User login
Imaging after bariatric surgery appears overdone
Nearly 70% of bariatric surgery patients received postoperative imaging, with more than one-third receiving CT imaging. This high level of screening resulted in symptom-related findings in only 23% of cases, and may be excessive, according to researchers who studied nearly 600 adults who underwent bariatric surgery.
As the volume of bariatric surgery has increased, so has the role of postoperative imaging, wrote Dana Haddad, MD, and her colleagues at Harlem Hospital Center, New York.
“However, there is a lack of well-defined postoperative imaging guidelines,” they said. “Detrimental aspects of postoperative imaging include the potential for false-positive findings leading to further and often unnecessary investigations, radiation exposure, and additional cost,” they added.
The primary outcomes were the numbers of initial postimaging studies and whether the findings supported subsequent studies.
The study population included 399 adults who underwent laparoscopic bypass and 144 who underwent sleeve gastrectomy. The average age of the patients was 41 years and 90% were women.
The researchers identified 907 imaging studies performed in 400 patients (69% of the study population). Of these, 38% were ultrasound, 36% were CT, 15% were x-ray, 6.6% were fluoroscopy, 3.3% were MRI, and .6% were nuclear medicine.
On review of the imaging findings, the researchers found that half (50%) were unremarkable, while 13% were either surgery related or symptom related, 6.8% were not related to surgery but might have explained patients’ symptoms, 4.3% were surgery-related but not likely to explain symptoms, and 26% were incidental. “Interestingly, no incidental findings were found to be of major clinical importance; all were benign,” according to the researchers.
However, incidental findings led to a total of 71 additional studies, and to 5 laparoscopic cholecystectomies.
A univariate analysis showed that the factors with a significant impact a patient’s odds of undergoing postoperative abdominal imaging included having a bypass procedure vs. a sleeve procedure, older age, and lower baseline body mass index. In addition, patients with a history of abdominal surgery or dyspepsia or those who had a routine postoperative upper gastrointestinal series were significantly more likely to undergo CT scans. Patients with history of ulcer or reflux were significantly less likely to undergo CT scans.
Although the study was limited by the retrospective design and lack of information about possible imaging of patients at other centers, “results suggest that nonroutine postoperative abdominal imaging in the bariatric population is common and requires streamlined protocols, with almost 70% of patients undergoing imaging and greater than 70% of findings being unrelated to symptoms or negative,” the researchers said.
A clinical algorithm for imaging of bariatric patients should be based on clinical parameters collected during a physical exam. “Once an algorithm is in place, further studies will be needed to validate its accuracy and efficiency,” the researchers stated.
Dr. Haddad and her colleagues had no financial conflicts to disclose.
Nearly 70% of bariatric surgery patients received postoperative imaging, with more than one-third receiving CT imaging. This high level of screening resulted in symptom-related findings in only 23% of cases, and may be excessive, according to researchers who studied nearly 600 adults who underwent bariatric surgery.
As the volume of bariatric surgery has increased, so has the role of postoperative imaging, wrote Dana Haddad, MD, and her colleagues at Harlem Hospital Center, New York.
“However, there is a lack of well-defined postoperative imaging guidelines,” they said. “Detrimental aspects of postoperative imaging include the potential for false-positive findings leading to further and often unnecessary investigations, radiation exposure, and additional cost,” they added.
The primary outcomes were the numbers of initial postimaging studies and whether the findings supported subsequent studies.
The study population included 399 adults who underwent laparoscopic bypass and 144 who underwent sleeve gastrectomy. The average age of the patients was 41 years and 90% were women.
The researchers identified 907 imaging studies performed in 400 patients (69% of the study population). Of these, 38% were ultrasound, 36% were CT, 15% were x-ray, 6.6% were fluoroscopy, 3.3% were MRI, and .6% were nuclear medicine.
On review of the imaging findings, the researchers found that half (50%) were unremarkable, while 13% were either surgery related or symptom related, 6.8% were not related to surgery but might have explained patients’ symptoms, 4.3% were surgery-related but not likely to explain symptoms, and 26% were incidental. “Interestingly, no incidental findings were found to be of major clinical importance; all were benign,” according to the researchers.
However, incidental findings led to a total of 71 additional studies, and to 5 laparoscopic cholecystectomies.
A univariate analysis showed that the factors with a significant impact a patient’s odds of undergoing postoperative abdominal imaging included having a bypass procedure vs. a sleeve procedure, older age, and lower baseline body mass index. In addition, patients with a history of abdominal surgery or dyspepsia or those who had a routine postoperative upper gastrointestinal series were significantly more likely to undergo CT scans. Patients with history of ulcer or reflux were significantly less likely to undergo CT scans.
Although the study was limited by the retrospective design and lack of information about possible imaging of patients at other centers, “results suggest that nonroutine postoperative abdominal imaging in the bariatric population is common and requires streamlined protocols, with almost 70% of patients undergoing imaging and greater than 70% of findings being unrelated to symptoms or negative,” the researchers said.
A clinical algorithm for imaging of bariatric patients should be based on clinical parameters collected during a physical exam. “Once an algorithm is in place, further studies will be needed to validate its accuracy and efficiency,” the researchers stated.
Dr. Haddad and her colleagues had no financial conflicts to disclose.
Nearly 70% of bariatric surgery patients received postoperative imaging, with more than one-third receiving CT imaging. This high level of screening resulted in symptom-related findings in only 23% of cases, and may be excessive, according to researchers who studied nearly 600 adults who underwent bariatric surgery.
As the volume of bariatric surgery has increased, so has the role of postoperative imaging, wrote Dana Haddad, MD, and her colleagues at Harlem Hospital Center, New York.
“However, there is a lack of well-defined postoperative imaging guidelines,” they said. “Detrimental aspects of postoperative imaging include the potential for false-positive findings leading to further and often unnecessary investigations, radiation exposure, and additional cost,” they added.
The primary outcomes were the numbers of initial postimaging studies and whether the findings supported subsequent studies.
The study population included 399 adults who underwent laparoscopic bypass and 144 who underwent sleeve gastrectomy. The average age of the patients was 41 years and 90% were women.
The researchers identified 907 imaging studies performed in 400 patients (69% of the study population). Of these, 38% were ultrasound, 36% were CT, 15% were x-ray, 6.6% were fluoroscopy, 3.3% were MRI, and .6% were nuclear medicine.
On review of the imaging findings, the researchers found that half (50%) were unremarkable, while 13% were either surgery related or symptom related, 6.8% were not related to surgery but might have explained patients’ symptoms, 4.3% were surgery-related but not likely to explain symptoms, and 26% were incidental. “Interestingly, no incidental findings were found to be of major clinical importance; all were benign,” according to the researchers.
However, incidental findings led to a total of 71 additional studies, and to 5 laparoscopic cholecystectomies.
A univariate analysis showed that the factors with a significant impact a patient’s odds of undergoing postoperative abdominal imaging included having a bypass procedure vs. a sleeve procedure, older age, and lower baseline body mass index. In addition, patients with a history of abdominal surgery or dyspepsia or those who had a routine postoperative upper gastrointestinal series were significantly more likely to undergo CT scans. Patients with history of ulcer or reflux were significantly less likely to undergo CT scans.
Although the study was limited by the retrospective design and lack of information about possible imaging of patients at other centers, “results suggest that nonroutine postoperative abdominal imaging in the bariatric population is common and requires streamlined protocols, with almost 70% of patients undergoing imaging and greater than 70% of findings being unrelated to symptoms or negative,” the researchers said.
A clinical algorithm for imaging of bariatric patients should be based on clinical parameters collected during a physical exam. “Once an algorithm is in place, further studies will be needed to validate its accuracy and efficiency,” the researchers stated.
Dr. Haddad and her colleagues had no financial conflicts to disclose.
FROM SURGERY FOR OBESITY AND RELATED DISEASES
Key clinical point: No well-defined guidelines exist for when to use postoperative imaging in bariatric surgery patients.
Major finding: Approximately 70% of postoperative imaging findings were not symptom related, and incidental findings led to 71 additional studies.
Data source: A review of 578 patients who underwent gastric bypass or sleeve gastrectomy.
Disclosures: The researchers had no financial conflicts to disclose.
Obeticholic acid fails to prevent liver damage in an animal model of short-bowel syndrome
Obeticholic acid failed to prevent the development of short-bowel syndrome–associated liver disease in a preliminary study using piglet models. The findings were published in the July issue of Cellular and Molecular Gastroenterology and Hepatology (doi: 10.1016/j.jcmgh.2017.02.008).
Current treatment options for short-bowel syndrome-associated liver disease are limited, wrote Prue M. Pereira-Fantini, PhD, of Murdoch Childrens Research Institute, Victoria, Australia, and colleagues. However, the farnesoid X receptor, which regulates genes involved in bile acid synthesis, absorption, and transport in the intestine and liver, has shown promise as a pharmaceutical target.
“Recently, we described SBS-ALD-associated alterations in bile acid composition associated with disrupted farnesoid X receptor (FXR) signaling mechanisms,” the researchers said. Obeticholic acid (OCA) has been shown to prevent liver disease in mouse models and human disease, and the researchers explored whether it would be effective in the context of short-bowel syndrome associated liver disease (SBS-ALD).
The researchers randomized piglets into four groups to receive small-bowel resection or sham surgery, and either a daily dose of 2.4 mg/kg per day of OCA or no treatment. The pigs were euthanized 2 weeks after their surgeries, and the researchers collected portal plasma samples, bile samples, and liver samples.
OCA treatment in piglets in the SBS surgery group was associated with decreased stool fat that suggested improved fat absorption, but impacted liver morphology, the researchers noted. “Untreated, sham-operated piglets showed normal liver histology when compared with SBS piglets who showed decreased hepatic lobule area and small clusters of inflammatory cells together with mild-to-moderate vesicular zone 2 lipidosis,” they wrote.
Overall, OCA treatment prevented the depletion of taurine; taurine concentration was approximately 8 ng/mL for piglets with SBS treated with OCA compared with 8 ng/mL in the sham group, 9 ng/mL in the sham plus OCA group, and 3 ng/mL in the SBS-only group. However, bile acid dysmetabolism occurred as shown by HDCA levels, which increased with OCA treatment compared to sham controls but were significantly reduced in SBS piglets treated with OCA vs. untreated SBS piglets.
In addition, the researchers found that small-bowel resection did not impact gene expression levels of FXR targets in the intestine or liver. However, “intestinal FXR gene expression was 11-fold higher in untreated SBS piglets when compared with untreated sham piglets,” they wrote. OCA treatment had no significant impact on FXR gene expression in the OCA-treated group vs. the untreated group and in the OCA-treated SBS group.
