User login
Parents support school-based HPV vaccination
Approximately 86% of middle school students were vaccinated against HPV in a school setting in a review of data from a service project involving more than 8,000 students.
“School-located vaccination programs (SLVPs) provide access to vaccination for those adolescents whose parents cannot miss work or other daytime commitments or those who have multiple after-school commitments,” wrote Dr. Amy Middleman of the University of Oklahoma Health Science Center, Oklahoma City, and her colleagues. Data from previous studies suggest reluctance on the part of parents to allow their children to receive the human papillomavirus vaccine (HPV) in a school setting, but such data may not reflect parents’ opinions when a school-based program is actually available, the researchers noted.

The researchers tested SLVPs at eight middle schools including 8,333 students; 80% were Hispanic, 17% were black, 1% were white, and the remainder of students’ ethnicities were not identified (Human Vaccines & Immunotherapeutics. 2016 Aug. doi: 10.1080/21645515.2016.1208326).
School-based vaccinations were scheduled for three times: September/October 2012, March/April 2013, and September/October 2013; the findings reflect the first two visits.
The SLVPs included the following vaccines: HPV, influenza, Tdap, meningococcal conjugate vaccine (MCV4), hepatitis A, varicella, and MMR. A total of 1,674 vaccines were administered in the fall of 2012, and 532 were administered in the spring of 2013. Overall, 449 of 524 (86%) students in the fall program and 161 of 188 (86%) in the spring program received the HPV vaccine.
The study was limited by several factors including the descriptive nature of the service project and the inability to obtain the vaccination status of all enrolled students. In addition, the schools were located in lower income areas, which might limit the generalizability of the findings, the researchers noted. However, the results suggest that “SLVPs may be more successful not only when they include all vaccines, but also when conducted in the fall prior to the onset of preparation for high-stakes state testing,” they said.
The study was supported by the Society for Adolescent Health through a grant from Merck. One study coauthor previously received salary support from Merck.
Approximately 86% of middle school students were vaccinated against HPV in a school setting in a review of data from a service project involving more than 8,000 students.
“School-located vaccination programs (SLVPs) provide access to vaccination for those adolescents whose parents cannot miss work or other daytime commitments or those who have multiple after-school commitments,” wrote Dr. Amy Middleman of the University of Oklahoma Health Science Center, Oklahoma City, and her colleagues. Data from previous studies suggest reluctance on the part of parents to allow their children to receive the human papillomavirus vaccine (HPV) in a school setting, but such data may not reflect parents’ opinions when a school-based program is actually available, the researchers noted.
The researchers tested SLVPs at eight middle schools including 8,333 students; 80% were Hispanic, 17% were black, 1% were white, and the remainder of students’ ethnicities were not identified (Human Vaccines & Immunotherapeutics. 2016 Aug. doi: 10.1080/21645515.2016.1208326).
School-based vaccinations were scheduled for three times: September/October 2012, March/April 2013, and September/October 2013; the findings reflect the first two visits.
The SLVPs included the following vaccines: HPV, influenza, Tdap, meningococcal conjugate vaccine (MCV4), hepatitis A, varicella, and MMR. A total of 1,674 vaccines were administered in the fall of 2012, and 532 were administered in the spring of 2013. Overall, 449 of 524 (86%) students in the fall program and 161 of 188 (86%) in the spring program received the HPV vaccine.
The study was limited by several factors including the descriptive nature of the service project and the inability to obtain the vaccination status of all enrolled students. In addition, the schools were located in lower income areas, which might limit the generalizability of the findings, the researchers noted. However, the results suggest that “SLVPs may be more successful not only when they include all vaccines, but also when conducted in the fall prior to the onset of preparation for high-stakes state testing,” they said.
The study was supported by the Society for Adolescent Health through a grant from Merck. One study coauthor previously received salary support from Merck.
Approximately 86% of middle school students were vaccinated against HPV in a school setting in a review of data from a service project involving more than 8,000 students.
“School-located vaccination programs (SLVPs) provide access to vaccination for those adolescents whose parents cannot miss work or other daytime commitments or those who have multiple after-school commitments,” wrote Dr. Amy Middleman of the University of Oklahoma Health Science Center, Oklahoma City, and her colleagues. Data from previous studies suggest reluctance on the part of parents to allow their children to receive the human papillomavirus vaccine (HPV) in a school setting, but such data may not reflect parents’ opinions when a school-based program is actually available, the researchers noted.
The researchers tested SLVPs at eight middle schools including 8,333 students; 80% were Hispanic, 17% were black, 1% were white, and the remainder of students’ ethnicities were not identified (Human Vaccines & Immunotherapeutics. 2016 Aug. doi: 10.1080/21645515.2016.1208326).
School-based vaccinations were scheduled for three times: September/October 2012, March/April 2013, and September/October 2013; the findings reflect the first two visits.
The SLVPs included the following vaccines: HPV, influenza, Tdap, meningococcal conjugate vaccine (MCV4), hepatitis A, varicella, and MMR. A total of 1,674 vaccines were administered in the fall of 2012, and 532 were administered in the spring of 2013. Overall, 449 of 524 (86%) students in the fall program and 161 of 188 (86%) in the spring program received the HPV vaccine.
The study was limited by several factors including the descriptive nature of the service project and the inability to obtain the vaccination status of all enrolled students. In addition, the schools were located in lower income areas, which might limit the generalizability of the findings, the researchers noted. However, the results suggest that “SLVPs may be more successful not only when they include all vaccines, but also when conducted in the fall prior to the onset of preparation for high-stakes state testing,” they said.
The study was supported by the Society for Adolescent Health through a grant from Merck. One study coauthor previously received salary support from Merck.
FROM HUMAN VACCINES & IMMUNOTHERAPEUTICS
Key clinical point: Parents already supportive of school-based vaccination are likely to support school-based HPV vaccination as well.
Major finding: Approximately 86% of adolescents participating in a school-based program received an HPV vaccine.
Data source: A descriptive study based on a service project that included 8,333 middle school students and parents.
Disclosures: The study was supported by the Society for Adolescent Health through a grant from Merck. One study coauthor previously received salary support from Merck.
Pediatric Hospital Medicine 2016 Wrap Up
Pediatric Hospital Medicine 2016, cosponsored by the American Academy of Pediatrics (AAP), the Academic Pediatric Association (APA), and the Society of Hospital Medicine (SHM), took place July 28–31 in Chicago. Didn’t make it? Here are all the news, research, and talking points you need to know.

Shape Your Brain to Avoid Burnout
Presenter: Lisa Zaoutis, MD, FHM
Amid the skyscrapers of the Windy City, Pediatric Hospital Medicine (PHM) 2016 swept into town, bringing with it the denizens of pediatric hospitalist programs across the country. Some 1,150 attendees, composed of hospitalists, PHM program leaders, and advanced-care practitioners, gathered to educate and inspire one another in the care of hospitalized children.
Lisa Zaoutis, MD, FHM, director of the pediatric residency program at The Children’s Hospital of Philadelphia, kicked off the conference with the opening plenary. Initially titled “North Star and Space,” she quickly changed the title to “Changing Our Minds.” Touching on the disconnect between positive experiences that bring physicians into pediatric hospital medicine and negative experiences that often drive behavior, she started with the beginning: the evolution of our brains.
“We are wired toward the negative,” Dr. Zaoutis said. “We are Teflon for positive experiences and Velcro for negative experiences.”
Delving deeper into neuroanatomy, Dr. Zaoutis spoke of “amygdala hijack,” where chronic stress inherent to the professional lives of pediatric hospitalists leads to anxiety responses that are faster, more robust, and more easily triggered.
But all is not lost, Dr. Zaoutis noted, as our brains are more plastic than previously known. The “neural Darwinism” of our brains, she said, leads to epigenetic intracellular changes, more sensitive synapses, improved blood flow, and even new cells as a result of experience-dependent neuroplasticity. For example, London taxi drivers have thicker white matter in their hippocampus as a result of learning London city streets, and mindfulness meditators have thicker gray matter in regions that control attention and self-insight.
Key Takeaways
The lesson for pediatric hospitalists, according Dr. Zaoutis, is that you can shape your brain for greater joy.
“Consciously choose activities” that counter our evolutionary negativity bias, Dr. Zaoutis said.
Here’s how to do it:
- Have a positive experience. (You can create one or retrieve a prior one.)
- Enrich it and install it by dwelling on it for at least 15–30 seconds.
- Absorb it into your body, which may require somatizing it. (Dr. Zaoutis presses her hand into her chest to aid in this.)
Further, spread this to your group by the old medical training technique of “see one, do one, teach one.” See if you can start your sign-out with the best thing that happened to you in the week. Most important, start with observing yourself.
Weijen Chang, MD, SFHM, is pediatric editor of The Hospitalist. He is associate clinical professor of medicine and pediatrics at the University of California, San Diego (UCSD) School of Medicine and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. Send comments and questions to wwch@ucsd.edu.

New AAP Guideline on Evaluating, Managing Febrile Infants
Presenter: Kenneth Roberts, MD
One of PHM16’s most highly attended sessions was an update on the anticipated AAP guidelines for febrile infants ages 7–90 days. The updated guidelines stress the need to separate individual components of serious bacterial infections (UTI, bacteremia, and meningitis) as the incidence and clinical course can vary greatly in this population.
The inclusion criteria for infants for this upcoming algorithm require an infant to be full-term (37–43 weeks’ gestation), aged 7–90 days, well-appearing, and presenting with a temperature of 38°C.
Exclusion criteria include perinatal/prenatal/neonatal maternal fever, infection, or antimicrobial treatment; the presence of any evident infection; being technology-dependent; and the presence of congenital anomalies.
The updated guideline will aim to stratify management by ages 7–28 days, 29–60 days, and 61–90 days to provide the most appropriate and directed treatment.
It will also include a role for inflammatory markers and allow for a “kinder, gentler” approach, including withholding certain treatments and procedures if infants are at low risk of infection. An active need for observation may be appropriate for certain infants as well. These guidelines should be tailored for individual patients to provide the best care possible while minimizing risk.
Key Takeaway
An updated AAP guideline algorithm for the management of well-appearing febrile infants ages 7–28 days, 29–60 days, and 60–90 days will be coming in the near future. It will help standardize care in this population but should not be used as a substitute for clinical judgment.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System and instructor of pediatrics at George Washington University School of Medicine & Health Sciences in Washington, D.C.

Promoting, Teaching Pediatric High-Value Care
Presenters: Lauren L. Walker, MD, FAAP; Alan Schroeder, MD, FAAP; Michael
Tchou, MD, FAAP; Jimmy Beck, MD, MEd; Lisa Herrmann, MD; Ricardo Quinonez, MD, FAAP
Pediatric hospitalists gathered to attend a fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high-value care are plenty and essentially universal to academic and community sites: We have had no formal teaching, there is cultural resistance, and there is lack of transparency on costs and charges.
The questions we perhaps should be asking ourselves, our trainees, and our families are:
- “What matters?” instead of “What’s the matter?”
- “Does that test benefit the patient? What are the harms of the test?” instead of “Will that test change our management?”
There is still a long way to go to move the pendulum to the side of value-based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary value; family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
Key Takeaway
This serves as an exciting time to unite and better our understanding about why we do what we do and deliberately think about downstream effects. High-value care curriculum for medical students, residents, fellows, and even faculty is an area ripe for further research.
Akshata Hopkins, MD, FAAP, is an academic hospitalist at Johns Hopkins All Children’s Hospital in St. Petersburg, Fla.

How to Design, Improve Educational Programs at Community Hospitals
Presenters: Christopher Russo, MD, FAAP; Laura Hodo, MD, and Lauren Wilson, MD
One session at PHM16 focused on ways to design and improve education within community hospital settings. It was done via a didactic session, breakout groups, and an electronic assessment tool. Facilitators included the workshop leaders and co-leaders along with current PHM fellows and educators from community and academic settings.
During the didactic session, a general background of the importance of education during times of increasing academic and community site affiliations was discussed. This included the strengths of community hospitals for learners such as “appropriate learner autonomy,” “exposure to different career paths,” and “transfer decision making.”
Some of the challenges discussed in regard to developing an educational structure in community settings included:
1. Logistics
- Making the case for education
- Legal framework (e.g., affiliation agreements, liability)
- Finances (e.g., GME funding)
- Paperwork burden (e.g., licensing, credentialing)
2. Learning environment
- Complementing clinical work with materials
- Autonomy/supervision balancing
- Developing clinical teachers
The didactic session also reviewed the six steps for curriculum development: general needs assessment, targeted needs assessment, goals and objectives, educational strategies, implementation, and evaluation/feedback. Each of these was described in further detail with relevant examples.
Groups were broken into small groups based on four learner types: medical students, family medicine residents, pediatric residents, and PHM fellows. Within each group, a “program development matrix” was distributed to assess the support from leadership and logistics within each setting. Each one of these was separated into subgroups such as credentialing, financial support, housing/travel, and preceptor recruitment.
A separate “curriculum development matrix” was used during breakout groups that focused on curriculum development. This matrix was broken into three areas: educational strategies, implementation, and evaluation/feedback. These were further broken down into subgroups such as content, identifying resources, and remediation planning. The group was asked to determine short- and long-term goals with action steps for both of these matrix subgroups.
Key Takeaway
Overall, the session presented a structured way of assessing the educational environment for learners in community settings. It gave tangible tools for sites that wish to develop or improve their current educational framework.
Francisco Alvarez, MD, FAAP, is a pediatric hospitalist and director of the Children’s National Health System Community Hospital Services in Washington, D.C.

Tips on Meeting Needs of Children with a Medical Complexity
Presenters: Mary L. Ehlenbach, MD, FAAP; Megan Z. Cardoso, MD, FAAP, and Christina Kleier, ARNP, PNP
This session at PHM16 was focused on logistical tips on how to build a pediatric complex-care program. Presenters opened with a discussion on how to define children with medical complexity. This involved reviewing different methods, including using research-based aggregation of ICD-10 codes, relying on referral from both families and other providers, and identifying patients by consumption of hospital resources. The presentation continued by highlighting that although medically complex children make up only a small percentage of the overall population of children, they account for about one-third of healthcare spending. Because of advances in technology and medicine, this group of children is growing in numbers. It currently makes up about 10% of all pediatric admissions.
Key Takeaways
1. Children with medical complexity are a growing population on which a large proportion of healthcare resources are utilized. A program dedicated to serving the needs of this population may be helpful in reducing costs and improving the patient and family experience during hospitalizations.
2. When working to initiate a complex-care program:
- Set clear guidelines about which children the program is intended to serve and in what capacity it will function.
- Ensure the team composition is sustainable and meets the needs of the patients.
- Aggregate data about if the program is helping. This may be difficult to quantify since these are mostly qualitative measures.
- Include team members who are nonclinical to aid in improving hospital revenue and highlighting program benefits to the institution.
Margaret Rush, MD, is a hospitalist fellow at Children’s National Medical Center in Washington, D.C.

