User login
New DES hailed for smallest coronary vessels
Paris – The first multicenter, prospective trial of a drug-eluting stent designed specifically to treat lesions in coronary vessels less than 2.25 mm in diameter showed excellent outcomes, with a 1-year target lesion failure rate of 5% for the Resolute Onyx 2.0 mm diameter zotarolimus-eluting stent.
This result in the pivotal trial easily surpassed the prespecified performance goal of a 19% target lesion failure rate, Matthew J. Price, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.

Hemodynamically significant lesions in such small vessels are “not uncommon, particularly in diabetic patients,” Dr. Price said in an interview. Indeed, 47% of patients in the clinical trial had diabetes.
At present, the only ways to treat coronary disease in arteries having a reference vessel diameter less than 2.25 mm are off-label placement of an oversized stent, with its attendant risk of complications; standard balloon angioplasty, which entails a particularly high restenosis rate in this setting; or medical management, the cardiologist noted.
He presented a multicenter, prospective, open-label, single-arm trial of 101 patients with documented ischemia-producing obstructions in coronary arteries having a reference vessel diameter less than 2.25 mm, a lesion length less than 27 mm, and evidence of ischemia attributable to the lesion, typically via fractional flow reserve. The mean diameter by quantitative coronary angiography was 1.91 mm.
The primary endpoint was the rate of target lesion failure at 12 months, a composite comprising cardiac death, target vessel MI, or clinically driven target lesion revascularization. This endpoint occurred in 5% of patients. There was a 3% target vessel MI rate and a 2% target lesion revascularization rate. There were no cardiac deaths.
“Importantly, the stent thrombosis rate in these patients with extremely small vessels was zero,” the cardiologist emphasized.
The mean angiographic in-stent late lumen loss at 13 months was 0.26 mm, which Dr. Price characterized as “quite good.” The in-segment binary angiographic restenosis rate was 20%.
“That’s slightly higher than you would expect to see in vessels with larger reference diameters. I think that’s because of the lack of headroom. You have a very small vessel, and, even with a very small stent, even a small amount of late loss will give you a larger percent diameter restenosis over time,” he explained.
The 19% target lesion failure rate selected as a performance goal in the trial was set somewhat arbitrarily. It wasn’t possible to randomize patients to a comparator arm because there are no approved stents for vessels less than 2.25 mm in diameter. The 19% figure was arrived at in discussion with the Food and Drug Administration on the basis of similarity to the performance goal used in clinical trials to gain approval of 2.25-mm, drug-eluting stents. Because the Onyx 2.0-mm-diameter trial was developed in collaboration with the FDA and the stent aced its primary endpoint and showed excellent clinical outcomes, Dr. Price anticipates the device will readily gain regulatory approval. In April 2017, the FDA approved the Resolute Onyx in sizes of 2.25- to 5.0-mm diameter.
The study met with an enthusiastic reception.
“That was terrific. It’s clearly an incredibly important unmet clinical need,” commented session cochair David R. Holmes Jr., MD, of the Mayo Clinic in Rochester, Minn.
Assuming the stent is approved, how should interventionalists put it into practice? he asked.
Dr. Price replied that, first, it’s important to step back and ask if percutaneous coronary intervention of a particular lesion in a very small coronary artery is clinically indicated. The stent itself is readily manipulatable. It is a thin-strut device constructed of a single strand of a cobalt alloy with enhanced radiopacity.
Investigators in the trial used the standard approach to dual antiplatelet therapy – at least 6 months, with 12 months preferable.
The 20% in-segment binary restenosis rate at 13 months provides a clear message for interventionalists, he continued. “What this tells me is that, while this is a very good stent, we can’t forget to treat the patient aggressively with medical therapy to stop the progression of prediabetes, diabetes, and small vessel disease in addition to treating obstructive lesions with a small stent.”
Asked if the lack of headroom in these extra-small arteries warrants liberal use of intraprocedural imaging to make sure the stent is perfectly apposed, Dr. Price replied that he doesn’t think so. He noted that intravascular ultrasound and optical coherence tomography were seldom used in the trial, yet the results were reassuringly excellent.
The study results were published simultaneously with Dr. Price’s presentation (JACC Cardiovasc Interv. 2017 May 17. doi: 10.1016/j.jcin.2017.05.004). The trial was sponsored by Medtronic. Dr. Price reported serving as a consultant and paid speaker on behalf of that company, as well as AstraZeneca, Boston Scientific, St. Jude Medical, and The Medicines Company.
Paris – The first multicenter, prospective trial of a drug-eluting stent designed specifically to treat lesions in coronary vessels less than 2.25 mm in diameter showed excellent outcomes, with a 1-year target lesion failure rate of 5% for the Resolute Onyx 2.0 mm diameter zotarolimus-eluting stent.
This result in the pivotal trial easily surpassed the prespecified performance goal of a 19% target lesion failure rate, Matthew J. Price, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Hemodynamically significant lesions in such small vessels are “not uncommon, particularly in diabetic patients,” Dr. Price said in an interview. Indeed, 47% of patients in the clinical trial had diabetes.
At present, the only ways to treat coronary disease in arteries having a reference vessel diameter less than 2.25 mm are off-label placement of an oversized stent, with its attendant risk of complications; standard balloon angioplasty, which entails a particularly high restenosis rate in this setting; or medical management, the cardiologist noted.
He presented a multicenter, prospective, open-label, single-arm trial of 101 patients with documented ischemia-producing obstructions in coronary arteries having a reference vessel diameter less than 2.25 mm, a lesion length less than 27 mm, and evidence of ischemia attributable to the lesion, typically via fractional flow reserve. The mean diameter by quantitative coronary angiography was 1.91 mm.
The primary endpoint was the rate of target lesion failure at 12 months, a composite comprising cardiac death, target vessel MI, or clinically driven target lesion revascularization. This endpoint occurred in 5% of patients. There was a 3% target vessel MI rate and a 2% target lesion revascularization rate. There were no cardiac deaths.
“Importantly, the stent thrombosis rate in these patients with extremely small vessels was zero,” the cardiologist emphasized.
The mean angiographic in-stent late lumen loss at 13 months was 0.26 mm, which Dr. Price characterized as “quite good.” The in-segment binary angiographic restenosis rate was 20%.
“That’s slightly higher than you would expect to see in vessels with larger reference diameters. I think that’s because of the lack of headroom. You have a very small vessel, and, even with a very small stent, even a small amount of late loss will give you a larger percent diameter restenosis over time,” he explained.
The 19% target lesion failure rate selected as a performance goal in the trial was set somewhat arbitrarily. It wasn’t possible to randomize patients to a comparator arm because there are no approved stents for vessels less than 2.25 mm in diameter. The 19% figure was arrived at in discussion with the Food and Drug Administration on the basis of similarity to the performance goal used in clinical trials to gain approval of 2.25-mm, drug-eluting stents. Because the Onyx 2.0-mm-diameter trial was developed in collaboration with the FDA and the stent aced its primary endpoint and showed excellent clinical outcomes, Dr. Price anticipates the device will readily gain regulatory approval. In April 2017, the FDA approved the Resolute Onyx in sizes of 2.25- to 5.0-mm diameter.
The study met with an enthusiastic reception.
“That was terrific. It’s clearly an incredibly important unmet clinical need,” commented session cochair David R. Holmes Jr., MD, of the Mayo Clinic in Rochester, Minn.
Assuming the stent is approved, how should interventionalists put it into practice? he asked.
Dr. Price replied that, first, it’s important to step back and ask if percutaneous coronary intervention of a particular lesion in a very small coronary artery is clinically indicated. The stent itself is readily manipulatable. It is a thin-strut device constructed of a single strand of a cobalt alloy with enhanced radiopacity.
Investigators in the trial used the standard approach to dual antiplatelet therapy – at least 6 months, with 12 months preferable.
The 20% in-segment binary restenosis rate at 13 months provides a clear message for interventionalists, he continued. “What this tells me is that, while this is a very good stent, we can’t forget to treat the patient aggressively with medical therapy to stop the progression of prediabetes, diabetes, and small vessel disease in addition to treating obstructive lesions with a small stent.”
Asked if the lack of headroom in these extra-small arteries warrants liberal use of intraprocedural imaging to make sure the stent is perfectly apposed, Dr. Price replied that he doesn’t think so. He noted that intravascular ultrasound and optical coherence tomography were seldom used in the trial, yet the results were reassuringly excellent.
The study results were published simultaneously with Dr. Price’s presentation (JACC Cardiovasc Interv. 2017 May 17. doi: 10.1016/j.jcin.2017.05.004). The trial was sponsored by Medtronic. Dr. Price reported serving as a consultant and paid speaker on behalf of that company, as well as AstraZeneca, Boston Scientific, St. Jude Medical, and The Medicines Company.
Paris – The first multicenter, prospective trial of a drug-eluting stent designed specifically to treat lesions in coronary vessels less than 2.25 mm in diameter showed excellent outcomes, with a 1-year target lesion failure rate of 5% for the Resolute Onyx 2.0 mm diameter zotarolimus-eluting stent.
This result in the pivotal trial easily surpassed the prespecified performance goal of a 19% target lesion failure rate, Matthew J. Price, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
Hemodynamically significant lesions in such small vessels are “not uncommon, particularly in diabetic patients,” Dr. Price said in an interview. Indeed, 47% of patients in the clinical trial had diabetes.
At present, the only ways to treat coronary disease in arteries having a reference vessel diameter less than 2.25 mm are off-label placement of an oversized stent, with its attendant risk of complications; standard balloon angioplasty, which entails a particularly high restenosis rate in this setting; or medical management, the cardiologist noted.
He presented a multicenter, prospective, open-label, single-arm trial of 101 patients with documented ischemia-producing obstructions in coronary arteries having a reference vessel diameter less than 2.25 mm, a lesion length less than 27 mm, and evidence of ischemia attributable to the lesion, typically via fractional flow reserve. The mean diameter by quantitative coronary angiography was 1.91 mm.
The primary endpoint was the rate of target lesion failure at 12 months, a composite comprising cardiac death, target vessel MI, or clinically driven target lesion revascularization. This endpoint occurred in 5% of patients. There was a 3% target vessel MI rate and a 2% target lesion revascularization rate. There were no cardiac deaths.
“Importantly, the stent thrombosis rate in these patients with extremely small vessels was zero,” the cardiologist emphasized.
The mean angiographic in-stent late lumen loss at 13 months was 0.26 mm, which Dr. Price characterized as “quite good.” The in-segment binary angiographic restenosis rate was 20%.
“That’s slightly higher than you would expect to see in vessels with larger reference diameters. I think that’s because of the lack of headroom. You have a very small vessel, and, even with a very small stent, even a small amount of late loss will give you a larger percent diameter restenosis over time,” he explained.
The 19% target lesion failure rate selected as a performance goal in the trial was set somewhat arbitrarily. It wasn’t possible to randomize patients to a comparator arm because there are no approved stents for vessels less than 2.25 mm in diameter. The 19% figure was arrived at in discussion with the Food and Drug Administration on the basis of similarity to the performance goal used in clinical trials to gain approval of 2.25-mm, drug-eluting stents. Because the Onyx 2.0-mm-diameter trial was developed in collaboration with the FDA and the stent aced its primary endpoint and showed excellent clinical outcomes, Dr. Price anticipates the device will readily gain regulatory approval. In April 2017, the FDA approved the Resolute Onyx in sizes of 2.25- to 5.0-mm diameter.
The study met with an enthusiastic reception.
“That was terrific. It’s clearly an incredibly important unmet clinical need,” commented session cochair David R. Holmes Jr., MD, of the Mayo Clinic in Rochester, Minn.
Assuming the stent is approved, how should interventionalists put it into practice? he asked.
Dr. Price replied that, first, it’s important to step back and ask if percutaneous coronary intervention of a particular lesion in a very small coronary artery is clinically indicated. The stent itself is readily manipulatable. It is a thin-strut device constructed of a single strand of a cobalt alloy with enhanced radiopacity.
Investigators in the trial used the standard approach to dual antiplatelet therapy – at least 6 months, with 12 months preferable.
The 20% in-segment binary restenosis rate at 13 months provides a clear message for interventionalists, he continued. “What this tells me is that, while this is a very good stent, we can’t forget to treat the patient aggressively with medical therapy to stop the progression of prediabetes, diabetes, and small vessel disease in addition to treating obstructive lesions with a small stent.”
Asked if the lack of headroom in these extra-small arteries warrants liberal use of intraprocedural imaging to make sure the stent is perfectly apposed, Dr. Price replied that he doesn’t think so. He noted that intravascular ultrasound and optical coherence tomography were seldom used in the trial, yet the results were reassuringly excellent.
The study results were published simultaneously with Dr. Price’s presentation (JACC Cardiovasc Interv. 2017 May 17. doi: 10.1016/j.jcin.2017.05.004). The trial was sponsored by Medtronic. Dr. Price reported serving as a consultant and paid speaker on behalf of that company, as well as AstraZeneca, Boston Scientific, St. Jude Medical, and The Medicines Company.
AT EUROPCR
Key clinical point:
Major finding: At 12 months’ follow-up, the key outcomes were a 3% rate of target vessel MI, a 2% rate of clinically driven target lesion revascularization, no stent thrombosis, and no cardiac deaths.
Data source: A prospective, multicenter, open-label trial in 101 patients who underwent percutaneous coronary intervention for coronary lesions with a reference vessel diameter of less than 2.25 mm.
Disclosures: The trial was sponsored by Medtronic. Dr. Price reported serving as a consultant to and paid speaker on behalf of that company as well as AstraZeneca, Boston Scientific, St. Jude Medical, and The Medicines Company.

Tweaking CBT may boost outcomes in hoarding disorder
SAN FRANCISCO – Cognitive-behavioral therapy for hoarding disorder leaves substantial room for improvement in efficacy, and additional therapeutic attention to maladaptive beliefs regarding perfectionism just might be the answer, Hannah C. Levy, PhD, said at the annual conference of the Anxiety and Depression Association of America.
