User login
Hyperthyroid? She sure doesn’t look like it
A 50-year-old woman returns for routine follow-up. She has a 15-year history of hypothyroidism, pernicious anemia, and celiac disease. She has had some recent abdominal pain, but no changes in her bowel patterns, and she has not experienced any problems with chest pain, palpitations, or weakness recently. The only medication she is taking is levothyroxine 125 mcg. She has reported no recent weight loss, her blood pressure is 100/60 mm Hg, pulse is 66 beats per minute, temperature is 36.8 degrees Celsius, body mass index is 20, and she does not have a neck goiter. Her cardiac exam was normal and her neurological exam revealed no tremor. Her lab for thyroid-stimulating hormone (TSH) was less than 0.03, and her lab for free thyroxine (FT4) was 2.2, while her TSH level had been 1.4 a year ago. Her levothyroxine dose was decreased to 100 mcg/day, and her repeat lab for TSH, which occurred 12 weeks later, was still less than 0.03. What is the best explanation for why this patient’s labs look like hyperthyroidism, but this patient clinically does not appear to have hyperthyroidism?
A) She was initially given too much levothyroxine; her TSH response is lagging to dose reduction.
B) She has Graves’ disease.
C) She has acute thyroiditis.
D) She is taking extra thyroid hormone.
E) She is taking biotin.

This patient has a history that includes multiple autoimmune diseases including hypothyroidism. It would be extremely unlikely that she would develop Graves' disease or develop acute thyroiditis in the setting of a gland that has been underfunctioning for years. She has no symptoms suggesting that she has hyperthyroidism, which makes taking more thyroid hormone than she is reporting less likely, although this could be possible. The TSH response can lag after dose adjustments of thyroid, but usually a 6-week interval is adequate. This patient’s testing was done 12 weeks after dose reduction making this very unlikely.
The cause for the labs that look like hyperthyroidism in this patient who appears clinically euthyroid is that she is taking biotin. Biotin (vitamin B7) has become a very popular supplement in the past few years for thin hair, brittle nails, and fatigue. The RDA for biotin is 30 mcg. It is widely available in high doses – 5,000-10,000 mcg – which are common doses for supplements.
Biotin has been used extensively as a key component of immunoassays. Streptavidin, a protein produced by the bacteria Streptomyces avidinii, binds biotin with an extremely high affinity, and this binding is utilized in a number of immunoassays, including the assays for thyroid hormone and TSH.1
High serum levels of biotin can make the assays inaccurate, with lower-than-actual TSH and higher-than-actual thyroid hormone levels. Multiple case reports have documented this happening clinically.1-3 I personally saw a case of this recently in my practice. Katzman and colleagues looked at the prevalence of biotin use in outpatients.4 They found that 7.7% were taking supplemental biotin, while 7.4% had levels of biotin in serum samples that were at a level that could interfere with biotin-based serum assays.
Theoretically, biotin can affect multiple other assays that use the streptavidin-biotin assay. The most concerning of these potential problems is with troponin assays. Biotin can falsely lower troponin assays and this can lead to missing the diagnosis of cardiac injury. The Food and Drug Administration released a warning about this and other biotin lab interactions in November 2017.5 Several studies have demonstrated that this effect can occur at serum levels achievable with available over-the-counter doses of biotin.6,7
Not all troponin assays are affected by high serum levels of biotin: The Gen 5 cTnT assay is the only troponin assay affected.7 I could not find any case reports that have been published where biotin had caused a clinical missed diagnosis with troponins.
Pearls
Consider biotin supplement use when you have patients whose labs look like hyperthyroidism, but clinically do not appear to be hyperthyroid.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at imnews@mdedge.com.
References
1. Charles S, Agrawal N, and Blum M. Erroneous thyroid diagnosis due to over-the-counter biotin. Nutrition 2019;57:257-8.
2. Elston MS et al. Factitious Graves’ disease due to a biotin immunoassay interference – a case and review of the literature. J Clin Endocrinol Metab 2016;101:3251-5.
3. Barbesino G. Misdiagnosis of Graves ’disease with apparent severe hyperthyroidism in a patient taking biotin megadoses. Thyroid 2016;26(6):860-3.
4. Katzman et al. Prevalence of biotin supplement usage in outpatients and plasma biotin concentrations in patients presenting to the emergency department. Clin Biochem. 2018 Sep;60:11-16.
5. “The FDA Warns that Biotin May Interfere with Lab Tests: FDA Safety Communication,” Nov. 28, 2017.
6. Trambas et al. Characterization of the scope and magnitude of biotin interference in susceptible Roche Elecsys competitive and sandwich immunoassays. Ann Clin Biochem. 2018 Mar;55(2):205-15.
7. Frame IJ et al. Susceptibility of cardiac troponin assays to biotin interference. Am J Clin Pathol. 2019 Apr 2;151(5):486-93.
A 50-year-old woman returns for routine follow-up. She has a 15-year history of hypothyroidism, pernicious anemia, and celiac disease. She has had some recent abdominal pain, but no changes in her bowel patterns, and she has not experienced any problems with chest pain, palpitations, or weakness recently. The only medication she is taking is levothyroxine 125 mcg. She has reported no recent weight loss, her blood pressure is 100/60 mm Hg, pulse is 66 beats per minute, temperature is 36.8 degrees Celsius, body mass index is 20, and she does not have a neck goiter. Her cardiac exam was normal and her neurological exam revealed no tremor. Her lab for thyroid-stimulating hormone (TSH) was less than 0.03, and her lab for free thyroxine (FT4) was 2.2, while her TSH level had been 1.4 a year ago. Her levothyroxine dose was decreased to 100 mcg/day, and her repeat lab for TSH, which occurred 12 weeks later, was still less than 0.03. What is the best explanation for why this patient’s labs look like hyperthyroidism, but this patient clinically does not appear to have hyperthyroidism?
A) She was initially given too much levothyroxine; her TSH response is lagging to dose reduction.
B) She has Graves’ disease.
C) She has acute thyroiditis.
D) She is taking extra thyroid hormone.
E) She is taking biotin.
This patient has a history that includes multiple autoimmune diseases including hypothyroidism. It would be extremely unlikely that she would develop Graves' disease or develop acute thyroiditis in the setting of a gland that has been underfunctioning for years. She has no symptoms suggesting that she has hyperthyroidism, which makes taking more thyroid hormone than she is reporting less likely, although this could be possible. The TSH response can lag after dose adjustments of thyroid, but usually a 6-week interval is adequate. This patient’s testing was done 12 weeks after dose reduction making this very unlikely.
The cause for the labs that look like hyperthyroidism in this patient who appears clinically euthyroid is that she is taking biotin. Biotin (vitamin B7) has become a very popular supplement in the past few years for thin hair, brittle nails, and fatigue. The RDA for biotin is 30 mcg. It is widely available in high doses – 5,000-10,000 mcg – which are common doses for supplements.
Biotin has been used extensively as a key component of immunoassays. Streptavidin, a protein produced by the bacteria Streptomyces avidinii, binds biotin with an extremely high affinity, and this binding is utilized in a number of immunoassays, including the assays for thyroid hormone and TSH.1
High serum levels of biotin can make the assays inaccurate, with lower-than-actual TSH and higher-than-actual thyroid hormone levels. Multiple case reports have documented this happening clinically.1-3 I personally saw a case of this recently in my practice. Katzman and colleagues looked at the prevalence of biotin use in outpatients.4 They found that 7.7% were taking supplemental biotin, while 7.4% had levels of biotin in serum samples that were at a level that could interfere with biotin-based serum assays.
Theoretically, biotin can affect multiple other assays that use the streptavidin-biotin assay. The most concerning of these potential problems is with troponin assays. Biotin can falsely lower troponin assays and this can lead to missing the diagnosis of cardiac injury. The Food and Drug Administration released a warning about this and other biotin lab interactions in November 2017.5 Several studies have demonstrated that this effect can occur at serum levels achievable with available over-the-counter doses of biotin.6,7
Not all troponin assays are affected by high serum levels of biotin: The Gen 5 cTnT assay is the only troponin assay affected.7 I could not find any case reports that have been published where biotin had caused a clinical missed diagnosis with troponins.
Pearls
Consider biotin supplement use when you have patients whose labs look like hyperthyroidism, but clinically do not appear to be hyperthyroid.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at imnews@mdedge.com.
References
1. Charles S, Agrawal N, and Blum M. Erroneous thyroid diagnosis due to over-the-counter biotin. Nutrition 2019;57:257-8.
2. Elston MS et al. Factitious Graves’ disease due to a biotin immunoassay interference – a case and review of the literature. J Clin Endocrinol Metab 2016;101:3251-5.
3. Barbesino G. Misdiagnosis of Graves ’disease with apparent severe hyperthyroidism in a patient taking biotin megadoses. Thyroid 2016;26(6):860-3.
4. Katzman et al. Prevalence of biotin supplement usage in outpatients and plasma biotin concentrations in patients presenting to the emergency department. Clin Biochem. 2018 Sep;60:11-16.
5. “The FDA Warns that Biotin May Interfere with Lab Tests: FDA Safety Communication,” Nov. 28, 2017.
6. Trambas et al. Characterization of the scope and magnitude of biotin interference in susceptible Roche Elecsys competitive and sandwich immunoassays. Ann Clin Biochem. 2018 Mar;55(2):205-15.
7. Frame IJ et al. Susceptibility of cardiac troponin assays to biotin interference. Am J Clin Pathol. 2019 Apr 2;151(5):486-93.
A 50-year-old woman returns for routine follow-up. She has a 15-year history of hypothyroidism, pernicious anemia, and celiac disease. She has had some recent abdominal pain, but no changes in her bowel patterns, and she has not experienced any problems with chest pain, palpitations, or weakness recently. The only medication she is taking is levothyroxine 125 mcg. She has reported no recent weight loss, her blood pressure is 100/60 mm Hg, pulse is 66 beats per minute, temperature is 36.8 degrees Celsius, body mass index is 20, and she does not have a neck goiter. Her cardiac exam was normal and her neurological exam revealed no tremor. Her lab for thyroid-stimulating hormone (TSH) was less than 0.03, and her lab for free thyroxine (FT4) was 2.2, while her TSH level had been 1.4 a year ago. Her levothyroxine dose was decreased to 100 mcg/day, and her repeat lab for TSH, which occurred 12 weeks later, was still less than 0.03. What is the best explanation for why this patient’s labs look like hyperthyroidism, but this patient clinically does not appear to have hyperthyroidism?
A) She was initially given too much levothyroxine; her TSH response is lagging to dose reduction.
B) She has Graves’ disease.
C) She has acute thyroiditis.
D) She is taking extra thyroid hormone.
E) She is taking biotin.
This patient has a history that includes multiple autoimmune diseases including hypothyroidism. It would be extremely unlikely that she would develop Graves' disease or develop acute thyroiditis in the setting of a gland that has been underfunctioning for years. She has no symptoms suggesting that she has hyperthyroidism, which makes taking more thyroid hormone than she is reporting less likely, although this could be possible. The TSH response can lag after dose adjustments of thyroid, but usually a 6-week interval is adequate. This patient’s testing was done 12 weeks after dose reduction making this very unlikely.
The cause for the labs that look like hyperthyroidism in this patient who appears clinically euthyroid is that she is taking biotin. Biotin (vitamin B7) has become a very popular supplement in the past few years for thin hair, brittle nails, and fatigue. The RDA for biotin is 30 mcg. It is widely available in high doses – 5,000-10,000 mcg – which are common doses for supplements.
Biotin has been used extensively as a key component of immunoassays. Streptavidin, a protein produced by the bacteria Streptomyces avidinii, binds biotin with an extremely high affinity, and this binding is utilized in a number of immunoassays, including the assays for thyroid hormone and TSH.1
High serum levels of biotin can make the assays inaccurate, with lower-than-actual TSH and higher-than-actual thyroid hormone levels. Multiple case reports have documented this happening clinically.1-3 I personally saw a case of this recently in my practice. Katzman and colleagues looked at the prevalence of biotin use in outpatients.4 They found that 7.7% were taking supplemental biotin, while 7.4% had levels of biotin in serum samples that were at a level that could interfere with biotin-based serum assays.
Theoretically, biotin can affect multiple other assays that use the streptavidin-biotin assay. The most concerning of these potential problems is with troponin assays. Biotin can falsely lower troponin assays and this can lead to missing the diagnosis of cardiac injury. The Food and Drug Administration released a warning about this and other biotin lab interactions in November 2017.5 Several studies have demonstrated that this effect can occur at serum levels achievable with available over-the-counter doses of biotin.6,7
Not all troponin assays are affected by high serum levels of biotin: The Gen 5 cTnT assay is the only troponin assay affected.7 I could not find any case reports that have been published where biotin had caused a clinical missed diagnosis with troponins.
Pearls
Consider biotin supplement use when you have patients whose labs look like hyperthyroidism, but clinically do not appear to be hyperthyroid.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. Contact Dr. Paauw at imnews@mdedge.com.
References
1. Charles S, Agrawal N, and Blum M. Erroneous thyroid diagnosis due to over-the-counter biotin. Nutrition 2019;57:257-8.
2. Elston MS et al. Factitious Graves’ disease due to a biotin immunoassay interference – a case and review of the literature. J Clin Endocrinol Metab 2016;101:3251-5.
3. Barbesino G. Misdiagnosis of Graves ’disease with apparent severe hyperthyroidism in a patient taking biotin megadoses. Thyroid 2016;26(6):860-3.
4. Katzman et al. Prevalence of biotin supplement usage in outpatients and plasma biotin concentrations in patients presenting to the emergency department. Clin Biochem. 2018 Sep;60:11-16.
5. “The FDA Warns that Biotin May Interfere with Lab Tests: FDA Safety Communication,” Nov. 28, 2017.
6. Trambas et al. Characterization of the scope and magnitude of biotin interference in susceptible Roche Elecsys competitive and sandwich immunoassays. Ann Clin Biochem. 2018 Mar;55(2):205-15.
7. Frame IJ et al. Susceptibility of cardiac troponin assays to biotin interference. Am J Clin Pathol. 2019 Apr 2;151(5):486-93.
I don’t have much use for evidence
.
Of course I am not against evidence. I respect and value evidence. I just have little day-to-day use for it. Maybe your practices are different from mine, but I spend my working days seeing cases ...
Where evidence is irrelevant:
- there is nothing wrong but the patient thinks there might be (an itch, a burning sensation, a mole that may or may not have changed).
- the condition is self-limiting and needs no therapy (viral rashes).
Where evidence could help, but there isn’t any:
- there is no useful available treatment (age-related hair thinning in women).
Where evidence may be statistically significant but clinically trivial:
- pills that make herpes simplex cold sores go away in 6 days instead of 7, acne cream that reduces lesions by 70% instead of 40% (so that after 12 weeks the patient has five pimples instead of eight).
Where evidence is unimpressive or unconvincing (to the patient, who often stops treatment because “it wasn’t working” or “it made me worse”):
- the condition is recurrent, and the patient interprets recurrence as failure (eczema, psoriasis).
- the condition (psoriasis, eczema, acne ) moves around, and the patient interprets success (fewer spots) as failure. (“It’s come in a new place it never came before” or “I never used to get pimples on my jawline.”)
- slam-dunk clearances are few, and instead, every possible permutation in the condition’s course happens – persistence, recurrence, extension, spontaneous involution, going away in one place while proliferating in another, etc. (warts, alopecia areata).
Where patients find other kinds of evidence more compelling than mine:
- “I stopped your cream because calendula/tea tree oil/Vicks VapoRub/apple cider vinegar/avoiding gluten works better” (eczema, rosacea, onychomycosis, etc.). This dynamic is not limited to dermatology. How many Crohn’s patients have I met who say they left their conventional physicians with their standard treatments and now see a naturopath or acupuncturist? Their doctors don’t know they left, or why, because it’s impossible to remember someone who isn’t there, and their patients never told them why they left. These patients tell me they are now “doing better.”
Where evidence is outweighed by other patient considerations:
- topical 5-fluorouracil or imiquimod for superficial basal cells or noninvasive squamous cells in a patient who can’t reach the spot, doesn’t want to be bothered, or just wants the damned thing cut off.
Then, of course, there are cases where evidence is crucial. It’s just that, at the moment, I can’t think of many. Besides which, I’ve lost count of all the patients who had exhaustive food or patch testing, been found sensitive to any number of chemicals and foods – exotic or otherwise – dutifully avoided all of same, yet still break out intermittently and inscrutably, just like all my other atopics.
I’ve concluded that it must be me, or at least the small slice of the planet I work in. Maybe if I practice for 70 years instead of 40, or on five continents instead of the corner of just one, I will figure it all out.

