User login
Itraconazole for BCC: Does it work?
CHICAGO – Justin J. Leitenberger, MD, declared at the annual meeting of the American College of Mohs Surgery.

The oral antifungal inhibits the hedgehog signaling pathway, a key driver of BCC. And while itraconazole is not as potent an inhibitor of hedgehog pathway expression as, say vismodegib (Erivedge), the antifungal acts at a separate site on the pathway, making it an attractive candidate for combination therapy, explained Dr. Leitenberger of Oregon Health & Science University, Portland.
Dermatologists at Stanford University have led the way in exploring oral itraconazole as a treatment for BCC. Among a series of 29 patients with one or more large but nonadvanced BCCs, 19 were treated using oral itraconazole at 200 mg b.i.d. for 1 month or 100 mg b.i.d. for an average of 2.3 months. Hedgehog pathway expression was reduced by 65% in the itraconazole-treated patients, as compared with the 90% reduction which is achieved with vismodegib.
Of more direct clinical relevance, however, itraconazole also reduced tumor area by 24%. Four of eight patients with 57 tumors achieved a partial response, and the other four had stable disease (J Clin Oncol. 2014 Mar 10;32[8]:745-51).
The Stanford group has also shown that combination therapy with oral itraconazole and intravenous arsenic trioxide reduces hedgehog pathway expression by 75%, up by an absolute 10% from itraconazole alone. The two agents inhibit the pathway at different sites.
Five patients with metastatic BCC who relapsed after treatment with vismodegib received intravenous arsenic trioxide for the first 5 days of every month, followed by oral itraconazole at 200 mg b.i.d. on days 6-28. Three patients completed three such cycles, while two discontinued early because of progressive disease or adverse events including a grade 3 infection and grade 2 transaminitis. All three patients who completed three treatment cycles achieved stable disease. The Stanford investigators speculated that concurrent continuous dosing might be required to obtain tumor shrinkage (JAMA Dermatol. 2016 Apr;152[4]:452-6).
Lots more work remains to be done in order to optimize combination therapy utilizing oral itraconazole for advanced BCC. Different dosing regimens and combinations of hedgehog pathway inhibitors need to be studied. Another important question is how effective itraconazole-based combinations will be in vismodegib-naive as compared with vismodegib-resistant patients, Dr. Leitenberger observed.
He reported having no financial conflicts regarding his presentation.
CHICAGO – Justin J. Leitenberger, MD, declared at the annual meeting of the American College of Mohs Surgery.
The oral antifungal inhibits the hedgehog signaling pathway, a key driver of BCC. And while itraconazole is not as potent an inhibitor of hedgehog pathway expression as, say vismodegib (Erivedge), the antifungal acts at a separate site on the pathway, making it an attractive candidate for combination therapy, explained Dr. Leitenberger of Oregon Health & Science University, Portland.
Dermatologists at Stanford University have led the way in exploring oral itraconazole as a treatment for BCC. Among a series of 29 patients with one or more large but nonadvanced BCCs, 19 were treated using oral itraconazole at 200 mg b.i.d. for 1 month or 100 mg b.i.d. for an average of 2.3 months. Hedgehog pathway expression was reduced by 65% in the itraconazole-treated patients, as compared with the 90% reduction which is achieved with vismodegib.
Of more direct clinical relevance, however, itraconazole also reduced tumor area by 24%. Four of eight patients with 57 tumors achieved a partial response, and the other four had stable disease (J Clin Oncol. 2014 Mar 10;32[8]:745-51).
The Stanford group has also shown that combination therapy with oral itraconazole and intravenous arsenic trioxide reduces hedgehog pathway expression by 75%, up by an absolute 10% from itraconazole alone. The two agents inhibit the pathway at different sites.
Five patients with metastatic BCC who relapsed after treatment with vismodegib received intravenous arsenic trioxide for the first 5 days of every month, followed by oral itraconazole at 200 mg b.i.d. on days 6-28. Three patients completed three such cycles, while two discontinued early because of progressive disease or adverse events including a grade 3 infection and grade 2 transaminitis. All three patients who completed three treatment cycles achieved stable disease. The Stanford investigators speculated that concurrent continuous dosing might be required to obtain tumor shrinkage (JAMA Dermatol. 2016 Apr;152[4]:452-6).
Lots more work remains to be done in order to optimize combination therapy utilizing oral itraconazole for advanced BCC. Different dosing regimens and combinations of hedgehog pathway inhibitors need to be studied. Another important question is how effective itraconazole-based combinations will be in vismodegib-naive as compared with vismodegib-resistant patients, Dr. Leitenberger observed.
He reported having no financial conflicts regarding his presentation.
CHICAGO – Justin J. Leitenberger, MD, declared at the annual meeting of the American College of Mohs Surgery.
The oral antifungal inhibits the hedgehog signaling pathway, a key driver of BCC. And while itraconazole is not as potent an inhibitor of hedgehog pathway expression as, say vismodegib (Erivedge), the antifungal acts at a separate site on the pathway, making it an attractive candidate for combination therapy, explained Dr. Leitenberger of Oregon Health & Science University, Portland.
Dermatologists at Stanford University have led the way in exploring oral itraconazole as a treatment for BCC. Among a series of 29 patients with one or more large but nonadvanced BCCs, 19 were treated using oral itraconazole at 200 mg b.i.d. for 1 month or 100 mg b.i.d. for an average of 2.3 months. Hedgehog pathway expression was reduced by 65% in the itraconazole-treated patients, as compared with the 90% reduction which is achieved with vismodegib.
Of more direct clinical relevance, however, itraconazole also reduced tumor area by 24%. Four of eight patients with 57 tumors achieved a partial response, and the other four had stable disease (J Clin Oncol. 2014 Mar 10;32[8]:745-51).
The Stanford group has also shown that combination therapy with oral itraconazole and intravenous arsenic trioxide reduces hedgehog pathway expression by 75%, up by an absolute 10% from itraconazole alone. The two agents inhibit the pathway at different sites.
Five patients with metastatic BCC who relapsed after treatment with vismodegib received intravenous arsenic trioxide for the first 5 days of every month, followed by oral itraconazole at 200 mg b.i.d. on days 6-28. Three patients completed three such cycles, while two discontinued early because of progressive disease or adverse events including a grade 3 infection and grade 2 transaminitis. All three patients who completed three treatment cycles achieved stable disease. The Stanford investigators speculated that concurrent continuous dosing might be required to obtain tumor shrinkage (JAMA Dermatol. 2016 Apr;152[4]:452-6).
Lots more work remains to be done in order to optimize combination therapy utilizing oral itraconazole for advanced BCC. Different dosing regimens and combinations of hedgehog pathway inhibitors need to be studied. Another important question is how effective itraconazole-based combinations will be in vismodegib-naive as compared with vismodegib-resistant patients, Dr. Leitenberger observed.
He reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM THE ACMS ANNUAL MEETING
ASCEND: Aspirin, fish oil flop in diabetes
MUNICH – In a double blow to the current, widespread routine use of low-dose aspirin and fish oil supplements for primary cardiovascular prevention in patients with diabetes, neither treatment provided any net clinical benefit in the massive, long-term ASCEND study, investigators reported at the annual congress of the European Society of Cardiology.
And, in yet another bitter pill to swallow, low-dose aspirin failed to reduce the incidence of GI cancer or any other type of cancer, compared with placebo in the study. Earlier, nondefinitive meta-analyses of much smaller randomized trials had raised the possibility of a roughly 30% reduction in the incidence of colorectal cancer in long-time users, said Jane Armitage, MD, professor of clinical trials and epidemiology at the University of Oxford (England).
“We saw no suggestion of an anticancer effect emerging over time,” Dr. Armitage said. “We did see a significant reduction in the risk of vascular events but also an increase in major bleeding such that the absolute benefits from avoiding a serious vascular event were largely counterbalanced by increased risk of bleeding. And there was no subgroup in which we could clearly define that the benefit outweighs the risk,” she added in a video interview.
ASCEND (A Study of Cardiovascular Events in Diabetes) was a randomized, blinded trial in which 15,480 U.K. patients with diabetes and no known cardiovascular disease were placed on 100 mg/day of enteric-coated aspirin or placebo and 1 g/day of omega-3 fatty acids in capsule form or placebo in a 2 x 2 factorial design and followed prospectively for a mean of 7.4 years.
The study was undertaken because, even though the value of low-dose aspirin for secondary prevention is supported by strong evidence, the medication’s value for primary prevention in patients with diabetes has long been uncertain. American Diabetes Association guidelines give a Grade C recommendation to consideration of low-dose aspirin as a primary prevention strategy in patients with diabetes having a 10-year cardiovascular risk estimated at 10% or greater.
The primary efficacy endpoint in ASCEND was the occurrence of a first serious vascular event, defined as MI, stroke, transient ischemic attack, or death from any vascular cause other than intracranial hemorrhage. The rate was 8.5% in the aspirin group and 9.6% with placebo, for a statistically significant 12% relative risk reduction. However, the rate of the primary composite safety endpoint, comprising intracranial hemorrhage, GI bleeding, sight-threatening bleeding in the eye, or other bleeding serious enough to entail a trip to the hospital, was 4.1% in the aspirin group and 3.2% with placebo, a 29% increase in risk.
Aspirin reduced the absolute risk of a serious vascular event by 1.1%, compared with placebo, while boosting the risk of major bleeding by an absolute 0.9% – essentially a wash. The number needed to treat to avoid a serious vascular event was 91 patients, with 112 being the number needed to cause a major bleeding event. The risk of major bleeding rose with increasing baseline 5-year vascular event risk.
ASCEND provided no support for a recent report suggesting the benefit of low-dose aspirin for cardioprotection is largely confined to individuals weighing less than 70 kg (Lancet. 2018; 392:387-99); in fact, the opposite appeared to be true, according to Dr. Armitage.
The incidence of cancer of the GI tract was 2.0% in both study arms. The overall cancer rate was 11.6% in the aspirin arm and 11.5% with placebo. Additional follow-up focused on cancer is planned for 5 and 10 years after the end of ASCEND in order to examine the possibility of a delayed anticancer effect, she added.
Dr. Armitage said one reason aspirin may have failed to show a significant net benefit was the high rate of background cardioprotective medication usage, especially statins and antihypertensive drugs.
“I think if your diabetes is well managed and you’ve got your other risk factors under control, you have to consider very carefully whether or not, for you, the benefits of aspirin outweigh the risks,” she concluded.
Cardiologists respond
ASCEND’s two designated discussants, both cardiologists, took a more positive view of the results than Dr. Armitage, who isn’t a cardiologist.

Sigrun Halvorsen, MD, professor of cardiology at the University of Oslo, noted that most ASCEND participants were at relatively low cardiovascular risk, with an event rate of about 1.3% per year. She indicated that she’d like to see more data on higher-risk individuals before excluding any role for aspirin in primary cardiovascular prevention in patients with diabetes.
“Serious vascular events and bleeding are not necessarily equally weighted,” she added. “Most major bleeds in ASCEND were GI bleeds, and these can be largely prevented by PPIs [proton pump inhibitors], in contrast to death and stroke, which are irreversible events.”
“I think this study could be interpreted more favorably,” agreed Christopher P. Cannon, MD, professor of medicine at Harvard Medical School, Boston. “Bleeds are reversible, but MIs and whatnot are not.”
Fish oil flounders in ASCEND

Louise Bowman, MD, also at the University of Oxford, presented the ASCEND fish oil findings. Over an average of 7.4 years, omega-3 fatty acid supplementation had no effect on the rate of serious vascular events, no effect on cancer, no impact on all-cause or cause-specific mortality, and raised no safety issues in patients with diabetes. She argued that current guidelines recommending fish oil supplements for cardiovascular prevention should be reconsidered.
“Certainly there doesn’t seem to be any justification for the use of this dose of omega-3 fatty acids – 1 g/day – for the prevention of cardiovascular disease,” Dr. Bowman said.
However, Dr. Cannon saw a sliver of hope within the ASCEND findings. One component of the serious vascular event composite endpoint – vascular death – occurred in 2.4% of the fish oil group and 2.9% of placebo-treated controls, for a statistically significant 19% relative risk reduction. It could be a fluke, given that none of the other vascular endpoints followed suit. But physicians and patients won’t have to wait long to find out. Another randomized trial of low-dose fish oil supplements for primary cardiovascular prevention – the nearly 26,000-patient VITAL trial – is due to report later in 2018.
In addition, two major, randomized trials of higher-dose fish oil supplementation for secondary prevention are ongoing. The roughly 8,000-patient REDUCE-IT trial is expected to report results later this year, and the STRENGTH trial, featuring more than 13,000 patients, should be completed in 2020. Both studies are heavily loaded with diabetes patients, Dr. Cannon noted.
Simultaneous with presentation of the ASCEND results at the ESC congress, the study was published online at the New England Journal of Medicine website (doi: 10.1056/NEJMoa1804988 and doi: 10.1056/NEJMoa1804989).
The ASCEND study was funded by the British Heart Foundation and the U.K. Medical Research Council with support provided by Abbott Laboratories, Bayer, Mylan, and Solvay. Dr. Armitage and Dr. Bowman reported receiving research grants from the Medicines Company, Bayer, and Mylan. Dr. Halvorsen reported no financial conflicts. Dr. Cannon reported serving as a consultant to roughly a dozen pharmaceutical companies, including the Amarin Corporation, which markets a fish oil supplement and sponsored the REDUCE-IT trial.
MUNICH – In a double blow to the current, widespread routine use of low-dose aspirin and fish oil supplements for primary cardiovascular prevention in patients with diabetes, neither treatment provided any net clinical benefit in the massive, long-term ASCEND study, investigators reported at the annual congress of the European Society of Cardiology.
And, in yet another bitter pill to swallow, low-dose aspirin failed to reduce the incidence of GI cancer or any other type of cancer, compared with placebo in the study. Earlier, nondefinitive meta-analyses of much smaller randomized trials had raised the possibility of a roughly 30% reduction in the incidence of colorectal cancer in long-time users, said Jane Armitage, MD, professor of clinical trials and epidemiology at the University of Oxford (England).
“We saw no suggestion of an anticancer effect emerging over time,” Dr. Armitage said. “We did see a significant reduction in the risk of vascular events but also an increase in major bleeding such that the absolute benefits from avoiding a serious vascular event were largely counterbalanced by increased risk of bleeding. And there was no subgroup in which we could clearly define that the benefit outweighs the risk,” she added in a video interview.
ASCEND (A Study of Cardiovascular Events in Diabetes) was a randomized, blinded trial in which 15,480 U.K. patients with diabetes and no known cardiovascular disease were placed on 100 mg/day of enteric-coated aspirin or placebo and 1 g/day of omega-3 fatty acids in capsule form or placebo in a 2 x 2 factorial design and followed prospectively for a mean of 7.4 years.
The study was undertaken because, even though the value of low-dose aspirin for secondary prevention is supported by strong evidence, the medication’s value for primary prevention in patients with diabetes has long been uncertain. American Diabetes Association guidelines give a Grade C recommendation to consideration of low-dose aspirin as a primary prevention strategy in patients with diabetes having a 10-year cardiovascular risk estimated at 10% or greater.
The primary efficacy endpoint in ASCEND was the occurrence of a first serious vascular event, defined as MI, stroke, transient ischemic attack, or death from any vascular cause other than intracranial hemorrhage. The rate was 8.5% in the aspirin group and 9.6% with placebo, for a statistically significant 12% relative risk reduction. However, the rate of the primary composite safety endpoint, comprising intracranial hemorrhage, GI bleeding, sight-threatening bleeding in the eye, or other bleeding serious enough to entail a trip to the hospital, was 4.1% in the aspirin group and 3.2% with placebo, a 29% increase in risk.
Aspirin reduced the absolute risk of a serious vascular event by 1.1%, compared with placebo, while boosting the risk of major bleeding by an absolute 0.9% – essentially a wash. The number needed to treat to avoid a serious vascular event was 91 patients, with 112 being the number needed to cause a major bleeding event. The risk of major bleeding rose with increasing baseline 5-year vascular event risk.
ASCEND provided no support for a recent report suggesting the benefit of low-dose aspirin for cardioprotection is largely confined to individuals weighing less than 70 kg (Lancet. 2018; 392:387-99); in fact, the opposite appeared to be true, according to Dr. Armitage.
The incidence of cancer of the GI tract was 2.0% in both study arms. The overall cancer rate was 11.6% in the aspirin arm and 11.5% with placebo. Additional follow-up focused on cancer is planned for 5 and 10 years after the end of ASCEND in order to examine the possibility of a delayed anticancer effect, she added.
