User login
More than half of pediatric residents feel burned out
More than half of all pediatric residents report feeling burned out, in a trend that has now reached 3 years.

“The stable 54%-56% rate of burnout found during 2016-2018 in this study is similar to burnout rates previously reported in U.S. studies of pediatric residents,” Kathi Kemper, MD, Ohio State University, Columbus, and colleagues wrote (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-1030).
The “alarming rate of physician burnout is a call to action on behalf of current trainees and future generations of doctors,” Jeanine Ronan, MD, of Children’s Hospital of Philadelphia, said in an accompanying editorial (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-3210), adding that “although this concern was identified more than a decade ago, little progress has been made.”
The findings were based on the Pediatric Resident Burnout and Resilience Study Consortium surveys completed at 34 residency programs in 2016 (1,664 residents participated in the survey), 43 in 2017 (2,153 participated), and 49 in 2018 (2,241 participated). The 22-item Maslach Burnout Inventory Human Services Survey was used to assess burnout.
However, researchers noted that there were “no consistent significant differences between residents meeting criteria for burnout and those not meeting criteria for burnout in terms of any demographic characteristic,” the authors added.
For example, residency year and program size were associated with burnout in some years but not others.
There “were significant differences in burnout rates among postgraduate year 1 (PGY1), postgraduate year 2 (PGY2), and postgraduate year 3 (PGY3) in 2016 and 2017, but not in 2018,” the authors stated.
For 2016, burnout rates in PGY1, PGY2 and PGY3 were 36%, 34%, and 30%, respectively. In 2017, the rates changed to 33%, 36%, and 31%, respectively, while in 2018, the rates were reported to be 35% in the first postgraduate year and 33% each for the second and third postgraduate years.
Other findings from the survey revealed that residents who met the criteria for burnout reported worse mental health, more sleepiness, and greater stress, as well as lower mindfulness and self-compassion scores, less confidence in providing compassionate care, and lower levels of empathy and resilience.
“Residents who met the criteria for burnout were more likely to be on high-acuity rotations,” the Dr. Kemper and colleagues observed. “They were approximately twice as likely to report recently having made a medical error, more likely to report a work-life conflict, less likely to have had a vacation within the past month, and less likely to have had a recent weekend off than those who did not meet the criteria for burnout.
Additionally, residents reporting burnout “consistently reported significantly less satisfaction with support from family, spouse, friends, faculty, and colleagues,” the report states. “They also reported significantly lower quality of life, less satisfaction with their choice to go into pediatrics, and less satisfaction with their balance between personal and professional life.”
Dr. Ronan also noted that the survey “showed the negative impact of the environment on trainee performance and ability to cope with stress. Residency training programs should evaluate different scheduling and staffing models to determine if there are opportunities to enhance the learning environment.”
She also noted that given the link between electronic health record usage and administrative tasks and burnout, lessening administrative task burden on trainees may help decrease the rate of burnout.
Dr. Ronan added that mental health services also must be made readily available to trainees.
“The high burnout rate among pediatric residents must be addressed,” she said. “A comprehensive approach would include developing evidence-based training in mindfulness and coping techniques for the individual resident, an institutional approach to improve resident engagement and increase joy in the workplace, and the availability of mental health services when needed to address both urgent and chronic concerns.”
SOURCE: Kemper K et al. Pediatrics 2019 Dec 16. doi: 10.1542/peds.2019-1030.
More than half of all pediatric residents report feeling burned out, in a trend that has now reached 3 years.
“The stable 54%-56% rate of burnout found during 2016-2018 in this study is similar to burnout rates previously reported in U.S. studies of pediatric residents,” Kathi Kemper, MD, Ohio State University, Columbus, and colleagues wrote (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-1030).
The “alarming rate of physician burnout is a call to action on behalf of current trainees and future generations of doctors,” Jeanine Ronan, MD, of Children’s Hospital of Philadelphia, said in an accompanying editorial (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-3210), adding that “although this concern was identified more than a decade ago, little progress has been made.”
The findings were based on the Pediatric Resident Burnout and Resilience Study Consortium surveys completed at 34 residency programs in 2016 (1,664 residents participated in the survey), 43 in 2017 (2,153 participated), and 49 in 2018 (2,241 participated). The 22-item Maslach Burnout Inventory Human Services Survey was used to assess burnout.
However, researchers noted that there were “no consistent significant differences between residents meeting criteria for burnout and those not meeting criteria for burnout in terms of any demographic characteristic,” the authors added.
For example, residency year and program size were associated with burnout in some years but not others.
There “were significant differences in burnout rates among postgraduate year 1 (PGY1), postgraduate year 2 (PGY2), and postgraduate year 3 (PGY3) in 2016 and 2017, but not in 2018,” the authors stated.
For 2016, burnout rates in PGY1, PGY2 and PGY3 were 36%, 34%, and 30%, respectively. In 2017, the rates changed to 33%, 36%, and 31%, respectively, while in 2018, the rates were reported to be 35% in the first postgraduate year and 33% each for the second and third postgraduate years.
Other findings from the survey revealed that residents who met the criteria for burnout reported worse mental health, more sleepiness, and greater stress, as well as lower mindfulness and self-compassion scores, less confidence in providing compassionate care, and lower levels of empathy and resilience.
“Residents who met the criteria for burnout were more likely to be on high-acuity rotations,” the Dr. Kemper and colleagues observed. “They were approximately twice as likely to report recently having made a medical error, more likely to report a work-life conflict, less likely to have had a vacation within the past month, and less likely to have had a recent weekend off than those who did not meet the criteria for burnout.
Additionally, residents reporting burnout “consistently reported significantly less satisfaction with support from family, spouse, friends, faculty, and colleagues,” the report states. “They also reported significantly lower quality of life, less satisfaction with their choice to go into pediatrics, and less satisfaction with their balance between personal and professional life.”
Dr. Ronan also noted that the survey “showed the negative impact of the environment on trainee performance and ability to cope with stress. Residency training programs should evaluate different scheduling and staffing models to determine if there are opportunities to enhance the learning environment.”
She also noted that given the link between electronic health record usage and administrative tasks and burnout, lessening administrative task burden on trainees may help decrease the rate of burnout.
Dr. Ronan added that mental health services also must be made readily available to trainees.
“The high burnout rate among pediatric residents must be addressed,” she said. “A comprehensive approach would include developing evidence-based training in mindfulness and coping techniques for the individual resident, an institutional approach to improve resident engagement and increase joy in the workplace, and the availability of mental health services when needed to address both urgent and chronic concerns.”
SOURCE: Kemper K et al. Pediatrics 2019 Dec 16. doi: 10.1542/peds.2019-1030.
More than half of all pediatric residents report feeling burned out, in a trend that has now reached 3 years.
“The stable 54%-56% rate of burnout found during 2016-2018 in this study is similar to burnout rates previously reported in U.S. studies of pediatric residents,” Kathi Kemper, MD, Ohio State University, Columbus, and colleagues wrote (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-1030).
The “alarming rate of physician burnout is a call to action on behalf of current trainees and future generations of doctors,” Jeanine Ronan, MD, of Children’s Hospital of Philadelphia, said in an accompanying editorial (Pediatrics. 2019 Dec. 16. doi: 10.1542/peds.2019-3210), adding that “although this concern was identified more than a decade ago, little progress has been made.”
The findings were based on the Pediatric Resident Burnout and Resilience Study Consortium surveys completed at 34 residency programs in 2016 (1,664 residents participated in the survey), 43 in 2017 (2,153 participated), and 49 in 2018 (2,241 participated). The 22-item Maslach Burnout Inventory Human Services Survey was used to assess burnout.
However, researchers noted that there were “no consistent significant differences between residents meeting criteria for burnout and those not meeting criteria for burnout in terms of any demographic characteristic,” the authors added.
For example, residency year and program size were associated with burnout in some years but not others.
There “were significant differences in burnout rates among postgraduate year 1 (PGY1), postgraduate year 2 (PGY2), and postgraduate year 3 (PGY3) in 2016 and 2017, but not in 2018,” the authors stated.
For 2016, burnout rates in PGY1, PGY2 and PGY3 were 36%, 34%, and 30%, respectively. In 2017, the rates changed to 33%, 36%, and 31%, respectively, while in 2018, the rates were reported to be 35% in the first postgraduate year and 33% each for the second and third postgraduate years.
Other findings from the survey revealed that residents who met the criteria for burnout reported worse mental health, more sleepiness, and greater stress, as well as lower mindfulness and self-compassion scores, less confidence in providing compassionate care, and lower levels of empathy and resilience.
“Residents who met the criteria for burnout were more likely to be on high-acuity rotations,” the Dr. Kemper and colleagues observed. “They were approximately twice as likely to report recently having made a medical error, more likely to report a work-life conflict, less likely to have had a vacation within the past month, and less likely to have had a recent weekend off than those who did not meet the criteria for burnout.
Additionally, residents reporting burnout “consistently reported significantly less satisfaction with support from family, spouse, friends, faculty, and colleagues,” the report states. “They also reported significantly lower quality of life, less satisfaction with their choice to go into pediatrics, and less satisfaction with their balance between personal and professional life.”
Dr. Ronan also noted that the survey “showed the negative impact of the environment on trainee performance and ability to cope with stress. Residency training programs should evaluate different scheduling and staffing models to determine if there are opportunities to enhance the learning environment.”
She also noted that given the link between electronic health record usage and administrative tasks and burnout, lessening administrative task burden on trainees may help decrease the rate of burnout.
Dr. Ronan added that mental health services also must be made readily available to trainees.
“The high burnout rate among pediatric residents must be addressed,” she said. “A comprehensive approach would include developing evidence-based training in mindfulness and coping techniques for the individual resident, an institutional approach to improve resident engagement and increase joy in the workplace, and the availability of mental health services when needed to address both urgent and chronic concerns.”
SOURCE: Kemper K et al. Pediatrics 2019 Dec 16. doi: 10.1542/peds.2019-1030.
FROM PEDIATRICS
House passes drug pricing bill, likely ending its journey
The House of Representatives passed a partisan drug pricing bill, a move that likely ends its legislative journey as Senate Majority Leader Mitch McConnell (R-Ky.) has already signaled he will not bring it to the Senate floor.

The Elijah E. Cummings Lower Drug Costs Now Act (H.R. 3) passed Dec. 12 on a near party-line vote of 230-192, with two Republicans crossing the aisle to join the Democrats in support of the bill, and no Democrats voting against it. Four members from each party did not record votes.
“The American people are fed up with paying 3, 4, or 10 times more than people in other countries for the exact same drug,” House Energy and Commerce Committee Chairman Frank Pallone (D-N.J) said in a statement following the passage. “I’m proud that the House took decisive action today to finally level the playing field and provide real relief to the American people.”
H.R. 3 would give the secretary of Health and Human Services the ability to negotiate with drug manufacturers on the price of pharmaceuticals in Medicare Part D (and available in the commercial markets) using an international pricing benchmark and would penalize manufacturers who do not negotiate or fail to lower prices to be more in line with generally lower costs internationally.
Drug prices would need to be within 120% of the average price in a reference group of six nations: Australia, Canada, France, Germany, Japan, and the United Kingdom.
Savings from the lower costs that result from negotiations would be reinvested into medical research.
Passage of H.R. 3 would “lower ... medication by 65%” per year for women with breast cancer, Rep. Haley Stevens (D-Mich.) said during the floor debate.
The Congressional Budget Office estimated that the drug price negotiation provision would lower spending on pharmaceuticals by $465 billion over the next 10 years, offset partially by an increase in spending by $358 billion associated with provisions to provide dental, vision, and hearing coverage.
