User login
Antirheumatic drugs don’t boost surgical infection risk
SAN DIEGO – Rheumatoid arthritis patients undergoing surgery who stayed on their antirheumatic medication perioperatively didn’t have a higher risk of early postoperative infection compared with those who temporarily stopped treatment before surgery, according to findings from a large national Veterans Affairs study.
Rheumatologists are frequently consulted about this issue. Evidence to guide practice has been scarce, however, and until now many rheumatologists and surgeons have taken a conservative approach, reasoning that the immunosuppressive drugs employed in controlling inflammation in rheumatoid arthritis might also increase the risk of surgical wound infection.

A common practice has been to have RA patients stop their medication a month ahead of elective surgery, or at least two drug half-lives beforehand, then start treatment again roughly a month after the operation, or when the wound has healed. The new Veterans Affairs (VA) study findings suggest this practice may be unnecessary, Dr. Zaki Abou Zahr said at the annual meeting of the American College of Rheumatology.
Dr. Bernard Ng, his senior coinvestigator in the study, added that temporarily stopping antirheumatic agents before surgery may actually be harmful in that it increases the risk of a flare of the RA, which in turn would impede postoperative rehabilitation.
But there is a major caveat regarding the VA study: Participation was restricted to RA patients on only a single conventional disease-modifying antirheumatic drug (DMARD) or biologic agent leading up to surgery. This restriction, imposed to make for a more clear-cut analysis, means that the study results can’t be extrapolated to patients on multidrug therapy. And multidrug therapy is quite common. Indeed, slightly more than half of RA patients in the VA health care system are on combination therapy, most often methotrexate plus a biologic agent, noted Dr. Ng, chief of rheumatology at the VA Puget Sound Health Care System, Seattle.
Dr. Abou Zahr presented the retrospective cohort study involving 6,548 RA patients in VA administrative databases, all of whom were on antirheumatic drug monotherapy prior to surgery. The surgery was of all types, including cardiothoracic, gastrointestinal, vascular, and orthopedic, as well as emergent and elective.

The primary endpoints were the rate of wound infections, both superficial and deep, within 30 days post surgery, and the general infection rate – including pneumonia, sepsis, and urinary tract infections – during the same time frame.
Sixty-two percent of the 1,480 RA patients on a single biologic agent did not stop taking it preoperatively. One key study finding was that neither their postoperative wound infection rate nor their general infection rate differed significantly from rates in patients who temporarily halted their biologic agent. The same held true among the 70% of patients on a single conventional DMARD who did not stop taking their medication preoperatively, according to Dr. Abou Zahr of Baylor College of Medicine, Houston.
Dr. Ng said the investigators plan to extend their work to include RA patients on multiple antirheumatic drugs that they do or don’t temporarily stop when undergoing surgery within the VA system. The researchers also plan to take a close look at patients undergoing specific types of surgery to see if the postoperative infection risk in patients who remain on treatment varies according to their operation.
Dr. Fehmida Zahabi, a rheumatologist from Plano, Tex., who chaired a press conference highlighting the VA study findings, said that while she’d like to see a confirmatory study, "I think we’re getting to the point where we’re saying we should cautiously keep these patients on their medications. That’s what the data suggest."

She noted that before the VA study, the very limited evidence available to guide practice in this area centered on a 12-year-old British randomized trial involving RA patients on methotrexate undergoing elective orthopedic surgery. Those assigned to stop the drug from 2 weeks before surgery to 2 weeks post surgery had significantly more infections, surgical complications, and RA flares within 6 weeks after surgery (Ann. Rheum. Dis. 2001;60:214-7).
As for patients on multidrug therapy who are scheduled for surgery, her inclination until evidence becomes available for guidance is to pare down the regimen preoperatively, while keeping the patient on one or two drugs.
The VA study was funded by the Department of Veterans Affairs. Dr. Abou Zahr and Dr. Ng reported having no conflicts of interest.
SAN DIEGO – Rheumatoid arthritis patients undergoing surgery who stayed on their antirheumatic medication perioperatively didn’t have a higher risk of early postoperative infection compared with those who temporarily stopped treatment before surgery, according to findings from a large national Veterans Affairs study.
Rheumatologists are frequently consulted about this issue. Evidence to guide practice has been scarce, however, and until now many rheumatologists and surgeons have taken a conservative approach, reasoning that the immunosuppressive drugs employed in controlling inflammation in rheumatoid arthritis might also increase the risk of surgical wound infection.
A common practice has been to have RA patients stop their medication a month ahead of elective surgery, or at least two drug half-lives beforehand, then start treatment again roughly a month after the operation, or when the wound has healed. The new Veterans Affairs (VA) study findings suggest this practice may be unnecessary, Dr. Zaki Abou Zahr said at the annual meeting of the American College of Rheumatology.
Dr. Bernard Ng, his senior coinvestigator in the study, added that temporarily stopping antirheumatic agents before surgery may actually be harmful in that it increases the risk of a flare of the RA, which in turn would impede postoperative rehabilitation.
But there is a major caveat regarding the VA study: Participation was restricted to RA patients on only a single conventional disease-modifying antirheumatic drug (DMARD) or biologic agent leading up to surgery. This restriction, imposed to make for a more clear-cut analysis, means that the study results can’t be extrapolated to patients on multidrug therapy. And multidrug therapy is quite common. Indeed, slightly more than half of RA patients in the VA health care system are on combination therapy, most often methotrexate plus a biologic agent, noted Dr. Ng, chief of rheumatology at the VA Puget Sound Health Care System, Seattle.
Dr. Abou Zahr presented the retrospective cohort study involving 6,548 RA patients in VA administrative databases, all of whom were on antirheumatic drug monotherapy prior to surgery. The surgery was of all types, including cardiothoracic, gastrointestinal, vascular, and orthopedic, as well as emergent and elective.
The primary endpoints were the rate of wound infections, both superficial and deep, within 30 days post surgery, and the general infection rate – including pneumonia, sepsis, and urinary tract infections – during the same time frame.
Sixty-two percent of the 1,480 RA patients on a single biologic agent did not stop taking it preoperatively. One key study finding was that neither their postoperative wound infection rate nor their general infection rate differed significantly from rates in patients who temporarily halted their biologic agent. The same held true among the 70% of patients on a single conventional DMARD who did not stop taking their medication preoperatively, according to Dr. Abou Zahr of Baylor College of Medicine, Houston.
Dr. Ng said the investigators plan to extend their work to include RA patients on multiple antirheumatic drugs that they do or don’t temporarily stop when undergoing surgery within the VA system. The researchers also plan to take a close look at patients undergoing specific types of surgery to see if the postoperative infection risk in patients who remain on treatment varies according to their operation.
Dr. Fehmida Zahabi, a rheumatologist from Plano, Tex., who chaired a press conference highlighting the VA study findings, said that while she’d like to see a confirmatory study, "I think we’re getting to the point where we’re saying we should cautiously keep these patients on their medications. That’s what the data suggest."
She noted that before the VA study, the very limited evidence available to guide practice in this area centered on a 12-year-old British randomized trial involving RA patients on methotrexate undergoing elective orthopedic surgery. Those assigned to stop the drug from 2 weeks before surgery to 2 weeks post surgery had significantly more infections, surgical complications, and RA flares within 6 weeks after surgery (Ann. Rheum. Dis. 2001;60:214-7).
As for patients on multidrug therapy who are scheduled for surgery, her inclination until evidence becomes available for guidance is to pare down the regimen preoperatively, while keeping the patient on one or two drugs.
The VA study was funded by the Department of Veterans Affairs. Dr. Abou Zahr and Dr. Ng reported having no conflicts of interest.
SAN DIEGO – Rheumatoid arthritis patients undergoing surgery who stayed on their antirheumatic medication perioperatively didn’t have a higher risk of early postoperative infection compared with those who temporarily stopped treatment before surgery, according to findings from a large national Veterans Affairs study.
Rheumatologists are frequently consulted about this issue. Evidence to guide practice has been scarce, however, and until now many rheumatologists and surgeons have taken a conservative approach, reasoning that the immunosuppressive drugs employed in controlling inflammation in rheumatoid arthritis might also increase the risk of surgical wound infection.
A common practice has been to have RA patients stop their medication a month ahead of elective surgery, or at least two drug half-lives beforehand, then start treatment again roughly a month after the operation, or when the wound has healed. The new Veterans Affairs (VA) study findings suggest this practice may be unnecessary, Dr. Zaki Abou Zahr said at the annual meeting of the American College of Rheumatology.
Dr. Bernard Ng, his senior coinvestigator in the study, added that temporarily stopping antirheumatic agents before surgery may actually be harmful in that it increases the risk of a flare of the RA, which in turn would impede postoperative rehabilitation.
But there is a major caveat regarding the VA study: Participation was restricted to RA patients on only a single conventional disease-modifying antirheumatic drug (DMARD) or biologic agent leading up to surgery. This restriction, imposed to make for a more clear-cut analysis, means that the study results can’t be extrapolated to patients on multidrug therapy. And multidrug therapy is quite common. Indeed, slightly more than half of RA patients in the VA health care system are on combination therapy, most often methotrexate plus a biologic agent, noted Dr. Ng, chief of rheumatology at the VA Puget Sound Health Care System, Seattle.
Dr. Abou Zahr presented the retrospective cohort study involving 6,548 RA patients in VA administrative databases, all of whom were on antirheumatic drug monotherapy prior to surgery. The surgery was of all types, including cardiothoracic, gastrointestinal, vascular, and orthopedic, as well as emergent and elective.
The primary endpoints were the rate of wound infections, both superficial and deep, within 30 days post surgery, and the general infection rate – including pneumonia, sepsis, and urinary tract infections – during the same time frame.
Sixty-two percent of the 1,480 RA patients on a single biologic agent did not stop taking it preoperatively. One key study finding was that neither their postoperative wound infection rate nor their general infection rate differed significantly from rates in patients who temporarily halted their biologic agent. The same held true among the 70% of patients on a single conventional DMARD who did not stop taking their medication preoperatively, according to Dr. Abou Zahr of Baylor College of Medicine, Houston.
Dr. Ng said the investigators plan to extend their work to include RA patients on multiple antirheumatic drugs that they do or don’t temporarily stop when undergoing surgery within the VA system. The researchers also plan to take a close look at patients undergoing specific types of surgery to see if the postoperative infection risk in patients who remain on treatment varies according to their operation.
Dr. Fehmida Zahabi, a rheumatologist from Plano, Tex., who chaired a press conference highlighting the VA study findings, said that while she’d like to see a confirmatory study, "I think we’re getting to the point where we’re saying we should cautiously keep these patients on their medications. That’s what the data suggest."
She noted that before the VA study, the very limited evidence available to guide practice in this area centered on a 12-year-old British randomized trial involving RA patients on methotrexate undergoing elective orthopedic surgery. Those assigned to stop the drug from 2 weeks before surgery to 2 weeks post surgery had significantly more infections, surgical complications, and RA flares within 6 weeks after surgery (Ann. Rheum. Dis. 2001;60:214-7).
As for patients on multidrug therapy who are scheduled for surgery, her inclination until evidence becomes available for guidance is to pare down the regimen preoperatively, while keeping the patient on one or two drugs.
The VA study was funded by the Department of Veterans Affairs. Dr. Abou Zahr and Dr. Ng reported having no conflicts of interest.
AT THE ACR ANNUAL MEETING
Major finding: Rheumatoid arthritis patients who remained on their antirheumatic medication while they underwent various types of surgery did not have a significantly different 30-day wound infection rate than those who stopped treatment temporarily prior to surgery.
Data source: This was a retrospective observational cohort study involving 6,548 rheumatoid arthritis patients undergoing various types of surgery.
Disclosures: The study was funded by the Department of Veterans Affairs. The presenters reported having no financial conflicts.

Systemic sclerosis brings sharply increased MI risk
SAN DIEGO – Patients with systemic sclerosis are at greater than eightfold increased risk of having an acute myocardial infarction during the first year after diagnosis, compared with matched controls, according to the first large population-based cohort study to look at the issue.
After that first year, the MI risk drops off over time. Still, during years 1-5 post diagnosis the MI risk remains more than triple that of the matched general population, Dr. J. Antonio Avina-Zubieta reported at the annual meeting of the American College of Rheumatology.
"Our findings support increased vigilance in cardiovascular disease prevention, surveillance, and risk modification in patients with systemic sclerosis," declared Dr. Avina-Zubieta, a rheumatologist at the University of British Columbia, Vancouver.