To be clear: I am not a therapeutic nihilist. I want to use verifiably effective treatments for my patients, just as I wish such to be used on me when I need treatment. It’s just that instances in which compelling, decisive evidence makes a crucial difference don’t come up all that often. Evidence applies to populations, whereas I treat people, one at a time.
Meantime, I will muddle along, concerned that one drawback of the emphasis on “evidence” (i.e. statistics) not often noted is its contribution to depersonalizing medical practice, reducing the therapeutic interaction between two people to iterated instances of quantifiable throughput. If you can’t measure it, you didn’t do it and it doesn’t exist. But it does exist. Like every clinician, I see and do it every day.
As Hippocrates supposedly said: Life is short, and art long, opportunity fleeting, experimentations perilous, and judgment difficult.
Evidence notwithstanding, judgment remains difficult, mine and the patient’s.
Now that I’m done with evidence, please stay tuned for future columns where I take on motherhood (unacceptably gendered!) and apple pie (fattening!)
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@mdedge.com.
.
Of course I am not against evidence. I respect and value evidence. I just have little day-to-day use for it. Maybe your practices are different from mine, but I spend my working days seeing cases ...
Where evidence is irrelevant:
- there is nothing wrong but the patient thinks there might be (an itch, a burning sensation, a mole that may or may not have changed).
- the condition is self-limiting and needs no therapy (viral rashes).
Where evidence could help, but there isn’t any:
- there is no useful available treatment (age-related hair thinning in women).
Where evidence may be statistically significant but clinically trivial:
- pills that make herpes simplex cold sores go away in 6 days instead of 7, acne cream that reduces lesions by 70% instead of 40% (so that after 12 weeks the patient has five pimples instead of eight).
Where evidence is unimpressive or unconvincing (to the patient, who often stops treatment because “it wasn’t working” or “it made me worse”):
- the condition is recurrent, and the patient interprets recurrence as failure (eczema, psoriasis).
- the condition (psoriasis, eczema, acne ) moves around, and the patient interprets success (fewer spots) as failure. (“It’s come in a new place it never came before” or “I never used to get pimples on my jawline.”)
- slam-dunk clearances are few, and instead, every possible permutation in the condition’s course happens – persistence, recurrence, extension, spontaneous involution, going away in one place while proliferating in another, etc. (warts, alopecia areata).
Where patients find other kinds of evidence more compelling than mine:
- “I stopped your cream because calendula/tea tree oil/Vicks VapoRub/apple cider vinegar/avoiding gluten works better” (eczema, rosacea, onychomycosis, etc.). This dynamic is not limited to dermatology. How many Crohn’s patients have I met who say they left their conventional physicians with their standard treatments and now see a naturopath or acupuncturist? Their doctors don’t know they left, or why, because it’s impossible to remember someone who isn’t there, and their patients never told them why they left. These patients tell me they are now “doing better.”
Where evidence is outweighed by other patient considerations:
- topical 5-fluorouracil or imiquimod for superficial basal cells or noninvasive squamous cells in a patient who can’t reach the spot, doesn’t want to be bothered, or just wants the damned thing cut off.
Then, of course, there are cases where evidence is crucial. It’s just that, at the moment, I can’t think of many. Besides which, I’ve lost count of all the patients who had exhaustive food or patch testing, been found sensitive to any number of chemicals and foods – exotic or otherwise – dutifully avoided all of same, yet still break out intermittently and inscrutably, just like all my other atopics.
I’ve concluded that it must be me, or at least the small slice of the planet I work in. Maybe if I practice for 70 years instead of 40, or on five continents instead of the corner of just one, I will figure it all out.
To be clear: I am not a therapeutic nihilist. I want to use verifiably effective treatments for my patients, just as I wish such to be used on me when I need treatment. It’s just that instances in which compelling, decisive evidence makes a crucial difference don’t come up all that often. Evidence applies to populations, whereas I treat people, one at a time.
Meantime, I will muddle along, concerned that one drawback of the emphasis on “evidence” (i.e. statistics) not often noted is its contribution to depersonalizing medical practice, reducing the therapeutic interaction between two people to iterated instances of quantifiable throughput. If you can’t measure it, you didn’t do it and it doesn’t exist. But it does exist. Like every clinician, I see and do it every day.
As Hippocrates supposedly said: Life is short, and art long, opportunity fleeting, experimentations perilous, and judgment difficult.
Evidence notwithstanding, judgment remains difficult, mine and the patient’s.
Now that I’m done with evidence, please stay tuned for future columns where I take on motherhood (unacceptably gendered!) and apple pie (fattening!)
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@mdedge.com.
.
Of course I am not against evidence. I respect and value evidence. I just have little day-to-day use for it. Maybe your practices are different from mine, but I spend my working days seeing cases ...
Where evidence is irrelevant:
- there is nothing wrong but the patient thinks there might be (an itch, a burning sensation, a mole that may or may not have changed).
- the condition is self-limiting and needs no therapy (viral rashes).
Where evidence could help, but there isn’t any:
- there is no useful available treatment (age-related hair thinning in women).
Where evidence may be statistically significant but clinically trivial:
- pills that make herpes simplex cold sores go away in 6 days instead of 7, acne cream that reduces lesions by 70% instead of 40% (so that after 12 weeks the patient has five pimples instead of eight).
Where evidence is unimpressive or unconvincing (to the patient, who often stops treatment because “it wasn’t working” or “it made me worse”):
- the condition is recurrent, and the patient interprets recurrence as failure (eczema, psoriasis).
- the condition (psoriasis, eczema, acne ) moves around, and the patient interprets success (fewer spots) as failure. (“It’s come in a new place it never came before” or “I never used to get pimples on my jawline.”)
- slam-dunk clearances are few, and instead, every possible permutation in the condition’s course happens – persistence, recurrence, extension, spontaneous involution, going away in one place while proliferating in another, etc. (warts, alopecia areata).
Where patients find other kinds of evidence more compelling than mine:
- “I stopped your cream because calendula/tea tree oil/Vicks VapoRub/apple cider vinegar/avoiding gluten works better” (eczema, rosacea, onychomycosis, etc.). This dynamic is not limited to dermatology. How many Crohn’s patients have I met who say they left their conventional physicians with their standard treatments and now see a naturopath or acupuncturist? Their doctors don’t know they left, or why, because it’s impossible to remember someone who isn’t there, and their patients never told them why they left. These patients tell me they are now “doing better.”
Where evidence is outweighed by other patient considerations:
- topical 5-fluorouracil or imiquimod for superficial basal cells or noninvasive squamous cells in a patient who can’t reach the spot, doesn’t want to be bothered, or just wants the damned thing cut off.
Then, of course, there are cases where evidence is crucial. It’s just that, at the moment, I can’t think of many. Besides which, I’ve lost count of all the patients who had exhaustive food or patch testing, been found sensitive to any number of chemicals and foods – exotic or otherwise – dutifully avoided all of same, yet still break out intermittently and inscrutably, just like all my other atopics.
I’ve concluded that it must be me, or at least the small slice of the planet I work in. Maybe if I practice for 70 years instead of 40, or on five continents instead of the corner of just one, I will figure it all out.
To be clear: I am not a therapeutic nihilist. I want to use verifiably effective treatments for my patients, just as I wish such to be used on me when I need treatment. It’s just that instances in which compelling, decisive evidence makes a crucial difference don’t come up all that often. Evidence applies to populations, whereas I treat people, one at a time.
Meantime, I will muddle along, concerned that one drawback of the emphasis on “evidence” (i.e. statistics) not often noted is its contribution to depersonalizing medical practice, reducing the therapeutic interaction between two people to iterated instances of quantifiable throughput. If you can’t measure it, you didn’t do it and it doesn’t exist. But it does exist. Like every clinician, I see and do it every day.
As Hippocrates supposedly said: Life is short, and art long, opportunity fleeting, experimentations perilous, and judgment difficult.
Evidence notwithstanding, judgment remains difficult, mine and the patient’s.
Now that I’m done with evidence, please stay tuned for future columns where I take on motherhood (unacceptably gendered!) and apple pie (fattening!)
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at dermnews@mdedge.com.
Whose needs come first – the patient’s or the trial’s?
Debra Banks (not her real name) had hope. There was a clinical trial open at an academic hospital 200 miles from where she lived. She would commute or find local housing. It would cost her, but this is what her savings were for, she reasoned. What expense could be more important than her life?
Next came the tests. Blood tests, an ultrasound of her heart, breathing tests. She gave vials of blood, lay in scanners, and eagerly jumped through every hoop placed before her. Then came the call from the trial coordinator. Her heart ultrasound showed a mild dysfunction in how it pumped. It excluded her from the trial.
“Not eligible.” The two words that took away everything reverberated in her mind. Her heart had never caused her any problems before. So after the shock wore off, she tried to bargain with the trial coordinator: Had the study drug been shown to cause or worsen heart damage? Could they repeat the ultrasound? Did this blip in her heart function really matter?
When the trial coordinator couldn’t answer all these questions, she encouraged Debra to come into the clinic and talk to the doctors directly. That’s where I met her.
Debra found herself in the middle of a painful crossroads she had no interest being in. What happens when the needs of an individual patient and the needs of medical research are at odds? From Debra’s perspective, she had one goal. She wanted the therapy that would give her the best chance of living.
But the aim of the trial was not to help Debra – not directly, at least. Clinical trials help patient populations. The goal is to add to a body of knowledge: To study new therapies, demonstrate safety and efficacy, and ultimately find better treatments. The bulk of benefit goes to future patients, not individual participants. If an individual participant does benefit, all the better. But this is a bonus, not a requirement.
In order to meet these goals, trials come with inclusion and exclusion criteria. These are often strict. Individuals with certain other medical conditions are frequently excluded, as the person needs to be able to tolerate the toxicities of the drug being tested.

This, of course, is very different from our usual approach to patient care. Outside of trials, the needs of the individual patient are our North Star. Instead of inclusion and exclusion criteria, we have guidelines: general goalposts that hint at the right answer, but are able to be bent based on individual circumstances. It’s something I love about medicine. Part science, part art. Part algorithmic, part creative.
I can give chemotherapy to a patient with a low platelet count, if I think it’s best. I can override an elevated bilirubin. I can simply not check a heart ultrasound in the first place, if I don’t believe it will change my management.
I understand why trial criteria exist. I fully support investing in novel therapies that will help future patients on a large scale. There will invariably be individuals for whom a clinical trial is unsafe or inappropriate for a multitude of reasons, and our job as oncologists is to make that call and convey that news.
Still, that can be hard to square with the human being sitting in front of you. Debra was only in her mid-50s. She was an artist, an educator, a parent. She was a person who was so, so not ready to die. That she would because of a glitch in her heart function – the significance of which nobody knew – was excruciating.
While we can’t enroll every patient in every trial, the least we can do is comb through trial criteria thoughtfully. With the role of clinical investigator comes great responsibility. Are we choosing a cutoff because it makes clinical sense – or because that’s how it was done before? Is there a medical justification behind each and every exclusion criterion? A careless cutoff is not just a line on a protocol. It can be the difference between someone’s last hope – and no more options.
Every time I saw Debra in clinic, she asked about the trial. Then one day she stopped asking. She was distracted by more pressing problems. Her breathing had worsened and her energy levels were so low she could hardly get out of bed. Debra became sicker and sicker until she could no longer request the last hope that might make her better.
A wonderful physician-scientist I worked with once said she split her time between patient care and medical research because they complement each other. Whenever she lost a patient, she turned that pain into motivation to delve deeper into her research. She coped with individual loss by helping to make small, incremental improvements for the needs of many.
I think about this, months later, as I look around the empty exam room where I first met Debra. I imagine a roomful of patients, alive and healthy, for whom the research she was excluded from has benefited.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz.
Debra Banks (not her real name) had hope. There was a clinical trial open at an academic hospital 200 miles from where she lived. She would commute or find local housing. It would cost her, but this is what her savings were for, she reasoned. What expense could be more important than her life?
Next came the tests. Blood tests, an ultrasound of her heart, breathing tests. She gave vials of blood, lay in scanners, and eagerly jumped through every hoop placed before her. Then came the call from the trial coordinator. Her heart ultrasound showed a mild dysfunction in how it pumped. It excluded her from the trial.
“Not eligible.” The two words that took away everything reverberated in her mind. Her heart had never caused her any problems before. So after the shock wore off, she tried to bargain with the trial coordinator: Had the study drug been shown to cause or worsen heart damage? Could they repeat the ultrasound? Did this blip in her heart function really matter?
When the trial coordinator couldn’t answer all these questions, she encouraged Debra to come into the clinic and talk to the doctors directly. That’s where I met her.
Debra found herself in the middle of a painful crossroads she had no interest being in. What happens when the needs of an individual patient and the needs of medical research are at odds? From Debra’s perspective, she had one goal. She wanted the therapy that would give her the best chance of living.
But the aim of the trial was not to help Debra – not directly, at least. Clinical trials help patient populations. The goal is to add to a body of knowledge: To study new therapies, demonstrate safety and efficacy, and ultimately find better treatments. The bulk of benefit goes to future patients, not individual participants. If an individual participant does benefit, all the better. But this is a bonus, not a requirement.
In order to meet these goals, trials come with inclusion and exclusion criteria. These are often strict. Individuals with certain other medical conditions are frequently excluded, as the person needs to be able to tolerate the toxicities of the drug being tested.
This, of course, is very different from our usual approach to patient care. Outside of trials, the needs of the individual patient are our North Star. Instead of inclusion and exclusion criteria, we have guidelines: general goalposts that hint at the right answer, but are able to be bent based on individual circumstances. It’s something I love about medicine. Part science, part art. Part algorithmic, part creative.
I can give chemotherapy to a patient with a low platelet count, if I think it’s best. I can override an elevated bilirubin. I can simply not check a heart ultrasound in the first place, if I don’t believe it will change my management.
I understand why trial criteria exist. I fully support investing in novel therapies that will help future patients on a large scale. There will invariably be individuals for whom a clinical trial is unsafe or inappropriate for a multitude of reasons, and our job as oncologists is to make that call and convey that news.
Still, that can be hard to square with the human being sitting in front of you. Debra was only in her mid-50s. She was an artist, an educator, a parent. She was a person who was so, so not ready to die. That she would because of a glitch in her heart function – the significance of which nobody knew – was excruciating.
While we can’t enroll every patient in every trial, the least we can do is comb through trial criteria thoughtfully. With the role of clinical investigator comes great responsibility. Are we choosing a cutoff because it makes clinical sense – or because that’s how it was done before? Is there a medical justification behind each and every exclusion criterion? A careless cutoff is not just a line on a protocol. It can be the difference between someone’s last hope – and no more options.
Every time I saw Debra in clinic, she asked about the trial. Then one day she stopped asking. She was distracted by more pressing problems. Her breathing had worsened and her energy levels were so low she could hardly get out of bed. Debra became sicker and sicker until she could no longer request the last hope that might make her better.
A wonderful physician-scientist I worked with once said she split her time between patient care and medical research because they complement each other. Whenever she lost a patient, she turned that pain into motivation to delve deeper into her research. She coped with individual loss by helping to make small, incremental improvements for the needs of many.
I think about this, months later, as I look around the empty exam room where I first met Debra. I imagine a roomful of patients, alive and healthy, for whom the research she was excluded from has benefited.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz.
Debra Banks (not her real name) had hope. There was a clinical trial open at an academic hospital 200 miles from where she lived. She would commute or find local housing. It would cost her, but this is what her savings were for, she reasoned. What expense could be more important than her life?
Next came the tests. Blood tests, an ultrasound of her heart, breathing tests. She gave vials of blood, lay in scanners, and eagerly jumped through every hoop placed before her. Then came the call from the trial coordinator. Her heart ultrasound showed a mild dysfunction in how it pumped. It excluded her from the trial.
“Not eligible.” The two words that took away everything reverberated in her mind. Her heart had never caused her any problems before. So after the shock wore off, she tried to bargain with the trial coordinator: Had the study drug been shown to cause or worsen heart damage? Could they repeat the ultrasound? Did this blip in her heart function really matter?
When the trial coordinator couldn’t answer all these questions, she encouraged Debra to come into the clinic and talk to the doctors directly. That’s where I met her.
Debra found herself in the middle of a painful crossroads she had no interest being in. What happens when the needs of an individual patient and the needs of medical research are at odds? From Debra’s perspective, she had one goal. She wanted the therapy that would give her the best chance of living.
But the aim of the trial was not to help Debra – not directly, at least. Clinical trials help patient populations. The goal is to add to a body of knowledge: To study new therapies, demonstrate safety and efficacy, and ultimately find better treatments. The bulk of benefit goes to future patients, not individual participants. If an individual participant does benefit, all the better. But this is a bonus, not a requirement.
In order to meet these goals, trials come with inclusion and exclusion criteria. These are often strict. Individuals with certain other medical conditions are frequently excluded, as the person needs to be able to tolerate the toxicities of the drug being tested.
This, of course, is very different from our usual approach to patient care. Outside of trials, the needs of the individual patient are our North Star. Instead of inclusion and exclusion criteria, we have guidelines: general goalposts that hint at the right answer, but are able to be bent based on individual circumstances. It’s something I love about medicine. Part science, part art. Part algorithmic, part creative.
I can give chemotherapy to a patient with a low platelet count, if I think it’s best. I can override an elevated bilirubin. I can simply not check a heart ultrasound in the first place, if I don’t believe it will change my management.
I understand why trial criteria exist. I fully support investing in novel therapies that will help future patients on a large scale. There will invariably be individuals for whom a clinical trial is unsafe or inappropriate for a multitude of reasons, and our job as oncologists is to make that call and convey that news.
Still, that can be hard to square with the human being sitting in front of you. Debra was only in her mid-50s. She was an artist, an educator, a parent. She was a person who was so, so not ready to die. That she would because of a glitch in her heart function – the significance of which nobody knew – was excruciating.
While we can’t enroll every patient in every trial, the least we can do is comb through trial criteria thoughtfully. With the role of clinical investigator comes great responsibility. Are we choosing a cutoff because it makes clinical sense – or because that’s how it was done before? Is there a medical justification behind each and every exclusion criterion? A careless cutoff is not just a line on a protocol. It can be the difference between someone’s last hope – and no more options.
Every time I saw Debra in clinic, she asked about the trial. Then one day she stopped asking. She was distracted by more pressing problems. Her breathing had worsened and her energy levels were so low she could hardly get out of bed. Debra became sicker and sicker until she could no longer request the last hope that might make her better.
A wonderful physician-scientist I worked with once said she split her time between patient care and medical research because they complement each other. Whenever she lost a patient, she turned that pain into motivation to delve deeper into her research. She coped with individual loss by helping to make small, incremental improvements for the needs of many.
I think about this, months later, as I look around the empty exam room where I first met Debra. I imagine a roomful of patients, alive and healthy, for whom the research she was excluded from has benefited.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz.
Wellness seminars won’t fix burnout
“Burnout” has been defined as long-term, unresolvable job stress that leads to exhaustion, depression, and in some tragic circumstances, suicide. One of our lead articles this month concerns an attempt to place a financial cost on physician burnout. More important, I think, is the toll burnout takes on an individual, their family, and their patients. In my role as Chief Clinical Officer of the University of Michigan Medical Group (our faculty and other clinical providers), I struggle to balance productivity demands with the increasing damage such demands are doing to our clinicians. Few primary care physicians at Michigan Medicine work full-time as clinicians (defined as 32 hours patient facing time per week for 46 weeks). Almost all request part-time status if they do not have protected, grant-funded time. They simply cannot keep up with the documentation required in our electronic health record, combined with our “patient-friendly” access via the electronic portal. One-third of the private practice group I helped build was part-time when I left in 2012, and it is not unusual to hear complaints about burnout from my ex-partners.

