User login
When school’s out, the obesity epidemic grows
NEW ORLEANS – All of the growth in the obesity epidemic in young American schoolchildren takes place during their summer vacations, Paul T. von Hippel, PhD, reported at Obesity Week 2016.
He presented an analysis from the Early Childhood Longitudinal Study, Kindergarten Class of 2010-2011 which included a nationally representative study population composed of 18,170 U.S. children in 970 schools who were followed with serial weight and height measurements from the start of kindergarten in 2010 through the end of second grade in 2013.
During the summer, the prevalence of both overweight and obesity increased by roughly 1 percentage point per month. In contrast, during the more than 9 months of each school year, the prevalence of overweight didn’t budge, while the prevalence of obesity decreased modestly, by 0.1 percentage points per month.
These data have far-reaching public health implications. The new evidence suggests that the major risk factors for obesity are located outside of schools. That helps explain why many school-based initiatives focused on improving the nutritional content of school lunches and promoting physical activity have had little impact on the pediatric obesity epidemic, said Dr. von Hippel of the University of Texas at Austin.
The data suggest it’s time to explore the potential of reshaping out-of-school behaviors by promoting summer school and summer camp, curbing food advertising directed at children, providing parental nutrition education, and other interventions, he added.
The explanation for the observed increase in body mass index during summer vacation is unclear. It’s known from other studies that children sleep less and engage in more screen time during summer, which may be relevant, according to Dr. von Hippel.
Simultaneous with Dr. von Hippel’s presentation at Obesity 2016, the study was published online in the journal Obesity (2016 Nov 2. doi: 10.1002/oby.21613).
He reported having no financial conflicts of interest regarding the study, which was funded by the Russell Sage Foundation.
NEW ORLEANS – All of the growth in the obesity epidemic in young American schoolchildren takes place during their summer vacations, Paul T. von Hippel, PhD, reported at Obesity Week 2016.
He presented an analysis from the Early Childhood Longitudinal Study, Kindergarten Class of 2010-2011 which included a nationally representative study population composed of 18,170 U.S. children in 970 schools who were followed with serial weight and height measurements from the start of kindergarten in 2010 through the end of second grade in 2013.
During the summer, the prevalence of both overweight and obesity increased by roughly 1 percentage point per month. In contrast, during the more than 9 months of each school year, the prevalence of overweight didn’t budge, while the prevalence of obesity decreased modestly, by 0.1 percentage points per month.
These data have far-reaching public health implications. The new evidence suggests that the major risk factors for obesity are located outside of schools. That helps explain why many school-based initiatives focused on improving the nutritional content of school lunches and promoting physical activity have had little impact on the pediatric obesity epidemic, said Dr. von Hippel of the University of Texas at Austin.
The data suggest it’s time to explore the potential of reshaping out-of-school behaviors by promoting summer school and summer camp, curbing food advertising directed at children, providing parental nutrition education, and other interventions, he added.
The explanation for the observed increase in body mass index during summer vacation is unclear. It’s known from other studies that children sleep less and engage in more screen time during summer, which may be relevant, according to Dr. von Hippel.
Simultaneous with Dr. von Hippel’s presentation at Obesity 2016, the study was published online in the journal Obesity (2016 Nov 2. doi: 10.1002/oby.21613).
He reported having no financial conflicts of interest regarding the study, which was funded by the Russell Sage Foundation.
NEW ORLEANS – All of the growth in the obesity epidemic in young American schoolchildren takes place during their summer vacations, Paul T. von Hippel, PhD, reported at Obesity Week 2016.
He presented an analysis from the Early Childhood Longitudinal Study, Kindergarten Class of 2010-2011 which included a nationally representative study population composed of 18,170 U.S. children in 970 schools who were followed with serial weight and height measurements from the start of kindergarten in 2010 through the end of second grade in 2013.
During the summer, the prevalence of both overweight and obesity increased by roughly 1 percentage point per month. In contrast, during the more than 9 months of each school year, the prevalence of overweight didn’t budge, while the prevalence of obesity decreased modestly, by 0.1 percentage points per month.
These data have far-reaching public health implications. The new evidence suggests that the major risk factors for obesity are located outside of schools. That helps explain why many school-based initiatives focused on improving the nutritional content of school lunches and promoting physical activity have had little impact on the pediatric obesity epidemic, said Dr. von Hippel of the University of Texas at Austin.
The data suggest it’s time to explore the potential of reshaping out-of-school behaviors by promoting summer school and summer camp, curbing food advertising directed at children, providing parental nutrition education, and other interventions, he added.
The explanation for the observed increase in body mass index during summer vacation is unclear. It’s known from other studies that children sleep less and engage in more screen time during summer, which may be relevant, according to Dr. von Hippel.
Simultaneous with Dr. von Hippel’s presentation at Obesity 2016, the study was published online in the journal Obesity (2016 Nov 2. doi: 10.1002/oby.21613).
He reported having no financial conflicts of interest regarding the study, which was funded by the Russell Sage Foundation.
AT OBESITY WEEK 2016
Key clinical point:
Major finding: Between the start of kindergarten and the end of second grade, the prevalence of overweight in a large group of U.S. children grew from 23.3% to 28.7%, with all of the increase coming during their two summer vacations.
Data source: The Early Childhood Longitudinal Study, Kindergarten Class of 2010-2011 included a nationally representative study population composed of more than 18,000 children who were followed with multiple weight and height measurements from the start of kindergarten through the end of second grade.
Disclosures: The study was funded by the Russell Sage Foundation. The presenter reported having no financial conflicts of interest.
New research in otitis media means new controversies
SAN FRANCISCO – As researchers have learned more about otitis media in the past decade, the guidelines have shifted accordingly for one of the most common conditions of childhood.
Yet some controversies remain, and the condition remains a challenge to properly identify, David Conrad, MD, of the University of California, San Francisco, said at the annual meeting of the American Academy of Pediatrics.
Pediatricians already know it’s the most common reason young children come into their offices and the most common reason they prescribe antibiotics. But they may know less about recognizing complications and long-term effects.
Complications and treatment
Ossicular erosion or tympanic membrane perforation are two complications; the latter’s rate is 5%-29% for untreated acute otitis media. It typically closes within hours to days, however, with a 95% closure rate within 4 weeks.
“The ear drum is pretty forgiving, pretty resilient, really,” Dr. Conrad said. The perforation occurs when pressure builds up and takes the path of least resistance through the drum, but that release of pressure also typically relieves the pain.
“Mastoiditis is one of the most feared complications, obviously,” Dr. Conrad noted, and it’s a clinical diagnosis that’s important to distinguish from mastoid effusion.
“Any child who has acute otitis media, and the middle ear fills up with fluid, which is under pressure, it will then migrate up the mastoid cavity; so, if you have an ear infection, you will have mastoid fluid – but that doesn’t necessarily mean you have mastoiditis,” he explained. “Mastoiditis is a very aggressive inflammatory process that destroys bone in the mastoid cavity. It’s often due to strep, and it’s usually a pyogenic organism that’s particularly virulent.”
Pus will then leak out from the mastoid cavity and form an abscess. If there is bone destruction, that is mastoiditis, which is treated with an ear tube or sometimes a mastoidectomy, in which a drill drains all the pus and other tissue.
Speech development and other controversies
Aside from the child’s pain, parental anxiety, and the other potential complications, researchers have learned more recently about speech delay with otitis media. The average child with recurrent otitis media or with otitis media with effusion will experience decreased hearing for about 3 or 4 months, which can affect speech, educational, and cognitive outcomes.
“If that process repeats itself, they could lose out on an entire year of not hearing well. It’s like walking around with an ear plug in,” Dr. Conrad said. It’s about a 25-35 dB hearing loss, he said, which can lead to trouble with speech discrimination, particularly with background noise, and can interfere with relationships with family, peers, and other adults.
Emerging data suggest educational difficulties, such as problems with reading comprehension, could result, and research is pivoting to look at potential cognitive development concerns, Dr. Conrad said.
“It has been noted that earlier onset of otitis media has a greater impact on educational and attention outcomes,” he said. Central auditory processing drives the development of the auditory cortex, and if that is impaired during a critical window of opportunity while synapses are forming, it could also have effects on speech.
“Otitis media and speech development is an area of controversy,” Dr. Conrad explained. Otitis media has been found to impact auditory processing skills, speech discrimination, auditory pattern recognition, and auditory temporal processing, “but there’s little evidence to support long-term language impairment,” he said.
But that’s being challenged now. Research in rats and cats in particular, however, has shown changes in the auditory cortex from ear infections.
“Most of the data are from animal models, and I think that will morph into more studies into educational outcomes in children who had a lot of ear infections when they were younger,” Dr. Conrad predicted.
Other areas of controversy relate to whether the use of the pneumococcal conjugate vaccine (PCV13), which has reduced ear infections, may have led to the rise of infections from Haemophilus influenzae and Moraxella catarrhalis, and what the duration of therapy should be for antibiotics.
If not doing watchful waiting, first-line treatment is amoxicillin or amoxicillin-clavulanate unless the child has a penicillin allergy, in which case cefdinir, cefuroxime, or cefpodoxime can be prescribed. After 48-72 hours of failed therapy, amoxicillin-clavulanate can be considered, or clindamycin or ceftriaxone, “obviously a popular option if the child has had multiple ear infections in the past month or so,” he said.
“If the child is older, we don’t treat as long,” Dr. Conrad noted. Current guidelines recommend a 10-day course if the infection resulted from strep, a 7-day or 10-day course in children aged 2-5 years, and a 5-7 day course for children older than 6 years.
Dr. Conrad reported no disclosures.
SAN FRANCISCO – As researchers have learned more about otitis media in the past decade, the guidelines have shifted accordingly for one of the most common conditions of childhood.
Yet some controversies remain, and the condition remains a challenge to properly identify, David Conrad, MD, of the University of California, San Francisco, said at the annual meeting of the American Academy of Pediatrics.
Pediatricians already know it’s the most common reason young children come into their offices and the most common reason they prescribe antibiotics. But they may know less about recognizing complications and long-term effects.
Complications and treatment
Ossicular erosion or tympanic membrane perforation are two complications; the latter’s rate is 5%-29% for untreated acute otitis media. It typically closes within hours to days, however, with a 95% closure rate within 4 weeks.
“The ear drum is pretty forgiving, pretty resilient, really,” Dr. Conrad said. The perforation occurs when pressure builds up and takes the path of least resistance through the drum, but that release of pressure also typically relieves the pain.
“Mastoiditis is one of the most feared complications, obviously,” Dr. Conrad noted, and it’s a clinical diagnosis that’s important to distinguish from mastoid effusion.
“Any child who has acute otitis media, and the middle ear fills up with fluid, which is under pressure, it will then migrate up the mastoid cavity; so, if you have an ear infection, you will have mastoid fluid – but that doesn’t necessarily mean you have mastoiditis,” he explained. “Mastoiditis is a very aggressive inflammatory process that destroys bone in the mastoid cavity. It’s often due to strep, and it’s usually a pyogenic organism that’s particularly virulent.”
Pus will then leak out from the mastoid cavity and form an abscess. If there is bone destruction, that is mastoiditis, which is treated with an ear tube or sometimes a mastoidectomy, in which a drill drains all the pus and other tissue.
Speech development and other controversies
Aside from the child’s pain, parental anxiety, and the other potential complications, researchers have learned more recently about speech delay with otitis media. The average child with recurrent otitis media or with otitis media with effusion will experience decreased hearing for about 3 or 4 months, which can affect speech, educational, and cognitive outcomes.
“If that process repeats itself, they could lose out on an entire year of not hearing well. It’s like walking around with an ear plug in,” Dr. Conrad said. It’s about a 25-35 dB hearing loss, he said, which can lead to trouble with speech discrimination, particularly with background noise, and can interfere with relationships with family, peers, and other adults.
Emerging data suggest educational difficulties, such as problems with reading comprehension, could result, and research is pivoting to look at potential cognitive development concerns, Dr. Conrad said.
“It has been noted that earlier onset of otitis media has a greater impact on educational and attention outcomes,” he said. Central auditory processing drives the development of the auditory cortex, and if that is impaired during a critical window of opportunity while synapses are forming, it could also have effects on speech.
“Otitis media and speech development is an area of controversy,” Dr. Conrad explained. Otitis media has been found to impact auditory processing skills, speech discrimination, auditory pattern recognition, and auditory temporal processing, “but there’s little evidence to support long-term language impairment,” he said.
But that’s being challenged now. Research in rats and cats in particular, however, has shown changes in the auditory cortex from ear infections.
“Most of the data are from animal models, and I think that will morph into more studies into educational outcomes in children who had a lot of ear infections when they were younger,” Dr. Conrad predicted.
Other areas of controversy relate to whether the use of the pneumococcal conjugate vaccine (PCV13), which has reduced ear infections, may have led to the rise of infections from Haemophilus influenzae and Moraxella catarrhalis, and what the duration of therapy should be for antibiotics.
If not doing watchful waiting, first-line treatment is amoxicillin or amoxicillin-clavulanate unless the child has a penicillin allergy, in which case cefdinir, cefuroxime, or cefpodoxime can be prescribed. After 48-72 hours of failed therapy, amoxicillin-clavulanate can be considered, or clindamycin or ceftriaxone, “obviously a popular option if the child has had multiple ear infections in the past month or so,” he said.
“If the child is older, we don’t treat as long,” Dr. Conrad noted. Current guidelines recommend a 10-day course if the infection resulted from strep, a 7-day or 10-day course in children aged 2-5 years, and a 5-7 day course for children older than 6 years.
Dr. Conrad reported no disclosures.
SAN FRANCISCO – As researchers have learned more about otitis media in the past decade, the guidelines have shifted accordingly for one of the most common conditions of childhood.
Yet some controversies remain, and the condition remains a challenge to properly identify, David Conrad, MD, of the University of California, San Francisco, said at the annual meeting of the American Academy of Pediatrics.
Pediatricians already know it’s the most common reason young children come into their offices and the most common reason they prescribe antibiotics. But they may know less about recognizing complications and long-term effects.
Complications and treatment
Ossicular erosion or tympanic membrane perforation are two complications; the latter’s rate is 5%-29% for untreated acute otitis media. It typically closes within hours to days, however, with a 95% closure rate within 4 weeks.
“The ear drum is pretty forgiving, pretty resilient, really,” Dr. Conrad said. The perforation occurs when pressure builds up and takes the path of least resistance through the drum, but that release of pressure also typically relieves the pain.
“Mastoiditis is one of the most feared complications, obviously,” Dr. Conrad noted, and it’s a clinical diagnosis that’s important to distinguish from mastoid effusion.
