User login
These umbilical lesions weren't granulomas after all
THE CASES
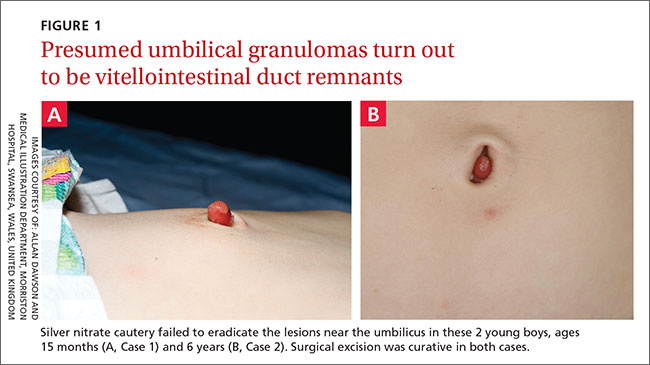
CASE 1 › A 15-month-old boy was brought to our center for plastic surgery after being referred by his general practitioner (GP). The patient had a non-healing lesion on his umbilicus that had been present since birth. It had remained the same size, but bled occasionally. The GP initially presumed the lesion was a granuloma and treated it with silver nitrate cautery, but this did not eradicate it.
After talking with the boy’s mother further, we learned that there had been a constant oozing from the area since birth and that the lesion protruded slightly from the abdomen when the child cried. The boy had congenital heart disease, but his bowel and genitourinary history were normal. A clinical examination revealed pink, moist tissue herniating from the umbilicus with surrounding abdominal fullness when the boy stood up (FIGURE 1A). An ultrasound showed a focal 19 x 7 mm complex area around the umbilicus with no definite track. The lesion was surgically removed. Histology revealed a completely excised vitellointestinal duct remnant.
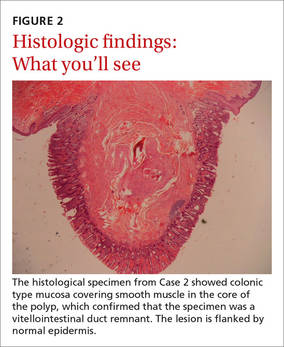
CASE 2 › A 6-year-old boy with a history of attention-deficit/hyperactivity disorder was brought to our clinic with a non-healing umbilical lesion after being referred by his GP. The lesion had been present since birth and had failed to resolve despite several attempts to treat it with silver nitrate cautery. Clinically, the patient appeared to have a granulomatous umbilical polyp (FIGURE 1B). The patient underwent surgical excision of the lesion. Histological analysis revealed a completely excised vitellointestinal duct remnant (FIGURE 2).
DISCUSSION
The vitellointestinal duct (VID), also called the omphalomesenteric duct (OMD), connects the alimentary canal and the yolk sac in early embryogenesis. Failure of involution of the duct results in abnormalities such as Meckel’s diverticulum, cysts, and polyps.
VID anomalies occur in approximately 2% of newborns; a small percentage of these have patent connections to the intestine.1 Parents are often the first to notice the abnormality and will typically see a reddish protrusion around the umbilicus or a persistent serous discharge around the umbilicus soon after birth.
VID remnants are similar in presentation to benign granulomas or granulation tissue, which are benign lesions that present in the first few weeks of life. Granulomas are reddish in color, bleed minimally when irritated by trauma, and respond well to silver nitrate cautery.2 When the lesion fails to respond to treatment, an alternative diagnosis should be investigated further.
Ultrasonography is the best way to evaluate a suspected VID remnant
A suspected VID remnant should first be assessed with ultrasonography to determine the extent of the remnant and guide surgical treatment. Ultrasonography can also delineate the relationship of these congenital remnants with the umbilicus and bladder.3
Potential complications that can arise from these lesions include an intestinal hernia, intussusception, volvulus, abdominal pain, or a persistent discharge that can lead to infection.3 Mortality following complications is significantly high.4
Although the etiology of patent VIDs and their remnants remains unknown, the presence of such ducts is associated with other congenital anomalies, including Down Syndrome, structural cardiac malformation, conduction abnormalities, and cleft lip and palate.5-7 Therefore, additional history taking and examinations may be required to identify these associated pathologies. In Case 1, the 15-month-old boy had congenital heart disease.
Surgical excision will prevent complications
A simple surgical excision should be performed for VID remnants. The prognosis is excellent when such procedures are performed in the non-acute setting. Some debate exists as to whether all remnants require formal abdominal exploration.8,9
Treatment of patent VIDs requires surgical excision of the duct, with or without a segment of the small bowel, to obliterate the connection.10 Reconstruction of the umbilicus is then performed, depending on the surgical technique used.
Our patients both made complete recoveries following their surgeries with resolution of their symptoms.
THE TAKEAWAY
Consider a VID remnant as part of the differential diagnosis for any patient who has what appears to be a granulomatous umbilical lesion. Order ultrasonography to evaluate a suspected VID, especially for lesions that fail to respond to 2 or 3 silver nitrate treatments. Surgical excision of a VID remnant is usually curative.
1. Vane DW, West KW, Grosfeld JL. Vitelline duct anomalies. Experience with 217 childhood cases. Arch Surg. 1987;122:542-547.
2. Piparsaliya S, Joshi M, Rajput N, et al. Patent vitellointestinal duct: A close differential diagnosis of umbilical granuloma: A case report and review of literature. Surgical Science. 2011;2:134-136.
3. Khati NJ, Enquist EG, Javitt MC. Imaging of the umbilicus and periumbilical region. Radiographics. 1998;18:413-431.
4. Yamada T, Seiki Y, Ueda M, et al. Patent omphalomesenteric duct: a case report and review of Japanese literature. Asia Oceania J Obstet Gynaecol. 1989;15:229-236.
5. Martin RH, Doublestein GL, Jarvis MR. Concurrent ectopic pregnancy, Meckel’s diverticulum with vitelline duct remnant, cecal volvulus, and congenital complete heart block: report of a case. J Am Osteopath Assoc. 1986;86:589-591.
6. Elebute EA, Ransome-Kuti O. Patent vitello-intestinal duct with ileal prolapse. Arch Surg. 1965;91:456-460.
7. Blair SP, Beasley SW. Intussusception of vitello-intestinal tract through an exomphalos in trisomy 13. Pediatric Surgery International. 1989;4:422-423.
8. Kutin ND, Allen JE, Jewett TC. The umbilical polyp. J Pediatr Surg. 1979;14:741-744.
9. Pacilli M, Sebire NJ, Maritsi D, et al. Umbilical polyp in infants and children. Eur J Pediatr Surg. 2007;17:397-399.
10. Storms P, Pexsters J, Vandekerkhof J. Small omphalocele with ileal prolapse through a patent omphalomesenteric duct. A case report and review of literature. Acta Chir Belg. 1988;88:392-394.
THE CASES
CASE 1 › A 15-month-old boy was brought to our center for plastic surgery after being referred by his general practitioner (GP). The patient had a non-healing lesion on his umbilicus that had been present since birth. It had remained the same size, but bled occasionally. The GP initially presumed the lesion was a granuloma and treated it with silver nitrate cautery, but this did not eradicate it.
After talking with the boy’s mother further, we learned that there had been a constant oozing from the area since birth and that the lesion protruded slightly from the abdomen when the child cried. The boy had congenital heart disease, but his bowel and genitourinary history were normal. A clinical examination revealed pink, moist tissue herniating from the umbilicus with surrounding abdominal fullness when the boy stood up (FIGURE 1A). An ultrasound showed a focal 19 x 7 mm complex area around the umbilicus with no definite track. The lesion was surgically removed. Histology revealed a completely excised vitellointestinal duct remnant.
CASE 2 › A 6-year-old boy with a history of attention-deficit/hyperactivity disorder was brought to our clinic with a non-healing umbilical lesion after being referred by his GP. The lesion had been present since birth and had failed to resolve despite several attempts to treat it with silver nitrate cautery. Clinically, the patient appeared to have a granulomatous umbilical polyp (FIGURE 1B). The patient underwent surgical excision of the lesion. Histological analysis revealed a completely excised vitellointestinal duct remnant (FIGURE 2).
DISCUSSION
The vitellointestinal duct (VID), also called the omphalomesenteric duct (OMD), connects the alimentary canal and the yolk sac in early embryogenesis. Failure of involution of the duct results in abnormalities such as Meckel’s diverticulum, cysts, and polyps.
VID anomalies occur in approximately 2% of newborns; a small percentage of these have patent connections to the intestine.1 Parents are often the first to notice the abnormality and will typically see a reddish protrusion around the umbilicus or a persistent serous discharge around the umbilicus soon after birth.
VID remnants are similar in presentation to benign granulomas or granulation tissue, which are benign lesions that present in the first few weeks of life. Granulomas are reddish in color, bleed minimally when irritated by trauma, and respond well to silver nitrate cautery.2 When the lesion fails to respond to treatment, an alternative diagnosis should be investigated further.
Ultrasonography is the best way to evaluate a suspected VID remnant
A suspected VID remnant should first be assessed with ultrasonography to determine the extent of the remnant and guide surgical treatment. Ultrasonography can also delineate the relationship of these congenital remnants with the umbilicus and bladder.3
Potential complications that can arise from these lesions include an intestinal hernia, intussusception, volvulus, abdominal pain, or a persistent discharge that can lead to infection.3 Mortality following complications is significantly high.4
Although the etiology of patent VIDs and their remnants remains unknown, the presence of such ducts is associated with other congenital anomalies, including Down Syndrome, structural cardiac malformation, conduction abnormalities, and cleft lip and palate.5-7 Therefore, additional history taking and examinations may be required to identify these associated pathologies. In Case 1, the 15-month-old boy had congenital heart disease.
Surgical excision will prevent complications
A simple surgical excision should be performed for VID remnants. The prognosis is excellent when such procedures are performed in the non-acute setting. Some debate exists as to whether all remnants require formal abdominal exploration.8,9
Treatment of patent VIDs requires surgical excision of the duct, with or without a segment of the small bowel, to obliterate the connection.10 Reconstruction of the umbilicus is then performed, depending on the surgical technique used.
Our patients both made complete recoveries following their surgeries with resolution of their symptoms.
THE TAKEAWAY
Consider a VID remnant as part of the differential diagnosis for any patient who has what appears to be a granulomatous umbilical lesion. Order ultrasonography to evaluate a suspected VID, especially for lesions that fail to respond to 2 or 3 silver nitrate treatments. Surgical excision of a VID remnant is usually curative.
THE CASES
CASE 1 › A 15-month-old boy was brought to our center for plastic surgery after being referred by his general practitioner (GP). The patient had a non-healing lesion on his umbilicus that had been present since birth. It had remained the same size, but bled occasionally. The GP initially presumed the lesion was a granuloma and treated it with silver nitrate cautery, but this did not eradicate it.
After talking with the boy’s mother further, we learned that there had been a constant oozing from the area since birth and that the lesion protruded slightly from the abdomen when the child cried. The boy had congenital heart disease, but his bowel and genitourinary history were normal. A clinical examination revealed pink, moist tissue herniating from the umbilicus with surrounding abdominal fullness when the boy stood up (FIGURE 1A). An ultrasound showed a focal 19 x 7 mm complex area around the umbilicus with no definite track. The lesion was surgically removed. Histology revealed a completely excised vitellointestinal duct remnant.
CASE 2 › A 6-year-old boy with a history of attention-deficit/hyperactivity disorder was brought to our clinic with a non-healing umbilical lesion after being referred by his GP. The lesion had been present since birth and had failed to resolve despite several attempts to treat it with silver nitrate cautery. Clinically, the patient appeared to have a granulomatous umbilical polyp (FIGURE 1B). The patient underwent surgical excision of the lesion. Histological analysis revealed a completely excised vitellointestinal duct remnant (FIGURE 2).
DISCUSSION
The vitellointestinal duct (VID), also called the omphalomesenteric duct (OMD), connects the alimentary canal and the yolk sac in early embryogenesis. Failure of involution of the duct results in abnormalities such as Meckel’s diverticulum, cysts, and polyps.
VID anomalies occur in approximately 2% of newborns; a small percentage of these have patent connections to the intestine.1 Parents are often the first to notice the abnormality and will typically see a reddish protrusion around the umbilicus or a persistent serous discharge around the umbilicus soon after birth.
VID remnants are similar in presentation to benign granulomas or granulation tissue, which are benign lesions that present in the first few weeks of life. Granulomas are reddish in color, bleed minimally when irritated by trauma, and respond well to silver nitrate cautery.2 When the lesion fails to respond to treatment, an alternative diagnosis should be investigated further.
Ultrasonography is the best way to evaluate a suspected VID remnant
A suspected VID remnant should first be assessed with ultrasonography to determine the extent of the remnant and guide surgical treatment. Ultrasonography can also delineate the relationship of these congenital remnants with the umbilicus and bladder.3
Potential complications that can arise from these lesions include an intestinal hernia, intussusception, volvulus, abdominal pain, or a persistent discharge that can lead to infection.3 Mortality following complications is significantly high.4
Although the etiology of patent VIDs and their remnants remains unknown, the presence of such ducts is associated with other congenital anomalies, including Down Syndrome, structural cardiac malformation, conduction abnormalities, and cleft lip and palate.5-7 Therefore, additional history taking and examinations may be required to identify these associated pathologies. In Case 1, the 15-month-old boy had congenital heart disease.
Surgical excision will prevent complications
A simple surgical excision should be performed for VID remnants. The prognosis is excellent when such procedures are performed in the non-acute setting. Some debate exists as to whether all remnants require formal abdominal exploration.8,9
Treatment of patent VIDs requires surgical excision of the duct, with or without a segment of the small bowel, to obliterate the connection.10 Reconstruction of the umbilicus is then performed, depending on the surgical technique used.
Our patients both made complete recoveries following their surgeries with resolution of their symptoms.
THE TAKEAWAY
Consider a VID remnant as part of the differential diagnosis for any patient who has what appears to be a granulomatous umbilical lesion. Order ultrasonography to evaluate a suspected VID, especially for lesions that fail to respond to 2 or 3 silver nitrate treatments. Surgical excision of a VID remnant is usually curative.
1. Vane DW, West KW, Grosfeld JL. Vitelline duct anomalies. Experience with 217 childhood cases. Arch Surg. 1987;122:542-547.
2. Piparsaliya S, Joshi M, Rajput N, et al. Patent vitellointestinal duct: A close differential diagnosis of umbilical granuloma: A case report and review of literature. Surgical Science. 2011;2:134-136.
3. Khati NJ, Enquist EG, Javitt MC. Imaging of the umbilicus and periumbilical region. Radiographics. 1998;18:413-431.
4. Yamada T, Seiki Y, Ueda M, et al. Patent omphalomesenteric duct: a case report and review of Japanese literature. Asia Oceania J Obstet Gynaecol. 1989;15:229-236.
5. Martin RH, Doublestein GL, Jarvis MR. Concurrent ectopic pregnancy, Meckel’s diverticulum with vitelline duct remnant, cecal volvulus, and congenital complete heart block: report of a case. J Am Osteopath Assoc. 1986;86:589-591.
6. Elebute EA, Ransome-Kuti O. Patent vitello-intestinal duct with ileal prolapse. Arch Surg. 1965;91:456-460.
7. Blair SP, Beasley SW. Intussusception of vitello-intestinal tract through an exomphalos in trisomy 13. Pediatric Surgery International. 1989;4:422-423.
8. Kutin ND, Allen JE, Jewett TC. The umbilical polyp. J Pediatr Surg. 1979;14:741-744.
9. Pacilli M, Sebire NJ, Maritsi D, et al. Umbilical polyp in infants and children. Eur J Pediatr Surg. 2007;17:397-399.
10. Storms P, Pexsters J, Vandekerkhof J. Small omphalocele with ileal prolapse through a patent omphalomesenteric duct. A case report and review of literature. Acta Chir Belg. 1988;88:392-394.
1. Vane DW, West KW, Grosfeld JL. Vitelline duct anomalies. Experience with 217 childhood cases. Arch Surg. 1987;122:542-547.
2. Piparsaliya S, Joshi M, Rajput N, et al. Patent vitellointestinal duct: A close differential diagnosis of umbilical granuloma: A case report and review of literature. Surgical Science. 2011;2:134-136.
3. Khati NJ, Enquist EG, Javitt MC. Imaging of the umbilicus and periumbilical region. Radiographics. 1998;18:413-431.
4. Yamada T, Seiki Y, Ueda M, et al. Patent omphalomesenteric duct: a case report and review of Japanese literature. Asia Oceania J Obstet Gynaecol. 1989;15:229-236.
5. Martin RH, Doublestein GL, Jarvis MR. Concurrent ectopic pregnancy, Meckel’s diverticulum with vitelline duct remnant, cecal volvulus, and congenital complete heart block: report of a case. J Am Osteopath Assoc. 1986;86:589-591.
6. Elebute EA, Ransome-Kuti O. Patent vitello-intestinal duct with ileal prolapse. Arch Surg. 1965;91:456-460.
7. Blair SP, Beasley SW. Intussusception of vitello-intestinal tract through an exomphalos in trisomy 13. Pediatric Surgery International. 1989;4:422-423.
8. Kutin ND, Allen JE, Jewett TC. The umbilical polyp. J Pediatr Surg. 1979;14:741-744.
9. Pacilli M, Sebire NJ, Maritsi D, et al. Umbilical polyp in infants and children. Eur J Pediatr Surg. 2007;17:397-399.
10. Storms P, Pexsters J, Vandekerkhof J. Small omphalocele with ileal prolapse through a patent omphalomesenteric duct. A case report and review of literature. Acta Chir Belg. 1988;88:392-394.

