User login
Obesity at Age 18 May Raise Risk of Later Psoriatic Arthritis
People who are obese at age 18 may be at an increased risk for psoriatic arthritis later in life, according to a report in the July issue of the Archives of Dermatology.
In a single-center study of 943 psoriasis patients, those who reported being obese at age 18 were three times more likely to develop psoriatic arthritis (PsA), compared with patients who reported having a normal body mass index at age 18, reported Dr. Razieh Soltani-Arabshahi and associates of the University of Utah School of Medicine, Salt Lake City.
In a previous study, the researchers found that patients with psoriasis had an increased BMI, compared with controls. So, they “set out to study if obesity increases the risk of PsA,” using data from a large cohort of subjects enrolled in the Utah Psoriasis Initiative, the researchers noted.
The cohort included consecutive patients older than 18 years who attended university-affiliated psoriasis clinics in 2002-2008 and provided detailed demographic and clinical data. A total of 250 (27%) of the 943 subjects included in the study reported having PsA.
Of the study patients, 14% had been overweight and 5% had been obese at age 18, according to self-reported height and weight measurements.
Higher BMI was associated with an increased risk of developing PsA, independent of other risk factors such as nail involvement. Each unit increase in BMI at age 18 corresponded to a 5% increase in risk of PsA.
In addition, patients who were obese at age 18 showed an earlier onset of PsA, compared with patients of normal weight at age 18. Twenty percent of those who had been overweight or obese at 18 years developed PsA by age 35. In comparison, among patients of normal weight at age 18, 20% did not develop PsA until age 48.
Moreover, patients who had been overweight or obese at age 18 were more likely to report having severe psoriasis (47% and 57%, respectively) than patients who were of normal weight at age 18 (39%).
The design of the study did not permit the investigators to infer causality. However, it is plausible that obesity and its associated inflammatory state might contribute to both psoriasis and PsA, Dr. Soltani-Arabshahi and colleagues reported (Arch. Dermatol. 2010;146:721-6).
“Evaluation of additional sample sets in an attempt to replicate these results is imperative for strong conclusions to be drawn,” they noted.
The study was limited in that it relied on subjects’ self-report of height and weight earlier in life, self-report of psoriasis severity, and self-report of diagnosis of PsA.
The study was supported in part by the Utah Psoriasis Initiative and the Benning Foundation. Dr. Soltani-Arabshahi’s associates reported numerous industry relationships.
People who are obese at age 18 may be at an increased risk for psoriatic arthritis later in life, according to a report in the July issue of the Archives of Dermatology.
In a single-center study of 943 psoriasis patients, those who reported being obese at age 18 were three times more likely to develop psoriatic arthritis (PsA), compared with patients who reported having a normal body mass index at age 18, reported Dr. Razieh Soltani-Arabshahi and associates of the University of Utah School of Medicine, Salt Lake City.
In a previous study, the researchers found that patients with psoriasis had an increased BMI, compared with controls. So, they “set out to study if obesity increases the risk of PsA,” using data from a large cohort of subjects enrolled in the Utah Psoriasis Initiative, the researchers noted.
The cohort included consecutive patients older than 18 years who attended university-affiliated psoriasis clinics in 2002-2008 and provided detailed demographic and clinical data. A total of 250 (27%) of the 943 subjects included in the study reported having PsA.
Of the study patients, 14% had been overweight and 5% had been obese at age 18, according to self-reported height and weight measurements.
Higher BMI was associated with an increased risk of developing PsA, independent of other risk factors such as nail involvement. Each unit increase in BMI at age 18 corresponded to a 5% increase in risk of PsA.
In addition, patients who were obese at age 18 showed an earlier onset of PsA, compared with patients of normal weight at age 18. Twenty percent of those who had been overweight or obese at 18 years developed PsA by age 35. In comparison, among patients of normal weight at age 18, 20% did not develop PsA until age 48.
Moreover, patients who had been overweight or obese at age 18 were more likely to report having severe psoriasis (47% and 57%, respectively) than patients who were of normal weight at age 18 (39%).
The design of the study did not permit the investigators to infer causality. However, it is plausible that obesity and its associated inflammatory state might contribute to both psoriasis and PsA, Dr. Soltani-Arabshahi and colleagues reported (Arch. Dermatol. 2010;146:721-6).
“Evaluation of additional sample sets in an attempt to replicate these results is imperative for strong conclusions to be drawn,” they noted.
The study was limited in that it relied on subjects’ self-report of height and weight earlier in life, self-report of psoriasis severity, and self-report of diagnosis of PsA.
The study was supported in part by the Utah Psoriasis Initiative and the Benning Foundation. Dr. Soltani-Arabshahi’s associates reported numerous industry relationships.
People who are obese at age 18 may be at an increased risk for psoriatic arthritis later in life, according to a report in the July issue of the Archives of Dermatology.
In a single-center study of 943 psoriasis patients, those who reported being obese at age 18 were three times more likely to develop psoriatic arthritis (PsA), compared with patients who reported having a normal body mass index at age 18, reported Dr. Razieh Soltani-Arabshahi and associates of the University of Utah School of Medicine, Salt Lake City.
In a previous study, the researchers found that patients with psoriasis had an increased BMI, compared with controls. So, they “set out to study if obesity increases the risk of PsA,” using data from a large cohort of subjects enrolled in the Utah Psoriasis Initiative, the researchers noted.
The cohort included consecutive patients older than 18 years who attended university-affiliated psoriasis clinics in 2002-2008 and provided detailed demographic and clinical data. A total of 250 (27%) of the 943 subjects included in the study reported having PsA.
Of the study patients, 14% had been overweight and 5% had been obese at age 18, according to self-reported height and weight measurements.
Higher BMI was associated with an increased risk of developing PsA, independent of other risk factors such as nail involvement. Each unit increase in BMI at age 18 corresponded to a 5% increase in risk of PsA.
In addition, patients who were obese at age 18 showed an earlier onset of PsA, compared with patients of normal weight at age 18. Twenty percent of those who had been overweight or obese at 18 years developed PsA by age 35. In comparison, among patients of normal weight at age 18, 20% did not develop PsA until age 48.
Moreover, patients who had been overweight or obese at age 18 were more likely to report having severe psoriasis (47% and 57%, respectively) than patients who were of normal weight at age 18 (39%).
The design of the study did not permit the investigators to infer causality. However, it is plausible that obesity and its associated inflammatory state might contribute to both psoriasis and PsA, Dr. Soltani-Arabshahi and colleagues reported (Arch. Dermatol. 2010;146:721-6).
“Evaluation of additional sample sets in an attempt to replicate these results is imperative for strong conclusions to be drawn,” they noted.
The study was limited in that it relied on subjects’ self-report of height and weight earlier in life, self-report of psoriasis severity, and self-report of diagnosis of PsA.
The study was supported in part by the Utah Psoriasis Initiative and the Benning Foundation. Dr. Soltani-Arabshahi’s associates reported numerous industry relationships.
More Evidence Ties Rheumatoid Arthritis to Increased MI Risk
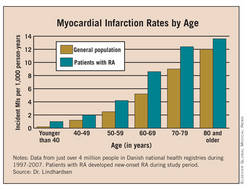
ROME - Adults with rheumatoid arthritis have a 65% higher rate of incident myocardial infarctions than does the general population, according to Danish data that strengthen the already significant evidence supporting a link between rheumatoid arthritis and elevated cardiovascular disease.
In addition, the new findings again showed that the heightened MI risk of RA patients matched the MI risk of patients with diabetes, Dr. Jesper Lindhardsen said at the annual European Congress of Rheumatology.
The new results also showed that the MI risk for RA patients at any age throughout adult life roughly matched the risk of a person without RA or diabetes who is 10 years older.
“An increased focus on the increased cardiovascular risk in patients with RA is warranted,” said Dr. Lindhardsen, a physician in the department of cardiology at Gentofte Hospital, Hellerup, Denmark. The attention paid to cardiovascular risk in RA patients should at least match the attention paid in diabetes patients, he added.
At last year’s European Congress of Rheumatology, a report from a task force convened by the European League Against Rheumatism declared that “rheumatoid arthritis should be regarded as a condition that is associated with higher risk for cardiovascular disease.” The report also spelled out 10 recommendations for cardiovascular disease risk management in RA patients. The report appeared in published form earlier this year (Ann. Rheum. Dis. 2010;69:325-1400).
The new findings by Dr. Lindhardsen and his associates took the prior evidence a step further by including RA patients with no prior diagnosis of cardiovascular disease, he said. The new study also provided a direct comparison of the risks conferred by RA and diabetes within the same background population, the entire Danish adult population during 1997-2007.

Dr. Lindhardsen and his associates used Danish national registry data during that period, a group of slightly more than 4 million people. During the decade studied, 10,547 adult Danes had newly diagnosed RA, and 132,868 had newly diagnosed diabetes, including both type 1 and type 2. The average age of those who developed RA was 56 years, and of those who developed diabetes it was 57 years, compared with an average age for everyone else of 46. Women constituted 71% of the incident RA cases, 46% of the incident diabetes cases, and 52% of the remaining population.
The researchers then tracked the rate of incident MIs in all three groups, with an average follow-up of 9 years in the general population, and 4 years following both the RA and diabetes diagnoses.
Compared with the rate of new-onset MI in the general population, RA patients had a 65% higher rate and patients with diabetes had a 73% higher rate, both statistically significant increases over the comparator group. This analysis adjusted for age, gender, cardiovascular pharmacotherapy, comorbidities, and socioeconomic status. About 400 people developed both RA and diabetes during the study period, and while their MI incidence was not additive, it significantly surpassed the rate among patients who had only RA or only diabetes, Dr. Lindhardsen said.
The analyses also provided insights into the interaction of age and gender with MI risk among RA patients. In general, the results showed that RA boosted MI risk regardless of age and gender. Among women younger than 50 years, RA and diabetes each boosted the MI risk sixfold, compared with similarly aged women without RA or diabetes. The impact on MI risk from either RA or diabetes fell substantially in women aged 50-65 years, and in women older than 65 years, although both RA and diabetes elevated the risk in both of these age groups. In men younger than 50 years, RA did not significantly raise MI risk but diabetes did. The biggest impact of RA on MI risk occurred in men aged 50-65, who had a twofold increased MI risk, compared with men who did not have RA or diabetes.
In another analysis that stratified all people studied by age, RA consistently boosted the MI rate across all age ranges, starting in people younger than 40 through those older than 80 (see chart above). This analysis showed that the presence of RA produced a MI rate roughly comparable to people who were 10 years older.
Disclosures: Dr. Lindhardsen said that he and his associates had no conflicts.
ROME - Adults with rheumatoid arthritis have a 65% higher rate of incident myocardial infarctions than does the general population, according to Danish data that strengthen the already significant evidence supporting a link between rheumatoid arthritis and elevated cardiovascular disease.
In addition, the new findings again showed that the heightened MI risk of RA patients matched the MI risk of patients with diabetes, Dr. Jesper Lindhardsen said at the annual European Congress of Rheumatology.
The new results also showed that the MI risk for RA patients at any age throughout adult life roughly matched the risk of a person without RA or diabetes who is 10 years older.
“An increased focus on the increased cardiovascular risk in patients with RA is warranted,” said Dr. Lindhardsen, a physician in the department of cardiology at Gentofte Hospital, Hellerup, Denmark. The attention paid to cardiovascular risk in RA patients should at least match the attention paid in diabetes patients, he added.
