User login
A healthy 8-year-old boy presents with several skin-colored, round 1-3 mm papules on the nose, forehead, and cheeks
A shave biopsy of one of the lesions was performed that showed a proliferation of nests of basaloid cells on the dermis with palisading and rare vacuolated clear cell change. A rare ductal structure with luminal proteinaceous contents was noted. The findings were consistent with a trichoepithelioma.

Trichoepitheliomas are rare, benign, adnexal skin tumors that can start in early childhood or during puberty. The lesions are most commonly seen in girls as skin color papules on the face, and sometimes on the trunk and the neck. Trichoepitheliomas can appear as a benign single lesion nonfamilial form or as a familial form with multiple lesions.1 Brooke-Spiegler syndrome (BSS) is a rare autosomal dominant condition where affected individuals have multiple trichoepitheliomas, cylindromas, and spiradenomas. Depending on the predominant type of lesion, phenotypic variants include multiple familial trichoepithelioma type 1 and familial cylindromatosis.2 BSS is caused by mutations within CYLD, a tumor-suppressor gene located on chromosome 16q12-q13.3 Our patient presented only with trichoepitheliomas with no other lesions on the scalp, neck, or torso.
Multiple trichoepitheliomas also can be seen in other syndromes including Rombo syndrome, which is characterized by basal cell carcinomas, milia, hypotrichosis, distal vasodilation, and atrophoderma vermiculata; none seen in our patient. Bazex-Dupré-Christol syndrome is an X-linked dominant condition in which affected individuals can present with multiple trichoepitheliomas, as well as milia, hypotrichosis, follicular atrophoderma, and basal cell carcinomas.
The differential diagnosis of skin color papules on the central face on a child should include acne, flat warts, and angiofibromas seen in tuberous sclerosis. Our patient’s lesions were monomorphous, and there were no comedones, pustules, or inflammatory papules characteristic of acne.
He had warts on his hands which could make it suspicious for the face lesions to be verrucous in nature. Flat warts also present as skin color papules, but characteristically are flat, not round and shiny as our patient’s lesions were. Angiofibromas, as seen in individuals with tuberous sclerosis, also can start at an early age in the same location as trichoepitheliomas in BSS, but clinically the lesions are pinker and redder rather than the skin-color, round shape papules characteristic of trichoepitheliomas. Patients may have other findings suggestive of tuberous sclerosis including confetti hypopigmentation, ash leaf spots, shagreen patch, and a history of seizures or developmental delay – none of which were present in our patient. Children with basal cell nevus syndrome can present with skin color to shiny telangiectatic papules (basal cell carcinomas) that can be single or multiple on the face, chest, and back. The lesions usually are not seen in clusters around the nose and central face as seen in patients with BSS. Patients with basal cell nevus syndrome can develop jaw bone cysts, brain tumors (medulloblastoma), and fibromas on the heart or ovaries, palmar pits and be macrocephalic.4
Trichoepitheliomas usually are treated surgically but other nonsurgical removing techniques include laser resurfacing, curettage, and electrocautery.5 Malignant transformation can occur in 5%-10% of the individuals and should be managed by a multidisciplinary team. Topical treatment with sirolimus previously has been reported to be effective in young patients.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email Dr. Matiz at pdnews@mdedge.com.
References
1. Acta Dermatovenerol Croat. 2018 Jun;26(2):162-5.
2. Eur J Med Genet. 2015;58(5):271-8.
3. Am J Dermatopathol. 2014;36(11):868-74.
4. Int J Dermatol. 2016 Apr;55(4):367-75.
5. Int J Dermatol. 2007;46(6):583-6.
6. Dermatol Ther. 2017 Mar. doi: 10.1111/dth.12458.
A shave biopsy of one of the lesions was performed that showed a proliferation of nests of basaloid cells on the dermis with palisading and rare vacuolated clear cell change. A rare ductal structure with luminal proteinaceous contents was noted. The findings were consistent with a trichoepithelioma.
Trichoepitheliomas are rare, benign, adnexal skin tumors that can start in early childhood or during puberty. The lesions are most commonly seen in girls as skin color papules on the face, and sometimes on the trunk and the neck. Trichoepitheliomas can appear as a benign single lesion nonfamilial form or as a familial form with multiple lesions.1 Brooke-Spiegler syndrome (BSS) is a rare autosomal dominant condition where affected individuals have multiple trichoepitheliomas, cylindromas, and spiradenomas. Depending on the predominant type of lesion, phenotypic variants include multiple familial trichoepithelioma type 1 and familial cylindromatosis.2 BSS is caused by mutations within CYLD, a tumor-suppressor gene located on chromosome 16q12-q13.3 Our patient presented only with trichoepitheliomas with no other lesions on the scalp, neck, or torso.
Multiple trichoepitheliomas also can be seen in other syndromes including Rombo syndrome, which is characterized by basal cell carcinomas, milia, hypotrichosis, distal vasodilation, and atrophoderma vermiculata; none seen in our patient. Bazex-Dupré-Christol syndrome is an X-linked dominant condition in which affected individuals can present with multiple trichoepitheliomas, as well as milia, hypotrichosis, follicular atrophoderma, and basal cell carcinomas.
The differential diagnosis of skin color papules on the central face on a child should include acne, flat warts, and angiofibromas seen in tuberous sclerosis. Our patient’s lesions were monomorphous, and there were no comedones, pustules, or inflammatory papules characteristic of acne.
He had warts on his hands which could make it suspicious for the face lesions to be verrucous in nature. Flat warts also present as skin color papules, but characteristically are flat, not round and shiny as our patient’s lesions were. Angiofibromas, as seen in individuals with tuberous sclerosis, also can start at an early age in the same location as trichoepitheliomas in BSS, but clinically the lesions are pinker and redder rather than the skin-color, round shape papules characteristic of trichoepitheliomas. Patients may have other findings suggestive of tuberous sclerosis including confetti hypopigmentation, ash leaf spots, shagreen patch, and a history of seizures or developmental delay – none of which were present in our patient. Children with basal cell nevus syndrome can present with skin color to shiny telangiectatic papules (basal cell carcinomas) that can be single or multiple on the face, chest, and back. The lesions usually are not seen in clusters around the nose and central face as seen in patients with BSS. Patients with basal cell nevus syndrome can develop jaw bone cysts, brain tumors (medulloblastoma), and fibromas on the heart or ovaries, palmar pits and be macrocephalic.4
Trichoepitheliomas usually are treated surgically but other nonsurgical removing techniques include laser resurfacing, curettage, and electrocautery.5 Malignant transformation can occur in 5%-10% of the individuals and should be managed by a multidisciplinary team. Topical treatment with sirolimus previously has been reported to be effective in young patients.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email Dr. Matiz at pdnews@mdedge.com.
References
1. Acta Dermatovenerol Croat. 2018 Jun;26(2):162-5.
2. Eur J Med Genet. 2015;58(5):271-8.
3. Am J Dermatopathol. 2014;36(11):868-74.
4. Int J Dermatol. 2016 Apr;55(4):367-75.
5. Int J Dermatol. 2007;46(6):583-6.
6. Dermatol Ther. 2017 Mar. doi: 10.1111/dth.12458.
A shave biopsy of one of the lesions was performed that showed a proliferation of nests of basaloid cells on the dermis with palisading and rare vacuolated clear cell change. A rare ductal structure with luminal proteinaceous contents was noted. The findings were consistent with a trichoepithelioma.
Trichoepitheliomas are rare, benign, adnexal skin tumors that can start in early childhood or during puberty. The lesions are most commonly seen in girls as skin color papules on the face, and sometimes on the trunk and the neck. Trichoepitheliomas can appear as a benign single lesion nonfamilial form or as a familial form with multiple lesions.1 Brooke-Spiegler syndrome (BSS) is a rare autosomal dominant condition where affected individuals have multiple trichoepitheliomas, cylindromas, and spiradenomas. Depending on the predominant type of lesion, phenotypic variants include multiple familial trichoepithelioma type 1 and familial cylindromatosis.2 BSS is caused by mutations within CYLD, a tumor-suppressor gene located on chromosome 16q12-q13.3 Our patient presented only with trichoepitheliomas with no other lesions on the scalp, neck, or torso.
Multiple trichoepitheliomas also can be seen in other syndromes including Rombo syndrome, which is characterized by basal cell carcinomas, milia, hypotrichosis, distal vasodilation, and atrophoderma vermiculata; none seen in our patient. Bazex-Dupré-Christol syndrome is an X-linked dominant condition in which affected individuals can present with multiple trichoepitheliomas, as well as milia, hypotrichosis, follicular atrophoderma, and basal cell carcinomas.
The differential diagnosis of skin color papules on the central face on a child should include acne, flat warts, and angiofibromas seen in tuberous sclerosis. Our patient’s lesions were monomorphous, and there were no comedones, pustules, or inflammatory papules characteristic of acne.
He had warts on his hands which could make it suspicious for the face lesions to be verrucous in nature. Flat warts also present as skin color papules, but characteristically are flat, not round and shiny as our patient’s lesions were. Angiofibromas, as seen in individuals with tuberous sclerosis, also can start at an early age in the same location as trichoepitheliomas in BSS, but clinically the lesions are pinker and redder rather than the skin-color, round shape papules characteristic of trichoepitheliomas. Patients may have other findings suggestive of tuberous sclerosis including confetti hypopigmentation, ash leaf spots, shagreen patch, and a history of seizures or developmental delay – none of which were present in our patient. Children with basal cell nevus syndrome can present with skin color to shiny telangiectatic papules (basal cell carcinomas) that can be single or multiple on the face, chest, and back. The lesions usually are not seen in clusters around the nose and central face as seen in patients with BSS. Patients with basal cell nevus syndrome can develop jaw bone cysts, brain tumors (medulloblastoma), and fibromas on the heart or ovaries, palmar pits and be macrocephalic.4
Trichoepitheliomas usually are treated surgically but other nonsurgical removing techniques include laser resurfacing, curettage, and electrocautery.5 Malignant transformation can occur in 5%-10% of the individuals and should be managed by a multidisciplinary team. Topical treatment with sirolimus previously has been reported to be effective in young patients.6
Dr. Matiz is a pediatric dermatologist at Southern California Permanente Medical Group, San Diego. She said she had no relevant financial disclosures. Email Dr. Matiz at pdnews@mdedge.com.
References
1. Acta Dermatovenerol Croat. 2018 Jun;26(2):162-5.
2. Eur J Med Genet. 2015;58(5):271-8.
3. Am J Dermatopathol. 2014;36(11):868-74.
4. Int J Dermatol. 2016 Apr;55(4):367-75.
5. Int J Dermatol. 2007;46(6):583-6.
6. Dermatol Ther. 2017 Mar. doi: 10.1111/dth.12458.
A white 8-year-old boy comes to our pediatric dermatology clinic with his mother for evaluation of acne. The lesions started about a year ago on his nose and now have spread to his cheeks. The bumps are not symptomatic. He has been applying over the counter salicylic acid and benzoyl peroxide gels with no help. The mother reports he has been growing well, denies any growth spurt, no axillary or genital hair or body odor noted.

None of the family members have a history of acne. The mother cannot recall any family members with similar lesions on the face. He has had some warts on his fingers for years and has been treated with over the counter salicylic acid. There is no family history of skin cancer.
On physical exam, he is a healthy young boy with several skin color, round papules 1-3 mm on the nose, forehead, and cheeks. There are no lesions on the scalp. He has abundant brown hair. He has few verrucous papules on the fingers. Axillary and genital hair is not noted. There is no body odor and he is Tanner stage I.
Improving self-confidence
The best way to ensure that I’ll run late in clinic is to start late. I avoid such delayed starts as scabies, yet, sometimes it’s unavoidable. I walked into my 1:30 appointment at 1:35. “Can I ask you a question?” my bony, patient with the long gray beard asked. “Sure.” I replied. “Is your time important to you?” he snapped.