“Any child who has acute otitis media, and the middle ear fills up with fluid, which is under pressure, it will then migrate up the mastoid cavity; so, if you have an ear infection, you will have mastoid fluid – but that doesn’t necessarily mean you have mastoiditis,” he explained. “Mastoiditis is a very aggressive inflammatory process that destroys bone in the mastoid cavity. It’s often due to strep, and it’s usually a pyogenic organism that’s particularly virulent.”
Pus will then leak out from the mastoid cavity and form an abscess. If there is bone destruction, that is mastoiditis, which is treated with an ear tube or sometimes a mastoidectomy, in which a drill drains all the pus and other tissue.
Speech development and other controversies
Aside from the child’s pain, parental anxiety, and the other potential complications, researchers have learned more recently about speech delay with otitis media. The average child with recurrent otitis media or with otitis media with effusion will experience decreased hearing for about 3 or 4 months, which can affect speech, educational, and cognitive outcomes.
“If that process repeats itself, they could lose out on an entire year of not hearing well. It’s like walking around with an ear plug in,” Dr. Conrad said. It’s about a 25-35 dB hearing loss, he said, which can lead to trouble with speech discrimination, particularly with background noise, and can interfere with relationships with family, peers, and other adults.
Emerging data suggest educational difficulties, such as problems with reading comprehension, could result, and research is pivoting to look at potential cognitive development concerns, Dr. Conrad said.
“It has been noted that earlier onset of otitis media has a greater impact on educational and attention outcomes,” he said. Central auditory processing drives the development of the auditory cortex, and if that is impaired during a critical window of opportunity while synapses are forming, it could also have effects on speech.
“Otitis media and speech development is an area of controversy,” Dr. Conrad explained. Otitis media has been found to impact auditory processing skills, speech discrimination, auditory pattern recognition, and auditory temporal processing, “but there’s little evidence to support long-term language impairment,” he said.
But that’s being challenged now. Research in rats and cats in particular, however, has shown changes in the auditory cortex from ear infections.
“Most of the data are from animal models, and I think that will morph into more studies into educational outcomes in children who had a lot of ear infections when they were younger,” Dr. Conrad predicted.
Other areas of controversy relate to whether the use of the pneumococcal conjugate vaccine (PCV13), which has reduced ear infections, may have led to the rise of infections from Haemophilus influenzae and Moraxella catarrhalis, and what the duration of therapy should be for antibiotics.
If not doing watchful waiting, first-line treatment is amoxicillin or amoxicillin-clavulanate unless the child has a penicillin allergy, in which case cefdinir, cefuroxime, or cefpodoxime can be prescribed. After 48-72 hours of failed therapy, amoxicillin-clavulanate can be considered, or clindamycin or ceftriaxone, “obviously a popular option if the child has had multiple ear infections in the past month or so,” he said.
“If the child is older, we don’t treat as long,” Dr. Conrad noted. Current guidelines recommend a 10-day course if the infection resulted from strep, a 7-day or 10-day course in children aged 2-5 years, and a 5-7 day course for children older than 6 years.
Dr. Conrad reported no disclosures.
Phase II data suggest IV zanamivir safe for severe flu in kids
NEW ORLEANS – The investigational intravenous formulation of the neuraminidase inhibitor zanamivir appears to be a safe influenza treatment for hospitalized children and adolescents at high risk of complications who can’t tolerate enteral therapy, according to findings from an open-label, multicenter, phase II study.
In 71 such patients with laboratory-confirmed flu, who presented within 7 days of illness onset and who received intravenous zanamivir (IVZ) for 5-10 days, 72% experienced adverse events (AEs), 21% experienced serious adverse events, and 5 deaths occurred, but none were considered by the investigators to be attributable to IVZ, Jeffrey Blumer, MD, reported at IDWeek, an annual scientific meeting on infectious diseases.
Rather, the adverse events were “fairly diverse. ... the kinds of things normally seen in critically ill pediatric populations,” he said.
The patients, who had a mean age of 7 years, were treated with IVZ doses selected to provide exposures comparable to 600 mg in adults – a dosage shown in prior studies to be safe and well-tolerated in adults. Patients aged 6 months to under age 6 years received twice-daily doses of 14 mg/kg, and those aged 6 years to less than 18 years received twice-daily doses of 12 mg/kg, not to exceed 600 mg. Doses were adjusted for renal function.
Patients were enrolled from five countries, and most (69%) had received prior treatment with oseltamivir. More than half (56%) had chronic medical conditions.
The median time from symptom onset to IVZ treatment was 4 days, Dr. Blumer of the University of Toledo (Ohio) said at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Infiltrate on chest x-ray was seen in 59% of patients, mechanical ventilation was required in 34% of patients, and extracorporeal membrane oxygenation was required in 6% of patients. Treatment in the intensive care unit was required in 65% of patients, and cumulative mortality was 4% at 14 days, and 7% at 28 days.
“Overall, the [IVZ] exposure and then the elimination profiles were consistent across the entire age cohort – unusual for most drugs, but it seemed to hold true, which makes zanamivir a lot easier for us to work with in pediatrics,” Dr. Blumer said.
While the numbers are small, exposure and response delineation didn’t seem to be impacted by mechanical ventilation, by extracorporeal membrane oxygenation, or by continuous renal replacement therapy, which is a good sign, he noted.
“So we generally had good, consistent experience here. ... Overall, 64 of the 71 patients survived, got better, left the ICU, and left the hospital,” Dr. Blumer said.
Of note, a treatment-emergent resistance substitution, E119G, was detected in a day 5 H1N1 isolate from an immunocompetent patient who improved clinically while on IVZ, he said, adding that no phenotype data were available as the sample could not be cultured.
The findings are important, because while zanamivir is currently labeled for patients older than 7 years, and the intravenous formulation currently in development has been shown to be safe for adults, there is a critical unmet need for an effective parenteral treatment for severe flu in children at high risk of complications who cannot tolerate enteral therapy.
“We need a drug that is available for the critically ill. We need a drug available for kids who are unable to take oral therapy, and for treatment of oseltamivir-resistant strains,” he said, adding that the current findings suggest that IVZ – with dose selection based on age, weight, and renal function – is a suitable treatment option for such patients.
“In conclusion, what we saw in this open-label trial was that the dose selection that we utilized gave us the kind of exposure we’d expect, and it seems it was an appropriate way to approach pediatric patients,” he said. “There wasn’t any safety signal attributable to the drug, and the overall pattern was more that of serious influenza, rather than of drug exposure.”
Dr. Blumer reported receiving research support from GlaxoSmithKline, which sponsored the study.
NEW ORLEANS – The investigational intravenous formulation of the neuraminidase inhibitor zanamivir appears to be a safe influenza treatment for hospitalized children and adolescents at high risk of complications who can’t tolerate enteral therapy, according to findings from an open-label, multicenter, phase II study.
In 71 such patients with laboratory-confirmed flu, who presented within 7 days of illness onset and who received intravenous zanamivir (IVZ) for 5-10 days, 72% experienced adverse events (AEs), 21% experienced serious adverse events, and 5 deaths occurred, but none were considered by the investigators to be attributable to IVZ, Jeffrey Blumer, MD, reported at IDWeek, an annual scientific meeting on infectious diseases.
Rather, the adverse events were “fairly diverse. ... the kinds of things normally seen in critically ill pediatric populations,” he said.
The patients, who had a mean age of 7 years, were treated with IVZ doses selected to provide exposures comparable to 600 mg in adults – a dosage shown in prior studies to be safe and well-tolerated in adults. Patients aged 6 months to under age 6 years received twice-daily doses of 14 mg/kg, and those aged 6 years to less than 18 years received twice-daily doses of 12 mg/kg, not to exceed 600 mg. Doses were adjusted for renal function.
Patients were enrolled from five countries, and most (69%) had received prior treatment with oseltamivir. More than half (56%) had chronic medical conditions.
The median time from symptom onset to IVZ treatment was 4 days, Dr. Blumer of the University of Toledo (Ohio) said at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Infiltrate on chest x-ray was seen in 59% of patients, mechanical ventilation was required in 34% of patients, and extracorporeal membrane oxygenation was required in 6% of patients. Treatment in the intensive care unit was required in 65% of patients, and cumulative mortality was 4% at 14 days, and 7% at 28 days.
“Overall, the [IVZ] exposure and then the elimination profiles were consistent across the entire age cohort – unusual for most drugs, but it seemed to hold true, which makes zanamivir a lot easier for us to work with in pediatrics,” Dr. Blumer said.
While the numbers are small, exposure and response delineation didn’t seem to be impacted by mechanical ventilation, by extracorporeal membrane oxygenation, or by continuous renal replacement therapy, which is a good sign, he noted.
“So we generally had good, consistent experience here. ... Overall, 64 of the 71 patients survived, got better, left the ICU, and left the hospital,” Dr. Blumer said.
Of note, a treatment-emergent resistance substitution, E119G, was detected in a day 5 H1N1 isolate from an immunocompetent patient who improved clinically while on IVZ, he said, adding that no phenotype data were available as the sample could not be cultured.
The findings are important, because while zanamivir is currently labeled for patients older than 7 years, and the intravenous formulation currently in development has been shown to be safe for adults, there is a critical unmet need for an effective parenteral treatment for severe flu in children at high risk of complications who cannot tolerate enteral therapy.
“We need a drug that is available for the critically ill. We need a drug available for kids who are unable to take oral therapy, and for treatment of oseltamivir-resistant strains,” he said, adding that the current findings suggest that IVZ – with dose selection based on age, weight, and renal function – is a suitable treatment option for such patients.
“In conclusion, what we saw in this open-label trial was that the dose selection that we utilized gave us the kind of exposure we’d expect, and it seems it was an appropriate way to approach pediatric patients,” he said. “There wasn’t any safety signal attributable to the drug, and the overall pattern was more that of serious influenza, rather than of drug exposure.”
Dr. Blumer reported receiving research support from GlaxoSmithKline, which sponsored the study.
NEW ORLEANS – The investigational intravenous formulation of the neuraminidase inhibitor zanamivir appears to be a safe influenza treatment for hospitalized children and adolescents at high risk of complications who can’t tolerate enteral therapy, according to findings from an open-label, multicenter, phase II study.
In 71 such patients with laboratory-confirmed flu, who presented within 7 days of illness onset and who received intravenous zanamivir (IVZ) for 5-10 days, 72% experienced adverse events (AEs), 21% experienced serious adverse events, and 5 deaths occurred, but none were considered by the investigators to be attributable to IVZ, Jeffrey Blumer, MD, reported at IDWeek, an annual scientific meeting on infectious diseases.
Rather, the adverse events were “fairly diverse. ... the kinds of things normally seen in critically ill pediatric populations,” he said.
The patients, who had a mean age of 7 years, were treated with IVZ doses selected to provide exposures comparable to 600 mg in adults – a dosage shown in prior studies to be safe and well-tolerated in adults. Patients aged 6 months to under age 6 years received twice-daily doses of 14 mg/kg, and those aged 6 years to less than 18 years received twice-daily doses of 12 mg/kg, not to exceed 600 mg. Doses were adjusted for renal function.
Patients were enrolled from five countries, and most (69%) had received prior treatment with oseltamivir. More than half (56%) had chronic medical conditions.
The median time from symptom onset to IVZ treatment was 4 days, Dr. Blumer of the University of Toledo (Ohio) said at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Infiltrate on chest x-ray was seen in 59% of patients, mechanical ventilation was required in 34% of patients, and extracorporeal membrane oxygenation was required in 6% of patients. Treatment in the intensive care unit was required in 65% of patients, and cumulative mortality was 4% at 14 days, and 7% at 28 days.
“Overall, the [IVZ] exposure and then the elimination profiles were consistent across the entire age cohort – unusual for most drugs, but it seemed to hold true, which makes zanamivir a lot easier for us to work with in pediatrics,” Dr. Blumer said.
While the numbers are small, exposure and response delineation didn’t seem to be impacted by mechanical ventilation, by extracorporeal membrane oxygenation, or by continuous renal replacement therapy, which is a good sign, he noted.
“So we generally had good, consistent experience here. ... Overall, 64 of the 71 patients survived, got better, left the ICU, and left the hospital,” Dr. Blumer said.
Of note, a treatment-emergent resistance substitution, E119G, was detected in a day 5 H1N1 isolate from an immunocompetent patient who improved clinically while on IVZ, he said, adding that no phenotype data were available as the sample could not be cultured.
The findings are important, because while zanamivir is currently labeled for patients older than 7 years, and the intravenous formulation currently in development has been shown to be safe for adults, there is a critical unmet need for an effective parenteral treatment for severe flu in children at high risk of complications who cannot tolerate enteral therapy.
“We need a drug that is available for the critically ill. We need a drug available for kids who are unable to take oral therapy, and for treatment of oseltamivir-resistant strains,” he said, adding that the current findings suggest that IVZ – with dose selection based on age, weight, and renal function – is a suitable treatment option for such patients.
“In conclusion, what we saw in this open-label trial was that the dose selection that we utilized gave us the kind of exposure we’d expect, and it seems it was an appropriate way to approach pediatric patients,” he said. “There wasn’t any safety signal attributable to the drug, and the overall pattern was more that of serious influenza, rather than of drug exposure.”
Dr. Blumer reported receiving research support from GlaxoSmithKline, which sponsored the study.
AT ID WEEK 2016
Key clinical point:
Major finding: A total of 72% of patients experienced adverse events and 21% experienced serious adverse events, but none were considered by the investigators to be attributable to intravenous zanamivir.
Data source: An open-label, multicenter, phase II study of 71 children with laboratory-confirmed influenza.
Disclosures: Dr. Blumer reported receiving research support from GlaxoSmithKline, which sponsored the study.
Research yields 5 key points about vaccine hesitancy
ATLANTA – While there is no question about the need to address pockets of increasing vaccine refusals, determining how to address it requires a better understanding of the forces underlying vaccine hesitancy.
This area of research is still young, but Glen Nowak, PhD, a visiting communication scientist at the National Vaccine Program Office and director of the Grady College Center for Health & Risk Communication at the University of Georgia in Athens, drew on multiple recent studies and an in-progress review of vaccine hesitancy and confidence literature to distill five key findings from recent research into vaccine hesitancy. He presented that summary at a conference sponsored by the Centers for Disease Control and Prevention.
The first insight: There is a lot of interest in understanding vaccine hesitancy and confidence. But the rub is that many inconsistencies and uncertainties exist, because efforts remain in the early stages of research.
Dr. Nowak referenced the November 2014 report of the World Health Organization’s Strategic Advisory Group of Experts (SAGE) on Immunization to define vaccine hesitancy as the “delay in acceptance or refusal of vaccines despite availability of vaccine services.” But that hesitancy is complex and context specific, varying across time, place, and type of vaccine, the report found.
