were in that facility.” The assignment for those who stayed behind ended on May 31.
On the opposite coast, Mercy’s sister ship, USNS Comfort, arrived in New York Harbor from Norfolk, Va., on March 30 and spent 3½ weeks assisting area hospitals in the COVID-19 pandemic fight. A few days into the mission, Comfort’s internal spaces were reconfigured to create separate COVID-negative and COVID-positive sections. Medical teams aboard the ship cared for a total of 182 patients during the assignment.
Looking back on Mercy’s mission, Cdr. Blevins marveled at the sense of teamwork that unfolded. “We have quarterly training exercises with a core set of personnel, [and] we train getting ready for activation in 5 days,” she said. “All of that training kicks in and it comes to fruition in a mission like this. It was terrific to see a group of very disparate subject matter experts from all over the country come together with one purpose: which was to serve our own country during the pandemic.”
Capt. Rotruck pointed out that the experience enabled enlisted and nonenlisted physicians to maintain their skill sets during a time when military and civilian hospitals had stopped doing elective procedures and routine appointments. “The fact that those people were able to come on board the ship and continue to conduct their medical practice and maintain their skills and competencies in an environment that they weren’t quite used to is great,” he said. “Otherwise, some of those medical personnel would have been sitting idle, wherever they were from. This is the power of Navy medicine on behalf of our country.”
When the hospital ship USNS Mercy departed San Diego’s Naval Station North Island on March 23, 2020, to support the Department of Defense efforts in Los Angeles during the coronavirus outbreak, Commander Erin Blevins remembers the crew’s excitement was palpable.
“We normally do partnerships abroad and respond to tsunamis and earthquakes,” said Cdr. Blevins, MD, a pediatric hematologist-oncologist who served as director of medical services for the mission. “This was a slight change in situation, but still disaster relief in the form of a pandemic. We switched our mindset to putting together the best experts for an infectious disease pandemic versus an earthquake disaster relief.”
A new mission
The 1,000-bed Mercy ship – a converted San Clemente–class oil tanker that was delivered in 1986 – spent nearly 50 days pier side in Los Angeles as a referral hospital for non–COVID-19 patients, so that clinicians at Los Angeles area hospitals could care for an anticipated surge of COVID-19 patients. “We went into it with expectations of, ‘We’ll treat as many patients as you need us to take,” Cdr. Blevins recalled. “I don’t even think Los Angeles [health officials] knew exactly where they were going to peak and what the need was going to be.”
Between March 29 and May 15, about 1,071 medical personnel aboard the Mercy cared for 77 patients with an average age of 53 years who were referred from 11 Los Angeles area hospitals. The physicians, nurses, and other medical support personnel were drawn from military treatment facilities across the country. “We had additional people join us as we scoped the mission to be more medically heavy and surgically light,” said Captain John Rotruck, MD, an anesthesiologist who is commanding officer of Mercy’s medical treatment facility. “We did adjust to make sure that we had the right staffing mix to meet the parameters that we were assigned. That was the crux of the change: a change in flavors of staffing to ensure that we focused on ICU and ward medical care as opposed to very heavy surgical care in support of a combat operation.”
About 10% of the team consisted of reservists who volunteered for the mission. “There’s no way you could have walked around the ship and known who was active duty and who was reservist,” said Capt. Rotruck, who was formerly chief of staff at Walter Reed National Military Medical Center, Bethesda, Md. “They worked together so well, and I think that marriage of active duty who are used to working in a military medical treatment facility – in our case, a Navy medical treatment facility – together with our reservist physician colleagues who work in civilian facilities around the country, was beneficial. It was a synergistic relationship. I think both sides walked away learning quite a bit from each other.”
Start with screening
All crew members underwent a temperature check and completed a health screening questionnaire: once before departing their home of record and again before boarding Mercy. Based on those results, crew members and medical staff were screened for COVID-19 and tested as needed in order to minimize the risk of an outbreak aboard the ship.
Fewer than 1% of crew members developed COVID-19 or tested positive for the virus during the mission, according to Capt. Rotruck. Affected individuals were isolated and quarantined. “All staff have recovered and are doing well,” he said.
Mercy personnel worked with local health officials to ensure that all patients transferred to the ship tested negative for COVID-19. Physicians aboard the Mercy then worked directly with the patients’ civilian physician to ensure a safe and thorough turnover process before the patients were transferred.
From basic medical to trauma care
Care aboard the ship, which consists of open-bay medical wards, ranged from basic medical and surgical care to critical care and trauma. The most common procedures were cholecystectomies and orthopedic procedures, and the average length of stay was 4-5 days, according to Cdr. Blevins. Over the course of the mission, the medical professionals conducted 36 surgeries, 77 x-ray exams, 26 CT scans, and administered hundreds of ancillary studies ranging from routine labs to high-end x-rays and blood transfusion support.
“Within our ICU, we did have some end-of-life patients who ended up dying on our ship in comfort care,” Cdr. Blevins said. “Fortunately, we had a wonderful ICU team who had a great deal of experience with end-of-life care and were able to take care of these patients very comfortably and ensure good communication with family and loved ones during that time. In most instances we tried to make sure that people got to FaceTime or video chat with their loved one before they passed away.”
The Mercy, which includes 12 operating rooms, four x-ray units, and one CAT-scan unit, was not equipped to deliver pediatric or obstetrical care. Other unavailable services included psychiatry, oncology, cardiac and thoracic surgery, nuclear medicine, MRI, mammography, electrophysiology, cardiac catheterization, negative-pressure isolation, speech therapy, and occupational therapy.
Not your typical hospital experience
But for patients who did receive medical care aboard the Mercy – which made three 150-day deployments in recent years for the military-led humanitarian response known as Pacific Partnership in 2015, 2016, and 2018 – it was an experience that they are unlikely to forget.
“Every time a patient left the ship, our team on the ground surveyed them to see how their experience was and see what we could do to improve,” Cdr. Blevins said. “Across the board, they were all very appreciative of the medical care. We had a couple of veterans on board. They got [USNS Mercy] hats on their way out and seemed to very much enjoy a slightly different experience than they would get at a regular hospital.”
Capt. Rotruck added that the enthusiasm crew members had for supporting fellow Americans “really energized our team and really saturated that caring aspect of the people who interacted directly with patients,” he said. “It wasn’t just the physicians and nurses, but it was the staff delivering the food and coming to take blood samples and every other interaction that the patients had with our team. I think they really felt that enthusiasm for being there and supporting our neighbors in LA [Los Angeles].”
