User login
Vaccine refusals and pediatrician dismissals increasing
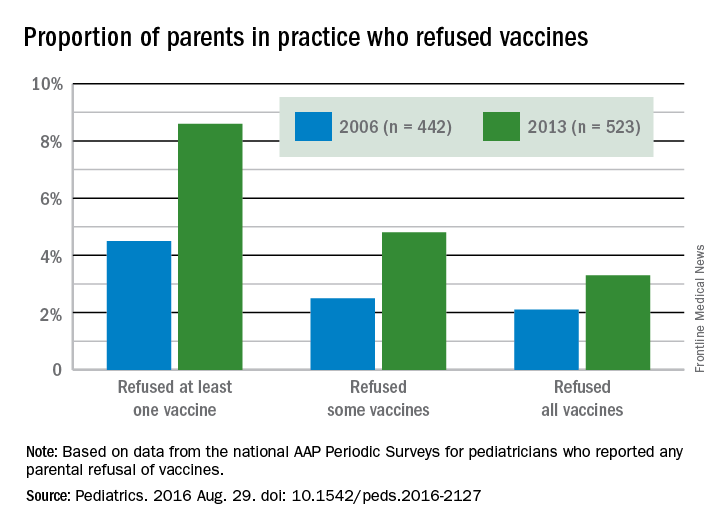
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).

“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.

Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).
“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.
Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
More parents have been refusing vaccines in recent years than a decade ago, according to surveys of pediatricians by the American Academy of Pediatrics published in Pediatrics Aug. 29.
“In a busy practice, vaccine refusals and delays occur daily (if not multiple times per day),” wrote Catherine Hough-Telford, MD, of the University of Alabama at Birmingham and her colleagues (Pediatrics. 2016 Aug. 29. doi: 10.1542/peds.2016-2127).
“From the perspective of the pediatricians, parents who delay vaccines may do so because of concern for their child’s discomfort and concern about immune system burden, whereas vaccine refusers are more likely to believe that vaccines are unnecessary,” the authors wrote. “Pediatricians report that they continue to provide education to vaccine-refusing and delaying parents at high rates.”
Dr. Hough-Telford’s team compared the national AAP Periodic Surveys of 2006 and 2013 that dealt exclusively with immunizations to learn how currently practicing pediatricians perceived three issues related to vaccination: the prevalence of vaccine refusals and delays, why parents refuse or delay vaccines, and the decision of doctors to dismiss families who refuse to vaccinate.
The researchers excluded pediatricians who did not routinely administer vaccines or otherwise adhere to the Centers for Disease Control and Prevention–recommended immunization schedule for their patients. The 2006 survey had a response rate of 52.6% and included 629 final respondents; the 2013 survey had a response rate of 52.7% and included 627 respondents.
The proportion of pediatricians reporting parental refusals in their practice increased from 74.5% in 2006 to 87% in 2013 (odds ratio, 2.29; P less than .001). These pediatricians estimated in 2013 that 8.6% of their patients refused at least one vaccine, compared with 4.5% in 2006. Similarly, 2.5% of parents refused some vaccines in 2006, the physicians reported, compared with 4.8% in 2013. Those refusing all vaccines increased from 2.1% in 2006 to 3.3% in 2013.
A perceived 73.1% of parents refused vaccines in 2013 because they regarded them as unnecessary, the pediatricians reported, compared with 63.4% in 2006. But parental concern over autism and/or thimerosal dropped from 74.2% of vaccine-refusing parents in 2006 to 64.3% in 2013. Further, the parents refusing vaccines because of safety/side effects concerns dropped from 73.7% in 2006 to 66.6% in 2013, and those worried about their children receiving too many shots more than halved from 42.1% in 2006 to 17% in 2013. Concern among parents about their baby being too small to receive vaccines also dropped.
Physicians estimated that 7.3% of their parents wanted to delay one vaccine, 7.1% wanted to delay multiple vaccines, and 4.3% wanted to delay all vaccines. Urban, inner-city pediatricians were less likely to have parents requesting delays than were parents in other areas, but requests for vaccine delays were geographically similar across different U.S. regions. Only the 2013 survey included questions on delaying vaccines.
Pediatricians reported that 75% of their patients wanted to delay vaccines to reduce discomfort to their child, and 72.5% wanted to delay because they perceived too many vaccines would overburden their child’s immune system.
The percentage of pediatricians who always dismiss patients who continue to refuse vaccines increased from 6.1% in 2006 to 11.7% in 2013; they cited a lack of trust between physician and patient as a major reason (87.4% in 2006; 79.9% in 2013). Further, 80.5% of pediatricians reported in 2013 (the only year asked) that they dismissed vaccine-refusing patients out of concern for their other patients.
Despite no notable geographic differences in dismissals in 2006, the 2013 survey revealed that pediatricians in the West had three to four times greater odds of dismissing patients than those in the Midwest and South. Suburban pediatricians had three times greater odds of dismissing patients than did urban physicians.
The research was funded by the AAP and the CDC Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
FROM PEDIATRICS
Key clinical point: More parents have been refusing vaccines, and more pediatricians have been dismissing vaccine-refusing patients, since 2006.
Major finding: 11.7% of pediatricians reported dismissing patients for refusing vaccines in 2013, compared with 6.1% in 2006, and 8.6% of parents refused at least one vaccine in 2013, compared with 4.5% in 2006.
Data source: The findings are based on surveys of practicing members of the American Academy of Pediatrics, with 629 pediatricians in 2006 and 627 pediatricians in 2013.
Disclosures: The research was funded by the AAP and the Centers for Disease Control and Prevention Childhood Immunization Support Program. Dr. Kimberlin was a site principal investigator for two multisite studies conducted by GlaxoSmithKline and Gilead.
Navigating the obstacle course of diagnosing, managing pediatric hypertension
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.

One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.

Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.

“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.

“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.
One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.
Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.
“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.
“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler
The clinical context of high blood pressure shifts abruptly when a person comes of age.
In adults 18 years old and up it’s fairly simple. Blood pressure above 140/90 mm Hg is generally a clear problem, less than 130/85 is probably okay for now, and in between is something to monitor. When pressure stays above 140/90 mm Hg despite lifestyle interventions it’s time to start treatment with any of several antihypertensive drug options that mostly have well-documented safety and efficacy track records in adults and widely agreed-on benefits that outweigh risks.
For pediatric practice, children and adolescents 3-17 years old, dealing with high blood pressure is much more an obstacle course of complex diagnostic criteria, challenges in pressure measurement, and seemingly inconsistent recommendations. Pediatric hypertension also often brings clinicians up against the child and adolescent obesity epidemic, which has made pediatric hypertension more common than ever.
Against this backdrop, a panel assembled by the American Academy of Pediatrics is revising the 2004 The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents, the reigning standard for pediatric blood pressure assessment and hypertension management and now more than a decade old. With new guidance from the AAP expected in the second half of 2017, best-practice approaches to pediatric hypertension are in flux and need updating just when the disorder is more prevalent than it’s ever been.
Diagnosing pediatric hypertension falls short
This shifting landscape and increasing burden of pediatric hypertension comes at a time when primary-care pediatricians and family practice physicians are failing to perform fully comprehensive blood pressure monitoring of their pediatric patients. Current practice recommendations from the National Heart Lung and Blood Institute (in the form of the 2004 Fourth Report), and from American Heart Association (most recently reiterated in a scientific statement in August 2016) call measuring blood pressure levels at every patient encounter starting at 3 years old, the approach also endorsed by the American Academy of Pediatrics.
But that’s often not done. “Results from plenty of studies show that we are not doing a great job” identifying children and adolescents with hypertension, said Tammy M. Brady, MD, a pediatric nephrologist at Johns Hopkins Medical Center in Baltimore.
One piece of evidence she cited was a study of more than 93,000 U.S. ambulatory pediatric visits during 2000-2009 in data collected by the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, and sampling that represented an average 142 million ambulatory visits each year by 3-18 year olds. The data showed blood pressure screening occurred during 35% of ambulatory visits, 67% of preventive visits, and during 84% of preventive visits for a child or adolescent who was overweight or obese (Pediatrics. 2012 October;130[4]:604-10).
While the numbers showed good practice with a reasonably high level of routine blood pressure measurement in overweight and obese patients, they also suggest that perhaps a third of all U.S. children and adolescents don’t have their blood pressure checked at least once a year. Statistical analyses from this study showed that blood pressure measurement was about twice as likely in children diagnosed as overweight or obese than normal-weight patients, and that blood pressure measurement was 2.6-fold more common in adolescents 13-18 years old compared with children 3-7 years old.
In a second, recent study of 29,000 2-17 years old seen at Children’s Hospital of Chicago, 3% had at least three elevated blood pressure measurements in their hospital record, but in this subset of patients at high risk of having hypertension 21% were actually identified in their medical record as having high blood pressure.
Dr. Brady pointed out that while many of the children and adolescents in this study with three or more high blood pressure readings may not actually have hypertension, defined as a sustained elevation of blood pressure, they are all at risk for development of hypertension and should be targeted for prevention.
“We do a bad job identifying when blood pressure is high,” Dr. Brady said in an interview. She cited a study she recently ran that examined the impact that EMR alerts could have on this diagnostic challenge. She reviewed records for 1,305 patient encounters done before or after institution of a EMR alert that warmed clinicians when a patient’s blood pressure measurement fell above the normal range. The results showed that for these patients, 3-21 years old, the rate of recognition of a high pressure measurement increased from 13% before the alert system started to 42% with the alert system in place (Clin Ped. 2015 June;54[7]:667-75). “That meant more than half the patients with high blood pressure measurements were still going unrecognized”, even with an EMR alert, Dr. Brady said.
“The U.S. clinical community falls way short” of adequately following blood pressure levels in children and adolescents, agreed Julia Steinberger, MD, professor and director of pediatric cardiology at the University of Minnesota in Minneapolis. She chalks this up to several factors: time-pressured clinicians who may let blood pressure slide when other aspects of a visit require more attention and the index of suspicion for elevated blood pressure is low, insufficient education to the primary-care community on how to proceed once an elevated blood pressure reading is made, the difficulty of measuring blood pressure in young or uncooperative patients, and lack of size-appropriate equipment.
Once a single high pressure is recorded, ideal follow-up means measuring and finding elevated blood pressures again on at least two subsequent visits, followed by even more confirmation with home monitoring or 24-hour ambulatory blood pressure monitoring (ABPM), now considered the gold standard for both diagnosing and following pediatric patients with hypertension, especially if they receive antihypertensive medications. In 2014, a scientific statement from the American Heart Association said routine APBM was indicated to confirm the diagnosis of hypertension in a patient with high casual blood pressure measurements. Not many primary-care physicians have ready access to or experience using and interpreting ABPM.
Other reasons for low diagnostic rates include therapeutic inertia, and the sheer complexity and time of identifying what is a high blood pressure reading, at least until automated calculation of high levels by EMRs became possible. “With a paper analysis you need to look at two different charts” and factor in the patient’s sex, age, and height to determine if a pressure reading is high or not for a particular patient. “Diagnosis has been a problem, especially in busy practice,” noted Dr. Brady. “I think we are addressing that with the EMR and pop-up alerts.”
Streamlining the diagnostic process
“We have a complex way to diagnose hypertension in kids,” admitted Bonita Falkner, MD, who chaired the Fourth Report panel that produced the complicated diagnostic process still used today. “It’s complex and tedious to calculate. There have been a number of reports of missed hypertension because of the complexity of the tables,” said Dr. Falkner, professor and director of hypertension and obesity research at Thomas Jefferson University in Philadelphia. “Because it’s so burdensome to diagnose the detection rate of hypertension is not as accurate as it should be. Hopefully this will be improved with the new guidelines. We plan to make them simpler, easier to use and more streamlined,” she said in an interview.
“One of the challenges is how to make high blood pressure identification simpler and more straightforward. Without question there are children and adolescents with persistently high blood pressures who fall through the cracks,” said Stephen R. Daniels, MD, professor and chairman of pediatrics at the University of Colorado in Aurora. “Recognizing hypertension in adults is much simpler, with a single set of values. The AAP is in the process of developing new guidelines and one goal is to make blood pressure measurement and recognition of hypertension as simple as possible. There is a tension between simplicity and precision. Finding the right balance will be the trick.”
Dr. Falkner highlighted two other new aspects the revised pediatric hypertension recommendations will address. The panel appears to be on track to recalculate the reference blood pressure tables to eliminate the contribution of overweight and obese children and adolescents. Because high blood pressure is defined statistically--pressures at or above the 95th percentile for a child’s sex, age and height--inclusion of overweight and obese children and adolescents in the databases that produced the original tables skewed the 95th percentile thresholds higher than they would be for those who are at normal-weights. “It will make the reference numbers somewhat lower, but not dramatically lower,” Dr. Falkner said.
When the 2004 Fourth Report was written and the calculation tables created “it was early in the obesity epidemic and we were not as tuned into it as a problem” for hypertension,” said Dr. Daniels, also a member of the Fourth Report panel.
Another new aspect will likely be highlighting the role of overweight in addition to obesity as a hypertension risk factor. “In 2004, obesity was a concern but overweight was considered just a risk factor for obesity. Now if a child is overweight we know they are also at increased risk for having high blood pressure,” said Dr. Falkner. “We’ve been trying to get an update of the Fourth Report going for some time; a lot has happened since 2004.”
The Preventive Services Task Force effect
One notable recent development in the field of pediatric hypertension was the 2013 statement by the U.S. Preventive Services Task Force that reinforced a similar conclusion the group had reached a decade before, in 2003. In 2013, the USPSTF said that following a review of the evidence “the USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for primary hypertension in asymptomatic children and adolescents to prevent subsequent cardiovascular disease in childhood or adulthood. (I statement)” (Pediatrics. 2013 Nov;132[5]:907-14).
The USPSTF’s 2013 reassertion of this position triggered several strong reactions from pediatric hypertension specialists, who critiqued the Task Force’s analysis as being overly restrictive. Among those weighing with comments that highlighted the flaws in the Task Force’s reasoning were Dr. Falkner, Dr. Brady, and Dr. Steinberger. Earlier in 2013, before the Task Force statement, Dr. Daniels wrote a commentary with similar arguments in favor of routine blood pressure measurements in response to a published assessment of pediatric blood pressure screening that largely presaged what the USPSTF said.
In brief, the USPSTF analysis “was flawed by an overly-narrow selection of evidence,” Dr. Steinberger said recently. “Short-term and observational studies were not considered. We think that in the absence of perfect data the practitioner must use common sense when superior evidence does not exist. The question of whether hypertension in adults can be prevented or modified by early intervention will never be answered unless we continue to measure blood pressure in children.”
“One of the problems with the USPSTF statement was the questions they addressed: Is blood pressure in children and adolescents clearly associated with hard cardiovascular disease outcomes in adults? That is a very tough question to answer. It would need studies that are 30, 40 years in duration, and is almost unanswerable,” said Dr. Daniels in an interview. “I think the USPSTF paid less attention to the fact that clearly a certain percentage of children and adolescents with hypertension already have developed left ventricular hypertrophy, increased carotid intimal-medial thickness and vascular stiffness. This shows that higher blood pressure in the short term is having several adverse effects on the cardiovascular system. If you insist on seeing a connection between pediatric blood pressure and adult outcomes there will always be insufficient evidence.”
Although, as Dr. Steinberger pointed out, the International Childhood Cardiovascular Cohort Consortium has been putting together long-term follow-up data from seven observational cohorts established in several different world regions. Collectively these seven cohorts include more than 340,000 people who have now been followed for about 40 years. This analysis may soon yield more definitive insight into the long-term consequences of childhood hypertension, Dr. Steinberger said.
Another relevant issue is that prevention of adult cardiovascular disease “is not why children are screened for hypertension, or at least not the primary reason,” Dr. Falkner said. “They are screened to find high blood pressure with an underlying cause, like coarctation of the aorta, which is only picked up by first noting a high blood pressure. Several other cardiovascular and renal disorders that can exist in childhood can also cause high blood pressure and measuring blood pressure is the only way to find them. It would be a tragedy to miss coarctation of the aorta by not measuring blood pressure.”
The family practice position
Despite rejection of the USPSTF analysis by many pediatric hypertension specialists, the USPSTF position has been officially embraced by the family practice community. The American Academy of Family Practice has adopted the USPSTF position as its own, although family practice physicians are also quick to point out that the USPSTF conclusion does not say that pediatric blood pressures should not be measured.
“An I level from the USPSTF doesn’t mean that screening is harmful or shouldn’t be done, just that more research is needed to fully evaluate if blood pressure screening in childhood has long-term health impacts,” said Margaret A. Riley, MD, a family practice physician at the University of Michigan in Ann Arbor with an interest in pediatric hypertension.
“I think the I rating has had little impact on practice. Measuring blood pressure is a routine and standard part of office practice. If the USPSTF had given blood pressure screening a D rating, causing more harm than good, that would be different. In my practice I screen blood pressure at every visit or at least once a year,” Dr. Riley said in an interview.
That’s the same approach taken by Wanda D. Filer, MD, a family practice physician in York, Pa. and president of the American Academy of Family Physicians. “This does not mean you don’t screen blood pressure, and it doesn’t mean you should screen. It says that data are not there either way. In my office we check everyone age 3 and up, and I think a lot of family practice physicians do that routinely.
“Most of us screen blood pressure, but the AAFP approach is to always look at the evidence. The AAFP stand is not opposite to other organizations [that have endorsed routine blood pressure measurements]. They take a stronger position in favor of screening than we do, but we don’t say do not screen. Other societies have relied on less direct evidence or expert opinion. Our approach is to see proof of benefit,” Dr. Filer said in an interview.
“I imagine most family practice physicians measure blood pressure in children aged 3 or older,” she added. “I work in a Federally-qualified health center, and we have a very diverse population. We routinely measure blood pressures because the patients are so diverse. Other family practice practices may come to a different decision. You need to look at your practice and your work flow and decide whether it is an appropriate use of time.
“I do it because I’m convinced there is a possibility of benefit from screening,” Dr. Filer said. “I am also convinced that the evidence is not there [to prove benefits]. But I won’t wait for the evidence to do this in my practice. For the mix of patients I see it is important to screen blood pressures, but I am comfortable if a family practice physician with a different patient population says that high blood pressure yields are not there; they never see them.”
Overweight and obesity raise a red flag
If there is one subgroup of the pediatric population that most everyone agrees needs close attention to blood pressure it’s the overweight or obese child or teenager. “Primary hypertension in children and adolescents is largely associated with obesity,” said Dr. Falkner. Study findings also suggest that obese children and teens with hypertension are much more likely to have or develop left ventricular hypertrophy than normal-weight patients with elevated blood pressures.
The consequences are two fold: First, it suggests that even if the entire pediatric population fails to get their blood pressures checked regularly diligent attention to blood pressure is a must for overweight and obese children and adolescents, many experts agree. “A child who is overweight as well as obese requires attention to their blood pressure. That is emerging as a guideline,” Dr. Falkner said.
Second, a growing number of U.S. clinical programs are geared to addressing hypertension in the overweight or obese pediatric patient using an aggressive and multidisciplinary treatment approach.
For example, a clinic devoted to the overweight or obese child or teen with hypertension, the ReNEW (Reversing the Negative Cardiovascular Effects of Weight) program, opened at Johns Hopkins Medical Center in February 2015.
“We were seeing a lot of obesity-related hypertension without an underlying secondary cause. And in a study we ran the only thing that could predict left ventricular hypertrophy in children with hypertension was body mass index,” said Dr. Brady, medical director for ReNEW. “This motivated me to try to find a better way to treat obesity and hypertension; the only real treatment for hypertension in obese patients is to treat the obesity.”
During its first year, the ReNEW program enrolled 35 patients 5-22 years old. “We assess them for any secondary cause of hypertension,” Dr. Brady said. “We do an echocardiography examination and assess left ventricular hypertrophy and the need for blood pressure reducing medications. We do interventions for weight loss, diet, exercise, a musculoskeletal assessment, psychiatric assessment and other comorbidity interventions such as for sleep apnea. We start blood pressure reducing drugs when appropriate.”
The average body mass index among the first 35 patients was 38 kg/m2, with an average 31 kg/m2 in kids 5-10 years old and 43 kg/m2 in those 18-21 years old. Fifty percent had obstructive sleep apnea, 33% had anxiety or depression, and about 25%-33% had diabetes. “These kids are at a really great risk for a cardiac event in early adulthood. They are probably one of the most vulnerable populations we see,” she said.
A major lesson she’s learned from the ReNEW experience so far is the spectrum of comorbidities that can affect these patients and the importance of behavioral change for the entire family to produce favorable changes in the patient. “Depression and anxiety are big factors that can affect a family’s success with weight loss. Many kids also have underlying orthopedic issues. There remains a lot of confusion about diet. We try to offer families a one-stop shop, a multidisciplinary clinic that can thoroughly address the patient’s full range of cardiovascular-disease risk factors.
“I’ve been how shocked by how complex these patients are. When there is a significant overweight or obesity problem the only way to succeed is to involve the whole family. And don’t forget about the role of mental health. That is a significant part of overweight and obesity,” Many of the psychiatric disorders that overweight and obese children and teenagers show results from learned family behaviors, Dr. Brady said.
Another U.S. clinic specifically targeted at obese children and adolescents also sees many patients with hypertension at the University of Minnesota, a program begun in about 2010 that now has treated more than 1,000 patients including “hundreds” with comorbid hypertension, as well as similar numbers with comorbid hyperlipidemia and comorbid diabetes , said Dr. Steinberger.
“There are very few of these programs in the U.S.; it is not widely available. The cardiovascular health promotion effort should include this approach because for the primary care physician there is insufficient time or expertise to do these evaluations and treatments. You need a group of clinicians with the needed expertise,” she said. “Our multidisciplinary approach to treating comorbidities like hypertension, dyslipidemia and elevated glucose uses specialists for each of these areas as well as dieticians, social workers, and other specialists.
“In general, when the primary care physician does not have the resources to further evaluate and treat overweight or obesity they should be able to refer the patient to a program like this. It is never too soon to refer and treat. To treat overweight you need to involve the whole family. Most children do not ‘grow out’ of overweight or obesity. The overweight or obese child will generally grow up to be the overweight or obese adult,” Dr. Steinberger said.
Targeting the greatest hypertension risk
The growing trend to focus multidisciplinary resources on hypertension in the overweight or obese pediatric patient may exemplify part of a new era of targeted attention for pediatric blood pressure screening.
“We have a hard time measuring blood pressure in kids, we know the importance of obesity [in causing hypertension] and we also know that first-line management for most hypertensive patients is non-drug, lifestyle interventions. Therefore, is it possible that a greater good can be achieved by addressing lifestyle and all the health issues that would reduce the risk for hypertension, such as making sure all children engage in more movement and exercise and get off devices rather than medicalizing the problem” with frequent blood pressure measurement, wondered Howard Trachtman, MD, a pediatric nephrologist at New York University.
“Routinely screening blood pressure in every child and adolescent is very burdensome and carries the potential cost of inconvenience and mislabeling errors. Could clinicians focus on the children and adolescents who really are at risk of high blood pressure? Can we use the EMR and alerts to make sure that repeated measures of blood pressure are done only when needed, after we identify who is at greatest risk?
“We need to become more precise in defining who is it in the age range of 8-17 years old who needs to be regularly screened for high blood pressure so we can focus our resources on these people and better avoid mislabeling and causing anxiety” for the many children and adolescents who have a very low risk for having hypertension, said Dr. Trachtman. He said that he is currently collaborating on a study that is examining whether data contained in a patient’s EMR can help in improving blood pressure assessment.
“We need to keep an open mind about who might have hypertension, but there are good data that it tracks with waist circumference, hypertriglyceridemia, and insulin resistance. The more of these you have the greater your risk. This is the kind of productive research I’m talking about, to determine whether you can be more thoughtful in identifying who is at risk of high blood pressure and who needs more systematic screening. Targeting blood pressure screening to overweight or obese kids is a step toward trying to be more methodical. The USPSTF statement should be a spur to pediatric nephrologists to make our case for blood pressure screening more cogently and to collect better data so that when we speak about this it is not based on speculation or extrapolation but on data,” Dr. Trachtman said.
“There are no arguments against optimizing health and reducing risk factors in all children, but that is not an acceptable rationale for not measuring blood pressure and attending to elevated levels in children,” responded Dr. Falkner. Dr Trachtman’s proposal to reduce health risks in all children “is a public health issue whereas the issue of detecting and managing hypertension in childhood is a clinical issue” faced by physicians as they see individual patients, she said.
Many pediatric hypertension specialists may not warm to a screening proposition that retreats from the notion that every child and teen 3 years old and up should have their blood pressure checked at least annually. But many of those specialists also realize that what’s now done has a lot of problems and that a more user-friendly approach is needed. As an expert panel works to produce a revision to the Fourth Report next year (which will not be the Fifth Report as the update is now outside the NHLBI purview), changes in how pediatric hypertension will be approached in the future seem likely.
Dr. Brady, Dr. Steinberger, Dr. Falkner, Dr. Daniels, Dr. Riley, Dr. Filer, and Dr. Trachtman had no disclosures.
On Twitter @mitchelzoler

