User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Gestational hypertension-diabetes combo signals CVD risk
Women who develop transient hypertensive disorders during their pregnancy are at risk for developing subsequent cardiovascular disease (CVD), particularly if this experienced at the same time as gestational diabetes.
In a large population-based study, the adjusted hazard ratios for developing CVD following a gestational hypertensive disorder (GHTD) alone were 1.90 (95% confidence interval, 1.151-2.25) within 5 years and 1.41 (95% CI, 1.12-1.76) after 5 years or more.
When gestational diabetes was added into the mix, however, the risk for CVD after 5 years more than doubled (aHR, 2.43; 95% CI, 1.60-3.67). Risk in the earlier postpartum period was also raised by the combination, but this was not significant (aHR, 1.42; 95% CI, 0.78-2.58).
Having gestational diabetes by itself did not seem to increase the risk for later CVD in the analysis, despite being linked to higher heart disease risk in other studies.
“These are women coming out of a pregnancy – young women of reproductive age – so this is not a group that typically has cardiovascular events,” said Ravi Retnakaran, MD, in an interview, an investigator in the new study, which is published in JAMA Network Open.
“If they are somebody who has both disorders concurrently in their pregnancy, they may be at even greater risk than a woman with one or the other disorder,” added Dr. Retnakaran, who is professor of medicine at the University of Toronto and an endocrinologist at the Leadership Sinai Centre for Diabetes, Mount Sinai Hospital, also in Toronto. “In other words, amongst already high-risk patients. This is identifying a subset at maybe an even higher risk.”
It doesn’t mean that there is a huge absolute risk, Dr. Retnakaran said, but it is showing that there is a heightened risk such that women and their clinicians need to be aware of and potentially the need for greater preventative care in the future.
“It is allowing you to identify future lifetime risk of cardiovascular disease,” he said.
Study rationale and design
GHTD is “a forerunner of hypertension,” and gestational diabetes is “a precursor of diabetes” – each associated with a high risk of developing CVD in the years after pregnancy, the investigators said. While studies have looked at their individual contributions to future CVD risk, not many had looked to see what risks having both may confer in the postpregnancy years.
For the analysis, data on 886,295 women with GHTD (43,861), gestational diabetes (54,061), both (4,975), or neither (783,398) were obtained from several Canadian administrative health databases.
The mean age was around 30 years across the groups, with those with both conditions or gestational diabetes alone more likely to be older than those with GTHD alone or neither condition (32 vs. 29 years, respectively, P < .001).
After a total follow-up period of 12 years, 1,999 CVD events were recorded, most of them (1,162) 5 years after the pregnancy.
Pregnancy is a stress test for the heart
“We know that what we call adverse pregnancy outcomes – things like gestational hypertension, and gestational diabetes, and preeclampsia – are on the rise globally,” Natalie A. Bello, MD, director of hypertension research at the Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, commented in an interview.

“People who are younger and of childbearing age who are going into pregnancy now are less healthy than they perhaps were in the past,” Dr. Bello suggested, with more hypertension, more obesity, and people being less physically active. “We think that’s translating into some of the pregnancy complications.”
That’s concerning for a number of reasons, said Dr. Bello, who is also the cochair of the American College of Cardiology’s Cardio-Obstetrics Workgroup, and the biggest one perhaps is the stress that these may conditions may be placing on the heart.
“We know that when individuals have an adverse pregnancy outcome like gestational hypertension, or gestational diabetes, their risk for heart disease is increased in the future compared to someone who has an uncomplicated pregnancy,” she said. “So, we sort of say pregnancy is like a stress test for your heart.”
Dr. Bello added that “these situations, these adverse pregnancy outcomes are an indicator for us as physicians, but also they should be for patients as well, to sort of make sure they’re talking to their doctor about their risk factors and modifying them whenever possible.”
The population studied came from quite a racially, ethnically, and economically diverse area of Canada, Dr. Bello pointed out, although because of the nature of an administrative database there wasn’t information on individual level risk factors.
“We don’t know things like smoking, or if individuals were obese when they were pregnant. So, there are some limitations that should be noted,” she said.
Also, the results don’t mean that isolated gestational diabetes “isn’t something we need to be concerned about,” Dr. Bello observed, adding that the study may have been underpowered to look at this association. “It may just be that it will take a longer time for individuals who have gestational diabetes who don’t make lifestyle changes to develop diabetes, and then develop heart disease.”
The main message is that the women who have a co-occurrence of gestational hypertension and gestational diabetes are at particularly high risk of cardiovascular disease in the future,” said Dr. Retnakaran.
“The way to look at it from a patient standpoint is that we are all on different tracks in terms of our cardiometabolic destiny,” and that these data give “some understanding of what kind of tracks they are on for future risk,” Dr. Retnakaran said.
“A history of either gestational hypertension, and/or gestational diabetes should be really a warning sign for physicians and for patients that they have a higher risk of heart disease,” said Dr. Bello.
She added that this is a signal “that we need to do things to modify their risk, because we know that about 80% of heart disease is modifiable and preventable with proper risk factor management.”
The study was funded by the Ontario Ministry of Health and Long-Term Care. Dr. Retnakaran has received grants and personal fees from Novo Nordisk and Merck, grants from Boehringer Ingelheim, and personal fees from Eli Lily Takeda, and Sanofi. Dr. Bello had no conflicts of interest to disclose.
Women who develop transient hypertensive disorders during their pregnancy are at risk for developing subsequent cardiovascular disease (CVD), particularly if this experienced at the same time as gestational diabetes.
In a large population-based study, the adjusted hazard ratios for developing CVD following a gestational hypertensive disorder (GHTD) alone were 1.90 (95% confidence interval, 1.151-2.25) within 5 years and 1.41 (95% CI, 1.12-1.76) after 5 years or more.
When gestational diabetes was added into the mix, however, the risk for CVD after 5 years more than doubled (aHR, 2.43; 95% CI, 1.60-3.67). Risk in the earlier postpartum period was also raised by the combination, but this was not significant (aHR, 1.42; 95% CI, 0.78-2.58).
Having gestational diabetes by itself did not seem to increase the risk for later CVD in the analysis, despite being linked to higher heart disease risk in other studies.
“These are women coming out of a pregnancy – young women of reproductive age – so this is not a group that typically has cardiovascular events,” said Ravi Retnakaran, MD, in an interview, an investigator in the new study, which is published in JAMA Network Open.
“If they are somebody who has both disorders concurrently in their pregnancy, they may be at even greater risk than a woman with one or the other disorder,” added Dr. Retnakaran, who is professor of medicine at the University of Toronto and an endocrinologist at the Leadership Sinai Centre for Diabetes, Mount Sinai Hospital, also in Toronto. “In other words, amongst already high-risk patients. This is identifying a subset at maybe an even higher risk.”
It doesn’t mean that there is a huge absolute risk, Dr. Retnakaran said, but it is showing that there is a heightened risk such that women and their clinicians need to be aware of and potentially the need for greater preventative care in the future.
“It is allowing you to identify future lifetime risk of cardiovascular disease,” he said.
Study rationale and design
GHTD is “a forerunner of hypertension,” and gestational diabetes is “a precursor of diabetes” – each associated with a high risk of developing CVD in the years after pregnancy, the investigators said. While studies have looked at their individual contributions to future CVD risk, not many had looked to see what risks having both may confer in the postpregnancy years.
For the analysis, data on 886,295 women with GHTD (43,861), gestational diabetes (54,061), both (4,975), or neither (783,398) were obtained from several Canadian administrative health databases.
The mean age was around 30 years across the groups, with those with both conditions or gestational diabetes alone more likely to be older than those with GTHD alone or neither condition (32 vs. 29 years, respectively, P < .001).
After a total follow-up period of 12 years, 1,999 CVD events were recorded, most of them (1,162) 5 years after the pregnancy.
Pregnancy is a stress test for the heart
“We know that what we call adverse pregnancy outcomes – things like gestational hypertension, and gestational diabetes, and preeclampsia – are on the rise globally,” Natalie A. Bello, MD, director of hypertension research at the Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, commented in an interview.
“People who are younger and of childbearing age who are going into pregnancy now are less healthy than they perhaps were in the past,” Dr. Bello suggested, with more hypertension, more obesity, and people being less physically active. “We think that’s translating into some of the pregnancy complications.”
That’s concerning for a number of reasons, said Dr. Bello, who is also the cochair of the American College of Cardiology’s Cardio-Obstetrics Workgroup, and the biggest one perhaps is the stress that these may conditions may be placing on the heart.
“We know that when individuals have an adverse pregnancy outcome like gestational hypertension, or gestational diabetes, their risk for heart disease is increased in the future compared to someone who has an uncomplicated pregnancy,” she said. “So, we sort of say pregnancy is like a stress test for your heart.”
Dr. Bello added that “these situations, these adverse pregnancy outcomes are an indicator for us as physicians, but also they should be for patients as well, to sort of make sure they’re talking to their doctor about their risk factors and modifying them whenever possible.”
The population studied came from quite a racially, ethnically, and economically diverse area of Canada, Dr. Bello pointed out, although because of the nature of an administrative database there wasn’t information on individual level risk factors.
“We don’t know things like smoking, or if individuals were obese when they were pregnant. So, there are some limitations that should be noted,” she said.
Also, the results don’t mean that isolated gestational diabetes “isn’t something we need to be concerned about,” Dr. Bello observed, adding that the study may have been underpowered to look at this association. “It may just be that it will take a longer time for individuals who have gestational diabetes who don’t make lifestyle changes to develop diabetes, and then develop heart disease.”
The main message is that the women who have a co-occurrence of gestational hypertension and gestational diabetes are at particularly high risk of cardiovascular disease in the future,” said Dr. Retnakaran.
“The way to look at it from a patient standpoint is that we are all on different tracks in terms of our cardiometabolic destiny,” and that these data give “some understanding of what kind of tracks they are on for future risk,” Dr. Retnakaran said.
“A history of either gestational hypertension, and/or gestational diabetes should be really a warning sign for physicians and for patients that they have a higher risk of heart disease,” said Dr. Bello.
She added that this is a signal “that we need to do things to modify their risk, because we know that about 80% of heart disease is modifiable and preventable with proper risk factor management.”
The study was funded by the Ontario Ministry of Health and Long-Term Care. Dr. Retnakaran has received grants and personal fees from Novo Nordisk and Merck, grants from Boehringer Ingelheim, and personal fees from Eli Lily Takeda, and Sanofi. Dr. Bello had no conflicts of interest to disclose.
Women who develop transient hypertensive disorders during their pregnancy are at risk for developing subsequent cardiovascular disease (CVD), particularly if this experienced at the same time as gestational diabetes.
In a large population-based study, the adjusted hazard ratios for developing CVD following a gestational hypertensive disorder (GHTD) alone were 1.90 (95% confidence interval, 1.151-2.25) within 5 years and 1.41 (95% CI, 1.12-1.76) after 5 years or more.
When gestational diabetes was added into the mix, however, the risk for CVD after 5 years more than doubled (aHR, 2.43; 95% CI, 1.60-3.67). Risk in the earlier postpartum period was also raised by the combination, but this was not significant (aHR, 1.42; 95% CI, 0.78-2.58).
Having gestational diabetes by itself did not seem to increase the risk for later CVD in the analysis, despite being linked to higher heart disease risk in other studies.
“These are women coming out of a pregnancy – young women of reproductive age – so this is not a group that typically has cardiovascular events,” said Ravi Retnakaran, MD, in an interview, an investigator in the new study, which is published in JAMA Network Open.
“If they are somebody who has both disorders concurrently in their pregnancy, they may be at even greater risk than a woman with one or the other disorder,” added Dr. Retnakaran, who is professor of medicine at the University of Toronto and an endocrinologist at the Leadership Sinai Centre for Diabetes, Mount Sinai Hospital, also in Toronto. “In other words, amongst already high-risk patients. This is identifying a subset at maybe an even higher risk.”
It doesn’t mean that there is a huge absolute risk, Dr. Retnakaran said, but it is showing that there is a heightened risk such that women and their clinicians need to be aware of and potentially the need for greater preventative care in the future.
“It is allowing you to identify future lifetime risk of cardiovascular disease,” he said.
Study rationale and design
GHTD is “a forerunner of hypertension,” and gestational diabetes is “a precursor of diabetes” – each associated with a high risk of developing CVD in the years after pregnancy, the investigators said. While studies have looked at their individual contributions to future CVD risk, not many had looked to see what risks having both may confer in the postpregnancy years.
For the analysis, data on 886,295 women with GHTD (43,861), gestational diabetes (54,061), both (4,975), or neither (783,398) were obtained from several Canadian administrative health databases.
The mean age was around 30 years across the groups, with those with both conditions or gestational diabetes alone more likely to be older than those with GTHD alone or neither condition (32 vs. 29 years, respectively, P < .001).
After a total follow-up period of 12 years, 1,999 CVD events were recorded, most of them (1,162) 5 years after the pregnancy.
Pregnancy is a stress test for the heart
“We know that what we call adverse pregnancy outcomes – things like gestational hypertension, and gestational diabetes, and preeclampsia – are on the rise globally,” Natalie A. Bello, MD, director of hypertension research at the Smidt Heart Institute, Cedars-Sinai Medical Center, Los Angeles, commented in an interview.
“People who are younger and of childbearing age who are going into pregnancy now are less healthy than they perhaps were in the past,” Dr. Bello suggested, with more hypertension, more obesity, and people being less physically active. “We think that’s translating into some of the pregnancy complications.”
That’s concerning for a number of reasons, said Dr. Bello, who is also the cochair of the American College of Cardiology’s Cardio-Obstetrics Workgroup, and the biggest one perhaps is the stress that these may conditions may be placing on the heart.
“We know that when individuals have an adverse pregnancy outcome like gestational hypertension, or gestational diabetes, their risk for heart disease is increased in the future compared to someone who has an uncomplicated pregnancy,” she said. “So, we sort of say pregnancy is like a stress test for your heart.”
Dr. Bello added that “these situations, these adverse pregnancy outcomes are an indicator for us as physicians, but also they should be for patients as well, to sort of make sure they’re talking to their doctor about their risk factors and modifying them whenever possible.”
The population studied came from quite a racially, ethnically, and economically diverse area of Canada, Dr. Bello pointed out, although because of the nature of an administrative database there wasn’t information on individual level risk factors.
“We don’t know things like smoking, or if individuals were obese when they were pregnant. So, there are some limitations that should be noted,” she said.
Also, the results don’t mean that isolated gestational diabetes “isn’t something we need to be concerned about,” Dr. Bello observed, adding that the study may have been underpowered to look at this association. “It may just be that it will take a longer time for individuals who have gestational diabetes who don’t make lifestyle changes to develop diabetes, and then develop heart disease.”
The main message is that the women who have a co-occurrence of gestational hypertension and gestational diabetes are at particularly high risk of cardiovascular disease in the future,” said Dr. Retnakaran.
“The way to look at it from a patient standpoint is that we are all on different tracks in terms of our cardiometabolic destiny,” and that these data give “some understanding of what kind of tracks they are on for future risk,” Dr. Retnakaran said.
“A history of either gestational hypertension, and/or gestational diabetes should be really a warning sign for physicians and for patients that they have a higher risk of heart disease,” said Dr. Bello.
She added that this is a signal “that we need to do things to modify their risk, because we know that about 80% of heart disease is modifiable and preventable with proper risk factor management.”
The study was funded by the Ontario Ministry of Health and Long-Term Care. Dr. Retnakaran has received grants and personal fees from Novo Nordisk and Merck, grants from Boehringer Ingelheim, and personal fees from Eli Lily Takeda, and Sanofi. Dr. Bello had no conflicts of interest to disclose.
FROM JAMA NETWORK OPEN

A new use for dating apps: Chasing STDs
Heather Meador and Anna Herber-Downey use dating apps on the job – and their boss knows it.
Both are public health nurses employed by Linn County Public Health in eastern Iowa. They’ve learned that dating apps are the most efficient way to inform users that people they previously met on the sites may have exposed them to sexually transmitted infections.
A nationwide surge in STIs, also known as STDs – with reported cases of gonorrhea and syphilis increasing 10% and 7%, respectively, from 2019 to 2020, according to the Centers for Disease Control and Prevention – isn’t sparing Iowa. The duo has found that the telephone call, a traditional method of contact tracing, no longer works well.
“When I started 12 years ago, we called everyone,” said Ms. Meador, the county health department’s clinical branch supervisor. “It’s getting harder and harder to just call someone on the phone.”
Even texting is ineffective, they said. And people aren’t necessarily answering messages on Facebook. The dating apps are where they’re at.
Because many people are meeting sex partners online – via sites like Grindr or Snapchat, which are headquartered in West Hollywood and Santa Monica, Calif., respectively – contact tracers often don’t have much information to go on, just a screen name or a picture.
So, about a year ago, Ms. Meador and her colleagues got approval from their bosses at the local level to build profiles on the app, through which they can contact the sex partners of infected people.
Traditionally, contact tracers interview people infected with an STI about their recent encounters and then reach out to those partners to tell them about the potential exposure.
Linn County contact tracers use the apps throughout their workday. Grindr, in particular, relies on geolocation, showing users matches who are close by. So the tracers use the apps when they’re out and about, hoping to wander into the same neighborhoods as the person diagnosed with an STI. Sometimes users “tap” the contract tracers to see whether they’re interested – in dating, that is.
When the public health officials spot someone they’re looking for, they send a message asking for a call. It’s a successful method: Ms. Herber-Downey estimated they make an initial contact 75% of the time.
Linn County’s decision to move online comes as STI rates rise nationally, funding to fight them falls, and people adopt new technologies to meet people and seek fun. “STIs are increasing way faster than the funding we have,” said Leo Parker, director of prevention programs for the National Coalition of STD Directors, all while public health departments – many underfunded – are grappling with new behaviors.
“Social media companies have billions; we have tens of thousands,” said Jeffrey Klausner, MD, MPH, a University of Southern California, Los Angeles, public health professor, who previously served as San Francisco’s director of STD prevention and control services. That funding disparity means few public health departments have staff members who can go online. “It’s only really in major cities that they have anyone who’s tasked for that,” Dr. Klausner said.
Even when departments have enough employees to take on the challenge, institutional support can be lacking. Some public health officials question employees who log into the apps. Dr. Klausner once testified on behalf of a Ventura County, Calif., contact tracer who was fired for using sex sites for work.
But with people migrating online to meet partners, following them there makes sense. “We’re now in a digital age,” Mr. Parker said. Individuals might not be out, or might be questioning their identity, making online venues comfortable, anonymous spaces for romance – which, in turn, means people are harder to reach face-to-face, at least at first.
What’s more, online spaces like Grindr are effective public health tools beyond contact tracing. They can be useful ways to get the word out about public health concerns.
Mr. Parker and the Linn County officials said public service announcements on dating apps – advocating for condom use or sharing the business hours for sexual health clinics – do seem to lead people to services. “We do have individuals coming in, saying, ‘I saw you had free testing. I saw it on Grindr,’ ” Mr. Parker said.
Grindr, which touts itself as the biggest dating app focused on LGBTQ+ people, pushes out messages and information to its members, said Jack Harrison-Quintana, director of Grindr for Equality. That engagement intensified during a 2015 meningitis outbreak among LGBTQ+ communities in Chicago, for example.
During that outbreak, the app sent citywide messages about vaccination. Then Mr. Harrison-Quintana took advantage of the service’s design: Using the site’s geolocating capabilities, Grindr workers targeted messages to specific neighborhoods. “We could go in and really go block to block and say, ‘Is this where the cases are showing up?’ ” he said. If so, they sent more messages to that area.
That campaign encouraged further efforts from the app, which regularly sends public health messages about everything from COVID-19 to monkeypox to the platform’s base of roughly 11 million monthly users. Grindr also allows users to display their HIV status and indicate whether they’re vaccinated against COVID, monkeypox, and meningitis.
There are a couple of things Grindr won’t do, however. The company won’t allow public health departments to create institutional accounts. And it won’t allow automated notifications about STI exposures to be sent to users.
That’s due to privacy concerns, the company said, despite calls from public health advocates to deploy better messaging features. Grindr believes that a government presence on the app would be too intrusive and that even anonymous notifications would allow users to trace infections back to their source. (When asked about public health officials who join the site on their own, company spokesperson Patrick Lenihan said: “Individuals are free to say something like ‘I’m a public health professional – ask me about my work!’ in their profile and are free to discuss sexual and public health matters however they see fit.”)
Grindr’s position – however disappointing to some in the public health world – reflects a longtime balancing act attempted by the private sector, which aims to square government concerns with users’ privacy interests.
Dr. Klausner pointed to a 1999 syphilis outbreak in San Francisco as one of the first times he saw how those interests could be at odds. The outbreak was traced to an AOL chatroom. Based on his research, Dr. Klausner said it seemed as though people could go online and “get a sex partner faster than you can get a pizza delivered.”
But persuading New York–based Time Warner, eventually AOL’s corporate parent, to cooperate was time-intensive and tricky – gaining entrée into the chatroom required help from the New York attorney general’s office.
The online industry has advanced since then, Dr. Klausner said. He helped one service develop a system to send digital postcards to potentially exposed people. “Congratulations, you got syphilis,” the postcards read. “They were edgy postcards,” he said, although some options were less “snarky.”
Overall, however, the dating app world is still “bifurcated,” he said. For public health efforts, apps that appeal to LGBTQ+ users are generally more helpful than those that predominantly cater to heterosexual clients.
That’s due to the community’s history with sexual health, explained Jen Hecht, a leader of Building Healthy Online Communities, a public health group partnering with dating apps. “Folks in the queer community have – what – 30, 40 years of thinking about HIV?” she said.
Even though STIs affect everyone, “the norm and the expectation is not there” for straight-focused dating apps, she said. Indeed, neither Match Group nor Bumble – the corporations with the biggest apps focused on heterosexual dating, both based in Texas – responded to multiple requests for comment from KHN.
But users, at least so far, seem to appreciate the app-based interventions. Mr. Harrison-Quintana said Grindr has landed on a just-the-facts approach to conveying health information. He has never received any backlash, “which has been very nice.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Heather Meador and Anna Herber-Downey use dating apps on the job – and their boss knows it.
