User login
Tofacitinib clears pediatric alopecia areata in small study
MINNEAPOLIS – The first study to evaluate tofacitinib’s effectiveness at treating severe alopecia areata in the pediatric population found that the janus kinase inhibitor was effective for more than half of the patients, and well tolerated by all.
Of a case series of 13 pediatric patients who had alopecia areata (AA) and were treated with tofacitinib, 9 (68%) experienced “clinically significant” regrowth of hair, with mean improvement in the Severity of Alopecia Tool (SALT) score of 88% for these responders. The nonresponding group, all of whom had alopecia universalis or totalis, saw essentially no response, with a 1% reduction in SALT score.
Lucy Y. Liu, a medical student at Yale University, New Haven, Conn., presented the findings at the annual meeting of the Society for Pediatric Dermatology.
Ms. Liu and her coinvestigators reported that all of the patients had severe AA by SALT scoring, with an overall mean pretreatment SALT score of 74. Eight of the patients (62%) had alopecia universalis, and two (15%) had alopecia totalis.
The patients ranged in age from 12 to 17 years, with a median age of 15. All but three were male, and patients were an average 9 years old at onset of AA. For patients with alopecia totalis or universalis, the duration of the current episode was a median 1.75 years.
Five patients (38%) had atopic dermatitis, while 1 (8%) had thyroid disease. Three patients (23%) had family members with AA; all but one patient, however, had a family history of autoimmune disease of some sort.
Patients were given tofacitinib 5 mg orally twice daily for 5 months. One patient developed new patches of alopecia during treatment, so the dosing for that patient was increased to 10 mg/5 mg daily.
Adverse events for participants included headaches, upper respiratory infections, and “mild, transient increases in transaminases,” wrote Dr. Lieu and her collaborators. No serious adverse events were reported.
Previous work at Yale had shown that tofacitinib reversed alopecia universalis in a patient who received the medication for plaque psoriasis, and that topical treatment with ruxolitinib, another janus kinase inhibitor, was effective in treating alopecia universalis.
Study limitations included the small sample size and the relatively short duration of follow-up, an important consideration because relapse has been observed after tofacitinib treatment in AA. Still, “Tofacitinib is a promising therapy for the treatment of severe AA in adolescents,” wrote Ms. Liu and her colleagues, recommending randomized clinical trials for further exploration of efficacy and safety in the pediatric population.
On Twitter @karioakes
MINNEAPOLIS – The first study to evaluate tofacitinib’s effectiveness at treating severe alopecia areata in the pediatric population found that the janus kinase inhibitor was effective for more than half of the patients, and well tolerated by all.
Of a case series of 13 pediatric patients who had alopecia areata (AA) and were treated with tofacitinib, 9 (68%) experienced “clinically significant” regrowth of hair, with mean improvement in the Severity of Alopecia Tool (SALT) score of 88% for these responders. The nonresponding group, all of whom had alopecia universalis or totalis, saw essentially no response, with a 1% reduction in SALT score.
Lucy Y. Liu, a medical student at Yale University, New Haven, Conn., presented the findings at the annual meeting of the Society for Pediatric Dermatology.
Ms. Liu and her coinvestigators reported that all of the patients had severe AA by SALT scoring, with an overall mean pretreatment SALT score of 74. Eight of the patients (62%) had alopecia universalis, and two (15%) had alopecia totalis.
The patients ranged in age from 12 to 17 years, with a median age of 15. All but three were male, and patients were an average 9 years old at onset of AA. For patients with alopecia totalis or universalis, the duration of the current episode was a median 1.75 years.
Five patients (38%) had atopic dermatitis, while 1 (8%) had thyroid disease. Three patients (23%) had family members with AA; all but one patient, however, had a family history of autoimmune disease of some sort.
Patients were given tofacitinib 5 mg orally twice daily for 5 months. One patient developed new patches of alopecia during treatment, so the dosing for that patient was increased to 10 mg/5 mg daily.
Adverse events for participants included headaches, upper respiratory infections, and “mild, transient increases in transaminases,” wrote Dr. Lieu and her collaborators. No serious adverse events were reported.
Previous work at Yale had shown that tofacitinib reversed alopecia universalis in a patient who received the medication for plaque psoriasis, and that topical treatment with ruxolitinib, another janus kinase inhibitor, was effective in treating alopecia universalis.
Study limitations included the small sample size and the relatively short duration of follow-up, an important consideration because relapse has been observed after tofacitinib treatment in AA. Still, “Tofacitinib is a promising therapy for the treatment of severe AA in adolescents,” wrote Ms. Liu and her colleagues, recommending randomized clinical trials for further exploration of efficacy and safety in the pediatric population.
On Twitter @karioakes
MINNEAPOLIS – The first study to evaluate tofacitinib’s effectiveness at treating severe alopecia areata in the pediatric population found that the janus kinase inhibitor was effective for more than half of the patients, and well tolerated by all.
Of a case series of 13 pediatric patients who had alopecia areata (AA) and were treated with tofacitinib, 9 (68%) experienced “clinically significant” regrowth of hair, with mean improvement in the Severity of Alopecia Tool (SALT) score of 88% for these responders. The nonresponding group, all of whom had alopecia universalis or totalis, saw essentially no response, with a 1% reduction in SALT score.
Lucy Y. Liu, a medical student at Yale University, New Haven, Conn., presented the findings at the annual meeting of the Society for Pediatric Dermatology.
Ms. Liu and her coinvestigators reported that all of the patients had severe AA by SALT scoring, with an overall mean pretreatment SALT score of 74. Eight of the patients (62%) had alopecia universalis, and two (15%) had alopecia totalis.
The patients ranged in age from 12 to 17 years, with a median age of 15. All but three were male, and patients were an average 9 years old at onset of AA. For patients with alopecia totalis or universalis, the duration of the current episode was a median 1.75 years.
Five patients (38%) had atopic dermatitis, while 1 (8%) had thyroid disease. Three patients (23%) had family members with AA; all but one patient, however, had a family history of autoimmune disease of some sort.
Patients were given tofacitinib 5 mg orally twice daily for 5 months. One patient developed new patches of alopecia during treatment, so the dosing for that patient was increased to 10 mg/5 mg daily.
Adverse events for participants included headaches, upper respiratory infections, and “mild, transient increases in transaminases,” wrote Dr. Lieu and her collaborators. No serious adverse events were reported.
Previous work at Yale had shown that tofacitinib reversed alopecia universalis in a patient who received the medication for plaque psoriasis, and that topical treatment with ruxolitinib, another janus kinase inhibitor, was effective in treating alopecia universalis.
Study limitations included the small sample size and the relatively short duration of follow-up, an important consideration because relapse has been observed after tofacitinib treatment in AA. Still, “Tofacitinib is a promising therapy for the treatment of severe AA in adolescents,” wrote Ms. Liu and her colleagues, recommending randomized clinical trials for further exploration of efficacy and safety in the pediatric population.
On Twitter @karioakes
AT THE SPD ANNUAL MEETING
Key clinical point: The JAK inhibitor tofacitinib resolved alopecia areata in 68% of pediatric patients.
Major finding: Among the responders, the Severity of Alopecia Tool score improved by a mean 88% over 5 months.
Data source: Case series of 13 pediatric patients with severe alopecia areata treated with tofacitinib at a single site.
Disclosures: Ms. Liu and her collaborators reported no conflicts of interest.
Portable device may underestimate FEV1 in children
The PiKo-1 device (nSpire Health) has limited utility in determining forced expiratory volume in 1 second (FEV1) in children with asthma, according to Jonathan M. Gaffin, MD, and his associates.
In a study of 242 children, spirometry and PiKo-1 devices were used to test FEV1. In the Bland-Altman analysis, it reported a mean difference between FEV1 measured by spirometry and PiKo-1 of 0.14 L. The PiKo-1 FEV1 was found to be moderately biased to underestimate FEV1 with increasing volumes, for every 1-liter increase in spirometry FEV1, having the difference between spirometry and PiKo-1 increased by 0.19 L (P < .001).
Researchers also used the pulmonary function test (PFT) and t showed variability was 0.4 L for spirometry at 2 SDs, a significant smaller range than seen in the PFT-PiKo confidence intervals (1.1 L). It is noted that this indicates that differences are credited to distinctions in the devices themselves and not within the techniques of the person using them. There was no effect on the order of PFT or PiKo-1 performance (P = .88).
“The findings from this study suggest that the PiKo-1 device has limited utility in assessing FEV1 in clinical or research settings in children with asthma,” researchers concluded. “Further investigation of its use in this respect and with different populations may prove the device more valuable.”
Find the full study in the Annals of Allergy, Asthma and Immunology (doi: 10.1016/j.anai.2016.06.022).
The PiKo-1 device (nSpire Health) has limited utility in determining forced expiratory volume in 1 second (FEV1) in children with asthma, according to Jonathan M. Gaffin, MD, and his associates.
In a study of 242 children, spirometry and PiKo-1 devices were used to test FEV1. In the Bland-Altman analysis, it reported a mean difference between FEV1 measured by spirometry and PiKo-1 of 0.14 L. The PiKo-1 FEV1 was found to be moderately biased to underestimate FEV1 with increasing volumes, for every 1-liter increase in spirometry FEV1, having the difference between spirometry and PiKo-1 increased by 0.19 L (P < .001).
Researchers also used the pulmonary function test (PFT) and t showed variability was 0.4 L for spirometry at 2 SDs, a significant smaller range than seen in the PFT-PiKo confidence intervals (1.1 L). It is noted that this indicates that differences are credited to distinctions in the devices themselves and not within the techniques of the person using them. There was no effect on the order of PFT or PiKo-1 performance (P = .88).
“The findings from this study suggest that the PiKo-1 device has limited utility in assessing FEV1 in clinical or research settings in children with asthma,” researchers concluded. “Further investigation of its use in this respect and with different populations may prove the device more valuable.”
Find the full study in the Annals of Allergy, Asthma and Immunology (doi: 10.1016/j.anai.2016.06.022).
The PiKo-1 device (nSpire Health) has limited utility in determining forced expiratory volume in 1 second (FEV1) in children with asthma, according to Jonathan M. Gaffin, MD, and his associates.
In a study of 242 children, spirometry and PiKo-1 devices were used to test FEV1. In the Bland-Altman analysis, it reported a mean difference between FEV1 measured by spirometry and PiKo-1 of 0.14 L. The PiKo-1 FEV1 was found to be moderately biased to underestimate FEV1 with increasing volumes, for every 1-liter increase in spirometry FEV1, having the difference between spirometry and PiKo-1 increased by 0.19 L (P < .001).