In adolescents, treat substance use disorder before ADHD
NEW YORK – When evaluating adolescents with substance use disorder (SUD), paying attention to frequently occurring comorbid conditions, such as attention-deficit/hyperactivity disorder (ADHD) and bipolar disorder, is essential for developing a successful treatment plan, according to an expert summary of current strategies that was presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“If you see SUD in a juvenile, think psychopathogy,” reported Dr. Timothy Wilens, chief of the division of child and adolescent psychiatry, Massachusetts General Hospital, Boston. Citing a series of studies published over the past 20 years, he said that the proportion of patients with SUD and overlapping psychopathology “is approaching 90%.”

The most significant predictor of SUD is conduct disorder whether or not it is linked to ADHD, according to Dr. Wilens. He emphasized the risk of SUD, which can range from a mild form consisting of intermittent use of alcohol or drugs to a severe form consisting of functional impairment and substance dependence, exceeds 80% in children and adolescents with a history of conduct disorder. ADHD specifically can be diagnosed in about 50% of children with SUD.
Overall, the presence of ADHD, mood disorders such as depression or anxiety, posttraumatic stress disorder (PTSD), and bipolar disorder all double the risk of SUD in children and adolescents. In most but not all cases, SUD should be treated first. According to Dr. Wilens, SUD can complicate efforts to treat comorbid psychopathology, particularly if pharmacologic agents such as stimulants are part of the therapy. One exception is bipolar disorder.
Bipolar disorder “is a different story. When I have bipolar kids who are using, I blast through the substance use,” said Dr. Wilens, referring to his strategy of treating this condition either first or in conjunction with treatment of SUD. While he indicated that control of bipolar disorder might be more important for achieving control of SUD than the other way around, he also cited data demonstrating a favorable influence of lithium relative to placebo on alcohol- or marijuana-associated SUD in adolescents. In another study of adolescents with SUD, quetiapine plus topiramate was associated with a significant reduction in marijuana use when compared with quetiapine and placebo.
In adolescents, marijuana is the most common form of SUD. Although alcohol is involved in about 70% of cases of SUD in adults, marijuana is also the most common type of SUD in the pediatric population, according to Dr. Wilens. Although the use of opioids has been trending upwards over the last 10 years in all age groups, use remains relatively low in children and adolescents. Still, 40% of adolescents reported narcotics to be fairly easy or very easy to obtain in a recent survey cited by Dr. Wilens.
“Most are getting the narcotics from family or friends,” reported Dr. Wilens, noting that these are too often found in the bathroom medicine cabinet. He suggested that parents could reduce risk of adolescent use of narcotics by either throwing away spare pills or putting them in a place where they are less likely to be found.
In a treatment plan for adolescents, harm reduction is the first concern, but Dr. Wilens also counseled that reasonable goals and a collaborative approach to treatment should be introduced long before a “tough love” strategy that includes total abstinence. In children with moderate to severe SUD, Dr. Wilens suggested that clinicians should work to define triggers and then negotiate reasonable strategies to change behavior.
In motivated children, one strategy is “sobriety sampling.” In this approach, the patient is challenged to abstain from substance use for a finite period, such as a month. According to Dr. Wilens, “kids often realize that they feel better,” which is a critical step toward success in avoiding triggers.
There are a number of psychotherapies, such as cognitive behavioral modification, and psychopharmacologic strategies, such as N-acetyl cysteine (NAC) and buspirone, associated with success in treating SUD, but dedicated treatment facilities may be the right answer when clinicians do not have the time or experience to provide care. Dr. Wilens suggested that a national treatment facility locator developed by the Substance Abuse and Mental Health Services Administration may be helpful. The locator tool can be found online (www.findtreatment.samhsa.gov).
One reason to treat SUD in adolescents is that the problem, if untreated, is likely to persist. Data suggest that 50% of adults with SUD developed this condition before the age of 18. For many patients, success in treatment will depend on strategies that ultimately addresses both SUD and the frequently occurring comorbid conditions. Overall, Dr. Wilens recommended a systematic but not a rigid approach.
“The ultimate goal of harm reduction is abstinence, but we are not saying you are a failure if you did not just stop,” Dr. Wilens said. Although a “tough love” approach may have value in some patients “it is not an first, second, third, fourth, or fifth intervention. It may be one, but it’s down the line.”
NEW YORK – When evaluating adolescents with substance use disorder (SUD), paying attention to frequently occurring comorbid conditions, such as attention-deficit/hyperactivity disorder (ADHD) and bipolar disorder, is essential for developing a successful treatment plan, according to an expert summary of current strategies that was presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“If you see SUD in a juvenile, think psychopathogy,” reported Dr. Timothy Wilens, chief of the division of child and adolescent psychiatry, Massachusetts General Hospital, Boston. Citing a series of studies published over the past 20 years, he said that the proportion of patients with SUD and overlapping psychopathology “is approaching 90%.”
The most significant predictor of SUD is conduct disorder whether or not it is linked to ADHD, according to Dr. Wilens. He emphasized the risk of SUD, which can range from a mild form consisting of intermittent use of alcohol or drugs to a severe form consisting of functional impairment and substance dependence, exceeds 80% in children and adolescents with a history of conduct disorder. ADHD specifically can be diagnosed in about 50% of children with SUD.
Overall, the presence of ADHD, mood disorders such as depression or anxiety, posttraumatic stress disorder (PTSD), and bipolar disorder all double the risk of SUD in children and adolescents. In most but not all cases, SUD should be treated first. According to Dr. Wilens, SUD can complicate efforts to treat comorbid psychopathology, particularly if pharmacologic agents such as stimulants are part of the therapy. One exception is bipolar disorder.
Bipolar disorder “is a different story. When I have bipolar kids who are using, I blast through the substance use,” said Dr. Wilens, referring to his strategy of treating this condition either first or in conjunction with treatment of SUD. While he indicated that control of bipolar disorder might be more important for achieving control of SUD than the other way around, he also cited data demonstrating a favorable influence of lithium relative to placebo on alcohol- or marijuana-associated SUD in adolescents. In another study of adolescents with SUD, quetiapine plus topiramate was associated with a significant reduction in marijuana use when compared with quetiapine and placebo.
In adolescents, marijuana is the most common form of SUD. Although alcohol is involved in about 70% of cases of SUD in adults, marijuana is also the most common type of SUD in the pediatric population, according to Dr. Wilens. Although the use of opioids has been trending upwards over the last 10 years in all age groups, use remains relatively low in children and adolescents. Still, 40% of adolescents reported narcotics to be fairly easy or very easy to obtain in a recent survey cited by Dr. Wilens.
“Most are getting the narcotics from family or friends,” reported Dr. Wilens, noting that these are too often found in the bathroom medicine cabinet. He suggested that parents could reduce risk of adolescent use of narcotics by either throwing away spare pills or putting them in a place where they are less likely to be found.
In a treatment plan for adolescents, harm reduction is the first concern, but Dr. Wilens also counseled that reasonable goals and a collaborative approach to treatment should be introduced long before a “tough love” strategy that includes total abstinence. In children with moderate to severe SUD, Dr. Wilens suggested that clinicians should work to define triggers and then negotiate reasonable strategies to change behavior.
In motivated children, one strategy is “sobriety sampling.” In this approach, the patient is challenged to abstain from substance use for a finite period, such as a month. According to Dr. Wilens, “kids often realize that they feel better,” which is a critical step toward success in avoiding triggers.
There are a number of psychotherapies, such as cognitive behavioral modification, and psychopharmacologic strategies, such as N-acetyl cysteine (NAC) and buspirone, associated with success in treating SUD, but dedicated treatment facilities may be the right answer when clinicians do not have the time or experience to provide care. Dr. Wilens suggested that a national treatment facility locator developed by the Substance Abuse and Mental Health Services Administration may be helpful. The locator tool can be found online (www.findtreatment.samhsa.gov).
One reason to treat SUD in adolescents is that the problem, if untreated, is likely to persist. Data suggest that 50% of adults with SUD developed this condition before the age of 18. For many patients, success in treatment will depend on strategies that ultimately addresses both SUD and the frequently occurring comorbid conditions. Overall, Dr. Wilens recommended a systematic but not a rigid approach.
“The ultimate goal of harm reduction is abstinence, but we are not saying you are a failure if you did not just stop,” Dr. Wilens said. Although a “tough love” approach may have value in some patients “it is not an first, second, third, fourth, or fifth intervention. It may be one, but it’s down the line.”
NEW YORK – When evaluating adolescents with substance use disorder (SUD), paying attention to frequently occurring comorbid conditions, such as attention-deficit/hyperactivity disorder (ADHD) and bipolar disorder, is essential for developing a successful treatment plan, according to an expert summary of current strategies that was presented at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“If you see SUD in a juvenile, think psychopathogy,” reported Dr. Timothy Wilens, chief of the division of child and adolescent psychiatry, Massachusetts General Hospital, Boston. Citing a series of studies published over the past 20 years, he said that the proportion of patients with SUD and overlapping psychopathology “is approaching 90%.”
The most significant predictor of SUD is conduct disorder whether or not it is linked to ADHD, according to Dr. Wilens. He emphasized the risk of SUD, which can range from a mild form consisting of intermittent use of alcohol or drugs to a severe form consisting of functional impairment and substance dependence, exceeds 80% in children and adolescents with a history of conduct disorder. ADHD specifically can be diagnosed in about 50% of children with SUD.
Overall, the presence of ADHD, mood disorders such as depression or anxiety, posttraumatic stress disorder (PTSD), and bipolar disorder all double the risk of SUD in children and adolescents. In most but not all cases, SUD should be treated first. According to Dr. Wilens, SUD can complicate efforts to treat comorbid psychopathology, particularly if pharmacologic agents such as stimulants are part of the therapy. One exception is bipolar disorder.
Bipolar disorder “is a different story. When I have bipolar kids who are using, I blast through the substance use,” said Dr. Wilens, referring to his strategy of treating this condition either first or in conjunction with treatment of SUD. While he indicated that control of bipolar disorder might be more important for achieving control of SUD than the other way around, he also cited data demonstrating a favorable influence of lithium relative to placebo on alcohol- or marijuana-associated SUD in adolescents. In another study of adolescents with SUD, quetiapine plus topiramate was associated with a significant reduction in marijuana use when compared with quetiapine and placebo.
In adolescents, marijuana is the most common form of SUD. Although alcohol is involved in about 70% of cases of SUD in adults, marijuana is also the most common type of SUD in the pediatric population, according to Dr. Wilens. Although the use of opioids has been trending upwards over the last 10 years in all age groups, use remains relatively low in children and adolescents. Still, 40% of adolescents reported narcotics to be fairly easy or very easy to obtain in a recent survey cited by Dr. Wilens.
“Most are getting the narcotics from family or friends,” reported Dr. Wilens, noting that these are too often found in the bathroom medicine cabinet. He suggested that parents could reduce risk of adolescent use of narcotics by either throwing away spare pills or putting them in a place where they are less likely to be found.
In a treatment plan for adolescents, harm reduction is the first concern, but Dr. Wilens also counseled that reasonable goals and a collaborative approach to treatment should be introduced long before a “tough love” strategy that includes total abstinence. In children with moderate to severe SUD, Dr. Wilens suggested that clinicians should work to define triggers and then negotiate reasonable strategies to change behavior.
In motivated children, one strategy is “sobriety sampling.” In this approach, the patient is challenged to abstain from substance use for a finite period, such as a month. According to Dr. Wilens, “kids often realize that they feel better,” which is a critical step toward success in avoiding triggers.
There are a number of psychotherapies, such as cognitive behavioral modification, and psychopharmacologic strategies, such as N-acetyl cysteine (NAC) and buspirone, associated with success in treating SUD, but dedicated treatment facilities may be the right answer when clinicians do not have the time or experience to provide care. Dr. Wilens suggested that a national treatment facility locator developed by the Substance Abuse and Mental Health Services Administration may be helpful. The locator tool can be found online (www.findtreatment.samhsa.gov).
One reason to treat SUD in adolescents is that the problem, if untreated, is likely to persist. Data suggest that 50% of adults with SUD developed this condition before the age of 18. For many patients, success in treatment will depend on strategies that ultimately addresses both SUD and the frequently occurring comorbid conditions. Overall, Dr. Wilens recommended a systematic but not a rigid approach.
“The ultimate goal of harm reduction is abstinence, but we are not saying you are a failure if you did not just stop,” Dr. Wilens said. Although a “tough love” approach may have value in some patients “it is not an first, second, third, fourth, or fifth intervention. It may be one, but it’s down the line.”
AT THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
Key clinical point: In adolescents with both attention-deficit/hyperactivity disorder and substance use disorder, control of substance use comes first.
Major finding: Nearly 90% of adolescents with substance use disorder have a comorbid psychopathology for which the order of treatment may affect likelihood of treatment success.
Data source: Clinical expert opinion.
Disclosures: Dr. Wilens reports financial relationship with Euthymics Bioscience, Ironshore Inc., Sunovion Pharmaceuticals, Theravance Biopharma, and Tris Pharma.

