User login
In Case You Missed It: COVID
Rapid establishment of therapeutic protocols during the pandemic
Summary
Evidence on emerging therapeutics and the treatment of COVID-19 and its complications has been incomplete, often contradictory, and rapidly changing. The brisk development of effective strategies aimed at identifying, isolating, and treating this disease requires an equally fluid response. At Dell Seton Medical Center, a safety-net hospital that serves Austin in central Texas, our hospitalists have led the formation of numerous collaborative work groups to address the appropriate triage, management, and operational processes during the COVID-19 evolving pandemic.
We created a hospitalist-led COVID Therapeutics and Informatics Committee composed of specialists (infectious disease, pulmonary and critical care, hematology/oncology, neurology), pharmacy, nursing leadership, and the hospital chief medical officer). This committee was formed to evaluate and reach consensus regarding therapeutic interventions in order to ensure appropriate and timely evidence-based treatment. The goal was to limit practice variation and create a shared mental model to deliver consistent value-based care without increasing complexity. We discuss how evidence was evaluated in an interprofessional setting, focusing on not just the quality of data, but its application in an environment of uncertainty and resource scarcity.
We review the use of electronic communication platforms to facilitate direct and rapid communication among interprofessional providers and hospital leadership. We also discuss the development of creative workarounds to build protocols into the electronic medical record to implement new therapeutic interventions in real time.
This approach allows the rapid establishment and adoption of therapeutic protocols based on expert and consensus opinion in the absence of comprehensive national guidelines. This model may also be adopted for other complex disease states that require coordinated interprofessional interventions and frequent revisions to the standard of care.
Key takeaways
1. Protocols improve care by creating a shared framework for approaching complex diseases and open communication within teams to personalize care.
2. Rapidly appraising evidence requires equipoise, thoughtful interpretation of retrospective data, and applying that specifically to a hospital’s local context.
3. Guidelines are best utilized when they are built into clinical care through Standardized Order Sets and disseminated in multiple modalities that reach their audience just in time.
4. The perfect can’t be the enemy of the good.
Protocolized care in progress: Rapid appraisal of evidence and standardization of practice in a pandemic
Live Q&A: Tuesday, Aug. 11, 1:00-2:00 p.m.
Dr. Brode and Dr. Busch are assistant professors in the department of internal medicine at Dell Medical School, University of Texas, Austin.
Summary
Evidence on emerging therapeutics and the treatment of COVID-19 and its complications has been incomplete, often contradictory, and rapidly changing. The brisk development of effective strategies aimed at identifying, isolating, and treating this disease requires an equally fluid response. At Dell Seton Medical Center, a safety-net hospital that serves Austin in central Texas, our hospitalists have led the formation of numerous collaborative work groups to address the appropriate triage, management, and operational processes during the COVID-19 evolving pandemic.
We created a hospitalist-led COVID Therapeutics and Informatics Committee composed of specialists (infectious disease, pulmonary and critical care, hematology/oncology, neurology), pharmacy, nursing leadership, and the hospital chief medical officer). This committee was formed to evaluate and reach consensus regarding therapeutic interventions in order to ensure appropriate and timely evidence-based treatment. The goal was to limit practice variation and create a shared mental model to deliver consistent value-based care without increasing complexity. We discuss how evidence was evaluated in an interprofessional setting, focusing on not just the quality of data, but its application in an environment of uncertainty and resource scarcity.
We review the use of electronic communication platforms to facilitate direct and rapid communication among interprofessional providers and hospital leadership. We also discuss the development of creative workarounds to build protocols into the electronic medical record to implement new therapeutic interventions in real time.
This approach allows the rapid establishment and adoption of therapeutic protocols based on expert and consensus opinion in the absence of comprehensive national guidelines. This model may also be adopted for other complex disease states that require coordinated interprofessional interventions and frequent revisions to the standard of care.
Key takeaways
1. Protocols improve care by creating a shared framework for approaching complex diseases and open communication within teams to personalize care.
2. Rapidly appraising evidence requires equipoise, thoughtful interpretation of retrospective data, and applying that specifically to a hospital’s local context.
3. Guidelines are best utilized when they are built into clinical care through Standardized Order Sets and disseminated in multiple modalities that reach their audience just in time.
4. The perfect can’t be the enemy of the good.
Protocolized care in progress: Rapid appraisal of evidence and standardization of practice in a pandemic
Live Q&A: Tuesday, Aug. 11, 1:00-2:00 p.m.
Dr. Brode and Dr. Busch are assistant professors in the department of internal medicine at Dell Medical School, University of Texas, Austin.
Summary
Evidence on emerging therapeutics and the treatment of COVID-19 and its complications has been incomplete, often contradictory, and rapidly changing. The brisk development of effective strategies aimed at identifying, isolating, and treating this disease requires an equally fluid response. At Dell Seton Medical Center, a safety-net hospital that serves Austin in central Texas, our hospitalists have led the formation of numerous collaborative work groups to address the appropriate triage, management, and operational processes during the COVID-19 evolving pandemic.
We created a hospitalist-led COVID Therapeutics and Informatics Committee composed of specialists (infectious disease, pulmonary and critical care, hematology/oncology, neurology), pharmacy, nursing leadership, and the hospital chief medical officer). This committee was formed to evaluate and reach consensus regarding therapeutic interventions in order to ensure appropriate and timely evidence-based treatment. The goal was to limit practice variation and create a shared mental model to deliver consistent value-based care without increasing complexity. We discuss how evidence was evaluated in an interprofessional setting, focusing on not just the quality of data, but its application in an environment of uncertainty and resource scarcity.
We review the use of electronic communication platforms to facilitate direct and rapid communication among interprofessional providers and hospital leadership. We also discuss the development of creative workarounds to build protocols into the electronic medical record to implement new therapeutic interventions in real time.
This approach allows the rapid establishment and adoption of therapeutic protocols based on expert and consensus opinion in the absence of comprehensive national guidelines. This model may also be adopted for other complex disease states that require coordinated interprofessional interventions and frequent revisions to the standard of care.
Key takeaways
1. Protocols improve care by creating a shared framework for approaching complex diseases and open communication within teams to personalize care.
2. Rapidly appraising evidence requires equipoise, thoughtful interpretation of retrospective data, and applying that specifically to a hospital’s local context.
3. Guidelines are best utilized when they are built into clinical care through Standardized Order Sets and disseminated in multiple modalities that reach their audience just in time.
4. The perfect can’t be the enemy of the good.
Protocolized care in progress: Rapid appraisal of evidence and standardization of practice in a pandemic
Live Q&A: Tuesday, Aug. 11, 1:00-2:00 p.m.
Dr. Brode and Dr. Busch are assistant professors in the department of internal medicine at Dell Medical School, University of Texas, Austin.
Cutaneous clues linked to COVID-19 coagulation risk
, new evidence suggests.
Researchers at Weill Cornell Medicine NewYork–Presbyterian Medical Center in New York linked livedoid and purpuric skin eruptions to a greater likelihood for occlusive vascular disease associated with SARS-CoV-2 infection in a small case series.
These skin signs could augment coagulation assays in this patient population. “Physicians should consider a hematology consult for potential anticoagulation in patients with these skin presentations and severe COVID-19,” senior author Joanna Harp, MD, said in an interview.
“Physicians should also consider D-dimer, fibrinogen, coagulation studies, and a skin biopsy given that there are other diagnoses on the differential as well.”
The research letter was published online on Aug. 5 in JAMA Dermatology.
The findings build on multiple previous reports of skin manifestations associated with COVID-19, including a study of 375 patients in Spain. Among people with suspected or confirmed SARS-CoV-2 infection, senior author of the Spanish research, Ignacio Garcia-Doval, MD, PhD, also observed livedoid and necrotic skin eruptions more commonly in severe disease.
“I think that this case series [from Harp and colleagues] confirms the findings of our previous paper – that patients with livedoid or necrotic lesions have a worse prognosis, as these are markers of vascular occlusion,” he said in an interview.
Dr. Harp and colleagues reported their observations with four patients aged 40-80 years. Each had severe COVID-19 with acute respiratory distress syndrome and required intubation. Treating clinicians requested a dermatology consult to assess acral fixed livedo racemosa and retiform purpura presentations.
D-dimer levels exceeded 3 mcg/mL in each case. All four patients had a suspected pulmonary embolism within 1-5 days of the dermatologic findings. Prophylactic anticoagulation at admission was changed to therapeutic anticoagulation because of increasing D-dimer levels and the suspected thrombotic events.
“I think that the paper is interesting because it shows the associated histopathological findings and has important clinical implications due to the association with pulmonary embolism,” said Dr. Garcia-Doval, a researcher at the Spanish Academy of Dermatology in Madrid. “These patients should probably be anticoagulated.”
Skin biopsy results
Punch biopsies revealed pauci-inflammatory thrombogenic vasculopathy involving capillaries, venules, arterioles, or small arteries.
Livedo racemosa skin findings point to partial occlusion of cutaneous blood vessels, whereas retiform purpura indicate full occlusion of cutaneous blood vessels.
An inability to confirm the exact timing of the onset of the skin rash was a limitation of the study.
“The findings suggest that clinicians caring for patients with COVID-19 should be aware of livedoid and purpuric rashes as potential manifestations of an underlying hypercoagulable state,” the authors noted. “If these skin findings are identified, a skin biopsy should be considered because the result may guide anticoagulation management.”
Observations during an outbreak
The researchers observed these cases between March 13 and April 3, during the peak of the COVID-19 outbreak in New York.
“We did see additional cases since our study period. However, it has decreased significantly with the falling number of COVID-19 cases in the city,” said Dr. Harp, a dermatologist at NewYork–Presbyterian.
Another contributing factor in the drop in cases was “implementation of earlier, more aggressive anticoagulation in many of these patients at our institution,” she added.
The investigators plan to continue the research. “We are working on a more formalized study,” lead author Caren Droesch, MD, said in an interview.
“But given very low patient numbers in our area we have not started recruiting patients,” said Dr. Droesch, a resident at Weill Cornell Medicine and NewYork–Presbyterian at the time of the study. She is now a dermatologist at Mass General Brigham in Wellesley, Mass.
Consider a dermatology consult
“This is a small case series of four patients, but mirrors what we have seen at our institution and what others have reported about individual patients around the world,” Anthony Fernandez, MD, PhD, a dermatologist at Cleveland Clinic, said in an interview. “The skin, like many other organ systems, can be affected by thrombotic events within the setting of COVID-19 disease.”
As in the current study, Dr. Fernandez observed skin manifestations in people with severe COVID-19 with elevated D-dimer levels. These patients typically require mechanical ventilation in the intensive care unit, he added.
“As these authors point out, it is important for all clinicians caring for COVID-19 patients to look for these rashes,” said Dr. Fernandez, who coauthored a report on skin manifestations in this patient population. “We also agree that clinicians should have a low threshold for consulting dermatology. A skin biopsy is minimally invasive and can be important in confirming or refuting that such rashes are truly reflective of thrombotic vasculopathy.”
Dr. Harp, Dr. Droesch and Dr. Garcia-Doval have disclosed no relevant financial relationships. Dr. Fernandez received funding from the Clinical and Translational Science Collaborative at Case Western Reserve University to study skin manifestations of COVID-19.
A version of this article originally appeared on Medscape.com.
, new evidence suggests.
Researchers at Weill Cornell Medicine NewYork–Presbyterian Medical Center in New York linked livedoid and purpuric skin eruptions to a greater likelihood for occlusive vascular disease associated with SARS-CoV-2 infection in a small case series.
These skin signs could augment coagulation assays in this patient population. “Physicians should consider a hematology consult for potential anticoagulation in patients with these skin presentations and severe COVID-19,” senior author Joanna Harp, MD, said in an interview.
“Physicians should also consider D-dimer, fibrinogen, coagulation studies, and a skin biopsy given that there are other diagnoses on the differential as well.”
The research letter was published online on Aug. 5 in JAMA Dermatology.
The findings build on multiple previous reports of skin manifestations associated with COVID-19, including a study of 375 patients in Spain. Among people with suspected or confirmed SARS-CoV-2 infection, senior author of the Spanish research, Ignacio Garcia-Doval, MD, PhD, also observed livedoid and necrotic skin eruptions more commonly in severe disease.
“I think that this case series [from Harp and colleagues] confirms the findings of our previous paper – that patients with livedoid or necrotic lesions have a worse prognosis, as these are markers of vascular occlusion,” he said in an interview.
Dr. Harp and colleagues reported their observations with four patients aged 40-80 years. Each had severe COVID-19 with acute respiratory distress syndrome and required intubation. Treating clinicians requested a dermatology consult to assess acral fixed livedo racemosa and retiform purpura presentations.
D-dimer levels exceeded 3 mcg/mL in each case. All four patients had a suspected pulmonary embolism within 1-5 days of the dermatologic findings. Prophylactic anticoagulation at admission was changed to therapeutic anticoagulation because of increasing D-dimer levels and the suspected thrombotic events.
“I think that the paper is interesting because it shows the associated histopathological findings and has important clinical implications due to the association with pulmonary embolism,” said Dr. Garcia-Doval, a researcher at the Spanish Academy of Dermatology in Madrid. “These patients should probably be anticoagulated.”
Skin biopsy results
Punch biopsies revealed pauci-inflammatory thrombogenic vasculopathy involving capillaries, venules, arterioles, or small arteries.
Livedo racemosa skin findings point to partial occlusion of cutaneous blood vessels, whereas retiform purpura indicate full occlusion of cutaneous blood vessels.
An inability to confirm the exact timing of the onset of the skin rash was a limitation of the study.
“The findings suggest that clinicians caring for patients with COVID-19 should be aware of livedoid and purpuric rashes as potential manifestations of an underlying hypercoagulable state,” the authors noted. “If these skin findings are identified, a skin biopsy should be considered because the result may guide anticoagulation management.”
Observations during an outbreak
The researchers observed these cases between March 13 and April 3, during the peak of the COVID-19 outbreak in New York.
“We did see additional cases since our study period. However, it has decreased significantly with the falling number of COVID-19 cases in the city,” said Dr. Harp, a dermatologist at NewYork–Presbyterian.
Another contributing factor in the drop in cases was “implementation of earlier, more aggressive anticoagulation in many of these patients at our institution,” she added.
The investigators plan to continue the research. “We are working on a more formalized study,” lead author Caren Droesch, MD, said in an interview.
“But given very low patient numbers in our area we have not started recruiting patients,” said Dr. Droesch, a resident at Weill Cornell Medicine and NewYork–Presbyterian at the time of the study. She is now a dermatologist at Mass General Brigham in Wellesley, Mass.
Consider a dermatology consult
“This is a small case series of four patients, but mirrors what we have seen at our institution and what others have reported about individual patients around the world,” Anthony Fernandez, MD, PhD, a dermatologist at Cleveland Clinic, said in an interview. “The skin, like many other organ systems, can be affected by thrombotic events within the setting of COVID-19 disease.”
As in the current study, Dr. Fernandez observed skin manifestations in people with severe COVID-19 with elevated D-dimer levels. These patients typically require mechanical ventilation in the intensive care unit, he added.
“As these authors point out, it is important for all clinicians caring for COVID-19 patients to look for these rashes,” said Dr. Fernandez, who coauthored a report on skin manifestations in this patient population. “We also agree that clinicians should have a low threshold for consulting dermatology. A skin biopsy is minimally invasive and can be important in confirming or refuting that such rashes are truly reflective of thrombotic vasculopathy.”
Dr. Harp, Dr. Droesch and Dr. Garcia-Doval have disclosed no relevant financial relationships. Dr. Fernandez received funding from the Clinical and Translational Science Collaborative at Case Western Reserve University to study skin manifestations of COVID-19.
A version of this article originally appeared on Medscape.com.
, new evidence suggests.
Researchers at Weill Cornell Medicine NewYork–Presbyterian Medical Center in New York linked livedoid and purpuric skin eruptions to a greater likelihood for occlusive vascular disease associated with SARS-CoV-2 infection in a small case series.
These skin signs could augment coagulation assays in this patient population. “Physicians should consider a hematology consult for potential anticoagulation in patients with these skin presentations and severe COVID-19,” senior author Joanna Harp, MD, said in an interview.
“Physicians should also consider D-dimer, fibrinogen, coagulation studies, and a skin biopsy given that there are other diagnoses on the differential as well.”
The research letter was published online on Aug. 5 in JAMA Dermatology.
The findings build on multiple previous reports of skin manifestations associated with COVID-19, including a study of 375 patients in Spain. Among people with suspected or confirmed SARS-CoV-2 infection, senior author of the Spanish research, Ignacio Garcia-Doval, MD, PhD, also observed livedoid and necrotic skin eruptions more commonly in severe disease.
“I think that this case series [from Harp and colleagues] confirms the findings of our previous paper – that patients with livedoid or necrotic lesions have a worse prognosis, as these are markers of vascular occlusion,” he said in an interview.
Dr. Harp and colleagues reported their observations with four patients aged 40-80 years. Each had severe COVID-19 with acute respiratory distress syndrome and required intubation. Treating clinicians requested a dermatology consult to assess acral fixed livedo racemosa and retiform purpura presentations.
D-dimer levels exceeded 3 mcg/mL in each case. All four patients had a suspected pulmonary embolism within 1-5 days of the dermatologic findings. Prophylactic anticoagulation at admission was changed to therapeutic anticoagulation because of increasing D-dimer levels and the suspected thrombotic events.
“I think that the paper is interesting because it shows the associated histopathological findings and has important clinical implications due to the association with pulmonary embolism,” said Dr. Garcia-Doval, a researcher at the Spanish Academy of Dermatology in Madrid. “These patients should probably be anticoagulated.”
Skin biopsy results
Punch biopsies revealed pauci-inflammatory thrombogenic vasculopathy involving capillaries, venules, arterioles, or small arteries.
Livedo racemosa skin findings point to partial occlusion of cutaneous blood vessels, whereas retiform purpura indicate full occlusion of cutaneous blood vessels.
An inability to confirm the exact timing of the onset of the skin rash was a limitation of the study.
“The findings suggest that clinicians caring for patients with COVID-19 should be aware of livedoid and purpuric rashes as potential manifestations of an underlying hypercoagulable state,” the authors noted. “If these skin findings are identified, a skin biopsy should be considered because the result may guide anticoagulation management.”
