User login
A ‘FRESH’ way to manage trauma
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
Flight, then fight

“Psychological first aid: emergency care for terrorism and disaster survivors” (Current Psychiatry, May 2004) touches on flight, fight, and fright as human reactions to disaster.
Since the Sept. 11, 2001 terrorist attacks, medical professionals have become much more interested in the immediate adverse effects of extreme acute stress and humans’ instinctual response to disaster. “Fight or flight,” a widely used catchphrase, has influenced the understanding and expectations of clinicians and patients for decades.
“Fight or flight,” however, does not reflect the many advances in understanding acute response to stress that have occurred since the phrase was coined in 1929.1 Indeed, as we note in two soon-to-be-published articles,2,3 the phrase is no longer accurate.
Gray described the correct sequence of universal hardwired responses to extreme stress caused by a life-threatening situation.4 Ethologists working with nonhuman primates have clearly established that sequence.
In all mammalian species studied, the urge to flee is the first normative fear response. If fleeing is not an option, the impulse to fight follows. Male and female mammals have demonstrated this response sequence. The belief that man’s first instinct is to fight is probably a misconception.
Thus, “flight or fight” is the proper order of responses. Recognizing this order may help us more effectively treat acute stress in emergency and other clinical settings. Understanding these responses as instinct might also help us ameliorate the guilt that plagues many military veterans who wonder why they fled rather than put up a fight.
H. Stefan Bracha, MD; Tyler C. Ralston, MA; Jennifer M. Matsukawa, MA
Department of Veterans Affairs
Pacific Islands Health Care System
Spark M. Matsunaga Medical Center, Honolulu, HI
Andrew E. Williams, MA
Department of psychology
University of Hawaii at Manoa, Honolulu, HI
Amnona B. Miller, NP
Emergency department
New York-Presbyterian Medical Center
New York, NY
- Cannon WB. Bodily changes in pain, hunger, fear and rage: An account of recent research into the function of emotional excitement (2nd ed). New York: Appleton-Century-Crofts, 1929.
- Bracha HS. Freeze-flight-fight-fright-faint: Adaptationist perspective on the acute stress response spectrum. CNS Spectrums 2004. In press.
- Bracha HS, Williams AE, Ralston TC, et al. “Fight or flight”: Does this 75 year-old term need updating? Psychosomatics 2004. In press.
- Gray JA. The psychology of fear and stress (2nd ed). New York: Cambridge University Press, 1988.
“Psychological first aid: emergency care for terrorism and disaster survivors” (Current Psychiatry, May 2004) touches on flight, fight, and fright as human reactions to disaster.
Since the Sept. 11, 2001 terrorist attacks, medical professionals have become much more interested in the immediate adverse effects of extreme acute stress and humans’ instinctual response to disaster. “Fight or flight,” a widely used catchphrase, has influenced the understanding and expectations of clinicians and patients for decades.
“Fight or flight,” however, does not reflect the many advances in understanding acute response to stress that have occurred since the phrase was coined in 1929.1 Indeed, as we note in two soon-to-be-published articles,2,3 the phrase is no longer accurate.
Gray described the correct sequence of universal hardwired responses to extreme stress caused by a life-threatening situation.4 Ethologists working with nonhuman primates have clearly established that sequence.
In all mammalian species studied, the urge to flee is the first normative fear response. If fleeing is not an option, the impulse to fight follows. Male and female mammals have demonstrated this response sequence. The belief that man’s first instinct is to fight is probably a misconception.
Thus, “flight or fight” is the proper order of responses. Recognizing this order may help us more effectively treat acute stress in emergency and other clinical settings. Understanding these responses as instinct might also help us ameliorate the guilt that plagues many military veterans who wonder why they fled rather than put up a fight.
H. Stefan Bracha, MD; Tyler C. Ralston, MA; Jennifer M. Matsukawa, MA
Department of Veterans Affairs
Pacific Islands Health Care System
Spark M. Matsunaga Medical Center, Honolulu, HI
Andrew E. Williams, MA
Department of psychology
University of Hawaii at Manoa, Honolulu, HI
Amnona B. Miller, NP
Emergency department
New York-Presbyterian Medical Center
New York, NY
- Cannon WB. Bodily changes in pain, hunger, fear and rage: An account of recent research into the function of emotional excitement (2nd ed). New York: Appleton-Century-Crofts, 1929.
- Bracha HS. Freeze-flight-fight-fright-faint: Adaptationist perspective on the acute stress response spectrum. CNS Spectrums 2004. In press.
- Bracha HS, Williams AE, Ralston TC, et al. “Fight or flight”: Does this 75 year-old term need updating? Psychosomatics 2004. In press.
- Gray JA. The psychology of fear and stress (2nd ed). New York: Cambridge University Press, 1988.
“Psychological first aid: emergency care for terrorism and disaster survivors” (Current Psychiatry, May 2004) touches on flight, fight, and fright as human reactions to disaster.
Since the Sept. 11, 2001 terrorist attacks, medical professionals have become much more interested in the immediate adverse effects of extreme acute stress and humans’ instinctual response to disaster. “Fight or flight,” a widely used catchphrase, has influenced the understanding and expectations of clinicians and patients for decades.
“Fight or flight,” however, does not reflect the many advances in understanding acute response to stress that have occurred since the phrase was coined in 1929.1 Indeed, as we note in two soon-to-be-published articles,2,3 the phrase is no longer accurate.
Gray described the correct sequence of universal hardwired responses to extreme stress caused by a life-threatening situation.4 Ethologists working with nonhuman primates have clearly established that sequence.
In all mammalian species studied, the urge to flee is the first normative fear response. If fleeing is not an option, the impulse to fight follows. Male and female mammals have demonstrated this response sequence. The belief that man’s first instinct is to fight is probably a misconception.
Thus, “flight or fight” is the proper order of responses. Recognizing this order may help us more effectively treat acute stress in emergency and other clinical settings. Understanding these responses as instinct might also help us ameliorate the guilt that plagues many military veterans who wonder why they fled rather than put up a fight.
H. Stefan Bracha, MD; Tyler C. Ralston, MA; Jennifer M. Matsukawa, MA
Department of Veterans Affairs
Pacific Islands Health Care System
Spark M. Matsunaga Medical Center, Honolulu, HI
Andrew E. Williams, MA
Department of psychology
University of Hawaii at Manoa, Honolulu, HI
Amnona B. Miller, NP
Emergency department
New York-Presbyterian Medical Center
New York, NY
- Cannon WB. Bodily changes in pain, hunger, fear and rage: An account of recent research into the function of emotional excitement (2nd ed). New York: Appleton-Century-Crofts, 1929.
- Bracha HS. Freeze-flight-fight-fright-faint: Adaptationist perspective on the acute stress response spectrum. CNS Spectrums 2004. In press.
- Bracha HS, Williams AE, Ralston TC, et al. “Fight or flight”: Does this 75 year-old term need updating? Psychosomatics 2004. In press.
- Gray JA. The psychology of fear and stress (2nd ed). New York: Cambridge University Press, 1988.
Posttraumatic stress disorder: Nature and nurture?
Posttraumatic stress disorder (PTSD) can be one of the most frustrating anxiety disorders for both the patient and clinician. Asymptomatic persons become haunted by an experience they can’t forget. Their resulting anxiety can sour what were once healthy relationships or disable someone who previously was productive.
In some cases, despite aggressive psychopharmacology and psychotherapy, the patient remains incapacitated by inappropriate and unremitting fear. The trauma seems to have broken something—changed something inside the brain—that can’t be fixed.
Brain imaging studies of patients with PTSD—combat veterans and women with histories of childhood sexual abuse—have shown smaller hippocampal volumes compared with patients without PTSD.1,2 This finding has led to speculation that stress hormones (glucocorticoids) adversely affect the hippocampus (Figure 1).
This line of reasoning suggests that prolonged stress causes increased production of glucocorticoids that are neurotoxic to the hippocampus, resulting in hippocampal atrophy.3 Studies of rodents and patients with Cushing’s syndrome support this hypothesis. The hippocampus, therefore, may have been irreversibly damaged in patients with severe PTSD.
Figure 1
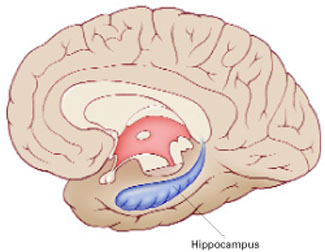
The hippocampus, a specialized type of cortex, is key to memory and emotion. As this medial view shows, it extends along the lateral ventricle floor on each side of the brain.
Illustration for Current Psychiatry by Marcia Hartsock, CMI Hippocampus
Intuitively, this theory makes sense, as the hippocampus is crucial for memory and emotion. However, a recent study of identical twins raises doubts.
Surprising evidence
Gilbertson et al recruited 40 pairs of twins, in which one was a Vietnam combat veteran and the other stayed home.4 Using MRI, the researchers measured hippocampal volume in each twin and assessed the presence and severity of PTSD in the combat-exposed twin.
Consistent with earlier reports, the authors found smaller hippocampal volumes in combat-exposed individuals diagnosed with PTSD. However, they found an almost identical correlation between the noncombat-exposed twin’s hippocampal volume and the combat-exposed twin’s PTSD score (Figure 2). In other words, the twin’s hippocampus size was a better predictor of the veteran’s hippocampus size than was the veteran’s trauma exposure or PTSD symptoms.
This finding puts a new spin on the association between small hippocampal volume and PTSD. The authors stated, “these data indicate that smaller hippocampi in PTSD represents a pre-existing, familial vulnerability factor rather than the neurotoxic product of trauma exposure per se.” Put another way, the small hippocampus is not created by stress and trauma but is a preexisting condition. Further, this study suggests that a larger hippocampus may protect a person from developing PTSD.
This study may help explain why different individuals exposed to the same trauma are frequently left with different symptoms.5,6 PTSD would seem to be an excellent example of the combined effects of nature (small hippocampus) and nurture (traumatic experience).
Figure 2 Hippocampal volume correlates with posttraumatic symptoms
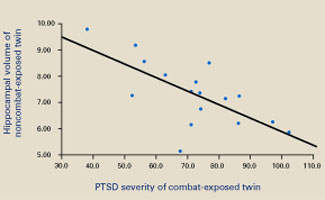
Smaller hippocampal volume in identical twins not exposed to combat was related to more-severe PTSD symptoms in their combat-exposed brothers (P = 0.002). Symptom severity was measured using Clinician-Administered PTSD Scale (CAPS) total scores.
Source: Reprinted with permission from Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nature Neurosci 2002;5:1242-7.
1. Bremner JD, Randall P, Scott TM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152:973-81.
2. Bremner JD, Vythilingam M, Vermetten E, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry 2003;160:924-32.
3. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
4. Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 2002;5:1242-7.
5. Macklin ML, Metzger LJ, Litz BT, et al. Lower precombat intelligence is a risk factor for posttraumatic stress disorder. J Consult Clin Psychol 1998;66:323-6.
6. Schlenger WE, Caddell JM, Ebert L, et al. Psychological reactions to terrorist attacks: findings from the National Study of Americans’ Reactions to September 11. JAMA 2002;288:581-8.
Posttraumatic stress disorder (PTSD) can be one of the most frustrating anxiety disorders for both the patient and clinician. Asymptomatic persons become haunted by an experience they can’t forget. Their resulting anxiety can sour what were once healthy relationships or disable someone who previously was productive.
In some cases, despite aggressive psychopharmacology and psychotherapy, the patient remains incapacitated by inappropriate and unremitting fear. The trauma seems to have broken something—changed something inside the brain—that can’t be fixed.
Brain imaging studies of patients with PTSD—combat veterans and women with histories of childhood sexual abuse—have shown smaller hippocampal volumes compared with patients without PTSD.1,2 This finding has led to speculation that stress hormones (glucocorticoids) adversely affect the hippocampus (Figure 1).
This line of reasoning suggests that prolonged stress causes increased production of glucocorticoids that are neurotoxic to the hippocampus, resulting in hippocampal atrophy.3 Studies of rodents and patients with Cushing’s syndrome support this hypothesis. The hippocampus, therefore, may have been irreversibly damaged in patients with severe PTSD.
Figure 1
The hippocampus, a specialized type of cortex, is key to memory and emotion. As this medial view shows, it extends along the lateral ventricle floor on each side of the brain.
Illustration for Current Psychiatry by Marcia Hartsock, CMI Hippocampus
Intuitively, this theory makes sense, as the hippocampus is crucial for memory and emotion. However, a recent study of identical twins raises doubts.
Surprising evidence
Gilbertson et al recruited 40 pairs of twins, in which one was a Vietnam combat veteran and the other stayed home.4 Using MRI, the researchers measured hippocampal volume in each twin and assessed the presence and severity of PTSD in the combat-exposed twin.
Consistent with earlier reports, the authors found smaller hippocampal volumes in combat-exposed individuals diagnosed with PTSD. However, they found an almost identical correlation between the noncombat-exposed twin’s hippocampal volume and the combat-exposed twin’s PTSD score (Figure 2). In other words, the twin’s hippocampus size was a better predictor of the veteran’s hippocampus size than was the veteran’s trauma exposure or PTSD symptoms.
This finding puts a new spin on the association between small hippocampal volume and PTSD. The authors stated, “these data indicate that smaller hippocampi in PTSD represents a pre-existing, familial vulnerability factor rather than the neurotoxic product of trauma exposure per se.” Put another way, the small hippocampus is not created by stress and trauma but is a preexisting condition. Further, this study suggests that a larger hippocampus may protect a person from developing PTSD.
This study may help explain why different individuals exposed to the same trauma are frequently left with different symptoms.5,6 PTSD would seem to be an excellent example of the combined effects of nature (small hippocampus) and nurture (traumatic experience).
Figure 2 Hippocampal volume correlates with posttraumatic symptoms
Smaller hippocampal volume in identical twins not exposed to combat was related to more-severe PTSD symptoms in their combat-exposed brothers (P = 0.002). Symptom severity was measured using Clinician-Administered PTSD Scale (CAPS) total scores.
Source: Reprinted with permission from Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nature Neurosci 2002;5:1242-7.
Posttraumatic stress disorder (PTSD) can be one of the most frustrating anxiety disorders for both the patient and clinician. Asymptomatic persons become haunted by an experience they can’t forget. Their resulting anxiety can sour what were once healthy relationships or disable someone who previously was productive.
In some cases, despite aggressive psychopharmacology and psychotherapy, the patient remains incapacitated by inappropriate and unremitting fear. The trauma seems to have broken something—changed something inside the brain—that can’t be fixed.
Brain imaging studies of patients with PTSD—combat veterans and women with histories of childhood sexual abuse—have shown smaller hippocampal volumes compared with patients without PTSD.1,2 This finding has led to speculation that stress hormones (glucocorticoids) adversely affect the hippocampus (Figure 1).
This line of reasoning suggests that prolonged stress causes increased production of glucocorticoids that are neurotoxic to the hippocampus, resulting in hippocampal atrophy.3 Studies of rodents and patients with Cushing’s syndrome support this hypothesis. The hippocampus, therefore, may have been irreversibly damaged in patients with severe PTSD.
Figure 1
The hippocampus, a specialized type of cortex, is key to memory and emotion. As this medial view shows, it extends along the lateral ventricle floor on each side of the brain.
Illustration for Current Psychiatry by Marcia Hartsock, CMI Hippocampus
Intuitively, this theory makes sense, as the hippocampus is crucial for memory and emotion. However, a recent study of identical twins raises doubts.
Surprising evidence
Gilbertson et al recruited 40 pairs of twins, in which one was a Vietnam combat veteran and the other stayed home.4 Using MRI, the researchers measured hippocampal volume in each twin and assessed the presence and severity of PTSD in the combat-exposed twin.
Consistent with earlier reports, the authors found smaller hippocampal volumes in combat-exposed individuals diagnosed with PTSD. However, they found an almost identical correlation between the noncombat-exposed twin’s hippocampal volume and the combat-exposed twin’s PTSD score (Figure 2). In other words, the twin’s hippocampus size was a better predictor of the veteran’s hippocampus size than was the veteran’s trauma exposure or PTSD symptoms.
This finding puts a new spin on the association between small hippocampal volume and PTSD. The authors stated, “these data indicate that smaller hippocampi in PTSD represents a pre-existing, familial vulnerability factor rather than the neurotoxic product of trauma exposure per se.” Put another way, the small hippocampus is not created by stress and trauma but is a preexisting condition. Further, this study suggests that a larger hippocampus may protect a person from developing PTSD.
This study may help explain why different individuals exposed to the same trauma are frequently left with different symptoms.5,6 PTSD would seem to be an excellent example of the combined effects of nature (small hippocampus) and nurture (traumatic experience).
Figure 2 Hippocampal volume correlates with posttraumatic symptoms
Smaller hippocampal volume in identical twins not exposed to combat was related to more-severe PTSD symptoms in their combat-exposed brothers (P = 0.002). Symptom severity was measured using Clinician-Administered PTSD Scale (CAPS) total scores.
Source: Reprinted with permission from Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nature Neurosci 2002;5:1242-7.
1. Bremner JD, Randall P, Scott TM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152:973-81.
2. Bremner JD, Vythilingam M, Vermetten E, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry 2003;160:924-32.
3. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
4. Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 2002;5:1242-7.
5. Macklin ML, Metzger LJ, Litz BT, et al. Lower precombat intelligence is a risk factor for posttraumatic stress disorder. J Consult Clin Psychol 1998;66:323-6.
6. Schlenger WE, Caddell JM, Ebert L, et al. Psychological reactions to terrorist attacks: findings from the National Study of Americans’ Reactions to September 11. JAMA 2002;288:581-8.
1. Bremner JD, Randall P, Scott TM, et al. MRI-based measurement of hippocampal volume in patients with combat-related posttraumatic stress disorder. Am J Psychiatry 1995;152:973-81.
2. Bremner JD, Vythilingam M, Vermetten E, et al. MRI and PET study of deficits in hippocampal structure and function in women with childhood sexual abuse and posttraumatic stress disorder. Am J Psychiatry 2003;160:924-32.
3. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
4. Gilbertson MW, Shenton ME, Ciszewski A, et al. Smaller hippocampal volume predicts pathologic vulnerability to psychological trauma. Nat Neurosci 2002;5:1242-7.
5. Macklin ML, Metzger LJ, Litz BT, et al. Lower precombat intelligence is a risk factor for posttraumatic stress disorder. J Consult Clin Psychol 1998;66:323-6.
6. Schlenger WE, Caddell JM, Ebert L, et al. Psychological reactions to terrorist attacks: findings from the National Study of Americans’ Reactions to September 11. JAMA 2002;288:581-8.
Psychological first aid: Emergency care for terrorism and disaster survivors
The night started like any other for Dr. Z. Kids in bed (too late) by 10:30, dog out by 11, fell asleep reading journal by 11:15. Sirens jolt her out of a solid stage 4. Her eyes widen, pulse quickens, mouth dries as she follows the glow of the TV into the living room. On TV, fire frames shots of tearful faces, body bags, and firefighters in protective suits. She catches the announcer’s voice: “…explosion at City Power and Light nuclear facility at 3:10 AM today. Fifty-five are known dead, and thousands are being told to evacuate. The blast’s cause is unknown, but terrorism is suspected.”
As her numbness slowly ebbs, Dr. Z’s questions rise insistently. How can I help the survivors? My patients? My children? What if the media call me? How could I have been better prepared for this?
Disaster shakes us to our human and biological core. More than any other clinical encounter, it reminds us that psychiatrists share the vulnerabilities of those we seek to help. Yet it also reminds us that even simple concepts and interventions can mobilize the healing process.
Are you ready to provide emergency psychiatric care following a disaster in your community—be it a nuclear accident, tornado, airplane crash, or terrorist act? Here is evidence—some counterintuitive—that can help you prepare.
Table 1
‘Psychological first aid’ for disaster survivors
Re-create sense of safety
|
Encourage social support
|
Re-establish sense of efficacy
|
Disaster’s psychobiology
Human reactions to disaster are often conceptualized as the mammalian survival response: flight, fight, and fright (freezing). In most cases, these reactions are adaptive and dissipate after safety is restored. Posttraumatic stress disorder (PTSD) develops in about 5% of natural disaster victims and 33% of mass shooting victims.1
Responses that do go awry appear to be associated with abnormally low cortisol and persistent adrenergic activation, leading to sensitization of the fear response.2 Reminders of trauma or persistent stressors—such as pain, problems with finances or housing, or bereavement—may exacerbate sensitization. On the other hand, preclinical studies suggest that social support3,4 and active coping5 mitigate physiologic stress responses, confirming numerous clinical observations that associate lack of social support and avoidant coping with eventual PTSD development.
Three basics. Just as our emergency medicine colleagues must often revert to life-support basics, we must remind ourselves of biology’s three basics for psychic resilience:
- safety (including—as much as possible—protection from reminders of trauma and ongoing stress)
- meaningful social connection
- re-establishing a sense of efficacy to overcome helplessness (Table 1).
Like the stress response, these protective factors seem hard-wired into our biological make-up. They form the foundation for all phases of disaster psychiatry interventions, from planning to immediate interventions through longterm follow-up.
Disaster planning
As a mental health professional, plan to operate within established disaster plans and agencies, not only for the sake of efficiency but also because structure and support are paramount in disaster situations. Check with the American Psychiatric Association’s local branch to determine if a disaster mental health plan exists. If not, explore how to work directly with local American Red Cross chapters and hospitals, which recruit personnel for the Disaster Medical Assistance Teams mobilized by the public health service.
Table 2
Normal reactions to disaster for adults and children
| All ages | |
| Emotional | Shock, fear, grief, anger, guilt, shame, helplessness, hopelessness, numbness, emptiness Decreased ability to feel interest, pleasure, love |
| Cognitive | Confusion, disorientation, indecisiveness, worry, shortened attention span, poor concentration, memory difficulties, unwanted memories, self-blame |
| Physical | Tension, fatigue, edginess, insomnia, generalized aches and pains, startling easily, rapid heartbeat, nausea, decreased appetite and sex drive |
| Interpersonal | Difficulties being intimate, being over-controlling, feeling rejected or abandoned |
| Children’s age-specific disaster responses | |
| Preschool | Separation fears, regression, fussiness, temper tantrums, somatization Sleep disturbances including nightmares, somnambulism, night terrors |
| School-age | May still have the above, as well as excessive guilt and worries about others’ safety, poor concentration and loss of school performance, repetitious re-telling or play related to trauma |
| Adolescent | Depression, acting out, wish for revenge, sleeping and eating disturbances, altered view of the future |
Immediate disaster mental health plans vary in detail according to local needs and resources but should at least address:
- providing on-site interventions
- disseminating information about responses to trauma
- identifying and publicizing local mental health resources.
Immediate interventions
Immediately following a disaster, psychiatrists are frequently asked to assist with on-site crisis and medical interventions, evaluate survivors with unusual or intense reactions, and provide public education about psychological reactions to disaster.
On-site response. All responders, regardless of discipline, should provide disaster survivors with “psychological first aid,” which is directed at reestablishing safety, connection, and efficacy. Basic crisis intervention principles are useful when support and reassurance are not enough.6
For example, relaxation exercises can reduce anxiety and improve sleep. Use focused, structured relaxation tools—such as progressive muscle relaxation and breathing training—as unstructured exercises can exacerbate dissociation and re-experiencing. Grounding techniques, by which survivors learn to focus all senses on immediate surroundings, often alleviate dissociation and flashbacks.
Care for children. Because children’s reactions to disaster greatly depend on their caregivers’ responses (social referencing), focus acute interventions for children on:
- re-connecting them with their families
- reducing caregivers’ distress
- educating caregivers about providing age appropriate information and support (see Related resources).
Medical care. As physicians, psychiatrists may be called upon to intervene medically. Although it is generally advisable to stay within our usual practice, medical personnel may be in short supply. Fortunately, Good Samaritan laws exist in every state, and the potential for a successful malpractice suit against a physician responding in a disaster is almost zero, unless the physician’s performance is grossly negligent (such as moving the neck of a patient with obvious head or neck injuries).7
Principles regarding informed consent and right to refuse treatment—along with the usual exceptions—apply during disasters.
Evaluating survivors in shelters and hospitals requires knowing the normal and abnormal responses to disaster, being able to differentially diagnose changes in mental status, and understanding risk factors for trauma’s psychiatric sequelae. Aside from PTSD, trauma’s long-term effects include other anxiety disorders, depression, substance abuse, and eating disorders. In addition to the usual components of a psychiatric evaluation, assessments must address event-related factors such as proximity to the disaster, loss of significant others or property, physical injuries, immediate needs, and social support.8
Normal stress reactions. Frequently described as “a normal response to an abnormal situation,” the normal stress reaction is multidimensional and depends on the person’s developmental level (Table 2). About 10% to 25% of survivors experience intense affect and dissociation, whereas a similar number may appear unusually calm.
Interventions beyond the“first aid” described above are not usually needed unless individuals:
- are a danger to themselves or others
- are psychotic
- have no social supports
- cannot perform tasks necessary for self-care and to begin the recovery process.
Always re-assess when there is any question about a survivor’s immediate reaction to trauma.
In DSM-IV-TR’s trauma-related diagnoses, the symptom clusters often do not capture many disaster survivors’ subjective experience: the shattering of fundamental beliefs regarding themselves (invulnerability), the world (predictability, safety), and others (trust, benevolence).9 By empathizing with these responses, you can help survivors feel less isolated and estranged.
Differential diagnosis. Survivors’ mental status changes may be manifestations of the stress response, but they also may represent:
- exacerbations of pre-existing psychiatric or general medical conditions
- hypoxemia, hypovolemia, or CNS trauma from physical injury
- responses to medications used for resuscitation or pain control, such as atropine, epinephrine, lidocaine, or morphine.
Effects of bioterrorism agents must also be considered. For example, organophosphorus compounds such as the nerve agents sarin and soman can cause impaired concentration, depression, and anxiety. Anthrax can cause rapidly progressing meningitis.10 Delirium must be differentiated from dissociation; patients with dissociation can be re-oriented, and changes will resolve with time rather than fluctuate.11
Psychopathology risk factors. Multiple studies have addressed risk factors for post-disaster psychiatric sequelae (usually PTSD). In general, risk increases with repeated trauma exposure (including TV viewing), prior trauma, lack of social support, injury, pre-existing psychiatric problems, traumatic bereavement (having witnessed the violent death of a loved one), avoidant coping, and having strong negative beliefs about the meanings of normal stress reactions such as tearfulness, anxiety, and insomnia.
Because a recent meta-analysis supports these observations,12 follow-up evaluation for signs of PTSD is recommended for:
- survivors with one or more of the risk factors discussed above
- vulnerable groups such as rescue workers, children, and dependent individuals
- survivors whose symptoms persist after 2 months.13
Decompensation immediately after a disaster seems to be the exception for psychiatric patients, despite their longer-term vulnerability. One psychiatrist who in 1989 survived Hurricane Hugo—the most intense storm to strike the Mid-Atlantic region in 100 years—noted that demand for inpatient psychiatric services did not increase in the storm’s aftermath. The only patient calls she received were inquiries about her own physical safety.14
Caregivers and rescue workers—including psychi-atrists—are also disaster survivors, and you need to tend to your needs for safety and support. Consult frequently with colleagues within and outside the disaster area, as much for support as for information and guidance.15 Remember also that rescue workers are occasionally targets for victims’ rage at their circumstances. Anticipating and explaining this displacement reduces its toxicity.
Using medications
Uses psychotropics judiciously in the first 48 hours of trauma. Medication effects may interfere with neurologic assessment of the injured, and monitoring and follow-up may not be possible.
However, drug therapy should start quickly when survivors are acutely psychotic or their behavior endangers themselves, others, or the milieu. Medications usually include a fast-acting benzodiazepine and/or an antipsychotic, as described in guidelines for managing agitation.16 Always provide structure and supervision for medicated patients.