She presented a secondary analysis of the relationship between cognitive-behavioral therapy (CBT) outcomes and baseline maladaptive beliefs in a wait list–controlled study of 36 patients with hoarding disorder (HD) who were not on psychiatric medication. Her purpose was to identify which cognitive domains predicted treatment outcome. This, in turn, could point the way to new treatment targets.

In contrast, the baseline strength of Saving Cognitions Inventory maladaptive beliefs about saving, such as emotional attachment to hoarded objects or a belief that keeping those objects is the only way to be able to remember an important event, proved unrelated to CBT outcomes. And this finding may help explain CBT’s limited effectiveness in HD.
“I think traditionally our CBT interventions are more focused on the maladaptive saving beliefs. We’re currently not doing a whole lot about the perfectionism ideas that people may be bringing in,” said Dr. Levy of the anxiety disorders center at the Institute of Living in Hartford, Conn.
A strong unmet need exists for novel targets for CBT in hoarding disorder to improve current less-than-stellar outcomes, she said. A recent meta-analysis demonstrated that while CBT did provide a statistically significant benefit for this common and often disabling disease, outcomes were far from optimal. Indeed, after completing their course of CBT, patients still scored an average of 3 standard deviations above mean normal for scores on the SI-R (Depress Anxiety. 2015 Mar;32[3]:158-66).
Other investigators have recognized the limitations of current CBT for HD and tried tweaking the therapy to boost efficacy. These efforts have included formal studies incorporating home visits, adding cognitive remediation to reduce the neuropsychological deficits often present in patients with HD, and/or extending the treatment duration to 26 weekly sessions from the current standard of 15 or 16.
Unfortunately, none of these innovations has really panned out when tested, Dr. Levy said. For example, in the 36-patient study analyzed by Dr. Levy, clinically significant improvement was seen in only 41% of subjects following 26 weeks of CBT (Depress Anxiety. 2010 May;27[5]:476-84). In contrast, published response rates for CBT in patients with obsessive-compulsive disorder – a related condition – are in the 85% range.
She described the perfectionism that often figures prominently in HD as a maladaptive belief that if something can’t be done perfectly, it’s not worth doing at all.
“People will say to me, ‘I can’t start discarding until I’ve got my organizational system down.’ They’re completely stymied. They can’t make any progress because their system isn’t fully coordinated yet,” the psychologist explained.
One way to potentially target this perfectionism more explicitly might be to incorporate cognitive restructuring or behavioral experiments that enable patients to test out and perhaps discard those beliefs, according to Dr. Levy.
She reported no financial conflicts regarding her analysis, which was based upon data collected in an earlier study sponsored by the National Institute of Mental Health.
SAN FRANCISCO – Cognitive-behavioral therapy for hoarding disorder leaves substantial room for improvement in efficacy, and additional therapeutic attention to maladaptive beliefs regarding perfectionism just might be the answer, Hannah C. Levy, PhD, said at the annual conference of the Anxiety and Depression Association of America.
She presented a secondary analysis of the relationship between cognitive-behavioral therapy (CBT) outcomes and baseline maladaptive beliefs in a wait list–controlled study of 36 patients with hoarding disorder (HD) who were not on psychiatric medication. Her purpose was to identify which cognitive domains predicted treatment outcome. This, in turn, could point the way to new treatment targets.
In contrast, the baseline strength of Saving Cognitions Inventory maladaptive beliefs about saving, such as emotional attachment to hoarded objects or a belief that keeping those objects is the only way to be able to remember an important event, proved unrelated to CBT outcomes. And this finding may help explain CBT’s limited effectiveness in HD.
“I think traditionally our CBT interventions are more focused on the maladaptive saving beliefs. We’re currently not doing a whole lot about the perfectionism ideas that people may be bringing in,” said Dr. Levy of the anxiety disorders center at the Institute of Living in Hartford, Conn.
A strong unmet need exists for novel targets for CBT in hoarding disorder to improve current less-than-stellar outcomes, she said. A recent meta-analysis demonstrated that while CBT did provide a statistically significant benefit for this common and often disabling disease, outcomes were far from optimal. Indeed, after completing their course of CBT, patients still scored an average of 3 standard deviations above mean normal for scores on the SI-R (Depress Anxiety. 2015 Mar;32[3]:158-66).
Other investigators have recognized the limitations of current CBT for HD and tried tweaking the therapy to boost efficacy. These efforts have included formal studies incorporating home visits, adding cognitive remediation to reduce the neuropsychological deficits often present in patients with HD, and/or extending the treatment duration to 26 weekly sessions from the current standard of 15 or 16.
Unfortunately, none of these innovations has really panned out when tested, Dr. Levy said. For example, in the 36-patient study analyzed by Dr. Levy, clinically significant improvement was seen in only 41% of subjects following 26 weeks of CBT (Depress Anxiety. 2010 May;27[5]:476-84). In contrast, published response rates for CBT in patients with obsessive-compulsive disorder – a related condition – are in the 85% range.
She described the perfectionism that often figures prominently in HD as a maladaptive belief that if something can’t be done perfectly, it’s not worth doing at all.
“People will say to me, ‘I can’t start discarding until I’ve got my organizational system down.’ They’re completely stymied. They can’t make any progress because their system isn’t fully coordinated yet,” the psychologist explained.
One way to potentially target this perfectionism more explicitly might be to incorporate cognitive restructuring or behavioral experiments that enable patients to test out and perhaps discard those beliefs, according to Dr. Levy.
She reported no financial conflicts regarding her analysis, which was based upon data collected in an earlier study sponsored by the National Institute of Mental Health.
SAN FRANCISCO – Cognitive-behavioral therapy for hoarding disorder leaves substantial room for improvement in efficacy, and additional therapeutic attention to maladaptive beliefs regarding perfectionism just might be the answer, Hannah C. Levy, PhD, said at the annual conference of the Anxiety and Depression Association of America.
She presented a secondary analysis of the relationship between cognitive-behavioral therapy (CBT) outcomes and baseline maladaptive beliefs in a wait list–controlled study of 36 patients with hoarding disorder (HD) who were not on psychiatric medication. Her purpose was to identify which cognitive domains predicted treatment outcome. This, in turn, could point the way to new treatment targets.
In contrast, the baseline strength of Saving Cognitions Inventory maladaptive beliefs about saving, such as emotional attachment to hoarded objects or a belief that keeping those objects is the only way to be able to remember an important event, proved unrelated to CBT outcomes. And this finding may help explain CBT’s limited effectiveness in HD.
“I think traditionally our CBT interventions are more focused on the maladaptive saving beliefs. We’re currently not doing a whole lot about the perfectionism ideas that people may be bringing in,” said Dr. Levy of the anxiety disorders center at the Institute of Living in Hartford, Conn.
A strong unmet need exists for novel targets for CBT in hoarding disorder to improve current less-than-stellar outcomes, she said. A recent meta-analysis demonstrated that while CBT did provide a statistically significant benefit for this common and often disabling disease, outcomes were far from optimal. Indeed, after completing their course of CBT, patients still scored an average of 3 standard deviations above mean normal for scores on the SI-R (Depress Anxiety. 2015 Mar;32[3]:158-66).
Other investigators have recognized the limitations of current CBT for HD and tried tweaking the therapy to boost efficacy. These efforts have included formal studies incorporating home visits, adding cognitive remediation to reduce the neuropsychological deficits often present in patients with HD, and/or extending the treatment duration to 26 weekly sessions from the current standard of 15 or 16.
Unfortunately, none of these innovations has really panned out when tested, Dr. Levy said. For example, in the 36-patient study analyzed by Dr. Levy, clinically significant improvement was seen in only 41% of subjects following 26 weeks of CBT (Depress Anxiety. 2010 May;27[5]:476-84). In contrast, published response rates for CBT in patients with obsessive-compulsive disorder – a related condition – are in the 85% range.
She described the perfectionism that often figures prominently in HD as a maladaptive belief that if something can’t be done perfectly, it’s not worth doing at all.
“People will say to me, ‘I can’t start discarding until I’ve got my organizational system down.’ They’re completely stymied. They can’t make any progress because their system isn’t fully coordinated yet,” the psychologist explained.
One way to potentially target this perfectionism more explicitly might be to incorporate cognitive restructuring or behavioral experiments that enable patients to test out and perhaps discard those beliefs, according to Dr. Levy.
She reported no financial conflicts regarding her analysis, which was based upon data collected in an earlier study sponsored by the National Institute of Mental Health.
AT ANXIETY AND DEPRESSION CONFERENCE 2017
Key clinical point:
Major finding: High baseline levels of perfectionism and rigidity of thinking were associated with lack of response to 26 weeks of CBT for hoarding disorder.
Data source: A secondary analysis of data from a prospective study of 36 patients with primary hoarding disorder.
Disclosures: The presenter reported no financial conflicts regarding her analysis, which was based upon data collected in an earlier study sponsored by the National Institute of Mental Health.
Novel Lotus valve outperforms CoreValve in REPRISE III
PARIS – The investigational mechanically expandable Lotus valve system for transcatheter aortic valve replacement proved significantly more effective than the commercially available CoreValve platform in patients with severe aortic stenosis deemed at high or extreme surgical risk in the randomized pivotal phase III REPRISE III trial, Ted E. Feldman, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The 1-year composite primary effectiveness endpoint comprised of all-cause mortality, disabling stroke, and moderate or greater paravalvular leak (PVL) occurred in 17% of patients randomized to the Lotus transcatheter aortic valve replacement (TAVR) device, compared with 29% of those in the CoreValve group, said Dr. Feldman, director of the cardiac catheterization laboratory at NorthShore University HealthSystem in Evanston, Ill.

A key finding was that the Lotus valve group had a 1-year rate of moderate or greater PVL of just 2% as assessed in a central core lab, compared with an 11% rate in patients randomized to the classic CoreValve or the subsequent-generation Evolut R device, he observed.
“With the Lotus valve there was no or only trace PVL in over 85% of patients. This is probably even more important than the low rate of moderate or severe PVL. The valve really does result in virtually no PVL in the vast majority of patients. That’s unique to this platform,” the cardiologist said in an interview.
The unprecedented low rate of moderate or severe PVL at 1 year postprocedure is attributable to the polymer seal delivered via the Lotus system for that express purpose, he explained.
REPRISE III was the first large randomized comparative clinical trial featuring two TAVR valves, an event that reflects the rapid expansion of the field. All previous major trials had compared TAVR with surgical aortic valve replacement.
REPRISE III randomized 912 TAVR patients at 55 centers 2:1 to the Lotus valve in its 23-, 25-, or 27-mm configurations or to a CoreValve at 26, 29, or 31 mm. Roughly half of the CoreValve group got the newer repositionable and retrievable Evolut R valve, while the earlier enrollees received the nonrepositionable classic CoreValve.
The Lotus valve group proved noninferior to the CoreValve recipients for the primary safety endpoint, a 30-day composite of all-cause mortality, stroke, major or life-threatening bleeding, major vascular complications, and stage 2 or 3 acute kidney injury. The rates were 20.3% in the Lotus arm and 17.2% with CoreValve.
The 1-year rate of disabling stroke was 3.6% in the Lotus group versus 7.3% in the CoreValve group. Dr. Feldman downplayed the importance of this difference, even though it was statistically significant. The Lotus valve performed as expected, but the disabling stroke rate in the CoreValve group was higher than in earlier studies for reasons unknown, most likely simply the play of chance, he said.
“I think the real message here is that the Lotus valve performed very well,” the cardiologist said. “There have been concerns that repositioning the valve into a better position during the deployment process might create excess stroke. It appears clear that’s not the case.”
The ability to reposition the Lotus device resulted in a significantly lower rate of repeat procedures at 1 year: 0.2% versus 2% with the CoreValve, as well as zero cases of aortic valve malposition and valve-in-valve deployment.
The need for a new pacemaker within 30 days after TAVR was strikingly more common in the Lotus valve group: 36%, compared with 20% with the CoreValve. Dr. Feldman attributed the high new pacemaker rate in the Lotus arm partly to the operators’ limited experience with the novel valve along with the fact that REPRISE III used a first-iteration device deployment mechanism. An improved deployment mechanism designed to minimize problematic contact with the left ventricular outflow tract was developed too late for inclusion in the trial. But in a recent European study using this proprietary deployment system, known as Depth Guard, the new pacemaker rate was below 20%.
The learning curve for the new Lotus valve system is “not at all challenging,” according to the cardiologist. He noted that U.S. operators participating in REPRISE III, who had no prior experience with the device, were allowed only two initial cases in order to gain experience; after that, every patient counted in the clinical trial results.
The REPRISE III results will be offered to the Food and Drug Administration to support regulatory approval of the device in high-surgical-risk patients. Dr. Feldman said Boston Scientific plans to conduct an additional clinical trial of the Lotus valve, this time in intermediate-risk patients, with the goal of gaining an expanded indication. This, too, will be a head-to-head comparison with a commercially available TAVR valve, probably the Edwards Sapien 3 valve.
REPRISE III was sponsored by Boston Scientific. Dr. Feldman reported serving as a consultant to that company, Abbott, and Edwards Lifesciences, and having received institutional research grants from those companies as well.
bjancin@frontlinemedcom.com
PARIS – The investigational mechanically expandable Lotus valve system for transcatheter aortic valve replacement proved significantly more effective than the commercially available CoreValve platform in patients with severe aortic stenosis deemed at high or extreme surgical risk in the randomized pivotal phase III REPRISE III trial, Ted E. Feldman, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The 1-year composite primary effectiveness endpoint comprised of all-cause mortality, disabling stroke, and moderate or greater paravalvular leak (PVL) occurred in 17% of patients randomized to the Lotus transcatheter aortic valve replacement (TAVR) device, compared with 29% of those in the CoreValve group, said Dr. Feldman, director of the cardiac catheterization laboratory at NorthShore University HealthSystem in Evanston, Ill.
A key finding was that the Lotus valve group had a 1-year rate of moderate or greater PVL of just 2% as assessed in a central core lab, compared with an 11% rate in patients randomized to the classic CoreValve or the subsequent-generation Evolut R device, he observed.
“With the Lotus valve there was no or only trace PVL in over 85% of patients. This is probably even more important than the low rate of moderate or severe PVL. The valve really does result in virtually no PVL in the vast majority of patients. That’s unique to this platform,” the cardiologist said in an interview.