The bill also includes mandatory rebates to the federal government when a drug’s price rises faster than the rate of inflation. It includes an annual cap on out-of-pocket spending on pharmaceuticals of $2,000 for Medicare Part D participants.
The bill was contentious from its introduction, which erased bipartisan work across the committees of jurisdiction, including a number of individual bills that passed at the committee level with bipartisan support.
The price negotiation scheme, using the international benchmark, was a key point of objection, which some argued was more akin to price-setting.
“Government price setting will kill innovation in clinical areas where it is most needed,” Rep. George Holding (R-N.C.) said during the floor debate. “The pricing scheme outlined in H.R. 3 would disincentivize research and development for drugs that are first in their class, such as the future cure for Alzheimer’s.”
The CBO estimates that if the bill were enacted, “8 fewer drugs would be introduced to the U.S. market over the 2020-2029 period, and about 30 fewer drugs over the subsequent decade.”
An amendment offered by House Energy and Commerce Committee Ranking Member Greg Walden (R-Ore.) attempted to replace the language of H.R. 3 with substitute language that collected all the individual drug pricing–related bills that had previously passed with bipartisan support at the committee level, but that was voted down by 223-201 vote with 12 members not voting.
Rep. Walden noted that policies within his substitute “unanimously passed the Energy and Commerce Committee earlier this year. They would have unanimously passed on this House floor had a poison pill not been put in up in the Rules Committee.”
Rep. Katie Porter (D-Calif.) countered that Rep. Walden’s amendment “doesn’t tackle the fundamental problem, which is reducing drug prices. This amendment fails to solve the main problem of actually lowering drug prices.”
The House of Representatives passed a partisan drug pricing bill, a move that likely ends its legislative journey as Senate Majority Leader Mitch McConnell (R-Ky.) has already signaled he will not bring it to the Senate floor.
The Elijah E. Cummings Lower Drug Costs Now Act (H.R. 3) passed Dec. 12 on a near party-line vote of 230-192, with two Republicans crossing the aisle to join the Democrats in support of the bill, and no Democrats voting against it. Four members from each party did not record votes.
“The American people are fed up with paying 3, 4, or 10 times more than people in other countries for the exact same drug,” House Energy and Commerce Committee Chairman Frank Pallone (D-N.J) said in a statement following the passage. “I’m proud that the House took decisive action today to finally level the playing field and provide real relief to the American people.”
H.R. 3 would give the secretary of Health and Human Services the ability to negotiate with drug manufacturers on the price of pharmaceuticals in Medicare Part D (and available in the commercial markets) using an international pricing benchmark and would penalize manufacturers who do not negotiate or fail to lower prices to be more in line with generally lower costs internationally.
Drug prices would need to be within 120% of the average price in a reference group of six nations: Australia, Canada, France, Germany, Japan, and the United Kingdom.
Savings from the lower costs that result from negotiations would be reinvested into medical research.
Passage of H.R. 3 would “lower ... medication by 65%” per year for women with breast cancer, Rep. Haley Stevens (D-Mich.) said during the floor debate.
The Congressional Budget Office estimated that the drug price negotiation provision would lower spending on pharmaceuticals by $465 billion over the next 10 years, offset partially by an increase in spending by $358 billion associated with provisions to provide dental, vision, and hearing coverage.
The bill also includes mandatory rebates to the federal government when a drug’s price rises faster than the rate of inflation. It includes an annual cap on out-of-pocket spending on pharmaceuticals of $2,000 for Medicare Part D participants.
The bill was contentious from its introduction, which erased bipartisan work across the committees of jurisdiction, including a number of individual bills that passed at the committee level with bipartisan support.
The price negotiation scheme, using the international benchmark, was a key point of objection, which some argued was more akin to price-setting.
“Government price setting will kill innovation in clinical areas where it is most needed,” Rep. George Holding (R-N.C.) said during the floor debate. “The pricing scheme outlined in H.R. 3 would disincentivize research and development for drugs that are first in their class, such as the future cure for Alzheimer’s.”
The CBO estimates that if the bill were enacted, “8 fewer drugs would be introduced to the U.S. market over the 2020-2029 period, and about 30 fewer drugs over the subsequent decade.”
An amendment offered by House Energy and Commerce Committee Ranking Member Greg Walden (R-Ore.) attempted to replace the language of H.R. 3 with substitute language that collected all the individual drug pricing–related bills that had previously passed with bipartisan support at the committee level, but that was voted down by 223-201 vote with 12 members not voting.
Rep. Walden noted that policies within his substitute “unanimously passed the Energy and Commerce Committee earlier this year. They would have unanimously passed on this House floor had a poison pill not been put in up in the Rules Committee.”
Rep. Katie Porter (D-Calif.) countered that Rep. Walden’s amendment “doesn’t tackle the fundamental problem, which is reducing drug prices. This amendment fails to solve the main problem of actually lowering drug prices.”
The House of Representatives passed a partisan drug pricing bill, a move that likely ends its legislative journey as Senate Majority Leader Mitch McConnell (R-Ky.) has already signaled he will not bring it to the Senate floor.
The Elijah E. Cummings Lower Drug Costs Now Act (H.R. 3) passed Dec. 12 on a near party-line vote of 230-192, with two Republicans crossing the aisle to join the Democrats in support of the bill, and no Democrats voting against it. Four members from each party did not record votes.
“The American people are fed up with paying 3, 4, or 10 times more than people in other countries for the exact same drug,” House Energy and Commerce Committee Chairman Frank Pallone (D-N.J) said in a statement following the passage. “I’m proud that the House took decisive action today to finally level the playing field and provide real relief to the American people.”
H.R. 3 would give the secretary of Health and Human Services the ability to negotiate with drug manufacturers on the price of pharmaceuticals in Medicare Part D (and available in the commercial markets) using an international pricing benchmark and would penalize manufacturers who do not negotiate or fail to lower prices to be more in line with generally lower costs internationally.
Drug prices would need to be within 120% of the average price in a reference group of six nations: Australia, Canada, France, Germany, Japan, and the United Kingdom.
Savings from the lower costs that result from negotiations would be reinvested into medical research.
Passage of H.R. 3 would “lower ... medication by 65%” per year for women with breast cancer, Rep. Haley Stevens (D-Mich.) said during the floor debate.
The Congressional Budget Office estimated that the drug price negotiation provision would lower spending on pharmaceuticals by $465 billion over the next 10 years, offset partially by an increase in spending by $358 billion associated with provisions to provide dental, vision, and hearing coverage.
The bill also includes mandatory rebates to the federal government when a drug’s price rises faster than the rate of inflation. It includes an annual cap on out-of-pocket spending on pharmaceuticals of $2,000 for Medicare Part D participants.
The bill was contentious from its introduction, which erased bipartisan work across the committees of jurisdiction, including a number of individual bills that passed at the committee level with bipartisan support.
The price negotiation scheme, using the international benchmark, was a key point of objection, which some argued was more akin to price-setting.
“Government price setting will kill innovation in clinical areas where it is most needed,” Rep. George Holding (R-N.C.) said during the floor debate. “The pricing scheme outlined in H.R. 3 would disincentivize research and development for drugs that are first in their class, such as the future cure for Alzheimer’s.”
The CBO estimates that if the bill were enacted, “8 fewer drugs would be introduced to the U.S. market over the 2020-2029 period, and about 30 fewer drugs over the subsequent decade.”
An amendment offered by House Energy and Commerce Committee Ranking Member Greg Walden (R-Ore.) attempted to replace the language of H.R. 3 with substitute language that collected all the individual drug pricing–related bills that had previously passed with bipartisan support at the committee level, but that was voted down by 223-201 vote with 12 members not voting.
Rep. Walden noted that policies within his substitute “unanimously passed the Energy and Commerce Committee earlier this year. They would have unanimously passed on this House floor had a poison pill not been put in up in the Rules Committee.”
Rep. Katie Porter (D-Calif.) countered that Rep. Walden’s amendment “doesn’t tackle the fundamental problem, which is reducing drug prices. This amendment fails to solve the main problem of actually lowering drug prices.”
Culture Change Needed Around Addiction Treatment in the Military
More work is needed to address how addiction is handled both within the military and for veterans after they serve. Removing the stigma around addiction treatment is key to addressing the issue, Anthony Dekker, DO, Northern Arizona VA Healthcare System, said at the AMSUS annual meeting on December 4, 2019.
“When we are talking about treating addiction in the military and the VA, those are 2 different issues,” Dr. Dekker said. “In the VA, it should be understood this is a service that needs to be provided. In the military, it is highly dependent on command. Some commands are in favor of treatment. Some commands are in favor of separation.”
But that separation comes with a cost. Dr. Dekker noted that the military spends about $200,000 to get a person from recruitment to an E-5 pay grade and about $400,000 to an O-5 pay grade. That can be a huge investment loss considering the cost of treatment for someone who is suffering from a use disorder.
“Treatment is going to cost about $44,000,” he said. “That will be treatment in a residential center. That was a person who is serious enough to come into a residential center, follow up with a partial hospital program and continue with ongoing [treatment] that would last a year.”
He touted some of the successes addiction treatment programs have had, recalling data from 2008-2009 from 110 military active-duty service members treated across 5 residential treatment centers in the Washington, DC, area. Within a year, 91% had separated from the military either because of a command decision before treatment or because of loss of recover.
“We know what works in addiction,” he said, noting that program changes that involved using a combination of medication-assisted treatments with regular substance use screenings and medical practitioner follow-up has helped to reduce the rate of lost recovery to 12%. He also noted that in 2013-2014, 41 active military members who received treatment in the same centers were able to be redeployed to Afghanistan and had no relapses during that deployment.
“We try to take the stigma away,” Dr. Dekker said. “So if you have leadership who has a stigma against addiction treatment, you are going to have a steep incline to work against, whereas if you have leadership that were, I would say, endowed with a different sense of knowledge and experience,” there is a much greater chance for helping both military service members and veterans alike.
He called on the US Department of Veterans Affairs (VA) to look more closely at how it is prescribing opioids. While acknowledging the opioid addiction epidemic, he noted that simply cutting back on prescribing may not be the right solution because it is having a ripple effect and causing other problems, namely that although the VA has written 60% fewer opioid prescriptions from 2012 to 2019, overdose rates have doubled as military members and veterans are seeking opioids from other sources outside of a controlled, safer medical environment.
It can be especially problematic for those who have a legitimate medical need for opioids but have a disqualifying event that causes the pain medication to be cut off.
“We need to have a different answer to this because termination of opioids because a patient is positive for marijuana or even positive for cocaine doesn’t mean you take services away. You ramp services up,” Dr. Dekker said. “If I have a patient who has a chronic pain syndrome, the only thing that is going to push him out of my system is if they threaten my staff.…The loss from recovery is not a reason to lose treatment. That is another concept that needs to be addressed and we need to really look at that.”
He also called on VA leadership to be more encouraging in prescribing buprenorphine, noting that many doctors and nurses have waivers to prescribe it, but there is a lot of reluctance to do so, even though there is a lot of success with that treatment.
More work is needed to address how addiction is handled both within the military and for veterans after they serve. Removing the stigma around addiction treatment is key to addressing the issue, Anthony Dekker, DO, Northern Arizona VA Healthcare System, said at the AMSUS annual meeting on December 4, 2019.
“When we are talking about treating addiction in the military and the VA, those are 2 different issues,” Dr. Dekker said. “In the VA, it should be understood this is a service that needs to be provided. In the military, it is highly dependent on command. Some commands are in favor of treatment. Some commands are in favor of separation.”