Primary care physicians diagnose most pediatric thyroid conditions
Primary care physicians can play an important role in managing thyroid disease in children and teens by proactive screening and evaluation, based on data from a literature review of 83 articles published between Jan. 1, 2010, and Dec. 31, 2015. The review was published online Aug. 29 in JAMA Pediatrics.
“Early diagnosis and treatment of thyroid hormone deficiency is crucial to ensure normal development and cognition,” wrote Dr. Patrick Hanley of the Children’s Hospital of Philadelphia and his colleagues.
Thyroid dysgenesis accounts for 80%-85% of cases of primary congenital hypothyroidism, and many newborns with the condition are asymptomatic at birth because of protection by maternal thyroid hormones. Early signs of thyroid problems include a hoarse cry, prolonged jaundice, lethargy, poor feeding, and constipation, the researchers said (JAMA Pediatr. 2016. doi:10.1001/jamapediatrics.2016.0486).
“Once the diagnosis has been made, additional testing can be considered to determine the etiology of the hypothyroidism so that the family can receive anticipatory guidance in regard to the potential need for lifelong thyroid hormone replacement therapy,” the researchers wrote.
The treatment of choice for congenital hypothyroidism is levothyroxine at a starting dose of 10-15 mcg/kg once daily, they noted.
Read the full study here: http://archpedi.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0486.
Primary care physicians can play an important role in managing thyroid disease in children and teens by proactive screening and evaluation, based on data from a literature review of 83 articles published between Jan. 1, 2010, and Dec. 31, 2015. The review was published online Aug. 29 in JAMA Pediatrics.
“Early diagnosis and treatment of thyroid hormone deficiency is crucial to ensure normal development and cognition,” wrote Dr. Patrick Hanley of the Children’s Hospital of Philadelphia and his colleagues.
Thyroid dysgenesis accounts for 80%-85% of cases of primary congenital hypothyroidism, and many newborns with the condition are asymptomatic at birth because of protection by maternal thyroid hormones. Early signs of thyroid problems include a hoarse cry, prolonged jaundice, lethargy, poor feeding, and constipation, the researchers said (JAMA Pediatr. 2016. doi:10.1001/jamapediatrics.2016.0486).
“Once the diagnosis has been made, additional testing can be considered to determine the etiology of the hypothyroidism so that the family can receive anticipatory guidance in regard to the potential need for lifelong thyroid hormone replacement therapy,” the researchers wrote.
The treatment of choice for congenital hypothyroidism is levothyroxine at a starting dose of 10-15 mcg/kg once daily, they noted.
Read the full study here: http://archpedi.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0486.
Primary care physicians can play an important role in managing thyroid disease in children and teens by proactive screening and evaluation, based on data from a literature review of 83 articles published between Jan. 1, 2010, and Dec. 31, 2015. The review was published online Aug. 29 in JAMA Pediatrics.
“Early diagnosis and treatment of thyroid hormone deficiency is crucial to ensure normal development and cognition,” wrote Dr. Patrick Hanley of the Children’s Hospital of Philadelphia and his colleagues.
Thyroid dysgenesis accounts for 80%-85% of cases of primary congenital hypothyroidism, and many newborns with the condition are asymptomatic at birth because of protection by maternal thyroid hormones. Early signs of thyroid problems include a hoarse cry, prolonged jaundice, lethargy, poor feeding, and constipation, the researchers said (JAMA Pediatr. 2016. doi:10.1001/jamapediatrics.2016.0486).
“Once the diagnosis has been made, additional testing can be considered to determine the etiology of the hypothyroidism so that the family can receive anticipatory guidance in regard to the potential need for lifelong thyroid hormone replacement therapy,” the researchers wrote.
The treatment of choice for congenital hypothyroidism is levothyroxine at a starting dose of 10-15 mcg/kg once daily, they noted.
Read the full study here: http://archpedi.jamanetwork.com/article.aspx?doi=10.1001/jamapediatrics.2016.0486.
FROM JAMA PEDIATRICS
Host RNA biosignatures distinguish bacterial from viral fever
RNA-expression biosignatures derived from the patient’s peripheral blood distinguish bacterial from viral causes of fever in young children, according to two separate preliminary studies published online Aug. 23 in JAMA.
Several studies have suggested that the source of infection in febrile children might be identified by examining the pattern of host genes that are either activated or suppressed during the body’s inflammatory response. Distinguishing the relatively few but potentially life-threatening bacterial infections from the more common but milder, self-resolving viral infections is difficult, and current practice is to admit “ill-appearing” febrile children to the hospital and administer parenteral antibiotics while awaiting the results of blood and tissue cultures. Those results are often ambiguous, and the whole process represents a large burden on health care resources as well as contributing to inappropriate antibiotic treatment.

Two multinational research groups developed different techniques for detecting RNA biosignatures in patients’ blood samples, then assessed the accuracy of those tests in validation cohorts. One group focused on ruling out bacterial infection as the source of fever in young children (median age, 19 months), while the other investigated whether the host responses of the youngest children (aged 60 days and younger), who have immature immune systems, are robust enough to allow detection of RNA biosignatures.
In the discovery phase of the first study, analysis of RNA gene expression was performed on blood samples obtained from 240 children at admission to hospitals in the United Kingdom, Spain, and the United States during a 4-year period. A total of 8,565 RNA transcript signatures were identified as potential biomarkers to discriminate between viral and bacterial infection. This was narrowed down to 38 transcript signatures, and then to only 2 – IFI44L and FAM89A – that were used to devise a Disease Risk Score (DRS) for each patient, said Jethro A. Herberg, PhD, of the division of infectious diseases, Imperial College London, and his associates.
IFI44L expression was increased in patients who had viral infection, while FAM89A expression was increased in those who had bacterial infection, as compared with healthy children. (In previous studies, IFI44L was reported to be up-regulated in interferon-mediated antiviral responses and FAM89A was reported to be elevated among children with septic shock.)
The DRS showed 90% sensitivity in distinguishing viral from bacterial infection in the discovery cohort. It then showed 96.4% sensitivity in a validation cohort of 130 febrile children (mean age, 17 months). The DRS also identified bacterial infection in a validation cohort of 24 children with meningococcal infection (91.7% sensitivity and 96.0% specificity), and distinguished it from inflammatory conditions in another cohort of 30 children with juvenile idiopathic arthritis and 18 with Henoch-Schönlein purpura (90.0% sensitivity and 95.8% specificity).
The DRS discriminated among viral, bacterial, and inflammatory diseases including systemic lupus erythematosus in a further validation cohort, a published dataset from children and adults who had all three types of illness. It was accurate regardless of the severity of infection and regardless of the duration of infection, as well as in cases where patients were coinfected with both virus and bacteria, the investigators said (JAMA. 2016 Aug 23. doi:10.1001/jama.2016.11236).
“The DRS signature, distinguishing viral from bacterial infections with only two transcripts, has potential to be translated into a clinically applicable test using current technology. Furthermore, new methods for rapid detection of nucleic acids, including nanoparticles and electrical impedance, have potential for low-cost, rapid analysis of multitranscript signatures,” Dr. Herberg and his associates noted.
Further research is needed to assess the accuracy and clinical utility of this technique in different settings, they added.
In the second study, RNA gene expression was analyzed from blood samples from 1,883 febrile infants (median age, 37 days) “who posed diagnostic quandaries” at admission to 22 emergency departments during a 2-year period. The discovery phase involved 89 of these infants who ultimately were found to have bacterial infections (bacteremia or UTIs), 190 who didn’t have bacterial infections (enterovirus, influenza, or other viruses), and 19 healthy control infants, said Prashant Mahajan, MD, division chief and research director, pediatric emergency medicine, Children’s Hospital of Michigan, Detroit, and his associates.