Dr. Armitage said one reason aspirin may have failed to show a significant net benefit was the high rate of background cardioprotective medication usage, especially statins and antihypertensive drugs.
“I think if your diabetes is well managed and you’ve got your other risk factors under control, you have to consider very carefully whether or not, for you, the benefits of aspirin outweigh the risks,” she concluded.
Cardiologists respond
ASCEND’s two designated discussants, both cardiologists, took a more positive view of the results than Dr. Armitage, who isn’t a cardiologist.
Sigrun Halvorsen, MD, professor of cardiology at the University of Oslo, noted that most ASCEND participants were at relatively low cardiovascular risk, with an event rate of about 1.3% per year. She indicated that she’d like to see more data on higher-risk individuals before excluding any role for aspirin in primary cardiovascular prevention in patients with diabetes.
“Serious vascular events and bleeding are not necessarily equally weighted,” she added. “Most major bleeds in ASCEND were GI bleeds, and these can be largely prevented by PPIs [proton pump inhibitors], in contrast to death and stroke, which are irreversible events.”
“I think this study could be interpreted more favorably,” agreed Christopher P. Cannon, MD, professor of medicine at Harvard Medical School, Boston. “Bleeds are reversible, but MIs and whatnot are not.”
Fish oil flounders in ASCEND
Louise Bowman, MD, also at the University of Oxford, presented the ASCEND fish oil findings. Over an average of 7.4 years, omega-3 fatty acid supplementation had no effect on the rate of serious vascular events, no effect on cancer, no impact on all-cause or cause-specific mortality, and raised no safety issues in patients with diabetes. She argued that current guidelines recommending fish oil supplements for cardiovascular prevention should be reconsidered.
“Certainly there doesn’t seem to be any justification for the use of this dose of omega-3 fatty acids – 1 g/day – for the prevention of cardiovascular disease,” Dr. Bowman said.
However, Dr. Cannon saw a sliver of hope within the ASCEND findings. One component of the serious vascular event composite endpoint – vascular death – occurred in 2.4% of the fish oil group and 2.9% of placebo-treated controls, for a statistically significant 19% relative risk reduction. It could be a fluke, given that none of the other vascular endpoints followed suit. But physicians and patients won’t have to wait long to find out. Another randomized trial of low-dose fish oil supplements for primary cardiovascular prevention – the nearly 26,000-patient VITAL trial – is due to report later in 2018.
In addition, two major, randomized trials of higher-dose fish oil supplementation for secondary prevention are ongoing. The roughly 8,000-patient REDUCE-IT trial is expected to report results later this year, and the STRENGTH trial, featuring more than 13,000 patients, should be completed in 2020. Both studies are heavily loaded with diabetes patients, Dr. Cannon noted.
Simultaneous with presentation of the ASCEND results at the ESC congress, the study was published online at the New England Journal of Medicine website (doi: 10.1056/NEJMoa1804988 and doi: 10.1056/NEJMoa1804989).
The ASCEND study was funded by the British Heart Foundation and the U.K. Medical Research Council with support provided by Abbott Laboratories, Bayer, Mylan, and Solvay. Dr. Armitage and Dr. Bowman reported receiving research grants from the Medicines Company, Bayer, and Mylan. Dr. Halvorsen reported no financial conflicts. Dr. Cannon reported serving as a consultant to roughly a dozen pharmaceutical companies, including the Amarin Corporation, which markets a fish oil supplement and sponsored the REDUCE-IT trial.
MUNICH – In a double blow to the current, widespread routine use of low-dose aspirin and fish oil supplements for primary cardiovascular prevention in patients with diabetes, neither treatment provided any net clinical benefit in the massive, long-term ASCEND study, investigators reported at the annual congress of the European Society of Cardiology.
And, in yet another bitter pill to swallow, low-dose aspirin failed to reduce the incidence of GI cancer or any other type of cancer, compared with placebo in the study. Earlier, nondefinitive meta-analyses of much smaller randomized trials had raised the possibility of a roughly 30% reduction in the incidence of colorectal cancer in long-time users, said Jane Armitage, MD, professor of clinical trials and epidemiology at the University of Oxford (England).
“We saw no suggestion of an anticancer effect emerging over time,” Dr. Armitage said. “We did see a significant reduction in the risk of vascular events but also an increase in major bleeding such that the absolute benefits from avoiding a serious vascular event were largely counterbalanced by increased risk of bleeding. And there was no subgroup in which we could clearly define that the benefit outweighs the risk,” she added in a video interview.
ASCEND (A Study of Cardiovascular Events in Diabetes) was a randomized, blinded trial in which 15,480 U.K. patients with diabetes and no known cardiovascular disease were placed on 100 mg/day of enteric-coated aspirin or placebo and 1 g/day of omega-3 fatty acids in capsule form or placebo in a 2 x 2 factorial design and followed prospectively for a mean of 7.4 years.
The study was undertaken because, even though the value of low-dose aspirin for secondary prevention is supported by strong evidence, the medication’s value for primary prevention in patients with diabetes has long been uncertain. American Diabetes Association guidelines give a Grade C recommendation to consideration of low-dose aspirin as a primary prevention strategy in patients with diabetes having a 10-year cardiovascular risk estimated at 10% or greater.
The primary efficacy endpoint in ASCEND was the occurrence of a first serious vascular event, defined as MI, stroke, transient ischemic attack, or death from any vascular cause other than intracranial hemorrhage. The rate was 8.5% in the aspirin group and 9.6% with placebo, for a statistically significant 12% relative risk reduction. However, the rate of the primary composite safety endpoint, comprising intracranial hemorrhage, GI bleeding, sight-threatening bleeding in the eye, or other bleeding serious enough to entail a trip to the hospital, was 4.1% in the aspirin group and 3.2% with placebo, a 29% increase in risk.
Aspirin reduced the absolute risk of a serious vascular event by 1.1%, compared with placebo, while boosting the risk of major bleeding by an absolute 0.9% – essentially a wash. The number needed to treat to avoid a serious vascular event was 91 patients, with 112 being the number needed to cause a major bleeding event. The risk of major bleeding rose with increasing baseline 5-year vascular event risk.
ASCEND provided no support for a recent report suggesting the benefit of low-dose aspirin for cardioprotection is largely confined to individuals weighing less than 70 kg (Lancet. 2018; 392:387-99); in fact, the opposite appeared to be true, according to Dr. Armitage.
The incidence of cancer of the GI tract was 2.0% in both study arms. The overall cancer rate was 11.6% in the aspirin arm and 11.5% with placebo. Additional follow-up focused on cancer is planned for 5 and 10 years after the end of ASCEND in order to examine the possibility of a delayed anticancer effect, she added.
Dr. Armitage said one reason aspirin may have failed to show a significant net benefit was the high rate of background cardioprotective medication usage, especially statins and antihypertensive drugs.
“I think if your diabetes is well managed and you’ve got your other risk factors under control, you have to consider very carefully whether or not, for you, the benefits of aspirin outweigh the risks,” she concluded.
Cardiologists respond
ASCEND’s two designated discussants, both cardiologists, took a more positive view of the results than Dr. Armitage, who isn’t a cardiologist.
Sigrun Halvorsen, MD, professor of cardiology at the University of Oslo, noted that most ASCEND participants were at relatively low cardiovascular risk, with an event rate of about 1.3% per year. She indicated that she’d like to see more data on higher-risk individuals before excluding any role for aspirin in primary cardiovascular prevention in patients with diabetes.
“Serious vascular events and bleeding are not necessarily equally weighted,” she added. “Most major bleeds in ASCEND were GI bleeds, and these can be largely prevented by PPIs [proton pump inhibitors], in contrast to death and stroke, which are irreversible events.”
“I think this study could be interpreted more favorably,” agreed Christopher P. Cannon, MD, professor of medicine at Harvard Medical School, Boston. “Bleeds are reversible, but MIs and whatnot are not.”
Fish oil flounders in ASCEND
Louise Bowman, MD, also at the University of Oxford, presented the ASCEND fish oil findings. Over an average of 7.4 years, omega-3 fatty acid supplementation had no effect on the rate of serious vascular events, no effect on cancer, no impact on all-cause or cause-specific mortality, and raised no safety issues in patients with diabetes. She argued that current guidelines recommending fish oil supplements for cardiovascular prevention should be reconsidered.
“Certainly there doesn’t seem to be any justification for the use of this dose of omega-3 fatty acids – 1 g/day – for the prevention of cardiovascular disease,” Dr. Bowman said.
However, Dr. Cannon saw a sliver of hope within the ASCEND findings. One component of the serious vascular event composite endpoint – vascular death – occurred in 2.4% of the fish oil group and 2.9% of placebo-treated controls, for a statistically significant 19% relative risk reduction. It could be a fluke, given that none of the other vascular endpoints followed suit. But physicians and patients won’t have to wait long to find out. Another randomized trial of low-dose fish oil supplements for primary cardiovascular prevention – the nearly 26,000-patient VITAL trial – is due to report later in 2018.
In addition, two major, randomized trials of higher-dose fish oil supplementation for secondary prevention are ongoing. The roughly 8,000-patient REDUCE-IT trial is expected to report results later this year, and the STRENGTH trial, featuring more than 13,000 patients, should be completed in 2020. Both studies are heavily loaded with diabetes patients, Dr. Cannon noted.
Simultaneous with presentation of the ASCEND results at the ESC congress, the study was published online at the New England Journal of Medicine website (doi: 10.1056/NEJMoa1804988 and doi: 10.1056/NEJMoa1804989).
The ASCEND study was funded by the British Heart Foundation and the U.K. Medical Research Council with support provided by Abbott Laboratories, Bayer, Mylan, and Solvay. Dr. Armitage and Dr. Bowman reported receiving research grants from the Medicines Company, Bayer, and Mylan. Dr. Halvorsen reported no financial conflicts. Dr. Cannon reported serving as a consultant to roughly a dozen pharmaceutical companies, including the Amarin Corporation, which markets a fish oil supplement and sponsored the REDUCE-IT trial.
REPORTING FROM THE ESC CONGRESS 2018
Key clinical point:
Major finding: Low-dose aspirin reduced the risk of serious vascular events by 12% versus placebo, but boosted major bleeding events by 29%.
Study details: This prospective, randomized trial included 15,480 patients with diabetes without known cardiovascular disease who were randomized to 100 mg/day of enteric-coated aspirin or placebo and 1 g/day of omega-3 fatty acids or placebo and followed for a mean of 7.4 years.
Disclosures: The study was funded by the British Heart Foundation and the U.K. Medical Research Council with support provided by Abbott Laboratories, Bayer, Mylan, and Solvay. The presenters reported receiving research grants from the Medicines Company, Bayer, and Mylan.

In geriatric urinary incontinence, think DIAPERS mnemonic
NEW ORLEANS – Neil M. Resnick, MD, has devoted more than 30 years of his career to refining the diagnosis and management of geriatric urinary incontinence. He has found it to be a deeply rewarding area of his medical practice. And he wants primary care physicians to share the joy.

Once you get the hang of it, you’re going to love it,” he promised at the annual meeting of the American College of Physicians.
“There is so much you have to offer, and it’s going to make you one happy, fulfilled, non–burned-out physician,” added Dr. Resnick, professor of medicine and chief of the division of geriatric medicine at the University of Pittsburgh.
He insisted that geriatric urinary incontinence belongs squarely in the province of primary care physicians, not just urologic surgeons. That’s because the condition is typically caused or exacerbated by medical diseases and drugs.
“These are things for which we are the experts, because they are conditions outside the bladder that our surgical colleagues aren’t always expert in,” the internist emphasized.
The seven reversible causes of geriatric urinary incontinence, which are categorized as transient urinary incontinence, can easily be remembered by busy primary care practitioners with the aid of a mnemonic of Dr. Resnick’s own devising: DIAPERS. It stands for Delirium, Infection, Atrophic urethritis/vaginitis, Pharmaceuticals, Excess urine output, Restricted mobility, and Stool impaction.
“Treatable causes of urinary incontinence are much more common in older people than in the young,” Dr. Resnick said. “If you just pay attention to these, and you can’t even spell ‘bladder,’ you can cure one-third of older patients. It’s pretty dramatic. And it improves the incontinence in all of the people in whom it’s still persistent, and that means improved responsiveness to further treatment addressing the urinary tract, improvement of other problems related to the incontinence, better quality of life, and it just makes patients better overall. This is really the joy and glory of geriatrics.”
He emphasized that urinary incontinence is never normal, no matter how advanced the patient’s age. The basic geriatric principle is that aging reduces resilience. Bladder sensation and contractility decrease with age. The prostate enlarges. Sphincter strength and urethral length decrease in older women. Involuntary bladder contractions occur in half of all elderly individuals. Nocturnal urine excretion increases. Postvoid urine volume creeps up to 50-100 mL. These are normal changes, but they predispose to tipping over into urinary incontinence in the setting of any additional challenges created by DIAPERS.
The scope of the problem
More than one-third of elderly individuals experience urinary incontinence with daily to weekly frequency. The associated morbidity includes cellulitis, perineal rashes, pressure ulcers, falls, fractures, anxiety, depression, and sexual dysfunction. The economic cost of geriatric urinary incontinence is believed to exceed that of coronary artery bypass surgery and renal dialysis combined.
“The morbidity is huge and the costs are astonishing,” the geriatrician declared.
Fewer than one-fifth and perhaps as few as one-tenth of affected patients actually require surgery.
Less than 20% of elderly patients with urinary incontinence volunteer that information to their primary care physician because of the stigma involved. So, it’s important to ask about it, he noted.
The lowdown on DIAPERS
- Delirium. “The last thing you want to do is refer a patient with urinary incontinence and delirium to a urologist for cystoscopy or urodynamic testing,” according to Dr. Resnick. “It misses the point: The problem is their brain is not working. If you address the causes of delirium, once the delirium subsides, the incontinence will abate.” However, addressing the cause of the acute confusional state can be challenging, he conceded, because delirium can result from virtually any drug or disease anywhere in the body.
- Infection. Acute urinary tract infection (UTI) is the cause of about only 3% of geriatric urinary incontinence. But when present, it’s simple enough to diagnosis and treat. Far more common is asymptomatic bacteriuria, which is present in about 20% of elderly men and 40% of elderly women but does not cause incontinence.
- “The key symptom is dysuria: If the patient [with bacteriuria] has new-onset urinary incontinence or worsened urinary incontinence that’s happened for only the last couple days, that’s an acute UTI that needs to be treated,” Dr. Resnick advised. “Other than that, don’t treat. All you’ll do is select for more virulent organisms, so when the patient does get an acute UTI, it’s tougher to treat.”
- Atrophic vaginitis/urethritis. A common condition when endogenous estrogen goes down. It is characterized by vaginal and urethral erosions and tissue friability. When an affected woman urinates, the acid urine gains exposure to the underlying subendothelial tissue, causing inflammation and irritation that prevent the urethra from closing properly. This condition, frequently mistaken for a UTI, responds well to low-dose topical estrogen in the form of either an easily implantable ring that lasts for 3 months or a topical estrogen cream applied once daily, after establishing the absence of breast or uterine cancer.
- “It takes weeks to months for this condition to remit,” he said. “So, if they’re doing cream, they do it every day for a month. Then every month, they pull back by one day. Eventually, they get to the point where they can be maintained with once- or twice-weekly application.”
- Pharmaceuticals. The list of potential offenders is lengthy. Dr. Resnick focused on six types of medications that are most often linked to increased risk of geriatric urinary incontinence. Those six include long-acting sedative hypnotics, including diazepam (Valium); loop diuretics; and anticholinergic agents, including sedating antihistamines, antipsychotics, tricyclic antidepressants, and tiotropium bromide (Spiriva).
- They also include adrenergic agents, with alpha-adrenergic blockers causing or contributing to urinary incontinence in women and alpha-adrenergic agonists – present in a vast number of OTC cold, sleep, and cough medications – being responsible for problems in men; drugs causing fluid accumulation, including the dihydropyridine calcium channel blockers, NSAIDs, some Parkinson’s agents, and gabapentin/pregabalin; and ACE inhibitors because of their side effect of cough.
- “The most common problem drugs in my practice are calcium channel blockers and gabapentin or pregabalin,” according to the geriatrician.