At last year’s European Congress of Rheumatology, a report from a task force convened by the European League Against Rheumatism declared that “rheumatoid arthritis should be regarded as a condition that is associated with higher risk for cardiovascular disease.” The report also spelled out 10 recommendations for cardiovascular disease risk management in RA patients. The report appeared in published form earlier this year (Ann. Rheum. Dis. 2010;69:325-1400).
The new findings by Dr. Lindhardsen and his associates took the prior evidence a step further by including RA patients with no prior diagnosis of cardiovascular disease, he said. The new study also provided a direct comparison of the risks conferred by RA and diabetes within the same background population, the entire Danish adult population during 1997-2007.
Dr. Lindhardsen and his associates used Danish national registry data during that period, a group of slightly more than 4 million people. During the decade studied, 10,547 adult Danes had newly diagnosed RA, and 132,868 had newly diagnosed diabetes, including both type 1 and type 2. The average age of those who developed RA was 56 years, and of those who developed diabetes it was 57 years, compared with an average age for everyone else of 46. Women constituted 71% of the incident RA cases, 46% of the incident diabetes cases, and 52% of the remaining population.
The researchers then tracked the rate of incident MIs in all three groups, with an average follow-up of 9 years in the general population, and 4 years following both the RA and diabetes diagnoses.
Compared with the rate of new-onset MI in the general population, RA patients had a 65% higher rate and patients with diabetes had a 73% higher rate, both statistically significant increases over the comparator group. This analysis adjusted for age, gender, cardiovascular pharmacotherapy, comorbidities, and socioeconomic status. About 400 people developed both RA and diabetes during the study period, and while their MI incidence was not additive, it significantly surpassed the rate among patients who had only RA or only diabetes, Dr. Lindhardsen said.
The analyses also provided insights into the interaction of age and gender with MI risk among RA patients. In general, the results showed that RA boosted MI risk regardless of age and gender. Among women younger than 50 years, RA and diabetes each boosted the MI risk sixfold, compared with similarly aged women without RA or diabetes. The impact on MI risk from either RA or diabetes fell substantially in women aged 50-65 years, and in women older than 65 years, although both RA and diabetes elevated the risk in both of these age groups. In men younger than 50 years, RA did not significantly raise MI risk but diabetes did. The biggest impact of RA on MI risk occurred in men aged 50-65, who had a twofold increased MI risk, compared with men who did not have RA or diabetes.
In another analysis that stratified all people studied by age, RA consistently boosted the MI rate across all age ranges, starting in people younger than 40 through those older than 80 (see chart above). This analysis showed that the presence of RA produced a MI rate roughly comparable to people who were 10 years older.
Disclosures: Dr. Lindhardsen said that he and his associates had no conflicts.
ROME - Adults with rheumatoid arthritis have a 65% higher rate of incident myocardial infarctions than does the general population, according to Danish data that strengthen the already significant evidence supporting a link between rheumatoid arthritis and elevated cardiovascular disease.
In addition, the new findings again showed that the heightened MI risk of RA patients matched the MI risk of patients with diabetes, Dr. Jesper Lindhardsen said at the annual European Congress of Rheumatology.
The new results also showed that the MI risk for RA patients at any age throughout adult life roughly matched the risk of a person without RA or diabetes who is 10 years older.
“An increased focus on the increased cardiovascular risk in patients with RA is warranted,” said Dr. Lindhardsen, a physician in the department of cardiology at Gentofte Hospital, Hellerup, Denmark. The attention paid to cardiovascular risk in RA patients should at least match the attention paid in diabetes patients, he added.
At last year’s European Congress of Rheumatology, a report from a task force convened by the European League Against Rheumatism declared that “rheumatoid arthritis should be regarded as a condition that is associated with higher risk for cardiovascular disease.” The report also spelled out 10 recommendations for cardiovascular disease risk management in RA patients. The report appeared in published form earlier this year (Ann. Rheum. Dis. 2010;69:325-1400).
The new findings by Dr. Lindhardsen and his associates took the prior evidence a step further by including RA patients with no prior diagnosis of cardiovascular disease, he said. The new study also provided a direct comparison of the risks conferred by RA and diabetes within the same background population, the entire Danish adult population during 1997-2007.
Dr. Lindhardsen and his associates used Danish national registry data during that period, a group of slightly more than 4 million people. During the decade studied, 10,547 adult Danes had newly diagnosed RA, and 132,868 had newly diagnosed diabetes, including both type 1 and type 2. The average age of those who developed RA was 56 years, and of those who developed diabetes it was 57 years, compared with an average age for everyone else of 46. Women constituted 71% of the incident RA cases, 46% of the incident diabetes cases, and 52% of the remaining population.
The researchers then tracked the rate of incident MIs in all three groups, with an average follow-up of 9 years in the general population, and 4 years following both the RA and diabetes diagnoses.
Compared with the rate of new-onset MI in the general population, RA patients had a 65% higher rate and patients with diabetes had a 73% higher rate, both statistically significant increases over the comparator group. This analysis adjusted for age, gender, cardiovascular pharmacotherapy, comorbidities, and socioeconomic status. About 400 people developed both RA and diabetes during the study period, and while their MI incidence was not additive, it significantly surpassed the rate among patients who had only RA or only diabetes, Dr. Lindhardsen said.
The analyses also provided insights into the interaction of age and gender with MI risk among RA patients. In general, the results showed that RA boosted MI risk regardless of age and gender. Among women younger than 50 years, RA and diabetes each boosted the MI risk sixfold, compared with similarly aged women without RA or diabetes. The impact on MI risk from either RA or diabetes fell substantially in women aged 50-65 years, and in women older than 65 years, although both RA and diabetes elevated the risk in both of these age groups. In men younger than 50 years, RA did not significantly raise MI risk but diabetes did. The biggest impact of RA on MI risk occurred in men aged 50-65, who had a twofold increased MI risk, compared with men who did not have RA or diabetes.
In another analysis that stratified all people studied by age, RA consistently boosted the MI rate across all age ranges, starting in people younger than 40 through those older than 80 (see chart above). This analysis showed that the presence of RA produced a MI rate roughly comparable to people who were 10 years older.
Disclosures: Dr. Lindhardsen said that he and his associates had no conflicts.
Alcohol Use Linked to Reduced Arthritis
ROME — Alcohol use was linked with a reduced risk for having several forms of arthritis in a case control study of about 1,000 arthritis patients and nearly 6,000 controls.
Patients with newly diagnosed arthritis—rheumatoid, psoriatic, or reactive arthritis, spondyloarthritis, or osteoarthritis had a significantly reduced prevalence of alcohol use, compared with a control population of adults who were free of arthritis.

In an analysis that controlled for age, gender, body mass index, and smoking, patients with arthritis had a roughly 70% reduced relative rate of being alcohol consumers, suggesting a protective effect from alcohol against a variety of arthritis types, Dr. Diane van der Woude said at the annual European Congress of Rheumatology.
However, she also gave an alternative, equally plausible explanation of the finding: reduced alcohol use was not the cause but the result of the arthritis. People with arthritis "do not feel well and so may be less physically capable of drinking, such as going to a pub, or they may not drink because they are on pain-killing medications," said Dr. van der Woude, of the rheumatology department of Leiden (the Netherlands) University Medical Center.
The new evidence confirms and expands a finding from a Swedish case control study published last year that found a link between a reduced prevalence of alcohol consumption and rheumatoid arthritis (Ann. Rheum. Dis. 2009;68:222-7). The Swedish study also showed a dose-response relationship, where people with the highest level of alcohol use had the lowest prevalence of rheumatoid arthritis. In contrast, Dr. van der Woude and her associates found no link between arthritis and quantity of alcohol in their analysis of the impact of amount of alcohol consumed. The significant relationship only held for whether or not the patients drank any alcohol, regardless of amount.
Dr. van der Woude’s study expanded the 2009 Swedish finding to arthritis types beyond rheumatoid.
Her study used 997 patients with arthritis of less than 2 years’ duration enrolled in the Leiden Early Arthritis Clinic, and 5,877 people with no history of arthritis from the Leiden area. The arthritis cohort included 651 patients with rheumatoid arthritis, 130 with psoriatic arthritis, 76 with spondyloarthritis, 73 with osteoarthritis, and 67 with reactive arthritis. When asked whether they drank any alcohol, 53%-68% of the arthritis patients said yes (the rate varied by arthritis type), compared with 83% of the controls. These are "large differences," Dr. van der Woude said in an interview.
The observation that alcohol use was low in patients with osteoarthritis reduced the likelihood that the link can be explained by alcohol having a protective, anti-inflammatory effect. In fact, low alcohol use among people with arthritis increased the possibility that the explanation is that arthritis reduced alcohol consumption. Dr. van der Woude plans to test this possibility by looking at other types of patients with chronic illness, such as inflammatory bowel disease, to see if a similar link exists. She also plans to study arthritis patients on successful treatment who have low disease activity to see whether their alcohol use is closer to control levels.
Dr. van der Woude said that she and her associates had no disclosures.
ROME — Alcohol use was linked with a reduced risk for having several forms of arthritis in a case control study of about 1,000 arthritis patients and nearly 6,000 controls.
Patients with newly diagnosed arthritis—rheumatoid, psoriatic, or reactive arthritis, spondyloarthritis, or osteoarthritis had a significantly reduced prevalence of alcohol use, compared with a control population of adults who were free of arthritis.
In an analysis that controlled for age, gender, body mass index, and smoking, patients with arthritis had a roughly 70% reduced relative rate of being alcohol consumers, suggesting a protective effect from alcohol against a variety of arthritis types, Dr. Diane van der Woude said at the annual European Congress of Rheumatology.
However, she also gave an alternative, equally plausible explanation of the finding: reduced alcohol use was not the cause but the result of the arthritis. People with arthritis "do not feel well and so may be less physically capable of drinking, such as going to a pub, or they may not drink because they are on pain-killing medications," said Dr. van der Woude, of the rheumatology department of Leiden (the Netherlands) University Medical Center.
The new evidence confirms and expands a finding from a Swedish case control study published last year that found a link between a reduced prevalence of alcohol consumption and rheumatoid arthritis (Ann. Rheum. Dis. 2009;68:222-7). The Swedish study also showed a dose-response relationship, where people with the highest level of alcohol use had the lowest prevalence of rheumatoid arthritis. In contrast, Dr. van der Woude and her associates found no link between arthritis and quantity of alcohol in their analysis of the impact of amount of alcohol consumed. The significant relationship only held for whether or not the patients drank any alcohol, regardless of amount.
Dr. van der Woude’s study expanded the 2009 Swedish finding to arthritis types beyond rheumatoid.
Her study used 997 patients with arthritis of less than 2 years’ duration enrolled in the Leiden Early Arthritis Clinic, and 5,877 people with no history of arthritis from the Leiden area. The arthritis cohort included 651 patients with rheumatoid arthritis, 130 with psoriatic arthritis, 76 with spondyloarthritis, 73 with osteoarthritis, and 67 with reactive arthritis. When asked whether they drank any alcohol, 53%-68% of the arthritis patients said yes (the rate varied by arthritis type), compared with 83% of the controls. These are "large differences," Dr. van der Woude said in an interview.