No guidelines exist for using medications to manage distressing—but less-severe—acute stress-related symptoms. Some experts advocate using adrenergic antagonists such as clonidine, guanfacine, and beta blockers to reduce excessive arousal. These drugs have not been adequately studied in this setting, however, and may harm those with cardiovascular instability from preexisting conditions or injuries.
Table 3
Psychoeducation: Simple messages for workers and trauma survivors
| Get adequate rest, food, sleep |
| Avoid exposure to trauma cues, including TV images |
| Seek support from loved ones and peers |
| Talk about events and feelings only if this feels comfortable and helpful |
| Return to normal routine as much as possible |
| Take action to rebuild, but at a reasonable pace |
| Reach out to others who may need assistance |
Get help:
|
Short-term (<1 week) benzodiazepine use for panic symptoms and severe insomnia is acceptable, but longer-term use may increase PTSD risk.17 A selective serotonin reuptake inhibitor may help individuals with pre-existing PTSD or depression, if you can arrange follow-up.
In the aftermath
‘Debriefing.’ Critical incident stress debriefing (CISD) is a structured, one-session group intervention in which survivors’ experiences and emotional reactions are discussed and education and follow-up recommendations are provided. Developed by Mitchell in 1983,18 CISD was widely used until systematic evaluations revealed that it did not alleviate psychological distress or prevent PTSD.19
Table 4
How to interact with news media during and after a disaster
| For organizations Identify a spokesperson with media experience beforehand Ensure that the spokesperson is well-informed about all aspects of the disaster |
| For spokespersons |
Always
|
Never
|
Thus, although survivor meetings may provide information, education, screening, and support, avoid detailed discussions of events and emotions. Any meetings should be conducted by mental health clinicians and should not be mandatory. Reserve the term “debriefing” for operational reviews by rescue personnel.20
Public education. Educate survivors, rescue workers, health care providers, teachers, and relief agency workers. Provide concise, simple messages as suggested in Table 3. News media provide our most effective means of reaching out to survivors, which is why having a pre-existing relationship is so important. Some guidelines for working with the media are presented in Table 4.
Outreach. Numerous educational resources are available for survivors and their caregivers (see Related resources). Other potentially useful outreach tools include:
- meetings with teachers’ organizations
- continuing medical education activities for primary care providers
- telephone hot lines.
Legal and ethical issues
Disaster scenes are chaotic and informal, and professionals must be flexible, often providing general support and information rather than specific clinical interventions. However, it is important in each encounter to decide whether a patient-physician relationship has begun.
As a general rule, a physician-patient relationship is established whenever diagnosis or treatment is discussed. Once that happens, briefly document:
- signs and symptoms
- working diagnosis
- suicide or violence potential
- treatment and/or follow-up plans.
Confidentiality may be difficult to preserve in chaotic situations involving workers from many agencies. Even in disasters, however, you must obtain permission before sharing information unless the individual’s situation is emergent.
Table 5
Keys to effective disaster psychiatry
Be prepared
|
Care for survivors
|
Care for yourself
|
Long-term interventions
Longer-term disaster interventions include continued outreach and education and needed follow-up services. Existing structures may provide effective follow-up, but additional resources are often needed.
Federal programs. Following a presidentialdeclared disaster, the Federal Emergency Management Agency (FEMA) provides funding for crisis counseling. Programs are typically funded for 9 to 15 months and administered through the emergency services and disaster relief branch of the Substance Abuse and Mental Health Services Administration (SAMHSA) and community mental health organizations. Examples include Project Heartland following the 1995 Oklahoma City federal building bombing and Project COPE following California’s 1989 Loma Prieta earthquake.
Cognitive-behavioral therapy. For adult survivors with acute stress disorder, specific cognitive-behavioral therapy (CBT) provided by trained therapists may prevent PTSD and other trauma sequelae, such as depression.21 CBT interventions may begin as early as 2 weeks after trauma and focus sequentially on anxiety management, cognitive restructuring, imaginal exposure followed by in vivo exposure, and relapse prevention.
Three controlled trials found 6-month PTSD rates of 14% to 20% among acute stress disorder patients treated with CBT, compared with 58% to 67% with supportive counseling.22-24 Although studies of interventions immediately following trauma are lacking, trauma-focused CBT is also recommended for children.25 Evidence-based treatments for PTSD are discussed in detail elsewhere.26
Not unprepared after all
With some reflection, Dr. Z realized she had the tools to help her community. Her feelings of helplessness receded as she envisioned how she could help survivors understand their experiences, re-create a sense of safety, restore important connections to loved ones, and begin to rebuild their lives (Table 5).
For clinicians
- Young BH, Ford JD, Ruzek JI, et al. Disaster mental health: a guidebook for clinicians and administrators. Washington, DC: National Center for Post-Traumatic Stress Disorder, 1998. http://ncptsd.org/publications/disaster/index.html
- Hillman JL. Crisis intervention and trauma: new approaches to evidence-based practice. New York: Kluwer Academic/Plenum Publishers, 2002.
- Office of the Surgeon General Web site on medical aspects of nuclear, biological, and chemical warfare. http://www.nbc-med.org
For survivors and clinicians
- National Center for Post-Traumatic Stress Disorder. Disaster mental health: Dealing with the aftereffects of terrorism. http://www.ncptsd.org/terrorism/index.html
- Substance Abuse and Mental Health Services Administration. Emergency mental health and traumatic stress. http://www.mentalhealth.org/cmhs/EmergencyServices/default.asp
- American Academy of Child and Adolescent Psychiatry. Talking to children about terrorism and war. http://www.aacap.org/publications/factsFam/87.htm
Drug brand names
- Clonidine • Catapres
- Guanfacine • Tenex
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Effects of traumatic stress in a disaster situation. Washington, DC: National Center for Post-Traumatic Stress Disorder. Department of Veterans Affairs, September 12, 2001 (Accessed March 31, 2004 at http://www.ncptsd.org/facts/disasters/fs_effects_disaster.html).
2. Yehuda R, McFarlane AC, Shalev AY. Predicting the development of post-traumatic stress disorder from the acute response to a traumatic event. Biol Psychiatry 1998;44:1305-13.
3. Levine S, Lyons DM, Schatzberg AF. Psychobiological consequences of social relationships. Ann NY Acad Sci 1997;807:210-18.
4. Uchino BN, Garvey TS. The availability of social support reduces cardiovascular reactivity to acute psychological stress. J Behav Med 1997;20:15-27.
5. LeDoux JE, Gorman JM. A call to action: overcoming anxiety through active coping. Am J Psychiatry 2001;158:1953-5.
6. Hillman JL. Crisis intervention and trauma: new approaches to evidence-based practice. New York: Kluwer Academic/Plenum Publishers, 2002.
7. Daniels G. Good Samaritan acts. Emerg Med Clin North Am 1999;17:491-504.
8. Mental-health intervention for disasters. Washington, DC: National Center for Post-Traumatic Stress Disorder, Department of Veterans Affairs, Sept. 12, 2001. (Accessed March 31, 2004 at http://www.ncptsd.org/facts/disasters/fs_treatment_disaster.html.)
9. Difede J, Apfeldorf WJ, Cloitre M, et al. Acute psychiatric responses to the explosion at the World Trade Center: a case series. J Nerv Ment Dis 1997;185:519-22.
10. DiGiovanni C. Domestic terrorism with chemical or biological agents: psychiatric aspects. Am J Psychiatry 1999;156:1500-5.
11. Rundle JR. Psychiatric issues in medical-surgical disaster casualties: consultation-liaison approach. Psychiatr Q 2000;71:245-58.
12. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for post-traumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000;68:748-66.
13. Mental health and mass violence: evidence-based early psychological intervention for victims/survivors of mass violence. Washington, DC: National Institute of Mental Health, Nov. 1, 2002 (Accessed Oct. 29, 2003 at http://www.nimh.nih.gov/research/massviolence.pdf.)
14. Austin LS. Organizing a disaster response program in one’s home community. In: Austin LS (ed). Responding to disaster: a guide for mental health professionals. Washington, DC: American Psychiatric Publishing, 1992;53-68.
15. Rousseau AW. Notes from Oklahoma City’s recovery. In: Hall RCW, Norwood AE (eds). Disaster psychiatry handbook. Washington, DC: American Psychiatric Association Committee on Psychiatric Dimensions of Disaster, undated:3-11. (Accessed Oct. 29, 2003 at http://www.psych.org/disasterpsych/pdfs/apadisasterhandbk.pdf.)
16. Yildiz A, Sachs GS, Turgay A. Pharmacological management of agitation in emergency settings. Emerg Med J 2003;20:339-46.
17. Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry 1996;57:390-4.
18. Mitchell JT. When disaster strikes. J Em Med Serv 1983;8:36-9.
19. Rose S, Bisson J, Wessely S. Psychological debriefing for preventing posttraumatic stress disorder (PTSD). Cochrane Database Syst Rev 2002;(2):CD000560.-
20. Black J. Forming the libidinal cocoon: the Dallas airplane crashes, the Guadalupe river drownings, and Hurricane Hugo in the Virgin Islands. In: Austin LS (ed). Responding to disaster: a guide for mental health professionals. Washington DC: American Psychiatric Publishing, 1992;169:84.-
21. Ehlers A, Clark DM. Early psychological interventions for adult survivors of trauma: a review. Biol Psychiatry 2003;53:817-26.
22. Bryant RA, Moulds M, Guthrie R, Nixon RD. Treating acute stress disorder following mild traumatic brain injury. Am J Psychiatry 2003;160:585-7.
23. Bryant RA, Sackville T, Dang ST, et al. Treating acute stress disorder: an evaluation of cognitive behavior therapy and supportive counseling techniques. Am J Psychiatry 1999;156:1780-6.
24. Bryant RA, Harvey AG, Dang ST, et al. Treatment of acute stress disorder: a comparison of cognitive-behavioral therapy and supportive counseling. J Consult Clin Psychol 1998;66:862-6.
25. Cohen JA. Treating acute posttraumatic reactions in children and adolescents. Biol Psychiatry 2003;53:827-33.
26. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD. New York: Guilford Press, 2000.
The night started like any other for Dr. Z. Kids in bed (too late) by 10:30, dog out by 11, fell asleep reading journal by 11:15. Sirens jolt her out of a solid stage 4. Her eyes widen, pulse quickens, mouth dries as she follows the glow of the TV into the living room. On TV, fire frames shots of tearful faces, body bags, and firefighters in protective suits. She catches the announcer’s voice: “…explosion at City Power and Light nuclear facility at 3:10 AM today. Fifty-five are known dead, and thousands are being told to evacuate. The blast’s cause is unknown, but terrorism is suspected.”
As her numbness slowly ebbs, Dr. Z’s questions rise insistently. How can I help the survivors? My patients? My children? What if the media call me? How could I have been better prepared for this?
Disaster shakes us to our human and biological core. More than any other clinical encounter, it reminds us that psychiatrists share the vulnerabilities of those we seek to help. Yet it also reminds us that even simple concepts and interventions can mobilize the healing process.
Are you ready to provide emergency psychiatric care following a disaster in your community—be it a nuclear accident, tornado, airplane crash, or terrorist act? Here is evidence—some counterintuitive—that can help you prepare.
Table 1
‘Psychological first aid’ for disaster survivors
Re-create sense of safety
|
Encourage social support
|
Re-establish sense of efficacy
|
Disaster’s psychobiology
Human reactions to disaster are often conceptualized as the mammalian survival response: flight, fight, and fright (freezing). In most cases, these reactions are adaptive and dissipate after safety is restored. Posttraumatic stress disorder (PTSD) develops in about 5% of natural disaster victims and 33% of mass shooting victims.1
Responses that do go awry appear to be associated with abnormally low cortisol and persistent adrenergic activation, leading to sensitization of the fear response.2 Reminders of trauma or persistent stressors—such as pain, problems with finances or housing, or bereavement—may exacerbate sensitization. On the other hand, preclinical studies suggest that social support3,4 and active coping5 mitigate physiologic stress responses, confirming numerous clinical observations that associate lack of social support and avoidant coping with eventual PTSD development.
Three basics. Just as our emergency medicine colleagues must often revert to life-support basics, we must remind ourselves of biology’s three basics for psychic resilience:
- safety (including—as much as possible—protection from reminders of trauma and ongoing stress)
- meaningful social connection
- re-establishing a sense of efficacy to overcome helplessness (Table 1).
Like the stress response, these protective factors seem hard-wired into our biological make-up. They form the foundation for all phases of disaster psychiatry interventions, from planning to immediate interventions through longterm follow-up.
Disaster planning
As a mental health professional, plan to operate within established disaster plans and agencies, not only for the sake of efficiency but also because structure and support are paramount in disaster situations. Check with the American Psychiatric Association’s local branch to determine if a disaster mental health plan exists. If not, explore how to work directly with local American Red Cross chapters and hospitals, which recruit personnel for the Disaster Medical Assistance Teams mobilized by the public health service.
Table 2
Normal reactions to disaster for adults and children
| All ages | |
| Emotional | Shock, fear, grief, anger, guilt, shame, helplessness, hopelessness, numbness, emptiness Decreased ability to feel interest, pleasure, love |
| Cognitive | Confusion, disorientation, indecisiveness, worry, shortened attention span, poor concentration, memory difficulties, unwanted memories, self-blame |
| Physical | Tension, fatigue, edginess, insomnia, generalized aches and pains, startling easily, rapid heartbeat, nausea, decreased appetite and sex drive |
| Interpersonal | Difficulties being intimate, being over-controlling, feeling rejected or abandoned |
| Children’s age-specific disaster responses | |
| Preschool | Separation fears, regression, fussiness, temper tantrums, somatization Sleep disturbances including nightmares, somnambulism, night terrors |
| School-age | May still have the above, as well as excessive guilt and worries about others’ safety, poor concentration and loss of school performance, repetitious re-telling or play related to trauma |
| Adolescent | Depression, acting out, wish for revenge, sleeping and eating disturbances, altered view of the future |
Immediate disaster mental health plans vary in detail according to local needs and resources but should at least address:
- providing on-site interventions
- disseminating information about responses to trauma
- identifying and publicizing local mental health resources.
Immediate interventions
Immediately following a disaster, psychiatrists are frequently asked to assist with on-site crisis and medical interventions, evaluate survivors with unusual or intense reactions, and provide public education about psychological reactions to disaster.
On-site response. All responders, regardless of discipline, should provide disaster survivors with “psychological first aid,” which is directed at reestablishing safety, connection, and efficacy. Basic crisis intervention principles are useful when support and reassurance are not enough.6
For example, relaxation exercises can reduce anxiety and improve sleep. Use focused, structured relaxation tools—such as progressive muscle relaxation and breathing training—as unstructured exercises can exacerbate dissociation and re-experiencing. Grounding techniques, by which survivors learn to focus all senses on immediate surroundings, often alleviate dissociation and flashbacks.
Care for children. Because children’s reactions to disaster greatly depend on their caregivers’ responses (social referencing), focus acute interventions for children on:
- re-connecting them with their families
- reducing caregivers’ distress
- educating caregivers about providing age appropriate information and support (see Related resources).
Medical care. As physicians, psychiatrists may be called upon to intervene medically. Although it is generally advisable to stay within our usual practice, medical personnel may be in short supply. Fortunately, Good Samaritan laws exist in every state, and the potential for a successful malpractice suit against a physician responding in a disaster is almost zero, unless the physician’s performance is grossly negligent (such as moving the neck of a patient with obvious head or neck injuries).7
Principles regarding informed consent and right to refuse treatment—along with the usual exceptions—apply during disasters.
Evaluating survivors in shelters and hospitals requires knowing the normal and abnormal responses to disaster, being able to differentially diagnose changes in mental status, and understanding risk factors for trauma’s psychiatric sequelae. Aside from PTSD, trauma’s long-term effects include other anxiety disorders, depression, substance abuse, and eating disorders. In addition to the usual components of a psychiatric evaluation, assessments must address event-related factors such as proximity to the disaster, loss of significant others or property, physical injuries, immediate needs, and social support.8
Normal stress reactions. Frequently described as “a normal response to an abnormal situation,” the normal stress reaction is multidimensional and depends on the person’s developmental level (Table 2). About 10% to 25% of survivors experience intense affect and dissociation, whereas a similar number may appear unusually calm.
Interventions beyond the“first aid” described above are not usually needed unless individuals:
- are a danger to themselves or others
- are psychotic
- have no social supports
- cannot perform tasks necessary for self-care and to begin the recovery process.
Always re-assess when there is any question about a survivor’s immediate reaction to trauma.
In DSM-IV-TR’s trauma-related diagnoses, the symptom clusters often do not capture many disaster survivors’ subjective experience: the shattering of fundamental beliefs regarding themselves (invulnerability), the world (predictability, safety), and others (trust, benevolence).9 By empathizing with these responses, you can help survivors feel less isolated and estranged.
Differential diagnosis. Survivors’ mental status changes may be manifestations of the stress response, but they also may represent:
- exacerbations of pre-existing psychiatric or general medical conditions
- hypoxemia, hypovolemia, or CNS trauma from physical injury
- responses to medications used for resuscitation or pain control, such as atropine, epinephrine, lidocaine, or morphine.
Effects of bioterrorism agents must also be considered. For example, organophosphorus compounds such as the nerve agents sarin and soman can cause impaired concentration, depression, and anxiety. Anthrax can cause rapidly progressing meningitis.10 Delirium must be differentiated from dissociation; patients with dissociation can be re-oriented, and changes will resolve with time rather than fluctuate.11
Psychopathology risk factors. Multiple studies have addressed risk factors for post-disaster psychiatric sequelae (usually PTSD). In general, risk increases with repeated trauma exposure (including TV viewing), prior trauma, lack of social support, injury, pre-existing psychiatric problems, traumatic bereavement (having witnessed the violent death of a loved one), avoidant coping, and having strong negative beliefs about the meanings of normal stress reactions such as tearfulness, anxiety, and insomnia.
Because a recent meta-analysis supports these observations,12 follow-up evaluation for signs of PTSD is recommended for:
- survivors with one or more of the risk factors discussed above
- vulnerable groups such as rescue workers, children, and dependent individuals
- survivors whose symptoms persist after 2 months.13
Decompensation immediately after a disaster seems to be the exception for psychiatric patients, despite their longer-term vulnerability. One psychiatrist who in 1989 survived Hurricane Hugo—the most intense storm to strike the Mid-Atlantic region in 100 years—noted that demand for inpatient psychiatric services did not increase in the storm’s aftermath. The only patient calls she received were inquiries about her own physical safety.14
Caregivers and rescue workers—including psychi-atrists—are also disaster survivors, and you need to tend to your needs for safety and support. Consult frequently with colleagues within and outside the disaster area, as much for support as for information and guidance.15 Remember also that rescue workers are occasionally targets for victims’ rage at their circumstances. Anticipating and explaining this displacement reduces its toxicity.
Using medications
Uses psychotropics judiciously in the first 48 hours of trauma. Medication effects may interfere with neurologic assessment of the injured, and monitoring and follow-up may not be possible.
However, drug therapy should start quickly when survivors are acutely psychotic or their behavior endangers themselves, others, or the milieu. Medications usually include a fast-acting benzodiazepine and/or an antipsychotic, as described in guidelines for managing agitation.16 Always provide structure and supervision for medicated patients.
No guidelines exist for using medications to manage distressing—but less-severe—acute stress-related symptoms. Some experts advocate using adrenergic antagonists such as clonidine, guanfacine, and beta blockers to reduce excessive arousal. These drugs have not been adequately studied in this setting, however, and may harm those with cardiovascular instability from preexisting conditions or injuries.
Table 3
Psychoeducation: Simple messages for workers and trauma survivors
| Get adequate rest, food, sleep |
| Avoid exposure to trauma cues, including TV images |
| Seek support from loved ones and peers |
| Talk about events and feelings only if this feels comfortable and helpful |
| Return to normal routine as much as possible |
| Take action to rebuild, but at a reasonable pace |
| Reach out to others who may need assistance |
Get help:
|
Short-term (<1 week) benzodiazepine use for panic symptoms and severe insomnia is acceptable, but longer-term use may increase PTSD risk.17 A selective serotonin reuptake inhibitor may help individuals with pre-existing PTSD or depression, if you can arrange follow-up.
In the aftermath
‘Debriefing.’ Critical incident stress debriefing (CISD) is a structured, one-session group intervention in which survivors’ experiences and emotional reactions are discussed and education and follow-up recommendations are provided. Developed by Mitchell in 1983,18 CISD was widely used until systematic evaluations revealed that it did not alleviate psychological distress or prevent PTSD.19
Table 4
How to interact with news media during and after a disaster
| For organizations Identify a spokesperson with media experience beforehand Ensure that the spokesperson is well-informed about all aspects of the disaster |
| For spokespersons |
Always
|
Never
|
Thus, although survivor meetings may provide information, education, screening, and support, avoid detailed discussions of events and emotions. Any meetings should be conducted by mental health clinicians and should not be mandatory. Reserve the term “debriefing” for operational reviews by rescue personnel.20
Public education. Educate survivors, rescue workers, health care providers, teachers, and relief agency workers. Provide concise, simple messages as suggested in Table 3. News media provide our most effective means of reaching out to survivors, which is why having a pre-existing relationship is so important. Some guidelines for working with the media are presented in Table 4.
Outreach. Numerous educational resources are available for survivors and their caregivers (see Related resources). Other potentially useful outreach tools include:
- meetings with teachers’ organizations
- continuing medical education activities for primary care providers
- telephone hot lines.
Legal and ethical issues
Disaster scenes are chaotic and informal, and professionals must be flexible, often providing general support and information rather than specific clinical interventions. However, it is important in each encounter to decide whether a patient-physician relationship has begun.
As a general rule, a physician-patient relationship is established whenever diagnosis or treatment is discussed. Once that happens, briefly document:
- signs and symptoms
- working diagnosis
- suicide or violence potential
- treatment and/or follow-up plans.
Confidentiality may be difficult to preserve in chaotic situations involving workers from many agencies. Even in disasters, however, you must obtain permission before sharing information unless the individual’s situation is emergent.
Table 5
Keys to effective disaster psychiatry
Be prepared
|
Care for survivors
|
Care for yourself
|
Long-term interventions
Longer-term disaster interventions include continued outreach and education and needed follow-up services. Existing structures may provide effective follow-up, but additional resources are often needed.
Federal programs. Following a presidentialdeclared disaster, the Federal Emergency Management Agency (FEMA) provides funding for crisis counseling. Programs are typically funded for 9 to 15 months and administered through the emergency services and disaster relief branch of the Substance Abuse and Mental Health Services Administration (SAMHSA) and community mental health organizations. Examples include Project Heartland following the 1995 Oklahoma City federal building bombing and Project COPE following California’s 1989 Loma Prieta earthquake.
Cognitive-behavioral therapy. For adult survivors with acute stress disorder, specific cognitive-behavioral therapy (CBT) provided by trained therapists may prevent PTSD and other trauma sequelae, such as depression.21 CBT interventions may begin as early as 2 weeks after trauma and focus sequentially on anxiety management, cognitive restructuring, imaginal exposure followed by in vivo exposure, and relapse prevention.
Three controlled trials found 6-month PTSD rates of 14% to 20% among acute stress disorder patients treated with CBT, compared with 58% to 67% with supportive counseling.22-24 Although studies of interventions immediately following trauma are lacking, trauma-focused CBT is also recommended for children.25 Evidence-based treatments for PTSD are discussed in detail elsewhere.26
Not unprepared after all
With some reflection, Dr. Z realized she had the tools to help her community. Her feelings of helplessness receded as she envisioned how she could help survivors understand their experiences, re-create a sense of safety, restore important connections to loved ones, and begin to rebuild their lives (Table 5).
For clinicians
- Young BH, Ford JD, Ruzek JI, et al. Disaster mental health: a guidebook for clinicians and administrators. Washington, DC: National Center for Post-Traumatic Stress Disorder, 1998. http://ncptsd.org/publications/disaster/index.html
- Hillman JL. Crisis intervention and trauma: new approaches to evidence-based practice. New York: Kluwer Academic/Plenum Publishers, 2002.
- Office of the Surgeon General Web site on medical aspects of nuclear, biological, and chemical warfare. http://www.nbc-med.org
For survivors and clinicians
- National Center for Post-Traumatic Stress Disorder. Disaster mental health: Dealing with the aftereffects of terrorism. http://www.ncptsd.org/terrorism/index.html
- Substance Abuse and Mental Health Services Administration. Emergency mental health and traumatic stress. http://www.mentalhealth.org/cmhs/EmergencyServices/default.asp
- American Academy of Child and Adolescent Psychiatry. Talking to children about terrorism and war. http://www.aacap.org/publications/factsFam/87.htm
Drug brand names
- Clonidine • Catapres
- Guanfacine • Tenex
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
The night started like any other for Dr. Z. Kids in bed (too late) by 10:30, dog out by 11, fell asleep reading journal by 11:15. Sirens jolt her out of a solid stage 4. Her eyes widen, pulse quickens, mouth dries as she follows the glow of the TV into the living room. On TV, fire frames shots of tearful faces, body bags, and firefighters in protective suits. She catches the announcer’s voice: “…explosion at City Power and Light nuclear facility at 3:10 AM today. Fifty-five are known dead, and thousands are being told to evacuate. The blast’s cause is unknown, but terrorism is suspected.”
As her numbness slowly ebbs, Dr. Z’s questions rise insistently. How can I help the survivors? My patients? My children? What if the media call me? How could I have been better prepared for this?
Disaster shakes us to our human and biological core. More than any other clinical encounter, it reminds us that psychiatrists share the vulnerabilities of those we seek to help. Yet it also reminds us that even simple concepts and interventions can mobilize the healing process.
Are you ready to provide emergency psychiatric care following a disaster in your community—be it a nuclear accident, tornado, airplane crash, or terrorist act? Here is evidence—some counterintuitive—that can help you prepare.
Table 1
‘Psychological first aid’ for disaster survivors
Re-create sense of safety
|
Encourage social support
|
Re-establish sense of efficacy
|
Disaster’s psychobiology
Human reactions to disaster are often conceptualized as the mammalian survival response: flight, fight, and fright (freezing). In most cases, these reactions are adaptive and dissipate after safety is restored. Posttraumatic stress disorder (PTSD) develops in about 5% of natural disaster victims and 33% of mass shooting victims.1
Responses that do go awry appear to be associated with abnormally low cortisol and persistent adrenergic activation, leading to sensitization of the fear response.2 Reminders of trauma or persistent stressors—such as pain, problems with finances or housing, or bereavement—may exacerbate sensitization. On the other hand, preclinical studies suggest that social support3,4 and active coping5 mitigate physiologic stress responses, confirming numerous clinical observations that associate lack of social support and avoidant coping with eventual PTSD development.
Three basics. Just as our emergency medicine colleagues must often revert to life-support basics, we must remind ourselves of biology’s three basics for psychic resilience:
- safety (including—as much as possible—protection from reminders of trauma and ongoing stress)
- meaningful social connection
- re-establishing a sense of efficacy to overcome helplessness (Table 1).
Like the stress response, these protective factors seem hard-wired into our biological make-up. They form the foundation for all phases of disaster psychiatry interventions, from planning to immediate interventions through longterm follow-up.
Disaster planning
As a mental health professional, plan to operate within established disaster plans and agencies, not only for the sake of efficiency but also because structure and support are paramount in disaster situations. Check with the American Psychiatric Association’s local branch to determine if a disaster mental health plan exists. If not, explore how to work directly with local American Red Cross chapters and hospitals, which recruit personnel for the Disaster Medical Assistance Teams mobilized by the public health service.
