User login
Not better late ...
You all know the statistics or at least have a sense of the scope of the problem. While 85% of mothers in this country intend to breastfeed their infants exclusively for at least 3 months, only slightly more than 30% achieve this goal. Among the dozens of reasons for this unfortunate shortfall is what some experts view as inadequate support by primary care physicians and their offices. In the May 2017 Pediatrics, two members of the American Academy of Pediatrics Section on Breastfeeding offer a clinical report that hopes to remedy this situation (“The Breastfeeding-Friendly Pediatric Office Practice.” Pediatrics. 2017 May. 139[5]:e20170647). It is a document that begins with an excellent review of the background and epidemiology of breastfeeding in the United States and a survey of the current initiatives targeted at improving our dismal performance. What follows is an extensive set of 19 evidence-based recommendations for the pediatric outpatient practice that hopes to “meet or exceed the AAP recommendations.”

A large part of the problem is the failure of the point person in the office, usually the receptionist, to realize that a tearful call from a new mother who is struggling with breastfeeding is an emergency, one that demands a response in minutes … not hours. Even when the call is eventually routed to someone with a compassionate voice who will call back with the right answers, if that process takes just an hour or two, that is enough time for a mother with a screaming and hungry newborn to reach for a bottle of formula.

I urge you to read this exhaustive clinical report in Pediatrics because it is very likely you will come across some things that you can include in your office practice to make it more breastfeeding friendly. However, Even if you and your staff have the right advice, this is not a situation of “better late than never.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
You all know the statistics or at least have a sense of the scope of the problem. While 85% of mothers in this country intend to breastfeed their infants exclusively for at least 3 months, only slightly more than 30% achieve this goal. Among the dozens of reasons for this unfortunate shortfall is what some experts view as inadequate support by primary care physicians and their offices. In the May 2017 Pediatrics, two members of the American Academy of Pediatrics Section on Breastfeeding offer a clinical report that hopes to remedy this situation (“The Breastfeeding-Friendly Pediatric Office Practice.” Pediatrics. 2017 May. 139[5]:e20170647). It is a document that begins with an excellent review of the background and epidemiology of breastfeeding in the United States and a survey of the current initiatives targeted at improving our dismal performance. What follows is an extensive set of 19 evidence-based recommendations for the pediatric outpatient practice that hopes to “meet or exceed the AAP recommendations.”
A large part of the problem is the failure of the point person in the office, usually the receptionist, to realize that a tearful call from a new mother who is struggling with breastfeeding is an emergency, one that demands a response in minutes … not hours. Even when the call is eventually routed to someone with a compassionate voice who will call back with the right answers, if that process takes just an hour or two, that is enough time for a mother with a screaming and hungry newborn to reach for a bottle of formula.
I urge you to read this exhaustive clinical report in Pediatrics because it is very likely you will come across some things that you can include in your office practice to make it more breastfeeding friendly. However, Even if you and your staff have the right advice, this is not a situation of “better late than never.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
You all know the statistics or at least have a sense of the scope of the problem. While 85% of mothers in this country intend to breastfeed their infants exclusively for at least 3 months, only slightly more than 30% achieve this goal. Among the dozens of reasons for this unfortunate shortfall is what some experts view as inadequate support by primary care physicians and their offices. In the May 2017 Pediatrics, two members of the American Academy of Pediatrics Section on Breastfeeding offer a clinical report that hopes to remedy this situation (“The Breastfeeding-Friendly Pediatric Office Practice.” Pediatrics. 2017 May. 139[5]:e20170647). It is a document that begins with an excellent review of the background and epidemiology of breastfeeding in the United States and a survey of the current initiatives targeted at improving our dismal performance. What follows is an extensive set of 19 evidence-based recommendations for the pediatric outpatient practice that hopes to “meet or exceed the AAP recommendations.”
A large part of the problem is the failure of the point person in the office, usually the receptionist, to realize that a tearful call from a new mother who is struggling with breastfeeding is an emergency, one that demands a response in minutes … not hours. Even when the call is eventually routed to someone with a compassionate voice who will call back with the right answers, if that process takes just an hour or two, that is enough time for a mother with a screaming and hungry newborn to reach for a bottle of formula.
I urge you to read this exhaustive clinical report in Pediatrics because it is very likely you will come across some things that you can include in your office practice to make it more breastfeeding friendly. However, Even if you and your staff have the right advice, this is not a situation of “better late than never.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Pulmonary Perspectives® China’s Pulmonary Crisis
Over the past 2 years, we had the opportunity to participate in an annual cross-cultural exchange that has broadened our horizons. Xi’an, the ancient capital of China and home of the Terracotta warriors, is a sprawling megapolis similar to Los Angeles. In the southern suburb of Huxian, US trained pulmonary, neurosurgical, and critical care physicians from Cooper University Hospital and Morehouse School of Medicine partnered with physicians of Ji-Ren Teaching Hospital to deliver a Chinese Medical Association accredited continuing medical education conference. The conference agenda included a variety of pulmonary and critical care topics highlighting sepsis, neurovascular disease, and lung cancer screening and diagnosis. We also provided a hands-on workshop for point of care ultrasound, and, in return, received education about Chinese medicine.
We found our hosts appreciative and hospitable, and they treated us with the highest level of respect (the cornerstone of Chinese culture). The audience was receptive and very interested in learning. However, while we were impressed with their rapid growth and interest in incorporating western medicine into their daily practice, it was impossible to overlook the major pulmonary health-care concerns threatening their communities. Tobacco use was omnipresent, and the haze of air pollution made the sky a constant shade of grey. In both public and private spaces, powerful echoes of a once familiar America resonated, and they served to underscore the obstacles the Chinese medical community now faces in caring for their country’s pulmonary health.
An Old, Familiar Foe
The China National Tobacco Corporation (CNTC) is the largest tobacco company in the world, as well as China’s most profitable state-owned enterprise (Pratt, A, et al. WHO Report. 2017. ISBN 9789290617907 [http://www.wpro.who.int/china/publications/2017_china_tobacco_control_report_en_web_final.pdf?ua=1]). As such, the CNTC controls every aspect of its production and supply chain with the force of the federal government and also exerts heavy influence over regulatory policy. It controls about 98% of domestic crop production and manages to price cigarettes just short of one American dollar per pack, yet contributes about $170 billion annually to the government (Rich, et al. Nicotine Tob Res. 2012;14[3]:258). This accounted for nearly 7% of total governmental revenue in 2015 (Pratt, 2017).
To date, nearly 44% of the world’s cigarettes are manufactured and consumed in China (Pratt 2017, Rich 2012). In 2015, more than 315 million Chinese adults were daily smokers, or about 28% of the adult population and nearly half of all men (Pratt, 2017). This is about double the proportion of US smokers (about 15.1%) and more than eight times the 36.5 million daily smokers in the United States (CDC Online Tobacco Use Report, 2016 [https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/]). However, to visit China is not only to know a love for tobacco, but also an overwhelming guest and gift culture. Gift giving and hospitality is central to the Chinese identity, from business meetings to afternoon tea. Given their economy and such rich supply, people gift cigarettes to one another at all times for nearly any occasion. Unfortunately, tobacco smoke in China is as inescapable as its health consequences.
The direct effects of smoking on China’s pulmonary health have been catastrophic. Cancers of the lung and bronchus constitute their most common malignancy across both sexes, accounting for the majority of the annual 4.3 million new cancer diagnoses (Chen et al. CA Cancer J Clin. 2016;66[2]:115). In Chinese men, lung cancer is the second most common cancer before the age of 60, and over the age of 75, it is the most common malignancy and also accounts for the majority of that group’s cancer mortality. Women fare only slightly better, with breast cancer being their most common malignancy, but with lung cancer remaining the most pervasive across all age groups, and, by far, the most deadly (Chen, 2016). All told, of the projected 2.8 million cancer deaths occurring in 2015 in China, 21% were directly a result of lung cancer.
Likewise, COPD also threatens China. The Global Burden of Disease study conducted in 2004 demonstrated that nearly 3 million people die of COPD each year. Chinese adults over the age of 40 had an overall prevalence of COPD of 9% for the last decade, though this may be higher given the high rate of underdiagnosis in rural China (Fang X, et al. Chest. 2011;139[4]:920). After 2004, the Chinese Ministry of Health affirmed that COPD was the fourth leading cause of mortality in urban areas, but third in rural ones (Fang, 2011). When investigators analyzed deaths secondary to cor pulmonale coexisting with COPD, they found COPD-related mortality increased to 179.9 for men and 141.3 for women per 100,000 persons, which is about double the COPD mortality for other countries in the Asian-Pacific region (Reilly K, et al. Am J Epidemiol. 2008;167[8]:998).

Both cancer and COPD in China disproportionately affect those in rural areas and with lower socioeconomic status, with smoking being the most potent causative exposure. On average, the annual direct and indirect per-patient cost of treating COPD amounted to about $2,000, comprising about 40% of a family’s total annual income (Fang, 2011). The cost of treating malignancy is even more expensive, but the higher likelihood of death results in an additional 10% to 20% reduction of family income when a working family member dies (Pratt, 2016). Taken together, and especially since rural Chinese citizens spend close to 20% of their income on tobacco products, the pulmonary health consequences of smoking are a significant driver of both health and economic inequality.
The Air We Breathe
Air pollution comprises a second pulmonary insult to China’s health. The International Agency for Research on Cancer designated particulate matter (PM) as a class I carcinogen (Kurt O, et al. Curr Opin Pulm Med. 2016;22[2]:138). PM forms from combustion of bio-mass fuel, as well as from dust storms or construction. Once particulates are smaller than 2.5 microns (PM2.5), they cause substantial harm to the pulmonary microenvironment. Guo and colleagues demonstrated markedly increased lung cancer risks associated with spatial mapping of ozone and PM2.5 concentrations (Guo Y, et al. Environ Res. 2016;144;60). PM2.5 also doubles the odds of contracting COPD in nonsmoking adults, conferring as much as a three-fold risk of contracting the disease in nonsmoking women (Fang, 2011).
Apart from causing pulmonary disease, studies also implicate air pollution as frequently causing exacerbations of existing disease. One study found an incremental increase in ED visits for respiratory illnesses for every 10 µg/m3 above the median PM2.5 level (Xu, et al. PLoS One. 2016;11(4): e0153099). In 2013, 83% of Chinese lived in places where PM2.5 levels exceeded China’s own ambient air standard. In this cohort, elevated PM2.5 levels contributed directly to 300,000 premature deaths from lung cancer and COPD, with PM2.5 causing 1.2 million premature deaths overall (Liu J, et al. Sci Total Environ. 2016;568;1253).
Moving Forward
The Chinese have few illusions about these pulmonary concerns, and they are making progress. The government recently introduced stricter smoking controls in Beijing and Shanghai and continues to explore ways to decrease emissions. President Xi has put forward strong initiatives to improve the health of the Chinese. However, the nation is trying to balance its national priorities in the context of a fluid, and, at times, perilous geopolitical climate. In some ways, their position is not too dissimilar from the US geopolitical and health-care situation of the 1970s. While challenging, the issue of Chinese health care should not overshadow the remarkable resources or the truly remarkable culture of their people. Friendship, cooperation, the reduction of suffering: these are ideals where all clinicians find common ground, regardless of nationality.
Dr. Mackay is Chief Fellow of Critical Care Medicine, Cooper University Hospital, Cooper Medical School of Rowan University, Camden, New Jersey; Dr. Flenaugh is Associate Professor of Medicine, Division Chief of Pulmonary and Critical Care Medicine, Director of Advance Diagnostic and Interventional Pulmonary, Morehouse School of Medicine, Atlanta, Georgia.
Editor’s Note
This excellent, up-close Pulmonary Perspective details observations of Drs. Mackay and Flenaugh as they have participated in cross-cultural exchanges in
The American College of Chest Physicians, likewise concerned about pulmonary health in China, has approached the problem on a different front, working closely with partners, such as the Chinese Thoracic Society, the Chinese Association of Chest Physicians, and the Chinese Medical Doctor Association, to implement China’s first ever fellowship program offering standardized training in PCCM for Chinese physicians. Read more at http://www.mdedge.com/chestphysician/article/131179/society-news/pccm-endorsed-pilot-subspecialty-chinese-national-health.
Nitin Puri, MD, FCCP, is the section editor of Pulmonary Perspectives.
Over the past 2 years, we had the opportunity to participate in an annual cross-cultural exchange that has broadened our horizons. Xi’an, the ancient capital of China and home of the Terracotta warriors, is a sprawling megapolis similar to Los Angeles. In the southern suburb of Huxian, US trained pulmonary, neurosurgical, and critical care physicians from Cooper University Hospital and Morehouse School of Medicine partnered with physicians of Ji-Ren Teaching Hospital to deliver a Chinese Medical Association accredited continuing medical education conference. The conference agenda included a variety of pulmonary and critical care topics highlighting sepsis, neurovascular disease, and lung cancer screening and diagnosis. We also provided a hands-on workshop for point of care ultrasound, and, in return, received education about Chinese medicine.
We found our hosts appreciative and hospitable, and they treated us with the highest level of respect (the cornerstone of Chinese culture). The audience was receptive and very interested in learning. However, while we were impressed with their rapid growth and interest in incorporating western medicine into their daily practice, it was impossible to overlook the major pulmonary health-care concerns threatening their communities. Tobacco use was omnipresent, and the haze of air pollution made the sky a constant shade of grey. In both public and private spaces, powerful echoes of a once familiar America resonated, and they served to underscore the obstacles the Chinese medical community now faces in caring for their country’s pulmonary health.
An Old, Familiar Foe
The China National Tobacco Corporation (CNTC) is the largest tobacco company in the world, as well as China’s most profitable state-owned enterprise (Pratt, A, et al. WHO Report. 2017. ISBN 9789290617907 [http://www.wpro.who.int/china/publications/2017_china_tobacco_control_report_en_web_final.pdf?ua=1]). As such, the CNTC controls every aspect of its production and supply chain with the force of the federal government and also exerts heavy influence over regulatory policy. It controls about 98% of domestic crop production and manages to price cigarettes just short of one American dollar per pack, yet contributes about $170 billion annually to the government (Rich, et al. Nicotine Tob Res. 2012;14[3]:258). This accounted for nearly 7% of total governmental revenue in 2015 (Pratt, 2017).
To date, nearly 44% of the world’s cigarettes are manufactured and consumed in China (Pratt 2017, Rich 2012). In 2015, more than 315 million Chinese adults were daily smokers, or about 28% of the adult population and nearly half of all men (Pratt, 2017). This is about double the proportion of US smokers (about 15.1%) and more than eight times the 36.5 million daily smokers in the United States (CDC Online Tobacco Use Report, 2016 [https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/]). However, to visit China is not only to know a love for tobacco, but also an overwhelming guest and gift culture. Gift giving and hospitality is central to the Chinese identity, from business meetings to afternoon tea. Given their economy and such rich supply, people gift cigarettes to one another at all times for nearly any occasion. Unfortunately, tobacco smoke in China is as inescapable as its health consequences.
The direct effects of smoking on China’s pulmonary health have been catastrophic. Cancers of the lung and bronchus constitute their most common malignancy across both sexes, accounting for the majority of the annual 4.3 million new cancer diagnoses (Chen et al. CA Cancer J Clin. 2016;66[2]:115). In Chinese men, lung cancer is the second most common cancer before the age of 60, and over the age of 75, it is the most common malignancy and also accounts for the majority of that group’s cancer mortality. Women fare only slightly better, with breast cancer being their most common malignancy, but with lung cancer remaining the most pervasive across all age groups, and, by far, the most deadly (Chen, 2016). All told, of the projected 2.8 million cancer deaths occurring in 2015 in China, 21% were directly a result of lung cancer.
Likewise, COPD also threatens China. The Global Burden of Disease study conducted in 2004 demonstrated that nearly 3 million people die of COPD each year. Chinese adults over the age of 40 had an overall prevalence of COPD of 9% for the last decade, though this may be higher given the high rate of underdiagnosis in rural China (Fang X, et al. Chest. 2011;139[4]:920). After 2004, the Chinese Ministry of Health affirmed that COPD was the fourth leading cause of mortality in urban areas, but third in rural ones (Fang, 2011). When investigators analyzed deaths secondary to cor pulmonale coexisting with COPD, they found COPD-related mortality increased to 179.9 for men and 141.3 for women per 100,000 persons, which is about double the COPD mortality for other countries in the Asian-Pacific region (Reilly K, et al. Am J Epidemiol. 2008;167[8]:998).
Both cancer and COPD in China disproportionately affect those in rural areas and with lower socioeconomic status, with smoking being the most potent causative exposure. On average, the annual direct and indirect per-patient cost of treating COPD amounted to about $2,000, comprising about 40% of a family’s total annual income (Fang, 2011). The cost of treating malignancy is even more expensive, but the higher likelihood of death results in an additional 10% to 20% reduction of family income when a working family member dies (Pratt, 2016). Taken together, and especially since rural Chinese citizens spend close to 20% of their income on tobacco products, the pulmonary health consequences of smoking are a significant driver of both health and economic inequality.
The Air We Breathe
Air pollution comprises a second pulmonary insult to China’s health. The International Agency for Research on Cancer designated particulate matter (PM) as a class I carcinogen (Kurt O, et al. Curr Opin Pulm Med. 2016;22[2]:138). PM forms from combustion of bio-mass fuel, as well as from dust storms or construction. Once particulates are smaller than 2.5 microns (PM2.5), they cause substantial harm to the pulmonary microenvironment. Guo and colleagues demonstrated markedly increased lung cancer risks associated with spatial mapping of ozone and PM2.5 concentrations (Guo Y, et al. Environ Res. 2016;144;60). PM2.5 also doubles the odds of contracting COPD in nonsmoking adults, conferring as much as a three-fold risk of contracting the disease in nonsmoking women (Fang, 2011).
Apart from causing pulmonary disease, studies also implicate air pollution as frequently causing exacerbations of existing disease. One study found an incremental increase in ED visits for respiratory illnesses for every 10 µg/m3 above the median PM2.5 level (Xu, et al. PLoS One. 2016;11(4): e0153099). In 2013, 83% of Chinese lived in places where PM2.5 levels exceeded China’s own ambient air standard. In this cohort, elevated PM2.5 levels contributed directly to 300,000 premature deaths from lung cancer and COPD, with PM2.5 causing 1.2 million premature deaths overall (Liu J, et al. Sci Total Environ. 2016;568;1253).
Moving Forward
The Chinese have few illusions about these pulmonary concerns, and they are making progress. The government recently introduced stricter smoking controls in Beijing and Shanghai and continues to explore ways to decrease emissions. President Xi has put forward strong initiatives to improve the health of the Chinese. However, the nation is trying to balance its national priorities in the context of a fluid, and, at times, perilous geopolitical climate. In some ways, their position is not too dissimilar from the US geopolitical and health-care situation of the 1970s. While challenging, the issue of Chinese health care should not overshadow the remarkable resources or the truly remarkable culture of their people. Friendship, cooperation, the reduction of suffering: these are ideals where all clinicians find common ground, regardless of nationality.
Dr. Mackay is Chief Fellow of Critical Care Medicine, Cooper University Hospital, Cooper Medical School of Rowan University, Camden, New Jersey; Dr. Flenaugh is Associate Professor of Medicine, Division Chief of Pulmonary and Critical Care Medicine, Director of Advance Diagnostic and Interventional Pulmonary, Morehouse School of Medicine, Atlanta, Georgia.
Editor’s Note
This excellent, up-close Pulmonary Perspective details observations of Drs. Mackay and Flenaugh as they have participated in cross-cultural exchanges in
The American College of Chest Physicians, likewise concerned about pulmonary health in China, has approached the problem on a different front, working closely with partners, such as the Chinese Thoracic Society, the Chinese Association of Chest Physicians, and the Chinese Medical Doctor Association, to implement China’s first ever fellowship program offering standardized training in PCCM for Chinese physicians. Read more at http://www.mdedge.com/chestphysician/article/131179/society-news/pccm-endorsed-pilot-subspecialty-chinese-national-health.
Nitin Puri, MD, FCCP, is the section editor of Pulmonary Perspectives.
