User login
Bryn Nelson is a former PhD microbiologist who decided he’d much rather write about microbes than mutate them. After seven years at the science desk of Newsday in New York, Nelson relocated to Seattle as a freelancer, where he has consumed far too much coffee and written features and stories for The Hospitalist, The New York Times, Nature, Scientific American, Science News for Students, Mosaic and many other print and online publications. In addition, he contributed a chapter to The Science Writers’ Handbook and edited two chapters for the six-volume Modernist Cuisine: The Art and Science of Cooking.
Where’s the Stimulus?
With much of the national discussion on healthcare policy still dominated by the Affordable Care Act, which was signed into law March 23, 2010, it’s easy to forget that the healthcare industry received a big influx of money through 2009’s federal stimulus. In all, the American Recovery and Reinvestment Act gave the go-ahead for roughly $160 billion in new health-related spending. So where has that money gone, and did it achieve the Obama administration’s overall goal of stimulating the economy?
As with all economic matters, there’s no simple answer, and economists may never reach consensus. Nor has all the money yet been spent, although the vast majority is now spoken for. Nevertheless, several reports and policy experts have provided at least a glimpse of whether certain monies were indeed well spent. Here’s a look at some of the main areas of interest to HM, including funding meant to expand access to care, boost research funding, and increase medical infrastructure.
$98 Billion for Medicaid
—Maggie Mahar, healthcare fellow, Century Foundation, Washington, D.C.
By far the biggest chunk of healthcare money went to states to help shore up their Medicaid programs, in exchange for assurances that they would not tighten eligibility requirements. Another sizable fraction went to help unemployed people maintain their health insurance coverage through the government’s COBRA program by subsidizing 65% of their premiums. Those subsidies eventually increased to $34.3 billion through subsequent legislation, according to the U.S. Congress Joint Committee on Taxation.
Both types of spending provide assistance for lower-income people, and studies have broadly concluded that stimulus spending is more effective when directed at poorer people who are more likely to spend than save additional income. James Feyrer, PhD, associate professor of economics at Dartmouth College and a research associate at the National Bureau of Economic Research, says the stimulus’ support for low-income households yielded more than two dollars for every dollar spent.
The key question, Dr. Feyrer says, is whether government spending changes behavior. “Any money that you spend that doesn’t change anybody’s behavior isn’t going to have any stimulus effect,” he says. Because the extra Medicaid funds were contingent on states maintaining their eligibility rules, they had no choice but to spend the new money. That infusion theoretically put more cash into the pockets of the poor, increasing their own propensity to spend and delivering a boost to the economy.
But this funding model comes with a major caveat: Now that the stimulus money has run out, Dr. Feyrer says a reverse effect could take place. “The hope is that the economy will come roaring back in such a fashion that when you pull the stimulus away, it will be less painful,” he says.
That hasn’t happened, however, meaning that the loss of stimulus funds is proving particularly painful for cash-strapped states. Looming budget gaps in Medicaid and other programs for the poor could result in economic contraction. A similar effect could be in play now that COBRA subsidies have lapsed.
$22.6 Billion for Health IT
A meta-analysis by the Office of the National Coordinator for Health Information Technology concludes that HIT has had a predominantly positive effect on healthcare, mainly on quality and efficiency. In principle, most observers agree that electronic health records (EHRs) are good for medicine. In reality, however, critics say the stimulus’ huge cash incentive to get doctors and hospitals to demonstrate “meaningful use” of the technology has exposed a major weakness.
Maggie Mahar, a healthcare fellow at the Century Foundation in Washington, D.C., contends the funds should have been kept in reserve until experts could better advise doctors and hospitals about which systems would work best for their specific practices, with an eye toward ensuring that the records could be linked.
“Instead, you’ve got this sort of laissez-faire chaos of people out there selling stuff, some of which is good, some of which isn’t, to people who don’t know much about what they’re buying. And that has created real problems,” Mahar says. “Some places have very good EHR in place, up and running. Other places have bought stuff that they’d now like to throw out the window and have to replace.”
$2.8 Billion for Community Healthcare Services
SHM has long supported efforts to address the nation’s PCP shortage. In October, federal officials announced that they had made some headway on that front by nearly tripling the size of the National Health Service Corps. The loan-repayment and scholarship program grants $60,000 awards to providers in exchange for two-year commitments to medically underserved communities. In 2008, about 3,600 clinicians, mainly PCPs, were enrolled in the corps. This year, the number surpassed 10,000, boosted by $300 million in stimulus money and $1.5 billion from the ACA.
As a matter of healthcare policy, then, the program has arguably been a big success. From a purely economics angle, however, Dr. Feyrer suggests the program’s effect is likely to be more modest, because the award acts like a two-year salary boost for doctors who would likely still be employed, just somewhere else.
Conversely, infrastructure projects like the building of hospitals and community centers could have generated a fairly robust economic boost if they wouldn’t have been completed in the absence of stimulus money. A May 27 report by the Connecticut General Assembly’s Office of Legislature Research, “Health Care Centers and Providers as Economic Drivers,” attempted to quantify the return on stimulus-funded investments in the state.
Among its conclusions, the report found that roughly $11.4 million in improvement grants yielded an estimated economic impact of $18.6 million. Similarly, $16.2 million in funds to renovate existing health centers or increase space through construction of new or expanded services sites yielded an impact of $26.3 million.
$10 Billion to the NIH
A big chunk of the National Institutes of Health’s monies went toward highly rated research projects stuck in backlog. As Dr. Feyrer points out, such funding is less likely to have a short-term stimulus effect. For a quick economic shot in the arm, the main question is whether funds will help create jobs that otherwise would not have existed. Over the long haul, however, Feyrer agrees that increased medical research can yield economic rewards.
Similarly, Mahar says comparative effectiveness research (CER) could provide sizable long-term returns. “Every penny we’re spending on comparative effectiveness research should, down the road, pay off in a big way,” she says. Already, stimulus-funded studies are beginning to emerge from such efforts as a Seattle-based research consortium focused on objectively analyzing cancer diagnostic tools, screening tests, and treatments.
Such research is not without its detractors, who have criticized what they view as government intrusion into personal healthcare decisions. CER also produces winners and losers, making it more politically vulnerable. “No one wants to see their revenue stream cut, even if their overpriced device is no better than other devices,” Mahar says.
Bottom Line
So has healthcare-related stimulus spending really paid off? If early indicators seem mixed, future economic studies may provide more clarity—to a point. After all, Feyrer says, no economist can know what a world without a stimulus would have looked like, meaning the arguments won’t end anytime soon.
Bryn Nelson is a freelance medical writer based in Seattle.
With much of the national discussion on healthcare policy still dominated by the Affordable Care Act, which was signed into law March 23, 2010, it’s easy to forget that the healthcare industry received a big influx of money through 2009’s federal stimulus. In all, the American Recovery and Reinvestment Act gave the go-ahead for roughly $160 billion in new health-related spending. So where has that money gone, and did it achieve the Obama administration’s overall goal of stimulating the economy?
As with all economic matters, there’s no simple answer, and economists may never reach consensus. Nor has all the money yet been spent, although the vast majority is now spoken for. Nevertheless, several reports and policy experts have provided at least a glimpse of whether certain monies were indeed well spent. Here’s a look at some of the main areas of interest to HM, including funding meant to expand access to care, boost research funding, and increase medical infrastructure.
$98 Billion for Medicaid
—Maggie Mahar, healthcare fellow, Century Foundation, Washington, D.C.
By far the biggest chunk of healthcare money went to states to help shore up their Medicaid programs, in exchange for assurances that they would not tighten eligibility requirements. Another sizable fraction went to help unemployed people maintain their health insurance coverage through the government’s COBRA program by subsidizing 65% of their premiums. Those subsidies eventually increased to $34.3 billion through subsequent legislation, according to the U.S. Congress Joint Committee on Taxation.
Both types of spending provide assistance for lower-income people, and studies have broadly concluded that stimulus spending is more effective when directed at poorer people who are more likely to spend than save additional income. James Feyrer, PhD, associate professor of economics at Dartmouth College and a research associate at the National Bureau of Economic Research, says the stimulus’ support for low-income households yielded more than two dollars for every dollar spent.
The key question, Dr. Feyrer says, is whether government spending changes behavior. “Any money that you spend that doesn’t change anybody’s behavior isn’t going to have any stimulus effect,” he says. Because the extra Medicaid funds were contingent on states maintaining their eligibility rules, they had no choice but to spend the new money. That infusion theoretically put more cash into the pockets of the poor, increasing their own propensity to spend and delivering a boost to the economy.
But this funding model comes with a major caveat: Now that the stimulus money has run out, Dr. Feyrer says a reverse effect could take place. “The hope is that the economy will come roaring back in such a fashion that when you pull the stimulus away, it will be less painful,” he says.
That hasn’t happened, however, meaning that the loss of stimulus funds is proving particularly painful for cash-strapped states. Looming budget gaps in Medicaid and other programs for the poor could result in economic contraction. A similar effect could be in play now that COBRA subsidies have lapsed.
$22.6 Billion for Health IT
A meta-analysis by the Office of the National Coordinator for Health Information Technology concludes that HIT has had a predominantly positive effect on healthcare, mainly on quality and efficiency. In principle, most observers agree that electronic health records (EHRs) are good for medicine. In reality, however, critics say the stimulus’ huge cash incentive to get doctors and hospitals to demonstrate “meaningful use” of the technology has exposed a major weakness.
Maggie Mahar, a healthcare fellow at the Century Foundation in Washington, D.C., contends the funds should have been kept in reserve until experts could better advise doctors and hospitals about which systems would work best for their specific practices, with an eye toward ensuring that the records could be linked.
“Instead, you’ve got this sort of laissez-faire chaos of people out there selling stuff, some of which is good, some of which isn’t, to people who don’t know much about what they’re buying. And that has created real problems,” Mahar says. “Some places have very good EHR in place, up and running. Other places have bought stuff that they’d now like to throw out the window and have to replace.”
$2.8 Billion for Community Healthcare Services
SHM has long supported efforts to address the nation’s PCP shortage. In October, federal officials announced that they had made some headway on that front by nearly tripling the size of the National Health Service Corps. The loan-repayment and scholarship program grants $60,000 awards to providers in exchange for two-year commitments to medically underserved communities. In 2008, about 3,600 clinicians, mainly PCPs, were enrolled in the corps. This year, the number surpassed 10,000, boosted by $300 million in stimulus money and $1.5 billion from the ACA.
As a matter of healthcare policy, then, the program has arguably been a big success. From a purely economics angle, however, Dr. Feyrer suggests the program’s effect is likely to be more modest, because the award acts like a two-year salary boost for doctors who would likely still be employed, just somewhere else.
Conversely, infrastructure projects like the building of hospitals and community centers could have generated a fairly robust economic boost if they wouldn’t have been completed in the absence of stimulus money. A May 27 report by the Connecticut General Assembly’s Office of Legislature Research, “Health Care Centers and Providers as Economic Drivers,” attempted to quantify the return on stimulus-funded investments in the state.
Among its conclusions, the report found that roughly $11.4 million in improvement grants yielded an estimated economic impact of $18.6 million. Similarly, $16.2 million in funds to renovate existing health centers or increase space through construction of new or expanded services sites yielded an impact of $26.3 million.
$10 Billion to the NIH
A big chunk of the National Institutes of Health’s monies went toward highly rated research projects stuck in backlog. As Dr. Feyrer points out, such funding is less likely to have a short-term stimulus effect. For a quick economic shot in the arm, the main question is whether funds will help create jobs that otherwise would not have existed. Over the long haul, however, Feyrer agrees that increased medical research can yield economic rewards.
Similarly, Mahar says comparative effectiveness research (CER) could provide sizable long-term returns. “Every penny we’re spending on comparative effectiveness research should, down the road, pay off in a big way,” she says. Already, stimulus-funded studies are beginning to emerge from such efforts as a Seattle-based research consortium focused on objectively analyzing cancer diagnostic tools, screening tests, and treatments.
Such research is not without its detractors, who have criticized what they view as government intrusion into personal healthcare decisions. CER also produces winners and losers, making it more politically vulnerable. “No one wants to see their revenue stream cut, even if their overpriced device is no better than other devices,” Mahar says.
Bottom Line
So has healthcare-related stimulus spending really paid off? If early indicators seem mixed, future economic studies may provide more clarity—to a point. After all, Feyrer says, no economist can know what a world without a stimulus would have looked like, meaning the arguments won’t end anytime soon.
Bryn Nelson is a freelance medical writer based in Seattle.
With much of the national discussion on healthcare policy still dominated by the Affordable Care Act, which was signed into law March 23, 2010, it’s easy to forget that the healthcare industry received a big influx of money through 2009’s federal stimulus. In all, the American Recovery and Reinvestment Act gave the go-ahead for roughly $160 billion in new health-related spending. So where has that money gone, and did it achieve the Obama administration’s overall goal of stimulating the economy?
As with all economic matters, there’s no simple answer, and economists may never reach consensus. Nor has all the money yet been spent, although the vast majority is now spoken for. Nevertheless, several reports and policy experts have provided at least a glimpse of whether certain monies were indeed well spent. Here’s a look at some of the main areas of interest to HM, including funding meant to expand access to care, boost research funding, and increase medical infrastructure.
$98 Billion for Medicaid
—Maggie Mahar, healthcare fellow, Century Foundation, Washington, D.C.
By far the biggest chunk of healthcare money went to states to help shore up their Medicaid programs, in exchange for assurances that they would not tighten eligibility requirements. Another sizable fraction went to help unemployed people maintain their health insurance coverage through the government’s COBRA program by subsidizing 65% of their premiums. Those subsidies eventually increased to $34.3 billion through subsequent legislation, according to the U.S. Congress Joint Committee on Taxation.
Both types of spending provide assistance for lower-income people, and studies have broadly concluded that stimulus spending is more effective when directed at poorer people who are more likely to spend than save additional income. James Feyrer, PhD, associate professor of economics at Dartmouth College and a research associate at the National Bureau of Economic Research, says the stimulus’ support for low-income households yielded more than two dollars for every dollar spent.
The key question, Dr. Feyrer says, is whether government spending changes behavior. “Any money that you spend that doesn’t change anybody’s behavior isn’t going to have any stimulus effect,” he says. Because the extra Medicaid funds were contingent on states maintaining their eligibility rules, they had no choice but to spend the new money. That infusion theoretically put more cash into the pockets of the poor, increasing their own propensity to spend and delivering a boost to the economy.
But this funding model comes with a major caveat: Now that the stimulus money has run out, Dr. Feyrer says a reverse effect could take place. “The hope is that the economy will come roaring back in such a fashion that when you pull the stimulus away, it will be less painful,” he says.
That hasn’t happened, however, meaning that the loss of stimulus funds is proving particularly painful for cash-strapped states. Looming budget gaps in Medicaid and other programs for the poor could result in economic contraction. A similar effect could be in play now that COBRA subsidies have lapsed.
$22.6 Billion for Health IT
A meta-analysis by the Office of the National Coordinator for Health Information Technology concludes that HIT has had a predominantly positive effect on healthcare, mainly on quality and efficiency. In principle, most observers agree that electronic health records (EHRs) are good for medicine. In reality, however, critics say the stimulus’ huge cash incentive to get doctors and hospitals to demonstrate “meaningful use” of the technology has exposed a major weakness.
Maggie Mahar, a healthcare fellow at the Century Foundation in Washington, D.C., contends the funds should have been kept in reserve until experts could better advise doctors and hospitals about which systems would work best for their specific practices, with an eye toward ensuring that the records could be linked.
“Instead, you’ve got this sort of laissez-faire chaos of people out there selling stuff, some of which is good, some of which isn’t, to people who don’t know much about what they’re buying. And that has created real problems,” Mahar says. “Some places have very good EHR in place, up and running. Other places have bought stuff that they’d now like to throw out the window and have to replace.”
$2.8 Billion for Community Healthcare Services
SHM has long supported efforts to address the nation’s PCP shortage. In October, federal officials announced that they had made some headway on that front by nearly tripling the size of the National Health Service Corps. The loan-repayment and scholarship program grants $60,000 awards to providers in exchange for two-year commitments to medically underserved communities. In 2008, about 3,600 clinicians, mainly PCPs, were enrolled in the corps. This year, the number surpassed 10,000, boosted by $300 million in stimulus money and $1.5 billion from the ACA.
As a matter of healthcare policy, then, the program has arguably been a big success. From a purely economics angle, however, Dr. Feyrer suggests the program’s effect is likely to be more modest, because the award acts like a two-year salary boost for doctors who would likely still be employed, just somewhere else.
Conversely, infrastructure projects like the building of hospitals and community centers could have generated a fairly robust economic boost if they wouldn’t have been completed in the absence of stimulus money. A May 27 report by the Connecticut General Assembly’s Office of Legislature Research, “Health Care Centers and Providers as Economic Drivers,” attempted to quantify the return on stimulus-funded investments in the state.
Among its conclusions, the report found that roughly $11.4 million in improvement grants yielded an estimated economic impact of $18.6 million. Similarly, $16.2 million in funds to renovate existing health centers or increase space through construction of new or expanded services sites yielded an impact of $26.3 million.
$10 Billion to the NIH
A big chunk of the National Institutes of Health’s monies went toward highly rated research projects stuck in backlog. As Dr. Feyrer points out, such funding is less likely to have a short-term stimulus effect. For a quick economic shot in the arm, the main question is whether funds will help create jobs that otherwise would not have existed. Over the long haul, however, Feyrer agrees that increased medical research can yield economic rewards.
Similarly, Mahar says comparative effectiveness research (CER) could provide sizable long-term returns. “Every penny we’re spending on comparative effectiveness research should, down the road, pay off in a big way,” she says. Already, stimulus-funded studies are beginning to emerge from such efforts as a Seattle-based research consortium focused on objectively analyzing cancer diagnostic tools, screening tests, and treatments.
Such research is not without its detractors, who have criticized what they view as government intrusion into personal healthcare decisions. CER also produces winners and losers, making it more politically vulnerable. “No one wants to see their revenue stream cut, even if their overpriced device is no better than other devices,” Mahar says.
Bottom Line
So has healthcare-related stimulus spending really paid off? If early indicators seem mixed, future economic studies may provide more clarity—to a point. After all, Feyrer says, no economist can know what a world without a stimulus would have looked like, meaning the arguments won’t end anytime soon.
Bryn Nelson is a freelance medical writer based in Seattle.
Does Hospital Medicine Reinforce the Pillars of Career Satisfaction?
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
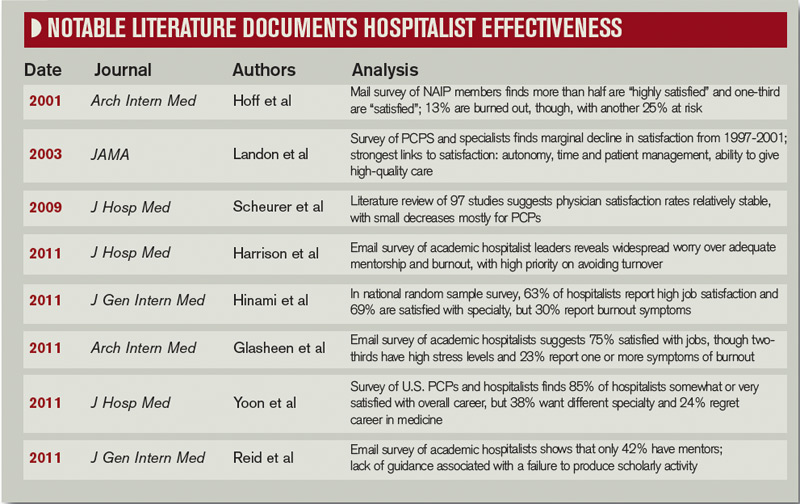
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.

—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
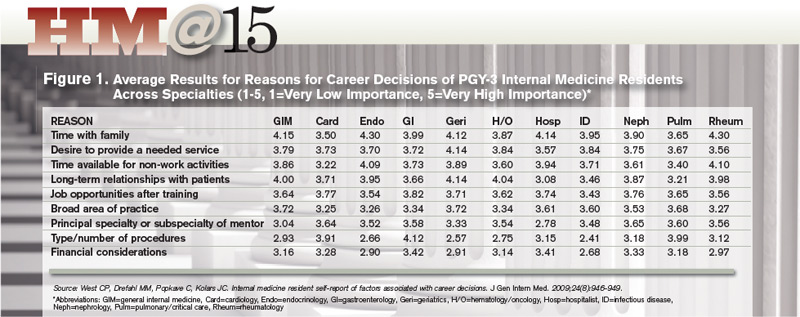
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.

—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic

Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.
—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.
—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic
Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.
—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.
—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic
Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
ONLINE EXCLUSIVE: A Loss of Meaning Vs. a Sense of Calling
Enter text here
Enter text here
Enter text here
Politics of Medicare Cuts
It reads like a brainteaser from hell: Twelve members of Congress must identify at least $1.2 trillion to cut from the federal budget over the next 10 years. Social Security cuts are a virtual nonstarter with Democrats. Tax hikes on the wealthy are anathema to Republicans. Significant Medicare cuts will invoke the wrath of seniors. The Joint Select Committee on Deficit Reduction, evenly split between both political parties, must somehow reach a majority agreement on what to trim by the Nov. 23 deadline. Then the full Congress must approve the committee’s recommendations by Dec. 23.
Here’s another caveat: In a Sept. 20 letter, SHM and 117 other medical groups urged the deficit reduction “super-committee” to “include a full repeal of the fatally flawed Medicare sustainable growth rate (SGR) formula in its final legislation.” Unless Congress repeals or delays the widely despised SGR mechanism, Medicare reimbursement rates for doctors will be cut by a catastrophic 29.4% in January. A full repeal, however, could cost $300 billion or more over 10 years, according to estimates by the nonpartisan Congressional Budget Office (CBO). If the super-committee takes up the SGR challenge, it will need to find at least $1.5 trillion worth of mutually agreeable cuts.