Table 2
Normal reactions to disaster for adults and children
| All ages | |
| Emotional | Shock, fear, grief, anger, guilt, shame, helplessness, hopelessness, numbness, emptiness Decreased ability to feel interest, pleasure, love |
| Cognitive | Confusion, disorientation, indecisiveness, worry, shortened attention span, poor concentration, memory difficulties, unwanted memories, self-blame |
| Physical | Tension, fatigue, edginess, insomnia, generalized aches and pains, startling easily, rapid heartbeat, nausea, decreased appetite and sex drive |
| Interpersonal | Difficulties being intimate, being over-controlling, feeling rejected or abandoned |
| Children’s age-specific disaster responses | |
| Preschool | Separation fears, regression, fussiness, temper tantrums, somatization Sleep disturbances including nightmares, somnambulism, night terrors |
| School-age | May still have the above, as well as excessive guilt and worries about others’ safety, poor concentration and loss of school performance, repetitious re-telling or play related to trauma |
| Adolescent | Depression, acting out, wish for revenge, sleeping and eating disturbances, altered view of the future |
Immediate disaster mental health plans vary in detail according to local needs and resources but should at least address:
- providing on-site interventions
- disseminating information about responses to trauma
- identifying and publicizing local mental health resources.
Immediate interventions
Immediately following a disaster, psychiatrists are frequently asked to assist with on-site crisis and medical interventions, evaluate survivors with unusual or intense reactions, and provide public education about psychological reactions to disaster.
On-site response. All responders, regardless of discipline, should provide disaster survivors with “psychological first aid,” which is directed at reestablishing safety, connection, and efficacy. Basic crisis intervention principles are useful when support and reassurance are not enough.6
For example, relaxation exercises can reduce anxiety and improve sleep. Use focused, structured relaxation tools—such as progressive muscle relaxation and breathing training—as unstructured exercises can exacerbate dissociation and re-experiencing. Grounding techniques, by which survivors learn to focus all senses on immediate surroundings, often alleviate dissociation and flashbacks.
Care for children. Because children’s reactions to disaster greatly depend on their caregivers’ responses (social referencing), focus acute interventions for children on:
- re-connecting them with their families
- reducing caregivers’ distress
- educating caregivers about providing age appropriate information and support (see Related resources).
Medical care. As physicians, psychiatrists may be called upon to intervene medically. Although it is generally advisable to stay within our usual practice, medical personnel may be in short supply. Fortunately, Good Samaritan laws exist in every state, and the potential for a successful malpractice suit against a physician responding in a disaster is almost zero, unless the physician’s performance is grossly negligent (such as moving the neck of a patient with obvious head or neck injuries).7
Principles regarding informed consent and right to refuse treatment—along with the usual exceptions—apply during disasters.
Evaluating survivors in shelters and hospitals requires knowing the normal and abnormal responses to disaster, being able to differentially diagnose changes in mental status, and understanding risk factors for trauma’s psychiatric sequelae. Aside from PTSD, trauma’s long-term effects include other anxiety disorders, depression, substance abuse, and eating disorders. In addition to the usual components of a psychiatric evaluation, assessments must address event-related factors such as proximity to the disaster, loss of significant others or property, physical injuries, immediate needs, and social support.8
Normal stress reactions. Frequently described as “a normal response to an abnormal situation,” the normal stress reaction is multidimensional and depends on the person’s developmental level (Table 2). About 10% to 25% of survivors experience intense affect and dissociation, whereas a similar number may appear unusually calm.
Interventions beyond the“first aid” described above are not usually needed unless individuals:
- are a danger to themselves or others
- are psychotic
- have no social supports
- cannot perform tasks necessary for self-care and to begin the recovery process.
Always re-assess when there is any question about a survivor’s immediate reaction to trauma.
In DSM-IV-TR’s trauma-related diagnoses, the symptom clusters often do not capture many disaster survivors’ subjective experience: the shattering of fundamental beliefs regarding themselves (invulnerability), the world (predictability, safety), and others (trust, benevolence).9 By empathizing with these responses, you can help survivors feel less isolated and estranged.
Differential diagnosis. Survivors’ mental status changes may be manifestations of the stress response, but they also may represent:
- exacerbations of pre-existing psychiatric or general medical conditions
- hypoxemia, hypovolemia, or CNS trauma from physical injury
- responses to medications used for resuscitation or pain control, such as atropine, epinephrine, lidocaine, or morphine.
Effects of bioterrorism agents must also be considered. For example, organophosphorus compounds such as the nerve agents sarin and soman can cause impaired concentration, depression, and anxiety. Anthrax can cause rapidly progressing meningitis.10 Delirium must be differentiated from dissociation; patients with dissociation can be re-oriented, and changes will resolve with time rather than fluctuate.11
Psychopathology risk factors. Multiple studies have addressed risk factors for post-disaster psychiatric sequelae (usually PTSD). In general, risk increases with repeated trauma exposure (including TV viewing), prior trauma, lack of social support, injury, pre-existing psychiatric problems, traumatic bereavement (having witnessed the violent death of a loved one), avoidant coping, and having strong negative beliefs about the meanings of normal stress reactions such as tearfulness, anxiety, and insomnia.
Because a recent meta-analysis supports these observations,12 follow-up evaluation for signs of PTSD is recommended for:
- survivors with one or more of the risk factors discussed above
- vulnerable groups such as rescue workers, children, and dependent individuals
- survivors whose symptoms persist after 2 months.13
Decompensation immediately after a disaster seems to be the exception for psychiatric patients, despite their longer-term vulnerability. One psychiatrist who in 1989 survived Hurricane Hugo—the most intense storm to strike the Mid-Atlantic region in 100 years—noted that demand for inpatient psychiatric services did not increase in the storm’s aftermath. The only patient calls she received were inquiries about her own physical safety.14
Caregivers and rescue workers—including psychi-atrists—are also disaster survivors, and you need to tend to your needs for safety and support. Consult frequently with colleagues within and outside the disaster area, as much for support as for information and guidance.15 Remember also that rescue workers are occasionally targets for victims’ rage at their circumstances. Anticipating and explaining this displacement reduces its toxicity.
Using medications
Uses psychotropics judiciously in the first 48 hours of trauma. Medication effects may interfere with neurologic assessment of the injured, and monitoring and follow-up may not be possible.
However, drug therapy should start quickly when survivors are acutely psychotic or their behavior endangers themselves, others, or the milieu. Medications usually include a fast-acting benzodiazepine and/or an antipsychotic, as described in guidelines for managing agitation.16 Always provide structure and supervision for medicated patients.
No guidelines exist for using medications to manage distressing—but less-severe—acute stress-related symptoms. Some experts advocate using adrenergic antagonists such as clonidine, guanfacine, and beta blockers to reduce excessive arousal. These drugs have not been adequately studied in this setting, however, and may harm those with cardiovascular instability from preexisting conditions or injuries.
Table 3
Psychoeducation: Simple messages for workers and trauma survivors
| Get adequate rest, food, sleep |
| Avoid exposure to trauma cues, including TV images |
| Seek support from loved ones and peers |
| Talk about events and feelings only if this feels comfortable and helpful |
| Return to normal routine as much as possible |
| Take action to rebuild, but at a reasonable pace |
| Reach out to others who may need assistance |
Get help:
|
Short-term (<1 week) benzodiazepine use for panic symptoms and severe insomnia is acceptable, but longer-term use may increase PTSD risk.17 A selective serotonin reuptake inhibitor may help individuals with pre-existing PTSD or depression, if you can arrange follow-up.
In the aftermath
‘Debriefing.’ Critical incident stress debriefing (CISD) is a structured, one-session group intervention in which survivors’ experiences and emotional reactions are discussed and education and follow-up recommendations are provided. Developed by Mitchell in 1983,18 CISD was widely used until systematic evaluations revealed that it did not alleviate psychological distress or prevent PTSD.19
Table 4
How to interact with news media during and after a disaster
| For organizations Identify a spokesperson with media experience beforehand Ensure that the spokesperson is well-informed about all aspects of the disaster |
| For spokespersons |
Always
|
Never
|
Thus, although survivor meetings may provide information, education, screening, and support, avoid detailed discussions of events and emotions. Any meetings should be conducted by mental health clinicians and should not be mandatory. Reserve the term “debriefing” for operational reviews by rescue personnel.20
Public education. Educate survivors, rescue workers, health care providers, teachers, and relief agency workers. Provide concise, simple messages as suggested in Table 3. News media provide our most effective means of reaching out to survivors, which is why having a pre-existing relationship is so important. Some guidelines for working with the media are presented in Table 4.
Outreach. Numerous educational resources are available for survivors and their caregivers (see Related resources). Other potentially useful outreach tools include:
- meetings with teachers’ organizations
- continuing medical education activities for primary care providers
- telephone hot lines.
Legal and ethical issues
Disaster scenes are chaotic and informal, and professionals must be flexible, often providing general support and information rather than specific clinical interventions. However, it is important in each encounter to decide whether a patient-physician relationship has begun.
As a general rule, a physician-patient relationship is established whenever diagnosis or treatment is discussed. Once that happens, briefly document:
- signs and symptoms
- working diagnosis
- suicide or violence potential
- treatment and/or follow-up plans.
Confidentiality may be difficult to preserve in chaotic situations involving workers from many agencies. Even in disasters, however, you must obtain permission before sharing information unless the individual’s situation is emergent.
Table 5
Keys to effective disaster psychiatry
Be prepared
|
Care for survivors
|
Care for yourself
|
Long-term interventions
Longer-term disaster interventions include continued outreach and education and needed follow-up services. Existing structures may provide effective follow-up, but additional resources are often needed.
Federal programs. Following a presidentialdeclared disaster, the Federal Emergency Management Agency (FEMA) provides funding for crisis counseling. Programs are typically funded for 9 to 15 months and administered through the emergency services and disaster relief branch of the Substance Abuse and Mental Health Services Administration (SAMHSA) and community mental health organizations. Examples include Project Heartland following the 1995 Oklahoma City federal building bombing and Project COPE following California’s 1989 Loma Prieta earthquake.
Cognitive-behavioral therapy. For adult survivors with acute stress disorder, specific cognitive-behavioral therapy (CBT) provided by trained therapists may prevent PTSD and other trauma sequelae, such as depression.21 CBT interventions may begin as early as 2 weeks after trauma and focus sequentially on anxiety management, cognitive restructuring, imaginal exposure followed by in vivo exposure, and relapse prevention.
Three controlled trials found 6-month PTSD rates of 14% to 20% among acute stress disorder patients treated with CBT, compared with 58% to 67% with supportive counseling.22-24 Although studies of interventions immediately following trauma are lacking, trauma-focused CBT is also recommended for children.25 Evidence-based treatments for PTSD are discussed in detail elsewhere.26
Not unprepared after all
With some reflection, Dr. Z realized she had the tools to help her community. Her feelings of helplessness receded as she envisioned how she could help survivors understand their experiences, re-create a sense of safety, restore important connections to loved ones, and begin to rebuild their lives (Table 5).
For clinicians
- Young BH, Ford JD, Ruzek JI, et al. Disaster mental health: a guidebook for clinicians and administrators. Washington, DC: National Center for Post-Traumatic Stress Disorder, 1998. http://ncptsd.org/publications/disaster/index.html
- Hillman JL. Crisis intervention and trauma: new approaches to evidence-based practice. New York: Kluwer Academic/Plenum Publishers, 2002.
- Office of the Surgeon General Web site on medical aspects of nuclear, biological, and chemical warfare. http://www.nbc-med.org
For survivors and clinicians
- National Center for Post-Traumatic Stress Disorder. Disaster mental health: Dealing with the aftereffects of terrorism. http://www.ncptsd.org/terrorism/index.html
- Substance Abuse and Mental Health Services Administration. Emergency mental health and traumatic stress. http://www.mentalhealth.org/cmhs/EmergencyServices/default.asp
- American Academy of Child and Adolescent Psychiatry. Talking to children about terrorism and war. http://www.aacap.org/publications/factsFam/87.htm
Drug brand names
- Clonidine • Catapres
- Guanfacine • Tenex
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Effects of traumatic stress in a disaster situation. Washington, DC: National Center for Post-Traumatic Stress Disorder. Department of Veterans Affairs, September 12, 2001 (Accessed March 31, 2004 at http://www.ncptsd.org/facts/disasters/fs_effects_disaster.html).
2. Yehuda R, McFarlane AC, Shalev AY. Predicting the development of post-traumatic stress disorder from the acute response to a traumatic event. Biol Psychiatry 1998;44:1305-13.
3. Levine S, Lyons DM, Schatzberg AF. Psychobiological consequences of social relationships. Ann NY Acad Sci 1997;807:210-18.
4. Uchino BN, Garvey TS. The availability of social support reduces cardiovascular reactivity to acute psychological stress. J Behav Med 1997;20:15-27.
5. LeDoux JE, Gorman JM. A call to action: overcoming anxiety through active coping. Am J Psychiatry 2001;158:1953-5.
6. Hillman JL. Crisis intervention and trauma: new approaches to evidence-based practice. New York: Kluwer Academic/Plenum Publishers, 2002.
7. Daniels G. Good Samaritan acts. Emerg Med Clin North Am 1999;17:491-504.
8. Mental-health intervention for disasters. Washington, DC: National Center for Post-Traumatic Stress Disorder, Department of Veterans Affairs, Sept. 12, 2001. (Accessed March 31, 2004 at http://www.ncptsd.org/facts/disasters/fs_treatment_disaster.html.)
9. Difede J, Apfeldorf WJ, Cloitre M, et al. Acute psychiatric responses to the explosion at the World Trade Center: a case series. J Nerv Ment Dis 1997;185:519-22.
10. DiGiovanni C. Domestic terrorism with chemical or biological agents: psychiatric aspects. Am J Psychiatry 1999;156:1500-5.
11. Rundle JR. Psychiatric issues in medical-surgical disaster casualties: consultation-liaison approach. Psychiatr Q 2000;71:245-58.
12. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for post-traumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000;68:748-66.
13. Mental health and mass violence: evidence-based early psychological intervention for victims/survivors of mass violence. Washington, DC: National Institute of Mental Health, Nov. 1, 2002 (Accessed Oct. 29, 2003 at http://www.nimh.nih.gov/research/massviolence.pdf.)
14. Austin LS. Organizing a disaster response program in one’s home community. In: Austin LS (ed). Responding to disaster: a guide for mental health professionals. Washington, DC: American Psychiatric Publishing, 1992;53-68.
15. Rousseau AW. Notes from Oklahoma City’s recovery. In: Hall RCW, Norwood AE (eds). Disaster psychiatry handbook. Washington, DC: American Psychiatric Association Committee on Psychiatric Dimensions of Disaster, undated:3-11. (Accessed Oct. 29, 2003 at http://www.psych.org/disasterpsych/pdfs/apadisasterhandbk.pdf.)
16. Yildiz A, Sachs GS, Turgay A. Pharmacological management of agitation in emergency settings. Emerg Med J 2003;20:339-46.
17. Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry 1996;57:390-4.
18. Mitchell JT. When disaster strikes. J Em Med Serv 1983;8:36-9.
19. Rose S, Bisson J, Wessely S. Psychological debriefing for preventing posttraumatic stress disorder (PTSD). Cochrane Database Syst Rev 2002;(2):CD000560.-
20. Black J. Forming the libidinal cocoon: the Dallas airplane crashes, the Guadalupe river drownings, and Hurricane Hugo in the Virgin Islands. In: Austin LS (ed). Responding to disaster: a guide for mental health professionals. Washington DC: American Psychiatric Publishing, 1992;169:84.-
21. Ehlers A, Clark DM. Early psychological interventions for adult survivors of trauma: a review. Biol Psychiatry 2003;53:817-26.
22. Bryant RA, Moulds M, Guthrie R, Nixon RD. Treating acute stress disorder following mild traumatic brain injury. Am J Psychiatry 2003;160:585-7.
23. Bryant RA, Sackville T, Dang ST, et al. Treating acute stress disorder: an evaluation of cognitive behavior therapy and supportive counseling techniques. Am J Psychiatry 1999;156:1780-6.
24. Bryant RA, Harvey AG, Dang ST, et al. Treatment of acute stress disorder: a comparison of cognitive-behavioral therapy and supportive counseling. J Consult Clin Psychol 1998;66:862-6.
25. Cohen JA. Treating acute posttraumatic reactions in children and adolescents. Biol Psychiatry 2003;53:827-33.
26. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD. New York: Guilford Press, 2000.
1. Effects of traumatic stress in a disaster situation. Washington, DC: National Center for Post-Traumatic Stress Disorder. Department of Veterans Affairs, September 12, 2001 (Accessed March 31, 2004 at http://www.ncptsd.org/facts/disasters/fs_effects_disaster.html).
2. Yehuda R, McFarlane AC, Shalev AY. Predicting the development of post-traumatic stress disorder from the acute response to a traumatic event. Biol Psychiatry 1998;44:1305-13.
3. Levine S, Lyons DM, Schatzberg AF. Psychobiological consequences of social relationships. Ann NY Acad Sci 1997;807:210-18.
4. Uchino BN, Garvey TS. The availability of social support reduces cardiovascular reactivity to acute psychological stress. J Behav Med 1997;20:15-27.
5. LeDoux JE, Gorman JM. A call to action: overcoming anxiety through active coping. Am J Psychiatry 2001;158:1953-5.
6. Hillman JL. Crisis intervention and trauma: new approaches to evidence-based practice. New York: Kluwer Academic/Plenum Publishers, 2002.
7. Daniels G. Good Samaritan acts. Emerg Med Clin North Am 1999;17:491-504.
8. Mental-health intervention for disasters. Washington, DC: National Center for Post-Traumatic Stress Disorder, Department of Veterans Affairs, Sept. 12, 2001. (Accessed March 31, 2004 at http://www.ncptsd.org/facts/disasters/fs_treatment_disaster.html.)
9. Difede J, Apfeldorf WJ, Cloitre M, et al. Acute psychiatric responses to the explosion at the World Trade Center: a case series. J Nerv Ment Dis 1997;185:519-22.
10. DiGiovanni C. Domestic terrorism with chemical or biological agents: psychiatric aspects. Am J Psychiatry 1999;156:1500-5.
11. Rundle JR. Psychiatric issues in medical-surgical disaster casualties: consultation-liaison approach. Psychiatr Q 2000;71:245-58.
12. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk factors for post-traumatic stress disorder in trauma-exposed adults. J Consult Clin Psychol 2000;68:748-66.
13. Mental health and mass violence: evidence-based early psychological intervention for victims/survivors of mass violence. Washington, DC: National Institute of Mental Health, Nov. 1, 2002 (Accessed Oct. 29, 2003 at http://www.nimh.nih.gov/research/massviolence.pdf.)
14. Austin LS. Organizing a disaster response program in one’s home community. In: Austin LS (ed). Responding to disaster: a guide for mental health professionals. Washington, DC: American Psychiatric Publishing, 1992;53-68.
15. Rousseau AW. Notes from Oklahoma City’s recovery. In: Hall RCW, Norwood AE (eds). Disaster psychiatry handbook. Washington, DC: American Psychiatric Association Committee on Psychiatric Dimensions of Disaster, undated:3-11. (Accessed Oct. 29, 2003 at http://www.psych.org/disasterpsych/pdfs/apadisasterhandbk.pdf.)
16. Yildiz A, Sachs GS, Turgay A. Pharmacological management of agitation in emergency settings. Emerg Med J 2003;20:339-46.
17. Gelpin E, Bonne O, Peri T, et al. Treatment of recent trauma survivors with benzodiazepines: a prospective study. J Clin Psychiatry 1996;57:390-4.
18. Mitchell JT. When disaster strikes. J Em Med Serv 1983;8:36-9.
19. Rose S, Bisson J, Wessely S. Psychological debriefing for preventing posttraumatic stress disorder (PTSD). Cochrane Database Syst Rev 2002;(2):CD000560.-
20. Black J. Forming the libidinal cocoon: the Dallas airplane crashes, the Guadalupe river drownings, and Hurricane Hugo in the Virgin Islands. In: Austin LS (ed). Responding to disaster: a guide for mental health professionals. Washington DC: American Psychiatric Publishing, 1992;169:84.-
21. Ehlers A, Clark DM. Early psychological interventions for adult survivors of trauma: a review. Biol Psychiatry 2003;53:817-26.
22. Bryant RA, Moulds M, Guthrie R, Nixon RD. Treating acute stress disorder following mild traumatic brain injury. Am J Psychiatry 2003;160:585-7.
23. Bryant RA, Sackville T, Dang ST, et al. Treating acute stress disorder: an evaluation of cognitive behavior therapy and supportive counseling techniques. Am J Psychiatry 1999;156:1780-6.
24. Bryant RA, Harvey AG, Dang ST, et al. Treatment of acute stress disorder: a comparison of cognitive-behavioral therapy and supportive counseling. J Consult Clin Psychol 1998;66:862-6.
25. Cohen JA. Treating acute posttraumatic reactions in children and adolescents. Biol Psychiatry 2003;53:827-33.
26. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD. New York: Guilford Press, 2000.
Are We Treating PTSD with Debridement and Lavage?
House Hearing Reassesses VA PTSD Programs
Posttraumatic Stress Disorder: A Sign of Weakness or of Strength?
Regression, depression, and the facts of life
HISTORY: New school, old problems
Mr. E, age 13, was diagnosed with Down syndrome at birth and has mild mental retardation and bilateral sensorineural hearing loss. His pediatrician referred him to our child and adolescent psychiatry clinic for regressed behavior, depression, and apparent psychotic symptoms. He was also having problems sleeping and had begun puberty 8 months earlier.
Five months before referral, Mr. E had graduated from a small elementary school, where he was fully mainstreamed, to a large junior high school, where he spent most of the school day in a functional skills class. About that time, Mr. E began exhibiting nocturnal and daytime enuresis, loss of previously mastered skills, intolerance of novelty and change, and separation difficulty. Although toilet trained at age 7, he started having “accidents” at home, school, and elsewhere. He was reluctant to dress himself, and he resisted going to school.
The youth also talked to himself often and appeared to respond to internal stimuli. He “relived” conversations aloud, described imaginary friends to family and teachers, and spoke to a stuffed dog called Goofy. He would sit and stare into space for up to a half-hour, appearing preoccupied. Family members said he had exhibited these behaviors in grade school but until now appeared to have “outgrown” them.
Once sociable, Mr. E had become increasingly moody, negativistic, and isolative. He spent hours alone in his room. His mother, with whom he was close, reported that he was often angry with her for no apparent reason.
With puberty, his mother noted, Mr. E had begun kissing other developmentally disabled children. He also masturbated, but at his parents’ urging he restricted this activity to his room.
On evaluation, Mr. E was pleasant and outgoing. He had the facial dysmorphia and stature typical of Down syndrome. He smiled often and interacted well, and he attended and adapted to transitions in conversation and activities. His speech was dysarthric (with hyperglossia) and telegraphic; he could speak only four- to five-word sentences.
Was Mr. E exhibiting an adjustment reaction, depression, or a normal developmental response to puberty? Do his psychotic symptoms signal onset of schizophrenia?
Dr. Krassner’s and Kraus’ observations
Because Down syndrome is the most common genetic cause of mental retardation—seen in approximately 1 in 1,000 live births1—pediatricians and child psychiatrists see this disorder fairly frequently.
Regression, a form of coping exhibited by many children, is extremely common in youths with Down syndrome2 and often has a definite—though sometimes unclear—precipitant. We felt Mr. E’s move from a highly responsive, familiar school environment to a far less responsive one that accentuated his differences contributed to many of his symptoms.
Psychosis is less common in Down syndrome than in other developmental disabilities.2 Schizophrenia may occur, but diagnosis is complicated by cognition impairments, test-taking skills, and—in Mr. E’s case—inability to describe disordered thoughts or hallucinations due to poor language skills.3
Self-talk is common in Down syndrome and might be mistaken for psychosis. Note that despite his chronologic age, Mr. E is developmentally a 6-year-old, and self-talk and imaginary friends are considered normal behaviors for a child that age. What’s more, the stress of changing schools may have further compromised his developmental skills.
The FDA’s recent advisory about reports of increased suicidality in youths taking selective serotonin reuptake inhibitors (SSRIs) and other antidepressants for major depressive disorder during clinical trials has raised questions about using these agents in children and adolescents. Until more data become available, however, SSRIs remain the preferred drug therapy for pediatric depression.
- Based on our experience, we recommend citalopram, escitalopram, fluoxetine, and sertraline as first-line medications for pediatric depression because their side effects are relatively benign. The reported link between increased risk of suicidal ideation and behavior and use of paroxetine in pediatric patients has not been clearly established, so we cannot extrapolate that possible risk to other SSRIs.
- Newer antidepressants should be considered with caution in pediatric patients. Bupropion is contraindicated in patients with a history of seizures, bulimia, or anorexia. Mirtazapine is extremely sedating, with side effects such as weight gain and, in rare cases, agranulocytosis. Nefazodone comes with a “black box” warning for risk of liver toxicity. Trazodone is also sedating and carries a risk of priapism in boys.
- Older antidepressants, such as tricyclics, require extreme caution before prescribing to children and adolescents. Tricyclics, with their cardiac side effects, are not recommended for patients with Down syndrome, many of whom have cardiac pathology.
By contrast, depression is fairly common in Down syndrome, although it is much less prevalent in children than in adults with the developmental disorder.2
Finally, children with Down syndrome often enter puberty early, but without the cognitive or emotional maturity or knowledge to deal with the physiologic changes of adolescence.3 Parents often are reluctant to recognize their developmentally disabled child’s sexuality or are uncomfortable providing sexuality education.4 Mr. E’s parents clearly were unconvinced that his sexual behavior was normal for an adolescent.
TREATMENT Antidepressants lead to improvement
We felt Mr. E regressed secondary to emotional stress caused by switching schools. We viewed his psychotic symptoms as part of an adjustment disorder and attributed most of his other symptoms to depression. We anticipated Mr. E’s psychotic symptoms would remit spontaneously and focused on treating his mood and sleep disturbances.
We prescribed sertraline liquid suspension, 10 mg/d titrated across 3 weeks to 40 mg/d. We based our medication choice on clinical experience, mindful of a recent FDA advisory about the use of antidepressants in pediatric patients (Box 1). Also, the liquid suspension is easier to titrate than the tablet form, and we feared Mr. E might have trouble swallowing a tablet.
Mr. E’s mood and sociability improved after 3 to 4 weeks. Within 6 weeks, he regained some of his previously mastered daily activities. We added zolpidem, 10 mg nightly, to address his sleeping difficulties but discontinued the agent after 2 weeks, when his sleep patterns normalized.
At 2, 4, and 6 weeks, Mr. E was pleasant and cooperative, his thinking less concrete, and his speech more intelligible. His parents reported he was happier and more involved with family activities. At his mother’s request, sertraline was changed to 37.5 mg/d in tablet form. The patient remained stable for another month, during which his self-talk, though decreased, continued.
Two weeks later, Mr. E’s mother reported that, during a routine dermatologic examination for a chronic, presacral rash, the dermatologist noticed strategic shaving on the boy’s thighs, calves, and scrotum. Strategic shaving has been reported among sexually active youths as a means of purportedly increasing their sexual pleasure.
The dermatologist then told Mr. E’s mother that her son likely was sexually molested. Based on the boy’s differential rates of pubic hair growth, the doctor suspected that the molestation was chronic, dating back at least 3 months and probably continuing until the week before the examination. Upon hearing this, Mr. E’s parents were stunned and angry.
What behavioral signs might have suggested sexual abuse? How do the dermatologist’s findings alter diagnosis and treatment?
Dr. Krassner’s and Kraus’ observations
Given the dermatologist’s findings, Mr. E’s parents asked us whether their son’s presenting psychiatric symptoms were manifestations of posttraumatic stress disorder (PTSD).
Until now, explaining Mr. E’s symptoms as a reaction to changing schools seemed plausible. His symptoms were improving with treatment, and his sexual behaviors and interest in sexual topics were physiologically normal for his chronologic age. Despite his earlier pubertal experimentations, nothing in his psychosocial history indicated risk for sexual abuse or exploitation.
