User login
Islet Cell Autografts Relieve Chronic Pancreatitis Pain
HOT SPRINGS, VA. – Despite the predominant view that islet cell transplantation is a radical procedure, it is effective for chronic pancreatitis when endoscopic duct drainage does not relieve the pain, according to researchers at the University of Minnesota, where the standard is to perform islet autotransplants in almost all cases of chronic pancreatitis.
The university began islet transplantation in 1977, but 60% of the procedures have been performed in the past 5 years. The total is now 374 adult cases and 57 pediatric cases. Dr. David Sutherland, professor of surgery at the university, presented data on the adult cases at the annual meeting of the Southern Surgical Association.
Islet autografts are still both a science and an art, said Dr. Sutherland. The pancreas is removed; importantly, the blood supply has to be preserved to the point of removal to avoid warm ischemia, he said. The islets are then isolated in a processing center. Each isolation must be adjusted to each individual’s diseased pancreas. The cells are then infused into the liver.
Minnesota’s case mix is very different from what is typical for pancreatitis. Seventy-three percent of the patients in the analysis were female, and only 7% of cases were due to alcoholism. In an interview after the presentation, Dr. Timothy Pruett, chief of the division of transplantation at the University of Minnesota, said that patients seem to be learning about the Minnesota procedure online and self-selecting to come to the university.
Some 41% of the cases were idiopathic in origin. Ninety-two percent did not have diabetes before transplantation.
Pain was a predominant factor for most patients. The average duration of pain was 9 years, and the duration of narcotic use was almost 4 years on average. This has many implications, including the central sensitization of pain and opioid-induced hyperalgesia.
The mortality rate for autotransplants has been low, with 97% of the most recent cohort (2006-2011) alive at 1 year. At 5 years, 86%-88% of the earlier transplant patients were still alive. Twenty-year survival is 66%, said Dr. Sutherland. Overall, 16% of patients have required reoperation; of those, about 10% needed surgery because of bleeding.
To assess the effectiveness of the islet autografts, the researchers looked at the 201 patients who had more than 1 year of follow-up. Regardless of the islet yield, 91% of the patients are C-peptide positive and 83% have a hemoglobin A1c level in the desired range of 7% or less. Higher islet yields produce better results, with fewer patients becoming diabetic.
At 3 years, 70% of patients who had a high yield of islet cells were insulin independent. Only 10%-20% of the patients who had lower yields of cells did not need insulin, however.
Pancreatitis pain resolved in 80%-90% of patients overall. In 60% of patients, narcotics were withdrawn by 2 years. It is a slow process, noted Dr. Sutherland.
The pain rating went down for most patients – from a 66 to a 44 on a 100-point scale. There was also improvement in all eight categories on the Short Form-36 quality of life survey, said Dr. Sutherland. Although pain scores improved more in the insulin-independent patients, significant pain improvement was also seen in the insulin-dependent group.
"There’s no doubt in my mind that this procedure is safe and effective in the management of intractable chronic pain associated with pancreatitis in selected patients," said Dr. David B. Adams, who commented on the presentation. However, it is not clear how to best identify patients who would benefit from the procedure, said Dr. Adams, a professor of surgery at the Medical University of South Carolina in Charleston. Calling the Minnesota report a "landmark paper," he added that while the procedure does not cure patients, it does improve quality of life, which is crucial in this group.
Dr. Kenneth L. Brayman, division chief of transplant surgery at the University of Virginia, Charlottesville, said that "islet autotransplantation has emerged as successful therapy." At his institution, 40%-50% of autograft patients are insulin free and 80% are pain free.
Noting the success at Virginia and in other programs, Dr. Brayman said that "it remains curious to me and others, why the management of chronic pancreatitis remains so controversial."
"The question of whether this is a radical procedure or not is in the eyes of the beholder," said Dr. Pruett. "It’s not radical in our hands. It is what we do."
Dr. Sutherland and Dr. Pruett reported no conflicts.
HOT SPRINGS, VA. – Despite the predominant view that islet cell transplantation is a radical procedure, it is effective for chronic pancreatitis when endoscopic duct drainage does not relieve the pain, according to researchers at the University of Minnesota, where the standard is to perform islet autotransplants in almost all cases of chronic pancreatitis.
The university began islet transplantation in 1977, but 60% of the procedures have been performed in the past 5 years. The total is now 374 adult cases and 57 pediatric cases. Dr. David Sutherland, professor of surgery at the university, presented data on the adult cases at the annual meeting of the Southern Surgical Association.
Islet autografts are still both a science and an art, said Dr. Sutherland. The pancreas is removed; importantly, the blood supply has to be preserved to the point of removal to avoid warm ischemia, he said. The islets are then isolated in a processing center. Each isolation must be adjusted to each individual’s diseased pancreas. The cells are then infused into the liver.
Minnesota’s case mix is very different from what is typical for pancreatitis. Seventy-three percent of the patients in the analysis were female, and only 7% of cases were due to alcoholism. In an interview after the presentation, Dr. Timothy Pruett, chief of the division of transplantation at the University of Minnesota, said that patients seem to be learning about the Minnesota procedure online and self-selecting to come to the university.
Some 41% of the cases were idiopathic in origin. Ninety-two percent did not have diabetes before transplantation.
Pain was a predominant factor for most patients. The average duration of pain was 9 years, and the duration of narcotic use was almost 4 years on average. This has many implications, including the central sensitization of pain and opioid-induced hyperalgesia.
The mortality rate for autotransplants has been low, with 97% of the most recent cohort (2006-2011) alive at 1 year. At 5 years, 86%-88% of the earlier transplant patients were still alive. Twenty-year survival is 66%, said Dr. Sutherland. Overall, 16% of patients have required reoperation; of those, about 10% needed surgery because of bleeding.
To assess the effectiveness of the islet autografts, the researchers looked at the 201 patients who had more than 1 year of follow-up. Regardless of the islet yield, 91% of the patients are C-peptide positive and 83% have a hemoglobin A1c level in the desired range of 7% or less. Higher islet yields produce better results, with fewer patients becoming diabetic.
At 3 years, 70% of patients who had a high yield of islet cells were insulin independent. Only 10%-20% of the patients who had lower yields of cells did not need insulin, however.
Pancreatitis pain resolved in 80%-90% of patients overall. In 60% of patients, narcotics were withdrawn by 2 years. It is a slow process, noted Dr. Sutherland.
The pain rating went down for most patients – from a 66 to a 44 on a 100-point scale. There was also improvement in all eight categories on the Short Form-36 quality of life survey, said Dr. Sutherland. Although pain scores improved more in the insulin-independent patients, significant pain improvement was also seen in the insulin-dependent group.
"There’s no doubt in my mind that this procedure is safe and effective in the management of intractable chronic pain associated with pancreatitis in selected patients," said Dr. David B. Adams, who commented on the presentation. However, it is not clear how to best identify patients who would benefit from the procedure, said Dr. Adams, a professor of surgery at the Medical University of South Carolina in Charleston. Calling the Minnesota report a "landmark paper," he added that while the procedure does not cure patients, it does improve quality of life, which is crucial in this group.
Dr. Kenneth L. Brayman, division chief of transplant surgery at the University of Virginia, Charlottesville, said that "islet autotransplantation has emerged as successful therapy." At his institution, 40%-50% of autograft patients are insulin free and 80% are pain free.
Noting the success at Virginia and in other programs, Dr. Brayman said that "it remains curious to me and others, why the management of chronic pancreatitis remains so controversial."
"The question of whether this is a radical procedure or not is in the eyes of the beholder," said Dr. Pruett. "It’s not radical in our hands. It is what we do."
Dr. Sutherland and Dr. Pruett reported no conflicts.
HOT SPRINGS, VA. – Despite the predominant view that islet cell transplantation is a radical procedure, it is effective for chronic pancreatitis when endoscopic duct drainage does not relieve the pain, according to researchers at the University of Minnesota, where the standard is to perform islet autotransplants in almost all cases of chronic pancreatitis.
The university began islet transplantation in 1977, but 60% of the procedures have been performed in the past 5 years. The total is now 374 adult cases and 57 pediatric cases. Dr. David Sutherland, professor of surgery at the university, presented data on the adult cases at the annual meeting of the Southern Surgical Association.
Islet autografts are still both a science and an art, said Dr. Sutherland. The pancreas is removed; importantly, the blood supply has to be preserved to the point of removal to avoid warm ischemia, he said. The islets are then isolated in a processing center. Each isolation must be adjusted to each individual’s diseased pancreas. The cells are then infused into the liver.
Minnesota’s case mix is very different from what is typical for pancreatitis. Seventy-three percent of the patients in the analysis were female, and only 7% of cases were due to alcoholism. In an interview after the presentation, Dr. Timothy Pruett, chief of the division of transplantation at the University of Minnesota, said that patients seem to be learning about the Minnesota procedure online and self-selecting to come to the university.
Some 41% of the cases were idiopathic in origin. Ninety-two percent did not have diabetes before transplantation.
Pain was a predominant factor for most patients. The average duration of pain was 9 years, and the duration of narcotic use was almost 4 years on average. This has many implications, including the central sensitization of pain and opioid-induced hyperalgesia.
The mortality rate for autotransplants has been low, with 97% of the most recent cohort (2006-2011) alive at 1 year. At 5 years, 86%-88% of the earlier transplant patients were still alive. Twenty-year survival is 66%, said Dr. Sutherland. Overall, 16% of patients have required reoperation; of those, about 10% needed surgery because of bleeding.
To assess the effectiveness of the islet autografts, the researchers looked at the 201 patients who had more than 1 year of follow-up. Regardless of the islet yield, 91% of the patients are C-peptide positive and 83% have a hemoglobin A1c level in the desired range of 7% or less. Higher islet yields produce better results, with fewer patients becoming diabetic.
At 3 years, 70% of patients who had a high yield of islet cells were insulin independent. Only 10%-20% of the patients who had lower yields of cells did not need insulin, however.
Pancreatitis pain resolved in 80%-90% of patients overall. In 60% of patients, narcotics were withdrawn by 2 years. It is a slow process, noted Dr. Sutherland.
The pain rating went down for most patients – from a 66 to a 44 on a 100-point scale. There was also improvement in all eight categories on the Short Form-36 quality of life survey, said Dr. Sutherland. Although pain scores improved more in the insulin-independent patients, significant pain improvement was also seen in the insulin-dependent group.
"There’s no doubt in my mind that this procedure is safe and effective in the management of intractable chronic pain associated with pancreatitis in selected patients," said Dr. David B. Adams, who commented on the presentation. However, it is not clear how to best identify patients who would benefit from the procedure, said Dr. Adams, a professor of surgery at the Medical University of South Carolina in Charleston. Calling the Minnesota report a "landmark paper," he added that while the procedure does not cure patients, it does improve quality of life, which is crucial in this group.
Dr. Kenneth L. Brayman, division chief of transplant surgery at the University of Virginia, Charlottesville, said that "islet autotransplantation has emerged as successful therapy." At his institution, 40%-50% of autograft patients are insulin free and 80% are pain free.
Noting the success at Virginia and in other programs, Dr. Brayman said that "it remains curious to me and others, why the management of chronic pancreatitis remains so controversial."
"The question of whether this is a radical procedure or not is in the eyes of the beholder," said Dr. Pruett. "It’s not radical in our hands. It is what we do."
Dr. Sutherland and Dr. Pruett reported no conflicts.
FROM THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Ninety-seven percent of autotransplant patients in the most recent cohort (2006-2011) were alive at 1 year. At 5 years, 86%-88% of the earlier transplants patients were still alive. Twenty-year survival is 66%. Pancreatitis pain resolved in 80%-90% of patients overall.
Data Source: Data gathered from 374 adult islet cell autografts done at the University of Minnesota since 1977.
Disclosures: Dr. Sutherland and Dr. Pruett reported no conflicts.
Older Age, Comorbidities Raise Readmission Risk After Colectomy
HOT SPRINGS, VA. – A shorter length of stay appears to be associated with a higher risk of readmission after colectomy, but only in patients who are older and have more preoperative comorbidities and perioperative complications, results of a large database review demonstrate.
Dr. Timothy Pawlik and his colleagues from Johns Hopkins Hospital, Baltimore, conducted a retrospective study of the Surveillance, Epidemiology, and End Results (SEER) database of 149,622 Medicare patients with a primary diagnosis of colorectal cancer who underwent colectomy from 1986 to 2005. The goal was to determine trends in readmission rates during the first 30 days.
"How do we begin to remedy the demonization of legitimate readmissions either politically, medically, or both?"
Increasingly, payers – especially Medicare – are penalizing hospitals for failing to prevent readmissions, which cost about $40 billion annually. Moreover, up to three-quarters of readmissions may be avoidable. In the meantime, many hospitals are fast-tracking patients for discharge after colorectal surgery.