The investigators identified 3,753 RNA transcript signatures that could potentially identify or rule out bacterial sources of infection, which they then narrowed down to 66. This set of 66 signatures showed 82% sensitivity and 88% specificity in the discovery cohort and 87% sensitivity and 89% specificity in a validation cohort.
“The bacterial RNA biosignature was notably more predictive of bacterial infection than clinical examination” and use of the Yale Observation Score, and it “added significantly to prediction beyond the YOS alone,” Dr. Mahajan and his associates said (JAMA. 2016 Aug 23. doi: 10.1001/jama.2016.9207).
“Despite the young age of the febrile infants evaluated, they carried robust RNA biosignatures and demonstrated that regardless of the etiology of the infections, their immune systems are programed to respond not only with shared elements induced by common microbes but also with specific patterns that allow discrimination by class of pathogen,” they noted.
Further research is needed to confirm and refine these preliminary results. “As technology advances, RNA biosignatures may prove to be an alternative and accurate method to identify infants with bacterial infections. This would help clinicians target evaluation and therapy when they are needed and avoid invasive procedures, antibiotics, and hospitalizations when they are not,” Dr. Mahajan and his associates said.
Dr. Herberg’s study was supported by the Imperial College Comprehensive Biomedical Research Center, the National Institutes of Health, the European Union’s Seventh Framework Program, and numerous other groups. Dr. Herberg reported having no relevant financial disclosures. Dr. Mahajan’s study was supported by the Health Resources and Services Administration, Emergency Services for Children, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Institutes of Health. Dr. Mahajan reported having no relevant financial disclosures.
The work by Herberg et al. and Mahajan et al. represents an important advance: the potential of genetics to help in the evaluation of febrile children.

|
Dr. Howard Bauchner |
Clearly RNA sequencing and other methods for RNA quantification are in the early days, and clinical applications must await further replication and refinement of these results in rigorous studies. But the day may soon arise when a parent of a febrile child may do a laboratory test at home, call a physician, and mutually decide whether the child should be seen for further evaluation.
Howard Bauchner, MD, is JAMA Editor in Chief. He reported having no relevant financial disclosures. Dr. Bauchner made these remarks in an editorial accompanying the two reports on RNA biosignatures (JAMA 2016;316:824-5).
The work by Herberg et al. and Mahajan et al. represents an important advance: the potential of genetics to help in the evaluation of febrile children.
|
|
Dr. Howard Bauchner |
Clearly RNA sequencing and other methods for RNA quantification are in the early days, and clinical applications must await further replication and refinement of these results in rigorous studies. But the day may soon arise when a parent of a febrile child may do a laboratory test at home, call a physician, and mutually decide whether the child should be seen for further evaluation.
Howard Bauchner, MD, is JAMA Editor in Chief. He reported having no relevant financial disclosures. Dr. Bauchner made these remarks in an editorial accompanying the two reports on RNA biosignatures (JAMA 2016;316:824-5).
The work by Herberg et al. and Mahajan et al. represents an important advance: the potential of genetics to help in the evaluation of febrile children.
|
|
Dr. Howard Bauchner |
Clearly RNA sequencing and other methods for RNA quantification are in the early days, and clinical applications must await further replication and refinement of these results in rigorous studies. But the day may soon arise when a parent of a febrile child may do a laboratory test at home, call a physician, and mutually decide whether the child should be seen for further evaluation.
Howard Bauchner, MD, is JAMA Editor in Chief. He reported having no relevant financial disclosures. Dr. Bauchner made these remarks in an editorial accompanying the two reports on RNA biosignatures (JAMA 2016;316:824-5).
RNA-expression biosignatures derived from the patient’s peripheral blood distinguish bacterial from viral causes of fever in young children, according to two separate preliminary studies published online Aug. 23 in JAMA.
Several studies have suggested that the source of infection in febrile children might be identified by examining the pattern of host genes that are either activated or suppressed during the body’s inflammatory response. Distinguishing the relatively few but potentially life-threatening bacterial infections from the more common but milder, self-resolving viral infections is difficult, and current practice is to admit “ill-appearing” febrile children to the hospital and administer parenteral antibiotics while awaiting the results of blood and tissue cultures. Those results are often ambiguous, and the whole process represents a large burden on health care resources as well as contributing to inappropriate antibiotic treatment.
Two multinational research groups developed different techniques for detecting RNA biosignatures in patients’ blood samples, then assessed the accuracy of those tests in validation cohorts. One group focused on ruling out bacterial infection as the source of fever in young children (median age, 19 months), while the other investigated whether the host responses of the youngest children (aged 60 days and younger), who have immature immune systems, are robust enough to allow detection of RNA biosignatures.
In the discovery phase of the first study, analysis of RNA gene expression was performed on blood samples obtained from 240 children at admission to hospitals in the United Kingdom, Spain, and the United States during a 4-year period. A total of 8,565 RNA transcript signatures were identified as potential biomarkers to discriminate between viral and bacterial infection. This was narrowed down to 38 transcript signatures, and then to only 2 – IFI44L and FAM89A – that were used to devise a Disease Risk Score (DRS) for each patient, said Jethro A. Herberg, PhD, of the division of infectious diseases, Imperial College London, and his associates.
IFI44L expression was increased in patients who had viral infection, while FAM89A expression was increased in those who had bacterial infection, as compared with healthy children. (In previous studies, IFI44L was reported to be up-regulated in interferon-mediated antiviral responses and FAM89A was reported to be elevated among children with septic shock.)
The DRS showed 90% sensitivity in distinguishing viral from bacterial infection in the discovery cohort. It then showed 96.4% sensitivity in a validation cohort of 130 febrile children (mean age, 17 months). The DRS also identified bacterial infection in a validation cohort of 24 children with meningococcal infection (91.7% sensitivity and 96.0% specificity), and distinguished it from inflammatory conditions in another cohort of 30 children with juvenile idiopathic arthritis and 18 with Henoch-Schönlein purpura (90.0% sensitivity and 95.8% specificity).
The DRS discriminated among viral, bacterial, and inflammatory diseases including systemic lupus erythematosus in a further validation cohort, a published dataset from children and adults who had all three types of illness. It was accurate regardless of the severity of infection and regardless of the duration of infection, as well as in cases where patients were coinfected with both virus and bacteria, the investigators said (JAMA. 2016 Aug 23. doi:10.1001/jama.2016.11236).
“The DRS signature, distinguishing viral from bacterial infections with only two transcripts, has potential to be translated into a clinically applicable test using current technology. Furthermore, new methods for rapid detection of nucleic acids, including nanoparticles and electrical impedance, have potential for low-cost, rapid analysis of multitranscript signatures,” Dr. Herberg and his associates noted.
Further research is needed to assess the accuracy and clinical utility of this technique in different settings, they added.
In the second study, RNA gene expression was analyzed from blood samples from 1,883 febrile infants (median age, 37 days) “who posed diagnostic quandaries” at admission to 22 emergency departments during a 2-year period. The discovery phase involved 89 of these infants who ultimately were found to have bacterial infections (bacteremia or UTIs), 190 who didn’t have bacterial infections (enterovirus, influenza, or other viruses), and 19 healthy control infants, said Prashant Mahajan, MD, division chief and research director, pediatric emergency medicine, Children’s Hospital of Michigan, Detroit, and his associates.
The investigators identified 3,753 RNA transcript signatures that could potentially identify or rule out bacterial sources of infection, which they then narrowed down to 66. This set of 66 signatures showed 82% sensitivity and 88% specificity in the discovery cohort and 87% sensitivity and 89% specificity in a validation cohort.
“The bacterial RNA biosignature was notably more predictive of bacterial infection than clinical examination” and use of the Yale Observation Score, and it “added significantly to prediction beyond the YOS alone,” Dr. Mahajan and his associates said (JAMA. 2016 Aug 23. doi: 10.1001/jama.2016.9207).
“Despite the young age of the febrile infants evaluated, they carried robust RNA biosignatures and demonstrated that regardless of the etiology of the infections, their immune systems are programed to respond not only with shared elements induced by common microbes but also with specific patterns that allow discrimination by class of pathogen,” they noted.
Further research is needed to confirm and refine these preliminary results. “As technology advances, RNA biosignatures may prove to be an alternative and accurate method to identify infants with bacterial infections. This would help clinicians target evaluation and therapy when they are needed and avoid invasive procedures, antibiotics, and hospitalizations when they are not,” Dr. Mahajan and his associates said.
Dr. Herberg’s study was supported by the Imperial College Comprehensive Biomedical Research Center, the National Institutes of Health, the European Union’s Seventh Framework Program, and numerous other groups. Dr. Herberg reported having no relevant financial disclosures. Dr. Mahajan’s study was supported by the Health Resources and Services Administration, Emergency Services for Children, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Institutes of Health. Dr. Mahajan reported having no relevant financial disclosures.
RNA-expression biosignatures derived from the patient’s peripheral blood distinguish bacterial from viral causes of fever in young children, according to two separate preliminary studies published online Aug. 23 in JAMA.
Several studies have suggested that the source of infection in febrile children might be identified by examining the pattern of host genes that are either activated or suppressed during the body’s inflammatory response. Distinguishing the relatively few but potentially life-threatening bacterial infections from the more common but milder, self-resolving viral infections is difficult, and current practice is to admit “ill-appearing” febrile children to the hospital and administer parenteral antibiotics while awaiting the results of blood and tissue cultures. Those results are often ambiguous, and the whole process represents a large burden on health care resources as well as contributing to inappropriate antibiotic treatment.
Two multinational research groups developed different techniques for detecting RNA biosignatures in patients’ blood samples, then assessed the accuracy of those tests in validation cohorts. One group focused on ruling out bacterial infection as the source of fever in young children (median age, 19 months), while the other investigated whether the host responses of the youngest children (aged 60 days and younger), who have immature immune systems, are robust enough to allow detection of RNA biosignatures.
In the discovery phase of the first study, analysis of RNA gene expression was performed on blood samples obtained from 240 children at admission to hospitals in the United Kingdom, Spain, and the United States during a 4-year period. A total of 8,565 RNA transcript signatures were identified as potential biomarkers to discriminate between viral and bacterial infection. This was narrowed down to 38 transcript signatures, and then to only 2 – IFI44L and FAM89A – that were used to devise a Disease Risk Score (DRS) for each patient, said Jethro A. Herberg, PhD, of the division of infectious diseases, Imperial College London, and his associates.
IFI44L expression was increased in patients who had viral infection, while FAM89A expression was increased in those who had bacterial infection, as compared with healthy children. (In previous studies, IFI44L was reported to be up-regulated in interferon-mediated antiviral responses and FAM89A was reported to be elevated among children with septic shock.)
The DRS showed 90% sensitivity in distinguishing viral from bacterial infection in the discovery cohort. It then showed 96.4% sensitivity in a validation cohort of 130 febrile children (mean age, 17 months). The DRS also identified bacterial infection in a validation cohort of 24 children with meningococcal infection (91.7% sensitivity and 96.0% specificity), and distinguished it from inflammatory conditions in another cohort of 30 children with juvenile idiopathic arthritis and 18 with Henoch-Schönlein purpura (90.0% sensitivity and 95.8% specificity).
The DRS discriminated among viral, bacterial, and inflammatory diseases including systemic lupus erythematosus in a further validation cohort, a published dataset from children and adults who had all three types of illness. It was accurate regardless of the severity of infection and regardless of the duration of infection, as well as in cases where patients were coinfected with both virus and bacteria, the investigators said (JAMA. 2016 Aug 23. doi:10.1001/jama.2016.11236).
“The DRS signature, distinguishing viral from bacterial infections with only two transcripts, has potential to be translated into a clinically applicable test using current technology. Furthermore, new methods for rapid detection of nucleic acids, including nanoparticles and electrical impedance, have potential for low-cost, rapid analysis of multitranscript signatures,” Dr. Herberg and his associates noted.
Further research is needed to assess the accuracy and clinical utility of this technique in different settings, they added.
In the second study, RNA gene expression was analyzed from blood samples from 1,883 febrile infants (median age, 37 days) “who posed diagnostic quandaries” at admission to 22 emergency departments during a 2-year period. The discovery phase involved 89 of these infants who ultimately were found to have bacterial infections (bacteremia or UTIs), 190 who didn’t have bacterial infections (enterovirus, influenza, or other viruses), and 19 healthy control infants, said Prashant Mahajan, MD, division chief and research director, pediatric emergency medicine, Children’s Hospital of Michigan, Detroit, and his associates.
The investigators identified 3,753 RNA transcript signatures that could potentially identify or rule out bacterial sources of infection, which they then narrowed down to 66. This set of 66 signatures showed 82% sensitivity and 88% specificity in the discovery cohort and 87% sensitivity and 89% specificity in a validation cohort.
“The bacterial RNA biosignature was notably more predictive of bacterial infection than clinical examination” and use of the Yale Observation Score, and it “added significantly to prediction beyond the YOS alone,” Dr. Mahajan and his associates said (JAMA. 2016 Aug 23. doi: 10.1001/jama.2016.9207).
“Despite the young age of the febrile infants evaluated, they carried robust RNA biosignatures and demonstrated that regardless of the etiology of the infections, their immune systems are programed to respond not only with shared elements induced by common microbes but also with specific patterns that allow discrimination by class of pathogen,” they noted.
Further research is needed to confirm and refine these preliminary results. “As technology advances, RNA biosignatures may prove to be an alternative and accurate method to identify infants with bacterial infections. This would help clinicians target evaluation and therapy when they are needed and avoid invasive procedures, antibiotics, and hospitalizations when they are not,” Dr. Mahajan and his associates said.
Dr. Herberg’s study was supported by the Imperial College Comprehensive Biomedical Research Center, the National Institutes of Health, the European Union’s Seventh Framework Program, and numerous other groups. Dr. Herberg reported having no relevant financial disclosures. Dr. Mahajan’s study was supported by the Health Resources and Services Administration, Emergency Services for Children, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Institutes of Health. Dr. Mahajan reported having no relevant financial disclosures.
FROM JAMA
Key clinical point: RNA biosignatures derived from the patient’s peripheral blood distinguish bacterial from viral causes of fever in young children.
Major finding: Study 1. The DRS showed 96.4% sensitivity in a validation cohort of 130 febrile children. Study 2. A set of 66 RNA transcript signatures showed 82% sensitivity and 88% specificity in the discovery cohort and 87% sensitivity and 89% specificity in a validation cohort.
Data source: Two separate preliminary studies developing and validating tests of host responses to infection, involving 240 and 279 patients, respectively.
Disclosures: Dr. Herberg’s study was supported by the Imperial College Comprehensive Biomedical Research Center, the National Institutes of Health, the European Union’s Seventh Framework Program, and numerous other groups. Dr. Herberg reported having no relevant financial disclosures. Dr. Mahajan’s study was supported by the Health Resources and Services Administration, Emergency Services for Children, the Eunice Kennedy Shriver National Institute of Child Health and Human Development, and the National Institutes of Health. Dr. Mahajan reported having no relevant financial disclosures.

CANDLE syndrome case highlights key features of this type 1 interferonopathy
BOSTON – Annular erythematous plaques in a child with fever and dense, atypical, mixed mononuclear and neutrophilic dermal infiltrate on biopsy could signal the recently described autoinflammatory disorder known as CANDLE Syndrome, according to Raegan Hunt, MD.
CANDLE, which stands for chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature, is a proteasome-associated autoinflammatory syndrome characterized by dysregulation of type 1 interferon signaling, Dr. Hunt of Baylor College of Medicine and Texas Children’s Hospital said during a presentation at the American Academy of Dermatology summer meeting.

She described a case involving a 12-year-old girl with erythematous, warm, tender, nonpruritic papules and plaques on the superior chest, neck, and upper back. Most had an annular configuration with central clearing and occasionally central duskiness and ulceration.
The child also sometimes had violaceous swelling of the eyelid, nodules on the ear, and figurate erythematous plaques on the upper arm.
“She’s been having these since she was an infant in periodic bursts, and carried a diagnosis of annular erythema of infancy,” Dr. Hunt said.
Other symptoms included recurrent fevers, myalgias, transient and migratory arthritis, elevated C-reactive protein and erythrocyte sedimentation rate, and aseptic meningitis requiring hospitalization.
She had no family history of autoimmune disease, immune deficiency, or other genetic diseases, Dr. Hunt said.