Let’s be clear, burnout is not going to be solved by increasing the resilience of our physicians or sending us to wellness seminars. That approach is a direct blame-the-victim paradigm. Physicians are burned out because of the constant assault on the core reasons we entered medicine – to help people (this assault has been termed “moral injury”). BPAs (best practice alerts), coding requirements, inbox demands, prior authorizations (see the practice management section of this issue), electronic-order entry, and most other practice enhancement tools rely on the willingness of physicians to sacrifice more time and energy and sit in front of a computer screen.
Salvation of our health care system will not come from mass retirements (although that is happening), concierge practices, part-time status, or other individual responses to this crisis. We will need a fundamental reorganization of our practice, where we (physicians) reduce our work to activities for which we trained combined with a shift of nonphysician work to others; better technology, virtual visits, and ancillary personnel. Patient expectations must be realistic and legal protections need strengthening. The politics of health care has focused on funds flow and ideology. We need a stronger voice that articulates the daily microaggressions that we each endure as we try to live Oslerian physician ideals.
John I. Allen, MD, MBA, AGAF
Editor in Chief
“Burnout” has been defined as long-term, unresolvable job stress that leads to exhaustion, depression, and in some tragic circumstances, suicide. One of our lead articles this month concerns an attempt to place a financial cost on physician burnout. More important, I think, is the toll burnout takes on an individual, their family, and their patients. In my role as Chief Clinical Officer of the University of Michigan Medical Group (our faculty and other clinical providers), I struggle to balance productivity demands with the increasing damage such demands are doing to our clinicians. Few primary care physicians at Michigan Medicine work full-time as clinicians (defined as 32 hours patient facing time per week for 46 weeks). Almost all request part-time status if they do not have protected, grant-funded time. They simply cannot keep up with the documentation required in our electronic health record, combined with our “patient-friendly” access via the electronic portal. One-third of the private practice group I helped build was part-time when I left in 2012, and it is not unusual to hear complaints about burnout from my ex-partners.
Let’s be clear, burnout is not going to be solved by increasing the resilience of our physicians or sending us to wellness seminars. That approach is a direct blame-the-victim paradigm. Physicians are burned out because of the constant assault on the core reasons we entered medicine – to help people (this assault has been termed “moral injury”). BPAs (best practice alerts), coding requirements, inbox demands, prior authorizations (see the practice management section of this issue), electronic-order entry, and most other practice enhancement tools rely on the willingness of physicians to sacrifice more time and energy and sit in front of a computer screen.
Salvation of our health care system will not come from mass retirements (although that is happening), concierge practices, part-time status, or other individual responses to this crisis. We will need a fundamental reorganization of our practice, where we (physicians) reduce our work to activities for which we trained combined with a shift of nonphysician work to others; better technology, virtual visits, and ancillary personnel. Patient expectations must be realistic and legal protections need strengthening. The politics of health care has focused on funds flow and ideology. We need a stronger voice that articulates the daily microaggressions that we each endure as we try to live Oslerian physician ideals.
John I. Allen, MD, MBA, AGAF
Editor in Chief
“Burnout” has been defined as long-term, unresolvable job stress that leads to exhaustion, depression, and in some tragic circumstances, suicide. One of our lead articles this month concerns an attempt to place a financial cost on physician burnout. More important, I think, is the toll burnout takes on an individual, their family, and their patients. In my role as Chief Clinical Officer of the University of Michigan Medical Group (our faculty and other clinical providers), I struggle to balance productivity demands with the increasing damage such demands are doing to our clinicians. Few primary care physicians at Michigan Medicine work full-time as clinicians (defined as 32 hours patient facing time per week for 46 weeks). Almost all request part-time status if they do not have protected, grant-funded time. They simply cannot keep up with the documentation required in our electronic health record, combined with our “patient-friendly” access via the electronic portal. One-third of the private practice group I helped build was part-time when I left in 2012, and it is not unusual to hear complaints about burnout from my ex-partners.
Let’s be clear, burnout is not going to be solved by increasing the resilience of our physicians or sending us to wellness seminars. That approach is a direct blame-the-victim paradigm. Physicians are burned out because of the constant assault on the core reasons we entered medicine – to help people (this assault has been termed “moral injury”). BPAs (best practice alerts), coding requirements, inbox demands, prior authorizations (see the practice management section of this issue), electronic-order entry, and most other practice enhancement tools rely on the willingness of physicians to sacrifice more time and energy and sit in front of a computer screen.
Salvation of our health care system will not come from mass retirements (although that is happening), concierge practices, part-time status, or other individual responses to this crisis. We will need a fundamental reorganization of our practice, where we (physicians) reduce our work to activities for which we trained combined with a shift of nonphysician work to others; better technology, virtual visits, and ancillary personnel. Patient expectations must be realistic and legal protections need strengthening. The politics of health care has focused on funds flow and ideology. We need a stronger voice that articulates the daily microaggressions that we each endure as we try to live Oslerian physician ideals.
John I. Allen, MD, MBA, AGAF
Editor in Chief

The 21st Century Cures Act: Tearing down fortresses to put patients first
"A fortress not only protects those inside of it, but it also enslaves them to work.”
– Anthony T. Hincks
As physicians, we spend a great deal of time intending to do our best for the people we serve. We believe fundamentally in the idea that our patients come first, and we toil daily to exercise that belief. We also want our patients to feel they are driving their care as active participants along the journey. Yet time and time again, despite our greatest attempts, those efforts are stymied by the state of modern medicine;

Over the past 10 years, we have done a tremendous job of constructing expensive fortresses around patient information known as electronic health records (EHRs). Billions of dollars have been spent implementing, upgrading, and optimizing. In spite of this, physicians are increasingly frustrated by EHRs (and in many cases, long to return to the days of paper). It isn’t surprising, then, that patients are frustrated as well. We use terms such as “patient-centered care,” but patients feel like they are not in the center at all. Instead, they can find themselves feeling like complete outsiders, at the mercy of the medical juggernaut to make sure they have the appropriate information when they need it. There are several issues that contribute to the frustrations of physicians and patients, but two in particular warrant attention. The first is the diversity of Health IT systems and ongoing issues with EHR interoperability. The second is a provincial attitude surrounding transparency and medical record ownership. We will discuss both of these here, as well as recent legislation designed to advance both concerns.
We have written in previous columns about the many challenges of interoperability. Electronic health records, sold by different vendors, typically won’t “talk” to each other. In spite of years of maturation, issues of compatibility remain. Patient data locked inside of one EHR is not easily accessible by a physician using a different EHR. While efforts have been made to streamline information sharing, there are still many fortresses that cannot be breached.
Bridging the moat
The 21st Century Cures Act, enacted by Congress in December of 2016, seeks to define and require interoperability while addressing many other significant problems in health care. According to the legislation, true interoperability means that health IT should enable the secure exchange of electronic health information with other electronic record systems without special effort on the part of the user; the process should be seamless and shouldn’t be cumbersome for physicians or patients. It also must be fully supported by EHR vendors, but those vendors have been expressing significant concerns with the ways in which the act is being interpreted.
In a recent blog post, the HIMSS Electronic Health Record Association – a consortium of vendors including Epic, Allscripts, eClinicalWorks, as well as several others – expressed “significant concerns regarding timelines, ambiguous language, disincentives for innovation, and definitions related to information blocking.”1 This is not surprising, as the onus for improving interoperability falls squarely on their shoulders, and the work to get there is arduous. Regardless of one’s interpretation, the goal of the Cures act is clear: Arrive at true interoperability in the shortest period of time, while eliminating barriers that prevent patients from accessing their health records. In other words, it asks for the avoidance of “information blocking.”
Breaching the gate
Information blocking, as defined by the Cures Act, is “a practice by a health care provider, health IT developer, health information exchange, or health information network that … is likely to interfere with, prevent, or materially discourage access, exchange, or use of electronic health information.”2 This practice is explicitly prohibited by the legislation – and is ethically wrong – yet it continues to occur implicitly every day as it has for many years. Even if unintentional and solely because of the growing complexity of our information systems, it makes accessing health information incredibly cumbersome for patients. Even worse, attempts to improve patients’ ability to access their health records have only created additional obstacles.
HIPAA (the Health Insurance Portability and Accountability Act of 1996) was designed to protect patient confidentiality and create security around protected health information. While noble in purpose, many have found it burdensome to work within the parameters set forth in the law. Physicians and patients needing legitimate access to clinical data discover endless release forms and convoluted processes standing in their way. Access to the information eventually comes in the form of reams of printed paper or faxed notes that cannot be easily consumed by or integrated into other systems.
The Meaningful Use initiative, while envisioned to improve data exchange and enhance population health, did little to help. Instead of enabling documentation efficiency and improving patient access, it promoted the proliferation of incompatible EHRs and poorly conceived patient portals. It also created heavy costs for both the federal government and physicians and was largely ineffective at producing systems whose use could be considered meaningful. The federal government paid out as much as $44,000 per physician to incentivize them to purchase medical records, while physicians often spent more than the $44,000 and, in many cases, wound up with EHRs that didn’t work well and had to be replaced.
Authors and supporters of the 21st Century Cures Act are hoping to avoid the shortcomings of prior legislation by attaching financial penalties to health care providers or IT vendors who engage in information blocking. While allowing for exceptions in appropriate cases, the law is clear: Patients deserve complete access to their medical records. While this goes against tradition, it has been proven to result in better outcomes.
Initiatives such as the OpenNotes movement have been pushing the value of full transparency for some time, and their website includes a long list of numerous examples to prove it. Indeed, several studies have demonstrated increased physician and patient satisfaction when both parties have ready access to health information. We believe that we, as physicians, should fully support the idea and lobby our EHR vendors to do the same.
It is time to tear down the impenetrable fortresses of traditional medicine, then work diligently to rebuild them with our patients safely inside.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
References
1. The Electronic Health Record Association blog
"A fortress not only protects those inside of it, but it also enslaves them to work.”
– Anthony T. Hincks
As physicians, we spend a great deal of time intending to do our best for the people we serve. We believe fundamentally in the idea that our patients come first, and we toil daily to exercise that belief. We also want our patients to feel they are driving their care as active participants along the journey. Yet time and time again, despite our greatest attempts, those efforts are stymied by the state of modern medicine;
Over the past 10 years, we have done a tremendous job of constructing expensive fortresses around patient information known as electronic health records (EHRs). Billions of dollars have been spent implementing, upgrading, and optimizing. In spite of this, physicians are increasingly frustrated by EHRs (and in many cases, long to return to the days of paper). It isn’t surprising, then, that patients are frustrated as well. We use terms such as “patient-centered care,” but patients feel like they are not in the center at all. Instead, they can find themselves feeling like complete outsiders, at the mercy of the medical juggernaut to make sure they have the appropriate information when they need it. There are several issues that contribute to the frustrations of physicians and patients, but two in particular warrant attention. The first is the diversity of Health IT systems and ongoing issues with EHR interoperability. The second is a provincial attitude surrounding transparency and medical record ownership. We will discuss both of these here, as well as recent legislation designed to advance both concerns.
We have written in previous columns about the many challenges of interoperability. Electronic health records, sold by different vendors, typically won’t “talk” to each other. In spite of years of maturation, issues of compatibility remain. Patient data locked inside of one EHR is not easily accessible by a physician using a different EHR. While efforts have been made to streamline information sharing, there are still many fortresses that cannot be breached.
Bridging the moat
The 21st Century Cures Act, enacted by Congress in December of 2016, seeks to define and require interoperability while addressing many other significant problems in health care. According to the legislation, true interoperability means that health IT should enable the secure exchange of electronic health information with other electronic record systems without special effort on the part of the user; the process should be seamless and shouldn’t be cumbersome for physicians or patients. It also must be fully supported by EHR vendors, but those vendors have been expressing significant concerns with the ways in which the act is being interpreted.
In a recent blog post, the HIMSS Electronic Health Record Association – a consortium of vendors including Epic, Allscripts, eClinicalWorks, as well as several others – expressed “significant concerns regarding timelines, ambiguous language, disincentives for innovation, and definitions related to information blocking.”1 This is not surprising, as the onus for improving interoperability falls squarely on their shoulders, and the work to get there is arduous. Regardless of one’s interpretation, the goal of the Cures act is clear: Arrive at true interoperability in the shortest period of time, while eliminating barriers that prevent patients from accessing their health records. In other words, it asks for the avoidance of “information blocking.”
Breaching the gate
Information blocking, as defined by the Cures Act, is “a practice by a health care provider, health IT developer, health information exchange, or health information network that … is likely to interfere with, prevent, or materially discourage access, exchange, or use of electronic health information.”2 This practice is explicitly prohibited by the legislation – and is ethically wrong – yet it continues to occur implicitly every day as it has for many years. Even if unintentional and solely because of the growing complexity of our information systems, it makes accessing health information incredibly cumbersome for patients. Even worse, attempts to improve patients’ ability to access their health records have only created additional obstacles.
HIPAA (the Health Insurance Portability and Accountability Act of 1996) was designed to protect patient confidentiality and create security around protected health information. While noble in purpose, many have found it burdensome to work within the parameters set forth in the law. Physicians and patients needing legitimate access to clinical data discover endless release forms and convoluted processes standing in their way. Access to the information eventually comes in the form of reams of printed paper or faxed notes that cannot be easily consumed by or integrated into other systems.
The Meaningful Use initiative, while envisioned to improve data exchange and enhance population health, did little to help. Instead of enabling documentation efficiency and improving patient access, it promoted the proliferation of incompatible EHRs and poorly conceived patient portals. It also created heavy costs for both the federal government and physicians and was largely ineffective at producing systems whose use could be considered meaningful. The federal government paid out as much as $44,000 per physician to incentivize them to purchase medical records, while physicians often spent more than the $44,000 and, in many cases, wound up with EHRs that didn’t work well and had to be replaced.
Authors and supporters of the 21st Century Cures Act are hoping to avoid the shortcomings of prior legislation by attaching financial penalties to health care providers or IT vendors who engage in information blocking. While allowing for exceptions in appropriate cases, the law is clear: Patients deserve complete access to their medical records. While this goes against tradition, it has been proven to result in better outcomes.
Initiatives such as the OpenNotes movement have been pushing the value of full transparency for some time, and their website includes a long list of numerous examples to prove it. Indeed, several studies have demonstrated increased physician and patient satisfaction when both parties have ready access to health information. We believe that we, as physicians, should fully support the idea and lobby our EHR vendors to do the same.
It is time to tear down the impenetrable fortresses of traditional medicine, then work diligently to rebuild them with our patients safely inside.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
References
1. The Electronic Health Record Association blog
"A fortress not only protects those inside of it, but it also enslaves them to work.”
– Anthony T. Hincks
As physicians, we spend a great deal of time intending to do our best for the people we serve. We believe fundamentally in the idea that our patients come first, and we toil daily to exercise that belief. We also want our patients to feel they are driving their care as active participants along the journey. Yet time and time again, despite our greatest attempts, those efforts are stymied by the state of modern medicine;
Over the past 10 years, we have done a tremendous job of constructing expensive fortresses around patient information known as electronic health records (EHRs). Billions of dollars have been spent implementing, upgrading, and optimizing. In spite of this, physicians are increasingly frustrated by EHRs (and in many cases, long to return to the days of paper). It isn’t surprising, then, that patients are frustrated as well. We use terms such as “patient-centered care,” but patients feel like they are not in the center at all. Instead, they can find themselves feeling like complete outsiders, at the mercy of the medical juggernaut to make sure they have the appropriate information when they need it. There are several issues that contribute to the frustrations of physicians and patients, but two in particular warrant attention. The first is the diversity of Health IT systems and ongoing issues with EHR interoperability. The second is a provincial attitude surrounding transparency and medical record ownership. We will discuss both of these here, as well as recent legislation designed to advance both concerns.
We have written in previous columns about the many challenges of interoperability. Electronic health records, sold by different vendors, typically won’t “talk” to each other. In spite of years of maturation, issues of compatibility remain. Patient data locked inside of one EHR is not easily accessible by a physician using a different EHR. While efforts have been made to streamline information sharing, there are still many fortresses that cannot be breached.
Bridging the moat
The 21st Century Cures Act, enacted by Congress in December of 2016, seeks to define and require interoperability while addressing many other significant problems in health care. According to the legislation, true interoperability means that health IT should enable the secure exchange of electronic health information with other electronic record systems without special effort on the part of the user; the process should be seamless and shouldn’t be cumbersome for physicians or patients. It also must be fully supported by EHR vendors, but those vendors have been expressing significant concerns with the ways in which the act is being interpreted.
In a recent blog post, the HIMSS Electronic Health Record Association – a consortium of vendors including Epic, Allscripts, eClinicalWorks, as well as several others – expressed “significant concerns regarding timelines, ambiguous language, disincentives for innovation, and definitions related to information blocking.”1 This is not surprising, as the onus for improving interoperability falls squarely on their shoulders, and the work to get there is arduous. Regardless of one’s interpretation, the goal of the Cures act is clear: Arrive at true interoperability in the shortest period of time, while eliminating barriers that prevent patients from accessing their health records. In other words, it asks for the avoidance of “information blocking.”
Breaching the gate
Information blocking, as defined by the Cures Act, is “a practice by a health care provider, health IT developer, health information exchange, or health information network that … is likely to interfere with, prevent, or materially discourage access, exchange, or use of electronic health information.”2 This practice is explicitly prohibited by the legislation – and is ethically wrong – yet it continues to occur implicitly every day as it has for many years. Even if unintentional and solely because of the growing complexity of our information systems, it makes accessing health information incredibly cumbersome for patients. Even worse, attempts to improve patients’ ability to access their health records have only created additional obstacles.
HIPAA (the Health Insurance Portability and Accountability Act of 1996) was designed to protect patient confidentiality and create security around protected health information. While noble in purpose, many have found it burdensome to work within the parameters set forth in the law. Physicians and patients needing legitimate access to clinical data discover endless release forms and convoluted processes standing in their way. Access to the information eventually comes in the form of reams of printed paper or faxed notes that cannot be easily consumed by or integrated into other systems.
The Meaningful Use initiative, while envisioned to improve data exchange and enhance population health, did little to help. Instead of enabling documentation efficiency and improving patient access, it promoted the proliferation of incompatible EHRs and poorly conceived patient portals. It also created heavy costs for both the federal government and physicians and was largely ineffective at producing systems whose use could be considered meaningful. The federal government paid out as much as $44,000 per physician to incentivize them to purchase medical records, while physicians often spent more than the $44,000 and, in many cases, wound up with EHRs that didn’t work well and had to be replaced.
Authors and supporters of the 21st Century Cures Act are hoping to avoid the shortcomings of prior legislation by attaching financial penalties to health care providers or IT vendors who engage in information blocking. While allowing for exceptions in appropriate cases, the law is clear: Patients deserve complete access to their medical records. While this goes against tradition, it has been proven to result in better outcomes.
Initiatives such as the OpenNotes movement have been pushing the value of full transparency for some time, and their website includes a long list of numerous examples to prove it. Indeed, several studies have demonstrated increased physician and patient satisfaction when both parties have ready access to health information. We believe that we, as physicians, should fully support the idea and lobby our EHR vendors to do the same.
It is time to tear down the impenetrable fortresses of traditional medicine, then work diligently to rebuild them with our patients safely inside.
Dr. Notte is a family physician and associate chief medical information officer for Abington (Pa.) Jefferson Health. Follow him on Twitter @doctornotte. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
References
1. The Electronic Health Record Association blog
Becoming a high-value care physician
‘Culture shift’ comes from collective efforts
It’s Monday morning, and Mrs. Jones still has abdominal pain. Your ward team decides to order a CT. On chart review you notice she’s had three other abdominal CTs for the same indication this year. How did this happen? What should you do?