Observations during an outbreak
The researchers observed these cases between March 13 and April 3, during the peak of the COVID-19 outbreak in New York.
“We did see additional cases since our study period. However, it has decreased significantly with the falling number of COVID-19 cases in the city,” said Dr. Harp, a dermatologist at NewYork–Presbyterian.
Another contributing factor in the drop in cases was “implementation of earlier, more aggressive anticoagulation in many of these patients at our institution,” she added.
The investigators plan to continue the research. “We are working on a more formalized study,” lead author Caren Droesch, MD, said in an interview.
“But given very low patient numbers in our area we have not started recruiting patients,” said Dr. Droesch, a resident at Weill Cornell Medicine and NewYork–Presbyterian at the time of the study. She is now a dermatologist at Mass General Brigham in Wellesley, Mass.
Consider a dermatology consult
“This is a small case series of four patients, but mirrors what we have seen at our institution and what others have reported about individual patients around the world,” Anthony Fernandez, MD, PhD, a dermatologist at Cleveland Clinic, said in an interview. “The skin, like many other organ systems, can be affected by thrombotic events within the setting of COVID-19 disease.”
As in the current study, Dr. Fernandez observed skin manifestations in people with severe COVID-19 with elevated D-dimer levels. These patients typically require mechanical ventilation in the intensive care unit, he added.
“As these authors point out, it is important for all clinicians caring for COVID-19 patients to look for these rashes,” said Dr. Fernandez, who coauthored a report on skin manifestations in this patient population. “We also agree that clinicians should have a low threshold for consulting dermatology. A skin biopsy is minimally invasive and can be important in confirming or refuting that such rashes are truly reflective of thrombotic vasculopathy.”
Dr. Harp, Dr. Droesch and Dr. Garcia-Doval have disclosed no relevant financial relationships. Dr. Fernandez received funding from the Clinical and Translational Science Collaborative at Case Western Reserve University to study skin manifestations of COVID-19.
A version of this article originally appeared on Medscape.com.
FROM JAMA DERMATOLOGY
When you see something ...
Over the last several decades science has fallen off this country’s radar screen. Yes, STEM (science, technology, engineering, and mathematics) has recently had a brief moment in the spotlight as a buzzword de jour. But the critical importance of careful and systematic investigation into the world around us using observation and trial and error is a tough sell to a large segment of our population.

The COVID-19 pandemic is providing an excellent opportunity for science and medicine to showcase their star qualities. Of course some people in leadership positions persist in disregarding the value of scientific investigation. But I get the feeling that the fear generated by the pandemic is creating some converts among many previous science skeptics. This gathering enthusiasm among the general population is a predictably slow process because that’s the way science works. It often doesn’t provide quick answers. And it is difficult for the nonscientist to see the beauty in the reality that the things we thought were true 2 months ago are likely to be proven wrong today as more observations accumulate.
A recent New York Times article examines the career of one such unscrupulous physician/scientist whose recent exploits threaten to undo much of the positive image the pandemic has cast on science (“The Doctor Behind the Disputed Covid Data,” by Ellen Gabler and Roni Caryn Rabin, The New York Times, July 27, 2020). The subject of the article is the physician who was responsible for providing some of the large data sets on which several papers were published about the apparent ineffectiveness and danger of using hydroxychloroquine in COVID-19 patients. The authenticity of the data sets recently has been seriously questioned, and the articles have been retracted by the journals in which they had appeared.
Based on numerous interviews with coworkers, the Times reporters present a strong case that this individual’s long history of unreliability make his association with allegedly fraudulent data set not surprising but maybe even predictable. At one point in his training, there appears to have been serious questions about advancing the physician to the next level. Despite these concerns, he was allowed to continue and complete his specialty training. It is of note that in his last year of clinical practice, the physician became the subject of three serious malpractice claims that question his competence.

I suspect that some of you have crossed paths with physicians whose competence and/or moral character you found concerning. Were they peers? Were you the individual’s supervisor or was he or she your mentor? How did you respond? Did anyone respond at all?
There has been a lot written and said in recent months about how and when to respond to respond to sexual harassment in the workplace. But I don’t recall reading any articles that discuss how one should respond to incompetence. Of course competency can be a relative term, but in most cases significant incompetence is hard to miss because it tends to be repeated.
It is easy for the airports and subway systems to post signs that say “If you see something say something.” It’s a different story for hospitals and medical schools that may have systems in place for reporting and following up on poor practice. But my sense is that there are too many cases that slip through the cracks.
This is another example of a problem for which I don’t have a solution. However, if this column prompts just one of you who sees something to say something then I have had a good day.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Over the last several decades science has fallen off this country’s radar screen. Yes, STEM (science, technology, engineering, and mathematics) has recently had a brief moment in the spotlight as a buzzword de jour. But the critical importance of careful and systematic investigation into the world around us using observation and trial and error is a tough sell to a large segment of our population.
The COVID-19 pandemic is providing an excellent opportunity for science and medicine to showcase their star qualities. Of course some people in leadership positions persist in disregarding the value of scientific investigation. But I get the feeling that the fear generated by the pandemic is creating some converts among many previous science skeptics. This gathering enthusiasm among the general population is a predictably slow process because that’s the way science works. It often doesn’t provide quick answers. And it is difficult for the nonscientist to see the beauty in the reality that the things we thought were true 2 months ago are likely to be proven wrong today as more observations accumulate.
A recent New York Times article examines the career of one such unscrupulous physician/scientist whose recent exploits threaten to undo much of the positive image the pandemic has cast on science (“The Doctor Behind the Disputed Covid Data,” by Ellen Gabler and Roni Caryn Rabin, The New York Times, July 27, 2020). The subject of the article is the physician who was responsible for providing some of the large data sets on which several papers were published about the apparent ineffectiveness and danger of using hydroxychloroquine in COVID-19 patients. The authenticity of the data sets recently has been seriously questioned, and the articles have been retracted by the journals in which they had appeared.
Based on numerous interviews with coworkers, the Times reporters present a strong case that this individual’s long history of unreliability make his association with allegedly fraudulent data set not surprising but maybe even predictable. At one point in his training, there appears to have been serious questions about advancing the physician to the next level. Despite these concerns, he was allowed to continue and complete his specialty training. It is of note that in his last year of clinical practice, the physician became the subject of three serious malpractice claims that question his competence.
I suspect that some of you have crossed paths with physicians whose competence and/or moral character you found concerning. Were they peers? Were you the individual’s supervisor or was he or she your mentor? How did you respond? Did anyone respond at all?
There has been a lot written and said in recent months about how and when to respond to respond to sexual harassment in the workplace. But I don’t recall reading any articles that discuss how one should respond to incompetence. Of course competency can be a relative term, but in most cases significant incompetence is hard to miss because it tends to be repeated.
It is easy for the airports and subway systems to post signs that say “If you see something say something.” It’s a different story for hospitals and medical schools that may have systems in place for reporting and following up on poor practice. But my sense is that there are too many cases that slip through the cracks.
This is another example of a problem for which I don’t have a solution. However, if this column prompts just one of you who sees something to say something then I have had a good day.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Over the last several decades science has fallen off this country’s radar screen. Yes, STEM (science, technology, engineering, and mathematics) has recently had a brief moment in the spotlight as a buzzword de jour. But the critical importance of careful and systematic investigation into the world around us using observation and trial and error is a tough sell to a large segment of our population.
The COVID-19 pandemic is providing an excellent opportunity for science and medicine to showcase their star qualities. Of course some people in leadership positions persist in disregarding the value of scientific investigation. But I get the feeling that the fear generated by the pandemic is creating some converts among many previous science skeptics. This gathering enthusiasm among the general population is a predictably slow process because that’s the way science works. It often doesn’t provide quick answers. And it is difficult for the nonscientist to see the beauty in the reality that the things we thought were true 2 months ago are likely to be proven wrong today as more observations accumulate.
A recent New York Times article examines the career of one such unscrupulous physician/scientist whose recent exploits threaten to undo much of the positive image the pandemic has cast on science (“The Doctor Behind the Disputed Covid Data,” by Ellen Gabler and Roni Caryn Rabin, The New York Times, July 27, 2020). The subject of the article is the physician who was responsible for providing some of the large data sets on which several papers were published about the apparent ineffectiveness and danger of using hydroxychloroquine in COVID-19 patients. The authenticity of the data sets recently has been seriously questioned, and the articles have been retracted by the journals in which they had appeared.
Based on numerous interviews with coworkers, the Times reporters present a strong case that this individual’s long history of unreliability make his association with allegedly fraudulent data set not surprising but maybe even predictable. At one point in his training, there appears to have been serious questions about advancing the physician to the next level. Despite these concerns, he was allowed to continue and complete his specialty training. It is of note that in his last year of clinical practice, the physician became the subject of three serious malpractice claims that question his competence.
I suspect that some of you have crossed paths with physicians whose competence and/or moral character you found concerning. Were they peers? Were you the individual’s supervisor or was he or she your mentor? How did you respond? Did anyone respond at all?
There has been a lot written and said in recent months about how and when to respond to respond to sexual harassment in the workplace. But I don’t recall reading any articles that discuss how one should respond to incompetence. Of course competency can be a relative term, but in most cases significant incompetence is hard to miss because it tends to be repeated.
It is easy for the airports and subway systems to post signs that say “If you see something say something.” It’s a different story for hospitals and medical schools that may have systems in place for reporting and following up on poor practice. But my sense is that there are too many cases that slip through the cracks.
This is another example of a problem for which I don’t have a solution. However, if this column prompts just one of you who sees something to say something then I have had a good day.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Value of palliative care shines clearly in a crisis
Hospitalists have played a key role
For some palliative care professionals, the COVID-19 pandemic, particularly in viral hot spots like New York City, represents a “moment” that could lead to greater awareness of what this service offers to seriously ill patients in a crisis.
They say it has provided an opportunity to show what palliative care teams can contribute to the difficult circumstances of patients with severe symptoms, isolated and alone in quarantined hospitals, with poor survival rates, perhaps sedated for extended stays on scarce ventilators – and for their family members, who are able to visit them only virtually via telephone or tablet.
But it has also highlighted gaps – including insufficient staffing for some palliative care teams. Hospitalists and other clinicians in the hospital need to learn the basics of primary palliative care, such as how to communicate bad news, initiate goals of care conversations, and address common symptoms of serious illness, such as pain. That way, they could shoulder more of the demand for this kind of care when palliative care specialists are in short supply.
Hospitalists, some of whom also have pursued a specialization in palliative care, have played key roles in clarifying and redefining the new role for palliative care, whom it is meant for, and who should provide it. Central to this new role is the greater use of telemedicine – for talking to hospitalized patients without increasing viral exposure, for linking up with family members who can’t visit their loved ones in the hospital, and for helping frontline hospital staff who need a palliative care consultation – or just a chance to debrief on what they are seeing.
A pandemic wake-up call
Elizabeth Gundersen, MD, FHM, FAAHPM, director of the hospice and palliative medicine fellowship program at the Charles E. Schmidt College of Medicine at Florida Atlantic University (FAU) in Boca Raton, practiced hospital medicine for 10 years before pursuing a fellowship in hospice and palliative medicine and working as an academic palliative medicine physician. She calls the pandemic a wake-up call for gaps in care and all the things that weren’t working well in the health care system.

“Now we are seeing more clearly what’s lacking – or broken – and what we will carry forward from this experience into the post-COVID world,” she said. Some hospitalists do palliative care very well, and others don’t feel as comfortable in having these difficult conversations with patients. But in the uncertain course of the virus they get thrust into it.
Although FAU’s associated hospitals were not as inundated with COVID-19 patients in the early weeks of the pandemic as were other regions, the volume of other patients plummeted, Dr. Gundersen said, adding that “there’s still been incredible intensity and worry about the virus. For me, the basic role of palliative care hasn’t changed, and the phrase I have always used when introducing myself – ‘we’re an extra layer of support for the patient and family’ – still holds true,” she said.
“I try to make it clear to people that palliative care is not synonymous with end-of-life care. We don’t want people to think that a palliative care referral implies imminent death. The goal is not to get more people to have a do not attempt resuscitation (DNAR) order, but to determine the patient and family’s treatment goals and whether a DNAR order fits those goals.”
The tough conversations
Dr. Gundersen is cochair of SHM’s Palliative Care Special Interest Group, along with Rab Razzak, MD, clinical director of palliative medicine at University Hospitals Cleveland Medical Center, one of the hospitals affiliated with Case Western University in Cleveland. (Connect with them on Twitter: @Top_Gundersen and @rabrazzak.)

Dr. Razzak also transitioned from hospital medicine to palliative medicine 10 years ago. “As a hospitalist, I enjoyed the tough conversations and bringing the human element into my health care interactions,” he explained. “To me, palliative care is a philosophy of care that puts the person we call the patient at the center of the interaction, while we try to figure out how to best care for them as a person.”
When the pandemic hit, University Hospitals made 20 ICU beds available for COVID-19 patients, Dr. Razzak said. This unit has since been full but not overflowing, while overall hospital census went down. The palliative care team at the hospital includes four inpatient doctors, nurse practitioners, and a chaplain, as well as an outpatient team primarily focused on oncology.
“In some settings, palliative care has been at the forefront of difficult conversations, when things aren’t going well for the patient and there’s much uncertainty,” Dr. Razzak said. The interface between hospital medicine and palliative care can be complementary, he added. “We talk about primary palliative care, which we want every discipline to be able to do – lead meaningful conversations, help manage symptoms.”
The take-home message for hospitalists, he said, is to get training in how to have these discussions, using such resources as VitalTalk (https://www.vitaltalk.org/), a nonprofit organization that disseminates education in communication skills for difficult conversations, and the Center to Advance Palliative Care (www.capc.org) at Icahn School of Medicine at Mount Sinai in New York City. “Once you’ve mastered the conversation, it will get easier. But ask for help when you need it, and learn how to know when you need it.”
Dr. Gundersen added that hospital medicine groups and palliative care teams could reach out to each other and talk about what they did in the crisis and how they can work together in the future. She recommends frequent ongoing support and collaboration that could range from formal conferences or training sessions to informal team interactions, perhaps with sandwiches in the doctor’s lounge – provided that there’s room for social distancing. She has recently started giving talks in the community and grand rounds presentations in hospitals about palliative care.
Other approaches and applications
In New York City, the initial epicenter for the pandemic in the United States, the adult palliative care service of Columbia University Medical Center (CUMC) experienced a sevenfold increase in consultation requests at the apex of the crisis, said its director, Craig Blinderman, MD. That demand was impossible to meet with existing staff. So Dr. Blinderman and colleagues established a virtual consultation model, recruiting and deploying volunteer out-of-state palliative care specialists to staff it.

An eight-bed palliative care unit was opened at CUMC for COVID-19 patients whose surrogates had opted not to initiate or continue intubation or life-sustaining treatments. This helped to relieve some of the pressures on the ICUs while making it possible for in-person visits to the hospice unit by families – in full PPE. Palliative care staff were embedded in various units in the hospital.
A palliative care response team composed of a hospice and palliative medicine fellow and four psychiatry residents or fellows, based in the emergency department and with supervision from the palliative care team, provided time-critical goals of care conversations with families using telemedicine – and a forum for listening to their suffering. Dr. Blinderman and colleagues also have found time to write up their experience for medical journals.1,2
There’s no reason to think that hospitalists, with a little basic training, couldn’t be having these same goals of care conversations, Dr. Blinderman said. “But the fact that hospitalists, at the pandemic’s peak, along with ICU doctors, were seeing an unprecedented magnitude of dying on a daily basis generated a lot of moral distress for them.”
Palliative care professionals, because they engage with these issues in a different way, may be somewhat better equipped to deal with the sheer emotional demands when so many are dying, as at the peak of the surge in New York. “We don’t see dying as a failure on our part but an opportunity to relieve suffering,” Dr. Blinderman said. And the palliative care field also emphasizes the importance of self-care for its practitioners.
“How do we meet the incredible palliative care needs in the epicenter of a pandemic? That question also applies to other kinds of crises we could imagine, for example, climate-related disasters,” Dr. Blinderman said. “What lessons have we learned about the value of palliative care and how to start incorporating it more integrally into the delivery of hospital care? Here we showed that we could work collaboratively with our colleagues at other major medical centers, bringing together their expertise to help us when we didn’t have the bandwidth to meet the demand,” he said.
Scripts can help
“Also, it won’t make sense to just go back to normal (after the crisis fades),” Dr. Blinderman said. “We need to take a close look at how our society is functioning in the wake of the pandemic and the ways the health care system has failed us. We have learned that we’re all interconnected and we need to work together to serve our communities – locally and nationally – applying basic distributive justice.”
Could there be, for example, a national infrastructure for mobilizing and deploying palliative care resources to areas of greatest need, similar to what was done in New York?
At Northwestern Medicine in Chicago, a number of palliative care clinicians at the system’s hospitals worked together to develop scripts designed to help other clinicians start goals of care conversations with patients and families, for use in the hospital as well as in outpatient primary care and other settings, with results integrated into the system’s electronic health record.
Front-line clinicians may not have the time to ask for formal consults from palliative care because of high volume and rapidly changing patient status, explained Eytan Szmuilowicz, MD, director of the section of palliative medicine at Northwestern Memorial Hospital. Or they may not have access to specialty-level palliative care in their settings.
The scripts are aimed at primary care, emergency physicians, and hospitalists needing to consider critical care placement or attempted resuscitation and to ICU clinicians helping families make decisions about life-sustaining treatments. They also can help facilitate advance care planning discussions. An example is “CALMER,” a six-step mnemonic guide to promote goals of care discussions with hospitalized patients. For more information on these scripts, contact Dr. Szmuilowicz: Eytan.Szmuilowicz@nm.org.
Eerily quiet
The COVID-19 crisis has been quite a whirlwind for hospital medicine, said Jeanie Youngwerth, MD, a hospitalist and program director of the palliative care service at the University of Colorado in Denver, which was a significant viral hotspot early on.
“When it first started, things seemed to change almost overnight – starting on Friday, March 13. People had to take action right away to develop work flows and the technology to allow us to see as many patients as possible,” she said. By the time Monday came, it was a whole new ballgame.
Dr. Youngwerth and two colleagues worked quickly to develop inpatient telemedicine capacity where none existed. “We knew we would not be going into patients’ rooms, but most of our team showed up in the hospital to work with the primary care teams. Our job was to see what we could do that actually made a difference,” she said.