“She was treated with methotrexate and prednisone, as well as IVIG [intravenous immunoglobulin] every 4 weeks. Her prednisone was never weaned successfully below 0.8 mg/kg. She had complications of chronic corticosteroid disease, including many fractures,” she said.
A biopsy showed a dense infiltrate of atypical, mixed mononuclear and neutrophilic dermal infiltrate.
“These taken together are suggestive of ... CANDLE,” she said.
Genetic testing confirmed the presence of a compound heterozygous mutation in the proteasome subunit beta type 9, or PSMB8 gene.
Key features of CANDLE syndrome, first described in a 2010 article and further described by Liu, et al in 2012, include early disease onset, recurrent febrile episodes, skin lesions – including recurrent attacks of erythematous annular plaques and violaceous swelling of the eyelids, delayed physical development, progressive lipodystrophy, arthralgias, systemic inflammation, and aseptic meningitis episodes.
“Our patient did have very, very subtle lipodystrophy, but overall not as quick onset as some other [cases in children] that have been described,” Dr. Hunt said.
The type 1 interferonopathy is of autosomal recessive inheritance, and involves either homozygous or compound heterozygous mutations in PSMB8, as found in this patient. PSMB8 is an immunoproteasome unit involved in proteolysis and maintenance of cell homeostasis, she explained.
Treatment of the syndrome involves high-dose corticosteroids (usually 1-2 mg/kg day), which helps improve cutaneous eruptions, joint pain, and fever, but it is important to remember that disease flares can occur with tapering, Dr. Hunt noted.
Response is typically poor in patients treated with steroid-sparing agents, such as methotrexate, cyclosporine, azathioprine, or IVIG, as well as with tumor necrosis factor–alpha inhibitors and interleukin-1 receptor antagonists.
“But there is an interesting molecule on the horizon for possibly treating this more specifically and that’s JAK inhibitors,” she said, noting that a National Institutes of Health compassionate use clinical research trial is evaluating the JAK 1/2 inhibitor, baricitinib.
Dr. Hunt reported having no relevant disclosures.
BOSTON – Annular erythematous plaques in a child with fever and dense, atypical, mixed mononuclear and neutrophilic dermal infiltrate on biopsy could signal the recently described autoinflammatory disorder known as CANDLE Syndrome, according to Raegan Hunt, MD.
CANDLE, which stands for chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature, is a proteasome-associated autoinflammatory syndrome characterized by dysregulation of type 1 interferon signaling, Dr. Hunt of Baylor College of Medicine and Texas Children’s Hospital said during a presentation at the American Academy of Dermatology summer meeting.
She described a case involving a 12-year-old girl with erythematous, warm, tender, nonpruritic papules and plaques on the superior chest, neck, and upper back. Most had an annular configuration with central clearing and occasionally central duskiness and ulceration.
The child also sometimes had violaceous swelling of the eyelid, nodules on the ear, and figurate erythematous plaques on the upper arm.
“She’s been having these since she was an infant in periodic bursts, and carried a diagnosis of annular erythema of infancy,” Dr. Hunt said.
Other symptoms included recurrent fevers, myalgias, transient and migratory arthritis, elevated C-reactive protein and erythrocyte sedimentation rate, and aseptic meningitis requiring hospitalization.
She had no family history of autoimmune disease, immune deficiency, or other genetic diseases, Dr. Hunt said.
“She was treated with methotrexate and prednisone, as well as IVIG [intravenous immunoglobulin] every 4 weeks. Her prednisone was never weaned successfully below 0.8 mg/kg. She had complications of chronic corticosteroid disease, including many fractures,” she said.
A biopsy showed a dense infiltrate of atypical, mixed mononuclear and neutrophilic dermal infiltrate.
“These taken together are suggestive of ... CANDLE,” she said.
Genetic testing confirmed the presence of a compound heterozygous mutation in the proteasome subunit beta type 9, or PSMB8 gene.
Key features of CANDLE syndrome, first described in a 2010 article and further described by Liu, et al in 2012, include early disease onset, recurrent febrile episodes, skin lesions – including recurrent attacks of erythematous annular plaques and violaceous swelling of the eyelids, delayed physical development, progressive lipodystrophy, arthralgias, systemic inflammation, and aseptic meningitis episodes.
“Our patient did have very, very subtle lipodystrophy, but overall not as quick onset as some other [cases in children] that have been described,” Dr. Hunt said.
The type 1 interferonopathy is of autosomal recessive inheritance, and involves either homozygous or compound heterozygous mutations in PSMB8, as found in this patient. PSMB8 is an immunoproteasome unit involved in proteolysis and maintenance of cell homeostasis, she explained.
Treatment of the syndrome involves high-dose corticosteroids (usually 1-2 mg/kg day), which helps improve cutaneous eruptions, joint pain, and fever, but it is important to remember that disease flares can occur with tapering, Dr. Hunt noted.
Response is typically poor in patients treated with steroid-sparing agents, such as methotrexate, cyclosporine, azathioprine, or IVIG, as well as with tumor necrosis factor–alpha inhibitors and interleukin-1 receptor antagonists.
“But there is an interesting molecule on the horizon for possibly treating this more specifically and that’s JAK inhibitors,” she said, noting that a National Institutes of Health compassionate use clinical research trial is evaluating the JAK 1/2 inhibitor, baricitinib.
Dr. Hunt reported having no relevant disclosures.
BOSTON – Annular erythematous plaques in a child with fever and dense, atypical, mixed mononuclear and neutrophilic dermal infiltrate on biopsy could signal the recently described autoinflammatory disorder known as CANDLE Syndrome, according to Raegan Hunt, MD.
CANDLE, which stands for chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature, is a proteasome-associated autoinflammatory syndrome characterized by dysregulation of type 1 interferon signaling, Dr. Hunt of Baylor College of Medicine and Texas Children’s Hospital said during a presentation at the American Academy of Dermatology summer meeting.
She described a case involving a 12-year-old girl with erythematous, warm, tender, nonpruritic papules and plaques on the superior chest, neck, and upper back. Most had an annular configuration with central clearing and occasionally central duskiness and ulceration.
The child also sometimes had violaceous swelling of the eyelid, nodules on the ear, and figurate erythematous plaques on the upper arm.
“She’s been having these since she was an infant in periodic bursts, and carried a diagnosis of annular erythema of infancy,” Dr. Hunt said.
Other symptoms included recurrent fevers, myalgias, transient and migratory arthritis, elevated C-reactive protein and erythrocyte sedimentation rate, and aseptic meningitis requiring hospitalization.
She had no family history of autoimmune disease, immune deficiency, or other genetic diseases, Dr. Hunt said.
“She was treated with methotrexate and prednisone, as well as IVIG [intravenous immunoglobulin] every 4 weeks. Her prednisone was never weaned successfully below 0.8 mg/kg. She had complications of chronic corticosteroid disease, including many fractures,” she said.
A biopsy showed a dense infiltrate of atypical, mixed mononuclear and neutrophilic dermal infiltrate.
“These taken together are suggestive of ... CANDLE,” she said.
Genetic testing confirmed the presence of a compound heterozygous mutation in the proteasome subunit beta type 9, or PSMB8 gene.
Key features of CANDLE syndrome, first described in a 2010 article and further described by Liu, et al in 2012, include early disease onset, recurrent febrile episodes, skin lesions – including recurrent attacks of erythematous annular plaques and violaceous swelling of the eyelids, delayed physical development, progressive lipodystrophy, arthralgias, systemic inflammation, and aseptic meningitis episodes.
“Our patient did have very, very subtle lipodystrophy, but overall not as quick onset as some other [cases in children] that have been described,” Dr. Hunt said.
The type 1 interferonopathy is of autosomal recessive inheritance, and involves either homozygous or compound heterozygous mutations in PSMB8, as found in this patient. PSMB8 is an immunoproteasome unit involved in proteolysis and maintenance of cell homeostasis, she explained.
Treatment of the syndrome involves high-dose corticosteroids (usually 1-2 mg/kg day), which helps improve cutaneous eruptions, joint pain, and fever, but it is important to remember that disease flares can occur with tapering, Dr. Hunt noted.
Response is typically poor in patients treated with steroid-sparing agents, such as methotrexate, cyclosporine, azathioprine, or IVIG, as well as with tumor necrosis factor–alpha inhibitors and interleukin-1 receptor antagonists.
“But there is an interesting molecule on the horizon for possibly treating this more specifically and that’s JAK inhibitors,” she said, noting that a National Institutes of Health compassionate use clinical research trial is evaluating the JAK 1/2 inhibitor, baricitinib.
Dr. Hunt reported having no relevant disclosures.
EXPERT ANALYSIS FROM THE AAD SUMMER ACADEMY 2016
Key clinical point: Annular erythematous plaques in a child with fever and dense, atypical, mixed mononuclear and neutrophilic dermal infiltrate on biopsy could signal the recently described autoinflammatory disorder known as CANDLE syndrome.
Major finding: Genetic testing confirmed the presence of a compound heterozygous mutation in the proteasome subunit beta type 9, or PSMB8 gene.
Data source: Expert analysis – case description.
Disclosures: Dr. Hunt reported having no disclosures.

Hepatitis B vaccine response suppressed by maternal antibodies
Maternal antibodies against hepatitis blunt the immune response to the hepatitis B vaccine in newborns, but the booster dose is unaffected by maternal antibodies, a study found.
Previous research also has identified a suppressed response to vaccination due to maternal antibodies with vaccines such as the measles, hepatitis A, mumps and tetanus vaccines.
“Maternal antibodies are a double-edged sword for infants,” wrote X. Chen of the Zhongnan Hospital of Wuhan (China) University, and colleagues (J Viral Hepat. 2016 Jul 29. doi: 10.1111/jvh.12572). “These neutralizing antibodies can protect neonates against most infectious diseases in early life; however, as shown in the study here, these antibodies can also suppress the immune response of infants to vaccines.”
The researchers first assessed transplacental transfer of antibodies by measuring anti–hepatitis B antibodies in 90 mothers and their newborns. The mothers were all positive for anti–hepatitis B antibodies with a median titer of 250. Before the infants had been vaccinated, 97% were positive for anti–hepatitis B antibodies. Among infants whose mothers had titers above 100 IU/L, 100% were positive for antibodies.
Then the researchers measured titers and rate of anti–hepatitis B positivity in 1,055 mothers and their 1,063 infants, aged 7-24 months, after the babies had received doses of the 10 mcg HBV vaccine at ages 0, 1 and 6 months, per the recommended schedule in China. In the United States, infants are recommended to receive the vaccine at birth, at 1-4 months, and then at 6-18 months.
Among the 405 mothers with antibodies of less than 10 IU/L, 89% of their newborns responded sufficiently to the vaccine to be positive for anti–hepatitis B antibodies. Among the 451 mothers with antibodies from 10-499 IU/L, 85% of the infants had positivity, and among the 207 mothers with antibodies of 500 IU/L and higher, 77% of the infants were positive for anti–hepatitis B antibodies.
Titers followed the same inverse pattern. The median titer was 169 in infants whose mothers had low titers, but the median titer was 79 in infants of mothers with high titers. When mothers with titers in the middle range, the infants’ median titer was 141.
Among 162 newborns who tested negative for anti–hepatitis B antibodies after receiving all three doses of the vaccine, 92% showed positivity for the antibodies after receiving a “catch-up” booster dose, without significant interference from maternal antibodies. Of another 11 infants still lacking positivity, 8 assessed 1 month later, achieved it after a second catch-up booster, suggesting “the suppression effects of the maternal anti-HBVs can be overcome.”
The research was funded by the Hongkong Zeshan Foundation, and the authors reported having no disclosures.
Maternal antibodies against hepatitis blunt the immune response to the hepatitis B vaccine in newborns, but the booster dose is unaffected by maternal antibodies, a study found.
Previous research also has identified a suppressed response to vaccination due to maternal antibodies with vaccines such as the measles, hepatitis A, mumps and tetanus vaccines.
“Maternal antibodies are a double-edged sword for infants,” wrote X. Chen of the Zhongnan Hospital of Wuhan (China) University, and colleagues (J Viral Hepat. 2016 Jul 29. doi: 10.1111/jvh.12572). “These neutralizing antibodies can protect neonates against most infectious diseases in early life; however, as shown in the study here, these antibodies can also suppress the immune response of infants to vaccines.”
The researchers first assessed transplacental transfer of antibodies by measuring anti–hepatitis B antibodies in 90 mothers and their newborns. The mothers were all positive for anti–hepatitis B antibodies with a median titer of 250. Before the infants had been vaccinated, 97% were positive for anti–hepatitis B antibodies. Among infants whose mothers had titers above 100 IU/L, 100% were positive for antibodies.
Then the researchers measured titers and rate of anti–hepatitis B positivity in 1,055 mothers and their 1,063 infants, aged 7-24 months, after the babies had received doses of the 10 mcg HBV vaccine at ages 0, 1 and 6 months, per the recommended schedule in China. In the United States, infants are recommended to receive the vaccine at birth, at 1-4 months, and then at 6-18 months.
Among the 405 mothers with antibodies of less than 10 IU/L, 89% of their newborns responded sufficiently to the vaccine to be positive for anti–hepatitis B antibodies. Among the 451 mothers with antibodies from 10-499 IU/L, 85% of the infants had positivity, and among the 207 mothers with antibodies of 500 IU/L and higher, 77% of the infants were positive for anti–hepatitis B antibodies.
Titers followed the same inverse pattern. The median titer was 169 in infants whose mothers had low titers, but the median titer was 79 in infants of mothers with high titers. When mothers with titers in the middle range, the infants’ median titer was 141.
Among 162 newborns who tested negative for anti–hepatitis B antibodies after receiving all three doses of the vaccine, 92% showed positivity for the antibodies after receiving a “catch-up” booster dose, without significant interference from maternal antibodies. Of another 11 infants still lacking positivity, 8 assessed 1 month later, achieved it after a second catch-up booster, suggesting “the suppression effects of the maternal anti-HBVs can be overcome.”
The research was funded by the Hongkong Zeshan Foundation, and the authors reported having no disclosures.
Maternal antibodies against hepatitis blunt the immune response to the hepatitis B vaccine in newborns, but the booster dose is unaffected by maternal antibodies, a study found.
Previous research also has identified a suppressed response to vaccination due to maternal antibodies with vaccines such as the measles, hepatitis A, mumps and tetanus vaccines.
“Maternal antibodies are a double-edged sword for infants,” wrote X. Chen of the Zhongnan Hospital of Wuhan (China) University, and colleagues (J Viral Hepat. 2016 Jul 29. doi: 10.1111/jvh.12572). “These neutralizing antibodies can protect neonates against most infectious diseases in early life; however, as shown in the study here, these antibodies can also suppress the immune response of infants to vaccines.”
The researchers first assessed transplacental transfer of antibodies by measuring anti–hepatitis B antibodies in 90 mothers and their newborns. The mothers were all positive for anti–hepatitis B antibodies with a median titer of 250. Before the infants had been vaccinated, 97% were positive for anti–hepatitis B antibodies. Among infants whose mothers had titers above 100 IU/L, 100% were positive for antibodies.
Then the researchers measured titers and rate of anti–hepatitis B positivity in 1,055 mothers and their 1,063 infants, aged 7-24 months, after the babies had received doses of the 10 mcg HBV vaccine at ages 0, 1 and 6 months, per the recommended schedule in China. In the United States, infants are recommended to receive the vaccine at birth, at 1-4 months, and then at 6-18 months.
Among the 405 mothers with antibodies of less than 10 IU/L, 89% of their newborns responded sufficiently to the vaccine to be positive for anti–hepatitis B antibodies. Among the 451 mothers with antibodies from 10-499 IU/L, 85% of the infants had positivity, and among the 207 mothers with antibodies of 500 IU/L and higher, 77% of the infants were positive for anti–hepatitis B antibodies.
Titers followed the same inverse pattern. The median titer was 169 in infants whose mothers had low titers, but the median titer was 79 in infants of mothers with high titers. When mothers with titers in the middle range, the infants’ median titer was 141.
Among 162 newborns who tested negative for anti–hepatitis B antibodies after receiving all three doses of the vaccine, 92% showed positivity for the antibodies after receiving a “catch-up” booster dose, without significant interference from maternal antibodies. Of another 11 infants still lacking positivity, 8 assessed 1 month later, achieved it after a second catch-up booster, suggesting “the suppression effects of the maternal anti-HBVs can be overcome.”
The research was funded by the Hongkong Zeshan Foundation, and the authors reported having no disclosures.
FROM THE JOURNAL OF VIRAL HEPATITIS
Key clinical point: Maternal immunity to hepatitis B suppresses infant response to vaccination.
Major finding: 89%, 85%, and 77% of newborns tested positive for anti–hepatitis B antibodies after a standard three-dose regimen when born to mothers with low, medium, and high titers, respectively.
Data source: The findings are based on titers and antibody positivity against hepatitis B in 1,055 mothers and 1,063 newborns at multiple centers in China from March 2012 to November 2015 before and after infant immunization against hepatitis B.
Disclosures: The research was funded by the Hongkong Zeshan Foundation, and the authors reported having no disclosures.
SHARE initiative releases consensus-based JDM management recommendations
Early and aggressive therapy may prevent or stabilize organ damage and disease-related complications in patients with juvenile dermatomyositis, according to new consensus-based recommendations for the management of the disorder.
Overall, the recommendations – a project of the Single Hub and Access Point for Pediatric Rheumatology in Europe (SHARE) initiative – include 7 overarching principles, 33 recommendations on diagnosis, and 19 recommendations on therapy that were accepted with greater than 80% agreement among experts. The recommendations, which address the assessment of skin, muscle, and major organ involvement and treatment suggestions at disease onset and in refractory cases, fill a void in the area of evidence-based guidelines for this rare disease within the group of pediatric rheumatic diseases, according to Felicitas Bellutti Enders, MD, of University Medical Center Utrecht (the Netherlands) and her colleagues.