- Excess urine output. Older people have smaller bladders. Dr. Resnick loathes the popular advice to drink 8 glasses of water per day. Every time that so-called health tip appears in the mass media, he sees a flurry of patients with new-onset geriatric urinary incontinence. Other causes of excess urine output include alcohol, caffeine, metabolic disorders including hyperglycemia, and peripheral edema attributable to heart failure or venous insufficiency.
- Restricted mobility. This often results from overlooked correctable conditions that bedevil older people, including poorly fitting shoes, calluses, bunions, and deformed toenails, as well as readily treatable disorders including depression, orthostatic or postprandial hypotension, and arthritis pain.
- Stool impaction. “The clinical key is new onset of double incontinence associated with bladder distension. One gloved finger will disimpact and cure both,” Dr. Resnick said.
- In patients whose urinary incontinence persists after systematic attention to the DIAPERS details, there are only four possible mechanisms, according to Dr. Resnick: an overactive detrusor or stress incontinence, which can be categorized as storage problems, or an underactive detrusor or a urethral obstruction, which can be considered emptying problems.
Dr. Resnick reported having no financial conflicts of interest regarding his presentation.
NEW ORLEANS – Neil M. Resnick, MD, has devoted more than 30 years of his career to refining the diagnosis and management of geriatric urinary incontinence. He has found it to be a deeply rewarding area of his medical practice. And he wants primary care physicians to share the joy.
Once you get the hang of it, you’re going to love it,” he promised at the annual meeting of the American College of Physicians.
“There is so much you have to offer, and it’s going to make you one happy, fulfilled, non–burned-out physician,” added Dr. Resnick, professor of medicine and chief of the division of geriatric medicine at the University of Pittsburgh.
He insisted that geriatric urinary incontinence belongs squarely in the province of primary care physicians, not just urologic surgeons. That’s because the condition is typically caused or exacerbated by medical diseases and drugs.
“These are things for which we are the experts, because they are conditions outside the bladder that our surgical colleagues aren’t always expert in,” the internist emphasized.
The seven reversible causes of geriatric urinary incontinence, which are categorized as transient urinary incontinence, can easily be remembered by busy primary care practitioners with the aid of a mnemonic of Dr. Resnick’s own devising: DIAPERS. It stands for Delirium, Infection, Atrophic urethritis/vaginitis, Pharmaceuticals, Excess urine output, Restricted mobility, and Stool impaction.
“Treatable causes of urinary incontinence are much more common in older people than in the young,” Dr. Resnick said. “If you just pay attention to these, and you can’t even spell ‘bladder,’ you can cure one-third of older patients. It’s pretty dramatic. And it improves the incontinence in all of the people in whom it’s still persistent, and that means improved responsiveness to further treatment addressing the urinary tract, improvement of other problems related to the incontinence, better quality of life, and it just makes patients better overall. This is really the joy and glory of geriatrics.”
He emphasized that urinary incontinence is never normal, no matter how advanced the patient’s age. The basic geriatric principle is that aging reduces resilience. Bladder sensation and contractility decrease with age. The prostate enlarges. Sphincter strength and urethral length decrease in older women. Involuntary bladder contractions occur in half of all elderly individuals. Nocturnal urine excretion increases. Postvoid urine volume creeps up to 50-100 mL. These are normal changes, but they predispose to tipping over into urinary incontinence in the setting of any additional challenges created by DIAPERS.
The scope of the problem
More than one-third of elderly individuals experience urinary incontinence with daily to weekly frequency. The associated morbidity includes cellulitis, perineal rashes, pressure ulcers, falls, fractures, anxiety, depression, and sexual dysfunction. The economic cost of geriatric urinary incontinence is believed to exceed that of coronary artery bypass surgery and renal dialysis combined.
“The morbidity is huge and the costs are astonishing,” the geriatrician declared.
Fewer than one-fifth and perhaps as few as one-tenth of affected patients actually require surgery.
Less than 20% of elderly patients with urinary incontinence volunteer that information to their primary care physician because of the stigma involved. So, it’s important to ask about it, he noted.
The lowdown on DIAPERS
- Delirium. “The last thing you want to do is refer a patient with urinary incontinence and delirium to a urologist for cystoscopy or urodynamic testing,” according to Dr. Resnick. “It misses the point: The problem is their brain is not working. If you address the causes of delirium, once the delirium subsides, the incontinence will abate.” However, addressing the cause of the acute confusional state can be challenging, he conceded, because delirium can result from virtually any drug or disease anywhere in the body.
- Infection. Acute urinary tract infection (UTI) is the cause of about only 3% of geriatric urinary incontinence. But when present, it’s simple enough to diagnosis and treat. Far more common is asymptomatic bacteriuria, which is present in about 20% of elderly men and 40% of elderly women but does not cause incontinence.
- “The key symptom is dysuria: If the patient [with bacteriuria] has new-onset urinary incontinence or worsened urinary incontinence that’s happened for only the last couple days, that’s an acute UTI that needs to be treated,” Dr. Resnick advised. “Other than that, don’t treat. All you’ll do is select for more virulent organisms, so when the patient does get an acute UTI, it’s tougher to treat.”
- Atrophic vaginitis/urethritis. A common condition when endogenous estrogen goes down. It is characterized by vaginal and urethral erosions and tissue friability. When an affected woman urinates, the acid urine gains exposure to the underlying subendothelial tissue, causing inflammation and irritation that prevent the urethra from closing properly. This condition, frequently mistaken for a UTI, responds well to low-dose topical estrogen in the form of either an easily implantable ring that lasts for 3 months or a topical estrogen cream applied once daily, after establishing the absence of breast or uterine cancer.
- “It takes weeks to months for this condition to remit,” he said. “So, if they’re doing cream, they do it every day for a month. Then every month, they pull back by one day. Eventually, they get to the point where they can be maintained with once- or twice-weekly application.”
- Pharmaceuticals. The list of potential offenders is lengthy. Dr. Resnick focused on six types of medications that are most often linked to increased risk of geriatric urinary incontinence. Those six include long-acting sedative hypnotics, including diazepam (Valium); loop diuretics; and anticholinergic agents, including sedating antihistamines, antipsychotics, tricyclic antidepressants, and tiotropium bromide (Spiriva).
- They also include adrenergic agents, with alpha-adrenergic blockers causing or contributing to urinary incontinence in women and alpha-adrenergic agonists – present in a vast number of OTC cold, sleep, and cough medications – being responsible for problems in men; drugs causing fluid accumulation, including the dihydropyridine calcium channel blockers, NSAIDs, some Parkinson’s agents, and gabapentin/pregabalin; and ACE inhibitors because of their side effect of cough.
- “The most common problem drugs in my practice are calcium channel blockers and gabapentin or pregabalin,” according to the geriatrician.
- Excess urine output. Older people have smaller bladders. Dr. Resnick loathes the popular advice to drink 8 glasses of water per day. Every time that so-called health tip appears in the mass media, he sees a flurry of patients with new-onset geriatric urinary incontinence. Other causes of excess urine output include alcohol, caffeine, metabolic disorders including hyperglycemia, and peripheral edema attributable to heart failure or venous insufficiency.
- Restricted mobility. This often results from overlooked correctable conditions that bedevil older people, including poorly fitting shoes, calluses, bunions, and deformed toenails, as well as readily treatable disorders including depression, orthostatic or postprandial hypotension, and arthritis pain.
- Stool impaction. “The clinical key is new onset of double incontinence associated with bladder distension. One gloved finger will disimpact and cure both,” Dr. Resnick said.
- In patients whose urinary incontinence persists after systematic attention to the DIAPERS details, there are only four possible mechanisms, according to Dr. Resnick: an overactive detrusor or stress incontinence, which can be categorized as storage problems, or an underactive detrusor or a urethral obstruction, which can be considered emptying problems.
Dr. Resnick reported having no financial conflicts of interest regarding his presentation.
NEW ORLEANS – Neil M. Resnick, MD, has devoted more than 30 years of his career to refining the diagnosis and management of geriatric urinary incontinence. He has found it to be a deeply rewarding area of his medical practice. And he wants primary care physicians to share the joy.
Once you get the hang of it, you’re going to love it,” he promised at the annual meeting of the American College of Physicians.
“There is so much you have to offer, and it’s going to make you one happy, fulfilled, non–burned-out physician,” added Dr. Resnick, professor of medicine and chief of the division of geriatric medicine at the University of Pittsburgh.
He insisted that geriatric urinary incontinence belongs squarely in the province of primary care physicians, not just urologic surgeons. That’s because the condition is typically caused or exacerbated by medical diseases and drugs.
“These are things for which we are the experts, because they are conditions outside the bladder that our surgical colleagues aren’t always expert in,” the internist emphasized.
The seven reversible causes of geriatric urinary incontinence, which are categorized as transient urinary incontinence, can easily be remembered by busy primary care practitioners with the aid of a mnemonic of Dr. Resnick’s own devising: DIAPERS. It stands for Delirium, Infection, Atrophic urethritis/vaginitis, Pharmaceuticals, Excess urine output, Restricted mobility, and Stool impaction.
“Treatable causes of urinary incontinence are much more common in older people than in the young,” Dr. Resnick said. “If you just pay attention to these, and you can’t even spell ‘bladder,’ you can cure one-third of older patients. It’s pretty dramatic. And it improves the incontinence in all of the people in whom it’s still persistent, and that means improved responsiveness to further treatment addressing the urinary tract, improvement of other problems related to the incontinence, better quality of life, and it just makes patients better overall. This is really the joy and glory of geriatrics.”
He emphasized that urinary incontinence is never normal, no matter how advanced the patient’s age. The basic geriatric principle is that aging reduces resilience. Bladder sensation and contractility decrease with age. The prostate enlarges. Sphincter strength and urethral length decrease in older women. Involuntary bladder contractions occur in half of all elderly individuals. Nocturnal urine excretion increases. Postvoid urine volume creeps up to 50-100 mL. These are normal changes, but they predispose to tipping over into urinary incontinence in the setting of any additional challenges created by DIAPERS.
The scope of the problem
More than one-third of elderly individuals experience urinary incontinence with daily to weekly frequency. The associated morbidity includes cellulitis, perineal rashes, pressure ulcers, falls, fractures, anxiety, depression, and sexual dysfunction. The economic cost of geriatric urinary incontinence is believed to exceed that of coronary artery bypass surgery and renal dialysis combined.
“The morbidity is huge and the costs are astonishing,” the geriatrician declared.
Fewer than one-fifth and perhaps as few as one-tenth of affected patients actually require surgery.
Less than 20% of elderly patients with urinary incontinence volunteer that information to their primary care physician because of the stigma involved. So, it’s important to ask about it, he noted.
The lowdown on DIAPERS
- Delirium. “The last thing you want to do is refer a patient with urinary incontinence and delirium to a urologist for cystoscopy or urodynamic testing,” according to Dr. Resnick. “It misses the point: The problem is their brain is not working. If you address the causes of delirium, once the delirium subsides, the incontinence will abate.” However, addressing the cause of the acute confusional state can be challenging, he conceded, because delirium can result from virtually any drug or disease anywhere in the body.
- Infection. Acute urinary tract infection (UTI) is the cause of about only 3% of geriatric urinary incontinence. But when present, it’s simple enough to diagnosis and treat. Far more common is asymptomatic bacteriuria, which is present in about 20% of elderly men and 40% of elderly women but does not cause incontinence.
- “The key symptom is dysuria: If the patient [with bacteriuria] has new-onset urinary incontinence or worsened urinary incontinence that’s happened for only the last couple days, that’s an acute UTI that needs to be treated,” Dr. Resnick advised. “Other than that, don’t treat. All you’ll do is select for more virulent organisms, so when the patient does get an acute UTI, it’s tougher to treat.”
- Atrophic vaginitis/urethritis. A common condition when endogenous estrogen goes down. It is characterized by vaginal and urethral erosions and tissue friability. When an affected woman urinates, the acid urine gains exposure to the underlying subendothelial tissue, causing inflammation and irritation that prevent the urethra from closing properly. This condition, frequently mistaken for a UTI, responds well to low-dose topical estrogen in the form of either an easily implantable ring that lasts for 3 months or a topical estrogen cream applied once daily, after establishing the absence of breast or uterine cancer.
- “It takes weeks to months for this condition to remit,” he said. “So, if they’re doing cream, they do it every day for a month. Then every month, they pull back by one day. Eventually, they get to the point where they can be maintained with once- or twice-weekly application.”
- Pharmaceuticals. The list of potential offenders is lengthy. Dr. Resnick focused on six types of medications that are most often linked to increased risk of geriatric urinary incontinence. Those six include long-acting sedative hypnotics, including diazepam (Valium); loop diuretics; and anticholinergic agents, including sedating antihistamines, antipsychotics, tricyclic antidepressants, and tiotropium bromide (Spiriva).
- They also include adrenergic agents, with alpha-adrenergic blockers causing or contributing to urinary incontinence in women and alpha-adrenergic agonists – present in a vast number of OTC cold, sleep, and cough medications – being responsible for problems in men; drugs causing fluid accumulation, including the dihydropyridine calcium channel blockers, NSAIDs, some Parkinson’s agents, and gabapentin/pregabalin; and ACE inhibitors because of their side effect of cough.
- “The most common problem drugs in my practice are calcium channel blockers and gabapentin or pregabalin,” according to the geriatrician.
- Excess urine output. Older people have smaller bladders. Dr. Resnick loathes the popular advice to drink 8 glasses of water per day. Every time that so-called health tip appears in the mass media, he sees a flurry of patients with new-onset geriatric urinary incontinence. Other causes of excess urine output include alcohol, caffeine, metabolic disorders including hyperglycemia, and peripheral edema attributable to heart failure or venous insufficiency.
- Restricted mobility. This often results from overlooked correctable conditions that bedevil older people, including poorly fitting shoes, calluses, bunions, and deformed toenails, as well as readily treatable disorders including depression, orthostatic or postprandial hypotension, and arthritis pain.
- Stool impaction. “The clinical key is new onset of double incontinence associated with bladder distension. One gloved finger will disimpact and cure both,” Dr. Resnick said.
- In patients whose urinary incontinence persists after systematic attention to the DIAPERS details, there are only four possible mechanisms, according to Dr. Resnick: an overactive detrusor or stress incontinence, which can be categorized as storage problems, or an underactive detrusor or a urethral obstruction, which can be considered emptying problems.
Dr. Resnick reported having no financial conflicts of interest regarding his presentation.
REPORTING FROM ACP INTERNAL MEDICINE
Mindfulness training for migraine just beginning to gather steam
SAN FRANCISCO – A brief course of mindfulness training for chronic migraine patients after their withdrawal from overuse of acute migraine medications proved as effective as prophylactic medication over the course of 12 months of follow-up, Frank Andrasik, PhD, reported at the annual meeting of the American Headache Society.
“The effects of mindfulness by and large rivaled those for medication alone. And although not specifically assessed, patients commented that mindfulness didn’t have side effects and promoted greater involvement and adherence,” said Dr. Andrasik, professor and chair, department of psychology, and director of the Center for Behavioral Medicine at the University of Memphis.
He noted that his recently published study (J Headache Pain. 2017 Dec;18[1]:15. doi: 10.1186/s10194-017-0728-z) is best considered exploratory because of its small size and nonrandomized design. Participants, after 5 days of structured acute medication withdrawal in a day hospital setting, got to choose whether to opt for pharmacologic prophylaxis for migraine – most often using botulinum toxin – or a brief course in mindfulness training entailing six once-weekly 45-minute sessions plus home practice for 7-10 minutes per day. And while this study design doesn’t rise to the status of level 1 randomized trial evidence, it does reflect real-world clinical practice, where patients often have a big say in choosing their treatment plan, the psychologist observed.
At baseline, all 44 patients met diagnostic criteria for chronic migraine with associated acute medication overuse. They averaged 20.5 headache days per month, with 18.4 days of acute migraine medication use.
At 3, 6, and 12 months of follow-up, the 22 patients in the mindfulness group averaged 8.3, 10.4, and 12.4 headache days per month, while the 22 on preventive migraine drugs averaged 8.8, 11, and 8.6 headache days per month. Both groups averaged similar 7- to 10-day reductions in days of acute migraine medication use per month.
Using the widely accepted endpoint of at least a 50% reduction in headache days per month, 50% of the mindfulness-only group and 52.6% of the prophylactic medication-only group met that standard at 12 months of follow-up. Moreover, at 12 months, 65% of the mindfulness therapy group and a similar 73.7% of the preventive medication group no longer met diagnostic criteria for chronic migraine.