High-value care has been defined by the Institute of Medicine as “the best care for the patient, with the optimal result for the circumstances, delivered at the right price.”1 With an estimated $700 billion dollars – 30% of medical expenditures – spent on wasted care, there are rising calls for a transformational shift.2
You are now asked to consider not just everything you can do for a patient, but also the benefits, harms, and costs associated with those choices. But where to start? We recommend that trainees integrate these tips for high-value care into their routine practice.
1. Use evidence-based resources that highlight value
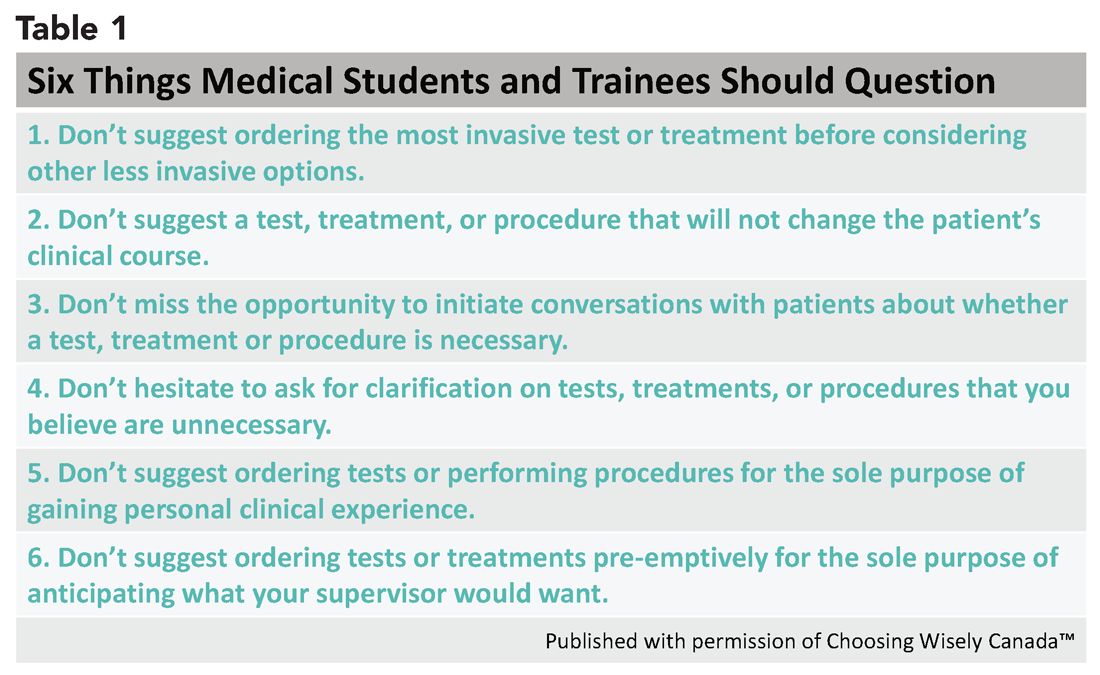
A great place to begin is the “Six Things Medical Students and Trainees Should Question,” originally published in Academic Medicine and created by Choosing Wisely Canada™. Recommendations range from avoiding tests or treatments that will not change a patient’s clinical course to holding off on ordering tests solely based on what you assume your preceptor will want (see the full list in Table 1).3