In the SEER data, the mean age was 75 years in the 1986-1990 period and 77 years in the later period of 2001-2005. Patients were sicker in the later time period, with 63% having a Charlson comorbidity score of 3 or greater, compared with only 53% in the earlier time frame.
Most patients (38%) had a right colectomy; 23% had a sigmoid procedure, 13% had a rectal procedure, and 11% had a left colectomy. Forty-six percent of patients had lymph node metastasis, and 17% had an emergent procedure.
Morbidity for the entire study period was 37%; most complications were gastrointestinal or related to bleeding or postoperative infection. Again, there was a significant difference between the earlier and the later time frames. Perioperative morbidity was 27% in the 1986-1990 time frame, vs. 40% in 2001-2005. Mortality, at 4%, remained stable over time.
The mean length of stay decreased from 14 to 10 days from the early time to the later time period. And, over time, the percentage of patients discharged to home decreased, while discharges to skilled nursing facilities increased.
Overall, there were 17,000 readmissions, for a rate of 11%. Readmissions also increased, from 10% early on to 14% in 2001-2005. During that later time frame, patients had a 46% increased risk of readmission. Almost half of the readmissions occurred within the first 7 days after surgery, primarily for complications, dehydration, or infection. The mortality rate associated with readmission was 8%.
Multivariate analysis showed that the factors most likely to impact readmission were multiple comorbidities or a history of any perioperative complication, said Dr. Pawlik. Early discharge alone was not associated with a higher risk of readmission.
The study shows that "ongoing initiatives to reduce risk of readmissions and the associated costs, morbidity, and mortality are needed," said Dr. Pawlik.
It also "provides data that we all know to be true: namely, that the patients we are operating on have more comorbidities and that length of stay increases the rate of readmissions," said Dr. Susan Galandiuk, the discussant at the meeting. However, payers have been using length of stay and readmissions as quality surrogates, said Dr. Galandiuk, professor of surgery at the University of Louisville, Ky.
Not readmitting an elderly patient with many comorbidities and complications "would be a quality of care issue, and not the other way around," she added. The problem now is, "How do we begin to remedy the demonization of legitimate readmissions either politically, medically, or both?" asked Dr. Galandiuk.
Dr. Pawlik agreed that readmissions should not necessarily be held to be all bad. "Blaming readmissions on length of stay is a gross oversimplification of what’s going on," he added. Surgeons are clearly operating on older and sicker patients, and are doing more complicated operations that may result in a higher rate of morbidity – all this "in a culture of being asked to send people home earlier," he said.
"Our data clearly show that early discharge is feasible in some patients, but it needs to be used judiciously, especially in an older population," said Dr. Pawlik.
Dr. Pawlik and Dr. Galandiuk reported no conflicts.
HOT SPRINGS, VA. – A shorter length of stay appears to be associated with a higher risk of readmission after colectomy, but only in patients who are older and have more preoperative comorbidities and perioperative complications, results of a large database review demonstrate.
Dr. Timothy Pawlik and his colleagues from Johns Hopkins Hospital, Baltimore, conducted a retrospective study of the Surveillance, Epidemiology, and End Results (SEER) database of 149,622 Medicare patients with a primary diagnosis of colorectal cancer who underwent colectomy from 1986 to 2005. The goal was to determine trends in readmission rates during the first 30 days.
"How do we begin to remedy the demonization of legitimate readmissions either politically, medically, or both?"
Increasingly, payers – especially Medicare – are penalizing hospitals for failing to prevent readmissions, which cost about $40 billion annually. Moreover, up to three-quarters of readmissions may be avoidable. In the meantime, many hospitals are fast-tracking patients for discharge after colorectal surgery.
In the SEER data, the mean age was 75 years in the 1986-1990 period and 77 years in the later period of 2001-2005. Patients were sicker in the later time period, with 63% having a Charlson comorbidity score of 3 or greater, compared with only 53% in the earlier time frame.
Most patients (38%) had a right colectomy; 23% had a sigmoid procedure, 13% had a rectal procedure, and 11% had a left colectomy. Forty-six percent of patients had lymph node metastasis, and 17% had an emergent procedure.
Morbidity for the entire study period was 37%; most complications were gastrointestinal or related to bleeding or postoperative infection. Again, there was a significant difference between the earlier and the later time frames. Perioperative morbidity was 27% in the 1986-1990 time frame, vs. 40% in 2001-2005. Mortality, at 4%, remained stable over time.
The mean length of stay decreased from 14 to 10 days from the early time to the later time period. And, over time, the percentage of patients discharged to home decreased, while discharges to skilled nursing facilities increased.
Overall, there were 17,000 readmissions, for a rate of 11%. Readmissions also increased, from 10% early on to 14% in 2001-2005. During that later time frame, patients had a 46% increased risk of readmission. Almost half of the readmissions occurred within the first 7 days after surgery, primarily for complications, dehydration, or infection. The mortality rate associated with readmission was 8%.
Multivariate analysis showed that the factors most likely to impact readmission were multiple comorbidities or a history of any perioperative complication, said Dr. Pawlik. Early discharge alone was not associated with a higher risk of readmission.
The study shows that "ongoing initiatives to reduce risk of readmissions and the associated costs, morbidity, and mortality are needed," said Dr. Pawlik.
It also "provides data that we all know to be true: namely, that the patients we are operating on have more comorbidities and that length of stay increases the rate of readmissions," said Dr. Susan Galandiuk, the discussant at the meeting. However, payers have been using length of stay and readmissions as quality surrogates, said Dr. Galandiuk, professor of surgery at the University of Louisville, Ky.
Not readmitting an elderly patient with many comorbidities and complications "would be a quality of care issue, and not the other way around," she added. The problem now is, "How do we begin to remedy the demonization of legitimate readmissions either politically, medically, or both?" asked Dr. Galandiuk.
Dr. Pawlik agreed that readmissions should not necessarily be held to be all bad. "Blaming readmissions on length of stay is a gross oversimplification of what’s going on," he added. Surgeons are clearly operating on older and sicker patients, and are doing more complicated operations that may result in a higher rate of morbidity – all this "in a culture of being asked to send people home earlier," he said.
"Our data clearly show that early discharge is feasible in some patients, but it needs to be used judiciously, especially in an older population," said Dr. Pawlik.
Dr. Pawlik and Dr. Galandiuk reported no conflicts.
HOT SPRINGS, VA. – A shorter length of stay appears to be associated with a higher risk of readmission after colectomy, but only in patients who are older and have more preoperative comorbidities and perioperative complications, results of a large database review demonstrate.
Dr. Timothy Pawlik and his colleagues from Johns Hopkins Hospital, Baltimore, conducted a retrospective study of the Surveillance, Epidemiology, and End Results (SEER) database of 149,622 Medicare patients with a primary diagnosis of colorectal cancer who underwent colectomy from 1986 to 2005. The goal was to determine trends in readmission rates during the first 30 days.
"How do we begin to remedy the demonization of legitimate readmissions either politically, medically, or both?"
Increasingly, payers – especially Medicare – are penalizing hospitals for failing to prevent readmissions, which cost about $40 billion annually. Moreover, up to three-quarters of readmissions may be avoidable. In the meantime, many hospitals are fast-tracking patients for discharge after colorectal surgery.
In the SEER data, the mean age was 75 years in the 1986-1990 period and 77 years in the later period of 2001-2005. Patients were sicker in the later time period, with 63% having a Charlson comorbidity score of 3 or greater, compared with only 53% in the earlier time frame.
Most patients (38%) had a right colectomy; 23% had a sigmoid procedure, 13% had a rectal procedure, and 11% had a left colectomy. Forty-six percent of patients had lymph node metastasis, and 17% had an emergent procedure.
Morbidity for the entire study period was 37%; most complications were gastrointestinal or related to bleeding or postoperative infection. Again, there was a significant difference between the earlier and the later time frames. Perioperative morbidity was 27% in the 1986-1990 time frame, vs. 40% in 2001-2005. Mortality, at 4%, remained stable over time.
The mean length of stay decreased from 14 to 10 days from the early time to the later time period. And, over time, the percentage of patients discharged to home decreased, while discharges to skilled nursing facilities increased.
Overall, there were 17,000 readmissions, for a rate of 11%. Readmissions also increased, from 10% early on to 14% in 2001-2005. During that later time frame, patients had a 46% increased risk of readmission. Almost half of the readmissions occurred within the first 7 days after surgery, primarily for complications, dehydration, or infection. The mortality rate associated with readmission was 8%.
Multivariate analysis showed that the factors most likely to impact readmission were multiple comorbidities or a history of any perioperative complication, said Dr. Pawlik. Early discharge alone was not associated with a higher risk of readmission.
The study shows that "ongoing initiatives to reduce risk of readmissions and the associated costs, morbidity, and mortality are needed," said Dr. Pawlik.
It also "provides data that we all know to be true: namely, that the patients we are operating on have more comorbidities and that length of stay increases the rate of readmissions," said Dr. Susan Galandiuk, the discussant at the meeting. However, payers have been using length of stay and readmissions as quality surrogates, said Dr. Galandiuk, professor of surgery at the University of Louisville, Ky.
Not readmitting an elderly patient with many comorbidities and complications "would be a quality of care issue, and not the other way around," she added. The problem now is, "How do we begin to remedy the demonization of legitimate readmissions either politically, medically, or both?" asked Dr. Galandiuk.
Dr. Pawlik agreed that readmissions should not necessarily be held to be all bad. "Blaming readmissions on length of stay is a gross oversimplification of what’s going on," he added. Surgeons are clearly operating on older and sicker patients, and are doing more complicated operations that may result in a higher rate of morbidity – all this "in a culture of being asked to send people home earlier," he said.
"Our data clearly show that early discharge is feasible in some patients, but it needs to be used judiciously, especially in an older population," said Dr. Pawlik.
Dr. Pawlik and Dr. Galandiuk reported no conflicts.
FROM THE SOUTHERN SURGICAL ASSOCIATION ANNUAL MEETING
Major Finding: An increase in readmissions from 10% in 1986-1990 to 14% in 2001-2005 corresponded to older age and higher comorbidities in the later time period.
Data Source: Retrospective study of the SEER database of 149,622 Medicare patients with a primary diagnosis of colorectal cancer.
Disclosures: Dr. Pawlik and Dr. Galandiuk reported no conflicts.
Stratify Patients for Opioid Misuse and Abuse Risk
NEW ORLEANS – Do you know which of your patients is likely to misuse or abuse opioid medications?
They can be stratified according to risk, but many physicians don’t know how or don’t take the time to do so, according to Dr. Lynn R. Webster, medical director of Lifetree Clinical Research in Salt Lake City and director at large for the American Academy of Pain Medicine.
It is important to try to prevent misuse or abuse, given that overdoses and deaths from prescription drugs are on the rise, said Dr. Webster at the American Medical Association House of Delegates Interim meeting.
According to the National Institute on Drug Abuse, emergency department visits involving nonmedical use of pharmaceuticals (either alone or in combination with another drug) increased 98% between 2004 and 2009, from 627,291 visits to 1.2 million visits. There was an 83% rise in emergency department visits involving adverse reactions to pharmaceuticals between 2005 and 2009, from 1.3 million to 2.3 million visits.
Opioids were the most frequently cited in those ED visits, accounting for about 50% of nonmedical use. Psychotherapeutic agents accounted for a third of the nonmedical use. According to the National Institute on Drug Abuse, the three most frequently cited drugs in those visits were hydrocodone (alone or in combination), accounting for 104,490 visits; oxycodone (alone or in combination), for 175,949 visits; and methadone, for 70,637 visits.
To properly assess and treat patients, physicians should understand and agree upon terminology, said Dr. Webster. Patients may "misuse" prescriptions if they are not taking them as directed. They aren’t seeking a high, they may just have undertreated pain, he said.
Abuse is the willful self-administration of a drug to get high. Addiction is a medical condition with complex genetic, psychosocial, and environmental factors that influence its development and manifestations. Addicts may have impaired control over drug use, compulsive use, or continued use despite harm.
"You don’t just put someone on an opioid and think you’ve done your job."
Pseudoaddiction results from undertreatment of pain, and may resolve with proper therapy. Patients in this state may manifest behavior that is misidentified as drug-seeking, according to Dr. Webster.
Even with chronic pain, "people prescribed opioids over a long period of time are going to have aberrant behavior," said Dr. Webster, noting that "it’s not a small problem." In research he conducted, up to 40% of patients in his chronic pain practice had aberrant behavior within a year of starting treatment.
But, he said, "only a small percent have the disease of addiction."
To prevent misuse and abuse, it’s important to understand patients’ motives, he said. Nonmedical users may have been prescribed pain medications, but they move on to recreational use and then, often, abuse.
Medical users generally are pain patients who are seeking more pain relief and end up misusing the drugs. They also may become abusers. In all, 40%-60% have other chronic conditions for which opioids provide relief, such as anxiety, said Dr. Webster. That use is obviously not appropriate, but it can only be prevented if physicians fully assess pain patients.