Over the past 2 years, we had the opportunity to participate in an annual cross-cultural exchange that has broadened our horizons. Xi’an, the ancient capital of China and home of the Terracotta warriors, is a sprawling megapolis similar to Los Angeles. In the southern suburb of Huxian, US trained pulmonary, neurosurgical, and critical care physicians from Cooper University Hospital and Morehouse School of Medicine partnered with physicians of Ji-Ren Teaching Hospital to deliver a Chinese Medical Association accredited continuing medical education conference. The conference agenda included a variety of pulmonary and critical care topics highlighting sepsis, neurovascular disease, and lung cancer screening and diagnosis. We also provided a hands-on workshop for point of care ultrasound, and, in return, received education about Chinese medicine.
We found our hosts appreciative and hospitable, and they treated us with the highest level of respect (the cornerstone of Chinese culture). The audience was receptive and very interested in learning. However, while we were impressed with their rapid growth and interest in incorporating western medicine into their daily practice, it was impossible to overlook the major pulmonary health-care concerns threatening their communities. Tobacco use was omnipresent, and the haze of air pollution made the sky a constant shade of grey. In both public and private spaces, powerful echoes of a once familiar America resonated, and they served to underscore the obstacles the Chinese medical community now faces in caring for their country’s pulmonary health.
An Old, Familiar Foe
The China National Tobacco Corporation (CNTC) is the largest tobacco company in the world, as well as China’s most profitable state-owned enterprise (Pratt, A, et al. WHO Report. 2017. ISBN 9789290617907 [http://www.wpro.who.int/china/publications/2017_china_tobacco_control_report_en_web_final.pdf?ua=1]). As such, the CNTC controls every aspect of its production and supply chain with the force of the federal government and also exerts heavy influence over regulatory policy. It controls about 98% of domestic crop production and manages to price cigarettes just short of one American dollar per pack, yet contributes about $170 billion annually to the government (Rich, et al. Nicotine Tob Res. 2012;14[3]:258). This accounted for nearly 7% of total governmental revenue in 2015 (Pratt, 2017).
To date, nearly 44% of the world’s cigarettes are manufactured and consumed in China (Pratt 2017, Rich 2012). In 2015, more than 315 million Chinese adults were daily smokers, or about 28% of the adult population and nearly half of all men (Pratt, 2017). This is about double the proportion of US smokers (about 15.1%) and more than eight times the 36.5 million daily smokers in the United States (CDC Online Tobacco Use Report, 2016 [https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/]). However, to visit China is not only to know a love for tobacco, but also an overwhelming guest and gift culture. Gift giving and hospitality is central to the Chinese identity, from business meetings to afternoon tea. Given their economy and such rich supply, people gift cigarettes to one another at all times for nearly any occasion. Unfortunately, tobacco smoke in China is as inescapable as its health consequences.
The direct effects of smoking on China’s pulmonary health have been catastrophic. Cancers of the lung and bronchus constitute their most common malignancy across both sexes, accounting for the majority of the annual 4.3 million new cancer diagnoses (Chen et al. CA Cancer J Clin. 2016;66[2]:115). In Chinese men, lung cancer is the second most common cancer before the age of 60, and over the age of 75, it is the most common malignancy and also accounts for the majority of that group’s cancer mortality. Women fare only slightly better, with breast cancer being their most common malignancy, but with lung cancer remaining the most pervasive across all age groups, and, by far, the most deadly (Chen, 2016). All told, of the projected 2.8 million cancer deaths occurring in 2015 in China, 21% were directly a result of lung cancer.
Likewise, COPD also threatens China. The Global Burden of Disease study conducted in 2004 demonstrated that nearly 3 million people die of COPD each year. Chinese adults over the age of 40 had an overall prevalence of COPD of 9% for the last decade, though this may be higher given the high rate of underdiagnosis in rural China (Fang X, et al. Chest. 2011;139[4]:920). After 2004, the Chinese Ministry of Health affirmed that COPD was the fourth leading cause of mortality in urban areas, but third in rural ones (Fang, 2011). When investigators analyzed deaths secondary to cor pulmonale coexisting with COPD, they found COPD-related mortality increased to 179.9 for men and 141.3 for women per 100,000 persons, which is about double the COPD mortality for other countries in the Asian-Pacific region (Reilly K, et al. Am J Epidemiol. 2008;167[8]:998).
Both cancer and COPD in China disproportionately affect those in rural areas and with lower socioeconomic status, with smoking being the most potent causative exposure. On average, the annual direct and indirect per-patient cost of treating COPD amounted to about $2,000, comprising about 40% of a family’s total annual income (Fang, 2011). The cost of treating malignancy is even more expensive, but the higher likelihood of death results in an additional 10% to 20% reduction of family income when a working family member dies (Pratt, 2016). Taken together, and especially since rural Chinese citizens spend close to 20% of their income on tobacco products, the pulmonary health consequences of smoking are a significant driver of both health and economic inequality.
The Air We Breathe
Air pollution comprises a second pulmonary insult to China’s health. The International Agency for Research on Cancer designated particulate matter (PM) as a class I carcinogen (Kurt O, et al. Curr Opin Pulm Med. 2016;22[2]:138). PM forms from combustion of bio-mass fuel, as well as from dust storms or construction. Once particulates are smaller than 2.5 microns (PM2.5), they cause substantial harm to the pulmonary microenvironment. Guo and colleagues demonstrated markedly increased lung cancer risks associated with spatial mapping of ozone and PM2.5 concentrations (Guo Y, et al. Environ Res. 2016;144;60). PM2.5 also doubles the odds of contracting COPD in nonsmoking adults, conferring as much as a three-fold risk of contracting the disease in nonsmoking women (Fang, 2011).
Apart from causing pulmonary disease, studies also implicate air pollution as frequently causing exacerbations of existing disease. One study found an incremental increase in ED visits for respiratory illnesses for every 10 µg/m3 above the median PM2.5 level (Xu, et al. PLoS One. 2016;11(4): e0153099). In 2013, 83% of Chinese lived in places where PM2.5 levels exceeded China’s own ambient air standard. In this cohort, elevated PM2.5 levels contributed directly to 300,000 premature deaths from lung cancer and COPD, with PM2.5 causing 1.2 million premature deaths overall (Liu J, et al. Sci Total Environ. 2016;568;1253).
Moving Forward
The Chinese have few illusions about these pulmonary concerns, and they are making progress. The government recently introduced stricter smoking controls in Beijing and Shanghai and continues to explore ways to decrease emissions. President Xi has put forward strong initiatives to improve the health of the Chinese. However, the nation is trying to balance its national priorities in the context of a fluid, and, at times, perilous geopolitical climate. In some ways, their position is not too dissimilar from the US geopolitical and health-care situation of the 1970s. While challenging, the issue of Chinese health care should not overshadow the remarkable resources or the truly remarkable culture of their people. Friendship, cooperation, the reduction of suffering: these are ideals where all clinicians find common ground, regardless of nationality.
Dr. Mackay is Chief Fellow of Critical Care Medicine, Cooper University Hospital, Cooper Medical School of Rowan University, Camden, New Jersey; Dr. Flenaugh is Associate Professor of Medicine, Division Chief of Pulmonary and Critical Care Medicine, Director of Advance Diagnostic and Interventional Pulmonary, Morehouse School of Medicine, Atlanta, Georgia.
Editor’s Note
This excellent, up-close Pulmonary Perspective details observations of Drs. Mackay and Flenaugh as they have participated in cross-cultural exchanges in
The American College of Chest Physicians, likewise concerned about pulmonary health in China, has approached the problem on a different front, working closely with partners, such as the Chinese Thoracic Society, the Chinese Association of Chest Physicians, and the Chinese Medical Doctor Association, to implement China’s first ever fellowship program offering standardized training in PCCM for Chinese physicians. Read more at http://www.mdedge.com/chestphysician/article/131179/society-news/pccm-endorsed-pilot-subspecialty-chinese-national-health.
Nitin Puri, MD, FCCP, is the section editor of Pulmonary Perspectives.
CHEST NetWorks Submassive PE, antibiotic resistance, advanced practice providers
Cardiovascular Medicine and Surgery
Catch 22 of Submassive Pulmonary Emboli
Venous thromboembolism (including deep vein thrombosis (DVT) and pulmonary embolism [PE]) occurs in approximately 1 per 1,000 patients (Piran S, Schulman S. Thromb J. 2016;14[S1]:23) and can be fatal. Pulmonary embolus severity is classified as low risk, intermediate-risk/submassive PE, and massive PE. There is significant controversy about the management of submassive PE, which is defined as PE with right-sided heart strain (elevated troponin or B-type natriuretic peptide, right-axis deviation on ECG, or e

David J. Nagel, MD
Steering Committee Member
Olivier Axler, MD, FCCP
Vice-Chair
Chest Infections
Antibiotic Resistance
One-hundred years ago, infectious diseases caused 5 of the 10 most common causes of deaths in the United States. In 2016, only one infection remained on this list (influenza/pneumonia) (MMWR Morb Mortal Wkly Rep. 2017;66:413).
How medicine has improved with antibiotics. An unfortunate and unintended consequence of widespread antibiotic use has been the progressive resistance to these drugs. It is estimated that, if current trends continue, 10 million lives a year will be at risk from resistant organisms by 2050 (O’Neill, J. (2016). https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf).
Pathogens acquire antibiotic resistance by passing genetic material to one another through plasmids, bacteriophages, or naked DNA. Once acquired, resistance manifests via a number of mechanisms under the stress imposed by antibiotics (Levy SB, et al. Nat Med. 2004;10:S122).
Among the best studied is enzymatic degradation of the antibiotic. This occurs when beta-lactamases degrade penicillin. A second mechanism alters cell transport, thereby blocking cell entry or actively ejecting the antibiotic from the cell. Finally, overexpression or alteration of the antibiotic target may render a drug ineffective at inhibiting any vital cell function.
At the pace with which resistance now develops, the medical community faces a crisis, whereby infections caused by evolving superbugs are no longer effectively controlled by the available menu of antimicrobial agents.
This challenge must be met collectively by the more prudent prescribing of antibiotics, potentially with the help of rapid diagnostics; isolation of patients potentially infected with resistant organisms; and a focus on developing newer drugs that defy known resistant mechanisms.
Marc Feinstein, MD, FCCP
Steering Committee Member
Clinical Pulmonary Medicine
COPD and sleep-disordered breathing; A missing comorbid condition
Subjective, as well as objective, sleep complaints are common in patients with COPD (Krachman S, et al. Proc Am Thorac Soc. 2008;5[4]:536), and sleeping difficulties are ranked the third most frequent complaint (behind dyspnea and fatigue) in patients with COPD (Kinsman RA, et al. Chest. 1983;83[5]:755). Also, sleep quality is poor, and patients with moderate to severe COPD may have higher-than-expected incidence of OSA (Soler X, et al. Ann Am Thorac Soc. 2015;12[8]:1219).
Unfortunately, sleep is usually not assessed during a COPD evaluation. Up to 27% of patients with COPD without hypoxia during wakefulness can experience important desaturation during sleep, so called nocturnal oxygen desaturation (NOD) (Fletcher EC, et al. Chest. 1987;92[4]:604), that may lead to pulmonary hypertension (Chaouat A, et a

Although identification and effective treatment of COPD comorbidities are becoming the cornerstone of COPD management, sleep-disordered breathing has not been identified in current guidelines yet as a true potential contributor in poor outcomes despite emergent clinical evidence. Multidisciplinary programs, such as pulmonary rehabilitation, that improve dyspnea, exercise capacity, and quality of life may also positively impact sleep (Soler X, et al. COPD. 2013;10[2]:156). Because of the background of the staff involved, the comprehensive approach to patient assessment, and access to number of COPD subjects, pulmonary rehabilitation may be an optimal opportunity to assess sleep and identify an important comorbid condition often overlooked in patients with more advanced COPD.
Xavier Soler, MD, PhD
Steering Committee Member
Interprofessional Team
Finding Home
Outside our internal medicine curriculum, there is no formal pulmonary training or post-masters fellowship in pulmonary medicine for Advanced Practice Providers (APPs). Because of this, APPs are left to their own devices to fill educational gaps. To perform at the level expected by the physicians I work for, journal reviews and memorizing guidelines were not going to be enough. Since there is no formal pulmonary APP society, there were no peers to reach out to either. Off to conferences I went.

At first, I found CHEST daunting. After all, it’s run by the American College of Chest “Physicians,” not Nurse Practitioners. I spent most of the first day with my nametag turned around worried I’d be found out as a nonphysician attendee who snuck in. And then the unthinkable happened, I ran into another unicorn—another APP seeking the same information, only her nametag was turned the right way. The best advice she gave was to attend the Interprofessional NetWork meeting. This was ground zero of the conference as far as I was concerned. There I found myself surrounded by RTs, RNs, NPs, PAs, and yes, even physicians.
Over the years, as I’ve gotten further involved with CHEST NetWorks, I have found from top to bottom CHEST striving to incorporate APPs and advance our education. From including us in the FCCP program, reducing conference pricing for APPs, and focusing this year’s conference theme around being team focused, CHEST is creating a home for APPs.
Corinne Preston Young, FNP, FCCP
Steering Committee Member
Cardiovascular Medicine and Surgery
Catch 22 of Submassive Pulmonary Emboli
Venous thromboembolism (including deep vein thrombosis (DVT) and pulmonary embolism [PE]) occurs in approximately 1 per 1,000 patients (Piran S, Schulman S. Thromb J. 2016;14[S1]:23) and can be fatal. Pulmonary embolus severity is classified as low risk, intermediate-risk/submassive PE, and massive PE. There is significant controversy about the management of submassive PE, which is defined as PE with right-sided heart strain (elevated troponin or B-type natriuretic peptide, right-axis deviation on ECG, or e
David J. Nagel, MD
Steering Committee Member
Olivier Axler, MD, FCCP
Vice-Chair
Chest Infections
Antibiotic Resistance
One-hundred years ago, infectious diseases caused 5 of the 10 most common causes of deaths in the United States. In 2016, only one infection remained on this list (influenza/pneumonia) (MMWR Morb Mortal Wkly Rep. 2017;66:413).
How medicine has improved with antibiotics. An unfortunate and unintended consequence of widespread antibiotic use has been the progressive resistance to these drugs. It is estimated that, if current trends continue, 10 million lives a year will be at risk from resistant organisms by 2050 (O’Neill, J. (2016). https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf).
Pathogens acquire antibiotic resistance by passing genetic material to one another through plasmids, bacteriophages, or naked DNA. Once acquired, resistance manifests via a number of mechanisms under the stress imposed by antibiotics (Levy SB, et al. Nat Med. 2004;10:S122).
Among the best studied is enzymatic degradation of the antibiotic. This occurs when beta-lactamases degrade penicillin. A second mechanism alters cell transport, thereby blocking cell entry or actively ejecting the antibiotic from the cell. Finally, overexpression or alteration of the antibiotic target may render a drug ineffective at inhibiting any vital cell function.
At the pace with which resistance now develops, the medical community faces a crisis, whereby infections caused by evolving superbugs are no longer effectively controlled by the available menu of antimicrobial agents.
This challenge must be met collectively by the more prudent prescribing of antibiotics, potentially with the help of rapid diagnostics; isolation of patients potentially infected with resistant organisms; and a focus on developing newer drugs that defy known resistant mechanisms.
Marc Feinstein, MD, FCCP
Steering Committee Member
Clinical Pulmonary Medicine
COPD and sleep-disordered breathing; A missing comorbid condition
Subjective, as well as objective, sleep complaints are common in patients with COPD (Krachman S, et al. Proc Am Thorac Soc. 2008;5[4]:536), and sleeping difficulties are ranked the third most frequent complaint (behind dyspnea and fatigue) in patients with COPD (Kinsman RA, et al. Chest. 1983;83[5]:755). Also, sleep quality is poor, and patients with moderate to severe COPD may have higher-than-expected incidence of OSA (Soler X, et al. Ann Am Thorac Soc. 2015;12[8]:1219).
Unfortunately, sleep is usually not assessed during a COPD evaluation. Up to 27% of patients with COPD without hypoxia during wakefulness can experience important desaturation during sleep, so called nocturnal oxygen desaturation (NOD) (Fletcher EC, et al. Chest. 1987;92[4]:604), that may lead to pulmonary hypertension (Chaouat A, et a
Although identification and effective treatment of COPD comorbidities are becoming the cornerstone of COPD management, sleep-disordered breathing has not been identified in current guidelines yet as a true potential contributor in poor outcomes despite emergent clinical evidence. Multidisciplinary programs, such as pulmonary rehabilitation, that improve dyspnea, exercise capacity, and quality of life may also positively impact sleep (Soler X, et al. COPD. 2013;10[2]:156). Because of the background of the staff involved, the comprehensive approach to patient assessment, and access to number of COPD subjects, pulmonary rehabilitation may be an optimal opportunity to assess sleep and identify an important comorbid condition often overlooked in patients with more advanced COPD.
Xavier Soler, MD, PhD
Steering Committee Member
Interprofessional Team
Finding Home
Outside our internal medicine curriculum, there is no formal pulmonary training or post-masters fellowship in pulmonary medicine for Advanced Practice Providers (APPs). Because of this, APPs are left to their own devices to fill educational gaps. To perform at the level expected by the physicians I work for, journal reviews and memorizing guidelines were not going to be enough. Since there is no formal pulmonary APP society, there were no peers to reach out to either. Off to conferences I went.
At first, I found CHEST daunting. After all, it’s run by the American College of Chest “Physicians,” not Nurse Practitioners. I spent most of the first day with my nametag turned around worried I’d be found out as a nonphysician attendee who snuck in. And then the unthinkable happened, I ran into another unicorn—another APP seeking the same information, only her nametag was turned the right way. The best advice she gave was to attend the Interprofessional NetWork meeting. This was ground zero of the conference as far as I was concerned. There I found myself surrounded by RTs, RNs, NPs, PAs, and yes, even physicians.
Over the years, as I’ve gotten further involved with CHEST NetWorks, I have found from top to bottom CHEST striving to incorporate APPs and advance our education. From including us in the FCCP program, reducing conference pricing for APPs, and focusing this year’s conference theme around being team focused, CHEST is creating a home for APPs.
Corinne Preston Young, FNP, FCCP
Steering Committee Member
Cardiovascular Medicine and Surgery
Catch 22 of Submassive Pulmonary Emboli
Venous thromboembolism (including deep vein thrombosis (DVT) and pulmonary embolism [PE]) occurs in approximately 1 per 1,000 patients (Piran S, Schulman S. Thromb J. 2016;14[S1]:23) and can be fatal. Pulmonary embolus severity is classified as low risk, intermediate-risk/submassive PE, and massive PE. There is significant controversy about the management of submassive PE, which is defined as PE with right-sided heart strain (elevated troponin or B-type natriuretic peptide, right-axis deviation on ECG, or e
David J. Nagel, MD
Steering Committee Member
Olivier Axler, MD, FCCP
Vice-Chair
Chest Infections
Antibiotic Resistance
One-hundred years ago, infectious diseases caused 5 of the 10 most common causes of deaths in the United States. In 2016, only one infection remained on this list (influenza/pneumonia) (MMWR Morb Mortal Wkly Rep. 2017;66:413).
How medicine has improved with antibiotics. An unfortunate and unintended consequence of widespread antibiotic use has been the progressive resistance to these drugs. It is estimated that, if current trends continue, 10 million lives a year will be at risk from resistant organisms by 2050 (O’Neill, J. (2016). https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf).
Pathogens acquire antibiotic resistance by passing genetic material to one another through plasmids, bacteriophages, or naked DNA. Once acquired, resistance manifests via a number of mechanisms under the stress imposed by antibiotics (Levy SB, et al. Nat Med. 2004;10:S122).
Among the best studied is enzymatic degradation of the antibiotic. This occurs when beta-lactamases degrade penicillin. A second mechanism alters cell transport, thereby blocking cell entry or actively ejecting the antibiotic from the cell. Finally, overexpression or alteration of the antibiotic target may render a drug ineffective at inhibiting any vital cell function.
At the pace with which resistance now develops, the medical community faces a crisis, whereby infections caused by evolving superbugs are no longer effectively controlled by the available menu of antimicrobial agents.