Oh, boy. Here we go.
“I’m sorry I’m running late and kept you waiting,” I offered, “but I had a sick patient this morning.” When he retorted that his time was important, too, I interrupted him.
“Please sit on the exam table and tell me how I can help you so we don’t waste any more of your time.” He went on to complain that the treatments for his facial seborrheic dermatitis did not resolve the problem. When he stops treatment, it flares. I explained that this was a chronic condition and that he could manage it with my help. He resisted, but with each parry, his aggressiveness weakened. We reviewed behavior, product, and medication options for him. By the end of the visit, he was (mostly) pleased and left with a plan and prescription to help.
Early in my career, this appointment might have been disastrous: It would have ruined my afternoon and possibly led to a formal patient complaint. His antagonistic comments and boorish behavior would have unsettled me. But it didn’t now.
I had the confidence to know his diagnosis and how to help him, despite his dissatisfaction. Those with strong self-confidence not only have better patient satisfaction and higher quality but also are more efficient and have high level of satisfaction with their career. When your confidence is low, medical decision making and managing patient expectations become difficult. This is particularly true when a patient comes “informed.” Often their knowledge is helpful but, as we know, sometimes it’s bogus, even detrimental. Although we ought to have come a long way from the brash doctor-knows-best days of our past, we also ought not capitulate to patients. Sometimes, you have to be the doctor. Balancing confidence with compassion is tricky yet essential to success.
When I meet with our young doctors, I try to provide feedback not only on their medical acumen but also on their confidence to deploy that expertise. Like a skill, self-confidence can be improved. The best way is to recognize difficult conversations and do not avoid them. When you feel your face flush and heart race, take a good belly breath and step into it. You don’t have to confront or argue with your patient, you do have to assert and negotiate. Helping a difficult patient can feel like you’ve done something wrong, but chances are, you haven’t. Reframe the situation, think of it as you doing the hard work to help them. Being confident is as important as getting the diagnosis right. Even when you don’t know the diagnosis, you can be most helpful when you are direct and say so. “I’m not sure what you have, but here is how I’m going to help you.”
To improve self-confidence you’ll have to practice. When you have a difficult visit that ultimately ended well, make a note of it. Reflect on it. The next time you have a challenging patient, remember your previous success and how you felt. Then breathe and do it again. After all, you are the doctor.
Dr. Benabio is director of health care transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
The best way to ensure that I’ll run late in clinic is to start late. I avoid such delayed starts as scabies, yet, sometimes it’s unavoidable. I walked into my 1:30 appointment at 1:35. “Can I ask you a question?” my bony, patient with the long gray beard asked. “Sure.” I replied. “Is your time important to you?” he snapped.
Oh, boy. Here we go.
“I’m sorry I’m running late and kept you waiting,” I offered, “but I had a sick patient this morning.” When he retorted that his time was important, too, I interrupted him.
“Please sit on the exam table and tell me how I can help you so we don’t waste any more of your time.” He went on to complain that the treatments for his facial seborrheic dermatitis did not resolve the problem. When he stops treatment, it flares. I explained that this was a chronic condition and that he could manage it with my help. He resisted, but with each parry, his aggressiveness weakened. We reviewed behavior, product, and medication options for him. By the end of the visit, he was (mostly) pleased and left with a plan and prescription to help.
Early in my career, this appointment might have been disastrous: It would have ruined my afternoon and possibly led to a formal patient complaint. His antagonistic comments and boorish behavior would have unsettled me. But it didn’t now.
I had the confidence to know his diagnosis and how to help him, despite his dissatisfaction. Those with strong self-confidence not only have better patient satisfaction and higher quality but also are more efficient and have high level of satisfaction with their career. When your confidence is low, medical decision making and managing patient expectations become difficult. This is particularly true when a patient comes “informed.” Often their knowledge is helpful but, as we know, sometimes it’s bogus, even detrimental. Although we ought to have come a long way from the brash doctor-knows-best days of our past, we also ought not capitulate to patients. Sometimes, you have to be the doctor. Balancing confidence with compassion is tricky yet essential to success.
When I meet with our young doctors, I try to provide feedback not only on their medical acumen but also on their confidence to deploy that expertise. Like a skill, self-confidence can be improved. The best way is to recognize difficult conversations and do not avoid them. When you feel your face flush and heart race, take a good belly breath and step into it. You don’t have to confront or argue with your patient, you do have to assert and negotiate. Helping a difficult patient can feel like you’ve done something wrong, but chances are, you haven’t. Reframe the situation, think of it as you doing the hard work to help them. Being confident is as important as getting the diagnosis right. Even when you don’t know the diagnosis, you can be most helpful when you are direct and say so. “I’m not sure what you have, but here is how I’m going to help you.”
To improve self-confidence you’ll have to practice. When you have a difficult visit that ultimately ended well, make a note of it. Reflect on it. The next time you have a challenging patient, remember your previous success and how you felt. Then breathe and do it again. After all, you are the doctor.
Dr. Benabio is director of health care transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
The best way to ensure that I’ll run late in clinic is to start late. I avoid such delayed starts as scabies, yet, sometimes it’s unavoidable. I walked into my 1:30 appointment at 1:35. “Can I ask you a question?” my bony, patient with the long gray beard asked. “Sure.” I replied. “Is your time important to you?” he snapped.
Oh, boy. Here we go.
“I’m sorry I’m running late and kept you waiting,” I offered, “but I had a sick patient this morning.” When he retorted that his time was important, too, I interrupted him.
“Please sit on the exam table and tell me how I can help you so we don’t waste any more of your time.” He went on to complain that the treatments for his facial seborrheic dermatitis did not resolve the problem. When he stops treatment, it flares. I explained that this was a chronic condition and that he could manage it with my help. He resisted, but with each parry, his aggressiveness weakened. We reviewed behavior, product, and medication options for him. By the end of the visit, he was (mostly) pleased and left with a plan and prescription to help.
Early in my career, this appointment might have been disastrous: It would have ruined my afternoon and possibly led to a formal patient complaint. His antagonistic comments and boorish behavior would have unsettled me. But it didn’t now.
I had the confidence to know his diagnosis and how to help him, despite his dissatisfaction. Those with strong self-confidence not only have better patient satisfaction and higher quality but also are more efficient and have high level of satisfaction with their career. When your confidence is low, medical decision making and managing patient expectations become difficult. This is particularly true when a patient comes “informed.” Often their knowledge is helpful but, as we know, sometimes it’s bogus, even detrimental. Although we ought to have come a long way from the brash doctor-knows-best days of our past, we also ought not capitulate to patients. Sometimes, you have to be the doctor. Balancing confidence with compassion is tricky yet essential to success.
When I meet with our young doctors, I try to provide feedback not only on their medical acumen but also on their confidence to deploy that expertise. Like a skill, self-confidence can be improved. The best way is to recognize difficult conversations and do not avoid them. When you feel your face flush and heart race, take a good belly breath and step into it. You don’t have to confront or argue with your patient, you do have to assert and negotiate. Helping a difficult patient can feel like you’ve done something wrong, but chances are, you haven’t. Reframe the situation, think of it as you doing the hard work to help them. Being confident is as important as getting the diagnosis right. Even when you don’t know the diagnosis, you can be most helpful when you are direct and say so. “I’m not sure what you have, but here is how I’m going to help you.”
To improve self-confidence you’ll have to practice. When you have a difficult visit that ultimately ended well, make a note of it. Reflect on it. The next time you have a challenging patient, remember your previous success and how you felt. Then breathe and do it again. After all, you are the doctor.
Dr. Benabio is director of health care transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Are nutritional supplements important in the treatment of female pattern hair loss?
Although genetics, hormones, age, environment, stress, and nutrition all play a role in the etiology of FPHL, the underlying pathophysiology is poorly understood. The only Food and Drug Administration–approved medication to treat FPHL is topical minoxidil. The armamentarium is limited so alternative treatments such as platelet-rich plasma, topical hair loss preparations, and nutritional supplements are now being used in an effort to slow down progression of this disease.

Hair follicles are metabolically active and thus nutrient deficiency as well as calorie and protein restriction impact the hair growth cycle. Patients often inquire if dietary changes or supplementation can help prevent the loss or increase the growth of the hair. Unfortunately, the quality of evidence on nutritional supplements for this use is poor. Furthermore, it is unclear whether patients with FPHL should be routinely tested for nutritional deficiencies, and which type and concentration of supplementation will be of benefit to patients.
Iron deficiency is one of the most well-known factors for hair loss. Risk factors include heavy bleeding during menses, gastrointestinal blood loss, and malabsorption. Studies have shown that iron supplementation does help increase hair growth in iron-deficient mice. Zinc is also a key mineral in hair follicle development, and zinc deficiency is seen in genetic diseases or malabsorption syndromes and has been linked to hair loss.
Deficiencies in selenium, essential fatty acids, vitamin D, vitamin A, vitamin E, folic acid, and biotin have been documented in relation to hair loss. However, no studies have effectively shown that supplementation of these nutrients helps hair growth in patients without a documented deficiency. Currently, it is difficult to ascertain which nutrients and in what concentrations are both safe and effective to correct hair loss.
In the vast hair supplement market, some of the more popular supplements for FPHL are DeeplyRooted (Hush & Hush), Viviscal, Nutrafol, and Nature’s Bounty and Sugarbearhair products. These supplements contain a combination of micronutrients (such as vitamin D, niacin, zinc, biotin, and selenium) and adaptogens (a natural substance that helps the body heal with stress and increased cortisol production during stress) that may stimulate the growth and health of the hair follicle and minimize the production of stress hormones and dihydrotestosterone.

In my practice, we see over 100 hair loss patients a week; 30%-40% are patients with FPHL who are often suffering from depression, anxiety, and emotional distress. Our combination treatments always include nutritional supplementation and we have had success not only halting subclinical shedding, but also increasing hair growth. Until the complex pathophysiology of FPHL is identified and new therapeutics are developed, practitioners should consider adding nutritional supplements for the treatment of women with FPHL. Monitoring of supplement use is essential given the risk of toxicity from some vitamins and supplements when taken without proper supervision. More research is also needed to help delineate both the guidelines of micronutrient testing and parameters for supplementation.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
Sources
Guo EL et al. Dermatol Pract Concept. 2017 Jan 31;7(1):1-10.
Goldberg LJ et al. Clin Dermatol. 2010 Jul-Aug;28(4):412-9.
Finner AM. Dermatol Clin. 2013 Jan;31(1):167-72.
St Pierre SA et al. J Am Acad Dermatol. 2010 Dec;63(6):1070-6.
Rasheed H et al. Skin Pharmacol Physiol. 2013;26(2):101-7.
Rogers NE et al. J Am Acad Dermatol. 2008 Oct;59(4):547-66.
Ablon G et al. J Drugs Dermatol. 2018 May 1;17(5):558-65.
Although genetics, hormones, age, environment, stress, and nutrition all play a role in the etiology of FPHL, the underlying pathophysiology is poorly understood. The only Food and Drug Administration–approved medication to treat FPHL is topical minoxidil. The armamentarium is limited so alternative treatments such as platelet-rich plasma, topical hair loss preparations, and nutritional supplements are now being used in an effort to slow down progression of this disease.
Hair follicles are metabolically active and thus nutrient deficiency as well as calorie and protein restriction impact the hair growth cycle. Patients often inquire if dietary changes or supplementation can help prevent the loss or increase the growth of the hair. Unfortunately, the quality of evidence on nutritional supplements for this use is poor. Furthermore, it is unclear whether patients with FPHL should be routinely tested for nutritional deficiencies, and which type and concentration of supplementation will be of benefit to patients.
Iron deficiency is one of the most well-known factors for hair loss. Risk factors include heavy bleeding during menses, gastrointestinal blood loss, and malabsorption. Studies have shown that iron supplementation does help increase hair growth in iron-deficient mice. Zinc is also a key mineral in hair follicle development, and zinc deficiency is seen in genetic diseases or malabsorption syndromes and has been linked to hair loss.
Deficiencies in selenium, essential fatty acids, vitamin D, vitamin A, vitamin E, folic acid, and biotin have been documented in relation to hair loss. However, no studies have effectively shown that supplementation of these nutrients helps hair growth in patients without a documented deficiency. Currently, it is difficult to ascertain which nutrients and in what concentrations are both safe and effective to correct hair loss.
In the vast hair supplement market, some of the more popular supplements for FPHL are DeeplyRooted (Hush & Hush), Viviscal, Nutrafol, and Nature’s Bounty and Sugarbearhair products. These supplements contain a combination of micronutrients (such as vitamin D, niacin, zinc, biotin, and selenium) and adaptogens (a natural substance that helps the body heal with stress and increased cortisol production during stress) that may stimulate the growth and health of the hair follicle and minimize the production of stress hormones and dihydrotestosterone.
In my practice, we see over 100 hair loss patients a week; 30%-40% are patients with FPHL who are often suffering from depression, anxiety, and emotional distress. Our combination treatments always include nutritional supplementation and we have had success not only halting subclinical shedding, but also increasing hair growth. Until the complex pathophysiology of FPHL is identified and new therapeutics are developed, practitioners should consider adding nutritional supplements for the treatment of women with FPHL. Monitoring of supplement use is essential given the risk of toxicity from some vitamins and supplements when taken without proper supervision. More research is also needed to help delineate both the guidelines of micronutrient testing and parameters for supplementation.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
Sources
Guo EL et al. Dermatol Pract Concept. 2017 Jan 31;7(1):1-10.
Goldberg LJ et al. Clin Dermatol. 2010 Jul-Aug;28(4):412-9.
Finner AM. Dermatol Clin. 2013 Jan;31(1):167-72.
St Pierre SA et al. J Am Acad Dermatol. 2010 Dec;63(6):1070-6.
Rasheed H et al. Skin Pharmacol Physiol. 2013;26(2):101-7.
Rogers NE et al. J Am Acad Dermatol. 2008 Oct;59(4):547-66.
Ablon G et al. J Drugs Dermatol. 2018 May 1;17(5):558-65.
Although genetics, hormones, age, environment, stress, and nutrition all play a role in the etiology of FPHL, the underlying pathophysiology is poorly understood. The only Food and Drug Administration–approved medication to treat FPHL is topical minoxidil. The armamentarium is limited so alternative treatments such as platelet-rich plasma, topical hair loss preparations, and nutritional supplements are now being used in an effort to slow down progression of this disease.
Hair follicles are metabolically active and thus nutrient deficiency as well as calorie and protein restriction impact the hair growth cycle. Patients often inquire if dietary changes or supplementation can help prevent the loss or increase the growth of the hair. Unfortunately, the quality of evidence on nutritional supplements for this use is poor. Furthermore, it is unclear whether patients with FPHL should be routinely tested for nutritional deficiencies, and which type and concentration of supplementation will be of benefit to patients.
Iron deficiency is one of the most well-known factors for hair loss. Risk factors include heavy bleeding during menses, gastrointestinal blood loss, and malabsorption. Studies have shown that iron supplementation does help increase hair growth in iron-deficient mice. Zinc is also a key mineral in hair follicle development, and zinc deficiency is seen in genetic diseases or malabsorption syndromes and has been linked to hair loss.
Deficiencies in selenium, essential fatty acids, vitamin D, vitamin A, vitamin E, folic acid, and biotin have been documented in relation to hair loss. However, no studies have effectively shown that supplementation of these nutrients helps hair growth in patients without a documented deficiency. Currently, it is difficult to ascertain which nutrients and in what concentrations are both safe and effective to correct hair loss.
In the vast hair supplement market, some of the more popular supplements for FPHL are DeeplyRooted (Hush & Hush), Viviscal, Nutrafol, and Nature’s Bounty and Sugarbearhair products. These supplements contain a combination of micronutrients (such as vitamin D, niacin, zinc, biotin, and selenium) and adaptogens (a natural substance that helps the body heal with stress and increased cortisol production during stress) that may stimulate the growth and health of the hair follicle and minimize the production of stress hormones and dihydrotestosterone.
In my practice, we see over 100 hair loss patients a week; 30%-40% are patients with FPHL who are often suffering from depression, anxiety, and emotional distress. Our combination treatments always include nutritional supplementation and we have had success not only halting subclinical shedding, but also increasing hair growth. Until the complex pathophysiology of FPHL is identified and new therapeutics are developed, practitioners should consider adding nutritional supplements for the treatment of women with FPHL. Monitoring of supplement use is essential given the risk of toxicity from some vitamins and supplements when taken without proper supervision. More research is also needed to help delineate both the guidelines of micronutrient testing and parameters for supplementation.
Dr. Talakoub and Dr. Wesley are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@mdedge.com. They had no relevant disclosures.
Sources
Guo EL et al. Dermatol Pract Concept. 2017 Jan 31;7(1):1-10.
Goldberg LJ et al. Clin Dermatol. 2010 Jul-Aug;28(4):412-9.
Finner AM. Dermatol Clin. 2013 Jan;31(1):167-72.
St Pierre SA et al. J Am Acad Dermatol. 2010 Dec;63(6):1070-6.
Rasheed H et al. Skin Pharmacol Physiol. 2013;26(2):101-7.
Rogers NE et al. J Am Acad Dermatol. 2008 Oct;59(4):547-66.
Ablon G et al. J Drugs Dermatol. 2018 May 1;17(5):558-65.
Sexual harassment: Prevention and defense
Unless you have been vacationing on some distant astral plane, you are well aware that sexual misconduct and harassment have dominated news coverage and social media forums over the past year or more. It has ended the careers of a number of formerly respectable celebrities, and the #MeToo movement has empowered many additional harassment victims to come forward with their stories.

Medical offices are far from immune from harassment, of course, and the problem is not limited to staff interactions. According to a Medscape poll, 27% of physicians have been targets of inappropriate behavior in a professional setting. In another poll, 47% of physicians and 71% of nurses reported being harassed (by stalking, persistent attempts at communication, or inappropriate social media contact) by a patient.
The reality is that , have an ethical and legal responsibility to provide a safe and respectful work environment for everyone involved.
The first step in meeting that responsibility is to develop a written policy, if you don’t already have one, starting with a clear definition of sexual harassment. The Equal Employment Opportunity Commission (EEOC) has a good summary on its website of what does and does not constitute harassment, and under what conditions employers may be liable. Once the problem has been defined, a good written policy will provide specific methods for reporting transgressions, along with outlines of investigative and corrective measures to be taken in response. Templates for such documents are available on many websites, if you don’t want to start from scratch.
The next step, once a written policy is in place (and vetted by your attorney), is training for your staff. In particular, you should ensure that those in supervisory roles understand their specific responsibilities, and that everyone knows how to report an incident.
Harassment prevention training is already mandated by law in some states, including New York, California (if you have five or more employees), Maine, Delaware, and Connecticut. Other states, such as Colorado, Florida, Massachusetts, Michigan, Oklahoma, Rhode Island, Tennessee, Utah, and Vermont, have laws that “encourage” employers to provide such training. Other legislation is pending; check for new laws in your state on a regular basis.
Federal EEOC guidelines suggest that all employers “conduct and reinforce” harassment prevention training, whether laws in your particular state require it or not. On a practical level, recent court decisions suggest that offices that do not train their employees may find it difficult to mount an effective defense of a harassment lawsuit, even when they have a written policy in place. They may also be more vulnerable to punitive damage awards.
OSHA and various private companies offer a variety of downloadable training videos at reasonable cost. (As always, I have no financial interest in any product or service mentioned here.)
Misconduct among office staff is a straightforward, zero-tolerance issue. Harassment by patients is more complex, and dealing with it often requires some creativity. No one in your office, however, should think it is something they must accept because it comes from a patient. Any physician or staffer should be empowered to speak up if anyone else’s behavior, including a patient’s, makes them uncomfortable. Even when there is a medical explanation – such as psychiatric or cognitive impairment – it is important (and in some states, mandatory) to call out the behavior and report the incident.
Once reported, it should be documented, so that colleagues and other providers will be aware of the problem, and to protect yourself should the patient ever make false accusations against your practice. At subsequent appointments, take common-sense precautions. Chaperones are always a good idea, but especially so in these situations.
With repeat offenders, everyone has their own barometer of what they can and cannot tolerate. My personal threshold is low; I give one polite warning, explaining that we must provide a respectful and welcoming environment for everyone in the office, and any unacceptable behavior in the future will be grounds for dismissal from my practice. Most get the message; those who don’t are dismissed, politely.