“The hospital became a very strange place. You’d walk down the hallway and it was eerily quiet. Everybody you came across was being so nice to each other.” Televisits became a powerful way to bring the human connection back to medical care.
“What we learned from families was that they were thirsting to have some kind of connection with their loved one, and to be able to talk about their loved one and who they were as a person,” she said. “We’d contact the family through video visits and then, when the family meeting ended, the nurse would bring an iPad into the patient’s room so the family could see their loved one on a ventilator. They would immediately start communicating with their loved one, praying aloud, singing, playing music. It would make a huge difference for the family – and for the staff.”
References
1. Nakagawa S et al. Pandemic palliative care consultations spanning state and institutional borders. J Am Geriatr Soc. 2020 May 22. doi: 10.1111/jgs.16643.
2. Lee J Abrukin L, Flores S. Early intervention of palliative care in the emergency department during the COVID-19 pandemic. JAMA Intern Med. 2020 Jun 5. doi: 10.1001/jamainternmed.2020.2713.
Hospitalists have played a key role
Hospitalists have played a key role
For some palliative care professionals, the COVID-19 pandemic, particularly in viral hot spots like New York City, represents a “moment” that could lead to greater awareness of what this service offers to seriously ill patients in a crisis.
They say it has provided an opportunity to show what palliative care teams can contribute to the difficult circumstances of patients with severe symptoms, isolated and alone in quarantined hospitals, with poor survival rates, perhaps sedated for extended stays on scarce ventilators – and for their family members, who are able to visit them only virtually via telephone or tablet.
But it has also highlighted gaps – including insufficient staffing for some palliative care teams. Hospitalists and other clinicians in the hospital need to learn the basics of primary palliative care, such as how to communicate bad news, initiate goals of care conversations, and address common symptoms of serious illness, such as pain. That way, they could shoulder more of the demand for this kind of care when palliative care specialists are in short supply.
Hospitalists, some of whom also have pursued a specialization in palliative care, have played key roles in clarifying and redefining the new role for palliative care, whom it is meant for, and who should provide it. Central to this new role is the greater use of telemedicine – for talking to hospitalized patients without increasing viral exposure, for linking up with family members who can’t visit their loved ones in the hospital, and for helping frontline hospital staff who need a palliative care consultation – or just a chance to debrief on what they are seeing.
A pandemic wake-up call
Elizabeth Gundersen, MD, FHM, FAAHPM, director of the hospice and palliative medicine fellowship program at the Charles E. Schmidt College of Medicine at Florida Atlantic University (FAU) in Boca Raton, practiced hospital medicine for 10 years before pursuing a fellowship in hospice and palliative medicine and working as an academic palliative medicine physician. She calls the pandemic a wake-up call for gaps in care and all the things that weren’t working well in the health care system.
“Now we are seeing more clearly what’s lacking – or broken – and what we will carry forward from this experience into the post-COVID world,” she said. Some hospitalists do palliative care very well, and others don’t feel as comfortable in having these difficult conversations with patients. But in the uncertain course of the virus they get thrust into it.
Although FAU’s associated hospitals were not as inundated with COVID-19 patients in the early weeks of the pandemic as were other regions, the volume of other patients plummeted, Dr. Gundersen said, adding that “there’s still been incredible intensity and worry about the virus. For me, the basic role of palliative care hasn’t changed, and the phrase I have always used when introducing myself – ‘we’re an extra layer of support for the patient and family’ – still holds true,” she said.
“I try to make it clear to people that palliative care is not synonymous with end-of-life care. We don’t want people to think that a palliative care referral implies imminent death. The goal is not to get more people to have a do not attempt resuscitation (DNAR) order, but to determine the patient and family’s treatment goals and whether a DNAR order fits those goals.”
The tough conversations
Dr. Gundersen is cochair of SHM’s Palliative Care Special Interest Group, along with Rab Razzak, MD, clinical director of palliative medicine at University Hospitals Cleveland Medical Center, one of the hospitals affiliated with Case Western University in Cleveland. (Connect with them on Twitter: @Top_Gundersen and @rabrazzak.)
Dr. Razzak also transitioned from hospital medicine to palliative medicine 10 years ago. “As a hospitalist, I enjoyed the tough conversations and bringing the human element into my health care interactions,” he explained. “To me, palliative care is a philosophy of care that puts the person we call the patient at the center of the interaction, while we try to figure out how to best care for them as a person.”
When the pandemic hit, University Hospitals made 20 ICU beds available for COVID-19 patients, Dr. Razzak said. This unit has since been full but not overflowing, while overall hospital census went down. The palliative care team at the hospital includes four inpatient doctors, nurse practitioners, and a chaplain, as well as an outpatient team primarily focused on oncology.
“In some settings, palliative care has been at the forefront of difficult conversations, when things aren’t going well for the patient and there’s much uncertainty,” Dr. Razzak said. The interface between hospital medicine and palliative care can be complementary, he added. “We talk about primary palliative care, which we want every discipline to be able to do – lead meaningful conversations, help manage symptoms.”
The take-home message for hospitalists, he said, is to get training in how to have these discussions, using such resources as VitalTalk (https://www.vitaltalk.org/), a nonprofit organization that disseminates education in communication skills for difficult conversations, and the Center to Advance Palliative Care (www.capc.org) at Icahn School of Medicine at Mount Sinai in New York City. “Once you’ve mastered the conversation, it will get easier. But ask for help when you need it, and learn how to know when you need it.”
Dr. Gundersen added that hospital medicine groups and palliative care teams could reach out to each other and talk about what they did in the crisis and how they can work together in the future. She recommends frequent ongoing support and collaboration that could range from formal conferences or training sessions to informal team interactions, perhaps with sandwiches in the doctor’s lounge – provided that there’s room for social distancing. She has recently started giving talks in the community and grand rounds presentations in hospitals about palliative care.
Other approaches and applications
In New York City, the initial epicenter for the pandemic in the United States, the adult palliative care service of Columbia University Medical Center (CUMC) experienced a sevenfold increase in consultation requests at the apex of the crisis, said its director, Craig Blinderman, MD. That demand was impossible to meet with existing staff. So Dr. Blinderman and colleagues established a virtual consultation model, recruiting and deploying volunteer out-of-state palliative care specialists to staff it.
An eight-bed palliative care unit was opened at CUMC for COVID-19 patients whose surrogates had opted not to initiate or continue intubation or life-sustaining treatments. This helped to relieve some of the pressures on the ICUs while making it possible for in-person visits to the hospice unit by families – in full PPE. Palliative care staff were embedded in various units in the hospital.
A palliative care response team composed of a hospice and palliative medicine fellow and four psychiatry residents or fellows, based in the emergency department and with supervision from the palliative care team, provided time-critical goals of care conversations with families using telemedicine – and a forum for listening to their suffering. Dr. Blinderman and colleagues also have found time to write up their experience for medical journals.1,2
There’s no reason to think that hospitalists, with a little basic training, couldn’t be having these same goals of care conversations, Dr. Blinderman said. “But the fact that hospitalists, at the pandemic’s peak, along with ICU doctors, were seeing an unprecedented magnitude of dying on a daily basis generated a lot of moral distress for them.”
Palliative care professionals, because they engage with these issues in a different way, may be somewhat better equipped to deal with the sheer emotional demands when so many are dying, as at the peak of the surge in New York. “We don’t see dying as a failure on our part but an opportunity to relieve suffering,” Dr. Blinderman said. And the palliative care field also emphasizes the importance of self-care for its practitioners.
“How do we meet the incredible palliative care needs in the epicenter of a pandemic? That question also applies to other kinds of crises we could imagine, for example, climate-related disasters,” Dr. Blinderman said. “What lessons have we learned about the value of palliative care and how to start incorporating it more integrally into the delivery of hospital care? Here we showed that we could work collaboratively with our colleagues at other major medical centers, bringing together their expertise to help us when we didn’t have the bandwidth to meet the demand,” he said.
Scripts can help
“Also, it won’t make sense to just go back to normal (after the crisis fades),” Dr. Blinderman said. “We need to take a close look at how our society is functioning in the wake of the pandemic and the ways the health care system has failed us. We have learned that we’re all interconnected and we need to work together to serve our communities – locally and nationally – applying basic distributive justice.”
Could there be, for example, a national infrastructure for mobilizing and deploying palliative care resources to areas of greatest need, similar to what was done in New York?
At Northwestern Medicine in Chicago, a number of palliative care clinicians at the system’s hospitals worked together to develop scripts designed to help other clinicians start goals of care conversations with patients and families, for use in the hospital as well as in outpatient primary care and other settings, with results integrated into the system’s electronic health record.
Front-line clinicians may not have the time to ask for formal consults from palliative care because of high volume and rapidly changing patient status, explained Eytan Szmuilowicz, MD, director of the section of palliative medicine at Northwestern Memorial Hospital. Or they may not have access to specialty-level palliative care in their settings.
The scripts are aimed at primary care, emergency physicians, and hospitalists needing to consider critical care placement or attempted resuscitation and to ICU clinicians helping families make decisions about life-sustaining treatments. They also can help facilitate advance care planning discussions. An example is “CALMER,” a six-step mnemonic guide to promote goals of care discussions with hospitalized patients. For more information on these scripts, contact Dr. Szmuilowicz: Eytan.Szmuilowicz@nm.org.
Eerily quiet
The COVID-19 crisis has been quite a whirlwind for hospital medicine, said Jeanie Youngwerth, MD, a hospitalist and program director of the palliative care service at the University of Colorado in Denver, which was a significant viral hotspot early on.
“When it first started, things seemed to change almost overnight – starting on Friday, March 13. People had to take action right away to develop work flows and the technology to allow us to see as many patients as possible,” she said. By the time Monday came, it was a whole new ballgame.
Dr. Youngwerth and two colleagues worked quickly to develop inpatient telemedicine capacity where none existed. “We knew we would not be going into patients’ rooms, but most of our team showed up in the hospital to work with the primary care teams. Our job was to see what we could do that actually made a difference,” she said.
“The hospital became a very strange place. You’d walk down the hallway and it was eerily quiet. Everybody you came across was being so nice to each other.” Televisits became a powerful way to bring the human connection back to medical care.
“What we learned from families was that they were thirsting to have some kind of connection with their loved one, and to be able to talk about their loved one and who they were as a person,” she said. “We’d contact the family through video visits and then, when the family meeting ended, the nurse would bring an iPad into the patient’s room so the family could see their loved one on a ventilator. They would immediately start communicating with their loved one, praying aloud, singing, playing music. It would make a huge difference for the family – and for the staff.”
References
1. Nakagawa S et al. Pandemic palliative care consultations spanning state and institutional borders. J Am Geriatr Soc. 2020 May 22. doi: 10.1111/jgs.16643.
2. Lee J Abrukin L, Flores S. Early intervention of palliative care in the emergency department during the COVID-19 pandemic. JAMA Intern Med. 2020 Jun 5. doi: 10.1001/jamainternmed.2020.2713.
For some palliative care professionals, the COVID-19 pandemic, particularly in viral hot spots like New York City, represents a “moment” that could lead to greater awareness of what this service offers to seriously ill patients in a crisis.
They say it has provided an opportunity to show what palliative care teams can contribute to the difficult circumstances of patients with severe symptoms, isolated and alone in quarantined hospitals, with poor survival rates, perhaps sedated for extended stays on scarce ventilators – and for their family members, who are able to visit them only virtually via telephone or tablet.
But it has also highlighted gaps – including insufficient staffing for some palliative care teams. Hospitalists and other clinicians in the hospital need to learn the basics of primary palliative care, such as how to communicate bad news, initiate goals of care conversations, and address common symptoms of serious illness, such as pain. That way, they could shoulder more of the demand for this kind of care when palliative care specialists are in short supply.
Hospitalists, some of whom also have pursued a specialization in palliative care, have played key roles in clarifying and redefining the new role for palliative care, whom it is meant for, and who should provide it. Central to this new role is the greater use of telemedicine – for talking to hospitalized patients without increasing viral exposure, for linking up with family members who can’t visit their loved ones in the hospital, and for helping frontline hospital staff who need a palliative care consultation – or just a chance to debrief on what they are seeing.
A pandemic wake-up call
Elizabeth Gundersen, MD, FHM, FAAHPM, director of the hospice and palliative medicine fellowship program at the Charles E. Schmidt College of Medicine at Florida Atlantic University (FAU) in Boca Raton, practiced hospital medicine for 10 years before pursuing a fellowship in hospice and palliative medicine and working as an academic palliative medicine physician. She calls the pandemic a wake-up call for gaps in care and all the things that weren’t working well in the health care system.
“Now we are seeing more clearly what’s lacking – or broken – and what we will carry forward from this experience into the post-COVID world,” she said. Some hospitalists do palliative care very well, and others don’t feel as comfortable in having these difficult conversations with patients. But in the uncertain course of the virus they get thrust into it.
Although FAU’s associated hospitals were not as inundated with COVID-19 patients in the early weeks of the pandemic as were other regions, the volume of other patients plummeted, Dr. Gundersen said, adding that “there’s still been incredible intensity and worry about the virus. For me, the basic role of palliative care hasn’t changed, and the phrase I have always used when introducing myself – ‘we’re an extra layer of support for the patient and family’ – still holds true,” she said.
“I try to make it clear to people that palliative care is not synonymous with end-of-life care. We don’t want people to think that a palliative care referral implies imminent death. The goal is not to get more people to have a do not attempt resuscitation (DNAR) order, but to determine the patient and family’s treatment goals and whether a DNAR order fits those goals.”
The tough conversations
Dr. Gundersen is cochair of SHM’s Palliative Care Special Interest Group, along with Rab Razzak, MD, clinical director of palliative medicine at University Hospitals Cleveland Medical Center, one of the hospitals affiliated with Case Western University in Cleveland. (Connect with them on Twitter: @Top_Gundersen and @rabrazzak.)
Dr. Razzak also transitioned from hospital medicine to palliative medicine 10 years ago. “As a hospitalist, I enjoyed the tough conversations and bringing the human element into my health care interactions,” he explained. “To me, palliative care is a philosophy of care that puts the person we call the patient at the center of the interaction, while we try to figure out how to best care for them as a person.”
When the pandemic hit, University Hospitals made 20 ICU beds available for COVID-19 patients, Dr. Razzak said. This unit has since been full but not overflowing, while overall hospital census went down. The palliative care team at the hospital includes four inpatient doctors, nurse practitioners, and a chaplain, as well as an outpatient team primarily focused on oncology.
“In some settings, palliative care has been at the forefront of difficult conversations, when things aren’t going well for the patient and there’s much uncertainty,” Dr. Razzak said. The interface between hospital medicine and palliative care can be complementary, he added. “We talk about primary palliative care, which we want every discipline to be able to do – lead meaningful conversations, help manage symptoms.”
The take-home message for hospitalists, he said, is to get training in how to have these discussions, using such resources as VitalTalk (https://www.vitaltalk.org/), a nonprofit organization that disseminates education in communication skills for difficult conversations, and the Center to Advance Palliative Care (www.capc.org) at Icahn School of Medicine at Mount Sinai in New York City. “Once you’ve mastered the conversation, it will get easier. But ask for help when you need it, and learn how to know when you need it.”
Dr. Gundersen added that hospital medicine groups and palliative care teams could reach out to each other and talk about what they did in the crisis and how they can work together in the future. She recommends frequent ongoing support and collaboration that could range from formal conferences or training sessions to informal team interactions, perhaps with sandwiches in the doctor’s lounge – provided that there’s room for social distancing. She has recently started giving talks in the community and grand rounds presentations in hospitals about palliative care.
Other approaches and applications
In New York City, the initial epicenter for the pandemic in the United States, the adult palliative care service of Columbia University Medical Center (CUMC) experienced a sevenfold increase in consultation requests at the apex of the crisis, said its director, Craig Blinderman, MD. That demand was impossible to meet with existing staff. So Dr. Blinderman and colleagues established a virtual consultation model, recruiting and deploying volunteer out-of-state palliative care specialists to staff it.
An eight-bed palliative care unit was opened at CUMC for COVID-19 patients whose surrogates had opted not to initiate or continue intubation or life-sustaining treatments. This helped to relieve some of the pressures on the ICUs while making it possible for in-person visits to the hospice unit by families – in full PPE. Palliative care staff were embedded in various units in the hospital.
A palliative care response team composed of a hospice and palliative medicine fellow and four psychiatry residents or fellows, based in the emergency department and with supervision from the palliative care team, provided time-critical goals of care conversations with families using telemedicine – and a forum for listening to their suffering. Dr. Blinderman and colleagues also have found time to write up their experience for medical journals.1,2
There’s no reason to think that hospitalists, with a little basic training, couldn’t be having these same goals of care conversations, Dr. Blinderman said. “But the fact that hospitalists, at the pandemic’s peak, along with ICU doctors, were seeing an unprecedented magnitude of dying on a daily basis generated a lot of moral distress for them.”
Palliative care professionals, because they engage with these issues in a different way, may be somewhat better equipped to deal with the sheer emotional demands when so many are dying, as at the peak of the surge in New York. “We don’t see dying as a failure on our part but an opportunity to relieve suffering,” Dr. Blinderman said. And the palliative care field also emphasizes the importance of self-care for its practitioners.
“How do we meet the incredible palliative care needs in the epicenter of a pandemic? That question also applies to other kinds of crises we could imagine, for example, climate-related disasters,” Dr. Blinderman said. “What lessons have we learned about the value of palliative care and how to start incorporating it more integrally into the delivery of hospital care? Here we showed that we could work collaboratively with our colleagues at other major medical centers, bringing together their expertise to help us when we didn’t have the bandwidth to meet the demand,” he said.
Scripts can help
“Also, it won’t make sense to just go back to normal (after the crisis fades),” Dr. Blinderman said. “We need to take a close look at how our society is functioning in the wake of the pandemic and the ways the health care system has failed us. We have learned that we’re all interconnected and we need to work together to serve our communities – locally and nationally – applying basic distributive justice.”
Could there be, for example, a national infrastructure for mobilizing and deploying palliative care resources to areas of greatest need, similar to what was done in New York?