Although the findings were limited by use of an animal model, the results suggest that OCA treatment may have clinical benefits for SBS patients by reducing fat malabsorption, which remains a challenge, the researchers wrote. However, OCA “did not prevent the development of SBS-ALD, thereby limiting the potential therapeutic benefit in patients with SBS,” they concluded.
The researchers had no financial conflicts to disclose. The study was supported in part by the National Health and Medical Research Council of Australia and by a research grant from the Science Foundation Ireland.
Obeticholic acid failed to prevent the development of short-bowel syndrome–associated liver disease in a preliminary study using piglet models. The findings were published in the July issue of Cellular and Molecular Gastroenterology and Hepatology (doi: 10.1016/j.jcmgh.2017.02.008).
Current treatment options for short-bowel syndrome-associated liver disease are limited, wrote Prue M. Pereira-Fantini, PhD, of Murdoch Childrens Research Institute, Victoria, Australia, and colleagues. However, the farnesoid X receptor, which regulates genes involved in bile acid synthesis, absorption, and transport in the intestine and liver, has shown promise as a pharmaceutical target.
“Recently, we described SBS-ALD-associated alterations in bile acid composition associated with disrupted farnesoid X receptor (FXR) signaling mechanisms,” the researchers said. Obeticholic acid (OCA) has been shown to prevent liver disease in mouse models and human disease, and the researchers explored whether it would be effective in the context of short-bowel syndrome associated liver disease (SBS-ALD).
The researchers randomized piglets into four groups to receive small-bowel resection or sham surgery, and either a daily dose of 2.4 mg/kg per day of OCA or no treatment. The pigs were euthanized 2 weeks after their surgeries, and the researchers collected portal plasma samples, bile samples, and liver samples.
OCA treatment in piglets in the SBS surgery group was associated with decreased stool fat that suggested improved fat absorption, but impacted liver morphology, the researchers noted. “Untreated, sham-operated piglets showed normal liver histology when compared with SBS piglets who showed decreased hepatic lobule area and small clusters of inflammatory cells together with mild-to-moderate vesicular zone 2 lipidosis,” they wrote.
Overall, OCA treatment prevented the depletion of taurine; taurine concentration was approximately 8 ng/mL for piglets with SBS treated with OCA compared with 8 ng/mL in the sham group, 9 ng/mL in the sham plus OCA group, and 3 ng/mL in the SBS-only group. However, bile acid dysmetabolism occurred as shown by HDCA levels, which increased with OCA treatment compared to sham controls but were significantly reduced in SBS piglets treated with OCA vs. untreated SBS piglets.
In addition, the researchers found that small-bowel resection did not impact gene expression levels of FXR targets in the intestine or liver. However, “intestinal FXR gene expression was 11-fold higher in untreated SBS piglets when compared with untreated sham piglets,” they wrote. OCA treatment had no significant impact on FXR gene expression in the OCA-treated group vs. the untreated group and in the OCA-treated SBS group.
Although the findings were limited by use of an animal model, the results suggest that OCA treatment may have clinical benefits for SBS patients by reducing fat malabsorption, which remains a challenge, the researchers wrote. However, OCA “did not prevent the development of SBS-ALD, thereby limiting the potential therapeutic benefit in patients with SBS,” they concluded.
The researchers had no financial conflicts to disclose. The study was supported in part by the National Health and Medical Research Council of Australia and by a research grant from the Science Foundation Ireland.
Obeticholic acid failed to prevent the development of short-bowel syndrome–associated liver disease in a preliminary study using piglet models. The findings were published in the July issue of Cellular and Molecular Gastroenterology and Hepatology (doi: 10.1016/j.jcmgh.2017.02.008).
Current treatment options for short-bowel syndrome-associated liver disease are limited, wrote Prue M. Pereira-Fantini, PhD, of Murdoch Childrens Research Institute, Victoria, Australia, and colleagues. However, the farnesoid X receptor, which regulates genes involved in bile acid synthesis, absorption, and transport in the intestine and liver, has shown promise as a pharmaceutical target.
“Recently, we described SBS-ALD-associated alterations in bile acid composition associated with disrupted farnesoid X receptor (FXR) signaling mechanisms,” the researchers said. Obeticholic acid (OCA) has been shown to prevent liver disease in mouse models and human disease, and the researchers explored whether it would be effective in the context of short-bowel syndrome associated liver disease (SBS-ALD).
The researchers randomized piglets into four groups to receive small-bowel resection or sham surgery, and either a daily dose of 2.4 mg/kg per day of OCA or no treatment. The pigs were euthanized 2 weeks after their surgeries, and the researchers collected portal plasma samples, bile samples, and liver samples.
OCA treatment in piglets in the SBS surgery group was associated with decreased stool fat that suggested improved fat absorption, but impacted liver morphology, the researchers noted. “Untreated, sham-operated piglets showed normal liver histology when compared with SBS piglets who showed decreased hepatic lobule area and small clusters of inflammatory cells together with mild-to-moderate vesicular zone 2 lipidosis,” they wrote.
Overall, OCA treatment prevented the depletion of taurine; taurine concentration was approximately 8 ng/mL for piglets with SBS treated with OCA compared with 8 ng/mL in the sham group, 9 ng/mL in the sham plus OCA group, and 3 ng/mL in the SBS-only group. However, bile acid dysmetabolism occurred as shown by HDCA levels, which increased with OCA treatment compared to sham controls but were significantly reduced in SBS piglets treated with OCA vs. untreated SBS piglets.
In addition, the researchers found that small-bowel resection did not impact gene expression levels of FXR targets in the intestine or liver. However, “intestinal FXR gene expression was 11-fold higher in untreated SBS piglets when compared with untreated sham piglets,” they wrote. OCA treatment had no significant impact on FXR gene expression in the OCA-treated group vs. the untreated group and in the OCA-treated SBS group.
Although the findings were limited by use of an animal model, the results suggest that OCA treatment may have clinical benefits for SBS patients by reducing fat malabsorption, which remains a challenge, the researchers wrote. However, OCA “did not prevent the development of SBS-ALD, thereby limiting the potential therapeutic benefit in patients with SBS,” they concluded.
The researchers had no financial conflicts to disclose. The study was supported in part by the National Health and Medical Research Council of Australia and by a research grant from the Science Foundation Ireland.
FROM CMGH
Key clinical point: Treatment with obeticholic acid improved absorption and altered bile acid, but did not prevent liver damage in a piglet model of short-bowel syndrome.
Major finding: Overall, taurine concentration was approximately 8 ng/mL for piglets with SBS treated with OCA compared with 8 ng/mL in the sham surgery group, 9 ng/mL in the sham treated with OCA group, and 3 ng/mL in the SBS-only group.
Data source: The data come from piglets treated with obeticholic acid or untreated, and randomized to a small-bowel resection or a sham surgery.
Disclosures: The researchers had no financial conflicts to disclose,
Proper catheter removal promotes colorectal surgery recovery
Adherence to guidelines for urinary catheter removal significantly reduced rates of urinary tract infection and length of hospital stay, based on data from almost 3,000 patients.
UTIs occurred in 0.8% of colonic surgery patients who were guideline compliant, compared with 4.1% of noncompliant patients. Similarly, UTIs were significantly less likely in rectal surgery patients who complied with guidelines, compared with those who did not (3.5% vs. 9.6%).
The Implementation of the Enhanced Recovery After Surgery (iERAS) program involved 15 academic hospitals in Ontario, Canada. The guidelines include prompt removal of catheters from colonic and rectal surgery patients. Recommended removal times ranged from 24 hours to 72 hours, depending on the procedure.
“Although numerous reports have documented the overall effectiveness of bundled ERAS interventions improving outcome, the contribution of individual components of the pathway in the context of an ERAS implementation program is uncertain,” wrote Allan Okrainec, MD, of the University of Toronto, and his colleagues.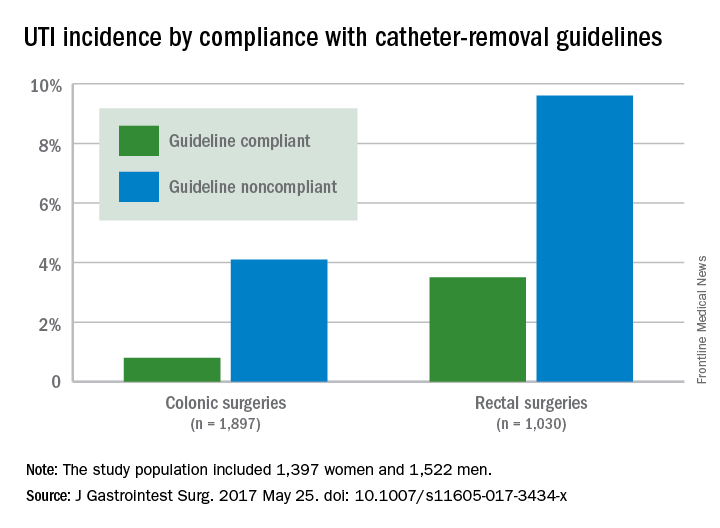
Overall, 53% of patients had catheters removed in compliance with the guidelines, including 47.2% of those with colonic resections and 69.5% of those with rectal resections.
The average length of hospital stay for colonic surgery patients who complied with the urinary catheter guideline was 4 days, compared with 5 days for noncompliant patients, a statistically significant difference. Similarly, the average length of stay was significantly shorter for compliant rectal surgery patients, compared with noncompliant patients (5 days vs. 8 days, respectively).
Reinsertion of the urinary catheter was needed for 6% of the patients, including 122 patients with suspected or confirmed urinary retention and 36 patients who had other indications for reinsertion.
“One of the concerns about early removal of catheters is that it might lead to an increased need for reinsertion,” the researchers noted. “In our study, guideline compliance was associated with an increased rate of catheter reinsertion, but [it] only increased the risk by 2%-3% in patients having rectal or colonic procedures,” the investigators said.
The study results were limited by a lack of information about reasons for noncompliance with the guidelines, the researchers added. However, the data support the value of early catheter removal for surgical patients. “It is noteworthy that, in our study, as well as others, urinary retention rates are relatively low,” they said.
The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
Adherence to guidelines for urinary catheter removal significantly reduced rates of urinary tract infection and length of hospital stay, based on data from almost 3,000 patients.
UTIs occurred in 0.8% of colonic surgery patients who were guideline compliant, compared with 4.1% of noncompliant patients. Similarly, UTIs were significantly less likely in rectal surgery patients who complied with guidelines, compared with those who did not (3.5% vs. 9.6%).