He and his coinvestigators harnessed comprehensive provincial medical databases to identify all 1,245 adults diagnosed with rheumatologist-confirmed systemic sclerosis (SSc) in British Columbia during 1996-2010. The SSc patients averaged 53 years of age at the time of their rheumatologic diagnosis. Eighty-three percent were women.
During a mean follow-up period of 3.5 years following diagnosis of SSc, 89 patients experienced an acute MI, as did 289 controls. This translated to an incidence rate of 20.2 cases per 1,000 person-years among patients with SSc, compared with 5.3 per 1,000 among controls.
The risk was 8.2-fold greater in SSc patients than controls during the first year after diagnosis and 3.5 times greater during years 1-5 after diagnosis, but once patients got more than 5 years out from diagnosis there was no longer any significant increase in MI risk.
Patients with SSc who were in the 45- to 59-year-old age group were at greatest risk: They were 7.4 times more likely than controls to have an MI. SSc patients aged 60-74 years had a 4.4-fold greater risk of MI than did controls, and those aged 75 years and older were at 5.6-fold increased risk.
The SSc patients remained at a 4.3-fold increased risk of MI, compared with controls, in a multivariate analysis extensively adjusted for baseline chronic obstructive pulmonary disease, angina, obesity, hormone replacement therapy, Charlson Comorbidity Index, number of hospitalizations during the 12 months prior to diagnosis, and the use of NSAIDs, COX-2 inhibitors, glucocorticoids, lipid-lowering drugs, and antidiabetic medications.
It is well established that patients with rheumatoid arthritis or systemic lupus erythematosus have an increased risk of premature atherosclerotic disease. Up until now, however, information about the risk of major adverse cardiovascular events in patients with SSc has been scarce and has come from nondefinitive studies in selected populations or cross-sectional studies lacking adequate adjustment for potential confounding factors, according to Dr. Avina-Zubieta, who also is a research scientist at the Arthritis Research Centre of Canada in Richmond, B.C.
Why the sharp increase in MI risk during the first year after diagnosis of SSc? He offered two hypotheses. One is that this is a time of particularly great inflammatory load as physicians work to get the disease under control. Also, there is a phenomenon Dr. Avina-Zubieta called "the depletion of susceptibles," whereby, once the patients at higher risk have had their MI early on, those who remain aren’t at sufficient risk to stand out from the general population.
The study was sponsored by the Arthritis Centre of Canada. Dr. Avina-Zubieta reported having no financial conflicts of interest.
SAN DIEGO – Patients with systemic sclerosis are at greater than eightfold increased risk of having an acute myocardial infarction during the first year after diagnosis, compared with matched controls, according to the first large population-based cohort study to look at the issue.
After that first year, the MI risk drops off over time. Still, during years 1-5 post diagnosis the MI risk remains more than triple that of the matched general population, Dr. J. Antonio Avina-Zubieta reported at the annual meeting of the American College of Rheumatology.
"Our findings support increased vigilance in cardiovascular disease prevention, surveillance, and risk modification in patients with systemic sclerosis," declared Dr. Avina-Zubieta, a rheumatologist at the University of British Columbia, Vancouver.
He and his coinvestigators harnessed comprehensive provincial medical databases to identify all 1,245 adults diagnosed with rheumatologist-confirmed systemic sclerosis (SSc) in British Columbia during 1996-2010. The SSc patients averaged 53 years of age at the time of their rheumatologic diagnosis. Eighty-three percent were women.
During a mean follow-up period of 3.5 years following diagnosis of SSc, 89 patients experienced an acute MI, as did 289 controls. This translated to an incidence rate of 20.2 cases per 1,000 person-years among patients with SSc, compared with 5.3 per 1,000 among controls.
The risk was 8.2-fold greater in SSc patients than controls during the first year after diagnosis and 3.5 times greater during years 1-5 after diagnosis, but once patients got more than 5 years out from diagnosis there was no longer any significant increase in MI risk.
Patients with SSc who were in the 45- to 59-year-old age group were at greatest risk: They were 7.4 times more likely than controls to have an MI. SSc patients aged 60-74 years had a 4.4-fold greater risk of MI than did controls, and those aged 75 years and older were at 5.6-fold increased risk.
The SSc patients remained at a 4.3-fold increased risk of MI, compared with controls, in a multivariate analysis extensively adjusted for baseline chronic obstructive pulmonary disease, angina, obesity, hormone replacement therapy, Charlson Comorbidity Index, number of hospitalizations during the 12 months prior to diagnosis, and the use of NSAIDs, COX-2 inhibitors, glucocorticoids, lipid-lowering drugs, and antidiabetic medications.
It is well established that patients with rheumatoid arthritis or systemic lupus erythematosus have an increased risk of premature atherosclerotic disease. Up until now, however, information about the risk of major adverse cardiovascular events in patients with SSc has been scarce and has come from nondefinitive studies in selected populations or cross-sectional studies lacking adequate adjustment for potential confounding factors, according to Dr. Avina-Zubieta, who also is a research scientist at the Arthritis Research Centre of Canada in Richmond, B.C.
Why the sharp increase in MI risk during the first year after diagnosis of SSc? He offered two hypotheses. One is that this is a time of particularly great inflammatory load as physicians work to get the disease under control. Also, there is a phenomenon Dr. Avina-Zubieta called "the depletion of susceptibles," whereby, once the patients at higher risk have had their MI early on, those who remain aren’t at sufficient risk to stand out from the general population.
The study was sponsored by the Arthritis Centre of Canada. Dr. Avina-Zubieta reported having no financial conflicts of interest.
SAN DIEGO – Patients with systemic sclerosis are at greater than eightfold increased risk of having an acute myocardial infarction during the first year after diagnosis, compared with matched controls, according to the first large population-based cohort study to look at the issue.
After that first year, the MI risk drops off over time. Still, during years 1-5 post diagnosis the MI risk remains more than triple that of the matched general population, Dr. J. Antonio Avina-Zubieta reported at the annual meeting of the American College of Rheumatology.
"Our findings support increased vigilance in cardiovascular disease prevention, surveillance, and risk modification in patients with systemic sclerosis," declared Dr. Avina-Zubieta, a rheumatologist at the University of British Columbia, Vancouver.
He and his coinvestigators harnessed comprehensive provincial medical databases to identify all 1,245 adults diagnosed with rheumatologist-confirmed systemic sclerosis (SSc) in British Columbia during 1996-2010. The SSc patients averaged 53 years of age at the time of their rheumatologic diagnosis. Eighty-three percent were women.
During a mean follow-up period of 3.5 years following diagnosis of SSc, 89 patients experienced an acute MI, as did 289 controls. This translated to an incidence rate of 20.2 cases per 1,000 person-years among patients with SSc, compared with 5.3 per 1,000 among controls.
The risk was 8.2-fold greater in SSc patients than controls during the first year after diagnosis and 3.5 times greater during years 1-5 after diagnosis, but once patients got more than 5 years out from diagnosis there was no longer any significant increase in MI risk.
Patients with SSc who were in the 45- to 59-year-old age group were at greatest risk: They were 7.4 times more likely than controls to have an MI. SSc patients aged 60-74 years had a 4.4-fold greater risk of MI than did controls, and those aged 75 years and older were at 5.6-fold increased risk.
The SSc patients remained at a 4.3-fold increased risk of MI, compared with controls, in a multivariate analysis extensively adjusted for baseline chronic obstructive pulmonary disease, angina, obesity, hormone replacement therapy, Charlson Comorbidity Index, number of hospitalizations during the 12 months prior to diagnosis, and the use of NSAIDs, COX-2 inhibitors, glucocorticoids, lipid-lowering drugs, and antidiabetic medications.
It is well established that patients with rheumatoid arthritis or systemic lupus erythematosus have an increased risk of premature atherosclerotic disease. Up until now, however, information about the risk of major adverse cardiovascular events in patients with SSc has been scarce and has come from nondefinitive studies in selected populations or cross-sectional studies lacking adequate adjustment for potential confounding factors, according to Dr. Avina-Zubieta, who also is a research scientist at the Arthritis Research Centre of Canada in Richmond, B.C.
Why the sharp increase in MI risk during the first year after diagnosis of SSc? He offered two hypotheses. One is that this is a time of particularly great inflammatory load as physicians work to get the disease under control. Also, there is a phenomenon Dr. Avina-Zubieta called "the depletion of susceptibles," whereby, once the patients at higher risk have had their MI early on, those who remain aren’t at sufficient risk to stand out from the general population.
The study was sponsored by the Arthritis Centre of Canada. Dr. Avina-Zubieta reported having no financial conflicts of interest.
AT THE ACR ANNUAL MEETING
Major finding: The incidence rate of acute MI following diagnosis of systemic sclerosis was 20.2 events per 1,000 person-years, compared with 5.3 per 1,000 in matched controls.
Data source: Population-based cohort study included all 1,245 adults diagnosed with systemic sclerosis in British Columbia in 1990-2010 and 12,678 matched controls drawn from the general population.
Disclosures: The study was sponsored by the Arthritis Centre of Canada. Dr. Avina-Zubieta reported having no financial conflicts of interest.

Apremilast promising for Behçet’s syndrome
ISTANBUL, TURKEY – The investigational oral phosphodiesterase-4 inhibitor apremilast showed dramatic efficacy in the treatment of oral and genital ulcers of Behçet’s syndrome in a randomized, double-blind clinical trial.
The multicenter phase II study included 111 Behçet’s syndrome patients with active oral ulcers. They were randomized to 12 weeks of double-blind apremilast at 30 mg twice daily or placebo followed by an additional 12 weeks of open-label apremilast for all, then 4 weeks of post-treatment observation.
Participants had a mean of 2.8 oral ulcers at baseline. The primary study endpoint was the number present at week 12: a mean of 0.5 in the apremilast group, compared with 2.1 in controls, Dr. Gülen Hatemi reported at the annual congress of the European Academy of Dermatology and Venereology.
A total of 71% of patients in the apremilast group were oral ulcer–free at week 12, as were 29% of controls, added Dr. Hatemi, a rheumatologist at Istanbul (Turkey) University.
The benefit of apremilast occurred rapidly. The full response was seen at week 2 and was then maintained throughout the remainder of the 12 weeks of double-blind therapy and the following 12 weeks of open-label apremilast. However, oral ulcers returned in full force quickly after treatment cessation.
Pain from oral ulcers on a 0-100 visual analog scale plummeted in the apremilast group by a mean 44.7 points from a baseline of score of 54. In contrast, pain scores in the control group improved by 16 points, which is less than the 20-point threshold accepted as being clinically meaningful.
Behçet’s syndrome is an immune-mediated small-vessel vasculitis. Its mucocutaneous manifestations can be disabling and resistant to conventional therapies, Dr. Hatemi noted.
Only 16 patients had genital ulcers. All 10 randomized to apremilast were free of the ulcers at week 12, as were three of six affected patients in the control group.
Average scores on the Behçet’s Disease Activity Index dropped from 3.4 at baseline to 2.0 at 12 weeks in the apremilast arm while remaining unchanged in controls. Mean scores on the Behçet’s Disease Quality of Life instrument decreased by 4.5 points from a baseline of 12.6 in apremilast-treated patients, compared with a 1.6-point reduction in controls.
The investigators said no serious adverse events were related to apremilast.
Dr. Hatemi received a research grant from Celgene, the study sponsor, which is also developing the oral drug as a possible treatment for psoriasis, psoriatic arthritis, and ankylosing spondylitis.
ISTANBUL, TURKEY – The investigational oral phosphodiesterase-4 inhibitor apremilast showed dramatic efficacy in the treatment of oral and genital ulcers of Behçet’s syndrome in a randomized, double-blind clinical trial.
The multicenter phase II study included 111 Behçet’s syndrome patients with active oral ulcers. They were randomized to 12 weeks of double-blind apremilast at 30 mg twice daily or placebo followed by an additional 12 weeks of open-label apremilast for all, then 4 weeks of post-treatment observation.
Participants had a mean of 2.8 oral ulcers at baseline. The primary study endpoint was the number present at week 12: a mean of 0.5 in the apremilast group, compared with 2.1 in controls, Dr. Gülen Hatemi reported at the annual congress of the European Academy of Dermatology and Venereology.
A total of 71% of patients in the apremilast group were oral ulcer–free at week 12, as were 29% of controls, added Dr. Hatemi, a rheumatologist at Istanbul (Turkey) University.
The benefit of apremilast occurred rapidly. The full response was seen at week 2 and was then maintained throughout the remainder of the 12 weeks of double-blind therapy and the following 12 weeks of open-label apremilast. However, oral ulcers returned in full force quickly after treatment cessation.
Pain from oral ulcers on a 0-100 visual analog scale plummeted in the apremilast group by a mean 44.7 points from a baseline of score of 54. In contrast, pain scores in the control group improved by 16 points, which is less than the 20-point threshold accepted as being clinically meaningful.
Behçet’s syndrome is an immune-mediated small-vessel vasculitis. Its mucocutaneous manifestations can be disabling and resistant to conventional therapies, Dr. Hatemi noted.
Only 16 patients had genital ulcers. All 10 randomized to apremilast were free of the ulcers at week 12, as were three of six affected patients in the control group.
Average scores on the Behçet’s Disease Activity Index dropped from 3.4 at baseline to 2.0 at 12 weeks in the apremilast arm while remaining unchanged in controls. Mean scores on the Behçet’s Disease Quality of Life instrument decreased by 4.5 points from a baseline of 12.6 in apremilast-treated patients, compared with a 1.6-point reduction in controls.
The investigators said no serious adverse events were related to apremilast.
Dr. Hatemi received a research grant from Celgene, the study sponsor, which is also developing the oral drug as a possible treatment for psoriasis, psoriatic arthritis, and ankylosing spondylitis.
ISTANBUL, TURKEY – The investigational oral phosphodiesterase-4 inhibitor apremilast showed dramatic efficacy in the treatment of oral and genital ulcers of Behçet’s syndrome in a randomized, double-blind clinical trial.
The multicenter phase II study included 111 Behçet’s syndrome patients with active oral ulcers. They were randomized to 12 weeks of double-blind apremilast at 30 mg twice daily or placebo followed by an additional 12 weeks of open-label apremilast for all, then 4 weeks of post-treatment observation.
Participants had a mean of 2.8 oral ulcers at baseline. The primary study endpoint was the number present at week 12: a mean of 0.5 in the apremilast group, compared with 2.1 in controls, Dr. Gülen Hatemi reported at the annual congress of the European Academy of Dermatology and Venereology.
A total of 71% of patients in the apremilast group were oral ulcer–free at week 12, as were 29% of controls, added Dr. Hatemi, a rheumatologist at Istanbul (Turkey) University.
The benefit of apremilast occurred rapidly. The full response was seen at week 2 and was then maintained throughout the remainder of the 12 weeks of double-blind therapy and the following 12 weeks of open-label apremilast. However, oral ulcers returned in full force quickly after treatment cessation.
Pain from oral ulcers on a 0-100 visual analog scale plummeted in the apremilast group by a mean 44.7 points from a baseline of score of 54. In contrast, pain scores in the control group improved by 16 points, which is less than the 20-point threshold accepted as being clinically meaningful.
Behçet’s syndrome is an immune-mediated small-vessel vasculitis. Its mucocutaneous manifestations can be disabling and resistant to conventional therapies, Dr. Hatemi noted.
Only 16 patients had genital ulcers. All 10 randomized to apremilast were free of the ulcers at week 12, as were three of six affected patients in the control group.
Average scores on the Behçet’s Disease Activity Index dropped from 3.4 at baseline to 2.0 at 12 weeks in the apremilast arm while remaining unchanged in controls. Mean scores on the Behçet’s Disease Quality of Life instrument decreased by 4.5 points from a baseline of 12.6 in apremilast-treated patients, compared with a 1.6-point reduction in controls.
The investigators said no serious adverse events were related to apremilast.
Dr. Hatemi received a research grant from Celgene, the study sponsor, which is also developing the oral drug as a possible treatment for psoriasis, psoriatic arthritis, and ankylosing spondylitis.
AT THE EADV CONGRESS
Major finding: The mean number of oral ulcers in Behçet’s syndrome patients treated with apremilast quickly dropped from 2.8 at baseline to 0.5, an improvement maintained during 24 weeks of therapy.
Data source: A randomized, double-blind, multicenter, 28-week phase II study involving 111 Behçet’s syndrome patients with active oral ulcers.
Disclosures: The presenter received a research grant from the study sponsor, Celgene.
Novel two-biomarker strategy permits early ACS rule-out
AMSTERDAM – An early rule-out strategy based upon using two cardiac biomarkers allowed for safe discharge within a couple hours from the emergency department for most low- to intermediate-risk patients who presented with suspected acute coronary syndrome, based on the results of a randomized, multicenter trial conducted in Europe.
Moreover, the 30-day rates of major adverse cardiovascular events in the Biomarkers in Cardiology-8 (BiC-8) study were similarly low in patients discharged from the ED using the early rule-out process and in those who received standard, guideline-recommended care, which includes 6-12 hours of serial ECGs and troponin measurements in the chest pain unit, Dr. Martin Moeckel reported at the annual congress of the European Society of Cardiology.