The observation that alcohol use was low in patients with osteoarthritis reduced the likelihood that the link can be explained by alcohol having a protective, anti-inflammatory effect. In fact, low alcohol use among people with arthritis increased the possibility that the explanation is that arthritis reduced alcohol consumption. Dr. van der Woude plans to test this possibility by looking at other types of patients with chronic illness, such as inflammatory bowel disease, to see if a similar link exists. She also plans to study arthritis patients on successful treatment who have low disease activity to see whether their alcohol use is closer to control levels.
Dr. van der Woude said that she and her associates had no disclosures.
ROME — Alcohol use was linked with a reduced risk for having several forms of arthritis in a case control study of about 1,000 arthritis patients and nearly 6,000 controls.
Patients with newly diagnosed arthritis—rheumatoid, psoriatic, or reactive arthritis, spondyloarthritis, or osteoarthritis had a significantly reduced prevalence of alcohol use, compared with a control population of adults who were free of arthritis.
In an analysis that controlled for age, gender, body mass index, and smoking, patients with arthritis had a roughly 70% reduced relative rate of being alcohol consumers, suggesting a protective effect from alcohol against a variety of arthritis types, Dr. Diane van der Woude said at the annual European Congress of Rheumatology.
However, she also gave an alternative, equally plausible explanation of the finding: reduced alcohol use was not the cause but the result of the arthritis. People with arthritis "do not feel well and so may be less physically capable of drinking, such as going to a pub, or they may not drink because they are on pain-killing medications," said Dr. van der Woude, of the rheumatology department of Leiden (the Netherlands) University Medical Center.
The new evidence confirms and expands a finding from a Swedish case control study published last year that found a link between a reduced prevalence of alcohol consumption and rheumatoid arthritis (Ann. Rheum. Dis. 2009;68:222-7). The Swedish study also showed a dose-response relationship, where people with the highest level of alcohol use had the lowest prevalence of rheumatoid arthritis. In contrast, Dr. van der Woude and her associates found no link between arthritis and quantity of alcohol in their analysis of the impact of amount of alcohol consumed. The significant relationship only held for whether or not the patients drank any alcohol, regardless of amount.
Dr. van der Woude’s study expanded the 2009 Swedish finding to arthritis types beyond rheumatoid.
Her study used 997 patients with arthritis of less than 2 years’ duration enrolled in the Leiden Early Arthritis Clinic, and 5,877 people with no history of arthritis from the Leiden area. The arthritis cohort included 651 patients with rheumatoid arthritis, 130 with psoriatic arthritis, 76 with spondyloarthritis, 73 with osteoarthritis, and 67 with reactive arthritis. When asked whether they drank any alcohol, 53%-68% of the arthritis patients said yes (the rate varied by arthritis type), compared with 83% of the controls. These are "large differences," Dr. van der Woude said in an interview.
The observation that alcohol use was low in patients with osteoarthritis reduced the likelihood that the link can be explained by alcohol having a protective, anti-inflammatory effect. In fact, low alcohol use among people with arthritis increased the possibility that the explanation is that arthritis reduced alcohol consumption. Dr. van der Woude plans to test this possibility by looking at other types of patients with chronic illness, such as inflammatory bowel disease, to see if a similar link exists. She also plans to study arthritis patients on successful treatment who have low disease activity to see whether their alcohol use is closer to control levels.
Dr. van der Woude said that she and her associates had no disclosures.
New Ankylosing Spondylitis Guidelines Highlight TNF Inhibitors
ROME — Revised recommendations for managing ankylosing spondylitis from two international societies set tumor necrosis factor inhibitors as the cornerstone of treatment for patients who fail to have an adequate response to treatment with NSAIDs.
The new recommendations also put new emphasis on the extra-articular manifestations of ankylosing spondylitis (AS) – psoriasis, uveitis, and inflammatory bowel disease – and stress that these manifestations should be managed in collaboration with other specialists, along with recognition that AS patients also face increased risks for cardiovascular disease and osteoporosis, Dr. Jürgen Braun said at the annual European Congress of Rheumatology.
AS patients who present with psoriasis, uveitis, or inflammatory bowel disease may do better on a monoclonal antibody–based TNF inhibitor because those forms seem to work better on the extra-articular manifestations than do soluble receptor–based TNF inhibitors, Dr. Braun said in an interview. On the other hand, soluble receptor–based anti-TNF drugs appear to be somewhat safer, in that they appear to pose a reduced risk for activating either latent tuberculosis or herpes zoster infections, he said.
In the treatment of AS, the main difference “compared with rheumatoid arthritis is that conventional disease-modifying antirheumatic drugs [DMARDs] do not work for axial symptoms,” which exist in the majority of AS patients. “This makes TNF inhibitors almost first-line agents, after [NSAIDs]. All TNF inhibitors work similarly well for the spine, peripheral joints, and entheses.” For AS patients whose major problem is peripheral joint disease, a conventional DMARD – specifically sulfasalazine – can be effective, said Dr. Braun, director of the Center for Rheumatic Diseases in Herne, Germany.
The new treatment guidelines complement the new classification criteria for AS and axial spondyloarthritis that were published by the ASAS (Assessment of Spondyloarthritis International Association) last year (Ann. Rheum. Dis. 2009;68:777-83). The new classification criteria mean that rheumatologists can “treat when they see inflammation on MRI” instead of having to wait for patients to develop radiographic changes, Dr. Braun noted. The new classification criteria – coupled with the new treatment recommendations – put treatment on a faster track, and give physicians backup to put those AS patients who don’t respond within a few weeks to NSAID therapy on a TNF inhibitor relatively early in the course of their disease.
A panel of 18 rheumatologists, two orthopedic surgeons, one physiotherapist, and four patients formed by ASAS and EULAR (European League Against Rheumatism) devised the new treatment recommendations over 2 days in February in Zurich. They based their decisions on a review of the published literature since 2005.
The recommendations consist of 11 specific AS management directives that cover everything from general treatment to surgery, and rule out other causes in patients who do respond to standard care. They will appear in an article the EULAR journal, Annals of the Rheumatic Diseases, in the near future.
The recommendations are as follows:
• General: Treatment of patients with AS should be tailored to their current disease manifestations; their current level of symptoms, clinical findings, and prognostic indicators; and the patient’s general clinical status, including age, gender, co-morbidities, concomitant medications, and psychosocial status.
• Disease monitoring:Monitoring should include a patient’s history, clinical parameters, laboratory tests, and imaging. Frequency of monitoring should be individualized based on the course of symptoms, symptom severity, and treatment.
• Non-pharmacologic treatment: The cornerstones are education about AS and regular exercise.
• Extra-articular manifestations: Psoriasis, uveitis, and inflammatory bowel disease need collaborative management by specialists. Rheumatologists should also be aware of the increased risk for cardiovascular disease and osteoporosis in AS patients.
• NSAIDs: NSAIDs, including selective cyclooxygenase-2 inhibitors (COXIBs), are the recommended first-line treatment for patients with AS who have pain and stiffness. Continuous NSAID treatment is preferred for patients with persistently active, symptomatic disease. A patient’s cardiovascular and gastrointestinal risks should be considered when prescribing NSAIDs.
• Analgesics: Pain medications such as paracetamol and opioids or opioid-like drugs might be considered to treat residual pain if previously recommended treatments failed, are contraindicated, or poorly tolerated.
• Corticosteroids: Consider local corticosteroid injections at sites of musculoskeletal inflammation. Systemic corticosteroids for treating axial disease is not supported by evidence.
• DMARDS: No evidence supports the efficacy of DMARDS, including sulfasalazine, for treating axial disease. Sulfasalazine may be considered for patients with peripheral arthritis.
• Biologic therapy: A TNF inhibitor should be given to patients with persistently high disease activity despite conventional treatments according to ASAS recommendations. No evidence supports the obligatory use of DMARDs before or during treatment with a TNF inhibitor in patients with axial AS. No evidence supports a difference in the efficacy of the various TNF inhibitors on axial and articular/entheseal disease manifestations. In patients with inflammatory bowel disease, differences in the gastrointestinal efficacy of the various TNF inhibitors should be taken into account. No evidence supports the efficacy of any other biologic agent aside from TNF inhibitors in AS patients. Switching to a second TNF inhibitor may benefit AS patients, especially those who lose response to the first drug they receive.
• Surgery: Consider total hip arthroplasty in patients with refractory pain or disability and radiographic evidence of structural damage independent of age. Spinal corrective osteotomy may be considered in patients with severe disabling deformity. AS patients with an acute vertebral fracture need a consultation with a spinal surgeon.
• If a patient has a significant change in disease course, other causes of inflammation, such as a spinal fracture, should be considered and an appropriate evaluation, including imaging, should be done.
Dr. Braun has received research support from, been a consultant to, and served as a speaker for Abbott Laboratories, Amgen Inc., Bristol-Myers Squibb Co., Centocor Inc., Merck/Schering-Plough Pharmaceuticals, Merck Sharp and Dohme Corp., Novartis, Pfizer Inc./Wyeth, and Roche.
ROME — Revised recommendations for managing ankylosing spondylitis from two international societies set tumor necrosis factor inhibitors as the cornerstone of treatment for patients who fail to have an adequate response to treatment with NSAIDs.
The new recommendations also put new emphasis on the extra-articular manifestations of ankylosing spondylitis (AS) – psoriasis, uveitis, and inflammatory bowel disease – and stress that these manifestations should be managed in collaboration with other specialists, along with recognition that AS patients also face increased risks for cardiovascular disease and osteoporosis, Dr. Jürgen Braun said at the annual European Congress of Rheumatology.
AS patients who present with psoriasis, uveitis, or inflammatory bowel disease may do better on a monoclonal antibody–based TNF inhibitor because those forms seem to work better on the extra-articular manifestations than do soluble receptor–based TNF inhibitors, Dr. Braun said in an interview. On the other hand, soluble receptor–based anti-TNF drugs appear to be somewhat safer, in that they appear to pose a reduced risk for activating either latent tuberculosis or herpes zoster infections, he said.
In the treatment of AS, the main difference “compared with rheumatoid arthritis is that conventional disease-modifying antirheumatic drugs [DMARDs] do not work for axial symptoms,” which exist in the majority of AS patients. “This makes TNF inhibitors almost first-line agents, after [NSAIDs]. All TNF inhibitors work similarly well for the spine, peripheral joints, and entheses.” For AS patients whose major problem is peripheral joint disease, a conventional DMARD – specifically sulfasalazine – can be effective, said Dr. Braun, director of the Center for Rheumatic Diseases in Herne, Germany.
The new treatment guidelines complement the new classification criteria for AS and axial spondyloarthritis that were published by the ASAS (Assessment of Spondyloarthritis International Association) last year (Ann. Rheum. Dis. 2009;68:777-83). The new classification criteria mean that rheumatologists can “treat when they see inflammation on MRI” instead of having to wait for patients to develop radiographic changes, Dr. Braun noted. The new classification criteria – coupled with the new treatment recommendations – put treatment on a faster track, and give physicians backup to put those AS patients who don’t respond within a few weeks to NSAID therapy on a TNF inhibitor relatively early in the course of their disease.
A panel of 18 rheumatologists, two orthopedic surgeons, one physiotherapist, and four patients formed by ASAS and EULAR (European League Against Rheumatism) devised the new treatment recommendations over 2 days in February in Zurich. They based their decisions on a review of the published literature since 2005.
The recommendations consist of 11 specific AS management directives that cover everything from general treatment to surgery, and rule out other causes in patients who do respond to standard care. They will appear in an article the EULAR journal, Annals of the Rheumatic Diseases, in the near future.