Proton radiotherapy effective for childhood medulloblastoma
Treatment of childhood medulloblastoma with proton radiotherapy resulted in acceptable toxicity, with no observed cardiac, pulmonary, or gastrointestinal late effects, and achieved outcomes that were similar to those of photon (x-ray)-based therapy.
At a median follow up of 5 years, the cumulative incidence of grade 3 to 4 hearing loss was 16% (95% confidence interval, 6-29). The Full Scale Intelligence Quotient decreased significantly, particularly in children younger than 8 years, driven mostly by drops in processing speed and verbal comprehension. The cumulative incidence of any hormone deficit at 7 years was 63% (95% CI, 48-75).
For all patients, progression-free survival (PFS) at 5 years was 80% (95% CI, 67-88) and overall survival (OS) was 83% (95% CI, 70-90). For patients with standard-risk disease, PFS was 85% (95% CI, 69-93) and OS was 86% (95% CI, 70-94); for intermediate-risk disease, PFS was 67% (95% CI, 19-90) and OS was 67% (95% CI, 19-90); for high-risk disease, PFS was 71% (95% CI, 41-88) and OS was 79% (95% CI, 47-93). These rates are similar to previously published outcomes of 81%-83% for PFS and 85%-86% for OS (Lancet Onc. 2016 Jan 29. doi: 10.1016/S1470-2045(15)00167-9).
“Therefore, the similar disease control coupled with similar patterns of failure should quell concerns raised about the differences in relative biologic effectiveness of passively scattered proton radiotherapy,” wrote Dr. Torunn Yock, chief of pediatric radiation oncology at Massachusetts General Hospital, Boston, and colleagues.
“Although there remain some effects of treatment on hearing, endocrine, and neurocognitive outcomes – particularly in younger patients – other late effects common in photon-treated patients, such as cardiac, pulmonary, and gastrointestinal toxic effects, were absent,” they said.
Medulloblastoma survivors often have treatment-related adverse late effects, and proton radiotherapy is used to mitigate late effects by decreasing the volume of normal tissue irradiated.
The estimated mean loss per year of IQ points, at –1.5, was less than IQ differences reported in previous studies, which ranged from –1.9 to –5.8 depending on age, craniospinal irradiation dosing, boost volumes, and length of follow-up.
There were no observed cardiac effects, and no patients had restrictive lung disease, which can occur in 24%-50% of long-term survivors treated with craniospinal photon irradiation. In addition, there were no new cases of gastrointestinal toxic effects that have occurred in up to 44% of photon-treated patients.
The prospective, nonrandomized phase II study carried out at Massachusetts General Hospital, Boston, evaluated 59 patients aged 3-21 years (median age 6.6 years) who had medulloblastoma (39 standard risk, 6 intermediate risk, and 14 high risk). All patients received chemotherapy and 55 had a near or gross total resection.
The prospective study by Dr. Yock and colleagues sets a new benchmark for treatment of medulloblastoma in pediatric patients and alludes to the clinical benefits of advanced radiation treatment. It becomes increasingly important for radiation oncologists to incorporate new findings in genomics and molecular subtyping for diseases such as medulloblastoma in the design of prospective studies, and to implement strategies to prevent cognitive decline in pediatric patients. The investigators demonstrate benefits of low-dose sparing afforded by proton therapy, but further improvements are possible. With newer delivery techniques, such as spot scanning proton therapy for the craniospinal component of treatment, more improvements in hearing outcomes can be expected.
The rarity of the disease, combined with the compelling results of Dr. Yock and colleagues, make randomized trials of photons versus protons for medulloblastoma unlikely. Without randomized trial data, some states require that all pediatric patients be treated with photon therapy, a requirement that could result higher rates of cardiovascular disease and other adverse effects. Radiation oncologists understand the potential for severe adverse effects of treatment, and many embrace new technologies that mitigate effects of radiation therapy on patients’ quality of life, a consideration that is particularly important in treatment of pediatric cancers.
Dr. David Grosshans is at the department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston. These remarks were part of an editorial accompanying the report by Dr. Yock and colleagues (Lancet Onc. 2016 Jan 29. doi: 10.1016/S1470-2045(15)00217-X. Dr. Grosshans reported having no disclosures.
The prospective study by Dr. Yock and colleagues sets a new benchmark for treatment of medulloblastoma in pediatric patients and alludes to the clinical benefits of advanced radiation treatment. It becomes increasingly important for radiation oncologists to incorporate new findings in genomics and molecular subtyping for diseases such as medulloblastoma in the design of prospective studies, and to implement strategies to prevent cognitive decline in pediatric patients. The investigators demonstrate benefits of low-dose sparing afforded by proton therapy, but further improvements are possible. With newer delivery techniques, such as spot scanning proton therapy for the craniospinal component of treatment, more improvements in hearing outcomes can be expected.
The rarity of the disease, combined with the compelling results of Dr. Yock and colleagues, make randomized trials of photons versus protons for medulloblastoma unlikely. Without randomized trial data, some states require that all pediatric patients be treated with photon therapy, a requirement that could result higher rates of cardiovascular disease and other adverse effects. Radiation oncologists understand the potential for severe adverse effects of treatment, and many embrace new technologies that mitigate effects of radiation therapy on patients’ quality of life, a consideration that is particularly important in treatment of pediatric cancers.
Dr. David Grosshans is at the department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston. These remarks were part of an editorial accompanying the report by Dr. Yock and colleagues (Lancet Onc. 2016 Jan 29. doi: 10.1016/S1470-2045(15)00217-X. Dr. Grosshans reported having no disclosures.
The prospective study by Dr. Yock and colleagues sets a new benchmark for treatment of medulloblastoma in pediatric patients and alludes to the clinical benefits of advanced radiation treatment. It becomes increasingly important for radiation oncologists to incorporate new findings in genomics and molecular subtyping for diseases such as medulloblastoma in the design of prospective studies, and to implement strategies to prevent cognitive decline in pediatric patients. The investigators demonstrate benefits of low-dose sparing afforded by proton therapy, but further improvements are possible. With newer delivery techniques, such as spot scanning proton therapy for the craniospinal component of treatment, more improvements in hearing outcomes can be expected.
The rarity of the disease, combined with the compelling results of Dr. Yock and colleagues, make randomized trials of photons versus protons for medulloblastoma unlikely. Without randomized trial data, some states require that all pediatric patients be treated with photon therapy, a requirement that could result higher rates of cardiovascular disease and other adverse effects. Radiation oncologists understand the potential for severe adverse effects of treatment, and many embrace new technologies that mitigate effects of radiation therapy on patients’ quality of life, a consideration that is particularly important in treatment of pediatric cancers.
Dr. David Grosshans is at the department of radiation oncology, University of Texas MD Anderson Cancer Center, Houston. These remarks were part of an editorial accompanying the report by Dr. Yock and colleagues (Lancet Onc. 2016 Jan 29. doi: 10.1016/S1470-2045(15)00217-X. Dr. Grosshans reported having no disclosures.
Treatment of childhood medulloblastoma with proton radiotherapy resulted in acceptable toxicity, with no observed cardiac, pulmonary, or gastrointestinal late effects, and achieved outcomes that were similar to those of photon (x-ray)-based therapy.
At a median follow up of 5 years, the cumulative incidence of grade 3 to 4 hearing loss was 16% (95% confidence interval, 6-29). The Full Scale Intelligence Quotient decreased significantly, particularly in children younger than 8 years, driven mostly by drops in processing speed and verbal comprehension. The cumulative incidence of any hormone deficit at 7 years was 63% (95% CI, 48-75).
For all patients, progression-free survival (PFS) at 5 years was 80% (95% CI, 67-88) and overall survival (OS) was 83% (95% CI, 70-90). For patients with standard-risk disease, PFS was 85% (95% CI, 69-93) and OS was 86% (95% CI, 70-94); for intermediate-risk disease, PFS was 67% (95% CI, 19-90) and OS was 67% (95% CI, 19-90); for high-risk disease, PFS was 71% (95% CI, 41-88) and OS was 79% (95% CI, 47-93). These rates are similar to previously published outcomes of 81%-83% for PFS and 85%-86% for OS (Lancet Onc. 2016 Jan 29. doi: 10.1016/S1470-2045(15)00167-9).
“Therefore, the similar disease control coupled with similar patterns of failure should quell concerns raised about the differences in relative biologic effectiveness of passively scattered proton radiotherapy,” wrote Dr. Torunn Yock, chief of pediatric radiation oncology at Massachusetts General Hospital, Boston, and colleagues.
“Although there remain some effects of treatment on hearing, endocrine, and neurocognitive outcomes – particularly in younger patients – other late effects common in photon-treated patients, such as cardiac, pulmonary, and gastrointestinal toxic effects, were absent,” they said.
Medulloblastoma survivors often have treatment-related adverse late effects, and proton radiotherapy is used to mitigate late effects by decreasing the volume of normal tissue irradiated.