At Northwestern Medicine in Chicago, a number of palliative care clinicians at the system’s hospitals worked together to develop scripts designed to help other clinicians start goals of care conversations with patients and families, for use in the hospital as well as in outpatient primary care and other settings, with results integrated into the system’s electronic health record.
Front-line clinicians may not have the time to ask for formal consults from palliative care because of high volume and rapidly changing patient status, explained Eytan Szmuilowicz, MD, director of the section of palliative medicine at Northwestern Memorial Hospital. Or they may not have access to specialty-level palliative care in their settings.
The scripts are aimed at primary care, emergency physicians, and hospitalists needing to consider critical care placement or attempted resuscitation and to ICU clinicians helping families make decisions about life-sustaining treatments. They also can help facilitate advance care planning discussions. An example is “CALMER,” a six-step mnemonic guide to promote goals of care discussions with hospitalized patients. For more information on these scripts, contact Dr. Szmuilowicz: Eytan.Szmuilowicz@nm.org.
Eerily quiet
The COVID-19 crisis has been quite a whirlwind for hospital medicine, said Jeanie Youngwerth, MD, a hospitalist and program director of the palliative care service at the University of Colorado in Denver, which was a significant viral hotspot early on.
“When it first started, things seemed to change almost overnight – starting on Friday, March 13. People had to take action right away to develop work flows and the technology to allow us to see as many patients as possible,” she said. By the time Monday came, it was a whole new ballgame.
Dr. Youngwerth and two colleagues worked quickly to develop inpatient telemedicine capacity where none existed. “We knew we would not be going into patients’ rooms, but most of our team showed up in the hospital to work with the primary care teams. Our job was to see what we could do that actually made a difference,” she said.
“The hospital became a very strange place. You’d walk down the hallway and it was eerily quiet. Everybody you came across was being so nice to each other.” Televisits became a powerful way to bring the human connection back to medical care.
“What we learned from families was that they were thirsting to have some kind of connection with their loved one, and to be able to talk about their loved one and who they were as a person,” she said. “We’d contact the family through video visits and then, when the family meeting ended, the nurse would bring an iPad into the patient’s room so the family could see their loved one on a ventilator. They would immediately start communicating with their loved one, praying aloud, singing, playing music. It would make a huge difference for the family – and for the staff.”
References
1. Nakagawa S et al. Pandemic palliative care consultations spanning state and institutional borders. J Am Geriatr Soc. 2020 May 22. doi: 10.1111/jgs.16643.
2. Lee J Abrukin L, Flores S. Early intervention of palliative care in the emergency department during the COVID-19 pandemic. JAMA Intern Med. 2020 Jun 5. doi: 10.1001/jamainternmed.2020.2713.
How three cardiac procedures changed in the COVID era
When Virginia’s governor directed the postponement of all elective surgeries in late March, Wayne Batchelor, MD and his colleagues at the Inova Heart and Vascular Institute in Falls Church, Va., canceled about two-thirds of their transcatheter aortic valve replacement (TAVR) procedures.

They then categorized patients by tiers to gauge which procedures could safely be postponed and to guide triaging. And while they did not deviate from the practice of having both an interventional cardiologist and a cardiothoracic surgeon present for TAVR, they slimmed down preprocedural testing when feasible and delayed some 30-day post-TAVR echocardiographic assessments. “It was a delicate dance, very difficult dance. But luckily, we were able to navigate the challenges effectively,” said Dr. Batchelor, the institute’s director of interventional cardiology and interventional cardiology research.
A “system capacity dashboard” that merged bed and staffing data from interventional cardiology spaces with cardiovascular and noncardiovascular ICU beds, operating rooms, and other resources – and daily cross-department meetings – enabled them to proceed with the most urgent TAVR procedures while “keeping a buffer of ICU beds to accommodate an anticipated surge of COVID-19,” he explained.
Such adaptations in cardiac procedures and processes are occurring in hospitals across the country as efforts are made to minimize the risk of COVID-19 exposure for patients and staff. Dr. Batchelor is one of four cardiologists who shared their experiences and advice on common cardiac procedures across three locales: TAVR in Virginia, percutaneous coronary intervention (PCI) in New York City, and atrial fibrillation (AFib) ablation in Kentucky.
More on TAVR in Virginia
Inova’s framework for triaging structural heart disease interventions (largely TAVR and/or percutaneous mitral valve repair) comprised three tiers. Tier 1 captured “emergent cases that had to be done, no questions asked,” Dr. Batchelor said. For TAVR, these were inpatients with severe to critical symptomatic aortic stenosis and advanced congestive heart failure who could not safely be discharged, as well as other patients “with refractory symptoms of heart failure that were compelling.” Many had associated left ventricular systolic dysfunction.
Those who could delay 14-30 days were placed in tier 2, and patients who “we felt were fairly stable and could wait at least 30 days” were placed in tier 3. “For TAVR, a tier 3 patient might be the one … who has severe aortic stenosis but is walking around and doing well at home with only stable exertional symptoms,” he said.
Patients whose procedures were delayed were contacted weekly by the valve clinic’s advanced practice practitioners through video visits or telephone calls, and tier categorization was reevaluated if symptoms worsened. “We had to keep in close contact with them,” Dr. Batchelor said. “These patients can deteriorate quite rapidly and sometimes without much warning.”
Virtual video visits were often used for 30-day postprocedural follow-ups, taking the place of in-person visits during which post-TAVR echocardiographic assessments would normally be performed. “For follow-up, we’d often just do a quick visit to check the vascular access site within 7-10 days, and then, if they were doing okay we’d delay the 30-day echo to a later time frame,” he said.
Preprocedural testing was streamlined to minimize the number of patient-provider interactions, with pulmonary function testing and pre-TAVR catheterization omitted unless absolutely necessary. “A TAVR CT angiogram [performed within the prior year] is the only test you really absolutely need,” Dr. Batchelor said. “We were much less likely to order a heart catheterization unless the patient was having angina and high risk or suspicion for significant coronary artery disease.”
This approach was not associated with any compromise in postprocedural outcomes, he noted. Prior to the pandemic, Inova routinely employed a minimalist approach to TAVR with moderate conscious sedation and avoiding transesophageal echocardiography – steps that were recommended for structural heart procedures in the COVID-19 era in a published review by the heart team at New York-Presbyterian Hospital/Columbia University Irving Medical Center.
The New York review is useful for cardiologists in areas with rising case burdens of COVID-19, Dr. Batchelor said, as is a position statement he coauthored from the American College of Cardiology and the Society for Cardiology and Angiography Interventions (SCAI) on triage considerations for structural heart disease interventions during the pandemic.
TAVR’s resource-heavy nature made the “system capacity dashboard” and daily meetings critical, Dr. Batchelor explained. At one point during the hold on elective procedures, the Falls Church INOVA facility had approximately 300 patients with COVID-19, a significant proportion of whom were in cardiac ICU beds.
“Everyone has to be flexible and learn,” he said. “We trained our cardiologists on managing ventilators in case some of the [critical care] staff got ill or were overwhelmed by the surge.”
More than 2 months after the surge eased and the ban on elective surgery was lifted, Dr. Batchelor and his colleagues are still using the dashboard and continue to meet daily to discuss COVID-19 prevalence in the hospital and the community as they work through the backlog of delayed procedures. They also routinely review the status of COVID-19 testing for inpatients and outpatients and the donning and doffing of personal protective equipment.
“You have to communicate early and often across the whole system of care because you’re competing for the same resources,” he advised. “And you have to be flexible and reassess. A policy that works at the beginning of the pandemic might have to change.”
PCI in New York
Before the pandemic, the cardiac catheterization laboratory at Mount Sinai Morningside Hospital in New York handled a monthly average of 140-150 PCIs, including 6-10 primary PCIs for ST-segment elevation myocardial infarction.

When electives were halted by the hospital in March and the City became the global epicenter for COVID-19, the cath lab went quiet. “Even though we were still able to do urgent cases or emergent cases, the case volume dropped tremendously,” said Jacqueline E. Tamis-Holland, MD, associate director of the cardiac catheterization laboratory and director of the interventional cardiology fellowship. “There weren’t many outpatients in our hospital … and by late March and through April, there wasn’t a single acute infarction.”
She and Tak W. Kwan, MD, director of the cardiac catheterization laboratory and professor of medicine at Icahn School of Medicine at Mount Sinai, New York, were prepared to move true STEMI patients into the cath lab for primary PCI without delay unless the staff or system were overrun.
That primary PCI should remain the first-line treatment for STEMI even in cases of confirmed or suspected COVID-19 was recommended by SCAI guidance issued in March and by a consensus statement released by the SCAI, ACC, and American College of Emergency Physicians in April – and “we were very much of the same frame of mind,” Dr. Tamis-Holland said.
Deciding which elective cases could not be delayed required a completely individualized approach, the cardiologists emphasized. Dr. Tamis-Holland had a few patients scheduled for elective PCI when the hold began, and “we spoke every few days or once a week in the beginning, then transitioned to once every 2 weeks,” she said. “With medical therapy and given that they were relatively sedentary, my patients did okay [with the delays].”
For subsequent patients, she considered their symptoms or stress test results. “If it’s someone who I’d [normally] wait until next week to schedule the cath, then we would wait 2 or 3 more weeks, or a month more with careful monitoring,” she said. “Certainly, there was a decrease in the number of abnormal stress tests that I referred to the cath lab during [the surge period].”
Dr. Kwan described one patient who had new-onset congestive heart failure in late March “with a markedly positive nuclear stress test.” The patient was monitored with twice-weekly telemedicine visits and office visits, and a cardiac catheterization was performed in early May as an urgent elective case. “He had severe three-vessel and left main disease,” he said. “Subsequently, [coronary artery bypass surgery] was done.”
There were no changes in the PCI procedure itself in terms of hospital stay (most elective cases at Mt. Sinai are same-day procedures) or in staffing, other than a ban on visiting students or residents. The most important changes during the surge – in addition to stocking enough personal protective equipment – concerned testing. Patients undergoing elective PCI are tested for the novel coronavirus 72 hours before the procedure, and rapid testing is performed in the emergency room for STEMI patients to determine patient disposition after the procedure.
“Until we have the results back we should treat all patients as if they are a patient under investigation or have COVID,” said Dr. Tamis-Holland, who helped develop emergency guidance on STEMI systems of care during the pandemic for the American Heart Association.
In early May, the hospital freed up additional space for cardiac care, allowing more “urgent-elective” PCIs to be done. Some patients were reluctant to proceed, the cardiologists said, because of a no-visitor policy. In mid-June, the hold on elective procedures was lifted, and around the same time, the hospital shifted to a one-visitor policy. Still, some patients opted to continue longer with medical therapy.
Patients need to feel comfortable, and “there is a lag time from the time everything opens up and when patients get their stress tests and their evaluations, and then arrive for PCI,” said Dr. Tamis-Holland.
By mid-July, the cardiologists were anticipating an increase in complications from infarctions among patients who “waited them out at home” – heart failure or mitral valve regurgitation, for instance – but, in their hospital at least, “we haven’t really seen that,” she added.
AFib ablation in Kentucky
As New York experienced its surge, John Mandrola, MD, and other electrophysiologists across the Baptist Health system in Kentucky reached a consensus on how to categorize their procedures. Electrophysiology interventions were classified urgent, emergent, and truly elective in the event that the state’s relatively low case burden of COVID-19 were to significantly worsen.
There was no doubt where AFib ablation sat. “It’s one of the most elective procedures there is” in terms of scheduling under normal circumstances, and it almost always requires an overnight stay and general anesthesia – factors that upped the ante on an elective classification, said Dr. Mandrola.
All AF ablations were deemed elective unless the patient required immediate hospitalization. For 8-10 weeks during the state’s shutdown of elective care, Dr. Mandrola and his partner successfully monitored patients with phone calls. “To be honest,” he said, “most patients did not want to have their AFib ablation anyway until the pandemic slowed and they knew it was safe.”
In some cases, patients reported that their symptoms were improving: “There are so many things to speculate about. ... Was it that everyone took their foot off the accelerator?” Dr. Mandrola thinks that postpandemic outcomes analyses may drive more scrutiny of the necessity of some AFib ablations and other procedures and tests. AFib ablation “has its place but is probably overused,” he said.
During the pause on electives, “the vast majority of procedures we did were pacemaker procedures,” he said. “We also did some atrial flutter ablations, and ablations for ventricular tachycardia and supraventricular tachycardia.” In mid-July, as the COVID-19 case burden in Kentucky remained relatively low, Dr. Mandrola was “up to 120%” of his pre-COVID electrophysiology volume – but ready to scale back again if needed.
Dr. Batchelor reported consulting fees from Boston Scientific, Abbott Medical, Medtronic, and V-wave. Dr. Kwan, Dr. Mandrola, and Dr. Tamis-Holland reported no relevant financial disclosures.
This article is a collaboration between Medscape and MDedge. A version of it originally appeared on Medscape.com.
When Virginia’s governor directed the postponement of all elective surgeries in late March, Wayne Batchelor, MD and his colleagues at the Inova Heart and Vascular Institute in Falls Church, Va., canceled about two-thirds of their transcatheter aortic valve replacement (TAVR) procedures.
They then categorized patients by tiers to gauge which procedures could safely be postponed and to guide triaging. And while they did not deviate from the practice of having both an interventional cardiologist and a cardiothoracic surgeon present for TAVR, they slimmed down preprocedural testing when feasible and delayed some 30-day post-TAVR echocardiographic assessments. “It was a delicate dance, very difficult dance. But luckily, we were able to navigate the challenges effectively,” said Dr. Batchelor, the institute’s director of interventional cardiology and interventional cardiology research.
A “system capacity dashboard” that merged bed and staffing data from interventional cardiology spaces with cardiovascular and noncardiovascular ICU beds, operating rooms, and other resources – and daily cross-department meetings – enabled them to proceed with the most urgent TAVR procedures while “keeping a buffer of ICU beds to accommodate an anticipated surge of COVID-19,” he explained.
Such adaptations in cardiac procedures and processes are occurring in hospitals across the country as efforts are made to minimize the risk of COVID-19 exposure for patients and staff. Dr. Batchelor is one of four cardiologists who shared their experiences and advice on common cardiac procedures across three locales: TAVR in Virginia, percutaneous coronary intervention (PCI) in New York City, and atrial fibrillation (AFib) ablation in Kentucky.
More on TAVR in Virginia
Inova’s framework for triaging structural heart disease interventions (largely TAVR and/or percutaneous mitral valve repair) comprised three tiers. Tier 1 captured “emergent cases that had to be done, no questions asked,” Dr. Batchelor said. For TAVR, these were inpatients with severe to critical symptomatic aortic stenosis and advanced congestive heart failure who could not safely be discharged, as well as other patients “with refractory symptoms of heart failure that were compelling.” Many had associated left ventricular systolic dysfunction.
Those who could delay 14-30 days were placed in tier 2, and patients who “we felt were fairly stable and could wait at least 30 days” were placed in tier 3. “For TAVR, a tier 3 patient might be the one … who has severe aortic stenosis but is walking around and doing well at home with only stable exertional symptoms,” he said.
Patients whose procedures were delayed were contacted weekly by the valve clinic’s advanced practice practitioners through video visits or telephone calls, and tier categorization was reevaluated if symptoms worsened. “We had to keep in close contact with them,” Dr. Batchelor said. “These patients can deteriorate quite rapidly and sometimes without much warning.”
Virtual video visits were often used for 30-day postprocedural follow-ups, taking the place of in-person visits during which post-TAVR echocardiographic assessments would normally be performed. “For follow-up, we’d often just do a quick visit to check the vascular access site within 7-10 days, and then, if they were doing okay we’d delay the 30-day echo to a later time frame,” he said.
Preprocedural testing was streamlined to minimize the number of patient-provider interactions, with pulmonary function testing and pre-TAVR catheterization omitted unless absolutely necessary. “A TAVR CT angiogram [performed within the prior year] is the only test you really absolutely need,” Dr. Batchelor said. “We were much less likely to order a heart catheterization unless the patient was having angina and high risk or suspicion for significant coronary artery disease.”
This approach was not associated with any compromise in postprocedural outcomes, he noted. Prior to the pandemic, Inova routinely employed a minimalist approach to TAVR with moderate conscious sedation and avoiding transesophageal echocardiography – steps that were recommended for structural heart procedures in the COVID-19 era in a published review by the heart team at New York-Presbyterian Hospital/Columbia University Irving Medical Center.
The New York review is useful for cardiologists in areas with rising case burdens of COVID-19, Dr. Batchelor said, as is a position statement he coauthored from the American College of Cardiology and the Society for Cardiology and Angiography Interventions (SCAI) on triage considerations for structural heart disease interventions during the pandemic.
TAVR’s resource-heavy nature made the “system capacity dashboard” and daily meetings critical, Dr. Batchelor explained. At one point during the hold on elective procedures, the Falls Church INOVA facility had approximately 300 patients with COVID-19, a significant proportion of whom were in cardiac ICU beds.
“Everyone has to be flexible and learn,” he said. “We trained our cardiologists on managing ventilators in case some of the [critical care] staff got ill or were overwhelmed by the surge.”
More than 2 months after the surge eased and the ban on elective surgery was lifted, Dr. Batchelor and his colleagues are still using the dashboard and continue to meet daily to discuss COVID-19 prevalence in the hospital and the community as they work through the backlog of delayed procedures. They also routinely review the status of COVID-19 testing for inpatients and outpatients and the donning and doffing of personal protective equipment.
“You have to communicate early and often across the whole system of care because you’re competing for the same resources,” he advised. “And you have to be flexible and reassess. A policy that works at the beginning of the pandemic might have to change.”
PCI in New York
Before the pandemic, the cardiac catheterization laboratory at Mount Sinai Morningside Hospital in New York handled a monthly average of 140-150 PCIs, including 6-10 primary PCIs for ST-segment elevation myocardial infarction.
When electives were halted by the hospital in March and the City became the global epicenter for COVID-19, the cath lab went quiet. “Even though we were still able to do urgent cases or emergent cases, the case volume dropped tremendously,” said Jacqueline E. Tamis-Holland, MD, associate director of the cardiac catheterization laboratory and director of the interventional cardiology fellowship. “There weren’t many outpatients in our hospital … and by late March and through April, there wasn’t a single acute infarction.”