Still, children with Down syndrome are at higher risk for sexual exploitation than other children,4 so the possibility should have been explored with the parents. Psychiatrists should watch for physical signs of sexual abuse in these patients during the first examination (Box 2).4
But how is sexual abuse defined in this case? Deficient language skills prevented Mr. E from describing what happened to him, so determining whether he initiated sexual relations and with whom is nearly impossible. The act clearly could be considered abuse if Mr. E had been with an adult or older child—even if Mr. E consented. However, if Mr. E had initiated contact with another mentally retarded child, then cause, blame, and semantics become unclear. Either way, the incident could have caused PTSD.5
Diagnosing PTSD in non- or semi-verbal or retarded children is extremely difficult.6,7 Unlike adults with PTSD, pre-verbal children might not have recurrent, distressing recollections of the trauma, but symbolic displacement may characterize repetitive play, during which themes are expressed.8
Scheeringa et al have recommended PTSD criteria for preschool children, including:
- social withdrawal
- extreme temper tantrums
- loss of developmental skills
- new separation anxiety
- new onset of aggression
- new fears without obvious links to the trauma.5,6
Treating PTSD in children with developmental disabilities is also difficult. Modalities applicable to adults or mainstream children—such as psychodynamic psychotherapy, cognitive-behavioral therapy (CBT), exposure therapy, and medications—often do not help developmentally disabled children. For example, Mr. E lacks the cognitive apparatus to respond to CBT.
On the other hand, behavioral therapy, reducing risk factors, minimizing dissociative triggers, and educating patients, parents, friends, and teachers about PTSD can help patients such as Mr. E.5 Attempting to provide structure and maintain routines is a cornerstone of any intervention.
- Aggression
- Anxiety
- Behavior, learning problems at school
- Depression
- Heightened somatic concerns
- Sexualized behavior
- Sleep disturbance
- Withdrawal
FURTHER TREATMENT A family in turmoil
We addressed Mr. E’s symptoms as PTSD-related, though his poor language skills kept us from identifying a trauma. Based on data regarding pediatric PTSD treatment,9 we increased sertraline to 50 mg/d and then to 75 mg/d across 2 weeks.
However, an intense legal investigation brought on by the parents, combined with ensuing tumult within the family, worsened Mr. E’s symptoms. His self-talk became more pronounced and his isolative behavior reappeared, suggesting that the intrusive, repetitive questioning caused him to re-experience the trauma.
We again increased sertraline, to 100 mg/d, and offered supportive therapy to Mr. E. We tried to educate his parents about understanding his symptoms and managing his behavior and strongly recommended that they undergo crisis therapy to keep their reactions and emotions from hurting Mr. E. The parents declined, however, and alleged that we did not adequately support their pursuit of a diagnosis or legal action, which for them had become synonymous with treatment.
Mr. E’s mother brought her son to a psychologist, who engaged him in play therapy. She followed her son around, noting everything he said. All the while, she failed to resolve her guilt and anger. When we explained to her that these actions were hurting Mr. E’s progress, she terminated therapy.
How would you have tried to keep Mr. E’s family in therapy?
Dr. Krassner’s and Kraus’ observations
Treating psychopathology in children carries the risk of strained relations with the patient’s family. The risk increases exponentially for developmentally disabled children, as they have little or no input and their parents are exquisitely sensitive to their needs. Further, the revelation that the parents might have somehow failed to avert or anticipate danger to the child complicates their emotional response.
Although the child is the patient, the parent is the consumer. Failure to gain or keep the parents’ confidence will hinder or destroy therapy.
We might have protected our working relationship with Mr. E’s parents by recognizing how fragile they were and how intensely they would react to any constructive criticism. Paradoxically, for the short-term we could have tolerated their detrimental behaviors toward Mr. E (such as repeated questioning) in the hopes of protecting a long-term relationship. Spending more time exploring the guilt, anger, and confusion that tormented Mr. E’s parents—particularly his mother—also might have helped.
Related resources
- Ryan RM. Recognition of psychosis in persons who do not use spoken communication. In: Ancill RJ, Holliday S, Higenbottam J (eds). Schizophrenia: exploring the spectrum of psychosis. New York: John Wiley & Sons, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zolpidem • Ambien
1. Pueschel S. Children with Down syndrome. In: Levine M, Carey W, Crocker A, Gross R (eds). Developmental-behavioral pediatrics. Philadelphia: WB Saunders, 1983.
2. Hodapp RM. Down syndrome: developmental, psychiatric, and management issues. Child Adolesc Psychiatr Clin North Am 1996;5:881-94.
3. Feinstein C, Reiss AL. Psychiatric disorder in mentally retarded children and adolescents. Child Adolesc Psychiatr Clin North Am 1996;5:827-52.
4. Wilgosh L. Sexual abuse of children with disabilities: intervention and treatment issues for parents. Developmental Disabil Bull. Available at: http://www.ualberta.ca/~jpdasddc/bulletin/articles/wilgosh1993.html. Accessed Nov. 10, 2003.
5. Ryan RM. Posttraumatic stress disorder in persons with developmental disabilities. Community Health J 1994;30:45-54.
6. Scheeringa MS, Seanah CH, Myers L, Putnam FW. New findings on alternative criteria for PTSD in preschool children. J Am Acad Child Adolesc Psychiatry 2003;42:561-70.
7. Diagnostic and Statistical Manual of Mental Disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
8. Lonigan CJ, Phillips BM, Richey JA. Posttraumatic stress disorder in children: diagnosis, assessment, and associated features. Child Adolesc Psychiatr Clin North Am 2003;12:171-94.
9. Donnelly CL. Pharmacological treatment approaches for children and adolescents with posttraumatic stress disorder. Child Adolesc Psychiatr Clin North Am 2003;12:251-69.
HISTORY: New school, old problems
Mr. E, age 13, was diagnosed with Down syndrome at birth and has mild mental retardation and bilateral sensorineural hearing loss. His pediatrician referred him to our child and adolescent psychiatry clinic for regressed behavior, depression, and apparent psychotic symptoms. He was also having problems sleeping and had begun puberty 8 months earlier.
Five months before referral, Mr. E had graduated from a small elementary school, where he was fully mainstreamed, to a large junior high school, where he spent most of the school day in a functional skills class. About that time, Mr. E began exhibiting nocturnal and daytime enuresis, loss of previously mastered skills, intolerance of novelty and change, and separation difficulty. Although toilet trained at age 7, he started having “accidents” at home, school, and elsewhere. He was reluctant to dress himself, and he resisted going to school.
The youth also talked to himself often and appeared to respond to internal stimuli. He “relived” conversations aloud, described imaginary friends to family and teachers, and spoke to a stuffed dog called Goofy. He would sit and stare into space for up to a half-hour, appearing preoccupied. Family members said he had exhibited these behaviors in grade school but until now appeared to have “outgrown” them.
Once sociable, Mr. E had become increasingly moody, negativistic, and isolative. He spent hours alone in his room. His mother, with whom he was close, reported that he was often angry with her for no apparent reason.
With puberty, his mother noted, Mr. E had begun kissing other developmentally disabled children. He also masturbated, but at his parents’ urging he restricted this activity to his room.
On evaluation, Mr. E was pleasant and outgoing. He had the facial dysmorphia and stature typical of Down syndrome. He smiled often and interacted well, and he attended and adapted to transitions in conversation and activities. His speech was dysarthric (with hyperglossia) and telegraphic; he could speak only four- to five-word sentences.
Was Mr. E exhibiting an adjustment reaction, depression, or a normal developmental response to puberty? Do his psychotic symptoms signal onset of schizophrenia?
Dr. Krassner’s and Kraus’ observations
Because Down syndrome is the most common genetic cause of mental retardation—seen in approximately 1 in 1,000 live births1—pediatricians and child psychiatrists see this disorder fairly frequently.
Regression, a form of coping exhibited by many children, is extremely common in youths with Down syndrome2 and often has a definite—though sometimes unclear—precipitant. We felt Mr. E’s move from a highly responsive, familiar school environment to a far less responsive one that accentuated his differences contributed to many of his symptoms.
Psychosis is less common in Down syndrome than in other developmental disabilities.2 Schizophrenia may occur, but diagnosis is complicated by cognition impairments, test-taking skills, and—in Mr. E’s case—inability to describe disordered thoughts or hallucinations due to poor language skills.3
Self-talk is common in Down syndrome and might be mistaken for psychosis. Note that despite his chronologic age, Mr. E is developmentally a 6-year-old, and self-talk and imaginary friends are considered normal behaviors for a child that age. What’s more, the stress of changing schools may have further compromised his developmental skills.
The FDA’s recent advisory about reports of increased suicidality in youths taking selective serotonin reuptake inhibitors (SSRIs) and other antidepressants for major depressive disorder during clinical trials has raised questions about using these agents in children and adolescents. Until more data become available, however, SSRIs remain the preferred drug therapy for pediatric depression.
- Based on our experience, we recommend citalopram, escitalopram, fluoxetine, and sertraline as first-line medications for pediatric depression because their side effects are relatively benign. The reported link between increased risk of suicidal ideation and behavior and use of paroxetine in pediatric patients has not been clearly established, so we cannot extrapolate that possible risk to other SSRIs.
- Newer antidepressants should be considered with caution in pediatric patients. Bupropion is contraindicated in patients with a history of seizures, bulimia, or anorexia. Mirtazapine is extremely sedating, with side effects such as weight gain and, in rare cases, agranulocytosis. Nefazodone comes with a “black box” warning for risk of liver toxicity. Trazodone is also sedating and carries a risk of priapism in boys.
- Older antidepressants, such as tricyclics, require extreme caution before prescribing to children and adolescents. Tricyclics, with their cardiac side effects, are not recommended for patients with Down syndrome, many of whom have cardiac pathology.
By contrast, depression is fairly common in Down syndrome, although it is much less prevalent in children than in adults with the developmental disorder.2
Finally, children with Down syndrome often enter puberty early, but without the cognitive or emotional maturity or knowledge to deal with the physiologic changes of adolescence.3 Parents often are reluctant to recognize their developmentally disabled child’s sexuality or are uncomfortable providing sexuality education.4 Mr. E’s parents clearly were unconvinced that his sexual behavior was normal for an adolescent.
TREATMENT Antidepressants lead to improvement
We felt Mr. E regressed secondary to emotional stress caused by switching schools. We viewed his psychotic symptoms as part of an adjustment disorder and attributed most of his other symptoms to depression. We anticipated Mr. E’s psychotic symptoms would remit spontaneously and focused on treating his mood and sleep disturbances.
We prescribed sertraline liquid suspension, 10 mg/d titrated across 3 weeks to 40 mg/d. We based our medication choice on clinical experience, mindful of a recent FDA advisory about the use of antidepressants in pediatric patients (Box 1). Also, the liquid suspension is easier to titrate than the tablet form, and we feared Mr. E might have trouble swallowing a tablet.
Mr. E’s mood and sociability improved after 3 to 4 weeks. Within 6 weeks, he regained some of his previously mastered daily activities. We added zolpidem, 10 mg nightly, to address his sleeping difficulties but discontinued the agent after 2 weeks, when his sleep patterns normalized.
At 2, 4, and 6 weeks, Mr. E was pleasant and cooperative, his thinking less concrete, and his speech more intelligible. His parents reported he was happier and more involved with family activities. At his mother’s request, sertraline was changed to 37.5 mg/d in tablet form. The patient remained stable for another month, during which his self-talk, though decreased, continued.
Two weeks later, Mr. E’s mother reported that, during a routine dermatologic examination for a chronic, presacral rash, the dermatologist noticed strategic shaving on the boy’s thighs, calves, and scrotum. Strategic shaving has been reported among sexually active youths as a means of purportedly increasing their sexual pleasure.
The dermatologist then told Mr. E’s mother that her son likely was sexually molested. Based on the boy’s differential rates of pubic hair growth, the doctor suspected that the molestation was chronic, dating back at least 3 months and probably continuing until the week before the examination. Upon hearing this, Mr. E’s parents were stunned and angry.
What behavioral signs might have suggested sexual abuse? How do the dermatologist’s findings alter diagnosis and treatment?
Dr. Krassner’s and Kraus’ observations
Given the dermatologist’s findings, Mr. E’s parents asked us whether their son’s presenting psychiatric symptoms were manifestations of posttraumatic stress disorder (PTSD).
Until now, explaining Mr. E’s symptoms as a reaction to changing schools seemed plausible. His symptoms were improving with treatment, and his sexual behaviors and interest in sexual topics were physiologically normal for his chronologic age. Despite his earlier pubertal experimentations, nothing in his psychosocial history indicated risk for sexual abuse or exploitation.
Still, children with Down syndrome are at higher risk for sexual exploitation than other children,4 so the possibility should have been explored with the parents. Psychiatrists should watch for physical signs of sexual abuse in these patients during the first examination (Box 2).4
But how is sexual abuse defined in this case? Deficient language skills prevented Mr. E from describing what happened to him, so determining whether he initiated sexual relations and with whom is nearly impossible. The act clearly could be considered abuse if Mr. E had been with an adult or older child—even if Mr. E consented. However, if Mr. E had initiated contact with another mentally retarded child, then cause, blame, and semantics become unclear. Either way, the incident could have caused PTSD.5
Diagnosing PTSD in non- or semi-verbal or retarded children is extremely difficult.6,7 Unlike adults with PTSD, pre-verbal children might not have recurrent, distressing recollections of the trauma, but symbolic displacement may characterize repetitive play, during which themes are expressed.8
Scheeringa et al have recommended PTSD criteria for preschool children, including:
- social withdrawal
- extreme temper tantrums
- loss of developmental skills
- new separation anxiety
- new onset of aggression
- new fears without obvious links to the trauma.5,6
Treating PTSD in children with developmental disabilities is also difficult. Modalities applicable to adults or mainstream children—such as psychodynamic psychotherapy, cognitive-behavioral therapy (CBT), exposure therapy, and medications—often do not help developmentally disabled children. For example, Mr. E lacks the cognitive apparatus to respond to CBT.
On the other hand, behavioral therapy, reducing risk factors, minimizing dissociative triggers, and educating patients, parents, friends, and teachers about PTSD can help patients such as Mr. E.5 Attempting to provide structure and maintain routines is a cornerstone of any intervention.
- Aggression
- Anxiety
- Behavior, learning problems at school
- Depression
- Heightened somatic concerns
- Sexualized behavior
- Sleep disturbance
- Withdrawal
FURTHER TREATMENT A family in turmoil
We addressed Mr. E’s symptoms as PTSD-related, though his poor language skills kept us from identifying a trauma. Based on data regarding pediatric PTSD treatment,9 we increased sertraline to 50 mg/d and then to 75 mg/d across 2 weeks.
However, an intense legal investigation brought on by the parents, combined with ensuing tumult within the family, worsened Mr. E’s symptoms. His self-talk became more pronounced and his isolative behavior reappeared, suggesting that the intrusive, repetitive questioning caused him to re-experience the trauma.
We again increased sertraline, to 100 mg/d, and offered supportive therapy to Mr. E. We tried to educate his parents about understanding his symptoms and managing his behavior and strongly recommended that they undergo crisis therapy to keep their reactions and emotions from hurting Mr. E. The parents declined, however, and alleged that we did not adequately support their pursuit of a diagnosis or legal action, which for them had become synonymous with treatment.
Mr. E’s mother brought her son to a psychologist, who engaged him in play therapy. She followed her son around, noting everything he said. All the while, she failed to resolve her guilt and anger. When we explained to her that these actions were hurting Mr. E’s progress, she terminated therapy.
How would you have tried to keep Mr. E’s family in therapy?
Dr. Krassner’s and Kraus’ observations
Treating psychopathology in children carries the risk of strained relations with the patient’s family. The risk increases exponentially for developmentally disabled children, as they have little or no input and their parents are exquisitely sensitive to their needs. Further, the revelation that the parents might have somehow failed to avert or anticipate danger to the child complicates their emotional response.
Although the child is the patient, the parent is the consumer. Failure to gain or keep the parents’ confidence will hinder or destroy therapy.
We might have protected our working relationship with Mr. E’s parents by recognizing how fragile they were and how intensely they would react to any constructive criticism. Paradoxically, for the short-term we could have tolerated their detrimental behaviors toward Mr. E (such as repeated questioning) in the hopes of protecting a long-term relationship. Spending more time exploring the guilt, anger, and confusion that tormented Mr. E’s parents—particularly his mother—also might have helped.
Related resources
- Ryan RM. Recognition of psychosis in persons who do not use spoken communication. In: Ancill RJ, Holliday S, Higenbottam J (eds). Schizophrenia: exploring the spectrum of psychosis. New York: John Wiley & Sons, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zolpidem • Ambien
HISTORY: New school, old problems
Mr. E, age 13, was diagnosed with Down syndrome at birth and has mild mental retardation and bilateral sensorineural hearing loss. His pediatrician referred him to our child and adolescent psychiatry clinic for regressed behavior, depression, and apparent psychotic symptoms. He was also having problems sleeping and had begun puberty 8 months earlier.
Five months before referral, Mr. E had graduated from a small elementary school, where he was fully mainstreamed, to a large junior high school, where he spent most of the school day in a functional skills class. About that time, Mr. E began exhibiting nocturnal and daytime enuresis, loss of previously mastered skills, intolerance of novelty and change, and separation difficulty. Although toilet trained at age 7, he started having “accidents” at home, school, and elsewhere. He was reluctant to dress himself, and he resisted going to school.
The youth also talked to himself often and appeared to respond to internal stimuli. He “relived” conversations aloud, described imaginary friends to family and teachers, and spoke to a stuffed dog called Goofy. He would sit and stare into space for up to a half-hour, appearing preoccupied. Family members said he had exhibited these behaviors in grade school but until now appeared to have “outgrown” them.
Once sociable, Mr. E had become increasingly moody, negativistic, and isolative. He spent hours alone in his room. His mother, with whom he was close, reported that he was often angry with her for no apparent reason.
With puberty, his mother noted, Mr. E had begun kissing other developmentally disabled children. He also masturbated, but at his parents’ urging he restricted this activity to his room.
On evaluation, Mr. E was pleasant and outgoing. He had the facial dysmorphia and stature typical of Down syndrome. He smiled often and interacted well, and he attended and adapted to transitions in conversation and activities. His speech was dysarthric (with hyperglossia) and telegraphic; he could speak only four- to five-word sentences.
Was Mr. E exhibiting an adjustment reaction, depression, or a normal developmental response to puberty? Do his psychotic symptoms signal onset of schizophrenia?
Dr. Krassner’s and Kraus’ observations
Because Down syndrome is the most common genetic cause of mental retardation—seen in approximately 1 in 1,000 live births1—pediatricians and child psychiatrists see this disorder fairly frequently.
Regression, a form of coping exhibited by many children, is extremely common in youths with Down syndrome2 and often has a definite—though sometimes unclear—precipitant. We felt Mr. E’s move from a highly responsive, familiar school environment to a far less responsive one that accentuated his differences contributed to many of his symptoms.
Psychosis is less common in Down syndrome than in other developmental disabilities.2 Schizophrenia may occur, but diagnosis is complicated by cognition impairments, test-taking skills, and—in Mr. E’s case—inability to describe disordered thoughts or hallucinations due to poor language skills.3
Self-talk is common in Down syndrome and might be mistaken for psychosis. Note that despite his chronologic age, Mr. E is developmentally a 6-year-old, and self-talk and imaginary friends are considered normal behaviors for a child that age. What’s more, the stress of changing schools may have further compromised his developmental skills.
The FDA’s recent advisory about reports of increased suicidality in youths taking selective serotonin reuptake inhibitors (SSRIs) and other antidepressants for major depressive disorder during clinical trials has raised questions about using these agents in children and adolescents. Until more data become available, however, SSRIs remain the preferred drug therapy for pediatric depression.
- Based on our experience, we recommend citalopram, escitalopram, fluoxetine, and sertraline as first-line medications for pediatric depression because their side effects are relatively benign. The reported link between increased risk of suicidal ideation and behavior and use of paroxetine in pediatric patients has not been clearly established, so we cannot extrapolate that possible risk to other SSRIs.
- Newer antidepressants should be considered with caution in pediatric patients. Bupropion is contraindicated in patients with a history of seizures, bulimia, or anorexia. Mirtazapine is extremely sedating, with side effects such as weight gain and, in rare cases, agranulocytosis. Nefazodone comes with a “black box” warning for risk of liver toxicity. Trazodone is also sedating and carries a risk of priapism in boys.
- Older antidepressants, such as tricyclics, require extreme caution before prescribing to children and adolescents. Tricyclics, with their cardiac side effects, are not recommended for patients with Down syndrome, many of whom have cardiac pathology.
By contrast, depression is fairly common in Down syndrome, although it is much less prevalent in children than in adults with the developmental disorder.2
Finally, children with Down syndrome often enter puberty early, but without the cognitive or emotional maturity or knowledge to deal with the physiologic changes of adolescence.3 Parents often are reluctant to recognize their developmentally disabled child’s sexuality or are uncomfortable providing sexuality education.4 Mr. E’s parents clearly were unconvinced that his sexual behavior was normal for an adolescent.
TREATMENT Antidepressants lead to improvement
We felt Mr. E regressed secondary to emotional stress caused by switching schools. We viewed his psychotic symptoms as part of an adjustment disorder and attributed most of his other symptoms to depression. We anticipated Mr. E’s psychotic symptoms would remit spontaneously and focused on treating his mood and sleep disturbances.
We prescribed sertraline liquid suspension, 10 mg/d titrated across 3 weeks to 40 mg/d. We based our medication choice on clinical experience, mindful of a recent FDA advisory about the use of antidepressants in pediatric patients (Box 1). Also, the liquid suspension is easier to titrate than the tablet form, and we feared Mr. E might have trouble swallowing a tablet.
Mr. E’s mood and sociability improved after 3 to 4 weeks. Within 6 weeks, he regained some of his previously mastered daily activities. We added zolpidem, 10 mg nightly, to address his sleeping difficulties but discontinued the agent after 2 weeks, when his sleep patterns normalized.
At 2, 4, and 6 weeks, Mr. E was pleasant and cooperative, his thinking less concrete, and his speech more intelligible. His parents reported he was happier and more involved with family activities. At his mother’s request, sertraline was changed to 37.5 mg/d in tablet form. The patient remained stable for another month, during which his self-talk, though decreased, continued.
Two weeks later, Mr. E’s mother reported that, during a routine dermatologic examination for a chronic, presacral rash, the dermatologist noticed strategic shaving on the boy’s thighs, calves, and scrotum. Strategic shaving has been reported among sexually active youths as a means of purportedly increasing their sexual pleasure.
The dermatologist then told Mr. E’s mother that her son likely was sexually molested. Based on the boy’s differential rates of pubic hair growth, the doctor suspected that the molestation was chronic, dating back at least 3 months and probably continuing until the week before the examination. Upon hearing this, Mr. E’s parents were stunned and angry.
What behavioral signs might have suggested sexual abuse? How do the dermatologist’s findings alter diagnosis and treatment?
Dr. Krassner’s and Kraus’ observations
Given the dermatologist’s findings, Mr. E’s parents asked us whether their son’s presenting psychiatric symptoms were manifestations of posttraumatic stress disorder (PTSD).
Until now, explaining Mr. E’s symptoms as a reaction to changing schools seemed plausible. His symptoms were improving with treatment, and his sexual behaviors and interest in sexual topics were physiologically normal for his chronologic age. Despite his earlier pubertal experimentations, nothing in his psychosocial history indicated risk for sexual abuse or exploitation.
Still, children with Down syndrome are at higher risk for sexual exploitation than other children,4 so the possibility should have been explored with the parents. Psychiatrists should watch for physical signs of sexual abuse in these patients during the first examination (Box 2).4
But how is sexual abuse defined in this case? Deficient language skills prevented Mr. E from describing what happened to him, so determining whether he initiated sexual relations and with whom is nearly impossible. The act clearly could be considered abuse if Mr. E had been with an adult or older child—even if Mr. E consented. However, if Mr. E had initiated contact with another mentally retarded child, then cause, blame, and semantics become unclear. Either way, the incident could have caused PTSD.5
Diagnosing PTSD in non- or semi-verbal or retarded children is extremely difficult.6,7 Unlike adults with PTSD, pre-verbal children might not have recurrent, distressing recollections of the trauma, but symbolic displacement may characterize repetitive play, during which themes are expressed.8
Scheeringa et al have recommended PTSD criteria for preschool children, including:
- social withdrawal
- extreme temper tantrums
- loss of developmental skills
- new separation anxiety
- new onset of aggression
- new fears without obvious links to the trauma.5,6
Treating PTSD in children with developmental disabilities is also difficult. Modalities applicable to adults or mainstream children—such as psychodynamic psychotherapy, cognitive-behavioral therapy (CBT), exposure therapy, and medications—often do not help developmentally disabled children. For example, Mr. E lacks the cognitive apparatus to respond to CBT.
On the other hand, behavioral therapy, reducing risk factors, minimizing dissociative triggers, and educating patients, parents, friends, and teachers about PTSD can help patients such as Mr. E.5 Attempting to provide structure and maintain routines is a cornerstone of any intervention.
- Aggression
- Anxiety
- Behavior, learning problems at school
- Depression
- Heightened somatic concerns
- Sexualized behavior
- Sleep disturbance
- Withdrawal
FURTHER TREATMENT A family in turmoil
We addressed Mr. E’s symptoms as PTSD-related, though his poor language skills kept us from identifying a trauma. Based on data regarding pediatric PTSD treatment,9 we increased sertraline to 50 mg/d and then to 75 mg/d across 2 weeks.
However, an intense legal investigation brought on by the parents, combined with ensuing tumult within the family, worsened Mr. E’s symptoms. His self-talk became more pronounced and his isolative behavior reappeared, suggesting that the intrusive, repetitive questioning caused him to re-experience the trauma.
We again increased sertraline, to 100 mg/d, and offered supportive therapy to Mr. E. We tried to educate his parents about understanding his symptoms and managing his behavior and strongly recommended that they undergo crisis therapy to keep their reactions and emotions from hurting Mr. E. The parents declined, however, and alleged that we did not adequately support their pursuit of a diagnosis or legal action, which for them had become synonymous with treatment.
Mr. E’s mother brought her son to a psychologist, who engaged him in play therapy. She followed her son around, noting everything he said. All the while, she failed to resolve her guilt and anger. When we explained to her that these actions were hurting Mr. E’s progress, she terminated therapy.
How would you have tried to keep Mr. E’s family in therapy?
Dr. Krassner’s and Kraus’ observations
Treating psychopathology in children carries the risk of strained relations with the patient’s family. The risk increases exponentially for developmentally disabled children, as they have little or no input and their parents are exquisitely sensitive to their needs. Further, the revelation that the parents might have somehow failed to avert or anticipate danger to the child complicates their emotional response.
Although the child is the patient, the parent is the consumer. Failure to gain or keep the parents’ confidence will hinder or destroy therapy.
We might have protected our working relationship with Mr. E’s parents by recognizing how fragile they were and how intensely they would react to any constructive criticism. Paradoxically, for the short-term we could have tolerated their detrimental behaviors toward Mr. E (such as repeated questioning) in the hopes of protecting a long-term relationship. Spending more time exploring the guilt, anger, and confusion that tormented Mr. E’s parents—particularly his mother—also might have helped.
Related resources
- Ryan RM. Recognition of psychosis in persons who do not use spoken communication. In: Ancill RJ, Holliday S, Higenbottam J (eds). Schizophrenia: exploring the spectrum of psychosis. New York: John Wiley & Sons, 1994.
Drug brand names
- Bupropion • Wellbutrin
- Citalopram • Celexa
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
- Zolpidem • Ambien
1. Pueschel S. Children with Down syndrome. In: Levine M, Carey W, Crocker A, Gross R (eds). Developmental-behavioral pediatrics. Philadelphia: WB Saunders, 1983.
