User login
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
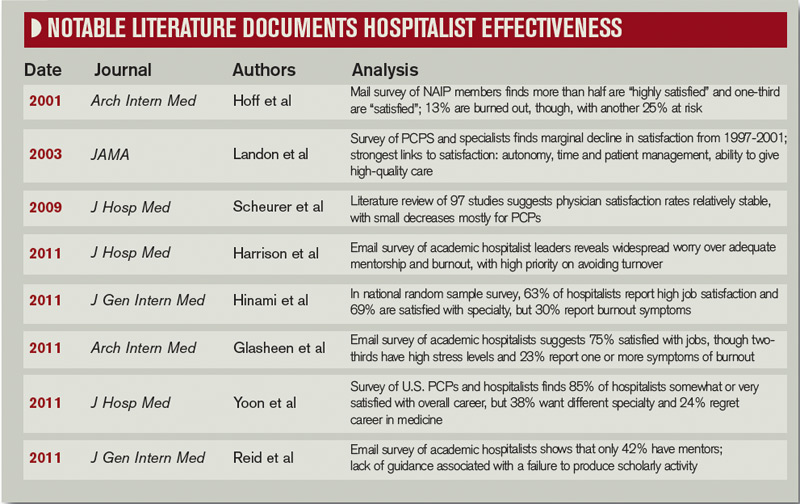
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.

—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
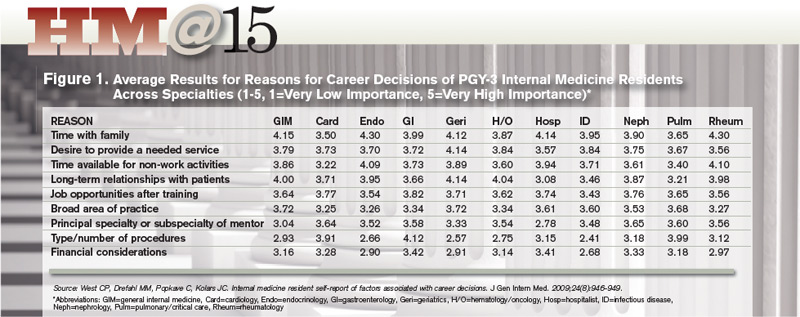
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.

—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic

Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.
—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.
—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic
Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.
Gregory Misky, MD, describes it as a “deer in the headlights” moment. About four years ago, Dr. Misky, assistant professor of medicine at the University of Colorado Denver, and Mark Reid, MD, assistant professor at Denver Health Medical Center, were trying to figure out what being an academic hospitalist was all about. What were the expectations of them, and how could they combine their clinical duties with scholarly work, especially given the significant lack of mentorship?
The duo wondered if other young hospitalists were feeling the same uncertainty about their chosen career, and whether there were any variables that might help predict success or burnout among their fellow doctors.
They haven’t been alone. Regardless of the practice model and location, physicians within the fastest-spreading medical specialty in the U.S. have noted both the promise and unsettled nature of HM. “We are still a relatively young profession, and I think over the past five to 10 years, we’ve been seeing the growing pains of the profession,” says Tosha Wetterneck, MD, MS, FACP, associate professor of medicine at the University of Wisconsin School of Medicine and Public Health in Madison.
In response to mounting concerns over multiple career-satisfaction-related issues, SHM assembled a Career Satisfaction Task Force that produced a detailed white paper at the end of 2006 (available from the “White Papers” tab under the “Publications” heading at www.hospitalmedicine.org).
One tangible outcome of the paper was the establishment of “Four Pillars of Career Satisfaction” for hospitalists:
- Reward and recognition;
- Workload and schedule;
- Autonomy and control; and
- Community and environment.
The paper included definitions for each pillar, and assembled scorecards, action steps, tools, and recommendations for both HM leaders and individual hospitalists to help shore up perceived weak spots.
So how strong are those pillars in practice? If hospitalists are the future of healthcare, as SHM and other medical groups assert, what do current studies suggest about the prospects of HM solidifying into a satisfying and sustainable career choice?