She and Tak W. Kwan, MD, director of the cardiac catheterization laboratory and professor of medicine at Icahn School of Medicine at Mount Sinai, New York, were prepared to move true STEMI patients into the cath lab for primary PCI without delay unless the staff or system were overrun.
That primary PCI should remain the first-line treatment for STEMI even in cases of confirmed or suspected COVID-19 was recommended by SCAI guidance issued in March and by a consensus statement released by the SCAI, ACC, and American College of Emergency Physicians in April – and “we were very much of the same frame of mind,” Dr. Tamis-Holland said.
Deciding which elective cases could not be delayed required a completely individualized approach, the cardiologists emphasized. Dr. Tamis-Holland had a few patients scheduled for elective PCI when the hold began, and “we spoke every few days or once a week in the beginning, then transitioned to once every 2 weeks,” she said. “With medical therapy and given that they were relatively sedentary, my patients did okay [with the delays].”
For subsequent patients, she considered their symptoms or stress test results. “If it’s someone who I’d [normally] wait until next week to schedule the cath, then we would wait 2 or 3 more weeks, or a month more with careful monitoring,” she said. “Certainly, there was a decrease in the number of abnormal stress tests that I referred to the cath lab during [the surge period].”
Dr. Kwan described one patient who had new-onset congestive heart failure in late March “with a markedly positive nuclear stress test.” The patient was monitored with twice-weekly telemedicine visits and office visits, and a cardiac catheterization was performed in early May as an urgent elective case. “He had severe three-vessel and left main disease,” he said. “Subsequently, [coronary artery bypass surgery] was done.”
There were no changes in the PCI procedure itself in terms of hospital stay (most elective cases at Mt. Sinai are same-day procedures) or in staffing, other than a ban on visiting students or residents. The most important changes during the surge – in addition to stocking enough personal protective equipment – concerned testing. Patients undergoing elective PCI are tested for the novel coronavirus 72 hours before the procedure, and rapid testing is performed in the emergency room for STEMI patients to determine patient disposition after the procedure.
“Until we have the results back we should treat all patients as if they are a patient under investigation or have COVID,” said Dr. Tamis-Holland, who helped develop emergency guidance on STEMI systems of care during the pandemic for the American Heart Association.
In early May, the hospital freed up additional space for cardiac care, allowing more “urgent-elective” PCIs to be done. Some patients were reluctant to proceed, the cardiologists said, because of a no-visitor policy. In mid-June, the hold on elective procedures was lifted, and around the same time, the hospital shifted to a one-visitor policy. Still, some patients opted to continue longer with medical therapy.
Patients need to feel comfortable, and “there is a lag time from the time everything opens up and when patients get their stress tests and their evaluations, and then arrive for PCI,” said Dr. Tamis-Holland.
By mid-July, the cardiologists were anticipating an increase in complications from infarctions among patients who “waited them out at home” – heart failure or mitral valve regurgitation, for instance – but, in their hospital at least, “we haven’t really seen that,” she added.
AFib ablation in Kentucky
As New York experienced its surge, John Mandrola, MD, and other electrophysiologists across the Baptist Health system in Kentucky reached a consensus on how to categorize their procedures. Electrophysiology interventions were classified urgent, emergent, and truly elective in the event that the state’s relatively low case burden of COVID-19 were to significantly worsen.
There was no doubt where AFib ablation sat. “It’s one of the most elective procedures there is” in terms of scheduling under normal circumstances, and it almost always requires an overnight stay and general anesthesia – factors that upped the ante on an elective classification, said Dr. Mandrola.
All AF ablations were deemed elective unless the patient required immediate hospitalization. For 8-10 weeks during the state’s shutdown of elective care, Dr. Mandrola and his partner successfully monitored patients with phone calls. “To be honest,” he said, “most patients did not want to have their AFib ablation anyway until the pandemic slowed and they knew it was safe.”
In some cases, patients reported that their symptoms were improving: “There are so many things to speculate about. ... Was it that everyone took their foot off the accelerator?” Dr. Mandrola thinks that postpandemic outcomes analyses may drive more scrutiny of the necessity of some AFib ablations and other procedures and tests. AFib ablation “has its place but is probably overused,” he said.
During the pause on electives, “the vast majority of procedures we did were pacemaker procedures,” he said. “We also did some atrial flutter ablations, and ablations for ventricular tachycardia and supraventricular tachycardia.” In mid-July, as the COVID-19 case burden in Kentucky remained relatively low, Dr. Mandrola was “up to 120%” of his pre-COVID electrophysiology volume – but ready to scale back again if needed.
Dr. Batchelor reported consulting fees from Boston Scientific, Abbott Medical, Medtronic, and V-wave. Dr. Kwan, Dr. Mandrola, and Dr. Tamis-Holland reported no relevant financial disclosures.
This article is a collaboration between Medscape and MDedge. A version of it originally appeared on Medscape.com.
When Virginia’s governor directed the postponement of all elective surgeries in late March, Wayne Batchelor, MD and his colleagues at the Inova Heart and Vascular Institute in Falls Church, Va., canceled about two-thirds of their transcatheter aortic valve replacement (TAVR) procedures.
They then categorized patients by tiers to gauge which procedures could safely be postponed and to guide triaging. And while they did not deviate from the practice of having both an interventional cardiologist and a cardiothoracic surgeon present for TAVR, they slimmed down preprocedural testing when feasible and delayed some 30-day post-TAVR echocardiographic assessments. “It was a delicate dance, very difficult dance. But luckily, we were able to navigate the challenges effectively,” said Dr. Batchelor, the institute’s director of interventional cardiology and interventional cardiology research.
A “system capacity dashboard” that merged bed and staffing data from interventional cardiology spaces with cardiovascular and noncardiovascular ICU beds, operating rooms, and other resources – and daily cross-department meetings – enabled them to proceed with the most urgent TAVR procedures while “keeping a buffer of ICU beds to accommodate an anticipated surge of COVID-19,” he explained.
Such adaptations in cardiac procedures and processes are occurring in hospitals across the country as efforts are made to minimize the risk of COVID-19 exposure for patients and staff. Dr. Batchelor is one of four cardiologists who shared their experiences and advice on common cardiac procedures across three locales: TAVR in Virginia, percutaneous coronary intervention (PCI) in New York City, and atrial fibrillation (AFib) ablation in Kentucky.
More on TAVR in Virginia
Inova’s framework for triaging structural heart disease interventions (largely TAVR and/or percutaneous mitral valve repair) comprised three tiers. Tier 1 captured “emergent cases that had to be done, no questions asked,” Dr. Batchelor said. For TAVR, these were inpatients with severe to critical symptomatic aortic stenosis and advanced congestive heart failure who could not safely be discharged, as well as other patients “with refractory symptoms of heart failure that were compelling.” Many had associated left ventricular systolic dysfunction.
Those who could delay 14-30 days were placed in tier 2, and patients who “we felt were fairly stable and could wait at least 30 days” were placed in tier 3. “For TAVR, a tier 3 patient might be the one … who has severe aortic stenosis but is walking around and doing well at home with only stable exertional symptoms,” he said.
Patients whose procedures were delayed were contacted weekly by the valve clinic’s advanced practice practitioners through video visits or telephone calls, and tier categorization was reevaluated if symptoms worsened. “We had to keep in close contact with them,” Dr. Batchelor said. “These patients can deteriorate quite rapidly and sometimes without much warning.”
Virtual video visits were often used for 30-day postprocedural follow-ups, taking the place of in-person visits during which post-TAVR echocardiographic assessments would normally be performed. “For follow-up, we’d often just do a quick visit to check the vascular access site within 7-10 days, and then, if they were doing okay we’d delay the 30-day echo to a later time frame,” he said.
Preprocedural testing was streamlined to minimize the number of patient-provider interactions, with pulmonary function testing and pre-TAVR catheterization omitted unless absolutely necessary. “A TAVR CT angiogram [performed within the prior year] is the only test you really absolutely need,” Dr. Batchelor said. “We were much less likely to order a heart catheterization unless the patient was having angina and high risk or suspicion for significant coronary artery disease.”
This approach was not associated with any compromise in postprocedural outcomes, he noted. Prior to the pandemic, Inova routinely employed a minimalist approach to TAVR with moderate conscious sedation and avoiding transesophageal echocardiography – steps that were recommended for structural heart procedures in the COVID-19 era in a published review by the heart team at New York-Presbyterian Hospital/Columbia University Irving Medical Center.
The New York review is useful for cardiologists in areas with rising case burdens of COVID-19, Dr. Batchelor said, as is a position statement he coauthored from the American College of Cardiology and the Society for Cardiology and Angiography Interventions (SCAI) on triage considerations for structural heart disease interventions during the pandemic.
TAVR’s resource-heavy nature made the “system capacity dashboard” and daily meetings critical, Dr. Batchelor explained. At one point during the hold on elective procedures, the Falls Church INOVA facility had approximately 300 patients with COVID-19, a significant proportion of whom were in cardiac ICU beds.
“Everyone has to be flexible and learn,” he said. “We trained our cardiologists on managing ventilators in case some of the [critical care] staff got ill or were overwhelmed by the surge.”
More than 2 months after the surge eased and the ban on elective surgery was lifted, Dr. Batchelor and his colleagues are still using the dashboard and continue to meet daily to discuss COVID-19 prevalence in the hospital and the community as they work through the backlog of delayed procedures. They also routinely review the status of COVID-19 testing for inpatients and outpatients and the donning and doffing of personal protective equipment.
“You have to communicate early and often across the whole system of care because you’re competing for the same resources,” he advised. “And you have to be flexible and reassess. A policy that works at the beginning of the pandemic might have to change.”
PCI in New York
Before the pandemic, the cardiac catheterization laboratory at Mount Sinai Morningside Hospital in New York handled a monthly average of 140-150 PCIs, including 6-10 primary PCIs for ST-segment elevation myocardial infarction.
When electives were halted by the hospital in March and the City became the global epicenter for COVID-19, the cath lab went quiet. “Even though we were still able to do urgent cases or emergent cases, the case volume dropped tremendously,” said Jacqueline E. Tamis-Holland, MD, associate director of the cardiac catheterization laboratory and director of the interventional cardiology fellowship. “There weren’t many outpatients in our hospital … and by late March and through April, there wasn’t a single acute infarction.”
She and Tak W. Kwan, MD, director of the cardiac catheterization laboratory and professor of medicine at Icahn School of Medicine at Mount Sinai, New York, were prepared to move true STEMI patients into the cath lab for primary PCI without delay unless the staff or system were overrun.
That primary PCI should remain the first-line treatment for STEMI even in cases of confirmed or suspected COVID-19 was recommended by SCAI guidance issued in March and by a consensus statement released by the SCAI, ACC, and American College of Emergency Physicians in April – and “we were very much of the same frame of mind,” Dr. Tamis-Holland said.
Deciding which elective cases could not be delayed required a completely individualized approach, the cardiologists emphasized. Dr. Tamis-Holland had a few patients scheduled for elective PCI when the hold began, and “we spoke every few days or once a week in the beginning, then transitioned to once every 2 weeks,” she said. “With medical therapy and given that they were relatively sedentary, my patients did okay [with the delays].”
For subsequent patients, she considered their symptoms or stress test results. “If it’s someone who I’d [normally] wait until next week to schedule the cath, then we would wait 2 or 3 more weeks, or a month more with careful monitoring,” she said. “Certainly, there was a decrease in the number of abnormal stress tests that I referred to the cath lab during [the surge period].”
Dr. Kwan described one patient who had new-onset congestive heart failure in late March “with a markedly positive nuclear stress test.” The patient was monitored with twice-weekly telemedicine visits and office visits, and a cardiac catheterization was performed in early May as an urgent elective case. “He had severe three-vessel and left main disease,” he said. “Subsequently, [coronary artery bypass surgery] was done.”
There were no changes in the PCI procedure itself in terms of hospital stay (most elective cases at Mt. Sinai are same-day procedures) or in staffing, other than a ban on visiting students or residents. The most important changes during the surge – in addition to stocking enough personal protective equipment – concerned testing. Patients undergoing elective PCI are tested for the novel coronavirus 72 hours before the procedure, and rapid testing is performed in the emergency room for STEMI patients to determine patient disposition after the procedure.
“Until we have the results back we should treat all patients as if they are a patient under investigation or have COVID,” said Dr. Tamis-Holland, who helped develop emergency guidance on STEMI systems of care during the pandemic for the American Heart Association.
In early May, the hospital freed up additional space for cardiac care, allowing more “urgent-elective” PCIs to be done. Some patients were reluctant to proceed, the cardiologists said, because of a no-visitor policy. In mid-June, the hold on elective procedures was lifted, and around the same time, the hospital shifted to a one-visitor policy. Still, some patients opted to continue longer with medical therapy.
Patients need to feel comfortable, and “there is a lag time from the time everything opens up and when patients get their stress tests and their evaluations, and then arrive for PCI,” said Dr. Tamis-Holland.
By mid-July, the cardiologists were anticipating an increase in complications from infarctions among patients who “waited them out at home” – heart failure or mitral valve regurgitation, for instance – but, in their hospital at least, “we haven’t really seen that,” she added.
AFib ablation in Kentucky
As New York experienced its surge, John Mandrola, MD, and other electrophysiologists across the Baptist Health system in Kentucky reached a consensus on how to categorize their procedures. Electrophysiology interventions were classified urgent, emergent, and truly elective in the event that the state’s relatively low case burden of COVID-19 were to significantly worsen.
There was no doubt where AFib ablation sat. “It’s one of the most elective procedures there is” in terms of scheduling under normal circumstances, and it almost always requires an overnight stay and general anesthesia – factors that upped the ante on an elective classification, said Dr. Mandrola.
All AF ablations were deemed elective unless the patient required immediate hospitalization. For 8-10 weeks during the state’s shutdown of elective care, Dr. Mandrola and his partner successfully monitored patients with phone calls. “To be honest,” he said, “most patients did not want to have their AFib ablation anyway until the pandemic slowed and they knew it was safe.”
In some cases, patients reported that their symptoms were improving: “There are so many things to speculate about. ... Was it that everyone took their foot off the accelerator?” Dr. Mandrola thinks that postpandemic outcomes analyses may drive more scrutiny of the necessity of some AFib ablations and other procedures and tests. AFib ablation “has its place but is probably overused,” he said.
During the pause on electives, “the vast majority of procedures we did were pacemaker procedures,” he said. “We also did some atrial flutter ablations, and ablations for ventricular tachycardia and supraventricular tachycardia.” In mid-July, as the COVID-19 case burden in Kentucky remained relatively low, Dr. Mandrola was “up to 120%” of his pre-COVID electrophysiology volume – but ready to scale back again if needed.
Dr. Batchelor reported consulting fees from Boston Scientific, Abbott Medical, Medtronic, and V-wave. Dr. Kwan, Dr. Mandrola, and Dr. Tamis-Holland reported no relevant financial disclosures.
This article is a collaboration between Medscape and MDedge. A version of it originally appeared on Medscape.com.
Web-based fellowship interviews in the era of COVID 19: Tips and tricks
Fellowship interviews are an essential step – arguably the most important step – in the process of matching candidates to training programs. Until recently, most programs relied exclusively on on-site face-to face interviews. Since the appearance of the COVID-19 pandemic, the medical field has utilized web-based platforms. Despite inherent limitations, virtual meetings appear to be effective in providing patient care and in conducting administrative meetings.1,2

Because of uncertainty related to the pandemic, including changing guidelines regarding social distancing and travel restrictions, fellowship programs are expected to comply with CDC,3 state, and federal recommendations to avoid nonessential travel. Therefore, conducting web-based interviews exclusively will likely become a necessity.
While there may be some disadvantages to web-based interviews, many candidates find the overall experience satisfactory, thereby allowing them to understand the programs, express themselves, and comfortably rank the programs, as two studies have shown.4,5 Programs and candidates are encouraged to adapt to this new reality in order to achieve a successful match. After all, there are many potential advantages of web-based interviews. In addition to eliminating the risk of COVID-19 acquisition, web-based interviews have been described as helping to improve scheduling flexibility, reduce the financial burden, and allow conducting more interviews for candidates and programs (Table 1).6-8
There are different styles to the web-based interview.9 Some programs choose to offer a single group interview (or the so-called panel interview) in which all the interviewing faculties invite each candidate at a time. Alternatively, programs might choose to conduct separate interviews by each faculty in which the candidates would alternate. For the latter option, the program could use a single invitation link or multiple invitation links for each session.
General tips for a successful interview:9
1. Be pleasant and professional: Your communication with the program should reflect excellent manners and a professional attitude with everyone (i.e., faculties, coordinators, and fellows).

2. Know yourself and what you want: Review your CV and personal statement and reflect on your achievements, strengths and weaknesses. Identify examples from your experience that would speak well of you as a person and as a physician.
3. Communication is key:
- Respond to the interview invitations promptly.
- Send a brief thank you email to the interviewers and the coordinator. Avoid being generic; mention specific points of discussion and show your interest in the program.
- Proofread your emails carefully. Well-written emails that are devoid of grammatical or spelling errors send a positive message about the candidate.
4. Do your homework:
- Read the information posted on the website carefully and take notes. This should provide you with useful information to use when you rank the programs and could lead to questions that you might want to ask your interviewers. Besides, asking questions that are answered on the website reflects poorly on the candidate.
- Pay attention to various clues that could reflect how organized and how academically oriented a program is. For example, a program that provides details about their didactic lectures sends a message that quality teaching is a priority. On the other hand, a program that has a website that hasn’t been updated for years could dissuade rather than recruit applicants.
- Read about the faculty, their areas of interests, and publications. Learn how their names are pronounced and use them during the interview.
- Read about the city where the program is. It shows interest in the area where you might be living and will help you to stand out among candidates.

5. Be prepared for the classics; be honest, genuine, and authentic. Think about these common prompts:
- Tell me about yourself.
- Why did you choose gastroenterology?
- Where do you see yourself in 5 years?
- Why would you like to come to the city where the program is?
- Are there any certain areas in gastroenterology that you’re interested in more (e.g., hepatology, motility, IBD, advanced endoscopy)?
6. It is likely your interviewer will ask if you have questions. Ask questions that further allow you to assess the program and your fit into the program.
- What aspects of the program are you most proud of?
- Where would you like to see this program in 5 years?
- What keeps you at this program?