A Picture Is Worth a Thousand Words
Presenter: Kenneth Roberts, MD
PHM16’s “Visual Diagnosis: Signs and Why They Matter” session was a review of case presentations in which visual clues were vital to establishing a diagnosis. Though much of the content was presented with pictures, the emphasis was placed on the importance of correct diagnosis to avoid both misdiagnoses or overdiagnoses and the potential harm that may result from inappropriate treatment. This may also translate into poor utilization of resources and significant financial burden that can result from the unnecessary hospitalization of a patient.
Many of the presented cases highlighted examples in which there was extensive workup, hospitalization, subspecialty evaluation, and even incorrect treatment of patients.
In other instances, such as with Henoch-Schonlein purpura, Waardenburg syndrome, or McCune-Albright syndrome, the correct diagnosis was necessary to help guide management and future treatment, including subspecialty evaluation.
Key Takeaway
Many diseases with visual presentations will have a benign course and require no treatment. Acknowledging this is important in providing reassurance to a family that may be very anxious over the physical appearance of their child.
This session underscores the need for experience and exposure to various signs not only with rare medical conditions but also in common illnesses such as Kawasaki disease and scarlet fever that may present similarly.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System and instructor of pediatrics at George Washington University School of Medicine & Health Sciences in Washington, D.C.
Pediatric Hospital Medicine 2016, cosponsored by the American Academy of Pediatrics (AAP), the Academic Pediatric Association (APA), and the Society of Hospital Medicine (SHM), took place July 28–31 in Chicago. Didn’t make it? Here are all the news, research, and talking points you need to know.
Shape Your Brain to Avoid Burnout
Presenter: Lisa Zaoutis, MD, FHM
Amid the skyscrapers of the Windy City, Pediatric Hospital Medicine (PHM) 2016 swept into town, bringing with it the denizens of pediatric hospitalist programs across the country. Some 1,150 attendees, composed of hospitalists, PHM program leaders, and advanced-care practitioners, gathered to educate and inspire one another in the care of hospitalized children.
Lisa Zaoutis, MD, FHM, director of the pediatric residency program at The Children’s Hospital of Philadelphia, kicked off the conference with the opening plenary. Initially titled “North Star and Space,” she quickly changed the title to “Changing Our Minds.” Touching on the disconnect between positive experiences that bring physicians into pediatric hospital medicine and negative experiences that often drive behavior, she started with the beginning: the evolution of our brains.
“We are wired toward the negative,” Dr. Zaoutis said. “We are Teflon for positive experiences and Velcro for negative experiences.”
Delving deeper into neuroanatomy, Dr. Zaoutis spoke of “amygdala hijack,” where chronic stress inherent to the professional lives of pediatric hospitalists leads to anxiety responses that are faster, more robust, and more easily triggered.
But all is not lost, Dr. Zaoutis noted, as our brains are more plastic than previously known. The “neural Darwinism” of our brains, she said, leads to epigenetic intracellular changes, more sensitive synapses, improved blood flow, and even new cells as a result of experience-dependent neuroplasticity. For example, London taxi drivers have thicker white matter in their hippocampus as a result of learning London city streets, and mindfulness meditators have thicker gray matter in regions that control attention and self-insight.
Key Takeaways
The lesson for pediatric hospitalists, according Dr. Zaoutis, is that you can shape your brain for greater joy.
“Consciously choose activities” that counter our evolutionary negativity bias, Dr. Zaoutis said.
Here’s how to do it:
- Have a positive experience. (You can create one or retrieve a prior one.)
- Enrich it and install it by dwelling on it for at least 15–30 seconds.
- Absorb it into your body, which may require somatizing it. (Dr. Zaoutis presses her hand into her chest to aid in this.)
Further, spread this to your group by the old medical training technique of “see one, do one, teach one.” See if you can start your sign-out with the best thing that happened to you in the week. Most important, start with observing yourself.
Weijen Chang, MD, SFHM, is pediatric editor of The Hospitalist. He is associate clinical professor of medicine and pediatrics at the University of California, San Diego (UCSD) School of Medicine and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. Send comments and questions to wwch@ucsd.edu.
New AAP Guideline on Evaluating, Managing Febrile Infants
Presenter: Kenneth Roberts, MD
One of PHM16’s most highly attended sessions was an update on the anticipated AAP guidelines for febrile infants ages 7–90 days. The updated guidelines stress the need to separate individual components of serious bacterial infections (UTI, bacteremia, and meningitis) as the incidence and clinical course can vary greatly in this population.
The inclusion criteria for infants for this upcoming algorithm require an infant to be full-term (37–43 weeks’ gestation), aged 7–90 days, well-appearing, and presenting with a temperature of 38°C.
Exclusion criteria include perinatal/prenatal/neonatal maternal fever, infection, or antimicrobial treatment; the presence of any evident infection; being technology-dependent; and the presence of congenital anomalies.
The updated guideline will aim to stratify management by ages 7–28 days, 29–60 days, and 61–90 days to provide the most appropriate and directed treatment.
It will also include a role for inflammatory markers and allow for a “kinder, gentler” approach, including withholding certain treatments and procedures if infants are at low risk of infection. An active need for observation may be appropriate for certain infants as well. These guidelines should be tailored for individual patients to provide the best care possible while minimizing risk.
Key Takeaway
An updated AAP guideline algorithm for the management of well-appearing febrile infants ages 7–28 days, 29–60 days, and 60–90 days will be coming in the near future. It will help standardize care in this population but should not be used as a substitute for clinical judgment.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System and instructor of pediatrics at George Washington University School of Medicine & Health Sciences in Washington, D.C.
Promoting, Teaching Pediatric High-Value Care
Presenters: Lauren L. Walker, MD, FAAP; Alan Schroeder, MD, FAAP; Michael
Tchou, MD, FAAP; Jimmy Beck, MD, MEd; Lisa Herrmann, MD; Ricardo Quinonez, MD, FAAP
Pediatric hospitalists gathered to attend a fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high-value care are plenty and essentially universal to academic and community sites: We have had no formal teaching, there is cultural resistance, and there is lack of transparency on costs and charges.
The questions we perhaps should be asking ourselves, our trainees, and our families are:
- “What matters?” instead of “What’s the matter?”
- “Does that test benefit the patient? What are the harms of the test?” instead of “Will that test change our management?”
There is still a long way to go to move the pendulum to the side of value-based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary value; family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
Key Takeaway
This serves as an exciting time to unite and better our understanding about why we do what we do and deliberately think about downstream effects. High-value care curriculum for medical students, residents, fellows, and even faculty is an area ripe for further research.
Akshata Hopkins, MD, FAAP, is an academic hospitalist at Johns Hopkins All Children’s Hospital in St. Petersburg, Fla.
How to Design, Improve Educational Programs at Community Hospitals
Presenters: Christopher Russo, MD, FAAP; Laura Hodo, MD, and Lauren Wilson, MD
One session at PHM16 focused on ways to design and improve education within community hospital settings. It was done via a didactic session, breakout groups, and an electronic assessment tool. Facilitators included the workshop leaders and co-leaders along with current PHM fellows and educators from community and academic settings.
During the didactic session, a general background of the importance of education during times of increasing academic and community site affiliations was discussed. This included the strengths of community hospitals for learners such as “appropriate learner autonomy,” “exposure to different career paths,” and “transfer decision making.”
Some of the challenges discussed in regard to developing an educational structure in community settings included:
1. Logistics
- Making the case for education
- Legal framework (e.g., affiliation agreements, liability)
- Finances (e.g., GME funding)
- Paperwork burden (e.g., licensing, credentialing)
2. Learning environment
- Complementing clinical work with materials
- Autonomy/supervision balancing
- Developing clinical teachers
The didactic session also reviewed the six steps for curriculum development: general needs assessment, targeted needs assessment, goals and objectives, educational strategies, implementation, and evaluation/feedback. Each of these was described in further detail with relevant examples.
Groups were broken into small groups based on four learner types: medical students, family medicine residents, pediatric residents, and PHM fellows. Within each group, a “program development matrix” was distributed to assess the support from leadership and logistics within each setting. Each one of these was separated into subgroups such as credentialing, financial support, housing/travel, and preceptor recruitment.
A separate “curriculum development matrix” was used during breakout groups that focused on curriculum development. This matrix was broken into three areas: educational strategies, implementation, and evaluation/feedback. These were further broken down into subgroups such as content, identifying resources, and remediation planning. The group was asked to determine short- and long-term goals with action steps for both of these matrix subgroups.
Key Takeaway
Overall, the session presented a structured way of assessing the educational environment for learners in community settings. It gave tangible tools for sites that wish to develop or improve their current educational framework.
Francisco Alvarez, MD, FAAP, is a pediatric hospitalist and director of the Children’s National Health System Community Hospital Services in Washington, D.C.
Tips on Meeting Needs of Children with a Medical Complexity
Presenters: Mary L. Ehlenbach, MD, FAAP; Megan Z. Cardoso, MD, FAAP, and Christina Kleier, ARNP, PNP
This session at PHM16 was focused on logistical tips on how to build a pediatric complex-care program. Presenters opened with a discussion on how to define children with medical complexity. This involved reviewing different methods, including using research-based aggregation of ICD-10 codes, relying on referral from both families and other providers, and identifying patients by consumption of hospital resources. The presentation continued by highlighting that although medically complex children make up only a small percentage of the overall population of children, they account for about one-third of healthcare spending. Because of advances in technology and medicine, this group of children is growing in numbers. It currently makes up about 10% of all pediatric admissions.
Key Takeaways
1. Children with medical complexity are a growing population on which a large proportion of healthcare resources are utilized. A program dedicated to serving the needs of this population may be helpful in reducing costs and improving the patient and family experience during hospitalizations.
2. When working to initiate a complex-care program:
- Set clear guidelines about which children the program is intended to serve and in what capacity it will function.
- Ensure the team composition is sustainable and meets the needs of the patients.
- Aggregate data about if the program is helping. This may be difficult to quantify since these are mostly qualitative measures.
- Include team members who are nonclinical to aid in improving hospital revenue and highlighting program benefits to the institution.
Margaret Rush, MD, is a hospitalist fellow at Children’s National Medical Center in Washington, D.C.
A Picture Is Worth a Thousand Words
Presenter: Kenneth Roberts, MD
PHM16’s “Visual Diagnosis: Signs and Why They Matter” session was a review of case presentations in which visual clues were vital to establishing a diagnosis. Though much of the content was presented with pictures, the emphasis was placed on the importance of correct diagnosis to avoid both misdiagnoses or overdiagnoses and the potential harm that may result from inappropriate treatment. This may also translate into poor utilization of resources and significant financial burden that can result from the unnecessary hospitalization of a patient.
Many of the presented cases highlighted examples in which there was extensive workup, hospitalization, subspecialty evaluation, and even incorrect treatment of patients.
In other instances, such as with Henoch-Schonlein purpura, Waardenburg syndrome, or McCune-Albright syndrome, the correct diagnosis was necessary to help guide management and future treatment, including subspecialty evaluation.
Key Takeaway
Many diseases with visual presentations will have a benign course and require no treatment. Acknowledging this is important in providing reassurance to a family that may be very anxious over the physical appearance of their child.
This session underscores the need for experience and exposure to various signs not only with rare medical conditions but also in common illnesses such as Kawasaki disease and scarlet fever that may present similarly.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System and instructor of pediatrics at George Washington University School of Medicine & Health Sciences in Washington, D.C.
Pediatric Hospital Medicine 2016, cosponsored by the American Academy of Pediatrics (AAP), the Academic Pediatric Association (APA), and the Society of Hospital Medicine (SHM), took place July 28–31 in Chicago. Didn’t make it? Here are all the news, research, and talking points you need to know.
Shape Your Brain to Avoid Burnout
Presenter: Lisa Zaoutis, MD, FHM
Amid the skyscrapers of the Windy City, Pediatric Hospital Medicine (PHM) 2016 swept into town, bringing with it the denizens of pediatric hospitalist programs across the country. Some 1,150 attendees, composed of hospitalists, PHM program leaders, and advanced-care practitioners, gathered to educate and inspire one another in the care of hospitalized children.
Lisa Zaoutis, MD, FHM, director of the pediatric residency program at The Children’s Hospital of Philadelphia, kicked off the conference with the opening plenary. Initially titled “North Star and Space,” she quickly changed the title to “Changing Our Minds.” Touching on the disconnect between positive experiences that bring physicians into pediatric hospital medicine and negative experiences that often drive behavior, she started with the beginning: the evolution of our brains.
“We are wired toward the negative,” Dr. Zaoutis said. “We are Teflon for positive experiences and Velcro for negative experiences.”
Delving deeper into neuroanatomy, Dr. Zaoutis spoke of “amygdala hijack,” where chronic stress inherent to the professional lives of pediatric hospitalists leads to anxiety responses that are faster, more robust, and more easily triggered.
But all is not lost, Dr. Zaoutis noted, as our brains are more plastic than previously known. The “neural Darwinism” of our brains, she said, leads to epigenetic intracellular changes, more sensitive synapses, improved blood flow, and even new cells as a result of experience-dependent neuroplasticity. For example, London taxi drivers have thicker white matter in their hippocampus as a result of learning London city streets, and mindfulness meditators have thicker gray matter in regions that control attention and self-insight.
Key Takeaways
The lesson for pediatric hospitalists, according Dr. Zaoutis, is that you can shape your brain for greater joy.
“Consciously choose activities” that counter our evolutionary negativity bias, Dr. Zaoutis said.
Here’s how to do it:
- Have a positive experience. (You can create one or retrieve a prior one.)
- Enrich it and install it by dwelling on it for at least 15–30 seconds.
- Absorb it into your body, which may require somatizing it. (Dr. Zaoutis presses her hand into her chest to aid in this.)
Further, spread this to your group by the old medical training technique of “see one, do one, teach one.” See if you can start your sign-out with the best thing that happened to you in the week. Most important, start with observing yourself.
Weijen Chang, MD, SFHM, is pediatric editor of The Hospitalist. He is associate clinical professor of medicine and pediatrics at the University of California, San Diego (UCSD) School of Medicine and a hospitalist at both UCSD Medical Center and Rady Children’s Hospital. Send comments and questions to wwch@ucsd.edu.
New AAP Guideline on Evaluating, Managing Febrile Infants
Presenter: Kenneth Roberts, MD
One of PHM16’s most highly attended sessions was an update on the anticipated AAP guidelines for febrile infants ages 7–90 days. The updated guidelines stress the need to separate individual components of serious bacterial infections (UTI, bacteremia, and meningitis) as the incidence and clinical course can vary greatly in this population.
The inclusion criteria for infants for this upcoming algorithm require an infant to be full-term (37–43 weeks’ gestation), aged 7–90 days, well-appearing, and presenting with a temperature of 38°C.
Exclusion criteria include perinatal/prenatal/neonatal maternal fever, infection, or antimicrobial treatment; the presence of any evident infection; being technology-dependent; and the presence of congenital anomalies.
The updated guideline will aim to stratify management by ages 7–28 days, 29–60 days, and 61–90 days to provide the most appropriate and directed treatment.
It will also include a role for inflammatory markers and allow for a “kinder, gentler” approach, including withholding certain treatments and procedures if infants are at low risk of infection. An active need for observation may be appropriate for certain infants as well. These guidelines should be tailored for individual patients to provide the best care possible while minimizing risk.
Key Takeaway
An updated AAP guideline algorithm for the management of well-appearing febrile infants ages 7–28 days, 29–60 days, and 60–90 days will be coming in the near future. It will help standardize care in this population but should not be used as a substitute for clinical judgment.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System and instructor of pediatrics at George Washington University School of Medicine & Health Sciences in Washington, D.C.
Promoting, Teaching Pediatric High-Value Care
Presenters: Lauren L. Walker, MD, FAAP; Alan Schroeder, MD, FAAP; Michael
Tchou, MD, FAAP; Jimmy Beck, MD, MEd; Lisa Herrmann, MD; Ricardo Quinonez, MD, FAAP
Pediatric hospitalists gathered to attend a fruitful discussion on not only how to change our way of thinking but also how to feed it forward to our trainees. The barriers to promoting and teaching high-value care are plenty and essentially universal to academic and community sites: We have had no formal teaching, there is cultural resistance, and there is lack of transparency on costs and charges.
The questions we perhaps should be asking ourselves, our trainees, and our families are:
- “What matters?” instead of “What’s the matter?”
- “Does that test benefit the patient? What are the harms of the test?” instead of “Will that test change our management?”
There is still a long way to go to move the pendulum to the side of value-based practice and teaching. There is still controversy on how and whether cost should be discussed with the family. Cost is more than just monetary value; family anxiety and patient harm may resonate more with families as we perfect our skills in shared decision making.
Key Takeaway
This serves as an exciting time to unite and better our understanding about why we do what we do and deliberately think about downstream effects. High-value care curriculum for medical students, residents, fellows, and even faculty is an area ripe for further research.
Akshata Hopkins, MD, FAAP, is an academic hospitalist at Johns Hopkins All Children’s Hospital in St. Petersburg, Fla.
How to Design, Improve Educational Programs at Community Hospitals
Presenters: Christopher Russo, MD, FAAP; Laura Hodo, MD, and Lauren Wilson, MD
One session at PHM16 focused on ways to design and improve education within community hospital settings. It was done via a didactic session, breakout groups, and an electronic assessment tool. Facilitators included the workshop leaders and co-leaders along with current PHM fellows and educators from community and academic settings.
During the didactic session, a general background of the importance of education during times of increasing academic and community site affiliations was discussed. This included the strengths of community hospitals for learners such as “appropriate learner autonomy,” “exposure to different career paths,” and “transfer decision making.”
Some of the challenges discussed in regard to developing an educational structure in community settings included:
1. Logistics
- Making the case for education
- Legal framework (e.g., affiliation agreements, liability)
- Finances (e.g., GME funding)
- Paperwork burden (e.g., licensing, credentialing)
2. Learning environment
- Complementing clinical work with materials
- Autonomy/supervision balancing
- Developing clinical teachers
The didactic session also reviewed the six steps for curriculum development: general needs assessment, targeted needs assessment, goals and objectives, educational strategies, implementation, and evaluation/feedback. Each of these was described in further detail with relevant examples.
Groups were broken into small groups based on four learner types: medical students, family medicine residents, pediatric residents, and PHM fellows. Within each group, a “program development matrix” was distributed to assess the support from leadership and logistics within each setting. Each one of these was separated into subgroups such as credentialing, financial support, housing/travel, and preceptor recruitment.
A separate “curriculum development matrix” was used during breakout groups that focused on curriculum development. This matrix was broken into three areas: educational strategies, implementation, and evaluation/feedback. These were further broken down into subgroups such as content, identifying resources, and remediation planning. The group was asked to determine short- and long-term goals with action steps for both of these matrix subgroups.
Key Takeaway
Overall, the session presented a structured way of assessing the educational environment for learners in community settings. It gave tangible tools for sites that wish to develop or improve their current educational framework.
Francisco Alvarez, MD, FAAP, is a pediatric hospitalist and director of the Children’s National Health System Community Hospital Services in Washington, D.C.
Tips on Meeting Needs of Children with a Medical Complexity
Presenters: Mary L. Ehlenbach, MD, FAAP; Megan Z. Cardoso, MD, FAAP, and Christina Kleier, ARNP, PNP
This session at PHM16 was focused on logistical tips on how to build a pediatric complex-care program. Presenters opened with a discussion on how to define children with medical complexity. This involved reviewing different methods, including using research-based aggregation of ICD-10 codes, relying on referral from both families and other providers, and identifying patients by consumption of hospital resources. The presentation continued by highlighting that although medically complex children make up only a small percentage of the overall population of children, they account for about one-third of healthcare spending. Because of advances in technology and medicine, this group of children is growing in numbers. It currently makes up about 10% of all pediatric admissions.
Key Takeaways
1. Children with medical complexity are a growing population on which a large proportion of healthcare resources are utilized. A program dedicated to serving the needs of this population may be helpful in reducing costs and improving the patient and family experience during hospitalizations.
2. When working to initiate a complex-care program:
- Set clear guidelines about which children the program is intended to serve and in what capacity it will function.
- Ensure the team composition is sustainable and meets the needs of the patients.
- Aggregate data about if the program is helping. This may be difficult to quantify since these are mostly qualitative measures.
- Include team members who are nonclinical to aid in improving hospital revenue and highlighting program benefits to the institution.
Margaret Rush, MD, is a hospitalist fellow at Children’s National Medical Center in Washington, D.C.
A Picture Is Worth a Thousand Words
Presenter: Kenneth Roberts, MD
PHM16’s “Visual Diagnosis: Signs and Why They Matter” session was a review of case presentations in which visual clues were vital to establishing a diagnosis. Though much of the content was presented with pictures, the emphasis was placed on the importance of correct diagnosis to avoid both misdiagnoses or overdiagnoses and the potential harm that may result from inappropriate treatment. This may also translate into poor utilization of resources and significant financial burden that can result from the unnecessary hospitalization of a patient.
Many of the presented cases highlighted examples in which there was extensive workup, hospitalization, subspecialty evaluation, and even incorrect treatment of patients.
In other instances, such as with Henoch-Schonlein purpura, Waardenburg syndrome, or McCune-Albright syndrome, the correct diagnosis was necessary to help guide management and future treatment, including subspecialty evaluation.
Key Takeaway
Many diseases with visual presentations will have a benign course and require no treatment. Acknowledging this is important in providing reassurance to a family that may be very anxious over the physical appearance of their child.
This session underscores the need for experience and exposure to various signs not only with rare medical conditions but also in common illnesses such as Kawasaki disease and scarlet fever that may present similarly.
Chandani DeZure, MD, FAAP, is a pediatric hospitalist at Children’s National Health System and instructor of pediatrics at George Washington University School of Medicine & Health Sciences in Washington, D.C.
FDA expands approval of blinatumomab