Both are public health nurses employed by Linn County Public Health in eastern Iowa. They’ve learned that dating apps are the most efficient way to inform users that people they previously met on the sites may have exposed them to sexually transmitted infections.
A nationwide surge in STIs, also known as STDs – with reported cases of gonorrhea and syphilis increasing 10% and 7%, respectively, from 2019 to 2020, according to the Centers for Disease Control and Prevention – isn’t sparing Iowa. The duo has found that the telephone call, a traditional method of contact tracing, no longer works well.
“When I started 12 years ago, we called everyone,” said Ms. Meador, the county health department’s clinical branch supervisor. “It’s getting harder and harder to just call someone on the phone.”
Even texting is ineffective, they said. And people aren’t necessarily answering messages on Facebook. The dating apps are where they’re at.
Because many people are meeting sex partners online – via sites like Grindr or Snapchat, which are headquartered in West Hollywood and Santa Monica, Calif., respectively – contact tracers often don’t have much information to go on, just a screen name or a picture.
So, about a year ago, Ms. Meador and her colleagues got approval from their bosses at the local level to build profiles on the app, through which they can contact the sex partners of infected people.
Traditionally, contact tracers interview people infected with an STI about their recent encounters and then reach out to those partners to tell them about the potential exposure.
Linn County contact tracers use the apps throughout their workday. Grindr, in particular, relies on geolocation, showing users matches who are close by. So the tracers use the apps when they’re out and about, hoping to wander into the same neighborhoods as the person diagnosed with an STI. Sometimes users “tap” the contract tracers to see whether they’re interested – in dating, that is.
When the public health officials spot someone they’re looking for, they send a message asking for a call. It’s a successful method: Ms. Herber-Downey estimated they make an initial contact 75% of the time.
Linn County’s decision to move online comes as STI rates rise nationally, funding to fight them falls, and people adopt new technologies to meet people and seek fun. “STIs are increasing way faster than the funding we have,” said Leo Parker, director of prevention programs for the National Coalition of STD Directors, all while public health departments – many underfunded – are grappling with new behaviors.
“Social media companies have billions; we have tens of thousands,” said Jeffrey Klausner, MD, MPH, a University of Southern California, Los Angeles, public health professor, who previously served as San Francisco’s director of STD prevention and control services. That funding disparity means few public health departments have staff members who can go online. “It’s only really in major cities that they have anyone who’s tasked for that,” Dr. Klausner said.
Even when departments have enough employees to take on the challenge, institutional support can be lacking. Some public health officials question employees who log into the apps. Dr. Klausner once testified on behalf of a Ventura County, Calif., contact tracer who was fired for using sex sites for work.
But with people migrating online to meet partners, following them there makes sense. “We’re now in a digital age,” Mr. Parker said. Individuals might not be out, or might be questioning their identity, making online venues comfortable, anonymous spaces for romance – which, in turn, means people are harder to reach face-to-face, at least at first.
What’s more, online spaces like Grindr are effective public health tools beyond contact tracing. They can be useful ways to get the word out about public health concerns.
Mr. Parker and the Linn County officials said public service announcements on dating apps – advocating for condom use or sharing the business hours for sexual health clinics – do seem to lead people to services. “We do have individuals coming in, saying, ‘I saw you had free testing. I saw it on Grindr,’ ” Mr. Parker said.
Grindr, which touts itself as the biggest dating app focused on LGBTQ+ people, pushes out messages and information to its members, said Jack Harrison-Quintana, director of Grindr for Equality. That engagement intensified during a 2015 meningitis outbreak among LGBTQ+ communities in Chicago, for example.
During that outbreak, the app sent citywide messages about vaccination. Then Mr. Harrison-Quintana took advantage of the service’s design: Using the site’s geolocating capabilities, Grindr workers targeted messages to specific neighborhoods. “We could go in and really go block to block and say, ‘Is this where the cases are showing up?’ ” he said. If so, they sent more messages to that area.
That campaign encouraged further efforts from the app, which regularly sends public health messages about everything from COVID-19 to monkeypox to the platform’s base of roughly 11 million monthly users. Grindr also allows users to display their HIV status and indicate whether they’re vaccinated against COVID, monkeypox, and meningitis.
There are a couple of things Grindr won’t do, however. The company won’t allow public health departments to create institutional accounts. And it won’t allow automated notifications about STI exposures to be sent to users.
That’s due to privacy concerns, the company said, despite calls from public health advocates to deploy better messaging features. Grindr believes that a government presence on the app would be too intrusive and that even anonymous notifications would allow users to trace infections back to their source. (When asked about public health officials who join the site on their own, company spokesperson Patrick Lenihan said: “Individuals are free to say something like ‘I’m a public health professional – ask me about my work!’ in their profile and are free to discuss sexual and public health matters however they see fit.”)
Grindr’s position – however disappointing to some in the public health world – reflects a longtime balancing act attempted by the private sector, which aims to square government concerns with users’ privacy interests.
Dr. Klausner pointed to a 1999 syphilis outbreak in San Francisco as one of the first times he saw how those interests could be at odds. The outbreak was traced to an AOL chatroom. Based on his research, Dr. Klausner said it seemed as though people could go online and “get a sex partner faster than you can get a pizza delivered.”
But persuading New York–based Time Warner, eventually AOL’s corporate parent, to cooperate was time-intensive and tricky – gaining entrée into the chatroom required help from the New York attorney general’s office.
The online industry has advanced since then, Dr. Klausner said. He helped one service develop a system to send digital postcards to potentially exposed people. “Congratulations, you got syphilis,” the postcards read. “They were edgy postcards,” he said, although some options were less “snarky.”
Overall, however, the dating app world is still “bifurcated,” he said. For public health efforts, apps that appeal to LGBTQ+ users are generally more helpful than those that predominantly cater to heterosexual clients.
That’s due to the community’s history with sexual health, explained Jen Hecht, a leader of Building Healthy Online Communities, a public health group partnering with dating apps. “Folks in the queer community have – what – 30, 40 years of thinking about HIV?” she said.
Even though STIs affect everyone, “the norm and the expectation is not there” for straight-focused dating apps, she said. Indeed, neither Match Group nor Bumble – the corporations with the biggest apps focused on heterosexual dating, both based in Texas – responded to multiple requests for comment from KHN.
But users, at least so far, seem to appreciate the app-based interventions. Mr. Harrison-Quintana said Grindr has landed on a just-the-facts approach to conveying health information. He has never received any backlash, “which has been very nice.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Heather Meador and Anna Herber-Downey use dating apps on the job – and their boss knows it.
Both are public health nurses employed by Linn County Public Health in eastern Iowa. They’ve learned that dating apps are the most efficient way to inform users that people they previously met on the sites may have exposed them to sexually transmitted infections.
A nationwide surge in STIs, also known as STDs – with reported cases of gonorrhea and syphilis increasing 10% and 7%, respectively, from 2019 to 2020, according to the Centers for Disease Control and Prevention – isn’t sparing Iowa. The duo has found that the telephone call, a traditional method of contact tracing, no longer works well.
“When I started 12 years ago, we called everyone,” said Ms. Meador, the county health department’s clinical branch supervisor. “It’s getting harder and harder to just call someone on the phone.”
Even texting is ineffective, they said. And people aren’t necessarily answering messages on Facebook. The dating apps are where they’re at.
Because many people are meeting sex partners online – via sites like Grindr or Snapchat, which are headquartered in West Hollywood and Santa Monica, Calif., respectively – contact tracers often don’t have much information to go on, just a screen name or a picture.
So, about a year ago, Ms. Meador and her colleagues got approval from their bosses at the local level to build profiles on the app, through which they can contact the sex partners of infected people.
Traditionally, contact tracers interview people infected with an STI about their recent encounters and then reach out to those partners to tell them about the potential exposure.
Linn County contact tracers use the apps throughout their workday. Grindr, in particular, relies on geolocation, showing users matches who are close by. So the tracers use the apps when they’re out and about, hoping to wander into the same neighborhoods as the person diagnosed with an STI. Sometimes users “tap” the contract tracers to see whether they’re interested – in dating, that is.
When the public health officials spot someone they’re looking for, they send a message asking for a call. It’s a successful method: Ms. Herber-Downey estimated they make an initial contact 75% of the time.
Linn County’s decision to move online comes as STI rates rise nationally, funding to fight them falls, and people adopt new technologies to meet people and seek fun. “STIs are increasing way faster than the funding we have,” said Leo Parker, director of prevention programs for the National Coalition of STD Directors, all while public health departments – many underfunded – are grappling with new behaviors.
“Social media companies have billions; we have tens of thousands,” said Jeffrey Klausner, MD, MPH, a University of Southern California, Los Angeles, public health professor, who previously served as San Francisco’s director of STD prevention and control services. That funding disparity means few public health departments have staff members who can go online. “It’s only really in major cities that they have anyone who’s tasked for that,” Dr. Klausner said.
Even when departments have enough employees to take on the challenge, institutional support can be lacking. Some public health officials question employees who log into the apps. Dr. Klausner once testified on behalf of a Ventura County, Calif., contact tracer who was fired for using sex sites for work.
But with people migrating online to meet partners, following them there makes sense. “We’re now in a digital age,” Mr. Parker said. Individuals might not be out, or might be questioning their identity, making online venues comfortable, anonymous spaces for romance – which, in turn, means people are harder to reach face-to-face, at least at first.
What’s more, online spaces like Grindr are effective public health tools beyond contact tracing. They can be useful ways to get the word out about public health concerns.
Mr. Parker and the Linn County officials said public service announcements on dating apps – advocating for condom use or sharing the business hours for sexual health clinics – do seem to lead people to services. “We do have individuals coming in, saying, ‘I saw you had free testing. I saw it on Grindr,’ ” Mr. Parker said.
Grindr, which touts itself as the biggest dating app focused on LGBTQ+ people, pushes out messages and information to its members, said Jack Harrison-Quintana, director of Grindr for Equality. That engagement intensified during a 2015 meningitis outbreak among LGBTQ+ communities in Chicago, for example.
During that outbreak, the app sent citywide messages about vaccination. Then Mr. Harrison-Quintana took advantage of the service’s design: Using the site’s geolocating capabilities, Grindr workers targeted messages to specific neighborhoods. “We could go in and really go block to block and say, ‘Is this where the cases are showing up?’ ” he said. If so, they sent more messages to that area.
That campaign encouraged further efforts from the app, which regularly sends public health messages about everything from COVID-19 to monkeypox to the platform’s base of roughly 11 million monthly users. Grindr also allows users to display their HIV status and indicate whether they’re vaccinated against COVID, monkeypox, and meningitis.
There are a couple of things Grindr won’t do, however. The company won’t allow public health departments to create institutional accounts. And it won’t allow automated notifications about STI exposures to be sent to users.
That’s due to privacy concerns, the company said, despite calls from public health advocates to deploy better messaging features. Grindr believes that a government presence on the app would be too intrusive and that even anonymous notifications would allow users to trace infections back to their source. (When asked about public health officials who join the site on their own, company spokesperson Patrick Lenihan said: “Individuals are free to say something like ‘I’m a public health professional – ask me about my work!’ in their profile and are free to discuss sexual and public health matters however they see fit.”)
Grindr’s position – however disappointing to some in the public health world – reflects a longtime balancing act attempted by the private sector, which aims to square government concerns with users’ privacy interests.
Dr. Klausner pointed to a 1999 syphilis outbreak in San Francisco as one of the first times he saw how those interests could be at odds. The outbreak was traced to an AOL chatroom. Based on his research, Dr. Klausner said it seemed as though people could go online and “get a sex partner faster than you can get a pizza delivered.”
But persuading New York–based Time Warner, eventually AOL’s corporate parent, to cooperate was time-intensive and tricky – gaining entrée into the chatroom required help from the New York attorney general’s office.
The online industry has advanced since then, Dr. Klausner said. He helped one service develop a system to send digital postcards to potentially exposed people. “Congratulations, you got syphilis,” the postcards read. “They were edgy postcards,” he said, although some options were less “snarky.”
Overall, however, the dating app world is still “bifurcated,” he said. For public health efforts, apps that appeal to LGBTQ+ users are generally more helpful than those that predominantly cater to heterosexual clients.
That’s due to the community’s history with sexual health, explained Jen Hecht, a leader of Building Healthy Online Communities, a public health group partnering with dating apps. “Folks in the queer community have – what – 30, 40 years of thinking about HIV?” she said.
Even though STIs affect everyone, “the norm and the expectation is not there” for straight-focused dating apps, she said. Indeed, neither Match Group nor Bumble – the corporations with the biggest apps focused on heterosexual dating, both based in Texas – responded to multiple requests for comment from KHN.
But users, at least so far, seem to appreciate the app-based interventions. Mr. Harrison-Quintana said Grindr has landed on a just-the-facts approach to conveying health information. He has never received any backlash, “which has been very nice.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Move faster, live longer? A little more effort goes a long way
If there’s one public health message Americans have heard loud and clear, it’s this one:
Move more.
Take more steps.
Spend more time doing physical activity – at least 150 minutes a week, according to the latest guidelines.
But hearing the message doesn’t mean we act on it. A whopping 25% of Americans don’t get any physical activity beyond what they do in their job, according to a CDC survey.
Just do what you’re already doing, but with a little more effort.
The study, which was published in the European Heart Journal, builds on growing evidence that suggests exercise intensity matters just as much as the amount. So, something as simple as turning a leisurely stroll into a brisk walk can, over time, lead to significant reductions in your risk of cardiovascular disease. No additional moves, steps, or minutes needed.
Step it up
Researchers at Cambridge University and the University of Leicester in England looked at data from 88,000 middle-aged adults who wore an activity tracking device for 7 days.
The devices tracked both the total amount of activity they did and the intensity of that movement – that is, how fast they walked or how hard they pushed themselves.
The researchers then calculated their physical activity energy expenditure (the number of calories they burned when they were up and moving) and the percentage that came from moderate to vigorous physical activity.
What’s the difference?
- Physical activity means any and every movement you do throughout the day. Mostly it’s mundane tasks like shopping, walking to the mailbox, playing with your dog, or cooking.
- Moderate-intensity physical activity includes things you do at a faster pace. Maybe you’re walking for exercise, doing yard work or household chores, or running late and just trying to get somewhere faster. You’re breathing a little harder and possibly working up a sweat.
- Vigorous-intensity physical activity is usually an exercise session – a run, a strenuous hike, a tough workout in the gym. It can also be an exhausting chore like shoveling snow, which feels like a workout. You’re definitely breathing harder, and you’re probably working up a sweat, even in the middle of winter.
Over the next 6 to 7 years, there were 4,000 new cases of cardiovascular disease among the people in the study.
Those who got at least 20% of their physical activity energy expenditure from moderate to vigorous activities had significantly less risk of heart disease, compared with those whose higher-effort activities were about 10%.
That was true even for those whose total activity was relatively low. As long as higher-effort activities reached 20% of their total, they were 14% less likely to be diagnosed with a heart condition.
And for those with relatively high activity levels, there was little extra benefit if their moderate and vigorous activities remained around 10%.
That finding surprised Paddy Dempsey, PhD, a medical research scientist at Cambridge and the study’s lead author. But it also makes sense.
“People can improve their cardiorespiratory fitness to a greater degree with higher-intensity activity,” he says. “More intensity will stress the system and lead to greater adaptation.”
The key is an increase in the amount of oxygen your heart and lungs can provide your muscles during exercise, a measure known as VO2max.
Raising your VO2max is the best way to reduce your risk of early death, especially death from heart disease. Simply moving up from the lowest conditioning category to a higher one will cut your risk of dying in any given year by as much as 60%.
Making strides
The study builds on previous research that shows the benefits of moving faster.
Walking faster will naturally increase your stride length, another predictor of longevity and future health. A review study published in 2021 found that older adults who took shorter steps were 26% more likely to have a disability, 34% more likely to have a major adverse event (like an injury that leads to a loss of independence), and 69% more likely to die over the next several years.
Quality versus quantity
We’ve focused so far on the quality of your physical activity – moving faster, taking longer strides.
But there’s still a lot to be said for movement quantity.
“It would be a mistake to say volume doesn’t matter,” Dr. Dempsey cautions.
A 2022 study in the journal The Lancet found that the risk of dying during a given period decreases with each increase in daily steps. The protective effect peaks at about 6,000 to 8,000 steps a day for adults 60 and over, and at 8,000 to 10,000 steps for those under 60.
“The relative value of the quality and quantity of exercise are very specific to a person’s goals,” says Chhanda Dutta, PhD, chief of the Clinical Gerontology Branch at the National Institute on Aging. “If performance is the goal, quality matters at least as much as quantity.”
Dr. Dempsey agrees that it’s not a cage match between two. Every step you take is a step in the right direction.
“People can choose or gravitate to an approach that works best for them,” he says. “It’s also helpful to think about where some everyday activities can be punctuated with intensity,” which could be as simple as walking faster when possible.
What matters most is that you choose something, Dr. Dutta says. “You have more to risk by not exercising.”
A version of this article first appeared on WebMD.com.
If there’s one public health message Americans have heard loud and clear, it’s this one:
Move more.
Take more steps.
Spend more time doing physical activity – at least 150 minutes a week, according to the latest guidelines.
But hearing the message doesn’t mean we act on it. A whopping 25% of Americans don’t get any physical activity beyond what they do in their job, according to a CDC survey.
Just do what you’re already doing, but with a little more effort.
The study, which was published in the European Heart Journal, builds on growing evidence that suggests exercise intensity matters just as much as the amount. So, something as simple as turning a leisurely stroll into a brisk walk can, over time, lead to significant reductions in your risk of cardiovascular disease. No additional moves, steps, or minutes needed.
Step it up
Researchers at Cambridge University and the University of Leicester in England looked at data from 88,000 middle-aged adults who wore an activity tracking device for 7 days.
The devices tracked both the total amount of activity they did and the intensity of that movement – that is, how fast they walked or how hard they pushed themselves.
The researchers then calculated their physical activity energy expenditure (the number of calories they burned when they were up and moving) and the percentage that came from moderate to vigorous physical activity.
What’s the difference?
- Physical activity means any and every movement you do throughout the day. Mostly it’s mundane tasks like shopping, walking to the mailbox, playing with your dog, or cooking.
- Moderate-intensity physical activity includes things you do at a faster pace. Maybe you’re walking for exercise, doing yard work or household chores, or running late and just trying to get somewhere faster. You’re breathing a little harder and possibly working up a sweat.
- Vigorous-intensity physical activity is usually an exercise session – a run, a strenuous hike, a tough workout in the gym. It can also be an exhausting chore like shoveling snow, which feels like a workout. You’re definitely breathing harder, and you’re probably working up a sweat, even in the middle of winter.
Over the next 6 to 7 years, there were 4,000 new cases of cardiovascular disease among the people in the study.
Those who got at least 20% of their physical activity energy expenditure from moderate to vigorous activities had significantly less risk of heart disease, compared with those whose higher-effort activities were about 10%.
That was true even for those whose total activity was relatively low. As long as higher-effort activities reached 20% of their total, they were 14% less likely to be diagnosed with a heart condition.
And for those with relatively high activity levels, there was little extra benefit if their moderate and vigorous activities remained around 10%.
That finding surprised Paddy Dempsey, PhD, a medical research scientist at Cambridge and the study’s lead author. But it also makes sense.
“People can improve their cardiorespiratory fitness to a greater degree with higher-intensity activity,” he says. “More intensity will stress the system and lead to greater adaptation.”
The key is an increase in the amount of oxygen your heart and lungs can provide your muscles during exercise, a measure known as VO2max.
Raising your VO2max is the best way to reduce your risk of early death, especially death from heart disease. Simply moving up from the lowest conditioning category to a higher one will cut your risk of dying in any given year by as much as 60%.
Making strides
The study builds on previous research that shows the benefits of moving faster.
Walking faster will naturally increase your stride length, another predictor of longevity and future health. A review study published in 2021 found that older adults who took shorter steps were 26% more likely to have a disability, 34% more likely to have a major adverse event (like an injury that leads to a loss of independence), and 69% more likely to die over the next several years.
Quality versus quantity
We’ve focused so far on the quality of your physical activity – moving faster, taking longer strides.
But there’s still a lot to be said for movement quantity.
“It would be a mistake to say volume doesn’t matter,” Dr. Dempsey cautions.
A 2022 study in the journal The Lancet found that the risk of dying during a given period decreases with each increase in daily steps. The protective effect peaks at about 6,000 to 8,000 steps a day for adults 60 and over, and at 8,000 to 10,000 steps for those under 60.
“The relative value of the quality and quantity of exercise are very specific to a person’s goals,” says Chhanda Dutta, PhD, chief of the Clinical Gerontology Branch at the National Institute on Aging. “If performance is the goal, quality matters at least as much as quantity.”
Dr. Dempsey agrees that it’s not a cage match between two. Every step you take is a step in the right direction.
“People can choose or gravitate to an approach that works best for them,” he says. “It’s also helpful to think about where some everyday activities can be punctuated with intensity,” which could be as simple as walking faster when possible.
What matters most is that you choose something, Dr. Dutta says. “You have more to risk by not exercising.”
A version of this article first appeared on WebMD.com.
If there’s one public health message Americans have heard loud and clear, it’s this one:
Move more.
Take more steps.
Spend more time doing physical activity – at least 150 minutes a week, according to the latest guidelines.
But hearing the message doesn’t mean we act on it. A whopping 25% of Americans don’t get any physical activity beyond what they do in their job, according to a CDC survey.
Just do what you’re already doing, but with a little more effort.
The study, which was published in the European Heart Journal, builds on growing evidence that suggests exercise intensity matters just as much as the amount. So, something as simple as turning a leisurely stroll into a brisk walk can, over time, lead to significant reductions in your risk of cardiovascular disease. No additional moves, steps, or minutes needed.
Step it up
Researchers at Cambridge University and the University of Leicester in England looked at data from 88,000 middle-aged adults who wore an activity tracking device for 7 days.