Crew life aboard the Mercy
Just as with any hospital on shore, personnel aboard the Mercy practiced preventive hygiene measures recommended by the Centers for Disease Control and Prevention to help prevent the spread of COVID-19, such as wearing cloth face masks, spacing out tables in the dining hall, closing indoor gyms, and devising creative ways to stay physically fit. Popular options included jogging around the perimeter of the ship and practicing yoga and calisthenics on the deck, “making sure you were physically distanced appropriately, and when you were done, putting your mask back on,” Cdr. Blevins said. Others supplemented their workouts with a pull-up bar on the deck. “In addition, we have a series of ramps that run on the starboard side of the ship that we can use for patient movement with litters on wheels or patient beds,” Capt. Rotruck said. “The uphill portion of those ramps represents a good workout opportunity as well.”
Downtime in an era of physical distancing also afforded crew members the opportunity to call or FaceTime with loved ones, watch streamed TV shows and movies, and work on their own professional development. Some continued with coursework for online degree programs offered by colleges and universities they were enrolled in, while some enlisted personnel used the time to complete the Navy Enlisted Warfare Qualification Programs Instruction, which issues the basic overarching requirements for the qualification and designation of all enlisted warfare programs.
“As you can imagine, people spend a lot of time learning how the ship works and how it integrates into larger naval forces and so forth,” Capt. Rotruck said. “Not just our ship but also other ships: their weapons systems and defense mechanisms and navigation systems. We had people spending a significant amount of time working on that. We had people complete their Enlisted Surface Warfare qualification while we were on the mission.”
End of the mission
Mercy returned to its home base in San Diego on May 15, but about 60 medical personnel stayed behind in Los Angeles to support Federal Emergency Management Agency (FEMA), state, and local health care professionals. Some worked at a site where clinicians provided care for COVID-19–positive patients who had been transferred from area skilled nursing facilities.
In addition, a team consisting of one nurse and five corpsmen “would go out to individual skilled nursing facilities and mainly conduct assessments and training, such as training in donning proper PPE [personal protective equipment] and determining what needs they had,” Capt. Rotruck said. “They met those needs if possible or [communicated with California officials] and let them know what the requirements were and what the needs were in that facility.” The assignment for those who stayed behind ended on May 31.
On the opposite coast, Mercy’s sister ship, USNS Comfort, arrived in New York Harbor from Norfolk, Va., on March 30 and spent 3½ weeks assisting area hospitals in the COVID-19 pandemic fight. A few days into the mission, Comfort’s internal spaces were reconfigured to create separate COVID-negative and COVID-positive sections. Medical teams aboard the ship cared for a total of 182 patients during the assignment.
Looking back on Mercy’s mission, Cdr. Blevins marveled at the sense of teamwork that unfolded. “We have quarterly training exercises with a core set of personnel, [and] we train getting ready for activation in 5 days,” she said. “All of that training kicks in and it comes to fruition in a mission like this. It was terrific to see a group of very disparate subject matter experts from all over the country come together with one purpose: which was to serve our own country during the pandemic.”
Capt. Rotruck pointed out that the experience enabled enlisted and nonenlisted physicians to maintain their skill sets during a time when military and civilian hospitals had stopped doing elective procedures and routine appointments. “The fact that those people were able to come on board the ship and continue to conduct their medical practice and maintain their skills and competencies in an environment that they weren’t quite used to is great,” he said. “Otherwise, some of those medical personnel would have been sitting idle, wherever they were from. This is the power of Navy medicine on behalf of our country.”
When the hospital ship USNS Mercy departed San Diego’s Naval Station North Island on March 23, 2020, to support the Department of Defense efforts in Los Angeles during the coronavirus outbreak, Commander Erin Blevins remembers the crew’s excitement was palpable.
“We normally do partnerships abroad and respond to tsunamis and earthquakes,” said Cdr. Blevins, MD, a pediatric hematologist-oncologist who served as director of medical services for the mission. “This was a slight change in situation, but still disaster relief in the form of a pandemic. We switched our mindset to putting together the best experts for an infectious disease pandemic versus an earthquake disaster relief.”
A new mission
The 1,000-bed Mercy ship – a converted San Clemente–class oil tanker that was delivered in 1986 – spent nearly 50 days pier side in Los Angeles as a referral hospital for non–COVID-19 patients, so that clinicians at Los Angeles area hospitals could care for an anticipated surge of COVID-19 patients. “We went into it with expectations of, ‘We’ll treat as many patients as you need us to take,” Cdr. Blevins recalled. “I don’t even think Los Angeles [health officials] knew exactly where they were going to peak and what the need was going to be.”
Between March 29 and May 15, about 1,071 medical personnel aboard the Mercy cared for 77 patients with an average age of 53 years who were referred from 11 Los Angeles area hospitals. The physicians, nurses, and other medical support personnel were drawn from military treatment facilities across the country. “We had additional people join us as we scoped the mission to be more medically heavy and surgically light,” said Captain John Rotruck, MD, an anesthesiologist who is commanding officer of Mercy’s medical treatment facility. “We did adjust to make sure that we had the right staffing mix to meet the parameters that we were assigned. That was the crux of the change: a change in flavors of staffing to ensure that we focused on ICU and ward medical care as opposed to very heavy surgical care in support of a combat operation.”
About 10% of the team consisted of reservists who volunteered for the mission. “There’s no way you could have walked around the ship and known who was active duty and who was reservist,” said Capt. Rotruck, who was formerly chief of staff at Walter Reed National Military Medical Center, Bethesda, Md. “They worked together so well, and I think that marriage of active duty who are used to working in a military medical treatment facility – in our case, a Navy medical treatment facility – together with our reservist physician colleagues who work in civilian facilities around the country, was beneficial. It was a synergistic relationship. I think both sides walked away learning quite a bit from each other.”
Start with screening
All crew members underwent a temperature check and completed a health screening questionnaire: once before departing their home of record and again before boarding Mercy. Based on those results, crew members and medical staff were screened for COVID-19 and tested as needed in order to minimize the risk of an outbreak aboard the ship.
Fewer than 1% of crew members developed COVID-19 or tested positive for the virus during the mission, according to Capt. Rotruck. Affected individuals were isolated and quarantined. “All staff have recovered and are doing well,” he said.
Mercy personnel worked with local health officials to ensure that all patients transferred to the ship tested negative for COVID-19. Physicians aboard the Mercy then worked directly with the patients’ civilian physician to ensure a safe and thorough turnover process before the patients were transferred.
From basic medical to trauma care
Care aboard the ship, which consists of open-bay medical wards, ranged from basic medical and surgical care to critical care and trauma. The most common procedures were cholecystectomies and orthopedic procedures, and the average length of stay was 4-5 days, according to Cdr. Blevins. Over the course of the mission, the medical professionals conducted 36 surgeries, 77 x-ray exams, 26 CT scans, and administered hundreds of ancillary studies ranging from routine labs to high-end x-rays and blood transfusion support.