Other ways to avoid low-value care include following the United States Choosing Wisely™ campaign, which has collected more than 500 specialty society recommendations. Likewise, the American College of Radiology Appropriateness Criteria are designed to assist providers with ordering the appropriate imaging tests (for a more extensive list see Table 2).
2. Express your clinical reasoning
One driver of health care expenditures that is especially prevalent in academia is the pressure to demonstrate knowledge by recommending extensive testing. While these tests may rule out obscure diagnoses, they often do not change management.
You can still demonstrate a mastery of your patients’ care by expressing your thought process overtly. For instance, “I considered secondary causes of the patient’s severe hypertension but felt it was most reasonable to first treat her pain and restart her home medications before pursuing a larger work-up. If the patient’s blood pressure remains elevated and she is hypokalemic, we could consider testing for hyperaldosteronism.” If you explain why you think a diagnosis is less likely and order tests accordingly, others will be encouraged to consider value in their own medical decision making.
3. Hone your communication skills
One of the most cited reasons for providing unnecessary care is the time required to discuss treatment plans with patients – it’s much faster to just order the test than to explain why it isn’t needed. Research, however, shows that these cost conversations take 68 seconds on average.4 Costs of Care (see Table 2) has an excellent video series that highlights how effective communication allows for shared decision making, which promotes both patient engagement and helps avoid wasteful care.
Physicians’ first instincts are often defensive when a patient asks for care we perceive as unnecessary. However, exploring what the patient hopes to gain from said test or treatment frequently reveals concern for a specific, missed diagnosis or complication. Addressing this underlying fear, rather than defending your ordering patterns, can create improved rapport and may serve to provide more reassurance than a test ever could.5
As a physician-in-training, try to observe others having these conversations and take every opportunity to practice. By focusing on this key skill set, you will increase your comfort with in-depth discussions on the value of care.
4. Get involved in a project related to high-value care
While you are developing your own practice patterns, you may be inspired to tackle areas of overuse and underuse at a more systemwide level. If your hospital does not have a committee for high-value care, perhaps a quality improvement leader can support your ideas to launch a project or participate in an ongoing initiative. Physicians-in-training have been identified as crucial to these projects’ success – your frontline insight can highlight potential problems and the nuances of workflow that are key to effective solutions.6
5. Embrace lifelong learning and reflection
The process of becoming a physician and of practicing high-value care is not a sprint but a marathon. Multiple barriers to high-value care exist, and you may feel these pressures differently at various points in your career. These include malpractice concerns, addressing patient expectations, and the desire to take action “just to be safe.”6
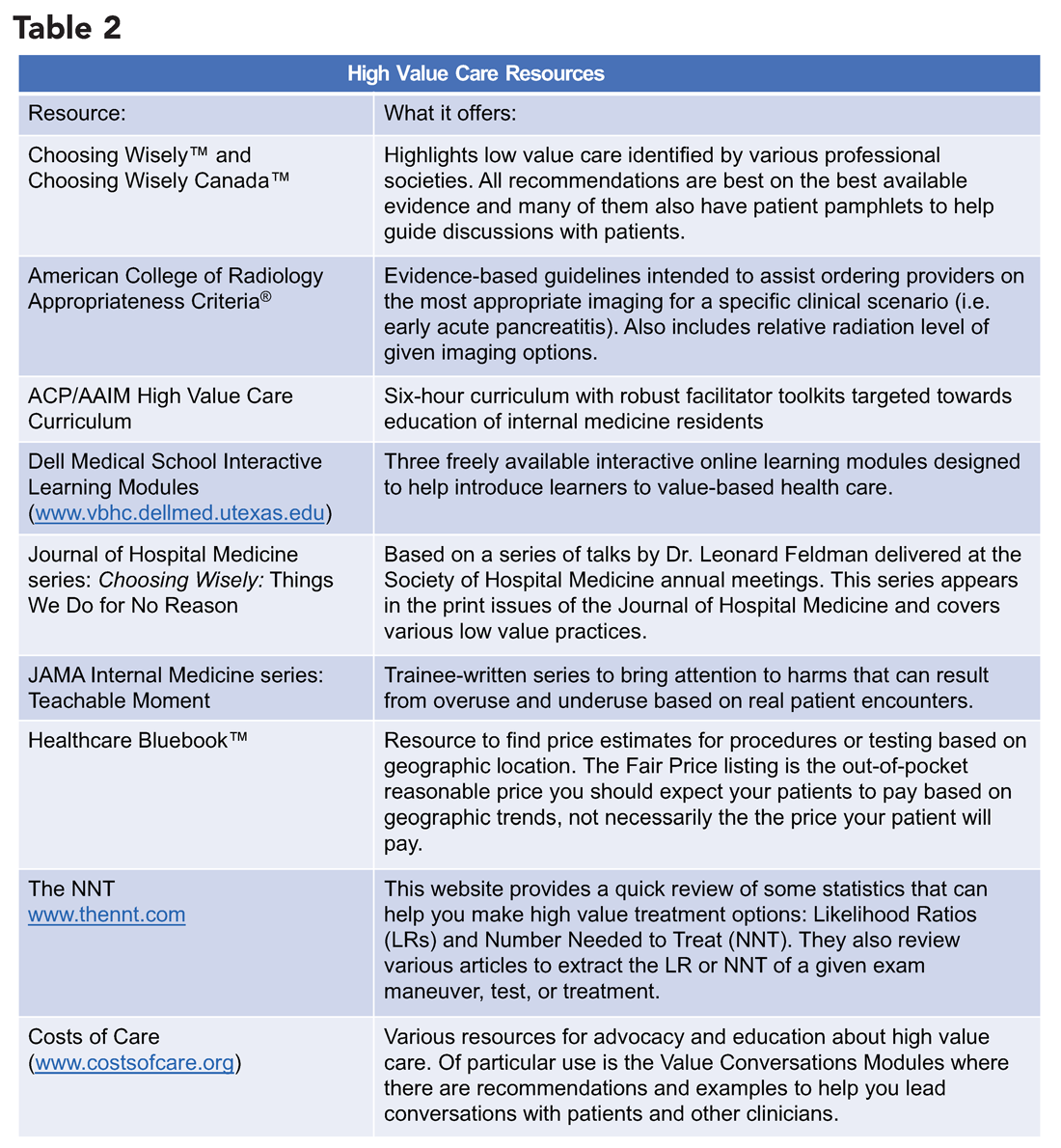
Interestingly, fear of malpractice does not seem to dissipate in areas where tort reform has provided stronger provider protections.7 Practitioners may also inaccurately assume a patient’s desire for additional work-up or treatment.8 Furthermore, be aware of the role of “commission bias” by which a provider regrets not doing something that could have helped a previous patient. This regret can prove to be a stronger motivator than the potential harm related to unnecessary diagnostic tests or treatments.9
While these barriers cannot be removed easily, learners and providers can practice active reflection by examining their own fears, biases, and motivations before and after they order additional testing or treatment.
As a physician-in-training, you may feel that your decisions do not have a major impact on the health care system as a whole. However, the culture shift needed to “bend the cost curve” will come from the collective efforts of individuals like you. Practicing high-value care is not just a matter of ordering fewer tests – appropriate ordering of an expensive test that expedites a diagnosis may be more cost-effective and enhance the quality of care provided. Increasing your own awareness of both necessary and unnecessary practices is a major step toward realizing system change. Your efforts to resist and reform the medical culture that propagates low value care will encourage your colleagues to follow suit.
Dr. Lacy is assistant professor and associate clerkship director at the University of New Mexico, Albuquerque, as well as division director of high-value care for the division of hospital medicine. Dr. Goetz is assistant professor at Rush University Medical Center, Chicago. They met as 2015 Copello Fellows at the National Physician Alliance. Both have been involved in numerous high-value care initiatives, curricular development, and medical education at their respective institutions.
References
1. Committee on the Learning Health Care System in America, Institute of Medicine. “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Edited by Smith M, Saunders R, Stuckhardt L, and McGinnis JM. (Washington: National Academies Press, 2013). http://www.ncbi.nlm.nih.gov/books/NBK207225/.
2. Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513-6.
3. Lakhani A et al. Choosing Wisely for Medical Education: Six things medical students and trainees should question. Acad Med. 2016 Oct;91(10):1374-8.
4. Hunter WG et al. Patient-physician discussions about costs: Definitions and impact on cost conversation incidence estimates. BMC Health Serv Res. 2016;16:108.
5. van Ravesteijn H et al. The reassuring value of diagnostic tests: a systematic review. Patient Educ Couns. 2012;86(1):3-8.
6. Moriates C, Wong BM. High-value care programmes from the bottom-up… and the top-down. BMJ Qual Saf. 2016;25(11):821-3.
7. Snyder Sulmasy L, Weinberger SE. Better care is the best defense: High-value clinical practice vs. defensive medicine. Cleve Clin J Med. 2014;81(8):464-7.
8. Mulley AG, Trimble C, Elwyn G. Stop the silent misdiagnosis: Patients’ preferences matter. BMJ. 2012;345:e6572.
9. Scott IA. Cognitive challenges to minimising low value care. Intern Med J. 2017;47(9):1079-1083.
‘Culture shift’ comes from collective efforts
‘Culture shift’ comes from collective efforts
It’s Monday morning, and Mrs. Jones still has abdominal pain. Your ward team decides to order a CT. On chart review you notice she’s had three other abdominal CTs for the same indication this year. How did this happen? What should you do?
High-value care has been defined by the Institute of Medicine as “the best care for the patient, with the optimal result for the circumstances, delivered at the right price.”1 With an estimated $700 billion dollars – 30% of medical expenditures – spent on wasted care, there are rising calls for a transformational shift.2
You are now asked to consider not just everything you can do for a patient, but also the benefits, harms, and costs associated with those choices. But where to start? We recommend that trainees integrate these tips for high-value care into their routine practice.
1. Use evidence-based resources that highlight value
A great place to begin is the “Six Things Medical Students and Trainees Should Question,” originally published in Academic Medicine and created by Choosing Wisely Canada™. Recommendations range from avoiding tests or treatments that will not change a patient’s clinical course to holding off on ordering tests solely based on what you assume your preceptor will want (see the full list in Table 1).3
Other ways to avoid low-value care include following the United States Choosing Wisely™ campaign, which has collected more than 500 specialty society recommendations. Likewise, the American College of Radiology Appropriateness Criteria are designed to assist providers with ordering the appropriate imaging tests (for a more extensive list see Table 2).
2. Express your clinical reasoning
One driver of health care expenditures that is especially prevalent in academia is the pressure to demonstrate knowledge by recommending extensive testing. While these tests may rule out obscure diagnoses, they often do not change management.
You can still demonstrate a mastery of your patients’ care by expressing your thought process overtly. For instance, “I considered secondary causes of the patient’s severe hypertension but felt it was most reasonable to first treat her pain and restart her home medications before pursuing a larger work-up. If the patient’s blood pressure remains elevated and she is hypokalemic, we could consider testing for hyperaldosteronism.” If you explain why you think a diagnosis is less likely and order tests accordingly, others will be encouraged to consider value in their own medical decision making.
3. Hone your communication skills
One of the most cited reasons for providing unnecessary care is the time required to discuss treatment plans with patients – it’s much faster to just order the test than to explain why it isn’t needed. Research, however, shows that these cost conversations take 68 seconds on average.4 Costs of Care (see Table 2) has an excellent video series that highlights how effective communication allows for shared decision making, which promotes both patient engagement and helps avoid wasteful care.
Physicians’ first instincts are often defensive when a patient asks for care we perceive as unnecessary. However, exploring what the patient hopes to gain from said test or treatment frequently reveals concern for a specific, missed diagnosis or complication. Addressing this underlying fear, rather than defending your ordering patterns, can create improved rapport and may serve to provide more reassurance than a test ever could.5
As a physician-in-training, try to observe others having these conversations and take every opportunity to practice. By focusing on this key skill set, you will increase your comfort with in-depth discussions on the value of care.
4. Get involved in a project related to high-value care
While you are developing your own practice patterns, you may be inspired to tackle areas of overuse and underuse at a more systemwide level. If your hospital does not have a committee for high-value care, perhaps a quality improvement leader can support your ideas to launch a project or participate in an ongoing initiative. Physicians-in-training have been identified as crucial to these projects’ success – your frontline insight can highlight potential problems and the nuances of workflow that are key to effective solutions.6
5. Embrace lifelong learning and reflection
The process of becoming a physician and of practicing high-value care is not a sprint but a marathon. Multiple barriers to high-value care exist, and you may feel these pressures differently at various points in your career. These include malpractice concerns, addressing patient expectations, and the desire to take action “just to be safe.”6
Interestingly, fear of malpractice does not seem to dissipate in areas where tort reform has provided stronger provider protections.7 Practitioners may also inaccurately assume a patient’s desire for additional work-up or treatment.8 Furthermore, be aware of the role of “commission bias” by which a provider regrets not doing something that could have helped a previous patient. This regret can prove to be a stronger motivator than the potential harm related to unnecessary diagnostic tests or treatments.9
While these barriers cannot be removed easily, learners and providers can practice active reflection by examining their own fears, biases, and motivations before and after they order additional testing or treatment.
As a physician-in-training, you may feel that your decisions do not have a major impact on the health care system as a whole. However, the culture shift needed to “bend the cost curve” will come from the collective efforts of individuals like you. Practicing high-value care is not just a matter of ordering fewer tests – appropriate ordering of an expensive test that expedites a diagnosis may be more cost-effective and enhance the quality of care provided. Increasing your own awareness of both necessary and unnecessary practices is a major step toward realizing system change. Your efforts to resist and reform the medical culture that propagates low value care will encourage your colleagues to follow suit.
Dr. Lacy is assistant professor and associate clerkship director at the University of New Mexico, Albuquerque, as well as division director of high-value care for the division of hospital medicine. Dr. Goetz is assistant professor at Rush University Medical Center, Chicago. They met as 2015 Copello Fellows at the National Physician Alliance. Both have been involved in numerous high-value care initiatives, curricular development, and medical education at their respective institutions.
References
1. Committee on the Learning Health Care System in America, Institute of Medicine. “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Edited by Smith M, Saunders R, Stuckhardt L, and McGinnis JM. (Washington: National Academies Press, 2013). http://www.ncbi.nlm.nih.gov/books/NBK207225/.
2. Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513-6.
3. Lakhani A et al. Choosing Wisely for Medical Education: Six things medical students and trainees should question. Acad Med. 2016 Oct;91(10):1374-8.
4. Hunter WG et al. Patient-physician discussions about costs: Definitions and impact on cost conversation incidence estimates. BMC Health Serv Res. 2016;16:108.
5. van Ravesteijn H et al. The reassuring value of diagnostic tests: a systematic review. Patient Educ Couns. 2012;86(1):3-8.
6. Moriates C, Wong BM. High-value care programmes from the bottom-up… and the top-down. BMJ Qual Saf. 2016;25(11):821-3.
7. Snyder Sulmasy L, Weinberger SE. Better care is the best defense: High-value clinical practice vs. defensive medicine. Cleve Clin J Med. 2014;81(8):464-7.
8. Mulley AG, Trimble C, Elwyn G. Stop the silent misdiagnosis: Patients’ preferences matter. BMJ. 2012;345:e6572.
9. Scott IA. Cognitive challenges to minimising low value care. Intern Med J. 2017;47(9):1079-1083.
It’s Monday morning, and Mrs. Jones still has abdominal pain. Your ward team decides to order a CT. On chart review you notice she’s had three other abdominal CTs for the same indication this year. How did this happen? What should you do?
High-value care has been defined by the Institute of Medicine as “the best care for the patient, with the optimal result for the circumstances, delivered at the right price.”1 With an estimated $700 billion dollars – 30% of medical expenditures – spent on wasted care, there are rising calls for a transformational shift.2
You are now asked to consider not just everything you can do for a patient, but also the benefits, harms, and costs associated with those choices. But where to start? We recommend that trainees integrate these tips for high-value care into their routine practice.
1. Use evidence-based resources that highlight value
A great place to begin is the “Six Things Medical Students and Trainees Should Question,” originally published in Academic Medicine and created by Choosing Wisely Canada™. Recommendations range from avoiding tests or treatments that will not change a patient’s clinical course to holding off on ordering tests solely based on what you assume your preceptor will want (see the full list in Table 1).3
Other ways to avoid low-value care include following the United States Choosing Wisely™ campaign, which has collected more than 500 specialty society recommendations. Likewise, the American College of Radiology Appropriateness Criteria are designed to assist providers with ordering the appropriate imaging tests (for a more extensive list see Table 2).
2. Express your clinical reasoning
One driver of health care expenditures that is especially prevalent in academia is the pressure to demonstrate knowledge by recommending extensive testing. While these tests may rule out obscure diagnoses, they often do not change management.
You can still demonstrate a mastery of your patients’ care by expressing your thought process overtly. For instance, “I considered secondary causes of the patient’s severe hypertension but felt it was most reasonable to first treat her pain and restart her home medications before pursuing a larger work-up. If the patient’s blood pressure remains elevated and she is hypokalemic, we could consider testing for hyperaldosteronism.” If you explain why you think a diagnosis is less likely and order tests accordingly, others will be encouraged to consider value in their own medical decision making.
3. Hone your communication skills
One of the most cited reasons for providing unnecessary care is the time required to discuss treatment plans with patients – it’s much faster to just order the test than to explain why it isn’t needed. Research, however, shows that these cost conversations take 68 seconds on average.4 Costs of Care (see Table 2) has an excellent video series that highlights how effective communication allows for shared decision making, which promotes both patient engagement and helps avoid wasteful care.
Physicians’ first instincts are often defensive when a patient asks for care we perceive as unnecessary. However, exploring what the patient hopes to gain from said test or treatment frequently reveals concern for a specific, missed diagnosis or complication. Addressing this underlying fear, rather than defending your ordering patterns, can create improved rapport and may serve to provide more reassurance than a test ever could.5
As a physician-in-training, try to observe others having these conversations and take every opportunity to practice. By focusing on this key skill set, you will increase your comfort with in-depth discussions on the value of care.
4. Get involved in a project related to high-value care
While you are developing your own practice patterns, you may be inspired to tackle areas of overuse and underuse at a more systemwide level. If your hospital does not have a committee for high-value care, perhaps a quality improvement leader can support your ideas to launch a project or participate in an ongoing initiative. Physicians-in-training have been identified as crucial to these projects’ success – your frontline insight can highlight potential problems and the nuances of workflow that are key to effective solutions.6
5. Embrace lifelong learning and reflection
The process of becoming a physician and of practicing high-value care is not a sprint but a marathon. Multiple barriers to high-value care exist, and you may feel these pressures differently at various points in your career. These include malpractice concerns, addressing patient expectations, and the desire to take action “just to be safe.”6
Interestingly, fear of malpractice does not seem to dissipate in areas where tort reform has provided stronger provider protections.7 Practitioners may also inaccurately assume a patient’s desire for additional work-up or treatment.8 Furthermore, be aware of the role of “commission bias” by which a provider regrets not doing something that could have helped a previous patient. This regret can prove to be a stronger motivator than the potential harm related to unnecessary diagnostic tests or treatments.9
While these barriers cannot be removed easily, learners and providers can practice active reflection by examining their own fears, biases, and motivations before and after they order additional testing or treatment.
As a physician-in-training, you may feel that your decisions do not have a major impact on the health care system as a whole. However, the culture shift needed to “bend the cost curve” will come from the collective efforts of individuals like you. Practicing high-value care is not just a matter of ordering fewer tests – appropriate ordering of an expensive test that expedites a diagnosis may be more cost-effective and enhance the quality of care provided. Increasing your own awareness of both necessary and unnecessary practices is a major step toward realizing system change. Your efforts to resist and reform the medical culture that propagates low value care will encourage your colleagues to follow suit.
Dr. Lacy is assistant professor and associate clerkship director at the University of New Mexico, Albuquerque, as well as division director of high-value care for the division of hospital medicine. Dr. Goetz is assistant professor at Rush University Medical Center, Chicago. They met as 2015 Copello Fellows at the National Physician Alliance. Both have been involved in numerous high-value care initiatives, curricular development, and medical education at their respective institutions.
References
1. Committee on the Learning Health Care System in America, Institute of Medicine. “Best Care at Lower Cost: The Path to Continuously Learning Health Care in America.” Edited by Smith M, Saunders R, Stuckhardt L, and McGinnis JM. (Washington: National Academies Press, 2013). http://www.ncbi.nlm.nih.gov/books/NBK207225/.
2. Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA. 2012;307(14):1513-6.
3. Lakhani A et al. Choosing Wisely for Medical Education: Six things medical students and trainees should question. Acad Med. 2016 Oct;91(10):1374-8.
4. Hunter WG et al. Patient-physician discussions about costs: Definitions and impact on cost conversation incidence estimates. BMC Health Serv Res. 2016;16:108.
5. van Ravesteijn H et al. The reassuring value of diagnostic tests: a systematic review. Patient Educ Couns. 2012;86(1):3-8.
6. Moriates C, Wong BM. High-value care programmes from the bottom-up… and the top-down. BMJ Qual Saf. 2016;25(11):821-3.
7. Snyder Sulmasy L, Weinberger SE. Better care is the best defense: High-value clinical practice vs. defensive medicine. Cleve Clin J Med. 2014;81(8):464-7.
8. Mulley AG, Trimble C, Elwyn G. Stop the silent misdiagnosis: Patients’ preferences matter. BMJ. 2012;345:e6572.
9. Scott IA. Cognitive challenges to minimising low value care. Intern Med J. 2017;47(9):1079-1083.
Why we need another article on suicide contracts
Every guideline and lecture on suicide risk assessment includes the message: “Do not use suicide contracts.” Yet, as forensic psychiatrists, we continue to see medical records that rely solely on the patient verbalizing, agreeing, or signing that they will be safe, in order to justify medical decision-making. A recent case we reviewed involving a grossly psychotic male spotlighted the meaninglessness of suicide contracts. In an attempt to understand the impulse by clinicians to use suicide contracts, we decided to review the topic.

Suicide risk assessment is a confusing and poorly explained skill in our field. Suicide risk assessment tools are well-intended. They are meant to identify and stratify risk, and help guide medical decision-making. Popular tools are startlingly different. How can two scales represent adequate psychiatric knowledge yet be completely different? SADPERSONS1 is widely used and still considered standard of care yet has nothing in common with the Columbia–Suicide Severity Rating Scale (CSSRS).2