But that separation comes with a cost. Dr. Dekker noted that the military spends about $200,000 to get a person from recruitment to an E-5 pay grade and about $400,000 to an O-5 pay grade. That can be a huge investment loss considering the cost of treatment for someone who is suffering from a use disorder.
“Treatment is going to cost about $44,000,” he said. “That will be treatment in a residential center. That was a person who is serious enough to come into a residential center, follow up with a partial hospital program and continue with ongoing [treatment] that would last a year.”
He touted some of the successes addiction treatment programs have had, recalling data from 2008-2009 from 110 military active-duty service members treated across 5 residential treatment centers in the Washington, DC, area. Within a year, 91% had separated from the military either because of a command decision before treatment or because of loss of recover.
“We know what works in addiction,” he said, noting that program changes that involved using a combination of medication-assisted treatments with regular substance use screenings and medical practitioner follow-up has helped to reduce the rate of lost recovery to 12%. He also noted that in 2013-2014, 41 active military members who received treatment in the same centers were able to be redeployed to Afghanistan and had no relapses during that deployment.
“We try to take the stigma away,” Dr. Dekker said. “So if you have leadership who has a stigma against addiction treatment, you are going to have a steep incline to work against, whereas if you have leadership that were, I would say, endowed with a different sense of knowledge and experience,” there is a much greater chance for helping both military service members and veterans alike.
He called on the US Department of Veterans Affairs (VA) to look more closely at how it is prescribing opioids. While acknowledging the opioid addiction epidemic, he noted that simply cutting back on prescribing may not be the right solution because it is having a ripple effect and causing other problems, namely that although the VA has written 60% fewer opioid prescriptions from 2012 to 2019, overdose rates have doubled as military members and veterans are seeking opioids from other sources outside of a controlled, safer medical environment.
It can be especially problematic for those who have a legitimate medical need for opioids but have a disqualifying event that causes the pain medication to be cut off.
“We need to have a different answer to this because termination of opioids because a patient is positive for marijuana or even positive for cocaine doesn’t mean you take services away. You ramp services up,” Dr. Dekker said. “If I have a patient who has a chronic pain syndrome, the only thing that is going to push him out of my system is if they threaten my staff.…The loss from recovery is not a reason to lose treatment. That is another concept that needs to be addressed and we need to really look at that.”
He also called on VA leadership to be more encouraging in prescribing buprenorphine, noting that many doctors and nurses have waivers to prescribe it, but there is a lot of reluctance to do so, even though there is a lot of success with that treatment.
More work is needed to address how addiction is handled both within the military and for veterans after they serve. Removing the stigma around addiction treatment is key to addressing the issue, Anthony Dekker, DO, Northern Arizona VA Healthcare System, said at the AMSUS annual meeting on December 4, 2019.
“When we are talking about treating addiction in the military and the VA, those are 2 different issues,” Dr. Dekker said. “In the VA, it should be understood this is a service that needs to be provided. In the military, it is highly dependent on command. Some commands are in favor of treatment. Some commands are in favor of separation.”
But that separation comes with a cost. Dr. Dekker noted that the military spends about $200,000 to get a person from recruitment to an E-5 pay grade and about $400,000 to an O-5 pay grade. That can be a huge investment loss considering the cost of treatment for someone who is suffering from a use disorder.
“Treatment is going to cost about $44,000,” he said. “That will be treatment in a residential center. That was a person who is serious enough to come into a residential center, follow up with a partial hospital program and continue with ongoing [treatment] that would last a year.”
He touted some of the successes addiction treatment programs have had, recalling data from 2008-2009 from 110 military active-duty service members treated across 5 residential treatment centers in the Washington, DC, area. Within a year, 91% had separated from the military either because of a command decision before treatment or because of loss of recover.
“We know what works in addiction,” he said, noting that program changes that involved using a combination of medication-assisted treatments with regular substance use screenings and medical practitioner follow-up has helped to reduce the rate of lost recovery to 12%. He also noted that in 2013-2014, 41 active military members who received treatment in the same centers were able to be redeployed to Afghanistan and had no relapses during that deployment.
“We try to take the stigma away,” Dr. Dekker said. “So if you have leadership who has a stigma against addiction treatment, you are going to have a steep incline to work against, whereas if you have leadership that were, I would say, endowed with a different sense of knowledge and experience,” there is a much greater chance for helping both military service members and veterans alike.
He called on the US Department of Veterans Affairs (VA) to look more closely at how it is prescribing opioids. While acknowledging the opioid addiction epidemic, he noted that simply cutting back on prescribing may not be the right solution because it is having a ripple effect and causing other problems, namely that although the VA has written 60% fewer opioid prescriptions from 2012 to 2019, overdose rates have doubled as military members and veterans are seeking opioids from other sources outside of a controlled, safer medical environment.
It can be especially problematic for those who have a legitimate medical need for opioids but have a disqualifying event that causes the pain medication to be cut off.
“We need to have a different answer to this because termination of opioids because a patient is positive for marijuana or even positive for cocaine doesn’t mean you take services away. You ramp services up,” Dr. Dekker said. “If I have a patient who has a chronic pain syndrome, the only thing that is going to push him out of my system is if they threaten my staff.…The loss from recovery is not a reason to lose treatment. That is another concept that needs to be addressed and we need to really look at that.”
He also called on VA leadership to be more encouraging in prescribing buprenorphine, noting that many doctors and nurses have waivers to prescribe it, but there is a lot of reluctance to do so, even though there is a lot of success with that treatment.
Docs push back on surprise billing compromise
Compromise bipartisan legislation to address surprise medical bills is getting push back from physician groups.

Leadership from the House Energy and Commerce Committee and the Senate Health, Education, Labor, and Pensions Committee on Dec. 9 unveiled a compromise bill that includes rate-setting for small surprise billing and arbitration for larger ones at a lower threshold than what was originally proposed.
The new bill, part of a broader Lower Health Care Costs Act, would protect patients from surprise medical bills related to emergency care, holding them responsible for in-network cost-sharing rates for out-of-network care provided at an in-network facility without their informed consent. Out-of-network surprise bills would be applied to the patient’s in-network deductible.
Under the legislation, providers would be paid at minimum the local, market-based median in-network negotiated rate for services, with a median rate under a $750 threshold. When the median exceeds $750, the provider or insurer would be allowed to choose arbitration process to resolve payment disputes.
The bill also protects patients by banning out-of-network facilities and providers from sending balance bills for more than in-network cost-sharing amounts.
Physician groups, however, see the legislation as a giveback to insurers that puts health care professionals at a disadvantage when negotiating to be included in insurer networks.
At issue is the $750 threshold for optional arbitration.
“If you set the arbitration system in such a way that limits the ability of a physician to go to arbitration to settle a dispute between a health plan and the doctor, and if you say that can only be done when there [are] bills that are greater than $750 for a particular service, then the vast majority of services provided by doctors will not be able to go to arbitration,” Christian Shalgian, director of advocacy and health policy at the American College of Surgeons, said in an interview.
Cynthia Moran, executive vice president of government relations and health policy at the American College of Radiology, agreed.
“This particular product is going in a direction that we’re not comfortable with so we can’t support it on the basis of the benchmarks and the independent dispute resolution (IDR) process with the $750 threshold,” she said in an interview. The services radiologists provide tend to be in the $100-200 range, she said, so that would automatically exclude them from accessing arbitration. She also said that it is her understanding that many physician services will fall under that $750 threshold.
“That $750 is really going to mean that the vast majority of this policy is a benchmark-driven policy,” she said. “It is not going to be an IDR-driven policy and that is the crux of our objection to it.”
And by taking arbitration off the table, insurers have no incentive to negotiate in good faith with doctors to ensure that doctors are getting paid for the services they perform.
“For those situations where there is an out-of-network physician at an in-network facility, we believe that the patient should not have to pay any more for those emergency situations where they patient doesn’t get to choose their doctor,” Mr. Shalgian said. “The dispute really comes down to how much does the health plan have to pay the doctor.”
He noted that the legislation ties the rate to median in-network rates “and that’s a problem for us as well because of the fact that [this is] going to allow the health plans to set median in-network rates as the rate that they can pay the doctors.”
If the bill becomes law, “when you have a situation where you have an in-network physician trying to negotiate with a health plan to stay in network, that health plan now has more power in that negotiation because if [the physician] is making more than median in-network rates, then the health plan can say, ‘go out of network because we will just pay you median in-network’ at that point. That is a significant concern to us as well.”
Mr. Shalgian said that the ideal solution would be to eliminate the threshold entirely and just send disputes to arbitration. Recognizing that it might not be practical, the $750 threshold should be lowered.
ACS supported a $300 threshold, he added.
The bill is expected to be tacked on to one of the mandatory spending bills that Congress needs to pass by the end of the year.
The $750 threshold would be a savings generator for the government and an important bill such as this should be passed on its own merits, Mr. Shalgian said.
Ms. Moran called for Congress to take its time with the legislation.
“We do think that this whole issue needs more time for everyone to understand what the impact is on this first run of the solution and we think it should be slowed down a bit,” she said. “It should not go to the floor until you hear more from the providers [after] the providers figure out what the impact will be.”
The American Medical Association also called for Congress to slow down.
“The current proposal relies on benchmark rate setting that would serve only to benefit the bottom line of insurance companies at the expense of patients seeking a robust network of physicians for their care,” AMA President Patrice Harris, MD, said in a statement. “Rather than rushing to meet arbitrary deadlines, it is important to get this legislation right.”
Compromise bipartisan legislation to address surprise medical bills is getting push back from physician groups.
Leadership from the House Energy and Commerce Committee and the Senate Health, Education, Labor, and Pensions Committee on Dec. 9 unveiled a compromise bill that includes rate-setting for small surprise billing and arbitration for larger ones at a lower threshold than what was originally proposed.
The new bill, part of a broader Lower Health Care Costs Act, would protect patients from surprise medical bills related to emergency care, holding them responsible for in-network cost-sharing rates for out-of-network care provided at an in-network facility without their informed consent. Out-of-network surprise bills would be applied to the patient’s in-network deductible.
Under the legislation, providers would be paid at minimum the local, market-based median in-network negotiated rate for services, with a median rate under a $750 threshold. When the median exceeds $750, the provider or insurer would be allowed to choose arbitration process to resolve payment disputes.
The bill also protects patients by banning out-of-network facilities and providers from sending balance bills for more than in-network cost-sharing amounts.
Physician groups, however, see the legislation as a giveback to insurers that puts health care professionals at a disadvantage when negotiating to be included in insurer networks.
At issue is the $750 threshold for optional arbitration.
“If you set the arbitration system in such a way that limits the ability of a physician to go to arbitration to settle a dispute between a health plan and the doctor, and if you say that can only be done when there [are] bills that are greater than $750 for a particular service, then the vast majority of services provided by doctors will not be able to go to arbitration,” Christian Shalgian, director of advocacy and health policy at the American College of Surgeons, said in an interview.
Cynthia Moran, executive vice president of government relations and health policy at the American College of Radiology, agreed.
“This particular product is going in a direction that we’re not comfortable with so we can’t support it on the basis of the benchmarks and the independent dispute resolution (IDR) process with the $750 threshold,” she said in an interview. The services radiologists provide tend to be in the $100-200 range, she said, so that would automatically exclude them from accessing arbitration. She also said that it is her understanding that many physician services will fall under that $750 threshold.
“That $750 is really going to mean that the vast majority of this policy is a benchmark-driven policy,” she said. “It is not going to be an IDR-driven policy and that is the crux of our objection to it.”