The recommendations are as follows:
• General: Treatment of patients with AS should be tailored to their current disease manifestations; their current level of symptoms, clinical findings, and prognostic indicators; and the patient’s general clinical status, including age, gender, co-morbidities, concomitant medications, and psychosocial status.
• Disease monitoring:Monitoring should include a patient’s history, clinical parameters, laboratory tests, and imaging. Frequency of monitoring should be individualized based on the course of symptoms, symptom severity, and treatment.
• Non-pharmacologic treatment: The cornerstones are education about AS and regular exercise.
• Extra-articular manifestations: Psoriasis, uveitis, and inflammatory bowel disease need collaborative management by specialists. Rheumatologists should also be aware of the increased risk for cardiovascular disease and osteoporosis in AS patients.
• NSAIDs: NSAIDs, including selective cyclooxygenase-2 inhibitors (COXIBs), are the recommended first-line treatment for patients with AS who have pain and stiffness. Continuous NSAID treatment is preferred for patients with persistently active, symptomatic disease. A patient’s cardiovascular and gastrointestinal risks should be considered when prescribing NSAIDs.
• Analgesics: Pain medications such as paracetamol and opioids or opioid-like drugs might be considered to treat residual pain if previously recommended treatments failed, are contraindicated, or poorly tolerated.
• Corticosteroids: Consider local corticosteroid injections at sites of musculoskeletal inflammation. Systemic corticosteroids for treating axial disease is not supported by evidence.
• DMARDS: No evidence supports the efficacy of DMARDS, including sulfasalazine, for treating axial disease. Sulfasalazine may be considered for patients with peripheral arthritis.
• Biologic therapy: A TNF inhibitor should be given to patients with persistently high disease activity despite conventional treatments according to ASAS recommendations. No evidence supports the obligatory use of DMARDs before or during treatment with a TNF inhibitor in patients with axial AS. No evidence supports a difference in the efficacy of the various TNF inhibitors on axial and articular/entheseal disease manifestations. In patients with inflammatory bowel disease, differences in the gastrointestinal efficacy of the various TNF inhibitors should be taken into account. No evidence supports the efficacy of any other biologic agent aside from TNF inhibitors in AS patients. Switching to a second TNF inhibitor may benefit AS patients, especially those who lose response to the first drug they receive.
• Surgery: Consider total hip arthroplasty in patients with refractory pain or disability and radiographic evidence of structural damage independent of age. Spinal corrective osteotomy may be considered in patients with severe disabling deformity. AS patients with an acute vertebral fracture need a consultation with a spinal surgeon.
• If a patient has a significant change in disease course, other causes of inflammation, such as a spinal fracture, should be considered and an appropriate evaluation, including imaging, should be done.
Dr. Braun has received research support from, been a consultant to, and served as a speaker for Abbott Laboratories, Amgen Inc., Bristol-Myers Squibb Co., Centocor Inc., Merck/Schering-Plough Pharmaceuticals, Merck Sharp and Dohme Corp., Novartis, Pfizer Inc./Wyeth, and Roche.
ROME — Revised recommendations for managing ankylosing spondylitis from two international societies set tumor necrosis factor inhibitors as the cornerstone of treatment for patients who fail to have an adequate response to treatment with NSAIDs.
The new recommendations also put new emphasis on the extra-articular manifestations of ankylosing spondylitis (AS) – psoriasis, uveitis, and inflammatory bowel disease – and stress that these manifestations should be managed in collaboration with other specialists, along with recognition that AS patients also face increased risks for cardiovascular disease and osteoporosis, Dr. Jürgen Braun said at the annual European Congress of Rheumatology.
AS patients who present with psoriasis, uveitis, or inflammatory bowel disease may do better on a monoclonal antibody–based TNF inhibitor because those forms seem to work better on the extra-articular manifestations than do soluble receptor–based TNF inhibitors, Dr. Braun said in an interview. On the other hand, soluble receptor–based anti-TNF drugs appear to be somewhat safer, in that they appear to pose a reduced risk for activating either latent tuberculosis or herpes zoster infections, he said.
In the treatment of AS, the main difference “compared with rheumatoid arthritis is that conventional disease-modifying antirheumatic drugs [DMARDs] do not work for axial symptoms,” which exist in the majority of AS patients. “This makes TNF inhibitors almost first-line agents, after [NSAIDs]. All TNF inhibitors work similarly well for the spine, peripheral joints, and entheses.” For AS patients whose major problem is peripheral joint disease, a conventional DMARD – specifically sulfasalazine – can be effective, said Dr. Braun, director of the Center for Rheumatic Diseases in Herne, Germany.
The new treatment guidelines complement the new classification criteria for AS and axial spondyloarthritis that were published by the ASAS (Assessment of Spondyloarthritis International Association) last year (Ann. Rheum. Dis. 2009;68:777-83). The new classification criteria mean that rheumatologists can “treat when they see inflammation on MRI” instead of having to wait for patients to develop radiographic changes, Dr. Braun noted. The new classification criteria – coupled with the new treatment recommendations – put treatment on a faster track, and give physicians backup to put those AS patients who don’t respond within a few weeks to NSAID therapy on a TNF inhibitor relatively early in the course of their disease.
A panel of 18 rheumatologists, two orthopedic surgeons, one physiotherapist, and four patients formed by ASAS and EULAR (European League Against Rheumatism) devised the new treatment recommendations over 2 days in February in Zurich. They based their decisions on a review of the published literature since 2005.
The recommendations consist of 11 specific AS management directives that cover everything from general treatment to surgery, and rule out other causes in patients who do respond to standard care. They will appear in an article the EULAR journal, Annals of the Rheumatic Diseases, in the near future.
The recommendations are as follows:
• General: Treatment of patients with AS should be tailored to their current disease manifestations; their current level of symptoms, clinical findings, and prognostic indicators; and the patient’s general clinical status, including age, gender, co-morbidities, concomitant medications, and psychosocial status.
• Disease monitoring:Monitoring should include a patient’s history, clinical parameters, laboratory tests, and imaging. Frequency of monitoring should be individualized based on the course of symptoms, symptom severity, and treatment.
• Non-pharmacologic treatment: The cornerstones are education about AS and regular exercise.
• Extra-articular manifestations: Psoriasis, uveitis, and inflammatory bowel disease need collaborative management by specialists. Rheumatologists should also be aware of the increased risk for cardiovascular disease and osteoporosis in AS patients.
• NSAIDs: NSAIDs, including selective cyclooxygenase-2 inhibitors (COXIBs), are the recommended first-line treatment for patients with AS who have pain and stiffness. Continuous NSAID treatment is preferred for patients with persistently active, symptomatic disease. A patient’s cardiovascular and gastrointestinal risks should be considered when prescribing NSAIDs.
• Analgesics: Pain medications such as paracetamol and opioids or opioid-like drugs might be considered to treat residual pain if previously recommended treatments failed, are contraindicated, or poorly tolerated.
• Corticosteroids: Consider local corticosteroid injections at sites of musculoskeletal inflammation. Systemic corticosteroids for treating axial disease is not supported by evidence.
• DMARDS: No evidence supports the efficacy of DMARDS, including sulfasalazine, for treating axial disease. Sulfasalazine may be considered for patients with peripheral arthritis.
• Biologic therapy: A TNF inhibitor should be given to patients with persistently high disease activity despite conventional treatments according to ASAS recommendations. No evidence supports the obligatory use of DMARDs before or during treatment with a TNF inhibitor in patients with axial AS. No evidence supports a difference in the efficacy of the various TNF inhibitors on axial and articular/entheseal disease manifestations. In patients with inflammatory bowel disease, differences in the gastrointestinal efficacy of the various TNF inhibitors should be taken into account. No evidence supports the efficacy of any other biologic agent aside from TNF inhibitors in AS patients. Switching to a second TNF inhibitor may benefit AS patients, especially those who lose response to the first drug they receive.
• Surgery: Consider total hip arthroplasty in patients with refractory pain or disability and radiographic evidence of structural damage independent of age. Spinal corrective osteotomy may be considered in patients with severe disabling deformity. AS patients with an acute vertebral fracture need a consultation with a spinal surgeon.
• If a patient has a significant change in disease course, other causes of inflammation, such as a spinal fracture, should be considered and an appropriate evaluation, including imaging, should be done.
Dr. Braun has received research support from, been a consultant to, and served as a speaker for Abbott Laboratories, Amgen Inc., Bristol-Myers Squibb Co., Centocor Inc., Merck/Schering-Plough Pharmaceuticals, Merck Sharp and Dohme Corp., Novartis, Pfizer Inc./Wyeth, and Roche.
Cutaneous Manifestations of Diabetes Mellitus: A Case Series
EULAR: Common Vaccinations Do Not Increase RA Risk
Immunization with common vaccines is not associated with an increased risk for rheumatoid arthritis, nor does it trigger the autoimmune disease in individuals who have established risk factors, according to an analysis of data that was presented by Camilla Bengtsson at the annual European Congress of Rheumatology on June 16.
Although anecdotal reports have suggested that common vaccinations might be inciting agents for rheumatoid arthritis, no sufficiently powered epidemiologic studies have addressed this concern, according to Ms. Bengtsson, a doctoral candidate at the Karolinska Institute in Stockholm.
Using data on 1,851 people with RA from the Swedish population-based EIRA (Epidemiological Investigation of Rheumatoid Arthritis) data set and 1,984 healthy matched controls, Ms. Bengtsson and her associates investigated the possible association between vaccinations that are commonly used in industrialized societies (influenza; tetanus; diphtheria; tick-borne encephalitis; hepatitis A, B, and C; polio; and pneumococcus) and the risk for RA, as well as the impact of vaccinations on two subsets of RA patients: those with and without antibodies to citrullinated peptides. Ms. Bengtsson discussed their findings on potential interactions between vaccination and smoking and between vaccination and the presence of HLA-DRB1 SE alleles with respect to RA risk, both of which have been implicated anecdotally as possible catalysts for the disease.
To evaluate these potential associations, the investigators compared the 582 individuals in the EIRA data set who had been vaccinated in the 5 years prior to disease onset with the 1,269 RA patients who had not been vaccinated within 5 years prior to disease onset. Among the control subjects, 617 had been vaccinated and 1,367 had not been vaccinated within the preceding 5 years.
Vaccine by vaccine, the odds ratio for developing RA after influenza vaccination was 1.1 (252 RA patients and 279 controls had received the flu vaccine during the period of interest). The OR for RA after tetanus vaccination was 1.0 (170 cases and 179 controls had received that vaccination). The OR was 1.0 for diphtheria vaccination (71 cases/71 controls). For tick-borne encephalitis, the OR was 0.8 (91 cases/122 controls). The OR for hepatitis A, B, and C was 0.9 (105 cases/124 controls). The OR for polio vaccination was 1.1 (29 cases/31 controls). The OR for pneumococcus was 1.0 (22 cases/22 controls). The RA OR for the unvaccinated was 1.0 (1,269 cases/1,367 controls).
There was no statistically significant difference among the outcomes. Based on the analysis, vaccinations did not increase the risk of RA overall. Being negative or positive for antibodies to citrullinated peptides did not alter the risk for RA among the vaccinated or unvaccinated subjects, according to Ms. Bengtsson. Additionally, there was no association between any specific vaccine and the risk of RA, nor did vaccinations increase the risk of RA among smokers or among carriers of HLA-DRB1 SE alleles, she said.