and solution for infusion
Photo courtesy of Amgen
The US Food and Drug Administration (FDA) has granted accelerated approval for blinatumomab (Blincyto®) to treat pediatric patients with Philadelphia chromosome-negative (Ph-) relapsed or refractory B-cell precursor acute lymphoblastic leukemia (BCP-ALL).
The approval is based on results from a phase 1/2 study.
Continued approval of blinatumomab for this indication may be contingent upon verification of clinical benefit in subsequent trials.
Blinatumomab is a bispecific, CD19-directed, CD3 T-cell engager (BiTE®) antibody construct that binds specifically to CD19 expressed on the surface of cells of B-lineage origin and CD3 expressed on the surface of T cells.
In 2014, blinatumomab received accelerated approval from the FDA to treat adults with Ph- relapsed or refractory BCP-ALL. The FDA has also granted the drug priority review, breakthrough therapy designation, and orphan drug designation.
Blinatumomab is being developed by Amgen. Full prescribing information is available at www.blincyto.com.
‘205 trial
The latest accelerated approval of blinatumomab is based on results from the phase 1/2 ‘205 trial, in which researchers evaluated blinatumomab in 93 pediatric patients with relapsed or refractory BCP-ALL.
Amgen said treatment in this study has been completed, subjects are being monitored for long-term efficacy, and the data will be submitted for publication.
Initial results from this study were presented at ASH 2014. The abstract included data on 39 patients with relapsed/refractory BCP-ALL and a median age of 9 (range, 2-16).
The patients received blinatumomab at a dose of 5-15 µg/m²/day. Nineteen patients completed 1 cycle of blinatumomab, 4 completed 2 cycles, and 2 completed 3 cycles.
During the first 2 treatment cycles, 12 patients achieved a complete response, 5 of whom were negative for minimal residual disease.
Six of the complete responders went on to transplant. The median relapse-free survival for complete responders was 5.6 months.
At 6 months of follow-up, the median overall survival for all 39 patients was 4.3 months.
All of the patients experienced adverse events. The most common were pyrexia (74%), anemia (33%), nausea (31%), headache (28%), hypertension (26%), increased alanine aminotransferase (23%), and cough (21%).
The most common grade 3 or higher events were anemia (26%), pyrexia (21%), increased alanine aminotransferase (18%), increased aspartate aminotransferase (18%), and febrile neutropenia (15%).
Three patients developed cytokine release syndrome (2 grade 3). ![]()
and solution for infusion
Photo courtesy of Amgen
The US Food and Drug Administration (FDA) has granted accelerated approval for blinatumomab (Blincyto®) to treat pediatric patients with Philadelphia chromosome-negative (Ph-) relapsed or refractory B-cell precursor acute lymphoblastic leukemia (BCP-ALL).
The approval is based on results from a phase 1/2 study.
Continued approval of blinatumomab for this indication may be contingent upon verification of clinical benefit in subsequent trials.
Blinatumomab is a bispecific, CD19-directed, CD3 T-cell engager (BiTE®) antibody construct that binds specifically to CD19 expressed on the surface of cells of B-lineage origin and CD3 expressed on the surface of T cells.
In 2014, blinatumomab received accelerated approval from the FDA to treat adults with Ph- relapsed or refractory BCP-ALL. The FDA has also granted the drug priority review, breakthrough therapy designation, and orphan drug designation.
Blinatumomab is being developed by Amgen. Full prescribing information is available at www.blincyto.com.
‘205 trial
The latest accelerated approval of blinatumomab is based on results from the phase 1/2 ‘205 trial, in which researchers evaluated blinatumomab in 93 pediatric patients with relapsed or refractory BCP-ALL.
Amgen said treatment in this study has been completed, subjects are being monitored for long-term efficacy, and the data will be submitted for publication.
Initial results from this study were presented at ASH 2014. The abstract included data on 39 patients with relapsed/refractory BCP-ALL and a median age of 9 (range, 2-16).
The patients received blinatumomab at a dose of 5-15 µg/m²/day. Nineteen patients completed 1 cycle of blinatumomab, 4 completed 2 cycles, and 2 completed 3 cycles.
During the first 2 treatment cycles, 12 patients achieved a complete response, 5 of whom were negative for minimal residual disease.
Six of the complete responders went on to transplant. The median relapse-free survival for complete responders was 5.6 months.
At 6 months of follow-up, the median overall survival for all 39 patients was 4.3 months.
All of the patients experienced adverse events. The most common were pyrexia (74%), anemia (33%), nausea (31%), headache (28%), hypertension (26%), increased alanine aminotransferase (23%), and cough (21%).
The most common grade 3 or higher events were anemia (26%), pyrexia (21%), increased alanine aminotransferase (18%), increased aspartate aminotransferase (18%), and febrile neutropenia (15%).
Three patients developed cytokine release syndrome (2 grade 3). ![]()
and solution for infusion
Photo courtesy of Amgen
The US Food and Drug Administration (FDA) has granted accelerated approval for blinatumomab (Blincyto®) to treat pediatric patients with Philadelphia chromosome-negative (Ph-) relapsed or refractory B-cell precursor acute lymphoblastic leukemia (BCP-ALL).
The approval is based on results from a phase 1/2 study.
Continued approval of blinatumomab for this indication may be contingent upon verification of clinical benefit in subsequent trials.
Blinatumomab is a bispecific, CD19-directed, CD3 T-cell engager (BiTE®) antibody construct that binds specifically to CD19 expressed on the surface of cells of B-lineage origin and CD3 expressed on the surface of T cells.
In 2014, blinatumomab received accelerated approval from the FDA to treat adults with Ph- relapsed or refractory BCP-ALL. The FDA has also granted the drug priority review, breakthrough therapy designation, and orphan drug designation.
Blinatumomab is being developed by Amgen. Full prescribing information is available at www.blincyto.com.
‘205 trial
The latest accelerated approval of blinatumomab is based on results from the phase 1/2 ‘205 trial, in which researchers evaluated blinatumomab in 93 pediatric patients with relapsed or refractory BCP-ALL.
Amgen said treatment in this study has been completed, subjects are being monitored for long-term efficacy, and the data will be submitted for publication.
Initial results from this study were presented at ASH 2014. The abstract included data on 39 patients with relapsed/refractory BCP-ALL and a median age of 9 (range, 2-16).
The patients received blinatumomab at a dose of 5-15 µg/m²/day. Nineteen patients completed 1 cycle of blinatumomab, 4 completed 2 cycles, and 2 completed 3 cycles.
During the first 2 treatment cycles, 12 patients achieved a complete response, 5 of whom were negative for minimal residual disease.
Six of the complete responders went on to transplant. The median relapse-free survival for complete responders was 5.6 months.
At 6 months of follow-up, the median overall survival for all 39 patients was 4.3 months.
All of the patients experienced adverse events. The most common were pyrexia (74%), anemia (33%), nausea (31%), headache (28%), hypertension (26%), increased alanine aminotransferase (23%), and cough (21%).
The most common grade 3 or higher events were anemia (26%), pyrexia (21%), increased alanine aminotransferase (18%), increased aspartate aminotransferase (18%), and febrile neutropenia (15%).
Three patients developed cytokine release syndrome (2 grade 3). ![]()
When should primary care physicians prescribe antibiotics to children with respiratory infection symptoms?
Duration of illness, age, and the presence of specific symptoms are key predictors of hospitalization risk due to respiratory infection, according to a study published in The Lancet. These demographic and clinical factors should guide a primary care physician’s decision to prescribe antibiotics.
“More than 80% of all health-service antibiotics [are] prescribed by primary care clinicians,” reported Alastair Hay, MD, of the University of Bristol, England, and his associates.

