User login
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
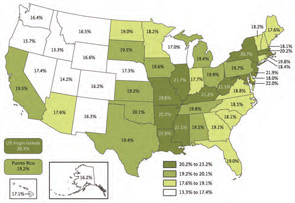
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.

Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).

On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.

“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.
Ten years ago, Stephen Jencks, MD, MPH, was hospitalized after taking a nasty spill and rupturing a kidney, breaking two ribs, and fracturing two transverse processes. The independent healthcare safety and quality consultant based in Baltimore still laughs ruefully at what happened next.
Dr. Jencks was stabilized and given OxyContin to treat his considerable pain, and then he was discharged—without his wife or another caregiver present, with a prescription for nothing more than Tylenol, and without any instructions on what to do if his condition worsened. Twelve hours after returning home, his pain re-emerged with such a vengeance that he experienced severe muscle spasms.
Dr. Jencks suspects his doctor was so focused on his ruptured kidney that pain management and follow-up fell by the wayside. “I am not an unassertive individual, so why didn’t I say something?” he asks. “The simple answer is that, at least for me, if I’m taking OxyContin, there are no problems. People tend not to be at the very top of their game when they’re on opioids and traumatized.”
He made it through the night at home and received better pain medication in the morning, but his experience, he says, “beautifully illustrates” the chronic problem of less-than-graceful transfers of care that can lead to unnecessary hospital readmissions. If it nearly happened to him, it can happen to anyone.
And, based on his research, it often does. In an influential 2009 New England Journal of Medicine study coauthored with Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and principal investigator of SHM’s Project BOOST, and Eric Coleman, MD, MPH, FACP, associate professor of medicine and director of the care transitions program at the University of Colorado Denver, Dr. Jencks helped uncover some startling statistics: During a 15-month period from 2003 to 2004, nearly 20% of the roughly 12 million Medicare beneficiaries discharged from hospitals were readmitted within 30 days (see “State-by-State Breakdown of 30-Day Rehospitalizations of Medicare Beneficiaries,” p. 7).1 Of those patients discharged to the community and then rehospitalized, half had not seen their own primary-care physician (PCP) in the interim. In all, the authors estimated Medicare’s financial toll from unplanned rehospitalizations at $17.4 billion for 2004 alone.
Surprisingly, Dr. Jencks’ study and a 2007 Medicare Payment Advisory Commission report to Congress provided the first estimates of the overall burden of rehospitalization in nearly a quarter-century. Since then, however, the topic has been a mainstay in conversations about the kinds of interventions that could yield major improvements in healthcare.
“The thing that has propelled this to the front is the recognition that we really can do better,” Dr. Jencks says. “What had tended to be seen as just an evitable consequence of people being sick is now increasingly seen as often being the consequence of not having done as good a job as we should have.”
Beyond the potential for poor patient outcomes and wasted money, healthcare experts say excessive readmissions have the potential to undermine the reputations of hospitalists just as they are moving to center stage in national quality-improvement (QI) efforts.
“I see, basically every day, patients that come back to the hospital because the discharge process is broken,” says Eric Howell, MD, SFHM, director of the hospitalist division at Johns Hopkins Bayview Medical Center in Baltimore. Dr. Howell says communication difficulties between the hospital and a nursing home have plagued one “revolving door” case involving a patient with a stomach ulcer that requires surgical resection. Hospital surgeons have repeatedly arranged to see her as an outpatient and schedule the surgery, but before the surgery can take place, the patient vomits up blood and is rehospitalized.
Another contributing factor, Dr. Howell argues, is the lack of incentives for both hospitals and hospitalists to work hard at preventing the next readmission. Although Dr. Jencks’ study suggests readmissions might not always be profitable, Dr. Howell and others say the sizeable contribution of rehospitalizations to overall admission numbers and the single-digit profit margins of most hospitals offer little motivation to change the status quo. “I think there are good people who want to fix it,” says Dr. Howell, an SHM board member and Project BOOST mentor. But changing the reimbursement system so that hospitalists can better focus on reducing readmissions, he adds, “will really go a long way.”
A New Landscape
Change is in the air. As part of the federal Affordable Care Act of 2010, the Centers for Medicare & Medicaid Services (CMS) is expanding a pilot project on bundling payments to doctors and hospitals around episodes of care. Starting Jan. 1, 2013, the bundling pilot will define “episodes” as all medical services administered three days before a hospital admission until 30 days after discharge. A rehospitalization within that timeframe would net reduced reimbursements.
CMS also has begun accepting applications for what’s known as the Community-Based Care Transitions Program, with $500 million over five years authorized by the healthcare reform act to fund collaborative, readmission-reducing efforts between hospitals and community-based organizations. Linda Magno, CMS director of the Medicare Demonstrations Program Group (www.cms.gov/CMSLeadership/19_Office_ORDI.asp), says program participants will form a learning network so the agency can quickly deliver information about who’s doing well and what approaches are working better than others. The participating organizations, she says, can then help teach best practices to other hospitals around the country.
CMS has adopted public reporting requirements as another tactic. The “Hospital Compare” website (www.hospitalcompare.hhs.gov/) set up by CMS, for example, uses discharge data to publish rehospitalization rates for heart failure, acute myocardial infarction, and pneumonia. More published rates will be added soon. More importantly, Medicare will begin penalizing poorly performing institutions in October 2012 by withholding a percentage of their payments, starting at 1% and rising to 3% within three years, as part of the value-based purchasing initiative.