"This biomarker strategy using a state-of-the-art quantitative troponin assay in combination with an ultrasensitive copeptin assay has the potential to change clinical practice with high patient safety," observed Dr. Moeckel of Charité Hospital, Berlin. The copeptin test is approved for use in the European Union but remains investigational in the United States.
Based upon the results of BiC-8, this dual biomarker for early rule-out of myocardial infarction (MI) is now standard clinical practice at Charité, he added.
The rationale for developing the early rule-out strategy tested in BiC-8 lies in the serious overcrowding that is now the norm in many EDs. This overcrowding has been shown to be in and of itself a risk factor for poor outcomes. The quandary is that nearly 12% of all patients who present to the ED do so because of chest pain, yet after an extensive and time-consuming evaluation only 1 in 10 of those patients is found to actually be having an acute MI.
"Rapid rule-out of acute MI is therefore a major clinical need, saving the health care system time and resources, and saving patients unnecessary stress, anxiety, and other risks," he said.
Copeptin is a marker for vasopressin, a hemodynamic stress indicator that shoots up immediately in an acute MI. In earlier studies, a negative result for both troponin and copeptin in an initial blood sample drawn at ED presentation had a 99% negative predictive value for MI.
The BiC-8 trial included 902 low- to intermediate-risk patients who presented with suspected acute coronary syndrome (ACS) to EDs in university medical centers. All had a negative initial cardiac troponin test. They were randomized to standard care in the chest pain unit, including serial troponin testing and ECGs, or to the experimental strategy, in which physicians were informed of the copeptin results from the same initial blood sample as the troponin. If the copeptin test was positive as defined by a level of 10 pmol/L or more, the patient was hospitalized for standard care. If the copeptin result was negative, however, the patient was immediately discharged with a scheduled outpatient visit within 72 hours.
Of the patients in the copeptin group, 66% were discharged directly from the ED, compared with 12% in the standard-care group.
The 30-day incidence of major adverse cardiovascular events (MACE) was 5.5% in the standard-care group and nearly identical at 5.46% in the copeptin group. However, physicians were permitted under the study protocol to overrule negative biomarker test results on the basis of their final clinical assessment, such as if their suspicions were aroused due to recurrent symptoms or new information about the patient’s history. In this per-protocol analysis, the 30-day MACE rate was 5.68% in the standard-care group and 3.18% in the copeptin group.
MACE was defined in BiC-8 as all-cause mortality, MI, rehospitalization for ACS, acute unplanned percutaneous coronary intervention (PCI), coronary artery bypass surgery, life-threatening arrhythmia, or resuscitation from cardiac arrest.
MACE occurred in 14 copeptin-negative patients. However, 12 of the 14 were not discharged early because physicians overruled the negative biomarker results and moved the patients into standard in-hospital management. Two patients, or 0.6% of those discharged from the ED on the basis of a negative copeptin test had adverse events: One was rehospitalized on day 23 and underwent acute unplanned PCI on the next day, and the other was rehospitalized on day 4 and underwent coronary artery bypass graft surgery on day 12.

American Heart Association Immediate Past President Donna K. Arnett, Ph.D., said in an interview that she’d really like to see a second, confirmatory randomized trial before this early rule-out strategy is widely adopted. She considers the lost-to-follow-up rate uncomfortably high: 63 patients in the intention-to-treat analysis, and another 75 not accounted for in the per-protocol analysis, noted Dr. Arnett, professor and chair of the epidemiology department at the University of Alabama, Birmingham.
BiC-8 coinvestigator Dr. Kurt Huber said in an interview that the dual-biomarker early rule-out strategy is now used routinely in the hospital where he practices. Yet like Dr. Arnett, he considers a confirmatory test "extremely important" before concluding that the strategy is ready for prime-time use in every ED.
"The most important message from BiC-8, I think, is that these were patients at low to intermediate risk; they’re not the high-risk patients. And it’s also important that the physician doesn’t rely only on the test result, but also takes a final look at the clinical situation before releasing the patient. There is some overruling when patients are biomarker-negative but have typical risk markers. No test is 100% accurate. Clinical judgment remains extremely important," emphasized Dr. Huber, professor and director of cardiology and emergency medicine at Wilhelminen Hospital, Vienna.
The BiC-8 trial was sponsored by ThermoFisher Scientific and six university medical centers in German-speaking Europe. Dr. Moeckel reported receiving a research grant from ThermoFisher and serving as a consultant to Bayer, AstraZeneca, and The Medicines Company. Dr. Arnett and Dr. Huber had no conflicts of interest to declare.
In an era of tight resource utilization, patient throughput problems with ED backlogs, and judicious placement of higher-acuity patients into the hospital, a risk-stratification system for acute coronary syndrome (ACS) that would allow for early discharge from the ED with outpatient follow-up rather than the current practice of an extended ED workup for two troponins 6 hours apart or hospital admission, has the potential to radically change care processes.
Hospitals have developed observation units to address the need to provide less-intensive services in these clinical situations, but these units have faced significant patient concerns due to higher copays for services provided that are billed by outpatient codes.

|
| Dr. Hiren Shah |
This study, using the novel biomarker called copeptin in addition to troponin, has shown equivalent 30-day incidence of major cardiovascular events when the early-discharge strategy is compared to current practice. I would note, however, that this assay was utilized only in low- to intermediate-risk patients, and that clinical assessment of cardiovascular risk should always supersede this new assay in the discharge decision-making process. Of course, the challenges in the determination of risk and the variability in individual physician clinical risk-assessment approaches remain significant barriers no matter which assay system is used.
Future larger studies and those with a lower lost-to-follow-up rate than the current one will yield important results that may better evaluate the copeptin assay. If the results are similar in a more thorough study, the potential to change clinical practice for our ACS patients and to affect hospital resource utilization remains very significant.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital. He is on the advisory board of Hospitalist News.
In an era of tight resource utilization, patient throughput problems with ED backlogs, and judicious placement of higher-acuity patients into the hospital, a risk-stratification system for acute coronary syndrome (ACS) that would allow for early discharge from the ED with outpatient follow-up rather than the current practice of an extended ED workup for two troponins 6 hours apart or hospital admission, has the potential to radically change care processes.
Hospitals have developed observation units to address the need to provide less-intensive services in these clinical situations, but these units have faced significant patient concerns due to higher copays for services provided that are billed by outpatient codes.
|
|
| Dr. Hiren Shah |
This study, using the novel biomarker called copeptin in addition to troponin, has shown equivalent 30-day incidence of major cardiovascular events when the early-discharge strategy is compared to current practice. I would note, however, that this assay was utilized only in low- to intermediate-risk patients, and that clinical assessment of cardiovascular risk should always supersede this new assay in the discharge decision-making process. Of course, the challenges in the determination of risk and the variability in individual physician clinical risk-assessment approaches remain significant barriers no matter which assay system is used.
Future larger studies and those with a lower lost-to-follow-up rate than the current one will yield important results that may better evaluate the copeptin assay. If the results are similar in a more thorough study, the potential to change clinical practice for our ACS patients and to affect hospital resource utilization remains very significant.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital. He is on the advisory board of Hospitalist News.
In an era of tight resource utilization, patient throughput problems with ED backlogs, and judicious placement of higher-acuity patients into the hospital, a risk-stratification system for acute coronary syndrome (ACS) that would allow for early discharge from the ED with outpatient follow-up rather than the current practice of an extended ED workup for two troponins 6 hours apart or hospital admission, has the potential to radically change care processes.
Hospitals have developed observation units to address the need to provide less-intensive services in these clinical situations, but these units have faced significant patient concerns due to higher copays for services provided that are billed by outpatient codes.
|
|
| Dr. Hiren Shah |
This study, using the novel biomarker called copeptin in addition to troponin, has shown equivalent 30-day incidence of major cardiovascular events when the early-discharge strategy is compared to current practice. I would note, however, that this assay was utilized only in low- to intermediate-risk patients, and that clinical assessment of cardiovascular risk should always supersede this new assay in the discharge decision-making process. Of course, the challenges in the determination of risk and the variability in individual physician clinical risk-assessment approaches remain significant barriers no matter which assay system is used.
Future larger studies and those with a lower lost-to-follow-up rate than the current one will yield important results that may better evaluate the copeptin assay. If the results are similar in a more thorough study, the potential to change clinical practice for our ACS patients and to affect hospital resource utilization remains very significant.
Dr. Hiren Shah is an assistant professor of medicine in the Feinberg School of Medicine, Northwestern University, Chicago, and a medical director of the Medicine and Cardiac Telemetry Hospitalist Unit at Northwestern Memorial Hospital. He is on the advisory board of Hospitalist News.
AMSTERDAM – An early rule-out strategy based upon using two cardiac biomarkers allowed for safe discharge within a couple hours from the emergency department for most low- to intermediate-risk patients who presented with suspected acute coronary syndrome, based on the results of a randomized, multicenter trial conducted in Europe.
Moreover, the 30-day rates of major adverse cardiovascular events in the Biomarkers in Cardiology-8 (BiC-8) study were similarly low in patients discharged from the ED using the early rule-out process and in those who received standard, guideline-recommended care, which includes 6-12 hours of serial ECGs and troponin measurements in the chest pain unit, Dr. Martin Moeckel reported at the annual congress of the European Society of Cardiology.
"This biomarker strategy using a state-of-the-art quantitative troponin assay in combination with an ultrasensitive copeptin assay has the potential to change clinical practice with high patient safety," observed Dr. Moeckel of Charité Hospital, Berlin. The copeptin test is approved for use in the European Union but remains investigational in the United States.
Based upon the results of BiC-8, this dual biomarker for early rule-out of myocardial infarction (MI) is now standard clinical practice at Charité, he added.
The rationale for developing the early rule-out strategy tested in BiC-8 lies in the serious overcrowding that is now the norm in many EDs. This overcrowding has been shown to be in and of itself a risk factor for poor outcomes. The quandary is that nearly 12% of all patients who present to the ED do so because of chest pain, yet after an extensive and time-consuming evaluation only 1 in 10 of those patients is found to actually be having an acute MI.
"Rapid rule-out of acute MI is therefore a major clinical need, saving the health care system time and resources, and saving patients unnecessary stress, anxiety, and other risks," he said.
Copeptin is a marker for vasopressin, a hemodynamic stress indicator that shoots up immediately in an acute MI. In earlier studies, a negative result for both troponin and copeptin in an initial blood sample drawn at ED presentation had a 99% negative predictive value for MI.
The BiC-8 trial included 902 low- to intermediate-risk patients who presented with suspected acute coronary syndrome (ACS) to EDs in university medical centers. All had a negative initial cardiac troponin test. They were randomized to standard care in the chest pain unit, including serial troponin testing and ECGs, or to the experimental strategy, in which physicians were informed of the copeptin results from the same initial blood sample as the troponin. If the copeptin test was positive as defined by a level of 10 pmol/L or more, the patient was hospitalized for standard care. If the copeptin result was negative, however, the patient was immediately discharged with a scheduled outpatient visit within 72 hours.
Of the patients in the copeptin group, 66% were discharged directly from the ED, compared with 12% in the standard-care group.
The 30-day incidence of major adverse cardiovascular events (MACE) was 5.5% in the standard-care group and nearly identical at 5.46% in the copeptin group. However, physicians were permitted under the study protocol to overrule negative biomarker test results on the basis of their final clinical assessment, such as if their suspicions were aroused due to recurrent symptoms or new information about the patient’s history. In this per-protocol analysis, the 30-day MACE rate was 5.68% in the standard-care group and 3.18% in the copeptin group.
MACE was defined in BiC-8 as all-cause mortality, MI, rehospitalization for ACS, acute unplanned percutaneous coronary intervention (PCI), coronary artery bypass surgery, life-threatening arrhythmia, or resuscitation from cardiac arrest.
MACE occurred in 14 copeptin-negative patients. However, 12 of the 14 were not discharged early because physicians overruled the negative biomarker results and moved the patients into standard in-hospital management. Two patients, or 0.6% of those discharged from the ED on the basis of a negative copeptin test had adverse events: One was rehospitalized on day 23 and underwent acute unplanned PCI on the next day, and the other was rehospitalized on day 4 and underwent coronary artery bypass graft surgery on day 12.
American Heart Association Immediate Past President Donna K. Arnett, Ph.D., said in an interview that she’d really like to see a second, confirmatory randomized trial before this early rule-out strategy is widely adopted. She considers the lost-to-follow-up rate uncomfortably high: 63 patients in the intention-to-treat analysis, and another 75 not accounted for in the per-protocol analysis, noted Dr. Arnett, professor and chair of the epidemiology department at the University of Alabama, Birmingham.
BiC-8 coinvestigator Dr. Kurt Huber said in an interview that the dual-biomarker early rule-out strategy is now used routinely in the hospital where he practices. Yet like Dr. Arnett, he considers a confirmatory test "extremely important" before concluding that the strategy is ready for prime-time use in every ED.
"The most important message from BiC-8, I think, is that these were patients at low to intermediate risk; they’re not the high-risk patients. And it’s also important that the physician doesn’t rely only on the test result, but also takes a final look at the clinical situation before releasing the patient. There is some overruling when patients are biomarker-negative but have typical risk markers. No test is 100% accurate. Clinical judgment remains extremely important," emphasized Dr. Huber, professor and director of cardiology and emergency medicine at Wilhelminen Hospital, Vienna.
The BiC-8 trial was sponsored by ThermoFisher Scientific and six university medical centers in German-speaking Europe. Dr. Moeckel reported receiving a research grant from ThermoFisher and serving as a consultant to Bayer, AstraZeneca, and The Medicines Company. Dr. Arnett and Dr. Huber had no conflicts of interest to declare.
AMSTERDAM – An early rule-out strategy based upon using two cardiac biomarkers allowed for safe discharge within a couple hours from the emergency department for most low- to intermediate-risk patients who presented with suspected acute coronary syndrome, based on the results of a randomized, multicenter trial conducted in Europe.
Moreover, the 30-day rates of major adverse cardiovascular events in the Biomarkers in Cardiology-8 (BiC-8) study were similarly low in patients discharged from the ED using the early rule-out process and in those who received standard, guideline-recommended care, which includes 6-12 hours of serial ECGs and troponin measurements in the chest pain unit, Dr. Martin Moeckel reported at the annual congress of the European Society of Cardiology.
"This biomarker strategy using a state-of-the-art quantitative troponin assay in combination with an ultrasensitive copeptin assay has the potential to change clinical practice with high patient safety," observed Dr. Moeckel of Charité Hospital, Berlin. The copeptin test is approved for use in the European Union but remains investigational in the United States.
Based upon the results of BiC-8, this dual biomarker for early rule-out of myocardial infarction (MI) is now standard clinical practice at Charité, he added.
The rationale for developing the early rule-out strategy tested in BiC-8 lies in the serious overcrowding that is now the norm in many EDs. This overcrowding has been shown to be in and of itself a risk factor for poor outcomes. The quandary is that nearly 12% of all patients who present to the ED do so because of chest pain, yet after an extensive and time-consuming evaluation only 1 in 10 of those patients is found to actually be having an acute MI.
"Rapid rule-out of acute MI is therefore a major clinical need, saving the health care system time and resources, and saving patients unnecessary stress, anxiety, and other risks," he said.
Copeptin is a marker for vasopressin, a hemodynamic stress indicator that shoots up immediately in an acute MI. In earlier studies, a negative result for both troponin and copeptin in an initial blood sample drawn at ED presentation had a 99% negative predictive value for MI.
The BiC-8 trial included 902 low- to intermediate-risk patients who presented with suspected acute coronary syndrome (ACS) to EDs in university medical centers. All had a negative initial cardiac troponin test. They were randomized to standard care in the chest pain unit, including serial troponin testing and ECGs, or to the experimental strategy, in which physicians were informed of the copeptin results from the same initial blood sample as the troponin. If the copeptin test was positive as defined by a level of 10 pmol/L or more, the patient was hospitalized for standard care. If the copeptin result was negative, however, the patient was immediately discharged with a scheduled outpatient visit within 72 hours.
Of the patients in the copeptin group, 66% were discharged directly from the ED, compared with 12% in the standard-care group.
The 30-day incidence of major adverse cardiovascular events (MACE) was 5.5% in the standard-care group and nearly identical at 5.46% in the copeptin group. However, physicians were permitted under the study protocol to overrule negative biomarker test results on the basis of their final clinical assessment, such as if their suspicions were aroused due to recurrent symptoms or new information about the patient’s history. In this per-protocol analysis, the 30-day MACE rate was 5.68% in the standard-care group and 3.18% in the copeptin group.
MACE was defined in BiC-8 as all-cause mortality, MI, rehospitalization for ACS, acute unplanned percutaneous coronary intervention (PCI), coronary artery bypass surgery, life-threatening arrhythmia, or resuscitation from cardiac arrest.
MACE occurred in 14 copeptin-negative patients. However, 12 of the 14 were not discharged early because physicians overruled the negative biomarker results and moved the patients into standard in-hospital management. Two patients, or 0.6% of those discharged from the ED on the basis of a negative copeptin test had adverse events: One was rehospitalized on day 23 and underwent acute unplanned PCI on the next day, and the other was rehospitalized on day 4 and underwent coronary artery bypass graft surgery on day 12.
American Heart Association Immediate Past President Donna K. Arnett, Ph.D., said in an interview that she’d really like to see a second, confirmatory randomized trial before this early rule-out strategy is widely adopted. She considers the lost-to-follow-up rate uncomfortably high: 63 patients in the intention-to-treat analysis, and another 75 not accounted for in the per-protocol analysis, noted Dr. Arnett, professor and chair of the epidemiology department at the University of Alabama, Birmingham.
BiC-8 coinvestigator Dr. Kurt Huber said in an interview that the dual-biomarker early rule-out strategy is now used routinely in the hospital where he practices. Yet like Dr. Arnett, he considers a confirmatory test "extremely important" before concluding that the strategy is ready for prime-time use in every ED.
"The most important message from BiC-8, I think, is that these were patients at low to intermediate risk; they’re not the high-risk patients. And it’s also important that the physician doesn’t rely only on the test result, but also takes a final look at the clinical situation before releasing the patient. There is some overruling when patients are biomarker-negative but have typical risk markers. No test is 100% accurate. Clinical judgment remains extremely important," emphasized Dr. Huber, professor and director of cardiology and emergency medicine at Wilhelminen Hospital, Vienna.
The BiC-8 trial was sponsored by ThermoFisher Scientific and six university medical centers in German-speaking Europe. Dr. Moeckel reported receiving a research grant from ThermoFisher and serving as a consultant to Bayer, AstraZeneca, and The Medicines Company. Dr. Arnett and Dr. Huber had no conflicts of interest to declare.
AT THE ESC CONGRESS 2013
Major finding: Of the patients in the copeptin group, 66% were discharged directly from the emergency department, compared with 12% in the standard-care group.
Data source: BiC-8, a prospective, randomized multicenter trial involving 902 low- to intermediate-risk patients who presented to emergency departments with suspected acute coronary syndrome and a negative initial troponin assay.
Disclosures: The BiC-8 trial was sponsored by ThermoFisher Scientific and six university medical centers in German-speaking Europe. Dr. Moeckel reported receiving a research grant from ThermoFisher and serving as a consultant to Bayer, AstraZeneca, and The Medicines Company. Dr. Arnett and Dr. Huber had no conflicts of interest to declare.