“Within our ICU, we did have some end-of-life patients who ended up dying on our ship in comfort care,” Cdr. Blevins said. “Fortunately, we had a wonderful ICU team who had a great deal of experience with end-of-life care and were able to take care of these patients very comfortably and ensure good communication with family and loved ones during that time. In most instances we tried to make sure that people got to FaceTime or video chat with their loved one before they passed away.”
The Mercy, which includes 12 operating rooms, four x-ray units, and one CAT-scan unit, was not equipped to deliver pediatric or obstetrical care. Other unavailable services included psychiatry, oncology, cardiac and thoracic surgery, nuclear medicine, MRI, mammography, electrophysiology, cardiac catheterization, negative-pressure isolation, speech therapy, and occupational therapy.
Not your typical hospital experience
But for patients who did receive medical care aboard the Mercy – which made three 150-day deployments in recent years for the military-led humanitarian response known as Pacific Partnership in 2015, 2016, and 2018 – it was an experience that they are unlikely to forget.
“Every time a patient left the ship, our team on the ground surveyed them to see how their experience was and see what we could do to improve,” Cdr. Blevins said. “Across the board, they were all very appreciative of the medical care. We had a couple of veterans on board. They got [USNS Mercy] hats on their way out and seemed to very much enjoy a slightly different experience than they would get at a regular hospital.”
Capt. Rotruck added that the enthusiasm crew members had for supporting fellow Americans “really energized our team and really saturated that caring aspect of the people who interacted directly with patients,” he said. “It wasn’t just the physicians and nurses, but it was the staff delivering the food and coming to take blood samples and every other interaction that the patients had with our team. I think they really felt that enthusiasm for being there and supporting our neighbors in LA [Los Angeles].”
Crew life aboard the Mercy
Just as with any hospital on shore, personnel aboard the Mercy practiced preventive hygiene measures recommended by the Centers for Disease Control and Prevention to help prevent the spread of COVID-19, such as wearing cloth face masks, spacing out tables in the dining hall, closing indoor gyms, and devising creative ways to stay physically fit. Popular options included jogging around the perimeter of the ship and practicing yoga and calisthenics on the deck, “making sure you were physically distanced appropriately, and when you were done, putting your mask back on,” Cdr. Blevins said. Others supplemented their workouts with a pull-up bar on the deck. “In addition, we have a series of ramps that run on the starboard side of the ship that we can use for patient movement with litters on wheels or patient beds,” Capt. Rotruck said. “The uphill portion of those ramps represents a good workout opportunity as well.”
Downtime in an era of physical distancing also afforded crew members the opportunity to call or FaceTime with loved ones, watch streamed TV shows and movies, and work on their own professional development. Some continued with coursework for online degree programs offered by colleges and universities they were enrolled in, while some enlisted personnel used the time to complete the Navy Enlisted Warfare Qualification Programs Instruction, which issues the basic overarching requirements for the qualification and designation of all enlisted warfare programs.
“As you can imagine, people spend a lot of time learning how the ship works and how it integrates into larger naval forces and so forth,” Capt. Rotruck said. “Not just our ship but also other ships: their weapons systems and defense mechanisms and navigation systems. We had people spending a significant amount of time working on that. We had people complete their Enlisted Surface Warfare qualification while we were on the mission.”
End of the mission
Mercy returned to its home base in San Diego on May 15, but about 60 medical personnel stayed behind in Los Angeles to support Federal Emergency Management Agency (FEMA), state, and local health care professionals. Some worked at a site where clinicians provided care for COVID-19–positive patients who had been transferred from area skilled nursing facilities.
In addition, a team consisting of one nurse and five corpsmen “would go out to individual skilled nursing facilities and mainly conduct assessments and training, such as training in donning proper PPE [personal protective equipment] and determining what needs they had,” Capt. Rotruck said. “They met those needs if possible or [communicated with California officials] and let them know what the requirements were and what the needs were in that facility.” The assignment for those who stayed behind ended on May 31.
On the opposite coast, Mercy’s sister ship, USNS Comfort, arrived in New York Harbor from Norfolk, Va., on March 30 and spent 3½ weeks assisting area hospitals in the COVID-19 pandemic fight. A few days into the mission, Comfort’s internal spaces were reconfigured to create separate COVID-negative and COVID-positive sections. Medical teams aboard the ship cared for a total of 182 patients during the assignment.
Looking back on Mercy’s mission, Cdr. Blevins marveled at the sense of teamwork that unfolded. “We have quarterly training exercises with a core set of personnel, [and] we train getting ready for activation in 5 days,” she said. “All of that training kicks in and it comes to fruition in a mission like this. It was terrific to see a group of very disparate subject matter experts from all over the country come together with one purpose: which was to serve our own country during the pandemic.”
Capt. Rotruck pointed out that the experience enabled enlisted and nonenlisted physicians to maintain their skill sets during a time when military and civilian hospitals had stopped doing elective procedures and routine appointments. “The fact that those people were able to come on board the ship and continue to conduct their medical practice and maintain their skills and competencies in an environment that they weren’t quite used to is great,” he said. “Otherwise, some of those medical personnel would have been sitting idle, wherever they were from. This is the power of Navy medicine on behalf of our country.”
Daily Recap: ED visits for life-threatening conditions plummet; COVID-19 imaging strategies for kids
Here are the stories our MDedge editors across specialties think you need to know about today:
ED visits drop for life-threatening conditions
Emergency department visits for myocardial infarction, stroke, and hyperglycemic crisis dropped substantially in the 10 weeks after COVID-19 was declared a national emergency, according to new research from the Centers for Disease Control and Prevention.
Compared with the 10-week period from Jan. 5 to March 14, ED visits were down by 23% for MI, 20% for stroke, and 10% for hyperglycemic crisis from March 15 to May 23.
“A short-term decline of this magnitude … is biologically implausible for MI and stroke, especially for older adults, and unlikely for hyperglycemic crisis, and the finding suggests that patients with these conditions either could not access care or were delaying or avoiding seeking care during the early pandemic period,” the researchers wrote in the Morbidity and Mortality Weekly Report. Read more.
Expert recommendations for pediatric COVID-19 imaging
A team of pulmonologists has synthesized the clinical and imaging characteristics of COVID-19 in children, and has issued recommendations for ordering imaging studies in suspected cases of the infection.
Current recommendations from the American College of Radiology (ACR) do not include chest computed tomography (CT) or chest radiography (CXR) as an upfront test to diagnose pediatric COVID-19, but the tests may still have a role in clinical monitoring, especially in patients with a moderate to severe disease course. The potential benefits of utilizing radiologic evaluation – such as establishing a baseline for monitoring disease progression – must be balanced with potential drawbacks, including radiation exposure and reduced availability of imaging resources owing to necessary cleaning and air turnover time.