This challenge must be met collectively by the more prudent prescribing of antibiotics, potentially with the help of rapid diagnostics; isolation of patients potentially infected with resistant organisms; and a focus on developing newer drugs that defy known resistant mechanisms.
Marc Feinstein, MD, FCCP
Steering Committee Member
Clinical Pulmonary Medicine
COPD and sleep-disordered breathing; A missing comorbid condition
Subjective, as well as objective, sleep complaints are common in patients with COPD (Krachman S, et al. Proc Am Thorac Soc. 2008;5[4]:536), and sleeping difficulties are ranked the third most frequent complaint (behind dyspnea and fatigue) in patients with COPD (Kinsman RA, et al. Chest. 1983;83[5]:755). Also, sleep quality is poor, and patients with moderate to severe COPD may have higher-than-expected incidence of OSA (Soler X, et al. Ann Am Thorac Soc. 2015;12[8]:1219).
Unfortunately, sleep is usually not assessed during a COPD evaluation. Up to 27% of patients with COPD without hypoxia during wakefulness can experience important desaturation during sleep, so called nocturnal oxygen desaturation (NOD) (Fletcher EC, et al. Chest. 1987;92[4]:604), that may lead to pulmonary hypertension (Chaouat A, et a
Although identification and effective treatment of COPD comorbidities are becoming the cornerstone of COPD management, sleep-disordered breathing has not been identified in current guidelines yet as a true potential contributor in poor outcomes despite emergent clinical evidence. Multidisciplinary programs, such as pulmonary rehabilitation, that improve dyspnea, exercise capacity, and quality of life may also positively impact sleep (Soler X, et al. COPD. 2013;10[2]:156). Because of the background of the staff involved, the comprehensive approach to patient assessment, and access to number of COPD subjects, pulmonary rehabilitation may be an optimal opportunity to assess sleep and identify an important comorbid condition often overlooked in patients with more advanced COPD.
Xavier Soler, MD, PhD
Steering Committee Member
Interprofessional Team
Finding Home
Outside our internal medicine curriculum, there is no formal pulmonary training or post-masters fellowship in pulmonary medicine for Advanced Practice Providers (APPs). Because of this, APPs are left to their own devices to fill educational gaps. To perform at the level expected by the physicians I work for, journal reviews and memorizing guidelines were not going to be enough. Since there is no formal pulmonary APP society, there were no peers to reach out to either. Off to conferences I went.
At first, I found CHEST daunting. After all, it’s run by the American College of Chest “Physicians,” not Nurse Practitioners. I spent most of the first day with my nametag turned around worried I’d be found out as a nonphysician attendee who snuck in. And then the unthinkable happened, I ran into another unicorn—another APP seeking the same information, only her nametag was turned the right way. The best advice she gave was to attend the Interprofessional NetWork meeting. This was ground zero of the conference as far as I was concerned. There I found myself surrounded by RTs, RNs, NPs, PAs, and yes, even physicians.
Over the years, as I’ve gotten further involved with CHEST NetWorks, I have found from top to bottom CHEST striving to incorporate APPs and advance our education. From including us in the FCCP program, reducing conference pricing for APPs, and focusing this year’s conference theme around being team focused, CHEST is creating a home for APPs.
Corinne Preston Young, FNP, FCCP
Steering Committee Member
Scheduling patterns: Time for a change?
Bob Wachter, MD, created buzz in March 2016 when, at the SHM annual meeting in San Diego, he displayed a slide titled “What did we get wrong?” The slide contained the copy, “Hospitalist shifts run 7 a.m.-7 p.m.; 10 a.m.-10 p.m. 7on/7off” circled in bold red.
Over the last several years, thought leaders in the hospital medicine field have expressed concern that this one-size-fits-all schedule model is a threat to the well-being of many physicians and, by extension, the sustainability of their hospital medicine groups. Despite this, the 2016 State of Hospital Medicine Report reveals relatively little change in the way hospital medicine groups schedule their physicians.

Night shifts echo this trend. There is an even greater number of groups utilizing the 12- to 13.9-hour shift length (79%), which has also varied less at just approximately 5% in either direction over the last two surveys. It is likely very hard to be creative with the shift length for your night physicians when the group is structured predominately around a 12-hour day position.
The 12-hour shift scheduled in long blocks is straightforward to employ for the scheduler, limits hand offs of care, and maximizes number of days off. So, why are Wachter et al. calling for change? Seven day stretches off may seem attractive when you are just starting out, but, as physicians mature, the very long day competes with family time that cannot be made up on weekday mornings when others are at school and work. Furthermore, the very long hours for 7 days straight lead to burn out and eventually retention issues as well. Some argue that this design promotes disengagement. It sets the expectation that, during “off” weeks, physicians might be unavailable for email responses, committee meetings, or participation in quality improvement initiatives, which disrupts integration into the larger hospital community and perhaps even our own career advancement.
Some groups are trying to address these concerns with innovative approaches to block scheduling. While the hallmark hospital medicine schedule of 7on/7off blocks remains the predominant model – 38.1% of all groups – this represents a drop of approximately 15%, compared with the prior survey. A new large contingent of groups entering the survey this year utilize a Monday-Friday model with rotating moonlighter/weekend coverage. This lifestyle and family-friendly model predominates in the Midwest. It is also found more in smaller groups, which may employ this model to keep the most system-knowledgeable worker around during high volume times, as well as to preserve the well-being and retention of their limited physician work force.
Of note, reconfiguring the 7on/7off model does not necessarily translate into more time off. The median number of shifts per year is also relatively stable at 182 which is the exact number of shifts per year in a strict 7on/7off schedule. This number does not vary by region of the country, group size, or teaching status. Some might argue that working 182 annual shifts is ideal, giving hospitalists a “vacation” every other week. However, this line of thought does not take into account the very long workdays, nor the 52 weekend days spent in the hospital – far more than most specialty peers who serve fewer weekend calls often with more limited in-house hours. In addition, one might argue that defining ourselves as available only during our 182 clinical “on” days is not in our own best interest, as it is the important nonclinical quality and committee service activities that are likely to lead to professional recognition and advancement.
Our hospital medicine group has deviated from this scheduling mainstay and requires only 160 shifts per year. We have set this number based on removal of the number of shifts equivalent to the vacation hours received by our medical group peers. The model poses a challenge in terms of matching our productivity up to benchmarks when talking to system leaders. This challenge pales in comparison to the increased buy-in from our physicians, as they feel equitable vacation time signifies respect from the medical group leadership.
In addition, our group has had success in being flexible around the number of days worked in a continuity stretch. We utilize everything from a 3-day block over holidays to a 7-day block. In general, we allow physicians to select their desired block length. The scheduler then works to accommodate that stretch as much as is feasible. The upfront work in this system is significant, but the downstream effect is decreased turnover costs. Even our own entrenched standard of 7on/7off schedules for house staff services (designed to protect continuity for the learner) have been the target of change. A pilot of alternating 4 and 5 day runs in a 4-week stretch has been implemented over the last few months. The number of days the residents are exposed to a given attending is the same in this model, but there is one additional switch day. The additional switch day puts the residents at risk of managing a change in care plan related to change in attending, but this was mitigated by paring attendings with very similar teaching and patient management styles. For our group, the extra administrative effort needed to work around the 7on/7off model has always paid off in terms of provider satisfaction and retention.
On the other hand, although I lead a large academic group, we have not yet developed flexibility around the shift length. Only one of the 29 roles our providers fill each 24-hour period is not a 12-hour shift. Over the years, I have tried to offer alternate models with shorter shifts to improve flow, reduce burn out, and increase family time. No matter how eloquent the reasoning, the response from the group was always the same: a resounding “no.” Most providers felt that they would wind up with a very similar work load and not actually leave the hospital earlier. Other reasons included not wanting to come in more days per month and concerns about increased handoffs/cross coverage.
There is some reason to think change may actually come. For one, burnout is high and may lead physicians to try a new model even with fear of the unknown. Our practice may be reconsidering this one-size-fits-all shift length in the very near future as an increasing percentage of candidates seeking to join our group express a strong interest in finding more accommodating hours.
Overall, I am hopeful that, in the coming years, my hospital medicine group, as well as many others, will heed the thoughts expressed by Dr. Wachter. Finding the flexibility to break out of these rigid scheduling models will be a first step in promoting both physician and system well being.
Dr. Eisenstock, MD, FHM, is clinical chief, division of hospital medicine, at the University of Massachusetts Memorial Health Care, Worcester.
Bob Wachter, MD, created buzz in March 2016 when, at the SHM annual meeting in San Diego, he displayed a slide titled “What did we get wrong?” The slide contained the copy, “Hospitalist shifts run 7 a.m.-7 p.m.; 10 a.m.-10 p.m. 7on/7off” circled in bold red.
Over the last several years, thought leaders in the hospital medicine field have expressed concern that this one-size-fits-all schedule model is a threat to the well-being of many physicians and, by extension, the sustainability of their hospital medicine groups. Despite this, the 2016 State of Hospital Medicine Report reveals relatively little change in the way hospital medicine groups schedule their physicians.
Night shifts echo this trend. There is an even greater number of groups utilizing the 12- to 13.9-hour shift length (79%), which has also varied less at just approximately 5% in either direction over the last two surveys. It is likely very hard to be creative with the shift length for your night physicians when the group is structured predominately around a 12-hour day position.
The 12-hour shift scheduled in long blocks is straightforward to employ for the scheduler, limits hand offs of care, and maximizes number of days off. So, why are Wachter et al. calling for change? Seven day stretches off may seem attractive when you are just starting out, but, as physicians mature, the very long day competes with family time that cannot be made up on weekday mornings when others are at school and work. Furthermore, the very long hours for 7 days straight lead to burn out and eventually retention issues as well. Some argue that this design promotes disengagement. It sets the expectation that, during “off” weeks, physicians might be unavailable for email responses, committee meetings, or participation in quality improvement initiatives, which disrupts integration into the larger hospital community and perhaps even our own career advancement.
Some groups are trying to address these concerns with innovative approaches to block scheduling. While the hallmark hospital medicine schedule of 7on/7off blocks remains the predominant model – 38.1% of all groups – this represents a drop of approximately 15%, compared with the prior survey. A new large contingent of groups entering the survey this year utilize a Monday-Friday model with rotating moonlighter/weekend coverage. This lifestyle and family-friendly model predominates in the Midwest. It is also found more in smaller groups, which may employ this model to keep the most system-knowledgeable worker around during high volume times, as well as to preserve the well-being and retention of their limited physician work force.
Of note, reconfiguring the 7on/7off model does not necessarily translate into more time off. The median number of shifts per year is also relatively stable at 182 which is the exact number of shifts per year in a strict 7on/7off schedule. This number does not vary by region of the country, group size, or teaching status. Some might argue that working 182 annual shifts is ideal, giving hospitalists a “vacation” every other week. However, this line of thought does not take into account the very long workdays, nor the 52 weekend days spent in the hospital – far more than most specialty peers who serve fewer weekend calls often with more limited in-house hours. In addition, one might argue that defining ourselves as available only during our 182 clinical “on” days is not in our own best interest, as it is the important nonclinical quality and committee service activities that are likely to lead to professional recognition and advancement.
Our hospital medicine group has deviated from this scheduling mainstay and requires only 160 shifts per year. We have set this number based on removal of the number of shifts equivalent to the vacation hours received by our medical group peers. The model poses a challenge in terms of matching our productivity up to benchmarks when talking to system leaders. This challenge pales in comparison to the increased buy-in from our physicians, as they feel equitable vacation time signifies respect from the medical group leadership.
In addition, our group has had success in being flexible around the number of days worked in a continuity stretch. We utilize everything from a 3-day block over holidays to a 7-day block. In general, we allow physicians to select their desired block length. The scheduler then works to accommodate that stretch as much as is feasible. The upfront work in this system is significant, but the downstream effect is decreased turnover costs. Even our own entrenched standard of 7on/7off schedules for house staff services (designed to protect continuity for the learner) have been the target of change. A pilot of alternating 4 and 5 day runs in a 4-week stretch has been implemented over the last few months. The number of days the residents are exposed to a given attending is the same in this model, but there is one additional switch day. The additional switch day puts the residents at risk of managing a change in care plan related to change in attending, but this was mitigated by paring attendings with very similar teaching and patient management styles. For our group, the extra administrative effort needed to work around the 7on/7off model has always paid off in terms of provider satisfaction and retention.
On the other hand, although I lead a large academic group, we have not yet developed flexibility around the shift length. Only one of the 29 roles our providers fill each 24-hour period is not a 12-hour shift. Over the years, I have tried to offer alternate models with shorter shifts to improve flow, reduce burn out, and increase family time. No matter how eloquent the reasoning, the response from the group was always the same: a resounding “no.” Most providers felt that they would wind up with a very similar work load and not actually leave the hospital earlier. Other reasons included not wanting to come in more days per month and concerns about increased handoffs/cross coverage.
There is some reason to think change may actually come. For one, burnout is high and may lead physicians to try a new model even with fear of the unknown. Our practice may be reconsidering this one-size-fits-all shift length in the very near future as an increasing percentage of candidates seeking to join our group express a strong interest in finding more accommodating hours.
Overall, I am hopeful that, in the coming years, my hospital medicine group, as well as many others, will heed the thoughts expressed by Dr. Wachter. Finding the flexibility to break out of these rigid scheduling models will be a first step in promoting both physician and system well being.
Dr. Eisenstock, MD, FHM, is clinical chief, division of hospital medicine, at the University of Massachusetts Memorial Health Care, Worcester.
Bob Wachter, MD, created buzz in March 2016 when, at the SHM annual meeting in San Diego, he displayed a slide titled “What did we get wrong?” The slide contained the copy, “Hospitalist shifts run 7 a.m.-7 p.m.; 10 a.m.-10 p.m. 7on/7off” circled in bold red.
Over the last several years, thought leaders in the hospital medicine field have expressed concern that this one-size-fits-all schedule model is a threat to the well-being of many physicians and, by extension, the sustainability of their hospital medicine groups. Despite this, the 2016 State of Hospital Medicine Report reveals relatively little change in the way hospital medicine groups schedule their physicians.
Night shifts echo this trend. There is an even greater number of groups utilizing the 12- to 13.9-hour shift length (79%), which has also varied less at just approximately 5% in either direction over the last two surveys. It is likely very hard to be creative with the shift length for your night physicians when the group is structured predominately around a 12-hour day position.
The 12-hour shift scheduled in long blocks is straightforward to employ for the scheduler, limits hand offs of care, and maximizes number of days off. So, why are Wachter et al. calling for change? Seven day stretches off may seem attractive when you are just starting out, but, as physicians mature, the very long day competes with family time that cannot be made up on weekday mornings when others are at school and work. Furthermore, the very long hours for 7 days straight lead to burn out and eventually retention issues as well. Some argue that this design promotes disengagement. It sets the expectation that, during “off” weeks, physicians might be unavailable for email responses, committee meetings, or participation in quality improvement initiatives, which disrupts integration into the larger hospital community and perhaps even our own career advancement.
Some groups are trying to address these concerns with innovative approaches to block scheduling. While the hallmark hospital medicine schedule of 7on/7off blocks remains the predominant model – 38.1% of all groups – this represents a drop of approximately 15%, compared with the prior survey. A new large contingent of groups entering the survey this year utilize a Monday-Friday model with rotating moonlighter/weekend coverage. This lifestyle and family-friendly model predominates in the Midwest. It is also found more in smaller groups, which may employ this model to keep the most system-knowledgeable worker around during high volume times, as well as to preserve the well-being and retention of their limited physician work force.
Of note, reconfiguring the 7on/7off model does not necessarily translate into more time off. The median number of shifts per year is also relatively stable at 182 which is the exact number of shifts per year in a strict 7on/7off schedule. This number does not vary by region of the country, group size, or teaching status. Some might argue that working 182 annual shifts is ideal, giving hospitalists a “vacation” every other week. However, this line of thought does not take into account the very long workdays, nor the 52 weekend days spent in the hospital – far more than most specialty peers who serve fewer weekend calls often with more limited in-house hours. In addition, one might argue that defining ourselves as available only during our 182 clinical “on” days is not in our own best interest, as it is the important nonclinical quality and committee service activities that are likely to lead to professional recognition and advancement.
Our hospital medicine group has deviated from this scheduling mainstay and requires only 160 shifts per year. We have set this number based on removal of the number of shifts equivalent to the vacation hours received by our medical group peers. The model poses a challenge in terms of matching our productivity up to benchmarks when talking to system leaders. This challenge pales in comparison to the increased buy-in from our physicians, as they feel equitable vacation time signifies respect from the medical group leadership.
In addition, our group has had success in being flexible around the number of days worked in a continuity stretch. We utilize everything from a 3-day block over holidays to a 7-day block. In general, we allow physicians to select their desired block length. The scheduler then works to accommodate that stretch as much as is feasible. The upfront work in this system is significant, but the downstream effect is decreased turnover costs. Even our own entrenched standard of 7on/7off schedules for house staff services (designed to protect continuity for the learner) have been the target of change. A pilot of alternating 4 and 5 day runs in a 4-week stretch has been implemented over the last few months. The number of days the residents are exposed to a given attending is the same in this model, but there is one additional switch day. The additional switch day puts the residents at risk of managing a change in care plan related to change in attending, but this was mitigated by paring attendings with very similar teaching and patient management styles. For our group, the extra administrative effort needed to work around the 7on/7off model has always paid off in terms of provider satisfaction and retention.
On the other hand, although I lead a large academic group, we have not yet developed flexibility around the shift length. Only one of the 29 roles our providers fill each 24-hour period is not a 12-hour shift. Over the years, I have tried to offer alternate models with shorter shifts to improve flow, reduce burn out, and increase family time. No matter how eloquent the reasoning, the response from the group was always the same: a resounding “no.” Most providers felt that they would wind up with a very similar work load and not actually leave the hospital earlier. Other reasons included not wanting to come in more days per month and concerns about increased handoffs/cross coverage.
There is some reason to think change may actually come. For one, burnout is high and may lead physicians to try a new model even with fear of the unknown. Our practice may be reconsidering this one-size-fits-all shift length in the very near future as an increasing percentage of candidates seeking to join our group express a strong interest in finding more accommodating hours.
Overall, I am hopeful that, in the coming years, my hospital medicine group, as well as many others, will heed the thoughts expressed by Dr. Wachter. Finding the flexibility to break out of these rigid scheduling models will be a first step in promoting both physician and system well being.
Dr. Eisenstock, MD, FHM, is clinical chief, division of hospital medicine, at the University of Massachusetts Memorial Health Care, Worcester.
Mitigating Burnout - Part 3
It is easy to look at the changes required to mitigate burnout and improve compassionate care and see the burden being placed mainly on the physician. Many of the proposed modifications seem to require the one commodity surgeons lack most, time. Any widespread effort to mitigate the burnout crisis must involve decreasing the barriers to patient care and reducing the physicians’ time constraints.
This may seem daunting, but broad changes in our healthcare system have been implemented in the name of quality, reducing errors, and alleviating trainee fatigue. Burnout can be a similar force for change. Much like the resident’s 80-hour workweek, however, in what manner this change is applied will be the ultimate determinant of the movement’s success.

This series of articles dealt with the adverse consequences of surgeon burnout on both clinicians and their patients, and then presented a conceptual framework to promote workforce well-being. Strategies that the SVS might adopt have been suggested. The central proposal is that helping physicians to deliver compassionate, collaborative care will not only mitigate burnout but also will enhance provider engagement, patient experience, and clinical outcomes, as well as improve the quality and safety of healthcare delivery. It seems reasonable to question if such broad strategic proposals are scalable to individual clinical settings.
The characteristics of compassionate care have been well described by patients, and, not surprisingly, only 53% reported that their last encounter with the health care system was compassionate. In 2014, a multidisciplinary consortium published recommendations for advancing compassionate person- and family-centered care. They detailed the attributes, values, and behaviors of such care, including focusing one’s attention, recognizing nonverbal clues, active listening, demonstrating nonjudgmental interest in the whole person, understanding the context of a person’s disease, and asking about the patient’s chief concerns in addition to their chief complaints. Most significantly, the authors outlined how these attributes could be integrated into existing competency documents such as those provided by the Association of American Medical Colleges (AAMC) Entrustable Professional Activities, or the milestones programs of the Accreditation Council of Graduate Medical Education (ACGME) and the American Board of Internal Medicine (ABIM).