The Implementation of the Enhanced Recovery After Surgery (iERAS) program involved 15 academic hospitals in Ontario, Canada. The guidelines include prompt removal of catheters from colonic and rectal surgery patients. Recommended removal times ranged from 24 hours to 72 hours, depending on the procedure.
“Although numerous reports have documented the overall effectiveness of bundled ERAS interventions improving outcome, the contribution of individual components of the pathway in the context of an ERAS implementation program is uncertain,” wrote Allan Okrainec, MD, of the University of Toronto, and his colleagues.
Overall, 53% of patients had catheters removed in compliance with the guidelines, including 47.2% of those with colonic resections and 69.5% of those with rectal resections.
The average length of hospital stay for colonic surgery patients who complied with the urinary catheter guideline was 4 days, compared with 5 days for noncompliant patients, a statistically significant difference. Similarly, the average length of stay was significantly shorter for compliant rectal surgery patients, compared with noncompliant patients (5 days vs. 8 days, respectively).
Reinsertion of the urinary catheter was needed for 6% of the patients, including 122 patients with suspected or confirmed urinary retention and 36 patients who had other indications for reinsertion.
“One of the concerns about early removal of catheters is that it might lead to an increased need for reinsertion,” the researchers noted. “In our study, guideline compliance was associated with an increased rate of catheter reinsertion, but [it] only increased the risk by 2%-3% in patients having rectal or colonic procedures,” the investigators said.
The study results were limited by a lack of information about reasons for noncompliance with the guidelines, the researchers added. However, the data support the value of early catheter removal for surgical patients. “It is noteworthy that, in our study, as well as others, urinary retention rates are relatively low,” they said.
The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
Adherence to guidelines for urinary catheter removal significantly reduced rates of urinary tract infection and length of hospital stay, based on data from almost 3,000 patients.
UTIs occurred in 0.8% of colonic surgery patients who were guideline compliant, compared with 4.1% of noncompliant patients. Similarly, UTIs were significantly less likely in rectal surgery patients who complied with guidelines, compared with those who did not (3.5% vs. 9.6%).
The Implementation of the Enhanced Recovery After Surgery (iERAS) program involved 15 academic hospitals in Ontario, Canada. The guidelines include prompt removal of catheters from colonic and rectal surgery patients. Recommended removal times ranged from 24 hours to 72 hours, depending on the procedure.
“Although numerous reports have documented the overall effectiveness of bundled ERAS interventions improving outcome, the contribution of individual components of the pathway in the context of an ERAS implementation program is uncertain,” wrote Allan Okrainec, MD, of the University of Toronto, and his colleagues.
Overall, 53% of patients had catheters removed in compliance with the guidelines, including 47.2% of those with colonic resections and 69.5% of those with rectal resections.
The average length of hospital stay for colonic surgery patients who complied with the urinary catheter guideline was 4 days, compared with 5 days for noncompliant patients, a statistically significant difference. Similarly, the average length of stay was significantly shorter for compliant rectal surgery patients, compared with noncompliant patients (5 days vs. 8 days, respectively).
Reinsertion of the urinary catheter was needed for 6% of the patients, including 122 patients with suspected or confirmed urinary retention and 36 patients who had other indications for reinsertion.
“One of the concerns about early removal of catheters is that it might lead to an increased need for reinsertion,” the researchers noted. “In our study, guideline compliance was associated with an increased rate of catheter reinsertion, but [it] only increased the risk by 2%-3% in patients having rectal or colonic procedures,” the investigators said.
The study results were limited by a lack of information about reasons for noncompliance with the guidelines, the researchers added. However, the data support the value of early catheter removal for surgical patients. “It is noteworthy that, in our study, as well as others, urinary retention rates are relatively low,” they said.
The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF GASTROINTESTINAL SURGERY
Key clinical point: Compliance with guidelines for urinary catheter removal significantly reduced hospital stay and UTI rates in colon and rectal surgery patients.
Major finding: UTI rates in colonic surgery patients were 0.8% and 4.1%, respectively, for those who were compliant and noncompliant with the guidelines. Rates were 3.5% and 9.6%, respectively, for compliant and noncompliant rectal surgery patients.
Data source: A prospective study of 2,927 adults who underwent colonic or rectal surgery between September 2012 and April 2015.
Disclosures: The Council of Academic Hospitals of Ontario funded the study. The researchers had no financial conflicts to disclose.
Breastfeeding may reduce moms’ stroke risk
Breastfeeding not only benefits babies; it also may lower the risk for a heart attack or stroke later in life for mothers who breastfeed more than for women who don’t.
The findings, which were published online June 21 in the Journal of the American Heart Association, are based on data from a prospective study of nearly 300,000 women in China.
To assess the impact of breastfeeding on maternal cardiovascular health, the researchers reviewed data from 289,573 women who were participating in the China Kadoorie Biobank study to assess their reproductive history and lifestyle. At the time of study enrollment, none of the women had a history of cardiovascular disease and 99% reported at least one live birth. The average age of the women at baseline was 51 years.
Of the women who had given birth, 97% reported ever breastfeeding, and 91% reported breastfeeding each child for at least 6 months. The median duration of breastfeeding was 12 months per child (J Am Heart Assoc. 2017 Jun 21. doi: JAHA/2017/006081-T2).
During an 8-year follow-up period, participants experienced 16,671 cases of coronary heart disease and 23,983 strokes.
Overall, women who breastfed babies had a 9% reduction in risk of coronary heart disease and an 8% reduction in risk of stroke, compared with women who never breastfed. The longer the duration of breastfeeding, the greater the risk reduction; for every additional 6 months of breastfeeding, researchers found a 4% reduction in heart disease risk and a 3% reduction in stroke risk. Mothers who breastfed for 2 years or more had the most protection – an 18% reduced risk of heart disease and a 17% reduced risk of stroke, compared with mothers who never breastfed.
The study was limited by several factors, including its observational nature, which cannot confirm a causal relationship between breastfeeding and CVD. However, the results suggest that, if causal, “interventions to increase the likelihood and duration of breastfeeding could have persistent benefits to maternal cardiovascular health,” they wrote.
The baseline study was funded by the Kadoorie Charitable Foundation in Hong Kong; long-term support came from the UK Wellcome Trust, Chinese Ministry of Science and Technology, and the Chinese National Natural Science Foundation. Other support came from the British Heart Foundation, UK Medical Research Council and Cancer Research UK, and the National Natural Science Foundation of China. Dr. Peters has received support from the British Heart Foundation.
Breastfeeding not only benefits babies; it also may lower the risk for a heart attack or stroke later in life for mothers who breastfeed more than for women who don’t.
The findings, which were published online June 21 in the Journal of the American Heart Association, are based on data from a prospective study of nearly 300,000 women in China.
To assess the impact of breastfeeding on maternal cardiovascular health, the researchers reviewed data from 289,573 women who were participating in the China Kadoorie Biobank study to assess their reproductive history and lifestyle. At the time of study enrollment, none of the women had a history of cardiovascular disease and 99% reported at least one live birth. The average age of the women at baseline was 51 years.
Of the women who had given birth, 97% reported ever breastfeeding, and 91% reported breastfeeding each child for at least 6 months. The median duration of breastfeeding was 12 months per child (J Am Heart Assoc. 2017 Jun 21. doi: JAHA/2017/006081-T2).
During an 8-year follow-up period, participants experienced 16,671 cases of coronary heart disease and 23,983 strokes.
Overall, women who breastfed babies had a 9% reduction in risk of coronary heart disease and an 8% reduction in risk of stroke, compared with women who never breastfed. The longer the duration of breastfeeding, the greater the risk reduction; for every additional 6 months of breastfeeding, researchers found a 4% reduction in heart disease risk and a 3% reduction in stroke risk. Mothers who breastfed for 2 years or more had the most protection – an 18% reduced risk of heart disease and a 17% reduced risk of stroke, compared with mothers who never breastfed.
The study was limited by several factors, including its observational nature, which cannot confirm a causal relationship between breastfeeding and CVD. However, the results suggest that, if causal, “interventions to increase the likelihood and duration of breastfeeding could have persistent benefits to maternal cardiovascular health,” they wrote.
The baseline study was funded by the Kadoorie Charitable Foundation in Hong Kong; long-term support came from the UK Wellcome Trust, Chinese Ministry of Science and Technology, and the Chinese National Natural Science Foundation. Other support came from the British Heart Foundation, UK Medical Research Council and Cancer Research UK, and the National Natural Science Foundation of China. Dr. Peters has received support from the British Heart Foundation.
Breastfeeding not only benefits babies; it also may lower the risk for a heart attack or stroke later in life for mothers who breastfeed more than for women who don’t.
The findings, which were published online June 21 in the Journal of the American Heart Association, are based on data from a prospective study of nearly 300,000 women in China.
To assess the impact of breastfeeding on maternal cardiovascular health, the researchers reviewed data from 289,573 women who were participating in the China Kadoorie Biobank study to assess their reproductive history and lifestyle. At the time of study enrollment, none of the women had a history of cardiovascular disease and 99% reported at least one live birth. The average age of the women at baseline was 51 years.
Of the women who had given birth, 97% reported ever breastfeeding, and 91% reported breastfeeding each child for at least 6 months. The median duration of breastfeeding was 12 months per child (J Am Heart Assoc. 2017 Jun 21. doi: JAHA/2017/006081-T2).
During an 8-year follow-up period, participants experienced 16,671 cases of coronary heart disease and 23,983 strokes.
Overall, women who breastfed babies had a 9% reduction in risk of coronary heart disease and an 8% reduction in risk of stroke, compared with women who never breastfed. The longer the duration of breastfeeding, the greater the risk reduction; for every additional 6 months of breastfeeding, researchers found a 4% reduction in heart disease risk and a 3% reduction in stroke risk. Mothers who breastfed for 2 years or more had the most protection – an 18% reduced risk of heart disease and a 17% reduced risk of stroke, compared with mothers who never breastfed.
The study was limited by several factors, including its observational nature, which cannot confirm a causal relationship between breastfeeding and CVD. However, the results suggest that, if causal, “interventions to increase the likelihood and duration of breastfeeding could have persistent benefits to maternal cardiovascular health,” they wrote.
The baseline study was funded by the Kadoorie Charitable Foundation in Hong Kong; long-term support came from the UK Wellcome Trust, Chinese Ministry of Science and Technology, and the Chinese National Natural Science Foundation. Other support came from the British Heart Foundation, UK Medical Research Council and Cancer Research UK, and the National Natural Science Foundation of China. Dr. Peters has received support from the British Heart Foundation.