Those who are hesitant about vaccines are not a homogeneous group, Dr. Nowak said. Their degree of indecision ranges from refusing all vaccines, refusing some and accepting others, or delaying some but not others, to full acceptance of all vaccines despite hesitancy. Their attitudes also vary about vaccination overall and about specific vaccines.
“Vaccines hesitancy is influenced by several factors: complacency, convenience, and confidence,” Dr. Nowak said.
“Generally speaking, the end goal of all of our efforts is vaccine coverage, and before that is vaccine acceptance,” he said. “Before acceptance is hesitancy, and confidence is considered the precursor to hesitancy.” But no clear definition or measure of “vaccine confidence” exists yet.
Dr. Nowak next highlighted the second key finding: that research has identified an association between vaccine hesitancy or vaccine-related hesitancy and vaccine acceptance.
A 2016 study found that scores from the Attitudes about Childhood Vaccines Survey predicted under-immunization in children at 19 months of age, and three studies from 2008 through 2012 found a greater likelihood to delay or refuse vaccines among parents who had vaccine-related doubts.
Focus groups have found that parents who express hesitation or a lack of trust in vaccines also tend to mention using “alternative schedules,” including delaying vaccines or only vaccinating their children with select vaccines instead of all the recommended immunizations.
The third key finding Dr. Nowak discussed returned to the idea of “vaccine confidence,” which has aroused more interest in research but which requires refinement before it can become a truly helpful concept. Studies have already found links between confidence and parents vaccinating their children, but the field lacks standard measures.
“There are all different definitions that are out there, but they have not been measured,” Dr. Nowak said.
For example, the 2015 National Vaccine Advisory Committee report defined vaccine confidence as parents’ or health care providers’ trust in three areas: the immunizations recommended by the CDC’s Advisory Committee on Immunization Practices, the providers who administer the vaccines, and the processes that lead to vaccine licensure and vaccine recommendations.
But other definitions might include having faith that a person will benefit from a vaccine or that they won’t experience harm, or lacking any concerns about potential adverse outcomes.
The fourth key finding of recent research delivered positive news, Dr. Nowak noted: “Vaccines do relatively well compared to other health-related products that parents of young children have to make decisions about, such as antibiotics, over-the-counter medicines and vitamins.”
For example, in one study, the mean score (scale 1-10) of parents’ confidence that their child will not have a bad or serious adverse reaction to a recommended vaccine was 6.6, the same as the confidence level for antibiotics and only slightly below the scores of 6.8 for OTC medications and 7.3 for vitamins. Vaccines and antibiotics tied for the highest score for parents’ confidence in their effectiveness: 7.1, compared with 6.3 for OTC medications and 5.8 for vitamins. And of all four products, parents had the highest faith in vaccines as benefiting their children’s health.
But it was the final finding Dr. Nowak discussed that can present some of the greatest challenges to addressing vaccine hesitancy: Parents’ direct and indirect experiences play a significant role in their confidence about vaccines.
One study found that nearly a quarter of parents reported knowing someone who had a “bad reaction” to a vaccine (aside from soreness, fever, redness, or swelling), compared with 16.7% reporting that someone they knew had a bad reaction to an OTC medication. About one-third of parents reported the same for antibiotics.
Similarly, the measles outbreak at Disneyland in 2015 increased parents’ confidence in the safety and effectiveness of the CDC-recommended childhood vaccination schedule, and in the belief that their child’s health would benefit from receiving all the recommended vaccines.
Dr. Nowak reported no disclosures.
ATLANTA – While there is no question about the need to address pockets of increasing vaccine refusals, determining how to address it requires a better understanding of the forces underlying vaccine hesitancy.
This area of research is still young, but Glen Nowak, PhD, a visiting communication scientist at the National Vaccine Program Office and director of the Grady College Center for Health & Risk Communication at the University of Georgia in Athens, drew on multiple recent studies and an in-progress review of vaccine hesitancy and confidence literature to distill five key findings from recent research into vaccine hesitancy. He presented that summary at a conference sponsored by the Centers for Disease Control and Prevention.
The first insight: There is a lot of interest in understanding vaccine hesitancy and confidence. But the rub is that many inconsistencies and uncertainties exist, because efforts remain in the early stages of research.
Dr. Nowak referenced the November 2014 report of the World Health Organization’s Strategic Advisory Group of Experts (SAGE) on Immunization to define vaccine hesitancy as the “delay in acceptance or refusal of vaccines despite availability of vaccine services.” But that hesitancy is complex and context specific, varying across time, place, and type of vaccine, the report found.
Those who are hesitant about vaccines are not a homogeneous group, Dr. Nowak said. Their degree of indecision ranges from refusing all vaccines, refusing some and accepting others, or delaying some but not others, to full acceptance of all vaccines despite hesitancy. Their attitudes also vary about vaccination overall and about specific vaccines.
“Vaccines hesitancy is influenced by several factors: complacency, convenience, and confidence,” Dr. Nowak said.
“Generally speaking, the end goal of all of our efforts is vaccine coverage, and before that is vaccine acceptance,” he said. “Before acceptance is hesitancy, and confidence is considered the precursor to hesitancy.” But no clear definition or measure of “vaccine confidence” exists yet.
Dr. Nowak next highlighted the second key finding: that research has identified an association between vaccine hesitancy or vaccine-related hesitancy and vaccine acceptance.
A 2016 study found that scores from the Attitudes about Childhood Vaccines Survey predicted under-immunization in children at 19 months of age, and three studies from 2008 through 2012 found a greater likelihood to delay or refuse vaccines among parents who had vaccine-related doubts.
Focus groups have found that parents who express hesitation or a lack of trust in vaccines also tend to mention using “alternative schedules,” including delaying vaccines or only vaccinating their children with select vaccines instead of all the recommended immunizations.
The third key finding Dr. Nowak discussed returned to the idea of “vaccine confidence,” which has aroused more interest in research but which requires refinement before it can become a truly helpful concept. Studies have already found links between confidence and parents vaccinating their children, but the field lacks standard measures.
“There are all different definitions that are out there, but they have not been measured,” Dr. Nowak said.
For example, the 2015 National Vaccine Advisory Committee report defined vaccine confidence as parents’ or health care providers’ trust in three areas: the immunizations recommended by the CDC’s Advisory Committee on Immunization Practices, the providers who administer the vaccines, and the processes that lead to vaccine licensure and vaccine recommendations.
But other definitions might include having faith that a person will benefit from a vaccine or that they won’t experience harm, or lacking any concerns about potential adverse outcomes.
The fourth key finding of recent research delivered positive news, Dr. Nowak noted: “Vaccines do relatively well compared to other health-related products that parents of young children have to make decisions about, such as antibiotics, over-the-counter medicines and vitamins.”
For example, in one study, the mean score (scale 1-10) of parents’ confidence that their child will not have a bad or serious adverse reaction to a recommended vaccine was 6.6, the same as the confidence level for antibiotics and only slightly below the scores of 6.8 for OTC medications and 7.3 for vitamins. Vaccines and antibiotics tied for the highest score for parents’ confidence in their effectiveness: 7.1, compared with 6.3 for OTC medications and 5.8 for vitamins. And of all four products, parents had the highest faith in vaccines as benefiting their children’s health.
But it was the final finding Dr. Nowak discussed that can present some of the greatest challenges to addressing vaccine hesitancy: Parents’ direct and indirect experiences play a significant role in their confidence about vaccines.
One study found that nearly a quarter of parents reported knowing someone who had a “bad reaction” to a vaccine (aside from soreness, fever, redness, or swelling), compared with 16.7% reporting that someone they knew had a bad reaction to an OTC medication. About one-third of parents reported the same for antibiotics.
Similarly, the measles outbreak at Disneyland in 2015 increased parents’ confidence in the safety and effectiveness of the CDC-recommended childhood vaccination schedule, and in the belief that their child’s health would benefit from receiving all the recommended vaccines.
Dr. Nowak reported no disclosures.
ATLANTA – While there is no question about the need to address pockets of increasing vaccine refusals, determining how to address it requires a better understanding of the forces underlying vaccine hesitancy.
This area of research is still young, but Glen Nowak, PhD, a visiting communication scientist at the National Vaccine Program Office and director of the Grady College Center for Health & Risk Communication at the University of Georgia in Athens, drew on multiple recent studies and an in-progress review of vaccine hesitancy and confidence literature to distill five key findings from recent research into vaccine hesitancy. He presented that summary at a conference sponsored by the Centers for Disease Control and Prevention.
The first insight: There is a lot of interest in understanding vaccine hesitancy and confidence. But the rub is that many inconsistencies and uncertainties exist, because efforts remain in the early stages of research.
Dr. Nowak referenced the November 2014 report of the World Health Organization’s Strategic Advisory Group of Experts (SAGE) on Immunization to define vaccine hesitancy as the “delay in acceptance or refusal of vaccines despite availability of vaccine services.” But that hesitancy is complex and context specific, varying across time, place, and type of vaccine, the report found.
Those who are hesitant about vaccines are not a homogeneous group, Dr. Nowak said. Their degree of indecision ranges from refusing all vaccines, refusing some and accepting others, or delaying some but not others, to full acceptance of all vaccines despite hesitancy. Their attitudes also vary about vaccination overall and about specific vaccines.
“Vaccines hesitancy is influenced by several factors: complacency, convenience, and confidence,” Dr. Nowak said.
“Generally speaking, the end goal of all of our efforts is vaccine coverage, and before that is vaccine acceptance,” he said. “Before acceptance is hesitancy, and confidence is considered the precursor to hesitancy.” But no clear definition or measure of “vaccine confidence” exists yet.
Dr. Nowak next highlighted the second key finding: that research has identified an association between vaccine hesitancy or vaccine-related hesitancy and vaccine acceptance.
A 2016 study found that scores from the Attitudes about Childhood Vaccines Survey predicted under-immunization in children at 19 months of age, and three studies from 2008 through 2012 found a greater likelihood to delay or refuse vaccines among parents who had vaccine-related doubts.
Focus groups have found that parents who express hesitation or a lack of trust in vaccines also tend to mention using “alternative schedules,” including delaying vaccines or only vaccinating their children with select vaccines instead of all the recommended immunizations.
The third key finding Dr. Nowak discussed returned to the idea of “vaccine confidence,” which has aroused more interest in research but which requires refinement before it can become a truly helpful concept. Studies have already found links between confidence and parents vaccinating their children, but the field lacks standard measures.
“There are all different definitions that are out there, but they have not been measured,” Dr. Nowak said.
For example, the 2015 National Vaccine Advisory Committee report defined vaccine confidence as parents’ or health care providers’ trust in three areas: the immunizations recommended by the CDC’s Advisory Committee on Immunization Practices, the providers who administer the vaccines, and the processes that lead to vaccine licensure and vaccine recommendations.
But other definitions might include having faith that a person will benefit from a vaccine or that they won’t experience harm, or lacking any concerns about potential adverse outcomes.
The fourth key finding of recent research delivered positive news, Dr. Nowak noted: “Vaccines do relatively well compared to other health-related products that parents of young children have to make decisions about, such as antibiotics, over-the-counter medicines and vitamins.”
For example, in one study, the mean score (scale 1-10) of parents’ confidence that their child will not have a bad or serious adverse reaction to a recommended vaccine was 6.6, the same as the confidence level for antibiotics and only slightly below the scores of 6.8 for OTC medications and 7.3 for vitamins. Vaccines and antibiotics tied for the highest score for parents’ confidence in their effectiveness: 7.1, compared with 6.3 for OTC medications and 5.8 for vitamins. And of all four products, parents had the highest faith in vaccines as benefiting their children’s health.
But it was the final finding Dr. Nowak discussed that can present some of the greatest challenges to addressing vaccine hesitancy: Parents’ direct and indirect experiences play a significant role in their confidence about vaccines.
One study found that nearly a quarter of parents reported knowing someone who had a “bad reaction” to a vaccine (aside from soreness, fever, redness, or swelling), compared with 16.7% reporting that someone they knew had a bad reaction to an OTC medication. About one-third of parents reported the same for antibiotics.
Similarly, the measles outbreak at Disneyland in 2015 increased parents’ confidence in the safety and effectiveness of the CDC-recommended childhood vaccination schedule, and in the belief that their child’s health would benefit from receiving all the recommended vaccines.
Dr. Nowak reported no disclosures.
Toddler gaze patterns heritable, stable over time
NEW YORK – A team of autism researchers has found that patterns of social-visual engagement are markedly more similar among identical twin toddlers than among fraternal twins.
Social-visual engagement (SVE), which can be measured using eye-tracking technology, is how humans give preferential attention to social stimuli – in particular, people’s eyes and mouths, which provide important information for communication.
Lower levels of SVE have been shown to be associated with the later development of autism, even in children just a few months old (Nature. 2013 Dec 19;504:427-31). “But what hasn’t been shown until now is that this measure relates to genetics,” said Natasha Marrus, MD, PhD, of the department of psychiatry at Washington University in St. Louis.
The identical twins, who share 100% of their genes, “showed much more similar levels of social-visual engagement than fraternal twins,” Dr. Marrus said, with an intraclass correlation coefficient (ICC) of 0.91 (95% confidence interval, 0.85-0.95) for time spent looking at eyes, compared with 0.35 (95% CI, 0.07-0.59) for fraternal twins. Similar results were obtained for the caregiver questionnaire, suggesting strong genetic influences on both early reciprocal social behavior and SVE, said Dr. Marrus, also of Washington University.
At 36 months, 69 of the twin pairs were reevaluated. The investigators again found significantly greater SVE concordance for the identical twins: ICC, 0.93 (95% CI, 0.75-0.98), compared with ICC, 0.25 (95% CI, 0.0-0.60) for fraternal twins. They also found SVE patterns strongly correlated between 21 and 36 months for individual twins, indicating traitlike stability of this behavior over time.
“These two measures that are heritable, like autism, can be measured in a general population sample, which means they show good variability – potentially allowing the detection of subtle differences that may correspond to levels of risk for autism,” Dr. Marrus said. “By 18-21 months, the risk markers for later autism are already there – if you use a nuanced enough measure to detect them.”
Dr. Marrus said that while some practitioners have been able to reliably diagnose autism in children younger than 24 months, “it’s usually with the most severe cases,” she said. “But 18 months is a big time for social as well as language development, which becomes easier to measure at that point.”
A future direction for study, she said, “would be to go earlier. If we’re seeing this at 18 months, maybe we’d see it at 12.”
With autism, “early intervention is key, and even 6 months could make a difference,” Dr. Marrus said. “These two measures stand a really good chance of telling us important things about autism – which at early ages means better diagnostic prediction, measurement of severity and risk, and the potential to monitor responses to interventions.”