Systemic sclerosis overlap syndromes called distinct entity
ISTANBUL – Systemic sclerosis overlap syndromes follow a path of disease progression distinctly different from that of limited or diffuse cutaneous systemic sclerosis, according to a new analysis from the German Network for Systemic Scleroderma.
"This study shows for the first time that patients suffering from systemic sclerosis overlap syndromes should be viewed as a distinct systemic sclerosis subset," Dr. Pia Moinzadeh noted at the annual congress of the European Academy of Dermatology and Venereology.
Those with systemic sclerosis overlap syndromes (SSc-OS) are a heterogeneous subgroup of patients who have the clinical features of SSc according to American College of Rheumatology criteria simultaneously with the characteristic findings of at least one other connective tissue disease, such as dermatomyositis, Sjögren’s syndrome, rheumatoid arthritis, or lupus erythematosus.
The registry of the German Network for Systemic Scleroderma is a uniquely large and inclusive ongoing prospective data base directed by a joint committee of dermatologists and rheumatologists. More than 6 years ago, when the investigators realized that a sizable fraction of patients enrolled in the national registry didn’t fit within the classic bimodal SSc categorization scheme composed of two subtypes – limited cutaneous and diffuse cutaneous SSc – they proposed three additional SSc subtypes. These are SSc-OS, undifferentiated scleroderma, and sclerosis sine scleroderma.
The focus of Dr. Moinzadeh’s EADV presentation was on SSc-OS. Of 3,240 SSc patients in the German registry, patients with OS comprise 11%, while those with limited cutaneous SSc make up 43%, those with diffuse cutaneous disease account for 31%, and the remainder of patients have undifferentiated scleroderma or sclerosis sine scleroderma.
The validity of the SSc-OS diagnostic construct has been controversial. Some experts have contended that patients with SSc-OS ought to be lumped under the headings of limited cutaneous SSc or diffuse cutaneous SSc, depending on the extent of skin involvement. However, the unparalleled size, inclusiveness, and long-term prospective follow-up provided by the German registry have resulted in evidence that argues to the contrary, according to Dr. Moinzadeh, a rheumatologist at the University of Cologne (Germany).
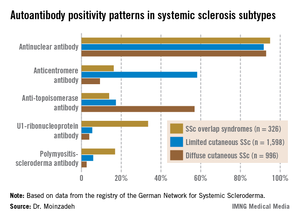
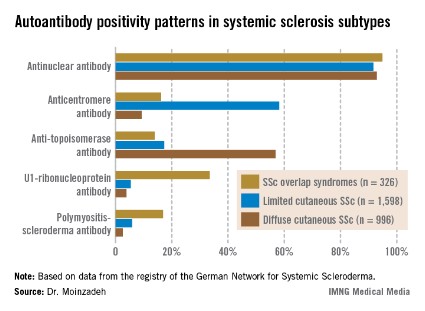
She reported on 326 patients with SSc-OS, 1,598 with limited cutaneous SSc, and 996 with diffuse cutaneous SSc prospectively followed through the German registry for a mean of 10.1 years. The follow-up data indicate SSc-OS evolves differently from either limited cutaneous SSc or diffuse cutaneous SSc. It also displays a distinctive pattern of organ involvement and autoantibody positivity, she noted.
The group with SSc-OS had a mean modified Rodnan skin score of 6.7, similar to the 7.2 score in the limited cutaneous SSc group and markedly less than the 15.8 in the diffuse cutaneous SSc patients. While this might suggest that patients with SSc-OS have a milder course of disease comparable to limited cutaneous SSc, in fact they progressed more rapidly, with earlier and more widespread significant organ involvement and a higher disease burden than the limited cutaneous SSc group, according to Dr. Moinzadeh.
Patients with SSc-OS developed musculoskeletal involvement far more frequently than others. Sixty-seven percent were affected, compared with 38% of patients with limited cutaneous SSc and 48% with diffuse cutaneous SSc. The patients in the SSc-OS group also developed musculoskeletal involvement earlier.
Lung fibrosis occurred in 38% of patients with SSc-OS, 27% of patients with limited cutaneous SSc, and 63% with diffuse cutaneous SSc. Cardiac involvement occurred in 15% with SSc-OS, 10% with limited cutaneous SSc, and 19% with diffuse cutaneous SSc. The onset of these manifestations of SSc in the SSc-OS subgroup was significantly earlier than in the limited cutaneous SSc patients but later than with diffuse cutaneous SSc.
Progression to esophageal and renal involvement, as well as pulmonary arterial hypertension, in the SSc-OS group occurred significantly earlier than in the limited cutaneous SSC patients, but again was later than with diffuse cutaneous SSC.
The autoantibody status of the three subgroups showed distinct differences (see graphic).
The German Network for Systemic Scleroderma is funded by the German Federal Ministry of Education and Research. Dr. Moinzadeh reported having no financial conflicts.
ISTANBUL – Systemic sclerosis overlap syndromes follow a path of disease progression distinctly different from that of limited or diffuse cutaneous systemic sclerosis, according to a new analysis from the German Network for Systemic Scleroderma.
"This study shows for the first time that patients suffering from systemic sclerosis overlap syndromes should be viewed as a distinct systemic sclerosis subset," Dr. Pia Moinzadeh noted at the annual congress of the European Academy of Dermatology and Venereology.
Those with systemic sclerosis overlap syndromes (SSc-OS) are a heterogeneous subgroup of patients who have the clinical features of SSc according to American College of Rheumatology criteria simultaneously with the characteristic findings of at least one other connective tissue disease, such as dermatomyositis, Sjögren’s syndrome, rheumatoid arthritis, or lupus erythematosus.
The registry of the German Network for Systemic Scleroderma is a uniquely large and inclusive ongoing prospective data base directed by a joint committee of dermatologists and rheumatologists. More than 6 years ago, when the investigators realized that a sizable fraction of patients enrolled in the national registry didn’t fit within the classic bimodal SSc categorization scheme composed of two subtypes – limited cutaneous and diffuse cutaneous SSc – they proposed three additional SSc subtypes. These are SSc-OS, undifferentiated scleroderma, and sclerosis sine scleroderma.
The focus of Dr. Moinzadeh’s EADV presentation was on SSc-OS. Of 3,240 SSc patients in the German registry, patients with OS comprise 11%, while those with limited cutaneous SSc make up 43%, those with diffuse cutaneous disease account for 31%, and the remainder of patients have undifferentiated scleroderma or sclerosis sine scleroderma.
The validity of the SSc-OS diagnostic construct has been controversial. Some experts have contended that patients with SSc-OS ought to be lumped under the headings of limited cutaneous SSc or diffuse cutaneous SSc, depending on the extent of skin involvement. However, the unparalleled size, inclusiveness, and long-term prospective follow-up provided by the German registry have resulted in evidence that argues to the contrary, according to Dr. Moinzadeh, a rheumatologist at the University of Cologne (Germany).
She reported on 326 patients with SSc-OS, 1,598 with limited cutaneous SSc, and 996 with diffuse cutaneous SSc prospectively followed through the German registry for a mean of 10.1 years. The follow-up data indicate SSc-OS evolves differently from either limited cutaneous SSc or diffuse cutaneous SSc. It also displays a distinctive pattern of organ involvement and autoantibody positivity, she noted.
The group with SSc-OS had a mean modified Rodnan skin score of 6.7, similar to the 7.2 score in the limited cutaneous SSc group and markedly less than the 15.8 in the diffuse cutaneous SSc patients. While this might suggest that patients with SSc-OS have a milder course of disease comparable to limited cutaneous SSc, in fact they progressed more rapidly, with earlier and more widespread significant organ involvement and a higher disease burden than the limited cutaneous SSc group, according to Dr. Moinzadeh.
Patients with SSc-OS developed musculoskeletal involvement far more frequently than others. Sixty-seven percent were affected, compared with 38% of patients with limited cutaneous SSc and 48% with diffuse cutaneous SSc. The patients in the SSc-OS group also developed musculoskeletal involvement earlier.
Lung fibrosis occurred in 38% of patients with SSc-OS, 27% of patients with limited cutaneous SSc, and 63% with diffuse cutaneous SSc. Cardiac involvement occurred in 15% with SSc-OS, 10% with limited cutaneous SSc, and 19% with diffuse cutaneous SSc. The onset of these manifestations of SSc in the SSc-OS subgroup was significantly earlier than in the limited cutaneous SSc patients but later than with diffuse cutaneous SSc.
Progression to esophageal and renal involvement, as well as pulmonary arterial hypertension, in the SSc-OS group occurred significantly earlier than in the limited cutaneous SSC patients, but again was later than with diffuse cutaneous SSC.
The autoantibody status of the three subgroups showed distinct differences (see graphic).
The German Network for Systemic Scleroderma is funded by the German Federal Ministry of Education and Research. Dr. Moinzadeh reported having no financial conflicts.
ISTANBUL – Systemic sclerosis overlap syndromes follow a path of disease progression distinctly different from that of limited or diffuse cutaneous systemic sclerosis, according to a new analysis from the German Network for Systemic Scleroderma.
"This study shows for the first time that patients suffering from systemic sclerosis overlap syndromes should be viewed as a distinct systemic sclerosis subset," Dr. Pia Moinzadeh noted at the annual congress of the European Academy of Dermatology and Venereology.
Those with systemic sclerosis overlap syndromes (SSc-OS) are a heterogeneous subgroup of patients who have the clinical features of SSc according to American College of Rheumatology criteria simultaneously with the characteristic findings of at least one other connective tissue disease, such as dermatomyositis, Sjögren’s syndrome, rheumatoid arthritis, or lupus erythematosus.
The registry of the German Network for Systemic Scleroderma is a uniquely large and inclusive ongoing prospective data base directed by a joint committee of dermatologists and rheumatologists. More than 6 years ago, when the investigators realized that a sizable fraction of patients enrolled in the national registry didn’t fit within the classic bimodal SSc categorization scheme composed of two subtypes – limited cutaneous and diffuse cutaneous SSc – they proposed three additional SSc subtypes. These are SSc-OS, undifferentiated scleroderma, and sclerosis sine scleroderma.
The focus of Dr. Moinzadeh’s EADV presentation was on SSc-OS. Of 3,240 SSc patients in the German registry, patients with OS comprise 11%, while those with limited cutaneous SSc make up 43%, those with diffuse cutaneous disease account for 31%, and the remainder of patients have undifferentiated scleroderma or sclerosis sine scleroderma.
The validity of the SSc-OS diagnostic construct has been controversial. Some experts have contended that patients with SSc-OS ought to be lumped under the headings of limited cutaneous SSc or diffuse cutaneous SSc, depending on the extent of skin involvement. However, the unparalleled size, inclusiveness, and long-term prospective follow-up provided by the German registry have resulted in evidence that argues to the contrary, according to Dr. Moinzadeh, a rheumatologist at the University of Cologne (Germany).
She reported on 326 patients with SSc-OS, 1,598 with limited cutaneous SSc, and 996 with diffuse cutaneous SSc prospectively followed through the German registry for a mean of 10.1 years. The follow-up data indicate SSc-OS evolves differently from either limited cutaneous SSc or diffuse cutaneous SSc. It also displays a distinctive pattern of organ involvement and autoantibody positivity, she noted.
The group with SSc-OS had a mean modified Rodnan skin score of 6.7, similar to the 7.2 score in the limited cutaneous SSc group and markedly less than the 15.8 in the diffuse cutaneous SSc patients. While this might suggest that patients with SSc-OS have a milder course of disease comparable to limited cutaneous SSc, in fact they progressed more rapidly, with earlier and more widespread significant organ involvement and a higher disease burden than the limited cutaneous SSc group, according to Dr. Moinzadeh.
Patients with SSc-OS developed musculoskeletal involvement far more frequently than others. Sixty-seven percent were affected, compared with 38% of patients with limited cutaneous SSc and 48% with diffuse cutaneous SSc. The patients in the SSc-OS group also developed musculoskeletal involvement earlier.
Lung fibrosis occurred in 38% of patients with SSc-OS, 27% of patients with limited cutaneous SSc, and 63% with diffuse cutaneous SSc. Cardiac involvement occurred in 15% with SSc-OS, 10% with limited cutaneous SSc, and 19% with diffuse cutaneous SSc. The onset of these manifestations of SSc in the SSc-OS subgroup was significantly earlier than in the limited cutaneous SSc patients but later than with diffuse cutaneous SSc.
Progression to esophageal and renal involvement, as well as pulmonary arterial hypertension, in the SSc-OS group occurred significantly earlier than in the limited cutaneous SSC patients, but again was later than with diffuse cutaneous SSC.
The autoantibody status of the three subgroups showed distinct differences (see graphic).
The German Network for Systemic Scleroderma is funded by the German Federal Ministry of Education and Research. Dr. Moinzadeh reported having no financial conflicts.
AT THE EADV CONGRESS
Major finding: Musculoskeletal involvement occurred in 67% of patients with systemic sclerosis overlap syndromes, compared with 38% of those with limited cutaneous systemic sclerosis and 48% with diffuse cutaneous systemic sclerosis.
Data source: This analysis from the ongoing prospective national registry maintained by the German Network for Systemic Scleroderma included nearly 3,000 patients with systemic sclerosis followed for a mean of 10.1 years.
Disclosures: The German Network for Systemic Scleroderma is funded by the German Federal Ministry of Education and Research. Dr. Moinzadeh reported having no financial conflicts.
Is PASI 90 becoming the new PASI 75?
ISTANBUL – With the majority of psoriasis patients now achieving PASI 90 responses in randomized trials of the latest-generation biologic agents, a push is on to replace PASI 75 with PASI 90 as the new goal defining treatment success. But some dermatologists have misgivings about raising the bar.
"More and more, editorialists are promoting the idea of silencing psoriasis in all patients. This is a tricky and challenging goal," Dr. Hervé Bachelez said at the annual congress of the European Academy of Dermatology and Venereology.