There is a constellation of risk factors that help determine potential for misuse and abuse, according to Dr. Webster.
The potency of a pharmacologic substance and how fast it works are important, as those factors help determine how much dopamine is released, and thus, the amount of reward the patient feels, said Dr. Webster. If the drug is readily available, that also determines its attractiveness.
One-fifth of the overall population is at risk for addiction. There is no on/off switch, but a continuum of risk, he explained. Biological, psychiatric, and social factors all play a role in where patients fall on that continuum. Age, gender, family history, cigarette smoking, pain severity and duration, and sleep disorders are all risk factors. Patients with a history of a psychiatric disorder, being sexual abused, or substance use disorder also are at higher risk. "We must assess mental health," said Dr. Webster, noting that patients with anxiety, depression, traumatic brain injury, and attention-deficit/hyperactivity disorder are at risk for self-medicating and overdose.
A history of legal problems and motor vehicle accidents, or poor family support and unemployment also are predictors, Dr. Webster said.
Aberrant behaviors are directly related to the duration and the intensity of pain. Patients who cannot completely eliminate their pain may resort to taking more medication, which they will see as less of a wrong than the pain itself, he said.
Physicians generally have not done a good job at evaluating these risks, and selecting and managing patients according to these factors. But how patients are managed can help determine whether they end up in the emergency room, "or going to a substance abuse treatment center or the morgue," he said.
There are tools that can be used to screen patients for risk. Among those are the Screener and Opioid Assessment for Patients With Pain (SOAPP); the Opioid Risk Tool (ORT); the Diagnosis, Intractability, Risk Efficacy (DIRE) test; and the Current Opioid Misuse Measure (COMM), which is used for patients already taking opioids.
These tests all are simple and take only 1 to 10 minutes to administer. They can be given by any physician, including primary care physicians, he said.
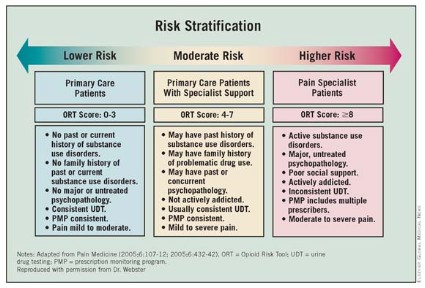
Once all the factors are taken into account, patients can be stratified according to risk. Lower-risk patients – those with moderate pain and no personal or family history of substance use disorders – can be managed by primary care physicians. Those at moderate risk may need the addition of a pain specialist. The higher-risk patients will need consultations with mental health professionals and pain physicians.
Monitoring higher-risk patients may require urine drug testing and prescription monitoring programs. Pharmacists should be kept in the loop to see whether patients are shopping around. Family and friends can be invaluable sources to help identify risky behaviors.
Physicians need to do a better job of titrating opioids and determining proper dosing. Many patients have died at initiation of opioid therapy, or from rotating from one drug to another, he said. Patients should not be allowed to determine how much of a long-acting medication they can take.
So how do doctors mitigate risk? The first order of business is to treat the pain. "Uncontrolled pain, untreated pain, I believe is the number one reason for aberrant behavior," said Dr. Webster. Physicians cannot eliminate all pain, however, so education also is crucial.
Physicians also have a duty to monitor pain patients. "You don’t just put someone on an opioid and think you’ve done your job," said Dr. Webster. A doctor would not stop managing a diabetic; pain patients need long-term management, he said.
Dr. Webster reported having no relevant conflicts of interest.
NEW ORLEANS – Do you know which of your patients is likely to misuse or abuse opioid medications?
They can be stratified according to risk, but many physicians don’t know how or don’t take the time to do so, according to Dr. Lynn R. Webster, medical director of Lifetree Clinical Research in Salt Lake City and director at large for the American Academy of Pain Medicine.
It is important to try to prevent misuse or abuse, given that overdoses and deaths from prescription drugs are on the rise, said Dr. Webster at the American Medical Association House of Delegates Interim meeting.
According to the National Institute on Drug Abuse, emergency department visits involving nonmedical use of pharmaceuticals (either alone or in combination with another drug) increased 98% between 2004 and 2009, from 627,291 visits to 1.2 million visits. There was an 83% rise in emergency department visits involving adverse reactions to pharmaceuticals between 2005 and 2009, from 1.3 million to 2.3 million visits.
Opioids were the most frequently cited in those ED visits, accounting for about 50% of nonmedical use. Psychotherapeutic agents accounted for a third of the nonmedical use. According to the National Institute on Drug Abuse, the three most frequently cited drugs in those visits were hydrocodone (alone or in combination), accounting for 104,490 visits; oxycodone (alone or in combination), for 175,949 visits; and methadone, for 70,637 visits.
To properly assess and treat patients, physicians should understand and agree upon terminology, said Dr. Webster. Patients may "misuse" prescriptions if they are not taking them as directed. They aren’t seeking a high, they may just have undertreated pain, he said.
Abuse is the willful self-administration of a drug to get high. Addiction is a medical condition with complex genetic, psychosocial, and environmental factors that influence its development and manifestations. Addicts may have impaired control over drug use, compulsive use, or continued use despite harm.
"You don’t just put someone on an opioid and think you’ve done your job."
Pseudoaddiction results from undertreatment of pain, and may resolve with proper therapy. Patients in this state may manifest behavior that is misidentified as drug-seeking, according to Dr. Webster.
Even with chronic pain, "people prescribed opioids over a long period of time are going to have aberrant behavior," said Dr. Webster, noting that "it’s not a small problem." In research he conducted, up to 40% of patients in his chronic pain practice had aberrant behavior within a year of starting treatment.
But, he said, "only a small percent have the disease of addiction."
To prevent misuse and abuse, it’s important to understand patients’ motives, he said. Nonmedical users may have been prescribed pain medications, but they move on to recreational use and then, often, abuse.
Medical users generally are pain patients who are seeking more pain relief and end up misusing the drugs. They also may become abusers. In all, 40%-60% have other chronic conditions for which opioids provide relief, such as anxiety, said Dr. Webster. That use is obviously not appropriate, but it can only be prevented if physicians fully assess pain patients.
There is a constellation of risk factors that help determine potential for misuse and abuse, according to Dr. Webster.
The potency of a pharmacologic substance and how fast it works are important, as those factors help determine how much dopamine is released, and thus, the amount of reward the patient feels, said Dr. Webster. If the drug is readily available, that also determines its attractiveness.
One-fifth of the overall population is at risk for addiction. There is no on/off switch, but a continuum of risk, he explained. Biological, psychiatric, and social factors all play a role in where patients fall on that continuum. Age, gender, family history, cigarette smoking, pain severity and duration, and sleep disorders are all risk factors. Patients with a history of a psychiatric disorder, being sexual abused, or substance use disorder also are at higher risk. "We must assess mental health," said Dr. Webster, noting that patients with anxiety, depression, traumatic brain injury, and attention-deficit/hyperactivity disorder are at risk for self-medicating and overdose.
A history of legal problems and motor vehicle accidents, or poor family support and unemployment also are predictors, Dr. Webster said.
Aberrant behaviors are directly related to the duration and the intensity of pain. Patients who cannot completely eliminate their pain may resort to taking more medication, which they will see as less of a wrong than the pain itself, he said.
Physicians generally have not done a good job at evaluating these risks, and selecting and managing patients according to these factors. But how patients are managed can help determine whether they end up in the emergency room, "or going to a substance abuse treatment center or the morgue," he said.
There are tools that can be used to screen patients for risk. Among those are the Screener and Opioid Assessment for Patients With Pain (SOAPP); the Opioid Risk Tool (ORT); the Diagnosis, Intractability, Risk Efficacy (DIRE) test; and the Current Opioid Misuse Measure (COMM), which is used for patients already taking opioids.
These tests all are simple and take only 1 to 10 minutes to administer. They can be given by any physician, including primary care physicians, he said.
Once all the factors are taken into account, patients can be stratified according to risk. Lower-risk patients – those with moderate pain and no personal or family history of substance use disorders – can be managed by primary care physicians. Those at moderate risk may need the addition of a pain specialist. The higher-risk patients will need consultations with mental health professionals and pain physicians.
Monitoring higher-risk patients may require urine drug testing and prescription monitoring programs. Pharmacists should be kept in the loop to see whether patients are shopping around. Family and friends can be invaluable sources to help identify risky behaviors.
Physicians need to do a better job of titrating opioids and determining proper dosing. Many patients have died at initiation of opioid therapy, or from rotating from one drug to another, he said. Patients should not be allowed to determine how much of a long-acting medication they can take.
So how do doctors mitigate risk? The first order of business is to treat the pain. "Uncontrolled pain, untreated pain, I believe is the number one reason for aberrant behavior," said Dr. Webster. Physicians cannot eliminate all pain, however, so education also is crucial.
Physicians also have a duty to monitor pain patients. "You don’t just put someone on an opioid and think you’ve done your job," said Dr. Webster. A doctor would not stop managing a diabetic; pain patients need long-term management, he said.
Dr. Webster reported having no relevant conflicts of interest.
NEW ORLEANS – Do you know which of your patients is likely to misuse or abuse opioid medications?
They can be stratified according to risk, but many physicians don’t know how or don’t take the time to do so, according to Dr. Lynn R. Webster, medical director of Lifetree Clinical Research in Salt Lake City and director at large for the American Academy of Pain Medicine.
It is important to try to prevent misuse or abuse, given that overdoses and deaths from prescription drugs are on the rise, said Dr. Webster at the American Medical Association House of Delegates Interim meeting.
According to the National Institute on Drug Abuse, emergency department visits involving nonmedical use of pharmaceuticals (either alone or in combination with another drug) increased 98% between 2004 and 2009, from 627,291 visits to 1.2 million visits. There was an 83% rise in emergency department visits involving adverse reactions to pharmaceuticals between 2005 and 2009, from 1.3 million to 2.3 million visits.
Opioids were the most frequently cited in those ED visits, accounting for about 50% of nonmedical use. Psychotherapeutic agents accounted for a third of the nonmedical use. According to the National Institute on Drug Abuse, the three most frequently cited drugs in those visits were hydrocodone (alone or in combination), accounting for 104,490 visits; oxycodone (alone or in combination), for 175,949 visits; and methadone, for 70,637 visits.
To properly assess and treat patients, physicians should understand and agree upon terminology, said Dr. Webster. Patients may "misuse" prescriptions if they are not taking them as directed. They aren’t seeking a high, they may just have undertreated pain, he said.
Abuse is the willful self-administration of a drug to get high. Addiction is a medical condition with complex genetic, psychosocial, and environmental factors that influence its development and manifestations. Addicts may have impaired control over drug use, compulsive use, or continued use despite harm.
"You don’t just put someone on an opioid and think you’ve done your job."
Pseudoaddiction results from undertreatment of pain, and may resolve with proper therapy. Patients in this state may manifest behavior that is misidentified as drug-seeking, according to Dr. Webster.
Even with chronic pain, "people prescribed opioids over a long period of time are going to have aberrant behavior," said Dr. Webster, noting that "it’s not a small problem." In research he conducted, up to 40% of patients in his chronic pain practice had aberrant behavior within a year of starting treatment.
But, he said, "only a small percent have the disease of addiction."
To prevent misuse and abuse, it’s important to understand patients’ motives, he said. Nonmedical users may have been prescribed pain medications, but they move on to recreational use and then, often, abuse.
Medical users generally are pain patients who are seeking more pain relief and end up misusing the drugs. They also may become abusers. In all, 40%-60% have other chronic conditions for which opioids provide relief, such as anxiety, said Dr. Webster. That use is obviously not appropriate, but it can only be prevented if physicians fully assess pain patients.
There is a constellation of risk factors that help determine potential for misuse and abuse, according to Dr. Webster.
The potency of a pharmacologic substance and how fast it works are important, as those factors help determine how much dopamine is released, and thus, the amount of reward the patient feels, said Dr. Webster. If the drug is readily available, that also determines its attractiveness.
One-fifth of the overall population is at risk for addiction. There is no on/off switch, but a continuum of risk, he explained. Biological, psychiatric, and social factors all play a role in where patients fall on that continuum. Age, gender, family history, cigarette smoking, pain severity and duration, and sleep disorders are all risk factors. Patients with a history of a psychiatric disorder, being sexual abused, or substance use disorder also are at higher risk. "We must assess mental health," said Dr. Webster, noting that patients with anxiety, depression, traumatic brain injury, and attention-deficit/hyperactivity disorder are at risk for self-medicating and overdose.
A history of legal problems and motor vehicle accidents, or poor family support and unemployment also are predictors, Dr. Webster said.