FROM THE JOURNAL OF THE AMERICAN HEART ASSOCIATION
Key clinical point: Interventions to encourage breastfeeding may benefit mothers’ cardiovascular health later in life.
Major finding: Women who breastfed their babies had a 10% reduction in risk of cardiovascular disease later in life.
Data source: A prospective study of approximately 300,000 women in China.
Disclosures: The baseline study was funded by the Kadoorie Charitable Foundation in Hong Kong; long-term support came from the UK Wellcome Trust, Chinese Ministry of Science and Technology, and the Chinese National Natural Science Foundation. Dr. Peters has received support from the British Heart Foundation.
Knee OA structural defects predict pain trajectories
The presence of bone marrow lesions and cartilage defects on baseline MRI scans of knee osteoarthritis (OA) patients may help to predict moderate to severe pain trajectories, based on data from a population-based study presented here at the European Congress of Rheumatology.
Three pain trajectories were identified: 52% of the patients reported stable mild pain over time, 33% reported moderate pain over time, and 15% reported fluctuating or severe pain over time.

“Knee pain is the most prominent symptom of knee osteoarthritis,” Dr. Pan said in an interview. “It is also a main reason for people to seek joint replacement. Despite this, the causes of knee pain are poorly understood. Therapy will only improve if we understand this better.”
Dr. Pan and his colleagues studied 1,099 adults with knee OA who participated in a population-based study. The mean age was 63 years (ranging from 51 to 81 years). A total of 875 participants were assessed using the knee pain components of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) at 2.6 years’ follow-up, 768 at 5.1 years’ follow-up, and 563 at 10.7 years’ follow-up.
Knee OA was assessed at baseline by x-ray, and T1-weighted or T2-weighted MRI scans of the right knee were used to assess knee structural pathology. The researchers applied group-based trajectory modeling to identify pain trajectories.
“We identified three distinct trajectories over time,” Dr. Pan said. “Remarkably, structural, environmental, sociodemographic, and psychological factors are associated with a more ‘severe pain’ trajectory, suggesting that pain course is determined by an integrated mix of all these factors.”
Dr. Pan added: “We already know that structural damage is a major driver in the development and maintenance of pain severity, but less is known about the other factors.”
The researchers found a significant dose-response relationship between the number of knee structural abnormalities, including cartilage defects and bone marrow lesions, and the ‘moderate pain’ and ‘severe pain’ trajectories (P less than .001 comparing both categories to the ‘mild pain’ trajectory).
Other factors that were significantly associated with both moderate and severe pain, compared with mild pain, included higher body mass index (overweight but not obese), emotional problems, and musculoskeletal diseases.
The findings provide support to the concept that “pain experience is both complex and individual in nature, suggesting the clinician should target treatments according to which of these factors predominate in the individual,” Dr. Pan said.
Future research may aim to develop “a predictive model that could be utilized in clinical practice and target therapies based on these trajectories.”
Dr. Pan had no financial conflicts to disclose.
The presence of bone marrow lesions and cartilage defects on baseline MRI scans of knee osteoarthritis (OA) patients may help to predict moderate to severe pain trajectories, based on data from a population-based study presented here at the European Congress of Rheumatology.
Three pain trajectories were identified: 52% of the patients reported stable mild pain over time, 33% reported moderate pain over time, and 15% reported fluctuating or severe pain over time.
“Knee pain is the most prominent symptom of knee osteoarthritis,” Dr. Pan said in an interview. “It is also a main reason for people to seek joint replacement. Despite this, the causes of knee pain are poorly understood. Therapy will only improve if we understand this better.”
Dr. Pan and his colleagues studied 1,099 adults with knee OA who participated in a population-based study. The mean age was 63 years (ranging from 51 to 81 years). A total of 875 participants were assessed using the knee pain components of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) at 2.6 years’ follow-up, 768 at 5.1 years’ follow-up, and 563 at 10.7 years’ follow-up.
Knee OA was assessed at baseline by x-ray, and T1-weighted or T2-weighted MRI scans of the right knee were used to assess knee structural pathology. The researchers applied group-based trajectory modeling to identify pain trajectories.
“We identified three distinct trajectories over time,” Dr. Pan said. “Remarkably, structural, environmental, sociodemographic, and psychological factors are associated with a more ‘severe pain’ trajectory, suggesting that pain course is determined by an integrated mix of all these factors.”
Dr. Pan added: “We already know that structural damage is a major driver in the development and maintenance of pain severity, but less is known about the other factors.”
The researchers found a significant dose-response relationship between the number of knee structural abnormalities, including cartilage defects and bone marrow lesions, and the ‘moderate pain’ and ‘severe pain’ trajectories (P less than .001 comparing both categories to the ‘mild pain’ trajectory).
Other factors that were significantly associated with both moderate and severe pain, compared with mild pain, included higher body mass index (overweight but not obese), emotional problems, and musculoskeletal diseases.
The findings provide support to the concept that “pain experience is both complex and individual in nature, suggesting the clinician should target treatments according to which of these factors predominate in the individual,” Dr. Pan said.
Future research may aim to develop “a predictive model that could be utilized in clinical practice and target therapies based on these trajectories.”
Dr. Pan had no financial conflicts to disclose.
The presence of bone marrow lesions and cartilage defects on baseline MRI scans of knee osteoarthritis (OA) patients may help to predict moderate to severe pain trajectories, based on data from a population-based study presented here at the European Congress of Rheumatology.
Three pain trajectories were identified: 52% of the patients reported stable mild pain over time, 33% reported moderate pain over time, and 15% reported fluctuating or severe pain over time.
“Knee pain is the most prominent symptom of knee osteoarthritis,” Dr. Pan said in an interview. “It is also a main reason for people to seek joint replacement. Despite this, the causes of knee pain are poorly understood. Therapy will only improve if we understand this better.”
Dr. Pan and his colleagues studied 1,099 adults with knee OA who participated in a population-based study. The mean age was 63 years (ranging from 51 to 81 years). A total of 875 participants were assessed using the knee pain components of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) at 2.6 years’ follow-up, 768 at 5.1 years’ follow-up, and 563 at 10.7 years’ follow-up.
Knee OA was assessed at baseline by x-ray, and T1-weighted or T2-weighted MRI scans of the right knee were used to assess knee structural pathology. The researchers applied group-based trajectory modeling to identify pain trajectories.
“We identified three distinct trajectories over time,” Dr. Pan said. “Remarkably, structural, environmental, sociodemographic, and psychological factors are associated with a more ‘severe pain’ trajectory, suggesting that pain course is determined by an integrated mix of all these factors.”
Dr. Pan added: “We already know that structural damage is a major driver in the development and maintenance of pain severity, but less is known about the other factors.”
The researchers found a significant dose-response relationship between the number of knee structural abnormalities, including cartilage defects and bone marrow lesions, and the ‘moderate pain’ and ‘severe pain’ trajectories (P less than .001 comparing both categories to the ‘mild pain’ trajectory).
Other factors that were significantly associated with both moderate and severe pain, compared with mild pain, included higher body mass index (overweight but not obese), emotional problems, and musculoskeletal diseases.
The findings provide support to the concept that “pain experience is both complex and individual in nature, suggesting the clinician should target treatments according to which of these factors predominate in the individual,” Dr. Pan said.
Future research may aim to develop “a predictive model that could be utilized in clinical practice and target therapies based on these trajectories.”
Dr. Pan had no financial conflicts to disclose.
FROM THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: Three pain trajectories were identified: stable mild pain (52% of patients), moderate pain (33%), and fluctuating or severe pain (15%).
Data source: Population-based cohort study of 1,099 patients with knee OA.
Disclosures: The presenter had no financial conflicts to disclose.
Aspirin triples major bleeding risk after age 75 years
Older adults who take aspirin daily are at greater risk for serious bleeding than previously thought, based on data from roughly 3,000 patients.
“The risk of upper gastrointestinal bleeding on antiplatelet treatment increases with age, but it is uncertain whether older age alone is a sufficient indicator of high risk to justify routine coprescription of PPIs [proton pump inhibitors],” wrote Linxin Li, DPhil, of the University of Oxford (England) and her colleagues.
To assess the rate of bleeding among older adults on long-term aspirin therapy, Dr. Li and her colleagues reviewed data from the Oxford Vascular Study, a prospective population-based study of 3,166 patients. Of those, 1,584 were younger than 75 years, with an average age of 61 years, and 1,582 were at least 75 years old, with average age of 83 years. Patients were followed at 30 days, 6 months, and 1, 5, and 10 years to determine bleeding, recurrent ischemic events, and disability (Lancet. 2017. doi: 10.1016/S0140-6736[17]30770-5).

In addition, more than twice the major upper GI bleeds were disabling or fatal in adults aged 75 years and older than in the younger patients (62% vs. 25%).
Only a third of the patients in the study were taking proton pump inhibitors (PPIs), partly because current clinical guidelines don’t specifically recommend their use and partly in the absence of an accepted definition of which patients are at high risk for upper GI bleeding, the researchers said. They estimated that the number needed to treat with PPIs to prevent a major GI bleed after 5 years decreased with age: “80 for patients younger than 65 years, 75 for patients aged 65-74 years, 23 for patients aged 75-84 years, and 21 for patients aged 85 years or older.” In addition, the number needed to treat with PPIs to prevent a disabling or fatal upper GI bleed after 5 years was 338 for patients younger than 65 years but dropped to 25 for patients aged 85 years and older.
The findings were limited by the observational nature of the study and inability to show that increased risk of bleeding was caused by aspirin alone, the researchers said. However, based on the data, “age 75 years would be an appropriate threshold to start a PPI both in patients newly initiated on antiplatelet drugs and in patients on established treatment,” they wrote.
The study data were taken from the Oxford Vascular Study, which was funded by the National Institute of Health Research and several other research institutions. Corresponding author Peter Rothwell, MD, disclosed financial relationships with Bayer.
In patients with stroke with a cardiac source of embolism who qualify for oral anticoagulation, we obsess about the association between benefit and bleeding risk. Specific risk scores were developed to assess the bleeding risk for patients with atrial fibrillation who qualified for anticoagulation. However, similar risk scores are not applied for patients who undergo long-term prevention with antiplatelet therapy.
On the basis of this study’s results, the benefit-risk association in long-term antiplatelet therapy should be evaluated every 3-5 years in patients older than 75 years, and PPIs should be used in patients on antiplatelet therapy who are at least 75 years old or in patients with a history of gastrointestinal bleeds.