It is but a small step to enhance current criteria for certification, clinical appointment, and privileging by including these professional attributes. Bear in mind that these skills are teachable and easily incorporated into health professional education and clinical care. As for metrics, the Schwartz Compassionate Care Scale is a validated patient-rated questionnaire that reliably measures physicians’ compassion and overall patient satisfaction and is available in the public domain. It also provides a metric that is important to clinicians and, when placed on the hospital dashboard, highlights that compassion is an organizational priority. Such priorities become the fabric of the workforce when organizational leadership installs programs such as values-based recruitment, retention, and promotion as Vivian Lee describes at the University of Utah Health System. Mitigating burnout requires changing the culture in which clinicians work and with whom they work.
Vascular surgeons and their professional surgical societies have a leadership opportunity to design high performing teams. Most patient care models have been structured around traditional medical and surgical departments. This paradigm overlooks the fact that patients do not “get sick” within traditional teaching disciplines but do so across varied medical and surgical specialties. Changes in organizational hierarchy are needed so that team-based care is supported. In addition to physician and nurse clinicians, the new teams would do well to expand to all “caregivers,” i.e. everyone who touches the patient (technologists, interpreters, pharmacists, transport workers, support staff, and administrators).
On the front line
On April 15, 2013, at 2:49 pm, two homemade bombs detonated near the finish line of the Boston Marathon killing three people at the scene and injuring 264 others; the most severe sustaining mutilating lower extremity injuries. Much has been written about the preparedness, the emergency response, and the fact that all those who made it to the hospital survived. Jeffrey Kalish, MD, a vascular surgeon at Boston Medical Center and SVS member, was on the front line that day. We asked him to share his personal experience of caring for the victims through the lens of compassionate collaborative care.
“It has been over four years since I went from being a spectator near the Boston Marathon finish line to rushing directly to the operating rooms at Boston Medical Center to help our teams perform lifesaving procedures on critically ill patients, including amputations and complex vascular repairs. While I have learned a tremendous amount since that experience with regard to limb salvage and amputation, reconstructive techniques, and prosthetics, I will focus here on the care the patients and their families received, the lessons our hospital learned from the weeks and months that followed, and how we modeled this care going forward for all amputation patients at Boston Medical Center.
"Based on lessons from the Boston Marathon bombings, I aligned a multidisciplinary team of health care providers in order to formalize and standardize best practices to benefit our amputation patients. STRONG (Surgery To Rehab Ongoing Needs Group) continues to strive toward the ultimate goal of improving and coordinating care for amputation patients and their families as they transition from the hospital setting to rehabilitation. Some of our guiding principles, along with their positive impacts on patient care and physician well-being, are highlighted below:
1. Sustaining hope with a new mindset: Although surgeons have historically considered amputation as a treatment failure, a more appropriate mindset is that amputation can often be a reconstructive procedure in the surgical armamentarium designed to restore a patient back to full function.
2. Seeing the patient in context: Shared decision making can occur more readily once a surgeon and the care team seek to understand the whole person and their family, including what that person does for work and leisure.
3. Communication with colleagues, patients, and families: Patient and family fear and confusion can often be reduced after establishment of a multi-disciplinary team with daily care coordination and consistent messaging. Breaking down traditional hospital silos to allow for improved coordination of care benefits both the patients and the practitioners.
4. Managing emotional and physical suffering: Introducing social workers, mental health professionals, or pastoral care advocates into the care team as soon as a patient is ready can help manage the emotional and psychosocial needs of patients and their families.
5. Sustaining long term surgeon/patient relationships: As clinicians, we can feel rewarded after restoring functional performance in our patients and by meeting the needs of our patients and families. This can occur both in the short-term during the acute hospital stay and in the long-term as we follow our patients’ progress towards achievement of their ultimate goals.
6. Attend to one’s own well-being and foster resilience. There will never be a substitute in our profession for the human connection between our patients and ourselves as their caregivers, and this connection should be one of the most treasured aspects of our work life. We should seek daily reminders of these positive interactions to nurture our ability to cope with a grueling and challenging field, where the outcomes are not always as ideal as we hope.
For me, STRONG is now a consistent and powerful reminder of why I originally became a doctor in the first place, and I strive to propagate this model of compassionate care to benefit future patients as we move forward together.”
We are at an inflexion point in health care. No amount of individual resilience can withstand a toxic or nonsupportive environment. It is unreasonable to think that simply by taking better care of ourselves we are going to resolve the issue of burnout. We need to rethink our current systems of care and focus our energy on developing those that support our ability to deliver the kind of care we know our patients need and deserve. We have an opportunity to alleviate the suffering many providers are experiencing as they strive to heal their patients. We have an opportunity to improve both physician and patient engagement, develop care delivery systems we know our patients deserve, and restore the deep sense of satisfaction that comes from practicing medicine and surgery. There is abundant expertise within our professional medical and surgical societies. The SVS has the courage and the duty to lead.
Drs. Colman, Kalish, and Sheahan extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, M.D., Scholar in Residence, Schwartz Center for Compassionate Care, Boston, Mass., and Clinical Professor of Orthopedics at Seattle Children’s Hospital.
Bibliography
1. Acad Med (2016) 91:338-344
2. Health Aff (2011) 30:1772-1778
3. Patient Educ Couns (2015) 98:1005-10
4. Acad Med (2016) 91:310-316
5. http://www.theschwartzcenter.org/media/Triple-C-Conference-Framework-Tables_FINAL.pdf
6. http://www.theschwartzcenter.org/media/Triple-C-Conference-Recommendations-Report_FINAL1.pdf
7. JAMA (2017) 317: 901-2
8. Clin Orthop Relat Res. (2017) 475:1309-14.
It is easy to look at the changes required to mitigate burnout and improve compassionate care and see the burden being placed mainly on the physician. Many of the proposed modifications seem to require the one commodity surgeons lack most, time. Any widespread effort to mitigate the burnout crisis must involve decreasing the barriers to patient care and reducing the physicians’ time constraints.
This may seem daunting, but broad changes in our healthcare system have been implemented in the name of quality, reducing errors, and alleviating trainee fatigue. Burnout can be a similar force for change. Much like the resident’s 80-hour workweek, however, in what manner this change is applied will be the ultimate determinant of the movement’s success.
This series of articles dealt with the adverse consequences of surgeon burnout on both clinicians and their patients, and then presented a conceptual framework to promote workforce well-being. Strategies that the SVS might adopt have been suggested. The central proposal is that helping physicians to deliver compassionate, collaborative care will not only mitigate burnout but also will enhance provider engagement, patient experience, and clinical outcomes, as well as improve the quality and safety of healthcare delivery. It seems reasonable to question if such broad strategic proposals are scalable to individual clinical settings.
The characteristics of compassionate care have been well described by patients, and, not surprisingly, only 53% reported that their last encounter with the health care system was compassionate. In 2014, a multidisciplinary consortium published recommendations for advancing compassionate person- and family-centered care. They detailed the attributes, values, and behaviors of such care, including focusing one’s attention, recognizing nonverbal clues, active listening, demonstrating nonjudgmental interest in the whole person, understanding the context of a person’s disease, and asking about the patient’s chief concerns in addition to their chief complaints. Most significantly, the authors outlined how these attributes could be integrated into existing competency documents such as those provided by the Association of American Medical Colleges (AAMC) Entrustable Professional Activities, or the milestones programs of the Accreditation Council of Graduate Medical Education (ACGME) and the American Board of Internal Medicine (ABIM).
It is but a small step to enhance current criteria for certification, clinical appointment, and privileging by including these professional attributes. Bear in mind that these skills are teachable and easily incorporated into health professional education and clinical care. As for metrics, the Schwartz Compassionate Care Scale is a validated patient-rated questionnaire that reliably measures physicians’ compassion and overall patient satisfaction and is available in the public domain. It also provides a metric that is important to clinicians and, when placed on the hospital dashboard, highlights that compassion is an organizational priority. Such priorities become the fabric of the workforce when organizational leadership installs programs such as values-based recruitment, retention, and promotion as Vivian Lee describes at the University of Utah Health System. Mitigating burnout requires changing the culture in which clinicians work and with whom they work.
Vascular surgeons and their professional surgical societies have a leadership opportunity to design high performing teams. Most patient care models have been structured around traditional medical and surgical departments. This paradigm overlooks the fact that patients do not “get sick” within traditional teaching disciplines but do so across varied medical and surgical specialties. Changes in organizational hierarchy are needed so that team-based care is supported. In addition to physician and nurse clinicians, the new teams would do well to expand to all “caregivers,” i.e. everyone who touches the patient (technologists, interpreters, pharmacists, transport workers, support staff, and administrators).
On the front line
On April 15, 2013, at 2:49 pm, two homemade bombs detonated near the finish line of the Boston Marathon killing three people at the scene and injuring 264 others; the most severe sustaining mutilating lower extremity injuries. Much has been written about the preparedness, the emergency response, and the fact that all those who made it to the hospital survived. Jeffrey Kalish, MD, a vascular surgeon at Boston Medical Center and SVS member, was on the front line that day. We asked him to share his personal experience of caring for the victims through the lens of compassionate collaborative care.
“It has been over four years since I went from being a spectator near the Boston Marathon finish line to rushing directly to the operating rooms at Boston Medical Center to help our teams perform lifesaving procedures on critically ill patients, including amputations and complex vascular repairs. While I have learned a tremendous amount since that experience with regard to limb salvage and amputation, reconstructive techniques, and prosthetics, I will focus here on the care the patients and their families received, the lessons our hospital learned from the weeks and months that followed, and how we modeled this care going forward for all amputation patients at Boston Medical Center.
"Based on lessons from the Boston Marathon bombings, I aligned a multidisciplinary team of health care providers in order to formalize and standardize best practices to benefit our amputation patients. STRONG (Surgery To Rehab Ongoing Needs Group) continues to strive toward the ultimate goal of improving and coordinating care for amputation patients and their families as they transition from the hospital setting to rehabilitation. Some of our guiding principles, along with their positive impacts on patient care and physician well-being, are highlighted below:
1. Sustaining hope with a new mindset: Although surgeons have historically considered amputation as a treatment failure, a more appropriate mindset is that amputation can often be a reconstructive procedure in the surgical armamentarium designed to restore a patient back to full function.
2. Seeing the patient in context: Shared decision making can occur more readily once a surgeon and the care team seek to understand the whole person and their family, including what that person does for work and leisure.
3. Communication with colleagues, patients, and families: Patient and family fear and confusion can often be reduced after establishment of a multi-disciplinary team with daily care coordination and consistent messaging. Breaking down traditional hospital silos to allow for improved coordination of care benefits both the patients and the practitioners.
4. Managing emotional and physical suffering: Introducing social workers, mental health professionals, or pastoral care advocates into the care team as soon as a patient is ready can help manage the emotional and psychosocial needs of patients and their families.
5. Sustaining long term surgeon/patient relationships: As clinicians, we can feel rewarded after restoring functional performance in our patients and by meeting the needs of our patients and families. This can occur both in the short-term during the acute hospital stay and in the long-term as we follow our patients’ progress towards achievement of their ultimate goals.
6. Attend to one’s own well-being and foster resilience. There will never be a substitute in our profession for the human connection between our patients and ourselves as their caregivers, and this connection should be one of the most treasured aspects of our work life. We should seek daily reminders of these positive interactions to nurture our ability to cope with a grueling and challenging field, where the outcomes are not always as ideal as we hope.
For me, STRONG is now a consistent and powerful reminder of why I originally became a doctor in the first place, and I strive to propagate this model of compassionate care to benefit future patients as we move forward together.”
We are at an inflexion point in health care. No amount of individual resilience can withstand a toxic or nonsupportive environment. It is unreasonable to think that simply by taking better care of ourselves we are going to resolve the issue of burnout. We need to rethink our current systems of care and focus our energy on developing those that support our ability to deliver the kind of care we know our patients need and deserve. We have an opportunity to alleviate the suffering many providers are experiencing as they strive to heal their patients. We have an opportunity to improve both physician and patient engagement, develop care delivery systems we know our patients deserve, and restore the deep sense of satisfaction that comes from practicing medicine and surgery. There is abundant expertise within our professional medical and surgical societies. The SVS has the courage and the duty to lead.
Drs. Colman, Kalish, and Sheahan extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, M.D., Scholar in Residence, Schwartz Center for Compassionate Care, Boston, Mass., and Clinical Professor of Orthopedics at Seattle Children’s Hospital.
Bibliography
1. Acad Med (2016) 91:338-344
2. Health Aff (2011) 30:1772-1778
3. Patient Educ Couns (2015) 98:1005-10
4. Acad Med (2016) 91:310-316
5. http://www.theschwartzcenter.org/media/Triple-C-Conference-Framework-Tables_FINAL.pdf
6. http://www.theschwartzcenter.org/media/Triple-C-Conference-Recommendations-Report_FINAL1.pdf
7. JAMA (2017) 317: 901-2
8. Clin Orthop Relat Res. (2017) 475:1309-14.
It is easy to look at the changes required to mitigate burnout and improve compassionate care and see the burden being placed mainly on the physician. Many of the proposed modifications seem to require the one commodity surgeons lack most, time. Any widespread effort to mitigate the burnout crisis must involve decreasing the barriers to patient care and reducing the physicians’ time constraints.
This may seem daunting, but broad changes in our healthcare system have been implemented in the name of quality, reducing errors, and alleviating trainee fatigue. Burnout can be a similar force for change. Much like the resident’s 80-hour workweek, however, in what manner this change is applied will be the ultimate determinant of the movement’s success.
This series of articles dealt with the adverse consequences of surgeon burnout on both clinicians and their patients, and then presented a conceptual framework to promote workforce well-being. Strategies that the SVS might adopt have been suggested. The central proposal is that helping physicians to deliver compassionate, collaborative care will not only mitigate burnout but also will enhance provider engagement, patient experience, and clinical outcomes, as well as improve the quality and safety of healthcare delivery. It seems reasonable to question if such broad strategic proposals are scalable to individual clinical settings.
The characteristics of compassionate care have been well described by patients, and, not surprisingly, only 53% reported that their last encounter with the health care system was compassionate. In 2014, a multidisciplinary consortium published recommendations for advancing compassionate person- and family-centered care. They detailed the attributes, values, and behaviors of such care, including focusing one’s attention, recognizing nonverbal clues, active listening, demonstrating nonjudgmental interest in the whole person, understanding the context of a person’s disease, and asking about the patient’s chief concerns in addition to their chief complaints. Most significantly, the authors outlined how these attributes could be integrated into existing competency documents such as those provided by the Association of American Medical Colleges (AAMC) Entrustable Professional Activities, or the milestones programs of the Accreditation Council of Graduate Medical Education (ACGME) and the American Board of Internal Medicine (ABIM).
It is but a small step to enhance current criteria for certification, clinical appointment, and privileging by including these professional attributes. Bear in mind that these skills are teachable and easily incorporated into health professional education and clinical care. As for metrics, the Schwartz Compassionate Care Scale is a validated patient-rated questionnaire that reliably measures physicians’ compassion and overall patient satisfaction and is available in the public domain. It also provides a metric that is important to clinicians and, when placed on the hospital dashboard, highlights that compassion is an organizational priority. Such priorities become the fabric of the workforce when organizational leadership installs programs such as values-based recruitment, retention, and promotion as Vivian Lee describes at the University of Utah Health System. Mitigating burnout requires changing the culture in which clinicians work and with whom they work.
Vascular surgeons and their professional surgical societies have a leadership opportunity to design high performing teams. Most patient care models have been structured around traditional medical and surgical departments. This paradigm overlooks the fact that patients do not “get sick” within traditional teaching disciplines but do so across varied medical and surgical specialties. Changes in organizational hierarchy are needed so that team-based care is supported. In addition to physician and nurse clinicians, the new teams would do well to expand to all “caregivers,” i.e. everyone who touches the patient (technologists, interpreters, pharmacists, transport workers, support staff, and administrators).
On the front line
On April 15, 2013, at 2:49 pm, two homemade bombs detonated near the finish line of the Boston Marathon killing three people at the scene and injuring 264 others; the most severe sustaining mutilating lower extremity injuries. Much has been written about the preparedness, the emergency response, and the fact that all those who made it to the hospital survived. Jeffrey Kalish, MD, a vascular surgeon at Boston Medical Center and SVS member, was on the front line that day. We asked him to share his personal experience of caring for the victims through the lens of compassionate collaborative care.
“It has been over four years since I went from being a spectator near the Boston Marathon finish line to rushing directly to the operating rooms at Boston Medical Center to help our teams perform lifesaving procedures on critically ill patients, including amputations and complex vascular repairs. While I have learned a tremendous amount since that experience with regard to limb salvage and amputation, reconstructive techniques, and prosthetics, I will focus here on the care the patients and their families received, the lessons our hospital learned from the weeks and months that followed, and how we modeled this care going forward for all amputation patients at Boston Medical Center.
"Based on lessons from the Boston Marathon bombings, I aligned a multidisciplinary team of health care providers in order to formalize and standardize best practices to benefit our amputation patients. STRONG (Surgery To Rehab Ongoing Needs Group) continues to strive toward the ultimate goal of improving and coordinating care for amputation patients and their families as they transition from the hospital setting to rehabilitation. Some of our guiding principles, along with their positive impacts on patient care and physician well-being, are highlighted below:
1. Sustaining hope with a new mindset: Although surgeons have historically considered amputation as a treatment failure, a more appropriate mindset is that amputation can often be a reconstructive procedure in the surgical armamentarium designed to restore a patient back to full function.
2. Seeing the patient in context: Shared decision making can occur more readily once a surgeon and the care team seek to understand the whole person and their family, including what that person does for work and leisure.
3. Communication with colleagues, patients, and families: Patient and family fear and confusion can often be reduced after establishment of a multi-disciplinary team with daily care coordination and consistent messaging. Breaking down traditional hospital silos to allow for improved coordination of care benefits both the patients and the practitioners.
4. Managing emotional and physical suffering: Introducing social workers, mental health professionals, or pastoral care advocates into the care team as soon as a patient is ready can help manage the emotional and psychosocial needs of patients and their families.
5. Sustaining long term surgeon/patient relationships: As clinicians, we can feel rewarded after restoring functional performance in our patients and by meeting the needs of our patients and families. This can occur both in the short-term during the acute hospital stay and in the long-term as we follow our patients’ progress towards achievement of their ultimate goals.
6. Attend to one’s own well-being and foster resilience. There will never be a substitute in our profession for the human connection between our patients and ourselves as their caregivers, and this connection should be one of the most treasured aspects of our work life. We should seek daily reminders of these positive interactions to nurture our ability to cope with a grueling and challenging field, where the outcomes are not always as ideal as we hope.
For me, STRONG is now a consistent and powerful reminder of why I originally became a doctor in the first place, and I strive to propagate this model of compassionate care to benefit future patients as we move forward together.”
We are at an inflexion point in health care. No amount of individual resilience can withstand a toxic or nonsupportive environment. It is unreasonable to think that simply by taking better care of ourselves we are going to resolve the issue of burnout. We need to rethink our current systems of care and focus our energy on developing those that support our ability to deliver the kind of care we know our patients need and deserve. We have an opportunity to alleviate the suffering many providers are experiencing as they strive to heal their patients. We have an opportunity to improve both physician and patient engagement, develop care delivery systems we know our patients deserve, and restore the deep sense of satisfaction that comes from practicing medicine and surgery. There is abundant expertise within our professional medical and surgical societies. The SVS has the courage and the duty to lead.
Drs. Colman, Kalish, and Sheahan extend their thanks and appreciation for the guidance, resources and support of Michael Goldberg, M.D., Scholar in Residence, Schwartz Center for Compassionate Care, Boston, Mass., and Clinical Professor of Orthopedics at Seattle Children’s Hospital.
Bibliography
1. Acad Med (2016) 91:338-344
2. Health Aff (2011) 30:1772-1778
3. Patient Educ Couns (2015) 98:1005-10
4. Acad Med (2016) 91:310-316
5. http://www.theschwartzcenter.org/media/Triple-C-Conference-Framework-Tables_FINAL.pdf
6. http://www.theschwartzcenter.org/media/Triple-C-Conference-Recommendations-Report_FINAL1.pdf
7. JAMA (2017) 317: 901-2
8. Clin Orthop Relat Res. (2017) 475:1309-14.
Will artificial intelligence make us better doctors?