Aberrant behaviors are directly related to the duration and the intensity of pain. Patients who cannot completely eliminate their pain may resort to taking more medication, which they will see as less of a wrong than the pain itself, he said.
Physicians generally have not done a good job at evaluating these risks, and selecting and managing patients according to these factors. But how patients are managed can help determine whether they end up in the emergency room, "or going to a substance abuse treatment center or the morgue," he said.
There are tools that can be used to screen patients for risk. Among those are the Screener and Opioid Assessment for Patients With Pain (SOAPP); the Opioid Risk Tool (ORT); the Diagnosis, Intractability, Risk Efficacy (DIRE) test; and the Current Opioid Misuse Measure (COMM), which is used for patients already taking opioids.
These tests all are simple and take only 1 to 10 minutes to administer. They can be given by any physician, including primary care physicians, he said.
Once all the factors are taken into account, patients can be stratified according to risk. Lower-risk patients – those with moderate pain and no personal or family history of substance use disorders – can be managed by primary care physicians. Those at moderate risk may need the addition of a pain specialist. The higher-risk patients will need consultations with mental health professionals and pain physicians.
Monitoring higher-risk patients may require urine drug testing and prescription monitoring programs. Pharmacists should be kept in the loop to see whether patients are shopping around. Family and friends can be invaluable sources to help identify risky behaviors.
Physicians need to do a better job of titrating opioids and determining proper dosing. Many patients have died at initiation of opioid therapy, or from rotating from one drug to another, he said. Patients should not be allowed to determine how much of a long-acting medication they can take.
So how do doctors mitigate risk? The first order of business is to treat the pain. "Uncontrolled pain, untreated pain, I believe is the number one reason for aberrant behavior," said Dr. Webster. Physicians cannot eliminate all pain, however, so education also is crucial.
Physicians also have a duty to monitor pain patients. "You don’t just put someone on an opioid and think you’ve done your job," said Dr. Webster. A doctor would not stop managing a diabetic; pain patients need long-term management, he said.
Dr. Webster reported having no relevant conflicts of interest.
FROM THE AMERICAN MEDICAL ASSOCIATION HOUSE OF DELEGATES INTERIM MEETING
FDA Advisers: iPLEDGE Needs More Tweaking
SILVER SPRING, MD. – The iPLEDGE risk management program for isotretinoin has reduced fetal exposure to the teratogen but still needs to be tweaked to reduce burdens on physicians and improve patient access, advisers to the Food and Drug Administration said Dec. 1.
The agency is required by law to bring at least one drug a year to its Drug Safety and Risk Management Advisory Committee to determine if the product’s risk management evaluation and mitigation strategy (REMS) is ensuring safe use. Isotretinoin was chosen for that exercise this year.
Three versions of isotretinoin currently are on the market: Amnesteem, Sotret, and Claravis. The makers of those products said at the meeting that they were already planning on making changes to the iPLEDGE program in 2012. It’s not clear whether the panels’ suggestions would be incorporated then.
"I’m exceedingly impressed with what has evolved over time," said Dr. Wilma F. Bergfeld, professor of dermatology and pathology at the Cleveland Clinic and a temporary voting panelist on the Dermatologic and Ophthalmology Drugs Advisory Committee. She said that that it seemed that manufacturers, the FDA, physicians, and pharmacists were working together to make the program even better. "With everyone working at this, I believe the risk will go down."

Dr. Andrea Zaenglein of the departments of dermatology and pediatrics at Pennsylvania State University at Hershey said that while she was personally happy with the iPLEDGE program, it did constitute somewhat of a burden for physicians.
She said she spends at least 30 minutes counseling patients at the initial visit and then at least 15-20 minutes at each subsequent visit. Dr. Zaenglein, who spoke on behalf of the American Academy of Dermatology Association during the public portion of the meeting, said that the organization wanted to have more physicians participate in the ongoing evaluation of iPLEDGE. And, she said, the AADA hoped to have men and women of non–childbearing potential taken out of the registration process.
Dr. Robert A. Silverman, past president of the Society for Pediatric Dermatology, said that Dr. Zaenglein’s estimate on time spent counseling was conservative. He said he counsels patients over two or three extended visits, and that often he holds separate meetings with parents.
"After-hours discussion in my practice is not uncommon," added Dr. Silverman of Georgetown University, Washington. Still he said, isotretinoin "is a miracle drug that saves lives."
The dermatologists’ concerns about physicians’ burdens were echoed by the FDA panelists.
The panelists noted that they were especially worried about what seemed to be a lack of understanding among patients and even physicians about birth control. Several wanted to see a clearer, more concrete presentation to patients on the relative merits and effectiveness of various contraceptive methods. They also asked for more data on why pregnancies were still occurring. And several panel members suggested that men and women who are shown to not be of child-bearing potential be removed from most of the restrictions imposed by iPLEDGE.
For the year ending February 2011, 569,385 women of childbearing potential, 45,484 women of non–childbearing potential, and 620,012 men had enrolled in iPLEDGE since its inception in 2006.
The committee was first asked to whether iPLEDGE is continuing to assure the safe use of isotretinoin. Overall, there have been 836 pregnancies since 2006; of those, 400 were terminated and 282 patients were lost to follow-up. A total of 45 live births were recorded; of those, 8 were children born with congenital anomalies.
In the year ending February 2011, there were 155 pregnancies, a decline from 186 the previous year, and 190 in 2008. Dr. Eric Davis, director of medical services for Mylan Pharmaceuticals, said that the pregnancy rate for iPLEDGE patients was 1.27/1,000, as compared with the 51/1,000 rate of unintended pregnancies in the general U.S. population.

James Shamp, director of risk management programs at United BioSource Corp., which helped develop iPLEDGE, said that analysis of program data had determined that some physicians were erroneously classifying women as being of non-childbearing potential. To mitigate against such errors, the iPLEDGE online system next year will include a "wizard" that will classify women as of childbearing potential or of non–childbearing potential based on a series of responses from the prescriber.
The panelists were also asked whether iPLEDGE was "unduly burdensome" for patients. FDA officials said that after iPLEDGE was introduced in 2006, there was a 29% drop in use by men and a 55% drop in use by women. Use among men recovered to pre-iPLEDGE levels within 7 months, but it took almost a year for usage to recover among women, according to Marta Wosinska, an analyst at the FDA Center for Drug Evaluation and Research. She said that iPLEDGE may have negatively affected patient access, but that the program also probably caused physicians to make more clinically appropriate prescribing decisions in certain cases.
Finally, the committee was asked to assess the burden on prescribers. According to data from Mylan, there are 14,444 registered prescribers in the iPLEDGE program, primarily with a specialty in dermatology (10,435, or 72%). Family physicians comprised the next largest group (2,095 prescribers 14%). Internists, ob.gyns., and pediatricians also were prescribers.
Mr. Shamp said that the program had become easier to manage for prescribers—a fact reflected by the declining volume of calls to the iPLEDGE call centers. Currently, there are about 20,000 calls a month, with an average hold time of a minute and an average time per call of just under 5 minutes, he said.
SILVER SPRING, MD. – The iPLEDGE risk management program for isotretinoin has reduced fetal exposure to the teratogen but still needs to be tweaked to reduce burdens on physicians and improve patient access, advisers to the Food and Drug Administration said Dec. 1.
The agency is required by law to bring at least one drug a year to its Drug Safety and Risk Management Advisory Committee to determine if the product’s risk management evaluation and mitigation strategy (REMS) is ensuring safe use. Isotretinoin was chosen for that exercise this year.
Three versions of isotretinoin currently are on the market: Amnesteem, Sotret, and Claravis. The makers of those products said at the meeting that they were already planning on making changes to the iPLEDGE program in 2012. It’s not clear whether the panels’ suggestions would be incorporated then.
"I’m exceedingly impressed with what has evolved over time," said Dr. Wilma F. Bergfeld, professor of dermatology and pathology at the Cleveland Clinic and a temporary voting panelist on the Dermatologic and Ophthalmology Drugs Advisory Committee. She said that that it seemed that manufacturers, the FDA, physicians, and pharmacists were working together to make the program even better. "With everyone working at this, I believe the risk will go down."
Dr. Andrea Zaenglein of the departments of dermatology and pediatrics at Pennsylvania State University at Hershey said that while she was personally happy with the iPLEDGE program, it did constitute somewhat of a burden for physicians.
She said she spends at least 30 minutes counseling patients at the initial visit and then at least 15-20 minutes at each subsequent visit. Dr. Zaenglein, who spoke on behalf of the American Academy of Dermatology Association during the public portion of the meeting, said that the organization wanted to have more physicians participate in the ongoing evaluation of iPLEDGE. And, she said, the AADA hoped to have men and women of non–childbearing potential taken out of the registration process.
Dr. Robert A. Silverman, past president of the Society for Pediatric Dermatology, said that Dr. Zaenglein’s estimate on time spent counseling was conservative. He said he counsels patients over two or three extended visits, and that often he holds separate meetings with parents.
"After-hours discussion in my practice is not uncommon," added Dr. Silverman of Georgetown University, Washington. Still he said, isotretinoin "is a miracle drug that saves lives."
The dermatologists’ concerns about physicians’ burdens were echoed by the FDA panelists.
The panelists noted that they were especially worried about what seemed to be a lack of understanding among patients and even physicians about birth control. Several wanted to see a clearer, more concrete presentation to patients on the relative merits and effectiveness of various contraceptive methods. They also asked for more data on why pregnancies were still occurring. And several panel members suggested that men and women who are shown to not be of child-bearing potential be removed from most of the restrictions imposed by iPLEDGE.
For the year ending February 2011, 569,385 women of childbearing potential, 45,484 women of non–childbearing potential, and 620,012 men had enrolled in iPLEDGE since its inception in 2006.
The committee was first asked to whether iPLEDGE is continuing to assure the safe use of isotretinoin. Overall, there have been 836 pregnancies since 2006; of those, 400 were terminated and 282 patients were lost to follow-up. A total of 45 live births were recorded; of those, 8 were children born with congenital anomalies.
In the year ending February 2011, there were 155 pregnancies, a decline from 186 the previous year, and 190 in 2008. Dr. Eric Davis, director of medical services for Mylan Pharmaceuticals, said that the pregnancy rate for iPLEDGE patients was 1.27/1,000, as compared with the 51/1,000 rate of unintended pregnancies in the general U.S. population.
James Shamp, director of risk management programs at United BioSource Corp., which helped develop iPLEDGE, said that analysis of program data had determined that some physicians were erroneously classifying women as being of non-childbearing potential. To mitigate against such errors, the iPLEDGE online system next year will include a "wizard" that will classify women as of childbearing potential or of non–childbearing potential based on a series of responses from the prescriber.
The panelists were also asked whether iPLEDGE was "unduly burdensome" for patients. FDA officials said that after iPLEDGE was introduced in 2006, there was a 29% drop in use by men and a 55% drop in use by women. Use among men recovered to pre-iPLEDGE levels within 7 months, but it took almost a year for usage to recover among women, according to Marta Wosinska, an analyst at the FDA Center for Drug Evaluation and Research. She said that iPLEDGE may have negatively affected patient access, but that the program also probably caused physicians to make more clinically appropriate prescribing decisions in certain cases.
Finally, the committee was asked to assess the burden on prescribers. According to data from Mylan, there are 14,444 registered prescribers in the iPLEDGE program, primarily with a specialty in dermatology (10,435, or 72%). Family physicians comprised the next largest group (2,095 prescribers 14%). Internists, ob.gyns., and pediatricians also were prescribers.
Mr. Shamp said that the program had become easier to manage for prescribers—a fact reflected by the declining volume of calls to the iPLEDGE call centers. Currently, there are about 20,000 calls a month, with an average hold time of a minute and an average time per call of just under 5 minutes, he said.
SILVER SPRING, MD. – The iPLEDGE risk management program for isotretinoin has reduced fetal exposure to the teratogen but still needs to be tweaked to reduce burdens on physicians and improve patient access, advisers to the Food and Drug Administration said Dec. 1.
The agency is required by law to bring at least one drug a year to its Drug Safety and Risk Management Advisory Committee to determine if the product’s risk management evaluation and mitigation strategy (REMS) is ensuring safe use. Isotretinoin was chosen for that exercise this year.
Three versions of isotretinoin currently are on the market: Amnesteem, Sotret, and Claravis. The makers of those products said at the meeting that they were already planning on making changes to the iPLEDGE program in 2012. It’s not clear whether the panels’ suggestions would be incorporated then.
"I’m exceedingly impressed with what has evolved over time," said Dr. Wilma F. Bergfeld, professor of dermatology and pathology at the Cleveland Clinic and a temporary voting panelist on the Dermatologic and Ophthalmology Drugs Advisory Committee. She said that that it seemed that manufacturers, the FDA, physicians, and pharmacists were working together to make the program even better. "With everyone working at this, I believe the risk will go down."