The estimated mean loss per year of IQ points, at –1.5, was less than IQ differences reported in previous studies, which ranged from –1.9 to –5.8 depending on age, craniospinal irradiation dosing, boost volumes, and length of follow-up.
There were no observed cardiac effects, and no patients had restrictive lung disease, which can occur in 24%-50% of long-term survivors treated with craniospinal photon irradiation. In addition, there were no new cases of gastrointestinal toxic effects that have occurred in up to 44% of photon-treated patients.
The prospective, nonrandomized phase II study carried out at Massachusetts General Hospital, Boston, evaluated 59 patients aged 3-21 years (median age 6.6 years) who had medulloblastoma (39 standard risk, 6 intermediate risk, and 14 high risk). All patients received chemotherapy and 55 had a near or gross total resection.
Treatment of childhood medulloblastoma with proton radiotherapy resulted in acceptable toxicity, with no observed cardiac, pulmonary, or gastrointestinal late effects, and achieved outcomes that were similar to those of photon (x-ray)-based therapy.
At a median follow up of 5 years, the cumulative incidence of grade 3 to 4 hearing loss was 16% (95% confidence interval, 6-29). The Full Scale Intelligence Quotient decreased significantly, particularly in children younger than 8 years, driven mostly by drops in processing speed and verbal comprehension. The cumulative incidence of any hormone deficit at 7 years was 63% (95% CI, 48-75).
For all patients, progression-free survival (PFS) at 5 years was 80% (95% CI, 67-88) and overall survival (OS) was 83% (95% CI, 70-90). For patients with standard-risk disease, PFS was 85% (95% CI, 69-93) and OS was 86% (95% CI, 70-94); for intermediate-risk disease, PFS was 67% (95% CI, 19-90) and OS was 67% (95% CI, 19-90); for high-risk disease, PFS was 71% (95% CI, 41-88) and OS was 79% (95% CI, 47-93). These rates are similar to previously published outcomes of 81%-83% for PFS and 85%-86% for OS (Lancet Onc. 2016 Jan 29. doi: 10.1016/S1470-2045(15)00167-9).
“Therefore, the similar disease control coupled with similar patterns of failure should quell concerns raised about the differences in relative biologic effectiveness of passively scattered proton radiotherapy,” wrote Dr. Torunn Yock, chief of pediatric radiation oncology at Massachusetts General Hospital, Boston, and colleagues.
“Although there remain some effects of treatment on hearing, endocrine, and neurocognitive outcomes – particularly in younger patients – other late effects common in photon-treated patients, such as cardiac, pulmonary, and gastrointestinal toxic effects, were absent,” they said.
Medulloblastoma survivors often have treatment-related adverse late effects, and proton radiotherapy is used to mitigate late effects by decreasing the volume of normal tissue irradiated.
The estimated mean loss per year of IQ points, at –1.5, was less than IQ differences reported in previous studies, which ranged from –1.9 to –5.8 depending on age, craniospinal irradiation dosing, boost volumes, and length of follow-up.
There were no observed cardiac effects, and no patients had restrictive lung disease, which can occur in 24%-50% of long-term survivors treated with craniospinal photon irradiation. In addition, there were no new cases of gastrointestinal toxic effects that have occurred in up to 44% of photon-treated patients.
The prospective, nonrandomized phase II study carried out at Massachusetts General Hospital, Boston, evaluated 59 patients aged 3-21 years (median age 6.6 years) who had medulloblastoma (39 standard risk, 6 intermediate risk, and 14 high risk). All patients received chemotherapy and 55 had a near or gross total resection.
FROM THE LANCET ONCOLOGY
Key clinical point: Proton radiotherapy for childhood medulloblastoma resulted in similar survival outcomes to those of photon-based therapy and had acceptable toxicity.
Major finding: At 5 years, the cumulative incidence of grade 3 to 4 hearing loss was 16%; 5-year progression-free and overall survival for patients with standard risk were 85% and 86%, respectively, and for those with high to intermediate risk, 70% and 75%, respectively.
Data source: A prospective, nonrandomized, phase II study with 59 patients aged 3-21 years who had medulloblastoma (39 standard risk, 6 intermediate risk, and 14 high risk).
Disclosures: Dr. Yock and coauthors reported having no disclosures.
FDA approves Adzenys XR-ODT for ADHD
An amphetamine-based extended-release orally disintegrating tablet for patients aged 6 years and older diagnosed with attention-deficit/hyperactivity disorder won Food and Drug Administration approval on Jan. 28.
Adzenys XR-ODT is the first and only extended-release orally disintegrating tablet for ADHD, Neos Therapeutics, the drug’s manufacturer, said in a statement. The newly approved agent is bioequivalent to Adderall XR, and patients taking Adderall can be switched to the new drug. Equivalent doses of the two drugs are outlined on the drug label.
“The novel features of an extended-release orally disintegrating tablet ... make Adzenys XR-ODT attractive for use in both children (6 and older) and adults,” Dr. Alice R. Mao, medical director, Memorial Park Psychiatry, Houston, said in the statement.
As a condition of the approval, Neos Therapeutics must report the status of three postmarketing studies annually of children diagnosed with ADHD taking Adzenys XR-ODT, according to the approval letter. One is a single-dose, open-label study of children aged 4 years to under 6 years; the second is a randomized, double-blind, placebo-controlled titration study of children aged 4-5 years; and the third is a 1-year, open-label safety study of patients aged 4-5 years.
For patients aged 6-17 years, the starting dose is 6.3 mg once daily in the morning, and for adults, it is 12.5 mg once daily in the morning, according to the label. The medication will be available in four other dose strengths: 3.1 mg, 9.4 mg, 15.7 mg, and 18.8 mg.
The most common adverse reactions to the drug among pediatric patients include loss of appetite, insomnia, and abdominal pain. Among adult patients, adverse reactions include dry mouth, loss of appetite, and insomnia.
An amphetamine-based extended-release orally disintegrating tablet for patients aged 6 years and older diagnosed with attention-deficit/hyperactivity disorder won Food and Drug Administration approval on Jan. 28.
Adzenys XR-ODT is the first and only extended-release orally disintegrating tablet for ADHD, Neos Therapeutics, the drug’s manufacturer, said in a statement. The newly approved agent is bioequivalent to Adderall XR, and patients taking Adderall can be switched to the new drug. Equivalent doses of the two drugs are outlined on the drug label.
“The novel features of an extended-release orally disintegrating tablet ... make Adzenys XR-ODT attractive for use in both children (6 and older) and adults,” Dr. Alice R. Mao, medical director, Memorial Park Psychiatry, Houston, said in the statement.
As a condition of the approval, Neos Therapeutics must report the status of three postmarketing studies annually of children diagnosed with ADHD taking Adzenys XR-ODT, according to the approval letter. One is a single-dose, open-label study of children aged 4 years to under 6 years; the second is a randomized, double-blind, placebo-controlled titration study of children aged 4-5 years; and the third is a 1-year, open-label safety study of patients aged 4-5 years.
For patients aged 6-17 years, the starting dose is 6.3 mg once daily in the morning, and for adults, it is 12.5 mg once daily in the morning, according to the label. The medication will be available in four other dose strengths: 3.1 mg, 9.4 mg, 15.7 mg, and 18.8 mg.
The most common adverse reactions to the drug among pediatric patients include loss of appetite, insomnia, and abdominal pain. Among adult patients, adverse reactions include dry mouth, loss of appetite, and insomnia.
An amphetamine-based extended-release orally disintegrating tablet for patients aged 6 years and older diagnosed with attention-deficit/hyperactivity disorder won Food and Drug Administration approval on Jan. 28.
Adzenys XR-ODT is the first and only extended-release orally disintegrating tablet for ADHD, Neos Therapeutics, the drug’s manufacturer, said in a statement. The newly approved agent is bioequivalent to Adderall XR, and patients taking Adderall can be switched to the new drug. Equivalent doses of the two drugs are outlined on the drug label.
“The novel features of an extended-release orally disintegrating tablet ... make Adzenys XR-ODT attractive for use in both children (6 and older) and adults,” Dr. Alice R. Mao, medical director, Memorial Park Psychiatry, Houston, said in the statement.
As a condition of the approval, Neos Therapeutics must report the status of three postmarketing studies annually of children diagnosed with ADHD taking Adzenys XR-ODT, according to the approval letter. One is a single-dose, open-label study of children aged 4 years to under 6 years; the second is a randomized, double-blind, placebo-controlled titration study of children aged 4-5 years; and the third is a 1-year, open-label safety study of patients aged 4-5 years.
For patients aged 6-17 years, the starting dose is 6.3 mg once daily in the morning, and for adults, it is 12.5 mg once daily in the morning, according to the label. The medication will be available in four other dose strengths: 3.1 mg, 9.4 mg, 15.7 mg, and 18.8 mg.
The most common adverse reactions to the drug among pediatric patients include loss of appetite, insomnia, and abdominal pain. Among adult patients, adverse reactions include dry mouth, loss of appetite, and insomnia.
Suicidal ideation in elderly depression patients linked to inhibitory response
Older depression patients with poorer ability to switch between inhibitory and noninhibitory responses are more likely to have higher levels of suicidal ideation, according to Dr. John Kasckow and his associates.
They analyzed data from 468 adults aged 60 or older with major depressive disorder who had undergone venlafaxine XR monotherapy for up to 16 weeks.