Hans-Christoph Diener, MD, of the department of neurology at the University Duisburg-Essen in Essen, Germany, made these remarks in an accompanying editorial (Lancet. 2017 Jun 13. doi: 10.1016/S0140-6736[17]31507-6). He disclosed relationships with multiple companies, including AstraZeneca, Bristol-Myers Squibb, GlaxoSmithKline, Merck, and Novartis.
In patients with stroke with a cardiac source of embolism who qualify for oral anticoagulation, we obsess about the association between benefit and bleeding risk. Specific risk scores were developed to assess the bleeding risk for patients with atrial fibrillation who qualified for anticoagulation. However, similar risk scores are not applied for patients who undergo long-term prevention with antiplatelet therapy.
On the basis of this study’s results, the benefit-risk association in long-term antiplatelet therapy should be evaluated every 3-5 years in patients older than 75 years, and PPIs should be used in patients on antiplatelet therapy who are at least 75 years old or in patients with a history of gastrointestinal bleeds.
Hans-Christoph Diener, MD, of the department of neurology at the University Duisburg-Essen in Essen, Germany, made these remarks in an accompanying editorial (Lancet. 2017 Jun 13. doi: 10.1016/S0140-6736[17]31507-6). He disclosed relationships with multiple companies, including AstraZeneca, Bristol-Myers Squibb, GlaxoSmithKline, Merck, and Novartis.
In patients with stroke with a cardiac source of embolism who qualify for oral anticoagulation, we obsess about the association between benefit and bleeding risk. Specific risk scores were developed to assess the bleeding risk for patients with atrial fibrillation who qualified for anticoagulation. However, similar risk scores are not applied for patients who undergo long-term prevention with antiplatelet therapy.
On the basis of this study’s results, the benefit-risk association in long-term antiplatelet therapy should be evaluated every 3-5 years in patients older than 75 years, and PPIs should be used in patients on antiplatelet therapy who are at least 75 years old or in patients with a history of gastrointestinal bleeds.
Hans-Christoph Diener, MD, of the department of neurology at the University Duisburg-Essen in Essen, Germany, made these remarks in an accompanying editorial (Lancet. 2017 Jun 13. doi: 10.1016/S0140-6736[17]31507-6). He disclosed relationships with multiple companies, including AstraZeneca, Bristol-Myers Squibb, GlaxoSmithKline, Merck, and Novartis.
Older adults who take aspirin daily are at greater risk for serious bleeding than previously thought, based on data from roughly 3,000 patients.
“The risk of upper gastrointestinal bleeding on antiplatelet treatment increases with age, but it is uncertain whether older age alone is a sufficient indicator of high risk to justify routine coprescription of PPIs [proton pump inhibitors],” wrote Linxin Li, DPhil, of the University of Oxford (England) and her colleagues.
To assess the rate of bleeding among older adults on long-term aspirin therapy, Dr. Li and her colleagues reviewed data from the Oxford Vascular Study, a prospective population-based study of 3,166 patients. Of those, 1,584 were younger than 75 years, with an average age of 61 years, and 1,582 were at least 75 years old, with average age of 83 years. Patients were followed at 30 days, 6 months, and 1, 5, and 10 years to determine bleeding, recurrent ischemic events, and disability (Lancet. 2017. doi: 10.1016/S0140-6736[17]30770-5).
In addition, more than twice the major upper GI bleeds were disabling or fatal in adults aged 75 years and older than in the younger patients (62% vs. 25%).
Only a third of the patients in the study were taking proton pump inhibitors (PPIs), partly because current clinical guidelines don’t specifically recommend their use and partly in the absence of an accepted definition of which patients are at high risk for upper GI bleeding, the researchers said. They estimated that the number needed to treat with PPIs to prevent a major GI bleed after 5 years decreased with age: “80 for patients younger than 65 years, 75 for patients aged 65-74 years, 23 for patients aged 75-84 years, and 21 for patients aged 85 years or older.” In addition, the number needed to treat with PPIs to prevent a disabling or fatal upper GI bleed after 5 years was 338 for patients younger than 65 years but dropped to 25 for patients aged 85 years and older.
The findings were limited by the observational nature of the study and inability to show that increased risk of bleeding was caused by aspirin alone, the researchers said. However, based on the data, “age 75 years would be an appropriate threshold to start a PPI both in patients newly initiated on antiplatelet drugs and in patients on established treatment,” they wrote.
The study data were taken from the Oxford Vascular Study, which was funded by the National Institute of Health Research and several other research institutions. Corresponding author Peter Rothwell, MD, disclosed financial relationships with Bayer.
Older adults who take aspirin daily are at greater risk for serious bleeding than previously thought, based on data from roughly 3,000 patients.
“The risk of upper gastrointestinal bleeding on antiplatelet treatment increases with age, but it is uncertain whether older age alone is a sufficient indicator of high risk to justify routine coprescription of PPIs [proton pump inhibitors],” wrote Linxin Li, DPhil, of the University of Oxford (England) and her colleagues.
To assess the rate of bleeding among older adults on long-term aspirin therapy, Dr. Li and her colleagues reviewed data from the Oxford Vascular Study, a prospective population-based study of 3,166 patients. Of those, 1,584 were younger than 75 years, with an average age of 61 years, and 1,582 were at least 75 years old, with average age of 83 years. Patients were followed at 30 days, 6 months, and 1, 5, and 10 years to determine bleeding, recurrent ischemic events, and disability (Lancet. 2017. doi: 10.1016/S0140-6736[17]30770-5).
In addition, more than twice the major upper GI bleeds were disabling or fatal in adults aged 75 years and older than in the younger patients (62% vs. 25%).
Only a third of the patients in the study were taking proton pump inhibitors (PPIs), partly because current clinical guidelines don’t specifically recommend their use and partly in the absence of an accepted definition of which patients are at high risk for upper GI bleeding, the researchers said. They estimated that the number needed to treat with PPIs to prevent a major GI bleed after 5 years decreased with age: “80 for patients younger than 65 years, 75 for patients aged 65-74 years, 23 for patients aged 75-84 years, and 21 for patients aged 85 years or older.” In addition, the number needed to treat with PPIs to prevent a disabling or fatal upper GI bleed after 5 years was 338 for patients younger than 65 years but dropped to 25 for patients aged 85 years and older.
The findings were limited by the observational nature of the study and inability to show that increased risk of bleeding was caused by aspirin alone, the researchers said. However, based on the data, “age 75 years would be an appropriate threshold to start a PPI both in patients newly initiated on antiplatelet drugs and in patients on established treatment,” they wrote.
The study data were taken from the Oxford Vascular Study, which was funded by the National Institute of Health Research and several other research institutions. Corresponding author Peter Rothwell, MD, disclosed financial relationships with Bayer.
FROM THE LANCET
Key clinical point:
Major finding: The annual rate of life-threatening or fatal bleeding episodes was less than 0.5% for patients younger than 65 years but rose to 1.5% in those aged 75-84 years and 2.5% in those aged 85 years and older.
Data source: A prospective, population-based cohort study of 3,166 adults who had one transient ischemic attack, ischemic stroke, or MI and who were treated with antiplatelet drugs.
Disclosures: The study data were taken from the Oxford Vascular Study, which was funded by the Wellcome Trust, Wolfson Foundation, British Heart Foundation, Dunhill Medical Trust, the National Institute of Health Research (NIHR), and the NIHR Oxford Biomedical Research Centre. Corresponding author Peter Rothwell, MD, disclosed financial relationships with Bayer.
Depression not responsible for teen weight gain, but SSRIs may be
Adolescents with major depressive disorder (MDD) were more likely to lose weight, but treatment with some SSRIs was associated with weight gain, based on data from a longitudinal study of 264 participants published online June 16 in Pediatrics.
MDD was associated with decrease in body mass index (BMI), fat mass index (FMI), and lean BMI (LBMI) z scores after controlling for factors including age, sex, physical activity, dietary intake, and length of study participation. However, dosage and duration of treatment with SSRIs were associated with increases in BMI, FMI, and LBMI z scores (Pediatrics. 2017. doi: 10.1542/peds.2016-3943).
The participants were part of a 2-year prospective study on the skeletal impact of SSRI use in older adolescents, and the average length of study participation was 1.5 years. After a baseline visit, they had follow-up visits, at which they completed the Inventory of Depressive Symptomatology (IDS), the Beck Depression Inventory (BDI-II), the Beck Anxiety Inventory (BAI), and the modified version of the Physical Activity Questionnaire for Adolescents, every four months. In addition, height, weight, and grip strength were measured. Body composition was measured using the BMI z score, FMI z score, LBMI z score, and visceral fat (Vfat) score.
Depression and anxiety, based on IDS and BAI scores, were inversely associated with changes in BMI z scores, and longer SSRI use was associated with increased BMI z scores. These changes remained significant when IDS scores and cumulative SSRI doses were included in the analysis.
In addition, use and duration of SSRIs each were significantly associated with increased FMI and LBMI scores after adjusting for standard confounding variables. SSRI use was associated with increased visceral fat mass, but the change was not significant.
When the researchers examined differences among individual drugs, they found that citalopram and escitalopram, but not sertraline, were associated with significant increases in both adiposity and lean mass. Fluoxetine showed a smaller, but still significant, effect.
SSRI use also impacted height over the study period (P less than .05), and fluoxetine had the greatest effect. Depression (IDS score) had no significant impact on height.
No significant differences appeared in the impact of SSRI use according to gender for LBMI, height z scores, or VFat. However, males had a significantly greater increase in BMI and FMI z scores, compared with females, over a longer period of SSRI use, a finding that deserves additional study, Dr. Calarge and associates noted.
The results were limited by several factors including the relatively small sample size, the use of self-reports, and the challenges of accurately documenting medication use, the researchers said.
Fat and lean mass were measured separately in this study, and, “to our surprise, SSRI use was positively associated with both outcome variables in a similar manner,” Dr. Calarge and associates noted. “When we specifically focused on VFat, the association with SSRI use remained positive, albeit weaker. This suggests that, over extended periods of use, SSRIs will cause an overall increase in BMI, comprising an increase in both fat and lean mass. Importantly, this is also associated with an increase in VFat, which is particularly detrimental to health,” and may contribute to the higher incidence of cardiovascular disease in MDD patients, they added. Future research should explore mechanisms of action and interventions to address treatment effects.
The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
Adolescents with major depressive disorder (MDD) were more likely to lose weight, but treatment with some SSRIs was associated with weight gain, based on data from a longitudinal study of 264 participants published online June 16 in Pediatrics.