The unprecedented low rate of moderate or severe PVL at 1 year postprocedure is attributable to the polymer seal delivered via the Lotus system for that express purpose, he explained.
REPRISE III was the first large randomized comparative clinical trial featuring two TAVR valves, an event that reflects the rapid expansion of the field. All previous major trials had compared TAVR with surgical aortic valve replacement.
REPRISE III randomized 912 TAVR patients at 55 centers 2:1 to the Lotus valve in its 23-, 25-, or 27-mm configurations or to a CoreValve at 26, 29, or 31 mm. Roughly half of the CoreValve group got the newer repositionable and retrievable Evolut R valve, while the earlier enrollees received the nonrepositionable classic CoreValve.
The Lotus valve group proved noninferior to the CoreValve recipients for the primary safety endpoint, a 30-day composite of all-cause mortality, stroke, major or life-threatening bleeding, major vascular complications, and stage 2 or 3 acute kidney injury. The rates were 20.3% in the Lotus arm and 17.2% with CoreValve.
The 1-year rate of disabling stroke was 3.6% in the Lotus group versus 7.3% in the CoreValve group. Dr. Feldman downplayed the importance of this difference, even though it was statistically significant. The Lotus valve performed as expected, but the disabling stroke rate in the CoreValve group was higher than in earlier studies for reasons unknown, most likely simply the play of chance, he said.
“I think the real message here is that the Lotus valve performed very well,” the cardiologist said. “There have been concerns that repositioning the valve into a better position during the deployment process might create excess stroke. It appears clear that’s not the case.”
The ability to reposition the Lotus device resulted in a significantly lower rate of repeat procedures at 1 year: 0.2% versus 2% with the CoreValve, as well as zero cases of aortic valve malposition and valve-in-valve deployment.
The need for a new pacemaker within 30 days after TAVR was strikingly more common in the Lotus valve group: 36%, compared with 20% with the CoreValve. Dr. Feldman attributed the high new pacemaker rate in the Lotus arm partly to the operators’ limited experience with the novel valve along with the fact that REPRISE III used a first-iteration device deployment mechanism. An improved deployment mechanism designed to minimize problematic contact with the left ventricular outflow tract was developed too late for inclusion in the trial. But in a recent European study using this proprietary deployment system, known as Depth Guard, the new pacemaker rate was below 20%.
The learning curve for the new Lotus valve system is “not at all challenging,” according to the cardiologist. He noted that U.S. operators participating in REPRISE III, who had no prior experience with the device, were allowed only two initial cases in order to gain experience; after that, every patient counted in the clinical trial results.
The REPRISE III results will be offered to the Food and Drug Administration to support regulatory approval of the device in high-surgical-risk patients. Dr. Feldman said Boston Scientific plans to conduct an additional clinical trial of the Lotus valve, this time in intermediate-risk patients, with the goal of gaining an expanded indication. This, too, will be a head-to-head comparison with a commercially available TAVR valve, probably the Edwards Sapien 3 valve.
REPRISE III was sponsored by Boston Scientific. Dr. Feldman reported serving as a consultant to that company, Abbott, and Edwards Lifesciences, and having received institutional research grants from those companies as well.
bjancin@frontlinemedcom.com
PARIS – The investigational mechanically expandable Lotus valve system for transcatheter aortic valve replacement proved significantly more effective than the commercially available CoreValve platform in patients with severe aortic stenosis deemed at high or extreme surgical risk in the randomized pivotal phase III REPRISE III trial, Ted E. Feldman, MD, reported at the annual congress of the European Association of Percutaneous Cardiovascular Interventions.
The 1-year composite primary effectiveness endpoint comprised of all-cause mortality, disabling stroke, and moderate or greater paravalvular leak (PVL) occurred in 17% of patients randomized to the Lotus transcatheter aortic valve replacement (TAVR) device, compared with 29% of those in the CoreValve group, said Dr. Feldman, director of the cardiac catheterization laboratory at NorthShore University HealthSystem in Evanston, Ill.
A key finding was that the Lotus valve group had a 1-year rate of moderate or greater PVL of just 2% as assessed in a central core lab, compared with an 11% rate in patients randomized to the classic CoreValve or the subsequent-generation Evolut R device, he observed.
“With the Lotus valve there was no or only trace PVL in over 85% of patients. This is probably even more important than the low rate of moderate or severe PVL. The valve really does result in virtually no PVL in the vast majority of patients. That’s unique to this platform,” the cardiologist said in an interview.
The unprecedented low rate of moderate or severe PVL at 1 year postprocedure is attributable to the polymer seal delivered via the Lotus system for that express purpose, he explained.
REPRISE III was the first large randomized comparative clinical trial featuring two TAVR valves, an event that reflects the rapid expansion of the field. All previous major trials had compared TAVR with surgical aortic valve replacement.
REPRISE III randomized 912 TAVR patients at 55 centers 2:1 to the Lotus valve in its 23-, 25-, or 27-mm configurations or to a CoreValve at 26, 29, or 31 mm. Roughly half of the CoreValve group got the newer repositionable and retrievable Evolut R valve, while the earlier enrollees received the nonrepositionable classic CoreValve.
The Lotus valve group proved noninferior to the CoreValve recipients for the primary safety endpoint, a 30-day composite of all-cause mortality, stroke, major or life-threatening bleeding, major vascular complications, and stage 2 or 3 acute kidney injury. The rates were 20.3% in the Lotus arm and 17.2% with CoreValve.
The 1-year rate of disabling stroke was 3.6% in the Lotus group versus 7.3% in the CoreValve group. Dr. Feldman downplayed the importance of this difference, even though it was statistically significant. The Lotus valve performed as expected, but the disabling stroke rate in the CoreValve group was higher than in earlier studies for reasons unknown, most likely simply the play of chance, he said.
“I think the real message here is that the Lotus valve performed very well,” the cardiologist said. “There have been concerns that repositioning the valve into a better position during the deployment process might create excess stroke. It appears clear that’s not the case.”
The ability to reposition the Lotus device resulted in a significantly lower rate of repeat procedures at 1 year: 0.2% versus 2% with the CoreValve, as well as zero cases of aortic valve malposition and valve-in-valve deployment.
The need for a new pacemaker within 30 days after TAVR was strikingly more common in the Lotus valve group: 36%, compared with 20% with the CoreValve. Dr. Feldman attributed the high new pacemaker rate in the Lotus arm partly to the operators’ limited experience with the novel valve along with the fact that REPRISE III used a first-iteration device deployment mechanism. An improved deployment mechanism designed to minimize problematic contact with the left ventricular outflow tract was developed too late for inclusion in the trial. But in a recent European study using this proprietary deployment system, known as Depth Guard, the new pacemaker rate was below 20%.
The learning curve for the new Lotus valve system is “not at all challenging,” according to the cardiologist. He noted that U.S. operators participating in REPRISE III, who had no prior experience with the device, were allowed only two initial cases in order to gain experience; after that, every patient counted in the clinical trial results.
The REPRISE III results will be offered to the Food and Drug Administration to support regulatory approval of the device in high-surgical-risk patients. Dr. Feldman said Boston Scientific plans to conduct an additional clinical trial of the Lotus valve, this time in intermediate-risk patients, with the goal of gaining an expanded indication. This, too, will be a head-to-head comparison with a commercially available TAVR valve, probably the Edwards Sapien 3 valve.
REPRISE III was sponsored by Boston Scientific. Dr. Feldman reported serving as a consultant to that company, Abbott, and Edwards Lifesciences, and having received institutional research grants from those companies as well.
bjancin@frontlinemedcom.com
AT EUROPCR
Key clinical point:
Major finding: The rate of the 1-year composite primary effectiveness endpoint comprised of all-cause mortality, disabling stroke, and moderate or greater paravalvular leak was 17% in patients randomized to the investigational Lotus transcatheter aortic valve replacement system, compared with 29% in recipients of the CoreValve.
Data source: REPRISE III, a prospective, multicenter, international clinical trial randomized 912 patients with severe aortic stenosis who were at high surgical risk to TAVR with the investigational Lotus valve or a commercially available CoreValve.
Disclosures: REPRISE III was sponsored by Boston Scientific. The study presenter reported serving as a consultant to that company as well as for Abbott and Edwards Lifesciences. He has also received institutional research grants from those companies.
Consider switch to clopidogrel for DAPT early post ACS
PARIS – A strategy of switching from prasugrel or ticagrelor to clopidogrel 1 month after percutaneous coronary intervention for acute coronary syndrome is superior to the guideline-recommended full 12 months of dual-antiplatelet therapy with either of the newer P2Y12 inhibitors, according to Thomas Cuisset, MD.
In the randomized TOPIC (Timing of Platelet Inhibition After Acute Coronary Syndrome) trial, this switch strategy resulted in a marked reduction in bleeding without an increased risk of ischemic events, compared with a full 12 months of standard dual-antiplatelet therapy (DAPT) using prasugrel (Effient) or ticagrelor (Brilinta).

He added that the cost savings of this switch strategy would be enormous, since generic clopidogrel is vastly less expensive than prasugrel or ticagrelor.
Twelve months of DAPT with aspirin plus either prasugrel or ticagrelor is the guideline-recommended DAPT regimen following PCI for ACS on the strength of the TRITON and PLATO trials, respectively, which showed that those agents were more effective than clopidogrel for the prevention of thrombotic events. But Dr. Cuisset and his coinvestigators noted that the risk of ischemic events was highest in the first month or so following ACS, while the risk of DAPT-related serious bleeding increased after the first month and continued for the duration.
“We need to use the new drugs, and we need to go for 1 year with DAPT. But does that mean we need to go for 1 year with the new drugs?” he asked.
This question was the impetus for TOPIC, an open-label, single-center randomized trial that included 646 ACS patients who were free of major adverse cardiovascular events during their first month on DAPT with prasugrel or ticagrelor. At that point they were randomized to remain on their standard regimen or switch to aspirin at 75 mg/day plus clopidogrel at 75 mg/day for months 2-12. The switch strategy is similar to the way pulmonary embolism is managed: an early phase of high-intensity therapy followed by a backing off to a less intensive regimen, said Dr. Cuisset, a cardiologist at Aix-Marseille University, Provence, France.
The primary endpoint in TOPIC was the cumulative 1-year rate of a composite of all-cause mortality, stroke, urgent revascularization, or clinically significant bleeding as reflected in a Bleeding Academic Research Consortium (BARC) grade 2 or greater bleeding. The primary endpoint occurred in 13.4% of the switch group, a 52% relative risk reduction, compared with the 26.3% cumulative incidence with standard DAPT.
This difference wasn’t due to any between-group disparity in ischemic events, but rather to a 70% reduction in the risk of BARC grade 2 or greater bleeding in the switch group: 4.0% vs. 14.9%.
Some physicians have already been switching to clopidogrel for DAPT after ACS, either because of safety or cost concerns. Now their practice is evidence based, Dr. Cuisset noted.
Asked why TOPIC didn’t use the more stringent bleeding endpoint of BARC grade 3-5 bleeding, the cardiologist replied that it would have required a larger trial to show a significant difference. Besides, he added, BARC grade 2 bleeding is clinically important because it has a negative impact on quality of life and can cause patients to discontinue DAPT, thereby increasing their risk of thrombosis.
The TOPIC protocol didn’t utilize a loading dose of clopidogrel when making the switch. Investigators started clopidogrel the day after stopping prasugrel and at least 12 hours after the final dose of ticagrelor.
Ideally, the novel TOPIC findings should be confirmed in a much larger, randomized, double-blind clinical trial capable of detecting any small differences in stent thrombosis or MI rates before physicians adopt a change in practice, but discussant Chaim Lotan, MD, director of the Heart Institute at Hadassah Medical Center in Jerusalem, dismissed that prospect as unlikely.
“I tried myself to do a similar study and found I got a lot of opposition from the pharma companies as well as from physicians who said, ‘How can you go against the guidelines?’ ” he said.
“I want to congratulate your team because I think this is a groundbreaking study that is going to dictate a changing of the guidelines,” he told Dr. Cuisset.
Dr. Cuisset reported having no financial conflicts regarding this investigator-driven study funded without commercial support.
Simultaneous with his presentation in Paris, the TOPIC findings were published online (Eur Heart J. 2017 May 16. doi: 10.1093/eurheartj/ehx175).
Dr. Cuisset reported no financial conflicts regarding this investigator-driven study funded without commercial support.
bjancin@frontlinemedcom.com
PARIS – A strategy of switching from prasugrel or ticagrelor to clopidogrel 1 month after percutaneous coronary intervention for acute coronary syndrome is superior to the guideline-recommended full 12 months of dual-antiplatelet therapy with either of the newer P2Y12 inhibitors, according to Thomas Cuisset, MD.
In the randomized TOPIC (Timing of Platelet Inhibition After Acute Coronary Syndrome) trial, this switch strategy resulted in a marked reduction in bleeding without an increased risk of ischemic events, compared with a full 12 months of standard dual-antiplatelet therapy (DAPT) using prasugrel (Effient) or ticagrelor (Brilinta).
He added that the cost savings of this switch strategy would be enormous, since generic clopidogrel is vastly less expensive than prasugrel or ticagrelor.
Twelve months of DAPT with aspirin plus either prasugrel or ticagrelor is the guideline-recommended DAPT regimen following PCI for ACS on the strength of the TRITON and PLATO trials, respectively, which showed that those agents were more effective than clopidogrel for the prevention of thrombotic events. But Dr. Cuisset and his coinvestigators noted that the risk of ischemic events was highest in the first month or so following ACS, while the risk of DAPT-related serious bleeding increased after the first month and continued for the duration.
“We need to use the new drugs, and we need to go for 1 year with DAPT. But does that mean we need to go for 1 year with the new drugs?” he asked.
This question was the impetus for TOPIC, an open-label, single-center randomized trial that included 646 ACS patients who were free of major adverse cardiovascular events during their first month on DAPT with prasugrel or ticagrelor. At that point they were randomized to remain on their standard regimen or switch to aspirin at 75 mg/day plus clopidogrel at 75 mg/day for months 2-12. The switch strategy is similar to the way pulmonary embolism is managed: an early phase of high-intensity therapy followed by a backing off to a less intensive regimen, said Dr. Cuisset, a cardiologist at Aix-Marseille University, Provence, France.