And by taking arbitration off the table, insurers have no incentive to negotiate in good faith with doctors to ensure that doctors are getting paid for the services they perform.
“For those situations where there is an out-of-network physician at an in-network facility, we believe that the patient should not have to pay any more for those emergency situations where they patient doesn’t get to choose their doctor,” Mr. Shalgian said. “The dispute really comes down to how much does the health plan have to pay the doctor.”
He noted that the legislation ties the rate to median in-network rates “and that’s a problem for us as well because of the fact that [this is] going to allow the health plans to set median in-network rates as the rate that they can pay the doctors.”
If the bill becomes law, “when you have a situation where you have an in-network physician trying to negotiate with a health plan to stay in network, that health plan now has more power in that negotiation because if [the physician] is making more than median in-network rates, then the health plan can say, ‘go out of network because we will just pay you median in-network’ at that point. That is a significant concern to us as well.”
Mr. Shalgian said that the ideal solution would be to eliminate the threshold entirely and just send disputes to arbitration. Recognizing that it might not be practical, the $750 threshold should be lowered.
ACS supported a $300 threshold, he added.
The bill is expected to be tacked on to one of the mandatory spending bills that Congress needs to pass by the end of the year.
The $750 threshold would be a savings generator for the government and an important bill such as this should be passed on its own merits, Mr. Shalgian said.
Ms. Moran called for Congress to take its time with the legislation.
“We do think that this whole issue needs more time for everyone to understand what the impact is on this first run of the solution and we think it should be slowed down a bit,” she said. “It should not go to the floor until you hear more from the providers [after] the providers figure out what the impact will be.”
The American Medical Association also called for Congress to slow down.
“The current proposal relies on benchmark rate setting that would serve only to benefit the bottom line of insurance companies at the expense of patients seeking a robust network of physicians for their care,” AMA President Patrice Harris, MD, said in a statement. “Rather than rushing to meet arbitrary deadlines, it is important to get this legislation right.”
Compromise bipartisan legislation to address surprise medical bills is getting push back from physician groups.
Leadership from the House Energy and Commerce Committee and the Senate Health, Education, Labor, and Pensions Committee on Dec. 9 unveiled a compromise bill that includes rate-setting for small surprise billing and arbitration for larger ones at a lower threshold than what was originally proposed.
The new bill, part of a broader Lower Health Care Costs Act, would protect patients from surprise medical bills related to emergency care, holding them responsible for in-network cost-sharing rates for out-of-network care provided at an in-network facility without their informed consent. Out-of-network surprise bills would be applied to the patient’s in-network deductible.
Under the legislation, providers would be paid at minimum the local, market-based median in-network negotiated rate for services, with a median rate under a $750 threshold. When the median exceeds $750, the provider or insurer would be allowed to choose arbitration process to resolve payment disputes.
The bill also protects patients by banning out-of-network facilities and providers from sending balance bills for more than in-network cost-sharing amounts.
Physician groups, however, see the legislation as a giveback to insurers that puts health care professionals at a disadvantage when negotiating to be included in insurer networks.
At issue is the $750 threshold for optional arbitration.
“If you set the arbitration system in such a way that limits the ability of a physician to go to arbitration to settle a dispute between a health plan and the doctor, and if you say that can only be done when there [are] bills that are greater than $750 for a particular service, then the vast majority of services provided by doctors will not be able to go to arbitration,” Christian Shalgian, director of advocacy and health policy at the American College of Surgeons, said in an interview.
Cynthia Moran, executive vice president of government relations and health policy at the American College of Radiology, agreed.
“This particular product is going in a direction that we’re not comfortable with so we can’t support it on the basis of the benchmarks and the independent dispute resolution (IDR) process with the $750 threshold,” she said in an interview. The services radiologists provide tend to be in the $100-200 range, she said, so that would automatically exclude them from accessing arbitration. She also said that it is her understanding that many physician services will fall under that $750 threshold.
“That $750 is really going to mean that the vast majority of this policy is a benchmark-driven policy,” she said. “It is not going to be an IDR-driven policy and that is the crux of our objection to it.”
And by taking arbitration off the table, insurers have no incentive to negotiate in good faith with doctors to ensure that doctors are getting paid for the services they perform.
“For those situations where there is an out-of-network physician at an in-network facility, we believe that the patient should not have to pay any more for those emergency situations where they patient doesn’t get to choose their doctor,” Mr. Shalgian said. “The dispute really comes down to how much does the health plan have to pay the doctor.”
He noted that the legislation ties the rate to median in-network rates “and that’s a problem for us as well because of the fact that [this is] going to allow the health plans to set median in-network rates as the rate that they can pay the doctors.”
If the bill becomes law, “when you have a situation where you have an in-network physician trying to negotiate with a health plan to stay in network, that health plan now has more power in that negotiation because if [the physician] is making more than median in-network rates, then the health plan can say, ‘go out of network because we will just pay you median in-network’ at that point. That is a significant concern to us as well.”
Mr. Shalgian said that the ideal solution would be to eliminate the threshold entirely and just send disputes to arbitration. Recognizing that it might not be practical, the $750 threshold should be lowered.
ACS supported a $300 threshold, he added.
The bill is expected to be tacked on to one of the mandatory spending bills that Congress needs to pass by the end of the year.
The $750 threshold would be a savings generator for the government and an important bill such as this should be passed on its own merits, Mr. Shalgian said.
Ms. Moran called for Congress to take its time with the legislation.
“We do think that this whole issue needs more time for everyone to understand what the impact is on this first run of the solution and we think it should be slowed down a bit,” she said. “It should not go to the floor until you hear more from the providers [after] the providers figure out what the impact will be.”
The American Medical Association also called for Congress to slow down.
“The current proposal relies on benchmark rate setting that would serve only to benefit the bottom line of insurance companies at the expense of patients seeking a robust network of physicians for their care,” AMA President Patrice Harris, MD, said in a statement. “Rather than rushing to meet arbitrary deadlines, it is important to get this legislation right.”
Health care: More uninsured as insurance costs grow faster
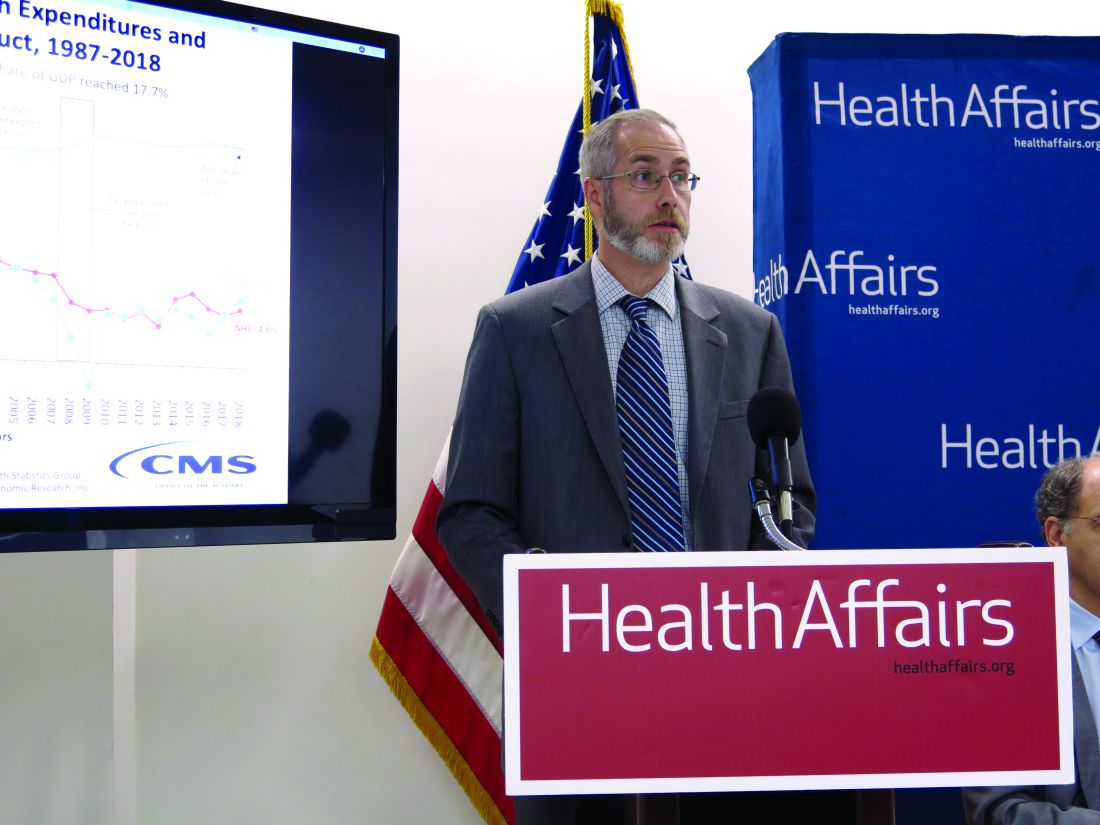
WASHINGTON – The number of uninsured grew in 2018 as the rate of health care spending grew, according to data from the Centers for Medicare & Medicaid Services.
A total of 30.7 million people in the United States were uninsured in 2018 – up 1 million from 2017. It was the second year in a row that the number of uninsured grew by that amount.
The newly uninsured came from the private insurance sector, which saw the number of insured decrease to 200.5 million in 2018 from 202.1 million in the previous year, partially offset by increases in Americans covered by Medicare and Medicaid.
The increase in uninsured people comes as the growth rate in health care spending rose to 4.6% in 2018 from 4.2% in 2017, though much of that growth in the rate of spending was attributed to the application of a health insurance tax in 2018 that Congress put a moratorium on in the previous year. The tax was part of the Affordable Care Act and was enacted in 2014.
“We see that health care spending reached $3.6 trillion, or $11,172 per person, and spending was faster,” Micah Hartman, statistician in the National Health Statistics Group in the CMS Office of the Actuary, said during a press conference to review the national health expenditure results. “The main reason for the acceleration was faster growth in the net cost of insurance, and that was particularly the case for private health insurance and also for Medicare.”
The net cost of insurance includes nonmedical expenses such as administration, taxes, and fees, as well as gains or losses for private health insurers. The ACA’s health insurance tax generated $14.3 billion in spending, according to Internal Revenue Service data.
Also contributing to the rise in the rate of growth was faster growth in medical prices, “and that was due to underlying economy-wide inflation, as well as the impacts of the tax,” Mr. Hartman said.
Despite this growth in the rate of spending, health care spending as a percentage of GDP fell slightly from 17.9% in 2017 in 17.7%, as the GDP grew faster than health care spending in 2018.
The faster growth in prices more than offset the slightly slower growth in the use and intensity of medical services, CMS reported.
The growth rate on spending on physician and clinical services slowed to 4.1% in 2018 from 4.7% in 2017. Overall spending on physician and clinical services in 2018 reached $725.6 billion and accounted for 20% of overall health care spending.
Spending on hospital services also slowed, but only slightly, dropping to a growth rate of 4.5% from 4.7% during this period. Hospital spending in 2018, at $1.2 trillion, accounted for 33% of overall health care spending.

On a personal level, overall growth in personal health care spending held steady with growth rate of 4.1% in 2018, the same as 2017, though individual components that feed into the figure varied. For example, growth rate in the spending on retail pharmaceuticals rose to 2.5% from 1.4% during this period. Spending on retail pharmaceuticals reached $335 billion and accounted for 9% of overall health care spending.
Another factor in the rising growth rate in spending came from employer-sponsored insurance.