The results indicate that “immunological provocation with common vaccines given to adults in their present form is not a major risk factor for RA, at least not vaccines administered [within 5 years] before onset of disease,” Ms. Bengtsson noted, suggesting that clinicians point to these findings to encourage patients to follow recommended immunization guidelines.
No conflicts of interest were reported.
Immunization with common vaccines is not associated with an increased risk for rheumatoid arthritis, nor does it trigger the autoimmune disease in individuals who have established risk factors, according to an analysis of data that was presented by Camilla Bengtsson at the annual European Congress of Rheumatology on June 16.
Although anecdotal reports have suggested that common vaccinations might be inciting agents for rheumatoid arthritis, no sufficiently powered epidemiologic studies have addressed this concern, according to Ms. Bengtsson, a doctoral candidate at the Karolinska Institute in Stockholm.
Using data on 1,851 people with RA from the Swedish population-based EIRA (Epidemiological Investigation of Rheumatoid Arthritis) data set and 1,984 healthy matched controls, Ms. Bengtsson and her associates investigated the possible association between vaccinations that are commonly used in industrialized societies (influenza; tetanus; diphtheria; tick-borne encephalitis; hepatitis A, B, and C; polio; and pneumococcus) and the risk for RA, as well as the impact of vaccinations on two subsets of RA patients: those with and without antibodies to citrullinated peptides. Ms. Bengtsson discussed their findings on potential interactions between vaccination and smoking and between vaccination and the presence of HLA-DRB1 SE alleles with respect to RA risk, both of which have been implicated anecdotally as possible catalysts for the disease.
To evaluate these potential associations, the investigators compared the 582 individuals in the EIRA data set who had been vaccinated in the 5 years prior to disease onset with the 1,269 RA patients who had not been vaccinated within 5 years prior to disease onset. Among the control subjects, 617 had been vaccinated and 1,367 had not been vaccinated within the preceding 5 years.
Vaccine by vaccine, the odds ratio for developing RA after influenza vaccination was 1.1 (252 RA patients and 279 controls had received the flu vaccine during the period of interest). The OR for RA after tetanus vaccination was 1.0 (170 cases and 179 controls had received that vaccination). The OR was 1.0 for diphtheria vaccination (71 cases/71 controls). For tick-borne encephalitis, the OR was 0.8 (91 cases/122 controls). The OR for hepatitis A, B, and C was 0.9 (105 cases/124 controls). The OR for polio vaccination was 1.1 (29 cases/31 controls). The OR for pneumococcus was 1.0 (22 cases/22 controls). The RA OR for the unvaccinated was 1.0 (1,269 cases/1,367 controls).
There was no statistically significant difference among the outcomes. Based on the analysis, vaccinations did not increase the risk of RA overall. Being negative or positive for antibodies to citrullinated peptides did not alter the risk for RA among the vaccinated or unvaccinated subjects, according to Ms. Bengtsson. Additionally, there was no association between any specific vaccine and the risk of RA, nor did vaccinations increase the risk of RA among smokers or among carriers of HLA-DRB1 SE alleles, she said.
The results indicate that “immunological provocation with common vaccines given to adults in their present form is not a major risk factor for RA, at least not vaccines administered [within 5 years] before onset of disease,” Ms. Bengtsson noted, suggesting that clinicians point to these findings to encourage patients to follow recommended immunization guidelines.
No conflicts of interest were reported.
Immunization with common vaccines is not associated with an increased risk for rheumatoid arthritis, nor does it trigger the autoimmune disease in individuals who have established risk factors, according to an analysis of data that was presented by Camilla Bengtsson at the annual European Congress of Rheumatology on June 16.
Although anecdotal reports have suggested that common vaccinations might be inciting agents for rheumatoid arthritis, no sufficiently powered epidemiologic studies have addressed this concern, according to Ms. Bengtsson, a doctoral candidate at the Karolinska Institute in Stockholm.
Using data on 1,851 people with RA from the Swedish population-based EIRA (Epidemiological Investigation of Rheumatoid Arthritis) data set and 1,984 healthy matched controls, Ms. Bengtsson and her associates investigated the possible association between vaccinations that are commonly used in industrialized societies (influenza; tetanus; diphtheria; tick-borne encephalitis; hepatitis A, B, and C; polio; and pneumococcus) and the risk for RA, as well as the impact of vaccinations on two subsets of RA patients: those with and without antibodies to citrullinated peptides. Ms. Bengtsson discussed their findings on potential interactions between vaccination and smoking and between vaccination and the presence of HLA-DRB1 SE alleles with respect to RA risk, both of which have been implicated anecdotally as possible catalysts for the disease.
To evaluate these potential associations, the investigators compared the 582 individuals in the EIRA data set who had been vaccinated in the 5 years prior to disease onset with the 1,269 RA patients who had not been vaccinated within 5 years prior to disease onset. Among the control subjects, 617 had been vaccinated and 1,367 had not been vaccinated within the preceding 5 years.
Vaccine by vaccine, the odds ratio for developing RA after influenza vaccination was 1.1 (252 RA patients and 279 controls had received the flu vaccine during the period of interest). The OR for RA after tetanus vaccination was 1.0 (170 cases and 179 controls had received that vaccination). The OR was 1.0 for diphtheria vaccination (71 cases/71 controls). For tick-borne encephalitis, the OR was 0.8 (91 cases/122 controls). The OR for hepatitis A, B, and C was 0.9 (105 cases/124 controls). The OR for polio vaccination was 1.1 (29 cases/31 controls). The OR for pneumococcus was 1.0 (22 cases/22 controls). The RA OR for the unvaccinated was 1.0 (1,269 cases/1,367 controls).
There was no statistically significant difference among the outcomes. Based on the analysis, vaccinations did not increase the risk of RA overall. Being negative or positive for antibodies to citrullinated peptides did not alter the risk for RA among the vaccinated or unvaccinated subjects, according to Ms. Bengtsson. Additionally, there was no association between any specific vaccine and the risk of RA, nor did vaccinations increase the risk of RA among smokers or among carriers of HLA-DRB1 SE alleles, she said.
The results indicate that “immunological provocation with common vaccines given to adults in their present form is not a major risk factor for RA, at least not vaccines administered [within 5 years] before onset of disease,” Ms. Bengtsson noted, suggesting that clinicians point to these findings to encourage patients to follow recommended immunization guidelines.
No conflicts of interest were reported.
EULAR: BLISS-76 Yields Positive Data on Belimumab in SLE
The complete set of data from the BLISS-76 study of belimumab in seropositive patients with systemic lupus erythematosus supports the efficacy of the B-lymphocyte stimulator inhibitor as a treatment for SLE, and provides encouraging safety data, according to Dr. Ronald van Vollenhoven, speaking to a standing-room-only session at the European Congress of Rheumatology on June 16.
In what was the first full presentation of the BLISS-76 (Belimumab in Subjects With Systemic Lupus Erythematosus–76) data at a scientific meeting, Dr. van Vollenhoven, a rheumatologist at the Karolinska Institute in Stockholm, discussed how belimumab plus standard therapy was effective in reducing disease activity and severe flares, as well as achieving a higher response rate, compared with standard care alone. The treatment and placebo groups had similar adverse events.
Two doses were studied: 1 mg/kg and 10 mg/kg administered intravenously once every 4 weeks. Efficacy according to the trial’s primary outcome was seen with the higher dose. Most of the trial’s secondary end points either achieved significance for at least one of the dosages vs. placebo, or showed trends in the right direction, he added.
Based on these data as well as those from the previously reported BLISS-52 trial with the same drug, “the clear conclusion is that belimumab is efficacious,” Dr. van Vollenhoven said in an interview. Although the magnitude of the differences in response rates between active drug and placebo could have been larger, BLISS-76 was a successful study, he noted.
Among the unanswered questions that may need to be explored further is whether doses between 1 mg/kg and 10 mg/kg might also be efficacious, he added. Additional analyses are ongoing to determine if any group of patients is more likely to benefit from the drug.
Human Genome Sciences Inc. (HGS) and GlaxoSmithKline (GSK) are developing belimumab, which inhibits the biological activity of B-lymphocyte stimulator (BLyS), as a treatment for SLE. HGS has filed for approval for the 10-mg/kg dose in the United States.
BLISS-76, a 76-week, double-blind, international study that compared the two belimumab doses vs. placebo in 819 seropositive patients with SLE, is one of the two pivotal studies to evaluate the safety and efficacy of belimumab in this population. Patients in the study had to have an antinuclear antibody ratio of at least 1:80 and/or anti–double-stranded DNA of at least 30 IU/mL, with a SELENA-SLEDAI (Safety of Estrogens in Lupus Erythematosus–National Assessment SLE Disease Activity Index) score of at least 6 on stable therapy.
Patients had had the disease for a mean of 7.5 years, 63% used antimalarials, 76% used steroids, and 56% used immunosuppressants. Patients received standard-of-care treatment and were randomized to receive either IV belimumab at days 0, 14, 28, and then every 28 days for 72 weeks, or placebo.
Some of the top-line BLISS-76 results were reported in November 2009 by HGS and GSK. At that time, the developers announced that the study had met its primary end point, which was the patient response rate as measured by the SLE Responder Index (SRI) at 52 weeks. In all, 43% of those on the higher dose and 41% of those on the lower dose met this end point, compared with 34% of those on placebo. The difference between the higher dose and placebo was statistically significant.
According to the SRI, which was developed in collaboration with the Food and Drug Administration, a patient response is defined as an improvement in the SELENA-SLEDAI score of 4 points or greater, with no clinically significant worsening on the either the BILAG (British Isles Lupus Assessment Group) index or the Physician’s Global Assessment (PGA).
Secondary end points included components of the primary end point. In all, 47% of those on the higher dose and 43% of those on the lower dose had at least a 4-point reduction in the SELENA-SLEDAI score at 52 weeks, compared with 36% among placebo. The difference between the higher dose and placebo was significant.
The proportion of patients who did not have a worsening in the PGA score greater than 0.3 points was 69% and 73% in the 10-mg/kg and 1-mg/kg groups, respectively, compared with 63% in the placebo group. The difference between the 1-mg/kg dose and placebo was significant. There were no statistically significant improvements in PGA or in steroid dose reductions among the two belimumab-treated groups, compared with placebo, according to Dr. van Vollenhoven.
In addition, 69% of those on the 10-mg/kg dose, 75% of those on the 1-mg/kg dose, and 65% of those on placebo had no new BILAG grade A or B scores. The difference between the 1-mg/kg dose and placebo was significant.
There were no significant differences between the three groups in the risk of having a flare, or in the median time to the first flare, based on the SELENA Flare Index (SFI). But the proportion of patients who had a severe SFI flare was lower in the two treatment groups (18% of those on the higher dose and 16% of those on the lower dose, compared with 24% of those on placebo), he said, noting that the difference was significant between the 1-mg/kg and placebo groups.
Other secondary end points included the mean in SF-36 Physical Component Summary (PCS) scores from baseline to week 52, which increased by a mean of 3.4, 4.4 and 2.9, in the 10-mg/kg, 1-mg/kg and placebo groups, respectively. The difference was significant only between placebo and the 1-mg/kg dose. The change in the FACIT-F (Functional Assessment of Chronic Illness Therapy–Fatigue) score from baseline at 52 weeks increased by a mean of 4.6, 5.7, and 2.9 respectively, with the difference being significant between the 1-mg/kg dose and placebo, Dr. van Vollenhoven said. “These data are important in that they reflect patient-reported aspects of the disease, namely physical function and fatigue, which are of major importance in terms of quality of life,” Dr. van Vollenhoven said in the interview. “In fact, fatigue has been identified by lupus patients in our unit as their most important symptom.”