The mindfulness protocol used in the study was based upon the popular mindfulness-based stress reduction program developed by Jon Kabat-Zinn, PhD.
Scores on the Migraine Disability Assessment (MIDAS) measure improved significantly and to a similar extent over baseline in both groups. So did scores on the Beck Depression Inventory. In contrast, scores on the State-Trait Anxiety Inventory didn’t change significantly in either study arm.
Both Dr. Andrasik and session chair Elizabeth K. Seng, PhD, cautioned that despite solid evidence of efficacy for mindfulness training in the treatment of depression and a number of chronic pain disorders, . Large randomized, controlled clinical trials are ongoing or in the planning stages, with no results yet available.
Dr. Seng, a clinical psychologist at Albert Einstein College of Medicine in New York, described mindfulness and acceptance as “third wave” behavioral treatments for migraine. The first wave therapies focused on fostering behavioral changes to reduce perceived stress in order to avoid triggering migraine attacks. The second wave involved therapeutic interactions aimed at helping patients reframe maladaptive automatic thoughts to reduce stress stemming from the daily hassles of life.
“The focus in the first- and second-wave therapies is, ‘Change something and your life will be better. Change your behaviors, clean up your act, change your thoughts because your thoughts are not helping you, and thereby reduce stress and reduce migraine.’ These mindfulness therapies are incredibly different from that,” she explained.

Indeed, the third-wave therapies aren’t trying to change daily hassles or automatic thoughts; instead, they seek to change the patient’s relationship to them such that they no longer create barriers to engaging in life activities that the patient finds nourishing and meaningful. It’s a matter of creating a willingness to experience pain in order to achieve worthwhile objectives, Dr. Seng continued.
It’s unclear that a reduction in migraine days – the traditional yardstick for therapeutic efficacy in migraine research – is the right primary outcome measure for third-wave therapies, according to the psychologist.
“So far, our evidence would suggest that mindfulness-based therapies do not reduce migraine days as much as other behavioral treatments, but what they’re doing is increasing migraine-related quality of life and reducing migraine-related disability to the same or possibly larger extent than our other behavioral treatments,“ she said. “Maybe what these third-wave therapies are actually doing is impacting our cognitive and emotional functioning, and that even if patients still experience similar levels of headache frequency, their reaction to those headache days no longer leads to a bunch of suffering. And that could be a clinically relevant outcome.”
Dr. Seng is particularly eager to formally study mindfulness therapies in a subgroup of migraine patients with high levels of depression. They might respond especially well, since mindfulness was originally developed as a treatment for severe depression. “Patients who are depressed have a hard time overcoming barriers to engaging in nourishing life activities, and when they have a headache day it’s even worse. That’s one of the things that’s leading them to have migraine-related disability,” she said.
Dr. Andrasik, whose study was supported by the European Commission and an Italian research foundation, reported having no financial conflicts of interest regarding his presentation. Dr. Seng reported serving as a consultant to GlaxoSmithKline.
SAN FRANCISCO – A brief course of mindfulness training for chronic migraine patients after their withdrawal from overuse of acute migraine medications proved as effective as prophylactic medication over the course of 12 months of follow-up, Frank Andrasik, PhD, reported at the annual meeting of the American Headache Society.
“The effects of mindfulness by and large rivaled those for medication alone. And although not specifically assessed, patients commented that mindfulness didn’t have side effects and promoted greater involvement and adherence,” said Dr. Andrasik, professor and chair, department of psychology, and director of the Center for Behavioral Medicine at the University of Memphis.
He noted that his recently published study (J Headache Pain. 2017 Dec;18[1]:15. doi: 10.1186/s10194-017-0728-z) is best considered exploratory because of its small size and nonrandomized design. Participants, after 5 days of structured acute medication withdrawal in a day hospital setting, got to choose whether to opt for pharmacologic prophylaxis for migraine – most often using botulinum toxin – or a brief course in mindfulness training entailing six once-weekly 45-minute sessions plus home practice for 7-10 minutes per day. And while this study design doesn’t rise to the status of level 1 randomized trial evidence, it does reflect real-world clinical practice, where patients often have a big say in choosing their treatment plan, the psychologist observed.
At baseline, all 44 patients met diagnostic criteria for chronic migraine with associated acute medication overuse. They averaged 20.5 headache days per month, with 18.4 days of acute migraine medication use.
At 3, 6, and 12 months of follow-up, the 22 patients in the mindfulness group averaged 8.3, 10.4, and 12.4 headache days per month, while the 22 on preventive migraine drugs averaged 8.8, 11, and 8.6 headache days per month. Both groups averaged similar 7- to 10-day reductions in days of acute migraine medication use per month.
Using the widely accepted endpoint of at least a 50% reduction in headache days per month, 50% of the mindfulness-only group and 52.6% of the prophylactic medication-only group met that standard at 12 months of follow-up. Moreover, at 12 months, 65% of the mindfulness therapy group and a similar 73.7% of the preventive medication group no longer met diagnostic criteria for chronic migraine.
The mindfulness protocol used in the study was based upon the popular mindfulness-based stress reduction program developed by Jon Kabat-Zinn, PhD.
Scores on the Migraine Disability Assessment (MIDAS) measure improved significantly and to a similar extent over baseline in both groups. So did scores on the Beck Depression Inventory. In contrast, scores on the State-Trait Anxiety Inventory didn’t change significantly in either study arm.
Both Dr. Andrasik and session chair Elizabeth K. Seng, PhD, cautioned that despite solid evidence of efficacy for mindfulness training in the treatment of depression and a number of chronic pain disorders, . Large randomized, controlled clinical trials are ongoing or in the planning stages, with no results yet available.
Dr. Seng, a clinical psychologist at Albert Einstein College of Medicine in New York, described mindfulness and acceptance as “third wave” behavioral treatments for migraine. The first wave therapies focused on fostering behavioral changes to reduce perceived stress in order to avoid triggering migraine attacks. The second wave involved therapeutic interactions aimed at helping patients reframe maladaptive automatic thoughts to reduce stress stemming from the daily hassles of life.
“The focus in the first- and second-wave therapies is, ‘Change something and your life will be better. Change your behaviors, clean up your act, change your thoughts because your thoughts are not helping you, and thereby reduce stress and reduce migraine.’ These mindfulness therapies are incredibly different from that,” she explained.
Indeed, the third-wave therapies aren’t trying to change daily hassles or automatic thoughts; instead, they seek to change the patient’s relationship to them such that they no longer create barriers to engaging in life activities that the patient finds nourishing and meaningful. It’s a matter of creating a willingness to experience pain in order to achieve worthwhile objectives, Dr. Seng continued.
It’s unclear that a reduction in migraine days – the traditional yardstick for therapeutic efficacy in migraine research – is the right primary outcome measure for third-wave therapies, according to the psychologist.
“So far, our evidence would suggest that mindfulness-based therapies do not reduce migraine days as much as other behavioral treatments, but what they’re doing is increasing migraine-related quality of life and reducing migraine-related disability to the same or possibly larger extent than our other behavioral treatments,“ she said. “Maybe what these third-wave therapies are actually doing is impacting our cognitive and emotional functioning, and that even if patients still experience similar levels of headache frequency, their reaction to those headache days no longer leads to a bunch of suffering. And that could be a clinically relevant outcome.”
Dr. Seng is particularly eager to formally study mindfulness therapies in a subgroup of migraine patients with high levels of depression. They might respond especially well, since mindfulness was originally developed as a treatment for severe depression. “Patients who are depressed have a hard time overcoming barriers to engaging in nourishing life activities, and when they have a headache day it’s even worse. That’s one of the things that’s leading them to have migraine-related disability,” she said.
Dr. Andrasik, whose study was supported by the European Commission and an Italian research foundation, reported having no financial conflicts of interest regarding his presentation. Dr. Seng reported serving as a consultant to GlaxoSmithKline.
SAN FRANCISCO – A brief course of mindfulness training for chronic migraine patients after their withdrawal from overuse of acute migraine medications proved as effective as prophylactic medication over the course of 12 months of follow-up, Frank Andrasik, PhD, reported at the annual meeting of the American Headache Society.
“The effects of mindfulness by and large rivaled those for medication alone. And although not specifically assessed, patients commented that mindfulness didn’t have side effects and promoted greater involvement and adherence,” said Dr. Andrasik, professor and chair, department of psychology, and director of the Center for Behavioral Medicine at the University of Memphis.
He noted that his recently published study (J Headache Pain. 2017 Dec;18[1]:15. doi: 10.1186/s10194-017-0728-z) is best considered exploratory because of its small size and nonrandomized design. Participants, after 5 days of structured acute medication withdrawal in a day hospital setting, got to choose whether to opt for pharmacologic prophylaxis for migraine – most often using botulinum toxin – or a brief course in mindfulness training entailing six once-weekly 45-minute sessions plus home practice for 7-10 minutes per day. And while this study design doesn’t rise to the status of level 1 randomized trial evidence, it does reflect real-world clinical practice, where patients often have a big say in choosing their treatment plan, the psychologist observed.
At baseline, all 44 patients met diagnostic criteria for chronic migraine with associated acute medication overuse. They averaged 20.5 headache days per month, with 18.4 days of acute migraine medication use.
At 3, 6, and 12 months of follow-up, the 22 patients in the mindfulness group averaged 8.3, 10.4, and 12.4 headache days per month, while the 22 on preventive migraine drugs averaged 8.8, 11, and 8.6 headache days per month. Both groups averaged similar 7- to 10-day reductions in days of acute migraine medication use per month.
Using the widely accepted endpoint of at least a 50% reduction in headache days per month, 50% of the mindfulness-only group and 52.6% of the prophylactic medication-only group met that standard at 12 months of follow-up. Moreover, at 12 months, 65% of the mindfulness therapy group and a similar 73.7% of the preventive medication group no longer met diagnostic criteria for chronic migraine.
The mindfulness protocol used in the study was based upon the popular mindfulness-based stress reduction program developed by Jon Kabat-Zinn, PhD.
Scores on the Migraine Disability Assessment (MIDAS) measure improved significantly and to a similar extent over baseline in both groups. So did scores on the Beck Depression Inventory. In contrast, scores on the State-Trait Anxiety Inventory didn’t change significantly in either study arm.
Both Dr. Andrasik and session chair Elizabeth K. Seng, PhD, cautioned that despite solid evidence of efficacy for mindfulness training in the treatment of depression and a number of chronic pain disorders, . Large randomized, controlled clinical trials are ongoing or in the planning stages, with no results yet available.
Dr. Seng, a clinical psychologist at Albert Einstein College of Medicine in New York, described mindfulness and acceptance as “third wave” behavioral treatments for migraine. The first wave therapies focused on fostering behavioral changes to reduce perceived stress in order to avoid triggering migraine attacks. The second wave involved therapeutic interactions aimed at helping patients reframe maladaptive automatic thoughts to reduce stress stemming from the daily hassles of life.
“The focus in the first- and second-wave therapies is, ‘Change something and your life will be better. Change your behaviors, clean up your act, change your thoughts because your thoughts are not helping you, and thereby reduce stress and reduce migraine.’ These mindfulness therapies are incredibly different from that,” she explained.
Indeed, the third-wave therapies aren’t trying to change daily hassles or automatic thoughts; instead, they seek to change the patient’s relationship to them such that they no longer create barriers to engaging in life activities that the patient finds nourishing and meaningful. It’s a matter of creating a willingness to experience pain in order to achieve worthwhile objectives, Dr. Seng continued.
It’s unclear that a reduction in migraine days – the traditional yardstick for therapeutic efficacy in migraine research – is the right primary outcome measure for third-wave therapies, according to the psychologist.
“So far, our evidence would suggest that mindfulness-based therapies do not reduce migraine days as much as other behavioral treatments, but what they’re doing is increasing migraine-related quality of life and reducing migraine-related disability to the same or possibly larger extent than our other behavioral treatments,“ she said. “Maybe what these third-wave therapies are actually doing is impacting our cognitive and emotional functioning, and that even if patients still experience similar levels of headache frequency, their reaction to those headache days no longer leads to a bunch of suffering. And that could be a clinically relevant outcome.”
Dr. Seng is particularly eager to formally study mindfulness therapies in a subgroup of migraine patients with high levels of depression. They might respond especially well, since mindfulness was originally developed as a treatment for severe depression. “Patients who are depressed have a hard time overcoming barriers to engaging in nourishing life activities, and when they have a headache day it’s even worse. That’s one of the things that’s leading them to have migraine-related disability,” she said.
Dr. Andrasik, whose study was supported by the European Commission and an Italian research foundation, reported having no financial conflicts of interest regarding his presentation. Dr. Seng reported serving as a consultant to GlaxoSmithKline.
REPORTING FROM THE AHS ANNUAL MEETING
BIO-RESORT trial: Synergy, Orsiro, Resolution stents go head to head to head
PARIS – Three contemporary yet very different drug-eluting stents – two very-thin-strut biodegradable devices and one that leaves behind a durable polymer – achieved similarly low target vessel failure rates through 2 years of prospective follow-up in the large, all-comers, randomized BIO-RESORT trial, Marlies M. Kok, MD, reported at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.

That being said, the study provided an intriguing signal that the Orsiro sirolimus-eluting stent might reduce the risk of revascularization after the first year of follow-up, compared with the Synergy everolimus-eluting stent and Resolute Integrity zotarolimus-eluting stent.
“This is a signal of great interest,” noted Dr. Kok, a cardiologist at Thoraxcentrum Twente in Enschede, the Netherlands.
The BIO-RESORT trial was a multicenter, three-arm, patient- and assessor-blinded Dutch study in which 3,514 patients undergoing percutaneous coronary intervention (PCI) were randomized to the Resolute Integrity, Synergy, or Orsiro stent. This was an all-comers trial in which everyone who needed PCI with a drug-eluting stent was included. Most (70%) patients had an acute coronary syndrome; 31% presented with ST-segment elevation MI. At 1 year of follow-up, 86% of patients were on dual-antiplatelet therapy. The 1-year safety and efficacy outcomes, previously reported, were reassuringly similar in the three groups (Lancet. 2016 Nov 26;388[10060]:2607-17).
This was the first randomized trial to examine the safety and efficacy of the Synergy stent in all comers. Dr. Kok presented the new 2-year results, featuring 99% patient follow-up. It’s important to look at outcomes well beyond 1 year, she said, because the three stents are so different.
The Synergy and Orsiro stents feature very-thin, flexible struts with an uncoated thickness of 74 mm and 60 mm, respectively, compared with 91 mm for the Resolute Integrity stent. While the Synergy and Orsiro stents both utilize biodegradable polymer frames, the two devices utilize different drugs with different drug-eluting and polymer-resorption times. The polymer coating of the Synergy stent is resorbed within 4 months, while the Orsiro stent’s polymer degrades after 12 months and is resorbed by 24 months. Everolimus is distributed abluminally in the Synergy stent, while the other two stents feature circumferential drug placement. The Synergy frame is platinum and chromium, while other two utilize cobalt-chromium frames.
The thinking has been that treatment of coronary artery disease with drug-eluting stents, such as the Resolute Integrity, might delay arterial healing as a consequence of the life-long presence of the polymer in the vessel. Very-thin-strut biodegradable polymer stents were developed as a means of getting around this problem. But, at 1 year, the primary endpoint of target vessel failure – a safety and efficacy composite comprising cardiac death, target vessel-related MI, or clinically driven target vessel revascularization – was 5% in all three groups.
Dr. Kok reported that, at 2 years, the target vessel failure rate remained nonsignificantly different between the three study arms: 8.3% with the zotarolimus-eluting Resolute Integrity stent, 6.8% with the everolimus-eluting Synergy stent, and 6.6% with the sirolimus-eluting Orsiro stent. Nor were there any significant differences in the individual components of the primary endpoint. However, the secondary endpoint of target lesion failure – comprising cardiac death, any MI, or clinically driven target lesion revascularization – was a different story. At 1 year, there were no significant between-group differences in this composite outcome. But, a landmark analysis showed that between years 1 and 2, the incidence was 2.4% in the Resolute Integrity group, 1.6% with the Synergy group, and 1.1% in patients randomized to the Orsiro stent. The difference in target lesion failure between the Resolute Integrity and Orsiro groups was statistically significant. This difference was driven in part by the rates of target lesion revascularization: 1.5% with the Resolute Integrity, 0.9% with the Synergy, and 0.6% with the Orsiro stent.
The 2-year rates of definite or probable stent thrombosis were low and similar in the three groups: 1.0% with the Synergy stent, 0.8% with the Resolute Integrity, and 0.6% with the Orsiro, she continued.