In a final twist, President Obama has threatened to veto any deficit reduction plan that slashes Medicare benefits and fails to raise taxes on the wealthy. The punchline is that unless the divided super-committee, a polarized Congress, and the president can all agree, $1.2 trillion in domestic and military spending cuts will automatically kick in, giving both political parties a lump of coal just in time for Christmas.
If any solution is possible, it might have to rely on some old numbers regarding potential cuts to Medicare and other federal programs. “There’s no time to develop new policy,” says Joseph Antos, PhD, a health policy expert at the American Enterprise Institute, a conservative think tank. “The old ideas that have been kicking around for years are scorable [by the CBO], and because they’ve been around for so long, it’s easier to write the legislative language.”
Here’s a look at perennial Medicare proposals and the chances of their inclusion in serious deficit-reduction negotiations.
—Joseph Antos, PhD, health policy expert, American Enterprise Institute, Washington, D.C.
Reduced Payments
Obama’s proposal to the super-committee includes $248 billion in Medicare cuts and savings. Of most direct relevance to hospitalists, about $57 billion comes from reduced payments to providers over 10 years. The proposal would reduce Indirect Medical Education add-on payments to teaching hospitals by 10%, end an add-on payment for hospitals and physicians in low-population states, and reduce payments to post-acute-care facilities.
Separately, the Medicare Payment Advisory Commission (MedPAC) released a proposal that would save $233 billion over 10 years—designed in large part to offset the costs necessary for a permanent SGR fix. Among its suggestions, the MedPAC proposal would freeze reimbursements for primary-care providers (PCPs) and trim payments to specialists by 5.9% per year for three years. Despite agreement by virtually everyone that the SGR has to go, groups like the Alliance of Specialty Medicine and American College of Surgeons have expressed concerns with MedPAC’s suggested offsets.
Dr. Antos says MedPAC has adopted the view that preventing the 29.4% cut in Medicare reimbursements will require spreading the pain more generally throughout the health sector. “That makes sense until you realize that politically, when you do that, you just generate lots of resistance from lots of organizations,” he says. So what about the SGR? Dr. Antos sees a permanent fix this year as “extremely unlikely,” especially given the general pessimism over the super-committee’s ability to agree on $1.2 trillion in cuts. Instead, he predicts a two-year fix that would require tens of billions in offsets but delay (yet again) more difficult political choices until after the 2012 elections. “They definitely do not want to be arguing about this next fall,” he says.
Drug Rebates
Under the president’s proposal, Medicare would receive the same rebates as Medicaid’s discount for brand name and generic drugs given to beneficiaries under the Medicare Low-Income Subsidy. This proposal alone is estimated to net some $135 billion in savings over 10 years, an inclusion that Judith Stein, executive director of the Center for Medicare Advocacy, says her organization was “delighted” to see. “We think that’s extremely reasonable, fair, good public policy, and good economic policy,” she says. Left-leaning groups are particularly vehement on this issue, given Medicare’s prohibition against negotiating with pharmaceutical companies on drug prices, a restriction that other bulk buyers, such as the Veterans Administration, don’t face.
Dr. Antos expects some form of the president’s proposal to be taken seriously. “This is something that is easy to do, and I think politically, it’s easier to go after a supplier of products—and drugs are the biggest one—than it is to go after doctors or hospitals,” he says. “And it’s hardest to go after beneficiaries.”
Premium Surcharges
Another element of President Obama’s proposal would save $20 billion by increasing wealthier beneficiaries’ insurance premiums on prescription drugs and doctors’ services. Beginning in 2017, income-based premiums for Medicare Part B and Part D both would rise by 15% for beneficiaries earning more than $85,000 annually.
AARP opposes the idea, and Stein says she’s concerned about the overall notion of basing Medicare premiums on income. “The problem is that we want to keep higher-income people satisfied with the Medicare program, because they’re the ones that get listened to,” Stein says.
Austin Frakt, PhD, a healthcare economist at Boston University, makes a similar point in a recent Health Affairs blog post: “The wealthy are a potential source of revenue for Medicare but also possess the means to finance the most strident challenge to it,” he writes. Even so, Stein says, “it’s easier to swallow than some other things,” especially if drug companies and others are required to share in the sacrifices.
Medicare Eligibility
President Obama’s proposal excludes any discussion about raising the age of Medicare eligibility, signaling a harder line on a change that Republicans and groups like the American Hospital Association have favored and that Obama himself floated as a trial balloon earlier this year. The Democratic base and AARP, however, rebelled against the notion, and Dr. Antos says the idea has “zero” chance of being included in the super-committee’s proposal. “This is the sort of thing that you don’t really want to bring up when you’re running for president, which is why the president backed off, and which is why the Republicans won’t be eager to see it, either,” he says.
Dr. Antos expects the eligible-age proposal to re-emerge in 2013, though he cautions against taking any “extravagant claims for savings” at face value. To be publicly acceptable, Medicare’s minimum age would need to rise slowly, he says, perhaps phased in over 20 years, and in a way that likely wouldn’t save a huge sum of money.
If Medicare raised its minimum age to 67 in 2014, the federal government would save roughly $5.7 billion, according to the nonprofit Center on Budget and Policy Priorities. In an “Incidental Economist” blog post, however, Dr. Frakt points out that the savings would simply shift the cost to beneficiaries, employers, private insurers, and others, a point echoed by Stein.
“All told, the cost to the system of raising the Medicare age to 67 would be $11.4 billion in 2014,” Dr. Frakt writes, “which is a high price to pay for $5.7 billion in federal savings.”
Bryn Nelson is a freelance medical writer based in Seattle.
It reads like a brainteaser from hell: Twelve members of Congress must identify at least $1.2 trillion to cut from the federal budget over the next 10 years. Social Security cuts are a virtual nonstarter with Democrats. Tax hikes on the wealthy are anathema to Republicans. Significant Medicare cuts will invoke the wrath of seniors. The Joint Select Committee on Deficit Reduction, evenly split between both political parties, must somehow reach a majority agreement on what to trim by the Nov. 23 deadline. Then the full Congress must approve the committee’s recommendations by Dec. 23.
Here’s another caveat: In a Sept. 20 letter, SHM and 117 other medical groups urged the deficit reduction “super-committee” to “include a full repeal of the fatally flawed Medicare sustainable growth rate (SGR) formula in its final legislation.” Unless Congress repeals or delays the widely despised SGR mechanism, Medicare reimbursement rates for doctors will be cut by a catastrophic 29.4% in January. A full repeal, however, could cost $300 billion or more over 10 years, according to estimates by the nonpartisan Congressional Budget Office (CBO). If the super-committee takes up the SGR challenge, it will need to find at least $1.5 trillion worth of mutually agreeable cuts.
In a final twist, President Obama has threatened to veto any deficit reduction plan that slashes Medicare benefits and fails to raise taxes on the wealthy. The punchline is that unless the divided super-committee, a polarized Congress, and the president can all agree, $1.2 trillion in domestic and military spending cuts will automatically kick in, giving both political parties a lump of coal just in time for Christmas.
If any solution is possible, it might have to rely on some old numbers regarding potential cuts to Medicare and other federal programs. “There’s no time to develop new policy,” says Joseph Antos, PhD, a health policy expert at the American Enterprise Institute, a conservative think tank. “The old ideas that have been kicking around for years are scorable [by the CBO], and because they’ve been around for so long, it’s easier to write the legislative language.”
Here’s a look at perennial Medicare proposals and the chances of their inclusion in serious deficit-reduction negotiations.
—Joseph Antos, PhD, health policy expert, American Enterprise Institute, Washington, D.C.
Reduced Payments
Obama’s proposal to the super-committee includes $248 billion in Medicare cuts and savings. Of most direct relevance to hospitalists, about $57 billion comes from reduced payments to providers over 10 years. The proposal would reduce Indirect Medical Education add-on payments to teaching hospitals by 10%, end an add-on payment for hospitals and physicians in low-population states, and reduce payments to post-acute-care facilities.
Separately, the Medicare Payment Advisory Commission (MedPAC) released a proposal that would save $233 billion over 10 years—designed in large part to offset the costs necessary for a permanent SGR fix. Among its suggestions, the MedPAC proposal would freeze reimbursements for primary-care providers (PCPs) and trim payments to specialists by 5.9% per year for three years. Despite agreement by virtually everyone that the SGR has to go, groups like the Alliance of Specialty Medicine and American College of Surgeons have expressed concerns with MedPAC’s suggested offsets.
Dr. Antos says MedPAC has adopted the view that preventing the 29.4% cut in Medicare reimbursements will require spreading the pain more generally throughout the health sector. “That makes sense until you realize that politically, when you do that, you just generate lots of resistance from lots of organizations,” he says. So what about the SGR? Dr. Antos sees a permanent fix this year as “extremely unlikely,” especially given the general pessimism over the super-committee’s ability to agree on $1.2 trillion in cuts. Instead, he predicts a two-year fix that would require tens of billions in offsets but delay (yet again) more difficult political choices until after the 2012 elections. “They definitely do not want to be arguing about this next fall,” he says.
Drug Rebates
Under the president’s proposal, Medicare would receive the same rebates as Medicaid’s discount for brand name and generic drugs given to beneficiaries under the Medicare Low-Income Subsidy. This proposal alone is estimated to net some $135 billion in savings over 10 years, an inclusion that Judith Stein, executive director of the Center for Medicare Advocacy, says her organization was “delighted” to see. “We think that’s extremely reasonable, fair, good public policy, and good economic policy,” she says. Left-leaning groups are particularly vehement on this issue, given Medicare’s prohibition against negotiating with pharmaceutical companies on drug prices, a restriction that other bulk buyers, such as the Veterans Administration, don’t face.
Dr. Antos expects some form of the president’s proposal to be taken seriously. “This is something that is easy to do, and I think politically, it’s easier to go after a supplier of products—and drugs are the biggest one—than it is to go after doctors or hospitals,” he says. “And it’s hardest to go after beneficiaries.”
Premium Surcharges
Another element of President Obama’s proposal would save $20 billion by increasing wealthier beneficiaries’ insurance premiums on prescription drugs and doctors’ services. Beginning in 2017, income-based premiums for Medicare Part B and Part D both would rise by 15% for beneficiaries earning more than $85,000 annually.
AARP opposes the idea, and Stein says she’s concerned about the overall notion of basing Medicare premiums on income. “The problem is that we want to keep higher-income people satisfied with the Medicare program, because they’re the ones that get listened to,” Stein says.
Austin Frakt, PhD, a healthcare economist at Boston University, makes a similar point in a recent Health Affairs blog post: “The wealthy are a potential source of revenue for Medicare but also possess the means to finance the most strident challenge to it,” he writes. Even so, Stein says, “it’s easier to swallow than some other things,” especially if drug companies and others are required to share in the sacrifices.
Medicare Eligibility
President Obama’s proposal excludes any discussion about raising the age of Medicare eligibility, signaling a harder line on a change that Republicans and groups like the American Hospital Association have favored and that Obama himself floated as a trial balloon earlier this year. The Democratic base and AARP, however, rebelled against the notion, and Dr. Antos says the idea has “zero” chance of being included in the super-committee’s proposal. “This is the sort of thing that you don’t really want to bring up when you’re running for president, which is why the president backed off, and which is why the Republicans won’t be eager to see it, either,” he says.
Dr. Antos expects the eligible-age proposal to re-emerge in 2013, though he cautions against taking any “extravagant claims for savings” at face value. To be publicly acceptable, Medicare’s minimum age would need to rise slowly, he says, perhaps phased in over 20 years, and in a way that likely wouldn’t save a huge sum of money.
If Medicare raised its minimum age to 67 in 2014, the federal government would save roughly $5.7 billion, according to the nonprofit Center on Budget and Policy Priorities. In an “Incidental Economist” blog post, however, Dr. Frakt points out that the savings would simply shift the cost to beneficiaries, employers, private insurers, and others, a point echoed by Stein.
“All told, the cost to the system of raising the Medicare age to 67 would be $11.4 billion in 2014,” Dr. Frakt writes, “which is a high price to pay for $5.7 billion in federal savings.”
Bryn Nelson is a freelance medical writer based in Seattle.
It reads like a brainteaser from hell: Twelve members of Congress must identify at least $1.2 trillion to cut from the federal budget over the next 10 years. Social Security cuts are a virtual nonstarter with Democrats. Tax hikes on the wealthy are anathema to Republicans. Significant Medicare cuts will invoke the wrath of seniors. The Joint Select Committee on Deficit Reduction, evenly split between both political parties, must somehow reach a majority agreement on what to trim by the Nov. 23 deadline. Then the full Congress must approve the committee’s recommendations by Dec. 23.
Here’s another caveat: In a Sept. 20 letter, SHM and 117 other medical groups urged the deficit reduction “super-committee” to “include a full repeal of the fatally flawed Medicare sustainable growth rate (SGR) formula in its final legislation.” Unless Congress repeals or delays the widely despised SGR mechanism, Medicare reimbursement rates for doctors will be cut by a catastrophic 29.4% in January. A full repeal, however, could cost $300 billion or more over 10 years, according to estimates by the nonpartisan Congressional Budget Office (CBO). If the super-committee takes up the SGR challenge, it will need to find at least $1.5 trillion worth of mutually agreeable cuts.
In a final twist, President Obama has threatened to veto any deficit reduction plan that slashes Medicare benefits and fails to raise taxes on the wealthy. The punchline is that unless the divided super-committee, a polarized Congress, and the president can all agree, $1.2 trillion in domestic and military spending cuts will automatically kick in, giving both political parties a lump of coal just in time for Christmas.
If any solution is possible, it might have to rely on some old numbers regarding potential cuts to Medicare and other federal programs. “There’s no time to develop new policy,” says Joseph Antos, PhD, a health policy expert at the American Enterprise Institute, a conservative think tank. “The old ideas that have been kicking around for years are scorable [by the CBO], and because they’ve been around for so long, it’s easier to write the legislative language.”
Here’s a look at perennial Medicare proposals and the chances of their inclusion in serious deficit-reduction negotiations.
—Joseph Antos, PhD, health policy expert, American Enterprise Institute, Washington, D.C.
Reduced Payments
Obama’s proposal to the super-committee includes $248 billion in Medicare cuts and savings. Of most direct relevance to hospitalists, about $57 billion comes from reduced payments to providers over 10 years. The proposal would reduce Indirect Medical Education add-on payments to teaching hospitals by 10%, end an add-on payment for hospitals and physicians in low-population states, and reduce payments to post-acute-care facilities.
Separately, the Medicare Payment Advisory Commission (MedPAC) released a proposal that would save $233 billion over 10 years—designed in large part to offset the costs necessary for a permanent SGR fix. Among its suggestions, the MedPAC proposal would freeze reimbursements for primary-care providers (PCPs) and trim payments to specialists by 5.9% per year for three years. Despite agreement by virtually everyone that the SGR has to go, groups like the Alliance of Specialty Medicine and American College of Surgeons have expressed concerns with MedPAC’s suggested offsets.
Dr. Antos says MedPAC has adopted the view that preventing the 29.4% cut in Medicare reimbursements will require spreading the pain more generally throughout the health sector. “That makes sense until you realize that politically, when you do that, you just generate lots of resistance from lots of organizations,” he says. So what about the SGR? Dr. Antos sees a permanent fix this year as “extremely unlikely,” especially given the general pessimism over the super-committee’s ability to agree on $1.2 trillion in cuts. Instead, he predicts a two-year fix that would require tens of billions in offsets but delay (yet again) more difficult political choices until after the 2012 elections. “They definitely do not want to be arguing about this next fall,” he says.
Drug Rebates
Under the president’s proposal, Medicare would receive the same rebates as Medicaid’s discount for brand name and generic drugs given to beneficiaries under the Medicare Low-Income Subsidy. This proposal alone is estimated to net some $135 billion in savings over 10 years, an inclusion that Judith Stein, executive director of the Center for Medicare Advocacy, says her organization was “delighted” to see. “We think that’s extremely reasonable, fair, good public policy, and good economic policy,” she says. Left-leaning groups are particularly vehement on this issue, given Medicare’s prohibition against negotiating with pharmaceutical companies on drug prices, a restriction that other bulk buyers, such as the Veterans Administration, don’t face.
Dr. Antos expects some form of the president’s proposal to be taken seriously. “This is something that is easy to do, and I think politically, it’s easier to go after a supplier of products—and drugs are the biggest one—than it is to go after doctors or hospitals,” he says. “And it’s hardest to go after beneficiaries.”
Premium Surcharges
Another element of President Obama’s proposal would save $20 billion by increasing wealthier beneficiaries’ insurance premiums on prescription drugs and doctors’ services. Beginning in 2017, income-based premiums for Medicare Part B and Part D both would rise by 15% for beneficiaries earning more than $85,000 annually.
AARP opposes the idea, and Stein says she’s concerned about the overall notion of basing Medicare premiums on income. “The problem is that we want to keep higher-income people satisfied with the Medicare program, because they’re the ones that get listened to,” Stein says.
Austin Frakt, PhD, a healthcare economist at Boston University, makes a similar point in a recent Health Affairs blog post: “The wealthy are a potential source of revenue for Medicare but also possess the means to finance the most strident challenge to it,” he writes. Even so, Stein says, “it’s easier to swallow than some other things,” especially if drug companies and others are required to share in the sacrifices.
Medicare Eligibility
President Obama’s proposal excludes any discussion about raising the age of Medicare eligibility, signaling a harder line on a change that Republicans and groups like the American Hospital Association have favored and that Obama himself floated as a trial balloon earlier this year. The Democratic base and AARP, however, rebelled against the notion, and Dr. Antos says the idea has “zero” chance of being included in the super-committee’s proposal. “This is the sort of thing that you don’t really want to bring up when you’re running for president, which is why the president backed off, and which is why the Republicans won’t be eager to see it, either,” he says.
Dr. Antos expects the eligible-age proposal to re-emerge in 2013, though he cautions against taking any “extravagant claims for savings” at face value. To be publicly acceptable, Medicare’s minimum age would need to rise slowly, he says, perhaps phased in over 20 years, and in a way that likely wouldn’t save a huge sum of money.
If Medicare raised its minimum age to 67 in 2014, the federal government would save roughly $5.7 billion, according to the nonprofit Center on Budget and Policy Priorities. In an “Incidental Economist” blog post, however, Dr. Frakt points out that the savings would simply shift the cost to beneficiaries, employers, private insurers, and others, a point echoed by Stein.
“All told, the cost to the system of raising the Medicare age to 67 would be $11.4 billion in 2014,” Dr. Frakt writes, “which is a high price to pay for $5.7 billion in federal savings.”
Bryn Nelson is a freelance medical writer based in Seattle.
ONLINE EXCLUSIVE: Listen to hospitalists Greg Misky and Tosha Wetterneck discuss career satisfaction
Click here to listen to Dr. Misky.
Click here to listen to Dr. Wetterneck.
Click here to listen to Dr. Misky.
Click here to listen to Dr. Wetterneck.
Click here to listen to Dr. Misky.
Click here to listen to Dr. Wetterneck.
HM@15 - Is Hospital Medicine a Good Bet for Improving Patient Satisfaction?
At first glance, the deck might seem hopelessly stacked against hospitalists with regard to patient satisfaction. HM practitioners lack the long-term relationship with patients that many primary-care physicians (PCPs) have established. Unlike surgeons and other specialists, they tend to care for those patients—more complicated, lacking a regular doctor, or admitted through the ED, for example—who are more inclined to rate their hospital stay unfavorably.1 They may not even be accurately remembered by patients who encounter multiple doctors during the course of their hospitalization.2 And hospital information systems can misidentify the treating physician, while the actual surveys used to gauge hospitalists have been imperfect at best.3
And yet, the hospitalist model has evolved substantially on the question of how it can impact patient perceptions of care.
Initially, hospitalist champions adopted a largely defensive posture: The model would not negatively impact patient satisfaction as it delivered on efficiency—and later on quality. The healthcare system, however, is beginning to recognize the hospitalist as part of a care “team” whose patient-centered approach might pay big dividends in the inpatient experience and, eventually, on satisfaction scores.
“I think the next phase, which is a focus on the hospitalist as a team member and team builder, is going to be key,” says William Southern, MD, MPH, SFHM, chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y.
Recent studies suggest that hospitalists are helping to design and test new tools that will not only improve satisfaction, but also more fairly assess the impact of individual doctors. As the maturation process continues, experts say, hospitalists have an opportunity to influence both provider-based interventions and more programmatic decision-making that can have far-reaching effects. Certainly, the hand dealt to hospitalists is looking more favorable even as the ante has been raised with Medicare programs like value-based purchasing, and its pot of money tied to patient perceptions of care.
So how have hospitalists played their cards so far?