Given the amount of time physicians spend entering data, clicking through screens, navigating pages, and logging in to computers, one would have hoped that substantial near-term payback for such efforts would have materialized.
Many of us believed this would take the form of health information exchange – the ability to easily access clinical information from hospitals or clinics other than our own, creating a more complete picture of the patient before us. To our disappointment, true information exchange has yet to materialize. (We won’t debate here whether politics or technology is culpable.) We are left to look elsewhere for the benefits of the digitization of the medical records and other sources of health care knowledge.
Lately, there has been a lot of talk about the promise of machine learning and artificial intelligence (AI) in health care. Much of the resurgence of interest in AI can be traced to IBM Watson’s appearance as a contestant on Jeopardy in 2011. Watson, a natural language supercomputer with enough power to process the equivalent of a million books per second, had access to 200 million pages of content, including the full text of Wikipedia, for Jeopardy.1 Watson handily outperformed its human opponents – two Jeopardy savants who were also the most successful contestants in game show history – taking the $1 million first prize but struggling in categories with clues containing only a few words.
MD Anderson and Watson: Dashed hopes follow initial promise
As a result of growing recognition of AI’s potential in health care, IBM began collaborations with a number of health care organizations to deploy Watson.
In 2013, MD Anderson Cancer Center and IBM began a pilot to develop an oncology clinical decision support technology tool powered by Watson to aid MD Anderson “in its mission to eradicate cancer.” Recently, it was announced that the project – which cost the cancer center $62 million – has been put on hold, and MD Anderson is looking for other contractors to replace IBM.
While administrative problems are at least partly responsible for the project’s challenges, the undertaking has raised issues with the quality and quantity of data in health care that call into question the ability of AI to work as well in health care as it did on Jeopardy, at least in the short term.
Health care: Not as data rich as you might think
“We are not ‘Big Data’ in health care, yet.” – Dale Sanders, Health Catalyst.2
In its quest for Jeopardy victory, Watson accessed a massive data storehouse subsuming a vast array of knowledge assembled over the course of human history. Conversely, for health care, Watson is limited to a few decades of scientific journals (that may not contribute to diagnosis and treatment as much as one might think), claims data geared to billing without much clinical information like outcomes, and clinical data from progress notes (plagued by inaccuracies, serial “copy and paste,” and nonstandardized language and numeric representations), and variable-format reports from lab, radiology, pathology, and other disciplines.
To articulate how data-poor health care is, Dale Sanders, executive vice president for software at Health Catalyst, notes that a Boeing 787 generates 500GB of data in a six hour flight while one patient may generate just 100MB of data in an entire year.2 He pointed out that, in the near term, AI platforms like Watson simply do not have enough data substrate to impact health care as many hoped it would. Over the longer term, he says, if health care can develop a coherent, standard approach to data content, AI may fulfill its promise. 
What can AI and related technologies achieve in the near-term?
“AI seems to have replaced Uber as the most overused word or phrase in digital health.” – Reporter Stephanie Baum, paraphrasing from an interview with Bob Kocher, Venrock Partners.3
My observations tell me that we have already made some progress and are likely to make more strides in the coming years, thanks to AI, machine learning, and natural language processing. A few areas of potential gain are:
Clinical documentation
Technology that can derive meaning from words or groups of words can help with more accurate clinical documentation. For example, if a patient has a documented UTI but also has in the record an 11 on the Glasgow Coma Scale, a systolic BP of 90, and a respiratory rate of 24, technology can alert the physician to document sepsis.
Quality measurement and reporting
Similarly, if technology can recognize words and numbers, it may be able to extract and report quality measures (for example, an ejection fraction of 35% in a heart failure patient) from progress notes without having a nurse-abstractor manually enter such data into structured fields for reporting, as is currently the case.
Predicting readmissions, mortality, other events
While machine learning has had mixed results in predicting future clinical events, this is likely to change as data integrity and algorithms improve. Best-of-breed technology will probably use both clinical and machine learning tools for predictive purposes in the future.
In 2015, I had the privilege of meeting Vinod Khosla, cofounder of SUN Microsystems and venture capitalist, who predicts that computers will largely supplant physicians in the future, at least in domains relying on access to data. As he puts it, “the core functions necessary for complex diagnoses, treatments, and monitoring will be driven by machine judgment instead of human judgment.”4
While the benefits of technology, especially in health care, are often oversold, I believe AI and related technologies will some day play a large role alongside physicians in the care of patients. However, for AI to deliver, we must first figure out how to collect and organize health care data so that computers are able to ingest, digest and use it in a purposeful way.
Note: Dr. Whitcomb is founder and advisor to Zato Health, which uses natural language processing and discovery technology in health care.
He is chief medical officer at Remedy Partners in Darien, Conn., and a cofounder and past president of SHM.
References
1. Zimmer, Ben. Is It Time to Welcome Our New Computer Overlords?. The Atlantic. https://www.theatlantic.com/technology/archive/2011/02/is-it-time-to-welcome-our-new-computer-overlords/71388/. Accessed 23 Apr 2017.
2. Sanders, Dale. The MD Anderson / IBM Watson Announcement: What does it mean for machine learning in healthcare? Webinar. https://www.slideshare.net/healthcatalyst1/the-md-anderson-ibm-watson-announcement-what-does-it-mean-for-machine-learning-in-healthcare. Accessed 23 Apr 2017.
3. Baum, Stephanie. Venrock survey predicts a flight to quality for digital health investments. MedCity News. 12 Apr 2017. http://medcitynews.com/2017/04/venrock-survey-predicts-flight-quality-digital-health-investment/. Accessed 22 Apr 2017.
4. Khosla, Vinod. The Reinvention Of Medicine: Dr. Algorithm V0-7 And Beyond. TechCrunch. 22 Sept 2014. https://techcrunch.com/2014/09/22/the-reinvention-of-medicine-dr-algorithm-version-0-7-and-beyond/. Accessed 22 Apr 2017.
Given the amount of time physicians spend entering data, clicking through screens, navigating pages, and logging in to computers, one would have hoped that substantial near-term payback for such efforts would have materialized.
Many of us believed this would take the form of health information exchange – the ability to easily access clinical information from hospitals or clinics other than our own, creating a more complete picture of the patient before us. To our disappointment, true information exchange has yet to materialize. (We won’t debate here whether politics or technology is culpable.) We are left to look elsewhere for the benefits of the digitization of the medical records and other sources of health care knowledge.
Lately, there has been a lot of talk about the promise of machine learning and artificial intelligence (AI) in health care. Much of the resurgence of interest in AI can be traced to IBM Watson’s appearance as a contestant on Jeopardy in 2011. Watson, a natural language supercomputer with enough power to process the equivalent of a million books per second, had access to 200 million pages of content, including the full text of Wikipedia, for Jeopardy.1 Watson handily outperformed its human opponents – two Jeopardy savants who were also the most successful contestants in game show history – taking the $1 million first prize but struggling in categories with clues containing only a few words.
MD Anderson and Watson: Dashed hopes follow initial promise
As a result of growing recognition of AI’s potential in health care, IBM began collaborations with a number of health care organizations to deploy Watson.
In 2013, MD Anderson Cancer Center and IBM began a pilot to develop an oncology clinical decision support technology tool powered by Watson to aid MD Anderson “in its mission to eradicate cancer.” Recently, it was announced that the project – which cost the cancer center $62 million – has been put on hold, and MD Anderson is looking for other contractors to replace IBM.
While administrative problems are at least partly responsible for the project’s challenges, the undertaking has raised issues with the quality and quantity of data in health care that call into question the ability of AI to work as well in health care as it did on Jeopardy, at least in the short term.
Health care: Not as data rich as you might think
“We are not ‘Big Data’ in health care, yet.” – Dale Sanders, Health Catalyst.2
In its quest for Jeopardy victory, Watson accessed a massive data storehouse subsuming a vast array of knowledge assembled over the course of human history. Conversely, for health care, Watson is limited to a few decades of scientific journals (that may not contribute to diagnosis and treatment as much as one might think), claims data geared to billing without much clinical information like outcomes, and clinical data from progress notes (plagued by inaccuracies, serial “copy and paste,” and nonstandardized language and numeric representations), and variable-format reports from lab, radiology, pathology, and other disciplines.
To articulate how data-poor health care is, Dale Sanders, executive vice president for software at Health Catalyst, notes that a Boeing 787 generates 500GB of data in a six hour flight while one patient may generate just 100MB of data in an entire year.2 He pointed out that, in the near term, AI platforms like Watson simply do not have enough data substrate to impact health care as many hoped it would. Over the longer term, he says, if health care can develop a coherent, standard approach to data content, AI may fulfill its promise.
What can AI and related technologies achieve in the near-term?
“AI seems to have replaced Uber as the most overused word or phrase in digital health.” – Reporter Stephanie Baum, paraphrasing from an interview with Bob Kocher, Venrock Partners.3
My observations tell me that we have already made some progress and are likely to make more strides in the coming years, thanks to AI, machine learning, and natural language processing. A few areas of potential gain are:
Clinical documentation
Technology that can derive meaning from words or groups of words can help with more accurate clinical documentation. For example, if a patient has a documented UTI but also has in the record an 11 on the Glasgow Coma Scale, a systolic BP of 90, and a respiratory rate of 24, technology can alert the physician to document sepsis.
Quality measurement and reporting
Similarly, if technology can recognize words and numbers, it may be able to extract and report quality measures (for example, an ejection fraction of 35% in a heart failure patient) from progress notes without having a nurse-abstractor manually enter such data into structured fields for reporting, as is currently the case.
Predicting readmissions, mortality, other events
While machine learning has had mixed results in predicting future clinical events, this is likely to change as data integrity and algorithms improve. Best-of-breed technology will probably use both clinical and machine learning tools for predictive purposes in the future.
In 2015, I had the privilege of meeting Vinod Khosla, cofounder of SUN Microsystems and venture capitalist, who predicts that computers will largely supplant physicians in the future, at least in domains relying on access to data. As he puts it, “the core functions necessary for complex diagnoses, treatments, and monitoring will be driven by machine judgment instead of human judgment.”4
While the benefits of technology, especially in health care, are often oversold, I believe AI and related technologies will some day play a large role alongside physicians in the care of patients. However, for AI to deliver, we must first figure out how to collect and organize health care data so that computers are able to ingest, digest and use it in a purposeful way.
Note: Dr. Whitcomb is founder and advisor to Zato Health, which uses natural language processing and discovery technology in health care.
He is chief medical officer at Remedy Partners in Darien, Conn., and a cofounder and past president of SHM.
References
1. Zimmer, Ben. Is It Time to Welcome Our New Computer Overlords?. The Atlantic. https://www.theatlantic.com/technology/archive/2011/02/is-it-time-to-welcome-our-new-computer-overlords/71388/. Accessed 23 Apr 2017.
2. Sanders, Dale. The MD Anderson / IBM Watson Announcement: What does it mean for machine learning in healthcare? Webinar. https://www.slideshare.net/healthcatalyst1/the-md-anderson-ibm-watson-announcement-what-does-it-mean-for-machine-learning-in-healthcare. Accessed 23 Apr 2017.
3. Baum, Stephanie. Venrock survey predicts a flight to quality for digital health investments. MedCity News. 12 Apr 2017. http://medcitynews.com/2017/04/venrock-survey-predicts-flight-quality-digital-health-investment/. Accessed 22 Apr 2017.
4. Khosla, Vinod. The Reinvention Of Medicine: Dr. Algorithm V0-7 And Beyond. TechCrunch. 22 Sept 2014. https://techcrunch.com/2014/09/22/the-reinvention-of-medicine-dr-algorithm-version-0-7-and-beyond/. Accessed 22 Apr 2017.
Given the amount of time physicians spend entering data, clicking through screens, navigating pages, and logging in to computers, one would have hoped that substantial near-term payback for such efforts would have materialized.
Many of us believed this would take the form of health information exchange – the ability to easily access clinical information from hospitals or clinics other than our own, creating a more complete picture of the patient before us. To our disappointment, true information exchange has yet to materialize. (We won’t debate here whether politics or technology is culpable.) We are left to look elsewhere for the benefits of the digitization of the medical records and other sources of health care knowledge.
Lately, there has been a lot of talk about the promise of machine learning and artificial intelligence (AI) in health care. Much of the resurgence of interest in AI can be traced to IBM Watson’s appearance as a contestant on Jeopardy in 2011. Watson, a natural language supercomputer with enough power to process the equivalent of a million books per second, had access to 200 million pages of content, including the full text of Wikipedia, for Jeopardy.1 Watson handily outperformed its human opponents – two Jeopardy savants who were also the most successful contestants in game show history – taking the $1 million first prize but struggling in categories with clues containing only a few words.
MD Anderson and Watson: Dashed hopes follow initial promise
As a result of growing recognition of AI’s potential in health care, IBM began collaborations with a number of health care organizations to deploy Watson.
In 2013, MD Anderson Cancer Center and IBM began a pilot to develop an oncology clinical decision support technology tool powered by Watson to aid MD Anderson “in its mission to eradicate cancer.” Recently, it was announced that the project – which cost the cancer center $62 million – has been put on hold, and MD Anderson is looking for other contractors to replace IBM.
While administrative problems are at least partly responsible for the project’s challenges, the undertaking has raised issues with the quality and quantity of data in health care that call into question the ability of AI to work as well in health care as it did on Jeopardy, at least in the short term.
Health care: Not as data rich as you might think
“We are not ‘Big Data’ in health care, yet.” – Dale Sanders, Health Catalyst.2
In its quest for Jeopardy victory, Watson accessed a massive data storehouse subsuming a vast array of knowledge assembled over the course of human history. Conversely, for health care, Watson is limited to a few decades of scientific journals (that may not contribute to diagnosis and treatment as much as one might think), claims data geared to billing without much clinical information like outcomes, and clinical data from progress notes (plagued by inaccuracies, serial “copy and paste,” and nonstandardized language and numeric representations), and variable-format reports from lab, radiology, pathology, and other disciplines.
To articulate how data-poor health care is, Dale Sanders, executive vice president for software at Health Catalyst, notes that a Boeing 787 generates 500GB of data in a six hour flight while one patient may generate just 100MB of data in an entire year.2 He pointed out that, in the near term, AI platforms like Watson simply do not have enough data substrate to impact health care as many hoped it would. Over the longer term, he says, if health care can develop a coherent, standard approach to data content, AI may fulfill its promise.
What can AI and related technologies achieve in the near-term?
“AI seems to have replaced Uber as the most overused word or phrase in digital health.” – Reporter Stephanie Baum, paraphrasing from an interview with Bob Kocher, Venrock Partners.3
My observations tell me that we have already made some progress and are likely to make more strides in the coming years, thanks to AI, machine learning, and natural language processing. A few areas of potential gain are:
Clinical documentation
Technology that can derive meaning from words or groups of words can help with more accurate clinical documentation. For example, if a patient has a documented UTI but also has in the record an 11 on the Glasgow Coma Scale, a systolic BP of 90, and a respiratory rate of 24, technology can alert the physician to document sepsis.
Quality measurement and reporting
Similarly, if technology can recognize words and numbers, it may be able to extract and report quality measures (for example, an ejection fraction of 35% in a heart failure patient) from progress notes without having a nurse-abstractor manually enter such data into structured fields for reporting, as is currently the case.
Predicting readmissions, mortality, other events
While machine learning has had mixed results in predicting future clinical events, this is likely to change as data integrity and algorithms improve. Best-of-breed technology will probably use both clinical and machine learning tools for predictive purposes in the future.
In 2015, I had the privilege of meeting Vinod Khosla, cofounder of SUN Microsystems and venture capitalist, who predicts that computers will largely supplant physicians in the future, at least in domains relying on access to data. As he puts it, “the core functions necessary for complex diagnoses, treatments, and monitoring will be driven by machine judgment instead of human judgment.”4
While the benefits of technology, especially in health care, are often oversold, I believe AI and related technologies will some day play a large role alongside physicians in the care of patients. However, for AI to deliver, we must first figure out how to collect and organize health care data so that computers are able to ingest, digest and use it in a purposeful way.
Note: Dr. Whitcomb is founder and advisor to Zato Health, which uses natural language processing and discovery technology in health care.
He is chief medical officer at Remedy Partners in Darien, Conn., and a cofounder and past president of SHM.
References
1. Zimmer, Ben. Is It Time to Welcome Our New Computer Overlords?. The Atlantic. https://www.theatlantic.com/technology/archive/2011/02/is-it-time-to-welcome-our-new-computer-overlords/71388/. Accessed 23 Apr 2017.
2. Sanders, Dale. The MD Anderson / IBM Watson Announcement: What does it mean for machine learning in healthcare? Webinar. https://www.slideshare.net/healthcatalyst1/the-md-anderson-ibm-watson-announcement-what-does-it-mean-for-machine-learning-in-healthcare. Accessed 23 Apr 2017.
3. Baum, Stephanie. Venrock survey predicts a flight to quality for digital health investments. MedCity News. 12 Apr 2017. http://medcitynews.com/2017/04/venrock-survey-predicts-flight-quality-digital-health-investment/. Accessed 22 Apr 2017.
4. Khosla, Vinod. The Reinvention Of Medicine: Dr. Algorithm V0-7 And Beyond. TechCrunch. 22 Sept 2014. https://techcrunch.com/2014/09/22/the-reinvention-of-medicine-dr-algorithm-version-0-7-and-beyond/. Accessed 22 Apr 2017.
Health inequities take a societal toll
Arguably one of the most important public health issues in our nation is the gap between high-quality care and the people who need it most. The passage of the Affordable Care Act was meant, in part, to reduce this gap and increase health equity in terms of both eligibility for, and access to, care. However, lower-income residents, especially those from minority groups, are more likely to be hospitalized for asthma, hypertension, heart disease, and diabetes, and to experience infertility, preterm birth, and fetal death.
Health disparities, or inequities, translate not only into greater suffering for certain segments of the population, but also to significantly greater health care costs for everyone. Racial health disparities are associated with an estimated $35 billion annually in excess expenditures, $10 billion in lost productivity, and nearly $200 billion in premature deaths, according to an article in the Harvard Business Review. A 2013 study estimated that reducing racial disparities in adverse pregnancy outcomes – preeclampsia, preterm birth, gestational diabetes mellitus, and fetal death/stillbirth – could generate health care cost savings of up to $214 million per year (Matern Child Health J. 2013 Oct;17[8]:1518-25).
Several years ago, the State of Maryland took a unique approach to reducing health disparities by passing the Maryland Health Improvement and Disparities Reduction Act. One of the major components of this legislation was the creation of Health Enterprise Zones (HEZs), distinct geographical areas across the state dedicated to addressing health disparities and improving access to high-quality care. This incentive-based program provides state-funded resources to primary care providers and community-based health organizations specifically to help the neighborhoods they serve. I was deeply honored to serve as chairman of the task force that recommended the establishment of the HEZs.

For this Master Class, I have invited Melissa A. Simon, MD, the George H. Gardner, MD, Professor of Clinical Gynecology and professor of obstetrics and gynecology at Northwestern University, Chicago, to provide some practical advice on how to create greater health equity.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Arguably one of the most important public health issues in our nation is the gap between high-quality care and the people who need it most. The passage of the Affordable Care Act was meant, in part, to reduce this gap and increase health equity in terms of both eligibility for, and access to, care. However, lower-income residents, especially those from minority groups, are more likely to be hospitalized for asthma, hypertension, heart disease, and diabetes, and to experience infertility, preterm birth, and fetal death.
Health disparities, or inequities, translate not only into greater suffering for certain segments of the population, but also to significantly greater health care costs for everyone. Racial health disparities are associated with an estimated $35 billion annually in excess expenditures, $10 billion in lost productivity, and nearly $200 billion in premature deaths, according to an article in the Harvard Business Review. A 2013 study estimated that reducing racial disparities in adverse pregnancy outcomes – preeclampsia, preterm birth, gestational diabetes mellitus, and fetal death/stillbirth – could generate health care cost savings of up to $214 million per year (Matern Child Health J. 2013 Oct;17[8]:1518-25).