He added, “All these instruments are blunt, however. It’s like having an old radio with a lot of background noise.”
In the study, treatment was well tolerated, with similar rates of deaths, adverse events, serious adverse events, infections, and laboratory abnormalities in the three groups. There was a modest increase in serious or severe infusion reactions among those on belimumab, compared with those on placebo, he noted. The overall infusion reaction rate was 13%-15% in the two belimumab groups, compared with 10% in the placebo group; the rate of severe infusion reactions was 1.1% in the 10-mg/kg group and 0.4% in the 1-mg/kg and placebo groups. Thus, the clinical response to the 10-mg dose appeared to be more robust. However, we need to learn more in the future about refining doses.”
There were six malignancies in the study, one in a patient on placebo, and five in the belimumab-treated patients. The infection rate was 72% in the two belimumab groups, compared with 67% in the placebo group; the serious infection rate was 7% in the 10-mg group, 6% in the 1-mg/kg group, and 5% in the placebo group, Dr. van Vollenhoven said.
Dr. van Vollenhoven was an investigator in the BLISS-76 study and is a consultant to HGS and GSK; he also served on the BLISS-52 and BLISS-76 steering committees. Some of the investigators on this trial are HGS employees.
The complete set of data from the BLISS-76 study of belimumab in seropositive patients with systemic lupus erythematosus supports the efficacy of the B-lymphocyte stimulator inhibitor as a treatment for SLE, and provides encouraging safety data, according to Dr. Ronald van Vollenhoven, speaking to a standing-room-only session at the European Congress of Rheumatology on June 16.
In what was the first full presentation of the BLISS-76 (Belimumab in Subjects With Systemic Lupus Erythematosus–76) data at a scientific meeting, Dr. van Vollenhoven, a rheumatologist at the Karolinska Institute in Stockholm, discussed how belimumab plus standard therapy was effective in reducing disease activity and severe flares, as well as achieving a higher response rate, compared with standard care alone. The treatment and placebo groups had similar adverse events.
Two doses were studied: 1 mg/kg and 10 mg/kg administered intravenously once every 4 weeks. Efficacy according to the trial’s primary outcome was seen with the higher dose. Most of the trial’s secondary end points either achieved significance for at least one of the dosages vs. placebo, or showed trends in the right direction, he added.
Based on these data as well as those from the previously reported BLISS-52 trial with the same drug, “the clear conclusion is that belimumab is efficacious,” Dr. van Vollenhoven said in an interview. Although the magnitude of the differences in response rates between active drug and placebo could have been larger, BLISS-76 was a successful study, he noted.
Among the unanswered questions that may need to be explored further is whether doses between 1 mg/kg and 10 mg/kg might also be efficacious, he added. Additional analyses are ongoing to determine if any group of patients is more likely to benefit from the drug.
Human Genome Sciences Inc. (HGS) and GlaxoSmithKline (GSK) are developing belimumab, which inhibits the biological activity of B-lymphocyte stimulator (BLyS), as a treatment for SLE. HGS has filed for approval for the 10-mg/kg dose in the United States.
BLISS-76, a 76-week, double-blind, international study that compared the two belimumab doses vs. placebo in 819 seropositive patients with SLE, is one of the two pivotal studies to evaluate the safety and efficacy of belimumab in this population. Patients in the study had to have an antinuclear antibody ratio of at least 1:80 and/or anti–double-stranded DNA of at least 30 IU/mL, with a SELENA-SLEDAI (Safety of Estrogens in Lupus Erythematosus–National Assessment SLE Disease Activity Index) score of at least 6 on stable therapy.
Patients had had the disease for a mean of 7.5 years, 63% used antimalarials, 76% used steroids, and 56% used immunosuppressants. Patients received standard-of-care treatment and were randomized to receive either IV belimumab at days 0, 14, 28, and then every 28 days for 72 weeks, or placebo.
Some of the top-line BLISS-76 results were reported in November 2009 by HGS and GSK. At that time, the developers announced that the study had met its primary end point, which was the patient response rate as measured by the SLE Responder Index (SRI) at 52 weeks. In all, 43% of those on the higher dose and 41% of those on the lower dose met this end point, compared with 34% of those on placebo. The difference between the higher dose and placebo was statistically significant.
According to the SRI, which was developed in collaboration with the Food and Drug Administration, a patient response is defined as an improvement in the SELENA-SLEDAI score of 4 points or greater, with no clinically significant worsening on the either the BILAG (British Isles Lupus Assessment Group) index or the Physician’s Global Assessment (PGA).
Secondary end points included components of the primary end point. In all, 47% of those on the higher dose and 43% of those on the lower dose had at least a 4-point reduction in the SELENA-SLEDAI score at 52 weeks, compared with 36% among placebo. The difference between the higher dose and placebo was significant.
The proportion of patients who did not have a worsening in the PGA score greater than 0.3 points was 69% and 73% in the 10-mg/kg and 1-mg/kg groups, respectively, compared with 63% in the placebo group. The difference between the 1-mg/kg dose and placebo was significant. There were no statistically significant improvements in PGA or in steroid dose reductions among the two belimumab-treated groups, compared with placebo, according to Dr. van Vollenhoven.
In addition, 69% of those on the 10-mg/kg dose, 75% of those on the 1-mg/kg dose, and 65% of those on placebo had no new BILAG grade A or B scores. The difference between the 1-mg/kg dose and placebo was significant.
There were no significant differences between the three groups in the risk of having a flare, or in the median time to the first flare, based on the SELENA Flare Index (SFI). But the proportion of patients who had a severe SFI flare was lower in the two treatment groups (18% of those on the higher dose and 16% of those on the lower dose, compared with 24% of those on placebo), he said, noting that the difference was significant between the 1-mg/kg and placebo groups.
Other secondary end points included the mean in SF-36 Physical Component Summary (PCS) scores from baseline to week 52, which increased by a mean of 3.4, 4.4 and 2.9, in the 10-mg/kg, 1-mg/kg and placebo groups, respectively. The difference was significant only between placebo and the 1-mg/kg dose. The change in the FACIT-F (Functional Assessment of Chronic Illness Therapy–Fatigue) score from baseline at 52 weeks increased by a mean of 4.6, 5.7, and 2.9 respectively, with the difference being significant between the 1-mg/kg dose and placebo, Dr. van Vollenhoven said. “These data are important in that they reflect patient-reported aspects of the disease, namely physical function and fatigue, which are of major importance in terms of quality of life,” Dr. van Vollenhoven said in the interview. “In fact, fatigue has been identified by lupus patients in our unit as their most important symptom.”
He added, “All these instruments are blunt, however. It’s like having an old radio with a lot of background noise.”
In the study, treatment was well tolerated, with similar rates of deaths, adverse events, serious adverse events, infections, and laboratory abnormalities in the three groups. There was a modest increase in serious or severe infusion reactions among those on belimumab, compared with those on placebo, he noted. The overall infusion reaction rate was 13%-15% in the two belimumab groups, compared with 10% in the placebo group; the rate of severe infusion reactions was 1.1% in the 10-mg/kg group and 0.4% in the 1-mg/kg and placebo groups. Thus, the clinical response to the 10-mg dose appeared to be more robust. However, we need to learn more in the future about refining doses.”
There were six malignancies in the study, one in a patient on placebo, and five in the belimumab-treated patients. The infection rate was 72% in the two belimumab groups, compared with 67% in the placebo group; the serious infection rate was 7% in the 10-mg group, 6% in the 1-mg/kg group, and 5% in the placebo group, Dr. van Vollenhoven said.
Dr. van Vollenhoven was an investigator in the BLISS-76 study and is a consultant to HGS and GSK; he also served on the BLISS-52 and BLISS-76 steering committees. Some of the investigators on this trial are HGS employees.
The complete set of data from the BLISS-76 study of belimumab in seropositive patients with systemic lupus erythematosus supports the efficacy of the B-lymphocyte stimulator inhibitor as a treatment for SLE, and provides encouraging safety data, according to Dr. Ronald van Vollenhoven, speaking to a standing-room-only session at the European Congress of Rheumatology on June 16.
In what was the first full presentation of the BLISS-76 (Belimumab in Subjects With Systemic Lupus Erythematosus–76) data at a scientific meeting, Dr. van Vollenhoven, a rheumatologist at the Karolinska Institute in Stockholm, discussed how belimumab plus standard therapy was effective in reducing disease activity and severe flares, as well as achieving a higher response rate, compared with standard care alone. The treatment and placebo groups had similar adverse events.
Two doses were studied: 1 mg/kg and 10 mg/kg administered intravenously once every 4 weeks. Efficacy according to the trial’s primary outcome was seen with the higher dose. Most of the trial’s secondary end points either achieved significance for at least one of the dosages vs. placebo, or showed trends in the right direction, he added.
Based on these data as well as those from the previously reported BLISS-52 trial with the same drug, “the clear conclusion is that belimumab is efficacious,” Dr. van Vollenhoven said in an interview. Although the magnitude of the differences in response rates between active drug and placebo could have been larger, BLISS-76 was a successful study, he noted.
Among the unanswered questions that may need to be explored further is whether doses between 1 mg/kg and 10 mg/kg might also be efficacious, he added. Additional analyses are ongoing to determine if any group of patients is more likely to benefit from the drug.
Human Genome Sciences Inc. (HGS) and GlaxoSmithKline (GSK) are developing belimumab, which inhibits the biological activity of B-lymphocyte stimulator (BLyS), as a treatment for SLE. HGS has filed for approval for the 10-mg/kg dose in the United States.
BLISS-76, a 76-week, double-blind, international study that compared the two belimumab doses vs. placebo in 819 seropositive patients with SLE, is one of the two pivotal studies to evaluate the safety and efficacy of belimumab in this population. Patients in the study had to have an antinuclear antibody ratio of at least 1:80 and/or anti–double-stranded DNA of at least 30 IU/mL, with a SELENA-SLEDAI (Safety of Estrogens in Lupus Erythematosus–National Assessment SLE Disease Activity Index) score of at least 6 on stable therapy.
Patients had had the disease for a mean of 7.5 years, 63% used antimalarials, 76% used steroids, and 56% used immunosuppressants. Patients received standard-of-care treatment and were randomized to receive either IV belimumab at days 0, 14, 28, and then every 28 days for 72 weeks, or placebo.
Some of the top-line BLISS-76 results were reported in November 2009 by HGS and GSK. At that time, the developers announced that the study had met its primary end point, which was the patient response rate as measured by the SLE Responder Index (SRI) at 52 weeks. In all, 43% of those on the higher dose and 41% of those on the lower dose met this end point, compared with 34% of those on placebo. The difference between the higher dose and placebo was statistically significant.
According to the SRI, which was developed in collaboration with the Food and Drug Administration, a patient response is defined as an improvement in the SELENA-SLEDAI score of 4 points or greater, with no clinically significant worsening on the either the BILAG (British Isles Lupus Assessment Group) index or the Physician’s Global Assessment (PGA).
Secondary end points included components of the primary end point. In all, 47% of those on the higher dose and 43% of those on the lower dose had at least a 4-point reduction in the SELENA-SLEDAI score at 52 weeks, compared with 36% among placebo. The difference between the higher dose and placebo was significant.