“Clear recommendations can help clinicians in the care of patients with JDM [juvenile dermatomyositis] as no international consensus regarding diagnosis and treatment is currently available and management therefore varies,” they wrote (Ann Rheum Dis. 2016 Aug 11. doi: 10.1136/annrheumdis-2016-209247).
The consensus committee, including 19 experienced pediatric rheumatologists and 2 experts in pediatric exercise physiology and physical therapy, developed recommendations based on a validated systematic literature review. The recommendations were evaluated by an online survey and then discussed at two subsequent consensus meetings.
The overarching principles accepted by more than 80% of respondents (100% in all but number 4 below), hold that:
1) All children with suspected idiopathic inflammatory myopathies should be referred to a specialized center.
2) High-risk patients need immediate/urgent referral to a specialized center.
3) Patient-/parent-reported outcomes measures are helpful when assessing disease activity and should be used at diagnosis and during disease monitoring.
4) Validated tools such as the Childhood Health Assessment Questionnaire, patient/parent visual analog scale and Juvenile Dermatomyositis Multi-dimensional Assessment Report should be used to measure health status.
5) All children with JDM should have disease activity (muscle, skin, major organ) assessed regularly in a standardized way, using tools such as the Disease Activity Score.
6) All children with JDM should have disease damage assessed at least yearly using a standardized disease damage measure, such as the Myositis Damage index.
7) All patients with JDM should have the opportunity to be registered within a research registry/repository such as the Euromyositis registry.
The consensus process also yielded both general and specific recommendations for diagnosis and management – also with 100% agreement in almost all cases – addressing investigations to consider in all those with a JDM diagnosis (muscle enzymes, full blood count, renal function and liver function tests, and infection screen – to name a few), ways that MRI can be used (both for diagnosis and disease activity monitoring), the use of muscle biopsy (use in all cases involving atypical presentation), and assessment of calcinosis and skin, lung, and cardiac involvement.
Treatment recommendations address sun protection (encourage routine use of sunblock), exercise (should be safe and appropriate and monitored by a physiotherapist), corticosteroid use (administer systematically either orally or intravenously in moderate to severe JDM and wean as the patient shows clinical improvement), use of intravenous immunoglobulin (a useful adjunct for resistant disease, especially when skin features are prominent), and the use of anti–tumor necrosis factor therapies (consider in refractory disease; infliximab or adalimumab are favored over etanercept), as well as other treatments.
The recommendations state that while there is no high-level evidence of when to stop therapy, consideration may be given to withdrawing treatment if a patient has been off steroids and in remission on methotrexate or an alternative disease-modifying antirheumatic drug [DMARD] for at least 1 year.
The management of JDM is complex and warrants a multidisciplinary approach, involving physiotherapists, specialist nurses, pediatric rheumatologists, and other specialists as needed, the authors wrote, noting that the mainstay of therapy is high-dose corticosteroids initially in combination with DMARDS.
However, the evidence base for treatment is limited and “often confined to small case-controlled studies, with the exception of two randomized controlled trials,” they said.
Similarly, there is no high-level evidence regarding when to stop immunosuppressive therapy, but the expert group suggested considering the withdrawal of methotrexate or alternative DMARD once the patient is in remission and off steroids for a minimum of 1 year.
The authors concluded that “this SHARE initiative is based on expert opinion informed by the best available evidence and provides recommendations ... with a view to improving the outcome for patients with JDM in Europe.
“It will now be important to broaden discussion and test acceptability of these to the wider community,” they wrote.
The SHARE initiative is funded by a grant from the European Agency for Health and Consumers. Dr. Enders disclosed a relationship with the Valeria e Ettore Bossi Foundation. Her coauthors reported financial or other relationships with Roche/Chugai, AbbVie, Pfizer, Novartis, Bristol-Myers Squibb, SOBI, Medac, The Myositis Association, Neopharm, GlaxoSmithKline, and/or Genzyme.
The consensus-based recommendations for the management of juvenile dermatomyositis published in Annals of Rheumatic Diseases again highlight the ability of the European and Canadian investigators to work together and pool the information from a large number of centers. Similar efforts to pool data and encourage the development of protocols to optimize care are occurring in the United States under the auspices of CARRA (the Childhood Arthritis and Rheumatology Research Alliance).
These working groups represent an important first step toward standardizing optimal care for children with rheumatic diseases. However, the protocols put forth by both groups suffer from failure to address the diversity of presentations within their diseases and a resultant lack of specificity in their recommendations. The authors of these guidelines make specific recommendations regarding diagnosis, but these fail to encompass the range of weakness that may be present initially. Is it truly appropriate to bolus every child diagnosed with dermatomyositis with high-dose corticosteroids and begin methotrexate? No mention is made of the hypertension, pancreatitis, or systemic infection that might result.
The guidelines and protocols being promulgated in pediatric rheumatology continue to suffer from the grouping of children with diverse disease presentations and probably diverse diseases under a single diagnosis. Charles Spencer and colleagues described the highly variable course of juvenile dermatomyositis and the presence of distinct subsets of patients more than 30 years ago (J Pediatr. 1984 Sep;105[3]:399-408), but this diversity is not reflected in the current protocol. Methods for better characterizing our patients based on gene activation and cytokine profiles have been developed. More effort should be placed on accurate characterization of our patients with many diseases before we attempt to treat them all the same way.
Thomas J.A. Lehman, MD, is chief of the division of pediatric rheumatology at the Hospital for Special Surgery, and professor of clinical pediatrics at Weill Medical Center, Cornell University, New York. He has no relevant disclosures.
The consensus-based recommendations for the management of juvenile dermatomyositis published in Annals of Rheumatic Diseases again highlight the ability of the European and Canadian investigators to work together and pool the information from a large number of centers. Similar efforts to pool data and encourage the development of protocols to optimize care are occurring in the United States under the auspices of CARRA (the Childhood Arthritis and Rheumatology Research Alliance).
These working groups represent an important first step toward standardizing optimal care for children with rheumatic diseases. However, the protocols put forth by both groups suffer from failure to address the diversity of presentations within their diseases and a resultant lack of specificity in their recommendations. The authors of these guidelines make specific recommendations regarding diagnosis, but these fail to encompass the range of weakness that may be present initially. Is it truly appropriate to bolus every child diagnosed with dermatomyositis with high-dose corticosteroids and begin methotrexate? No mention is made of the hypertension, pancreatitis, or systemic infection that might result.
The guidelines and protocols being promulgated in pediatric rheumatology continue to suffer from the grouping of children with diverse disease presentations and probably diverse diseases under a single diagnosis. Charles Spencer and colleagues described the highly variable course of juvenile dermatomyositis and the presence of distinct subsets of patients more than 30 years ago (J Pediatr. 1984 Sep;105[3]:399-408), but this diversity is not reflected in the current protocol. Methods for better characterizing our patients based on gene activation and cytokine profiles have been developed. More effort should be placed on accurate characterization of our patients with many diseases before we attempt to treat them all the same way.
Thomas J.A. Lehman, MD, is chief of the division of pediatric rheumatology at the Hospital for Special Surgery, and professor of clinical pediatrics at Weill Medical Center, Cornell University, New York. He has no relevant disclosures.
The consensus-based recommendations for the management of juvenile dermatomyositis published in Annals of Rheumatic Diseases again highlight the ability of the European and Canadian investigators to work together and pool the information from a large number of centers. Similar efforts to pool data and encourage the development of protocols to optimize care are occurring in the United States under the auspices of CARRA (the Childhood Arthritis and Rheumatology Research Alliance).
These working groups represent an important first step toward standardizing optimal care for children with rheumatic diseases. However, the protocols put forth by both groups suffer from failure to address the diversity of presentations within their diseases and a resultant lack of specificity in their recommendations. The authors of these guidelines make specific recommendations regarding diagnosis, but these fail to encompass the range of weakness that may be present initially. Is it truly appropriate to bolus every child diagnosed with dermatomyositis with high-dose corticosteroids and begin methotrexate? No mention is made of the hypertension, pancreatitis, or systemic infection that might result.
The guidelines and protocols being promulgated in pediatric rheumatology continue to suffer from the grouping of children with diverse disease presentations and probably diverse diseases under a single diagnosis. Charles Spencer and colleagues described the highly variable course of juvenile dermatomyositis and the presence of distinct subsets of patients more than 30 years ago (J Pediatr. 1984 Sep;105[3]:399-408), but this diversity is not reflected in the current protocol. Methods for better characterizing our patients based on gene activation and cytokine profiles have been developed. More effort should be placed on accurate characterization of our patients with many diseases before we attempt to treat them all the same way.
Thomas J.A. Lehman, MD, is chief of the division of pediatric rheumatology at the Hospital for Special Surgery, and professor of clinical pediatrics at Weill Medical Center, Cornell University, New York. He has no relevant disclosures.
Early and aggressive therapy may prevent or stabilize organ damage and disease-related complications in patients with juvenile dermatomyositis, according to new consensus-based recommendations for the management of the disorder.
Overall, the recommendations – a project of the Single Hub and Access Point for Pediatric Rheumatology in Europe (SHARE) initiative – include 7 overarching principles, 33 recommendations on diagnosis, and 19 recommendations on therapy that were accepted with greater than 80% agreement among experts. The recommendations, which address the assessment of skin, muscle, and major organ involvement and treatment suggestions at disease onset and in refractory cases, fill a void in the area of evidence-based guidelines for this rare disease within the group of pediatric rheumatic diseases, according to Felicitas Bellutti Enders, MD, of University Medical Center Utrecht (the Netherlands) and her colleagues.
“Clear recommendations can help clinicians in the care of patients with JDM [juvenile dermatomyositis] as no international consensus regarding diagnosis and treatment is currently available and management therefore varies,” they wrote (Ann Rheum Dis. 2016 Aug 11. doi: 10.1136/annrheumdis-2016-209247).
The consensus committee, including 19 experienced pediatric rheumatologists and 2 experts in pediatric exercise physiology and physical therapy, developed recommendations based on a validated systematic literature review. The recommendations were evaluated by an online survey and then discussed at two subsequent consensus meetings.
The overarching principles accepted by more than 80% of respondents (100% in all but number 4 below), hold that:
1) All children with suspected idiopathic inflammatory myopathies should be referred to a specialized center.
2) High-risk patients need immediate/urgent referral to a specialized center.
3) Patient-/parent-reported outcomes measures are helpful when assessing disease activity and should be used at diagnosis and during disease monitoring.
4) Validated tools such as the Childhood Health Assessment Questionnaire, patient/parent visual analog scale and Juvenile Dermatomyositis Multi-dimensional Assessment Report should be used to measure health status.
5) All children with JDM should have disease activity (muscle, skin, major organ) assessed regularly in a standardized way, using tools such as the Disease Activity Score.
6) All children with JDM should have disease damage assessed at least yearly using a standardized disease damage measure, such as the Myositis Damage index.
7) All patients with JDM should have the opportunity to be registered within a research registry/repository such as the Euromyositis registry.
The consensus process also yielded both general and specific recommendations for diagnosis and management – also with 100% agreement in almost all cases – addressing investigations to consider in all those with a JDM diagnosis (muscle enzymes, full blood count, renal function and liver function tests, and infection screen – to name a few), ways that MRI can be used (both for diagnosis and disease activity monitoring), the use of muscle biopsy (use in all cases involving atypical presentation), and assessment of calcinosis and skin, lung, and cardiac involvement.
Treatment recommendations address sun protection (encourage routine use of sunblock), exercise (should be safe and appropriate and monitored by a physiotherapist), corticosteroid use (administer systematically either orally or intravenously in moderate to severe JDM and wean as the patient shows clinical improvement), use of intravenous immunoglobulin (a useful adjunct for resistant disease, especially when skin features are prominent), and the use of anti–tumor necrosis factor therapies (consider in refractory disease; infliximab or adalimumab are favored over etanercept), as well as other treatments.
The recommendations state that while there is no high-level evidence of when to stop therapy, consideration may be given to withdrawing treatment if a patient has been off steroids and in remission on methotrexate or an alternative disease-modifying antirheumatic drug [DMARD] for at least 1 year.
The management of JDM is complex and warrants a multidisciplinary approach, involving physiotherapists, specialist nurses, pediatric rheumatologists, and other specialists as needed, the authors wrote, noting that the mainstay of therapy is high-dose corticosteroids initially in combination with DMARDS.
However, the evidence base for treatment is limited and “often confined to small case-controlled studies, with the exception of two randomized controlled trials,” they said.
Similarly, there is no high-level evidence regarding when to stop immunosuppressive therapy, but the expert group suggested considering the withdrawal of methotrexate or alternative DMARD once the patient is in remission and off steroids for a minimum of 1 year.
The authors concluded that “this SHARE initiative is based on expert opinion informed by the best available evidence and provides recommendations ... with a view to improving the outcome for patients with JDM in Europe.
“It will now be important to broaden discussion and test acceptability of these to the wider community,” they wrote.
The SHARE initiative is funded by a grant from the European Agency for Health and Consumers. Dr. Enders disclosed a relationship with the Valeria e Ettore Bossi Foundation. Her coauthors reported financial or other relationships with Roche/Chugai, AbbVie, Pfizer, Novartis, Bristol-Myers Squibb, SOBI, Medac, The Myositis Association, Neopharm, GlaxoSmithKline, and/or Genzyme.
Early and aggressive therapy may prevent or stabilize organ damage and disease-related complications in patients with juvenile dermatomyositis, according to new consensus-based recommendations for the management of the disorder.
Overall, the recommendations – a project of the Single Hub and Access Point for Pediatric Rheumatology in Europe (SHARE) initiative – include 7 overarching principles, 33 recommendations on diagnosis, and 19 recommendations on therapy that were accepted with greater than 80% agreement among experts. The recommendations, which address the assessment of skin, muscle, and major organ involvement and treatment suggestions at disease onset and in refractory cases, fill a void in the area of evidence-based guidelines for this rare disease within the group of pediatric rheumatic diseases, according to Felicitas Bellutti Enders, MD, of University Medical Center Utrecht (the Netherlands) and her colleagues.
“Clear recommendations can help clinicians in the care of patients with JDM [juvenile dermatomyositis] as no international consensus regarding diagnosis and treatment is currently available and management therefore varies,” they wrote (Ann Rheum Dis. 2016 Aug 11. doi: 10.1136/annrheumdis-2016-209247).
The consensus committee, including 19 experienced pediatric rheumatologists and 2 experts in pediatric exercise physiology and physical therapy, developed recommendations based on a validated systematic literature review. The recommendations were evaluated by an online survey and then discussed at two subsequent consensus meetings.
The overarching principles accepted by more than 80% of respondents (100% in all but number 4 below), hold that:
1) All children with suspected idiopathic inflammatory myopathies should be referred to a specialized center.
2) High-risk patients need immediate/urgent referral to a specialized center.
3) Patient-/parent-reported outcomes measures are helpful when assessing disease activity and should be used at diagnosis and during disease monitoring.
4) Validated tools such as the Childhood Health Assessment Questionnaire, patient/parent visual analog scale and Juvenile Dermatomyositis Multi-dimensional Assessment Report should be used to measure health status.
5) All children with JDM should have disease activity (muscle, skin, major organ) assessed regularly in a standardized way, using tools such as the Disease Activity Score.
6) All children with JDM should have disease damage assessed at least yearly using a standardized disease damage measure, such as the Myositis Damage index.
7) All patients with JDM should have the opportunity to be registered within a research registry/repository such as the Euromyositis registry.
The consensus process also yielded both general and specific recommendations for diagnosis and management – also with 100% agreement in almost all cases – addressing investigations to consider in all those with a JDM diagnosis (muscle enzymes, full blood count, renal function and liver function tests, and infection screen – to name a few), ways that MRI can be used (both for diagnosis and disease activity monitoring), the use of muscle biopsy (use in all cases involving atypical presentation), and assessment of calcinosis and skin, lung, and cardiac involvement.
Treatment recommendations address sun protection (encourage routine use of sunblock), exercise (should be safe and appropriate and monitored by a physiotherapist), corticosteroid use (administer systematically either orally or intravenously in moderate to severe JDM and wean as the patient shows clinical improvement), use of intravenous immunoglobulin (a useful adjunct for resistant disease, especially when skin features are prominent), and the use of anti–tumor necrosis factor therapies (consider in refractory disease; infliximab or adalimumab are favored over etanercept), as well as other treatments.
The recommendations state that while there is no high-level evidence of when to stop therapy, consideration may be given to withdrawing treatment if a patient has been off steroids and in remission on methotrexate or an alternative disease-modifying antirheumatic drug [DMARD] for at least 1 year.
The management of JDM is complex and warrants a multidisciplinary approach, involving physiotherapists, specialist nurses, pediatric rheumatologists, and other specialists as needed, the authors wrote, noting that the mainstay of therapy is high-dose corticosteroids initially in combination with DMARDS.
However, the evidence base for treatment is limited and “often confined to small case-controlled studies, with the exception of two randomized controlled trials,” they said.
Similarly, there is no high-level evidence regarding when to stop immunosuppressive therapy, but the expert group suggested considering the withdrawal of methotrexate or alternative DMARD once the patient is in remission and off steroids for a minimum of 1 year.
The authors concluded that “this SHARE initiative is based on expert opinion informed by the best available evidence and provides recommendations ... with a view to improving the outcome for patients with JDM in Europe.
“It will now be important to broaden discussion and test acceptability of these to the wider community,” they wrote.
The SHARE initiative is funded by a grant from the European Agency for Health and Consumers. Dr. Enders disclosed a relationship with the Valeria e Ettore Bossi Foundation. Her coauthors reported financial or other relationships with Roche/Chugai, AbbVie, Pfizer, Novartis, Bristol-Myers Squibb, SOBI, Medac, The Myositis Association, Neopharm, GlaxoSmithKline, and/or Genzyme.
FROM ANNALS OF THE RHEUMATIC DISEASES