“Antibiotic prescribing in primary care is increasing and directly affects antimicrobial resistance,” the researchers noted, adding that many primary care clinicians prescribe antibiotics to pediatric patients with respiratory tract infections and/or cough to “mitigate perceived risk of future hospital admission and complications.”
A total of 8,394 pediatric patients who presented with acute cough and one or more other symptoms of respiratory tract infection (such as fever and coryza) were enrolled in the study by primary care physicians at 247 clinical sites in England. All eligible patients were between the ages of 3 months and 16 years; children were excluded if they presented with noninfective exacerbation of asthma, were at high risk of serious infection, or required a throat swab. The study’s primary outcome was hospital admission for any respiratory tract infection within 30 days of enrollment; the data were collected from a review of electronic medical records (Lancet. 2016. Sept 1. doi: 10.1016/S2213-2600[16]30223-5).

The median age of the pediatric cohort was 3 years, 52% were male, and 78% were white. A total of 3,121 patients (37%) were prescribed an antibiotic by their primary care physicians, but only 78 patients (0.9%) were admitted to the hospital, and 27% of discharge diagnoses suggested a possible bacterial cause (lower respiratory tract infection, tonsillitis, and pneumonia).
Multivariate modeling with bootstrap validation demonstrated that duration of illness, age, and the presence or absence of specific respiratory symptoms were the key factors that should be used to identify children at low, normal, and high risk for hospitalization due to respiratory infection. Younger patients with shorter illness durations who presented with wheeze, fever, vomiting, intercostal or subcostal recession, and/or asthma were at higher risk for hospitalization.
“Our data show that 1,846 (33%) of the very-low-risk stratum children received antibiotics. Because these children represent the majority (67%) of all the participants, a 10% overall reduction in antibiotic prescription would be achieved if prescription in this group halved, remained static in the normal risk stratum, and increased to 90% in the high risk stratum, resulting in a similar effect size to other contemporary antimicrobial stewardship interventions,” Dr. Hay and his associates concluded.
This study received funding and sponsorship from the National Institute for Health Research and the University of Bristol. Two investigators reported receiving financial compensation or honoraria from multiple companies including companies with an interest in diagnostic microbiology in respiratory tract infections.
On Twitter @jessnicolecraig
Duration of illness, age, and the presence of specific symptoms are key predictors of hospitalization risk due to respiratory infection, according to a study published in The Lancet. These demographic and clinical factors should guide a primary care physician’s decision to prescribe antibiotics.
“More than 80% of all health-service antibiotics [are] prescribed by primary care clinicians,” reported Alastair Hay, MD, of the University of Bristol, England, and his associates.
“Antibiotic prescribing in primary care is increasing and directly affects antimicrobial resistance,” the researchers noted, adding that many primary care clinicians prescribe antibiotics to pediatric patients with respiratory tract infections and/or cough to “mitigate perceived risk of future hospital admission and complications.”
A total of 8,394 pediatric patients who presented with acute cough and one or more other symptoms of respiratory tract infection (such as fever and coryza) were enrolled in the study by primary care physicians at 247 clinical sites in England. All eligible patients were between the ages of 3 months and 16 years; children were excluded if they presented with noninfective exacerbation of asthma, were at high risk of serious infection, or required a throat swab. The study’s primary outcome was hospital admission for any respiratory tract infection within 30 days of enrollment; the data were collected from a review of electronic medical records (Lancet. 2016. Sept 1. doi: 10.1016/S2213-2600[16]30223-5).
The median age of the pediatric cohort was 3 years, 52% were male, and 78% were white. A total of 3,121 patients (37%) were prescribed an antibiotic by their primary care physicians, but only 78 patients (0.9%) were admitted to the hospital, and 27% of discharge diagnoses suggested a possible bacterial cause (lower respiratory tract infection, tonsillitis, and pneumonia).
Multivariate modeling with bootstrap validation demonstrated that duration of illness, age, and the presence or absence of specific respiratory symptoms were the key factors that should be used to identify children at low, normal, and high risk for hospitalization due to respiratory infection. Younger patients with shorter illness durations who presented with wheeze, fever, vomiting, intercostal or subcostal recession, and/or asthma were at higher risk for hospitalization.
“Our data show that 1,846 (33%) of the very-low-risk stratum children received antibiotics. Because these children represent the majority (67%) of all the participants, a 10% overall reduction in antibiotic prescription would be achieved if prescription in this group halved, remained static in the normal risk stratum, and increased to 90% in the high risk stratum, resulting in a similar effect size to other contemporary antimicrobial stewardship interventions,” Dr. Hay and his associates concluded.
This study received funding and sponsorship from the National Institute for Health Research and the University of Bristol. Two investigators reported receiving financial compensation or honoraria from multiple companies including companies with an interest in diagnostic microbiology in respiratory tract infections.
On Twitter @jessnicolecraig
Duration of illness, age, and the presence of specific symptoms are key predictors of hospitalization risk due to respiratory infection, according to a study published in The Lancet. These demographic and clinical factors should guide a primary care physician’s decision to prescribe antibiotics.
“More than 80% of all health-service antibiotics [are] prescribed by primary care clinicians,” reported Alastair Hay, MD, of the University of Bristol, England, and his associates.
“Antibiotic prescribing in primary care is increasing and directly affects antimicrobial resistance,” the researchers noted, adding that many primary care clinicians prescribe antibiotics to pediatric patients with respiratory tract infections and/or cough to “mitigate perceived risk of future hospital admission and complications.”
A total of 8,394 pediatric patients who presented with acute cough and one or more other symptoms of respiratory tract infection (such as fever and coryza) were enrolled in the study by primary care physicians at 247 clinical sites in England. All eligible patients were between the ages of 3 months and 16 years; children were excluded if they presented with noninfective exacerbation of asthma, were at high risk of serious infection, or required a throat swab. The study’s primary outcome was hospital admission for any respiratory tract infection within 30 days of enrollment; the data were collected from a review of electronic medical records (Lancet. 2016. Sept 1. doi: 10.1016/S2213-2600[16]30223-5).
The median age of the pediatric cohort was 3 years, 52% were male, and 78% were white. A total of 3,121 patients (37%) were prescribed an antibiotic by their primary care physicians, but only 78 patients (0.9%) were admitted to the hospital, and 27% of discharge diagnoses suggested a possible bacterial cause (lower respiratory tract infection, tonsillitis, and pneumonia).
Multivariate modeling with bootstrap validation demonstrated that duration of illness, age, and the presence or absence of specific respiratory symptoms were the key factors that should be used to identify children at low, normal, and high risk for hospitalization due to respiratory infection. Younger patients with shorter illness durations who presented with wheeze, fever, vomiting, intercostal or subcostal recession, and/or asthma were at higher risk for hospitalization.
“Our data show that 1,846 (33%) of the very-low-risk stratum children received antibiotics. Because these children represent the majority (67%) of all the participants, a 10% overall reduction in antibiotic prescription would be achieved if prescription in this group halved, remained static in the normal risk stratum, and increased to 90% in the high risk stratum, resulting in a similar effect size to other contemporary antimicrobial stewardship interventions,” Dr. Hay and his associates concluded.
This study received funding and sponsorship from the National Institute for Health Research and the University of Bristol. Two investigators reported receiving financial compensation or honoraria from multiple companies including companies with an interest in diagnostic microbiology in respiratory tract infections.
On Twitter @jessnicolecraig
FROM THE LANCET
Key clinical point: Duration of illness, age, and the presence of specific symptoms are key predictors of hospitalization risk due to respiratory infection. These factors should guide a primary care physician’s decision to prescribe antibiotics.
Major finding: Younger patients with shorter illness durations who presented with wheeze, fever, vomiting, intercostal or subcostal recession, and/or asthma are at higher risk for hospitalization.
Data source: A prospective, prognostic cohort study of 8,394 children.
Disclosures: This study received funding and sponsorship from the National Institute for Health Research and the University of Bristol. Two investigators reported receiving financial compensation or honoraria from multiple companies, including those with an interest in diagnostic microbiology in respiratory tract infections.

PCV vaccines less prominent in children with meningitis
Pneumococcal conjugate vaccines 7-valent and 13-valent (PCV7/PCV13) in children younger than 5 years of age in Israel were less prominent in meningitis than in nonmeningitis invasive pneumococcal disease (nm-IPD), according to S. Ben-Shimol, MD, and associates.
Between July 2000 and June 2015, 4,168 IPD episodes were reported; 426 (10.2%) were meningitis. The PCV13 serotype (13VT) meningitis rates significantly declined by 93% (incidence rate ratio = 0.07), from 3.6 ± 1.3 in the pre-PCV period to 0.3 in the last year of the study. Also, the 13VT nm-IPD rates significantly declined by 95% (IRR = 0.05), from a rate of 40.0 ± 5.4 in the pre-PCV period to 1.9. The non-13VT meningitis rates significantly increased by 273% (IRR = 3.73), from 0.8 ± 0.3 in the pre-PCV period to 3.0. And the non-13VT nm-IPD rates also significantly increased by 162% (IRR = 2.62), from 4.5 ± 0.8 in the pre-PCV period to 11.8.

The researchers noted that the increase in non-13VT meningitis was partially driven by a sharp and significant increase of serotype 12F, along with the other predominant non-13VT serotypes that caused meningitis: 15B/C, 24F, and 27. The serotypes also were predominant in non-13VT nm-IPD, as were additional serotypes 8, 10A, 33F, 7B and 10B.
“This finding may be attributed to the younger age of children with meningitis and differences in causative serotypes between the two groups, as the decline of the incidence of meningitis and nm-IPD caused by vaccine-serotypes is similar,” researchers concluded. “Continuous monitoring of meningitis and nm-IPD is warranted.”
Find the full study in Vaccine (doi: 10.1016/j.vaccine.2016.07.038).
Pneumococcal conjugate vaccines 7-valent and 13-valent (PCV7/PCV13) in children younger than 5 years of age in Israel were less prominent in meningitis than in nonmeningitis invasive pneumococcal disease (nm-IPD), according to S. Ben-Shimol, MD, and associates.
Between July 2000 and June 2015, 4,168 IPD episodes were reported; 426 (10.2%) were meningitis. The PCV13 serotype (13VT) meningitis rates significantly declined by 93% (incidence rate ratio = 0.07), from 3.6 ± 1.3 in the pre-PCV period to 0.3 in the last year of the study. Also, the 13VT nm-IPD rates significantly declined by 95% (IRR = 0.05), from a rate of 40.0 ± 5.4 in the pre-PCV period to 1.9. The non-13VT meningitis rates significantly increased by 273% (IRR = 3.73), from 0.8 ± 0.3 in the pre-PCV period to 3.0. And the non-13VT nm-IPD rates also significantly increased by 162% (IRR = 2.62), from 4.5 ± 0.8 in the pre-PCV period to 11.8.
The researchers noted that the increase in non-13VT meningitis was partially driven by a sharp and significant increase of serotype 12F, along with the other predominant non-13VT serotypes that caused meningitis: 15B/C, 24F, and 27. The serotypes also were predominant in non-13VT nm-IPD, as were additional serotypes 8, 10A, 33F, 7B and 10B.
“This finding may be attributed to the younger age of children with meningitis and differences in causative serotypes between the two groups, as the decline of the incidence of meningitis and nm-IPD caused by vaccine-serotypes is similar,” researchers concluded. “Continuous monitoring of meningitis and nm-IPD is warranted.”
Find the full study in Vaccine (doi: 10.1016/j.vaccine.2016.07.038).
Pneumococcal conjugate vaccines 7-valent and 13-valent (PCV7/PCV13) in children younger than 5 years of age in Israel were less prominent in meningitis than in nonmeningitis invasive pneumococcal disease (nm-IPD), according to S. Ben-Shimol, MD, and associates.
Between July 2000 and June 2015, 4,168 IPD episodes were reported; 426 (10.2%) were meningitis. The PCV13 serotype (13VT) meningitis rates significantly declined by 93% (incidence rate ratio = 0.07), from 3.6 ± 1.3 in the pre-PCV period to 0.3 in the last year of the study. Also, the 13VT nm-IPD rates significantly declined by 95% (IRR = 0.05), from a rate of 40.0 ± 5.4 in the pre-PCV period to 1.9. The non-13VT meningitis rates significantly increased by 273% (IRR = 3.73), from 0.8 ± 0.3 in the pre-PCV period to 3.0. And the non-13VT nm-IPD rates also significantly increased by 162% (IRR = 2.62), from 4.5 ± 0.8 in the pre-PCV period to 11.8.
The researchers noted that the increase in non-13VT meningitis was partially driven by a sharp and significant increase of serotype 12F, along with the other predominant non-13VT serotypes that caused meningitis: 15B/C, 24F, and 27. The serotypes also were predominant in non-13VT nm-IPD, as were additional serotypes 8, 10A, 33F, 7B and 10B.
“This finding may be attributed to the younger age of children with meningitis and differences in causative serotypes between the two groups, as the decline of the incidence of meningitis and nm-IPD caused by vaccine-serotypes is similar,” researchers concluded. “Continuous monitoring of meningitis and nm-IPD is warranted.”
Find the full study in Vaccine (doi: 10.1016/j.vaccine.2016.07.038).
FROM VACCINE