The central point is to prevent harassment whenever possible, and to take every complaint seriously and address it promptly. An effective misconduct policy goes beyond simply avoiding legal liability. Patients and staffers alike should be secure in the knowledge that inappropriate verbal or physical interactions are not acceptable in your office under any circumstances, and will not be ignored or tolerated.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com .
Unless you have been vacationing on some distant astral plane, you are well aware that sexual misconduct and harassment have dominated news coverage and social media forums over the past year or more. It has ended the careers of a number of formerly respectable celebrities, and the #MeToo movement has empowered many additional harassment victims to come forward with their stories.
Medical offices are far from immune from harassment, of course, and the problem is not limited to staff interactions. According to a Medscape poll, 27% of physicians have been targets of inappropriate behavior in a professional setting. In another poll, 47% of physicians and 71% of nurses reported being harassed (by stalking, persistent attempts at communication, or inappropriate social media contact) by a patient.
The reality is that , have an ethical and legal responsibility to provide a safe and respectful work environment for everyone involved.
The first step in meeting that responsibility is to develop a written policy, if you don’t already have one, starting with a clear definition of sexual harassment. The Equal Employment Opportunity Commission (EEOC) has a good summary on its website of what does and does not constitute harassment, and under what conditions employers may be liable. Once the problem has been defined, a good written policy will provide specific methods for reporting transgressions, along with outlines of investigative and corrective measures to be taken in response. Templates for such documents are available on many websites, if you don’t want to start from scratch.
The next step, once a written policy is in place (and vetted by your attorney), is training for your staff. In particular, you should ensure that those in supervisory roles understand their specific responsibilities, and that everyone knows how to report an incident.
Harassment prevention training is already mandated by law in some states, including New York, California (if you have five or more employees), Maine, Delaware, and Connecticut. Other states, such as Colorado, Florida, Massachusetts, Michigan, Oklahoma, Rhode Island, Tennessee, Utah, and Vermont, have laws that “encourage” employers to provide such training. Other legislation is pending; check for new laws in your state on a regular basis.
Federal EEOC guidelines suggest that all employers “conduct and reinforce” harassment prevention training, whether laws in your particular state require it or not. On a practical level, recent court decisions suggest that offices that do not train their employees may find it difficult to mount an effective defense of a harassment lawsuit, even when they have a written policy in place. They may also be more vulnerable to punitive damage awards.
OSHA and various private companies offer a variety of downloadable training videos at reasonable cost. (As always, I have no financial interest in any product or service mentioned here.)
Misconduct among office staff is a straightforward, zero-tolerance issue. Harassment by patients is more complex, and dealing with it often requires some creativity. No one in your office, however, should think it is something they must accept because it comes from a patient. Any physician or staffer should be empowered to speak up if anyone else’s behavior, including a patient’s, makes them uncomfortable. Even when there is a medical explanation – such as psychiatric or cognitive impairment – it is important (and in some states, mandatory) to call out the behavior and report the incident.
Once reported, it should be documented, so that colleagues and other providers will be aware of the problem, and to protect yourself should the patient ever make false accusations against your practice. At subsequent appointments, take common-sense precautions. Chaperones are always a good idea, but especially so in these situations.
With repeat offenders, everyone has their own barometer of what they can and cannot tolerate. My personal threshold is low; I give one polite warning, explaining that we must provide a respectful and welcoming environment for everyone in the office, and any unacceptable behavior in the future will be grounds for dismissal from my practice. Most get the message; those who don’t are dismissed, politely.
The central point is to prevent harassment whenever possible, and to take every complaint seriously and address it promptly. An effective misconduct policy goes beyond simply avoiding legal liability. Patients and staffers alike should be secure in the knowledge that inappropriate verbal or physical interactions are not acceptable in your office under any circumstances, and will not be ignored or tolerated.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com .
Unless you have been vacationing on some distant astral plane, you are well aware that sexual misconduct and harassment have dominated news coverage and social media forums over the past year or more. It has ended the careers of a number of formerly respectable celebrities, and the #MeToo movement has empowered many additional harassment victims to come forward with their stories.
Medical offices are far from immune from harassment, of course, and the problem is not limited to staff interactions. According to a Medscape poll, 27% of physicians have been targets of inappropriate behavior in a professional setting. In another poll, 47% of physicians and 71% of nurses reported being harassed (by stalking, persistent attempts at communication, or inappropriate social media contact) by a patient.
The reality is that , have an ethical and legal responsibility to provide a safe and respectful work environment for everyone involved.
The first step in meeting that responsibility is to develop a written policy, if you don’t already have one, starting with a clear definition of sexual harassment. The Equal Employment Opportunity Commission (EEOC) has a good summary on its website of what does and does not constitute harassment, and under what conditions employers may be liable. Once the problem has been defined, a good written policy will provide specific methods for reporting transgressions, along with outlines of investigative and corrective measures to be taken in response. Templates for such documents are available on many websites, if you don’t want to start from scratch.
The next step, once a written policy is in place (and vetted by your attorney), is training for your staff. In particular, you should ensure that those in supervisory roles understand their specific responsibilities, and that everyone knows how to report an incident.
Harassment prevention training is already mandated by law in some states, including New York, California (if you have five or more employees), Maine, Delaware, and Connecticut. Other states, such as Colorado, Florida, Massachusetts, Michigan, Oklahoma, Rhode Island, Tennessee, Utah, and Vermont, have laws that “encourage” employers to provide such training. Other legislation is pending; check for new laws in your state on a regular basis.
Federal EEOC guidelines suggest that all employers “conduct and reinforce” harassment prevention training, whether laws in your particular state require it or not. On a practical level, recent court decisions suggest that offices that do not train their employees may find it difficult to mount an effective defense of a harassment lawsuit, even when they have a written policy in place. They may also be more vulnerable to punitive damage awards.
OSHA and various private companies offer a variety of downloadable training videos at reasonable cost. (As always, I have no financial interest in any product or service mentioned here.)
Misconduct among office staff is a straightforward, zero-tolerance issue. Harassment by patients is more complex, and dealing with it often requires some creativity. No one in your office, however, should think it is something they must accept because it comes from a patient. Any physician or staffer should be empowered to speak up if anyone else’s behavior, including a patient’s, makes them uncomfortable. Even when there is a medical explanation – such as psychiatric or cognitive impairment – it is important (and in some states, mandatory) to call out the behavior and report the incident.
Once reported, it should be documented, so that colleagues and other providers will be aware of the problem, and to protect yourself should the patient ever make false accusations against your practice. At subsequent appointments, take common-sense precautions. Chaperones are always a good idea, but especially so in these situations.
With repeat offenders, everyone has their own barometer of what they can and cannot tolerate. My personal threshold is low; I give one polite warning, explaining that we must provide a respectful and welcoming environment for everyone in the office, and any unacceptable behavior in the future will be grounds for dismissal from my practice. Most get the message; those who don’t are dismissed, politely.
The central point is to prevent harassment whenever possible, and to take every complaint seriously and address it promptly. An effective misconduct policy goes beyond simply avoiding legal liability. Patients and staffers alike should be secure in the knowledge that inappropriate verbal or physical interactions are not acceptable in your office under any circumstances, and will not be ignored or tolerated.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com .

A “Ray of light”
Finding inspiration in our patients
I rush into the room at 4:30 p.m., hoping for a quick visit and maybe an early exit from the hospital; I had been asked to see Mr. Bryant in room 6765 with sigmoid volvulus.