The devices tracked both the total amount of activity they did and the intensity of that movement – that is, how fast they walked or how hard they pushed themselves.
The researchers then calculated their physical activity energy expenditure (the number of calories they burned when they were up and moving) and the percentage that came from moderate to vigorous physical activity.
What’s the difference?
- Physical activity means any and every movement you do throughout the day. Mostly it’s mundane tasks like shopping, walking to the mailbox, playing with your dog, or cooking.
- Moderate-intensity physical activity includes things you do at a faster pace. Maybe you’re walking for exercise, doing yard work or household chores, or running late and just trying to get somewhere faster. You’re breathing a little harder and possibly working up a sweat.
- Vigorous-intensity physical activity is usually an exercise session – a run, a strenuous hike, a tough workout in the gym. It can also be an exhausting chore like shoveling snow, which feels like a workout. You’re definitely breathing harder, and you’re probably working up a sweat, even in the middle of winter.
Over the next 6 to 7 years, there were 4,000 new cases of cardiovascular disease among the people in the study.
Those who got at least 20% of their physical activity energy expenditure from moderate to vigorous activities had significantly less risk of heart disease, compared with those whose higher-effort activities were about 10%.
That was true even for those whose total activity was relatively low. As long as higher-effort activities reached 20% of their total, they were 14% less likely to be diagnosed with a heart condition.
And for those with relatively high activity levels, there was little extra benefit if their moderate and vigorous activities remained around 10%.
That finding surprised Paddy Dempsey, PhD, a medical research scientist at Cambridge and the study’s lead author. But it also makes sense.
“People can improve their cardiorespiratory fitness to a greater degree with higher-intensity activity,” he says. “More intensity will stress the system and lead to greater adaptation.”
The key is an increase in the amount of oxygen your heart and lungs can provide your muscles during exercise, a measure known as VO2max.
Raising your VO2max is the best way to reduce your risk of early death, especially death from heart disease. Simply moving up from the lowest conditioning category to a higher one will cut your risk of dying in any given year by as much as 60%.
Making strides
The study builds on previous research that shows the benefits of moving faster.
Walking faster will naturally increase your stride length, another predictor of longevity and future health. A review study published in 2021 found that older adults who took shorter steps were 26% more likely to have a disability, 34% more likely to have a major adverse event (like an injury that leads to a loss of independence), and 69% more likely to die over the next several years.
Quality versus quantity
We’ve focused so far on the quality of your physical activity – moving faster, taking longer strides.
But there’s still a lot to be said for movement quantity.
“It would be a mistake to say volume doesn’t matter,” Dr. Dempsey cautions.
A 2022 study in the journal The Lancet found that the risk of dying during a given period decreases with each increase in daily steps. The protective effect peaks at about 6,000 to 8,000 steps a day for adults 60 and over, and at 8,000 to 10,000 steps for those under 60.
“The relative value of the quality and quantity of exercise are very specific to a person’s goals,” says Chhanda Dutta, PhD, chief of the Clinical Gerontology Branch at the National Institute on Aging. “If performance is the goal, quality matters at least as much as quantity.”
Dr. Dempsey agrees that it’s not a cage match between two. Every step you take is a step in the right direction.
“People can choose or gravitate to an approach that works best for them,” he says. “It’s also helpful to think about where some everyday activities can be punctuated with intensity,” which could be as simple as walking faster when possible.
What matters most is that you choose something, Dr. Dutta says. “You have more to risk by not exercising.”
A version of this article first appeared on WebMD.com.
FROM EUROPEAN HEART JOURNAL
The TikTok trend that triggered a diabetes drug shortage
Weight loss advice is everywhere you look on social media, but one trend sweeping TikTok has led to shortages of an important diabetes drug.
Ozempic, a weekly injection that helps boost insulin sensitivity in people with type 2 diabetes, also suppresses appetite, which leads to weight loss. Stories of celebrities using the drug off-label to lose a few pounds have led to an explosion of interest. And now people with diabetes – people whose lives could be saved by the drug – are having trouble finding it.
Kim Kardashian and Elon Musk
In the spring, Kim Kardashian pulled off a dramatic weight loss to fit into Marilyn Monroe’s dress for the Met Gala. Soon rumors began to circulate that she’d used Ozempic to do it. Just this week, new Twitter owner Elon Musk tweeted about his own use of Ozempic and its sibling drug, Wegovy.
Variety dubbed Ozempic “the worst kept secret in Hollywood – especially given that its most enthusiastic users are not prediabetic and do not require the drug.” The rich and famous are spending $1,200 to $1,500 a month to get access.
As so often happens, high-profile use sparked a trend. Videos on TikTok hashtagged #ozempic have amassed more than 275 million views, and #ozempicweightloss has more than 110 million.
This raises concerns about who, exactly, is watching these videos, and what message they’re receiving.
“Forty-two percent of Americans have obesity, and even more have overweight. That’s affecting our younger people and our adolescents,” says Caroline Apovian, MD, codirector of the Center for Weight Management and Wellness at the Brigham and Women’s Hospital in Boston. “They’re looking at TikTok and other social media outlets for help.”
A new study shows how damaging this can be: Researchers analyzed 1,000 videos with nutrition, food, and weight-related hashtags, with over 1 billion views combined. They found that nearly all included messages glorifying weight loss and thinness.
At last, an effective weight-loss drug
Ozempic is Danish drug company Novo Nordisk’s brand name for semaglutide, which works by mimicking a naturally occurring hormone known as GLP-1. It travels to your brain and helps you feel full on less food. That leads to weight loss. In one 68-week study, semaglutide helped people lose an average of 15% of their body weight. But it’s not a miracle drug: You still have to change your eating habits and stay physically active.
The FDA approved Ozempic to treat people with type 2 diabetes in 2017. Four years later, Novo Nordisk received the green light for a higher-dose version meant specifically for people with obesity. Wegovy is approved for use only if you have a BMI of at least 27 with one or more weight-related ailments, or a BMI of 30 or more with none.
“These drugs are dominating my practice, because they’re so effective,” says Amanda Velazquez, MD, director of obesity medicine at Cedars-Sinai Medical Center in Los Angeles. The drug is considered safe, “so the majority of patients are good candidates.”
More demand than supply
As word spread about how well Ozempic and Wegovy worked, social media posts helped drive even more people to seek out the drugs. Now demand is outpacing the supply – according to the FDA, starter doses of Ozempic will have limited availability through January.
“In Hollywood, people are losing 10 pounds, getting it for $1,500 a month, and depleting stores for people who have such severe obesity that they have congestive heart failure and diabetes,” Dr. Apovian says. “These are people who are going to die, and you’re taking it away just for cosmetic weight loss. That is deplorable.”
In addition to huge demand, Wegovy also had a disruption in its supply chain. Right now, it isn’t available at all in lower doses, which is helping to spike off-label demand for Ozempic. Novo Nordisk expects to have these problems sorted out by the end of the year, with distribution following soon after.
The price of access
With a list price of $1,350 a month, Wegovy costs as much as many mortgages. And Medicaid, Medicare, and many insurance companies don’t cover it. Although obesity is a disease, the insurance industry treats weight loss as more of a vanity issue – so even if you could find the drug, you might not be able to afford it.
“We’re seeing that roughly half the prescriptions we write aren’t being covered,” Dr. Apovian says. “And for the half that are covered, we have to do prior authorization, which takes days, and it’s laborious.” In some instances, she says, insurance companies withdraw authorization after 3 months if they don’t see enough weight coming off.
It’s not like you can take Wegovy for 3 months, lose some weight, and expect it to stay off, either. The medication requires a real commitment, potentially for life. That’s because once the semaglutide leaves your system, your appetite returns. In one study, people regained two-thirds of the weight they’d lost within a year of stopping.
Many see a double standard in the insurance companies’ refusal to cover a drug that could prevent serious illness or death.
“They’re saying it’s not cost-effective to give the 42% of Americans who have a BMI over 30 Wegovy. Did they say this when statins came out?” Dr. Apovian says. “Why are they doing this with antiobesity agents? It’s the culture. The culture isn’t ready to adopt obesity as the disease that it is.”
Unpleasant side effects
Let’s assume you’re one of the lucky ones – your insurance covers Wegovy, and you can actually find some. You might discover that using it is no walk in the park. Common side effects include gastrointestinal issues like nausea, vomiting, and diarrhea.
“The way we counteract that is to start very slowly at a low dose of these medications,” Dr. Apovian says. “We only go up when the patient doesn’t have nausea or it gets better.”
Elise Davenport was excited to try Wegovy. “I did my online research. I’m the type who’s interested in early adoption, tech gadgets and stuff,” says the 40-year-old technical writer. “I wanted to try it because I’d tried so many other things that failed, or hadn’t worked long-term.”
With a BMI over 30, Ms. Davenport qualified for the drug. She signed up for an online program that guaranteed insurance coverage and started taking it in October 2021. At first, the side effects were mild, just a touch of nausea and diarrhea. And the results were impressive. She found it easy to feel satisfied with smaller portions and lost her cravings for sugar and highly processed foods. The weight fell off, roughly 5 pounds a week.
It turns out, that’s too much, too fast. Dr. Apovian and Dr. Velazquez say their patients lose more like 2 pounds each week, with careful monitoring.
By early December, Ms. Davenport’s side effects were ramping up. Because of shortages in lower dosages, the online program wasn’t able to adjust hers right away. She felt nauseated all the time, bad enough that brushing her teeth made her vomit and she had to force herself to eat. Some weeks, she managed less than 500 calories a day. Her sleep patterns became erratic. And then her depression, which medication had kept under control for years, spiraled.
“I remember sitting on the floor of my bathroom crying, thinking I’d rather carry the extra weight,” she says. “I used to take a lot of enjoyment from food, and I had none of that anymore. It was such a joyless experience at that point.”
Eventually, her dosage was reduced and the symptoms let up, but her primary care doctor encouraged her to stop. By the time she did, in March, she’d lost 55 pounds. So far, she’s gained back about 10.
More than just weight loss
Even though Ms. Davenport’s experience wasn’t a good one, with better monitoring, she’d be willing to try again. For one thing, seeing how easy it was to eat less with medical help helped to undo years of shame.
“Our culture treats obesity like a moral failing. I realized I’d been made to feel that way by doctors and programs – that I wasn’t doing enough,” she says. “This drug made me realize there are legit physiological things going on in my body, things that are often excluded from the conversation.”
Dr. Apovian and Dr. Velazquez say their patients regularly discover similar things.
“Obesity is not a disease of willpower. Medications are not the easy way out,” Dr. Velazquez says. “This is a chronic, relapsing medical condition, and because of that, we should treat it how we treat diabetes, high blood pressure, all these other conditions. We’d never hold back medication for individuals coming in with high blood pressure, tell them to work on willpower and withhold drugs they’d qualify for.”
A version of this article first appeared on WebMD.com.
Weight loss advice is everywhere you look on social media, but one trend sweeping TikTok has led to shortages of an important diabetes drug.
Ozempic, a weekly injection that helps boost insulin sensitivity in people with type 2 diabetes, also suppresses appetite, which leads to weight loss. Stories of celebrities using the drug off-label to lose a few pounds have led to an explosion of interest. And now people with diabetes – people whose lives could be saved by the drug – are having trouble finding it.
Kim Kardashian and Elon Musk
In the spring, Kim Kardashian pulled off a dramatic weight loss to fit into Marilyn Monroe’s dress for the Met Gala. Soon rumors began to circulate that she’d used Ozempic to do it. Just this week, new Twitter owner Elon Musk tweeted about his own use of Ozempic and its sibling drug, Wegovy.
Variety dubbed Ozempic “the worst kept secret in Hollywood – especially given that its most enthusiastic users are not prediabetic and do not require the drug.” The rich and famous are spending $1,200 to $1,500 a month to get access.
As so often happens, high-profile use sparked a trend. Videos on TikTok hashtagged #ozempic have amassed more than 275 million views, and #ozempicweightloss has more than 110 million.
This raises concerns about who, exactly, is watching these videos, and what message they’re receiving.
“Forty-two percent of Americans have obesity, and even more have overweight. That’s affecting our younger people and our adolescents,” says Caroline Apovian, MD, codirector of the Center for Weight Management and Wellness at the Brigham and Women’s Hospital in Boston. “They’re looking at TikTok and other social media outlets for help.”
A new study shows how damaging this can be: Researchers analyzed 1,000 videos with nutrition, food, and weight-related hashtags, with over 1 billion views combined. They found that nearly all included messages glorifying weight loss and thinness.
At last, an effective weight-loss drug
Ozempic is Danish drug company Novo Nordisk’s brand name for semaglutide, which works by mimicking a naturally occurring hormone known as GLP-1. It travels to your brain and helps you feel full on less food. That leads to weight loss. In one 68-week study, semaglutide helped people lose an average of 15% of their body weight. But it’s not a miracle drug: You still have to change your eating habits and stay physically active.
The FDA approved Ozempic to treat people with type 2 diabetes in 2017. Four years later, Novo Nordisk received the green light for a higher-dose version meant specifically for people with obesity. Wegovy is approved for use only if you have a BMI of at least 27 with one or more weight-related ailments, or a BMI of 30 or more with none.
“These drugs are dominating my practice, because they’re so effective,” says Amanda Velazquez, MD, director of obesity medicine at Cedars-Sinai Medical Center in Los Angeles. The drug is considered safe, “so the majority of patients are good candidates.”
More demand than supply
As word spread about how well Ozempic and Wegovy worked, social media posts helped drive even more people to seek out the drugs. Now demand is outpacing the supply – according to the FDA, starter doses of Ozempic will have limited availability through January.
“In Hollywood, people are losing 10 pounds, getting it for $1,500 a month, and depleting stores for people who have such severe obesity that they have congestive heart failure and diabetes,” Dr. Apovian says. “These are people who are going to die, and you’re taking it away just for cosmetic weight loss. That is deplorable.”
In addition to huge demand, Wegovy also had a disruption in its supply chain. Right now, it isn’t available at all in lower doses, which is helping to spike off-label demand for Ozempic. Novo Nordisk expects to have these problems sorted out by the end of the year, with distribution following soon after.
The price of access
With a list price of $1,350 a month, Wegovy costs as much as many mortgages. And Medicaid, Medicare, and many insurance companies don’t cover it. Although obesity is a disease, the insurance industry treats weight loss as more of a vanity issue – so even if you could find the drug, you might not be able to afford it.
“We’re seeing that roughly half the prescriptions we write aren’t being covered,” Dr. Apovian says. “And for the half that are covered, we have to do prior authorization, which takes days, and it’s laborious.” In some instances, she says, insurance companies withdraw authorization after 3 months if they don’t see enough weight coming off.
It’s not like you can take Wegovy for 3 months, lose some weight, and expect it to stay off, either. The medication requires a real commitment, potentially for life. That’s because once the semaglutide leaves your system, your appetite returns. In one study, people regained two-thirds of the weight they’d lost within a year of stopping.
Many see a double standard in the insurance companies’ refusal to cover a drug that could prevent serious illness or death.
“They’re saying it’s not cost-effective to give the 42% of Americans who have a BMI over 30 Wegovy. Did they say this when statins came out?” Dr. Apovian says. “Why are they doing this with antiobesity agents? It’s the culture. The culture isn’t ready to adopt obesity as the disease that it is.”
Unpleasant side effects
Let’s assume you’re one of the lucky ones – your insurance covers Wegovy, and you can actually find some. You might discover that using it is no walk in the park. Common side effects include gastrointestinal issues like nausea, vomiting, and diarrhea.
“The way we counteract that is to start very slowly at a low dose of these medications,” Dr. Apovian says. “We only go up when the patient doesn’t have nausea or it gets better.”
Elise Davenport was excited to try Wegovy. “I did my online research. I’m the type who’s interested in early adoption, tech gadgets and stuff,” says the 40-year-old technical writer. “I wanted to try it because I’d tried so many other things that failed, or hadn’t worked long-term.”
With a BMI over 30, Ms. Davenport qualified for the drug. She signed up for an online program that guaranteed insurance coverage and started taking it in October 2021. At first, the side effects were mild, just a touch of nausea and diarrhea. And the results were impressive. She found it easy to feel satisfied with smaller portions and lost her cravings for sugar and highly processed foods. The weight fell off, roughly 5 pounds a week.
It turns out, that’s too much, too fast. Dr. Apovian and Dr. Velazquez say their patients lose more like 2 pounds each week, with careful monitoring.
By early December, Ms. Davenport’s side effects were ramping up. Because of shortages in lower dosages, the online program wasn’t able to adjust hers right away. She felt nauseated all the time, bad enough that brushing her teeth made her vomit and she had to force herself to eat. Some weeks, she managed less than 500 calories a day. Her sleep patterns became erratic. And then her depression, which medication had kept under control for years, spiraled.
“I remember sitting on the floor of my bathroom crying, thinking I’d rather carry the extra weight,” she says. “I used to take a lot of enjoyment from food, and I had none of that anymore. It was such a joyless experience at that point.”
Eventually, her dosage was reduced and the symptoms let up, but her primary care doctor encouraged her to stop. By the time she did, in March, she’d lost 55 pounds. So far, she’s gained back about 10.
More than just weight loss
Even though Ms. Davenport’s experience wasn’t a good one, with better monitoring, she’d be willing to try again. For one thing, seeing how easy it was to eat less with medical help helped to undo years of shame.
“Our culture treats obesity like a moral failing. I realized I’d been made to feel that way by doctors and programs – that I wasn’t doing enough,” she says. “This drug made me realize there are legit physiological things going on in my body, things that are often excluded from the conversation.”
Dr. Apovian and Dr. Velazquez say their patients regularly discover similar things.
“Obesity is not a disease of willpower. Medications are not the easy way out,” Dr. Velazquez says. “This is a chronic, relapsing medical condition, and because of that, we should treat it how we treat diabetes, high blood pressure, all these other conditions. We’d never hold back medication for individuals coming in with high blood pressure, tell them to work on willpower and withhold drugs they’d qualify for.”
A version of this article first appeared on WebMD.com.
Weight loss advice is everywhere you look on social media, but one trend sweeping TikTok has led to shortages of an important diabetes drug.
Ozempic, a weekly injection that helps boost insulin sensitivity in people with type 2 diabetes, also suppresses appetite, which leads to weight loss. Stories of celebrities using the drug off-label to lose a few pounds have led to an explosion of interest. And now people with diabetes – people whose lives could be saved by the drug – are having trouble finding it.
Kim Kardashian and Elon Musk
In the spring, Kim Kardashian pulled off a dramatic weight loss to fit into Marilyn Monroe’s dress for the Met Gala. Soon rumors began to circulate that she’d used Ozempic to do it. Just this week, new Twitter owner Elon Musk tweeted about his own use of Ozempic and its sibling drug, Wegovy.
Variety dubbed Ozempic “the worst kept secret in Hollywood – especially given that its most enthusiastic users are not prediabetic and do not require the drug.” The rich and famous are spending $1,200 to $1,500 a month to get access.
As so often happens, high-profile use sparked a trend. Videos on TikTok hashtagged #ozempic have amassed more than 275 million views, and #ozempicweightloss has more than 110 million.
This raises concerns about who, exactly, is watching these videos, and what message they’re receiving.
“Forty-two percent of Americans have obesity, and even more have overweight. That’s affecting our younger people and our adolescents,” says Caroline Apovian, MD, codirector of the Center for Weight Management and Wellness at the Brigham and Women’s Hospital in Boston. “They’re looking at TikTok and other social media outlets for help.”
A new study shows how damaging this can be: Researchers analyzed 1,000 videos with nutrition, food, and weight-related hashtags, with over 1 billion views combined. They found that nearly all included messages glorifying weight loss and thinness.
At last, an effective weight-loss drug
Ozempic is Danish drug company Novo Nordisk’s brand name for semaglutide, which works by mimicking a naturally occurring hormone known as GLP-1. It travels to your brain and helps you feel full on less food. That leads to weight loss. In one 68-week study, semaglutide helped people lose an average of 15% of their body weight. But it’s not a miracle drug: You still have to change your eating habits and stay physically active.
The FDA approved Ozempic to treat people with type 2 diabetes in 2017. Four years later, Novo Nordisk received the green light for a higher-dose version meant specifically for people with obesity. Wegovy is approved for use only if you have a BMI of at least 27 with one or more weight-related ailments, or a BMI of 30 or more with none.
“These drugs are dominating my practice, because they’re so effective,” says Amanda Velazquez, MD, director of obesity medicine at Cedars-Sinai Medical Center in Los Angeles. The drug is considered safe, “so the majority of patients are good candidates.”
More demand than supply
As word spread about how well Ozempic and Wegovy worked, social media posts helped drive even more people to seek out the drugs. Now demand is outpacing the supply – according to the FDA, starter doses of Ozempic will have limited availability through January.
“In Hollywood, people are losing 10 pounds, getting it for $1,500 a month, and depleting stores for people who have such severe obesity that they have congestive heart failure and diabetes,” Dr. Apovian says. “These are people who are going to die, and you’re taking it away just for cosmetic weight loss. That is deplorable.”
In addition to huge demand, Wegovy also had a disruption in its supply chain. Right now, it isn’t available at all in lower doses, which is helping to spike off-label demand for Ozempic. Novo Nordisk expects to have these problems sorted out by the end of the year, with distribution following soon after.
The price of access
With a list price of $1,350 a month, Wegovy costs as much as many mortgages. And Medicaid, Medicare, and many insurance companies don’t cover it. Although obesity is a disease, the insurance industry treats weight loss as more of a vanity issue – so even if you could find the drug, you might not be able to afford it.
“We’re seeing that roughly half the prescriptions we write aren’t being covered,” Dr. Apovian says. “And for the half that are covered, we have to do prior authorization, which takes days, and it’s laborious.” In some instances, she says, insurance companies withdraw authorization after 3 months if they don’t see enough weight coming off.
It’s not like you can take Wegovy for 3 months, lose some weight, and expect it to stay off, either. The medication requires a real commitment, potentially for life. That’s because once the semaglutide leaves your system, your appetite returns. In one study, people regained two-thirds of the weight they’d lost within a year of stopping.