For those of us working in forensic settings, we are aghast that neither assessment is modified for use in correctional settings or accounts for essential risk factors of suicide in jails and prisons (placement in solitary, significant charges, homeless, etc.) Yet, they are widely used in jails and prisons across the country. This can be extrapolated to all of us who work with specific populations yet are asked to follow generic scales by administrators.
In reviewing the literature, we are surprised to see the lack of acknowledgment that many tools used in suicide risk assessment have little to no evidence. Despite their numerous appearances in medical records that we review, we are not aware of existing evidence for asking patients whether patients are suicidal on an hourly basis, for psychotropic treatment other than lithium and clozapine (Clozaril), and for safety plans that involve telling the patient to call 911. Of even greater concern, suicide risk assessments themselves may have limited value because of a lack of evidence as suggested by large study findings. It may surprise some to learn that the National Institute for Health and Care Excellence (NICE) in the United Kingdom includes the following statement in its guidelines: “Do not use risk assessment tools and scales to predict future suicide or repetition of self-harm.”3
In 2017, Carter et al.4 reviewed 70 studies using suicide risk scales to stratify patients in higher-risk groups for self-harm or suicide, during a follow-up period. The study reviewed biological tests such as the dexamethasone suppression test and 5-hydroxyindoleacetic acid; as well as psychological scales, including Buglass & Horton, SADPERSONS, the Beck Hopelessness Scale, the Beck’s Depression Inventory, Manchester Self Harm Rule, and the Edinburgh Risk Rating Scale. Their conclusion was clear: “No individual predictive instrument or pooled subgroups of instruments were able to classify patients as being at high risk of suicidal behavior with a level of accuracy suitable to be used to allocate treatment.”
Despite the bad reputation, one must admit that suicide contracts intuitively feel right. Just as we ask patients whether they believe they will stay sober in the future, or ask patients if they will be compliant with their psychotropics, asking them if they feel that they can maintain safety seems relevant. Reading through the literature, one can even find articles promoting this approach. In 2011, researchers simply asked 147 patients in psychiatric hospitals considered to be high risk for suicide whether they would engage in self-harm in the following weeks. They followed those patients for 15 weeks after their discharge for acts of self-harm. They concluded that “self-perceptions of risk seem to perform as well as the best [standardized assessment tools] the field has to offer” for the prediction of self-harm.5 We are unconvinced that juries would find suicide contracts irrelevant despite the lack of evidence. American society values individual autonomy and self-decision making. Patients telling their clinicians, “I will be OK” is relevant to suicide risk assessment. One can argue that the problem is not with the suicide contract itself, but with its blind use as a marker of safety.
The standard of care dictates that we try to assess suicide risk using evidence-based techniques. To the providers who see merit in asking patients whether they will be able to maintain their safety, we empathize with this impulse despite the lack of evidence. This will contribute in our shared effort to minimize suicide.
We acknowledge that the evidence of any assessment is limited and might miss a greater point in this entire discussion: Why are new iterations of suicide risk assessments not an improvement on the prior ones but a competing theory? New assessments emphasizing different facets of suicidal thinking do not include key demographic factors, while older tools do not include more recent understanding, such as the importance of hopelessness. From a provider’s perspective, the debate appears to be a battle of trends, theories, and acronyms rather than comprehensive analysis of the latest evidence. We, therefore, are concerned by “suicide experts” who advocate for any one assessment as the only gold standard and give false hopes about its efficacy.
As suicide rates continue to climb across the country, one wonders what we, as psychiatrists, are trying to achieve. Promises of zero suicides by hospitals,6 academic institutions,7 and even governments8 are well-meaning but possibly misleading to families and patients. Psychiatry should advocate within the standard of care for reasonable attempts at suicide risk assessment, including demographic factors (see SADPERSONS), as well as examination of the actual suicidality (see the CSSRS). Our professional organizations should clarify expectations for clinicians while also clarifying the limitations of our current knowledge base.
References
1. Patterson WM et al. Evaluation of suicidal patients: the SADPERSONS scale. Psychosomatics. 1983 Apr;24[4]:343-5, 348-9.
2. Posner K et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011 Dec;168(12):1266-77.
3. Kendall T et al. Longer term management of self harm: summary of NICE guidance. BMJ. 2011;343. doi: 10.1136/bmj.d7073.
4. Carter G et al. Predicting suicidal behaviors using clinical instruments: systematic review and meta-analysis of positive predictive values for risk scales. Br J Psychiatry. 2017 Jun;210(6):387-95.
5. Peterson J et al. If you want to know, consider asking: How likely is it that patients will hurt themselves in the future? Psychol Assess. 2011 Sep;23(3):626-34.
5. Byrne JM et al. Implementation and impact of the central district of California’s suicide prevention program for crime defendants. Federal Probation. 2012 Jun;76(1):3-13.
6. “R.I.’s Butler Hospital sets ‘zero suicide’ goal for patients”/audio. Providence Journal. May 15, 2018.
7. “NIMH funds 3 ‘zero suicide’ grants.” National Institute of Mental Health. Sep 16, 2016.
8. Rothschild N. “Is it possible to eliminate suicide?” Atlantic. Jun 5, 2015.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. Dr. Rao is a San Diego–based board-certified psychiatrist with expertise in forensic psychiatry, correctional psychiatry, telepsychiatry, and inpatient psychiatry.
Every guideline and lecture on suicide risk assessment includes the message: “Do not use suicide contracts.” Yet, as forensic psychiatrists, we continue to see medical records that rely solely on the patient verbalizing, agreeing, or signing that they will be safe, in order to justify medical decision-making. A recent case we reviewed involving a grossly psychotic male spotlighted the meaninglessness of suicide contracts. In an attempt to understand the impulse by clinicians to use suicide contracts, we decided to review the topic.
Suicide risk assessment is a confusing and poorly explained skill in our field. Suicide risk assessment tools are well-intended. They are meant to identify and stratify risk, and help guide medical decision-making. Popular tools are startlingly different. How can two scales represent adequate psychiatric knowledge yet be completely different? SADPERSONS1 is widely used and still considered standard of care yet has nothing in common with the Columbia–Suicide Severity Rating Scale (CSSRS).2
For those of us working in forensic settings, we are aghast that neither assessment is modified for use in correctional settings or accounts for essential risk factors of suicide in jails and prisons (placement in solitary, significant charges, homeless, etc.) Yet, they are widely used in jails and prisons across the country. This can be extrapolated to all of us who work with specific populations yet are asked to follow generic scales by administrators.
In reviewing the literature, we are surprised to see the lack of acknowledgment that many tools used in suicide risk assessment have little to no evidence. Despite their numerous appearances in medical records that we review, we are not aware of existing evidence for asking patients whether patients are suicidal on an hourly basis, for psychotropic treatment other than lithium and clozapine (Clozaril), and for safety plans that involve telling the patient to call 911. Of even greater concern, suicide risk assessments themselves may have limited value because of a lack of evidence as suggested by large study findings. It may surprise some to learn that the National Institute for Health and Care Excellence (NICE) in the United Kingdom includes the following statement in its guidelines: “Do not use risk assessment tools and scales to predict future suicide or repetition of self-harm.”3
In 2017, Carter et al.4 reviewed 70 studies using suicide risk scales to stratify patients in higher-risk groups for self-harm or suicide, during a follow-up period. The study reviewed biological tests such as the dexamethasone suppression test and 5-hydroxyindoleacetic acid; as well as psychological scales, including Buglass & Horton, SADPERSONS, the Beck Hopelessness Scale, the Beck’s Depression Inventory, Manchester Self Harm Rule, and the Edinburgh Risk Rating Scale. Their conclusion was clear: “No individual predictive instrument or pooled subgroups of instruments were able to classify patients as being at high risk of suicidal behavior with a level of accuracy suitable to be used to allocate treatment.”
Despite the bad reputation, one must admit that suicide contracts intuitively feel right. Just as we ask patients whether they believe they will stay sober in the future, or ask patients if they will be compliant with their psychotropics, asking them if they feel that they can maintain safety seems relevant. Reading through the literature, one can even find articles promoting this approach. In 2011, researchers simply asked 147 patients in psychiatric hospitals considered to be high risk for suicide whether they would engage in self-harm in the following weeks. They followed those patients for 15 weeks after their discharge for acts of self-harm. They concluded that “self-perceptions of risk seem to perform as well as the best [standardized assessment tools] the field has to offer” for the prediction of self-harm.5 We are unconvinced that juries would find suicide contracts irrelevant despite the lack of evidence. American society values individual autonomy and self-decision making. Patients telling their clinicians, “I will be OK” is relevant to suicide risk assessment. One can argue that the problem is not with the suicide contract itself, but with its blind use as a marker of safety.
The standard of care dictates that we try to assess suicide risk using evidence-based techniques. To the providers who see merit in asking patients whether they will be able to maintain their safety, we empathize with this impulse despite the lack of evidence. This will contribute in our shared effort to minimize suicide.
We acknowledge that the evidence of any assessment is limited and might miss a greater point in this entire discussion: Why are new iterations of suicide risk assessments not an improvement on the prior ones but a competing theory? New assessments emphasizing different facets of suicidal thinking do not include key demographic factors, while older tools do not include more recent understanding, such as the importance of hopelessness. From a provider’s perspective, the debate appears to be a battle of trends, theories, and acronyms rather than comprehensive analysis of the latest evidence. We, therefore, are concerned by “suicide experts” who advocate for any one assessment as the only gold standard and give false hopes about its efficacy.
As suicide rates continue to climb across the country, one wonders what we, as psychiatrists, are trying to achieve. Promises of zero suicides by hospitals,6 academic institutions,7 and even governments8 are well-meaning but possibly misleading to families and patients. Psychiatry should advocate within the standard of care for reasonable attempts at suicide risk assessment, including demographic factors (see SADPERSONS), as well as examination of the actual suicidality (see the CSSRS). Our professional organizations should clarify expectations for clinicians while also clarifying the limitations of our current knowledge base.
References
1. Patterson WM et al. Evaluation of suicidal patients: the SADPERSONS scale. Psychosomatics. 1983 Apr;24[4]:343-5, 348-9.
2. Posner K et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011 Dec;168(12):1266-77.
3. Kendall T et al. Longer term management of self harm: summary of NICE guidance. BMJ. 2011;343. doi: 10.1136/bmj.d7073.
4. Carter G et al. Predicting suicidal behaviors using clinical instruments: systematic review and meta-analysis of positive predictive values for risk scales. Br J Psychiatry. 2017 Jun;210(6):387-95.
5. Peterson J et al. If you want to know, consider asking: How likely is it that patients will hurt themselves in the future? Psychol Assess. 2011 Sep;23(3):626-34.
5. Byrne JM et al. Implementation and impact of the central district of California’s suicide prevention program for crime defendants. Federal Probation. 2012 Jun;76(1):3-13.
6. “R.I.’s Butler Hospital sets ‘zero suicide’ goal for patients”/audio. Providence Journal. May 15, 2018.
7. “NIMH funds 3 ‘zero suicide’ grants.” National Institute of Mental Health. Sep 16, 2016.
8. Rothschild N. “Is it possible to eliminate suicide?” Atlantic. Jun 5, 2015.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. Dr. Rao is a San Diego–based board-certified psychiatrist with expertise in forensic psychiatry, correctional psychiatry, telepsychiatry, and inpatient psychiatry.
Every guideline and lecture on suicide risk assessment includes the message: “Do not use suicide contracts.” Yet, as forensic psychiatrists, we continue to see medical records that rely solely on the patient verbalizing, agreeing, or signing that they will be safe, in order to justify medical decision-making. A recent case we reviewed involving a grossly psychotic male spotlighted the meaninglessness of suicide contracts. In an attempt to understand the impulse by clinicians to use suicide contracts, we decided to review the topic.
Suicide risk assessment is a confusing and poorly explained skill in our field. Suicide risk assessment tools are well-intended. They are meant to identify and stratify risk, and help guide medical decision-making. Popular tools are startlingly different. How can two scales represent adequate psychiatric knowledge yet be completely different? SADPERSONS1 is widely used and still considered standard of care yet has nothing in common with the Columbia–Suicide Severity Rating Scale (CSSRS).2
For those of us working in forensic settings, we are aghast that neither assessment is modified for use in correctional settings or accounts for essential risk factors of suicide in jails and prisons (placement in solitary, significant charges, homeless, etc.) Yet, they are widely used in jails and prisons across the country. This can be extrapolated to all of us who work with specific populations yet are asked to follow generic scales by administrators.
In reviewing the literature, we are surprised to see the lack of acknowledgment that many tools used in suicide risk assessment have little to no evidence. Despite their numerous appearances in medical records that we review, we are not aware of existing evidence for asking patients whether patients are suicidal on an hourly basis, for psychotropic treatment other than lithium and clozapine (Clozaril), and for safety plans that involve telling the patient to call 911. Of even greater concern, suicide risk assessments themselves may have limited value because of a lack of evidence as suggested by large study findings. It may surprise some to learn that the National Institute for Health and Care Excellence (NICE) in the United Kingdom includes the following statement in its guidelines: “Do not use risk assessment tools and scales to predict future suicide or repetition of self-harm.”3
In 2017, Carter et al.4 reviewed 70 studies using suicide risk scales to stratify patients in higher-risk groups for self-harm or suicide, during a follow-up period. The study reviewed biological tests such as the dexamethasone suppression test and 5-hydroxyindoleacetic acid; as well as psychological scales, including Buglass & Horton, SADPERSONS, the Beck Hopelessness Scale, the Beck’s Depression Inventory, Manchester Self Harm Rule, and the Edinburgh Risk Rating Scale. Their conclusion was clear: “No individual predictive instrument or pooled subgroups of instruments were able to classify patients as being at high risk of suicidal behavior with a level of accuracy suitable to be used to allocate treatment.”
Despite the bad reputation, one must admit that suicide contracts intuitively feel right. Just as we ask patients whether they believe they will stay sober in the future, or ask patients if they will be compliant with their psychotropics, asking them if they feel that they can maintain safety seems relevant. Reading through the literature, one can even find articles promoting this approach. In 2011, researchers simply asked 147 patients in psychiatric hospitals considered to be high risk for suicide whether they would engage in self-harm in the following weeks. They followed those patients for 15 weeks after their discharge for acts of self-harm. They concluded that “self-perceptions of risk seem to perform as well as the best [standardized assessment tools] the field has to offer” for the prediction of self-harm.5 We are unconvinced that juries would find suicide contracts irrelevant despite the lack of evidence. American society values individual autonomy and self-decision making. Patients telling their clinicians, “I will be OK” is relevant to suicide risk assessment. One can argue that the problem is not with the suicide contract itself, but with its blind use as a marker of safety.
The standard of care dictates that we try to assess suicide risk using evidence-based techniques. To the providers who see merit in asking patients whether they will be able to maintain their safety, we empathize with this impulse despite the lack of evidence. This will contribute in our shared effort to minimize suicide.
We acknowledge that the evidence of any assessment is limited and might miss a greater point in this entire discussion: Why are new iterations of suicide risk assessments not an improvement on the prior ones but a competing theory? New assessments emphasizing different facets of suicidal thinking do not include key demographic factors, while older tools do not include more recent understanding, such as the importance of hopelessness. From a provider’s perspective, the debate appears to be a battle of trends, theories, and acronyms rather than comprehensive analysis of the latest evidence. We, therefore, are concerned by “suicide experts” who advocate for any one assessment as the only gold standard and give false hopes about its efficacy.
As suicide rates continue to climb across the country, one wonders what we, as psychiatrists, are trying to achieve. Promises of zero suicides by hospitals,6 academic institutions,7 and even governments8 are well-meaning but possibly misleading to families and patients. Psychiatry should advocate within the standard of care for reasonable attempts at suicide risk assessment, including demographic factors (see SADPERSONS), as well as examination of the actual suicidality (see the CSSRS). Our professional organizations should clarify expectations for clinicians while also clarifying the limitations of our current knowledge base.
References
1. Patterson WM et al. Evaluation of suicidal patients: the SADPERSONS scale. Psychosomatics. 1983 Apr;24[4]:343-5, 348-9.
2. Posner K et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011 Dec;168(12):1266-77.
3. Kendall T et al. Longer term management of self harm: summary of NICE guidance. BMJ. 2011;343. doi: 10.1136/bmj.d7073.
4. Carter G et al. Predicting suicidal behaviors using clinical instruments: systematic review and meta-analysis of positive predictive values for risk scales. Br J Psychiatry. 2017 Jun;210(6):387-95.
5. Peterson J et al. If you want to know, consider asking: How likely is it that patients will hurt themselves in the future? Psychol Assess. 2011 Sep;23(3):626-34.
5. Byrne JM et al. Implementation and impact of the central district of California’s suicide prevention program for crime defendants. Federal Probation. 2012 Jun;76(1):3-13.
6. “R.I.’s Butler Hospital sets ‘zero suicide’ goal for patients”/audio. Providence Journal. May 15, 2018.
7. “NIMH funds 3 ‘zero suicide’ grants.” National Institute of Mental Health. Sep 16, 2016.
8. Rothschild N. “Is it possible to eliminate suicide?” Atlantic. Jun 5, 2015.
Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at the University of California, San Diego, and the University of San Diego. Dr. Rao is a San Diego–based board-certified psychiatrist with expertise in forensic psychiatry, correctional psychiatry, telepsychiatry, and inpatient psychiatry.
Lack of CBD oil regulations hearkens back to patent medicines
My vet sells cannabidiol (CBD) oil for dogs and cats.

So does the vape store down the street, the pharmacy around the corner ... and pretty much every place these days.
I probably have more patients ask me about CBD than any other drug, usually because a friend/cousin/in-law/child/parent/spouse/neighbor/coworker “said I should ask you about this.” That’s the power of the Internet: The most marginally proven treatments are portrayed as definitive cures, while some of the most effective treatments (like vaccines) are treated like a lethal-injection drug.
Nothing is, or ever will be, a miracle cure. There will always be nonresponders and those who have adverse effects. In that respect, what goes for one treatment goes for all of them.
But that doesn’t stop these things from being pushed in the most unreliable ways. On Yelp, Groupon, Facebook, and countless other nonmedical sites that aren’t required to back up their claims with hard evidence.
Anything I prescribe, and all over-the-counter medications, are subject to far more scrutiny. They have known risks and benefits. They’ve been through trials, and most have years of data to review when questions arise.