Longer-term follow-up is planned.
The latest BIO-RESORT results received a skeptical reception from the session’s discussion panel. Nick E. J. West, MD, of Royal Papworth Hospital in Cambridge, England, praised the study as large and well run, yet, “notwithstanding some post hoc statistical nitty-gritty, there are essentially no differences. Have we come as far as we’re going to go with metallic stents in terms of the devices, and is it now a bit more about implantation, about accuracy, about dual-antiplatelet therapy?” he asked.
Mirvat Al Alasnag, MD, an interventional cardiologist at King Fahd Armed Forces Hospital in Jeddah, Saudi Arabia, said, “An all-comers trial design does not necessarily tell you that something is good for everyone. We try and make everything simple, and it is not that simple. I do believe that stent choice decisions should be individualized.”
The BIO-RESORT trial was funded by institutional research grants from Biotronik, Boston Scientific, and Medtronic.
PARIS – Three contemporary yet very different drug-eluting stents – two very-thin-strut biodegradable devices and one that leaves behind a durable polymer – achieved similarly low target vessel failure rates through 2 years of prospective follow-up in the large, all-comers, randomized BIO-RESORT trial, Marlies M. Kok, MD, reported at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
That being said, the study provided an intriguing signal that the Orsiro sirolimus-eluting stent might reduce the risk of revascularization after the first year of follow-up, compared with the Synergy everolimus-eluting stent and Resolute Integrity zotarolimus-eluting stent.
“This is a signal of great interest,” noted Dr. Kok, a cardiologist at Thoraxcentrum Twente in Enschede, the Netherlands.
The BIO-RESORT trial was a multicenter, three-arm, patient- and assessor-blinded Dutch study in which 3,514 patients undergoing percutaneous coronary intervention (PCI) were randomized to the Resolute Integrity, Synergy, or Orsiro stent. This was an all-comers trial in which everyone who needed PCI with a drug-eluting stent was included. Most (70%) patients had an acute coronary syndrome; 31% presented with ST-segment elevation MI. At 1 year of follow-up, 86% of patients were on dual-antiplatelet therapy. The 1-year safety and efficacy outcomes, previously reported, were reassuringly similar in the three groups (Lancet. 2016 Nov 26;388[10060]:2607-17).
This was the first randomized trial to examine the safety and efficacy of the Synergy stent in all comers. Dr. Kok presented the new 2-year results, featuring 99% patient follow-up. It’s important to look at outcomes well beyond 1 year, she said, because the three stents are so different.
The Synergy and Orsiro stents feature very-thin, flexible struts with an uncoated thickness of 74 mm and 60 mm, respectively, compared with 91 mm for the Resolute Integrity stent. While the Synergy and Orsiro stents both utilize biodegradable polymer frames, the two devices utilize different drugs with different drug-eluting and polymer-resorption times. The polymer coating of the Synergy stent is resorbed within 4 months, while the Orsiro stent’s polymer degrades after 12 months and is resorbed by 24 months. Everolimus is distributed abluminally in the Synergy stent, while the other two stents feature circumferential drug placement. The Synergy frame is platinum and chromium, while other two utilize cobalt-chromium frames.
The thinking has been that treatment of coronary artery disease with drug-eluting stents, such as the Resolute Integrity, might delay arterial healing as a consequence of the life-long presence of the polymer in the vessel. Very-thin-strut biodegradable polymer stents were developed as a means of getting around this problem. But, at 1 year, the primary endpoint of target vessel failure – a safety and efficacy composite comprising cardiac death, target vessel-related MI, or clinically driven target vessel revascularization – was 5% in all three groups.
Dr. Kok reported that, at 2 years, the target vessel failure rate remained nonsignificantly different between the three study arms: 8.3% with the zotarolimus-eluting Resolute Integrity stent, 6.8% with the everolimus-eluting Synergy stent, and 6.6% with the sirolimus-eluting Orsiro stent. Nor were there any significant differences in the individual components of the primary endpoint. However, the secondary endpoint of target lesion failure – comprising cardiac death, any MI, or clinically driven target lesion revascularization – was a different story. At 1 year, there were no significant between-group differences in this composite outcome. But, a landmark analysis showed that between years 1 and 2, the incidence was 2.4% in the Resolute Integrity group, 1.6% with the Synergy group, and 1.1% in patients randomized to the Orsiro stent. The difference in target lesion failure between the Resolute Integrity and Orsiro groups was statistically significant. This difference was driven in part by the rates of target lesion revascularization: 1.5% with the Resolute Integrity, 0.9% with the Synergy, and 0.6% with the Orsiro stent.
The 2-year rates of definite or probable stent thrombosis were low and similar in the three groups: 1.0% with the Synergy stent, 0.8% with the Resolute Integrity, and 0.6% with the Orsiro, she continued.
Longer-term follow-up is planned.
The latest BIO-RESORT results received a skeptical reception from the session’s discussion panel. Nick E. J. West, MD, of Royal Papworth Hospital in Cambridge, England, praised the study as large and well run, yet, “notwithstanding some post hoc statistical nitty-gritty, there are essentially no differences. Have we come as far as we’re going to go with metallic stents in terms of the devices, and is it now a bit more about implantation, about accuracy, about dual-antiplatelet therapy?” he asked.
Mirvat Al Alasnag, MD, an interventional cardiologist at King Fahd Armed Forces Hospital in Jeddah, Saudi Arabia, said, “An all-comers trial design does not necessarily tell you that something is good for everyone. We try and make everything simple, and it is not that simple. I do believe that stent choice decisions should be individualized.”
The BIO-RESORT trial was funded by institutional research grants from Biotronik, Boston Scientific, and Medtronic.
PARIS – Three contemporary yet very different drug-eluting stents – two very-thin-strut biodegradable devices and one that leaves behind a durable polymer – achieved similarly low target vessel failure rates through 2 years of prospective follow-up in the large, all-comers, randomized BIO-RESORT trial, Marlies M. Kok, MD, reported at the annual meeting of the European Association of Percutaneous Cardiovascular Interventions.
That being said, the study provided an intriguing signal that the Orsiro sirolimus-eluting stent might reduce the risk of revascularization after the first year of follow-up, compared with the Synergy everolimus-eluting stent and Resolute Integrity zotarolimus-eluting stent.
“This is a signal of great interest,” noted Dr. Kok, a cardiologist at Thoraxcentrum Twente in Enschede, the Netherlands.
The BIO-RESORT trial was a multicenter, three-arm, patient- and assessor-blinded Dutch study in which 3,514 patients undergoing percutaneous coronary intervention (PCI) were randomized to the Resolute Integrity, Synergy, or Orsiro stent. This was an all-comers trial in which everyone who needed PCI with a drug-eluting stent was included. Most (70%) patients had an acute coronary syndrome; 31% presented with ST-segment elevation MI. At 1 year of follow-up, 86% of patients were on dual-antiplatelet therapy. The 1-year safety and efficacy outcomes, previously reported, were reassuringly similar in the three groups (Lancet. 2016 Nov 26;388[10060]:2607-17).
This was the first randomized trial to examine the safety and efficacy of the Synergy stent in all comers. Dr. Kok presented the new 2-year results, featuring 99% patient follow-up. It’s important to look at outcomes well beyond 1 year, she said, because the three stents are so different.
The Synergy and Orsiro stents feature very-thin, flexible struts with an uncoated thickness of 74 mm and 60 mm, respectively, compared with 91 mm for the Resolute Integrity stent. While the Synergy and Orsiro stents both utilize biodegradable polymer frames, the two devices utilize different drugs with different drug-eluting and polymer-resorption times. The polymer coating of the Synergy stent is resorbed within 4 months, while the Orsiro stent’s polymer degrades after 12 months and is resorbed by 24 months. Everolimus is distributed abluminally in the Synergy stent, while the other two stents feature circumferential drug placement. The Synergy frame is platinum and chromium, while other two utilize cobalt-chromium frames.
The thinking has been that treatment of coronary artery disease with drug-eluting stents, such as the Resolute Integrity, might delay arterial healing as a consequence of the life-long presence of the polymer in the vessel. Very-thin-strut biodegradable polymer stents were developed as a means of getting around this problem. But, at 1 year, the primary endpoint of target vessel failure – a safety and efficacy composite comprising cardiac death, target vessel-related MI, or clinically driven target vessel revascularization – was 5% in all three groups.
Dr. Kok reported that, at 2 years, the target vessel failure rate remained nonsignificantly different between the three study arms: 8.3% with the zotarolimus-eluting Resolute Integrity stent, 6.8% with the everolimus-eluting Synergy stent, and 6.6% with the sirolimus-eluting Orsiro stent. Nor were there any significant differences in the individual components of the primary endpoint. However, the secondary endpoint of target lesion failure – comprising cardiac death, any MI, or clinically driven target lesion revascularization – was a different story. At 1 year, there were no significant between-group differences in this composite outcome. But, a landmark analysis showed that between years 1 and 2, the incidence was 2.4% in the Resolute Integrity group, 1.6% with the Synergy group, and 1.1% in patients randomized to the Orsiro stent. The difference in target lesion failure between the Resolute Integrity and Orsiro groups was statistically significant. This difference was driven in part by the rates of target lesion revascularization: 1.5% with the Resolute Integrity, 0.9% with the Synergy, and 0.6% with the Orsiro stent.
The 2-year rates of definite or probable stent thrombosis were low and similar in the three groups: 1.0% with the Synergy stent, 0.8% with the Resolute Integrity, and 0.6% with the Orsiro, she continued.
Longer-term follow-up is planned.
The latest BIO-RESORT results received a skeptical reception from the session’s discussion panel. Nick E. J. West, MD, of Royal Papworth Hospital in Cambridge, England, praised the study as large and well run, yet, “notwithstanding some post hoc statistical nitty-gritty, there are essentially no differences. Have we come as far as we’re going to go with metallic stents in terms of the devices, and is it now a bit more about implantation, about accuracy, about dual-antiplatelet therapy?” he asked.
Mirvat Al Alasnag, MD, an interventional cardiologist at King Fahd Armed Forces Hospital in Jeddah, Saudi Arabia, said, “An all-comers trial design does not necessarily tell you that something is good for everyone. We try and make everything simple, and it is not that simple. I do believe that stent choice decisions should be individualized.”
The BIO-RESORT trial was funded by institutional research grants from Biotronik, Boston Scientific, and Medtronic.
REPORTING FROM EUROPCR 2018
Key clinical point: Three contemporary, very dissimilar drug-eluting stents show impressively low 2-year target vessel failure rates.
Major finding:
Study details: This was a multicenter, randomized trial with 99% 2-year follow-up of 3,514 patients, deemed to need PCI, who were randomized to one of three contemporary drug-eluting stents.
Disclosures: The study was funded by institutional research grants from Biotronik, Boston Scientific, and Medtronic.
Should PCPs take over chronic HCV treatment?
ESTES PARK, COLO. – Direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection has progressed to the point that it’s time for primary care physicians to take on the treatment of all affected patients who don’t have advanced fibrosis or other complex forms of the disease, Michael Kriss, MD, asserted at a conference on internal medicine sponsored by the University of Colorado.

declared Dr. Kriss, a gastroenterologist at the university.
Referral to a specialist should be reserved for those more complex patients with stage 3 or 4 fibrosis, hepatocellular carcinoma, coinfection with HIV or hepatitis B virus, end-stage organ disease being considered for transplantation, prior exposure to an NS5A inhibitor, or concomitant secondary liver disease, such as nonalcoholic steatohepatitis, he continued.
Treatment of chronic HCV now entails just 8-12 weeks of DAA therapy, with a cure rate greater than 95% and almost no side effects. The costs have come down, too, because of increased competition.
The epidemiology of HCV infection is changing. The opioid epidemic is driving an increased incidence of acute infection, with nearly 34,000 new cases per year, most of which will go on to chronic infection. Moreover, 93% of acutely infected individuals and half of the estimated 3.5 million Americans with chronic HCV are unaware they are infected. The scope of the problem is too big for gastroenterologists and infectious disease specialists to handle alone, according to Dr. Kriss.
Contemporary treatment of HCV involves a 6-step program that’s simpler than that of many of the diseases primary care physicians currently manage.
1) Confirm chronicity by two measurements of HCV RNA obtained 6 months apart.
2) Stage the patient’s fibrosis.
3) Order a baseline cross-sectional ultrasound to exclude cirrhosis or hepatocellular carcinoma, since the fibrosis staging methods aren’t foolproof.
4) Make sure the patient is still positive for HCV RNA prior to therapy.
5) Commence DAA therapy. The simplest regimen is 8 weeks of glecaprevir/pibrentasvir (Mavyret), provided it’s approved by the patient’s insurance.
6) Get a repeat HCV RNA 12 weeks after conclusion of treatment to confirm there is a sustained virologic response.
The critical part is step 2 because that’s how primary care physicians will decide which patients to treat in their office and which to refer to a specialist. Many biomarkers are available, some proprietary and others gratis. Dr. Kriss is particularly partial to the free Fibrosis-4 (Fib-4) calculator, which provides an estimate of the amount of liver scarring based upon the patient’s age, liver enzyme levels, and platelet count.
“This is really a valuable, extremely well-validated tool that any of you can use in your clinic,” he said.
The American Association for the Study of Liver Disease/Infectious Diseases Society of America hepatitis C guidelines state that the nonproprietary biomarker assays are equivalent to transient elastography for staging fibrosis. Those guidelines are an “outstanding” and extremely user-friendly resource for primary care physicians interested in taking on the treatment of chronic HCV, Dr. Kriss added.
In selecting a DAA, another key resource is the HEP Drug Interactions website, which enables physicians to identify potentially problematic drug-drug interactions. The two most important interactions involve statins or proton pump inhibitors.
Recent studies have shown that the benefits of achieving a sustained virologic response include a clinically meaningful regression of advanced fibrosis at 1 year after treatment in roughly half of patients (Dig Dis Sci. 2018 Feb;63[2]:486-92) and a reduced risk of developing hepatocellular carcinoma (Hepatology. 2018 Jun;67[6]:2244-53).
Models of remote consultation pathways to link primary care providers with consultant HCV specialists are being developed. In a study of 600 patients at federally qualified community health centers in Washington, the risk-adjusted cure rate was 90.4% among patients assigned to a nurse practitioner, 87.6% if DAA therapy was prescribed by a primary care physician, and 84.8% if treated by a specialist. Treatment visit adherence followed the same pattern and correlated with cure rates (Ann Intern Med. 2017 Sep 5;167[5]:311-8).
“Patients might be better off seeing someone they know instead of somebody like me who they’re only going to see one time,” Dr. Kriss observed.
Turning to a couple of controversial expansions of DAA into new populations, Dr. Kriss noted that the AASLD/IDSA guidelines state that active intravenous drug use should not be considered a contraindication to HCV therapy.
“Scaling up HCV treatment in persons who inject drugs is necessary to positively impact the HCV epidemic in the U.S. and globally,” according to the guidelines.
This message was recently underscored by the positive results of the seven-country SIMPLIFY trial, in which 12 weeks of velpatasvir-sofosbuvir (Epclusa) in a population of recent IV drug users achieved a 97% cure rate, with only one reinfection in this high-risk population (Lancet Gastroenterol Hepatol. 2018 Mar;3[3]:153-61).
The hottest controversy in hepatology has been whether to place HCV-positive donor organs in HCV-negative recipients.
“This is intentionally giving hepatitis C to the recipient knowing that he can be cured. Because treatment cure rates are so high, I predict this will become the standard of care in the next year or two,” Dr. Kriss said.
He reported having no financial conflicts regarding his presentation.
.
ESTES PARK, COLO. – Direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection has progressed to the point that it’s time for primary care physicians to take on the treatment of all affected patients who don’t have advanced fibrosis or other complex forms of the disease, Michael Kriss, MD, asserted at a conference on internal medicine sponsored by the University of Colorado.
declared Dr. Kriss, a gastroenterologist at the university.
Referral to a specialist should be reserved for those more complex patients with stage 3 or 4 fibrosis, hepatocellular carcinoma, coinfection with HIV or hepatitis B virus, end-stage organ disease being considered for transplantation, prior exposure to an NS5A inhibitor, or concomitant secondary liver disease, such as nonalcoholic steatohepatitis, he continued.
Treatment of chronic HCV now entails just 8-12 weeks of DAA therapy, with a cure rate greater than 95% and almost no side effects. The costs have come down, too, because of increased competition.