The primary endpoint in TOPIC was the cumulative 1-year rate of a composite of all-cause mortality, stroke, urgent revascularization, or clinically significant bleeding as reflected in a Bleeding Academic Research Consortium (BARC) grade 2 or greater bleeding. The primary endpoint occurred in 13.4% of the switch group, a 52% relative risk reduction, compared with the 26.3% cumulative incidence with standard DAPT.
This difference wasn’t due to any between-group disparity in ischemic events, but rather to a 70% reduction in the risk of BARC grade 2 or greater bleeding in the switch group: 4.0% vs. 14.9%.
Some physicians have already been switching to clopidogrel for DAPT after ACS, either because of safety or cost concerns. Now their practice is evidence based, Dr. Cuisset noted.
Asked why TOPIC didn’t use the more stringent bleeding endpoint of BARC grade 3-5 bleeding, the cardiologist replied that it would have required a larger trial to show a significant difference. Besides, he added, BARC grade 2 bleeding is clinically important because it has a negative impact on quality of life and can cause patients to discontinue DAPT, thereby increasing their risk of thrombosis.
The TOPIC protocol didn’t utilize a loading dose of clopidogrel when making the switch. Investigators started clopidogrel the day after stopping prasugrel and at least 12 hours after the final dose of ticagrelor.
Ideally, the novel TOPIC findings should be confirmed in a much larger, randomized, double-blind clinical trial capable of detecting any small differences in stent thrombosis or MI rates before physicians adopt a change in practice, but discussant Chaim Lotan, MD, director of the Heart Institute at Hadassah Medical Center in Jerusalem, dismissed that prospect as unlikely.
“I tried myself to do a similar study and found I got a lot of opposition from the pharma companies as well as from physicians who said, ‘How can you go against the guidelines?’ ” he said.
“I want to congratulate your team because I think this is a groundbreaking study that is going to dictate a changing of the guidelines,” he told Dr. Cuisset.
Dr. Cuisset reported having no financial conflicts regarding this investigator-driven study funded without commercial support.
Simultaneous with his presentation in Paris, the TOPIC findings were published online (Eur Heart J. 2017 May 16. doi: 10.1093/eurheartj/ehx175).
Dr. Cuisset reported no financial conflicts regarding this investigator-driven study funded without commercial support.
bjancin@frontlinemedcom.com
PARIS – A strategy of switching from prasugrel or ticagrelor to clopidogrel 1 month after percutaneous coronary intervention for acute coronary syndrome is superior to the guideline-recommended full 12 months of dual-antiplatelet therapy with either of the newer P2Y12 inhibitors, according to Thomas Cuisset, MD.
In the randomized TOPIC (Timing of Platelet Inhibition After Acute Coronary Syndrome) trial, this switch strategy resulted in a marked reduction in bleeding without an increased risk of ischemic events, compared with a full 12 months of standard dual-antiplatelet therapy (DAPT) using prasugrel (Effient) or ticagrelor (Brilinta).
He added that the cost savings of this switch strategy would be enormous, since generic clopidogrel is vastly less expensive than prasugrel or ticagrelor.
Twelve months of DAPT with aspirin plus either prasugrel or ticagrelor is the guideline-recommended DAPT regimen following PCI for ACS on the strength of the TRITON and PLATO trials, respectively, which showed that those agents were more effective than clopidogrel for the prevention of thrombotic events. But Dr. Cuisset and his coinvestigators noted that the risk of ischemic events was highest in the first month or so following ACS, while the risk of DAPT-related serious bleeding increased after the first month and continued for the duration.
“We need to use the new drugs, and we need to go for 1 year with DAPT. But does that mean we need to go for 1 year with the new drugs?” he asked.
This question was the impetus for TOPIC, an open-label, single-center randomized trial that included 646 ACS patients who were free of major adverse cardiovascular events during their first month on DAPT with prasugrel or ticagrelor. At that point they were randomized to remain on their standard regimen or switch to aspirin at 75 mg/day plus clopidogrel at 75 mg/day for months 2-12. The switch strategy is similar to the way pulmonary embolism is managed: an early phase of high-intensity therapy followed by a backing off to a less intensive regimen, said Dr. Cuisset, a cardiologist at Aix-Marseille University, Provence, France.
The primary endpoint in TOPIC was the cumulative 1-year rate of a composite of all-cause mortality, stroke, urgent revascularization, or clinically significant bleeding as reflected in a Bleeding Academic Research Consortium (BARC) grade 2 or greater bleeding. The primary endpoint occurred in 13.4% of the switch group, a 52% relative risk reduction, compared with the 26.3% cumulative incidence with standard DAPT.
This difference wasn’t due to any between-group disparity in ischemic events, but rather to a 70% reduction in the risk of BARC grade 2 or greater bleeding in the switch group: 4.0% vs. 14.9%.
Some physicians have already been switching to clopidogrel for DAPT after ACS, either because of safety or cost concerns. Now their practice is evidence based, Dr. Cuisset noted.
Asked why TOPIC didn’t use the more stringent bleeding endpoint of BARC grade 3-5 bleeding, the cardiologist replied that it would have required a larger trial to show a significant difference. Besides, he added, BARC grade 2 bleeding is clinically important because it has a negative impact on quality of life and can cause patients to discontinue DAPT, thereby increasing their risk of thrombosis.
The TOPIC protocol didn’t utilize a loading dose of clopidogrel when making the switch. Investigators started clopidogrel the day after stopping prasugrel and at least 12 hours after the final dose of ticagrelor.
Ideally, the novel TOPIC findings should be confirmed in a much larger, randomized, double-blind clinical trial capable of detecting any small differences in stent thrombosis or MI rates before physicians adopt a change in practice, but discussant Chaim Lotan, MD, director of the Heart Institute at Hadassah Medical Center in Jerusalem, dismissed that prospect as unlikely.
“I tried myself to do a similar study and found I got a lot of opposition from the pharma companies as well as from physicians who said, ‘How can you go against the guidelines?’ ” he said.
“I want to congratulate your team because I think this is a groundbreaking study that is going to dictate a changing of the guidelines,” he told Dr. Cuisset.
Dr. Cuisset reported having no financial conflicts regarding this investigator-driven study funded without commercial support.
Simultaneous with his presentation in Paris, the TOPIC findings were published online (Eur Heart J. 2017 May 16. doi: 10.1093/eurheartj/ehx175).
Dr. Cuisset reported no financial conflicts regarding this investigator-driven study funded without commercial support.
bjancin@frontlinemedcom.com
AT EuroPCR
Key clinical point:
Major finding: The cumulative 1-year incidence of all-cause mortality, stroke, urgent revascularization, or clinically significant bleeding was 13.4% in acute coronary syndrome patients who switched to clopidogrel after 1 month on prasugrel or ticagrelor for dual-antiplatelet therapy, compared with 26.3% in those who didn’t switch.
Data source: An open-label, single-center, randomized trial including 646 ACS patients.
Disclosures: The presenter reported no financial conflicts regarding this investigator-driven study funded without commercial support.
Chemoprevention: Thinking outside the box
WAILEA, HAWAII – Nicotinamide is one of the rare proposed agents for skin cancer chemoprevention distinguished by dirt cheap cost combined with a highly reassuring safety profile plus evidence of efficacy – which, together, make it a reasonable option in high risk patients, according to Daniel M. Siegel, MD.
Other agents that fit into that category include the tropical rainforest fern Polypodium leucotomos and milk thistle, added Dr. Siegel, a dermatologist at the State University of New York, Brooklyn.
“That’s a really interesting one. I don’t know if, 5 years from now, we’ll all be taking low-dose rapamycin as an antiaging drug, but we might, especially if someone figures out the ideal dose,” he said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Research Foundation.
Nicotinamide
In the case of nicotinamide, the efficacy is actually supported by published level 1 evidence in the form of a highly positive 1-year, double-blind, randomized, placebo-controlled phase III clinical trial.
“You can Google ‘nicotinamide’ and find it at places like Costco and Trader Joe’s for less than 6 cents per day. That makes for a really good risk/benefit ratio. A nickel a day: That’s a cheap one. That’s one where I’d say, ‘Why not?’ It seems to be safe,” Dr. Siegel said.
In the phase III ONTRAC trial, Australian investigators randomized 386 patients who averaged roughly eight nonmelanoma skin cancers in the past 5 years to either 500 mg of oral nicotinamide twice daily or matched placebo for 12 months. During the study period, the nicotinamide group had a statistically significant and clinically meaningful 23% reduction in new nonmelanoma skin cancers, compared with the control group. They also had 13% fewer actinic keratoses at 12 months than controls. And the side effect profile mirrored that of placebo (N Engl J Med. 2015 Oct 22;373[17]:1618-26).
“Nicotinamide is vitamin B3. It’s not niacin. It doesn’t cause flushing and other vasodilatory effects. It’s actually pretty innocuous,” Dr. Siegel said.
In laboratory studies, nicotinamide has been shown to enhance DNA repair following UV exposure, as well as curb UV-induced immunosuppression.
Polypodium leucotomos Samambaia
This plant, commonly known as calaguala in the Spanish-speaking tropics and samambaia in Brazil, has a centuries-long tradition of safe medicinal use. It is commercially available over-the-counter (OTC) as a standardized product called Heliocare, designed to avoid the guesswork involved in topical sunscreen application. Each capsule contains 240 mg of an extract of P. leucotomos. Dr. Siegel said he takes it daily when he’s in a sunny locale, such as Hawaii.
Milk thistle
This plant, known as Silybum marianum, has silymarin as its bioactive compound. Dermatologist Haines Ely, MD, of the University of California, Davis, has reported therapeutic success using it in porphyria cutanea tarda and other conditions. It has been shown to inhibit photocarcinogenesis in animal studies.
Dr. Siegel said that, while Dr. Ely has told him his preferred preparation is a German OTC product, milk thistle seeds can be found in health food stores, ground to a powder using a coffee bean grinder, and used as a food supplement. Like Polypodium leucotomos and nicotinamide, milk thistle is nontoxic.
Rapamycin
This macrolide compound is produced by the bacterium Streptomyces hygroscopicus. Rapamycin is an immunosuppressant used to coat coronary stents and prevent rejection of transplanted organs. It is an mechanistic target of rapamycin signaling pathway inhibitor being studied as a cancer prevention and antiaging agent.
Science magazine called the discovery that rapamycin increased the lifespan of mice one of the top scientific breakthroughs of 2009. Subsequent animal studies have established that the extended lifespan wasn’t solely the result of rapamycin’s antineoplastic effects but of across-the-board delayed onset of all the major age-related diseases. Thus, rapamycin could turn out to be a true antiaging agent, in Dr. Siegel’s view.
Studies in humans are underway. Researchers at Novartis have reported that a rapamycin-related compound curbed the typical decline in immune function that accompanies aging as reflected in a 20% enhancement in the response to influenza vaccine in elderly volunteers (Sci Transl Med. 2014 Dec 24;6[268]:268ra179).
Dr. Siegel reported serving as a consultant to Ferndale, which markets Heliocare. The SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – Nicotinamide is one of the rare proposed agents for skin cancer chemoprevention distinguished by dirt cheap cost combined with a highly reassuring safety profile plus evidence of efficacy – which, together, make it a reasonable option in high risk patients, according to Daniel M. Siegel, MD.
Other agents that fit into that category include the tropical rainforest fern Polypodium leucotomos and milk thistle, added Dr. Siegel, a dermatologist at the State University of New York, Brooklyn.
“That’s a really interesting one. I don’t know if, 5 years from now, we’ll all be taking low-dose rapamycin as an antiaging drug, but we might, especially if someone figures out the ideal dose,” he said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Research Foundation.
Nicotinamide
In the case of nicotinamide, the efficacy is actually supported by published level 1 evidence in the form of a highly positive 1-year, double-blind, randomized, placebo-controlled phase III clinical trial.
“You can Google ‘nicotinamide’ and find it at places like Costco and Trader Joe’s for less than 6 cents per day. That makes for a really good risk/benefit ratio. A nickel a day: That’s a cheap one. That’s one where I’d say, ‘Why not?’ It seems to be safe,” Dr. Siegel said.
In the phase III ONTRAC trial, Australian investigators randomized 386 patients who averaged roughly eight nonmelanoma skin cancers in the past 5 years to either 500 mg of oral nicotinamide twice daily or matched placebo for 12 months. During the study period, the nicotinamide group had a statistically significant and clinically meaningful 23% reduction in new nonmelanoma skin cancers, compared with the control group. They also had 13% fewer actinic keratoses at 12 months than controls. And the side effect profile mirrored that of placebo (N Engl J Med. 2015 Oct 22;373[17]:1618-26).
“Nicotinamide is vitamin B3. It’s not niacin. It doesn’t cause flushing and other vasodilatory effects. It’s actually pretty innocuous,” Dr. Siegel said.
In laboratory studies, nicotinamide has been shown to enhance DNA repair following UV exposure, as well as curb UV-induced immunosuppression.
Polypodium leucotomos Samambaia
This plant, commonly known as calaguala in the Spanish-speaking tropics and samambaia in Brazil, has a centuries-long tradition of safe medicinal use. It is commercially available over-the-counter (OTC) as a standardized product called Heliocare, designed to avoid the guesswork involved in topical sunscreen application. Each capsule contains 240 mg of an extract of P. leucotomos. Dr. Siegel said he takes it daily when he’s in a sunny locale, such as Hawaii.
Milk thistle
This plant, known as Silybum marianum, has silymarin as its bioactive compound. Dermatologist Haines Ely, MD, of the University of California, Davis, has reported therapeutic success using it in porphyria cutanea tarda and other conditions. It has been shown to inhibit photocarcinogenesis in animal studies.
Dr. Siegel said that, while Dr. Ely has told him his preferred preparation is a German OTC product, milk thistle seeds can be found in health food stores, ground to a powder using a coffee bean grinder, and used as a food supplement. Like Polypodium leucotomos and nicotinamide, milk thistle is nontoxic.