The proportion of patients who did not have a worsening in the PGA score greater than 0.3 points was 69% and 73% in the 10-mg/kg and 1-mg/kg groups, respectively, compared with 63% in the placebo group. The difference between the 1-mg/kg dose and placebo was significant. There were no statistically significant improvements in PGA or in steroid dose reductions among the two belimumab-treated groups, compared with placebo, according to Dr. van Vollenhoven.
In addition, 69% of those on the 10-mg/kg dose, 75% of those on the 1-mg/kg dose, and 65% of those on placebo had no new BILAG grade A or B scores. The difference between the 1-mg/kg dose and placebo was significant.
There were no significant differences between the three groups in the risk of having a flare, or in the median time to the first flare, based on the SELENA Flare Index (SFI). But the proportion of patients who had a severe SFI flare was lower in the two treatment groups (18% of those on the higher dose and 16% of those on the lower dose, compared with 24% of those on placebo), he said, noting that the difference was significant between the 1-mg/kg and placebo groups.
Other secondary end points included the mean in SF-36 Physical Component Summary (PCS) scores from baseline to week 52, which increased by a mean of 3.4, 4.4 and 2.9, in the 10-mg/kg, 1-mg/kg and placebo groups, respectively. The difference was significant only between placebo and the 1-mg/kg dose. The change in the FACIT-F (Functional Assessment of Chronic Illness Therapy–Fatigue) score from baseline at 52 weeks increased by a mean of 4.6, 5.7, and 2.9 respectively, with the difference being significant between the 1-mg/kg dose and placebo, Dr. van Vollenhoven said. “These data are important in that they reflect patient-reported aspects of the disease, namely physical function and fatigue, which are of major importance in terms of quality of life,” Dr. van Vollenhoven said in the interview. “In fact, fatigue has been identified by lupus patients in our unit as their most important symptom.”
He added, “All these instruments are blunt, however. It’s like having an old radio with a lot of background noise.”
In the study, treatment was well tolerated, with similar rates of deaths, adverse events, serious adverse events, infections, and laboratory abnormalities in the three groups. There was a modest increase in serious or severe infusion reactions among those on belimumab, compared with those on placebo, he noted. The overall infusion reaction rate was 13%-15% in the two belimumab groups, compared with 10% in the placebo group; the rate of severe infusion reactions was 1.1% in the 10-mg/kg group and 0.4% in the 1-mg/kg and placebo groups. Thus, the clinical response to the 10-mg dose appeared to be more robust. However, we need to learn more in the future about refining doses.”
There were six malignancies in the study, one in a patient on placebo, and five in the belimumab-treated patients. The infection rate was 72% in the two belimumab groups, compared with 67% in the placebo group; the serious infection rate was 7% in the 10-mg group, 6% in the 1-mg/kg group, and 5% in the placebo group, Dr. van Vollenhoven said.
Dr. van Vollenhoven was an investigator in the BLISS-76 study and is a consultant to HGS and GSK; he also served on the BLISS-52 and BLISS-76 steering committees. Some of the investigators on this trial are HGS employees.
NICE Okays Three TNF Inhibitors for Psoriatic Arthritis
The clinical effectiveness agency for England and Wales said it plans to formally recommend three tumor necrosis factor inhibitors – etanercept, infliximab, and adalimumab – interchangeably for the treatment of psoriatic arthritis, saying the evidence suggests that they are equally safe and work equally well.
Current National Institute for Health and Clinical Excellence guidance mandates that infliximab be prescribed only in the event that etanercept or adalimumab (the two less expensive drugs) were contraindicated.
In draft guidance published June 11, NICE reviewers proposed that all three drugs be made available according to which is cheapest in a particular treatment setting.
People with active and progressive psoriatic arthritis who have peripheral arthritis with three or more tender joints, three or more swollen joints, and no response to at least two standard disease-modifying antirheumatic drugs (usually methotrexate and sulfasalazine, alone or in combination) are eligible for the treatments.
After examining data from randomized, controlled trials, the NICE reviewers determined that infliximab was associated with the highest probability of achieving a response for both the skin and joint symptoms in people with psoriatic arthritis.
The probability of response in joint disease was higher with etanercept than with adalimumab, they noted, and the probability of response in skin disease was higher with adalimumab than with etanercept. However, they urged that price be the sole determinant of TNF-inhibitor choice in each clinical setting.
Etanercept and adalimumab carry a similar price tag of about £9,300 each for the first treatment year, compared with £10,910 for infliximab. However, the NICE reviewers noted, “vial sharing arrangements for infliximab are available in some clinical settings and may reduce drug wastage by up to 50%,” and may make infliximab the cost-effective choice.
With any of the three drugs, NICE said, treatment should be terminated after 12 weeks if there is no adequate joint response, according to established criteria for psoriatic arthritis, although a dermatologist may find continuing treatment to be appropriate on the basis of skin response.
Final guidance on etanercept, infliximab, and adalimumab is expected in July, the agency said.
The clinical effectiveness agency for England and Wales said it plans to formally recommend three tumor necrosis factor inhibitors – etanercept, infliximab, and adalimumab – interchangeably for the treatment of psoriatic arthritis, saying the evidence suggests that they are equally safe and work equally well.
Current National Institute for Health and Clinical Excellence guidance mandates that infliximab be prescribed only in the event that etanercept or adalimumab (the two less expensive drugs) were contraindicated.
In draft guidance published June 11, NICE reviewers proposed that all three drugs be made available according to which is cheapest in a particular treatment setting.
People with active and progressive psoriatic arthritis who have peripheral arthritis with three or more tender joints, three or more swollen joints, and no response to at least two standard disease-modifying antirheumatic drugs (usually methotrexate and sulfasalazine, alone or in combination) are eligible for the treatments.
After examining data from randomized, controlled trials, the NICE reviewers determined that infliximab was associated with the highest probability of achieving a response for both the skin and joint symptoms in people with psoriatic arthritis.
The probability of response in joint disease was higher with etanercept than with adalimumab, they noted, and the probability of response in skin disease was higher with adalimumab than with etanercept. However, they urged that price be the sole determinant of TNF-inhibitor choice in each clinical setting.
Etanercept and adalimumab carry a similar price tag of about £9,300 each for the first treatment year, compared with £10,910 for infliximab. However, the NICE reviewers noted, “vial sharing arrangements for infliximab are available in some clinical settings and may reduce drug wastage by up to 50%,” and may make infliximab the cost-effective choice.
With any of the three drugs, NICE said, treatment should be terminated after 12 weeks if there is no adequate joint response, according to established criteria for psoriatic arthritis, although a dermatologist may find continuing treatment to be appropriate on the basis of skin response.
Final guidance on etanercept, infliximab, and adalimumab is expected in July, the agency said.
The clinical effectiveness agency for England and Wales said it plans to formally recommend three tumor necrosis factor inhibitors – etanercept, infliximab, and adalimumab – interchangeably for the treatment of psoriatic arthritis, saying the evidence suggests that they are equally safe and work equally well.
Current National Institute for Health and Clinical Excellence guidance mandates that infliximab be prescribed only in the event that etanercept or adalimumab (the two less expensive drugs) were contraindicated.
In draft guidance published June 11, NICE reviewers proposed that all three drugs be made available according to which is cheapest in a particular treatment setting.
People with active and progressive psoriatic arthritis who have peripheral arthritis with three or more tender joints, three or more swollen joints, and no response to at least two standard disease-modifying antirheumatic drugs (usually methotrexate and sulfasalazine, alone or in combination) are eligible for the treatments.
After examining data from randomized, controlled trials, the NICE reviewers determined that infliximab was associated with the highest probability of achieving a response for both the skin and joint symptoms in people with psoriatic arthritis.
The probability of response in joint disease was higher with etanercept than with adalimumab, they noted, and the probability of response in skin disease was higher with adalimumab than with etanercept. However, they urged that price be the sole determinant of TNF-inhibitor choice in each clinical setting.
Etanercept and adalimumab carry a similar price tag of about £9,300 each for the first treatment year, compared with £10,910 for infliximab. However, the NICE reviewers noted, “vial sharing arrangements for infliximab are available in some clinical settings and may reduce drug wastage by up to 50%,” and may make infliximab the cost-effective choice.
With any of the three drugs, NICE said, treatment should be terminated after 12 weeks if there is no adequate joint response, according to established criteria for psoriatic arthritis, although a dermatologist may find continuing treatment to be appropriate on the basis of skin response.
Final guidance on etanercept, infliximab, and adalimumab is expected in July, the agency said.
Doctors Concerned About Shrinking Supply of Unapproved Colchicine
As URL Pharma Inc. and other drug companies battle in court over access to the U.S. colchicine market, the supply of unapproved colchicine is beginning to decline, and patients in at least one small town are scrambling to find what’s left.
“It’s harder to get,” Dr. Christopher Morris, a rheumatologist in Kingsport, Tenn., said in an interview. “Some [patients] have had to go to two or three different pharmacies to find it. Some are going online to find it. Some pharmacies only have Colcrys available,” he added.
The situation started last summer when the Food and Drug Administration approved URL’s colchicine (Colcrys) for gout and familial Mediterranean fever.
URL was the first company to submit colchicine for approval and, under FDA regulations, the company was granted multiyear marketing exclusivity for its efforts.
After the approval, URL went to court to end its competitors’ sales on the grounds that by marketing their colchicine, they falsely imply that it is FDA approved.
Instead, unapproved colchicine was grandfathered into the marketplace by the Food, Drug, and Cosmetic Act of 1938.
Two manufacturers of unbranded colchicine, Vision Pharma LLC and Excellium Pharmaceuticals Inc., were no longer supplying the U.S. market at the end of April, according to the American Society of Health System Pharmacists’ drug shortage Web site.
A third, West-Ward Pharmaceutical Corp., was still doing so, according to the Web site.
The unapproved colchicine business had been growing until now; 1.2 million retail prescriptions were written for it in the first 4 months of this year, compared with 1.1 million for the same period last year and 1 million during the first 4 months of 2008, according to SDI Health LLC, a health care market insight and analytics firm.
Meanwhile, the price of unbranded colchicine has gone from a nationwide average of 19 cents per pill in 2008 to 44 cents, according to SDI.
West-Ward, Vision, and Excellium declined to comment for this story, citing ongoing litigation.
Stocking up
Physicians are bracing for an unbranded colchicine shortage.
Physicians in Cleveland; Austin, Tex.; and New York City said in interviews that although patients are complaining about the higher cost, they can still get the pills.
But anticipating dwindling supplies, Dr. Edward Fudman, a rheumatologist in Austin, said he is writing larger than usual prescriptions to help his patients stock up.
Dr. Brian Mandell, a Cleveland Clinic rheumatologist, said he will refer patients to the Internet and Canadian pharmacies if they run into trouble.
Two companies, Euro-Pharm International Canada Inc. and Odan Laboratories Ltd., sell colchicine in Canada, according to Gary Holub, a Health Canada spokesman.
Another Alternative
Colcrys sells for about $5 per pill, according to DestinationRx.com.
But URL has both a patient assistance program and a copay coupon program to help eligible patients. In this way, the company has taken steps to “ensure everyone in need of Colcrys therapy can get it regardless of income level,” a spokesperson said.
The Colcrys patient assistance program is tiered. A 30-day supply of Colcrys, for example, is free for households with an annual income of up to three times the federal poverty level ($66,150 per year for a family of four), a URL spokesperson said.
Assistance is available for households up to six times the federal poverty level ($132,000 per year for a four-member family).