Based on the most recent international guidelines for pediatric COVID-19 patient management, the authors developed an algorithm for performing imaging studies in suspected cases of COVID-19 pneumonia. The purpose of the tool is to support clinical decision-making around the utilization of CXR and CT to evaluate pediatric COVID-19 pneumonia. “The step by step algorithm addresses the selection, sequence and timing of imaging studies with multiple images illustrating key findings of COVID-19 pneumonia in the pediatric age group,” said Mary Cataletto, MD, of NYU Langone Health in Mineola, N.Y. Read more.
Cortisol levels on COVID-19 admission may be a marker of severity
Patients with COVID-19 who have high levels of the steroid hormone cortisol on admission to the hospital have a substantially increased risk of dying, according to new study findings.
Researchers assessed 535 patients admitted to major London hospitals. Of these, 403 patients were diagnosed with COVID-19 based on a positive result on real-time polymerase chain reaction testing or a strong clinical and radiological suspicion, despite a negative test. Mean cortisol concentrations in patients with COVID-19 were significantly higher than those not diagnosed with the virus and as of May 8, significantly more patients with COVID-19 died than those without (27.8% vs 6.8%).
Measuring cortisol on admission is potentially “another simple marker to use alongside oxygen saturation levels to help us identify which patients need to be admitted immediately, and which may not,” said Waljit S. Dhillo, MBBS, PhD, head of the division of diabetes, endocrinology and metabolism at Imperial College London.
“Having an early indicator of which patients may deteriorate more quickly will help us with providing the best level of care as quickly as possible. In addition, we can also take cortisol levels into account when we are working out how best to treat our patients,” he said. Read more.
Normal-weight prediabetes patients can benefit from lifestyle changes
Adults of normal weight with prediabetes may derive at least as much benefit from lifestyle health coaching programs as adults who are overweight or obese, results of a recent nonrandomized, real-world study show.
Fasting plasma glucose (FPG) normalized in about 63% of prediabetic adults with normal body mass index (BMI) participating in a personalized coaching program that emphasized exercise, nutrition, and weight management. In contrast, FPG normalized in about 52% of overweight and 44% of obese prediabetic individuals participating in the program.
“It is interesting to note that, although the normal weight group lost the least amount of weight, they still benefited from the lifestyle health coaching program... having a resultant greatest decrease in fasting plasma glucose and normalization to a range of someone without prediabetes,” said researcher Mandy Salmon, MS, a medical student at the University of Pennsylvania, Philadelphia. She presented the findings at the virtual annual scientific sessions of the American Diabetes Association. Read more.
Diabetes-related amputations rise in older adults
The recent resurgence in diabetes-related lower-extremity amputations in the United States is not limited to younger adults, according to the author of a recent study that documents similar increases among an older population of Medicare beneficiaries.
While the rate of amputations fell among these older adults from 2000 to 2009, it increased significantly from 2009 to 2017, albeit at a “less severe rate” than recently reported in younger populations, according to study investigator Jessica Harding, PhD, an assistant professor in the department of surgery at Emory University, Atlanta. Dr. Harding reported the results at the virtual annual scientific sessions of the American Diabetes Association.
The rate of nontraumatic lower extremity amputation (NLEA) was ticking upward by more than 1% per year over the 2009-2017 period. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
ED visits drop for life-threatening conditions
Emergency department visits for myocardial infarction, stroke, and hyperglycemic crisis dropped substantially in the 10 weeks after COVID-19 was declared a national emergency, according to new research from the Centers for Disease Control and Prevention.
Compared with the 10-week period from Jan. 5 to March 14, ED visits were down by 23% for MI, 20% for stroke, and 10% for hyperglycemic crisis from March 15 to May 23.
“A short-term decline of this magnitude … is biologically implausible for MI and stroke, especially for older adults, and unlikely for hyperglycemic crisis, and the finding suggests that patients with these conditions either could not access care or were delaying or avoiding seeking care during the early pandemic period,” the researchers wrote in the Morbidity and Mortality Weekly Report. Read more.
Expert recommendations for pediatric COVID-19 imaging
A team of pulmonologists has synthesized the clinical and imaging characteristics of COVID-19 in children, and has issued recommendations for ordering imaging studies in suspected cases of the infection.
Current recommendations from the American College of Radiology (ACR) do not include chest computed tomography (CT) or chest radiography (CXR) as an upfront test to diagnose pediatric COVID-19, but the tests may still have a role in clinical monitoring, especially in patients with a moderate to severe disease course. The potential benefits of utilizing radiologic evaluation – such as establishing a baseline for monitoring disease progression – must be balanced with potential drawbacks, including radiation exposure and reduced availability of imaging resources owing to necessary cleaning and air turnover time.
Based on the most recent international guidelines for pediatric COVID-19 patient management, the authors developed an algorithm for performing imaging studies in suspected cases of COVID-19 pneumonia. The purpose of the tool is to support clinical decision-making around the utilization of CXR and CT to evaluate pediatric COVID-19 pneumonia. “The step by step algorithm addresses the selection, sequence and timing of imaging studies with multiple images illustrating key findings of COVID-19 pneumonia in the pediatric age group,” said Mary Cataletto, MD, of NYU Langone Health in Mineola, N.Y. Read more.
Cortisol levels on COVID-19 admission may be a marker of severity
Patients with COVID-19 who have high levels of the steroid hormone cortisol on admission to the hospital have a substantially increased risk of dying, according to new study findings.
Researchers assessed 535 patients admitted to major London hospitals. Of these, 403 patients were diagnosed with COVID-19 based on a positive result on real-time polymerase chain reaction testing or a strong clinical and radiological suspicion, despite a negative test. Mean cortisol concentrations in patients with COVID-19 were significantly higher than those not diagnosed with the virus and as of May 8, significantly more patients with COVID-19 died than those without (27.8% vs 6.8%).
Measuring cortisol on admission is potentially “another simple marker to use alongside oxygen saturation levels to help us identify which patients need to be admitted immediately, and which may not,” said Waljit S. Dhillo, MBBS, PhD, head of the division of diabetes, endocrinology and metabolism at Imperial College London.
“Having an early indicator of which patients may deteriorate more quickly will help us with providing the best level of care as quickly as possible. In addition, we can also take cortisol levels into account when we are working out how best to treat our patients,” he said. Read more.
Normal-weight prediabetes patients can benefit from lifestyle changes
Adults of normal weight with prediabetes may derive at least as much benefit from lifestyle health coaching programs as adults who are overweight or obese, results of a recent nonrandomized, real-world study show.