Which SSRIs most effectively treat depression in adolescents?
EVIDENCE-BASED ANSWER:
We don’t know which selective serotonin reuptake inhibitors (SSRIs) are the most effective and safe because no studies have compared these antidepressants with each other.
Three SSRI antidepressant medications—fluoxetine, sertraline, and escitalopram—produce modest improvements (about 5% to 10%) in standardized depression scores without a significant increase in the risk of suicide-related outcomes (suicidal behavior or ideation) in adolescent patients with major depression of moderate severity. As a group, however, the newer-generation antidepressants, including SSRIs, increase suicide-related outcomes by 50%. Citalopram, paroxetine, venlafaxine, and mirtazapine don’t improve depression scores (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
An updated national guideline recommends specific psychological therapy for adolescents with mild depression and combined psychotherapy and fluoxetine for moderate or severe depression, with sertraline or citalopram as second-line agents (SOR: A, RCTs).
EVIDENCE SUMMARY
A Cochrane systematic review (19 RCTs; 3335 patients, total) of newer-generation antidepressants for treating depression in adolescents found that, overall, they produced both a small decrease in symptom severity scores and an increased risk of suicide-related outcomes.1
Three SSRIs slightly lower one symptom severity score
Investigators performed a meta-analysis of all trials (14 RCTs; 2490 patients, total) that used the same standardized symptom severity score (the Children’s Depression Rating Scale—Revised [CDRS-R], range 17 to 113 points) to evaluate the following medications: fluoxetine, sertraline, escitalopram, citalopram, paroxetine, venlafaxine, and mirtazapine.1
All participants were outpatients who met criteria for a primary diagnosis of major depression, excluding comorbid conditions. The CDRS-R scores were evaluated by clinicians; the mean baseline score was 57 (40 is considered a threshold score for diagnosis, and above 60 indicates severe symptoms). Only 5 trials reported patients’ self-rated depression symptom severity (in patients taking fluoxetine and paroxetine) and none reported improvement. Treatment courses ranged from 8 to 12 weeks.
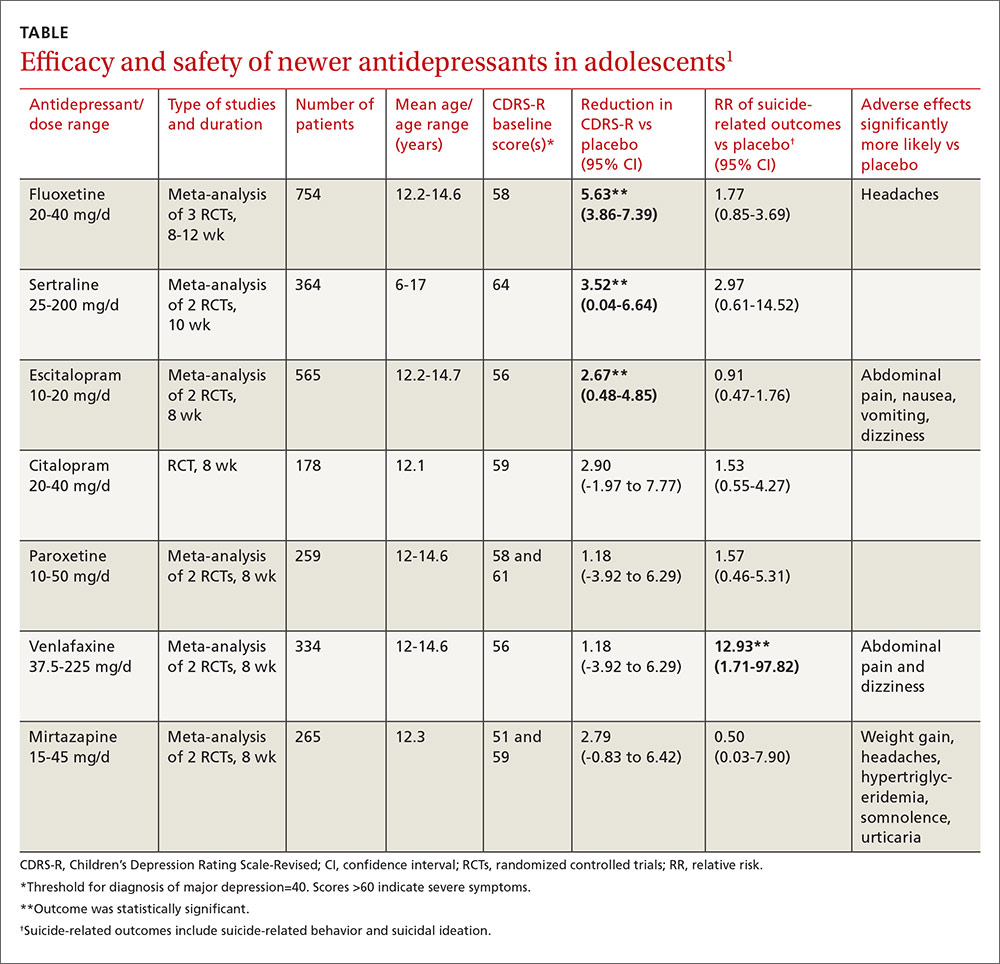
As a group, the newer antidepressants slightly reduced CDRS-R scores in adolescents (by 4.21 points, 95% confidence interval [CI], 0.41-5.95) but increased suicide-related outcomes (relative risk [RR]=1.47; 95% CI, 0.99-2.19). The individual antidepressants fluoxetine, sertraline, and escitalopram each produced statistically significant but clinically small reductions in CDRS-R scores of 5% to 10% without significantly increasing suicide-related outcomes (TABLE1). The other medications evaluated individually didn’t improve CDRS-R scores, and only venlafaxine increased suicide-related outcomes.
Other symptom severity scores show no improvement with SSRIs
Five additional RCTs not included in the meta-analysis that used standardized symptom severity scores other than the CDRS-R (Schedule for Affective Disorders and Schizophrenia for School-Aged Children [K-SADS], Montgomery-Asberg Depression Rating Scale [MADR], and Hamilton Depression Rating Scale [HAM-D]) found no improvement with fluoxetine (2 RCTs; 63 patients, total), citalopram (one RCT, 233 patients), or paroxetine (2 RCTs; 466 patients, total).
Certain drugs cause significantly more adverse events than placebo
Ten RCTs evaluated adverse events in adolescents treated with fluoxetine, escitalopram, citalopram, and paroxetine and reported a small increase over placebo when all medications were combined as a group (RR=1.11; 95% CI, 1.05-1.17). Investigators reported that the individual antidepressants fluoxetine, escitalopram, venlafaxine, and mirtazapine produced significantly more adverse events than placebo (P values not given). No studies compared antidepressant medications against each other for either efficacy or potential harms.
RECOMMENDATIONS
A newly revised expert guideline recommends treating mildly depressed adolescents with a specific psychological therapy—individual cognitive behavioral therapy, interpersonal therapy, family therapy, or psychodynamic psychotherapy—for at least 3 months.2
For adolescents with moderate to severe depression, the guideline advocates psychotherapy with the option of adding fluoxetine, although using antidepressants in adolescents who haven’t at least tried psychotherapy is outside of the drug’s indications.
The guideline also recommends careful monitoring for adverse effects and close review of mental state—weekly for the first 4 weeks of treatment, for example. If fluoxetine doesn’t help, sertraline and citalopram are recommended as alternatives.
1. Hetrick SE, McKenzie JE, Cox GR, et al. Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database Syst Rev. 2012;11:CD004851.
2. Hopkins K, Crosland P, Elliott N, et al. Diagnosis and management of depression in children and young people: summary of updated NICE guidance. BMJ. 2015;350:h824.
EVIDENCE-BASED ANSWER:
We don’t know which selective serotonin reuptake inhibitors (SSRIs) are the most effective and safe because no studies have compared these antidepressants with each other.
Three SSRI antidepressant medications—fluoxetine, sertraline, and escitalopram—produce modest improvements (about 5% to 10%) in standardized depression scores without a significant increase in the risk of suicide-related outcomes (suicidal behavior or ideation) in adolescent patients with major depression of moderate severity. As a group, however, the newer-generation antidepressants, including SSRIs, increase suicide-related outcomes by 50%. Citalopram, paroxetine, venlafaxine, and mirtazapine don’t improve depression scores (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
An updated national guideline recommends specific psychological therapy for adolescents with mild depression and combined psychotherapy and fluoxetine for moderate or severe depression, with sertraline or citalopram as second-line agents (SOR: A, RCTs).
EVIDENCE SUMMARY
A Cochrane systematic review (19 RCTs; 3335 patients, total) of newer-generation antidepressants for treating depression in adolescents found that, overall, they produced both a small decrease in symptom severity scores and an increased risk of suicide-related outcomes.1
Three SSRIs slightly lower one symptom severity score
Investigators performed a meta-analysis of all trials (14 RCTs; 2490 patients, total) that used the same standardized symptom severity score (the Children’s Depression Rating Scale—Revised [CDRS-R], range 17 to 113 points) to evaluate the following medications: fluoxetine, sertraline, escitalopram, citalopram, paroxetine, venlafaxine, and mirtazapine.1
All participants were outpatients who met criteria for a primary diagnosis of major depression, excluding comorbid conditions. The CDRS-R scores were evaluated by clinicians; the mean baseline score was 57 (40 is considered a threshold score for diagnosis, and above 60 indicates severe symptoms). Only 5 trials reported patients’ self-rated depression symptom severity (in patients taking fluoxetine and paroxetine) and none reported improvement. Treatment courses ranged from 8 to 12 weeks.
As a group, the newer antidepressants slightly reduced CDRS-R scores in adolescents (by 4.21 points, 95% confidence interval [CI], 0.41-5.95) but increased suicide-related outcomes (relative risk [RR]=1.47; 95% CI, 0.99-2.19). The individual antidepressants fluoxetine, sertraline, and escitalopram each produced statistically significant but clinically small reductions in CDRS-R scores of 5% to 10% without significantly increasing suicide-related outcomes (TABLE1). The other medications evaluated individually didn’t improve CDRS-R scores, and only venlafaxine increased suicide-related outcomes.
Other symptom severity scores show no improvement with SSRIs
Five additional RCTs not included in the meta-analysis that used standardized symptom severity scores other than the CDRS-R (Schedule for Affective Disorders and Schizophrenia for School-Aged Children [K-SADS], Montgomery-Asberg Depression Rating Scale [MADR], and Hamilton Depression Rating Scale [HAM-D]) found no improvement with fluoxetine (2 RCTs; 63 patients, total), citalopram (one RCT, 233 patients), or paroxetine (2 RCTs; 466 patients, total).
Certain drugs cause significantly more adverse events than placebo
Ten RCTs evaluated adverse events in adolescents treated with fluoxetine, escitalopram, citalopram, and paroxetine and reported a small increase over placebo when all medications were combined as a group (RR=1.11; 95% CI, 1.05-1.17). Investigators reported that the individual antidepressants fluoxetine, escitalopram, venlafaxine, and mirtazapine produced significantly more adverse events than placebo (P values not given). No studies compared antidepressant medications against each other for either efficacy or potential harms.
RECOMMENDATIONS
A newly revised expert guideline recommends treating mildly depressed adolescents with a specific psychological therapy—individual cognitive behavioral therapy, interpersonal therapy, family therapy, or psychodynamic psychotherapy—for at least 3 months.2
For adolescents with moderate to severe depression, the guideline advocates psychotherapy with the option of adding fluoxetine, although using antidepressants in adolescents who haven’t at least tried psychotherapy is outside of the drug’s indications.
The guideline also recommends careful monitoring for adverse effects and close review of mental state—weekly for the first 4 weeks of treatment, for example. If fluoxetine doesn’t help, sertraline and citalopram are recommended as alternatives.
EVIDENCE-BASED ANSWER:
We don’t know which selective serotonin reuptake inhibitors (SSRIs) are the most effective and safe because no studies have compared these antidepressants with each other.
Three SSRI antidepressant medications—fluoxetine, sertraline, and escitalopram—produce modest improvements (about 5% to 10%) in standardized depression scores without a significant increase in the risk of suicide-related outcomes (suicidal behavior or ideation) in adolescent patients with major depression of moderate severity. As a group, however, the newer-generation antidepressants, including SSRIs, increase suicide-related outcomes by 50%. Citalopram, paroxetine, venlafaxine, and mirtazapine don’t improve depression scores (strength of recommendation [SOR]: A, meta-analyses of randomized controlled trials [RCTs]).
An updated national guideline recommends specific psychological therapy for adolescents with mild depression and combined psychotherapy and fluoxetine for moderate or severe depression, with sertraline or citalopram as second-line agents (SOR: A, RCTs).
EVIDENCE SUMMARY
A Cochrane systematic review (19 RCTs; 3335 patients, total) of newer-generation antidepressants for treating depression in adolescents found that, overall, they produced both a small decrease in symptom severity scores and an increased risk of suicide-related outcomes.1
Three SSRIs slightly lower one symptom severity score
Investigators performed a meta-analysis of all trials (14 RCTs; 2490 patients, total) that used the same standardized symptom severity score (the Children’s Depression Rating Scale—Revised [CDRS-R], range 17 to 113 points) to evaluate the following medications: fluoxetine, sertraline, escitalopram, citalopram, paroxetine, venlafaxine, and mirtazapine.1
All participants were outpatients who met criteria for a primary diagnosis of major depression, excluding comorbid conditions. The CDRS-R scores were evaluated by clinicians; the mean baseline score was 57 (40 is considered a threshold score for diagnosis, and above 60 indicates severe symptoms). Only 5 trials reported patients’ self-rated depression symptom severity (in patients taking fluoxetine and paroxetine) and none reported improvement. Treatment courses ranged from 8 to 12 weeks.
As a group, the newer antidepressants slightly reduced CDRS-R scores in adolescents (by 4.21 points, 95% confidence interval [CI], 0.41-5.95) but increased suicide-related outcomes (relative risk [RR]=1.47; 95% CI, 0.99-2.19). The individual antidepressants fluoxetine, sertraline, and escitalopram each produced statistically significant but clinically small reductions in CDRS-R scores of 5% to 10% without significantly increasing suicide-related outcomes (TABLE1). The other medications evaluated individually didn’t improve CDRS-R scores, and only venlafaxine increased suicide-related outcomes.
Other symptom severity scores show no improvement with SSRIs
Five additional RCTs not included in the meta-analysis that used standardized symptom severity scores other than the CDRS-R (Schedule for Affective Disorders and Schizophrenia for School-Aged Children [K-SADS], Montgomery-Asberg Depression Rating Scale [MADR], and Hamilton Depression Rating Scale [HAM-D]) found no improvement with fluoxetine (2 RCTs; 63 patients, total), citalopram (one RCT, 233 patients), or paroxetine (2 RCTs; 466 patients, total).
Certain drugs cause significantly more adverse events than placebo
Ten RCTs evaluated adverse events in adolescents treated with fluoxetine, escitalopram, citalopram, and paroxetine and reported a small increase over placebo when all medications were combined as a group (RR=1.11; 95% CI, 1.05-1.17). Investigators reported that the individual antidepressants fluoxetine, escitalopram, venlafaxine, and mirtazapine produced significantly more adverse events than placebo (P values not given). No studies compared antidepressant medications against each other for either efficacy or potential harms.
RECOMMENDATIONS
A newly revised expert guideline recommends treating mildly depressed adolescents with a specific psychological therapy—individual cognitive behavioral therapy, interpersonal therapy, family therapy, or psychodynamic psychotherapy—for at least 3 months.2
For adolescents with moderate to severe depression, the guideline advocates psychotherapy with the option of adding fluoxetine, although using antidepressants in adolescents who haven’t at least tried psychotherapy is outside of the drug’s indications.
The guideline also recommends careful monitoring for adverse effects and close review of mental state—weekly for the first 4 weeks of treatment, for example. If fluoxetine doesn’t help, sertraline and citalopram are recommended as alternatives.
1. Hetrick SE, McKenzie JE, Cox GR, et al. Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database Syst Rev. 2012;11:CD004851.
2. Hopkins K, Crosland P, Elliott N, et al. Diagnosis and management of depression in children and young people: summary of updated NICE guidance. BMJ. 2015;350:h824.
1. Hetrick SE, McKenzie JE, Cox GR, et al. Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database Syst Rev. 2012;11:CD004851.
2. Hopkins K, Crosland P, Elliott N, et al. Diagnosis and management of depression in children and young people: summary of updated NICE guidance. BMJ. 2015;350:h824.
Evidence-based answers from the Family Physicians Inquiries Network