For hospitals, the looming deadline has prompted widespread concern about the potential financial impact. With a growing number of models and projects springing up around the country, however, hospitalists and other healthcare providers are finding encouraging signs that even relatively simple interventions might help profoundly change the trajectory of care transitions.
Rachel George, MD, MBA, FHM, regional medical director and vice president of operations for West Cogent Healthcare Inc., says Cogent has found success with one tactic—ensuring that all patients are called after being discharged. The call helps to verify that prescribed medications have been picked up and that other care-related questions have been answered. Even before discharge, Dr. George says, Cogent also tries to ensure that a follow-up appointment with every patient’s PCP is on the calendar.
Debbie White, project coordinator for the Little Rock, Ark.-based National Transitions of Care Coalition (NTOCC), says it helps to frame the entire process as a transition plan rather than a discharge. White says patients—and often their family caregivers—are the one constant in every transition. “Some older Americans, including the baby boomers, came from a culture where you don’t question your physician or even an RN,” White says. “So they’ve had a hard time speaking up and learning to ask for a list of their medications, or who’s going to make their next follow-up appointment.” Among its tools, NTOCC offers resources to teach patients how to take more responsibility for their own care (see “Patient Interaction,” p. 5).
On the other side of the equation, the most downloaded tool on the coalition’s website is an evaluation and implementation plan that helps healthcare professionals find the gaps in care transitions. Other tools, including case scenarios and checklists, help healthcare providers consider specific steps, and a compendium of evidence offers a look at successful models and projects.
Dr. Bradley M. Sherman, MD, FHM, chairman of the department of medicine at Glen Cove Hospital/North Shore-LIJ University Health System in New York, led one such project, sponsored by the Greater New York Hospital Association. Dr. Sherman targeted heart failure, the condition with the highest readmission rate for both Glen Cove Hospital and the North Shore/LIJ system. By placing special emphasis on medication compliance, dietary adherence, and physician follow-up, Dr. Sherman says, the hospital cut its readmission rates by more than half, to well below the national average.
Another effort led by Johns Hopkins’ Dr. Howell, known as Safe and Successful Transition of Elderly Patients (Safe STEP), used a collaborative staff approach in general medicine wards overseen by hospitalists to reduce 30-day readmission rates from 22% to 14%. The encouraging results, first reported at SHM’s annual meeting in 2008, provided the impetus for a project called Better Outcomes for Older Adults through Safe Transitions, or Project BOOST (www.hospitalmedicine.org/BOOST).
Developed by SHM, BOOST features a yearlong mentoring program to help sites implement the QI project. It began at six hospitals and has since spread to 62 active mentor sites. Enrollment may swell to between 100 and 120 sites by the end of 2011, according to project director Tina Budnitz, MPH. Data from the first phase revealed a 21% reduction in 30-day readmission rates at the six pilot sites, to 11.2% from 14.2%. Follow-up data from the larger cohort are expected this spring.
Eric Siegal, MD, SFHM, an SHM board member, past chair of SHM’s Public Policy Committee, and a clinical assistant professor of medicine at the University of Wisconsin School of Medicine and Public Health, says BOOST has benefited from being solidly in place at the right time, gaining momentum and garnering significant national attention as the focus on better care transitions has intensified.
“If BOOST demonstrates substantial and reproducible decreases in rehospitalizations, improvements in quality, and presumed projected cost reductions, I think that it’s going to go off like a bomb,” he says, “in a good way.”
Lakshmi Halasyamani, MD, SFHM, vice president for medical affairs for the Saint Joseph Mercy Health System in Michigan and an SHM board member, says BOOST encourages hospitalists to think about ways in which a discharge might fail. “And then we need to actively mitigate those risks,” she says.
National Collaborations
CMS has tapped a network of technical assistance and QI contractors in all 50 states, known as quality-improvement organizations (QIOs), for its own project addressing rehospitalizations. In 2008, these QIOs began working with communities in 14 states to implement what’s known as the Care Transitions Program.
The program has helped community leaders highlight three root causes of high readmission rates: patients’ lack of knowledge and understanding about their chronic conditions, lack of communication among providers, and the healthcare system’s lack of known standards.
The 14 communities, 70 hospitals, and 1.25 million Medicare beneficiaries being followed to date suggest that 30-day readmission rates can be significantly decreased, says Paul McGann, MD, CMS deputy chief medical officer. Preliminary data based on the number of readmissions per 1,000 Medicare beneficiaries, he says, show that participating communities have improved by an average of 4.7% over the first two years of the project, with the top performer improving 14% (for more information, visit www.cfmc.org/caretransitions).
Dr. Halasyamani says no single program has necessarily found the “secret sauce” to improve readmission rates across the board. “And we definitely haven’t figured out how to implement that in as cost-effective a way as possible,” she says.
But optimism is clearly building. With the initial focus on coaching low-performing institutions to improve their rates, Medicare could tap programs that demonstrate early promise as the main go-to teaching aids.
More importantly, hospitals around the country are finding what it takes to help their own patients.
“The question isn’t, ‘Is our number better than St. Elsewhere’s down the street?’ ” Dr. Jencks concludes. “The real question is, ‘Are there things we could reasonably have done for this patient and could do for the next patient that will keep this from happening to them?’ ” TH
Bryn Nelson is a freelance medical writer based in Seattle.
Reference
- Jencks SJ, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418-1428.