Granted, CBD oil has been approved, as Epidiolex, for different forms of epilepsy. That kind of regulation is a step forward, but the majority of people selling CBD oil are doing so with unregulated OTC forms.
These may work, but the lack of regulation means every one of these places can make their own formulations, purities, and strengths. In some respects it’s a throwback to the era of patent medicines, where each pharmacy was free to whip up their own concoctions, label them as treatments for whatever they wished, and advertise and sell them.
The Food and Drug Administration, however, continues to take an ostrich approach. At their level these OTC agents are illegal and cannot be sold or marketed. At the same time, though, the restrictions overall are not being enforced. This gives the impression that there is nothing wrong with selling them.
Let’s look at morphine, an effective pain reliever and controlled substance. It’s tightly regulated, as it should be. But what if those regulations were ignored? What if, in addition to it being available by prescription, it were sold OTC in perhaps weaker but unregulated strengths and forms, with a variety of unscientific claims made for its benefits?
I don’t see anyone getting away with doing that.
Like I said earlier, I have nothing against CBD oil. But I do think it should have to go through the same approval process as any other medication, with specific strengths, dosing, benefits, and side effects determined, and enforceable regulations around its manufacturing, sale, and use.
Anything less is snake oil.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
My vet sells cannabidiol (CBD) oil for dogs and cats.
So does the vape store down the street, the pharmacy around the corner ... and pretty much every place these days.
I probably have more patients ask me about CBD than any other drug, usually because a friend/cousin/in-law/child/parent/spouse/neighbor/coworker “said I should ask you about this.” That’s the power of the Internet: The most marginally proven treatments are portrayed as definitive cures, while some of the most effective treatments (like vaccines) are treated like a lethal-injection drug.
Nothing is, or ever will be, a miracle cure. There will always be nonresponders and those who have adverse effects. In that respect, what goes for one treatment goes for all of them.
But that doesn’t stop these things from being pushed in the most unreliable ways. On Yelp, Groupon, Facebook, and countless other nonmedical sites that aren’t required to back up their claims with hard evidence.
Anything I prescribe, and all over-the-counter medications, are subject to far more scrutiny. They have known risks and benefits. They’ve been through trials, and most have years of data to review when questions arise.
Granted, CBD oil has been approved, as Epidiolex, for different forms of epilepsy. That kind of regulation is a step forward, but the majority of people selling CBD oil are doing so with unregulated OTC forms.
These may work, but the lack of regulation means every one of these places can make their own formulations, purities, and strengths. In some respects it’s a throwback to the era of patent medicines, where each pharmacy was free to whip up their own concoctions, label them as treatments for whatever they wished, and advertise and sell them.
The Food and Drug Administration, however, continues to take an ostrich approach. At their level these OTC agents are illegal and cannot be sold or marketed. At the same time, though, the restrictions overall are not being enforced. This gives the impression that there is nothing wrong with selling them.
Let’s look at morphine, an effective pain reliever and controlled substance. It’s tightly regulated, as it should be. But what if those regulations were ignored? What if, in addition to it being available by prescription, it were sold OTC in perhaps weaker but unregulated strengths and forms, with a variety of unscientific claims made for its benefits?
I don’t see anyone getting away with doing that.
Like I said earlier, I have nothing against CBD oil. But I do think it should have to go through the same approval process as any other medication, with specific strengths, dosing, benefits, and side effects determined, and enforceable regulations around its manufacturing, sale, and use.
Anything less is snake oil.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
My vet sells cannabidiol (CBD) oil for dogs and cats.
So does the vape store down the street, the pharmacy around the corner ... and pretty much every place these days.
I probably have more patients ask me about CBD than any other drug, usually because a friend/cousin/in-law/child/parent/spouse/neighbor/coworker “said I should ask you about this.” That’s the power of the Internet: The most marginally proven treatments are portrayed as definitive cures, while some of the most effective treatments (like vaccines) are treated like a lethal-injection drug.
Nothing is, or ever will be, a miracle cure. There will always be nonresponders and those who have adverse effects. In that respect, what goes for one treatment goes for all of them.
But that doesn’t stop these things from being pushed in the most unreliable ways. On Yelp, Groupon, Facebook, and countless other nonmedical sites that aren’t required to back up their claims with hard evidence.
Anything I prescribe, and all over-the-counter medications, are subject to far more scrutiny. They have known risks and benefits. They’ve been through trials, and most have years of data to review when questions arise.
Granted, CBD oil has been approved, as Epidiolex, for different forms of epilepsy. That kind of regulation is a step forward, but the majority of people selling CBD oil are doing so with unregulated OTC forms.
These may work, but the lack of regulation means every one of these places can make their own formulations, purities, and strengths. In some respects it’s a throwback to the era of patent medicines, where each pharmacy was free to whip up their own concoctions, label them as treatments for whatever they wished, and advertise and sell them.
The Food and Drug Administration, however, continues to take an ostrich approach. At their level these OTC agents are illegal and cannot be sold or marketed. At the same time, though, the restrictions overall are not being enforced. This gives the impression that there is nothing wrong with selling them.
Let’s look at morphine, an effective pain reliever and controlled substance. It’s tightly regulated, as it should be. But what if those regulations were ignored? What if, in addition to it being available by prescription, it were sold OTC in perhaps weaker but unregulated strengths and forms, with a variety of unscientific claims made for its benefits?
I don’t see anyone getting away with doing that.
Like I said earlier, I have nothing against CBD oil. But I do think it should have to go through the same approval process as any other medication, with specific strengths, dosing, benefits, and side effects determined, and enforceable regulations around its manufacturing, sale, and use.
Anything less is snake oil.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Scoring below the cut but still depressed: What to do?
Depression is one of the most common mental health conditions in childhood, especially during socially turbulent adolescence when the brain is rapidly changing and parent-child relationships are strained by the teen’s striving for independence and identity. Often parents of teens call me worrying about possible depression, but in the next breath say “but maybe it is just puberty.” Because suicide is one of the most common causes of death among teens and is often associated with depression, we pediatricians have the scary job of sorting out symptoms and making a plan.
The Guidelines for Adolescent Depression in Primary Care (GLAD-PC)1,2 were revised in 2018 to help. This expert consensus document contains specific and practical guidance for all levels of depression. But for mild depression, GLAD-PC now advises pediatricians in Recommendation II to go beyond “watchful waiting.” It states, “After initial diagnosis,
Although a little vague, mild depression is diagnosed when there are “closer to 5” significant symptoms of depression, with “distressing but manageable” severity and only “mildly impaired” functioning. The most commonly used self-report adolescent depression screen, the Patient Health Questionnaire–Modified–9 (PHQ-9), has a recommended cut score of greater than 10, but 5-9 is considered mild depression symptoms. A clinical interview also is always required.
So what is this “active support” being recommended? After making an assessment of symptoms, severity, and impact – and ruling out significant suicide risk – the task is rather familiar to us from other medical conditions. We need to talk clearly and empathetically with the teen (and parents with consent) about depression and its neurological etiology, ask about contributing stress and genetic factors, and describe the typical course with optimism. This discussion is critical to pushing guilt or blame aside to rally family support. Substance use – (including alcohol) both a cause and attempted coping strategy for depression – must be addressed because it adds to risk for suicide or crashes and because it interacts with medicines.
Perhaps the biggest difference between active support for depression versus that for other conditions is that teens are likely reluctant, hopeless, and/or lacking energy to participate in the plan. The plan, therefore, needs to be approached in smaller steps and build on prior teen strengths, goals, or talents to motivate them and create reward to counteract general lethargy. You may know this teen used to play basketball, or sing at church, or love playing with a baby sister – all activities to try to reawaken. Parents can help recall these and are key to setting up opportunities.
GLAD-PC provides a “Self-Care Success!” worksheet of categories for goal setting for active support. These goals include:
- Stay physically active. Specified days/month, minutes/session, and dates and times.
- Engage spirituality and fun activities. Specify times/week, when, and with whom).
- Eat balanced meals. Specify number/day and names of foods.
- Spend time with people who can support you. Specify number/month, minutes/time, with whom, and doing what.
- Spend time relaxing. Specify days/week, minutes/time, and doing what.
- Determine small goals and simple steps. Establish these for a specified problem.
There is now evidence for these you can share with your teen patients and families.
Exercise
Exercise has a moderate effect size of 0.56 on depression, comparable to medications for mild to moderate depression and a useful adjunct to medications. The national Office of Disease Prevention and Health Promotion recommends that 6- to 17-year-olds get 60 minutes/day of moderate exercise or undertake vigorous “out of breath” exercise three times a week to maintain health. A meta-analysis of studies of yoga for people with depressive symptoms (not necessarily diagnosed depression) found reduced symptoms in 14 of 23 studies.
Pleasure
Advising fun has to include acknowledgment that a depressed teen is not motivated to do formerly fun things and may not get as much/any pleasure from it. You need to explain that “doing precedes feeling.” While what is fun is personal, new findings indicate that 2 hours/week “in nature” lowers stress, boosts mental health, and increases sense of well-being.
Nutrition
The MIND diet (Mediterranean-type diet high in leafy vegetables and berries but low in red meat) has evidence for lower odds of depression and psychological distress. Fatty acid supplements, specifically eicosapentaenoic acid at greater than 800 mg/day (930 mg), is better than placebo (P less than .001) for reducing mild depression within as little as 4 weeks. Natural S-Adenosyl-L-methionine (SAMe) has many studies showing benefit, according to National Center for Complementary and Alternative Medicine, a government-run website. NCCAM notes that St. John’s Wort has evidence for effectiveness equal to prescribed antidepressants for mild depression but with dangerous potential side effects, such as worsening of psychotic symptoms in bipolar disorder or schizophrenia, plus potentially life threatening drug interactions. While safe, valerian and probiotics have no evidence for reducing depression.
Social support
Family is usually the most important support for depressed teens even though they may be pushing family away, may refuse to come on outings, or may even refuse to come out of the bedroom. We should encourage parents and siblings to “hang out,” sitting quietly, available to listen rather than probing, cajoling, or nagging as they may have been doing. Parents also provide support by assuring adherence to visits, goals, and medications. Peer support helps a teen feel less alone and may increase social skills, but it can be difficult to sustain because friends may find depression threatening or give up when the teen avoids them and refuses activities. The National Association for Mental Illness has an online support group (www.strengthofus.org), as well as many excellent family resources. Sometimes medical efforts to be nonsectarian result in failure to recognize and remind teens and families of the value of religion, which is free and universally available, as a source of social support.
Relaxation
An evaluation of 15 studies concluded that relaxation techniques reduced depressive symptoms better than no treatment but not as much cognitive-behavior therapy (CBT). Yoga is another source of relaxation training. Mindfulness includes relaxation and specifies working to stay nonjudgmental about thoughts passing through one’s mind, recognizing and “arguing” with negative thinking, which is also part of CBT. Guided relaxation with a person, audiotape, or app (Calm or Headspace, among others) may be better for depressed teens because it inserts a voice to guide thoughts, which could potentially fend off ruminating on sad things.
Setting goals to address problems
In mild depression, compared with more endogenous moderate to severe major depressive disorder, a specific life stressor or relationship issue may be the precipitant. Identifying such factors (never forgetting possible trauma or abuse, which are harder to reveal), empathizing with the pain, and addressing them such as using Problem Solving Treatment for Primary Care (PST-PC) are within primary care skills. PST-PC involves four to six 30-minute sessions over 6-10 weeks during which you can provide perspective, help your patient set realistic goals and solutions to try out for situations that can be changed or coping strategies for emotion-focused unchangeable issues, iteratively check on progress via calls or televisits (the monitoring component), and renew problem-solving efforts as needed.

If mild depression fails to improve over several months or worsens, GLAD-PC describes evidence-based treatments. Even if it remits, your active support and monitoring should continue because depression tends to recur. You may not realize how valuable these seemingly simple active supports are to keeping mild depression in your teen patients at bay.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
References
1. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4081.
2. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4082.
Depression is one of the most common mental health conditions in childhood, especially during socially turbulent adolescence when the brain is rapidly changing and parent-child relationships are strained by the teen’s striving for independence and identity. Often parents of teens call me worrying about possible depression, but in the next breath say “but maybe it is just puberty.” Because suicide is one of the most common causes of death among teens and is often associated with depression, we pediatricians have the scary job of sorting out symptoms and making a plan.
The Guidelines for Adolescent Depression in Primary Care (GLAD-PC)1,2 were revised in 2018 to help. This expert consensus document contains specific and practical guidance for all levels of depression. But for mild depression, GLAD-PC now advises pediatricians in Recommendation II to go beyond “watchful waiting.” It states, “After initial diagnosis,
Although a little vague, mild depression is diagnosed when there are “closer to 5” significant symptoms of depression, with “distressing but manageable” severity and only “mildly impaired” functioning. The most commonly used self-report adolescent depression screen, the Patient Health Questionnaire–Modified–9 (PHQ-9), has a recommended cut score of greater than 10, but 5-9 is considered mild depression symptoms. A clinical interview also is always required.
So what is this “active support” being recommended? After making an assessment of symptoms, severity, and impact – and ruling out significant suicide risk – the task is rather familiar to us from other medical conditions. We need to talk clearly and empathetically with the teen (and parents with consent) about depression and its neurological etiology, ask about contributing stress and genetic factors, and describe the typical course with optimism. This discussion is critical to pushing guilt or blame aside to rally family support. Substance use – (including alcohol) both a cause and attempted coping strategy for depression – must be addressed because it adds to risk for suicide or crashes and because it interacts with medicines.
Perhaps the biggest difference between active support for depression versus that for other conditions is that teens are likely reluctant, hopeless, and/or lacking energy to participate in the plan. The plan, therefore, needs to be approached in smaller steps and build on prior teen strengths, goals, or talents to motivate them and create reward to counteract general lethargy. You may know this teen used to play basketball, or sing at church, or love playing with a baby sister – all activities to try to reawaken. Parents can help recall these and are key to setting up opportunities.
GLAD-PC provides a “Self-Care Success!” worksheet of categories for goal setting for active support. These goals include:
- Stay physically active. Specified days/month, minutes/session, and dates and times.
- Engage spirituality and fun activities. Specify times/week, when, and with whom).
- Eat balanced meals. Specify number/day and names of foods.
- Spend time with people who can support you. Specify number/month, minutes/time, with whom, and doing what.
- Spend time relaxing. Specify days/week, minutes/time, and doing what.
- Determine small goals and simple steps. Establish these for a specified problem.
There is now evidence for these you can share with your teen patients and families.
Exercise
Exercise has a moderate effect size of 0.56 on depression, comparable to medications for mild to moderate depression and a useful adjunct to medications. The national Office of Disease Prevention and Health Promotion recommends that 6- to 17-year-olds get 60 minutes/day of moderate exercise or undertake vigorous “out of breath” exercise three times a week to maintain health. A meta-analysis of studies of yoga for people with depressive symptoms (not necessarily diagnosed depression) found reduced symptoms in 14 of 23 studies.
Pleasure
Advising fun has to include acknowledgment that a depressed teen is not motivated to do formerly fun things and may not get as much/any pleasure from it. You need to explain that “doing precedes feeling.” While what is fun is personal, new findings indicate that 2 hours/week “in nature” lowers stress, boosts mental health, and increases sense of well-being.
Nutrition
The MIND diet (Mediterranean-type diet high in leafy vegetables and berries but low in red meat) has evidence for lower odds of depression and psychological distress. Fatty acid supplements, specifically eicosapentaenoic acid at greater than 800 mg/day (930 mg), is better than placebo (P less than .001) for reducing mild depression within as little as 4 weeks. Natural S-Adenosyl-L-methionine (SAMe) has many studies showing benefit, according to National Center for Complementary and Alternative Medicine, a government-run website. NCCAM notes that St. John’s Wort has evidence for effectiveness equal to prescribed antidepressants for mild depression but with dangerous potential side effects, such as worsening of psychotic symptoms in bipolar disorder or schizophrenia, plus potentially life threatening drug interactions. While safe, valerian and probiotics have no evidence for reducing depression.
Social support
Family is usually the most important support for depressed teens even though they may be pushing family away, may refuse to come on outings, or may even refuse to come out of the bedroom. We should encourage parents and siblings to “hang out,” sitting quietly, available to listen rather than probing, cajoling, or nagging as they may have been doing. Parents also provide support by assuring adherence to visits, goals, and medications. Peer support helps a teen feel less alone and may increase social skills, but it can be difficult to sustain because friends may find depression threatening or give up when the teen avoids them and refuses activities. The National Association for Mental Illness has an online support group (www.strengthofus.org), as well as many excellent family resources. Sometimes medical efforts to be nonsectarian result in failure to recognize and remind teens and families of the value of religion, which is free and universally available, as a source of social support.
Relaxation
An evaluation of 15 studies concluded that relaxation techniques reduced depressive symptoms better than no treatment but not as much cognitive-behavior therapy (CBT). Yoga is another source of relaxation training. Mindfulness includes relaxation and specifies working to stay nonjudgmental about thoughts passing through one’s mind, recognizing and “arguing” with negative thinking, which is also part of CBT. Guided relaxation with a person, audiotape, or app (Calm or Headspace, among others) may be better for depressed teens because it inserts a voice to guide thoughts, which could potentially fend off ruminating on sad things.
Setting goals to address problems
In mild depression, compared with more endogenous moderate to severe major depressive disorder, a specific life stressor or relationship issue may be the precipitant. Identifying such factors (never forgetting possible trauma or abuse, which are harder to reveal), empathizing with the pain, and addressing them such as using Problem Solving Treatment for Primary Care (PST-PC) are within primary care skills. PST-PC involves four to six 30-minute sessions over 6-10 weeks during which you can provide perspective, help your patient set realistic goals and solutions to try out for situations that can be changed or coping strategies for emotion-focused unchangeable issues, iteratively check on progress via calls or televisits (the monitoring component), and renew problem-solving efforts as needed.
If mild depression fails to improve over several months or worsens, GLAD-PC describes evidence-based treatments. Even if it remits, your active support and monitoring should continue because depression tends to recur. You may not realize how valuable these seemingly simple active supports are to keeping mild depression in your teen patients at bay.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
References
1. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4081.
2. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4082.
Depression is one of the most common mental health conditions in childhood, especially during socially turbulent adolescence when the brain is rapidly changing and parent-child relationships are strained by the teen’s striving for independence and identity. Often parents of teens call me worrying about possible depression, but in the next breath say “but maybe it is just puberty.” Because suicide is one of the most common causes of death among teens and is often associated with depression, we pediatricians have the scary job of sorting out symptoms and making a plan.
The Guidelines for Adolescent Depression in Primary Care (GLAD-PC)1,2 were revised in 2018 to help. This expert consensus document contains specific and practical guidance for all levels of depression. But for mild depression, GLAD-PC now advises pediatricians in Recommendation II to go beyond “watchful waiting.” It states, “After initial diagnosis,
Although a little vague, mild depression is diagnosed when there are “closer to 5” significant symptoms of depression, with “distressing but manageable” severity and only “mildly impaired” functioning. The most commonly used self-report adolescent depression screen, the Patient Health Questionnaire–Modified–9 (PHQ-9), has a recommended cut score of greater than 10, but 5-9 is considered mild depression symptoms. A clinical interview also is always required.
So what is this “active support” being recommended? After making an assessment of symptoms, severity, and impact – and ruling out significant suicide risk – the task is rather familiar to us from other medical conditions. We need to talk clearly and empathetically with the teen (and parents with consent) about depression and its neurological etiology, ask about contributing stress and genetic factors, and describe the typical course with optimism. This discussion is critical to pushing guilt or blame aside to rally family support. Substance use – (including alcohol) both a cause and attempted coping strategy for depression – must be addressed because it adds to risk for suicide or crashes and because it interacts with medicines.
Perhaps the biggest difference between active support for depression versus that for other conditions is that teens are likely reluctant, hopeless, and/or lacking energy to participate in the plan. The plan, therefore, needs to be approached in smaller steps and build on prior teen strengths, goals, or talents to motivate them and create reward to counteract general lethargy. You may know this teen used to play basketball, or sing at church, or love playing with a baby sister – all activities to try to reawaken. Parents can help recall these and are key to setting up opportunities.
GLAD-PC provides a “Self-Care Success!” worksheet of categories for goal setting for active support. These goals include:
- Stay physically active. Specified days/month, minutes/session, and dates and times.
- Engage spirituality and fun activities. Specify times/week, when, and with whom).
- Eat balanced meals. Specify number/day and names of foods.
- Spend time with people who can support you. Specify number/month, minutes/time, with whom, and doing what.
- Spend time relaxing. Specify days/week, minutes/time, and doing what.
- Determine small goals and simple steps. Establish these for a specified problem.
There is now evidence for these you can share with your teen patients and families.
Exercise
Exercise has a moderate effect size of 0.56 on depression, comparable to medications for mild to moderate depression and a useful adjunct to medications. The national Office of Disease Prevention and Health Promotion recommends that 6- to 17-year-olds get 60 minutes/day of moderate exercise or undertake vigorous “out of breath” exercise three times a week to maintain health. A meta-analysis of studies of yoga for people with depressive symptoms (not necessarily diagnosed depression) found reduced symptoms in 14 of 23 studies.
Pleasure
Advising fun has to include acknowledgment that a depressed teen is not motivated to do formerly fun things and may not get as much/any pleasure from it. You need to explain that “doing precedes feeling.” While what is fun is personal, new findings indicate that 2 hours/week “in nature” lowers stress, boosts mental health, and increases sense of well-being.
Nutrition
The MIND diet (Mediterranean-type diet high in leafy vegetables and berries but low in red meat) has evidence for lower odds of depression and psychological distress. Fatty acid supplements, specifically eicosapentaenoic acid at greater than 800 mg/day (930 mg), is better than placebo (P less than .001) for reducing mild depression within as little as 4 weeks. Natural S-Adenosyl-L-methionine (SAMe) has many studies showing benefit, according to National Center for Complementary and Alternative Medicine, a government-run website. NCCAM notes that St. John’s Wort has evidence for effectiveness equal to prescribed antidepressants for mild depression but with dangerous potential side effects, such as worsening of psychotic symptoms in bipolar disorder or schizophrenia, plus potentially life threatening drug interactions. While safe, valerian and probiotics have no evidence for reducing depression.
Social support
Family is usually the most important support for depressed teens even though they may be pushing family away, may refuse to come on outings, or may even refuse to come out of the bedroom. We should encourage parents and siblings to “hang out,” sitting quietly, available to listen rather than probing, cajoling, or nagging as they may have been doing. Parents also provide support by assuring adherence to visits, goals, and medications. Peer support helps a teen feel less alone and may increase social skills, but it can be difficult to sustain because friends may find depression threatening or give up when the teen avoids them and refuses activities. The National Association for Mental Illness has an online support group (www.strengthofus.org), as well as many excellent family resources. Sometimes medical efforts to be nonsectarian result in failure to recognize and remind teens and families of the value of religion, which is free and universally available, as a source of social support.
Relaxation
An evaluation of 15 studies concluded that relaxation techniques reduced depressive symptoms better than no treatment but not as much cognitive-behavior therapy (CBT). Yoga is another source of relaxation training. Mindfulness includes relaxation and specifies working to stay nonjudgmental about thoughts passing through one’s mind, recognizing and “arguing” with negative thinking, which is also part of CBT. Guided relaxation with a person, audiotape, or app (Calm or Headspace, among others) may be better for depressed teens because it inserts a voice to guide thoughts, which could potentially fend off ruminating on sad things.
Setting goals to address problems
In mild depression, compared with more endogenous moderate to severe major depressive disorder, a specific life stressor or relationship issue may be the precipitant. Identifying such factors (never forgetting possible trauma or abuse, which are harder to reveal), empathizing with the pain, and addressing them such as using Problem Solving Treatment for Primary Care (PST-PC) are within primary care skills. PST-PC involves four to six 30-minute sessions over 6-10 weeks during which you can provide perspective, help your patient set realistic goals and solutions to try out for situations that can be changed or coping strategies for emotion-focused unchangeable issues, iteratively check on progress via calls or televisits (the monitoring component), and renew problem-solving efforts as needed.
If mild depression fails to improve over several months or worsens, GLAD-PC describes evidence-based treatments. Even if it remits, your active support and monitoring should continue because depression tends to recur. You may not realize how valuable these seemingly simple active supports are to keeping mild depression in your teen patients at bay.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to MDedge News. E-mail her at pdnews@mdedge.com.
References
1. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4081.
2. Pediatrics. 2018 Mar 1. doi: 10.1542/peds.2017-4082.
The right of conscientious objection
This particularly is true for those who consider medicine a vocation, or a calling, rather than just a job.