Researchers also used the pulmonary function test (PFT) and t showed variability was 0.4 L for spirometry at 2 SDs, a significant smaller range than seen in the PFT-PiKo confidence intervals (1.1 L). It is noted that this indicates that differences are credited to distinctions in the devices themselves and not within the techniques of the person using them. There was no effect on the order of PFT or PiKo-1 performance (P = .88).
“The findings from this study suggest that the PiKo-1 device has limited utility in assessing FEV1 in clinical or research settings in children with asthma,” researchers concluded. “Further investigation of its use in this respect and with different populations may prove the device more valuable.”
Find the full study in the Annals of Allergy, Asthma and Immunology (doi: 10.1016/j.anai.2016.06.022).
FROM THE ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Sunscreens safe in babies, children
BOSTON – Despite what some popular online media outlets report, sunscreens are safe in children and can even be used on infants under 6 months of age when sun avoidance – the best approach to protecting babies from the damaging effects of the sun – is not possible, according to Mercedes E. Gonzalez, MD.
A quick Google search reveals numerous, widely-shared articles about the dangers lurking in one’s beach bag, and while many product labels recommend asking a doctor about whether the product is safe for babies under age 6 months, that’s only because most product safety studies didn’t include that age group, Dr. Gonzalez of the University of Miami said at the American Academy of Dermatology summer meeting.

In fact, there is “nothing magical that happens” in infant skin after 6 months that makes sunscreen use safer, she said, explaining that infant skin is structurally and functionally different from adult skin, and that while gradual maturation takes place over time, thereby reducing susceptibility to percutaneous absorption of topically applied products, the risk is minimal even in babies younger than age 6 months.
The skin characteristics that make younger skin more susceptible to percutaneous absorption also make babies and children unusually susceptible to ultraviolet radiation and ultraviolet radiation–induced immunosuppression, for which the consequences are not fully understood, she said.
Among the more commonly cited sunscreen ingredients of concern are oxybenzone, or benzonephenone-3, and nanoparticles, she noted.
However, the overall consensus based on studies of oxybenzone is that aside from causing some cases of allergic and irritant contact dermatitis, the compound is safe; no harmful cause and effect relationship with oxybenzone and systemic side effects in humans have been reported, and periodic reviews by European, Australian and U.S. safety panels all conclude that it is safe.
Numerous studies of nanoparticles – such as nanosized zinc oxide and titanium dioxide – have shown that absorption is confined to the level of stratum corneum – even when skin barrier function has been altered, she said, noting that most are coated with aluminum oxide and SiO2 to minimize contact.
However, the safety of sunscreen shouldn’t be seen as license to ignore sun-exposure recommendations; sunscreen in infants should be considered “the last layer of protection,” used only on exposed areas when adequate clothing and shade are not available, according to a 2011 American Academy of Pediatrics statement (Pediatrics. 2011 Feb. doi: 10.1542/peds.2010-3501).
Efforts should be made to keep babies in the shade when outdoors whenever possible, especially during peak sun hours. Use sun-protective clothing, including hats, sunglasses, and long-sleeved shirts, Dr. Gonzalez advised.
When sunscreen is required, a broad-spectrum water-resistant product with an SPF of more than 30 is preferable.
“But the best sunscreen is the one you and your child will use,” she said.
Mineral-based products are less irritating and thus may be a preferred option for children with atopic dermatitis, she added.
Advise parents to apply sunscreen to all areas not protected by their child’s clothing, paying particular attention to vulnerable areas, including the back of the neck, ears, and dorsal feet. Reapply before going outdoors, and then again every 2 hours, she advised.
“So the overall answer to the parents’ question, ‘Are sunscreens safe?’ ... the overwhelming answer here is yes, and the weight of the evidence shows there is no proven harm from sunscreen use especially when used properly,” she said.
Provide specific guidance for pediatric sunscreen use
In the face of conflicting information about sunscreen safety and efficacy, parents with questions about sunscreen are looking for specific direction, Dr. Gonzalez said.
She said she finds it helpful to teach them about the importance of reading labels. That is, looking at the ingredients, and looking for SPF above 30, broad-spectrum coverage, and water resistance. She also recommends providing a list or images of good options, and circling the specific preferred products.
For babies, she finds stick sunscreens most useful for application.
“I generally don’t recommend sprays, but if they’re going to use a spray – and parents love sprays because they are easy to apply – I recommend the ones that have some zinc oxide in them, so that when they apply them they can see where they’re going on the skin,” Dr. Gonzalez said.
Tell patients to apply sunscreen before leaving the house, she advised, adding that making sunscreen application part of a daily routine helps encourage healthy behaviors, as does allowing children, at the right age, to participate in sunscreen application.
For adolescents, avoid scare tactics such as warning about skin cancer. Rather, focus on benefits of avoiding the sun, help them find a product they like by finding out why they don’t like a particular product and recommending an alternative, then following up on that when they come back in, she suggested.
“I really try to address it at every visit,” Dr. Gonzalez said.
“Finally, the most important message is that sunscreen is really just one part of complete sun protection,” she said, noting that specific information about where to buy sun-protective clothing and hats is also important.
Dr. Gonzalez reported serving as a speaker and/or advisory board member and receiving honoraria from Pierre Fabre Dermatologie, Anacor Pharmaceuticals, Encore Dermatology, and PuraCap Pharmaceutical.
BOSTON – Despite what some popular online media outlets report, sunscreens are safe in children and can even be used on infants under 6 months of age when sun avoidance – the best approach to protecting babies from the damaging effects of the sun – is not possible, according to Mercedes E. Gonzalez, MD.
A quick Google search reveals numerous, widely-shared articles about the dangers lurking in one’s beach bag, and while many product labels recommend asking a doctor about whether the product is safe for babies under age 6 months, that’s only because most product safety studies didn’t include that age group, Dr. Gonzalez of the University of Miami said at the American Academy of Dermatology summer meeting.
In fact, there is “nothing magical that happens” in infant skin after 6 months that makes sunscreen use safer, she said, explaining that infant skin is structurally and functionally different from adult skin, and that while gradual maturation takes place over time, thereby reducing susceptibility to percutaneous absorption of topically applied products, the risk is minimal even in babies younger than age 6 months.
The skin characteristics that make younger skin more susceptible to percutaneous absorption also make babies and children unusually susceptible to ultraviolet radiation and ultraviolet radiation–induced immunosuppression, for which the consequences are not fully understood, she said.
Among the more commonly cited sunscreen ingredients of concern are oxybenzone, or benzonephenone-3, and nanoparticles, she noted.
However, the overall consensus based on studies of oxybenzone is that aside from causing some cases of allergic and irritant contact dermatitis, the compound is safe; no harmful cause and effect relationship with oxybenzone and systemic side effects in humans have been reported, and periodic reviews by European, Australian and U.S. safety panels all conclude that it is safe.
Numerous studies of nanoparticles – such as nanosized zinc oxide and titanium dioxide – have shown that absorption is confined to the level of stratum corneum – even when skin barrier function has been altered, she said, noting that most are coated with aluminum oxide and SiO2 to minimize contact.
However, the safety of sunscreen shouldn’t be seen as license to ignore sun-exposure recommendations; sunscreen in infants should be considered “the last layer of protection,” used only on exposed areas when adequate clothing and shade are not available, according to a 2011 American Academy of Pediatrics statement (Pediatrics. 2011 Feb. doi: 10.1542/peds.2010-3501).
Efforts should be made to keep babies in the shade when outdoors whenever possible, especially during peak sun hours. Use sun-protective clothing, including hats, sunglasses, and long-sleeved shirts, Dr. Gonzalez advised.
When sunscreen is required, a broad-spectrum water-resistant product with an SPF of more than 30 is preferable.
“But the best sunscreen is the one you and your child will use,” she said.
Mineral-based products are less irritating and thus may be a preferred option for children with atopic dermatitis, she added.
Advise parents to apply sunscreen to all areas not protected by their child’s clothing, paying particular attention to vulnerable areas, including the back of the neck, ears, and dorsal feet. Reapply before going outdoors, and then again every 2 hours, she advised.
“So the overall answer to the parents’ question, ‘Are sunscreens safe?’ ... the overwhelming answer here is yes, and the weight of the evidence shows there is no proven harm from sunscreen use especially when used properly,” she said.
Provide specific guidance for pediatric sunscreen use
In the face of conflicting information about sunscreen safety and efficacy, parents with questions about sunscreen are looking for specific direction, Dr. Gonzalez said.
She said she finds it helpful to teach them about the importance of reading labels. That is, looking at the ingredients, and looking for SPF above 30, broad-spectrum coverage, and water resistance. She also recommends providing a list or images of good options, and circling the specific preferred products.
For babies, she finds stick sunscreens most useful for application.
“I generally don’t recommend sprays, but if they’re going to use a spray – and parents love sprays because they are easy to apply – I recommend the ones that have some zinc oxide in them, so that when they apply them they can see where they’re going on the skin,” Dr. Gonzalez said.
Tell patients to apply sunscreen before leaving the house, she advised, adding that making sunscreen application part of a daily routine helps encourage healthy behaviors, as does allowing children, at the right age, to participate in sunscreen application.
For adolescents, avoid scare tactics such as warning about skin cancer. Rather, focus on benefits of avoiding the sun, help them find a product they like by finding out why they don’t like a particular product and recommending an alternative, then following up on that when they come back in, she suggested.
“I really try to address it at every visit,” Dr. Gonzalez said.
“Finally, the most important message is that sunscreen is really just one part of complete sun protection,” she said, noting that specific information about where to buy sun-protective clothing and hats is also important.
Dr. Gonzalez reported serving as a speaker and/or advisory board member and receiving honoraria from Pierre Fabre Dermatologie, Anacor Pharmaceuticals, Encore Dermatology, and PuraCap Pharmaceutical.
BOSTON – Despite what some popular online media outlets report, sunscreens are safe in children and can even be used on infants under 6 months of age when sun avoidance – the best approach to protecting babies from the damaging effects of the sun – is not possible, according to Mercedes E. Gonzalez, MD.
A quick Google search reveals numerous, widely-shared articles about the dangers lurking in one’s beach bag, and while many product labels recommend asking a doctor about whether the product is safe for babies under age 6 months, that’s only because most product safety studies didn’t include that age group, Dr. Gonzalez of the University of Miami said at the American Academy of Dermatology summer meeting.
In fact, there is “nothing magical that happens” in infant skin after 6 months that makes sunscreen use safer, she said, explaining that infant skin is structurally and functionally different from adult skin, and that while gradual maturation takes place over time, thereby reducing susceptibility to percutaneous absorption of topically applied products, the risk is minimal even in babies younger than age 6 months.
The skin characteristics that make younger skin more susceptible to percutaneous absorption also make babies and children unusually susceptible to ultraviolet radiation and ultraviolet radiation–induced immunosuppression, for which the consequences are not fully understood, she said.