Rapamycin
This macrolide compound is produced by the bacterium Streptomyces hygroscopicus. Rapamycin is an immunosuppressant used to coat coronary stents and prevent rejection of transplanted organs. It is an mechanistic target of rapamycin signaling pathway inhibitor being studied as a cancer prevention and antiaging agent.
Science magazine called the discovery that rapamycin increased the lifespan of mice one of the top scientific breakthroughs of 2009. Subsequent animal studies have established that the extended lifespan wasn’t solely the result of rapamycin’s antineoplastic effects but of across-the-board delayed onset of all the major age-related diseases. Thus, rapamycin could turn out to be a true antiaging agent, in Dr. Siegel’s view.
Studies in humans are underway. Researchers at Novartis have reported that a rapamycin-related compound curbed the typical decline in immune function that accompanies aging as reflected in a 20% enhancement in the response to influenza vaccine in elderly volunteers (Sci Transl Med. 2014 Dec 24;6[268]:268ra179).
Dr. Siegel reported serving as a consultant to Ferndale, which markets Heliocare. The SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – Nicotinamide is one of the rare proposed agents for skin cancer chemoprevention distinguished by dirt cheap cost combined with a highly reassuring safety profile plus evidence of efficacy – which, together, make it a reasonable option in high risk patients, according to Daniel M. Siegel, MD.
Other agents that fit into that category include the tropical rainforest fern Polypodium leucotomos and milk thistle, added Dr. Siegel, a dermatologist at the State University of New York, Brooklyn.
“That’s a really interesting one. I don’t know if, 5 years from now, we’ll all be taking low-dose rapamycin as an antiaging drug, but we might, especially if someone figures out the ideal dose,” he said at the Hawaii Dermatology Seminar provided by Global Academy for Medical Education/Skin Disease Research Foundation.
Nicotinamide
In the case of nicotinamide, the efficacy is actually supported by published level 1 evidence in the form of a highly positive 1-year, double-blind, randomized, placebo-controlled phase III clinical trial.
“You can Google ‘nicotinamide’ and find it at places like Costco and Trader Joe’s for less than 6 cents per day. That makes for a really good risk/benefit ratio. A nickel a day: That’s a cheap one. That’s one where I’d say, ‘Why not?’ It seems to be safe,” Dr. Siegel said.
In the phase III ONTRAC trial, Australian investigators randomized 386 patients who averaged roughly eight nonmelanoma skin cancers in the past 5 years to either 500 mg of oral nicotinamide twice daily or matched placebo for 12 months. During the study period, the nicotinamide group had a statistically significant and clinically meaningful 23% reduction in new nonmelanoma skin cancers, compared with the control group. They also had 13% fewer actinic keratoses at 12 months than controls. And the side effect profile mirrored that of placebo (N Engl J Med. 2015 Oct 22;373[17]:1618-26).
“Nicotinamide is vitamin B3. It’s not niacin. It doesn’t cause flushing and other vasodilatory effects. It’s actually pretty innocuous,” Dr. Siegel said.
In laboratory studies, nicotinamide has been shown to enhance DNA repair following UV exposure, as well as curb UV-induced immunosuppression.
Polypodium leucotomos Samambaia
This plant, commonly known as calaguala in the Spanish-speaking tropics and samambaia in Brazil, has a centuries-long tradition of safe medicinal use. It is commercially available over-the-counter (OTC) as a standardized product called Heliocare, designed to avoid the guesswork involved in topical sunscreen application. Each capsule contains 240 mg of an extract of P. leucotomos. Dr. Siegel said he takes it daily when he’s in a sunny locale, such as Hawaii.
Milk thistle
This plant, known as Silybum marianum, has silymarin as its bioactive compound. Dermatologist Haines Ely, MD, of the University of California, Davis, has reported therapeutic success using it in porphyria cutanea tarda and other conditions. It has been shown to inhibit photocarcinogenesis in animal studies.
Dr. Siegel said that, while Dr. Ely has told him his preferred preparation is a German OTC product, milk thistle seeds can be found in health food stores, ground to a powder using a coffee bean grinder, and used as a food supplement. Like Polypodium leucotomos and nicotinamide, milk thistle is nontoxic.
Rapamycin
This macrolide compound is produced by the bacterium Streptomyces hygroscopicus. Rapamycin is an immunosuppressant used to coat coronary stents and prevent rejection of transplanted organs. It is an mechanistic target of rapamycin signaling pathway inhibitor being studied as a cancer prevention and antiaging agent.
Science magazine called the discovery that rapamycin increased the lifespan of mice one of the top scientific breakthroughs of 2009. Subsequent animal studies have established that the extended lifespan wasn’t solely the result of rapamycin’s antineoplastic effects but of across-the-board delayed onset of all the major age-related diseases. Thus, rapamycin could turn out to be a true antiaging agent, in Dr. Siegel’s view.
Studies in humans are underway. Researchers at Novartis have reported that a rapamycin-related compound curbed the typical decline in immune function that accompanies aging as reflected in a 20% enhancement in the response to influenza vaccine in elderly volunteers (Sci Transl Med. 2014 Dec 24;6[268]:268ra179).
Dr. Siegel reported serving as a consultant to Ferndale, which markets Heliocare. The SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
Illness-induced PTSD is common, understudied
SAN FRANCISCO – Posttraumatic stress disorder symptoms triggered by a life-threatening medical illness differ from the more common PTSD, the source of which is an external trauma such as an assault or natural disaster, according to Renee El-Gabalawy, PhD.
“This suggests implications for diagnostic classification. Maybe, in future editions of the DSM, we should think of this as a subtype of PTSD or potentially as a new diagnostic category, although it’s far too early to make any conclusions about that,” Dr. El-Gabalawy said at the annual conference of the Anxiety and Depression Association of America.

It’s estimated that PTSD occurs in 12%-25% of people who experience a life-threatening medical event.
“This is a fairly staggering proportion of people, and unfortunately this is a very overlooked area in the PTSD literature, almost all of which has been done in critical care units or oncology settings,” said Dr. El-Gabalawy, a psychologist at the University of Manitoba in Winnipeg.
She presented an analysis of data from the 2012-2013 National Epidemiologic Survey on Alcohol and Related Conditions, in which a nationally representative sample composed of 36,309 U.S. adults were interviewed face to face, with the current DSM-5 diagnostic criteria for PTSD being applied using the Alcohol Use Disorder and Association Disabilities Interview Schedule–5 (AUDADIS-5).
A total of 1,779 subjects (4.9%) indicated they had experienced physician-diagnosed PTSD during the previous year. Of those, 6.5% said their PTSD was triggered by an acute life-threatening medical event. The rest were attributed to nonmedical trauma.
There were sharp demographic differences between the two groups. Individuals with medical illness–induced PTSD were older – 35 years old at onset of their first episode, compared with age 23 in the others – with later onset of their PTSD. They were more likely to be men: 45.7% were male, compared with 31.8% for subjects with nonmedical PTSD. Comorbid depression was present in 25.4% of those with medical illness–induced PTSD, and comorbid panic disorder was present in 17%, significantly lower than the 37% and 24.5% rates in individuals with other triggers of PTSD.
Quality of life as measured by the Short Form-12 was similar in the two groups, after the investigators controlled for the number of medical conditions patients had.
Of people with medical illness–induced PTSD, 41% attributed their PTSD to a digestive disease, most often inflammatory bowel disease. In contrast, a digestive condition was present in 19.2% of subjects with nonmedical trauma as the source of their PTSD. Thus, a serious digestive disorder was associated with a 2.4-times increased risk of medical illness–induced PTSD in an analysis adjusted for socioeconomic factors and number of health conditions. Cancer, which was the trigger for 16.1% of cases of medical illness–induced PTSD and which had a prevalence of 5.8% in those with nonmedical sources of PTSD, was associated with a 2.64-times increased risk of medical illness–related PTSD.
“Those odds ratios are quite high for a population-based sample. This was a very dramatic effect,” Dr. El-Gabalawy commented.
The two groups of participants with PTSD had similar intensity of core PTSD symptom clusters with the exception of negative mood/cognition, which figured more prominently in those with medical illness–induced PTSD.
“This is very much in line with my clinical experience, that what’s really predominant in these folks are the maladaptive cognitions, their fear about their future health trajectory,” she said. “I tend to use cognitive processing therapy in these patients. It really taps into those maladaptive cognitions, and I’ve found that my patients are very receptive to this. Cognitive processing therapy might be more advantageous in this situation than prolonged exposure therapy .”
Dr. El-Gabalawy said she is a fan of the Enduring Somatic Threat model of medical illness–induced PTSD developed by Donald Edmondson, PhD, of Columbia University in New York (Soc Personal Psychol Compass. 2014 Mar 5;8[3]:118-34).
“It aligns with the literature and my own clinical experience,” she explained.
Dr. Edmondson’s model draws conceptual distinctions between medical illness–induced PTSD and other causes of PTSD. In medical illness–related PTSD, the trauma has a somatic source, the trauma tends to be chronic, and intrusive thoughts tend to be future oriented and highly cognitive in nature.
“It’s not uncommon that I’ll hear my patients with medical illness–induced PTSD say, ‘I’m really scared my disease is going to get worse.’ And behavioral avoidance is really difficult. Whereas, in the traditional conceptualization of PTSD, the intrusions are often past oriented and elicited by external triggers. Behavioral avoidance of those triggers is possible, but, in illness-related PTSD, arousal is keyed to internal triggers, often somatic in nature, such as heart palpitations,” according to the psychologist.
Her study was supported by the Canadian National Institutes of Health Research and the University of Manitoba. She reported having no financial conflicts.
SAN FRANCISCO – Posttraumatic stress disorder symptoms triggered by a life-threatening medical illness differ from the more common PTSD, the source of which is an external trauma such as an assault or natural disaster, according to Renee El-Gabalawy, PhD.
“This suggests implications for diagnostic classification. Maybe, in future editions of the DSM, we should think of this as a subtype of PTSD or potentially as a new diagnostic category, although it’s far too early to make any conclusions about that,” Dr. El-Gabalawy said at the annual conference of the Anxiety and Depression Association of America.
It’s estimated that PTSD occurs in 12%-25% of people who experience a life-threatening medical event.
“This is a fairly staggering proportion of people, and unfortunately this is a very overlooked area in the PTSD literature, almost all of which has been done in critical care units or oncology settings,” said Dr. El-Gabalawy, a psychologist at the University of Manitoba in Winnipeg.
She presented an analysis of data from the 2012-2013 National Epidemiologic Survey on Alcohol and Related Conditions, in which a nationally representative sample composed of 36,309 U.S. adults were interviewed face to face, with the current DSM-5 diagnostic criteria for PTSD being applied using the Alcohol Use Disorder and Association Disabilities Interview Schedule–5 (AUDADIS-5).
A total of 1,779 subjects (4.9%) indicated they had experienced physician-diagnosed PTSD during the previous year. Of those, 6.5% said their PTSD was triggered by an acute life-threatening medical event. The rest were attributed to nonmedical trauma.
There were sharp demographic differences between the two groups. Individuals with medical illness–induced PTSD were older – 35 years old at onset of their first episode, compared with age 23 in the others – with later onset of their PTSD. They were more likely to be men: 45.7% were male, compared with 31.8% for subjects with nonmedical PTSD. Comorbid depression was present in 25.4% of those with medical illness–induced PTSD, and comorbid panic disorder was present in 17%, significantly lower than the 37% and 24.5% rates in individuals with other triggers of PTSD.
Quality of life as measured by the Short Form-12 was similar in the two groups, after the investigators controlled for the number of medical conditions patients had.
Of people with medical illness–induced PTSD, 41% attributed their PTSD to a digestive disease, most often inflammatory bowel disease. In contrast, a digestive condition was present in 19.2% of subjects with nonmedical trauma as the source of their PTSD. Thus, a serious digestive disorder was associated with a 2.4-times increased risk of medical illness–induced PTSD in an analysis adjusted for socioeconomic factors and number of health conditions. Cancer, which was the trigger for 16.1% of cases of medical illness–induced PTSD and which had a prevalence of 5.8% in those with nonmedical sources of PTSD, was associated with a 2.64-times increased risk of medical illness–related PTSD.
“Those odds ratios are quite high for a population-based sample. This was a very dramatic effect,” Dr. El-Gabalawy commented.
The two groups of participants with PTSD had similar intensity of core PTSD symptom clusters with the exception of negative mood/cognition, which figured more prominently in those with medical illness–induced PTSD.
“This is very much in line with my clinical experience, that what’s really predominant in these folks are the maladaptive cognitions, their fear about their future health trajectory,” she said. “I tend to use cognitive processing therapy in these patients. It really taps into those maladaptive cognitions, and I’ve found that my patients are very receptive to this. Cognitive processing therapy might be more advantageous in this situation than prolonged exposure therapy .”
Dr. El-Gabalawy said she is a fan of the Enduring Somatic Threat model of medical illness–induced PTSD developed by Donald Edmondson, PhD, of Columbia University in New York (Soc Personal Psychol Compass. 2014 Mar 5;8[3]:118-34).
“It aligns with the literature and my own clinical experience,” she explained.
Dr. Edmondson’s model draws conceptual distinctions between medical illness–induced PTSD and other causes of PTSD. In medical illness–related PTSD, the trauma has a somatic source, the trauma tends to be chronic, and intrusive thoughts tend to be future oriented and highly cognitive in nature.
“It’s not uncommon that I’ll hear my patients with medical illness–induced PTSD say, ‘I’m really scared my disease is going to get worse.’ And behavioral avoidance is really difficult. Whereas, in the traditional conceptualization of PTSD, the intrusions are often past oriented and elicited by external triggers. Behavioral avoidance of those triggers is possible, but, in illness-related PTSD, arousal is keyed to internal triggers, often somatic in nature, such as heart palpitations,” according to the psychologist.
Her study was supported by the Canadian National Institutes of Health Research and the University of Manitoba. She reported having no financial conflicts.
