User login
Sharon Worcester is an award-winning medical journalist for MDedge News. She has been with the company since 1996, first as the Southeast Bureau Chief (1996-2009) when the company was known as International Medical News Group, then as a freelance writer (2010-2015) before returning as a reporter in 2015. She previously worked as a daily newspaper reporter covering health and local government. Sharon currently reports primarily on oncology and hematology. She has a BA from Eckerd College and an MA in Mass Communication/Print Journalism from the University of Florida. Connect with her via LinkedIn and follow her on twitter @SW_MedReporter.
Metformin May Lower Pancreatic Cancer Risk in Women
Metformin use was associated with a decreased risk of pancreatic cancer in women, but not in men, in a large case-control study involving more than 19,300 U.K. primary care patients.
Additionally, use of insulin and sulfonylureas was found in the study to be associated with increased risk of pancreatic cancer in both men and women, Dr. Michael Bodmer of the University of Basel, Switzerland, and his colleagues reported online in the Jan. 31 issue of the American Journal of Gastroenterology.
Overall, metformin use was not found to be associated with pancreatic cancer in 2,763 patients with a first-time diagnosis of pancreatic cancer, compared with 16,578 matched controls with no such diagnosis – all from the U.K.-based General Practice Research Database, which includes data on more than 8 million individuals (adjusted odds ratios, 1.01, 0.92, and 0.87 for those who received 1-9, 10-29, and 30 or more metformin prescriptions, respectively), the investigators said.
The findings were similar when analysis was restricted to cases with pancreatic surgery, radio/chemotherapy, or with a specific oncology code, and also when analysis was restricted to diabetic patients. However, in an analysis by gender, long-term metformin use was associated with a decreased risk of pancreatic cancer in women (adjusted OR, 0.43), but not in men (adjusted OR, 1.59), they found (Am. J. Gastroenterol. 2012 Jan. 31 [doi10.1038/ajg.2011.483]).
As for long-term use of sulfonylureas and insulin, the overall analysis demonstrated a "materially increased risk of pancreatic cancer (adjusted OR, 1.90 and 2.29, respectively), and as with metformin, the findings were closely similar in those with pancreatic surgery, radio/chemotherapy, or an oncology code, while in the analysis restricted to patients with diabetes, the adjusted odds ratios for long-term use of sulfonylureas and insulin were 1.59 and 1.69, respectively.
In contrast with the findings regarding metformin, the increased risk of pancreatic cancer among long-term users of sulfonylureas was mainly restricted to women (adjusted OR, 3.05), the investigators said.
Cases in this study were individuals with a first-time diagnosis of pancreatic cancer before the age of 90 years between 1995 and 2009. Controls had no diagnosis of pancreatic cancer and were matched based on calendar time, age, sex, general practice, and number of years of active history in the database before the index date. The average age was 70 years, and 46% were men.
The analyses were conducted using the index date shifted back in time by 2 years to account for cancer latency, the investigators explained.
Using that same shifted index date, the investigators also looked for a link between diabetes history and the risk of pancreatic cancer, and found one. "Overall, the adjusted odds ratio of pancreatic cancer associated with a recorded diagnosis of diabetes mellitus was 1.22. When we stratified the risk of pancreatic cancer by diabetes duration, the odds ratio decreased with increasing duration of diabetes; the odds ratios for a diabetes history of less than 2, 2-5, 5-10, or greater than 10 years were 1.71, 1.21, 0.94, and 0.71, respectively," they said.
In the analysis using the recorded index date, rather than the shifted date, the overall odds ratio for pancreatic cancer in diabetic patients compared with nondiabetic patients was 1.60, and for those with disease duration of less than 2 years, 2-5 years, 5-10 years, and greater than 10 years were 3.30, 1.13, 0.72, and 0.56, respectively.
The finding of an effect modification by gender for the use of metformin was "somewhat unexpected and could not be explained by confounding by use of estrogens," the investigators said, noting that the finding should be interpreted with caution since it is based on a limited number of exposed cases and controls, and since there is no obvious pathophysiologic explanation.
Also, the findings regarding metformin differed somewhat from those of prior smaller studies showing an overall decrease in pancreatic cancer with long-term metformin use.
The findings regarding sulfonylureas and insulin, however, support those of prior studies, and as with metformin, effect modification by gender seemed to have a role: The increased risk with long-term use of sulfonylureas was mainly seen in women, and the increased risk with insulin was mainly seen in men.
"Of importance, in our study, neither short-term use of metformin or sulfonylureas, nor insulin was associated with altered relative risk estimates for pancreatic cancer, indicating that our study design effectively eliminated detection bias and/or bias by intensification of antidiabetic therapy due to undiagnosed pancreatic cancer," they said.
Also the finding of a link between diabetes mellitus and increased risk for pancreatic cancer, which was restricted to those with newly diagnosed diabetes, strongly supports the hypothesis suggested by other authors that short-term diabetes mellitus is likely caused by pancreatic cancer.
"Although uncontrolled confounding by dietary habits or physical activity may be of importance, these findings do not support a causative role for diabetes mellitus for development of pancreatic cancer," they noted.
This study was partially funded by the Swiss Cancer League and the Research Fund of the University of Basel, Switzerland. None of the authors had relevant disclosures.
Metformin use was associated with a decreased risk of pancreatic cancer in women, but not in men, in a large case-control study involving more than 19,300 U.K. primary care patients.
Additionally, use of insulin and sulfonylureas was found in the study to be associated with increased risk of pancreatic cancer in both men and women, Dr. Michael Bodmer of the University of Basel, Switzerland, and his colleagues reported online in the Jan. 31 issue of the American Journal of Gastroenterology.
Overall, metformin use was not found to be associated with pancreatic cancer in 2,763 patients with a first-time diagnosis of pancreatic cancer, compared with 16,578 matched controls with no such diagnosis – all from the U.K.-based General Practice Research Database, which includes data on more than 8 million individuals (adjusted odds ratios, 1.01, 0.92, and 0.87 for those who received 1-9, 10-29, and 30 or more metformin prescriptions, respectively), the investigators said.
The findings were similar when analysis was restricted to cases with pancreatic surgery, radio/chemotherapy, or with a specific oncology code, and also when analysis was restricted to diabetic patients. However, in an analysis by gender, long-term metformin use was associated with a decreased risk of pancreatic cancer in women (adjusted OR, 0.43), but not in men (adjusted OR, 1.59), they found (Am. J. Gastroenterol. 2012 Jan. 31 [doi10.1038/ajg.2011.483]).
As for long-term use of sulfonylureas and insulin, the overall analysis demonstrated a "materially increased risk of pancreatic cancer (adjusted OR, 1.90 and 2.29, respectively), and as with metformin, the findings were closely similar in those with pancreatic surgery, radio/chemotherapy, or an oncology code, while in the analysis restricted to patients with diabetes, the adjusted odds ratios for long-term use of sulfonylureas and insulin were 1.59 and 1.69, respectively.
In contrast with the findings regarding metformin, the increased risk of pancreatic cancer among long-term users of sulfonylureas was mainly restricted to women (adjusted OR, 3.05), the investigators said.
Cases in this study were individuals with a first-time diagnosis of pancreatic cancer before the age of 90 years between 1995 and 2009. Controls had no diagnosis of pancreatic cancer and were matched based on calendar time, age, sex, general practice, and number of years of active history in the database before the index date. The average age was 70 years, and 46% were men.
The analyses were conducted using the index date shifted back in time by 2 years to account for cancer latency, the investigators explained.
Using that same shifted index date, the investigators also looked for a link between diabetes history and the risk of pancreatic cancer, and found one. "Overall, the adjusted odds ratio of pancreatic cancer associated with a recorded diagnosis of diabetes mellitus was 1.22. When we stratified the risk of pancreatic cancer by diabetes duration, the odds ratio decreased with increasing duration of diabetes; the odds ratios for a diabetes history of less than 2, 2-5, 5-10, or greater than 10 years were 1.71, 1.21, 0.94, and 0.71, respectively," they said.
In the analysis using the recorded index date, rather than the shifted date, the overall odds ratio for pancreatic cancer in diabetic patients compared with nondiabetic patients was 1.60, and for those with disease duration of less than 2 years, 2-5 years, 5-10 years, and greater than 10 years were 3.30, 1.13, 0.72, and 0.56, respectively.
The finding of an effect modification by gender for the use of metformin was "somewhat unexpected and could not be explained by confounding by use of estrogens," the investigators said, noting that the finding should be interpreted with caution since it is based on a limited number of exposed cases and controls, and since there is no obvious pathophysiologic explanation.
Also, the findings regarding metformin differed somewhat from those of prior smaller studies showing an overall decrease in pancreatic cancer with long-term metformin use.
The findings regarding sulfonylureas and insulin, however, support those of prior studies, and as with metformin, effect modification by gender seemed to have a role: The increased risk with long-term use of sulfonylureas was mainly seen in women, and the increased risk with insulin was mainly seen in men.
"Of importance, in our study, neither short-term use of metformin or sulfonylureas, nor insulin was associated with altered relative risk estimates for pancreatic cancer, indicating that our study design effectively eliminated detection bias and/or bias by intensification of antidiabetic therapy due to undiagnosed pancreatic cancer," they said.
Also the finding of a link between diabetes mellitus and increased risk for pancreatic cancer, which was restricted to those with newly diagnosed diabetes, strongly supports the hypothesis suggested by other authors that short-term diabetes mellitus is likely caused by pancreatic cancer.
"Although uncontrolled confounding by dietary habits or physical activity may be of importance, these findings do not support a causative role for diabetes mellitus for development of pancreatic cancer," they noted.
This study was partially funded by the Swiss Cancer League and the Research Fund of the University of Basel, Switzerland. None of the authors had relevant disclosures.
Metformin use was associated with a decreased risk of pancreatic cancer in women, but not in men, in a large case-control study involving more than 19,300 U.K. primary care patients.
Additionally, use of insulin and sulfonylureas was found in the study to be associated with increased risk of pancreatic cancer in both men and women, Dr. Michael Bodmer of the University of Basel, Switzerland, and his colleagues reported online in the Jan. 31 issue of the American Journal of Gastroenterology.
Overall, metformin use was not found to be associated with pancreatic cancer in 2,763 patients with a first-time diagnosis of pancreatic cancer, compared with 16,578 matched controls with no such diagnosis – all from the U.K.-based General Practice Research Database, which includes data on more than 8 million individuals (adjusted odds ratios, 1.01, 0.92, and 0.87 for those who received 1-9, 10-29, and 30 or more metformin prescriptions, respectively), the investigators said.
The findings were similar when analysis was restricted to cases with pancreatic surgery, radio/chemotherapy, or with a specific oncology code, and also when analysis was restricted to diabetic patients. However, in an analysis by gender, long-term metformin use was associated with a decreased risk of pancreatic cancer in women (adjusted OR, 0.43), but not in men (adjusted OR, 1.59), they found (Am. J. Gastroenterol. 2012 Jan. 31 [doi10.1038/ajg.2011.483]).
As for long-term use of sulfonylureas and insulin, the overall analysis demonstrated a "materially increased risk of pancreatic cancer (adjusted OR, 1.90 and 2.29, respectively), and as with metformin, the findings were closely similar in those with pancreatic surgery, radio/chemotherapy, or an oncology code, while in the analysis restricted to patients with diabetes, the adjusted odds ratios for long-term use of sulfonylureas and insulin were 1.59 and 1.69, respectively.
In contrast with the findings regarding metformin, the increased risk of pancreatic cancer among long-term users of sulfonylureas was mainly restricted to women (adjusted OR, 3.05), the investigators said.
Cases in this study were individuals with a first-time diagnosis of pancreatic cancer before the age of 90 years between 1995 and 2009. Controls had no diagnosis of pancreatic cancer and were matched based on calendar time, age, sex, general practice, and number of years of active history in the database before the index date. The average age was 70 years, and 46% were men.
The analyses were conducted using the index date shifted back in time by 2 years to account for cancer latency, the investigators explained.
Using that same shifted index date, the investigators also looked for a link between diabetes history and the risk of pancreatic cancer, and found one. "Overall, the adjusted odds ratio of pancreatic cancer associated with a recorded diagnosis of diabetes mellitus was 1.22. When we stratified the risk of pancreatic cancer by diabetes duration, the odds ratio decreased with increasing duration of diabetes; the odds ratios for a diabetes history of less than 2, 2-5, 5-10, or greater than 10 years were 1.71, 1.21, 0.94, and 0.71, respectively," they said.
In the analysis using the recorded index date, rather than the shifted date, the overall odds ratio for pancreatic cancer in diabetic patients compared with nondiabetic patients was 1.60, and for those with disease duration of less than 2 years, 2-5 years, 5-10 years, and greater than 10 years were 3.30, 1.13, 0.72, and 0.56, respectively.
The finding of an effect modification by gender for the use of metformin was "somewhat unexpected and could not be explained by confounding by use of estrogens," the investigators said, noting that the finding should be interpreted with caution since it is based on a limited number of exposed cases and controls, and since there is no obvious pathophysiologic explanation.
Also, the findings regarding metformin differed somewhat from those of prior smaller studies showing an overall decrease in pancreatic cancer with long-term metformin use.
The findings regarding sulfonylureas and insulin, however, support those of prior studies, and as with metformin, effect modification by gender seemed to have a role: The increased risk with long-term use of sulfonylureas was mainly seen in women, and the increased risk with insulin was mainly seen in men.
"Of importance, in our study, neither short-term use of metformin or sulfonylureas, nor insulin was associated with altered relative risk estimates for pancreatic cancer, indicating that our study design effectively eliminated detection bias and/or bias by intensification of antidiabetic therapy due to undiagnosed pancreatic cancer," they said.
Also the finding of a link between diabetes mellitus and increased risk for pancreatic cancer, which was restricted to those with newly diagnosed diabetes, strongly supports the hypothesis suggested by other authors that short-term diabetes mellitus is likely caused by pancreatic cancer.
"Although uncontrolled confounding by dietary habits or physical activity may be of importance, these findings do not support a causative role for diabetes mellitus for development of pancreatic cancer," they noted.
This study was partially funded by the Swiss Cancer League and the Research Fund of the University of Basel, Switzerland. None of the authors had relevant disclosures.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY
Major Finding: Overall, metformin use was not found to be associated with pancreatic cancer in 2,763 patients with a first-time diagnosis, compared with 16,578 matched controls with no such diagnosis (adjusted odds ratios, 1.01, 0.92, and 0.87 for those who received 1-9, 10-29, and 30 or more metformin prescriptions, respectively). However, in an analysis by gender, long-term metformin use was associated with a decreased risk of pancreatic cancer in women (adjusted OR, 0.43), but not in men (adjusted OR, 1.59).
Data Source: A large case-control study using the U.K.-based General Practice Research Database.
Disclosures: This study was partially funded by the Swiss Cancer League and the Research Fund of the University of Basel, Switzerland. None of the authors had relevant disclosures.
Epidural-Related Fever Linked With Adverse Neonatal Outcomes
Epidural-related maternal temperature elevation is associated with an increased risk of adverse neonatal outcomes, a retrospective cohort study involving more than 3,200 women has shown.
Because randomized and observational studies consistently demonstrate an association between epidural use and maternal fever during labor – with greater than 90% of fever in labor related to epidural use in low-risk women at term, the findings are concerning, Elizabeth A. Greenwell, Sc.D., of the Harvard School of Public Health, Boston, and her colleagues reported Jan. 30 in Pediatrics. Dr. Greenwell is currently a postdoctoral fellow at the University of Colorado at Denver.
Of 3,209 women in the study population, 2,784 received epidural anesthesia and 425 did not. A temperature greater than 99.5 F developed after admission for delivery in 1,246 (44.8%) of those who received an epidural and in 62 (14.6%) of those who did not. A temperature greater than 100.4° F developed during labor in 535 (19.2%) of those who received epidural anesthesia and in 10 (2.4%) of those who did not.
In the absence of intrapartum temperature, no significant differences were seen in regard to adverse neonatal outcomes between those who did and did not receive epidural anesthesia. However, a trend was seen between the maximum maternal temperature and a significant increase in the incidence of hypotonia, assisted ventilation, 1- and 5-minute Apgar scores less than 7, and early-onset seizures in those with temperature elevation who received an epidural, the investigators said (Pediatrics 2012;129:e447-54).
On regression analysis, the risk of these adverse outcomes was two- to six-fold greater among infants born to women with a fever greater than 101° F.
For example, the proportion of infants with transitional hypotonia increased from 10.8% to 25.2% when maternal temperature was less than or equal to 99.5 F, compared with a temperature greater than 101° F. Similarly, the proportion of infants with hypotonia lasting greater than 15 minutes increased from 0.6% to 2.5% when maternal temperature was less than or equal to 99.5 F, compared with a temperature greater than 101° F, they said.
"Maternal fever exceeding 101 F was associated with a twofold increase in the risk of transitional hypotonia, a threefold increased risk of hypotonia lasting greater than 15 minutes, and a twofold increased risk for assisted ventilation. ... Infants of mothers with fever greater than 101° F were also 6.5 times more likely to have a seizure compared with infants of mothers with a maximum temperature less than or equal to 99.5 ° F," they said.
Study participants were low-risk nulliparous women with singleton pregnancies who were delivered at 37 or more weeks’ gestation in 2000, and who had their temperature recorded. Those with a temperature above 99.5° F at admission were excluded, as were those who received spinal anesthesia and those with infants who had conditions that might be associated with adverse neonatal outcomes.
The findings suggest that epidural analgesia without accompanying maternal fever does not have an immediate effect on neonatal status, but that epidural analgesia with fever could have an impact on the fetus.
"Our finding of an increase in unexplained seizures among infants of women with fever greater than 101° F is of concern," they said, noting that even though the findings were based on a relatively small number of seizures (n = 8), the finding is consistent with other studies demonstrating a link between intrapartum maternal fever and neonatal encephalopathy.
"Studies hypothesizing an association between neonatal encephalopathy or seizures and intrapartum maternal fever have assumed the fever resulted from infection such as chorioamnionitis. However, data suggest that among women delivering at term, most fever is related to epidural use rather than infection," they said.
Findings in this study also support those from prior studies suggesting an association between maternal fever and neonatal stroke in term infants, which along with other data demonstrating that clinical chorioamnionitis – primarily diagnosed by the presence of intrapartum fever – is associated with a substantially increased risk of cerebral palsy in term infants suggest that "exposure to intrapartum fever may not only increase the risk of adverse effects at birth but could potentially contribute to the development of long-term neurologic morbidity," they said.
The mechanism by which epidural analgesia may cause maternal fever, and by which fever might increase risk for adverse neonatal outcomes, remains unclear, they said, noting: "Our recent work, as well as that of others, suggests an inflammatory response accompanying epidural-related fever. ...
"Cytokines released in response to inflammation or infection can act as mediators of neurologic injury, and have been linked to neonatal encephalopathy and brain damage in newborns," they explained.
It remains unclear whether control of fever would ameliorate adverse effects.
Although limited by several factors, including the fact that few women (n = 10) not receiving an epidural developed fever in this study, thereby precluding meaningful analysis of neonatal outcomes in that group, and by the fact that undiagnosed neonatal or maternal infections may have caused the increase in adverse neonatal outcomes, the findings raise important concerns about the risks of epidural-related intrapartum maternal temperature.
"Although many of the specific outcomes we found associated with elevated maternal temperature may be transient, it is possible that particularly the increase in early-onset neonatal seizures could have implications for longer-term health of the infant," they concluded.
This study was supported in part by a Predoctoral Individual Ruth L. Kerschstein National Research Service Award from the National Institute of Child Health and Human Development to Dr. Greenwell.
Epidural-related maternal temperature elevation is associated with an increased risk of adverse neonatal outcomes, a retrospective cohort study involving more than 3,200 women has shown.
Because randomized and observational studies consistently demonstrate an association between epidural use and maternal fever during labor – with greater than 90% of fever in labor related to epidural use in low-risk women at term, the findings are concerning, Elizabeth A. Greenwell, Sc.D., of the Harvard School of Public Health, Boston, and her colleagues reported Jan. 30 in Pediatrics. Dr. Greenwell is currently a postdoctoral fellow at the University of Colorado at Denver.
Of 3,209 women in the study population, 2,784 received epidural anesthesia and 425 did not. A temperature greater than 99.5 F developed after admission for delivery in 1,246 (44.8%) of those who received an epidural and in 62 (14.6%) of those who did not. A temperature greater than 100.4° F developed during labor in 535 (19.2%) of those who received epidural anesthesia and in 10 (2.4%) of those who did not.
In the absence of intrapartum temperature, no significant differences were seen in regard to adverse neonatal outcomes between those who did and did not receive epidural anesthesia. However, a trend was seen between the maximum maternal temperature and a significant increase in the incidence of hypotonia, assisted ventilation, 1- and 5-minute Apgar scores less than 7, and early-onset seizures in those with temperature elevation who received an epidural, the investigators said (Pediatrics 2012;129:e447-54).
On regression analysis, the risk of these adverse outcomes was two- to six-fold greater among infants born to women with a fever greater than 101° F.
For example, the proportion of infants with transitional hypotonia increased from 10.8% to 25.2% when maternal temperature was less than or equal to 99.5 F, compared with a temperature greater than 101° F. Similarly, the proportion of infants with hypotonia lasting greater than 15 minutes increased from 0.6% to 2.5% when maternal temperature was less than or equal to 99.5 F, compared with a temperature greater than 101° F, they said.