Depigmented patches, mild scaling on newborn • Dx?
THE CASE
A 21-year-old G3P2 mother gave birth to an African American girl via vaginal delivery. Labor had been induced due to gestational hypertension at term. She’d also had a stillborn at term at the age of 16 followed by a second live term birth 3 years ago. During this most recent pregnancy, she’d received adequate prenatal care and had been treated for chlamydia with a single dose of oral azithromycin 1 g.
The newborn had an Apgar score of 9 out of 9 and weighed 6.7 pounds at birth. During a physical examination in the nursery, the infant was found to have large areas of smooth depigmentation on her forehead, right forearm, lower abdomen, and left thigh, with surrounding areas of thickened skin that had mild scaling and hyperpigmentation (FIGURE). The depigmented areas involved approximately 15% of the newborn’s body. The father and paternal grandmother, who were present at the time of delivery, also had depigmented areas of their skin.
The newborn’s tongue was pink and her mucus membranes were moist. No macules or patches were noted on either the oral or vaginal mucosa. Cardiac, pulmonary, and ocular examinations (including evaluation of the retina by ophthalmoscopy) were normal. There was no nystagmus or strabismus. The newborn’s extremities were normal, symmetric, and moveable, and she was easily consoled.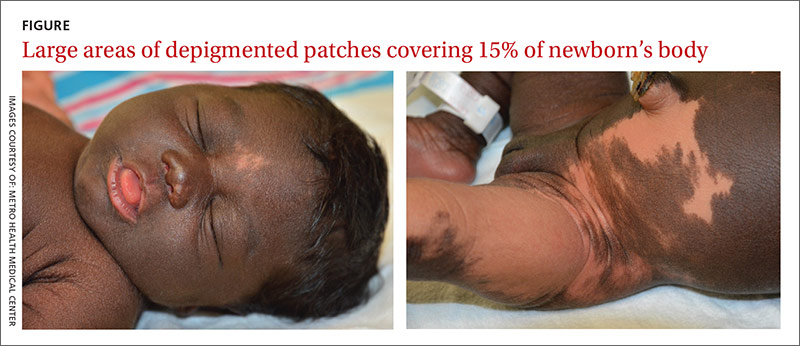
THE DIAGNOSIS
We diagnosed the newborn with piebaldism based on her appearance. Piebaldism consists of hypopigmented/depigmented areas and is a clinical diagnosis; no testing is required.
Concerned about the areas of hyperpigmentation, we decided to get a dermatologist’s opinion. The dermatology team briefly considered the diagnosis of a large melanocytic nevus with sparing of some areas, but a skin biopsy of a hyperpigmented area on the left leg came back with a normal number of melanocytes.
DISCUSSION
Piebaldism is a rare autosomal dominant disorder characterized by the congenital absence of melanocytes in affected areas of the skin and hair due to mutations of the c-kit gene. The c-kit gene affects the differentiation and migration of melanoblasts from the neural crest during embryonic life.1 The incidence of piebaldism is estimated to be less than one in 20,000.2 Both males and females are equally affected, and no race is spared.2,3
Affected individuals present with a white forelock and relatively stable, persistent depigmentation of skin with a characteristic distribution from birth.3 A white forelock arising from a triangular, elongated, or diamond-shaped midline or depigmented macule on the forehead may be the only manifestation in 80% to 90% of cases.3 The characteristic distribution of depigmented macules includes a central macule on the forehead, the anterior abdomen extending to the chest, the lateral trunk sparing the dorsal spine, and the mid-arms and legs sparing the hands and feet.2
Depigmented macules are rectangular, rhomboid, or irregular in shape and usually have a symmetrical distribution. Typically, islands of hyperpigmentation are present within and at the border of depigmented areas.4 Piebaldism is associated in rare instances with neurofibromatosis type 1, Hirschsprung’s disease, hearing loss, and Waardenburg syndrome.4
Histologically, melanocytes are absent or considerably reduced in the depigmented areas and are normal in number in the hyperpigmented areas.5
The differential diagnosis of piebaldism includes mosaicism, albinism, and vitiligo.
Cutaneous mosaicism stems from a gene mutation that occurs during embryogenesis and the lesions are distributed along certain patterns and forms. A chromosomal analysis of our patient showed a normal female karyotype that excluded mosaicism.
Albinism is a genetically inherited disorder characterized by partial or complete absence of melanin production in the skin, hair, and eyes.6 Eye and fundus examinations were normal in our patient, which excluded albinism.
Vitiligo is rarely present at birth but is usually acquired later in life. It results from an immune-mediated destruction of melanocytes and is not genetically inherited, although familial incidence has been reported.7
There are no effective therapies
A combination of dermabrasion and grafting of pigmented skin into depigmented areas, with or without phototherapy, has been used in select patients, although no solid data are available on its effectiveness.3 The lack of effective and safe therapies can make treatment challenging. Piebaldism is usually not medically harmful, but the emotional and psychological effects on the family and the patient as they grow up can be devastating. Therefore, supportive counseling is recommended.
Our patient. Supportive counseling and a follow-up appointment with a dermatologist was planned for our patient and her family.
THE TAKEAWAY
The clinical diagnosis of piebaldism is straightforward based on the presence of a white forelock in the frontal region, the appearance of depigmented macules since birth that stay relatively stable, and the presence of a similar pattern of depigmented macules in other family members. Histologic or genetic testing is not necessary to establish the diagnosis. Rarely, cases of piebaldism are associated with hearing loss, necessitating a hearing assessment and an audiology exam. Unfortunately, there are no effective treatments for piebaldism.
1. Ward KA, Moss C, Sanders DS. Human piebaldism: relationship between phenotype and site of kit gene mutation. Br J Dermatol. 1995;132:929-935.
2. Agarwal S, Ojha A. Piebaldism: A brief report and review of the literature. Indian Dermatol Online J. 2012;3:144-147.
3. Oiso N, Fukai K, Kawada A, et al. Piebaldism. J Dermatol. 2013;40:330-335.
4. Spritz RA, Itin PH, Gutmann DH. Piebaldism and neurofibromatosis type 1: horses of very different colors. J Invest Dermatol. 2004;122:xxxiv-xxxv.
5. Makino T, Yanagihara M, Oiso N, et al. Repigmentation of the epidermis around the acrosyringium in piebald skin: an ultrastructural examination. Br J Dermatol. 2013;168:910-912.
6. Karaman A. Oculocutaneous albinism type 1A: a case report. Dermatol Online J. 2008;14:13.
7. Plensdorf S, Martinez J. Common pigmentation disorders. Am Fam Physician. 2009;79:109-116.
THE CASE
A 21-year-old G3P2 mother gave birth to an African American girl via vaginal delivery. Labor had been induced due to gestational hypertension at term. She’d also had a stillborn at term at the age of 16 followed by a second live term birth 3 years ago. During this most recent pregnancy, she’d received adequate prenatal care and had been treated for chlamydia with a single dose of oral azithromycin 1 g.
The newborn had an Apgar score of 9 out of 9 and weighed 6.7 pounds at birth. During a physical examination in the nursery, the infant was found to have large areas of smooth depigmentation on her forehead, right forearm, lower abdomen, and left thigh, with surrounding areas of thickened skin that had mild scaling and hyperpigmentation (FIGURE). The depigmented areas involved approximately 15% of the newborn’s body. The father and paternal grandmother, who were present at the time of delivery, also had depigmented areas of their skin.
The newborn’s tongue was pink and her mucus membranes were moist. No macules or patches were noted on either the oral or vaginal mucosa. Cardiac, pulmonary, and ocular examinations (including evaluation of the retina by ophthalmoscopy) were normal. There was no nystagmus or strabismus. The newborn’s extremities were normal, symmetric, and moveable, and she was easily consoled.
THE DIAGNOSIS
We diagnosed the newborn with piebaldism based on her appearance. Piebaldism consists of hypopigmented/depigmented areas and is a clinical diagnosis; no testing is required.
Concerned about the areas of hyperpigmentation, we decided to get a dermatologist’s opinion. The dermatology team briefly considered the diagnosis of a large melanocytic nevus with sparing of some areas, but a skin biopsy of a hyperpigmented area on the left leg came back with a normal number of melanocytes.
DISCUSSION
Piebaldism is a rare autosomal dominant disorder characterized by the congenital absence of melanocytes in affected areas of the skin and hair due to mutations of the c-kit gene. The c-kit gene affects the differentiation and migration of melanoblasts from the neural crest during embryonic life.1 The incidence of piebaldism is estimated to be less than one in 20,000.2 Both males and females are equally affected, and no race is spared.2,3
Affected individuals present with a white forelock and relatively stable, persistent depigmentation of skin with a characteristic distribution from birth.3 A white forelock arising from a triangular, elongated, or diamond-shaped midline or depigmented macule on the forehead may be the only manifestation in 80% to 90% of cases.3 The characteristic distribution of depigmented macules includes a central macule on the forehead, the anterior abdomen extending to the chest, the lateral trunk sparing the dorsal spine, and the mid-arms and legs sparing the hands and feet.2
Depigmented macules are rectangular, rhomboid, or irregular in shape and usually have a symmetrical distribution. Typically, islands of hyperpigmentation are present within and at the border of depigmented areas.4 Piebaldism is associated in rare instances with neurofibromatosis type 1, Hirschsprung’s disease, hearing loss, and Waardenburg syndrome.4
Histologically, melanocytes are absent or considerably reduced in the depigmented areas and are normal in number in the hyperpigmented areas.5
The differential diagnosis of piebaldism includes mosaicism, albinism, and vitiligo.
Cutaneous mosaicism stems from a gene mutation that occurs during embryogenesis and the lesions are distributed along certain patterns and forms. A chromosomal analysis of our patient showed a normal female karyotype that excluded mosaicism.
Albinism is a genetically inherited disorder characterized by partial or complete absence of melanin production in the skin, hair, and eyes.6 Eye and fundus examinations were normal in our patient, which excluded albinism.
Vitiligo is rarely present at birth but is usually acquired later in life. It results from an immune-mediated destruction of melanocytes and is not genetically inherited, although familial incidence has been reported.7
There are no effective therapies
A combination of dermabrasion and grafting of pigmented skin into depigmented areas, with or without phototherapy, has been used in select patients, although no solid data are available on its effectiveness.3 The lack of effective and safe therapies can make treatment challenging. Piebaldism is usually not medically harmful, but the emotional and psychological effects on the family and the patient as they grow up can be devastating. Therefore, supportive counseling is recommended.
Our patient. Supportive counseling and a follow-up appointment with a dermatologist was planned for our patient and her family.
THE TAKEAWAY
The clinical diagnosis of piebaldism is straightforward based on the presence of a white forelock in the frontal region, the appearance of depigmented macules since birth that stay relatively stable, and the presence of a similar pattern of depigmented macules in other family members. Histologic or genetic testing is not necessary to establish the diagnosis. Rarely, cases of piebaldism are associated with hearing loss, necessitating a hearing assessment and an audiology exam. Unfortunately, there are no effective treatments for piebaldism.
THE CASE
A 21-year-old G3P2 mother gave birth to an African American girl via vaginal delivery. Labor had been induced due to gestational hypertension at term. She’d also had a stillborn at term at the age of 16 followed by a second live term birth 3 years ago. During this most recent pregnancy, she’d received adequate prenatal care and had been treated for chlamydia with a single dose of oral azithromycin 1 g.
The newborn had an Apgar score of 9 out of 9 and weighed 6.7 pounds at birth. During a physical examination in the nursery, the infant was found to have large areas of smooth depigmentation on her forehead, right forearm, lower abdomen, and left thigh, with surrounding areas of thickened skin that had mild scaling and hyperpigmentation (FIGURE). The depigmented areas involved approximately 15% of the newborn’s body. The father and paternal grandmother, who were present at the time of delivery, also had depigmented areas of their skin.
The newborn’s tongue was pink and her mucus membranes were moist. No macules or patches were noted on either the oral or vaginal mucosa. Cardiac, pulmonary, and ocular examinations (including evaluation of the retina by ophthalmoscopy) were normal. There was no nystagmus or strabismus. The newborn’s extremities were normal, symmetric, and moveable, and she was easily consoled.
THE DIAGNOSIS
We diagnosed the newborn with piebaldism based on her appearance. Piebaldism consists of hypopigmented/depigmented areas and is a clinical diagnosis; no testing is required.
Concerned about the areas of hyperpigmentation, we decided to get a dermatologist’s opinion. The dermatology team briefly considered the diagnosis of a large melanocytic nevus with sparing of some areas, but a skin biopsy of a hyperpigmented area on the left leg came back with a normal number of melanocytes.
DISCUSSION
Piebaldism is a rare autosomal dominant disorder characterized by the congenital absence of melanocytes in affected areas of the skin and hair due to mutations of the c-kit gene. The c-kit gene affects the differentiation and migration of melanoblasts from the neural crest during embryonic life.1 The incidence of piebaldism is estimated to be less than one in 20,000.2 Both males and females are equally affected, and no race is spared.2,3
Affected individuals present with a white forelock and relatively stable, persistent depigmentation of skin with a characteristic distribution from birth.3 A white forelock arising from a triangular, elongated, or diamond-shaped midline or depigmented macule on the forehead may be the only manifestation in 80% to 90% of cases.3 The characteristic distribution of depigmented macules includes a central macule on the forehead, the anterior abdomen extending to the chest, the lateral trunk sparing the dorsal spine, and the mid-arms and legs sparing the hands and feet.2
Depigmented macules are rectangular, rhomboid, or irregular in shape and usually have a symmetrical distribution. Typically, islands of hyperpigmentation are present within and at the border of depigmented areas.4 Piebaldism is associated in rare instances with neurofibromatosis type 1, Hirschsprung’s disease, hearing loss, and Waardenburg syndrome.4
Histologically, melanocytes are absent or considerably reduced in the depigmented areas and are normal in number in the hyperpigmented areas.5
The differential diagnosis of piebaldism includes mosaicism, albinism, and vitiligo.
Cutaneous mosaicism stems from a gene mutation that occurs during embryogenesis and the lesions are distributed along certain patterns and forms. A chromosomal analysis of our patient showed a normal female karyotype that excluded mosaicism.
Albinism is a genetically inherited disorder characterized by partial or complete absence of melanin production in the skin, hair, and eyes.6 Eye and fundus examinations were normal in our patient, which excluded albinism.
Vitiligo is rarely present at birth but is usually acquired later in life. It results from an immune-mediated destruction of melanocytes and is not genetically inherited, although familial incidence has been reported.7
There are no effective therapies
A combination of dermabrasion and grafting of pigmented skin into depigmented areas, with or without phototherapy, has been used in select patients, although no solid data are available on its effectiveness.3 The lack of effective and safe therapies can make treatment challenging. Piebaldism is usually not medically harmful, but the emotional and psychological effects on the family and the patient as they grow up can be devastating. Therefore, supportive counseling is recommended.
Our patient. Supportive counseling and a follow-up appointment with a dermatologist was planned for our patient and her family.
THE TAKEAWAY
The clinical diagnosis of piebaldism is straightforward based on the presence of a white forelock in the frontal region, the appearance of depigmented macules since birth that stay relatively stable, and the presence of a similar pattern of depigmented macules in other family members. Histologic or genetic testing is not necessary to establish the diagnosis. Rarely, cases of piebaldism are associated with hearing loss, necessitating a hearing assessment and an audiology exam. Unfortunately, there are no effective treatments for piebaldism.
1. Ward KA, Moss C, Sanders DS. Human piebaldism: relationship between phenotype and site of kit gene mutation. Br J Dermatol. 1995;132:929-935.
2. Agarwal S, Ojha A. Piebaldism: A brief report and review of the literature. Indian Dermatol Online J. 2012;3:144-147.
3. Oiso N, Fukai K, Kawada A, et al. Piebaldism. J Dermatol. 2013;40:330-335.
4. Spritz RA, Itin PH, Gutmann DH. Piebaldism and neurofibromatosis type 1: horses of very different colors. J Invest Dermatol. 2004;122:xxxiv-xxxv.
5. Makino T, Yanagihara M, Oiso N, et al. Repigmentation of the epidermis around the acrosyringium in piebald skin: an ultrastructural examination. Br J Dermatol. 2013;168:910-912.
6. Karaman A. Oculocutaneous albinism type 1A: a case report. Dermatol Online J. 2008;14:13.
7. Plensdorf S, Martinez J. Common pigmentation disorders. Am Fam Physician. 2009;79:109-116.
1. Ward KA, Moss C, Sanders DS. Human piebaldism: relationship between phenotype and site of kit gene mutation. Br J Dermatol. 1995;132:929-935.
2. Agarwal S, Ojha A. Piebaldism: A brief report and review of the literature. Indian Dermatol Online J. 2012;3:144-147.
3. Oiso N, Fukai K, Kawada A, et al. Piebaldism. J Dermatol. 2013;40:330-335.
4. Spritz RA, Itin PH, Gutmann DH. Piebaldism and neurofibromatosis type 1: horses of very different colors. J Invest Dermatol. 2004;122:xxxiv-xxxv.
5. Makino T, Yanagihara M, Oiso N, et al. Repigmentation of the epidermis around the acrosyringium in piebald skin: an ultrastructural examination. Br J Dermatol. 2013;168:910-912.
6. Karaman A. Oculocutaneous albinism type 1A: a case report. Dermatol Online J. 2008;14:13.
7. Plensdorf S, Martinez J. Common pigmentation disorders. Am Fam Physician. 2009;79:109-116.
Adding salmeterol to steroids didn’t boost kids’ serious asthma events
Adding the long-acting beta-agonist salmeterol to fluticasone in a fixed-dose combination didn’t increase serious asthma-related events among children aged 4-11 years, according to a report published online Sept. 1 in the New England Journal of Medicine.
After long-acting beta-agonists were introduced as add-on therapy for uncontrolled asthma, two large studies involving adults linked the treatment to an increase in asthma-related death. Other studies found no such association.
The FDA mandated that all four manufacturers of those agents in the United States perform large postmarketing safety trials to establish the noninferiority of the approach. In response, GlaxoSmithKline, the only maker of a long-acting beta-agonist with a pediatric indication (salmeterol), performed this international randomized, double-blind, controlled trial at 567 medical centers in 32 countries, said David A. Stempel, MD, of Respiratory Clinical Development, GSK, Research Triangle Park, N.C., and his associates.
The trial involved 6,208 children aged 4-11 years who had controlled or uncontrolled asthma with a history of exacerbations during the preceding year. The participants were randomly assigned to receive 26 weeks of a lower fixed-dose combination of salmeterol plus fluticasone, a higher fixed-dose combination, a lower dose of fluticasone alone, or a higher dose of fluticasone alone, delivered twice daily via a disk device.
The primary safety endpoint was a composite of death, endotracheal intubation, and hospitalization. No deaths or intubations occurred.
A total of 27 patients taking combined therapy and 21 taking fluticasone alone required hospitalization for asthma (hazard ratio, 1.28). The number of severe asthma exacerbations was 14% lower when salmeterol was added to fluticasone, a nonsignificant difference.
The results demonstrate the noninferiority of the combined therapy, Dr. Stempel and his associates said (N Engl J Med. 2016 Sep 1;375[9]:840-9).
The percentage of children who withdrew from the study because of asthma exacerbations was identical in the two groups (1.1% of each), and the percentage who had a serious adverse event was nearly identical (1.8% vs 1.7%, respectively). The mean percentage of rescue therapy–free days also was similar (83.0% vs 81.9%), as was the mean percentage of days in which asthma was controlled (74.8% vs. 73.4%).
At the conclusion of the study, 88.1% of the fluticasone-plus-salmeterol group had controlled asthma, as did 88.5% of the fluticasone-only group. Meaningful differences between the two treatments could not be identified among various subgroups of patients – defined by age, sex, and race – because the overall number of adverse events was so low, the investigators added.
They cautioned that the trial excluded children who had a history of multiple asthma-related hospitalizations and intubations. Therefore, the findings may not be applicable to patients with very severe asthma, the researchers cautioned.
GlaxoSmithKline sponsored the trial in response to a Food and Drug Administration mandate for large postmarketing safety studies from the marketers of long-acting beta agonist–containing products sold in the United States. Dr. Stempel is an employee of GSK; his associates reported ties to numerous industry sources.
These study findings provide reassuring evidence that combination inhalers are safe for the unusual child with asthma who needs more than inhaled glucocorticoids to control the disease or who has persistent, objectively documented variable airflow obstruction.