"You’ve probably noticed that PASI 90 and even PASI 100 are becoming important as secondary endpoints in virtually all clinical trials. It’s good, it’s legitimate, and the PASI 90 probably better reflects the wishes of the patient and the physician than the PASI 75. But we have to wait and see what the caveats of this are. You can say, ‘Let’s push the response rate up to PASI 100 in all patients,’ but the danger is that if you cross a line, you may be unable to precisely regulate the level of immunosuppression in some patients. Basically you can expect some safety issues in real life that you would not see in clinical trials," cautioned Dr. Bachelez, professor of dermatology and head of the inflammatory skin diseases unit at Saint Louis University Hospital, Paris.
Not so many years ago the notion of PASI 90 responses in high double figures seemed a pipedream, he observed. For example, the week-12 PASI 90 rate in published randomized trials of methotrexate was only 9%, while for the first-generation tumor necrosis factor inhibitor etanercept, the rates were 19%-23%. In contrast, among the highlights of this year’s EADV congress were the presentation of results from clinical trials of two investigational interleukin-17 inhibitors: In the pivotal Phase III FIXTURE trial, secukinumab-treated patients had a PASI 90 response rate of 72% at week 16, while the week-16 PASI 90 rate in the Phase II OLE trial was 87% in patients on brodalimab, and even out to week 96, it was 78%.
Underscoring Dr. Bachelez’ concern that the randomized trial experience likely underestimates the true extent of safety hazards posed by potent therapies in daily clinical practice was a report by a consortium of 13 Spanish dermatology departments responsible for the BIOBADADERM registry. The Spanish registry is focused on safety and includes only psoriasis patients on systemic therapy, whether biologics or classic drugs. Among the first 1,042 enrollees receiving systemic therapy, fully 30% would not have been eligible for participation in randomized controlled trials for various reasons, including age greater than 70 years, having chronic kidney or liver disease, a history of hepatitis B or C, HIV infection, or cancer, or having psoriasis of a type other than chronic plaque disease.
The disturbing finding was that during 2,179 person-years of prospective follow-up, the large group of patients ineligible for randomized trials had a 2.7-fold increased risk of serious adverse events compared with patients on systemic therapy who were eligible for study participation.
The number needed to harm was calculated as follows: For every 40 patients treated with systemic therapy for 2.1 years despite not being eligible for randomized trials, one additional serious adverse event can be expected compared with similar treatment in randomized trial-eligible patients, according to the investigators (Arch. Dermatol. 2012;148:463-70). And that’s without pushing the envelope by trying to aim for a PASI 90 response, Dr. Bachelez noted.
A contrary view regarding PASI 90 as an emerging standard of treatment excellence was put forth elsewhere at the meeting by Dr. Peter van de Kerkhof, professor and head of the department of dermatology at Radboud University in Nijmegen, the Netherlands.
He cited multiple studies demonstrating that substantial PASI reductions may not translate into tangible improvements in patients’ quality of life. For example, among psoriasis patients who achieved a PASI 75 response in one European study, 65% still had a Dermatology Life Quality Index (DLQI) score of 2 or more (Eur. J. Dermatol. 2010;20:62-7).
"This implies that there is something more to be wished for by patients, even when PASI 75 is reached," according to Dr. van de Kerkhof.
Moreover, in another trial, even among patients with a PASI score of 0 at week 24, only 70% had an optimal DLQI of 0, not 100% as most dermatologists might expect (Br. J. Dermatol. 2006;154:1161-8).

A recent survey of 2,151 European psoriasis patients and their dermatologists highlighted a substantial degree of dissatisfaction with current therapies. Patients on biologics had higher rates of improvement from severe to moderate or mild disease than did those on any other forms of psoriasis therapy, yet 41% of patients on biologics were dissatisfied with their treatment (J. Dermatolog. Treat. 2013;24:193-8).
"I think it’s extremely important that we continue to innovate treatment possibilities for psoriasis in order to improve outcomes for our patients," Dr. van de Kerkhof said.
What patients really want, surveys suggest, are treatments that render them clear or nearly clear, and do so quickly. In one survey, patients rated as the most important characteristic about a therapy the rapidity with which it could achieve a moderate 50% improvement in symptoms. They rated that as higher in importance to them than the therapy’s long-term risks (Arch. Dermatol. 2007;143:1175-9), Dr. van de Kerkhof noted.
Patients also place a high priority on improvement of a broad array of symptoms that aren’t captured by either the PASI or the DLQI, Dr. Bruce E. Strober noted in a separate presentation. These include itching, plaque-related pain, altered skin appearance, flaking, and bleeding.
For this reason, he and a group of his coworkers have created and are now validating a new tool for the assessment of patient-related outcomes in psoriasis called the Psoriasis Symptom Diary (Value Health 2013;16:1014-22). The 16-item tool takes less than 5 minutes for a patient to fill out and is designed to replace the DLQI both in clinical trials and everyday practice. The goal is to be able to walk into the examination room, take a quick look at the Psoriasis Symptom Diary, and know from that how a patient is currently doing even before asking for the patient to disrobe.
"Let’s face it: Outside of skin cancer, when we’re doing dermatology, we’re in the quality of life business. That means we’re asking patients how they’re doing at every visit for psoriasis, atopic dermatitis, or severe acne. The DLQI does that, but it’s not psoriasis specific," said Dr. Strober, vice chair and director of the clinical trials unit in the department of dermatology at the University of Connecticut, Farmington.

As for the PASI, he doesn’t use it except in structured clinical trials. It’s too time consuming and has a high rate of inter- and intrarater variability.
"In the United States, dermatologists never do PASI scores in their clinics. The PASI score has numerous drawbacks that make it impractical in a regular practice setting," Dr. Strober said. "In my own practice, I routinely do a 5-point Physician’s Global Assessment along with an estimate of involved body surface area. I think that gives you a good picture of the objective level of psoriasis severity."
Dr. Bachelez, Dr. van de Kerkhof, and Dr. Strober each reported receiving research grants from and serving on advisory boards for 9-14 pharmaceutical companies engaged in developing new treatments for psoriasis.
ISTANBUL – With the majority of psoriasis patients now achieving PASI 90 responses in randomized trials of the latest-generation biologic agents, a push is on to replace PASI 75 with PASI 90 as the new goal defining treatment success. But some dermatologists have misgivings about raising the bar.
"More and more, editorialists are promoting the idea of silencing psoriasis in all patients. This is a tricky and challenging goal," Dr. Hervé Bachelez said at the annual congress of the European Academy of Dermatology and Venereology.
"You’ve probably noticed that PASI 90 and even PASI 100 are becoming important as secondary endpoints in virtually all clinical trials. It’s good, it’s legitimate, and the PASI 90 probably better reflects the wishes of the patient and the physician than the PASI 75. But we have to wait and see what the caveats of this are. You can say, ‘Let’s push the response rate up to PASI 100 in all patients,’ but the danger is that if you cross a line, you may be unable to precisely regulate the level of immunosuppression in some patients. Basically you can expect some safety issues in real life that you would not see in clinical trials," cautioned Dr. Bachelez, professor of dermatology and head of the inflammatory skin diseases unit at Saint Louis University Hospital, Paris.
Not so many years ago the notion of PASI 90 responses in high double figures seemed a pipedream, he observed. For example, the week-12 PASI 90 rate in published randomized trials of methotrexate was only 9%, while for the first-generation tumor necrosis factor inhibitor etanercept, the rates were 19%-23%. In contrast, among the highlights of this year’s EADV congress were the presentation of results from clinical trials of two investigational interleukin-17 inhibitors: In the pivotal Phase III FIXTURE trial, secukinumab-treated patients had a PASI 90 response rate of 72% at week 16, while the week-16 PASI 90 rate in the Phase II OLE trial was 87% in patients on brodalimab, and even out to week 96, it was 78%.
Underscoring Dr. Bachelez’ concern that the randomized trial experience likely underestimates the true extent of safety hazards posed by potent therapies in daily clinical practice was a report by a consortium of 13 Spanish dermatology departments responsible for the BIOBADADERM registry. The Spanish registry is focused on safety and includes only psoriasis patients on systemic therapy, whether biologics or classic drugs. Among the first 1,042 enrollees receiving systemic therapy, fully 30% would not have been eligible for participation in randomized controlled trials for various reasons, including age greater than 70 years, having chronic kidney or liver disease, a history of hepatitis B or C, HIV infection, or cancer, or having psoriasis of a type other than chronic plaque disease.
The disturbing finding was that during 2,179 person-years of prospective follow-up, the large group of patients ineligible for randomized trials had a 2.7-fold increased risk of serious adverse events compared with patients on systemic therapy who were eligible for study participation.
The number needed to harm was calculated as follows: For every 40 patients treated with systemic therapy for 2.1 years despite not being eligible for randomized trials, one additional serious adverse event can be expected compared with similar treatment in randomized trial-eligible patients, according to the investigators (Arch. Dermatol. 2012;148:463-70). And that’s without pushing the envelope by trying to aim for a PASI 90 response, Dr. Bachelez noted.
A contrary view regarding PASI 90 as an emerging standard of treatment excellence was put forth elsewhere at the meeting by Dr. Peter van de Kerkhof, professor and head of the department of dermatology at Radboud University in Nijmegen, the Netherlands.
He cited multiple studies demonstrating that substantial PASI reductions may not translate into tangible improvements in patients’ quality of life. For example, among psoriasis patients who achieved a PASI 75 response in one European study, 65% still had a Dermatology Life Quality Index (DLQI) score of 2 or more (Eur. J. Dermatol. 2010;20:62-7).
"This implies that there is something more to be wished for by patients, even when PASI 75 is reached," according to Dr. van de Kerkhof.
Moreover, in another trial, even among patients with a PASI score of 0 at week 24, only 70% had an optimal DLQI of 0, not 100% as most dermatologists might expect (Br. J. Dermatol. 2006;154:1161-8).
A recent survey of 2,151 European psoriasis patients and their dermatologists highlighted a substantial degree of dissatisfaction with current therapies. Patients on biologics had higher rates of improvement from severe to moderate or mild disease than did those on any other forms of psoriasis therapy, yet 41% of patients on biologics were dissatisfied with their treatment (J. Dermatolog. Treat. 2013;24:193-8).
"I think it’s extremely important that we continue to innovate treatment possibilities for psoriasis in order to improve outcomes for our patients," Dr. van de Kerkhof said.
What patients really want, surveys suggest, are treatments that render them clear or nearly clear, and do so quickly. In one survey, patients rated as the most important characteristic about a therapy the rapidity with which it could achieve a moderate 50% improvement in symptoms. They rated that as higher in importance to them than the therapy’s long-term risks (Arch. Dermatol. 2007;143:1175-9), Dr. van de Kerkhof noted.
Patients also place a high priority on improvement of a broad array of symptoms that aren’t captured by either the PASI or the DLQI, Dr. Bruce E. Strober noted in a separate presentation. These include itching, plaque-related pain, altered skin appearance, flaking, and bleeding.
For this reason, he and a group of his coworkers have created and are now validating a new tool for the assessment of patient-related outcomes in psoriasis called the Psoriasis Symptom Diary (Value Health 2013;16:1014-22). The 16-item tool takes less than 5 minutes for a patient to fill out and is designed to replace the DLQI both in clinical trials and everyday practice. The goal is to be able to walk into the examination room, take a quick look at the Psoriasis Symptom Diary, and know from that how a patient is currently doing even before asking for the patient to disrobe.
"Let’s face it: Outside of skin cancer, when we’re doing dermatology, we’re in the quality of life business. That means we’re asking patients how they’re doing at every visit for psoriasis, atopic dermatitis, or severe acne. The DLQI does that, but it’s not psoriasis specific," said Dr. Strober, vice chair and director of the clinical trials unit in the department of dermatology at the University of Connecticut, Farmington.
As for the PASI, he doesn’t use it except in structured clinical trials. It’s too time consuming and has a high rate of inter- and intrarater variability.
"In the United States, dermatologists never do PASI scores in their clinics. The PASI score has numerous drawbacks that make it impractical in a regular practice setting," Dr. Strober said. "In my own practice, I routinely do a 5-point Physician’s Global Assessment along with an estimate of involved body surface area. I think that gives you a good picture of the objective level of psoriasis severity."
Dr. Bachelez, Dr. van de Kerkhof, and Dr. Strober each reported receiving research grants from and serving on advisory boards for 9-14 pharmaceutical companies engaged in developing new treatments for psoriasis.
ISTANBUL – With the majority of psoriasis patients now achieving PASI 90 responses in randomized trials of the latest-generation biologic agents, a push is on to replace PASI 75 with PASI 90 as the new goal defining treatment success. But some dermatologists have misgivings about raising the bar.
"More and more, editorialists are promoting the idea of silencing psoriasis in all patients. This is a tricky and challenging goal," Dr. Hervé Bachelez said at the annual congress of the European Academy of Dermatology and Venereology.
"You’ve probably noticed that PASI 90 and even PASI 100 are becoming important as secondary endpoints in virtually all clinical trials. It’s good, it’s legitimate, and the PASI 90 probably better reflects the wishes of the patient and the physician than the PASI 75. But we have to wait and see what the caveats of this are. You can say, ‘Let’s push the response rate up to PASI 100 in all patients,’ but the danger is that if you cross a line, you may be unable to precisely regulate the level of immunosuppression in some patients. Basically you can expect some safety issues in real life that you would not see in clinical trials," cautioned Dr. Bachelez, professor of dermatology and head of the inflammatory skin diseases unit at Saint Louis University Hospital, Paris.
Not so many years ago the notion of PASI 90 responses in high double figures seemed a pipedream, he observed. For example, the week-12 PASI 90 rate in published randomized trials of methotrexate was only 9%, while for the first-generation tumor necrosis factor inhibitor etanercept, the rates were 19%-23%. In contrast, among the highlights of this year’s EADV congress were the presentation of results from clinical trials of two investigational interleukin-17 inhibitors: In the pivotal Phase III FIXTURE trial, secukinumab-treated patients had a PASI 90 response rate of 72% at week 16, while the week-16 PASI 90 rate in the Phase II OLE trial was 87% in patients on brodalimab, and even out to week 96, it was 78%.
Underscoring Dr. Bachelez’ concern that the randomized trial experience likely underestimates the true extent of safety hazards posed by potent therapies in daily clinical practice was a report by a consortium of 13 Spanish dermatology departments responsible for the BIOBADADERM registry. The Spanish registry is focused on safety and includes only psoriasis patients on systemic therapy, whether biologics or classic drugs. Among the first 1,042 enrollees receiving systemic therapy, fully 30% would not have been eligible for participation in randomized controlled trials for various reasons, including age greater than 70 years, having chronic kidney or liver disease, a history of hepatitis B or C, HIV infection, or cancer, or having psoriasis of a type other than chronic plaque disease.
The disturbing finding was that during 2,179 person-years of prospective follow-up, the large group of patients ineligible for randomized trials had a 2.7-fold increased risk of serious adverse events compared with patients on systemic therapy who were eligible for study participation.
The number needed to harm was calculated as follows: For every 40 patients treated with systemic therapy for 2.1 years despite not being eligible for randomized trials, one additional serious adverse event can be expected compared with similar treatment in randomized trial-eligible patients, according to the investigators (Arch. Dermatol. 2012;148:463-70). And that’s without pushing the envelope by trying to aim for a PASI 90 response, Dr. Bachelez noted.
A contrary view regarding PASI 90 as an emerging standard of treatment excellence was put forth elsewhere at the meeting by Dr. Peter van de Kerkhof, professor and head of the department of dermatology at Radboud University in Nijmegen, the Netherlands.
He cited multiple studies demonstrating that substantial PASI reductions may not translate into tangible improvements in patients’ quality of life. For example, among psoriasis patients who achieved a PASI 75 response in one European study, 65% still had a Dermatology Life Quality Index (DLQI) score of 2 or more (Eur. J. Dermatol. 2010;20:62-7).
"This implies that there is something more to be wished for by patients, even when PASI 75 is reached," according to Dr. van de Kerkhof.
Moreover, in another trial, even among patients with a PASI score of 0 at week 24, only 70% had an optimal DLQI of 0, not 100% as most dermatologists might expect (Br. J. Dermatol. 2006;154:1161-8).
A recent survey of 2,151 European psoriasis patients and their dermatologists highlighted a substantial degree of dissatisfaction with current therapies. Patients on biologics had higher rates of improvement from severe to moderate or mild disease than did those on any other forms of psoriasis therapy, yet 41% of patients on biologics were dissatisfied with their treatment (J. Dermatolog. Treat. 2013;24:193-8).
"I think it’s extremely important that we continue to innovate treatment possibilities for psoriasis in order to improve outcomes for our patients," Dr. van de Kerkhof said.
What patients really want, surveys suggest, are treatments that render them clear or nearly clear, and do so quickly. In one survey, patients rated as the most important characteristic about a therapy the rapidity with which it could achieve a moderate 50% improvement in symptoms. They rated that as higher in importance to them than the therapy’s long-term risks (Arch. Dermatol. 2007;143:1175-9), Dr. van de Kerkhof noted.
Patients also place a high priority on improvement of a broad array of symptoms that aren’t captured by either the PASI or the DLQI, Dr. Bruce E. Strober noted in a separate presentation. These include itching, plaque-related pain, altered skin appearance, flaking, and bleeding.
For this reason, he and a group of his coworkers have created and are now validating a new tool for the assessment of patient-related outcomes in psoriasis called the Psoriasis Symptom Diary (Value Health 2013;16:1014-22). The 16-item tool takes less than 5 minutes for a patient to fill out and is designed to replace the DLQI both in clinical trials and everyday practice. The goal is to be able to walk into the examination room, take a quick look at the Psoriasis Symptom Diary, and know from that how a patient is currently doing even before asking for the patient to disrobe.
"Let’s face it: Outside of skin cancer, when we’re doing dermatology, we’re in the quality of life business. That means we’re asking patients how they’re doing at every visit for psoriasis, atopic dermatitis, or severe acne. The DLQI does that, but it’s not psoriasis specific," said Dr. Strober, vice chair and director of the clinical trials unit in the department of dermatology at the University of Connecticut, Farmington.
As for the PASI, he doesn’t use it except in structured clinical trials. It’s too time consuming and has a high rate of inter- and intrarater variability.
"In the United States, dermatologists never do PASI scores in their clinics. The PASI score has numerous drawbacks that make it impractical in a regular practice setting," Dr. Strober said. "In my own practice, I routinely do a 5-point Physician’s Global Assessment along with an estimate of involved body surface area. I think that gives you a good picture of the objective level of psoriasis severity."
Dr. Bachelez, Dr. van de Kerkhof, and Dr. Strober each reported receiving research grants from and serving on advisory boards for 9-14 pharmaceutical companies engaged in developing new treatments for psoriasis.
EXPERT ANALYSIS FROM THE eadv CONGRESS