Those who had “high and persistent” suicidal ideation scored significantly worse on the Color/Word “inhibition/switching” subtest of the Delis-Kaplan Executive Function Scale, compared with patients with “rapidly decreasing” suicidal ideation, reported Dr. Kasckow of the VA Pittsburgh Healthcare System.
In addition, patients with “high and persistent” suicidal ideation performed worse on the attention index section of the Repeatable Battery for the Assessment of Neuropsychological Status, and worse on the RBANS overall than did other major depressive disorder patients.
“This is the first study that reports that worse executive dysfunction, attention, and global cognition are associated with high and persistent suicidal ideation in older depressed adults adequately treated with antidepressant medication. These findings need to be reproduced,” the investigators noted.
Find the study in the Journal of Psychiatric Research (doi: 10.1016/j.jpsychires.2015.11.004).
Older depression patients with poorer ability to switch between inhibitory and noninhibitory responses are more likely to have higher levels of suicidal ideation, according to Dr. John Kasckow and his associates.
They analyzed data from 468 adults aged 60 or older with major depressive disorder who had undergone venlafaxine XR monotherapy for up to 16 weeks.
Those who had “high and persistent” suicidal ideation scored significantly worse on the Color/Word “inhibition/switching” subtest of the Delis-Kaplan Executive Function Scale, compared with patients with “rapidly decreasing” suicidal ideation, reported Dr. Kasckow of the VA Pittsburgh Healthcare System.
In addition, patients with “high and persistent” suicidal ideation performed worse on the attention index section of the Repeatable Battery for the Assessment of Neuropsychological Status, and worse on the RBANS overall than did other major depressive disorder patients.
“This is the first study that reports that worse executive dysfunction, attention, and global cognition are associated with high and persistent suicidal ideation in older depressed adults adequately treated with antidepressant medication. These findings need to be reproduced,” the investigators noted.
Find the study in the Journal of Psychiatric Research (doi: 10.1016/j.jpsychires.2015.11.004).
Older depression patients with poorer ability to switch between inhibitory and noninhibitory responses are more likely to have higher levels of suicidal ideation, according to Dr. John Kasckow and his associates.
They analyzed data from 468 adults aged 60 or older with major depressive disorder who had undergone venlafaxine XR monotherapy for up to 16 weeks.
Those who had “high and persistent” suicidal ideation scored significantly worse on the Color/Word “inhibition/switching” subtest of the Delis-Kaplan Executive Function Scale, compared with patients with “rapidly decreasing” suicidal ideation, reported Dr. Kasckow of the VA Pittsburgh Healthcare System.
In addition, patients with “high and persistent” suicidal ideation performed worse on the attention index section of the Repeatable Battery for the Assessment of Neuropsychological Status, and worse on the RBANS overall than did other major depressive disorder patients.
“This is the first study that reports that worse executive dysfunction, attention, and global cognition are associated with high and persistent suicidal ideation in older depressed adults adequately treated with antidepressant medication. These findings need to be reproduced,” the investigators noted.
Find the study in the Journal of Psychiatric Research (doi: 10.1016/j.jpsychires.2015.11.004).
FROM THE JOURNAL OF PSYCHIATRIC RESEARCH

AES: Development of unobtrusive seizure-detection devices continues
PHILADELPHIA – Reliable, externally worn seizure-detection devices for epilepsy patients have been eagerly sought but elusive. New results from the pivotal trial of an arm-mounted device that works by analyzing skin electromyography showed promise when tested in 142 adults and children with epilepsy who also underwent video EEG monitoring, Dr. José E. Cavazos reported in a poster at the annual meeting of the American Epilepsy Society.
More than 7,000 hours of simultaneous surface electromyography with the investigational device, worn on the patient’s upper arm, and video EEG monitoring as the gold standard for seizure detection showed that the device correctly identified all 29 generalized tonic-clonic seizures experienced by the 142 patients studied. This level of detection came with a false-positive rate of 1.47 false events during every 24 hours of monitoring, with most of the false positives occurring when the device was being placed or removed.

The results made Dr. Cavazos hopeful that the Food and Drug Administration would clear the device, the Brain Sentinel Seizure Detection and Warning System, for U.S. marketing in 2016. The FDA first received the marketing-clearance application in late 2014, said Dr. Cavazos, an epileptologist and professor of neurology at the University of Texas Health Science Center in San Antonio.
But Dr. Cavazos also conceded that receiving FDA clearance for U.S. sale of the device is just the next step in an ongoing process to prove its clinical value.
“Currently, clinical decisions for epilepsy patients are often based on patient-reported seizure counts. There is a clear need for objective data on seizure frequency,” something now obtainable only by running an expensive visual-monitoring study, said Dr. Cavazos, who is also founder of and a stockholder in the company that is developing this device. “We definitely need to show in future studies that monitoring [with the worn device] has a positive impact on patient care, by reducing hospitalizations and producing improved patient outcomes,” he said in an interview. “These data may be enough to get regulatory clearance to sell the device, but insurers may not want to reimburse for it until we can prove its value.”
When the device detects a generalized tonic-clonic seizure, it produces an audible alert and also starts recording both surface EMG data and local audible sounds for use in future analysis of the patient’s status. In the study, seizure detection occurred an average of 14 seconds following seizure onset as judged by visual EEG monitoring adjudicated by three epileptologists. The study also included an additional 31 patients who initially entered the study and began wearing the device but did not complete the monitoring protocol because of an adverse effect while wearing the monitor, usually mild or moderate skin irritation.
The results from this study come in a context of extensive research efforts aimed trying to find reliable and unobtrusive methods to quickly detect seizures short of running an observational study. The best results so far have come when using devices that monitor brain EEG signals with electrode-containing caps or implanted electrodes. But patients have voiced substantially reduced interest in having to resort to such stigmatizing methods, noted Dr. Elizabeth Donner during a separate talk at the meeting.
“Patients don’t want what looks like an EEG-detection device. We need devices that suit our patients’ needs,” said Dr. Donner, an epileptologist at the Hospital for Sick Children in Toronto. Aside from direct measurement of EEG, other approaches involve measurement of heart rate or movement, she noted.
“There are very good techniques for detecting seizures without using EEG,” said Dr. Gregory L. Krauss, a professor of neurology at Johns Hopkins University in Baltimore who joined Dr. Donner in a discussion of the pros and cons of current methods for seizure detection. He specifically cited a heart-rate based detection scheme reported last year by a Belgian team (Seizure. 2015 Nov;[32]:52-61). But like all detection methods, the heart rate–based approach showed a marked trade-off between sensitivity and specificity: A heart-rate threshold of at least 50% above baseline had a sensitivity of 82% while identifying one false positive every hour. Raising the detection threshold to at least 30% above baseline boosted the sensitivity to 91%, but with the cost of flagging 3.5 false positives each hour.
Dr. Krauss is currently trying to develop a motion-based approach to identifying seizure onset using an Apple watch, He concluded that, as of now, development of seizure-detection devices that do not rely on direct measurement of brain EEG patterns remains a work in progress, with no prospectively collected data, although he made this assessment prior to the poster report by Dr. Cavazos at the meeting.
On Twitter @mitchelzoler
PHILADELPHIA – Reliable, externally worn seizure-detection devices for epilepsy patients have been eagerly sought but elusive. New results from the pivotal trial of an arm-mounted device that works by analyzing skin electromyography showed promise when tested in 142 adults and children with epilepsy who also underwent video EEG monitoring, Dr. José E. Cavazos reported in a poster at the annual meeting of the American Epilepsy Society.
More than 7,000 hours of simultaneous surface electromyography with the investigational device, worn on the patient’s upper arm, and video EEG monitoring as the gold standard for seizure detection showed that the device correctly identified all 29 generalized tonic-clonic seizures experienced by the 142 patients studied. This level of detection came with a false-positive rate of 1.47 false events during every 24 hours of monitoring, with most of the false positives occurring when the device was being placed or removed.
The results made Dr. Cavazos hopeful that the Food and Drug Administration would clear the device, the Brain Sentinel Seizure Detection and Warning System, for U.S. marketing in 2016. The FDA first received the marketing-clearance application in late 2014, said Dr. Cavazos, an epileptologist and professor of neurology at the University of Texas Health Science Center in San Antonio.
But Dr. Cavazos also conceded that receiving FDA clearance for U.S. sale of the device is just the next step in an ongoing process to prove its clinical value.
“Currently, clinical decisions for epilepsy patients are often based on patient-reported seizure counts. There is a clear need for objective data on seizure frequency,” something now obtainable only by running an expensive visual-monitoring study, said Dr. Cavazos, who is also founder of and a stockholder in the company that is developing this device. “We definitely need to show in future studies that monitoring [with the worn device] has a positive impact on patient care, by reducing hospitalizations and producing improved patient outcomes,” he said in an interview. “These data may be enough to get regulatory clearance to sell the device, but insurers may not want to reimburse for it until we can prove its value.”
When the device detects a generalized tonic-clonic seizure, it produces an audible alert and also starts recording both surface EMG data and local audible sounds for use in future analysis of the patient’s status. In the study, seizure detection occurred an average of 14 seconds following seizure onset as judged by visual EEG monitoring adjudicated by three epileptologists. The study also included an additional 31 patients who initially entered the study and began wearing the device but did not complete the monitoring protocol because of an adverse effect while wearing the monitor, usually mild or moderate skin irritation.
The results from this study come in a context of extensive research efforts aimed trying to find reliable and unobtrusive methods to quickly detect seizures short of running an observational study. The best results so far have come when using devices that monitor brain EEG signals with electrode-containing caps or implanted electrodes. But patients have voiced substantially reduced interest in having to resort to such stigmatizing methods, noted Dr. Elizabeth Donner during a separate talk at the meeting.
“Patients don’t want what looks like an EEG-detection device. We need devices that suit our patients’ needs,” said Dr. Donner, an epileptologist at the Hospital for Sick Children in Toronto. Aside from direct measurement of EEG, other approaches involve measurement of heart rate or movement, she noted.
“There are very good techniques for detecting seizures without using EEG,” said Dr. Gregory L. Krauss, a professor of neurology at Johns Hopkins University in Baltimore who joined Dr. Donner in a discussion of the pros and cons of current methods for seizure detection. He specifically cited a heart-rate based detection scheme reported last year by a Belgian team (Seizure. 2015 Nov;[32]:52-61). But like all detection methods, the heart rate–based approach showed a marked trade-off between sensitivity and specificity: A heart-rate threshold of at least 50% above baseline had a sensitivity of 82% while identifying one false positive every hour. Raising the detection threshold to at least 30% above baseline boosted the sensitivity to 91%, but with the cost of flagging 3.5 false positives each hour.
Dr. Krauss is currently trying to develop a motion-based approach to identifying seizure onset using an Apple watch, He concluded that, as of now, development of seizure-detection devices that do not rely on direct measurement of brain EEG patterns remains a work in progress, with no prospectively collected data, although he made this assessment prior to the poster report by Dr. Cavazos at the meeting.
On Twitter @mitchelzoler
PHILADELPHIA – Reliable, externally worn seizure-detection devices for epilepsy patients have been eagerly sought but elusive. New results from the pivotal trial of an arm-mounted device that works by analyzing skin electromyography showed promise when tested in 142 adults and children with epilepsy who also underwent video EEG monitoring, Dr. José E. Cavazos reported in a poster at the annual meeting of the American Epilepsy Society.
More than 7,000 hours of simultaneous surface electromyography with the investigational device, worn on the patient’s upper arm, and video EEG monitoring as the gold standard for seizure detection showed that the device correctly identified all 29 generalized tonic-clonic seizures experienced by the 142 patients studied. This level of detection came with a false-positive rate of 1.47 false events during every 24 hours of monitoring, with most of the false positives occurring when the device was being placed or removed.
The results made Dr. Cavazos hopeful that the Food and Drug Administration would clear the device, the Brain Sentinel Seizure Detection and Warning System, for U.S. marketing in 2016. The FDA first received the marketing-clearance application in late 2014, said Dr. Cavazos, an epileptologist and professor of neurology at the University of Texas Health Science Center in San Antonio.
But Dr. Cavazos also conceded that receiving FDA clearance for U.S. sale of the device is just the next step in an ongoing process to prove its clinical value.
“Currently, clinical decisions for epilepsy patients are often based on patient-reported seizure counts. There is a clear need for objective data on seizure frequency,” something now obtainable only by running an expensive visual-monitoring study, said Dr. Cavazos, who is also founder of and a stockholder in the company that is developing this device. “We definitely need to show in future studies that monitoring [with the worn device] has a positive impact on patient care, by reducing hospitalizations and producing improved patient outcomes,” he said in an interview. “These data may be enough to get regulatory clearance to sell the device, but insurers may not want to reimburse for it until we can prove its value.”
When the device detects a generalized tonic-clonic seizure, it produces an audible alert and also starts recording both surface EMG data and local audible sounds for use in future analysis of the patient’s status. In the study, seizure detection occurred an average of 14 seconds following seizure onset as judged by visual EEG monitoring adjudicated by three epileptologists. The study also included an additional 31 patients who initially entered the study and began wearing the device but did not complete the monitoring protocol because of an adverse effect while wearing the monitor, usually mild or moderate skin irritation.
The results from this study come in a context of extensive research efforts aimed trying to find reliable and unobtrusive methods to quickly detect seizures short of running an observational study. The best results so far have come when using devices that monitor brain EEG signals with electrode-containing caps or implanted electrodes. But patients have voiced substantially reduced interest in having to resort to such stigmatizing methods, noted Dr. Elizabeth Donner during a separate talk at the meeting.
“Patients don’t want what looks like an EEG-detection device. We need devices that suit our patients’ needs,” said Dr. Donner, an epileptologist at the Hospital for Sick Children in Toronto. Aside from direct measurement of EEG, other approaches involve measurement of heart rate or movement, she noted.
“There are very good techniques for detecting seizures without using EEG,” said Dr. Gregory L. Krauss, a professor of neurology at Johns Hopkins University in Baltimore who joined Dr. Donner in a discussion of the pros and cons of current methods for seizure detection. He specifically cited a heart-rate based detection scheme reported last year by a Belgian team (Seizure. 2015 Nov;[32]:52-61). But like all detection methods, the heart rate–based approach showed a marked trade-off between sensitivity and specificity: A heart-rate threshold of at least 50% above baseline had a sensitivity of 82% while identifying one false positive every hour. Raising the detection threshold to at least 30% above baseline boosted the sensitivity to 91%, but with the cost of flagging 3.5 false positives each hour.
Dr. Krauss is currently trying to develop a motion-based approach to identifying seizure onset using an Apple watch, He concluded that, as of now, development of seizure-detection devices that do not rely on direct measurement of brain EEG patterns remains a work in progress, with no prospectively collected data, although he made this assessment prior to the poster report by Dr. Cavazos at the meeting.
On Twitter @mitchelzoler
AT AES 2015
Key clinical point: A seizure-detection device worn on the arm showed good sensitivity and reasonable specificity, but no data yet exist on its clinical utility.
Major finding: The Brain Sentinel device had 100% sensitivity while resulting in 1.47 false-positive alarms every 24 hours.
Data source: The pivotal trial for the Brain Sentinel device, which collected detection data from 142 adults and children with a history of seizures.
Disclosures: The study was sponsored by Brain Sentinel, which is developing the device. Dr. Cavazos is a founder of the company, holds stock in the company and is a consultant to the company. Dr. Donner had no disclosures. Dr. Krauss has been a consultant to SK Life Science, Acorda Therapeutics, and Sunovion and has received research support from Upsher-Smith, SK Life Science, UCB, Novartis, and Pfizer.