The National Institutes of Health supported the study through a grant to Dr. Constantino, and Dr. Marrus’s work was supported with a postdoctoral fellowship from the Autism Science Foundation. The investigators declared no relevant financial conflicts.
NEW YORK – A team of autism researchers has found that patterns of social-visual engagement are markedly more similar among identical twin toddlers than among fraternal twins.
Social-visual engagement (SVE), which can be measured using eye-tracking technology, is how humans give preferential attention to social stimuli – in particular, people’s eyes and mouths, which provide important information for communication.
Lower levels of SVE have been shown to be associated with the later development of autism, even in children just a few months old (Nature. 2013 Dec 19;504:427-31). “But what hasn’t been shown until now is that this measure relates to genetics,” said Natasha Marrus, MD, PhD, of the department of psychiatry at Washington University in St. Louis.
The identical twins, who share 100% of their genes, “showed much more similar levels of social-visual engagement than fraternal twins,” Dr. Marrus said, with an intraclass correlation coefficient (ICC) of 0.91 (95% confidence interval, 0.85-0.95) for time spent looking at eyes, compared with 0.35 (95% CI, 0.07-0.59) for fraternal twins. Similar results were obtained for the caregiver questionnaire, suggesting strong genetic influences on both early reciprocal social behavior and SVE, said Dr. Marrus, also of Washington University.
At 36 months, 69 of the twin pairs were reevaluated. The investigators again found significantly greater SVE concordance for the identical twins: ICC, 0.93 (95% CI, 0.75-0.98), compared with ICC, 0.25 (95% CI, 0.0-0.60) for fraternal twins. They also found SVE patterns strongly correlated between 21 and 36 months for individual twins, indicating traitlike stability of this behavior over time.
“These two measures that are heritable, like autism, can be measured in a general population sample, which means they show good variability – potentially allowing the detection of subtle differences that may correspond to levels of risk for autism,” Dr. Marrus said. “By 18-21 months, the risk markers for later autism are already there – if you use a nuanced enough measure to detect them.”
Dr. Marrus said that while some practitioners have been able to reliably diagnose autism in children younger than 24 months, “it’s usually with the most severe cases,” she said. “But 18 months is a big time for social as well as language development, which becomes easier to measure at that point.”
A future direction for study, she said, “would be to go earlier. If we’re seeing this at 18 months, maybe we’d see it at 12.”
With autism, “early intervention is key, and even 6 months could make a difference,” Dr. Marrus said. “These two measures stand a really good chance of telling us important things about autism – which at early ages means better diagnostic prediction, measurement of severity and risk, and the potential to monitor responses to interventions.”
The National Institutes of Health supported the study through a grant to Dr. Constantino, and Dr. Marrus’s work was supported with a postdoctoral fellowship from the Autism Science Foundation. The investigators declared no relevant financial conflicts.
NEW YORK – A team of autism researchers has found that patterns of social-visual engagement are markedly more similar among identical twin toddlers than among fraternal twins.
Social-visual engagement (SVE), which can be measured using eye-tracking technology, is how humans give preferential attention to social stimuli – in particular, people’s eyes and mouths, which provide important information for communication.
Lower levels of SVE have been shown to be associated with the later development of autism, even in children just a few months old (Nature. 2013 Dec 19;504:427-31). “But what hasn’t been shown until now is that this measure relates to genetics,” said Natasha Marrus, MD, PhD, of the department of psychiatry at Washington University in St. Louis.
The identical twins, who share 100% of their genes, “showed much more similar levels of social-visual engagement than fraternal twins,” Dr. Marrus said, with an intraclass correlation coefficient (ICC) of 0.91 (95% confidence interval, 0.85-0.95) for time spent looking at eyes, compared with 0.35 (95% CI, 0.07-0.59) for fraternal twins. Similar results were obtained for the caregiver questionnaire, suggesting strong genetic influences on both early reciprocal social behavior and SVE, said Dr. Marrus, also of Washington University.
At 36 months, 69 of the twin pairs were reevaluated. The investigators again found significantly greater SVE concordance for the identical twins: ICC, 0.93 (95% CI, 0.75-0.98), compared with ICC, 0.25 (95% CI, 0.0-0.60) for fraternal twins. They also found SVE patterns strongly correlated between 21 and 36 months for individual twins, indicating traitlike stability of this behavior over time.
“These two measures that are heritable, like autism, can be measured in a general population sample, which means they show good variability – potentially allowing the detection of subtle differences that may correspond to levels of risk for autism,” Dr. Marrus said. “By 18-21 months, the risk markers for later autism are already there – if you use a nuanced enough measure to detect them.”
Dr. Marrus said that while some practitioners have been able to reliably diagnose autism in children younger than 24 months, “it’s usually with the most severe cases,” she said. “But 18 months is a big time for social as well as language development, which becomes easier to measure at that point.”
A future direction for study, she said, “would be to go earlier. If we’re seeing this at 18 months, maybe we’d see it at 12.”
With autism, “early intervention is key, and even 6 months could make a difference,” Dr. Marrus said. “These two measures stand a really good chance of telling us important things about autism – which at early ages means better diagnostic prediction, measurement of severity and risk, and the potential to monitor responses to interventions.”
The National Institutes of Health supported the study through a grant to Dr. Constantino, and Dr. Marrus’s work was supported with a postdoctoral fellowship from the Autism Science Foundation. The investigators declared no relevant financial conflicts.
AT AACAP 2016
Clindamycin, TMP-SMX both of benefit for small abscesses
NEW ORLEANS – Both clindamycin and trimethoprim-sulfamethoxazole (TMP-SMX) were superior to placebo when used after incision and drainage for the treatment of small, uncomplicated abscesses in children and adults in a prospective, randomized, placebo-controlled study.
Further, the cure rates were similar with both antibiotics, except in subjects with a clindamycin-resistant Staphylococcus aureus isolate, in whom the cure rate was lower, Robert S. Daum, MD, of the University of Chicago reported at an annual scientific meeting on infectious diseases.
Small, uncomplicated skin abscesses are common in ambulatory settings, but the optimal treatment strategy in the era of community-acquired methicillin-resistant S. aureus has been unclear. A prior study showed that clindamycin and TMP-SMX are both of benefit in the setting of large skin abscesses. The current findings further demonstrate that they also are of benefit when used in conjunction with incision and drainage for the treatment of small abscesses.
In 786 outpatient subjects, including 505 adults and 281 children who were randomized to receive 10 days of treatment with either clindamycin, TMP-SMX, or placebo following incision and drainage, mean cure rates at the 10-day posttherapy test of cure visit were 83% in the clindamycin group, 82% in the TMP-SMX group, and 69% in the placebo group, he said, noting that the differences were statistically significant for both treatments vs. placebo.
Study participants had a single skin abscess of 5 cm or less in diameter. Those with significant comorbidity, such as diabetes, were excluded.
S. aureus was isolated from 527 subjects (67%), and methicillin-resistant S. aureus was isolated from 388 (49%).
In clindamycin-treated subjects with an S. aureus lesion, 54% with a clindamycin-resistant isolate were cured, compared with 85% with a clindamycin-susceptible isolate.
Of note, subjects without S. aureus did not do better with antibiotics vs. placebo, Dr. Daum said.
“Staph aureus matters,” he said. People who did not grow Staph aureus did not do better with placebo than with antibiotic ... incision and drainage was basically all that was needed [in those patients],” he said.
Adverse events were more common in the clindamycin group (22% vs. 11% with TMP-SMX and 12.5% with placebo), but all events were mild and resolved without sequelae, and among those who were cured initially, fewer new skin infections were noted at a 1-month follow-up visit among clindamycin recipients, compared with those who received TMP-SMX or placebo, he noted at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
No cases of Clostridium difficile-associated diarrhea were reported among study subjects.
Dr. Daum reported having no disclosures.
NEW ORLEANS – Both clindamycin and trimethoprim-sulfamethoxazole (TMP-SMX) were superior to placebo when used after incision and drainage for the treatment of small, uncomplicated abscesses in children and adults in a prospective, randomized, placebo-controlled study.
Further, the cure rates were similar with both antibiotics, except in subjects with a clindamycin-resistant Staphylococcus aureus isolate, in whom the cure rate was lower, Robert S. Daum, MD, of the University of Chicago reported at an annual scientific meeting on infectious diseases.
Small, uncomplicated skin abscesses are common in ambulatory settings, but the optimal treatment strategy in the era of community-acquired methicillin-resistant S. aureus has been unclear. A prior study showed that clindamycin and TMP-SMX are both of benefit in the setting of large skin abscesses. The current findings further demonstrate that they also are of benefit when used in conjunction with incision and drainage for the treatment of small abscesses.
In 786 outpatient subjects, including 505 adults and 281 children who were randomized to receive 10 days of treatment with either clindamycin, TMP-SMX, or placebo following incision and drainage, mean cure rates at the 10-day posttherapy test of cure visit were 83% in the clindamycin group, 82% in the TMP-SMX group, and 69% in the placebo group, he said, noting that the differences were statistically significant for both treatments vs. placebo.
Study participants had a single skin abscess of 5 cm or less in diameter. Those with significant comorbidity, such as diabetes, were excluded.
S. aureus was isolated from 527 subjects (67%), and methicillin-resistant S. aureus was isolated from 388 (49%).
In clindamycin-treated subjects with an S. aureus lesion, 54% with a clindamycin-resistant isolate were cured, compared with 85% with a clindamycin-susceptible isolate.
Of note, subjects without S. aureus did not do better with antibiotics vs. placebo, Dr. Daum said.
“Staph aureus matters,” he said. People who did not grow Staph aureus did not do better with placebo than with antibiotic ... incision and drainage was basically all that was needed [in those patients],” he said.
Adverse events were more common in the clindamycin group (22% vs. 11% with TMP-SMX and 12.5% with placebo), but all events were mild and resolved without sequelae, and among those who were cured initially, fewer new skin infections were noted at a 1-month follow-up visit among clindamycin recipients, compared with those who received TMP-SMX or placebo, he noted at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
No cases of Clostridium difficile-associated diarrhea were reported among study subjects.
Dr. Daum reported having no disclosures.
NEW ORLEANS – Both clindamycin and trimethoprim-sulfamethoxazole (TMP-SMX) were superior to placebo when used after incision and drainage for the treatment of small, uncomplicated abscesses in children and adults in a prospective, randomized, placebo-controlled study.
Further, the cure rates were similar with both antibiotics, except in subjects with a clindamycin-resistant Staphylococcus aureus isolate, in whom the cure rate was lower, Robert S. Daum, MD, of the University of Chicago reported at an annual scientific meeting on infectious diseases.
Small, uncomplicated skin abscesses are common in ambulatory settings, but the optimal treatment strategy in the era of community-acquired methicillin-resistant S. aureus has been unclear. A prior study showed that clindamycin and TMP-SMX are both of benefit in the setting of large skin abscesses. The current findings further demonstrate that they also are of benefit when used in conjunction with incision and drainage for the treatment of small abscesses.
In 786 outpatient subjects, including 505 adults and 281 children who were randomized to receive 10 days of treatment with either clindamycin, TMP-SMX, or placebo following incision and drainage, mean cure rates at the 10-day posttherapy test of cure visit were 83% in the clindamycin group, 82% in the TMP-SMX group, and 69% in the placebo group, he said, noting that the differences were statistically significant for both treatments vs. placebo.
Study participants had a single skin abscess of 5 cm or less in diameter. Those with significant comorbidity, such as diabetes, were excluded.
S. aureus was isolated from 527 subjects (67%), and methicillin-resistant S. aureus was isolated from 388 (49%).
In clindamycin-treated subjects with an S. aureus lesion, 54% with a clindamycin-resistant isolate were cured, compared with 85% with a clindamycin-susceptible isolate.
Of note, subjects without S. aureus did not do better with antibiotics vs. placebo, Dr. Daum said.
“Staph aureus matters,” he said. People who did not grow Staph aureus did not do better with placebo than with antibiotic ... incision and drainage was basically all that was needed [in those patients],” he said.
Adverse events were more common in the clindamycin group (22% vs. 11% with TMP-SMX and 12.5% with placebo), but all events were mild and resolved without sequelae, and among those who were cured initially, fewer new skin infections were noted at a 1-month follow-up visit among clindamycin recipients, compared with those who received TMP-SMX or placebo, he noted at the combined annual meetings of the Infectious Diseases Society of America, the Society of Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
No cases of Clostridium difficile-associated diarrhea were reported among study subjects.
Dr. Daum reported having no disclosures.
AT IDWEEK 2016
Key clinical point:
Major finding: Mean cure rates were 83%, 82%, and 69% with clindamycin, TMP-SMX, and placebo, respectively.
Data source: A randomized, placebo-controlled, multicenter study of 786 subjects.
Disclosures: Dr. Daum reported having no disclosures.
Wide spectrum of feeding problems poses challenge for clinicians
SAN FRANCISCO – Clinicians are likely to encounter diverse feeding problems in daily practice that will challenge their diagnostic and treatment acumen, Dr. Irene Chatoor told attendees of the annual meeting of the American Academy of Pediatrics.
These problems run the gamut from the most prevalent but least serious picky eating, to the least prevalent but most serious feeding disorders, she noted. Correspondingly, management will range from simple reassurance of parents to more intensive behavioral and medical interventions.
Assessment

“When you assess a feeding problem, you have to look at both the mother and father, and the child,” she advised. The parents are evaluated for their feeding style, while the child is evaluated for three feeding problems: limited appetite, selective intake, and fear of feeding (Pediatrics. 2015;135[2]:344-53).
Clinicians must be alert for organic red flags, such as dysphagia, aspiration, and vomiting, and for behavioral red flags, such as food fixation, abrupt cessation of feeding after a trigger event, and anticipatory gagging. An overarching red flag is failure to thrive.
Sometimes, a child will have both an organic condition and a behavioral feeding disorder at the same time. “It’s very important that you don’t think one excludes the other,” she cautioned.
Diagnosis
“To delineate milder feeding difficulties from feeding disorders, there must be some form of impairment caused by the feeding problem,” Dr. Chatoor commented. “Why is this important? For two reasons. One is for the insurance companies, because they don’t pay unless there is a disorder. And then there is research: you cannot do research unless you clearly define what you are studying.”
Children are considered to have impairment if they have weight loss or growth faltering, considerable nutritional deficiency, or a marked interference with psychosocial functioning.
“When we diagnose feeding problems, it is best done with a multidisciplinary team,” Dr. Chatoor maintained. “I have learned many years ago that I’m not effective in helping parents deal with the feeding disorder if they are still in the back of their mind worried that the child has something organically wrong and that’s why the child does not want to eat.”
