User login
Bryn Nelson is a former PhD microbiologist who decided he’d much rather write about microbes than mutate them. After seven years at the science desk of Newsday in New York, Nelson relocated to Seattle as a freelancer, where he has consumed far too much coffee and written features and stories for The Hospitalist, The New York Times, Nature, Scientific American, Science News for Students, Mosaic and many other print and online publications. In addition, he contributed a chapter to The Science Writers’ Handbook and edited two chapters for the six-volume Modernist Cuisine: The Art and Science of Cooking.
Paid For Being Special

It’s official. I am a “recognized” hospitalist. I’m certified. I’m special.
Although I’ve always felt that HM was special, that it’s a field with its own defined body of knowledge, area of expertise, and dedicated providers, it is now official. It is special; I am special. I got the letter in the mail the other day to prove it.
The correspondence arrived in an important-looking white envelope, with a return address stamped with the “American Board of Internal Medicine” insignia. The letter itself congratulated me on becoming a member of the first class of internists to complete their Maintenance of Certification (MOC) with Recognition of Focused Practice in Hospital Medicine (FPHM). As you’ve no doubt heard, the ABIM developed this MOC process to recognize hospitalists who’ve been in practice for at least three years after their initial certification in internal medicine (IM).
This is the first ABIM certification program that recognizes physician expertise in a field that is not tied directly to either residency or specialty fellowship training. In other words, unlike the cardiology certification exam, which requires a physician to have completed a fellowship training program, the FPHM allows for clinical experience to substitute for fellowship training. While the FPHM does not confer true “specialty status” (like the cardiology certification exam does), it does, as the moniker implies, recognize that we have focused our practice.
Implicit within that is the understanding that this focus brings with it a level of expertise that distinguishes hospitalists from nonhospitalists. This is a massive step forward for HM, as it lends significant credibility to the work we do and helps the public better understand what a hospitalist is and does. Most important, it helps set apart that cadre of true hospitalists who are dedicating their careers to fundamentally improving the care and outcomes of hospitalized patients.
It is this last point that came to mind as I reviewed this month’s cover story on value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” p. 1).
Sticky Yet Crucial Point
One of the sticking points that I’ve heard from some hospitalists is that the FPHM requires a three-year cycle of self-evaluation. For those new to this process, let’s clear up some of the nomenclature. When IM residents graduate, they are eligible to sit for the ABIM certification exam. Upon passage, they are board-certified internists and can choose to enter into the maintenance of certification process. This is a 10-year process whereby diplomates (ABIM-speak for those certified as a specialist, with a diploma in medicine; not to be confused with a diplomat—a person who conducts negotiations and maintains political rest through the tactful handling of delicate situations, something perhaps more appropriate to the bulk of patient situations we encounter) must complete self-evaluation of medical knowledge modules, self-evaluation of practice performance, and ultimately a secure exam. This is where the FPHM differs.
The 10-year cycle for MOC is maintained for FPHM, such that diplomates only recertify every 10 years. However, the self-evaluation must occur every three years to maintain one’s certification. In other words, fail to keep up with the self-evaluation process, and your FPHM is revoked. This is different than the MOC for IM, and it is why some hospitalists are choosing not to enroll in the FPHM. This is a mistake.
Unnecessary Burden?
For many hospitalists, this extra evaluation, especially the practice improvement, is seen as an undue burden. Why is it that hospitalists should have to do more frequent self-evaluation than other specialists? My answer is that this is an important part of what defines our hospitalist specialty—that is, our ability to go beyond the individual patient encounter to fundamentally improve outcomes for the patients under our care. This is not done through “good doctoring.” Hospitalists are not necessarily better doctors than nonhospitalists. Rather, we have embodied a commitment to process and quality improvement within the hospital. This is what our patients need from us. This is what makes us hospitalists. This is what makes us special.
And this brings me back to value-based purchasing.
The Next Phase: Purchasing Value
For those of you, like me, who struggle to comprehend what buying value actually means, take a few minutes to peruse Bryn Nelson’s cover story this month. Not only will it help you understand the healthcare reform bill, it will help you understand the future of our field. I’ve personally witnessed HM traverse three distinct phases.
In the late 1990s and early 2000s, HM growth was driven by the need to improve efficiency. In most ways, this was code for reducing costs. Hospital executives recognized that hospitalists could reduce the overall costs of a patient admission, thus turning the balance of the prospective payment into profit. In other words, the amount of money a hospital receives for a patient stay is most often fixed and determined up front (prospectively), such that more efficiently moving patients through the system equates to more profit (or less loss).
This growth phase was quickly supplanted by the volume phase—a phase that was driven by the relative departure of primary-care physicians and subspecialists from the hospital. Although some of these doctors still admit their own patients, most of them now take advantage of hospitalist programs to focus their own practice to the outpatient or procedural arenas. Effectively, many of the other doctors have left the house, and hospitalists have had to back-fill this patient volume. To a certain degree, we are all still filling this need.
Connect the Dots
However, it is clear that the next HM driver is going to be quality. And it is programs like VBP that will drive it. Essentially, VBP means that hospitals will be competing with each other to be the best. By best, I mean “most able” to achieve pre-determined quality, safety, and patient-satisfaction indicators. By competing, I mean the reimbursement pie is fixed and those who achieve will get more, and those who fall short will get less.
When you consider that as much as 2% of a hospital’s Medicare reimbursement will soon be at risk, we are talking about millions of dollars per hospital per year. To hospitals with a 1% to 2% profit margin, this is the difference between being in or out of business. It also is interestingly close to the amount of support most hospitals give their HM groups; the exact groups that touch the majority of the patients that will determine their VBP outcomes. Connect the dots, and you can see that your hospitalist group—indeed, your paycheck—is very much at risk.
Which brings me back to the FPHM. In a serendipitous turn of events, the FPHM not only recognizes hospitalists as “special,” but, more important, it also gives us the opportunity to simultaneously enhance both our patients’ outcomes and our compensation. If we get this right, the every-three-year improvement projects required to maintain your certification are exactly the type of work you’ll need to be doing to achieve the outcomes your hospital needs to maintain its Medicare payments. In turn, this will ensure your group maintains its hospital support, and you, your paycheck.
It’s the kind of work that will ensure the best possible outcomes for our patients. And in the end, that, more than an ABIM certificate, is what truly makes us special. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
It’s official. I am a “recognized” hospitalist. I’m certified. I’m special.
Although I’ve always felt that HM was special, that it’s a field with its own defined body of knowledge, area of expertise, and dedicated providers, it is now official. It is special; I am special. I got the letter in the mail the other day to prove it.
The correspondence arrived in an important-looking white envelope, with a return address stamped with the “American Board of Internal Medicine” insignia. The letter itself congratulated me on becoming a member of the first class of internists to complete their Maintenance of Certification (MOC) with Recognition of Focused Practice in Hospital Medicine (FPHM). As you’ve no doubt heard, the ABIM developed this MOC process to recognize hospitalists who’ve been in practice for at least three years after their initial certification in internal medicine (IM).
This is the first ABIM certification program that recognizes physician expertise in a field that is not tied directly to either residency or specialty fellowship training. In other words, unlike the cardiology certification exam, which requires a physician to have completed a fellowship training program, the FPHM allows for clinical experience to substitute for fellowship training. While the FPHM does not confer true “specialty status” (like the cardiology certification exam does), it does, as the moniker implies, recognize that we have focused our practice.
Implicit within that is the understanding that this focus brings with it a level of expertise that distinguishes hospitalists from nonhospitalists. This is a massive step forward for HM, as it lends significant credibility to the work we do and helps the public better understand what a hospitalist is and does. Most important, it helps set apart that cadre of true hospitalists who are dedicating their careers to fundamentally improving the care and outcomes of hospitalized patients.
It is this last point that came to mind as I reviewed this month’s cover story on value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” p. 1).
Sticky Yet Crucial Point
One of the sticking points that I’ve heard from some hospitalists is that the FPHM requires a three-year cycle of self-evaluation. For those new to this process, let’s clear up some of the nomenclature. When IM residents graduate, they are eligible to sit for the ABIM certification exam. Upon passage, they are board-certified internists and can choose to enter into the maintenance of certification process. This is a 10-year process whereby diplomates (ABIM-speak for those certified as a specialist, with a diploma in medicine; not to be confused with a diplomat—a person who conducts negotiations and maintains political rest through the tactful handling of delicate situations, something perhaps more appropriate to the bulk of patient situations we encounter) must complete self-evaluation of medical knowledge modules, self-evaluation of practice performance, and ultimately a secure exam. This is where the FPHM differs.
The 10-year cycle for MOC is maintained for FPHM, such that diplomates only recertify every 10 years. However, the self-evaluation must occur every three years to maintain one’s certification. In other words, fail to keep up with the self-evaluation process, and your FPHM is revoked. This is different than the MOC for IM, and it is why some hospitalists are choosing not to enroll in the FPHM. This is a mistake.
Unnecessary Burden?
For many hospitalists, this extra evaluation, especially the practice improvement, is seen as an undue burden. Why is it that hospitalists should have to do more frequent self-evaluation than other specialists? My answer is that this is an important part of what defines our hospitalist specialty—that is, our ability to go beyond the individual patient encounter to fundamentally improve outcomes for the patients under our care. This is not done through “good doctoring.” Hospitalists are not necessarily better doctors than nonhospitalists. Rather, we have embodied a commitment to process and quality improvement within the hospital. This is what our patients need from us. This is what makes us hospitalists. This is what makes us special.
And this brings me back to value-based purchasing.
The Next Phase: Purchasing Value
For those of you, like me, who struggle to comprehend what buying value actually means, take a few minutes to peruse Bryn Nelson’s cover story this month. Not only will it help you understand the healthcare reform bill, it will help you understand the future of our field. I’ve personally witnessed HM traverse three distinct phases.
In the late 1990s and early 2000s, HM growth was driven by the need to improve efficiency. In most ways, this was code for reducing costs. Hospital executives recognized that hospitalists could reduce the overall costs of a patient admission, thus turning the balance of the prospective payment into profit. In other words, the amount of money a hospital receives for a patient stay is most often fixed and determined up front (prospectively), such that more efficiently moving patients through the system equates to more profit (or less loss).
This growth phase was quickly supplanted by the volume phase—a phase that was driven by the relative departure of primary-care physicians and subspecialists from the hospital. Although some of these doctors still admit their own patients, most of them now take advantage of hospitalist programs to focus their own practice to the outpatient or procedural arenas. Effectively, many of the other doctors have left the house, and hospitalists have had to back-fill this patient volume. To a certain degree, we are all still filling this need.
Connect the Dots
However, it is clear that the next HM driver is going to be quality. And it is programs like VBP that will drive it. Essentially, VBP means that hospitals will be competing with each other to be the best. By best, I mean “most able” to achieve pre-determined quality, safety, and patient-satisfaction indicators. By competing, I mean the reimbursement pie is fixed and those who achieve will get more, and those who fall short will get less.
When you consider that as much as 2% of a hospital’s Medicare reimbursement will soon be at risk, we are talking about millions of dollars per hospital per year. To hospitals with a 1% to 2% profit margin, this is the difference between being in or out of business. It also is interestingly close to the amount of support most hospitals give their HM groups; the exact groups that touch the majority of the patients that will determine their VBP outcomes. Connect the dots, and you can see that your hospitalist group—indeed, your paycheck—is very much at risk.
Which brings me back to the FPHM. In a serendipitous turn of events, the FPHM not only recognizes hospitalists as “special,” but, more important, it also gives us the opportunity to simultaneously enhance both our patients’ outcomes and our compensation. If we get this right, the every-three-year improvement projects required to maintain your certification are exactly the type of work you’ll need to be doing to achieve the outcomes your hospital needs to maintain its Medicare payments. In turn, this will ensure your group maintains its hospital support, and you, your paycheck.
It’s the kind of work that will ensure the best possible outcomes for our patients. And in the end, that, more than an ABIM certificate, is what truly makes us special. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
It’s official. I am a “recognized” hospitalist. I’m certified. I’m special.
Although I’ve always felt that HM was special, that it’s a field with its own defined body of knowledge, area of expertise, and dedicated providers, it is now official. It is special; I am special. I got the letter in the mail the other day to prove it.
The correspondence arrived in an important-looking white envelope, with a return address stamped with the “American Board of Internal Medicine” insignia. The letter itself congratulated me on becoming a member of the first class of internists to complete their Maintenance of Certification (MOC) with Recognition of Focused Practice in Hospital Medicine (FPHM). As you’ve no doubt heard, the ABIM developed this MOC process to recognize hospitalists who’ve been in practice for at least three years after their initial certification in internal medicine (IM).
This is the first ABIM certification program that recognizes physician expertise in a field that is not tied directly to either residency or specialty fellowship training. In other words, unlike the cardiology certification exam, which requires a physician to have completed a fellowship training program, the FPHM allows for clinical experience to substitute for fellowship training. While the FPHM does not confer true “specialty status” (like the cardiology certification exam does), it does, as the moniker implies, recognize that we have focused our practice.
Implicit within that is the understanding that this focus brings with it a level of expertise that distinguishes hospitalists from nonhospitalists. This is a massive step forward for HM, as it lends significant credibility to the work we do and helps the public better understand what a hospitalist is and does. Most important, it helps set apart that cadre of true hospitalists who are dedicating their careers to fundamentally improving the care and outcomes of hospitalized patients.
It is this last point that came to mind as I reviewed this month’s cover story on value-based purchasing (see “Value-Based Purchasing Raises the Stakes,” p. 1).
Sticky Yet Crucial Point
One of the sticking points that I’ve heard from some hospitalists is that the FPHM requires a three-year cycle of self-evaluation. For those new to this process, let’s clear up some of the nomenclature. When IM residents graduate, they are eligible to sit for the ABIM certification exam. Upon passage, they are board-certified internists and can choose to enter into the maintenance of certification process. This is a 10-year process whereby diplomates (ABIM-speak for those certified as a specialist, with a diploma in medicine; not to be confused with a diplomat—a person who conducts negotiations and maintains political rest through the tactful handling of delicate situations, something perhaps more appropriate to the bulk of patient situations we encounter) must complete self-evaluation of medical knowledge modules, self-evaluation of practice performance, and ultimately a secure exam. This is where the FPHM differs.
The 10-year cycle for MOC is maintained for FPHM, such that diplomates only recertify every 10 years. However, the self-evaluation must occur every three years to maintain one’s certification. In other words, fail to keep up with the self-evaluation process, and your FPHM is revoked. This is different than the MOC for IM, and it is why some hospitalists are choosing not to enroll in the FPHM. This is a mistake.
Unnecessary Burden?
For many hospitalists, this extra evaluation, especially the practice improvement, is seen as an undue burden. Why is it that hospitalists should have to do more frequent self-evaluation than other specialists? My answer is that this is an important part of what defines our hospitalist specialty—that is, our ability to go beyond the individual patient encounter to fundamentally improve outcomes for the patients under our care. This is not done through “good doctoring.” Hospitalists are not necessarily better doctors than nonhospitalists. Rather, we have embodied a commitment to process and quality improvement within the hospital. This is what our patients need from us. This is what makes us hospitalists. This is what makes us special.
And this brings me back to value-based purchasing.
The Next Phase: Purchasing Value
For those of you, like me, who struggle to comprehend what buying value actually means, take a few minutes to peruse Bryn Nelson’s cover story this month. Not only will it help you understand the healthcare reform bill, it will help you understand the future of our field. I’ve personally witnessed HM traverse three distinct phases.
In the late 1990s and early 2000s, HM growth was driven by the need to improve efficiency. In most ways, this was code for reducing costs. Hospital executives recognized that hospitalists could reduce the overall costs of a patient admission, thus turning the balance of the prospective payment into profit. In other words, the amount of money a hospital receives for a patient stay is most often fixed and determined up front (prospectively), such that more efficiently moving patients through the system equates to more profit (or less loss).