Among the more commonly cited sunscreen ingredients of concern are oxybenzone, or benzonephenone-3, and nanoparticles, she noted.
However, the overall consensus based on studies of oxybenzone is that aside from causing some cases of allergic and irritant contact dermatitis, the compound is safe; no harmful cause and effect relationship with oxybenzone and systemic side effects in humans have been reported, and periodic reviews by European, Australian and U.S. safety panels all conclude that it is safe.
Numerous studies of nanoparticles – such as nanosized zinc oxide and titanium dioxide – have shown that absorption is confined to the level of stratum corneum – even when skin barrier function has been altered, she said, noting that most are coated with aluminum oxide and SiO2 to minimize contact.
However, the safety of sunscreen shouldn’t be seen as license to ignore sun-exposure recommendations; sunscreen in infants should be considered “the last layer of protection,” used only on exposed areas when adequate clothing and shade are not available, according to a 2011 American Academy of Pediatrics statement (Pediatrics. 2011 Feb. doi: 10.1542/peds.2010-3501).
Efforts should be made to keep babies in the shade when outdoors whenever possible, especially during peak sun hours. Use sun-protective clothing, including hats, sunglasses, and long-sleeved shirts, Dr. Gonzalez advised.
When sunscreen is required, a broad-spectrum water-resistant product with an SPF of more than 30 is preferable.
“But the best sunscreen is the one you and your child will use,” she said.
Mineral-based products are less irritating and thus may be a preferred option for children with atopic dermatitis, she added.
Advise parents to apply sunscreen to all areas not protected by their child’s clothing, paying particular attention to vulnerable areas, including the back of the neck, ears, and dorsal feet. Reapply before going outdoors, and then again every 2 hours, she advised.
“So the overall answer to the parents’ question, ‘Are sunscreens safe?’ ... the overwhelming answer here is yes, and the weight of the evidence shows there is no proven harm from sunscreen use especially when used properly,” she said.
Provide specific guidance for pediatric sunscreen use
In the face of conflicting information about sunscreen safety and efficacy, parents with questions about sunscreen are looking for specific direction, Dr. Gonzalez said.
She said she finds it helpful to teach them about the importance of reading labels. That is, looking at the ingredients, and looking for SPF above 30, broad-spectrum coverage, and water resistance. She also recommends providing a list or images of good options, and circling the specific preferred products.
For babies, she finds stick sunscreens most useful for application.
“I generally don’t recommend sprays, but if they’re going to use a spray – and parents love sprays because they are easy to apply – I recommend the ones that have some zinc oxide in them, so that when they apply them they can see where they’re going on the skin,” Dr. Gonzalez said.
Tell patients to apply sunscreen before leaving the house, she advised, adding that making sunscreen application part of a daily routine helps encourage healthy behaviors, as does allowing children, at the right age, to participate in sunscreen application.
For adolescents, avoid scare tactics such as warning about skin cancer. Rather, focus on benefits of avoiding the sun, help them find a product they like by finding out why they don’t like a particular product and recommending an alternative, then following up on that when they come back in, she suggested.
“I really try to address it at every visit,” Dr. Gonzalez said.
“Finally, the most important message is that sunscreen is really just one part of complete sun protection,” she said, noting that specific information about where to buy sun-protective clothing and hats is also important.
Dr. Gonzalez reported serving as a speaker and/or advisory board member and receiving honoraria from Pierre Fabre Dermatologie, Anacor Pharmaceuticals, Encore Dermatology, and PuraCap Pharmaceutical.
EXPERT ANALYSIS FROM THE AAD SUMMER ACADEMY 2016

CDC reports two new cases of Zika-related birth defects
Two live-born infants with Zika virus–related birth defects were reported the week ending Aug. 4, 2016, bringing the U.S. total to 17, the Centers for Disease Control and Prevention reported.
One of the two infants was born in the 50 states and the District of Columbia, and the other was the first live-born infant with Zika-related birth defects born in the U.S. territories. State- or territorial-level data are not being reported to protect the privacy of affected women and children, the CDC said.
There were no new pregnancy losses among Zika-infected women in the territories, keeping the total at one for the year, but the CDC seems to have adjusted the number of pregnancy losses for the states and D.C., as the most recent total for the year is now five, after six were reported the previous week.
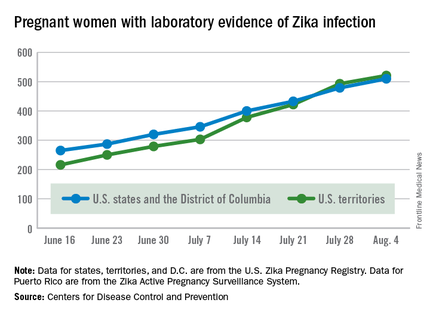
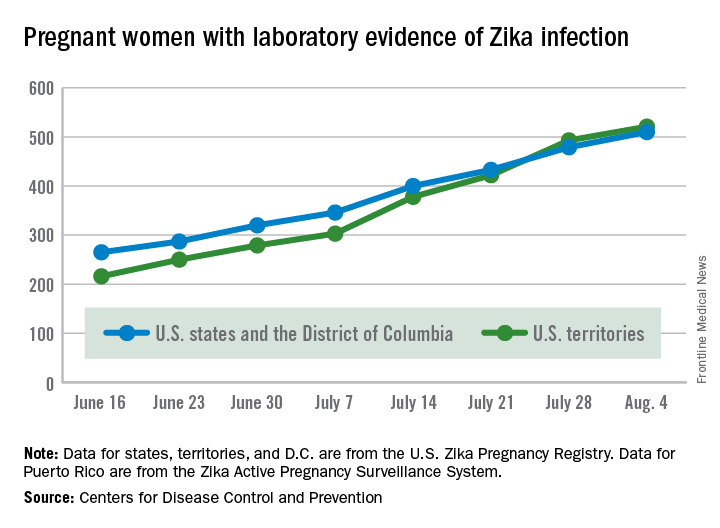
A total of 59 new cases of Zika infection in pregnant women were reported for the week ending Aug. 4: 31 new cases in the states/D.C. and 28 in the territories. For the year, there have been 510 cases of pregnant women with laboratory evidence of Zika infection in the states/D.C. and 521 in the territories, for a U.S. total of 1,031, the CDC reported.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika virus–related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Two live-born infants with Zika virus–related birth defects were reported the week ending Aug. 4, 2016, bringing the U.S. total to 17, the Centers for Disease Control and Prevention reported.
One of the two infants was born in the 50 states and the District of Columbia, and the other was the first live-born infant with Zika-related birth defects born in the U.S. territories. State- or territorial-level data are not being reported to protect the privacy of affected women and children, the CDC said.
There were no new pregnancy losses among Zika-infected women in the territories, keeping the total at one for the year, but the CDC seems to have adjusted the number of pregnancy losses for the states and D.C., as the most recent total for the year is now five, after six were reported the previous week.
A total of 59 new cases of Zika infection in pregnant women were reported for the week ending Aug. 4: 31 new cases in the states/D.C. and 28 in the territories. For the year, there have been 510 cases of pregnant women with laboratory evidence of Zika infection in the states/D.C. and 521 in the territories, for a U.S. total of 1,031, the CDC reported.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika virus–related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
Two live-born infants with Zika virus–related birth defects were reported the week ending Aug. 4, 2016, bringing the U.S. total to 17, the Centers for Disease Control and Prevention reported.
One of the two infants was born in the 50 states and the District of Columbia, and the other was the first live-born infant with Zika-related birth defects born in the U.S. territories. State- or territorial-level data are not being reported to protect the privacy of affected women and children, the CDC said.
There were no new pregnancy losses among Zika-infected women in the territories, keeping the total at one for the year, but the CDC seems to have adjusted the number of pregnancy losses for the states and D.C., as the most recent total for the year is now five, after six were reported the previous week.
A total of 59 new cases of Zika infection in pregnant women were reported for the week ending Aug. 4: 31 new cases in the states/D.C. and 28 in the territories. For the year, there have been 510 cases of pregnant women with laboratory evidence of Zika infection in the states/D.C. and 521 in the territories, for a U.S. total of 1,031, the CDC reported.
The figures for states, territories, and D.C. reflect reporting to the U.S. Zika Pregnancy Registry; data for Puerto Rico are reported to the U.S. Zika Active Pregnancy Surveillance System.
Zika virus–related birth defects recorded by the CDC could include microcephaly, calcium deposits in the brain indicating possible brain damage, excess fluid in the brain cavities and surrounding the brain, absent or poorly formed brain structures, abnormal eye development, or other problems resulting from brain damage that affect nerves, muscles, and bones. The pregnancy losses encompass any miscarriage, stillbirth, and termination with evidence of birth defects.
FDA approves generic version of Tamiflu
The Food and Drug Administration has approved the first generic version of Tamiflu (oseltamivir phosphate), a medication for the treatment of influenza A and B.
The announcement was made Aug. 3, 2016, on the Drugs@FDA website and in an email from the FDA’s Division of Drug Information (DDI). Tamiflu was first approved in 1999.
Oseltamivir phosphate is intended for use in patients 2 weeks of age and older who have had flu symptoms for no more than 48 hours, and for prevention of influenza in patients 1 year of age and older. According to the FDA, the drug does not treat or prevent illness caused by viral infections other than the influenza virus, and does not prevent bacterial infections that may happen with the flu.

Products in the FDA generic approval application submitted by Natco Pharma Ltd., an India-based drug company, include the oral capsule form of the drug, in 30-, 45-, and 75-mg strengths.
The FDA acknowledged in its approval that it does not know if oseltamivir phosphate is effective in patients who start treatment after 2 days of developing symptoms, or have weakened immune systems. The most common side effects reported by patients using oseltamivir phosphate in clinical trials included nausea and vomiting.
For more information on oseltamivir phosphate, see the Tamiflu drug label.
On Twitter @richpizzi
The Food and Drug Administration has approved the first generic version of Tamiflu (oseltamivir phosphate), a medication for the treatment of influenza A and B.
The announcement was made Aug. 3, 2016, on the Drugs@FDA website and in an email from the FDA’s Division of Drug Information (DDI). Tamiflu was first approved in 1999.
Oseltamivir phosphate is intended for use in patients 2 weeks of age and older who have had flu symptoms for no more than 48 hours, and for prevention of influenza in patients 1 year of age and older. According to the FDA, the drug does not treat or prevent illness caused by viral infections other than the influenza virus, and does not prevent bacterial infections that may happen with the flu.
Products in the FDA generic approval application submitted by Natco Pharma Ltd., an India-based drug company, include the oral capsule form of the drug, in 30-, 45-, and 75-mg strengths.
The FDA acknowledged in its approval that it does not know if oseltamivir phosphate is effective in patients who start treatment after 2 days of developing symptoms, or have weakened immune systems. The most common side effects reported by patients using oseltamivir phosphate in clinical trials included nausea and vomiting.
For more information on oseltamivir phosphate, see the Tamiflu drug label.
On Twitter @richpizzi
The Food and Drug Administration has approved the first generic version of Tamiflu (oseltamivir phosphate), a medication for the treatment of influenza A and B.
The announcement was made Aug. 3, 2016, on the Drugs@FDA website and in an email from the FDA’s Division of Drug Information (DDI). Tamiflu was first approved in 1999.
Oseltamivir phosphate is intended for use in patients 2 weeks of age and older who have had flu symptoms for no more than 48 hours, and for prevention of influenza in patients 1 year of age and older. According to the FDA, the drug does not treat or prevent illness caused by viral infections other than the influenza virus, and does not prevent bacterial infections that may happen with the flu.
Products in the FDA generic approval application submitted by Natco Pharma Ltd., an India-based drug company, include the oral capsule form of the drug, in 30-, 45-, and 75-mg strengths.
The FDA acknowledged in its approval that it does not know if oseltamivir phosphate is effective in patients who start treatment after 2 days of developing symptoms, or have weakened immune systems. The most common side effects reported by patients using oseltamivir phosphate in clinical trials included nausea and vomiting.
For more information on oseltamivir phosphate, see the Tamiflu drug label.
On Twitter @richpizzi

Hypoxia of obstructive sleep apnea aggravates NAFLD, NASH in adolescents
A new study has found that a strong association exists in adolescents who have obstructive sleep apnea, and their risks of developing more highly progressed forms of nonalcoholic fatty liver disease (NAFLD) or nonalcoholic steatohepatitis (NASH).
“Substantial evidence suggests oxidative stress is a central mediator in NAFLD pathogenesis and progression, although the specific trigger for reactive oxygen species (ROS) generation has not been clearly delineated,” wrote the authors, led by Shikha S. Sundaram, MD of the University of Colorado at Denver, Aurora, adding that “Emerging evidence demonstrates that obesity-related obstructive sleep apnea (OSA) and intermittent nocturnal hypoxia are associated with NAFLD progression.”
Dr. Sundaram and her coinvestigators looked at patients admitted to the Children’s Hospital Colorado Pediatric Liver Center from June 2009 through January 2014. Subjects included were children ages 8-18 years, male and female, who were classified as Tanner stage 2-4 with liver biopsy evidence of NAFLD.
“In our center, a clinical liver biopsy for suspected NAFLD is performed in overweight or obese children (body mass index greater than 85% for age and gender) with chronically elevated aminotransferases in whom a diagnosis is unclear based on serologic testing,” Dr. Sundaram and her coauthors clarified regarding the screening process.
Additionally, age-matched “lean” children, that is, those with a body mass index lower than 85%, were also enrolled as controls; these subjects were included if they had no evidence of hepatomegaly or liver disease – translated to AST and ALT levels of 640 IU/L – and were also Tanner stage 2-4. The authors explained that this Tanner stage range was chosen in order to “minimize variations in insulin sensitivity that may confound the interpretation of potential associations between OSA/hypoxia and NAFLD.”
Ultimately, 36 NAFLD adolescent subjects and 14 controls completed the study. A total of 25 of the 36 NAFLD subjects (69.4%) had OSA and/or nocturnal hypoxia; of these, 15 were classified as having isolated OSA, 9 had both OSA and hypoxia, and 1 had isolated hypoxia. Polysomnograms found that all NAFLD subjects spent more than 12% of their total time asleep in REM sleep, which was deemed adequate enough to consider the findings valid.
Based on liver histology scoring, laboratory testing, urine F2-isoprostanes, and 4-hydroxynonenal liver immunohistochemistry tests that were conducted on all subjects, Dr. Sundaram and her coinvestigators found that subjects with OSA or hypoxia had more severe fibrosis than did those without. While the latter cohort were 100% stage 0-2, only 64% of those with OSA/hypoxia were stage 0-2, while the remaining 36% were stage 3 (P = .03). Additionally, higher F2-isoprostanes – used to measure lipid peroxidation – correlated with apnea/hypoxia index (r = 0.39; P = .03), and the most severe OSA/hypoxia occurred in subjects that had the greatest 4-hydroxynonenal staining (P = .03). Furthermore, an increase in both F2-isoprostanes and 4-hydroxynonenal hepatic staining was shown to lead to a higher risk of worse steatosis: r = 0.32 and r = 0.47, respectively (P = .04 and P = .007).
“These data support sleep disordered breathing as an important trigger of oxidative stress that promotes progression of pediatric NAFLD to NASH,” the authors concluded, adding that “this study confirms that OSA/hypoxia is common in pediatric NAFLD and that more severe OSA/hypoxia is associated with elevated aminotransferases, hepatic steatosis, inflammation, NAS [NAFLD activity score], and fibrosis.”
Dr. Sundaram and her coauthors call for further research to examine if “prevention or reversal of NASH following effective therapy of OSA and nocturnal hypoxia in obese patients” is viable.
This study was supported by funding from the National Institutes of Health. Dr. Sundaram and her coinvestigators did not report any relevant financial disclosures.
A new study has found that a strong association exists in adolescents who have obstructive sleep apnea, and their risks of developing more highly progressed forms of nonalcoholic fatty liver disease (NAFLD) or nonalcoholic steatohepatitis (NASH).
“Substantial evidence suggests oxidative stress is a central mediator in NAFLD pathogenesis and progression, although the specific trigger for reactive oxygen species (ROS) generation has not been clearly delineated,” wrote the authors, led by Shikha S. Sundaram, MD of the University of Colorado at Denver, Aurora, adding that “Emerging evidence demonstrates that obesity-related obstructive sleep apnea (OSA) and intermittent nocturnal hypoxia are associated with NAFLD progression.”
Dr. Sundaram and her coinvestigators looked at patients admitted to the Children’s Hospital Colorado Pediatric Liver Center from June 2009 through January 2014. Subjects included were children ages 8-18 years, male and female, who were classified as Tanner stage 2-4 with liver biopsy evidence of NAFLD.
“In our center, a clinical liver biopsy for suspected NAFLD is performed in overweight or obese children (body mass index greater than 85% for age and gender) with chronically elevated aminotransferases in whom a diagnosis is unclear based on serologic testing,” Dr. Sundaram and her coauthors clarified regarding the screening process.
Additionally, age-matched “lean” children, that is, those with a body mass index lower than 85%, were also enrolled as controls; these subjects were included if they had no evidence of hepatomegaly or liver disease – translated to AST and ALT levels of 640 IU/L – and were also Tanner stage 2-4. The authors explained that this Tanner stage range was chosen in order to “minimize variations in insulin sensitivity that may confound the interpretation of potential associations between OSA/hypoxia and NAFLD.”
Ultimately, 36 NAFLD adolescent subjects and 14 controls completed the study. A total of 25 of the 36 NAFLD subjects (69.4%) had OSA and/or nocturnal hypoxia; of these, 15 were classified as having isolated OSA, 9 had both OSA and hypoxia, and 1 had isolated hypoxia. Polysomnograms found that all NAFLD subjects spent more than 12% of their total time asleep in REM sleep, which was deemed adequate enough to consider the findings valid.
Based on liver histology scoring, laboratory testing, urine F2-isoprostanes, and 4-hydroxynonenal liver immunohistochemistry tests that were conducted on all subjects, Dr. Sundaram and her coinvestigators found that subjects with OSA or hypoxia had more severe fibrosis than did those without. While the latter cohort were 100% stage 0-2, only 64% of those with OSA/hypoxia were stage 0-2, while the remaining 36% were stage 3 (P = .03). Additionally, higher F2-isoprostanes – used to measure lipid peroxidation – correlated with apnea/hypoxia index (r = 0.39; P = .03), and the most severe OSA/hypoxia occurred in subjects that had the greatest 4-hydroxynonenal staining (P = .03). Furthermore, an increase in both F2-isoprostanes and 4-hydroxynonenal hepatic staining was shown to lead to a higher risk of worse steatosis: r = 0.32 and r = 0.47, respectively (P = .04 and P = .007).
“These data support sleep disordered breathing as an important trigger of oxidative stress that promotes progression of pediatric NAFLD to NASH,” the authors concluded, adding that “this study confirms that OSA/hypoxia is common in pediatric NAFLD and that more severe OSA/hypoxia is associated with elevated aminotransferases, hepatic steatosis, inflammation, NAS [NAFLD activity score], and fibrosis.”
Dr. Sundaram and her coauthors call for further research to examine if “prevention or reversal of NASH following effective therapy of OSA and nocturnal hypoxia in obese patients” is viable.
This study was supported by funding from the National Institutes of Health. Dr. Sundaram and her coinvestigators did not report any relevant financial disclosures.
A new study has found that a strong association exists in adolescents who have obstructive sleep apnea, and their risks of developing more highly progressed forms of nonalcoholic fatty liver disease (NAFLD) or nonalcoholic steatohepatitis (NASH).
“Substantial evidence suggests oxidative stress is a central mediator in NAFLD pathogenesis and progression, although the specific trigger for reactive oxygen species (ROS) generation has not been clearly delineated,” wrote the authors, led by Shikha S. Sundaram, MD of the University of Colorado at Denver, Aurora, adding that “Emerging evidence demonstrates that obesity-related obstructive sleep apnea (OSA) and intermittent nocturnal hypoxia are associated with NAFLD progression.”
Dr. Sundaram and her coinvestigators looked at patients admitted to the Children’s Hospital Colorado Pediatric Liver Center from June 2009 through January 2014. Subjects included were children ages 8-18 years, male and female, who were classified as Tanner stage 2-4 with liver biopsy evidence of NAFLD.
“In our center, a clinical liver biopsy for suspected NAFLD is performed in overweight or obese children (body mass index greater than 85% for age and gender) with chronically elevated aminotransferases in whom a diagnosis is unclear based on serologic testing,” Dr. Sundaram and her coauthors clarified regarding the screening process.
Additionally, age-matched “lean” children, that is, those with a body mass index lower than 85%, were also enrolled as controls; these subjects were included if they had no evidence of hepatomegaly or liver disease – translated to AST and ALT levels of 640 IU/L – and were also Tanner stage 2-4. The authors explained that this Tanner stage range was chosen in order to “minimize variations in insulin sensitivity that may confound the interpretation of potential associations between OSA/hypoxia and NAFLD.”
Ultimately, 36 NAFLD adolescent subjects and 14 controls completed the study. A total of 25 of the 36 NAFLD subjects (69.4%) had OSA and/or nocturnal hypoxia; of these, 15 were classified as having isolated OSA, 9 had both OSA and hypoxia, and 1 had isolated hypoxia. Polysomnograms found that all NAFLD subjects spent more than 12% of their total time asleep in REM sleep, which was deemed adequate enough to consider the findings valid.
Based on liver histology scoring, laboratory testing, urine F2-isoprostanes, and 4-hydroxynonenal liver immunohistochemistry tests that were conducted on all subjects, Dr. Sundaram and her coinvestigators found that subjects with OSA or hypoxia had more severe fibrosis than did those without. While the latter cohort were 100% stage 0-2, only 64% of those with OSA/hypoxia were stage 0-2, while the remaining 36% were stage 3 (P = .03). Additionally, higher F2-isoprostanes – used to measure lipid peroxidation – correlated with apnea/hypoxia index (r = 0.39; P = .03), and the most severe OSA/hypoxia occurred in subjects that had the greatest 4-hydroxynonenal staining (P = .03). Furthermore, an increase in both F2-isoprostanes and 4-hydroxynonenal hepatic staining was shown to lead to a higher risk of worse steatosis: r = 0.32 and r = 0.47, respectively (P = .04 and P = .007).
“These data support sleep disordered breathing as an important trigger of oxidative stress that promotes progression of pediatric NAFLD to NASH,” the authors concluded, adding that “this study confirms that OSA/hypoxia is common in pediatric NAFLD and that more severe OSA/hypoxia is associated with elevated aminotransferases, hepatic steatosis, inflammation, NAS [NAFLD activity score], and fibrosis.”
Dr. Sundaram and her coauthors call for further research to examine if “prevention or reversal of NASH following effective therapy of OSA and nocturnal hypoxia in obese patients” is viable.
This study was supported by funding from the National Institutes of Health. Dr. Sundaram and her coinvestigators did not report any relevant financial disclosures.
FROM THE JOURNAL OF HEPATOLOGY
Key clinical point: Adolescents with obstructive sleep apnea have a higher risk for nonalcoholic fatty liver disease, because of liver tissue scarring.
Major finding: The cohort of subjects with OSA had more severe fibrosis (64%, stages 0-2; 36% stage 3) than those without OSA (100%, stages 0-2) (P = .03).
Data source: Prospective cohort study of 36 adolescents with NAFLD and 14 lean controls.
Disclosures: Funding provided by the NIH. Authors reported no relevant financial disclosures.
Pediatric Hospital Medicine Meetings Foster Engagement, Growth
Kris Rehm, MD, is associate professor of clinical pediatrics and director of the Division of Hospital Medicine at the Vanderbilt University School of Medicine in Nashville. Dr. Rehm also serves as a pediatric hospitalist at the Monroe Carell Jr. Children’s Hospital at Vanderbilt, chairs the Society of Hospital Medicine’s Pediatrics Committee, and is chair of the 2017 Pediatric Hospital Medicine meeting.

The Hospitalist recently spoke with Dr. Rehm about her career path to pediatric hospital medicine, the impact SHM has had on her career, and how she balances the busy schedule of a hospitalist with her family and personal life.
Question: How did you arrive at a career in pediatric hospital medicine?
Answer: In 2001, as a resident in the Boston Combined Residency Program in pediatrics at Boston Children’s Hospital, I knew that I preferred caring for patients who were acutely ill. I also enjoyed collaborating with subspecialists as we worked to diagnose and treat patients with some of the most complicated disease processes at a tertiary-care center. At this time, hospital medicine was still quite a young specialty.
After my residency, my husband and I moved from Boston to Nashville, and I worked in general pediatrics in the community for three years. In 2005, Vanderbilt was ready to begin a hospital medicine program. It was perfect timing for me, as I had just delivered my first set of twins. (Yes, that’s right—I have two sets of twins!)
I started to work part-time in hospital medicine—what a great opportunity! I was able to work in the acute-care setting, which I loved, with residents, students, and subspecialists that I loved, and also be home with my 1-year-old sons, Jackson and Lucas.
As time passed, I gradually moved from part-time to full-time. In addition, opportunities to advance in administrative leadership have helped me broaden my career, working as the medical director of hospital operations as well as the division director of hospital medicine.
Q: What is the most memorable moment in your career as a pediatric hospitalist?
A: Honestly, the most amazing memories that I have are when those in my division are successful—and that has happened a lot! In our division, we now have the dean of students at the medical school, the two faculty voted as best teachers by our residents last year, and the director of our Quality Academy at Vanderbilt. In fact, earlier this year, a member of our division won the teaching award voted on by residents—the third year in a row for her and our group. I am so proud of those members in my division. … They do incredible things at work and beyond.
While completing our annual reviews this spring, I had a chance to talk with faculty about contributions they have each made in making a diagnosis, comforting a patient, or assisting a family member through a difficult time. Moments like these truly inspire me to keep doing what I do.
Q: What do you find most valuable about your work with SHM?
A: Being involved in a national organization like SHM has opened tremendous doors for me, both personally and professionally. It has helped my academic promotion to associate professor, it has allowed me networking opportunities with leaders in both pediatric and adult hospital medicine, and it has had a tremendous impact on my life as an academic leader in hospital medicine.
The SHM Pediatrics Committee is another example of a truly collaborative group of individuals trying to make a difference every day for the children we care for and the hospital medicine specialty through our professional “home” of SHM. As chair of the Pediatrics Committee, I have had the chance to empower our new committee members who articulate willingness to take leadership to become active, engaged members of the society. Watching Drs. Charlotte Brown and Akshata Hopkins present the top articles in the Pediatric Hospital Medicine talk at HM16 in San Diego was an awesome example.
At the moment, we are jumping into planning for PHM17, and I am honored and excited to serve as chair of this meeting. I have attended annually since 2005, and to watch the meeting grow and take on many issues has been truly unbelievable. The meeting now draws nearly 1,000 pediatric hospitalists and is an invaluable opportunity for attendees to learn from each other.
SHM provides our members with the opportunity to become as engaged as you are able with committees, training opportunities, annual meetings, and more. So jump in!
Q: How do you balance your demanding schedule with your husband, children, and leisure?
A: Raising four young boys, now ages 9 and 12, with my husband and working full-time as a pediatric hospitalist is so challenging but so rewarding. (My husband and I are experts at Outlook invitations to coordinate a busy schedule of sporting events and school functions as well as night shifts for me and travel for him.) As a family, we spend lots of nights at the soccer field or basketball court, and we love to travel, ski, and swim. And personally, I run. That is my time to unwind. I just ask for one hour a day to exercise, which doubles as my therapy.
I run for Nashville Running Company, a local running store. Some of the other ladies and I meet most mornings at 5 a.m. This year, I ran in the St. George Marathon in Utah as well as the L.A. Marathon. Super fun! I’m planning to run the Chicago Marathon this fall, and Boston’s in the spring of 2017.
Q: As we celebrate the 20th anniversary of hospital medicine, how do you see HM evolving over the next 20 years?
A: What an interesting idea to consider! PHM is moving toward a board certification process, which will be exciting for our field. Similar to other specialties, such as pediatric emergency medicine, adolescent medicine, or child abuse pediatrics, it will be wonderful to watch our specialty gain recognition as a boarded specialty.
HM providers are positioned for leadership throughout organizations, and as we strive to provide the highest-value care, I believe we will continue to grow in this regard. PHM providers now serve as department chairs and hospital CEOs, CMOs, and many other leadership positions. At Vanderbilt, we are seeing some other divisions, such as pediatric neurology, hire neurologists who have inpatient versus outpatient interests. We may see this trend continue over time through other fields as well, with physicians providing specialty-specific hospital care expertise in very defined areas. TH
Brett Radler is SHM’s communications specialist.
Kris Rehm, MD, is associate professor of clinical pediatrics and director of the Division of Hospital Medicine at the Vanderbilt University School of Medicine in Nashville. Dr. Rehm also serves as a pediatric hospitalist at the Monroe Carell Jr. Children’s Hospital at Vanderbilt, chairs the Society of Hospital Medicine’s Pediatrics Committee, and is chair of the 2017 Pediatric Hospital Medicine meeting.
The Hospitalist recently spoke with Dr. Rehm about her career path to pediatric hospital medicine, the impact SHM has had on her career, and how she balances the busy schedule of a hospitalist with her family and personal life.
Question: How did you arrive at a career in pediatric hospital medicine?
Answer: In 2001, as a resident in the Boston Combined Residency Program in pediatrics at Boston Children’s Hospital, I knew that I preferred caring for patients who were acutely ill. I also enjoyed collaborating with subspecialists as we worked to diagnose and treat patients with some of the most complicated disease processes at a tertiary-care center. At this time, hospital medicine was still quite a young specialty.
After my residency, my husband and I moved from Boston to Nashville, and I worked in general pediatrics in the community for three years. In 2005, Vanderbilt was ready to begin a hospital medicine program. It was perfect timing for me, as I had just delivered my first set of twins. (Yes, that’s right—I have two sets of twins!)
I started to work part-time in hospital medicine—what a great opportunity! I was able to work in the acute-care setting, which I loved, with residents, students, and subspecialists that I loved, and also be home with my 1-year-old sons, Jackson and Lucas.
As time passed, I gradually moved from part-time to full-time. In addition, opportunities to advance in administrative leadership have helped me broaden my career, working as the medical director of hospital operations as well as the division director of hospital medicine.
Q: What is the most memorable moment in your career as a pediatric hospitalist?
A: Honestly, the most amazing memories that I have are when those in my division are successful—and that has happened a lot! In our division, we now have the dean of students at the medical school, the two faculty voted as best teachers by our residents last year, and the director of our Quality Academy at Vanderbilt. In fact, earlier this year, a member of our division won the teaching award voted on by residents—the third year in a row for her and our group. I am so proud of those members in my division. … They do incredible things at work and beyond.
While completing our annual reviews this spring, I had a chance to talk with faculty about contributions they have each made in making a diagnosis, comforting a patient, or assisting a family member through a difficult time. Moments like these truly inspire me to keep doing what I do.
Q: What do you find most valuable about your work with SHM?
A: Being involved in a national organization like SHM has opened tremendous doors for me, both personally and professionally. It has helped my academic promotion to associate professor, it has allowed me networking opportunities with leaders in both pediatric and adult hospital medicine, and it has had a tremendous impact on my life as an academic leader in hospital medicine.
The SHM Pediatrics Committee is another example of a truly collaborative group of individuals trying to make a difference every day for the children we care for and the hospital medicine specialty through our professional “home” of SHM. As chair of the Pediatrics Committee, I have had the chance to empower our new committee members who articulate willingness to take leadership to become active, engaged members of the society. Watching Drs. Charlotte Brown and Akshata Hopkins present the top articles in the Pediatric Hospital Medicine talk at HM16 in San Diego was an awesome example.
At the moment, we are jumping into planning for PHM17, and I am honored and excited to serve as chair of this meeting. I have attended annually since 2005, and to watch the meeting grow and take on many issues has been truly unbelievable. The meeting now draws nearly 1,000 pediatric hospitalists and is an invaluable opportunity for attendees to learn from each other.
SHM provides our members with the opportunity to become as engaged as you are able with committees, training opportunities, annual meetings, and more. So jump in!
Q: How do you balance your demanding schedule with your husband, children, and leisure?
A: Raising four young boys, now ages 9 and 12, with my husband and working full-time as a pediatric hospitalist is so challenging but so rewarding. (My husband and I are experts at Outlook invitations to coordinate a busy schedule of sporting events and school functions as well as night shifts for me and travel for him.) As a family, we spend lots of nights at the soccer field or basketball court, and we love to travel, ski, and swim. And personally, I run. That is my time to unwind. I just ask for one hour a day to exercise, which doubles as my therapy.
I run for Nashville Running Company, a local running store. Some of the other ladies and I meet most mornings at 5 a.m. This year, I ran in the St. George Marathon in Utah as well as the L.A. Marathon. Super fun! I’m planning to run the Chicago Marathon this fall, and Boston’s in the spring of 2017.
Q: As we celebrate the 20th anniversary of hospital medicine, how do you see HM evolving over the next 20 years?
A: What an interesting idea to consider! PHM is moving toward a board certification process, which will be exciting for our field. Similar to other specialties, such as pediatric emergency medicine, adolescent medicine, or child abuse pediatrics, it will be wonderful to watch our specialty gain recognition as a boarded specialty.
HM providers are positioned for leadership throughout organizations, and as we strive to provide the highest-value care, I believe we will continue to grow in this regard. PHM providers now serve as department chairs and hospital CEOs, CMOs, and many other leadership positions. At Vanderbilt, we are seeing some other divisions, such as pediatric neurology, hire neurologists who have inpatient versus outpatient interests. We may see this trend continue over time through other fields as well, with physicians providing specialty-specific hospital care expertise in very defined areas. TH
Brett Radler is SHM’s communications specialist.
Kris Rehm, MD, is associate professor of clinical pediatrics and director of the Division of Hospital Medicine at the Vanderbilt University School of Medicine in Nashville. Dr. Rehm also serves as a pediatric hospitalist at the Monroe Carell Jr. Children’s Hospital at Vanderbilt, chairs the Society of Hospital Medicine’s Pediatrics Committee, and is chair of the 2017 Pediatric Hospital Medicine meeting.
The Hospitalist recently spoke with Dr. Rehm about her career path to pediatric hospital medicine, the impact SHM has had on her career, and how she balances the busy schedule of a hospitalist with her family and personal life.
Question: How did you arrive at a career in pediatric hospital medicine?
Answer: In 2001, as a resident in the Boston Combined Residency Program in pediatrics at Boston Children’s Hospital, I knew that I preferred caring for patients who were acutely ill. I also enjoyed collaborating with subspecialists as we worked to diagnose and treat patients with some of the most complicated disease processes at a tertiary-care center. At this time, hospital medicine was still quite a young specialty.
After my residency, my husband and I moved from Boston to Nashville, and I worked in general pediatrics in the community for three years. In 2005, Vanderbilt was ready to begin a hospital medicine program. It was perfect timing for me, as I had just delivered my first set of twins. (Yes, that’s right—I have two sets of twins!)
I started to work part-time in hospital medicine—what a great opportunity! I was able to work in the acute-care setting, which I loved, with residents, students, and subspecialists that I loved, and also be home with my 1-year-old sons, Jackson and Lucas.
As time passed, I gradually moved from part-time to full-time. In addition, opportunities to advance in administrative leadership have helped me broaden my career, working as the medical director of hospital operations as well as the division director of hospital medicine.
Q: What is the most memorable moment in your career as a pediatric hospitalist?
A: Honestly, the most amazing memories that I have are when those in my division are successful—and that has happened a lot! In our division, we now have the dean of students at the medical school, the two faculty voted as best teachers by our residents last year, and the director of our Quality Academy at Vanderbilt. In fact, earlier this year, a member of our division won the teaching award voted on by residents—the third year in a row for her and our group. I am so proud of those members in my division. … They do incredible things at work and beyond.
While completing our annual reviews this spring, I had a chance to talk with faculty about contributions they have each made in making a diagnosis, comforting a patient, or assisting a family member through a difficult time. Moments like these truly inspire me to keep doing what I do.
Q: What do you find most valuable about your work with SHM?
A: Being involved in a national organization like SHM has opened tremendous doors for me, both personally and professionally. It has helped my academic promotion to associate professor, it has allowed me networking opportunities with leaders in both pediatric and adult hospital medicine, and it has had a tremendous impact on my life as an academic leader in hospital medicine.
The SHM Pediatrics Committee is another example of a truly collaborative group of individuals trying to make a difference every day for the children we care for and the hospital medicine specialty through our professional “home” of SHM. As chair of the Pediatrics Committee, I have had the chance to empower our new committee members who articulate willingness to take leadership to become active, engaged members of the society. Watching Drs. Charlotte Brown and Akshata Hopkins present the top articles in the Pediatric Hospital Medicine talk at HM16 in San Diego was an awesome example.
At the moment, we are jumping into planning for PHM17, and I am honored and excited to serve as chair of this meeting. I have attended annually since 2005, and to watch the meeting grow and take on many issues has been truly unbelievable. The meeting now draws nearly 1,000 pediatric hospitalists and is an invaluable opportunity for attendees to learn from each other.
SHM provides our members with the opportunity to become as engaged as you are able with committees, training opportunities, annual meetings, and more. So jump in!
Q: How do you balance your demanding schedule with your husband, children, and leisure?
A: Raising four young boys, now ages 9 and 12, with my husband and working full-time as a pediatric hospitalist is so challenging but so rewarding. (My husband and I are experts at Outlook invitations to coordinate a busy schedule of sporting events and school functions as well as night shifts for me and travel for him.) As a family, we spend lots of nights at the soccer field or basketball court, and we love to travel, ski, and swim. And personally, I run. That is my time to unwind. I just ask for one hour a day to exercise, which doubles as my therapy.
I run for Nashville Running Company, a local running store. Some of the other ladies and I meet most mornings at 5 a.m. This year, I ran in the St. George Marathon in Utah as well as the L.A. Marathon. Super fun! I’m planning to run the Chicago Marathon this fall, and Boston’s in the spring of 2017.
Q: As we celebrate the 20th anniversary of hospital medicine, how do you see HM evolving over the next 20 years?
A: What an interesting idea to consider! PHM is moving toward a board certification process, which will be exciting for our field. Similar to other specialties, such as pediatric emergency medicine, adolescent medicine, or child abuse pediatrics, it will be wonderful to watch our specialty gain recognition as a boarded specialty.
HM providers are positioned for leadership throughout organizations, and as we strive to provide the highest-value care, I believe we will continue to grow in this regard. PHM providers now serve as department chairs and hospital CEOs, CMOs, and many other leadership positions. At Vanderbilt, we are seeing some other divisions, such as pediatric neurology, hire neurologists who have inpatient versus outpatient interests. We may see this trend continue over time through other fields as well, with physicians providing specialty-specific hospital care expertise in very defined areas. TH
Brett Radler is SHM’s communications specialist.
Epilepsy has wide-ranging psychosocial impact on youth
The psychosocial impact of epilepsy on children and adolescents is profound, ranging from a sense of vulnerability and disempowerment to discrimination, results from a systematic review of medical literature suggest.
“Children and adolescents perceive that epilepsy forces them to relinquish their sense of privacy, bodily control, normality, freedom, and confidence to participate in school and social activities,” researchers led by Lauren Chong wrote in a study published online Aug. 10 in Pediatrics. “They are overwhelmed by the daily uncertainties attributed to the unpredictable timing and potential harm from seizures, side effects of ongoing treatment, and the impermanence of remission.”

In an effort to describe the perspectives of children and adolescents with epilepsy, Ms. Chong of the Sydney School of Public Health at the University of Sydney, New South Wales, Australia, and her associates searched Medline and other key databases for qualitative primary studies on children’s experience of epilepsy from inception to August 2015 (Pediatrics. 2016;138[3]:e20160658. doi: 10.1542/peds.2016-0658). They used thematic synthesis to analyze their findings. The final analysis included 43 articles involving 951 children and adolescents aged 3-21 years from 21 different countries. Articles written in a language other than English were excluded.
The researchers identified six themes: loss of bodily control such as a sense of being overtaken and alertness to mortality; loss of privacy such as humiliating involuntary function and unwanted special attention; inescapable inferiority and discrimination such as vulnerability to prejudice and inability to achieve academically; therapeutic burden and futility such as financial burden and insurmountable side effects; navigating health care such as unexpected necessity of transition as well as fragmented and inconsistent care; and recontextualizing to regain normality such as distinguishing disease from identity and gaining perspective and maturity.
The researchers observed some differences in experiences and perspectives based on patient age and disease severity. For example, “feelings of loss and abnormality tended to be expressed more strongly by older adolescent patients,” they wrote. “As young adults, they were aware of the potentially serious ramifications of epilepsy on their future, including their independence, school performance, vocation, and relationships. Teenage patients were more frustrated by social limitations on partying, drinking, and sleepovers that differentiated them from their peers.” Patients with more severe disease, meanwhile, “contended with disempowerment and seemed less able to delineate epilepsy from their identity. They seemed more willing to trial therapies that may work and some, on being told they would not achieve remission, chose to disengage from the health care system, deeming further treatment or follow-up to be futile.”
Suggestions for clinical practice based on the analysis include providing access to support groups of other epilepsy sufferers or other children/adolescents with chronic disease; facilitating liaisons between clinicians, families, and school teachers, and delivering coordinated care with psychologists and psychiatrists to address psychosocial aspects of epilepsy.
“Treatment and management should address the psychosocial needs of patients regarding stigma, present lifestyle limitations, and future concerns,” the researchers wrote. “These suggestions may inform strategies for practice and research that may contribute toward the improved [quality of life], therapeutic satisfaction, and health outcomes of children and adolescents with epilepsy.”
Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
The psychosocial impact of epilepsy on children and adolescents is profound, ranging from a sense of vulnerability and disempowerment to discrimination, results from a systematic review of medical literature suggest.
“Children and adolescents perceive that epilepsy forces them to relinquish their sense of privacy, bodily control, normality, freedom, and confidence to participate in school and social activities,” researchers led by Lauren Chong wrote in a study published online Aug. 10 in Pediatrics. “They are overwhelmed by the daily uncertainties attributed to the unpredictable timing and potential harm from seizures, side effects of ongoing treatment, and the impermanence of remission.”
In an effort to describe the perspectives of children and adolescents with epilepsy, Ms. Chong of the Sydney School of Public Health at the University of Sydney, New South Wales, Australia, and her associates searched Medline and other key databases for qualitative primary studies on children’s experience of epilepsy from inception to August 2015 (Pediatrics. 2016;138[3]:e20160658. doi: 10.1542/peds.2016-0658). They used thematic synthesis to analyze their findings. The final analysis included 43 articles involving 951 children and adolescents aged 3-21 years from 21 different countries. Articles written in a language other than English were excluded.
The researchers identified six themes: loss of bodily control such as a sense of being overtaken and alertness to mortality; loss of privacy such as humiliating involuntary function and unwanted special attention; inescapable inferiority and discrimination such as vulnerability to prejudice and inability to achieve academically; therapeutic burden and futility such as financial burden and insurmountable side effects; navigating health care such as unexpected necessity of transition as well as fragmented and inconsistent care; and recontextualizing to regain normality such as distinguishing disease from identity and gaining perspective and maturity.
The researchers observed some differences in experiences and perspectives based on patient age and disease severity. For example, “feelings of loss and abnormality tended to be expressed more strongly by older adolescent patients,” they wrote. “As young adults, they were aware of the potentially serious ramifications of epilepsy on their future, including their independence, school performance, vocation, and relationships. Teenage patients were more frustrated by social limitations on partying, drinking, and sleepovers that differentiated them from their peers.” Patients with more severe disease, meanwhile, “contended with disempowerment and seemed less able to delineate epilepsy from their identity. They seemed more willing to trial therapies that may work and some, on being told they would not achieve remission, chose to disengage from the health care system, deeming further treatment or follow-up to be futile.”
Suggestions for clinical practice based on the analysis include providing access to support groups of other epilepsy sufferers or other children/adolescents with chronic disease; facilitating liaisons between clinicians, families, and school teachers, and delivering coordinated care with psychologists and psychiatrists to address psychosocial aspects of epilepsy.
“Treatment and management should address the psychosocial needs of patients regarding stigma, present lifestyle limitations, and future concerns,” the researchers wrote. “These suggestions may inform strategies for practice and research that may contribute toward the improved [quality of life], therapeutic satisfaction, and health outcomes of children and adolescents with epilepsy.”
Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
The psychosocial impact of epilepsy on children and adolescents is profound, ranging from a sense of vulnerability and disempowerment to discrimination, results from a systematic review of medical literature suggest.
“Children and adolescents perceive that epilepsy forces them to relinquish their sense of privacy, bodily control, normality, freedom, and confidence to participate in school and social activities,” researchers led by Lauren Chong wrote in a study published online Aug. 10 in Pediatrics. “They are overwhelmed by the daily uncertainties attributed to the unpredictable timing and potential harm from seizures, side effects of ongoing treatment, and the impermanence of remission.”
In an effort to describe the perspectives of children and adolescents with epilepsy, Ms. Chong of the Sydney School of Public Health at the University of Sydney, New South Wales, Australia, and her associates searched Medline and other key databases for qualitative primary studies on children’s experience of epilepsy from inception to August 2015 (Pediatrics. 2016;138[3]:e20160658. doi: 10.1542/peds.2016-0658). They used thematic synthesis to analyze their findings. The final analysis included 43 articles involving 951 children and adolescents aged 3-21 years from 21 different countries. Articles written in a language other than English were excluded.
The researchers identified six themes: loss of bodily control such as a sense of being overtaken and alertness to mortality; loss of privacy such as humiliating involuntary function and unwanted special attention; inescapable inferiority and discrimination such as vulnerability to prejudice and inability to achieve academically; therapeutic burden and futility such as financial burden and insurmountable side effects; navigating health care such as unexpected necessity of transition as well as fragmented and inconsistent care; and recontextualizing to regain normality such as distinguishing disease from identity and gaining perspective and maturity.
The researchers observed some differences in experiences and perspectives based on patient age and disease severity. For example, “feelings of loss and abnormality tended to be expressed more strongly by older adolescent patients,” they wrote. “As young adults, they were aware of the potentially serious ramifications of epilepsy on their future, including their independence, school performance, vocation, and relationships. Teenage patients were more frustrated by social limitations on partying, drinking, and sleepovers that differentiated them from their peers.” Patients with more severe disease, meanwhile, “contended with disempowerment and seemed less able to delineate epilepsy from their identity. They seemed more willing to trial therapies that may work and some, on being told they would not achieve remission, chose to disengage from the health care system, deeming further treatment or follow-up to be futile.”
Suggestions for clinical practice based on the analysis include providing access to support groups of other epilepsy sufferers or other children/adolescents with chronic disease; facilitating liaisons between clinicians, families, and school teachers, and delivering coordinated care with psychologists and psychiatrists to address psychosocial aspects of epilepsy.
“Treatment and management should address the psychosocial needs of patients regarding stigma, present lifestyle limitations, and future concerns,” the researchers wrote. “These suggestions may inform strategies for practice and research that may contribute toward the improved [quality of life], therapeutic satisfaction, and health outcomes of children and adolescents with epilepsy.”
Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
FROM PEDIATRICS
Key clinical point: Addressing stigma, future independence, and fear of death may improve the overall well-being of children with epilepsy.
Major finding: Children with epilepsy experience vulnerability, disempowerment, and discrimination.
Data source: A meta-analysis of 43 articles involving 951 children and adolescents with epilepsy aged 3-21 years.
Disclosures: Ms. Chong is supported by the University of Sydney Neuroscience Network Research Scholarship. Another coauthor, Allison Tong, PhD, is supported by the National Health and Medical Research Council Fellowship. The researchers reported having no financial disclosures.
Study evaluates Zika syndrome with joint contractures
Congenital Zika syndrome should be added to the differential diagnosis of congenital infections and arthrogryposis (joint contractures), results from a case series study in Brazil suggest.
“Brain impairment in the presence of microcephaly is the main characteristic of a congenital Zika virus syndrome,” researchers led by Vanessa van der Linden, MD, wrote in a study published online Aug. 9 in the BMJ. “However, little is still known about this condition and its clinical spectrum, which also concerns newborns with a normal head circumference. Two studies have described the association between arthrogryposis and microcephaly in newborns presumed to have congenital Zika virus infection [See Morb Mortal Wkly. Rep. 2016;65:59-62 and Ultrasound Obstet Gynecol. 2016;47:6-7].” The authors went on to note that while arthrogryposis might be considered more of a sign than a specific disease, “it might be associated with several disorders. However, there are no reports in the literature about other congenital infections in humans associated with arthrogryposis.”

Dr. van der Linden, a pediatric neurologist with the Association for Assistance of Disabled Children, Recife, Brazil, and her associates retrospectively evaluated the medical records of seven patients with arthrogryposis associated with congenital infection believed to be caused by Zika virus, during the Brazilian microcephaly epidemic (BMJ. 2016;354:i3899). The main outcomes of interest were clinical, radiologic, and electromyographic findings, and likely collaboration between clinical and primary neurological abnormalities.
The researchers reported that brain images of all seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%). In addition, hip x-rays showed bilateral dislocation in all seven children and subluxation of the knee associated with genu valgus in three (43%). No evidence of abnormalities was seen on high-definition ultrasonography of the joints, but moderate signs of remodeling of the motor units and a reduced recruitment pattern were found on needle electromyography. Results from brain computed tomography conducted in all seven patients and magnetic resonance imaging conducted in five revealed malformations of cortical development, calcifications predominantly in the cortex and subcortical white matter, reduction in brain volume, ventriculomegaly, and hypoplasia of the brainstem and cerebellum. Spinal MRI conducted in four children showed apparent thinning of the cord and reduced ventral roots.
“Further research is needed with a larger number of cases to study the neurological abnormalities behind arthrogryposis, including histopathology of autopsy samples or tissues from stillborn babies,” the researchers concluded. “As we do not know the potential implications of congenital Zika virus infection as it evolves, children must receive orthopedic follow-up, even those with a standard first orthopedic evaluation, because they could develop musculoskeletal deformities secondary to neurological impairment, central or peripheral, or both, as these occur in patients with cerebral palsy and other chronic encephalopathies.”
The researchers reported having no financial disclosures.
Congenital Zika syndrome should be added to the differential diagnosis of congenital infections and arthrogryposis (joint contractures), results from a case series study in Brazil suggest.
“Brain impairment in the presence of microcephaly is the main characteristic of a congenital Zika virus syndrome,” researchers led by Vanessa van der Linden, MD, wrote in a study published online Aug. 9 in the BMJ. “However, little is still known about this condition and its clinical spectrum, which also concerns newborns with a normal head circumference. Two studies have described the association between arthrogryposis and microcephaly in newborns presumed to have congenital Zika virus infection [See Morb Mortal Wkly. Rep. 2016;65:59-62 and Ultrasound Obstet Gynecol. 2016;47:6-7].” The authors went on to note that while arthrogryposis might be considered more of a sign than a specific disease, “it might be associated with several disorders. However, there are no reports in the literature about other congenital infections in humans associated with arthrogryposis.”
Dr. van der Linden, a pediatric neurologist with the Association for Assistance of Disabled Children, Recife, Brazil, and her associates retrospectively evaluated the medical records of seven patients with arthrogryposis associated with congenital infection believed to be caused by Zika virus, during the Brazilian microcephaly epidemic (BMJ. 2016;354:i3899). The main outcomes of interest were clinical, radiologic, and electromyographic findings, and likely collaboration between clinical and primary neurological abnormalities.
The researchers reported that brain images of all seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%). In addition, hip x-rays showed bilateral dislocation in all seven children and subluxation of the knee associated with genu valgus in three (43%). No evidence of abnormalities was seen on high-definition ultrasonography of the joints, but moderate signs of remodeling of the motor units and a reduced recruitment pattern were found on needle electromyography. Results from brain computed tomography conducted in all seven patients and magnetic resonance imaging conducted in five revealed malformations of cortical development, calcifications predominantly in the cortex and subcortical white matter, reduction in brain volume, ventriculomegaly, and hypoplasia of the brainstem and cerebellum. Spinal MRI conducted in four children showed apparent thinning of the cord and reduced ventral roots.
“Further research is needed with a larger number of cases to study the neurological abnormalities behind arthrogryposis, including histopathology of autopsy samples or tissues from stillborn babies,” the researchers concluded. “As we do not know the potential implications of congenital Zika virus infection as it evolves, children must receive orthopedic follow-up, even those with a standard first orthopedic evaluation, because they could develop musculoskeletal deformities secondary to neurological impairment, central or peripheral, or both, as these occur in patients with cerebral palsy and other chronic encephalopathies.”
The researchers reported having no financial disclosures.
Congenital Zika syndrome should be added to the differential diagnosis of congenital infections and arthrogryposis (joint contractures), results from a case series study in Brazil suggest.
“Brain impairment in the presence of microcephaly is the main characteristic of a congenital Zika virus syndrome,” researchers led by Vanessa van der Linden, MD, wrote in a study published online Aug. 9 in the BMJ. “However, little is still known about this condition and its clinical spectrum, which also concerns newborns with a normal head circumference. Two studies have described the association between arthrogryposis and microcephaly in newborns presumed to have congenital Zika virus infection [See Morb Mortal Wkly. Rep. 2016;65:59-62 and Ultrasound Obstet Gynecol. 2016;47:6-7].” The authors went on to note that while arthrogryposis might be considered more of a sign than a specific disease, “it might be associated with several disorders. However, there are no reports in the literature about other congenital infections in humans associated with arthrogryposis.”
Dr. van der Linden, a pediatric neurologist with the Association for Assistance of Disabled Children, Recife, Brazil, and her associates retrospectively evaluated the medical records of seven patients with arthrogryposis associated with congenital infection believed to be caused by Zika virus, during the Brazilian microcephaly epidemic (BMJ. 2016;354:i3899). The main outcomes of interest were clinical, radiologic, and electromyographic findings, and likely collaboration between clinical and primary neurological abnormalities.
The researchers reported that brain images of all seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%). In addition, hip x-rays showed bilateral dislocation in all seven children and subluxation of the knee associated with genu valgus in three (43%). No evidence of abnormalities was seen on high-definition ultrasonography of the joints, but moderate signs of remodeling of the motor units and a reduced recruitment pattern were found on needle electromyography. Results from brain computed tomography conducted in all seven patients and magnetic resonance imaging conducted in five revealed malformations of cortical development, calcifications predominantly in the cortex and subcortical white matter, reduction in brain volume, ventriculomegaly, and hypoplasia of the brainstem and cerebellum. Spinal MRI conducted in four children showed apparent thinning of the cord and reduced ventral roots.
“Further research is needed with a larger number of cases to study the neurological abnormalities behind arthrogryposis, including histopathology of autopsy samples or tissues from stillborn babies,” the researchers concluded. “As we do not know the potential implications of congenital Zika virus infection as it evolves, children must receive orthopedic follow-up, even those with a standard first orthopedic evaluation, because they could develop musculoskeletal deformities secondary to neurological impairment, central or peripheral, or both, as these occur in patients with cerebral palsy and other chronic encephalopathies.”
The researchers reported having no financial disclosures.
FROM BMJ
Key clinical point: The differential diagnosis of congenital infections and arthrogryposis should include congenital Zika syndrome.
Major finding: All seven children revealed characteristics of congenital infection and arthrogryposis. Two children (29%) tested positive for IgM antibody for Zika virus in the cerebrospinal fluid, while arthrogryposis was present in the arms and legs of six children (86%) and in the legs of one child (14%).
Data source: A retrospective case series study of seven children with arthrogryposis associated with congenital infection believed to be caused by Zika virus.
Disclosures: The researchers reported having no financial disclosures.
Two-dose HPV vaccines at younger age are noninferior to standard three-dose vaccine
“The licensed vaccines HPV-16/18 AS04–adjuvanted (Cervarix; GSK Vaccines) and HPV-6/11/16/18 (Gardasil; Merck) were first approved as regimen including three doses (3D) with administration over a 6-month period,” reported Thanyawee Puthanakit, MD, of Chulalongkorn University in Bangkok, and her associates. “Reduced dose schedules could make vaccination easier to implement and more affordable, creating the potential for higher vaccination coverage and improved cervical cancer protection (J Infect Dis. 2016;214:525-36).”

The investigators enrolled girls aged 9-25 years starting in June 2011, from 33 clinical sites in Canada, Germany, Italy, Taiwan, and Thailand. The study lasted through January 2013, during which time 1,447 girls were enrolled and 1,428 were randomized into one of three cohorts: one receiving the two-dose, 6-month regimen; one receiving the two-dose, 12-month regime; and one receiving the three-dose, 6-month regimen. In the former two cohorts, girls aged 9-14 years would receive their doses at 0 months and either 6 or 12 months, depending on the cohort. In the three-dose regimen, girls aged 15-25 years received doses at 0, 1, and 6 months. At enrollment, 550 girls were randomized into the two-dose, 6-month regimen; 415 girls into the two-dose, 12-month regimen; and 482 girls into the three-dose, 6-month regimen. Follow-up occurred at 1 month after they received the final dose for all three cohorts.
Ultimately, 534 girls in the two-dose, 6-month cohort; 394 in the two-dose, 12-month cohort; and 427 in the three-dose, 6-month cohort completed the study through the 1-month follow-up. Serologic testing indicated that girls in both the two-dose cohorts were not immunologically worse off than those who were in the three-dose cohort, with seroconversion differences of 0.00 when comparing HPV-16 and HPV-18 antibodies between any two of the three regimens. Furthermore, geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% confidence interval, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for the 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI, 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs.three-dose, indicating little statistically significant difference.
“The flexibility around the timing of the second dose, giving the option of annual vaccination over 2 consecutive years, is an added benefit [because] reduced dose schedules of HPV vaccines may facilitate vaccination implementation and reduce cost, allowing for higher vaccination coverage and potentially more girls being protected from cervical cancer,” the investigators noted.
The study was supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.
“The licensed vaccines HPV-16/18 AS04–adjuvanted (Cervarix; GSK Vaccines) and HPV-6/11/16/18 (Gardasil; Merck) were first approved as regimen including three doses (3D) with administration over a 6-month period,” reported Thanyawee Puthanakit, MD, of Chulalongkorn University in Bangkok, and her associates. “Reduced dose schedules could make vaccination easier to implement and more affordable, creating the potential for higher vaccination coverage and improved cervical cancer protection (J Infect Dis. 2016;214:525-36).”
The investigators enrolled girls aged 9-25 years starting in June 2011, from 33 clinical sites in Canada, Germany, Italy, Taiwan, and Thailand. The study lasted through January 2013, during which time 1,447 girls were enrolled and 1,428 were randomized into one of three cohorts: one receiving the two-dose, 6-month regimen; one receiving the two-dose, 12-month regime; and one receiving the three-dose, 6-month regimen. In the former two cohorts, girls aged 9-14 years would receive their doses at 0 months and either 6 or 12 months, depending on the cohort. In the three-dose regimen, girls aged 15-25 years received doses at 0, 1, and 6 months. At enrollment, 550 girls were randomized into the two-dose, 6-month regimen; 415 girls into the two-dose, 12-month regimen; and 482 girls into the three-dose, 6-month regimen. Follow-up occurred at 1 month after they received the final dose for all three cohorts.
Ultimately, 534 girls in the two-dose, 6-month cohort; 394 in the two-dose, 12-month cohort; and 427 in the three-dose, 6-month cohort completed the study through the 1-month follow-up. Serologic testing indicated that girls in both the two-dose cohorts were not immunologically worse off than those who were in the three-dose cohort, with seroconversion differences of 0.00 when comparing HPV-16 and HPV-18 antibodies between any two of the three regimens. Furthermore, geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% confidence interval, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for the 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI, 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs.three-dose, indicating little statistically significant difference.
“The flexibility around the timing of the second dose, giving the option of annual vaccination over 2 consecutive years, is an added benefit [because] reduced dose schedules of HPV vaccines may facilitate vaccination implementation and reduce cost, allowing for higher vaccination coverage and potentially more girls being protected from cervical cancer,” the investigators noted.
The study was supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.
“The licensed vaccines HPV-16/18 AS04–adjuvanted (Cervarix; GSK Vaccines) and HPV-6/11/16/18 (Gardasil; Merck) were first approved as regimen including three doses (3D) with administration over a 6-month period,” reported Thanyawee Puthanakit, MD, of Chulalongkorn University in Bangkok, and her associates. “Reduced dose schedules could make vaccination easier to implement and more affordable, creating the potential for higher vaccination coverage and improved cervical cancer protection (J Infect Dis. 2016;214:525-36).”
The investigators enrolled girls aged 9-25 years starting in June 2011, from 33 clinical sites in Canada, Germany, Italy, Taiwan, and Thailand. The study lasted through January 2013, during which time 1,447 girls were enrolled and 1,428 were randomized into one of three cohorts: one receiving the two-dose, 6-month regimen; one receiving the two-dose, 12-month regime; and one receiving the three-dose, 6-month regimen. In the former two cohorts, girls aged 9-14 years would receive their doses at 0 months and either 6 or 12 months, depending on the cohort. In the three-dose regimen, girls aged 15-25 years received doses at 0, 1, and 6 months. At enrollment, 550 girls were randomized into the two-dose, 6-month regimen; 415 girls into the two-dose, 12-month regimen; and 482 girls into the three-dose, 6-month regimen. Follow-up occurred at 1 month after they received the final dose for all three cohorts.
Ultimately, 534 girls in the two-dose, 6-month cohort; 394 in the two-dose, 12-month cohort; and 427 in the three-dose, 6-month cohort completed the study through the 1-month follow-up. Serologic testing indicated that girls in both the two-dose cohorts were not immunologically worse off than those who were in the three-dose cohort, with seroconversion differences of 0.00 when comparing HPV-16 and HPV-18 antibodies between any two of the three regimens. Furthermore, geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% confidence interval, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for the 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI, 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs.three-dose, indicating little statistically significant difference.
“The flexibility around the timing of the second dose, giving the option of annual vaccination over 2 consecutive years, is an added benefit [because] reduced dose schedules of HPV vaccines may facilitate vaccination implementation and reduce cost, allowing for higher vaccination coverage and potentially more girls being protected from cervical cancer,” the investigators noted.
The study was supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.
FROM THE JOURNAL OF INFECTIOUS DISEASES
Key clinical point: Girls receiving 2-dose HPV-16/18 AS04-adjuvanted vaccine at age 9-14 years over a 6- or 12-month timespan appear to be equally protected against HPV than those receiving 3-dose HPV vaccine schedules at age 15-25 years.
Major finding: Geometric mean antibody titer ratios for HPV-16 and HPV-18 were 1.09 (95% CI, 0.97-1.22) and 0.85 (95% CI, 0.76-0.95) for 6-month two-dose regimen vs. three-dose, and 0.89 (95% CI 0.79-1.01) and 0.75 (95% CI, 0.67-0.85) for 12-month two-dose regimen vs. three-dose.
Data source: A randomized, open trial of 1,447 vaccinated girls aged 9-25 years.
Disclosures: Study supported by GlaxoSmithKline Biologicals SA. Dr. Puthanakit received a grant from GSK through her institution. Some of her many coauthors disclosed relationships with GSK and/or other pharmaceutical companies.