Many see a double standard in the insurance companies’ refusal to cover a drug that could prevent serious illness or death.
“They’re saying it’s not cost-effective to give the 42% of Americans who have a BMI over 30 Wegovy. Did they say this when statins came out?” Dr. Apovian says. “Why are they doing this with antiobesity agents? It’s the culture. The culture isn’t ready to adopt obesity as the disease that it is.”
Unpleasant side effects
Let’s assume you’re one of the lucky ones – your insurance covers Wegovy, and you can actually find some. You might discover that using it is no walk in the park. Common side effects include gastrointestinal issues like nausea, vomiting, and diarrhea.
“The way we counteract that is to start very slowly at a low dose of these medications,” Dr. Apovian says. “We only go up when the patient doesn’t have nausea or it gets better.”
Elise Davenport was excited to try Wegovy. “I did my online research. I’m the type who’s interested in early adoption, tech gadgets and stuff,” says the 40-year-old technical writer. “I wanted to try it because I’d tried so many other things that failed, or hadn’t worked long-term.”
With a BMI over 30, Ms. Davenport qualified for the drug. She signed up for an online program that guaranteed insurance coverage and started taking it in October 2021. At first, the side effects were mild, just a touch of nausea and diarrhea. And the results were impressive. She found it easy to feel satisfied with smaller portions and lost her cravings for sugar and highly processed foods. The weight fell off, roughly 5 pounds a week.
It turns out, that’s too much, too fast. Dr. Apovian and Dr. Velazquez say their patients lose more like 2 pounds each week, with careful monitoring.
By early December, Ms. Davenport’s side effects were ramping up. Because of shortages in lower dosages, the online program wasn’t able to adjust hers right away. She felt nauseated all the time, bad enough that brushing her teeth made her vomit and she had to force herself to eat. Some weeks, she managed less than 500 calories a day. Her sleep patterns became erratic. And then her depression, which medication had kept under control for years, spiraled.
“I remember sitting on the floor of my bathroom crying, thinking I’d rather carry the extra weight,” she says. “I used to take a lot of enjoyment from food, and I had none of that anymore. It was such a joyless experience at that point.”
Eventually, her dosage was reduced and the symptoms let up, but her primary care doctor encouraged her to stop. By the time she did, in March, she’d lost 55 pounds. So far, she’s gained back about 10.
More than just weight loss
Even though Ms. Davenport’s experience wasn’t a good one, with better monitoring, she’d be willing to try again. For one thing, seeing how easy it was to eat less with medical help helped to undo years of shame.
“Our culture treats obesity like a moral failing. I realized I’d been made to feel that way by doctors and programs – that I wasn’t doing enough,” she says. “This drug made me realize there are legit physiological things going on in my body, things that are often excluded from the conversation.”
Dr. Apovian and Dr. Velazquez say their patients regularly discover similar things.
“Obesity is not a disease of willpower. Medications are not the easy way out,” Dr. Velazquez says. “This is a chronic, relapsing medical condition, and because of that, we should treat it how we treat diabetes, high blood pressure, all these other conditions. We’d never hold back medication for individuals coming in with high blood pressure, tell them to work on willpower and withhold drugs they’d qualify for.”
A version of this article first appeared on WebMD.com.
With type 1 diabetes delay possible, focus now on screening
The recent approval of teplizumab-mzwv (Tzield, Provention Bio) for the delay of type 1 diabetes by the Food and Drug Administration is expected to advance efforts to increase screening to cost effectively identify those at risk for the condition who would be eligible to receive the new treatment.
The anti-CD3 monoclonal antibody was approved Nov. 17 as the first disease-modifying therapy for impeding progression of type 1 diabetes. In a clinical trial, teplizumab delayed the onset of clinical (stage 3) type 1 diabetes by approximately 2 years, and longer in some cases.
It is administered by intravenous infusion once daily for 14 consecutive days and is expected to cost in the region of $200,000 for the course of treatment.
The specific indication is “to delay the onset of stage 3 type 1 diabetes in adults and pediatric patients 8 years and older who currently have stage 2 type 1 diabetes.” In stage 2 type 1 diabetes, the individual has two or more islet autoantibodies and abnormal glycemia but is as yet asymptomatic. It is associated with a nearly 100% lifetime risk of progression to clinical (stage 3) type 1 diabetes and a 75% risk of developing the condition within 5 years.
Currently, most people who are screened for type 1 diabetes autoantibodies are first-degree relatives of those with the condition through TrialNet, other local programs, or more recently, a $55 test offered by the research and advocacy organization JDRF.
But because 85%-90% of people who develop type 1 diabetes don’t have first-degree relatives with the condition, broader population screening will be necessary to identify eligible candidates for teplizumab.
During an investor call on Nov. 18, Provention Bio chief commercial officer Jason Hoitt said that among the company’s “strategic initiatives” were “advancing awareness and screening for autoantibodies in at-risk individuals, and ultimately, routine screening during pediatric well visits for the general population,” as well as “[health care provider] belief in teplizumab and desire to prescribe it for their patients.”
Without broad population-based screening, first-degree relatives of people with type 1 diabetes are likely to be the first to be screened and those with stage 2 identified for receipt of teplizumab. Today, that population is estimated at about 30,000 in the United States, Mr. Hoitt said, adding, “with this approval we hope that more stage 2 patients can be readily identified so the course of the disease can be changed.”
During the call, Mr. Hoitt also announced that the wholesale acquisition cost of Tzield would be $13,850 per vial, which translates to $193,900 per 14-vial continuous regimen, anticipated to be a sufficient dose for most patients. The company also launched a program called COMPASS to help patients navigate insurance reimbursement, as well as provide some with financial assistance.
Cost aside, JDRF CEO Aaron Kowalski, PhD, said in an interview that clinicians shouldn’t doubt the value of delaying type 1 diabetes onset, even if not completely preventing it. “This is the first drug ever to treat the underlying disease. There is this undercurrent that insulin is enough. Why would you undertake an additional risk of an immunotherapy? Type 1 is hard to live with. I think sometimes the clinical community doesn’t appreciate that insulin is not enough. It’s very difficult, and opening this door is important. ... We believe very strongly that the delay of onset of type 1 diabetes is clinically meaningful. We hear that from every family we’ve talked to. Clinicians should appreciate this and not discount it.”
How would screening happen?
While the path to universal screening for type 1 diabetes risk isn’t yet clear, quite a bit of thought and research has gone into it even before teplizumab and other immune-modulating agents showed promise in forestalling the condition.
Data from a universal screening program of schoolchildren implemented in Bavaria, Germany, and a screening program in Denver, suggest that even without such an intervention, identifying people at high risk for developing type 1 diabetes could be cost effective by allowing for education of the individual and family members about the signs of type 1 diabetes, thereby reducing the likelihood that the person would progress to developing diabetic ketoacidosis (DKA) prior to diagnosis.
Another study that used data from the United States and Western Europe, found that screening children for type 1 diabetes–associated islet autoantibodies at ages 2 and 6 years would identify most of those who go on to develop the disease by midadolescence.
However, using a genetic risk score at birth to identify those who would go on to autoantibody testing is potentially a more cost-effective approach, William A. Hagopian, MD, PhD, director of diabetes programs, Pacific Northwest Research Institute, Seattle, said in an interview.
The score – based on human leukocyte antigen haplotypes and their interactions as well as non-HLA genes – can stratify nearly 80% of childhood type 1 diabetes within the top 10% of all newborns. Thus, only the top 10% would then go on to receive the more expensive autoantibody testing.
“I’ve been working with U.K. colleagues for the past 3-4 years to develop a strategy using genetic risk scores followed by autoantibody screening. I feel strongly that that’s the cost-effective way to go. It’s relatively inexpensive, scalable, and can be applied commercially in newborn screening labs. To be successful an approach must be cost effective. Payors are willing to pay for newborn screening, but not so much on testing 100% of kids for antibodies,” Dr. Hagopian said.
He is now working with Washington State newborn screening labs to demonstrate feasibility of the approach using dried blood samples from actual neonatal screening after obtaining informed consent from the mothers in postpartum wards in several hospitals. Those found to be at high risk using the genetic risk score are contacted for follow-up with autoantibody screening. The program will continue for another year and a half. “I think it actually has a chance of being accepted into their regular program,” he said.
And then, he hopes, other states will follow, and eventually, the strategy will be added to the Recommended Uniform Screening Panel for universal newborn screening programs, as recommended by the Department of Health & Human Services.
“New newborn screenings for additional diseases are implemented regularly,” Dr. Hagopian said. “Most are far less common than type 1 diabetes. So even if our approach is less than 100% sensitive, this condition is a lot more common than the many inborn errors of metabolism, so we’re still going to be identifying a lot of cases. ... This is my hope for how universal type 1 diabetes screening will unfold. I see a way this may work quite well.”
A two-pronged approach to screening could work best
Meanwhile, JDRF, which supported the teplizumab research as well as others working in the space, is focusing on both genetic and autoantibody screening, Dr. Kowalski said.
“JDRF is working on both pathways – testing kids at birth for genetic predisposition and also antibody screening. We have huge programs focused on general population antibody screening.”
Dr. Kowalski said that, while the two-pronged approach certainly is worth exploring – and JDRF is doing that – he also thinks that universal autoantibody screening could be cost effective if done efficiently, such as with less expensive assays than the one used in TrialNet.
“We have programs where you do the genetic screening and keep an eye on people. We also have programs, like the one we’re funding in Germany, that are doing broad autoantibody screening of all kids. We’re hopeful that will be very cost effective if we move to cheaper assays.”
He noted that the proportion of children with new-onset type 1 diabetes who present in DKA rose from 40% pre–COVID-19 to 50% during the early days of the pandemic. On the other hand, “With screening you can get that to near zero, like they did in Bavaria. Here [in the United States], one ICU visit for DKA [costs] $100,000.”
While JDRF and others have been working on this for years, the new availability of teplizumab will be “multifold in helping things along. ... I think you’re going to see a lot of work on the cost-effectiveness of teplizumab. I think the case will be pretty straightforward that there’s huge upside to delaying the disease from a near-term and a long-term cost perspective. This is the first time we’ve had a drug out there with a price attached to it.”
But it may not happen quickly, Kowalski cautioned. “I feel there’s a ... series of events that has to happen to drive towards universal screening. Here in the U.S. it’s complicated because we have a very discrepant health care system with all these different payers, public and private.”
During the investor call, Mr. Hoitt said that Provention Bio is also exploring use of Tzield in younger patients and newly diagnosed patients, and the potential benefit of redosing or combining with other treatments.
Mr. Hoitt is an employee of Provention Bio. Dr. Kowalski is an employee of JDRF. Dr. Hagopian has reported receiving study funding from Janssen.
A version of this article first appeared on Medscape.com.
The recent approval of teplizumab-mzwv (Tzield, Provention Bio) for the delay of type 1 diabetes by the Food and Drug Administration is expected to advance efforts to increase screening to cost effectively identify those at risk for the condition who would be eligible to receive the new treatment.
The anti-CD3 monoclonal antibody was approved Nov. 17 as the first disease-modifying therapy for impeding progression of type 1 diabetes. In a clinical trial, teplizumab delayed the onset of clinical (stage 3) type 1 diabetes by approximately 2 years, and longer in some cases.
It is administered by intravenous infusion once daily for 14 consecutive days and is expected to cost in the region of $200,000 for the course of treatment.
The specific indication is “to delay the onset of stage 3 type 1 diabetes in adults and pediatric patients 8 years and older who currently have stage 2 type 1 diabetes.” In stage 2 type 1 diabetes, the individual has two or more islet autoantibodies and abnormal glycemia but is as yet asymptomatic. It is associated with a nearly 100% lifetime risk of progression to clinical (stage 3) type 1 diabetes and a 75% risk of developing the condition within 5 years.
Currently, most people who are screened for type 1 diabetes autoantibodies are first-degree relatives of those with the condition through TrialNet, other local programs, or more recently, a $55 test offered by the research and advocacy organization JDRF.
But because 85%-90% of people who develop type 1 diabetes don’t have first-degree relatives with the condition, broader population screening will be necessary to identify eligible candidates for teplizumab.
During an investor call on Nov. 18, Provention Bio chief commercial officer Jason Hoitt said that among the company’s “strategic initiatives” were “advancing awareness and screening for autoantibodies in at-risk individuals, and ultimately, routine screening during pediatric well visits for the general population,” as well as “[health care provider] belief in teplizumab and desire to prescribe it for their patients.”
Without broad population-based screening, first-degree relatives of people with type 1 diabetes are likely to be the first to be screened and those with stage 2 identified for receipt of teplizumab. Today, that population is estimated at about 30,000 in the United States, Mr. Hoitt said, adding, “with this approval we hope that more stage 2 patients can be readily identified so the course of the disease can be changed.”
During the call, Mr. Hoitt also announced that the wholesale acquisition cost of Tzield would be $13,850 per vial, which translates to $193,900 per 14-vial continuous regimen, anticipated to be a sufficient dose for most patients. The company also launched a program called COMPASS to help patients navigate insurance reimbursement, as well as provide some with financial assistance.
Cost aside, JDRF CEO Aaron Kowalski, PhD, said in an interview that clinicians shouldn’t doubt the value of delaying type 1 diabetes onset, even if not completely preventing it. “This is the first drug ever to treat the underlying disease. There is this undercurrent that insulin is enough. Why would you undertake an additional risk of an immunotherapy? Type 1 is hard to live with. I think sometimes the clinical community doesn’t appreciate that insulin is not enough. It’s very difficult, and opening this door is important. ... We believe very strongly that the delay of onset of type 1 diabetes is clinically meaningful. We hear that from every family we’ve talked to. Clinicians should appreciate this and not discount it.”
How would screening happen?
While the path to universal screening for type 1 diabetes risk isn’t yet clear, quite a bit of thought and research has gone into it even before teplizumab and other immune-modulating agents showed promise in forestalling the condition.
Data from a universal screening program of schoolchildren implemented in Bavaria, Germany, and a screening program in Denver, suggest that even without such an intervention, identifying people at high risk for developing type 1 diabetes could be cost effective by allowing for education of the individual and family members about the signs of type 1 diabetes, thereby reducing the likelihood that the person would progress to developing diabetic ketoacidosis (DKA) prior to diagnosis.
Another study that used data from the United States and Western Europe, found that screening children for type 1 diabetes–associated islet autoantibodies at ages 2 and 6 years would identify most of those who go on to develop the disease by midadolescence.
However, using a genetic risk score at birth to identify those who would go on to autoantibody testing is potentially a more cost-effective approach, William A. Hagopian, MD, PhD, director of diabetes programs, Pacific Northwest Research Institute, Seattle, said in an interview.
The score – based on human leukocyte antigen haplotypes and their interactions as well as non-HLA genes – can stratify nearly 80% of childhood type 1 diabetes within the top 10% of all newborns. Thus, only the top 10% would then go on to receive the more expensive autoantibody testing.
“I’ve been working with U.K. colleagues for the past 3-4 years to develop a strategy using genetic risk scores followed by autoantibody screening. I feel strongly that that’s the cost-effective way to go. It’s relatively inexpensive, scalable, and can be applied commercially in newborn screening labs. To be successful an approach must be cost effective. Payors are willing to pay for newborn screening, but not so much on testing 100% of kids for antibodies,” Dr. Hagopian said.
He is now working with Washington State newborn screening labs to demonstrate feasibility of the approach using dried blood samples from actual neonatal screening after obtaining informed consent from the mothers in postpartum wards in several hospitals. Those found to be at high risk using the genetic risk score are contacted for follow-up with autoantibody screening. The program will continue for another year and a half. “I think it actually has a chance of being accepted into their regular program,” he said.
And then, he hopes, other states will follow, and eventually, the strategy will be added to the Recommended Uniform Screening Panel for universal newborn screening programs, as recommended by the Department of Health & Human Services.
“New newborn screenings for additional diseases are implemented regularly,” Dr. Hagopian said. “Most are far less common than type 1 diabetes. So even if our approach is less than 100% sensitive, this condition is a lot more common than the many inborn errors of metabolism, so we’re still going to be identifying a lot of cases. ... This is my hope for how universal type 1 diabetes screening will unfold. I see a way this may work quite well.”
A two-pronged approach to screening could work best
Meanwhile, JDRF, which supported the teplizumab research as well as others working in the space, is focusing on both genetic and autoantibody screening, Dr. Kowalski said.
“JDRF is working on both pathways – testing kids at birth for genetic predisposition and also antibody screening. We have huge programs focused on general population antibody screening.”
Dr. Kowalski said that, while the two-pronged approach certainly is worth exploring – and JDRF is doing that – he also thinks that universal autoantibody screening could be cost effective if done efficiently, such as with less expensive assays than the one used in TrialNet.
“We have programs where you do the genetic screening and keep an eye on people. We also have programs, like the one we’re funding in Germany, that are doing broad autoantibody screening of all kids. We’re hopeful that will be very cost effective if we move to cheaper assays.”
He noted that the proportion of children with new-onset type 1 diabetes who present in DKA rose from 40% pre–COVID-19 to 50% during the early days of the pandemic. On the other hand, “With screening you can get that to near zero, like they did in Bavaria. Here [in the United States], one ICU visit for DKA [costs] $100,000.”
While JDRF and others have been working on this for years, the new availability of teplizumab will be “multifold in helping things along. ... I think you’re going to see a lot of work on the cost-effectiveness of teplizumab. I think the case will be pretty straightforward that there’s huge upside to delaying the disease from a near-term and a long-term cost perspective. This is the first time we’ve had a drug out there with a price attached to it.”
But it may not happen quickly, Kowalski cautioned. “I feel there’s a ... series of events that has to happen to drive towards universal screening. Here in the U.S. it’s complicated because we have a very discrepant health care system with all these different payers, public and private.”
During the investor call, Mr. Hoitt said that Provention Bio is also exploring use of Tzield in younger patients and newly diagnosed patients, and the potential benefit of redosing or combining with other treatments.
Mr. Hoitt is an employee of Provention Bio. Dr. Kowalski is an employee of JDRF. Dr. Hagopian has reported receiving study funding from Janssen.
A version of this article first appeared on Medscape.com.
The recent approval of teplizumab-mzwv (Tzield, Provention Bio) for the delay of type 1 diabetes by the Food and Drug Administration is expected to advance efforts to increase screening to cost effectively identify those at risk for the condition who would be eligible to receive the new treatment.
The anti-CD3 monoclonal antibody was approved Nov. 17 as the first disease-modifying therapy for impeding progression of type 1 diabetes. In a clinical trial, teplizumab delayed the onset of clinical (stage 3) type 1 diabetes by approximately 2 years, and longer in some cases.
It is administered by intravenous infusion once daily for 14 consecutive days and is expected to cost in the region of $200,000 for the course of treatment.
The specific indication is “to delay the onset of stage 3 type 1 diabetes in adults and pediatric patients 8 years and older who currently have stage 2 type 1 diabetes.” In stage 2 type 1 diabetes, the individual has two or more islet autoantibodies and abnormal glycemia but is as yet asymptomatic. It is associated with a nearly 100% lifetime risk of progression to clinical (stage 3) type 1 diabetes and a 75% risk of developing the condition within 5 years.
Currently, most people who are screened for type 1 diabetes autoantibodies are first-degree relatives of those with the condition through TrialNet, other local programs, or more recently, a $55 test offered by the research and advocacy organization JDRF.
But because 85%-90% of people who develop type 1 diabetes don’t have first-degree relatives with the condition, broader population screening will be necessary to identify eligible candidates for teplizumab.
During an investor call on Nov. 18, Provention Bio chief commercial officer Jason Hoitt said that among the company’s “strategic initiatives” were “advancing awareness and screening for autoantibodies in at-risk individuals, and ultimately, routine screening during pediatric well visits for the general population,” as well as “[health care provider] belief in teplizumab and desire to prescribe it for their patients.”
Without broad population-based screening, first-degree relatives of people with type 1 diabetes are likely to be the first to be screened and those with stage 2 identified for receipt of teplizumab. Today, that population is estimated at about 30,000 in the United States, Mr. Hoitt said, adding, “with this approval we hope that more stage 2 patients can be readily identified so the course of the disease can be changed.”
During the call, Mr. Hoitt also announced that the wholesale acquisition cost of Tzield would be $13,850 per vial, which translates to $193,900 per 14-vial continuous regimen, anticipated to be a sufficient dose for most patients. The company also launched a program called COMPASS to help patients navigate insurance reimbursement, as well as provide some with financial assistance.
Cost aside, JDRF CEO Aaron Kowalski, PhD, said in an interview that clinicians shouldn’t doubt the value of delaying type 1 diabetes onset, even if not completely preventing it. “This is the first drug ever to treat the underlying disease. There is this undercurrent that insulin is enough. Why would you undertake an additional risk of an immunotherapy? Type 1 is hard to live with. I think sometimes the clinical community doesn’t appreciate that insulin is not enough. It’s very difficult, and opening this door is important. ... We believe very strongly that the delay of onset of type 1 diabetes is clinically meaningful. We hear that from every family we’ve talked to. Clinicians should appreciate this and not discount it.”
How would screening happen?
While the path to universal screening for type 1 diabetes risk isn’t yet clear, quite a bit of thought and research has gone into it even before teplizumab and other immune-modulating agents showed promise in forestalling the condition.
Data from a universal screening program of schoolchildren implemented in Bavaria, Germany, and a screening program in Denver, suggest that even without such an intervention, identifying people at high risk for developing type 1 diabetes could be cost effective by allowing for education of the individual and family members about the signs of type 1 diabetes, thereby reducing the likelihood that the person would progress to developing diabetic ketoacidosis (DKA) prior to diagnosis.
Another study that used data from the United States and Western Europe, found that screening children for type 1 diabetes–associated islet autoantibodies at ages 2 and 6 years would identify most of those who go on to develop the disease by midadolescence.
However, using a genetic risk score at birth to identify those who would go on to autoantibody testing is potentially a more cost-effective approach, William A. Hagopian, MD, PhD, director of diabetes programs, Pacific Northwest Research Institute, Seattle, said in an interview.
The score – based on human leukocyte antigen haplotypes and their interactions as well as non-HLA genes – can stratify nearly 80% of childhood type 1 diabetes within the top 10% of all newborns. Thus, only the top 10% would then go on to receive the more expensive autoantibody testing.
“I’ve been working with U.K. colleagues for the past 3-4 years to develop a strategy using genetic risk scores followed by autoantibody screening. I feel strongly that that’s the cost-effective way to go. It’s relatively inexpensive, scalable, and can be applied commercially in newborn screening labs. To be successful an approach must be cost effective. Payors are willing to pay for newborn screening, but not so much on testing 100% of kids for antibodies,” Dr. Hagopian said.
He is now working with Washington State newborn screening labs to demonstrate feasibility of the approach using dried blood samples from actual neonatal screening after obtaining informed consent from the mothers in postpartum wards in several hospitals. Those found to be at high risk using the genetic risk score are contacted for follow-up with autoantibody screening. The program will continue for another year and a half. “I think it actually has a chance of being accepted into their regular program,” he said.
And then, he hopes, other states will follow, and eventually, the strategy will be added to the Recommended Uniform Screening Panel for universal newborn screening programs, as recommended by the Department of Health & Human Services.
“New newborn screenings for additional diseases are implemented regularly,” Dr. Hagopian said. “Most are far less common than type 1 diabetes. So even if our approach is less than 100% sensitive, this condition is a lot more common than the many inborn errors of metabolism, so we’re still going to be identifying a lot of cases. ... This is my hope for how universal type 1 diabetes screening will unfold. I see a way this may work quite well.”
A two-pronged approach to screening could work best
Meanwhile, JDRF, which supported the teplizumab research as well as others working in the space, is focusing on both genetic and autoantibody screening, Dr. Kowalski said.
“JDRF is working on both pathways – testing kids at birth for genetic predisposition and also antibody screening. We have huge programs focused on general population antibody screening.”
Dr. Kowalski said that, while the two-pronged approach certainly is worth exploring – and JDRF is doing that – he also thinks that universal autoantibody screening could be cost effective if done efficiently, such as with less expensive assays than the one used in TrialNet.
“We have programs where you do the genetic screening and keep an eye on people. We also have programs, like the one we’re funding in Germany, that are doing broad autoantibody screening of all kids. We’re hopeful that will be very cost effective if we move to cheaper assays.”
He noted that the proportion of children with new-onset type 1 diabetes who present in DKA rose from 40% pre–COVID-19 to 50% during the early days of the pandemic. On the other hand, “With screening you can get that to near zero, like they did in Bavaria. Here [in the United States], one ICU visit for DKA [costs] $100,000.”
While JDRF and others have been working on this for years, the new availability of teplizumab will be “multifold in helping things along. ... I think you’re going to see a lot of work on the cost-effectiveness of teplizumab. I think the case will be pretty straightforward that there’s huge upside to delaying the disease from a near-term and a long-term cost perspective. This is the first time we’ve had a drug out there with a price attached to it.”
But it may not happen quickly, Kowalski cautioned. “I feel there’s a ... series of events that has to happen to drive towards universal screening. Here in the U.S. it’s complicated because we have a very discrepant health care system with all these different payers, public and private.”
During the investor call, Mr. Hoitt said that Provention Bio is also exploring use of Tzield in younger patients and newly diagnosed patients, and the potential benefit of redosing or combining with other treatments.
Mr. Hoitt is an employee of Provention Bio. Dr. Kowalski is an employee of JDRF. Dr. Hagopian has reported receiving study funding from Janssen.
A version of this article first appeared on Medscape.com.
Both potatoes and beans reduced insulin resistance, weight in controlled study
Low energy–density diets that are based either on potatoes or beans similarly reduced insulin resistance in adults with poor blood glucose control, according to a controlled feeding study in 36 individuals.

Potatoes have gotten a bad rap for their high glycemic index, but they have little fat and a low energy density, wrote the study investigators. In fact, “cooling of gelatinized potatoes generates appreciable levels of slowly digested starch (resistant starch type 3) and substantially lowers the blood glucose response that potatoes elicit.”
“There is a view that potatoes are a less healthy plant food, but there is very little empirical data from randomized trials to support this view,” senior investigator John P. Kirwan, PhD, said in an interview.
Dry beans and peas (known as pulses) also contain resistant starch that improves insulin sensitivity and glucose tolerance, and multiple studies support pulses as part of a low-glycemic diet to improve glucose control in adults, the researchers explained, but because the density of food often guides how much people eat, they hypothesized that potatoes could substitute for beans and provide similar glucose control benefits.
In a study published in the Journal of Medicinal Food, the researchers randomized 36 adults aged 18-60 years with insulin resistance to 8 weeks of a low energy–density diet (1 kcal/g) high in either potatoes or beans. The baseline body mass index ranged from 25 to 40 kg/m2. Insulin resistance was defined using the homeostatic model assessment of insulin resistance (HOMA-IR) with a score greater than 2.
The controlled diet consisted of 50%-55% carbohydrates, 30%-35% fats, and 15%-20% protein. Each meal in the potato group included a side of potatoes, and each meal in the bean group included a side of beans.
The primary outcome was the mean change in blood glucose concentration; the researchers also assessed weight loss.
A total of 14 individuals in the potato group and 17 in the bean group completed the study; but data from the 18 individuals in each group were included in an intent-to-treat analysis.
Among study completers, HOMA-IR in the bean group showed an average decrease of 1.4 from baseline (P = .02 ); a similar decrease of 1.3 occurred in the potato group (P < .05) with no significant difference between the two diets.
Overall compliance with both diets was roughly 88%. Body weight reductions were similar in both groups and significantly reduced from baseline over the study period, with average reductions in intent-to-treat analysis of 5.82 kg in the potato group and 4.0 kg in the bean group. BMI also was significantly reduced from baseline in both potato and bean groups (2.04 kg/m2 and 1.35 kg/m2, respectively). Although baseline differences were not significant, “BMI at baseline was higher and the reduction in response to the treatment was significantly greater in the potato diet compared with the bean diet,” the researchers noted. The effect on blood glucose response was not significantly different between the two groups or from baseline, they said.
The findings were limited by several factors including the small size, relatively short study period, and controlled nature of the study diet, the researchers noted. “The addition of a typical Western diet would have enhanced our understanding of the effect of low energy–dense diets on metabolic outcomes,” they noted in their discussion.
However, both diets led to a reduction in body weight, and the low energy density of both potato and bean diets promoted weight loss without affecting appetite or requiring calorie restriction, the researchers explained. Therefore, “this weight loss if sustained over time could have a substantial impact on body weight,” they said.
“We hypothesized that there would be equivalence between the potato and bean diet and this hypothesis proved to be correct,” said Dr. Kirwan, of the Pennington Biomedical Research Center, Baton Rouge, La., in an interview.
The take-home message for clinicians is that, though small, the study was very well-controlled, Dr. Kirwan emphasized. “Clinicians ought to consider the health benefits of the potato when it is cooked and served appropriately.”
Looking ahead, larger randomized controlled trials with additional control arms, longer time of at least 12 weeks, and different patient populations are needed, Dr. Kirwan added.
Findings mitigate food myths
The debate continues about whether there are foods that are “good” or “evil;” or foods that one “should not eat” or “should eat,” said Amy Rothberg, MD, associate professor of internal medicine and of nutritional sciences at the University of Michigan, Ann Arbor, in an interview.
“This study dispels the myth that incorporating a small portion of potato into the diet (although these are not potatoes that are fried, or are topped with cheese, bacon, sour cream, etc.) results in deleterious metabolic outcomes when compared to a diet that is comprised of beans (pulses) as part of a low energy–dense diet,” she explained.
“The diet in both groups was of low energy density, which has been shown to result in fewer calories consumed, weight loss, and improvement in insulin resistance,” so the similarity in results was not so surprising, said Dr. Rothberg.
For the clinical takeaway, Dr. Rothberg agreed with the study authors: “Clinicians may counsel their patients that they can still consume a small potato (with the caveat above regarding cooking methods and toppings) as part of a balanced meal so long as they are keeping their overall calories low and not exceeding their metabolic requirements based on body weight/BMI,” she said.
As for additional research, studies with a longer time frame and a larger and more diverse study population are needed, including populations with common insulin resistance comorbidities such as type 2 diabetes, fatty liver disease, and cardiovascular disease, Dr. Rothberg noted.
Consumer considerations, with caveats
The key message for consumers is that, “based on this very small study of short duration, consuming a small portion of potato as part of an overall balanced, low-energy diet did not produce adverse effects on glucose or insulin when compared to a diet of pulses known to have favorable effects on glucose and insulin,” Dr. Rothberg told this news organization. However, “consumers should note that, although the results from this small study are encouraging, it would be premature to extrapolate the findings from this study to other populations,” she said. Also, keep in mind that the study was supported in part by the Alliance for Potato Research, although the authors stated that none of the funders (Alliance for Potato Research and Education and the National Institutes of Health) had any role in the design, analysis, or writing of the article, she added.
The study was supported in part by the Alliance for Potato Research and Education and the National Institutes of Health, which funds the Louisiana Clinical and Translational Science Center. The researchers and Dr. Rothberg had no financial conflicts to disclose.
Low energy–density diets that are based either on potatoes or beans similarly reduced insulin resistance in adults with poor blood glucose control, according to a controlled feeding study in 36 individuals.
Potatoes have gotten a bad rap for their high glycemic index, but they have little fat and a low energy density, wrote the study investigators. In fact, “cooling of gelatinized potatoes generates appreciable levels of slowly digested starch (resistant starch type 3) and substantially lowers the blood glucose response that potatoes elicit.”
“There is a view that potatoes are a less healthy plant food, but there is very little empirical data from randomized trials to support this view,” senior investigator John P. Kirwan, PhD, said in an interview.
Dry beans and peas (known as pulses) also contain resistant starch that improves insulin sensitivity and glucose tolerance, and multiple studies support pulses as part of a low-glycemic diet to improve glucose control in adults, the researchers explained, but because the density of food often guides how much people eat, they hypothesized that potatoes could substitute for beans and provide similar glucose control benefits.
In a study published in the Journal of Medicinal Food, the researchers randomized 36 adults aged 18-60 years with insulin resistance to 8 weeks of a low energy–density diet (1 kcal/g) high in either potatoes or beans. The baseline body mass index ranged from 25 to 40 kg/m2. Insulin resistance was defined using the homeostatic model assessment of insulin resistance (HOMA-IR) with a score greater than 2.
The controlled diet consisted of 50%-55% carbohydrates, 30%-35% fats, and 15%-20% protein. Each meal in the potato group included a side of potatoes, and each meal in the bean group included a side of beans.
The primary outcome was the mean change in blood glucose concentration; the researchers also assessed weight loss.
A total of 14 individuals in the potato group and 17 in the bean group completed the study; but data from the 18 individuals in each group were included in an intent-to-treat analysis.
Among study completers, HOMA-IR in the bean group showed an average decrease of 1.4 from baseline (P = .02 ); a similar decrease of 1.3 occurred in the potato group (P < .05) with no significant difference between the two diets.
Overall compliance with both diets was roughly 88%. Body weight reductions were similar in both groups and significantly reduced from baseline over the study period, with average reductions in intent-to-treat analysis of 5.82 kg in the potato group and 4.0 kg in the bean group. BMI also was significantly reduced from baseline in both potato and bean groups (2.04 kg/m2 and 1.35 kg/m2, respectively). Although baseline differences were not significant, “BMI at baseline was higher and the reduction in response to the treatment was significantly greater in the potato diet compared with the bean diet,” the researchers noted. The effect on blood glucose response was not significantly different between the two groups or from baseline, they said.
The findings were limited by several factors including the small size, relatively short study period, and controlled nature of the study diet, the researchers noted. “The addition of a typical Western diet would have enhanced our understanding of the effect of low energy–dense diets on metabolic outcomes,” they noted in their discussion.
However, both diets led to a reduction in body weight, and the low energy density of both potato and bean diets promoted weight loss without affecting appetite or requiring calorie restriction, the researchers explained. Therefore, “this weight loss if sustained over time could have a substantial impact on body weight,” they said.
“We hypothesized that there would be equivalence between the potato and bean diet and this hypothesis proved to be correct,” said Dr. Kirwan, of the Pennington Biomedical Research Center, Baton Rouge, La., in an interview.
The take-home message for clinicians is that, though small, the study was very well-controlled, Dr. Kirwan emphasized. “Clinicians ought to consider the health benefits of the potato when it is cooked and served appropriately.”
Looking ahead, larger randomized controlled trials with additional control arms, longer time of at least 12 weeks, and different patient populations are needed, Dr. Kirwan added.
Findings mitigate food myths
The debate continues about whether there are foods that are “good” or “evil;” or foods that one “should not eat” or “should eat,” said Amy Rothberg, MD, associate professor of internal medicine and of nutritional sciences at the University of Michigan, Ann Arbor, in an interview.
“This study dispels the myth that incorporating a small portion of potato into the diet (although these are not potatoes that are fried, or are topped with cheese, bacon, sour cream, etc.) results in deleterious metabolic outcomes when compared to a diet that is comprised of beans (pulses) as part of a low energy–dense diet,” she explained.
“The diet in both groups was of low energy density, which has been shown to result in fewer calories consumed, weight loss, and improvement in insulin resistance,” so the similarity in results was not so surprising, said Dr. Rothberg.
For the clinical takeaway, Dr. Rothberg agreed with the study authors: “Clinicians may counsel their patients that they can still consume a small potato (with the caveat above regarding cooking methods and toppings) as part of a balanced meal so long as they are keeping their overall calories low and not exceeding their metabolic requirements based on body weight/BMI,” she said.
As for additional research, studies with a longer time frame and a larger and more diverse study population are needed, including populations with common insulin resistance comorbidities such as type 2 diabetes, fatty liver disease, and cardiovascular disease, Dr. Rothberg noted.
Consumer considerations, with caveats
The key message for consumers is that, “based on this very small study of short duration, consuming a small portion of potato as part of an overall balanced, low-energy diet did not produce adverse effects on glucose or insulin when compared to a diet of pulses known to have favorable effects on glucose and insulin,” Dr. Rothberg told this news organization. However, “consumers should note that, although the results from this small study are encouraging, it would be premature to extrapolate the findings from this study to other populations,” she said. Also, keep in mind that the study was supported in part by the Alliance for Potato Research, although the authors stated that none of the funders (Alliance for Potato Research and Education and the National Institutes of Health) had any role in the design, analysis, or writing of the article, she added.
The study was supported in part by the Alliance for Potato Research and Education and the National Institutes of Health, which funds the Louisiana Clinical and Translational Science Center. The researchers and Dr. Rothberg had no financial conflicts to disclose.
Low energy–density diets that are based either on potatoes or beans similarly reduced insulin resistance in adults with poor blood glucose control, according to a controlled feeding study in 36 individuals.
Potatoes have gotten a bad rap for their high glycemic index, but they have little fat and a low energy density, wrote the study investigators. In fact, “cooling of gelatinized potatoes generates appreciable levels of slowly digested starch (resistant starch type 3) and substantially lowers the blood glucose response that potatoes elicit.”
“There is a view that potatoes are a less healthy plant food, but there is very little empirical data from randomized trials to support this view,” senior investigator John P. Kirwan, PhD, said in an interview.
Dry beans and peas (known as pulses) also contain resistant starch that improves insulin sensitivity and glucose tolerance, and multiple studies support pulses as part of a low-glycemic diet to improve glucose control in adults, the researchers explained, but because the density of food often guides how much people eat, they hypothesized that potatoes could substitute for beans and provide similar glucose control benefits.
In a study published in the Journal of Medicinal Food, the researchers randomized 36 adults aged 18-60 years with insulin resistance to 8 weeks of a low energy–density diet (1 kcal/g) high in either potatoes or beans. The baseline body mass index ranged from 25 to 40 kg/m2. Insulin resistance was defined using the homeostatic model assessment of insulin resistance (HOMA-IR) with a score greater than 2.
The controlled diet consisted of 50%-55% carbohydrates, 30%-35% fats, and 15%-20% protein. Each meal in the potato group included a side of potatoes, and each meal in the bean group included a side of beans.
The primary outcome was the mean change in blood glucose concentration; the researchers also assessed weight loss.
A total of 14 individuals in the potato group and 17 in the bean group completed the study; but data from the 18 individuals in each group were included in an intent-to-treat analysis.
Among study completers, HOMA-IR in the bean group showed an average decrease of 1.4 from baseline (P = .02 ); a similar decrease of 1.3 occurred in the potato group (P < .05) with no significant difference between the two diets.
Overall compliance with both diets was roughly 88%. Body weight reductions were similar in both groups and significantly reduced from baseline over the study period, with average reductions in intent-to-treat analysis of 5.82 kg in the potato group and 4.0 kg in the bean group. BMI also was significantly reduced from baseline in both potato and bean groups (2.04 kg/m2 and 1.35 kg/m2, respectively). Although baseline differences were not significant, “BMI at baseline was higher and the reduction in response to the treatment was significantly greater in the potato diet compared with the bean diet,” the researchers noted. The effect on blood glucose response was not significantly different between the two groups or from baseline, they said.
The findings were limited by several factors including the small size, relatively short study period, and controlled nature of the study diet, the researchers noted. “The addition of a typical Western diet would have enhanced our understanding of the effect of low energy–dense diets on metabolic outcomes,” they noted in their discussion.
However, both diets led to a reduction in body weight, and the low energy density of both potato and bean diets promoted weight loss without affecting appetite or requiring calorie restriction, the researchers explained. Therefore, “this weight loss if sustained over time could have a substantial impact on body weight,” they said.
“We hypothesized that there would be equivalence between the potato and bean diet and this hypothesis proved to be correct,” said Dr. Kirwan, of the Pennington Biomedical Research Center, Baton Rouge, La., in an interview.
The take-home message for clinicians is that, though small, the study was very well-controlled, Dr. Kirwan emphasized. “Clinicians ought to consider the health benefits of the potato when it is cooked and served appropriately.”
Looking ahead, larger randomized controlled trials with additional control arms, longer time of at least 12 weeks, and different patient populations are needed, Dr. Kirwan added.
Findings mitigate food myths
The debate continues about whether there are foods that are “good” or “evil;” or foods that one “should not eat” or “should eat,” said Amy Rothberg, MD, associate professor of internal medicine and of nutritional sciences at the University of Michigan, Ann Arbor, in an interview.
“This study dispels the myth that incorporating a small portion of potato into the diet (although these are not potatoes that are fried, or are topped with cheese, bacon, sour cream, etc.) results in deleterious metabolic outcomes when compared to a diet that is comprised of beans (pulses) as part of a low energy–dense diet,” she explained.
“The diet in both groups was of low energy density, which has been shown to result in fewer calories consumed, weight loss, and improvement in insulin resistance,” so the similarity in results was not so surprising, said Dr. Rothberg.
For the clinical takeaway, Dr. Rothberg agreed with the study authors: “Clinicians may counsel their patients that they can still consume a small potato (with the caveat above regarding cooking methods and toppings) as part of a balanced meal so long as they are keeping their overall calories low and not exceeding their metabolic requirements based on body weight/BMI,” she said.
As for additional research, studies with a longer time frame and a larger and more diverse study population are needed, including populations with common insulin resistance comorbidities such as type 2 diabetes, fatty liver disease, and cardiovascular disease, Dr. Rothberg noted.
Consumer considerations, with caveats
The key message for consumers is that, “based on this very small study of short duration, consuming a small portion of potato as part of an overall balanced, low-energy diet did not produce adverse effects on glucose or insulin when compared to a diet of pulses known to have favorable effects on glucose and insulin,” Dr. Rothberg told this news organization. However, “consumers should note that, although the results from this small study are encouraging, it would be premature to extrapolate the findings from this study to other populations,” she said. Also, keep in mind that the study was supported in part by the Alliance for Potato Research, although the authors stated that none of the funders (Alliance for Potato Research and Education and the National Institutes of Health) had any role in the design, analysis, or writing of the article, she added.
The study was supported in part by the Alliance for Potato Research and Education and the National Institutes of Health, which funds the Louisiana Clinical and Translational Science Center. The researchers and Dr. Rothberg had no financial conflicts to disclose.
FROM THE JOURNAL OF MEDICINAL FOOD
What is the genetic influence on the severity of COVID-19?
A striking characteristic of COVID-19 is that the severity of clinical outcomes is remarkably variable. Establishing a prognosis for individuals infected with COVID-19 remains a challenge.
Since the start of the COVID-19 pandemic, the heterogeneity of individuals who progress toward severe disease or death, along with the fact that individuals directly exposed to the virus do not necessarily become sick, supports the hypothesis that genetic risk or protective factors are at play.
In an interview with this news organization, Mayana Zatz, PhD, head professor of genetics and coordinator of the Human Genome and Stem Cell Study Center at the University of São Paulo, explained: “The first case that caught my eye was the case of my neighbors, a couple. He presented COVID-19 symptoms, but his wife, who took care of him, had absolutely no symptoms. I thought that it was strange, but we received 3,000 emails from people saying, ‘This happened to me, too.’”
Reports in the media about seven pairs of monozygotic (MZ) twins who died from COVID-19 within days of one another in Brazil also stood out, said the researcher.
, as well as their pathology. Dr. Zatz’s team analyzed the case of a 31-year-old Brazilian MZ twin brother pair who presented simultaneously with severe COVID-19 and the need for oxygen support, despite their age and good health conditions. Curiously, they were admitted and intubated on the same day, but neither of the twins knew about the other’s situation; they found out only when they were extubated.
The study was carried out at the USP with the collaboration of the State University of São Paulo. The authors mapped the genetic profile (by sequencing the genome responsible for coding proteins, or whole-exome sequencing) and the immune cell profile to evaluate innate and adaptive immunity.
The MZ twin brothers shared the same two rare genetic mutations, which may be associated with their increased risk of developing severe COVID-19. However, since these variants were not studied at the protein or functional level, their pathogenicity has yet to be determined. The twins also had [human leukocyte antigen (HLA)] alleles associated with severe COVID-19, which are important candidates for the mechanisms of innate and adaptive immunity and susceptibility to COVID-19 infection and manifestation.
But one particular oddity stood out to the researchers: One of the brothers required longer hospitalization, and only he reported symptoms of long COVID.
In the authors’ eyes, even though the patients shared genetic mutations potentially associated with the risk of developing severe COVID-19, the differences in clinical progression emphasize that, beyond genetic risk factors, continuous exposure to pathogens over a lifetime and other environmental factors mean that each individual’s immune response is unique, even in twins.
“There is no doubt that genetics contribute to the severity of COVID-19, and environmental factors sometimes give us the opportunity to study the disease, too. Such [is the case with] MZ twins who have genetic similarities, even with changes that take place over a lifetime,” José Eduardo Krieger, MD, PhD, professor of molecular medicine at the University of São Paulo Medical School (FMUSP), told this news organization. “Examining MZ twins is a strategy that may help, but, with n = 2, luck really needs to be on your side to get straight to the problem. You need to combine [these findings] with other studies to solve this conundrum,” said Dr. Krieger, who did not take part in the research.
Large cohorts
Genomic and computer resources allow for the study of large sets of data from thousands of individuals. In each of those sets of data, the signal offered by thousands of markers distributed throughout the genome can be studied. This is the possibility offered by various genomic studies of large cohorts of patients with different clinical manifestations.
“Researchers examine thousands of genetic variants throughout the genome from a large sample of individuals and have the chance, for example, to identify genetic variants that are more prevalent in patients who have presented with severe disease than in those who presented with milder disease,” said Dr. Krieger. “These associations highlight a chromosome region in which one or more genes explain, at least in part, the differences observed.”
Genomewide association studies have identified some genetic variants that indicate severity of COVID-19, with potential impact on the virus entering the cell, the immune response, or the development of cytokine storms.
One of these studies, COVID-19 Host Genetics Initiative (COVID-19 HGI), is an international, open-science collaboration for sharing scientific methods and resources with research groups across the world, with the goal of robustly mapping the host genetic determinants of SARS-CoV-2 infection and the severity of the resulting COVID-19 disease. At the start of 2021, the COVID-19 HGI combined genetic data from 49,562 cases and 2 million controls from 46 studies in 19 countries. A total of 853 samples from the BRACOVID study were included in the meta-analysis. The endeavor enabled the identification of 13 genomewide significant loci that are associated with SARS-CoV-2 infection or severe manifestations of COVID-19.
The BRACOVID study, in which Dr. Krieger participates, aims to identify host genetic factors that determine the severity of COVID-19. It is currently the largest project of its kind in Latin America. An article provides the analysis of the first 5,233 participants in the BRACOVID study, who were recruited in São Paulo. Of these participants, 3,533 had been infected with COVID-19 and hospitalized at either the Heart Institute or the Central Institute of the FMUSP General Hospital. The remaining 1,700 made up the control group, which included health care professionals and members of the general population. The controls were recruited through serology assays or PCR tests for SARS-CoV-2.
The researchers discovered a region of chromosome 1 that could play a role in modulating immune response and that could lead to an increase in the likelihood of hospitalization across a wide range of COVID-19 risk factors. This region of chromosome 1 was observed only in Brazilians with a strong European ancestry; however, this finding had not been mentioned in previous studies, suggesting that it could harbor a risk allele specific to the Brazilian population.
The study also confirmed most, but not all, of the regions recorded in the literature, which may be significant in identifying factors determining severity that are specific to a given population.
Including information from the BRACOVID study, other studies have enhanced the knowledge on affected organs. Combined data from 14,000 patients from nine countries evaluated a region of a single chromosome and found that carriers of a certain allele had a higher probability of experiencing various COVID-19 complications, such as severe respiratory failure, venous thromboembolism, and liver damage. The risk was even higher for individuals aged 60 years and over.
Discordant couples
Smaller sample sizes of underrepresented populations also provide relevant data for genomic studies. Dr. Zatz’s team carried out genomic studies on smaller groups, comparing serodiscordant couples (where one was infected and symptomatic while the partner remained asymptomatic and seronegative despite sharing the same bedroom during the infection). Their research found genetic variants related to immune response that were associated with susceptibility to infection and progression to severe COVID-19.
The team also went on to study a group of patients older than 90 years who recovered from COVID-19 with mild symptoms or who remained asymptomatic following a positive test for SARS-CoV-2. They compared these patients with a sample of elderly patients from the same city (São Paulo), sampled before the current pandemic. The researchers identified a genetic variant related to mucin production. “In individuals with mild COVID-19, the degradation of these mucins would be more efficient,” said Dr. Zatz. It is possible for this variant to interfere not only with the production of mucus, but also in its composition, as there is an exchange of amino acids in the protein.
“We continued the study by comparing the extremes, i.e., those in their 90s with mild COVID-19 and younger patients with severe COVID-19, including several who died,” said Dr. Zatz.
More personalized medicine
The specialists agreed that a genetic test to predict COVID-19 severity is still a long way away. The genetic component is too little understood to enable the evaluation of individual risk. It has been possible to identify several important areas but, as Dr. Krieger pointed out, a variant identified in a certain chromosome interval may not be just one gene. There may be various candidate genes, or there may be a regulatory sequence for a distant gene. Furthermore, there are regions with genes that make sense as moderators of COVID-19 severity, because they regulate an inflammatory or immunologic reaction, but evidence is still lacking.
Reaching the molecular mechanism would, in future, allow a medicine to be chosen for a given patient, as already happens with other diseases. It also could enable the discovery of new medicines following as-yet-unexplored lines of research. Dr. Zatz also considers the possibility of genetic therapy.
Even with the knowledge of human genetics, one part of the equation is missing: viral genetics. “Many of the individuals who were resistant to the Delta variant were later affected by Omicron,” she pointed out.
Significance of Brazil
“We have an infinite amount of genomic data worldwide, but the vast majority originates from White Americans of European origin,” said Dr. Krieger. Moreover, genomic associations of COVID-19 severity discovered in the Chinese population were not significant in the European population. Besides underscoring the importance of collaborating with international studies, this situation supports scientists’ interest in carrying out genetic studies within Brazil, he added.
“In the genomic study of the Brazilian population, we found 2 million variants that were not present in the European populations,” said Dr. Zatz.
Dr. Krieger mentioned a technical advantage that Brazil has. “Having been colonized by different ethnic groups and mixed many generations ago, Brazil has a population with a unique genetic structure; the recombinations are different. When preparing the samples, the regions break differently.” This factor could help to separate, in a candidate region, the gene that is significant from those that might not be.
In general, severe COVID-19 would be a complex phenomenon involving several genes and interactions with environmental factors. The Brazilian studies tried to find a factor that was unique to Brazil, but the significance of the differences remained unclear. “We found some signs that were specific to our population,” concluded Dr. Krieger. “But the reason that more people in Brazil died as a result of COVID-19 was not genetic,” he added.
Dr. Zatz and Dr. Krieger reported no conflicts of interest. This article was translated from the Medscape Portuguese edition.
A version of this article first appeared on Medscape.com.
A striking characteristic of COVID-19 is that the severity of clinical outcomes is remarkably variable. Establishing a prognosis for individuals infected with COVID-19 remains a challenge.
Since the start of the COVID-19 pandemic, the heterogeneity of individuals who progress toward severe disease or death, along with the fact that individuals directly exposed to the virus do not necessarily become sick, supports the hypothesis that genetic risk or protective factors are at play.
In an interview with this news organization, Mayana Zatz, PhD, head professor of genetics and coordinator of the Human Genome and Stem Cell Study Center at the University of São Paulo, explained: “The first case that caught my eye was the case of my neighbors, a couple. He presented COVID-19 symptoms, but his wife, who took care of him, had absolutely no symptoms. I thought that it was strange, but we received 3,000 emails from people saying, ‘This happened to me, too.’”
Reports in the media about seven pairs of monozygotic (MZ) twins who died from COVID-19 within days of one another in Brazil also stood out, said the researcher.
, as well as their pathology. Dr. Zatz’s team analyzed the case of a 31-year-old Brazilian MZ twin brother pair who presented simultaneously with severe COVID-19 and the need for oxygen support, despite their age and good health conditions. Curiously, they were admitted and intubated on the same day, but neither of the twins knew about the other’s situation; they found out only when they were extubated.
The study was carried out at the USP with the collaboration of the State University of São Paulo. The authors mapped the genetic profile (by sequencing the genome responsible for coding proteins, or whole-exome sequencing) and the immune cell profile to evaluate innate and adaptive immunity.
The MZ twin brothers shared the same two rare genetic mutations, which may be associated with their increased risk of developing severe COVID-19. However, since these variants were not studied at the protein or functional level, their pathogenicity has yet to be determined. The twins also had [human leukocyte antigen (HLA)] alleles associated with severe COVID-19, which are important candidates for the mechanisms of innate and adaptive immunity and susceptibility to COVID-19 infection and manifestation.
But one particular oddity stood out to the researchers: One of the brothers required longer hospitalization, and only he reported symptoms of long COVID.
In the authors’ eyes, even though the patients shared genetic mutations potentially associated with the risk of developing severe COVID-19, the differences in clinical progression emphasize that, beyond genetic risk factors, continuous exposure to pathogens over a lifetime and other environmental factors mean that each individual’s immune response is unique, even in twins.
“There is no doubt that genetics contribute to the severity of COVID-19, and environmental factors sometimes give us the opportunity to study the disease, too. Such [is the case with] MZ twins who have genetic similarities, even with changes that take place over a lifetime,” José Eduardo Krieger, MD, PhD, professor of molecular medicine at the University of São Paulo Medical School (FMUSP), told this news organization. “Examining MZ twins is a strategy that may help, but, with n = 2, luck really needs to be on your side to get straight to the problem. You need to combine [these findings] with other studies to solve this conundrum,” said Dr. Krieger, who did not take part in the research.
Large cohorts
Genomic and computer resources allow for the study of large sets of data from thousands of individuals. In each of those sets of data, the signal offered by thousands of markers distributed throughout the genome can be studied. This is the possibility offered by various genomic studies of large cohorts of patients with different clinical manifestations.
“Researchers examine thousands of genetic variants throughout the genome from a large sample of individuals and have the chance, for example, to identify genetic variants that are more prevalent in patients who have presented with severe disease than in those who presented with milder disease,” said Dr. Krieger. “These associations highlight a chromosome region in which one or more genes explain, at least in part, the differences observed.”
Genomewide association studies have identified some genetic variants that indicate severity of COVID-19, with potential impact on the virus entering the cell, the immune response, or the development of cytokine storms.
One of these studies, COVID-19 Host Genetics Initiative (COVID-19 HGI), is an international, open-science collaboration for sharing scientific methods and resources with research groups across the world, with the goal of robustly mapping the host genetic determinants of SARS-CoV-2 infection and the severity of the resulting COVID-19 disease. At the start of 2021, the COVID-19 HGI combined genetic data from 49,562 cases and 2 million controls from 46 studies in 19 countries. A total of 853 samples from the BRACOVID study were included in the meta-analysis. The endeavor enabled the identification of 13 genomewide significant loci that are associated with SARS-CoV-2 infection or severe manifestations of COVID-19.
The BRACOVID study, in which Dr. Krieger participates, aims to identify host genetic factors that determine the severity of COVID-19. It is currently the largest project of its kind in Latin America. An article provides the analysis of the first 5,233 participants in the BRACOVID study, who were recruited in São Paulo. Of these participants, 3,533 had been infected with COVID-19 and hospitalized at either the Heart Institute or the Central Institute of the FMUSP General Hospital. The remaining 1,700 made up the control group, which included health care professionals and members of the general population. The controls were recruited through serology assays or PCR tests for SARS-CoV-2.
The researchers discovered a region of chromosome 1 that could play a role in modulating immune response and that could lead to an increase in the likelihood of hospitalization across a wide range of COVID-19 risk factors. This region of chromosome 1 was observed only in Brazilians with a strong European ancestry; however, this finding had not been mentioned in previous studies, suggesting that it could harbor a risk allele specific to the Brazilian population.
The study also confirmed most, but not all, of the regions recorded in the literature, which may be significant in identifying factors determining severity that are specific to a given population.
Including information from the BRACOVID study, other studies have enhanced the knowledge on affected organs. Combined data from 14,000 patients from nine countries evaluated a region of a single chromosome and found that carriers of a certain allele had a higher probability of experiencing various COVID-19 complications, such as severe respiratory failure, venous thromboembolism, and liver damage. The risk was even higher for individuals aged 60 years and over.
Discordant couples
Smaller sample sizes of underrepresented populations also provide relevant data for genomic studies. Dr. Zatz’s team carried out genomic studies on smaller groups, comparing serodiscordant couples (where one was infected and symptomatic while the partner remained asymptomatic and seronegative despite sharing the same bedroom during the infection). Their research found genetic variants related to immune response that were associated with susceptibility to infection and progression to severe COVID-19.
The team also went on to study a group of patients older than 90 years who recovered from COVID-19 with mild symptoms or who remained asymptomatic following a positive test for SARS-CoV-2. They compared these patients with a sample of elderly patients from the same city (São Paulo), sampled before the current pandemic. The researchers identified a genetic variant related to mucin production. “In individuals with mild COVID-19, the degradation of these mucins would be more efficient,” said Dr. Zatz. It is possible for this variant to interfere not only with the production of mucus, but also in its composition, as there is an exchange of amino acids in the protein.
“We continued the study by comparing the extremes, i.e., those in their 90s with mild COVID-19 and younger patients with severe COVID-19, including several who died,” said Dr. Zatz.
More personalized medicine
The specialists agreed that a genetic test to predict COVID-19 severity is still a long way away. The genetic component is too little understood to enable the evaluation of individual risk. It has been possible to identify several important areas but, as Dr. Krieger pointed out, a variant identified in a certain chromosome interval may not be just one gene. There may be various candidate genes, or there may be a regulatory sequence for a distant gene. Furthermore, there are regions with genes that make sense as moderators of COVID-19 severity, because they regulate an inflammatory or immunologic reaction, but evidence is still lacking.
Reaching the molecular mechanism would, in future, allow a medicine to be chosen for a given patient, as already happens with other diseases. It also could enable the discovery of new medicines following as-yet-unexplored lines of research. Dr. Zatz also considers the possibility of genetic therapy.
Even with the knowledge of human genetics, one part of the equation is missing: viral genetics. “Many of the individuals who were resistant to the Delta variant were later affected by Omicron,” she pointed out.
Significance of Brazil
“We have an infinite amount of genomic data worldwide, but the vast majority originates from White Americans of European origin,” said Dr. Krieger. Moreover, genomic associations of COVID-19 severity discovered in the Chinese population were not significant in the European population. Besides underscoring the importance of collaborating with international studies, this situation supports scientists’ interest in carrying out genetic studies within Brazil, he added.
“In the genomic study of the Brazilian population, we found 2 million variants that were not present in the European populations,” said Dr. Zatz.
Dr. Krieger mentioned a technical advantage that Brazil has. “Having been colonized by different ethnic groups and mixed many generations ago, Brazil has a population with a unique genetic structure; the recombinations are different. When preparing the samples, the regions break differently.” This factor could help to separate, in a candidate region, the gene that is significant from those that might not be.
In general, severe COVID-19 would be a complex phenomenon involving several genes and interactions with environmental factors. The Brazilian studies tried to find a factor that was unique to Brazil, but the significance of the differences remained unclear. “We found some signs that were specific to our population,” concluded Dr. Krieger. “But the reason that more people in Brazil died as a result of COVID-19 was not genetic,” he added.
Dr. Zatz and Dr. Krieger reported no conflicts of interest. This article was translated from the Medscape Portuguese edition.
A version of this article first appeared on Medscape.com.
A striking characteristic of COVID-19 is that the severity of clinical outcomes is remarkably variable. Establishing a prognosis for individuals infected with COVID-19 remains a challenge.
Since the start of the COVID-19 pandemic, the heterogeneity of individuals who progress toward severe disease or death, along with the fact that individuals directly exposed to the virus do not necessarily become sick, supports the hypothesis that genetic risk or protective factors are at play.
In an interview with this news organization, Mayana Zatz, PhD, head professor of genetics and coordinator of the Human Genome and Stem Cell Study Center at the University of São Paulo, explained: “The first case that caught my eye was the case of my neighbors, a couple. He presented COVID-19 symptoms, but his wife, who took care of him, had absolutely no symptoms. I thought that it was strange, but we received 3,000 emails from people saying, ‘This happened to me, too.’”
Reports in the media about seven pairs of monozygotic (MZ) twins who died from COVID-19 within days of one another in Brazil also stood out, said the researcher.
, as well as their pathology. Dr. Zatz’s team analyzed the case of a 31-year-old Brazilian MZ twin brother pair who presented simultaneously with severe COVID-19 and the need for oxygen support, despite their age and good health conditions. Curiously, they were admitted and intubated on the same day, but neither of the twins knew about the other’s situation; they found out only when they were extubated.
The study was carried out at the USP with the collaboration of the State University of São Paulo. The authors mapped the genetic profile (by sequencing the genome responsible for coding proteins, or whole-exome sequencing) and the immune cell profile to evaluate innate and adaptive immunity.
The MZ twin brothers shared the same two rare genetic mutations, which may be associated with their increased risk of developing severe COVID-19. However, since these variants were not studied at the protein or functional level, their pathogenicity has yet to be determined. The twins also had [human leukocyte antigen (HLA)] alleles associated with severe COVID-19, which are important candidates for the mechanisms of innate and adaptive immunity and susceptibility to COVID-19 infection and manifestation.
But one particular oddity stood out to the researchers: One of the brothers required longer hospitalization, and only he reported symptoms of long COVID.
In the authors’ eyes, even though the patients shared genetic mutations potentially associated with the risk of developing severe COVID-19, the differences in clinical progression emphasize that, beyond genetic risk factors, continuous exposure to pathogens over a lifetime and other environmental factors mean that each individual’s immune response is unique, even in twins.
“There is no doubt that genetics contribute to the severity of COVID-19, and environmental factors sometimes give us the opportunity to study the disease, too. Such [is the case with] MZ twins who have genetic similarities, even with changes that take place over a lifetime,” José Eduardo Krieger, MD, PhD, professor of molecular medicine at the University of São Paulo Medical School (FMUSP), told this news organization. “Examining MZ twins is a strategy that may help, but, with n = 2, luck really needs to be on your side to get straight to the problem. You need to combine [these findings] with other studies to solve this conundrum,” said Dr. Krieger, who did not take part in the research.
Large cohorts
Genomic and computer resources allow for the study of large sets of data from thousands of individuals. In each of those sets of data, the signal offered by thousands of markers distributed throughout the genome can be studied. This is the possibility offered by various genomic studies of large cohorts of patients with different clinical manifestations.
“Researchers examine thousands of genetic variants throughout the genome from a large sample of individuals and have the chance, for example, to identify genetic variants that are more prevalent in patients who have presented with severe disease than in those who presented with milder disease,” said Dr. Krieger. “These associations highlight a chromosome region in which one or more genes explain, at least in part, the differences observed.”
Genomewide association studies have identified some genetic variants that indicate severity of COVID-19, with potential impact on the virus entering the cell, the immune response, or the development of cytokine storms.
One of these studies, COVID-19 Host Genetics Initiative (COVID-19 HGI), is an international, open-science collaboration for sharing scientific methods and resources with research groups across the world, with the goal of robustly mapping the host genetic determinants of SARS-CoV-2 infection and the severity of the resulting COVID-19 disease. At the start of 2021, the COVID-19 HGI combined genetic data from 49,562 cases and 2 million controls from 46 studies in 19 countries. A total of 853 samples from the BRACOVID study were included in the meta-analysis. The endeavor enabled the identification of 13 genomewide significant loci that are associated with SARS-CoV-2 infection or severe manifestations of COVID-19.
The BRACOVID study, in which Dr. Krieger participates, aims to identify host genetic factors that determine the severity of COVID-19. It is currently the largest project of its kind in Latin America. An article provides the analysis of the first 5,233 participants in the BRACOVID study, who were recruited in São Paulo. Of these participants, 3,533 had been infected with COVID-19 and hospitalized at either the Heart Institute or the Central Institute of the FMUSP General Hospital. The remaining 1,700 made up the control group, which included health care professionals and members of the general population. The controls were recruited through serology assays or PCR tests for SARS-CoV-2.
The researchers discovered a region of chromosome 1 that could play a role in modulating immune response and that could lead to an increase in the likelihood of hospitalization across a wide range of COVID-19 risk factors. This region of chromosome 1 was observed only in Brazilians with a strong European ancestry; however, this finding had not been mentioned in previous studies, suggesting that it could harbor a risk allele specific to the Brazilian population.
The study also confirmed most, but not all, of the regions recorded in the literature, which may be significant in identifying factors determining severity that are specific to a given population.
Including information from the BRACOVID study, other studies have enhanced the knowledge on affected organs. Combined data from 14,000 patients from nine countries evaluated a region of a single chromosome and found that carriers of a certain allele had a higher probability of experiencing various COVID-19 complications, such as severe respiratory failure, venous thromboembolism, and liver damage. The risk was even higher for individuals aged 60 years and over.
Discordant couples
Smaller sample sizes of underrepresented populations also provide relevant data for genomic studies. Dr. Zatz’s team carried out genomic studies on smaller groups, comparing serodiscordant couples (where one was infected and symptomatic while the partner remained asymptomatic and seronegative despite sharing the same bedroom during the infection). Their research found genetic variants related to immune response that were associated with susceptibility to infection and progression to severe COVID-19.
The team also went on to study a group of patients older than 90 years who recovered from COVID-19 with mild symptoms or who remained asymptomatic following a positive test for SARS-CoV-2. They compared these patients with a sample of elderly patients from the same city (São Paulo), sampled before the current pandemic. The researchers identified a genetic variant related to mucin production. “In individuals with mild COVID-19, the degradation of these mucins would be more efficient,” said Dr. Zatz. It is possible for this variant to interfere not only with the production of mucus, but also in its composition, as there is an exchange of amino acids in the protein.
“We continued the study by comparing the extremes, i.e., those in their 90s with mild COVID-19 and younger patients with severe COVID-19, including several who died,” said Dr. Zatz.
More personalized medicine
The specialists agreed that a genetic test to predict COVID-19 severity is still a long way away. The genetic component is too little understood to enable the evaluation of individual risk. It has been possible to identify several important areas but, as Dr. Krieger pointed out, a variant identified in a certain chromosome interval may not be just one gene. There may be various candidate genes, or there may be a regulatory sequence for a distant gene. Furthermore, there are regions with genes that make sense as moderators of COVID-19 severity, because they regulate an inflammatory or immunologic reaction, but evidence is still lacking.
Reaching the molecular mechanism would, in future, allow a medicine to be chosen for a given patient, as already happens with other diseases. It also could enable the discovery of new medicines following as-yet-unexplored lines of research. Dr. Zatz also considers the possibility of genetic therapy.
Even with the knowledge of human genetics, one part of the equation is missing: viral genetics. “Many of the individuals who were resistant to the Delta variant were later affected by Omicron,” she pointed out.
Significance of Brazil
“We have an infinite amount of genomic data worldwide, but the vast majority originates from White Americans of European origin,” said Dr. Krieger. Moreover, genomic associations of COVID-19 severity discovered in the Chinese population were not significant in the European population. Besides underscoring the importance of collaborating with international studies, this situation supports scientists’ interest in carrying out genetic studies within Brazil, he added.
“In the genomic study of the Brazilian population, we found 2 million variants that were not present in the European populations,” said Dr. Zatz.
Dr. Krieger mentioned a technical advantage that Brazil has. “Having been colonized by different ethnic groups and mixed many generations ago, Brazil has a population with a unique genetic structure; the recombinations are different. When preparing the samples, the regions break differently.” This factor could help to separate, in a candidate region, the gene that is significant from those that might not be.
In general, severe COVID-19 would be a complex phenomenon involving several genes and interactions with environmental factors. The Brazilian studies tried to find a factor that was unique to Brazil, but the significance of the differences remained unclear. “We found some signs that were specific to our population,” concluded Dr. Krieger. “But the reason that more people in Brazil died as a result of COVID-19 was not genetic,” he added.
Dr. Zatz and Dr. Krieger reported no conflicts of interest. This article was translated from the Medscape Portuguese edition.
A version of this article first appeared on Medscape.com.
Lp(a) tied to more early CV events than familial hypercholesterolemia
Many more people are at risk for early cardiovascular events because of raised lipoprotein(a) levels than from having familial hypercholesterolemia (FH), a new study suggests.
The Danish study set out to try and establish a level of Lp(a) that would be associated with a cardiovascular risk similar to that seen with FH. As there are many different definitions of FH, results showed a large range of Lp(a) values that corresponded to risk levels of the different FH definitions.
However, if considering one of the broadest FH definitions (from MEDPED – Make Early Diagnoses, Prevent Early Deaths), which is the one most commonly used in the United States, results showed that the level of cardiovascular risk in patients with this definition of FH is similar to that associated with Lp(a) levels of around 70 mg/dL (0.7 g/L).
“While FH is fairly unusual, occurring in less than 1% of the population, levels of Lp(a) of 70 mg/dL or above are much more common, occurring in around 10% of the White population,” Børge Nordestgaard, MD, Copenhagen University Hospital, said in an interview. Around 20% of the Black population have such high levels, while levels in Hispanics are in between.
“Our results suggest that there will be many more individuals at risk of premature MI or cardiovascular death because of raised Lp(a) levels than because of FH,” added Dr. Nordestgaard, the senior author of the current study.
Dr. Nordestgaard explained that FH is well established to be a serious condition. “We consider FH to be the genetic disease that causes the most cases of early heart disease and early death worldwide.”
“But we know now that raised levels of Lp(a), which is also genetically determined, can also lead to an increased risk of cardiovascular events relatively early in life, and when you look into the numbers, it seems like high levels of Lp(a) could be more common than FH. We wanted to try and find the levels of Lp(a) that corresponded to similar cardiovascular risk as FH.”
The Danish study was published in the Journal of the American College of Cardiology.
The authors note that the 2019 joint European Society of Cardiology and European Atherosclerosis Society guidelines suggested that an Lp(a) level greater than 180 mg/dL (0.8 g/L) may confer a lifetime risk for heart disease equivalent to the risk associated with heterozygous FH, but they point out that this value was speculative and not based on a direct comparison of risk associated with the two conditions in the same population.
For their study, Dr. Nordestgaard and colleagues analyzed information from a large database of the Danish population, the Copenhagen General Population Study, including 69,644 individuals for whom data on FH and Lp(a) levels were available. As these conditions are genetically determined, and the study held records on individuals going back several decades, the researchers were able to analyze event rates over a median follow up time of 42 years. During this time, there were 4,166 cases of myocardial infarction and 11,464 cases of atherosclerotic cardiovascular disease (ASCVD).
Results showed that Lp(a) levels associated with MI risk equivalent to that of clinical FH ranged from 67 to 402 mg/dL depending on the definition used for FH. The Lp(a) level corresponding to the MI risk of genetically determined FH was 180 mg/dL.
In terms of risk of ASCVD events, the levels of Lp(a) corresponding to the risk associated with clinical FH ranged from 130 to 391 mg/dL, and the Lp(a) level corresponding to the ASCVD risk of genetically determined FH was 175 mg/dL.
“All these different definitions of FH may cause some confusion, but basically we are saying that if an individual is found to have an Lp(a) above 70 mg/dL, then they have a similar level of cardiovascular risk as that associated with the broadest definition of FH, and they should be taken as seriously as a patient diagnosed with FH,” Dr. Nordestgaard said.
He estimated that these individuals have approximately a doubling of cardiovascular risk, compared with the general population, and risk increases further with rising Lp(a) levels.
The researchers also found that if an individual has both FH and raised Lp(a) they are at very high risk, as these two conditions are independent of each other.
Although a specific treatment for lowering Lp(a) levels is not yet available, Dr. Nordestgaard stresses that it is still worth identifying individuals with raised Lp(a) as efforts can be made to address other cardiovascular risk factors.
“We know raised Lp(a) increases cardiovascular risk, but there are also many other factors that likewise increase this risk, and they are all additive. So, it is very important that individuals with raised Lp(a) levels address these other risk factors,” he said. “These include stopping smoking, being at healthy weight, exercising regularly, eating a heart-healthy diet, and aggressive treatment of raised LDL, hypertension, and diabetes. All these things will lower their overall risk of cardiovascular disease.”
And there is the promise of new drugs to lower Lp(a) on the horizon, with several such products now in clinical development.
Dr. Nordestgaard also points out that as Lp(a) is genetically determined, cascade screening of close relatives of the individual with raised Lp(a) should also take place to detect others who may be at risk.
Although a level of Lp(a) of around 70 mg/dL confers similar cardiovascular risk than some definitions of FH, Dr. Nordestgaard says lower levels than this should also be a signal for concern.
“We usually say Lp(a) levels of 50 mg/dL are when we need to start to take this seriously. And it’s estimated that about 20% of the White population will have levels of 50 mg/dL or over and even more in the Black population,” he added.
‘Screen for both conditions’
In an accompanying editorial, Pamela Morris, MD, Medical University of South Carolina, Charleston; Jagat Narula, MD, Icahn School of Medicine, New York; and Sotirios Tsimikas, MD, University of California, San Diego, say “the weight of evidence strongly supports that both genetic lipid disorders, elevated Lp(a) levels and FH, are causally associated with an increased risk of premature ASCVD and should be carefully considered in risk assessment and management for ASCVD risk reduction.”

Dr. Morris told this news organization that the current study found a very large range of Lp(a) levels that conferred a similar cardiovascular risk to FH, because of the many different definitions of FH in use.
“But this should not take away the importance of screening for raised Lp(a) levels,” she stressed.
“We know that increased Lp(a) levels signal a high risk of cardiovascular disease. A diagnosis of FH is also a high-risk condition,” she said. “Both are important, and we need to screen for both, but it is difficult to directly compare the two conditions because the different definitions of FH get in the way.”
Dr. Morris agrees with Dr. Nordestgaard that raised levels of Lp(a) may actually be more important for the population risk of cardiovascular disease than FH, as the prevalence of increased Lp(a) levels is higher.
“Because raised Lp(a) levels are more prevalent than confirmed FH, the risk to the population is greater,” she said.
Dr. Morris points out that cardiovascular risk starts to increase at Lp(a) levels of 30 mg/dL (75 nmol/L).
The editorialists recommend that “in addition to performing a lipid panel periodically according to evidence-based guidelines, measurement of Lp(a) levels should also be performed at least once in an individual’s lifetime for ASCVD risk assessment.”
They conclude that “it is vital to continue to raise awareness among clinicians and patients of these high-risk genetic lipid disorders. Our understanding of both disorders is rapidly expanding, and promising novel therapeutics may offer hope for prevention of cardiovascular disease in patients with elevated Lp(a) levels in the future.”
This work was supported by Copenhagen University Hospital – Herlev Gentofte, Denmark, and the Danish Beckett-Foundation. The Copenhagen General Population Study is supported by the Copenhagen County Foundation and Copenhagen University Hospital – Herlev Gentofte. Dr. Nordestgaard has been a consultant and a speaker for AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Silence Therapeutics, Abbott, and Esperion.
A version of this article first appeared on Medscape.com.
Many more people are at risk for early cardiovascular events because of raised lipoprotein(a) levels than from having familial hypercholesterolemia (FH), a new study suggests.
The Danish study set out to try and establish a level of Lp(a) that would be associated with a cardiovascular risk similar to that seen with FH. As there are many different definitions of FH, results showed a large range of Lp(a) values that corresponded to risk levels of the different FH definitions.
However, if considering one of the broadest FH definitions (from MEDPED – Make Early Diagnoses, Prevent Early Deaths), which is the one most commonly used in the United States, results showed that the level of cardiovascular risk in patients with this definition of FH is similar to that associated with Lp(a) levels of around 70 mg/dL (0.7 g/L).
“While FH is fairly unusual, occurring in less than 1% of the population, levels of Lp(a) of 70 mg/dL or above are much more common, occurring in around 10% of the White population,” Børge Nordestgaard, MD, Copenhagen University Hospital, said in an interview. Around 20% of the Black population have such high levels, while levels in Hispanics are in between.
“Our results suggest that there will be many more individuals at risk of premature MI or cardiovascular death because of raised Lp(a) levels than because of FH,” added Dr. Nordestgaard, the senior author of the current study.
Dr. Nordestgaard explained that FH is well established to be a serious condition. “We consider FH to be the genetic disease that causes the most cases of early heart disease and early death worldwide.”
“But we know now that raised levels of Lp(a), which is also genetically determined, can also lead to an increased risk of cardiovascular events relatively early in life, and when you look into the numbers, it seems like high levels of Lp(a) could be more common than FH. We wanted to try and find the levels of Lp(a) that corresponded to similar cardiovascular risk as FH.”
The Danish study was published in the Journal of the American College of Cardiology.
The authors note that the 2019 joint European Society of Cardiology and European Atherosclerosis Society guidelines suggested that an Lp(a) level greater than 180 mg/dL (0.8 g/L) may confer a lifetime risk for heart disease equivalent to the risk associated with heterozygous FH, but they point out that this value was speculative and not based on a direct comparison of risk associated with the two conditions in the same population.
For their study, Dr. Nordestgaard and colleagues analyzed information from a large database of the Danish population, the Copenhagen General Population Study, including 69,644 individuals for whom data on FH and Lp(a) levels were available. As these conditions are genetically determined, and the study held records on individuals going back several decades, the researchers were able to analyze event rates over a median follow up time of 42 years. During this time, there were 4,166 cases of myocardial infarction and 11,464 cases of atherosclerotic cardiovascular disease (ASCVD).
Results showed that Lp(a) levels associated with MI risk equivalent to that of clinical FH ranged from 67 to 402 mg/dL depending on the definition used for FH. The Lp(a) level corresponding to the MI risk of genetically determined FH was 180 mg/dL.
In terms of risk of ASCVD events, the levels of Lp(a) corresponding to the risk associated with clinical FH ranged from 130 to 391 mg/dL, and the Lp(a) level corresponding to the ASCVD risk of genetically determined FH was 175 mg/dL.
“All these different definitions of FH may cause some confusion, but basically we are saying that if an individual is found to have an Lp(a) above 70 mg/dL, then they have a similar level of cardiovascular risk as that associated with the broadest definition of FH, and they should be taken as seriously as a patient diagnosed with FH,” Dr. Nordestgaard said.
He estimated that these individuals have approximately a doubling of cardiovascular risk, compared with the general population, and risk increases further with rising Lp(a) levels.
The researchers also found that if an individual has both FH and raised Lp(a) they are at very high risk, as these two conditions are independent of each other.
Although a specific treatment for lowering Lp(a) levels is not yet available, Dr. Nordestgaard stresses that it is still worth identifying individuals with raised Lp(a) as efforts can be made to address other cardiovascular risk factors.
“We know raised Lp(a) increases cardiovascular risk, but there are also many other factors that likewise increase this risk, and they are all additive. So, it is very important that individuals with raised Lp(a) levels address these other risk factors,” he said. “These include stopping smoking, being at healthy weight, exercising regularly, eating a heart-healthy diet, and aggressive treatment of raised LDL, hypertension, and diabetes. All these things will lower their overall risk of cardiovascular disease.”
And there is the promise of new drugs to lower Lp(a) on the horizon, with several such products now in clinical development.
Dr. Nordestgaard also points out that as Lp(a) is genetically determined, cascade screening of close relatives of the individual with raised Lp(a) should also take place to detect others who may be at risk.
Although a level of Lp(a) of around 70 mg/dL confers similar cardiovascular risk than some definitions of FH, Dr. Nordestgaard says lower levels than this should also be a signal for concern.
“We usually say Lp(a) levels of 50 mg/dL are when we need to start to take this seriously. And it’s estimated that about 20% of the White population will have levels of 50 mg/dL or over and even more in the Black population,” he added.
‘Screen for both conditions’
In an accompanying editorial, Pamela Morris, MD, Medical University of South Carolina, Charleston; Jagat Narula, MD, Icahn School of Medicine, New York; and Sotirios Tsimikas, MD, University of California, San Diego, say “the weight of evidence strongly supports that both genetic lipid disorders, elevated Lp(a) levels and FH, are causally associated with an increased risk of premature ASCVD and should be carefully considered in risk assessment and management for ASCVD risk reduction.”
Dr. Morris told this news organization that the current study found a very large range of Lp(a) levels that conferred a similar cardiovascular risk to FH, because of the many different definitions of FH in use.
“But this should not take away the importance of screening for raised Lp(a) levels,” she stressed.
“We know that increased Lp(a) levels signal a high risk of cardiovascular disease. A diagnosis of FH is also a high-risk condition,” she said. “Both are important, and we need to screen for both, but it is difficult to directly compare the two conditions because the different definitions of FH get in the way.”
Dr. Morris agrees with Dr. Nordestgaard that raised levels of Lp(a) may actually be more important for the population risk of cardiovascular disease than FH, as the prevalence of increased Lp(a) levels is higher.
“Because raised Lp(a) levels are more prevalent than confirmed FH, the risk to the population is greater,” she said.
Dr. Morris points out that cardiovascular risk starts to increase at Lp(a) levels of 30 mg/dL (75 nmol/L).
The editorialists recommend that “in addition to performing a lipid panel periodically according to evidence-based guidelines, measurement of Lp(a) levels should also be performed at least once in an individual’s lifetime for ASCVD risk assessment.”
They conclude that “it is vital to continue to raise awareness among clinicians and patients of these high-risk genetic lipid disorders. Our understanding of both disorders is rapidly expanding, and promising novel therapeutics may offer hope for prevention of cardiovascular disease in patients with elevated Lp(a) levels in the future.”
This work was supported by Copenhagen University Hospital – Herlev Gentofte, Denmark, and the Danish Beckett-Foundation. The Copenhagen General Population Study is supported by the Copenhagen County Foundation and Copenhagen University Hospital – Herlev Gentofte. Dr. Nordestgaard has been a consultant and a speaker for AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Silence Therapeutics, Abbott, and Esperion.
A version of this article first appeared on Medscape.com.
Many more people are at risk for early cardiovascular events because of raised lipoprotein(a) levels than from having familial hypercholesterolemia (FH), a new study suggests.
The Danish study set out to try and establish a level of Lp(a) that would be associated with a cardiovascular risk similar to that seen with FH. As there are many different definitions of FH, results showed a large range of Lp(a) values that corresponded to risk levels of the different FH definitions.
However, if considering one of the broadest FH definitions (from MEDPED – Make Early Diagnoses, Prevent Early Deaths), which is the one most commonly used in the United States, results showed that the level of cardiovascular risk in patients with this definition of FH is similar to that associated with Lp(a) levels of around 70 mg/dL (0.7 g/L).
“While FH is fairly unusual, occurring in less than 1% of the population, levels of Lp(a) of 70 mg/dL or above are much more common, occurring in around 10% of the White population,” Børge Nordestgaard, MD, Copenhagen University Hospital, said in an interview. Around 20% of the Black population have such high levels, while levels in Hispanics are in between.
“Our results suggest that there will be many more individuals at risk of premature MI or cardiovascular death because of raised Lp(a) levels than because of FH,” added Dr. Nordestgaard, the senior author of the current study.
Dr. Nordestgaard explained that FH is well established to be a serious condition. “We consider FH to be the genetic disease that causes the most cases of early heart disease and early death worldwide.”
“But we know now that raised levels of Lp(a), which is also genetically determined, can also lead to an increased risk of cardiovascular events relatively early in life, and when you look into the numbers, it seems like high levels of Lp(a) could be more common than FH. We wanted to try and find the levels of Lp(a) that corresponded to similar cardiovascular risk as FH.”
The Danish study was published in the Journal of the American College of Cardiology.
The authors note that the 2019 joint European Society of Cardiology and European Atherosclerosis Society guidelines suggested that an Lp(a) level greater than 180 mg/dL (0.8 g/L) may confer a lifetime risk for heart disease equivalent to the risk associated with heterozygous FH, but they point out that this value was speculative and not based on a direct comparison of risk associated with the two conditions in the same population.
For their study, Dr. Nordestgaard and colleagues analyzed information from a large database of the Danish population, the Copenhagen General Population Study, including 69,644 individuals for whom data on FH and Lp(a) levels were available. As these conditions are genetically determined, and the study held records on individuals going back several decades, the researchers were able to analyze event rates over a median follow up time of 42 years. During this time, there were 4,166 cases of myocardial infarction and 11,464 cases of atherosclerotic cardiovascular disease (ASCVD).
Results showed that Lp(a) levels associated with MI risk equivalent to that of clinical FH ranged from 67 to 402 mg/dL depending on the definition used for FH. The Lp(a) level corresponding to the MI risk of genetically determined FH was 180 mg/dL.
In terms of risk of ASCVD events, the levels of Lp(a) corresponding to the risk associated with clinical FH ranged from 130 to 391 mg/dL, and the Lp(a) level corresponding to the ASCVD risk of genetically determined FH was 175 mg/dL.
“All these different definitions of FH may cause some confusion, but basically we are saying that if an individual is found to have an Lp(a) above 70 mg/dL, then they have a similar level of cardiovascular risk as that associated with the broadest definition of FH, and they should be taken as seriously as a patient diagnosed with FH,” Dr. Nordestgaard said.
He estimated that these individuals have approximately a doubling of cardiovascular risk, compared with the general population, and risk increases further with rising Lp(a) levels.
The researchers also found that if an individual has both FH and raised Lp(a) they are at very high risk, as these two conditions are independent of each other.
Although a specific treatment for lowering Lp(a) levels is not yet available, Dr. Nordestgaard stresses that it is still worth identifying individuals with raised Lp(a) as efforts can be made to address other cardiovascular risk factors.
“We know raised Lp(a) increases cardiovascular risk, but there are also many other factors that likewise increase this risk, and they are all additive. So, it is very important that individuals with raised Lp(a) levels address these other risk factors,” he said. “These include stopping smoking, being at healthy weight, exercising regularly, eating a heart-healthy diet, and aggressive treatment of raised LDL, hypertension, and diabetes. All these things will lower their overall risk of cardiovascular disease.”
And there is the promise of new drugs to lower Lp(a) on the horizon, with several such products now in clinical development.
Dr. Nordestgaard also points out that as Lp(a) is genetically determined, cascade screening of close relatives of the individual with raised Lp(a) should also take place to detect others who may be at risk.
Although a level of Lp(a) of around 70 mg/dL confers similar cardiovascular risk than some definitions of FH, Dr. Nordestgaard says lower levels than this should also be a signal for concern.
“We usually say Lp(a) levels of 50 mg/dL are when we need to start to take this seriously. And it’s estimated that about 20% of the White population will have levels of 50 mg/dL or over and even more in the Black population,” he added.
‘Screen for both conditions’
In an accompanying editorial, Pamela Morris, MD, Medical University of South Carolina, Charleston; Jagat Narula, MD, Icahn School of Medicine, New York; and Sotirios Tsimikas, MD, University of California, San Diego, say “the weight of evidence strongly supports that both genetic lipid disorders, elevated Lp(a) levels and FH, are causally associated with an increased risk of premature ASCVD and should be carefully considered in risk assessment and management for ASCVD risk reduction.”
Dr. Morris told this news organization that the current study found a very large range of Lp(a) levels that conferred a similar cardiovascular risk to FH, because of the many different definitions of FH in use.
“But this should not take away the importance of screening for raised Lp(a) levels,” she stressed.
“We know that increased Lp(a) levels signal a high risk of cardiovascular disease. A diagnosis of FH is also a high-risk condition,” she said. “Both are important, and we need to screen for both, but it is difficult to directly compare the two conditions because the different definitions of FH get in the way.”
Dr. Morris agrees with Dr. Nordestgaard that raised levels of Lp(a) may actually be more important for the population risk of cardiovascular disease than FH, as the prevalence of increased Lp(a) levels is higher.
“Because raised Lp(a) levels are more prevalent than confirmed FH, the risk to the population is greater,” she said.
Dr. Morris points out that cardiovascular risk starts to increase at Lp(a) levels of 30 mg/dL (75 nmol/L).
The editorialists recommend that “in addition to performing a lipid panel periodically according to evidence-based guidelines, measurement of Lp(a) levels should also be performed at least once in an individual’s lifetime for ASCVD risk assessment.”
They conclude that “it is vital to continue to raise awareness among clinicians and patients of these high-risk genetic lipid disorders. Our understanding of both disorders is rapidly expanding, and promising novel therapeutics may offer hope for prevention of cardiovascular disease in patients with elevated Lp(a) levels in the future.”
This work was supported by Copenhagen University Hospital – Herlev Gentofte, Denmark, and the Danish Beckett-Foundation. The Copenhagen General Population Study is supported by the Copenhagen County Foundation and Copenhagen University Hospital – Herlev Gentofte. Dr. Nordestgaard has been a consultant and a speaker for AstraZeneca, Sanofi, Regeneron, Akcea, Amgen, Kowa, Denka, Amarin, Novartis, Novo Nordisk, Silence Therapeutics, Abbott, and Esperion.
A version of this article first appeared on Medscape.com.
New studies change beliefs about cardiovascular disease
This transcript has been edited for clarity.
I’m going to review a few of these.
The first is the TIME study. The TIME study looked at whether it matters if you give antihypertensive agents in the morning or the evening. This was a prospective, pragmatic, parallel-group study that was performed in the U.K. and published in The Lancet.
Their question was whether evening dosing of antihypertensives has benefit in cardiovascular outcomes in adults. They enrolled over 21,000 people with hypertension who were taking at least one antihypertensive medication. Patients were randomized to morning or evening dosing.
The primary outcome was death or hospitalization due to myocardial infarction or stroke. There was no difference. It doesn’t matter if you take your antihypertensive agent in the morning or the evening. I think this is important because, clinically, the simpler the regimen for the patient, the greater the adherence, leading to better outcomes.
I know I can safely ask a patient when they would rather take their medicine. For many people, that may be the morning because they’re brushing their teeth and they remember. If they want to take it in the evening, that’s fine, too. We’re no longer slave to telling a patient to take their antihypertensive medications in the evening.
At the meeting of the American Society of Nephrology, results from a study on the use of renin-angiotensin system (RAS) inhibitors in advanced CKD was presented, called the STOP ACEi trial. Again, another interesting trial asking a simple question. This was a randomized controlled trial (RCT) in patients who had an estimated glomerular filtration rate (eGFR) less than 30, and they were randomized to stop or continue therapy with their RAS inhibitors.
The primary outcome was the eGFR at 3 years. They enrolled 411 patients with a median baseline eGFR of 18. At 3 years, there was no difference in the eGFR between the groups. In the discontinuation group, the eGFR was 12.6 versus 13.3 in the continuation group. There were no differences in complications or anything else. Their conclusion was that among patients with advanced and progressive CKD, the discontinuation of a RAS inhibitor was not associated with a significant difference in the long-term rate of decrease in eGFR.
I think this is important because it changes our paradigm a bit. You can stop the RAS inhibitor; reduce the need for excessive medication in these patients; and, hopefully, focus on some newer medications that have been shown to prevent the decline in eGFR that are now available.
Next is from a letter published in JAMA, which asks the following question: Is diabetes itself an equivalent cardiovascular risk factor to those who have had a prior cardiovascular event?
We used to put having diabetes in that same high-risk category as people who’d already had a cardiovascular disease event. Well, have we made that any different? These authors are from Canada, and they did a retrospective population-based study looking at administrative health claims from Ontario, Canada, to assess the association of diabetes and prior cardiovascular disease with cardiovascular events from 1994 to 2014.
What I think is kind of cool, because I’m a diabetologist, is that over time the magnitude of the association between diabetes and cardiovascular event rates decreased. In somebody with diabetes, they don’t have the same high risk that a person who’s already had a cardiovascular event rate does. Diabetes is less of a risk factor for cardiovascular disease than having established cardiovascular disease, which means we’re treating diabetes better and reducing the risk for cardiovascular disease.
If you look at people with diabetes and a prior cardiovascular event, that’s still the very highest risk. The risk of people having another event who have established cardiovascular disease is pretty flat. Those people didn’t get better and the people with preexisting diabetes and cardiovascular events at baseline didn’t get much better, but those who had diabetes alone did improve in terms of looking at cardiovascular event rates.
I think this is good news because diabetes itself isn’t as high a cardiovascular risk factor as we once thought. It doesn’t mean that it isn’t a cardiovascular risk factor, but I think we’ve done better at mitigating the risk.
Finally, there is a relatively small study that was presented at the American Heart Association and published in the Journal of the American College of Cardiology, which asks whether supplements that are often used to lower LDL cholesterol are equivalent to a statin.
They compared six supplements with a placebo and with rosuvastatin, and looked to see what happened. This is not an outcome study, but a very short study, at 28 days, that used a placebo. They included 190 people with no history of cardiovascular disease but an increased 10-year risk for sclerotic cardiovascular disease.
The agents studied were rosuvastatin, placebo, fish oil, cinnamon, garlic, turmeric, plant sterols, and red yeast rice. Well, not surprisingly, rosuvastatin worked. It showed a 35% reduction in LDL cholesterol, and there was no significant impact on cholesterol levels with any of the other agents. The supplements yielded a similar response, as did the placebo. Side effects were similar, but they were most common with plant sterols and red yeast rice.
Clearly, a statin is better if you want to lower cholesterol levels. My approach, when patients want to take supplements, is to tell them what I know factually, which basically is that they don’t really cause much in the way of LDL cholesterol lowering. If I think the supplement isn’t going to hurt someone, I don’t tell them not to use it. I certainly tell them that they need to use agents that we know can actually reduce cardiovascular risk.
I think these studies really go through the gamut of asking questions. When can we stop an agent? What time of day do we need to give an agent? What, really, is the risk for type 2 diabetes with regard to cardiovascular events? What’s the value of supplements?
I think this is interesting, because I really encourage researchers to ask and answer these kinds of questions because it helps us clinically decide what’s best for treating our patients.
Thank you.
Dr. Peters is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She reported conflicts of interest with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to review a few of these.
The first is the TIME study. The TIME study looked at whether it matters if you give antihypertensive agents in the morning or the evening. This was a prospective, pragmatic, parallel-group study that was performed in the U.K. and published in The Lancet.
Their question was whether evening dosing of antihypertensives has benefit in cardiovascular outcomes in adults. They enrolled over 21,000 people with hypertension who were taking at least one antihypertensive medication. Patients were randomized to morning or evening dosing.
The primary outcome was death or hospitalization due to myocardial infarction or stroke. There was no difference. It doesn’t matter if you take your antihypertensive agent in the morning or the evening. I think this is important because, clinically, the simpler the regimen for the patient, the greater the adherence, leading to better outcomes.
I know I can safely ask a patient when they would rather take their medicine. For many people, that may be the morning because they’re brushing their teeth and they remember. If they want to take it in the evening, that’s fine, too. We’re no longer slave to telling a patient to take their antihypertensive medications in the evening.
At the meeting of the American Society of Nephrology, results from a study on the use of renin-angiotensin system (RAS) inhibitors in advanced CKD was presented, called the STOP ACEi trial. Again, another interesting trial asking a simple question. This was a randomized controlled trial (RCT) in patients who had an estimated glomerular filtration rate (eGFR) less than 30, and they were randomized to stop or continue therapy with their RAS inhibitors.
The primary outcome was the eGFR at 3 years. They enrolled 411 patients with a median baseline eGFR of 18. At 3 years, there was no difference in the eGFR between the groups. In the discontinuation group, the eGFR was 12.6 versus 13.3 in the continuation group. There were no differences in complications or anything else. Their conclusion was that among patients with advanced and progressive CKD, the discontinuation of a RAS inhibitor was not associated with a significant difference in the long-term rate of decrease in eGFR.
I think this is important because it changes our paradigm a bit. You can stop the RAS inhibitor; reduce the need for excessive medication in these patients; and, hopefully, focus on some newer medications that have been shown to prevent the decline in eGFR that are now available.
Next is from a letter published in JAMA, which asks the following question: Is diabetes itself an equivalent cardiovascular risk factor to those who have had a prior cardiovascular event?
We used to put having diabetes in that same high-risk category as people who’d already had a cardiovascular disease event. Well, have we made that any different? These authors are from Canada, and they did a retrospective population-based study looking at administrative health claims from Ontario, Canada, to assess the association of diabetes and prior cardiovascular disease with cardiovascular events from 1994 to 2014.
What I think is kind of cool, because I’m a diabetologist, is that over time the magnitude of the association between diabetes and cardiovascular event rates decreased. In somebody with diabetes, they don’t have the same high risk that a person who’s already had a cardiovascular event rate does. Diabetes is less of a risk factor for cardiovascular disease than having established cardiovascular disease, which means we’re treating diabetes better and reducing the risk for cardiovascular disease.
If you look at people with diabetes and a prior cardiovascular event, that’s still the very highest risk. The risk of people having another event who have established cardiovascular disease is pretty flat. Those people didn’t get better and the people with preexisting diabetes and cardiovascular events at baseline didn’t get much better, but those who had diabetes alone did improve in terms of looking at cardiovascular event rates.
I think this is good news because diabetes itself isn’t as high a cardiovascular risk factor as we once thought. It doesn’t mean that it isn’t a cardiovascular risk factor, but I think we’ve done better at mitigating the risk.
Finally, there is a relatively small study that was presented at the American Heart Association and published in the Journal of the American College of Cardiology, which asks whether supplements that are often used to lower LDL cholesterol are equivalent to a statin.
They compared six supplements with a placebo and with rosuvastatin, and looked to see what happened. This is not an outcome study, but a very short study, at 28 days, that used a placebo. They included 190 people with no history of cardiovascular disease but an increased 10-year risk for sclerotic cardiovascular disease.
The agents studied were rosuvastatin, placebo, fish oil, cinnamon, garlic, turmeric, plant sterols, and red yeast rice. Well, not surprisingly, rosuvastatin worked. It showed a 35% reduction in LDL cholesterol, and there was no significant impact on cholesterol levels with any of the other agents. The supplements yielded a similar response, as did the placebo. Side effects were similar, but they were most common with plant sterols and red yeast rice.
Clearly, a statin is better if you want to lower cholesterol levels. My approach, when patients want to take supplements, is to tell them what I know factually, which basically is that they don’t really cause much in the way of LDL cholesterol lowering. If I think the supplement isn’t going to hurt someone, I don’t tell them not to use it. I certainly tell them that they need to use agents that we know can actually reduce cardiovascular risk.
I think these studies really go through the gamut of asking questions. When can we stop an agent? What time of day do we need to give an agent? What, really, is the risk for type 2 diabetes with regard to cardiovascular events? What’s the value of supplements?
I think this is interesting, because I really encourage researchers to ask and answer these kinds of questions because it helps us clinically decide what’s best for treating our patients.
Thank you.
Dr. Peters is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She reported conflicts of interest with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
I’m going to review a few of these.
The first is the TIME study. The TIME study looked at whether it matters if you give antihypertensive agents in the morning or the evening. This was a prospective, pragmatic, parallel-group study that was performed in the U.K. and published in The Lancet.
Their question was whether evening dosing of antihypertensives has benefit in cardiovascular outcomes in adults. They enrolled over 21,000 people with hypertension who were taking at least one antihypertensive medication. Patients were randomized to morning or evening dosing.
The primary outcome was death or hospitalization due to myocardial infarction or stroke. There was no difference. It doesn’t matter if you take your antihypertensive agent in the morning or the evening. I think this is important because, clinically, the simpler the regimen for the patient, the greater the adherence, leading to better outcomes.
I know I can safely ask a patient when they would rather take their medicine. For many people, that may be the morning because they’re brushing their teeth and they remember. If they want to take it in the evening, that’s fine, too. We’re no longer slave to telling a patient to take their antihypertensive medications in the evening.
At the meeting of the American Society of Nephrology, results from a study on the use of renin-angiotensin system (RAS) inhibitors in advanced CKD was presented, called the STOP ACEi trial. Again, another interesting trial asking a simple question. This was a randomized controlled trial (RCT) in patients who had an estimated glomerular filtration rate (eGFR) less than 30, and they were randomized to stop or continue therapy with their RAS inhibitors.
The primary outcome was the eGFR at 3 years. They enrolled 411 patients with a median baseline eGFR of 18. At 3 years, there was no difference in the eGFR between the groups. In the discontinuation group, the eGFR was 12.6 versus 13.3 in the continuation group. There were no differences in complications or anything else. Their conclusion was that among patients with advanced and progressive CKD, the discontinuation of a RAS inhibitor was not associated with a significant difference in the long-term rate of decrease in eGFR.
I think this is important because it changes our paradigm a bit. You can stop the RAS inhibitor; reduce the need for excessive medication in these patients; and, hopefully, focus on some newer medications that have been shown to prevent the decline in eGFR that are now available.
Next is from a letter published in JAMA, which asks the following question: Is diabetes itself an equivalent cardiovascular risk factor to those who have had a prior cardiovascular event?
We used to put having diabetes in that same high-risk category as people who’d already had a cardiovascular disease event. Well, have we made that any different? These authors are from Canada, and they did a retrospective population-based study looking at administrative health claims from Ontario, Canada, to assess the association of diabetes and prior cardiovascular disease with cardiovascular events from 1994 to 2014.
What I think is kind of cool, because I’m a diabetologist, is that over time the magnitude of the association between diabetes and cardiovascular event rates decreased. In somebody with diabetes, they don’t have the same high risk that a person who’s already had a cardiovascular event rate does. Diabetes is less of a risk factor for cardiovascular disease than having established cardiovascular disease, which means we’re treating diabetes better and reducing the risk for cardiovascular disease.
If you look at people with diabetes and a prior cardiovascular event, that’s still the very highest risk. The risk of people having another event who have established cardiovascular disease is pretty flat. Those people didn’t get better and the people with preexisting diabetes and cardiovascular events at baseline didn’t get much better, but those who had diabetes alone did improve in terms of looking at cardiovascular event rates.
I think this is good news because diabetes itself isn’t as high a cardiovascular risk factor as we once thought. It doesn’t mean that it isn’t a cardiovascular risk factor, but I think we’ve done better at mitigating the risk.
Finally, there is a relatively small study that was presented at the American Heart Association and published in the Journal of the American College of Cardiology, which asks whether supplements that are often used to lower LDL cholesterol are equivalent to a statin.
They compared six supplements with a placebo and with rosuvastatin, and looked to see what happened. This is not an outcome study, but a very short study, at 28 days, that used a placebo. They included 190 people with no history of cardiovascular disease but an increased 10-year risk for sclerotic cardiovascular disease.
The agents studied were rosuvastatin, placebo, fish oil, cinnamon, garlic, turmeric, plant sterols, and red yeast rice. Well, not surprisingly, rosuvastatin worked. It showed a 35% reduction in LDL cholesterol, and there was no significant impact on cholesterol levels with any of the other agents. The supplements yielded a similar response, as did the placebo. Side effects were similar, but they were most common with plant sterols and red yeast rice.
Clearly, a statin is better if you want to lower cholesterol levels. My approach, when patients want to take supplements, is to tell them what I know factually, which basically is that they don’t really cause much in the way of LDL cholesterol lowering. If I think the supplement isn’t going to hurt someone, I don’t tell them not to use it. I certainly tell them that they need to use agents that we know can actually reduce cardiovascular risk.
I think these studies really go through the gamut of asking questions. When can we stop an agent? What time of day do we need to give an agent? What, really, is the risk for type 2 diabetes with regard to cardiovascular events? What’s the value of supplements?
I think this is interesting, because I really encourage researchers to ask and answer these kinds of questions because it helps us clinically decide what’s best for treating our patients.
Thank you.
Dr. Peters is a professor of medicine at the University of Southern California, Los Angeles, and director of the USC clinical diabetes programs. She reported conflicts of interest with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
U.S. flu activity already at mid-season levels
according to the Centers of Disease Control and Prevention.
Nationally, 6% of all outpatient visits were because of flu or flu-like illness for the week of Nov. 13-19, up from 5.8% the previous week, the CDC’s Influenza Division said in its weekly FluView report.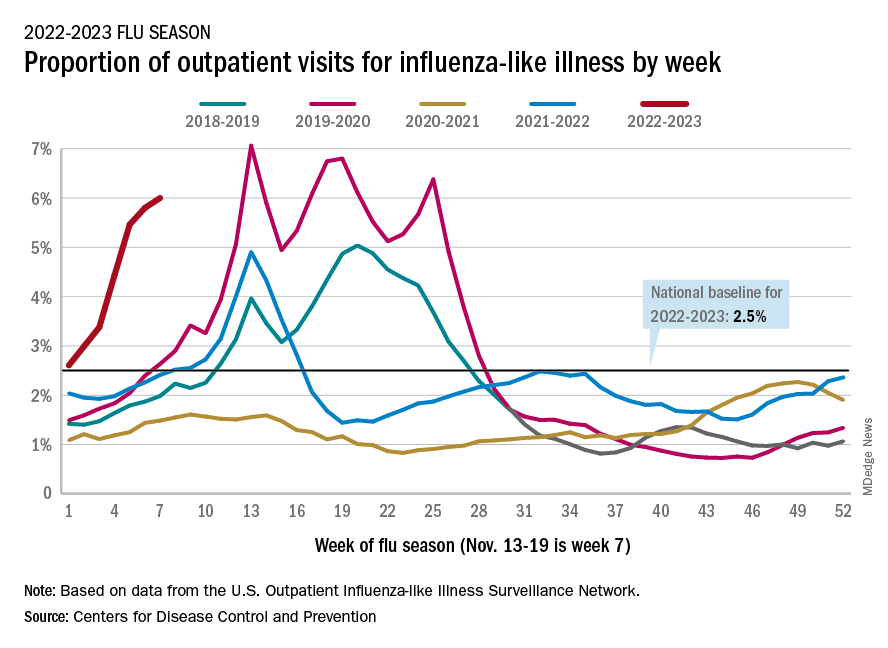
Those figures are the highest recorded in November since 2009, but the peak of the 2009-10 flu season occurred even earlier – the week of Oct. 18-24 – and the rate of flu-like illness had already dropped to just over 4.0% by Nov. 15-21 that year and continued to drop thereafter.
Although COVID-19 and respiratory syncytial virus (RSV) are included in the data from the CDC’s Outpatient Influenza-like Illness Surveillance Network, the agency did note that “seasonal influenza activity is elevated across the country” and estimated that “there have been at least 6.2 million illnesses, 53,000 hospitalizations, and 2,900 deaths from flu” during the 2022-23 season.
Total flu deaths include 11 reported in children as of Nov. 19, and children ages 0-4 had a higher proportion of visits for flu like-illness than other age groups.
The agency also said the cumulative hospitalization rate of 11.3 per 100,000 population “is higher than the rate observed in [the corresponding week of] every previous season since 2010-2011.” Adults 65 years and older have the highest cumulative rate, 25.9 per 100,000, for this year, compared with 20.7 for children 0-4; 11.1 for adults 50-64; 10.3 for children 5-17; and 5.6 for adults 18-49 years old, the CDC said.
A version of this article first appeared on WebMD.com.
according to the Centers of Disease Control and Prevention.
Nationally, 6% of all outpatient visits were because of flu or flu-like illness for the week of Nov. 13-19, up from 5.8% the previous week, the CDC’s Influenza Division said in its weekly FluView report.
Those figures are the highest recorded in November since 2009, but the peak of the 2009-10 flu season occurred even earlier – the week of Oct. 18-24 – and the rate of flu-like illness had already dropped to just over 4.0% by Nov. 15-21 that year and continued to drop thereafter.
Although COVID-19 and respiratory syncytial virus (RSV) are included in the data from the CDC’s Outpatient Influenza-like Illness Surveillance Network, the agency did note that “seasonal influenza activity is elevated across the country” and estimated that “there have been at least 6.2 million illnesses, 53,000 hospitalizations, and 2,900 deaths from flu” during the 2022-23 season.
Total flu deaths include 11 reported in children as of Nov. 19, and children ages 0-4 had a higher proportion of visits for flu like-illness than other age groups.
The agency also said the cumulative hospitalization rate of 11.3 per 100,000 population “is higher than the rate observed in [the corresponding week of] every previous season since 2010-2011.” Adults 65 years and older have the highest cumulative rate, 25.9 per 100,000, for this year, compared with 20.7 for children 0-4; 11.1 for adults 50-64; 10.3 for children 5-17; and 5.6 for adults 18-49 years old, the CDC said.
A version of this article first appeared on WebMD.com.
according to the Centers of Disease Control and Prevention.
Nationally, 6% of all outpatient visits were because of flu or flu-like illness for the week of Nov. 13-19, up from 5.8% the previous week, the CDC’s Influenza Division said in its weekly FluView report.
Those figures are the highest recorded in November since 2009, but the peak of the 2009-10 flu season occurred even earlier – the week of Oct. 18-24 – and the rate of flu-like illness had already dropped to just over 4.0% by Nov. 15-21 that year and continued to drop thereafter.
Although COVID-19 and respiratory syncytial virus (RSV) are included in the data from the CDC’s Outpatient Influenza-like Illness Surveillance Network, the agency did note that “seasonal influenza activity is elevated across the country” and estimated that “there have been at least 6.2 million illnesses, 53,000 hospitalizations, and 2,900 deaths from flu” during the 2022-23 season.
Total flu deaths include 11 reported in children as of Nov. 19, and children ages 0-4 had a higher proportion of visits for flu like-illness than other age groups.
The agency also said the cumulative hospitalization rate of 11.3 per 100,000 population “is higher than the rate observed in [the corresponding week of] every previous season since 2010-2011.” Adults 65 years and older have the highest cumulative rate, 25.9 per 100,000, for this year, compared with 20.7 for children 0-4; 11.1 for adults 50-64; 10.3 for children 5-17; and 5.6 for adults 18-49 years old, the CDC said.
A version of this article first appeared on WebMD.com.