This growth phase was quickly supplanted by the volume phase—a phase that was driven by the relative departure of primary-care physicians and subspecialists from the hospital. Although some of these doctors still admit their own patients, most of them now take advantage of hospitalist programs to focus their own practice to the outpatient or procedural arenas. Effectively, many of the other doctors have left the house, and hospitalists have had to back-fill this patient volume. To a certain degree, we are all still filling this need.
Connect the Dots
However, it is clear that the next HM driver is going to be quality. And it is programs like VBP that will drive it. Essentially, VBP means that hospitals will be competing with each other to be the best. By best, I mean “most able” to achieve pre-determined quality, safety, and patient-satisfaction indicators. By competing, I mean the reimbursement pie is fixed and those who achieve will get more, and those who fall short will get less.
When you consider that as much as 2% of a hospital’s Medicare reimbursement will soon be at risk, we are talking about millions of dollars per hospital per year. To hospitals with a 1% to 2% profit margin, this is the difference between being in or out of business. It also is interestingly close to the amount of support most hospitals give their HM groups; the exact groups that touch the majority of the patients that will determine their VBP outcomes. Connect the dots, and you can see that your hospitalist group—indeed, your paycheck—is very much at risk.
Which brings me back to the FPHM. In a serendipitous turn of events, the FPHM not only recognizes hospitalists as “special,” but, more important, it also gives us the opportunity to simultaneously enhance both our patients’ outcomes and our compensation. If we get this right, the every-three-year improvement projects required to maintain your certification are exactly the type of work you’ll need to be doing to achieve the outcomes your hospital needs to maintain its Medicare payments. In turn, this will ensure your group maintains its hospital support, and you, your paycheck.
It’s the kind of work that will ensure the best possible outcomes for our patients. And in the end, that, more than an ABIM certificate, is what truly makes us special. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
The GOP Viewpoint
A two-time cancer survivor and obstetrician who has delivered thousands of babies, U.S. Sen. Tom Coburn (R-Okla.) has a unique perspective on healthcare as a provider, recipient, and influential advocate for change. Minutes after voting to repeal the Patient Protection and Affordable Care Act of 2010—an effort that ultimately failed in the Democratic-controlled Senate—Dr. Coburn talked with The Hospitalist about his objections to the existing law, his views on the main drivers of upwardly spiraling healthcare costs, and the Republican Party’s alternatives for achieving the elusive goals of better quality and cost control.
Question: What are your main concerns about the healthcare reform law?
Answer: I think, first of all, the healthcare reform bill doesn’t fix the problem, and the question is, what is the problem in healthcare in America? Is it quality, is it outcome, is it access, or is it cost?
And the problem is we spend twice as much per capita as anybody else in the world on healthcare to get 30% better outcomes on average. So the problem with healthcare in our country is it costs too much, and there’s a lot of reasons it costs too much. But the number-one reason is that everybody in the country, except those without insurance, thinks somebody else is paying their bill. So there’s no consumer discretionary choices that are made once you’ve met your deductible.
Having practiced for a long period of time and cared for the Amish, they always bought healthcare about 40% to 60% less than everybody else, because they pay cash for it and they deal [with] it, and they ask, “Why am I having this test?” and “Where can I get this test done more cheaply?” and “Are you sure I need this test?”
Being trained in the early 1980s and late ’70s as a physician, we’re trained different than the way doctors are trained today. Doctors today don’t think a thing about utilization. … What this bill did was expand coverage but didn’t fix the system, except that Washington’s now going to tell your hospitalists who they’re going to treat, how they’re going to treat them, and when they’re going to treat them.
Q: How do we fix the right problem?
A: You have to reconnect the purchaser with the payment; that’s No. 1. No. 2 is, you cannot continue to allow people to think somebody else is paying their bill, even when they’re not. If you work for a large company or you work for the government, the fact is, you’re paying money out every year for your portion of the coverage, and your employer is paying it out. They’re paying, in most instances, the vast majority of it, and so once you’ve met a deductible, you’re no longer a discretionary consumer because your assumption is, it’s going to get paid for.
And the other side of this is, how do we put in the doctors’ hands cost consciousness? In other words, can I do this and get the same outcome without spending this money? And quite frankly, we’ve trained a generation-and-a-half of physicians not to think about that.
Q: How else can we reduce costs?
A: It’s amazing what could happen if we start driving toward cost reduction. We have veterans who have to drive … to get to a VA. Give the veteran a card. If you’re service-connected, you can go wherever you want. Why should a veteran only be able to get access at a veterans’ healthcare center where the care isn’t as good, the outcomes aren’t as good, when they can go in their own hometown and buy something that’s better? So, you know, it’s about real freedom of choice and it’s about letting markets allocate scarce resources.
We’ve got a whole host of things that we’ve talked about on how to do this. The [Patients’ Freedom to Choose Act], it saves the states billions in terms of cost.
Q: Do you have any optimism that Congress can work together in a bipartisan way to address some of your concerns with the existing law?
A: No. This isn’t fixable in the way that they have it. To make this fixable, you have to take out the individual mandate, you have to take out the employer mandate, and you have to go to a system of risk reallocation on the insurance industry. If you want to really cover people with pre-existing illnesses, what you have to do is keep the insurance industry from cherry-picking. And what they tried to do is to get everybody covered so you could actually indemnify the whole population.
Our other problem is we’re spending money. You know, if we spent a lot of money on prevention that actually worked, we would in fact save some dollars. But we haven’t created a situation where the insurance industry is interested in keeping you as a long-term insuree, so, therefore, I don’t have any incentive to work on your wellness. Now they’re doing a little bit of that, but they’re not to a great extent. And if you knew you could buy your health insurance over a period of 20 years and be with the same company and they’d actually help teach you, get the things that are going to lower your risk and your cost, they’d both save money.
So there are all sorts of things, but what we’ve done is we’ve abandoned the thing that we use in the rest of the country to allocate scarce resources, and that’s market forces. Ask yourself why the best hospitalists in the country get paid the same as the worst. Well, why wouldn’t we want to incentivize and pay for higher quality and pay less for poorer quality and poorer outcomes, to the point where we promote excellence rather than mediocrity? But we don’t do that.
Q: What’s the next step for Republicans in trying to push forward some of your own ideas?
A: We’re going to take our [Patients’ Freedom to Choose Act] and we’re going to modify it somewhat and we’re going to introduce it and have, you know, “Here’s what we believe. You all believe this, we believe in individual freedom and personal responsibility and accountability,” and we’re going to try to do that. That won’t go anywhere because we don’t have the votes to have it go anywhere. What we’re going to wait for if the court cases. My suspicion is the president loses the court case when it gets to the Supreme Court.
Q: Do you believe the entire act will be struck down or just the individual mandate?
A: No, no. I think the entire act will be struck. The bill doesn’t work without the individual mandate because you don’t get enough revenues in to cover what—and the bill is scored so stupidly anyhow. I don’t know if you know much about government budgeting, but this thing’s a farce in terms of its cost. It’s going to cost fully $600 billion to a trillion dollars more in the first year [2014] than they’re saying it will.
Q: What’s your view on accountable-care organizations?
A: Accountable-care organizations (ACOs) aren’t going to work, and let me tell you why they’re not going to work: because the ACOs are going to be grouped in the large metropolitan areas and you’re going to have less competition rather than more. And so what you’re doing is you’re seeing hospitals buy physician practices, and then they’re going to get into this accountable care, and what they’re going to find is it’s not going to save them any money because you’ve got less competition.
Just go look at Boston; it’s happening right now. Prices aren’t going to go down with ACOs—they’re going to go up because you’re forcing.
What we really need is groups of physicians who say, “We’ll bid outside of the hospital; we’ll bid to make this care available.” In other words, you take 100 cardiologists and say, “Here are our rates to do these things for these people, on average.”
Let the physicians compete outside of being owned by the hospital. If you know anything about hospitals, their bureaucracy is amazing. It looks just like the federal government.
Q: What about bundling payments around episodes of care as a way to try to align incentives?
A: Well, why not let cost and outcome align incentives and let individuals do it? In other words, you’re talking about: “Here’s another system. The American consumer isn’t smart enough to buy their healthcare, so therefore, we have to have somebody else tell us how to do it.” And I would tell you, if we had no insurance in this country, none whatsoever, and we had no Medicare and people were buying their healthcare, I guarantee the prices would go down drastically, and we’d eliminate all this bureaucracy.
So what you’re suggesting is: “Here’s all these things that we can do because of the problem,” but that’s fixing the wrong problem. The problem is there’s no market force in play to control or check the cost. We’re just always looking for another gimmick. TH
Bryn Nelson is a freelance medical writer based in Seattle.
A two-time cancer survivor and obstetrician who has delivered thousands of babies, U.S. Sen. Tom Coburn (R-Okla.) has a unique perspective on healthcare as a provider, recipient, and influential advocate for change. Minutes after voting to repeal the Patient Protection and Affordable Care Act of 2010—an effort that ultimately failed in the Democratic-controlled Senate—Dr. Coburn talked with The Hospitalist about his objections to the existing law, his views on the main drivers of upwardly spiraling healthcare costs, and the Republican Party’s alternatives for achieving the elusive goals of better quality and cost control.
Question: What are your main concerns about the healthcare reform law?
Answer: I think, first of all, the healthcare reform bill doesn’t fix the problem, and the question is, what is the problem in healthcare in America? Is it quality, is it outcome, is it access, or is it cost?
And the problem is we spend twice as much per capita as anybody else in the world on healthcare to get 30% better outcomes on average. So the problem with healthcare in our country is it costs too much, and there’s a lot of reasons it costs too much. But the number-one reason is that everybody in the country, except those without insurance, thinks somebody else is paying their bill. So there’s no consumer discretionary choices that are made once you’ve met your deductible.
Having practiced for a long period of time and cared for the Amish, they always bought healthcare about 40% to 60% less than everybody else, because they pay cash for it and they deal [with] it, and they ask, “Why am I having this test?” and “Where can I get this test done more cheaply?” and “Are you sure I need this test?”
Being trained in the early 1980s and late ’70s as a physician, we’re trained different than the way doctors are trained today. Doctors today don’t think a thing about utilization. … What this bill did was expand coverage but didn’t fix the system, except that Washington’s now going to tell your hospitalists who they’re going to treat, how they’re going to treat them, and when they’re going to treat them.
Q: How do we fix the right problem?
A: You have to reconnect the purchaser with the payment; that’s No. 1. No. 2 is, you cannot continue to allow people to think somebody else is paying their bill, even when they’re not. If you work for a large company or you work for the government, the fact is, you’re paying money out every year for your portion of the coverage, and your employer is paying it out. They’re paying, in most instances, the vast majority of it, and so once you’ve met a deductible, you’re no longer a discretionary consumer because your assumption is, it’s going to get paid for.
And the other side of this is, how do we put in the doctors’ hands cost consciousness? In other words, can I do this and get the same outcome without spending this money? And quite frankly, we’ve trained a generation-and-a-half of physicians not to think about that.
Q: How else can we reduce costs?
A: It’s amazing what could happen if we start driving toward cost reduction. We have veterans who have to drive … to get to a VA. Give the veteran a card. If you’re service-connected, you can go wherever you want. Why should a veteran only be able to get access at a veterans’ healthcare center where the care isn’t as good, the outcomes aren’t as good, when they can go in their own hometown and buy something that’s better? So, you know, it’s about real freedom of choice and it’s about letting markets allocate scarce resources.
We’ve got a whole host of things that we’ve talked about on how to do this. The [Patients’ Freedom to Choose Act], it saves the states billions in terms of cost.
Q: Do you have any optimism that Congress can work together in a bipartisan way to address some of your concerns with the existing law?
A: No. This isn’t fixable in the way that they have it. To make this fixable, you have to take out the individual mandate, you have to take out the employer mandate, and you have to go to a system of risk reallocation on the insurance industry. If you want to really cover people with pre-existing illnesses, what you have to do is keep the insurance industry from cherry-picking. And what they tried to do is to get everybody covered so you could actually indemnify the whole population.
Our other problem is we’re spending money. You know, if we spent a lot of money on prevention that actually worked, we would in fact save some dollars. But we haven’t created a situation where the insurance industry is interested in keeping you as a long-term insuree, so, therefore, I don’t have any incentive to work on your wellness. Now they’re doing a little bit of that, but they’re not to a great extent. And if you knew you could buy your health insurance over a period of 20 years and be with the same company and they’d actually help teach you, get the things that are going to lower your risk and your cost, they’d both save money.
So there are all sorts of things, but what we’ve done is we’ve abandoned the thing that we use in the rest of the country to allocate scarce resources, and that’s market forces. Ask yourself why the best hospitalists in the country get paid the same as the worst. Well, why wouldn’t we want to incentivize and pay for higher quality and pay less for poorer quality and poorer outcomes, to the point where we promote excellence rather than mediocrity? But we don’t do that.
Q: What’s the next step for Republicans in trying to push forward some of your own ideas?
A: We’re going to take our [Patients’ Freedom to Choose Act] and we’re going to modify it somewhat and we’re going to introduce it and have, you know, “Here’s what we believe. You all believe this, we believe in individual freedom and personal responsibility and accountability,” and we’re going to try to do that. That won’t go anywhere because we don’t have the votes to have it go anywhere. What we’re going to wait for if the court cases. My suspicion is the president loses the court case when it gets to the Supreme Court.
Q: Do you believe the entire act will be struck down or just the individual mandate?
A: No, no. I think the entire act will be struck. The bill doesn’t work without the individual mandate because you don’t get enough revenues in to cover what—and the bill is scored so stupidly anyhow. I don’t know if you know much about government budgeting, but this thing’s a farce in terms of its cost. It’s going to cost fully $600 billion to a trillion dollars more in the first year [2014] than they’re saying it will.
Q: What’s your view on accountable-care organizations?
A: Accountable-care organizations (ACOs) aren’t going to work, and let me tell you why they’re not going to work: because the ACOs are going to be grouped in the large metropolitan areas and you’re going to have less competition rather than more. And so what you’re doing is you’re seeing hospitals buy physician practices, and then they’re going to get into this accountable care, and what they’re going to find is it’s not going to save them any money because you’ve got less competition.
Just go look at Boston; it’s happening right now. Prices aren’t going to go down with ACOs—they’re going to go up because you’re forcing.
What we really need is groups of physicians who say, “We’ll bid outside of the hospital; we’ll bid to make this care available.” In other words, you take 100 cardiologists and say, “Here are our rates to do these things for these people, on average.”
Let the physicians compete outside of being owned by the hospital. If you know anything about hospitals, their bureaucracy is amazing. It looks just like the federal government.
Q: What about bundling payments around episodes of care as a way to try to align incentives?
A: Well, why not let cost and outcome align incentives and let individuals do it? In other words, you’re talking about: “Here’s another system. The American consumer isn’t smart enough to buy their healthcare, so therefore, we have to have somebody else tell us how to do it.” And I would tell you, if we had no insurance in this country, none whatsoever, and we had no Medicare and people were buying their healthcare, I guarantee the prices would go down drastically, and we’d eliminate all this bureaucracy.
So what you’re suggesting is: “Here’s all these things that we can do because of the problem,” but that’s fixing the wrong problem. The problem is there’s no market force in play to control or check the cost. We’re just always looking for another gimmick. TH
Bryn Nelson is a freelance medical writer based in Seattle.
A two-time cancer survivor and obstetrician who has delivered thousands of babies, U.S. Sen. Tom Coburn (R-Okla.) has a unique perspective on healthcare as a provider, recipient, and influential advocate for change. Minutes after voting to repeal the Patient Protection and Affordable Care Act of 2010—an effort that ultimately failed in the Democratic-controlled Senate—Dr. Coburn talked with The Hospitalist about his objections to the existing law, his views on the main drivers of upwardly spiraling healthcare costs, and the Republican Party’s alternatives for achieving the elusive goals of better quality and cost control.