Dr. Andrea Zaenglein of the departments of dermatology and pediatrics at Pennsylvania State University at Hershey said that while she was personally happy with the iPLEDGE program, it did constitute somewhat of a burden for physicians.
She said she spends at least 30 minutes counseling patients at the initial visit and then at least 15-20 minutes at each subsequent visit. Dr. Zaenglein, who spoke on behalf of the American Academy of Dermatology Association during the public portion of the meeting, said that the organization wanted to have more physicians participate in the ongoing evaluation of iPLEDGE. And, she said, the AADA hoped to have men and women of non–childbearing potential taken out of the registration process.
Dr. Robert A. Silverman, past president of the Society for Pediatric Dermatology, said that Dr. Zaenglein’s estimate on time spent counseling was conservative. He said he counsels patients over two or three extended visits, and that often he holds separate meetings with parents.
"After-hours discussion in my practice is not uncommon," added Dr. Silverman of Georgetown University, Washington. Still he said, isotretinoin "is a miracle drug that saves lives."
The dermatologists’ concerns about physicians’ burdens were echoed by the FDA panelists.
The panelists noted that they were especially worried about what seemed to be a lack of understanding among patients and even physicians about birth control. Several wanted to see a clearer, more concrete presentation to patients on the relative merits and effectiveness of various contraceptive methods. They also asked for more data on why pregnancies were still occurring. And several panel members suggested that men and women who are shown to not be of child-bearing potential be removed from most of the restrictions imposed by iPLEDGE.
For the year ending February 2011, 569,385 women of childbearing potential, 45,484 women of non–childbearing potential, and 620,012 men had enrolled in iPLEDGE since its inception in 2006.
The committee was first asked to whether iPLEDGE is continuing to assure the safe use of isotretinoin. Overall, there have been 836 pregnancies since 2006; of those, 400 were terminated and 282 patients were lost to follow-up. A total of 45 live births were recorded; of those, 8 were children born with congenital anomalies.
In the year ending February 2011, there were 155 pregnancies, a decline from 186 the previous year, and 190 in 2008. Dr. Eric Davis, director of medical services for Mylan Pharmaceuticals, said that the pregnancy rate for iPLEDGE patients was 1.27/1,000, as compared with the 51/1,000 rate of unintended pregnancies in the general U.S. population.
James Shamp, director of risk management programs at United BioSource Corp., which helped develop iPLEDGE, said that analysis of program data had determined that some physicians were erroneously classifying women as being of non-childbearing potential. To mitigate against such errors, the iPLEDGE online system next year will include a "wizard" that will classify women as of childbearing potential or of non–childbearing potential based on a series of responses from the prescriber.
The panelists were also asked whether iPLEDGE was "unduly burdensome" for patients. FDA officials said that after iPLEDGE was introduced in 2006, there was a 29% drop in use by men and a 55% drop in use by women. Use among men recovered to pre-iPLEDGE levels within 7 months, but it took almost a year for usage to recover among women, according to Marta Wosinska, an analyst at the FDA Center for Drug Evaluation and Research. She said that iPLEDGE may have negatively affected patient access, but that the program also probably caused physicians to make more clinically appropriate prescribing decisions in certain cases.
Finally, the committee was asked to assess the burden on prescribers. According to data from Mylan, there are 14,444 registered prescribers in the iPLEDGE program, primarily with a specialty in dermatology (10,435, or 72%). Family physicians comprised the next largest group (2,095 prescribers 14%). Internists, ob.gyns., and pediatricians also were prescribers.
Mr. Shamp said that the program had become easier to manage for prescribers—a fact reflected by the declining volume of calls to the iPLEDGE call centers. Currently, there are about 20,000 calls a month, with an average hold time of a minute and an average time per call of just under 5 minutes, he said.
FROM A JOINT MEETING OF THE FDA DRUG SAFETY AND RISK MANAGEMENT AND DERMATOLOGIC AND OPHTHALMIC DRUGS ADVISORY COMMITTEES
Census Bureau Confirms Huge Growth in Over-65 Population
From 2000 to 2010, the nation’s over-65 population grew at a faster rate than the overall population, according to data released by the Census Bureau on Nov. 30.
The numbers have implications for Social Security, Medicare, and Medicaid, as well as the physicians who will be serving an increasingly aging population.
The over-65 group grew 15%, to 40 million, while the nation’s overall population grew about 10% to 308 million. In all, 13% of Americans are over age 65; that is the highest proportion of seniors since 1900, Census Bureau Statistician Carrie Werner said during a press briefing.
The Census reported that there are 1.3 million people over age 65 (3% of that age group) who lived in skilled-nursing facilities in 2010.
There has also been a big increase in the number of Americans in the older age groups, in particular for those over age 85. There was a 30% increase in the number of 85- to 94-year-olds from 2000 to 2010. For those aged 95 or older, there was a 26% increase over the last decade. There are now an estimated 5.1 million Americans over age 85 and 400,000 over age 95.
And there are more than 50,000 Americans who are older than 100.
There was a slight decline in the number of Americans aged 75 to 79, mostly because there were fewer births during the early 1930s.
Although women still edge out men in terms of longevity, more men are living longer, Ms. Werner said. There was a 20% increase in the number of men over age 65, to 17.4 million. By contrast, there were about 23 million women over age 65 in 2010, which represented an 11% increase from 2000.
For every 10-year age group, the percentage growth in the number of men outstrips that for women.
While the Census Bureau does not analyze underlying reasons for the population shifts, Ms. Werner said that it appears to reflect data that shows that men have had improving life expectancy.
In terms of absolute numbers, the South and the Midwest have more elderly than any other region. But the Northeast has the greatest percentage of over-65 residents, at 14%. The Midwest and the South each have about 13% of their population as over 65. The Northeast and Midwest have the largest proportions of over-85 residents.
The states with the largest numbers of people over 65 are also the five most-populous states: California, Florida, New York, Texas, and Pennsylvania. But when it comes to proportion of elderly residents, the top five shift: Florida, West Virginia, Maine, Pennsylvania, and Iowa.
But the data shows that, increasingly, Americans over 65, and 85, are moving to the South and West. Three of the top five counties with percentage of residents over age 65 are in Florida. The Great Plains states and the Rocky Mountain states also have large percentages of residents over age 65.
The main areas of growth in the senior population are in the Sierra Nevada mountains and the Rocky Mountain states, said Ms. Werner. There was also notable growth in Texas, Georgia, Alaska, and Virginia, she said.
The Census Bureau data did not break out the data according to race or ethnicity, said Ms. Werner.
senior population statistics, skilled-nursing facilities
From 2000 to 2010, the nation’s over-65 population grew at a faster rate than the overall population, according to data released by the Census Bureau on Nov. 30.
The numbers have implications for Social Security, Medicare, and Medicaid, as well as the physicians who will be serving an increasingly aging population.
The over-65 group grew 15%, to 40 million, while the nation’s overall population grew about 10% to 308 million. In all, 13% of Americans are over age 65; that is the highest proportion of seniors since 1900, Census Bureau Statistician Carrie Werner said during a press briefing.
The Census reported that there are 1.3 million people over age 65 (3% of that age group) who lived in skilled-nursing facilities in 2010.
There has also been a big increase in the number of Americans in the older age groups, in particular for those over age 85. There was a 30% increase in the number of 85- to 94-year-olds from 2000 to 2010. For those aged 95 or older, there was a 26% increase over the last decade. There are now an estimated 5.1 million Americans over age 85 and 400,000 over age 95.
And there are more than 50,000 Americans who are older than 100.
There was a slight decline in the number of Americans aged 75 to 79, mostly because there were fewer births during the early 1930s.
Although women still edge out men in terms of longevity, more men are living longer, Ms. Werner said. There was a 20% increase in the number of men over age 65, to 17.4 million. By contrast, there were about 23 million women over age 65 in 2010, which represented an 11% increase from 2000.
For every 10-year age group, the percentage growth in the number of men outstrips that for women.
While the Census Bureau does not analyze underlying reasons for the population shifts, Ms. Werner said that it appears to reflect data that shows that men have had improving life expectancy.
In terms of absolute numbers, the South and the Midwest have more elderly than any other region. But the Northeast has the greatest percentage of over-65 residents, at 14%. The Midwest and the South each have about 13% of their population as over 65. The Northeast and Midwest have the largest proportions of over-85 residents.
The states with the largest numbers of people over 65 are also the five most-populous states: California, Florida, New York, Texas, and Pennsylvania. But when it comes to proportion of elderly residents, the top five shift: Florida, West Virginia, Maine, Pennsylvania, and Iowa.
But the data shows that, increasingly, Americans over 65, and 85, are moving to the South and West. Three of the top five counties with percentage of residents over age 65 are in Florida. The Great Plains states and the Rocky Mountain states also have large percentages of residents over age 65.
The main areas of growth in the senior population are in the Sierra Nevada mountains and the Rocky Mountain states, said Ms. Werner. There was also notable growth in Texas, Georgia, Alaska, and Virginia, she said.
The Census Bureau data did not break out the data according to race or ethnicity, said Ms. Werner.
From 2000 to 2010, the nation’s over-65 population grew at a faster rate than the overall population, according to data released by the Census Bureau on Nov. 30.
The numbers have implications for Social Security, Medicare, and Medicaid, as well as the physicians who will be serving an increasingly aging population.
The over-65 group grew 15%, to 40 million, while the nation’s overall population grew about 10% to 308 million. In all, 13% of Americans are over age 65; that is the highest proportion of seniors since 1900, Census Bureau Statistician Carrie Werner said during a press briefing.
The Census reported that there are 1.3 million people over age 65 (3% of that age group) who lived in skilled-nursing facilities in 2010.
There has also been a big increase in the number of Americans in the older age groups, in particular for those over age 85. There was a 30% increase in the number of 85- to 94-year-olds from 2000 to 2010. For those aged 95 or older, there was a 26% increase over the last decade. There are now an estimated 5.1 million Americans over age 85 and 400,000 over age 95.
And there are more than 50,000 Americans who are older than 100.
There was a slight decline in the number of Americans aged 75 to 79, mostly because there were fewer births during the early 1930s.
Although women still edge out men in terms of longevity, more men are living longer, Ms. Werner said. There was a 20% increase in the number of men over age 65, to 17.4 million. By contrast, there were about 23 million women over age 65 in 2010, which represented an 11% increase from 2000.
For every 10-year age group, the percentage growth in the number of men outstrips that for women.
While the Census Bureau does not analyze underlying reasons for the population shifts, Ms. Werner said that it appears to reflect data that shows that men have had improving life expectancy.
In terms of absolute numbers, the South and the Midwest have more elderly than any other region. But the Northeast has the greatest percentage of over-65 residents, at 14%. The Midwest and the South each have about 13% of their population as over 65. The Northeast and Midwest have the largest proportions of over-85 residents.
The states with the largest numbers of people over 65 are also the five most-populous states: California, Florida, New York, Texas, and Pennsylvania. But when it comes to proportion of elderly residents, the top five shift: Florida, West Virginia, Maine, Pennsylvania, and Iowa.
But the data shows that, increasingly, Americans over 65, and 85, are moving to the South and West. Three of the top five counties with percentage of residents over age 65 are in Florida. The Great Plains states and the Rocky Mountain states also have large percentages of residents over age 65.
The main areas of growth in the senior population are in the Sierra Nevada mountains and the Rocky Mountain states, said Ms. Werner. There was also notable growth in Texas, Georgia, Alaska, and Virginia, she said.
The Census Bureau data did not break out the data according to race or ethnicity, said Ms. Werner.
senior population statistics, skilled-nursing facilities
senior population statistics, skilled-nursing facilities
FROM A U.S. CENSUS BUREAU REPORT
AMA Delegates to Push for Private Medicare Contracting
NEW ORLEANS – The American Medical Association's policy-making body wrapped up 2½ days of meetings Nov. 15 by calling for a delay in implementation of the ICD-10 coding system, and reiterating its intention to seek the ability to privately broker fees with Medicare patients.
Physicians have long sought to be allowed to engage in so-called “private contracting” with Medicare patients. Under that scenario, Medicare patients could use their benefits to see a physician that does not accept Medicare. Currently, patients have to pay for the entire visit out of pocket if their physicians do not accept Medicare.
The AMA says private contracting will empower patients, and the group is supporting legislation sponsored by Rep. Tom Price (R-Ga.) that would allow it. The Medicare Patient Empowerment Act (H.R. 1700) was introduced in May; a companion bill was quickly introduced in the Senate by Lisa Murkowski (R-Alaska).
The AMA House of Delegates reaffirmed support of the legislation, but also called upon the AMA to start a grassroots campaign to get patients involved.
“This is a directive to take action,” said Dr. Corey Howard, chair of the Florida delegation, which initiated the resolution seeking a public campaign. “It's time to start planting those seeds to help the public begin to look at this in a favorable way.”