“Growth in health spending by private business was due to faster growth in employer contributions to private health insurance premiums,” Anne B. Martin, economist in the National Health Statistics Group, said during the press conference. There also was faster growth in spending by the federal government, “driven mainly by faster growth in the federally funded portions of Medicare and Medicaid.”
Spending by private health insurance grew at a rate of 5.8% and reached $1.2 trillion in 2018. Medicare spending grew by 6.4% and reached $750.2 billion, while Medicaid spending grew 3.0%, reaching $597.4 billion.
SOURCE: Hartman M et al. Health Affairs. 2019. doi: 10.1377/hlthaff.2019.00451
WASHINGTON – The number of uninsured grew in 2018 as the rate of health care spending grew, according to data from the Centers for Medicare & Medicaid Services.
A total of 30.7 million people in the United States were uninsured in 2018 – up 1 million from 2017. It was the second year in a row that the number of uninsured grew by that amount.
The newly uninsured came from the private insurance sector, which saw the number of insured decrease to 200.5 million in 2018 from 202.1 million in the previous year, partially offset by increases in Americans covered by Medicare and Medicaid.
The increase in uninsured people comes as the growth rate in health care spending rose to 4.6% in 2018 from 4.2% in 2017, though much of that growth in the rate of spending was attributed to the application of a health insurance tax in 2018 that Congress put a moratorium on in the previous year. The tax was part of the Affordable Care Act and was enacted in 2014.
“We see that health care spending reached $3.6 trillion, or $11,172 per person, and spending was faster,” Micah Hartman, statistician in the National Health Statistics Group in the CMS Office of the Actuary, said during a press conference to review the national health expenditure results. “The main reason for the acceleration was faster growth in the net cost of insurance, and that was particularly the case for private health insurance and also for Medicare.”
The net cost of insurance includes nonmedical expenses such as administration, taxes, and fees, as well as gains or losses for private health insurers. The ACA’s health insurance tax generated $14.3 billion in spending, according to Internal Revenue Service data.
Also contributing to the rise in the rate of growth was faster growth in medical prices, “and that was due to underlying economy-wide inflation, as well as the impacts of the tax,” Mr. Hartman said.
Despite this growth in the rate of spending, health care spending as a percentage of GDP fell slightly from 17.9% in 2017 in 17.7%, as the GDP grew faster than health care spending in 2018.
The faster growth in prices more than offset the slightly slower growth in the use and intensity of medical services, CMS reported.
The growth rate on spending on physician and clinical services slowed to 4.1% in 2018 from 4.7% in 2017. Overall spending on physician and clinical services in 2018 reached $725.6 billion and accounted for 20% of overall health care spending.
Spending on hospital services also slowed, but only slightly, dropping to a growth rate of 4.5% from 4.7% during this period. Hospital spending in 2018, at $1.2 trillion, accounted for 33% of overall health care spending.
On a personal level, overall growth in personal health care spending held steady with growth rate of 4.1% in 2018, the same as 2017, though individual components that feed into the figure varied. For example, growth rate in the spending on retail pharmaceuticals rose to 2.5% from 1.4% during this period. Spending on retail pharmaceuticals reached $335 billion and accounted for 9% of overall health care spending.
Another factor in the rising growth rate in spending came from employer-sponsored insurance.
“Growth in health spending by private business was due to faster growth in employer contributions to private health insurance premiums,” Anne B. Martin, economist in the National Health Statistics Group, said during the press conference. There also was faster growth in spending by the federal government, “driven mainly by faster growth in the federally funded portions of Medicare and Medicaid.”
Spending by private health insurance grew at a rate of 5.8% and reached $1.2 trillion in 2018. Medicare spending grew by 6.4% and reached $750.2 billion, while Medicaid spending grew 3.0%, reaching $597.4 billion.
SOURCE: Hartman M et al. Health Affairs. 2019. doi: 10.1377/hlthaff.2019.00451
WASHINGTON – The number of uninsured grew in 2018 as the rate of health care spending grew, according to data from the Centers for Medicare & Medicaid Services.
A total of 30.7 million people in the United States were uninsured in 2018 – up 1 million from 2017. It was the second year in a row that the number of uninsured grew by that amount.
The newly uninsured came from the private insurance sector, which saw the number of insured decrease to 200.5 million in 2018 from 202.1 million in the previous year, partially offset by increases in Americans covered by Medicare and Medicaid.
The increase in uninsured people comes as the growth rate in health care spending rose to 4.6% in 2018 from 4.2% in 2017, though much of that growth in the rate of spending was attributed to the application of a health insurance tax in 2018 that Congress put a moratorium on in the previous year. The tax was part of the Affordable Care Act and was enacted in 2014.
“We see that health care spending reached $3.6 trillion, or $11,172 per person, and spending was faster,” Micah Hartman, statistician in the National Health Statistics Group in the CMS Office of the Actuary, said during a press conference to review the national health expenditure results. “The main reason for the acceleration was faster growth in the net cost of insurance, and that was particularly the case for private health insurance and also for Medicare.”
The net cost of insurance includes nonmedical expenses such as administration, taxes, and fees, as well as gains or losses for private health insurers. The ACA’s health insurance tax generated $14.3 billion in spending, according to Internal Revenue Service data.
Also contributing to the rise in the rate of growth was faster growth in medical prices, “and that was due to underlying economy-wide inflation, as well as the impacts of the tax,” Mr. Hartman said.
Despite this growth in the rate of spending, health care spending as a percentage of GDP fell slightly from 17.9% in 2017 in 17.7%, as the GDP grew faster than health care spending in 2018.
The faster growth in prices more than offset the slightly slower growth in the use and intensity of medical services, CMS reported.
The growth rate on spending on physician and clinical services slowed to 4.1% in 2018 from 4.7% in 2017. Overall spending on physician and clinical services in 2018 reached $725.6 billion and accounted for 20% of overall health care spending.
Spending on hospital services also slowed, but only slightly, dropping to a growth rate of 4.5% from 4.7% during this period. Hospital spending in 2018, at $1.2 trillion, accounted for 33% of overall health care spending.
On a personal level, overall growth in personal health care spending held steady with growth rate of 4.1% in 2018, the same as 2017, though individual components that feed into the figure varied. For example, growth rate in the spending on retail pharmaceuticals rose to 2.5% from 1.4% during this period. Spending on retail pharmaceuticals reached $335 billion and accounted for 9% of overall health care spending.
Another factor in the rising growth rate in spending came from employer-sponsored insurance.
“Growth in health spending by private business was due to faster growth in employer contributions to private health insurance premiums,” Anne B. Martin, economist in the National Health Statistics Group, said during the press conference. There also was faster growth in spending by the federal government, “driven mainly by faster growth in the federally funded portions of Medicare and Medicaid.”
Spending by private health insurance grew at a rate of 5.8% and reached $1.2 trillion in 2018. Medicare spending grew by 6.4% and reached $750.2 billion, while Medicaid spending grew 3.0%, reaching $597.4 billion.
SOURCE: Hartman M et al. Health Affairs. 2019. doi: 10.1377/hlthaff.2019.00451
Improving Veteran Care With the Mission Act
NATIONAL HARBOR, MD–The US Department of Veterans Affairs (VA) is in the midst of a significant change in the way it will deliver care to veterans. Agency officials remain optimistic that the change will be for the better, and early indications are positive.
The change is being driven by the VA Maintaining Internal Systems and Strengthening Integrated Outside Networks (Mission) Act of 2018, a bill that opens health services options for veterans and integrates VA-administered care and care from community-based providers.
“This is change that is enhancing their experience in the system, and this is enhancing their options and the quality of the options in the system,” Jennifer MacDonald, MD, chief consultant to the principal deputy undersecretary for health at the VA, said during a December 3 session at the AMSUS 2019 annual meeting. “We need also for our workforce to understand how important they are to us across this degree of change.”
Dr. MacDonald highlighted integration with community-based care, including a community urgent care provision that allows veterans to access urgent care facilities and receive care without the need for prior authorization.
“The important piece about that is that we are also looking at the way this care has been accessed,” she said. “By and large, what we have seen from the data is that veterans are indeed seeking community urgent care at a site close to home. This may be CVS or Walgreens. It may be a stand-alone urgent care with a bit more functionality than those Minute Clinics tend to have. We are seeing veterans typically access care through those sites for those minor concerns and illnesses.”
However, she noted that this type of access does not alter the role the VA plays in administration of health care services.
“We are seeing them come back to VA for the majority of their care and for their core care–when there are serious issues, when insulin needs to be adjusted for diabetes, when there are heart disease medications that need to be refilled–we are seeing veterans not seek out urgent care, but come to us, and that is exactly what we want,” she said. “We want the continuity of care to continue and we want to help guide people to the right care, right place, right time.”
Dr. MacDonald also highlighted the expansion of a program that provides a stipend to caregivers that allows veterans to avoid institutionalization and remain within the community under that caregiver’s (a family or friend) supervision. This will expand by year’s end to Vietnam War-era veterans and within 2 years, to veterans that fall between the Vietnam War-era and the September 11, 2001, terrorist attacks.
“We wanted to do this equitably across all eras of veterans,” she said. “This now gives us that opportunity.”
Telehealth also plays a key role.
“For the first time ever, VA now has what we term ‘anywhere-to-anywhere’ telehealth under the Mission Act, an enormous opportunity for us,” she said. “Since we stretch … from New York City to Guam, we need the opportunity to provide care where it may be difficult to recruit and retain providers wherever veterans choose to live,” she said. “We believe that we should be able to meet people where they are regardless of where they choose to live. That’s an aspirational vision, but it is one we believe is exceptionally important and indeed we are moving toward that.”
These are just the beginning; the full implementation of the act goes out to 2034.
According to Dr. MacDonald, the agency is working hard to engage both veterans and the workforce to keep tabs on how the implementation is going.
“It’s a fundamental change in the day-to-day business that they’ve been doing, sometimes for years, and so extremely important across this change is that we have set up processes and now a joint operations center and a number of forums to hear directly from our front line and make sure that their issues are our issues in central office, in DC here, and that they feel heard and that they know that when they have needs, those needs are actioned,” she said.
The VA, under the Mission Act, is also working hard to engage health care providers in the community, including making VA training to community partners, including training on opioid use, suicide prevent and military culture.
However, all these change are for naught if the veterans are not on board. But so far, Dr. MacDonald said the early feedback is very positive.
She cited a VFW survey that asked a question about the Mission Act changes so far and whether they would recommend the VA to other veterans. Ninety percent of the respondents answered they would.
“That’s our marker that we are getting somewhere with these changes and the way we do business,” she said. “That is what we want to see continue to increase.”
NATIONAL HARBOR, MD–The US Department of Veterans Affairs (VA) is in the midst of a significant change in the way it will deliver care to veterans. Agency officials remain optimistic that the change will be for the better, and early indications are positive.
The change is being driven by the VA Maintaining Internal Systems and Strengthening Integrated Outside Networks (Mission) Act of 2018, a bill that opens health services options for veterans and integrates VA-administered care and care from community-based providers.
“This is change that is enhancing their experience in the system, and this is enhancing their options and the quality of the options in the system,” Jennifer MacDonald, MD, chief consultant to the principal deputy undersecretary for health at the VA, said during a December 3 session at the AMSUS 2019 annual meeting. “We need also for our workforce to understand how important they are to us across this degree of change.”
Dr. MacDonald highlighted integration with community-based care, including a community urgent care provision that allows veterans to access urgent care facilities and receive care without the need for prior authorization.