Fasting plasma glucose (FPG) normalized in about 63% of prediabetic adults with normal body mass index (BMI) participating in a personalized coaching program that emphasized exercise, nutrition, and weight management. In contrast, FPG normalized in about 52% of overweight and 44% of obese prediabetic individuals participating in the program.
“It is interesting to note that, although the normal weight group lost the least amount of weight, they still benefited from the lifestyle health coaching program... having a resultant greatest decrease in fasting plasma glucose and normalization to a range of someone without prediabetes,” said researcher Mandy Salmon, MS, a medical student at the University of Pennsylvania, Philadelphia. She presented the findings at the virtual annual scientific sessions of the American Diabetes Association. Read more.
Diabetes-related amputations rise in older adults
The recent resurgence in diabetes-related lower-extremity amputations in the United States is not limited to younger adults, according to the author of a recent study that documents similar increases among an older population of Medicare beneficiaries.
While the rate of amputations fell among these older adults from 2000 to 2009, it increased significantly from 2009 to 2017, albeit at a “less severe rate” than recently reported in younger populations, according to study investigator Jessica Harding, PhD, an assistant professor in the department of surgery at Emory University, Atlanta. Dr. Harding reported the results at the virtual annual scientific sessions of the American Diabetes Association.
The rate of nontraumatic lower extremity amputation (NLEA) was ticking upward by more than 1% per year over the 2009-2017 period. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Here are the stories our MDedge editors across specialties think you need to know about today:
ED visits drop for life-threatening conditions
Emergency department visits for myocardial infarction, stroke, and hyperglycemic crisis dropped substantially in the 10 weeks after COVID-19 was declared a national emergency, according to new research from the Centers for Disease Control and Prevention.
Compared with the 10-week period from Jan. 5 to March 14, ED visits were down by 23% for MI, 20% for stroke, and 10% for hyperglycemic crisis from March 15 to May 23.
“A short-term decline of this magnitude … is biologically implausible for MI and stroke, especially for older adults, and unlikely for hyperglycemic crisis, and the finding suggests that patients with these conditions either could not access care or were delaying or avoiding seeking care during the early pandemic period,” the researchers wrote in the Morbidity and Mortality Weekly Report. Read more.
Expert recommendations for pediatric COVID-19 imaging
A team of pulmonologists has synthesized the clinical and imaging characteristics of COVID-19 in children, and has issued recommendations for ordering imaging studies in suspected cases of the infection.
Current recommendations from the American College of Radiology (ACR) do not include chest computed tomography (CT) or chest radiography (CXR) as an upfront test to diagnose pediatric COVID-19, but the tests may still have a role in clinical monitoring, especially in patients with a moderate to severe disease course. The potential benefits of utilizing radiologic evaluation – such as establishing a baseline for monitoring disease progression – must be balanced with potential drawbacks, including radiation exposure and reduced availability of imaging resources owing to necessary cleaning and air turnover time.
Based on the most recent international guidelines for pediatric COVID-19 patient management, the authors developed an algorithm for performing imaging studies in suspected cases of COVID-19 pneumonia. The purpose of the tool is to support clinical decision-making around the utilization of CXR and CT to evaluate pediatric COVID-19 pneumonia. “The step by step algorithm addresses the selection, sequence and timing of imaging studies with multiple images illustrating key findings of COVID-19 pneumonia in the pediatric age group,” said Mary Cataletto, MD, of NYU Langone Health in Mineola, N.Y. Read more.
Cortisol levels on COVID-19 admission may be a marker of severity
Patients with COVID-19 who have high levels of the steroid hormone cortisol on admission to the hospital have a substantially increased risk of dying, according to new study findings.
Researchers assessed 535 patients admitted to major London hospitals. Of these, 403 patients were diagnosed with COVID-19 based on a positive result on real-time polymerase chain reaction testing or a strong clinical and radiological suspicion, despite a negative test. Mean cortisol concentrations in patients with COVID-19 were significantly higher than those not diagnosed with the virus and as of May 8, significantly more patients with COVID-19 died than those without (27.8% vs 6.8%).
Measuring cortisol on admission is potentially “another simple marker to use alongside oxygen saturation levels to help us identify which patients need to be admitted immediately, and which may not,” said Waljit S. Dhillo, MBBS, PhD, head of the division of diabetes, endocrinology and metabolism at Imperial College London.
“Having an early indicator of which patients may deteriorate more quickly will help us with providing the best level of care as quickly as possible. In addition, we can also take cortisol levels into account when we are working out how best to treat our patients,” he said. Read more.
Normal-weight prediabetes patients can benefit from lifestyle changes
Adults of normal weight with prediabetes may derive at least as much benefit from lifestyle health coaching programs as adults who are overweight or obese, results of a recent nonrandomized, real-world study show.
Fasting plasma glucose (FPG) normalized in about 63% of prediabetic adults with normal body mass index (BMI) participating in a personalized coaching program that emphasized exercise, nutrition, and weight management. In contrast, FPG normalized in about 52% of overweight and 44% of obese prediabetic individuals participating in the program.
“It is interesting to note that, although the normal weight group lost the least amount of weight, they still benefited from the lifestyle health coaching program... having a resultant greatest decrease in fasting plasma glucose and normalization to a range of someone without prediabetes,” said researcher Mandy Salmon, MS, a medical student at the University of Pennsylvania, Philadelphia. She presented the findings at the virtual annual scientific sessions of the American Diabetes Association. Read more.
Diabetes-related amputations rise in older adults
The recent resurgence in diabetes-related lower-extremity amputations in the United States is not limited to younger adults, according to the author of a recent study that documents similar increases among an older population of Medicare beneficiaries.
While the rate of amputations fell among these older adults from 2000 to 2009, it increased significantly from 2009 to 2017, albeit at a “less severe rate” than recently reported in younger populations, according to study investigator Jessica Harding, PhD, an assistant professor in the department of surgery at Emory University, Atlanta. Dr. Harding reported the results at the virtual annual scientific sessions of the American Diabetes Association.
The rate of nontraumatic lower extremity amputation (NLEA) was ticking upward by more than 1% per year over the 2009-2017 period. Read more.
For more on COVID-19, visit our Resource Center. All of our latest news is available on MDedge.com.
Guidance on infection prevention for health care personnel
As we reopen our offices we are faced with the challenge of determining the best way to do it safely – protecting ourselves, our staff, and our patients.

In this column we will focus on selected details of the recommendations from IDSA and the CDC that may be helpful in primary care offices.