Alabama delegate Dr. Jeff Terry, president of the Medical Association of the State of Alabama, said that a grassroots campaign “will allow our politicians to do the right thing.” Such a campaign will let politicians know “that we don't want our congressmen to walk out on a political limb not supported by the public.”
The emphasis on private contracting was in part a symptom of the high-pressure environment physicians find themselves in, facing a potential 27% cut in Medicare payments as well as high-cost requirements to implement electronic medical records, said Dr. Robert Wah, chairman of the AMA Board of Trustees.
“The fact that patients may be able to take their benefit where they'd like to, to see the doctors they want to see, is a potential safety valve to all this pressure being exerted on physician practices and patients in the Medicare system,” Dr. Wah said in an interview. “So we're actively pushing at the local level for people to go to their congressmen and ask them to sign on to this legislation.”
The push back against the coming implementation of the new ICD-10 coding system in 2013 is also a sign that physicians feel overwhelmed by their changing practice environment, Dr. Wah said. The House approved a resolution sponsored by the Alabama and Mississippi delegations, along with the American Urological Association and American Association of Clinical Urologists, to take action to stop the implementation.
The ICD-10 will consist of 69,000 codes, compared with the 14,000 in the current ICD-9.
“At a time when we are working to get the best value possible for our health care dollar, this massive and expensive undertaking will add administrative expense and create unnecessary workflow disruptions,” AMA President Peter W. Carmel said in a statement.
NEW ORLEANS – The American Medical Association's policy-making body wrapped up 2½ days of meetings Nov. 15 by calling for a delay in implementation of the ICD-10 coding system, and reiterating its intention to seek the ability to privately broker fees with Medicare patients.
Physicians have long sought to be allowed to engage in so-called “private contracting” with Medicare patients. Under that scenario, Medicare patients could use their benefits to see a physician that does not accept Medicare. Currently, patients have to pay for the entire visit out of pocket if their physicians do not accept Medicare.
The AMA says private contracting will empower patients, and the group is supporting legislation sponsored by Rep. Tom Price (R-Ga.) that would allow it. The Medicare Patient Empowerment Act (H.R. 1700) was introduced in May; a companion bill was quickly introduced in the Senate by Lisa Murkowski (R-Alaska).
The AMA House of Delegates reaffirmed support of the legislation, but also called upon the AMA to start a grassroots campaign to get patients involved.
“This is a directive to take action,” said Dr. Corey Howard, chair of the Florida delegation, which initiated the resolution seeking a public campaign. “It's time to start planting those seeds to help the public begin to look at this in a favorable way.”
Alabama delegate Dr. Jeff Terry, president of the Medical Association of the State of Alabama, said that a grassroots campaign “will allow our politicians to do the right thing.” Such a campaign will let politicians know “that we don't want our congressmen to walk out on a political limb not supported by the public.”
The emphasis on private contracting was in part a symptom of the high-pressure environment physicians find themselves in, facing a potential 27% cut in Medicare payments as well as high-cost requirements to implement electronic medical records, said Dr. Robert Wah, chairman of the AMA Board of Trustees.
“The fact that patients may be able to take their benefit where they'd like to, to see the doctors they want to see, is a potential safety valve to all this pressure being exerted on physician practices and patients in the Medicare system,” Dr. Wah said in an interview. “So we're actively pushing at the local level for people to go to their congressmen and ask them to sign on to this legislation.”
The push back against the coming implementation of the new ICD-10 coding system in 2013 is also a sign that physicians feel overwhelmed by their changing practice environment, Dr. Wah said. The House approved a resolution sponsored by the Alabama and Mississippi delegations, along with the American Urological Association and American Association of Clinical Urologists, to take action to stop the implementation.
The ICD-10 will consist of 69,000 codes, compared with the 14,000 in the current ICD-9.
“At a time when we are working to get the best value possible for our health care dollar, this massive and expensive undertaking will add administrative expense and create unnecessary workflow disruptions,” AMA President Peter W. Carmel said in a statement.
NEW ORLEANS – The American Medical Association's policy-making body wrapped up 2½ days of meetings Nov. 15 by calling for a delay in implementation of the ICD-10 coding system, and reiterating its intention to seek the ability to privately broker fees with Medicare patients.
Physicians have long sought to be allowed to engage in so-called “private contracting” with Medicare patients. Under that scenario, Medicare patients could use their benefits to see a physician that does not accept Medicare. Currently, patients have to pay for the entire visit out of pocket if their physicians do not accept Medicare.
The AMA says private contracting will empower patients, and the group is supporting legislation sponsored by Rep. Tom Price (R-Ga.) that would allow it. The Medicare Patient Empowerment Act (H.R. 1700) was introduced in May; a companion bill was quickly introduced in the Senate by Lisa Murkowski (R-Alaska).
The AMA House of Delegates reaffirmed support of the legislation, but also called upon the AMA to start a grassroots campaign to get patients involved.
“This is a directive to take action,” said Dr. Corey Howard, chair of the Florida delegation, which initiated the resolution seeking a public campaign. “It's time to start planting those seeds to help the public begin to look at this in a favorable way.”
Alabama delegate Dr. Jeff Terry, president of the Medical Association of the State of Alabama, said that a grassroots campaign “will allow our politicians to do the right thing.” Such a campaign will let politicians know “that we don't want our congressmen to walk out on a political limb not supported by the public.”
The emphasis on private contracting was in part a symptom of the high-pressure environment physicians find themselves in, facing a potential 27% cut in Medicare payments as well as high-cost requirements to implement electronic medical records, said Dr. Robert Wah, chairman of the AMA Board of Trustees.
“The fact that patients may be able to take their benefit where they'd like to, to see the doctors they want to see, is a potential safety valve to all this pressure being exerted on physician practices and patients in the Medicare system,” Dr. Wah said in an interview. “So we're actively pushing at the local level for people to go to their congressmen and ask them to sign on to this legislation.”
The push back against the coming implementation of the new ICD-10 coding system in 2013 is also a sign that physicians feel overwhelmed by their changing practice environment, Dr. Wah said. The House approved a resolution sponsored by the Alabama and Mississippi delegations, along with the American Urological Association and American Association of Clinical Urologists, to take action to stop the implementation.
The ICD-10 will consist of 69,000 codes, compared with the 14,000 in the current ICD-9.
“At a time when we are working to get the best value possible for our health care dollar, this massive and expensive undertaking will add administrative expense and create unnecessary workflow disruptions,” AMA President Peter W. Carmel said in a statement.
From the Interim Meeting of the American Medical Association House of Delegates
President Obama Nominates New Medicare Chief
President Obama on Nov. 23 nominated Marilyn B. Tavenner to be the new administrator of the Centers for Medicare and Medicaid Services.
The current CMS chief, Dr. Donald Berwick,was expected to stay in his position only until the end of this year. He was never confirmed by the Senate. Republican senators had blocked the confirmation, stating concerns that he might favor rationing care.
Dr. Berwick strenuously denied those charges.

When his confirmation failed, President Obama made a recess appointment, which meant that Dr. Berwick would have the position only for a short time.
The appointment of Ms. Tavenner to take his place is not a surprise, as she has been the principal deputy administrator of the CMS since February 2010. She also served as acting administrator from February to July 2010.
Before that, Ms. Tavenner was the Commonwealth of Virginia’s Secretary of Health and Human Resources, serving under former Gov. Tim Kaine (D).
Ms. Tavenner holds a B.S. in nursing and an M.A. in health administration, both from the Virginia Commonwealth University, Richmond.
She will have to be confirmed by the Senate.
President Obama on Nov. 23 nominated Marilyn B. Tavenner to be the new administrator of the Centers for Medicare and Medicaid Services.
The current CMS chief, Dr. Donald Berwick,was expected to stay in his position only until the end of this year. He was never confirmed by the Senate. Republican senators had blocked the confirmation, stating concerns that he might favor rationing care.
Dr. Berwick strenuously denied those charges.
When his confirmation failed, President Obama made a recess appointment, which meant that Dr. Berwick would have the position only for a short time.
The appointment of Ms. Tavenner to take his place is not a surprise, as she has been the principal deputy administrator of the CMS since February 2010. She also served as acting administrator from February to July 2010.
Before that, Ms. Tavenner was the Commonwealth of Virginia’s Secretary of Health and Human Resources, serving under former Gov. Tim Kaine (D).
Ms. Tavenner holds a B.S. in nursing and an M.A. in health administration, both from the Virginia Commonwealth University, Richmond.
She will have to be confirmed by the Senate.
President Obama on Nov. 23 nominated Marilyn B. Tavenner to be the new administrator of the Centers for Medicare and Medicaid Services.
The current CMS chief, Dr. Donald Berwick,was expected to stay in his position only until the end of this year. He was never confirmed by the Senate. Republican senators had blocked the confirmation, stating concerns that he might favor rationing care.
Dr. Berwick strenuously denied those charges.
When his confirmation failed, President Obama made a recess appointment, which meant that Dr. Berwick would have the position only for a short time.
The appointment of Ms. Tavenner to take his place is not a surprise, as she has been the principal deputy administrator of the CMS since February 2010. She also served as acting administrator from February to July 2010.
Before that, Ms. Tavenner was the Commonwealth of Virginia’s Secretary of Health and Human Resources, serving under former Gov. Tim Kaine (D).
Ms. Tavenner holds a B.S. in nursing and an M.A. in health administration, both from the Virginia Commonwealth University, Richmond.
She will have to be confirmed by the Senate.
AMA House: Regulate Med Spas
NEW ORLEANS – The American Medical Association’s House of Delegates has passed a resolution urging physician organizations to push for stricter state regulation of medical spas. The vote came at the Delegates’ interim meeting, held in New Orleans.
The resolution seeks to ensure that cosmetic medical procedures have the same safeguards as do medically necessary procedures. That includes appropriate training, supervision, and oversight.
The resolution also stated that cosmetic procedures, including botulinum toxin injections, dermal filler injections, and laser and intense pulsed-light procedures, should be considered the practice of medicine.
The Medical Student Section of the House brought the resolution forward, stating that patient safety was a growing concern. The resolution also urged the AMA to increase public awareness about potential dangers presented by unregulated spas and to work to help create a formal complaint procedure for patients.
NEW ORLEANS – The American Medical Association’s House of Delegates has passed a resolution urging physician organizations to push for stricter state regulation of medical spas. The vote came at the Delegates’ interim meeting, held in New Orleans.
The resolution seeks to ensure that cosmetic medical procedures have the same safeguards as do medically necessary procedures. That includes appropriate training, supervision, and oversight.
The resolution also stated that cosmetic procedures, including botulinum toxin injections, dermal filler injections, and laser and intense pulsed-light procedures, should be considered the practice of medicine.
The Medical Student Section of the House brought the resolution forward, stating that patient safety was a growing concern. The resolution also urged the AMA to increase public awareness about potential dangers presented by unregulated spas and to work to help create a formal complaint procedure for patients.
NEW ORLEANS – The American Medical Association’s House of Delegates has passed a resolution urging physician organizations to push for stricter state regulation of medical spas. The vote came at the Delegates’ interim meeting, held in New Orleans.
The resolution seeks to ensure that cosmetic medical procedures have the same safeguards as do medically necessary procedures. That includes appropriate training, supervision, and oversight.
The resolution also stated that cosmetic procedures, including botulinum toxin injections, dermal filler injections, and laser and intense pulsed-light procedures, should be considered the practice of medicine.
The Medical Student Section of the House brought the resolution forward, stating that patient safety was a growing concern. The resolution also urged the AMA to increase public awareness about potential dangers presented by unregulated spas and to work to help create a formal complaint procedure for patients.
CMS Issues Final Rule on ACOs
Use of electronic health records is no longer a condition for participating in an accountable care organization, according to the Oct. 20 final rule that will govern how ACOs are constructed and how they will be paid. The change is just one of many in the long-awaited regulation.
The 696-page final rule contains many significant changes that were made in response to the 1,320 comments the agency received on its proposed rule, issued in late March and published April 7 in the Federal Register.
Many physician groups and hospitals complained about various aspects of the proposed rule. They met repeatedly with the agency, CMS Administrator Don Berwick said during a press briefing.
"Thanks to the generous input of ideas from so many Americans, we’ve been able to fine-tune and improve these rules to better meet the needs of a range of stakeholders," Dr. Berwick said.
"When folks see the rules and see the many changes, they will see that CMS listened," Jonathan Blum, CMS deputy administrator and director of the Center for Medicare, said during the briefing.
In the proposed rule, half of primary care physicians in an ACO had to meet the meaningful use criteria for EHRs by the second year of what will be 3-year contracts with the CMS. Under the final rule, EHRs will not be required, but instead be heavily weighted as a measure of quality of care.
The final rule also pushes back the program’s starting dates. Originally, the CMS envisioned a start date of January 2012 for organizations that wanted to participate.