The epidemiology of HCV infection is changing. The opioid epidemic is driving an increased incidence of acute infection, with nearly 34,000 new cases per year, most of which will go on to chronic infection. Moreover, 93% of acutely infected individuals and half of the estimated 3.5 million Americans with chronic HCV are unaware they are infected. The scope of the problem is too big for gastroenterologists and infectious disease specialists to handle alone, according to Dr. Kriss.
Contemporary treatment of HCV involves a 6-step program that’s simpler than that of many of the diseases primary care physicians currently manage.
1) Confirm chronicity by two measurements of HCV RNA obtained 6 months apart.
2) Stage the patient’s fibrosis.
3) Order a baseline cross-sectional ultrasound to exclude cirrhosis or hepatocellular carcinoma, since the fibrosis staging methods aren’t foolproof.
4) Make sure the patient is still positive for HCV RNA prior to therapy.
5) Commence DAA therapy. The simplest regimen is 8 weeks of glecaprevir/pibrentasvir (Mavyret), provided it’s approved by the patient’s insurance.
6) Get a repeat HCV RNA 12 weeks after conclusion of treatment to confirm there is a sustained virologic response.
The critical part is step 2 because that’s how primary care physicians will decide which patients to treat in their office and which to refer to a specialist. Many biomarkers are available, some proprietary and others gratis. Dr. Kriss is particularly partial to the free Fibrosis-4 (Fib-4) calculator, which provides an estimate of the amount of liver scarring based upon the patient’s age, liver enzyme levels, and platelet count.
“This is really a valuable, extremely well-validated tool that any of you can use in your clinic,” he said.
The American Association for the Study of Liver Disease/Infectious Diseases Society of America hepatitis C guidelines state that the nonproprietary biomarker assays are equivalent to transient elastography for staging fibrosis. Those guidelines are an “outstanding” and extremely user-friendly resource for primary care physicians interested in taking on the treatment of chronic HCV, Dr. Kriss added.
In selecting a DAA, another key resource is the HEP Drug Interactions website, which enables physicians to identify potentially problematic drug-drug interactions. The two most important interactions involve statins or proton pump inhibitors.
Recent studies have shown that the benefits of achieving a sustained virologic response include a clinically meaningful regression of advanced fibrosis at 1 year after treatment in roughly half of patients (Dig Dis Sci. 2018 Feb;63[2]:486-92) and a reduced risk of developing hepatocellular carcinoma (Hepatology. 2018 Jun;67[6]:2244-53).
Models of remote consultation pathways to link primary care providers with consultant HCV specialists are being developed. In a study of 600 patients at federally qualified community health centers in Washington, the risk-adjusted cure rate was 90.4% among patients assigned to a nurse practitioner, 87.6% if DAA therapy was prescribed by a primary care physician, and 84.8% if treated by a specialist. Treatment visit adherence followed the same pattern and correlated with cure rates (Ann Intern Med. 2017 Sep 5;167[5]:311-8).
“Patients might be better off seeing someone they know instead of somebody like me who they’re only going to see one time,” Dr. Kriss observed.
Turning to a couple of controversial expansions of DAA into new populations, Dr. Kriss noted that the AASLD/IDSA guidelines state that active intravenous drug use should not be considered a contraindication to HCV therapy.
“Scaling up HCV treatment in persons who inject drugs is necessary to positively impact the HCV epidemic in the U.S. and globally,” according to the guidelines.
This message was recently underscored by the positive results of the seven-country SIMPLIFY trial, in which 12 weeks of velpatasvir-sofosbuvir (Epclusa) in a population of recent IV drug users achieved a 97% cure rate, with only one reinfection in this high-risk population (Lancet Gastroenterol Hepatol. 2018 Mar;3[3]:153-61).
The hottest controversy in hepatology has been whether to place HCV-positive donor organs in HCV-negative recipients.
“This is intentionally giving hepatitis C to the recipient knowing that he can be cured. Because treatment cure rates are so high, I predict this will become the standard of care in the next year or two,” Dr. Kriss said.
He reported having no financial conflicts regarding his presentation.
.
ESTES PARK, COLO. – Direct-acting antiviral (DAA) therapy for chronic hepatitis C virus (HCV) infection has progressed to the point that it’s time for primary care physicians to take on the treatment of all affected patients who don’t have advanced fibrosis or other complex forms of the disease, Michael Kriss, MD, asserted at a conference on internal medicine sponsored by the University of Colorado.
declared Dr. Kriss, a gastroenterologist at the university.
Referral to a specialist should be reserved for those more complex patients with stage 3 or 4 fibrosis, hepatocellular carcinoma, coinfection with HIV or hepatitis B virus, end-stage organ disease being considered for transplantation, prior exposure to an NS5A inhibitor, or concomitant secondary liver disease, such as nonalcoholic steatohepatitis, he continued.
Treatment of chronic HCV now entails just 8-12 weeks of DAA therapy, with a cure rate greater than 95% and almost no side effects. The costs have come down, too, because of increased competition.
The epidemiology of HCV infection is changing. The opioid epidemic is driving an increased incidence of acute infection, with nearly 34,000 new cases per year, most of which will go on to chronic infection. Moreover, 93% of acutely infected individuals and half of the estimated 3.5 million Americans with chronic HCV are unaware they are infected. The scope of the problem is too big for gastroenterologists and infectious disease specialists to handle alone, according to Dr. Kriss.
Contemporary treatment of HCV involves a 6-step program that’s simpler than that of many of the diseases primary care physicians currently manage.
1) Confirm chronicity by two measurements of HCV RNA obtained 6 months apart.
2) Stage the patient’s fibrosis.
3) Order a baseline cross-sectional ultrasound to exclude cirrhosis or hepatocellular carcinoma, since the fibrosis staging methods aren’t foolproof.
4) Make sure the patient is still positive for HCV RNA prior to therapy.
5) Commence DAA therapy. The simplest regimen is 8 weeks of glecaprevir/pibrentasvir (Mavyret), provided it’s approved by the patient’s insurance.
6) Get a repeat HCV RNA 12 weeks after conclusion of treatment to confirm there is a sustained virologic response.
The critical part is step 2 because that’s how primary care physicians will decide which patients to treat in their office and which to refer to a specialist. Many biomarkers are available, some proprietary and others gratis. Dr. Kriss is particularly partial to the free Fibrosis-4 (Fib-4) calculator, which provides an estimate of the amount of liver scarring based upon the patient’s age, liver enzyme levels, and platelet count.
“This is really a valuable, extremely well-validated tool that any of you can use in your clinic,” he said.
The American Association for the Study of Liver Disease/Infectious Diseases Society of America hepatitis C guidelines state that the nonproprietary biomarker assays are equivalent to transient elastography for staging fibrosis. Those guidelines are an “outstanding” and extremely user-friendly resource for primary care physicians interested in taking on the treatment of chronic HCV, Dr. Kriss added.
In selecting a DAA, another key resource is the HEP Drug Interactions website, which enables physicians to identify potentially problematic drug-drug interactions. The two most important interactions involve statins or proton pump inhibitors.
Recent studies have shown that the benefits of achieving a sustained virologic response include a clinically meaningful regression of advanced fibrosis at 1 year after treatment in roughly half of patients (Dig Dis Sci. 2018 Feb;63[2]:486-92) and a reduced risk of developing hepatocellular carcinoma (Hepatology. 2018 Jun;67[6]:2244-53).
Models of remote consultation pathways to link primary care providers with consultant HCV specialists are being developed. In a study of 600 patients at federally qualified community health centers in Washington, the risk-adjusted cure rate was 90.4% among patients assigned to a nurse practitioner, 87.6% if DAA therapy was prescribed by a primary care physician, and 84.8% if treated by a specialist. Treatment visit adherence followed the same pattern and correlated with cure rates (Ann Intern Med. 2017 Sep 5;167[5]:311-8).
“Patients might be better off seeing someone they know instead of somebody like me who they’re only going to see one time,” Dr. Kriss observed.
Turning to a couple of controversial expansions of DAA into new populations, Dr. Kriss noted that the AASLD/IDSA guidelines state that active intravenous drug use should not be considered a contraindication to HCV therapy.
“Scaling up HCV treatment in persons who inject drugs is necessary to positively impact the HCV epidemic in the U.S. and globally,” according to the guidelines.
This message was recently underscored by the positive results of the seven-country SIMPLIFY trial, in which 12 weeks of velpatasvir-sofosbuvir (Epclusa) in a population of recent IV drug users achieved a 97% cure rate, with only one reinfection in this high-risk population (Lancet Gastroenterol Hepatol. 2018 Mar;3[3]:153-61).
The hottest controversy in hepatology has been whether to place HCV-positive donor organs in HCV-negative recipients.
“This is intentionally giving hepatitis C to the recipient knowing that he can be cured. Because treatment cure rates are so high, I predict this will become the standard of care in the next year or two,” Dr. Kriss said.
He reported having no financial conflicts regarding his presentation.
.
REPORTING FROM COLORADO IM
High autonomic dysfunction distinguishes persistent posttraumatic headache
SAN FRANCISCO – Symptoms of autonomic dysfunction are significantly greater in patients with persistent posttraumatic headache than in migraine, raising the welcome possibility that this characteristic might serve to reliably differentiate the two disorders, Levi Howard, MD, said at the annual meeting of the American Headache Society.

“Interestingly enough, in looking at other studies evaluating dysautonomia, the [autonomic dysfunction scores] in our persistent posttraumatic headache group were on a par with scores previously reported for patients with diseases such as small-fiber polyneuropathy and postural orthostatic tachycardia syndrome,” observed Dr. Howard, an active duty military physician assigned to obtain neurology training at the Mayo Clinic Arizona in Phoenix.
“This brings up two questions: Do autonomic symptoms contribute to accurate classification of persistent posttraumatic headache versus migraine? And if we treat this autonomic dysfunction, does the headache also improve? In our clinical observation, this appears to be the case,” he continued.
Right now, posttraumatic headache (PTH) is defined on the basis of its temporal relationship to head injury. At this time, PTH has no defining clinical characteristics, although most often it has a phenotype that meets diagnostic criteria for migraine.
However, Dr. Howard and his coinvestigators have observed anecdotally in clinical practice that persistent PTH – defined as PTH lasting longer than 3 months – is often accompanied by orthostatic intolerance. This observation, coupled with reports in multiple prior studies that dysautonomia is common in patients with mild traumatic brain injury (TBI) and postconcussion syndrome, prompted Dr. Howard and his coworkers to conduct a cross-sectional cohort study. It included 56 patients with persistent PTH due to mild TBI, 30 patients with migraine, and 36 healthy controls. Most of the persistent PTH group were military veterans with mild TBI due to blast injuries.
All subjects were assessed for autonomic dysfunction using the well-validated COMPASS-31 questionnaire. This instrument assesses six domains of autonomic function: orthostatic intolerance, bladder, gastrointestinal, vasomotor, secretomotor, and pupillomotor.
Scores in each of the six domains were numerically higher in the persistent PTH group, with the differences achieving statistical significance in the orthostatic intolerance and bladder domains.
Of note, the migraine group had a greater headache burden, with a mean 23-year headache history, compared with 10.56 years in the persistent PTH group. The migraine patients also averaged 21.1 headache days per month, versus 16.2 in the persistent PTH group. Yet the investigators found no strong association between autonomic dysfunction and headache burden as reflected in headache duration or headache days per month.
The study was funded by the Department of Defense. Dr. Howard reported having no financial conflicts of interest.
SOURCE: Howard L et al. AHS 2018, Abstract FHM03.
SAN FRANCISCO – Symptoms of autonomic dysfunction are significantly greater in patients with persistent posttraumatic headache than in migraine, raising the welcome possibility that this characteristic might serve to reliably differentiate the two disorders, Levi Howard, MD, said at the annual meeting of the American Headache Society.
“Interestingly enough, in looking at other studies evaluating dysautonomia, the [autonomic dysfunction scores] in our persistent posttraumatic headache group were on a par with scores previously reported for patients with diseases such as small-fiber polyneuropathy and postural orthostatic tachycardia syndrome,” observed Dr. Howard, an active duty military physician assigned to obtain neurology training at the Mayo Clinic Arizona in Phoenix.
“This brings up two questions: Do autonomic symptoms contribute to accurate classification of persistent posttraumatic headache versus migraine? And if we treat this autonomic dysfunction, does the headache also improve? In our clinical observation, this appears to be the case,” he continued.
Right now, posttraumatic headache (PTH) is defined on the basis of its temporal relationship to head injury. At this time, PTH has no defining clinical characteristics, although most often it has a phenotype that meets diagnostic criteria for migraine.
However, Dr. Howard and his coinvestigators have observed anecdotally in clinical practice that persistent PTH – defined as PTH lasting longer than 3 months – is often accompanied by orthostatic intolerance. This observation, coupled with reports in multiple prior studies that dysautonomia is common in patients with mild traumatic brain injury (TBI) and postconcussion syndrome, prompted Dr. Howard and his coworkers to conduct a cross-sectional cohort study. It included 56 patients with persistent PTH due to mild TBI, 30 patients with migraine, and 36 healthy controls. Most of the persistent PTH group were military veterans with mild TBI due to blast injuries.
All subjects were assessed for autonomic dysfunction using the well-validated COMPASS-31 questionnaire. This instrument assesses six domains of autonomic function: orthostatic intolerance, bladder, gastrointestinal, vasomotor, secretomotor, and pupillomotor.
Scores in each of the six domains were numerically higher in the persistent PTH group, with the differences achieving statistical significance in the orthostatic intolerance and bladder domains.
Of note, the migraine group had a greater headache burden, with a mean 23-year headache history, compared with 10.56 years in the persistent PTH group. The migraine patients also averaged 21.1 headache days per month, versus 16.2 in the persistent PTH group. Yet the investigators found no strong association between autonomic dysfunction and headache burden as reflected in headache duration or headache days per month.
The study was funded by the Department of Defense. Dr. Howard reported having no financial conflicts of interest.
SOURCE: Howard L et al. AHS 2018, Abstract FHM03.
SAN FRANCISCO – Symptoms of autonomic dysfunction are significantly greater in patients with persistent posttraumatic headache than in migraine, raising the welcome possibility that this characteristic might serve to reliably differentiate the two disorders, Levi Howard, MD, said at the annual meeting of the American Headache Society.
“Interestingly enough, in looking at other studies evaluating dysautonomia, the [autonomic dysfunction scores] in our persistent posttraumatic headache group were on a par with scores previously reported for patients with diseases such as small-fiber polyneuropathy and postural orthostatic tachycardia syndrome,” observed Dr. Howard, an active duty military physician assigned to obtain neurology training at the Mayo Clinic Arizona in Phoenix.
“This brings up two questions: Do autonomic symptoms contribute to accurate classification of persistent posttraumatic headache versus migraine? And if we treat this autonomic dysfunction, does the headache also improve? In our clinical observation, this appears to be the case,” he continued.
Right now, posttraumatic headache (PTH) is defined on the basis of its temporal relationship to head injury. At this time, PTH has no defining clinical characteristics, although most often it has a phenotype that meets diagnostic criteria for migraine.
However, Dr. Howard and his coinvestigators have observed anecdotally in clinical practice that persistent PTH – defined as PTH lasting longer than 3 months – is often accompanied by orthostatic intolerance. This observation, coupled with reports in multiple prior studies that dysautonomia is common in patients with mild traumatic brain injury (TBI) and postconcussion syndrome, prompted Dr. Howard and his coworkers to conduct a cross-sectional cohort study. It included 56 patients with persistent PTH due to mild TBI, 30 patients with migraine, and 36 healthy controls. Most of the persistent PTH group were military veterans with mild TBI due to blast injuries.
All subjects were assessed for autonomic dysfunction using the well-validated COMPASS-31 questionnaire. This instrument assesses six domains of autonomic function: orthostatic intolerance, bladder, gastrointestinal, vasomotor, secretomotor, and pupillomotor.
Scores in each of the six domains were numerically higher in the persistent PTH group, with the differences achieving statistical significance in the orthostatic intolerance and bladder domains.
Of note, the migraine group had a greater headache burden, with a mean 23-year headache history, compared with 10.56 years in the persistent PTH group. The migraine patients also averaged 21.1 headache days per month, versus 16.2 in the persistent PTH group. Yet the investigators found no strong association between autonomic dysfunction and headache burden as reflected in headache duration or headache days per month.
The study was funded by the Department of Defense. Dr. Howard reported having no financial conflicts of interest.