"Maternal fever exceeding 101 F was associated with a twofold increase in the risk of transitional hypotonia, a threefold increased risk of hypotonia lasting greater than 15 minutes, and a twofold increased risk for assisted ventilation. ... Infants of mothers with fever greater than 101° F were also 6.5 times more likely to have a seizure compared with infants of mothers with a maximum temperature less than or equal to 99.5 ° F," they said.
Study participants were low-risk nulliparous women with singleton pregnancies who were delivered at 37 or more weeks’ gestation in 2000, and who had their temperature recorded. Those with a temperature above 99.5° F at admission were excluded, as were those who received spinal anesthesia and those with infants who had conditions that might be associated with adverse neonatal outcomes.
The findings suggest that epidural analgesia without accompanying maternal fever does not have an immediate effect on neonatal status, but that epidural analgesia with fever could have an impact on the fetus.
"Our finding of an increase in unexplained seizures among infants of women with fever greater than 101° F is of concern," they said, noting that even though the findings were based on a relatively small number of seizures (n = 8), the finding is consistent with other studies demonstrating a link between intrapartum maternal fever and neonatal encephalopathy.
"Studies hypothesizing an association between neonatal encephalopathy or seizures and intrapartum maternal fever have assumed the fever resulted from infection such as chorioamnionitis. However, data suggest that among women delivering at term, most fever is related to epidural use rather than infection," they said.
Findings in this study also support those from prior studies suggesting an association between maternal fever and neonatal stroke in term infants, which along with other data demonstrating that clinical chorioamnionitis – primarily diagnosed by the presence of intrapartum fever – is associated with a substantially increased risk of cerebral palsy in term infants suggest that "exposure to intrapartum fever may not only increase the risk of adverse effects at birth but could potentially contribute to the development of long-term neurologic morbidity," they said.
The mechanism by which epidural analgesia may cause maternal fever, and by which fever might increase risk for adverse neonatal outcomes, remains unclear, they said, noting: "Our recent work, as well as that of others, suggests an inflammatory response accompanying epidural-related fever. ...
"Cytokines released in response to inflammation or infection can act as mediators of neurologic injury, and have been linked to neonatal encephalopathy and brain damage in newborns," they explained.
It remains unclear whether control of fever would ameliorate adverse effects.
Although limited by several factors, including the fact that few women (n = 10) not receiving an epidural developed fever in this study, thereby precluding meaningful analysis of neonatal outcomes in that group, and by the fact that undiagnosed neonatal or maternal infections may have caused the increase in adverse neonatal outcomes, the findings raise important concerns about the risks of epidural-related intrapartum maternal temperature.
"Although many of the specific outcomes we found associated with elevated maternal temperature may be transient, it is possible that particularly the increase in early-onset neonatal seizures could have implications for longer-term health of the infant," they concluded.
This study was supported in part by a Predoctoral Individual Ruth L. Kerschstein National Research Service Award from the National Institute of Child Health and Human Development to Dr. Greenwell.
Epidural-related maternal temperature elevation is associated with an increased risk of adverse neonatal outcomes, a retrospective cohort study involving more than 3,200 women has shown.
Because randomized and observational studies consistently demonstrate an association between epidural use and maternal fever during labor – with greater than 90% of fever in labor related to epidural use in low-risk women at term, the findings are concerning, Elizabeth A. Greenwell, Sc.D., of the Harvard School of Public Health, Boston, and her colleagues reported Jan. 30 in Pediatrics. Dr. Greenwell is currently a postdoctoral fellow at the University of Colorado at Denver.
Of 3,209 women in the study population, 2,784 received epidural anesthesia and 425 did not. A temperature greater than 99.5 F developed after admission for delivery in 1,246 (44.8%) of those who received an epidural and in 62 (14.6%) of those who did not. A temperature greater than 100.4° F developed during labor in 535 (19.2%) of those who received epidural anesthesia and in 10 (2.4%) of those who did not.
In the absence of intrapartum temperature, no significant differences were seen in regard to adverse neonatal outcomes between those who did and did not receive epidural anesthesia. However, a trend was seen between the maximum maternal temperature and a significant increase in the incidence of hypotonia, assisted ventilation, 1- and 5-minute Apgar scores less than 7, and early-onset seizures in those with temperature elevation who received an epidural, the investigators said (Pediatrics 2012;129:e447-54).
On regression analysis, the risk of these adverse outcomes was two- to six-fold greater among infants born to women with a fever greater than 101° F.
For example, the proportion of infants with transitional hypotonia increased from 10.8% to 25.2% when maternal temperature was less than or equal to 99.5 F, compared with a temperature greater than 101° F. Similarly, the proportion of infants with hypotonia lasting greater than 15 minutes increased from 0.6% to 2.5% when maternal temperature was less than or equal to 99.5 F, compared with a temperature greater than 101° F, they said.
"Maternal fever exceeding 101 F was associated with a twofold increase in the risk of transitional hypotonia, a threefold increased risk of hypotonia lasting greater than 15 minutes, and a twofold increased risk for assisted ventilation. ... Infants of mothers with fever greater than 101° F were also 6.5 times more likely to have a seizure compared with infants of mothers with a maximum temperature less than or equal to 99.5 ° F," they said.
Study participants were low-risk nulliparous women with singleton pregnancies who were delivered at 37 or more weeks’ gestation in 2000, and who had their temperature recorded. Those with a temperature above 99.5° F at admission were excluded, as were those who received spinal anesthesia and those with infants who had conditions that might be associated with adverse neonatal outcomes.
The findings suggest that epidural analgesia without accompanying maternal fever does not have an immediate effect on neonatal status, but that epidural analgesia with fever could have an impact on the fetus.
"Our finding of an increase in unexplained seizures among infants of women with fever greater than 101° F is of concern," they said, noting that even though the findings were based on a relatively small number of seizures (n = 8), the finding is consistent with other studies demonstrating a link between intrapartum maternal fever and neonatal encephalopathy.
"Studies hypothesizing an association between neonatal encephalopathy or seizures and intrapartum maternal fever have assumed the fever resulted from infection such as chorioamnionitis. However, data suggest that among women delivering at term, most fever is related to epidural use rather than infection," they said.
Findings in this study also support those from prior studies suggesting an association between maternal fever and neonatal stroke in term infants, which along with other data demonstrating that clinical chorioamnionitis – primarily diagnosed by the presence of intrapartum fever – is associated with a substantially increased risk of cerebral palsy in term infants suggest that "exposure to intrapartum fever may not only increase the risk of adverse effects at birth but could potentially contribute to the development of long-term neurologic morbidity," they said.
The mechanism by which epidural analgesia may cause maternal fever, and by which fever might increase risk for adverse neonatal outcomes, remains unclear, they said, noting: "Our recent work, as well as that of others, suggests an inflammatory response accompanying epidural-related fever. ...
"Cytokines released in response to inflammation or infection can act as mediators of neurologic injury, and have been linked to neonatal encephalopathy and brain damage in newborns," they explained.
It remains unclear whether control of fever would ameliorate adverse effects.
Although limited by several factors, including the fact that few women (n = 10) not receiving an epidural developed fever in this study, thereby precluding meaningful analysis of neonatal outcomes in that group, and by the fact that undiagnosed neonatal or maternal infections may have caused the increase in adverse neonatal outcomes, the findings raise important concerns about the risks of epidural-related intrapartum maternal temperature.
"Although many of the specific outcomes we found associated with elevated maternal temperature may be transient, it is possible that particularly the increase in early-onset neonatal seizures could have implications for longer-term health of the infant," they concluded.
This study was supported in part by a Predoctoral Individual Ruth L. Kerschstein National Research Service Award from the National Institute of Child Health and Human Development to Dr. Greenwell.
FROM PEDIATRICS
Major Finding: In the absence of intrapartum temperature, no significant differences were seen in regard to adverse neonatal outcomes between those who did and did not receive epidural anesthesia. However, a trend was seen between the maximum maternal temperature and a significant increase in the incidence of hypotonia, assisted ventilation, 1- and 5-minute Apgar scores less than 7, and early-onset seizures in those with temperature elevation who received an epidural.
Data Source: A retrospective cohort study involving more than 3,200 women.
Disclosures: This study was supported in part by a Predoctoral Individual Ruth L. Kerschstein National Research Service Award from the National Institute of Child Health and Human Development to Dr. Greenwell.
Study Supports Oral Antibiotics for Acute Pyelonephritis
The incidence of renal scarring did not differ significantly in children with acute pyelonephritis and scintigraphy-documented acute lesions who were treated with oral antibiotics, compared with those treated with sequential intravenous and oral antibiotics in a prospective multicenter trial.
Although the trial wasn’t statistically powered to demonstrate noninferiority of oral treatment, compared with sequential intravenous/oral treatment, the findings confirm those of prior studies and support the use of oral antibiotics for primary acute pyelonephritis (APN) in this population, Dr. Nathalie Bocquet of Assistance Publique-Hôpitaux de Paris and her colleagues reported Jan. 30 in Pediatrics.
In 85 children randomized to receive treatment with oral antibiotics and in 86 randomized to receive sequential treatment with intravenous and oral antibiotics, the incidence of renal scarring based on per protocol analysis was 30.8% and 27.3%, respectively, the investigators said (Pediatrics 2012;129:e269-75).
Participants were infants and children aged 1-36 months who presented with a first case of febrile urinary tract infection (UTI) between August 2004 and April 2008 and who were found to have renal involvement based on serum procalcitonin measurement. All had normal ultrasound findings prenatally, no known uropathy, and no suspected uropathy after ultrasound examination at study inclusion. Dimercaptosuccinic acid (DMSA) scintigraphy was performed within 8 days of inclusion, and those found to have acute lesions underwent follow-up and scintigraphy 6-8 months later.
Treatment for those in the oral antibiotics group included 10 days of cefixime, consisting of an initial double dose of 8 mg/kg administered in the emergency department, followed by 4 mg/kg twice daily. Those in the sequential treatment group received 50 mg/kg of IV ceftriaxone for 4 days followed by oral cefixime at a dose of 4 mg/kg twice daily for 6 days.
After the initial 10-day treatment, antibiotic prophylaxis with co-trimoxazole or another antibiotic adapted to prevent bacterial resistance was continued for up to 1 month until voiding cystography (VCG) could be performed; prophylaxis was discontinued if the VCG findings were normal.
"The frequencies of renal scarring in our treatment groups are comparable with those of previous trials, which reported renal scarring frequencies of 15%-20% and 45%-60%," the investigators noted.
Because high serum procalcitonin concentrations have been shown in prior studies to correlate with acute renal defects on DMSA scintigraphy, they used serum procalcitonin to identify children at high risk for renal involvement.
"Because one of our inclusion criteria was a PCT [procalcitonin] greater than or equal to 0.5 ng/mL, 85.4% of the patients in our study had positive acute phase scintigraphies," they said, noting that in the prior studies, the rates ranged from 60.5% to 63.3%.
"Consistent with what has been previously reported, we found that serum PCT concentrations were significantly higher in children who developed scars than in those who had acute abnormalities but no definitive damage. For this reason, monitoring PCT levels in children afflicted with APN could help to identify those at risk for renal complications even in the absence of a suspected or documented uropathy," they said.
Additionally, they noted that all pathogens isolated in this study were Escherichia coli, which is usually the main pathogen isolated in UTI.
"Antimicrobial treatment with cefixime is a safe choice as long as the likelihood of infection with an E. coli strain that is resistant to third-generation cephalosporins remains low," they said, adding: "Our results support the use of a completely oral cefixime treatment for initial episodes of APN involving a gram-negative bacteria strain in infants and children aged 1 month to 3 years who are without urological abnormalities and without clinical hemodynamic impairment."
This approach to treatment can be proposed for children with serum PCT concentrations greater than 0.5 ng/mL who are at high risk for renal involvement, as well as for those with lower PCT concentrations, despite their low risk for acute renal involvement, they said.
"Oral treatment can facilitate outpatient management of young children with APN because it reduces cost, familial disruption, and nosocomial disease exposure," they concluded.
This study was supported by the Ministry of Health, the Direction de la Recherche Clinique, and the Unit of Clinical Research in Hospital Necker. Only one of the study authors, Dr. Vincent Gajdos, had disclosures to report: He has received consulting fees from GlaxoSmithKline.
The findings by Dr. Bocquet and her colleagues provide additional support for the guidelines published last summer by the American Academy of Pediatrics for the treatment of infants and children with a first febrile UTI (Pediatrics 2011;128:e749-70), Dr. Daniel T. Coghlin said in an interview.
The guidelines note that oral antibiotics are just as effective as intravenous antibiotics are and in this study no significant difference was seen in regard to the rates of kidney scarring with oral vs. sequential intravenous/oral antibiotic treatment. Other studies that have looked at this same outcome from different angles all have come to the same conclusion, he said.
"What’s different is that in this study the authors looked at children with elevated serum levels of procalcitonin, indicating elevated risk for pyelonephritis and even, with this increased risk, no difference in renal scarring was evident between the treatment groups," he said, noting that although the study was too small to definitively show noninferiority, the weight of the available evidence is in favor of this approach.
Some have argued that the guidelines are not proactive enough in advocating the kind of testing that has been done traditionally and thus may lead to missing children who could potentially benefit from aggressive therapies that could be initiated sooner to help prevent kidney injury.
"In fact, most studies over the past 5-10 years have shown that we have probably been over-testing and over-treating children with UTI," he said.
In one study published last year by Salo et al. (Pediatrics 2011;128:840-7), the investigators found no link between chronic UTIs in childhood and chronic kidney injury in adulthood. Of those cases showing even a possible link, all had some kind of structural problem that would have been found on ultrasound. This suggests that even if a difference in the rates of renal scarring was found in this new study, it’s not obvious that that matters, Dr. Coghlin said.
"The guidelines are the best tool for pediatricians to reference when they are deciding how to work up a first- time febrile UTI in an infant, and this study is supportive of those guidelines," he added.
Dr. Coghlin is assistant professor of pediatrics at Brown University, and a pediatric hospitalist at Hasbro Children’s Hospital, both in Providence, R.I. He said he had no disclosures to report.
The findings by Dr. Bocquet and her colleagues provide additional support for the guidelines published last summer by the American Academy of Pediatrics for the treatment of infants and children with a first febrile UTI (Pediatrics 2011;128:e749-70), Dr. Daniel T. Coghlin said in an interview.
The guidelines note that oral antibiotics are just as effective as intravenous antibiotics are and in this study no significant difference was seen in regard to the rates of kidney scarring with oral vs. sequential intravenous/oral antibiotic treatment. Other studies that have looked at this same outcome from different angles all have come to the same conclusion, he said.
"What’s different is that in this study the authors looked at children with elevated serum levels of procalcitonin, indicating elevated risk for pyelonephritis and even, with this increased risk, no difference in renal scarring was evident between the treatment groups," he said, noting that although the study was too small to definitively show noninferiority, the weight of the available evidence is in favor of this approach.
Some have argued that the guidelines are not proactive enough in advocating the kind of testing that has been done traditionally and thus may lead to missing children who could potentially benefit from aggressive therapies that could be initiated sooner to help prevent kidney injury.
"In fact, most studies over the past 5-10 years have shown that we have probably been over-testing and over-treating children with UTI," he said.
In one study published last year by Salo et al. (Pediatrics 2011;128:840-7), the investigators found no link between chronic UTIs in childhood and chronic kidney injury in adulthood. Of those cases showing even a possible link, all had some kind of structural problem that would have been found on ultrasound. This suggests that even if a difference in the rates of renal scarring was found in this new study, it’s not obvious that that matters, Dr. Coghlin said.
"The guidelines are the best tool for pediatricians to reference when they are deciding how to work up a first- time febrile UTI in an infant, and this study is supportive of those guidelines," he added.
Dr. Coghlin is assistant professor of pediatrics at Brown University, and a pediatric hospitalist at Hasbro Children’s Hospital, both in Providence, R.I. He said he had no disclosures to report.
The findings by Dr. Bocquet and her colleagues provide additional support for the guidelines published last summer by the American Academy of Pediatrics for the treatment of infants and children with a first febrile UTI (Pediatrics 2011;128:e749-70), Dr. Daniel T. Coghlin said in an interview.
The guidelines note that oral antibiotics are just as effective as intravenous antibiotics are and in this study no significant difference was seen in regard to the rates of kidney scarring with oral vs. sequential intravenous/oral antibiotic treatment. Other studies that have looked at this same outcome from different angles all have come to the same conclusion, he said.
"What’s different is that in this study the authors looked at children with elevated serum levels of procalcitonin, indicating elevated risk for pyelonephritis and even, with this increased risk, no difference in renal scarring was evident between the treatment groups," he said, noting that although the study was too small to definitively show noninferiority, the weight of the available evidence is in favor of this approach.
Some have argued that the guidelines are not proactive enough in advocating the kind of testing that has been done traditionally and thus may lead to missing children who could potentially benefit from aggressive therapies that could be initiated sooner to help prevent kidney injury.
"In fact, most studies over the past 5-10 years have shown that we have probably been over-testing and over-treating children with UTI," he said.
In one study published last year by Salo et al. (Pediatrics 2011;128:840-7), the investigators found no link between chronic UTIs in childhood and chronic kidney injury in adulthood. Of those cases showing even a possible link, all had some kind of structural problem that would have been found on ultrasound. This suggests that even if a difference in the rates of renal scarring was found in this new study, it’s not obvious that that matters, Dr. Coghlin said.
"The guidelines are the best tool for pediatricians to reference when they are deciding how to work up a first- time febrile UTI in an infant, and this study is supportive of those guidelines," he added.
Dr. Coghlin is assistant professor of pediatrics at Brown University, and a pediatric hospitalist at Hasbro Children’s Hospital, both in Providence, R.I. He said he had no disclosures to report.
The incidence of renal scarring did not differ significantly in children with acute pyelonephritis and scintigraphy-documented acute lesions who were treated with oral antibiotics, compared with those treated with sequential intravenous and oral antibiotics in a prospective multicenter trial.
Although the trial wasn’t statistically powered to demonstrate noninferiority of oral treatment, compared with sequential intravenous/oral treatment, the findings confirm those of prior studies and support the use of oral antibiotics for primary acute pyelonephritis (APN) in this population, Dr. Nathalie Bocquet of Assistance Publique-Hôpitaux de Paris and her colleagues reported Jan. 30 in Pediatrics.
In 85 children randomized to receive treatment with oral antibiotics and in 86 randomized to receive sequential treatment with intravenous and oral antibiotics, the incidence of renal scarring based on per protocol analysis was 30.8% and 27.3%, respectively, the investigators said (Pediatrics 2012;129:e269-75).
Participants were infants and children aged 1-36 months who presented with a first case of febrile urinary tract infection (UTI) between August 2004 and April 2008 and who were found to have renal involvement based on serum procalcitonin measurement. All had normal ultrasound findings prenatally, no known uropathy, and no suspected uropathy after ultrasound examination at study inclusion. Dimercaptosuccinic acid (DMSA) scintigraphy was performed within 8 days of inclusion, and those found to have acute lesions underwent follow-up and scintigraphy 6-8 months later.
Treatment for those in the oral antibiotics group included 10 days of cefixime, consisting of an initial double dose of 8 mg/kg administered in the emergency department, followed by 4 mg/kg twice daily. Those in the sequential treatment group received 50 mg/kg of IV ceftriaxone for 4 days followed by oral cefixime at a dose of 4 mg/kg twice daily for 6 days.
After the initial 10-day treatment, antibiotic prophylaxis with co-trimoxazole or another antibiotic adapted to prevent bacterial resistance was continued for up to 1 month until voiding cystography (VCG) could be performed; prophylaxis was discontinued if the VCG findings were normal.
"The frequencies of renal scarring in our treatment groups are comparable with those of previous trials, which reported renal scarring frequencies of 15%-20% and 45%-60%," the investigators noted.
Because high serum procalcitonin concentrations have been shown in prior studies to correlate with acute renal defects on DMSA scintigraphy, they used serum procalcitonin to identify children at high risk for renal involvement.
"Because one of our inclusion criteria was a PCT [procalcitonin] greater than or equal to 0.5 ng/mL, 85.4% of the patients in our study had positive acute phase scintigraphies," they said, noting that in the prior studies, the rates ranged from 60.5% to 63.3%.
"Consistent with what has been previously reported, we found that serum PCT concentrations were significantly higher in children who developed scars than in those who had acute abnormalities but no definitive damage. For this reason, monitoring PCT levels in children afflicted with APN could help to identify those at risk for renal complications even in the absence of a suspected or documented uropathy," they said.
Additionally, they noted that all pathogens isolated in this study were Escherichia coli, which is usually the main pathogen isolated in UTI.
"Antimicrobial treatment with cefixime is a safe choice as long as the likelihood of infection with an E. coli strain that is resistant to third-generation cephalosporins remains low," they said, adding: "Our results support the use of a completely oral cefixime treatment for initial episodes of APN involving a gram-negative bacteria strain in infants and children aged 1 month to 3 years who are without urological abnormalities and without clinical hemodynamic impairment."
This approach to treatment can be proposed for children with serum PCT concentrations greater than 0.5 ng/mL who are at high risk for renal involvement, as well as for those with lower PCT concentrations, despite their low risk for acute renal involvement, they said.