“Hey, Dr. Hass, my brother!” he says with a huge smile. Somehow, he must have gotten a glimpse of me before I could see him. I peek over the nurse’s shoulder, and then I see that unforgettable smile with only a few teeth and big bright eyes. Immediately I recognize him and think, “How could I have forgotten his name? Ray – like a beam of light.” He certainly had not forgotten me.
“It’s been more than a year since I was last here,” he says proudly.
When we met during his last hospitalization, I was struck by a thought that implanted itself deep in my brain: This guy is the happiest person I have ever met. And after what must have been 18 hard months for him, he is still smiling – and more than that, he is radiating love.
The fact that he is the “happiest person” is made more remarkable by all the hardship he has endured. Ray was born with cerebral palsy and didn’t walk until he was 10. The continuous spasms in his muscles led to severe cervical disc disease. His worsening pain and weakness were missed by his health care providers until he had lost significant strength in his hands and legs. When he finally got an MRI and then emergency surgery, it was too late. He never regained the dexterity of his hands or the ability to walk. He can climb onto his scooter chair only with the help of a lift.
“Wow! How you been, Ray?”
He replies with a phrase that jumped back out from my memory as he was saying it: “I just wake up every day and think about what I can do to make people happy.”
The goosebumps rise on my arms; I remember feeling this same sense of awe the last time we met – a feeling of real spiritual love for this guy.
“Today I feel so much better, too. I want to thank y’all who helped my stomach go down. Man, it got so huge, I thought I might blow up.” One of the consequences of the nerve damage he sustained is a very slow gut that has led to a stretched-out colon. The other day, his big, floppy colon got twisted, and neither our gastroenterologist nor radiologist was able to untwist it. He still has a tube in his rectum to help decompress his bowel.
Ray fills me in on the details in the slightly strained and slurred speech that sometimes comes with cerebral palsy. As he relays his story, my mind goes to work trying to diagnosis this mysterious case of happiness. How can I not try to get to the origins of this wellspring of love? I can’t help but thinking: Was it Ray’s joy and his speech impediment that made him seem childlike, or was it some brain injury that blessedly knocked out his self-pity? I would be wallowing in self-pity if I were as gravely disabled as him.
After a moment’s reflection, I recall the research on the amazing stability of our happiness set point: Good things and bad only move our happiness for a while before we return to our innate level of happiness. I see I had likely fallen prey to a stereotype of the disabled as heroic for just being themselves. Ray’s happiness is largely because of his lack of self-absorption and his focus on service and love.
Finishing our conversation and leaving the room feeling enlivened, I realize that Ray‘s generous spirit is a gift.
That night, my heart aches. I think about the inadequate care that led to Ray’s profound loss of function, leading to a surge of anger toward our flawed health care system – one that routinely lets down the most vulnerable among us.
The next day, two sisters and an aunt join Ray in his room. They ask for hugs, and I happily supply them. “Ray told us about you,” says Sheila, one of his sisters.
“Well, we have been talking about him here at the hospital, because he brightens everyone’s day. He is truly amazing. Has Ray always been so full of love?” I say, hoping to get some insight into his remarkable spirit.
Tonya, his aunt, responds first. “We were raised that way – to look for the good and keep love in our hearts. But Ray has always been the best. He never, ever complains. He brings joy to so many people. You should see him every day out on his scooter. That’s how he got that big sore on his butt.”
Ray indeed had developed a pressure sore, one that was going to need some thoughtful, ongoing care.
“But I finally got the right kind of cushion, before it was real hard,” he says.
I move from hospitalist mode to primary care mode and ask about his home equipment and his dental care. But they all want to keep talking about love.
“If doctors showed more love and their human side, they could bring more healing,” his sister says.
After 20 minutes of chatting, I pause. It is my last day on service, I had run out of medical reason to stay and I have others to see. So, I reluctantly give my goodbye hugs and leave. At the door, I turn back around. “Hey, Ray, can I get a picture with you?”
“Yeah, I want one with you, too!”
So, not surprisingly, Ray never complains. Maybe his spinal cord injury wasn’t from negligent care. Maybe he was so accustomed to looking past discomfort and too busy with his ministry of love, it didn’t occur to him to seek care.
Still, such a tragedy that he lost so much of the little mobility he did have. But maybe not so bad. His injury brought him back in contact with me and our staff. He is still waking up trying to make people happy and I can see his efforts are working. “He made my day!” I hear from a nurse. There is a healthy buzz at the nurses’ station after visits to his room.
Before walking out the door, he gives me an awkward fist bump from the bed and says, “I want to thank y’all again for everything. And I want you to know I love you.”
I find myself tearing up. “I love you too, my brother. And I am the one who should be grateful, Ray.” Saying it, I feel myself playing a part in the cycle of gratitude. Even small gifts put us under an obligation to give back. With great gifts, the desire to give is inescapable.
There is only one Ray, but he has given me something to aspire toward and what feels like urgency to do it. I want to “wake up each day thinking about ways to make other people happy.”
And understanding the potency of the gift from him has alerted me to the value of looking for other gifts and other inspirations from those I care for – something those of us who tend to be in the “doing” part of the provider-patient relationship can easy miss.
I will never be the beacon of light and love that Ray is, but being compelled to be my most authentic caring self with him, I see that for years I have held back – in the name of professionalism – the positive emotions that naturally arise from the work I do. I will try to shine and try to connect with that “Ray of light” residing in all my patients. I hope, too, that the cycle of giving Ray started will continue spreading to all those I care for.
Dr. Hass is a hospitalist at Sutter Health in Oakland, Calif. This article appeared originally in SHM's official blog The Hospital Leader. Read more recent posts here.
Finding inspiration in our patients
Finding inspiration in our patients
I rush into the room at 4:30 p.m., hoping for a quick visit and maybe an early exit from the hospital; I had been asked to see Mr. Bryant in room 6765 with sigmoid volvulus.
“Hey, Dr. Hass, my brother!” he says with a huge smile. Somehow, he must have gotten a glimpse of me before I could see him. I peek over the nurse’s shoulder, and then I see that unforgettable smile with only a few teeth and big bright eyes. Immediately I recognize him and think, “How could I have forgotten his name? Ray – like a beam of light.” He certainly had not forgotten me.
“It’s been more than a year since I was last here,” he says proudly.
When we met during his last hospitalization, I was struck by a thought that implanted itself deep in my brain: This guy is the happiest person I have ever met. And after what must have been 18 hard months for him, he is still smiling – and more than that, he is radiating love.
The fact that he is the “happiest person” is made more remarkable by all the hardship he has endured. Ray was born with cerebral palsy and didn’t walk until he was 10. The continuous spasms in his muscles led to severe cervical disc disease. His worsening pain and weakness were missed by his health care providers until he had lost significant strength in his hands and legs. When he finally got an MRI and then emergency surgery, it was too late. He never regained the dexterity of his hands or the ability to walk. He can climb onto his scooter chair only with the help of a lift.
“Wow! How you been, Ray?”
He replies with a phrase that jumped back out from my memory as he was saying it: “I just wake up every day and think about what I can do to make people happy.”
The goosebumps rise on my arms; I remember feeling this same sense of awe the last time we met – a feeling of real spiritual love for this guy.
“Today I feel so much better, too. I want to thank y’all who helped my stomach go down. Man, it got so huge, I thought I might blow up.” One of the consequences of the nerve damage he sustained is a very slow gut that has led to a stretched-out colon. The other day, his big, floppy colon got twisted, and neither our gastroenterologist nor radiologist was able to untwist it. He still has a tube in his rectum to help decompress his bowel.
Ray fills me in on the details in the slightly strained and slurred speech that sometimes comes with cerebral palsy. As he relays his story, my mind goes to work trying to diagnosis this mysterious case of happiness. How can I not try to get to the origins of this wellspring of love? I can’t help but thinking: Was it Ray’s joy and his speech impediment that made him seem childlike, or was it some brain injury that blessedly knocked out his self-pity? I would be wallowing in self-pity if I were as gravely disabled as him.
After a moment’s reflection, I recall the research on the amazing stability of our happiness set point: Good things and bad only move our happiness for a while before we return to our innate level of happiness. I see I had likely fallen prey to a stereotype of the disabled as heroic for just being themselves. Ray’s happiness is largely because of his lack of self-absorption and his focus on service and love.
Finishing our conversation and leaving the room feeling enlivened, I realize that Ray‘s generous spirit is a gift.
That night, my heart aches. I think about the inadequate care that led to Ray’s profound loss of function, leading to a surge of anger toward our flawed health care system – one that routinely lets down the most vulnerable among us.
The next day, two sisters and an aunt join Ray in his room. They ask for hugs, and I happily supply them. “Ray told us about you,” says Sheila, one of his sisters.
“Well, we have been talking about him here at the hospital, because he brightens everyone’s day. He is truly amazing. Has Ray always been so full of love?” I say, hoping to get some insight into his remarkable spirit.
Tonya, his aunt, responds first. “We were raised that way – to look for the good and keep love in our hearts. But Ray has always been the best. He never, ever complains. He brings joy to so many people. You should see him every day out on his scooter. That’s how he got that big sore on his butt.”
Ray indeed had developed a pressure sore, one that was going to need some thoughtful, ongoing care.
“But I finally got the right kind of cushion, before it was real hard,” he says.
I move from hospitalist mode to primary care mode and ask about his home equipment and his dental care. But they all want to keep talking about love.
“If doctors showed more love and their human side, they could bring more healing,” his sister says.
After 20 minutes of chatting, I pause. It is my last day on service, I had run out of medical reason to stay and I have others to see. So, I reluctantly give my goodbye hugs and leave. At the door, I turn back around. “Hey, Ray, can I get a picture with you?”
“Yeah, I want one with you, too!”
So, not surprisingly, Ray never complains. Maybe his spinal cord injury wasn’t from negligent care. Maybe he was so accustomed to looking past discomfort and too busy with his ministry of love, it didn’t occur to him to seek care.
Still, such a tragedy that he lost so much of the little mobility he did have. But maybe not so bad. His injury brought him back in contact with me and our staff. He is still waking up trying to make people happy and I can see his efforts are working. “He made my day!” I hear from a nurse. There is a healthy buzz at the nurses’ station after visits to his room.
Before walking out the door, he gives me an awkward fist bump from the bed and says, “I want to thank y’all again for everything. And I want you to know I love you.”
I find myself tearing up. “I love you too, my brother. And I am the one who should be grateful, Ray.” Saying it, I feel myself playing a part in the cycle of gratitude. Even small gifts put us under an obligation to give back. With great gifts, the desire to give is inescapable.
There is only one Ray, but he has given me something to aspire toward and what feels like urgency to do it. I want to “wake up each day thinking about ways to make other people happy.”
And understanding the potency of the gift from him has alerted me to the value of looking for other gifts and other inspirations from those I care for – something those of us who tend to be in the “doing” part of the provider-patient relationship can easy miss.
I will never be the beacon of light and love that Ray is, but being compelled to be my most authentic caring self with him, I see that for years I have held back – in the name of professionalism – the positive emotions that naturally arise from the work I do. I will try to shine and try to connect with that “Ray of light” residing in all my patients. I hope, too, that the cycle of giving Ray started will continue spreading to all those I care for.
Dr. Hass is a hospitalist at Sutter Health in Oakland, Calif. This article appeared originally in SHM's official blog The Hospital Leader. Read more recent posts here.
I rush into the room at 4:30 p.m., hoping for a quick visit and maybe an early exit from the hospital; I had been asked to see Mr. Bryant in room 6765 with sigmoid volvulus.
“Hey, Dr. Hass, my brother!” he says with a huge smile. Somehow, he must have gotten a glimpse of me before I could see him. I peek over the nurse’s shoulder, and then I see that unforgettable smile with only a few teeth and big bright eyes. Immediately I recognize him and think, “How could I have forgotten his name? Ray – like a beam of light.” He certainly had not forgotten me.
“It’s been more than a year since I was last here,” he says proudly.
When we met during his last hospitalization, I was struck by a thought that implanted itself deep in my brain: This guy is the happiest person I have ever met. And after what must have been 18 hard months for him, he is still smiling – and more than that, he is radiating love.
The fact that he is the “happiest person” is made more remarkable by all the hardship he has endured. Ray was born with cerebral palsy and didn’t walk until he was 10. The continuous spasms in his muscles led to severe cervical disc disease. His worsening pain and weakness were missed by his health care providers until he had lost significant strength in his hands and legs. When he finally got an MRI and then emergency surgery, it was too late. He never regained the dexterity of his hands or the ability to walk. He can climb onto his scooter chair only with the help of a lift.
“Wow! How you been, Ray?”
He replies with a phrase that jumped back out from my memory as he was saying it: “I just wake up every day and think about what I can do to make people happy.”
The goosebumps rise on my arms; I remember feeling this same sense of awe the last time we met – a feeling of real spiritual love for this guy.
“Today I feel so much better, too. I want to thank y’all who helped my stomach go down. Man, it got so huge, I thought I might blow up.” One of the consequences of the nerve damage he sustained is a very slow gut that has led to a stretched-out colon. The other day, his big, floppy colon got twisted, and neither our gastroenterologist nor radiologist was able to untwist it. He still has a tube in his rectum to help decompress his bowel.
Ray fills me in on the details in the slightly strained and slurred speech that sometimes comes with cerebral palsy. As he relays his story, my mind goes to work trying to diagnosis this mysterious case of happiness. How can I not try to get to the origins of this wellspring of love? I can’t help but thinking: Was it Ray’s joy and his speech impediment that made him seem childlike, or was it some brain injury that blessedly knocked out his self-pity? I would be wallowing in self-pity if I were as gravely disabled as him.
After a moment’s reflection, I recall the research on the amazing stability of our happiness set point: Good things and bad only move our happiness for a while before we return to our innate level of happiness. I see I had likely fallen prey to a stereotype of the disabled as heroic for just being themselves. Ray’s happiness is largely because of his lack of self-absorption and his focus on service and love.
Finishing our conversation and leaving the room feeling enlivened, I realize that Ray‘s generous spirit is a gift.
That night, my heart aches. I think about the inadequate care that led to Ray’s profound loss of function, leading to a surge of anger toward our flawed health care system – one that routinely lets down the most vulnerable among us.
The next day, two sisters and an aunt join Ray in his room. They ask for hugs, and I happily supply them. “Ray told us about you,” says Sheila, one of his sisters.
“Well, we have been talking about him here at the hospital, because he brightens everyone’s day. He is truly amazing. Has Ray always been so full of love?” I say, hoping to get some insight into his remarkable spirit.
Tonya, his aunt, responds first. “We were raised that way – to look for the good and keep love in our hearts. But Ray has always been the best. He never, ever complains. He brings joy to so many people. You should see him every day out on his scooter. That’s how he got that big sore on his butt.”
Ray indeed had developed a pressure sore, one that was going to need some thoughtful, ongoing care.
“But I finally got the right kind of cushion, before it was real hard,” he says.
I move from hospitalist mode to primary care mode and ask about his home equipment and his dental care. But they all want to keep talking about love.
“If doctors showed more love and their human side, they could bring more healing,” his sister says.
After 20 minutes of chatting, I pause. It is my last day on service, I had run out of medical reason to stay and I have others to see. So, I reluctantly give my goodbye hugs and leave. At the door, I turn back around. “Hey, Ray, can I get a picture with you?”
“Yeah, I want one with you, too!”
So, not surprisingly, Ray never complains. Maybe his spinal cord injury wasn’t from negligent care. Maybe he was so accustomed to looking past discomfort and too busy with his ministry of love, it didn’t occur to him to seek care.
Still, such a tragedy that he lost so much of the little mobility he did have. But maybe not so bad. His injury brought him back in contact with me and our staff. He is still waking up trying to make people happy and I can see his efforts are working. “He made my day!” I hear from a nurse. There is a healthy buzz at the nurses’ station after visits to his room.
Before walking out the door, he gives me an awkward fist bump from the bed and says, “I want to thank y’all again for everything. And I want you to know I love you.”
I find myself tearing up. “I love you too, my brother. And I am the one who should be grateful, Ray.” Saying it, I feel myself playing a part in the cycle of gratitude. Even small gifts put us under an obligation to give back. With great gifts, the desire to give is inescapable.
There is only one Ray, but he has given me something to aspire toward and what feels like urgency to do it. I want to “wake up each day thinking about ways to make other people happy.”
And understanding the potency of the gift from him has alerted me to the value of looking for other gifts and other inspirations from those I care for – something those of us who tend to be in the “doing” part of the provider-patient relationship can easy miss.
I will never be the beacon of light and love that Ray is, but being compelled to be my most authentic caring self with him, I see that for years I have held back – in the name of professionalism – the positive emotions that naturally arise from the work I do. I will try to shine and try to connect with that “Ray of light” residing in all my patients. I hope, too, that the cycle of giving Ray started will continue spreading to all those I care for.
Dr. Hass is a hospitalist at Sutter Health in Oakland, Calif. This article appeared originally in SHM's official blog The Hospital Leader. Read more recent posts here.
Get patients vaccinated: Avoid unwelcome international travel souvenirs
Summer officially began June 21, 2019, but many of your patients already may have departed or will soon be headed to international destinations. Reasons for travel are as variable as their destinations and include but are not limited to family vacations, mission trips, study abroad, parental job relocation, and visiting friends and relatives. The majority of the trips are planned at least 3 months in advance; however, for many travelers and their parents, they suddenly get an aha moment and realize there is/are specific vaccines required to obtain a visa or entry to their final destination. Unfortunately, too much emphasis is focused on required vaccines. The well-informed traveler knows that they may be exposed to multiple diseases and many are vaccine preventable.

The accompanying table lists vaccines traditionally considered to be travel vaccines. Several require multiple doses administered over 21-28 days to provide protection. Others such as cholera and yellow fever must be completed at least 10 days prior to departure to be effective. Typhoid has two formulations: The oral and injectable typhoid vaccines should be completed 1 and 2 weeks, respectively, prior to travel. Several vaccines have age limitations. Routine immunization of all infants against hepatitis A was recommended in 2006. Depending on your region, there may be adolescents who have not been immunized. Fortunately, hepatitis A vaccine works immediately.
One of the challenges you face is identifying someone in your area that provides travel medicine advice and immunizations to children and adolescents. Most children and teens travel with their parents, but today many adolescents travel independently with organized groups. Most of the vaccines listed are not routinely administered at your office, yet you most likely will be the first call a parent makes seeking travel advice.
Let me tell you about a few vaccines in particular.
Japanese encephalitis
This is most common cause of encephalitis in Asia and parts of the western Pacific. Risk generally is limited to rural agricultural areas where the causative virus is transmitted by a mosquito. Fatality rates are 20%-30%. Among survivors, 30%-50% have significant neurologic, cognitive, and psychiatric sequelae. Candidates for this vaccine are long-term travelers and short-term travelers with extensive outdoor rural activities.
Meningococcal conjugate vaccines (MCV4)
All travelers to the Hajj Pilgrimage (Aug. 9-14, 2019) and/or Umrah must show proof of immunization. Vaccine must be received at least 10 days prior to and no greater than 5 years prior to arrival to Saudi Arabia. Conjugate vaccine must clearly be documented for validity of 5 years. For all health entry requirements, go to www.moh.gov.sa/en/hajj/pages/healthregulations.aspx.
Measles
The Advisory Committee on Immunization Practices recommends all infants 6-11 months old receive one dose of MMR prior to international travel regardless of the destination. This should be followed by two additional countable doses. All persons at least 12 months of age and born after 1956 should receive two doses of MMR at least 28 days apart prior to international travel.
Rabies
Rabies is a viral disease endemic in more than 150 countries with approximately 60,000 fatal cases worldwide each year. Asia and Africa are the areas with the highest risk of exposure, and dogs are the principal hosts. Human rabies is almost always fatal once symptoms develop. Preexposure vaccine is recommended for persons with prolonged and/or remote travel to countries where rabies immunoglobulin is unavailable and the occurrence of animal rabies is high. Post exposure vaccination on days 0 and 3 still would be required.*
Typhoid
A bacterial infection caused by Salmonella enterica serotype Typhi and Paratyphi manifests with fever, headache, abdominal pain, diarrhea, or constipation. When bacteremia occurs, it usually is referred to as enteric fever. It is acquired by consumption of food/water contaminated with human feces. Highest risk areas include Africa, Southern Asia, and Southeast Asia
Yellow fever
Risk is limited to sub-Saharan Africa and the tropical areas of South America. It is transmitted by the bite of an infected mosquito. The vaccine is required for entry into at least 16 countries. In a country where yellow fever is present, persons transiting through for more than 12 hours to reach their final destination may actually cause a change in the entry requirements for the destination country. For example, travel from the United States to Tanzania requires no yellow fever vaccine while travel from the United States to Nairobi (more than 12 hours) to Tanzania requires yellow fever vaccine for entry into Tanzania. Travel sequence and duration is extremely important. Check the Centers for Disease Control and Prevention yellow fever site and/or the consulate for the most up-to-date yellow fever vaccine requirements.