Face masks
Many clinicians have asked whether a physician should use a mask while seeing patients without COVID-19 in the office, and if yes, which type. The IDSA guideline states that mask usage is imperative for reducing the risk of health care workers contracting COVID-19.1 The evidence is derived from a number of sources, including a retrospective study from Wuhan (China) University that examined two groups of health care workers during the outbreak. The first group wore N95 masks and washed their hands frequently, while the second group did not wear masks and washed their hands less frequently. In the group that took greater actions to protect themselves, none of the 493 staff members contracted COVID-19, compared with 10 of 213 staff members in the other group. The decrease in infection rate occurred in the group that wore masks despite the fact that this group had 733% more exposure to COVID-19 patients.2 Further evidence came from a case-control study done in hospitals in Hong Kong during the 2003 SARS-CoV outbreak.3 This study showed that mask wearing was the most significant intervention for reducing infection, followed by gowning, and then handwashing. These findings make it clear that mask usage is a must for all health care providers who may be caring for patients who could have COVID-19.
The guideline also reviews evidence about the use of surgical masks versus N95 masks. On reviewing indirect evidence from the SARS-CoV epidemic, IDSA found that wearing any mask – surgical or N95 – led to a large reduction in the risk of developing an infection. In this systematic review of five observational studies in health care personnel, for those wearing surgical masks, the odds ratio for developing an infection was 0.13 (95% CI, 0.03-0.62), and for those wearing N95 masks, the odds ratio was 0.12 (95% CI, 0.06-0.26). There was not a significant difference between risk reductions for those who wore surgical masks and N95 masks, respectively.1,4 The IDSA guideline panel recommended “that health care personnel caring for patients with suspected or known COVID-19 use either a surgical mask or N95 respirator ... as part of appropriate PPE.” Since there is not a significant difference in outcomes between those who use surgical masks and those who use N95 respirators, and the IDSA guideline states either type of mask is considered appropriate when taking care of patients with suspected or known COVID-19, in our opinion, use of surgical masks rather than N95s is sufficient when performing low-risk activities. Such activities include seeing patients who do not have a high likelihood of COVID-19 in the office setting.

The IDSA recommendation also discusses universal masking, defined as both patients and clinicians wearing masks. The recommendation is supported by the findings of a study in which universal mask usage was used to prevent the spread of H1N 1 during the 2009 outbreak. In this study of staff members and patients exposed to H1N1 who all wore masks, only 0.48% of 836 acquired infection. In the same study, not wearing a mask by either the provider or patient increased the risk of infection.5 Also, in a prospective study of hematopoietic stem cell transplant patients, universal masking caused infection rates to drop from 10.3% to 4.4%.6
The IDSA guideline states the following: “There may be some, albeit uncertain, benefit to universal masking in the absence of resource constraints. However, the benefits of universal masking with surgical masks should be weighed against the risk of increasing the PPE burn rate and contextualized to the background COVID-19 prevalence rate for asymptomatic or minimally symptomatic HCPs [health care providers] and visitors.”1
The CDC’s guidance statement says the following: “Continued community transmission has increased the number of individuals potentially exposed to and infectious with SARS-CoV-2. Fever and symptom screening have proven to be relatively ineffective in identifying all infected individuals, including HCPs. Symptom screening also will not identify individuals who are infected but otherwise asymptomatic or pre-symptomatic; additional interventions are needed to limit the unrecognized introduction of SARS-CoV-2 into healthcare settings by these individuals. As part of aggressive source control measures, healthcare facilities should consider implementing policies requiring everyone entering the facility to wear a cloth face covering (if tolerated) while in the building, regardless of symptoms.”7
It is our opinion, based on the CDC and IDSA recommendations, that both clinicians and patients should be required to wear masks when patients are seen in the office if possible. Many offices have instituted a policy that says, if a patient refuses to wear a mask during an office visit, then the patient will not be seen.
Eye protection
Many clinicians are uncertain about whether eye protection needs to be used when seeing asymptomatic patients. The IDSA acknowledges that there are not studies that have looked critically at eye protection, but the society also acknowledges “appropriate personal protective equipment includes, in addition to a mask or respirator, eye protection, gown and gloves.”1 In addition, the CDC recommends that, for healthcare workers located in areas with moderate or higher prevalence of COVID-19, HCPs should wear eye protection in addition to facemasks since they may encounter asymptomatic individuals with COVID-19.
Gowns and gloves
Gowns and gloves are recommended as a part of personal protective gear when caring for patients who have COVID-19. The IDSA guideline is clear in its recommendations, but does not cite evidence for having no gloves versus having gloves. Furthermore, they state that the evidence is insufficient to recommend double gloves, with the top glove used to take off a personal protective gown, and the inner glove discarded after the gown is removed. The CDC do not make recommendations for routine use of gloves in the care of patients who do not have COVID-19, even in areas where there may be asymptomatic COVID-19, and recommends standard precautions, specifically practicing hand hygiene before and after patient contact.8
The Bottom Line
When seeing patients with COVID-19, N-95 masks, goggles or face shields, gowns, and gloves should be used, with hand hygiene routinely practiced before and after seeing patients. For offices seeing patients not suspected of having COVID-19, the IDSA guideline clarifies that there is not a statistical difference in acquisition of infection with the use of surgical face masks vs N95 respirators. According to the CDC recommendations, eye protection in addition to facemasks should be used by the health care provider, and masks should be worn by patients. Hand hygiene should be used routinely before and after all patient contact. With use of these approaches, it should be safe for offices to reopen and see patients.
Neil Skolnik, MD, is professor of family and community medicine at the Thomas Jefferson University, Philadelphia, and associate director of the Family Medicine Residency Program at Abington (Pa.) Jefferson Health. Jeffrey Matthews, DO, is a second-year resident in the Family Medicine Residency at Abington Jefferson Health. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Lynch JB, Davitkov P, Anderson DJ, et al. COVID-19 Guideline, Part 2: Infection Prevention. IDSA Home. https://www.idsociety.org/practice-guideline/covid-19-guideline-infection-prevention/. April 27, 2020. Accessed June 10, 2020.
2. J Hosp Infect. 2020 May;105(1):104-5.
3. Lancet. 2003;361(9368):1519-20.
4. Influenza Other Respir Viruses. 2020 Apr 4. doi: 2020;10.1111/irv.12745.
5. J Hosp Infect. 2010;74(3):271-7.
6. Clin Infect Dis. 2016;63(8):999-1006.
7. Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed Jun 16, 2020.
8. Centers for Disease Control and Prevention. Healthcare Infection Prevention and Control FAQs for COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-faq.html. Accessed June 15, 2020.
As we reopen our offices we are faced with the challenge of determining the best way to do it safely – protecting ourselves, our staff, and our patients.
In this column we will focus on selected details of the recommendations from IDSA and the CDC that may be helpful in primary care offices.