Under the coupon program, the cost is no more than $25 for prescription of 30 pills or more, the spokesman said.
With Changes Come Tension
Even so, the changes in the U.S. colchicine market have brought tension, with strong opinions among those involved.
Doctors have said that their patients have safely used unapproved colchicine for decades, and that the higher price of Colcrys will limit patient access and drain public health programs (N. Engl. J. Med. 2010 April 21 [doi:10.1056/NEJMp 1003126]).
There have also been calls for the FDA to tighten its marketing exclusivity regulations, and concern that the agency will remove unapproved colchicine from the market as part of its goal to ensure that drugs sold in the United States are tested for safety and efficacy.
In response, URL asserts that the marketing of unbranded colchicine is illegal.
The company also points to a March letter from Dr. Janet Woodcock, director of the FDA’s Center for Drug Evaluation and Research, to the American College of Rheumatology. The letter stated that Colcrys approval studies generated important new information about how to safely use colchicine, and that the safety, purity, and efficacy of unapproved drugs cannot be guaranteed.
Because of the latter reason, unbranded colchicine was pulled from Medicare part D formularies this year, and was replaced by Colcrys.
Whatever the outcome of the court battles, the situation isn’t permanent.
URL’s marketing exclusivity for Colcrys’s gout indications expires July 30, 2012. The familial Mediterranean fever indication expires July 29, 2016, according to the FDA’s Web site.
Information about URL’s Colcrys patient assistance program and copayment coupons are available by visiting Colcrys.com or by calling 888-811-8423. Copayment coupons can be downloaded at the Web site.
Dr. Fudman said that he had no relevant disclosures. Dr. Morris disclosed that he is on the speakers’ bureau for Takeda, Eli Lilly, and Forest Pharmaceuticals. Dr. Mandell disclosed that he is an advisor to Takeda and URL Pharma, and was a clinical investigator for Savient Pharmaceuticals.
As URL Pharma Inc. and other drug companies battle in court over access to the U.S. colchicine market, the supply of unapproved colchicine is beginning to decline, and patients in at least one small town are scrambling to find what’s left.
“It’s harder to get,” Dr. Christopher Morris, a rheumatologist in Kingsport, Tenn., said in an interview. “Some [patients] have had to go to two or three different pharmacies to find it. Some are going online to find it. Some pharmacies only have Colcrys available,” he added.
The situation started last summer when the Food and Drug Administration approved URL’s colchicine (Colcrys) for gout and familial Mediterranean fever.
URL was the first company to submit colchicine for approval and, under FDA regulations, the company was granted multiyear marketing exclusivity for its efforts.
After the approval, URL went to court to end its competitors’ sales on the grounds that by marketing their colchicine, they falsely imply that it is FDA approved.
Instead, unapproved colchicine was grandfathered into the marketplace by the Food, Drug, and Cosmetic Act of 1938.
Two manufacturers of unbranded colchicine, Vision Pharma LLC and Excellium Pharmaceuticals Inc., were no longer supplying the U.S. market at the end of April, according to the American Society of Health System Pharmacists’ drug shortage Web site.
A third, West-Ward Pharmaceutical Corp., was still doing so, according to the Web site.
The unapproved colchicine business had been growing until now; 1.2 million retail prescriptions were written for it in the first 4 months of this year, compared with 1.1 million for the same period last year and 1 million during the first 4 months of 2008, according to SDI Health LLC, a health care market insight and analytics firm.
Meanwhile, the price of unbranded colchicine has gone from a nationwide average of 19 cents per pill in 2008 to 44 cents, according to SDI.
West-Ward, Vision, and Excellium declined to comment for this story, citing ongoing litigation.
Stocking up
Physicians are bracing for an unbranded colchicine shortage.
Physicians in Cleveland; Austin, Tex.; and New York City said in interviews that although patients are complaining about the higher cost, they can still get the pills.
But anticipating dwindling supplies, Dr. Edward Fudman, a rheumatologist in Austin, said he is writing larger than usual prescriptions to help his patients stock up.
Dr. Brian Mandell, a Cleveland Clinic rheumatologist, said he will refer patients to the Internet and Canadian pharmacies if they run into trouble.
Two companies, Euro-Pharm International Canada Inc. and Odan Laboratories Ltd., sell colchicine in Canada, according to Gary Holub, a Health Canada spokesman.
Another Alternative
Colcrys sells for about $5 per pill, according to DestinationRx.com.
But URL has both a patient assistance program and a copay coupon program to help eligible patients. In this way, the company has taken steps to “ensure everyone in need of Colcrys therapy can get it regardless of income level,” a spokesperson said.
The Colcrys patient assistance program is tiered. A 30-day supply of Colcrys, for example, is free for households with an annual income of up to three times the federal poverty level ($66,150 per year for a family of four), a URL spokesperson said.
Assistance is available for households up to six times the federal poverty level ($132,000 per year for a four-member family).
Under the coupon program, the cost is no more than $25 for prescription of 30 pills or more, the spokesman said.
With Changes Come Tension
Even so, the changes in the U.S. colchicine market have brought tension, with strong opinions among those involved.
Doctors have said that their patients have safely used unapproved colchicine for decades, and that the higher price of Colcrys will limit patient access and drain public health programs (N. Engl. J. Med. 2010 April 21 [doi:10.1056/NEJMp 1003126]).
There have also been calls for the FDA to tighten its marketing exclusivity regulations, and concern that the agency will remove unapproved colchicine from the market as part of its goal to ensure that drugs sold in the United States are tested for safety and efficacy.
In response, URL asserts that the marketing of unbranded colchicine is illegal.
The company also points to a March letter from Dr. Janet Woodcock, director of the FDA’s Center for Drug Evaluation and Research, to the American College of Rheumatology. The letter stated that Colcrys approval studies generated important new information about how to safely use colchicine, and that the safety, purity, and efficacy of unapproved drugs cannot be guaranteed.
Because of the latter reason, unbranded colchicine was pulled from Medicare part D formularies this year, and was replaced by Colcrys.
Whatever the outcome of the court battles, the situation isn’t permanent.
URL’s marketing exclusivity for Colcrys’s gout indications expires July 30, 2012. The familial Mediterranean fever indication expires July 29, 2016, according to the FDA’s Web site.
Information about URL’s Colcrys patient assistance program and copayment coupons are available by visiting Colcrys.com or by calling 888-811-8423. Copayment coupons can be downloaded at the Web site.
Dr. Fudman said that he had no relevant disclosures. Dr. Morris disclosed that he is on the speakers’ bureau for Takeda, Eli Lilly, and Forest Pharmaceuticals. Dr. Mandell disclosed that he is an advisor to Takeda and URL Pharma, and was a clinical investigator for Savient Pharmaceuticals.
As URL Pharma Inc. and other drug companies battle in court over access to the U.S. colchicine market, the supply of unapproved colchicine is beginning to decline, and patients in at least one small town are scrambling to find what’s left.
“It’s harder to get,” Dr. Christopher Morris, a rheumatologist in Kingsport, Tenn., said in an interview. “Some [patients] have had to go to two or three different pharmacies to find it. Some are going online to find it. Some pharmacies only have Colcrys available,” he added.
The situation started last summer when the Food and Drug Administration approved URL’s colchicine (Colcrys) for gout and familial Mediterranean fever.
URL was the first company to submit colchicine for approval and, under FDA regulations, the company was granted multiyear marketing exclusivity for its efforts.
After the approval, URL went to court to end its competitors’ sales on the grounds that by marketing their colchicine, they falsely imply that it is FDA approved.
Instead, unapproved colchicine was grandfathered into the marketplace by the Food, Drug, and Cosmetic Act of 1938.
Two manufacturers of unbranded colchicine, Vision Pharma LLC and Excellium Pharmaceuticals Inc., were no longer supplying the U.S. market at the end of April, according to the American Society of Health System Pharmacists’ drug shortage Web site.
A third, West-Ward Pharmaceutical Corp., was still doing so, according to the Web site.
The unapproved colchicine business had been growing until now; 1.2 million retail prescriptions were written for it in the first 4 months of this year, compared with 1.1 million for the same period last year and 1 million during the first 4 months of 2008, according to SDI Health LLC, a health care market insight and analytics firm.
Meanwhile, the price of unbranded colchicine has gone from a nationwide average of 19 cents per pill in 2008 to 44 cents, according to SDI.
West-Ward, Vision, and Excellium declined to comment for this story, citing ongoing litigation.
Stocking up
Physicians are bracing for an unbranded colchicine shortage.
Physicians in Cleveland; Austin, Tex.; and New York City said in interviews that although patients are complaining about the higher cost, they can still get the pills.
But anticipating dwindling supplies, Dr. Edward Fudman, a rheumatologist in Austin, said he is writing larger than usual prescriptions to help his patients stock up.
Dr. Brian Mandell, a Cleveland Clinic rheumatologist, said he will refer patients to the Internet and Canadian pharmacies if they run into trouble.
Two companies, Euro-Pharm International Canada Inc. and Odan Laboratories Ltd., sell colchicine in Canada, according to Gary Holub, a Health Canada spokesman.
Another Alternative
Colcrys sells for about $5 per pill, according to DestinationRx.com.
But URL has both a patient assistance program and a copay coupon program to help eligible patients. In this way, the company has taken steps to “ensure everyone in need of Colcrys therapy can get it regardless of income level,” a spokesperson said.
The Colcrys patient assistance program is tiered. A 30-day supply of Colcrys, for example, is free for households with an annual income of up to three times the federal poverty level ($66,150 per year for a family of four), a URL spokesperson said.
Assistance is available for households up to six times the federal poverty level ($132,000 per year for a four-member family).
Under the coupon program, the cost is no more than $25 for prescription of 30 pills or more, the spokesman said.
With Changes Come Tension
Even so, the changes in the U.S. colchicine market have brought tension, with strong opinions among those involved.
Doctors have said that their patients have safely used unapproved colchicine for decades, and that the higher price of Colcrys will limit patient access and drain public health programs (N. Engl. J. Med. 2010 April 21 [doi:10.1056/NEJMp 1003126]).
There have also been calls for the FDA to tighten its marketing exclusivity regulations, and concern that the agency will remove unapproved colchicine from the market as part of its goal to ensure that drugs sold in the United States are tested for safety and efficacy.
In response, URL asserts that the marketing of unbranded colchicine is illegal.
The company also points to a March letter from Dr. Janet Woodcock, director of the FDA’s Center for Drug Evaluation and Research, to the American College of Rheumatology. The letter stated that Colcrys approval studies generated important new information about how to safely use colchicine, and that the safety, purity, and efficacy of unapproved drugs cannot be guaranteed.
Because of the latter reason, unbranded colchicine was pulled from Medicare part D formularies this year, and was replaced by Colcrys.
Whatever the outcome of the court battles, the situation isn’t permanent.
URL’s marketing exclusivity for Colcrys’s gout indications expires July 30, 2012. The familial Mediterranean fever indication expires July 29, 2016, according to the FDA’s Web site.
Information about URL’s Colcrys patient assistance program and copayment coupons are available by visiting Colcrys.com or by calling 888-811-8423. Copayment coupons can be downloaded at the Web site.
Dr. Fudman said that he had no relevant disclosures. Dr. Morris disclosed that he is on the speakers’ bureau for Takeda, Eli Lilly, and Forest Pharmaceuticals. Dr. Mandell disclosed that he is an advisor to Takeda and URL Pharma, and was a clinical investigator for Savient Pharmaceuticals.