MDD was associated with decrease in body mass index (BMI), fat mass index (FMI), and lean BMI (LBMI) z scores after controlling for factors including age, sex, physical activity, dietary intake, and length of study participation. However, dosage and duration of treatment with SSRIs were associated with increases in BMI, FMI, and LBMI z scores (Pediatrics. 2017. doi: 10.1542/peds.2016-3943).
The participants were part of a 2-year prospective study on the skeletal impact of SSRI use in older adolescents, and the average length of study participation was 1.5 years. After a baseline visit, they had follow-up visits, at which they completed the Inventory of Depressive Symptomatology (IDS), the Beck Depression Inventory (BDI-II), the Beck Anxiety Inventory (BAI), and the modified version of the Physical Activity Questionnaire for Adolescents, every four months. In addition, height, weight, and grip strength were measured. Body composition was measured using the BMI z score, FMI z score, LBMI z score, and visceral fat (Vfat) score.
Depression and anxiety, based on IDS and BAI scores, were inversely associated with changes in BMI z scores, and longer SSRI use was associated with increased BMI z scores. These changes remained significant when IDS scores and cumulative SSRI doses were included in the analysis.
In addition, use and duration of SSRIs each were significantly associated with increased FMI and LBMI scores after adjusting for standard confounding variables. SSRI use was associated with increased visceral fat mass, but the change was not significant.
When the researchers examined differences among individual drugs, they found that citalopram and escitalopram, but not sertraline, were associated with significant increases in both adiposity and lean mass. Fluoxetine showed a smaller, but still significant, effect.
SSRI use also impacted height over the study period (P less than .05), and fluoxetine had the greatest effect. Depression (IDS score) had no significant impact on height.
No significant differences appeared in the impact of SSRI use according to gender for LBMI, height z scores, or VFat. However, males had a significantly greater increase in BMI and FMI z scores, compared with females, over a longer period of SSRI use, a finding that deserves additional study, Dr. Calarge and associates noted.
The results were limited by several factors including the relatively small sample size, the use of self-reports, and the challenges of accurately documenting medication use, the researchers said.
Fat and lean mass were measured separately in this study, and, “to our surprise, SSRI use was positively associated with both outcome variables in a similar manner,” Dr. Calarge and associates noted. “When we specifically focused on VFat, the association with SSRI use remained positive, albeit weaker. This suggests that, over extended periods of use, SSRIs will cause an overall increase in BMI, comprising an increase in both fat and lean mass. Importantly, this is also associated with an increase in VFat, which is particularly detrimental to health,” and may contribute to the higher incidence of cardiovascular disease in MDD patients, they added. Future research should explore mechanisms of action and interventions to address treatment effects.
The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
Adolescents with major depressive disorder (MDD) were more likely to lose weight, but treatment with some SSRIs was associated with weight gain, based on data from a longitudinal study of 264 participants published online June 16 in Pediatrics.
MDD was associated with decrease in body mass index (BMI), fat mass index (FMI), and lean BMI (LBMI) z scores after controlling for factors including age, sex, physical activity, dietary intake, and length of study participation. However, dosage and duration of treatment with SSRIs were associated with increases in BMI, FMI, and LBMI z scores (Pediatrics. 2017. doi: 10.1542/peds.2016-3943).
The participants were part of a 2-year prospective study on the skeletal impact of SSRI use in older adolescents, and the average length of study participation was 1.5 years. After a baseline visit, they had follow-up visits, at which they completed the Inventory of Depressive Symptomatology (IDS), the Beck Depression Inventory (BDI-II), the Beck Anxiety Inventory (BAI), and the modified version of the Physical Activity Questionnaire for Adolescents, every four months. In addition, height, weight, and grip strength were measured. Body composition was measured using the BMI z score, FMI z score, LBMI z score, and visceral fat (Vfat) score.
Depression and anxiety, based on IDS and BAI scores, were inversely associated with changes in BMI z scores, and longer SSRI use was associated with increased BMI z scores. These changes remained significant when IDS scores and cumulative SSRI doses were included in the analysis.
In addition, use and duration of SSRIs each were significantly associated with increased FMI and LBMI scores after adjusting for standard confounding variables. SSRI use was associated with increased visceral fat mass, but the change was not significant.
When the researchers examined differences among individual drugs, they found that citalopram and escitalopram, but not sertraline, were associated with significant increases in both adiposity and lean mass. Fluoxetine showed a smaller, but still significant, effect.
SSRI use also impacted height over the study period (P less than .05), and fluoxetine had the greatest effect. Depression (IDS score) had no significant impact on height.
No significant differences appeared in the impact of SSRI use according to gender for LBMI, height z scores, or VFat. However, males had a significantly greater increase in BMI and FMI z scores, compared with females, over a longer period of SSRI use, a finding that deserves additional study, Dr. Calarge and associates noted.
The results were limited by several factors including the relatively small sample size, the use of self-reports, and the challenges of accurately documenting medication use, the researchers said.
Fat and lean mass were measured separately in this study, and, “to our surprise, SSRI use was positively associated with both outcome variables in a similar manner,” Dr. Calarge and associates noted. “When we specifically focused on VFat, the association with SSRI use remained positive, albeit weaker. This suggests that, over extended periods of use, SSRIs will cause an overall increase in BMI, comprising an increase in both fat and lean mass. Importantly, this is also associated with an increase in VFat, which is particularly detrimental to health,” and may contribute to the higher incidence of cardiovascular disease in MDD patients, they added. Future research should explore mechanisms of action and interventions to address treatment effects.
The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
FROM PEDIATRICS
Key clinical point: Major depressive disorder failed to promote changes in BMI in older adolescents.
Major finding: (P less than .003).
Data source: The data came from a longitudinal study of 264 adolescents aged 15-20 years.
Disclosures: The researchers had no relevant financial disclosures. The study was funded by the National Institutes of Health, the National Institute of Mental Health, and the National Center for Research Resources.
Experts endorse routine screening for pediatric psoriasis comorbidities
Pediatric psoriasis patients should be screened regularly to identify risk factors for comorbidities including depression, gastrointestinal problems, diabetes, and dyslipidemia, according to the debut guidelines issued by an expert panel.
The National Psoriasis Foundation and the Pediatric Dermatology Research Alliance joined forces to assess the literature and develop recommendations for screening comorbidities for children with psoriasis. The National Psoriasis Foundation has guidelines for comorbidity screening in adults with psoriasis, but no guidelines previously existed for children, wrote Emily Osier, MD, of Eastern Virginia Medical School, Norfolk, and her colleagues (JAMA Dermatol 2017 May 17. doi: 10.1001/jamadermatol.2017.0499).
The panelists reviewed the literature on psoriasis and comorbidities published between 1999 and 2015 and identified 153 studies, 26 of which involved children.
“The screening recommendations derived are largely consistent with those endorsed by the AAP for the general pediatric patient,” the researchers noted.
Although many young children are screened for a range of comorbid conditions at annual checkups, preteens and teenagers may be less likely to receive preventive services in primary care, they said. “Thus, all health care providers caring for patients with pediatric psoriasis should help assess and ensure that appropriate screening has been performed,” they emphasized.
Some notable recommendations include the following:
• Screen children with psoriasis for overweight and obesity annually using body mass index percentiles.
• Screen for diabetes every 3 years starting at age 10 years.
• Perform universal lipid screening at ages 9-11 years and 17-21 years.
• Screen for nonalcoholic fatty liver disease every 2-3 years starting at age 9-11 years.
• Screen for hypertension annually starting at age 3 years.
• Screen for arthritis at the time of psoriasis diagnosis and periodically.
• Screen yearly for depression and anxiety at all ages, with yearly screening for substance abuse starting at age 11 years.
Uveitis screening is recommended only for children with psoriatic arthritis, the researchers said.
In addition, clinicians “should recognize the profound psychosocial ramifications of psoriasis and the potential significant impact on quality of life of patients and caregivers,” the researchers wrote. Clinicians may consider a formal quality of life measurement, such as the Children’s Dermatology Life Quality Index, or at least asking questions about the impact of psoriasis on the child’s life at home, at school, and during other activities.
Awareness of comorbidities also impacts potential psoriasis treatment, the researchers said. “Direct baseline screening and monitoring tests should be performed as indicated by each individual’s therapeutic plan,” they said.
The consensus statement is a starting point for screening that will be refined over time, and may include stratifying patients by age, disease subtype, or disease severity, the researchers noted.
“Communication and collaboration between dermatologists, primary care providers, and other pediatric specialists will be critical to accomplish the recommended screenings and to limit the sequelae of this disorder,” they wrote.
The National Psoriasis Foundation and the University of California, San Diego, Eczema and Inflammatory Skin Disease Center supported the study. Dr. Osier was supported in part by a Medical Dermatology Research Fellowship grant from the National Psoriasis Foundation in 2014-2016, but she had no financial conflicts to disclose.
Pediatric psoriasis patients should be screened regularly to identify risk factors for comorbidities including depression, gastrointestinal problems, diabetes, and dyslipidemia, according to the debut guidelines issued by an expert panel.
The National Psoriasis Foundation and the Pediatric Dermatology Research Alliance joined forces to assess the literature and develop recommendations for screening comorbidities for children with psoriasis. The National Psoriasis Foundation has guidelines for comorbidity screening in adults with psoriasis, but no guidelines previously existed for children, wrote Emily Osier, MD, of Eastern Virginia Medical School, Norfolk, and her colleagues (JAMA Dermatol 2017 May 17. doi: 10.1001/jamadermatol.2017.0499).
The panelists reviewed the literature on psoriasis and comorbidities published between 1999 and 2015 and identified 153 studies, 26 of which involved children.
“The screening recommendations derived are largely consistent with those endorsed by the AAP for the general pediatric patient,” the researchers noted.
Although many young children are screened for a range of comorbid conditions at annual checkups, preteens and teenagers may be less likely to receive preventive services in primary care, they said. “Thus, all health care providers caring for patients with pediatric psoriasis should help assess and ensure that appropriate screening has been performed,” they emphasized.
Some notable recommendations include the following:
• Screen children with psoriasis for overweight and obesity annually using body mass index percentiles.
• Screen for diabetes every 3 years starting at age 10 years.
• Perform universal lipid screening at ages 9-11 years and 17-21 years.
• Screen for nonalcoholic fatty liver disease every 2-3 years starting at age 9-11 years.
• Screen for hypertension annually starting at age 3 years.
• Screen for arthritis at the time of psoriasis diagnosis and periodically.
• Screen yearly for depression and anxiety at all ages, with yearly screening for substance abuse starting at age 11 years.