|
Dr. Andrew Bush |
But it’s important to emphasize that a combined inhaler is never indicated as first-line preventive therapy in children, because such use is increasingly creeping into practice. And monotherapy with a long-acting beta-agonist in a child should be considered medical negligence.
Andrew Bush, MD, is in the department of respiratory medicine at Royal Brompton Hospital, London. Urs Frey, MD, PhD, is in the department of pediatrics at the University of Basel (Switzerland) Children’s Hospital. They reported having no relevant financial disclosures. Dr. Bush and Dr. Frey made these remarks in an editorial accompanying Dr. Stempel’s report (N Engl J Med. 2016 Sep 1;375[9]:889-91).
These study findings provide reassuring evidence that combination inhalers are safe for the unusual child with asthma who needs more than inhaled glucocorticoids to control the disease or who has persistent, objectively documented variable airflow obstruction.
|
|
Dr. Andrew Bush |
But it’s important to emphasize that a combined inhaler is never indicated as first-line preventive therapy in children, because such use is increasingly creeping into practice. And monotherapy with a long-acting beta-agonist in a child should be considered medical negligence.
Andrew Bush, MD, is in the department of respiratory medicine at Royal Brompton Hospital, London. Urs Frey, MD, PhD, is in the department of pediatrics at the University of Basel (Switzerland) Children’s Hospital. They reported having no relevant financial disclosures. Dr. Bush and Dr. Frey made these remarks in an editorial accompanying Dr. Stempel’s report (N Engl J Med. 2016 Sep 1;375[9]:889-91).
These study findings provide reassuring evidence that combination inhalers are safe for the unusual child with asthma who needs more than inhaled glucocorticoids to control the disease or who has persistent, objectively documented variable airflow obstruction.
|
|
Dr. Andrew Bush |
But it’s important to emphasize that a combined inhaler is never indicated as first-line preventive therapy in children, because such use is increasingly creeping into practice. And monotherapy with a long-acting beta-agonist in a child should be considered medical negligence.
Andrew Bush, MD, is in the department of respiratory medicine at Royal Brompton Hospital, London. Urs Frey, MD, PhD, is in the department of pediatrics at the University of Basel (Switzerland) Children’s Hospital. They reported having no relevant financial disclosures. Dr. Bush and Dr. Frey made these remarks in an editorial accompanying Dr. Stempel’s report (N Engl J Med. 2016 Sep 1;375[9]:889-91).
Adding the long-acting beta-agonist salmeterol to fluticasone in a fixed-dose combination didn’t increase serious asthma-related events among children aged 4-11 years, according to a report published online Sept. 1 in the New England Journal of Medicine.
After long-acting beta-agonists were introduced as add-on therapy for uncontrolled asthma, two large studies involving adults linked the treatment to an increase in asthma-related death. Other studies found no such association.
The FDA mandated that all four manufacturers of those agents in the United States perform large postmarketing safety trials to establish the noninferiority of the approach. In response, GlaxoSmithKline, the only maker of a long-acting beta-agonist with a pediatric indication (salmeterol), performed this international randomized, double-blind, controlled trial at 567 medical centers in 32 countries, said David A. Stempel, MD, of Respiratory Clinical Development, GSK, Research Triangle Park, N.C., and his associates.
The trial involved 6,208 children aged 4-11 years who had controlled or uncontrolled asthma with a history of exacerbations during the preceding year. The participants were randomly assigned to receive 26 weeks of a lower fixed-dose combination of salmeterol plus fluticasone, a higher fixed-dose combination, a lower dose of fluticasone alone, or a higher dose of fluticasone alone, delivered twice daily via a disk device.
The primary safety endpoint was a composite of death, endotracheal intubation, and hospitalization. No deaths or intubations occurred.
A total of 27 patients taking combined therapy and 21 taking fluticasone alone required hospitalization for asthma (hazard ratio, 1.28). The number of severe asthma exacerbations was 14% lower when salmeterol was added to fluticasone, a nonsignificant difference.
The results demonstrate the noninferiority of the combined therapy, Dr. Stempel and his associates said (N Engl J Med. 2016 Sep 1;375[9]:840-9).
The percentage of children who withdrew from the study because of asthma exacerbations was identical in the two groups (1.1% of each), and the percentage who had a serious adverse event was nearly identical (1.8% vs 1.7%, respectively). The mean percentage of rescue therapy–free days also was similar (83.0% vs 81.9%), as was the mean percentage of days in which asthma was controlled (74.8% vs. 73.4%).
At the conclusion of the study, 88.1% of the fluticasone-plus-salmeterol group had controlled asthma, as did 88.5% of the fluticasone-only group. Meaningful differences between the two treatments could not be identified among various subgroups of patients – defined by age, sex, and race – because the overall number of adverse events was so low, the investigators added.
They cautioned that the trial excluded children who had a history of multiple asthma-related hospitalizations and intubations. Therefore, the findings may not be applicable to patients with very severe asthma, the researchers cautioned.
GlaxoSmithKline sponsored the trial in response to a Food and Drug Administration mandate for large postmarketing safety studies from the marketers of long-acting beta agonist–containing products sold in the United States. Dr. Stempel is an employee of GSK; his associates reported ties to numerous industry sources.
Adding the long-acting beta-agonist salmeterol to fluticasone in a fixed-dose combination didn’t increase serious asthma-related events among children aged 4-11 years, according to a report published online Sept. 1 in the New England Journal of Medicine.
After long-acting beta-agonists were introduced as add-on therapy for uncontrolled asthma, two large studies involving adults linked the treatment to an increase in asthma-related death. Other studies found no such association.
The FDA mandated that all four manufacturers of those agents in the United States perform large postmarketing safety trials to establish the noninferiority of the approach. In response, GlaxoSmithKline, the only maker of a long-acting beta-agonist with a pediatric indication (salmeterol), performed this international randomized, double-blind, controlled trial at 567 medical centers in 32 countries, said David A. Stempel, MD, of Respiratory Clinical Development, GSK, Research Triangle Park, N.C., and his associates.
The trial involved 6,208 children aged 4-11 years who had controlled or uncontrolled asthma with a history of exacerbations during the preceding year. The participants were randomly assigned to receive 26 weeks of a lower fixed-dose combination of salmeterol plus fluticasone, a higher fixed-dose combination, a lower dose of fluticasone alone, or a higher dose of fluticasone alone, delivered twice daily via a disk device.
The primary safety endpoint was a composite of death, endotracheal intubation, and hospitalization. No deaths or intubations occurred.
A total of 27 patients taking combined therapy and 21 taking fluticasone alone required hospitalization for asthma (hazard ratio, 1.28). The number of severe asthma exacerbations was 14% lower when salmeterol was added to fluticasone, a nonsignificant difference.
The results demonstrate the noninferiority of the combined therapy, Dr. Stempel and his associates said (N Engl J Med. 2016 Sep 1;375[9]:840-9).
The percentage of children who withdrew from the study because of asthma exacerbations was identical in the two groups (1.1% of each), and the percentage who had a serious adverse event was nearly identical (1.8% vs 1.7%, respectively). The mean percentage of rescue therapy–free days also was similar (83.0% vs 81.9%), as was the mean percentage of days in which asthma was controlled (74.8% vs. 73.4%).
At the conclusion of the study, 88.1% of the fluticasone-plus-salmeterol group had controlled asthma, as did 88.5% of the fluticasone-only group. Meaningful differences between the two treatments could not be identified among various subgroups of patients – defined by age, sex, and race – because the overall number of adverse events was so low, the investigators added.
They cautioned that the trial excluded children who had a history of multiple asthma-related hospitalizations and intubations. Therefore, the findings may not be applicable to patients with very severe asthma, the researchers cautioned.
GlaxoSmithKline sponsored the trial in response to a Food and Drug Administration mandate for large postmarketing safety studies from the marketers of long-acting beta agonist–containing products sold in the United States. Dr. Stempel is an employee of GSK; his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Adding salmeterol to fluticasone therapy didn’t increase serious asthma-related events among children.
Major finding: 27 patients taking combined therapy and 21 taking fluticasone alone required hospitalization for asthma (HR, 1.28).
Data source: A 26-week international randomized, double-blind trial involving 6,208 patients aged 4-11 years.
Disclosures: GlaxoSmithKline sponsored the trial in response to a Food and Drug Administration mandate for large postmarketing safety studies from the marketers of long-acting beta agonist–containing products sold in the United States. Dr. Stempel is an employee of GSK; his associates reported ties to numerous industry sources.