The Evidence
One outgrowth of Dr. Misky and Dr. Reid’s frustration was a study in which they and their collaborators emailed a 61-question survey to hospitalists at 20 academic medical centers. Among the results, the researchers found that 75% of respondents reported either “high” or “somewhat high” satisfaction with their current job. At the same time, though, 67% felt “high” or “somewhat high” stress levels at work, and nearly 1 in 4 (24%) reported some degree of burnout, based on their own definition of the word.1
As one of the first hospitalists in his group, Dr. Misky recalls the stress he felt over whether the hospital, division, and department would all buy into the idea of an academic hospitalist, and what his role would be. “I think we spent a lot of our early years trying to carve out our niche and proving ourselves and trying to balance the clinical needs that people had for us with other expectations of being an academic,” he says. Dr. Misky likens the experience to the adrenaline rush of mountain-biking straight down a hill. The feeling that too many things are going on at once, though, might also partially explain the apparent dichotomy of high overall satisfaction but a worrisome degree of burnout.
The profession hasn’t been around long enough for good longitudinal studies, and surveys have worded questions on satisfaction and burnout in different ways, complicating attempts at direct comparisons over time. A 2001 study, for example, reported that 12.9% of community and academic hospitalists were burned out, with another 25% at risk, but the survey was limited to dues-paying members of the National Association of Inpatient Physicians, the precursor to SHM.2
Nor has it been easy to compare hospitalist satisfaction and burnout levels to those of other specialists. “We haven’t really defined what a sustained, long-term career in hospital medicine is going to be,” Dr. Wetterneck says. “And in that way, it’s hard to say, ‘Compared to other professions, are we happier or not?’”
One of her recent studies, however, generally agrees with the handful of surveys addressing satisfaction and burnout among hospitalists. Overall, 63% of respondents reported high satisfaction with their job, while 69% were highly satisfied with their specialty. Roughly 30%, however, also reported feeling symptom of job burnout.3
Kelki Hinami, MD, MS, assistant of professor of medicine at Northwestern University Feinberg School of Medicine in Chicago and a coauthor of the study, says one take-home message is that hospitalists do fairly well in finding jobs that match their individual needs. “To further illustrate this, we found that hospitalists working in various practice models have different ideas about what is most important to their job,” he says.
Autonomy, for example, is considered most important by more local group hospitalists than by those of any other model, while recognition by leaders and having a variety of tasks at work are particularly important to academic hospitalists. Unlike other hospitalists, however, fewer academics consider pay to be the most important job characteristic.
A third study, led by John Yoon, MD, assistant professor in the section of hospital medicine at the University of Chicago, has examined career satisfaction, burnout, and morale among primary-care physicians (PCPs) and hospitalists. So far, the results he reported at HM11 largely agree with the other recent surveys: Combined, 85% of hospitalists report being either somewhat or very satisfied with their overall career. Conversely, 24% of hospitalists regretted choosing medicine as a career and 38% say they would have chosen a different medical specialty if they had to do it over again.4
Dr. Yoon says his data, compiled from two survey samples of about 1,000 generalists each, have revealed few differences between hospitalists and PCPs. “I thought hospitalists would be more satisfied than primary-care physicians, given the declining satisfaction rates of PCPs that we know about, and that students and trainees are less likely to go into primary care,” he says. Even burnout rates are similar, however; Dr. Yoon says he’s noticed a trend toward hospitalists reporting less burnout than PCPs, but the difference is not yet statistically significant.
Choice of a New Generation?
HM’s attractiveness to medical residents offers other clues about its ability to provide a sustainable and satisfying career choice. Salary, part of the “reward and recognition” pillar, has long been one perceived weakness. Anecdotally, however, Dr. Yoon says many general medicine residents see HM as a better financial option than primary care. “Some of the residents I work with, when I asked them, ‘Will you be a primary-care physician or a hospitalist?’ a lot of them say, ‘Probably hospitalist,’” he says. “And generally the reason is because they have to pay off their debt.”
It’s true that hospitalists’ salaries lag behind that of most of other specialists. Nevertheless, researchers like Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., say many medical residents are prioritizing financial considerations as relatively low on the scale of general preferences.
—John Yoon, MD, assistant professor, section of hospital medicine, University of Chicago
Dr. West, an associate program director for the internal-medicine residency program at Mayo, sees a generational sea change in the career considerations deemed most important. Based on a career decision survey filled out by nearly 15,000 internal-medical residents, he found that roughly 70% of respondents said time with family was of “high” or “very high” importance to their career decisions.5 The category, which relates to SHM’s “workload and schedule” pillar, beat out eight others as the most important factor overall, while global financial considerations scored relatively low.