2. Hodapp RM. Down syndrome: developmental, psychiatric, and management issues. Child Adolesc Psychiatr Clin North Am 1996;5:881-94.
3. Feinstein C, Reiss AL. Psychiatric disorder in mentally retarded children and adolescents. Child Adolesc Psychiatr Clin North Am 1996;5:827-52.
4. Wilgosh L. Sexual abuse of children with disabilities: intervention and treatment issues for parents. Developmental Disabil Bull. Available at: http://www.ualberta.ca/~jpdasddc/bulletin/articles/wilgosh1993.html. Accessed Nov. 10, 2003.
5. Ryan RM. Posttraumatic stress disorder in persons with developmental disabilities. Community Health J 1994;30:45-54.
6. Scheeringa MS, Seanah CH, Myers L, Putnam FW. New findings on alternative criteria for PTSD in preschool children. J Am Acad Child Adolesc Psychiatry 2003;42:561-70.
7. Diagnostic and Statistical Manual of Mental Disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
8. Lonigan CJ, Phillips BM, Richey JA. Posttraumatic stress disorder in children: diagnosis, assessment, and associated features. Child Adolesc Psychiatr Clin North Am 2003;12:171-94.
9. Donnelly CL. Pharmacological treatment approaches for children and adolescents with posttraumatic stress disorder. Child Adolesc Psychiatr Clin North Am 2003;12:251-69.
1. Pueschel S. Children with Down syndrome. In: Levine M, Carey W, Crocker A, Gross R (eds). Developmental-behavioral pediatrics. Philadelphia: WB Saunders, 1983.
2. Hodapp RM. Down syndrome: developmental, psychiatric, and management issues. Child Adolesc Psychiatr Clin North Am 1996;5:881-94.
3. Feinstein C, Reiss AL. Psychiatric disorder in mentally retarded children and adolescents. Child Adolesc Psychiatr Clin North Am 1996;5:827-52.
4. Wilgosh L. Sexual abuse of children with disabilities: intervention and treatment issues for parents. Developmental Disabil Bull. Available at: http://www.ualberta.ca/~jpdasddc/bulletin/articles/wilgosh1993.html. Accessed Nov. 10, 2003.
5. Ryan RM. Posttraumatic stress disorder in persons with developmental disabilities. Community Health J 1994;30:45-54.
6. Scheeringa MS, Seanah CH, Myers L, Putnam FW. New findings on alternative criteria for PTSD in preschool children. J Am Acad Child Adolesc Psychiatry 2003;42:561-70.
7. Diagnostic and Statistical Manual of Mental Disorders (4th ed-text revision). Washington, DC: American Psychiatric Association, 2000.
8. Lonigan CJ, Phillips BM, Richey JA. Posttraumatic stress disorder in children: diagnosis, assessment, and associated features. Child Adolesc Psychiatr Clin North Am 2003;12:171-94.
9. Donnelly CL. Pharmacological treatment approaches for children and adolescents with posttraumatic stress disorder. Child Adolesc Psychiatr Clin North Am 2003;12:251-69.
Posttraumatic stress disorder: How to meet women’s specific needs
Posttraumatic stress disorder (PTSD) was first recognized as a diagnosis in male Vietnam War veterans, but studies since then have consistently found PTSD to be more common in women than in men. Understanding the gender-related differences in PTSD’s presentation can help us craft optimal treatment for women suffering with this persistent disorder.
Data from the National Comorbidity Survey suggest a lifetime PTSD prevalence of 10.4% in women and 5.0% in men.1 PTSD also tends to be more chronic in women. In one study of patients with PTSD, median time from symptom onset to remission was 4 years for women and 1 year for men.2
Evidence suggests that women:
- experience more or different types of trauma than men, including labor and delivery, rape, and childhood sexual abuse
- may react to trauma more often and more robustly than men because of sex hormones, cultural gender roles, or some combination of those factors.
How women experience trauma
Among studies that show gender differences in response to specific trauma, nearly all have found higher PTSD rates in women than in men. This pattern emerges early in life and is seen in children and adults.
A meta-analysis comparing PTSD symptoms in females and males of all ages after specific traumas3 found that females were much more likely than males to report PTSD symptoms after some types of trauma but not others. None of the trauma types predicted PTSD more often for males than for females.
Amount of trauma. Men are more likely than women to be exposed to traumatic events, such as violent assault, during their lifetimes.4 However, the types of trauma that women experience predominantly or exclusively—such as childhood sexual abuse, traumatic labor and delivery, pregnancy loss, severe health problems in a newborn, and prostitution—are rarely included in trauma questionnaires (Table 1). As a result, the full range of traumatic experiences in women’s lives is likely underestimated.
Instruments designed to measure trauma may inadvertently introduce gender bias in other ways.5 For example, questionnaires asking about single traumatic events may underestimate the impact of repetitive traumas, such as childhood sexual abuse and domestic violence, which are more frequently experienced by girls and women. Further, women may not acknowledge sexually linked traumas—such as childhood sexual abuse and rape—unless the questions are asked in a sensitive manner and describe specific behaviors.
Table 1
TRAUMAS THAT CAUSE PTSD PREDOMINANTLY IN WOMEN
| Rape |
| Childhood sexual abuse |
| Domestic violence |
| Pregnancy loss |
| Labor and delivery |
| Neonatal complications |
| Sexual abuse of a child |
| Prostitution |
Types of trauma. Certain types of trauma are associated with especially high conditional risk of PTSD, defined as the risk of developing PTSD after being exposed to the trauma. Childhood sexual abuse, domestic violence, and rape are among the traumas with the highest conditional risk, and women are more likely to be exposed to these trauma types than men.6
Childhood sexual abuse has a particularly high conditional risk of PTSD.7 Such abuse happens over long periods during developmentally vulnerable stages of life. Sexual abuse perpetrated by a family member creates a greater sense of betrayal than does trauma at the hands of a stranger or an impersonal force of nature. In many cases, the victims blame themselves.
Domestic violence, like sexual abuse, has a high conditional PTSD risk because of the intimate nature of the relationship and the usual pattern of multiple assaults over time.
Rape carries the highest conditional risk of any trauma,8 possibly because of the degree to which rape violates a victim’s assumptions about the world as a reasonably safe place.3 PTSD risk after rape is intensified when the victim blames himself or herself and when society—such as the family or court system—reinforces this tendency toward self-blame.9
Influence of sex hormones. Neurophysiologic systems that lie beneath stress responses are closely linked with reproductive physiology.10 Evolution may have favored this association, allowing reproductive efforts to shut down during extreme stress.
Key components of the primary stress-activated hormonal system—corticotropin-releasing hormone, adrenocorticotropic hormone, and the glucocorticoids—inhibit secretion of gonadotropin-releasing hormone and the gonadotropins, the major reproductive hormones. In turn, sex hormones modulate hypothalamic-pituitary adrenal (HPA) axis activity, stress-linked neurotransmitter changes, and behavioral responses to stress.
This intertwining of stress and reproductive hormones suggests that men’s and women’s physiologic response to trauma may differ. Women’s vulnerability to PTSD also may vary at different parts of their menstrual cycles, during pregnancy, or postpartum.
Several animal studies have shown a more intense HPA axis response to stress in females than in males’.11 To date, however, studies have not shown clear gender differences in human physiologic response to trauma. Increased sympathetic nervous system activity, enhanced dexamethasone suppression of cortisol, and hippocampal atrophy have been found in both men and women with PTSD.11,12
Some human studies suggest gender differences in PTSD-related neurophysiologic changes. For example, activation of both the sympathetic and adrenocortical systems (epinephrine and cortisol) has been seen in women with PTSD from childhood sexual abuse, whereas activation of only the sympathetic system (epinephrine but not cortisol) has been seen in men with combat-related PTSD.13 Research with improved methodology is investigating whether sex hormones modulate human response to trauma.
Gender role differences. Because of cultural expectations, women may more easily acknowledge and report distress and feelings of being traumatized.14 This behavioral difference may contribute to higher PTSD prevalence rates in women than in men. Women also may develop more negative beliefs in response to some types of trauma, such as nonsexual assault by a stranger.3
Treating PTSD in women
Drug therapy. Antidepressants—including tricyclics, monoamine oxidase inhibitors, and selective serotonin reuptake inhibitors (SSRIs)—have shown efficacy in treating PTSD. Some studies have found that women respond more robustly to SSRI antidepressants than men.15
Cognitive-behavioral therapy. Trauma victims tend to avoid reminders of the trauma. Although this coping strategy can provide short-term relief, it can also constrict a person’s life and preclude opportunities to correct distorted information. For example, a person may attribute danger to benign stimuli that were coincidentally associated with the trauma, such as fearing all men with mustaches after being raped by a man with a mustache.3
Table 2
MALADAPTIVE REACTIONS DURING LABOR AND DELIVERY
| Reaction type | Description |
|---|---|
| Fighting |
|
| Regression |
|
| Dissociation |
|
| Over-control |
|
Cognitive-behavioral therapy (CBT) for PTSD aims to activate and correct information by prolonged exposure to traumatic stimuli and to restructure incorrect cognitions. CBT approaches to PTSD include exposure therapy, cognitive therapy, cognitive processing, stress inoculation training, assertiveness training, systematic desensitization, biofeedback, and relaxation training. Of these, exposure therapy has been studied the most systematically and found to work especially well for female rape victims.16 Exposure therapy consists of confronting feared stimuli—such as returning to the scene of a rape or recalling detailed memories of childhood sexual abuse—until anxiety diminishes.
Psychodynamic therapy aims to re-engage normal adaptive mechanisms by introducing the unconscious into consciousness in tolerable doses.17 Therapy serves as a means of processing traumatic events, such as childhood sexual abuse, and exploring the psychological meanings of traumas.18 Few well-controlled studies have examined psychodynamic therapy in PTSD, in part because of the difficulty in operationally defining and assessing mechanisms of change. However, at least one relatively controlled study found reduced avoidance symptoms with psychodynamic therapy, compared with wait list and active treatment groups.19
EMDR. During eye movement desensitization and reprocessing (EMDR), the patient focuses on a disturbing image, a negative cognition, and somatic sensations associated with the trauma while tracking the movement of the clinician’s finger within her visual field.20 The procedure is repeated until the patient’s distress is reduced and she develops more adaptive thoughts about the trauma.
Most EMDR practitioners recommend its use primarily for single-event traumas, such as rape or traumatic labor and delivery. Meta-analyses have suggested that EMDR may be as effective as other exposure therapy,21 although methodologic problems in several studies limit our ability to determine EMDR’s efficacy in treating women with PTSD.22
Treating and preventing perinatal PTSD
Historically, common outcomes of giving birth included death or chronic disability. Despite advances in obstetric care, labor and delivery remains painful, frightening, and potentially dangerous. Although childbirth is a normative experience for many women, an estimated 2.8 to 5.6% of new mothers develop labor-related PTSD.23-25 Risk of PTSD is increased in women with:
- high general anxiety levels prior to labor
- a history of mental illness
- unplanned pregnancy
- absence of partner during labor and delivery
- the perception that obstetric staff is unsupportive or ineffective
- a need for obstetric interventions, including episiotomy, emergency cesarean section, or use of forceps
- a perception of lack of control.
Table 3
LABOR INTERVENTIONS FOR VICTIMS OF CHILDHOOD SEXUAL ABUSE
|
Untreated PTSD may impair the woman’s functional ability and compromise her relationship with the infant:
Avoidance can extend to subsequent health care (such as not attending the postpartum checkup), sexual relationships, caring for the baby, and future pregnancies. Some women request general anesthesia and cesarean sections for future deliveries.
Arousal may intensify postpartum sleep disturbance and fatigue and may cause a mother to be hypervigilant about her baby.
Flashbacks can influence feelings about the baby, such as when the mother has repeated, vivid memories of the newborn being limp and blue after delivery, even though the infant is healthy now.
Preventive interventions that can minimize PTSD risk after labor and dshlivery include:
- explaining to women before the onset of labor that emergency obstetric interventions might be necessary
- providing adequate social support during labor and delivery
- ensuring that the obstetric staff communicates clearly with the patient
- effectively managing pain to minimize trauma.
Postpartum, it is important to screen for PTSD symptoms among high-risk women. Prompt intervention can alleviate symptoms and minimize adverse effects on the family and the mother-infant relationship.
Role of sexual abuse in perinatal PTSD. For a woman who was sexually abused as a child, even an uncomplicated labor and delivery may trigger memories, flashbacks, and emotions associated with the abuse.26 Physical sensations associated with gynecologic examinations and labor contractions may remind her of abuse-related sensations. Some women with sexual abuse histories react adversely to the loss of control and need to depend on others during labor and delivery.
Unrecognized posttraumatic reactions during labor may result in maladaptive behaviors (Table 2).26 Obstetric staff who encounter these behaviors without being aware of their origins may think the patient is oppositional or noncompliant and may regard her as an adversary to be defeated or bypassed in order to safely deliver the baby.27 The psychiatrist can minimize this problem early in labor by alerting the staff to signs of possible sexual abuse-related PTSD. These may include:
- little or no prenatal care (due to fear of obstetric procedures)
- unusual fears of needles, intravenous lines, etc.
- recoiling when touched during obstetric examinations
- insistence on female obstetric staff
- extreme sensitivity about bodily exposure.26,28
Table 4
USE OF ANTIDEPRESSANTS FOR PTSD DURING BREAST FEEDING
| Medication | Nursling dose range* | Reported nursling side effects |
|---|---|---|
| Citalopram | 0.7 to 9.0% | Uneasy sleep |
| Fluoxetine | 1.2 to 12.0% | Vomiting, watery stools, excessive crying, difficulty sleeping, tremor, somnolence, hypotonia, decreased weight gain |
| Mirtazapine | Not known | Not known |
| Nefazodone | 0.45% | Drowsiness, poor feeding, difficulty maintaining body temperature |
| Paroxetine | 0.1 to 4.3% | None |
| Sertraline | 0.4 to 1.0% | None |
| Venlafaxine | 5.2 to 7.4% | None |
| *Weight-adjusted estimated percent of mother’s dose ingested by a nursing infant | ||
Intervention. Once abuse-related perinatal PTSD is diagnosed, the interventions in Table 3 can help a woman through labor and delivery.26,28 When successful, they can turn childbirth into a healing experience that promotes the mother’s sense of accomplishment, positive association with sexuality, and a new relationship with her body.28
Breastfeeding can also trigger flashbacks and frightening emotions in a woman who was sexually abused as a child.29 She may confuse normal sensations of skin-to-skin contact with the baby or the milk ejection reflex with unpleasant sexually-linked feelings. In such cases, it may help to:
- explain the normal sensations associated with breastfeeding and normal behaviors of breastfeeding infants
- show her how to gently redirect her baby if it does something she finds uncomfortable
- identify situations that are especially difficult for her (such as nighttime feedings) and substitute bottle feeding at those times.
These measures may promote feelings of self-efficacy and help more in the long run than prematurely giving up on breastfeeding.
Prescribing to the nursing woman. When prescribing medication for PTSD in a breast-feeding woman, minimize potential infant side effects by choosing agents that produce relatively low drug levels in breast milk (Table 4).30-34 Sertraline—the first medication to receive Food and Drug Administration approval for treating PTSD—is recommended during breastfeeding.35
Pregnancy loss. Although the prevalence of PTSD in response to miscarriage or stillbirth is unknown, some women clearly develop PTSD after pregnancy loss. The degree of associated physical trauma—and of social and professional support—influence anxiety levels in response to miscarriage36 and may also influence the likelihood of developing PTSD. Pregnancy loss after the first trimester may be more likely to result in PTSD than earlier loss, and subsequent pregnancies may exacerbate PTSD symptoms. In one study, spontaneous fetal loss after the 18th week of gestation led to high rates of PTSD symptoms in a subsequent pregnancy and up to 1 year postpartum.37
Asking a woman how she wants to grieve her pregnancy loss and helping her in that process may minimize her risk of subsequent PTSD. Couples counseling may help in some cases, as each partner may have a different grieving style.
Related resources
- Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
- Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002.
- Madison Institute of Medicine. Facts for Health: posttraumatic stress disorder. www.ptsd.factsforhealth.org
Drug brand names
- Citalopram • Celexa
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Sonnega A, Bromet E, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
2. Breslau N, Kessler R, Chilcoat H, Schulz L, Davis G, Andreski P. Trauma and post-traumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:627-32.
3. Tolin DF, Foa EB. Gender and PTSD: a cognitive model. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;76-97.
4. Breslau N, Chilcoat HD, Kessler RC, Peterson EL, Lucia VC. Vulnerability to assaultive violence: further specification of the sex difference in post-traumatic stress disorder. Psychol Med 1999;29:813-21.
5. Cusack K, Falsetti S, de Arellano M. Gender considerations in the psychometric assessment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;150-76.
6. Norris F, Foster JD, Weisshaar DL. The epidemiology of sex differences in PTSD across developmental, societal, and research contexts. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;3-42.
7. DePrince AP, Freyd JJ. The intersection of gender and betrayal in trauma. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;98-113.
8. Breslau N, Davis G, Andreski P, Peterson E. Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry 1991;48:216-22.
9. Best CL, Dansky BS, Kilpatrick DG. Medical students’ attitudes about female rape victims. J Interpersonal Violence 1992;7:175-88.
10. Rubinow DR, Schmidt PJ. The neuroendocrinology of menstrual cycle mood disorders. Ann NY Acad Sci 1995;771:648-59.
11. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
12. Rasmusson AM, Friedman MJ. Gender issues in the neurobiology of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;43-75.
13. Lemieux AM, Coe CL. Abuse-related posttraumatic stress disorder: evidence for chronic neuroendocrine activation in women. Psychosomatic Med 1995;57:105-15.
14. Saxe G, Wolfe J. Gender and posttraumatic stress disorder. In: Saigh P, Bremner JD (eds). Posttraumatic stress disorder: A comprehensive text. Boston: Allyn & Bacon, 1999;160-79.
15. Brady KT, Back SE. Gender and the psychopharmacological treatment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;335-48.
16. Foa EB, Rothbaum BO, Riggs DS, Murdock TB. Treatment of posttraumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedures and counseling. J Consult Clin Psychol 1991;59:715-23.
17. Kudler HS, Blank AS, Krupnick JL. Psychodynamic therapy. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;176-98.
18. Krupnick JL. Brief psychodynamic treatment of PTSD. J Clin Psychol 2002;58:919-32.
19. Brom D, Kleber RJ, Defares PB. Brief psychotherapy for posttraumatic stress disorders. J Consult Clin Psychol 1989;57:607-12.
20. Chemtob CM, Tolin DF, van der Kolk BA, Pitman RK. Eye movement desensitization and reprocessing. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;333-5.
21. Davidson PR, Parker CH. Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol 2001;69:305-16.
22. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
23. Creedy D, Shochet I, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000;27:104-11.
24. Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br J Clin Psychol 2000;39:35-51.
25. Ayers S, Pickering AD. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001;28:111-18.
26. Rhodes N, Hutchinson S. Labor experiences of childhood sexual abuse survivors. Birth 1994;21:213-20.
27. Josephs L. Women and trauma: a contemporary psychodynamic approach to traumatization for patients in the OB/GYN psychological consultation clinic. Bull Menninger Clin 1996;60:22-8.
28. Burian J. Helping survivors of sexual abuse through labor. MCN 1995;20:252-6.
29. Kendall-Tackett K. Breastfeeding and the sexual abuse survivor. J Hum Lact 1998;14:125-30.
30. Ilett KF, Kristensen JH, Hackett LP, Paech M, Kohan R, Rampono J. Distribution of venlafaxine and its O-desmethyl metabolite in human milk and their effects in breastfed infants. Br J Clin Pharmacol 2002;53:17-22.
31. Kristensen JH, Ilett KF, Yapp P, Paech M, Begg EJ. Distribution and excretion of fluoxetine and norfluoxetine in human milk. Br J Clin Pharmacol 1999;48:521-7.
32. Misri S, Kim J, Riggs KW, Kostaras X. Paroxetine levels in postpartum depressed women, breast milk, and infant serum. J Clin Psychiatry 2000;61:828-32.
33. Ohmann R, Hagg S, Carleborg L, Spigset O. Excretion of paroxetine into breast milk. J Clin Psychiatry 1999;60:519-23.
34. Yapp P, Ilett KF, Kristensen JH, Hackett LP, Paech MJ, Rampono J. Drowsiness and poor feeding in a breast-fed infant: association with nefazodone and its metabolites. Ann Pharmacother 2000;34:1269-72.
35. Altshuler LL, Cohen LS, Moline ML, Kahn DA, Carpenter D, Docherty JR. The Expert Consensus Guideline Series. Treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-107.
36. Lee C, Slade P. Miscarriage as a traumatic event: a review of the literature and new implications for intervention. J Psychosom Res 1996;40:225-44.
37. Turton P, Hughes P, Evans CDH, Fainman D. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry 2001;178:556-60.
Posttraumatic stress disorder (PTSD) was first recognized as a diagnosis in male Vietnam War veterans, but studies since then have consistently found PTSD to be more common in women than in men. Understanding the gender-related differences in PTSD’s presentation can help us craft optimal treatment for women suffering with this persistent disorder.
Data from the National Comorbidity Survey suggest a lifetime PTSD prevalence of 10.4% in women and 5.0% in men.1 PTSD also tends to be more chronic in women. In one study of patients with PTSD, median time from symptom onset to remission was 4 years for women and 1 year for men.2
Evidence suggests that women:
- experience more or different types of trauma than men, including labor and delivery, rape, and childhood sexual abuse
- may react to trauma more often and more robustly than men because of sex hormones, cultural gender roles, or some combination of those factors.
How women experience trauma
Among studies that show gender differences in response to specific trauma, nearly all have found higher PTSD rates in women than in men. This pattern emerges early in life and is seen in children and adults.
A meta-analysis comparing PTSD symptoms in females and males of all ages after specific traumas3 found that females were much more likely than males to report PTSD symptoms after some types of trauma but not others. None of the trauma types predicted PTSD more often for males than for females.
Amount of trauma. Men are more likely than women to be exposed to traumatic events, such as violent assault, during their lifetimes.4 However, the types of trauma that women experience predominantly or exclusively—such as childhood sexual abuse, traumatic labor and delivery, pregnancy loss, severe health problems in a newborn, and prostitution—are rarely included in trauma questionnaires (Table 1). As a result, the full range of traumatic experiences in women’s lives is likely underestimated.
Instruments designed to measure trauma may inadvertently introduce gender bias in other ways.5 For example, questionnaires asking about single traumatic events may underestimate the impact of repetitive traumas, such as childhood sexual abuse and domestic violence, which are more frequently experienced by girls and women. Further, women may not acknowledge sexually linked traumas—such as childhood sexual abuse and rape—unless the questions are asked in a sensitive manner and describe specific behaviors.
Table 1
TRAUMAS THAT CAUSE PTSD PREDOMINANTLY IN WOMEN
| Rape |
| Childhood sexual abuse |
| Domestic violence |
| Pregnancy loss |
| Labor and delivery |
| Neonatal complications |
| Sexual abuse of a child |
| Prostitution |
Types of trauma. Certain types of trauma are associated with especially high conditional risk of PTSD, defined as the risk of developing PTSD after being exposed to the trauma. Childhood sexual abuse, domestic violence, and rape are among the traumas with the highest conditional risk, and women are more likely to be exposed to these trauma types than men.6
Childhood sexual abuse has a particularly high conditional risk of PTSD.7 Such abuse happens over long periods during developmentally vulnerable stages of life. Sexual abuse perpetrated by a family member creates a greater sense of betrayal than does trauma at the hands of a stranger or an impersonal force of nature. In many cases, the victims blame themselves.
Domestic violence, like sexual abuse, has a high conditional PTSD risk because of the intimate nature of the relationship and the usual pattern of multiple assaults over time.
Rape carries the highest conditional risk of any trauma,8 possibly because of the degree to which rape violates a victim’s assumptions about the world as a reasonably safe place.3 PTSD risk after rape is intensified when the victim blames himself or herself and when society—such as the family or court system—reinforces this tendency toward self-blame.9
Influence of sex hormones. Neurophysiologic systems that lie beneath stress responses are closely linked with reproductive physiology.10 Evolution may have favored this association, allowing reproductive efforts to shut down during extreme stress.
Key components of the primary stress-activated hormonal system—corticotropin-releasing hormone, adrenocorticotropic hormone, and the glucocorticoids—inhibit secretion of gonadotropin-releasing hormone and the gonadotropins, the major reproductive hormones. In turn, sex hormones modulate hypothalamic-pituitary adrenal (HPA) axis activity, stress-linked neurotransmitter changes, and behavioral responses to stress.
This intertwining of stress and reproductive hormones suggests that men’s and women’s physiologic response to trauma may differ. Women’s vulnerability to PTSD also may vary at different parts of their menstrual cycles, during pregnancy, or postpartum.
Several animal studies have shown a more intense HPA axis response to stress in females than in males’.11 To date, however, studies have not shown clear gender differences in human physiologic response to trauma. Increased sympathetic nervous system activity, enhanced dexamethasone suppression of cortisol, and hippocampal atrophy have been found in both men and women with PTSD.11,12
Some human studies suggest gender differences in PTSD-related neurophysiologic changes. For example, activation of both the sympathetic and adrenocortical systems (epinephrine and cortisol) has been seen in women with PTSD from childhood sexual abuse, whereas activation of only the sympathetic system (epinephrine but not cortisol) has been seen in men with combat-related PTSD.13 Research with improved methodology is investigating whether sex hormones modulate human response to trauma.
Gender role differences. Because of cultural expectations, women may more easily acknowledge and report distress and feelings of being traumatized.14 This behavioral difference may contribute to higher PTSD prevalence rates in women than in men. Women also may develop more negative beliefs in response to some types of trauma, such as nonsexual assault by a stranger.3
Treating PTSD in women
Drug therapy. Antidepressants—including tricyclics, monoamine oxidase inhibitors, and selective serotonin reuptake inhibitors (SSRIs)—have shown efficacy in treating PTSD. Some studies have found that women respond more robustly to SSRI antidepressants than men.15
Cognitive-behavioral therapy. Trauma victims tend to avoid reminders of the trauma. Although this coping strategy can provide short-term relief, it can also constrict a person’s life and preclude opportunities to correct distorted information. For example, a person may attribute danger to benign stimuli that were coincidentally associated with the trauma, such as fearing all men with mustaches after being raped by a man with a mustache.3
Table 2
MALADAPTIVE REACTIONS DURING LABOR AND DELIVERY
| Reaction type | Description |
|---|---|
| Fighting |
|
| Regression |
|
| Dissociation |
|
| Over-control |
|
Cognitive-behavioral therapy (CBT) for PTSD aims to activate and correct information by prolonged exposure to traumatic stimuli and to restructure incorrect cognitions. CBT approaches to PTSD include exposure therapy, cognitive therapy, cognitive processing, stress inoculation training, assertiveness training, systematic desensitization, biofeedback, and relaxation training. Of these, exposure therapy has been studied the most systematically and found to work especially well for female rape victims.16 Exposure therapy consists of confronting feared stimuli—such as returning to the scene of a rape or recalling detailed memories of childhood sexual abuse—until anxiety diminishes.
Psychodynamic therapy aims to re-engage normal adaptive mechanisms by introducing the unconscious into consciousness in tolerable doses.17 Therapy serves as a means of processing traumatic events, such as childhood sexual abuse, and exploring the psychological meanings of traumas.18 Few well-controlled studies have examined psychodynamic therapy in PTSD, in part because of the difficulty in operationally defining and assessing mechanisms of change. However, at least one relatively controlled study found reduced avoidance symptoms with psychodynamic therapy, compared with wait list and active treatment groups.19
EMDR. During eye movement desensitization and reprocessing (EMDR), the patient focuses on a disturbing image, a negative cognition, and somatic sensations associated with the trauma while tracking the movement of the clinician’s finger within her visual field.20 The procedure is repeated until the patient’s distress is reduced and she develops more adaptive thoughts about the trauma.