Zika could soon infect 4 million; U.S. impact likely to be much smaller
The Zika virus continues to spread, with the potential to infect up to 4 million people throughout the Americas.
But although locally transmitted infections are all almost certainly inevitable in the United States, federal health officials don’t expect large-scale infections.
“We do expect to see local transmission, but we are not likely to see widespread outbreaks,” Dr. Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said during a press briefing on Jan. 28. “We think these would occur in pockets, similar to what we now see with dengue and chikungunya. We are not being cavalier about this; we are preparing. But large-scale outbreaks are not something we are likely to see, based on our experience with dengue and chikungunya.”

Dr. Fauci’s comments were in contrast to warnings issued simultaneously by the World Health Organization and the Pan American Health Organization (PAHO), WHO’s South American arm.
On Jan. 28, the WHO announced it would convene a meeting of its International Health Regulations Emergency Committee. WHO Director-General Margaret Chan said the virus is now present in 23 countries and territories in the region, as well as in parts of the South Pacific.
“The level of alarm is extremely high,” she said during the meeting. Although a causal link between the virus and outbreaks of microcephaly and Guillain-Barré syndrome is yet unproven, she said it is strongly suspected. “The possible links, only recently suspected, have rapidly changed the risk profile of Zika, from a mild threat to one of alarming proportions.”
Dr. Marcos Espinal, PAHO’s director of communicable diseases and health analysis, outlined the potential spread. His agency expects to see 3-4 million cases throughout North and South America, which could occur in any region that has endemic dengue fever. Both viruses are carried by mosquitoes of the Aedes genus. Two of these, the Asian tiger mosquito and the yellow fever mosquito, are commonly found in the United States, particularly in warmer regions.
Thus far, 31 cases of Zika virus have been confirmed in the United States (11 states and Washington), Dr. Anne Schuchat, principal deputy director for the Centers for Disease Control and Prevention, said in that agency’s briefing. All of these cases have been associated with travel to endemic areas, she said. She was unable to say how many cases had occurred in pregnant women.
There have been 19 confirmed cases in Puerto Rico and 1 in the U.S. Virgin Islands. These could be locally acquired cases, although that has not been confirmed. However, Zika infection is now a notifiable illness and any confirmed cases must be reported to CDC, she said.
Nearly a million cases have been laboratory confirmed in South America since 2015, Dr. Espinal noted. The vast majority of those have caused mild, transient symptoms. But in Brazil alone – the epicenter of the epidemic – there has been a substantial increase in newborn microcephaly. Almost 4,000 cases of this rare birth defect have been identified since October, when tracking began. Although the cases coincide with the rise of Zika infections, no one knows how many were related or what pathology could be mediating the association.
This is just one question muddying the Zika waters right now, Dr. Chan of the WHO said. Several difficult-to-address issues are hampering an effective response, including the widespread range of the mosquito vectors, which allows international spread; a lack of population immunity; and the absence of rapid diagnostic tests, effective treatment, and any vaccine.
Another concern is the potential for illness-potentiating coinfection. In the lab, Zika virus has shown cross-reactions with dengue types 1-4, yellow fever, and West Nile virus – all of which are carried by Aedes mosquitoes.
Scientists at the CDC and National Institutes of Health are working on the problem now, Dr. Fauci said. Efforts include the creation of animal models to study disease transmission and its effect on pre- and postnatal outcomes, and of diagnostic platforms that could easily and quickly identify Zika infections. These would quickly differentiate Zika from dengue infections, which are also caused by a strain of flavivirus.
An effective vaccine will not be quickly forthcoming, he cautioned, although a phase I trial is in the works and could begin later this year. The candidate is a DNA-based vaccine similar to the one now used to protect against dengue. It would almost certainly not be approved in less than 2 years, Dr Fauci added.