SAN FRANCISCO – Posttraumatic stress disorder symptoms triggered by a life-threatening medical illness differ from the more common PTSD, the source of which is an external trauma such as an assault or natural disaster, according to Renee El-Gabalawy, PhD.
“This suggests implications for diagnostic classification. Maybe, in future editions of the DSM, we should think of this as a subtype of PTSD or potentially as a new diagnostic category, although it’s far too early to make any conclusions about that,” Dr. El-Gabalawy said at the annual conference of the Anxiety and Depression Association of America.
It’s estimated that PTSD occurs in 12%-25% of people who experience a life-threatening medical event.
“This is a fairly staggering proportion of people, and unfortunately this is a very overlooked area in the PTSD literature, almost all of which has been done in critical care units or oncology settings,” said Dr. El-Gabalawy, a psychologist at the University of Manitoba in Winnipeg.
She presented an analysis of data from the 2012-2013 National Epidemiologic Survey on Alcohol and Related Conditions, in which a nationally representative sample composed of 36,309 U.S. adults were interviewed face to face, with the current DSM-5 diagnostic criteria for PTSD being applied using the Alcohol Use Disorder and Association Disabilities Interview Schedule–5 (AUDADIS-5).
A total of 1,779 subjects (4.9%) indicated they had experienced physician-diagnosed PTSD during the previous year. Of those, 6.5% said their PTSD was triggered by an acute life-threatening medical event. The rest were attributed to nonmedical trauma.
There were sharp demographic differences between the two groups. Individuals with medical illness–induced PTSD were older – 35 years old at onset of their first episode, compared with age 23 in the others – with later onset of their PTSD. They were more likely to be men: 45.7% were male, compared with 31.8% for subjects with nonmedical PTSD. Comorbid depression was present in 25.4% of those with medical illness–induced PTSD, and comorbid panic disorder was present in 17%, significantly lower than the 37% and 24.5% rates in individuals with other triggers of PTSD.
Quality of life as measured by the Short Form-12 was similar in the two groups, after the investigators controlled for the number of medical conditions patients had.
Of people with medical illness–induced PTSD, 41% attributed their PTSD to a digestive disease, most often inflammatory bowel disease. In contrast, a digestive condition was present in 19.2% of subjects with nonmedical trauma as the source of their PTSD. Thus, a serious digestive disorder was associated with a 2.4-times increased risk of medical illness–induced PTSD in an analysis adjusted for socioeconomic factors and number of health conditions. Cancer, which was the trigger for 16.1% of cases of medical illness–induced PTSD and which had a prevalence of 5.8% in those with nonmedical sources of PTSD, was associated with a 2.64-times increased risk of medical illness–related PTSD.
“Those odds ratios are quite high for a population-based sample. This was a very dramatic effect,” Dr. El-Gabalawy commented.
The two groups of participants with PTSD had similar intensity of core PTSD symptom clusters with the exception of negative mood/cognition, which figured more prominently in those with medical illness–induced PTSD.
“This is very much in line with my clinical experience, that what’s really predominant in these folks are the maladaptive cognitions, their fear about their future health trajectory,” she said. “I tend to use cognitive processing therapy in these patients. It really taps into those maladaptive cognitions, and I’ve found that my patients are very receptive to this. Cognitive processing therapy might be more advantageous in this situation than prolonged exposure therapy .”
Dr. El-Gabalawy said she is a fan of the Enduring Somatic Threat model of medical illness–induced PTSD developed by Donald Edmondson, PhD, of Columbia University in New York (Soc Personal Psychol Compass. 2014 Mar 5;8[3]:118-34).
“It aligns with the literature and my own clinical experience,” she explained.
Dr. Edmondson’s model draws conceptual distinctions between medical illness–induced PTSD and other causes of PTSD. In medical illness–related PTSD, the trauma has a somatic source, the trauma tends to be chronic, and intrusive thoughts tend to be future oriented and highly cognitive in nature.
“It’s not uncommon that I’ll hear my patients with medical illness–induced PTSD say, ‘I’m really scared my disease is going to get worse.’ And behavioral avoidance is really difficult. Whereas, in the traditional conceptualization of PTSD, the intrusions are often past oriented and elicited by external triggers. Behavioral avoidance of those triggers is possible, but, in illness-related PTSD, arousal is keyed to internal triggers, often somatic in nature, such as heart palpitations,” according to the psychologist.
Her study was supported by the Canadian National Institutes of Health Research and the University of Manitoba. She reported having no financial conflicts.
AT ANXIETY AND DEPRESSION CONFERENCE 2017
Key clinical point:
Major finding: Individuals with PTSD and a serious digestive disease were 2.4-times more likely to have medical illness–induced PTSD than PTSD triggered by a nonmedical cause.
Data source: A cross-sectional study of a nationally representative sample of more than 36,000 U.S. adults, 4.9% of whom met DSM 5 criteria for PTSD.
Disclosures: The presenter reported no financial conflicts regarding her study, which was supported by the Canadian National Institutes of Health Research and the University of Manitoba.
Knee injuries in youth sports bring double whammy
LAS VEGAS – Young people who sustain an intra-articular knee injury while participating in youth sports are not only at increased risk for early posttraumatic osteoarthritis 3-10 years later as young adults, but they also are more prone to develop obesity and other modifiable risk factors for osteoarthritis, according to Jackie Whittaker, PhD.
“It appears that some of these young active individuals, after sustaining an injury which is itself a risk factor for osteoarthritis, are going down a pathway where they’re developing a second risk factor for the disease. This may accelerate the rate at which they get the disease and may very well also accelerate the rate at which the disease progresses after its onset,” Dr. Whittaker of the University of Alberta, Edmonton, said at the World Congress on Osteoarthritis.

It’s well established from other studies that roughly 50% of youth who have a significant knee joint injury for which they seek medical attention go on to develop knee osteoarthritis within 10-15 years. The Alberta study focuses on the years between injury and OA onset in an effort to identify modifiable risk factors and develop interventions to delay or halt progression to the disease. There is a paucity of research regarding this crucial time period, Dr. Whittaker explained at the congress sponsored by the Osteoarthritis Research Society International.
“In Canada, we know that injury during sport and recreation is the No. 1 reason that youth between the ages of 11 and 18 seek medical attention, with an alarming one in three doing so. Knee injuries are among the most common of those injuries,” she said.
At follow-up, 29% of the group with a history of knee injury and 4% of controls already had OA as defined by MRI. The likelihood of MRI evidence of OA was 13.5-fold greater in patients who underwent knee surgery for their injury, compared with controls.
“We saw the highest risk, as expected, in patients with ACL [anterior cruciate ligament] and/or meniscal tears, but we also saw a twofold increased risk of OA in those with seemingly less severe injuries, like grade 1-3 medial and collateral ligament injuries,” said Dr. Whittaker.
“I don’t think we were really shocked that knee injury can lead to structural changes that can be associated with future symptomatic OA, but we were surprised to be seeing that as early as 3-10 years post injury. And we were also seeing greater adiposity, a higher rate of being overweight or obese, reduced physical activity, weaker knee muscular strength, and poorer performance on balance and physical function tests,” she continued.
Indeed, at follow-up the subjects with a history of a youth sports knee injury were 4.4-fold more likely to be in the top quartile of fat mass index, compared with uninjured controls, 5.7-fold more likely to be in the highest quartile for abdominal fat, 2.1 times more likely to be in the lowest quartile for total weekly physical activity, and 2.4-fold more likely to be overweight or obese by body mass index (BMI). They were significantly less aerobically fit as reflected in their performance on the 20-meter shuttle run. And they scored significantly worse on the validated Knee Injury and Osteoarthritis Outcome Score (KOOS), particularly on the knee-related quality of life, pain, and symptom subscales.
“The study is ongoing, but it has already contributed to identification of who we’re probably going to need to target for secondary prevention strategies: obviously, individuals who have torn their ACL and/or their meniscus, as was already well known, but perhaps also individuals that have had less severe injuries, those who have a high BMI or some other indicator of adiposity, and those at risk of becoming physically inactive,” Dr. Whittaker said.
She added that a key take-away message from the study, for which she is coprincipal investigator, is that reduced physical activity on the part of someone with a history of a youth sports knee injury is a big red flag. These patients need to address their modifiable risk factors for OA via physical therapy and rehabilitation, along with receiving education reinforcing the importance of lifelong musculoskeletal health.
“Reduced physical activity is a warning sign. Don’t wait for knee pain,” she emphasized.
The Alberta Youth Prevention in Early OA study is funded by the Canadian Institutes of Health Research and nonprofit organizations. Dr. Whittaker reported having no financial conflicts.
LAS VEGAS – Young people who sustain an intra-articular knee injury while participating in youth sports are not only at increased risk for early posttraumatic osteoarthritis 3-10 years later as young adults, but they also are more prone to develop obesity and other modifiable risk factors for osteoarthritis, according to Jackie Whittaker, PhD.
“It appears that some of these young active individuals, after sustaining an injury which is itself a risk factor for osteoarthritis, are going down a pathway where they’re developing a second risk factor for the disease. This may accelerate the rate at which they get the disease and may very well also accelerate the rate at which the disease progresses after its onset,” Dr. Whittaker of the University of Alberta, Edmonton, said at the World Congress on Osteoarthritis.
It’s well established from other studies that roughly 50% of youth who have a significant knee joint injury for which they seek medical attention go on to develop knee osteoarthritis within 10-15 years. The Alberta study focuses on the years between injury and OA onset in an effort to identify modifiable risk factors and develop interventions to delay or halt progression to the disease. There is a paucity of research regarding this crucial time period, Dr. Whittaker explained at the congress sponsored by the Osteoarthritis Research Society International.
“In Canada, we know that injury during sport and recreation is the No. 1 reason that youth between the ages of 11 and 18 seek medical attention, with an alarming one in three doing so. Knee injuries are among the most common of those injuries,” she said.
At follow-up, 29% of the group with a history of knee injury and 4% of controls already had OA as defined by MRI. The likelihood of MRI evidence of OA was 13.5-fold greater in patients who underwent knee surgery for their injury, compared with controls.
“We saw the highest risk, as expected, in patients with ACL [anterior cruciate ligament] and/or meniscal tears, but we also saw a twofold increased risk of OA in those with seemingly less severe injuries, like grade 1-3 medial and collateral ligament injuries,” said Dr. Whittaker.
“I don’t think we were really shocked that knee injury can lead to structural changes that can be associated with future symptomatic OA, but we were surprised to be seeing that as early as 3-10 years post injury. And we were also seeing greater adiposity, a higher rate of being overweight or obese, reduced physical activity, weaker knee muscular strength, and poorer performance on balance and physical function tests,” she continued.
Indeed, at follow-up the subjects with a history of a youth sports knee injury were 4.4-fold more likely to be in the top quartile of fat mass index, compared with uninjured controls, 5.7-fold more likely to be in the highest quartile for abdominal fat, 2.1 times more likely to be in the lowest quartile for total weekly physical activity, and 2.4-fold more likely to be overweight or obese by body mass index (BMI). They were significantly less aerobically fit as reflected in their performance on the 20-meter shuttle run. And they scored significantly worse on the validated Knee Injury and Osteoarthritis Outcome Score (KOOS), particularly on the knee-related quality of life, pain, and symptom subscales.
“The study is ongoing, but it has already contributed to identification of who we’re probably going to need to target for secondary prevention strategies: obviously, individuals who have torn their ACL and/or their meniscus, as was already well known, but perhaps also individuals that have had less severe injuries, those who have a high BMI or some other indicator of adiposity, and those at risk of becoming physically inactive,” Dr. Whittaker said.
She added that a key take-away message from the study, for which she is coprincipal investigator, is that reduced physical activity on the part of someone with a history of a youth sports knee injury is a big red flag. These patients need to address their modifiable risk factors for OA via physical therapy and rehabilitation, along with receiving education reinforcing the importance of lifelong musculoskeletal health.
“Reduced physical activity is a warning sign. Don’t wait for knee pain,” she emphasized.
The Alberta Youth Prevention in Early OA study is funded by the Canadian Institutes of Health Research and nonprofit organizations. Dr. Whittaker reported having no financial conflicts.
LAS VEGAS – Young people who sustain an intra-articular knee injury while participating in youth sports are not only at increased risk for early posttraumatic osteoarthritis 3-10 years later as young adults, but they also are more prone to develop obesity and other modifiable risk factors for osteoarthritis, according to Jackie Whittaker, PhD.
“It appears that some of these young active individuals, after sustaining an injury which is itself a risk factor for osteoarthritis, are going down a pathway where they’re developing a second risk factor for the disease. This may accelerate the rate at which they get the disease and may very well also accelerate the rate at which the disease progresses after its onset,” Dr. Whittaker of the University of Alberta, Edmonton, said at the World Congress on Osteoarthritis.
It’s well established from other studies that roughly 50% of youth who have a significant knee joint injury for which they seek medical attention go on to develop knee osteoarthritis within 10-15 years. The Alberta study focuses on the years between injury and OA onset in an effort to identify modifiable risk factors and develop interventions to delay or halt progression to the disease. There is a paucity of research regarding this crucial time period, Dr. Whittaker explained at the congress sponsored by the Osteoarthritis Research Society International.
“In Canada, we know that injury during sport and recreation is the No. 1 reason that youth between the ages of 11 and 18 seek medical attention, with an alarming one in three doing so. Knee injuries are among the most common of those injuries,” she said.
At follow-up, 29% of the group with a history of knee injury and 4% of controls already had OA as defined by MRI. The likelihood of MRI evidence of OA was 13.5-fold greater in patients who underwent knee surgery for their injury, compared with controls.
“We saw the highest risk, as expected, in patients with ACL [anterior cruciate ligament] and/or meniscal tears, but we also saw a twofold increased risk of OA in those with seemingly less severe injuries, like grade 1-3 medial and collateral ligament injuries,” said Dr. Whittaker.
“I don’t think we were really shocked that knee injury can lead to structural changes that can be associated with future symptomatic OA, but we were surprised to be seeing that as early as 3-10 years post injury. And we were also seeing greater adiposity, a higher rate of being overweight or obese, reduced physical activity, weaker knee muscular strength, and poorer performance on balance and physical function tests,” she continued.