Most EMDR practitioners recommend its use primarily for single-event traumas, such as rape or traumatic labor and delivery. Meta-analyses have suggested that EMDR may be as effective as other exposure therapy,21 although methodologic problems in several studies limit our ability to determine EMDR’s efficacy in treating women with PTSD.22
Treating and preventing perinatal PTSD
Historically, common outcomes of giving birth included death or chronic disability. Despite advances in obstetric care, labor and delivery remains painful, frightening, and potentially dangerous. Although childbirth is a normative experience for many women, an estimated 2.8 to 5.6% of new mothers develop labor-related PTSD.23-25 Risk of PTSD is increased in women with:
- high general anxiety levels prior to labor
- a history of mental illness
- unplanned pregnancy
- absence of partner during labor and delivery
- the perception that obstetric staff is unsupportive or ineffective
- a need for obstetric interventions, including episiotomy, emergency cesarean section, or use of forceps
- a perception of lack of control.
Table 3
LABOR INTERVENTIONS FOR VICTIMS OF CHILDHOOD SEXUAL ABUSE
|
Untreated PTSD may impair the woman’s functional ability and compromise her relationship with the infant:
Avoidance can extend to subsequent health care (such as not attending the postpartum checkup), sexual relationships, caring for the baby, and future pregnancies. Some women request general anesthesia and cesarean sections for future deliveries.
Arousal may intensify postpartum sleep disturbance and fatigue and may cause a mother to be hypervigilant about her baby.
Flashbacks can influence feelings about the baby, such as when the mother has repeated, vivid memories of the newborn being limp and blue after delivery, even though the infant is healthy now.
Preventive interventions that can minimize PTSD risk after labor and dshlivery include:
- explaining to women before the onset of labor that emergency obstetric interventions might be necessary
- providing adequate social support during labor and delivery
- ensuring that the obstetric staff communicates clearly with the patient
- effectively managing pain to minimize trauma.
Postpartum, it is important to screen for PTSD symptoms among high-risk women. Prompt intervention can alleviate symptoms and minimize adverse effects on the family and the mother-infant relationship.
Role of sexual abuse in perinatal PTSD. For a woman who was sexually abused as a child, even an uncomplicated labor and delivery may trigger memories, flashbacks, and emotions associated with the abuse.26 Physical sensations associated with gynecologic examinations and labor contractions may remind her of abuse-related sensations. Some women with sexual abuse histories react adversely to the loss of control and need to depend on others during labor and delivery.
Unrecognized posttraumatic reactions during labor may result in maladaptive behaviors (Table 2).26 Obstetric staff who encounter these behaviors without being aware of their origins may think the patient is oppositional or noncompliant and may regard her as an adversary to be defeated or bypassed in order to safely deliver the baby.27 The psychiatrist can minimize this problem early in labor by alerting the staff to signs of possible sexual abuse-related PTSD. These may include:
- little or no prenatal care (due to fear of obstetric procedures)
- unusual fears of needles, intravenous lines, etc.
- recoiling when touched during obstetric examinations
- insistence on female obstetric staff
- extreme sensitivity about bodily exposure.26,28
Table 4
USE OF ANTIDEPRESSANTS FOR PTSD DURING BREAST FEEDING
| Medication | Nursling dose range* | Reported nursling side effects |
|---|---|---|
| Citalopram | 0.7 to 9.0% | Uneasy sleep |
| Fluoxetine | 1.2 to 12.0% | Vomiting, watery stools, excessive crying, difficulty sleeping, tremor, somnolence, hypotonia, decreased weight gain |
| Mirtazapine | Not known | Not known |
| Nefazodone | 0.45% | Drowsiness, poor feeding, difficulty maintaining body temperature |
| Paroxetine | 0.1 to 4.3% | None |
| Sertraline | 0.4 to 1.0% | None |
| Venlafaxine | 5.2 to 7.4% | None |
| *Weight-adjusted estimated percent of mother’s dose ingested by a nursing infant | ||
Intervention. Once abuse-related perinatal PTSD is diagnosed, the interventions in Table 3 can help a woman through labor and delivery.26,28 When successful, they can turn childbirth into a healing experience that promotes the mother’s sense of accomplishment, positive association with sexuality, and a new relationship with her body.28
Breastfeeding can also trigger flashbacks and frightening emotions in a woman who was sexually abused as a child.29 She may confuse normal sensations of skin-to-skin contact with the baby or the milk ejection reflex with unpleasant sexually-linked feelings. In such cases, it may help to:
- explain the normal sensations associated with breastfeeding and normal behaviors of breastfeeding infants
- show her how to gently redirect her baby if it does something she finds uncomfortable
- identify situations that are especially difficult for her (such as nighttime feedings) and substitute bottle feeding at those times.
These measures may promote feelings of self-efficacy and help more in the long run than prematurely giving up on breastfeeding.
Prescribing to the nursing woman. When prescribing medication for PTSD in a breast-feeding woman, minimize potential infant side effects by choosing agents that produce relatively low drug levels in breast milk (Table 4).30-34 Sertraline—the first medication to receive Food and Drug Administration approval for treating PTSD—is recommended during breastfeeding.35
Pregnancy loss. Although the prevalence of PTSD in response to miscarriage or stillbirth is unknown, some women clearly develop PTSD after pregnancy loss. The degree of associated physical trauma—and of social and professional support—influence anxiety levels in response to miscarriage36 and may also influence the likelihood of developing PTSD. Pregnancy loss after the first trimester may be more likely to result in PTSD than earlier loss, and subsequent pregnancies may exacerbate PTSD symptoms. In one study, spontaneous fetal loss after the 18th week of gestation led to high rates of PTSD symptoms in a subsequent pregnancy and up to 1 year postpartum.37
Asking a woman how she wants to grieve her pregnancy loss and helping her in that process may minimize her risk of subsequent PTSD. Couples counseling may help in some cases, as each partner may have a different grieving style.
Related resources
- Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
- Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002.
- Madison Institute of Medicine. Facts for Health: posttraumatic stress disorder. www.ptsd.factsforhealth.org
Drug brand names
- Citalopram • Celexa
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Posttraumatic stress disorder (PTSD) was first recognized as a diagnosis in male Vietnam War veterans, but studies since then have consistently found PTSD to be more common in women than in men. Understanding the gender-related differences in PTSD’s presentation can help us craft optimal treatment for women suffering with this persistent disorder.
Data from the National Comorbidity Survey suggest a lifetime PTSD prevalence of 10.4% in women and 5.0% in men.1 PTSD also tends to be more chronic in women. In one study of patients with PTSD, median time from symptom onset to remission was 4 years for women and 1 year for men.2
Evidence suggests that women:
- experience more or different types of trauma than men, including labor and delivery, rape, and childhood sexual abuse
- may react to trauma more often and more robustly than men because of sex hormones, cultural gender roles, or some combination of those factors.
How women experience trauma
Among studies that show gender differences in response to specific trauma, nearly all have found higher PTSD rates in women than in men. This pattern emerges early in life and is seen in children and adults.
A meta-analysis comparing PTSD symptoms in females and males of all ages after specific traumas3 found that females were much more likely than males to report PTSD symptoms after some types of trauma but not others. None of the trauma types predicted PTSD more often for males than for females.
Amount of trauma. Men are more likely than women to be exposed to traumatic events, such as violent assault, during their lifetimes.4 However, the types of trauma that women experience predominantly or exclusively—such as childhood sexual abuse, traumatic labor and delivery, pregnancy loss, severe health problems in a newborn, and prostitution—are rarely included in trauma questionnaires (Table 1). As a result, the full range of traumatic experiences in women’s lives is likely underestimated.
Instruments designed to measure trauma may inadvertently introduce gender bias in other ways.5 For example, questionnaires asking about single traumatic events may underestimate the impact of repetitive traumas, such as childhood sexual abuse and domestic violence, which are more frequently experienced by girls and women. Further, women may not acknowledge sexually linked traumas—such as childhood sexual abuse and rape—unless the questions are asked in a sensitive manner and describe specific behaviors.
Table 1
TRAUMAS THAT CAUSE PTSD PREDOMINANTLY IN WOMEN
| Rape |
| Childhood sexual abuse |
| Domestic violence |
| Pregnancy loss |
| Labor and delivery |
| Neonatal complications |
| Sexual abuse of a child |
| Prostitution |
Types of trauma. Certain types of trauma are associated with especially high conditional risk of PTSD, defined as the risk of developing PTSD after being exposed to the trauma. Childhood sexual abuse, domestic violence, and rape are among the traumas with the highest conditional risk, and women are more likely to be exposed to these trauma types than men.6
Childhood sexual abuse has a particularly high conditional risk of PTSD.7 Such abuse happens over long periods during developmentally vulnerable stages of life. Sexual abuse perpetrated by a family member creates a greater sense of betrayal than does trauma at the hands of a stranger or an impersonal force of nature. In many cases, the victims blame themselves.
Domestic violence, like sexual abuse, has a high conditional PTSD risk because of the intimate nature of the relationship and the usual pattern of multiple assaults over time.
Rape carries the highest conditional risk of any trauma,8 possibly because of the degree to which rape violates a victim’s assumptions about the world as a reasonably safe place.3 PTSD risk after rape is intensified when the victim blames himself or herself and when society—such as the family or court system—reinforces this tendency toward self-blame.9
Influence of sex hormones. Neurophysiologic systems that lie beneath stress responses are closely linked with reproductive physiology.10 Evolution may have favored this association, allowing reproductive efforts to shut down during extreme stress.
Key components of the primary stress-activated hormonal system—corticotropin-releasing hormone, adrenocorticotropic hormone, and the glucocorticoids—inhibit secretion of gonadotropin-releasing hormone and the gonadotropins, the major reproductive hormones. In turn, sex hormones modulate hypothalamic-pituitary adrenal (HPA) axis activity, stress-linked neurotransmitter changes, and behavioral responses to stress.
This intertwining of stress and reproductive hormones suggests that men’s and women’s physiologic response to trauma may differ. Women’s vulnerability to PTSD also may vary at different parts of their menstrual cycles, during pregnancy, or postpartum.
Several animal studies have shown a more intense HPA axis response to stress in females than in males’.11 To date, however, studies have not shown clear gender differences in human physiologic response to trauma. Increased sympathetic nervous system activity, enhanced dexamethasone suppression of cortisol, and hippocampal atrophy have been found in both men and women with PTSD.11,12
Some human studies suggest gender differences in PTSD-related neurophysiologic changes. For example, activation of both the sympathetic and adrenocortical systems (epinephrine and cortisol) has been seen in women with PTSD from childhood sexual abuse, whereas activation of only the sympathetic system (epinephrine but not cortisol) has been seen in men with combat-related PTSD.13 Research with improved methodology is investigating whether sex hormones modulate human response to trauma.
Gender role differences. Because of cultural expectations, women may more easily acknowledge and report distress and feelings of being traumatized.14 This behavioral difference may contribute to higher PTSD prevalence rates in women than in men. Women also may develop more negative beliefs in response to some types of trauma, such as nonsexual assault by a stranger.3
Treating PTSD in women
Drug therapy. Antidepressants—including tricyclics, monoamine oxidase inhibitors, and selective serotonin reuptake inhibitors (SSRIs)—have shown efficacy in treating PTSD. Some studies have found that women respond more robustly to SSRI antidepressants than men.15
Cognitive-behavioral therapy. Trauma victims tend to avoid reminders of the trauma. Although this coping strategy can provide short-term relief, it can also constrict a person’s life and preclude opportunities to correct distorted information. For example, a person may attribute danger to benign stimuli that were coincidentally associated with the trauma, such as fearing all men with mustaches after being raped by a man with a mustache.3
Table 2
MALADAPTIVE REACTIONS DURING LABOR AND DELIVERY
| Reaction type | Description |
|---|---|
| Fighting |
|
| Regression |
|
| Dissociation |
|
| Over-control |
|
Cognitive-behavioral therapy (CBT) for PTSD aims to activate and correct information by prolonged exposure to traumatic stimuli and to restructure incorrect cognitions. CBT approaches to PTSD include exposure therapy, cognitive therapy, cognitive processing, stress inoculation training, assertiveness training, systematic desensitization, biofeedback, and relaxation training. Of these, exposure therapy has been studied the most systematically and found to work especially well for female rape victims.16 Exposure therapy consists of confronting feared stimuli—such as returning to the scene of a rape or recalling detailed memories of childhood sexual abuse—until anxiety diminishes.
Psychodynamic therapy aims to re-engage normal adaptive mechanisms by introducing the unconscious into consciousness in tolerable doses.17 Therapy serves as a means of processing traumatic events, such as childhood sexual abuse, and exploring the psychological meanings of traumas.18 Few well-controlled studies have examined psychodynamic therapy in PTSD, in part because of the difficulty in operationally defining and assessing mechanisms of change. However, at least one relatively controlled study found reduced avoidance symptoms with psychodynamic therapy, compared with wait list and active treatment groups.19
EMDR. During eye movement desensitization and reprocessing (EMDR), the patient focuses on a disturbing image, a negative cognition, and somatic sensations associated with the trauma while tracking the movement of the clinician’s finger within her visual field.20 The procedure is repeated until the patient’s distress is reduced and she develops more adaptive thoughts about the trauma.
Most EMDR practitioners recommend its use primarily for single-event traumas, such as rape or traumatic labor and delivery. Meta-analyses have suggested that EMDR may be as effective as other exposure therapy,21 although methodologic problems in several studies limit our ability to determine EMDR’s efficacy in treating women with PTSD.22
Treating and preventing perinatal PTSD
Historically, common outcomes of giving birth included death or chronic disability. Despite advances in obstetric care, labor and delivery remains painful, frightening, and potentially dangerous. Although childbirth is a normative experience for many women, an estimated 2.8 to 5.6% of new mothers develop labor-related PTSD.23-25 Risk of PTSD is increased in women with:
- high general anxiety levels prior to labor
- a history of mental illness
- unplanned pregnancy
- absence of partner during labor and delivery
- the perception that obstetric staff is unsupportive or ineffective
- a need for obstetric interventions, including episiotomy, emergency cesarean section, or use of forceps
- a perception of lack of control.
Table 3
LABOR INTERVENTIONS FOR VICTIMS OF CHILDHOOD SEXUAL ABUSE
|
Untreated PTSD may impair the woman’s functional ability and compromise her relationship with the infant:
Avoidance can extend to subsequent health care (such as not attending the postpartum checkup), sexual relationships, caring for the baby, and future pregnancies. Some women request general anesthesia and cesarean sections for future deliveries.
Arousal may intensify postpartum sleep disturbance and fatigue and may cause a mother to be hypervigilant about her baby.
Flashbacks can influence feelings about the baby, such as when the mother has repeated, vivid memories of the newborn being limp and blue after delivery, even though the infant is healthy now.
Preventive interventions that can minimize PTSD risk after labor and dshlivery include:
- explaining to women before the onset of labor that emergency obstetric interventions might be necessary
- providing adequate social support during labor and delivery
- ensuring that the obstetric staff communicates clearly with the patient
- effectively managing pain to minimize trauma.
Postpartum, it is important to screen for PTSD symptoms among high-risk women. Prompt intervention can alleviate symptoms and minimize adverse effects on the family and the mother-infant relationship.
Role of sexual abuse in perinatal PTSD. For a woman who was sexually abused as a child, even an uncomplicated labor and delivery may trigger memories, flashbacks, and emotions associated with the abuse.26 Physical sensations associated with gynecologic examinations and labor contractions may remind her of abuse-related sensations. Some women with sexual abuse histories react adversely to the loss of control and need to depend on others during labor and delivery.
Unrecognized posttraumatic reactions during labor may result in maladaptive behaviors (Table 2).26 Obstetric staff who encounter these behaviors without being aware of their origins may think the patient is oppositional or noncompliant and may regard her as an adversary to be defeated or bypassed in order to safely deliver the baby.27 The psychiatrist can minimize this problem early in labor by alerting the staff to signs of possible sexual abuse-related PTSD. These may include:
- little or no prenatal care (due to fear of obstetric procedures)
- unusual fears of needles, intravenous lines, etc.
- recoiling when touched during obstetric examinations
- insistence on female obstetric staff
- extreme sensitivity about bodily exposure.26,28
Table 4
USE OF ANTIDEPRESSANTS FOR PTSD DURING BREAST FEEDING
| Medication | Nursling dose range* | Reported nursling side effects |
|---|---|---|
| Citalopram | 0.7 to 9.0% | Uneasy sleep |
| Fluoxetine | 1.2 to 12.0% | Vomiting, watery stools, excessive crying, difficulty sleeping, tremor, somnolence, hypotonia, decreased weight gain |
| Mirtazapine | Not known | Not known |
| Nefazodone | 0.45% | Drowsiness, poor feeding, difficulty maintaining body temperature |
| Paroxetine | 0.1 to 4.3% | None |
| Sertraline | 0.4 to 1.0% | None |
| Venlafaxine | 5.2 to 7.4% | None |
| *Weight-adjusted estimated percent of mother’s dose ingested by a nursing infant | ||
Intervention. Once abuse-related perinatal PTSD is diagnosed, the interventions in Table 3 can help a woman through labor and delivery.26,28 When successful, they can turn childbirth into a healing experience that promotes the mother’s sense of accomplishment, positive association with sexuality, and a new relationship with her body.28
Breastfeeding can also trigger flashbacks and frightening emotions in a woman who was sexually abused as a child.29 She may confuse normal sensations of skin-to-skin contact with the baby or the milk ejection reflex with unpleasant sexually-linked feelings. In such cases, it may help to:
- explain the normal sensations associated with breastfeeding and normal behaviors of breastfeeding infants
- show her how to gently redirect her baby if it does something she finds uncomfortable
- identify situations that are especially difficult for her (such as nighttime feedings) and substitute bottle feeding at those times.
These measures may promote feelings of self-efficacy and help more in the long run than prematurely giving up on breastfeeding.
Prescribing to the nursing woman. When prescribing medication for PTSD in a breast-feeding woman, minimize potential infant side effects by choosing agents that produce relatively low drug levels in breast milk (Table 4).30-34 Sertraline—the first medication to receive Food and Drug Administration approval for treating PTSD—is recommended during breastfeeding.35
Pregnancy loss. Although the prevalence of PTSD in response to miscarriage or stillbirth is unknown, some women clearly develop PTSD after pregnancy loss. The degree of associated physical trauma—and of social and professional support—influence anxiety levels in response to miscarriage36 and may also influence the likelihood of developing PTSD. Pregnancy loss after the first trimester may be more likely to result in PTSD than earlier loss, and subsequent pregnancies may exacerbate PTSD symptoms. In one study, spontaneous fetal loss after the 18th week of gestation led to high rates of PTSD symptoms in a subsequent pregnancy and up to 1 year postpartum.37
Asking a woman how she wants to grieve her pregnancy loss and helping her in that process may minimize her risk of subsequent PTSD. Couples counseling may help in some cases, as each partner may have a different grieving style.
Related resources
- Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
- Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002.
- Madison Institute of Medicine. Facts for Health: posttraumatic stress disorder. www.ptsd.factsforhealth.org
Drug brand names
- Citalopram • Celexa
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Sonnega A, Bromet E, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
2. Breslau N, Kessler R, Chilcoat H, Schulz L, Davis G, Andreski P. Trauma and post-traumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:627-32.
3. Tolin DF, Foa EB. Gender and PTSD: a cognitive model. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;76-97.
4. Breslau N, Chilcoat HD, Kessler RC, Peterson EL, Lucia VC. Vulnerability to assaultive violence: further specification of the sex difference in post-traumatic stress disorder. Psychol Med 1999;29:813-21.
5. Cusack K, Falsetti S, de Arellano M. Gender considerations in the psychometric assessment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;150-76.
6. Norris F, Foster JD, Weisshaar DL. The epidemiology of sex differences in PTSD across developmental, societal, and research contexts. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;3-42.
7. DePrince AP, Freyd JJ. The intersection of gender and betrayal in trauma. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;98-113.
8. Breslau N, Davis G, Andreski P, Peterson E. Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry 1991;48:216-22.
9. Best CL, Dansky BS, Kilpatrick DG. Medical students’ attitudes about female rape victims. J Interpersonal Violence 1992;7:175-88.
10. Rubinow DR, Schmidt PJ. The neuroendocrinology of menstrual cycle mood disorders. Ann NY Acad Sci 1995;771:648-59.
11. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
12. Rasmusson AM, Friedman MJ. Gender issues in the neurobiology of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;43-75.
13. Lemieux AM, Coe CL. Abuse-related posttraumatic stress disorder: evidence for chronic neuroendocrine activation in women. Psychosomatic Med 1995;57:105-15.
14. Saxe G, Wolfe J. Gender and posttraumatic stress disorder. In: Saigh P, Bremner JD (eds). Posttraumatic stress disorder: A comprehensive text. Boston: Allyn & Bacon, 1999;160-79.
15. Brady KT, Back SE. Gender and the psychopharmacological treatment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;335-48.
16. Foa EB, Rothbaum BO, Riggs DS, Murdock TB. Treatment of posttraumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedures and counseling. J Consult Clin Psychol 1991;59:715-23.
17. Kudler HS, Blank AS, Krupnick JL. Psychodynamic therapy. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;176-98.
18. Krupnick JL. Brief psychodynamic treatment of PTSD. J Clin Psychol 2002;58:919-32.
19. Brom D, Kleber RJ, Defares PB. Brief psychotherapy for posttraumatic stress disorders. J Consult Clin Psychol 1989;57:607-12.
20. Chemtob CM, Tolin DF, van der Kolk BA, Pitman RK. Eye movement desensitization and reprocessing. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;333-5.
21. Davidson PR, Parker CH. Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol 2001;69:305-16.
22. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
23. Creedy D, Shochet I, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000;27:104-11.
24. Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br J Clin Psychol 2000;39:35-51.
25. Ayers S, Pickering AD. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001;28:111-18.
26. Rhodes N, Hutchinson S. Labor experiences of childhood sexual abuse survivors. Birth 1994;21:213-20.
27. Josephs L. Women and trauma: a contemporary psychodynamic approach to traumatization for patients in the OB/GYN psychological consultation clinic. Bull Menninger Clin 1996;60:22-8.
28. Burian J. Helping survivors of sexual abuse through labor. MCN 1995;20:252-6.
29. Kendall-Tackett K. Breastfeeding and the sexual abuse survivor. J Hum Lact 1998;14:125-30.
30. Ilett KF, Kristensen JH, Hackett LP, Paech M, Kohan R, Rampono J. Distribution of venlafaxine and its O-desmethyl metabolite in human milk and their effects in breastfed infants. Br J Clin Pharmacol 2002;53:17-22.
31. Kristensen JH, Ilett KF, Yapp P, Paech M, Begg EJ. Distribution and excretion of fluoxetine and norfluoxetine in human milk. Br J Clin Pharmacol 1999;48:521-7.
32. Misri S, Kim J, Riggs KW, Kostaras X. Paroxetine levels in postpartum depressed women, breast milk, and infant serum. J Clin Psychiatry 2000;61:828-32.
33. Ohmann R, Hagg S, Carleborg L, Spigset O. Excretion of paroxetine into breast milk. J Clin Psychiatry 1999;60:519-23.
34. Yapp P, Ilett KF, Kristensen JH, Hackett LP, Paech MJ, Rampono J. Drowsiness and poor feeding in a breast-fed infant: association with nefazodone and its metabolites. Ann Pharmacother 2000;34:1269-72.
35. Altshuler LL, Cohen LS, Moline ML, Kahn DA, Carpenter D, Docherty JR. The Expert Consensus Guideline Series. Treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-107.
36. Lee C, Slade P. Miscarriage as a traumatic event: a review of the literature and new implications for intervention. J Psychosom Res 1996;40:225-44.
37. Turton P, Hughes P, Evans CDH, Fainman D. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry 2001;178:556-60.
1. Kessler RC, Sonnega A, Bromet E, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
2. Breslau N, Kessler R, Chilcoat H, Schulz L, Davis G, Andreski P. Trauma and post-traumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:627-32.
3. Tolin DF, Foa EB. Gender and PTSD: a cognitive model. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;76-97.
4. Breslau N, Chilcoat HD, Kessler RC, Peterson EL, Lucia VC. Vulnerability to assaultive violence: further specification of the sex difference in post-traumatic stress disorder. Psychol Med 1999;29:813-21.
5. Cusack K, Falsetti S, de Arellano M. Gender considerations in the psychometric assessment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;150-76.
6. Norris F, Foster JD, Weisshaar DL. The epidemiology of sex differences in PTSD across developmental, societal, and research contexts. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;3-42.
7. DePrince AP, Freyd JJ. The intersection of gender and betrayal in trauma. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;98-113.
8. Breslau N, Davis G, Andreski P, Peterson E. Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry 1991;48:216-22.
9. Best CL, Dansky BS, Kilpatrick DG. Medical students’ attitudes about female rape victims. J Interpersonal Violence 1992;7:175-88.
10. Rubinow DR, Schmidt PJ. The neuroendocrinology of menstrual cycle mood disorders. Ann NY Acad Sci 1995;771:648-59.
11. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
12. Rasmusson AM, Friedman MJ. Gender issues in the neurobiology of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;43-75.
13. Lemieux AM, Coe CL. Abuse-related posttraumatic stress disorder: evidence for chronic neuroendocrine activation in women. Psychosomatic Med 1995;57:105-15.
14. Saxe G, Wolfe J. Gender and posttraumatic stress disorder. In: Saigh P, Bremner JD (eds). Posttraumatic stress disorder: A comprehensive text. Boston: Allyn & Bacon, 1999;160-79.
15. Brady KT, Back SE. Gender and the psychopharmacological treatment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;335-48.
16. Foa EB, Rothbaum BO, Riggs DS, Murdock TB. Treatment of posttraumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedures and counseling. J Consult Clin Psychol 1991;59:715-23.
17. Kudler HS, Blank AS, Krupnick JL. Psychodynamic therapy. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;176-98.
18. Krupnick JL. Brief psychodynamic treatment of PTSD. J Clin Psychol 2002;58:919-32.
19. Brom D, Kleber RJ, Defares PB. Brief psychotherapy for posttraumatic stress disorders. J Consult Clin Psychol 1989;57:607-12.
20. Chemtob CM, Tolin DF, van der Kolk BA, Pitman RK. Eye movement desensitization and reprocessing. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;333-5.
21. Davidson PR, Parker CH. Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol 2001;69:305-16.
22. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
23. Creedy D, Shochet I, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000;27:104-11.
24. Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br J Clin Psychol 2000;39:35-51.
25. Ayers S, Pickering AD. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001;28:111-18.
26. Rhodes N, Hutchinson S. Labor experiences of childhood sexual abuse survivors. Birth 1994;21:213-20.
27. Josephs L. Women and trauma: a contemporary psychodynamic approach to traumatization for patients in the OB/GYN psychological consultation clinic. Bull Menninger Clin 1996;60:22-8.
28. Burian J. Helping survivors of sexual abuse through labor. MCN 1995;20:252-6.
29. Kendall-Tackett K. Breastfeeding and the sexual abuse survivor. J Hum Lact 1998;14:125-30.
30. Ilett KF, Kristensen JH, Hackett LP, Paech M, Kohan R, Rampono J. Distribution of venlafaxine and its O-desmethyl metabolite in human milk and their effects in breastfed infants. Br J Clin Pharmacol 2002;53:17-22.
31. Kristensen JH, Ilett KF, Yapp P, Paech M, Begg EJ. Distribution and excretion of fluoxetine and norfluoxetine in human milk. Br J Clin Pharmacol 1999;48:521-7.
32. Misri S, Kim J, Riggs KW, Kostaras X. Paroxetine levels in postpartum depressed women, breast milk, and infant serum. J Clin Psychiatry 2000;61:828-32.
33. Ohmann R, Hagg S, Carleborg L, Spigset O. Excretion of paroxetine into breast milk. J Clin Psychiatry 1999;60:519-23.