YF-Vax (yellow fever vaccine) produced by Sanofi Pasteur in the United States currently is unavailable. The company is building a new facility, and vaccine will not be available for the remainder of 2019. To assure vaccine for U.S. travelers, Stamaril, a yellow fever vaccine produced by Sanofi Pasteur in France has been made available at more than 250 sites nationwide. Because Stamaril is offered at a limited number of locations, persons in need of vaccine should not delay seeking it. Because of increased demand related to summer travel, travelers in some areas have reported delays of several weeks in scheduling an appointment. To locate a Stamaril site in your area, go to wwwnc.cdc.gov/travel/page/search-for-stamaril-clinics.
There are several other diseases transmitted by mosquitoes and ticks including malaria, dengue, Zika and rickettsial diseases. Vigilant use of mosquito repellents is a must. Prophylactic medication is available for only malaria and should be initiated prior to exposure. Frequency and duration depends on the medication selected.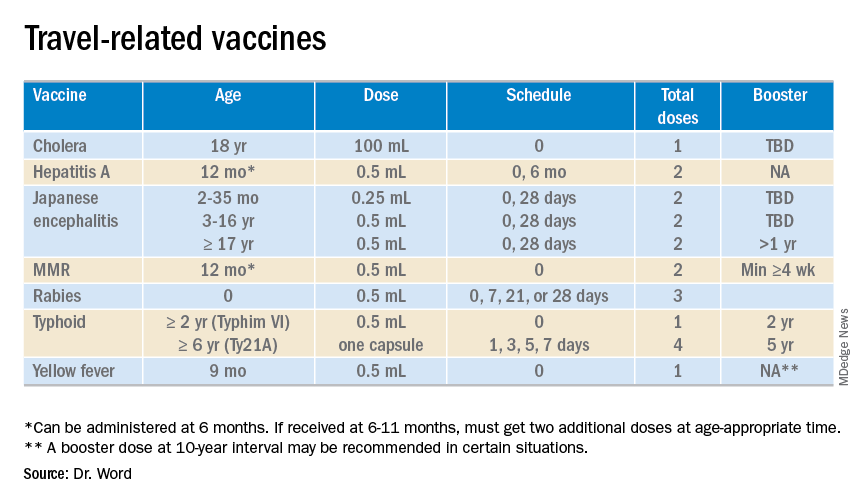
So how do you assist your patients?
Once you’ve identified a travel medicine facility in your area, encourage them to seek pretravel advice 4-6 weeks prior to international travel and make sure their routine immunizations are up to date. Generally, this is not an issue. One challenge is the early administration of MMR. While most practitioners know that early administration for international travel has been recommended for years, many office staff are accustomed to administration at only the 12 month and 4 year visit. When parents call requesting immunization, they often are informed that is it unnecessary and the appointment denied. This is a challenge, especially when coordination of administration of another live vaccine, such as yellow fever, is planned. Familiarizing all members of the health care team with current vaccine recommendations is critical.
For country-specific information, up-to-date travel alerts, and to locate a travel medicine clinic, visit www.cdc.gov/travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Email her at pdnews@mdedge.com.
*This article was updated 6/18/2019.
Summer officially began June 21, 2019, but many of your patients already may have departed or will soon be headed to international destinations. Reasons for travel are as variable as their destinations and include but are not limited to family vacations, mission trips, study abroad, parental job relocation, and visiting friends and relatives. The majority of the trips are planned at least 3 months in advance; however, for many travelers and their parents, they suddenly get an aha moment and realize there is/are specific vaccines required to obtain a visa or entry to their final destination. Unfortunately, too much emphasis is focused on required vaccines. The well-informed traveler knows that they may be exposed to multiple diseases and many are vaccine preventable.
The accompanying table lists vaccines traditionally considered to be travel vaccines. Several require multiple doses administered over 21-28 days to provide protection. Others such as cholera and yellow fever must be completed at least 10 days prior to departure to be effective. Typhoid has two formulations: The oral and injectable typhoid vaccines should be completed 1 and 2 weeks, respectively, prior to travel. Several vaccines have age limitations. Routine immunization of all infants against hepatitis A was recommended in 2006. Depending on your region, there may be adolescents who have not been immunized. Fortunately, hepatitis A vaccine works immediately.
One of the challenges you face is identifying someone in your area that provides travel medicine advice and immunizations to children and adolescents. Most children and teens travel with their parents, but today many adolescents travel independently with organized groups. Most of the vaccines listed are not routinely administered at your office, yet you most likely will be the first call a parent makes seeking travel advice.
Let me tell you about a few vaccines in particular.
Japanese encephalitis
This is most common cause of encephalitis in Asia and parts of the western Pacific. Risk generally is limited to rural agricultural areas where the causative virus is transmitted by a mosquito. Fatality rates are 20%-30%. Among survivors, 30%-50% have significant neurologic, cognitive, and psychiatric sequelae. Candidates for this vaccine are long-term travelers and short-term travelers with extensive outdoor rural activities.
Meningococcal conjugate vaccines (MCV4)
All travelers to the Hajj Pilgrimage (Aug. 9-14, 2019) and/or Umrah must show proof of immunization. Vaccine must be received at least 10 days prior to and no greater than 5 years prior to arrival to Saudi Arabia. Conjugate vaccine must clearly be documented for validity of 5 years. For all health entry requirements, go to www.moh.gov.sa/en/hajj/pages/healthregulations.aspx.
Measles
The Advisory Committee on Immunization Practices recommends all infants 6-11 months old receive one dose of MMR prior to international travel regardless of the destination. This should be followed by two additional countable doses. All persons at least 12 months of age and born after 1956 should receive two doses of MMR at least 28 days apart prior to international travel.
Rabies
Rabies is a viral disease endemic in more than 150 countries with approximately 60,000 fatal cases worldwide each year. Asia and Africa are the areas with the highest risk of exposure, and dogs are the principal hosts. Human rabies is almost always fatal once symptoms develop. Preexposure vaccine is recommended for persons with prolonged and/or remote travel to countries where rabies immunoglobulin is unavailable and the occurrence of animal rabies is high. Post exposure vaccination on days 0 and 3 still would be required.*
Typhoid
A bacterial infection caused by Salmonella enterica serotype Typhi and Paratyphi manifests with fever, headache, abdominal pain, diarrhea, or constipation. When bacteremia occurs, it usually is referred to as enteric fever. It is acquired by consumption of food/water contaminated with human feces. Highest risk areas include Africa, Southern Asia, and Southeast Asia
Yellow fever
Risk is limited to sub-Saharan Africa and the tropical areas of South America. It is transmitted by the bite of an infected mosquito. The vaccine is required for entry into at least 16 countries. In a country where yellow fever is present, persons transiting through for more than 12 hours to reach their final destination may actually cause a change in the entry requirements for the destination country. For example, travel from the United States to Tanzania requires no yellow fever vaccine while travel from the United States to Nairobi (more than 12 hours) to Tanzania requires yellow fever vaccine for entry into Tanzania. Travel sequence and duration is extremely important. Check the Centers for Disease Control and Prevention yellow fever site and/or the consulate for the most up-to-date yellow fever vaccine requirements.
YF-Vax (yellow fever vaccine) produced by Sanofi Pasteur in the United States currently is unavailable. The company is building a new facility, and vaccine will not be available for the remainder of 2019. To assure vaccine for U.S. travelers, Stamaril, a yellow fever vaccine produced by Sanofi Pasteur in France has been made available at more than 250 sites nationwide. Because Stamaril is offered at a limited number of locations, persons in need of vaccine should not delay seeking it. Because of increased demand related to summer travel, travelers in some areas have reported delays of several weeks in scheduling an appointment. To locate a Stamaril site in your area, go to wwwnc.cdc.gov/travel/page/search-for-stamaril-clinics.
There are several other diseases transmitted by mosquitoes and ticks including malaria, dengue, Zika and rickettsial diseases. Vigilant use of mosquito repellents is a must. Prophylactic medication is available for only malaria and should be initiated prior to exposure. Frequency and duration depends on the medication selected.
So how do you assist your patients?
Once you’ve identified a travel medicine facility in your area, encourage them to seek pretravel advice 4-6 weeks prior to international travel and make sure their routine immunizations are up to date. Generally, this is not an issue. One challenge is the early administration of MMR. While most practitioners know that early administration for international travel has been recommended for years, many office staff are accustomed to administration at only the 12 month and 4 year visit. When parents call requesting immunization, they often are informed that is it unnecessary and the appointment denied. This is a challenge, especially when coordination of administration of another live vaccine, such as yellow fever, is planned. Familiarizing all members of the health care team with current vaccine recommendations is critical.
For country-specific information, up-to-date travel alerts, and to locate a travel medicine clinic, visit www.cdc.gov/travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Email her at pdnews@mdedge.com.
*This article was updated 6/18/2019.
Summer officially began June 21, 2019, but many of your patients already may have departed or will soon be headed to international destinations. Reasons for travel are as variable as their destinations and include but are not limited to family vacations, mission trips, study abroad, parental job relocation, and visiting friends and relatives. The majority of the trips are planned at least 3 months in advance; however, for many travelers and their parents, they suddenly get an aha moment and realize there is/are specific vaccines required to obtain a visa or entry to their final destination. Unfortunately, too much emphasis is focused on required vaccines. The well-informed traveler knows that they may be exposed to multiple diseases and many are vaccine preventable.
The accompanying table lists vaccines traditionally considered to be travel vaccines. Several require multiple doses administered over 21-28 days to provide protection. Others such as cholera and yellow fever must be completed at least 10 days prior to departure to be effective. Typhoid has two formulations: The oral and injectable typhoid vaccines should be completed 1 and 2 weeks, respectively, prior to travel. Several vaccines have age limitations. Routine immunization of all infants against hepatitis A was recommended in 2006. Depending on your region, there may be adolescents who have not been immunized. Fortunately, hepatitis A vaccine works immediately.
One of the challenges you face is identifying someone in your area that provides travel medicine advice and immunizations to children and adolescents. Most children and teens travel with their parents, but today many adolescents travel independently with organized groups. Most of the vaccines listed are not routinely administered at your office, yet you most likely will be the first call a parent makes seeking travel advice.
Let me tell you about a few vaccines in particular.
Japanese encephalitis
This is most common cause of encephalitis in Asia and parts of the western Pacific. Risk generally is limited to rural agricultural areas where the causative virus is transmitted by a mosquito. Fatality rates are 20%-30%. Among survivors, 30%-50% have significant neurologic, cognitive, and psychiatric sequelae. Candidates for this vaccine are long-term travelers and short-term travelers with extensive outdoor rural activities.
Meningococcal conjugate vaccines (MCV4)
All travelers to the Hajj Pilgrimage (Aug. 9-14, 2019) and/or Umrah must show proof of immunization. Vaccine must be received at least 10 days prior to and no greater than 5 years prior to arrival to Saudi Arabia. Conjugate vaccine must clearly be documented for validity of 5 years. For all health entry requirements, go to www.moh.gov.sa/en/hajj/pages/healthregulations.aspx.
Measles
The Advisory Committee on Immunization Practices recommends all infants 6-11 months old receive one dose of MMR prior to international travel regardless of the destination. This should be followed by two additional countable doses. All persons at least 12 months of age and born after 1956 should receive two doses of MMR at least 28 days apart prior to international travel.
Rabies
Rabies is a viral disease endemic in more than 150 countries with approximately 60,000 fatal cases worldwide each year. Asia and Africa are the areas with the highest risk of exposure, and dogs are the principal hosts. Human rabies is almost always fatal once symptoms develop. Preexposure vaccine is recommended for persons with prolonged and/or remote travel to countries where rabies immunoglobulin is unavailable and the occurrence of animal rabies is high. Post exposure vaccination on days 0 and 3 still would be required.*
Typhoid
A bacterial infection caused by Salmonella enterica serotype Typhi and Paratyphi manifests with fever, headache, abdominal pain, diarrhea, or constipation. When bacteremia occurs, it usually is referred to as enteric fever. It is acquired by consumption of food/water contaminated with human feces. Highest risk areas include Africa, Southern Asia, and Southeast Asia
Yellow fever
Risk is limited to sub-Saharan Africa and the tropical areas of South America. It is transmitted by the bite of an infected mosquito. The vaccine is required for entry into at least 16 countries. In a country where yellow fever is present, persons transiting through for more than 12 hours to reach their final destination may actually cause a change in the entry requirements for the destination country. For example, travel from the United States to Tanzania requires no yellow fever vaccine while travel from the United States to Nairobi (more than 12 hours) to Tanzania requires yellow fever vaccine for entry into Tanzania. Travel sequence and duration is extremely important. Check the Centers for Disease Control and Prevention yellow fever site and/or the consulate for the most up-to-date yellow fever vaccine requirements.
YF-Vax (yellow fever vaccine) produced by Sanofi Pasteur in the United States currently is unavailable. The company is building a new facility, and vaccine will not be available for the remainder of 2019. To assure vaccine for U.S. travelers, Stamaril, a yellow fever vaccine produced by Sanofi Pasteur in France has been made available at more than 250 sites nationwide. Because Stamaril is offered at a limited number of locations, persons in need of vaccine should not delay seeking it. Because of increased demand related to summer travel, travelers in some areas have reported delays of several weeks in scheduling an appointment. To locate a Stamaril site in your area, go to wwwnc.cdc.gov/travel/page/search-for-stamaril-clinics.
There are several other diseases transmitted by mosquitoes and ticks including malaria, dengue, Zika and rickettsial diseases. Vigilant use of mosquito repellents is a must. Prophylactic medication is available for only malaria and should be initiated prior to exposure. Frequency and duration depends on the medication selected.
So how do you assist your patients?
Once you’ve identified a travel medicine facility in your area, encourage them to seek pretravel advice 4-6 weeks prior to international travel and make sure their routine immunizations are up to date. Generally, this is not an issue. One challenge is the early administration of MMR. While most practitioners know that early administration for international travel has been recommended for years, many office staff are accustomed to administration at only the 12 month and 4 year visit. When parents call requesting immunization, they often are informed that is it unnecessary and the appointment denied. This is a challenge, especially when coordination of administration of another live vaccine, such as yellow fever, is planned. Familiarizing all members of the health care team with current vaccine recommendations is critical.
For country-specific information, up-to-date travel alerts, and to locate a travel medicine clinic, visit www.cdc.gov/travel.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She had no relevant financial disclosures. Email her at pdnews@mdedge.com.
*This article was updated 6/18/2019.
What makes a mass murderer?
‘A Dark Night in Aurora’ gives view into one killer’s mind
It was an unthinkable crime; on July 20, 2012, a 24-year-old neuroscience graduate student* walked into a movie theatre in Aurora, Colo., and began shooting people he had never before seen. Twelve people died and 70 were wounded in this calculated and intricately planned massacre that challenged everything we know about the intersection of mental illness and evil.
So much has been written about mass shooters as we’ve struggled to understand what motivates someone to kill strangers in a public place. The hope is that if we can understand it, then we can prevent it. The topic has been one of great interest to me because it gets quickly linked to advocacy for involuntary psychiatric care: Half of mass murderers suffer from psychiatric disorders and if we could force them to get treatment, then we could prevent these horrific events.