Until some of these questions have been answered, or until the epidemic slows, the CDC continues to caution pregnant women against travel to endemic areas. For those who do travel or who live in endemic areas, Dr. Schuchat reiterated CDC’s long-held advice to take precautions against mosquito bites: long-sleeved shirts and long pants; staying inside; and using an effective insect repellent. Those containing DEET are most effective and are safe for pregnant women to use, Dr. Schuchat said.
For now, the CDC’s Zika travel alert includes Puerto Rico, Barbados, Bolivia, Brazil, Cape Verde, Colombia, Ecuador, El Salvador, French Guiana, Guadeloupe, Guatemala, Guyana, Haiti, Honduras, Martinique, Mexico, Panama, Paraguay, Saint Martin, Samoa, Suriname, Venezuela, the U.S. Virgin Islands, and the Dominican Republic.
A transcript of the press briefing is available online.
This article was updated 2/1/2016.
On Twitter @Alz_Gal
The Zika virus continues to spread, with the potential to infect up to 4 million people throughout the Americas.
But although locally transmitted infections are all almost certainly inevitable in the United States, federal health officials don’t expect large-scale infections.
“We do expect to see local transmission, but we are not likely to see widespread outbreaks,” Dr. Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said during a press briefing on Jan. 28. “We think these would occur in pockets, similar to what we now see with dengue and chikungunya. We are not being cavalier about this; we are preparing. But large-scale outbreaks are not something we are likely to see, based on our experience with dengue and chikungunya.”
Dr. Fauci’s comments were in contrast to warnings issued simultaneously by the World Health Organization and the Pan American Health Organization (PAHO), WHO’s South American arm.
On Jan. 28, the WHO announced it would convene a meeting of its International Health Regulations Emergency Committee. WHO Director-General Margaret Chan said the virus is now present in 23 countries and territories in the region, as well as in parts of the South Pacific.
“The level of alarm is extremely high,” she said during the meeting. Although a causal link between the virus and outbreaks of microcephaly and Guillain-Barré syndrome is yet unproven, she said it is strongly suspected. “The possible links, only recently suspected, have rapidly changed the risk profile of Zika, from a mild threat to one of alarming proportions.”
Dr. Marcos Espinal, PAHO’s director of communicable diseases and health analysis, outlined the potential spread. His agency expects to see 3-4 million cases throughout North and South America, which could occur in any region that has endemic dengue fever. Both viruses are carried by mosquitoes of the Aedes genus. Two of these, the Asian tiger mosquito and the yellow fever mosquito, are commonly found in the United States, particularly in warmer regions.
Thus far, 31 cases of Zika virus have been confirmed in the United States (11 states and Washington), Dr. Anne Schuchat, principal deputy director for the Centers for Disease Control and Prevention, said in that agency’s briefing. All of these cases have been associated with travel to endemic areas, she said. She was unable to say how many cases had occurred in pregnant women.
There have been 19 confirmed cases in Puerto Rico and 1 in the U.S. Virgin Islands. These could be locally acquired cases, although that has not been confirmed. However, Zika infection is now a notifiable illness and any confirmed cases must be reported to CDC, she said.
Nearly a million cases have been laboratory confirmed in South America since 2015, Dr. Espinal noted. The vast majority of those have caused mild, transient symptoms. But in Brazil alone – the epicenter of the epidemic – there has been a substantial increase in newborn microcephaly. Almost 4,000 cases of this rare birth defect have been identified since October, when tracking began. Although the cases coincide with the rise of Zika infections, no one knows how many were related or what pathology could be mediating the association.
This is just one question muddying the Zika waters right now, Dr. Chan of the WHO said. Several difficult-to-address issues are hampering an effective response, including the widespread range of the mosquito vectors, which allows international spread; a lack of population immunity; and the absence of rapid diagnostic tests, effective treatment, and any vaccine.
Another concern is the potential for illness-potentiating coinfection. In the lab, Zika virus has shown cross-reactions with dengue types 1-4, yellow fever, and West Nile virus – all of which are carried by Aedes mosquitoes.
Scientists at the CDC and National Institutes of Health are working on the problem now, Dr. Fauci said. Efforts include the creation of animal models to study disease transmission and its effect on pre- and postnatal outcomes, and of diagnostic platforms that could easily and quickly identify Zika infections. These would quickly differentiate Zika from dengue infections, which are also caused by a strain of flavivirus.
An effective vaccine will not be quickly forthcoming, he cautioned, although a phase I trial is in the works and could begin later this year. The candidate is a DNA-based vaccine similar to the one now used to protect against dengue. It would almost certainly not be approved in less than 2 years, Dr Fauci added.
Until some of these questions have been answered, or until the epidemic slows, the CDC continues to caution pregnant women against travel to endemic areas. For those who do travel or who live in endemic areas, Dr. Schuchat reiterated CDC’s long-held advice to take precautions against mosquito bites: long-sleeved shirts and long pants; staying inside; and using an effective insect repellent. Those containing DEET are most effective and are safe for pregnant women to use, Dr. Schuchat said.
For now, the CDC’s Zika travel alert includes Puerto Rico, Barbados, Bolivia, Brazil, Cape Verde, Colombia, Ecuador, El Salvador, French Guiana, Guadeloupe, Guatemala, Guyana, Haiti, Honduras, Martinique, Mexico, Panama, Paraguay, Saint Martin, Samoa, Suriname, Venezuela, the U.S. Virgin Islands, and the Dominican Republic.
A transcript of the press briefing is available online.
This article was updated 2/1/2016.
On Twitter @Alz_Gal
The Zika virus continues to spread, with the potential to infect up to 4 million people throughout the Americas.
But although locally transmitted infections are all almost certainly inevitable in the United States, federal health officials don’t expect large-scale infections.
“We do expect to see local transmission, but we are not likely to see widespread outbreaks,” Dr. Anthony S. Fauci, director of the National Institute of Allergy and Infectious Diseases, said during a press briefing on Jan. 28. “We think these would occur in pockets, similar to what we now see with dengue and chikungunya. We are not being cavalier about this; we are preparing. But large-scale outbreaks are not something we are likely to see, based on our experience with dengue and chikungunya.”
Dr. Fauci’s comments were in contrast to warnings issued simultaneously by the World Health Organization and the Pan American Health Organization (PAHO), WHO’s South American arm.
On Jan. 28, the WHO announced it would convene a meeting of its International Health Regulations Emergency Committee. WHO Director-General Margaret Chan said the virus is now present in 23 countries and territories in the region, as well as in parts of the South Pacific.
“The level of alarm is extremely high,” she said during the meeting. Although a causal link between the virus and outbreaks of microcephaly and Guillain-Barré syndrome is yet unproven, she said it is strongly suspected. “The possible links, only recently suspected, have rapidly changed the risk profile of Zika, from a mild threat to one of alarming proportions.”
Dr. Marcos Espinal, PAHO’s director of communicable diseases and health analysis, outlined the potential spread. His agency expects to see 3-4 million cases throughout North and South America, which could occur in any region that has endemic dengue fever. Both viruses are carried by mosquitoes of the Aedes genus. Two of these, the Asian tiger mosquito and the yellow fever mosquito, are commonly found in the United States, particularly in warmer regions.
Thus far, 31 cases of Zika virus have been confirmed in the United States (11 states and Washington), Dr. Anne Schuchat, principal deputy director for the Centers for Disease Control and Prevention, said in that agency’s briefing. All of these cases have been associated with travel to endemic areas, she said. She was unable to say how many cases had occurred in pregnant women.
There have been 19 confirmed cases in Puerto Rico and 1 in the U.S. Virgin Islands. These could be locally acquired cases, although that has not been confirmed. However, Zika infection is now a notifiable illness and any confirmed cases must be reported to CDC, she said.
Nearly a million cases have been laboratory confirmed in South America since 2015, Dr. Espinal noted. The vast majority of those have caused mild, transient symptoms. But in Brazil alone – the epicenter of the epidemic – there has been a substantial increase in newborn microcephaly. Almost 4,000 cases of this rare birth defect have been identified since October, when tracking began. Although the cases coincide with the rise of Zika infections, no one knows how many were related or what pathology could be mediating the association.
This is just one question muddying the Zika waters right now, Dr. Chan of the WHO said. Several difficult-to-address issues are hampering an effective response, including the widespread range of the mosquito vectors, which allows international spread; a lack of population immunity; and the absence of rapid diagnostic tests, effective treatment, and any vaccine.
Another concern is the potential for illness-potentiating coinfection. In the lab, Zika virus has shown cross-reactions with dengue types 1-4, yellow fever, and West Nile virus – all of which are carried by Aedes mosquitoes.
Scientists at the CDC and National Institutes of Health are working on the problem now, Dr. Fauci said. Efforts include the creation of animal models to study disease transmission and its effect on pre- and postnatal outcomes, and of diagnostic platforms that could easily and quickly identify Zika infections. These would quickly differentiate Zika from dengue infections, which are also caused by a strain of flavivirus.
An effective vaccine will not be quickly forthcoming, he cautioned, although a phase I trial is in the works and could begin later this year. The candidate is a DNA-based vaccine similar to the one now used to protect against dengue. It would almost certainly not be approved in less than 2 years, Dr Fauci added.
Until some of these questions have been answered, or until the epidemic slows, the CDC continues to caution pregnant women against travel to endemic areas. For those who do travel or who live in endemic areas, Dr. Schuchat reiterated CDC’s long-held advice to take precautions against mosquito bites: long-sleeved shirts and long pants; staying inside; and using an effective insect repellent. Those containing DEET are most effective and are safe for pregnant women to use, Dr. Schuchat said.
For now, the CDC’s Zika travel alert includes Puerto Rico, Barbados, Bolivia, Brazil, Cape Verde, Colombia, Ecuador, El Salvador, French Guiana, Guadeloupe, Guatemala, Guyana, Haiti, Honduras, Martinique, Mexico, Panama, Paraguay, Saint Martin, Samoa, Suriname, Venezuela, the U.S. Virgin Islands, and the Dominican Republic.
A transcript of the press briefing is available online.
This article was updated 2/1/2016.
On Twitter @Alz_Gal

Telemental health reaches underserved children, builds partnerships
The patient, a 10-year-old girl, was exhibiting defiant and angry behavior at home. Her pediatrician in rural Vermont was not able to support the family optimally, so he referred her to Dr. David C. Rettew.
Dr. Rettew soon learned that the girl blamed herself for her father’s absence, and she interpreted efforts by her mother to set limits as evidence that her mom didn’t love her.

“During the course of the interview, it became clear that the girl had some specific thoughts that were likely fueling her anger,” said Dr. Rettew, director of the Pediatric Psychiatry Clinic at the University of Vermont, Burlington. “She also met criteria clearly for ADHD, which had never been diagnosed. The consultation recommendations not only included some possible medications to try, but also some specific areas that could be addressed for psychotherapy that could really help the relationship between this child and her mother.”
The successful intervention took place via a secure, two-way videoconference. It is one example of how physicians at the University of Vermont are using telemental health to treat children in underserved areas. As part of a state-funded training program, child psychiatry fellows at the university consult with primary care doctors at federally qualified health centers across the state. The primary care physicians discuss patient cases with fellows via phone or email and can refer patients for in-person or telemental health assessments.
The program has been running for about 5 years and so far has yielded countless benefits, said Dr. Rettew, who directs the university’s Child and Adolescent Psychiatry Fellowship Program. “It helps keep the care housed and centered within the primary care home. That can help coordination of services so that care isn’t fragmented around multiple centers. It also allows evaluations to happen that wouldn’t happen otherwise because it’s too much of a hardship for families to travel long distances and come for regular follow-up appointments.”

University of Vermont physicians also use telemedicine to consult with other mental health clinicians across the state. Child psychiatrist Allison Y. Hall provides in-person training to clinicians and then counsels and supervises their efforts through a telemedicine unit.
“For this purpose, it’s great,” said Dr. Hall, who practices at the Vermont Center for Children, Youth, and Families, which is housed within the university’s psychiatry department. “There’s more confidentiality than Skype, for instance. It’s wonderful to be able to reach clinicians at a great distance.”
On a broader scale, telemental health is a promising tool to address the shortage of mental health providers in the United States, said Dr. Robert C. Gunther, a pediatrician at the University of Virginia Health System in Fishersville. Recent research found that one in three children receiving outpatient care for mental health conditions saw only their primary care doctor for care (Pediatrics. 2015 Nov;136;e1178-85).

“There is a tremendous need for pediatric mental health care,” Dr. Gunther said in an interview. “There is a great shortage of child psychiatrists and other child mental health specialists. Telemental health can help in areas where geography or financial barriers exist to accessing care.”
Data from the Children’s ADHD Telemental Health Treatment Study (CATTS) illustrates the impact that telemental health can have on children facing such barriers to care. Researchers randomized 223 children referred by 88 primary care providers in seven underserved communities into two study groups. Children in the first group were seen by child psychiatrists via videoconference six times over 22 weeks; treatment included pharmacotherapy. Their caregivers received behavior training provided in person by community therapists who were supervised remotely. Children in the second group were treated by their primary care physicians and received one telepsychiatry consult.
Children in both groups improved; however, those randomized to the telemental health model improved “significantly more than patients in the augmented primary care arm” (J Am Acad Child Adolesc Psychiatry. 2015 Apr;54[4]:263-74).