Lower serum IgE level tied to better treatment response in atopic dermatitis
ISTANBUL – Baseline total serum immunoglobulin E shows promise as a biomarker predictive of long-term treatment outcomes in atopic dermatitis patients.
In a retrospective study involving 175 Finnish patients with atopic dermatitis followed for a mean of 4.2 years, total clearance was achieved in 54% of patients with a baseline total serum IgE below 1,000 IU/mL, 38% of those with a baseline value of 1,000-10,000 IU/mL, and in a mere 8.3% with a baseline total serum IgE in excess of 10,000 IU/mL, Dr. Ville Kiiski reported at the annual congress of the European Academy of Dermatology and Venereology.
Similarly, treatment response, a lower bar as an endpoint in that it was defined as a lasting reduction in atopic dermatitis severity but not necessarily total clearance, occurred in 93% of those with a baseline total serum IgE below 1,000 IU/mL, compared with 64% of patients with a baseline of 1,000-10,000 IU/mL and 13% with a baseline level greater than 10,000 IU/mL, added Dr. Kiiski of Helsinki University.
Of note, this was largely an adult patient population, with a mean age of 32 years, although the range was 3-78 years. And these patients had atopic dermatitis of sufficient severity that it brought them to a specialized outpatient atopic dermatitis clinic at the Helsinki Skin and Allergy Hospital, where their baseline total serum IgE was measured.
Maintenance therapy during more than 4 years of follow-up was topical tacrolimus (Protopic) in 122 patients and topical corticosteroids and tacrolimus in 53.
Treatment had only a modest effect on total serum IgE levels over time. The median value was 1,472 IU/mL at baseline and 1,114 IU/mL more than 4 years later.
This retrospective study was free of commercial sponsorship, and Dr. Kiiski reported having no financial conflicts of interest.
ISTANBUL – Baseline total serum immunoglobulin E shows promise as a biomarker predictive of long-term treatment outcomes in atopic dermatitis patients.
In a retrospective study involving 175 Finnish patients with atopic dermatitis followed for a mean of 4.2 years, total clearance was achieved in 54% of patients with a baseline total serum IgE below 1,000 IU/mL, 38% of those with a baseline value of 1,000-10,000 IU/mL, and in a mere 8.3% with a baseline total serum IgE in excess of 10,000 IU/mL, Dr. Ville Kiiski reported at the annual congress of the European Academy of Dermatology and Venereology.
Similarly, treatment response, a lower bar as an endpoint in that it was defined as a lasting reduction in atopic dermatitis severity but not necessarily total clearance, occurred in 93% of those with a baseline total serum IgE below 1,000 IU/mL, compared with 64% of patients with a baseline of 1,000-10,000 IU/mL and 13% with a baseline level greater than 10,000 IU/mL, added Dr. Kiiski of Helsinki University.
Of note, this was largely an adult patient population, with a mean age of 32 years, although the range was 3-78 years. And these patients had atopic dermatitis of sufficient severity that it brought them to a specialized outpatient atopic dermatitis clinic at the Helsinki Skin and Allergy Hospital, where their baseline total serum IgE was measured.
Maintenance therapy during more than 4 years of follow-up was topical tacrolimus (Protopic) in 122 patients and topical corticosteroids and tacrolimus in 53.
Treatment had only a modest effect on total serum IgE levels over time. The median value was 1,472 IU/mL at baseline and 1,114 IU/mL more than 4 years later.
This retrospective study was free of commercial sponsorship, and Dr. Kiiski reported having no financial conflicts of interest.
ISTANBUL – Baseline total serum immunoglobulin E shows promise as a biomarker predictive of long-term treatment outcomes in atopic dermatitis patients.
In a retrospective study involving 175 Finnish patients with atopic dermatitis followed for a mean of 4.2 years, total clearance was achieved in 54% of patients with a baseline total serum IgE below 1,000 IU/mL, 38% of those with a baseline value of 1,000-10,000 IU/mL, and in a mere 8.3% with a baseline total serum IgE in excess of 10,000 IU/mL, Dr. Ville Kiiski reported at the annual congress of the European Academy of Dermatology and Venereology.
Similarly, treatment response, a lower bar as an endpoint in that it was defined as a lasting reduction in atopic dermatitis severity but not necessarily total clearance, occurred in 93% of those with a baseline total serum IgE below 1,000 IU/mL, compared with 64% of patients with a baseline of 1,000-10,000 IU/mL and 13% with a baseline level greater than 10,000 IU/mL, added Dr. Kiiski of Helsinki University.
Of note, this was largely an adult patient population, with a mean age of 32 years, although the range was 3-78 years. And these patients had atopic dermatitis of sufficient severity that it brought them to a specialized outpatient atopic dermatitis clinic at the Helsinki Skin and Allergy Hospital, where their baseline total serum IgE was measured.
Maintenance therapy during more than 4 years of follow-up was topical tacrolimus (Protopic) in 122 patients and topical corticosteroids and tacrolimus in 53.
Treatment had only a modest effect on total serum IgE levels over time. The median value was 1,472 IU/mL at baseline and 1,114 IU/mL more than 4 years later.
This retrospective study was free of commercial sponsorship, and Dr. Kiiski reported having no financial conflicts of interest.
AT THE EADV CONGRESS
Major finding: A reduction in atopic dermatitis severity during 4.2 years of topical therapy occurred in 93% of patients with a baseline total serum IgE level below 1,000 IU/mL, compared with 64% of those with a baseline IgE of 1,000-10,000 IU/mL, and just 13% of patients with a baseline value greater than 10,000 IU/mL.
Data source: This was a retrospective study involving 175 patients with atopic dermatitis followed for a mean of 4.2 years of treatment.
Disclosures: This retrospective study was free of commercial sponsorship, and Dr. Kiiski reported having no financial conflicts of interest.
Azelaic acid 15% gel tames women’s acne
ISTANBUL, TURKEY – Azelaic acid 15% gel constitutes an effective and well-tolerated treatment option for women with adult acne, according to the findings of an investigator-blinded, 9-month, randomized clinical trial.
The results showed azelaic acid 15% gel was similar in effectiveness to adapalene 0.1% gel, a widely prescribed treatment for this common condition, Dr. Anja Thielitz reported at the annual congress of the European Academy of Dermatology and Venereology.
However, azelaic acid 15% gel had a clear advantage in terms of tolerability. Median scores for skin redness, dryness, and scaling were significantly lower in the azelaic acid–treated group, added Dr. Thielitz of Otto von Guericke University in Magdeburg, Germany.
The single-center study involved 55 women aged 18-45 years, all with mild to moderate adult acne. They were randomized to one of three study arms: azelaic acid 15% gel twice daily for 9 months; adapalene 0.1% gel once daily, or 3 months of twice-daily azelaic acid 15% gel followed by 6 months of observation with no treatment.
Inflammatory and noninflammatory acne lesion counts, microcomedones, acne grading scale scores, and Dermatology Life Quality Index scores improved similarly in all three groups after 3 months. For example, median total lesion counts decreased from approximately 50 to 20, and median scores on the Leeds revised acne grading system dropped from 4 to roughly 2.5. Similar degrees of additional improvement were seen during months 4-9 in the two groups who remained on active treatment.
In contrast, some backsliding – although less than Dr. Thielitz had anticipated occurred during the untreated observation period among patients who halted the azelaic acid 15% gel after 3 months. By month 9, their total lesion count was 31% greater than the group that stayed on the topical therapy for the full 9 months.
Of note, azelaic acid 15% gel is technically an off-label therapy for adult female acne. The medication’s approved indication is in treating mild to moderate rosacea.
Dr. Thielitz reported having no financial conflicts in this investigator-initiated randomized trial.
ISTANBUL, TURKEY – Azelaic acid 15% gel constitutes an effective and well-tolerated treatment option for women with adult acne, according to the findings of an investigator-blinded, 9-month, randomized clinical trial.
The results showed azelaic acid 15% gel was similar in effectiveness to adapalene 0.1% gel, a widely prescribed treatment for this common condition, Dr. Anja Thielitz reported at the annual congress of the European Academy of Dermatology and Venereology.
However, azelaic acid 15% gel had a clear advantage in terms of tolerability. Median scores for skin redness, dryness, and scaling were significantly lower in the azelaic acid–treated group, added Dr. Thielitz of Otto von Guericke University in Magdeburg, Germany.
The single-center study involved 55 women aged 18-45 years, all with mild to moderate adult acne. They were randomized to one of three study arms: azelaic acid 15% gel twice daily for 9 months; adapalene 0.1% gel once daily, or 3 months of twice-daily azelaic acid 15% gel followed by 6 months of observation with no treatment.
Inflammatory and noninflammatory acne lesion counts, microcomedones, acne grading scale scores, and Dermatology Life Quality Index scores improved similarly in all three groups after 3 months. For example, median total lesion counts decreased from approximately 50 to 20, and median scores on the Leeds revised acne grading system dropped from 4 to roughly 2.5. Similar degrees of additional improvement were seen during months 4-9 in the two groups who remained on active treatment.
In contrast, some backsliding – although less than Dr. Thielitz had anticipated occurred during the untreated observation period among patients who halted the azelaic acid 15% gel after 3 months. By month 9, their total lesion count was 31% greater than the group that stayed on the topical therapy for the full 9 months.
Of note, azelaic acid 15% gel is technically an off-label therapy for adult female acne. The medication’s approved indication is in treating mild to moderate rosacea.
Dr. Thielitz reported having no financial conflicts in this investigator-initiated randomized trial.
ISTANBUL, TURKEY – Azelaic acid 15% gel constitutes an effective and well-tolerated treatment option for women with adult acne, according to the findings of an investigator-blinded, 9-month, randomized clinical trial.
The results showed azelaic acid 15% gel was similar in effectiveness to adapalene 0.1% gel, a widely prescribed treatment for this common condition, Dr. Anja Thielitz reported at the annual congress of the European Academy of Dermatology and Venereology.
However, azelaic acid 15% gel had a clear advantage in terms of tolerability. Median scores for skin redness, dryness, and scaling were significantly lower in the azelaic acid–treated group, added Dr. Thielitz of Otto von Guericke University in Magdeburg, Germany.
The single-center study involved 55 women aged 18-45 years, all with mild to moderate adult acne. They were randomized to one of three study arms: azelaic acid 15% gel twice daily for 9 months; adapalene 0.1% gel once daily, or 3 months of twice-daily azelaic acid 15% gel followed by 6 months of observation with no treatment.
Inflammatory and noninflammatory acne lesion counts, microcomedones, acne grading scale scores, and Dermatology Life Quality Index scores improved similarly in all three groups after 3 months. For example, median total lesion counts decreased from approximately 50 to 20, and median scores on the Leeds revised acne grading system dropped from 4 to roughly 2.5. Similar degrees of additional improvement were seen during months 4-9 in the two groups who remained on active treatment.
In contrast, some backsliding – although less than Dr. Thielitz had anticipated occurred during the untreated observation period among patients who halted the azelaic acid 15% gel after 3 months. By month 9, their total lesion count was 31% greater than the group that stayed on the topical therapy for the full 9 months.
Of note, azelaic acid 15% gel is technically an off-label therapy for adult female acne. The medication’s approved indication is in treating mild to moderate rosacea.
Dr. Thielitz reported having no financial conflicts in this investigator-initiated randomized trial.
AT THE EADV CONGRESS
Major finding: Azelaic acid 15% gel and adapalene 0.1% gel displayed comparable efficacy in treating women with adult acne, with median scores on the Leeds Revised Acne Grading Scale dropping from 4 to roughly 2.5 at 3 months and 2 at 9 months.
Data source: An investigator-blinded, randomized, 9-month study of 55 women with mild to moderate acne.
Disclosures: The presenter reported having no financial conflicts regarding this single-center, investigator-initiated study.
Hidradenitis Suppurativa Linked to Metabolic Syndrome
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
ISTANBUL, TURKEY – Patients with hidradenitis suppurativa have a sharply increased prevalence of the metabolic syndrome, according to the first case-control study to examine the relationship.
Metabolic syndrome is known to be associated with increased cardiovascular risk, which may be particularly high in patients with hidradenitis suppurativa (HS), a dermatologic disease with an estimated prevalence of 1%-4%, because they develop metabolic syndrome at a much younger age than do individuals without the dermatologic disease, Dr. Wolfram Sterry said at the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights from a single-center, case-control study that comprised 80 patients with HS with a mean 12-year disease duration and 100 age- and gender-matched controls. Patients’ mean age was 40 years (PLoS One 2012 [doi:10.1371/journal.pone.0031810]).
The prevalence of metabolic syndrome was 40% in the HS group and 13% in controls, for an adjusted 4.5-fold increased likelihood, reported Dr. Sterry, professor and chairman of the department of dermatology at Charité University Hospital, Berlin.
Of the five metabolic derangements used in defining the metabolic syndrome, four were significantly more prevalent in subjects with HS. They were 5.9-fold more likely than were matched controls to have central obesity, 4.1-fold more likely to have hyperglycemia, 4.6-fold more likely to have low HDL cholesterol, and 2.2-fold more likely to be hypertriglyceridemic. Hypertension was present in 48% of HS patients and 35% of controls, a difference that did not achieve statistical significance.