Face masks
Many clinicians have asked whether a physician should use a mask while seeing patients without COVID-19 in the office, and if yes, which type. The IDSA guideline states that mask usage is imperative for reducing the risk of health care workers contracting COVID-19.1 The evidence is derived from a number of sources, including a retrospective study from Wuhan (China) University that examined two groups of health care workers during the outbreak. The first group wore N95 masks and washed their hands frequently, while the second group did not wear masks and washed their hands less frequently. In the group that took greater actions to protect themselves, none of the 493 staff members contracted COVID-19, compared with 10 of 213 staff members in the other group. The decrease in infection rate occurred in the group that wore masks despite the fact that this group had 733% more exposure to COVID-19 patients.2 Further evidence came from a case-control study done in hospitals in Hong Kong during the 2003 SARS-CoV outbreak.3 This study showed that mask wearing was the most significant intervention for reducing infection, followed by gowning, and then handwashing. These findings make it clear that mask usage is a must for all health care providers who may be caring for patients who could have COVID-19.
The guideline also reviews evidence about the use of surgical masks versus N95 masks. On reviewing indirect evidence from the SARS-CoV epidemic, IDSA found that wearing any mask – surgical or N95 – led to a large reduction in the risk of developing an infection. In this systematic review of five observational studies in health care personnel, for those wearing surgical masks, the odds ratio for developing an infection was 0.13 (95% CI, 0.03-0.62), and for those wearing N95 masks, the odds ratio was 0.12 (95% CI, 0.06-0.26). There was not a significant difference between risk reductions for those who wore surgical masks and N95 masks, respectively.1,4 The IDSA guideline panel recommended “that health care personnel caring for patients with suspected or known COVID-19 use either a surgical mask or N95 respirator ... as part of appropriate PPE.” Since there is not a significant difference in outcomes between those who use surgical masks and those who use N95 respirators, and the IDSA guideline states either type of mask is considered appropriate when taking care of patients with suspected or known COVID-19, in our opinion, use of surgical masks rather than N95s is sufficient when performing low-risk activities. Such activities include seeing patients who do not have a high likelihood of COVID-19 in the office setting.
The IDSA recommendation also discusses universal masking, defined as both patients and clinicians wearing masks. The recommendation is supported by the findings of a study in which universal mask usage was used to prevent the spread of H1N 1 during the 2009 outbreak. In this study of staff members and patients exposed to H1N1 who all wore masks, only 0.48% of 836 acquired infection. In the same study, not wearing a mask by either the provider or patient increased the risk of infection.5 Also, in a prospective study of hematopoietic stem cell transplant patients, universal masking caused infection rates to drop from 10.3% to 4.4%.6
The IDSA guideline states the following: “There may be some, albeit uncertain, benefit to universal masking in the absence of resource constraints. However, the benefits of universal masking with surgical masks should be weighed against the risk of increasing the PPE burn rate and contextualized to the background COVID-19 prevalence rate for asymptomatic or minimally symptomatic HCPs [health care providers] and visitors.”1
The CDC’s guidance statement says the following: “Continued community transmission has increased the number of individuals potentially exposed to and infectious with SARS-CoV-2. Fever and symptom screening have proven to be relatively ineffective in identifying all infected individuals, including HCPs. Symptom screening also will not identify individuals who are infected but otherwise asymptomatic or pre-symptomatic; additional interventions are needed to limit the unrecognized introduction of SARS-CoV-2 into healthcare settings by these individuals. As part of aggressive source control measures, healthcare facilities should consider implementing policies requiring everyone entering the facility to wear a cloth face covering (if tolerated) while in the building, regardless of symptoms.”7
It is our opinion, based on the CDC and IDSA recommendations, that both clinicians and patients should be required to wear masks when patients are seen in the office if possible. Many offices have instituted a policy that says, if a patient refuses to wear a mask during an office visit, then the patient will not be seen.
Eye protection
Many clinicians are uncertain about whether eye protection needs to be used when seeing asymptomatic patients. The IDSA acknowledges that there are not studies that have looked critically at eye protection, but the society also acknowledges “appropriate personal protective equipment includes, in addition to a mask or respirator, eye protection, gown and gloves.”1 In addition, the CDC recommends that, for healthcare workers located in areas with moderate or higher prevalence of COVID-19, HCPs should wear eye protection in addition to facemasks since they may encounter asymptomatic individuals with COVID-19.
Gowns and gloves
Gowns and gloves are recommended as a part of personal protective gear when caring for patients who have COVID-19. The IDSA guideline is clear in its recommendations, but does not cite evidence for having no gloves versus having gloves. Furthermore, they state that the evidence is insufficient to recommend double gloves, with the top glove used to take off a personal protective gown, and the inner glove discarded after the gown is removed. The CDC do not make recommendations for routine use of gloves in the care of patients who do not have COVID-19, even in areas where there may be asymptomatic COVID-19, and recommends standard precautions, specifically practicing hand hygiene before and after patient contact.8
The Bottom Line
When seeing patients with COVID-19, N-95 masks, goggles or face shields, gowns, and gloves should be used, with hand hygiene routinely practiced before and after seeing patients. For offices seeing patients not suspected of having COVID-19, the IDSA guideline clarifies that there is not a statistical difference in acquisition of infection with the use of surgical face masks vs N95 respirators. According to the CDC recommendations, eye protection in addition to facemasks should be used by the health care provider, and masks should be worn by patients. Hand hygiene should be used routinely before and after all patient contact. With use of these approaches, it should be safe for offices to reopen and see patients.
Neil Skolnik, MD, is professor of family and community medicine at the Thomas Jefferson University, Philadelphia, and associate director of the Family Medicine Residency Program at Abington (Pa.) Jefferson Health. Jeffrey Matthews, DO, is a second-year resident in the Family Medicine Residency at Abington Jefferson Health. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Lynch JB, Davitkov P, Anderson DJ, et al. COVID-19 Guideline, Part 2: Infection Prevention. IDSA Home. https://www.idsociety.org/practice-guideline/covid-19-guideline-infection-prevention/. April 27, 2020. Accessed June 10, 2020.
2. J Hosp Infect. 2020 May;105(1):104-5.
3. Lancet. 2003;361(9368):1519-20.
4. Influenza Other Respir Viruses. 2020 Apr 4. doi: 2020;10.1111/irv.12745.
5. J Hosp Infect. 2010;74(3):271-7.
6. Clin Infect Dis. 2016;63(8):999-1006.
7. Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed Jun 16, 2020.
8. Centers for Disease Control and Prevention. Healthcare Infection Prevention and Control FAQs for COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-faq.html. Accessed June 15, 2020.
As we reopen our offices we are faced with the challenge of determining the best way to do it safely – protecting ourselves, our staff, and our patients.
In this column we will focus on selected details of the recommendations from IDSA and the CDC that may be helpful in primary care offices.