“The important piece about that is that we are also looking at the way this care has been accessed,” she said. “By and large, what we have seen from the data is that veterans are indeed seeking community urgent care at a site close to home. This may be CVS or Walgreens. It may be a stand-alone urgent care with a bit more functionality than those Minute Clinics tend to have. We are seeing veterans typically access care through those sites for those minor concerns and illnesses.”
However, she noted that this type of access does not alter the role the VA plays in administration of health care services.
“We are seeing them come back to VA for the majority of their care and for their core care–when there are serious issues, when insulin needs to be adjusted for diabetes, when there are heart disease medications that need to be refilled–we are seeing veterans not seek out urgent care, but come to us, and that is exactly what we want,” she said. “We want the continuity of care to continue and we want to help guide people to the right care, right place, right time.”
Dr. MacDonald also highlighted the expansion of a program that provides a stipend to caregivers that allows veterans to avoid institutionalization and remain within the community under that caregiver’s (a family or friend) supervision. This will expand by year’s end to Vietnam War-era veterans and within 2 years, to veterans that fall between the Vietnam War-era and the September 11, 2001, terrorist attacks.
“We wanted to do this equitably across all eras of veterans,” she said. “This now gives us that opportunity.”
Telehealth also plays a key role.
“For the first time ever, VA now has what we term ‘anywhere-to-anywhere’ telehealth under the Mission Act, an enormous opportunity for us,” she said. “Since we stretch … from New York City to Guam, we need the opportunity to provide care where it may be difficult to recruit and retain providers wherever veterans choose to live,” she said. “We believe that we should be able to meet people where they are regardless of where they choose to live. That’s an aspirational vision, but it is one we believe is exceptionally important and indeed we are moving toward that.”
These are just the beginning; the full implementation of the act goes out to 2034.
According to Dr. MacDonald, the agency is working hard to engage both veterans and the workforce to keep tabs on how the implementation is going.
“It’s a fundamental change in the day-to-day business that they’ve been doing, sometimes for years, and so extremely important across this change is that we have set up processes and now a joint operations center and a number of forums to hear directly from our front line and make sure that their issues are our issues in central office, in DC here, and that they feel heard and that they know that when they have needs, those needs are actioned,” she said.
The VA, under the Mission Act, is also working hard to engage health care providers in the community, including making VA training to community partners, including training on opioid use, suicide prevent and military culture.
However, all these change are for naught if the veterans are not on board. But so far, Dr. MacDonald said the early feedback is very positive.
She cited a VFW survey that asked a question about the Mission Act changes so far and whether they would recommend the VA to other veterans. Ninety percent of the respondents answered they would.
“That’s our marker that we are getting somewhere with these changes and the way we do business,” she said. “That is what we want to see continue to increase.”
NATIONAL HARBOR, MD–The US Department of Veterans Affairs (VA) is in the midst of a significant change in the way it will deliver care to veterans. Agency officials remain optimistic that the change will be for the better, and early indications are positive.
The change is being driven by the VA Maintaining Internal Systems and Strengthening Integrated Outside Networks (Mission) Act of 2018, a bill that opens health services options for veterans and integrates VA-administered care and care from community-based providers.
“This is change that is enhancing their experience in the system, and this is enhancing their options and the quality of the options in the system,” Jennifer MacDonald, MD, chief consultant to the principal deputy undersecretary for health at the VA, said during a December 3 session at the AMSUS 2019 annual meeting. “We need also for our workforce to understand how important they are to us across this degree of change.”
Dr. MacDonald highlighted integration with community-based care, including a community urgent care provision that allows veterans to access urgent care facilities and receive care without the need for prior authorization.
“The important piece about that is that we are also looking at the way this care has been accessed,” she said. “By and large, what we have seen from the data is that veterans are indeed seeking community urgent care at a site close to home. This may be CVS or Walgreens. It may be a stand-alone urgent care with a bit more functionality than those Minute Clinics tend to have. We are seeing veterans typically access care through those sites for those minor concerns and illnesses.”
However, she noted that this type of access does not alter the role the VA plays in administration of health care services.
“We are seeing them come back to VA for the majority of their care and for their core care–when there are serious issues, when insulin needs to be adjusted for diabetes, when there are heart disease medications that need to be refilled–we are seeing veterans not seek out urgent care, but come to us, and that is exactly what we want,” she said. “We want the continuity of care to continue and we want to help guide people to the right care, right place, right time.”
Dr. MacDonald also highlighted the expansion of a program that provides a stipend to caregivers that allows veterans to avoid institutionalization and remain within the community under that caregiver’s (a family or friend) supervision. This will expand by year’s end to Vietnam War-era veterans and within 2 years, to veterans that fall between the Vietnam War-era and the September 11, 2001, terrorist attacks.
“We wanted to do this equitably across all eras of veterans,” she said. “This now gives us that opportunity.”
Telehealth also plays a key role.
“For the first time ever, VA now has what we term ‘anywhere-to-anywhere’ telehealth under the Mission Act, an enormous opportunity for us,” she said. “Since we stretch … from New York City to Guam, we need the opportunity to provide care where it may be difficult to recruit and retain providers wherever veterans choose to live,” she said. “We believe that we should be able to meet people where they are regardless of where they choose to live. That’s an aspirational vision, but it is one we believe is exceptionally important and indeed we are moving toward that.”
These are just the beginning; the full implementation of the act goes out to 2034.
According to Dr. MacDonald, the agency is working hard to engage both veterans and the workforce to keep tabs on how the implementation is going.
“It’s a fundamental change in the day-to-day business that they’ve been doing, sometimes for years, and so extremely important across this change is that we have set up processes and now a joint operations center and a number of forums to hear directly from our front line and make sure that their issues are our issues in central office, in DC here, and that they feel heard and that they know that when they have needs, those needs are actioned,” she said.
The VA, under the Mission Act, is also working hard to engage health care providers in the community, including making VA training to community partners, including training on opioid use, suicide prevent and military culture.
However, all these change are for naught if the veterans are not on board. But so far, Dr. MacDonald said the early feedback is very positive.
She cited a VFW survey that asked a question about the Mission Act changes so far and whether they would recommend the VA to other veterans. Ninety percent of the respondents answered they would.
“That’s our marker that we are getting somewhere with these changes and the way we do business,” she said. “That is what we want to see continue to increase.”
Better Planning Needed to Help Veterans During, After Service
NATIONAL HARBOR, MD – More work and planning is needed for veterans after they serve in the Armed Forces, Rep. Brad Wenstrup, MD (R-Ohio), told attendees of the 2019 AMSUS annual meeting.
Rep. Wenstrup, in his December 3 keynote address, suggested that in addition to recruiters asking about what enlistees want to do in the military, they also should be asking what they want to do after military service.
“Let’s plan for that right now because it’s so much better, it’s so much healthier when you have a plan,” he said, noting that many military members struggle when integrating back into civilian life: They don’t have a plan, and they don’t feel “essential” and part of a team the way they did while serving. He pointed to graduating college students who have made plans for their next steps.
“We need to do the same thing for our troops who serve us [and] prepare them for what is next,” he said.
In addition to ensuring the health and well-being of service members when they come home, Rep. Wenstrup also discussed the need to ensure that medical staff are prepared for emergencies, identifying it as one of the challenges of military medicine right now.
“It’s a challenge for a lot in the active component when we are not at war … to sustain those skills, and it is very frustrating to the providers all the way around,” Rep. Wenstrup said. He noted that a lot of military medical staff help keep and refine those skills by working in the trauma department of major city hospitals.
“We are working together to try and bring our military assets, our civilian assets, DEA, whatever we can, together so that we make sure that we can provide and be ready,” he said. “And the importance of building these bridges is key to the future of medicine,” especially in a time of domestic crisis, so that all medical personnel, civilian and military, can work together for the common good of providing that service. “These are bridges we have to build.”
Rep. Wenstrup also talked about the need to do more to ensure a healthier population.
“The key is how do we live healthier, longer, because that is the real savings. A healthy nation is a stronger nation,” he said.
When comparing the amounts paid to providers for surgery with those paid for health and wellness, he contended that high payments for surgeons are due to the high skill set required for difficult procedures. However, health and wellness providers are paid poorly, as is payment for the management of chronic illness. “We don’t pay very well to the doctor who works with the patient and prevents the need to do open heart surgery,” he said. “Let’s start looking at that. Let’s start keeping people healthier longer.”
gtwachtman@mdedge.com
NATIONAL HARBOR, MD – More work and planning is needed for veterans after they serve in the Armed Forces, Rep. Brad Wenstrup, MD (R-Ohio), told attendees of the 2019 AMSUS annual meeting.
Rep. Wenstrup, in his December 3 keynote address, suggested that in addition to recruiters asking about what enlistees want to do in the military, they also should be asking what they want to do after military service.
“Let’s plan for that right now because it’s so much better, it’s so much healthier when you have a plan,” he said, noting that many military members struggle when integrating back into civilian life: They don’t have a plan, and they don’t feel “essential” and part of a team the way they did while serving. He pointed to graduating college students who have made plans for their next steps.
“We need to do the same thing for our troops who serve us [and] prepare them for what is next,” he said.
In addition to ensuring the health and well-being of service members when they come home, Rep. Wenstrup also discussed the need to ensure that medical staff are prepared for emergencies, identifying it as one of the challenges of military medicine right now.
“It’s a challenge for a lot in the active component when we are not at war … to sustain those skills, and it is very frustrating to the providers all the way around,” Rep. Wenstrup said. He noted that a lot of military medical staff help keep and refine those skills by working in the trauma department of major city hospitals.
“We are working together to try and bring our military assets, our civilian assets, DEA, whatever we can, together so that we make sure that we can provide and be ready,” he said. “And the importance of building these bridges is key to the future of medicine,” especially in a time of domestic crisis, so that all medical personnel, civilian and military, can work together for the common good of providing that service. “These are bridges we have to build.”
Rep. Wenstrup also talked about the need to do more to ensure a healthier population.
“The key is how do we live healthier, longer, because that is the real savings. A healthy nation is a stronger nation,” he said.
When comparing the amounts paid to providers for surgery with those paid for health and wellness, he contended that high payments for surgeons are due to the high skill set required for difficult procedures. However, health and wellness providers are paid poorly, as is payment for the management of chronic illness. “We don’t pay very well to the doctor who works with the patient and prevents the need to do open heart surgery,” he said. “Let’s start looking at that. Let’s start keeping people healthier longer.”
gtwachtman@mdedge.com
NATIONAL HARBOR, MD – More work and planning is needed for veterans after they serve in the Armed Forces, Rep. Brad Wenstrup, MD (R-Ohio), told attendees of the 2019 AMSUS annual meeting.
Rep. Wenstrup, in his December 3 keynote address, suggested that in addition to recruiters asking about what enlistees want to do in the military, they also should be asking what they want to do after military service.
“Let’s plan for that right now because it’s so much better, it’s so much healthier when you have a plan,” he said, noting that many military members struggle when integrating back into civilian life: They don’t have a plan, and they don’t feel “essential” and part of a team the way they did while serving. He pointed to graduating college students who have made plans for their next steps.
“We need to do the same thing for our troops who serve us [and] prepare them for what is next,” he said.
In addition to ensuring the health and well-being of service members when they come home, Rep. Wenstrup also discussed the need to ensure that medical staff are prepared for emergencies, identifying it as one of the challenges of military medicine right now.
“It’s a challenge for a lot in the active component when we are not at war … to sustain those skills, and it is very frustrating to the providers all the way around,” Rep. Wenstrup said. He noted that a lot of military medical staff help keep and refine those skills by working in the trauma department of major city hospitals.