Of note, HS patients with metabolic syndrome had more pronounced metabolic abnormalities than did controls with metabolic syndrome. While the definition of metabolic syndrome requires the presence of at least three of five metabolic alterations, half of all HS patients with metabolic syndrome met four or more of the criteria, compared with 39% of controls.
Moreover, metabolic syndrome occurred at a much younger age in subjects with HS than is typical in the general population or than was seen in controls. Indeed, 40% of HS patients under age 35 had metabolic syndrome, compared with none of the matched controls. Thus, the odds ratio for metabolic syndrome in HS patients aged 34 years or less was increased more than 20-fold compared with controls, while in the 35- to 44-year-old age group it was increased 6.2-fold, and in HS patients aged 45 and older it was 2-fold higher.
An increased prevalence of metabolic syndrome also has been documented in patients with psoriasis. But the prevalence of metabolic syndrome appears to be higher in HS patients and the metabolic disorder occurs at an earlier age than in psoriasis.
There was no correlation between duration or severity of HS and the prevalence of metabolic syndrome, according to Dr. Sterry. That’s an important message for physicians who see patients with the skin disease because it means such patients should be evaluated for metabolic syndrome early on, even if they have only moderate skin disease. After all, the elements of the metabolic syndrome are modifiable cardiovascular risk factors.
The lack of correlation between HS severity or duration and metabolic syndrome prevalence also has implications for the mechanism underlying the increased risk of metabolic syndrome in HS. When Dr. Sterry and coworkers compared the levels of metabolic syndrome parameters in the 42 patients with prior surgical treatment of their HS to the 38 patients who had not undergone surgery, they found no significant differences even though the surgical patients presumably had less inflammatory load. This led them to speculate that chronic inflammation may not be the major driver of the metabolic abnormalities in HS patients.
"It must be that a genetic predisposition for metabolic syndrome then induces the development of acne inversa [hidradenitis suppurativa] in predisposed individuals," Dr. Sterry said.
The proposed mechanism involves metabolic syndrome–induced poor blood circulation in the intertriginous axillary, perianal, and inguinal skin where HS most often occurs, with resultant increased interleukin-10 production by CD4-positive T cells. Interleukin-10, in turn, inhibits keratinocyte production of interleukins-20 and -22, which induce antimicrobial proteins in the skin. This would set the stage for HS, which is characterized by bacterial persistence in obstructed hair follicles, nodules, and fistulating sinuses.
Of course, this is speculation, Dr. Sterry was quick to acknowledge.
"Acne inversa is also known as hidradenitis suppurativa, apocrine acne, pyoderma fistulans significa ... If a disease has that many names, that’s always a sign that we don’t know too much about it," the dermatologist observed.
In a separate study presented at the EADV, investigators found that the most common comorbid conditions in a cohort of 154 patients with HS enrolled in a clinical trial of adalimumab (Humira) therapy were depression as defined by a score of 10 or more on the Patient Health Questionnaire–9, which had a prevalence of 42%; severe obesity marked by a body mass index of at least 40 kg/m2, present in 28% of patients; and uncontrolled hypertension, which was present in 27%. However, the investigators did not look at metabolic syndrome.
Dr. Sterry reported having no financial conflicts regarding this unfunded case-control study.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
ISTANBUL, TURKEY – Patients with hidradenitis suppurativa have a sharply increased prevalence of the metabolic syndrome, according to the first case-control study to examine the relationship.
Metabolic syndrome is known to be associated with increased cardiovascular risk, which may be particularly high in patients with hidradenitis suppurativa (HS), a dermatologic disease with an estimated prevalence of 1%-4%, because they develop metabolic syndrome at a much younger age than do individuals without the dermatologic disease, Dr. Wolfram Sterry said at the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights from a single-center, case-control study that comprised 80 patients with HS with a mean 12-year disease duration and 100 age- and gender-matched controls. Patients’ mean age was 40 years (PLoS One 2012 [doi:10.1371/journal.pone.0031810]).
The prevalence of metabolic syndrome was 40% in the HS group and 13% in controls, for an adjusted 4.5-fold increased likelihood, reported Dr. Sterry, professor and chairman of the department of dermatology at Charité University Hospital, Berlin.
Of the five metabolic derangements used in defining the metabolic syndrome, four were significantly more prevalent in subjects with HS. They were 5.9-fold more likely than were matched controls to have central obesity, 4.1-fold more likely to have hyperglycemia, 4.6-fold more likely to have low HDL cholesterol, and 2.2-fold more likely to be hypertriglyceridemic. Hypertension was present in 48% of HS patients and 35% of controls, a difference that did not achieve statistical significance.
Of note, HS patients with metabolic syndrome had more pronounced metabolic abnormalities than did controls with metabolic syndrome. While the definition of metabolic syndrome requires the presence of at least three of five metabolic alterations, half of all HS patients with metabolic syndrome met four or more of the criteria, compared with 39% of controls.
Moreover, metabolic syndrome occurred at a much younger age in subjects with HS than is typical in the general population or than was seen in controls. Indeed, 40% of HS patients under age 35 had metabolic syndrome, compared with none of the matched controls. Thus, the odds ratio for metabolic syndrome in HS patients aged 34 years or less was increased more than 20-fold compared with controls, while in the 35- to 44-year-old age group it was increased 6.2-fold, and in HS patients aged 45 and older it was 2-fold higher.
An increased prevalence of metabolic syndrome also has been documented in patients with psoriasis. But the prevalence of metabolic syndrome appears to be higher in HS patients and the metabolic disorder occurs at an earlier age than in psoriasis.
There was no correlation between duration or severity of HS and the prevalence of metabolic syndrome, according to Dr. Sterry. That’s an important message for physicians who see patients with the skin disease because it means such patients should be evaluated for metabolic syndrome early on, even if they have only moderate skin disease. After all, the elements of the metabolic syndrome are modifiable cardiovascular risk factors.
The lack of correlation between HS severity or duration and metabolic syndrome prevalence also has implications for the mechanism underlying the increased risk of metabolic syndrome in HS. When Dr. Sterry and coworkers compared the levels of metabolic syndrome parameters in the 42 patients with prior surgical treatment of their HS to the 38 patients who had not undergone surgery, they found no significant differences even though the surgical patients presumably had less inflammatory load. This led them to speculate that chronic inflammation may not be the major driver of the metabolic abnormalities in HS patients.
"It must be that a genetic predisposition for metabolic syndrome then induces the development of acne inversa [hidradenitis suppurativa] in predisposed individuals," Dr. Sterry said.
The proposed mechanism involves metabolic syndrome–induced poor blood circulation in the intertriginous axillary, perianal, and inguinal skin where HS most often occurs, with resultant increased interleukin-10 production by CD4-positive T cells. Interleukin-10, in turn, inhibits keratinocyte production of interleukins-20 and -22, which induce antimicrobial proteins in the skin. This would set the stage for HS, which is characterized by bacterial persistence in obstructed hair follicles, nodules, and fistulating sinuses.
Of course, this is speculation, Dr. Sterry was quick to acknowledge.
"Acne inversa is also known as hidradenitis suppurativa, apocrine acne, pyoderma fistulans significa ... If a disease has that many names, that’s always a sign that we don’t know too much about it," the dermatologist observed.
In a separate study presented at the EADV, investigators found that the most common comorbid conditions in a cohort of 154 patients with HS enrolled in a clinical trial of adalimumab (Humira) therapy were depression as defined by a score of 10 or more on the Patient Health Questionnaire–9, which had a prevalence of 42%; severe obesity marked by a body mass index of at least 40 kg/m2, present in 28% of patients; and uncontrolled hypertension, which was present in 27%. However, the investigators did not look at metabolic syndrome.
Dr. Sterry reported having no financial conflicts regarding this unfunded case-control study.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
Earn 0.25 hours AMA PRA Category 1 credit: Read this article, and click the link at the end to take the post-test.
ISTANBUL, TURKEY – Patients with hidradenitis suppurativa have a sharply increased prevalence of the metabolic syndrome, according to the first case-control study to examine the relationship.
Metabolic syndrome is known to be associated with increased cardiovascular risk, which may be particularly high in patients with hidradenitis suppurativa (HS), a dermatologic disease with an estimated prevalence of 1%-4%, because they develop metabolic syndrome at a much younger age than do individuals without the dermatologic disease, Dr. Wolfram Sterry said at the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights from a single-center, case-control study that comprised 80 patients with HS with a mean 12-year disease duration and 100 age- and gender-matched controls. Patients’ mean age was 40 years (PLoS One 2012 [doi:10.1371/journal.pone.0031810]).
The prevalence of metabolic syndrome was 40% in the HS group and 13% in controls, for an adjusted 4.5-fold increased likelihood, reported Dr. Sterry, professor and chairman of the department of dermatology at Charité University Hospital, Berlin.
Of the five metabolic derangements used in defining the metabolic syndrome, four were significantly more prevalent in subjects with HS. They were 5.9-fold more likely than were matched controls to have central obesity, 4.1-fold more likely to have hyperglycemia, 4.6-fold more likely to have low HDL cholesterol, and 2.2-fold more likely to be hypertriglyceridemic. Hypertension was present in 48% of HS patients and 35% of controls, a difference that did not achieve statistical significance.
Of note, HS patients with metabolic syndrome had more pronounced metabolic abnormalities than did controls with metabolic syndrome. While the definition of metabolic syndrome requires the presence of at least three of five metabolic alterations, half of all HS patients with metabolic syndrome met four or more of the criteria, compared with 39% of controls.
Moreover, metabolic syndrome occurred at a much younger age in subjects with HS than is typical in the general population or than was seen in controls. Indeed, 40% of HS patients under age 35 had metabolic syndrome, compared with none of the matched controls. Thus, the odds ratio for metabolic syndrome in HS patients aged 34 years or less was increased more than 20-fold compared with controls, while in the 35- to 44-year-old age group it was increased 6.2-fold, and in HS patients aged 45 and older it was 2-fold higher.
An increased prevalence of metabolic syndrome also has been documented in patients with psoriasis. But the prevalence of metabolic syndrome appears to be higher in HS patients and the metabolic disorder occurs at an earlier age than in psoriasis.
There was no correlation between duration or severity of HS and the prevalence of metabolic syndrome, according to Dr. Sterry. That’s an important message for physicians who see patients with the skin disease because it means such patients should be evaluated for metabolic syndrome early on, even if they have only moderate skin disease. After all, the elements of the metabolic syndrome are modifiable cardiovascular risk factors.
The lack of correlation between HS severity or duration and metabolic syndrome prevalence also has implications for the mechanism underlying the increased risk of metabolic syndrome in HS. When Dr. Sterry and coworkers compared the levels of metabolic syndrome parameters in the 42 patients with prior surgical treatment of their HS to the 38 patients who had not undergone surgery, they found no significant differences even though the surgical patients presumably had less inflammatory load. This led them to speculate that chronic inflammation may not be the major driver of the metabolic abnormalities in HS patients.
"It must be that a genetic predisposition for metabolic syndrome then induces the development of acne inversa [hidradenitis suppurativa] in predisposed individuals," Dr. Sterry said.
The proposed mechanism involves metabolic syndrome–induced poor blood circulation in the intertriginous axillary, perianal, and inguinal skin where HS most often occurs, with resultant increased interleukin-10 production by CD4-positive T cells. Interleukin-10, in turn, inhibits keratinocyte production of interleukins-20 and -22, which induce antimicrobial proteins in the skin. This would set the stage for HS, which is characterized by bacterial persistence in obstructed hair follicles, nodules, and fistulating sinuses.
Of course, this is speculation, Dr. Sterry was quick to acknowledge.
"Acne inversa is also known as hidradenitis suppurativa, apocrine acne, pyoderma fistulans significa ... If a disease has that many names, that’s always a sign that we don’t know too much about it," the dermatologist observed.
In a separate study presented at the EADV, investigators found that the most common comorbid conditions in a cohort of 154 patients with HS enrolled in a clinical trial of adalimumab (Humira) therapy were depression as defined by a score of 10 or more on the Patient Health Questionnaire–9, which had a prevalence of 42%; severe obesity marked by a body mass index of at least 40 kg/m2, present in 28% of patients; and uncontrolled hypertension, which was present in 27%. However, the investigators did not look at metabolic syndrome.
Dr. Sterry reported having no financial conflicts regarding this unfunded case-control study.
To earn 0.25 hours AMA PRA Category 1 credit after reading this article, take the post-test here.
AT THE EADV CONGRESS