Accordingly, various team members perform a medical examination, a nutritional assessment, an oral motor and sensory evaluation, and a psychiatric or psychological assessment to identify the root cause or causes of the problem.
When it comes to behavioral etiologies, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) now groups all feeding and eating disorders together in one section, reflecting the fact that disorders starting early in life can and often do track into adolescence and adulthood, according to Dr. Chatoor.
The manual also features a new diagnosis, avoidant/restrictive food intake disorder (ARFID). Key criteria include the presence of an eating or feeding disturbance that cannot be better explained by lack of available food, culturally sanctioned practices, or a concurrent medical condition or another mental disorder.
The child must have a persistent failure to meet appropriate nutritional and/or energy needs, associated with any of four findings: significant weight loss or failure to achieve expected weight gain or growth, significant nutritional deficiencies, dependence on enteral feeding or oral nutritional supplements, and marked interference with psychosocial functioning.
“You need to have at least one but often you have a combination of nutritional and emotional impairment in the same child,” she commented.
ARFID and its treatment
There are three subtypes of ARFID having different features, treatments, and prognosis, although they all share in common food refusal, according to Dr. Chatoor.
The first subtype – apparent lack of interest in eating or food – emerges by 3 years of age, most often during the transition to self-feeding between 9 and 18 months. Affected children refuse to eat an adequate amount of food for at least 1 month, rarely communicate hunger, lack interest in food, and prefer to play or talk. They typically present with growth deficiency.
“If you have a child who refuses to eat, it generates anxiety in the mother. The mother does things she would not normally do with the child who is eating well. She starts to distract, to cajole, to sometimes even force-feed the child,” Dr. Chatoor explained. “And the more she engages in these behaviors, the more resistant the child becomes. So they become trapped in this vicious cycle.”
Treatment is aimed at removing this conflict with three approaches: explaining to parents the infant’s special temperament (notably, high arousal and difficulty turning off excitement); addressing their background, including any eating issues of their own, and difficulty with setting limits; and providing specific feeding guidelines and a time-out procedure.
The guidelines stress regular feeding, withholding of all snacks, keeping the child at the table for 20 to 30 minutes, and not using any distractions or pressure. Also, importantly, the parents should have dinner with their child. “I always tell the parents what is good for the child is good for you. It’s good for your whole family,” she said. “If they have other children, these rules apply to everybody. Young children learn to eat by watching their parents eating.”
With early and consistent use of these interventions, about two-thirds of children outgrow this eating/feeding disturbance by mid-childhood, according to Dr. Chatoor.
Children with the second subtype of ARFID – avoidance based on the sensory characteristics of food – consistently refuse to eat certain foods having specific tastes, textures, temperatures, smells, and/or appearances. Onset occurs during the toddler years, when a new or different food is introduced.
“Not only do they refuse the same foods that were aversive, but they also generalize it. So these children are afraid to try other foods and they may end up limiting food groups – they don’t eat any vegetables and some of them don’t eat any meats,” she explained. “They are a challenge because this always causes a nutritional deficiency and they also have problems socially as they get older.”
Treatment varies by age, with gradual desensitization for infants and parent modeling of eating new foods for toddlers. A multifaceted approach is used for preschoolers, combining modeling, giving foods attractive shapes and names, having the child participate in food preparation, and using focused play therapy, such as feeding dolls who are “brave” and try new foods.
Clinicians can explain to affected school-aged children that they are “supertasters,” having more taste buds and therefore experiencing food more intensely, and that they can help their taste buds not react so strongly by starting to eat small amounts of new foods and gradually increasing over time. Parents can let the child make a list of 10 foods they would like to eat, and award them points for “courage” for every bite of a new food they try.
Prognosis of this type of ARFID varies, according to Dr. Chatoor. “Through gradual exposure, young children can expand the variety of foods they eat,” she elaborated. However, “some children become very rigid and brand sensitive in regard to the food they are willing to eat and begin to experience social problems during mid-childhood and adolescence. Some children grow up eating a limited diet, but finding ways to compensate nutritionally and socially.”
Children with the third subtype of ARFID – concern about aversive consequences of eating – have an acute onset of consistent food refusal at any age, from infancy onward, after experiencing a traumatic event or repeated traumatic insults to the oropharynx or gastrointestinal tract that trigger distress in the child. These children often have comorbidities such as gastroesophageal reflux, eosinophilic gastroenteritis, or anxiety disorder.
“Treatment involves gradual desensitization to feared objects: the highchair, bib, bottle, or spoon,” Dr. Chatoor explained. “It also involves training of the mother in behavioral techniques to feed the child in spite of the child’s fear and distress.”
Any underlying medical condition causing pain or distress should be treated. Additional measures may include, for example, use of a graduated approach, starting with liquids and progressing to purees, if the child fears solid foods, and prescribing anxiolytic medication in cases of severe anxiety.
Dr. Chatoor disclosed that she has lectured internationally at conferences on feeding disorders that were organized by Abbott Nutrition International and that the company provided a research grant for a study on feeding.
SAN FRANCISCO – Clinicians are likely to encounter diverse feeding problems in daily practice that will challenge their diagnostic and treatment acumen, Dr. Irene Chatoor told attendees of the annual meeting of the American Academy of Pediatrics.
These problems run the gamut from the most prevalent but least serious picky eating, to the least prevalent but most serious feeding disorders, she noted. Correspondingly, management will range from simple reassurance of parents to more intensive behavioral and medical interventions.
Assessment
“When you assess a feeding problem, you have to look at both the mother and father, and the child,” she advised. The parents are evaluated for their feeding style, while the child is evaluated for three feeding problems: limited appetite, selective intake, and fear of feeding (Pediatrics. 2015;135[2]:344-53).
Clinicians must be alert for organic red flags, such as dysphagia, aspiration, and vomiting, and for behavioral red flags, such as food fixation, abrupt cessation of feeding after a trigger event, and anticipatory gagging. An overarching red flag is failure to thrive.
Sometimes, a child will have both an organic condition and a behavioral feeding disorder at the same time. “It’s very important that you don’t think one excludes the other,” she cautioned.
Diagnosis
“To delineate milder feeding difficulties from feeding disorders, there must be some form of impairment caused by the feeding problem,” Dr. Chatoor commented. “Why is this important? For two reasons. One is for the insurance companies, because they don’t pay unless there is a disorder. And then there is research: you cannot do research unless you clearly define what you are studying.”
Children are considered to have impairment if they have weight loss or growth faltering, considerable nutritional deficiency, or a marked interference with psychosocial functioning.
“When we diagnose feeding problems, it is best done with a multidisciplinary team,” Dr. Chatoor maintained. “I have learned many years ago that I’m not effective in helping parents deal with the feeding disorder if they are still in the back of their mind worried that the child has something organically wrong and that’s why the child does not want to eat.”
Accordingly, various team members perform a medical examination, a nutritional assessment, an oral motor and sensory evaluation, and a psychiatric or psychological assessment to identify the root cause or causes of the problem.
When it comes to behavioral etiologies, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) now groups all feeding and eating disorders together in one section, reflecting the fact that disorders starting early in life can and often do track into adolescence and adulthood, according to Dr. Chatoor.
The manual also features a new diagnosis, avoidant/restrictive food intake disorder (ARFID). Key criteria include the presence of an eating or feeding disturbance that cannot be better explained by lack of available food, culturally sanctioned practices, or a concurrent medical condition or another mental disorder.
The child must have a persistent failure to meet appropriate nutritional and/or energy needs, associated with any of four findings: significant weight loss or failure to achieve expected weight gain or growth, significant nutritional deficiencies, dependence on enteral feeding or oral nutritional supplements, and marked interference with psychosocial functioning.
“You need to have at least one but often you have a combination of nutritional and emotional impairment in the same child,” she commented.
ARFID and its treatment
There are three subtypes of ARFID having different features, treatments, and prognosis, although they all share in common food refusal, according to Dr. Chatoor.
The first subtype – apparent lack of interest in eating or food – emerges by 3 years of age, most often during the transition to self-feeding between 9 and 18 months. Affected children refuse to eat an adequate amount of food for at least 1 month, rarely communicate hunger, lack interest in food, and prefer to play or talk. They typically present with growth deficiency.
“If you have a child who refuses to eat, it generates anxiety in the mother. The mother does things she would not normally do with the child who is eating well. She starts to distract, to cajole, to sometimes even force-feed the child,” Dr. Chatoor explained. “And the more she engages in these behaviors, the more resistant the child becomes. So they become trapped in this vicious cycle.”
Treatment is aimed at removing this conflict with three approaches: explaining to parents the infant’s special temperament (notably, high arousal and difficulty turning off excitement); addressing their background, including any eating issues of their own, and difficulty with setting limits; and providing specific feeding guidelines and a time-out procedure.
The guidelines stress regular feeding, withholding of all snacks, keeping the child at the table for 20 to 30 minutes, and not using any distractions or pressure. Also, importantly, the parents should have dinner with their child. “I always tell the parents what is good for the child is good for you. It’s good for your whole family,” she said. “If they have other children, these rules apply to everybody. Young children learn to eat by watching their parents eating.”
With early and consistent use of these interventions, about two-thirds of children outgrow this eating/feeding disturbance by mid-childhood, according to Dr. Chatoor.
Children with the second subtype of ARFID – avoidance based on the sensory characteristics of food – consistently refuse to eat certain foods having specific tastes, textures, temperatures, smells, and/or appearances. Onset occurs during the toddler years, when a new or different food is introduced.
“Not only do they refuse the same foods that were aversive, but they also generalize it. So these children are afraid to try other foods and they may end up limiting food groups – they don’t eat any vegetables and some of them don’t eat any meats,” she explained. “They are a challenge because this always causes a nutritional deficiency and they also have problems socially as they get older.”
Treatment varies by age, with gradual desensitization for infants and parent modeling of eating new foods for toddlers. A multifaceted approach is used for preschoolers, combining modeling, giving foods attractive shapes and names, having the child participate in food preparation, and using focused play therapy, such as feeding dolls who are “brave” and try new foods.
Clinicians can explain to affected school-aged children that they are “supertasters,” having more taste buds and therefore experiencing food more intensely, and that they can help their taste buds not react so strongly by starting to eat small amounts of new foods and gradually increasing over time. Parents can let the child make a list of 10 foods they would like to eat, and award them points for “courage” for every bite of a new food they try.
Prognosis of this type of ARFID varies, according to Dr. Chatoor. “Through gradual exposure, young children can expand the variety of foods they eat,” she elaborated. However, “some children become very rigid and brand sensitive in regard to the food they are willing to eat and begin to experience social problems during mid-childhood and adolescence. Some children grow up eating a limited diet, but finding ways to compensate nutritionally and socially.”
Children with the third subtype of ARFID – concern about aversive consequences of eating – have an acute onset of consistent food refusal at any age, from infancy onward, after experiencing a traumatic event or repeated traumatic insults to the oropharynx or gastrointestinal tract that trigger distress in the child. These children often have comorbidities such as gastroesophageal reflux, eosinophilic gastroenteritis, or anxiety disorder.
“Treatment involves gradual desensitization to feared objects: the highchair, bib, bottle, or spoon,” Dr. Chatoor explained. “It also involves training of the mother in behavioral techniques to feed the child in spite of the child’s fear and distress.”
Any underlying medical condition causing pain or distress should be treated. Additional measures may include, for example, use of a graduated approach, starting with liquids and progressing to purees, if the child fears solid foods, and prescribing anxiolytic medication in cases of severe anxiety.
Dr. Chatoor disclosed that she has lectured internationally at conferences on feeding disorders that were organized by Abbott Nutrition International and that the company provided a research grant for a study on feeding.
SAN FRANCISCO – Clinicians are likely to encounter diverse feeding problems in daily practice that will challenge their diagnostic and treatment acumen, Dr. Irene Chatoor told attendees of the annual meeting of the American Academy of Pediatrics.
These problems run the gamut from the most prevalent but least serious picky eating, to the least prevalent but most serious feeding disorders, she noted. Correspondingly, management will range from simple reassurance of parents to more intensive behavioral and medical interventions.
Assessment
“When you assess a feeding problem, you have to look at both the mother and father, and the child,” she advised. The parents are evaluated for their feeding style, while the child is evaluated for three feeding problems: limited appetite, selective intake, and fear of feeding (Pediatrics. 2015;135[2]:344-53).
Clinicians must be alert for organic red flags, such as dysphagia, aspiration, and vomiting, and for behavioral red flags, such as food fixation, abrupt cessation of feeding after a trigger event, and anticipatory gagging. An overarching red flag is failure to thrive.
Sometimes, a child will have both an organic condition and a behavioral feeding disorder at the same time. “It’s very important that you don’t think one excludes the other,” she cautioned.
Diagnosis
“To delineate milder feeding difficulties from feeding disorders, there must be some form of impairment caused by the feeding problem,” Dr. Chatoor commented. “Why is this important? For two reasons. One is for the insurance companies, because they don’t pay unless there is a disorder. And then there is research: you cannot do research unless you clearly define what you are studying.”
Children are considered to have impairment if they have weight loss or growth faltering, considerable nutritional deficiency, or a marked interference with psychosocial functioning.
“When we diagnose feeding problems, it is best done with a multidisciplinary team,” Dr. Chatoor maintained. “I have learned many years ago that I’m not effective in helping parents deal with the feeding disorder if they are still in the back of their mind worried that the child has something organically wrong and that’s why the child does not want to eat.”
Accordingly, various team members perform a medical examination, a nutritional assessment, an oral motor and sensory evaluation, and a psychiatric or psychological assessment to identify the root cause or causes of the problem.
When it comes to behavioral etiologies, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) now groups all feeding and eating disorders together in one section, reflecting the fact that disorders starting early in life can and often do track into adolescence and adulthood, according to Dr. Chatoor.
The manual also features a new diagnosis, avoidant/restrictive food intake disorder (ARFID). Key criteria include the presence of an eating or feeding disturbance that cannot be better explained by lack of available food, culturally sanctioned practices, or a concurrent medical condition or another mental disorder.
The child must have a persistent failure to meet appropriate nutritional and/or energy needs, associated with any of four findings: significant weight loss or failure to achieve expected weight gain or growth, significant nutritional deficiencies, dependence on enteral feeding or oral nutritional supplements, and marked interference with psychosocial functioning.
“You need to have at least one but often you have a combination of nutritional and emotional impairment in the same child,” she commented.
ARFID and its treatment
There are three subtypes of ARFID having different features, treatments, and prognosis, although they all share in common food refusal, according to Dr. Chatoor.
The first subtype – apparent lack of interest in eating or food – emerges by 3 years of age, most often during the transition to self-feeding between 9 and 18 months. Affected children refuse to eat an adequate amount of food for at least 1 month, rarely communicate hunger, lack interest in food, and prefer to play or talk. They typically present with growth deficiency.