Tips for a successful web-based interview9,10 (Table 2):
1. Pay attention to the time zone of the city of the program. Be ready at least 10 minutes before the interview.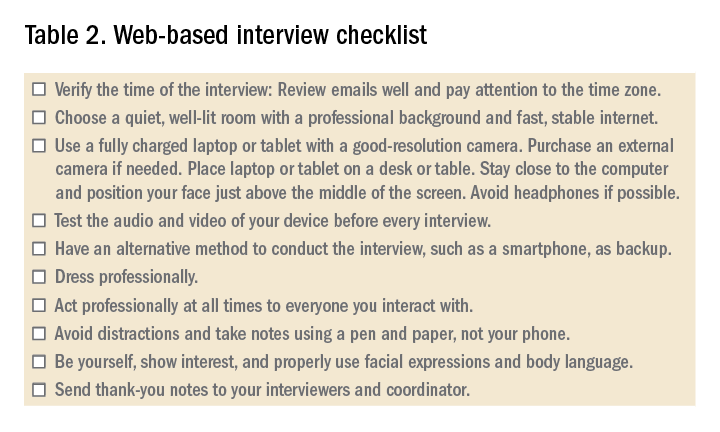
2. Ensure a fast and stable Internet service for an uninterrupted interview experience. Consider using an ethernet cable. Have a back-up plan such as using a phone as a hotspot.
3. Use a quiet and private room, preferably at home. Be aware of the background. A simple decoration is acceptable.
4. Consider recording yourself using the same device you’ll use for the interview to make sure audio and video are functioning properly.
5. When scheduling more than one interview in 1 day, allow at least 2 hours between interviews to avoid scheduling conflicts caused by unanticipated delays related to technical issues.

6. Have immediate access to the invitation link(s) that you received. Add the interviews to your device’s calendar. Note that sometimes a new invitation link is generated last minute because of technical issues.
7. While the advice for physical interviews is to turn off your phone (and smart watch), you’ll have to keep your phone on but on silent for the virtual interviews. Sometimes, you’ll receive a phone call from the program to update you about any last-minute changes.
7. It is recommended that a laptop or a tablet with a camera with good resolution and a microphone be used rather than using a phone. A wide screen allows better communication. Disable notification on that device to avoid interruptions.
8. Sit comfortably with the device being at or just below eye level. Avoid distractions and maintain eye contact.
9. Familiarize yourself with the platform used and its functions. Double check the audio and video before each interview.
10. Put your device on a desk or table to improve stability; don’t hold it in your hand.
11. Find a place where the view is best and your face appears in the middle of the screen; not too far or too close. Use a well-lit room but don’t have a source of light behind you. Many platforms allow you to select a background or blur the background. A background that is monochromatic and not distracting is recommended.
12. Use a pen and a paper to take notes during the interview. You would use these notes to generate “thank you” or “interest in program” emails. Additionally, they will be a helpful reference when ranking programs.
13. Do not type. Typing is much louder to the interviewer and can be distracting.
14. Dress professionally, just as you dress for an on-site interview. You never know when you might have to stand up during the interview for unplanned reasons.
15. Do a practice interview. Have a colleague set up a virtual web session using any available platform. This will allow you to get feedback on your dress, background, acoustics, and general ability to answer questions.
References
1. Dig Dis Sci. 2019;64:1150-7.
2. BMJ Open. 2017;7:e016242.
3. Centers for Disease Control and Prevention. Coronavirus and Travel in the United States, 2020.
4. J Bone Joint Surg Am. 2017;99:e114.
5. Am J Gastroenterol. 2014;109:155-9.
6. West J Emerg Med. 2018;19:80-6.
7. Int J Med Educ. 2016;7:102-8.
8. Aparajit Naram M. How COVID-19 changed our fellowship interview process for the better. KevinMD.com. April 17, 2020.
9. Association of American Medical Colleges. Virtual interviews: Tips for medical school applicants, 2020. Updated May 14, 2020.
10. Top 5 video interviewing tips for residency and fellowship programs. Thalamus: Connecting the Docs. April 2, 2020, 2020.
Dr. Kiwan is chief fellow in gastroenterology, division of gastroenterology, at Wayne State University, Detroit Medical Center, John D. Dingell VA Medical Center, all in Detroit. Dr. Judd is an assistant professor and associate program director in the division of gastroenterology, Wayne State University, Detroit Medical Center, John D. Dingell VA Medical Center. Dr. Al Masalmeh is in the department of internal medicine, Wayne State University, Detroit Medical Center. Dr. Levine is professor and the vice chair for education, Wayne State University, Detroit Medical Center.
Fellowship interviews are an essential step – arguably the most important step – in the process of matching candidates to training programs. Until recently, most programs relied exclusively on on-site face-to face interviews. Since the appearance of the COVID-19 pandemic, the medical field has utilized web-based platforms. Despite inherent limitations, virtual meetings appear to be effective in providing patient care and in conducting administrative meetings.1,2
Because of uncertainty related to the pandemic, including changing guidelines regarding social distancing and travel restrictions, fellowship programs are expected to comply with CDC,3 state, and federal recommendations to avoid nonessential travel. Therefore, conducting web-based interviews exclusively will likely become a necessity.
While there may be some disadvantages to web-based interviews, many candidates find the overall experience satisfactory, thereby allowing them to understand the programs, express themselves, and comfortably rank the programs, as two studies have shown.4,5 Programs and candidates are encouraged to adapt to this new reality in order to achieve a successful match. After all, there are many potential advantages of web-based interviews. In addition to eliminating the risk of COVID-19 acquisition, web-based interviews have been described as helping to improve scheduling flexibility, reduce the financial burden, and allow conducting more interviews for candidates and programs (Table 1).6-8
There are different styles to the web-based interview.9 Some programs choose to offer a single group interview (or the so-called panel interview) in which all the interviewing faculties invite each candidate at a time. Alternatively, programs might choose to conduct separate interviews by each faculty in which the candidates would alternate. For the latter option, the program could use a single invitation link or multiple invitation links for each session.
General tips for a successful interview:9
1. Be pleasant and professional: Your communication with the program should reflect excellent manners and a professional attitude with everyone (i.e., faculties, coordinators, and fellows).
2. Know yourself and what you want: Review your CV and personal statement and reflect on your achievements, strengths and weaknesses. Identify examples from your experience that would speak well of you as a person and as a physician.
3. Communication is key:
- Respond to the interview invitations promptly.
- Send a brief thank you email to the interviewers and the coordinator. Avoid being generic; mention specific points of discussion and show your interest in the program.
- Proofread your emails carefully. Well-written emails that are devoid of grammatical or spelling errors send a positive message about the candidate.
4. Do your homework:
- Read the information posted on the website carefully and take notes. This should provide you with useful information to use when you rank the programs and could lead to questions that you might want to ask your interviewers. Besides, asking questions that are answered on the website reflects poorly on the candidate.
- Pay attention to various clues that could reflect how organized and how academically oriented a program is. For example, a program that provides details about their didactic lectures sends a message that quality teaching is a priority. On the other hand, a program that has a website that hasn’t been updated for years could dissuade rather than recruit applicants.
- Read about the faculty, their areas of interests, and publications. Learn how their names are pronounced and use them during the interview.
- Read about the city where the program is. It shows interest in the area where you might be living and will help you to stand out among candidates.
5. Be prepared for the classics; be honest, genuine, and authentic. Think about these common prompts:
- Tell me about yourself.
- Why did you choose gastroenterology?
- Where do you see yourself in 5 years?
- Why would you like to come to the city where the program is?
- Are there any certain areas in gastroenterology that you’re interested in more (e.g., hepatology, motility, IBD, advanced endoscopy)?
6. It is likely your interviewer will ask if you have questions. Ask questions that further allow you to assess the program and your fit into the program.
- What aspects of the program are you most proud of?
- Where would you like to see this program in 5 years?
- What keeps you at this program?
Tips for a successful web-based interview9,10 (Table 2):
1. Pay attention to the time zone of the city of the program. Be ready at least 10 minutes before the interview.
2. Ensure a fast and stable Internet service for an uninterrupted interview experience. Consider using an ethernet cable. Have a back-up plan such as using a phone as a hotspot.
3. Use a quiet and private room, preferably at home. Be aware of the background. A simple decoration is acceptable.
4. Consider recording yourself using the same device you’ll use for the interview to make sure audio and video are functioning properly.
5. When scheduling more than one interview in 1 day, allow at least 2 hours between interviews to avoid scheduling conflicts caused by unanticipated delays related to technical issues.
6. Have immediate access to the invitation link(s) that you received. Add the interviews to your device’s calendar. Note that sometimes a new invitation link is generated last minute because of technical issues.
7. While the advice for physical interviews is to turn off your phone (and smart watch), you’ll have to keep your phone on but on silent for the virtual interviews. Sometimes, you’ll receive a phone call from the program to update you about any last-minute changes.
7. It is recommended that a laptop or a tablet with a camera with good resolution and a microphone be used rather than using a phone. A wide screen allows better communication. Disable notification on that device to avoid interruptions.
8. Sit comfortably with the device being at or just below eye level. Avoid distractions and maintain eye contact.
9. Familiarize yourself with the platform used and its functions. Double check the audio and video before each interview.
10. Put your device on a desk or table to improve stability; don’t hold it in your hand.
11. Find a place where the view is best and your face appears in the middle of the screen; not too far or too close. Use a well-lit room but don’t have a source of light behind you. Many platforms allow you to select a background or blur the background. A background that is monochromatic and not distracting is recommended.
12. Use a pen and a paper to take notes during the interview. You would use these notes to generate “thank you” or “interest in program” emails. Additionally, they will be a helpful reference when ranking programs.
13. Do not type. Typing is much louder to the interviewer and can be distracting.
14. Dress professionally, just as you dress for an on-site interview. You never know when you might have to stand up during the interview for unplanned reasons.
15. Do a practice interview. Have a colleague set up a virtual web session using any available platform. This will allow you to get feedback on your dress, background, acoustics, and general ability to answer questions.
References
1. Dig Dis Sci. 2019;64:1150-7.
2. BMJ Open. 2017;7:e016242.
3. Centers for Disease Control and Prevention. Coronavirus and Travel in the United States, 2020.
4. J Bone Joint Surg Am. 2017;99:e114.
5. Am J Gastroenterol. 2014;109:155-9.
6. West J Emerg Med. 2018;19:80-6.
7. Int J Med Educ. 2016;7:102-8.
8. Aparajit Naram M. How COVID-19 changed our fellowship interview process for the better. KevinMD.com. April 17, 2020.
9. Association of American Medical Colleges. Virtual interviews: Tips for medical school applicants, 2020. Updated May 14, 2020.
10. Top 5 video interviewing tips for residency and fellowship programs. Thalamus: Connecting the Docs. April 2, 2020, 2020.
Dr. Kiwan is chief fellow in gastroenterology, division of gastroenterology, at Wayne State University, Detroit Medical Center, John D. Dingell VA Medical Center, all in Detroit. Dr. Judd is an assistant professor and associate program director in the division of gastroenterology, Wayne State University, Detroit Medical Center, John D. Dingell VA Medical Center. Dr. Al Masalmeh is in the department of internal medicine, Wayne State University, Detroit Medical Center. Dr. Levine is professor and the vice chair for education, Wayne State University, Detroit Medical Center.
Fellowship interviews are an essential step – arguably the most important step – in the process of matching candidates to training programs. Until recently, most programs relied exclusively on on-site face-to face interviews. Since the appearance of the COVID-19 pandemic, the medical field has utilized web-based platforms. Despite inherent limitations, virtual meetings appear to be effective in providing patient care and in conducting administrative meetings.1,2
Because of uncertainty related to the pandemic, including changing guidelines regarding social distancing and travel restrictions, fellowship programs are expected to comply with CDC,3 state, and federal recommendations to avoid nonessential travel. Therefore, conducting web-based interviews exclusively will likely become a necessity.
While there may be some disadvantages to web-based interviews, many candidates find the overall experience satisfactory, thereby allowing them to understand the programs, express themselves, and comfortably rank the programs, as two studies have shown.4,5 Programs and candidates are encouraged to adapt to this new reality in order to achieve a successful match. After all, there are many potential advantages of web-based interviews. In addition to eliminating the risk of COVID-19 acquisition, web-based interviews have been described as helping to improve scheduling flexibility, reduce the financial burden, and allow conducting more interviews for candidates and programs (Table 1).6-8
There are different styles to the web-based interview.9 Some programs choose to offer a single group interview (or the so-called panel interview) in which all the interviewing faculties invite each candidate at a time. Alternatively, programs might choose to conduct separate interviews by each faculty in which the candidates would alternate. For the latter option, the program could use a single invitation link or multiple invitation links for each session.
General tips for a successful interview:9
1. Be pleasant and professional: Your communication with the program should reflect excellent manners and a professional attitude with everyone (i.e., faculties, coordinators, and fellows).
2. Know yourself and what you want: Review your CV and personal statement and reflect on your achievements, strengths and weaknesses. Identify examples from your experience that would speak well of you as a person and as a physician.
3. Communication is key:
- Respond to the interview invitations promptly.
- Send a brief thank you email to the interviewers and the coordinator. Avoid being generic; mention specific points of discussion and show your interest in the program.
- Proofread your emails carefully. Well-written emails that are devoid of grammatical or spelling errors send a positive message about the candidate.
4. Do your homework:
- Read the information posted on the website carefully and take notes. This should provide you with useful information to use when you rank the programs and could lead to questions that you might want to ask your interviewers. Besides, asking questions that are answered on the website reflects poorly on the candidate.
- Pay attention to various clues that could reflect how organized and how academically oriented a program is. For example, a program that provides details about their didactic lectures sends a message that quality teaching is a priority. On the other hand, a program that has a website that hasn’t been updated for years could dissuade rather than recruit applicants.
- Read about the faculty, their areas of interests, and publications. Learn how their names are pronounced and use them during the interview.
- Read about the city where the program is. It shows interest in the area where you might be living and will help you to stand out among candidates.
5. Be prepared for the classics; be honest, genuine, and authentic. Think about these common prompts:
- Tell me about yourself.
- Why did you choose gastroenterology?
- Where do you see yourself in 5 years?
- Why would you like to come to the city where the program is?
- Are there any certain areas in gastroenterology that you’re interested in more (e.g., hepatology, motility, IBD, advanced endoscopy)?
6. It is likely your interviewer will ask if you have questions. Ask questions that further allow you to assess the program and your fit into the program.
- What aspects of the program are you most proud of?
- Where would you like to see this program in 5 years?
- What keeps you at this program?
Tips for a successful web-based interview9,10 (Table 2):
1. Pay attention to the time zone of the city of the program. Be ready at least 10 minutes before the interview.
2. Ensure a fast and stable Internet service for an uninterrupted interview experience. Consider using an ethernet cable. Have a back-up plan such as using a phone as a hotspot.
3. Use a quiet and private room, preferably at home. Be aware of the background. A simple decoration is acceptable.
4. Consider recording yourself using the same device you’ll use for the interview to make sure audio and video are functioning properly.
5. When scheduling more than one interview in 1 day, allow at least 2 hours between interviews to avoid scheduling conflicts caused by unanticipated delays related to technical issues.
6. Have immediate access to the invitation link(s) that you received. Add the interviews to your device’s calendar. Note that sometimes a new invitation link is generated last minute because of technical issues.
7. While the advice for physical interviews is to turn off your phone (and smart watch), you’ll have to keep your phone on but on silent for the virtual interviews. Sometimes, you’ll receive a phone call from the program to update you about any last-minute changes.
7. It is recommended that a laptop or a tablet with a camera with good resolution and a microphone be used rather than using a phone. A wide screen allows better communication. Disable notification on that device to avoid interruptions.
8. Sit comfortably with the device being at or just below eye level. Avoid distractions and maintain eye contact.
9. Familiarize yourself with the platform used and its functions. Double check the audio and video before each interview.
10. Put your device on a desk or table to improve stability; don’t hold it in your hand.
11. Find a place where the view is best and your face appears in the middle of the screen; not too far or too close. Use a well-lit room but don’t have a source of light behind you. Many platforms allow you to select a background or blur the background. A background that is monochromatic and not distracting is recommended.
12. Use a pen and a paper to take notes during the interview. You would use these notes to generate “thank you” or “interest in program” emails. Additionally, they will be a helpful reference when ranking programs.
13. Do not type. Typing is much louder to the interviewer and can be distracting.
14. Dress professionally, just as you dress for an on-site interview. You never know when you might have to stand up during the interview for unplanned reasons.
15. Do a practice interview. Have a colleague set up a virtual web session using any available platform. This will allow you to get feedback on your dress, background, acoustics, and general ability to answer questions.
References
1. Dig Dis Sci. 2019;64:1150-7.
2. BMJ Open. 2017;7:e016242.
3. Centers for Disease Control and Prevention. Coronavirus and Travel in the United States, 2020.
4. J Bone Joint Surg Am. 2017;99:e114.
5. Am J Gastroenterol. 2014;109:155-9.
6. West J Emerg Med. 2018;19:80-6.
7. Int J Med Educ. 2016;7:102-8.
8. Aparajit Naram M. How COVID-19 changed our fellowship interview process for the better. KevinMD.com. April 17, 2020.
9. Association of American Medical Colleges. Virtual interviews: Tips for medical school applicants, 2020. Updated May 14, 2020.
10. Top 5 video interviewing tips for residency and fellowship programs. Thalamus: Connecting the Docs. April 2, 2020, 2020.
Dr. Kiwan is chief fellow in gastroenterology, division of gastroenterology, at Wayne State University, Detroit Medical Center, John D. Dingell VA Medical Center, all in Detroit. Dr. Judd is an assistant professor and associate program director in the division of gastroenterology, Wayne State University, Detroit Medical Center, John D. Dingell VA Medical Center. Dr. Al Masalmeh is in the department of internal medicine, Wayne State University, Detroit Medical Center. Dr. Levine is professor and the vice chair for education, Wayne State University, Detroit Medical Center.
Global study to track COVID-19’s impact on the brain
At its annual meeting, the Alzheimer’s Association announced the launch of a global study to examine the impact of COVID-19 on the brain, as well as policy recommendations to better address the COVID-19 crisis in long-term care facilities. The study will be led by researchers at the Alzheimer’s Association and the University of Texas Health, San Antonio, with participation from more than 30 countries and technical guidance from the World Health Organization.