Residents who placed high value on time with family were more likely to choose careers in more predictable, outpatient-based specialties, such as endocrinology or rheumatology. HM also fared well in this category. Dr. West says the results suggest that residents considering a hospitalist career are attracted to the specialty’s flexibility and predictability of the largely shift-based scheduling.
William Cors, MD, chief medical quality officer at Pocono Health System in East Stroudsburg, Pa., says more physicians are looking for job security, predictable shifts, and a better work-life balance. As HM matures and demonstrates that it can address those needs, Dr. Cors sees it becoming more attractive for medical students and residents.
In practice, though, other research suggests a career in HM doesn’t always meet expectations. Dr. Wetterneck and Dr. Hinami, for example, highlighted both compensation and work-life balance as points of concern in their study: For both factors, only about 30% of hospitalists were optimally satisfied.
Separately, Dr. Misky and his colleagues reported that roughly half of academic hospitalists were satisfied with the ability to control their schedule, and with their amount of personal and family time. Those who were unsatisfied with either of these categories, the survey found, were at higher risk for burnout. Similarly, Dr. Yoon found that physicians who reported having no control over their work hours or their call schedule, part of SHM’s “autonomy and control” pillar, were more likely to report burnout.
So why is HM stumbling on perceived selling points like family friendliness and autonomy? Dr. Wetterneck believes too many unfilled jobs and rapid turnover could be putting more pressure on existing hospitalists and interfering with their ability to balance home and work life. “There’s a huge need for hospitalists everywhere,” she says, and reliance on them has been especially acute at academic centers and large community hospitals contending with the recently imposed limits on residents’ work hours.
The Hospitalist: A People Person
Another shift may be occurring in the types of relationships necessary for a satisfying work environment, a big part of the “community and environment” pillar. Although Dr. Yoon says long-term connections with students and trainees have added meaning to his job, he is mourning the absence of other bonds. “One loss I’m starting to feel keenly as an academic hospitalist, having spent my early training years as a primary-care doc, really is the loss of having long-term relationships with patients,” he says. “My clinical encounters with patients these days as a hospitalist are very intense, but also very brief.”
Dr. Yoon has pondered whether the HM field can rearrange practice settings to promote more satisfying relationships. Such a change, he says, might occur through innovative models that aid coordination with medical homes, or provide more chronic care for high-risk patients. “In my view, the trajectory of hospital medicine is pretty wide open for creativity and new models of care,” he says. “I think it will be partly driven by the need to want to have more meaningful interactions with patients.”
Those relationships need not be long-term, however. One recent study found high satisfaction among hospitalists and laborists working within the fast-growing OBGYN hospitalist field.6
Dr. Hinami says collaborative care that involves close working relationships with specialists and other care providers might help propel the hospitalist movement forward. In his survey with Dr. Wetterneck, hospitalists ranked relationships with staff and colleagues among the most satisfying of any of the domains; hospitalists also indicated high levels of satisfaction with their patient relationships. “Clearly, relationships are critical to overall job satisfaction, and hospitalists, I think, are doing a fairly good job at maintaining those relationships,” Dr. Hinami says.
—Keiki Hinami, MD, assistant professor of medicine, Northwestern University Feinberg School of Medicine, Chicago
A 2002 survey-based study reinforces the importance of such bonds. Job burnout and intent to remain in the hospitalist career, its authors concluded, were more highly influenced by “favorable social relations” involving colleagues, coworkers, and patients than by such factors as reduced autonomy and the use of financial incentives.7
The focus on maintaining multiple relationships fits well with the collaborative approach to care that many hospitalists say they value highly. One big satisfier for hospitalists, Dr. Cors says, will be “a sense that they’re really part of a healthcare team and not just punching the clock and doing their shifts.”
The Verdict
Despite the difficulty in discerning long-term trends, studies suggest that overall satisfaction with the specialty of hospital medicine remains high, a promising sign for the maturing field. Career hospitalists also seem adept at relationships with peers and other providers, a skill that will serve them well as collaborative-care models gain steam.
Nonetheless, surveys also suggest a worrisome rate of burnout and less-than-optimal satisfaction with elements that should be the strong suits of HM, such as work-life balance and autonomy. Academics are searching for their own clinical-research balance. And Dr. West says the jury’s still out on the future pitfalls that might get in the way of a sustainable career path for older practitioners, such as overnight shifts.