Several years ago, the State of Maryland took a unique approach to reducing health disparities by passing the Maryland Health Improvement and Disparities Reduction Act. One of the major components of this legislation was the creation of Health Enterprise Zones (HEZs), distinct geographical areas across the state dedicated to addressing health disparities and improving access to high-quality care. This incentive-based program provides state-funded resources to primary care providers and community-based health organizations specifically to help the neighborhoods they serve. I was deeply honored to serve as chairman of the task force that recommended the establishment of the HEZs.
For this Master Class, I have invited Melissa A. Simon, MD, the George H. Gardner, MD, Professor of Clinical Gynecology and professor of obstetrics and gynecology at Northwestern University, Chicago, to provide some practical advice on how to create greater health equity.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Arguably one of the most important public health issues in our nation is the gap between high-quality care and the people who need it most. The passage of the Affordable Care Act was meant, in part, to reduce this gap and increase health equity in terms of both eligibility for, and access to, care. However, lower-income residents, especially those from minority groups, are more likely to be hospitalized for asthma, hypertension, heart disease, and diabetes, and to experience infertility, preterm birth, and fetal death.
Health disparities, or inequities, translate not only into greater suffering for certain segments of the population, but also to significantly greater health care costs for everyone. Racial health disparities are associated with an estimated $35 billion annually in excess expenditures, $10 billion in lost productivity, and nearly $200 billion in premature deaths, according to an article in the Harvard Business Review. A 2013 study estimated that reducing racial disparities in adverse pregnancy outcomes – preeclampsia, preterm birth, gestational diabetes mellitus, and fetal death/stillbirth – could generate health care cost savings of up to $214 million per year (Matern Child Health J. 2013 Oct;17[8]:1518-25).
Several years ago, the State of Maryland took a unique approach to reducing health disparities by passing the Maryland Health Improvement and Disparities Reduction Act. One of the major components of this legislation was the creation of Health Enterprise Zones (HEZs), distinct geographical areas across the state dedicated to addressing health disparities and improving access to high-quality care. This incentive-based program provides state-funded resources to primary care providers and community-based health organizations specifically to help the neighborhoods they serve. I was deeply honored to serve as chairman of the task force that recommended the establishment of the HEZs.
For this Master Class, I have invited Melissa A. Simon, MD, the George H. Gardner, MD, Professor of Clinical Gynecology and professor of obstetrics and gynecology at Northwestern University, Chicago, to provide some practical advice on how to create greater health equity.
Dr. Reece, who specializes in maternal-fetal medicine, is vice president for medical affairs at the University of Maryland, Baltimore, as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. Dr. Reece said he had no relevant financial disclosures. He is the medical editor of this column. Contact him at obnews@frontlinemedcom.com.
Moving toward health equity in practice
Of all the medical professions, obstetrics and gynecology should be the strongest champion for equity in women’s health in this country and globally. The question is, what does this mean in the reality of 2017 and moving forward in the 21st century? What does it mean in the context of our own practices and in the landscape of current policy and politics?
Finding answers to these questions requires both a deep understanding of the meaning of health equity and a willingness to rethink the architecture and engineering of how we currently provide care.
The terms equity and equality are sometimes used interchangeably, but they actually have quite different meanings. Imagine three women of different heights standing underneath the lowest branch of a tall apple tree. None of the three women are tall enough to pick an apple from the branch.
If we think about equality, we would assist each woman by giving her a box to stand on, and all three boxes would be the same size. This means that while the tallest woman will now be able to pick an apple, the medium-height woman may be able to touch but not pick the apple, and the shortest woman still may not be able to reach the apple at all.
However, if we think about equity, we’d acknowledge that each woman needs her own personalized box to be able to pick the apple. For instance, the shortest woman may need a box that is three times the height of the box used by the tallest woman.
Achieving true population health for all women requires that we similarly eliminate inequities by providing each patient with her own personalized care plan to help her reach and maintain her health.

Women from minority groups have higher rates of low birth weight, preterm birth, stillbirth, gestational diabetes and its complications, HIV, breast cancer mortality and cervical cancer incidence and mortality, infertility and response to fertility treatment, and maternal mortality.
Yet inequity runs deeper than racial/ethnic labels; disparities also are created by a host of other factors, from cognitive or physical disabilities to gender or sexual identity or orientation, one’s ZIP code, working environment, language, and health literacy.
More than ever, the art of medicine involves understanding how to meet every patient where she is – given her own context and beliefs and levels of support – so that every woman has the opportunity to stand on the right-sized box and pick the apple and thrive.
Our practices
Provider bias and stereotyping can impact health care and health outcomes, and it is important that we work to prevent this in ourselves and in our staff. This means not making assumptions. It means really listening to our patients in ways that we may not have before.
Women who have experienced health inequity may have unique barriers to success. Therefore, we must listen for cues and inquire about our patients’ environment and circumstances, as well as their partnerships and support – or lack thereof. We should then acknowledge and communicate that certain social and environmental factors may impact our ability to achieve a desired outcome.
How can we impact the diet of a patient with gestational diabetes, for instance, if we have not adequately communicated what medical nutritional therapy means in the context of her own culture and ability to access food? If she lives in a food desert or has food insecurity or lives in a violence-ridden neighborhood that keeps her from going to a grocery store regularly, we must think outside the box. Ob.gyns. and their clinical care teams can work with women who have less access to nutritious foods, or who have certain cultural food staples, to suggest recipes and grocery lists that make sense with respect to the types of stores they shop in or their cultural preferences.
When it comes to cancer prevention and treatment, how can we expect a woman to be compliant with screening if we cannot help her understand that she can get screening services for free with her health insurance? How can we help a woman who has coverage for, or access to, free screening but then no funding or coverage for a diagnostic test or cancer treatment? How can we support a patient with abnormal cancer screening results who hasn’t followed up for months because she is afraid to leave home without her partner’s permission?
Such questions and circumstances often involve what we call “social determinants of health,” and they force us to rethink how we can better deliver and optimize care. Re-engineering our practices for health equity may involve employing a more diverse practice staff, linking patients with community resources, modifying our practice hours to align better with working women’s schedules, or finding creative ways to discern patients’ motivating factors and then piggyback on these factors.
We may also need to modify how we approach the number of return visits that we request of women so that follow-up care aligns better with their ability to leave work or find childcare. Simply put, we should strive to set up our patients for success, not failure.
We can pointedly ask patients about the kinds of information and support they want and need. We might ask, for instance: What do you need, and how can I work with you, so that you can effectively monitor and control your glucose levels? How can I work with you to help you get onto a trajectory to stop smoking? How can I help you better understand what tests and procedures are covered under your insurance plan, or whether you qualify for free services?
Patients with lower health literacy may need teach-back methods to validate understanding, or messaging that is more focused and limited at any one time. Self-efficacy through patient-centered education and support should be our goal.
Practices and clinics may also be able to adapt elements of the National Cancer Institute’s multicenter Patient Navigation Research Program, in which community health workers or other “patient navigators” address women’s personal barriers to the timely follow-up of abnormal breast and cervical cancer screening results. Patient navigation through this program and similar projects, including programs that we’ve adapted for different racial and ethnic communities in and around Chicago, has reduced or eliminated delays in diagnostic resolution of gynecologic cancer (Cancer. 2015 Nov 15;121[22]:4025-34, Breast Cancer Res Treat. 2016 Aug;158[3]:523-34, Am J Public Health. 2015 May;105[5]:e87-94).
The patient navigation model is increasingly being adapted and used in a variety of contexts outside of cancer care as well. In a postpartum patient navigation program that we tested at Northwestern University’s Medicaid-based outpatient clinic, a navigator was hired to communicate with patients and support them between delivery and completion of their postpartum care. Patients were reminded through calls and/or texts of their postpartum visits and of the benefits of breastfeeding, effective contraception, and other postpartum practices.
The demonstration project was impactful: Women who were enrolled in the program were more likely to return for postpartum care, to receive World Health Organization Tier 1 or 2 contraception, and to have postpartum screening and vaccinations, compared with women who received care before the program began (Obstet Gynecol. 2017 May;129[5]:925-33).
Connections to our patients will help us to achieve health equity. This includes connections between the primary care we provide and the specialty care our patients sometimes require, both inside and outside of our field. We may refer a patient to an oncology team, for instance, and in the process, unwittingly transfer her care such that other conditions that we’ve been managing – hypertension, depression, or diabetes – fall by the wayside.
Instead, we have to re-engineer our processes so that we maintain personalized connections back to these patients. For example, the referring ob.gyn. could develop and send to the oncologist or gynecologic-oncologist a care plan that includes the patient’s comorbid conditions and how they could be managed. This would allow for clearer communication.
Our communities
As ob.gyns., we have a common goal of championing health equity and true population health for every woman, regardless of whether she lives in rural, urban, or suburban America and regardless of whether she has conservative or liberal values. To do so, we must extend ourselves beyond our own practices.
In a committee opinion on Racial and Ethnic Disparities in Obstetrics and Gynecology, the American College of Obstetricians and Gynecologists advises that ob.gyns. take a number of actions to increase health equity. These include raising awareness about inequity and its effects on health outcomes, promoting quality improvement projects that target disparities, working with public health leadership, and helping recruit ob.gyns. and other health care providers from racial and ethnic minority groups (Obstet Gynecol 2015;126:e130-4).
In Chicago, where 1 out of 5 people lives in poverty and 1 out of 10 lives in deep poverty, we are still in our infancy in combating health inequities. However, with partnerships between academic institutions, departments of health, and other organizations across various sectors, we are beginning to move the needle on these entrenched health inequities.
For example, in 2007, there was a 60% difference in breast cancer mortality between black and white women in Chicago. This disparity sparked the development of the Metropolitan Chicago Breast Cancer Task Force and a series of on-the-ground patient navigator programs, along with several key policy changes and new state laws.
State actions included requiring quality reporting on mammography and increasing the Medicaid reimbursement rate for mammography to the Medicare rate. Nationally, beneficial changes were made to Medicare’s quality metrics and to the National Breast and Cervical Cancer Early Detection Program. All told, through a combination of studies and initiatives focused on improving knowledge, trust, access to care, and quality of care, we have been able to decrease the breast cancer mortality gap by 20%.
We also have a role to play in nurturing and developing a workforce that better aligns with our evolving demographics. This involves redesigning how we plant seeds of opportunity among high school students, undergraduates, and young medical students, and how we seek job applicants. Moreover, when we help people get to the next step in their careers, we need to make sure there is continuous support to retain them and help propel them to the next level.
We should think creatively to establish programs or launch initiatives that can help level the playing field for all women. For example, I created a Massive Open Online Course called “Career 911: Your Future Job in Medicine and Healthcare” as a free workforce development pipeline program. It is accessible on a global platform (https://www.coursera.org/learn/healthcarejobs) and is one example of how we as ob.gyns. can leverage our skills and resources.
Along the way, we also need to train our students and residents – and ourselves – to be more familiar with, and articulate about, health care policy. We need to understand how policy is made and modified and how we can be good communicators and thought leaders.
Right now, our ability to articulate our patients’ stories to policy makers and to the public seems underdeveloped and undertapped. The onus is on us to write and speak about how all women must have the opportunity to not only access care but to access high-quality care and preventive services that are important for full health. Providing health equity isn’t about giving someone a handout, but about giving her a helping hand to take control of her health.
Achieving health equity will involve changing our approach to research. If medical research on women’s health continues to be dominated by studies in which participants are homogeneous and from mainly white or well-resourced populations, we will never have output that is generalizable. As practicing ob.gyns., we can look for opportunities to advocate for diversity in research. We can also acknowledge that, for some women, there is historically-rooted distrust of the health care system that serves as a barrier both to obtaining care and enrolling in trials.
By meeting women where they are, and by tailoring their individual boxes as best we can – in research, in workforce development, and in clinical care delivery – we can work toward solutions.
Strategies for achieving women’s health equity
• Modify office hours/dates to allow flexibility for women who have challenges scheduling childcare and time off from work.
• Ensure handouts, educational materials, and all communications are at appropriate health literacy levels.
• Acknowledge and understand an individual woman’s barriers to care, including social determinants of health, and create a care plan that is achievable for her.
• Learn about and refer women to local community resources needed to overcome barriers to care, such as childcare, social services support, support services for intimate partner violence, and substance abuse counseling.
• Examine office processes to optimize the number of visits women have to attend for a particular health issue. Are there ways to explain results and next steps in a care plan without having to make her come back for an office visit?
Dr. Simon is the George H. Gardner Professor of Clinical Gynecology at Northwestern University, Chicago, and director of the Chicago Cancer Health Equity Collaborative. She is a member of the U.S. Preventive Services Task Force, but the views expressed in this piece are her own.
Of all the medical professions, obstetrics and gynecology should be the strongest champion for equity in women’s health in this country and globally. The question is, what does this mean in the reality of 2017 and moving forward in the 21st century? What does it mean in the context of our own practices and in the landscape of current policy and politics?
Finding answers to these questions requires both a deep understanding of the meaning of health equity and a willingness to rethink the architecture and engineering of how we currently provide care.
The terms equity and equality are sometimes used interchangeably, but they actually have quite different meanings. Imagine three women of different heights standing underneath the lowest branch of a tall apple tree. None of the three women are tall enough to pick an apple from the branch.
If we think about equality, we would assist each woman by giving her a box to stand on, and all three boxes would be the same size. This means that while the tallest woman will now be able to pick an apple, the medium-height woman may be able to touch but not pick the apple, and the shortest woman still may not be able to reach the apple at all.
However, if we think about equity, we’d acknowledge that each woman needs her own personalized box to be able to pick the apple. For instance, the shortest woman may need a box that is three times the height of the box used by the tallest woman.
Achieving true population health for all women requires that we similarly eliminate inequities by providing each patient with her own personalized care plan to help her reach and maintain her health.
Women from minority groups have higher rates of low birth weight, preterm birth, stillbirth, gestational diabetes and its complications, HIV, breast cancer mortality and cervical cancer incidence and mortality, infertility and response to fertility treatment, and maternal mortality.
Yet inequity runs deeper than racial/ethnic labels; disparities also are created by a host of other factors, from cognitive or physical disabilities to gender or sexual identity or orientation, one’s ZIP code, working environment, language, and health literacy.
More than ever, the art of medicine involves understanding how to meet every patient where she is – given her own context and beliefs and levels of support – so that every woman has the opportunity to stand on the right-sized box and pick the apple and thrive.
Our practices
Provider bias and stereotyping can impact health care and health outcomes, and it is important that we work to prevent this in ourselves and in our staff. This means not making assumptions. It means really listening to our patients in ways that we may not have before.
Women who have experienced health inequity may have unique barriers to success. Therefore, we must listen for cues and inquire about our patients’ environment and circumstances, as well as their partnerships and support – or lack thereof. We should then acknowledge and communicate that certain social and environmental factors may impact our ability to achieve a desired outcome.
How can we impact the diet of a patient with gestational diabetes, for instance, if we have not adequately communicated what medical nutritional therapy means in the context of her own culture and ability to access food? If she lives in a food desert or has food insecurity or lives in a violence-ridden neighborhood that keeps her from going to a grocery store regularly, we must think outside the box. Ob.gyns. and their clinical care teams can work with women who have less access to nutritious foods, or who have certain cultural food staples, to suggest recipes and grocery lists that make sense with respect to the types of stores they shop in or their cultural preferences.
When it comes to cancer prevention and treatment, how can we expect a woman to be compliant with screening if we cannot help her understand that she can get screening services for free with her health insurance? How can we help a woman who has coverage for, or access to, free screening but then no funding or coverage for a diagnostic test or cancer treatment? How can we support a patient with abnormal cancer screening results who hasn’t followed up for months because she is afraid to leave home without her partner’s permission?
Such questions and circumstances often involve what we call “social determinants of health,” and they force us to rethink how we can better deliver and optimize care. Re-engineering our practices for health equity may involve employing a more diverse practice staff, linking patients with community resources, modifying our practice hours to align better with working women’s schedules, or finding creative ways to discern patients’ motivating factors and then piggyback on these factors.
We may also need to modify how we approach the number of return visits that we request of women so that follow-up care aligns better with their ability to leave work or find childcare. Simply put, we should strive to set up our patients for success, not failure.
We can pointedly ask patients about the kinds of information and support they want and need. We might ask, for instance: What do you need, and how can I work with you, so that you can effectively monitor and control your glucose levels? How can I work with you to help you get onto a trajectory to stop smoking? How can I help you better understand what tests and procedures are covered under your insurance plan, or whether you qualify for free services?
Patients with lower health literacy may need teach-back methods to validate understanding, or messaging that is more focused and limited at any one time. Self-efficacy through patient-centered education and support should be our goal.
Practices and clinics may also be able to adapt elements of the National Cancer Institute’s multicenter Patient Navigation Research Program, in which community health workers or other “patient navigators” address women’s personal barriers to the timely follow-up of abnormal breast and cervical cancer screening results. Patient navigation through this program and similar projects, including programs that we’ve adapted for different racial and ethnic communities in and around Chicago, has reduced or eliminated delays in diagnostic resolution of gynecologic cancer (Cancer. 2015 Nov 15;121[22]:4025-34, Breast Cancer Res Treat. 2016 Aug;158[3]:523-34, Am J Public Health. 2015 May;105[5]:e87-94).
The patient navigation model is increasingly being adapted and used in a variety of contexts outside of cancer care as well. In a postpartum patient navigation program that we tested at Northwestern University’s Medicaid-based outpatient clinic, a navigator was hired to communicate with patients and support them between delivery and completion of their postpartum care. Patients were reminded through calls and/or texts of their postpartum visits and of the benefits of breastfeeding, effective contraception, and other postpartum practices.
The demonstration project was impactful: Women who were enrolled in the program were more likely to return for postpartum care, to receive World Health Organization Tier 1 or 2 contraception, and to have postpartum screening and vaccinations, compared with women who received care before the program began (Obstet Gynecol. 2017 May;129[5]:925-33).
Connections to our patients will help us to achieve health equity. This includes connections between the primary care we provide and the specialty care our patients sometimes require, both inside and outside of our field. We may refer a patient to an oncology team, for instance, and in the process, unwittingly transfer her care such that other conditions that we’ve been managing – hypertension, depression, or diabetes – fall by the wayside.
Instead, we have to re-engineer our processes so that we maintain personalized connections back to these patients. For example, the referring ob.gyn. could develop and send to the oncologist or gynecologic-oncologist a care plan that includes the patient’s comorbid conditions and how they could be managed. This would allow for clearer communication.
Our communities
As ob.gyns., we have a common goal of championing health equity and true population health for every woman, regardless of whether she lives in rural, urban, or suburban America and regardless of whether she has conservative or liberal values. To do so, we must extend ourselves beyond our own practices.
In a committee opinion on Racial and Ethnic Disparities in Obstetrics and Gynecology, the American College of Obstetricians and Gynecologists advises that ob.gyns. take a number of actions to increase health equity. These include raising awareness about inequity and its effects on health outcomes, promoting quality improvement projects that target disparities, working with public health leadership, and helping recruit ob.gyns. and other health care providers from racial and ethnic minority groups (Obstet Gynecol 2015;126:e130-4).
In Chicago, where 1 out of 5 people lives in poverty and 1 out of 10 lives in deep poverty, we are still in our infancy in combating health inequities. However, with partnerships between academic institutions, departments of health, and other organizations across various sectors, we are beginning to move the needle on these entrenched health inequities.
For example, in 2007, there was a 60% difference in breast cancer mortality between black and white women in Chicago. This disparity sparked the development of the Metropolitan Chicago Breast Cancer Task Force and a series of on-the-ground patient navigator programs, along with several key policy changes and new state laws.
State actions included requiring quality reporting on mammography and increasing the Medicaid reimbursement rate for mammography to the Medicare rate. Nationally, beneficial changes were made to Medicare’s quality metrics and to the National Breast and Cervical Cancer Early Detection Program. All told, through a combination of studies and initiatives focused on improving knowledge, trust, access to care, and quality of care, we have been able to decrease the breast cancer mortality gap by 20%.
We also have a role to play in nurturing and developing a workforce that better aligns with our evolving demographics. This involves redesigning how we plant seeds of opportunity among high school students, undergraduates, and young medical students, and how we seek job applicants. Moreover, when we help people get to the next step in their careers, we need to make sure there is continuous support to retain them and help propel them to the next level.