“If you have a child who refuses to eat, it generates anxiety in the mother. The mother does things she would not normally do with the child who is eating well. She starts to distract, to cajole, to sometimes even force-feed the child,” Dr. Chatoor explained. “And the more she engages in these behaviors, the more resistant the child becomes. So they become trapped in this vicious cycle.”
Treatment is aimed at removing this conflict with three approaches: explaining to parents the infant’s special temperament (notably, high arousal and difficulty turning off excitement); addressing their background, including any eating issues of their own, and difficulty with setting limits; and providing specific feeding guidelines and a time-out procedure.
The guidelines stress regular feeding, withholding of all snacks, keeping the child at the table for 20 to 30 minutes, and not using any distractions or pressure. Also, importantly, the parents should have dinner with their child. “I always tell the parents what is good for the child is good for you. It’s good for your whole family,” she said. “If they have other children, these rules apply to everybody. Young children learn to eat by watching their parents eating.”
With early and consistent use of these interventions, about two-thirds of children outgrow this eating/feeding disturbance by mid-childhood, according to Dr. Chatoor.
Children with the second subtype of ARFID – avoidance based on the sensory characteristics of food – consistently refuse to eat certain foods having specific tastes, textures, temperatures, smells, and/or appearances. Onset occurs during the toddler years, when a new or different food is introduced.
“Not only do they refuse the same foods that were aversive, but they also generalize it. So these children are afraid to try other foods and they may end up limiting food groups – they don’t eat any vegetables and some of them don’t eat any meats,” she explained. “They are a challenge because this always causes a nutritional deficiency and they also have problems socially as they get older.”
Treatment varies by age, with gradual desensitization for infants and parent modeling of eating new foods for toddlers. A multifaceted approach is used for preschoolers, combining modeling, giving foods attractive shapes and names, having the child participate in food preparation, and using focused play therapy, such as feeding dolls who are “brave” and try new foods.
Clinicians can explain to affected school-aged children that they are “supertasters,” having more taste buds and therefore experiencing food more intensely, and that they can help their taste buds not react so strongly by starting to eat small amounts of new foods and gradually increasing over time. Parents can let the child make a list of 10 foods they would like to eat, and award them points for “courage” for every bite of a new food they try.
Prognosis of this type of ARFID varies, according to Dr. Chatoor. “Through gradual exposure, young children can expand the variety of foods they eat,” she elaborated. However, “some children become very rigid and brand sensitive in regard to the food they are willing to eat and begin to experience social problems during mid-childhood and adolescence. Some children grow up eating a limited diet, but finding ways to compensate nutritionally and socially.”
Children with the third subtype of ARFID – concern about aversive consequences of eating – have an acute onset of consistent food refusal at any age, from infancy onward, after experiencing a traumatic event or repeated traumatic insults to the oropharynx or gastrointestinal tract that trigger distress in the child. These children often have comorbidities such as gastroesophageal reflux, eosinophilic gastroenteritis, or anxiety disorder.
“Treatment involves gradual desensitization to feared objects: the highchair, bib, bottle, or spoon,” Dr. Chatoor explained. “It also involves training of the mother in behavioral techniques to feed the child in spite of the child’s fear and distress.”
Any underlying medical condition causing pain or distress should be treated. Additional measures may include, for example, use of a graduated approach, starting with liquids and progressing to purees, if the child fears solid foods, and prescribing anxiolytic medication in cases of severe anxiety.
Dr. Chatoor disclosed that she has lectured internationally at conferences on feeding disorders that were organized by Abbott Nutrition International and that the company provided a research grant for a study on feeding.
EXPERT ANALYSIS FROM AAP 16
Addiction potential
By nature, my wife and I are risk-averse people. Our investment strategy is just a few baby steps short of hiding our money under the mattress. We have never tried marijuana, though to some extent this is because we were out of college and already married when its popularity surged across this country’s campuses. We do drink alcohol, which was so ubiquitous when we were teenagers that it seemed innocuous.
Given my personality, you can understand why I have trouble understanding why anyone would ever try heroin or any opiate. I realize that many of the young addicts don’t follow the news closely enough to realize the risks. But the epidemic of addiction is so entrenched here in rural Maine that they must have known someone who has died of an overdose.

A recent op-ed piece in the New York Times describes a program that attempts to do just that (“The 4 Traits That Put Kids at Risk for Addiction,” by Maia Szalavitz, Sept. 29, 2016). The program is called Preventure and is the result of some work by Patricia Conrod, a psychiatry professor at the University of Montreal. It has been tried in Britain, Canada, Australia, and the Netherlands with some success in reducing binge drinking. In other studies, it reduced symptoms of depression, panic attacks, and impulsive behavior.
The program begins with testing middle school students and focuses on the traits of hopelessness, sensation-seeking, impulsiveness, and anxiety sensitivity. Hopeless is not a surprising choice given that many of the areas of this country with highest rates of opiate addiction are economically depressed. And it is easy to see why impulsivity and sensation-seeking are related to addiction potential. Anxiety-sensitivity is a less intuitive choice.
With the results of this testing in hand, the program administrators wait several months before approaching the outliers. The next step offers two 90-minute workshops to the entire school with the stated goal of showing how the students can channel their personalities toward success. Although the workshops are advertised as being open to everyone but limited in number of attendees, only the students identified as being at the highest risk are actually selected. It is hoped that this deception will avoid having the participants feel that they have been labeled. However, if a student asks about the selection process, he is given an honest answer. The workshops are targeted to the students’ specific emotional and behavioral vulnerabilities, and teaches cognitive behavioral techniques on how they can be managed.
While I think the deceptive selection process is a clever to wrinkle to avoid labeling, I wonder how long the ruse will survive should the program become more universally adopted. With increased popularity and publicity, every parent and most of the children in a school will realize why the test is being administered and what being selected for the workshop means. There is the threat that being identified as at risk for addiction will become a self-fulfilling prophecy and a trigger for depression.
Preventure sounds like a program worth watching. If larger series and long-term outcomes continue to be favorable, it will remain to be seen whether labeling is a hazard worth worrying about.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
By nature, my wife and I are risk-averse people. Our investment strategy is just a few baby steps short of hiding our money under the mattress. We have never tried marijuana, though to some extent this is because we were out of college and already married when its popularity surged across this country’s campuses. We do drink alcohol, which was so ubiquitous when we were teenagers that it seemed innocuous.
Given my personality, you can understand why I have trouble understanding why anyone would ever try heroin or any opiate. I realize that many of the young addicts don’t follow the news closely enough to realize the risks. But the epidemic of addiction is so entrenched here in rural Maine that they must have known someone who has died of an overdose.
A recent op-ed piece in the New York Times describes a program that attempts to do just that (“The 4 Traits That Put Kids at Risk for Addiction,” by Maia Szalavitz, Sept. 29, 2016). The program is called Preventure and is the result of some work by Patricia Conrod, a psychiatry professor at the University of Montreal. It has been tried in Britain, Canada, Australia, and the Netherlands with some success in reducing binge drinking. In other studies, it reduced symptoms of depression, panic attacks, and impulsive behavior.
The program begins with testing middle school students and focuses on the traits of hopelessness, sensation-seeking, impulsiveness, and anxiety sensitivity. Hopeless is not a surprising choice given that many of the areas of this country with highest rates of opiate addiction are economically depressed. And it is easy to see why impulsivity and sensation-seeking are related to addiction potential. Anxiety-sensitivity is a less intuitive choice.
With the results of this testing in hand, the program administrators wait several months before approaching the outliers. The next step offers two 90-minute workshops to the entire school with the stated goal of showing how the students can channel their personalities toward success. Although the workshops are advertised as being open to everyone but limited in number of attendees, only the students identified as being at the highest risk are actually selected. It is hoped that this deception will avoid having the participants feel that they have been labeled. However, if a student asks about the selection process, he is given an honest answer. The workshops are targeted to the students’ specific emotional and behavioral vulnerabilities, and teaches cognitive behavioral techniques on how they can be managed.
While I think the deceptive selection process is a clever to wrinkle to avoid labeling, I wonder how long the ruse will survive should the program become more universally adopted. With increased popularity and publicity, every parent and most of the children in a school will realize why the test is being administered and what being selected for the workshop means. There is the threat that being identified as at risk for addiction will become a self-fulfilling prophecy and a trigger for depression.
Preventure sounds like a program worth watching. If larger series and long-term outcomes continue to be favorable, it will remain to be seen whether labeling is a hazard worth worrying about.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
By nature, my wife and I are risk-averse people. Our investment strategy is just a few baby steps short of hiding our money under the mattress. We have never tried marijuana, though to some extent this is because we were out of college and already married when its popularity surged across this country’s campuses. We do drink alcohol, which was so ubiquitous when we were teenagers that it seemed innocuous.
Given my personality, you can understand why I have trouble understanding why anyone would ever try heroin or any opiate. I realize that many of the young addicts don’t follow the news closely enough to realize the risks. But the epidemic of addiction is so entrenched here in rural Maine that they must have known someone who has died of an overdose.
A recent op-ed piece in the New York Times describes a program that attempts to do just that (“The 4 Traits That Put Kids at Risk for Addiction,” by Maia Szalavitz, Sept. 29, 2016). The program is called Preventure and is the result of some work by Patricia Conrod, a psychiatry professor at the University of Montreal. It has been tried in Britain, Canada, Australia, and the Netherlands with some success in reducing binge drinking. In other studies, it reduced symptoms of depression, panic attacks, and impulsive behavior.
The program begins with testing middle school students and focuses on the traits of hopelessness, sensation-seeking, impulsiveness, and anxiety sensitivity. Hopeless is not a surprising choice given that many of the areas of this country with highest rates of opiate addiction are economically depressed. And it is easy to see why impulsivity and sensation-seeking are related to addiction potential. Anxiety-sensitivity is a less intuitive choice.
With the results of this testing in hand, the program administrators wait several months before approaching the outliers. The next step offers two 90-minute workshops to the entire school with the stated goal of showing how the students can channel their personalities toward success. Although the workshops are advertised as being open to everyone but limited in number of attendees, only the students identified as being at the highest risk are actually selected. It is hoped that this deception will avoid having the participants feel that they have been labeled. However, if a student asks about the selection process, he is given an honest answer. The workshops are targeted to the students’ specific emotional and behavioral vulnerabilities, and teaches cognitive behavioral techniques on how they can be managed.
While I think the deceptive selection process is a clever to wrinkle to avoid labeling, I wonder how long the ruse will survive should the program become more universally adopted. With increased popularity and publicity, every parent and most of the children in a school will realize why the test is being administered and what being selected for the workshop means. There is the threat that being identified as at risk for addiction will become a self-fulfilling prophecy and a trigger for depression.
Preventure sounds like a program worth watching. If larger series and long-term outcomes continue to be favorable, it will remain to be seen whether labeling is a hazard worth worrying about.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Panobinostat might treat high-risk ALL subtype

Photo courtesy of Novartis
Researchers say they have identified a high-risk subtype of acute lymphoblastic leukemia (ALL) that may respond to treatment with the histone deacetylase (HDAC) inhibitor panobinostat.
The ALL subtype is characterized by chromosomal rearrangements that involve the MEF2D gene and 1 of 6 partner genes, most often BCL9.
The researchers described this subtype, known as MEF2D-rearranged ALL, in Nature Communications.
“MEF2D is a transcription factor that switches on expression of other genes during normal development,” said study author Charles Mullighan, MD, MBBS, of the St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We found that MEF2D chromosomal rearrangements disrupt expression of those genes and create a vulnerability to at least one targeted therapy, the drug panobinostat.”
Dr Mullighan and his colleagues performed genomic analyses on samples from a total of 1724 children, adolescents, and adults with ALL. This revealed 52 patients with MEF2D rearrangements.
MEF2D-rearranged ALL
The researchers calculated that MEF2D-rearranged ALL accounted for 5.3% of the ALL cases whose genetic basis was unknown.
The team also noted that MEF2D-rearranged ALL occurred most frequently in adolescents. Although, overall, ALL occurs most often in children between 3 and 5 years old, the average patient with MEF2D-rearranged ALL was 14.
In addition, MEF2D-rearranged ALL was associated with reduced survival when compared to some other ALL subtypes. The 5-year cancer-free survival for MEF2D-rearranged ALL patients was 71.6%.
The researchers also found that a fusion protein resulting from the MEF2D rearrangement led to sustained growth of mouse cells when compared to wild-type MEF2D or other proteins.
“That indicates the MEF2D fusion is a key step in transforming a normal white blood cell with a finite lifespan into a leukemic cell that is immortal,” Dr Mullighan said.
Role for panobinostat
MEF2D-rearranged leukemic cells produced high levels of HDAC9, which is targeted by panobinostat.
The researchers tested panobinostat in the lab and found the drug stopped proliferation of human MEF2D-rearranged leukemic cells.
Dr Mullighan said MEF2D-rearranged leukemic cells were exquisitely sensitive to panobinostat, which suggested the drug might function in a more targeted manner against cells with the rearrangement.
“If further testing of panobinostat, either alone or in combination therapy, confirms the anti-proliferative activity, that would lay the foundation for a clinical trial in patients, particularly patients with high-risk disease or those who have relapsed,” he said. ![]()
Photo courtesy of Novartis
Researchers say they have identified a high-risk subtype of acute lymphoblastic leukemia (ALL) that may respond to treatment with the histone deacetylase (HDAC) inhibitor panobinostat.
The ALL subtype is characterized by chromosomal rearrangements that involve the MEF2D gene and 1 of 6 partner genes, most often BCL9.
The researchers described this subtype, known as MEF2D-rearranged ALL, in Nature Communications.
“MEF2D is a transcription factor that switches on expression of other genes during normal development,” said study author Charles Mullighan, MD, MBBS, of the St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We found that MEF2D chromosomal rearrangements disrupt expression of those genes and create a vulnerability to at least one targeted therapy, the drug panobinostat.”
Dr Mullighan and his colleagues performed genomic analyses on samples from a total of 1724 children, adolescents, and adults with ALL. This revealed 52 patients with MEF2D rearrangements.
MEF2D-rearranged ALL
The researchers calculated that MEF2D-rearranged ALL accounted for 5.3% of the ALL cases whose genetic basis was unknown.
The team also noted that MEF2D-rearranged ALL occurred most frequently in adolescents. Although, overall, ALL occurs most often in children between 3 and 5 years old, the average patient with MEF2D-rearranged ALL was 14.
In addition, MEF2D-rearranged ALL was associated with reduced survival when compared to some other ALL subtypes. The 5-year cancer-free survival for MEF2D-rearranged ALL patients was 71.6%.