Nonpharmacologic AD therapy: Strongest evidence supports moisturizers
BOSTON – Moisturizers are “a cornerstone” of therapy for children with atopic dermatitis, according to Julie V. Schaffer, MD.
Moisturizers improve skin hydration, increase the time between flares, and reduce xerosis and pruritus, Dr. Schaffer of Hackensack (N.J.) University Medical Group said at the American Academy of Dermatology summer meeting.

In 2014, the AAD released guidelines that “very strongly” recommended moisturizers as an important nonpharmacologic intervention for patients with AD, stating that moisturizer use decreases disease severity and can reduce the need for pharmacologic intervention, she said.
In fact, the recommendation for moisturizer was based on “strength A, level 1 evidence,” she noted.
The role of bathing is a bit less clear; bathing is suggested as part of treatment and maintenance, but no standard exists with respect to frequency or duration for those with AD (evidence level: III, strength of recommendation: C). In general, the AAD recommends daily or less frequent bathing in warm water for 5-10 minutes, but surveys suggest that bathing recommendations vary widely among specialists and primary care providers, Dr. Schaffer said.
She noted that she sometimes sees children who have been told to bathe only once a week.
“They will come in just covered with disgusting gunk and it can’t be good for them,” she said. Bathing, especially if they have crusting and scaling, removes irritants and potential allergens, and provides hydration. It can also improve penetration of topical medications, as well as tolerance of those medications so that they burn less.
“So I give a thumbs up to daily bathing,” she said.
It is generally agreed that moisturizers should be applied soon after bathing (after applying medication) to improve skin hydration in patients with AD, Dr. Schaffer said.
The AAD says that moisturizers should be applied liberally and frequently, but the ideal frequency and type of moisturizer remains “a bit of an art form rather than a precise science,” she added.
The ideal moisturizer is one that is safe, effective, and free of fragrance, irritants, and potential sensitizers, she said, noting that “an individualized approach to moisturizer and vehicle selection can be very helpful.”
For young children, it is important that the product doesn’t sting; an ointment may be preferable in this population. Preteens and teenagers may dislike greasiness, so that is an important consideration, she said.
Dr. Schaffer pointed out that lotion formulations typically have water content that is too high to be helpful for patients with substantial xerosis. Creams or ointments may be a better bet, but take care to avoid contamination in large jars of such products, she advised.
“I’ve had a couple times when patients were getting recurrent infections, and we traced it down to a nasty jar that had a little too much bacteria in it,” she said, noting that using a clean scoop or pump can help prevent contamination.
As for cleansers, the “pretty clear winner” is a nonsoap cleanser, Dr. Schaffer said.
The AAD recommends limited use of hypoallergenic, fragrance-free, nonsoap cleansers with neutral to low pH, but the evidence is insufficient for recommending the addition of bath oils, emollients, oatmeal, and most other additives to bath water, as well as for the use of acidic spring water, she said (evidence level: III, strength of recommendation: C). An exception is bleach baths, as adding a small amount of bleach to bath water has been shown to improve symptoms, but the other products have not been shown to be beneficial.
The AAD notes that wet wrap therapy, either with or without a topical corticosteroid, can be recommended for patients with moderate to severe AD, as this can decrease disease severity and water loss during flares (evidence level: II, strength of recommendation: B).
Use moisturizer in newborns at risk for AD
Moisturizers don’t just help improve atopic dermatitis in children, they may also prevent the condition in at risk newborns.
Parents of a child with eczema who are concerned about the condition developing in their next child may find hope in the findings from two studies published in 2014, Dr. Schaffer said.
In a study of 124 newborns at high risk for AD who were randomized to daily emollient therapy or usual infant skin care started by age 3 weeks, the incidence of AD over 6 months was 43% in the control group, vs. 22% in the emollient group, a relative risk reduction of 50% (J Allergy Clin Immunol. 2014 Oct;134[4]:818-23). Parents in the emollient therapy group were allowed to choose between sunflower oil, Cetaphil cream, or Aquaphor Healing Ointment.
In a similar Japanese study of 118 high risk infants who were randomized to daily treatment with an emulsion-type emollient or usual skin care starting the first week of life, the AD/eczema rates at 32 weeks were 47% and 32% in the control and emollient groups, respectively (J Allergy Clin Immunol. 2014 Oct;134[4], 824-30). Both groups were allowed to use petroleum jelly.
“So that is something you can potentially make a recommendation for,” she said.
Dr. Schaffer reported having no conflicts of interest.
BOSTON – Moisturizers are “a cornerstone” of therapy for children with atopic dermatitis, according to Julie V. Schaffer, MD.
Moisturizers improve skin hydration, increase the time between flares, and reduce xerosis and pruritus, Dr. Schaffer of Hackensack (N.J.) University Medical Group said at the American Academy of Dermatology summer meeting.
In 2014, the AAD released guidelines that “very strongly” recommended moisturizers as an important nonpharmacologic intervention for patients with AD, stating that moisturizer use decreases disease severity and can reduce the need for pharmacologic intervention, she said.
In fact, the recommendation for moisturizer was based on “strength A, level 1 evidence,” she noted.
The role of bathing is a bit less clear; bathing is suggested as part of treatment and maintenance, but no standard exists with respect to frequency or duration for those with AD (evidence level: III, strength of recommendation: C). In general, the AAD recommends daily or less frequent bathing in warm water for 5-10 minutes, but surveys suggest that bathing recommendations vary widely among specialists and primary care providers, Dr. Schaffer said.
She noted that she sometimes sees children who have been told to bathe only once a week.
“They will come in just covered with disgusting gunk and it can’t be good for them,” she said. Bathing, especially if they have crusting and scaling, removes irritants and potential allergens, and provides hydration. It can also improve penetration of topical medications, as well as tolerance of those medications so that they burn less.
“So I give a thumbs up to daily bathing,” she said.
It is generally agreed that moisturizers should be applied soon after bathing (after applying medication) to improve skin hydration in patients with AD, Dr. Schaffer said.
The AAD says that moisturizers should be applied liberally and frequently, but the ideal frequency and type of moisturizer remains “a bit of an art form rather than a precise science,” she added.
The ideal moisturizer is one that is safe, effective, and free of fragrance, irritants, and potential sensitizers, she said, noting that “an individualized approach to moisturizer and vehicle selection can be very helpful.”
For young children, it is important that the product doesn’t sting; an ointment may be preferable in this population. Preteens and teenagers may dislike greasiness, so that is an important consideration, she said.
Dr. Schaffer pointed out that lotion formulations typically have water content that is too high to be helpful for patients with substantial xerosis. Creams or ointments may be a better bet, but take care to avoid contamination in large jars of such products, she advised.
“I’ve had a couple times when patients were getting recurrent infections, and we traced it down to a nasty jar that had a little too much bacteria in it,” she said, noting that using a clean scoop or pump can help prevent contamination.
As for cleansers, the “pretty clear winner” is a nonsoap cleanser, Dr. Schaffer said.
The AAD recommends limited use of hypoallergenic, fragrance-free, nonsoap cleansers with neutral to low pH, but the evidence is insufficient for recommending the addition of bath oils, emollients, oatmeal, and most other additives to bath water, as well as for the use of acidic spring water, she said (evidence level: III, strength of recommendation: C). An exception is bleach baths, as adding a small amount of bleach to bath water has been shown to improve symptoms, but the other products have not been shown to be beneficial.
The AAD notes that wet wrap therapy, either with or without a topical corticosteroid, can be recommended for patients with moderate to severe AD, as this can decrease disease severity and water loss during flares (evidence level: II, strength of recommendation: B).
Use moisturizer in newborns at risk for AD
Moisturizers don’t just help improve atopic dermatitis in children, they may also prevent the condition in at risk newborns.
Parents of a child with eczema who are concerned about the condition developing in their next child may find hope in the findings from two studies published in 2014, Dr. Schaffer said.
In a study of 124 newborns at high risk for AD who were randomized to daily emollient therapy or usual infant skin care started by age 3 weeks, the incidence of AD over 6 months was 43% in the control group, vs. 22% in the emollient group, a relative risk reduction of 50% (J Allergy Clin Immunol. 2014 Oct;134[4]:818-23). Parents in the emollient therapy group were allowed to choose between sunflower oil, Cetaphil cream, or Aquaphor Healing Ointment.
In a similar Japanese study of 118 high risk infants who were randomized to daily treatment with an emulsion-type emollient or usual skin care starting the first week of life, the AD/eczema rates at 32 weeks were 47% and 32% in the control and emollient groups, respectively (J Allergy Clin Immunol. 2014 Oct;134[4], 824-30). Both groups were allowed to use petroleum jelly.
“So that is something you can potentially make a recommendation for,” she said.
Dr. Schaffer reported having no conflicts of interest.
BOSTON – Moisturizers are “a cornerstone” of therapy for children with atopic dermatitis, according to Julie V. Schaffer, MD.
Moisturizers improve skin hydration, increase the time between flares, and reduce xerosis and pruritus, Dr. Schaffer of Hackensack (N.J.) University Medical Group said at the American Academy of Dermatology summer meeting.
In 2014, the AAD released guidelines that “very strongly” recommended moisturizers as an important nonpharmacologic intervention for patients with AD, stating that moisturizer use decreases disease severity and can reduce the need for pharmacologic intervention, she said.
In fact, the recommendation for moisturizer was based on “strength A, level 1 evidence,” she noted.
The role of bathing is a bit less clear; bathing is suggested as part of treatment and maintenance, but no standard exists with respect to frequency or duration for those with AD (evidence level: III, strength of recommendation: C). In general, the AAD recommends daily or less frequent bathing in warm water for 5-10 minutes, but surveys suggest that bathing recommendations vary widely among specialists and primary care providers, Dr. Schaffer said.
She noted that she sometimes sees children who have been told to bathe only once a week.
“They will come in just covered with disgusting gunk and it can’t be good for them,” she said. Bathing, especially if they have crusting and scaling, removes irritants and potential allergens, and provides hydration. It can also improve penetration of topical medications, as well as tolerance of those medications so that they burn less.
“So I give a thumbs up to daily bathing,” she said.
It is generally agreed that moisturizers should be applied soon after bathing (after applying medication) to improve skin hydration in patients with AD, Dr. Schaffer said.
The AAD says that moisturizers should be applied liberally and frequently, but the ideal frequency and type of moisturizer remains “a bit of an art form rather than a precise science,” she added.
The ideal moisturizer is one that is safe, effective, and free of fragrance, irritants, and potential sensitizers, she said, noting that “an individualized approach to moisturizer and vehicle selection can be very helpful.”
For young children, it is important that the product doesn’t sting; an ointment may be preferable in this population. Preteens and teenagers may dislike greasiness, so that is an important consideration, she said.
Dr. Schaffer pointed out that lotion formulations typically have water content that is too high to be helpful for patients with substantial xerosis. Creams or ointments may be a better bet, but take care to avoid contamination in large jars of such products, she advised.
“I’ve had a couple times when patients were getting recurrent infections, and we traced it down to a nasty jar that had a little too much bacteria in it,” she said, noting that using a clean scoop or pump can help prevent contamination.
As for cleansers, the “pretty clear winner” is a nonsoap cleanser, Dr. Schaffer said.
The AAD recommends limited use of hypoallergenic, fragrance-free, nonsoap cleansers with neutral to low pH, but the evidence is insufficient for recommending the addition of bath oils, emollients, oatmeal, and most other additives to bath water, as well as for the use of acidic spring water, she said (evidence level: III, strength of recommendation: C). An exception is bleach baths, as adding a small amount of bleach to bath water has been shown to improve symptoms, but the other products have not been shown to be beneficial.
The AAD notes that wet wrap therapy, either with or without a topical corticosteroid, can be recommended for patients with moderate to severe AD, as this can decrease disease severity and water loss during flares (evidence level: II, strength of recommendation: B).
Use moisturizer in newborns at risk for AD
Moisturizers don’t just help improve atopic dermatitis in children, they may also prevent the condition in at risk newborns.
Parents of a child with eczema who are concerned about the condition developing in their next child may find hope in the findings from two studies published in 2014, Dr. Schaffer said.
In a study of 124 newborns at high risk for AD who were randomized to daily emollient therapy or usual infant skin care started by age 3 weeks, the incidence of AD over 6 months was 43% in the control group, vs. 22% in the emollient group, a relative risk reduction of 50% (J Allergy Clin Immunol. 2014 Oct;134[4]:818-23). Parents in the emollient therapy group were allowed to choose between sunflower oil, Cetaphil cream, or Aquaphor Healing Ointment.
In a similar Japanese study of 118 high risk infants who were randomized to daily treatment with an emulsion-type emollient or usual skin care starting the first week of life, the AD/eczema rates at 32 weeks were 47% and 32% in the control and emollient groups, respectively (J Allergy Clin Immunol. 2014 Oct;134[4], 824-30). Both groups were allowed to use petroleum jelly.
“So that is something you can potentially make a recommendation for,” she said.
Dr. Schaffer reported having no conflicts of interest.
EXPERT ANALYSIS FROM THE AAD SUMMER ACADEMY 2016

Summer flu? Think variant swine influenza virus infection
Two children presented with influenza, and both recovered without the need for hospitalization. This scenario would fail to pique the interest of any pediatrician in January. But what about when it happens in July?
In early August, public health authorities in Ohio announced that two children had tested positive for the variant swine influenza virus H3N2v. Both children had direct contact with pigs at the Clark County Fair in late July. Along with a handful of cases diagnosed in Michigan, these represent the first H3N2v cases in the United States in 2016.