SOURCE: Howard L et al. AHS 2018, Abstract FHM03.
REPORTING FROM THE AHS ANNUAL MEETING
Key clinical point: New evidence that patients with persistent posttraumatic headache have high levels of autonomic dysfunction could open the door to novel treatments.
Major finding: Scores on the COMPASS-31 questionnaire, a measure of autonomic dysfunction, averaged 37.22 in patients with persistent posttraumatic headache, indicative of significantly greater impairment than the 27.15 in migraine patients and 11.67 in healthy controls.
Study details: This cross-sectional cohort study included 56 patients with persistent posttraumatic headache, 30 with migraine, and 36 healthy controls.
Disclosures: The study was sponsored by the Department of Defense and presented by an active duty military physician.
Source: Howard L et al. AHS 2018, Abstract FHM03
Prescription opioid epidemic hits migraine patients hard
SAN FRANCISCO –

“Given the opioid epidemic in the U.S. and the high prevalence of opioid use in migraine patients shown in our study, especially in those with chronic migraine, our results suggest that improved management of treatment is needed to optimize care,” said Justin S. Yu, PharmD.
“We’re seeing a lot of opioid use in these migraine patients. It may not all be due to migraine – some had comorbid nonheadache pain conditions – but this still represents an opportunity to look at these patients more closely, maybe treat them better, because there are opportunities to improve their care, their outcomes, and their quality of life,” added Dr. Yu of Allergan in Irvine, Calif.
He presented an in-depth retrospective observational study of opioid use in 129 chronic migraine patients as defined by more than 15 headache days per month (at least 8 of which fulfilled the diagnostic criteria for migraine) and 63 others with less frequent episodic migraine. In the previous 12 months, according to claims data, 54% of the chronic migraine patients and 37% of the episodic migraine patient filled one or more prescriptions for an opioid.
More impressively, fully one-third of the chronic migraine group and 16% of episodic migraineurs filled three or more opioid prescriptions within that 12-month interval. In fact, the mean number of filled opioid prescriptions over the year was 4.0 among all chronic migraine patients and 2.8 in the overall episodic migraine cohort.
“Opioids have been used for acute treatment of chronic migraine and episodic migraine but are not recommended for regular use due to the risk of medication overuse, tolerance, dependence, and opioid hyperalgesia,” Dr. Yu noted.

Separately, Richard B. Lipton, MD, presented an analysis of 3,930 migraine patients currently using acute oral prescription headache medications who were among the larger group of 15,133 migraineurs who participated in the massive MAST (Migraine in America Symptoms and Treatment) study, an Internet-based epidemiologic survey of a nationally representative sample of patients with the disorder.
Topping the list of the most frequently used oral prescription acute headache medications were the oral triptans, used by 46% of subjects, followed by prescription NSAIDs, taken by 36%, and oral prescription opioids, used by 33.1%. And that eyebrow-raising rate of prescription opioid use is apparently par for the course.
“In lots of survey data now we’re seeing that among people with migraine who take acute prescription drugs, this one-third number is not unusual, although at least from my perspective it’s certainly a problem. Also, of people using oral acute prescription agents, a full 66% were also using OTC headache medications,” said Dr. Lipton, professor and vice chair of the department of neurology at Albert Einstein College of Medicine and director of the Montefiore Headache Center in New York.
In addition, oral prescription barbiturates were used for acute treatment of migraine by 11.2% of the MAST participants.
Acute medication overuse, as defined by use of oral prescription opioids and/or barbiturates on an average of more than 10 days per month, was identified in 8.1% of the total group. For them, the appropriate course of action is withdrawal of the overused medication, addition of a preventive agent – such drugs weren’t being used by the great majority of patients on acute prescription medications for migraine – and replacement of the opioid or barbiturate with a less problematic class of acute therapy, Dr. Lipton advised.
The MAST analysis identified a bevy of major unmet needs in people with migraine who are using acute prescription medications to treat their headaches. Fifty-three percent of participants said their severe headache attacks come on very rapidly, 50% indicated their attacks reach peak intensity in less than 2 hours no matter what they do, 39% said their head pain returns less than 24 hours after initial pain relief, and 41% complained of severe headache upon awakening. Nausea interfering with daily activities was frequently cited. Seventy-six percent of the sample had at least one of these major unmet needs.
Dr. Lipton stressed that although some of his colleagues have reacted defensively to these data highlighting numerous major unmet treatment needs in migraine patients, the MAST findings certainly aren’t an indictment that headache specialists are doing a poor job.
“I am not saying that. Of course, the vast majority of these people aren’t treated by headache specialists, they’re treated by primary care physicians. What I am saying is there are lots of opportunities to use new and emerging tools to improve the lives of our patients,” the neurologist said.
Dr. Yu noted that in his study, 14.7% of patients with chronic migraine and 15.9% with episodic migraine had been diagnosed with an anxiety disorder within the previous 12 months. Also, 24% with chronic and 11.1% with episodic migraine had been diagnosed with depression. A diagnosis of a comorbid nonheadache pain disorder was present in 13% of the chronic migraineurs and 8% of those with episodic migraine.
The MAST study was sponsored by Promius Pharma, a subsidiary of Dr. Reddy’s Laboratories. Dr. Lipton reported receiving research funding from and/or honoraria from that company and more than a dozen others.
Dr. Yu is employed by Allergan, which sponsored his study.
SOURCE: AHS annual meeting, Yu JS et al., Abstract PF11, and Lipton RB et al., Abstract OR02.
SAN FRANCISCO –
“Given the opioid epidemic in the U.S. and the high prevalence of opioid use in migraine patients shown in our study, especially in those with chronic migraine, our results suggest that improved management of treatment is needed to optimize care,” said Justin S. Yu, PharmD.
“We’re seeing a lot of opioid use in these migraine patients. It may not all be due to migraine – some had comorbid nonheadache pain conditions – but this still represents an opportunity to look at these patients more closely, maybe treat them better, because there are opportunities to improve their care, their outcomes, and their quality of life,” added Dr. Yu of Allergan in Irvine, Calif.
He presented an in-depth retrospective observational study of opioid use in 129 chronic migraine patients as defined by more than 15 headache days per month (at least 8 of which fulfilled the diagnostic criteria for migraine) and 63 others with less frequent episodic migraine. In the previous 12 months, according to claims data, 54% of the chronic migraine patients and 37% of the episodic migraine patient filled one or more prescriptions for an opioid.
More impressively, fully one-third of the chronic migraine group and 16% of episodic migraineurs filled three or more opioid prescriptions within that 12-month interval. In fact, the mean number of filled opioid prescriptions over the year was 4.0 among all chronic migraine patients and 2.8 in the overall episodic migraine cohort.
“Opioids have been used for acute treatment of chronic migraine and episodic migraine but are not recommended for regular use due to the risk of medication overuse, tolerance, dependence, and opioid hyperalgesia,” Dr. Yu noted.
Separately, Richard B. Lipton, MD, presented an analysis of 3,930 migraine patients currently using acute oral prescription headache medications who were among the larger group of 15,133 migraineurs who participated in the massive MAST (Migraine in America Symptoms and Treatment) study, an Internet-based epidemiologic survey of a nationally representative sample of patients with the disorder.
Topping the list of the most frequently used oral prescription acute headache medications were the oral triptans, used by 46% of subjects, followed by prescription NSAIDs, taken by 36%, and oral prescription opioids, used by 33.1%. And that eyebrow-raising rate of prescription opioid use is apparently par for the course.
“In lots of survey data now we’re seeing that among people with migraine who take acute prescription drugs, this one-third number is not unusual, although at least from my perspective it’s certainly a problem. Also, of people using oral acute prescription agents, a full 66% were also using OTC headache medications,” said Dr. Lipton, professor and vice chair of the department of neurology at Albert Einstein College of Medicine and director of the Montefiore Headache Center in New York.
In addition, oral prescription barbiturates were used for acute treatment of migraine by 11.2% of the MAST participants.
Acute medication overuse, as defined by use of oral prescription opioids and/or barbiturates on an average of more than 10 days per month, was identified in 8.1% of the total group. For them, the appropriate course of action is withdrawal of the overused medication, addition of a preventive agent – such drugs weren’t being used by the great majority of patients on acute prescription medications for migraine – and replacement of the opioid or barbiturate with a less problematic class of acute therapy, Dr. Lipton advised.
The MAST analysis identified a bevy of major unmet needs in people with migraine who are using acute prescription medications to treat their headaches. Fifty-three percent of participants said their severe headache attacks come on very rapidly, 50% indicated their attacks reach peak intensity in less than 2 hours no matter what they do, 39% said their head pain returns less than 24 hours after initial pain relief, and 41% complained of severe headache upon awakening. Nausea interfering with daily activities was frequently cited. Seventy-six percent of the sample had at least one of these major unmet needs.
Dr. Lipton stressed that although some of his colleagues have reacted defensively to these data highlighting numerous major unmet treatment needs in migraine patients, the MAST findings certainly aren’t an indictment that headache specialists are doing a poor job.
“I am not saying that. Of course, the vast majority of these people aren’t treated by headache specialists, they’re treated by primary care physicians. What I am saying is there are lots of opportunities to use new and emerging tools to improve the lives of our patients,” the neurologist said.
Dr. Yu noted that in his study, 14.7% of patients with chronic migraine and 15.9% with episodic migraine had been diagnosed with an anxiety disorder within the previous 12 months. Also, 24% with chronic and 11.1% with episodic migraine had been diagnosed with depression. A diagnosis of a comorbid nonheadache pain disorder was present in 13% of the chronic migraineurs and 8% of those with episodic migraine.
The MAST study was sponsored by Promius Pharma, a subsidiary of Dr. Reddy’s Laboratories. Dr. Lipton reported receiving research funding from and/or honoraria from that company and more than a dozen others.
Dr. Yu is employed by Allergan, which sponsored his study.
SOURCE: AHS annual meeting, Yu JS et al., Abstract PF11, and Lipton RB et al., Abstract OR02.
SAN FRANCISCO –
“Given the opioid epidemic in the U.S. and the high prevalence of opioid use in migraine patients shown in our study, especially in those with chronic migraine, our results suggest that improved management of treatment is needed to optimize care,” said Justin S. Yu, PharmD.
“We’re seeing a lot of opioid use in these migraine patients. It may not all be due to migraine – some had comorbid nonheadache pain conditions – but this still represents an opportunity to look at these patients more closely, maybe treat them better, because there are opportunities to improve their care, their outcomes, and their quality of life,” added Dr. Yu of Allergan in Irvine, Calif.
He presented an in-depth retrospective observational study of opioid use in 129 chronic migraine patients as defined by more than 15 headache days per month (at least 8 of which fulfilled the diagnostic criteria for migraine) and 63 others with less frequent episodic migraine. In the previous 12 months, according to claims data, 54% of the chronic migraine patients and 37% of the episodic migraine patient filled one or more prescriptions for an opioid.
More impressively, fully one-third of the chronic migraine group and 16% of episodic migraineurs filled three or more opioid prescriptions within that 12-month interval. In fact, the mean number of filled opioid prescriptions over the year was 4.0 among all chronic migraine patients and 2.8 in the overall episodic migraine cohort.
“Opioids have been used for acute treatment of chronic migraine and episodic migraine but are not recommended for regular use due to the risk of medication overuse, tolerance, dependence, and opioid hyperalgesia,” Dr. Yu noted.
Separately, Richard B. Lipton, MD, presented an analysis of 3,930 migraine patients currently using acute oral prescription headache medications who were among the larger group of 15,133 migraineurs who participated in the massive MAST (Migraine in America Symptoms and Treatment) study, an Internet-based epidemiologic survey of a nationally representative sample of patients with the disorder.
Topping the list of the most frequently used oral prescription acute headache medications were the oral triptans, used by 46% of subjects, followed by prescription NSAIDs, taken by 36%, and oral prescription opioids, used by 33.1%. And that eyebrow-raising rate of prescription opioid use is apparently par for the course.
“In lots of survey data now we’re seeing that among people with migraine who take acute prescription drugs, this one-third number is not unusual, although at least from my perspective it’s certainly a problem. Also, of people using oral acute prescription agents, a full 66% were also using OTC headache medications,” said Dr. Lipton, professor and vice chair of the department of neurology at Albert Einstein College of Medicine and director of the Montefiore Headache Center in New York.
In addition, oral prescription barbiturates were used for acute treatment of migraine by 11.2% of the MAST participants.
Acute medication overuse, as defined by use of oral prescription opioids and/or barbiturates on an average of more than 10 days per month, was identified in 8.1% of the total group. For them, the appropriate course of action is withdrawal of the overused medication, addition of a preventive agent – such drugs weren’t being used by the great majority of patients on acute prescription medications for migraine – and replacement of the opioid or barbiturate with a less problematic class of acute therapy, Dr. Lipton advised.
The MAST analysis identified a bevy of major unmet needs in people with migraine who are using acute prescription medications to treat their headaches. Fifty-three percent of participants said their severe headache attacks come on very rapidly, 50% indicated their attacks reach peak intensity in less than 2 hours no matter what they do, 39% said their head pain returns less than 24 hours after initial pain relief, and 41% complained of severe headache upon awakening. Nausea interfering with daily activities was frequently cited. Seventy-six percent of the sample had at least one of these major unmet needs.
Dr. Lipton stressed that although some of his colleagues have reacted defensively to these data highlighting numerous major unmet treatment needs in migraine patients, the MAST findings certainly aren’t an indictment that headache specialists are doing a poor job.
“I am not saying that. Of course, the vast majority of these people aren’t treated by headache specialists, they’re treated by primary care physicians. What I am saying is there are lots of opportunities to use new and emerging tools to improve the lives of our patients,” the neurologist said.
Dr. Yu noted that in his study, 14.7% of patients with chronic migraine and 15.9% with episodic migraine had been diagnosed with an anxiety disorder within the previous 12 months. Also, 24% with chronic and 11.1% with episodic migraine had been diagnosed with depression. A diagnosis of a comorbid nonheadache pain disorder was present in 13% of the chronic migraineurs and 8% of those with episodic migraine.
The MAST study was sponsored by Promius Pharma, a subsidiary of Dr. Reddy’s Laboratories. Dr. Lipton reported receiving research funding from and/or honoraria from that company and more than a dozen others.
Dr. Yu is employed by Allergan, which sponsored his study.
SOURCE: AHS annual meeting, Yu JS et al., Abstract PF11, and Lipton RB et al., Abstract OR02.
REPORTING FROM THE AHS ANNUAL MEETING
New Valsalva maneuver for SVT beats all others
NEW ORLEANS – , according to Jeet Mehta, MD, a resident in the combined medicine/pediatrics program at the University of Kansas, Wichita.
The 2015 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines recommended vagal maneuvers as first-line treatment of supraventricular tachycardia, but added that there was no gold standard method. Since then, the situation has changed. Two well-conducted randomized clinical trials have been published that bring clarity as to the vagal maneuver of choice, Dr. Mehta reported at the annual meeting of the American College of Physicians.
He and his coinvestigators performed a meta-analysis of the three pre-2000 randomized controlled trials that compared the standard Valsalva maneuver to carotid sinus massage plus the two newer studies, both of which systematically compared a modified Valsalva maneuver with the standard version.
The clear winner in terms of efficacy was the modified Valsalva maneuver, in which patients with supraventricular tachycardia (SVT) performed a standardized strain while in a semirecumbent position, then immediately laid flat and had their legs raised to 45 degrees for 15 seconds before returning to the semirecumbent position. The purpose of this postural modification is to boost relaxation phase venous return and vagal stimulation.
In the 433-patient multicenter REVERT trial in the United Kingdom, 43% of those assigned to the modified Valsalva maneuver returned to sinus rhythm 1 minute after completing the task, compared with 17% of those randomized to the standard semirecumbent Valsalva maneuver. This resulted in significantly less need for adenosine and other treatments. Although REVERT investigators had the patients blow into a manometer at 40 mm Hg for 15 seconds, they noted that the same intensity of strain can be achieved more practically by blowing into a 10-mL syringe sufficient to just move the plunger (Lancet. 2015 Oct 31;386[10005]:1747-53).
The REVERT findings were confirmed by a second trial conducted by Turkish investigators, in which the modified Valsalva maneuver was successful in 43% of patients, compared with 11% in the standard Valsalva maneuver group (Am J Emerg Med. 2017 Nov;35[11]:1662-5).