Question: What are your main concerns about the healthcare reform law?
Answer: I think, first of all, the healthcare reform bill doesn’t fix the problem, and the question is, what is the problem in healthcare in America? Is it quality, is it outcome, is it access, or is it cost?
And the problem is we spend twice as much per capita as anybody else in the world on healthcare to get 30% better outcomes on average. So the problem with healthcare in our country is it costs too much, and there’s a lot of reasons it costs too much. But the number-one reason is that everybody in the country, except those without insurance, thinks somebody else is paying their bill. So there’s no consumer discretionary choices that are made once you’ve met your deductible.
Having practiced for a long period of time and cared for the Amish, they always bought healthcare about 40% to 60% less than everybody else, because they pay cash for it and they deal [with] it, and they ask, “Why am I having this test?” and “Where can I get this test done more cheaply?” and “Are you sure I need this test?”
Being trained in the early 1980s and late ’70s as a physician, we’re trained different than the way doctors are trained today. Doctors today don’t think a thing about utilization. … What this bill did was expand coverage but didn’t fix the system, except that Washington’s now going to tell your hospitalists who they’re going to treat, how they’re going to treat them, and when they’re going to treat them.
Q: How do we fix the right problem?
A: You have to reconnect the purchaser with the payment; that’s No. 1. No. 2 is, you cannot continue to allow people to think somebody else is paying their bill, even when they’re not. If you work for a large company or you work for the government, the fact is, you’re paying money out every year for your portion of the coverage, and your employer is paying it out. They’re paying, in most instances, the vast majority of it, and so once you’ve met a deductible, you’re no longer a discretionary consumer because your assumption is, it’s going to get paid for.
And the other side of this is, how do we put in the doctors’ hands cost consciousness? In other words, can I do this and get the same outcome without spending this money? And quite frankly, we’ve trained a generation-and-a-half of physicians not to think about that.
Q: How else can we reduce costs?
A: It’s amazing what could happen if we start driving toward cost reduction. We have veterans who have to drive … to get to a VA. Give the veteran a card. If you’re service-connected, you can go wherever you want. Why should a veteran only be able to get access at a veterans’ healthcare center where the care isn’t as good, the outcomes aren’t as good, when they can go in their own hometown and buy something that’s better? So, you know, it’s about real freedom of choice and it’s about letting markets allocate scarce resources.
We’ve got a whole host of things that we’ve talked about on how to do this. The [Patients’ Freedom to Choose Act], it saves the states billions in terms of cost.
Q: Do you have any optimism that Congress can work together in a bipartisan way to address some of your concerns with the existing law?
A: No. This isn’t fixable in the way that they have it. To make this fixable, you have to take out the individual mandate, you have to take out the employer mandate, and you have to go to a system of risk reallocation on the insurance industry. If you want to really cover people with pre-existing illnesses, what you have to do is keep the insurance industry from cherry-picking. And what they tried to do is to get everybody covered so you could actually indemnify the whole population.
Our other problem is we’re spending money. You know, if we spent a lot of money on prevention that actually worked, we would in fact save some dollars. But we haven’t created a situation where the insurance industry is interested in keeping you as a long-term insuree, so, therefore, I don’t have any incentive to work on your wellness. Now they’re doing a little bit of that, but they’re not to a great extent. And if you knew you could buy your health insurance over a period of 20 years and be with the same company and they’d actually help teach you, get the things that are going to lower your risk and your cost, they’d both save money.
So there are all sorts of things, but what we’ve done is we’ve abandoned the thing that we use in the rest of the country to allocate scarce resources, and that’s market forces. Ask yourself why the best hospitalists in the country get paid the same as the worst. Well, why wouldn’t we want to incentivize and pay for higher quality and pay less for poorer quality and poorer outcomes, to the point where we promote excellence rather than mediocrity? But we don’t do that.
Q: What’s the next step for Republicans in trying to push forward some of your own ideas?
A: We’re going to take our [Patients’ Freedom to Choose Act] and we’re going to modify it somewhat and we’re going to introduce it and have, you know, “Here’s what we believe. You all believe this, we believe in individual freedom and personal responsibility and accountability,” and we’re going to try to do that. That won’t go anywhere because we don’t have the votes to have it go anywhere. What we’re going to wait for if the court cases. My suspicion is the president loses the court case when it gets to the Supreme Court.
Q: Do you believe the entire act will be struck down or just the individual mandate?
A: No, no. I think the entire act will be struck. The bill doesn’t work without the individual mandate because you don’t get enough revenues in to cover what—and the bill is scored so stupidly anyhow. I don’t know if you know much about government budgeting, but this thing’s a farce in terms of its cost. It’s going to cost fully $600 billion to a trillion dollars more in the first year [2014] than they’re saying it will.
Q: What’s your view on accountable-care organizations?
A: Accountable-care organizations (ACOs) aren’t going to work, and let me tell you why they’re not going to work: because the ACOs are going to be grouped in the large metropolitan areas and you’re going to have less competition rather than more. And so what you’re doing is you’re seeing hospitals buy physician practices, and then they’re going to get into this accountable care, and what they’re going to find is it’s not going to save them any money because you’ve got less competition.
Just go look at Boston; it’s happening right now. Prices aren’t going to go down with ACOs—they’re going to go up because you’re forcing.
What we really need is groups of physicians who say, “We’ll bid outside of the hospital; we’ll bid to make this care available.” In other words, you take 100 cardiologists and say, “Here are our rates to do these things for these people, on average.”
Let the physicians compete outside of being owned by the hospital. If you know anything about hospitals, their bureaucracy is amazing. It looks just like the federal government.
Q: What about bundling payments around episodes of care as a way to try to align incentives?
A: Well, why not let cost and outcome align incentives and let individuals do it? In other words, you’re talking about: “Here’s another system. The American consumer isn’t smart enough to buy their healthcare, so therefore, we have to have somebody else tell us how to do it.” And I would tell you, if we had no insurance in this country, none whatsoever, and we had no Medicare and people were buying their healthcare, I guarantee the prices would go down drastically, and we’d eliminate all this bureaucracy.
So what you’re suggesting is: “Here’s all these things that we can do because of the problem,” but that’s fixing the wrong problem. The problem is there’s no market force in play to control or check the cost. We’re just always looking for another gimmick. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Health Reform Turns 1
As America’s love-hate relationship with healthcare reform approaches its first anniversary, the law is proving just as divisive now as it was during the midterm elections. Fittingly, the Patient Protection and Affordable Care Act of 2010 (ACA), which has polarized the country, is moving forward along three separate tracks.
“Usually, at this point of the game one would only be worrying about the implementation,” says Leighton Ku, a health-policy analyst at George Washington University. “But, obviously, there’s been enough discord that the political route and the legal route are now equally important.”
Here’s a look at where the ACA stands from practical, political, and legal standpoints, along with the major players involved in the ongoing tussle.
The Battle of Public Perception
America is hopelessly divided. Despite pollsters’ best efforts to break the stalemate, the collective numbers still suggest that roughly equal numbers of respondents favor and oppose healthcare reform (with a slight advantage to opponents). It’s a trend line that has barely budged since the bill’s enactment last March.
In January, the Republican-led House of Representatives voted to repeal the entire reform act in what analysts have called a largely symbolic gesture, given that the repeal effort subsequently failed in the Democratic-controlled Senate. Even so, Ku says, the vote fulfills a Republican campaign promise and sends a strong signal to the party’s political base. “What’s driving the Republicans is that their constituencies really don’t like it,” agrees Robert J. Blendon, a professor of health policy and political analysis at the Harvard School of Public Health. “Almost all Republican congressmen who ran had on their website, ‘I will repeal this bill if elected.’ ”
But opposition doesn’t necessarily mean voters want everything repealed, a caveat also borne out by recent polling. “Where the public stands is a little more ambiguous than what the campaign rhetoric is,” Ku says. That ambiguity could present an opportunity for both parties to reframe the debate in the coming months in an effort to win over a clear majority of the public. With the economy of paramount concern, Republicans have cast healthcare reform as a “job-destroying” act that will speed the country’s descent into bankruptcy.
If the economy improves, however, opposition to the law is likely to soften. And with their “no” vote behind them, Republicans in the House will be expected to craft a coherent alternative to the legislation. “Now comes the tough part,” Ku says.
Democrats, meanwhile, have largely regrouped and are being more vocal about the law’s necessity—after a campaign season in which many conservative Democrats largely avoided talking about it, or even touted their opposition to it, and were beaten anyway.
In the absence of wholesale repeal, a few individual provisions might be stripped away. Most key elements cannot be defunded, although Republicans could cut funding streams to Health and Human Services (HHS) or the IRS to hamper implementation. Congress also could choose not to appropriate money to the estimated $106 billion worth of new spending authorizations. A sizable percentage of that pool covers popular pre-existing programs, however, which makes a “no” vote politically more risky.
A Matter of Time
The nonpartisan Congressional Budget Office has predicted that repealing the healthcare reform legislation would increase the federal deficit by $230 billion over the next decade. Even so, the law’s supporters are finding little traction among voters who have heard repeated claims by Republicans that the act itself will push the country deeper into debt (many Republicans say the CBO estimate is based on faulty numbers provided by the law’s supporters). One big reason why: The tanking economy has eroded public trust in the government. “The ratings of trust in the federal government are so low,” Blendon says, “you need a stethoscope to try to hear them.”
And then there’s the matter of time. Because the act’s biggest provisions don’t go into effect until 2014, there are no made-for-media moments—like the large numbers of previously uninsured receiving health insurance cards—to counter the dire predictions that patients will lose their doctors. Instead, the White House has tried to make the most of smaller provisions now in effect, such as one that allows children to stay on a parent’s insurance until their 26th birthday, another that lifts the lifetime caps on insurance coverage, and a third that bans insurers from dropping children with pre-existing conditions (a video explaining what the ACA does and doesn’t do, produced by the Kaiser Family Foundation, is available at http://healthreform.kff.org/The Animation.aspx).
In mid-January, on the eve of the House vote to repeal the entire act, the White House released an HHS study to bolster its contention that the law will eventually aid tens of millions, and, conversely, that any repeal would harm them (www.healthcare.gov/center/reports/preexisting.html). The study estimates that 50 million to 129 million Americans under the age of 65 have pre-existing conditions that would, theoretically, make it harder for them to buy insurance in the absence of regulations requiring coverage. But the study also reports that up to 82 million of these people already have employer-provided insurance, meaning they wouldn’t be affected either way unless they switch jobs or become unemployed.
The White House’s case has been made harder by the confluence of a poor economy, growing concern over the deficit, and the ongoing battle over whether and how to fix the Medicare reimbursement rate paid to doctors, according to Blendon. When the rate paid to doctors temporarily nosedived last June, stories about doctors refusing to see Medicare beneficiaries proliferated among alarmed seniors (Congress eventually passed another short-term patch). The memory of that lack of medical access is now being conflated with the potential side effects of the new law by the constituency most likely to vote (seniors) and most skeptical in general about healthcare reform.
Legal Limbo
More than half the states have now joined lawsuits challenging the ACA’s constitutionality. In the first of what observers expect to be a multitude of legal decisions, federal judges in two cases upheld the law, and the individual mandate requiring people to buy health insurance was ruled unconstitutional in a third.
Ultimately, most experts believe the Supreme Court will have the final say, likely before the 2012 elections. Ku says analysts already are talking about a possible 5-4 decision, with Justice Anthony Kennedy as the potential swing vote—though so far, he’s given no clear hints about which way he may be leaning. Even if the individual mandate component is struck down, Ku says, the court could uphold everything else, changing its overall impact but not the implementation of most provisions. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Key Players in the Healthcare Debate

John Boehner (R-Ohio), the new Speaker of the House, is the public face of many Republican talking points on healthcare reform and the leader in trying to maintain a unified front against the existing law.
Paul Ryan (R-Wis.), chairman of the House Budget Committee and a senior member of the Ways and Means Committee, delivered the GOP response to President Obama’s State of the Union address. He will help the party craft a coherent ACA alternative.
Many conservative “Blue Dog” Democrats either actively opposed the law or stayed silent about it—and got routed in November anyway. Most remaining Blue Dogs have since rejoined the party in highlighting the ACA’s benefits. If Republicans pass an alternative measure, it would need to attract some Democratic support to be seen as bipartisan.

Although Sen. Majority Leader Harry Reid (D-Nev.) is opposing any attempt to bring up a vote on repealing the law, Minority Leader Mitch McConnell (R-Ky.) has kept the pressure on, vowing to find a way to force a vote on repealing what he told Fox News Sunday was “the single worst piece of legislation passed in my time in the Senate.” Obama was criticized by other Democrats for not being more vocal about healthcare reform’s benefits in the leadup to the November elections. The repeal effort gives him another chance to make his case.

HHS Secretary Kathleen Sebelius likely will testify repeatedly in hearings called by the Republican leadership to scrutinize how the law is being implemented.
Supreme Court Justice Anthony Kennedy, appointed by President Reagan, is expected to be the swing vote in a closely divided court. The issue: whether an individual mandate requiring people to buy insurance is constitutional. So far, he has given little indication as to how he might rule.
—BN
As America’s love-hate relationship with healthcare reform approaches its first anniversary, the law is proving just as divisive now as it was during the midterm elections. Fittingly, the Patient Protection and Affordable Care Act of 2010 (ACA), which has polarized the country, is moving forward along three separate tracks.
“Usually, at this point of the game one would only be worrying about the implementation,” says Leighton Ku, a health-policy analyst at George Washington University. “But, obviously, there’s been enough discord that the political route and the legal route are now equally important.”
Here’s a look at where the ACA stands from practical, political, and legal standpoints, along with the major players involved in the ongoing tussle.
The Battle of Public Perception
America is hopelessly divided. Despite pollsters’ best efforts to break the stalemate, the collective numbers still suggest that roughly equal numbers of respondents favor and oppose healthcare reform (with a slight advantage to opponents). It’s a trend line that has barely budged since the bill’s enactment last March.
In January, the Republican-led House of Representatives voted to repeal the entire reform act in what analysts have called a largely symbolic gesture, given that the repeal effort subsequently failed in the Democratic-controlled Senate. Even so, Ku says, the vote fulfills a Republican campaign promise and sends a strong signal to the party’s political base. “What’s driving the Republicans is that their constituencies really don’t like it,” agrees Robert J. Blendon, a professor of health policy and political analysis at the Harvard School of Public Health. “Almost all Republican congressmen who ran had on their website, ‘I will repeal this bill if elected.’ ”
But opposition doesn’t necessarily mean voters want everything repealed, a caveat also borne out by recent polling. “Where the public stands is a little more ambiguous than what the campaign rhetoric is,” Ku says. That ambiguity could present an opportunity for both parties to reframe the debate in the coming months in an effort to win over a clear majority of the public. With the economy of paramount concern, Republicans have cast healthcare reform as a “job-destroying” act that will speed the country’s descent into bankruptcy.
If the economy improves, however, opposition to the law is likely to soften. And with their “no” vote behind them, Republicans in the House will be expected to craft a coherent alternative to the legislation. “Now comes the tough part,” Ku says.
Democrats, meanwhile, have largely regrouped and are being more vocal about the law’s necessity—after a campaign season in which many conservative Democrats largely avoided talking about it, or even touted their opposition to it, and were beaten anyway.
In the absence of wholesale repeal, a few individual provisions might be stripped away. Most key elements cannot be defunded, although Republicans could cut funding streams to Health and Human Services (HHS) or the IRS to hamper implementation. Congress also could choose not to appropriate money to the estimated $106 billion worth of new spending authorizations. A sizable percentage of that pool covers popular pre-existing programs, however, which makes a “no” vote politically more risky.
A Matter of Time
The nonpartisan Congressional Budget Office has predicted that repealing the healthcare reform legislation would increase the federal deficit by $230 billion over the next decade. Even so, the law’s supporters are finding little traction among voters who have heard repeated claims by Republicans that the act itself will push the country deeper into debt (many Republicans say the CBO estimate is based on faulty numbers provided by the law’s supporters). One big reason why: The tanking economy has eroded public trust in the government. “The ratings of trust in the federal government are so low,” Blendon says, “you need a stethoscope to try to hear them.”
And then there’s the matter of time. Because the act’s biggest provisions don’t go into effect until 2014, there are no made-for-media moments—like the large numbers of previously uninsured receiving health insurance cards—to counter the dire predictions that patients will lose their doctors. Instead, the White House has tried to make the most of smaller provisions now in effect, such as one that allows children to stay on a parent’s insurance until their 26th birthday, another that lifts the lifetime caps on insurance coverage, and a third that bans insurers from dropping children with pre-existing conditions (a video explaining what the ACA does and doesn’t do, produced by the Kaiser Family Foundation, is available at http://healthreform.kff.org/The Animation.aspx).
In mid-January, on the eve of the House vote to repeal the entire act, the White House released an HHS study to bolster its contention that the law will eventually aid tens of millions, and, conversely, that any repeal would harm them (www.healthcare.gov/center/reports/preexisting.html). The study estimates that 50 million to 129 million Americans under the age of 65 have pre-existing conditions that would, theoretically, make it harder for them to buy insurance in the absence of regulations requiring coverage. But the study also reports that up to 82 million of these people already have employer-provided insurance, meaning they wouldn’t be affected either way unless they switch jobs or become unemployed.
The White House’s case has been made harder by the confluence of a poor economy, growing concern over the deficit, and the ongoing battle over whether and how to fix the Medicare reimbursement rate paid to doctors, according to Blendon. When the rate paid to doctors temporarily nosedived last June, stories about doctors refusing to see Medicare beneficiaries proliferated among alarmed seniors (Congress eventually passed another short-term patch). The memory of that lack of medical access is now being conflated with the potential side effects of the new law by the constituency most likely to vote (seniors) and most skeptical in general about healthcare reform.
Legal Limbo
More than half the states have now joined lawsuits challenging the ACA’s constitutionality. In the first of what observers expect to be a multitude of legal decisions, federal judges in two cases upheld the law, and the individual mandate requiring people to buy health insurance was ruled unconstitutional in a third.
Ultimately, most experts believe the Supreme Court will have the final say, likely before the 2012 elections. Ku says analysts already are talking about a possible 5-4 decision, with Justice Anthony Kennedy as the potential swing vote—though so far, he’s given no clear hints about which way he may be leaning. Even if the individual mandate component is struck down, Ku says, the court could uphold everything else, changing its overall impact but not the implementation of most provisions. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Key Players in the Healthcare Debate
John Boehner (R-Ohio), the new Speaker of the House, is the public face of many Republican talking points on healthcare reform and the leader in trying to maintain a unified front against the existing law.
Paul Ryan (R-Wis.), chairman of the House Budget Committee and a senior member of the Ways and Means Committee, delivered the GOP response to President Obama’s State of the Union address. He will help the party craft a coherent ACA alternative.
Many conservative “Blue Dog” Democrats either actively opposed the law or stayed silent about it—and got routed in November anyway. Most remaining Blue Dogs have since rejoined the party in highlighting the ACA’s benefits. If Republicans pass an alternative measure, it would need to attract some Democratic support to be seen as bipartisan.
Although Sen. Majority Leader Harry Reid (D-Nev.) is opposing any attempt to bring up a vote on repealing the law, Minority Leader Mitch McConnell (R-Ky.) has kept the pressure on, vowing to find a way to force a vote on repealing what he told Fox News Sunday was “the single worst piece of legislation passed in my time in the Senate.” Obama was criticized by other Democrats for not being more vocal about healthcare reform’s benefits in the leadup to the November elections. The repeal effort gives him another chance to make his case.
HHS Secretary Kathleen Sebelius likely will testify repeatedly in hearings called by the Republican leadership to scrutinize how the law is being implemented.
Supreme Court Justice Anthony Kennedy, appointed by President Reagan, is expected to be the swing vote in a closely divided court. The issue: whether an individual mandate requiring people to buy insurance is constitutional. So far, he has given little indication as to how he might rule.
—BN
As America’s love-hate relationship with healthcare reform approaches its first anniversary, the law is proving just as divisive now as it was during the midterm elections. Fittingly, the Patient Protection and Affordable Care Act of 2010 (ACA), which has polarized the country, is moving forward along three separate tracks.
“Usually, at this point of the game one would only be worrying about the implementation,” says Leighton Ku, a health-policy analyst at George Washington University. “But, obviously, there’s been enough discord that the political route and the legal route are now equally important.”
Here’s a look at where the ACA stands from practical, political, and legal standpoints, along with the major players involved in the ongoing tussle.
The Battle of Public Perception
America is hopelessly divided. Despite pollsters’ best efforts to break the stalemate, the collective numbers still suggest that roughly equal numbers of respondents favor and oppose healthcare reform (with a slight advantage to opponents). It’s a trend line that has barely budged since the bill’s enactment last March.
In January, the Republican-led House of Representatives voted to repeal the entire reform act in what analysts have called a largely symbolic gesture, given that the repeal effort subsequently failed in the Democratic-controlled Senate. Even so, Ku says, the vote fulfills a Republican campaign promise and sends a strong signal to the party’s political base. “What’s driving the Republicans is that their constituencies really don’t like it,” agrees Robert J. Blendon, a professor of health policy and political analysis at the Harvard School of Public Health. “Almost all Republican congressmen who ran had on their website, ‘I will repeal this bill if elected.’ ”
But opposition doesn’t necessarily mean voters want everything repealed, a caveat also borne out by recent polling. “Where the public stands is a little more ambiguous than what the campaign rhetoric is,” Ku says. That ambiguity could present an opportunity for both parties to reframe the debate in the coming months in an effort to win over a clear majority of the public. With the economy of paramount concern, Republicans have cast healthcare reform as a “job-destroying” act that will speed the country’s descent into bankruptcy.
If the economy improves, however, opposition to the law is likely to soften. And with their “no” vote behind them, Republicans in the House will be expected to craft a coherent alternative to the legislation. “Now comes the tough part,” Ku says.
Democrats, meanwhile, have largely regrouped and are being more vocal about the law’s necessity—after a campaign season in which many conservative Democrats largely avoided talking about it, or even touted their opposition to it, and were beaten anyway.
In the absence of wholesale repeal, a few individual provisions might be stripped away. Most key elements cannot be defunded, although Republicans could cut funding streams to Health and Human Services (HHS) or the IRS to hamper implementation. Congress also could choose not to appropriate money to the estimated $106 billion worth of new spending authorizations. A sizable percentage of that pool covers popular pre-existing programs, however, which makes a “no” vote politically more risky.
A Matter of Time
The nonpartisan Congressional Budget Office has predicted that repealing the healthcare reform legislation would increase the federal deficit by $230 billion over the next decade. Even so, the law’s supporters are finding little traction among voters who have heard repeated claims by Republicans that the act itself will push the country deeper into debt (many Republicans say the CBO estimate is based on faulty numbers provided by the law’s supporters). One big reason why: The tanking economy has eroded public trust in the government. “The ratings of trust in the federal government are so low,” Blendon says, “you need a stethoscope to try to hear them.”
And then there’s the matter of time. Because the act’s biggest provisions don’t go into effect until 2014, there are no made-for-media moments—like the large numbers of previously uninsured receiving health insurance cards—to counter the dire predictions that patients will lose their doctors. Instead, the White House has tried to make the most of smaller provisions now in effect, such as one that allows children to stay on a parent’s insurance until their 26th birthday, another that lifts the lifetime caps on insurance coverage, and a third that bans insurers from dropping children with pre-existing conditions (a video explaining what the ACA does and doesn’t do, produced by the Kaiser Family Foundation, is available at http://healthreform.kff.org/The Animation.aspx).
In mid-January, on the eve of the House vote to repeal the entire act, the White House released an HHS study to bolster its contention that the law will eventually aid tens of millions, and, conversely, that any repeal would harm them (www.healthcare.gov/center/reports/preexisting.html). The study estimates that 50 million to 129 million Americans under the age of 65 have pre-existing conditions that would, theoretically, make it harder for them to buy insurance in the absence of regulations requiring coverage. But the study also reports that up to 82 million of these people already have employer-provided insurance, meaning they wouldn’t be affected either way unless they switch jobs or become unemployed.
The White House’s case has been made harder by the confluence of a poor economy, growing concern over the deficit, and the ongoing battle over whether and how to fix the Medicare reimbursement rate paid to doctors, according to Blendon. When the rate paid to doctors temporarily nosedived last June, stories about doctors refusing to see Medicare beneficiaries proliferated among alarmed seniors (Congress eventually passed another short-term patch). The memory of that lack of medical access is now being conflated with the potential side effects of the new law by the constituency most likely to vote (seniors) and most skeptical in general about healthcare reform.
Legal Limbo
More than half the states have now joined lawsuits challenging the ACA’s constitutionality. In the first of what observers expect to be a multitude of legal decisions, federal judges in two cases upheld the law, and the individual mandate requiring people to buy health insurance was ruled unconstitutional in a third.
Ultimately, most experts believe the Supreme Court will have the final say, likely before the 2012 elections. Ku says analysts already are talking about a possible 5-4 decision, with Justice Anthony Kennedy as the potential swing vote—though so far, he’s given no clear hints about which way he may be leaning. Even if the individual mandate component is struck down, Ku says, the court could uphold everything else, changing its overall impact but not the implementation of most provisions. TH
Bryn Nelson is a freelance medical writer based in Seattle.
Key Players in the Healthcare Debate
John Boehner (R-Ohio), the new Speaker of the House, is the public face of many Republican talking points on healthcare reform and the leader in trying to maintain a unified front against the existing law.
Paul Ryan (R-Wis.), chairman of the House Budget Committee and a senior member of the Ways and Means Committee, delivered the GOP response to President Obama’s State of the Union address. He will help the party craft a coherent ACA alternative.
Many conservative “Blue Dog” Democrats either actively opposed the law or stayed silent about it—and got routed in November anyway. Most remaining Blue Dogs have since rejoined the party in highlighting the ACA’s benefits. If Republicans pass an alternative measure, it would need to attract some Democratic support to be seen as bipartisan.
Although Sen. Majority Leader Harry Reid (D-Nev.) is opposing any attempt to bring up a vote on repealing the law, Minority Leader Mitch McConnell (R-Ky.) has kept the pressure on, vowing to find a way to force a vote on repealing what he told Fox News Sunday was “the single worst piece of legislation passed in my time in the Senate.” Obama was criticized by other Democrats for not being more vocal about healthcare reform’s benefits in the leadup to the November elections. The repeal effort gives him another chance to make his case.
HHS Secretary Kathleen Sebelius likely will testify repeatedly in hearings called by the Republican leadership to scrutinize how the law is being implemented.
Supreme Court Justice Anthony Kennedy, appointed by President Reagan, is expected to be the swing vote in a closely divided court. The issue: whether an individual mandate requiring people to buy insurance is constitutional. So far, he has given little indication as to how he might rule.
—BN
Obama’s SGR Fix Gets Mixed Reviews
President Obama's budget proposal for a two-year, $54 billion extension of the temporary fix to the reimbursement rate that Medicare pays doctors is getting a mixed reception from doctors as well as legislators on Capitol Hill.
"It's not ideal, but it's better than what we've been dealing with," says Ron Greeno, MD, SFHM, chief medical officer for Cogent Healthcare, and a member of SHM's Public Policy Committee. "The question is, will it remain part of the budget that gets passed?"
Last year, Congress approved five temporary extensions preventing draconian rate cuts mandated by Medicare's sustainable growth rate (SGR) formula, including a one-year, $19 billion extension passed with bipartisan support during the lame-duck session. The new proposal would further delay the cut, now at 25%, until September 2013. To pay for the patch, the budget suggests $62 billion in cuts that would transfer more of the Medicaid burden to states, recoup "erroneous" payments to insurers, and speed the process of getting generic drugs to market at the expense of major pharmaceutical companies, among other targets.
Republicans, however, have objected to the spend-now, save-later mechanism paying for the fix, with spending over two years counterbalanced by projected savings over an entire decade. And the proposal is silent on how the fix would be funded for the eight years beyond 2013, an extension the budget suggests would require an additional $316 billion.
Both Democrats and Republicans agree that the current SGR formula is unworkable. But Dr. Greeno says neither party wants to make a move that would add hundreds of billions to the debt amid heightened concern over the rising deficit.
"I think we need to change the way we pay, and I haven't figured out exactly how," Sen. Tom Coburn (R-Okla.) told The Hospitalist in an interview earlier this month. "But the SGR's a joke; it's never worked. It was a gimmick from the time it started in 1997 forward. It's never going to work."
Nevertheless, Republicans like Sen. Coburn have signaled that they understand allowing the rate cut to take place is untenable. "What I would tell your physicians is … they won't see any cuts, but they're not going to see any increases," he said. "The country is broke."
If Congress ultimately agrees to a two-year solution, Dr. Greeno says, it could buy the administration some wait-and-see time amid ongoing efforts aimed at repealing parts of the healthcare reform law or having it declared unconstitutional. A two-year extension also could buy more time for the Centers for Medicare & Medicaid Services' new Center for Medicare and Medicaid Innovation to figure out how to transition out of a total fee-for-service healthcare environment. "But that," Dr. Greeno says, "is going to take years."
President Obama's budget proposal for a two-year, $54 billion extension of the temporary fix to the reimbursement rate that Medicare pays doctors is getting a mixed reception from doctors as well as legislators on Capitol Hill.
"It's not ideal, but it's better than what we've been dealing with," says Ron Greeno, MD, SFHM, chief medical officer for Cogent Healthcare, and a member of SHM's Public Policy Committee. "The question is, will it remain part of the budget that gets passed?"
Last year, Congress approved five temporary extensions preventing draconian rate cuts mandated by Medicare's sustainable growth rate (SGR) formula, including a one-year, $19 billion extension passed with bipartisan support during the lame-duck session. The new proposal would further delay the cut, now at 25%, until September 2013. To pay for the patch, the budget suggests $62 billion in cuts that would transfer more of the Medicaid burden to states, recoup "erroneous" payments to insurers, and speed the process of getting generic drugs to market at the expense of major pharmaceutical companies, among other targets.
Republicans, however, have objected to the spend-now, save-later mechanism paying for the fix, with spending over two years counterbalanced by projected savings over an entire decade. And the proposal is silent on how the fix would be funded for the eight years beyond 2013, an extension the budget suggests would require an additional $316 billion.
Both Democrats and Republicans agree that the current SGR formula is unworkable. But Dr. Greeno says neither party wants to make a move that would add hundreds of billions to the debt amid heightened concern over the rising deficit.
"I think we need to change the way we pay, and I haven't figured out exactly how," Sen. Tom Coburn (R-Okla.) told The Hospitalist in an interview earlier this month. "But the SGR's a joke; it's never worked. It was a gimmick from the time it started in 1997 forward. It's never going to work."
Nevertheless, Republicans like Sen. Coburn have signaled that they understand allowing the rate cut to take place is untenable. "What I would tell your physicians is … they won't see any cuts, but they're not going to see any increases," he said. "The country is broke."
If Congress ultimately agrees to a two-year solution, Dr. Greeno says, it could buy the administration some wait-and-see time amid ongoing efforts aimed at repealing parts of the healthcare reform law or having it declared unconstitutional. A two-year extension also could buy more time for the Centers for Medicare & Medicaid Services' new Center for Medicare and Medicaid Innovation to figure out how to transition out of a total fee-for-service healthcare environment. "But that," Dr. Greeno says, "is going to take years."
President Obama's budget proposal for a two-year, $54 billion extension of the temporary fix to the reimbursement rate that Medicare pays doctors is getting a mixed reception from doctors as well as legislators on Capitol Hill.
"It's not ideal, but it's better than what we've been dealing with," says Ron Greeno, MD, SFHM, chief medical officer for Cogent Healthcare, and a member of SHM's Public Policy Committee. "The question is, will it remain part of the budget that gets passed?"
Last year, Congress approved five temporary extensions preventing draconian rate cuts mandated by Medicare's sustainable growth rate (SGR) formula, including a one-year, $19 billion extension passed with bipartisan support during the lame-duck session. The new proposal would further delay the cut, now at 25%, until September 2013. To pay for the patch, the budget suggests $62 billion in cuts that would transfer more of the Medicaid burden to states, recoup "erroneous" payments to insurers, and speed the process of getting generic drugs to market at the expense of major pharmaceutical companies, among other targets.
Republicans, however, have objected to the spend-now, save-later mechanism paying for the fix, with spending over two years counterbalanced by projected savings over an entire decade. And the proposal is silent on how the fix would be funded for the eight years beyond 2013, an extension the budget suggests would require an additional $316 billion.
Both Democrats and Republicans agree that the current SGR formula is unworkable. But Dr. Greeno says neither party wants to make a move that would add hundreds of billions to the debt amid heightened concern over the rising deficit.
"I think we need to change the way we pay, and I haven't figured out exactly how," Sen. Tom Coburn (R-Okla.) told The Hospitalist in an interview earlier this month. "But the SGR's a joke; it's never worked. It was a gimmick from the time it started in 1997 forward. It's never going to work."
Nevertheless, Republicans like Sen. Coburn have signaled that they understand allowing the rate cut to take place is untenable. "What I would tell your physicians is … they won't see any cuts, but they're not going to see any increases," he said. "The country is broke."
If Congress ultimately agrees to a two-year solution, Dr. Greeno says, it could buy the administration some wait-and-see time amid ongoing efforts aimed at repealing parts of the healthcare reform law or having it declared unconstitutional. A two-year extension also could buy more time for the Centers for Medicare & Medicaid Services' new Center for Medicare and Medicaid Innovation to figure out how to transition out of a total fee-for-service healthcare environment. "But that," Dr. Greeno says, "is going to take years."
All Aboard
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.

Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).

On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.

“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
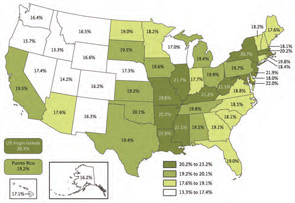
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
On the Road Again?
Necessity, as they say, is the mother of invention, and the growing focus on the need for high-quality and cost-effective care is bringing a host of new innovations to light. One that hospitalists are likely to hear about far more about is the evolving role of an “extensivist,” an inpatient provider who ventures to outpatient settings to assist with care transitions.
In many ways, the expanding discussion of what extensivists are and do reflects the success of hospitalists in coordinating inpatient care and improving such metrics as length of stay (LOS). Why should that coordination end upon discharge? healthcare experts have wondered. Instead of a pure hospitalist system, could the experience and training of hospitalists be extended to include transitional or interim settings that provide a safety net between the hospital and a primary-care physician (PCP)? Might that improved inpatient-outpatient coordination help with other metrics, such as reduced rehospitalizations (see “All Aboard,” p. 1)?

One tangible result of those questions has been the growth of high-risk clinics. Hospitalist programs can provide clinic referrals for discharged patients who still require hands-on care, while PCPs can likewise refer some of their more complex patients. The clinic, then, becomes an alternative to hospitalization, or a preventive measure to avoid rehospitalization.
Philip Sanger, MD, founder and former CEO of Houston-based Inpatient Medical Services (now Intercede Health), is credited with one of the first uses of the term “extensivist.” Initially, it only described a hospitalist or other care provider who sees high-risk patients in an outpatient clinic.
Writing in Managed Healthcare Executive in 2002, Dr. Sanger explained: “To move from generally sick to generally well, high-risk patients need something extra—more attention than a busy PCP can offer [and] more individualized care than most protocol-driven disease management programs can provide. A high-risk clinic system is one way to fill this care gap. Also referred to as transitional-care clinics, these outpatient clinics focus on preventing hospital admissions and stabilizing high-risk patients.”1
Measured Improvements
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Co., says this extensivist model provides a respite for hospitalists, who typically spend a month at a time in these transitional clinics before heading back into the fray of the hospital. As hospitals, independent physician associations, and managed-care organizations try out new models of care, though, the definition of an extensivist has broadened to include providers in a range of outpatient settings, such as skilled nursing facilities, assistant living communities, and even home health services. California’s CareMore Medicare Advantage plan, in particular, has been cited by the Agency for Healthcare Research and Quality (AHRQ) for using hospitalists as extensivists in both outpatient clinics and skilled nursing facilities to reduce hospital readmission rates, LOS, and inpatient resource use.
The CareMore model reduces the caseload of its hospitalists to about six or eight patients per half-day, giving doctors more time to talk to patients and their family members. Based on those conversations, the extensivist works with a case manager to provide needed resources to each patient after discharge. The doctors also spend roughly half of each day in clinics seeing their own recently discharged patients, and one or two days each week in a skilled nursing facility to visit patients transferred from the hospital (for more details, visit www.innovations.ahrq.gov/content.aspx?id=2903).
Average inpatient LOS among the plan’s 44,000 members dipped to 3.2 days, compared with 5.8 days for Medicare fee-for-service providers and 4.5 days for traditional HM programs in the state. Last April, CareMore’s 30-day readmission rate averaged 13.4%, compared with a 19.6% rate for Medicare.
Baltimore-based Bravo Health has begun opening its own transitional advanced-care centers for members of its Medicare Advantage program, offering case management for complex conditions and immediate care when a PCP is unavailable. Another model has been advanced through team approaches practiced by the likes of Kaiser Permanente, though hospitalists aren’t necessarily the ones providing outpatient follow-up care. No matter what the model is called, Dr. Singer says, the main point is the same: “trying to connect the dots so that we get patients continuing to get better along the continuum without having to be readmitted.”
In December, IPC did some more dot-connecting of its own with its announced acquisition of Senior Care of Colorado, which operates more than 200 geriatric-care facilities in the Denver area. Don Murphy, MD, IPC’s practice group leader for Senior Care of Colorado, says the model emphasizes a continuum of care and information flow from hospitalists in the hospital to affiliated providers in skilled nursing facilities and other outpatient settings. “We think that model, where we tie everything together, will be one of the best that we can do,” Dr. Murphy says.
From Dr. Singer’s perspective, the growing opportunities have sprung from efforts to address a persistent challenge. “We write an order of discharge to a skilled nursing facility, and patients go off into the community and we have no idea where they’re going, who they’re going to, what’s the quality of care out there, what’s the capacity of care,” he says. One of the central ideas of healthcare reform—creating true accountability around an episode of care—will require doctors to be linked “not just during what used to be the episode of care in the hospital,” he adds, “but throughout the continuum until that patient is really returned healthy back to wherever they’re going to be living.”
With a new emphasis on avoidable hospitalizations, hospitals will increasingly need to team up with other providers to avoid fragmentation of care. Using extensivists to help avoid gaps might be a good fit for accountable-care organizations, and Dr. Murphy says the process may be easier for big systems, such as Ochsner in New Orleans or the Cleveland Clinic, which are working in a confined geographic area with a defined patient population.
“The real challenge will be those of us out there in larger metropolitan areas where we’re not under the roof of one big conglomerate but still having to work together creatively and effectively to smooth the continuum,” Dr. Singer says.
Emerging Trends
Other trends are making inpatient-outpatient partnerships, whether formal or informal, an increasingly necessary part of providing high-quality healthcare. “We are seeing folks come out of the hospitals who 30 years ago clearly would have been in the hospital for a prolonged stay,” Dr. Murphy says. “A lot of these [patients], instead of going to SNFs, are going back to their homes and to assisted living with additional services; they require a lot of follow-up.”
Dr. Singer says he’s seeing another trend in which PCPs are likewise transitioning to newly created extensivist roles in sub-acute settings such as nursing homes. The position, he says, offers the attraction of a high-impact, longer-term relationship with patients without the high overhead of standalone clinics. The blurring of lines between outpatient and inpatient providers has created questions for hospitalists, too. For example, at what point does a hospitalist working much of the time in an outpatient clinic or skilled nursing facility no longer fit the traditional definition of a hospitalist? Does that detract from the doctor’s hospital duties? TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Sanger, P. Health plans juggle precarious patients. Managed Healthcare Executive. 2002:40-41.
Necessity, as they say, is the mother of invention, and the growing focus on the need for high-quality and cost-effective care is bringing a host of new innovations to light. One that hospitalists are likely to hear about far more about is the evolving role of an “extensivist,” an inpatient provider who ventures to outpatient settings to assist with care transitions.
In many ways, the expanding discussion of what extensivists are and do reflects the success of hospitalists in coordinating inpatient care and improving such metrics as length of stay (LOS). Why should that coordination end upon discharge? healthcare experts have wondered. Instead of a pure hospitalist system, could the experience and training of hospitalists be extended to include transitional or interim settings that provide a safety net between the hospital and a primary-care physician (PCP)? Might that improved inpatient-outpatient coordination help with other metrics, such as reduced rehospitalizations (see “All Aboard,” p. 1)?
One tangible result of those questions has been the growth of high-risk clinics. Hospitalist programs can provide clinic referrals for discharged patients who still require hands-on care, while PCPs can likewise refer some of their more complex patients. The clinic, then, becomes an alternative to hospitalization, or a preventive measure to avoid rehospitalization.
Philip Sanger, MD, founder and former CEO of Houston-based Inpatient Medical Services (now Intercede Health), is credited with one of the first uses of the term “extensivist.” Initially, it only described a hospitalist or other care provider who sees high-risk patients in an outpatient clinic.
Writing in Managed Healthcare Executive in 2002, Dr. Sanger explained: “To move from generally sick to generally well, high-risk patients need something extra—more attention than a busy PCP can offer [and] more individualized care than most protocol-driven disease management programs can provide. A high-risk clinic system is one way to fill this care gap. Also referred to as transitional-care clinics, these outpatient clinics focus on preventing hospital admissions and stabilizing high-risk patients.”1
Measured Improvements
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Co., says this extensivist model provides a respite for hospitalists, who typically spend a month at a time in these transitional clinics before heading back into the fray of the hospital. As hospitals, independent physician associations, and managed-care organizations try out new models of care, though, the definition of an extensivist has broadened to include providers in a range of outpatient settings, such as skilled nursing facilities, assistant living communities, and even home health services. California’s CareMore Medicare Advantage plan, in particular, has been cited by the Agency for Healthcare Research and Quality (AHRQ) for using hospitalists as extensivists in both outpatient clinics and skilled nursing facilities to reduce hospital readmission rates, LOS, and inpatient resource use.
The CareMore model reduces the caseload of its hospitalists to about six or eight patients per half-day, giving doctors more time to talk to patients and their family members. Based on those conversations, the extensivist works with a case manager to provide needed resources to each patient after discharge. The doctors also spend roughly half of each day in clinics seeing their own recently discharged patients, and one or two days each week in a skilled nursing facility to visit patients transferred from the hospital (for more details, visit www.innovations.ahrq.gov/content.aspx?id=2903).
Average inpatient LOS among the plan’s 44,000 members dipped to 3.2 days, compared with 5.8 days for Medicare fee-for-service providers and 4.5 days for traditional HM programs in the state. Last April, CareMore’s 30-day readmission rate averaged 13.4%, compared with a 19.6% rate for Medicare.
Baltimore-based Bravo Health has begun opening its own transitional advanced-care centers for members of its Medicare Advantage program, offering case management for complex conditions and immediate care when a PCP is unavailable. Another model has been advanced through team approaches practiced by the likes of Kaiser Permanente, though hospitalists aren’t necessarily the ones providing outpatient follow-up care. No matter what the model is called, Dr. Singer says, the main point is the same: “trying to connect the dots so that we get patients continuing to get better along the continuum without having to be readmitted.”
In December, IPC did some more dot-connecting of its own with its announced acquisition of Senior Care of Colorado, which operates more than 200 geriatric-care facilities in the Denver area. Don Murphy, MD, IPC’s practice group leader for Senior Care of Colorado, says the model emphasizes a continuum of care and information flow from hospitalists in the hospital to affiliated providers in skilled nursing facilities and other outpatient settings. “We think that model, where we tie everything together, will be one of the best that we can do,” Dr. Murphy says.
From Dr. Singer’s perspective, the growing opportunities have sprung from efforts to address a persistent challenge. “We write an order of discharge to a skilled nursing facility, and patients go off into the community and we have no idea where they’re going, who they’re going to, what’s the quality of care out there, what’s the capacity of care,” he says. One of the central ideas of healthcare reform—creating true accountability around an episode of care—will require doctors to be linked “not just during what used to be the episode of care in the hospital,” he adds, “but throughout the continuum until that patient is really returned healthy back to wherever they’re going to be living.”
With a new emphasis on avoidable hospitalizations, hospitals will increasingly need to team up with other providers to avoid fragmentation of care. Using extensivists to help avoid gaps might be a good fit for accountable-care organizations, and Dr. Murphy says the process may be easier for big systems, such as Ochsner in New Orleans or the Cleveland Clinic, which are working in a confined geographic area with a defined patient population.
“The real challenge will be those of us out there in larger metropolitan areas where we’re not under the roof of one big conglomerate but still having to work together creatively and effectively to smooth the continuum,” Dr. Singer says.
Emerging Trends
Other trends are making inpatient-outpatient partnerships, whether formal or informal, an increasingly necessary part of providing high-quality healthcare. “We are seeing folks come out of the hospitals who 30 years ago clearly would have been in the hospital for a prolonged stay,” Dr. Murphy says. “A lot of these [patients], instead of going to SNFs, are going back to their homes and to assisted living with additional services; they require a lot of follow-up.”
Dr. Singer says he’s seeing another trend in which PCPs are likewise transitioning to newly created extensivist roles in sub-acute settings such as nursing homes. The position, he says, offers the attraction of a high-impact, longer-term relationship with patients without the high overhead of standalone clinics. The blurring of lines between outpatient and inpatient providers has created questions for hospitalists, too. For example, at what point does a hospitalist working much of the time in an outpatient clinic or skilled nursing facility no longer fit the traditional definition of a hospitalist? Does that detract from the doctor’s hospital duties? TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Sanger, P. Health plans juggle precarious patients. Managed Healthcare Executive. 2002:40-41.
Necessity, as they say, is the mother of invention, and the growing focus on the need for high-quality and cost-effective care is bringing a host of new innovations to light. One that hospitalists are likely to hear about far more about is the evolving role of an “extensivist,” an inpatient provider who ventures to outpatient settings to assist with care transitions.
In many ways, the expanding discussion of what extensivists are and do reflects the success of hospitalists in coordinating inpatient care and improving such metrics as length of stay (LOS). Why should that coordination end upon discharge? healthcare experts have wondered. Instead of a pure hospitalist system, could the experience and training of hospitalists be extended to include transitional or interim settings that provide a safety net between the hospital and a primary-care physician (PCP)? Might that improved inpatient-outpatient coordination help with other metrics, such as reduced rehospitalizations (see “All Aboard,” p. 1)?
One tangible result of those questions has been the growth of high-risk clinics. Hospitalist programs can provide clinic referrals for discharged patients who still require hands-on care, while PCPs can likewise refer some of their more complex patients. The clinic, then, becomes an alternative to hospitalization, or a preventive measure to avoid rehospitalization.
Philip Sanger, MD, founder and former CEO of Houston-based Inpatient Medical Services (now Intercede Health), is credited with one of the first uses of the term “extensivist.” Initially, it only described a hospitalist or other care provider who sees high-risk patients in an outpatient clinic.
Writing in Managed Healthcare Executive in 2002, Dr. Sanger explained: “To move from generally sick to generally well, high-risk patients need something extra—more attention than a busy PCP can offer [and] more individualized care than most protocol-driven disease management programs can provide. A high-risk clinic system is one way to fill this care gap. Also referred to as transitional-care clinics, these outpatient clinics focus on preventing hospital admissions and stabilizing high-risk patients.”1
Measured Improvements
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Co., says this extensivist model provides a respite for hospitalists, who typically spend a month at a time in these transitional clinics before heading back into the fray of the hospital. As hospitals, independent physician associations, and managed-care organizations try out new models of care, though, the definition of an extensivist has broadened to include providers in a range of outpatient settings, such as skilled nursing facilities, assistant living communities, and even home health services. California’s CareMore Medicare Advantage plan, in particular, has been cited by the Agency for Healthcare Research and Quality (AHRQ) for using hospitalists as extensivists in both outpatient clinics and skilled nursing facilities to reduce hospital readmission rates, LOS, and inpatient resource use.
The CareMore model reduces the caseload of its hospitalists to about six or eight patients per half-day, giving doctors more time to talk to patients and their family members. Based on those conversations, the extensivist works with a case manager to provide needed resources to each patient after discharge. The doctors also spend roughly half of each day in clinics seeing their own recently discharged patients, and one or two days each week in a skilled nursing facility to visit patients transferred from the hospital (for more details, visit www.innovations.ahrq.gov/content.aspx?id=2903).
Average inpatient LOS among the plan’s 44,000 members dipped to 3.2 days, compared with 5.8 days for Medicare fee-for-service providers and 4.5 days for traditional HM programs in the state. Last April, CareMore’s 30-day readmission rate averaged 13.4%, compared with a 19.6% rate for Medicare.
Baltimore-based Bravo Health has begun opening its own transitional advanced-care centers for members of its Medicare Advantage program, offering case management for complex conditions and immediate care when a PCP is unavailable. Another model has been advanced through team approaches practiced by the likes of Kaiser Permanente, though hospitalists aren’t necessarily the ones providing outpatient follow-up care. No matter what the model is called, Dr. Singer says, the main point is the same: “trying to connect the dots so that we get patients continuing to get better along the continuum without having to be readmitted.”
In December, IPC did some more dot-connecting of its own with its announced acquisition of Senior Care of Colorado, which operates more than 200 geriatric-care facilities in the Denver area. Don Murphy, MD, IPC’s practice group leader for Senior Care of Colorado, says the model emphasizes a continuum of care and information flow from hospitalists in the hospital to affiliated providers in skilled nursing facilities and other outpatient settings. “We think that model, where we tie everything together, will be one of the best that we can do,” Dr. Murphy says.
From Dr. Singer’s perspective, the growing opportunities have sprung from efforts to address a persistent challenge. “We write an order of discharge to a skilled nursing facility, and patients go off into the community and we have no idea where they’re going, who they’re going to, what’s the quality of care out there, what’s the capacity of care,” he says. One of the central ideas of healthcare reform—creating true accountability around an episode of care—will require doctors to be linked “not just during what used to be the episode of care in the hospital,” he adds, “but throughout the continuum until that patient is really returned healthy back to wherever they’re going to be living.”
With a new emphasis on avoidable hospitalizations, hospitals will increasingly need to team up with other providers to avoid fragmentation of care. Using extensivists to help avoid gaps might be a good fit for accountable-care organizations, and Dr. Murphy says the process may be easier for big systems, such as Ochsner in New Orleans or the Cleveland Clinic, which are working in a confined geographic area with a defined patient population.
“The real challenge will be those of us out there in larger metropolitan areas where we’re not under the roof of one big conglomerate but still having to work together creatively and effectively to smooth the continuum,” Dr. Singer says.
Emerging Trends
Other trends are making inpatient-outpatient partnerships, whether formal or informal, an increasingly necessary part of providing high-quality healthcare. “We are seeing folks come out of the hospitals who 30 years ago clearly would have been in the hospital for a prolonged stay,” Dr. Murphy says. “A lot of these [patients], instead of going to SNFs, are going back to their homes and to assisted living with additional services; they require a lot of follow-up.”
Dr. Singer says he’s seeing another trend in which PCPs are likewise transitioning to newly created extensivist roles in sub-acute settings such as nursing homes. The position, he says, offers the attraction of a high-impact, longer-term relationship with patients without the high overhead of standalone clinics. The blurring of lines between outpatient and inpatient providers has created questions for hospitalists, too. For example, at what point does a hospitalist working much of the time in an outpatient clinic or skilled nursing facility no longer fit the traditional definition of a hospitalist? Does that detract from the doctor’s hospital duties? TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Sanger, P. Health plans juggle precarious patients. Managed Healthcare Executive. 2002:40-41.
ONLINE EXCLUSIVE: Listen to Stephen Jencks, MD, and hospitalist Brad Sherman, MD, FHM, chat about readmission problems and solutions
Listen to Stephen Jencks, MD, MPH, discuss why the issue of hospital readmissions has caught the attention of doctors and professional societies.
Listen to veteran hospitalist Bradley Sherman, MD, FHM, chairman of the Department of Medicine at Glen Cove Hospital, part of the North Shore/LIJ Health System in New York, talk about what you can do both now and over the next year to help your institutions decrease readmission rates.
Listen to Stephen Jencks, MD, MPH, discuss why the issue of hospital readmissions has caught the attention of doctors and professional societies.
Listen to veteran hospitalist Bradley Sherman, MD, FHM, chairman of the Department of Medicine at Glen Cove Hospital, part of the North Shore/LIJ Health System in New York, talk about what you can do both now and over the next year to help your institutions decrease readmission rates.
Listen to Stephen Jencks, MD, MPH, discuss why the issue of hospital readmissions has caught the attention of doctors and professional societies.
Listen to veteran hospitalist Bradley Sherman, MD, FHM, chairman of the Department of Medicine at Glen Cove Hospital, part of the North Shore/LIJ Health System in New York, talk about what you can do both now and over the next year to help your institutions decrease readmission rates.
ONLINE EXCLUSIVE: The Exception or the Rule? Targeting the Right Patient Populations
Which patients are you most likely to see again? It’s a particularly vexing question for hospitalists amid the heightened focus on lowering hospital readmissions, and one that several recent studies have sought to address.
One Journal of Hospital Medicine analysis of more than 10,300 admissions found that unplanned rehospitalizations within 30 days of discharge were far more likely for African-American patients and those on high-risk medications like narcotics and corticosteroids.1 Patients with such chronic conditions as cancer, renal failure, and congestive heart failure also were at increased risk.
A second, smaller study of 142 inpatients who had been hospitalized within the preceding six months found that chronic disease, depression, and being underweight or obese all predicted a higher risk of another readmission within the next six months.2
And a third report in the Journal of Urban Health examined more than 36,000 Medicare patients admitted to urban public hospitals to assess which were most likely to return within the following year. Chronic medical conditions, substance abuse, and homelessness all contributed to increased odds.3

Most efforts aimed at reducing rehospitalizations, such as SHM’s Project BOOST, include a risk assessment that can point to potential trouble spots for individual patients. For certain populations, research has highlighted socioeconomic and racial disparities in access to healthcare that likely lead to unnecessary hospitalizations. But it’s one thing to identify the factors associated with higher rates, and quite another to actively manage them, especially when many crop up well beyond a hospital’s walls. Anxiety over these contributing factors is steadily building in anticipation of Medicare penalties for excessively high readmission rates set to begin in 2012.
“Whenever there is a program that has financial incentives, people always get concerned that they have patients who are somehow different,” says Lakshmi Halasyamani, MD, SFHM, SHM board member and vice president for medical affairs at Saint Joseph Mercy Health System in Ann Arbor, Mich. “Inherent in that assumption is: more difficult to manage or sicker or more complicated.”
Stephen Jencks, MD, MPH, an independent healthcare safety and quality consultant based in Baltimore, says he’s heard the same complaint for three decades. “It’s what we call the 'Lake Wobegon effect': All of our patients are sicker than average.
“I think it’s just a really poor way to go about what is a very human sort of question,” he adds. “If Mrs. Jones is back in the hospital because she didn’t understand the discharge instructions, the question is not ‘Does my population have more literacy problems than somebody else’s population of patients?’ The question is ‘What can we do for Mrs. Jones so she can understand this stuff?’ ” (For help communicating with patients, check out SHM's on-demand webinar, "Implementing Teach Back as a System-Wide Patient Communication Strategy.")
Healthcare experts say it’s not difficult to find challenges unique to particular urban areas or populations. Florida Hospital Association President Bruce Rueben, MBA, says many Floridians speak English as a second language, making clear communication critical. The state also has one of the highest percentages of elderly residents and is in a funding crisis that has required providers to do more with less. But instead of worrying about exceptions or anomalies, Rueben says, focusing on the best overall readmission-reducing approaches will help ensure that all patients are being treated and discharged effectively.
What about dealing with specific conditions? Paul McGann, MD, deputy chief medical officer at the Centers for Medicare & Medicaid Services (CMS), says good evidence exists for the effectiveness of interventions aimed at diseases ranging from congestive heart failure and cancer to chronic obstructive lung disease, ulcers, and stroke. But data from Medicare’s Care Transitions Program, he says, suggest that even if all hospitals pursued the dozens of disease-specific interventions collectively implemented by the program’s participants, they still wouldn’t address more than about half of the causes of readmission. Based on that finding, he says, project leaders have insisted on an all-cause focus.
Dr. Halasyamani says it’s only natural to sometimes focus on the exception rather than the rule. “And we’ve all had those experiences where, boy, you feel like you’ve done everything you can and the patient still comes back,” she says. “But having said that, we also have opportunities where we haven’t done everything that we can and the patient comes back. So I think we need to focus on that first, rather than say, ‘Well, this isn’t fixable based on all of the patient-level issues.’”
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says it all comes down to perspective. “Instead of looking at what’s the percentage that we can’t deal with,” she says, “let’s look at the patient population that we can affect.”
Bryn Nelson is a freelance medical writer based in Seattle.
References
1. Allaudeen N, Vidyarthi A, Maselli J, Auerbach A. Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6(2):54-60.
2. Mudge AM, Kasper KM, Clair, A, et al. Recurrent readmissions in medical patients: a prospective study. J Hosp Med. 2011;6(2):61-67.
3. Raven, MC, Billings, JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urb Health. 2009;86(2):230-241.
Which patients are you most likely to see again? It’s a particularly vexing question for hospitalists amid the heightened focus on lowering hospital readmissions, and one that several recent studies have sought to address.
One Journal of Hospital Medicine analysis of more than 10,300 admissions found that unplanned rehospitalizations within 30 days of discharge were far more likely for African-American patients and those on high-risk medications like narcotics and corticosteroids.1 Patients with such chronic conditions as cancer, renal failure, and congestive heart failure also were at increased risk.
A second, smaller study of 142 inpatients who had been hospitalized within the preceding six months found that chronic disease, depression, and being underweight or obese all predicted a higher risk of another readmission within the next six months.2
And a third report in the Journal of Urban Health examined more than 36,000 Medicare patients admitted to urban public hospitals to assess which were most likely to return within the following year. Chronic medical conditions, substance abuse, and homelessness all contributed to increased odds.3
Most efforts aimed at reducing rehospitalizations, such as SHM’s Project BOOST, include a risk assessment that can point to potential trouble spots for individual patients. For certain populations, research has highlighted socioeconomic and racial disparities in access to healthcare that likely lead to unnecessary hospitalizations. But it’s one thing to identify the factors associated with higher rates, and quite another to actively manage them, especially when many crop up well beyond a hospital’s walls. Anxiety over these contributing factors is steadily building in anticipation of Medicare penalties for excessively high readmission rates set to begin in 2012.
“Whenever there is a program that has financial incentives, people always get concerned that they have patients who are somehow different,” says Lakshmi Halasyamani, MD, SFHM, SHM board member and vice president for medical affairs at Saint Joseph Mercy Health System in Ann Arbor, Mich. “Inherent in that assumption is: more difficult to manage or sicker or more complicated.”
Stephen Jencks, MD, MPH, an independent healthcare safety and quality consultant based in Baltimore, says he’s heard the same complaint for three decades. “It’s what we call the 'Lake Wobegon effect': All of our patients are sicker than average.
“I think it’s just a really poor way to go about what is a very human sort of question,” he adds. “If Mrs. Jones is back in the hospital because she didn’t understand the discharge instructions, the question is not ‘Does my population have more literacy problems than somebody else’s population of patients?’ The question is ‘What can we do for Mrs. Jones so she can understand this stuff?’ ” (For help communicating with patients, check out SHM's on-demand webinar, "Implementing Teach Back as a System-Wide Patient Communication Strategy.")
Healthcare experts say it’s not difficult to find challenges unique to particular urban areas or populations. Florida Hospital Association President Bruce Rueben, MBA, says many Floridians speak English as a second language, making clear communication critical. The state also has one of the highest percentages of elderly residents and is in a funding crisis that has required providers to do more with less. But instead of worrying about exceptions or anomalies, Rueben says, focusing on the best overall readmission-reducing approaches will help ensure that all patients are being treated and discharged effectively.
What about dealing with specific conditions? Paul McGann, MD, deputy chief medical officer at the Centers for Medicare & Medicaid Services (CMS), says good evidence exists for the effectiveness of interventions aimed at diseases ranging from congestive heart failure and cancer to chronic obstructive lung disease, ulcers, and stroke. But data from Medicare’s Care Transitions Program, he says, suggest that even if all hospitals pursued the dozens of disease-specific interventions collectively implemented by the program’s participants, they still wouldn’t address more than about half of the causes of readmission. Based on that finding, he says, project leaders have insisted on an all-cause focus.
Dr. Halasyamani says it’s only natural to sometimes focus on the exception rather than the rule. “And we’ve all had those experiences where, boy, you feel like you’ve done everything you can and the patient still comes back,” she says. “But having said that, we also have opportunities where we haven’t done everything that we can and the patient comes back. So I think we need to focus on that first, rather than say, ‘Well, this isn’t fixable based on all of the patient-level issues.’”
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says it all comes down to perspective. “Instead of looking at what’s the percentage that we can’t deal with,” she says, “let’s look at the patient population that we can affect.”
Bryn Nelson is a freelance medical writer based in Seattle.
References
1. Allaudeen N, Vidyarthi A, Maselli J, Auerbach A. Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6(2):54-60.
2. Mudge AM, Kasper KM, Clair, A, et al. Recurrent readmissions in medical patients: a prospective study. J Hosp Med. 2011;6(2):61-67.
3. Raven, MC, Billings, JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urb Health. 2009;86(2):230-241.
Which patients are you most likely to see again? It’s a particularly vexing question for hospitalists amid the heightened focus on lowering hospital readmissions, and one that several recent studies have sought to address.
One Journal of Hospital Medicine analysis of more than 10,300 admissions found that unplanned rehospitalizations within 30 days of discharge were far more likely for African-American patients and those on high-risk medications like narcotics and corticosteroids.1 Patients with such chronic conditions as cancer, renal failure, and congestive heart failure also were at increased risk.
A second, smaller study of 142 inpatients who had been hospitalized within the preceding six months found that chronic disease, depression, and being underweight or obese all predicted a higher risk of another readmission within the next six months.2
And a third report in the Journal of Urban Health examined more than 36,000 Medicare patients admitted to urban public hospitals to assess which were most likely to return within the following year. Chronic medical conditions, substance abuse, and homelessness all contributed to increased odds.3
Most efforts aimed at reducing rehospitalizations, such as SHM’s Project BOOST, include a risk assessment that can point to potential trouble spots for individual patients. For certain populations, research has highlighted socioeconomic and racial disparities in access to healthcare that likely lead to unnecessary hospitalizations. But it’s one thing to identify the factors associated with higher rates, and quite another to actively manage them, especially when many crop up well beyond a hospital’s walls. Anxiety over these contributing factors is steadily building in anticipation of Medicare penalties for excessively high readmission rates set to begin in 2012.