“We are working together to try and bring our military assets, our civilian assets, DEA, whatever we can, together so that we make sure that we can provide and be ready,” he said. “And the importance of building these bridges is key to the future of medicine,” especially in a time of domestic crisis, so that all medical personnel, civilian and military, can work together for the common good of providing that service. “These are bridges we have to build.”
Rep. Wenstrup also talked about the need to do more to ensure a healthier population.
“The key is how do we live healthier, longer, because that is the real savings. A healthy nation is a stronger nation,” he said.
When comparing the amounts paid to providers for surgery with those paid for health and wellness, he contended that high payments for surgeons are due to the high skill set required for difficult procedures. However, health and wellness providers are paid poorly, as is payment for the management of chronic illness. “We don’t pay very well to the doctor who works with the patient and prevents the need to do open heart surgery,” he said. “Let’s start looking at that. Let’s start keeping people healthier longer.”
gtwachtman@mdedge.com
Quantifying the EHR connection to burnout
While plenty of anecdotal and other evidence exists to connect the use of electronic health records to physician burnout, new research puts a more standard, quantifiable measure to it in an effort to help measure progress in improving the usability of EHRs.
Researchers used the System Usability Scale (SUS), “favored as an industry standard as a short, simple, and reliable measurement of technology usability with solid benchmarks to easily interpret its results, as the measure in this research, Edward Melnick, MD, of Yale University, New Haven, Conn., and colleagues wrote in Mayo Clinic Proceedings.
“The previous studies have definitely hinted at [the link between EHRs and burnout], but never really quantified it,” Dr. Melnick said in an interview.
Among the 870 physicians evaluating their EHRs’ usability, the mean score on a scale of 0-100 (higher being more usable) was 45.9. As a point of comparison, Microsoft Excel has an SUS score of 57, digital video recorders score 74, Amazon scores 82, microwave ovens score 87, and Google search scores 93.
“A score of 45.9 is in the bottom 9% of usability scores across studies in other industries and is categorized as in the ‘not acceptable’ range with a grade of F,” the authors wrote. “In aggregate, 733 of 870 (84.2%) of respondents rated their EHR less than 68 on the SUS, the average score across industries.”
In tying the SUS results to burnout, which was measured using the Maslach Burnout Inventory, the authors noted that the scores “were strongly and independently associated with physician burnout in a dose-response relationship. The odds of burnout were lower for each 1 point more favorable SUS score, a finding that persisted after adjusting for an extensive array of other personal and professional characteristics. The relationship between SUS score and burnout also persisted when emotional exhaustion and depersonalization were treated as continuous variables.”
The authors did note that, despite the strong relationship, they could not determine a causation given the cross-sectional nature of the data.
“I’m hoping that this paper will spark conversation and drive change and be a way of tracking improvements,” Dr. Melnick said. “So, if you bring in something new and say this is going to be better, how do you know it is going to be better? Well maybe you measure it using the System Usability Scale” to give it a quantifiable measure of improvement. He said it is an advantage “of having a metric that has been standardized and used in other industries,” allowing EHR stakeholders to measure improvement. “Once you can measure it, you can manage it and make improvements faster.”
The findings “will not come as a surprise to anyone who practices medicine,” Patrice Harris, MD, president of the American Medical Association, said in a statement. “It is a national imperative to overhaul the design and use of EHRs and reframe the technology to focus primarily on its most critical function: helping physicians care for patients. Significantly enhancing EHR usability is key and the AMA is working to ensure a new generation of EHRs are designed to prioritize time with patients, rather than overload physicians with type-and-click tasks.”
Funding for the study was provided by the Stanford Medicine WebMD Center, AMA, and the Mayo Clinic Department of Medicine Program on Physician Well-Being. No conflicts of interest were reported by the authors.
SOURCE: Melnick E et al. Mayo Clinic Proceedings 2019 Nov 14. doi: 10.1016/j.mayocp.2019.09.024.
While plenty of anecdotal and other evidence exists to connect the use of electronic health records to physician burnout, new research puts a more standard, quantifiable measure to it in an effort to help measure progress in improving the usability of EHRs.
Researchers used the System Usability Scale (SUS), “favored as an industry standard as a short, simple, and reliable measurement of technology usability with solid benchmarks to easily interpret its results, as the measure in this research, Edward Melnick, MD, of Yale University, New Haven, Conn., and colleagues wrote in Mayo Clinic Proceedings.
“The previous studies have definitely hinted at [the link between EHRs and burnout], but never really quantified it,” Dr. Melnick said in an interview.
Among the 870 physicians evaluating their EHRs’ usability, the mean score on a scale of 0-100 (higher being more usable) was 45.9. As a point of comparison, Microsoft Excel has an SUS score of 57, digital video recorders score 74, Amazon scores 82, microwave ovens score 87, and Google search scores 93.
“A score of 45.9 is in the bottom 9% of usability scores across studies in other industries and is categorized as in the ‘not acceptable’ range with a grade of F,” the authors wrote. “In aggregate, 733 of 870 (84.2%) of respondents rated their EHR less than 68 on the SUS, the average score across industries.”
In tying the SUS results to burnout, which was measured using the Maslach Burnout Inventory, the authors noted that the scores “were strongly and independently associated with physician burnout in a dose-response relationship. The odds of burnout were lower for each 1 point more favorable SUS score, a finding that persisted after adjusting for an extensive array of other personal and professional characteristics. The relationship between SUS score and burnout also persisted when emotional exhaustion and depersonalization were treated as continuous variables.”
The authors did note that, despite the strong relationship, they could not determine a causation given the cross-sectional nature of the data.
“I’m hoping that this paper will spark conversation and drive change and be a way of tracking improvements,” Dr. Melnick said. “So, if you bring in something new and say this is going to be better, how do you know it is going to be better? Well maybe you measure it using the System Usability Scale” to give it a quantifiable measure of improvement. He said it is an advantage “of having a metric that has been standardized and used in other industries,” allowing EHR stakeholders to measure improvement. “Once you can measure it, you can manage it and make improvements faster.”
The findings “will not come as a surprise to anyone who practices medicine,” Patrice Harris, MD, president of the American Medical Association, said in a statement. “It is a national imperative to overhaul the design and use of EHRs and reframe the technology to focus primarily on its most critical function: helping physicians care for patients. Significantly enhancing EHR usability is key and the AMA is working to ensure a new generation of EHRs are designed to prioritize time with patients, rather than overload physicians with type-and-click tasks.”
Funding for the study was provided by the Stanford Medicine WebMD Center, AMA, and the Mayo Clinic Department of Medicine Program on Physician Well-Being. No conflicts of interest were reported by the authors.
SOURCE: Melnick E et al. Mayo Clinic Proceedings 2019 Nov 14. doi: 10.1016/j.mayocp.2019.09.024.
While plenty of anecdotal and other evidence exists to connect the use of electronic health records to physician burnout, new research puts a more standard, quantifiable measure to it in an effort to help measure progress in improving the usability of EHRs.
Researchers used the System Usability Scale (SUS), “favored as an industry standard as a short, simple, and reliable measurement of technology usability with solid benchmarks to easily interpret its results, as the measure in this research, Edward Melnick, MD, of Yale University, New Haven, Conn., and colleagues wrote in Mayo Clinic Proceedings.
“The previous studies have definitely hinted at [the link between EHRs and burnout], but never really quantified it,” Dr. Melnick said in an interview.
Among the 870 physicians evaluating their EHRs’ usability, the mean score on a scale of 0-100 (higher being more usable) was 45.9. As a point of comparison, Microsoft Excel has an SUS score of 57, digital video recorders score 74, Amazon scores 82, microwave ovens score 87, and Google search scores 93.
“A score of 45.9 is in the bottom 9% of usability scores across studies in other industries and is categorized as in the ‘not acceptable’ range with a grade of F,” the authors wrote. “In aggregate, 733 of 870 (84.2%) of respondents rated their EHR less than 68 on the SUS, the average score across industries.”
In tying the SUS results to burnout, which was measured using the Maslach Burnout Inventory, the authors noted that the scores “were strongly and independently associated with physician burnout in a dose-response relationship. The odds of burnout were lower for each 1 point more favorable SUS score, a finding that persisted after adjusting for an extensive array of other personal and professional characteristics. The relationship between SUS score and burnout also persisted when emotional exhaustion and depersonalization were treated as continuous variables.”
The authors did note that, despite the strong relationship, they could not determine a causation given the cross-sectional nature of the data.
“I’m hoping that this paper will spark conversation and drive change and be a way of tracking improvements,” Dr. Melnick said. “So, if you bring in something new and say this is going to be better, how do you know it is going to be better? Well maybe you measure it using the System Usability Scale” to give it a quantifiable measure of improvement. He said it is an advantage “of having a metric that has been standardized and used in other industries,” allowing EHR stakeholders to measure improvement. “Once you can measure it, you can manage it and make improvements faster.”
The findings “will not come as a surprise to anyone who practices medicine,” Patrice Harris, MD, president of the American Medical Association, said in a statement. “It is a national imperative to overhaul the design and use of EHRs and reframe the technology to focus primarily on its most critical function: helping physicians care for patients. Significantly enhancing EHR usability is key and the AMA is working to ensure a new generation of EHRs are designed to prioritize time with patients, rather than overload physicians with type-and-click tasks.”
Funding for the study was provided by the Stanford Medicine WebMD Center, AMA, and the Mayo Clinic Department of Medicine Program on Physician Well-Being. No conflicts of interest were reported by the authors.
SOURCE: Melnick E et al. Mayo Clinic Proceedings 2019 Nov 14. doi: 10.1016/j.mayocp.2019.09.024.
FROM MAYO CLINIC PROCEEDINGS
CMS announces application process for Direct Contracting model
The Centers for Medicare & Medicaid Services will be accepting letters of intent from physician practices interested in participating in the Direct Contracting model, a new payment model aimed at practices serving at least 5,000 Medicare beneficiaries.

First announced in April 2019, the Direct Contracting program is an advanced alternative payment model designed for organizations that are ready to take on more financial risk and have experience managing large populations through accountable care organizations or working with Medicare Advantage plans.
Interested practices will be able to choose from the Professional population-based payment, which has a lower risk-sharing arrangement (50% savings/losses), and the Global model, which offers a 100% savings/loss risk-sharing arrangement.
“The payment model options available under Direct Contracting aim to reduce expenditures while preserving or enhancing quality of care for beneficiaries,” agency officials said on a web page detailing information for the payment model.
The model offers a prospectively determined and predictable revenue stream for participants and aims to transform risk-sharing arrangements through capitated and partially capitated population-based payments, open up participation in alternative payment models to more physicians, and reduce clinician burden by using smaller sets of quality measures and waivers to help facilitate the delivery of care.
Letters of intent are due to the agency by Dec. 10. CMS noted that submission of a letter of intent will not bind the organization to participating in the program.
The Centers for Medicare & Medicaid Services will be accepting letters of intent from physician practices interested in participating in the Direct Contracting model, a new payment model aimed at practices serving at least 5,000 Medicare beneficiaries.
First announced in April 2019, the Direct Contracting program is an advanced alternative payment model designed for organizations that are ready to take on more financial risk and have experience managing large populations through accountable care organizations or working with Medicare Advantage plans.
Interested practices will be able to choose from the Professional population-based payment, which has a lower risk-sharing arrangement (50% savings/losses), and the Global model, which offers a 100% savings/loss risk-sharing arrangement.
“The payment model options available under Direct Contracting aim to reduce expenditures while preserving or enhancing quality of care for beneficiaries,” agency officials said on a web page detailing information for the payment model.