“The CATTS trial demonstrated the effectiveness of a telehealth service model to treat ADHD in communities with limited access to specialty mental health services,” investigators concluded.
But Dr. Joshua J. Alexander, chair of the American Academy of Pediatrics Section on Telehealth Care, notes that some mental health conditions fit more smoothly within the telemental health model than others. ADHD is the most common condition treated by telemental health, he said. The model also has shown success in the treatment of childhood adjustment disorders, anxiety, oppositional defiant disorder, mood disorders, anxiety, and depression.
“I think you have to be careful in determining where telemental health would be beneficial to use and in which cases it might not be an appropriate method to deliver care,” Dr. Alexander said in an interview.
Developing trust and rapport with patients through videoconferencing also can be a challenge, added Dr. Alexander, who is director of the TelAbility telehealth program at the University of North Carolina at Chapel Hill. He recommends that specialists use the technology to continue an existing doctor-patient relationship or to provide care in a consultative model in which the child’s primary care doctor is present along with the patient and patient’s family.
The AAP advocates for the use of telemedicine so long as it is conducted within the context of the medical home. Fragmented telemedicine services that could disrupt continuity of care should be avoided, according to a 2015 AAP policy statement (Pediatrics. 2015 Jun. doi: 10.1542/peds.2015-1253). The academy also calls for the expansion of pediatric telemedicine to increase access to care for underserved communities and improve quality of care for children.
More partnerships between mental health specialists and primary care providers are a key step in delivering high quality pediatric telemental care, Dr. Alexander said.
“Some larger pediatric practices already do this by hiring and colocating individuals at their practice site, but other, smaller practices might not have the room, finances, sufficient patient population, or enough local providers to make this happen,” he said. “A telemedicine program, located within the practice, could enable this specialized service to be provided in a convenient, coordinated setting.”
On Twitter @legal_med
The patient, a 10-year-old girl, was exhibiting defiant and angry behavior at home. Her pediatrician in rural Vermont was not able to support the family optimally, so he referred her to Dr. David C. Rettew.
Dr. Rettew soon learned that the girl blamed herself for her father’s absence, and she interpreted efforts by her mother to set limits as evidence that her mom didn’t love her.
“During the course of the interview, it became clear that the girl had some specific thoughts that were likely fueling her anger,” said Dr. Rettew, director of the Pediatric Psychiatry Clinic at the University of Vermont, Burlington. “She also met criteria clearly for ADHD, which had never been diagnosed. The consultation recommendations not only included some possible medications to try, but also some specific areas that could be addressed for psychotherapy that could really help the relationship between this child and her mother.”
The successful intervention took place via a secure, two-way videoconference. It is one example of how physicians at the University of Vermont are using telemental health to treat children in underserved areas. As part of a state-funded training program, child psychiatry fellows at the university consult with primary care doctors at federally qualified health centers across the state. The primary care physicians discuss patient cases with fellows via phone or email and can refer patients for in-person or telemental health assessments.
The program has been running for about 5 years and so far has yielded countless benefits, said Dr. Rettew, who directs the university’s Child and Adolescent Psychiatry Fellowship Program. “It helps keep the care housed and centered within the primary care home. That can help coordination of services so that care isn’t fragmented around multiple centers. It also allows evaluations to happen that wouldn’t happen otherwise because it’s too much of a hardship for families to travel long distances and come for regular follow-up appointments.”
University of Vermont physicians also use telemedicine to consult with other mental health clinicians across the state. Child psychiatrist Allison Y. Hall provides in-person training to clinicians and then counsels and supervises their efforts through a telemedicine unit.
“For this purpose, it’s great,” said Dr. Hall, who practices at the Vermont Center for Children, Youth, and Families, which is housed within the university’s psychiatry department. “There’s more confidentiality than Skype, for instance. It’s wonderful to be able to reach clinicians at a great distance.”
On a broader scale, telemental health is a promising tool to address the shortage of mental health providers in the United States, said Dr. Robert C. Gunther, a pediatrician at the University of Virginia Health System in Fishersville. Recent research found that one in three children receiving outpatient care for mental health conditions saw only their primary care doctor for care (Pediatrics. 2015 Nov;136;e1178-85).
“There is a tremendous need for pediatric mental health care,” Dr. Gunther said in an interview. “There is a great shortage of child psychiatrists and other child mental health specialists. Telemental health can help in areas where geography or financial barriers exist to accessing care.”
Data from the Children’s ADHD Telemental Health Treatment Study (CATTS) illustrates the impact that telemental health can have on children facing such barriers to care. Researchers randomized 223 children referred by 88 primary care providers in seven underserved communities into two study groups. Children in the first group were seen by child psychiatrists via videoconference six times over 22 weeks; treatment included pharmacotherapy. Their caregivers received behavior training provided in person by community therapists who were supervised remotely. Children in the second group were treated by their primary care physicians and received one telepsychiatry consult.
Children in both groups improved; however, those randomized to the telemental health model improved “significantly more than patients in the augmented primary care arm” (J Am Acad Child Adolesc Psychiatry. 2015 Apr;54[4]:263-74).
“The CATTS trial demonstrated the effectiveness of a telehealth service model to treat ADHD in communities with limited access to specialty mental health services,” investigators concluded.
But Dr. Joshua J. Alexander, chair of the American Academy of Pediatrics Section on Telehealth Care, notes that some mental health conditions fit more smoothly within the telemental health model than others. ADHD is the most common condition treated by telemental health, he said. The model also has shown success in the treatment of childhood adjustment disorders, anxiety, oppositional defiant disorder, mood disorders, anxiety, and depression.
“I think you have to be careful in determining where telemental health would be beneficial to use and in which cases it might not be an appropriate method to deliver care,” Dr. Alexander said in an interview.
Developing trust and rapport with patients through videoconferencing also can be a challenge, added Dr. Alexander, who is director of the TelAbility telehealth program at the University of North Carolina at Chapel Hill. He recommends that specialists use the technology to continue an existing doctor-patient relationship or to provide care in a consultative model in which the child’s primary care doctor is present along with the patient and patient’s family.
The AAP advocates for the use of telemedicine so long as it is conducted within the context of the medical home. Fragmented telemedicine services that could disrupt continuity of care should be avoided, according to a 2015 AAP policy statement (Pediatrics. 2015 Jun. doi: 10.1542/peds.2015-1253). The academy also calls for the expansion of pediatric telemedicine to increase access to care for underserved communities and improve quality of care for children.
More partnerships between mental health specialists and primary care providers are a key step in delivering high quality pediatric telemental care, Dr. Alexander said.
“Some larger pediatric practices already do this by hiring and colocating individuals at their practice site, but other, smaller practices might not have the room, finances, sufficient patient population, or enough local providers to make this happen,” he said. “A telemedicine program, located within the practice, could enable this specialized service to be provided in a convenient, coordinated setting.”
On Twitter @legal_med
The patient, a 10-year-old girl, was exhibiting defiant and angry behavior at home. Her pediatrician in rural Vermont was not able to support the family optimally, so he referred her to Dr. David C. Rettew.
Dr. Rettew soon learned that the girl blamed herself for her father’s absence, and she interpreted efforts by her mother to set limits as evidence that her mom didn’t love her.
“During the course of the interview, it became clear that the girl had some specific thoughts that were likely fueling her anger,” said Dr. Rettew, director of the Pediatric Psychiatry Clinic at the University of Vermont, Burlington. “She also met criteria clearly for ADHD, which had never been diagnosed. The consultation recommendations not only included some possible medications to try, but also some specific areas that could be addressed for psychotherapy that could really help the relationship between this child and her mother.”
The successful intervention took place via a secure, two-way videoconference. It is one example of how physicians at the University of Vermont are using telemental health to treat children in underserved areas. As part of a state-funded training program, child psychiatry fellows at the university consult with primary care doctors at federally qualified health centers across the state. The primary care physicians discuss patient cases with fellows via phone or email and can refer patients for in-person or telemental health assessments.
The program has been running for about 5 years and so far has yielded countless benefits, said Dr. Rettew, who directs the university’s Child and Adolescent Psychiatry Fellowship Program. “It helps keep the care housed and centered within the primary care home. That can help coordination of services so that care isn’t fragmented around multiple centers. It also allows evaluations to happen that wouldn’t happen otherwise because it’s too much of a hardship for families to travel long distances and come for regular follow-up appointments.”
University of Vermont physicians also use telemedicine to consult with other mental health clinicians across the state. Child psychiatrist Allison Y. Hall provides in-person training to clinicians and then counsels and supervises their efforts through a telemedicine unit.
“For this purpose, it’s great,” said Dr. Hall, who practices at the Vermont Center for Children, Youth, and Families, which is housed within the university’s psychiatry department. “There’s more confidentiality than Skype, for instance. It’s wonderful to be able to reach clinicians at a great distance.”
On a broader scale, telemental health is a promising tool to address the shortage of mental health providers in the United States, said Dr. Robert C. Gunther, a pediatrician at the University of Virginia Health System in Fishersville. Recent research found that one in three children receiving outpatient care for mental health conditions saw only their primary care doctor for care (Pediatrics. 2015 Nov;136;e1178-85).
“There is a tremendous need for pediatric mental health care,” Dr. Gunther said in an interview. “There is a great shortage of child psychiatrists and other child mental health specialists. Telemental health can help in areas where geography or financial barriers exist to accessing care.”
Data from the Children’s ADHD Telemental Health Treatment Study (CATTS) illustrates the impact that telemental health can have on children facing such barriers to care. Researchers randomized 223 children referred by 88 primary care providers in seven underserved communities into two study groups. Children in the first group were seen by child psychiatrists via videoconference six times over 22 weeks; treatment included pharmacotherapy. Their caregivers received behavior training provided in person by community therapists who were supervised remotely. Children in the second group were treated by their primary care physicians and received one telepsychiatry consult.
Children in both groups improved; however, those randomized to the telemental health model improved “significantly more than patients in the augmented primary care arm” (J Am Acad Child Adolesc Psychiatry. 2015 Apr;54[4]:263-74).
“The CATTS trial demonstrated the effectiveness of a telehealth service model to treat ADHD in communities with limited access to specialty mental health services,” investigators concluded.
But Dr. Joshua J. Alexander, chair of the American Academy of Pediatrics Section on Telehealth Care, notes that some mental health conditions fit more smoothly within the telemental health model than others. ADHD is the most common condition treated by telemental health, he said. The model also has shown success in the treatment of childhood adjustment disorders, anxiety, oppositional defiant disorder, mood disorders, anxiety, and depression.
“I think you have to be careful in determining where telemental health would be beneficial to use and in which cases it might not be an appropriate method to deliver care,” Dr. Alexander said in an interview.
Developing trust and rapport with patients through videoconferencing also can be a challenge, added Dr. Alexander, who is director of the TelAbility telehealth program at the University of North Carolina at Chapel Hill. He recommends that specialists use the technology to continue an existing doctor-patient relationship or to provide care in a consultative model in which the child’s primary care doctor is present along with the patient and patient’s family.
The AAP advocates for the use of telemedicine so long as it is conducted within the context of the medical home. Fragmented telemedicine services that could disrupt continuity of care should be avoided, according to a 2015 AAP policy statement (Pediatrics. 2015 Jun. doi: 10.1542/peds.2015-1253). The academy also calls for the expansion of pediatric telemedicine to increase access to care for underserved communities and improve quality of care for children.
More partnerships between mental health specialists and primary care providers are a key step in delivering high quality pediatric telemental care, Dr. Alexander said.
“Some larger pediatric practices already do this by hiring and colocating individuals at their practice site, but other, smaller practices might not have the room, finances, sufficient patient population, or enough local providers to make this happen,” he said. “A telemedicine program, located within the practice, could enable this specialized service to be provided in a convenient, coordinated setting.”
On Twitter @legal_med

VIDEO: N-acetylcysteine for ichthyosis, OCD behaviors
GRAND CAYMAN – N-acetylcysteine is reemerging as a treatment for ichthyosis, and even some compulsive behaviors like skin picking. In an interview at this year’s Caribbean Dermatology Symposium, Dr. Albert C. Yan, section chief of dermatology at the Children’s Hospital of Philadelphia, discusses in this video interview the use of this agent as an effective treatment for these indications in children.
The meeting is provided by Global Academy for Medical Education. Global Academy and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
GRAND CAYMAN – N-acetylcysteine is reemerging as a treatment for ichthyosis, and even some compulsive behaviors like skin picking. In an interview at this year’s Caribbean Dermatology Symposium, Dr. Albert C. Yan, section chief of dermatology at the Children’s Hospital of Philadelphia, discusses in this video interview the use of this agent as an effective treatment for these indications in children.
The meeting is provided by Global Academy for Medical Education. Global Academy and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
GRAND CAYMAN – N-acetylcysteine is reemerging as a treatment for ichthyosis, and even some compulsive behaviors like skin picking. In an interview at this year’s Caribbean Dermatology Symposium, Dr. Albert C. Yan, section chief of dermatology at the Children’s Hospital of Philadelphia, discusses in this video interview the use of this agent as an effective treatment for these indications in children.
The meeting is provided by Global Academy for Medical Education. Global Academy and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
AT THE CARIBBEAN DERMATOLOGY SYMPOSIUM

VIDEO: Prophylaxis for atopic dermatitis
GRAND CAYMAN – What simple prophylactic measures can you recommend to parents of children at risk of atopic dermatitis? In an interview at this year’s Caribbean Dermatology Symposium, Dr. Albert C. Yan, section chief of dermatology at the Children’s Hospital of Philadelphia and professor of pediatrics and dermatology, University of Pennsylvania, Philadelphia, discusses the evidence indicating that early use of moisturizers reduces the risk of atopic dermatitis in children at risk.
The meeting is provided by Global Academy for Medical Education. Global Academy and this news organization are owned by the same parent company.
On Twitter @whitneymcknight
GRAND CAYMAN – What simple prophylactic measures can you recommend to parents of children at risk of atopic dermatitis? In an interview at this year’s Caribbean Dermatology Symposium, Dr. Albert C. Yan, section chief of dermatology at the Children’s Hospital of Philadelphia and professor of pediatrics and dermatology, University of Pennsylvania, Philadelphia, discusses the evidence indicating that early use of moisturizers reduces the risk of atopic dermatitis in children at risk.
The meeting is provided by Global Academy for Medical Education. Global Academy and this news organization are owned by the same parent company.
On Twitter @whitneymcknight
GRAND CAYMAN – What simple prophylactic measures can you recommend to parents of children at risk of atopic dermatitis? In an interview at this year’s Caribbean Dermatology Symposium, Dr. Albert C. Yan, section chief of dermatology at the Children’s Hospital of Philadelphia and professor of pediatrics and dermatology, University of Pennsylvania, Philadelphia, discusses the evidence indicating that early use of moisturizers reduces the risk of atopic dermatitis in children at risk.
The meeting is provided by Global Academy for Medical Education. Global Academy and this news organization are owned by the same parent company.
On Twitter @whitneymcknight
AT THE CARIBBEAN DERMATOLOGY SYMPOSIUM