Face masks
Many clinicians have asked whether a physician should use a mask while seeing patients without COVID-19 in the office, and if yes, which type. The IDSA guideline states that mask usage is imperative for reducing the risk of health care workers contracting COVID-19.1 The evidence is derived from a number of sources, including a retrospective study from Wuhan (China) University that examined two groups of health care workers during the outbreak. The first group wore N95 masks and washed their hands frequently, while the second group did not wear masks and washed their hands less frequently. In the group that took greater actions to protect themselves, none of the 493 staff members contracted COVID-19, compared with 10 of 213 staff members in the other group. The decrease in infection rate occurred in the group that wore masks despite the fact that this group had 733% more exposure to COVID-19 patients.2 Further evidence came from a case-control study done in hospitals in Hong Kong during the 2003 SARS-CoV outbreak.3 This study showed that mask wearing was the most significant intervention for reducing infection, followed by gowning, and then handwashing. These findings make it clear that mask usage is a must for all health care providers who may be caring for patients who could have COVID-19.
The guideline also reviews evidence about the use of surgical masks versus N95 masks. On reviewing indirect evidence from the SARS-CoV epidemic, IDSA found that wearing any mask – surgical or N95 – led to a large reduction in the risk of developing an infection. In this systematic review of five observational studies in health care personnel, for those wearing surgical masks, the odds ratio for developing an infection was 0.13 (95% CI, 0.03-0.62), and for those wearing N95 masks, the odds ratio was 0.12 (95% CI, 0.06-0.26). There was not a significant difference between risk reductions for those who wore surgical masks and N95 masks, respectively.1,4 The IDSA guideline panel recommended “that health care personnel caring for patients with suspected or known COVID-19 use either a surgical mask or N95 respirator ... as part of appropriate PPE.” Since there is not a significant difference in outcomes between those who use surgical masks and those who use N95 respirators, and the IDSA guideline states either type of mask is considered appropriate when taking care of patients with suspected or known COVID-19, in our opinion, use of surgical masks rather than N95s is sufficient when performing low-risk activities. Such activities include seeing patients who do not have a high likelihood of COVID-19 in the office setting.
The IDSA recommendation also discusses universal masking, defined as both patients and clinicians wearing masks. The recommendation is supported by the findings of a study in which universal mask usage was used to prevent the spread of H1N 1 during the 2009 outbreak. In this study of staff members and patients exposed to H1N1 who all wore masks, only 0.48% of 836 acquired infection. In the same study, not wearing a mask by either the provider or patient increased the risk of infection.5 Also, in a prospective study of hematopoietic stem cell transplant patients, universal masking caused infection rates to drop from 10.3% to 4.4%.6
The IDSA guideline states the following: “There may be some, albeit uncertain, benefit to universal masking in the absence of resource constraints. However, the benefits of universal masking with surgical masks should be weighed against the risk of increasing the PPE burn rate and contextualized to the background COVID-19 prevalence rate for asymptomatic or minimally symptomatic HCPs [health care providers] and visitors.”1
The CDC’s guidance statement says the following: “Continued community transmission has increased the number of individuals potentially exposed to and infectious with SARS-CoV-2. Fever and symptom screening have proven to be relatively ineffective in identifying all infected individuals, including HCPs. Symptom screening also will not identify individuals who are infected but otherwise asymptomatic or pre-symptomatic; additional interventions are needed to limit the unrecognized introduction of SARS-CoV-2 into healthcare settings by these individuals. As part of aggressive source control measures, healthcare facilities should consider implementing policies requiring everyone entering the facility to wear a cloth face covering (if tolerated) while in the building, regardless of symptoms.”7
It is our opinion, based on the CDC and IDSA recommendations, that both clinicians and patients should be required to wear masks when patients are seen in the office if possible. Many offices have instituted a policy that says, if a patient refuses to wear a mask during an office visit, then the patient will not be seen.
Eye protection
Many clinicians are uncertain about whether eye protection needs to be used when seeing asymptomatic patients. The IDSA acknowledges that there are not studies that have looked critically at eye protection, but the society also acknowledges “appropriate personal protective equipment includes, in addition to a mask or respirator, eye protection, gown and gloves.”1 In addition, the CDC recommends that, for healthcare workers located in areas with moderate or higher prevalence of COVID-19, HCPs should wear eye protection in addition to facemasks since they may encounter asymptomatic individuals with COVID-19.
Gowns and gloves
Gowns and gloves are recommended as a part of personal protective gear when caring for patients who have COVID-19. The IDSA guideline is clear in its recommendations, but does not cite evidence for having no gloves versus having gloves. Furthermore, they state that the evidence is insufficient to recommend double gloves, with the top glove used to take off a personal protective gown, and the inner glove discarded after the gown is removed. The CDC do not make recommendations for routine use of gloves in the care of patients who do not have COVID-19, even in areas where there may be asymptomatic COVID-19, and recommends standard precautions, specifically practicing hand hygiene before and after patient contact.8
The Bottom Line
When seeing patients with COVID-19, N-95 masks, goggles or face shields, gowns, and gloves should be used, with hand hygiene routinely practiced before and after seeing patients. For offices seeing patients not suspected of having COVID-19, the IDSA guideline clarifies that there is not a statistical difference in acquisition of infection with the use of surgical face masks vs N95 respirators. According to the CDC recommendations, eye protection in addition to facemasks should be used by the health care provider, and masks should be worn by patients. Hand hygiene should be used routinely before and after all patient contact. With use of these approaches, it should be safe for offices to reopen and see patients.
Neil Skolnik, MD, is professor of family and community medicine at the Thomas Jefferson University, Philadelphia, and associate director of the Family Medicine Residency Program at Abington (Pa.) Jefferson Health. Jeffrey Matthews, DO, is a second-year resident in the Family Medicine Residency at Abington Jefferson Health. For questions or comments, feel free to contact Dr. Skolnik on Twitter @NeilSkolnik.
References
1. Lynch JB, Davitkov P, Anderson DJ, et al. COVID-19 Guideline, Part 2: Infection Prevention. IDSA Home. https://www.idsociety.org/practice-guideline/covid-19-guideline-infection-prevention/. April 27, 2020. Accessed June 10, 2020.
2. J Hosp Infect. 2020 May;105(1):104-5.
3. Lancet. 2003;361(9368):1519-20.
4. Influenza Other Respir Viruses. 2020 Apr 4. doi: 2020;10.1111/irv.12745.
5. J Hosp Infect. 2010;74(3):271-7.
6. Clin Infect Dis. 2016;63(8):999-1006.
7. Centers for Disease Control and Prevention. Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html. Accessed Jun 16, 2020.
8. Centers for Disease Control and Prevention. Healthcare Infection Prevention and Control FAQs for COVID-19. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-faq.html. Accessed June 15, 2020.