Now, the program will be established by January 2012 with the initial agreements starting in April or July of that year. The first performance "year" will be 18 or 21 months in length, rather than 12 months.
Under the final rule, there are two components to the ACO program: the Shared Savings Program and the Advanced Payment Model.
To be eligible to participate in the Shared Savings Program, ACOs must be able to be held accountable for at least 5,000 beneficiaries a year for each of the 3 years of the agreement. Only certain parties may sponsor an ACO: physicians in group practices, individual practitioner networks, or hospitals. That list was expanded in the final rule to include collaborations between Rural Health Clinics and Federally Qualified Health Centers.
To earn shared savings, ACO participants will have to report on measures that span four quality domains: quality standards, care coordination, preventive health, and at-risk populations. The final rule substantially reduces the number of quality measures, from 65 in five domains to 33 in four domains. In the first year, ACOs that are sharing savings will be required to report only on these measures to receive payment. In the second year, they will need to meet pay-for-performance standards on 25 of the measures, growing to 32 measures in the third year.
In the proposed rule, ACOs could share savings only in the third year of the 3-year agreement. Now, they can share beginning in the first. The CMS says this will help less-experienced organizations gain know-how before they more fully participate in the program. Fuller participation would have ACOs sharing losses, as well.
The savings-only route has ACOs splitting up to 50% of the savings with the CMS. If an ACO chooses to also share losses, it will get up to 60% of the savings. Under the proposed rule, the CMS could withhold 25% of pay-for-performance bonuses, but that has been removed from the final rule.
Also, under the proposed rule, ACOs would start sharing in the savings only after they had passed a minimum threshold set by the CMS. That threshold was established to ensure that the savings weren’t just random, Dr. Berwick said. The minimum still exists under the final rule, but now, if the savings aren’t just due to a random variation in costs, the ACO can share in savings starting with the first dollar, Dr. Berwick said.
The final rule made some changes to how Medicare beneficiaries would be assigned to ACOs, noting that "determination of whether an Accountable Care Organization was responsible for coordinating care for a beneficiary will be based on whether that person received most of their primary care services from the organization."
To spur participation in the Shared Savings Program, the CMS also announced that it would make money available to physicians, hospitals, and others for major capital investments under the Advanced Payment Model.
This model will pay a portion of future savings to eligible participants. Once they begin sharing in savings, they will have to repay the money. According to the final rule, eligible ACOs will either receive an upfront, fixed payment; an upfront, variable payment; or a monthly payment of varying amount depending on of the number of Medicare beneficiaries historically attributed to the ACO. More information on eligibility and requirements is at the agency’s innovation centers website.
Simultaneously with the announcement of the final rule, several federal agencies issued additional guidance on how ACOs could steer clear of violating antitrust laws and other measures designed to keep medicine competitive.
The HHS Office of Inspector General also issued an interim final rule on how the ACOs could stay within the antikickback rules.
In the proposed rule, ACOs were required to seek antitrust review from the Federal Trade Commission and the Department of Justice. The final rule lifts that requirement, and instead advises potential ACOs to seek review. Those two agencies issued a final policy statement outlining enforcement plans and indicating that voluntary reviews would likely take about 90 days.
In true bureaucratic style our government has issued a 696- page document to tell us how to create a 3-letter organization! If you are unlucky enough to be
invited into one of these money-losing propositions, I would suggest that you first hire a lawyer, second take a deep breath, and third reconsider why you still want to be a doctor!
Russell H. Samson, M.D., is a Clinical Associate Professor of Surgery (Vascular) at Florida State University Medical School, and Attending Vascular Surgeon, Sarasota Vascular Specialists.
In true bureaucratic style our government has issued a 696- page document to tell us how to create a 3-letter organization! If you are unlucky enough to be
invited into one of these money-losing propositions, I would suggest that you first hire a lawyer, second take a deep breath, and third reconsider why you still want to be a doctor!
Russell H. Samson, M.D., is a Clinical Associate Professor of Surgery (Vascular) at Florida State University Medical School, and Attending Vascular Surgeon, Sarasota Vascular Specialists.
In true bureaucratic style our government has issued a 696- page document to tell us how to create a 3-letter organization! If you are unlucky enough to be
invited into one of these money-losing propositions, I would suggest that you first hire a lawyer, second take a deep breath, and third reconsider why you still want to be a doctor!
Russell H. Samson, M.D., is a Clinical Associate Professor of Surgery (Vascular) at Florida State University Medical School, and Attending Vascular Surgeon, Sarasota Vascular Specialists.
Use of electronic health records is no longer a condition for participating in an accountable care organization, according to the Oct. 20 final rule that will govern how ACOs are constructed and how they will be paid. The change is just one of many in the long-awaited regulation.
The 696-page final rule contains many significant changes that were made in response to the 1,320 comments the agency received on its proposed rule, issued in late March and published April 7 in the Federal Register.
Many physician groups and hospitals complained about various aspects of the proposed rule. They met repeatedly with the agency, CMS Administrator Don Berwick said during a press briefing.
"Thanks to the generous input of ideas from so many Americans, we’ve been able to fine-tune and improve these rules to better meet the needs of a range of stakeholders," Dr. Berwick said.
"When folks see the rules and see the many changes, they will see that CMS listened," Jonathan Blum, CMS deputy administrator and director of the Center for Medicare, said during the briefing.
In the proposed rule, half of primary care physicians in an ACO had to meet the meaningful use criteria for EHRs by the second year of what will be 3-year contracts with the CMS. Under the final rule, EHRs will not be required, but instead be heavily weighted as a measure of quality of care.
The final rule also pushes back the program’s starting dates. Originally, the CMS envisioned a start date of January 2012 for organizations that wanted to participate.
Now, the program will be established by January 2012 with the initial agreements starting in April or July of that year. The first performance "year" will be 18 or 21 months in length, rather than 12 months.
Under the final rule, there are two components to the ACO program: the Shared Savings Program and the Advanced Payment Model.
To be eligible to participate in the Shared Savings Program, ACOs must be able to be held accountable for at least 5,000 beneficiaries a year for each of the 3 years of the agreement. Only certain parties may sponsor an ACO: physicians in group practices, individual practitioner networks, or hospitals. That list was expanded in the final rule to include collaborations between Rural Health Clinics and Federally Qualified Health Centers.
To earn shared savings, ACO participants will have to report on measures that span four quality domains: quality standards, care coordination, preventive health, and at-risk populations. The final rule substantially reduces the number of quality measures, from 65 in five domains to 33 in four domains. In the first year, ACOs that are sharing savings will be required to report only on these measures to receive payment. In the second year, they will need to meet pay-for-performance standards on 25 of the measures, growing to 32 measures in the third year.
In the proposed rule, ACOs could share savings only in the third year of the 3-year agreement. Now, they can share beginning in the first. The CMS says this will help less-experienced organizations gain know-how before they more fully participate in the program. Fuller participation would have ACOs sharing losses, as well.
The savings-only route has ACOs splitting up to 50% of the savings with the CMS. If an ACO chooses to also share losses, it will get up to 60% of the savings. Under the proposed rule, the CMS could withhold 25% of pay-for-performance bonuses, but that has been removed from the final rule.
Also, under the proposed rule, ACOs would start sharing in the savings only after they had passed a minimum threshold set by the CMS. That threshold was established to ensure that the savings weren’t just random, Dr. Berwick said. The minimum still exists under the final rule, but now, if the savings aren’t just due to a random variation in costs, the ACO can share in savings starting with the first dollar, Dr. Berwick said.
The final rule made some changes to how Medicare beneficiaries would be assigned to ACOs, noting that "determination of whether an Accountable Care Organization was responsible for coordinating care for a beneficiary will be based on whether that person received most of their primary care services from the organization."
To spur participation in the Shared Savings Program, the CMS also announced that it would make money available to physicians, hospitals, and others for major capital investments under the Advanced Payment Model.
This model will pay a portion of future savings to eligible participants. Once they begin sharing in savings, they will have to repay the money. According to the final rule, eligible ACOs will either receive an upfront, fixed payment; an upfront, variable payment; or a monthly payment of varying amount depending on of the number of Medicare beneficiaries historically attributed to the ACO. More information on eligibility and requirements is at the agency’s innovation centers website.
Simultaneously with the announcement of the final rule, several federal agencies issued additional guidance on how ACOs could steer clear of violating antitrust laws and other measures designed to keep medicine competitive.
The HHS Office of Inspector General also issued an interim final rule on how the ACOs could stay within the antikickback rules.
In the proposed rule, ACOs were required to seek antitrust review from the Federal Trade Commission and the Department of Justice. The final rule lifts that requirement, and instead advises potential ACOs to seek review. Those two agencies issued a final policy statement outlining enforcement plans and indicating that voluntary reviews would likely take about 90 days.
Use of electronic health records is no longer a condition for participating in an accountable care organization, according to the Oct. 20 final rule that will govern how ACOs are constructed and how they will be paid. The change is just one of many in the long-awaited regulation.
The 696-page final rule contains many significant changes that were made in response to the 1,320 comments the agency received on its proposed rule, issued in late March and published April 7 in the Federal Register.
Many physician groups and hospitals complained about various aspects of the proposed rule. They met repeatedly with the agency, CMS Administrator Don Berwick said during a press briefing.
"Thanks to the generous input of ideas from so many Americans, we’ve been able to fine-tune and improve these rules to better meet the needs of a range of stakeholders," Dr. Berwick said.
"When folks see the rules and see the many changes, they will see that CMS listened," Jonathan Blum, CMS deputy administrator and director of the Center for Medicare, said during the briefing.
In the proposed rule, half of primary care physicians in an ACO had to meet the meaningful use criteria for EHRs by the second year of what will be 3-year contracts with the CMS. Under the final rule, EHRs will not be required, but instead be heavily weighted as a measure of quality of care.
The final rule also pushes back the program’s starting dates. Originally, the CMS envisioned a start date of January 2012 for organizations that wanted to participate.
Now, the program will be established by January 2012 with the initial agreements starting in April or July of that year. The first performance "year" will be 18 or 21 months in length, rather than 12 months.
Under the final rule, there are two components to the ACO program: the Shared Savings Program and the Advanced Payment Model.
To be eligible to participate in the Shared Savings Program, ACOs must be able to be held accountable for at least 5,000 beneficiaries a year for each of the 3 years of the agreement. Only certain parties may sponsor an ACO: physicians in group practices, individual practitioner networks, or hospitals. That list was expanded in the final rule to include collaborations between Rural Health Clinics and Federally Qualified Health Centers.
To earn shared savings, ACO participants will have to report on measures that span four quality domains: quality standards, care coordination, preventive health, and at-risk populations. The final rule substantially reduces the number of quality measures, from 65 in five domains to 33 in four domains. In the first year, ACOs that are sharing savings will be required to report only on these measures to receive payment. In the second year, they will need to meet pay-for-performance standards on 25 of the measures, growing to 32 measures in the third year.
In the proposed rule, ACOs could share savings only in the third year of the 3-year agreement. Now, they can share beginning in the first. The CMS says this will help less-experienced organizations gain know-how before they more fully participate in the program. Fuller participation would have ACOs sharing losses, as well.
The savings-only route has ACOs splitting up to 50% of the savings with the CMS. If an ACO chooses to also share losses, it will get up to 60% of the savings. Under the proposed rule, the CMS could withhold 25% of pay-for-performance bonuses, but that has been removed from the final rule.
Also, under the proposed rule, ACOs would start sharing in the savings only after they had passed a minimum threshold set by the CMS. That threshold was established to ensure that the savings weren’t just random, Dr. Berwick said. The minimum still exists under the final rule, but now, if the savings aren’t just due to a random variation in costs, the ACO can share in savings starting with the first dollar, Dr. Berwick said.
The final rule made some changes to how Medicare beneficiaries would be assigned to ACOs, noting that "determination of whether an Accountable Care Organization was responsible for coordinating care for a beneficiary will be based on whether that person received most of their primary care services from the organization."
To spur participation in the Shared Savings Program, the CMS also announced that it would make money available to physicians, hospitals, and others for major capital investments under the Advanced Payment Model.
This model will pay a portion of future savings to eligible participants. Once they begin sharing in savings, they will have to repay the money. According to the final rule, eligible ACOs will either receive an upfront, fixed payment; an upfront, variable payment; or a monthly payment of varying amount depending on of the number of Medicare beneficiaries historically attributed to the ACO. More information on eligibility and requirements is at the agency’s innovation centers website.
Simultaneously with the announcement of the final rule, several federal agencies issued additional guidance on how ACOs could steer clear of violating antitrust laws and other measures designed to keep medicine competitive.
The HHS Office of Inspector General also issued an interim final rule on how the ACOs could stay within the antikickback rules.
In the proposed rule, ACOs were required to seek antitrust review from the Federal Trade Commission and the Department of Justice. The final rule lifts that requirement, and instead advises potential ACOs to seek review. Those two agencies issued a final policy statement outlining enforcement plans and indicating that voluntary reviews would likely take about 90 days.