The model offers a prospectively determined and predictable revenue stream for participants and aims to transform risk-sharing arrangements through capitated and partially capitated population-based payments, open up participation in alternative payment models to more physicians, and reduce clinician burden by using smaller sets of quality measures and waivers to help facilitate the delivery of care.
Letters of intent are due to the agency by Dec. 10. CMS noted that submission of a letter of intent will not bind the organization to participating in the program.
The Centers for Medicare & Medicaid Services will be accepting letters of intent from physician practices interested in participating in the Direct Contracting model, a new payment model aimed at practices serving at least 5,000 Medicare beneficiaries.
First announced in April 2019, the Direct Contracting program is an advanced alternative payment model designed for organizations that are ready to take on more financial risk and have experience managing large populations through accountable care organizations or working with Medicare Advantage plans.
Interested practices will be able to choose from the Professional population-based payment, which has a lower risk-sharing arrangement (50% savings/losses), and the Global model, which offers a 100% savings/loss risk-sharing arrangement.
“The payment model options available under Direct Contracting aim to reduce expenditures while preserving or enhancing quality of care for beneficiaries,” agency officials said on a web page detailing information for the payment model.
The model offers a prospectively determined and predictable revenue stream for participants and aims to transform risk-sharing arrangements through capitated and partially capitated population-based payments, open up participation in alternative payment models to more physicians, and reduce clinician burden by using smaller sets of quality measures and waivers to help facilitate the delivery of care.
Letters of intent are due to the agency by Dec. 10. CMS noted that submission of a letter of intent will not bind the organization to participating in the program.
ASCO releases revised version of its Patient-Centered Oncology Payment model
The American Society of Clinical Oncology has made some adjustments to its Patient-Centered Oncology Payment (PCOP) advanced alternative payment model and will now be looking to gain approval from the Physician-Focused Payment Model Technical Advisory Committee (PTAC).

PTAC reviews physician-developed advanced alternative payment models and sends those APMs that are approved to the Centers for Medicare & Medicaid Services’ Center for Medicare & Medicaid Innovation (CMMI) to determine if there will be further testing and possible implementation for use by physicians as part of the APM track of the Quality Payment Program.
Even if approved by PTAC, the ASCO model faces an uphill battle. CMS already has its own Oncology Care Model (OCM), and given the agency’s track record of not testing APMs that have been approved by PTAC, the deck may be stacked against ASCO in terms of getting its model into Medicare.
But officials at ASCO are hoping a PTAC vetting and approval will open the door to its implementation by commercial payers.
“We are now ready to take this to PTAC,” Jeffery Ward, MD, past chair of ASCO’s government relations committee, said in an interview. “I don’t expect any trouble getting through PTAC. The other question is whether CMMI would decide to actually test a model like this, and so far, they have seemed pretty much a one-trick pony, as in they’ve got their Oncology Care Model and they are going to run with it.”
However, Dr. Ward, a medical oncologist at Swedish Cancer Institute of Edmonds, Wash., said that PCOP has been designed with the commercial market in mind and the PTAC recommendation will help validate the model and make it more appealing to commercial payers.
A key feature of the adjusted payment model is that it has taken a lesson learned from CMS’s Oncology Care Model in terms of how to account for the price of drugs. Including the price of drugs in a value-based payment model – the approach taken by the OCM – creates too much variability, Dr. Ward noted. He used lung cancer as an example, noting that the type of lung cancer could have more of an impact on physician spending than any specific treatment decisions a physician can make because the treatment choices may not be there.
“When that happens, whether you are successful or not depends on the luck of the draw instead of the choices you make,” he said.
In an effort not to penalize practices because of their patient mix, PCOP takes the cost of drugs out of the value mix.
“What this model does is it doesn’t hold practices responsible for the cost of the drugs. It holds them responsible for how they utilize the drugs,” he said. “It really begins to make me responsible for making value-based decisions as opposed to just getting lucky and having a cheaper panel of patients.”
Overall, Dr. Ward described the PCOP model as accomplishing the goals of CMS’s APMs by encouraging physicians to treat patients through high-value treatments.
“This model does that by including quality measures that play a role in how much you get paid,” he said. “There are pathways that are value-based pathways and your ability to follow those pathways plays a role in how much you get paid. The amount of care that you send to the ER or the hospital plays a role in how much you get paid. Those things are then used in adjusting what is our fee-for-service model of medicine. So you are still getting paid a base rate based on the care that you give on a fee-for-service model, but that gets adjusted up or down depending on those other characteristics.”
But for the model to have the biggest impact, it needs to be adopted by all payers in a given state or region and used by all physicians, who by the design of the payment model, will have a role in shaping the implementation details.
Savings could come from lower administrative costs at the physician office because there would be no need for separate contracts between payers, something that could generate savings of up to 8%, compared with the current system, Dr. Ward noted.
“This is designed to be a multipayer and multipractice initiative,” he said. “In its grandest form, a state or states would implement this and it would be participated in by all the oncology practices and all of the payers.”
The American Society of Clinical Oncology has made some adjustments to its Patient-Centered Oncology Payment (PCOP) advanced alternative payment model and will now be looking to gain approval from the Physician-Focused Payment Model Technical Advisory Committee (PTAC).
PTAC reviews physician-developed advanced alternative payment models and sends those APMs that are approved to the Centers for Medicare & Medicaid Services’ Center for Medicare & Medicaid Innovation (CMMI) to determine if there will be further testing and possible implementation for use by physicians as part of the APM track of the Quality Payment Program.
Even if approved by PTAC, the ASCO model faces an uphill battle. CMS already has its own Oncology Care Model (OCM), and given the agency’s track record of not testing APMs that have been approved by PTAC, the deck may be stacked against ASCO in terms of getting its model into Medicare.
But officials at ASCO are hoping a PTAC vetting and approval will open the door to its implementation by commercial payers.
“We are now ready to take this to PTAC,” Jeffery Ward, MD, past chair of ASCO’s government relations committee, said in an interview. “I don’t expect any trouble getting through PTAC. The other question is whether CMMI would decide to actually test a model like this, and so far, they have seemed pretty much a one-trick pony, as in they’ve got their Oncology Care Model and they are going to run with it.”
However, Dr. Ward, a medical oncologist at Swedish Cancer Institute of Edmonds, Wash., said that PCOP has been designed with the commercial market in mind and the PTAC recommendation will help validate the model and make it more appealing to commercial payers.
A key feature of the adjusted payment model is that it has taken a lesson learned from CMS’s Oncology Care Model in terms of how to account for the price of drugs. Including the price of drugs in a value-based payment model – the approach taken by the OCM – creates too much variability, Dr. Ward noted. He used lung cancer as an example, noting that the type of lung cancer could have more of an impact on physician spending than any specific treatment decisions a physician can make because the treatment choices may not be there.
“When that happens, whether you are successful or not depends on the luck of the draw instead of the choices you make,” he said.
In an effort not to penalize practices because of their patient mix, PCOP takes the cost of drugs out of the value mix.
“What this model does is it doesn’t hold practices responsible for the cost of the drugs. It holds them responsible for how they utilize the drugs,” he said. “It really begins to make me responsible for making value-based decisions as opposed to just getting lucky and having a cheaper panel of patients.”
Overall, Dr. Ward described the PCOP model as accomplishing the goals of CMS’s APMs by encouraging physicians to treat patients through high-value treatments.
“This model does that by including quality measures that play a role in how much you get paid,” he said. “There are pathways that are value-based pathways and your ability to follow those pathways plays a role in how much you get paid. The amount of care that you send to the ER or the hospital plays a role in how much you get paid. Those things are then used in adjusting what is our fee-for-service model of medicine. So you are still getting paid a base rate based on the care that you give on a fee-for-service model, but that gets adjusted up or down depending on those other characteristics.”
But for the model to have the biggest impact, it needs to be adopted by all payers in a given state or region and used by all physicians, who by the design of the payment model, will have a role in shaping the implementation details.
Savings could come from lower administrative costs at the physician office because there would be no need for separate contracts between payers, something that could generate savings of up to 8%, compared with the current system, Dr. Ward noted.
“This is designed to be a multipayer and multipractice initiative,” he said. “In its grandest form, a state or states would implement this and it would be participated in by all the oncology practices and all of the payers.”
The American Society of Clinical Oncology has made some adjustments to its Patient-Centered Oncology Payment (PCOP) advanced alternative payment model and will now be looking to gain approval from the Physician-Focused Payment Model Technical Advisory Committee (PTAC).
PTAC reviews physician-developed advanced alternative payment models and sends those APMs that are approved to the Centers for Medicare & Medicaid Services’ Center for Medicare & Medicaid Innovation (CMMI) to determine if there will be further testing and possible implementation for use by physicians as part of the APM track of the Quality Payment Program.
Even if approved by PTAC, the ASCO model faces an uphill battle. CMS already has its own Oncology Care Model (OCM), and given the agency’s track record of not testing APMs that have been approved by PTAC, the deck may be stacked against ASCO in terms of getting its model into Medicare.
But officials at ASCO are hoping a PTAC vetting and approval will open the door to its implementation by commercial payers.
“We are now ready to take this to PTAC,” Jeffery Ward, MD, past chair of ASCO’s government relations committee, said in an interview. “I don’t expect any trouble getting through PTAC. The other question is whether CMMI would decide to actually test a model like this, and so far, they have seemed pretty much a one-trick pony, as in they’ve got their Oncology Care Model and they are going to run with it.”
However, Dr. Ward, a medical oncologist at Swedish Cancer Institute of Edmonds, Wash., said that PCOP has been designed with the commercial market in mind and the PTAC recommendation will help validate the model and make it more appealing to commercial payers.
A key feature of the adjusted payment model is that it has taken a lesson learned from CMS’s Oncology Care Model in terms of how to account for the price of drugs. Including the price of drugs in a value-based payment model – the approach taken by the OCM – creates too much variability, Dr. Ward noted. He used lung cancer as an example, noting that the type of lung cancer could have more of an impact on physician spending than any specific treatment decisions a physician can make because the treatment choices may not be there.
“When that happens, whether you are successful or not depends on the luck of the draw instead of the choices you make,” he said.
In an effort not to penalize practices because of their patient mix, PCOP takes the cost of drugs out of the value mix.
“What this model does is it doesn’t hold practices responsible for the cost of the drugs. It holds them responsible for how they utilize the drugs,” he said. “It really begins to make me responsible for making value-based decisions as opposed to just getting lucky and having a cheaper panel of patients.”
Overall, Dr. Ward described the PCOP model as accomplishing the goals of CMS’s APMs by encouraging physicians to treat patients through high-value treatments.
“This model does that by including quality measures that play a role in how much you get paid,” he said. “There are pathways that are value-based pathways and your ability to follow those pathways plays a role in how much you get paid. The amount of care that you send to the ER or the hospital plays a role in how much you get paid. Those things are then used in adjusting what is our fee-for-service model of medicine. So you are still getting paid a base rate based on the care that you give on a fee-for-service model, but that gets adjusted up or down depending on those other characteristics.”
But for the model to have the biggest impact, it needs to be adopted by all payers in a given state or region and used by all physicians, who by the design of the payment model, will have a role in shaping the implementation details.
Savings could come from lower administrative costs at the physician office because there would be no need for separate contracts between payers, something that could generate savings of up to 8%, compared with the current system, Dr. Ward noted.
“This is designed to be a multipayer and multipractice initiative,” he said. “In its grandest form, a state or states would implement this and it would be participated in by all the oncology practices and all of the payers.”