A Look at the Evidence
In its early years, the HM model faced a persistent criticism: Replacing traditional caregivers with these new inpatient providers in the name of efficiency would increase handoffs and, therefore, discontinuities of care delivered by a succession of unfamiliar faces. If patients didn’t see their PCP in the hospital, the thinking went, they might be more disgruntled at being tended to by hospitalists, leading to lower satisfaction scores.4
A particularly heated exchange played out in 1999 in the New England Journal of Medicine. Farris A. Manian, MD, MPH, of Infectious Disease Consultants in St. Louis wrote in one letter, “I am particularly concerned about what impressionable house-staff members will learn from hospitalists who place an inordinate emphasis on cost rather than the quality of patient care or teaching.”5
A few subsequent studies, however, hinted that such concerns might be overstated. A 2000 analysis in the American Journal of Medicine that examined North Mississippi Health Services in Tupelo, for instance, found that care administered by hospitalists led to a shorter length of stay and lower costs than care delivered by internists. Importantly, the study found that patient satisfaction was similar for both models, while quality metrics were likewise equal or even tilted slightly toward hospitalists.6
In their influential 2002 review of a profession that was only a half-decade old, Robert Wachter, MD, MHM, and Lee Goldman, MD, MPH, FACP from the University of California at San Francisco reinforced the message that HM wouldn’t lead to unhappy patients. “Empirical research supports the premise that hospitalists improve inpatient efficiency without harmful effects on quality or patient satisfaction,” they asserted.7
Among pediatric patients, a 2005 review found that “none of the four studies that evaluated patient satisfaction found statistically significant differences in satisfaction with inpatient care. However, two of the three evaluations that did assess parents’ satisfaction with care provided to their children found that parents were more satisfied with some aspects of care provided by hospitalists.”8

—William Southern, MD, chief, division of hospital medicine, Montefiore Medical Center, Bronx, N.Y.
Similar findings were popping up around the country: Replacing an internal medicine residency program with a physician assistant/hospitalist model at Brooklyn, N.Y.’s Coney Island Hospital did not adversely impact patient satisfaction, while it significantly improved mortality.9 Brigham & Women’s Hospital in Boston likewise reported no change in patient satisfaction in a study comparing a physician assistant/hospitalist service with traditional house staff services.10
The shift toward a more proactive position on patient satisfaction is exemplified within a 2008 white paper, “Hospitalists Meeting the Challenge of Patient Satisfaction,” written by a group of 19 private-practice HM experts known as The Phoenix Group.3 The paper acknowledged the flaws and limitations of existing survey methodologies, including Medicare’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores. Even so, the authors urged practice groups to adopt a team-oriented approach to communicate to hospital administrations “the belief that hospitalists are in the best position to improve survey scores overall for the facility.”
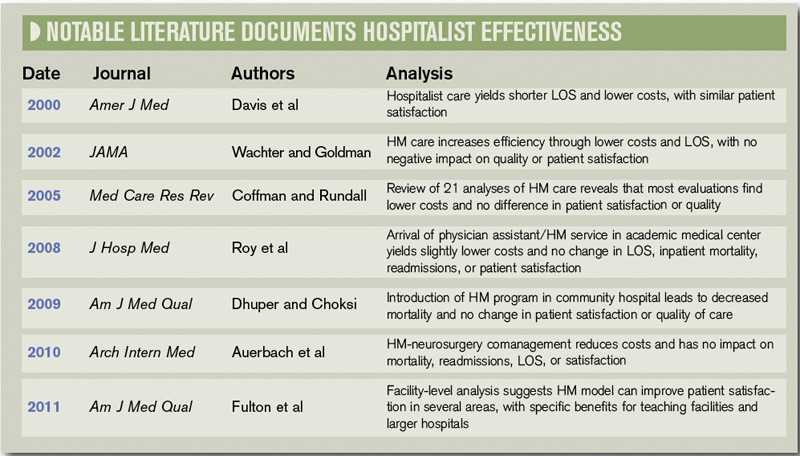
Carle Foundation Hospital in Urbana, Ill., is now publicly advertising its HM service’s contribution to high patient satisfaction scores on its website, and underscoring the hospitalists’ consistency, accessibility, and communication skills. “The hospital is never without a hospitalist, and our nurses know that they can rely on them,” says Lynn Barnes, vice president of hospital operations. “They’re available, they’re within a few minutes away, and patients’ needs get met very efficiently and rapidly.”
As a result, she says, their presence can lead to higher scores in patients’ perceptions of communication.
Hospitalists also have been central to several safety initiatives at Carle. Napoleon Knight, MD, medical director of hospital medicine and associate vice president for quality, says the HM team has helped address undiagnosed sleep apnea and implement rapid responses, such as “Code Speed.” Caregivers or family members can use the code to immediately call for help if they detect a downturn in a patient’s condition.
The ongoing initiatives, Dr. Knight and Barnes say, are helping the hospital improve how patients and their loved ones perceive care as Carle adapts to a rapidly shifting healthcare landscape. “With all of the changes that seem to be coming from the external environment weekly, we want to work collaboratively to make sure we’re connected and aligned and communicating in an ongoing fashion so we can react to all of these changes,” Dr. Knight says.
Continued below...
A Hopeful Trend
So far, evidence that the HM model is more broadly raising patient satisfaction scores is largely anecdotal. But a few analyses suggest the trend is moving in the right direction. A recent study in the American Journal of Medical Quality, for instance, concludes that facilities with hospitalists might have an advantage in patient satisfaction with nursing and such personal issues as privacy, emotional needs, and response to complaints.11 The study also posits that teaching facilities employing hospitalists could see benefits in overall satisfaction, while large facilities with hospitalists might see gains in satisfaction with admissions, nursing, and tests and treatments.
Brad Fulton, PhD, a researcher at South Bend, Ind.-based healthcare consulting firm Press Ganey and the study’s lead author, says the 30,000-foot view of patient satisfaction at the facility level can get foggy in a hurry due to differences in the kind and size of hospitalist programs. “And despite all of that fog, we’re still able to see through that and find something,” he says.
One limitation is that the study findings could also reflect differences in the culture of facilities that choose to add hospitalists. That caveat means it might not be possible to completely untangle the effect of an HM group on inpatient care from the larger, hospitalwide values that have allowed the group to set up shop. The wrinkle brings its own fascinating questions, according to Fulton. For example, is that kind of culture necessary for hospitalists to function as well as they do?

—Lynn Barnes, vice president of hospital operations, Carle Foundation Hospital, Urbana, Ill.
Such considerations will become more important as the healthcare system places additional emphasis on patient satisfaction, as Medicare’s value-based purchasing program is doing through its HCAHPS scores. With all the changes, success or failure on the patient experience front is going to carry “not just a reputational import, but also a financial impact,” says Ethan Cumbler, MD, FACP, director of Acute Care for the Elderly (ACE) Service at the University of Colorado Denver.
So how can HM fairly and accurately assess its own practitioners? “I think one starts by trying to apply some of the rigor that we have learned from our experience as hospitalists in quality improvement to the more warm and fuzzy field of patient experience,” Dr. Cumbler says. Many hospitals employ surveys supplied by consultants like Press Ganey to track the global patient satisfaction for their institution, he says.
“But for an individual hospitalist or hospitalist group, that kind of tool often lacks both the specificity and the timeliness necessary to make good decisions about impact of interventions on patient satisfaction,” he says.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, agrees that such imprecision could lead to unfair assessments. “You can imagine a scenario where a patient actually liked their hospitalist very much,” he says, “but when they got the survey, they said [their stay] was terrible and the reasons being because maybe the nurse call button was not answered and the food was terrible and medications were given to them incorrectly, or it was noisy at night so they couldn’t sleep.”
A recent study by Dr. Williams and his colleagues, in which they employed a new assessment method called the Communication Assessment Tool (CAT), confirmed the group’s suspicions: “that the results from the Press Ganey didn’t match up with the CAT, which was a direct assessment of the patient’s perception of the hospitalist’s communication skills,” he says.12
The validated tool, he adds, provides directed feedback to the physician based on the percentage of patients rating that provider as excellent, instead of on the average total score. Hospitalists have felt vindicated by the results. “They were very nervous because the hospital talked about basing an incentive off of the Press Ganey scores, and we said, ‘You can’t do that,’ because we didn’t feel they were accurate, and this study proved that,” Dr. Williams explains.
Fortunately, the message has reached researchers and consultants alike, and better tools are starting to reach hospitals around the country. At HM11 in May, Press Ganey unveiled a new survey designed to help patients assess the care delivered by two hospitalists, the average for inpatient stays. The item set is specific to HM functions, and includes the photo and name of each hospitalist, which Fulton says should improve the validity and accuracy of the data.
“The early response looks really good,” Fulton says, though it’s too early to say whether the tool, called Hospitalist Insight, will live up to its billing. If it proves its mettle, Fulton says, the survey could be used to reward top-performing hospitalists, and the growing dataset could allow hospitals to compare themselves with appropriate peer groups for fairer comparisons.
Meanwhile, researchers are testing out checklists to score hospitalist etiquette, and tracking and paging systems to help ensure continuity of care. They have found increased patient satisfaction when doctors engage in verbal communication during a discharge, in interdisciplinary team rounding, and in efforts to address religious and spiritual concerns.
Since 2000, when Montefiore’s hospitalist program began, Dr. Southern says the hospital has explained to patients the tradeoff accompanying the HM model. “I say something like this to every patient: ‘I know I’m not the doctor that you know, and you’re just meeting me. The downside is that you haven’t met me before and I’m a new face, but the upside is that if you need me during the day, I’m here all the time, I’m not someplace else. And so if you need something, I can be here quickly.’ ”
Being very explicit about that tradeoff, he says, has made patients very comfortable with the model of care, especially during a crisis moment in their lives. “I think it’s really important to say, ‘I know you don’t know me, but here’s the upside.’ And my experience is that patients easily understand that tradeoff and are very positive,” Dr. Southern says.
The Verdict
Available evidence suggests that practitioners of the HM model have pivoted from defending against early criticism that they may harm patient satisfaction to pitching themselves as team leaders who can boost facilitywide perceptions of care. So far, too little research has been conducted to suggest whether that optimism is fully warranted, but early signs look promising.
At facilities like Chicago’s Northwestern Memorial Hospital, medical floors staffed by hospitalists are beginning to beat out surgical floors for the traveling patient satisfaction award. And experts like Dr. Cumbler are pondering how ongoing initiatives to boost scores can follow in the footsteps of efficiency and quality-raising efforts by making the transition from focusing on individual doctors to adopting a more programmatic approach. “What’s happening to that patient during the 23 hours and 45 minutes of their hospital day that you are not sitting by the bedside? And what influence should a hospitalist have in affecting that other 23 hours and 45 minutes?” he says.
Handoffs, discharges, communication with PCPs, and other potential weak points in maintaining high levels of patient satisfaction, Dr. Cumbler says, all are amenable to systems-based improvement. “As hospitalists, we are in a unique position to influence not only our one-one-one interaction with the patient, but also to influence that system of care in a way that patients will notice in a real and tangible way,” he says. “I think we’ve recognized for some time that a healthy heart but a miserable patient is not a healthy person.”
Teaching Hospitals Gain Ground in Patient Satisfaction

One widely accepted truism about teaching facilities is that they’re known to have lower patient satisfaction scores than nonteaching hospitals. Brad Fulton, researcher for South Bend, Ind.-based consultant firm Press Ganey, attributes the difference in part to the fact that many doctors at teaching facilities must divide their time among patient care, education, and research. Such hospitals also tend to have some of the more medically difficult patients, he says, some of who may be more apt to feel like they’re on display with the abundance of students and residents.
In one of his recent studies, however, teaching facilities with hospitalists scored higher on patient satisfaction than nonteaching facilities or teaching facilities that lacked hospitalists. One potential follow-up question could have broad implications: “What is it about having hospitalists in teaching facilities that works so well in terms of patient satisfaction?” Can that be replicated elsewhere, he wonders? And is there an essential element that could be applied to nonteaching facilities?
A separate study also defied expectations by finding that teaching bedside procedures to inexperienced residents can be reassuring to patients, if done correctly. In a teaching model instituted at the University of California San Francisco, an experienced hospitalist with extra training supervises a novice during bedside procedures such as lumbar punctures and paracentesis. Study coauthor Diane Sliwka, MD, associate clinical professor of medicine and a hospitalist, says the feedback so far suggests that the model can improve safety, boost education, and deliver a positive patient experience.
Patients may be hesitant about having trainees do procedures, she says, but surveys suggest those patients are reassured when they know an expert is in the room and watching. They also want to hear what will happen next to counteract the anxiety of feeling pain or encountering something unexpected.
As the study suggested, what patients may find to be the most difficult or nerve-wracking can be quite different from what doctors expect. “You would think it was actually the procedure that was most painful part, but actually that was after we had given lidocaine,” Dr. Sliwka says. Patients repeatedly reacted to the doctors using a plastic pen cap to imprint the site where they would insert a needle. “Over and over we would hear people say, ‘That is actually the most painful part and you didn’t warn me about that,’ ” she recalls. “And we didn’t warn people about that because we didn’t think it was a big deal.”
Procedures can take longer with trainees, another tradeoff that can leading to lower satisfaction scores. But what the study also showed is that in academic settings, involving residents doesn’t harm the overall patient experience and can in fact improve it. “Anecdotally, what we hear from patients a lot is, ‘Oh, I had this procedure done before and it went horribly.’ They would tell stories of previous bad experiences, and then really be thankful for the experience that they had in our setting,” Dr. Sliwka says.
The extended face-to-face time can yield another positive effect. Dr. Sliwka found that hospitalists and residents often learned medical and historical information about the patient that the primary care team hadn’t yet had an opportunity to glean. “Patients just start to tell you about their families, their lives, their medical problems, their experiences,” she says, a product of building more rapport with them. “We would often find ourselves telling the primary medical team, ‘By the way, we found this out and you should probably know it: the patient is very concerned about this that’s been going on,’ and the patient hasn’t had a chance to tell the team because there isn’t that kind of time.”
Even without the specific model, Dr. Sliwka says, several principles can be applied to daily interactions. Framing things appropriately, she says, helps patients gain confidence in the doctors and allows them to safely conduct bedside teaching and openly discuss procedures. Even correcting mistakes can be a positive experience. “That actually makes the patient feel more confident in you than less confident,” Dr. Sliwka says.
Ultimately, the teaching experience can help residents broaden their thinking about patient satisfaction. “I think when trainees are starting, their real focus is, ‘How do I deal with this correctly?’ ” Dr. Sliwka says. “It takes a level of comfort with the basic skills to then go beyond that and start thinking about, ‘How is the patient perceiving this?’”
Bryn Nelson is a freelance medical journalist based in Seattle.
References
- Williams M, Flanders SA, Whitcomb WF. Comprehensive hospital medicine: an evidence based approach. Elsevier;2007:971-976.
- Arora V, Gangireddy S, Mehrotra A, Ginde R, Tormey M, Meltzer D. Ability of hospitalized patients to identify their in-hospital physicians. Arch Intern Med. 2009;169(2):199-201.
- Singer AS, et al. Hospitalists meeting the challenge of patient satisfaction. The Phoenix Group. 2008;1-5.
- Manian FA. Whither continuity of care? N Engl J Med. 1999;340:1362-1363.
- Correspondence. Whither continuity of care? N Engl J Med. 1999;341:850-852.
- Davis KM, Koch KE, Harvey JK, et al. Effects of hospitalists on cost, outcomes, and patient satisfaction in a rural health system. Amer J Med. 2000;108(8):621-626.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Coffman J, Rundall TG. The impact of hospitalists on the cost and quality of inpatient care in the United States (a research synthesis). Med Care Res Rev. 2005;62:379–406.
- Dhuper S, Choksi S. Replacing an academic internal medicine residency program with a physician assistant-hospitalist model: a comparative analysis study. Am J Med Qual. 2009;24(2):132-139.
- Roy CL, Liang CL, Lund M, et al. Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes. J Hosp Med. 2008;3(5):361-368.
- Fulton BR, Drevs KE, Ayala LJ, Malott DL Jr. Patient satisfaction with hospitalists: facility-level analyses. Am J Med Qual. 2011;26(2):95-102.
- Ferranti DE, Makoul G, Forth VE, Rauworth J, Lee J, Williams MV. Assessing patient perceptions of hospitalist communication skills using the Communication Assessment Tool (CAT). J Hosp Med. 2010;5(9):522-527.
At first glance, the deck might seem hopelessly stacked against hospitalists with regard to patient satisfaction. HM practitioners lack the long-term relationship with patients that many primary-care physicians (PCPs) have established. Unlike surgeons and other specialists, they tend to care for those patients—more complicated, lacking a regular doctor, or admitted through the ED, for example—who are more inclined to rate their hospital stay unfavorably.1 They may not even be accurately remembered by patients who encounter multiple doctors during the course of their hospitalization.2 And hospital information systems can misidentify the treating physician, while the actual surveys used to gauge hospitalists have been imperfect at best.3
And yet, the hospitalist model has evolved substantially on the question of how it can impact patient perceptions of care.
Initially, hospitalist champions adopted a largely defensive posture: The model would not negatively impact patient satisfaction as it delivered on efficiency—and later on quality. The healthcare system, however, is beginning to recognize the hospitalist as part of a care “team” whose patient-centered approach might pay big dividends in the inpatient experience and, eventually, on satisfaction scores.
“I think the next phase, which is a focus on the hospitalist as a team member and team builder, is going to be key,” says William Southern, MD, MPH, SFHM, chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y.
Recent studies suggest that hospitalists are helping to design and test new tools that will not only improve satisfaction, but also more fairly assess the impact of individual doctors. As the maturation process continues, experts say, hospitalists have an opportunity to influence both provider-based interventions and more programmatic decision-making that can have far-reaching effects. Certainly, the hand dealt to hospitalists is looking more favorable even as the ante has been raised with Medicare programs like value-based purchasing, and its pot of money tied to patient perceptions of care.
So how have hospitalists played their cards so far?
A Look at the Evidence
In its early years, the HM model faced a persistent criticism: Replacing traditional caregivers with these new inpatient providers in the name of efficiency would increase handoffs and, therefore, discontinuities of care delivered by a succession of unfamiliar faces. If patients didn’t see their PCP in the hospital, the thinking went, they might be more disgruntled at being tended to by hospitalists, leading to lower satisfaction scores.4
A particularly heated exchange played out in 1999 in the New England Journal of Medicine. Farris A. Manian, MD, MPH, of Infectious Disease Consultants in St. Louis wrote in one letter, “I am particularly concerned about what impressionable house-staff members will learn from hospitalists who place an inordinate emphasis on cost rather than the quality of patient care or teaching.”5
A few subsequent studies, however, hinted that such concerns might be overstated. A 2000 analysis in the American Journal of Medicine that examined North Mississippi Health Services in Tupelo, for instance, found that care administered by hospitalists led to a shorter length of stay and lower costs than care delivered by internists. Importantly, the study found that patient satisfaction was similar for both models, while quality metrics were likewise equal or even tilted slightly toward hospitalists.6
In their influential 2002 review of a profession that was only a half-decade old, Robert Wachter, MD, MHM, and Lee Goldman, MD, MPH, FACP from the University of California at San Francisco reinforced the message that HM wouldn’t lead to unhappy patients. “Empirical research supports the premise that hospitalists improve inpatient efficiency without harmful effects on quality or patient satisfaction,” they asserted.7
Among pediatric patients, a 2005 review found that “none of the four studies that evaluated patient satisfaction found statistically significant differences in satisfaction with inpatient care. However, two of the three evaluations that did assess parents’ satisfaction with care provided to their children found that parents were more satisfied with some aspects of care provided by hospitalists.”8
—William Southern, MD, chief, division of hospital medicine, Montefiore Medical Center, Bronx, N.Y.
Similar findings were popping up around the country: Replacing an internal medicine residency program with a physician assistant/hospitalist model at Brooklyn, N.Y.’s Coney Island Hospital did not adversely impact patient satisfaction, while it significantly improved mortality.9 Brigham & Women’s Hospital in Boston likewise reported no change in patient satisfaction in a study comparing a physician assistant/hospitalist service with traditional house staff services.10
The shift toward a more proactive position on patient satisfaction is exemplified within a 2008 white paper, “Hospitalists Meeting the Challenge of Patient Satisfaction,” written by a group of 19 private-practice HM experts known as The Phoenix Group.3 The paper acknowledged the flaws and limitations of existing survey methodologies, including Medicare’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores. Even so, the authors urged practice groups to adopt a team-oriented approach to communicate to hospital administrations “the belief that hospitalists are in the best position to improve survey scores overall for the facility.”
Carle Foundation Hospital in Urbana, Ill., is now publicly advertising its HM service’s contribution to high patient satisfaction scores on its website, and underscoring the hospitalists’ consistency, accessibility, and communication skills. “The hospital is never without a hospitalist, and our nurses know that they can rely on them,” says Lynn Barnes, vice president of hospital operations. “They’re available, they’re within a few minutes away, and patients’ needs get met very efficiently and rapidly.”
As a result, she says, their presence can lead to higher scores in patients’ perceptions of communication.
Hospitalists also have been central to several safety initiatives at Carle. Napoleon Knight, MD, medical director of hospital medicine and associate vice president for quality, says the HM team has helped address undiagnosed sleep apnea and implement rapid responses, such as “Code Speed.” Caregivers or family members can use the code to immediately call for help if they detect a downturn in a patient’s condition.
The ongoing initiatives, Dr. Knight and Barnes say, are helping the hospital improve how patients and their loved ones perceive care as Carle adapts to a rapidly shifting healthcare landscape. “With all of the changes that seem to be coming from the external environment weekly, we want to work collaboratively to make sure we’re connected and aligned and communicating in an ongoing fashion so we can react to all of these changes,” Dr. Knight says.
Continued below...
A Hopeful Trend
So far, evidence that the HM model is more broadly raising patient satisfaction scores is largely anecdotal. But a few analyses suggest the trend is moving in the right direction. A recent study in the American Journal of Medical Quality, for instance, concludes that facilities with hospitalists might have an advantage in patient satisfaction with nursing and such personal issues as privacy, emotional needs, and response to complaints.11 The study also posits that teaching facilities employing hospitalists could see benefits in overall satisfaction, while large facilities with hospitalists might see gains in satisfaction with admissions, nursing, and tests and treatments.
Brad Fulton, PhD, a researcher at South Bend, Ind.-based healthcare consulting firm Press Ganey and the study’s lead author, says the 30,000-foot view of patient satisfaction at the facility level can get foggy in a hurry due to differences in the kind and size of hospitalist programs. “And despite all of that fog, we’re still able to see through that and find something,” he says.