Indeed, at follow-up the subjects with a history of a youth sports knee injury were 4.4-fold more likely to be in the top quartile of fat mass index, compared with uninjured controls, 5.7-fold more likely to be in the highest quartile for abdominal fat, 2.1 times more likely to be in the lowest quartile for total weekly physical activity, and 2.4-fold more likely to be overweight or obese by body mass index (BMI). They were significantly less aerobically fit as reflected in their performance on the 20-meter shuttle run. And they scored significantly worse on the validated Knee Injury and Osteoarthritis Outcome Score (KOOS), particularly on the knee-related quality of life, pain, and symptom subscales.
“The study is ongoing, but it has already contributed to identification of who we’re probably going to need to target for secondary prevention strategies: obviously, individuals who have torn their ACL and/or their meniscus, as was already well known, but perhaps also individuals that have had less severe injuries, those who have a high BMI or some other indicator of adiposity, and those at risk of becoming physically inactive,” Dr. Whittaker said.
She added that a key take-away message from the study, for which she is coprincipal investigator, is that reduced physical activity on the part of someone with a history of a youth sports knee injury is a big red flag. These patients need to address their modifiable risk factors for OA via physical therapy and rehabilitation, along with receiving education reinforcing the importance of lifelong musculoskeletal health.
“Reduced physical activity is a warning sign. Don’t wait for knee pain,” she emphasized.
The Alberta Youth Prevention in Early OA study is funded by the Canadian Institutes of Health Research and nonprofit organizations. Dr. Whittaker reported having no financial conflicts.
Key clinical point:
Major finding: Just 3-10 years after sustaining a knee injury while participating in youth sports, 29% of young people already have MRI evidence of knee osteoarthritis.
Data source: The Alberta Youth Prevention in Early OA study, an ongoing prospective 200-subject longitudinal cohort study of the long-term consequences of sports-related knee injury.
Disclosures: The study is funded by the Canadian Institutes of Health Research and nonprofit organizations. The presenter reported having no financial conflicts.
Children exposed to violence show accelerated cellular aging
SAN FRANCISCO – Children exposed to high levels of urban violence demonstrate accelerated cellular aging beyond their chronologic years, Vasiliki Michopoulos, PhD, reported at the annual conference of the Anxiety and Depression Association of America.
This fast-running cellular biologic clock is not a good thing. Neither is their blunted heart rate variability in response to stress, an indicator of autonomic dysfunction that constitutes a cardiovascular risk factor, she added.

Accelerated cellular aging as measured by DNA methylation in blood or saliva samples has become a red hot research area. Investigators have shown that a person’s DNA methylation age, also known as epigenetic age, predicts all-cause mortality risk in later life. In adults, accelerated cellular aging as reflected in a 5-year discrepancy between DNA methylation age and chronologic age is predictive of an adjusted 16% increased mortality risk independent of social class, education level, lifestyle factors, and chronic diseases, including diabetes and cardiovascular disease (Genome Biol. 2015 Jan 30;16:25).
Lifetime exposure to stress has been convincingly shown to accelerate epigenetic aging, as reflected by DNA methylation level. But, prior to Dr. Michopoulos’s study, it wasn’t known if exposure to violence during childhood influences epigenetic aging or if perhaps only later-life trauma is relevant.
To address this question, she and her coinvestigators recruited 101 African American children aged 6-11 years and their mothers. Of note, medical attention wasn’t being sought for the children. Rather, their mothers were approached regarding study participation while attending primary care clinics at Atlanta’s Grady Memorial Hospital. Children were not eligible to participate if they had been diagnosed with autism spectrum disorder, bipolar disorder, cognitive impairment, or a psychotic disorder.
The children had been exposed to a lot of violence, both witnessed and directly experienced, as reflected in their mean total score of 18.9 on the Violence Exposure Scale for Children-Revised (VEX-R). More than 80% of the children had witnessed an assault and 30% a murder. Stabbings, shootings, drug trafficking, and arrests were other common exposures.
One-quarter of the children showed accelerated cellular aging. They had experienced twice as much violence exposure as reflected in their VEX-R scores, compared with children whose epigenetic and chronologic ages were the same.
The children with accelerated cellular aging also demonstrated decreased heart rate variability in response to a standardized stressor, which involved a startle experience in a darkened room. Their heart rate in the stressor situation shot up on average by 17 bpm less than the children whose cellular age as measured by DNA methylation matched their chronologic age.
“Our data suggest that DNA methylation may serve as a biomarker by which to identify at-risk individuals who may benefit from interventions that decrease risk for cardiometabolic disorders in adulthood,” Dr. Michopoulos said. “It’ll be really interesting to see, as these kids grow up and develop, whether their phenotype stays static, reverses, or changes completely.”
Dr. Michopoulos reported having no financial conflicts regarding the study, conducted as part of the Grady Trauma Project (www.gradytraumaproject.com) with funding from the National Institute of Mental Health and Emory University and Grady Memorial Hospital, both in Atlanta.
SAN FRANCISCO – Children exposed to high levels of urban violence demonstrate accelerated cellular aging beyond their chronologic years, Vasiliki Michopoulos, PhD, reported at the annual conference of the Anxiety and Depression Association of America.
This fast-running cellular biologic clock is not a good thing. Neither is their blunted heart rate variability in response to stress, an indicator of autonomic dysfunction that constitutes a cardiovascular risk factor, she added.
Accelerated cellular aging as measured by DNA methylation in blood or saliva samples has become a red hot research area. Investigators have shown that a person’s DNA methylation age, also known as epigenetic age, predicts all-cause mortality risk in later life. In adults, accelerated cellular aging as reflected in a 5-year discrepancy between DNA methylation age and chronologic age is predictive of an adjusted 16% increased mortality risk independent of social class, education level, lifestyle factors, and chronic diseases, including diabetes and cardiovascular disease (Genome Biol. 2015 Jan 30;16:25).
Lifetime exposure to stress has been convincingly shown to accelerate epigenetic aging, as reflected by DNA methylation level. But, prior to Dr. Michopoulos’s study, it wasn’t known if exposure to violence during childhood influences epigenetic aging or if perhaps only later-life trauma is relevant.
To address this question, she and her coinvestigators recruited 101 African American children aged 6-11 years and their mothers. Of note, medical attention wasn’t being sought for the children. Rather, their mothers were approached regarding study participation while attending primary care clinics at Atlanta’s Grady Memorial Hospital. Children were not eligible to participate if they had been diagnosed with autism spectrum disorder, bipolar disorder, cognitive impairment, or a psychotic disorder.
The children had been exposed to a lot of violence, both witnessed and directly experienced, as reflected in their mean total score of 18.9 on the Violence Exposure Scale for Children-Revised (VEX-R). More than 80% of the children had witnessed an assault and 30% a murder. Stabbings, shootings, drug trafficking, and arrests were other common exposures.
One-quarter of the children showed accelerated cellular aging. They had experienced twice as much violence exposure as reflected in their VEX-R scores, compared with children whose epigenetic and chronologic ages were the same.
The children with accelerated cellular aging also demonstrated decreased heart rate variability in response to a standardized stressor, which involved a startle experience in a darkened room. Their heart rate in the stressor situation shot up on average by 17 bpm less than the children whose cellular age as measured by DNA methylation matched their chronologic age.
“Our data suggest that DNA methylation may serve as a biomarker by which to identify at-risk individuals who may benefit from interventions that decrease risk for cardiometabolic disorders in adulthood,” Dr. Michopoulos said. “It’ll be really interesting to see, as these kids grow up and develop, whether their phenotype stays static, reverses, or changes completely.”
Dr. Michopoulos reported having no financial conflicts regarding the study, conducted as part of the Grady Trauma Project (www.gradytraumaproject.com) with funding from the National Institute of Mental Health and Emory University and Grady Memorial Hospital, both in Atlanta.
SAN FRANCISCO – Children exposed to high levels of urban violence demonstrate accelerated cellular aging beyond their chronologic years, Vasiliki Michopoulos, PhD, reported at the annual conference of the Anxiety and Depression Association of America.
This fast-running cellular biologic clock is not a good thing. Neither is their blunted heart rate variability in response to stress, an indicator of autonomic dysfunction that constitutes a cardiovascular risk factor, she added.
Accelerated cellular aging as measured by DNA methylation in blood or saliva samples has become a red hot research area. Investigators have shown that a person’s DNA methylation age, also known as epigenetic age, predicts all-cause mortality risk in later life. In adults, accelerated cellular aging as reflected in a 5-year discrepancy between DNA methylation age and chronologic age is predictive of an adjusted 16% increased mortality risk independent of social class, education level, lifestyle factors, and chronic diseases, including diabetes and cardiovascular disease (Genome Biol. 2015 Jan 30;16:25).
Lifetime exposure to stress has been convincingly shown to accelerate epigenetic aging, as reflected by DNA methylation level. But, prior to Dr. Michopoulos’s study, it wasn’t known if exposure to violence during childhood influences epigenetic aging or if perhaps only later-life trauma is relevant.
To address this question, she and her coinvestigators recruited 101 African American children aged 6-11 years and their mothers. Of note, medical attention wasn’t being sought for the children. Rather, their mothers were approached regarding study participation while attending primary care clinics at Atlanta’s Grady Memorial Hospital. Children were not eligible to participate if they had been diagnosed with autism spectrum disorder, bipolar disorder, cognitive impairment, or a psychotic disorder.
The children had been exposed to a lot of violence, both witnessed and directly experienced, as reflected in their mean total score of 18.9 on the Violence Exposure Scale for Children-Revised (VEX-R). More than 80% of the children had witnessed an assault and 30% a murder. Stabbings, shootings, drug trafficking, and arrests were other common exposures.
One-quarter of the children showed accelerated cellular aging. They had experienced twice as much violence exposure as reflected in their VEX-R scores, compared with children whose epigenetic and chronologic ages were the same.
The children with accelerated cellular aging also demonstrated decreased heart rate variability in response to a standardized stressor, which involved a startle experience in a darkened room. Their heart rate in the stressor situation shot up on average by 17 bpm less than the children whose cellular age as measured by DNA methylation matched their chronologic age.
“Our data suggest that DNA methylation may serve as a biomarker by which to identify at-risk individuals who may benefit from interventions that decrease risk for cardiometabolic disorders in adulthood,” Dr. Michopoulos said. “It’ll be really interesting to see, as these kids grow up and develop, whether their phenotype stays static, reverses, or changes completely.”
Dr. Michopoulos reported having no financial conflicts regarding the study, conducted as part of the Grady Trauma Project (www.gradytraumaproject.com) with funding from the National Institute of Mental Health and Emory University and Grady Memorial Hospital, both in Atlanta.
AT THE ANXIETY AND DEPRESSION CONFERENCE 2017
Key clinical point:
Major finding: Children who demonstrated advanced cellular aging based on DNA methylation levels had experienced twice as much exposure to violence as those whose epigenetic and chronologic ages matched.
Data source: This cross-sectional study included 101 urban African American children aged 6-11 years.
Disclosures: The presenter reported having no financial conflicts regarding the study, which was funded by the National Institute of Mental Health and Emory University and Grady Memorial Hospital, both in Atlanta.
Think twice before recommending partial meniscectomy
LAS VEGAS – Patients with knee osteoarthritis (OA) and a meniscal tear who underwent arthroscopic partial meniscectomy (APM) subsequently experienced accelerated structural progression of their OA, compared with those randomized to physical therapy alone in the randomized METEOR trial.
“In discussing treatment options for symptomatic meniscal tear, patients and providers must weigh the potential benefits and risks of arthroscopic partial meniscectomy, including this increased risk of structural progression,” Jamie E. Collins, PhD, said at the World Congress on Osteoarthritis.

A thorough physician-patient discussion also needs to mention that several large randomized trials have suggested that patients with meniscal tear and osteoarthritic changes experience similar pain relief with APM plus physical therapy (PT) as compared with PT alone, she added at the congress sponsored by the Osteoarthritis Research Society International.
The METEOR trial was a seven-center U.S. randomized trial of APM plus PT or PT alone in patients with MRI or radiographic evidence of OA changes, a meniscal tear on MRI, and mechanical knee symptoms. Dr. Collins reported on 176 randomized patients with baseline and 18-month follow-up MRIs read by a specialist musculoskeletal radiologist. This analysis excluded the 37 patients in the PT group who crossed over to APM within 6 months after randomization.
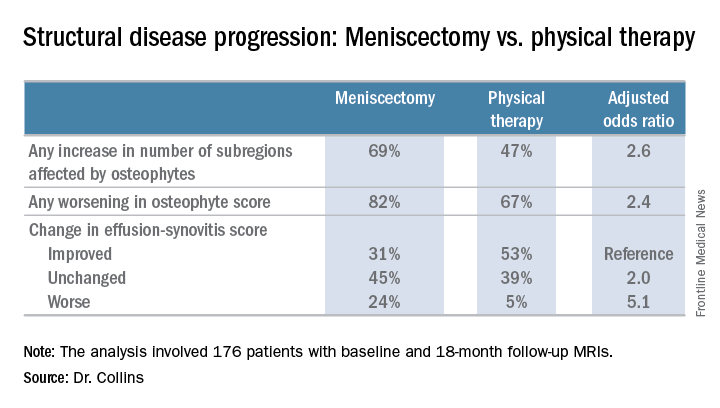
There was no significant difference between the two treatment groups in changes in bone marrow lesions or Hoffa-synovitis.
A secondary analysis that incorporated the 37 crossovers from PT to APM within 6 months showed similarly accelerated OA progression after arthroscopic surgery.
“Future work should focus on determining whether this accelerated structural progression is associated with changes in symptoms and ultimately with a higher risk of total knee replacement. In other words, is 2+ structural worsening something that’s noticeable or important for patients?” Dr. Collins concluded.
She reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
LAS VEGAS – Patients with knee osteoarthritis (OA) and a meniscal tear who underwent arthroscopic partial meniscectomy (APM) subsequently experienced accelerated structural progression of their OA, compared with those randomized to physical therapy alone in the randomized METEOR trial.