We should think creatively to establish programs or launch initiatives that can help level the playing field for all women. For example, I created a Massive Open Online Course called “Career 911: Your Future Job in Medicine and Healthcare” as a free workforce development pipeline program. It is accessible on a global platform (https://www.coursera.org/learn/healthcarejobs) and is one example of how we as ob.gyns. can leverage our skills and resources.
Along the way, we also need to train our students and residents – and ourselves – to be more familiar with, and articulate about, health care policy. We need to understand how policy is made and modified and how we can be good communicators and thought leaders.
Right now, our ability to articulate our patients’ stories to policy makers and to the public seems underdeveloped and undertapped. The onus is on us to write and speak about how all women must have the opportunity to not only access care but to access high-quality care and preventive services that are important for full health. Providing health equity isn’t about giving someone a handout, but about giving her a helping hand to take control of her health.
Achieving health equity will involve changing our approach to research. If medical research on women’s health continues to be dominated by studies in which participants are homogeneous and from mainly white or well-resourced populations, we will never have output that is generalizable. As practicing ob.gyns., we can look for opportunities to advocate for diversity in research. We can also acknowledge that, for some women, there is historically-rooted distrust of the health care system that serves as a barrier both to obtaining care and enrolling in trials.
By meeting women where they are, and by tailoring their individual boxes as best we can – in research, in workforce development, and in clinical care delivery – we can work toward solutions.
Strategies for achieving women’s health equity
• Modify office hours/dates to allow flexibility for women who have challenges scheduling childcare and time off from work.
• Ensure handouts, educational materials, and all communications are at appropriate health literacy levels.
• Acknowledge and understand an individual woman’s barriers to care, including social determinants of health, and create a care plan that is achievable for her.
• Learn about and refer women to local community resources needed to overcome barriers to care, such as childcare, social services support, support services for intimate partner violence, and substance abuse counseling.
• Examine office processes to optimize the number of visits women have to attend for a particular health issue. Are there ways to explain results and next steps in a care plan without having to make her come back for an office visit?
Dr. Simon is the George H. Gardner Professor of Clinical Gynecology at Northwestern University, Chicago, and director of the Chicago Cancer Health Equity Collaborative. She is a member of the U.S. Preventive Services Task Force, but the views expressed in this piece are her own.
Of all the medical professions, obstetrics and gynecology should be the strongest champion for equity in women’s health in this country and globally. The question is, what does this mean in the reality of 2017 and moving forward in the 21st century? What does it mean in the context of our own practices and in the landscape of current policy and politics?
Finding answers to these questions requires both a deep understanding of the meaning of health equity and a willingness to rethink the architecture and engineering of how we currently provide care.
The terms equity and equality are sometimes used interchangeably, but they actually have quite different meanings. Imagine three women of different heights standing underneath the lowest branch of a tall apple tree. None of the three women are tall enough to pick an apple from the branch.
If we think about equality, we would assist each woman by giving her a box to stand on, and all three boxes would be the same size. This means that while the tallest woman will now be able to pick an apple, the medium-height woman may be able to touch but not pick the apple, and the shortest woman still may not be able to reach the apple at all.
However, if we think about equity, we’d acknowledge that each woman needs her own personalized box to be able to pick the apple. For instance, the shortest woman may need a box that is three times the height of the box used by the tallest woman.
Achieving true population health for all women requires that we similarly eliminate inequities by providing each patient with her own personalized care plan to help her reach and maintain her health.
Women from minority groups have higher rates of low birth weight, preterm birth, stillbirth, gestational diabetes and its complications, HIV, breast cancer mortality and cervical cancer incidence and mortality, infertility and response to fertility treatment, and maternal mortality.
Yet inequity runs deeper than racial/ethnic labels; disparities also are created by a host of other factors, from cognitive or physical disabilities to gender or sexual identity or orientation, one’s ZIP code, working environment, language, and health literacy.
More than ever, the art of medicine involves understanding how to meet every patient where she is – given her own context and beliefs and levels of support – so that every woman has the opportunity to stand on the right-sized box and pick the apple and thrive.
Our practices
Provider bias and stereotyping can impact health care and health outcomes, and it is important that we work to prevent this in ourselves and in our staff. This means not making assumptions. It means really listening to our patients in ways that we may not have before.
Women who have experienced health inequity may have unique barriers to success. Therefore, we must listen for cues and inquire about our patients’ environment and circumstances, as well as their partnerships and support – or lack thereof. We should then acknowledge and communicate that certain social and environmental factors may impact our ability to achieve a desired outcome.
How can we impact the diet of a patient with gestational diabetes, for instance, if we have not adequately communicated what medical nutritional therapy means in the context of her own culture and ability to access food? If she lives in a food desert or has food insecurity or lives in a violence-ridden neighborhood that keeps her from going to a grocery store regularly, we must think outside the box. Ob.gyns. and their clinical care teams can work with women who have less access to nutritious foods, or who have certain cultural food staples, to suggest recipes and grocery lists that make sense with respect to the types of stores they shop in or their cultural preferences.
When it comes to cancer prevention and treatment, how can we expect a woman to be compliant with screening if we cannot help her understand that she can get screening services for free with her health insurance? How can we help a woman who has coverage for, or access to, free screening but then no funding or coverage for a diagnostic test or cancer treatment? How can we support a patient with abnormal cancer screening results who hasn’t followed up for months because she is afraid to leave home without her partner’s permission?
Such questions and circumstances often involve what we call “social determinants of health,” and they force us to rethink how we can better deliver and optimize care. Re-engineering our practices for health equity may involve employing a more diverse practice staff, linking patients with community resources, modifying our practice hours to align better with working women’s schedules, or finding creative ways to discern patients’ motivating factors and then piggyback on these factors.
We may also need to modify how we approach the number of return visits that we request of women so that follow-up care aligns better with their ability to leave work or find childcare. Simply put, we should strive to set up our patients for success, not failure.
We can pointedly ask patients about the kinds of information and support they want and need. We might ask, for instance: What do you need, and how can I work with you, so that you can effectively monitor and control your glucose levels? How can I work with you to help you get onto a trajectory to stop smoking? How can I help you better understand what tests and procedures are covered under your insurance plan, or whether you qualify for free services?
Patients with lower health literacy may need teach-back methods to validate understanding, or messaging that is more focused and limited at any one time. Self-efficacy through patient-centered education and support should be our goal.
Practices and clinics may also be able to adapt elements of the National Cancer Institute’s multicenter Patient Navigation Research Program, in which community health workers or other “patient navigators” address women’s personal barriers to the timely follow-up of abnormal breast and cervical cancer screening results. Patient navigation through this program and similar projects, including programs that we’ve adapted for different racial and ethnic communities in and around Chicago, has reduced or eliminated delays in diagnostic resolution of gynecologic cancer (Cancer. 2015 Nov 15;121[22]:4025-34, Breast Cancer Res Treat. 2016 Aug;158[3]:523-34, Am J Public Health. 2015 May;105[5]:e87-94).
The patient navigation model is increasingly being adapted and used in a variety of contexts outside of cancer care as well. In a postpartum patient navigation program that we tested at Northwestern University’s Medicaid-based outpatient clinic, a navigator was hired to communicate with patients and support them between delivery and completion of their postpartum care. Patients were reminded through calls and/or texts of their postpartum visits and of the benefits of breastfeeding, effective contraception, and other postpartum practices.
The demonstration project was impactful: Women who were enrolled in the program were more likely to return for postpartum care, to receive World Health Organization Tier 1 or 2 contraception, and to have postpartum screening and vaccinations, compared with women who received care before the program began (Obstet Gynecol. 2017 May;129[5]:925-33).
Connections to our patients will help us to achieve health equity. This includes connections between the primary care we provide and the specialty care our patients sometimes require, both inside and outside of our field. We may refer a patient to an oncology team, for instance, and in the process, unwittingly transfer her care such that other conditions that we’ve been managing – hypertension, depression, or diabetes – fall by the wayside.
Instead, we have to re-engineer our processes so that we maintain personalized connections back to these patients. For example, the referring ob.gyn. could develop and send to the oncologist or gynecologic-oncologist a care plan that includes the patient’s comorbid conditions and how they could be managed. This would allow for clearer communication.
Our communities
As ob.gyns., we have a common goal of championing health equity and true population health for every woman, regardless of whether she lives in rural, urban, or suburban America and regardless of whether she has conservative or liberal values. To do so, we must extend ourselves beyond our own practices.
In a committee opinion on Racial and Ethnic Disparities in Obstetrics and Gynecology, the American College of Obstetricians and Gynecologists advises that ob.gyns. take a number of actions to increase health equity. These include raising awareness about inequity and its effects on health outcomes, promoting quality improvement projects that target disparities, working with public health leadership, and helping recruit ob.gyns. and other health care providers from racial and ethnic minority groups (Obstet Gynecol 2015;126:e130-4).
In Chicago, where 1 out of 5 people lives in poverty and 1 out of 10 lives in deep poverty, we are still in our infancy in combating health inequities. However, with partnerships between academic institutions, departments of health, and other organizations across various sectors, we are beginning to move the needle on these entrenched health inequities.
For example, in 2007, there was a 60% difference in breast cancer mortality between black and white women in Chicago. This disparity sparked the development of the Metropolitan Chicago Breast Cancer Task Force and a series of on-the-ground patient navigator programs, along with several key policy changes and new state laws.
State actions included requiring quality reporting on mammography and increasing the Medicaid reimbursement rate for mammography to the Medicare rate. Nationally, beneficial changes were made to Medicare’s quality metrics and to the National Breast and Cervical Cancer Early Detection Program. All told, through a combination of studies and initiatives focused on improving knowledge, trust, access to care, and quality of care, we have been able to decrease the breast cancer mortality gap by 20%.
We also have a role to play in nurturing and developing a workforce that better aligns with our evolving demographics. This involves redesigning how we plant seeds of opportunity among high school students, undergraduates, and young medical students, and how we seek job applicants. Moreover, when we help people get to the next step in their careers, we need to make sure there is continuous support to retain them and help propel them to the next level.
We should think creatively to establish programs or launch initiatives that can help level the playing field for all women. For example, I created a Massive Open Online Course called “Career 911: Your Future Job in Medicine and Healthcare” as a free workforce development pipeline program. It is accessible on a global platform (https://www.coursera.org/learn/healthcarejobs) and is one example of how we as ob.gyns. can leverage our skills and resources.
Along the way, we also need to train our students and residents – and ourselves – to be more familiar with, and articulate about, health care policy. We need to understand how policy is made and modified and how we can be good communicators and thought leaders.
Right now, our ability to articulate our patients’ stories to policy makers and to the public seems underdeveloped and undertapped. The onus is on us to write and speak about how all women must have the opportunity to not only access care but to access high-quality care and preventive services that are important for full health. Providing health equity isn’t about giving someone a handout, but about giving her a helping hand to take control of her health.
Achieving health equity will involve changing our approach to research. If medical research on women’s health continues to be dominated by studies in which participants are homogeneous and from mainly white or well-resourced populations, we will never have output that is generalizable. As practicing ob.gyns., we can look for opportunities to advocate for diversity in research. We can also acknowledge that, for some women, there is historically-rooted distrust of the health care system that serves as a barrier both to obtaining care and enrolling in trials.
By meeting women where they are, and by tailoring their individual boxes as best we can – in research, in workforce development, and in clinical care delivery – we can work toward solutions.
Strategies for achieving women’s health equity
• Modify office hours/dates to allow flexibility for women who have challenges scheduling childcare and time off from work.
• Ensure handouts, educational materials, and all communications are at appropriate health literacy levels.
• Acknowledge and understand an individual woman’s barriers to care, including social determinants of health, and create a care plan that is achievable for her.
• Learn about and refer women to local community resources needed to overcome barriers to care, such as childcare, social services support, support services for intimate partner violence, and substance abuse counseling.
• Examine office processes to optimize the number of visits women have to attend for a particular health issue. Are there ways to explain results and next steps in a care plan without having to make her come back for an office visit?
Dr. Simon is the George H. Gardner Professor of Clinical Gynecology at Northwestern University, Chicago, and director of the Chicago Cancer Health Equity Collaborative. She is a member of the U.S. Preventive Services Task Force, but the views expressed in this piece are her own.
Consider neurodevelopmental impacts of hyperemesis gravidarum
Hyperemesis gravidarum (HG) affects just 1%-2% of pregnant women, but it’s clinical consequences are significant, with excess vomiting and dehydration, hospitalization, and the need for intravenous fluids being common in that group. In extreme cases, repeated vomiting has led to tears in the esophagus and severe dehydration has caused acute renal failure. All of that leaves aside the obvious suffering and distress it causes for women with the condition.
While studies continue to support the long-held theory that mild-to-moderate nausea and vomiting has a protective effect in pregnancy, that does not appear to be true for HG. Rather, the medical literature shows that HG is associated with small-for-gestational-age neonates, low birth weight, higher rates of preterm birth, and lower Apgar scores at 5 minutes.

I was one of the investigators on a study that prospectively followed more than 200 women with nausea and vomiting in pregnancy from 2006 to 2012. We found that children whose mothers were hospitalized for their symptoms – 22 in all – had significantly lower IQ scores at 3.5 years to 7 years, compared with children whose mothers were not hospitalized. Verbal IQ scores were 107.2 points vs. 112.7 (P = .04), performance IQ scores were 105.6 vs. 112.3 (P = .03), and full scale IQ was 108.7 vs. 114.2 (P = .05).
The study cohort included three groups: women treated with more than four tablets per day of doxylamine/pyridoxine (Diclegis); women treated with up to four tablets per day of the drug; and women who did not receive pharmacotherapy (Obstet Gynecol. 2015. doi: 10.1097/01.AOG.0000463229.81803.1a).
Hospitalized women in the study received antiemetics about a week later, experienced more severe symptoms, and were more likely to report depression. Overall, we found that duration of hospitalization, maternal depression, and maternal IQ all were significant predictors for these outcomes. However, daily antiemetic therapy was not associated with adverse outcomes.

Another study, published the same year, found that children exposed to HG had a more than three times increased risk for a neurodevelopmental diagnosis, including attention disorders, speech and language delays, and sensory disorders. The changes were more prevalent when women experienced symptoms early in pregnancy – prior to 5 weeks of gestation (Eur J Obstet Gynecol Reprod Biol. 2015 Jun;189:79-84).
The study compared neurodevelopmental outcomes for 312 children from 203 women with HG, with 169 children from 89 unaffected mothers. The findings are similar to those of our study, despite the differences in methodologies. Both studies found that the antiemetics were not associated with adverse outcomes, but the symptoms of HG appear to be the culprit.
While more research is needed to confirm these findings, it makes sense that the nutritional deficiencies created by excess vomiting and inability to eat are having an impact on the fetus.
It also raises an important question for the ob.gyn. about when to intervene in these women. Often, clinicians take a wait-and-see approach to nausea and vomiting in pregnancy, but the developing research suggests that earlier intervention would lead to better outcomes for mother and baby. One guide to determining that preventive antiemetics are necessary is to consider whether your patient has had HG in a previous pregnancy or if her mother or sister has experienced HG.
Another consideration is treating the nutritional deficiency that develops in women whose HG symptoms persist. These women are not simply in need of fluids and electrolytes but are missing essential vitamins and proteins. This is an area where much more research is needed, but clinicians can take a proactive approach by providing team care that includes consultation with a dietitians or nutritionist.
Finally, we cannot forget that maternal depression also appears to be significant predictor of poor fetal outcomes, so providing appropriate psychiatric treatment is essential.
Dr. Koren is professor of physiology/pharmacology and pediatrics at Western University in Ontario. He is the founder of the Motherisk Program. Dr. Koren was a principal investigator in the U.S. study that resulted in the approval of Diclegis, marketed by Duchesnay USA, and has served as a consultant to Duchesnay.
Hyperemesis gravidarum (HG) affects just 1%-2% of pregnant women, but it’s clinical consequences are significant, with excess vomiting and dehydration, hospitalization, and the need for intravenous fluids being common in that group. In extreme cases, repeated vomiting has led to tears in the esophagus and severe dehydration has caused acute renal failure. All of that leaves aside the obvious suffering and distress it causes for women with the condition.
While studies continue to support the long-held theory that mild-to-moderate nausea and vomiting has a protective effect in pregnancy, that does not appear to be true for HG. Rather, the medical literature shows that HG is associated with small-for-gestational-age neonates, low birth weight, higher rates of preterm birth, and lower Apgar scores at 5 minutes.
I was one of the investigators on a study that prospectively followed more than 200 women with nausea and vomiting in pregnancy from 2006 to 2012. We found that children whose mothers were hospitalized for their symptoms – 22 in all – had significantly lower IQ scores at 3.5 years to 7 years, compared with children whose mothers were not hospitalized. Verbal IQ scores were 107.2 points vs. 112.7 (P = .04), performance IQ scores were 105.6 vs. 112.3 (P = .03), and full scale IQ was 108.7 vs. 114.2 (P = .05).
The study cohort included three groups: women treated with more than four tablets per day of doxylamine/pyridoxine (Diclegis); women treated with up to four tablets per day of the drug; and women who did not receive pharmacotherapy (Obstet Gynecol. 2015. doi: 10.1097/01.AOG.0000463229.81803.1a).
Hospitalized women in the study received antiemetics about a week later, experienced more severe symptoms, and were more likely to report depression. Overall, we found that duration of hospitalization, maternal depression, and maternal IQ all were significant predictors for these outcomes. However, daily antiemetic therapy was not associated with adverse outcomes.
Another study, published the same year, found that children exposed to HG had a more than three times increased risk for a neurodevelopmental diagnosis, including attention disorders, speech and language delays, and sensory disorders. The changes were more prevalent when women experienced symptoms early in pregnancy – prior to 5 weeks of gestation (Eur J Obstet Gynecol Reprod Biol. 2015 Jun;189:79-84).
The study compared neurodevelopmental outcomes for 312 children from 203 women with HG, with 169 children from 89 unaffected mothers. The findings are similar to those of our study, despite the differences in methodologies. Both studies found that the antiemetics were not associated with adverse outcomes, but the symptoms of HG appear to be the culprit.
While more research is needed to confirm these findings, it makes sense that the nutritional deficiencies created by excess vomiting and inability to eat are having an impact on the fetus.
It also raises an important question for the ob.gyn. about when to intervene in these women. Often, clinicians take a wait-and-see approach to nausea and vomiting in pregnancy, but the developing research suggests that earlier intervention would lead to better outcomes for mother and baby. One guide to determining that preventive antiemetics are necessary is to consider whether your patient has had HG in a previous pregnancy or if her mother or sister has experienced HG.
Another consideration is treating the nutritional deficiency that develops in women whose HG symptoms persist. These women are not simply in need of fluids and electrolytes but are missing essential vitamins and proteins. This is an area where much more research is needed, but clinicians can take a proactive approach by providing team care that includes consultation with a dietitians or nutritionist.
Finally, we cannot forget that maternal depression also appears to be significant predictor of poor fetal outcomes, so providing appropriate psychiatric treatment is essential.
Dr. Koren is professor of physiology/pharmacology and pediatrics at Western University in Ontario. He is the founder of the Motherisk Program. Dr. Koren was a principal investigator in the U.S. study that resulted in the approval of Diclegis, marketed by Duchesnay USA, and has served as a consultant to Duchesnay.
Hyperemesis gravidarum (HG) affects just 1%-2% of pregnant women, but it’s clinical consequences are significant, with excess vomiting and dehydration, hospitalization, and the need for intravenous fluids being common in that group. In extreme cases, repeated vomiting has led to tears in the esophagus and severe dehydration has caused acute renal failure. All of that leaves aside the obvious suffering and distress it causes for women with the condition.
While studies continue to support the long-held theory that mild-to-moderate nausea and vomiting has a protective effect in pregnancy, that does not appear to be true for HG. Rather, the medical literature shows that HG is associated with small-for-gestational-age neonates, low birth weight, higher rates of preterm birth, and lower Apgar scores at 5 minutes.