One limitation is that the study findings could also reflect differences in the culture of facilities that choose to add hospitalists. That caveat means it might not be possible to completely untangle the effect of an HM group on inpatient care from the larger, hospitalwide values that have allowed the group to set up shop. The wrinkle brings its own fascinating questions, according to Fulton. For example, is that kind of culture necessary for hospitalists to function as well as they do?
—Lynn Barnes, vice president of hospital operations, Carle Foundation Hospital, Urbana, Ill.
Such considerations will become more important as the healthcare system places additional emphasis on patient satisfaction, as Medicare’s value-based purchasing program is doing through its HCAHPS scores. With all the changes, success or failure on the patient experience front is going to carry “not just a reputational import, but also a financial impact,” says Ethan Cumbler, MD, FACP, director of Acute Care for the Elderly (ACE) Service at the University of Colorado Denver.
So how can HM fairly and accurately assess its own practitioners? “I think one starts by trying to apply some of the rigor that we have learned from our experience as hospitalists in quality improvement to the more warm and fuzzy field of patient experience,” Dr. Cumbler says. Many hospitals employ surveys supplied by consultants like Press Ganey to track the global patient satisfaction for their institution, he says.
“But for an individual hospitalist or hospitalist group, that kind of tool often lacks both the specificity and the timeliness necessary to make good decisions about impact of interventions on patient satisfaction,” he says.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, agrees that such imprecision could lead to unfair assessments. “You can imagine a scenario where a patient actually liked their hospitalist very much,” he says, “but when they got the survey, they said [their stay] was terrible and the reasons being because maybe the nurse call button was not answered and the food was terrible and medications were given to them incorrectly, or it was noisy at night so they couldn’t sleep.”
A recent study by Dr. Williams and his colleagues, in which they employed a new assessment method called the Communication Assessment Tool (CAT), confirmed the group’s suspicions: “that the results from the Press Ganey didn’t match up with the CAT, which was a direct assessment of the patient’s perception of the hospitalist’s communication skills,” he says.12
The validated tool, he adds, provides directed feedback to the physician based on the percentage of patients rating that provider as excellent, instead of on the average total score. Hospitalists have felt vindicated by the results. “They were very nervous because the hospital talked about basing an incentive off of the Press Ganey scores, and we said, ‘You can’t do that,’ because we didn’t feel they were accurate, and this study proved that,” Dr. Williams explains.
Fortunately, the message has reached researchers and consultants alike, and better tools are starting to reach hospitals around the country. At HM11 in May, Press Ganey unveiled a new survey designed to help patients assess the care delivered by two hospitalists, the average for inpatient stays. The item set is specific to HM functions, and includes the photo and name of each hospitalist, which Fulton says should improve the validity and accuracy of the data.
“The early response looks really good,” Fulton says, though it’s too early to say whether the tool, called Hospitalist Insight, will live up to its billing. If it proves its mettle, Fulton says, the survey could be used to reward top-performing hospitalists, and the growing dataset could allow hospitals to compare themselves with appropriate peer groups for fairer comparisons.
Meanwhile, researchers are testing out checklists to score hospitalist etiquette, and tracking and paging systems to help ensure continuity of care. They have found increased patient satisfaction when doctors engage in verbal communication during a discharge, in interdisciplinary team rounding, and in efforts to address religious and spiritual concerns.
Since 2000, when Montefiore’s hospitalist program began, Dr. Southern says the hospital has explained to patients the tradeoff accompanying the HM model. “I say something like this to every patient: ‘I know I’m not the doctor that you know, and you’re just meeting me. The downside is that you haven’t met me before and I’m a new face, but the upside is that if you need me during the day, I’m here all the time, I’m not someplace else. And so if you need something, I can be here quickly.’ ”
Being very explicit about that tradeoff, he says, has made patients very comfortable with the model of care, especially during a crisis moment in their lives. “I think it’s really important to say, ‘I know you don’t know me, but here’s the upside.’ And my experience is that patients easily understand that tradeoff and are very positive,” Dr. Southern says.
The Verdict
Available evidence suggests that practitioners of the HM model have pivoted from defending against early criticism that they may harm patient satisfaction to pitching themselves as team leaders who can boost facilitywide perceptions of care. So far, too little research has been conducted to suggest whether that optimism is fully warranted, but early signs look promising.
At facilities like Chicago’s Northwestern Memorial Hospital, medical floors staffed by hospitalists are beginning to beat out surgical floors for the traveling patient satisfaction award. And experts like Dr. Cumbler are pondering how ongoing initiatives to boost scores can follow in the footsteps of efficiency and quality-raising efforts by making the transition from focusing on individual doctors to adopting a more programmatic approach. “What’s happening to that patient during the 23 hours and 45 minutes of their hospital day that you are not sitting by the bedside? And what influence should a hospitalist have in affecting that other 23 hours and 45 minutes?” he says.
Handoffs, discharges, communication with PCPs, and other potential weak points in maintaining high levels of patient satisfaction, Dr. Cumbler says, all are amenable to systems-based improvement. “As hospitalists, we are in a unique position to influence not only our one-one-one interaction with the patient, but also to influence that system of care in a way that patients will notice in a real and tangible way,” he says. “I think we’ve recognized for some time that a healthy heart but a miserable patient is not a healthy person.”
Teaching Hospitals Gain Ground in Patient Satisfaction
One widely accepted truism about teaching facilities is that they’re known to have lower patient satisfaction scores than nonteaching hospitals. Brad Fulton, researcher for South Bend, Ind.-based consultant firm Press Ganey, attributes the difference in part to the fact that many doctors at teaching facilities must divide their time among patient care, education, and research. Such hospitals also tend to have some of the more medically difficult patients, he says, some of who may be more apt to feel like they’re on display with the abundance of students and residents.
In one of his recent studies, however, teaching facilities with hospitalists scored higher on patient satisfaction than nonteaching facilities or teaching facilities that lacked hospitalists. One potential follow-up question could have broad implications: “What is it about having hospitalists in teaching facilities that works so well in terms of patient satisfaction?” Can that be replicated elsewhere, he wonders? And is there an essential element that could be applied to nonteaching facilities?
A separate study also defied expectations by finding that teaching bedside procedures to inexperienced residents can be reassuring to patients, if done correctly. In a teaching model instituted at the University of California San Francisco, an experienced hospitalist with extra training supervises a novice during bedside procedures such as lumbar punctures and paracentesis. Study coauthor Diane Sliwka, MD, associate clinical professor of medicine and a hospitalist, says the feedback so far suggests that the model can improve safety, boost education, and deliver a positive patient experience.
Patients may be hesitant about having trainees do procedures, she says, but surveys suggest those patients are reassured when they know an expert is in the room and watching. They also want to hear what will happen next to counteract the anxiety of feeling pain or encountering something unexpected.
As the study suggested, what patients may find to be the most difficult or nerve-wracking can be quite different from what doctors expect. “You would think it was actually the procedure that was most painful part, but actually that was after we had given lidocaine,” Dr. Sliwka says. Patients repeatedly reacted to the doctors using a plastic pen cap to imprint the site where they would insert a needle. “Over and over we would hear people say, ‘That is actually the most painful part and you didn’t warn me about that,’ ” she recalls. “And we didn’t warn people about that because we didn’t think it was a big deal.”
Procedures can take longer with trainees, another tradeoff that can leading to lower satisfaction scores. But what the study also showed is that in academic settings, involving residents doesn’t harm the overall patient experience and can in fact improve it. “Anecdotally, what we hear from patients a lot is, ‘Oh, I had this procedure done before and it went horribly.’ They would tell stories of previous bad experiences, and then really be thankful for the experience that they had in our setting,” Dr. Sliwka says.
The extended face-to-face time can yield another positive effect. Dr. Sliwka found that hospitalists and residents often learned medical and historical information about the patient that the primary care team hadn’t yet had an opportunity to glean. “Patients just start to tell you about their families, their lives, their medical problems, their experiences,” she says, a product of building more rapport with them. “We would often find ourselves telling the primary medical team, ‘By the way, we found this out and you should probably know it: the patient is very concerned about this that’s been going on,’ and the patient hasn’t had a chance to tell the team because there isn’t that kind of time.”
Even without the specific model, Dr. Sliwka says, several principles can be applied to daily interactions. Framing things appropriately, she says, helps patients gain confidence in the doctors and allows them to safely conduct bedside teaching and openly discuss procedures. Even correcting mistakes can be a positive experience. “That actually makes the patient feel more confident in you than less confident,” Dr. Sliwka says.
Ultimately, the teaching experience can help residents broaden their thinking about patient satisfaction. “I think when trainees are starting, their real focus is, ‘How do I deal with this correctly?’ ” Dr. Sliwka says. “It takes a level of comfort with the basic skills to then go beyond that and start thinking about, ‘How is the patient perceiving this?’”
Bryn Nelson is a freelance medical journalist based in Seattle.
References
- Williams M, Flanders SA, Whitcomb WF. Comprehensive hospital medicine: an evidence based approach. Elsevier;2007:971-976.
- Arora V, Gangireddy S, Mehrotra A, Ginde R, Tormey M, Meltzer D. Ability of hospitalized patients to identify their in-hospital physicians. Arch Intern Med. 2009;169(2):199-201.
- Singer AS, et al. Hospitalists meeting the challenge of patient satisfaction. The Phoenix Group. 2008;1-5.
- Manian FA. Whither continuity of care? N Engl J Med. 1999;340:1362-1363.
- Correspondence. Whither continuity of care? N Engl J Med. 1999;341:850-852.
- Davis KM, Koch KE, Harvey JK, et al. Effects of hospitalists on cost, outcomes, and patient satisfaction in a rural health system. Amer J Med. 2000;108(8):621-626.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Coffman J, Rundall TG. The impact of hospitalists on the cost and quality of inpatient care in the United States (a research synthesis). Med Care Res Rev. 2005;62:379–406.
- Dhuper S, Choksi S. Replacing an academic internal medicine residency program with a physician assistant-hospitalist model: a comparative analysis study. Am J Med Qual. 2009;24(2):132-139.
- Roy CL, Liang CL, Lund M, et al. Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes. J Hosp Med. 2008;3(5):361-368.
- Fulton BR, Drevs KE, Ayala LJ, Malott DL Jr. Patient satisfaction with hospitalists: facility-level analyses. Am J Med Qual. 2011;26(2):95-102.
- Ferranti DE, Makoul G, Forth VE, Rauworth J, Lee J, Williams MV. Assessing patient perceptions of hospitalist communication skills using the Communication Assessment Tool (CAT). J Hosp Med. 2010;5(9):522-527.
At first glance, the deck might seem hopelessly stacked against hospitalists with regard to patient satisfaction. HM practitioners lack the long-term relationship with patients that many primary-care physicians (PCPs) have established. Unlike surgeons and other specialists, they tend to care for those patients—more complicated, lacking a regular doctor, or admitted through the ED, for example—who are more inclined to rate their hospital stay unfavorably.1 They may not even be accurately remembered by patients who encounter multiple doctors during the course of their hospitalization.2 And hospital information systems can misidentify the treating physician, while the actual surveys used to gauge hospitalists have been imperfect at best.3
And yet, the hospitalist model has evolved substantially on the question of how it can impact patient perceptions of care.
Initially, hospitalist champions adopted a largely defensive posture: The model would not negatively impact patient satisfaction as it delivered on efficiency—and later on quality. The healthcare system, however, is beginning to recognize the hospitalist as part of a care “team” whose patient-centered approach might pay big dividends in the inpatient experience and, eventually, on satisfaction scores.
“I think the next phase, which is a focus on the hospitalist as a team member and team builder, is going to be key,” says William Southern, MD, MPH, SFHM, chief of the division of hospital medicine at Montefiore Medical Center in Bronx, N.Y.
Recent studies suggest that hospitalists are helping to design and test new tools that will not only improve satisfaction, but also more fairly assess the impact of individual doctors. As the maturation process continues, experts say, hospitalists have an opportunity to influence both provider-based interventions and more programmatic decision-making that can have far-reaching effects. Certainly, the hand dealt to hospitalists is looking more favorable even as the ante has been raised with Medicare programs like value-based purchasing, and its pot of money tied to patient perceptions of care.
So how have hospitalists played their cards so far?
A Look at the Evidence
In its early years, the HM model faced a persistent criticism: Replacing traditional caregivers with these new inpatient providers in the name of efficiency would increase handoffs and, therefore, discontinuities of care delivered by a succession of unfamiliar faces. If patients didn’t see their PCP in the hospital, the thinking went, they might be more disgruntled at being tended to by hospitalists, leading to lower satisfaction scores.4
A particularly heated exchange played out in 1999 in the New England Journal of Medicine. Farris A. Manian, MD, MPH, of Infectious Disease Consultants in St. Louis wrote in one letter, “I am particularly concerned about what impressionable house-staff members will learn from hospitalists who place an inordinate emphasis on cost rather than the quality of patient care or teaching.”5
A few subsequent studies, however, hinted that such concerns might be overstated. A 2000 analysis in the American Journal of Medicine that examined North Mississippi Health Services in Tupelo, for instance, found that care administered by hospitalists led to a shorter length of stay and lower costs than care delivered by internists. Importantly, the study found that patient satisfaction was similar for both models, while quality metrics were likewise equal or even tilted slightly toward hospitalists.6
In their influential 2002 review of a profession that was only a half-decade old, Robert Wachter, MD, MHM, and Lee Goldman, MD, MPH, FACP from the University of California at San Francisco reinforced the message that HM wouldn’t lead to unhappy patients. “Empirical research supports the premise that hospitalists improve inpatient efficiency without harmful effects on quality or patient satisfaction,” they asserted.7
Among pediatric patients, a 2005 review found that “none of the four studies that evaluated patient satisfaction found statistically significant differences in satisfaction with inpatient care. However, two of the three evaluations that did assess parents’ satisfaction with care provided to their children found that parents were more satisfied with some aspects of care provided by hospitalists.”8
—William Southern, MD, chief, division of hospital medicine, Montefiore Medical Center, Bronx, N.Y.
Similar findings were popping up around the country: Replacing an internal medicine residency program with a physician assistant/hospitalist model at Brooklyn, N.Y.’s Coney Island Hospital did not adversely impact patient satisfaction, while it significantly improved mortality.9 Brigham & Women’s Hospital in Boston likewise reported no change in patient satisfaction in a study comparing a physician assistant/hospitalist service with traditional house staff services.10
The shift toward a more proactive position on patient satisfaction is exemplified within a 2008 white paper, “Hospitalists Meeting the Challenge of Patient Satisfaction,” written by a group of 19 private-practice HM experts known as The Phoenix Group.3 The paper acknowledged the flaws and limitations of existing survey methodologies, including Medicare’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) scores. Even so, the authors urged practice groups to adopt a team-oriented approach to communicate to hospital administrations “the belief that hospitalists are in the best position to improve survey scores overall for the facility.”
Carle Foundation Hospital in Urbana, Ill., is now publicly advertising its HM service’s contribution to high patient satisfaction scores on its website, and underscoring the hospitalists’ consistency, accessibility, and communication skills. “The hospital is never without a hospitalist, and our nurses know that they can rely on them,” says Lynn Barnes, vice president of hospital operations. “They’re available, they’re within a few minutes away, and patients’ needs get met very efficiently and rapidly.”
As a result, she says, their presence can lead to higher scores in patients’ perceptions of communication.
Hospitalists also have been central to several safety initiatives at Carle. Napoleon Knight, MD, medical director of hospital medicine and associate vice president for quality, says the HM team has helped address undiagnosed sleep apnea and implement rapid responses, such as “Code Speed.” Caregivers or family members can use the code to immediately call for help if they detect a downturn in a patient’s condition.
The ongoing initiatives, Dr. Knight and Barnes say, are helping the hospital improve how patients and their loved ones perceive care as Carle adapts to a rapidly shifting healthcare landscape. “With all of the changes that seem to be coming from the external environment weekly, we want to work collaboratively to make sure we’re connected and aligned and communicating in an ongoing fashion so we can react to all of these changes,” Dr. Knight says.
Continued below...
A Hopeful Trend
So far, evidence that the HM model is more broadly raising patient satisfaction scores is largely anecdotal. But a few analyses suggest the trend is moving in the right direction. A recent study in the American Journal of Medical Quality, for instance, concludes that facilities with hospitalists might have an advantage in patient satisfaction with nursing and such personal issues as privacy, emotional needs, and response to complaints.11 The study also posits that teaching facilities employing hospitalists could see benefits in overall satisfaction, while large facilities with hospitalists might see gains in satisfaction with admissions, nursing, and tests and treatments.
Brad Fulton, PhD, a researcher at South Bend, Ind.-based healthcare consulting firm Press Ganey and the study’s lead author, says the 30,000-foot view of patient satisfaction at the facility level can get foggy in a hurry due to differences in the kind and size of hospitalist programs. “And despite all of that fog, we’re still able to see through that and find something,” he says.
One limitation is that the study findings could also reflect differences in the culture of facilities that choose to add hospitalists. That caveat means it might not be possible to completely untangle the effect of an HM group on inpatient care from the larger, hospitalwide values that have allowed the group to set up shop. The wrinkle brings its own fascinating questions, according to Fulton. For example, is that kind of culture necessary for hospitalists to function as well as they do?
—Lynn Barnes, vice president of hospital operations, Carle Foundation Hospital, Urbana, Ill.
Such considerations will become more important as the healthcare system places additional emphasis on patient satisfaction, as Medicare’s value-based purchasing program is doing through its HCAHPS scores. With all the changes, success or failure on the patient experience front is going to carry “not just a reputational import, but also a financial impact,” says Ethan Cumbler, MD, FACP, director of Acute Care for the Elderly (ACE) Service at the University of Colorado Denver.
So how can HM fairly and accurately assess its own practitioners? “I think one starts by trying to apply some of the rigor that we have learned from our experience as hospitalists in quality improvement to the more warm and fuzzy field of patient experience,” Dr. Cumbler says. Many hospitals employ surveys supplied by consultants like Press Ganey to track the global patient satisfaction for their institution, he says.
“But for an individual hospitalist or hospitalist group, that kind of tool often lacks both the specificity and the timeliness necessary to make good decisions about impact of interventions on patient satisfaction,” he says.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, agrees that such imprecision could lead to unfair assessments. “You can imagine a scenario where a patient actually liked their hospitalist very much,” he says, “but when they got the survey, they said [their stay] was terrible and the reasons being because maybe the nurse call button was not answered and the food was terrible and medications were given to them incorrectly, or it was noisy at night so they couldn’t sleep.”
A recent study by Dr. Williams and his colleagues, in which they employed a new assessment method called the Communication Assessment Tool (CAT), confirmed the group’s suspicions: “that the results from the Press Ganey didn’t match up with the CAT, which was a direct assessment of the patient’s perception of the hospitalist’s communication skills,” he says.12
The validated tool, he adds, provides directed feedback to the physician based on the percentage of patients rating that provider as excellent, instead of on the average total score. Hospitalists have felt vindicated by the results. “They were very nervous because the hospital talked about basing an incentive off of the Press Ganey scores, and we said, ‘You can’t do that,’ because we didn’t feel they were accurate, and this study proved that,” Dr. Williams explains.
Fortunately, the message has reached researchers and consultants alike, and better tools are starting to reach hospitals around the country. At HM11 in May, Press Ganey unveiled a new survey designed to help patients assess the care delivered by two hospitalists, the average for inpatient stays. The item set is specific to HM functions, and includes the photo and name of each hospitalist, which Fulton says should improve the validity and accuracy of the data.
“The early response looks really good,” Fulton says, though it’s too early to say whether the tool, called Hospitalist Insight, will live up to its billing. If it proves its mettle, Fulton says, the survey could be used to reward top-performing hospitalists, and the growing dataset could allow hospitals to compare themselves with appropriate peer groups for fairer comparisons.
Meanwhile, researchers are testing out checklists to score hospitalist etiquette, and tracking and paging systems to help ensure continuity of care. They have found increased patient satisfaction when doctors engage in verbal communication during a discharge, in interdisciplinary team rounding, and in efforts to address religious and spiritual concerns.
Since 2000, when Montefiore’s hospitalist program began, Dr. Southern says the hospital has explained to patients the tradeoff accompanying the HM model. “I say something like this to every patient: ‘I know I’m not the doctor that you know, and you’re just meeting me. The downside is that you haven’t met me before and I’m a new face, but the upside is that if you need me during the day, I’m here all the time, I’m not someplace else. And so if you need something, I can be here quickly.’ ”
Being very explicit about that tradeoff, he says, has made patients very comfortable with the model of care, especially during a crisis moment in their lives. “I think it’s really important to say, ‘I know you don’t know me, but here’s the upside.’ And my experience is that patients easily understand that tradeoff and are very positive,” Dr. Southern says.
The Verdict
Available evidence suggests that practitioners of the HM model have pivoted from defending against early criticism that they may harm patient satisfaction to pitching themselves as team leaders who can boost facilitywide perceptions of care. So far, too little research has been conducted to suggest whether that optimism is fully warranted, but early signs look promising.
At facilities like Chicago’s Northwestern Memorial Hospital, medical floors staffed by hospitalists are beginning to beat out surgical floors for the traveling patient satisfaction award. And experts like Dr. Cumbler are pondering how ongoing initiatives to boost scores can follow in the footsteps of efficiency and quality-raising efforts by making the transition from focusing on individual doctors to adopting a more programmatic approach. “What’s happening to that patient during the 23 hours and 45 minutes of their hospital day that you are not sitting by the bedside? And what influence should a hospitalist have in affecting that other 23 hours and 45 minutes?” he says.