Many mass shooters die at the scene. Not only did the Aurora shooter survive, but his case went to trial – also a rarity – providing insights we have not had with other similar cases. With information gained through this court case comes “A Dark Night In Aurora” (Skyhorse Press, 2018), a careful dissection of the Aurora shooter by William H. Reid, MD, MPH. There are many books about crimes and criminals, but what caught my attention about this book was the author. Dr. Reid is one of five expert/forensic psychiatrists retained for the case and he was brought on by the judge as a second nonpartisan psychiatrist. Dr. Reid interviewed the defendant for more than 20 hours, he video-recorded the interviews, and he had access to, “... the existing seventy-five thousand pages of evidence, hundreds of audio and video files, and access to the defendants and scores of witnesses, experts, and others associated with the case ...” Dr. Reid notes that when the defendant placed his sanity in question, all confidentiality was waived.
In this case, the perpetrator had been treated by a therapist and two psychiatrists at his university counseling center in the semester before the shooting. There were video recordings of the defendant in his cell, a correctional psychiatrist in the local jail; psychiatric records from an admission to Denver Health Medical Center and two admissions to the Colorado Health Institute at Pueblo (a secure, forensic setting); and neuropsychological testing done by psychologists hired for the case. In all, there was a lot of mental health data, and I’m not aware of any other book that has been written by a psychiatrist about a criminal case where the author testified in the case.
Let me start by saying that the book is well written, very readable, and fascinating. I’d followed parts of the case in the news and had even watched some of the trial being live-streamed, so not all of the information was new, but Dr. Reid has put together the many facts of a perplexing case together in a cohesive way. There’s no literary descriptions or flowery writing; Dr. Reid is a focused writer. He also does a good job of explaining the specifics of Colorado state law to the forensic aspects of the case. In the end, there were nuances of how the shooter came to be found both competent and sane but was spared the death penalty by a single vote. Overall, I found the book haunting, and it would have been a more comfortable read if it were fiction. There was something terribly disconcerting about following along this miserable journey, all the while knowing that the killer ultimately would destroy so many lives and then watching his disconnected existence after the massacre.
As a general adult psychiatrist, I wanted to learn something very specific from this book: What is the recipe for creating a mass murderer and what are the warning signs a psychiatrist should catch? I would like my career to be free of patients who kill. The Aurora shooter’s family life sounded fairly pedestrian. His parents are professionals; there was a boy and a girl in an intact family with attentive parents, and no findings of abuse, torture, neglect, bullying, or anything out of the ordinary.
As a child, the shooter was noted for his kindness, and he was particularly caring toward his younger sister. As he grew older, reports about his personality were conflicting: Some saw him as awkward, and later even as odd, while others described him as normal, especially within a cohort of studious kids. He played on sports teams, was an excellent student, liked nonviolent video games, and while he was not outgoing, he always had some friends, though he shunned them during the semester before the shooting. He was not comfortable with women, but he had one girlfriend in graduate school, and when that relationship broke up, he texted with another classmate about how “hot” she was and that they went hiking together. The breakup may have contributed to the shooter’s unraveling, but if it did, Dr. Reid did not present this as the precipitant, and many young men are awkward with women – and endure breakups and rejection.
While the media said the shooter failed out of school, this was not the case. He did well in his classes but chose not to study for an important oral exam while he devoted his time to gathering weapons for his mission to kill, planning out the details, learning to use firearms, and rigging up a complex explosive system around his apartment. When he failed the oral exam, he was told he could study and retake it in a few weeks. He chose, instead, to withdraw from graduate school.
What stood out for me was that this young man talked about thoughts of killing people. He did so to the point of worrying his psychiatrist: She called in a second psychiatrist for a consultation, alerted the university’s threat assessment team, contacted an out-of-state parent, and considered admitting him on an involuntary hold. While many patients say they might hurt someone if provoked or threatened, few discuss thoughts of killing indiscriminately. But when people do talk about killing, we do our best to flush out their intentions, whether it is a fantasy or a plan, if they’ve been violent before. This shooter had no history of violence, and he hid from the psychiatrist the fact that he was acquiring weapons and actually planning a massacre. His psychiatrist diagnosed him with social anxiety, obsessive-compulsive disorder, and possible schizotypal personality disorder. He was prescribed an antidepressant, and later offered an antipsychotic, which he refused.
Three of the four psychiatrists who evaluated the defendant for the legal proceedings made a diagnosis of schizoaffective disorder. (The fifth psychiatrist for the prosecution never examined the defendant.) Dr. Reid made a diagnosis of schizotypal personality disorder. Everyone agreed that the shooter had a mental illness that influenced his actions. When it came to ascertaining the defendant’s mental state at the time of the crime, there was a glitch: The first psychiatrist for the defense examined the defendant only once, days after the shooting, and not again until 3 years later, right before the trial. His exam was limited: The defense attorney was present in the room, and he had instructed the psychiatrist not to ask about the shooting. The attorney interrupted the interview twice, and it’s not the usual practice to place these conditions on a forensic evaluation. After that exam, there was some misunderstanding about who was in charge of the treatment, and the defendant refused the services of the jail psychiatrist. It was not until 4 months later when the inmate became dehydrated, delirious, and psychotic that he finally was evaluated and treated. Despite the abundance of psychiatric information available, no direct and complete assessment was made by a psychiatrist immediately before the shooting, or in the months right after.
When we try to understand what motivates someone to commit such a heinous act, we look for psychosis. If the person suffers from paranoid delusions and believes his behavior is in self-defense, the behavior becomes understandable and justifiable. Even if it’s less organized, if it is the clear result of a psychotic thought process, we often attribute the behavior to illness. Usually, people with psychosis are too disorganized to enact complex plans, to acquire and learn to use ammunition, to plot out when and where there will be potential victims, and to plot out this degree of planning.
This shooter had an odd belief that if he killed people, he would attain “human capital.” Their deaths might fortify him, increase his value and decrease his suffering, and thereby prevent him from dying by suicide. Dr. Reid talks about whether it’s a delusion, an overvalued idea, or just an unusual belief. The shooter was aware that others don’t agree with this, that they would see it as wrong and criminal, and he thought there was only a 50% chance that it would work. If this were a delusion, it was not one we typically see, nor was it accompanied by more usual perceptual phenomena. Ultimately, there was no consensus on whether the patient was psychotic at the time of the shooting. On antipsychotic medication, he continued to believe that if he killed people that he would attain their human capital. In his book, Dr. Reid concluded that he remained dangerous.
Because the shooter told the university health center psychiatrist that he did not want to be locked up, she considered involuntary hospitalization, but she did not believe he would meet criteria for commitment. I saw nothing that indicated whether he was offered voluntary inpatient care with an explanation that hospital treatment is not the same as being locked up and might help alleviate his suffering. We don’t know if he could have been persuaded to enter the hospital willingly, but I suspect that this would have been difficult to justify to an insurer. There’s nothing to indicate that a hospitalization would have prevented this massacre.

From my perspective, I concluded that if individuals say they are thinking about killing strangers, they may be at risk of violence. This is a much smaller group of people to target for intervention than everyone with mental illness or everyone who is odd. This particular shooter appears to suffer from some type of mental derangement that does not fit neatly into our current psychiatric nomenclature or respond to our current treatments, and thoughtful psychiatric intervention – which he had – could not prevent his actions. It seems the only thing that would have changed this outcome is if someone had discovered his arsenal before July 20, 2012.
*Please note: The shooter’s name is intentionally omitted from my review.
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
‘A Dark Night in Aurora’ gives view into one killer’s mind
‘A Dark Night in Aurora’ gives view into one killer’s mind
It was an unthinkable crime; on July 20, 2012, a 24-year-old neuroscience graduate student* walked into a movie theatre in Aurora, Colo., and began shooting people he had never before seen. Twelve people died and 70 were wounded in this calculated and intricately planned massacre that challenged everything we know about the intersection of mental illness and evil.
So much has been written about mass shooters as we’ve struggled to understand what motivates someone to kill strangers in a public place. The hope is that if we can understand it, then we can prevent it. The topic has been one of great interest to me because it gets quickly linked to advocacy for involuntary psychiatric care: Half of mass murderers suffer from psychiatric disorders and if we could force them to get treatment, then we could prevent these horrific events.
Many mass shooters die at the scene. Not only did the Aurora shooter survive, but his case went to trial – also a rarity – providing insights we have not had with other similar cases. With information gained through this court case comes “A Dark Night In Aurora” (Skyhorse Press, 2018), a careful dissection of the Aurora shooter by William H. Reid, MD, MPH. There are many books about crimes and criminals, but what caught my attention about this book was the author. Dr. Reid is one of five expert/forensic psychiatrists retained for the case and he was brought on by the judge as a second nonpartisan psychiatrist. Dr. Reid interviewed the defendant for more than 20 hours, he video-recorded the interviews, and he had access to, “... the existing seventy-five thousand pages of evidence, hundreds of audio and video files, and access to the defendants and scores of witnesses, experts, and others associated with the case ...” Dr. Reid notes that when the defendant placed his sanity in question, all confidentiality was waived.
In this case, the perpetrator had been treated by a therapist and two psychiatrists at his university counseling center in the semester before the shooting. There were video recordings of the defendant in his cell, a correctional psychiatrist in the local jail; psychiatric records from an admission to Denver Health Medical Center and two admissions to the Colorado Health Institute at Pueblo (a secure, forensic setting); and neuropsychological testing done by psychologists hired for the case. In all, there was a lot of mental health data, and I’m not aware of any other book that has been written by a psychiatrist about a criminal case where the author testified in the case.
Let me start by saying that the book is well written, very readable, and fascinating. I’d followed parts of the case in the news and had even watched some of the trial being live-streamed, so not all of the information was new, but Dr. Reid has put together the many facts of a perplexing case together in a cohesive way. There’s no literary descriptions or flowery writing; Dr. Reid is a focused writer. He also does a good job of explaining the specifics of Colorado state law to the forensic aspects of the case. In the end, there were nuances of how the shooter came to be found both competent and sane but was spared the death penalty by a single vote. Overall, I found the book haunting, and it would have been a more comfortable read if it were fiction. There was something terribly disconcerting about following along this miserable journey, all the while knowing that the killer ultimately would destroy so many lives and then watching his disconnected existence after the massacre.
As a general adult psychiatrist, I wanted to learn something very specific from this book: What is the recipe for creating a mass murderer and what are the warning signs a psychiatrist should catch? I would like my career to be free of patients who kill. The Aurora shooter’s family life sounded fairly pedestrian. His parents are professionals; there was a boy and a girl in an intact family with attentive parents, and no findings of abuse, torture, neglect, bullying, or anything out of the ordinary.
As a child, the shooter was noted for his kindness, and he was particularly caring toward his younger sister. As he grew older, reports about his personality were conflicting: Some saw him as awkward, and later even as odd, while others described him as normal, especially within a cohort of studious kids. He played on sports teams, was an excellent student, liked nonviolent video games, and while he was not outgoing, he always had some friends, though he shunned them during the semester before the shooting. He was not comfortable with women, but he had one girlfriend in graduate school, and when that relationship broke up, he texted with another classmate about how “hot” she was and that they went hiking together. The breakup may have contributed to the shooter’s unraveling, but if it did, Dr. Reid did not present this as the precipitant, and many young men are awkward with women – and endure breakups and rejection.
While the media said the shooter failed out of school, this was not the case. He did well in his classes but chose not to study for an important oral exam while he devoted his time to gathering weapons for his mission to kill, planning out the details, learning to use firearms, and rigging up a complex explosive system around his apartment. When he failed the oral exam, he was told he could study and retake it in a few weeks. He chose, instead, to withdraw from graduate school.
What stood out for me was that this young man talked about thoughts of killing people. He did so to the point of worrying his psychiatrist: She called in a second psychiatrist for a consultation, alerted the university’s threat assessment team, contacted an out-of-state parent, and considered admitting him on an involuntary hold. While many patients say they might hurt someone if provoked or threatened, few discuss thoughts of killing indiscriminately. But when people do talk about killing, we do our best to flush out their intentions, whether it is a fantasy or a plan, if they’ve been violent before. This shooter had no history of violence, and he hid from the psychiatrist the fact that he was acquiring weapons and actually planning a massacre. His psychiatrist diagnosed him with social anxiety, obsessive-compulsive disorder, and possible schizotypal personality disorder. He was prescribed an antidepressant, and later offered an antipsychotic, which he refused.
Three of the four psychiatrists who evaluated the defendant for the legal proceedings made a diagnosis of schizoaffective disorder. (The fifth psychiatrist for the prosecution never examined the defendant.) Dr. Reid made a diagnosis of schizotypal personality disorder. Everyone agreed that the shooter had a mental illness that influenced his actions. When it came to ascertaining the defendant’s mental state at the time of the crime, there was a glitch: The first psychiatrist for the defense examined the defendant only once, days after the shooting, and not again until 3 years later, right before the trial. His exam was limited: The defense attorney was present in the room, and he had instructed the psychiatrist not to ask about the shooting. The attorney interrupted the interview twice, and it’s not the usual practice to place these conditions on a forensic evaluation. After that exam, there was some misunderstanding about who was in charge of the treatment, and the defendant refused the services of the jail psychiatrist. It was not until 4 months later when the inmate became dehydrated, delirious, and psychotic that he finally was evaluated and treated. Despite the abundance of psychiatric information available, no direct and complete assessment was made by a psychiatrist immediately before the shooting, or in the months right after.
When we try to understand what motivates someone to commit such a heinous act, we look for psychosis. If the person suffers from paranoid delusions and believes his behavior is in self-defense, the behavior becomes understandable and justifiable. Even if it’s less organized, if it is the clear result of a psychotic thought process, we often attribute the behavior to illness. Usually, people with psychosis are too disorganized to enact complex plans, to acquire and learn to use ammunition, to plot out when and where there will be potential victims, and to plot out this degree of planning.
This shooter had an odd belief that if he killed people, he would attain “human capital.” Their deaths might fortify him, increase his value and decrease his suffering, and thereby prevent him from dying by suicide. Dr. Reid talks about whether it’s a delusion, an overvalued idea, or just an unusual belief. The shooter was aware that others don’t agree with this, that they would see it as wrong and criminal, and he thought there was only a 50% chance that it would work. If this were a delusion, it was not one we typically see, nor was it accompanied by more usual perceptual phenomena. Ultimately, there was no consensus on whether the patient was psychotic at the time of the shooting. On antipsychotic medication, he continued to believe that if he killed people that he would attain their human capital. In his book, Dr. Reid concluded that he remained dangerous.
Because the shooter told the university health center psychiatrist that he did not want to be locked up, she considered involuntary hospitalization, but she did not believe he would meet criteria for commitment. I saw nothing that indicated whether he was offered voluntary inpatient care with an explanation that hospital treatment is not the same as being locked up and might help alleviate his suffering. We don’t know if he could have been persuaded to enter the hospital willingly, but I suspect that this would have been difficult to justify to an insurer. There’s nothing to indicate that a hospitalization would have prevented this massacre.
From my perspective, I concluded that if individuals say they are thinking about killing strangers, they may be at risk of violence. This is a much smaller group of people to target for intervention than everyone with mental illness or everyone who is odd. This particular shooter appears to suffer from some type of mental derangement that does not fit neatly into our current psychiatric nomenclature or respond to our current treatments, and thoughtful psychiatric intervention – which he had – could not prevent his actions. It seems the only thing that would have changed this outcome is if someone had discovered his arsenal before July 20, 2012.
*Please note: The shooter’s name is intentionally omitted from my review.
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
It was an unthinkable crime; on July 20, 2012, a 24-year-old neuroscience graduate student* walked into a movie theatre in Aurora, Colo., and began shooting people he had never before seen. Twelve people died and 70 were wounded in this calculated and intricately planned massacre that challenged everything we know about the intersection of mental illness and evil.
So much has been written about mass shooters as we’ve struggled to understand what motivates someone to kill strangers in a public place. The hope is that if we can understand it, then we can prevent it. The topic has been one of great interest to me because it gets quickly linked to advocacy for involuntary psychiatric care: Half of mass murderers suffer from psychiatric disorders and if we could force them to get treatment, then we could prevent these horrific events.
Many mass shooters die at the scene. Not only did the Aurora shooter survive, but his case went to trial – also a rarity – providing insights we have not had with other similar cases. With information gained through this court case comes “A Dark Night In Aurora” (Skyhorse Press, 2018), a careful dissection of the Aurora shooter by William H. Reid, MD, MPH. There are many books about crimes and criminals, but what caught my attention about this book was the author. Dr. Reid is one of five expert/forensic psychiatrists retained for the case and he was brought on by the judge as a second nonpartisan psychiatrist. Dr. Reid interviewed the defendant for more than 20 hours, he video-recorded the interviews, and he had access to, “... the existing seventy-five thousand pages of evidence, hundreds of audio and video files, and access to the defendants and scores of witnesses, experts, and others associated with the case ...” Dr. Reid notes that when the defendant placed his sanity in question, all confidentiality was waived.
In this case, the perpetrator had been treated by a therapist and two psychiatrists at his university counseling center in the semester before the shooting. There were video recordings of the defendant in his cell, a correctional psychiatrist in the local jail; psychiatric records from an admission to Denver Health Medical Center and two admissions to the Colorado Health Institute at Pueblo (a secure, forensic setting); and neuropsychological testing done by psychologists hired for the case. In all, there was a lot of mental health data, and I’m not aware of any other book that has been written by a psychiatrist about a criminal case where the author testified in the case.
Let me start by saying that the book is well written, very readable, and fascinating. I’d followed parts of the case in the news and had even watched some of the trial being live-streamed, so not all of the information was new, but Dr. Reid has put together the many facts of a perplexing case together in a cohesive way. There’s no literary descriptions or flowery writing; Dr. Reid is a focused writer. He also does a good job of explaining the specifics of Colorado state law to the forensic aspects of the case. In the end, there were nuances of how the shooter came to be found both competent and sane but was spared the death penalty by a single vote. Overall, I found the book haunting, and it would have been a more comfortable read if it were fiction. There was something terribly disconcerting about following along this miserable journey, all the while knowing that the killer ultimately would destroy so many lives and then watching his disconnected existence after the massacre.
As a general adult psychiatrist, I wanted to learn something very specific from this book: What is the recipe for creating a mass murderer and what are the warning signs a psychiatrist should catch? I would like my career to be free of patients who kill. The Aurora shooter’s family life sounded fairly pedestrian. His parents are professionals; there was a boy and a girl in an intact family with attentive parents, and no findings of abuse, torture, neglect, bullying, or anything out of the ordinary.
As a child, the shooter was noted for his kindness, and he was particularly caring toward his younger sister. As he grew older, reports about his personality were conflicting: Some saw him as awkward, and later even as odd, while others described him as normal, especially within a cohort of studious kids. He played on sports teams, was an excellent student, liked nonviolent video games, and while he was not outgoing, he always had some friends, though he shunned them during the semester before the shooting. He was not comfortable with women, but he had one girlfriend in graduate school, and when that relationship broke up, he texted with another classmate about how “hot” she was and that they went hiking together. The breakup may have contributed to the shooter’s unraveling, but if it did, Dr. Reid did not present this as the precipitant, and many young men are awkward with women – and endure breakups and rejection.
While the media said the shooter failed out of school, this was not the case. He did well in his classes but chose not to study for an important oral exam while he devoted his time to gathering weapons for his mission to kill, planning out the details, learning to use firearms, and rigging up a complex explosive system around his apartment. When he failed the oral exam, he was told he could study and retake it in a few weeks. He chose, instead, to withdraw from graduate school.
What stood out for me was that this young man talked about thoughts of killing people. He did so to the point of worrying his psychiatrist: She called in a second psychiatrist for a consultation, alerted the university’s threat assessment team, contacted an out-of-state parent, and considered admitting him on an involuntary hold. While many patients say they might hurt someone if provoked or threatened, few discuss thoughts of killing indiscriminately. But when people do talk about killing, we do our best to flush out their intentions, whether it is a fantasy or a plan, if they’ve been violent before. This shooter had no history of violence, and he hid from the psychiatrist the fact that he was acquiring weapons and actually planning a massacre. His psychiatrist diagnosed him with social anxiety, obsessive-compulsive disorder, and possible schizotypal personality disorder. He was prescribed an antidepressant, and later offered an antipsychotic, which he refused.
Three of the four psychiatrists who evaluated the defendant for the legal proceedings made a diagnosis of schizoaffective disorder. (The fifth psychiatrist for the prosecution never examined the defendant.) Dr. Reid made a diagnosis of schizotypal personality disorder. Everyone agreed that the shooter had a mental illness that influenced his actions. When it came to ascertaining the defendant’s mental state at the time of the crime, there was a glitch: The first psychiatrist for the defense examined the defendant only once, days after the shooting, and not again until 3 years later, right before the trial. His exam was limited: The defense attorney was present in the room, and he had instructed the psychiatrist not to ask about the shooting. The attorney interrupted the interview twice, and it’s not the usual practice to place these conditions on a forensic evaluation. After that exam, there was some misunderstanding about who was in charge of the treatment, and the defendant refused the services of the jail psychiatrist. It was not until 4 months later when the inmate became dehydrated, delirious, and psychotic that he finally was evaluated and treated. Despite the abundance of psychiatric information available, no direct and complete assessment was made by a psychiatrist immediately before the shooting, or in the months right after.
When we try to understand what motivates someone to commit such a heinous act, we look for psychosis. If the person suffers from paranoid delusions and believes his behavior is in self-defense, the behavior becomes understandable and justifiable. Even if it’s less organized, if it is the clear result of a psychotic thought process, we often attribute the behavior to illness. Usually, people with psychosis are too disorganized to enact complex plans, to acquire and learn to use ammunition, to plot out when and where there will be potential victims, and to plot out this degree of planning.
This shooter had an odd belief that if he killed people, he would attain “human capital.” Their deaths might fortify him, increase his value and decrease his suffering, and thereby prevent him from dying by suicide. Dr. Reid talks about whether it’s a delusion, an overvalued idea, or just an unusual belief. The shooter was aware that others don’t agree with this, that they would see it as wrong and criminal, and he thought there was only a 50% chance that it would work. If this were a delusion, it was not one we typically see, nor was it accompanied by more usual perceptual phenomena. Ultimately, there was no consensus on whether the patient was psychotic at the time of the shooting. On antipsychotic medication, he continued to believe that if he killed people that he would attain their human capital. In his book, Dr. Reid concluded that he remained dangerous.
Because the shooter told the university health center psychiatrist that he did not want to be locked up, she considered involuntary hospitalization, but she did not believe he would meet criteria for commitment. I saw nothing that indicated whether he was offered voluntary inpatient care with an explanation that hospital treatment is not the same as being locked up and might help alleviate his suffering. We don’t know if he could have been persuaded to enter the hospital willingly, but I suspect that this would have been difficult to justify to an insurer. There’s nothing to indicate that a hospitalization would have prevented this massacre.
From my perspective, I concluded that if individuals say they are thinking about killing strangers, they may be at risk of violence. This is a much smaller group of people to target for intervention than everyone with mental illness or everyone who is odd. This particular shooter appears to suffer from some type of mental derangement that does not fit neatly into our current psychiatric nomenclature or respond to our current treatments, and thoughtful psychiatric intervention – which he had – could not prevent his actions. It seems the only thing that would have changed this outcome is if someone had discovered his arsenal before July 20, 2012.
*Please note: The shooter’s name is intentionally omitted from my review.
Dr. Miller is coauthor with Annette Hanson, MD, of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University Press, 2016).
The answer is early follow-up
Rachel Pearson – writing in an article on the vulnerable child syndrome in The New Yorker – claims that “scheduling an early follow-up is as important as doing a detailed exam and having a broad differential diagnosis” (“The Durable Feeling That a Child is Always at Risk,” June 10, 2019) At first blush that may sound like a rather radical observation. How many medical school instructors and house office mentors would begin a teaching session by telling their trainees that doing a complete exam and developing an inclusive list of diagnoses really wasn’t all that important?