Influenza viruses that normally circulate in swine are designated as “variant” when they infect humans. According to the Centers for Disease Control and Prevention (CDC), human infections with H1N1v, H1N2v, and H3N2v have been identified in the United States. Influenza A H3N2v viruses carrying the matrix gene from the 2009 H1N1 pandemic virus were first detected in pigs in 2010, and in people in the summer of 2011. Since that time, 357 human cases have been reported from 14 states, with nearly 75% occurring in Indiana and Ohio. Most infections occurred after prolonged exposure to pigs at agricultural fairs.
Fortunately, most H3N2v infections have been mild: Since July 2012, only 21 individuals have required hospitalization and a single case resulted in death. Notably, though, many of the hospitalizations involved children.
On Aug. 15, the Centers for Disease Control and Prevention released Interim Guidance for Clinicians on Human Infections with Variant Influenza Viruses.
Because variant virus infection is indistinguishable from seasonal influenza or any other virus that cause influenzalike illness (think fever, cough, sore throat), physicians and other frontline providers need to maintain an index of suspicion. The key is eliciting a history of swine exposure in the week before illness onset. Practically, this means asking about direct contact with pigs, indirect contact with pigs, or close contact with an ill person who has had contact with pigs. Kudos to the astute clinicians in Ohio who thought to send the appropriate influenza testing in July.
When variant influenza virus is suspected, a nasopharyngeal swab or aspirate should be obtained for testing at a state public health lab or the CDC. Rapid antigen tests for influenza may be falsely negative in the setting of H3N2v infection, just as they may be with seasonal influenza infection. Molecular tests such as reverse transcription polymerase chain reaction (RT-PCR) are likely more sensitive, but cannot distinguish variant influenza A viruses from seasonal influenza A viruses.
The Kentucky State Fair opened on Aug. 18, making the CDC guidance especially timely for health care providers in my area. I called a friend who is a pediatric emergency medicine physician to ask if she and her colleagues were routinely screening patients for encounters of the porcine kind.
“For example, are you asking, ‘Have you been showing, raising or feeding swine? Have you been to the pig barn at the fair?’ ”
When my friend quit laughing, I confessed to her that I had not been doing that routinely either. The exposure history is often the most interesting part of the infectious disease evaluation and in the last month, I’ve asked about exposure to sheep (a risk factor for Q fever), exposure to chickens (a risk factor for Salmonella infections), and exposure to beaver dams (a risk factor for blastomycosis). But I’ve not asked about exposure to pigs.
“The emergency medicine approach is to avoid a lot of viral diagnostic testing unless it is going to impact management,” she said. “Tell me how this changes management of my patient.”
From the patient perspective, making a presumptive diagnosis of H3N2v infection would open the door to empiric treatment with antivirals, at least for individuals who are hospitalized, have severe or progressive disease, or who at high risk for complications of influenza. Neuraminidase inhibitors, including oral oseltamivir, inhaled zanamivir, and intravenous peramivir, can be used for treatment of H3N2v infections.
From a societal perspective, making the diagnosis gives public health experts the opportunity to investigate and potentially prevent further infections by isolating sick pigs. Human to human transmission of H3N2v is rare, but has occasionally occurred in households and in one instance, a child care setting. Careful surveillance of each swine flu case in a human is important to exclude the possibility that the virus has developed the ability to spread efficiently from person to person, creating the risk for an epidemic.
Seasonal influenza vaccine does not prevent infection with variant viruses, so avoidance is key. Those at high risk for complications from influenza infection, including children younger than 5 years of age and those with asthma, diabetes, heart disease, immunocompromised conditions, and neurologic or neurodevelopmental disorders, are urged to avoid pigs and swine barns when visiting fairs where the animals are present. Everyone else needs to follow common sense measures to prevent the spread of infection.
• Don’t take food or drink into pig areas; don’t eat, drink or put anything in your mouth in pig areas.
• Don’t take toys, pacifiers, cups, baby bottles, strollers, or similar items into pig areas.
• Wash your hands often with soap and running water before and after exposure to pigs. If soap and water are not available, use an alcohol-based hand rub.
• Avoid close contact with pigs that look or act ill.
• Take protective measures if you must come in contact with pigs that are known or suspected to be sick. This includes wearing personal protective equipment like protective clothing, gloves, and masks that cover your mouth and nose when contact is required.
• To further reduce the risk of infection, minimize contact with pigs in the pig barn and arenas.
It shouldn’t be surprising that flu viruses spread from pigs to people in the same way that regular seasonal influenza spread from person to person. An infected pig coughs or sneezes influenza-containing droplets, and these droplets are inhaled or swallowed by a susceptible human. That makes avoiding contact with pigs that look or act ill especially important. For the record, a pig with flu might have fever, depression, cough, nasal or eye discharge, eye redness, or a poor appetite.
On the bright side, you can’t get H3N2v or any other variant virus from eating properly prepared pork meat. Fairgoers can feel free to indulge in a deep-fried pork chop or one of this year’s featured food items: a basket of French fries topped with smoked pork, cheddar cheese sauce, red onions, jalapeño peppers and barbecue sauce.
Or maybe not. The CDC has a web page devoted to food safety at fairs and festivals. It notes that cases of foodborne illness increase during summer months, and usual safety controls “like monitoring of food temperatures, refrigeration, workers trained in food safety and washing facilities, may not be available when cooking and dining at fairs and festivals.”
The public is urged to seek out “healthy options” from fair vendors first. If healthy options aren’t available, we’re advised to consider bringing food from home to save money and calories.
Sigh. I remember when summer used to be more fun.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville, Ky. and Kosair Children’s Hospital, also in Louisville.
Two children presented with influenza, and both recovered without the need for hospitalization. This scenario would fail to pique the interest of any pediatrician in January. But what about when it happens in July?
In early August, public health authorities in Ohio announced that two children had tested positive for the variant swine influenza virus H3N2v. Both children had direct contact with pigs at the Clark County Fair in late July. Along with a handful of cases diagnosed in Michigan, these represent the first H3N2v cases in the United States in 2016.
Influenza viruses that normally circulate in swine are designated as “variant” when they infect humans. According to the Centers for Disease Control and Prevention (CDC), human infections with H1N1v, H1N2v, and H3N2v have been identified in the United States. Influenza A H3N2v viruses carrying the matrix gene from the 2009 H1N1 pandemic virus were first detected in pigs in 2010, and in people in the summer of 2011. Since that time, 357 human cases have been reported from 14 states, with nearly 75% occurring in Indiana and Ohio. Most infections occurred after prolonged exposure to pigs at agricultural fairs.
Fortunately, most H3N2v infections have been mild: Since July 2012, only 21 individuals have required hospitalization and a single case resulted in death. Notably, though, many of the hospitalizations involved children.
On Aug. 15, the Centers for Disease Control and Prevention released Interim Guidance for Clinicians on Human Infections with Variant Influenza Viruses.
Because variant virus infection is indistinguishable from seasonal influenza or any other virus that cause influenzalike illness (think fever, cough, sore throat), physicians and other frontline providers need to maintain an index of suspicion. The key is eliciting a history of swine exposure in the week before illness onset. Practically, this means asking about direct contact with pigs, indirect contact with pigs, or close contact with an ill person who has had contact with pigs. Kudos to the astute clinicians in Ohio who thought to send the appropriate influenza testing in July.
When variant influenza virus is suspected, a nasopharyngeal swab or aspirate should be obtained for testing at a state public health lab or the CDC. Rapid antigen tests for influenza may be falsely negative in the setting of H3N2v infection, just as they may be with seasonal influenza infection. Molecular tests such as reverse transcription polymerase chain reaction (RT-PCR) are likely more sensitive, but cannot distinguish variant influenza A viruses from seasonal influenza A viruses.
The Kentucky State Fair opened on Aug. 18, making the CDC guidance especially timely for health care providers in my area. I called a friend who is a pediatric emergency medicine physician to ask if she and her colleagues were routinely screening patients for encounters of the porcine kind.
“For example, are you asking, ‘Have you been showing, raising or feeding swine? Have you been to the pig barn at the fair?’ ”
When my friend quit laughing, I confessed to her that I had not been doing that routinely either. The exposure history is often the most interesting part of the infectious disease evaluation and in the last month, I’ve asked about exposure to sheep (a risk factor for Q fever), exposure to chickens (a risk factor for Salmonella infections), and exposure to beaver dams (a risk factor for blastomycosis). But I’ve not asked about exposure to pigs.
“The emergency medicine approach is to avoid a lot of viral diagnostic testing unless it is going to impact management,” she said. “Tell me how this changes management of my patient.”
From the patient perspective, making a presumptive diagnosis of H3N2v infection would open the door to empiric treatment with antivirals, at least for individuals who are hospitalized, have severe or progressive disease, or who at high risk for complications of influenza. Neuraminidase inhibitors, including oral oseltamivir, inhaled zanamivir, and intravenous peramivir, can be used for treatment of H3N2v infections.
From a societal perspective, making the diagnosis gives public health experts the opportunity to investigate and potentially prevent further infections by isolating sick pigs. Human to human transmission of H3N2v is rare, but has occasionally occurred in households and in one instance, a child care setting. Careful surveillance of each swine flu case in a human is important to exclude the possibility that the virus has developed the ability to spread efficiently from person to person, creating the risk for an epidemic.
Seasonal influenza vaccine does not prevent infection with variant viruses, so avoidance is key. Those at high risk for complications from influenza infection, including children younger than 5 years of age and those with asthma, diabetes, heart disease, immunocompromised conditions, and neurologic or neurodevelopmental disorders, are urged to avoid pigs and swine barns when visiting fairs where the animals are present. Everyone else needs to follow common sense measures to prevent the spread of infection.
• Don’t take food or drink into pig areas; don’t eat, drink or put anything in your mouth in pig areas.
• Don’t take toys, pacifiers, cups, baby bottles, strollers, or similar items into pig areas.
• Wash your hands often with soap and running water before and after exposure to pigs. If soap and water are not available, use an alcohol-based hand rub.
• Avoid close contact with pigs that look or act ill.
• Take protective measures if you must come in contact with pigs that are known or suspected to be sick. This includes wearing personal protective equipment like protective clothing, gloves, and masks that cover your mouth and nose when contact is required.
• To further reduce the risk of infection, minimize contact with pigs in the pig barn and arenas.
It shouldn’t be surprising that flu viruses spread from pigs to people in the same way that regular seasonal influenza spread from person to person. An infected pig coughs or sneezes influenza-containing droplets, and these droplets are inhaled or swallowed by a susceptible human. That makes avoiding contact with pigs that look or act ill especially important. For the record, a pig with flu might have fever, depression, cough, nasal or eye discharge, eye redness, or a poor appetite.
On the bright side, you can’t get H3N2v or any other variant virus from eating properly prepared pork meat. Fairgoers can feel free to indulge in a deep-fried pork chop or one of this year’s featured food items: a basket of French fries topped with smoked pork, cheddar cheese sauce, red onions, jalapeño peppers and barbecue sauce.
Or maybe not. The CDC has a web page devoted to food safety at fairs and festivals. It notes that cases of foodborne illness increase during summer months, and usual safety controls “like monitoring of food temperatures, refrigeration, workers trained in food safety and washing facilities, may not be available when cooking and dining at fairs and festivals.”
The public is urged to seek out “healthy options” from fair vendors first. If healthy options aren’t available, we’re advised to consider bringing food from home to save money and calories.
Sigh. I remember when summer used to be more fun.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville, Ky. and Kosair Children’s Hospital, also in Louisville.
Two children presented with influenza, and both recovered without the need for hospitalization. This scenario would fail to pique the interest of any pediatrician in January. But what about when it happens in July?
In early August, public health authorities in Ohio announced that two children had tested positive for the variant swine influenza virus H3N2v. Both children had direct contact with pigs at the Clark County Fair in late July. Along with a handful of cases diagnosed in Michigan, these represent the first H3N2v cases in the United States in 2016.
Influenza viruses that normally circulate in swine are designated as “variant” when they infect humans. According to the Centers for Disease Control and Prevention (CDC), human infections with H1N1v, H1N2v, and H3N2v have been identified in the United States. Influenza A H3N2v viruses carrying the matrix gene from the 2009 H1N1 pandemic virus were first detected in pigs in 2010, and in people in the summer of 2011. Since that time, 357 human cases have been reported from 14 states, with nearly 75% occurring in Indiana and Ohio. Most infections occurred after prolonged exposure to pigs at agricultural fairs.
Fortunately, most H3N2v infections have been mild: Since July 2012, only 21 individuals have required hospitalization and a single case resulted in death. Notably, though, many of the hospitalizations involved children.
On Aug. 15, the Centers for Disease Control and Prevention released Interim Guidance for Clinicians on Human Infections with Variant Influenza Viruses.
Because variant virus infection is indistinguishable from seasonal influenza or any other virus that cause influenzalike illness (think fever, cough, sore throat), physicians and other frontline providers need to maintain an index of suspicion. The key is eliciting a history of swine exposure in the week before illness onset. Practically, this means asking about direct contact with pigs, indirect contact with pigs, or close contact with an ill person who has had contact with pigs. Kudos to the astute clinicians in Ohio who thought to send the appropriate influenza testing in July.
When variant influenza virus is suspected, a nasopharyngeal swab or aspirate should be obtained for testing at a state public health lab or the CDC. Rapid antigen tests for influenza may be falsely negative in the setting of H3N2v infection, just as they may be with seasonal influenza infection. Molecular tests such as reverse transcription polymerase chain reaction (RT-PCR) are likely more sensitive, but cannot distinguish variant influenza A viruses from seasonal influenza A viruses.
The Kentucky State Fair opened on Aug. 18, making the CDC guidance especially timely for health care providers in my area. I called a friend who is a pediatric emergency medicine physician to ask if she and her colleagues were routinely screening patients for encounters of the porcine kind.
“For example, are you asking, ‘Have you been showing, raising or feeding swine? Have you been to the pig barn at the fair?’ ”
When my friend quit laughing, I confessed to her that I had not been doing that routinely either. The exposure history is often the most interesting part of the infectious disease evaluation and in the last month, I’ve asked about exposure to sheep (a risk factor for Q fever), exposure to chickens (a risk factor for Salmonella infections), and exposure to beaver dams (a risk factor for blastomycosis). But I’ve not asked about exposure to pigs.
“The emergency medicine approach is to avoid a lot of viral diagnostic testing unless it is going to impact management,” she said. “Tell me how this changes management of my patient.”
From the patient perspective, making a presumptive diagnosis of H3N2v infection would open the door to empiric treatment with antivirals, at least for individuals who are hospitalized, have severe or progressive disease, or who at high risk for complications of influenza. Neuraminidase inhibitors, including oral oseltamivir, inhaled zanamivir, and intravenous peramivir, can be used for treatment of H3N2v infections.
From a societal perspective, making the diagnosis gives public health experts the opportunity to investigate and potentially prevent further infections by isolating sick pigs. Human to human transmission of H3N2v is rare, but has occasionally occurred in households and in one instance, a child care setting. Careful surveillance of each swine flu case in a human is important to exclude the possibility that the virus has developed the ability to spread efficiently from person to person, creating the risk for an epidemic.
Seasonal influenza vaccine does not prevent infection with variant viruses, so avoidance is key. Those at high risk for complications from influenza infection, including children younger than 5 years of age and those with asthma, diabetes, heart disease, immunocompromised conditions, and neurologic or neurodevelopmental disorders, are urged to avoid pigs and swine barns when visiting fairs where the animals are present. Everyone else needs to follow common sense measures to prevent the spread of infection.
• Don’t take food or drink into pig areas; don’t eat, drink or put anything in your mouth in pig areas.
• Don’t take toys, pacifiers, cups, baby bottles, strollers, or similar items into pig areas.
• Wash your hands often with soap and running water before and after exposure to pigs. If soap and water are not available, use an alcohol-based hand rub.
• Avoid close contact with pigs that look or act ill.
• Take protective measures if you must come in contact with pigs that are known or suspected to be sick. This includes wearing personal protective equipment like protective clothing, gloves, and masks that cover your mouth and nose when contact is required.
• To further reduce the risk of infection, minimize contact with pigs in the pig barn and arenas.
It shouldn’t be surprising that flu viruses spread from pigs to people in the same way that regular seasonal influenza spread from person to person. An infected pig coughs or sneezes influenza-containing droplets, and these droplets are inhaled or swallowed by a susceptible human. That makes avoiding contact with pigs that look or act ill especially important. For the record, a pig with flu might have fever, depression, cough, nasal or eye discharge, eye redness, or a poor appetite.
On the bright side, you can’t get H3N2v or any other variant virus from eating properly prepared pork meat. Fairgoers can feel free to indulge in a deep-fried pork chop or one of this year’s featured food items: a basket of French fries topped with smoked pork, cheddar cheese sauce, red onions, jalapeño peppers and barbecue sauce.
Or maybe not. The CDC has a web page devoted to food safety at fairs and festivals. It notes that cases of foodborne illness increase during summer months, and usual safety controls “like monitoring of food temperatures, refrigeration, workers trained in food safety and washing facilities, may not be available when cooking and dining at fairs and festivals.”
The public is urged to seek out “healthy options” from fair vendors first. If healthy options aren’t available, we’re advised to consider bringing food from home to save money and calories.
Sigh. I remember when summer used to be more fun.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville, Ky. and Kosair Children’s Hospital, also in Louisville.