Handoffs, discharges, communication with PCPs, and other potential weak points in maintaining high levels of patient satisfaction, Dr. Cumbler says, all are amenable to systems-based improvement. “As hospitalists, we are in a unique position to influence not only our one-one-one interaction with the patient, but also to influence that system of care in a way that patients will notice in a real and tangible way,” he says. “I think we’ve recognized for some time that a healthy heart but a miserable patient is not a healthy person.”
Teaching Hospitals Gain Ground in Patient Satisfaction
One widely accepted truism about teaching facilities is that they’re known to have lower patient satisfaction scores than nonteaching hospitals. Brad Fulton, researcher for South Bend, Ind.-based consultant firm Press Ganey, attributes the difference in part to the fact that many doctors at teaching facilities must divide their time among patient care, education, and research. Such hospitals also tend to have some of the more medically difficult patients, he says, some of who may be more apt to feel like they’re on display with the abundance of students and residents.
In one of his recent studies, however, teaching facilities with hospitalists scored higher on patient satisfaction than nonteaching facilities or teaching facilities that lacked hospitalists. One potential follow-up question could have broad implications: “What is it about having hospitalists in teaching facilities that works so well in terms of patient satisfaction?” Can that be replicated elsewhere, he wonders? And is there an essential element that could be applied to nonteaching facilities?
A separate study also defied expectations by finding that teaching bedside procedures to inexperienced residents can be reassuring to patients, if done correctly. In a teaching model instituted at the University of California San Francisco, an experienced hospitalist with extra training supervises a novice during bedside procedures such as lumbar punctures and paracentesis. Study coauthor Diane Sliwka, MD, associate clinical professor of medicine and a hospitalist, says the feedback so far suggests that the model can improve safety, boost education, and deliver a positive patient experience.
Patients may be hesitant about having trainees do procedures, she says, but surveys suggest those patients are reassured when they know an expert is in the room and watching. They also want to hear what will happen next to counteract the anxiety of feeling pain or encountering something unexpected.
As the study suggested, what patients may find to be the most difficult or nerve-wracking can be quite different from what doctors expect. “You would think it was actually the procedure that was most painful part, but actually that was after we had given lidocaine,” Dr. Sliwka says. Patients repeatedly reacted to the doctors using a plastic pen cap to imprint the site where they would insert a needle. “Over and over we would hear people say, ‘That is actually the most painful part and you didn’t warn me about that,’ ” she recalls. “And we didn’t warn people about that because we didn’t think it was a big deal.”
Procedures can take longer with trainees, another tradeoff that can leading to lower satisfaction scores. But what the study also showed is that in academic settings, involving residents doesn’t harm the overall patient experience and can in fact improve it. “Anecdotally, what we hear from patients a lot is, ‘Oh, I had this procedure done before and it went horribly.’ They would tell stories of previous bad experiences, and then really be thankful for the experience that they had in our setting,” Dr. Sliwka says.
The extended face-to-face time can yield another positive effect. Dr. Sliwka found that hospitalists and residents often learned medical and historical information about the patient that the primary care team hadn’t yet had an opportunity to glean. “Patients just start to tell you about their families, their lives, their medical problems, their experiences,” she says, a product of building more rapport with them. “We would often find ourselves telling the primary medical team, ‘By the way, we found this out and you should probably know it: the patient is very concerned about this that’s been going on,’ and the patient hasn’t had a chance to tell the team because there isn’t that kind of time.”
Even without the specific model, Dr. Sliwka says, several principles can be applied to daily interactions. Framing things appropriately, she says, helps patients gain confidence in the doctors and allows them to safely conduct bedside teaching and openly discuss procedures. Even correcting mistakes can be a positive experience. “That actually makes the patient feel more confident in you than less confident,” Dr. Sliwka says.
Ultimately, the teaching experience can help residents broaden their thinking about patient satisfaction. “I think when trainees are starting, their real focus is, ‘How do I deal with this correctly?’ ” Dr. Sliwka says. “It takes a level of comfort with the basic skills to then go beyond that and start thinking about, ‘How is the patient perceiving this?’”
Bryn Nelson is a freelance medical journalist based in Seattle.
References
- Williams M, Flanders SA, Whitcomb WF. Comprehensive hospital medicine: an evidence based approach. Elsevier;2007:971-976.
- Arora V, Gangireddy S, Mehrotra A, Ginde R, Tormey M, Meltzer D. Ability of hospitalized patients to identify their in-hospital physicians. Arch Intern Med. 2009;169(2):199-201.
- Singer AS, et al. Hospitalists meeting the challenge of patient satisfaction. The Phoenix Group. 2008;1-5.
- Manian FA. Whither continuity of care? N Engl J Med. 1999;340:1362-1363.
- Correspondence. Whither continuity of care? N Engl J Med. 1999;341:850-852.
- Davis KM, Koch KE, Harvey JK, et al. Effects of hospitalists on cost, outcomes, and patient satisfaction in a rural health system. Amer J Med. 2000;108(8):621-626.
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Coffman J, Rundall TG. The impact of hospitalists on the cost and quality of inpatient care in the United States (a research synthesis). Med Care Res Rev. 2005;62:379–406.
- Dhuper S, Choksi S. Replacing an academic internal medicine residency program with a physician assistant-hospitalist model: a comparative analysis study. Am J Med Qual. 2009;24(2):132-139.
- Roy CL, Liang CL, Lund M, et al. Implementation of a physician assistant/hospitalist service in an academic medical center: impact on efficiency and patient outcomes. J Hosp Med. 2008;3(5):361-368.
- Fulton BR, Drevs KE, Ayala LJ, Malott DL Jr. Patient satisfaction with hospitalists: facility-level analyses. Am J Med Qual. 2011;26(2):95-102.
- Ferranti DE, Makoul G, Forth VE, Rauworth J, Lee J, Williams MV. Assessing patient perceptions of hospitalist communication skills using the Communication Assessment Tool (CAT). J Hosp Med. 2010;5(9):522-527.
Small-Town Tonic
In mid-August, the White House released its “Jobs and Economic Security for Rural America” report (www.whitehouse.gov), which underlines what most hospitalists already know: Rural healthcare is ailing. As the report points out, rural residents are more likely to be uninsured or be covered through public sources, while mortality rates have dropped more slowly in rural areas than in urban ones.
One troubling statistic in particular highlights the disparity in access: In 2008, the report notes, rural counties had 62 primary-care physicians (PCPs) per 100,000 residents, while urban areas counted an average of 79.5 PCPs (28% more). Although a number of initiatives have specifically sought to narrow that gap, a lesser-known dynamic between primary care and HM might be exacerbating the shortage.
Over the past few years, several reports and media accounts have suggested that medical students increasingly want practices that are either hospital-based or office-based, but not both. The presence of hospitalists, then, helps rural facilities create an attractive office-hospital divide and place PCPs in practices frequently owned by the hospital. Hospitalists, in other words, might be necessary prerequisites to help lure and retain PCPs.

—Louis J. O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, P.C., Honesdale, Pa.
Meanwhile, many physicians already in private rural practices are burning out. According to the 2009 Rural Hospitalist Study by the Illinois Critical Access Health Network, “primary-care physicians in rural areas are throwing in the towel of managing their hospitalized patients. More and more, these PCPs unilaterally are announcing to their patients and to the local hospitals they will neither continue to take responsibility for hospitalized patients nor continue to ‘take call.’ ”
Ome Nwanze, MD, one of two hospitalists at the 42-bed Greenville Regional Hospital in Greenville, Ill., says the biggest benefit to being a rural hospitalist is the ability to make a difference in the lives of everyone in the community. Along with patients, Dr. Nwanze includes other doctors as beneficiaries: “The primary-care physicians and specialists are very happy with the program and the difference it makes in their lives.”
Competitive Business
If hospitalists are a natural solution, though, there’s a key problem: Rural communities are struggling to attract them as well. One sign of the difficulty is median salary. Similar to what surveys consistently show for other specialties, rural hospitalists outpace their urban counterparts in median annual salary, at roughly $206,000 versus $187,000, according to Becker’s Hospital Review (overall, hospitalists rank behind most other specialties in salary). The rural-urban divide can be attributed to that old real estate adage: location, location, location. Competition for hospitalist jobs in large cities is generally fierce, while rural communities often have to offer more incentives to attract and retain the doctors they need.
“The two biggest issues that I can see are recruitment and night coverage,” says Louis J. O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine (AIM), P.C., in Honesdale, Pa. He and AIM’s four other hospitalists work exclusively with the town’s 98-bed Wayne Memorial Hospital. “It is easier to recruit to a larger city, closer to more activities and residency programs,” Dr. O’Boyle says. “To get someone to come to our area almost always requires some form of local connection. That makes retention paramount.”
Night call can be a particular sticking point: Most rural hospitals aren’t busy enough to justify an FTE nocturnist, he says, putting the onus of night call on full-time hospitalists. Wayne Memorial Hospital is fortunate in that regard, as it averages only one or two admissions a day after 10 p.m., leaving the hospitalists “fresh enough to round the next day,” Dr. O’Boyle says. “However, this still makes rural programs less attractive compared to places that can boast a nocturnist team that eliminates night call.”
Government Assistance
So what has the government done to help address the growing need for more rural hospitalists and other healthcare providers? If the Affordable Care Act’s (ACA) measures proceed as expected, most experts predict a significant drop in the number of uninsured individuals—meaning a surge in both rural and urban demand for care.
According to the White House report, the Department of Health and Human Services has funded 444 rural community health centers since 2009. The ACA has expanded and extended the Medicare Rural Community Hospital Demonstration, providing “an estimated $52 million in enhanced reimbursement for inpatient services at 25 rural hospitals.” And the administration has expanded funding for the National Health Service Corps, which offers doctors scholarships and loan repayment in exchange for a commitment to practice medicine at underserved communities. The corps website boasts that more than 8,000 clinicians are in place, but it also notes that there are “more than 9,000 job vacancies for NHSC primary care medical, dental, and mental health clinicians.” (View the full report at http://nhsc.hrsa.gov/about.) Clearly, loan forgiveness isn’t enough.
Furthermore, the government might be facing a perception problem. Dr. Nwanze describes government support to rural programs as “poor,” while Dr. O’Boyle says he’s not aware of any specific efforts to support rural hospitalists. “There may be some areas, such as giving grants for telemedicine and other tertiary support, but I don’t think those of us in rural programs can sense any impact,” Dr. O’Boyle says. Wayne Memorial Hospital is in an underserved area, he says, and PCPs there do receive loan forgiveness. “However, I was disappointed to learn that those programs are not open to hospitalists.”
Meanwhile, many rural hospitalists face daunting responsibilities. Dr. Nwanze cites “the need to be a jack-of-all-trades and master of all,” and notes the pressure of providing a wide range of services and handling almost all situations with little or no specialist support.
But Dr. O’Boyle also sees opportunity in the autonomy, such as the ability to play a larger role in hospital management and more independence. “We don’t have a plethora of subspecialists looking for business,” he says. “That means much greater responsibility for our hospitalists, who will take care of much sicker patients without specialist backup being readily available.” As a result, advanced duties like ventilator management and the care of complex patients with such diagnoses as acute renal failure or new malignancies are all within the realm of the hospitalist.
“This is an attractive prospect for certain hospitalists who like the idea of taking care of patients without feeling like a captain who merely delegates to multiple specialists,” Dr. O’Boyle says. “Also, the group integrates into hospital committees at every level, and has an overall much larger say in the day-to-day operations, something largely out of the control of a hospitalist group at a large tertiary facility.”
Tech Solutions
Despite the challenges, many rural hospitals are gaining new tools to help them survive, and tech-savvy hospitalists might be big assets. Smaller facilities are increasingly gaining access to electronic health records, while many also are using video links to allow specialists hundreds of miles away to help with diagnoses without having to transfer the patients.
Recent research also suggests that hospital discharges could be better in rural communities.
Bryn Nelson is a freelance medical writer based in Seattle.
In mid-August, the White House released its “Jobs and Economic Security for Rural America” report (www.whitehouse.gov), which underlines what most hospitalists already know: Rural healthcare is ailing. As the report points out, rural residents are more likely to be uninsured or be covered through public sources, while mortality rates have dropped more slowly in rural areas than in urban ones.
One troubling statistic in particular highlights the disparity in access: In 2008, the report notes, rural counties had 62 primary-care physicians (PCPs) per 100,000 residents, while urban areas counted an average of 79.5 PCPs (28% more). Although a number of initiatives have specifically sought to narrow that gap, a lesser-known dynamic between primary care and HM might be exacerbating the shortage.
Over the past few years, several reports and media accounts have suggested that medical students increasingly want practices that are either hospital-based or office-based, but not both. The presence of hospitalists, then, helps rural facilities create an attractive office-hospital divide and place PCPs in practices frequently owned by the hospital. Hospitalists, in other words, might be necessary prerequisites to help lure and retain PCPs.
—Louis J. O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, P.C., Honesdale, Pa.
Meanwhile, many physicians already in private rural practices are burning out. According to the 2009 Rural Hospitalist Study by the Illinois Critical Access Health Network, “primary-care physicians in rural areas are throwing in the towel of managing their hospitalized patients. More and more, these PCPs unilaterally are announcing to their patients and to the local hospitals they will neither continue to take responsibility for hospitalized patients nor continue to ‘take call.’ ”
Ome Nwanze, MD, one of two hospitalists at the 42-bed Greenville Regional Hospital in Greenville, Ill., says the biggest benefit to being a rural hospitalist is the ability to make a difference in the lives of everyone in the community. Along with patients, Dr. Nwanze includes other doctors as beneficiaries: “The primary-care physicians and specialists are very happy with the program and the difference it makes in their lives.”
Competitive Business
If hospitalists are a natural solution, though, there’s a key problem: Rural communities are struggling to attract them as well. One sign of the difficulty is median salary. Similar to what surveys consistently show for other specialties, rural hospitalists outpace their urban counterparts in median annual salary, at roughly $206,000 versus $187,000, according to Becker’s Hospital Review (overall, hospitalists rank behind most other specialties in salary). The rural-urban divide can be attributed to that old real estate adage: location, location, location. Competition for hospitalist jobs in large cities is generally fierce, while rural communities often have to offer more incentives to attract and retain the doctors they need.
“The two biggest issues that I can see are recruitment and night coverage,” says Louis J. O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine (AIM), P.C., in Honesdale, Pa. He and AIM’s four other hospitalists work exclusively with the town’s 98-bed Wayne Memorial Hospital. “It is easier to recruit to a larger city, closer to more activities and residency programs,” Dr. O’Boyle says. “To get someone to come to our area almost always requires some form of local connection. That makes retention paramount.”
Night call can be a particular sticking point: Most rural hospitals aren’t busy enough to justify an FTE nocturnist, he says, putting the onus of night call on full-time hospitalists. Wayne Memorial Hospital is fortunate in that regard, as it averages only one or two admissions a day after 10 p.m., leaving the hospitalists “fresh enough to round the next day,” Dr. O’Boyle says. “However, this still makes rural programs less attractive compared to places that can boast a nocturnist team that eliminates night call.”
Government Assistance
So what has the government done to help address the growing need for more rural hospitalists and other healthcare providers? If the Affordable Care Act’s (ACA) measures proceed as expected, most experts predict a significant drop in the number of uninsured individuals—meaning a surge in both rural and urban demand for care.
According to the White House report, the Department of Health and Human Services has funded 444 rural community health centers since 2009. The ACA has expanded and extended the Medicare Rural Community Hospital Demonstration, providing “an estimated $52 million in enhanced reimbursement for inpatient services at 25 rural hospitals.” And the administration has expanded funding for the National Health Service Corps, which offers doctors scholarships and loan repayment in exchange for a commitment to practice medicine at underserved communities. The corps website boasts that more than 8,000 clinicians are in place, but it also notes that there are “more than 9,000 job vacancies for NHSC primary care medical, dental, and mental health clinicians.” (View the full report at http://nhsc.hrsa.gov/about.) Clearly, loan forgiveness isn’t enough.
Furthermore, the government might be facing a perception problem. Dr. Nwanze describes government support to rural programs as “poor,” while Dr. O’Boyle says he’s not aware of any specific efforts to support rural hospitalists. “There may be some areas, such as giving grants for telemedicine and other tertiary support, but I don’t think those of us in rural programs can sense any impact,” Dr. O’Boyle says. Wayne Memorial Hospital is in an underserved area, he says, and PCPs there do receive loan forgiveness. “However, I was disappointed to learn that those programs are not open to hospitalists.”
Meanwhile, many rural hospitalists face daunting responsibilities. Dr. Nwanze cites “the need to be a jack-of-all-trades and master of all,” and notes the pressure of providing a wide range of services and handling almost all situations with little or no specialist support.
But Dr. O’Boyle also sees opportunity in the autonomy, such as the ability to play a larger role in hospital management and more independence. “We don’t have a plethora of subspecialists looking for business,” he says. “That means much greater responsibility for our hospitalists, who will take care of much sicker patients without specialist backup being readily available.” As a result, advanced duties like ventilator management and the care of complex patients with such diagnoses as acute renal failure or new malignancies are all within the realm of the hospitalist.
“This is an attractive prospect for certain hospitalists who like the idea of taking care of patients without feeling like a captain who merely delegates to multiple specialists,” Dr. O’Boyle says. “Also, the group integrates into hospital committees at every level, and has an overall much larger say in the day-to-day operations, something largely out of the control of a hospitalist group at a large tertiary facility.”
Tech Solutions
Despite the challenges, many rural hospitals are gaining new tools to help them survive, and tech-savvy hospitalists might be big assets. Smaller facilities are increasingly gaining access to electronic health records, while many also are using video links to allow specialists hundreds of miles away to help with diagnoses without having to transfer the patients.
Recent research also suggests that hospital discharges could be better in rural communities.
Bryn Nelson is a freelance medical writer based in Seattle.
In mid-August, the White House released its “Jobs and Economic Security for Rural America” report (www.whitehouse.gov), which underlines what most hospitalists already know: Rural healthcare is ailing. As the report points out, rural residents are more likely to be uninsured or be covered through public sources, while mortality rates have dropped more slowly in rural areas than in urban ones.
One troubling statistic in particular highlights the disparity in access: In 2008, the report notes, rural counties had 62 primary-care physicians (PCPs) per 100,000 residents, while urban areas counted an average of 79.5 PCPs (28% more). Although a number of initiatives have specifically sought to narrow that gap, a lesser-known dynamic between primary care and HM might be exacerbating the shortage.
Over the past few years, several reports and media accounts have suggested that medical students increasingly want practices that are either hospital-based or office-based, but not both. The presence of hospitalists, then, helps rural facilities create an attractive office-hospital divide and place PCPs in practices frequently owned by the hospital. Hospitalists, in other words, might be necessary prerequisites to help lure and retain PCPs.
—Louis J. O’Boyle, DO, FACP, FHM, medical director, Advanced Inpatient Medicine, P.C., Honesdale, Pa.
Meanwhile, many physicians already in private rural practices are burning out. According to the 2009 Rural Hospitalist Study by the Illinois Critical Access Health Network, “primary-care physicians in rural areas are throwing in the towel of managing their hospitalized patients. More and more, these PCPs unilaterally are announcing to their patients and to the local hospitals they will neither continue to take responsibility for hospitalized patients nor continue to ‘take call.’ ”
Ome Nwanze, MD, one of two hospitalists at the 42-bed Greenville Regional Hospital in Greenville, Ill., says the biggest benefit to being a rural hospitalist is the ability to make a difference in the lives of everyone in the community. Along with patients, Dr. Nwanze includes other doctors as beneficiaries: “The primary-care physicians and specialists are very happy with the program and the difference it makes in their lives.”
Competitive Business
If hospitalists are a natural solution, though, there’s a key problem: Rural communities are struggling to attract them as well. One sign of the difficulty is median salary. Similar to what surveys consistently show for other specialties, rural hospitalists outpace their urban counterparts in median annual salary, at roughly $206,000 versus $187,000, according to Becker’s Hospital Review (overall, hospitalists rank behind most other specialties in salary). The rural-urban divide can be attributed to that old real estate adage: location, location, location. Competition for hospitalist jobs in large cities is generally fierce, while rural communities often have to offer more incentives to attract and retain the doctors they need.
“The two biggest issues that I can see are recruitment and night coverage,” says Louis J. O’Boyle, DO, FACP, FHM, medical director of Advanced Inpatient Medicine (AIM), P.C., in Honesdale, Pa. He and AIM’s four other hospitalists work exclusively with the town’s 98-bed Wayne Memorial Hospital. “It is easier to recruit to a larger city, closer to more activities and residency programs,” Dr. O’Boyle says. “To get someone to come to our area almost always requires some form of local connection. That makes retention paramount.”
Night call can be a particular sticking point: Most rural hospitals aren’t busy enough to justify an FTE nocturnist, he says, putting the onus of night call on full-time hospitalists. Wayne Memorial Hospital is fortunate in that regard, as it averages only one or two admissions a day after 10 p.m., leaving the hospitalists “fresh enough to round the next day,” Dr. O’Boyle says. “However, this still makes rural programs less attractive compared to places that can boast a nocturnist team that eliminates night call.”
Government Assistance
So what has the government done to help address the growing need for more rural hospitalists and other healthcare providers? If the Affordable Care Act’s (ACA) measures proceed as expected, most experts predict a significant drop in the number of uninsured individuals—meaning a surge in both rural and urban demand for care.
According to the White House report, the Department of Health and Human Services has funded 444 rural community health centers since 2009. The ACA has expanded and extended the Medicare Rural Community Hospital Demonstration, providing “an estimated $52 million in enhanced reimbursement for inpatient services at 25 rural hospitals.” And the administration has expanded funding for the National Health Service Corps, which offers doctors scholarships and loan repayment in exchange for a commitment to practice medicine at underserved communities. The corps website boasts that more than 8,000 clinicians are in place, but it also notes that there are “more than 9,000 job vacancies for NHSC primary care medical, dental, and mental health clinicians.” (View the full report at http://nhsc.hrsa.gov/about.) Clearly, loan forgiveness isn’t enough.