"Oral treatment can facilitate outpatient management of young children with APN because it reduces cost, familial disruption, and nosocomial disease exposure," they concluded.
This study was supported by the Ministry of Health, the Direction de la Recherche Clinique, and the Unit of Clinical Research in Hospital Necker. Only one of the study authors, Dr. Vincent Gajdos, had disclosures to report: He has received consulting fees from GlaxoSmithKline.
The incidence of renal scarring did not differ significantly in children with acute pyelonephritis and scintigraphy-documented acute lesions who were treated with oral antibiotics, compared with those treated with sequential intravenous and oral antibiotics in a prospective multicenter trial.
Although the trial wasn’t statistically powered to demonstrate noninferiority of oral treatment, compared with sequential intravenous/oral treatment, the findings confirm those of prior studies and support the use of oral antibiotics for primary acute pyelonephritis (APN) in this population, Dr. Nathalie Bocquet of Assistance Publique-Hôpitaux de Paris and her colleagues reported Jan. 30 in Pediatrics.
In 85 children randomized to receive treatment with oral antibiotics and in 86 randomized to receive sequential treatment with intravenous and oral antibiotics, the incidence of renal scarring based on per protocol analysis was 30.8% and 27.3%, respectively, the investigators said (Pediatrics 2012;129:e269-75).
Participants were infants and children aged 1-36 months who presented with a first case of febrile urinary tract infection (UTI) between August 2004 and April 2008 and who were found to have renal involvement based on serum procalcitonin measurement. All had normal ultrasound findings prenatally, no known uropathy, and no suspected uropathy after ultrasound examination at study inclusion. Dimercaptosuccinic acid (DMSA) scintigraphy was performed within 8 days of inclusion, and those found to have acute lesions underwent follow-up and scintigraphy 6-8 months later.
Treatment for those in the oral antibiotics group included 10 days of cefixime, consisting of an initial double dose of 8 mg/kg administered in the emergency department, followed by 4 mg/kg twice daily. Those in the sequential treatment group received 50 mg/kg of IV ceftriaxone for 4 days followed by oral cefixime at a dose of 4 mg/kg twice daily for 6 days.
After the initial 10-day treatment, antibiotic prophylaxis with co-trimoxazole or another antibiotic adapted to prevent bacterial resistance was continued for up to 1 month until voiding cystography (VCG) could be performed; prophylaxis was discontinued if the VCG findings were normal.
"The frequencies of renal scarring in our treatment groups are comparable with those of previous trials, which reported renal scarring frequencies of 15%-20% and 45%-60%," the investigators noted.
Because high serum procalcitonin concentrations have been shown in prior studies to correlate with acute renal defects on DMSA scintigraphy, they used serum procalcitonin to identify children at high risk for renal involvement.
"Because one of our inclusion criteria was a PCT [procalcitonin] greater than or equal to 0.5 ng/mL, 85.4% of the patients in our study had positive acute phase scintigraphies," they said, noting that in the prior studies, the rates ranged from 60.5% to 63.3%.
"Consistent with what has been previously reported, we found that serum PCT concentrations were significantly higher in children who developed scars than in those who had acute abnormalities but no definitive damage. For this reason, monitoring PCT levels in children afflicted with APN could help to identify those at risk for renal complications even in the absence of a suspected or documented uropathy," they said.
Additionally, they noted that all pathogens isolated in this study were Escherichia coli, which is usually the main pathogen isolated in UTI.
"Antimicrobial treatment with cefixime is a safe choice as long as the likelihood of infection with an E. coli strain that is resistant to third-generation cephalosporins remains low," they said, adding: "Our results support the use of a completely oral cefixime treatment for initial episodes of APN involving a gram-negative bacteria strain in infants and children aged 1 month to 3 years who are without urological abnormalities and without clinical hemodynamic impairment."
This approach to treatment can be proposed for children with serum PCT concentrations greater than 0.5 ng/mL who are at high risk for renal involvement, as well as for those with lower PCT concentrations, despite their low risk for acute renal involvement, they said.
"Oral treatment can facilitate outpatient management of young children with APN because it reduces cost, familial disruption, and nosocomial disease exposure," they concluded.
This study was supported by the Ministry of Health, the Direction de la Recherche Clinique, and the Unit of Clinical Research in Hospital Necker. Only one of the study authors, Dr. Vincent Gajdos, had disclosures to report: He has received consulting fees from GlaxoSmithKline.
FROM PEDIATRICS
Major Finding: In 85 children randomized to receive treatment with oral antibiotics and 86 randomized to receive sequential treatment with intravenous and oral antibiotics, the incidence of renal scarring based on per-protocol analysis was 30.8% and 27.3%, respectively.
Data Source: A prospective randomized multicenter trial.
Disclosures: This study was supported by the Ministry of Health, the Direction de la Recherche Clinique, and the Unit of Clinical Research in Hospital Necker. Only one of the study authors, Dr. Vincent Gajdos, had disclosures to report: He has received consulting fees from GlaxoSmithKline.
Risk Factors, Not Race, Determine Lifetime Heart Risks
Adults with an optimal cardiovascular risk profile at age 55 have a substantially lower risk of death from cardiovascular disease through age 80 years, and a lower lifetime risk of fatal coronary heart disease, nonfatal myocardial infarction, and stroke, compared with those who have two or more major risk factors, according to a meta-analysis of 18 studies involving more than 257,000 adults.
The findings, which have important disease prevention and public health implications, were consistent across race and diverse birth cohorts, Dr. Jarett D. Berry of the University of Texas Southwestern Medical Center, Dallas and his colleagues report in the Jan. 26 issue of The New England Journal of Medicine.
The investigators conducted their meta-analysis at the individual level using data from studies that included black men and women and white men and women who were assessed for cardiovascular risk factors at ages 45, 55, 65, and 75 years. Patients were stratified into five mutually exclusive risk categories based on blood pressure, cholesterol level, smoking status, and diabetes status; only about 5% of participants comprised the optimal risk category, and about two-thirds comprised the two highest-risk groups.
The risk of cardiovascular disease-related death through age 80 years was 4.7% and 6.4% in men and women, respectively, who were nonsmokers without diabetes, and who had a total cholesterol level of less than 80 mg/dL, and blood pressure less than 120 mm Hg systolic and 80 mm Hg diastolic at age 55 years. The risk was 30% and 21% in men and women, respectively, with two or more major risk factors at that age, they said (N. Engl. J. Med. 2012;366:321-9).
The risk of fatal coronary heart disease or nonfatal MI was 3.6% and less than 1% in men and women, respectively, with the optimal risk factor profile, compared with 37.5% and 18.3% in men and women, respectively, with two or more major risk factors. The risk of fatal or nonfatal stroke was 2.3% and 5.3% in men and women with the optimal profile, compared with 8.3% and 10.7% in those with at least two major risk factors.
Similar patterns were seen based on assessments at other ages.
Significant, but expected, differences in the burden of risk factors were seen between older and younger birth cohorts, such as a higher prevalence of diabetes, a lower prevalence of smoking, and lower mean total cholesterol and systolic blood pressure in 55-year-old men born after 1920, compared with those born before 1920. Also, the burden of risk factors was higher among blacks than among whites, when participants were stratified according to race.
This approach to characterizing the lifetime risk of cardiovascular disease provides a more comprehensive assessment of overall disease burden in the general population than does the more common approach that calculates global, 10-year risk estimates, the investigators said, explaining that the majority of adults in the U.S. who are considered to be at low risk in the short-term, are actually at high risk across their lifespan.
According to the investigators, the findings "strongly reinforce the influence of traditional risk factors on the lifetime risk of cardiovascular disease" and despite the development of notable secular trends in the prevalence of risk factors over the past 4 decades, the effect of those risk factors remained remarkably consistent across birth cohorts, they said.
In fact, they concluded that it is the presence or absence of traditional risk factors, rather than race or birth cohort, that appears to be the most consistent determinant of long-term cardiovascular disease risk – a conclusion based in part on a finding that despite an overall higher prevalence of risk factors in black than in whites, the lifetime risks of end points related to cardiovascular disease were similar in blacks and whites when risk factor profiles were similar.
The findings, according to the investigators, have important implications for clinical disease prevention and public health practice.
"First, the effect of untreated risk factors has been fairly constant for decades. Therefore, the present estimates of lifetime risk, made on the basis of current or projected risk-factor levels, may be important in estimating the future burden of cardiovascular disease in the general population. Second, efforts to lower the burden of cardiovascular disease will require prevention of the development of risk factors (primordial prevention) rather than the sole reliance on the treatment of existing risk factors (primary prevention)," they wrote.
Also, the findings are consistent with prior observations that the decline in cardiovascular event rates in the general population reflect changes in risk factor prevalence as opposed to treatment effects alone.
"For example, 44.3% of the overall decline in the U.S rates of death from coronary heart disease in 1980 and 2000 was attributed to population changes in levels of serum total cholesterol (24.2%) and systolic blood pressure (20.1%). The effects of clinical treatment on these risk factors were more modest, with statin and antihypertensive therapy accounting for 4.9% and 7.0% of the decline, respectively."
"These observations were extended to long-term risk estimates, showing that changes in the prevalence of risk factor profiles strongly influence lifetime risk estimates in the general population," the authors wrote.
This study was supported by grants from the National Heart, Lung, and Blood Institute and the American Heart Association, and by funding from the Dedman Family Scholar in Clinical Care endowment at the University of Texas Southwestern Medical Center. Dr. Thompson is a consultant, has done research, or has received speaking honoraria numerous manufacturers of lipid-lowering drugs, including GlaxoSmithKline, Merck, Pfizer, and AstraZeneca. Individual author disclosures are available with the full text of the article at NEJM.org.
I applaud the approach taken by the investigators of this meta-analysis. Many in the field have been troubled by the tendency to use 10-year risk estimates.
Nobody wants to live just 10 years, so it’s important to be able to provide younger patients with a broader picture of lifetime risk. This study does not give us the ability to calculate 20- and 30-year risk, but it does introduce that concept.
It also introduces the intriguing and somewhat novel concept of primordial prevention, that is, preventing the development of risk factors.
The study’s findings that the effects of traditional risk factors are consistent between races and across birth cohorts is not surprising. In fact, they emphasizes the classic risk factor model we’ve talked about all along, and debunks some myths about age, race, and other factors. I think that’s a useful message.
However, although the concept of primordial prevention is intriguing, the findings don’t obviate the need for maintaining a focus on primary prevention. The treatment effects mentioned by the investigators are small, but given the number of patients who get heart disease, they represent an enormous effect.
Paul D. Thompson, M.D., is director of cardiology at Hartford Hospital. He is a consultant, has done research, or has received speaking honoraria numerous manufacturers of lipid-lowering drugs, including GlaxoSmithKline, Merck, Pfizer, and AstraZeneca.
I applaud the approach taken by the investigators of this meta-analysis. Many in the field have been troubled by the tendency to use 10-year risk estimates.
Nobody wants to live just 10 years, so it’s important to be able to provide younger patients with a broader picture of lifetime risk. This study does not give us the ability to calculate 20- and 30-year risk, but it does introduce that concept.
It also introduces the intriguing and somewhat novel concept of primordial prevention, that is, preventing the development of risk factors.
The study’s findings that the effects of traditional risk factors are consistent between races and across birth cohorts is not surprising. In fact, they emphasizes the classic risk factor model we’ve talked about all along, and debunks some myths about age, race, and other factors. I think that’s a useful message.
However, although the concept of primordial prevention is intriguing, the findings don’t obviate the need for maintaining a focus on primary prevention. The treatment effects mentioned by the investigators are small, but given the number of patients who get heart disease, they represent an enormous effect.
Paul D. Thompson, M.D., is director of cardiology at Hartford Hospital. He is a consultant, has done research, or has received speaking honoraria numerous manufacturers of lipid-lowering drugs, including GlaxoSmithKline, Merck, Pfizer, and AstraZeneca.
I applaud the approach taken by the investigators of this meta-analysis. Many in the field have been troubled by the tendency to use 10-year risk estimates.
Nobody wants to live just 10 years, so it’s important to be able to provide younger patients with a broader picture of lifetime risk. This study does not give us the ability to calculate 20- and 30-year risk, but it does introduce that concept.
It also introduces the intriguing and somewhat novel concept of primordial prevention, that is, preventing the development of risk factors.
The study’s findings that the effects of traditional risk factors are consistent between races and across birth cohorts is not surprising. In fact, they emphasizes the classic risk factor model we’ve talked about all along, and debunks some myths about age, race, and other factors. I think that’s a useful message.
However, although the concept of primordial prevention is intriguing, the findings don’t obviate the need for maintaining a focus on primary prevention. The treatment effects mentioned by the investigators are small, but given the number of patients who get heart disease, they represent an enormous effect.
Paul D. Thompson, M.D., is director of cardiology at Hartford Hospital. He is a consultant, has done research, or has received speaking honoraria numerous manufacturers of lipid-lowering drugs, including GlaxoSmithKline, Merck, Pfizer, and AstraZeneca.
Adults with an optimal cardiovascular risk profile at age 55 have a substantially lower risk of death from cardiovascular disease through age 80 years, and a lower lifetime risk of fatal coronary heart disease, nonfatal myocardial infarction, and stroke, compared with those who have two or more major risk factors, according to a meta-analysis of 18 studies involving more than 257,000 adults.
The findings, which have important disease prevention and public health implications, were consistent across race and diverse birth cohorts, Dr. Jarett D. Berry of the University of Texas Southwestern Medical Center, Dallas and his colleagues report in the Jan. 26 issue of The New England Journal of Medicine.
The investigators conducted their meta-analysis at the individual level using data from studies that included black men and women and white men and women who were assessed for cardiovascular risk factors at ages 45, 55, 65, and 75 years. Patients were stratified into five mutually exclusive risk categories based on blood pressure, cholesterol level, smoking status, and diabetes status; only about 5% of participants comprised the optimal risk category, and about two-thirds comprised the two highest-risk groups.
The risk of cardiovascular disease-related death through age 80 years was 4.7% and 6.4% in men and women, respectively, who were nonsmokers without diabetes, and who had a total cholesterol level of less than 80 mg/dL, and blood pressure less than 120 mm Hg systolic and 80 mm Hg diastolic at age 55 years. The risk was 30% and 21% in men and women, respectively, with two or more major risk factors at that age, they said (N. Engl. J. Med. 2012;366:321-9).
The risk of fatal coronary heart disease or nonfatal MI was 3.6% and less than 1% in men and women, respectively, with the optimal risk factor profile, compared with 37.5% and 18.3% in men and women, respectively, with two or more major risk factors. The risk of fatal or nonfatal stroke was 2.3% and 5.3% in men and women with the optimal profile, compared with 8.3% and 10.7% in those with at least two major risk factors.
Similar patterns were seen based on assessments at other ages.
Significant, but expected, differences in the burden of risk factors were seen between older and younger birth cohorts, such as a higher prevalence of diabetes, a lower prevalence of smoking, and lower mean total cholesterol and systolic blood pressure in 55-year-old men born after 1920, compared with those born before 1920. Also, the burden of risk factors was higher among blacks than among whites, when participants were stratified according to race.
This approach to characterizing the lifetime risk of cardiovascular disease provides a more comprehensive assessment of overall disease burden in the general population than does the more common approach that calculates global, 10-year risk estimates, the investigators said, explaining that the majority of adults in the U.S. who are considered to be at low risk in the short-term, are actually at high risk across their lifespan.
According to the investigators, the findings "strongly reinforce the influence of traditional risk factors on the lifetime risk of cardiovascular disease" and despite the development of notable secular trends in the prevalence of risk factors over the past 4 decades, the effect of those risk factors remained remarkably consistent across birth cohorts, they said.
In fact, they concluded that it is the presence or absence of traditional risk factors, rather than race or birth cohort, that appears to be the most consistent determinant of long-term cardiovascular disease risk – a conclusion based in part on a finding that despite an overall higher prevalence of risk factors in black than in whites, the lifetime risks of end points related to cardiovascular disease were similar in blacks and whites when risk factor profiles were similar.
The findings, according to the investigators, have important implications for clinical disease prevention and public health practice.
"First, the effect of untreated risk factors has been fairly constant for decades. Therefore, the present estimates of lifetime risk, made on the basis of current or projected risk-factor levels, may be important in estimating the future burden of cardiovascular disease in the general population. Second, efforts to lower the burden of cardiovascular disease will require prevention of the development of risk factors (primordial prevention) rather than the sole reliance on the treatment of existing risk factors (primary prevention)," they wrote.
Also, the findings are consistent with prior observations that the decline in cardiovascular event rates in the general population reflect changes in risk factor prevalence as opposed to treatment effects alone.
"For example, 44.3% of the overall decline in the U.S rates of death from coronary heart disease in 1980 and 2000 was attributed to population changes in levels of serum total cholesterol (24.2%) and systolic blood pressure (20.1%). The effects of clinical treatment on these risk factors were more modest, with statin and antihypertensive therapy accounting for 4.9% and 7.0% of the decline, respectively."
"These observations were extended to long-term risk estimates, showing that changes in the prevalence of risk factor profiles strongly influence lifetime risk estimates in the general population," the authors wrote.
This study was supported by grants from the National Heart, Lung, and Blood Institute and the American Heart Association, and by funding from the Dedman Family Scholar in Clinical Care endowment at the University of Texas Southwestern Medical Center. Dr. Thompson is a consultant, has done research, or has received speaking honoraria numerous manufacturers of lipid-lowering drugs, including GlaxoSmithKline, Merck, Pfizer, and AstraZeneca. Individual author disclosures are available with the full text of the article at NEJM.org.
Adults with an optimal cardiovascular risk profile at age 55 have a substantially lower risk of death from cardiovascular disease through age 80 years, and a lower lifetime risk of fatal coronary heart disease, nonfatal myocardial infarction, and stroke, compared with those who have two or more major risk factors, according to a meta-analysis of 18 studies involving more than 257,000 adults.
The findings, which have important disease prevention and public health implications, were consistent across race and diverse birth cohorts, Dr. Jarett D. Berry of the University of Texas Southwestern Medical Center, Dallas and his colleagues report in the Jan. 26 issue of The New England Journal of Medicine.
The investigators conducted their meta-analysis at the individual level using data from studies that included black men and women and white men and women who were assessed for cardiovascular risk factors at ages 45, 55, 65, and 75 years. Patients were stratified into five mutually exclusive risk categories based on blood pressure, cholesterol level, smoking status, and diabetes status; only about 5% of participants comprised the optimal risk category, and about two-thirds comprised the two highest-risk groups.
The risk of cardiovascular disease-related death through age 80 years was 4.7% and 6.4% in men and women, respectively, who were nonsmokers without diabetes, and who had a total cholesterol level of less than 80 mg/dL, and blood pressure less than 120 mm Hg systolic and 80 mm Hg diastolic at age 55 years. The risk was 30% and 21% in men and women, respectively, with two or more major risk factors at that age, they said (N. Engl. J. Med. 2012;366:321-9).
The risk of fatal coronary heart disease or nonfatal MI was 3.6% and less than 1% in men and women, respectively, with the optimal risk factor profile, compared with 37.5% and 18.3% in men and women, respectively, with two or more major risk factors. The risk of fatal or nonfatal stroke was 2.3% and 5.3% in men and women with the optimal profile, compared with 8.3% and 10.7% in those with at least two major risk factors.
Similar patterns were seen based on assessments at other ages.
Significant, but expected, differences in the burden of risk factors were seen between older and younger birth cohorts, such as a higher prevalence of diabetes, a lower prevalence of smoking, and lower mean total cholesterol and systolic blood pressure in 55-year-old men born after 1920, compared with those born before 1920. Also, the burden of risk factors was higher among blacks than among whites, when participants were stratified according to race.
This approach to characterizing the lifetime risk of cardiovascular disease provides a more comprehensive assessment of overall disease burden in the general population than does the more common approach that calculates global, 10-year risk estimates, the investigators said, explaining that the majority of adults in the U.S. who are considered to be at low risk in the short-term, are actually at high risk across their lifespan.
According to the investigators, the findings "strongly reinforce the influence of traditional risk factors on the lifetime risk of cardiovascular disease" and despite the development of notable secular trends in the prevalence of risk factors over the past 4 decades, the effect of those risk factors remained remarkably consistent across birth cohorts, they said.
In fact, they concluded that it is the presence or absence of traditional risk factors, rather than race or birth cohort, that appears to be the most consistent determinant of long-term cardiovascular disease risk – a conclusion based in part on a finding that despite an overall higher prevalence of risk factors in black than in whites, the lifetime risks of end points related to cardiovascular disease were similar in blacks and whites when risk factor profiles were similar.
The findings, according to the investigators, have important implications for clinical disease prevention and public health practice.
"First, the effect of untreated risk factors has been fairly constant for decades. Therefore, the present estimates of lifetime risk, made on the basis of current or projected risk-factor levels, may be important in estimating the future burden of cardiovascular disease in the general population. Second, efforts to lower the burden of cardiovascular disease will require prevention of the development of risk factors (primordial prevention) rather than the sole reliance on the treatment of existing risk factors (primary prevention)," they wrote.
Also, the findings are consistent with prior observations that the decline in cardiovascular event rates in the general population reflect changes in risk factor prevalence as opposed to treatment effects alone.
"For example, 44.3% of the overall decline in the U.S rates of death from coronary heart disease in 1980 and 2000 was attributed to population changes in levels of serum total cholesterol (24.2%) and systolic blood pressure (20.1%). The effects of clinical treatment on these risk factors were more modest, with statin and antihypertensive therapy accounting for 4.9% and 7.0% of the decline, respectively."