I was one of the investigators on a study that prospectively followed more than 200 women with nausea and vomiting in pregnancy from 2006 to 2012. We found that children whose mothers were hospitalized for their symptoms – 22 in all – had significantly lower IQ scores at 3.5 years to 7 years, compared with children whose mothers were not hospitalized. Verbal IQ scores were 107.2 points vs. 112.7 (P = .04), performance IQ scores were 105.6 vs. 112.3 (P = .03), and full scale IQ was 108.7 vs. 114.2 (P = .05).
The study cohort included three groups: women treated with more than four tablets per day of doxylamine/pyridoxine (Diclegis); women treated with up to four tablets per day of the drug; and women who did not receive pharmacotherapy (Obstet Gynecol. 2015. doi: 10.1097/01.AOG.0000463229.81803.1a).
Hospitalized women in the study received antiemetics about a week later, experienced more severe symptoms, and were more likely to report depression. Overall, we found that duration of hospitalization, maternal depression, and maternal IQ all were significant predictors for these outcomes. However, daily antiemetic therapy was not associated with adverse outcomes.
Another study, published the same year, found that children exposed to HG had a more than three times increased risk for a neurodevelopmental diagnosis, including attention disorders, speech and language delays, and sensory disorders. The changes were more prevalent when women experienced symptoms early in pregnancy – prior to 5 weeks of gestation (Eur J Obstet Gynecol Reprod Biol. 2015 Jun;189:79-84).
The study compared neurodevelopmental outcomes for 312 children from 203 women with HG, with 169 children from 89 unaffected mothers. The findings are similar to those of our study, despite the differences in methodologies. Both studies found that the antiemetics were not associated with adverse outcomes, but the symptoms of HG appear to be the culprit.
While more research is needed to confirm these findings, it makes sense that the nutritional deficiencies created by excess vomiting and inability to eat are having an impact on the fetus.
It also raises an important question for the ob.gyn. about when to intervene in these women. Often, clinicians take a wait-and-see approach to nausea and vomiting in pregnancy, but the developing research suggests that earlier intervention would lead to better outcomes for mother and baby. One guide to determining that preventive antiemetics are necessary is to consider whether your patient has had HG in a previous pregnancy or if her mother or sister has experienced HG.
Another consideration is treating the nutritional deficiency that develops in women whose HG symptoms persist. These women are not simply in need of fluids and electrolytes but are missing essential vitamins and proteins. This is an area where much more research is needed, but clinicians can take a proactive approach by providing team care that includes consultation with a dietitians or nutritionist.
Finally, we cannot forget that maternal depression also appears to be significant predictor of poor fetal outcomes, so providing appropriate psychiatric treatment is essential.
Dr. Koren is professor of physiology/pharmacology and pediatrics at Western University in Ontario. He is the founder of the Motherisk Program. Dr. Koren was a principal investigator in the U.S. study that resulted in the approval of Diclegis, marketed by Duchesnay USA, and has served as a consultant to Duchesnay.
PARP inhibitors: New developments in ovarian cancer treatment
Ovarian cancer remains the leading cause of death from gynecologic cancer worldwide and one of the five leading causes of death from cancer in women in the United States. In addition to surgery, treatment consists of combination platinum and taxane chemotherapy that offers a high response rate; however, a majority of women will develop persistent or recurrent disease.
A clinical practice statement released by the Society of Gynecologic Oncology in October 2014 states that “women diagnosed with epithelial ovarian, tubal, and peritoneal cancers should receive genetic counseling and be offered genetic testing, even in the absence of family history.” Patients should be informed that this genetic testing serves to prognosticate, inform about personal and familial cancer risk, but also aids in choices of novel therapeutic agents, specifically Poly (ADP-ribose) polymerase (PARP) inhibitors.

Genetic involvement of BRCA
A small proportion of ovarian cancers are attributable to genetic mutations, with approximately 10%-15% of cases caused by germline mutations of BRCA1 and BRCA2. BRCA1 deleterious mutations confer an ovarian cancer risk of approximately 39%-46%; and the risk of ovarian cancer is roughly 12%-20% for patients with BRCA2 deleterious mutations. As a tumor suppressor gene, BRCA is involved in the DNA repair process. Specifically, it is involved in homologous recombination (a form of double-stranded DNA repair mechanism). Thus, cells with defective BRCA proteins cannot repair double-stranded breaks (DSB) in DNA.
The homologous recombination pathway is complex and involves a number of genes. Deficiencies in this pathway confer a sensitivity to PARP inhibition. Tumors that share dysfunction in the homologous recombination pathway, but do not contain mutations in the BRCA gene, are classified as tumors with “BRCAness.”
Generally, the inheritance of a defective BRCA1 or BRCA2 allele (a germline mutation) alone is not enough to cause the development of cancer. Instead, once the second, functioning allele becomes nonfunctional, cancer can arise through an accumulation of mutations in the genetic code.
Furthermore, regardless of germline BRCA status, cancers have high rates of genetic mutation. As a result of the mutation rate, tumors can develop noninherited, noninheritable alterations in BRCA1 or BRCA2 genes (a somatic mutation).

Mechanism of PARP inhibitor activity
The PARP family of enzymes hold a vital role in the repair of DNA and the stabilization of the human genome through the repair of single-stranded breaks (SSB) in DNA. PARP inhibitors were originally developed as a chemosensitizing agent for other cytotoxic agents. It was only later discovered that ovarian cancer cells and mouse models that were deficient in BRCA proteins were especially sensitive to PARP inhibition. Eventually, the clinical development strategy became to employ PARP inhibitors in selected patients with BRCA mutations.
As previously mentioned, cells deficient in the tumor suppressor genes (BRCA1 and BRCA2) have an inability to repair DSBs. Inhibiting PARP enzymes will therefore cause an increase in SSB. During cell replication, these SSBs are converted to DSBs. Ultimately, the accumulation of DSBs leads to cell death. The concept that these two deficiencies – which alone are nonlethal – can be combined to induce cell death is described as synthetic lethality.
The exact mechanism through which PARP inhibitors function is not fully understood; however, four models currently exist to explain how PARP inhibitors instigate synthetic lethality. PARP inhibitors may block base excision repair mechanisms, trap PARP enzymes on damaged DNA, reduce the affinity of functioning BRCA enzymes to damaged DNA, and suppress nonhomologous end joining repair mechanisms.1 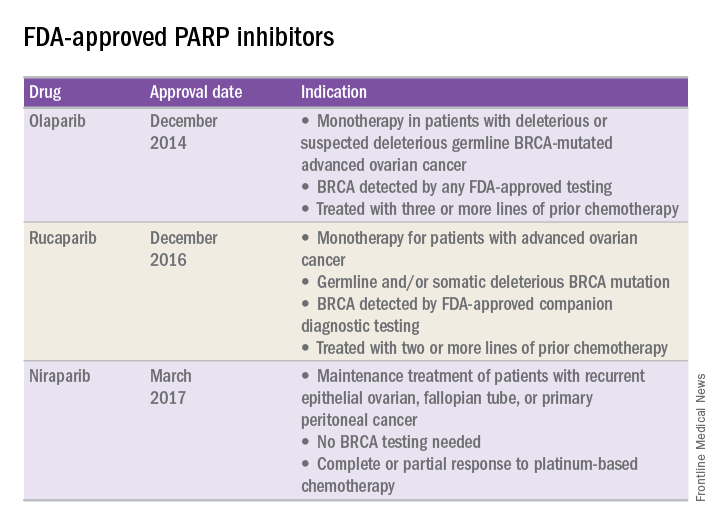
FDA approval of PARP inhibitors
In recent years, the Food and Drug Administration has approved three PARP inhibitors in the treatment of ovarian cancer in slightly different clinical scenarios.
Olaparib was tested in a trial of 193 patients who harbored a deleterious or suspected deleterious germline BRCA-associated ovarian cancer who had received prior therapies.2 Overall, the response rate in this population was 41% (95% confidence interval, 28-54) with a median duration of response of 8.0 months. These results led to the FDA approval of olaparib for ovarian cancer treatment as fourth-line therapy in patients with BRCA mutations.
Two separate trials using rucaparib showed an overall response rate of 54% and a duration of response of 9.2 months.3,4 These early results allowed the FDA to grant accelerated approval to another PARP inhibitor for use in ovarian cancer.
More recently, a phase III trial of niraparib maintenance therapy versus placebo enrolled 553 women with recurrent epithelial ovarian cancer.5 Women with germline BRCA mutations had recurrence-free intervals of 21 months on niraparib, compared with 5.5 months for those on placebo. Even without germline BRCA mutations, women benefited from a recurrence-free interval of 9.3 months, compared with 3.9 months for placebo.
PARP inhibitors represent a novel targeted therapy for ovarian cancer, particularly those with deleterious germline or somatic BRCA mutations. When combined with genetic testing for BRCA mutations, PARP inhibitors represent an example of a predictive biomarker paired with a tailored therapeutic. Maturing data from ongoing trials will likely expand the opportunity to use PARP inhibitors for the treatment of ovarian cancer.
References
1. Br J Cancer. 2016 Nov 8;115(10):1157-73.
2. J Clin Oncol. 2015 Jan 20;33(3):244-50.
3. Clin Cancer Res. 2017 Mar 6. pii: clincanres.2796.2016. doi: 10.1158/1078-0432.CCR-16-2796.
4. Lancet Oncol. 2017 Jan;18(1):75-87.
5. N Engl J Med 2016; 375:2154-64.
Dr. Tran is a gynecologic oncology fellow in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Rossi is an assistant professor in the division of gynecologic oncology at UNC-Chapel Hill. They reported having no relevant financial disclosures.
Ovarian cancer remains the leading cause of death from gynecologic cancer worldwide and one of the five leading causes of death from cancer in women in the United States. In addition to surgery, treatment consists of combination platinum and taxane chemotherapy that offers a high response rate; however, a majority of women will develop persistent or recurrent disease.
A clinical practice statement released by the Society of Gynecologic Oncology in October 2014 states that “women diagnosed with epithelial ovarian, tubal, and peritoneal cancers should receive genetic counseling and be offered genetic testing, even in the absence of family history.” Patients should be informed that this genetic testing serves to prognosticate, inform about personal and familial cancer risk, but also aids in choices of novel therapeutic agents, specifically Poly (ADP-ribose) polymerase (PARP) inhibitors.
Genetic involvement of BRCA
A small proportion of ovarian cancers are attributable to genetic mutations, with approximately 10%-15% of cases caused by germline mutations of BRCA1 and BRCA2. BRCA1 deleterious mutations confer an ovarian cancer risk of approximately 39%-46%; and the risk of ovarian cancer is roughly 12%-20% for patients with BRCA2 deleterious mutations. As a tumor suppressor gene, BRCA is involved in the DNA repair process. Specifically, it is involved in homologous recombination (a form of double-stranded DNA repair mechanism). Thus, cells with defective BRCA proteins cannot repair double-stranded breaks (DSB) in DNA.
The homologous recombination pathway is complex and involves a number of genes. Deficiencies in this pathway confer a sensitivity to PARP inhibition. Tumors that share dysfunction in the homologous recombination pathway, but do not contain mutations in the BRCA gene, are classified as tumors with “BRCAness.”
Generally, the inheritance of a defective BRCA1 or BRCA2 allele (a germline mutation) alone is not enough to cause the development of cancer. Instead, once the second, functioning allele becomes nonfunctional, cancer can arise through an accumulation of mutations in the genetic code.
Furthermore, regardless of germline BRCA status, cancers have high rates of genetic mutation. As a result of the mutation rate, tumors can develop noninherited, noninheritable alterations in BRCA1 or BRCA2 genes (a somatic mutation).
Mechanism of PARP inhibitor activity
The PARP family of enzymes hold a vital role in the repair of DNA and the stabilization of the human genome through the repair of single-stranded breaks (SSB) in DNA. PARP inhibitors were originally developed as a chemosensitizing agent for other cytotoxic agents. It was only later discovered that ovarian cancer cells and mouse models that were deficient in BRCA proteins were especially sensitive to PARP inhibition. Eventually, the clinical development strategy became to employ PARP inhibitors in selected patients with BRCA mutations.
As previously mentioned, cells deficient in the tumor suppressor genes (BRCA1 and BRCA2) have an inability to repair DSBs. Inhibiting PARP enzymes will therefore cause an increase in SSB. During cell replication, these SSBs are converted to DSBs. Ultimately, the accumulation of DSBs leads to cell death. The concept that these two deficiencies – which alone are nonlethal – can be combined to induce cell death is described as synthetic lethality.
The exact mechanism through which PARP inhibitors function is not fully understood; however, four models currently exist to explain how PARP inhibitors instigate synthetic lethality. PARP inhibitors may block base excision repair mechanisms, trap PARP enzymes on damaged DNA, reduce the affinity of functioning BRCA enzymes to damaged DNA, and suppress nonhomologous end joining repair mechanisms.1
FDA approval of PARP inhibitors
In recent years, the Food and Drug Administration has approved three PARP inhibitors in the treatment of ovarian cancer in slightly different clinical scenarios.
Olaparib was tested in a trial of 193 patients who harbored a deleterious or suspected deleterious germline BRCA-associated ovarian cancer who had received prior therapies.2 Overall, the response rate in this population was 41% (95% confidence interval, 28-54) with a median duration of response of 8.0 months. These results led to the FDA approval of olaparib for ovarian cancer treatment as fourth-line therapy in patients with BRCA mutations.
Two separate trials using rucaparib showed an overall response rate of 54% and a duration of response of 9.2 months.3,4 These early results allowed the FDA to grant accelerated approval to another PARP inhibitor for use in ovarian cancer.
More recently, a phase III trial of niraparib maintenance therapy versus placebo enrolled 553 women with recurrent epithelial ovarian cancer.5 Women with germline BRCA mutations had recurrence-free intervals of 21 months on niraparib, compared with 5.5 months for those on placebo. Even without germline BRCA mutations, women benefited from a recurrence-free interval of 9.3 months, compared with 3.9 months for placebo.
PARP inhibitors represent a novel targeted therapy for ovarian cancer, particularly those with deleterious germline or somatic BRCA mutations. When combined with genetic testing for BRCA mutations, PARP inhibitors represent an example of a predictive biomarker paired with a tailored therapeutic. Maturing data from ongoing trials will likely expand the opportunity to use PARP inhibitors for the treatment of ovarian cancer.
References
1. Br J Cancer. 2016 Nov 8;115(10):1157-73.
2. J Clin Oncol. 2015 Jan 20;33(3):244-50.
3. Clin Cancer Res. 2017 Mar 6. pii: clincanres.2796.2016. doi: 10.1158/1078-0432.CCR-16-2796.
4. Lancet Oncol. 2017 Jan;18(1):75-87.
5. N Engl J Med 2016; 375:2154-64.
Dr. Tran is a gynecologic oncology fellow in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Rossi is an assistant professor in the division of gynecologic oncology at UNC-Chapel Hill. They reported having no relevant financial disclosures.
Ovarian cancer remains the leading cause of death from gynecologic cancer worldwide and one of the five leading causes of death from cancer in women in the United States. In addition to surgery, treatment consists of combination platinum and taxane chemotherapy that offers a high response rate; however, a majority of women will develop persistent or recurrent disease.
A clinical practice statement released by the Society of Gynecologic Oncology in October 2014 states that “women diagnosed with epithelial ovarian, tubal, and peritoneal cancers should receive genetic counseling and be offered genetic testing, even in the absence of family history.” Patients should be informed that this genetic testing serves to prognosticate, inform about personal and familial cancer risk, but also aids in choices of novel therapeutic agents, specifically Poly (ADP-ribose) polymerase (PARP) inhibitors.
Genetic involvement of BRCA
A small proportion of ovarian cancers are attributable to genetic mutations, with approximately 10%-15% of cases caused by germline mutations of BRCA1 and BRCA2. BRCA1 deleterious mutations confer an ovarian cancer risk of approximately 39%-46%; and the risk of ovarian cancer is roughly 12%-20% for patients with BRCA2 deleterious mutations. As a tumor suppressor gene, BRCA is involved in the DNA repair process. Specifically, it is involved in homologous recombination (a form of double-stranded DNA repair mechanism). Thus, cells with defective BRCA proteins cannot repair double-stranded breaks (DSB) in DNA.
The homologous recombination pathway is complex and involves a number of genes. Deficiencies in this pathway confer a sensitivity to PARP inhibition. Tumors that share dysfunction in the homologous recombination pathway, but do not contain mutations in the BRCA gene, are classified as tumors with “BRCAness.”
Generally, the inheritance of a defective BRCA1 or BRCA2 allele (a germline mutation) alone is not enough to cause the development of cancer. Instead, once the second, functioning allele becomes nonfunctional, cancer can arise through an accumulation of mutations in the genetic code.
Furthermore, regardless of germline BRCA status, cancers have high rates of genetic mutation. As a result of the mutation rate, tumors can develop noninherited, noninheritable alterations in BRCA1 or BRCA2 genes (a somatic mutation).
Mechanism of PARP inhibitor activity
The PARP family of enzymes hold a vital role in the repair of DNA and the stabilization of the human genome through the repair of single-stranded breaks (SSB) in DNA. PARP inhibitors were originally developed as a chemosensitizing agent for other cytotoxic agents. It was only later discovered that ovarian cancer cells and mouse models that were deficient in BRCA proteins were especially sensitive to PARP inhibition. Eventually, the clinical development strategy became to employ PARP inhibitors in selected patients with BRCA mutations.
As previously mentioned, cells deficient in the tumor suppressor genes (BRCA1 and BRCA2) have an inability to repair DSBs. Inhibiting PARP enzymes will therefore cause an increase in SSB. During cell replication, these SSBs are converted to DSBs. Ultimately, the accumulation of DSBs leads to cell death. The concept that these two deficiencies – which alone are nonlethal – can be combined to induce cell death is described as synthetic lethality.
The exact mechanism through which PARP inhibitors function is not fully understood; however, four models currently exist to explain how PARP inhibitors instigate synthetic lethality. PARP inhibitors may block base excision repair mechanisms, trap PARP enzymes on damaged DNA, reduce the affinity of functioning BRCA enzymes to damaged DNA, and suppress nonhomologous end joining repair mechanisms.1
FDA approval of PARP inhibitors
In recent years, the Food and Drug Administration has approved three PARP inhibitors in the treatment of ovarian cancer in slightly different clinical scenarios.
Olaparib was tested in a trial of 193 patients who harbored a deleterious or suspected deleterious germline BRCA-associated ovarian cancer who had received prior therapies.2 Overall, the response rate in this population was 41% (95% confidence interval, 28-54) with a median duration of response of 8.0 months. These results led to the FDA approval of olaparib for ovarian cancer treatment as fourth-line therapy in patients with BRCA mutations.
Two separate trials using rucaparib showed an overall response rate of 54% and a duration of response of 9.2 months.3,4 These early results allowed the FDA to grant accelerated approval to another PARP inhibitor for use in ovarian cancer.
More recently, a phase III trial of niraparib maintenance therapy versus placebo enrolled 553 women with recurrent epithelial ovarian cancer.5 Women with germline BRCA mutations had recurrence-free intervals of 21 months on niraparib, compared with 5.5 months for those on placebo. Even without germline BRCA mutations, women benefited from a recurrence-free interval of 9.3 months, compared with 3.9 months for placebo.
PARP inhibitors represent a novel targeted therapy for ovarian cancer, particularly those with deleterious germline or somatic BRCA mutations. When combined with genetic testing for BRCA mutations, PARP inhibitors represent an example of a predictive biomarker paired with a tailored therapeutic. Maturing data from ongoing trials will likely expand the opportunity to use PARP inhibitors for the treatment of ovarian cancer.
References
1. Br J Cancer. 2016 Nov 8;115(10):1157-73.
2. J Clin Oncol. 2015 Jan 20;33(3):244-50.
3. Clin Cancer Res. 2017 Mar 6. pii: clincanres.2796.2016. doi: 10.1158/1078-0432.CCR-16-2796.
4. Lancet Oncol. 2017 Jan;18(1):75-87.
5. N Engl J Med 2016; 375:2154-64.
Dr. Tran is a gynecologic oncology fellow in the department of obstetrics and gynecology at the University of North Carolina at Chapel Hill. Dr. Rossi is an assistant professor in the division of gynecologic oncology at UNC-Chapel Hill. They reported having no relevant financial disclosures.