Furthermore, the government might be facing a perception problem. Dr. Nwanze describes government support to rural programs as “poor,” while Dr. O’Boyle says he’s not aware of any specific efforts to support rural hospitalists. “There may be some areas, such as giving grants for telemedicine and other tertiary support, but I don’t think those of us in rural programs can sense any impact,” Dr. O’Boyle says. Wayne Memorial Hospital is in an underserved area, he says, and PCPs there do receive loan forgiveness. “However, I was disappointed to learn that those programs are not open to hospitalists.”
Meanwhile, many rural hospitalists face daunting responsibilities. Dr. Nwanze cites “the need to be a jack-of-all-trades and master of all,” and notes the pressure of providing a wide range of services and handling almost all situations with little or no specialist support.
But Dr. O’Boyle also sees opportunity in the autonomy, such as the ability to play a larger role in hospital management and more independence. “We don’t have a plethora of subspecialists looking for business,” he says. “That means much greater responsibility for our hospitalists, who will take care of much sicker patients without specialist backup being readily available.” As a result, advanced duties like ventilator management and the care of complex patients with such diagnoses as acute renal failure or new malignancies are all within the realm of the hospitalist.
“This is an attractive prospect for certain hospitalists who like the idea of taking care of patients without feeling like a captain who merely delegates to multiple specialists,” Dr. O’Boyle says. “Also, the group integrates into hospital committees at every level, and has an overall much larger say in the day-to-day operations, something largely out of the control of a hospitalist group at a large tertiary facility.”
Tech Solutions
Despite the challenges, many rural hospitals are gaining new tools to help them survive, and tech-savvy hospitalists might be big assets. Smaller facilities are increasingly gaining access to electronic health records, while many also are using video links to allow specialists hundreds of miles away to help with diagnoses without having to transfer the patients.
Recent research also suggests that hospital discharges could be better in rural communities.
Bryn Nelson is a freelance medical writer based in Seattle.
ONLINE EXCLUSIVE: Hospitalists discuss how HM can improve patient satisfaction
HM@15 - Are You Living Up to High Expectations of Efficiency?
In 2002, a summary article in the Journal of the American Medical Association helped put the relatively small but rapidly growing HM profession on the map. Reviewing the available data, Robert Wachter, MD, MHM, and Lee Goldman, MD, MPH, of the University of California at San Francisco (UCSF) concluded that implementing a hospitalist program yielded an average savings of 13.4% in hospital costs and a 16.6% reduction in the length of stay (LOS).1
A decade later, the idea of efficiency has become so intertwined with hospitalists that SHM has included the concept in its definition of a profession that now comprises more than 30,000 doctors, nurses, and other care providers. HM practitioners work to enhance hospital and healthcare performance, in part, through “efficient use of hospital and healthcare resources,” according to SHM.
The growth of any profession can create exceptions and outliers, and observers point out that HM programs have become as varied as the hospitals in which they reside, complicating any attempt at broad generalizations. As a core part of the job description, though, efficiency and its implied benefit on costs have been widely promoted as arguments for expanding HM’s reach.
So are hospitalists meeting the lofty expectations?
A Look at the Evidence
A large retrospective study that examined outcomes of care for nearly 77,000 patients in 45 hospitals found that those cared for by hospitalists had a “modestly shorter” stay (by 0.4 days) in the hospital than those cared for by either general internists or family physicians.2 Hospitalists saved about $270 per hospitalization compared with general internists but only about $125 per stay compared with family physicians, the latter of which was not deemed statistically significant.
A more recent review of 33 studies found general agreement that hospitalist care led to reduced costs and length of stay but revealed less uniformity in the impacts on quality and patient outcomes.3
A more dramatic—albeit smaller—affirmation of HM as an efficient force has come from a study of patients admitted to 200-bed Olive View-UCLA Medical Center in Sylmar, Calif. The study, led by assistant medical director Scott Lundberg, MD, concluded that the arrival of an academic hospitalist program led to a one-year increase of $2.3 million in reimbursements from Medi-Cal, California’s Medicaid program.4
“Most other places that have demonstrated the cost-effectiveness of hospitalists generally point to reducing length of stay, which therefore reduces the costs,” Dr. Lundberg says. Under Medicare’s diagnosis-based reimbursement (DRG) system, hospitals could get paid the same amount whether the patient stays one day or five.
Medi-Cal, however, uses a straight-up per diem reimbursement system. “So reducing someone’s length of stay is not necessarily desirable if Medi-Cal would have paid you for all of those days,” Dr. Lundberg says. The state’s Medicare program also can deny coverage for days deemed medically unnecessary after a review of patient charts.
Hospitalists, he says, helped boost revenue in two ways. First, the program helped the hospital avoid denied coverage days by ensuring that patients stayed only as long as necessary. Average LOS, in fact, dropped to 1.92 days from 2.48 days, decreasing the Medi-Cal denial rate to 31.8% (from 43.8%) and bumping up the average reimbursement per inpatient day to $955 from $787.
Hospitalists also helped alleviate the work-hour limits for residents imposed by the Accreditation Council for Graduate Medical Education (ACGME), which had effectively capped the number of inpatients the center could admit. Because Olive View-UCLA receives per diem payments from Medi-Cal, making room to accept more patients into the hospital has meant increased revenues. Among the other benefits, the program has improved patient satisfaction and relieved some of the pressure on teaching teams.
With $310,000 for salary outlay in the hospitalist program’s first year, the study found a net cost benefit of $2 million. “One of the real challenges in getting this hospitalist thing going was getting our administrators to shell out the money for the salaries,” Dr. Lundberg says. The study demonstrated that a hospitalist program not only pays for itself, but also can substantially ramp up revenue. “I’m guessing that others, especially at public hospitals, face the same challenges,” he says. “I’m hoping they can point to this analysis and say, ‘Look, here’s what L.A. County did. They were able to show a net increase in revenue from this hospitalist service.’ ”
On the opposite side of the country, hospitalists are pointing to a success story in pediatric care. At the 120-bed Children’s Hospital at Montefiore at Albert Einstein College of Medicine in the Bronx, N.Y., a recent study concluded that establishing a pediatric HM program led to a significant reduction in LOS for patients with asthma or bronchiolitis.5 Nora Esteban-Cruciani, MD, MS, assistant director of pediatric hospital medicine and lead author of the report, which was presented at HM11, says it’s the first study to demonstrate such an effect for asthma in an inner-city academic setting.
Compared to a traditional resident-attending team, care administered by a resident-physician’s assistant-hospitalist team reduced LOS for bronchiolitis by 15.5% and asthma by 11.8%. With the 378 hospital-bed days saved annually, Children’s Hospital at Montefiore achieved an estimated savings of about $944,000 before taking salaries into account. “We anticipate seeing similar benefits in other groups of patients, and the total savings will far exceed the hospitalist salaries,” Dr. Esteban-Cruciani says.
After the pediatric HM program launched, her study also documented a 17% to 25% decrease in rehospitalizations among asthmatic children at four, six, and 12 months after their initial hospital discharge. As a result of the demonstrated value, Dr. Esteban-Cruciani says, the children’s hospital is expanding its HM program and hiring another 4.5 full-time equivalents.
So how did hospitalists achieve the positive results?
“Knowing the most up-to-date and evidence-based treatment plans, understanding how to use the hospital systems in the most efficient manner, being on the ward for eight to 12 hours per day to respond to issues that arise, as well as 24-hour availability by phone for the residents,” she says. “The day-to-day continuity, as well as the ability to consistently improve systems of care, are distinctive advantages to hospital medicine.”
The case for HM as a model of efficiency comes with a major caveat, however. David Meltzer, MD, PhD, FHM, chief of the section of hospital medicine and an economist and public-policy expert at the University of Chicago, points out that healthcare costs don’t end with a patient’s hospital discharge. Could savings achieved during inpatient care be offset by greater costs afterward?
A new study in the Annals of Internal Medicine by researchers at the University of Texas Medical Branch in Galveston has sharpened that question with the suggestion that, at least in some cases, hospitalist-procured savings might not last.6 When compared to care delivered by primary-care physicians (PCPs), the researchers found that hospitalist care yielded an average inpatient savings of $282 per Medicare beneficiary. But that reduction was wiped out by an extra $332 average cost in the month after discharge, due to higher readmissions, more emergency department visits, and more patients sent to nursing facilities instead of to their own homes. An accompanying editorial raises the uncomfortable question: “Are hospitalists discharging their patients more quickly but less appropriately, such that some of their patients bounce back?”7

—David Meltzer, MD, PhD, FHM, chief, section of hospital medicine, economist, University of Chicago
The study itself has its own share of caveats: Data were collected only until 2006, before reducing 30-day readmissions became a widespread focal point. The editorial also highlights the possibility that hospitalists might care for patients whose weaker relationships with outpatient providers could be the true driver of increased readmissions. In a statement, SHM President Joe Li, MD, SFHM, adds that constructive talks about healthcare costs must include the notion of quality, something the organization has worked to improve with interventions like Project BOOST.
At the very least, the new research highlights the importance of context when considering HM impacts on cost and quality. Separate studies, meanwhile, suggest that the jury is still out on whether other hospitalist-led models can consistently improve outcomes and costs. At academic centers, for instance, work-hour limits for medical residents have provided a strong impetus for joint-care arrangements, such as comanagement systems. A 2004 study found that an orthopedics-hospitalist comanagement structure led to a modest reduction in complications after elective hip and knee surgery. But the report documented no difference in costs or actual length of stay.8

More recently, a study of nearly 7,600 patients at UCSF Medical Center found that an HM-neurosurgery comanagement model had no significant impact on the center’s patient mortality, readmissions, LOS, or patient satisfaction. The comanagement system, however, yielded an average savings of $1,439 per hospitalization and boosted physicians’ perceptions of quality and safety.9
Andrew Auerbach, MD, MPH, SFHM, associate professor of medicine at UCSF Medical Center, says the savings, while not dramatic, nevertheless can add up when applied to the thousands of patients seen by the service every year. “That’s compelling because I think one of the things that you’re arguing when you’re doing these services is what the return on investment is going to be,” he says. “Traditionally, these have been implemented without any specific financial return on investment being applied, but the large expectation that clinical improvement is going to happen.”
His study at UCSF found just the opposite: no clinical improvement but a net cost benefit. “We were a little disappointed in some ways, but in other ways not surprised because there are very few data out in the community that suggest comanagement improves any outcomes,” Dr. Auerbach says. Among complicated neurosurgery patients, the strongest determinants of outcome might be beyond the scope of hospitalist-aided medical care.
With hospitals nervously eyeing their bottom lines, however, any financial improvement that does not adversely affect quality can still be seen as a positive development, and Dr. Auerbach says his study was the first to demonstrate that benefit. At UCSF Medical Center, at least, comanagement has proven compelling enough to spur plans for extending the service to orthopedic surgery patients.
Regardless of the care model, other studies suggest that specific interventions at key moments can yield substantial savings. A small, randomized controlled study led by hospitalists at Johns Hopkins University in Baltimore, for example, supports the idea that “simply showing providers the cost of some diagnostic tests at the time of order entry can affect behavior.”10 Although the study didn’t focus exclusively on hospitalists, experts say they’re in the best position to take the lead in curbing unnecessary costs.
“Hospitalists, I think, have a better understanding of the impact of resource utilization on the total cost of care and can be more prudent in the use of technologies,” says Kenneth Epstein, MD, MBA, FHM, FACP, chief medical officer for Traverse City, Mich.-based Hospitalist Consultants Inc. One reason is that hospitalists aren’t beholden to any specific technology, whether endoscopies or cardiac catheterization.

—Scott Lundberg, MD, assistant medical director, Olive View-UCLA Medical Center, Sylmar, Calif.
Mark Graban, author of the book “Lean Hospitals: Improving Quality, Patient Safety, and Employee Satisfaction,” says hospitalists can play another critical role in controlling costs by mapping out and simplifying the discharge processes. He recalls how hospitalists helped coordinate the effort by one of his hospital clients to prevent discharge delays that would have unnecessarily kept patients in the hospital for an additional night or two.
“That length-of-stay reduction, especially in a fixed-reimbursement setting, can have a huge financial impact,” Graban says. “And, inarguably, it’s the right thing to do for the patient, because it’s patients that are medically ready to be discharged. It gets them home and it reduces their increased risk of picking up infections or being involved in hospital errors.”
Focusing on patient safety could translate into big cost savings under the new Medicare system that penalizes providers for certain hospital-acquired conditions, such as skin ulcers and urinary tract infections, Dr. Epstein says. “There’s an emphasis by hospitalists in understanding the system and being willing to put energy into things like documenting ‘present on admission,’ which then has a huge impact on the hospital,” he says. Close monitoring of patients and developing standardization of care can likewise minimize the risk of conditions, such as catheter-associated infections, from cropping up in the hospital.
Dr. Meltzer says his own research suggests that experienced hospitalists are most effective at controlling costs. “So a program that is structured in such a way as to hire or retain experienced hospitalists is likely to have a higher cost savings than one that doesn’t,” he says.
In a broader sense, the maturation of the HM model and more widespread adoption of effective methods by practitioners might be boosting the overall impact of hospitalist care. A study that examined nearly 2 million Medicare admissions over six years found that the effects of the hospitalist care model on LOS became progressively more pronounced over time, from an average reduction of only 0.02 inpatient days in 2001-2002 to a decrease of 0.35 days by 2005-2006.11
Interestingly, the study’s authors suggest that effects attributable to hospitalists were most pronounced among older, complicated, nonsurgical patients cared for at nonprofit community hospitals.
The Verdict
Despite the variable design and scope of individual programs, experts say, HM’s overall net positive on the efficiency of inpatient care is fairly well documented. Future considerations of hospitalists’ true effects on costs, however, will demand an accounting of healthcare across an entire system, where the HM impact is decidedly less certain. “The right comparison in some sense is, What are the total costs of care for a patient cared for in a system that uses hospitalists versus the totals costs of similar patients cared for in a system that doesn’t use hospitalists?” Dr. Meltzer says.
David Mitchell, MD, PhD, a hospitalist at Sibley Memorial Hospital in Washington, D.C., and a member of SHM’s Performance Standards Committee, is among those with an additional concern: Providers may not be taking full advantage of their position to control costs.
“The reason is primarily that the reimbursement structure is not set up to incentivize us to cut costs,” he says. Dr. Mitchell, who has worked in 12 hospitals in six states, argues that hospitalists still are too detached from the true price of ordered tests. “That’s what I fear in hospital medicine, that we just become robots: chest pain means CT scan without thinking,” he says. “This just doesn’t make sense.” Dr. Mitchell also contends that the focus of some HM programs on seeing as many patients as possible to maximize reimbursements is leading to less efficiency. At HM11 in May, he met another hospitalist who said he regularly saw 40 to 45 patients every day. “I know there’s absolutely no way you can see that many patients and do an efficient job,” Dr. Mitchell says.
If one of the clearest areas of success for hospitalists has been in reducing length of stay within a hospital, experts acknowledge that it may no longer be enough. “In the new payment model, success is going to be defined differently, and it will be in terms of reducing the total cost of care,” Dr. Meltzer says.
Over the next decade, hospitalists will need to respond to new set of incentives. “And I think one of the really interesting questions will be how hospitalists can best do that, and the extent to which it causes them to rethink the ways in which they organize their practice,” he says.
Bryn Nelson is a freelance medical writer based in Seattle.
References
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Lindenauer PK, Rothberg MB, Pekow PS, Kenwood C, Benjamin EM, Auerbach AD. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007;357:2589-2600.
- Peterson MC. A systematic review of outcomes and quality measures in adult patients cared for by hospitalists vs nonhospitalists. Mayo Clin Proc. 2009;84(3): 248-254.
- Lundberg S, Balingit P, Wali S, Cope D. Cost-effectiveness of a hospitalist service in a public teaching hospital. Acad Med. 2010;85(8):1312-1315.
- Esteban-Cruciani N, Montejo J, Azzarone G, Douglas L, et al. Impact of a pediatric hospital medicine program on resource utilization for children with respiratory disorders. J Hosp Med. 2011;6(4)Supp 2:S27.
- Kuo Y-F, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3): 152-159.
- Chen LM, Saint S. Moments in time. Ann Intern Med. 2011;155(3):194-195.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Auerbach AD, Wachter RM, Cheng HQ, et al. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22): 2004-2010.
- Feldman L, Thiemann D, Brotman D. Financial impact of presenting lab cost data to providers at the time of order entry: a randomized controlled clinical trial. J Hosp Med. 2011;6(4)Supp 2:S93.
- Kuo Y-F, Goodwin JS. Effect of hospitalists on length of stay in the Medicare population: variation according to hospital and patient characteristics. J Am Geriatr Soc. 2010;58:1649-1657.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-8.
- Chandra S, Howell E, Wright S. CICLE: Creating incentives and continuity leading to efficiency. J Hosp Med. 2011;6(4)Supp 2:S17
In 2002, a summary article in the Journal of the American Medical Association helped put the relatively small but rapidly growing HM profession on the map. Reviewing the available data, Robert Wachter, MD, MHM, and Lee Goldman, MD, MPH, of the University of California at San Francisco (UCSF) concluded that implementing a hospitalist program yielded an average savings of 13.4% in hospital costs and a 16.6% reduction in the length of stay (LOS).1
A decade later, the idea of efficiency has become so intertwined with hospitalists that SHM has included the concept in its definition of a profession that now comprises more than 30,000 doctors, nurses, and other care providers. HM practitioners work to enhance hospital and healthcare performance, in part, through “efficient use of hospital and healthcare resources,” according to SHM.
The growth of any profession can create exceptions and outliers, and observers point out that HM programs have become as varied as the hospitals in which they reside, complicating any attempt at broad generalizations. As a core part of the job description, though, efficiency and its implied benefit on costs have been widely promoted as arguments for expanding HM’s reach.
So are hospitalists meeting the lofty expectations?
A Look at the Evidence
A large retrospective study that examined outcomes of care for nearly 77,000 patients in 45 hospitals found that those cared for by hospitalists had a “modestly shorter” stay (by 0.4 days) in the hospital than those cared for by either general internists or family physicians.2 Hospitalists saved about $270 per hospitalization compared with general internists but only about $125 per stay compared with family physicians, the latter of which was not deemed statistically significant.
A more recent review of 33 studies found general agreement that hospitalist care led to reduced costs and length of stay but revealed less uniformity in the impacts on quality and patient outcomes.3
A more dramatic—albeit smaller—affirmation of HM as an efficient force has come from a study of patients admitted to 200-bed Olive View-UCLA Medical Center in Sylmar, Calif. The study, led by assistant medical director Scott Lundberg, MD, concluded that the arrival of an academic hospitalist program led to a one-year increase of $2.3 million in reimbursements from Medi-Cal, California’s Medicaid program.4
“Most other places that have demonstrated the cost-effectiveness of hospitalists generally point to reducing length of stay, which therefore reduces the costs,” Dr. Lundberg says. Under Medicare’s diagnosis-based reimbursement (DRG) system, hospitals could get paid the same amount whether the patient stays one day or five.
Medi-Cal, however, uses a straight-up per diem reimbursement system. “So reducing someone’s length of stay is not necessarily desirable if Medi-Cal would have paid you for all of those days,” Dr. Lundberg says. The state’s Medicare program also can deny coverage for days deemed medically unnecessary after a review of patient charts.
Hospitalists, he says, helped boost revenue in two ways. First, the program helped the hospital avoid denied coverage days by ensuring that patients stayed only as long as necessary. Average LOS, in fact, dropped to 1.92 days from 2.48 days, decreasing the Medi-Cal denial rate to 31.8% (from 43.8%) and bumping up the average reimbursement per inpatient day to $955 from $787.
Hospitalists also helped alleviate the work-hour limits for residents imposed by the Accreditation Council for Graduate Medical Education (ACGME), which had effectively capped the number of inpatients the center could admit. Because Olive View-UCLA receives per diem payments from Medi-Cal, making room to accept more patients into the hospital has meant increased revenues. Among the other benefits, the program has improved patient satisfaction and relieved some of the pressure on teaching teams.
With $310,000 for salary outlay in the hospitalist program’s first year, the study found a net cost benefit of $2 million. “One of the real challenges in getting this hospitalist thing going was getting our administrators to shell out the money for the salaries,” Dr. Lundberg says. The study demonstrated that a hospitalist program not only pays for itself, but also can substantially ramp up revenue. “I’m guessing that others, especially at public hospitals, face the same challenges,” he says. “I’m hoping they can point to this analysis and say, ‘Look, here’s what L.A. County did. They were able to show a net increase in revenue from this hospitalist service.’ ”
On the opposite side of the country, hospitalists are pointing to a success story in pediatric care. At the 120-bed Children’s Hospital at Montefiore at Albert Einstein College of Medicine in the Bronx, N.Y., a recent study concluded that establishing a pediatric HM program led to a significant reduction in LOS for patients with asthma or bronchiolitis.5 Nora Esteban-Cruciani, MD, MS, assistant director of pediatric hospital medicine and lead author of the report, which was presented at HM11, says it’s the first study to demonstrate such an effect for asthma in an inner-city academic setting.
Compared to a traditional resident-attending team, care administered by a resident-physician’s assistant-hospitalist team reduced LOS for bronchiolitis by 15.5% and asthma by 11.8%. With the 378 hospital-bed days saved annually, Children’s Hospital at Montefiore achieved an estimated savings of about $944,000 before taking salaries into account. “We anticipate seeing similar benefits in other groups of patients, and the total savings will far exceed the hospitalist salaries,” Dr. Esteban-Cruciani says.