"These observations were extended to long-term risk estimates, showing that changes in the prevalence of risk factor profiles strongly influence lifetime risk estimates in the general population," the authors wrote.
This study was supported by grants from the National Heart, Lung, and Blood Institute and the American Heart Association, and by funding from the Dedman Family Scholar in Clinical Care endowment at the University of Texas Southwestern Medical Center. Dr. Thompson is a consultant, has done research, or has received speaking honoraria numerous manufacturers of lipid-lowering drugs, including GlaxoSmithKline, Merck, Pfizer, and AstraZeneca. Individual author disclosures are available with the full text of the article at NEJM.org.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: The risk of cardiovascular disease-related death through age 80 years was 4.7% and 6.4% among men and women, respectively, who were nonsmokers without diabetes, a total cholesterol level of less than 80 mg/dL, and blood pressure less than 120 mm Hg systolic and 80 mm Hg diastolic at age 55 years. The risks were 30% and 21% in men and women, respectively, with at least two major risk factors at that age.
Data Source: A meta-analysis using data from 18 cohort studies.
Disclosures: This study was supported by grants from the National Heart, Lung, and Blood Institute and the American Heart Association, and by funding from the Dedman Family Scholar in Clinical Care endowment at the University of Texas Southwestern Medical Center. Individual author disclosures are available with the full text of the article at NEJM.org.
Bevacizumab Boosts Treatment Responses in Early Breast Cancer
Adding bevacizumab to neoadjuvant chemotherapy in patients with early-stage HER2-negative breast cancer significantly improves pathological complete response, according to preliminary reports from two large randomized clinical trials.
The published results are likely to reopen debate over the recent U.S. Food and Drug Administration decision to revoke an indication for bevacizumab (Avastin) in metastatic breast cancer and the use of surrogate end points for survival in breast cancer trials.
Findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-40 trial and the GeparQuinto (GBG44) trial appear in the Jan. 26 issue of The New England Journal of Medicine.
Docetaxel-Based Chemo in NSABP B-40
In NSABP B-40, 1,206 patients were enrolled between Jan. 5, 2007 and June 20, 2101 and randomly assigned to receive docetaxel (Taxotere), docetaxel plus capecitabine (Xeloda), or docetaxel plus gemcitabine (Gemzar) for four cycles. All groups received doxorubicin and cyclophosphamide for an additional four cycles, and the participants were additionally assigned to receive or not receive bevacizumab (Avastin) – an antiangiogenic monoclonal antibody against vascular endothelial growth factor (VEGF), for the first 6 of the 8 treatment cycles.
The addition of the antimetabolites capecitabine or gemcitabine had no significant effect on pathological complete response in the breast, with, respectively 29.7% and 31.8% of patients achieving that primary end point, compared with 32.7% of those receiving only docetaxel, Dr. Harry D. Bear of Virginia Commonwealth University, Richmond and his colleagues reported (N. Engl. J. Med. 2012;366:310-20).
Adding bevacizumab, however, increased the rate of pathological complete response in the breast significantly from 28.2% to 34.5%. Subgroup analysis indicated the effect was more pronounced in patients with hormone receptor–positive tumors (the rate increasing significantly from 15.1% without bevacizumab to 23.2% with bevacizumab) than in hormone receptor–negative tumors (47.1% and 51.5%, respectively), the investigators said. The benefit of bevacizumab tended to be seen more in patients with a high tumor grade.
Epirubicin-based Chemo in GeparQuinto
In the GeparQuinto trial, 1,948 patients were enrolled from November 2007 through June 2010 and randomized to receive neoadjuvant epirubicin (Ellence) and cyclophosphamide followed by docetaxel either with or without bevacizumab.

Pathological complete response occurred in 18.4% of those who received bevacizumab, compared with 14.9% of those who did not (odds ratio, 1.29), Dr. Gunter von Minckwitz of the German Breast Group, Neu-Isenburg, Germany and his colleagues reported. (N. Engl. J. Med. 2012;366:299-309). After adjusting for age, clinical tumor and nodal stage, hormone-receptor status, tumor grade, and histologic type, the odds ratio was 1.36.
In contrast with the findings from NSABP B-40, the greatest effects of bevacizumab in GBG44 were seen in the 633 patients with triple-negative tumors (27.9% without vs. 39.3% with bevacizumab), compared with the 1,262 patients with hormone-receptor-positive tumors (7.8% and 7.7%, respectively). The test for interaction for this finding was not significant, but the study was not powered to show these differential effects, the investigators noted.
Investigators from both trials suggested that possible reasons for the divergent findings between the studies include differences in inclusion criteria and drug dosing and/or sequencing.
The NSABP B-40 investigators noted that "the increased rate of pathological complete response in patients with hormone receptor–positive tumors is encouraging, since this group tends to have low rates of pathological complete response with chemotherapy."
Bevacizumab was associated with toxic effects in both studies, including hand-foot syndrome, mucositis, hypertension, and left ventricular systolic dysfunction in NSABP B-40, and with bleeding, febrile neutropenia, mucositis, hand-foot syndrome, infection, and hypertension in GBG44.
Survival Results Pending
The NSABP B-40 investigators said that the potential for bevacizumab to improve patient outcomes should be clarified when disease-free and overall survival results become available for those who underwent surgery in this study, and for those in other ongoing studies.
They also noted that "the collection of tissue samples from all our patients before treatment, a major advantage of the neoadjuvant approach, offers an opportunity to discover molecular markers that might predict a benefit from bevacizumab."
The GBG44 investigators noted that because of the short follow-up in their study, it cannot be confirmed that the observed increases in the rate of pathological complete response will translate into a survival advantage.
"However, given that pathological complete response has been shown to be highly correlated with outcome, particularly in patients with triple-negative disease, we speculate that the beneficial effects will be sustained," they said, adding, "Long-term follow-up data are needed before this treatment option can be fully understood."
Dosing in the studies was as follows:
In NSABP B-40, docetaxel was administered intravenously at 100 mg/m2 on day 1 of the cycle every 3 weeks in the docetaxel-only group, followed by four cycles of doxorubicin-cyclophosphamide at 60 mg/m2 and 600 mg/m2, respectively, administered intravenously every 3 weeks. Docetaxel was administered at a dose of 75 mg/m2 on day 1 in the docetaxel plus capecitabine or gemcitabine groups followed by the doxorubicin-cyclophosphamide. The capecitabine dose was 825 mg/m2 twice daily on days 1-14; the gemcitabine dose was 1,000 mg/m2 on days 1 and 8. The bevacizumab dose was 15 mg/kg administered intravenously for the first six cycles.
In GBG44, epirubicin was administered at a dose of 90 mg/m2and cyclophosphamide was administered at a dose of 600 mg/m2– both on day 1, every 3 weeks for four cycles, followed by four cycles of docetaxel a dose of 100 mg/m2 on day 1, every 3 weeks. As in NSABP B-40, bevacizumab was administered at a dose of 15 mg/kg intravenously. In this study, however, it was administered every 3 weeks starting on day 1 of the first epirubicin-cyclophosphamide cycle for 8 cycles.
NSABP B-40 was supported by grants from the National Cancer Institute, the Department of Health and Human Services, the Public Health Service, F. Hoffman-La Roche, Genentech USA, and Eli Lilly. GeparQuinto was supported by grants from Sanofi-Aventis and Roche, Germany. Detailed individual author disclosures are available with the full text of the articles at NEJM.org.
While the results of these studies are particularly timely given the U.S. Food and Drug Administration’s revocation in November of its 2008 approval of bevacizumab in combination with paclitaxel for the treatment of metastatic breast cancer, they do little to quell the controversy surrounding bevacizumab, Dr. Alberto J. Montero and Dr. Charles Vogel said in an accompanying editorial.
The studies were designed based on the "plausible assumption" that a surrogate clinical end point such as progression-free survival – the end point used in the trials on which bevacizumab was initially approved – should be used in cases of metastatic breast cancer.
"The unresolved issue is whether significant improvements in a surrogate end point ... in the absence of a benefit for overall survival, are potentially predictive of curative benefits in patients with earlier-stage breast cancer," they said; only data on recurrence and survival from ongoing trials will resolve this issue (N. Engl. J. Med. 2012;366:374-5).
The controversy also involves broader questions about the use of surrogate end points, as well as about economic factors such as the ever-increasing cost of new cancer drugs.
"It is through this lens that the NSABP B-40 and GBG44 trials should be viewed, since each of these trials reports a significant improvement with bevacizumab in another putative surrogate clinical end point: pathological complete response," they said, adding that if such surrogate end points are ultimately shown to predict survival benefits in earlier-stage disease, their use in clinical research will be vindicated – and the FDA’s recent action will be further called into question.
"However, in the context of unsustainable expenditures for cancer care in the United States, any survival benefit of bevacizumab, or other molecularly targeted drugs, will be balanced against the considerable development costs of modern molecularly targeted oncology drugs," they said.
Dr. Montero and Dr. Vogel are with the University of Miami Sylvester Comprehensive Cancer Center. Dr. Vogel had several disclosures. The complete list is available with the full text of the editorial at NEJM.org.
While the results of these studies are particularly timely given the U.S. Food and Drug Administration’s revocation in November of its 2008 approval of bevacizumab in combination with paclitaxel for the treatment of metastatic breast cancer, they do little to quell the controversy surrounding bevacizumab, Dr. Alberto J. Montero and Dr. Charles Vogel said in an accompanying editorial.
The studies were designed based on the "plausible assumption" that a surrogate clinical end point such as progression-free survival – the end point used in the trials on which bevacizumab was initially approved – should be used in cases of metastatic breast cancer.
"The unresolved issue is whether significant improvements in a surrogate end point ... in the absence of a benefit for overall survival, are potentially predictive of curative benefits in patients with earlier-stage breast cancer," they said; only data on recurrence and survival from ongoing trials will resolve this issue (N. Engl. J. Med. 2012;366:374-5).
The controversy also involves broader questions about the use of surrogate end points, as well as about economic factors such as the ever-increasing cost of new cancer drugs.
"It is through this lens that the NSABP B-40 and GBG44 trials should be viewed, since each of these trials reports a significant improvement with bevacizumab in another putative surrogate clinical end point: pathological complete response," they said, adding that if such surrogate end points are ultimately shown to predict survival benefits in earlier-stage disease, their use in clinical research will be vindicated – and the FDA’s recent action will be further called into question.
"However, in the context of unsustainable expenditures for cancer care in the United States, any survival benefit of bevacizumab, or other molecularly targeted drugs, will be balanced against the considerable development costs of modern molecularly targeted oncology drugs," they said.
Dr. Montero and Dr. Vogel are with the University of Miami Sylvester Comprehensive Cancer Center. Dr. Vogel had several disclosures. The complete list is available with the full text of the editorial at NEJM.org.
While the results of these studies are particularly timely given the U.S. Food and Drug Administration’s revocation in November of its 2008 approval of bevacizumab in combination with paclitaxel for the treatment of metastatic breast cancer, they do little to quell the controversy surrounding bevacizumab, Dr. Alberto J. Montero and Dr. Charles Vogel said in an accompanying editorial.
The studies were designed based on the "plausible assumption" that a surrogate clinical end point such as progression-free survival – the end point used in the trials on which bevacizumab was initially approved – should be used in cases of metastatic breast cancer.
"The unresolved issue is whether significant improvements in a surrogate end point ... in the absence of a benefit for overall survival, are potentially predictive of curative benefits in patients with earlier-stage breast cancer," they said; only data on recurrence and survival from ongoing trials will resolve this issue (N. Engl. J. Med. 2012;366:374-5).
The controversy also involves broader questions about the use of surrogate end points, as well as about economic factors such as the ever-increasing cost of new cancer drugs.
"It is through this lens that the NSABP B-40 and GBG44 trials should be viewed, since each of these trials reports a significant improvement with bevacizumab in another putative surrogate clinical end point: pathological complete response," they said, adding that if such surrogate end points are ultimately shown to predict survival benefits in earlier-stage disease, their use in clinical research will be vindicated – and the FDA’s recent action will be further called into question.
"However, in the context of unsustainable expenditures for cancer care in the United States, any survival benefit of bevacizumab, or other molecularly targeted drugs, will be balanced against the considerable development costs of modern molecularly targeted oncology drugs," they said.
Dr. Montero and Dr. Vogel are with the University of Miami Sylvester Comprehensive Cancer Center. Dr. Vogel had several disclosures. The complete list is available with the full text of the editorial at NEJM.org.
Adding bevacizumab to neoadjuvant chemotherapy in patients with early-stage HER2-negative breast cancer significantly improves pathological complete response, according to preliminary reports from two large randomized clinical trials.
The published results are likely to reopen debate over the recent U.S. Food and Drug Administration decision to revoke an indication for bevacizumab (Avastin) in metastatic breast cancer and the use of surrogate end points for survival in breast cancer trials.
Findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-40 trial and the GeparQuinto (GBG44) trial appear in the Jan. 26 issue of The New England Journal of Medicine.
Docetaxel-Based Chemo in NSABP B-40
In NSABP B-40, 1,206 patients were enrolled between Jan. 5, 2007 and June 20, 2101 and randomly assigned to receive docetaxel (Taxotere), docetaxel plus capecitabine (Xeloda), or docetaxel plus gemcitabine (Gemzar) for four cycles. All groups received doxorubicin and cyclophosphamide for an additional four cycles, and the participants were additionally assigned to receive or not receive bevacizumab (Avastin) – an antiangiogenic monoclonal antibody against vascular endothelial growth factor (VEGF), for the first 6 of the 8 treatment cycles.
The addition of the antimetabolites capecitabine or gemcitabine had no significant effect on pathological complete response in the breast, with, respectively 29.7% and 31.8% of patients achieving that primary end point, compared with 32.7% of those receiving only docetaxel, Dr. Harry D. Bear of Virginia Commonwealth University, Richmond and his colleagues reported (N. Engl. J. Med. 2012;366:310-20).
Adding bevacizumab, however, increased the rate of pathological complete response in the breast significantly from 28.2% to 34.5%. Subgroup analysis indicated the effect was more pronounced in patients with hormone receptor–positive tumors (the rate increasing significantly from 15.1% without bevacizumab to 23.2% with bevacizumab) than in hormone receptor–negative tumors (47.1% and 51.5%, respectively), the investigators said. The benefit of bevacizumab tended to be seen more in patients with a high tumor grade.
Epirubicin-based Chemo in GeparQuinto
In the GeparQuinto trial, 1,948 patients were enrolled from November 2007 through June 2010 and randomized to receive neoadjuvant epirubicin (Ellence) and cyclophosphamide followed by docetaxel either with or without bevacizumab.
Pathological complete response occurred in 18.4% of those who received bevacizumab, compared with 14.9% of those who did not (odds ratio, 1.29), Dr. Gunter von Minckwitz of the German Breast Group, Neu-Isenburg, Germany and his colleagues reported. (N. Engl. J. Med. 2012;366:299-309). After adjusting for age, clinical tumor and nodal stage, hormone-receptor status, tumor grade, and histologic type, the odds ratio was 1.36.
In contrast with the findings from NSABP B-40, the greatest effects of bevacizumab in GBG44 were seen in the 633 patients with triple-negative tumors (27.9% without vs. 39.3% with bevacizumab), compared with the 1,262 patients with hormone-receptor-positive tumors (7.8% and 7.7%, respectively). The test for interaction for this finding was not significant, but the study was not powered to show these differential effects, the investigators noted.
Investigators from both trials suggested that possible reasons for the divergent findings between the studies include differences in inclusion criteria and drug dosing and/or sequencing.
The NSABP B-40 investigators noted that "the increased rate of pathological complete response in patients with hormone receptor–positive tumors is encouraging, since this group tends to have low rates of pathological complete response with chemotherapy."
Bevacizumab was associated with toxic effects in both studies, including hand-foot syndrome, mucositis, hypertension, and left ventricular systolic dysfunction in NSABP B-40, and with bleeding, febrile neutropenia, mucositis, hand-foot syndrome, infection, and hypertension in GBG44.
Survival Results Pending
The NSABP B-40 investigators said that the potential for bevacizumab to improve patient outcomes should be clarified when disease-free and overall survival results become available for those who underwent surgery in this study, and for those in other ongoing studies.
They also noted that "the collection of tissue samples from all our patients before treatment, a major advantage of the neoadjuvant approach, offers an opportunity to discover molecular markers that might predict a benefit from bevacizumab."
The GBG44 investigators noted that because of the short follow-up in their study, it cannot be confirmed that the observed increases in the rate of pathological complete response will translate into a survival advantage.
"However, given that pathological complete response has been shown to be highly correlated with outcome, particularly in patients with triple-negative disease, we speculate that the beneficial effects will be sustained," they said, adding, "Long-term follow-up data are needed before this treatment option can be fully understood."
Dosing in the studies was as follows:
In NSABP B-40, docetaxel was administered intravenously at 100 mg/m2 on day 1 of the cycle every 3 weeks in the docetaxel-only group, followed by four cycles of doxorubicin-cyclophosphamide at 60 mg/m2 and 600 mg/m2, respectively, administered intravenously every 3 weeks. Docetaxel was administered at a dose of 75 mg/m2 on day 1 in the docetaxel plus capecitabine or gemcitabine groups followed by the doxorubicin-cyclophosphamide. The capecitabine dose was 825 mg/m2 twice daily on days 1-14; the gemcitabine dose was 1,000 mg/m2 on days 1 and 8. The bevacizumab dose was 15 mg/kg administered intravenously for the first six cycles.
In GBG44, epirubicin was administered at a dose of 90 mg/m2and cyclophosphamide was administered at a dose of 600 mg/m2– both on day 1, every 3 weeks for four cycles, followed by four cycles of docetaxel a dose of 100 mg/m2 on day 1, every 3 weeks. As in NSABP B-40, bevacizumab was administered at a dose of 15 mg/kg intravenously. In this study, however, it was administered every 3 weeks starting on day 1 of the first epirubicin-cyclophosphamide cycle for 8 cycles.
NSABP B-40 was supported by grants from the National Cancer Institute, the Department of Health and Human Services, the Public Health Service, F. Hoffman-La Roche, Genentech USA, and Eli Lilly. GeparQuinto was supported by grants from Sanofi-Aventis and Roche, Germany. Detailed individual author disclosures are available with the full text of the articles at NEJM.org.
Adding bevacizumab to neoadjuvant chemotherapy in patients with early-stage HER2-negative breast cancer significantly improves pathological complete response, according to preliminary reports from two large randomized clinical trials.
The published results are likely to reopen debate over the recent U.S. Food and Drug Administration decision to revoke an indication for bevacizumab (Avastin) in metastatic breast cancer and the use of surrogate end points for survival in breast cancer trials.
Findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-40 trial and the GeparQuinto (GBG44) trial appear in the Jan. 26 issue of The New England Journal of Medicine.
Docetaxel-Based Chemo in NSABP B-40
In NSABP B-40, 1,206 patients were enrolled between Jan. 5, 2007 and June 20, 2101 and randomly assigned to receive docetaxel (Taxotere), docetaxel plus capecitabine (Xeloda), or docetaxel plus gemcitabine (Gemzar) for four cycles. All groups received doxorubicin and cyclophosphamide for an additional four cycles, and the participants were additionally assigned to receive or not receive bevacizumab (Avastin) – an antiangiogenic monoclonal antibody against vascular endothelial growth factor (VEGF), for the first 6 of the 8 treatment cycles.
The addition of the antimetabolites capecitabine or gemcitabine had no significant effect on pathological complete response in the breast, with, respectively 29.7% and 31.8% of patients achieving that primary end point, compared with 32.7% of those receiving only docetaxel, Dr. Harry D. Bear of Virginia Commonwealth University, Richmond and his colleagues reported (N. Engl. J. Med. 2012;366:310-20).
Adding bevacizumab, however, increased the rate of pathological complete response in the breast significantly from 28.2% to 34.5%. Subgroup analysis indicated the effect was more pronounced in patients with hormone receptor–positive tumors (the rate increasing significantly from 15.1% without bevacizumab to 23.2% with bevacizumab) than in hormone receptor–negative tumors (47.1% and 51.5%, respectively), the investigators said. The benefit of bevacizumab tended to be seen more in patients with a high tumor grade.
Epirubicin-based Chemo in GeparQuinto
In the GeparQuinto trial, 1,948 patients were enrolled from November 2007 through June 2010 and randomized to receive neoadjuvant epirubicin (Ellence) and cyclophosphamide followed by docetaxel either with or without bevacizumab.
Pathological complete response occurred in 18.4% of those who received bevacizumab, compared with 14.9% of those who did not (odds ratio, 1.29), Dr. Gunter von Minckwitz of the German Breast Group, Neu-Isenburg, Germany and his colleagues reported. (N. Engl. J. Med. 2012;366:299-309). After adjusting for age, clinical tumor and nodal stage, hormone-receptor status, tumor grade, and histologic type, the odds ratio was 1.36.
In contrast with the findings from NSABP B-40, the greatest effects of bevacizumab in GBG44 were seen in the 633 patients with triple-negative tumors (27.9% without vs. 39.3% with bevacizumab), compared with the 1,262 patients with hormone-receptor-positive tumors (7.8% and 7.7%, respectively). The test for interaction for this finding was not significant, but the study was not powered to show these differential effects, the investigators noted.
Investigators from both trials suggested that possible reasons for the divergent findings between the studies include differences in inclusion criteria and drug dosing and/or sequencing.
The NSABP B-40 investigators noted that "the increased rate of pathological complete response in patients with hormone receptor–positive tumors is encouraging, since this group tends to have low rates of pathological complete response with chemotherapy."
Bevacizumab was associated with toxic effects in both studies, including hand-foot syndrome, mucositis, hypertension, and left ventricular systolic dysfunction in NSABP B-40, and with bleeding, febrile neutropenia, mucositis, hand-foot syndrome, infection, and hypertension in GBG44.
Survival Results Pending
The NSABP B-40 investigators said that the potential for bevacizumab to improve patient outcomes should be clarified when disease-free and overall survival results become available for those who underwent surgery in this study, and for those in other ongoing studies.
They also noted that "the collection of tissue samples from all our patients before treatment, a major advantage of the neoadjuvant approach, offers an opportunity to discover molecular markers that might predict a benefit from bevacizumab."
The GBG44 investigators noted that because of the short follow-up in their study, it cannot be confirmed that the observed increases in the rate of pathological complete response will translate into a survival advantage.
"However, given that pathological complete response has been shown to be highly correlated with outcome, particularly in patients with triple-negative disease, we speculate that the beneficial effects will be sustained," they said, adding, "Long-term follow-up data are needed before this treatment option can be fully understood."
Dosing in the studies was as follows:
In NSABP B-40, docetaxel was administered intravenously at 100 mg/m2 on day 1 of the cycle every 3 weeks in the docetaxel-only group, followed by four cycles of doxorubicin-cyclophosphamide at 60 mg/m2 and 600 mg/m2, respectively, administered intravenously every 3 weeks. Docetaxel was administered at a dose of 75 mg/m2 on day 1 in the docetaxel plus capecitabine or gemcitabine groups followed by the doxorubicin-cyclophosphamide. The capecitabine dose was 825 mg/m2 twice daily on days 1-14; the gemcitabine dose was 1,000 mg/m2 on days 1 and 8. The bevacizumab dose was 15 mg/kg administered intravenously for the first six cycles.
In GBG44, epirubicin was administered at a dose of 90 mg/m2and cyclophosphamide was administered at a dose of 600 mg/m2– both on day 1, every 3 weeks for four cycles, followed by four cycles of docetaxel a dose of 100 mg/m2 on day 1, every 3 weeks. As in NSABP B-40, bevacizumab was administered at a dose of 15 mg/kg intravenously. In this study, however, it was administered every 3 weeks starting on day 1 of the first epirubicin-cyclophosphamide cycle for 8 cycles.
NSABP B-40 was supported by grants from the National Cancer Institute, the Department of Health and Human Services, the Public Health Service, F. Hoffman-La Roche, Genentech USA, and Eli Lilly. GeparQuinto was supported by grants from Sanofi-Aventis and Roche, Germany. Detailed individual author disclosures are available with the full text of the articles at NEJM.org.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: Adding bevacizumab to neoadjuvant chemotherapy increased the rate of pathological complete response from 28.2% to 34.5% in one study and from 14.9% to 18.4% in another.
Data Source: The results come from two large randomized phase III trials – the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-40 trial and the GeparQuinto (GBG44) trial.
Disclosures: NSABP B-40 was supported by grants from the National Cancer Institute, the Department of Health and Human Services, the Public Health Service, F. Hoffman-La Roche, Genentech USA, and Eli Lilly. GeparQuinto was supported by grants from Sanofi-Aventis and Roche, Germany. Detailed individual author disclosures are available with the full text of the articles at NEJM.org.
BRCA1/2 Mutations Tied to Better Ovarian Cancer Survival
Germline mutations in the tumor suppressor genes BRCA1 and BRCA2 – and particularly those in BRCA2 – are associated with higher 5-year overall survival rates among patients with confirmed invasive epithelial ovarian cancer, according to a pooled analysis of data from 26 observational studies involving nearly 3,900 women.
The 5-year overall-survival rate was 36% for 2,666 non-BRCA carriers, 44% for 909 BRCA1 carriers, and 52% for 304 BRCA2 carriers, Kelly L. Bolton, Ph.D., of the National Cancer Institute, Bethesda, Md., and her colleagues reported on behalf of EMBRACE, KConFab Investigators, and the Cancer Genome Atlas Research Network.
The findings are reported in the Jan. 25 issue of JAMA.
After adjustment for study and year of diagnosis, BRCA1 carriers were significantly more like to survive than were noncarriers (hazard ratio, 0.78), and their advantage improved slightly after additional adjustment for stage, grade, histology, and age at diagnosis (HR, 0.73), the investigators said (JAMA 2012;307:382-90).
BRCA2 carriers had an even greater advantage when compared with noncarriers (HR, 0.61), particularly after adjustment for other prognostic factors (HR, 0.49). The differences between BRCA1 and BRCA2 carriers were statistically significant.
Although prior smaller studies have also demonstrated survival advantages among invasive epithelial ovarian cancer patients with BRCA2, with some also showing an advantage for those with BRCA1, the current study is the largest to date to assess survival in patients with invasive epithelial ovarian cancer based on BRCA1/2 carrier status.
The studies used in the analysis were reported as 10 from the United States, 6 from Europe, 2 from Israel, 1 each from Hong Kong, Canada, and Australia, and 5 from the United Kingdom. Participants were enrolled between 1987 and 2010 and were actively followed for a mean of 38 months.
Several significant differences were seen in regard to clinical features of BRCA1 and BRCA2 carriers compared with noncarriers. For example, tumors in carriers were more likely to be of serous histology and less likely to be of mucinous histology, and carriers were more likely to have stage III/IV tumors and poorly differentiated or undifferentiated tumors, compared with noncarriers. BRCA2 carriers were more likely than were BRCA1 carriers to have stage III/IV tumors. Also, BRCA1 carriers were younger at diagnosis than noncarriers, and BRCA2 carriers were slightly older.
The investigators also found that the survival advantage of BRCA1/2 carriers, compared with noncarriers, was attenuated in women who had a family history of ovarian cancer, breast cancer, or both.
"The improved survival or BRCA1/2 carriers relative to noncarriers, and the survival advantage of BRCA2 carriers relative to BRCA1 carriers, could be related to intrinsic biological differences, their response to therapeutic agents, or both," the investigators said, noting that in addition to differences in stage, grade, and histology, BRCA1/2 carriers could have differences in other aspects of tumor biology that were not measured in this study.
Although the study is limited by factors associated with the study design such as a heterogeneous population, the sample size and the magnitude of the differences observed between carriers and noncarriers are a testament to the robustness of the findings, they said.
The results have potentially important implications for the clinical management of patients with epithelial ovarian cancer, including immediate use by health care professionals for patient counseling regarding expected survival, they said, adding:
"BRCA1 and BRCA2 carriers with EOC respond better than noncarriers to platinum-based chemotherapies and have improved survival despite the fact that the disease is generally diagnosed at a later stage and higher grade. If patients could be stratified based on their BRCA status, their treatment could be tailored to reflect this, with noncarriers targeted for more aggressive treatment."
Epithelial ovarian cancer clinical trials should be stratified by BRCA status, they said, explaining that this would not only allow more appropriately targeted therapy, but also would allow avoidance of potential bias introduced by unequal numbers of carriers in treatment groups or between study cohorts.
"Furthermore, given the important prognostic information provided by BRCA1 and BRCA2 status and the potential for personalized treatment in carriers, the routine testing of women presenting with high-grade serous EOC may now be warranted," they said.
Numerous funding sources and author disclosures were reported. The complete list is available with the full text of the article at jama.com.
The findings of this study provide "the latest evidence that ovarian cancer is a much more genetically and biologically heterogeneous disease than previously appreciated," Dr. David M. Hyman and Dr. David R. Spriggs wrote in an accompanying editorial.
The paper –"by far, the largest study of BRCA-associated ovarian cancer outcomes reported to date" – has important implications for the future of ovarian cancer research and treatment, they said:
"Phase [III] studies that do not stratify by BRCA mutation status or account for this factor in a preplanned statistical analysis risk possible confounding because approximately 15% of unselected patients with serous ovarian cancer will carry germline BRCA1/2 mutations."
The findings also provide impetus for rethinking the current approach to the development of targeted agents in molecularly defined subsets of ovarian cancer, according to the editorial (JAMA 2012;307:408-10). Trials of poly (ADP-ribose) polymerase (PARP) inhibitors, which block base excision repair, have shown promise in BRCA-associated and sporadic ovarian cancers. Investigators should consider whether the unknown mechanisms underpinning the differences in survival of BRCA1- and BRCA2-associated ovarian cancers, as demonstrated in this study, "may also result in differential sensitivity to agents that target the resultant homologous recombination defects."
"In the future, even germline BRCA status may not be sufficient to fully subclassify ovarian cancers and select the best treatment," said Dr. Hyman and Dr. Spriggs.
Additional study, in similarly large data sets, is needed to improve the understanding of the effects of somatic and epigenetic alterations in BRCA gene function and the complex interactions with other inherited alleles, they added, concluding that "the accelerating availability of detailed somatic and germline genetic information will challenge all physicians who stand at the bedside of patients with cancer and struggle to deliver compassionate, individualized care."
Dr. Hyman and Dr. Spriggs are with Memorial Sloan-Kettering Cancer Center and Cornell University, both in New York. Neither had disclosures to report.
The findings of this study provide "the latest evidence that ovarian cancer is a much more genetically and biologically heterogeneous disease than previously appreciated," Dr. David M. Hyman and Dr. David R. Spriggs wrote in an accompanying editorial.
The paper –"by far, the largest study of BRCA-associated ovarian cancer outcomes reported to date" – has important implications for the future of ovarian cancer research and treatment, they said:
"Phase [III] studies that do not stratify by BRCA mutation status or account for this factor in a preplanned statistical analysis risk possible confounding because approximately 15% of unselected patients with serous ovarian cancer will carry germline BRCA1/2 mutations."
The findings also provide impetus for rethinking the current approach to the development of targeted agents in molecularly defined subsets of ovarian cancer, according to the editorial (JAMA 2012;307:408-10). Trials of poly (ADP-ribose) polymerase (PARP) inhibitors, which block base excision repair, have shown promise in BRCA-associated and sporadic ovarian cancers. Investigators should consider whether the unknown mechanisms underpinning the differences in survival of BRCA1- and BRCA2-associated ovarian cancers, as demonstrated in this study, "may also result in differential sensitivity to agents that target the resultant homologous recombination defects."
"In the future, even germline BRCA status may not be sufficient to fully subclassify ovarian cancers and select the best treatment," said Dr. Hyman and Dr. Spriggs.
Additional study, in similarly large data sets, is needed to improve the understanding of the effects of somatic and epigenetic alterations in BRCA gene function and the complex interactions with other inherited alleles, they added, concluding that "the accelerating availability of detailed somatic and germline genetic information will challenge all physicians who stand at the bedside of patients with cancer and struggle to deliver compassionate, individualized care."
Dr. Hyman and Dr. Spriggs are with Memorial Sloan-Kettering Cancer Center and Cornell University, both in New York. Neither had disclosures to report.
The findings of this study provide "the latest evidence that ovarian cancer is a much more genetically and biologically heterogeneous disease than previously appreciated," Dr. David M. Hyman and Dr. David R. Spriggs wrote in an accompanying editorial.
The paper –"by far, the largest study of BRCA-associated ovarian cancer outcomes reported to date" – has important implications for the future of ovarian cancer research and treatment, they said:
"Phase [III] studies that do not stratify by BRCA mutation status or account for this factor in a preplanned statistical analysis risk possible confounding because approximately 15% of unselected patients with serous ovarian cancer will carry germline BRCA1/2 mutations."
The findings also provide impetus for rethinking the current approach to the development of targeted agents in molecularly defined subsets of ovarian cancer, according to the editorial (JAMA 2012;307:408-10). Trials of poly (ADP-ribose) polymerase (PARP) inhibitors, which block base excision repair, have shown promise in BRCA-associated and sporadic ovarian cancers. Investigators should consider whether the unknown mechanisms underpinning the differences in survival of BRCA1- and BRCA2-associated ovarian cancers, as demonstrated in this study, "may also result in differential sensitivity to agents that target the resultant homologous recombination defects."
"In the future, even germline BRCA status may not be sufficient to fully subclassify ovarian cancers and select the best treatment," said Dr. Hyman and Dr. Spriggs.
Additional study, in similarly large data sets, is needed to improve the understanding of the effects of somatic and epigenetic alterations in BRCA gene function and the complex interactions with other inherited alleles, they added, concluding that "the accelerating availability of detailed somatic and germline genetic information will challenge all physicians who stand at the bedside of patients with cancer and struggle to deliver compassionate, individualized care."
Dr. Hyman and Dr. Spriggs are with Memorial Sloan-Kettering Cancer Center and Cornell University, both in New York. Neither had disclosures to report.
Germline mutations in the tumor suppressor genes BRCA1 and BRCA2 – and particularly those in BRCA2 – are associated with higher 5-year overall survival rates among patients with confirmed invasive epithelial ovarian cancer, according to a pooled analysis of data from 26 observational studies involving nearly 3,900 women.
The 5-year overall-survival rate was 36% for 2,666 non-BRCA carriers, 44% for 909 BRCA1 carriers, and 52% for 304 BRCA2 carriers, Kelly L. Bolton, Ph.D., of the National Cancer Institute, Bethesda, Md., and her colleagues reported on behalf of EMBRACE, KConFab Investigators, and the Cancer Genome Atlas Research Network.
The findings are reported in the Jan. 25 issue of JAMA.
After adjustment for study and year of diagnosis, BRCA1 carriers were significantly more like to survive than were noncarriers (hazard ratio, 0.78), and their advantage improved slightly after additional adjustment for stage, grade, histology, and age at diagnosis (HR, 0.73), the investigators said (JAMA 2012;307:382-90).
BRCA2 carriers had an even greater advantage when compared with noncarriers (HR, 0.61), particularly after adjustment for other prognostic factors (HR, 0.49). The differences between BRCA1 and BRCA2 carriers were statistically significant.
Although prior smaller studies have also demonstrated survival advantages among invasive epithelial ovarian cancer patients with BRCA2, with some also showing an advantage for those with BRCA1, the current study is the largest to date to assess survival in patients with invasive epithelial ovarian cancer based on BRCA1/2 carrier status.
The studies used in the analysis were reported as 10 from the United States, 6 from Europe, 2 from Israel, 1 each from Hong Kong, Canada, and Australia, and 5 from the United Kingdom. Participants were enrolled between 1987 and 2010 and were actively followed for a mean of 38 months.
Several significant differences were seen in regard to clinical features of BRCA1 and BRCA2 carriers compared with noncarriers. For example, tumors in carriers were more likely to be of serous histology and less likely to be of mucinous histology, and carriers were more likely to have stage III/IV tumors and poorly differentiated or undifferentiated tumors, compared with noncarriers. BRCA2 carriers were more likely than were BRCA1 carriers to have stage III/IV tumors. Also, BRCA1 carriers were younger at diagnosis than noncarriers, and BRCA2 carriers were slightly older.
The investigators also found that the survival advantage of BRCA1/2 carriers, compared with noncarriers, was attenuated in women who had a family history of ovarian cancer, breast cancer, or both.
"The improved survival or BRCA1/2 carriers relative to noncarriers, and the survival advantage of BRCA2 carriers relative to BRCA1 carriers, could be related to intrinsic biological differences, their response to therapeutic agents, or both," the investigators said, noting that in addition to differences in stage, grade, and histology, BRCA1/2 carriers could have differences in other aspects of tumor biology that were not measured in this study.
Although the study is limited by factors associated with the study design such as a heterogeneous population, the sample size and the magnitude of the differences observed between carriers and noncarriers are a testament to the robustness of the findings, they said.
The results have potentially important implications for the clinical management of patients with epithelial ovarian cancer, including immediate use by health care professionals for patient counseling regarding expected survival, they said, adding:
"BRCA1 and BRCA2 carriers with EOC respond better than noncarriers to platinum-based chemotherapies and have improved survival despite the fact that the disease is generally diagnosed at a later stage and higher grade. If patients could be stratified based on their BRCA status, their treatment could be tailored to reflect this, with noncarriers targeted for more aggressive treatment."
Epithelial ovarian cancer clinical trials should be stratified by BRCA status, they said, explaining that this would not only allow more appropriately targeted therapy, but also would allow avoidance of potential bias introduced by unequal numbers of carriers in treatment groups or between study cohorts.
"Furthermore, given the important prognostic information provided by BRCA1 and BRCA2 status and the potential for personalized treatment in carriers, the routine testing of women presenting with high-grade serous EOC may now be warranted," they said.
Numerous funding sources and author disclosures were reported. The complete list is available with the full text of the article at jama.com.
Germline mutations in the tumor suppressor genes BRCA1 and BRCA2 – and particularly those in BRCA2 – are associated with higher 5-year overall survival rates among patients with confirmed invasive epithelial ovarian cancer, according to a pooled analysis of data from 26 observational studies involving nearly 3,900 women.
The 5-year overall-survival rate was 36% for 2,666 non-BRCA carriers, 44% for 909 BRCA1 carriers, and 52% for 304 BRCA2 carriers, Kelly L. Bolton, Ph.D., of the National Cancer Institute, Bethesda, Md., and her colleagues reported on behalf of EMBRACE, KConFab Investigators, and the Cancer Genome Atlas Research Network.
The findings are reported in the Jan. 25 issue of JAMA.
After adjustment for study and year of diagnosis, BRCA1 carriers were significantly more like to survive than were noncarriers (hazard ratio, 0.78), and their advantage improved slightly after additional adjustment for stage, grade, histology, and age at diagnosis (HR, 0.73), the investigators said (JAMA 2012;307:382-90).
BRCA2 carriers had an even greater advantage when compared with noncarriers (HR, 0.61), particularly after adjustment for other prognostic factors (HR, 0.49). The differences between BRCA1 and BRCA2 carriers were statistically significant.
Although prior smaller studies have also demonstrated survival advantages among invasive epithelial ovarian cancer patients with BRCA2, with some also showing an advantage for those with BRCA1, the current study is the largest to date to assess survival in patients with invasive epithelial ovarian cancer based on BRCA1/2 carrier status.
The studies used in the analysis were reported as 10 from the United States, 6 from Europe, 2 from Israel, 1 each from Hong Kong, Canada, and Australia, and 5 from the United Kingdom. Participants were enrolled between 1987 and 2010 and were actively followed for a mean of 38 months.
Several significant differences were seen in regard to clinical features of BRCA1 and BRCA2 carriers compared with noncarriers. For example, tumors in carriers were more likely to be of serous histology and less likely to be of mucinous histology, and carriers were more likely to have stage III/IV tumors and poorly differentiated or undifferentiated tumors, compared with noncarriers. BRCA2 carriers were more likely than were BRCA1 carriers to have stage III/IV tumors. Also, BRCA1 carriers were younger at diagnosis than noncarriers, and BRCA2 carriers were slightly older.
The investigators also found that the survival advantage of BRCA1/2 carriers, compared with noncarriers, was attenuated in women who had a family history of ovarian cancer, breast cancer, or both.
"The improved survival or BRCA1/2 carriers relative to noncarriers, and the survival advantage of BRCA2 carriers relative to BRCA1 carriers, could be related to intrinsic biological differences, their response to therapeutic agents, or both," the investigators said, noting that in addition to differences in stage, grade, and histology, BRCA1/2 carriers could have differences in other aspects of tumor biology that were not measured in this study.
Although the study is limited by factors associated with the study design such as a heterogeneous population, the sample size and the magnitude of the differences observed between carriers and noncarriers are a testament to the robustness of the findings, they said.
The results have potentially important implications for the clinical management of patients with epithelial ovarian cancer, including immediate use by health care professionals for patient counseling regarding expected survival, they said, adding:
"BRCA1 and BRCA2 carriers with EOC respond better than noncarriers to platinum-based chemotherapies and have improved survival despite the fact that the disease is generally diagnosed at a later stage and higher grade. If patients could be stratified based on their BRCA status, their treatment could be tailored to reflect this, with noncarriers targeted for more aggressive treatment."
Epithelial ovarian cancer clinical trials should be stratified by BRCA status, they said, explaining that this would not only allow more appropriately targeted therapy, but also would allow avoidance of potential bias introduced by unequal numbers of carriers in treatment groups or between study cohorts.
"Furthermore, given the important prognostic information provided by BRCA1 and BRCA2 status and the potential for personalized treatment in carriers, the routine testing of women presenting with high-grade serous EOC may now be warranted," they said.
Numerous funding sources and author disclosures were reported. The complete list is available with the full text of the article at jama.com.
FROM JAMA
Major Finding: The 5-year overall-survival rate was 36% for 2,666 non-BRCA carriers, 44% for 909 BRCA1 carriers, and 52% for 304 BRCA2 carriers.
Data Source: A pooled analysis of 26 observational studies.
Disclosures: Numerous funding sources and author disclosures were reported. The complete list is available with the full text of the article at www.jama.com.
Lansoprazole Disappoints for Poorly Controlled Asthma in Kids
The proton pump inhibitor lansoprazole was no better than placebo for improving symptoms and lung function in a randomized, placebo-controlled trial involving more than 300 children with poorly controlled asthma without overt gastroesophageal reflux.
Those treated with lansoprazole did, however, experience significantly more respiratory infections (relative risk, 1.3), sore throats (RR, 1.3), and episodes of bronchitis (RR, 2.2) than did those receiving placebo during the course of the 24-week study. The treatment group also experienced more activity-related bone fractures (6 vs. 1 in treatment vs. placebo groups, respectively), although this difference did not reach significance, Dr. Nicola Hanania and his* colleagues from the Writing Committee for the American Lung Association Asthma Clinical Research Centers reported in the Jan. 25 issue of JAMA.
The mean difference in change in Asthma Control Questionnaire scores between the 149 children treated with 15-30 mg/day of lansoprazole depending on weight and the 157 who received placebo in the Study of Acid Reflux in Children With Asthma was 0.2 units, which was less than the meaningful clinically important difference in both groups (–0.1 for lansoprazole, and –0.2 for placebo), and was not statistically significant. Mean differences in change for secondary outcomes, including forced expiratory volume in the first second, asthma-related quality of life, and rate of episodes of poor asthma control, also did not differ significantly between the groups, Dr. Hanania of Baylor College of Medicine, Houston, and his colleagues reported (JAMA 2012;307:373-81).
Additionally, lansoprazole had no treatment effect, compared with placebo, in a subanalysis of 49 study participants (20 in the placebo group and 29 in the lansoprazole group) who were found on esophageal pH studies to have gastroesophageal reflux (GER), they noted.
Untreated GER has been considered a possible cause of inadequate asthma control in children treated with inhaled corticosteroids, but proton pump inhibitors (PPIs) have not been well studied with respect to their use for asymptomatic GER in children with refractory asthma.
For the current double-masked study, children were enrolled between April 2007 and September 2010 at 19 academic clinical centers throughout the United States. They had a mean age of 11 years (range 6-17 years), 50% were black, 65% were boys, and all were using inhaled corticosteroids. Most had required an intervention for asthma symptoms in the year prior to enrollment, and the mean Asthma Control Questionnaire score was high, at 1.6 for both groups, which is consistent with poor asthma control.
The lansoprazole dose used for the study was based on weight, with patients weighing less than 30 kg receiving 15 mg/day, and those weighing 30 kg or more receiving 30 mg/day.
The findings indicate that the drug has no effect on asthma control measures, the investigators wrote. "This was the case even though GER was prevalent in the study sample," they noted. It was also the case in subgroups defined by markers of asthma severity.
"The results of this clinical trial are uniformly negative regarding the benefit of acid suppression therapy on symptom relief, lung function, airways reactivity, or quality of life," they said, concluding that in light of previous negative findings from a study of omeprazole, the use of PPI therapy in children with poorly controlled asthma is unwarranted.
The findings also raise important questions about the adverse effects of lansoprazole in children, and along with other concerning data that have led to two Food and Drug Administration Advisory Board Reviews in the past 2 years, they underscore the need for continued study of PPI safety in children, they said.
Although the activity-related fractures in the lansoprazole group were not significantly more common than in the placebo group (6 of 149 [4%] vs. 1 of 157 [less than 1%]; P = .06), they are a cause for concern. Of the seven fractures, one occurred on the day of randomization; the others occurred after 2 months (n = 1), 5 months (n = 3), and 6 months (n = 2) of follow-up. The affected children were 7-14 years old, and all had been taking inhaled corticosteroids during the trial; two had taken oral prednisone as well (one in each group).
This study was supported by the American Lung Association Asthma Clinical Research Centers, as well as by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute. Lansoprazole and placebo were provided by Takeda Pharmaceuticals; albuterol was provided by GlaxoSmithKline. Dr. Hanania and his coauthors had no disclosures to report.
*Correction, 1/27/2012: An earlier version of this story had an incorrect pronoun referencing Dr. Hanania.
Despite "unimpressive evidence" derived largely from anecdotal experience in regard to a consistent role of gastroesophageal reflux in asthma morbidity, children with asthma often are treated with antireflux medications. One study demonstrated that 13- to 14-year-old children with asthma were more than eight times more likely to be treated with antireflux therapy than those without asthma, Dr. Fernando D. Martinez said.
The practice represents "therapeutic creep" – or the extension of the use of a treatment with real or suggestive therapeutic effects observed in a certain age group or certain disease phenotype to other patients in whom the efficacy has never been demonstrated – and its perils and costs are highlighted in this study by Dr. Hanania and his colleagues, Dr. Martinez said.
Children in the study who were treated with lansoprazole were more likely than those treated with placebo to experience a number of adverse effects, including respiratory infections – without any improvement in asthma symptoms. Of even greater concern was a finding of increased activity-related bone fractures in the lansoprazole group, Dr. Martinez said, noting that this is the first large randomized controlled trial to look at this potential complication of proton pump inhibitors (PPIs) in children.
Although the finding didn’t reach statistical significance, it should be considered "in the framework of a substantial body of evidence that has prompted the U.S. Food and Drug Administration to issue an advisory about the risk of fractures in adults taking PPIs chronically," he said.
The findings of this study should strongly discourage the generalized use of PPIs for treating asthma, and a tentative recommendation by the current National Heart, Lung, and Blood Institute guidelines for an empirical trial of antireflux therapy in patients with poorly controlled asthma – based on the few data available at the time the guidelines were written – should be promptly revised, he concluded.
Dr. Martinez is at the Arizona Respiratory Center, BIO5 Institute and Clinical and Translational Science Institute at the University of Arizona, Tucson. He commented in an accompanying editorial (JAMA 2012;307:406-7). He has served as a consultant to MedImmune and has presented at an Abbott-sponsored seminar.
Asthma Control Questionnaire scores, Acid Reflux,
Despite "unimpressive evidence" derived largely from anecdotal experience in regard to a consistent role of gastroesophageal reflux in asthma morbidity, children with asthma often are treated with antireflux medications. One study demonstrated that 13- to 14-year-old children with asthma were more than eight times more likely to be treated with antireflux therapy than those without asthma, Dr. Fernando D. Martinez said.
The practice represents "therapeutic creep" – or the extension of the use of a treatment with real or suggestive therapeutic effects observed in a certain age group or certain disease phenotype to other patients in whom the efficacy has never been demonstrated – and its perils and costs are highlighted in this study by Dr. Hanania and his colleagues, Dr. Martinez said.
Children in the study who were treated with lansoprazole were more likely than those treated with placebo to experience a number of adverse effects, including respiratory infections – without any improvement in asthma symptoms. Of even greater concern was a finding of increased activity-related bone fractures in the lansoprazole group, Dr. Martinez said, noting that this is the first large randomized controlled trial to look at this potential complication of proton pump inhibitors (PPIs) in children.
Although the finding didn’t reach statistical significance, it should be considered "in the framework of a substantial body of evidence that has prompted the U.S. Food and Drug Administration to issue an advisory about the risk of fractures in adults taking PPIs chronically," he said.
The findings of this study should strongly discourage the generalized use of PPIs for treating asthma, and a tentative recommendation by the current National Heart, Lung, and Blood Institute guidelines for an empirical trial of antireflux therapy in patients with poorly controlled asthma – based on the few data available at the time the guidelines were written – should be promptly revised, he concluded.
Dr. Martinez is at the Arizona Respiratory Center, BIO5 Institute and Clinical and Translational Science Institute at the University of Arizona, Tucson. He commented in an accompanying editorial (JAMA 2012;307:406-7). He has served as a consultant to MedImmune and has presented at an Abbott-sponsored seminar.
Despite "unimpressive evidence" derived largely from anecdotal experience in regard to a consistent role of gastroesophageal reflux in asthma morbidity, children with asthma often are treated with antireflux medications. One study demonstrated that 13- to 14-year-old children with asthma were more than eight times more likely to be treated with antireflux therapy than those without asthma, Dr. Fernando D. Martinez said.
The practice represents "therapeutic creep" – or the extension of the use of a treatment with real or suggestive therapeutic effects observed in a certain age group or certain disease phenotype to other patients in whom the efficacy has never been demonstrated – and its perils and costs are highlighted in this study by Dr. Hanania and his colleagues, Dr. Martinez said.
Children in the study who were treated with lansoprazole were more likely than those treated with placebo to experience a number of adverse effects, including respiratory infections – without any improvement in asthma symptoms. Of even greater concern was a finding of increased activity-related bone fractures in the lansoprazole group, Dr. Martinez said, noting that this is the first large randomized controlled trial to look at this potential complication of proton pump inhibitors (PPIs) in children.
Although the finding didn’t reach statistical significance, it should be considered "in the framework of a substantial body of evidence that has prompted the U.S. Food and Drug Administration to issue an advisory about the risk of fractures in adults taking PPIs chronically," he said.
The findings of this study should strongly discourage the generalized use of PPIs for treating asthma, and a tentative recommendation by the current National Heart, Lung, and Blood Institute guidelines for an empirical trial of antireflux therapy in patients with poorly controlled asthma – based on the few data available at the time the guidelines were written – should be promptly revised, he concluded.
Dr. Martinez is at the Arizona Respiratory Center, BIO5 Institute and Clinical and Translational Science Institute at the University of Arizona, Tucson. He commented in an accompanying editorial (JAMA 2012;307:406-7). He has served as a consultant to MedImmune and has presented at an Abbott-sponsored seminar.
The proton pump inhibitor lansoprazole was no better than placebo for improving symptoms and lung function in a randomized, placebo-controlled trial involving more than 300 children with poorly controlled asthma without overt gastroesophageal reflux.
Those treated with lansoprazole did, however, experience significantly more respiratory infections (relative risk, 1.3), sore throats (RR, 1.3), and episodes of bronchitis (RR, 2.2) than did those receiving placebo during the course of the 24-week study. The treatment group also experienced more activity-related bone fractures (6 vs. 1 in treatment vs. placebo groups, respectively), although this difference did not reach significance, Dr. Nicola Hanania and his* colleagues from the Writing Committee for the American Lung Association Asthma Clinical Research Centers reported in the Jan. 25 issue of JAMA.
The mean difference in change in Asthma Control Questionnaire scores between the 149 children treated with 15-30 mg/day of lansoprazole depending on weight and the 157 who received placebo in the Study of Acid Reflux in Children With Asthma was 0.2 units, which was less than the meaningful clinically important difference in both groups (–0.1 for lansoprazole, and –0.2 for placebo), and was not statistically significant. Mean differences in change for secondary outcomes, including forced expiratory volume in the first second, asthma-related quality of life, and rate of episodes of poor asthma control, also did not differ significantly between the groups, Dr. Hanania of Baylor College of Medicine, Houston, and his colleagues reported (JAMA 2012;307:373-81).
Additionally, lansoprazole had no treatment effect, compared with placebo, in a subanalysis of 49 study participants (20 in the placebo group and 29 in the lansoprazole group) who were found on esophageal pH studies to have gastroesophageal reflux (GER), they noted.
Untreated GER has been considered a possible cause of inadequate asthma control in children treated with inhaled corticosteroids, but proton pump inhibitors (PPIs) have not been well studied with respect to their use for asymptomatic GER in children with refractory asthma.
For the current double-masked study, children were enrolled between April 2007 and September 2010 at 19 academic clinical centers throughout the United States. They had a mean age of 11 years (range 6-17 years), 50% were black, 65% were boys, and all were using inhaled corticosteroids. Most had required an intervention for asthma symptoms in the year prior to enrollment, and the mean Asthma Control Questionnaire score was high, at 1.6 for both groups, which is consistent with poor asthma control.
The lansoprazole dose used for the study was based on weight, with patients weighing less than 30 kg receiving 15 mg/day, and those weighing 30 kg or more receiving 30 mg/day.
The findings indicate that the drug has no effect on asthma control measures, the investigators wrote. "This was the case even though GER was prevalent in the study sample," they noted. It was also the case in subgroups defined by markers of asthma severity.
"The results of this clinical trial are uniformly negative regarding the benefit of acid suppression therapy on symptom relief, lung function, airways reactivity, or quality of life," they said, concluding that in light of previous negative findings from a study of omeprazole, the use of PPI therapy in children with poorly controlled asthma is unwarranted.
The findings also raise important questions about the adverse effects of lansoprazole in children, and along with other concerning data that have led to two Food and Drug Administration Advisory Board Reviews in the past 2 years, they underscore the need for continued study of PPI safety in children, they said.
Although the activity-related fractures in the lansoprazole group were not significantly more common than in the placebo group (6 of 149 [4%] vs. 1 of 157 [less than 1%]; P = .06), they are a cause for concern. Of the seven fractures, one occurred on the day of randomization; the others occurred after 2 months (n = 1), 5 months (n = 3), and 6 months (n = 2) of follow-up. The affected children were 7-14 years old, and all had been taking inhaled corticosteroids during the trial; two had taken oral prednisone as well (one in each group).
This study was supported by the American Lung Association Asthma Clinical Research Centers, as well as by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute. Lansoprazole and placebo were provided by Takeda Pharmaceuticals; albuterol was provided by GlaxoSmithKline. Dr. Hanania and his coauthors had no disclosures to report.
*Correction, 1/27/2012: An earlier version of this story had an incorrect pronoun referencing Dr. Hanania.
The proton pump inhibitor lansoprazole was no better than placebo for improving symptoms and lung function in a randomized, placebo-controlled trial involving more than 300 children with poorly controlled asthma without overt gastroesophageal reflux.
Those treated with lansoprazole did, however, experience significantly more respiratory infections (relative risk, 1.3), sore throats (RR, 1.3), and episodes of bronchitis (RR, 2.2) than did those receiving placebo during the course of the 24-week study. The treatment group also experienced more activity-related bone fractures (6 vs. 1 in treatment vs. placebo groups, respectively), although this difference did not reach significance, Dr. Nicola Hanania and his* colleagues from the Writing Committee for the American Lung Association Asthma Clinical Research Centers reported in the Jan. 25 issue of JAMA.
The mean difference in change in Asthma Control Questionnaire scores between the 149 children treated with 15-30 mg/day of lansoprazole depending on weight and the 157 who received placebo in the Study of Acid Reflux in Children With Asthma was 0.2 units, which was less than the meaningful clinically important difference in both groups (–0.1 for lansoprazole, and –0.2 for placebo), and was not statistically significant. Mean differences in change for secondary outcomes, including forced expiratory volume in the first second, asthma-related quality of life, and rate of episodes of poor asthma control, also did not differ significantly between the groups, Dr. Hanania of Baylor College of Medicine, Houston, and his colleagues reported (JAMA 2012;307:373-81).
Additionally, lansoprazole had no treatment effect, compared with placebo, in a subanalysis of 49 study participants (20 in the placebo group and 29 in the lansoprazole group) who were found on esophageal pH studies to have gastroesophageal reflux (GER), they noted.
Untreated GER has been considered a possible cause of inadequate asthma control in children treated with inhaled corticosteroids, but proton pump inhibitors (PPIs) have not been well studied with respect to their use for asymptomatic GER in children with refractory asthma.
For the current double-masked study, children were enrolled between April 2007 and September 2010 at 19 academic clinical centers throughout the United States. They had a mean age of 11 years (range 6-17 years), 50% were black, 65% were boys, and all were using inhaled corticosteroids. Most had required an intervention for asthma symptoms in the year prior to enrollment, and the mean Asthma Control Questionnaire score was high, at 1.6 for both groups, which is consistent with poor asthma control.
The lansoprazole dose used for the study was based on weight, with patients weighing less than 30 kg receiving 15 mg/day, and those weighing 30 kg or more receiving 30 mg/day.
The findings indicate that the drug has no effect on asthma control measures, the investigators wrote. "This was the case even though GER was prevalent in the study sample," they noted. It was also the case in subgroups defined by markers of asthma severity.
"The results of this clinical trial are uniformly negative regarding the benefit of acid suppression therapy on symptom relief, lung function, airways reactivity, or quality of life," they said, concluding that in light of previous negative findings from a study of omeprazole, the use of PPI therapy in children with poorly controlled asthma is unwarranted.
The findings also raise important questions about the adverse effects of lansoprazole in children, and along with other concerning data that have led to two Food and Drug Administration Advisory Board Reviews in the past 2 years, they underscore the need for continued study of PPI safety in children, they said.
Although the activity-related fractures in the lansoprazole group were not significantly more common than in the placebo group (6 of 149 [4%] vs. 1 of 157 [less than 1%]; P = .06), they are a cause for concern. Of the seven fractures, one occurred on the day of randomization; the others occurred after 2 months (n = 1), 5 months (n = 3), and 6 months (n = 2) of follow-up. The affected children were 7-14 years old, and all had been taking inhaled corticosteroids during the trial; two had taken oral prednisone as well (one in each group).
This study was supported by the American Lung Association Asthma Clinical Research Centers, as well as by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute. Lansoprazole and placebo were provided by Takeda Pharmaceuticals; albuterol was provided by GlaxoSmithKline. Dr. Hanania and his coauthors had no disclosures to report.
*Correction, 1/27/2012: An earlier version of this story had an incorrect pronoun referencing Dr. Hanania.
Asthma Control Questionnaire scores, Acid Reflux,
Asthma Control Questionnaire scores, Acid Reflux,
FROM JAMA
Major Finding: The mean difference in change in Asthma Control Questionnaire score between the 149 children treated with 15-30 mg/day of lansoprazole and the 157 who received placebo during the course of the Study of Acid Reflux in Children With Asthma was 0.2 units, which was less than the meaningful clinically important difference in both groups (–0.1 for lansoprazole, and –0.2 for placebo), and was not statistically significant.
Data Source: A randomized, double-masked, placebo-controlled trial.
Disclosures: This study was supported by the American Lung Association Asthma Clinical Research Centers, as well as by grants from the National Institutes of Health/National Heart, Lung, and Blood Institute. Lansoprazole and placebo were provided by Takeda Pharmaceuticals; albuterol was provided by GlaxoSmithKline. The authors had no disclosures to report.
Depressive Symptoms Common, Neglected in Early Schizophrenia
Depressive symptoms are common and tend to be neglected in patients with first episode schizophrenia spectrum disorders, according to a medical file audit involving records for more than 400 patients.
Of 405 patients with an available baseline Clinical Global Impressions-Severity of Illness Scale-Bipolar Illness (CGI-BP) depression score, 106 (26.2%) had moderate to severe depression at service entry, Sue M. Cotton, Ph.D., of the University of Melbourne, and her colleagues report in the January issue of Schizophrenia Research.
Among the characteristics of patients with moderate to severe depression at service entry, compared with those without depressive symptoms, were a significantly greater likelihood of a past history of major depressive disorder (MDD; odds ratio, 2.58) and suicide attempts (OR, 1.55), a family history of psychiatric disorder (OR, 1.40), and significantly reduced likelihood of a past history of substance use disorder (OR, 0.67), the investigators found (Schizophr. Research 2012;134:20-6).
The patients with depressive symptoms also were more likely to have current MDD (OR, 5.52), and to have partial/full insight into their psychotic disorder (OR, 0.68), and they were less likely to have a current substance use disorder (OR, 0.65).
During treatment they were less likely to be admitted to the hospital (OR, 0.79), with a lower number of admission (OR, 0.84), and were less likely to be using substances (OR, 0.40).At discharge they were more likely to be depressed and to have partial/full insight to their illness (OR, 2.04 and 0.70, respectively), the investigators said.
Data on antidepressant medication use were available for 254 patients, and of those with moderate to severe depressive symptoms, 45 (55.6%) were prescribed antidepressants; these patients had significantly higher CGI-BP depression scores than did those with depressive symptoms who were not prescribed antidepressants.
The audit also provided descriptive characteristics of the 15 patients with persistent depressive symptoms and the 91 without persistent depressive symptoms (of the 105 patients with moderate to severe depressive symptoms at service entry). For example, those with persistent symptoms were significantly more likely to have a past diagnosis of personality disorder, as well as a diagnosis of a personality disorder at service entry (OR, 10.88 and 3.81, respectively).
Personality disorder diagnoses at service entry included borderline personality disorder, schizotypal, antisocial personality disorder, and personality disorder not otherwise specified.
Patients with persistent depression were also significantly more likely to have a past history of suicide attempts as compared with the two other groups (OR, 2.54).
Those patients with persistent depression had a shorter duration of treatment, all were noncompliant with treatment, and they were more likely to have ongoing substance use. At discharge, they had a significantly higher CGI symptom severity score, a lower global assessment of functioning mean score, and were less likely to be working, the investigators noted.
Of 81 patients with depression for whom antidepressant treatment information was available, 4 had persistent depressive symptoms and 77 did not. All four of those with persistent symptoms received treatment, and 41 of those without persistent symptoms received treatment.
The findings regarding the prevalence of depressive symptoms support the notion that the condition is common in early schizophrenia, and the fact that only about 29% of those with depressive symptoms had a comorbid clinical diagnosis of major depressive disorder at service entry might reflect underdiagnosis or underreporting of MDD. That finding also might be a sign that depressive symptoms are neglected in first episode of schizophrenia (FES) treatment, with more emphasis being placed on management of positive and negative symptoms, the investigators suggested.
"This may also be compounded by the lack of detail in clinical guidelines regarding the best treatments (including antidepressant use and psychotherapy) for depressive symptoms in FES," they said.
The findings underscore the need for assessing FES patients for depression at service entry, and for monitoring those with a history of depression, suicidality, and greater insight into their psychotic illness for depression over time, they added.
Although data on therapeutic interventions for those with depression in FES are scant, available data suggest that pharmacotherapy might be indicated. Requirements for such therapy might vary depending on the stage of the psychotic illness.
"For example, during the acute psychotic episode, antipsychotic medication may be the best treatment option, as observational studies have indicated that depression often subsides when the acute psychotic symptoms are treated," the investigators noted.
Cognitive therapies might also be useful and should focus on shifting negative appraisals of the self and the diagnosis of postpsychotic depression.
"Undoubtedly, controlled trials are needed to help determine the efficacy of pharmacological and psychological therapies for depressive symptoms in FES. Importantly, the findings of the current study are helpful for characterizing the appropriate target groups for such studies," they added, noting that understanding the nature and characteristics of depression in FES has important clinical implication for both early intervention and outcome in FES patients, particularly in regard to quality of life.
The findings of this study must be considered in the context of the medical file audit methodology used – an approach potentially limited by medical record quality and lack of inter-rater reliability, but the widely used methodology also offers several benefits, including the fact that a highly representative sample of patients can be obtained, the investigators said.
Future prospective research should focus on "mapping the trajectory of depressive symptoms against the course of positive and negative symptoms, insight, and substance use," they concluded, noting that such studies will improve understanding of the phenomenology and trajectory of depressive pathology in FES and inform the development of targeted interventions.
This study was supported by grants from Eli Lilly & Co. Australia and the Leenaards Foundation, Switzerland. Dr. Cotton is supported by the Ronald Phillip Griffith Fellowship, the University of Melbourne. Several other study authors reported that they serve on Eli Lilly’s speakers board.
Depressive symptoms are common and tend to be neglected in patients with first episode schizophrenia spectrum disorders, according to a medical file audit involving records for more than 400 patients.
Of 405 patients with an available baseline Clinical Global Impressions-Severity of Illness Scale-Bipolar Illness (CGI-BP) depression score, 106 (26.2%) had moderate to severe depression at service entry, Sue M. Cotton, Ph.D., of the University of Melbourne, and her colleagues report in the January issue of Schizophrenia Research.
Among the characteristics of patients with moderate to severe depression at service entry, compared with those without depressive symptoms, were a significantly greater likelihood of a past history of major depressive disorder (MDD; odds ratio, 2.58) and suicide attempts (OR, 1.55), a family history of psychiatric disorder (OR, 1.40), and significantly reduced likelihood of a past history of substance use disorder (OR, 0.67), the investigators found (Schizophr. Research 2012;134:20-6).
The patients with depressive symptoms also were more likely to have current MDD (OR, 5.52), and to have partial/full insight into their psychotic disorder (OR, 0.68), and they were less likely to have a current substance use disorder (OR, 0.65).
During treatment they were less likely to be admitted to the hospital (OR, 0.79), with a lower number of admission (OR, 0.84), and were less likely to be using substances (OR, 0.40).At discharge they were more likely to be depressed and to have partial/full insight to their illness (OR, 2.04 and 0.70, respectively), the investigators said.
Data on antidepressant medication use were available for 254 patients, and of those with moderate to severe depressive symptoms, 45 (55.6%) were prescribed antidepressants; these patients had significantly higher CGI-BP depression scores than did those with depressive symptoms who were not prescribed antidepressants.
The audit also provided descriptive characteristics of the 15 patients with persistent depressive symptoms and the 91 without persistent depressive symptoms (of the 105 patients with moderate to severe depressive symptoms at service entry). For example, those with persistent symptoms were significantly more likely to have a past diagnosis of personality disorder, as well as a diagnosis of a personality disorder at service entry (OR, 10.88 and 3.81, respectively).
Personality disorder diagnoses at service entry included borderline personality disorder, schizotypal, antisocial personality disorder, and personality disorder not otherwise specified.
Patients with persistent depression were also significantly more likely to have a past history of suicide attempts as compared with the two other groups (OR, 2.54).
Those patients with persistent depression had a shorter duration of treatment, all were noncompliant with treatment, and they were more likely to have ongoing substance use. At discharge, they had a significantly higher CGI symptom severity score, a lower global assessment of functioning mean score, and were less likely to be working, the investigators noted.
Of 81 patients with depression for whom antidepressant treatment information was available, 4 had persistent depressive symptoms and 77 did not. All four of those with persistent symptoms received treatment, and 41 of those without persistent symptoms received treatment.
The findings regarding the prevalence of depressive symptoms support the notion that the condition is common in early schizophrenia, and the fact that only about 29% of those with depressive symptoms had a comorbid clinical diagnosis of major depressive disorder at service entry might reflect underdiagnosis or underreporting of MDD. That finding also might be a sign that depressive symptoms are neglected in first episode of schizophrenia (FES) treatment, with more emphasis being placed on management of positive and negative symptoms, the investigators suggested.
"This may also be compounded by the lack of detail in clinical guidelines regarding the best treatments (including antidepressant use and psychotherapy) for depressive symptoms in FES," they said.
The findings underscore the need for assessing FES patients for depression at service entry, and for monitoring those with a history of depression, suicidality, and greater insight into their psychotic illness for depression over time, they added.
Although data on therapeutic interventions for those with depression in FES are scant, available data suggest that pharmacotherapy might be indicated. Requirements for such therapy might vary depending on the stage of the psychotic illness.
"For example, during the acute psychotic episode, antipsychotic medication may be the best treatment option, as observational studies have indicated that depression often subsides when the acute psychotic symptoms are treated," the investigators noted.
Cognitive therapies might also be useful and should focus on shifting negative appraisals of the self and the diagnosis of postpsychotic depression.
"Undoubtedly, controlled trials are needed to help determine the efficacy of pharmacological and psychological therapies for depressive symptoms in FES. Importantly, the findings of the current study are helpful for characterizing the appropriate target groups for such studies," they added, noting that understanding the nature and characteristics of depression in FES has important clinical implication for both early intervention and outcome in FES patients, particularly in regard to quality of life.
The findings of this study must be considered in the context of the medical file audit methodology used – an approach potentially limited by medical record quality and lack of inter-rater reliability, but the widely used methodology also offers several benefits, including the fact that a highly representative sample of patients can be obtained, the investigators said.
Future prospective research should focus on "mapping the trajectory of depressive symptoms against the course of positive and negative symptoms, insight, and substance use," they concluded, noting that such studies will improve understanding of the phenomenology and trajectory of depressive pathology in FES and inform the development of targeted interventions.
This study was supported by grants from Eli Lilly & Co. Australia and the Leenaards Foundation, Switzerland. Dr. Cotton is supported by the Ronald Phillip Griffith Fellowship, the University of Melbourne. Several other study authors reported that they serve on Eli Lilly’s speakers board.
Depressive symptoms are common and tend to be neglected in patients with first episode schizophrenia spectrum disorders, according to a medical file audit involving records for more than 400 patients.
Of 405 patients with an available baseline Clinical Global Impressions-Severity of Illness Scale-Bipolar Illness (CGI-BP) depression score, 106 (26.2%) had moderate to severe depression at service entry, Sue M. Cotton, Ph.D., of the University of Melbourne, and her colleagues report in the January issue of Schizophrenia Research.
Among the characteristics of patients with moderate to severe depression at service entry, compared with those without depressive symptoms, were a significantly greater likelihood of a past history of major depressive disorder (MDD; odds ratio, 2.58) and suicide attempts (OR, 1.55), a family history of psychiatric disorder (OR, 1.40), and significantly reduced likelihood of a past history of substance use disorder (OR, 0.67), the investigators found (Schizophr. Research 2012;134:20-6).
The patients with depressive symptoms also were more likely to have current MDD (OR, 5.52), and to have partial/full insight into their psychotic disorder (OR, 0.68), and they were less likely to have a current substance use disorder (OR, 0.65).
During treatment they were less likely to be admitted to the hospital (OR, 0.79), with a lower number of admission (OR, 0.84), and were less likely to be using substances (OR, 0.40).At discharge they were more likely to be depressed and to have partial/full insight to their illness (OR, 2.04 and 0.70, respectively), the investigators said.
Data on antidepressant medication use were available for 254 patients, and of those with moderate to severe depressive symptoms, 45 (55.6%) were prescribed antidepressants; these patients had significantly higher CGI-BP depression scores than did those with depressive symptoms who were not prescribed antidepressants.
The audit also provided descriptive characteristics of the 15 patients with persistent depressive symptoms and the 91 without persistent depressive symptoms (of the 105 patients with moderate to severe depressive symptoms at service entry). For example, those with persistent symptoms were significantly more likely to have a past diagnosis of personality disorder, as well as a diagnosis of a personality disorder at service entry (OR, 10.88 and 3.81, respectively).
Personality disorder diagnoses at service entry included borderline personality disorder, schizotypal, antisocial personality disorder, and personality disorder not otherwise specified.
Patients with persistent depression were also significantly more likely to have a past history of suicide attempts as compared with the two other groups (OR, 2.54).
Those patients with persistent depression had a shorter duration of treatment, all were noncompliant with treatment, and they were more likely to have ongoing substance use. At discharge, they had a significantly higher CGI symptom severity score, a lower global assessment of functioning mean score, and were less likely to be working, the investigators noted.
Of 81 patients with depression for whom antidepressant treatment information was available, 4 had persistent depressive symptoms and 77 did not. All four of those with persistent symptoms received treatment, and 41 of those without persistent symptoms received treatment.
The findings regarding the prevalence of depressive symptoms support the notion that the condition is common in early schizophrenia, and the fact that only about 29% of those with depressive symptoms had a comorbid clinical diagnosis of major depressive disorder at service entry might reflect underdiagnosis or underreporting of MDD. That finding also might be a sign that depressive symptoms are neglected in first episode of schizophrenia (FES) treatment, with more emphasis being placed on management of positive and negative symptoms, the investigators suggested.
"This may also be compounded by the lack of detail in clinical guidelines regarding the best treatments (including antidepressant use and psychotherapy) for depressive symptoms in FES," they said.
The findings underscore the need for assessing FES patients for depression at service entry, and for monitoring those with a history of depression, suicidality, and greater insight into their psychotic illness for depression over time, they added.
Although data on therapeutic interventions for those with depression in FES are scant, available data suggest that pharmacotherapy might be indicated. Requirements for such therapy might vary depending on the stage of the psychotic illness.
"For example, during the acute psychotic episode, antipsychotic medication may be the best treatment option, as observational studies have indicated that depression often subsides when the acute psychotic symptoms are treated," the investigators noted.
Cognitive therapies might also be useful and should focus on shifting negative appraisals of the self and the diagnosis of postpsychotic depression.
"Undoubtedly, controlled trials are needed to help determine the efficacy of pharmacological and psychological therapies for depressive symptoms in FES. Importantly, the findings of the current study are helpful for characterizing the appropriate target groups for such studies," they added, noting that understanding the nature and characteristics of depression in FES has important clinical implication for both early intervention and outcome in FES patients, particularly in regard to quality of life.
The findings of this study must be considered in the context of the medical file audit methodology used – an approach potentially limited by medical record quality and lack of inter-rater reliability, but the widely used methodology also offers several benefits, including the fact that a highly representative sample of patients can be obtained, the investigators said.
Future prospective research should focus on "mapping the trajectory of depressive symptoms against the course of positive and negative symptoms, insight, and substance use," they concluded, noting that such studies will improve understanding of the phenomenology and trajectory of depressive pathology in FES and inform the development of targeted interventions.
This study was supported by grants from Eli Lilly & Co. Australia and the Leenaards Foundation, Switzerland. Dr. Cotton is supported by the Ronald Phillip Griffith Fellowship, the University of Melbourne. Several other study authors reported that they serve on Eli Lilly’s speakers board.
FROM SCHIZOPHRENIA RESEARCH
Major Finding: Of 405 patients with an available baseline Clinical Global Impressions-Severity of Illness Scale-Bipolar Illness (CGI-BP) depression score, 106 (26.2%) had moderate to severe depressive symptoms at service entry.
Data Source: A medical file audit.
Disclosures: This study was supported by grants from Eli Lilly & Co. Australia and the Leenaards Foundation, Switzerland. Dr. Cotton is supported by the Ronald Phillip Griffith Fellowship, the University of Melbourne. Several other study authors reported that they serve on Eli Lilly’s speakers board.
Cognitive Engagement Associated With Less of an Alzheimer's Protein
Cognitively stimulating activity, particularly in early and midlife, is associated with lower brain deposition of the major protein constituent of amyloid plaques in Alzheimer’s disease later in life, based on findings from a cross-sectional clinical study.
The study’s direct association between cognitive activity and beta-amyloid (A-beta) protein suggests that the lifestyles of those with greater cognitive engagement may play a role in the onset and progression of Alzheimer’s disease (AD), particularly because participation in cognitively stimulating activities has been linked with other lifestyle practices associated with reduced Alzheimer’s disease risk, Susan M. Landau, Ph.D., of the University of California, Berkeley, and her colleagues reported online Jan. 23 in Archives of Neurology.

PET imaging of the binding of the radiopharmaceutical carbon 11–labeled Pittsburgh Compound B ([11C]PiB) to A-beta protein showed comparable A-beta deposition in older adults in the highest cognitive activity tertile and young controls. On the other hand, older adults in the lowest cognitive activity tertile had mean cortical [11C]PiB uptake comparable with the Alzheimer’s patients, the investigators said (Arch. Neurol. 2012 Jan. 23 [doi:10.1001/archneurol.2011.2748]).
The researchers defined cognitively demanding activities in terms of activities that depended minimally on socioeconomic status, such as reading books or newspapers, writing letters or e-mails, and playing games.
The greatest association was seen between higher past cognitive activity scores (based on levels from ages 6 to 40 years, compared with those from ages 40 and older) and lower [11C]PiB uptake, but the association between cognitive activity and lower [11C]PiB uptake existed across the life span after age, sex, and years of education were taken into account, the investigators noted.
Although previous epidemiologic studies have also demonstrated a link between cognitive stimulation throughout life and a reduced risk of cognitive decline and Alzheimer’s disease, these findings "suggest a novel mechanism in which increased cognitive activity may play a direct role in reducing A-beta before disease onset," they wrote.
The notion that cognitive activity influences the development of Alzheimer’s disease pathology is supported by recent findings of reduced hippocampal atrophy – another biomarker of Alzheimer’s pathology – in cognitively normal older adults with greater lifelong complex mental activity levels, they said.
"Our cognitive activity measurement is likely just one of a variety of interrelated lifestyle factors that are difficult to quantify. Cognitive activity and (marginally) years of education were associated with [11C]PiB uptake (although cognitive activity and years of education were not related to one another), suggesting that these measurements may reflect a broader underlying tendency to engage in intellectual, occupational, social, and recreational activities," Dr. Landau and her coauthors wrote.
The study’s 75 older adults included 65 healthy participants with normal cognition and a mean age of 76 years and 10 with Alzheimer’s disease who had a mean age of 75 years. A total of 11 young control participants had a mean age of 24.5 years.
The healthy older adults underwent [11C]PiB PET imaging and completed an extensive neuropsychological battery between Oct. 31, 2005, and Feb. 22, 2011. They self-reported their levels of cognitively demanding activities and physical activity.
Although physical activity was associated with cognitive activity in this study, it was not associated with [11C]PiB uptake. The addition of physical activity to the model also did not reduce the association between cognitive activity and PiB. This indicates that cognitive activity was the primary variable driving the association because physical activity was measured as a current function and cognitive activity was assessed as a lifelong engagement. Dr. Landau and her associates then proposed that the association between [11C]PiB and cognitive (but not physical) activity "may thus reflect a time-sensitive neural process in which early- and midlife practices have a greater influence on AD pathology than later-life practices."
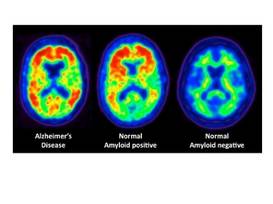
It is plausible, they said, that people who participate in a variety of cognitively stimulating activities throughout life may develop more efficient neural processing that results in less A-beta deposition – an idea supported by findings in transgenic A-beta–expressing mice.
"It is unlikely that our results reflect a single unitary cause of AD, which is a complex disease with many potential pathogenetic processes. ... However, the present findings extend previous findings that link cognitive stimulation and AD risk (an indirect downstream effect of A-beta) by providing evidence that is consistent with a model in which cognitive stimulation is linked directly to the AD-related pathology itself," they concluded.
This study was supported by grants from the National Institutes of Health and the Alzheimer’s Association. The authors reported no relevant financial disclosures.
Cognitively stimulating activity, particularly in early and midlife, is associated with lower brain deposition of the major protein constituent of amyloid plaques in Alzheimer’s disease later in life, based on findings from a cross-sectional clinical study.
The study’s direct association between cognitive activity and beta-amyloid (A-beta) protein suggests that the lifestyles of those with greater cognitive engagement may play a role in the onset and progression of Alzheimer’s disease (AD), particularly because participation in cognitively stimulating activities has been linked with other lifestyle practices associated with reduced Alzheimer’s disease risk, Susan M. Landau, Ph.D., of the University of California, Berkeley, and her colleagues reported online Jan. 23 in Archives of Neurology.
PET imaging of the binding of the radiopharmaceutical carbon 11–labeled Pittsburgh Compound B ([11C]PiB) to A-beta protein showed comparable A-beta deposition in older adults in the highest cognitive activity tertile and young controls. On the other hand, older adults in the lowest cognitive activity tertile had mean cortical [11C]PiB uptake comparable with the Alzheimer’s patients, the investigators said (Arch. Neurol. 2012 Jan. 23 [doi:10.1001/archneurol.2011.2748]).
The researchers defined cognitively demanding activities in terms of activities that depended minimally on socioeconomic status, such as reading books or newspapers, writing letters or e-mails, and playing games.
The greatest association was seen between higher past cognitive activity scores (based on levels from ages 6 to 40 years, compared with those from ages 40 and older) and lower [11C]PiB uptake, but the association between cognitive activity and lower [11C]PiB uptake existed across the life span after age, sex, and years of education were taken into account, the investigators noted.
Although previous epidemiologic studies have also demonstrated a link between cognitive stimulation throughout life and a reduced risk of cognitive decline and Alzheimer’s disease, these findings "suggest a novel mechanism in which increased cognitive activity may play a direct role in reducing A-beta before disease onset," they wrote.
The notion that cognitive activity influences the development of Alzheimer’s disease pathology is supported by recent findings of reduced hippocampal atrophy – another biomarker of Alzheimer’s pathology – in cognitively normal older adults with greater lifelong complex mental activity levels, they said.
"Our cognitive activity measurement is likely just one of a variety of interrelated lifestyle factors that are difficult to quantify. Cognitive activity and (marginally) years of education were associated with [11C]PiB uptake (although cognitive activity and years of education were not related to one another), suggesting that these measurements may reflect a broader underlying tendency to engage in intellectual, occupational, social, and recreational activities," Dr. Landau and her coauthors wrote.
The study’s 75 older adults included 65 healthy participants with normal cognition and a mean age of 76 years and 10 with Alzheimer’s disease who had a mean age of 75 years. A total of 11 young control participants had a mean age of 24.5 years.
The healthy older adults underwent [11C]PiB PET imaging and completed an extensive neuropsychological battery between Oct. 31, 2005, and Feb. 22, 2011. They self-reported their levels of cognitively demanding activities and physical activity.
Although physical activity was associated with cognitive activity in this study, it was not associated with [11C]PiB uptake. The addition of physical activity to the model also did not reduce the association between cognitive activity and PiB. This indicates that cognitive activity was the primary variable driving the association because physical activity was measured as a current function and cognitive activity was assessed as a lifelong engagement. Dr. Landau and her associates then proposed that the association between [11C]PiB and cognitive (but not physical) activity "may thus reflect a time-sensitive neural process in which early- and midlife practices have a greater influence on AD pathology than later-life practices."
It is plausible, they said, that people who participate in a variety of cognitively stimulating activities throughout life may develop more efficient neural processing that results in less A-beta deposition – an idea supported by findings in transgenic A-beta–expressing mice.
"It is unlikely that our results reflect a single unitary cause of AD, which is a complex disease with many potential pathogenetic processes. ... However, the present findings extend previous findings that link cognitive stimulation and AD risk (an indirect downstream effect of A-beta) by providing evidence that is consistent with a model in which cognitive stimulation is linked directly to the AD-related pathology itself," they concluded.
This study was supported by grants from the National Institutes of Health and the Alzheimer’s Association. The authors reported no relevant financial disclosures.
Cognitively stimulating activity, particularly in early and midlife, is associated with lower brain deposition of the major protein constituent of amyloid plaques in Alzheimer’s disease later in life, based on findings from a cross-sectional clinical study.
The study’s direct association between cognitive activity and beta-amyloid (A-beta) protein suggests that the lifestyles of those with greater cognitive engagement may play a role in the onset and progression of Alzheimer’s disease (AD), particularly because participation in cognitively stimulating activities has been linked with other lifestyle practices associated with reduced Alzheimer’s disease risk, Susan M. Landau, Ph.D., of the University of California, Berkeley, and her colleagues reported online Jan. 23 in Archives of Neurology.
PET imaging of the binding of the radiopharmaceutical carbon 11–labeled Pittsburgh Compound B ([11C]PiB) to A-beta protein showed comparable A-beta deposition in older adults in the highest cognitive activity tertile and young controls. On the other hand, older adults in the lowest cognitive activity tertile had mean cortical [11C]PiB uptake comparable with the Alzheimer’s patients, the investigators said (Arch. Neurol. 2012 Jan. 23 [doi:10.1001/archneurol.2011.2748]).
The researchers defined cognitively demanding activities in terms of activities that depended minimally on socioeconomic status, such as reading books or newspapers, writing letters or e-mails, and playing games.
The greatest association was seen between higher past cognitive activity scores (based on levels from ages 6 to 40 years, compared with those from ages 40 and older) and lower [11C]PiB uptake, but the association between cognitive activity and lower [11C]PiB uptake existed across the life span after age, sex, and years of education were taken into account, the investigators noted.
Although previous epidemiologic studies have also demonstrated a link between cognitive stimulation throughout life and a reduced risk of cognitive decline and Alzheimer’s disease, these findings "suggest a novel mechanism in which increased cognitive activity may play a direct role in reducing A-beta before disease onset," they wrote.
The notion that cognitive activity influences the development of Alzheimer’s disease pathology is supported by recent findings of reduced hippocampal atrophy – another biomarker of Alzheimer’s pathology – in cognitively normal older adults with greater lifelong complex mental activity levels, they said.
"Our cognitive activity measurement is likely just one of a variety of interrelated lifestyle factors that are difficult to quantify. Cognitive activity and (marginally) years of education were associated with [11C]PiB uptake (although cognitive activity and years of education were not related to one another), suggesting that these measurements may reflect a broader underlying tendency to engage in intellectual, occupational, social, and recreational activities," Dr. Landau and her coauthors wrote.
The study’s 75 older adults included 65 healthy participants with normal cognition and a mean age of 76 years and 10 with Alzheimer’s disease who had a mean age of 75 years. A total of 11 young control participants had a mean age of 24.5 years.
The healthy older adults underwent [11C]PiB PET imaging and completed an extensive neuropsychological battery between Oct. 31, 2005, and Feb. 22, 2011. They self-reported their levels of cognitively demanding activities and physical activity.
Although physical activity was associated with cognitive activity in this study, it was not associated with [11C]PiB uptake. The addition of physical activity to the model also did not reduce the association between cognitive activity and PiB. This indicates that cognitive activity was the primary variable driving the association because physical activity was measured as a current function and cognitive activity was assessed as a lifelong engagement. Dr. Landau and her associates then proposed that the association between [11C]PiB and cognitive (but not physical) activity "may thus reflect a time-sensitive neural process in which early- and midlife practices have a greater influence on AD pathology than later-life practices."
It is plausible, they said, that people who participate in a variety of cognitively stimulating activities throughout life may develop more efficient neural processing that results in less A-beta deposition – an idea supported by findings in transgenic A-beta–expressing mice.
"It is unlikely that our results reflect a single unitary cause of AD, which is a complex disease with many potential pathogenetic processes. ... However, the present findings extend previous findings that link cognitive stimulation and AD risk (an indirect downstream effect of A-beta) by providing evidence that is consistent with a model in which cognitive stimulation is linked directly to the AD-related pathology itself," they concluded.
This study was supported by grants from the National Institutes of Health and the Alzheimer’s Association. The authors reported no relevant financial disclosures.
FROM ARCHIVES OF NEUROLOGY
Major Finding: The greatest association was seen between higher past cognitive activity scores (based on levels from ages 6 to 40 years, compared with those from ages 40 and older) and lower [11C]PiB uptake, but the association between cognitive activity and lower [11C]PiB uptake existed across the life span after accounting for age, sex, and years of education.
Data Source: A cross-sectional clinical study of 75 older adults and 11 young healthy control participants.
Disclosures: This study was supported by grants from the National Institutes of Health and the Alzheimer’s Association. The authors reported no relevant financial disclosures.
Meta-Analysis Outlines Lithium Toxicity Profile
Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but, despite widespread belief to the contrary, it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function, according to findings from a systematic review and meta-analysis of data from 385 studies.
The review was undertaken in part because new evidence confirming the efficacy of lithium in bipolar disorder has led to suggestions that it be used more widely. Although it is considered an effective long-term therapy for bipolar disorder, its use has declined in recent years as new, more commercially promoted – but not always equally or more effective – drugs have become available. Concerns about potential teratogenic and other adverse effects, particularly on renal function, and have also contributed to declining use, Dr. Rebecca F. McKnight of the University of Oxford (England) and her colleagues reported online in the Jan. 20 issue of the Lancet.
To provide clinicians and patients with accurate evidence of lithium’s harms and benefits, the investigators set out to provide "a clinically informative systematic toxicity profile for lithium" they said (Lancet 2012 Jan. 20 [doi: 10.1016/S0140-6736(11)61516-X]).
Based on a hierarchy of evidence from the 22 randomized controlled trials, 197 cohort studies and case-control studies, and 166 case reports included in the review and meta-analysis, the investigators found that overall, glomerular filtration was reduced by –6.22 mL/min and urinary concentrating ability was reduced by 15% of normal maximum in patients receiving lithium, compared with controls.
"Data for the most clinically important outcome, renal failure, were scarce," the investigators said, noting that the only substantial cohort study showed that only 0.5% of patients receiving lithium were treated with renal replacement therapy.
As for clinical hypothyroidism, those taking lithium were significantly more likely than those on a placebo to develop the condition (odds ratio, 5.78), and based on a meta-analysis of the case-control studies, thyroid-stimulating hormone (TSH) concentrations were also significantly greater in those taking lithium (weighted mean difference, 4.00 IU/mL). Also, based on findings from 60 studies, blood calcium and parathyroid hormone levels were increased by about 10% over normal values in those taking lithium.
Clinically significant weight gain was also more frequent among those taking lithium than in controls (OR, 1.89), the investigators noted.
The evidence indicated, however, that lithium has little effect on hair or skin, with no significant difference seen in the incidence of alopecia in 24 publications reporting on the condition, and with no significant difference found in the prevalence of skin disorders between those taking lithium and controls in a meta-analysis of 77 publications.
Of note, six case-control studies that measured the association between Ebstein’s anomaly and lithium exposure found no link between the two. Although those estimates are unstable because of the low number of events, a case-control study of nearly 10,700 infants with a major congenital abnormality and more than 21,500 healthy controls also showed no significant association between lithium and congenital abnormalities.
Though limited by the quality and quantity of the primary evidence used in this study, which involved the screening of nearly 6,000 abstracts, the findings represent a "reasonable amount of evidence that allows cautious conclusions to be drawn about the safety of lithium," according to the investigators.
"This review provides a comprehensive synthesis of the evidence of harm that should inform clinical decision and draw attention to key questions in urgent need of further clarification," they said.
Based on their findings, the investigators developed the following recommendations for monitoring of lithium in clinical practice:
Before the start of lithium therapy, the risk of major adverse events should be discussed with the patient, a serum calcium level should be added to baseline blood tests, and uncertainty about the risk of congenital malformations to women of childbearing age should be explained. The latter two of these recommendations mark a change from current U.K. guidelines, the authors noted.
Also, during lithium therapy, renal, parathyroid, and thyroid function (at least glomerular filtration rate, TSH, and calcium) should be repeated at least every 12 months – and more frequently if an abnormal result is found or if the patient has a family history of endocrine disease; blood tests should all be repeated immediately in the event of a change in mood state; the occurrence of adverse effects should be routinely recorded; and women who would like to conceive or who have become pregnant during therapy should be advised that the increased risk of congenital malformation is uncertain, and the balance of risks between harm to the baby and maternal mood instability should be discussed before making a decision to discontinue lithium. All but the recommendation regarding repeat blood tests in the setting of mood state changes mark a change from current U.K. guidelines.
This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.
The authors of this review should be congratulated for the systematic quantification of the potential risks associated with lithium, Dr. Gin S. Malhi and Dr. Michael Berk wrote in an editorial that accompanied the report by Dr. McKnight and her colleagues in the Lancet.
This detailed review and analysis provides meaningful and reassuring advice for clinicians and identifies areas in need of additional research in regard to the safety of lithium, said Dr. Malhi and Dr. Berk. While the available evidence is far from ideal, the study – in the context of efficacy data upgrading the ranking of lithium, and new data that "recalibrate the safety risks of alternative drugs" – provides "timely clarification of the toxicity associated with lithium therapy, and on balance, reaffirms its role as a treatment of choice for bipolar disorder," they noted (Lancet 2012 Jan. 20 [doi:10.1016/S0140-6736(11)61703-0]).
"The renal side-effects of lithium are of greatest concern to both clinicians and patients, and in this regard, the analysis is reassuring in that, even with long-term lithium use, the risk of renal toxicity, specifically end-stage renal failure, is fairly low (0.53% compared to 0.2% in the general population)," they noted.
However, since the data on dosing and its relationship with toxicity were insufficient, matters of dose-related side-effects cannot be informed by the findings.
"Instead, the study provides useful guidance for clinicians considering lithium treatment, and redirects the focus of research to dosage and safety monitoring," said Dr. Malhi and Dr. Berk.
Dr. Malhi is with the University of Sydney. Dr. Berk is with the University of Melbourne. Dr. Malhi has received research support from, and/or served as a speaker or consultant for AstraZeneca, Eli Lilly, Organon, Pfizer, Servier, Wyeth, Janssen-Cilag, Lundbeck, and Ranbaxy. Dr. Berk has received research support from, and/or served as a speaker or consultant for Medical Benefits Funds of Australia, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Organon, Novartis, Mayne Pharma, Servier, Janssen-Cilag, Lundbeck, Merck, Pfizer, Sanofi-Synthelabo, Solvay, and Wyeth.
The authors of this review should be congratulated for the systematic quantification of the potential risks associated with lithium, Dr. Gin S. Malhi and Dr. Michael Berk wrote in an editorial that accompanied the report by Dr. McKnight and her colleagues in the Lancet.
This detailed review and analysis provides meaningful and reassuring advice for clinicians and identifies areas in need of additional research in regard to the safety of lithium, said Dr. Malhi and Dr. Berk. While the available evidence is far from ideal, the study – in the context of efficacy data upgrading the ranking of lithium, and new data that "recalibrate the safety risks of alternative drugs" – provides "timely clarification of the toxicity associated with lithium therapy, and on balance, reaffirms its role as a treatment of choice for bipolar disorder," they noted (Lancet 2012 Jan. 20 [doi:10.1016/S0140-6736(11)61703-0]).
"The renal side-effects of lithium are of greatest concern to both clinicians and patients, and in this regard, the analysis is reassuring in that, even with long-term lithium use, the risk of renal toxicity, specifically end-stage renal failure, is fairly low (0.53% compared to 0.2% in the general population)," they noted.
However, since the data on dosing and its relationship with toxicity were insufficient, matters of dose-related side-effects cannot be informed by the findings.
"Instead, the study provides useful guidance for clinicians considering lithium treatment, and redirects the focus of research to dosage and safety monitoring," said Dr. Malhi and Dr. Berk.
Dr. Malhi is with the University of Sydney. Dr. Berk is with the University of Melbourne. Dr. Malhi has received research support from, and/or served as a speaker or consultant for AstraZeneca, Eli Lilly, Organon, Pfizer, Servier, Wyeth, Janssen-Cilag, Lundbeck, and Ranbaxy. Dr. Berk has received research support from, and/or served as a speaker or consultant for Medical Benefits Funds of Australia, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Organon, Novartis, Mayne Pharma, Servier, Janssen-Cilag, Lundbeck, Merck, Pfizer, Sanofi-Synthelabo, Solvay, and Wyeth.
The authors of this review should be congratulated for the systematic quantification of the potential risks associated with lithium, Dr. Gin S. Malhi and Dr. Michael Berk wrote in an editorial that accompanied the report by Dr. McKnight and her colleagues in the Lancet.
This detailed review and analysis provides meaningful and reassuring advice for clinicians and identifies areas in need of additional research in regard to the safety of lithium, said Dr. Malhi and Dr. Berk. While the available evidence is far from ideal, the study – in the context of efficacy data upgrading the ranking of lithium, and new data that "recalibrate the safety risks of alternative drugs" – provides "timely clarification of the toxicity associated with lithium therapy, and on balance, reaffirms its role as a treatment of choice for bipolar disorder," they noted (Lancet 2012 Jan. 20 [doi:10.1016/S0140-6736(11)61703-0]).
"The renal side-effects of lithium are of greatest concern to both clinicians and patients, and in this regard, the analysis is reassuring in that, even with long-term lithium use, the risk of renal toxicity, specifically end-stage renal failure, is fairly low (0.53% compared to 0.2% in the general population)," they noted.
However, since the data on dosing and its relationship with toxicity were insufficient, matters of dose-related side-effects cannot be informed by the findings.
"Instead, the study provides useful guidance for clinicians considering lithium treatment, and redirects the focus of research to dosage and safety monitoring," said Dr. Malhi and Dr. Berk.
Dr. Malhi is with the University of Sydney. Dr. Berk is with the University of Melbourne. Dr. Malhi has received research support from, and/or served as a speaker or consultant for AstraZeneca, Eli Lilly, Organon, Pfizer, Servier, Wyeth, Janssen-Cilag, Lundbeck, and Ranbaxy. Dr. Berk has received research support from, and/or served as a speaker or consultant for Medical Benefits Funds of Australia, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Organon, Novartis, Mayne Pharma, Servier, Janssen-Cilag, Lundbeck, Merck, Pfizer, Sanofi-Synthelabo, Solvay, and Wyeth.
Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but, despite widespread belief to the contrary, it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function, according to findings from a systematic review and meta-analysis of data from 385 studies.
The review was undertaken in part because new evidence confirming the efficacy of lithium in bipolar disorder has led to suggestions that it be used more widely. Although it is considered an effective long-term therapy for bipolar disorder, its use has declined in recent years as new, more commercially promoted – but not always equally or more effective – drugs have become available. Concerns about potential teratogenic and other adverse effects, particularly on renal function, and have also contributed to declining use, Dr. Rebecca F. McKnight of the University of Oxford (England) and her colleagues reported online in the Jan. 20 issue of the Lancet.
To provide clinicians and patients with accurate evidence of lithium’s harms and benefits, the investigators set out to provide "a clinically informative systematic toxicity profile for lithium" they said (Lancet 2012 Jan. 20 [doi: 10.1016/S0140-6736(11)61516-X]).
Based on a hierarchy of evidence from the 22 randomized controlled trials, 197 cohort studies and case-control studies, and 166 case reports included in the review and meta-analysis, the investigators found that overall, glomerular filtration was reduced by –6.22 mL/min and urinary concentrating ability was reduced by 15% of normal maximum in patients receiving lithium, compared with controls.
"Data for the most clinically important outcome, renal failure, were scarce," the investigators said, noting that the only substantial cohort study showed that only 0.5% of patients receiving lithium were treated with renal replacement therapy.
As for clinical hypothyroidism, those taking lithium were significantly more likely than those on a placebo to develop the condition (odds ratio, 5.78), and based on a meta-analysis of the case-control studies, thyroid-stimulating hormone (TSH) concentrations were also significantly greater in those taking lithium (weighted mean difference, 4.00 IU/mL). Also, based on findings from 60 studies, blood calcium and parathyroid hormone levels were increased by about 10% over normal values in those taking lithium.
Clinically significant weight gain was also more frequent among those taking lithium than in controls (OR, 1.89), the investigators noted.
The evidence indicated, however, that lithium has little effect on hair or skin, with no significant difference seen in the incidence of alopecia in 24 publications reporting on the condition, and with no significant difference found in the prevalence of skin disorders between those taking lithium and controls in a meta-analysis of 77 publications.
Of note, six case-control studies that measured the association between Ebstein’s anomaly and lithium exposure found no link between the two. Although those estimates are unstable because of the low number of events, a case-control study of nearly 10,700 infants with a major congenital abnormality and more than 21,500 healthy controls also showed no significant association between lithium and congenital abnormalities.
Though limited by the quality and quantity of the primary evidence used in this study, which involved the screening of nearly 6,000 abstracts, the findings represent a "reasonable amount of evidence that allows cautious conclusions to be drawn about the safety of lithium," according to the investigators.
"This review provides a comprehensive synthesis of the evidence of harm that should inform clinical decision and draw attention to key questions in urgent need of further clarification," they said.
Based on their findings, the investigators developed the following recommendations for monitoring of lithium in clinical practice:
Before the start of lithium therapy, the risk of major adverse events should be discussed with the patient, a serum calcium level should be added to baseline blood tests, and uncertainty about the risk of congenital malformations to women of childbearing age should be explained. The latter two of these recommendations mark a change from current U.K. guidelines, the authors noted.
Also, during lithium therapy, renal, parathyroid, and thyroid function (at least glomerular filtration rate, TSH, and calcium) should be repeated at least every 12 months – and more frequently if an abnormal result is found or if the patient has a family history of endocrine disease; blood tests should all be repeated immediately in the event of a change in mood state; the occurrence of adverse effects should be routinely recorded; and women who would like to conceive or who have become pregnant during therapy should be advised that the increased risk of congenital malformation is uncertain, and the balance of risks between harm to the baby and maternal mood instability should be discussed before making a decision to discontinue lithium. All but the recommendation regarding repeat blood tests in the setting of mood state changes mark a change from current U.K. guidelines.
This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.
Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but, despite widespread belief to the contrary, it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function, according to findings from a systematic review and meta-analysis of data from 385 studies.
The review was undertaken in part because new evidence confirming the efficacy of lithium in bipolar disorder has led to suggestions that it be used more widely. Although it is considered an effective long-term therapy for bipolar disorder, its use has declined in recent years as new, more commercially promoted – but not always equally or more effective – drugs have become available. Concerns about potential teratogenic and other adverse effects, particularly on renal function, and have also contributed to declining use, Dr. Rebecca F. McKnight of the University of Oxford (England) and her colleagues reported online in the Jan. 20 issue of the Lancet.
To provide clinicians and patients with accurate evidence of lithium’s harms and benefits, the investigators set out to provide "a clinically informative systematic toxicity profile for lithium" they said (Lancet 2012 Jan. 20 [doi: 10.1016/S0140-6736(11)61516-X]).
Based on a hierarchy of evidence from the 22 randomized controlled trials, 197 cohort studies and case-control studies, and 166 case reports included in the review and meta-analysis, the investigators found that overall, glomerular filtration was reduced by –6.22 mL/min and urinary concentrating ability was reduced by 15% of normal maximum in patients receiving lithium, compared with controls.
"Data for the most clinically important outcome, renal failure, were scarce," the investigators said, noting that the only substantial cohort study showed that only 0.5% of patients receiving lithium were treated with renal replacement therapy.
As for clinical hypothyroidism, those taking lithium were significantly more likely than those on a placebo to develop the condition (odds ratio, 5.78), and based on a meta-analysis of the case-control studies, thyroid-stimulating hormone (TSH) concentrations were also significantly greater in those taking lithium (weighted mean difference, 4.00 IU/mL). Also, based on findings from 60 studies, blood calcium and parathyroid hormone levels were increased by about 10% over normal values in those taking lithium.
Clinically significant weight gain was also more frequent among those taking lithium than in controls (OR, 1.89), the investigators noted.
The evidence indicated, however, that lithium has little effect on hair or skin, with no significant difference seen in the incidence of alopecia in 24 publications reporting on the condition, and with no significant difference found in the prevalence of skin disorders between those taking lithium and controls in a meta-analysis of 77 publications.
Of note, six case-control studies that measured the association between Ebstein’s anomaly and lithium exposure found no link between the two. Although those estimates are unstable because of the low number of events, a case-control study of nearly 10,700 infants with a major congenital abnormality and more than 21,500 healthy controls also showed no significant association between lithium and congenital abnormalities.
Though limited by the quality and quantity of the primary evidence used in this study, which involved the screening of nearly 6,000 abstracts, the findings represent a "reasonable amount of evidence that allows cautious conclusions to be drawn about the safety of lithium," according to the investigators.
"This review provides a comprehensive synthesis of the evidence of harm that should inform clinical decision and draw attention to key questions in urgent need of further clarification," they said.
Based on their findings, the investigators developed the following recommendations for monitoring of lithium in clinical practice:
Before the start of lithium therapy, the risk of major adverse events should be discussed with the patient, a serum calcium level should be added to baseline blood tests, and uncertainty about the risk of congenital malformations to women of childbearing age should be explained. The latter two of these recommendations mark a change from current U.K. guidelines, the authors noted.
Also, during lithium therapy, renal, parathyroid, and thyroid function (at least glomerular filtration rate, TSH, and calcium) should be repeated at least every 12 months – and more frequently if an abnormal result is found or if the patient has a family history of endocrine disease; blood tests should all be repeated immediately in the event of a change in mood state; the occurrence of adverse effects should be routinely recorded; and women who would like to conceive or who have become pregnant during therapy should be advised that the increased risk of congenital malformation is uncertain, and the balance of risks between harm to the baby and maternal mood instability should be discussed before making a decision to discontinue lithium. All but the recommendation regarding repeat blood tests in the setting of mood state changes mark a change from current U.K. guidelines.
This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.
FROM THE LANCET
Major Finding: Lithium is associated with an increased risk of reduced urinary concentrating ability, hypothyroidism, hyperparathyroidism, and weight gain, but it may not be associated with congenital malformations, alopecia, skin disorders, or clinically significant reductions in renal function.
Data Source: A systematic review and meta-analysis of randomized controlled trials and observational studies.
Disclosures: This study was funded by the National Institute for Health Research Programme Grant for Applied Research. The authors had no disclosures to report.