Uveitis screening is recommended only for children with psoriatic arthritis, the researchers said.
In addition, clinicians “should recognize the profound psychosocial ramifications of psoriasis and the potential significant impact on quality of life of patients and caregivers,” the researchers wrote. Clinicians may consider a formal quality of life measurement, such as the Children’s Dermatology Life Quality Index, or at least asking questions about the impact of psoriasis on the child’s life at home, at school, and during other activities.
Awareness of comorbidities also impacts potential psoriasis treatment, the researchers said. “Direct baseline screening and monitoring tests should be performed as indicated by each individual’s therapeutic plan,” they said.
The consensus statement is a starting point for screening that will be refined over time, and may include stratifying patients by age, disease subtype, or disease severity, the researchers noted.
“Communication and collaboration between dermatologists, primary care providers, and other pediatric specialists will be critical to accomplish the recommended screenings and to limit the sequelae of this disorder,” they wrote.
The National Psoriasis Foundation and the University of California, San Diego, Eczema and Inflammatory Skin Disease Center supported the study. Dr. Osier was supported in part by a Medical Dermatology Research Fellowship grant from the National Psoriasis Foundation in 2014-2016, but she had no financial conflicts to disclose.
Pediatric psoriasis patients should be screened regularly to identify risk factors for comorbidities including depression, gastrointestinal problems, diabetes, and dyslipidemia, according to the debut guidelines issued by an expert panel.
The National Psoriasis Foundation and the Pediatric Dermatology Research Alliance joined forces to assess the literature and develop recommendations for screening comorbidities for children with psoriasis. The National Psoriasis Foundation has guidelines for comorbidity screening in adults with psoriasis, but no guidelines previously existed for children, wrote Emily Osier, MD, of Eastern Virginia Medical School, Norfolk, and her colleagues (JAMA Dermatol 2017 May 17. doi: 10.1001/jamadermatol.2017.0499).
The panelists reviewed the literature on psoriasis and comorbidities published between 1999 and 2015 and identified 153 studies, 26 of which involved children.
“The screening recommendations derived are largely consistent with those endorsed by the AAP for the general pediatric patient,” the researchers noted.
Although many young children are screened for a range of comorbid conditions at annual checkups, preteens and teenagers may be less likely to receive preventive services in primary care, they said. “Thus, all health care providers caring for patients with pediatric psoriasis should help assess and ensure that appropriate screening has been performed,” they emphasized.
Some notable recommendations include the following:
• Screen children with psoriasis for overweight and obesity annually using body mass index percentiles.
• Screen for diabetes every 3 years starting at age 10 years.
• Perform universal lipid screening at ages 9-11 years and 17-21 years.
• Screen for nonalcoholic fatty liver disease every 2-3 years starting at age 9-11 years.
• Screen for hypertension annually starting at age 3 years.
• Screen for arthritis at the time of psoriasis diagnosis and periodically.
• Screen yearly for depression and anxiety at all ages, with yearly screening for substance abuse starting at age 11 years.
Uveitis screening is recommended only for children with psoriatic arthritis, the researchers said.
In addition, clinicians “should recognize the profound psychosocial ramifications of psoriasis and the potential significant impact on quality of life of patients and caregivers,” the researchers wrote. Clinicians may consider a formal quality of life measurement, such as the Children’s Dermatology Life Quality Index, or at least asking questions about the impact of psoriasis on the child’s life at home, at school, and during other activities.
Awareness of comorbidities also impacts potential psoriasis treatment, the researchers said. “Direct baseline screening and monitoring tests should be performed as indicated by each individual’s therapeutic plan,” they said.
The consensus statement is a starting point for screening that will be refined over time, and may include stratifying patients by age, disease subtype, or disease severity, the researchers noted.
“Communication and collaboration between dermatologists, primary care providers, and other pediatric specialists will be critical to accomplish the recommended screenings and to limit the sequelae of this disorder,” they wrote.
The National Psoriasis Foundation and the University of California, San Diego, Eczema and Inflammatory Skin Disease Center supported the study. Dr. Osier was supported in part by a Medical Dermatology Research Fellowship grant from the National Psoriasis Foundation in 2014-2016, but she had no financial conflicts to disclose.
FROM JAMA DERMATOLOGY
Osteoarthritis contributes more to difficulty walking than do diabetes, CVD
Hip and knee osteoarthritis on their own predict difficulty walking in adults aged 55 years and older to a greater extent than do diabetes or cardiovascular disease individually, according to findings from a Canadian population-based study.
The ability of hip and knee osteoarthritis (OA) to predict difficulty walking also increased with the number of joints affected and acted additively with either diabetes or cardiovascular disease (CVD) or both to raise the odds for walking problems, reported Lauren K. King, MBBS, of the University of Toronto, and colleagues.
To determine the impact of hip and knee OA on difficulty walking, the researchers reviewed data from 18,490 adults recruited between 1996 and 1998. The average age of the participants was 68 years, 60% were women, and 25% reported difficulty with walking during the past 3 months (Arthritis Care Res. 2017 May 17 doi: 10.1002/acr.23250). They completed questionnaires about their health conditions, and the researchers developed a clinical nomogram using their final multivariate logistic model.
The researchers calculated that the predicted probability of difficulty walking for a 60-year-old, middle-income, normal-weight woman with no health conditions was 5%-10%. However, the probability of walking problems was 10%-20% for the same woman with diabetes and CVD; 40% with osteoarthritis in two hips/knees; 60%-70% with diabetes, CVD, and osteoarthritis in two hips/knees; and 80% with diabetes, CVD, and osteoarthritis in all hips/knees.
Overall, 10% of the participants met criteria for hip OA and 15% met criteria for knee OA. The most common chronic conditions were hypertension (43%), diabetes (11%), and CVD (11%).
In a multivariate analysis, individuals with knee or hip OA had the highest odds of reporting walking difficulty, and the odds increased with the number of joints affected.
The results were limited by the cross-sectional nature of the study and the use of self-reports, the researchers noted.
However, “Given the high prevalence of OA and the substantial physical, social, and psychological consequences of walking difficulty, we believe our findings have high clinical relevance to primary care physicians and internal medicine specialists beyond rheumatology,” they said.
“Further research is warranted to understand the mechanisms by which chronic conditions affect mobility, physical activity, and sedentary behavior, and to elucidate safe and effective management approaches to reduce OA-related walking difficulty,” they added.
None of the investigators had relevant financial disclosures to report.
Hip and knee osteoarthritis on their own predict difficulty walking in adults aged 55 years and older to a greater extent than do diabetes or cardiovascular disease individually, according to findings from a Canadian population-based study.
The ability of hip and knee osteoarthritis (OA) to predict difficulty walking also increased with the number of joints affected and acted additively with either diabetes or cardiovascular disease (CVD) or both to raise the odds for walking problems, reported Lauren K. King, MBBS, of the University of Toronto, and colleagues.
To determine the impact of hip and knee OA on difficulty walking, the researchers reviewed data from 18,490 adults recruited between 1996 and 1998. The average age of the participants was 68 years, 60% were women, and 25% reported difficulty with walking during the past 3 months (Arthritis Care Res. 2017 May 17 doi: 10.1002/acr.23250). They completed questionnaires about their health conditions, and the researchers developed a clinical nomogram using their final multivariate logistic model.
The researchers calculated that the predicted probability of difficulty walking for a 60-year-old, middle-income, normal-weight woman with no health conditions was 5%-10%. However, the probability of walking problems was 10%-20% for the same woman with diabetes and CVD; 40% with osteoarthritis in two hips/knees; 60%-70% with diabetes, CVD, and osteoarthritis in two hips/knees; and 80% with diabetes, CVD, and osteoarthritis in all hips/knees.
Overall, 10% of the participants met criteria for hip OA and 15% met criteria for knee OA. The most common chronic conditions were hypertension (43%), diabetes (11%), and CVD (11%).
In a multivariate analysis, individuals with knee or hip OA had the highest odds of reporting walking difficulty, and the odds increased with the number of joints affected.
The results were limited by the cross-sectional nature of the study and the use of self-reports, the researchers noted.
However, “Given the high prevalence of OA and the substantial physical, social, and psychological consequences of walking difficulty, we believe our findings have high clinical relevance to primary care physicians and internal medicine specialists beyond rheumatology,” they said.
“Further research is warranted to understand the mechanisms by which chronic conditions affect mobility, physical activity, and sedentary behavior, and to elucidate safe and effective management approaches to reduce OA-related walking difficulty,” they added.
None of the investigators had relevant financial disclosures to report.
Hip and knee osteoarthritis on their own predict difficulty walking in adults aged 55 years and older to a greater extent than do diabetes or cardiovascular disease individually, according to findings from a Canadian population-based study.
The ability of hip and knee osteoarthritis (OA) to predict difficulty walking also increased with the number of joints affected and acted additively with either diabetes or cardiovascular disease (CVD) or both to raise the odds for walking problems, reported Lauren K. King, MBBS, of the University of Toronto, and colleagues.
To determine the impact of hip and knee OA on difficulty walking, the researchers reviewed data from 18,490 adults recruited between 1996 and 1998. The average age of the participants was 68 years, 60% were women, and 25% reported difficulty with walking during the past 3 months (Arthritis Care Res. 2017 May 17 doi: 10.1002/acr.23250). They completed questionnaires about their health conditions, and the researchers developed a clinical nomogram using their final multivariate logistic model.
The researchers calculated that the predicted probability of difficulty walking for a 60-year-old, middle-income, normal-weight woman with no health conditions was 5%-10%. However, the probability of walking problems was 10%-20% for the same woman with diabetes and CVD; 40% with osteoarthritis in two hips/knees; 60%-70% with diabetes, CVD, and osteoarthritis in two hips/knees; and 80% with diabetes, CVD, and osteoarthritis in all hips/knees.
Overall, 10% of the participants met criteria for hip OA and 15% met criteria for knee OA. The most common chronic conditions were hypertension (43%), diabetes (11%), and CVD (11%).
In a multivariate analysis, individuals with knee or hip OA had the highest odds of reporting walking difficulty, and the odds increased with the number of joints affected.
The results were limited by the cross-sectional nature of the study and the use of self-reports, the researchers noted.
However, “Given the high prevalence of OA and the substantial physical, social, and psychological consequences of walking difficulty, we believe our findings have high clinical relevance to primary care physicians and internal medicine specialists beyond rheumatology,” they said.
“Further research is warranted to understand the mechanisms by which chronic conditions affect mobility, physical activity, and sedentary behavior, and to elucidate safe and effective management approaches to reduce OA-related walking difficulty,” they added.