After the pediatric HM program launched, her study also documented a 17% to 25% decrease in rehospitalizations among asthmatic children at four, six, and 12 months after their initial hospital discharge. As a result of the demonstrated value, Dr. Esteban-Cruciani says, the children’s hospital is expanding its HM program and hiring another 4.5 full-time equivalents.
So how did hospitalists achieve the positive results?
“Knowing the most up-to-date and evidence-based treatment plans, understanding how to use the hospital systems in the most efficient manner, being on the ward for eight to 12 hours per day to respond to issues that arise, as well as 24-hour availability by phone for the residents,” she says. “The day-to-day continuity, as well as the ability to consistently improve systems of care, are distinctive advantages to hospital medicine.”
The case for HM as a model of efficiency comes with a major caveat, however. David Meltzer, MD, PhD, FHM, chief of the section of hospital medicine and an economist and public-policy expert at the University of Chicago, points out that healthcare costs don’t end with a patient’s hospital discharge. Could savings achieved during inpatient care be offset by greater costs afterward?
A new study in the Annals of Internal Medicine by researchers at the University of Texas Medical Branch in Galveston has sharpened that question with the suggestion that, at least in some cases, hospitalist-procured savings might not last.6 When compared to care delivered by primary-care physicians (PCPs), the researchers found that hospitalist care yielded an average inpatient savings of $282 per Medicare beneficiary. But that reduction was wiped out by an extra $332 average cost in the month after discharge, due to higher readmissions, more emergency department visits, and more patients sent to nursing facilities instead of to their own homes. An accompanying editorial raises the uncomfortable question: “Are hospitalists discharging their patients more quickly but less appropriately, such that some of their patients bounce back?”7
—David Meltzer, MD, PhD, FHM, chief, section of hospital medicine, economist, University of Chicago
The study itself has its own share of caveats: Data were collected only until 2006, before reducing 30-day readmissions became a widespread focal point. The editorial also highlights the possibility that hospitalists might care for patients whose weaker relationships with outpatient providers could be the true driver of increased readmissions. In a statement, SHM President Joe Li, MD, SFHM, adds that constructive talks about healthcare costs must include the notion of quality, something the organization has worked to improve with interventions like Project BOOST.
At the very least, the new research highlights the importance of context when considering HM impacts on cost and quality. Separate studies, meanwhile, suggest that the jury is still out on whether other hospitalist-led models can consistently improve outcomes and costs. At academic centers, for instance, work-hour limits for medical residents have provided a strong impetus for joint-care arrangements, such as comanagement systems. A 2004 study found that an orthopedics-hospitalist comanagement structure led to a modest reduction in complications after elective hip and knee surgery. But the report documented no difference in costs or actual length of stay.8
More recently, a study of nearly 7,600 patients at UCSF Medical Center found that an HM-neurosurgery comanagement model had no significant impact on the center’s patient mortality, readmissions, LOS, or patient satisfaction. The comanagement system, however, yielded an average savings of $1,439 per hospitalization and boosted physicians’ perceptions of quality and safety.9
Andrew Auerbach, MD, MPH, SFHM, associate professor of medicine at UCSF Medical Center, says the savings, while not dramatic, nevertheless can add up when applied to the thousands of patients seen by the service every year. “That’s compelling because I think one of the things that you’re arguing when you’re doing these services is what the return on investment is going to be,” he says. “Traditionally, these have been implemented without any specific financial return on investment being applied, but the large expectation that clinical improvement is going to happen.”
His study at UCSF found just the opposite: no clinical improvement but a net cost benefit. “We were a little disappointed in some ways, but in other ways not surprised because there are very few data out in the community that suggest comanagement improves any outcomes,” Dr. Auerbach says. Among complicated neurosurgery patients, the strongest determinants of outcome might be beyond the scope of hospitalist-aided medical care.
With hospitals nervously eyeing their bottom lines, however, any financial improvement that does not adversely affect quality can still be seen as a positive development, and Dr. Auerbach says his study was the first to demonstrate that benefit. At UCSF Medical Center, at least, comanagement has proven compelling enough to spur plans for extending the service to orthopedic surgery patients.
Regardless of the care model, other studies suggest that specific interventions at key moments can yield substantial savings. A small, randomized controlled study led by hospitalists at Johns Hopkins University in Baltimore, for example, supports the idea that “simply showing providers the cost of some diagnostic tests at the time of order entry can affect behavior.”10 Although the study didn’t focus exclusively on hospitalists, experts say they’re in the best position to take the lead in curbing unnecessary costs.
“Hospitalists, I think, have a better understanding of the impact of resource utilization on the total cost of care and can be more prudent in the use of technologies,” says Kenneth Epstein, MD, MBA, FHM, FACP, chief medical officer for Traverse City, Mich.-based Hospitalist Consultants Inc. One reason is that hospitalists aren’t beholden to any specific technology, whether endoscopies or cardiac catheterization.
—Scott Lundberg, MD, assistant medical director, Olive View-UCLA Medical Center, Sylmar, Calif.
Mark Graban, author of the book “Lean Hospitals: Improving Quality, Patient Safety, and Employee Satisfaction,” says hospitalists can play another critical role in controlling costs by mapping out and simplifying the discharge processes. He recalls how hospitalists helped coordinate the effort by one of his hospital clients to prevent discharge delays that would have unnecessarily kept patients in the hospital for an additional night or two.
“That length-of-stay reduction, especially in a fixed-reimbursement setting, can have a huge financial impact,” Graban says. “And, inarguably, it’s the right thing to do for the patient, because it’s patients that are medically ready to be discharged. It gets them home and it reduces their increased risk of picking up infections or being involved in hospital errors.”
Focusing on patient safety could translate into big cost savings under the new Medicare system that penalizes providers for certain hospital-acquired conditions, such as skin ulcers and urinary tract infections, Dr. Epstein says. “There’s an emphasis by hospitalists in understanding the system and being willing to put energy into things like documenting ‘present on admission,’ which then has a huge impact on the hospital,” he says. Close monitoring of patients and developing standardization of care can likewise minimize the risk of conditions, such as catheter-associated infections, from cropping up in the hospital.
Dr. Meltzer says his own research suggests that experienced hospitalists are most effective at controlling costs. “So a program that is structured in such a way as to hire or retain experienced hospitalists is likely to have a higher cost savings than one that doesn’t,” he says.
In a broader sense, the maturation of the HM model and more widespread adoption of effective methods by practitioners might be boosting the overall impact of hospitalist care. A study that examined nearly 2 million Medicare admissions over six years found that the effects of the hospitalist care model on LOS became progressively more pronounced over time, from an average reduction of only 0.02 inpatient days in 2001-2002 to a decrease of 0.35 days by 2005-2006.11
Interestingly, the study’s authors suggest that effects attributable to hospitalists were most pronounced among older, complicated, nonsurgical patients cared for at nonprofit community hospitals.
The Verdict
Despite the variable design and scope of individual programs, experts say, HM’s overall net positive on the efficiency of inpatient care is fairly well documented. Future considerations of hospitalists’ true effects on costs, however, will demand an accounting of healthcare across an entire system, where the HM impact is decidedly less certain. “The right comparison in some sense is, What are the total costs of care for a patient cared for in a system that uses hospitalists versus the totals costs of similar patients cared for in a system that doesn’t use hospitalists?” Dr. Meltzer says.
David Mitchell, MD, PhD, a hospitalist at Sibley Memorial Hospital in Washington, D.C., and a member of SHM’s Performance Standards Committee, is among those with an additional concern: Providers may not be taking full advantage of their position to control costs.
“The reason is primarily that the reimbursement structure is not set up to incentivize us to cut costs,” he says. Dr. Mitchell, who has worked in 12 hospitals in six states, argues that hospitalists still are too detached from the true price of ordered tests. “That’s what I fear in hospital medicine, that we just become robots: chest pain means CT scan without thinking,” he says. “This just doesn’t make sense.” Dr. Mitchell also contends that the focus of some HM programs on seeing as many patients as possible to maximize reimbursements is leading to less efficiency. At HM11 in May, he met another hospitalist who said he regularly saw 40 to 45 patients every day. “I know there’s absolutely no way you can see that many patients and do an efficient job,” Dr. Mitchell says.
If one of the clearest areas of success for hospitalists has been in reducing length of stay within a hospital, experts acknowledge that it may no longer be enough. “In the new payment model, success is going to be defined differently, and it will be in terms of reducing the total cost of care,” Dr. Meltzer says.
Over the next decade, hospitalists will need to respond to new set of incentives. “And I think one of the really interesting questions will be how hospitalists can best do that, and the extent to which it causes them to rethink the ways in which they organize their practice,” he says.
Bryn Nelson is a freelance medical writer based in Seattle.
References
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Lindenauer PK, Rothberg MB, Pekow PS, Kenwood C, Benjamin EM, Auerbach AD. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007;357:2589-2600.
- Peterson MC. A systematic review of outcomes and quality measures in adult patients cared for by hospitalists vs nonhospitalists. Mayo Clin Proc. 2009;84(3): 248-254.
- Lundberg S, Balingit P, Wali S, Cope D. Cost-effectiveness of a hospitalist service in a public teaching hospital. Acad Med. 2010;85(8):1312-1315.
- Esteban-Cruciani N, Montejo J, Azzarone G, Douglas L, et al. Impact of a pediatric hospital medicine program on resource utilization for children with respiratory disorders. J Hosp Med. 2011;6(4)Supp 2:S27.
- Kuo Y-F, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3): 152-159.
- Chen LM, Saint S. Moments in time. Ann Intern Med. 2011;155(3):194-195.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Auerbach AD, Wachter RM, Cheng HQ, et al. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22): 2004-2010.
- Feldman L, Thiemann D, Brotman D. Financial impact of presenting lab cost data to providers at the time of order entry: a randomized controlled clinical trial. J Hosp Med. 2011;6(4)Supp 2:S93.
- Kuo Y-F, Goodwin JS. Effect of hospitalists on length of stay in the Medicare population: variation according to hospital and patient characteristics. J Am Geriatr Soc. 2010;58:1649-1657.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-8.
- Chandra S, Howell E, Wright S. CICLE: Creating incentives and continuity leading to efficiency. J Hosp Med. 2011;6(4)Supp 2:S17
In 2002, a summary article in the Journal of the American Medical Association helped put the relatively small but rapidly growing HM profession on the map. Reviewing the available data, Robert Wachter, MD, MHM, and Lee Goldman, MD, MPH, of the University of California at San Francisco (UCSF) concluded that implementing a hospitalist program yielded an average savings of 13.4% in hospital costs and a 16.6% reduction in the length of stay (LOS).1
A decade later, the idea of efficiency has become so intertwined with hospitalists that SHM has included the concept in its definition of a profession that now comprises more than 30,000 doctors, nurses, and other care providers. HM practitioners work to enhance hospital and healthcare performance, in part, through “efficient use of hospital and healthcare resources,” according to SHM.
The growth of any profession can create exceptions and outliers, and observers point out that HM programs have become as varied as the hospitals in which they reside, complicating any attempt at broad generalizations. As a core part of the job description, though, efficiency and its implied benefit on costs have been widely promoted as arguments for expanding HM’s reach.
So are hospitalists meeting the lofty expectations?
A Look at the Evidence
A large retrospective study that examined outcomes of care for nearly 77,000 patients in 45 hospitals found that those cared for by hospitalists had a “modestly shorter” stay (by 0.4 days) in the hospital than those cared for by either general internists or family physicians.2 Hospitalists saved about $270 per hospitalization compared with general internists but only about $125 per stay compared with family physicians, the latter of which was not deemed statistically significant.
A more recent review of 33 studies found general agreement that hospitalist care led to reduced costs and length of stay but revealed less uniformity in the impacts on quality and patient outcomes.3
A more dramatic—albeit smaller—affirmation of HM as an efficient force has come from a study of patients admitted to 200-bed Olive View-UCLA Medical Center in Sylmar, Calif. The study, led by assistant medical director Scott Lundberg, MD, concluded that the arrival of an academic hospitalist program led to a one-year increase of $2.3 million in reimbursements from Medi-Cal, California’s Medicaid program.4
“Most other places that have demonstrated the cost-effectiveness of hospitalists generally point to reducing length of stay, which therefore reduces the costs,” Dr. Lundberg says. Under Medicare’s diagnosis-based reimbursement (DRG) system, hospitals could get paid the same amount whether the patient stays one day or five.
Medi-Cal, however, uses a straight-up per diem reimbursement system. “So reducing someone’s length of stay is not necessarily desirable if Medi-Cal would have paid you for all of those days,” Dr. Lundberg says. The state’s Medicare program also can deny coverage for days deemed medically unnecessary after a review of patient charts.
Hospitalists, he says, helped boost revenue in two ways. First, the program helped the hospital avoid denied coverage days by ensuring that patients stayed only as long as necessary. Average LOS, in fact, dropped to 1.92 days from 2.48 days, decreasing the Medi-Cal denial rate to 31.8% (from 43.8%) and bumping up the average reimbursement per inpatient day to $955 from $787.
Hospitalists also helped alleviate the work-hour limits for residents imposed by the Accreditation Council for Graduate Medical Education (ACGME), which had effectively capped the number of inpatients the center could admit. Because Olive View-UCLA receives per diem payments from Medi-Cal, making room to accept more patients into the hospital has meant increased revenues. Among the other benefits, the program has improved patient satisfaction and relieved some of the pressure on teaching teams.
With $310,000 for salary outlay in the hospitalist program’s first year, the study found a net cost benefit of $2 million. “One of the real challenges in getting this hospitalist thing going was getting our administrators to shell out the money for the salaries,” Dr. Lundberg says. The study demonstrated that a hospitalist program not only pays for itself, but also can substantially ramp up revenue. “I’m guessing that others, especially at public hospitals, face the same challenges,” he says. “I’m hoping they can point to this analysis and say, ‘Look, here’s what L.A. County did. They were able to show a net increase in revenue from this hospitalist service.’ ”
On the opposite side of the country, hospitalists are pointing to a success story in pediatric care. At the 120-bed Children’s Hospital at Montefiore at Albert Einstein College of Medicine in the Bronx, N.Y., a recent study concluded that establishing a pediatric HM program led to a significant reduction in LOS for patients with asthma or bronchiolitis.5 Nora Esteban-Cruciani, MD, MS, assistant director of pediatric hospital medicine and lead author of the report, which was presented at HM11, says it’s the first study to demonstrate such an effect for asthma in an inner-city academic setting.
Compared to a traditional resident-attending team, care administered by a resident-physician’s assistant-hospitalist team reduced LOS for bronchiolitis by 15.5% and asthma by 11.8%. With the 378 hospital-bed days saved annually, Children’s Hospital at Montefiore achieved an estimated savings of about $944,000 before taking salaries into account. “We anticipate seeing similar benefits in other groups of patients, and the total savings will far exceed the hospitalist salaries,” Dr. Esteban-Cruciani says.
After the pediatric HM program launched, her study also documented a 17% to 25% decrease in rehospitalizations among asthmatic children at four, six, and 12 months after their initial hospital discharge. As a result of the demonstrated value, Dr. Esteban-Cruciani says, the children’s hospital is expanding its HM program and hiring another 4.5 full-time equivalents.
So how did hospitalists achieve the positive results?
“Knowing the most up-to-date and evidence-based treatment plans, understanding how to use the hospital systems in the most efficient manner, being on the ward for eight to 12 hours per day to respond to issues that arise, as well as 24-hour availability by phone for the residents,” she says. “The day-to-day continuity, as well as the ability to consistently improve systems of care, are distinctive advantages to hospital medicine.”
The case for HM as a model of efficiency comes with a major caveat, however. David Meltzer, MD, PhD, FHM, chief of the section of hospital medicine and an economist and public-policy expert at the University of Chicago, points out that healthcare costs don’t end with a patient’s hospital discharge. Could savings achieved during inpatient care be offset by greater costs afterward?
A new study in the Annals of Internal Medicine by researchers at the University of Texas Medical Branch in Galveston has sharpened that question with the suggestion that, at least in some cases, hospitalist-procured savings might not last.6 When compared to care delivered by primary-care physicians (PCPs), the researchers found that hospitalist care yielded an average inpatient savings of $282 per Medicare beneficiary. But that reduction was wiped out by an extra $332 average cost in the month after discharge, due to higher readmissions, more emergency department visits, and more patients sent to nursing facilities instead of to their own homes. An accompanying editorial raises the uncomfortable question: “Are hospitalists discharging their patients more quickly but less appropriately, such that some of their patients bounce back?”7
—David Meltzer, MD, PhD, FHM, chief, section of hospital medicine, economist, University of Chicago
The study itself has its own share of caveats: Data were collected only until 2006, before reducing 30-day readmissions became a widespread focal point. The editorial also highlights the possibility that hospitalists might care for patients whose weaker relationships with outpatient providers could be the true driver of increased readmissions. In a statement, SHM President Joe Li, MD, SFHM, adds that constructive talks about healthcare costs must include the notion of quality, something the organization has worked to improve with interventions like Project BOOST.
At the very least, the new research highlights the importance of context when considering HM impacts on cost and quality. Separate studies, meanwhile, suggest that the jury is still out on whether other hospitalist-led models can consistently improve outcomes and costs. At academic centers, for instance, work-hour limits for medical residents have provided a strong impetus for joint-care arrangements, such as comanagement systems. A 2004 study found that an orthopedics-hospitalist comanagement structure led to a modest reduction in complications after elective hip and knee surgery. But the report documented no difference in costs or actual length of stay.8
More recently, a study of nearly 7,600 patients at UCSF Medical Center found that an HM-neurosurgery comanagement model had no significant impact on the center’s patient mortality, readmissions, LOS, or patient satisfaction. The comanagement system, however, yielded an average savings of $1,439 per hospitalization and boosted physicians’ perceptions of quality and safety.9
Andrew Auerbach, MD, MPH, SFHM, associate professor of medicine at UCSF Medical Center, says the savings, while not dramatic, nevertheless can add up when applied to the thousands of patients seen by the service every year. “That’s compelling because I think one of the things that you’re arguing when you’re doing these services is what the return on investment is going to be,” he says. “Traditionally, these have been implemented without any specific financial return on investment being applied, but the large expectation that clinical improvement is going to happen.”
His study at UCSF found just the opposite: no clinical improvement but a net cost benefit. “We were a little disappointed in some ways, but in other ways not surprised because there are very few data out in the community that suggest comanagement improves any outcomes,” Dr. Auerbach says. Among complicated neurosurgery patients, the strongest determinants of outcome might be beyond the scope of hospitalist-aided medical care.
With hospitals nervously eyeing their bottom lines, however, any financial improvement that does not adversely affect quality can still be seen as a positive development, and Dr. Auerbach says his study was the first to demonstrate that benefit. At UCSF Medical Center, at least, comanagement has proven compelling enough to spur plans for extending the service to orthopedic surgery patients.
Regardless of the care model, other studies suggest that specific interventions at key moments can yield substantial savings. A small, randomized controlled study led by hospitalists at Johns Hopkins University in Baltimore, for example, supports the idea that “simply showing providers the cost of some diagnostic tests at the time of order entry can affect behavior.”10 Although the study didn’t focus exclusively on hospitalists, experts say they’re in the best position to take the lead in curbing unnecessary costs.
“Hospitalists, I think, have a better understanding of the impact of resource utilization on the total cost of care and can be more prudent in the use of technologies,” says Kenneth Epstein, MD, MBA, FHM, FACP, chief medical officer for Traverse City, Mich.-based Hospitalist Consultants Inc. One reason is that hospitalists aren’t beholden to any specific technology, whether endoscopies or cardiac catheterization.
—Scott Lundberg, MD, assistant medical director, Olive View-UCLA Medical Center, Sylmar, Calif.
Mark Graban, author of the book “Lean Hospitals: Improving Quality, Patient Safety, and Employee Satisfaction,” says hospitalists can play another critical role in controlling costs by mapping out and simplifying the discharge processes. He recalls how hospitalists helped coordinate the effort by one of his hospital clients to prevent discharge delays that would have unnecessarily kept patients in the hospital for an additional night or two.
“That length-of-stay reduction, especially in a fixed-reimbursement setting, can have a huge financial impact,” Graban says. “And, inarguably, it’s the right thing to do for the patient, because it’s patients that are medically ready to be discharged. It gets them home and it reduces their increased risk of picking up infections or being involved in hospital errors.”
Focusing on patient safety could translate into big cost savings under the new Medicare system that penalizes providers for certain hospital-acquired conditions, such as skin ulcers and urinary tract infections, Dr. Epstein says. “There’s an emphasis by hospitalists in understanding the system and being willing to put energy into things like documenting ‘present on admission,’ which then has a huge impact on the hospital,” he says. Close monitoring of patients and developing standardization of care can likewise minimize the risk of conditions, such as catheter-associated infections, from cropping up in the hospital.
Dr. Meltzer says his own research suggests that experienced hospitalists are most effective at controlling costs. “So a program that is structured in such a way as to hire or retain experienced hospitalists is likely to have a higher cost savings than one that doesn’t,” he says.
In a broader sense, the maturation of the HM model and more widespread adoption of effective methods by practitioners might be boosting the overall impact of hospitalist care. A study that examined nearly 2 million Medicare admissions over six years found that the effects of the hospitalist care model on LOS became progressively more pronounced over time, from an average reduction of only 0.02 inpatient days in 2001-2002 to a decrease of 0.35 days by 2005-2006.11
Interestingly, the study’s authors suggest that effects attributable to hospitalists were most pronounced among older, complicated, nonsurgical patients cared for at nonprofit community hospitals.
The Verdict
Despite the variable design and scope of individual programs, experts say, HM’s overall net positive on the efficiency of inpatient care is fairly well documented. Future considerations of hospitalists’ true effects on costs, however, will demand an accounting of healthcare across an entire system, where the HM impact is decidedly less certain. “The right comparison in some sense is, What are the total costs of care for a patient cared for in a system that uses hospitalists versus the totals costs of similar patients cared for in a system that doesn’t use hospitalists?” Dr. Meltzer says.