34. Yapp P, Ilett KF, Kristensen JH, Hackett LP, Paech MJ, Rampono J. Drowsiness and poor feeding in a breast-fed infant: association with nefazodone and its metabolites. Ann Pharmacother 2000;34:1269-72.
35. Altshuler LL, Cohen LS, Moline ML, Kahn DA, Carpenter D, Docherty JR. The Expert Consensus Guideline Series. Treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-107.
36. Lee C, Slade P. Miscarriage as a traumatic event: a review of the literature and new implications for intervention. J Psychosom Res 1996;40:225-44.
37. Turton P, Hughes P, Evans CDH, Fainman D. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry 2001;178:556-60.
Posttraumatic stress disorder: How to meet women’s specific needs
Posttraumatic stress disorder (PTSD) was first recognized as a diagnosis in male Vietnam War veterans, but studies since then have consistently found PTSD to be more common in women than in men. Understanding the gender-related differences in PTSD’s presentation can help us craft optimal treatment for women suffering with this persistent disorder.
Data from the National Comorbidity Survey suggest a lifetime PTSD prevalence of 10.4% in women and 5.0% in men.1 PTSD also tends to be more chronic in women. In one study of patients with PTSD, median time from symptom onset to remission was 4 years for women and 1 year for men.2
Evidence suggests that women:
- experience more or different types of trauma than men, including labor and delivery, rape, and childhood sexual abuse
- may react to trauma more often and more robustly than men because of sex hormones, cultural gender roles, or some combination of those factors.
How women experience trauma
Among studies that show gender differences in response to specific trauma, nearly all have found higher PTSD rates in women than in men. This pattern emerges early in life and is seen in children and adults.
A meta-analysis comparing PTSD symptoms in females and males of all ages after specific traumas3 found that females were much more likely than males to report PTSD symptoms after some types of trauma but not others. None of the trauma types predicted PTSD more often for males than for females.
Amount of trauma. Men are more likely than women to be exposed to traumatic events, such as violent assault, during their lifetimes.4 However, the types of trauma that women experience predominantly or exclusively—such as childhood sexual abuse, traumatic labor and delivery, pregnancy loss, severe health problems in a newborn, and prostitution—are rarely included in trauma questionnaires (Table 1). As a result, the full range of traumatic experiences in women’s lives is likely underestimated.
Instruments designed to measure trauma may inadvertently introduce gender bias in other ways.5 For example, questionnaires asking about single traumatic events may underestimate the impact of repetitive traumas, such as childhood sexual abuse and domestic violence, which are more frequently experienced by girls and women. Further, women may not acknowledge sexually linked traumas—such as childhood sexual abuse and rape—unless the questions are asked in a sensitive manner and describe specific behaviors.
Table 1
TRAUMAS THAT CAUSE PTSD PREDOMINANTLY IN WOMEN
| Rape |
| Childhood sexual abuse |
| Domestic violence |
| Pregnancy loss |
| Labor and delivery |
| Neonatal complications |
| Sexual abuse of a child |
| Prostitution |
Types of trauma. Certain types of trauma are associated with especially high conditional risk of PTSD, defined as the risk of developing PTSD after being exposed to the trauma. Childhood sexual abuse, domestic violence, and rape are among the traumas with the highest conditional risk, and women are more likely to be exposed to these trauma types than men.6
Childhood sexual abuse has a particularly high conditional risk of PTSD.7 Such abuse happens over long periods during developmentally vulnerable stages of life. Sexual abuse perpetrated by a family member creates a greater sense of betrayal than does trauma at the hands of a stranger or an impersonal force of nature. In many cases, the victims blame themselves.
Domestic violence, like sexual abuse, has a high conditional PTSD risk because of the intimate nature of the relationship and the usual pattern of multiple assaults over time.
Rape carries the highest conditional risk of any trauma,8 possibly because of the degree to which rape violates a victim’s assumptions about the world as a reasonably safe place.3 PTSD risk after rape is intensified when the victim blames himself or herself and when society—such as the family or court system—reinforces this tendency toward self-blame.9
Influence of sex hormones. Neurophysiologic systems that lie beneath stress responses are closely linked with reproductive physiology.10 Evolution may have favored this association, allowing reproductive efforts to shut down during extreme stress.
Key components of the primary stress-activated hormonal system—corticotropin-releasing hormone, adrenocorticotropic hormone, and the glucocorticoids—inhibit secretion of gonadotropin-releasing hormone and the gonadotropins, the major reproductive hormones. In turn, sex hormones modulate hypothalamic-pituitary adrenal (HPA) axis activity, stress-linked neurotransmitter changes, and behavioral responses to stress.
This intertwining of stress and reproductive hormones suggests that men’s and women’s physiologic response to trauma may differ. Women’s vulnerability to PTSD also may vary at different parts of their menstrual cycles, during pregnancy, or postpartum.
Several animal studies have shown a more intense HPA axis response to stress in females than in males’.11 To date, however, studies have not shown clear gender differences in human physiologic response to trauma. Increased sympathetic nervous system activity, enhanced dexamethasone suppression of cortisol, and hippocampal atrophy have been found in both men and women with PTSD.11,12
Some human studies suggest gender differences in PTSD-related neurophysiologic changes. For example, activation of both the sympathetic and adrenocortical systems (epinephrine and cortisol) has been seen in women with PTSD from childhood sexual abuse, whereas activation of only the sympathetic system (epinephrine but not cortisol) has been seen in men with combat-related PTSD.13 Research with improved methodology is investigating whether sex hormones modulate human response to trauma.
Gender role differences. Because of cultural expectations, women may more easily acknowledge and report distress and feelings of being traumatized.14 This behavioral difference may contribute to higher PTSD prevalence rates in women than in men. Women also may develop more negative beliefs in response to some types of trauma, such as nonsexual assault by a stranger.3
Treating PTSD in women
Drug therapy. Antidepressants—including tricyclics, monoamine oxidase inhibitors, and selective serotonin reuptake inhibitors (SSRIs)—have shown efficacy in treating PTSD. Some studies have found that women respond more robustly to SSRI antidepressants than men.15
Cognitive-behavioral therapy. Trauma victims tend to avoid reminders of the trauma. Although this coping strategy can provide short-term relief, it can also constrict a person’s life and preclude opportunities to correct distorted information. For example, a person may attribute danger to benign stimuli that were coincidentally associated with the trauma, such as fearing all men with mustaches after being raped by a man with a mustache.3
Table 2
MALADAPTIVE REACTIONS DURING LABOR AND DELIVERY
| Reaction type | Description |
|---|---|
| Fighting |
|
| Regression |
|
| Dissociation |
|
| Over-control |
|
Cognitive-behavioral therapy (CBT) for PTSD aims to activate and correct information by prolonged exposure to traumatic stimuli and to restructure incorrect cognitions. CBT approaches to PTSD include exposure therapy, cognitive therapy, cognitive processing, stress inoculation training, assertiveness training, systematic desensitization, biofeedback, and relaxation training. Of these, exposure therapy has been studied the most systematically and found to work especially well for female rape victims.16 Exposure therapy consists of confronting feared stimuli—such as returning to the scene of a rape or recalling detailed memories of childhood sexual abuse—until anxiety diminishes.
Psychodynamic therapy aims to re-engage normal adaptive mechanisms by introducing the unconscious into consciousness in tolerable doses.17 Therapy serves as a means of processing traumatic events, such as childhood sexual abuse, and exploring the psychological meanings of traumas.18 Few well-controlled studies have examined psychodynamic therapy in PTSD, in part because of the difficulty in operationally defining and assessing mechanisms of change. However, at least one relatively controlled study found reduced avoidance symptoms with psychodynamic therapy, compared with wait list and active treatment groups.19
EMDR. During eye movement desensitization and reprocessing (EMDR), the patient focuses on a disturbing image, a negative cognition, and somatic sensations associated with the trauma while tracking the movement of the clinician’s finger within her visual field.20 The procedure is repeated until the patient’s distress is reduced and she develops more adaptive thoughts about the trauma.
Most EMDR practitioners recommend its use primarily for single-event traumas, such as rape or traumatic labor and delivery. Meta-analyses have suggested that EMDR may be as effective as other exposure therapy,21 although methodologic problems in several studies limit our ability to determine EMDR’s efficacy in treating women with PTSD.22
Treating and preventing perinatal PTSD
Historically, common outcomes of giving birth included death or chronic disability. Despite advances in obstetric care, labor and delivery remains painful, frightening, and potentially dangerous. Although childbirth is a normative experience for many women, an estimated 2.8 to 5.6% of new mothers develop labor-related PTSD.23-25 Risk of PTSD is increased in women with:
- high general anxiety levels prior to labor
- a history of mental illness
- unplanned pregnancy
- absence of partner during labor and delivery
- the perception that obstetric staff is unsupportive or ineffective
- a need for obstetric interventions, including episiotomy, emergency cesarean section, or use of forceps
- a perception of lack of control.
Table 3
LABOR INTERVENTIONS FOR VICTIMS OF CHILDHOOD SEXUAL ABUSE
|
Untreated PTSD may impair the woman’s functional ability and compromise her relationship with the infant:
Avoidance can extend to subsequent health care (such as not attending the postpartum checkup), sexual relationships, caring for the baby, and future pregnancies. Some women request general anesthesia and cesarean sections for future deliveries.
Arousal may intensify postpartum sleep disturbance and fatigue and may cause a mother to be hypervigilant about her baby.
Flashbacks can influence feelings about the baby, such as when the mother has repeated, vivid memories of the newborn being limp and blue after delivery, even though the infant is healthy now.
Preventive interventions that can minimize PTSD risk after labor and dshlivery include:
- explaining to women before the onset of labor that emergency obstetric interventions might be necessary
- providing adequate social support during labor and delivery
- ensuring that the obstetric staff communicates clearly with the patient
- effectively managing pain to minimize trauma.
Postpartum, it is important to screen for PTSD symptoms among high-risk women. Prompt intervention can alleviate symptoms and minimize adverse effects on the family and the mother-infant relationship.
Role of sexual abuse in perinatal PTSD. For a woman who was sexually abused as a child, even an uncomplicated labor and delivery may trigger memories, flashbacks, and emotions associated with the abuse.26 Physical sensations associated with gynecologic examinations and labor contractions may remind her of abuse-related sensations. Some women with sexual abuse histories react adversely to the loss of control and need to depend on others during labor and delivery.
Unrecognized posttraumatic reactions during labor may result in maladaptive behaviors (Table 2).26 Obstetric staff who encounter these behaviors without being aware of their origins may think the patient is oppositional or noncompliant and may regard her as an adversary to be defeated or bypassed in order to safely deliver the baby.27 The psychiatrist can minimize this problem early in labor by alerting the staff to signs of possible sexual abuse-related PTSD. These may include:
- little or no prenatal care (due to fear of obstetric procedures)
- unusual fears of needles, intravenous lines, etc.
- recoiling when touched during obstetric examinations
- insistence on female obstetric staff
- extreme sensitivity about bodily exposure.26,28
Table 4
USE OF ANTIDEPRESSANTS FOR PTSD DURING BREAST FEEDING
| Medication | Nursling dose range* | Reported nursling side effects |
|---|---|---|
| Citalopram | 0.7 to 9.0% | Uneasy sleep |
| Fluoxetine | 1.2 to 12.0% | Vomiting, watery stools, excessive crying, difficulty sleeping, tremor, somnolence, hypotonia, decreased weight gain |
| Mirtazapine | Not known | Not known |
| Nefazodone | 0.45% | Drowsiness, poor feeding, difficulty maintaining body temperature |
| Paroxetine | 0.1 to 4.3% | None |
| Sertraline | 0.4 to 1.0% | None |
| Venlafaxine | 5.2 to 7.4% | None |
| *Weight-adjusted estimated percent of mother’s dose ingested by a nursing infant | ||
Intervention. Once abuse-related perinatal PTSD is diagnosed, the interventions in Table 3 can help a woman through labor and delivery.26,28 When successful, they can turn childbirth into a healing experience that promotes the mother’s sense of accomplishment, positive association with sexuality, and a new relationship with her body.28
Breastfeeding can also trigger flashbacks and frightening emotions in a woman who was sexually abused as a child.29 She may confuse normal sensations of skin-to-skin contact with the baby or the milk ejection reflex with unpleasant sexually-linked feelings. In such cases, it may help to:
- explain the normal sensations associated with breastfeeding and normal behaviors of breastfeeding infants
- show her how to gently redirect her baby if it does something she finds uncomfortable
- identify situations that are especially difficult for her (such as nighttime feedings) and substitute bottle feeding at those times.
These measures may promote feelings of self-efficacy and help more in the long run than prematurely giving up on breastfeeding.
Prescribing to the nursing woman. When prescribing medication for PTSD in a breast-feeding woman, minimize potential infant side effects by choosing agents that produce relatively low drug levels in breast milk (Table 4).30-34 Sertraline—the first medication to receive Food and Drug Administration approval for treating PTSD—is recommended during breastfeeding.35
Pregnancy loss. Although the prevalence of PTSD in response to miscarriage or stillbirth is unknown, some women clearly develop PTSD after pregnancy loss. The degree of associated physical trauma—and of social and professional support—influence anxiety levels in response to miscarriage36 and may also influence the likelihood of developing PTSD. Pregnancy loss after the first trimester may be more likely to result in PTSD than earlier loss, and subsequent pregnancies may exacerbate PTSD symptoms. In one study, spontaneous fetal loss after the 18th week of gestation led to high rates of PTSD symptoms in a subsequent pregnancy and up to 1 year postpartum.37
Asking a woman how she wants to grieve her pregnancy loss and helping her in that process may minimize her risk of subsequent PTSD. Couples counseling may help in some cases, as each partner may have a different grieving style.
Related resources
- Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
- Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002.
- Madison Institute of Medicine. Facts for Health: posttraumatic stress disorder. www.ptsd.factsforhealth.org
Drug brand names
- Citalopram • Celexa
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Sonnega A, Bromet E, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
2. Breslau N, Kessler R, Chilcoat H, Schulz L, Davis G, Andreski P. Trauma and post-traumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:627-32.
3. Tolin DF, Foa EB. Gender and PTSD: a cognitive model. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;76-97.
4. Breslau N, Chilcoat HD, Kessler RC, Peterson EL, Lucia VC. Vulnerability to assaultive violence: further specification of the sex difference in post-traumatic stress disorder. Psychol Med 1999;29:813-21.
5. Cusack K, Falsetti S, de Arellano M. Gender considerations in the psychometric assessment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;150-76.
6. Norris F, Foster JD, Weisshaar DL. The epidemiology of sex differences in PTSD across developmental, societal, and research contexts. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;3-42.
7. DePrince AP, Freyd JJ. The intersection of gender and betrayal in trauma. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;98-113.
8. Breslau N, Davis G, Andreski P, Peterson E. Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry 1991;48:216-22.
9. Best CL, Dansky BS, Kilpatrick DG. Medical students’ attitudes about female rape victims. J Interpersonal Violence 1992;7:175-88.
10. Rubinow DR, Schmidt PJ. The neuroendocrinology of menstrual cycle mood disorders. Ann NY Acad Sci 1995;771:648-59.
11. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
12. Rasmusson AM, Friedman MJ. Gender issues in the neurobiology of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;43-75.
13. Lemieux AM, Coe CL. Abuse-related posttraumatic stress disorder: evidence for chronic neuroendocrine activation in women. Psychosomatic Med 1995;57:105-15.
14. Saxe G, Wolfe J. Gender and posttraumatic stress disorder. In: Saigh P, Bremner JD (eds). Posttraumatic stress disorder: A comprehensive text. Boston: Allyn & Bacon, 1999;160-79.
15. Brady KT, Back SE. Gender and the psychopharmacological treatment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;335-48.
16. Foa EB, Rothbaum BO, Riggs DS, Murdock TB. Treatment of posttraumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedures and counseling. J Consult Clin Psychol 1991;59:715-23.
17. Kudler HS, Blank AS, Krupnick JL. Psychodynamic therapy. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;176-98.
18. Krupnick JL. Brief psychodynamic treatment of PTSD. J Clin Psychol 2002;58:919-32.
19. Brom D, Kleber RJ, Defares PB. Brief psychotherapy for posttraumatic stress disorders. J Consult Clin Psychol 1989;57:607-12.
20. Chemtob CM, Tolin DF, van der Kolk BA, Pitman RK. Eye movement desensitization and reprocessing. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;333-5.
21. Davidson PR, Parker CH. Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol 2001;69:305-16.
22. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
23. Creedy D, Shochet I, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000;27:104-11.
24. Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br J Clin Psychol 2000;39:35-51.
25. Ayers S, Pickering AD. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001;28:111-18.
26. Rhodes N, Hutchinson S. Labor experiences of childhood sexual abuse survivors. Birth 1994;21:213-20.
27. Josephs L. Women and trauma: a contemporary psychodynamic approach to traumatization for patients in the OB/GYN psychological consultation clinic. Bull Menninger Clin 1996;60:22-8.
28. Burian J. Helping survivors of sexual abuse through labor. MCN 1995;20:252-6.
29. Kendall-Tackett K. Breastfeeding and the sexual abuse survivor. J Hum Lact 1998;14:125-30.
30. Ilett KF, Kristensen JH, Hackett LP, Paech M, Kohan R, Rampono J. Distribution of venlafaxine and its O-desmethyl metabolite in human milk and their effects in breastfed infants. Br J Clin Pharmacol 2002;53:17-22.
31. Kristensen JH, Ilett KF, Yapp P, Paech M, Begg EJ. Distribution and excretion of fluoxetine and norfluoxetine in human milk. Br J Clin Pharmacol 1999;48:521-7.
32. Misri S, Kim J, Riggs KW, Kostaras X. Paroxetine levels in postpartum depressed women, breast milk, and infant serum. J Clin Psychiatry 2000;61:828-32.
33. Ohmann R, Hagg S, Carleborg L, Spigset O. Excretion of paroxetine into breast milk. J Clin Psychiatry 1999;60:519-23.
34. Yapp P, Ilett KF, Kristensen JH, Hackett LP, Paech MJ, Rampono J. Drowsiness and poor feeding in a breast-fed infant: association with nefazodone and its metabolites. Ann Pharmacother 2000;34:1269-72.
35. Altshuler LL, Cohen LS, Moline ML, Kahn DA, Carpenter D, Docherty JR. The Expert Consensus Guideline Series. Treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-107.
36. Lee C, Slade P. Miscarriage as a traumatic event: a review of the literature and new implications for intervention. J Psychosom Res 1996;40:225-44.
37. Turton P, Hughes P, Evans CDH, Fainman D. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry 2001;178:556-60.
Posttraumatic stress disorder (PTSD) was first recognized as a diagnosis in male Vietnam War veterans, but studies since then have consistently found PTSD to be more common in women than in men. Understanding the gender-related differences in PTSD’s presentation can help us craft optimal treatment for women suffering with this persistent disorder.
Data from the National Comorbidity Survey suggest a lifetime PTSD prevalence of 10.4% in women and 5.0% in men.1 PTSD also tends to be more chronic in women. In one study of patients with PTSD, median time from symptom onset to remission was 4 years for women and 1 year for men.2
Evidence suggests that women:
- experience more or different types of trauma than men, including labor and delivery, rape, and childhood sexual abuse
- may react to trauma more often and more robustly than men because of sex hormones, cultural gender roles, or some combination of those factors.
How women experience trauma
Among studies that show gender differences in response to specific trauma, nearly all have found higher PTSD rates in women than in men. This pattern emerges early in life and is seen in children and adults.
A meta-analysis comparing PTSD symptoms in females and males of all ages after specific traumas3 found that females were much more likely than males to report PTSD symptoms after some types of trauma but not others. None of the trauma types predicted PTSD more often for males than for females.
Amount of trauma. Men are more likely than women to be exposed to traumatic events, such as violent assault, during their lifetimes.4 However, the types of trauma that women experience predominantly or exclusively—such as childhood sexual abuse, traumatic labor and delivery, pregnancy loss, severe health problems in a newborn, and prostitution—are rarely included in trauma questionnaires (Table 1). As a result, the full range of traumatic experiences in women’s lives is likely underestimated.
Instruments designed to measure trauma may inadvertently introduce gender bias in other ways.5 For example, questionnaires asking about single traumatic events may underestimate the impact of repetitive traumas, such as childhood sexual abuse and domestic violence, which are more frequently experienced by girls and women. Further, women may not acknowledge sexually linked traumas—such as childhood sexual abuse and rape—unless the questions are asked in a sensitive manner and describe specific behaviors.
Table 1
TRAUMAS THAT CAUSE PTSD PREDOMINANTLY IN WOMEN
| Rape |
| Childhood sexual abuse |
| Domestic violence |
| Pregnancy loss |
| Labor and delivery |
| Neonatal complications |
| Sexual abuse of a child |
| Prostitution |
Types of trauma. Certain types of trauma are associated with especially high conditional risk of PTSD, defined as the risk of developing PTSD after being exposed to the trauma. Childhood sexual abuse, domestic violence, and rape are among the traumas with the highest conditional risk, and women are more likely to be exposed to these trauma types than men.6
Childhood sexual abuse has a particularly high conditional risk of PTSD.7 Such abuse happens over long periods during developmentally vulnerable stages of life. Sexual abuse perpetrated by a family member creates a greater sense of betrayal than does trauma at the hands of a stranger or an impersonal force of nature. In many cases, the victims blame themselves.
Domestic violence, like sexual abuse, has a high conditional PTSD risk because of the intimate nature of the relationship and the usual pattern of multiple assaults over time.
Rape carries the highest conditional risk of any trauma,8 possibly because of the degree to which rape violates a victim’s assumptions about the world as a reasonably safe place.3 PTSD risk after rape is intensified when the victim blames himself or herself and when society—such as the family or court system—reinforces this tendency toward self-blame.9
Influence of sex hormones. Neurophysiologic systems that lie beneath stress responses are closely linked with reproductive physiology.10 Evolution may have favored this association, allowing reproductive efforts to shut down during extreme stress.
Key components of the primary stress-activated hormonal system—corticotropin-releasing hormone, adrenocorticotropic hormone, and the glucocorticoids—inhibit secretion of gonadotropin-releasing hormone and the gonadotropins, the major reproductive hormones. In turn, sex hormones modulate hypothalamic-pituitary adrenal (HPA) axis activity, stress-linked neurotransmitter changes, and behavioral responses to stress.
This intertwining of stress and reproductive hormones suggests that men’s and women’s physiologic response to trauma may differ. Women’s vulnerability to PTSD also may vary at different parts of their menstrual cycles, during pregnancy, or postpartum.
Several animal studies have shown a more intense HPA axis response to stress in females than in males’.11 To date, however, studies have not shown clear gender differences in human physiologic response to trauma. Increased sympathetic nervous system activity, enhanced dexamethasone suppression of cortisol, and hippocampal atrophy have been found in both men and women with PTSD.11,12
Some human studies suggest gender differences in PTSD-related neurophysiologic changes. For example, activation of both the sympathetic and adrenocortical systems (epinephrine and cortisol) has been seen in women with PTSD from childhood sexual abuse, whereas activation of only the sympathetic system (epinephrine but not cortisol) has been seen in men with combat-related PTSD.13 Research with improved methodology is investigating whether sex hormones modulate human response to trauma.
Gender role differences. Because of cultural expectations, women may more easily acknowledge and report distress and feelings of being traumatized.14 This behavioral difference may contribute to higher PTSD prevalence rates in women than in men. Women also may develop more negative beliefs in response to some types of trauma, such as nonsexual assault by a stranger.3
Treating PTSD in women
Drug therapy. Antidepressants—including tricyclics, monoamine oxidase inhibitors, and selective serotonin reuptake inhibitors (SSRIs)—have shown efficacy in treating PTSD. Some studies have found that women respond more robustly to SSRI antidepressants than men.15
Cognitive-behavioral therapy. Trauma victims tend to avoid reminders of the trauma. Although this coping strategy can provide short-term relief, it can also constrict a person’s life and preclude opportunities to correct distorted information. For example, a person may attribute danger to benign stimuli that were coincidentally associated with the trauma, such as fearing all men with mustaches after being raped by a man with a mustache.3
Table 2
MALADAPTIVE REACTIONS DURING LABOR AND DELIVERY
| Reaction type | Description |
|---|---|
| Fighting |
|
| Regression |
|
| Dissociation |
|
| Over-control |
|
Cognitive-behavioral therapy (CBT) for PTSD aims to activate and correct information by prolonged exposure to traumatic stimuli and to restructure incorrect cognitions. CBT approaches to PTSD include exposure therapy, cognitive therapy, cognitive processing, stress inoculation training, assertiveness training, systematic desensitization, biofeedback, and relaxation training. Of these, exposure therapy has been studied the most systematically and found to work especially well for female rape victims.16 Exposure therapy consists of confronting feared stimuli—such as returning to the scene of a rape or recalling detailed memories of childhood sexual abuse—until anxiety diminishes.
Psychodynamic therapy aims to re-engage normal adaptive mechanisms by introducing the unconscious into consciousness in tolerable doses.17 Therapy serves as a means of processing traumatic events, such as childhood sexual abuse, and exploring the psychological meanings of traumas.18 Few well-controlled studies have examined psychodynamic therapy in PTSD, in part because of the difficulty in operationally defining and assessing mechanisms of change. However, at least one relatively controlled study found reduced avoidance symptoms with psychodynamic therapy, compared with wait list and active treatment groups.19
EMDR. During eye movement desensitization and reprocessing (EMDR), the patient focuses on a disturbing image, a negative cognition, and somatic sensations associated with the trauma while tracking the movement of the clinician’s finger within her visual field.20 The procedure is repeated until the patient’s distress is reduced and she develops more adaptive thoughts about the trauma.
Most EMDR practitioners recommend its use primarily for single-event traumas, such as rape or traumatic labor and delivery. Meta-analyses have suggested that EMDR may be as effective as other exposure therapy,21 although methodologic problems in several studies limit our ability to determine EMDR’s efficacy in treating women with PTSD.22
Treating and preventing perinatal PTSD
Historically, common outcomes of giving birth included death or chronic disability. Despite advances in obstetric care, labor and delivery remains painful, frightening, and potentially dangerous. Although childbirth is a normative experience for many women, an estimated 2.8 to 5.6% of new mothers develop labor-related PTSD.23-25 Risk of PTSD is increased in women with:
- high general anxiety levels prior to labor
- a history of mental illness
- unplanned pregnancy
- absence of partner during labor and delivery
- the perception that obstetric staff is unsupportive or ineffective
- a need for obstetric interventions, including episiotomy, emergency cesarean section, or use of forceps
- a perception of lack of control.
Table 3
LABOR INTERVENTIONS FOR VICTIMS OF CHILDHOOD SEXUAL ABUSE
|
Untreated PTSD may impair the woman’s functional ability and compromise her relationship with the infant:
Avoidance can extend to subsequent health care (such as not attending the postpartum checkup), sexual relationships, caring for the baby, and future pregnancies. Some women request general anesthesia and cesarean sections for future deliveries.
Arousal may intensify postpartum sleep disturbance and fatigue and may cause a mother to be hypervigilant about her baby.
Flashbacks can influence feelings about the baby, such as when the mother has repeated, vivid memories of the newborn being limp and blue after delivery, even though the infant is healthy now.
Preventive interventions that can minimize PTSD risk after labor and dshlivery include:
- explaining to women before the onset of labor that emergency obstetric interventions might be necessary
- providing adequate social support during labor and delivery
- ensuring that the obstetric staff communicates clearly with the patient
- effectively managing pain to minimize trauma.
Postpartum, it is important to screen for PTSD symptoms among high-risk women. Prompt intervention can alleviate symptoms and minimize adverse effects on the family and the mother-infant relationship.