Trauma CT Saves Lives - If Scans Are Read in Time
SAN FRANCISCO – With radiology assistance often taking hours, more physicians should know the basics of reading a trauma CT to identify injuries that require immediate action, Dr. Andrew D. Perron said.
"At 3 a.m., I have to know without calling someone whether I need to get moving," said Dr. Perron, an emergency physician at Maine Medical Center, Portland. It is crucial to be able to identify which diagnoses could kill a patient within an hour, so focus on detecting a handful of potentially life-threatening injuries in the head, chest, abdomen, and pelvis, he said at the Scientific Assembly of the American College of Emergency Physicians.

For trauma victims, CT scans have become almost automatic. Currently in the United States, 60-70 million CT scans are conducted each year, compared with only 3 million in 1980, Dr. Perron said. A quarter of the scans are of the head.
When reading a CT of the head, look for epidural hematoma, subdural hematoma, skull fracture, contusions, head pressure and shift, and neck injuries. An epidural hematoma will be lens shaped and does not cross the sutures. A clot will appear as bright white on the scan; if an area is on its way to clotting, it will be gray. Epidural hematomas have low mortality if the patient is treated before he or she loses consciousness.
Subdural hematomas are sickle-shaped and do cross the sutures but not the midline. Subdurals have an 80% mortality rate. Even if a neurosurgeon suctions out the clot, the brain may not recover, Dr. Perron said.
Any area of the skull can sustain a fracture, but skull fractures sometimes aren’t readily visible on plain film or CT. The give-away on imaging is if there is blood instead of air in the mastoid cells, he said.
Although brain contusions are not readily treatable, it is important to know they are there, Dr. Perron said. A contusion will appear as a high-density area on the scan. They commonly result from a sudden deceleration, as in a motor vehicle collision. CT scans can be used to show high pressure within the skull, but there is divergence in the literature about CT’s true utility for these cases, Dr. Perron said.
In the neck, look for fracture and dislocation. CT is 98% sensitive for neck fractures and is especially good for diagnosing fractures located either high or low in the neck. Vertebral body fractures are the most common and account for about a third of neck fractures. Axial views provide the most data on the state of the spinal canal, but a coronal view is easier to read if the physician is more experienced with plain x-rays.
Dislocation is most common, but easier to miss, at C5-6 and C6-7. Dislocations are usually accompanied by torn ligaments. The injury comes from a rotational deceleration in most cases. Vascular injury can occur with dislocation or subluxation, with an attendant risk for dissection. An angiogram should be considered for patients with a C1-3 fracture and subluxation or fracture of the foramen transversarium.
In the chest, the main concerns are aortic injury, pneumothorax, and hemothorax. Like contusions, aortic injuries often are caused by sudden deceleration. Most patients with an aortic injury die in the field. If they survive to the hospital and are scanned, leaking contrast material seen on imaging indicates a ruptured aorta, Dr. Perron said.
A chest x-ray can miss a small pneumothorax, but they are easy to see on CT, with a black space demonstrating where air is outside the lung. A hemothorax cannot be detected by x-ray until at least 250 cc of blood has accumulated, but CT is more sensitive for these as well.
The spleen, liver, kidneys, pancreas, and blood in the abdomen are the areas of greatest concern in abdominal trauma. When scanning the abdomen, Dr. Perron generally uses intravenous contrast because it helps identify the major blood vessels and shows active bleeding. He starts with a supine and coronal view, as axial orientations are more difficult to read.
There should never be blood visible in the middle of the spleen. The liver has more vascularity on a normal view. Lacerations are the most common injury in the liver, and lacerations to the kidneys are also often seen. CT may detect an absence of blood flow to the liver or kidney, indicating severe injury. The main issue with these organs is to be sure they are in one piece and functioning.
The sensitivity of CT is only 68% for pancreatic injuries. This pancreas can be damaged when it is compressed against the spine, which may occur in a bicycle- or sports-related impact. CT can be used to spot active bleeding; the active extravasation of IV contrast is the hallmark, but it may be subtle.
In the pelvis, fractures and other bony injuries and free fluid are the biggest concerns. Pelvic fractures, which are generally easy to see on imaging, suggest that the body sustained a large amount of force. Free fluid in the pelvis can indicate a solid organ injury, a mesenteric injury, a bowel injury, or even a preexisting condition such as ascites.
Dr. Perron reported no conflicts of interest.
SAN FRANCISCO – With radiology assistance often taking hours, more physicians should know the basics of reading a trauma CT to identify injuries that require immediate action, Dr. Andrew D. Perron said.
"At 3 a.m., I have to know without calling someone whether I need to get moving," said Dr. Perron, an emergency physician at Maine Medical Center, Portland. It is crucial to be able to identify which diagnoses could kill a patient within an hour, so focus on detecting a handful of potentially life-threatening injuries in the head, chest, abdomen, and pelvis, he said at the Scientific Assembly of the American College of Emergency Physicians.
For trauma victims, CT scans have become almost automatic. Currently in the United States, 60-70 million CT scans are conducted each year, compared with only 3 million in 1980, Dr. Perron said. A quarter of the scans are of the head.
When reading a CT of the head, look for epidural hematoma, subdural hematoma, skull fracture, contusions, head pressure and shift, and neck injuries. An epidural hematoma will be lens shaped and does not cross the sutures. A clot will appear as bright white on the scan; if an area is on its way to clotting, it will be gray. Epidural hematomas have low mortality if the patient is treated before he or she loses consciousness.
Subdural hematomas are sickle-shaped and do cross the sutures but not the midline. Subdurals have an 80% mortality rate. Even if a neurosurgeon suctions out the clot, the brain may not recover, Dr. Perron said.
Any area of the skull can sustain a fracture, but skull fractures sometimes aren’t readily visible on plain film or CT. The give-away on imaging is if there is blood instead of air in the mastoid cells, he said.
Although brain contusions are not readily treatable, it is important to know they are there, Dr. Perron said. A contusion will appear as a high-density area on the scan. They commonly result from a sudden deceleration, as in a motor vehicle collision. CT scans can be used to show high pressure within the skull, but there is divergence in the literature about CT’s true utility for these cases, Dr. Perron said.
In the neck, look for fracture and dislocation. CT is 98% sensitive for neck fractures and is especially good for diagnosing fractures located either high or low in the neck. Vertebral body fractures are the most common and account for about a third of neck fractures. Axial views provide the most data on the state of the spinal canal, but a coronal view is easier to read if the physician is more experienced with plain x-rays.
Dislocation is most common, but easier to miss, at C5-6 and C6-7. Dislocations are usually accompanied by torn ligaments. The injury comes from a rotational deceleration in most cases. Vascular injury can occur with dislocation or subluxation, with an attendant risk for dissection. An angiogram should be considered for patients with a C1-3 fracture and subluxation or fracture of the foramen transversarium.
In the chest, the main concerns are aortic injury, pneumothorax, and hemothorax. Like contusions, aortic injuries often are caused by sudden deceleration. Most patients with an aortic injury die in the field. If they survive to the hospital and are scanned, leaking contrast material seen on imaging indicates a ruptured aorta, Dr. Perron said.
A chest x-ray can miss a small pneumothorax, but they are easy to see on CT, with a black space demonstrating where air is outside the lung. A hemothorax cannot be detected by x-ray until at least 250 cc of blood has accumulated, but CT is more sensitive for these as well.
The spleen, liver, kidneys, pancreas, and blood in the abdomen are the areas of greatest concern in abdominal trauma. When scanning the abdomen, Dr. Perron generally uses intravenous contrast because it helps identify the major blood vessels and shows active bleeding. He starts with a supine and coronal view, as axial orientations are more difficult to read.
There should never be blood visible in the middle of the spleen. The liver has more vascularity on a normal view. Lacerations are the most common injury in the liver, and lacerations to the kidneys are also often seen. CT may detect an absence of blood flow to the liver or kidney, indicating severe injury. The main issue with these organs is to be sure they are in one piece and functioning.
The sensitivity of CT is only 68% for pancreatic injuries. This pancreas can be damaged when it is compressed against the spine, which may occur in a bicycle- or sports-related impact. CT can be used to spot active bleeding; the active extravasation of IV contrast is the hallmark, but it may be subtle.
In the pelvis, fractures and other bony injuries and free fluid are the biggest concerns. Pelvic fractures, which are generally easy to see on imaging, suggest that the body sustained a large amount of force. Free fluid in the pelvis can indicate a solid organ injury, a mesenteric injury, a bowel injury, or even a preexisting condition such as ascites.
Dr. Perron reported no conflicts of interest.
SAN FRANCISCO – With radiology assistance often taking hours, more physicians should know the basics of reading a trauma CT to identify injuries that require immediate action, Dr. Andrew D. Perron said.
"At 3 a.m., I have to know without calling someone whether I need to get moving," said Dr. Perron, an emergency physician at Maine Medical Center, Portland. It is crucial to be able to identify which diagnoses could kill a patient within an hour, so focus on detecting a handful of potentially life-threatening injuries in the head, chest, abdomen, and pelvis, he said at the Scientific Assembly of the American College of Emergency Physicians.
For trauma victims, CT scans have become almost automatic. Currently in the United States, 60-70 million CT scans are conducted each year, compared with only 3 million in 1980, Dr. Perron said. A quarter of the scans are of the head.
When reading a CT of the head, look for epidural hematoma, subdural hematoma, skull fracture, contusions, head pressure and shift, and neck injuries. An epidural hematoma will be lens shaped and does not cross the sutures. A clot will appear as bright white on the scan; if an area is on its way to clotting, it will be gray. Epidural hematomas have low mortality if the patient is treated before he or she loses consciousness.
Subdural hematomas are sickle-shaped and do cross the sutures but not the midline. Subdurals have an 80% mortality rate. Even if a neurosurgeon suctions out the clot, the brain may not recover, Dr. Perron said.
Any area of the skull can sustain a fracture, but skull fractures sometimes aren’t readily visible on plain film or CT. The give-away on imaging is if there is blood instead of air in the mastoid cells, he said.
Although brain contusions are not readily treatable, it is important to know they are there, Dr. Perron said. A contusion will appear as a high-density area on the scan. They commonly result from a sudden deceleration, as in a motor vehicle collision. CT scans can be used to show high pressure within the skull, but there is divergence in the literature about CT’s true utility for these cases, Dr. Perron said.
In the neck, look for fracture and dislocation. CT is 98% sensitive for neck fractures and is especially good for diagnosing fractures located either high or low in the neck. Vertebral body fractures are the most common and account for about a third of neck fractures. Axial views provide the most data on the state of the spinal canal, but a coronal view is easier to read if the physician is more experienced with plain x-rays.
Dislocation is most common, but easier to miss, at C5-6 and C6-7. Dislocations are usually accompanied by torn ligaments. The injury comes from a rotational deceleration in most cases. Vascular injury can occur with dislocation or subluxation, with an attendant risk for dissection. An angiogram should be considered for patients with a C1-3 fracture and subluxation or fracture of the foramen transversarium.
In the chest, the main concerns are aortic injury, pneumothorax, and hemothorax. Like contusions, aortic injuries often are caused by sudden deceleration. Most patients with an aortic injury die in the field. If they survive to the hospital and are scanned, leaking contrast material seen on imaging indicates a ruptured aorta, Dr. Perron said.
A chest x-ray can miss a small pneumothorax, but they are easy to see on CT, with a black space demonstrating where air is outside the lung. A hemothorax cannot be detected by x-ray until at least 250 cc of blood has accumulated, but CT is more sensitive for these as well.
The spleen, liver, kidneys, pancreas, and blood in the abdomen are the areas of greatest concern in abdominal trauma. When scanning the abdomen, Dr. Perron generally uses intravenous contrast because it helps identify the major blood vessels and shows active bleeding. He starts with a supine and coronal view, as axial orientations are more difficult to read.
There should never be blood visible in the middle of the spleen. The liver has more vascularity on a normal view. Lacerations are the most common injury in the liver, and lacerations to the kidneys are also often seen. CT may detect an absence of blood flow to the liver or kidney, indicating severe injury. The main issue with these organs is to be sure they are in one piece and functioning.
The sensitivity of CT is only 68% for pancreatic injuries. This pancreas can be damaged when it is compressed against the spine, which may occur in a bicycle- or sports-related impact. CT can be used to spot active bleeding; the active extravasation of IV contrast is the hallmark, but it may be subtle.
In the pelvis, fractures and other bony injuries and free fluid are the biggest concerns. Pelvic fractures, which are generally easy to see on imaging, suggest that the body sustained a large amount of force. Free fluid in the pelvis can indicate a solid organ injury, a mesenteric injury, a bowel injury, or even a preexisting condition such as ascites.
Dr. Perron reported no conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS