User login
Mortality rates higher among influenza B patients than influenza A patients
Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A, investigators found.
Among those with influenza B, patients aged 10-16 years were most likely to require ICU admission, suggesting this subpopulation may be a target for immunization programs.

The percentage of clinical cases attributed to influenza B range from less than 1% to 44%, according to data published by the Centers for Disease Control and Prevention. However, influenza B is considered less virulent and less capable of causing pandemics and has therefore been less studied and outcomes of its disease less characterized, Dat Tran, MD, MSc, of the Hospital for Sick Children in Canada and his associates reported (Pediatrics. 2016 August. doi: 10.1542/peds.2015-4643).
The purpose of this study was to further understand the prevalence and severity of influenza B cases in comparison with influenza A and to identify pediatric subpopulations most at risk for contracting influenza B.
Children aged 16 years or younger hospitalized from laboratory-confirmed influenza A or B from September 2004 to June 2013 (excluding the pandemic year 2009-2010) were identified through active surveillance of admissions at the 12 pediatric referral centers of the Canadian Immunization Monitoring Program Active (IMPACT), a national surveillance initiative. Information regarding demographics, health status, vaccination status, presenting signs and symptoms, illness severity and mortality, treatment regimens, and ICU admission were collected and analyzed.
Of 4,155 influenza-related admissions during this time period, influenza B accounted for 1,510 (36.3%) cases and influenza A accounted for 2,645 (63.7%) cases.
Children admitted with influenza B tended to be older with a median age 3.9 years (interquartile range, 1.4-7.2), compared with a median of 2 years (IQR, 0.6-4.8 years) for children admitted with influenza A.
Children admitted with influenza B, compared with influenza A, had higher odds of having a vaccine-indicated condition (odds ratio, 1.30; 95% confidence interval, 1.14-1.47) and lower odds of having no underlying medical condition (OR, 0.80; 95% CI, 0.71-0.91), Dr. Tran and his associates reported.
“Compared with influenza A cases, children admitted with influenza B had greater adjusted odds of presenting with headache, abdominal pain, and myalgia, ranging from 1.38 for abdominal pain to 3.19 for myalgia,” they added. “There were no significant differences in antiviral or antibiotic prescription or use between influenza A and B cases.”
There was no significant difference in the proportion of influenza A or B patients admitted to the ICU (12.7% vs. 12.6%). Rather, multivariate modeling identified age and presence of an underlying condition as independent predictors of ICU admission.
Finally, influenza-attributable mortality was significantly greater in children with influenza B (adjusted OR, 2.65; 95% CI, 1.18-5.94). Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. All-cause mortality followed a similar trend.
“Among hospitalized children, influenza A and B infections resulted in similar morbidity while mortality was greater for influenza B disease. Among healthy children hospitalized with influenza B, those aged 10-16 years were most likely to require ICU admission,” the investigators summarized.
“These children should be considered at high risk for complicated influenza B infection and be specifically targeted by immunization programs to receive influenza vaccination, and in particular, a [quadrivalent influenza vaccine],” they recommended.
This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.
Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A, investigators found.
Among those with influenza B, patients aged 10-16 years were most likely to require ICU admission, suggesting this subpopulation may be a target for immunization programs.
The percentage of clinical cases attributed to influenza B range from less than 1% to 44%, according to data published by the Centers for Disease Control and Prevention. However, influenza B is considered less virulent and less capable of causing pandemics and has therefore been less studied and outcomes of its disease less characterized, Dat Tran, MD, MSc, of the Hospital for Sick Children in Canada and his associates reported (Pediatrics. 2016 August. doi: 10.1542/peds.2015-4643).
The purpose of this study was to further understand the prevalence and severity of influenza B cases in comparison with influenza A and to identify pediatric subpopulations most at risk for contracting influenza B.
Children aged 16 years or younger hospitalized from laboratory-confirmed influenza A or B from September 2004 to June 2013 (excluding the pandemic year 2009-2010) were identified through active surveillance of admissions at the 12 pediatric referral centers of the Canadian Immunization Monitoring Program Active (IMPACT), a national surveillance initiative. Information regarding demographics, health status, vaccination status, presenting signs and symptoms, illness severity and mortality, treatment regimens, and ICU admission were collected and analyzed.
Of 4,155 influenza-related admissions during this time period, influenza B accounted for 1,510 (36.3%) cases and influenza A accounted for 2,645 (63.7%) cases.
Children admitted with influenza B tended to be older with a median age 3.9 years (interquartile range, 1.4-7.2), compared with a median of 2 years (IQR, 0.6-4.8 years) for children admitted with influenza A.
Children admitted with influenza B, compared with influenza A, had higher odds of having a vaccine-indicated condition (odds ratio, 1.30; 95% confidence interval, 1.14-1.47) and lower odds of having no underlying medical condition (OR, 0.80; 95% CI, 0.71-0.91), Dr. Tran and his associates reported.
“Compared with influenza A cases, children admitted with influenza B had greater adjusted odds of presenting with headache, abdominal pain, and myalgia, ranging from 1.38 for abdominal pain to 3.19 for myalgia,” they added. “There were no significant differences in antiviral or antibiotic prescription or use between influenza A and B cases.”
There was no significant difference in the proportion of influenza A or B patients admitted to the ICU (12.7% vs. 12.6%). Rather, multivariate modeling identified age and presence of an underlying condition as independent predictors of ICU admission.
Finally, influenza-attributable mortality was significantly greater in children with influenza B (adjusted OR, 2.65; 95% CI, 1.18-5.94). Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. All-cause mortality followed a similar trend.
“Among hospitalized children, influenza A and B infections resulted in similar morbidity while mortality was greater for influenza B disease. Among healthy children hospitalized with influenza B, those aged 10-16 years were most likely to require ICU admission,” the investigators summarized.
“These children should be considered at high risk for complicated influenza B infection and be specifically targeted by immunization programs to receive influenza vaccination, and in particular, a [quadrivalent influenza vaccine],” they recommended.
This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.
Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A, investigators found.
Among those with influenza B, patients aged 10-16 years were most likely to require ICU admission, suggesting this subpopulation may be a target for immunization programs.
The percentage of clinical cases attributed to influenza B range from less than 1% to 44%, according to data published by the Centers for Disease Control and Prevention. However, influenza B is considered less virulent and less capable of causing pandemics and has therefore been less studied and outcomes of its disease less characterized, Dat Tran, MD, MSc, of the Hospital for Sick Children in Canada and his associates reported (Pediatrics. 2016 August. doi: 10.1542/peds.2015-4643).
The purpose of this study was to further understand the prevalence and severity of influenza B cases in comparison with influenza A and to identify pediatric subpopulations most at risk for contracting influenza B.
Children aged 16 years or younger hospitalized from laboratory-confirmed influenza A or B from September 2004 to June 2013 (excluding the pandemic year 2009-2010) were identified through active surveillance of admissions at the 12 pediatric referral centers of the Canadian Immunization Monitoring Program Active (IMPACT), a national surveillance initiative. Information regarding demographics, health status, vaccination status, presenting signs and symptoms, illness severity and mortality, treatment regimens, and ICU admission were collected and analyzed.
Of 4,155 influenza-related admissions during this time period, influenza B accounted for 1,510 (36.3%) cases and influenza A accounted for 2,645 (63.7%) cases.
Children admitted with influenza B tended to be older with a median age 3.9 years (interquartile range, 1.4-7.2), compared with a median of 2 years (IQR, 0.6-4.8 years) for children admitted with influenza A.
Children admitted with influenza B, compared with influenza A, had higher odds of having a vaccine-indicated condition (odds ratio, 1.30; 95% confidence interval, 1.14-1.47) and lower odds of having no underlying medical condition (OR, 0.80; 95% CI, 0.71-0.91), Dr. Tran and his associates reported.
“Compared with influenza A cases, children admitted with influenza B had greater adjusted odds of presenting with headache, abdominal pain, and myalgia, ranging from 1.38 for abdominal pain to 3.19 for myalgia,” they added. “There were no significant differences in antiviral or antibiotic prescription or use between influenza A and B cases.”
There was no significant difference in the proportion of influenza A or B patients admitted to the ICU (12.7% vs. 12.6%). Rather, multivariate modeling identified age and presence of an underlying condition as independent predictors of ICU admission.
Finally, influenza-attributable mortality was significantly greater in children with influenza B (adjusted OR, 2.65; 95% CI, 1.18-5.94). Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. All-cause mortality followed a similar trend.
“Among hospitalized children, influenza A and B infections resulted in similar morbidity while mortality was greater for influenza B disease. Among healthy children hospitalized with influenza B, those aged 10-16 years were most likely to require ICU admission,” the investigators summarized.
“These children should be considered at high risk for complicated influenza B infection and be specifically targeted by immunization programs to receive influenza vaccination, and in particular, a [quadrivalent influenza vaccine],” they recommended.
This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.
FROM PEDIATRICS
Key clinical point: Influenza-attributable mortality was significantly greater in children with influenza B, compared with influenza A.
Major finding: Influenza-attributable mortality occurred in 16 (1.1%) children with influenza B and only 10 (0.4%) children with influenza A. Influenza-attributable mortality was significantly greater in children with influenza B (adjusted odds ratio, 2.65, 95% confidence interval, 1.18-5.94).
Data source: An observational study of 4,155 children admitted to the hospital with influenza A or B during nonpandemic years between September 2004 and June 2013.
Disclosures: This study was funded by GlaxoSmithKline Biologicals SA. The Canadian Immunization Monitoring Program Active is funded by the Public Health Agency of Canada. The investigators reported having no relevant disclosures.

Routine screening unwarranted in siblings of food-allergic children
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
Siblings of children with food allergy should not be screened routinely for such allergies before food introduction, results of a large cohort study suggest.
In a study of 478 food-allergic children and 642 of their siblings, 53% of the siblings were sensitized without clinical reactivity and only 13.6% were found to have a clinically reactive food allergy, wrote Ruchi S. Gupta, MD, of Northwestern University, Chicago, and her associates.

The investigators noted that their findings support current guidelines from the National Institute of Allergy and Infectious Diseases to not screen siblings based on another sibling having a food allergy.
“Given the lack of a dramatically increased risk of food allergy in siblings, compared with that of the general population, as well as the high rate of what are falsely positive diagnostic test results among siblings of a food allergic child, [these siblings] should not have routine screening for food allergy before food introduction,” the investigators concluded. “Such siblings are likely to be mislabeled as allergic when they are actually tolerant to the food, which may lead to an increased risk of developing allergy via avoidance,” and both quality of life and nutrition may be adversely impacted.
Dr. Gupta has received research support from Mylan, Food Allergy Research and Education, and United Health Care.
Read the full study here (http://dx.doi.org/10.1016/j.jaip.2016.04.009)
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
Siblings of children with food allergy should not be screened routinely for such allergies before food introduction, results of a large cohort study suggest.
In a study of 478 food-allergic children and 642 of their siblings, 53% of the siblings were sensitized without clinical reactivity and only 13.6% were found to have a clinically reactive food allergy, wrote Ruchi S. Gupta, MD, of Northwestern University, Chicago, and her associates.
The investigators noted that their findings support current guidelines from the National Institute of Allergy and Infectious Diseases to not screen siblings based on another sibling having a food allergy.
“Given the lack of a dramatically increased risk of food allergy in siblings, compared with that of the general population, as well as the high rate of what are falsely positive diagnostic test results among siblings of a food allergic child, [these siblings] should not have routine screening for food allergy before food introduction,” the investigators concluded. “Such siblings are likely to be mislabeled as allergic when they are actually tolerant to the food, which may lead to an increased risk of developing allergy via avoidance,” and both quality of life and nutrition may be adversely impacted.
Dr. Gupta has received research support from Mylan, Food Allergy Research and Education, and United Health Care.
Read the full study here (http://dx.doi.org/10.1016/j.jaip.2016.04.009)
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
Siblings of children with food allergy should not be screened routinely for such allergies before food introduction, results of a large cohort study suggest.
In a study of 478 food-allergic children and 642 of their siblings, 53% of the siblings were sensitized without clinical reactivity and only 13.6% were found to have a clinically reactive food allergy, wrote Ruchi S. Gupta, MD, of Northwestern University, Chicago, and her associates.
The investigators noted that their findings support current guidelines from the National Institute of Allergy and Infectious Diseases to not screen siblings based on another sibling having a food allergy.
“Given the lack of a dramatically increased risk of food allergy in siblings, compared with that of the general population, as well as the high rate of what are falsely positive diagnostic test results among siblings of a food allergic child, [these siblings] should not have routine screening for food allergy before food introduction,” the investigators concluded. “Such siblings are likely to be mislabeled as allergic when they are actually tolerant to the food, which may lead to an increased risk of developing allergy via avoidance,” and both quality of life and nutrition may be adversely impacted.
Dr. Gupta has received research support from Mylan, Food Allergy Research and Education, and United Health Care.
Read the full study here (http://dx.doi.org/10.1016/j.jaip.2016.04.009)

Pulmonary complications affect cancer survivors long-term

Photo by Bill Branson
A new study suggests that survivors of childhood cancer may be plagued by pulmonary complications related to treatment well into their adult lives.
The research indicated that the cumulative incidence of pulmonary complications continues to increase up to 25 years from a patient’s initial cancer diagnosis.
In addition, platinum-based chemotherapy and higher doses of radiation were linked to an increased risk of death from pulmonary causes.
Andrew C. Dietz, MD, of Children’s Hospital Los Angeles in California, and his colleagues reported these findings in Cancer.
The researchers analyzed data from 20,690 five-year cancer survivors who participated in the Childhood Cancer Survivor Study to determine the incidence of death from pulmonary causes.
The team also assessed the incidence of various pulmonary complications in 14,316 of those cancer survivors (who completed a baseline survey and/or 1 of 2 follow-up surveys years later), comparing the results to those seen in a control group of 4027 cancer survivor siblings.
About 34% of the 14,316 cancer survivors had been diagnosed with acute leukemia, and about 21% were diagnosed with Hodgkin or non-Hodgkin lymphoma.
The cancer survivors’ median age at diagnosis was 7 (range, 0-21), and their median age at evaluation was 32 (range, 6-59). The median time from diagnosis was 25 years (range, 5-39).
Compared with controls, cancer survivors were more likely to be male, black, and Hispanic. Cancer survivors were slightly younger and more likely to report a history of congestive heart failure, but they were less likely to be overweight/obese or have ever smoked at the time of the baseline survey.
Results
By age 45, the cumulative incidence of any pulmonary condition was 29.6% among cancer survivors and 26.5% among controls (P=0.001).
The cancer survivors were more likely than controls to report chronic cough (rate ratio [RR]=1.6), the need for extra oxygen (RR=1.8), lung fibrosis (RR=3.5), and recurrent pneumonia (RR=2.0).
Among cancer survivors, the risk of asthma was significantly associated with exposure to asparaginase. Chronic cough was significantly associated with chest wall or lung surgery, anthracyclines, hydroxyurea, and lung radiation doses ≥15 Gy.
Emphysema was significantly associated with lomustine. The need for extra oxygen was significantly associated with hematopoietic stem cell transplant, chest wall or lung surgery, and lung radiation doses ≥10 Gy.
Lung fibrosis was significantly associated with chest wall or lung surgery, asparaginase, platinum-based chemotherapy, and lung radiation doses ≥10 Gy. Recurrent pneumonia was significantly associated with lung radiation doses ≥15 Gy.
The standardized mortality ratio for death from pulmonary causes among all eligible cancer survivors (n=20,690) was 5.9. Pulmonary death was significantly associated with exposure to platinum-based agents and lung radiation doses ≥10 Gy.
“This study adds to our understanding of specific, long-term risks to pulmonary health for survivors of childhood cancer and will help refine guidelines for appropriate screening, health surveillance, and counseling,” said study author Daniel A. Mulrooney, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
He added that this knowledge could potentially contribute to the design and testing of better, targeted interventions to decrease adverse pulmonary events in this population. ![]()
Photo by Bill Branson
A new study suggests that survivors of childhood cancer may be plagued by pulmonary complications related to treatment well into their adult lives.
The research indicated that the cumulative incidence of pulmonary complications continues to increase up to 25 years from a patient’s initial cancer diagnosis.
In addition, platinum-based chemotherapy and higher doses of radiation were linked to an increased risk of death from pulmonary causes.
Andrew C. Dietz, MD, of Children’s Hospital Los Angeles in California, and his colleagues reported these findings in Cancer.
The researchers analyzed data from 20,690 five-year cancer survivors who participated in the Childhood Cancer Survivor Study to determine the incidence of death from pulmonary causes.
The team also assessed the incidence of various pulmonary complications in 14,316 of those cancer survivors (who completed a baseline survey and/or 1 of 2 follow-up surveys years later), comparing the results to those seen in a control group of 4027 cancer survivor siblings.
About 34% of the 14,316 cancer survivors had been diagnosed with acute leukemia, and about 21% were diagnosed with Hodgkin or non-Hodgkin lymphoma.
The cancer survivors’ median age at diagnosis was 7 (range, 0-21), and their median age at evaluation was 32 (range, 6-59). The median time from diagnosis was 25 years (range, 5-39).
Compared with controls, cancer survivors were more likely to be male, black, and Hispanic. Cancer survivors were slightly younger and more likely to report a history of congestive heart failure, but they were less likely to be overweight/obese or have ever smoked at the time of the baseline survey.
Results
By age 45, the cumulative incidence of any pulmonary condition was 29.6% among cancer survivors and 26.5% among controls (P=0.001).
The cancer survivors were more likely than controls to report chronic cough (rate ratio [RR]=1.6), the need for extra oxygen (RR=1.8), lung fibrosis (RR=3.5), and recurrent pneumonia (RR=2.0).
Among cancer survivors, the risk of asthma was significantly associated with exposure to asparaginase. Chronic cough was significantly associated with chest wall or lung surgery, anthracyclines, hydroxyurea, and lung radiation doses ≥15 Gy.
Emphysema was significantly associated with lomustine. The need for extra oxygen was significantly associated with hematopoietic stem cell transplant, chest wall or lung surgery, and lung radiation doses ≥10 Gy.
Lung fibrosis was significantly associated with chest wall or lung surgery, asparaginase, platinum-based chemotherapy, and lung radiation doses ≥10 Gy. Recurrent pneumonia was significantly associated with lung radiation doses ≥15 Gy.
The standardized mortality ratio for death from pulmonary causes among all eligible cancer survivors (n=20,690) was 5.9. Pulmonary death was significantly associated with exposure to platinum-based agents and lung radiation doses ≥10 Gy.
“This study adds to our understanding of specific, long-term risks to pulmonary health for survivors of childhood cancer and will help refine guidelines for appropriate screening, health surveillance, and counseling,” said study author Daniel A. Mulrooney, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
He added that this knowledge could potentially contribute to the design and testing of better, targeted interventions to decrease adverse pulmonary events in this population. ![]()
Photo by Bill Branson
A new study suggests that survivors of childhood cancer may be plagued by pulmonary complications related to treatment well into their adult lives.
The research indicated that the cumulative incidence of pulmonary complications continues to increase up to 25 years from a patient’s initial cancer diagnosis.
In addition, platinum-based chemotherapy and higher doses of radiation were linked to an increased risk of death from pulmonary causes.
Andrew C. Dietz, MD, of Children’s Hospital Los Angeles in California, and his colleagues reported these findings in Cancer.
The researchers analyzed data from 20,690 five-year cancer survivors who participated in the Childhood Cancer Survivor Study to determine the incidence of death from pulmonary causes.
The team also assessed the incidence of various pulmonary complications in 14,316 of those cancer survivors (who completed a baseline survey and/or 1 of 2 follow-up surveys years later), comparing the results to those seen in a control group of 4027 cancer survivor siblings.
About 34% of the 14,316 cancer survivors had been diagnosed with acute leukemia, and about 21% were diagnosed with Hodgkin or non-Hodgkin lymphoma.
The cancer survivors’ median age at diagnosis was 7 (range, 0-21), and their median age at evaluation was 32 (range, 6-59). The median time from diagnosis was 25 years (range, 5-39).
Compared with controls, cancer survivors were more likely to be male, black, and Hispanic. Cancer survivors were slightly younger and more likely to report a history of congestive heart failure, but they were less likely to be overweight/obese or have ever smoked at the time of the baseline survey.
Results
By age 45, the cumulative incidence of any pulmonary condition was 29.6% among cancer survivors and 26.5% among controls (P=0.001).
The cancer survivors were more likely than controls to report chronic cough (rate ratio [RR]=1.6), the need for extra oxygen (RR=1.8), lung fibrosis (RR=3.5), and recurrent pneumonia (RR=2.0).
Among cancer survivors, the risk of asthma was significantly associated with exposure to asparaginase. Chronic cough was significantly associated with chest wall or lung surgery, anthracyclines, hydroxyurea, and lung radiation doses ≥15 Gy.
Emphysema was significantly associated with lomustine. The need for extra oxygen was significantly associated with hematopoietic stem cell transplant, chest wall or lung surgery, and lung radiation doses ≥10 Gy.
Lung fibrosis was significantly associated with chest wall or lung surgery, asparaginase, platinum-based chemotherapy, and lung radiation doses ≥10 Gy. Recurrent pneumonia was significantly associated with lung radiation doses ≥15 Gy.
The standardized mortality ratio for death from pulmonary causes among all eligible cancer survivors (n=20,690) was 5.9. Pulmonary death was significantly associated with exposure to platinum-based agents and lung radiation doses ≥10 Gy.
“This study adds to our understanding of specific, long-term risks to pulmonary health for survivors of childhood cancer and will help refine guidelines for appropriate screening, health surveillance, and counseling,” said study author Daniel A. Mulrooney, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
He added that this knowledge could potentially contribute to the design and testing of better, targeted interventions to decrease adverse pulmonary events in this population. ![]()
LAIV no better than IIV for influenza protection in children
Live attenuated influenza vaccine (LAIV) was no more effective than inactivated influenza vaccine (IIV) in small, compact, rural communities, according to Mark Loeb, MD, and his associates.
For the study, vaccinations were given to children aged 36 months to 15 years living in Hutterite colonies in Canada. Hutterite colonies are isolated, their residents live communally, and influenza is prevalent, making them suited for this cluster randomized trial.
Of the 1,186 children included in the study, mean coverage was 76.7% in the LAIV group, compared with 72.4% in the IIV group. Incidence of influenza was 5.3% in the LAIV group and 5.2% in the IIV group. Compared to IIV, the hazard ratio for LAIV for influenza A or B was 1.03.
Children vaccinated with LAIV were at a higher risk for influenza A (hazard ratio, 1.62), but were at lower risk for influenza B (HR, 0.66). Influenza attack rates were similar in children younger and older than 6 years old. Adverse reactions were more likely in the IIV group than in the LAIV group, but no serious adverse events were reported.
“Although influenza transmission networks in Hutterite communities may differ from that in other communities, there are no data to confirm this. In fact, there may be more variability in social networks between urban and rural communities – or even among various urban communities – than between Hutterite and other (rural) communities. Even if variability exists, if a clear benefit of LAIV over IIV in reducing influenza-associated illness cannot be detected in this setting it is unlikely to be seen in other communities,” the investigators noted.
Find the full study in Annals of Internal Medicine (doi: 10.7326/M16-0513).
Live attenuated influenza vaccine (LAIV) was no more effective than inactivated influenza vaccine (IIV) in small, compact, rural communities, according to Mark Loeb, MD, and his associates.
For the study, vaccinations were given to children aged 36 months to 15 years living in Hutterite colonies in Canada. Hutterite colonies are isolated, their residents live communally, and influenza is prevalent, making them suited for this cluster randomized trial.
Of the 1,186 children included in the study, mean coverage was 76.7% in the LAIV group, compared with 72.4% in the IIV group. Incidence of influenza was 5.3% in the LAIV group and 5.2% in the IIV group. Compared to IIV, the hazard ratio for LAIV for influenza A or B was 1.03.
Children vaccinated with LAIV were at a higher risk for influenza A (hazard ratio, 1.62), but were at lower risk for influenza B (HR, 0.66). Influenza attack rates were similar in children younger and older than 6 years old. Adverse reactions were more likely in the IIV group than in the LAIV group, but no serious adverse events were reported.
“Although influenza transmission networks in Hutterite communities may differ from that in other communities, there are no data to confirm this. In fact, there may be more variability in social networks between urban and rural communities – or even among various urban communities – than between Hutterite and other (rural) communities. Even if variability exists, if a clear benefit of LAIV over IIV in reducing influenza-associated illness cannot be detected in this setting it is unlikely to be seen in other communities,” the investigators noted.
Find the full study in Annals of Internal Medicine (doi: 10.7326/M16-0513).
Live attenuated influenza vaccine (LAIV) was no more effective than inactivated influenza vaccine (IIV) in small, compact, rural communities, according to Mark Loeb, MD, and his associates.
For the study, vaccinations were given to children aged 36 months to 15 years living in Hutterite colonies in Canada. Hutterite colonies are isolated, their residents live communally, and influenza is prevalent, making them suited for this cluster randomized trial.
Of the 1,186 children included in the study, mean coverage was 76.7% in the LAIV group, compared with 72.4% in the IIV group. Incidence of influenza was 5.3% in the LAIV group and 5.2% in the IIV group. Compared to IIV, the hazard ratio for LAIV for influenza A or B was 1.03.
Children vaccinated with LAIV were at a higher risk for influenza A (hazard ratio, 1.62), but were at lower risk for influenza B (HR, 0.66). Influenza attack rates were similar in children younger and older than 6 years old. Adverse reactions were more likely in the IIV group than in the LAIV group, but no serious adverse events were reported.
“Although influenza transmission networks in Hutterite communities may differ from that in other communities, there are no data to confirm this. In fact, there may be more variability in social networks between urban and rural communities – or even among various urban communities – than between Hutterite and other (rural) communities. Even if variability exists, if a clear benefit of LAIV over IIV in reducing influenza-associated illness cannot be detected in this setting it is unlikely to be seen in other communities,” the investigators noted.
Find the full study in Annals of Internal Medicine (doi: 10.7326/M16-0513).
FROM ANNALS OF INTERNAL MEDICINE
Topical timolol improves thinnest infantile hemangiomas
Topical timolol maleate acts as an effective alternate to oral propranolol for treatment of certain infantile hemangiomas (IHs), based on data from a retrospective study of 731 children. The findings were published online August 15 in Pediatrics.
“Superficial, relatively thin IHs, regardless of pretreatment surface or body site, are likely to respond reasonably well to several months of treatment with modest, but definite improvements in color and size,” wrote Katherine Püttgen, MD, of Johns Hopkins University in Baltimore, Md., and colleagues in the Hemangioma Investigator Group (Pediatrics 2016;138:e20160355 [doi: 10.1052/peds.2016-0355]).

Although topical timolol maleate (TTM) has been used off label to treat infantile hemangiomas since 2010, “there is very limited information regarding off-label safety and pharmacokinetic data when used on hemangioma-affected skin,” the researchers noted.
The researchers reviewed data from 731 children treated at nine pediatric centers in the United States. Patients were treated for at least 30 days; the average treatment duration was 9 months. Most of the children (41%) began treatment between ages 0 and 3 months, and 86% were treatment naïve.
About 85% of the children received TTM 0.5% GFS (gel-forming solution), with parents instructed to apply 1 drop twice daily to the IH; 15% were prescribed 4 drops or more of TTM daily. Treatment response was assessed based on visual analog scales for color (VAS-C) and for size, extent, and volume (VAS-SEV).
Overall, 70% of children showed improvement of at least 10% from baseline on the VAS-C after 1-3 months of treatment, and 92% showed meaningful improvement from baseline after 6-9 months of treatment. VAS-SEV scores improved at least 10% from baseline in 39% of children after 1-3 months and meaningful improvement in 76% after 6-9 months.
Independent predictors of treatment success included longer treatment time and thinner, superficial IH at baseline.
Adverse events were observed in 3% of the patients, approximately half of which were reports of scaly skin. No patients discontinued the study because of adverse events, and no cardiovascular adverse events were reported.
The results were limited by several factors including the lack of controls and the retrospective nature of the study, the researchers noted. In addition, they cautioned against the use of However, the findings suggest that “TTM can be recommended as an initial, and often sole, treatment modality for many relatively superficial His without aggressive growth or threat of functional impairment,” they said. However, the researchers cautioned against TTM in cases of ulcerated IHs because of the potential for increased drug absorption.
Dr. Püttgen and several coauthors disclosed serving as consultants to Pierre Fabre.
Topical timolol maleate acts as an effective alternate to oral propranolol for treatment of certain infantile hemangiomas (IHs), based on data from a retrospective study of 731 children. The findings were published online August 15 in Pediatrics.
“Superficial, relatively thin IHs, regardless of pretreatment surface or body site, are likely to respond reasonably well to several months of treatment with modest, but definite improvements in color and size,” wrote Katherine Püttgen, MD, of Johns Hopkins University in Baltimore, Md., and colleagues in the Hemangioma Investigator Group (Pediatrics 2016;138:e20160355 [doi: 10.1052/peds.2016-0355]).
Although topical timolol maleate (TTM) has been used off label to treat infantile hemangiomas since 2010, “there is very limited information regarding off-label safety and pharmacokinetic data when used on hemangioma-affected skin,” the researchers noted.
The researchers reviewed data from 731 children treated at nine pediatric centers in the United States. Patients were treated for at least 30 days; the average treatment duration was 9 months. Most of the children (41%) began treatment between ages 0 and 3 months, and 86% were treatment naïve.
About 85% of the children received TTM 0.5% GFS (gel-forming solution), with parents instructed to apply 1 drop twice daily to the IH; 15% were prescribed 4 drops or more of TTM daily. Treatment response was assessed based on visual analog scales for color (VAS-C) and for size, extent, and volume (VAS-SEV).
Overall, 70% of children showed improvement of at least 10% from baseline on the VAS-C after 1-3 months of treatment, and 92% showed meaningful improvement from baseline after 6-9 months of treatment. VAS-SEV scores improved at least 10% from baseline in 39% of children after 1-3 months and meaningful improvement in 76% after 6-9 months.
Independent predictors of treatment success included longer treatment time and thinner, superficial IH at baseline.
Adverse events were observed in 3% of the patients, approximately half of which were reports of scaly skin. No patients discontinued the study because of adverse events, and no cardiovascular adverse events were reported.
The results were limited by several factors including the lack of controls and the retrospective nature of the study, the researchers noted. In addition, they cautioned against the use of However, the findings suggest that “TTM can be recommended as an initial, and often sole, treatment modality for many relatively superficial His without aggressive growth or threat of functional impairment,” they said. However, the researchers cautioned against TTM in cases of ulcerated IHs because of the potential for increased drug absorption.
Dr. Püttgen and several coauthors disclosed serving as consultants to Pierre Fabre.
Topical timolol maleate acts as an effective alternate to oral propranolol for treatment of certain infantile hemangiomas (IHs), based on data from a retrospective study of 731 children. The findings were published online August 15 in Pediatrics.
“Superficial, relatively thin IHs, regardless of pretreatment surface or body site, are likely to respond reasonably well to several months of treatment with modest, but definite improvements in color and size,” wrote Katherine Püttgen, MD, of Johns Hopkins University in Baltimore, Md., and colleagues in the Hemangioma Investigator Group (Pediatrics 2016;138:e20160355 [doi: 10.1052/peds.2016-0355]).
Although topical timolol maleate (TTM) has been used off label to treat infantile hemangiomas since 2010, “there is very limited information regarding off-label safety and pharmacokinetic data when used on hemangioma-affected skin,” the researchers noted.
The researchers reviewed data from 731 children treated at nine pediatric centers in the United States. Patients were treated for at least 30 days; the average treatment duration was 9 months. Most of the children (41%) began treatment between ages 0 and 3 months, and 86% were treatment naïve.
About 85% of the children received TTM 0.5% GFS (gel-forming solution), with parents instructed to apply 1 drop twice daily to the IH; 15% were prescribed 4 drops or more of TTM daily. Treatment response was assessed based on visual analog scales for color (VAS-C) and for size, extent, and volume (VAS-SEV).
Overall, 70% of children showed improvement of at least 10% from baseline on the VAS-C after 1-3 months of treatment, and 92% showed meaningful improvement from baseline after 6-9 months of treatment. VAS-SEV scores improved at least 10% from baseline in 39% of children after 1-3 months and meaningful improvement in 76% after 6-9 months.
Independent predictors of treatment success included longer treatment time and thinner, superficial IH at baseline.
Adverse events were observed in 3% of the patients, approximately half of which were reports of scaly skin. No patients discontinued the study because of adverse events, and no cardiovascular adverse events were reported.
The results were limited by several factors including the lack of controls and the retrospective nature of the study, the researchers noted. In addition, they cautioned against the use of However, the findings suggest that “TTM can be recommended as an initial, and often sole, treatment modality for many relatively superficial His without aggressive growth or threat of functional impairment,” they said. However, the researchers cautioned against TTM in cases of ulcerated IHs because of the potential for increased drug absorption.
Dr. Püttgen and several coauthors disclosed serving as consultants to Pierre Fabre.
FROM PEDIATRICS
Key clinical point: Superficial, thin infantile hemangiomas responded positively to several months of treatment with topical timolol maleate.
Major finding: After 1-3 months of treatment, approximately 70% of patients showed at least 10% improvement from baseline on measures of color.
Data source: A retrospective, multicenter study of 731 children aged younger than 12 months.
Disclosures: Dr. Puttgen and several coauthors disclosed serving as consultants to Pierre Fabre.

Most infants still face SIDS risk factors
Most infants sleep in environments with risk factors for sudden infant death syndrome (SIDS), even when parents know that they are being recorded on cameras placed in their homes, according to a study published online Aug. 15 by Pediatrics.
Most infants slept with objects that were loose or not approved by the American Academy of Pediatrics: 91% at 1 month of age, 87% at 3 months, and 93% at 6 months. Items included loose bedding, bumper pads, pillows or cushions, and stuffed animals. Three 6-month-olds were allowed to sleep with pets, and two slept with loose cords or electrical wire, reported Erich K. Batra, MD, and his associates at the Penn State University, Hershey.

Smaller percentages of infants slept on nonapproved surfaces such as adult beds, car seats, or swings: 21% at 1 month of age, 10% at 3 months, and 12% at 6 months. Fourteen percent of infants were placed in a nonsupine position at 1 month, 18% at 3 months, and 33% at 6 months of age, Dr. Batra and his associates said (Pediatrics. 2016 Aug 15;138[3]:e20161533).
The results of the study “suggest that current public education and health care provider guidance related to safe infant sleep are not being carefully adhered to, even in a relatively educated, affluent patient population,” they wrote.
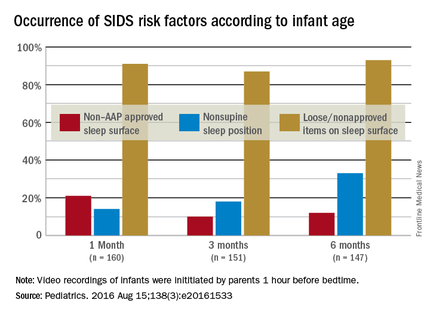
Almost 70% of mothers and fathers were college graduates, and the median family income was $60,000. Of the 167 infants enrolled in the study, 160 had videos available at 1 month of age, 151 had 3-month videos, and 147 had 6-month videos. At each of the three time points, “video recordings were initiated by parents 1 hour before the start of bedtime. Recordings continued throughout the night until the infant was fully awake in the morning,” Dr. Batra and his associates noted.
The investigators said that they had no conflicts to disclose, and the study was funded by the National Institutes of Health.
Most infants sleep in environments with risk factors for sudden infant death syndrome (SIDS), even when parents know that they are being recorded on cameras placed in their homes, according to a study published online Aug. 15 by Pediatrics.
Most infants slept with objects that were loose or not approved by the American Academy of Pediatrics: 91% at 1 month of age, 87% at 3 months, and 93% at 6 months. Items included loose bedding, bumper pads, pillows or cushions, and stuffed animals. Three 6-month-olds were allowed to sleep with pets, and two slept with loose cords or electrical wire, reported Erich K. Batra, MD, and his associates at the Penn State University, Hershey.
Smaller percentages of infants slept on nonapproved surfaces such as adult beds, car seats, or swings: 21% at 1 month of age, 10% at 3 months, and 12% at 6 months. Fourteen percent of infants were placed in a nonsupine position at 1 month, 18% at 3 months, and 33% at 6 months of age, Dr. Batra and his associates said (Pediatrics. 2016 Aug 15;138[3]:e20161533).
The results of the study “suggest that current public education and health care provider guidance related to safe infant sleep are not being carefully adhered to, even in a relatively educated, affluent patient population,” they wrote.
Almost 70% of mothers and fathers were college graduates, and the median family income was $60,000. Of the 167 infants enrolled in the study, 160 had videos available at 1 month of age, 151 had 3-month videos, and 147 had 6-month videos. At each of the three time points, “video recordings were initiated by parents 1 hour before the start of bedtime. Recordings continued throughout the night until the infant was fully awake in the morning,” Dr. Batra and his associates noted.
The investigators said that they had no conflicts to disclose, and the study was funded by the National Institutes of Health.
Most infants sleep in environments with risk factors for sudden infant death syndrome (SIDS), even when parents know that they are being recorded on cameras placed in their homes, according to a study published online Aug. 15 by Pediatrics.
Most infants slept with objects that were loose or not approved by the American Academy of Pediatrics: 91% at 1 month of age, 87% at 3 months, and 93% at 6 months. Items included loose bedding, bumper pads, pillows or cushions, and stuffed animals. Three 6-month-olds were allowed to sleep with pets, and two slept with loose cords or electrical wire, reported Erich K. Batra, MD, and his associates at the Penn State University, Hershey.
Smaller percentages of infants slept on nonapproved surfaces such as adult beds, car seats, or swings: 21% at 1 month of age, 10% at 3 months, and 12% at 6 months. Fourteen percent of infants were placed in a nonsupine position at 1 month, 18% at 3 months, and 33% at 6 months of age, Dr. Batra and his associates said (Pediatrics. 2016 Aug 15;138[3]:e20161533).
The results of the study “suggest that current public education and health care provider guidance related to safe infant sleep are not being carefully adhered to, even in a relatively educated, affluent patient population,” they wrote.
Almost 70% of mothers and fathers were college graduates, and the median family income was $60,000. Of the 167 infants enrolled in the study, 160 had videos available at 1 month of age, 151 had 3-month videos, and 147 had 6-month videos. At each of the three time points, “video recordings were initiated by parents 1 hour before the start of bedtime. Recordings continued throughout the night until the infant was fully awake in the morning,” Dr. Batra and his associates noted.
The investigators said that they had no conflicts to disclose, and the study was funded by the National Institutes of Health.
FROM PEDIATRICS

Hematuria a common finding in pediatric hemophilia
ORLANDO – Screening urinalysis should be a part of routine care for children and young adults with hemophilia, although the clinical significance of the finding is still unclear, investigators say.
Among 93 boys and young men with hemophilia A or B followed at a hemophilia treatment center, nearly half were found to have hematuria on routine screening, a possible indicator for future renal problems, said Kyle Davis, MD, and Amy Dunn, MD, from the division of hematology at Nationwide Children’s Hospital in Columbus, Ohio.
“It’s not routine for all centers to screen for hematuria, so there is likely a large number of patients that are underrecognized, who have hematuria but we don’t even know it,” Dr. Davis said in an interview at the World Federation of Hemophilia World Congress.
Hematuria is a recognized complication in patients with hemophilia A and B, second only to joint damage in frequency. In addition, adults with hemophilia have been shown to have a higher prevalence of renal disease than the general population, suggesting that hematuria might be a marker or harbinger of later renal disease, the authors proposed in a scientific poster.
The investigators conducted their study as part of a quality improvement program at their center aimed at increasing the frequency of urine screening in patients with hemophilia during annual comprehensive visits.
They looked at urinalysis results collected from all male patients older than 2 years with hemophilia A or B seen at their center from August 2011 through September 2015. They defined hematuria as the presence of three or more red blood cells on at least one urinalysis sample.
They also performed univariate logistic regression to evaluate the association of hematuria with patient age, race, hemophilia type and severity, treatment regimen, and history of inhibitory antibodies.
A total of 93 patients, 67 with hemophilia A and 26 with hemophilia B, were included. In all, 43 patients (47%) were identified as having hematuria, with a median of seven red cells. Hematuria was seen in 37 patients with hemophilia A (55%), and in 6 patients with hemophilia B (23%).
Characteristics associated with risk for hematuria included older age and hemophilia A.
Imaging studies available on 24 of the 93 patients showed renal calculi in 3 patients, minor pelviectasis in 1, and congenital dysplastic left kidney, ureterocele, and right hydroureter in 1 patient.
Dr. Davis and Dr. Dunn said that while screening urinalysis could be considered as a part of routine hemophilia, additional studies are needed to replicate the finding in other treatment centers and to determine whether urinalysis results can be predictive of future renal disease, and if so, whether interventions might help.
“For example, there is the potential that if you recognize hematuria in a patient and that patient is currently on an on-demand treatment process, should we switch to prophylaxis?” Dr Davis said.
Dr. Dunn noted that “certainly there are high-risk populations who should be screened, like our patients who have an active inhibitor or even a tolerized inhibitor. Our data suggest that we ought to be looking a bit more closely at those patients, and perhaps that will help us tease out the cause of this. Can we blame it all on hemophilia, or is there something else going on?”
The study was internally funded. Dr. Davis and Dr. Dunn reported no relevant disclosures.
ORLANDO – Screening urinalysis should be a part of routine care for children and young adults with hemophilia, although the clinical significance of the finding is still unclear, investigators say.
Among 93 boys and young men with hemophilia A or B followed at a hemophilia treatment center, nearly half were found to have hematuria on routine screening, a possible indicator for future renal problems, said Kyle Davis, MD, and Amy Dunn, MD, from the division of hematology at Nationwide Children’s Hospital in Columbus, Ohio.
“It’s not routine for all centers to screen for hematuria, so there is likely a large number of patients that are underrecognized, who have hematuria but we don’t even know it,” Dr. Davis said in an interview at the World Federation of Hemophilia World Congress.
Hematuria is a recognized complication in patients with hemophilia A and B, second only to joint damage in frequency. In addition, adults with hemophilia have been shown to have a higher prevalence of renal disease than the general population, suggesting that hematuria might be a marker or harbinger of later renal disease, the authors proposed in a scientific poster.
The investigators conducted their study as part of a quality improvement program at their center aimed at increasing the frequency of urine screening in patients with hemophilia during annual comprehensive visits.
They looked at urinalysis results collected from all male patients older than 2 years with hemophilia A or B seen at their center from August 2011 through September 2015. They defined hematuria as the presence of three or more red blood cells on at least one urinalysis sample.
They also performed univariate logistic regression to evaluate the association of hematuria with patient age, race, hemophilia type and severity, treatment regimen, and history of inhibitory antibodies.
A total of 93 patients, 67 with hemophilia A and 26 with hemophilia B, were included. In all, 43 patients (47%) were identified as having hematuria, with a median of seven red cells. Hematuria was seen in 37 patients with hemophilia A (55%), and in 6 patients with hemophilia B (23%).
Characteristics associated with risk for hematuria included older age and hemophilia A.
Imaging studies available on 24 of the 93 patients showed renal calculi in 3 patients, minor pelviectasis in 1, and congenital dysplastic left kidney, ureterocele, and right hydroureter in 1 patient.
Dr. Davis and Dr. Dunn said that while screening urinalysis could be considered as a part of routine hemophilia, additional studies are needed to replicate the finding in other treatment centers and to determine whether urinalysis results can be predictive of future renal disease, and if so, whether interventions might help.
“For example, there is the potential that if you recognize hematuria in a patient and that patient is currently on an on-demand treatment process, should we switch to prophylaxis?” Dr Davis said.
Dr. Dunn noted that “certainly there are high-risk populations who should be screened, like our patients who have an active inhibitor or even a tolerized inhibitor. Our data suggest that we ought to be looking a bit more closely at those patients, and perhaps that will help us tease out the cause of this. Can we blame it all on hemophilia, or is there something else going on?”
The study was internally funded. Dr. Davis and Dr. Dunn reported no relevant disclosures.
ORLANDO – Screening urinalysis should be a part of routine care for children and young adults with hemophilia, although the clinical significance of the finding is still unclear, investigators say.
Among 93 boys and young men with hemophilia A or B followed at a hemophilia treatment center, nearly half were found to have hematuria on routine screening, a possible indicator for future renal problems, said Kyle Davis, MD, and Amy Dunn, MD, from the division of hematology at Nationwide Children’s Hospital in Columbus, Ohio.
“It’s not routine for all centers to screen for hematuria, so there is likely a large number of patients that are underrecognized, who have hematuria but we don’t even know it,” Dr. Davis said in an interview at the World Federation of Hemophilia World Congress.
Hematuria is a recognized complication in patients with hemophilia A and B, second only to joint damage in frequency. In addition, adults with hemophilia have been shown to have a higher prevalence of renal disease than the general population, suggesting that hematuria might be a marker or harbinger of later renal disease, the authors proposed in a scientific poster.
The investigators conducted their study as part of a quality improvement program at their center aimed at increasing the frequency of urine screening in patients with hemophilia during annual comprehensive visits.
They looked at urinalysis results collected from all male patients older than 2 years with hemophilia A or B seen at their center from August 2011 through September 2015. They defined hematuria as the presence of three or more red blood cells on at least one urinalysis sample.
They also performed univariate logistic regression to evaluate the association of hematuria with patient age, race, hemophilia type and severity, treatment regimen, and history of inhibitory antibodies.
A total of 93 patients, 67 with hemophilia A and 26 with hemophilia B, were included. In all, 43 patients (47%) were identified as having hematuria, with a median of seven red cells. Hematuria was seen in 37 patients with hemophilia A (55%), and in 6 patients with hemophilia B (23%).
Characteristics associated with risk for hematuria included older age and hemophilia A.
Imaging studies available on 24 of the 93 patients showed renal calculi in 3 patients, minor pelviectasis in 1, and congenital dysplastic left kidney, ureterocele, and right hydroureter in 1 patient.
Dr. Davis and Dr. Dunn said that while screening urinalysis could be considered as a part of routine hemophilia, additional studies are needed to replicate the finding in other treatment centers and to determine whether urinalysis results can be predictive of future renal disease, and if so, whether interventions might help.
“For example, there is the potential that if you recognize hematuria in a patient and that patient is currently on an on-demand treatment process, should we switch to prophylaxis?” Dr Davis said.
Dr. Dunn noted that “certainly there are high-risk populations who should be screened, like our patients who have an active inhibitor or even a tolerized inhibitor. Our data suggest that we ought to be looking a bit more closely at those patients, and perhaps that will help us tease out the cause of this. Can we blame it all on hemophilia, or is there something else going on?”
The study was internally funded. Dr. Davis and Dr. Dunn reported no relevant disclosures.
AT WFH 2016 WORLD CONGRESS
Key clinical point:. Hematuria is a common finding in children with hemophilia A or B.
Major finding: Of 93 patients with hemophilia, 43 (47%) had hematuria findings on routine urinalysis.
Data source:. Prospective study in 67 patients with hemophilia A and 26 with hemophilia B.
Disclosures: The study was internally funded. Dr. Davis and Dr. Dunn reported no relevant disclosures
Distinguish between autoinflammatory, autoimmune disorders in children
Boston – Autoinflammatory and autoimmune disorders in children have many overlapping features, but the former represents a malfunction of the innate immune system, and the latter a malfunction of the adaptive immune system. Fevers, skin eruptions, joint pain and swelling, fatigue, and growth failure can occur in both, but it is important to identify the underlying problem, according to Raegan Hunt, MD.
Autoinflammatory disorders can be difficult to detect, so it is important to maintain a high index of suspicion for them, Dr. Hunt of Baylor College of Medicine and Texas Children’s Hospital, Houston, said at the American Academy of Dermatology annual summer meeting.
She discussed five signs of possible autoinflammatory disease in children, as described in a recent report by Hal M. Hoffman, MD, and Lori Broderick, MD, of Children’s Hospital of San Diego, La Jolla, Calif. (J Allergy Clin Immunol. July 2016; 138:3-14)*:
1. More than three episodes of fever over 101 degrees Farenheit with no explained infectious etiology.
2. Having predictable patterns of characteristic course of each episode.
3. Having specific symptoms during episodes, including nonpruritic skin eruptions, joint or bone pain, severe abdominal pain, and conjunctivitis, with no upper respiratory infection symptoms.
4. Episodes may be triggered by specific stimuli, such as cold exposure or vaccines.
5. A family history of autoinflammatory disease or amyloidosis.
The authors “propose that two or more of these might suggest that an autoinflammatory disorder is possible and should be investigated,” Dr. Hunt said.
Dr. Hunt reported having no relevant disclosures.
sworcester@frontlinemedcom.com
*Correction, 8/16/16: An earlier version of this article failed to note that Dr. Lori Broderick was a co-investigator in the cited report.
Boston – Autoinflammatory and autoimmune disorders in children have many overlapping features, but the former represents a malfunction of the innate immune system, and the latter a malfunction of the adaptive immune system. Fevers, skin eruptions, joint pain and swelling, fatigue, and growth failure can occur in both, but it is important to identify the underlying problem, according to Raegan Hunt, MD.
Autoinflammatory disorders can be difficult to detect, so it is important to maintain a high index of suspicion for them, Dr. Hunt of Baylor College of Medicine and Texas Children’s Hospital, Houston, said at the American Academy of Dermatology annual summer meeting.
She discussed five signs of possible autoinflammatory disease in children, as described in a recent report by Hal M. Hoffman, MD, and Lori Broderick, MD, of Children’s Hospital of San Diego, La Jolla, Calif. (J Allergy Clin Immunol. July 2016; 138:3-14)*:
1. More than three episodes of fever over 101 degrees Farenheit with no explained infectious etiology.
2. Having predictable patterns of characteristic course of each episode.
3. Having specific symptoms during episodes, including nonpruritic skin eruptions, joint or bone pain, severe abdominal pain, and conjunctivitis, with no upper respiratory infection symptoms.
4. Episodes may be triggered by specific stimuli, such as cold exposure or vaccines.
5. A family history of autoinflammatory disease or amyloidosis.
The authors “propose that two or more of these might suggest that an autoinflammatory disorder is possible and should be investigated,” Dr. Hunt said.
Dr. Hunt reported having no relevant disclosures.
sworcester@frontlinemedcom.com
*Correction, 8/16/16: An earlier version of this article failed to note that Dr. Lori Broderick was a co-investigator in the cited report.
Boston – Autoinflammatory and autoimmune disorders in children have many overlapping features, but the former represents a malfunction of the innate immune system, and the latter a malfunction of the adaptive immune system. Fevers, skin eruptions, joint pain and swelling, fatigue, and growth failure can occur in both, but it is important to identify the underlying problem, according to Raegan Hunt, MD.
Autoinflammatory disorders can be difficult to detect, so it is important to maintain a high index of suspicion for them, Dr. Hunt of Baylor College of Medicine and Texas Children’s Hospital, Houston, said at the American Academy of Dermatology annual summer meeting.
She discussed five signs of possible autoinflammatory disease in children, as described in a recent report by Hal M. Hoffman, MD, and Lori Broderick, MD, of Children’s Hospital of San Diego, La Jolla, Calif. (J Allergy Clin Immunol. July 2016; 138:3-14)*:
1. More than three episodes of fever over 101 degrees Farenheit with no explained infectious etiology.
2. Having predictable patterns of characteristic course of each episode.
3. Having specific symptoms during episodes, including nonpruritic skin eruptions, joint or bone pain, severe abdominal pain, and conjunctivitis, with no upper respiratory infection symptoms.
4. Episodes may be triggered by specific stimuli, such as cold exposure or vaccines.
5. A family history of autoinflammatory disease or amyloidosis.
The authors “propose that two or more of these might suggest that an autoinflammatory disorder is possible and should be investigated,” Dr. Hunt said.
Dr. Hunt reported having no relevant disclosures.
sworcester@frontlinemedcom.com
*Correction, 8/16/16: An earlier version of this article failed to note that Dr. Lori Broderick was a co-investigator in the cited report.
Expert Analysis from the AAD Summer Academy 2016
Mycobiome much more diverse in children than in adults
The normal fungal communities that inhabit healthy skin are much more diverse in children than adults, a new study has discovered.
That diversity dwindles, however, around puberty, when the lipophilic taxa Malassezia surges in abundance. This is probably mediated by the increase in sebaceous gland activation and sebum composition that occurs around sexual maturity, Jay-Hyun Jo, PhD, wrote (J Invest Dermatol. 2016 Jul 28; doi: 10.1016/j.jid.2016.05.130).
The diversity of the childhood mycobiome may also play into the larger prevalence of fungal skin diseases in children, wrote Dr. Jo of the National Cancer Institute.
“Several fungal skin infections (dermatophytoses), such as tinea capitis and tinea corporis, are more frequently seen in children. This epidemiological dichotomy in fungal infections may relate to the physiologic characteristics of younger skin, which appears more permissive to colonization by diverse fungi.”
The researchers used the fungal internal transcribed spacer–1 (ITS1) sequence to pinpoint the taxonomic details of the mycobiome of 14 healthy children and 19 healthy adults. They looked at samples from 10 sites on each subject: the external auditory canal, forehead, occiput, retroauricular crease, back, manubrium, antecubital fossa, inguinal crease, volar forearm, and nares.
Malassezia monopolized the adult samples, constituting 80%-99% of the communities on each skin site. In children, however, Malassezia was much less common, comprising 35%-76% of the samples of each site.
However, children boasted a much more diverse mycobiome. Other constituents included members of the Ascomycota, Aspergillus, Epicoccum, and Phoma taxae. Ascomycota species were found on 40% of samples from children, compared with 9.5% of samples from adults. Children also played host to communities of Epicoccum, Cladosporium, and Cryptococcus.
There were individual variations in diversity, however, the authors noted. “For clinical samples from children, decreased diversity was correlated with increased relative abundance of Malassezia, especially on sebaceous sites. Given the predominance of Malassezia on sebaceous skin, it is possible that reduction in diversity was attributed to relative overexpansion of Malassezia.”
The team also discovered gender differences in the mycobiome of children. The sebaceous skin sites of boys were much more likely to host species of Epicoccum and Cryptococcus. Girls showed an early enrichment of Malassezia. “These results suggested that gender may affect mycobiome structures during sexual maturation.”
“Since Malassezia is an obligatory lipophilic fungus, differential Malassezia abundance might be due to the full activation of sebaceous glands during puberty,” they theorized. “Therefore, it would be intriguing to identify the sebaceous gland activity and sebum signatures during childhood in conjunction with sequence-based mycobiome analysis.”
The National Institutes of Health funded the study. Dr. Jo had no financial disclosures.
On Twitter @Alz_Gal
The normal fungal communities that inhabit healthy skin are much more diverse in children than adults, a new study has discovered.
That diversity dwindles, however, around puberty, when the lipophilic taxa Malassezia surges in abundance. This is probably mediated by the increase in sebaceous gland activation and sebum composition that occurs around sexual maturity, Jay-Hyun Jo, PhD, wrote (J Invest Dermatol. 2016 Jul 28; doi: 10.1016/j.jid.2016.05.130).
The diversity of the childhood mycobiome may also play into the larger prevalence of fungal skin diseases in children, wrote Dr. Jo of the National Cancer Institute.
“Several fungal skin infections (dermatophytoses), such as tinea capitis and tinea corporis, are more frequently seen in children. This epidemiological dichotomy in fungal infections may relate to the physiologic characteristics of younger skin, which appears more permissive to colonization by diverse fungi.”
The researchers used the fungal internal transcribed spacer–1 (ITS1) sequence to pinpoint the taxonomic details of the mycobiome of 14 healthy children and 19 healthy adults. They looked at samples from 10 sites on each subject: the external auditory canal, forehead, occiput, retroauricular crease, back, manubrium, antecubital fossa, inguinal crease, volar forearm, and nares.
Malassezia monopolized the adult samples, constituting 80%-99% of the communities on each skin site. In children, however, Malassezia was much less common, comprising 35%-76% of the samples of each site.
However, children boasted a much more diverse mycobiome. Other constituents included members of the Ascomycota, Aspergillus, Epicoccum, and Phoma taxae. Ascomycota species were found on 40% of samples from children, compared with 9.5% of samples from adults. Children also played host to communities of Epicoccum, Cladosporium, and Cryptococcus.
There were individual variations in diversity, however, the authors noted. “For clinical samples from children, decreased diversity was correlated with increased relative abundance of Malassezia, especially on sebaceous sites. Given the predominance of Malassezia on sebaceous skin, it is possible that reduction in diversity was attributed to relative overexpansion of Malassezia.”
The team also discovered gender differences in the mycobiome of children. The sebaceous skin sites of boys were much more likely to host species of Epicoccum and Cryptococcus. Girls showed an early enrichment of Malassezia. “These results suggested that gender may affect mycobiome structures during sexual maturation.”
“Since Malassezia is an obligatory lipophilic fungus, differential Malassezia abundance might be due to the full activation of sebaceous glands during puberty,” they theorized. “Therefore, it would be intriguing to identify the sebaceous gland activity and sebum signatures during childhood in conjunction with sequence-based mycobiome analysis.”
The National Institutes of Health funded the study. Dr. Jo had no financial disclosures.
On Twitter @Alz_Gal
The normal fungal communities that inhabit healthy skin are much more diverse in children than adults, a new study has discovered.
That diversity dwindles, however, around puberty, when the lipophilic taxa Malassezia surges in abundance. This is probably mediated by the increase in sebaceous gland activation and sebum composition that occurs around sexual maturity, Jay-Hyun Jo, PhD, wrote (J Invest Dermatol. 2016 Jul 28; doi: 10.1016/j.jid.2016.05.130).
The diversity of the childhood mycobiome may also play into the larger prevalence of fungal skin diseases in children, wrote Dr. Jo of the National Cancer Institute.
“Several fungal skin infections (dermatophytoses), such as tinea capitis and tinea corporis, are more frequently seen in children. This epidemiological dichotomy in fungal infections may relate to the physiologic characteristics of younger skin, which appears more permissive to colonization by diverse fungi.”
The researchers used the fungal internal transcribed spacer–1 (ITS1) sequence to pinpoint the taxonomic details of the mycobiome of 14 healthy children and 19 healthy adults. They looked at samples from 10 sites on each subject: the external auditory canal, forehead, occiput, retroauricular crease, back, manubrium, antecubital fossa, inguinal crease, volar forearm, and nares.
Malassezia monopolized the adult samples, constituting 80%-99% of the communities on each skin site. In children, however, Malassezia was much less common, comprising 35%-76% of the samples of each site.
However, children boasted a much more diverse mycobiome. Other constituents included members of the Ascomycota, Aspergillus, Epicoccum, and Phoma taxae. Ascomycota species were found on 40% of samples from children, compared with 9.5% of samples from adults. Children also played host to communities of Epicoccum, Cladosporium, and Cryptococcus.
There were individual variations in diversity, however, the authors noted. “For clinical samples from children, decreased diversity was correlated with increased relative abundance of Malassezia, especially on sebaceous sites. Given the predominance of Malassezia on sebaceous skin, it is possible that reduction in diversity was attributed to relative overexpansion of Malassezia.”
The team also discovered gender differences in the mycobiome of children. The sebaceous skin sites of boys were much more likely to host species of Epicoccum and Cryptococcus. Girls showed an early enrichment of Malassezia. “These results suggested that gender may affect mycobiome structures during sexual maturation.”
“Since Malassezia is an obligatory lipophilic fungus, differential Malassezia abundance might be due to the full activation of sebaceous glands during puberty,” they theorized. “Therefore, it would be intriguing to identify the sebaceous gland activity and sebum signatures during childhood in conjunction with sequence-based mycobiome analysis.”
The National Institutes of Health funded the study. Dr. Jo had no financial disclosures.
On Twitter @Alz_Gal
FROM THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
Key clinical point: The mycobiome of children is much more diverse than that of adults.
Major finding: Malassezia species comprised 80%-99% the adult mycobiome, while numerous other taxae were found on children’s skin.
Data source: The taxonomic analysis comprised 19 healthy adults and 14 healthy children.
Disclosures: The National Institutes of Health funded the study. Dr. Jo had no financial disclosures.
Candida auris in Venezuela outbreak is triazole-resistant, opportunistic
BOSTON – An investigation into 18 nosocomial Candida auris infections at a tertiary care center in Venezuela showed that isolates of the emerging fungal pathogen obtained during the outbreak were resistant to fluconazole and voriconazole. However, the isolates were intermediately susceptible to amphotericin B and susceptible to 5-fluorocitosine, and demonstrated high susceptibility to the candin antifungal anidulafungin.
Dr. Belinda Calvo, an infectious disease specialist at the University of Maracaibo, Venezuela, and her collaborators reported these findings, related to a 2012-2013 C. auris outbreak at the hospital. Dr. Calvo and her coinvestigators noted that other invasive C. auris outbreaks have been reported in India, Korea, and South Africa, but that “the real prevalence of this organism may be underestimated,” since common rapid microbial identification techniques may misidentify the species.
In a poster session at the annual meeting of the American Society of Microbiology, Dr. Calvo and her collaborators reported that the 18 patients involved in the Venezuelan outbreak were critically ill, of whom 11 were pediatric, and all had central venous catheter placement. All but two of the pediatric patients were neonates, and all had serious underlying morbidities; several had significant congenital anomalies. The median patient age was 26 days (range, 2 days to 72 years), reflecting the high number of neonates affected. One of the adult patients had esophageal carcinoma. Overall, 10/18 patients (56%) had undergone surgical procedures, and all had received antibiotics.
As has been reported in other C. auris outbreaks, isolates from blood cultures of affected individuals were initially reported as C. haemulonii by the Vitek 2 C automated microbial identification system. Molecular identification was completed by sequencing the internal transcribed spacer (ITS) of the rDNA gene, with analysis aided by the National Institutes of Health’s GenBank and the Netherland’s CBS Fungal Diversity Centre , in order to confirm the identity of the fungal isolates as C. auris. Dr. Calvo and her associates were able to generate a dendrogram of the 18 isolates, showing high clonality, a trait shared with other nosocomial C. auris outbreaks.
Susceptibility testing of the C. auris cultured from blood samples of the affected patients showed that fluconazole had a minimum inhibitory concentration to inhibit the growth of 50% of the organisms (MIC50) of greater than 64 mcg/mL. For fluconazole, the MIC90, range, and geometric mean were all also above 64 mcg/mL, indicating a high level of resistance. For voriconazole, the MICs, range, and mean were all 4 mcg/mL. For amphotericin B, the MIC50 was 1 mcg/mL, the MIC90 was 2 mcg/mL, the range was 1-2, and the geometric mean was 1.414 mcg/mL.
The high number of pediatric patients affected, as well as early pathogen identification with speedy and appropriate antifungal therapy and prompt removal of central venous catheters, likely contributed to the relatively low 30-day crude mortality rate of 28%, said Dr. Calvo and her coauthors.
“C. auris should be considered an emergent multiresistant species,” wrote Dr. Calbo and her collaborators, noting that the opportunistic pathogen has a “high potential for nosocomial horizontal transmission.”
In June 2016, the Centers for Disease Control issued a clinical alert to U.S. healthcare facilities regarding the global emergence of invasive infections caused by C. auris.
The study authors reported no external sources of funding and no conflicts of interest.
On Twitter @karioakes
BOSTON – An investigation into 18 nosocomial Candida auris infections at a tertiary care center in Venezuela showed that isolates of the emerging fungal pathogen obtained during the outbreak were resistant to fluconazole and voriconazole. However, the isolates were intermediately susceptible to amphotericin B and susceptible to 5-fluorocitosine, and demonstrated high susceptibility to the candin antifungal anidulafungin.
Dr. Belinda Calvo, an infectious disease specialist at the University of Maracaibo, Venezuela, and her collaborators reported these findings, related to a 2012-2013 C. auris outbreak at the hospital. Dr. Calvo and her coinvestigators noted that other invasive C. auris outbreaks have been reported in India, Korea, and South Africa, but that “the real prevalence of this organism may be underestimated,” since common rapid microbial identification techniques may misidentify the species.
In a poster session at the annual meeting of the American Society of Microbiology, Dr. Calvo and her collaborators reported that the 18 patients involved in the Venezuelan outbreak were critically ill, of whom 11 were pediatric, and all had central venous catheter placement. All but two of the pediatric patients were neonates, and all had serious underlying morbidities; several had significant congenital anomalies. The median patient age was 26 days (range, 2 days to 72 years), reflecting the high number of neonates affected. One of the adult patients had esophageal carcinoma. Overall, 10/18 patients (56%) had undergone surgical procedures, and all had received antibiotics.
As has been reported in other C. auris outbreaks, isolates from blood cultures of affected individuals were initially reported as C. haemulonii by the Vitek 2 C automated microbial identification system. Molecular identification was completed by sequencing the internal transcribed spacer (ITS) of the rDNA gene, with analysis aided by the National Institutes of Health’s GenBank and the Netherland’s CBS Fungal Diversity Centre , in order to confirm the identity of the fungal isolates as C. auris. Dr. Calvo and her associates were able to generate a dendrogram of the 18 isolates, showing high clonality, a trait shared with other nosocomial C. auris outbreaks.
Susceptibility testing of the C. auris cultured from blood samples of the affected patients showed that fluconazole had a minimum inhibitory concentration to inhibit the growth of 50% of the organisms (MIC50) of greater than 64 mcg/mL. For fluconazole, the MIC90, range, and geometric mean were all also above 64 mcg/mL, indicating a high level of resistance. For voriconazole, the MICs, range, and mean were all 4 mcg/mL. For amphotericin B, the MIC50 was 1 mcg/mL, the MIC90 was 2 mcg/mL, the range was 1-2, and the geometric mean was 1.414 mcg/mL.
The high number of pediatric patients affected, as well as early pathogen identification with speedy and appropriate antifungal therapy and prompt removal of central venous catheters, likely contributed to the relatively low 30-day crude mortality rate of 28%, said Dr. Calvo and her coauthors.
“C. auris should be considered an emergent multiresistant species,” wrote Dr. Calbo and her collaborators, noting that the opportunistic pathogen has a “high potential for nosocomial horizontal transmission.”
In June 2016, the Centers for Disease Control issued a clinical alert to U.S. healthcare facilities regarding the global emergence of invasive infections caused by C. auris.
The study authors reported no external sources of funding and no conflicts of interest.
On Twitter @karioakes
BOSTON – An investigation into 18 nosocomial Candida auris infections at a tertiary care center in Venezuela showed that isolates of the emerging fungal pathogen obtained during the outbreak were resistant to fluconazole and voriconazole. However, the isolates were intermediately susceptible to amphotericin B and susceptible to 5-fluorocitosine, and demonstrated high susceptibility to the candin antifungal anidulafungin.
Dr. Belinda Calvo, an infectious disease specialist at the University of Maracaibo, Venezuela, and her collaborators reported these findings, related to a 2012-2013 C. auris outbreak at the hospital. Dr. Calvo and her coinvestigators noted that other invasive C. auris outbreaks have been reported in India, Korea, and South Africa, but that “the real prevalence of this organism may be underestimated,” since common rapid microbial identification techniques may misidentify the species.
In a poster session at the annual meeting of the American Society of Microbiology, Dr. Calvo and her collaborators reported that the 18 patients involved in the Venezuelan outbreak were critically ill, of whom 11 were pediatric, and all had central venous catheter placement. All but two of the pediatric patients were neonates, and all had serious underlying morbidities; several had significant congenital anomalies. The median patient age was 26 days (range, 2 days to 72 years), reflecting the high number of neonates affected. One of the adult patients had esophageal carcinoma. Overall, 10/18 patients (56%) had undergone surgical procedures, and all had received antibiotics.
As has been reported in other C. auris outbreaks, isolates from blood cultures of affected individuals were initially reported as C. haemulonii by the Vitek 2 C automated microbial identification system. Molecular identification was completed by sequencing the internal transcribed spacer (ITS) of the rDNA gene, with analysis aided by the National Institutes of Health’s GenBank and the Netherland’s CBS Fungal Diversity Centre , in order to confirm the identity of the fungal isolates as C. auris. Dr. Calvo and her associates were able to generate a dendrogram of the 18 isolates, showing high clonality, a trait shared with other nosocomial C. auris outbreaks.
Susceptibility testing of the C. auris cultured from blood samples of the affected patients showed that fluconazole had a minimum inhibitory concentration to inhibit the growth of 50% of the organisms (MIC50) of greater than 64 mcg/mL. For fluconazole, the MIC90, range, and geometric mean were all also above 64 mcg/mL, indicating a high level of resistance. For voriconazole, the MICs, range, and mean were all 4 mcg/mL. For amphotericin B, the MIC50 was 1 mcg/mL, the MIC90 was 2 mcg/mL, the range was 1-2, and the geometric mean was 1.414 mcg/mL.
The high number of pediatric patients affected, as well as early pathogen identification with speedy and appropriate antifungal therapy and prompt removal of central venous catheters, likely contributed to the relatively low 30-day crude mortality rate of 28%, said Dr. Calvo and her coauthors.
“C. auris should be considered an emergent multiresistant species,” wrote Dr. Calbo and her collaborators, noting that the opportunistic pathogen has a “high potential for nosocomial horizontal transmission.”
In June 2016, the Centers for Disease Control issued a clinical alert to U.S. healthcare facilities regarding the global emergence of invasive infections caused by C. auris.
The study authors reported no external sources of funding and no conflicts of interest.
On Twitter @karioakes
AT ASM 2016
Key clinical point: Isolates in an outbreak of nosocomially acquired Candida auris were fluconazole-resistant.
Major finding: All C. auris isolates were resistant to fluconazole, with geometric mean minimum inhibitory concentrations greater than 64 mcg/mL.
Data source: Retrospective, single-center study of 18 pediatric and adult patients with C. auris infections at a tertiary care center in Venezuela.
Disclosures: The study investigators reported no outside sources of funding and no disclosures.