None of the investigators had relevant financial disclosures to report.
FROM ARTHRITIS CARE & RESEARCH
Key clinical point:
Major finding: The probability of difficulty walking was 40% for a 60-year-old, middle-income, normal-weight woman with OA in two hips or knees vs. 5% in the same woman with no health conditions.
Data source: A population-based cohort study of 18,490 adults aged 55 years and older.
Disclosures: None of the investigators had relevant financial disclosures to report.
Benefits, safety of dupilumab-steroid combination in adults with AD sustained
Dupilumab significantly improved symptoms when used in conjunction with topical steroids over one year in a phase III randomized trial of adults with moderate to severe atopic dermatitis (AD) conducted at 161 centers in 14 countries.
The study is “the first large, randomized, double-blinded placebo-controlled study of long-term systemic treatment in patients with moderate-to-severe atopic dermatitis,” wrote Andrew Blauvelt, MD, president of the Oregon Medical Research Center, Portland, and his coauthors. “These results validate the fundamental role for interleukin 4 and interleukin 13 in the pathogenesis of atopic dermatitis,” they added. The findings were published online (Lancet. 2017 May 4. doi: 10.1016/S0140-6736[17]31191-1).
Dupilumab (Dupixent), a monoclonal antibody that inhibits signaling of both interleukin-4 and interleukin-13, was approved by the Food and Drug Administration in March for treating moderate-to-severe AD in adults.
In the study, known as LIBERTY AD CHRONOS, 740 patients were enrolled and 1-year data were available for 270 adults who received 300 mg of dupilumab once a week plus topical corticosteroids, 89 patients who received 300 mg of dupilumab every two weeks plus topical corticosteroids, and 264 patients who received a placebo plus topical corticosteroids. The two efficacy endpoints were the percent of patients with Investigator’s Global Assessment (IGA) of 0/1 and a 2-point or higher improvement from baseline and a 75% improvement from baseline on the Eczema Area and Severity Index.
At week 16, significantly more patients who received dupilumab plus topical corticosteroids achieved IGA 0/1 (39% of weekly dupilumab plus topical corticosteroids and 39% of those who received dupilumab every 2 weeks plus topical corticosteroids), compared with 12% of placebo/corticosteroid patients. The percentages of patients in each group who met the EASI-75 endpoint were 64%, 69%, and 23%, respectively (P less than .0001).
“The improvement was sustained over the 52-week treatment period,” and the combination therapy was also associated with improvements in “several other measures of clinical signs and symptoms of atopic dermatitis including pruritus, as well as symptoms of anxiety and depression and health-related quality of life, over the 52-week treatment period,” they wrote.
Adverse events were similar among the groups, with 83%, 88%, and 84% of patients in the weekly dupilumab, biweekly dupilumab, and placebo groups, respectively, reporting at least one adverse event. Nonherpetic skin infections were less common among dupilumab patients than among placebo patients, but conjunctivitis was more common among those on dupilumab (14%-19% vs. 8%). “Dupilumab might be the first targeted immune biologic that is neither immunosuppressive nor associated with increased risk of infection but, rather, restorative of barrier and immune function,” the researchers noted.
The results were limited by several factors including the challenges of determining how much topical medication was actually used by patients across multiple study sites, they wrote. However, the data suggest that “the emerging benefit-to-risk profile in this 52-week study supports the role of dupilumab as a primary targeted biologic therapy for up to 1 year in patients with moderate-to-severe atopic dermatitis who are not controlled with topical medications alone,” they said.
The study was funded by Sanofi and Regeneron Pharmaceuticals. Dr. Blauvelt and coauthors disclosed relationships with companies including Sanofi and Regeneron. Several authors were employees of the two companies.
Dupilumab significantly improved symptoms when used in conjunction with topical steroids over one year in a phase III randomized trial of adults with moderate to severe atopic dermatitis (AD) conducted at 161 centers in 14 countries.
The study is “the first large, randomized, double-blinded placebo-controlled study of long-term systemic treatment in patients with moderate-to-severe atopic dermatitis,” wrote Andrew Blauvelt, MD, president of the Oregon Medical Research Center, Portland, and his coauthors. “These results validate the fundamental role for interleukin 4 and interleukin 13 in the pathogenesis of atopic dermatitis,” they added. The findings were published online (Lancet. 2017 May 4. doi: 10.1016/S0140-6736[17]31191-1).
Dupilumab (Dupixent), a monoclonal antibody that inhibits signaling of both interleukin-4 and interleukin-13, was approved by the Food and Drug Administration in March for treating moderate-to-severe AD in adults.
In the study, known as LIBERTY AD CHRONOS, 740 patients were enrolled and 1-year data were available for 270 adults who received 300 mg of dupilumab once a week plus topical corticosteroids, 89 patients who received 300 mg of dupilumab every two weeks plus topical corticosteroids, and 264 patients who received a placebo plus topical corticosteroids. The two efficacy endpoints were the percent of patients with Investigator’s Global Assessment (IGA) of 0/1 and a 2-point or higher improvement from baseline and a 75% improvement from baseline on the Eczema Area and Severity Index.
At week 16, significantly more patients who received dupilumab plus topical corticosteroids achieved IGA 0/1 (39% of weekly dupilumab plus topical corticosteroids and 39% of those who received dupilumab every 2 weeks plus topical corticosteroids), compared with 12% of placebo/corticosteroid patients. The percentages of patients in each group who met the EASI-75 endpoint were 64%, 69%, and 23%, respectively (P less than .0001).
“The improvement was sustained over the 52-week treatment period,” and the combination therapy was also associated with improvements in “several other measures of clinical signs and symptoms of atopic dermatitis including pruritus, as well as symptoms of anxiety and depression and health-related quality of life, over the 52-week treatment period,” they wrote.
Adverse events were similar among the groups, with 83%, 88%, and 84% of patients in the weekly dupilumab, biweekly dupilumab, and placebo groups, respectively, reporting at least one adverse event. Nonherpetic skin infections were less common among dupilumab patients than among placebo patients, but conjunctivitis was more common among those on dupilumab (14%-19% vs. 8%). “Dupilumab might be the first targeted immune biologic that is neither immunosuppressive nor associated with increased risk of infection but, rather, restorative of barrier and immune function,” the researchers noted.
The results were limited by several factors including the challenges of determining how much topical medication was actually used by patients across multiple study sites, they wrote. However, the data suggest that “the emerging benefit-to-risk profile in this 52-week study supports the role of dupilumab as a primary targeted biologic therapy for up to 1 year in patients with moderate-to-severe atopic dermatitis who are not controlled with topical medications alone,” they said.
The study was funded by Sanofi and Regeneron Pharmaceuticals. Dr. Blauvelt and coauthors disclosed relationships with companies including Sanofi and Regeneron. Several authors were employees of the two companies.
Dupilumab significantly improved symptoms when used in conjunction with topical steroids over one year in a phase III randomized trial of adults with moderate to severe atopic dermatitis (AD) conducted at 161 centers in 14 countries.
The study is “the first large, randomized, double-blinded placebo-controlled study of long-term systemic treatment in patients with moderate-to-severe atopic dermatitis,” wrote Andrew Blauvelt, MD, president of the Oregon Medical Research Center, Portland, and his coauthors. “These results validate the fundamental role for interleukin 4 and interleukin 13 in the pathogenesis of atopic dermatitis,” they added. The findings were published online (Lancet. 2017 May 4. doi: 10.1016/S0140-6736[17]31191-1).
Dupilumab (Dupixent), a monoclonal antibody that inhibits signaling of both interleukin-4 and interleukin-13, was approved by the Food and Drug Administration in March for treating moderate-to-severe AD in adults.
In the study, known as LIBERTY AD CHRONOS, 740 patients were enrolled and 1-year data were available for 270 adults who received 300 mg of dupilumab once a week plus topical corticosteroids, 89 patients who received 300 mg of dupilumab every two weeks plus topical corticosteroids, and 264 patients who received a placebo plus topical corticosteroids. The two efficacy endpoints were the percent of patients with Investigator’s Global Assessment (IGA) of 0/1 and a 2-point or higher improvement from baseline and a 75% improvement from baseline on the Eczema Area and Severity Index.
At week 16, significantly more patients who received dupilumab plus topical corticosteroids achieved IGA 0/1 (39% of weekly dupilumab plus topical corticosteroids and 39% of those who received dupilumab every 2 weeks plus topical corticosteroids), compared with 12% of placebo/corticosteroid patients. The percentages of patients in each group who met the EASI-75 endpoint were 64%, 69%, and 23%, respectively (P less than .0001).
“The improvement was sustained over the 52-week treatment period,” and the combination therapy was also associated with improvements in “several other measures of clinical signs and symptoms of atopic dermatitis including pruritus, as well as symptoms of anxiety and depression and health-related quality of life, over the 52-week treatment period,” they wrote.
Adverse events were similar among the groups, with 83%, 88%, and 84% of patients in the weekly dupilumab, biweekly dupilumab, and placebo groups, respectively, reporting at least one adverse event. Nonherpetic skin infections were less common among dupilumab patients than among placebo patients, but conjunctivitis was more common among those on dupilumab (14%-19% vs. 8%). “Dupilumab might be the first targeted immune biologic that is neither immunosuppressive nor associated with increased risk of infection but, rather, restorative of barrier and immune function,” the researchers noted.
The results were limited by several factors including the challenges of determining how much topical medication was actually used by patients across multiple study sites, they wrote. However, the data suggest that “the emerging benefit-to-risk profile in this 52-week study supports the role of dupilumab as a primary targeted biologic therapy for up to 1 year in patients with moderate-to-severe atopic dermatitis who are not controlled with topical medications alone,” they said.
The study was funded by Sanofi and Regeneron Pharmaceuticals. Dr. Blauvelt and coauthors disclosed relationships with companies including Sanofi and Regeneron. Several authors were employees of the two companies.
FROM THE LANCET
Key clinical point: One year data on the efficacy and safety of dupilumab, combined with topical steroids, in adults with atopic dermatitis reflected the positive 16-week results, with encouraging safety data.
Major finding: After 16 weeks, 39% of atopic dermatitis patients who received dupilumab in addition to topical steroids met endpoints for improved symptoms, vs. 12% of patients who received topical steroids plus placebo. These benefits were sustained through one year.
Data source: An international phase III randomized trial of adults with moderate to severe atopic dermatitis.
Disclosures: The study was funded by Sanofi and Regeneron Pharmaceuticals. The lead author and coauthors disclosed relationships with companies including Sanofi and Regeneron. Several authors were employees of the two companies.