The target sample size is 20,000-40,000 total participants.
Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, announced the study’s launch during a COVID-19–focused panel discussion at the virtual annual meeting of the Alzheimer’s Association International Conference 2020.
“To build a strong foundation for this research, we will align with existing studies, such as the Framingham Heart Study, and clinicians from around the world on how the data are going to be collected, obtained, and shared. We are going to have cross-study collaborations to understand the impact of the virus on the brain directly,” said Dr. Carrillo. “We will have some very good data to present next year at AAIC.”
‘Frightening’ headlines
As previously reported, mounting evidence suggests that SARS-CoV-2 invades the central nervous system, causing a wide range of neurologic and neuropsychiatric complications, including stroke, psychosis, altered mental state, and dementia-like syndrome. It’s likely that “dementia does not increase the risk for COVID-19, just like dementia does not increase risk for the flu. But increased age, being in a long-term care setting, and common health conditions that often accompany dementia may increase the risk,” Dr. Carrillo said.
Panel member Beth Kallmyer, MSW, vice president of care and support at the Alzheimer’s Association, spoke about the ongoing challenges long-term care facilities are facing during the pandemic. “You’ve all seen the headlines, and they’re frightening, frankly,” she said. An estimated 59,000 residents and employees of long-term care have died as a result of COVID-19, which is 42% of all U.S. deaths.
The long-term care community is being impacted at “significantly greater rates than the rest of society and yet we don’t have things in place to protect them. We also know that individuals living with dementia make up a large percentage of those that are living in long-term care,” Ms. Kallmyer said.
She noted that infection control is always a challenge in long-term care settings, but infection control during a pandemic “takes it to a whole other level.” Quarantining is hard for anyone, “but when you layer dementia on top of that we have a real challenge.” One long-term care provider told Ms. Kallmyer that “we might be saving them from COVID, but we’re losing them to social isolation and cognitive decline.”
New recommendations
Ms. Kallmyer outlined new policy recommendations from the Alzheimer’s Association to address the COVID-19 crisis in long-term and community-based care settings. They include:
- Testing every resident, employee, and visitor each time they leave and come back, so residents would not need to be confined to their own rooms
- Having a single portal that is easy and efficient for reporting cases
- Developing “surge activation” protocols to respond to hot spots, including the possibility of “strike teams” that go in and help during an outbreak
- Making sure all long-term care providers have full access to all needed personal protective equipment (PPE)
“Five months in and long-term care providers still don’t have adequate PPE. This is unacceptable,” said Ms. Kallmyer. “We have to be able to provide them with PPE.”
Panel member Gregory A. Jicha, MD, PhD, Sanders-Brown Center on Aging, University of Kentucky, Lexington, spoke about the critical need to continue Alzheimer’s disease research during the pandemic, noting that the number of promising targets for Alzheimer’s disease and related dementias has “never been higher or more comprehensive.”
Measures to ensure safety of researchers and participants include screening for symptoms (50% effective), social distancing (93% effective), minimizing exposure time (50% effective), limiting staff to 50% (50% effective), cloth/paper masks (80% effective), and testing (99.25% effective), Dr. Jicha noted.
With no safety measures in place, the risk of getting COVID-19 from a research visit is 1 in 20; when all these safety measures are combined, the risk is 1 in over 1.5 million, so “we can essentially eradicate or minimize the risks for COVID to less that of a lightning strike,” he said.
Dr. Carrillo, Ms. Kallmyer, and Dr. Jicha disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
At its annual meeting, the Alzheimer’s Association announced the launch of a global study to examine the impact of COVID-19 on the brain, as well as policy recommendations to better address the COVID-19 crisis in long-term care facilities. The study will be led by researchers at the Alzheimer’s Association and the University of Texas Health, San Antonio, with participation from more than 30 countries and technical guidance from the World Health Organization.
The target sample size is 20,000-40,000 total participants.
Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, announced the study’s launch during a COVID-19–focused panel discussion at the virtual annual meeting of the Alzheimer’s Association International Conference 2020.
“To build a strong foundation for this research, we will align with existing studies, such as the Framingham Heart Study, and clinicians from around the world on how the data are going to be collected, obtained, and shared. We are going to have cross-study collaborations to understand the impact of the virus on the brain directly,” said Dr. Carrillo. “We will have some very good data to present next year at AAIC.”
‘Frightening’ headlines
As previously reported, mounting evidence suggests that SARS-CoV-2 invades the central nervous system, causing a wide range of neurologic and neuropsychiatric complications, including stroke, psychosis, altered mental state, and dementia-like syndrome. It’s likely that “dementia does not increase the risk for COVID-19, just like dementia does not increase risk for the flu. But increased age, being in a long-term care setting, and common health conditions that often accompany dementia may increase the risk,” Dr. Carrillo said.
Panel member Beth Kallmyer, MSW, vice president of care and support at the Alzheimer’s Association, spoke about the ongoing challenges long-term care facilities are facing during the pandemic. “You’ve all seen the headlines, and they’re frightening, frankly,” she said. An estimated 59,000 residents and employees of long-term care have died as a result of COVID-19, which is 42% of all U.S. deaths.
The long-term care community is being impacted at “significantly greater rates than the rest of society and yet we don’t have things in place to protect them. We also know that individuals living with dementia make up a large percentage of those that are living in long-term care,” Ms. Kallmyer said.
She noted that infection control is always a challenge in long-term care settings, but infection control during a pandemic “takes it to a whole other level.” Quarantining is hard for anyone, “but when you layer dementia on top of that we have a real challenge.” One long-term care provider told Ms. Kallmyer that “we might be saving them from COVID, but we’re losing them to social isolation and cognitive decline.”
New recommendations
Ms. Kallmyer outlined new policy recommendations from the Alzheimer’s Association to address the COVID-19 crisis in long-term and community-based care settings. They include:
- Testing every resident, employee, and visitor each time they leave and come back, so residents would not need to be confined to their own rooms
- Having a single portal that is easy and efficient for reporting cases
- Developing “surge activation” protocols to respond to hot spots, including the possibility of “strike teams” that go in and help during an outbreak
- Making sure all long-term care providers have full access to all needed personal protective equipment (PPE)
“Five months in and long-term care providers still don’t have adequate PPE. This is unacceptable,” said Ms. Kallmyer. “We have to be able to provide them with PPE.”
Panel member Gregory A. Jicha, MD, PhD, Sanders-Brown Center on Aging, University of Kentucky, Lexington, spoke about the critical need to continue Alzheimer’s disease research during the pandemic, noting that the number of promising targets for Alzheimer’s disease and related dementias has “never been higher or more comprehensive.”
Measures to ensure safety of researchers and participants include screening for symptoms (50% effective), social distancing (93% effective), minimizing exposure time (50% effective), limiting staff to 50% (50% effective), cloth/paper masks (80% effective), and testing (99.25% effective), Dr. Jicha noted.
With no safety measures in place, the risk of getting COVID-19 from a research visit is 1 in 20; when all these safety measures are combined, the risk is 1 in over 1.5 million, so “we can essentially eradicate or minimize the risks for COVID to less that of a lightning strike,” he said.
Dr. Carrillo, Ms. Kallmyer, and Dr. Jicha disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
At its annual meeting, the Alzheimer’s Association announced the launch of a global study to examine the impact of COVID-19 on the brain, as well as policy recommendations to better address the COVID-19 crisis in long-term care facilities. The study will be led by researchers at the Alzheimer’s Association and the University of Texas Health, San Antonio, with participation from more than 30 countries and technical guidance from the World Health Organization.
The target sample size is 20,000-40,000 total participants.
Maria C. Carrillo, PhD, chief science officer for the Alzheimer’s Association, announced the study’s launch during a COVID-19–focused panel discussion at the virtual annual meeting of the Alzheimer’s Association International Conference 2020.
“To build a strong foundation for this research, we will align with existing studies, such as the Framingham Heart Study, and clinicians from around the world on how the data are going to be collected, obtained, and shared. We are going to have cross-study collaborations to understand the impact of the virus on the brain directly,” said Dr. Carrillo. “We will have some very good data to present next year at AAIC.”
‘Frightening’ headlines
As previously reported, mounting evidence suggests that SARS-CoV-2 invades the central nervous system, causing a wide range of neurologic and neuropsychiatric complications, including stroke, psychosis, altered mental state, and dementia-like syndrome. It’s likely that “dementia does not increase the risk for COVID-19, just like dementia does not increase risk for the flu. But increased age, being in a long-term care setting, and common health conditions that often accompany dementia may increase the risk,” Dr. Carrillo said.
Panel member Beth Kallmyer, MSW, vice president of care and support at the Alzheimer’s Association, spoke about the ongoing challenges long-term care facilities are facing during the pandemic. “You’ve all seen the headlines, and they’re frightening, frankly,” she said. An estimated 59,000 residents and employees of long-term care have died as a result of COVID-19, which is 42% of all U.S. deaths.
The long-term care community is being impacted at “significantly greater rates than the rest of society and yet we don’t have things in place to protect them. We also know that individuals living with dementia make up a large percentage of those that are living in long-term care,” Ms. Kallmyer said.
She noted that infection control is always a challenge in long-term care settings, but infection control during a pandemic “takes it to a whole other level.” Quarantining is hard for anyone, “but when you layer dementia on top of that we have a real challenge.” One long-term care provider told Ms. Kallmyer that “we might be saving them from COVID, but we’re losing them to social isolation and cognitive decline.”
New recommendations
Ms. Kallmyer outlined new policy recommendations from the Alzheimer’s Association to address the COVID-19 crisis in long-term and community-based care settings. They include:
- Testing every resident, employee, and visitor each time they leave and come back, so residents would not need to be confined to their own rooms
- Having a single portal that is easy and efficient for reporting cases
- Developing “surge activation” protocols to respond to hot spots, including the possibility of “strike teams” that go in and help during an outbreak
- Making sure all long-term care providers have full access to all needed personal protective equipment (PPE)
“Five months in and long-term care providers still don’t have adequate PPE. This is unacceptable,” said Ms. Kallmyer. “We have to be able to provide them with PPE.”
Panel member Gregory A. Jicha, MD, PhD, Sanders-Brown Center on Aging, University of Kentucky, Lexington, spoke about the critical need to continue Alzheimer’s disease research during the pandemic, noting that the number of promising targets for Alzheimer’s disease and related dementias has “never been higher or more comprehensive.”
Measures to ensure safety of researchers and participants include screening for symptoms (50% effective), social distancing (93% effective), minimizing exposure time (50% effective), limiting staff to 50% (50% effective), cloth/paper masks (80% effective), and testing (99.25% effective), Dr. Jicha noted.
With no safety measures in place, the risk of getting COVID-19 from a research visit is 1 in 20; when all these safety measures are combined, the risk is 1 in over 1.5 million, so “we can essentially eradicate or minimize the risks for COVID to less that of a lightning strike,” he said.
Dr. Carrillo, Ms. Kallmyer, and Dr. Jicha disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM AAIC 2020
COVID-19 taking financial toll on people in U.S. with diabetes
The COVID-19 pandemic is taking a particularly severe financial toll on people with diabetes, new research from the United States suggests.
Results from a national online survey of 5,000 people with diabetes conducted between June 26 and July 1, 2020, were posted July 29 on the American Diabetes Association website.
The survey, conducted by the diabetes research company dQ&A in association with the ADA, revealed that Americans with diabetes are experiencing extreme financial pressures, leading to medication and supply rationing.
A high proportion of respondents had either lost income or are working in jobs that place them at risk for catching the novel coronavirus.
“These new numbers show the urgency needed to adopt measures to protect and assist the millions of people with diabetes who are suffering through this pandemic,” Tracey D. Brown, CEO of the ADA, said in a statement.
She called for states to extend health care coverage to people who have lost their jobs, for the eradication of insulin copays during the pandemic, and for increased COVID-19 testing capacity in high-risk communities.
“If these actions aren’t taken immediately, we will continue to see devastating impacts and outcomes for millions of vulnerable Americans,” Ms. Brown stressed.
COVID-19 has worsened financial pressures for people with diabetes
In the survey, 24% of respondents reported having used savings, loans, or stimulus check money to pay for diabetes care in the past 3 months. Among those who have lost income, half are using savings or stimulus money.
A quarter of respondents said they have been self-rationing supplies to cut costs.
Extrapolating to the entire U.S. population with diabetes, dQ&A estimated that roughly 650,000 are skipping insulin doses or taking less than prescribed, and 3 million are skipping blood glucose tests.
In June, the unemployment rate for people with diabetes was 18%, higher than the national rate of 12%.
Also higher is the proportion of those working prior to the pandemic who have since lost income: 33%, compared with 29% for the general population.
Among those who are self-employed, 7 in 10 of those with diabetes have lost some or all of their income.
Many with diabetes who are employed are vulnerable to exposure
Of those who remain employed, half said they can’t work from home.
Of those, 60% work in essential industries, with 22% in health care. A large majority, 90%, reported lack of social distancing at work and nearly a third work in places that don’t require masks.
“People with diabetes are helping to provide the services we all depend on during this pandemic, even as it puts their own well-being at risk,” the report said.
It concluded that “these numbers represent a conservative estimate of the pandemic’s impact. They are generated from an ongoing online study of the diabetes population amongst people who have opted in to participate.”
A version of this article originally appeared on Medscape.com.
The COVID-19 pandemic is taking a particularly severe financial toll on people with diabetes, new research from the United States suggests.
Results from a national online survey of 5,000 people with diabetes conducted between June 26 and July 1, 2020, were posted July 29 on the American Diabetes Association website.
The survey, conducted by the diabetes research company dQ&A in association with the ADA, revealed that Americans with diabetes are experiencing extreme financial pressures, leading to medication and supply rationing.
A high proportion of respondents had either lost income or are working in jobs that place them at risk for catching the novel coronavirus.
“These new numbers show the urgency needed to adopt measures to protect and assist the millions of people with diabetes who are suffering through this pandemic,” Tracey D. Brown, CEO of the ADA, said in a statement.
She called for states to extend health care coverage to people who have lost their jobs, for the eradication of insulin copays during the pandemic, and for increased COVID-19 testing capacity in high-risk communities.
“If these actions aren’t taken immediately, we will continue to see devastating impacts and outcomes for millions of vulnerable Americans,” Ms. Brown stressed.
COVID-19 has worsened financial pressures for people with diabetes
In the survey, 24% of respondents reported having used savings, loans, or stimulus check money to pay for diabetes care in the past 3 months. Among those who have lost income, half are using savings or stimulus money.
A quarter of respondents said they have been self-rationing supplies to cut costs.
Extrapolating to the entire U.S. population with diabetes, dQ&A estimated that roughly 650,000 are skipping insulin doses or taking less than prescribed, and 3 million are skipping blood glucose tests.
In June, the unemployment rate for people with diabetes was 18%, higher than the national rate of 12%.
Also higher is the proportion of those working prior to the pandemic who have since lost income: 33%, compared with 29% for the general population.
Among those who are self-employed, 7 in 10 of those with diabetes have lost some or all of their income.
Many with diabetes who are employed are vulnerable to exposure
Of those who remain employed, half said they can’t work from home.
Of those, 60% work in essential industries, with 22% in health care. A large majority, 90%, reported lack of social distancing at work and nearly a third work in places that don’t require masks.
“People with diabetes are helping to provide the services we all depend on during this pandemic, even as it puts their own well-being at risk,” the report said.
It concluded that “these numbers represent a conservative estimate of the pandemic’s impact. They are generated from an ongoing online study of the diabetes population amongst people who have opted in to participate.”
A version of this article originally appeared on Medscape.com.
The COVID-19 pandemic is taking a particularly severe financial toll on people with diabetes, new research from the United States suggests.
Results from a national online survey of 5,000 people with diabetes conducted between June 26 and July 1, 2020, were posted July 29 on the American Diabetes Association website.
The survey, conducted by the diabetes research company dQ&A in association with the ADA, revealed that Americans with diabetes are experiencing extreme financial pressures, leading to medication and supply rationing.
A high proportion of respondents had either lost income or are working in jobs that place them at risk for catching the novel coronavirus.
“These new numbers show the urgency needed to adopt measures to protect and assist the millions of people with diabetes who are suffering through this pandemic,” Tracey D. Brown, CEO of the ADA, said in a statement.
She called for states to extend health care coverage to people who have lost their jobs, for the eradication of insulin copays during the pandemic, and for increased COVID-19 testing capacity in high-risk communities.
“If these actions aren’t taken immediately, we will continue to see devastating impacts and outcomes for millions of vulnerable Americans,” Ms. Brown stressed.
COVID-19 has worsened financial pressures for people with diabetes
In the survey, 24% of respondents reported having used savings, loans, or stimulus check money to pay for diabetes care in the past 3 months. Among those who have lost income, half are using savings or stimulus money.
A quarter of respondents said they have been self-rationing supplies to cut costs.
Extrapolating to the entire U.S. population with diabetes, dQ&A estimated that roughly 650,000 are skipping insulin doses or taking less than prescribed, and 3 million are skipping blood glucose tests.
In June, the unemployment rate for people with diabetes was 18%, higher than the national rate of 12%.
Also higher is the proportion of those working prior to the pandemic who have since lost income: 33%, compared with 29% for the general population.
Among those who are self-employed, 7 in 10 of those with diabetes have lost some or all of their income.
Many with diabetes who are employed are vulnerable to exposure
Of those who remain employed, half said they can’t work from home.
Of those, 60% work in essential industries, with 22% in health care. A large majority, 90%, reported lack of social distancing at work and nearly a third work in places that don’t require masks.
“People with diabetes are helping to provide the services we all depend on during this pandemic, even as it puts their own well-being at risk,” the report said.
It concluded that “these numbers represent a conservative estimate of the pandemic’s impact. They are generated from an ongoing online study of the diabetes population amongst people who have opted in to participate.”
A version of this article originally appeared on Medscape.com.
Why are we still talking about hydroxychloroquine?
This is getting pretty ridiculous. The number of well-done, evidence-based trials of hydroxychloroquine in COVID-19 showing minimal-to-no benefit is increasing. There are still studies that show benefit in certain cases, but many of them are small-scale or even anecdotal.

How long is this going to go on? If the evidence supporting its use were to be put through the standard Food and Drug Administration approval panels it wouldn’t have a chance.