Hidradenitis suppurativa linked to metabolic syndrome
ISTANBUL, TURKEY – Patients with hidradenitis suppurativa have a sharply increased prevalence of the metabolic syndrome, according to the first case-control study to examine the relationship.
Metabolic syndrome is known to be associated with increased cardiovascular risk, which may be particularly high in patients with hidradenitis suppurativa (HS), a dermatologic disease with an estimated prevalence of 1%-4%, because they develop metabolic syndrome at a much younger age than do individuals without the dermatologic disease, Dr. Wolfram Sterry said at the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights from a single-center, case-control study that comprised 80 patients with HS with a mean 12-year disease duration and 100 age- and gender-matched controls. Patients’ mean age was 40 years (PLoS One 2012 [doi:10.1371/journal.pone.0031810]).

The prevalence of metabolic syndrome was 40% in the HS group and 13% in controls, for an adjusted 4.5-fold increased likelihood, reported Dr. Sterry, professor and chairman of the department of dermatology at Charité University Hospital, Berlin.
Of the five metabolic derangements used in defining the metabolic syndrome, four were significantly more prevalent in subjects with HS. They were 5.9-fold more likely than were matched controls to have central obesity, 4.1-fold more likely to have hyperglycemia, 4.6-fold more likely to have low HDL cholesterol, and 2.2-fold more likely to be hypertriglyceridemic. Hypertension was present in 48% of HS patients and 35% of controls, a difference that did not achieve statistical significance.
Of note, HS patients with metabolic syndrome had more pronounced metabolic abnormalities than did controls with metabolic syndrome. While the definition of metabolic syndrome requires the presence of at least three of five metabolic alterations, half of all HS patients with metabolic syndrome met four or more of the criteria, compared with 39% of controls.
Moreover, metabolic syndrome occurred at a much younger age in subjects with HS than is typical in the general population or than was seen in controls. Indeed, 40% of HS patients under age 35 had metabolic syndrome, compared with none of the matched controls. Thus, the odds ratio for metabolic syndrome in HS patients aged 34 years or less was increased more than 20-fold compared with controls, while in the 35- to 44-year-old age group it was increased 6.2-fold, and in HS patients aged 45 and older it was 2-fold higher.
An increased prevalence of metabolic syndrome also has been documented in patients with psoriasis. But the prevalence of metabolic syndrome appears to be higher in HS patients and the metabolic disorder occurs at an earlier age than in psoriasis.
There was no correlation between duration or severity of HS and the prevalence of metabolic syndrome, according to Dr. Sterry. That’s an important message for physicians who see patients with the skin disease because it means such patients should be evaluated for metabolic syndrome early on, even if they have only moderate skin disease. After all, the elements of the metabolic syndrome are modifiable cardiovascular risk factors.
The lack of correlation between HS severity or duration and metabolic syndrome prevalence also has implications for the mechanism underlying the increased risk of metabolic syndrome in HS. When Dr. Sterry and coworkers compared the levels of metabolic syndrome parameters in the 42 patients with prior surgical treatment of their HS to the 38 patients who had not undergone surgery, they found no significant differences even though the surgical patients presumably had less inflammatory load. This led them to speculate that chronic inflammation may not be the major driver of the metabolic abnormalities in HS patients.
"It must be that a genetic predisposition for metabolic syndrome then induces the development of acne inversa [hidradenitis suppurativa] in predisposed individuals," Dr. Sterry said.
The proposed mechanism involves metabolic syndrome–induced poor blood circulation in the intertriginous axillary, perianal, and inguinal skin where HS most often occurs, with resultant increased interleukin-10 production by CD4-positive T cells. Interleukin-10, in turn, inhibits keratinocyte production of interleukins-20 and -22, which induce antimicrobial proteins in the skin. This would set the stage for HS, which is characterized by bacterial persistence in obstructed hair follicles, nodules, and fistulating sinuses.
Of course, this is speculation, Dr. Sterry was quick to acknowledge.
"Acne inversa is also known as hidradenitis suppurativa, apocrine acne, pyoderma fistulans significa ... If a disease has that many names, that’s always a sign that we don’t know too much about it," the dermatologist observed.
In a separate study presented at the EADV, investigators found that the most common comorbid conditions in a cohort of 154 patients with HS enrolled in a clinical trial of adalimumab (Humira) therapy were depression as defined by a score of 10 or more on the Patient Health Questionnaire–9, which had a prevalence of 42%; severe obesity marked by a body mass index of at least 40 kg/m2, present in 28% of patients; and uncontrolled hypertension, which was present in 27%. However, the investigators did not look at metabolic syndrome.
Dr. Sterry reported having no financial conflicts regarding this unfunded case-control study.
ISTANBUL, TURKEY – Patients with hidradenitis suppurativa have a sharply increased prevalence of the metabolic syndrome, according to the first case-control study to examine the relationship.
Metabolic syndrome is known to be associated with increased cardiovascular risk, which may be particularly high in patients with hidradenitis suppurativa (HS), a dermatologic disease with an estimated prevalence of 1%-4%, because they develop metabolic syndrome at a much younger age than do individuals without the dermatologic disease, Dr. Wolfram Sterry said at the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights from a single-center, case-control study that comprised 80 patients with HS with a mean 12-year disease duration and 100 age- and gender-matched controls. Patients’ mean age was 40 years (PLoS One 2012 [doi:10.1371/journal.pone.0031810]).
The prevalence of metabolic syndrome was 40% in the HS group and 13% in controls, for an adjusted 4.5-fold increased likelihood, reported Dr. Sterry, professor and chairman of the department of dermatology at Charité University Hospital, Berlin.
Of the five metabolic derangements used in defining the metabolic syndrome, four were significantly more prevalent in subjects with HS. They were 5.9-fold more likely than were matched controls to have central obesity, 4.1-fold more likely to have hyperglycemia, 4.6-fold more likely to have low HDL cholesterol, and 2.2-fold more likely to be hypertriglyceridemic. Hypertension was present in 48% of HS patients and 35% of controls, a difference that did not achieve statistical significance.
Of note, HS patients with metabolic syndrome had more pronounced metabolic abnormalities than did controls with metabolic syndrome. While the definition of metabolic syndrome requires the presence of at least three of five metabolic alterations, half of all HS patients with metabolic syndrome met four or more of the criteria, compared with 39% of controls.
Moreover, metabolic syndrome occurred at a much younger age in subjects with HS than is typical in the general population or than was seen in controls. Indeed, 40% of HS patients under age 35 had metabolic syndrome, compared with none of the matched controls. Thus, the odds ratio for metabolic syndrome in HS patients aged 34 years or less was increased more than 20-fold compared with controls, while in the 35- to 44-year-old age group it was increased 6.2-fold, and in HS patients aged 45 and older it was 2-fold higher.
An increased prevalence of metabolic syndrome also has been documented in patients with psoriasis. But the prevalence of metabolic syndrome appears to be higher in HS patients and the metabolic disorder occurs at an earlier age than in psoriasis.
There was no correlation between duration or severity of HS and the prevalence of metabolic syndrome, according to Dr. Sterry. That’s an important message for physicians who see patients with the skin disease because it means such patients should be evaluated for metabolic syndrome early on, even if they have only moderate skin disease. After all, the elements of the metabolic syndrome are modifiable cardiovascular risk factors.
The lack of correlation between HS severity or duration and metabolic syndrome prevalence also has implications for the mechanism underlying the increased risk of metabolic syndrome in HS. When Dr. Sterry and coworkers compared the levels of metabolic syndrome parameters in the 42 patients with prior surgical treatment of their HS to the 38 patients who had not undergone surgery, they found no significant differences even though the surgical patients presumably had less inflammatory load. This led them to speculate that chronic inflammation may not be the major driver of the metabolic abnormalities in HS patients.
"It must be that a genetic predisposition for metabolic syndrome then induces the development of acne inversa [hidradenitis suppurativa] in predisposed individuals," Dr. Sterry said.
The proposed mechanism involves metabolic syndrome–induced poor blood circulation in the intertriginous axillary, perianal, and inguinal skin where HS most often occurs, with resultant increased interleukin-10 production by CD4-positive T cells. Interleukin-10, in turn, inhibits keratinocyte production of interleukins-20 and -22, which induce antimicrobial proteins in the skin. This would set the stage for HS, which is characterized by bacterial persistence in obstructed hair follicles, nodules, and fistulating sinuses.
Of course, this is speculation, Dr. Sterry was quick to acknowledge.
"Acne inversa is also known as hidradenitis suppurativa, apocrine acne, pyoderma fistulans significa ... If a disease has that many names, that’s always a sign that we don’t know too much about it," the dermatologist observed.
In a separate study presented at the EADV, investigators found that the most common comorbid conditions in a cohort of 154 patients with HS enrolled in a clinical trial of adalimumab (Humira) therapy were depression as defined by a score of 10 or more on the Patient Health Questionnaire–9, which had a prevalence of 42%; severe obesity marked by a body mass index of at least 40 kg/m2, present in 28% of patients; and uncontrolled hypertension, which was present in 27%. However, the investigators did not look at metabolic syndrome.
Dr. Sterry reported having no financial conflicts regarding this unfunded case-control study.
ISTANBUL, TURKEY – Patients with hidradenitis suppurativa have a sharply increased prevalence of the metabolic syndrome, according to the first case-control study to examine the relationship.
Metabolic syndrome is known to be associated with increased cardiovascular risk, which may be particularly high in patients with hidradenitis suppurativa (HS), a dermatologic disease with an estimated prevalence of 1%-4%, because they develop metabolic syndrome at a much younger age than do individuals without the dermatologic disease, Dr. Wolfram Sterry said at the annual congress of the European Academy of Dermatology and Venereology.
He presented highlights from a single-center, case-control study that comprised 80 patients with HS with a mean 12-year disease duration and 100 age- and gender-matched controls. Patients’ mean age was 40 years (PLoS One 2012 [doi:10.1371/journal.pone.0031810]).
The prevalence of metabolic syndrome was 40% in the HS group and 13% in controls, for an adjusted 4.5-fold increased likelihood, reported Dr. Sterry, professor and chairman of the department of dermatology at Charité University Hospital, Berlin.
Of the five metabolic derangements used in defining the metabolic syndrome, four were significantly more prevalent in subjects with HS. They were 5.9-fold more likely than were matched controls to have central obesity, 4.1-fold more likely to have hyperglycemia, 4.6-fold more likely to have low HDL cholesterol, and 2.2-fold more likely to be hypertriglyceridemic. Hypertension was present in 48% of HS patients and 35% of controls, a difference that did not achieve statistical significance.
Of note, HS patients with metabolic syndrome had more pronounced metabolic abnormalities than did controls with metabolic syndrome. While the definition of metabolic syndrome requires the presence of at least three of five metabolic alterations, half of all HS patients with metabolic syndrome met four or more of the criteria, compared with 39% of controls.
Moreover, metabolic syndrome occurred at a much younger age in subjects with HS than is typical in the general population or than was seen in controls. Indeed, 40% of HS patients under age 35 had metabolic syndrome, compared with none of the matched controls. Thus, the odds ratio for metabolic syndrome in HS patients aged 34 years or less was increased more than 20-fold compared with controls, while in the 35- to 44-year-old age group it was increased 6.2-fold, and in HS patients aged 45 and older it was 2-fold higher.
An increased prevalence of metabolic syndrome also has been documented in patients with psoriasis. But the prevalence of metabolic syndrome appears to be higher in HS patients and the metabolic disorder occurs at an earlier age than in psoriasis.
There was no correlation between duration or severity of HS and the prevalence of metabolic syndrome, according to Dr. Sterry. That’s an important message for physicians who see patients with the skin disease because it means such patients should be evaluated for metabolic syndrome early on, even if they have only moderate skin disease. After all, the elements of the metabolic syndrome are modifiable cardiovascular risk factors.
The lack of correlation between HS severity or duration and metabolic syndrome prevalence also has implications for the mechanism underlying the increased risk of metabolic syndrome in HS. When Dr. Sterry and coworkers compared the levels of metabolic syndrome parameters in the 42 patients with prior surgical treatment of their HS to the 38 patients who had not undergone surgery, they found no significant differences even though the surgical patients presumably had less inflammatory load. This led them to speculate that chronic inflammation may not be the major driver of the metabolic abnormalities in HS patients.
"It must be that a genetic predisposition for metabolic syndrome then induces the development of acne inversa [hidradenitis suppurativa] in predisposed individuals," Dr. Sterry said.
The proposed mechanism involves metabolic syndrome–induced poor blood circulation in the intertriginous axillary, perianal, and inguinal skin where HS most often occurs, with resultant increased interleukin-10 production by CD4-positive T cells. Interleukin-10, in turn, inhibits keratinocyte production of interleukins-20 and -22, which induce antimicrobial proteins in the skin. This would set the stage for HS, which is characterized by bacterial persistence in obstructed hair follicles, nodules, and fistulating sinuses.
Of course, this is speculation, Dr. Sterry was quick to acknowledge.
"Acne inversa is also known as hidradenitis suppurativa, apocrine acne, pyoderma fistulans significa ... If a disease has that many names, that’s always a sign that we don’t know too much about it," the dermatologist observed.
In a separate study presented at the EADV, investigators found that the most common comorbid conditions in a cohort of 154 patients with HS enrolled in a clinical trial of adalimumab (Humira) therapy were depression as defined by a score of 10 or more on the Patient Health Questionnaire–9, which had a prevalence of 42%; severe obesity marked by a body mass index of at least 40 kg/m2, present in 28% of patients; and uncontrolled hypertension, which was present in 27%. However, the investigators did not look at metabolic syndrome.
Dr. Sterry reported having no financial conflicts regarding this unfunded case-control study.
AT THE EADV CONGRESS
Major finding: The prevalence of metabolic syndrome was 40% in a cohort of patients with hidradenitis suppurativa compared with 13% in matched controls.
Data source: A case-control study involving 80 patients with hidradenitis suppurativa and 100 age- and gender-matched controls.
Disclosures: Dr. Sterry, the presenter of this unfunded investigation, reported having no financial conflicts of interest.