“Whenever there is a program that has financial incentives, people always get concerned that they have patients who are somehow different,” says Lakshmi Halasyamani, MD, SFHM, SHM board member and vice president for medical affairs at Saint Joseph Mercy Health System in Ann Arbor, Mich. “Inherent in that assumption is: more difficult to manage or sicker or more complicated.”
Stephen Jencks, MD, MPH, an independent healthcare safety and quality consultant based in Baltimore, says he’s heard the same complaint for three decades. “It’s what we call the 'Lake Wobegon effect': All of our patients are sicker than average.
“I think it’s just a really poor way to go about what is a very human sort of question,” he adds. “If Mrs. Jones is back in the hospital because she didn’t understand the discharge instructions, the question is not ‘Does my population have more literacy problems than somebody else’s population of patients?’ The question is ‘What can we do for Mrs. Jones so she can understand this stuff?’ ” (For help communicating with patients, check out SHM's on-demand webinar, "Implementing Teach Back as a System-Wide Patient Communication Strategy.")
Healthcare experts say it’s not difficult to find challenges unique to particular urban areas or populations. Florida Hospital Association President Bruce Rueben, MBA, says many Floridians speak English as a second language, making clear communication critical. The state also has one of the highest percentages of elderly residents and is in a funding crisis that has required providers to do more with less. But instead of worrying about exceptions or anomalies, Rueben says, focusing on the best overall readmission-reducing approaches will help ensure that all patients are being treated and discharged effectively.
What about dealing with specific conditions? Paul McGann, MD, deputy chief medical officer at the Centers for Medicare & Medicaid Services (CMS), says good evidence exists for the effectiveness of interventions aimed at diseases ranging from congestive heart failure and cancer to chronic obstructive lung disease, ulcers, and stroke. But data from Medicare’s Care Transitions Program, he says, suggest that even if all hospitals pursued the dozens of disease-specific interventions collectively implemented by the program’s participants, they still wouldn’t address more than about half of the causes of readmission. Based on that finding, he says, project leaders have insisted on an all-cause focus.
Dr. Halasyamani says it’s only natural to sometimes focus on the exception rather than the rule. “And we’ve all had those experiences where, boy, you feel like you’ve done everything you can and the patient still comes back,” she says. “But having said that, we also have opportunities where we haven’t done everything that we can and the patient comes back. So I think we need to focus on that first, rather than say, ‘Well, this isn’t fixable based on all of the patient-level issues.’”
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says it all comes down to perspective. “Instead of looking at what’s the percentage that we can’t deal with,” she says, “let’s look at the patient population that we can affect.”
Bryn Nelson is a freelance medical writer based in Seattle.
References
1. Allaudeen N, Vidyarthi A, Maselli J, Auerbach A. Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6(2):54-60.
2. Mudge AM, Kasper KM, Clair, A, et al. Recurrent readmissions in medical patients: a prospective study. J Hosp Med. 2011;6(2):61-67.
3. Raven, MC, Billings, JC, Goldfrank LR, Manheimer ED, Gourevitch MN. Medicaid patients at high risk for frequent hospital admission: real-time identification and remediable risks. J Urb Health. 2009;86(2):230-241.

A New Year’s Resolution to Crack Down on Opioids?
Sometime early this year, after two years of controversy, the FDA might finally release its revised proposal for more stringent regulations on opioid pain relievers. The following are the key questions—and answers—surrounding new regulations, as well as a look at other recent FDA actions, including increased scrutiny of diabetes and obesity drugs due to heart concerns.
Question: What’s the latest on the FDA release of new regulations for prescription opioids?
Answer: First, the back story: The controversy concerns the creation of a Risk Evaluation and Mitigation Strategy (REMS) for opioid analgesics amid a troubling boom in prescription drug abuse, addiction, and overdose, and an accompanying spike in deaths from opioid overdoses. Under a 2007 law, the FDA can require drug and medical device manufacturers to adopt a REMS to ensure that the benefits outweigh the risks of continued use and that patients are adequately informed. In this case, the strategy could impact how nearly 4 million patients receive long-acting and extended-release opioids annually, according to FDA statistics.
In February 2009, the FDA sent a letter to manufacturers of opioid pain relievers, proposing a classwide REMS that would require certification by a physician or pharmacist and restrict distribution of the drugs, among other provisions. In response, many healthcare providers and medical organizations warned of an increased regulatory burden that would negatively impact patients. Among the concerns: fewer primary-care physicians (PCPs) willing to manage patients with chronic pain, reduced access to medically necessary drugs in underserved communities, undermedicated cancer patients, and increased use of other drugs with less stringent oversight.
In response, the FDA dropped its proposal for a prescriber accreditation program and another for a patient registry. But an FDA advisory panel soundly rejected a revised REMS proposal in July, by a vote of 25-10. The panel criticized the new plans as being too lax, lacking a formal requirement f

Q: What will the new REMS likely include?
A: Based on the criticisms of FDA panelists in July, the revised REMS could mandate a training requirement for all prescribers. The program would likely be created by the FDA and not by the drug industry, as had first been proposed (many doctors have agreed that a centralized, standardized program would be far preferable to dealing with programs set up independently by drug manufacturers). The strategy also might govern immediate-release opioids, in addition to extended-release and long-acting formulations. The FDA could propose linking doctor education to an existing Drug Enforcement Administration registration, but that would require congressional approval.
Q: What was the outcome of safety deliberations over the diabetes drug rosiglitazone (Avandia)?
A: After several years of concern over a heightened risk of heart attacks and other heart problems among patients taking rosiglitazone for type 2 diabetes mellitus, the FDA sharply restricted its availability in September and required the manufacturer, GlaxoSmithKline, to submit a REMS. When implemented, the REMS will limit new prescriptions to patients who cannot achieve glycemic control with other medications and decide not to take the alternative (pioglitazone) for medical reasons.1 Other diabetes drugs have faced similar scrutiny: In October, the FDA rejected an extended-release form of the diabetes drug exenatide (Bydureon) due to safety concerns, citing the need for more studies from manufacturer Eli Lilly about its effect on heart rate.
Q: What’s the upshot of recent FDA actions on weight-loss drugs and supplements?
A: The FDA also cracked down on weight-loss formulations in 2010, declining to approve several new drugs, overseeing the withdrawal of Abbott Laboratory’s Meridia in October, and announcing a December recall of capsules marketed online as Fruta Planta. Safety concerns over the latter two were linked to sibutramine, a drug that is “known to increase blood pressure and/or pulse rate in some patients and may present a serious risk for patients with a history of coronary artery disease, congestive heart failure, arrhythmias or stroke,” according to the FDA. Additionally, the drug can interact “in life-threatening ways” with other medications, reinforcing the idea that hospitalists and other doctors should delve into patients’ recent history of weight-loss drug or supplement use.
Q: What should we expect from the FDA in the next year?
A: Analysts will be keeping an eye on the number of new drugs approved in 2011 to discern any new trends. As reported by The Wall Street Journal and other publications, the FDA gave 21 drugs the go-ahead in 2010, down from 26 cleared in 2009 and 25 approved in 2008. The dip has concerned some drug industry representatives, who warn that an overly cautious approach could lead to more delays in new drugs reaching patients. Of course, the lower number also could reflect a continued dry spell in the pipelines of many pharmaceutical companies. On the flipside, consumer watchdogs have expressed optimism that the FDA might be devoting more attention to safety. In November, for example, the FDA oversaw the pulling of popular painkiller propoxyphene (marketed as Darvon and Darvocet) after evidence accumulated that the medication can cause potentially fatal heart damage and rhythm abnormalities.
Bryn Nelson is a freelance medical writer based in Seattle.
References
1. Woodcock J, Sharfstein JM, Hamburg M. Regulatory action on rosiglitazone by the U.S. Food and Drug Administration. N Engl J Med. 2010;363(16):1489-1491.
Sometime early this year, after two years of controversy, the FDA might finally release its revised proposal for more stringent regulations on opioid pain relievers. The following are the key questions—and answers—surrounding new regulations, as well as a look at other recent FDA actions, including increased scrutiny of diabetes and obesity drugs due to heart concerns.
Question: What’s the latest on the FDA release of new regulations for prescription opioids?
Answer: First, the back story: The controversy concerns the creation of a Risk Evaluation and Mitigation Strategy (REMS) for opioid analgesics amid a troubling boom in prescription drug abuse, addiction, and overdose, and an accompanying spike in deaths from opioid overdoses. Under a 2007 law, the FDA can require drug and medical device manufacturers to adopt a REMS to ensure that the benefits outweigh the risks of continued use and that patients are adequately informed. In this case, the strategy could impact how nearly 4 million patients receive long-acting and extended-release opioids annually, according to FDA statistics.
In February 2009, the FDA sent a letter to manufacturers of opioid pain relievers, proposing a classwide REMS that would require certification by a physician or pharmacist and restrict distribution of the drugs, among other provisions. In response, many healthcare providers and medical organizations warned of an increased regulatory burden that would negatively impact patients. Among the concerns: fewer primary-care physicians (PCPs) willing to manage patients with chronic pain, reduced access to medically necessary drugs in underserved communities, undermedicated cancer patients, and increased use of other drugs with less stringent oversight.
In response, the FDA dropped its proposal for a prescriber accreditation program and another for a patient registry. But an FDA advisory panel soundly rejected a revised REMS proposal in July, by a vote of 25-10. The panel criticized the new plans as being too lax, lacking a formal requirement f
Q: What will the new REMS likely include?
A: Based on the criticisms of FDA panelists in July, the revised REMS could mandate a training requirement for all prescribers. The program would likely be created by the FDA and not by the drug industry, as had first been proposed (many doctors have agreed that a centralized, standardized program would be far preferable to dealing with programs set up independently by drug manufacturers). The strategy also might govern immediate-release opioids, in addition to extended-release and long-acting formulations. The FDA could propose linking doctor education to an existing Drug Enforcement Administration registration, but that would require congressional approval.
Q: What was the outcome of safety deliberations over the diabetes drug rosiglitazone (Avandia)?
A: After several years of concern over a heightened risk of heart attacks and other heart problems among patients taking rosiglitazone for type 2 diabetes mellitus, the FDA sharply restricted its availability in September and required the manufacturer, GlaxoSmithKline, to submit a REMS. When implemented, the REMS will limit new prescriptions to patients who cannot achieve glycemic control with other medications and decide not to take the alternative (pioglitazone) for medical reasons.1 Other diabetes drugs have faced similar scrutiny: In October, the FDA rejected an extended-release form of the diabetes drug exenatide (Bydureon) due to safety concerns, citing the need for more studies from manufacturer Eli Lilly about its effect on heart rate.
Q: What’s the upshot of recent FDA actions on weight-loss drugs and supplements?
A: The FDA also cracked down on weight-loss formulations in 2010, declining to approve several new drugs, overseeing the withdrawal of Abbott Laboratory’s Meridia in October, and announcing a December recall of capsules marketed online as Fruta Planta. Safety concerns over the latter two were linked to sibutramine, a drug that is “known to increase blood pressure and/or pulse rate in some patients and may present a serious risk for patients with a history of coronary artery disease, congestive heart failure, arrhythmias or stroke,” according to the FDA. Additionally, the drug can interact “in life-threatening ways” with other medications, reinforcing the idea that hospitalists and other doctors should delve into patients’ recent history of weight-loss drug or supplement use.
Q: What should we expect from the FDA in the next year?
A: Analysts will be keeping an eye on the number of new drugs approved in 2011 to discern any new trends. As reported by The Wall Street Journal and other publications, the FDA gave 21 drugs the go-ahead in 2010, down from 26 cleared in 2009 and 25 approved in 2008. The dip has concerned some drug industry representatives, who warn that an overly cautious approach could lead to more delays in new drugs reaching patients. Of course, the lower number also could reflect a continued dry spell in the pipelines of many pharmaceutical companies. On the flipside, consumer watchdogs have expressed optimism that the FDA might be devoting more attention to safety. In November, for example, the FDA oversaw the pulling of popular painkiller propoxyphene (marketed as Darvon and Darvocet) after evidence accumulated that the medication can cause potentially fatal heart damage and rhythm abnormalities.
Bryn Nelson is a freelance medical writer based in Seattle.
References
1. Woodcock J, Sharfstein JM, Hamburg M. Regulatory action on rosiglitazone by the U.S. Food and Drug Administration. N Engl J Med. 2010;363(16):1489-1491.
Sometime early this year, after two years of controversy, the FDA might finally release its revised proposal for more stringent regulations on opioid pain relievers. The following are the key questions—and answers—surrounding new regulations, as well as a look at other recent FDA actions, including increased scrutiny of diabetes and obesity drugs due to heart concerns.
Question: What’s the latest on the FDA release of new regulations for prescription opioids?
Answer: First, the back story: The controversy concerns the creation of a Risk Evaluation and Mitigation Strategy (REMS) for opioid analgesics amid a troubling boom in prescription drug abuse, addiction, and overdose, and an accompanying spike in deaths from opioid overdoses. Under a 2007 law, the FDA can require drug and medical device manufacturers to adopt a REMS to ensure that the benefits outweigh the risks of continued use and that patients are adequately informed. In this case, the strategy could impact how nearly 4 million patients receive long-acting and extended-release opioids annually, according to FDA statistics.
In February 2009, the FDA sent a letter to manufacturers of opioid pain relievers, proposing a classwide REMS that would require certification by a physician or pharmacist and restrict distribution of the drugs, among other provisions. In response, many healthcare providers and medical organizations warned of an increased regulatory burden that would negatively impact patients. Among the concerns: fewer primary-care physicians (PCPs) willing to manage patients with chronic pain, reduced access to medically necessary drugs in underserved communities, undermedicated cancer patients, and increased use of other drugs with less stringent oversight.
In response, the FDA dropped its proposal for a prescriber accreditation program and another for a patient registry. But an FDA advisory panel soundly rejected a revised REMS proposal in July, by a vote of 25-10. The panel criticized the new plans as being too lax, lacking a formal requirement f
Q: What will the new REMS likely include?
A: Based on the criticisms of FDA panelists in July, the revised REMS could mandate a training requirement for all prescribers. The program would likely be created by the FDA and not by the drug industry, as had first been proposed (many doctors have agreed that a centralized, standardized program would be far preferable to dealing with programs set up independently by drug manufacturers). The strategy also might govern immediate-release opioids, in addition to extended-release and long-acting formulations. The FDA could propose linking doctor education to an existing Drug Enforcement Administration registration, but that would require congressional approval.
Q: What was the outcome of safety deliberations over the diabetes drug rosiglitazone (Avandia)?
A: After several years of concern over a heightened risk of heart attacks and other heart problems among patients taking rosiglitazone for type 2 diabetes mellitus, the FDA sharply restricted its availability in September and required the manufacturer, GlaxoSmithKline, to submit a REMS. When implemented, the REMS will limit new prescriptions to patients who cannot achieve glycemic control with other medications and decide not to take the alternative (pioglitazone) for medical reasons.1 Other diabetes drugs have faced similar scrutiny: In October, the FDA rejected an extended-release form of the diabetes drug exenatide (Bydureon) due to safety concerns, citing the need for more studies from manufacturer Eli Lilly about its effect on heart rate.
Q: What’s the upshot of recent FDA actions on weight-loss drugs and supplements?