“In discussing treatment options for symptomatic meniscal tear, patients and providers must weigh the potential benefits and risks of arthroscopic partial meniscectomy, including this increased risk of structural progression,” Jamie E. Collins, PhD, said at the World Congress on Osteoarthritis.
A thorough physician-patient discussion also needs to mention that several large randomized trials have suggested that patients with meniscal tear and osteoarthritic changes experience similar pain relief with APM plus physical therapy (PT) as compared with PT alone, she added at the congress sponsored by the Osteoarthritis Research Society International.
The METEOR trial was a seven-center U.S. randomized trial of APM plus PT or PT alone in patients with MRI or radiographic evidence of OA changes, a meniscal tear on MRI, and mechanical knee symptoms. Dr. Collins reported on 176 randomized patients with baseline and 18-month follow-up MRIs read by a specialist musculoskeletal radiologist. This analysis excluded the 37 patients in the PT group who crossed over to APM within 6 months after randomization.
There was no significant difference between the two treatment groups in changes in bone marrow lesions or Hoffa-synovitis.
A secondary analysis that incorporated the 37 crossovers from PT to APM within 6 months showed similarly accelerated OA progression after arthroscopic surgery.
“Future work should focus on determining whether this accelerated structural progression is associated with changes in symptoms and ultimately with a higher risk of total knee replacement. In other words, is 2+ structural worsening something that’s noticeable or important for patients?” Dr. Collins concluded.
She reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
LAS VEGAS – Patients with knee osteoarthritis (OA) and a meniscal tear who underwent arthroscopic partial meniscectomy (APM) subsequently experienced accelerated structural progression of their OA, compared with those randomized to physical therapy alone in the randomized METEOR trial.
“In discussing treatment options for symptomatic meniscal tear, patients and providers must weigh the potential benefits and risks of arthroscopic partial meniscectomy, including this increased risk of structural progression,” Jamie E. Collins, PhD, said at the World Congress on Osteoarthritis.
A thorough physician-patient discussion also needs to mention that several large randomized trials have suggested that patients with meniscal tear and osteoarthritic changes experience similar pain relief with APM plus physical therapy (PT) as compared with PT alone, she added at the congress sponsored by the Osteoarthritis Research Society International.
The METEOR trial was a seven-center U.S. randomized trial of APM plus PT or PT alone in patients with MRI or radiographic evidence of OA changes, a meniscal tear on MRI, and mechanical knee symptoms. Dr. Collins reported on 176 randomized patients with baseline and 18-month follow-up MRIs read by a specialist musculoskeletal radiologist. This analysis excluded the 37 patients in the PT group who crossed over to APM within 6 months after randomization.
There was no significant difference between the two treatment groups in changes in bone marrow lesions or Hoffa-synovitis.
A secondary analysis that incorporated the 37 crossovers from PT to APM within 6 months showed similarly accelerated OA progression after arthroscopic surgery.
“Future work should focus on determining whether this accelerated structural progression is associated with changes in symptoms and ultimately with a higher risk of total knee replacement. In other words, is 2+ structural worsening something that’s noticeable or important for patients?” Dr. Collins concluded.
She reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
AT OARSI 2017
Key clinical point:
Major finding: Surgically treated patients were 2.6 times more likely to demonstrate MRI evidence of structural disease progression at 18 months than those who received physical therapy alone.
Data source: This analysis from the multicenter METEOR trial included 176 patients with a symptomatic meniscal tear.
Disclosures: The presenter reported having no financial conflicts regarding her study, which was sponsored by Brigham and Women’s Hospital.
New evidence bisphosphonates may prevent OA
LAS VEGAS – Bisphosphonates may slow the onset and progression of osteoarthritis (OA), according to data from the National Institutes of Health–sponsored Osteoarthritis Initiative. “Bisphosphonates warrant further study as potential disease-modifying agents in osteoarthritis,” Tuhina Neogi, MD, declared in presenting the study findings at the World Congress on Osteoarthritis.
In addition to the promising signal of a preventive effect for bisphosphonates, her analysis of Osteoarthritis Initiative data yielded two other major findings: Changes over time in the MRI-based three-dimensional bone shape of the knee constitute a novel structural imaging biomarker that appears to be of value in monitoring patients with OA or at high risk for the joint disease, and bisphosphonate-induced suppression of bone turnover had no adverse long-term impact on osteoarthritis risk.
“While bisphosphonates may have beneficial articular cartilage effects, there are potential theoretical concerns regarding long-term effects of bone turnover. This issue hasn’t previously been addressed. Bone turnover suppression may lead to more bone deposition and bone stiffness, with adverse biomechanical consequences. But it did not appear, in this sample at least, that suppression of bone turnover had a negative impact over the long term,” said Dr. Neogi, professor of medicine at Boston University.
The Osteoarthritis Initiative is a multicenter, longitudinal, prospective, observational study of knee osteoarthritis launched by the NIH in 2002. Dr. Neogi’s analysis was limited to the 1,071 female participants free of radiographic knee OA at baseline and who had 3-Tesla MRIs of the right knee at baseline and annually thereafter for 4 years. They were at increased risk for OA on the basis of their age – a mean of 62 years – along with their mean body mass index of 28.3 kg/m2. Just under one-quarter of the women were on bisphosphonate therapy.
Prior studies of the effects of bisphosphonates in patients with knee OA have yielded conflicting results, in part because radiographic findings are a relatively crude indicator of bone and joint changes. 3D bone shape of the knee has been shown to change much more quickly than traditional radiographic measures. These changes predict the incidence of knee OA even years later, the rheumatologist explained at the congress sponsored by the Osteoarthritis Research Society International.
Using bone shape analytic software developed by England-based Imorphics, she and her coinvestigators categorized the women into three distinct groups on the basis of the trajectory of MRI changes toward a more osteoarthritic bone shape over time. Of them, 23% fell into the fast-change group, 49% were in the intermediate group, and 28% were in the slowest-changing group. The rate of MRI bone shape progression toward knee OA was 2.7-times higher in the fastest, compared with the slowest, group.
The incidence of radiographic OA during 4 years of prospective follow-up was 14% in the fastest bone shape-changing group, 8% in the intermediate-speed group, and 4% in the slowest-changing group.
In a multivariate analysis adjusted for age, BMI, education, race, quadriceps strength, and history of knee injury, bisphosphonate users were 41% less likely to be in the fastest bone shape–changing group and 32% less likely to be in the intermediate group, compared with the slowest-changing group.
As a rheumatologist with a PhD in epidemiology, Dr. Neogi was readily prepared to critique her own study. The major limitation in her view was the potential for residual confounding, which is inherent in observational studies. In this instance, the possibility of confounding by indication cannot be excluded. Also, bone mineral density data wasn’t collected in the Osteoarthritis Initiative. Future studies should evaluate the impact over time of new-onset bisphosphonate therapy as a means of altering the slope of the trajectory of MRI-based 3D bone shape of the knee, Dr. Neogi said.
She reported having no financial conflicts regarding the NIH-sponsored study.
LAS VEGAS – Bisphosphonates may slow the onset and progression of osteoarthritis (OA), according to data from the National Institutes of Health–sponsored Osteoarthritis Initiative. “Bisphosphonates warrant further study as potential disease-modifying agents in osteoarthritis,” Tuhina Neogi, MD, declared in presenting the study findings at the World Congress on Osteoarthritis.
In addition to the promising signal of a preventive effect for bisphosphonates, her analysis of Osteoarthritis Initiative data yielded two other major findings: Changes over time in the MRI-based three-dimensional bone shape of the knee constitute a novel structural imaging biomarker that appears to be of value in monitoring patients with OA or at high risk for the joint disease, and bisphosphonate-induced suppression of bone turnover had no adverse long-term impact on osteoarthritis risk.
“While bisphosphonates may have beneficial articular cartilage effects, there are potential theoretical concerns regarding long-term effects of bone turnover. This issue hasn’t previously been addressed. Bone turnover suppression may lead to more bone deposition and bone stiffness, with adverse biomechanical consequences. But it did not appear, in this sample at least, that suppression of bone turnover had a negative impact over the long term,” said Dr. Neogi, professor of medicine at Boston University.
The Osteoarthritis Initiative is a multicenter, longitudinal, prospective, observational study of knee osteoarthritis launched by the NIH in 2002. Dr. Neogi’s analysis was limited to the 1,071 female participants free of radiographic knee OA at baseline and who had 3-Tesla MRIs of the right knee at baseline and annually thereafter for 4 years. They were at increased risk for OA on the basis of their age – a mean of 62 years – along with their mean body mass index of 28.3 kg/m2. Just under one-quarter of the women were on bisphosphonate therapy.
Prior studies of the effects of bisphosphonates in patients with knee OA have yielded conflicting results, in part because radiographic findings are a relatively crude indicator of bone and joint changes. 3D bone shape of the knee has been shown to change much more quickly than traditional radiographic measures. These changes predict the incidence of knee OA even years later, the rheumatologist explained at the congress sponsored by the Osteoarthritis Research Society International.
Using bone shape analytic software developed by England-based Imorphics, she and her coinvestigators categorized the women into three distinct groups on the basis of the trajectory of MRI changes toward a more osteoarthritic bone shape over time. Of them, 23% fell into the fast-change group, 49% were in the intermediate group, and 28% were in the slowest-changing group. The rate of MRI bone shape progression toward knee OA was 2.7-times higher in the fastest, compared with the slowest, group.
The incidence of radiographic OA during 4 years of prospective follow-up was 14% in the fastest bone shape-changing group, 8% in the intermediate-speed group, and 4% in the slowest-changing group.
In a multivariate analysis adjusted for age, BMI, education, race, quadriceps strength, and history of knee injury, bisphosphonate users were 41% less likely to be in the fastest bone shape–changing group and 32% less likely to be in the intermediate group, compared with the slowest-changing group.
As a rheumatologist with a PhD in epidemiology, Dr. Neogi was readily prepared to critique her own study. The major limitation in her view was the potential for residual confounding, which is inherent in observational studies. In this instance, the possibility of confounding by indication cannot be excluded. Also, bone mineral density data wasn’t collected in the Osteoarthritis Initiative. Future studies should evaluate the impact over time of new-onset bisphosphonate therapy as a means of altering the slope of the trajectory of MRI-based 3D bone shape of the knee, Dr. Neogi said.
She reported having no financial conflicts regarding the NIH-sponsored study.
LAS VEGAS – Bisphosphonates may slow the onset and progression of osteoarthritis (OA), according to data from the National Institutes of Health–sponsored Osteoarthritis Initiative. “Bisphosphonates warrant further study as potential disease-modifying agents in osteoarthritis,” Tuhina Neogi, MD, declared in presenting the study findings at the World Congress on Osteoarthritis.
In addition to the promising signal of a preventive effect for bisphosphonates, her analysis of Osteoarthritis Initiative data yielded two other major findings: Changes over time in the MRI-based three-dimensional bone shape of the knee constitute a novel structural imaging biomarker that appears to be of value in monitoring patients with OA or at high risk for the joint disease, and bisphosphonate-induced suppression of bone turnover had no adverse long-term impact on osteoarthritis risk.
“While bisphosphonates may have beneficial articular cartilage effects, there are potential theoretical concerns regarding long-term effects of bone turnover. This issue hasn’t previously been addressed. Bone turnover suppression may lead to more bone deposition and bone stiffness, with adverse biomechanical consequences. But it did not appear, in this sample at least, that suppression of bone turnover had a negative impact over the long term,” said Dr. Neogi, professor of medicine at Boston University.
The Osteoarthritis Initiative is a multicenter, longitudinal, prospective, observational study of knee osteoarthritis launched by the NIH in 2002. Dr. Neogi’s analysis was limited to the 1,071 female participants free of radiographic knee OA at baseline and who had 3-Tesla MRIs of the right knee at baseline and annually thereafter for 4 years. They were at increased risk for OA on the basis of their age – a mean of 62 years – along with their mean body mass index of 28.3 kg/m2. Just under one-quarter of the women were on bisphosphonate therapy.
Prior studies of the effects of bisphosphonates in patients with knee OA have yielded conflicting results, in part because radiographic findings are a relatively crude indicator of bone and joint changes. 3D bone shape of the knee has been shown to change much more quickly than traditional radiographic measures. These changes predict the incidence of knee OA even years later, the rheumatologist explained at the congress sponsored by the Osteoarthritis Research Society International.
Using bone shape analytic software developed by England-based Imorphics, she and her coinvestigators categorized the women into three distinct groups on the basis of the trajectory of MRI changes toward a more osteoarthritic bone shape over time. Of them, 23% fell into the fast-change group, 49% were in the intermediate group, and 28% were in the slowest-changing group. The rate of MRI bone shape progression toward knee OA was 2.7-times higher in the fastest, compared with the slowest, group.
The incidence of radiographic OA during 4 years of prospective follow-up was 14% in the fastest bone shape-changing group, 8% in the intermediate-speed group, and 4% in the slowest-changing group.
In a multivariate analysis adjusted for age, BMI, education, race, quadriceps strength, and history of knee injury, bisphosphonate users were 41% less likely to be in the fastest bone shape–changing group and 32% less likely to be in the intermediate group, compared with the slowest-changing group.
As a rheumatologist with a PhD in epidemiology, Dr. Neogi was readily prepared to critique her own study. The major limitation in her view was the potential for residual confounding, which is inherent in observational studies. In this instance, the possibility of confounding by indication cannot be excluded. Also, bone mineral density data wasn’t collected in the Osteoarthritis Initiative. Future studies should evaluate the impact over time of new-onset bisphosphonate therapy as a means of altering the slope of the trajectory of MRI-based 3D bone shape of the knee, Dr. Neogi said.
She reported having no financial conflicts regarding the NIH-sponsored study.
AT OARSI 2017
Key clinical point:
Major finding: Bisphosphonate users were 41% less likely to be in the group with the fastest trajectory of changes in bone shape known to be highly predictive of knee osteoarthritis.
Data source: This analysis of MRI-based changes in 3D bone shape of the knee over 4 years of follow-up included 1,071 female participants in the multicenter, prospective, observational Osteoarthritis Initiative.
Disclosures: The presenter reported having no financial conflicts regarding the NIH-sponsored study.