Role of sexual abuse in perinatal PTSD. For a woman who was sexually abused as a child, even an uncomplicated labor and delivery may trigger memories, flashbacks, and emotions associated with the abuse.26 Physical sensations associated with gynecologic examinations and labor contractions may remind her of abuse-related sensations. Some women with sexual abuse histories react adversely to the loss of control and need to depend on others during labor and delivery.
Unrecognized posttraumatic reactions during labor may result in maladaptive behaviors (Table 2).26 Obstetric staff who encounter these behaviors without being aware of their origins may think the patient is oppositional or noncompliant and may regard her as an adversary to be defeated or bypassed in order to safely deliver the baby.27 The psychiatrist can minimize this problem early in labor by alerting the staff to signs of possible sexual abuse-related PTSD. These may include:
- little or no prenatal care (due to fear of obstetric procedures)
- unusual fears of needles, intravenous lines, etc.
- recoiling when touched during obstetric examinations
- insistence on female obstetric staff
- extreme sensitivity about bodily exposure.26,28
Table 4
USE OF ANTIDEPRESSANTS FOR PTSD DURING BREAST FEEDING
| Medication | Nursling dose range* | Reported nursling side effects |
|---|---|---|
| Citalopram | 0.7 to 9.0% | Uneasy sleep |
| Fluoxetine | 1.2 to 12.0% | Vomiting, watery stools, excessive crying, difficulty sleeping, tremor, somnolence, hypotonia, decreased weight gain |
| Mirtazapine | Not known | Not known |
| Nefazodone | 0.45% | Drowsiness, poor feeding, difficulty maintaining body temperature |
| Paroxetine | 0.1 to 4.3% | None |
| Sertraline | 0.4 to 1.0% | None |
| Venlafaxine | 5.2 to 7.4% | None |
| *Weight-adjusted estimated percent of mother’s dose ingested by a nursing infant | ||
Intervention. Once abuse-related perinatal PTSD is diagnosed, the interventions in Table 3 can help a woman through labor and delivery.26,28 When successful, they can turn childbirth into a healing experience that promotes the mother’s sense of accomplishment, positive association with sexuality, and a new relationship with her body.28
Breastfeeding can also trigger flashbacks and frightening emotions in a woman who was sexually abused as a child.29 She may confuse normal sensations of skin-to-skin contact with the baby or the milk ejection reflex with unpleasant sexually-linked feelings. In such cases, it may help to:
- explain the normal sensations associated with breastfeeding and normal behaviors of breastfeeding infants
- show her how to gently redirect her baby if it does something she finds uncomfortable
- identify situations that are especially difficult for her (such as nighttime feedings) and substitute bottle feeding at those times.
These measures may promote feelings of self-efficacy and help more in the long run than prematurely giving up on breastfeeding.
Prescribing to the nursing woman. When prescribing medication for PTSD in a breast-feeding woman, minimize potential infant side effects by choosing agents that produce relatively low drug levels in breast milk (Table 4).30-34 Sertraline—the first medication to receive Food and Drug Administration approval for treating PTSD—is recommended during breastfeeding.35
Pregnancy loss. Although the prevalence of PTSD in response to miscarriage or stillbirth is unknown, some women clearly develop PTSD after pregnancy loss. The degree of associated physical trauma—and of social and professional support—influence anxiety levels in response to miscarriage36 and may also influence the likelihood of developing PTSD. Pregnancy loss after the first trimester may be more likely to result in PTSD than earlier loss, and subsequent pregnancies may exacerbate PTSD symptoms. In one study, spontaneous fetal loss after the 18th week of gestation led to high rates of PTSD symptoms in a subsequent pregnancy and up to 1 year postpartum.37
Asking a woman how she wants to grieve her pregnancy loss and helping her in that process may minimize her risk of subsequent PTSD. Couples counseling may help in some cases, as each partner may have a different grieving style.
Related resources
- Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
- Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002.
- Madison Institute of Medicine. Facts for Health: posttraumatic stress disorder. www.ptsd.factsforhealth.org
Drug brand names
- Citalopram • Celexa
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Posttraumatic stress disorder (PTSD) was first recognized as a diagnosis in male Vietnam War veterans, but studies since then have consistently found PTSD to be more common in women than in men. Understanding the gender-related differences in PTSD’s presentation can help us craft optimal treatment for women suffering with this persistent disorder.
Data from the National Comorbidity Survey suggest a lifetime PTSD prevalence of 10.4% in women and 5.0% in men.1 PTSD also tends to be more chronic in women. In one study of patients with PTSD, median time from symptom onset to remission was 4 years for women and 1 year for men.2
Evidence suggests that women:
- experience more or different types of trauma than men, including labor and delivery, rape, and childhood sexual abuse
- may react to trauma more often and more robustly than men because of sex hormones, cultural gender roles, or some combination of those factors.
How women experience trauma
Among studies that show gender differences in response to specific trauma, nearly all have found higher PTSD rates in women than in men. This pattern emerges early in life and is seen in children and adults.
A meta-analysis comparing PTSD symptoms in females and males of all ages after specific traumas3 found that females were much more likely than males to report PTSD symptoms after some types of trauma but not others. None of the trauma types predicted PTSD more often for males than for females.
Amount of trauma. Men are more likely than women to be exposed to traumatic events, such as violent assault, during their lifetimes.4 However, the types of trauma that women experience predominantly or exclusively—such as childhood sexual abuse, traumatic labor and delivery, pregnancy loss, severe health problems in a newborn, and prostitution—are rarely included in trauma questionnaires (Table 1). As a result, the full range of traumatic experiences in women’s lives is likely underestimated.
Instruments designed to measure trauma may inadvertently introduce gender bias in other ways.5 For example, questionnaires asking about single traumatic events may underestimate the impact of repetitive traumas, such as childhood sexual abuse and domestic violence, which are more frequently experienced by girls and women. Further, women may not acknowledge sexually linked traumas—such as childhood sexual abuse and rape—unless the questions are asked in a sensitive manner and describe specific behaviors.
Table 1
TRAUMAS THAT CAUSE PTSD PREDOMINANTLY IN WOMEN
| Rape |
| Childhood sexual abuse |
| Domestic violence |
| Pregnancy loss |
| Labor and delivery |
| Neonatal complications |
| Sexual abuse of a child |
| Prostitution |
Types of trauma. Certain types of trauma are associated with especially high conditional risk of PTSD, defined as the risk of developing PTSD after being exposed to the trauma. Childhood sexual abuse, domestic violence, and rape are among the traumas with the highest conditional risk, and women are more likely to be exposed to these trauma types than men.6
Childhood sexual abuse has a particularly high conditional risk of PTSD.7 Such abuse happens over long periods during developmentally vulnerable stages of life. Sexual abuse perpetrated by a family member creates a greater sense of betrayal than does trauma at the hands of a stranger or an impersonal force of nature. In many cases, the victims blame themselves.
Domestic violence, like sexual abuse, has a high conditional PTSD risk because of the intimate nature of the relationship and the usual pattern of multiple assaults over time.
Rape carries the highest conditional risk of any trauma,8 possibly because of the degree to which rape violates a victim’s assumptions about the world as a reasonably safe place.3 PTSD risk after rape is intensified when the victim blames himself or herself and when society—such as the family or court system—reinforces this tendency toward self-blame.9
Influence of sex hormones. Neurophysiologic systems that lie beneath stress responses are closely linked with reproductive physiology.10 Evolution may have favored this association, allowing reproductive efforts to shut down during extreme stress.
Key components of the primary stress-activated hormonal system—corticotropin-releasing hormone, adrenocorticotropic hormone, and the glucocorticoids—inhibit secretion of gonadotropin-releasing hormone and the gonadotropins, the major reproductive hormones. In turn, sex hormones modulate hypothalamic-pituitary adrenal (HPA) axis activity, stress-linked neurotransmitter changes, and behavioral responses to stress.
This intertwining of stress and reproductive hormones suggests that men’s and women’s physiologic response to trauma may differ. Women’s vulnerability to PTSD also may vary at different parts of their menstrual cycles, during pregnancy, or postpartum.
Several animal studies have shown a more intense HPA axis response to stress in females than in males’.11 To date, however, studies have not shown clear gender differences in human physiologic response to trauma. Increased sympathetic nervous system activity, enhanced dexamethasone suppression of cortisol, and hippocampal atrophy have been found in both men and women with PTSD.11,12
Some human studies suggest gender differences in PTSD-related neurophysiologic changes. For example, activation of both the sympathetic and adrenocortical systems (epinephrine and cortisol) has been seen in women with PTSD from childhood sexual abuse, whereas activation of only the sympathetic system (epinephrine but not cortisol) has been seen in men with combat-related PTSD.13 Research with improved methodology is investigating whether sex hormones modulate human response to trauma.
Gender role differences. Because of cultural expectations, women may more easily acknowledge and report distress and feelings of being traumatized.14 This behavioral difference may contribute to higher PTSD prevalence rates in women than in men. Women also may develop more negative beliefs in response to some types of trauma, such as nonsexual assault by a stranger.3
Treating PTSD in women
Drug therapy. Antidepressants—including tricyclics, monoamine oxidase inhibitors, and selective serotonin reuptake inhibitors (SSRIs)—have shown efficacy in treating PTSD. Some studies have found that women respond more robustly to SSRI antidepressants than men.15
Cognitive-behavioral therapy. Trauma victims tend to avoid reminders of the trauma. Although this coping strategy can provide short-term relief, it can also constrict a person’s life and preclude opportunities to correct distorted information. For example, a person may attribute danger to benign stimuli that were coincidentally associated with the trauma, such as fearing all men with mustaches after being raped by a man with a mustache.3
Table 2
MALADAPTIVE REACTIONS DURING LABOR AND DELIVERY
| Reaction type | Description |
|---|---|
| Fighting |
|
| Regression |
|
| Dissociation |
|
| Over-control |
|
Cognitive-behavioral therapy (CBT) for PTSD aims to activate and correct information by prolonged exposure to traumatic stimuli and to restructure incorrect cognitions. CBT approaches to PTSD include exposure therapy, cognitive therapy, cognitive processing, stress inoculation training, assertiveness training, systematic desensitization, biofeedback, and relaxation training. Of these, exposure therapy has been studied the most systematically and found to work especially well for female rape victims.16 Exposure therapy consists of confronting feared stimuli—such as returning to the scene of a rape or recalling detailed memories of childhood sexual abuse—until anxiety diminishes.
Psychodynamic therapy aims to re-engage normal adaptive mechanisms by introducing the unconscious into consciousness in tolerable doses.17 Therapy serves as a means of processing traumatic events, such as childhood sexual abuse, and exploring the psychological meanings of traumas.18 Few well-controlled studies have examined psychodynamic therapy in PTSD, in part because of the difficulty in operationally defining and assessing mechanisms of change. However, at least one relatively controlled study found reduced avoidance symptoms with psychodynamic therapy, compared with wait list and active treatment groups.19
EMDR. During eye movement desensitization and reprocessing (EMDR), the patient focuses on a disturbing image, a negative cognition, and somatic sensations associated with the trauma while tracking the movement of the clinician’s finger within her visual field.20 The procedure is repeated until the patient’s distress is reduced and she develops more adaptive thoughts about the trauma.
Most EMDR practitioners recommend its use primarily for single-event traumas, such as rape or traumatic labor and delivery. Meta-analyses have suggested that EMDR may be as effective as other exposure therapy,21 although methodologic problems in several studies limit our ability to determine EMDR’s efficacy in treating women with PTSD.22
Treating and preventing perinatal PTSD
Historically, common outcomes of giving birth included death or chronic disability. Despite advances in obstetric care, labor and delivery remains painful, frightening, and potentially dangerous. Although childbirth is a normative experience for many women, an estimated 2.8 to 5.6% of new mothers develop labor-related PTSD.23-25 Risk of PTSD is increased in women with:
- high general anxiety levels prior to labor
- a history of mental illness
- unplanned pregnancy
- absence of partner during labor and delivery
- the perception that obstetric staff is unsupportive or ineffective
- a need for obstetric interventions, including episiotomy, emergency cesarean section, or use of forceps
- a perception of lack of control.
Table 3
LABOR INTERVENTIONS FOR VICTIMS OF CHILDHOOD SEXUAL ABUSE
|
Untreated PTSD may impair the woman’s functional ability and compromise her relationship with the infant:
Avoidance can extend to subsequent health care (such as not attending the postpartum checkup), sexual relationships, caring for the baby, and future pregnancies. Some women request general anesthesia and cesarean sections for future deliveries.
Arousal may intensify postpartum sleep disturbance and fatigue and may cause a mother to be hypervigilant about her baby.
Flashbacks can influence feelings about the baby, such as when the mother has repeated, vivid memories of the newborn being limp and blue after delivery, even though the infant is healthy now.
Preventive interventions that can minimize PTSD risk after labor and dshlivery include:
- explaining to women before the onset of labor that emergency obstetric interventions might be necessary
- providing adequate social support during labor and delivery
- ensuring that the obstetric staff communicates clearly with the patient
- effectively managing pain to minimize trauma.
Postpartum, it is important to screen for PTSD symptoms among high-risk women. Prompt intervention can alleviate symptoms and minimize adverse effects on the family and the mother-infant relationship.
Role of sexual abuse in perinatal PTSD. For a woman who was sexually abused as a child, even an uncomplicated labor and delivery may trigger memories, flashbacks, and emotions associated with the abuse.26 Physical sensations associated with gynecologic examinations and labor contractions may remind her of abuse-related sensations. Some women with sexual abuse histories react adversely to the loss of control and need to depend on others during labor and delivery.
Unrecognized posttraumatic reactions during labor may result in maladaptive behaviors (Table 2).26 Obstetric staff who encounter these behaviors without being aware of their origins may think the patient is oppositional or noncompliant and may regard her as an adversary to be defeated or bypassed in order to safely deliver the baby.27 The psychiatrist can minimize this problem early in labor by alerting the staff to signs of possible sexual abuse-related PTSD. These may include:
- little or no prenatal care (due to fear of obstetric procedures)
- unusual fears of needles, intravenous lines, etc.
- recoiling when touched during obstetric examinations
- insistence on female obstetric staff
- extreme sensitivity about bodily exposure.26,28
Table 4
USE OF ANTIDEPRESSANTS FOR PTSD DURING BREAST FEEDING
| Medication | Nursling dose range* | Reported nursling side effects |
|---|---|---|
| Citalopram | 0.7 to 9.0% | Uneasy sleep |
| Fluoxetine | 1.2 to 12.0% | Vomiting, watery stools, excessive crying, difficulty sleeping, tremor, somnolence, hypotonia, decreased weight gain |
| Mirtazapine | Not known | Not known |
| Nefazodone | 0.45% | Drowsiness, poor feeding, difficulty maintaining body temperature |
| Paroxetine | 0.1 to 4.3% | None |
| Sertraline | 0.4 to 1.0% | None |
| Venlafaxine | 5.2 to 7.4% | None |
| *Weight-adjusted estimated percent of mother’s dose ingested by a nursing infant | ||
Intervention. Once abuse-related perinatal PTSD is diagnosed, the interventions in Table 3 can help a woman through labor and delivery.26,28 When successful, they can turn childbirth into a healing experience that promotes the mother’s sense of accomplishment, positive association with sexuality, and a new relationship with her body.28
Breastfeeding can also trigger flashbacks and frightening emotions in a woman who was sexually abused as a child.29 She may confuse normal sensations of skin-to-skin contact with the baby or the milk ejection reflex with unpleasant sexually-linked feelings. In such cases, it may help to:
- explain the normal sensations associated with breastfeeding and normal behaviors of breastfeeding infants
- show her how to gently redirect her baby if it does something she finds uncomfortable
- identify situations that are especially difficult for her (such as nighttime feedings) and substitute bottle feeding at those times.
These measures may promote feelings of self-efficacy and help more in the long run than prematurely giving up on breastfeeding.
Prescribing to the nursing woman. When prescribing medication for PTSD in a breast-feeding woman, minimize potential infant side effects by choosing agents that produce relatively low drug levels in breast milk (Table 4).30-34 Sertraline—the first medication to receive Food and Drug Administration approval for treating PTSD—is recommended during breastfeeding.35
Pregnancy loss. Although the prevalence of PTSD in response to miscarriage or stillbirth is unknown, some women clearly develop PTSD after pregnancy loss. The degree of associated physical trauma—and of social and professional support—influence anxiety levels in response to miscarriage36 and may also influence the likelihood of developing PTSD. Pregnancy loss after the first trimester may be more likely to result in PTSD than earlier loss, and subsequent pregnancies may exacerbate PTSD symptoms. In one study, spontaneous fetal loss after the 18th week of gestation led to high rates of PTSD symptoms in a subsequent pregnancy and up to 1 year postpartum.37
Asking a woman how she wants to grieve her pregnancy loss and helping her in that process may minimize her risk of subsequent PTSD. Couples counseling may help in some cases, as each partner may have a different grieving style.
Related resources
- Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
- Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002.
- Madison Institute of Medicine. Facts for Health: posttraumatic stress disorder. www.ptsd.factsforhealth.org
Drug brand names
- Citalopram • Celexa
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Nefazodone • Serzone
- Paroxetine • Paxil
- Sertraline • Zoloft
- Venlafaxine • Effexor
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Kessler RC, Sonnega A, Bromet E, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
2. Breslau N, Kessler R, Chilcoat H, Schulz L, Davis G, Andreski P. Trauma and post-traumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:627-32.
3. Tolin DF, Foa EB. Gender and PTSD: a cognitive model. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;76-97.
4. Breslau N, Chilcoat HD, Kessler RC, Peterson EL, Lucia VC. Vulnerability to assaultive violence: further specification of the sex difference in post-traumatic stress disorder. Psychol Med 1999;29:813-21.
5. Cusack K, Falsetti S, de Arellano M. Gender considerations in the psychometric assessment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;150-76.
6. Norris F, Foster JD, Weisshaar DL. The epidemiology of sex differences in PTSD across developmental, societal, and research contexts. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;3-42.
7. DePrince AP, Freyd JJ. The intersection of gender and betrayal in trauma. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;98-113.
8. Breslau N, Davis G, Andreski P, Peterson E. Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry 1991;48:216-22.
9. Best CL, Dansky BS, Kilpatrick DG. Medical students’ attitudes about female rape victims. J Interpersonal Violence 1992;7:175-88.
10. Rubinow DR, Schmidt PJ. The neuroendocrinology of menstrual cycle mood disorders. Ann NY Acad Sci 1995;771:648-59.
11. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
12. Rasmusson AM, Friedman MJ. Gender issues in the neurobiology of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;43-75.
13. Lemieux AM, Coe CL. Abuse-related posttraumatic stress disorder: evidence for chronic neuroendocrine activation in women. Psychosomatic Med 1995;57:105-15.
14. Saxe G, Wolfe J. Gender and posttraumatic stress disorder. In: Saigh P, Bremner JD (eds). Posttraumatic stress disorder: A comprehensive text. Boston: Allyn & Bacon, 1999;160-79.
15. Brady KT, Back SE. Gender and the psychopharmacological treatment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;335-48.
16. Foa EB, Rothbaum BO, Riggs DS, Murdock TB. Treatment of posttraumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedures and counseling. J Consult Clin Psychol 1991;59:715-23.
17. Kudler HS, Blank AS, Krupnick JL. Psychodynamic therapy. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;176-98.
18. Krupnick JL. Brief psychodynamic treatment of PTSD. J Clin Psychol 2002;58:919-32.
19. Brom D, Kleber RJ, Defares PB. Brief psychotherapy for posttraumatic stress disorders. J Consult Clin Psychol 1989;57:607-12.
20. Chemtob CM, Tolin DF, van der Kolk BA, Pitman RK. Eye movement desensitization and reprocessing. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;333-5.
21. Davidson PR, Parker CH. Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol 2001;69:305-16.
22. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
23. Creedy D, Shochet I, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000;27:104-11.
24. Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br J Clin Psychol 2000;39:35-51.
25. Ayers S, Pickering AD. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001;28:111-18.
26. Rhodes N, Hutchinson S. Labor experiences of childhood sexual abuse survivors. Birth 1994;21:213-20.
27. Josephs L. Women and trauma: a contemporary psychodynamic approach to traumatization for patients in the OB/GYN psychological consultation clinic. Bull Menninger Clin 1996;60:22-8.
28. Burian J. Helping survivors of sexual abuse through labor. MCN 1995;20:252-6.
29. Kendall-Tackett K. Breastfeeding and the sexual abuse survivor. J Hum Lact 1998;14:125-30.
30. Ilett KF, Kristensen JH, Hackett LP, Paech M, Kohan R, Rampono J. Distribution of venlafaxine and its O-desmethyl metabolite in human milk and their effects in breastfed infants. Br J Clin Pharmacol 2002;53:17-22.
31. Kristensen JH, Ilett KF, Yapp P, Paech M, Begg EJ. Distribution and excretion of fluoxetine and norfluoxetine in human milk. Br J Clin Pharmacol 1999;48:521-7.
32. Misri S, Kim J, Riggs KW, Kostaras X. Paroxetine levels in postpartum depressed women, breast milk, and infant serum. J Clin Psychiatry 2000;61:828-32.
33. Ohmann R, Hagg S, Carleborg L, Spigset O. Excretion of paroxetine into breast milk. J Clin Psychiatry 1999;60:519-23.
34. Yapp P, Ilett KF, Kristensen JH, Hackett LP, Paech MJ, Rampono J. Drowsiness and poor feeding in a breast-fed infant: association with nefazodone and its metabolites. Ann Pharmacother 2000;34:1269-72.
35. Altshuler LL, Cohen LS, Moline ML, Kahn DA, Carpenter D, Docherty JR. The Expert Consensus Guideline Series. Treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-107.
36. Lee C, Slade P. Miscarriage as a traumatic event: a review of the literature and new implications for intervention. J Psychosom Res 1996;40:225-44.
37. Turton P, Hughes P, Evans CDH, Fainman D. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry 2001;178:556-60.
1. Kessler RC, Sonnega A, Bromet E, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Survey. Arch Gen Psychiatry 1995;52:1048-60.
2. Breslau N, Kessler R, Chilcoat H, Schulz L, Davis G, Andreski P. Trauma and post-traumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry 1998;55:627-32.
3. Tolin DF, Foa EB. Gender and PTSD: a cognitive model. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;76-97.
4. Breslau N, Chilcoat HD, Kessler RC, Peterson EL, Lucia VC. Vulnerability to assaultive violence: further specification of the sex difference in post-traumatic stress disorder. Psychol Med 1999;29:813-21.
5. Cusack K, Falsetti S, de Arellano M. Gender considerations in the psychometric assessment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;150-76.
6. Norris F, Foster JD, Weisshaar DL. The epidemiology of sex differences in PTSD across developmental, societal, and research contexts. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;3-42.
7. DePrince AP, Freyd JJ. The intersection of gender and betrayal in trauma. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;98-113.
8. Breslau N, Davis G, Andreski P, Peterson E. Traumatic events and posttraumatic stress disorder in an urban population of young adults. Arch Gen Psychiatry 1991;48:216-22.
9. Best CL, Dansky BS, Kilpatrick DG. Medical students’ attitudes about female rape victims. J Interpersonal Violence 1992;7:175-88.
10. Rubinow DR, Schmidt PJ. The neuroendocrinology of menstrual cycle mood disorders. Ann NY Acad Sci 1995;771:648-59.
11. Sapolsky RM. Glucocorticoids and hippocampal atrophy in neuropsychiatric disorders. Arch Gen Psychiatry 2000;57:925-35.
12. Rasmusson AM, Friedman MJ. Gender issues in the neurobiology of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;43-75.
13. Lemieux AM, Coe CL. Abuse-related posttraumatic stress disorder: evidence for chronic neuroendocrine activation in women. Psychosomatic Med 1995;57:105-15.
14. Saxe G, Wolfe J. Gender and posttraumatic stress disorder. In: Saigh P, Bremner JD (eds). Posttraumatic stress disorder: A comprehensive text. Boston: Allyn & Bacon, 1999;160-79.
15. Brady KT, Back SE. Gender and the psychopharmacological treatment of PTSD. In: Kimerling R, Ouimette P, Wolfe J (eds). Gender and PTSD. New York: Guilford Publications, 2002;335-48.
16. Foa EB, Rothbaum BO, Riggs DS, Murdock TB. Treatment of posttraumatic stress disorder in rape victims: a comparison between cognitive-behavioral procedures and counseling. J Consult Clin Psychol 1991;59:715-23.
17. Kudler HS, Blank AS, Krupnick JL. Psychodynamic therapy. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;176-98.
18. Krupnick JL. Brief psychodynamic treatment of PTSD. J Clin Psychol 2002;58:919-32.
19. Brom D, Kleber RJ, Defares PB. Brief psychotherapy for posttraumatic stress disorders. J Consult Clin Psychol 1989;57:607-12.
20. Chemtob CM, Tolin DF, van der Kolk BA, Pitman RK. Eye movement desensitization and reprocessing. In: Foa EB, Keane TM, Friedman MJ (eds). Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000;333-5.
21. Davidson PR, Parker CH. Eye movement desensitization and reprocessing (EMDR): a meta-analysis. J Consult Clin Psychol 2001;69:305-16.
22. Foa EB, Keane TM, Friedman MJ. Effective treatments for PTSD: practice guidelines from the International Society for Traumatic Stress studies. New York: Guilford Publications, 2000.
23. Creedy D, Shochet I, Horsfall J. Childbirth and the development of acute trauma symptoms: incidence and contributing factors. Birth 2000;27:104-11.
24. Czarnocka J, Slade P. Prevalence and predictors of post-traumatic stress symptoms following childbirth. Br J Clin Psychol 2000;39:35-51.
25. Ayers S, Pickering AD. Do women get posttraumatic stress disorder as a result of childbirth? A prospective study of incidence. Birth 2001;28:111-18.
26. Rhodes N, Hutchinson S. Labor experiences of childhood sexual abuse survivors. Birth 1994;21:213-20.
27. Josephs L. Women and trauma: a contemporary psychodynamic approach to traumatization for patients in the OB/GYN psychological consultation clinic. Bull Menninger Clin 1996;60:22-8.
28. Burian J. Helping survivors of sexual abuse through labor. MCN 1995;20:252-6.
29. Kendall-Tackett K. Breastfeeding and the sexual abuse survivor. J Hum Lact 1998;14:125-30.
30. Ilett KF, Kristensen JH, Hackett LP, Paech M, Kohan R, Rampono J. Distribution of venlafaxine and its O-desmethyl metabolite in human milk and their effects in breastfed infants. Br J Clin Pharmacol 2002;53:17-22.
31. Kristensen JH, Ilett KF, Yapp P, Paech M, Begg EJ. Distribution and excretion of fluoxetine and norfluoxetine in human milk. Br J Clin Pharmacol 1999;48:521-7.
32. Misri S, Kim J, Riggs KW, Kostaras X. Paroxetine levels in postpartum depressed women, breast milk, and infant serum. J Clin Psychiatry 2000;61:828-32.
33. Ohmann R, Hagg S, Carleborg L, Spigset O. Excretion of paroxetine into breast milk. J Clin Psychiatry 1999;60:519-23.
34. Yapp P, Ilett KF, Kristensen JH, Hackett LP, Paech MJ, Rampono J. Drowsiness and poor feeding in a breast-fed infant: association with nefazodone and its metabolites. Ann Pharmacother 2000;34:1269-72.
35. Altshuler LL, Cohen LS, Moline ML, Kahn DA, Carpenter D, Docherty JR. The Expert Consensus Guideline Series. Treatment of depression in women. Postgrad Med 2001 Mar;(Spec No):1-107.
36. Lee C, Slade P. Miscarriage as a traumatic event: a review of the literature and new implications for intervention. J Psychosom Res 1996;40:225-44.
37. Turton P, Hughes P, Evans CDH, Fainman D. Incidence, correlates and predictors of post-traumatic stress disorder in the pregnancy after stillbirth. Br J Psychiatry 2001;178:556-60.