School refusal
As summer winds down, it is routine for children and adolescents to feel a little melancholy or even worried about the approaching start of school. But for some students, anxiety about school is more than routine; it is insurmountable. School refusal is a serious behavioral problem: without assertive management, it can become a pattern which is very difficult to alter. Whether a child is complaining of vague somatic concerns or is explicitly refusing to go to school, the pediatrician’s office is often the first place a parent will turn to for help. If you can recognize the true nature of the problem, help to determine its cause, and facilitate the needed management, you will have effectively treated what can become a disabling problem for vulnerable young people.
School refusal is happening when a child has major difficulty attending school, associated with intense emotional distress. It can be a refusal to attend school or difficulty remaining in school for an entire day. It is distinct (but not mutually exclusive) from truancy, which is a failure to attend school associated with antisocial behavior or other conduct problems. In the pediatrician’s office, school refusal sounds like, “He was moaning about a stomachache yesterday, I kept him home, but he had no fever and ate okay. Then it all repeated again this morning.” Or you might hear, “She was whining about a headache, but when I said she had to go to school, she started crying and couldn’t stop. She was hysterical!” In teenagers, there may be somatic complaints or just a sleepy, sulky refusal to get out of bed. Children with truancy might fake illness (as compared with feeling sick), or simply leave school. Truant children often want to be out of school doing other things, and may keep their whereabouts a secret from their parents. While it might seem like just one tough morning that can be shrugged off, true school refusal will continue or escalate unless it is properly managed.

School refusal affects approximately 5% of all children annually, affecting girls and boys in equal numbers and with peaks in incidence at the ages of 5 to 6 years and again at 10 to 11 years. Approximately half of children and teenagers with school refusal have a treatable psychiatric illness. In the Great Smoky Mountain Study of 2003, where more than 1,400 children were observed, they categorized children as being anxious school refusers, truant, or “mixed school refusers,” with features of both truancy and anxiety. In children with truancy or anxious school refusal, 25% had a psychiatric illness. In the mixed school refusers, they found 88% had at least one psychiatric diagnosis and 42% had somatic complaints. While pure truancy will require different management strategies from school and parents, those young people who display features of both anxiety and truancy around school attendance are most likely to be suffering from a psychiatric illness. Those illnesses most commonly associated with difficulty attending school include anxiety disorders (separation anxiety, social phobia, generalized anxiety disorder) and depression.
While psychiatric illness is a common factor, there is also always a behavioral component to school refusal. This simply means that children are either avoiding unpleasant feelings associated with school, such as anxiety, or escaping uncomfortable situations, such as bullying or the stress of performance. On the positive side, children may be refusing school because they are pursuing the attention of important people (parents, peers) or pursuing pleasurable activities (playing video games, surfing the web or hanging out in town). Beyond an internal anxiety disorder, some children may be facing bullying or threats at school or may have to walk through a dangerous neighborhood to get to school. Some children may be missing school because of significant stress or transitions at home, such as financial difficulties or divorce. Other children may be staying home to take care of younger siblings because of a parent’s medical illness or substance abuse problem. Children who are being abused may be kept home to prevent suspicion about bruises. Lastly, some children feel they have to stay home to be with a lonely or depressed parent. Gently asking about these very real concerns will help determine the necessary course of action.

Pediatricians can play a central role in the management of school refusal. Often, the most important step is helping parents to understand that there is not an insidious medical problem driving the morning stomachaches and headaches. It is critical to clarify that (usually) their child is not feigning illness, but that there is significant distress around school that has led to this behavioral problem. Even children who have a genuine medical problem also can have school refusal. Once parents understand that without proper management, this behavior will continue or worsen, they usually are ready to collaborate on effective management. Their child may need a thorough psychiatric evaluation to rule out a treatable underlying psychiatric diagnosis, particularly if they have both anxious and truant behaviors. Most of the psychiatric problems associated with school refusal will require therapy and some may require medications for effective treatment.
Successfully getting children back to school will require a behavior plan that is agreed upon by the parents and the school, and then used consistently. This plan will simply detail strategies to “demagnetize” the home and “remagnetize” the school. Such strategies might include ensuring that children are not allowed “screen time” when home from school, and that their homework expectations continue. It should support healthy routines, including a regular sleep schedule and exercise. It should facilitate their being able to gradually manage any anxiety associated with school (shorter days initially, the option to have time-outs in a favorite part of the school or with a favorite teacher). A behavior plan should detail strategies for the child to manage stress (relaxation strategies, connecting with supportive individuals, even singing a favorite song). This plan can detail reasonable accommodations for a medical or psychiatric condition and appropriate rewards for regular attendance, such as being able to go on a class trip.
Through all of this, the pediatrician is in a uniquely authoritative position to provide support and reassurance to parents of a school refusing child. The pediatrician has a unique ability to clarify for parents the seriousness of the behavioral problem, even if there is no medical problem. Compassionately acknowledging how much a child is suffering (and the parents, as well) is powerful. Remind parents that accommodating anxiety only shows a child you don’t think they can master it, and often keeps them from trying. Express confidence that this is a relatively common and treatable phenomenon. If a pediatrician’s and parents’ efforts do not work quickly, in a matter of a few days, urgent referral to a mental health consultant is indicated, as falling behind in school and any acceptance of staying home makes return to school more difficult every day.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston.
As summer winds down, it is routine for children and adolescents to feel a little melancholy or even worried about the approaching start of school. But for some students, anxiety about school is more than routine; it is insurmountable. School refusal is a serious behavioral problem: without assertive management, it can become a pattern which is very difficult to alter. Whether a child is complaining of vague somatic concerns or is explicitly refusing to go to school, the pediatrician’s office is often the first place a parent will turn to for help. If you can recognize the true nature of the problem, help to determine its cause, and facilitate the needed management, you will have effectively treated what can become a disabling problem for vulnerable young people.
School refusal is happening when a child has major difficulty attending school, associated with intense emotional distress. It can be a refusal to attend school or difficulty remaining in school for an entire day. It is distinct (but not mutually exclusive) from truancy, which is a failure to attend school associated with antisocial behavior or other conduct problems. In the pediatrician’s office, school refusal sounds like, “He was moaning about a stomachache yesterday, I kept him home, but he had no fever and ate okay. Then it all repeated again this morning.” Or you might hear, “She was whining about a headache, but when I said she had to go to school, she started crying and couldn’t stop. She was hysterical!” In teenagers, there may be somatic complaints or just a sleepy, sulky refusal to get out of bed. Children with truancy might fake illness (as compared with feeling sick), or simply leave school. Truant children often want to be out of school doing other things, and may keep their whereabouts a secret from their parents. While it might seem like just one tough morning that can be shrugged off, true school refusal will continue or escalate unless it is properly managed.
School refusal affects approximately 5% of all children annually, affecting girls and boys in equal numbers and with peaks in incidence at the ages of 5 to 6 years and again at 10 to 11 years. Approximately half of children and teenagers with school refusal have a treatable psychiatric illness. In the Great Smoky Mountain Study of 2003, where more than 1,400 children were observed, they categorized children as being anxious school refusers, truant, or “mixed school refusers,” with features of both truancy and anxiety. In children with truancy or anxious school refusal, 25% had a psychiatric illness. In the mixed school refusers, they found 88% had at least one psychiatric diagnosis and 42% had somatic complaints. While pure truancy will require different management strategies from school and parents, those young people who display features of both anxiety and truancy around school attendance are most likely to be suffering from a psychiatric illness. Those illnesses most commonly associated with difficulty attending school include anxiety disorders (separation anxiety, social phobia, generalized anxiety disorder) and depression.
While psychiatric illness is a common factor, there is also always a behavioral component to school refusal. This simply means that children are either avoiding unpleasant feelings associated with school, such as anxiety, or escaping uncomfortable situations, such as bullying or the stress of performance. On the positive side, children may be refusing school because they are pursuing the attention of important people (parents, peers) or pursuing pleasurable activities (playing video games, surfing the web or hanging out in town). Beyond an internal anxiety disorder, some children may be facing bullying or threats at school or may have to walk through a dangerous neighborhood to get to school. Some children may be missing school because of significant stress or transitions at home, such as financial difficulties or divorce. Other children may be staying home to take care of younger siblings because of a parent’s medical illness or substance abuse problem. Children who are being abused may be kept home to prevent suspicion about bruises. Lastly, some children feel they have to stay home to be with a lonely or depressed parent. Gently asking about these very real concerns will help determine the necessary course of action.
Pediatricians can play a central role in the management of school refusal. Often, the most important step is helping parents to understand that there is not an insidious medical problem driving the morning stomachaches and headaches. It is critical to clarify that (usually) their child is not feigning illness, but that there is significant distress around school that has led to this behavioral problem. Even children who have a genuine medical problem also can have school refusal. Once parents understand that without proper management, this behavior will continue or worsen, they usually are ready to collaborate on effective management. Their child may need a thorough psychiatric evaluation to rule out a treatable underlying psychiatric diagnosis, particularly if they have both anxious and truant behaviors. Most of the psychiatric problems associated with school refusal will require therapy and some may require medications for effective treatment.
Successfully getting children back to school will require a behavior plan that is agreed upon by the parents and the school, and then used consistently. This plan will simply detail strategies to “demagnetize” the home and “remagnetize” the school. Such strategies might include ensuring that children are not allowed “screen time” when home from school, and that their homework expectations continue. It should support healthy routines, including a regular sleep schedule and exercise. It should facilitate their being able to gradually manage any anxiety associated with school (shorter days initially, the option to have time-outs in a favorite part of the school or with a favorite teacher). A behavior plan should detail strategies for the child to manage stress (relaxation strategies, connecting with supportive individuals, even singing a favorite song). This plan can detail reasonable accommodations for a medical or psychiatric condition and appropriate rewards for regular attendance, such as being able to go on a class trip.
Through all of this, the pediatrician is in a uniquely authoritative position to provide support and reassurance to parents of a school refusing child. The pediatrician has a unique ability to clarify for parents the seriousness of the behavioral problem, even if there is no medical problem. Compassionately acknowledging how much a child is suffering (and the parents, as well) is powerful. Remind parents that accommodating anxiety only shows a child you don’t think they can master it, and often keeps them from trying. Express confidence that this is a relatively common and treatable phenomenon. If a pediatrician’s and parents’ efforts do not work quickly, in a matter of a few days, urgent referral to a mental health consultant is indicated, as falling behind in school and any acceptance of staying home makes return to school more difficult every day.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston.
As summer winds down, it is routine for children and adolescents to feel a little melancholy or even worried about the approaching start of school. But for some students, anxiety about school is more than routine; it is insurmountable. School refusal is a serious behavioral problem: without assertive management, it can become a pattern which is very difficult to alter. Whether a child is complaining of vague somatic concerns or is explicitly refusing to go to school, the pediatrician’s office is often the first place a parent will turn to for help. If you can recognize the true nature of the problem, help to determine its cause, and facilitate the needed management, you will have effectively treated what can become a disabling problem for vulnerable young people.
School refusal is happening when a child has major difficulty attending school, associated with intense emotional distress. It can be a refusal to attend school or difficulty remaining in school for an entire day. It is distinct (but not mutually exclusive) from truancy, which is a failure to attend school associated with antisocial behavior or other conduct problems. In the pediatrician’s office, school refusal sounds like, “He was moaning about a stomachache yesterday, I kept him home, but he had no fever and ate okay. Then it all repeated again this morning.” Or you might hear, “She was whining about a headache, but when I said she had to go to school, she started crying and couldn’t stop. She was hysterical!” In teenagers, there may be somatic complaints or just a sleepy, sulky refusal to get out of bed. Children with truancy might fake illness (as compared with feeling sick), or simply leave school. Truant children often want to be out of school doing other things, and may keep their whereabouts a secret from their parents. While it might seem like just one tough morning that can be shrugged off, true school refusal will continue or escalate unless it is properly managed.
School refusal affects approximately 5% of all children annually, affecting girls and boys in equal numbers and with peaks in incidence at the ages of 5 to 6 years and again at 10 to 11 years. Approximately half of children and teenagers with school refusal have a treatable psychiatric illness. In the Great Smoky Mountain Study of 2003, where more than 1,400 children were observed, they categorized children as being anxious school refusers, truant, or “mixed school refusers,” with features of both truancy and anxiety. In children with truancy or anxious school refusal, 25% had a psychiatric illness. In the mixed school refusers, they found 88% had at least one psychiatric diagnosis and 42% had somatic complaints. While pure truancy will require different management strategies from school and parents, those young people who display features of both anxiety and truancy around school attendance are most likely to be suffering from a psychiatric illness. Those illnesses most commonly associated with difficulty attending school include anxiety disorders (separation anxiety, social phobia, generalized anxiety disorder) and depression.
While psychiatric illness is a common factor, there is also always a behavioral component to school refusal. This simply means that children are either avoiding unpleasant feelings associated with school, such as anxiety, or escaping uncomfortable situations, such as bullying or the stress of performance. On the positive side, children may be refusing school because they are pursuing the attention of important people (parents, peers) or pursuing pleasurable activities (playing video games, surfing the web or hanging out in town). Beyond an internal anxiety disorder, some children may be facing bullying or threats at school or may have to walk through a dangerous neighborhood to get to school. Some children may be missing school because of significant stress or transitions at home, such as financial difficulties or divorce. Other children may be staying home to take care of younger siblings because of a parent’s medical illness or substance abuse problem. Children who are being abused may be kept home to prevent suspicion about bruises. Lastly, some children feel they have to stay home to be with a lonely or depressed parent. Gently asking about these very real concerns will help determine the necessary course of action.
Pediatricians can play a central role in the management of school refusal. Often, the most important step is helping parents to understand that there is not an insidious medical problem driving the morning stomachaches and headaches. It is critical to clarify that (usually) their child is not feigning illness, but that there is significant distress around school that has led to this behavioral problem. Even children who have a genuine medical problem also can have school refusal. Once parents understand that without proper management, this behavior will continue or worsen, they usually are ready to collaborate on effective management. Their child may need a thorough psychiatric evaluation to rule out a treatable underlying psychiatric diagnosis, particularly if they have both anxious and truant behaviors. Most of the psychiatric problems associated with school refusal will require therapy and some may require medications for effective treatment.
Successfully getting children back to school will require a behavior plan that is agreed upon by the parents and the school, and then used consistently. This plan will simply detail strategies to “demagnetize” the home and “remagnetize” the school. Such strategies might include ensuring that children are not allowed “screen time” when home from school, and that their homework expectations continue. It should support healthy routines, including a regular sleep schedule and exercise. It should facilitate their being able to gradually manage any anxiety associated with school (shorter days initially, the option to have time-outs in a favorite part of the school or with a favorite teacher). A behavior plan should detail strategies for the child to manage stress (relaxation strategies, connecting with supportive individuals, even singing a favorite song). This plan can detail reasonable accommodations for a medical or psychiatric condition and appropriate rewards for regular attendance, such as being able to go on a class trip.
Through all of this, the pediatrician is in a uniquely authoritative position to provide support and reassurance to parents of a school refusing child. The pediatrician has a unique ability to clarify for parents the seriousness of the behavioral problem, even if there is no medical problem. Compassionately acknowledging how much a child is suffering (and the parents, as well) is powerful. Remind parents that accommodating anxiety only shows a child you don’t think they can master it, and often keeps them from trying. Express confidence that this is a relatively common and treatable phenomenon. If a pediatrician’s and parents’ efforts do not work quickly, in a matter of a few days, urgent referral to a mental health consultant is indicated, as falling behind in school and any acceptance of staying home makes return to school more difficult every day.
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston.