Hospitalist-led efforts, however, may be starting to pay dividends. At the University of California at San Francisco, a faculty development program for first-year hospitalists has included a coaching relationship with a senior faculty member, a teaching course, newly established divisional grand rounds, and a framework for meeting scholarly expectations. Upon its implementation, the program has led to higher job satisfaction, skill-set comfort, and academic production among participants.8
Given the expanding range of HM duties and practice models, hospitals, division chiefs, and team leaders cannot rely on a single recipe for happy and productive hospitalists. “I don’t know if there is a cookbook; I think it’s highly variable depending on your institution and the needs of the academic facility where you are,” Dr. Misky says.
SHM’s 2006 white paper stated that the best career satisfaction strategy is to find a job that fits an individual’s preferences and attitudes. “People who are unhappy with their job don’t tend to stay in it, and from what we know about hospital medicine right now, you can find pretty much any type of job anywhere you want, so the job market is very open,” Dr. Wetterneck says.
Ensuring the right fit for doctors within HM, though, will require institutional support. “It’s going to be up to hospitals and hospitalist programs to create jobs that are sustainable that people like,” she says, “so that hospitalists will stay long in their job and in the profession.”
Bryn Nelson is a freelance medical writer based in Seattle.
More Mentorship in Hospital Medicine? It’s Academic
Within the 2011 State of Hospital Medicine report, one statistic in particular points to the youth of the medical specialty: Just over 10% of surveyed hospitalists had reached the rank of associate professor or higher.
How might the potential lack of mentorship within this immature field affect the ability of hospitalists to successfully navigate academia? So asked Gregory Misky, MD, assistant professor of medicine at the University of Colorado Denver, and his colleagues in a survey-based study. The results agree with other recent assessments that mentors are in short supply. “Academic hospital medicine groups have an acute need for mentoring and career development programs,” one study concludes.
The research of Dr. Misky and his collaborators found that only 42% of academic hospitalists could identify a mentor, while only 31% reported that they were mentoring another academic hospitalist.1 Based on sheer numbers and experience, the pool of mentors may significantly expand as the field matures. But Dr. Misky also urges some flexibility, noting that his own mentor is a non-hospitalist.
In his own research, Colin West, MD, PhD, associate professor of medicine and biostatistics at the Mayo Clinic in Rochester, Minn., found that residents considering a career in HM placed less emphasis on the specialty or subspecialty of their mentor.5 Why? Very likely, he says, there just weren’t enough hospitalist mentors around to get a sense of what the career was all about.
Dr. West hopes the numbers suggest otherwise in the near future. “You want to recruit bright people into your specialty, but at the same time, you also want to recruit the right people,” he says. “And that means that you need to be able to expose people to a full breadth of what a decision to pursue a certain specialty really means.”
References
- Glasheen JJ, Misky GJ, Reid MB, Harrison RA, Sharpe B, Auerbach A. Career satisfaction and burnout in academic hospital medicine. Arch Intern Med. 2011;171(8) 782-785.
- Hoff TH, Whitcomb WF, Williams K, Nelson JR, Cheesman RA. Characteristics and work experiences of hospitalists in the United States. Arch Intern Med. 2001;161(6):851-858.
- Hinami K, Whelan CT, Wolosin RJ, Miller JA, Wetterneck TB. Worklife and satisfaction of hospitalists: toward flourishing careers [published online ahead of print July 20, 2011]. J Gen Intern Med. doi:10.1007/s116060-011-1780-z.
- Yoon J, Miller A, Rasinski K, Curlin F. Burnout, sense of calling, and career resilience among hospitalists and primary care physicians: a national survey. J Hosp Med. 2011;6(4):S90-S91.
- West CP, Drefahl MM, Popkave C, Kolars JC. Internal medicine resident self-report of factors associated with career decisions. J Gen Intern Med. 2009;24(8):946-949.
- Funk C, Anderson BL, Schulkin J, Weinstein L. Survey of obstetric and gynecologic hospitalists and laborists. Am J Obstet Gynecol. 2010;203(2):177.e1-177.e4.
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. J Health Soc Behav. 2002;43(1):72-91.
- Sehgal NL, Sharpe BA, Auerbach AA, Wachter RM. Investing in the future: Building an academic hospitalist faculty development program. J Hosp Med. 2011;6(3):161-166.