David Mitchell, MD, PhD, a hospitalist at Sibley Memorial Hospital in Washington, D.C., and a member of SHM’s Performance Standards Committee, is among those with an additional concern: Providers may not be taking full advantage of their position to control costs.
“The reason is primarily that the reimbursement structure is not set up to incentivize us to cut costs,” he says. Dr. Mitchell, who has worked in 12 hospitals in six states, argues that hospitalists still are too detached from the true price of ordered tests. “That’s what I fear in hospital medicine, that we just become robots: chest pain means CT scan without thinking,” he says. “This just doesn’t make sense.” Dr. Mitchell also contends that the focus of some HM programs on seeing as many patients as possible to maximize reimbursements is leading to less efficiency. At HM11 in May, he met another hospitalist who said he regularly saw 40 to 45 patients every day. “I know there’s absolutely no way you can see that many patients and do an efficient job,” Dr. Mitchell says.
If one of the clearest areas of success for hospitalists has been in reducing length of stay within a hospital, experts acknowledge that it may no longer be enough. “In the new payment model, success is going to be defined differently, and it will be in terms of reducing the total cost of care,” Dr. Meltzer says.
Over the next decade, hospitalists will need to respond to new set of incentives. “And I think one of the really interesting questions will be how hospitalists can best do that, and the extent to which it causes them to rethink the ways in which they organize their practice,” he says.
Bryn Nelson is a freelance medical writer based in Seattle.
References
- Wachter RM, Goldman L. The hospitalist movement 5 years later. JAMA. 2002;287(4):487-494.
- Lindenauer PK, Rothberg MB, Pekow PS, Kenwood C, Benjamin EM, Auerbach AD. Outcomes of care by hospitalists, general internists, and family physicians. N Engl J Med. 2007;357:2589-2600.
- Peterson MC. A systematic review of outcomes and quality measures in adult patients cared for by hospitalists vs nonhospitalists. Mayo Clin Proc. 2009;84(3): 248-254.
- Lundberg S, Balingit P, Wali S, Cope D. Cost-effectiveness of a hospitalist service in a public teaching hospital. Acad Med. 2010;85(8):1312-1315.
- Esteban-Cruciani N, Montejo J, Azzarone G, Douglas L, et al. Impact of a pediatric hospital medicine program on resource utilization for children with respiratory disorders. J Hosp Med. 2011;6(4)Supp 2:S27.
- Kuo Y-F, Goodwin JS. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3): 152-159.
- Chen LM, Saint S. Moments in time. Ann Intern Med. 2011;155(3):194-195.
- Huddleston JM, Long KH, Naessens JM, et al. Medical and surgical comanagement after elective hip and knee arthroplasty: a randomized, controlled trial. Ann Intern Med. 2004;141(1):28-38.
- Auerbach AD, Wachter RM, Cheng HQ, et al. Comanagement of surgical patients between neurosurgeons and hospitalists. Arch Intern Med. 2010;170(22): 2004-2010.
- Feldman L, Thiemann D, Brotman D. Financial impact of presenting lab cost data to providers at the time of order entry: a randomized controlled clinical trial. J Hosp Med. 2011;6(4)Supp 2:S93.
- Kuo Y-F, Goodwin JS. Effect of hospitalists on length of stay in the Medicare population: variation according to hospital and patient characteristics. J Am Geriatr Soc. 2010;58:1649-1657.
- Epstein K, Juarez E, Epstein A, Loya K, Singer A. The impact of fragmentation of hospitalist care on length of stay. J Hosp Med. 2010;5(6):335-8.
- Chandra S, Howell E, Wright S. CICLE: Creating incentives and continuity leading to efficiency. J Hosp Med. 2011;6(4)Supp 2:S17
Exchange Anxiety
A 224-page document full of regulatory jargon might not be a fun summer read. Nevertheless, the U.S. Department of Health and Human Service’s (HHS) mid-July release of proposed rules for state-run health insurance exchanges (HIE) represents a major step toward expanding an insurance pool that could grow by an estimated 24 million Americans over the next eight years.
When the exchanges arrive in 2014, the single biggest impact is likely to be a major expansion of access, with 8.9 million individuals expected to sign up in the first year alone, according to projections by the Congressional Budget Office. A new report by PwC US Health Research Institute forecasts that a stunning 97% of those expected participants will be individuals who currently lack health insurance. A major driver of the new enrollments will be sliding-scale federal subsidies for individuals who earn from 138% to 400% of the federal poverty level, helping them buy insurance through the exchanges.
Experts say the exchanges also could directly impact hospitalists by bringing big changes to hospitals’ reimbursement revenue streams, spurring efforts to improve patient satisfaction metrics and increasing the momentum toward clinical comanagement agreements.
First, though, the public will get a chance to weigh in over rules that have been alternately lauded and derided, largely following the fault lines over the broader package of healthcare reforms. At a news conference set in front of a hardware store, HHS Secretary Kathleen Sebelius said competition on a level playing field would increase the purchasing power and drive down costs for individuals and small businesses. Websites for each of the exchanges would allow consumers to comparison-shop, with HHS ensuring that plans provide minimum standards for coverage. Patient groups, consumer organizations, and some small-business associations have welcomed the HHS rules, despite some concern that the exchanges could be tilted too far in favor of insurers. Overall, many analysts say, the rules have provided a fair amount of latitude over how the HIEs will be established and governed. Some business lobbyists, however, contend that the complex requirements will increase healthcare costs instead of lowering them. A July 16 editorial in the Wall Street Journal blasted the exchange rules as poorly designed and offering too little flexibility for states.
Two state-run ex-changes already exist, in Massachusetts and Utah. As of mid-July, however, states that had enacted laws to establish their own HIEs were outnumbered by those whose legislatures or governors had specifically blocked efforts to do likewise, according to the National Conference of State Legislatures. If states cannot or will not set up an exchange, HHS will step in and do it for them.
Reversal of Fortune?
Regardless of who ultimately oversees the exchanges, studies have begun suggesting who the most likely participants might be. An analysis by the Kaiser Family Foundation suggests that the newly insured are likely to be relatively older, less educated, more racially diverse, and in poorer health than those who currently carry private insurance but have fewer diagnosed conditions (www.kff.org/health reform/8147.cfm). Just as analysts, such as PwC, say that insurers will need to change their business strategy to lure and retain consumers, hospitals might need to redouble efforts to ensure high quality and patient satisfaction among a patient demographic that might be harder to please.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, says the shift could represent a boon for hospitals that have been forced to maximize efficiency. “In general, those hospitals that have a poorer payor mix have tended to become very efficient, and so they make money off of Medicare patients,” Dr. Williams, a former SHM president, says. “This is fascinating because, on the one hand, there may be a lot of patients for whom hospitalists can now get paid because they’re insured. But I personally think that, simultaneously, we’re going to be seeing cutbacks in payments for other patients who have private insurance.”
For some hospitals, the net effect on revenue might not be materially different, though Dr. Williams sees a potentially sizable benefit for “safety net” hospitals that care for a large proportion of uninsured patients and excel in making the most of limited resources. Some investors apparently agree. Last December, Nashville, Tenn.-based Vanguard Health Systems finalized a deal to buy Detroit Medical Center, with a total investment of nearly $1.5 billion. Dr. Williams says the expectation is that the medical center will suddenly see many more insured patients via an HIE. The result could be a dramatic boost to its finances.
Wealthier hospitals, by contrast, have had less incentive to maximize efficiency—and now are worried by the potential financial impacts of insurance exchanges. “Your classic, highly profitable community hospital that has a good payor mix loses money on Medicare patients and tends to subsidize that with their private patients,” Dr. Williams says. “The wealthier hospitals are nervous because they’re worried that this entire health insurance exchange is going to put downward pressure on reimbursements from the private insurers.”

—Mark Williams, MD, FACP, SFHM, chief, division of hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Satisfaction Times Two
With Medicare’s value-based purchasing initiative on its way, hospitals are ramping up their attention to patient satisfaction scores. So how will an influx of potentially older and sicker patients insured through the exchanges affect hospitalists’ scores? No one knows, but because hospitalists already are known for their expertise in treating this very demographic, some experts expect hospitals to lean on them more for leading quality and satisfaction initiatives. This reliance could represent a major opportunity for HM, but faulty performance metrics could also bring danger (read more about this topic in next month’s The Hospitalist).
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., says the expected shift in the nature of inpatients could accelerate efforts to be more accurate about physicians’ performance measures. “Patients who may be in the ICU are at a higher level of crisis than a person who’s in and out for an appendectomy, and yet we’re using the same tool of satisfaction,” she says. Furthermore, she adds, many factors that contribute to patient satisfaction are highly subjective and have nothing to do with a specific physician. “We have to really question the tools now, moreso than only questioning the participation and the outcome,” she says. As with other aspects of healthcare reform, Murer says, the looming arrival of exchanges also should be prompting hospitalists to ask themselves: “What’s our game plan now?” One compelling answer, she contends, is a clinical comanagement agreement that takes a longer-term view of doctors’ relationships with hospitals and gives them more control over decision-making. After all, if HM is taking care of “the sickest of the sick patients,” she says, a comanagement agreement can mean more say in factors that will directly impact their jobs over the long haul. Strategic direction of product lines, space, and equipment-buying decisions are just a few examples.
Murer ultimately sees clinical comanagement as a precursor to more widespread bundling of payments to hospitals and physicians. The mix of private and public insurance reimbursements, already in flux, might be further clouded by the arrival of HIEs. But solidifying hospital-hospitalist alignment with a flexible comanagement agreement, she says, can offer some reassurance over job structure, rewards, and authority as healthcare continues hurtling toward profound change.
Bryn Nelson is a freelance medical writer based in Seattle.
A 224-page document full of regulatory jargon might not be a fun summer read. Nevertheless, the U.S. Department of Health and Human Service’s (HHS) mid-July release of proposed rules for state-run health insurance exchanges (HIE) represents a major step toward expanding an insurance pool that could grow by an estimated 24 million Americans over the next eight years.
When the exchanges arrive in 2014, the single biggest impact is likely to be a major expansion of access, with 8.9 million individuals expected to sign up in the first year alone, according to projections by the Congressional Budget Office. A new report by PwC US Health Research Institute forecasts that a stunning 97% of those expected participants will be individuals who currently lack health insurance. A major driver of the new enrollments will be sliding-scale federal subsidies for individuals who earn from 138% to 400% of the federal poverty level, helping them buy insurance through the exchanges.
Experts say the exchanges also could directly impact hospitalists by bringing big changes to hospitals’ reimbursement revenue streams, spurring efforts to improve patient satisfaction metrics and increasing the momentum toward clinical comanagement agreements.
First, though, the public will get a chance to weigh in over rules that have been alternately lauded and derided, largely following the fault lines over the broader package of healthcare reforms. At a news conference set in front of a hardware store, HHS Secretary Kathleen Sebelius said competition on a level playing field would increase the purchasing power and drive down costs for individuals and small businesses. Websites for each of the exchanges would allow consumers to comparison-shop, with HHS ensuring that plans provide minimum standards for coverage. Patient groups, consumer organizations, and some small-business associations have welcomed the HHS rules, despite some concern that the exchanges could be tilted too far in favor of insurers. Overall, many analysts say, the rules have provided a fair amount of latitude over how the HIEs will be established and governed. Some business lobbyists, however, contend that the complex requirements will increase healthcare costs instead of lowering them. A July 16 editorial in the Wall Street Journal blasted the exchange rules as poorly designed and offering too little flexibility for states.
Two state-run ex-changes already exist, in Massachusetts and Utah. As of mid-July, however, states that had enacted laws to establish their own HIEs were outnumbered by those whose legislatures or governors had specifically blocked efforts to do likewise, according to the National Conference of State Legislatures. If states cannot or will not set up an exchange, HHS will step in and do it for them.
Reversal of Fortune?
Regardless of who ultimately oversees the exchanges, studies have begun suggesting who the most likely participants might be. An analysis by the Kaiser Family Foundation suggests that the newly insured are likely to be relatively older, less educated, more racially diverse, and in poorer health than those who currently carry private insurance but have fewer diagnosed conditions (www.kff.org/health reform/8147.cfm). Just as analysts, such as PwC, say that insurers will need to change their business strategy to lure and retain consumers, hospitals might need to redouble efforts to ensure high quality and patient satisfaction among a patient demographic that might be harder to please.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, says the shift could represent a boon for hospitals that have been forced to maximize efficiency. “In general, those hospitals that have a poorer payor mix have tended to become very efficient, and so they make money off of Medicare patients,” Dr. Williams, a former SHM president, says. “This is fascinating because, on the one hand, there may be a lot of patients for whom hospitalists can now get paid because they’re insured. But I personally think that, simultaneously, we’re going to be seeing cutbacks in payments for other patients who have private insurance.”
For some hospitals, the net effect on revenue might not be materially different, though Dr. Williams sees a potentially sizable benefit for “safety net” hospitals that care for a large proportion of uninsured patients and excel in making the most of limited resources. Some investors apparently agree. Last December, Nashville, Tenn.-based Vanguard Health Systems finalized a deal to buy Detroit Medical Center, with a total investment of nearly $1.5 billion. Dr. Williams says the expectation is that the medical center will suddenly see many more insured patients via an HIE. The result could be a dramatic boost to its finances.
Wealthier hospitals, by contrast, have had less incentive to maximize efficiency—and now are worried by the potential financial impacts of insurance exchanges. “Your classic, highly profitable community hospital that has a good payor mix loses money on Medicare patients and tends to subsidize that with their private patients,” Dr. Williams says. “The wealthier hospitals are nervous because they’re worried that this entire health insurance exchange is going to put downward pressure on reimbursements from the private insurers.”
—Mark Williams, MD, FACP, SFHM, chief, division of hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Satisfaction Times Two
With Medicare’s value-based purchasing initiative on its way, hospitals are ramping up their attention to patient satisfaction scores. So how will an influx of potentially older and sicker patients insured through the exchanges affect hospitalists’ scores? No one knows, but because hospitalists already are known for their expertise in treating this very demographic, some experts expect hospitals to lean on them more for leading quality and satisfaction initiatives. This reliance could represent a major opportunity for HM, but faulty performance metrics could also bring danger (read more about this topic in next month’s The Hospitalist).
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., says the expected shift in the nature of inpatients could accelerate efforts to be more accurate about physicians’ performance measures. “Patients who may be in the ICU are at a higher level of crisis than a person who’s in and out for an appendectomy, and yet we’re using the same tool of satisfaction,” she says. Furthermore, she adds, many factors that contribute to patient satisfaction are highly subjective and have nothing to do with a specific physician. “We have to really question the tools now, moreso than only questioning the participation and the outcome,” she says. As with other aspects of healthcare reform, Murer says, the looming arrival of exchanges also should be prompting hospitalists to ask themselves: “What’s our game plan now?” One compelling answer, she contends, is a clinical comanagement agreement that takes a longer-term view of doctors’ relationships with hospitals and gives them more control over decision-making. After all, if HM is taking care of “the sickest of the sick patients,” she says, a comanagement agreement can mean more say in factors that will directly impact their jobs over the long haul. Strategic direction of product lines, space, and equipment-buying decisions are just a few examples.
Murer ultimately sees clinical comanagement as a precursor to more widespread bundling of payments to hospitals and physicians. The mix of private and public insurance reimbursements, already in flux, might be further clouded by the arrival of HIEs. But solidifying hospital-hospitalist alignment with a flexible comanagement agreement, she says, can offer some reassurance over job structure, rewards, and authority as healthcare continues hurtling toward profound change.
Bryn Nelson is a freelance medical writer based in Seattle.
A 224-page document full of regulatory jargon might not be a fun summer read. Nevertheless, the U.S. Department of Health and Human Service’s (HHS) mid-July release of proposed rules for state-run health insurance exchanges (HIE) represents a major step toward expanding an insurance pool that could grow by an estimated 24 million Americans over the next eight years.
When the exchanges arrive in 2014, the single biggest impact is likely to be a major expansion of access, with 8.9 million individuals expected to sign up in the first year alone, according to projections by the Congressional Budget Office. A new report by PwC US Health Research Institute forecasts that a stunning 97% of those expected participants will be individuals who currently lack health insurance. A major driver of the new enrollments will be sliding-scale federal subsidies for individuals who earn from 138% to 400% of the federal poverty level, helping them buy insurance through the exchanges.
Experts say the exchanges also could directly impact hospitalists by bringing big changes to hospitals’ reimbursement revenue streams, spurring efforts to improve patient satisfaction metrics and increasing the momentum toward clinical comanagement agreements.
First, though, the public will get a chance to weigh in over rules that have been alternately lauded and derided, largely following the fault lines over the broader package of healthcare reforms. At a news conference set in front of a hardware store, HHS Secretary Kathleen Sebelius said competition on a level playing field would increase the purchasing power and drive down costs for individuals and small businesses. Websites for each of the exchanges would allow consumers to comparison-shop, with HHS ensuring that plans provide minimum standards for coverage. Patient groups, consumer organizations, and some small-business associations have welcomed the HHS rules, despite some concern that the exchanges could be tilted too far in favor of insurers. Overall, many analysts say, the rules have provided a fair amount of latitude over how the HIEs will be established and governed. Some business lobbyists, however, contend that the complex requirements will increase healthcare costs instead of lowering them. A July 16 editorial in the Wall Street Journal blasted the exchange rules as poorly designed and offering too little flexibility for states.
Two state-run ex-changes already exist, in Massachusetts and Utah. As of mid-July, however, states that had enacted laws to establish their own HIEs were outnumbered by those whose legislatures or governors had specifically blocked efforts to do likewise, according to the National Conference of State Legislatures. If states cannot or will not set up an exchange, HHS will step in and do it for them.
Reversal of Fortune?
Regardless of who ultimately oversees the exchanges, studies have begun suggesting who the most likely participants might be. An analysis by the Kaiser Family Foundation suggests that the newly insured are likely to be relatively older, less educated, more racially diverse, and in poorer health than those who currently carry private insurance but have fewer diagnosed conditions (www.kff.org/health reform/8147.cfm). Just as analysts, such as PwC, say that insurers will need to change their business strategy to lure and retain consumers, hospitals might need to redouble efforts to ensure high quality and patient satisfaction among a patient demographic that might be harder to please.
Mark Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, says the shift could represent a boon for hospitals that have been forced to maximize efficiency. “In general, those hospitals that have a poorer payor mix have tended to become very efficient, and so they make money off of Medicare patients,” Dr. Williams, a former SHM president, says. “This is fascinating because, on the one hand, there may be a lot of patients for whom hospitalists can now get paid because they’re insured. But I personally think that, simultaneously, we’re going to be seeing cutbacks in payments for other patients who have private insurance.”
For some hospitals, the net effect on revenue might not be materially different, though Dr. Williams sees a potentially sizable benefit for “safety net” hospitals that care for a large proportion of uninsured patients and excel in making the most of limited resources. Some investors apparently agree. Last December, Nashville, Tenn.-based Vanguard Health Systems finalized a deal to buy Detroit Medical Center, with a total investment of nearly $1.5 billion. Dr. Williams says the expectation is that the medical center will suddenly see many more insured patients via an HIE. The result could be a dramatic boost to its finances.
Wealthier hospitals, by contrast, have had less incentive to maximize efficiency—and now are worried by the potential financial impacts of insurance exchanges. “Your classic, highly profitable community hospital that has a good payor mix loses money on Medicare patients and tends to subsidize that with their private patients,” Dr. Williams says. “The wealthier hospitals are nervous because they’re worried that this entire health insurance exchange is going to put downward pressure on reimbursements from the private insurers.”
—Mark Williams, MD, FACP, SFHM, chief, division of hospital medicine, Feinberg School of Medicine, Northwestern University, Chicago
Satisfaction Times Two
With Medicare’s value-based purchasing initiative on its way, hospitals are ramping up their attention to patient satisfaction scores. So how will an influx of potentially older and sicker patients insured through the exchanges affect hospitalists’ scores? No one knows, but because hospitalists already are known for their expertise in treating this very demographic, some experts expect hospitals to lean on them more for leading quality and satisfaction initiatives. This reliance could represent a major opportunity for HM, but faulty performance metrics could also bring danger (read more about this topic in next month’s The Hospitalist).
Cherilyn Murer, president and CEO of Joliet, Ill.-based Murer Consultants Inc., says the expected shift in the nature of inpatients could accelerate efforts to be more accurate about physicians’ performance measures. “Patients who may be in the ICU are at a higher level of crisis than a person who’s in and out for an appendectomy, and yet we’re using the same tool of satisfaction,” she says. Furthermore, she adds, many factors that contribute to patient satisfaction are highly subjective and have nothing to do with a specific physician. “We have to really question the tools now, moreso than only questioning the participation and the outcome,” she says. As with other aspects of healthcare reform, Murer says, the looming arrival of exchanges also should be prompting hospitalists to ask themselves: “What’s our game plan now?” One compelling answer, she contends, is a clinical comanagement agreement that takes a longer-term view of doctors’ relationships with hospitals and gives them more control over decision-making. After all, if HM is taking care of “the sickest of the sick patients,” she says, a comanagement agreement can mean more say in factors that will directly impact their jobs over the long haul. Strategic direction of product lines, space, and equipment-buying decisions are just a few examples.
Murer ultimately sees clinical comanagement as a precursor to more widespread bundling of payments to hospitals and physicians. The mix of private and public insurance reimbursements, already in flux, might be further clouded by the arrival of HIEs. But solidifying hospital-hospitalist alignment with a flexible comanagement agreement, she says, can offer some reassurance over job structure, rewards, and authority as healthcare continues hurtling toward profound change.
Bryn Nelson is a freelance medical writer based in Seattle.