A: The FDA also cracked down on weight-loss formulations in 2010, declining to approve several new drugs, overseeing the withdrawal of Abbott Laboratory’s Meridia in October, and announcing a December recall of capsules marketed online as Fruta Planta. Safety concerns over the latter two were linked to sibutramine, a drug that is “known to increase blood pressure and/or pulse rate in some patients and may present a serious risk for patients with a history of coronary artery disease, congestive heart failure, arrhythmias or stroke,” according to the FDA. Additionally, the drug can interact “in life-threatening ways” with other medications, reinforcing the idea that hospitalists and other doctors should delve into patients’ recent history of weight-loss drug or supplement use.
Q: What should we expect from the FDA in the next year?
A: Analysts will be keeping an eye on the number of new drugs approved in 2011 to discern any new trends. As reported by The Wall Street Journal and other publications, the FDA gave 21 drugs the go-ahead in 2010, down from 26 cleared in 2009 and 25 approved in 2008. The dip has concerned some drug industry representatives, who warn that an overly cautious approach could lead to more delays in new drugs reaching patients. Of course, the lower number also could reflect a continued dry spell in the pipelines of many pharmaceutical companies. On the flipside, consumer watchdogs have expressed optimism that the FDA might be devoting more attention to safety. In November, for example, the FDA oversaw the pulling of popular painkiller propoxyphene (marketed as Darvon and Darvocet) after evidence accumulated that the medication can cause potentially fatal heart damage and rhythm abnormalities.
Bryn Nelson is a freelance medical writer based in Seattle.
References
1. Woodcock J, Sharfstein JM, Hamburg M. Regulatory action on rosiglitazone by the U.S. Food and Drug Administration. N Engl J Med. 2010;363(16):1489-1491.

Turbulence Ahead
After the wild ride of 2010, public-policy watchers could be forgiven for fervently hoping that 2011 offers a calmer year on the healthcare front.
Fat chance.
The turbulence could begin immediately, with the seating of the 112th Congress on Jan. 3. “I think the first question that’s on everybody’s mind is, ‘What will the Republican majority in the House do to Obama’s healthcare reform initiative?’ ” says Eric Siegal, MD, SFHM, a member of SHM’s Public Policy Committee (PPC) and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health.
For most issues of direct concern to hospitalists, he says, especially those centered on healthcare delivery, “the wheels were in motion” long before the reform bill became law. Dr. Siegal also says most healthcare experts support the substance of accountable care organizations (ACOs), pay for performance, and reforming Medicare in ways that reward quality instead of quantity. “I think that ship is out of the harbor,” he says.
Throughout the year, the PPC will focus on three priorities identified in the Affordable Care Act: hospital value-based purchasing, bundled payments including ACOs, and hospital readmissions and transitions of care.
—Bill Vaughan, senior policy analyst, Consumers Union, Washington, D.C.
Debate, Delay, Defund?
There are several ways that Congress can delay or thwart the launch of specific reform initiatives. The first is to hold hearings about reform measures, Dr. Siegal says, “with the hope that they can somehow undermine it by raising questions about either the finances of it or about the implications for average Americans in terms of what kind of healthcare they’re going to get.” Such tactics carry significant risk, however, because highlighting specific aspects of the reform law could actually increase overall public support. “It has the potential to backfire on them,” he says.
“Repeal won’t happen anytime soon,” predicts Pat Conway, MD, chair of the PPC and director of hospital medicine at Cincinnati Children’s Hospital. “However, Congress could gut or significantly reduce funding to multiple programs within the bill, and then if you significantly reduce the funding, this may make it nearly impossible for those programs to be successful.”
Rough estimates suggest that some $150 billion worth of programs over the 10-year life of the healthcare reform act remain unfunded and are at risk. As an example, Dr. Conway cites wording in the bill that authorizes a program to help ease patient transitions in and out of the hospital. “If you reduce that funding to near zero, hospitals and hospitalists may still be successful, but you’ve essentially removed the program to learn how to be successful,” he says.
Bill Vaughan, a senior policy analyst in healthcare with the Washington, D.C.-based organization Consumers Union, says targeted riders could be added to appropriations bills. For instance, one rider could prohibit the Centers for Medicare & Medicaid Services (CMS) from spending any money to help develop government-supported insurance exchanges. Another could prevent the IRS from collecting money to be channeled into the trust fund for the Patient-Centered Outcomes Research Institute and its focus on comparative-effectiveness research. “There’s no end to mischief,” Vaughan says. “There are as many opportunities as the day is long.”
A major confrontation could arrive in March or April, when the U.S. runs into its debt ceiling. A continuing resolution would then be required to continue the appropriations process (and increase the U.S. debt ceiling past its current limit of $14.3 trillion). At that point or soon thereafter, Vaughan says, an opportunity could arise for legislators to say they won’t vote for a critical appropriations bill unless it includes certain spending reductions cited by one of several commissions tasked with recommending ways to reduce the deficit. “That could include hospital cuts, more doctor cuts, significant cost shifting to beneficiaries, higher copays,” he says.
Amid a “firestorm of ideas” on how to further cut Medicare and Medicaid spending, ideas once deemed radical could gain more traction. Some legislators have tossed around the idea of shutting down the government, if need be. “There’s nothing on the radar scope but static and fuzz,” Vaughan says. “It is totally unclear what is going to happen.”
Dearth of Drugs
Another trend generating both uncertainty and headaches in the nation’s hospitals is an unprecedented prescription drug shortage that could last well into the New Year, based on the number of medicines now in scarce supply across the country. In mid-November, for example, the American Society of Clinical Oncology announced “severe and worsening shortages of many critical therapies,” including doxorubicin, leucovorin, etoposide, nitrogen mustard, vincristine, propofol, and morphine.
Valerie Jensen, associate director of the FDA’s drug shortage program, told the Associated Press that her agency was seeing a record number of drug shortfalls in 2010. In mid-November, the FDA’s Current Drug Shortages list (www.fda.gov/Drugs/DrugSafety/DrugShortages/ucm050792.htm) included multiple formulations of 50 different medicines. Why so many? Jensen blamed the scarcity, in part, on the fact that many older drugs are not as profitable as newer ones. Manufacturing issues or delays and increased demand were the two biggest official reasons, though the FDA reported that at least eight formulations had been pulled or held from the market.
Vaughan says he’s heard plenty of buzz about the problem showing up quickly and unexpectedly in hospitals. Drug companies are supposed to give the FDA six months’ notice if they stop producing a drug, he says, but there’s no penalty if they don’t. “It’s amazing the number of people who are starting to worry about it,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
After the wild ride of 2010, public-policy watchers could be forgiven for fervently hoping that 2011 offers a calmer year on the healthcare front.
Fat chance.
The turbulence could begin immediately, with the seating of the 112th Congress on Jan. 3. “I think the first question that’s on everybody’s mind is, ‘What will the Republican majority in the House do to Obama’s healthcare reform initiative?’ ” says Eric Siegal, MD, SFHM, a member of SHM’s Public Policy Committee (PPC) and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health.
For most issues of direct concern to hospitalists, he says, especially those centered on healthcare delivery, “the wheels were in motion” long before the reform bill became law. Dr. Siegal also says most healthcare experts support the substance of accountable care organizations (ACOs), pay for performance, and reforming Medicare in ways that reward quality instead of quantity. “I think that ship is out of the harbor,” he says.
Throughout the year, the PPC will focus on three priorities identified in the Affordable Care Act: hospital value-based purchasing, bundled payments including ACOs, and hospital readmissions and transitions of care.
—Bill Vaughan, senior policy analyst, Consumers Union, Washington, D.C.
Debate, Delay, Defund?
There are several ways that Congress can delay or thwart the launch of specific reform initiatives. The first is to hold hearings about reform measures, Dr. Siegal says, “with the hope that they can somehow undermine it by raising questions about either the finances of it or about the implications for average Americans in terms of what kind of healthcare they’re going to get.” Such tactics carry significant risk, however, because highlighting specific aspects of the reform law could actually increase overall public support. “It has the potential to backfire on them,” he says.
“Repeal won’t happen anytime soon,” predicts Pat Conway, MD, chair of the PPC and director of hospital medicine at Cincinnati Children’s Hospital. “However, Congress could gut or significantly reduce funding to multiple programs within the bill, and then if you significantly reduce the funding, this may make it nearly impossible for those programs to be successful.”
Rough estimates suggest that some $150 billion worth of programs over the 10-year life of the healthcare reform act remain unfunded and are at risk. As an example, Dr. Conway cites wording in the bill that authorizes a program to help ease patient transitions in and out of the hospital. “If you reduce that funding to near zero, hospitals and hospitalists may still be successful, but you’ve essentially removed the program to learn how to be successful,” he says.
Bill Vaughan, a senior policy analyst in healthcare with the Washington, D.C.-based organization Consumers Union, says targeted riders could be added to appropriations bills. For instance, one rider could prohibit the Centers for Medicare & Medicaid Services (CMS) from spending any money to help develop government-supported insurance exchanges. Another could prevent the IRS from collecting money to be channeled into the trust fund for the Patient-Centered Outcomes Research Institute and its focus on comparative-effectiveness research. “There’s no end to mischief,” Vaughan says. “There are as many opportunities as the day is long.”
A major confrontation could arrive in March or April, when the U.S. runs into its debt ceiling. A continuing resolution would then be required to continue the appropriations process (and increase the U.S. debt ceiling past its current limit of $14.3 trillion). At that point or soon thereafter, Vaughan says, an opportunity could arise for legislators to say they won’t vote for a critical appropriations bill unless it includes certain spending reductions cited by one of several commissions tasked with recommending ways to reduce the deficit. “That could include hospital cuts, more doctor cuts, significant cost shifting to beneficiaries, higher copays,” he says.
Amid a “firestorm of ideas” on how to further cut Medicare and Medicaid spending, ideas once deemed radical could gain more traction. Some legislators have tossed around the idea of shutting down the government, if need be. “There’s nothing on the radar scope but static and fuzz,” Vaughan says. “It is totally unclear what is going to happen.”
Dearth of Drugs
Another trend generating both uncertainty and headaches in the nation’s hospitals is an unprecedented prescription drug shortage that could last well into the New Year, based on the number of medicines now in scarce supply across the country. In mid-November, for example, the American Society of Clinical Oncology announced “severe and worsening shortages of many critical therapies,” including doxorubicin, leucovorin, etoposide, nitrogen mustard, vincristine, propofol, and morphine.
Valerie Jensen, associate director of the FDA’s drug shortage program, told the Associated Press that her agency was seeing a record number of drug shortfalls in 2010. In mid-November, the FDA’s Current Drug Shortages list (www.fda.gov/Drugs/DrugSafety/DrugShortages/ucm050792.htm) included multiple formulations of 50 different medicines. Why so many? Jensen blamed the scarcity, in part, on the fact that many older drugs are not as profitable as newer ones. Manufacturing issues or delays and increased demand were the two biggest official reasons, though the FDA reported that at least eight formulations had been pulled or held from the market.
Vaughan says he’s heard plenty of buzz about the problem showing up quickly and unexpectedly in hospitals. Drug companies are supposed to give the FDA six months’ notice if they stop producing a drug, he says, but there’s no penalty if they don’t. “It’s amazing the number of people who are starting to worry about it,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.
After the wild ride of 2010, public-policy watchers could be forgiven for fervently hoping that 2011 offers a calmer year on the healthcare front.
Fat chance.
The turbulence could begin immediately, with the seating of the 112th Congress on Jan. 3. “I think the first question that’s on everybody’s mind is, ‘What will the Republican majority in the House do to Obama’s healthcare reform initiative?’ ” says Eric Siegal, MD, SFHM, a member of SHM’s Public Policy Committee (PPC) and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health.
For most issues of direct concern to hospitalists, he says, especially those centered on healthcare delivery, “the wheels were in motion” long before the reform bill became law. Dr. Siegal also says most healthcare experts support the substance of accountable care organizations (ACOs), pay for performance, and reforming Medicare in ways that reward quality instead of quantity. “I think that ship is out of the harbor,” he says.
Throughout the year, the PPC will focus on three priorities identified in the Affordable Care Act: hospital value-based purchasing, bundled payments including ACOs, and hospital readmissions and transitions of care.
—Bill Vaughan, senior policy analyst, Consumers Union, Washington, D.C.
Debate, Delay, Defund?
There are several ways that Congress can delay or thwart the launch of specific reform initiatives. The first is to hold hearings about reform measures, Dr. Siegal says, “with the hope that they can somehow undermine it by raising questions about either the finances of it or about the implications for average Americans in terms of what kind of healthcare they’re going to get.” Such tactics carry significant risk, however, because highlighting specific aspects of the reform law could actually increase overall public support. “It has the potential to backfire on them,” he says.
“Repeal won’t happen anytime soon,” predicts Pat Conway, MD, chair of the PPC and director of hospital medicine at Cincinnati Children’s Hospital. “However, Congress could gut or significantly reduce funding to multiple programs within the bill, and then if you significantly reduce the funding, this may make it nearly impossible for those programs to be successful.”
Rough estimates suggest that some $150 billion worth of programs over the 10-year life of the healthcare reform act remain unfunded and are at risk. As an example, Dr. Conway cites wording in the bill that authorizes a program to help ease patient transitions in and out of the hospital. “If you reduce that funding to near zero, hospitals and hospitalists may still be successful, but you’ve essentially removed the program to learn how to be successful,” he says.
Bill Vaughan, a senior policy analyst in healthcare with the Washington, D.C.-based organization Consumers Union, says targeted riders could be added to appropriations bills. For instance, one rider could prohibit the Centers for Medicare & Medicaid Services (CMS) from spending any money to help develop government-supported insurance exchanges. Another could prevent the IRS from collecting money to be channeled into the trust fund for the Patient-Centered Outcomes Research Institute and its focus on comparative-effectiveness research. “There’s no end to mischief,” Vaughan says. “There are as many opportunities as the day is long.”
A major confrontation could arrive in March or April, when the U.S. runs into its debt ceiling. A continuing resolution would then be required to continue the appropriations process (and increase the U.S. debt ceiling past its current limit of $14.3 trillion). At that point or soon thereafter, Vaughan says, an opportunity could arise for legislators to say they won’t vote for a critical appropriations bill unless it includes certain spending reductions cited by one of several commissions tasked with recommending ways to reduce the deficit. “That could include hospital cuts, more doctor cuts, significant cost shifting to beneficiaries, higher copays,” he says.
Amid a “firestorm of ideas” on how to further cut Medicare and Medicaid spending, ideas once deemed radical could gain more traction. Some legislators have tossed around the idea of shutting down the government, if need be. “There’s nothing on the radar scope but static and fuzz,” Vaughan says. “It is totally unclear what is going to happen.”
Dearth of Drugs
Another trend generating both uncertainty and headaches in the nation’s hospitals is an unprecedented prescription drug shortage that could last well into the New Year, based on the number of medicines now in scarce supply across the country. In mid-November, for example, the American Society of Clinical Oncology announced “severe and worsening shortages of many critical therapies,” including doxorubicin, leucovorin, etoposide, nitrogen mustard, vincristine, propofol, and morphine.
Valerie Jensen, associate director of the FDA’s drug shortage program, told the Associated Press that her agency was seeing a record number of drug shortfalls in 2010. In mid-November, the FDA’s Current Drug Shortages list (www.fda.gov/Drugs/DrugSafety/DrugShortages/ucm050792.htm) included multiple formulations of 50 different medicines. Why so many? Jensen blamed the scarcity, in part, on the fact that many older drugs are not as profitable as newer ones. Manufacturing issues or delays and increased demand were the two biggest official reasons, though the FDA reported that at least eight formulations had been pulled or held from the market.
Vaughan says he’s heard plenty of buzz about the problem showing up quickly and unexpectedly in hospitals. Drug companies are supposed to give the FDA six months’ notice if they stop producing a drug, he says, but there’s no penalty if they don’t. “It’s amazing the number of people who are starting to worry about it,” he says. TH
Bryn Nelson is a freelance medical writer based in Seattle.