Extrapolating from the published evidence, including a Cochrane Collaboration review (Cochrane Database Syst Rev. 2015 Feb 18;[2]:CD009502. doi: 10.1002/14651858.CD009502.pub3), Dr. Mehta and his coinvestigators ranked the likelihood of successful conversion of SVT to sinus rhythm from a high of 48% for the modified Valsalva maneuver, descending to 43% for a supine Valsalva maneuver, 36% for a standard semirecumbent Valsalva, 21% for a seated Valsalva, 19% for a standing one, and just 11% for carotid sinus massage.
“Based on evidence of high quality, we encourage that the modified Valsalva maneuver be done due its safety and low cost,” Dr. Mehta concluded.
He reported having no financial conflicts regarding his study, conducted free of commercial support.
NEW ORLEANS – , according to Jeet Mehta, MD, a resident in the combined medicine/pediatrics program at the University of Kansas, Wichita.
The 2015 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines recommended vagal maneuvers as first-line treatment of supraventricular tachycardia, but added that there was no gold standard method. Since then, the situation has changed. Two well-conducted randomized clinical trials have been published that bring clarity as to the vagal maneuver of choice, Dr. Mehta reported at the annual meeting of the American College of Physicians.
He and his coinvestigators performed a meta-analysis of the three pre-2000 randomized controlled trials that compared the standard Valsalva maneuver to carotid sinus massage plus the two newer studies, both of which systematically compared a modified Valsalva maneuver with the standard version.
The clear winner in terms of efficacy was the modified Valsalva maneuver, in which patients with supraventricular tachycardia (SVT) performed a standardized strain while in a semirecumbent position, then immediately laid flat and had their legs raised to 45 degrees for 15 seconds before returning to the semirecumbent position. The purpose of this postural modification is to boost relaxation phase venous return and vagal stimulation.
In the 433-patient multicenter REVERT trial in the United Kingdom, 43% of those assigned to the modified Valsalva maneuver returned to sinus rhythm 1 minute after completing the task, compared with 17% of those randomized to the standard semirecumbent Valsalva maneuver. This resulted in significantly less need for adenosine and other treatments. Although REVERT investigators had the patients blow into a manometer at 40 mm Hg for 15 seconds, they noted that the same intensity of strain can be achieved more practically by blowing into a 10-mL syringe sufficient to just move the plunger (Lancet. 2015 Oct 31;386[10005]:1747-53).
The REVERT findings were confirmed by a second trial conducted by Turkish investigators, in which the modified Valsalva maneuver was successful in 43% of patients, compared with 11% in the standard Valsalva maneuver group (Am J Emerg Med. 2017 Nov;35[11]:1662-5).
Extrapolating from the published evidence, including a Cochrane Collaboration review (Cochrane Database Syst Rev. 2015 Feb 18;[2]:CD009502. doi: 10.1002/14651858.CD009502.pub3), Dr. Mehta and his coinvestigators ranked the likelihood of successful conversion of SVT to sinus rhythm from a high of 48% for the modified Valsalva maneuver, descending to 43% for a supine Valsalva maneuver, 36% for a standard semirecumbent Valsalva, 21% for a seated Valsalva, 19% for a standing one, and just 11% for carotid sinus massage.
“Based on evidence of high quality, we encourage that the modified Valsalva maneuver be done due its safety and low cost,” Dr. Mehta concluded.
He reported having no financial conflicts regarding his study, conducted free of commercial support.
NEW ORLEANS – , according to Jeet Mehta, MD, a resident in the combined medicine/pediatrics program at the University of Kansas, Wichita.
The 2015 American College of Cardiology/American Heart Association/Heart Rhythm Society guidelines recommended vagal maneuvers as first-line treatment of supraventricular tachycardia, but added that there was no gold standard method. Since then, the situation has changed. Two well-conducted randomized clinical trials have been published that bring clarity as to the vagal maneuver of choice, Dr. Mehta reported at the annual meeting of the American College of Physicians.
He and his coinvestigators performed a meta-analysis of the three pre-2000 randomized controlled trials that compared the standard Valsalva maneuver to carotid sinus massage plus the two newer studies, both of which systematically compared a modified Valsalva maneuver with the standard version.
The clear winner in terms of efficacy was the modified Valsalva maneuver, in which patients with supraventricular tachycardia (SVT) performed a standardized strain while in a semirecumbent position, then immediately laid flat and had their legs raised to 45 degrees for 15 seconds before returning to the semirecumbent position. The purpose of this postural modification is to boost relaxation phase venous return and vagal stimulation.
In the 433-patient multicenter REVERT trial in the United Kingdom, 43% of those assigned to the modified Valsalva maneuver returned to sinus rhythm 1 minute after completing the task, compared with 17% of those randomized to the standard semirecumbent Valsalva maneuver. This resulted in significantly less need for adenosine and other treatments. Although REVERT investigators had the patients blow into a manometer at 40 mm Hg for 15 seconds, they noted that the same intensity of strain can be achieved more practically by blowing into a 10-mL syringe sufficient to just move the plunger (Lancet. 2015 Oct 31;386[10005]:1747-53).
The REVERT findings were confirmed by a second trial conducted by Turkish investigators, in which the modified Valsalva maneuver was successful in 43% of patients, compared with 11% in the standard Valsalva maneuver group (Am J Emerg Med. 2017 Nov;35[11]:1662-5).
Extrapolating from the published evidence, including a Cochrane Collaboration review (Cochrane Database Syst Rev. 2015 Feb 18;[2]:CD009502. doi: 10.1002/14651858.CD009502.pub3), Dr. Mehta and his coinvestigators ranked the likelihood of successful conversion of SVT to sinus rhythm from a high of 48% for the modified Valsalva maneuver, descending to 43% for a supine Valsalva maneuver, 36% for a standard semirecumbent Valsalva, 21% for a seated Valsalva, 19% for a standing one, and just 11% for carotid sinus massage.
“Based on evidence of high quality, we encourage that the modified Valsalva maneuver be done due its safety and low cost,” Dr. Mehta concluded.
He reported having no financial conflicts regarding his study, conducted free of commercial support.
REPORTING FROM ACP INTERNAL MEDICINE
Key clinical point: A simple postural modification to the standard Valsalva maneuver boosts conversion rate.
Major finding: Nearly half of patients in SVT converted to sinus rhythm in response to a modified Valsalva maneuver.
Study details: This was a meta-analysis of five randomized clinical trials of vagal maneuvers for conversion of supraventricular tachycardia to sinus rhythm.
Disclosures: The presenter reported having no financial conflicts regarding the study, conducted free of commercial support.
A new, simple, inexpensive DVT diagnostic aid
NEW ORLEANS – Both the neutrophil-to-lymphocyte ratio and the platelet-to-lymphocyte ratio proved to be better predictors of the presence or absence of deep vein thrombosis than the ubiquitous D-dimer test in a retrospective study, Jason Mouabbi, MD, reported at the annual meeting of the American College of Physicians.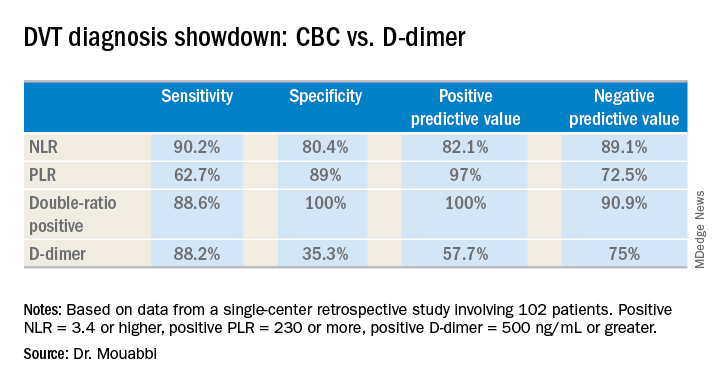
What’s more, both the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) can be readily calculated from the readout of a complete blood count (CBC) with differential. A CBC costs an average of $16, and everybody that comes through a hospital emergency department gets one. In contrast, the average charge for a D-dimer test is about $231 nationwide, and depending upon the specific test used the results can take up to a couple of hours to come back, noted Dr. Mouabbi of St. John Hospital and Medical Center in Detroit.
“The NLR and PLR ratios offer a new, powerful, affordable, simple, and readily available tool in the hands of clinicians to help them in the diagnosis of DVT,” he said. “The NLR can be useful to rule out DVT when it’s negative, whereas PLR can be useful in ruling DVT when positive.”
Investigators in a variety of fields are looking at the NLR and PLR as emerging practical, easily obtainable biomarkers for systemic inflammation. And DVT is thought to be an inflammatory process, he explained.
Dr. Mouabbi presented a single-center retrospective study of 102 matched patients who presented with lower extremity swelling and had a CBC drawn, as well as a D-dimer test, on the same day they underwent a lower extremity Doppler ultrasound evaluation. In 51 patients, the ultrasound revealed the presence of DVT and anticoagulation was started. In the other 51 patients, the ultrasound exam was negative and they weren’t anticoagulated. Since the study purpose was to assess the implications of a primary elevation of NLR and/or PLR, patients with rheumatic diseases, inflammatory bowel disease, recent surgery, chronic renal or liver disease, inherited thrombophilia, infection, or other possible secondary causes of altered ratios were excluded from the study.
A positive NLR was considered 3.4 or higher, a positive PLR was a ratio of 230 or more, and a positive D-dimer level was 500 ng/mL or greater. The NLR and PLR collectively outperformed the D-dimer test in terms of sensitivity, specificity, positive predictive value, and negative predictive value.
In addition, 89% of the DVT group were classified as “double-positive,” meaning they were both NLR and PLR positive. That combination provided the best diagnostic value of all, since none of the controls were double-positive and only 2% were PLR positive.
While the results are encouraging, before NLR and PLR can supplant D-dimer in patients with suspected DVT in clinical practice a confirmatory prospective study should be carried out, according to Dr. Mouabbi. Ideally it should include the use of the Wells score, which is part of most diagnostic algorithms as a preliminary means of categorizing DVT probability as low, moderate, or high. However, the popularity of the Wells score has fallen off in the face of reports that the results are subjective and variable. Indeed, the Wells score was included in the electronic medical record of so few participants in Dr. Mouabbi’s study that he couldn’t evaluate its utility.
He reported having no financial conflicts regarding his study, which was conducted free of commercial support.
NEW ORLEANS – Both the neutrophil-to-lymphocyte ratio and the platelet-to-lymphocyte ratio proved to be better predictors of the presence or absence of deep vein thrombosis than the ubiquitous D-dimer test in a retrospective study, Jason Mouabbi, MD, reported at the annual meeting of the American College of Physicians.
What’s more, both the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) can be readily calculated from the readout of a complete blood count (CBC) with differential. A CBC costs an average of $16, and everybody that comes through a hospital emergency department gets one. In contrast, the average charge for a D-dimer test is about $231 nationwide, and depending upon the specific test used the results can take up to a couple of hours to come back, noted Dr. Mouabbi of St. John Hospital and Medical Center in Detroit.
“The NLR and PLR ratios offer a new, powerful, affordable, simple, and readily available tool in the hands of clinicians to help them in the diagnosis of DVT,” he said. “The NLR can be useful to rule out DVT when it’s negative, whereas PLR can be useful in ruling DVT when positive.”
Investigators in a variety of fields are looking at the NLR and PLR as emerging practical, easily obtainable biomarkers for systemic inflammation. And DVT is thought to be an inflammatory process, he explained.
Dr. Mouabbi presented a single-center retrospective study of 102 matched patients who presented with lower extremity swelling and had a CBC drawn, as well as a D-dimer test, on the same day they underwent a lower extremity Doppler ultrasound evaluation. In 51 patients, the ultrasound revealed the presence of DVT and anticoagulation was started. In the other 51 patients, the ultrasound exam was negative and they weren’t anticoagulated. Since the study purpose was to assess the implications of a primary elevation of NLR and/or PLR, patients with rheumatic diseases, inflammatory bowel disease, recent surgery, chronic renal or liver disease, inherited thrombophilia, infection, or other possible secondary causes of altered ratios were excluded from the study.
A positive NLR was considered 3.4 or higher, a positive PLR was a ratio of 230 or more, and a positive D-dimer level was 500 ng/mL or greater. The NLR and PLR collectively outperformed the D-dimer test in terms of sensitivity, specificity, positive predictive value, and negative predictive value.
In addition, 89% of the DVT group were classified as “double-positive,” meaning they were both NLR and PLR positive. That combination provided the best diagnostic value of all, since none of the controls were double-positive and only 2% were PLR positive.
While the results are encouraging, before NLR and PLR can supplant D-dimer in patients with suspected DVT in clinical practice a confirmatory prospective study should be carried out, according to Dr. Mouabbi. Ideally it should include the use of the Wells score, which is part of most diagnostic algorithms as a preliminary means of categorizing DVT probability as low, moderate, or high. However, the popularity of the Wells score has fallen off in the face of reports that the results are subjective and variable. Indeed, the Wells score was included in the electronic medical record of so few participants in Dr. Mouabbi’s study that he couldn’t evaluate its utility.
He reported having no financial conflicts regarding his study, which was conducted free of commercial support.
NEW ORLEANS – Both the neutrophil-to-lymphocyte ratio and the platelet-to-lymphocyte ratio proved to be better predictors of the presence or absence of deep vein thrombosis than the ubiquitous D-dimer test in a retrospective study, Jason Mouabbi, MD, reported at the annual meeting of the American College of Physicians.
What’s more, both the neutrophil-to-lymphocyte ratio (NLR) and the platelet-to-lymphocyte ratio (PLR) can be readily calculated from the readout of a complete blood count (CBC) with differential. A CBC costs an average of $16, and everybody that comes through a hospital emergency department gets one. In contrast, the average charge for a D-dimer test is about $231 nationwide, and depending upon the specific test used the results can take up to a couple of hours to come back, noted Dr. Mouabbi of St. John Hospital and Medical Center in Detroit.
“The NLR and PLR ratios offer a new, powerful, affordable, simple, and readily available tool in the hands of clinicians to help them in the diagnosis of DVT,” he said. “The NLR can be useful to rule out DVT when it’s negative, whereas PLR can be useful in ruling DVT when positive.”
Investigators in a variety of fields are looking at the NLR and PLR as emerging practical, easily obtainable biomarkers for systemic inflammation. And DVT is thought to be an inflammatory process, he explained.
Dr. Mouabbi presented a single-center retrospective study of 102 matched patients who presented with lower extremity swelling and had a CBC drawn, as well as a D-dimer test, on the same day they underwent a lower extremity Doppler ultrasound evaluation. In 51 patients, the ultrasound revealed the presence of DVT and anticoagulation was started. In the other 51 patients, the ultrasound exam was negative and they weren’t anticoagulated. Since the study purpose was to assess the implications of a primary elevation of NLR and/or PLR, patients with rheumatic diseases, inflammatory bowel disease, recent surgery, chronic renal or liver disease, inherited thrombophilia, infection, or other possible secondary causes of altered ratios were excluded from the study.
A positive NLR was considered 3.4 or higher, a positive PLR was a ratio of 230 or more, and a positive D-dimer level was 500 ng/mL or greater. The NLR and PLR collectively outperformed the D-dimer test in terms of sensitivity, specificity, positive predictive value, and negative predictive value.
In addition, 89% of the DVT group were classified as “double-positive,” meaning they were both NLR and PLR positive. That combination provided the best diagnostic value of all, since none of the controls were double-positive and only 2% were PLR positive.
While the results are encouraging, before NLR and PLR can supplant D-dimer in patients with suspected DVT in clinical practice a confirmatory prospective study should be carried out, according to Dr. Mouabbi. Ideally it should include the use of the Wells score, which is part of most diagnostic algorithms as a preliminary means of categorizing DVT probability as low, moderate, or high. However, the popularity of the Wells score has fallen off in the face of reports that the results are subjective and variable. Indeed, the Wells score was included in the electronic medical record of so few participants in Dr. Mouabbi’s study that he couldn’t evaluate its utility.
He reported having no financial conflicts regarding his study, which was conducted free of commercial support.
REPORTING FROM ACP INTERNAL MEDICINE
Key clinical point:
Major finding: The neutrophil-to-lymphocyte ratio was better than the D-dimer test at helping to rule out DVT, while the platelet-to-lymphocyte ratio bested the D-dimer at ruling in DVT.
Study details: A retrospective study of 102 patients with suspected DVT.
Disclosures: Dr. Mouabbi reported no financial conflicts regarding his study, which was conducted free of commercial support.