But I completely agree with Dr. Pearson’s observation. An early follow-up is the answer when you don’t have clue what is causing the patient’s symptoms. Or you have too many clues, but don’t have the time to sort them out. Or you have a solid diagnosis, but you don’t have the time to adequately explain it to the patient. Or maybe you have the time, but you sense that the patient is uncomfortable with your opinion. Early follow-up also is the answer when the patient’s illness is one that can worsen before it begins to improve. You may have warned the patient of this phenomenon, but scheduling an early follow-up visit can allay their concerns.
Scheduling an early follow-up may allow you to sleep better when you are concerned about the patient’s condition. Particularly in the situation in which the patient isn’t quite sick enough to warrant the risks and expense of a hospitalization. If you and your office staff feel as though you are drowning in phone calls, a liberal use of timely follow-ups can dramatically reduce your phone interruptions. Particularly if you have earned a reputation of keeping your promises. If you are worried about being sued for malpractice, early follow-ups are far better protection than shotgun ordering of lab and imaging studies. And if you are the new guy or gal in town, early follow-ups are one of the most potent practice builders I know.

Does an early follow-up have to be an office visit? It depends on the situation. Most patients quickly realize when your scheduled follow-up visits aren’t necessary. You and your staff should be sensitive to the inconvenience and expense that an office visit may create. Would a phone call be just as effective? This is a particularly knotty question when it comes to newborns. On one hand, office visits can be very disruptive to sleep and nursing schedules of sleep-deprived parents. However, I have seen too many situations in which a physician’s office has relied too heavily on the observations of inexperienced parents when an eyeball in the office or by a visiting nurse would have headed off disaster.
And who should make the call? Never underestimate the power of your voice, even if it’s just a message on an answering machine or smartphone. It leaves an impression. “You know my doctor calls me to check to see how I am?” I think whenever possible, the provider should make the first call. If you fail to connect, your staff can make subsequent attempts.
Finally, you may ask what is an “early” follow-up? The better descriptor would be “timely.” You won’t find this answer in a text book. This is another case in which art trumps medicine in the practice of medicine. The “when” of a timely follow-up depends on the patient’s illness, what is its usual course from your experience. How anxious is the patient? How anxious are you? The answer is that scheduling the follow-up should err on the early side. Another can always be scheduled if the situation is still fluid. At worst, it will demonstrate you are a caring physician.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Rachel Pearson – writing in an article on the vulnerable child syndrome in The New Yorker – claims that “scheduling an early follow-up is as important as doing a detailed exam and having a broad differential diagnosis” (“The Durable Feeling That a Child is Always at Risk,” June 10, 2019) At first blush that may sound like a rather radical observation. How many medical school instructors and house office mentors would begin a teaching session by telling their trainees that doing a complete exam and developing an inclusive list of diagnoses really wasn’t all that important?
But I completely agree with Dr. Pearson’s observation. An early follow-up is the answer when you don’t have clue what is causing the patient’s symptoms. Or you have too many clues, but don’t have the time to sort them out. Or you have a solid diagnosis, but you don’t have the time to adequately explain it to the patient. Or maybe you have the time, but you sense that the patient is uncomfortable with your opinion. Early follow-up also is the answer when the patient’s illness is one that can worsen before it begins to improve. You may have warned the patient of this phenomenon, but scheduling an early follow-up visit can allay their concerns.
Scheduling an early follow-up may allow you to sleep better when you are concerned about the patient’s condition. Particularly in the situation in which the patient isn’t quite sick enough to warrant the risks and expense of a hospitalization. If you and your office staff feel as though you are drowning in phone calls, a liberal use of timely follow-ups can dramatically reduce your phone interruptions. Particularly if you have earned a reputation of keeping your promises. If you are worried about being sued for malpractice, early follow-ups are far better protection than shotgun ordering of lab and imaging studies. And if you are the new guy or gal in town, early follow-ups are one of the most potent practice builders I know.
Does an early follow-up have to be an office visit? It depends on the situation. Most patients quickly realize when your scheduled follow-up visits aren’t necessary. You and your staff should be sensitive to the inconvenience and expense that an office visit may create. Would a phone call be just as effective? This is a particularly knotty question when it comes to newborns. On one hand, office visits can be very disruptive to sleep and nursing schedules of sleep-deprived parents. However, I have seen too many situations in which a physician’s office has relied too heavily on the observations of inexperienced parents when an eyeball in the office or by a visiting nurse would have headed off disaster.
And who should make the call? Never underestimate the power of your voice, even if it’s just a message on an answering machine or smartphone. It leaves an impression. “You know my doctor calls me to check to see how I am?” I think whenever possible, the provider should make the first call. If you fail to connect, your staff can make subsequent attempts.
Finally, you may ask what is an “early” follow-up? The better descriptor would be “timely.” You won’t find this answer in a text book. This is another case in which art trumps medicine in the practice of medicine. The “when” of a timely follow-up depends on the patient’s illness, what is its usual course from your experience. How anxious is the patient? How anxious are you? The answer is that scheduling the follow-up should err on the early side. Another can always be scheduled if the situation is still fluid. At worst, it will demonstrate you are a caring physician.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Rachel Pearson – writing in an article on the vulnerable child syndrome in The New Yorker – claims that “scheduling an early follow-up is as important as doing a detailed exam and having a broad differential diagnosis” (“The Durable Feeling That a Child is Always at Risk,” June 10, 2019) At first blush that may sound like a rather radical observation. How many medical school instructors and house office mentors would begin a teaching session by telling their trainees that doing a complete exam and developing an inclusive list of diagnoses really wasn’t all that important?
But I completely agree with Dr. Pearson’s observation. An early follow-up is the answer when you don’t have clue what is causing the patient’s symptoms. Or you have too many clues, but don’t have the time to sort them out. Or you have a solid diagnosis, but you don’t have the time to adequately explain it to the patient. Or maybe you have the time, but you sense that the patient is uncomfortable with your opinion. Early follow-up also is the answer when the patient’s illness is one that can worsen before it begins to improve. You may have warned the patient of this phenomenon, but scheduling an early follow-up visit can allay their concerns.
Scheduling an early follow-up may allow you to sleep better when you are concerned about the patient’s condition. Particularly in the situation in which the patient isn’t quite sick enough to warrant the risks and expense of a hospitalization. If you and your office staff feel as though you are drowning in phone calls, a liberal use of timely follow-ups can dramatically reduce your phone interruptions. Particularly if you have earned a reputation of keeping your promises. If you are worried about being sued for malpractice, early follow-ups are far better protection than shotgun ordering of lab and imaging studies. And if you are the new guy or gal in town, early follow-ups are one of the most potent practice builders I know.
Does an early follow-up have to be an office visit? It depends on the situation. Most patients quickly realize when your scheduled follow-up visits aren’t necessary. You and your staff should be sensitive to the inconvenience and expense that an office visit may create. Would a phone call be just as effective? This is a particularly knotty question when it comes to newborns. On one hand, office visits can be very disruptive to sleep and nursing schedules of sleep-deprived parents. However, I have seen too many situations in which a physician’s office has relied too heavily on the observations of inexperienced parents when an eyeball in the office or by a visiting nurse would have headed off disaster.
And who should make the call? Never underestimate the power of your voice, even if it’s just a message on an answering machine or smartphone. It leaves an impression. “You know my doctor calls me to check to see how I am?” I think whenever possible, the provider should make the first call. If you fail to connect, your staff can make subsequent attempts.
Finally, you may ask what is an “early” follow-up? The better descriptor would be “timely.” You won’t find this answer in a text book. This is another case in which art trumps medicine in the practice of medicine. The “when” of a timely follow-up depends on the patient’s illness, what is its usual course from your experience. How anxious is the patient? How anxious are you? The answer is that scheduling the follow-up should err on the early side. Another can always be scheduled if the situation is still fluid. At worst, it will demonstrate you are a caring physician.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
One hundred thousand reasons to donate to your political action committee (PAC)
Payment policy for physicians is now set at the federal level. The Centers for Medicare and Medicaid Services generates a yearly final rule and a fee schedule, and all the Medicare carriers, AND the Medicare Advantage plans AND the private insurers use the rule and fee schedule as a payment guide.

Sometimes these rules can be at odds with best practices for dermatology patients. That is why lobbying is so critically important for us and for our patients.
Each year, SkinPAC contributes up to $5,000 a year to individual congressional races. The extent of contributions is based on an impartial scorecard that ranks congressional members by leadership position as well as the member’s understanding and history of support on our critical issues. I want to emphasize that the personal political leanings of the SkinPAC board members have no bearing on the level of support. We contribute to campaigns based on the congressional members’ positions on our issues, period. Full disclosure: I am the chair of SkinPAC for 2019-2021. This is an unpaid volunteer position.
To dermatologists who question the effectiveness of lobbying, I can attest that I have seen your political action committee contributions in action.
When Congress planned on tightening the Stark exceptions 5 years ago, our Washington office was able to gain access to key legislators. As a result of our good long-term relationships with these congress members and their staff, our lobbying group was able to explain the importance for dermatologists to be able to read their own slides and the value of global periods. Imagine the disasters of being unable to read our own dermatopathology slides, not performing diagnostic frozen sections before Mohs, and charging patients for suture removals. Lobbying efforts averted those potential catastrophes.
Unfortunately, the same issues are coming back. In the most recent Federal Register proposals, CMS again wanted to eliminate global periods and modifier 25, which allows you to bill for a procedure on the same day as an evaluation and management code. This action has been delayed for 2 years but will come back up for consideration next year.
Global periods are follow-up visits that are embedded in the destruction, excision, and repair codes that you currently use. For example, $42 of the $72 you get for destroying a premalignant lesion or a wart is a prepayment for the follow-up visit. Sure, if the global period is eliminated, you can bill the patient for the follow-up visit, but imagine the difficulty of collecting additional copays and deductibles. And imagine the impact of those additional costs on our patients.