On May 2, 2019, the Department of Health and Human Services made public a 440-page document known as the Final Conscience Rule.1 It isn’t quite final. And the state of California already is suing to stop it.2 But the document represents the culmination of years of legal wrangling over whether physicians are allowed to have consciences or whether they must function as automatons providing any legally permitted care that a patient might demand. This comprehensive document provides a history of the issues, but was written in dense legalese, as if it expected to be answering challenges in court.
The short answer in the United States is that religious liberty continues to triumph over editorials in the New England Journal of Medicine. Consciences are allowed. The Final Conscience Rule begins with “The United States has a long history of providing protections in health care for individuals and entities on the basis of religious beliefs or moral convictions.” That history includes the Religious Freedom and Restoration Act of 1993.3 RFRA was introduced into the Senate by Sen. Ted Kennedy (D-Mass.), a bastion of liberal health care policies, and passed by a 97-3 vote. It was introduced into the House by then-Rep. Chuck Schumer (D-N.Y.) and passed by a unanimous voice vote. RFRA is not the invention of Republican fundamentalists.
For my colleagues in Canada, the Ontario Court of Appeals (ONCA, the highest provincial court) decided on May 15, 2019, that the opposite situation is the law in Canada. A recent Ontario law concerning medical assistance in dying (also known as physician-assisted suicide) requires Ontario physicians to either provide the assistance when requested or to make an effective referral, defined as “a referral made in good faith, to a non-objecting, available, and accessible physician, other health-care professional, or agency.” Some Canadian physicians objected to this requirement as a violation of their consciences and their Hippocratic Oaths. They lost. The ONCA decision is 74 readable, double-spaced pages and spells out the ethics and legal principles. In summary, the ONCA said the policies on requiring an effective referral “strike a reasonable balance between patients’ interests and physicians’ Charter-protected religious freedom. In short, they are reasonable limits prescribed by law that are demonstrably justified in a free and democratic society.”4
The California physician-assisted dying law, known as the End of Life Option Act, which became effective in 2016, has policies which are very different from the Ontario policies. The California law has clear protections for the consciences of physicians. The law empowers them to avoid being compelled or coerced into cooperating with these deaths. “Participation in activities authorized pursuant to this part shall be voluntary. … A person or entity that elects, for reasons of conscience, morality, or ethics, not to engage in activities authorized pursuant to this part is not required to take any action in support of an individual’s decision under this part.”5 If it seems strange that California would strongly protect conscience with its own statute but challenge the new federal regulations, welcome to tribal politics.

The point is that the role of physicians in abortion, physician aid in dying, and other controversial practices is not going to be decided by philosophical discussions about the ideal scope and purpose of medicine. Compromises are involved that reflect the values of society. Canada is more anticlerical than the United States, and Ontario chose a different path. French culture is even more extreme. Recently, mayors in two towns in France told their elementary schools to stop offering alternative entrées on days when pork was served for hot lunches. Secular schools were not to provide accommodation for students (Muslim and Jewish) who religiously objected to pork. Since the French Revolution, the emphasis is on assimilation and laïcité (France’s principle of secularism in public affairs). The cathedral Notre-Dame de Paris – recently damaged by fire – is owned by the state, not the Catholic Church. The United States has a different history and culture. It has supported religious liberty and reasonable accommodations. That is the loving thing to do. But as a reminder, the Peace of Westphalia in 1648, which ended European religious wars between Protestants and Catholics, was not a result of enlightened thinking and agapeic love. The fighting parties looked in the abyss of mutual annihilation and opted for coexistence instead.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. Department of Health and Human Services, “HHS Announces Final Conscience Rule Protecting Health Care Entities and Individuals,” May 2, 2019.
2. “California sues Trump administration over ‘conscience rule’ that could limit abortions,” Los Angeles Times, May 21, 2019.
3. Wikipedia, “Religious Freedom Restoration Act of 1993”
4. Christian Medical and Dental Society of Canada v. College of Physicians and Surgeons of Ontario, 2019 ONCA 393.
5. California Assembly Bill No. 15, End of Life Option Act.
The article was updated on June 21, 2019.
This particularly is true for those who consider medicine a vocation, or a calling, rather than just a job.
On May 2, 2019, the Department of Health and Human Services made public a 440-page document known as the Final Conscience Rule.1 It isn’t quite final. And the state of California already is suing to stop it.2 But the document represents the culmination of years of legal wrangling over whether physicians are allowed to have consciences or whether they must function as automatons providing any legally permitted care that a patient might demand. This comprehensive document provides a history of the issues, but was written in dense legalese, as if it expected to be answering challenges in court.
The short answer in the United States is that religious liberty continues to triumph over editorials in the New England Journal of Medicine. Consciences are allowed. The Final Conscience Rule begins with “The United States has a long history of providing protections in health care for individuals and entities on the basis of religious beliefs or moral convictions.” That history includes the Religious Freedom and Restoration Act of 1993.3 RFRA was introduced into the Senate by Sen. Ted Kennedy (D-Mass.), a bastion of liberal health care policies, and passed by a 97-3 vote. It was introduced into the House by then-Rep. Chuck Schumer (D-N.Y.) and passed by a unanimous voice vote. RFRA is not the invention of Republican fundamentalists.
For my colleagues in Canada, the Ontario Court of Appeals (ONCA, the highest provincial court) decided on May 15, 2019, that the opposite situation is the law in Canada. A recent Ontario law concerning medical assistance in dying (also known as physician-assisted suicide) requires Ontario physicians to either provide the assistance when requested or to make an effective referral, defined as “a referral made in good faith, to a non-objecting, available, and accessible physician, other health-care professional, or agency.” Some Canadian physicians objected to this requirement as a violation of their consciences and their Hippocratic Oaths. They lost. The ONCA decision is 74 readable, double-spaced pages and spells out the ethics and legal principles. In summary, the ONCA said the policies on requiring an effective referral “strike a reasonable balance between patients’ interests and physicians’ Charter-protected religious freedom. In short, they are reasonable limits prescribed by law that are demonstrably justified in a free and democratic society.”4
The California physician-assisted dying law, known as the End of Life Option Act, which became effective in 2016, has policies which are very different from the Ontario policies. The California law has clear protections for the consciences of physicians. The law empowers them to avoid being compelled or coerced into cooperating with these deaths. “Participation in activities authorized pursuant to this part shall be voluntary. … A person or entity that elects, for reasons of conscience, morality, or ethics, not to engage in activities authorized pursuant to this part is not required to take any action in support of an individual’s decision under this part.”5 If it seems strange that California would strongly protect conscience with its own statute but challenge the new federal regulations, welcome to tribal politics.
The point is that the role of physicians in abortion, physician aid in dying, and other controversial practices is not going to be decided by philosophical discussions about the ideal scope and purpose of medicine. Compromises are involved that reflect the values of society. Canada is more anticlerical than the United States, and Ontario chose a different path. French culture is even more extreme. Recently, mayors in two towns in France told their elementary schools to stop offering alternative entrées on days when pork was served for hot lunches. Secular schools were not to provide accommodation for students (Muslim and Jewish) who religiously objected to pork. Since the French Revolution, the emphasis is on assimilation and laïcité (France’s principle of secularism in public affairs). The cathedral Notre-Dame de Paris – recently damaged by fire – is owned by the state, not the Catholic Church. The United States has a different history and culture. It has supported religious liberty and reasonable accommodations. That is the loving thing to do. But as a reminder, the Peace of Westphalia in 1648, which ended European religious wars between Protestants and Catholics, was not a result of enlightened thinking and agapeic love. The fighting parties looked in the abyss of mutual annihilation and opted for coexistence instead.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. Department of Health and Human Services, “HHS Announces Final Conscience Rule Protecting Health Care Entities and Individuals,” May 2, 2019.
2. “California sues Trump administration over ‘conscience rule’ that could limit abortions,” Los Angeles Times, May 21, 2019.
3. Wikipedia, “Religious Freedom Restoration Act of 1993”
4. Christian Medical and Dental Society of Canada v. College of Physicians and Surgeons of Ontario, 2019 ONCA 393.
5. California Assembly Bill No. 15, End of Life Option Act.
The article was updated on June 21, 2019.
This particularly is true for those who consider medicine a vocation, or a calling, rather than just a job.
On May 2, 2019, the Department of Health and Human Services made public a 440-page document known as the Final Conscience Rule.1 It isn’t quite final. And the state of California already is suing to stop it.2 But the document represents the culmination of years of legal wrangling over whether physicians are allowed to have consciences or whether they must function as automatons providing any legally permitted care that a patient might demand. This comprehensive document provides a history of the issues, but was written in dense legalese, as if it expected to be answering challenges in court.
The short answer in the United States is that religious liberty continues to triumph over editorials in the New England Journal of Medicine. Consciences are allowed. The Final Conscience Rule begins with “The United States has a long history of providing protections in health care for individuals and entities on the basis of religious beliefs or moral convictions.” That history includes the Religious Freedom and Restoration Act of 1993.3 RFRA was introduced into the Senate by Sen. Ted Kennedy (D-Mass.), a bastion of liberal health care policies, and passed by a 97-3 vote. It was introduced into the House by then-Rep. Chuck Schumer (D-N.Y.) and passed by a unanimous voice vote. RFRA is not the invention of Republican fundamentalists.
For my colleagues in Canada, the Ontario Court of Appeals (ONCA, the highest provincial court) decided on May 15, 2019, that the opposite situation is the law in Canada. A recent Ontario law concerning medical assistance in dying (also known as physician-assisted suicide) requires Ontario physicians to either provide the assistance when requested or to make an effective referral, defined as “a referral made in good faith, to a non-objecting, available, and accessible physician, other health-care professional, or agency.” Some Canadian physicians objected to this requirement as a violation of their consciences and their Hippocratic Oaths. They lost. The ONCA decision is 74 readable, double-spaced pages and spells out the ethics and legal principles. In summary, the ONCA said the policies on requiring an effective referral “strike a reasonable balance between patients’ interests and physicians’ Charter-protected religious freedom. In short, they are reasonable limits prescribed by law that are demonstrably justified in a free and democratic society.”4
The California physician-assisted dying law, known as the End of Life Option Act, which became effective in 2016, has policies which are very different from the Ontario policies. The California law has clear protections for the consciences of physicians. The law empowers them to avoid being compelled or coerced into cooperating with these deaths. “Participation in activities authorized pursuant to this part shall be voluntary. … A person or entity that elects, for reasons of conscience, morality, or ethics, not to engage in activities authorized pursuant to this part is not required to take any action in support of an individual’s decision under this part.”5 If it seems strange that California would strongly protect conscience with its own statute but challenge the new federal regulations, welcome to tribal politics.
The point is that the role of physicians in abortion, physician aid in dying, and other controversial practices is not going to be decided by philosophical discussions about the ideal scope and purpose of medicine. Compromises are involved that reflect the values of society. Canada is more anticlerical than the United States, and Ontario chose a different path. French culture is even more extreme. Recently, mayors in two towns in France told their elementary schools to stop offering alternative entrées on days when pork was served for hot lunches. Secular schools were not to provide accommodation for students (Muslim and Jewish) who religiously objected to pork. Since the French Revolution, the emphasis is on assimilation and laïcité (France’s principle of secularism in public affairs). The cathedral Notre-Dame de Paris – recently damaged by fire – is owned by the state, not the Catholic Church. The United States has a different history and culture. It has supported religious liberty and reasonable accommodations. That is the loving thing to do. But as a reminder, the Peace of Westphalia in 1648, which ended European religious wars between Protestants and Catholics, was not a result of enlightened thinking and agapeic love. The fighting parties looked in the abyss of mutual annihilation and opted for coexistence instead.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
References
1. Department of Health and Human Services, “HHS Announces Final Conscience Rule Protecting Health Care Entities and Individuals,” May 2, 2019.
2. “California sues Trump administration over ‘conscience rule’ that could limit abortions,” Los Angeles Times, May 21, 2019.
3. Wikipedia, “Religious Freedom Restoration Act of 1993”
4. Christian Medical and Dental Society of Canada v. College of Physicians and Surgeons of Ontario, 2019 ONCA 393.
5. California Assembly Bill No. 15, End of Life Option Act.
The article was updated on June 21, 2019.