Yet, because it’s become a political football (like masks), science and rational research are tossed out the window. At the end of July we were all treated to videos of Dr. Stella Immanuel claiming the drug is a cure. Dr. Immanuel may have medical credentials, but she also supports beliefs that space aliens and the Illuminati are involved in running governments, and that multiple gynecologic disorders are caused by sexual relations with demons and witches during dreams.
Even so, her hydroxychloroquine statements were given heavy play during a news cycle, then endorsed by the president and his supporters, all with very little immediate background provided for other claims she’s made in the past.
Medicine is a science. Politics shouldn’t be. Continuing to give it to sick people, despite the growing evidence against it, violates the “do-no-harm” tenet of our field.
There was no shame in trying it and failing. This is the process through which all treatments are tested. If they work (such as with penicillin, for example) that’s wonderful. If they fail (such as with countless Alzheimer’s trials) we learn what doesn’t work and move on.
But to keep claiming success where there isn’t any moves beyond science and into things that whiff of a hoax, such as 1989’s cold fusion or recurrent claims of capturing Bigfoot.
With an implacable enemy such as COVID-19 at the door, money and effort need to be focused on finding what works, not on putting stale milk back in the refrigerator and hoping it comes out fresh.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This is getting pretty ridiculous. The number of well-done, evidence-based trials of hydroxychloroquine in COVID-19 showing minimal-to-no benefit is increasing. There are still studies that show benefit in certain cases, but many of them are small-scale or even anecdotal.
How long is this going to go on? If the evidence supporting its use were to be put through the standard Food and Drug Administration approval panels it wouldn’t have a chance.
Yet, because it’s become a political football (like masks), science and rational research are tossed out the window. At the end of July we were all treated to videos of Dr. Stella Immanuel claiming the drug is a cure. Dr. Immanuel may have medical credentials, but she also supports beliefs that space aliens and the Illuminati are involved in running governments, and that multiple gynecologic disorders are caused by sexual relations with demons and witches during dreams.
Even so, her hydroxychloroquine statements were given heavy play during a news cycle, then endorsed by the president and his supporters, all with very little immediate background provided for other claims she’s made in the past.
Medicine is a science. Politics shouldn’t be. Continuing to give it to sick people, despite the growing evidence against it, violates the “do-no-harm” tenet of our field.
There was no shame in trying it and failing. This is the process through which all treatments are tested. If they work (such as with penicillin, for example) that’s wonderful. If they fail (such as with countless Alzheimer’s trials) we learn what doesn’t work and move on.
But to keep claiming success where there isn’t any moves beyond science and into things that whiff of a hoax, such as 1989’s cold fusion or recurrent claims of capturing Bigfoot.
With an implacable enemy such as COVID-19 at the door, money and effort need to be focused on finding what works, not on putting stale milk back in the refrigerator and hoping it comes out fresh.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This is getting pretty ridiculous. The number of well-done, evidence-based trials of hydroxychloroquine in COVID-19 showing minimal-to-no benefit is increasing. There are still studies that show benefit in certain cases, but many of them are small-scale or even anecdotal.
How long is this going to go on? If the evidence supporting its use were to be put through the standard Food and Drug Administration approval panels it wouldn’t have a chance.
Yet, because it’s become a political football (like masks), science and rational research are tossed out the window. At the end of July we were all treated to videos of Dr. Stella Immanuel claiming the drug is a cure. Dr. Immanuel may have medical credentials, but she also supports beliefs that space aliens and the Illuminati are involved in running governments, and that multiple gynecologic disorders are caused by sexual relations with demons and witches during dreams.
Even so, her hydroxychloroquine statements were given heavy play during a news cycle, then endorsed by the president and his supporters, all with very little immediate background provided for other claims she’s made in the past.
Medicine is a science. Politics shouldn’t be. Continuing to give it to sick people, despite the growing evidence against it, violates the “do-no-harm” tenet of our field.
There was no shame in trying it and failing. This is the process through which all treatments are tested. If they work (such as with penicillin, for example) that’s wonderful. If they fail (such as with countless Alzheimer’s trials) we learn what doesn’t work and move on.
But to keep claiming success where there isn’t any moves beyond science and into things that whiff of a hoax, such as 1989’s cold fusion or recurrent claims of capturing Bigfoot.
With an implacable enemy such as COVID-19 at the door, money and effort need to be focused on finding what works, not on putting stale milk back in the refrigerator and hoping it comes out fresh.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Enduring the ordeal of a quadruple threat is especially arduous for psychiatric patients
These are unusually stressful days for everyone, especially our patients. We are all experiencing a turbulent mix of emotions as we try to cope with a confluence of threats to both our lives and to life as we know it. Peace of mind has become so elusive due to the relentless overlapping waves of fear, sadness, anger, and uncertainty. We are all grieving in a different way, but our psychiatric patients are suffering the most.
Fear. It only takes 1 traumatic event to trigger posttraumatic stress disorder (PTSD). Yet over the past few months, we have been afflicted by 4 jarring traumatic events, individually and as a society. Just a few months ago, it would have been impossible to imagine the conflux of 4 concurrent seismic threats to our well-being. A toxic political zeitgeist was the backdrop, which we bemoaned and tried to compartmentalize, despite the corrosive political environment shrouding the country. Then the deadly coronavirus disease 2019 (COVID-19) pandemic suddenly arrived, imposing draconian health-preserving measures that impacted every individual’s daily life in countless detrimental ways. Fear prevailed as we all sheltered at home, stopped commuting to work, canceled all trips, distanced ourselves from our friends and relatives, and watched depressing and anxiety-provoking television and read online news throughout our waking hours. Hoarding food and household supplies became endemic due to fear about survival.
Sadness. The agonizing prospect of a national financial necrosis followed the threat of serious illness or death. The economy came to a screeching halt, hemorrhaging millions of jobs. Unemployed parents stayed home with their morose children whose schools were shuttered, leaving them deprived of socializing with their friends. The government hurried with financial chemotherapy, printing trillions of dollars to prevent economic collapse, to avert potential poverty and hunger for many. The fear of the pandemic became coupled with sadness over the loss of livelihoods and grief for the loss of liberty and the ability to pursue happiness, or even small pleasures.
Anger. Then a tsunami of anger was generated by the brutal and sadistic death of a black man in police custody. This was a spark that ignited a massive amount of previously dormant racial tension dating back to the dark days of slavery. Peaceful protests were marred by destructive riots. The explosive fury was perhaps intensified by the protestors having been being locked up for weeks and having to wear masks, both of which were symbolic of being held down and “unable to breathe,” like the murdered Mr. George Floyd.
An epidemic of destroying statues followed. Heavy statues that appeared invincible for decades were dismantled from their plinth in a matter of minutes, signifying extreme frustration with the social injustice that remains despite the transformational laws of the Civil Rights Acts of 1960 and 1964. Suddenly—like falling dominoes—statues, flags, names of military bases, and previously venerated monuments were removed, changed, vandalized, or threatened with destruction. The founders of the republic were also maligned because they were slave owners 2 centuries ago. The paradigm shift spawned by the rage over racial inequality was disconcerting and dramatic. The anger and rampage spawned a sense that a tipping point in our society has been reached.
Uncertainty. The confluence of political instability, a deadly pandemic, economic collapse, and racial tensions were like the 4 horsemen of mass PTSD. The result was an agonizing uncertainty about the impact of these changes, and whether a sense of normalcy will ever return. It became apparent to all of us that our social structure has changed forever across multiple fundamental domains: public health, social, political, and financial. The wait for a vaccine for COVID-19 seems interminable, and racial healing and harmony seems elusive. Economic recovery may be possible, but political detoxification appears unlikely. The fate of police departments, condemned because of the deplorable and illegal acts of a few, and the safety of citizens, usually guaranteed by law and order, seem uncertain. Like COVID-19, angst has rapidly spread across the population.
The price our patients pay
The ingredients of a large-scale societal PTSD, similar to what probably happens during a world war, are now in place. Even resilient individuals may buckle during quadruple ordeals such as this one. So imagine what is happening to our patients, rendered fragile and vulnerable to threats by their pre-existing psychiatric illness. They all pay a heavy price. Patients with anxiety disorders will decompensate, with more panic attacks. Patients burdened by depression will worsen, with more hopelessness, despair, and suicidal ideation due to anxiety and loneliness. Patients with bipolar disorder will become more labile and irritable, and their comorbid anxiety will intensify. Patients with schizophrenia will become more paranoid, depressed, and anxious. Patients with autism will become more agitated and aggressive because their cherished daily routines are disrupted. Patients with obsessive-compulsive disorder will react to their germaphobia by washing their hands and cleaning everything around them even more frequently, and they (along with everyone else) will become hoarders.
Hope and healing
As psychiatrists, we are determined to transcend our own stress, rise above it all, and attend to the pervasive sadness, grief, anger, and uncertainty all around us, but especially among our patients, for whom the anguish of a psychiatric disorder is further compounded by 4 additional ordeals. This is our moment of truth as healers of our patients’ souls, because they look to us to provide them with hope to help navigate these trying times into full health. And we psychiatrists, along with fellow mental health professionals, are up to this unprecedented challenge.
These are unusually stressful days for everyone, especially our patients. We are all experiencing a turbulent mix of emotions as we try to cope with a confluence of threats to both our lives and to life as we know it. Peace of mind has become so elusive due to the relentless overlapping waves of fear, sadness, anger, and uncertainty. We are all grieving in a different way, but our psychiatric patients are suffering the most.
Fear. It only takes 1 traumatic event to trigger posttraumatic stress disorder (PTSD). Yet over the past few months, we have been afflicted by 4 jarring traumatic events, individually and as a society. Just a few months ago, it would have been impossible to imagine the conflux of 4 concurrent seismic threats to our well-being. A toxic political zeitgeist was the backdrop, which we bemoaned and tried to compartmentalize, despite the corrosive political environment shrouding the country. Then the deadly coronavirus disease 2019 (COVID-19) pandemic suddenly arrived, imposing draconian health-preserving measures that impacted every individual’s daily life in countless detrimental ways. Fear prevailed as we all sheltered at home, stopped commuting to work, canceled all trips, distanced ourselves from our friends and relatives, and watched depressing and anxiety-provoking television and read online news throughout our waking hours. Hoarding food and household supplies became endemic due to fear about survival.
Sadness. The agonizing prospect of a national financial necrosis followed the threat of serious illness or death. The economy came to a screeching halt, hemorrhaging millions of jobs. Unemployed parents stayed home with their morose children whose schools were shuttered, leaving them deprived of socializing with their friends. The government hurried with financial chemotherapy, printing trillions of dollars to prevent economic collapse, to avert potential poverty and hunger for many. The fear of the pandemic became coupled with sadness over the loss of livelihoods and grief for the loss of liberty and the ability to pursue happiness, or even small pleasures.
Anger. Then a tsunami of anger was generated by the brutal and sadistic death of a black man in police custody. This was a spark that ignited a massive amount of previously dormant racial tension dating back to the dark days of slavery. Peaceful protests were marred by destructive riots. The explosive fury was perhaps intensified by the protestors having been being locked up for weeks and having to wear masks, both of which were symbolic of being held down and “unable to breathe,” like the murdered Mr. George Floyd.
An epidemic of destroying statues followed. Heavy statues that appeared invincible for decades were dismantled from their plinth in a matter of minutes, signifying extreme frustration with the social injustice that remains despite the transformational laws of the Civil Rights Acts of 1960 and 1964. Suddenly—like falling dominoes—statues, flags, names of military bases, and previously venerated monuments were removed, changed, vandalized, or threatened with destruction. The founders of the republic were also maligned because they were slave owners 2 centuries ago. The paradigm shift spawned by the rage over racial inequality was disconcerting and dramatic. The anger and rampage spawned a sense that a tipping point in our society has been reached.
Uncertainty. The confluence of political instability, a deadly pandemic, economic collapse, and racial tensions were like the 4 horsemen of mass PTSD. The result was an agonizing uncertainty about the impact of these changes, and whether a sense of normalcy will ever return. It became apparent to all of us that our social structure has changed forever across multiple fundamental domains: public health, social, political, and financial. The wait for a vaccine for COVID-19 seems interminable, and racial healing and harmony seems elusive. Economic recovery may be possible, but political detoxification appears unlikely. The fate of police departments, condemned because of the deplorable and illegal acts of a few, and the safety of citizens, usually guaranteed by law and order, seem uncertain. Like COVID-19, angst has rapidly spread across the population.
The price our patients pay
The ingredients of a large-scale societal PTSD, similar to what probably happens during a world war, are now in place. Even resilient individuals may buckle during quadruple ordeals such as this one. So imagine what is happening to our patients, rendered fragile and vulnerable to threats by their pre-existing psychiatric illness. They all pay a heavy price. Patients with anxiety disorders will decompensate, with more panic attacks. Patients burdened by depression will worsen, with more hopelessness, despair, and suicidal ideation due to anxiety and loneliness. Patients with bipolar disorder will become more labile and irritable, and their comorbid anxiety will intensify. Patients with schizophrenia will become more paranoid, depressed, and anxious. Patients with autism will become more agitated and aggressive because their cherished daily routines are disrupted. Patients with obsessive-compulsive disorder will react to their germaphobia by washing their hands and cleaning everything around them even more frequently, and they (along with everyone else) will become hoarders.
Hope and healing
As psychiatrists, we are determined to transcend our own stress, rise above it all, and attend to the pervasive sadness, grief, anger, and uncertainty all around us, but especially among our patients, for whom the anguish of a psychiatric disorder is further compounded by 4 additional ordeals. This is our moment of truth as healers of our patients’ souls, because they look to us to provide them with hope to help navigate these trying times into full health. And we psychiatrists, along with fellow mental health professionals, are up to this unprecedented challenge.
These are unusually stressful days for everyone, especially our patients. We are all experiencing a turbulent mix of emotions as we try to cope with a confluence of threats to both our lives and to life as we know it. Peace of mind has become so elusive due to the relentless overlapping waves of fear, sadness, anger, and uncertainty. We are all grieving in a different way, but our psychiatric patients are suffering the most.
Fear. It only takes 1 traumatic event to trigger posttraumatic stress disorder (PTSD). Yet over the past few months, we have been afflicted by 4 jarring traumatic events, individually and as a society. Just a few months ago, it would have been impossible to imagine the conflux of 4 concurrent seismic threats to our well-being. A toxic political zeitgeist was the backdrop, which we bemoaned and tried to compartmentalize, despite the corrosive political environment shrouding the country. Then the deadly coronavirus disease 2019 (COVID-19) pandemic suddenly arrived, imposing draconian health-preserving measures that impacted every individual’s daily life in countless detrimental ways. Fear prevailed as we all sheltered at home, stopped commuting to work, canceled all trips, distanced ourselves from our friends and relatives, and watched depressing and anxiety-provoking television and read online news throughout our waking hours. Hoarding food and household supplies became endemic due to fear about survival.
Sadness. The agonizing prospect of a national financial necrosis followed the threat of serious illness or death. The economy came to a screeching halt, hemorrhaging millions of jobs. Unemployed parents stayed home with their morose children whose schools were shuttered, leaving them deprived of socializing with their friends. The government hurried with financial chemotherapy, printing trillions of dollars to prevent economic collapse, to avert potential poverty and hunger for many. The fear of the pandemic became coupled with sadness over the loss of livelihoods and grief for the loss of liberty and the ability to pursue happiness, or even small pleasures.
Anger. Then a tsunami of anger was generated by the brutal and sadistic death of a black man in police custody. This was a spark that ignited a massive amount of previously dormant racial tension dating back to the dark days of slavery. Peaceful protests were marred by destructive riots. The explosive fury was perhaps intensified by the protestors having been being locked up for weeks and having to wear masks, both of which were symbolic of being held down and “unable to breathe,” like the murdered Mr. George Floyd.
An epidemic of destroying statues followed. Heavy statues that appeared invincible for decades were dismantled from their plinth in a matter of minutes, signifying extreme frustration with the social injustice that remains despite the transformational laws of the Civil Rights Acts of 1960 and 1964. Suddenly—like falling dominoes—statues, flags, names of military bases, and previously venerated monuments were removed, changed, vandalized, or threatened with destruction. The founders of the republic were also maligned because they were slave owners 2 centuries ago. The paradigm shift spawned by the rage over racial inequality was disconcerting and dramatic. The anger and rampage spawned a sense that a tipping point in our society has been reached.
Uncertainty. The confluence of political instability, a deadly pandemic, economic collapse, and racial tensions were like the 4 horsemen of mass PTSD. The result was an agonizing uncertainty about the impact of these changes, and whether a sense of normalcy will ever return. It became apparent to all of us that our social structure has changed forever across multiple fundamental domains: public health, social, political, and financial. The wait for a vaccine for COVID-19 seems interminable, and racial healing and harmony seems elusive. Economic recovery may be possible, but political detoxification appears unlikely. The fate of police departments, condemned because of the deplorable and illegal acts of a few, and the safety of citizens, usually guaranteed by law and order, seem uncertain. Like COVID-19, angst has rapidly spread across the population.
The price our patients pay
The ingredients of a large-scale societal PTSD, similar to what probably happens during a world war, are now in place. Even resilient individuals may buckle during quadruple ordeals such as this one. So imagine what is happening to our patients, rendered fragile and vulnerable to threats by their pre-existing psychiatric illness. They all pay a heavy price. Patients with anxiety disorders will decompensate, with more panic attacks. Patients burdened by depression will worsen, with more hopelessness, despair, and suicidal ideation due to anxiety and loneliness. Patients with bipolar disorder will become more labile and irritable, and their comorbid anxiety will intensify. Patients with schizophrenia will become more paranoid, depressed, and anxious. Patients with autism will become more agitated and aggressive because their cherished daily routines are disrupted. Patients with obsessive-compulsive disorder will react to their germaphobia by washing their hands and cleaning everything around them even more frequently, and they (along with everyone else) will become hoarders.
Hope and healing
As psychiatrists, we are determined to transcend our own stress, rise above it all, and attend to the pervasive sadness, grief, anger, and uncertainty all around us, but especially among our patients, for whom the anguish of a psychiatric disorder is further compounded by 4 additional ordeals. This is our moment of truth as healers of our patients’ souls, because they look to us to provide them with hope to help navigate these trying times into full health. And we psychiatrists, along with fellow mental health professionals, are up to this unprecedented challenge.