This brings me to your 100,000 reasons to contribute to your PAC. In Medicare alone, elimination of global periods and modifier 25 will shift $1.4 billion dollars per year away from dermatology. Assuming you will be able to recoup some payment from follow-up visits and by rescheduling some procedures, you are still looking at $1 billion or so, per year, cut from about 10,000 dermatologists with the expense shifted to patients. That’s a $100,000 loss per dermatologist per year and a $1 billion per year additional responsibility for Medicare insureds.
Yes, this will require a legislative fix. And unless it is fixed, the results will be viewed as price gouging by patients with disastrous implications for the physician-patient relationship. Imagine what your patient will say when you charge them to remove their sutures.
Your SkinPAC contribution should be viewed as a disaster insurance policy, just like any other insurance you buy. It covers the very real possibility of not a hurricane or a tornado, but a catastrophic blunder that will put you out of business as surely as any natural disaster. Support your SkinPAC! Support your patients and yourself.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Dr. Coldiron is the chair of SkinPAC for 2019-2021; this is an unpaid volunteer position. Write to him at dermnews@mdedge.com.
Payment policy for physicians is now set at the federal level. The Centers for Medicare and Medicaid Services generates a yearly final rule and a fee schedule, and all the Medicare carriers, AND the Medicare Advantage plans AND the private insurers use the rule and fee schedule as a payment guide.
Sometimes these rules can be at odds with best practices for dermatology patients. That is why lobbying is so critically important for us and for our patients.
Each year, SkinPAC contributes up to $5,000 a year to individual congressional races. The extent of contributions is based on an impartial scorecard that ranks congressional members by leadership position as well as the member’s understanding and history of support on our critical issues. I want to emphasize that the personal political leanings of the SkinPAC board members have no bearing on the level of support. We contribute to campaigns based on the congressional members’ positions on our issues, period. Full disclosure: I am the chair of SkinPAC for 2019-2021. This is an unpaid volunteer position.
To dermatologists who question the effectiveness of lobbying, I can attest that I have seen your political action committee contributions in action.
When Congress planned on tightening the Stark exceptions 5 years ago, our Washington office was able to gain access to key legislators. As a result of our good long-term relationships with these congress members and their staff, our lobbying group was able to explain the importance for dermatologists to be able to read their own slides and the value of global periods. Imagine the disasters of being unable to read our own dermatopathology slides, not performing diagnostic frozen sections before Mohs, and charging patients for suture removals. Lobbying efforts averted those potential catastrophes.
Unfortunately, the same issues are coming back. In the most recent Federal Register proposals, CMS again wanted to eliminate global periods and modifier 25, which allows you to bill for a procedure on the same day as an evaluation and management code. This action has been delayed for 2 years but will come back up for consideration next year.
Global periods are follow-up visits that are embedded in the destruction, excision, and repair codes that you currently use. For example, $42 of the $72 you get for destroying a premalignant lesion or a wart is a prepayment for the follow-up visit. Sure, if the global period is eliminated, you can bill the patient for the follow-up visit, but imagine the difficulty of collecting additional copays and deductibles. And imagine the impact of those additional costs on our patients.
This brings me to your 100,000 reasons to contribute to your PAC. In Medicare alone, elimination of global periods and modifier 25 will shift $1.4 billion dollars per year away from dermatology. Assuming you will be able to recoup some payment from follow-up visits and by rescheduling some procedures, you are still looking at $1 billion or so, per year, cut from about 10,000 dermatologists with the expense shifted to patients. That’s a $100,000 loss per dermatologist per year and a $1 billion per year additional responsibility for Medicare insureds.
Yes, this will require a legislative fix. And unless it is fixed, the results will be viewed as price gouging by patients with disastrous implications for the physician-patient relationship. Imagine what your patient will say when you charge them to remove their sutures.
Your SkinPAC contribution should be viewed as a disaster insurance policy, just like any other insurance you buy. It covers the very real possibility of not a hurricane or a tornado, but a catastrophic blunder that will put you out of business as surely as any natural disaster. Support your SkinPAC! Support your patients and yourself.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Dr. Coldiron is the chair of SkinPAC for 2019-2021; this is an unpaid volunteer position. Write to him at dermnews@mdedge.com.
Payment policy for physicians is now set at the federal level. The Centers for Medicare and Medicaid Services generates a yearly final rule and a fee schedule, and all the Medicare carriers, AND the Medicare Advantage plans AND the private insurers use the rule and fee schedule as a payment guide.
Sometimes these rules can be at odds with best practices for dermatology patients. That is why lobbying is so critically important for us and for our patients.
Each year, SkinPAC contributes up to $5,000 a year to individual congressional races. The extent of contributions is based on an impartial scorecard that ranks congressional members by leadership position as well as the member’s understanding and history of support on our critical issues. I want to emphasize that the personal political leanings of the SkinPAC board members have no bearing on the level of support. We contribute to campaigns based on the congressional members’ positions on our issues, period. Full disclosure: I am the chair of SkinPAC for 2019-2021. This is an unpaid volunteer position.
To dermatologists who question the effectiveness of lobbying, I can attest that I have seen your political action committee contributions in action.
When Congress planned on tightening the Stark exceptions 5 years ago, our Washington office was able to gain access to key legislators. As a result of our good long-term relationships with these congress members and their staff, our lobbying group was able to explain the importance for dermatologists to be able to read their own slides and the value of global periods. Imagine the disasters of being unable to read our own dermatopathology slides, not performing diagnostic frozen sections before Mohs, and charging patients for suture removals. Lobbying efforts averted those potential catastrophes.
Unfortunately, the same issues are coming back. In the most recent Federal Register proposals, CMS again wanted to eliminate global periods and modifier 25, which allows you to bill for a procedure on the same day as an evaluation and management code. This action has been delayed for 2 years but will come back up for consideration next year.
Global periods are follow-up visits that are embedded in the destruction, excision, and repair codes that you currently use. For example, $42 of the $72 you get for destroying a premalignant lesion or a wart is a prepayment for the follow-up visit. Sure, if the global period is eliminated, you can bill the patient for the follow-up visit, but imagine the difficulty of collecting additional copays and deductibles. And imagine the impact of those additional costs on our patients.
This brings me to your 100,000 reasons to contribute to your PAC. In Medicare alone, elimination of global periods and modifier 25 will shift $1.4 billion dollars per year away from dermatology. Assuming you will be able to recoup some payment from follow-up visits and by rescheduling some procedures, you are still looking at $1 billion or so, per year, cut from about 10,000 dermatologists with the expense shifted to patients. That’s a $100,000 loss per dermatologist per year and a $1 billion per year additional responsibility for Medicare insureds.
Yes, this will require a legislative fix. And unless it is fixed, the results will be viewed as price gouging by patients with disastrous implications for the physician-patient relationship. Imagine what your patient will say when you charge them to remove their sutures.
Your SkinPAC contribution should be viewed as a disaster insurance policy, just like any other insurance you buy. It covers the very real possibility of not a hurricane or a tornado, but a catastrophic blunder that will put you out of business as surely as any natural disaster. Support your SkinPAC! Support your patients and yourself.
Dr. Coldiron is in private practice but maintains a clinical assistant professorship at the University of Cincinnati. He cares for patients, teaches medical students and residents, and has several active clinical research projects. Dr. Coldiron is the author of more than 80 scientific letters, papers, and several book chapters, and he speaks frequently on a variety of topics. He is a past president of the American Academy of Dermatology. Dr. Coldiron is the chair of SkinPAC for 2019-2021; this is an unpaid volunteer position. Write to him at dermnews@mdedge.com.
Were the voices really tied to voodoo?
Culture can affect patients’ understanding of symptoms
The other day, I saw a patient who really brought home the importance of considering culture in psychiatry. The patient’s chief complaint was that he had been hearing the voice of an “invisible man.” I noticed he had an accent I was familiar with, and it sounded like he was from Haiti. Indeed, he was born there.

Accordingly, I asked him about voodoo. He said he is not a voodoo worshiper but he believes in voodoo – and he thought that that was what was happening to him. He reported this was the second time he heard the voices – the last time was less than a year ago. He said he came to the hospital because he was trying to wash dishes when he felt some invisible force holding him down. The patient got upset, and he broke the dishes he was washing. Of course, a big melee ensued, and the police were called. They brought the patient to my hospital.
When I spoke with him, he said he was doing pretty well with his Parkinson’s disease but he was a little stiff. The patient was on carbidopa-levodopa 25-100 mg 1.5 t.i.d. for his Parkinson’s, quetiapine 50 mg b.i.d. for his psychotic symptoms, amantadine 100 mg b.i.d. to stimulate his dopamine, ropinirole 1 mg t.i.d. for restless legs, and baclofen 10 mg t.i.d. for muscle spasms.
This is a 66-year-old male who was appropriately groomed and who was cooperative with the interview. He was not hyperactive or lethargic. His mood was euthymic, and he had a wide range of affect as he was able to smile, get serious, and be sad (about his problems). His speech was relevant, linear, and goal directed. His thought processes did not show any signs of loose associations, tangentiality or circumstantiality, but he did have delusions, and current auditory and visual hallucinations. His thought content was surrounding his problems, which because of the culture he is from, were attributed by him to voodoo. He was attentive, and his recent and remote memory were intact. Clinical estimate of his intelligence was average. Despite my explaining to him that his psychotic symptoms were caused by the medication he was taking, his judgment and insight were fair as he explained to me the things that were happening to him were so tangible they had to be real. He had no suicidal or homicidal ideation.
I decided to leave his meds as is, and I gave him 25 mg loxapine at h.s.
When I saw him a few days later, I asked him how he was doing, and he reported that the invisible man and all of his shenanigans were gone. I again explained that the medication he was taking for his Parkinson’s was causing his psychotic symptoms, and now I had proof. He looked skeptical.
This struck me as a perfect example of the importance of culture in psychiatry, and I thought it instructive to share.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit; clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago; former president/CEO of the Community Mental Health Council; and former director of the Institute for Juvenile Research (birthplace of child psychiatry), all in Chicago. He is recipient of the American Psychiatric Association’s 2019 Adolph Meyer Award for Lifetime Achievement in Psychiatric Research. Check out Dr. Bell’s new book, Fetal Alcohol Exposure in the African-American Community, at https://thirdworldpressfoundation.org/product/pre-order-fetal-alcohol-exposure-in-the-african-american-community.
Culture can affect patients’ understanding of symptoms
Culture can affect patients’ understanding of symptoms
The other day, I saw a patient who really brought home the importance of considering culture in psychiatry. The patient’s chief complaint was that he had been hearing the voice of an “invisible man.” I noticed he had an accent I was familiar with, and it sounded like he was from Haiti. Indeed, he was born there.
Accordingly, I asked him about voodoo. He said he is not a voodoo worshiper but he believes in voodoo – and he thought that that was what was happening to him. He reported this was the second time he heard the voices – the last time was less than a year ago. He said he came to the hospital because he was trying to wash dishes when he felt some invisible force holding him down. The patient got upset, and he broke the dishes he was washing. Of course, a big melee ensued, and the police were called. They brought the patient to my hospital.
When I spoke with him, he said he was doing pretty well with his Parkinson’s disease but he was a little stiff. The patient was on carbidopa-levodopa 25-100 mg 1.5 t.i.d. for his Parkinson’s, quetiapine 50 mg b.i.d. for his psychotic symptoms, amantadine 100 mg b.i.d. to stimulate his dopamine, ropinirole 1 mg t.i.d. for restless legs, and baclofen 10 mg t.i.d. for muscle spasms.
This is a 66-year-old male who was appropriately groomed and who was cooperative with the interview. He was not hyperactive or lethargic. His mood was euthymic, and he had a wide range of affect as he was able to smile, get serious, and be sad (about his problems). His speech was relevant, linear, and goal directed. His thought processes did not show any signs of loose associations, tangentiality or circumstantiality, but he did have delusions, and current auditory and visual hallucinations. His thought content was surrounding his problems, which because of the culture he is from, were attributed by him to voodoo. He was attentive, and his recent and remote memory were intact. Clinical estimate of his intelligence was average. Despite my explaining to him that his psychotic symptoms were caused by the medication he was taking, his judgment and insight were fair as he explained to me the things that were happening to him were so tangible they had to be real. He had no suicidal or homicidal ideation.
I decided to leave his meds as is, and I gave him 25 mg loxapine at h.s.
When I saw him a few days later, I asked him how he was doing, and he reported that the invisible man and all of his shenanigans were gone. I again explained that the medication he was taking for his Parkinson’s was causing his psychotic symptoms, and now I had proof. He looked skeptical.
This struck me as a perfect example of the importance of culture in psychiatry, and I thought it instructive to share.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit; clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago; former president/CEO of the Community Mental Health Council; and former director of the Institute for Juvenile Research (birthplace of child psychiatry), all in Chicago. He is recipient of the American Psychiatric Association’s 2019 Adolph Meyer Award for Lifetime Achievement in Psychiatric Research. Check out Dr. Bell’s new book, Fetal Alcohol Exposure in the African-American Community, at https://thirdworldpressfoundation.org/product/pre-order-fetal-alcohol-exposure-in-the-african-american-community.
The other day, I saw a patient who really brought home the importance of considering culture in psychiatry. The patient’s chief complaint was that he had been hearing the voice of an “invisible man.” I noticed he had an accent I was familiar with, and it sounded like he was from Haiti. Indeed, he was born there.
Accordingly, I asked him about voodoo. He said he is not a voodoo worshiper but he believes in voodoo – and he thought that that was what was happening to him. He reported this was the second time he heard the voices – the last time was less than a year ago. He said he came to the hospital because he was trying to wash dishes when he felt some invisible force holding him down. The patient got upset, and he broke the dishes he was washing. Of course, a big melee ensued, and the police were called. They brought the patient to my hospital.
When I spoke with him, he said he was doing pretty well with his Parkinson’s disease but he was a little stiff. The patient was on carbidopa-levodopa 25-100 mg 1.5 t.i.d. for his Parkinson’s, quetiapine 50 mg b.i.d. for his psychotic symptoms, amantadine 100 mg b.i.d. to stimulate his dopamine, ropinirole 1 mg t.i.d. for restless legs, and baclofen 10 mg t.i.d. for muscle spasms.
This is a 66-year-old male who was appropriately groomed and who was cooperative with the interview. He was not hyperactive or lethargic. His mood was euthymic, and he had a wide range of affect as he was able to smile, get serious, and be sad (about his problems). His speech was relevant, linear, and goal directed. His thought processes did not show any signs of loose associations, tangentiality or circumstantiality, but he did have delusions, and current auditory and visual hallucinations. His thought content was surrounding his problems, which because of the culture he is from, were attributed by him to voodoo. He was attentive, and his recent and remote memory were intact. Clinical estimate of his intelligence was average. Despite my explaining to him that his psychotic symptoms were caused by the medication he was taking, his judgment and insight were fair as he explained to me the things that were happening to him were so tangible they had to be real. He had no suicidal or homicidal ideation.
I decided to leave his meds as is, and I gave him 25 mg loxapine at h.s.
When I saw him a few days later, I asked him how he was doing, and he reported that the invisible man and all of his shenanigans were gone. I again explained that the medication he was taking for his Parkinson’s was causing his psychotic symptoms, and now I had proof. He looked skeptical.
This struck me as a perfect example of the importance of culture in psychiatry, and I thought it instructive to share.
Dr. Bell is a staff psychiatrist at Jackson Park Hospital’s Medical/Surgical-Psychiatry Inpatient Unit; clinical psychiatrist emeritus in the department of psychiatry at the University of Illinois at Chicago; former president/CEO of the Community Mental Health Council; and former director of the Institute for Juvenile Research (birthplace of child psychiatry), all in Chicago. He is recipient of the American Psychiatric Association’s 2019 Adolph Meyer Award for Lifetime Achievement in Psychiatric Research. Check out Dr. Bell’s new book, Fetal Alcohol Exposure in the African-American Community, at https://thirdworldpressfoundation.org/product/pre-order-fetal-alcohol-exposure-in-the-african-american-community.