The researchers also found that a fusion protein resulting from the MEF2D rearrangement led to sustained growth of mouse cells when compared to wild-type MEF2D or other proteins.
“That indicates the MEF2D fusion is a key step in transforming a normal white blood cell with a finite lifespan into a leukemic cell that is immortal,” Dr Mullighan said.
Role for panobinostat
MEF2D-rearranged leukemic cells produced high levels of HDAC9, which is targeted by panobinostat.
The researchers tested panobinostat in the lab and found the drug stopped proliferation of human MEF2D-rearranged leukemic cells.
Dr Mullighan said MEF2D-rearranged leukemic cells were exquisitely sensitive to panobinostat, which suggested the drug might function in a more targeted manner against cells with the rearrangement.
“If further testing of panobinostat, either alone or in combination therapy, confirms the anti-proliferative activity, that would lay the foundation for a clinical trial in patients, particularly patients with high-risk disease or those who have relapsed,” he said. ![]()
Photo courtesy of Novartis
Researchers say they have identified a high-risk subtype of acute lymphoblastic leukemia (ALL) that may respond to treatment with the histone deacetylase (HDAC) inhibitor panobinostat.
The ALL subtype is characterized by chromosomal rearrangements that involve the MEF2D gene and 1 of 6 partner genes, most often BCL9.
The researchers described this subtype, known as MEF2D-rearranged ALL, in Nature Communications.
“MEF2D is a transcription factor that switches on expression of other genes during normal development,” said study author Charles Mullighan, MD, MBBS, of the St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We found that MEF2D chromosomal rearrangements disrupt expression of those genes and create a vulnerability to at least one targeted therapy, the drug panobinostat.”
Dr Mullighan and his colleagues performed genomic analyses on samples from a total of 1724 children, adolescents, and adults with ALL. This revealed 52 patients with MEF2D rearrangements.
MEF2D-rearranged ALL
The researchers calculated that MEF2D-rearranged ALL accounted for 5.3% of the ALL cases whose genetic basis was unknown.
The team also noted that MEF2D-rearranged ALL occurred most frequently in adolescents. Although, overall, ALL occurs most often in children between 3 and 5 years old, the average patient with MEF2D-rearranged ALL was 14.
In addition, MEF2D-rearranged ALL was associated with reduced survival when compared to some other ALL subtypes. The 5-year cancer-free survival for MEF2D-rearranged ALL patients was 71.6%.
The researchers also found that a fusion protein resulting from the MEF2D rearrangement led to sustained growth of mouse cells when compared to wild-type MEF2D or other proteins.
“That indicates the MEF2D fusion is a key step in transforming a normal white blood cell with a finite lifespan into a leukemic cell that is immortal,” Dr Mullighan said.
Role for panobinostat
MEF2D-rearranged leukemic cells produced high levels of HDAC9, which is targeted by panobinostat.
The researchers tested panobinostat in the lab and found the drug stopped proliferation of human MEF2D-rearranged leukemic cells.
Dr Mullighan said MEF2D-rearranged leukemic cells were exquisitely sensitive to panobinostat, which suggested the drug might function in a more targeted manner against cells with the rearrangement.
“If further testing of panobinostat, either alone or in combination therapy, confirms the anti-proliferative activity, that would lay the foundation for a clinical trial in patients, particularly patients with high-risk disease or those who have relapsed,” he said. ![]()
Flushing Lesion on 4-Month-Old Boy
IN THIS ARTICLE
- Clinical presentation
- Disease triggers
- Outcome for the case patient
A 4-month-old white boy is brought to the allergy office for evaluation of a lesion on his back, first noticed when he was one month old. His parents report that on two separate occasions he developed a bright red, whole-body rash that resolved on its own. He is described as a “fussy” baby who has been on both milk- and soy-based formulas. Aside from mild eczema and infantile seborrheic dermatitis, his medical history is unremarkable.
Physical examination reveals a reddish, 3-cm plaque on his left upper back that, when stroked, exhibits an immediate urticarial response. The patient is given cetirizine in the office and within 45 minutes, the flushing resolves. A normal tryptase level is obtained. The patient is diagnosed with a solitary mastocytoma.

DISCUSSION
Mast cells play a central role in allergic rhinitis, asthma, eczema, and anaphylaxis; they are also a vital component in the inflammatory process. Cutaneous mastocytosis is a pathologic increase in mast cells that, when degranulated, release histamine and tryptase.1 Histamine is produced equally by both mast cells and basophils, while the production of tryptase is relatively specific to mast cells. An elevated tryptase level is indicative of mast cell activation. The signs and symptoms associated with cutaneous mastocytosis are due to the release of these mediators.2
While there is no gender bias for cutaneous mastocytosis, there is a bimodal distribution: Children from birth to age 2 account for 55% of cases, whereas 35% of cases occur in those older than 15—the remaining 10% are between these ages.1 During the first year of life, 60% to 80% of patients with cutaneous mastocytosis will develop lesions. Familial cases are rare.2
Clinical presentation
The presentation of cutaneous mastocytosis can vary. It is often mistaken for common childhood rashes such as poison ivy, eczema, or hives. The effects of histamine and tryptase cause children to present with pruritus, flushing, and headache. Gastrointestinal symptoms, such as abdominal pain and diarrhea, can also occur as a result of histamine release. Symptoms can occur spontaneously or be induced by certain triggers (see Table).3
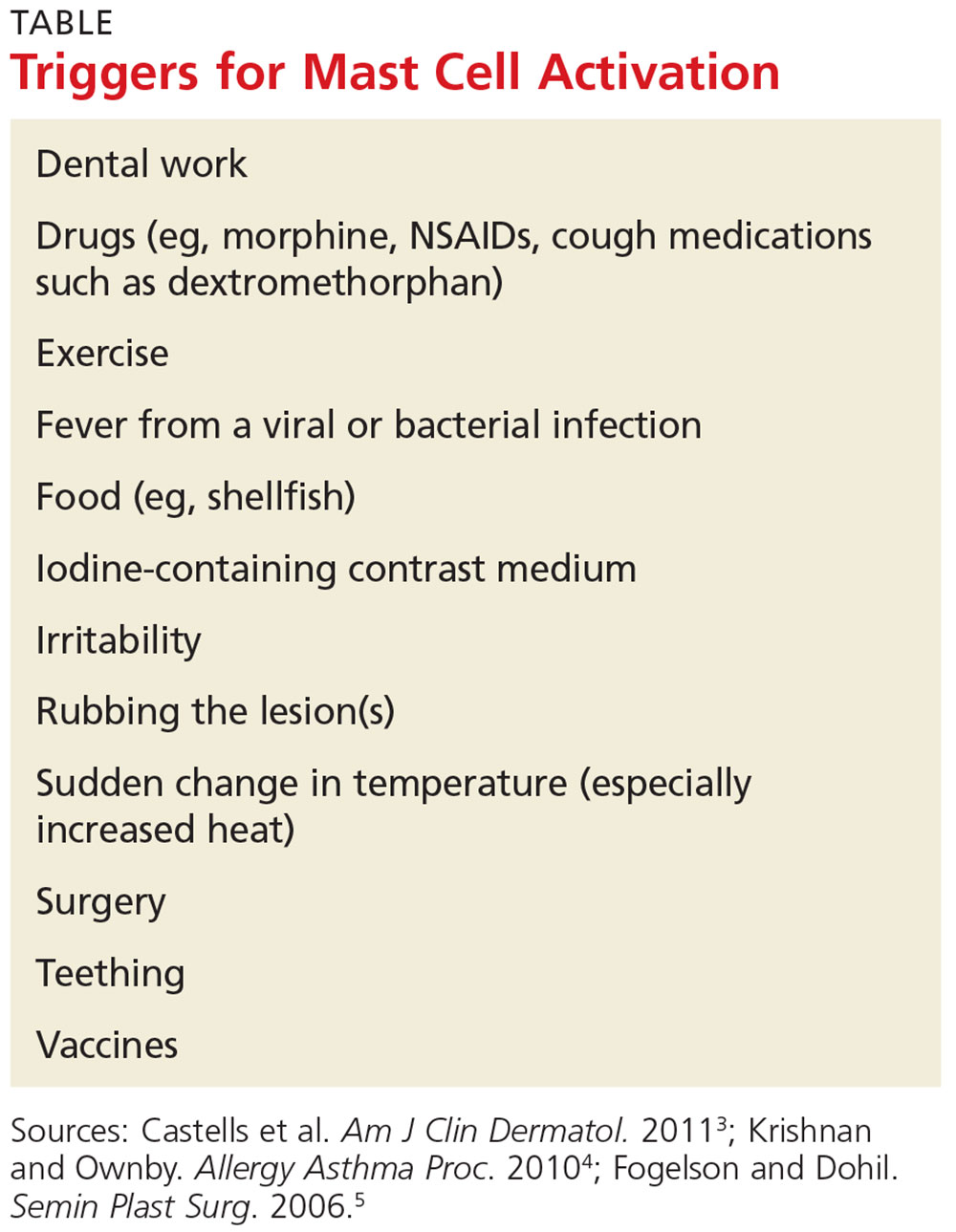
There are three types of cutaneous mastocytosis: urticarial pigmentosa (UP), solitary mastocytoma, and diffuse cutaneous mastocytosis (DCM). UP is the most common, representing 70% to 90% of all cases.3 It typically manifests as multiple red, brown, or yellow lesions that are small (usually < 2 cm). A positive Darier sign (the formation of a wheal and flare after stroking one or several lesions) is common in these patients.2,3
Solitary mastocytomas are single, indurated, red-brown macules, papules, or plaques.4 Frequently seen on the trunk, extremities, head, or neck, these lesions resemble UP but are larger (up to several centimeters in diameter).2,4 A positive Darier sign is elicited in approximately 50% of these patients.4 Solitary mastocytomas are seen in 10% to 15% of children with cutaneous mastocytosis.4
DCM accounts for only 1% to 3% of cases and typically involves the entire skin, which is usually thick, with a normal or yellowish brown color.3 Affected patients may experience blistering and bullae. Severe symptoms, including whole-body flushing, pruritus, diarrhea, intestinal bleeding, hypotension, anemia, and hypovolemic shock, can occur; deaths have been reported.2
Diagnostic evaluation
Following a thorough history and physical exam, the diagnosis of cutaneous mastocytosis can be made based on clinical findings.5 It can be confirmed by a punch biopsy of the lesion and measurement of serum tryptase levels; higher levels have been shown to correlate to the number of mast cells in the skin and the child’s cutaneous disease burden.2,4 Ordering baseline tryptase levels can also help distinguish children at risk for severe episodes of mast cell activation from those who may just have a mild case.6
If the patient exhibits symptoms suggestive of systemic mastocytosis (an abnormal increase in mast cells in extracutaneous organs, including bone marrow) or there is suspicion for malignancy, efforts must be made to rule out these more serious diagnoses. A complete white blood cell count with differential, metabolic profile with liver enzymes, and sedimentation rate should be obtained.4
Treatment
The treatment of cutaneous mastocytosis is symptomatic, as it is typically a benign disease. The goal of therapy is to prevent mast cell activation, and hence the symptoms that occur when mast cells release their mediators, by avoiding obvious triggers.4
NSAIDs have been reported to cause mast cell mediator release and should therefore be avoided. Since extremes in temperature—particularly heat—can lead to mast cell activation, it is important to control the temperature of a bath or swimming pool and to be wary of exposure to air conditioning. Though easier said than done, soothing crying babies and children is also helpful, as irritability is a known trigger. Management of anxiety and avoidance of stress when possible is recommended.2
Treatment usually begins with H1 and H2 blockers. Cetirizine and diphenhydramine work to control the itching, while ranitidine and famotidine help manage gastric acid secretion when there are symptoms of abdominal pain and peptic ulcer disease.3 Hydroxyzine is effective in controlling both itch and gastric acid secretion.4 Water-soluble cromolyn sodium cream helps to decrease the itch and flare of a mastocytoma; the oral form is also effective.3 Another option to relieve itching is to apply topical corticosteroids with an occlusive dressing.
An epinephrine auto-injector is recommended due to the risk for anaphylaxis; this risk, however, has not been clearly established in cutaneous mastocytosis, specifically in DCM. During an acute and severe flare that induces hypotension, wheezing, and/or laryngeal edema, epinephrine should be administered while the child is lying down.3,4
Surgical excision can be considered when other treatment options fail, or if the lesion is located on the scalp, flexure area, palm, or sole.3,4
Prognosis
The prognosis for a child with a solitary mastocytoma is extremely good. By the time the child reaches puberty, there is typically spontaneous regression.
If any type of mastocytoma persists beyond adolescence, or tryptase levels continue to rise after puberty, however, that raises concern for progression to systemic mastocytosis. Although this diagnosis is rare in children, bone marrow studies may be necessary to determine the patient’s course.1
OUTCOME FOR THE CASE PATIENT
The patient was placed on daily cetirizine. His parents were advised not to irritate the lesion and were educated on possible triggers, including the need to avoid NSAIDs. They were also trained in the use of an epinephrine auto-injector.
CONCLUSION
Cutaneous mastocytosis should be included in the differential diagnosis of rashes and skin lesions in pediatric patients. It is important to be able to recognize the presenting signs and symptoms of a mastocytoma and to monitor the lesion over time.4 Educating the child’s parents, teachers, and caregivers about potential triggers and treatment of a mast cell activation attack can help minimize the symptoms.
1. Frieri M, Quershi M. Pediatric mastocytosis: a review of the literature. Pediatr Allergy Immunol Pulmonol. 2013;26(4):175-180.
2. Castells M, Metcalfe DD, Escribano L. Guidelines for the diagnosis and treatment of cutaneous mastocytosis in children. Am J Clin Dermatol. 2011;12(4):259-270.
3. Castells M, Metcalfe DD, Escribano L. Diagnosis and treatment of cutaneous mastocytosis in children: practical recommendations. Am J Clin Dermatol. 2011;12(4):259-270.
4. Krishnan K, Ownby DR. A solitary mastocytoma presenting with urticaria and angioedema in a 14-year-old boy. Allergy Asthma Proc. 2010;31(6):520-523.
5. Fogelson SK, Dohil MA. Papular and nodular skin lesions in children. Semin Plast Surg. 2006;20(3):180-191.
6. Alvarez-Twose I, Vañó-Galván S, Sánchez-Muñoz L, et al. Increased serum baseline tryptase levels and extensive skin involvement are predictors for the severity of mast cell activation episodes in children with mastocytosis. Allergy. 2012;67(6):813-821.