AAP: MenB vaccines are safe for healthy adolescents, young adults
The serotype B meningococcal vaccines MenB-FHbp and MenB-4C are safe and can be administered to healthy people aged 10-25 years, according to a policy statement from the American Academy of Pediatrics Committee on Infectious Diseases.
The AAP recommends that people older than 10 years at increased risk for serogroup B meningococcal disease (category A) should receive MenB vaccines regularly. Category A includes people with persistent complement component deficiencies, people with anatomic or functional asplenia, and healthy people at increased risk because of a disease outbreak.

Young adults aged 16-23 years old may receive a vaccination, but it is not routinely recommended (category B), with a preferred vaccination age between 16 and 18 years.
Annual incidence of serogroup B meningococcal disease in people aged 11-24 years in the United States is about 50-60 cases per year, and a routine vaccination program would prevent 15-29 cases and 2-5 deaths per year, the researchers noted. The cost of routine vaccination in the general population would range from $3.7 million per quality-adjusted life year (QALY) to $9.4 million per QALY.
Both MenB-FHbp and MenB-4C have been safely administered in clinical trials, with no deaths related to either vaccine. Data on duration of immunogenicity and proportion of MenB strains covered by vaccines in different geographic regions remain incomplete, and both vaccine manufacturers must complete postmarketing studies to determine overall vaccine effectiveness.
“Pediatricians are encouraged to discuss the availability of the MenB vaccines with families. Discussion should include the low incidence of MenB disease and the unknown efficacy of the vaccines... The treating clinician should discuss the benefits, risks, and costs with patients and their families and then work with them to determine what is in their best interest,” the AAP committee noted.
Find the full study in Pediatrics (doi: 10.1542/peds.2016-1890).
The serotype B meningococcal vaccines MenB-FHbp and MenB-4C are safe and can be administered to healthy people aged 10-25 years, according to a policy statement from the American Academy of Pediatrics Committee on Infectious Diseases.
The AAP recommends that people older than 10 years at increased risk for serogroup B meningococcal disease (category A) should receive MenB vaccines regularly. Category A includes people with persistent complement component deficiencies, people with anatomic or functional asplenia, and healthy people at increased risk because of a disease outbreak.
Young adults aged 16-23 years old may receive a vaccination, but it is not routinely recommended (category B), with a preferred vaccination age between 16 and 18 years.
Annual incidence of serogroup B meningococcal disease in people aged 11-24 years in the United States is about 50-60 cases per year, and a routine vaccination program would prevent 15-29 cases and 2-5 deaths per year, the researchers noted. The cost of routine vaccination in the general population would range from $3.7 million per quality-adjusted life year (QALY) to $9.4 million per QALY.
Both MenB-FHbp and MenB-4C have been safely administered in clinical trials, with no deaths related to either vaccine. Data on duration of immunogenicity and proportion of MenB strains covered by vaccines in different geographic regions remain incomplete, and both vaccine manufacturers must complete postmarketing studies to determine overall vaccine effectiveness.
“Pediatricians are encouraged to discuss the availability of the MenB vaccines with families. Discussion should include the low incidence of MenB disease and the unknown efficacy of the vaccines... The treating clinician should discuss the benefits, risks, and costs with patients and their families and then work with them to determine what is in their best interest,” the AAP committee noted.
Find the full study in Pediatrics (doi: 10.1542/peds.2016-1890).
The serotype B meningococcal vaccines MenB-FHbp and MenB-4C are safe and can be administered to healthy people aged 10-25 years, according to a policy statement from the American Academy of Pediatrics Committee on Infectious Diseases.
The AAP recommends that people older than 10 years at increased risk for serogroup B meningococcal disease (category A) should receive MenB vaccines regularly. Category A includes people with persistent complement component deficiencies, people with anatomic or functional asplenia, and healthy people at increased risk because of a disease outbreak.
Young adults aged 16-23 years old may receive a vaccination, but it is not routinely recommended (category B), with a preferred vaccination age between 16 and 18 years.
Annual incidence of serogroup B meningococcal disease in people aged 11-24 years in the United States is about 50-60 cases per year, and a routine vaccination program would prevent 15-29 cases and 2-5 deaths per year, the researchers noted. The cost of routine vaccination in the general population would range from $3.7 million per quality-adjusted life year (QALY) to $9.4 million per QALY.
Both MenB-FHbp and MenB-4C have been safely administered in clinical trials, with no deaths related to either vaccine. Data on duration of immunogenicity and proportion of MenB strains covered by vaccines in different geographic regions remain incomplete, and both vaccine manufacturers must complete postmarketing studies to determine overall vaccine effectiveness.
“Pediatricians are encouraged to discuss the availability of the MenB vaccines with families. Discussion should include the low incidence of MenB disease and the unknown efficacy of the vaccines... The treating clinician should discuss the benefits, risks, and costs with patients and their families and then work with them to determine what is in their best interest,” the AAP committee noted.
Find the full study in Pediatrics (doi: 10.1542/peds.2016-1890).
FROM PEDIATRICS

Pediatric questionnaire sorts out psychosocial effects of skin conditions
MINNEAPOLIS – A new screening tool may help dermatologists address the psychosocial issues relating to appearance and body image in children and adolescents.
The Pediatric Dermatology Psychosocial Screen (PDPS), is being developed as a standardized tool to evaluate psychosocial stress related to birthmarks, skin diseases, and conditions affecting pigmentation or hair growth. Elizabeth Tocci, MD, and her colleagues, who have been involved with the development of the PDPS, envision it as a useful tool to provide support for pediatric dermatology patients and to help dermatologists decide when mental health consults are warranted in their pediatric patients.
Dr. Tocci, a resident in dermatology at Roger Williams Medical Center, Providence, R.I., and her colleagues described the tool and initial testing results in a poster session at the annual meeting of the Society for Pediatric Dermatology.
The PDPS is a refinement of a pilot survey, created by the coauthors in consultation with experts in neurodermatitis and body dysmorphic disorder (BDD). Following preliminary validity analysis of the pilot questionnaire, a revised PDPS was administered to 105 children, aged 8-19 years, who were patients at a pediatric dermatology clinic. In addition to completing the PDPS, they also filled out psychological questionnaires that assessed for depression, self-esteem, and social problems.
The PDPS asks general questions about the skin diagnosis and any treatments the patient may have used, such as over-the-counter products, prescription medications, and procedures, as well as the use of makeup. In addition, the PDPS asks what social and psychological supports or online resources the patient might have tried, including support groups and appointments with school counselors or mental health providers.
Psychosocial aspects of the skin condition are explored by asking how upset patients are about social sequelae of having a visible skin condition, and whether they are asked about the condition and whether they are made fun of, stared at, or avoided because of the condition. Other questions pertain to whether they notice others’ skin, are hyperobservant of their own skin condition, or feel their popularity and their willingness to date are affected by their skin condition.
Respondent resiliency as it relates to the skin condition is explored by asking whether the respondent found it difficult to move on after a negative social interaction related to the skin condition, and how long the feeling of upset persisted after a negative incident.
Of the 105 surveys, 87 were complete enough to allow analysis. The analysis showed that higher self-reported resiliency was associated with higher positive scores on other psychosocial factors, such as self-esteem, body image, fewer negative and more positive social supports, less self-consciousness, less negative affect, and less BDD. “Self-reported resilience was a significant predictor and determinant of all the psychosocial factors measured,” Dr. Tocci and her associates wrote.
Results indicate that the PDPS is useful to evaluate children and teens in a busy clinic setting, and is “an excellent self-reporting tool for measuring resilience versus psychosocial distress,” they added.
The test is not yet available; the next steps include refining the length and wording of the PDPS, with further validation and testing.
Dr. Tocci and her collaborators reported no conflicts of interest.
On Twitter @karioakes
MINNEAPOLIS – A new screening tool may help dermatologists address the psychosocial issues relating to appearance and body image in children and adolescents.
The Pediatric Dermatology Psychosocial Screen (PDPS), is being developed as a standardized tool to evaluate psychosocial stress related to birthmarks, skin diseases, and conditions affecting pigmentation or hair growth. Elizabeth Tocci, MD, and her colleagues, who have been involved with the development of the PDPS, envision it as a useful tool to provide support for pediatric dermatology patients and to help dermatologists decide when mental health consults are warranted in their pediatric patients.
Dr. Tocci, a resident in dermatology at Roger Williams Medical Center, Providence, R.I., and her colleagues described the tool and initial testing results in a poster session at the annual meeting of the Society for Pediatric Dermatology.
The PDPS is a refinement of a pilot survey, created by the coauthors in consultation with experts in neurodermatitis and body dysmorphic disorder (BDD). Following preliminary validity analysis of the pilot questionnaire, a revised PDPS was administered to 105 children, aged 8-19 years, who were patients at a pediatric dermatology clinic. In addition to completing the PDPS, they also filled out psychological questionnaires that assessed for depression, self-esteem, and social problems.
The PDPS asks general questions about the skin diagnosis and any treatments the patient may have used, such as over-the-counter products, prescription medications, and procedures, as well as the use of makeup. In addition, the PDPS asks what social and psychological supports or online resources the patient might have tried, including support groups and appointments with school counselors or mental health providers.
Psychosocial aspects of the skin condition are explored by asking how upset patients are about social sequelae of having a visible skin condition, and whether they are asked about the condition and whether they are made fun of, stared at, or avoided because of the condition. Other questions pertain to whether they notice others’ skin, are hyperobservant of their own skin condition, or feel their popularity and their willingness to date are affected by their skin condition.
Respondent resiliency as it relates to the skin condition is explored by asking whether the respondent found it difficult to move on after a negative social interaction related to the skin condition, and how long the feeling of upset persisted after a negative incident.
Of the 105 surveys, 87 were complete enough to allow analysis. The analysis showed that higher self-reported resiliency was associated with higher positive scores on other psychosocial factors, such as self-esteem, body image, fewer negative and more positive social supports, less self-consciousness, less negative affect, and less BDD. “Self-reported resilience was a significant predictor and determinant of all the psychosocial factors measured,” Dr. Tocci and her associates wrote.
Results indicate that the PDPS is useful to evaluate children and teens in a busy clinic setting, and is “an excellent self-reporting tool for measuring resilience versus psychosocial distress,” they added.
The test is not yet available; the next steps include refining the length and wording of the PDPS, with further validation and testing.
Dr. Tocci and her collaborators reported no conflicts of interest.
On Twitter @karioakes
MINNEAPOLIS – A new screening tool may help dermatologists address the psychosocial issues relating to appearance and body image in children and adolescents.
The Pediatric Dermatology Psychosocial Screen (PDPS), is being developed as a standardized tool to evaluate psychosocial stress related to birthmarks, skin diseases, and conditions affecting pigmentation or hair growth. Elizabeth Tocci, MD, and her colleagues, who have been involved with the development of the PDPS, envision it as a useful tool to provide support for pediatric dermatology patients and to help dermatologists decide when mental health consults are warranted in their pediatric patients.
Dr. Tocci, a resident in dermatology at Roger Williams Medical Center, Providence, R.I., and her colleagues described the tool and initial testing results in a poster session at the annual meeting of the Society for Pediatric Dermatology.
The PDPS is a refinement of a pilot survey, created by the coauthors in consultation with experts in neurodermatitis and body dysmorphic disorder (BDD). Following preliminary validity analysis of the pilot questionnaire, a revised PDPS was administered to 105 children, aged 8-19 years, who were patients at a pediatric dermatology clinic. In addition to completing the PDPS, they also filled out psychological questionnaires that assessed for depression, self-esteem, and social problems.
The PDPS asks general questions about the skin diagnosis and any treatments the patient may have used, such as over-the-counter products, prescription medications, and procedures, as well as the use of makeup. In addition, the PDPS asks what social and psychological supports or online resources the patient might have tried, including support groups and appointments with school counselors or mental health providers.
Psychosocial aspects of the skin condition are explored by asking how upset patients are about social sequelae of having a visible skin condition, and whether they are asked about the condition and whether they are made fun of, stared at, or avoided because of the condition. Other questions pertain to whether they notice others’ skin, are hyperobservant of their own skin condition, or feel their popularity and their willingness to date are affected by their skin condition.
Respondent resiliency as it relates to the skin condition is explored by asking whether the respondent found it difficult to move on after a negative social interaction related to the skin condition, and how long the feeling of upset persisted after a negative incident.
Of the 105 surveys, 87 were complete enough to allow analysis. The analysis showed that higher self-reported resiliency was associated with higher positive scores on other psychosocial factors, such as self-esteem, body image, fewer negative and more positive social supports, less self-consciousness, less negative affect, and less BDD. “Self-reported resilience was a significant predictor and determinant of all the psychosocial factors measured,” Dr. Tocci and her associates wrote.
Results indicate that the PDPS is useful to evaluate children and teens in a busy clinic setting, and is “an excellent self-reporting tool for measuring resilience versus psychosocial distress,” they added.
The test is not yet available; the next steps include refining the length and wording of the PDPS, with further validation and testing.
Dr. Tocci and her collaborators reported no conflicts of interest.
On Twitter @karioakes
EXPERT ANALYSIS FROM THE SPD ANNUAL MEETING