IN THIS ARTICLE
- Clinical presentation
- Disease triggers
- Outcome for the case patient
A 4-month-old white boy is brought to the allergy office for evaluation of a lesion on his back, first noticed when he was one month old. His parents report that on two separate occasions he developed a bright red, whole-body rash that resolved on its own. He is described as a “fussy” baby who has been on both milk- and soy-based formulas. Aside from mild eczema and infantile seborrheic dermatitis, his medical history is unremarkable.
Physical examination reveals a reddish, 3-cm plaque on his left upper back that, when stroked, exhibits an immediate urticarial response. The patient is given cetirizine in the office and within 45 minutes, the flushing resolves. A normal tryptase level is obtained. The patient is diagnosed with a solitary mastocytoma.
DISCUSSION
Mast cells play a central role in allergic rhinitis, asthma, eczema, and anaphylaxis; they are also a vital component in the inflammatory process. Cutaneous mastocytosis is a pathologic increase in mast cells that, when degranulated, release histamine and tryptase.1 Histamine is produced equally by both mast cells and basophils, while the production of tryptase is relatively specific to mast cells. An elevated tryptase level is indicative of mast cell activation. The signs and symptoms associated with cutaneous mastocytosis are due to the release of these mediators.2
While there is no gender bias for cutaneous mastocytosis, there is a bimodal distribution: Children from birth to age 2 account for 55% of cases, whereas 35% of cases occur in those older than 15—the remaining 10% are between these ages.1 During the first year of life, 60% to 80% of patients with cutaneous mastocytosis will develop lesions. Familial cases are rare.2
Clinical presentation
The presentation of cutaneous mastocytosis can vary. It is often mistaken for common childhood rashes such as poison ivy, eczema, or hives. The effects of histamine and tryptase cause children to present with pruritus, flushing, and headache. Gastrointestinal symptoms, such as abdominal pain and diarrhea, can also occur as a result of histamine release. Symptoms can occur spontaneously or be induced by certain triggers (see Table).3
There are three types of cutaneous mastocytosis: urticarial pigmentosa (UP), solitary mastocytoma, and diffuse cutaneous mastocytosis (DCM). UP is the most common, representing 70% to 90% of all cases.3 It typically manifests as multiple red, brown, or yellow lesions that are small (usually < 2 cm). A positive Darier sign (the formation of a wheal and flare after stroking one or several lesions) is common in these patients.2,3
Solitary mastocytomas are single, indurated, red-brown macules, papules, or plaques.4 Frequently seen on the trunk, extremities, head, or neck, these lesions resemble UP but are larger (up to several centimeters in diameter).2,4 A positive Darier sign is elicited in approximately 50% of these patients.4 Solitary mastocytomas are seen in 10% to 15% of children with cutaneous mastocytosis.4
DCM accounts for only 1% to 3% of cases and typically involves the entire skin, which is usually thick, with a normal or yellowish brown color.3 Affected patients may experience blistering and bullae. Severe symptoms, including whole-body flushing, pruritus, diarrhea, intestinal bleeding, hypotension, anemia, and hypovolemic shock, can occur; deaths have been reported.2
Diagnostic evaluation
Following a thorough history and physical exam, the diagnosis of cutaneous mastocytosis can be made based on clinical findings.5 It can be confirmed by a punch biopsy of the lesion and measurement of serum tryptase levels; higher levels have been shown to correlate to the number of mast cells in the skin and the child’s cutaneous disease burden.2,4 Ordering baseline tryptase levels can also help distinguish children at risk for severe episodes of mast cell activation from those who may just have a mild case.6
If the patient exhibits symptoms suggestive of systemic mastocytosis (an abnormal increase in mast cells in extracutaneous organs, including bone marrow) or there is suspicion for malignancy, efforts must be made to rule out these more serious diagnoses. A complete white blood cell count with differential, metabolic profile with liver enzymes, and sedimentation rate should be obtained.4
Treatment
The treatment of cutaneous mastocytosis is symptomatic, as it is typically a benign disease. The goal of therapy is to prevent mast cell activation, and hence the symptoms that occur when mast cells release their mediators, by avoiding obvious triggers.4
NSAIDs have been reported to cause mast cell mediator release and should therefore be avoided. Since extremes in temperature—particularly heat—can lead to mast cell activation, it is important to control the temperature of a bath or swimming pool and to be wary of exposure to air conditioning. Though easier said than done, soothing crying babies and children is also helpful, as irritability is a known trigger. Management of anxiety and avoidance of stress when possible is recommended.2
Treatment usually begins with H1 and H2 blockers. Cetirizine and diphenhydramine work to control the itching, while ranitidine and famotidine help manage gastric acid secretion when there are symptoms of abdominal pain and peptic ulcer disease.3 Hydroxyzine is effective in controlling both itch and gastric acid secretion.4 Water-soluble cromolyn sodium cream helps to decrease the itch and flare of a mastocytoma; the oral form is also effective.3 Another option to relieve itching is to apply topical corticosteroids with an occlusive dressing.
An epinephrine auto-injector is recommended due to the risk for anaphylaxis; this risk, however, has not been clearly established in cutaneous mastocytosis, specifically in DCM. During an acute and severe flare that induces hypotension, wheezing, and/or laryngeal edema, epinephrine should be administered while the child is lying down.3,4
Surgical excision can be considered when other treatment options fail, or if the lesion is located on the scalp, flexure area, palm, or sole.3,4
Prognosis
The prognosis for a child with a solitary mastocytoma is extremely good. By the time the child reaches puberty, there is typically spontaneous regression.
If any type of mastocytoma persists beyond adolescence, or tryptase levels continue to rise after puberty, however, that raises concern for progression to systemic mastocytosis. Although this diagnosis is rare in children, bone marrow studies may be necessary to determine the patient’s course.1
OUTCOME FOR THE CASE PATIENT
The patient was placed on daily cetirizine. His parents were advised not to irritate the lesion and were educated on possible triggers, including the need to avoid NSAIDs. They were also trained in the use of an epinephrine auto-injector.
CONCLUSION
Cutaneous mastocytosis should be included in the differential diagnosis of rashes and skin lesions in pediatric patients. It is important to be able to recognize the presenting signs and symptoms of a mastocytoma and to monitor the lesion over time.4 Educating the child’s parents, teachers, and caregivers about potential triggers and treatment of a mast cell activation attack can help minimize the symptoms.
IN THIS ARTICLE
- Clinical presentation
- Disease triggers
- Outcome for the case patient
A 4-month-old white boy is brought to the allergy office for evaluation of a lesion on his back, first noticed when he was one month old. His parents report that on two separate occasions he developed a bright red, whole-body rash that resolved on its own. He is described as a “fussy” baby who has been on both milk- and soy-based formulas. Aside from mild eczema and infantile seborrheic dermatitis, his medical history is unremarkable.
Physical examination reveals a reddish, 3-cm plaque on his left upper back that, when stroked, exhibits an immediate urticarial response. The patient is given cetirizine in the office and within 45 minutes, the flushing resolves. A normal tryptase level is obtained. The patient is diagnosed with a solitary mastocytoma.
DISCUSSION
Mast cells play a central role in allergic rhinitis, asthma, eczema, and anaphylaxis; they are also a vital component in the inflammatory process. Cutaneous mastocytosis is a pathologic increase in mast cells that, when degranulated, release histamine and tryptase.1 Histamine is produced equally by both mast cells and basophils, while the production of tryptase is relatively specific to mast cells. An elevated tryptase level is indicative of mast cell activation. The signs and symptoms associated with cutaneous mastocytosis are due to the release of these mediators.2
While there is no gender bias for cutaneous mastocytosis, there is a bimodal distribution: Children from birth to age 2 account for 55% of cases, whereas 35% of cases occur in those older than 15—the remaining 10% are between these ages.1 During the first year of life, 60% to 80% of patients with cutaneous mastocytosis will develop lesions. Familial cases are rare.2
Clinical presentation
The presentation of cutaneous mastocytosis can vary. It is often mistaken for common childhood rashes such as poison ivy, eczema, or hives. The effects of histamine and tryptase cause children to present with pruritus, flushing, and headache. Gastrointestinal symptoms, such as abdominal pain and diarrhea, can also occur as a result of histamine release. Symptoms can occur spontaneously or be induced by certain triggers (see Table).3
There are three types of cutaneous mastocytosis: urticarial pigmentosa (UP), solitary mastocytoma, and diffuse cutaneous mastocytosis (DCM). UP is the most common, representing 70% to 90% of all cases.3 It typically manifests as multiple red, brown, or yellow lesions that are small (usually < 2 cm). A positive Darier sign (the formation of a wheal and flare after stroking one or several lesions) is common in these patients.2,3
Solitary mastocytomas are single, indurated, red-brown macules, papules, or plaques.4 Frequently seen on the trunk, extremities, head, or neck, these lesions resemble UP but are larger (up to several centimeters in diameter).2,4 A positive Darier sign is elicited in approximately 50% of these patients.4 Solitary mastocytomas are seen in 10% to 15% of children with cutaneous mastocytosis.4
DCM accounts for only 1% to 3% of cases and typically involves the entire skin, which is usually thick, with a normal or yellowish brown color.3 Affected patients may experience blistering and bullae. Severe symptoms, including whole-body flushing, pruritus, diarrhea, intestinal bleeding, hypotension, anemia, and hypovolemic shock, can occur; deaths have been reported.2
Diagnostic evaluation
Following a thorough history and physical exam, the diagnosis of cutaneous mastocytosis can be made based on clinical findings.5 It can be confirmed by a punch biopsy of the lesion and measurement of serum tryptase levels; higher levels have been shown to correlate to the number of mast cells in the skin and the child’s cutaneous disease burden.2,4 Ordering baseline tryptase levels can also help distinguish children at risk for severe episodes of mast cell activation from those who may just have a mild case.6
If the patient exhibits symptoms suggestive of systemic mastocytosis (an abnormal increase in mast cells in extracutaneous organs, including bone marrow) or there is suspicion for malignancy, efforts must be made to rule out these more serious diagnoses. A complete white blood cell count with differential, metabolic profile with liver enzymes, and sedimentation rate should be obtained.4
Treatment
The treatment of cutaneous mastocytosis is symptomatic, as it is typically a benign disease. The goal of therapy is to prevent mast cell activation, and hence the symptoms that occur when mast cells release their mediators, by avoiding obvious triggers.4
NSAIDs have been reported to cause mast cell mediator release and should therefore be avoided. Since extremes in temperature—particularly heat—can lead to mast cell activation, it is important to control the temperature of a bath or swimming pool and to be wary of exposure to air conditioning. Though easier said than done, soothing crying babies and children is also helpful, as irritability is a known trigger. Management of anxiety and avoidance of stress when possible is recommended.2
Treatment usually begins with H1 and H2 blockers. Cetirizine and diphenhydramine work to control the itching, while ranitidine and famotidine help manage gastric acid secretion when there are symptoms of abdominal pain and peptic ulcer disease.3 Hydroxyzine is effective in controlling both itch and gastric acid secretion.4 Water-soluble cromolyn sodium cream helps to decrease the itch and flare of a mastocytoma; the oral form is also effective.3 Another option to relieve itching is to apply topical corticosteroids with an occlusive dressing.
An epinephrine auto-injector is recommended due to the risk for anaphylaxis; this risk, however, has not been clearly established in cutaneous mastocytosis, specifically in DCM. During an acute and severe flare that induces hypotension, wheezing, and/or laryngeal edema, epinephrine should be administered while the child is lying down.3,4
Surgical excision can be considered when other treatment options fail, or if the lesion is located on the scalp, flexure area, palm, or sole.3,4
Prognosis
The prognosis for a child with a solitary mastocytoma is extremely good. By the time the child reaches puberty, there is typically spontaneous regression.
If any type of mastocytoma persists beyond adolescence, or tryptase levels continue to rise after puberty, however, that raises concern for progression to systemic mastocytosis. Although this diagnosis is rare in children, bone marrow studies may be necessary to determine the patient’s course.1
OUTCOME FOR THE CASE PATIENT
The patient was placed on daily cetirizine. His parents were advised not to irritate the lesion and were educated on possible triggers, including the need to avoid NSAIDs. They were also trained in the use of an epinephrine auto-injector.
CONCLUSION
Cutaneous mastocytosis should be included in the differential diagnosis of rashes and skin lesions in pediatric patients. It is important to be able to recognize the presenting signs and symptoms of a mastocytoma and to monitor the lesion over time.4 Educating the child’s parents, teachers, and caregivers about potential triggers and treatment of a mast cell activation attack can help minimize the symptoms.
1. Frieri M, Quershi M. Pediatric mastocytosis: a review of the literature. Pediatr Allergy Immunol Pulmonol. 2013;26(4):175-180.
2. Castells M, Metcalfe DD, Escribano L. Guidelines for the diagnosis and treatment of cutaneous mastocytosis in children. Am J Clin Dermatol. 2011;12(4):259-270.
3. Castells M, Metcalfe DD, Escribano L. Diagnosis and treatment of cutaneous mastocytosis in children: practical recommendations. Am J Clin Dermatol. 2011;12(4):259-270.
4. Krishnan K, Ownby DR. A solitary mastocytoma presenting with urticaria and angioedema in a 14-year-old boy. Allergy Asthma Proc. 2010;31(6):520-523.
5. Fogelson SK, Dohil MA. Papular and nodular skin lesions in children. Semin Plast Surg. 2006;20(3):180-191.
6. Alvarez-Twose I, Vañó-Galván S, Sánchez-Muñoz L, et al. Increased serum baseline tryptase levels and extensive skin involvement are predictors for the severity of mast cell activation episodes in children with mastocytosis. Allergy. 2012;67(6):813-821.
1. Frieri M, Quershi M. Pediatric mastocytosis: a review of the literature. Pediatr Allergy Immunol Pulmonol. 2013;26(4):175-180.
2. Castells M, Metcalfe DD, Escribano L. Guidelines for the diagnosis and treatment of cutaneous mastocytosis in children. Am J Clin Dermatol. 2011;12(4):259-270.
3. Castells M, Metcalfe DD, Escribano L. Diagnosis and treatment of cutaneous mastocytosis in children: practical recommendations. Am J Clin Dermatol. 2011;12(4):259-270.
4. Krishnan K, Ownby DR. A solitary mastocytoma presenting with urticaria and angioedema in a 14-year-old boy. Allergy Asthma Proc. 2010;31(6):520-523.
5. Fogelson SK, Dohil MA. Papular and nodular skin lesions in children. Semin Plast Surg. 2006;20(3):180-191.
6. Alvarez-Twose I, Vañó-Galván S, Sánchez-Muñoz L, et al. Increased serum baseline tryptase levels and extensive skin involvement are predictors for the severity of mast cell activation episodes in children with mastocytosis. Allergy. 2012;67(6):813-821.
